User login
Study supports giving anticoagulants ‘as needed’

Photo courtesy of the CDC
SAN FRANCISCO—New research suggests patients with atrial fibrillation (AF) may benefit from receiving novel oral anticoagulants on an “as-needed” basis.
The study indicated that anticoagulant therapy guided by diligent pulse monitoring can be a safe and effective alternative to long-term anticoagulant therapy for lowering the overall risk of stroke in AF patients.
This finding was presented at the Heart Rhythm Society’s 37th Annual Scientific Session (abstract AB21-06).
The researchers studied 100 AF patients, ages 45 to 78, who had significant stroke risk. All patients had no AF recurrences during an extended period of telemetry monitoring before the study began.
Eighty-four patients had been ablated, 16 were being treated with drug therapy, and 3 had implanted devices that served as a quality control check.
Each patient was instructed to monitor his or her pulse—manually or by using a smartphone—twice a day and take an anticoagulant as needed. The patients were provided with novel oral anticoagulants and were instructed to start taking the medication if they suspected or detected an AF episode lasting longer than 1 hour.
“This kind of approach to anticoagulation therapy requires an open line of communication between the patient and the care team and calls for a specific type of patient,” said Monica Pammer, a physician assistant at the Hospital of the University of Pennsylvania in Philadelphia.
“We call them ‘highly motivated patients.’ These are patients who were actively seeking, preparing for, and are committed to the alternate treatment method, and who are informed about how to diligently and effectively monitor their pulse throughout the day.”
The researchers followed the patients for approximately 23 months.
During this time, 28 patients started taking an anticoagulant at least once for a suspected or detected AF episode, and 10 patients transitioned back to chronic oral anticoagulation therapy for recurrent AF.
None of the patients experienced a stroke or transient ischemic attack, but there was 1 mild bleeding incident that required medical attention.
“It is extremely common for patients with AF to seek treatment that does not involve the use of chronic oral anticoagulants therapy, as there are other risks associated with their long-term use,” said Francis E. Marchlinski, MD, of the University of Pennsylvania Health System.
“The goal of this study was to find a safe and effective treatment option, and our initial results support ‘as-needed’ blood thinners and pulse monitoring as the alternative.”
“While this is an observational study with a relatively small patient sample, further research is certainly needed to better understand alternate treatment options,” Pammer said. “And we stress that ‘as-needed’ blood thinners should not be considered unless the patient qualifies as highly motivated.” ![]()
Photo courtesy of the CDC
SAN FRANCISCO—New research suggests patients with atrial fibrillation (AF) may benefit from receiving novel oral anticoagulants on an “as-needed” basis.
The study indicated that anticoagulant therapy guided by diligent pulse monitoring can be a safe and effective alternative to long-term anticoagulant therapy for lowering the overall risk of stroke in AF patients.
This finding was presented at the Heart Rhythm Society’s 37th Annual Scientific Session (abstract AB21-06).
The researchers studied 100 AF patients, ages 45 to 78, who had significant stroke risk. All patients had no AF recurrences during an extended period of telemetry monitoring before the study began.
Eighty-four patients had been ablated, 16 were being treated with drug therapy, and 3 had implanted devices that served as a quality control check.
Each patient was instructed to monitor his or her pulse—manually or by using a smartphone—twice a day and take an anticoagulant as needed. The patients were provided with novel oral anticoagulants and were instructed to start taking the medication if they suspected or detected an AF episode lasting longer than 1 hour.
“This kind of approach to anticoagulation therapy requires an open line of communication between the patient and the care team and calls for a specific type of patient,” said Monica Pammer, a physician assistant at the Hospital of the University of Pennsylvania in Philadelphia.
“We call them ‘highly motivated patients.’ These are patients who were actively seeking, preparing for, and are committed to the alternate treatment method, and who are informed about how to diligently and effectively monitor their pulse throughout the day.”
The researchers followed the patients for approximately 23 months.
During this time, 28 patients started taking an anticoagulant at least once for a suspected or detected AF episode, and 10 patients transitioned back to chronic oral anticoagulation therapy for recurrent AF.
None of the patients experienced a stroke or transient ischemic attack, but there was 1 mild bleeding incident that required medical attention.
“It is extremely common for patients with AF to seek treatment that does not involve the use of chronic oral anticoagulants therapy, as there are other risks associated with their long-term use,” said Francis E. Marchlinski, MD, of the University of Pennsylvania Health System.
“The goal of this study was to find a safe and effective treatment option, and our initial results support ‘as-needed’ blood thinners and pulse monitoring as the alternative.”
“While this is an observational study with a relatively small patient sample, further research is certainly needed to better understand alternate treatment options,” Pammer said. “And we stress that ‘as-needed’ blood thinners should not be considered unless the patient qualifies as highly motivated.” ![]()
Photo courtesy of the CDC
SAN FRANCISCO—New research suggests patients with atrial fibrillation (AF) may benefit from receiving novel oral anticoagulants on an “as-needed” basis.
The study indicated that anticoagulant therapy guided by diligent pulse monitoring can be a safe and effective alternative to long-term anticoagulant therapy for lowering the overall risk of stroke in AF patients.
This finding was presented at the Heart Rhythm Society’s 37th Annual Scientific Session (abstract AB21-06).
The researchers studied 100 AF patients, ages 45 to 78, who had significant stroke risk. All patients had no AF recurrences during an extended period of telemetry monitoring before the study began.
Eighty-four patients had been ablated, 16 were being treated with drug therapy, and 3 had implanted devices that served as a quality control check.
Each patient was instructed to monitor his or her pulse—manually or by using a smartphone—twice a day and take an anticoagulant as needed. The patients were provided with novel oral anticoagulants and were instructed to start taking the medication if they suspected or detected an AF episode lasting longer than 1 hour.
“This kind of approach to anticoagulation therapy requires an open line of communication between the patient and the care team and calls for a specific type of patient,” said Monica Pammer, a physician assistant at the Hospital of the University of Pennsylvania in Philadelphia.
“We call them ‘highly motivated patients.’ These are patients who were actively seeking, preparing for, and are committed to the alternate treatment method, and who are informed about how to diligently and effectively monitor their pulse throughout the day.”
The researchers followed the patients for approximately 23 months.
During this time, 28 patients started taking an anticoagulant at least once for a suspected or detected AF episode, and 10 patients transitioned back to chronic oral anticoagulation therapy for recurrent AF.
None of the patients experienced a stroke or transient ischemic attack, but there was 1 mild bleeding incident that required medical attention.
“It is extremely common for patients with AF to seek treatment that does not involve the use of chronic oral anticoagulants therapy, as there are other risks associated with their long-term use,” said Francis E. Marchlinski, MD, of the University of Pennsylvania Health System.
“The goal of this study was to find a safe and effective treatment option, and our initial results support ‘as-needed’ blood thinners and pulse monitoring as the alternative.”
“While this is an observational study with a relatively small patient sample, further research is certainly needed to better understand alternate treatment options,” Pammer said. “And we stress that ‘as-needed’ blood thinners should not be considered unless the patient qualifies as highly motivated.” ![]()
Peptides show promise for treating thalassemia, PV

Preclinical research suggests synthetic peptides called minihepcidins could potentially treat beta-thalassemia and polycythemia vera (PV).
Investigators found that minihepcidin helped to restore normal levels of red blood cells (RBCs) and reduced spleen enlargement in mouse models of beta-thalassemia and PV.
Minihepcidin also controlled the accumulation of excess iron in the mice.
“It seems counterintuitive that one compound could treat two diseases that are quite different, but by restricting iron absorption, it also helps to normalize red blood cell levels in animals,” said study author Stefano Rivella, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
“If these preclinical results translate to humans, this could represent a new treatment for both disorders.”
Dr Rivella and his colleagues described the results in Blood.
The investigators used minihepcidins, modified versions of the naturally occurring hormone hepcidin, which regulates iron. Minihepcidins are smaller than the full-length hormone but have long-term stability and long-lasting biological activity when administered to animals.
Previous research showed that minihepcidin treatment can prevent iron overload in mouse models of hemochromatosis.
So Dr Rivella and his colleagues wanted to determine how minihepcidins affect beta-thalassemia and PV in mice separately engineered to model each disease.
The team found that, in young mice that modelled beta-thalassemia, minihepcidin treatment normalized RBC levels and relieved both anemia and iron overload.
In older mice, minihepcidin improved RBC production and did not interfere with a chelating drug used to remove excess iron deposits.
In mice expressing the orthologous JAK2 mutation causing human PV, minihepcidin normalized RBC production.
Because increased iron absorption in PV keeps RBC production in overdrive, when minihepcidin curtailed iron absorption, it lowered the abnormally high numbers of RBCs, which also reduced spleen enlargement.
Dr Rivella noted that if minihepcidins prove successful in clinical trials, they may provide an important tool in treating these blood disorders.
“In animals affected by beta-thalassemia, the compound blocks iron from getting into organs but doesn’t remove excess iron already in organs and tissues,” Dr Rivella said. “If minihepcidins are used in older patients, they would need to be combined with existing chelating drugs that remove the already-accumulated iron.”
However, he added that, in beta-thalassemia, providing minihepcidins in childhood might halt iron accumulation and prevent more severe adult disease.
In PV, minihepcidins may help normalize a patient’s RBC production but, as in beta-thalassemia, would not treat the underlying disease-causing mutations.
Merganser Biotech Inc. is developing minihepcidins as novel therapies for rare hematologic diseases. Merganser’s lead compound, M012, is now under evaluation in a phase 1 clinical program as a potential therapy for beta-thalassemia, low-risk myelodysplasia, PV, alpha-thalassemia, and sickle cell disease.
The company’s chief executive officer, Brian MacDonald, MB ChB, PhD, is a co-author of the current study. Dr Rivella is a paid consultant on Merganser Biotech’s clinical trial, owns restricted stocks in Merganser, and is a member of its scientific advisory board. ![]()
Preclinical research suggests synthetic peptides called minihepcidins could potentially treat beta-thalassemia and polycythemia vera (PV).
Investigators found that minihepcidin helped to restore normal levels of red blood cells (RBCs) and reduced spleen enlargement in mouse models of beta-thalassemia and PV.
Minihepcidin also controlled the accumulation of excess iron in the mice.
“It seems counterintuitive that one compound could treat two diseases that are quite different, but by restricting iron absorption, it also helps to normalize red blood cell levels in animals,” said study author Stefano Rivella, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
“If these preclinical results translate to humans, this could represent a new treatment for both disorders.”
Dr Rivella and his colleagues described the results in Blood.
The investigators used minihepcidins, modified versions of the naturally occurring hormone hepcidin, which regulates iron. Minihepcidins are smaller than the full-length hormone but have long-term stability and long-lasting biological activity when administered to animals.
Previous research showed that minihepcidin treatment can prevent iron overload in mouse models of hemochromatosis.
So Dr Rivella and his colleagues wanted to determine how minihepcidins affect beta-thalassemia and PV in mice separately engineered to model each disease.
The team found that, in young mice that modelled beta-thalassemia, minihepcidin treatment normalized RBC levels and relieved both anemia and iron overload.
In older mice, minihepcidin improved RBC production and did not interfere with a chelating drug used to remove excess iron deposits.
In mice expressing the orthologous JAK2 mutation causing human PV, minihepcidin normalized RBC production.
Because increased iron absorption in PV keeps RBC production in overdrive, when minihepcidin curtailed iron absorption, it lowered the abnormally high numbers of RBCs, which also reduced spleen enlargement.
Dr Rivella noted that if minihepcidins prove successful in clinical trials, they may provide an important tool in treating these blood disorders.
“In animals affected by beta-thalassemia, the compound blocks iron from getting into organs but doesn’t remove excess iron already in organs and tissues,” Dr Rivella said. “If minihepcidins are used in older patients, they would need to be combined with existing chelating drugs that remove the already-accumulated iron.”
However, he added that, in beta-thalassemia, providing minihepcidins in childhood might halt iron accumulation and prevent more severe adult disease.
In PV, minihepcidins may help normalize a patient’s RBC production but, as in beta-thalassemia, would not treat the underlying disease-causing mutations.
Merganser Biotech Inc. is developing minihepcidins as novel therapies for rare hematologic diseases. Merganser’s lead compound, M012, is now under evaluation in a phase 1 clinical program as a potential therapy for beta-thalassemia, low-risk myelodysplasia, PV, alpha-thalassemia, and sickle cell disease.
The company’s chief executive officer, Brian MacDonald, MB ChB, PhD, is a co-author of the current study. Dr Rivella is a paid consultant on Merganser Biotech’s clinical trial, owns restricted stocks in Merganser, and is a member of its scientific advisory board. ![]()
Preclinical research suggests synthetic peptides called minihepcidins could potentially treat beta-thalassemia and polycythemia vera (PV).
Investigators found that minihepcidin helped to restore normal levels of red blood cells (RBCs) and reduced spleen enlargement in mouse models of beta-thalassemia and PV.
Minihepcidin also controlled the accumulation of excess iron in the mice.
“It seems counterintuitive that one compound could treat two diseases that are quite different, but by restricting iron absorption, it also helps to normalize red blood cell levels in animals,” said study author Stefano Rivella, PhD, of The Children’s Hospital of Philadelphia in Pennsylvania.
“If these preclinical results translate to humans, this could represent a new treatment for both disorders.”
Dr Rivella and his colleagues described the results in Blood.
The investigators used minihepcidins, modified versions of the naturally occurring hormone hepcidin, which regulates iron. Minihepcidins are smaller than the full-length hormone but have long-term stability and long-lasting biological activity when administered to animals.
Previous research showed that minihepcidin treatment can prevent iron overload in mouse models of hemochromatosis.
So Dr Rivella and his colleagues wanted to determine how minihepcidins affect beta-thalassemia and PV in mice separately engineered to model each disease.
The team found that, in young mice that modelled beta-thalassemia, minihepcidin treatment normalized RBC levels and relieved both anemia and iron overload.
In older mice, minihepcidin improved RBC production and did not interfere with a chelating drug used to remove excess iron deposits.
In mice expressing the orthologous JAK2 mutation causing human PV, minihepcidin normalized RBC production.
Because increased iron absorption in PV keeps RBC production in overdrive, when minihepcidin curtailed iron absorption, it lowered the abnormally high numbers of RBCs, which also reduced spleen enlargement.
Dr Rivella noted that if minihepcidins prove successful in clinical trials, they may provide an important tool in treating these blood disorders.
“In animals affected by beta-thalassemia, the compound blocks iron from getting into organs but doesn’t remove excess iron already in organs and tissues,” Dr Rivella said. “If minihepcidins are used in older patients, they would need to be combined with existing chelating drugs that remove the already-accumulated iron.”
However, he added that, in beta-thalassemia, providing minihepcidins in childhood might halt iron accumulation and prevent more severe adult disease.
In PV, minihepcidins may help normalize a patient’s RBC production but, as in beta-thalassemia, would not treat the underlying disease-causing mutations.
Merganser Biotech Inc. is developing minihepcidins as novel therapies for rare hematologic diseases. Merganser’s lead compound, M012, is now under evaluation in a phase 1 clinical program as a potential therapy for beta-thalassemia, low-risk myelodysplasia, PV, alpha-thalassemia, and sickle cell disease.
The company’s chief executive officer, Brian MacDonald, MB ChB, PhD, is a co-author of the current study. Dr Rivella is a paid consultant on Merganser Biotech’s clinical trial, owns restricted stocks in Merganser, and is a member of its scientific advisory board. ![]()
Group isolates Tregs to treat GVHD

Image by Kathryn T. Iacono
Researchers say they have devised a method for harvesting regulatory T cells (Tregs) on a large scale, and they are currently testing these Tregs in a trial of patients with graft-versus-host disease (GVHD).
The team described the harvesting method in the Journal of Immunotherapy.
“A Tregs-based therapy could help reduce the risk of GVHD, but Tregs are a very rare population amongst blood cells,” said study author Sebastian Bertin-Maghit, PhD, of the Agency for Science, Technology and Research (A*STAR) in Singapore.
“For our therapy to work, we needed a large supply of pure, ‘untouched’ Tregs that are uncontaminated with other cell types.”
However, when it came to isolating pure Tregs on a large scale, the researchers found existing isolation methods inefficient.
So rather than isolating the cells by “plucking” them out of a donor sample—a method that comes with the risk of unwanted modification or activation of some cells—the team devised a depletion method for selecting Tregs in their pure, untouched state.
“We depleted all unwanted cells in donor samples using isolation reagents,” Dr Bertin-Maghit said. “This allowed us to harvest Tregs in their natural state. We took great care to wash out the isolation reagents in the final product.”
The researchers have since proven that this single-step depletion process can be scaled up to harvest highly pure Tregs at levels suitable for clinical trials, and their procedure complies with current trial standards.
Furthermore, while previous attempts to collect Tregs produced a final product with 60% pure Tregs, this new method generates over 90% pure Tregs.
“The first clinical trial using our Treg product is currently ongoing at the Singapore General Hospital,” Dr Bertin-Maghit said. “We are assessing the safety of Tregs in the treatment of GVHD in 12 leukemia patients. We believe our procedure will open doors to a new era in cell therapy.” ![]()
Image by Kathryn T. Iacono
Researchers say they have devised a method for harvesting regulatory T cells (Tregs) on a large scale, and they are currently testing these Tregs in a trial of patients with graft-versus-host disease (GVHD).
The team described the harvesting method in the Journal of Immunotherapy.
“A Tregs-based therapy could help reduce the risk of GVHD, but Tregs are a very rare population amongst blood cells,” said study author Sebastian Bertin-Maghit, PhD, of the Agency for Science, Technology and Research (A*STAR) in Singapore.
“For our therapy to work, we needed a large supply of pure, ‘untouched’ Tregs that are uncontaminated with other cell types.”
However, when it came to isolating pure Tregs on a large scale, the researchers found existing isolation methods inefficient.
So rather than isolating the cells by “plucking” them out of a donor sample—a method that comes with the risk of unwanted modification or activation of some cells—the team devised a depletion method for selecting Tregs in their pure, untouched state.
“We depleted all unwanted cells in donor samples using isolation reagents,” Dr Bertin-Maghit said. “This allowed us to harvest Tregs in their natural state. We took great care to wash out the isolation reagents in the final product.”
The researchers have since proven that this single-step depletion process can be scaled up to harvest highly pure Tregs at levels suitable for clinical trials, and their procedure complies with current trial standards.
Furthermore, while previous attempts to collect Tregs produced a final product with 60% pure Tregs, this new method generates over 90% pure Tregs.
“The first clinical trial using our Treg product is currently ongoing at the Singapore General Hospital,” Dr Bertin-Maghit said. “We are assessing the safety of Tregs in the treatment of GVHD in 12 leukemia patients. We believe our procedure will open doors to a new era in cell therapy.” ![]()
Image by Kathryn T. Iacono
Researchers say they have devised a method for harvesting regulatory T cells (Tregs) on a large scale, and they are currently testing these Tregs in a trial of patients with graft-versus-host disease (GVHD).
The team described the harvesting method in the Journal of Immunotherapy.
“A Tregs-based therapy could help reduce the risk of GVHD, but Tregs are a very rare population amongst blood cells,” said study author Sebastian Bertin-Maghit, PhD, of the Agency for Science, Technology and Research (A*STAR) in Singapore.
“For our therapy to work, we needed a large supply of pure, ‘untouched’ Tregs that are uncontaminated with other cell types.”
However, when it came to isolating pure Tregs on a large scale, the researchers found existing isolation methods inefficient.
So rather than isolating the cells by “plucking” them out of a donor sample—a method that comes with the risk of unwanted modification or activation of some cells—the team devised a depletion method for selecting Tregs in their pure, untouched state.
“We depleted all unwanted cells in donor samples using isolation reagents,” Dr Bertin-Maghit said. “This allowed us to harvest Tregs in their natural state. We took great care to wash out the isolation reagents in the final product.”
The researchers have since proven that this single-step depletion process can be scaled up to harvest highly pure Tregs at levels suitable for clinical trials, and their procedure complies with current trial standards.
Furthermore, while previous attempts to collect Tregs produced a final product with 60% pure Tregs, this new method generates over 90% pure Tregs.
“The first clinical trial using our Treg product is currently ongoing at the Singapore General Hospital,” Dr Bertin-Maghit said. “We are assessing the safety of Tregs in the treatment of GVHD in 12 leukemia patients. We believe our procedure will open doors to a new era in cell therapy.” ![]()
Warfarin indication, TTR linked to dementia risk

Photo courtesy of NIGMS
SAN FRANCISCO—Patients with atrial fibrillation (AF) who are on warfarin long-term have a higher risk of dementia than non-AF patients on long-term warfarin therapy, according to a new study.
The AF patients studied had higher rates of dementia, Alzheimer’s disease, and vascular dementia than their non-AF counterparts.
However, both groups of patients had a greater risk of dementia if they had lower percentages of time in therapeutic range (TTR).
“Our study results are the first to show that there are significant cognitive risk factors for patients treated with warfarin over a long period of time, regardless of the indication for anticoagulation,” said T. Jared Bunch, MD, of the Intermountain Medical Center Heart Institute in Salt Lake City, Utah.
Dr Bunch and his colleagues presented this research at the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract MP01-04).
The researchers enrolled 10,537 patients, age 18 and older, with no history of dementia prior to the study. They were receiving long-term warfarin for AF (n=4460), thromboembolism (n=5868), or mechanical heart valves (n=209).
The AF patients were older and had higher rates of hypertension, diabetes, heart failure, and stroke than the non-AF patients.
During a follow-up of approximately 7 years, the researchers found that all types of dementia increased in the AF group more than the non-AF group.
AF patients experienced higher rates of total dementia (5.8% vs 1.6%, P<0.0001), Alzheimer’s disease (2.8% vs 0.9%, P<0.0001), and vascular dementia (1.0% vs 0.2%, P<0.0001).
The researchers performed a propensity analysis of 6030 patients to account for the differences in baseline characteristics. And the risk of dementia remained significantly higher in AF patients than non-AF patients.
The hazard ratio (HR) was 2.42 for all types of dementia (P<0.0001), 2.04 for Alzheimer’s disease (P<0.0001), and 2.46 for senility (P<0.0001).
However, both AF and non-AF patients saw an increase in the risk of dementia if they had a low percent TTR.
In multivariate analysis, with the TTR >75% group as the reference, the HR for dementia in AF patients was:
- 1.30 for the 51%-75% TTR group (P=0.10)
- 1.57 for the 26%-50% TTR group (P=0.02)
- 1.92 for the ≤25% TTR group (P=0.005).
The HR for dementia in non-AF patients was:
- 1.57 for the 51%-75% TTR group (P=0.13)
- 2.69 for the 26%-50% TTR group (P=0.002)
- 3.87 for the ≤25% TTR group (P<0.0001).
Dr Bunch and his colleagues believe these findings have implications for treatment.
“First, as physicians, we have to understand that, although we need to use anticoagulants for many reasons, including to prevent stroke in AF patients, at that same time, there are risks that need to be considered, some of which we are only right now beginning to understand,” Dr Bunch said.
“In this regard, only those that absolutely need blood thinners should be placed on them long-term. Second, other medications like aspirin that may increase the blood thinner’s effect should be avoided unless there is a specific medical need. Finally, in people that are on warfarin in which the levels are erratic or difficult to control, switching to newer agents that are more predictable may lower risk.” ![]()
Photo courtesy of NIGMS
SAN FRANCISCO—Patients with atrial fibrillation (AF) who are on warfarin long-term have a higher risk of dementia than non-AF patients on long-term warfarin therapy, according to a new study.
The AF patients studied had higher rates of dementia, Alzheimer’s disease, and vascular dementia than their non-AF counterparts.
However, both groups of patients had a greater risk of dementia if they had lower percentages of time in therapeutic range (TTR).
“Our study results are the first to show that there are significant cognitive risk factors for patients treated with warfarin over a long period of time, regardless of the indication for anticoagulation,” said T. Jared Bunch, MD, of the Intermountain Medical Center Heart Institute in Salt Lake City, Utah.
Dr Bunch and his colleagues presented this research at the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract MP01-04).
The researchers enrolled 10,537 patients, age 18 and older, with no history of dementia prior to the study. They were receiving long-term warfarin for AF (n=4460), thromboembolism (n=5868), or mechanical heart valves (n=209).
The AF patients were older and had higher rates of hypertension, diabetes, heart failure, and stroke than the non-AF patients.
During a follow-up of approximately 7 years, the researchers found that all types of dementia increased in the AF group more than the non-AF group.
AF patients experienced higher rates of total dementia (5.8% vs 1.6%, P<0.0001), Alzheimer’s disease (2.8% vs 0.9%, P<0.0001), and vascular dementia (1.0% vs 0.2%, P<0.0001).
The researchers performed a propensity analysis of 6030 patients to account for the differences in baseline characteristics. And the risk of dementia remained significantly higher in AF patients than non-AF patients.
The hazard ratio (HR) was 2.42 for all types of dementia (P<0.0001), 2.04 for Alzheimer’s disease (P<0.0001), and 2.46 for senility (P<0.0001).
However, both AF and non-AF patients saw an increase in the risk of dementia if they had a low percent TTR.
In multivariate analysis, with the TTR >75% group as the reference, the HR for dementia in AF patients was:
- 1.30 for the 51%-75% TTR group (P=0.10)
- 1.57 for the 26%-50% TTR group (P=0.02)
- 1.92 for the ≤25% TTR group (P=0.005).
The HR for dementia in non-AF patients was:
- 1.57 for the 51%-75% TTR group (P=0.13)
- 2.69 for the 26%-50% TTR group (P=0.002)
- 3.87 for the ≤25% TTR group (P<0.0001).
Dr Bunch and his colleagues believe these findings have implications for treatment.
“First, as physicians, we have to understand that, although we need to use anticoagulants for many reasons, including to prevent stroke in AF patients, at that same time, there are risks that need to be considered, some of which we are only right now beginning to understand,” Dr Bunch said.
“In this regard, only those that absolutely need blood thinners should be placed on them long-term. Second, other medications like aspirin that may increase the blood thinner’s effect should be avoided unless there is a specific medical need. Finally, in people that are on warfarin in which the levels are erratic or difficult to control, switching to newer agents that are more predictable may lower risk.” ![]()
Photo courtesy of NIGMS
SAN FRANCISCO—Patients with atrial fibrillation (AF) who are on warfarin long-term have a higher risk of dementia than non-AF patients on long-term warfarin therapy, according to a new study.
The AF patients studied had higher rates of dementia, Alzheimer’s disease, and vascular dementia than their non-AF counterparts.
However, both groups of patients had a greater risk of dementia if they had lower percentages of time in therapeutic range (TTR).
“Our study results are the first to show that there are significant cognitive risk factors for patients treated with warfarin over a long period of time, regardless of the indication for anticoagulation,” said T. Jared Bunch, MD, of the Intermountain Medical Center Heart Institute in Salt Lake City, Utah.
Dr Bunch and his colleagues presented this research at the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract MP01-04).
The researchers enrolled 10,537 patients, age 18 and older, with no history of dementia prior to the study. They were receiving long-term warfarin for AF (n=4460), thromboembolism (n=5868), or mechanical heart valves (n=209).
The AF patients were older and had higher rates of hypertension, diabetes, heart failure, and stroke than the non-AF patients.
During a follow-up of approximately 7 years, the researchers found that all types of dementia increased in the AF group more than the non-AF group.
AF patients experienced higher rates of total dementia (5.8% vs 1.6%, P<0.0001), Alzheimer’s disease (2.8% vs 0.9%, P<0.0001), and vascular dementia (1.0% vs 0.2%, P<0.0001).
The researchers performed a propensity analysis of 6030 patients to account for the differences in baseline characteristics. And the risk of dementia remained significantly higher in AF patients than non-AF patients.
The hazard ratio (HR) was 2.42 for all types of dementia (P<0.0001), 2.04 for Alzheimer’s disease (P<0.0001), and 2.46 for senility (P<0.0001).
However, both AF and non-AF patients saw an increase in the risk of dementia if they had a low percent TTR.
In multivariate analysis, with the TTR >75% group as the reference, the HR for dementia in AF patients was:
- 1.30 for the 51%-75% TTR group (P=0.10)
- 1.57 for the 26%-50% TTR group (P=0.02)
- 1.92 for the ≤25% TTR group (P=0.005).
The HR for dementia in non-AF patients was:
- 1.57 for the 51%-75% TTR group (P=0.13)
- 2.69 for the 26%-50% TTR group (P=0.002)
- 3.87 for the ≤25% TTR group (P<0.0001).
Dr Bunch and his colleagues believe these findings have implications for treatment.
“First, as physicians, we have to understand that, although we need to use anticoagulants for many reasons, including to prevent stroke in AF patients, at that same time, there are risks that need to be considered, some of which we are only right now beginning to understand,” Dr Bunch said.
“In this regard, only those that absolutely need blood thinners should be placed on them long-term. Second, other medications like aspirin that may increase the blood thinner’s effect should be avoided unless there is a specific medical need. Finally, in people that are on warfarin in which the levels are erratic or difficult to control, switching to newer agents that are more predictable may lower risk.” ![]()
US docs call for single-payer health reform

Photo by Matthew Lester
A group of US physicians has called for the creation of a publicly financed, single-payer national health program that would cover all Americans for all medically necessary care.
The proposal, which was drafted by a panel of 39 physicians, was announced in an editorial published in the American Journal of Public Health.
The proposal currently has more than 2000 signatures from physicians practicing in 48 states and the District of Columbia.
“Our nation is at a crossroads,” said Adam Gaffney, MD, a pulmonary disease and critical care specialist in Boston, Massachusetts, who is lead author of the editorial and co-chair of the working group that drafted the proposal.
“Despite the passage of the Affordable Care Act 6 years ago, 30 million Americans remain uninsured, an even greater number are underinsured, financial barriers to care like co-pays and deductibles are rising, bureaucracy is growing, provider networks are narrowing, and medical costs are continuing to climb.”
Dr Gaffney and his colleagues described their publicly financed, single-payer national health program (NHP) as follows.
Patients could choose to visit any doctor and hospital. Most hospitals and clinics would remain privately owned and operated, receiving a budget from the NHP to cover all operating costs. Physicians could continue to practice on a fee-for-service basis or receive salaries from group practices, hospitals, or clinics.
The program would be paid for by combining current sources of government health spending into a single fund with new taxes that would be fully offset by reductions in premiums and out-of-pocket spending. Co-pays and deductibles would be eliminated.
The single-payer program would save about $500 billion annually by eliminating the high overhead and profits of insurance firms and the paperwork they require from hospitals and doctors.
The administrative savings of the system would fully offset the costs of covering the uninsured and upgraded coverage for everyone else—eg, full coverage of prescription drugs, dental care, and long-term care. Savings would also be redirected to currently underfunded health priorities, particularly public health.
The “single payer” would be in a position to negotiate lower prices for medications and other medical supplies.
More details and documents related to the physicians’ proposal are available on the Physicians for a National Health Program website.
The Physicians for a National Health Program is a nonpartisan, nonprofit research and education organization founded in 1987. The organization had no role in funding the aforementioned proposal or editorial. ![]()
Photo by Matthew Lester
A group of US physicians has called for the creation of a publicly financed, single-payer national health program that would cover all Americans for all medically necessary care.
The proposal, which was drafted by a panel of 39 physicians, was announced in an editorial published in the American Journal of Public Health.
The proposal currently has more than 2000 signatures from physicians practicing in 48 states and the District of Columbia.
“Our nation is at a crossroads,” said Adam Gaffney, MD, a pulmonary disease and critical care specialist in Boston, Massachusetts, who is lead author of the editorial and co-chair of the working group that drafted the proposal.
“Despite the passage of the Affordable Care Act 6 years ago, 30 million Americans remain uninsured, an even greater number are underinsured, financial barriers to care like co-pays and deductibles are rising, bureaucracy is growing, provider networks are narrowing, and medical costs are continuing to climb.”
Dr Gaffney and his colleagues described their publicly financed, single-payer national health program (NHP) as follows.
Patients could choose to visit any doctor and hospital. Most hospitals and clinics would remain privately owned and operated, receiving a budget from the NHP to cover all operating costs. Physicians could continue to practice on a fee-for-service basis or receive salaries from group practices, hospitals, or clinics.
The program would be paid for by combining current sources of government health spending into a single fund with new taxes that would be fully offset by reductions in premiums and out-of-pocket spending. Co-pays and deductibles would be eliminated.
The single-payer program would save about $500 billion annually by eliminating the high overhead and profits of insurance firms and the paperwork they require from hospitals and doctors.
The administrative savings of the system would fully offset the costs of covering the uninsured and upgraded coverage for everyone else—eg, full coverage of prescription drugs, dental care, and long-term care. Savings would also be redirected to currently underfunded health priorities, particularly public health.
The “single payer” would be in a position to negotiate lower prices for medications and other medical supplies.
More details and documents related to the physicians’ proposal are available on the Physicians for a National Health Program website.
The Physicians for a National Health Program is a nonpartisan, nonprofit research and education organization founded in 1987. The organization had no role in funding the aforementioned proposal or editorial. ![]()
Photo by Matthew Lester
A group of US physicians has called for the creation of a publicly financed, single-payer national health program that would cover all Americans for all medically necessary care.
The proposal, which was drafted by a panel of 39 physicians, was announced in an editorial published in the American Journal of Public Health.
The proposal currently has more than 2000 signatures from physicians practicing in 48 states and the District of Columbia.
“Our nation is at a crossroads,” said Adam Gaffney, MD, a pulmonary disease and critical care specialist in Boston, Massachusetts, who is lead author of the editorial and co-chair of the working group that drafted the proposal.
“Despite the passage of the Affordable Care Act 6 years ago, 30 million Americans remain uninsured, an even greater number are underinsured, financial barriers to care like co-pays and deductibles are rising, bureaucracy is growing, provider networks are narrowing, and medical costs are continuing to climb.”
Dr Gaffney and his colleagues described their publicly financed, single-payer national health program (NHP) as follows.
Patients could choose to visit any doctor and hospital. Most hospitals and clinics would remain privately owned and operated, receiving a budget from the NHP to cover all operating costs. Physicians could continue to practice on a fee-for-service basis or receive salaries from group practices, hospitals, or clinics.
The program would be paid for by combining current sources of government health spending into a single fund with new taxes that would be fully offset by reductions in premiums and out-of-pocket spending. Co-pays and deductibles would be eliminated.
The single-payer program would save about $500 billion annually by eliminating the high overhead and profits of insurance firms and the paperwork they require from hospitals and doctors.
The administrative savings of the system would fully offset the costs of covering the uninsured and upgraded coverage for everyone else—eg, full coverage of prescription drugs, dental care, and long-term care. Savings would also be redirected to currently underfunded health priorities, particularly public health.
The “single payer” would be in a position to negotiate lower prices for medications and other medical supplies.
More details and documents related to the physicians’ proposal are available on the Physicians for a National Health Program website.
The Physicians for a National Health Program is a nonpartisan, nonprofit research and education organization founded in 1987. The organization had no role in funding the aforementioned proposal or editorial. ![]()
A new paper-based test for the Zika virus
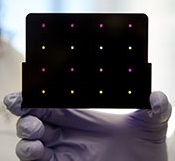
based test for Zika virus.
Purple dots indicate samples
infected with Zika, and yellow
dots indicate Zika-free samples.
Photo courtesy of the Wyss
Institute at Harvard University
A new paper-based test can diagnose Zika virus infection within a few hours, according to research published in Cell.
The test is based on technology previously developed to detect the Ebola virus.
In October 2014, researchers demonstrated that they could create synthetic gene networks and embed them on small discs of paper.
These gene networks can be programmed to detect a particular genetic sequence, which causes the paper to change color.
Upon learning about the Zika outbreak, the researchers decided to try adapting this technology to diagnose Zika.
“In a small number of weeks, we developed and validated a relatively rapid, inexpensive Zika diagnostic platform,” said study author James Collins, PhD, of the Massachusetts Institute of Technology in Cambridge.
Dr Collins and his colleagues developed sensors, embedded in the paper discs, that can detect 24 different RNA sequences found in the Zika viral genome. When the target RNA sequence is present, it initiates a series of interactions that turns the paper from yellow to purple.
This color change can be seen with the naked eye, but the researchers also developed an electronic reader that makes it easier to quantify the change, especially in cases where the sensor is detecting more than one RNA sequence.
All of the cellular components necessary for this process—including proteins, nucleic acids, and ribosomes—can be extracted from living cells and freeze-dried onto paper.
These paper discs can be stored at room temperature, making it easy to ship them to any location. Once rehydrated, all of the components function just as they would inside a living cell.
The researchers also incorporated a step that boosts the amount of viral RNA in the blood sample before exposing it to the sensor, using a system called nucleic acid sequence based amplification (NASBA). This amplification step, which takes 1 to 2 hours, increases the test’s sensitivity 1 million-fold.
The team tested this diagnostic platform using synthesized RNA sequences corresponding to the Zika genome, which were then added to human blood serum.
They found the test could detect very low viral RNA concentrations in those samples and could also distinguish Zika from dengue.
The researchers then tested samples taken from monkeys infected with the Zika virus. (Samples from humans affected by the current Zika outbreak were too difficult to obtain.)
The team found that, in these samples, the test could detect viral RNA concentrations as low as 2 or 3 parts per quadrillion.
The researchers believe this approach could also be adapted to other viruses that may emerge in the future. Dr Collins hopes to team up with other scientists to further develop the technology for diagnosing Zika.
“Here, we’ve done a nice proof-of-principle demonstration, but more work and additional testing would be needed to ensure safety and efficacy before actual deployment,” he said. “We’re not far off.” ![]()
based test for Zika virus.
Purple dots indicate samples
infected with Zika, and yellow
dots indicate Zika-free samples.
Photo courtesy of the Wyss
Institute at Harvard University
A new paper-based test can diagnose Zika virus infection within a few hours, according to research published in Cell.
The test is based on technology previously developed to detect the Ebola virus.
In October 2014, researchers demonstrated that they could create synthetic gene networks and embed them on small discs of paper.
These gene networks can be programmed to detect a particular genetic sequence, which causes the paper to change color.
Upon learning about the Zika outbreak, the researchers decided to try adapting this technology to diagnose Zika.
“In a small number of weeks, we developed and validated a relatively rapid, inexpensive Zika diagnostic platform,” said study author James Collins, PhD, of the Massachusetts Institute of Technology in Cambridge.
Dr Collins and his colleagues developed sensors, embedded in the paper discs, that can detect 24 different RNA sequences found in the Zika viral genome. When the target RNA sequence is present, it initiates a series of interactions that turns the paper from yellow to purple.
This color change can be seen with the naked eye, but the researchers also developed an electronic reader that makes it easier to quantify the change, especially in cases where the sensor is detecting more than one RNA sequence.
All of the cellular components necessary for this process—including proteins, nucleic acids, and ribosomes—can be extracted from living cells and freeze-dried onto paper.
These paper discs can be stored at room temperature, making it easy to ship them to any location. Once rehydrated, all of the components function just as they would inside a living cell.
The researchers also incorporated a step that boosts the amount of viral RNA in the blood sample before exposing it to the sensor, using a system called nucleic acid sequence based amplification (NASBA). This amplification step, which takes 1 to 2 hours, increases the test’s sensitivity 1 million-fold.
The team tested this diagnostic platform using synthesized RNA sequences corresponding to the Zika genome, which were then added to human blood serum.
They found the test could detect very low viral RNA concentrations in those samples and could also distinguish Zika from dengue.
The researchers then tested samples taken from monkeys infected with the Zika virus. (Samples from humans affected by the current Zika outbreak were too difficult to obtain.)
The team found that, in these samples, the test could detect viral RNA concentrations as low as 2 or 3 parts per quadrillion.
The researchers believe this approach could also be adapted to other viruses that may emerge in the future. Dr Collins hopes to team up with other scientists to further develop the technology for diagnosing Zika.
“Here, we’ve done a nice proof-of-principle demonstration, but more work and additional testing would be needed to ensure safety and efficacy before actual deployment,” he said. “We’re not far off.” ![]()
based test for Zika virus.
Purple dots indicate samples
infected with Zika, and yellow
dots indicate Zika-free samples.
Photo courtesy of the Wyss
Institute at Harvard University
A new paper-based test can diagnose Zika virus infection within a few hours, according to research published in Cell.
The test is based on technology previously developed to detect the Ebola virus.
In October 2014, researchers demonstrated that they could create synthetic gene networks and embed them on small discs of paper.
These gene networks can be programmed to detect a particular genetic sequence, which causes the paper to change color.
Upon learning about the Zika outbreak, the researchers decided to try adapting this technology to diagnose Zika.
“In a small number of weeks, we developed and validated a relatively rapid, inexpensive Zika diagnostic platform,” said study author James Collins, PhD, of the Massachusetts Institute of Technology in Cambridge.
Dr Collins and his colleagues developed sensors, embedded in the paper discs, that can detect 24 different RNA sequences found in the Zika viral genome. When the target RNA sequence is present, it initiates a series of interactions that turns the paper from yellow to purple.
This color change can be seen with the naked eye, but the researchers also developed an electronic reader that makes it easier to quantify the change, especially in cases where the sensor is detecting more than one RNA sequence.
All of the cellular components necessary for this process—including proteins, nucleic acids, and ribosomes—can be extracted from living cells and freeze-dried onto paper.
These paper discs can be stored at room temperature, making it easy to ship them to any location. Once rehydrated, all of the components function just as they would inside a living cell.
The researchers also incorporated a step that boosts the amount of viral RNA in the blood sample before exposing it to the sensor, using a system called nucleic acid sequence based amplification (NASBA). This amplification step, which takes 1 to 2 hours, increases the test’s sensitivity 1 million-fold.
The team tested this diagnostic platform using synthesized RNA sequences corresponding to the Zika genome, which were then added to human blood serum.
They found the test could detect very low viral RNA concentrations in those samples and could also distinguish Zika from dengue.
The researchers then tested samples taken from monkeys infected with the Zika virus. (Samples from humans affected by the current Zika outbreak were too difficult to obtain.)
The team found that, in these samples, the test could detect viral RNA concentrations as low as 2 or 3 parts per quadrillion.
The researchers believe this approach could also be adapted to other viruses that may emerge in the future. Dr Collins hopes to team up with other scientists to further develop the technology for diagnosing Zika.
“Here, we’ve done a nice proof-of-principle demonstration, but more work and additional testing would be needed to ensure safety and efficacy before actual deployment,” he said. “We’re not far off.” ![]()
Animal model recapitulates human MM, other neoplasms

Researchers say they have developed an animal model that allows them to better understand the mechanisms leading to multiple myeloma (MM) and other plasma cell neoplasms.
The group described this model in Scientific Reports.
“So far, there have not been animal models of malignant plasma cell diseases that allow us to study their stepwise progression and fully understand the complex cellular mechanisms,” said study author Stephen D. Nimer, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami in Florida.
“Now that we have a proper model of the disease, we’ll be able to more effectively study multiple myeloma as well as potential treatments.”
To create this model, the researchers crossed 2 genetically modified mice: mice lacking the Mef gene and mice with a Rad50 gene mutation (Rad50s).
Mef, also called Elf4, is a transcription factor known to both promote and suppress cancer formation. Rad50 is a component of a sensor of DNA damage induced by various stresses, and it regulates the DNA damage response pathways in cells.
The researchers found that Mef−/−Rad50s/s mice initially had abnormal plasma cell proliferation and monoclonal protein production.
Then, they developed anemia and a decreased bone mineral density. And 70% of these mice died from MM or other plasma cell neoplasms.
“We also found that the phenotype of these mice is not linked to activation of a specific oncogene or inactivation of a specific tumor suppressor, other than Mef,” said study author Takashi Asai, MD, PhD, also of the Sylvester Comprehensive Cancer Center.
Considering their findings together, the researchers said this model recapitulates the systemic manifestations of human MM and other plasma cell neoplasms. And their work suggests the Rad50s and Mef/Elf4 pathways cooperate to initiate myelomagenic mutations that promote plasma cell transformation.
“Although outcomes for multiple myeloma patients have greatly improved, it remains an incurable disease, despite the availability of newer treatments,” Dr Nimer noted.
“Several animal models of multiple myeloma have been reported, including models of human myeloma cells. However, these models imperfectly mimic the human disease. Developing more reliable and accurate animal models that help us better understand myeloma and test new treatments will take us to the next level on the long and challenging road to a cure.” ![]()
Researchers say they have developed an animal model that allows them to better understand the mechanisms leading to multiple myeloma (MM) and other plasma cell neoplasms.
The group described this model in Scientific Reports.
“So far, there have not been animal models of malignant plasma cell diseases that allow us to study their stepwise progression and fully understand the complex cellular mechanisms,” said study author Stephen D. Nimer, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami in Florida.
“Now that we have a proper model of the disease, we’ll be able to more effectively study multiple myeloma as well as potential treatments.”
To create this model, the researchers crossed 2 genetically modified mice: mice lacking the Mef gene and mice with a Rad50 gene mutation (Rad50s).
Mef, also called Elf4, is a transcription factor known to both promote and suppress cancer formation. Rad50 is a component of a sensor of DNA damage induced by various stresses, and it regulates the DNA damage response pathways in cells.
The researchers found that Mef−/−Rad50s/s mice initially had abnormal plasma cell proliferation and monoclonal protein production.
Then, they developed anemia and a decreased bone mineral density. And 70% of these mice died from MM or other plasma cell neoplasms.
“We also found that the phenotype of these mice is not linked to activation of a specific oncogene or inactivation of a specific tumor suppressor, other than Mef,” said study author Takashi Asai, MD, PhD, also of the Sylvester Comprehensive Cancer Center.
Considering their findings together, the researchers said this model recapitulates the systemic manifestations of human MM and other plasma cell neoplasms. And their work suggests the Rad50s and Mef/Elf4 pathways cooperate to initiate myelomagenic mutations that promote plasma cell transformation.
“Although outcomes for multiple myeloma patients have greatly improved, it remains an incurable disease, despite the availability of newer treatments,” Dr Nimer noted.
“Several animal models of multiple myeloma have been reported, including models of human myeloma cells. However, these models imperfectly mimic the human disease. Developing more reliable and accurate animal models that help us better understand myeloma and test new treatments will take us to the next level on the long and challenging road to a cure.” ![]()
Researchers say they have developed an animal model that allows them to better understand the mechanisms leading to multiple myeloma (MM) and other plasma cell neoplasms.
The group described this model in Scientific Reports.
“So far, there have not been animal models of malignant plasma cell diseases that allow us to study their stepwise progression and fully understand the complex cellular mechanisms,” said study author Stephen D. Nimer, MD, of the Sylvester Comprehensive Cancer Center at the University of Miami in Florida.
“Now that we have a proper model of the disease, we’ll be able to more effectively study multiple myeloma as well as potential treatments.”
To create this model, the researchers crossed 2 genetically modified mice: mice lacking the Mef gene and mice with a Rad50 gene mutation (Rad50s).
Mef, also called Elf4, is a transcription factor known to both promote and suppress cancer formation. Rad50 is a component of a sensor of DNA damage induced by various stresses, and it regulates the DNA damage response pathways in cells.
The researchers found that Mef−/−Rad50s/s mice initially had abnormal plasma cell proliferation and monoclonal protein production.
Then, they developed anemia and a decreased bone mineral density. And 70% of these mice died from MM or other plasma cell neoplasms.
“We also found that the phenotype of these mice is not linked to activation of a specific oncogene or inactivation of a specific tumor suppressor, other than Mef,” said study author Takashi Asai, MD, PhD, also of the Sylvester Comprehensive Cancer Center.
Considering their findings together, the researchers said this model recapitulates the systemic manifestations of human MM and other plasma cell neoplasms. And their work suggests the Rad50s and Mef/Elf4 pathways cooperate to initiate myelomagenic mutations that promote plasma cell transformation.
“Although outcomes for multiple myeloma patients have greatly improved, it remains an incurable disease, despite the availability of newer treatments,” Dr Nimer noted.
“Several animal models of multiple myeloma have been reported, including models of human myeloma cells. However, these models imperfectly mimic the human disease. Developing more reliable and accurate animal models that help us better understand myeloma and test new treatments will take us to the next level on the long and challenging road to a cure.”
Warfarin management linked to kidney function

SAN FRANCISCO—Patients with atrial fibrillation (AF) who are taking warfarin have a higher risk of kidney problems if their anticoagulation levels are not properly managed, according to a new study.
Researchers found that patients who had low times in therapeutic range were significantly more likely to develop renal dysfunction and experience renal failure.
Furthermore, all patients were at risk of developing renal dysfunction, whether they began the study with healthy kidney function or moderate to severe kidney disease.
T. Jared Bunch, MD, of Intermountain Medical Center Heart Institute in Salt Lake City, Utah, and his colleagues presented these findings during the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract PO02-210).
The researchers studied 2753 AF patients who were anticoagulated with warfarin and managed by Intermountain Healthcare Clinical Pharmacist Anticoagulation Services.
The patients’ mean age was 74.7±10.7, and 50.3% were male. The patients had a baseline creatinine level of less than 2.0 mg/dL or a glomerular filtration rate greater than 30 and serial renal function studies.
Dr Bunch and his colleagues stratified patients into 4 categories based on the amount of time their international normalized ratio levels were determined to be in the therapeutic range (TTR): >75%, 51% to 75%, 26% to 50%, and <25%.
The researchers then performed multivariate, adjusted analyses to calculate odds ratios (ORs) for renal dysfunction and hazard ratios (HRs) for renal failure based on TTR group. The >75% group was the reference.
Among patients with baseline creatinine ≤2.0 mg/dL, the OR for a 25% increase in creatinine was:
- 1.35 for the 51%-75% TTR group (P=0.06)
- 1.80 for the 26-50% TTR group (P=0.003)
- 2.34 for the ≤25% TTR group (P=0.003).
Among patients with baseline creatinine ≤2.0 mg/dL, the HR for renal failure was:
- 1.72 for the 51%-75% TTR group (P=0.001)
- 2.36 for the 26-50% TTR group (P<0.0001)
- 2.38 for the ≤25% TTR group (P<0.0001).
Among patients with baseline glomerular filtration rate >30, the OR for a 25% decrease in glomerular filtration rate was:
- 1.45 for the 51%-75% TTR group (P=0.03)
- 1.46 for the 26-50% TTR group (P=0.08)
- 1.52 for the ≤25% TTR group (P=0.20).
Among patients with a baseline glomerular filtration rate >30, the HR for renal failure was:
- 1.88 for the 51%-75% TTR group (P<0.0001)
- 2.40 for the 26-50% TTR group (P<0.0001)
- 2.60 for the ≤25% TTR group (P<0.0001).
The researchers said these results suggest the quality of anticoagulation management is associated with renal dysfunction and failure, so improving anticoagulation control might improve the long-term risk of end-organ injury in AF patients.
“Patients who use warfarin as part of their anticoagulation treatment for atrial fibrillation should have their anticoagulation levels closely monitored to ensure proper levels,” Dr Bunch said.
“Those who have erratic levels of warfarin despite close monitoring and care should consider other approaches such as newer anticoagulants that have more predictable blood effects, even if they have moderate kidney disease, and non drug-based methods to lower clot risk with atrial fibrillation.”
SAN FRANCISCO—Patients with atrial fibrillation (AF) who are taking warfarin have a higher risk of kidney problems if their anticoagulation levels are not properly managed, according to a new study.
Researchers found that patients who had low times in therapeutic range were significantly more likely to develop renal dysfunction and experience renal failure.
Furthermore, all patients were at risk of developing renal dysfunction, whether they began the study with healthy kidney function or moderate to severe kidney disease.
T. Jared Bunch, MD, of Intermountain Medical Center Heart Institute in Salt Lake City, Utah, and his colleagues presented these findings during the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract PO02-210).
The researchers studied 2753 AF patients who were anticoagulated with warfarin and managed by Intermountain Healthcare Clinical Pharmacist Anticoagulation Services.
The patients’ mean age was 74.7±10.7, and 50.3% were male. The patients had a baseline creatinine level of less than 2.0 mg/dL or a glomerular filtration rate greater than 30 and serial renal function studies.
Dr Bunch and his colleagues stratified patients into 4 categories based on the amount of time their international normalized ratio levels were determined to be in the therapeutic range (TTR): >75%, 51% to 75%, 26% to 50%, and <25%.
The researchers then performed multivariate, adjusted analyses to calculate odds ratios (ORs) for renal dysfunction and hazard ratios (HRs) for renal failure based on TTR group. The >75% group was the reference.
Among patients with baseline creatinine ≤2.0 mg/dL, the OR for a 25% increase in creatinine was:
- 1.35 for the 51%-75% TTR group (P=0.06)
- 1.80 for the 26-50% TTR group (P=0.003)
- 2.34 for the ≤25% TTR group (P=0.003).
Among patients with baseline creatinine ≤2.0 mg/dL, the HR for renal failure was:
- 1.72 for the 51%-75% TTR group (P=0.001)
- 2.36 for the 26-50% TTR group (P<0.0001)
- 2.38 for the ≤25% TTR group (P<0.0001).
Among patients with baseline glomerular filtration rate >30, the OR for a 25% decrease in glomerular filtration rate was:
- 1.45 for the 51%-75% TTR group (P=0.03)
- 1.46 for the 26-50% TTR group (P=0.08)
- 1.52 for the ≤25% TTR group (P=0.20).
Among patients with a baseline glomerular filtration rate >30, the HR for renal failure was:
- 1.88 for the 51%-75% TTR group (P<0.0001)
- 2.40 for the 26-50% TTR group (P<0.0001)
- 2.60 for the ≤25% TTR group (P<0.0001).
The researchers said these results suggest the quality of anticoagulation management is associated with renal dysfunction and failure, so improving anticoagulation control might improve the long-term risk of end-organ injury in AF patients.
“Patients who use warfarin as part of their anticoagulation treatment for atrial fibrillation should have their anticoagulation levels closely monitored to ensure proper levels,” Dr Bunch said.
“Those who have erratic levels of warfarin despite close monitoring and care should consider other approaches such as newer anticoagulants that have more predictable blood effects, even if they have moderate kidney disease, and non drug-based methods to lower clot risk with atrial fibrillation.”
SAN FRANCISCO—Patients with atrial fibrillation (AF) who are taking warfarin have a higher risk of kidney problems if their anticoagulation levels are not properly managed, according to a new study.
Researchers found that patients who had low times in therapeutic range were significantly more likely to develop renal dysfunction and experience renal failure.
Furthermore, all patients were at risk of developing renal dysfunction, whether they began the study with healthy kidney function or moderate to severe kidney disease.
T. Jared Bunch, MD, of Intermountain Medical Center Heart Institute in Salt Lake City, Utah, and his colleagues presented these findings during the Heart Rhythm Society’s 37th Annual Scientific Sessions (abstract PO02-210).
The researchers studied 2753 AF patients who were anticoagulated with warfarin and managed by Intermountain Healthcare Clinical Pharmacist Anticoagulation Services.
The patients’ mean age was 74.7±10.7, and 50.3% were male. The patients had a baseline creatinine level of less than 2.0 mg/dL or a glomerular filtration rate greater than 30 and serial renal function studies.
Dr Bunch and his colleagues stratified patients into 4 categories based on the amount of time their international normalized ratio levels were determined to be in the therapeutic range (TTR): >75%, 51% to 75%, 26% to 50%, and <25%.
The researchers then performed multivariate, adjusted analyses to calculate odds ratios (ORs) for renal dysfunction and hazard ratios (HRs) for renal failure based on TTR group. The >75% group was the reference.
Among patients with baseline creatinine ≤2.0 mg/dL, the OR for a 25% increase in creatinine was:
- 1.35 for the 51%-75% TTR group (P=0.06)
- 1.80 for the 26-50% TTR group (P=0.003)
- 2.34 for the ≤25% TTR group (P=0.003).
Among patients with baseline creatinine ≤2.0 mg/dL, the HR for renal failure was:
- 1.72 for the 51%-75% TTR group (P=0.001)
- 2.36 for the 26-50% TTR group (P<0.0001)
- 2.38 for the ≤25% TTR group (P<0.0001).
Among patients with baseline glomerular filtration rate >30, the OR for a 25% decrease in glomerular filtration rate was:
- 1.45 for the 51%-75% TTR group (P=0.03)
- 1.46 for the 26-50% TTR group (P=0.08)
- 1.52 for the ≤25% TTR group (P=0.20).
Among patients with a baseline glomerular filtration rate >30, the HR for renal failure was:
- 1.88 for the 51%-75% TTR group (P<0.0001)
- 2.40 for the 26-50% TTR group (P<0.0001)
- 2.60 for the ≤25% TTR group (P<0.0001).
The researchers said these results suggest the quality of anticoagulation management is associated with renal dysfunction and failure, so improving anticoagulation control might improve the long-term risk of end-organ injury in AF patients.
“Patients who use warfarin as part of their anticoagulation treatment for atrial fibrillation should have their anticoagulation levels closely monitored to ensure proper levels,” Dr Bunch said.
“Those who have erratic levels of warfarin despite close monitoring and care should consider other approaches such as newer anticoagulants that have more predictable blood effects, even if they have moderate kidney disease, and non drug-based methods to lower clot risk with atrial fibrillation.”
Stockings don’t reduce risk of PTS, study suggests

Image by Andre E.X. Brown
Results of a meta-analysis suggest elastic compression stockings do not significantly reduce the risk of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).
Investigators analyzed more than 600 past reports and studies involving elastic compression stockings, including the SOX trial.
And the results showed no significant difference in PTS incidence between patients who wore these stockings and those who did not.
Riyaz Bashir, MD, of Temple University Hospital in Philadelphia, Pennsylvania, and his colleagues performed the analysis and reported the results in The Lancet Haematology.
The investigators analyzed 674 reports, which included 6 randomized trials and a total of 1462 patients. The patients’ mean age was 59.5, and 56% were men.
All of the studies used stockings with a pressure range of 20 mm Hg to 40 mm Hg. Patient compliance varied from 55.6% to 91.6% and often decreased during follow-up. In most of the studies, the control group did not wear stockings, but, in 2 studies, the control group wore placebo stockings.
The data showed that use of elastic compression stockings was not associated with PTS prevention. The incidence of PTS was 36% (269/739) among patients who wore the stockings and 45% (322/723) among controls. The odds ratio (OR) was 0.56 (P=0.12).
The investigators observed similar results in subgroup analyses, when they tried to account for patient heterogeneity (27% vs 37%, OR=0.63, P=0.23) or diagnosis by Villalta scoring (43% vs 45%, OR=0.81, P=0.62) and when they looked at patients randomized within 1 month of DVT diagnosis (41% vs 49%, OR=0.57, P=0.24).
Furthermore, there was no significant difference between the treatment groups with regard to mortality or DVT recurrence.
The mortality incidence was 10% in both groups (OR 0.98, P=0.92), while the incidence of DVT recurrence was 6.4% in the compression stocking group and 6.8% in controls (OR=0.93, P=0.69).
“Many questions remain, such as whether certain groups of patients—like females or elderly patients—benefit from [compression stockings] or whether the timing of the intervention would make a difference,” Dr Bashir said.
“Based on the results of our study, we believe it’s too early to recommend that physicians stop using compression stockings and therefore should not give up on this modality of treatment yet. This study also highlights that there is a real need for new and more effective therapies for the treatment and prevention of post-thrombotic syndrome.”
Image by Andre E.X. Brown
Results of a meta-analysis suggest elastic compression stockings do not significantly reduce the risk of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).
Investigators analyzed more than 600 past reports and studies involving elastic compression stockings, including the SOX trial.
And the results showed no significant difference in PTS incidence between patients who wore these stockings and those who did not.
Riyaz Bashir, MD, of Temple University Hospital in Philadelphia, Pennsylvania, and his colleagues performed the analysis and reported the results in The Lancet Haematology.
The investigators analyzed 674 reports, which included 6 randomized trials and a total of 1462 patients. The patients’ mean age was 59.5, and 56% were men.
All of the studies used stockings with a pressure range of 20 mm Hg to 40 mm Hg. Patient compliance varied from 55.6% to 91.6% and often decreased during follow-up. In most of the studies, the control group did not wear stockings, but, in 2 studies, the control group wore placebo stockings.
The data showed that use of elastic compression stockings was not associated with PTS prevention. The incidence of PTS was 36% (269/739) among patients who wore the stockings and 45% (322/723) among controls. The odds ratio (OR) was 0.56 (P=0.12).
The investigators observed similar results in subgroup analyses, when they tried to account for patient heterogeneity (27% vs 37%, OR=0.63, P=0.23) or diagnosis by Villalta scoring (43% vs 45%, OR=0.81, P=0.62) and when they looked at patients randomized within 1 month of DVT diagnosis (41% vs 49%, OR=0.57, P=0.24).
Furthermore, there was no significant difference between the treatment groups with regard to mortality or DVT recurrence.
The mortality incidence was 10% in both groups (OR 0.98, P=0.92), while the incidence of DVT recurrence was 6.4% in the compression stocking group and 6.8% in controls (OR=0.93, P=0.69).
“Many questions remain, such as whether certain groups of patients—like females or elderly patients—benefit from [compression stockings] or whether the timing of the intervention would make a difference,” Dr Bashir said.
“Based on the results of our study, we believe it’s too early to recommend that physicians stop using compression stockings and therefore should not give up on this modality of treatment yet. This study also highlights that there is a real need for new and more effective therapies for the treatment and prevention of post-thrombotic syndrome.”
Image by Andre E.X. Brown
Results of a meta-analysis suggest elastic compression stockings do not significantly reduce the risk of post-thrombotic syndrome (PTS) after deep vein thrombosis (DVT).
Investigators analyzed more than 600 past reports and studies involving elastic compression stockings, including the SOX trial.
And the results showed no significant difference in PTS incidence between patients who wore these stockings and those who did not.
Riyaz Bashir, MD, of Temple University Hospital in Philadelphia, Pennsylvania, and his colleagues performed the analysis and reported the results in The Lancet Haematology.
The investigators analyzed 674 reports, which included 6 randomized trials and a total of 1462 patients. The patients’ mean age was 59.5, and 56% were men.
All of the studies used stockings with a pressure range of 20 mm Hg to 40 mm Hg. Patient compliance varied from 55.6% to 91.6% and often decreased during follow-up. In most of the studies, the control group did not wear stockings, but, in 2 studies, the control group wore placebo stockings.
The data showed that use of elastic compression stockings was not associated with PTS prevention. The incidence of PTS was 36% (269/739) among patients who wore the stockings and 45% (322/723) among controls. The odds ratio (OR) was 0.56 (P=0.12).
The investigators observed similar results in subgroup analyses, when they tried to account for patient heterogeneity (27% vs 37%, OR=0.63, P=0.23) or diagnosis by Villalta scoring (43% vs 45%, OR=0.81, P=0.62) and when they looked at patients randomized within 1 month of DVT diagnosis (41% vs 49%, OR=0.57, P=0.24).
Furthermore, there was no significant difference between the treatment groups with regard to mortality or DVT recurrence.
The mortality incidence was 10% in both groups (OR 0.98, P=0.92), while the incidence of DVT recurrence was 6.4% in the compression stocking group and 6.8% in controls (OR=0.93, P=0.69).
“Many questions remain, such as whether certain groups of patients—like females or elderly patients—benefit from [compression stockings] or whether the timing of the intervention would make a difference,” Dr Bashir said.
“Based on the results of our study, we believe it’s too early to recommend that physicians stop using compression stockings and therefore should not give up on this modality of treatment yet. This study also highlights that there is a real need for new and more effective therapies for the treatment and prevention of post-thrombotic syndrome.”
Tools may aid transition from pediatric to adult care

Photo courtesy of the CDC
WASHINGTON, DC—The American Society of Hematology (ASH) has created a toolkit to help hematologists aid patients who are transitioning from pediatric to adult practices.
The toolkit contains general resources for all hematologic conditions, as well as specific resources for patients with hemophilia and sickle cell disease.
It includes 2 types of forms—a transition-readiness assessment and a clinical summary.
The toolkit was presented at the American College of Physicians (ACP) Internal Medicine Meeting 2016.
“Transitioning from pediatric to adult healthcare practices is often a challenge for patients with chronic medical issues because it can be difficult to adhere to a treatment regimen or attend regular appointments without the assistance of a parent or guardian,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
“ASH recognizes that understanding a patient’s preparedness to take control of his or her medical condition in adulthood can make a huge difference in quality of care, which is why we are pleased to join the American College of Physicians and partner societies in this important initiative.”
ASH joined more than 2 dozen groups to participate in the ACP’s Pediatric to Adult Care Transition Initiative. The goal of this initiative was to develop guidance and tools that both primary care internal medicine and subspecialty practices can use for patients who are transitioning from pediatric/adolescent practices to adult care.
An ASH Transitions Work Group, made up of society members from pediatric and adult practices, developed 3 segments of the hematology-specific toolkit:
- generic forms for patients with any hematologic condition, with an addendum that includes links to additional condition-specific guidelines and resources
- specific forms for hemophilia
- specific forms for sickle cell disease.
For each segment, there are 2 types of forms— a transition-readiness assessment and a clinical summary.
The transition-readiness assessment should be completed by the patient. It assesses the patient’s readiness for the transition to adult care by evaluating the patient’s understanding of his or her condition and ability to manage medications, appointments, insurance, and medical privacy issues.
This assessment should be used by the adult care team to assess any remaining gaps in the patient’s self-care knowledge or additional issues that should be addressed to ensure optimal care.
The clinical summary is a medical record summary to be completed by the referring provider and the patient. The summary contains essential clinical information regarding the patient’s condition that is to be included in the patient’s medical record upon transfer to the adult practice.
More information on the ACP Pediatric to Adult Care Transitions Initiative is available on the ACP website. The forms for the ASH transitions toolkit are available in the “Hematology” section of the Condition-Specific Tools page.
Photo courtesy of the CDC
WASHINGTON, DC—The American Society of Hematology (ASH) has created a toolkit to help hematologists aid patients who are transitioning from pediatric to adult practices.
The toolkit contains general resources for all hematologic conditions, as well as specific resources for patients with hemophilia and sickle cell disease.
It includes 2 types of forms—a transition-readiness assessment and a clinical summary.
The toolkit was presented at the American College of Physicians (ACP) Internal Medicine Meeting 2016.
“Transitioning from pediatric to adult healthcare practices is often a challenge for patients with chronic medical issues because it can be difficult to adhere to a treatment regimen or attend regular appointments without the assistance of a parent or guardian,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
“ASH recognizes that understanding a patient’s preparedness to take control of his or her medical condition in adulthood can make a huge difference in quality of care, which is why we are pleased to join the American College of Physicians and partner societies in this important initiative.”
ASH joined more than 2 dozen groups to participate in the ACP’s Pediatric to Adult Care Transition Initiative. The goal of this initiative was to develop guidance and tools that both primary care internal medicine and subspecialty practices can use for patients who are transitioning from pediatric/adolescent practices to adult care.
An ASH Transitions Work Group, made up of society members from pediatric and adult practices, developed 3 segments of the hematology-specific toolkit:
- generic forms for patients with any hematologic condition, with an addendum that includes links to additional condition-specific guidelines and resources
- specific forms for hemophilia
- specific forms for sickle cell disease.
For each segment, there are 2 types of forms— a transition-readiness assessment and a clinical summary.
The transition-readiness assessment should be completed by the patient. It assesses the patient’s readiness for the transition to adult care by evaluating the patient’s understanding of his or her condition and ability to manage medications, appointments, insurance, and medical privacy issues.
This assessment should be used by the adult care team to assess any remaining gaps in the patient’s self-care knowledge or additional issues that should be addressed to ensure optimal care.
The clinical summary is a medical record summary to be completed by the referring provider and the patient. The summary contains essential clinical information regarding the patient’s condition that is to be included in the patient’s medical record upon transfer to the adult practice.
More information on the ACP Pediatric to Adult Care Transitions Initiative is available on the ACP website. The forms for the ASH transitions toolkit are available in the “Hematology” section of the Condition-Specific Tools page.
Photo courtesy of the CDC
WASHINGTON, DC—The American Society of Hematology (ASH) has created a toolkit to help hematologists aid patients who are transitioning from pediatric to adult practices.
The toolkit contains general resources for all hematologic conditions, as well as specific resources for patients with hemophilia and sickle cell disease.
It includes 2 types of forms—a transition-readiness assessment and a clinical summary.
The toolkit was presented at the American College of Physicians (ACP) Internal Medicine Meeting 2016.
“Transitioning from pediatric to adult healthcare practices is often a challenge for patients with chronic medical issues because it can be difficult to adhere to a treatment regimen or attend regular appointments without the assistance of a parent or guardian,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
“ASH recognizes that understanding a patient’s preparedness to take control of his or her medical condition in adulthood can make a huge difference in quality of care, which is why we are pleased to join the American College of Physicians and partner societies in this important initiative.”
ASH joined more than 2 dozen groups to participate in the ACP’s Pediatric to Adult Care Transition Initiative. The goal of this initiative was to develop guidance and tools that both primary care internal medicine and subspecialty practices can use for patients who are transitioning from pediatric/adolescent practices to adult care.
An ASH Transitions Work Group, made up of society members from pediatric and adult practices, developed 3 segments of the hematology-specific toolkit:
- generic forms for patients with any hematologic condition, with an addendum that includes links to additional condition-specific guidelines and resources
- specific forms for hemophilia
- specific forms for sickle cell disease.
For each segment, there are 2 types of forms— a transition-readiness assessment and a clinical summary.
The transition-readiness assessment should be completed by the patient. It assesses the patient’s readiness for the transition to adult care by evaluating the patient’s understanding of his or her condition and ability to manage medications, appointments, insurance, and medical privacy issues.
This assessment should be used by the adult care team to assess any remaining gaps in the patient’s self-care knowledge or additional issues that should be addressed to ensure optimal care.
The clinical summary is a medical record summary to be completed by the referring provider and the patient. The summary contains essential clinical information regarding the patient’s condition that is to be included in the patient’s medical record upon transfer to the adult practice.
More information on the ACP Pediatric to Adult Care Transitions Initiative is available on the ACP website. The forms for the ASH transitions toolkit are available in the “Hematology” section of the Condition-Specific Tools page.