User login
FDA approves recombinant product for VWD
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
The US Food and Drug Administration (FDA) has approved a recombinant von Willebrand factor product, Vonvendi (formerly BAX 111), for use in adults with von Willebrand disease (VWD).
Vonvendi is the first FDA-approved recombinant von Willebrand factor.
It is now approved for the on-demand treatment and control of bleeding episodes in VWD patients 18 years of age and older.
Vonvendi is expected to be broadly available in the US in late 2016.
Compared to other marketed von Willebrand factor concentrates, Vonvendi contains a more consistent concentration of ultra-large-molecular-weight multimers. And the product is developed using a plasma- and albumin-free manufacturing method.
Vonvendi is the first von Willebrand factor concentrate in the US that contains only trace amounts of factor VIII (FVIII), offering the flexibility to administer FVIII only when needed.
The FDA’s approval of Vonvendi was based on results from a phase 3 trial recently published in Blood. The study included 49 patients with WWD who received Vonvendi with and without recombinant FVIII.
All participants reported successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) achieved an “excellent” efficacy rating.
Most bleeds (81.8%) were resolved with a single infusion of Vonvendi, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events considered related to Vonvendi, but only 2 of these were serious. One patient experienced 2 simultaneous serious adverse events—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against von Willebrand factor, and no neutralizing antibodies against FVIII.
Vonvendi is manufactured by Baxalta Incorporated. Baxalta said it is building a robust clinical development program to optimize patient access to Vonvendi worldwide. A series of clinical programs are planned to evaluate its use for prophylaxis, surgical, and pediatric indications.
Baxalta expects to file for regulatory approvals in Europe in 2017 and in other markets around the world.
For more details on Vonvendi, see the product information. ![]()
Antiplatelet agent proves ineffective in SCD

Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Treatment with the antiplatelet agent prasugrel does not significantly reduce the rate of pain crises or severe lung complications in children with sickle cell disease (SCD), according to one of the largest and most geographically diverse international trials on SCD to date.
The DOVE trial was a double blind, randomized, placebo-controlled phase 3 study conducted at 51 sites across 13 nations in the Americas, Europe, the Middle East, Asia, and Africa.
“Although we were disappointed that prasugrel does not appear to ease the suffering of children with sickle cell disease, the fact that this study incorporated patients in the wide range of countries where the disease occurs is hugely significant,” said Carolyn Hoppe, MD, of UCSF Benioff Children’s Hospital Oakland in California.
“The logistical challenges that we addressed in designing and implementing the study can serve as a model for future research.”
The results of the study were published in NEJM. The research was sponsored by Daiichi Sankyo Company, Ltd. and Eli Lilly and Company.
The goal of the DOVE trial was to determine whether prasugrel could significantly reduce the rate of vaso-occlusive crises (VOCs)—defined as pain crises or acute chest syndrome—in children with SCD.
The trial enrolled 341 patients. About half of them (n=170) received daily oral prasugrel for between 9 and 24 months at individualized, blinded doses intended to maintain a selected target range of platelet activity. The remaining patients received a placebo.
All patients were monitored for VOCs prompting medical visits and for any increased risk of bleeding due to reduced platelet activity. In addition, patients 4 years old and older kept a daily electronic pain diary to aid in the reporting of painful events between visits.
At the end of the study period, there was no significant difference between the treatment arms in the overall rate of VOCs. The rate was 2.3 episodes per person-year in the prasugrel arm and 2.8 episodes per person-year in the placebo arm (P=0.12).
Similarly, prasugrel did not have a significant effect on the trial’s secondary outcome measures—VOC-related hospitalization rate, duration of hospitalization, time between VOCs, incidence of ischemic attack or ischemic stroke, transfusion rate, rate of pain, intensity of pain, use of analgesics, or missed school due to SCD-related pain.
The data did reveal a trend toward reduced VOC rates among patients ages 12 to 18 (P=0.06) and among patients who were not taking hydroxyurea (P=0.06). However, these trends were not statistically significant and require further research to determine their validity.
The investigators noted no adverse events related to prasugrel.
“Even though prasugrel did not achieve significant results, the findings should not detract from the fact that this team successfully completed a rigorous, sophisticated trial in a disease where the barriers to conducting large-scale international, patient-focused research are quite high,” said Matthew M. Heeney, MD, of the Dana–Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts.
To conduct the study successfully on such a broad geographical scale, the investigators had to address several obstacles, such as varying standards of care, local technological resources, and infrastructure challenges, such as a lack of reliable electrical power. ![]()
RBC storage duration doesn’t affect outcomes in kids

Photo by Elise Amendola
ORLANDO, FL—The storage duration of red blood cells (RBCs) doesn’t affect transfusion outcomes in children with lactic acidosis due to severe anemia, according to a new study.
Investigators found no significant differences in lactate levels, 30-day recovery, survival, or adverse events between children who received RBCs stored for 25 to 35 days and children who received RBCs stored for 1 to 10 days.
These results were published in JAMA and presented at the 2015 ASH Annual Meeting as abstract 769.
Christine Cserti-Gazdewich, MD, of University Health Network in Toronto, Canada, provided insights on the data during a press conference at ASH.
A concern of the investigators, according to Dr Cserti-Gazdewich, was that previous studies on blood storage were conducted in “high-income countries in high-technology care settings with blood inventory wealth, and findings may not be generalizable to the other half of the world.”
She pointed out that, in less developed countries, the shortfall in blood availability compared to the need is up to 3-fold.
So the investigators examined whether longer-stored red blood cells actually deliver oxygen in a manner not worse than shorter-stored or fresh blood and examined it at the extremes of storage duration in the context of a very high-dose need.
The team evaluated 290 children (aged 6 months to 60 months) with elevated blood lactate levels due to severe anemia who presented at a university-affiliated national referral hospital in Kampala, Uganda.
The children were randomized to receive RBC units stored for 25 to 35 days (longer-storage group, n=145) or RBCs stored for 1 to 10 days (shorter-storage group, n=145).
All units were leukoreduced prior to storage. All patients received 10 mL/kg of RBCs during hours 0 through 2 and, if indicated per protocol, an additional 10 mL/kg during hours 4 through 6.
In the entire population, the mean presenting hemoglobin level was 3.7 g/dL, and the mean lactate level was 9.3 mmol/L. The median RBC unit storage duration was 8 days (range, 7-9) for the shorter-storage group and 32 days (range, 30-34) for the longer-storage group.
Results
The investigators found that RBC units maintained under standard storage conditions for 25 to 35 days were not inferior to RBC units stored for up to 10 days.
The study’s primary endpoint was the proportion of patients with a lactate level of 3 mmol/L or lower at 8 hours, using a margin of noninferiority equal to an absolute difference of 25%.
The proportion of patients meeting this endpoint was 0.61 in the longer-storage group and 0.58 in the shorter-storage group (P<0.001 for noninferiority).
Average lactate levels were not statistically different between the 2 groups at 0, 2, 4, 6, 8, or 24 hours. And there was no statistical difference in the median time to achieve a blood lactate of 3 mmol/L or lower at 4 hours (hazard ratio=0.99, P=0.92).
Cerebral tissue oxygen saturation rose significantly during transfusion, but there was no significant difference between the 2 storage groups. The median area under the curve of cerebral tissue oxygen saturation during transfusion was 679 (range, 334-1156) for the longer-storage group and 521 (range, 303-835) for the shorter-storage group (P=0.25).
There was no significant difference between the longer-storage group and the shorter-storage group in the persistence of stupor or coma 8 hours after transfusion (12.6% and 19.6%, respectively, P=0.11) or the persistence of respiratory distress at 8 hours (28.7% and 30%, respectively, P=0.79).
The median length of hospital stay was 4 days (range, 2-6) in the longer-storage group and 4 days (range, 3-7) in the shorter-storage group.
There were 8 deaths, 3 in the longer-storage group and 5 in the shorter-storage group, during the 24 hours from the start of transfusion. Four additional patients, 2 in each group, died in the hospital after the initial 24-hour observation period.
The proportion of patients who had returned to good health by 30 days was 86% of the longer-storage group and 93% of the shorter-storage group (P=0.13).
“By every single measure we explored, and we explored many, we found that long-stored blood was not inferior . . . ,” Dr Csert-Gazdewich said. “We truly found no justification to shorten the current storage duration of red cells as judged by the fundamental role to deliver oxygen.” ![]()
Photo by Elise Amendola
ORLANDO, FL—The storage duration of red blood cells (RBCs) doesn’t affect transfusion outcomes in children with lactic acidosis due to severe anemia, according to a new study.
Investigators found no significant differences in lactate levels, 30-day recovery, survival, or adverse events between children who received RBCs stored for 25 to 35 days and children who received RBCs stored for 1 to 10 days.
These results were published in JAMA and presented at the 2015 ASH Annual Meeting as abstract 769.
Christine Cserti-Gazdewich, MD, of University Health Network in Toronto, Canada, provided insights on the data during a press conference at ASH.
A concern of the investigators, according to Dr Cserti-Gazdewich, was that previous studies on blood storage were conducted in “high-income countries in high-technology care settings with blood inventory wealth, and findings may not be generalizable to the other half of the world.”
She pointed out that, in less developed countries, the shortfall in blood availability compared to the need is up to 3-fold.
So the investigators examined whether longer-stored red blood cells actually deliver oxygen in a manner not worse than shorter-stored or fresh blood and examined it at the extremes of storage duration in the context of a very high-dose need.
The team evaluated 290 children (aged 6 months to 60 months) with elevated blood lactate levels due to severe anemia who presented at a university-affiliated national referral hospital in Kampala, Uganda.
The children were randomized to receive RBC units stored for 25 to 35 days (longer-storage group, n=145) or RBCs stored for 1 to 10 days (shorter-storage group, n=145).
All units were leukoreduced prior to storage. All patients received 10 mL/kg of RBCs during hours 0 through 2 and, if indicated per protocol, an additional 10 mL/kg during hours 4 through 6.
In the entire population, the mean presenting hemoglobin level was 3.7 g/dL, and the mean lactate level was 9.3 mmol/L. The median RBC unit storage duration was 8 days (range, 7-9) for the shorter-storage group and 32 days (range, 30-34) for the longer-storage group.
Results
The investigators found that RBC units maintained under standard storage conditions for 25 to 35 days were not inferior to RBC units stored for up to 10 days.
The study’s primary endpoint was the proportion of patients with a lactate level of 3 mmol/L or lower at 8 hours, using a margin of noninferiority equal to an absolute difference of 25%.
The proportion of patients meeting this endpoint was 0.61 in the longer-storage group and 0.58 in the shorter-storage group (P<0.001 for noninferiority).
Average lactate levels were not statistically different between the 2 groups at 0, 2, 4, 6, 8, or 24 hours. And there was no statistical difference in the median time to achieve a blood lactate of 3 mmol/L or lower at 4 hours (hazard ratio=0.99, P=0.92).
Cerebral tissue oxygen saturation rose significantly during transfusion, but there was no significant difference between the 2 storage groups. The median area under the curve of cerebral tissue oxygen saturation during transfusion was 679 (range, 334-1156) for the longer-storage group and 521 (range, 303-835) for the shorter-storage group (P=0.25).
There was no significant difference between the longer-storage group and the shorter-storage group in the persistence of stupor or coma 8 hours after transfusion (12.6% and 19.6%, respectively, P=0.11) or the persistence of respiratory distress at 8 hours (28.7% and 30%, respectively, P=0.79).
The median length of hospital stay was 4 days (range, 2-6) in the longer-storage group and 4 days (range, 3-7) in the shorter-storage group.
There were 8 deaths, 3 in the longer-storage group and 5 in the shorter-storage group, during the 24 hours from the start of transfusion. Four additional patients, 2 in each group, died in the hospital after the initial 24-hour observation period.
The proportion of patients who had returned to good health by 30 days was 86% of the longer-storage group and 93% of the shorter-storage group (P=0.13).
“By every single measure we explored, and we explored many, we found that long-stored blood was not inferior . . . ,” Dr Csert-Gazdewich said. “We truly found no justification to shorten the current storage duration of red cells as judged by the fundamental role to deliver oxygen.” ![]()
Photo by Elise Amendola
ORLANDO, FL—The storage duration of red blood cells (RBCs) doesn’t affect transfusion outcomes in children with lactic acidosis due to severe anemia, according to a new study.
Investigators found no significant differences in lactate levels, 30-day recovery, survival, or adverse events between children who received RBCs stored for 25 to 35 days and children who received RBCs stored for 1 to 10 days.
These results were published in JAMA and presented at the 2015 ASH Annual Meeting as abstract 769.
Christine Cserti-Gazdewich, MD, of University Health Network in Toronto, Canada, provided insights on the data during a press conference at ASH.
A concern of the investigators, according to Dr Cserti-Gazdewich, was that previous studies on blood storage were conducted in “high-income countries in high-technology care settings with blood inventory wealth, and findings may not be generalizable to the other half of the world.”
She pointed out that, in less developed countries, the shortfall in blood availability compared to the need is up to 3-fold.
So the investigators examined whether longer-stored red blood cells actually deliver oxygen in a manner not worse than shorter-stored or fresh blood and examined it at the extremes of storage duration in the context of a very high-dose need.
The team evaluated 290 children (aged 6 months to 60 months) with elevated blood lactate levels due to severe anemia who presented at a university-affiliated national referral hospital in Kampala, Uganda.
The children were randomized to receive RBC units stored for 25 to 35 days (longer-storage group, n=145) or RBCs stored for 1 to 10 days (shorter-storage group, n=145).
All units were leukoreduced prior to storage. All patients received 10 mL/kg of RBCs during hours 0 through 2 and, if indicated per protocol, an additional 10 mL/kg during hours 4 through 6.
In the entire population, the mean presenting hemoglobin level was 3.7 g/dL, and the mean lactate level was 9.3 mmol/L. The median RBC unit storage duration was 8 days (range, 7-9) for the shorter-storage group and 32 days (range, 30-34) for the longer-storage group.
Results
The investigators found that RBC units maintained under standard storage conditions for 25 to 35 days were not inferior to RBC units stored for up to 10 days.
The study’s primary endpoint was the proportion of patients with a lactate level of 3 mmol/L or lower at 8 hours, using a margin of noninferiority equal to an absolute difference of 25%.
The proportion of patients meeting this endpoint was 0.61 in the longer-storage group and 0.58 in the shorter-storage group (P<0.001 for noninferiority).
Average lactate levels were not statistically different between the 2 groups at 0, 2, 4, 6, 8, or 24 hours. And there was no statistical difference in the median time to achieve a blood lactate of 3 mmol/L or lower at 4 hours (hazard ratio=0.99, P=0.92).
Cerebral tissue oxygen saturation rose significantly during transfusion, but there was no significant difference between the 2 storage groups. The median area under the curve of cerebral tissue oxygen saturation during transfusion was 679 (range, 334-1156) for the longer-storage group and 521 (range, 303-835) for the shorter-storage group (P=0.25).
There was no significant difference between the longer-storage group and the shorter-storage group in the persistence of stupor or coma 8 hours after transfusion (12.6% and 19.6%, respectively, P=0.11) or the persistence of respiratory distress at 8 hours (28.7% and 30%, respectively, P=0.79).
The median length of hospital stay was 4 days (range, 2-6) in the longer-storage group and 4 days (range, 3-7) in the shorter-storage group.
There were 8 deaths, 3 in the longer-storage group and 5 in the shorter-storage group, during the 24 hours from the start of transfusion. Four additional patients, 2 in each group, died in the hospital after the initial 24-hour observation period.
The proportion of patients who had returned to good health by 30 days was 86% of the longer-storage group and 93% of the shorter-storage group (P=0.13).
“By every single measure we explored, and we explored many, we found that long-stored blood was not inferior . . . ,” Dr Csert-Gazdewich said. “We truly found no justification to shorten the current storage duration of red cells as judged by the fundamental role to deliver oxygen.” ![]()
Engineers create ‘smart wound dressing’
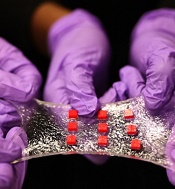
a matrix of polymer islands
(red) that can encapsulate
electronic components
Photo by Melanie Gonick/MIT
Engineers say they have designed “smart wound dressing,” a sticky, stretchy, gel-like material that can incorporate temperature sensors, LED lights, and other electronics, as well as tiny, drug-delivering reservoirs and channels.
The dressing releases medicine in response to changes in skin temperature and can be designed to light up if, say, medicine is running low.
When the dressing is applied to a highly flexible area, such as the elbow or knee, it stretches with the body, keeping the embedded electronics functional and intact.
The key to the design is a hydrogel matrix designed by Xuanhe Zhao, PhD, of the Massachusetts Institute of Technology in Cambridge.
The hydrogel, which was describe in Nature Materials last month, is a rubbery material, mostly composed of water, designed to bond strongly to surfaces such as gold, titanium, aluminum, silicon, glass, and ceramic.
In a paper published in Advanced Materials, Dr Zhao and his colleagues described embedding various electronics within the hydrogel, such as conductive wires, semiconductor chips, LED lights, and temperature sensors.
Dr Zhao said electronics coated in hydrogel may be used not just on the surface of the skin but also inside the body; for example, as implanted, biocompatible glucose sensors, or even soft, compliant neural probes.
“Electronics are usually hard and dry, but the human body is soft and wet,” Dr Zhao said. “These two systems have drastically different properties. If you want to put electronics in close contact with the human body for applications such as healthcare monitoring and drug delivery, it is highly desirable to make the electronic devices soft and stretchable to fit the environment of the human body. That’s the motivation for stretchable hydrogel electronics.”
A strong and stretchy bond
Typical synthetic hydrogels are brittle, barely stretchable, and adhere weakly to other surfaces.
“They’re often used as degradable biomaterials at the current stage,” Dr Zhao said. “If you want to make an electronic device out of hydrogels, you need to think of long-term stability of the hydrogels and interfaces.”
To get around these challenges, his team came up with a design strategy for robust hydrogels, mixing water with a small amount of selected biopolymers to create soft, stretchy materials with a stiffness of 10 to 100 kilopascals—about the range of human soft tissues. The researchers also devised a method to strongly bond the hydrogel to various nonporous surfaces.
In the new study, the researchers applied their techniques to demonstrate several uses for the hydrogel, including encapsulating a titanium wire to form a transparent, stretchable conductor. In experiments, they stretched the encapsulated wire multiple times and found it maintained constant electrical conductivity.
Dr Zhao also created an array of LED lights embedded in a sheet of hydrogel. When attached to different regions of the body, the array continued working, even when stretched across highly deformable areas such as the knee and elbow.
A versatile matrix
Finally, the group embedded various electronic components within a sheet of hydrogel to create a “smart wound dressing,” comprising regularly spaced temperature sensors and tiny drug reservoirs.
The researchers also created pathways for drugs to flow through the hydrogel, by either inserting patterned tubes or drilling tiny holes through the matrix. They placed the dressing over various regions of the body and found that, even when highly stretched, the dressing continued to monitor skin temperature and release drugs according to the sensor readings.
An immediate application of the technology may be as a stretchable, on-demand treatment for burns or other skin conditions, said Hyunwoo Yuk, a graduate student at MIT.
“It’s a very versatile matrix,” Yuk said. “The unique capability here is, when a sensor senses something different, like an abnormal increase in temperature, the device can, on demand, release drugs to that specific location and select a specific drug from one of the reservoirs, which can diffuse in the hydrogel matrix for sustained release over time.”
Delving deeper, Dr Zhao envisions hydrogel to be an ideal, biocompatible vehicle for delivering electronics inside the body. He is currently exploring hydrogel’s potential as a carrier for glucose sensors as well as neural probes. ![]()
a matrix of polymer islands
(red) that can encapsulate
electronic components
Photo by Melanie Gonick/MIT
Engineers say they have designed “smart wound dressing,” a sticky, stretchy, gel-like material that can incorporate temperature sensors, LED lights, and other electronics, as well as tiny, drug-delivering reservoirs and channels.
The dressing releases medicine in response to changes in skin temperature and can be designed to light up if, say, medicine is running low.
When the dressing is applied to a highly flexible area, such as the elbow or knee, it stretches with the body, keeping the embedded electronics functional and intact.
The key to the design is a hydrogel matrix designed by Xuanhe Zhao, PhD, of the Massachusetts Institute of Technology in Cambridge.
The hydrogel, which was describe in Nature Materials last month, is a rubbery material, mostly composed of water, designed to bond strongly to surfaces such as gold, titanium, aluminum, silicon, glass, and ceramic.
In a paper published in Advanced Materials, Dr Zhao and his colleagues described embedding various electronics within the hydrogel, such as conductive wires, semiconductor chips, LED lights, and temperature sensors.
Dr Zhao said electronics coated in hydrogel may be used not just on the surface of the skin but also inside the body; for example, as implanted, biocompatible glucose sensors, or even soft, compliant neural probes.
“Electronics are usually hard and dry, but the human body is soft and wet,” Dr Zhao said. “These two systems have drastically different properties. If you want to put electronics in close contact with the human body for applications such as healthcare monitoring and drug delivery, it is highly desirable to make the electronic devices soft and stretchable to fit the environment of the human body. That’s the motivation for stretchable hydrogel electronics.”
A strong and stretchy bond
Typical synthetic hydrogels are brittle, barely stretchable, and adhere weakly to other surfaces.
“They’re often used as degradable biomaterials at the current stage,” Dr Zhao said. “If you want to make an electronic device out of hydrogels, you need to think of long-term stability of the hydrogels and interfaces.”
To get around these challenges, his team came up with a design strategy for robust hydrogels, mixing water with a small amount of selected biopolymers to create soft, stretchy materials with a stiffness of 10 to 100 kilopascals—about the range of human soft tissues. The researchers also devised a method to strongly bond the hydrogel to various nonporous surfaces.
In the new study, the researchers applied their techniques to demonstrate several uses for the hydrogel, including encapsulating a titanium wire to form a transparent, stretchable conductor. In experiments, they stretched the encapsulated wire multiple times and found it maintained constant electrical conductivity.
Dr Zhao also created an array of LED lights embedded in a sheet of hydrogel. When attached to different regions of the body, the array continued working, even when stretched across highly deformable areas such as the knee and elbow.
A versatile matrix
Finally, the group embedded various electronic components within a sheet of hydrogel to create a “smart wound dressing,” comprising regularly spaced temperature sensors and tiny drug reservoirs.
The researchers also created pathways for drugs to flow through the hydrogel, by either inserting patterned tubes or drilling tiny holes through the matrix. They placed the dressing over various regions of the body and found that, even when highly stretched, the dressing continued to monitor skin temperature and release drugs according to the sensor readings.
An immediate application of the technology may be as a stretchable, on-demand treatment for burns or other skin conditions, said Hyunwoo Yuk, a graduate student at MIT.
“It’s a very versatile matrix,” Yuk said. “The unique capability here is, when a sensor senses something different, like an abnormal increase in temperature, the device can, on demand, release drugs to that specific location and select a specific drug from one of the reservoirs, which can diffuse in the hydrogel matrix for sustained release over time.”
Delving deeper, Dr Zhao envisions hydrogel to be an ideal, biocompatible vehicle for delivering electronics inside the body. He is currently exploring hydrogel’s potential as a carrier for glucose sensors as well as neural probes. ![]()
a matrix of polymer islands
(red) that can encapsulate
electronic components
Photo by Melanie Gonick/MIT
Engineers say they have designed “smart wound dressing,” a sticky, stretchy, gel-like material that can incorporate temperature sensors, LED lights, and other electronics, as well as tiny, drug-delivering reservoirs and channels.
The dressing releases medicine in response to changes in skin temperature and can be designed to light up if, say, medicine is running low.
When the dressing is applied to a highly flexible area, such as the elbow or knee, it stretches with the body, keeping the embedded electronics functional and intact.
The key to the design is a hydrogel matrix designed by Xuanhe Zhao, PhD, of the Massachusetts Institute of Technology in Cambridge.
The hydrogel, which was describe in Nature Materials last month, is a rubbery material, mostly composed of water, designed to bond strongly to surfaces such as gold, titanium, aluminum, silicon, glass, and ceramic.
In a paper published in Advanced Materials, Dr Zhao and his colleagues described embedding various electronics within the hydrogel, such as conductive wires, semiconductor chips, LED lights, and temperature sensors.
Dr Zhao said electronics coated in hydrogel may be used not just on the surface of the skin but also inside the body; for example, as implanted, biocompatible glucose sensors, or even soft, compliant neural probes.
“Electronics are usually hard and dry, but the human body is soft and wet,” Dr Zhao said. “These two systems have drastically different properties. If you want to put electronics in close contact with the human body for applications such as healthcare monitoring and drug delivery, it is highly desirable to make the electronic devices soft and stretchable to fit the environment of the human body. That’s the motivation for stretchable hydrogel electronics.”
A strong and stretchy bond
Typical synthetic hydrogels are brittle, barely stretchable, and adhere weakly to other surfaces.
“They’re often used as degradable biomaterials at the current stage,” Dr Zhao said. “If you want to make an electronic device out of hydrogels, you need to think of long-term stability of the hydrogels and interfaces.”
To get around these challenges, his team came up with a design strategy for robust hydrogels, mixing water with a small amount of selected biopolymers to create soft, stretchy materials with a stiffness of 10 to 100 kilopascals—about the range of human soft tissues. The researchers also devised a method to strongly bond the hydrogel to various nonporous surfaces.
In the new study, the researchers applied their techniques to demonstrate several uses for the hydrogel, including encapsulating a titanium wire to form a transparent, stretchable conductor. In experiments, they stretched the encapsulated wire multiple times and found it maintained constant electrical conductivity.
Dr Zhao also created an array of LED lights embedded in a sheet of hydrogel. When attached to different regions of the body, the array continued working, even when stretched across highly deformable areas such as the knee and elbow.
A versatile matrix
Finally, the group embedded various electronic components within a sheet of hydrogel to create a “smart wound dressing,” comprising regularly spaced temperature sensors and tiny drug reservoirs.
The researchers also created pathways for drugs to flow through the hydrogel, by either inserting patterned tubes or drilling tiny holes through the matrix. They placed the dressing over various regions of the body and found that, even when highly stretched, the dressing continued to monitor skin temperature and release drugs according to the sensor readings.
An immediate application of the technology may be as a stretchable, on-demand treatment for burns or other skin conditions, said Hyunwoo Yuk, a graduate student at MIT.
“It’s a very versatile matrix,” Yuk said. “The unique capability here is, when a sensor senses something different, like an abnormal increase in temperature, the device can, on demand, release drugs to that specific location and select a specific drug from one of the reservoirs, which can diffuse in the hydrogel matrix for sustained release over time.”
Delving deeper, Dr Zhao envisions hydrogel to be an ideal, biocompatible vehicle for delivering electronics inside the body. He is currently exploring hydrogel’s potential as a carrier for glucose sensors as well as neural probes. ![]()
Cancer drug prices vary widely from country to country

Photo by Bill Branson
The price of cancer drugs varies widely between European countries, Australia, and New Zealand, according to a study published in The Lancet Oncology.
The study indicates that, overall, the UK and Mediterranean countries such as Greece, Spain, and Portugal pay the lowest average unit manufacturer prices for a group of 31 originator cancer drugs (new drugs under patent).
And Sweden, Switzerland, and Germany pay the highest prices.
The greatest differences in price were noted for gemcitabine, which costs €209 per vial in New Zealand and €43 in Australia, and zoledronic acid, which costs €330 per vial in New Zealand but €128 in Greece.*
“Public payers in Germany are paying 223% more in terms of official prices for interferon alfa 2b for melanoma and leukemia treatment than those in Greece,” noted study author Sabine Vogler, PhD, of the WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies in Vienna, Austria.
“For gefitinib to treat non-small-lung cancer, the price in Germany is 172% higher than in New Zealand.”
To uncover these price differences, Dr Vogler and her colleagues reviewed official drug price data from the Pharma Price Information (PPI) service of the Austrian Public Health Institute for 16 European countries**, and from the pharmaceutical schedules in Australia and New Zealand.
The researchers compared what manufacturers charged for a unit (ie, price per tablet or vial) of 31 originator cancer drugs in June 2013.
None of these drugs had a unit price lower than €10. Four drugs (13%) had an average unit manufacturer price between €250 and €500, and 2 drugs (6%) had an average unit price between €500 and €1000.
Seven drugs (23%) had an average unit price higher than €1000. For example, plerixafor cost over €5000 per injection.
The price differences between the highest- and lowest-priced countries ranged from 28% to 50% for a third of the drugs sampled, between 50% and 100% for half of the drugs, and between 100% and 200% for 3 drugs (10%).
The researchers noted that information on real drug prices is scarce. The cancer drug prices they surveyed did not include confidential discounts such as those agreed upon in managed-entry arrangements that are increasingly used in countries such as Australia, Italy, the UK, and the Netherlands.
“Some high-income countries have managed to barter the manufacturers down to lower prices, but these agreements, including the agreed prices, are confidential,” Dr Vogler explained.
“Although these agreements ensure patient access to new drugs, other countries risk overpaying when setting drug prices through the common practice of external price referencing, or international price comparison, because they can only use the official undiscounted prices as a benchmark. There needs to be far more transparency.”
“We hope that our findings will provide concrete evidence for policymakers to take action to address high prices and ensure more transparency in cancer drug pricing so that costs and access to new drugs does not depend on where a patient lives.” ![]()
*Gemcitabine and zoledronic acid have generic versions in several countries, and originator prices were decreased in some countries following patent expiry but not in others.
**Austria, Belgium, Denmark, Germany, Greece, Finland, France, Italy, Ireland, the Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the UK.
Photo by Bill Branson
The price of cancer drugs varies widely between European countries, Australia, and New Zealand, according to a study published in The Lancet Oncology.
The study indicates that, overall, the UK and Mediterranean countries such as Greece, Spain, and Portugal pay the lowest average unit manufacturer prices for a group of 31 originator cancer drugs (new drugs under patent).
And Sweden, Switzerland, and Germany pay the highest prices.
The greatest differences in price were noted for gemcitabine, which costs €209 per vial in New Zealand and €43 in Australia, and zoledronic acid, which costs €330 per vial in New Zealand but €128 in Greece.*
“Public payers in Germany are paying 223% more in terms of official prices for interferon alfa 2b for melanoma and leukemia treatment than those in Greece,” noted study author Sabine Vogler, PhD, of the WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies in Vienna, Austria.
“For gefitinib to treat non-small-lung cancer, the price in Germany is 172% higher than in New Zealand.”
To uncover these price differences, Dr Vogler and her colleagues reviewed official drug price data from the Pharma Price Information (PPI) service of the Austrian Public Health Institute for 16 European countries**, and from the pharmaceutical schedules in Australia and New Zealand.
The researchers compared what manufacturers charged for a unit (ie, price per tablet or vial) of 31 originator cancer drugs in June 2013.
None of these drugs had a unit price lower than €10. Four drugs (13%) had an average unit manufacturer price between €250 and €500, and 2 drugs (6%) had an average unit price between €500 and €1000.
Seven drugs (23%) had an average unit price higher than €1000. For example, plerixafor cost over €5000 per injection.
The price differences between the highest- and lowest-priced countries ranged from 28% to 50% for a third of the drugs sampled, between 50% and 100% for half of the drugs, and between 100% and 200% for 3 drugs (10%).
The researchers noted that information on real drug prices is scarce. The cancer drug prices they surveyed did not include confidential discounts such as those agreed upon in managed-entry arrangements that are increasingly used in countries such as Australia, Italy, the UK, and the Netherlands.
“Some high-income countries have managed to barter the manufacturers down to lower prices, but these agreements, including the agreed prices, are confidential,” Dr Vogler explained.
“Although these agreements ensure patient access to new drugs, other countries risk overpaying when setting drug prices through the common practice of external price referencing, or international price comparison, because they can only use the official undiscounted prices as a benchmark. There needs to be far more transparency.”
“We hope that our findings will provide concrete evidence for policymakers to take action to address high prices and ensure more transparency in cancer drug pricing so that costs and access to new drugs does not depend on where a patient lives.” ![]()
*Gemcitabine and zoledronic acid have generic versions in several countries, and originator prices were decreased in some countries following patent expiry but not in others.
**Austria, Belgium, Denmark, Germany, Greece, Finland, France, Italy, Ireland, the Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the UK.
Photo by Bill Branson
The price of cancer drugs varies widely between European countries, Australia, and New Zealand, according to a study published in The Lancet Oncology.
The study indicates that, overall, the UK and Mediterranean countries such as Greece, Spain, and Portugal pay the lowest average unit manufacturer prices for a group of 31 originator cancer drugs (new drugs under patent).
And Sweden, Switzerland, and Germany pay the highest prices.
The greatest differences in price were noted for gemcitabine, which costs €209 per vial in New Zealand and €43 in Australia, and zoledronic acid, which costs €330 per vial in New Zealand but €128 in Greece.*
“Public payers in Germany are paying 223% more in terms of official prices for interferon alfa 2b for melanoma and leukemia treatment than those in Greece,” noted study author Sabine Vogler, PhD, of the WHO Collaborating Centre for Pharmaceutical Pricing and Reimbursement Policies in Vienna, Austria.
“For gefitinib to treat non-small-lung cancer, the price in Germany is 172% higher than in New Zealand.”
To uncover these price differences, Dr Vogler and her colleagues reviewed official drug price data from the Pharma Price Information (PPI) service of the Austrian Public Health Institute for 16 European countries**, and from the pharmaceutical schedules in Australia and New Zealand.
The researchers compared what manufacturers charged for a unit (ie, price per tablet or vial) of 31 originator cancer drugs in June 2013.
None of these drugs had a unit price lower than €10. Four drugs (13%) had an average unit manufacturer price between €250 and €500, and 2 drugs (6%) had an average unit price between €500 and €1000.
Seven drugs (23%) had an average unit price higher than €1000. For example, plerixafor cost over €5000 per injection.
The price differences between the highest- and lowest-priced countries ranged from 28% to 50% for a third of the drugs sampled, between 50% and 100% for half of the drugs, and between 100% and 200% for 3 drugs (10%).
The researchers noted that information on real drug prices is scarce. The cancer drug prices they surveyed did not include confidential discounts such as those agreed upon in managed-entry arrangements that are increasingly used in countries such as Australia, Italy, the UK, and the Netherlands.
“Some high-income countries have managed to barter the manufacturers down to lower prices, but these agreements, including the agreed prices, are confidential,” Dr Vogler explained.
“Although these agreements ensure patient access to new drugs, other countries risk overpaying when setting drug prices through the common practice of external price referencing, or international price comparison, because they can only use the official undiscounted prices as a benchmark. There needs to be far more transparency.”
“We hope that our findings will provide concrete evidence for policymakers to take action to address high prices and ensure more transparency in cancer drug pricing so that costs and access to new drugs does not depend on where a patient lives.” ![]()
*Gemcitabine and zoledronic acid have generic versions in several countries, and originator prices were decreased in some countries following patent expiry but not in others.
**Austria, Belgium, Denmark, Germany, Greece, Finland, France, Italy, Ireland, the Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the UK.
Fish-related findings may have implications for HSCT

Photo by Richard Ling
Research involving the stonefish—an animal that protects itself using razor-sharp, venom-filled spines—has provided unexpected insight into the human immune response that causes hematopoietic stem cell transplants (HSCTs) to fail.
The insight is now being used to develop immunosuppressants that could potentially improve the success rate of HSCTs.
Researchers explained this surprising connection in PNAS.
Their study indicated that the lethal component of stonefish venom, a protein called stonustoxin, is an ancient relative of the human immune protein perforin.
The body unleashes perforin to destroy virally infected and cancerous cells. Unwanted or excessive perforin activity is responsible for a range of medical problems, including the rejection of HSCTs.
Perforin proteins attach themselves to a cell and assemble to form giant pores on the cell surface. Each pore contains around 20 perforin proteins that stick together in a symmetrical fashion. The pores are big enough to allow toxins to enter the cell, killing it from within.
How these pores form is a mystery, but the current study has revealed a key part of the pore-assembly mechanism.
To make this discovery, the researchers used synchrotron radiation to visualize the atomic structure of stonustoxin. They found the toxin contains 2 perforin-like proteins stuck together.
Seeing how these 2 proteins interact has helped the researchers on their way to understanding how the full assembly of 20 perforin molecules forms a complete pore.
The team is also using their new insight to develop perforin inhibitors.
“Already, the structure of stonustoxin is starting to inform our drug development program, and we now understand the very first stages of perforin pore formation,” said James Whisstock, PhD, of Monash University in Melbourne, Victoria, Australia.
“This type of mechanistic information is extremely useful in developing new strategies to inhibit perforin itself.” ![]()
Photo by Richard Ling
Research involving the stonefish—an animal that protects itself using razor-sharp, venom-filled spines—has provided unexpected insight into the human immune response that causes hematopoietic stem cell transplants (HSCTs) to fail.
The insight is now being used to develop immunosuppressants that could potentially improve the success rate of HSCTs.
Researchers explained this surprising connection in PNAS.
Their study indicated that the lethal component of stonefish venom, a protein called stonustoxin, is an ancient relative of the human immune protein perforin.
The body unleashes perforin to destroy virally infected and cancerous cells. Unwanted or excessive perforin activity is responsible for a range of medical problems, including the rejection of HSCTs.
Perforin proteins attach themselves to a cell and assemble to form giant pores on the cell surface. Each pore contains around 20 perforin proteins that stick together in a symmetrical fashion. The pores are big enough to allow toxins to enter the cell, killing it from within.
How these pores form is a mystery, but the current study has revealed a key part of the pore-assembly mechanism.
To make this discovery, the researchers used synchrotron radiation to visualize the atomic structure of stonustoxin. They found the toxin contains 2 perforin-like proteins stuck together.
Seeing how these 2 proteins interact has helped the researchers on their way to understanding how the full assembly of 20 perforin molecules forms a complete pore.
The team is also using their new insight to develop perforin inhibitors.
“Already, the structure of stonustoxin is starting to inform our drug development program, and we now understand the very first stages of perforin pore formation,” said James Whisstock, PhD, of Monash University in Melbourne, Victoria, Australia.
“This type of mechanistic information is extremely useful in developing new strategies to inhibit perforin itself.” ![]()
Photo by Richard Ling
Research involving the stonefish—an animal that protects itself using razor-sharp, venom-filled spines—has provided unexpected insight into the human immune response that causes hematopoietic stem cell transplants (HSCTs) to fail.
The insight is now being used to develop immunosuppressants that could potentially improve the success rate of HSCTs.
Researchers explained this surprising connection in PNAS.
Their study indicated that the lethal component of stonefish venom, a protein called stonustoxin, is an ancient relative of the human immune protein perforin.
The body unleashes perforin to destroy virally infected and cancerous cells. Unwanted or excessive perforin activity is responsible for a range of medical problems, including the rejection of HSCTs.
Perforin proteins attach themselves to a cell and assemble to form giant pores on the cell surface. Each pore contains around 20 perforin proteins that stick together in a symmetrical fashion. The pores are big enough to allow toxins to enter the cell, killing it from within.
How these pores form is a mystery, but the current study has revealed a key part of the pore-assembly mechanism.
To make this discovery, the researchers used synchrotron radiation to visualize the atomic structure of stonustoxin. They found the toxin contains 2 perforin-like proteins stuck together.
Seeing how these 2 proteins interact has helped the researchers on their way to understanding how the full assembly of 20 perforin molecules forms a complete pore.
The team is also using their new insight to develop perforin inhibitors.
“Already, the structure of stonustoxin is starting to inform our drug development program, and we now understand the very first stages of perforin pore formation,” said James Whisstock, PhD, of Monash University in Melbourne, Victoria, Australia.
“This type of mechanistic information is extremely useful in developing new strategies to inhibit perforin itself.” ![]()
FDA approves generic imatinib

Photo by Steven Harbour
The US Food and Drug Administration (FDA) has approved the use of imatinib mesylate, a generic version of Novartis’s Gleevec being developed by a subsidiary of Sun Pharmaceuticals Limited.
Under the terms of a settlement agreement with Novartis, the Sun Pharma subsidiary is allowed to launch its generic imatinib in the US on February 1, 2016.
The drug will be available in 100 mg and 400 mg tablets.
The Sun Pharma subsidiary was the first company to file an abbreviated new drug application for generic imatinib with a para IV certification and is therefore eligible for 180 days of marketing exclusivity in the US.
Sun Pharma’s imatinib mesylate is approved for the following indications:
- Newly diagnosed adult and pediatric patients with Philadelphia chromosome positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with (Ph+ CML) in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adult patients with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adult patients with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adult patients with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukemia (CEL) who have the FIP1L1-PDGFRα fusion kinase and for patients with HES and/or CEL who are FIP1L1- PDGFRα fusion kinase negative or unknown
- Adult patients with unresectable, recurrent and/or metastatic dermatofibrosarcoma protuberans.
The drug is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors. ![]()
Photo by Steven Harbour
The US Food and Drug Administration (FDA) has approved the use of imatinib mesylate, a generic version of Novartis’s Gleevec being developed by a subsidiary of Sun Pharmaceuticals Limited.
Under the terms of a settlement agreement with Novartis, the Sun Pharma subsidiary is allowed to launch its generic imatinib in the US on February 1, 2016.
The drug will be available in 100 mg and 400 mg tablets.
The Sun Pharma subsidiary was the first company to file an abbreviated new drug application for generic imatinib with a para IV certification and is therefore eligible for 180 days of marketing exclusivity in the US.
Sun Pharma’s imatinib mesylate is approved for the following indications:
- Newly diagnosed adult and pediatric patients with Philadelphia chromosome positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with (Ph+ CML) in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adult patients with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adult patients with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adult patients with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukemia (CEL) who have the FIP1L1-PDGFRα fusion kinase and for patients with HES and/or CEL who are FIP1L1- PDGFRα fusion kinase negative or unknown
- Adult patients with unresectable, recurrent and/or metastatic dermatofibrosarcoma protuberans.
The drug is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors. ![]()
Photo by Steven Harbour
The US Food and Drug Administration (FDA) has approved the use of imatinib mesylate, a generic version of Novartis’s Gleevec being developed by a subsidiary of Sun Pharmaceuticals Limited.
Under the terms of a settlement agreement with Novartis, the Sun Pharma subsidiary is allowed to launch its generic imatinib in the US on February 1, 2016.
The drug will be available in 100 mg and 400 mg tablets.
The Sun Pharma subsidiary was the first company to file an abbreviated new drug application for generic imatinib with a para IV certification and is therefore eligible for 180 days of marketing exclusivity in the US.
Sun Pharma’s imatinib mesylate is approved for the following indications:
- Newly diagnosed adult and pediatric patients with Philadelphia chromosome positive chronic myeloid leukemia (Ph+ CML) in chronic phase
- Patients with (Ph+ CML) in blast crisis, accelerated phase, or in chronic phase after failure of interferon-alpha therapy
- Adult patients with relapsed or refractory Ph+ acute lymphoblastic leukemia
- Adult patients with myelodysplastic/myeloproliferative diseases associated with PDGFR gene re-arrangements
- Adult patients with aggressive systemic mastocytosis without the D816V c-Kit mutation or with c-Kit mutational status unknown
- Adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukemia (CEL) who have the FIP1L1-PDGFRα fusion kinase and for patients with HES and/or CEL who are FIP1L1- PDGFRα fusion kinase negative or unknown
- Adult patients with unresectable, recurrent and/or metastatic dermatofibrosarcoma protuberans.
The drug is not approved to treat patients with KIT (CD117)-positive unresectable and/or metastatic malignant gastrointestinal stromal tumors.
Combo could target LSCs, treat CML

Image by Difu Wu
Researchers say they have identified a mechanism governing malignant reprogramming of progenitors into self-renewing leukemia stem cells (LSCs).
And their discovery has revealed a potential new therapeutic approach for chronic myeloid leukemia (CML).
Experiments in mice showed that a targeted monoclonal antibody could impair LSCs’ ability to regenerate and made them easier to eradicate with a tyrosine kinase inhibitor.
Catriona Jamieson, MD, PhD, of the University of California, San Diego, and her colleagues described this research in PNAS.
The researchers found that downregulation of Muscleblind-like 3 (MBNL3) RNA binding proteins resulted in re-expression of a human embryonic stem cell-specific alternative splicing gene regulatory network—a mechanism that controls embryonic stem cell pluripotency and fate. One effect of this was reprogramming of progenitor cells into LSCs in blast crisis CML.
“This is the first description of cancer stem cell generation through decreased expression of a transcriptional repressor of an embryonic pattern of alternative splicing that enhances stem cell self-renewal and survival,” Dr Jamieson said.
“Rather than acquiring multiple DNA mutations, as was previously thought, cancer stem cells in chronic myeloid leukemia switch to embryonic RNA splicing, which enhances their capacity to self-renew or clone themselves.”
“If we can detect and turn off embryonic splicing, we may be able to prevent cancer stem cells from propagating themselves. Also, if we target embryonic versions of proteins that are re-expressed by cancer, like CD44 variant 3, with specific antibodies together with tyrosine kinase inhibitors, we may be able to circumvent cancer relapse—a leading cause of cancer-related mortality.”
The researchers tested this theory in mice. They found that treatment with a humanized pan-CD44 monoclonal antibody and a targeted tyrosine kinase antagonist disrupted the development of LSCs in their protected microenvironment.
This forced the cells to enter the bloodstream, where dasatinib could effectively target them.
Image by Difu Wu
Researchers say they have identified a mechanism governing malignant reprogramming of progenitors into self-renewing leukemia stem cells (LSCs).
And their discovery has revealed a potential new therapeutic approach for chronic myeloid leukemia (CML).
Experiments in mice showed that a targeted monoclonal antibody could impair LSCs’ ability to regenerate and made them easier to eradicate with a tyrosine kinase inhibitor.
Catriona Jamieson, MD, PhD, of the University of California, San Diego, and her colleagues described this research in PNAS.
The researchers found that downregulation of Muscleblind-like 3 (MBNL3) RNA binding proteins resulted in re-expression of a human embryonic stem cell-specific alternative splicing gene regulatory network—a mechanism that controls embryonic stem cell pluripotency and fate. One effect of this was reprogramming of progenitor cells into LSCs in blast crisis CML.
“This is the first description of cancer stem cell generation through decreased expression of a transcriptional repressor of an embryonic pattern of alternative splicing that enhances stem cell self-renewal and survival,” Dr Jamieson said.
“Rather than acquiring multiple DNA mutations, as was previously thought, cancer stem cells in chronic myeloid leukemia switch to embryonic RNA splicing, which enhances their capacity to self-renew or clone themselves.”
“If we can detect and turn off embryonic splicing, we may be able to prevent cancer stem cells from propagating themselves. Also, if we target embryonic versions of proteins that are re-expressed by cancer, like CD44 variant 3, with specific antibodies together with tyrosine kinase inhibitors, we may be able to circumvent cancer relapse—a leading cause of cancer-related mortality.”
The researchers tested this theory in mice. They found that treatment with a humanized pan-CD44 monoclonal antibody and a targeted tyrosine kinase antagonist disrupted the development of LSCs in their protected microenvironment.
This forced the cells to enter the bloodstream, where dasatinib could effectively target them.
Image by Difu Wu
Researchers say they have identified a mechanism governing malignant reprogramming of progenitors into self-renewing leukemia stem cells (LSCs).
And their discovery has revealed a potential new therapeutic approach for chronic myeloid leukemia (CML).
Experiments in mice showed that a targeted monoclonal antibody could impair LSCs’ ability to regenerate and made them easier to eradicate with a tyrosine kinase inhibitor.
Catriona Jamieson, MD, PhD, of the University of California, San Diego, and her colleagues described this research in PNAS.
The researchers found that downregulation of Muscleblind-like 3 (MBNL3) RNA binding proteins resulted in re-expression of a human embryonic stem cell-specific alternative splicing gene regulatory network—a mechanism that controls embryonic stem cell pluripotency and fate. One effect of this was reprogramming of progenitor cells into LSCs in blast crisis CML.
“This is the first description of cancer stem cell generation through decreased expression of a transcriptional repressor of an embryonic pattern of alternative splicing that enhances stem cell self-renewal and survival,” Dr Jamieson said.
“Rather than acquiring multiple DNA mutations, as was previously thought, cancer stem cells in chronic myeloid leukemia switch to embryonic RNA splicing, which enhances their capacity to self-renew or clone themselves.”
“If we can detect and turn off embryonic splicing, we may be able to prevent cancer stem cells from propagating themselves. Also, if we target embryonic versions of proteins that are re-expressed by cancer, like CD44 variant 3, with specific antibodies together with tyrosine kinase inhibitors, we may be able to circumvent cancer relapse—a leading cause of cancer-related mortality.”
The researchers tested this theory in mice. They found that treatment with a humanized pan-CD44 monoclonal antibody and a targeted tyrosine kinase antagonist disrupted the development of LSCs in their protected microenvironment.
This forced the cells to enter the bloodstream, where dasatinib could effectively target them.
Bone can reactivate dormant MM cells, study suggests

to the tibia of a mouse
Image courtesy of the Garvan
Institute of Medical Research
Cancer cells that lie dormant in the bone can be “woken up” by changes in their surroundings, according to researchers.
The group used microscopy techniques to study multiple myeloma (MM) cells that lay “sleeping” in mouse bones.
The experiment revealed that dormant cells can be reactivated when bone tissue is broken down around them, suggesting new possibilities for
treating metastatic cancers in bone.
“Once a cancer spreads to bone, it becomes notoriously difficult to treat,” said study author Peter Croucher, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia.
“So it’s important to establish exactly what wakes those cells in bone. Is it some signal within the cells themselves, or is it a change in their environment?”
The researchers set out to discover which scenario is correct and reported their findings in Nature Communications.
Using a technique called intravital 2-photon microscopy, the team tracked the fate of dormant MM cells in the tibia of living mice.
They introduced MM cells into the mice and watched as a small number of the cells lodged in the tibia and “went to sleep.” These cells could be detected because they contained a fluorescent dye that was quickly lost from dividing cells.
“Because we were looking at a long bone like a tibia, we could watch the same sleeping cancer cells, in the same bone, in the same mouse, over a long period of time, and this is something that hasn’t been done before,” said Tri Giang Phan, PhD, of the Garvan Institute of Medical Research.
Dr Croucher said that studying the same set of cells over a period of months revealed vital clues about what caused them to reactivate.
“Because we’ve done it this way, we can show that there are a great many dormant cells, yet only some of them get woken up, and those that do wake, wake at different times,” he noted.
“We even saw some cells that woke then went back to sleep again. The fact that these myeloma cells behave so differently, despite coming from the same cancer cell line, gave us our first clue that it is a signal from outside the cells that is controlling when they wake.”
Explaining the phenomenon
The researchers’ next challenge was to determine the precise nature of the “wake-up call” from bone.
“[W]e’ve shown that bone’s dynamic process of building up and breaking down can send signals to cancer cells to stay sleeping or to wake,” said Michelle McDonald, PhD, of the Garvan Institute of Medical Research.
“We were able to show that myeloma cells are usually kept asleep by close association with a layer of osteoblast-like cells, called bone-lining cells, in the endosteum. The bone-lining cells are essentially inactive, so we can think of them as providing a quiet environment in which myeloma cells sleep undisturbed.”
“Crucially, we can wake those myeloma cells by activating osteoclasts, which break down bone tissue. We think the osteoclasts are physically changing the local environment of the cancer cells and waking them up in the process, as if they were literally throwing them out of bed.”
“We know that bone remodeling is going on in all of us. So a myeloma cell could be woken in an essentially random fashion, by having its local environment remodeled by osteoclasts. Essentially, a cancer cell could be woken by being in the wrong place at the wrong time.”
Implications for treatment
So what do these findings mean for treating secondary cancers in bone?
“Now we can see that the cancer cells are woken by changes in the surrounding bone, we can think in a whole new way about treating bone metastasis,” Dr Croucher said. “And there are 2 treatment approaches in particular that have promise.”
“The first is that we could inhibit the breakdown of bone by osteoclasts so as to keep cancer cells in long-term hibernation. In fact, there are already drugs that can do this, such as bisphosphonates, and there’s already evidence that these drugs do improve survival in breast cancer patients.”
“The other, more radical, option is to do the opposite—to wake the sleeping cells by activating osteoclasts and driving the breakdown of bone. Most cancer treatments target active, dividing cells. So waking the sleeping cells should make them susceptible to those therapies and, ultimately, could eradicate any residual disease.”
to the tibia of a mouse
Image courtesy of the Garvan
Institute of Medical Research
Cancer cells that lie dormant in the bone can be “woken up” by changes in their surroundings, according to researchers.
The group used microscopy techniques to study multiple myeloma (MM) cells that lay “sleeping” in mouse bones.
The experiment revealed that dormant cells can be reactivated when bone tissue is broken down around them, suggesting new possibilities for
treating metastatic cancers in bone.
“Once a cancer spreads to bone, it becomes notoriously difficult to treat,” said study author Peter Croucher, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia.
“So it’s important to establish exactly what wakes those cells in bone. Is it some signal within the cells themselves, or is it a change in their environment?”
The researchers set out to discover which scenario is correct and reported their findings in Nature Communications.
Using a technique called intravital 2-photon microscopy, the team tracked the fate of dormant MM cells in the tibia of living mice.
They introduced MM cells into the mice and watched as a small number of the cells lodged in the tibia and “went to sleep.” These cells could be detected because they contained a fluorescent dye that was quickly lost from dividing cells.
“Because we were looking at a long bone like a tibia, we could watch the same sleeping cancer cells, in the same bone, in the same mouse, over a long period of time, and this is something that hasn’t been done before,” said Tri Giang Phan, PhD, of the Garvan Institute of Medical Research.
Dr Croucher said that studying the same set of cells over a period of months revealed vital clues about what caused them to reactivate.
“Because we’ve done it this way, we can show that there are a great many dormant cells, yet only some of them get woken up, and those that do wake, wake at different times,” he noted.
“We even saw some cells that woke then went back to sleep again. The fact that these myeloma cells behave so differently, despite coming from the same cancer cell line, gave us our first clue that it is a signal from outside the cells that is controlling when they wake.”
Explaining the phenomenon
The researchers’ next challenge was to determine the precise nature of the “wake-up call” from bone.
“[W]e’ve shown that bone’s dynamic process of building up and breaking down can send signals to cancer cells to stay sleeping or to wake,” said Michelle McDonald, PhD, of the Garvan Institute of Medical Research.
“We were able to show that myeloma cells are usually kept asleep by close association with a layer of osteoblast-like cells, called bone-lining cells, in the endosteum. The bone-lining cells are essentially inactive, so we can think of them as providing a quiet environment in which myeloma cells sleep undisturbed.”
“Crucially, we can wake those myeloma cells by activating osteoclasts, which break down bone tissue. We think the osteoclasts are physically changing the local environment of the cancer cells and waking them up in the process, as if they were literally throwing them out of bed.”
“We know that bone remodeling is going on in all of us. So a myeloma cell could be woken in an essentially random fashion, by having its local environment remodeled by osteoclasts. Essentially, a cancer cell could be woken by being in the wrong place at the wrong time.”
Implications for treatment
So what do these findings mean for treating secondary cancers in bone?
“Now we can see that the cancer cells are woken by changes in the surrounding bone, we can think in a whole new way about treating bone metastasis,” Dr Croucher said. “And there are 2 treatment approaches in particular that have promise.”
“The first is that we could inhibit the breakdown of bone by osteoclasts so as to keep cancer cells in long-term hibernation. In fact, there are already drugs that can do this, such as bisphosphonates, and there’s already evidence that these drugs do improve survival in breast cancer patients.”
“The other, more radical, option is to do the opposite—to wake the sleeping cells by activating osteoclasts and driving the breakdown of bone. Most cancer treatments target active, dividing cells. So waking the sleeping cells should make them susceptible to those therapies and, ultimately, could eradicate any residual disease.”
to the tibia of a mouse
Image courtesy of the Garvan
Institute of Medical Research
Cancer cells that lie dormant in the bone can be “woken up” by changes in their surroundings, according to researchers.
The group used microscopy techniques to study multiple myeloma (MM) cells that lay “sleeping” in mouse bones.
The experiment revealed that dormant cells can be reactivated when bone tissue is broken down around them, suggesting new possibilities for
treating metastatic cancers in bone.
“Once a cancer spreads to bone, it becomes notoriously difficult to treat,” said study author Peter Croucher, PhD, of the Garvan Institute of Medical Research in Sydney, New South Wales, Australia.
“So it’s important to establish exactly what wakes those cells in bone. Is it some signal within the cells themselves, or is it a change in their environment?”
The researchers set out to discover which scenario is correct and reported their findings in Nature Communications.
Using a technique called intravital 2-photon microscopy, the team tracked the fate of dormant MM cells in the tibia of living mice.
They introduced MM cells into the mice and watched as a small number of the cells lodged in the tibia and “went to sleep.” These cells could be detected because they contained a fluorescent dye that was quickly lost from dividing cells.
“Because we were looking at a long bone like a tibia, we could watch the same sleeping cancer cells, in the same bone, in the same mouse, over a long period of time, and this is something that hasn’t been done before,” said Tri Giang Phan, PhD, of the Garvan Institute of Medical Research.
Dr Croucher said that studying the same set of cells over a period of months revealed vital clues about what caused them to reactivate.
“Because we’ve done it this way, we can show that there are a great many dormant cells, yet only some of them get woken up, and those that do wake, wake at different times,” he noted.
“We even saw some cells that woke then went back to sleep again. The fact that these myeloma cells behave so differently, despite coming from the same cancer cell line, gave us our first clue that it is a signal from outside the cells that is controlling when they wake.”
Explaining the phenomenon
The researchers’ next challenge was to determine the precise nature of the “wake-up call” from bone.
“[W]e’ve shown that bone’s dynamic process of building up and breaking down can send signals to cancer cells to stay sleeping or to wake,” said Michelle McDonald, PhD, of the Garvan Institute of Medical Research.
“We were able to show that myeloma cells are usually kept asleep by close association with a layer of osteoblast-like cells, called bone-lining cells, in the endosteum. The bone-lining cells are essentially inactive, so we can think of them as providing a quiet environment in which myeloma cells sleep undisturbed.”
“Crucially, we can wake those myeloma cells by activating osteoclasts, which break down bone tissue. We think the osteoclasts are physically changing the local environment of the cancer cells and waking them up in the process, as if they were literally throwing them out of bed.”
“We know that bone remodeling is going on in all of us. So a myeloma cell could be woken in an essentially random fashion, by having its local environment remodeled by osteoclasts. Essentially, a cancer cell could be woken by being in the wrong place at the wrong time.”
Implications for treatment
So what do these findings mean for treating secondary cancers in bone?
“Now we can see that the cancer cells are woken by changes in the surrounding bone, we can think in a whole new way about treating bone metastasis,” Dr Croucher said. “And there are 2 treatment approaches in particular that have promise.”
“The first is that we could inhibit the breakdown of bone by osteoclasts so as to keep cancer cells in long-term hibernation. In fact, there are already drugs that can do this, such as bisphosphonates, and there’s already evidence that these drugs do improve survival in breast cancer patients.”
“The other, more radical, option is to do the opposite—to wake the sleeping cells by activating osteoclasts and driving the breakdown of bone. Most cancer treatments target active, dividing cells. So waking the sleeping cells should make them susceptible to those therapies and, ultimately, could eradicate any residual disease.”
Antibody shows early promise for hemophilia A

Results observed in healthy subjects suggest ACE910, a factor VIIIa-mimetic bispecific antibody, may be safe and effective for patients with severe hemophilia A.
The data indicate that a weekly injection of ACE910 may prevent excessive bleeding, whereas existing hemophilia treatments require 2 to 3 injections per week.
Furthermore, ACE910 may be less likely to prompt factor VIII inhibitors, and the drug may be effective in patients who already have inhibitors.
Researchers reported the results of this phase 1 trial in Blood.
The team enrolled healthy male volunteers (ages 20 to 44), 40 of whom were Japanese and 24 of whom were Caucasian.
In part A of the study, the Japanese volunteers were randomized to receive 1 of 5 doses of ACE910 (ranging from 0.001 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects per ACE910 dose group and 10 subjects who received placebo.
In part B, the Caucasian volunteers were randomized to receive 1 of 3 doses (ranging from 0.1 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects in each group.
The volunteers were monitored based on their dose group, ranging from 4 weeks of observation for 0.001 mg/kg to 24 weeks for 1 mg/kg.
In all 48, subjects received ACE910. The researchers said that doses up to 1 mg/kg appeared to be safe. There were 15 adverse events (AEs) in 13 (27.1%) subjects receiving ACE910, compared to 6 AEs in 4 (25%) subjects receiving placebo.
There was 1 moderate AE (nasopharyngitis in 1 Caucasian subject receiving ACE910 at 0.1 mg/kg), but all other events were mild. There were no serious AEs or AEs that led to study withdrawal. The incidence of AEs did not differ according to dose or ethnicity.
The researchers did not observe any cases of hypercoagulability, hypersensitivity, serum cytokine concentration abnormality, or injection site reaction.
ACE910 absorbed into the plasma at a steady rate similar for both Japanese and Caucasian volunteers and remained in the blood with a half-life of 4 to 5 weeks, suggesting the drug’s therapeutic effects could be sustained with once-weekly subcutaneous dosing of ACE910.
Two subjects (1 Japanese and 1 Caucasian) were positive for anti-ACE910 antibodies. One subject was positive for antibodies before and after receiving ACE910, and the other was only positive after.
“These data are very encouraging for patients with severe hemophilia A, irrespective of the presence of factor VIII inhibitors, as ACE910 has the potential to offer the opportunity to live more normal lives without constantly planning around the next injection,” said study author Midori Shima, MD, PhD, of Nara Medical University in Kashihara, Japan.
“The first clinical investigation of this drug in hemophilia A patients with or without factor VIII inhibitors has already been implemented, and phase 3 studies are being planned to start in the near future.”
Interim results of a phase 1 study of ACE910 in hemophilia A patients (with and without inhibitors) were presented at ISTH 2015. And ACE910 was recently granted breakthrough designation from the US Food and Drug Administration.
Results observed in healthy subjects suggest ACE910, a factor VIIIa-mimetic bispecific antibody, may be safe and effective for patients with severe hemophilia A.
The data indicate that a weekly injection of ACE910 may prevent excessive bleeding, whereas existing hemophilia treatments require 2 to 3 injections per week.
Furthermore, ACE910 may be less likely to prompt factor VIII inhibitors, and the drug may be effective in patients who already have inhibitors.
Researchers reported the results of this phase 1 trial in Blood.
The team enrolled healthy male volunteers (ages 20 to 44), 40 of whom were Japanese and 24 of whom were Caucasian.
In part A of the study, the Japanese volunteers were randomized to receive 1 of 5 doses of ACE910 (ranging from 0.001 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects per ACE910 dose group and 10 subjects who received placebo.
In part B, the Caucasian volunteers were randomized to receive 1 of 3 doses (ranging from 0.1 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects in each group.
The volunteers were monitored based on their dose group, ranging from 4 weeks of observation for 0.001 mg/kg to 24 weeks for 1 mg/kg.
In all 48, subjects received ACE910. The researchers said that doses up to 1 mg/kg appeared to be safe. There were 15 adverse events (AEs) in 13 (27.1%) subjects receiving ACE910, compared to 6 AEs in 4 (25%) subjects receiving placebo.
There was 1 moderate AE (nasopharyngitis in 1 Caucasian subject receiving ACE910 at 0.1 mg/kg), but all other events were mild. There were no serious AEs or AEs that led to study withdrawal. The incidence of AEs did not differ according to dose or ethnicity.
The researchers did not observe any cases of hypercoagulability, hypersensitivity, serum cytokine concentration abnormality, or injection site reaction.
ACE910 absorbed into the plasma at a steady rate similar for both Japanese and Caucasian volunteers and remained in the blood with a half-life of 4 to 5 weeks, suggesting the drug’s therapeutic effects could be sustained with once-weekly subcutaneous dosing of ACE910.
Two subjects (1 Japanese and 1 Caucasian) were positive for anti-ACE910 antibodies. One subject was positive for antibodies before and after receiving ACE910, and the other was only positive after.
“These data are very encouraging for patients with severe hemophilia A, irrespective of the presence of factor VIII inhibitors, as ACE910 has the potential to offer the opportunity to live more normal lives without constantly planning around the next injection,” said study author Midori Shima, MD, PhD, of Nara Medical University in Kashihara, Japan.
“The first clinical investigation of this drug in hemophilia A patients with or without factor VIII inhibitors has already been implemented, and phase 3 studies are being planned to start in the near future.”
Interim results of a phase 1 study of ACE910 in hemophilia A patients (with and without inhibitors) were presented at ISTH 2015. And ACE910 was recently granted breakthrough designation from the US Food and Drug Administration.
Results observed in healthy subjects suggest ACE910, a factor VIIIa-mimetic bispecific antibody, may be safe and effective for patients with severe hemophilia A.
The data indicate that a weekly injection of ACE910 may prevent excessive bleeding, whereas existing hemophilia treatments require 2 to 3 injections per week.
Furthermore, ACE910 may be less likely to prompt factor VIII inhibitors, and the drug may be effective in patients who already have inhibitors.
Researchers reported the results of this phase 1 trial in Blood.
The team enrolled healthy male volunteers (ages 20 to 44), 40 of whom were Japanese and 24 of whom were Caucasian.
In part A of the study, the Japanese volunteers were randomized to receive 1 of 5 doses of ACE910 (ranging from 0.001 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects per ACE910 dose group and 10 subjects who received placebo.
In part B, the Caucasian volunteers were randomized to receive 1 of 3 doses (ranging from 0.1 to 1 mg/kg) or placebo subcutaneously. There were 6 subjects in each group.
The volunteers were monitored based on their dose group, ranging from 4 weeks of observation for 0.001 mg/kg to 24 weeks for 1 mg/kg.
In all 48, subjects received ACE910. The researchers said that doses up to 1 mg/kg appeared to be safe. There were 15 adverse events (AEs) in 13 (27.1%) subjects receiving ACE910, compared to 6 AEs in 4 (25%) subjects receiving placebo.
There was 1 moderate AE (nasopharyngitis in 1 Caucasian subject receiving ACE910 at 0.1 mg/kg), but all other events were mild. There were no serious AEs or AEs that led to study withdrawal. The incidence of AEs did not differ according to dose or ethnicity.
The researchers did not observe any cases of hypercoagulability, hypersensitivity, serum cytokine concentration abnormality, or injection site reaction.
ACE910 absorbed into the plasma at a steady rate similar for both Japanese and Caucasian volunteers and remained in the blood with a half-life of 4 to 5 weeks, suggesting the drug’s therapeutic effects could be sustained with once-weekly subcutaneous dosing of ACE910.
Two subjects (1 Japanese and 1 Caucasian) were positive for anti-ACE910 antibodies. One subject was positive for antibodies before and after receiving ACE910, and the other was only positive after.
“These data are very encouraging for patients with severe hemophilia A, irrespective of the presence of factor VIII inhibitors, as ACE910 has the potential to offer the opportunity to live more normal lives without constantly planning around the next injection,” said study author Midori Shima, MD, PhD, of Nara Medical University in Kashihara, Japan.
“The first clinical investigation of this drug in hemophilia A patients with or without factor VIII inhibitors has already been implemented, and phase 3 studies are being planned to start in the near future.”
Interim results of a phase 1 study of ACE910 in hemophilia A patients (with and without inhibitors) were presented at ISTH 2015. And ACE910 was recently granted breakthrough designation from the US Food and Drug Administration.