User login
Pediatric Procedural Sedation, Analgesia, and Anxiolysis
For many years, pediatric patients undergoing procedures in the ED have received inadequate pain management and sedation. Children’s (and parents’) anxieties and distress leading up to and during a potentially painful or anxiety-inducing procedure are now more easily mitigated by the appropriate use of a variety of pediatric-appropriate analgesics, sedatives, and anxiolytics. The ability to provide adequate, minimally invasive sedation and analgesia is critically important to performing successful procedures in children, and is a hallmark of excellent pediatric emergency care.
The following case vignettes, based on actual cases, illustrate the range and routes of medications available to provide appropriate analgesia, sedation, and anxiolysis.
Cases
Case 1
A 4-year-old boy presented to the ED for evaluation of a fractured wrist sustained after he fell off his bed during a temper tantrum. At presentation, the patient’s vital signs were: blood pressure (BP), 110/70 mm Hg; heart rate (HR), 100 beats/min; respiratory rate (RR), 28 breaths/min; and temperature (T), 99.5°F. Oxygen saturation on room air was within normal limits. The patient’s weight was within normal range for his age and height at 15 kg (33 lb).
Upon examination, the child appeared agitated and in significant distress; his anxiety increased after an initial attempt at placing an intravenous (IV) line in his uninjured arm failed.
The emergency physician (EP) considered several options to ameliorate the child’s anxiety and facilitate evaluation and treatment.
Case 2
After accidentally running into a pole, a 6-year-old girl presented to the ED for evaluation and suturing of a large laceration to her forehead. At presentation, the patient’s vital signs were: BP, 115/70 mm Hg; HR, 95 beats/min; RR, 24 breaths/min; and T, 98.6°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 20 kg (44 lb).
On examination, the patient was awake, alert, and in no acute distress. However, she immediately became tearful and visibly upset when she learned that an IV line was about to be placed in her arm.
The physician instead decided to employ an IV/needle-free strategy for this wound repair, as well as anxiolysis.
Case 3
A 5-year-old girl was brought to a community hospital ED by emergency medical services after falling from a balance beam and landing headfirst on the ground during a gymnastics class. Prior to presentation, emergency medical technicians had placed the patient in a cervical collar. At presentation, the patient’s vital signs were: BP, 105/75 mm Hg; HR, 115 beats/min; RR, 28 breaths/min; and T, 99.1°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 18 kg (39.6 lb).
Although the neurological examination was normal, the patient had persistent midline cervical tenderness as well as hemotympanum. The EP ordered a head and neck computed tomography (CT) scan, but shortly after the patient arrived at radiology, the CT technician informed the EP that she was unable to perform the scan because the patient kept moving and would not stay still.
The EP considered several sedatives to facilitate the CT study.
Case 4
A febrile, but nontoxic-appearing 3-week-old girl was referred to the ED by her pediatrician for a lumbar puncture (LP) to diagnose or exclude meningitis. However, the mother’s own recent negative experience with an epidural analgesia during the patient’s delivery, made the neonate’s mother extremely anxious that the procedure might be too painful for her daughter.
The EP considered the best choice of medication to provide analgesia and allay the mother’s concerns prior to performing the LP in this neonatal patient.
Overview and Definitions
Analgesia describes the alleviation of pain without intentional sedation. However, pediatric patients typically receive sedative hypnotics (anxiolytics) both for analgesia and for anxiolysis to modify behavior (eg, enhance immobility) and to allow for the safe completion of a procedure.1 The ultimate goal of procedural sedation and analgesia is to provide a depressed level of consciousness and pain relief while the patient maintains a patent airway and spontaneous ventilation.2
Sedation Continuum
The American Society of Anesthesiologists (ASA) classifies procedural sedation and analgesia based on a sedation continuum that affects overall responsiveness, airway, ventilation, and cardiovascular (CV) function.3 Procedural sedation is subcategorized into minimal, moderate, and deep sedation.
Minimal Sedation. Formally referred to as anxiolysis, minimal sedation is a state in which the patient is responsive but somewhat cognitively impaired, while maintaining all other functions rated in the sedation continuum.
Moderate Sedation. Previously referred to as “conscious sedation,” moderate sedation is a state of drug-induced depression of consciousness that still enables the patient to maintain purposeful responses to age-appropriate verbal commands and tactile stimulation, spontaneous ventilation, and CV integrity.
Deep Sedation. Deep sedation causes a drug-induced depression of consciousness that may potentially impair spontaneous ventilation and independent airway patency, while maintaining CV function. A deeply sedated patient is usually arousable with repeated painful stimulation.
Dissociative Sedation. This level of sedation induces a unique, trance-like cataleptic state characterized by profound analgesia and amnesia, with retention of protective airway reflexes, spontaneous respirations, and cardiopulmonary stability. The dissociative state can facilitate the performance of moderate-to-severe painful procedures, as well as procedures requiring immobilization in uncooperative patients.4
Contraindications to Procedural Sedation
Though there are no absolute contraindications to procedural sedation in children, its use is generally determined based on ASA’s patient physical status classification system. In this grading system, procedural sedation is appropriate for pediatric patients with a physical status of Class I (normally healthy patient) or Class II (a patient with mild systemic disease—eg, mild asthma).5 The EP should consult with a pediatric anesthesiologist prior to sedating a patient with an ASA status of Class II or higher, or a patient with a known laryngotracheal pathology.1
Pre- and Postsedation Considerations
History and Physical Examination
Prior to patient sedation, the EP should perform a focused history, including a determination of the patient’s last meal and/or drink, and a physical examination. The history should also include known allergies and past or current medication use—specifically any history of adverse events associated with prior sedation. Pregnancy status should be determined in every postpubertal female patient.
The physical examination should focus on the cardiac and respiratory systems, with particular attention to any airway abnormalities or possible sources of obstruction.1,3
Fasting
A need for fasting prior to procedural sedation remains controversial: Current ASA guidelines for fasting call for fasting times of 2 hours for clear liquids, 4 hours after breastfeeding, 6 hours for nonhuman milk or formula feeding, and 8 hours for solids.6
Fasting prior to general anesthesia has become a common requirement because of the risk of adverse respiratory events, including apnea, stridor, bronchospasm, emesis, and pulmonary aspiration of gastric contents. However, these events rarely occur during pediatric procedural sedation in the ED, and it is important to note that the American College of Emergency Physicians’ standards do not require delaying procedural sedation based on fasting times. There is no strong evidence that the duration of preprocedural sedation-fasting reduces or prevents emesis or aspiration.7
Equipment
In 2016, the American Academy of Pediatrics (AAP) updated its “Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures,”1 including the essential equipment required for the safe administration of sedation, which can be remembered using the following “SOAPME” mnemonic:
Size: appropriate suction catheters and a functioning suction apparatus (eg, Yankauer-type suction);
Oxygen: An adequate oxygen supply and functioning flow meters or other devices to allow its delivery;
Airway: Size-appropriate equipment (eg, bag-valve-mask or equivalent device [functioning]), nasopharyngeal and oropharyngeal airways, laryngeal mask airway, laryngoscope blades (checked and functioning), endotracheal tubes, stylets, face mask;
Pharmacy: All the basic drugs needed to support life during an emergency, including antagonists as indicated;
Monitors: Functioning pulse oximeter with size-appropriate oximeter probes, end-tidal carbon dioxide monitor, and other monitors as appropriate for the procedure (eg, noninvasive blood pressure, electrocardiogram, stethoscope); and
Equipment: Special equipment or drugs for a particular case (eg, defibrillator).1
Personnel
The 2016 AAP guidelines1 also indicate the number and type of personnel needed for sedation—in addition to the physician performing the procedure—which is primarily determined by the intended level of sedation as follows:
Minimal Sedation. Though there are no set guidelines for minimal sedation, all providers must be capable of caring for a child who progresses to moderate sedation.
Moderate Sedation. Intentional moderate sedation necessitates two practitioners: one practitioner to oversee the sedation and monitor the patient’s vital signs, who is capable of rescuing the patient from deep sedation if it occurs; and a second provider proficient at least in basic life support to monitor vital signs and assist in a resuscitation as needed.
Deep Sedation. For patients requiring deep sedation, the practitioner administering or supervising sedative drug administration should have no other responsibilities other than observing the patient. Moreover, there must be at least one other individual present who is certified in advanced life support and airway management.1
Discharge Criteria
Prior to discharge, pediatric patients must meet predetermined criteria that include easy arousability, a return to baseline mental status, stable age-appropriate vital signs, and the ability to remain hydrated.1,3 In addition, while late postsedation complications are rare, caregivers should be provided with specific symptoms that would warrant immediate return to the ED.
Available Options for Analgesia and Sedation
Several different methods of providing analgesia and pediatric procedural sedation are available, ranging from nonpharmacological methods to topical and parenteral medication administration.
Nonpharmacological Options: Child-Life Specialists
Child-life specialists can be particularly helpful with pediatric emergency patients. With a background in normal child development, child-life specialists utilize myriad distraction techniques and coping strategies to help patients within the stressful environment of an ED. Studies have shown that the presence of a child-life specialist may reduce the depth of sedation needed for certain procedures.1
Sucrose
Several studies have identified the benefits of sucrose as a pain reliever in neonates. Available as a 12% to 25% solution, sucrose decreases noxious stimuli and is a useful analgesic for such common neonatal procedures as venipuncture, circumcision, heel sticks, Foley catheter insertion, and LP. Efficacy of sucrose for these procedures is greatest in newborns, and decreases gradually after 6 months of age. The effectiveness of sucrose is enhanced when it is given in conjunction with nonnutritive sucking or maternal “skin-to-skin” techniques. There are no contraindications to the use of sucrose.8
Nonopioid Systemic Analgesia
Nonopioid oral analgesics (NOAs), such as acetaminophen and the nonsteroidal anti-inflammatory drug (NSAID) ibuprofen, are appropriate for mild-to-moderate procedural pain. The NOAs can be given alone or in conjunction with an opioid to enhance the analgesic effect for patients with severe pain.
Acetaminophen. Acetaminophen, which also has antipyretic properties, can be administered orally, rectally, or IV. Since acetaminophen is not an NSAID and does not affect platelet function, it is a good choice for treating patients with gastrointestinal (GI) pain.
Adverse effects of acetaminophen, which is metabolized by the liver, include hepatotoxicity in toxic doses. The suggested oral dose for infants and children weighing less than 60 kg (132 lb) is 10 to 15 mg/kg per dose every 4 to 6 hours as needed, with a maximum dose of 75 mg/kg/d for infants and 100 mg/kg/d for children. Rectal dosing for infants and children weighing less than 60 kg (132 lb) is 10 to 20 mg/kg every 6 hours as needed, with a maximum daily dose of 75 mg/kg/d in infants, and 100 mg/kg/d in children.
Ibuprofen. Ibuprofen, an NSAID with both antipyretic and anti-inflammatory properties, acts as a prostaglandin inhibitor and is indicated for use in patients over 6 months of age. Since ibuprofen inhibits platelet function, it can cause GI bleeding with chronic use. The suggested pediatric dose for ibuprofen is 5 to 10 mg/kg per dose every 6 to 8 hours orally, with a maximum dose of 40 mg/kg/d.9
Local Anesthesia
Local anesthetics administered via the topical or subcutaneous (SC) route provide anesthesia by temporarily blocking peripheral or central nerve conduction at the sodium channel.
LET Gel. This topical anesthetic combination composed of 4% lidocaine, 0.1% epinephrine, and 0.5% tetracaine (LET gel) is commonly used on patients prior to repair of a skin laceration. Its peak onset of action occurs in 30 minutes, with an anesthetic duration of 45 minutes. The epinephrine component of LET reduces blood flow to the anesthetized area, which increases duration of action but also creates a small risk of vasoconstriction in the areas supplied by end arteries, such as in the penis, nose, digits, and pinna.9
EMLA and LMX4. Topical lidocaine anesthetics are extremely useful in the ED because their application can help reduce the pain of minor procedures, when they are applied in adequate time prior to initiating the procedure to reach peak effect. Eutectic mixture of 2.5% lidocaine and 2.5% prilocaine (EMLA) and liposomal 4% lidocaine (LMX4) are the most commonly used topical lidocaine anesthetics. The peak analgesic effect of EMLA occurs within 60 minutes, with a duration of 90 minutes; LMX4 reaches its analgesic peak after 30 minutes with duration of up to 60 minutes.
Because of the slight delay of the time-to-peak effect, these topical anesthetics are not useful for emergent procedures. Further, neither EMLA nor LMX4 is approved for nonintact skin injuries such as lacerations.9 Both LMX4 and EMLA are approved for use in intact skin, providing effective analgesia for procedures such as venipuncture, circumcision, LP, and abscess drainage.
Subcutaneous Lidocaine. When SC injection of lidocaine is preferred, a useful technique to reduce the pain of administration is to warm the lidocaine, alkalinize the solution with 1 mL (1 mEq) sodium bicarbonate to 9 mL lidocaine,6 prior to injecting it slowly with a small-gauge needle.8Vapocoolant Lidocaine. Vapocoolant sprays produce an immediate cold sensation that is effective in reducing localized pain in adults. Studies looking at its efficacy in children are not as convincing, with some studies suggesting the cold sensation is quite distressing for many children.8
Opioids
Opioids are commonly chosen for pediatric procedural sedation because of their short onset of action and ability to produce significant analgesia with varying amounts of sedation. Fentanyl and morphine are the most widely used opioid analgesics to manage moderate-to-severe procedural pain in children.
Morphine. Morphine remains the gold standard for pediatric opioid analgesia, partly because it can be administered SC, IV, intramuscularly (IM), and orally. Its properties are more quickly achieved via the IV route, as the onset of action is 4 to 6 minutes. The standard IV dose of morphine is 0.1 mg/kg per dose, and can provide analgesia for up to 4 hours.
Adverse effects of morphine include dependence (though not an issue with a single emergency dose), respiratory depression, nausea, vomiting, constipation, urinary retention, hypotension, and bradycardia. Naloxone can rapidly reverse these adverse effects.
Fentanyl. Fentanyl, which is 100 times more potent than morphine, can be administered IV, transdermally, or transmucosally. When given IV, the onset of action of fentanyl is 2 to 3 minutes, and duration of action of 30 to 60 minutes. For sedation and analgesia, the suggested IV dose of fentanyl in neonates and young infants is 1 to 4 mcg/kg every 2 to 4 hours as needed, and for older infants and children, 1 to 2 mcg/kg every 30 to 60 minutes as needed.
Adverse effects of fentanyl are respiratory depression and chest wall rigidity,9 which can be rapidly reversed with naloxone (the dose of naloxone by patient weight is the same as that given to reverse adverse effects of morphine and fentanyl).
Codeine. A weaker opioid analgesic, codeine is not recommended for routine pediatric use because of its significant potential to hypermetabolize to morphine in some children, leading to overdose.6
Benzodiazepines: Midazolam
Benzodiazepines, which act on the type A gamma-aminobutyric acid receptor, causing muscle relaxation, anxiolysis, and anterograde amnesia, are useful for pediatric procedural sedation. Due to its short half-life, midazolam is the most common benzodiazepine used in pediatric patients. Midazolam can be delivered via different routes of administration, including orally, IM, IV, and transmucosally.
Intramuscular Route. Intramuscular midazolam has been shown to cause deep sedation at doses of 0.3 mg/kg, with maximum sedation occurring at 45 minutes, recovery beginning by 60 minutes, and the most common side effect being euphoria.10
Intravenous Route. Intravenous midazolam is used extensively in pediatric procedural sedation and is usually given at a dose of 0.05 to 0.1 mg/kg, with a maximum dose of 2 mg.
Even among small children, midazolam is usually quite safe when given alone, but because it does not provide effective analgesia, it often requires combination with an opioid for effective procedural sedation. Flumazenil may be given for rapid reversal of known benzodiazepine-induced respiratory depression, but it should be avoided in children with seizure disorders.
Propofol
Propofol is now frequently employed for pediatric sedation outside of the operating room. Propofol has excellent sedation properties but, like midazolam, does not provide analgesia and necessitates a second agent such as ketamine or an opioid for successful completion of more painful procedures. However, for children in whom sedation is required to facilitate simple neuroimaging of the head or spine, propofol is a very useful agent given the child’s quick return to his/her baseline mental status following the procedure.
Regarding contraindications, since propofol contains egg lecithin and soybean oil, it was once considered inappropriate for use in patients with an egg or soy allergy. Recent data, however, have refuted this belief, and while the package insert for propofol still lists patient allergy to egg, egg products, soy, or soybeans as a contraindication to use,11 the American Academy of Allergy, Asthma and Immunology recently concluded that patients with soy allergy or egg allergy can receive propofol without any special precautions.12
Since propofol is a powerful sedative and can cause a greater depth of sedation than that intended, providers must be comfortable with both monitoring and managing the pediatric airway. The induction dose of propofol is 1 mg/kg with repeated doses of 0.5 mg/kg to achieve the desired level of sedation. One emergency medicine-specific study by Jasiak et al13 found a mean cumulative propofol dose of 2.1 mg/kg for pediatric procedures given in a median of three boluses, with younger children requiring an overall higher mg/kg induction dose. Another study by Young et al14 showed an induction dose of 2 mg/kg to be well tolerated and without increased adverse events for pediatric procedural sedation.
When used properly, propofol has been shown to be safe and effective in pediatric patients. A recent review by Mallory et al15 looking at 25,433 cases of EP administration of propofol to pediatric patients noted serious complications in only 2% of patients, including one unplanned intubation, one cardiac arrest, and two aspirations.
Ketamine
Dissociative procedural sedation is frequently utilized in pediatric patients, for which ketamine is usually the agent of choice given its fast onset of action, multiple modes of administration, and robust pediatric safety data. Ketamine is a unique agent because of its sedative, analgesic, and paralytic-like properties. A phencyclidine derivative, ketamine exerts its effect by binding to the N-methyl-D-aspartate receptor, and may be given IM or IV, with usual dosing of 1 to 1.5 mg/kg IV, or 2 to 4 mg/kg IM. Unlike other sedatives, there is a “dissociation threshold” for ketamine, and further dosing does not increase its effects.16
Because of multiple observations and reported cases of airway complications in infants younger than 3 months of age, it is not recommended for routine use in this age group. While ketamine-associated infant airway events are thought by some experts to not be specific to ketamine (and more representative of infant differences in airway anatomy and laryngeal excitability), risks seem to outweigh benefits for routine use in this cohort.16
Ketamine is known to exaggerate protective airway reflexes and can cause laryngospasm, so it is best avoided during procedures that cause a large amount of pharyngeal stimulation. The overall rate of ketamine-induced pediatric laryngospasm is low in the general population (0.3%), and when it does occur, can usually be treated easily with assisted ventilation and oxygenation.17
Prior concerns of ketamine increasing intracranial pressure (ICP) have been shown not to be the case by recent data, which in fact demonstrate that ketamine may instead actually lower ICP.18
For many pediatric centers, including the authors’, ketamine is a first-line agent to facilitate head and/or neck CT in otherwise uncooperative children. Emesis is the most common side effect of ketamine, but the incidence can be significantly reduced by pretreating the patient with ondansetron.19 Though ketamine may also be combined with propofol, there is no robust pediatric-specific evidence showing any benefits of this practice.
Nitrous Oxide
Nitrous oxide (N2O), the most commonly used inhaled anesthetic agent used in the pediatric ED, provides analgesia, sedation, anterograde amnesia, and anxiolysis. It can be given in mixtures of 30% to 70% N2O with oxygen, has a rapid onset of action (<1 minute), and there is rapid recovery after cessation. In patients older than 5 years of age, N2O is usually given via a demand valve system, which will fall off the patient’s face if he or she becomes overly sedated.
Nitrous oxide is usually very well tolerated with few serious events, the most common being emesis.20 Absolute contraindications to its use are few and include pneumothorax, pulmonary blebs, bowel obstruction, air embolus, and a recent history of intracranial or middle ear surgery.
Intranasal Analgesia
Intranasal (IN) analgesics are becoming increasingly popular for pediatric procedures because of their rapid onset of action compared with oral medications, without the need for IV or “needle” access prior to administration.
Intranasal Fentanyl. The EP should use a mucosal atomizer when administering midazolam or fentanyl via the IN route. The atomizer transforms these liquid drugs into a fine spray, which increases surface area, improving mucosal absorption and central nervous system concentrations when compared with IN administration via dropper.21
In a study by Klein et al,22 IN midazolam effectively provided sedation, with more effective diminution of activity and better overall patient satisfaction than with either oral or buccal midazolam. Intranasal midazolam causes a slight burning sensation, and some patients report initial discomfort after administration. The half-lives of IN and IV midazolam are very similar (2.2 vs 2.4 hours).23Intranasal Fentanyl. IN fentanyl is an excellent alternative to IV pain medications for patients in whom there is no IV access. When given at a dose of 1.7 mcg/kg, IN fentanyl produces analgesic effects similar to that of morphine 0.1 mg/kg.
The only reported adverse effect associated with IN fentanyl has been a bad taste in the mouth.24 Another study of children aged 1 to 3 years showed a significant decrease in pain in 93% of children at 10 minutes, and 98% of children at 30 minutes, with no significant side effects.25
Intranasal fentanyl is a great choice for initial and immediate pain control in children with suspected long bone fractures, and is especially useful in facilitating their comfort during radiographic imaging.
Managing a Child for Radiographic Imaging
To facilitate a relatively rapid procedure such as obtaining plain films or a CT scan, anxiolysis, rather than analgesia, is required. Given its quick and predictable onset of action, IN midazolam is an excellent choice for pediatric patients requiring imaging studies. If, however, a mucosal atomizer is not available for IN drug delivery and the patient is already in radiology and requires emergent imaging studies, oral midazolam should not be given as an alternative because of its delayed onset of action. In such cases, placing an IV line and administering IV propofol offers the best chance of achieving quick and effective anxiolysis to obtain the images required to exclude clinically important injuries.
In hospitals that restrict the use of propofol in young children outside of the operating room—and when there are no findings suggestive of impending cerebral herniation—a safe and effective alternative is IV ketamine at a dose of 1.5 mg/kg.
Cases Continued
Case 1
[The 4-year-old boy with the fractured wrist.]
Recognizing that repeated attempts at IV placement in a child with a contralateral extremity fracture often leads to escalating distress and anxiety, the EP decided against further attempts to place an IV line. Instead, he gave the child fentanyl via the IN route, which immediately relieved the patient’s pain and facilitated radiographic evaluation. After administrating the fentanyl IN, the EP instructed a member of the ED staff to apply LMX4 cream to several potential IV sites and then cover each site with occlusive dressings. Afterward, the patient was taken to radiology, and X-ray images of the fracture were easily obtained. When the patient returned from imaging, the ED nurse was able to place an IV line at one of the sites that had been previously anesthetized with LMX4 cream.
The EP consulted with the orthopedist, who determined that the child’s distal radius fracture necessitated closed reduction. To facilitate the procedure, the patient was given 1.5 mg/kg of ketamine. After a successful closed reduction, the orthopedic chief resident recommended the EP discharge the 15-kg (33-lb) patient home in the care of his parents, with a prescription for 5 mL oral acetaminophen and codeine suspension four times a day as needed for pain (5 mL = acetaminophen 120 mg/codeine 12 mg, and codeine dosed at 0.5-1 mg/kg per dose). Prior to discharge, the EP counseled the patient’s parents on the risks of codeine hypermetabolism in children. However, based on the parents’ expressed concerns, the EP instead discharged the patient home with a prescription for 4 cc oral acetaminophen-hydrocodone elixir every 4 to 6 hours as needed for pain instead (dosing is 0.27 mL/kg; elixir is hydrocodone bitartrate 7.5 mg/acetaminophen 325 mg/15 mL).
Case 2
[The 6-year-old girl with a large laceration to her forehead.]
The type of laceration sustained by this patient was appropriate for treatment with a local anesthetic combined with an agent for non-IV anxiolysis. Thirty minutes prior to suturing, LET gel was applied over the open wound site, and 5 minutes prior to initiating closure of the wound, the patient received IN midazolam. Since the LET cream was placed on the wound 30 minutes prior to the procedure, the site was well anesthetized for both irrigation and closure. The anxiolytic effects of the IN midazolam resulted in a calm patient, who was happy and playful throughout the procedure.
After successfully closing the wound, the physician discharged the patient home in the care of her parents, with instructions to apply bacitracin ointment to the wound site three times a day for the next 3 days, and give the patient over-the-counter acetaminophen elixir for any mild discomfort.
Case 3
[The 5-year-old boy who suffered cervical spine injuries after falling head-first off of a balance beam during gymnastics.]
Since no mucosal atomizer was available for IN drug delivery, and hospital policy restricted the use of propofol in young children outside of the operating room, the patient was given 1.5 mg/kg of IV ketamine. Within 45 seconds of ketamine administration, the child had adequate dissociative sedation, which allowed for high-quality CT scans of both the head and neck without incident.
Case 4
[The febrile 3-week-old female neonate referred by her pediatrician for evaluation and LP.]
Since this neonate did not appear toxic, the EP delayed the LP by 30 minutes to allow time for application of a topical anesthetic to minimize associated procedural pain. Thirty minutes prior to the LP, LMX4 cream was applied to the patient’s L4 spinal interspace, and just prior to the procedure, the patient was given a pacifier that had been dipped in a solution of 4% sucrose. The neonate was then positioned appropriately for the LP and barely squirmed when the spinal needle was introduced, allowing the EP to obtain a nontraumatic cerebrospinal fluid sample on the first attempt.
Conclusion
Addressing pediatric pain and anxiety, especially preceding and during procedures and radiographic imaging, is a serious challenge in the ED. Several means are now available to provide safe and effective sedation, analgesia, and anxiolysis in the ED, with or without IV access. Many of the medications utilized, however, can cause significant respiratory and CV depression, making proper patient selection and monitoring, and training of involved personnel imperative to ensure safe use in the ED. Appropriate use of the agents and strategies discussed above will allow EPs to reduce both procedural pain and anxiety for our youngest patients—and their parents.
1. Coté CJ, Wilson S; American academy of pediatrics; American Academy of Pediatric Dentistry. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatrics. 2016;138(1). doi:10.1542/peds.2016-1212. http://pediatrics.aappublications.org/content/pediatrics/early/2016/06/24/peds.2016-1212.full.pdf
2. Mace SE, Barata IA, Cravero JP, et al; American College of Emergency Physicians. Clinical policy: evidence-based approach to pharmacologic agents used in pediatric sedation and analgesia in the emergency department. Ann Emerg Med. 2004;44(4):342-377. doi:10.1016/S0196064404004214.
3. American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1004-1017. http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1944958. Accessed July 31, 2017.
4. Godwin SA, Burton JH, Gerardo CJ, et al; American College of Emergency Physicians. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63(2):247-258.e18. doi:10.1016/j.annemergmed.2013.10.015.
5. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006; 367(9512):766-780. doi:10.1016/S0140-6736(06)68230-5.
6. Berger J, Koszela KB. Analgesia and procedural sedation. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:136-155.
7. Milne K. Procedural Sedation Delays and NPO Status for Pediatric Patients in the Emergency Department. ACEP Now. http://www.acepnow.com/article/procedural-sedation-delays-npo-status-pediatric-patients-emergency-department/. Published January 22, 2017. Accessed July 25, 2017.
8. Fein JA, Zempsky WT, Cravero JP; Committee on Pediatric Emergency Medicine and Section on Anesthesiology and Pain Medicine; American Academy of Pediatrics. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2012;130(5):e1391-e1405. doi:10.1542/peds.2012-2536.
9. Lee CKK. Drug dosages. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:732-1109.
10. Ghane MR, Musavi Vaezi SY, Hedayati Asl AA, Javadzadeh HR, Mahmoudi S, Saburi A. Intramuscular midazolam for pediatric sedation in the emergency department: a short communication on clinical safety and effectiveness. Trauma Mon. 2012;17(1):233-235. doi:10.5812/traumamon.3458.
11. Diprivan [package insert]. Lake Zurich, IL: Fresenius Kabi USA, LLC; 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019627s066lbl.pdf. Accessed July 31, 2017.
12. American Academy of Allergy Asthma & Immunology. Soy-allergic and egg-allergic patients can safely receive anesthesia. https://www.aaaai.org/conditions-and-treatments/library/allergy-library/soy-egg-anesthesia. Accessed July 31, 2017.
13. Jasiak KD, Phan H, Christich AC, Edwards CJ, Skrepnek GH, Patanwala AE. Induction dose of propofol for pediatric patients undergoing procedural sedation in the emergency department. Pediatr Emerg Care. 2012;28(5):440-442. doi:10.1097/PEC.0b013e3182531a9b.
14. Young TP, Lim JJ, Kim TY, Thorp AW, Brown L. Pediatric procedural sedation with propofol using a higher initial bolus dose. Pediatr Emerg Care. 2014;30(10):689-693. doi:10.1097/PEC.0000000000000229.
15. Mallory MD, Baxter AL, Yanosky DJ, Cravero JP; Pediatric Sedation Research Consortium. Emergency physician-administered propofol sedation: a report on 25,433 sedations from the pediatric sedation research consortium. Ann Emerg Med. 2011;57(5):462-468.e1. doi:10.1016/j.annemergmed.2011.03.008.
16. Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57(5):449-461. doi:10.1016/j.annemergmed.2010.11.030.
17. Green SM, Roback MG, Krauss B, et al; Emergency Department Ketamine Meta-Analysis Study Group. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158-168.e1-4. doi:10.1016/j.annemergmed.2008.12.011.
18. Von der Brelie C, Seifert M, Rot S, et al. Sedation of patients with acute aneurysmal subarachnoid hemorrhage with ketamine is safe and might influence the occurrence of cerebral infarctions associated with delayed cerebral ischemia. World Neurosurg. 2017;97:374-382. doi:10.1016/j.wneu.2016.09.121.
19. Langston WT, Wathen JE, Roback MG, Bajaj L. Effect of ondansetron on the incidence of vomiting associated with ketamine sedation in children: a double-blind, randomized, placebo-controlled trial. Ann Emerg Med. 2008;52(1):30-34. doi:10.1016/j.annemergmed.2008.01.326.
20. Babl FE, Oakley E, Seaman C, Barnett P, Sharwood LN. High-concentration nitrous oxide for procedural sedation in children: adverse events and depth of sedation. Pediatrics. 2008;121(3):e528-e532. doi:10.1542/peds.2007-1044.
21. Henry RJ, Ruano N, Casto D, Wolf RH. A pharmacokinetic study of midazolam in dogs: nasal drop vs. atomizer administration. Pediatr Dent. 1998;20(5):321-326.
22. Klein EJ, Brown JC, Kobayashi A, Osincup D, Seidel K. A randomized clinical trial comparing oral, aerosolized intranasal, and aerosolized buccal midazolam. Ann Emerg Med. 2011;58(4):323-329. doi:10.1016/j.annemergmed.2011.05.016.
23. Rey E, Delaunay L, Pons G, et al. Pharmacokinetics of midazolam in children: comparative study of intranasal and intravenous administration. Eur J Clin Pharmacol. 1991;41(4):355-357. doi:10.1007/BF00314967.
24. Borland M, Jacobs I, King B, O’Brien D. A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med. 2007;49(3):335-340. doi:10.1016/j.annemergmed.2006.06.016.
25. Cole J, Shepherd M, Young P. Intranasal fentanyl in 1-3-year-olds: a prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas. 2009;21(5):395-400. doi:10.1111/j.1742-6723.2009.01216.x.
For many years, pediatric patients undergoing procedures in the ED have received inadequate pain management and sedation. Children’s (and parents’) anxieties and distress leading up to and during a potentially painful or anxiety-inducing procedure are now more easily mitigated by the appropriate use of a variety of pediatric-appropriate analgesics, sedatives, and anxiolytics. The ability to provide adequate, minimally invasive sedation and analgesia is critically important to performing successful procedures in children, and is a hallmark of excellent pediatric emergency care.
The following case vignettes, based on actual cases, illustrate the range and routes of medications available to provide appropriate analgesia, sedation, and anxiolysis.
Cases
Case 1
A 4-year-old boy presented to the ED for evaluation of a fractured wrist sustained after he fell off his bed during a temper tantrum. At presentation, the patient’s vital signs were: blood pressure (BP), 110/70 mm Hg; heart rate (HR), 100 beats/min; respiratory rate (RR), 28 breaths/min; and temperature (T), 99.5°F. Oxygen saturation on room air was within normal limits. The patient’s weight was within normal range for his age and height at 15 kg (33 lb).
Upon examination, the child appeared agitated and in significant distress; his anxiety increased after an initial attempt at placing an intravenous (IV) line in his uninjured arm failed.
The emergency physician (EP) considered several options to ameliorate the child’s anxiety and facilitate evaluation and treatment.
Case 2
After accidentally running into a pole, a 6-year-old girl presented to the ED for evaluation and suturing of a large laceration to her forehead. At presentation, the patient’s vital signs were: BP, 115/70 mm Hg; HR, 95 beats/min; RR, 24 breaths/min; and T, 98.6°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 20 kg (44 lb).
On examination, the patient was awake, alert, and in no acute distress. However, she immediately became tearful and visibly upset when she learned that an IV line was about to be placed in her arm.
The physician instead decided to employ an IV/needle-free strategy for this wound repair, as well as anxiolysis.
Case 3
A 5-year-old girl was brought to a community hospital ED by emergency medical services after falling from a balance beam and landing headfirst on the ground during a gymnastics class. Prior to presentation, emergency medical technicians had placed the patient in a cervical collar. At presentation, the patient’s vital signs were: BP, 105/75 mm Hg; HR, 115 beats/min; RR, 28 breaths/min; and T, 99.1°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 18 kg (39.6 lb).
Although the neurological examination was normal, the patient had persistent midline cervical tenderness as well as hemotympanum. The EP ordered a head and neck computed tomography (CT) scan, but shortly after the patient arrived at radiology, the CT technician informed the EP that she was unable to perform the scan because the patient kept moving and would not stay still.
The EP considered several sedatives to facilitate the CT study.
Case 4
A febrile, but nontoxic-appearing 3-week-old girl was referred to the ED by her pediatrician for a lumbar puncture (LP) to diagnose or exclude meningitis. However, the mother’s own recent negative experience with an epidural analgesia during the patient’s delivery, made the neonate’s mother extremely anxious that the procedure might be too painful for her daughter.
The EP considered the best choice of medication to provide analgesia and allay the mother’s concerns prior to performing the LP in this neonatal patient.
Overview and Definitions
Analgesia describes the alleviation of pain without intentional sedation. However, pediatric patients typically receive sedative hypnotics (anxiolytics) both for analgesia and for anxiolysis to modify behavior (eg, enhance immobility) and to allow for the safe completion of a procedure.1 The ultimate goal of procedural sedation and analgesia is to provide a depressed level of consciousness and pain relief while the patient maintains a patent airway and spontaneous ventilation.2
Sedation Continuum
The American Society of Anesthesiologists (ASA) classifies procedural sedation and analgesia based on a sedation continuum that affects overall responsiveness, airway, ventilation, and cardiovascular (CV) function.3 Procedural sedation is subcategorized into minimal, moderate, and deep sedation.
Minimal Sedation. Formally referred to as anxiolysis, minimal sedation is a state in which the patient is responsive but somewhat cognitively impaired, while maintaining all other functions rated in the sedation continuum.
Moderate Sedation. Previously referred to as “conscious sedation,” moderate sedation is a state of drug-induced depression of consciousness that still enables the patient to maintain purposeful responses to age-appropriate verbal commands and tactile stimulation, spontaneous ventilation, and CV integrity.
Deep Sedation. Deep sedation causes a drug-induced depression of consciousness that may potentially impair spontaneous ventilation and independent airway patency, while maintaining CV function. A deeply sedated patient is usually arousable with repeated painful stimulation.
Dissociative Sedation. This level of sedation induces a unique, trance-like cataleptic state characterized by profound analgesia and amnesia, with retention of protective airway reflexes, spontaneous respirations, and cardiopulmonary stability. The dissociative state can facilitate the performance of moderate-to-severe painful procedures, as well as procedures requiring immobilization in uncooperative patients.4
Contraindications to Procedural Sedation
Though there are no absolute contraindications to procedural sedation in children, its use is generally determined based on ASA’s patient physical status classification system. In this grading system, procedural sedation is appropriate for pediatric patients with a physical status of Class I (normally healthy patient) or Class II (a patient with mild systemic disease—eg, mild asthma).5 The EP should consult with a pediatric anesthesiologist prior to sedating a patient with an ASA status of Class II or higher, or a patient with a known laryngotracheal pathology.1
Pre- and Postsedation Considerations
History and Physical Examination
Prior to patient sedation, the EP should perform a focused history, including a determination of the patient’s last meal and/or drink, and a physical examination. The history should also include known allergies and past or current medication use—specifically any history of adverse events associated with prior sedation. Pregnancy status should be determined in every postpubertal female patient.
The physical examination should focus on the cardiac and respiratory systems, with particular attention to any airway abnormalities or possible sources of obstruction.1,3
Fasting
A need for fasting prior to procedural sedation remains controversial: Current ASA guidelines for fasting call for fasting times of 2 hours for clear liquids, 4 hours after breastfeeding, 6 hours for nonhuman milk or formula feeding, and 8 hours for solids.6
Fasting prior to general anesthesia has become a common requirement because of the risk of adverse respiratory events, including apnea, stridor, bronchospasm, emesis, and pulmonary aspiration of gastric contents. However, these events rarely occur during pediatric procedural sedation in the ED, and it is important to note that the American College of Emergency Physicians’ standards do not require delaying procedural sedation based on fasting times. There is no strong evidence that the duration of preprocedural sedation-fasting reduces or prevents emesis or aspiration.7
Equipment
In 2016, the American Academy of Pediatrics (AAP) updated its “Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures,”1 including the essential equipment required for the safe administration of sedation, which can be remembered using the following “SOAPME” mnemonic:
Size: appropriate suction catheters and a functioning suction apparatus (eg, Yankauer-type suction);
Oxygen: An adequate oxygen supply and functioning flow meters or other devices to allow its delivery;
Airway: Size-appropriate equipment (eg, bag-valve-mask or equivalent device [functioning]), nasopharyngeal and oropharyngeal airways, laryngeal mask airway, laryngoscope blades (checked and functioning), endotracheal tubes, stylets, face mask;
Pharmacy: All the basic drugs needed to support life during an emergency, including antagonists as indicated;
Monitors: Functioning pulse oximeter with size-appropriate oximeter probes, end-tidal carbon dioxide monitor, and other monitors as appropriate for the procedure (eg, noninvasive blood pressure, electrocardiogram, stethoscope); and
Equipment: Special equipment or drugs for a particular case (eg, defibrillator).1
Personnel
The 2016 AAP guidelines1 also indicate the number and type of personnel needed for sedation—in addition to the physician performing the procedure—which is primarily determined by the intended level of sedation as follows:
Minimal Sedation. Though there are no set guidelines for minimal sedation, all providers must be capable of caring for a child who progresses to moderate sedation.
Moderate Sedation. Intentional moderate sedation necessitates two practitioners: one practitioner to oversee the sedation and monitor the patient’s vital signs, who is capable of rescuing the patient from deep sedation if it occurs; and a second provider proficient at least in basic life support to monitor vital signs and assist in a resuscitation as needed.
Deep Sedation. For patients requiring deep sedation, the practitioner administering or supervising sedative drug administration should have no other responsibilities other than observing the patient. Moreover, there must be at least one other individual present who is certified in advanced life support and airway management.1
Discharge Criteria
Prior to discharge, pediatric patients must meet predetermined criteria that include easy arousability, a return to baseline mental status, stable age-appropriate vital signs, and the ability to remain hydrated.1,3 In addition, while late postsedation complications are rare, caregivers should be provided with specific symptoms that would warrant immediate return to the ED.
Available Options for Analgesia and Sedation
Several different methods of providing analgesia and pediatric procedural sedation are available, ranging from nonpharmacological methods to topical and parenteral medication administration.
Nonpharmacological Options: Child-Life Specialists
Child-life specialists can be particularly helpful with pediatric emergency patients. With a background in normal child development, child-life specialists utilize myriad distraction techniques and coping strategies to help patients within the stressful environment of an ED. Studies have shown that the presence of a child-life specialist may reduce the depth of sedation needed for certain procedures.1
Sucrose
Several studies have identified the benefits of sucrose as a pain reliever in neonates. Available as a 12% to 25% solution, sucrose decreases noxious stimuli and is a useful analgesic for such common neonatal procedures as venipuncture, circumcision, heel sticks, Foley catheter insertion, and LP. Efficacy of sucrose for these procedures is greatest in newborns, and decreases gradually after 6 months of age. The effectiveness of sucrose is enhanced when it is given in conjunction with nonnutritive sucking or maternal “skin-to-skin” techniques. There are no contraindications to the use of sucrose.8
Nonopioid Systemic Analgesia
Nonopioid oral analgesics (NOAs), such as acetaminophen and the nonsteroidal anti-inflammatory drug (NSAID) ibuprofen, are appropriate for mild-to-moderate procedural pain. The NOAs can be given alone or in conjunction with an opioid to enhance the analgesic effect for patients with severe pain.
Acetaminophen. Acetaminophen, which also has antipyretic properties, can be administered orally, rectally, or IV. Since acetaminophen is not an NSAID and does not affect platelet function, it is a good choice for treating patients with gastrointestinal (GI) pain.
Adverse effects of acetaminophen, which is metabolized by the liver, include hepatotoxicity in toxic doses. The suggested oral dose for infants and children weighing less than 60 kg (132 lb) is 10 to 15 mg/kg per dose every 4 to 6 hours as needed, with a maximum dose of 75 mg/kg/d for infants and 100 mg/kg/d for children. Rectal dosing for infants and children weighing less than 60 kg (132 lb) is 10 to 20 mg/kg every 6 hours as needed, with a maximum daily dose of 75 mg/kg/d in infants, and 100 mg/kg/d in children.
Ibuprofen. Ibuprofen, an NSAID with both antipyretic and anti-inflammatory properties, acts as a prostaglandin inhibitor and is indicated for use in patients over 6 months of age. Since ibuprofen inhibits platelet function, it can cause GI bleeding with chronic use. The suggested pediatric dose for ibuprofen is 5 to 10 mg/kg per dose every 6 to 8 hours orally, with a maximum dose of 40 mg/kg/d.9
Local Anesthesia
Local anesthetics administered via the topical or subcutaneous (SC) route provide anesthesia by temporarily blocking peripheral or central nerve conduction at the sodium channel.
LET Gel. This topical anesthetic combination composed of 4% lidocaine, 0.1% epinephrine, and 0.5% tetracaine (LET gel) is commonly used on patients prior to repair of a skin laceration. Its peak onset of action occurs in 30 minutes, with an anesthetic duration of 45 minutes. The epinephrine component of LET reduces blood flow to the anesthetized area, which increases duration of action but also creates a small risk of vasoconstriction in the areas supplied by end arteries, such as in the penis, nose, digits, and pinna.9
EMLA and LMX4. Topical lidocaine anesthetics are extremely useful in the ED because their application can help reduce the pain of minor procedures, when they are applied in adequate time prior to initiating the procedure to reach peak effect. Eutectic mixture of 2.5% lidocaine and 2.5% prilocaine (EMLA) and liposomal 4% lidocaine (LMX4) are the most commonly used topical lidocaine anesthetics. The peak analgesic effect of EMLA occurs within 60 minutes, with a duration of 90 minutes; LMX4 reaches its analgesic peak after 30 minutes with duration of up to 60 minutes.
Because of the slight delay of the time-to-peak effect, these topical anesthetics are not useful for emergent procedures. Further, neither EMLA nor LMX4 is approved for nonintact skin injuries such as lacerations.9 Both LMX4 and EMLA are approved for use in intact skin, providing effective analgesia for procedures such as venipuncture, circumcision, LP, and abscess drainage.
Subcutaneous Lidocaine. When SC injection of lidocaine is preferred, a useful technique to reduce the pain of administration is to warm the lidocaine, alkalinize the solution with 1 mL (1 mEq) sodium bicarbonate to 9 mL lidocaine,6 prior to injecting it slowly with a small-gauge needle.8Vapocoolant Lidocaine. Vapocoolant sprays produce an immediate cold sensation that is effective in reducing localized pain in adults. Studies looking at its efficacy in children are not as convincing, with some studies suggesting the cold sensation is quite distressing for many children.8
Opioids
Opioids are commonly chosen for pediatric procedural sedation because of their short onset of action and ability to produce significant analgesia with varying amounts of sedation. Fentanyl and morphine are the most widely used opioid analgesics to manage moderate-to-severe procedural pain in children.
Morphine. Morphine remains the gold standard for pediatric opioid analgesia, partly because it can be administered SC, IV, intramuscularly (IM), and orally. Its properties are more quickly achieved via the IV route, as the onset of action is 4 to 6 minutes. The standard IV dose of morphine is 0.1 mg/kg per dose, and can provide analgesia for up to 4 hours.
Adverse effects of morphine include dependence (though not an issue with a single emergency dose), respiratory depression, nausea, vomiting, constipation, urinary retention, hypotension, and bradycardia. Naloxone can rapidly reverse these adverse effects.
Fentanyl. Fentanyl, which is 100 times more potent than morphine, can be administered IV, transdermally, or transmucosally. When given IV, the onset of action of fentanyl is 2 to 3 minutes, and duration of action of 30 to 60 minutes. For sedation and analgesia, the suggested IV dose of fentanyl in neonates and young infants is 1 to 4 mcg/kg every 2 to 4 hours as needed, and for older infants and children, 1 to 2 mcg/kg every 30 to 60 minutes as needed.
Adverse effects of fentanyl are respiratory depression and chest wall rigidity,9 which can be rapidly reversed with naloxone (the dose of naloxone by patient weight is the same as that given to reverse adverse effects of morphine and fentanyl).
Codeine. A weaker opioid analgesic, codeine is not recommended for routine pediatric use because of its significant potential to hypermetabolize to morphine in some children, leading to overdose.6
Benzodiazepines: Midazolam
Benzodiazepines, which act on the type A gamma-aminobutyric acid receptor, causing muscle relaxation, anxiolysis, and anterograde amnesia, are useful for pediatric procedural sedation. Due to its short half-life, midazolam is the most common benzodiazepine used in pediatric patients. Midazolam can be delivered via different routes of administration, including orally, IM, IV, and transmucosally.
Intramuscular Route. Intramuscular midazolam has been shown to cause deep sedation at doses of 0.3 mg/kg, with maximum sedation occurring at 45 minutes, recovery beginning by 60 minutes, and the most common side effect being euphoria.10
Intravenous Route. Intravenous midazolam is used extensively in pediatric procedural sedation and is usually given at a dose of 0.05 to 0.1 mg/kg, with a maximum dose of 2 mg.
Even among small children, midazolam is usually quite safe when given alone, but because it does not provide effective analgesia, it often requires combination with an opioid for effective procedural sedation. Flumazenil may be given for rapid reversal of known benzodiazepine-induced respiratory depression, but it should be avoided in children with seizure disorders.
Propofol
Propofol is now frequently employed for pediatric sedation outside of the operating room. Propofol has excellent sedation properties but, like midazolam, does not provide analgesia and necessitates a second agent such as ketamine or an opioid for successful completion of more painful procedures. However, for children in whom sedation is required to facilitate simple neuroimaging of the head or spine, propofol is a very useful agent given the child’s quick return to his/her baseline mental status following the procedure.
Regarding contraindications, since propofol contains egg lecithin and soybean oil, it was once considered inappropriate for use in patients with an egg or soy allergy. Recent data, however, have refuted this belief, and while the package insert for propofol still lists patient allergy to egg, egg products, soy, or soybeans as a contraindication to use,11 the American Academy of Allergy, Asthma and Immunology recently concluded that patients with soy allergy or egg allergy can receive propofol without any special precautions.12
Since propofol is a powerful sedative and can cause a greater depth of sedation than that intended, providers must be comfortable with both monitoring and managing the pediatric airway. The induction dose of propofol is 1 mg/kg with repeated doses of 0.5 mg/kg to achieve the desired level of sedation. One emergency medicine-specific study by Jasiak et al13 found a mean cumulative propofol dose of 2.1 mg/kg for pediatric procedures given in a median of three boluses, with younger children requiring an overall higher mg/kg induction dose. Another study by Young et al14 showed an induction dose of 2 mg/kg to be well tolerated and without increased adverse events for pediatric procedural sedation.
When used properly, propofol has been shown to be safe and effective in pediatric patients. A recent review by Mallory et al15 looking at 25,433 cases of EP administration of propofol to pediatric patients noted serious complications in only 2% of patients, including one unplanned intubation, one cardiac arrest, and two aspirations.
Ketamine
Dissociative procedural sedation is frequently utilized in pediatric patients, for which ketamine is usually the agent of choice given its fast onset of action, multiple modes of administration, and robust pediatric safety data. Ketamine is a unique agent because of its sedative, analgesic, and paralytic-like properties. A phencyclidine derivative, ketamine exerts its effect by binding to the N-methyl-D-aspartate receptor, and may be given IM or IV, with usual dosing of 1 to 1.5 mg/kg IV, or 2 to 4 mg/kg IM. Unlike other sedatives, there is a “dissociation threshold” for ketamine, and further dosing does not increase its effects.16
Because of multiple observations and reported cases of airway complications in infants younger than 3 months of age, it is not recommended for routine use in this age group. While ketamine-associated infant airway events are thought by some experts to not be specific to ketamine (and more representative of infant differences in airway anatomy and laryngeal excitability), risks seem to outweigh benefits for routine use in this cohort.16
Ketamine is known to exaggerate protective airway reflexes and can cause laryngospasm, so it is best avoided during procedures that cause a large amount of pharyngeal stimulation. The overall rate of ketamine-induced pediatric laryngospasm is low in the general population (0.3%), and when it does occur, can usually be treated easily with assisted ventilation and oxygenation.17
Prior concerns of ketamine increasing intracranial pressure (ICP) have been shown not to be the case by recent data, which in fact demonstrate that ketamine may instead actually lower ICP.18
For many pediatric centers, including the authors’, ketamine is a first-line agent to facilitate head and/or neck CT in otherwise uncooperative children. Emesis is the most common side effect of ketamine, but the incidence can be significantly reduced by pretreating the patient with ondansetron.19 Though ketamine may also be combined with propofol, there is no robust pediatric-specific evidence showing any benefits of this practice.
Nitrous Oxide
Nitrous oxide (N2O), the most commonly used inhaled anesthetic agent used in the pediatric ED, provides analgesia, sedation, anterograde amnesia, and anxiolysis. It can be given in mixtures of 30% to 70% N2O with oxygen, has a rapid onset of action (<1 minute), and there is rapid recovery after cessation. In patients older than 5 years of age, N2O is usually given via a demand valve system, which will fall off the patient’s face if he or she becomes overly sedated.
Nitrous oxide is usually very well tolerated with few serious events, the most common being emesis.20 Absolute contraindications to its use are few and include pneumothorax, pulmonary blebs, bowel obstruction, air embolus, and a recent history of intracranial or middle ear surgery.
Intranasal Analgesia
Intranasal (IN) analgesics are becoming increasingly popular for pediatric procedures because of their rapid onset of action compared with oral medications, without the need for IV or “needle” access prior to administration.
Intranasal Fentanyl. The EP should use a mucosal atomizer when administering midazolam or fentanyl via the IN route. The atomizer transforms these liquid drugs into a fine spray, which increases surface area, improving mucosal absorption and central nervous system concentrations when compared with IN administration via dropper.21
In a study by Klein et al,22 IN midazolam effectively provided sedation, with more effective diminution of activity and better overall patient satisfaction than with either oral or buccal midazolam. Intranasal midazolam causes a slight burning sensation, and some patients report initial discomfort after administration. The half-lives of IN and IV midazolam are very similar (2.2 vs 2.4 hours).23Intranasal Fentanyl. IN fentanyl is an excellent alternative to IV pain medications for patients in whom there is no IV access. When given at a dose of 1.7 mcg/kg, IN fentanyl produces analgesic effects similar to that of morphine 0.1 mg/kg.
The only reported adverse effect associated with IN fentanyl has been a bad taste in the mouth.24 Another study of children aged 1 to 3 years showed a significant decrease in pain in 93% of children at 10 minutes, and 98% of children at 30 minutes, with no significant side effects.25
Intranasal fentanyl is a great choice for initial and immediate pain control in children with suspected long bone fractures, and is especially useful in facilitating their comfort during radiographic imaging.
Managing a Child for Radiographic Imaging
To facilitate a relatively rapid procedure such as obtaining plain films or a CT scan, anxiolysis, rather than analgesia, is required. Given its quick and predictable onset of action, IN midazolam is an excellent choice for pediatric patients requiring imaging studies. If, however, a mucosal atomizer is not available for IN drug delivery and the patient is already in radiology and requires emergent imaging studies, oral midazolam should not be given as an alternative because of its delayed onset of action. In such cases, placing an IV line and administering IV propofol offers the best chance of achieving quick and effective anxiolysis to obtain the images required to exclude clinically important injuries.
In hospitals that restrict the use of propofol in young children outside of the operating room—and when there are no findings suggestive of impending cerebral herniation—a safe and effective alternative is IV ketamine at a dose of 1.5 mg/kg.
Cases Continued
Case 1
[The 4-year-old boy with the fractured wrist.]
Recognizing that repeated attempts at IV placement in a child with a contralateral extremity fracture often leads to escalating distress and anxiety, the EP decided against further attempts to place an IV line. Instead, he gave the child fentanyl via the IN route, which immediately relieved the patient’s pain and facilitated radiographic evaluation. After administrating the fentanyl IN, the EP instructed a member of the ED staff to apply LMX4 cream to several potential IV sites and then cover each site with occlusive dressings. Afterward, the patient was taken to radiology, and X-ray images of the fracture were easily obtained. When the patient returned from imaging, the ED nurse was able to place an IV line at one of the sites that had been previously anesthetized with LMX4 cream.
The EP consulted with the orthopedist, who determined that the child’s distal radius fracture necessitated closed reduction. To facilitate the procedure, the patient was given 1.5 mg/kg of ketamine. After a successful closed reduction, the orthopedic chief resident recommended the EP discharge the 15-kg (33-lb) patient home in the care of his parents, with a prescription for 5 mL oral acetaminophen and codeine suspension four times a day as needed for pain (5 mL = acetaminophen 120 mg/codeine 12 mg, and codeine dosed at 0.5-1 mg/kg per dose). Prior to discharge, the EP counseled the patient’s parents on the risks of codeine hypermetabolism in children. However, based on the parents’ expressed concerns, the EP instead discharged the patient home with a prescription for 4 cc oral acetaminophen-hydrocodone elixir every 4 to 6 hours as needed for pain instead (dosing is 0.27 mL/kg; elixir is hydrocodone bitartrate 7.5 mg/acetaminophen 325 mg/15 mL).
Case 2
[The 6-year-old girl with a large laceration to her forehead.]
The type of laceration sustained by this patient was appropriate for treatment with a local anesthetic combined with an agent for non-IV anxiolysis. Thirty minutes prior to suturing, LET gel was applied over the open wound site, and 5 minutes prior to initiating closure of the wound, the patient received IN midazolam. Since the LET cream was placed on the wound 30 minutes prior to the procedure, the site was well anesthetized for both irrigation and closure. The anxiolytic effects of the IN midazolam resulted in a calm patient, who was happy and playful throughout the procedure.
After successfully closing the wound, the physician discharged the patient home in the care of her parents, with instructions to apply bacitracin ointment to the wound site three times a day for the next 3 days, and give the patient over-the-counter acetaminophen elixir for any mild discomfort.
Case 3
[The 5-year-old boy who suffered cervical spine injuries after falling head-first off of a balance beam during gymnastics.]
Since no mucosal atomizer was available for IN drug delivery, and hospital policy restricted the use of propofol in young children outside of the operating room, the patient was given 1.5 mg/kg of IV ketamine. Within 45 seconds of ketamine administration, the child had adequate dissociative sedation, which allowed for high-quality CT scans of both the head and neck without incident.
Case 4
[The febrile 3-week-old female neonate referred by her pediatrician for evaluation and LP.]
Since this neonate did not appear toxic, the EP delayed the LP by 30 minutes to allow time for application of a topical anesthetic to minimize associated procedural pain. Thirty minutes prior to the LP, LMX4 cream was applied to the patient’s L4 spinal interspace, and just prior to the procedure, the patient was given a pacifier that had been dipped in a solution of 4% sucrose. The neonate was then positioned appropriately for the LP and barely squirmed when the spinal needle was introduced, allowing the EP to obtain a nontraumatic cerebrospinal fluid sample on the first attempt.
Conclusion
Addressing pediatric pain and anxiety, especially preceding and during procedures and radiographic imaging, is a serious challenge in the ED. Several means are now available to provide safe and effective sedation, analgesia, and anxiolysis in the ED, with or without IV access. Many of the medications utilized, however, can cause significant respiratory and CV depression, making proper patient selection and monitoring, and training of involved personnel imperative to ensure safe use in the ED. Appropriate use of the agents and strategies discussed above will allow EPs to reduce both procedural pain and anxiety for our youngest patients—and their parents.
For many years, pediatric patients undergoing procedures in the ED have received inadequate pain management and sedation. Children’s (and parents’) anxieties and distress leading up to and during a potentially painful or anxiety-inducing procedure are now more easily mitigated by the appropriate use of a variety of pediatric-appropriate analgesics, sedatives, and anxiolytics. The ability to provide adequate, minimally invasive sedation and analgesia is critically important to performing successful procedures in children, and is a hallmark of excellent pediatric emergency care.
The following case vignettes, based on actual cases, illustrate the range and routes of medications available to provide appropriate analgesia, sedation, and anxiolysis.
Cases
Case 1
A 4-year-old boy presented to the ED for evaluation of a fractured wrist sustained after he fell off his bed during a temper tantrum. At presentation, the patient’s vital signs were: blood pressure (BP), 110/70 mm Hg; heart rate (HR), 100 beats/min; respiratory rate (RR), 28 breaths/min; and temperature (T), 99.5°F. Oxygen saturation on room air was within normal limits. The patient’s weight was within normal range for his age and height at 15 kg (33 lb).
Upon examination, the child appeared agitated and in significant distress; his anxiety increased after an initial attempt at placing an intravenous (IV) line in his uninjured arm failed.
The emergency physician (EP) considered several options to ameliorate the child’s anxiety and facilitate evaluation and treatment.
Case 2
After accidentally running into a pole, a 6-year-old girl presented to the ED for evaluation and suturing of a large laceration to her forehead. At presentation, the patient’s vital signs were: BP, 115/70 mm Hg; HR, 95 beats/min; RR, 24 breaths/min; and T, 98.6°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 20 kg (44 lb).
On examination, the patient was awake, alert, and in no acute distress. However, she immediately became tearful and visibly upset when she learned that an IV line was about to be placed in her arm.
The physician instead decided to employ an IV/needle-free strategy for this wound repair, as well as anxiolysis.
Case 3
A 5-year-old girl was brought to a community hospital ED by emergency medical services after falling from a balance beam and landing headfirst on the ground during a gymnastics class. Prior to presentation, emergency medical technicians had placed the patient in a cervical collar. At presentation, the patient’s vital signs were: BP, 105/75 mm Hg; HR, 115 beats/min; RR, 28 breaths/min; and T, 99.1°F. Oxygen saturation on room air was within normal limits. The patient’s body weight was normal for her age and height at 18 kg (39.6 lb).
Although the neurological examination was normal, the patient had persistent midline cervical tenderness as well as hemotympanum. The EP ordered a head and neck computed tomography (CT) scan, but shortly after the patient arrived at radiology, the CT technician informed the EP that she was unable to perform the scan because the patient kept moving and would not stay still.
The EP considered several sedatives to facilitate the CT study.
Case 4
A febrile, but nontoxic-appearing 3-week-old girl was referred to the ED by her pediatrician for a lumbar puncture (LP) to diagnose or exclude meningitis. However, the mother’s own recent negative experience with an epidural analgesia during the patient’s delivery, made the neonate’s mother extremely anxious that the procedure might be too painful for her daughter.
The EP considered the best choice of medication to provide analgesia and allay the mother’s concerns prior to performing the LP in this neonatal patient.
Overview and Definitions
Analgesia describes the alleviation of pain without intentional sedation. However, pediatric patients typically receive sedative hypnotics (anxiolytics) both for analgesia and for anxiolysis to modify behavior (eg, enhance immobility) and to allow for the safe completion of a procedure.1 The ultimate goal of procedural sedation and analgesia is to provide a depressed level of consciousness and pain relief while the patient maintains a patent airway and spontaneous ventilation.2
Sedation Continuum
The American Society of Anesthesiologists (ASA) classifies procedural sedation and analgesia based on a sedation continuum that affects overall responsiveness, airway, ventilation, and cardiovascular (CV) function.3 Procedural sedation is subcategorized into minimal, moderate, and deep sedation.
Minimal Sedation. Formally referred to as anxiolysis, minimal sedation is a state in which the patient is responsive but somewhat cognitively impaired, while maintaining all other functions rated in the sedation continuum.
Moderate Sedation. Previously referred to as “conscious sedation,” moderate sedation is a state of drug-induced depression of consciousness that still enables the patient to maintain purposeful responses to age-appropriate verbal commands and tactile stimulation, spontaneous ventilation, and CV integrity.
Deep Sedation. Deep sedation causes a drug-induced depression of consciousness that may potentially impair spontaneous ventilation and independent airway patency, while maintaining CV function. A deeply sedated patient is usually arousable with repeated painful stimulation.
Dissociative Sedation. This level of sedation induces a unique, trance-like cataleptic state characterized by profound analgesia and amnesia, with retention of protective airway reflexes, spontaneous respirations, and cardiopulmonary stability. The dissociative state can facilitate the performance of moderate-to-severe painful procedures, as well as procedures requiring immobilization in uncooperative patients.4
Contraindications to Procedural Sedation
Though there are no absolute contraindications to procedural sedation in children, its use is generally determined based on ASA’s patient physical status classification system. In this grading system, procedural sedation is appropriate for pediatric patients with a physical status of Class I (normally healthy patient) or Class II (a patient with mild systemic disease—eg, mild asthma).5 The EP should consult with a pediatric anesthesiologist prior to sedating a patient with an ASA status of Class II or higher, or a patient with a known laryngotracheal pathology.1
Pre- and Postsedation Considerations
History and Physical Examination
Prior to patient sedation, the EP should perform a focused history, including a determination of the patient’s last meal and/or drink, and a physical examination. The history should also include known allergies and past or current medication use—specifically any history of adverse events associated with prior sedation. Pregnancy status should be determined in every postpubertal female patient.
The physical examination should focus on the cardiac and respiratory systems, with particular attention to any airway abnormalities or possible sources of obstruction.1,3
Fasting
A need for fasting prior to procedural sedation remains controversial: Current ASA guidelines for fasting call for fasting times of 2 hours for clear liquids, 4 hours after breastfeeding, 6 hours for nonhuman milk or formula feeding, and 8 hours for solids.6
Fasting prior to general anesthesia has become a common requirement because of the risk of adverse respiratory events, including apnea, stridor, bronchospasm, emesis, and pulmonary aspiration of gastric contents. However, these events rarely occur during pediatric procedural sedation in the ED, and it is important to note that the American College of Emergency Physicians’ standards do not require delaying procedural sedation based on fasting times. There is no strong evidence that the duration of preprocedural sedation-fasting reduces or prevents emesis or aspiration.7
Equipment
In 2016, the American Academy of Pediatrics (AAP) updated its “Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures,”1 including the essential equipment required for the safe administration of sedation, which can be remembered using the following “SOAPME” mnemonic:
Size: appropriate suction catheters and a functioning suction apparatus (eg, Yankauer-type suction);
Oxygen: An adequate oxygen supply and functioning flow meters or other devices to allow its delivery;
Airway: Size-appropriate equipment (eg, bag-valve-mask or equivalent device [functioning]), nasopharyngeal and oropharyngeal airways, laryngeal mask airway, laryngoscope blades (checked and functioning), endotracheal tubes, stylets, face mask;
Pharmacy: All the basic drugs needed to support life during an emergency, including antagonists as indicated;
Monitors: Functioning pulse oximeter with size-appropriate oximeter probes, end-tidal carbon dioxide monitor, and other monitors as appropriate for the procedure (eg, noninvasive blood pressure, electrocardiogram, stethoscope); and
Equipment: Special equipment or drugs for a particular case (eg, defibrillator).1
Personnel
The 2016 AAP guidelines1 also indicate the number and type of personnel needed for sedation—in addition to the physician performing the procedure—which is primarily determined by the intended level of sedation as follows:
Minimal Sedation. Though there are no set guidelines for minimal sedation, all providers must be capable of caring for a child who progresses to moderate sedation.
Moderate Sedation. Intentional moderate sedation necessitates two practitioners: one practitioner to oversee the sedation and monitor the patient’s vital signs, who is capable of rescuing the patient from deep sedation if it occurs; and a second provider proficient at least in basic life support to monitor vital signs and assist in a resuscitation as needed.
Deep Sedation. For patients requiring deep sedation, the practitioner administering or supervising sedative drug administration should have no other responsibilities other than observing the patient. Moreover, there must be at least one other individual present who is certified in advanced life support and airway management.1
Discharge Criteria
Prior to discharge, pediatric patients must meet predetermined criteria that include easy arousability, a return to baseline mental status, stable age-appropriate vital signs, and the ability to remain hydrated.1,3 In addition, while late postsedation complications are rare, caregivers should be provided with specific symptoms that would warrant immediate return to the ED.
Available Options for Analgesia and Sedation
Several different methods of providing analgesia and pediatric procedural sedation are available, ranging from nonpharmacological methods to topical and parenteral medication administration.
Nonpharmacological Options: Child-Life Specialists
Child-life specialists can be particularly helpful with pediatric emergency patients. With a background in normal child development, child-life specialists utilize myriad distraction techniques and coping strategies to help patients within the stressful environment of an ED. Studies have shown that the presence of a child-life specialist may reduce the depth of sedation needed for certain procedures.1
Sucrose
Several studies have identified the benefits of sucrose as a pain reliever in neonates. Available as a 12% to 25% solution, sucrose decreases noxious stimuli and is a useful analgesic for such common neonatal procedures as venipuncture, circumcision, heel sticks, Foley catheter insertion, and LP. Efficacy of sucrose for these procedures is greatest in newborns, and decreases gradually after 6 months of age. The effectiveness of sucrose is enhanced when it is given in conjunction with nonnutritive sucking or maternal “skin-to-skin” techniques. There are no contraindications to the use of sucrose.8
Nonopioid Systemic Analgesia
Nonopioid oral analgesics (NOAs), such as acetaminophen and the nonsteroidal anti-inflammatory drug (NSAID) ibuprofen, are appropriate for mild-to-moderate procedural pain. The NOAs can be given alone or in conjunction with an opioid to enhance the analgesic effect for patients with severe pain.
Acetaminophen. Acetaminophen, which also has antipyretic properties, can be administered orally, rectally, or IV. Since acetaminophen is not an NSAID and does not affect platelet function, it is a good choice for treating patients with gastrointestinal (GI) pain.
Adverse effects of acetaminophen, which is metabolized by the liver, include hepatotoxicity in toxic doses. The suggested oral dose for infants and children weighing less than 60 kg (132 lb) is 10 to 15 mg/kg per dose every 4 to 6 hours as needed, with a maximum dose of 75 mg/kg/d for infants and 100 mg/kg/d for children. Rectal dosing for infants and children weighing less than 60 kg (132 lb) is 10 to 20 mg/kg every 6 hours as needed, with a maximum daily dose of 75 mg/kg/d in infants, and 100 mg/kg/d in children.
Ibuprofen. Ibuprofen, an NSAID with both antipyretic and anti-inflammatory properties, acts as a prostaglandin inhibitor and is indicated for use in patients over 6 months of age. Since ibuprofen inhibits platelet function, it can cause GI bleeding with chronic use. The suggested pediatric dose for ibuprofen is 5 to 10 mg/kg per dose every 6 to 8 hours orally, with a maximum dose of 40 mg/kg/d.9
Local Anesthesia
Local anesthetics administered via the topical or subcutaneous (SC) route provide anesthesia by temporarily blocking peripheral or central nerve conduction at the sodium channel.
LET Gel. This topical anesthetic combination composed of 4% lidocaine, 0.1% epinephrine, and 0.5% tetracaine (LET gel) is commonly used on patients prior to repair of a skin laceration. Its peak onset of action occurs in 30 minutes, with an anesthetic duration of 45 minutes. The epinephrine component of LET reduces blood flow to the anesthetized area, which increases duration of action but also creates a small risk of vasoconstriction in the areas supplied by end arteries, such as in the penis, nose, digits, and pinna.9
EMLA and LMX4. Topical lidocaine anesthetics are extremely useful in the ED because their application can help reduce the pain of minor procedures, when they are applied in adequate time prior to initiating the procedure to reach peak effect. Eutectic mixture of 2.5% lidocaine and 2.5% prilocaine (EMLA) and liposomal 4% lidocaine (LMX4) are the most commonly used topical lidocaine anesthetics. The peak analgesic effect of EMLA occurs within 60 minutes, with a duration of 90 minutes; LMX4 reaches its analgesic peak after 30 minutes with duration of up to 60 minutes.
Because of the slight delay of the time-to-peak effect, these topical anesthetics are not useful for emergent procedures. Further, neither EMLA nor LMX4 is approved for nonintact skin injuries such as lacerations.9 Both LMX4 and EMLA are approved for use in intact skin, providing effective analgesia for procedures such as venipuncture, circumcision, LP, and abscess drainage.
Subcutaneous Lidocaine. When SC injection of lidocaine is preferred, a useful technique to reduce the pain of administration is to warm the lidocaine, alkalinize the solution with 1 mL (1 mEq) sodium bicarbonate to 9 mL lidocaine,6 prior to injecting it slowly with a small-gauge needle.8Vapocoolant Lidocaine. Vapocoolant sprays produce an immediate cold sensation that is effective in reducing localized pain in adults. Studies looking at its efficacy in children are not as convincing, with some studies suggesting the cold sensation is quite distressing for many children.8
Opioids
Opioids are commonly chosen for pediatric procedural sedation because of their short onset of action and ability to produce significant analgesia with varying amounts of sedation. Fentanyl and morphine are the most widely used opioid analgesics to manage moderate-to-severe procedural pain in children.
Morphine. Morphine remains the gold standard for pediatric opioid analgesia, partly because it can be administered SC, IV, intramuscularly (IM), and orally. Its properties are more quickly achieved via the IV route, as the onset of action is 4 to 6 minutes. The standard IV dose of morphine is 0.1 mg/kg per dose, and can provide analgesia for up to 4 hours.
Adverse effects of morphine include dependence (though not an issue with a single emergency dose), respiratory depression, nausea, vomiting, constipation, urinary retention, hypotension, and bradycardia. Naloxone can rapidly reverse these adverse effects.
Fentanyl. Fentanyl, which is 100 times more potent than morphine, can be administered IV, transdermally, or transmucosally. When given IV, the onset of action of fentanyl is 2 to 3 minutes, and duration of action of 30 to 60 minutes. For sedation and analgesia, the suggested IV dose of fentanyl in neonates and young infants is 1 to 4 mcg/kg every 2 to 4 hours as needed, and for older infants and children, 1 to 2 mcg/kg every 30 to 60 minutes as needed.
Adverse effects of fentanyl are respiratory depression and chest wall rigidity,9 which can be rapidly reversed with naloxone (the dose of naloxone by patient weight is the same as that given to reverse adverse effects of morphine and fentanyl).
Codeine. A weaker opioid analgesic, codeine is not recommended for routine pediatric use because of its significant potential to hypermetabolize to morphine in some children, leading to overdose.6
Benzodiazepines: Midazolam
Benzodiazepines, which act on the type A gamma-aminobutyric acid receptor, causing muscle relaxation, anxiolysis, and anterograde amnesia, are useful for pediatric procedural sedation. Due to its short half-life, midazolam is the most common benzodiazepine used in pediatric patients. Midazolam can be delivered via different routes of administration, including orally, IM, IV, and transmucosally.
Intramuscular Route. Intramuscular midazolam has been shown to cause deep sedation at doses of 0.3 mg/kg, with maximum sedation occurring at 45 minutes, recovery beginning by 60 minutes, and the most common side effect being euphoria.10
Intravenous Route. Intravenous midazolam is used extensively in pediatric procedural sedation and is usually given at a dose of 0.05 to 0.1 mg/kg, with a maximum dose of 2 mg.
Even among small children, midazolam is usually quite safe when given alone, but because it does not provide effective analgesia, it often requires combination with an opioid for effective procedural sedation. Flumazenil may be given for rapid reversal of known benzodiazepine-induced respiratory depression, but it should be avoided in children with seizure disorders.
Propofol
Propofol is now frequently employed for pediatric sedation outside of the operating room. Propofol has excellent sedation properties but, like midazolam, does not provide analgesia and necessitates a second agent such as ketamine or an opioid for successful completion of more painful procedures. However, for children in whom sedation is required to facilitate simple neuroimaging of the head or spine, propofol is a very useful agent given the child’s quick return to his/her baseline mental status following the procedure.
Regarding contraindications, since propofol contains egg lecithin and soybean oil, it was once considered inappropriate for use in patients with an egg or soy allergy. Recent data, however, have refuted this belief, and while the package insert for propofol still lists patient allergy to egg, egg products, soy, or soybeans as a contraindication to use,11 the American Academy of Allergy, Asthma and Immunology recently concluded that patients with soy allergy or egg allergy can receive propofol without any special precautions.12
Since propofol is a powerful sedative and can cause a greater depth of sedation than that intended, providers must be comfortable with both monitoring and managing the pediatric airway. The induction dose of propofol is 1 mg/kg with repeated doses of 0.5 mg/kg to achieve the desired level of sedation. One emergency medicine-specific study by Jasiak et al13 found a mean cumulative propofol dose of 2.1 mg/kg for pediatric procedures given in a median of three boluses, with younger children requiring an overall higher mg/kg induction dose. Another study by Young et al14 showed an induction dose of 2 mg/kg to be well tolerated and without increased adverse events for pediatric procedural sedation.
When used properly, propofol has been shown to be safe and effective in pediatric patients. A recent review by Mallory et al15 looking at 25,433 cases of EP administration of propofol to pediatric patients noted serious complications in only 2% of patients, including one unplanned intubation, one cardiac arrest, and two aspirations.
Ketamine
Dissociative procedural sedation is frequently utilized in pediatric patients, for which ketamine is usually the agent of choice given its fast onset of action, multiple modes of administration, and robust pediatric safety data. Ketamine is a unique agent because of its sedative, analgesic, and paralytic-like properties. A phencyclidine derivative, ketamine exerts its effect by binding to the N-methyl-D-aspartate receptor, and may be given IM or IV, with usual dosing of 1 to 1.5 mg/kg IV, or 2 to 4 mg/kg IM. Unlike other sedatives, there is a “dissociation threshold” for ketamine, and further dosing does not increase its effects.16
Because of multiple observations and reported cases of airway complications in infants younger than 3 months of age, it is not recommended for routine use in this age group. While ketamine-associated infant airway events are thought by some experts to not be specific to ketamine (and more representative of infant differences in airway anatomy and laryngeal excitability), risks seem to outweigh benefits for routine use in this cohort.16
Ketamine is known to exaggerate protective airway reflexes and can cause laryngospasm, so it is best avoided during procedures that cause a large amount of pharyngeal stimulation. The overall rate of ketamine-induced pediatric laryngospasm is low in the general population (0.3%), and when it does occur, can usually be treated easily with assisted ventilation and oxygenation.17
Prior concerns of ketamine increasing intracranial pressure (ICP) have been shown not to be the case by recent data, which in fact demonstrate that ketamine may instead actually lower ICP.18
For many pediatric centers, including the authors’, ketamine is a first-line agent to facilitate head and/or neck CT in otherwise uncooperative children. Emesis is the most common side effect of ketamine, but the incidence can be significantly reduced by pretreating the patient with ondansetron.19 Though ketamine may also be combined with propofol, there is no robust pediatric-specific evidence showing any benefits of this practice.
Nitrous Oxide
Nitrous oxide (N2O), the most commonly used inhaled anesthetic agent used in the pediatric ED, provides analgesia, sedation, anterograde amnesia, and anxiolysis. It can be given in mixtures of 30% to 70% N2O with oxygen, has a rapid onset of action (<1 minute), and there is rapid recovery after cessation. In patients older than 5 years of age, N2O is usually given via a demand valve system, which will fall off the patient’s face if he or she becomes overly sedated.
Nitrous oxide is usually very well tolerated with few serious events, the most common being emesis.20 Absolute contraindications to its use are few and include pneumothorax, pulmonary blebs, bowel obstruction, air embolus, and a recent history of intracranial or middle ear surgery.
Intranasal Analgesia
Intranasal (IN) analgesics are becoming increasingly popular for pediatric procedures because of their rapid onset of action compared with oral medications, without the need for IV or “needle” access prior to administration.
Intranasal Fentanyl. The EP should use a mucosal atomizer when administering midazolam or fentanyl via the IN route. The atomizer transforms these liquid drugs into a fine spray, which increases surface area, improving mucosal absorption and central nervous system concentrations when compared with IN administration via dropper.21
In a study by Klein et al,22 IN midazolam effectively provided sedation, with more effective diminution of activity and better overall patient satisfaction than with either oral or buccal midazolam. Intranasal midazolam causes a slight burning sensation, and some patients report initial discomfort after administration. The half-lives of IN and IV midazolam are very similar (2.2 vs 2.4 hours).23Intranasal Fentanyl. IN fentanyl is an excellent alternative to IV pain medications for patients in whom there is no IV access. When given at a dose of 1.7 mcg/kg, IN fentanyl produces analgesic effects similar to that of morphine 0.1 mg/kg.
The only reported adverse effect associated with IN fentanyl has been a bad taste in the mouth.24 Another study of children aged 1 to 3 years showed a significant decrease in pain in 93% of children at 10 minutes, and 98% of children at 30 minutes, with no significant side effects.25
Intranasal fentanyl is a great choice for initial and immediate pain control in children with suspected long bone fractures, and is especially useful in facilitating their comfort during radiographic imaging.
Managing a Child for Radiographic Imaging
To facilitate a relatively rapid procedure such as obtaining plain films or a CT scan, anxiolysis, rather than analgesia, is required. Given its quick and predictable onset of action, IN midazolam is an excellent choice for pediatric patients requiring imaging studies. If, however, a mucosal atomizer is not available for IN drug delivery and the patient is already in radiology and requires emergent imaging studies, oral midazolam should not be given as an alternative because of its delayed onset of action. In such cases, placing an IV line and administering IV propofol offers the best chance of achieving quick and effective anxiolysis to obtain the images required to exclude clinically important injuries.
In hospitals that restrict the use of propofol in young children outside of the operating room—and when there are no findings suggestive of impending cerebral herniation—a safe and effective alternative is IV ketamine at a dose of 1.5 mg/kg.
Cases Continued
Case 1
[The 4-year-old boy with the fractured wrist.]
Recognizing that repeated attempts at IV placement in a child with a contralateral extremity fracture often leads to escalating distress and anxiety, the EP decided against further attempts to place an IV line. Instead, he gave the child fentanyl via the IN route, which immediately relieved the patient’s pain and facilitated radiographic evaluation. After administrating the fentanyl IN, the EP instructed a member of the ED staff to apply LMX4 cream to several potential IV sites and then cover each site with occlusive dressings. Afterward, the patient was taken to radiology, and X-ray images of the fracture were easily obtained. When the patient returned from imaging, the ED nurse was able to place an IV line at one of the sites that had been previously anesthetized with LMX4 cream.
The EP consulted with the orthopedist, who determined that the child’s distal radius fracture necessitated closed reduction. To facilitate the procedure, the patient was given 1.5 mg/kg of ketamine. After a successful closed reduction, the orthopedic chief resident recommended the EP discharge the 15-kg (33-lb) patient home in the care of his parents, with a prescription for 5 mL oral acetaminophen and codeine suspension four times a day as needed for pain (5 mL = acetaminophen 120 mg/codeine 12 mg, and codeine dosed at 0.5-1 mg/kg per dose). Prior to discharge, the EP counseled the patient’s parents on the risks of codeine hypermetabolism in children. However, based on the parents’ expressed concerns, the EP instead discharged the patient home with a prescription for 4 cc oral acetaminophen-hydrocodone elixir every 4 to 6 hours as needed for pain instead (dosing is 0.27 mL/kg; elixir is hydrocodone bitartrate 7.5 mg/acetaminophen 325 mg/15 mL).
Case 2
[The 6-year-old girl with a large laceration to her forehead.]
The type of laceration sustained by this patient was appropriate for treatment with a local anesthetic combined with an agent for non-IV anxiolysis. Thirty minutes prior to suturing, LET gel was applied over the open wound site, and 5 minutes prior to initiating closure of the wound, the patient received IN midazolam. Since the LET cream was placed on the wound 30 minutes prior to the procedure, the site was well anesthetized for both irrigation and closure. The anxiolytic effects of the IN midazolam resulted in a calm patient, who was happy and playful throughout the procedure.
After successfully closing the wound, the physician discharged the patient home in the care of her parents, with instructions to apply bacitracin ointment to the wound site three times a day for the next 3 days, and give the patient over-the-counter acetaminophen elixir for any mild discomfort.
Case 3
[The 5-year-old boy who suffered cervical spine injuries after falling head-first off of a balance beam during gymnastics.]
Since no mucosal atomizer was available for IN drug delivery, and hospital policy restricted the use of propofol in young children outside of the operating room, the patient was given 1.5 mg/kg of IV ketamine. Within 45 seconds of ketamine administration, the child had adequate dissociative sedation, which allowed for high-quality CT scans of both the head and neck without incident.
Case 4
[The febrile 3-week-old female neonate referred by her pediatrician for evaluation and LP.]
Since this neonate did not appear toxic, the EP delayed the LP by 30 minutes to allow time for application of a topical anesthetic to minimize associated procedural pain. Thirty minutes prior to the LP, LMX4 cream was applied to the patient’s L4 spinal interspace, and just prior to the procedure, the patient was given a pacifier that had been dipped in a solution of 4% sucrose. The neonate was then positioned appropriately for the LP and barely squirmed when the spinal needle was introduced, allowing the EP to obtain a nontraumatic cerebrospinal fluid sample on the first attempt.
Conclusion
Addressing pediatric pain and anxiety, especially preceding and during procedures and radiographic imaging, is a serious challenge in the ED. Several means are now available to provide safe and effective sedation, analgesia, and anxiolysis in the ED, with or without IV access. Many of the medications utilized, however, can cause significant respiratory and CV depression, making proper patient selection and monitoring, and training of involved personnel imperative to ensure safe use in the ED. Appropriate use of the agents and strategies discussed above will allow EPs to reduce both procedural pain and anxiety for our youngest patients—and their parents.
1. Coté CJ, Wilson S; American academy of pediatrics; American Academy of Pediatric Dentistry. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatrics. 2016;138(1). doi:10.1542/peds.2016-1212. http://pediatrics.aappublications.org/content/pediatrics/early/2016/06/24/peds.2016-1212.full.pdf
2. Mace SE, Barata IA, Cravero JP, et al; American College of Emergency Physicians. Clinical policy: evidence-based approach to pharmacologic agents used in pediatric sedation and analgesia in the emergency department. Ann Emerg Med. 2004;44(4):342-377. doi:10.1016/S0196064404004214.
3. American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1004-1017. http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1944958. Accessed July 31, 2017.
4. Godwin SA, Burton JH, Gerardo CJ, et al; American College of Emergency Physicians. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63(2):247-258.e18. doi:10.1016/j.annemergmed.2013.10.015.
5. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006; 367(9512):766-780. doi:10.1016/S0140-6736(06)68230-5.
6. Berger J, Koszela KB. Analgesia and procedural sedation. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:136-155.
7. Milne K. Procedural Sedation Delays and NPO Status for Pediatric Patients in the Emergency Department. ACEP Now. http://www.acepnow.com/article/procedural-sedation-delays-npo-status-pediatric-patients-emergency-department/. Published January 22, 2017. Accessed July 25, 2017.
8. Fein JA, Zempsky WT, Cravero JP; Committee on Pediatric Emergency Medicine and Section on Anesthesiology and Pain Medicine; American Academy of Pediatrics. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2012;130(5):e1391-e1405. doi:10.1542/peds.2012-2536.
9. Lee CKK. Drug dosages. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:732-1109.
10. Ghane MR, Musavi Vaezi SY, Hedayati Asl AA, Javadzadeh HR, Mahmoudi S, Saburi A. Intramuscular midazolam for pediatric sedation in the emergency department: a short communication on clinical safety and effectiveness. Trauma Mon. 2012;17(1):233-235. doi:10.5812/traumamon.3458.
11. Diprivan [package insert]. Lake Zurich, IL: Fresenius Kabi USA, LLC; 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019627s066lbl.pdf. Accessed July 31, 2017.
12. American Academy of Allergy Asthma & Immunology. Soy-allergic and egg-allergic patients can safely receive anesthesia. https://www.aaaai.org/conditions-and-treatments/library/allergy-library/soy-egg-anesthesia. Accessed July 31, 2017.
13. Jasiak KD, Phan H, Christich AC, Edwards CJ, Skrepnek GH, Patanwala AE. Induction dose of propofol for pediatric patients undergoing procedural sedation in the emergency department. Pediatr Emerg Care. 2012;28(5):440-442. doi:10.1097/PEC.0b013e3182531a9b.
14. Young TP, Lim JJ, Kim TY, Thorp AW, Brown L. Pediatric procedural sedation with propofol using a higher initial bolus dose. Pediatr Emerg Care. 2014;30(10):689-693. doi:10.1097/PEC.0000000000000229.
15. Mallory MD, Baxter AL, Yanosky DJ, Cravero JP; Pediatric Sedation Research Consortium. Emergency physician-administered propofol sedation: a report on 25,433 sedations from the pediatric sedation research consortium. Ann Emerg Med. 2011;57(5):462-468.e1. doi:10.1016/j.annemergmed.2011.03.008.
16. Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57(5):449-461. doi:10.1016/j.annemergmed.2010.11.030.
17. Green SM, Roback MG, Krauss B, et al; Emergency Department Ketamine Meta-Analysis Study Group. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158-168.e1-4. doi:10.1016/j.annemergmed.2008.12.011.
18. Von der Brelie C, Seifert M, Rot S, et al. Sedation of patients with acute aneurysmal subarachnoid hemorrhage with ketamine is safe and might influence the occurrence of cerebral infarctions associated with delayed cerebral ischemia. World Neurosurg. 2017;97:374-382. doi:10.1016/j.wneu.2016.09.121.
19. Langston WT, Wathen JE, Roback MG, Bajaj L. Effect of ondansetron on the incidence of vomiting associated with ketamine sedation in children: a double-blind, randomized, placebo-controlled trial. Ann Emerg Med. 2008;52(1):30-34. doi:10.1016/j.annemergmed.2008.01.326.
20. Babl FE, Oakley E, Seaman C, Barnett P, Sharwood LN. High-concentration nitrous oxide for procedural sedation in children: adverse events and depth of sedation. Pediatrics. 2008;121(3):e528-e532. doi:10.1542/peds.2007-1044.
21. Henry RJ, Ruano N, Casto D, Wolf RH. A pharmacokinetic study of midazolam in dogs: nasal drop vs. atomizer administration. Pediatr Dent. 1998;20(5):321-326.
22. Klein EJ, Brown JC, Kobayashi A, Osincup D, Seidel K. A randomized clinical trial comparing oral, aerosolized intranasal, and aerosolized buccal midazolam. Ann Emerg Med. 2011;58(4):323-329. doi:10.1016/j.annemergmed.2011.05.016.
23. Rey E, Delaunay L, Pons G, et al. Pharmacokinetics of midazolam in children: comparative study of intranasal and intravenous administration. Eur J Clin Pharmacol. 1991;41(4):355-357. doi:10.1007/BF00314967.
24. Borland M, Jacobs I, King B, O’Brien D. A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med. 2007;49(3):335-340. doi:10.1016/j.annemergmed.2006.06.016.
25. Cole J, Shepherd M, Young P. Intranasal fentanyl in 1-3-year-olds: a prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas. 2009;21(5):395-400. doi:10.1111/j.1742-6723.2009.01216.x.
1. Coté CJ, Wilson S; American academy of pediatrics; American Academy of Pediatric Dentistry. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: update 2016. Pediatrics. 2016;138(1). doi:10.1542/peds.2016-1212. http://pediatrics.aappublications.org/content/pediatrics/early/2016/06/24/peds.2016-1212.full.pdf
2. Mace SE, Barata IA, Cravero JP, et al; American College of Emergency Physicians. Clinical policy: evidence-based approach to pharmacologic agents used in pediatric sedation and analgesia in the emergency department. Ann Emerg Med. 2004;44(4):342-377. doi:10.1016/S0196064404004214.
3. American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1004-1017. http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1944958. Accessed July 31, 2017.
4. Godwin SA, Burton JH, Gerardo CJ, et al; American College of Emergency Physicians. Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2014;63(2):247-258.e18. doi:10.1016/j.annemergmed.2013.10.015.
5. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006; 367(9512):766-780. doi:10.1016/S0140-6736(06)68230-5.
6. Berger J, Koszela KB. Analgesia and procedural sedation. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:136-155.
7. Milne K. Procedural Sedation Delays and NPO Status for Pediatric Patients in the Emergency Department. ACEP Now. http://www.acepnow.com/article/procedural-sedation-delays-npo-status-pediatric-patients-emergency-department/. Published January 22, 2017. Accessed July 25, 2017.
8. Fein JA, Zempsky WT, Cravero JP; Committee on Pediatric Emergency Medicine and Section on Anesthesiology and Pain Medicine; American Academy of Pediatrics. Relief of pain and anxiety in pediatric patients in emergency medical systems. Pediatrics. 2012;130(5):e1391-e1405. doi:10.1542/peds.2012-2536.
9. Lee CKK. Drug dosages. In: Hughes HK, Kahl LK, eds. The Harriet Lane Handbook. 21st ed. Philadelphia, PA: Elsevier; 2018:732-1109.
10. Ghane MR, Musavi Vaezi SY, Hedayati Asl AA, Javadzadeh HR, Mahmoudi S, Saburi A. Intramuscular midazolam for pediatric sedation in the emergency department: a short communication on clinical safety and effectiveness. Trauma Mon. 2012;17(1):233-235. doi:10.5812/traumamon.3458.
11. Diprivan [package insert]. Lake Zurich, IL: Fresenius Kabi USA, LLC; 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/019627s066lbl.pdf. Accessed July 31, 2017.
12. American Academy of Allergy Asthma & Immunology. Soy-allergic and egg-allergic patients can safely receive anesthesia. https://www.aaaai.org/conditions-and-treatments/library/allergy-library/soy-egg-anesthesia. Accessed July 31, 2017.
13. Jasiak KD, Phan H, Christich AC, Edwards CJ, Skrepnek GH, Patanwala AE. Induction dose of propofol for pediatric patients undergoing procedural sedation in the emergency department. Pediatr Emerg Care. 2012;28(5):440-442. doi:10.1097/PEC.0b013e3182531a9b.
14. Young TP, Lim JJ, Kim TY, Thorp AW, Brown L. Pediatric procedural sedation with propofol using a higher initial bolus dose. Pediatr Emerg Care. 2014;30(10):689-693. doi:10.1097/PEC.0000000000000229.
15. Mallory MD, Baxter AL, Yanosky DJ, Cravero JP; Pediatric Sedation Research Consortium. Emergency physician-administered propofol sedation: a report on 25,433 sedations from the pediatric sedation research consortium. Ann Emerg Med. 2011;57(5):462-468.e1. doi:10.1016/j.annemergmed.2011.03.008.
16. Green SM, Roback MG, Kennedy RM, Krauss B. Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update. Ann Emerg Med. 2011;57(5):449-461. doi:10.1016/j.annemergmed.2010.11.030.
17. Green SM, Roback MG, Krauss B, et al; Emergency Department Ketamine Meta-Analysis Study Group. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54(2):158-168.e1-4. doi:10.1016/j.annemergmed.2008.12.011.
18. Von der Brelie C, Seifert M, Rot S, et al. Sedation of patients with acute aneurysmal subarachnoid hemorrhage with ketamine is safe and might influence the occurrence of cerebral infarctions associated with delayed cerebral ischemia. World Neurosurg. 2017;97:374-382. doi:10.1016/j.wneu.2016.09.121.
19. Langston WT, Wathen JE, Roback MG, Bajaj L. Effect of ondansetron on the incidence of vomiting associated with ketamine sedation in children: a double-blind, randomized, placebo-controlled trial. Ann Emerg Med. 2008;52(1):30-34. doi:10.1016/j.annemergmed.2008.01.326.
20. Babl FE, Oakley E, Seaman C, Barnett P, Sharwood LN. High-concentration nitrous oxide for procedural sedation in children: adverse events and depth of sedation. Pediatrics. 2008;121(3):e528-e532. doi:10.1542/peds.2007-1044.
21. Henry RJ, Ruano N, Casto D, Wolf RH. A pharmacokinetic study of midazolam in dogs: nasal drop vs. atomizer administration. Pediatr Dent. 1998;20(5):321-326.
22. Klein EJ, Brown JC, Kobayashi A, Osincup D, Seidel K. A randomized clinical trial comparing oral, aerosolized intranasal, and aerosolized buccal midazolam. Ann Emerg Med. 2011;58(4):323-329. doi:10.1016/j.annemergmed.2011.05.016.
23. Rey E, Delaunay L, Pons G, et al. Pharmacokinetics of midazolam in children: comparative study of intranasal and intravenous administration. Eur J Clin Pharmacol. 1991;41(4):355-357. doi:10.1007/BF00314967.
24. Borland M, Jacobs I, King B, O’Brien D. A randomized controlled trial comparing intranasal fentanyl to intravenous morphine for managing acute pain in children in the emergency department. Ann Emerg Med. 2007;49(3):335-340. doi:10.1016/j.annemergmed.2006.06.016.
25. Cole J, Shepherd M, Young P. Intranasal fentanyl in 1-3-year-olds: a prospective study of the effectiveness of intranasal fentanyl as acute analgesia. Emerg Med Australas. 2009;21(5):395-400. doi:10.1111/j.1742-6723.2009.01216.x.

Pediatric Heat-Related Illnesses
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
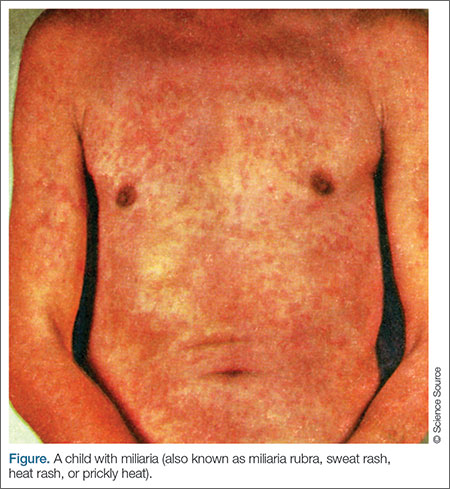
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
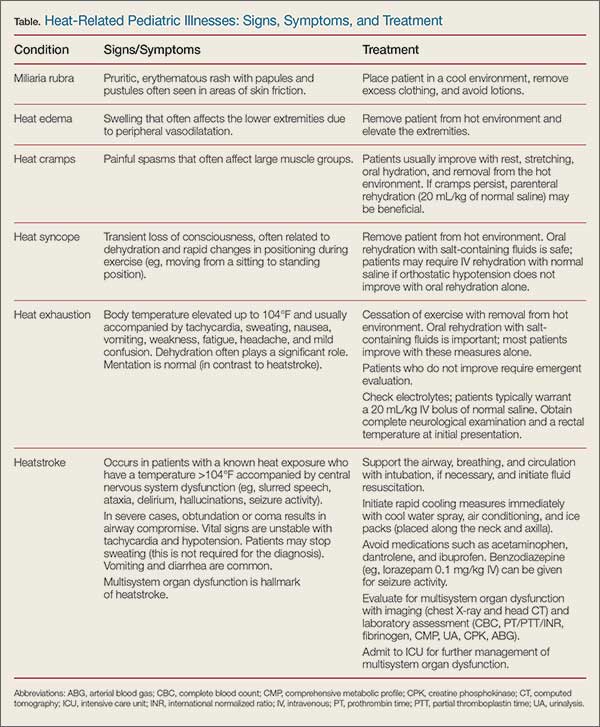
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.

Current Management of Acute Bronchiolitis: An Evidence-Based Approach
Case
An 8-week-old male infant was brought to the ED by his parents after an episode in which it appeared the baby had stopped breathing. The parents stated that while lying on his mother’s lap at home, the patient stopped breathing for approximately 10 to 15 seconds, during which time his face exhibited a bluish color. They further noted that the patient began breathing again after gentle stimulation and had been acting normally since.
The patient was born at 39 weeks gestation via normal vaginal delivery and without any complications. His parents further stated that prior to the cessation of breathing incident, his symptoms of nasal congestion, decreased energy level, and fast breathing had gradually worsened over the past 2 days. The parents also noted that the infant had not been feeding as well over the past 2 days.
Upon arrival, the patient’s vital signs were: heart rate, 140 beats/minute; respiratory rate (RR), 72 beats/minute; and temperature 101.3°F. Oxygen saturation was 92% on room air. On physical examination, the infant had significant rhinorrhea, moderate intercostal and supraclavicular retractions, ausculatory wheezes, and transmitted upper airway noises throughout.
Overview
Bronchiolitis, a disorder caused by a viral lower respiratory tract infection, is the most common lower respiratory infection in children younger than age 2 years.1 In 2014, the American Academy of Pediatrics (AAP) characterized bronchiolitis as “rhinitis, cough, tachypnea, wheezing, rales, use of accessory muscles, and/or nasal flaring in children under 24 months of age.”2 This condition is the most common cause of hospitalization in the first 12 months of life. It is responsible for over 100,000 admissions annually at an estimated cost to the healthcare system of $1.73 billion.3
Etiology and Pathophysiology
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis. In the United States, the highest incidence of infection occurs during the months of December through March, with some degree of regional variability.4 A number of other viruses that can cause bronchiolitis include human metapneumovirus, parainfluenza virus, and influenza virus.1 Infection with RSV does not grant permanent immunity, and reinfection is common throughout life.2
Pathophysiologically, bronchiolitis is characterized by an invasion of bronchial epithelial cells that lead to to cell death and sloughing into the bronchial lumen. This, coupled with increased mucous production and submucosal edema, leads to a narrowing of the bronchial lumen and obstruction of airflow.5
Clinical Manifestations
Bronchiolitis represents a constellation of signs and symptoms beginning with those of an upper respiratory tract infection, including nasal congestion and rhinorrhea with mild cough. On days 3 to 5, the following symptoms develop: tachypnea, wheezing, rales, and signs of respiratory distress (eg, grunting, nasal flaring, inter-/subcostal retractions). Approximately two-thirds of patients will develop a fever.2 Recovery tends to begin around days 5 to 7, with the median duration of illness being 12 days.1 It should be noted that bronchiolitis represents a highly variable and dynamic disease state. Transient episodes of improvement and worsening are common, emphasizing the importance of serial examinations and assessments. Though rare, progression to respiratory failure and death do occur.2
History and Risk Stratification
The focus of the initial history by the clinician should serve two primary purposes. First, it is important to differentiate infants with probable bronchiolitis from those with other disease states having similar clinical manifestations. One of the most challenging diseases to differentiate from bronchiolitis is that of reactive airway disease (RAD). Eliciting a history of allergic rhinitis, eczema, or a family history of asthma may be helpful in determining the precise etiology of the patient’s symptoms. Although no longer recommended for children with bronchiolitis (as will be later discussed), a trial of a bronchodilation may be beneficial in the setting of familial atopy.
The second—and perhaps most important—aspect of patient history is to determine the presence of risk factors for both apnea and the development of severe bronchiolitis. Regarding the risk factors for apnea, Willwerth et al6 developed a set of criteria to identify patients at high risk for apnea in the inpatient setting. Patients were considered high risk if they were born at full term and were younger than 1 month of age; if they were born preterm (<37 weeks gestation) and were younger than 48 weeks postconception; and/or if the infant’s parents or a clinician had already witnessed an episode of apnea during the patient’s illness. In this study, all patients who developed apnea were correctly identified by the risk criteria.6 Risk factors for severe bronchiolitis include the following: patient age younger than 12 weeks; patient prematurity younger than 37 weeks gestation; and an underlying hemodynamically significant congenital heart disease, chronic lung disease/bronchopulmonary dysplasia, or an immunocompromised state.1
Diagnosis
In 2014, the AAP updated its guidelines on the diagnosis, management, and prevention of bronchiolitis. One of the strongest statements in these guidelines emphasize that the diagnosis of bronchiolitis should be based almost exclusively on the history and physical examination.2 In children younger than age 2 years, historical features such as a viral prodrome, followed by progressively worsening increased respiratory effort and signs and symptoms of lower respiratory-tract disease (eg, wheezing), should guide clinicians to the diagnosis of bronchiolitis. Although nonspecific, physical examination findings such as rhinorrhea, cough, tachypnea, wheezing, rales, and increased respiratory effort—when coupled with a good history—can be beneficial in the diagnosis of bronchiolitis.
Pulse Oximetry
Pulse oximetry has become a standard part of the clinical assessment of patients with bronchiolitis. This is based on data suggesting that pulse oximetry detects hypoxia in cases where it was not suspected on physical examination alone.7 However, the effectiveness of pulse oximetry in predicting clinical outcomes is limited. Pulse oximetry should not be used as a proxy for respiratory distress, as studies have shown poor correlation between respiratory distress and oxygen saturations in infants with lower respiratory tract infection.8
Radiographic Evaluation
Regarding the diagnosis of bronchiolitis, the AAP notes, “radiographic and laboratory studies should not be obtained routinely.”2 While many children with bronchiolitis may have abnormalities on radiographs, there is insufficient data to suggest that chest radiographs correlate with disease severity. In addition, several studies, including a prospective cohort study by Schuh et al,9 have shown that infants with suspected lower respiratory tract infections who undergo radiography are more likely to receive antibiotics without any difference in outcomes.
Laboratory Studies
As stated in the AAP guidelines, routine laboratory testing, particularly virologic studies for RSV, have little role in the diagnosis of bronchiolitis. Since numerous viruses can cause bronchiolitis and have similar clinical presentations, the absence of identification of a particular virologic agent does not exclude the diagnosis of bronchiolitis and is moreover unlikely to alter management.
Although routine laboratory evaluation is not recommended in infants with bronchiolitis, one subgroup in which it may be beneficial is in the assessment of serious bacterial infections (SBIs) in febrile infants with bronchiolitis who are younger than 60 days old. Levine et al10 conducted a large, multicenter, prospective, cross-sectional study of young, febrile infants to determine the risk of SBI in those with RSV bronchiolitis versus those without RSV bronchiolitis. They found that overall febrile infants younger than age 60 days with RSV bronchiolitis have a lower rate of SBI than those without RSV (7% v 12.5%, respectively).10 In infants between age 28 and 60 days with RSV bronchiolitis, the origin of all SBIs in the study were urinary tract infections. In patients younger than 28 days of age, the risk of developing an SBI was found to be no different between the RSV-positive and RSV-negative groups.10
Based on the findings in this study, it is recommended that, at the very least, urinalysis for bacterial infection be performed in all infants with RSV bronchiolitis who are younger than age 60 days. Furthermore, since there was no difference in the rates of SBI in patients younger than age 28 days, infants in this age range should undergo a full septic work-up (blood, urine, and cerebrospinal fluid)—regardless of RSV infection status. For infants between ages 28 and 60 days, there is not enough evidence to recommend for or against further laboratory evaluation other than urinalysis.
Treatment


Nasal Suctioning
Nasal suctioning has become the first-line treatment for infants with bronchiolitis. It is used to clear secretions from the nasal passages to aid in respiration, which is particularly important in younger infants—who are obligate nose breathers. Current recommendations are to perform suctioning with increasing respiratory effort, before feeding and before laying the infant down to sleep.1
Bronchodilators
In the past, bronchodilators such as the β-agonist albuterol have been used to treat bronchiolitis with the idea that bronchial smooth muscle relaxation would improve clinical symptoms. In its 2006 guidelines, the AAP had recommended a trial of albuterol and continuation only if there was a documented objective response. In the 2014 updated guidelines, however, the AAP no longer recommends the use of albuterol in any capacity.
Although several meta-analyses and systematic reviews have demonstrated that bronchodilators may improve clinical symptoms scores, they did not affect disease resolution, need for hospitalization, or length of hospital stay.2 In addition, a recent Cochrane systematic review noted no benefit in the clinical course of infants with bronchiolitis treated with bronchodilators, and cited the potential adverse events (tachycardia and tremors) as outweighing any potential benefit.11 In addition to albuterol, the AAP no longer recommends the use of nebulized epinephrine in the treatment of bronchiolitis.2
Hypertonic Saline
Although hypertonic saline (HTS) has been increasingly studied for the treatment of bronchiolitis, the AAP does not recommend its use in the ED. Despite evidence that HTS may reduce hospital length of stay after 24 hours of use in settings where the typical duration of hospitalization exceeds 3 days, it has not been shown to reduce the rate of hospitalization when used in an emergency setting.2
Corticosteroids
While there is good evidence that corticosteroids are beneficial in treating some respiratory diseases, such as asthma and croup, numerous studies have repeatedly failed to show a benefit in treating bronchiolitis. One of the largest studies, a multicenter, randomized, controlled trial of dexamethasone for bronchiolitis by the Pediatric Emergency Care Applied Research Network, did not show any alteration in admission rates, respiratory status after 4 hours of observation, or length of hospital stay.12 Accordingly, the AAP strongly recommends against the administration of corticosteroids for bronchiolitis in any setting.2
Oxygen Therapy
Oxygen therapy is often necessary in patients with bronchiolitis who demonstrate hypoxia. The definition of hypoxia in this patient population has remained variable. The AAP has established a threshold of oxyhemoglobin saturation (SpO2) of less than 90% to define hypoxia and has empowered clinicians to not administer oxygen if the SpO2 exceeds 90%. Based on the oxyhemoglobin dissociation curve, the authors of the AAP guidelines note that when the SpO2 is less than 90%, small decreases in the arterial partial pressure of oxygen (PaO2) result in large decreases in the SpO2. When SpO2 is greater than 90%, however, large increases in PaO2 are associated with only small increased in SpO2. The AAP guidelines note, “In infants and children with bronchiolitis, no data exist to suggest that such increases [in PaO2 and SpO2] result in any clinically significant differences in physiologic function, patient symptoms, or clinical outcomes.”2
A relatively new method of administration of oxygen to infants with bronchiolitis is via a humidified, heated, high-flow nasal cannula (HHHFNC). This therapy has been shown to generate continuous positive airway pressure, which improves respiratory effort, reduces the work of breathing, and may decrease the need for intubation.2
Patient Disposition
One of the most challenging tasks for emergency physicians (EPs) is determining the appropriate disposition of infants with bronchiolitis. The variable presentation and dynamic nature of the disease make this particularly difficult. Patients at high risk for apnea should be admitted to the hospital for observation and further care as needed. Admission also should be strongly considered for those with significantly increased work of breathing and tachypnea that does not improve with suctioning—especially when these interfere with feeding. Infants with poor feeding or evidence of dehydration should be admitted to the hospital for intravenous (IV) fluid hydration or nasogastric feedings. Patients with hypoxia (SpO2 saturations <90%) should also be admitted for supplemental oxygen therapy. It should be noted, however, the AAP recommends “spot-checks” over continuous pulse oximetry in patients who do not require oxygen therapy.2
Another important factor affecting patient disposition is the ability of the caregiver to provide basic patient care and ensure close outpatient follow-up. Prior to discharge, caregivers should be educated on the highly dynamic nature of bronchiolitis and the signs and symptoms that would require prompt return to the ED—especially if the infant has risk factors for the development of severe disease.
Case Conclusion
Based on the patient’s symptoms, history (most notably, the recent incident of sleep apnea at home), and physical examination, the EP quickly identified this infant was at a high risk for both severe bronchiolitis and apnea and required aggressive management. Nasal suctioning was immediately performed to help clear the patient’s secretions; this, however, only slightly improved his RR and work of breathing. Although the infant’s SpO2 was greater than 90% on room air, the EP administered oxygen via HHHFNC at 6 L per minute, which produced a significant improvement in both RR and effort.
Given the patient’s age and the presence of a fever, a urinalysis was also obtained, the results of which showed no evidence of infection. Since the patient was only able to bottle-feed for a few minutes at a time, the EP initiated IV fluid hydration and contacted the hospitalist team for inpatient admission.
The infant was gradually weaned from HHHFNC on hospital day 2 but remained with suboptimal oral intake for another 24 hours. By hospital day 4, his work of breathing had improved significantly, and he was feeding well with through the assistance of pre-feeding nasal syringe suctioning. The patient was discharged home in the care of his parents later that same day with only mild tachypnea over baseline. At discharge, the EP emphasized the importance of providing close follow-up with their son’s pediatrician. The infant continued to gradually improve as an outpatient, with resolution of nasal congestion by day 12 of his illness; he returned to his baseline breathing and feeding pattern on day 14.
Dr Schneider is a pediatric emergency medicine fellow, Eastern Virginia Medical School, Children’s Hospital of The King’s Daughters, Norfolk. Dr Clingenpeel is a fellowship director of pediatric emergency medicine, and an associate professor of pediatrics, Eastern Virginia Medical School, Norfolk.
- Joseph M. Evidence-based assessment and management of acute bronchiolitis in the emergency department. Pediatr Emerg Med Pract. 2011;8(3):1-20.
- Ralston SL, Lieberthal AS, Meissner HC, et al; American Academy of Pediatrics. Clinical practice guidelines: the diagnosis, management, and prevention of bronchiolitis [Published correction appears in Pediatrics. 2014;134(5):e1474-e1502]. Pediatrics. 2014;134:5 e1474-e1502.
- Hasegawa K, Tsugawa Y, Brown DF, Mansbach JM, Camargo CA Jr. Trends in bronchiolitis hospitalizations in the United States, 2000-20009. Pediatrics. 2013;32(1):28-36.
- Centers for Disease Control and Prevention (CDC). Respiratory syncytial virus activity—United States, July 2011-January 2013. MMWR Morb Mortal Wkly Rep. 2013;62(8):141-144.
- Harper MB, Fleisher GR. Infectious emergencies. In: Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2010:916-917.
- Willwerth BM, Harper MB, Greenes DS. Identifying hospitalized infants who have bronchiolitis and are at high risk for apnea. Ann Emerg Med. 2006;48(4):441-447.
- Shaw KN, Bell LM, Sherman NH. Outpatient assessment of infants with bronchiolitis. Am J Dis Child. 1991;145(2):151-155.
- Wang EE, Milner RA, Navas L, Maj H. Observer agreement for respiratory signs and oximetry in infants hospitalized with lower respiratory infections. Am Rev Respir Dis. 1992;145(1):106-109.
- Schuh S, Lalani A, Allen U, et al. Evaluation of the utility of radiography in acute bronchiolitis. J Pediatr. 2007;150(4):429-433.
- Levine DA, Platt SL, Dayan PS, et al; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infection. Pediatrics. 2004;113(6):1728-1734.
- Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;(6):CD001266.
- Corneli HM, Zorc JJ, Majahan P, et al; Bronchiolitis Study Group of the Pediatric Emergency Care Applied Research Network (PECARN). A multicenter, randomized, controlled trial of dexamethasone for bronchiolitis. N Engl J Med. 2007;357(4):331-339.
Case
An 8-week-old male infant was brought to the ED by his parents after an episode in which it appeared the baby had stopped breathing. The parents stated that while lying on his mother’s lap at home, the patient stopped breathing for approximately 10 to 15 seconds, during which time his face exhibited a bluish color. They further noted that the patient began breathing again after gentle stimulation and had been acting normally since.
The patient was born at 39 weeks gestation via normal vaginal delivery and without any complications. His parents further stated that prior to the cessation of breathing incident, his symptoms of nasal congestion, decreased energy level, and fast breathing had gradually worsened over the past 2 days. The parents also noted that the infant had not been feeding as well over the past 2 days.
Upon arrival, the patient’s vital signs were: heart rate, 140 beats/minute; respiratory rate (RR), 72 beats/minute; and temperature 101.3°F. Oxygen saturation was 92% on room air. On physical examination, the infant had significant rhinorrhea, moderate intercostal and supraclavicular retractions, ausculatory wheezes, and transmitted upper airway noises throughout.
Overview
Bronchiolitis, a disorder caused by a viral lower respiratory tract infection, is the most common lower respiratory infection in children younger than age 2 years.1 In 2014, the American Academy of Pediatrics (AAP) characterized bronchiolitis as “rhinitis, cough, tachypnea, wheezing, rales, use of accessory muscles, and/or nasal flaring in children under 24 months of age.”2 This condition is the most common cause of hospitalization in the first 12 months of life. It is responsible for over 100,000 admissions annually at an estimated cost to the healthcare system of $1.73 billion.3
Etiology and Pathophysiology
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis. In the United States, the highest incidence of infection occurs during the months of December through March, with some degree of regional variability.4 A number of other viruses that can cause bronchiolitis include human metapneumovirus, parainfluenza virus, and influenza virus.1 Infection with RSV does not grant permanent immunity, and reinfection is common throughout life.2
Pathophysiologically, bronchiolitis is characterized by an invasion of bronchial epithelial cells that lead to to cell death and sloughing into the bronchial lumen. This, coupled with increased mucous production and submucosal edema, leads to a narrowing of the bronchial lumen and obstruction of airflow.5
Clinical Manifestations
Bronchiolitis represents a constellation of signs and symptoms beginning with those of an upper respiratory tract infection, including nasal congestion and rhinorrhea with mild cough. On days 3 to 5, the following symptoms develop: tachypnea, wheezing, rales, and signs of respiratory distress (eg, grunting, nasal flaring, inter-/subcostal retractions). Approximately two-thirds of patients will develop a fever.2 Recovery tends to begin around days 5 to 7, with the median duration of illness being 12 days.1 It should be noted that bronchiolitis represents a highly variable and dynamic disease state. Transient episodes of improvement and worsening are common, emphasizing the importance of serial examinations and assessments. Though rare, progression to respiratory failure and death do occur.2
History and Risk Stratification
The focus of the initial history by the clinician should serve two primary purposes. First, it is important to differentiate infants with probable bronchiolitis from those with other disease states having similar clinical manifestations. One of the most challenging diseases to differentiate from bronchiolitis is that of reactive airway disease (RAD). Eliciting a history of allergic rhinitis, eczema, or a family history of asthma may be helpful in determining the precise etiology of the patient’s symptoms. Although no longer recommended for children with bronchiolitis (as will be later discussed), a trial of a bronchodilation may be beneficial in the setting of familial atopy.
The second—and perhaps most important—aspect of patient history is to determine the presence of risk factors for both apnea and the development of severe bronchiolitis. Regarding the risk factors for apnea, Willwerth et al6 developed a set of criteria to identify patients at high risk for apnea in the inpatient setting. Patients were considered high risk if they were born at full term and were younger than 1 month of age; if they were born preterm (<37 weeks gestation) and were younger than 48 weeks postconception; and/or if the infant’s parents or a clinician had already witnessed an episode of apnea during the patient’s illness. In this study, all patients who developed apnea were correctly identified by the risk criteria.6 Risk factors for severe bronchiolitis include the following: patient age younger than 12 weeks; patient prematurity younger than 37 weeks gestation; and an underlying hemodynamically significant congenital heart disease, chronic lung disease/bronchopulmonary dysplasia, or an immunocompromised state.1
Diagnosis
In 2014, the AAP updated its guidelines on the diagnosis, management, and prevention of bronchiolitis. One of the strongest statements in these guidelines emphasize that the diagnosis of bronchiolitis should be based almost exclusively on the history and physical examination.2 In children younger than age 2 years, historical features such as a viral prodrome, followed by progressively worsening increased respiratory effort and signs and symptoms of lower respiratory-tract disease (eg, wheezing), should guide clinicians to the diagnosis of bronchiolitis. Although nonspecific, physical examination findings such as rhinorrhea, cough, tachypnea, wheezing, rales, and increased respiratory effort—when coupled with a good history—can be beneficial in the diagnosis of bronchiolitis.
Pulse Oximetry
Pulse oximetry has become a standard part of the clinical assessment of patients with bronchiolitis. This is based on data suggesting that pulse oximetry detects hypoxia in cases where it was not suspected on physical examination alone.7 However, the effectiveness of pulse oximetry in predicting clinical outcomes is limited. Pulse oximetry should not be used as a proxy for respiratory distress, as studies have shown poor correlation between respiratory distress and oxygen saturations in infants with lower respiratory tract infection.8
Radiographic Evaluation
Regarding the diagnosis of bronchiolitis, the AAP notes, “radiographic and laboratory studies should not be obtained routinely.”2 While many children with bronchiolitis may have abnormalities on radiographs, there is insufficient data to suggest that chest radiographs correlate with disease severity. In addition, several studies, including a prospective cohort study by Schuh et al,9 have shown that infants with suspected lower respiratory tract infections who undergo radiography are more likely to receive antibiotics without any difference in outcomes.
Laboratory Studies
As stated in the AAP guidelines, routine laboratory testing, particularly virologic studies for RSV, have little role in the diagnosis of bronchiolitis. Since numerous viruses can cause bronchiolitis and have similar clinical presentations, the absence of identification of a particular virologic agent does not exclude the diagnosis of bronchiolitis and is moreover unlikely to alter management.
Although routine laboratory evaluation is not recommended in infants with bronchiolitis, one subgroup in which it may be beneficial is in the assessment of serious bacterial infections (SBIs) in febrile infants with bronchiolitis who are younger than 60 days old. Levine et al10 conducted a large, multicenter, prospective, cross-sectional study of young, febrile infants to determine the risk of SBI in those with RSV bronchiolitis versus those without RSV bronchiolitis. They found that overall febrile infants younger than age 60 days with RSV bronchiolitis have a lower rate of SBI than those without RSV (7% v 12.5%, respectively).10 In infants between age 28 and 60 days with RSV bronchiolitis, the origin of all SBIs in the study were urinary tract infections. In patients younger than 28 days of age, the risk of developing an SBI was found to be no different between the RSV-positive and RSV-negative groups.10
Based on the findings in this study, it is recommended that, at the very least, urinalysis for bacterial infection be performed in all infants with RSV bronchiolitis who are younger than age 60 days. Furthermore, since there was no difference in the rates of SBI in patients younger than age 28 days, infants in this age range should undergo a full septic work-up (blood, urine, and cerebrospinal fluid)—regardless of RSV infection status. For infants between ages 28 and 60 days, there is not enough evidence to recommend for or against further laboratory evaluation other than urinalysis.
Treatment
Nasal Suctioning
Nasal suctioning has become the first-line treatment for infants with bronchiolitis. It is used to clear secretions from the nasal passages to aid in respiration, which is particularly important in younger infants—who are obligate nose breathers. Current recommendations are to perform suctioning with increasing respiratory effort, before feeding and before laying the infant down to sleep.1
Bronchodilators
In the past, bronchodilators such as the β-agonist albuterol have been used to treat bronchiolitis with the idea that bronchial smooth muscle relaxation would improve clinical symptoms. In its 2006 guidelines, the AAP had recommended a trial of albuterol and continuation only if there was a documented objective response. In the 2014 updated guidelines, however, the AAP no longer recommends the use of albuterol in any capacity.
Although several meta-analyses and systematic reviews have demonstrated that bronchodilators may improve clinical symptoms scores, they did not affect disease resolution, need for hospitalization, or length of hospital stay.2 In addition, a recent Cochrane systematic review noted no benefit in the clinical course of infants with bronchiolitis treated with bronchodilators, and cited the potential adverse events (tachycardia and tremors) as outweighing any potential benefit.11 In addition to albuterol, the AAP no longer recommends the use of nebulized epinephrine in the treatment of bronchiolitis.2
Hypertonic Saline
Although hypertonic saline (HTS) has been increasingly studied for the treatment of bronchiolitis, the AAP does not recommend its use in the ED. Despite evidence that HTS may reduce hospital length of stay after 24 hours of use in settings where the typical duration of hospitalization exceeds 3 days, it has not been shown to reduce the rate of hospitalization when used in an emergency setting.2
Corticosteroids
While there is good evidence that corticosteroids are beneficial in treating some respiratory diseases, such as asthma and croup, numerous studies have repeatedly failed to show a benefit in treating bronchiolitis. One of the largest studies, a multicenter, randomized, controlled trial of dexamethasone for bronchiolitis by the Pediatric Emergency Care Applied Research Network, did not show any alteration in admission rates, respiratory status after 4 hours of observation, or length of hospital stay.12 Accordingly, the AAP strongly recommends against the administration of corticosteroids for bronchiolitis in any setting.2
Oxygen Therapy
Oxygen therapy is often necessary in patients with bronchiolitis who demonstrate hypoxia. The definition of hypoxia in this patient population has remained variable. The AAP has established a threshold of oxyhemoglobin saturation (SpO2) of less than 90% to define hypoxia and has empowered clinicians to not administer oxygen if the SpO2 exceeds 90%. Based on the oxyhemoglobin dissociation curve, the authors of the AAP guidelines note that when the SpO2 is less than 90%, small decreases in the arterial partial pressure of oxygen (PaO2) result in large decreases in the SpO2. When SpO2 is greater than 90%, however, large increases in PaO2 are associated with only small increased in SpO2. The AAP guidelines note, “In infants and children with bronchiolitis, no data exist to suggest that such increases [in PaO2 and SpO2] result in any clinically significant differences in physiologic function, patient symptoms, or clinical outcomes.”2
A relatively new method of administration of oxygen to infants with bronchiolitis is via a humidified, heated, high-flow nasal cannula (HHHFNC). This therapy has been shown to generate continuous positive airway pressure, which improves respiratory effort, reduces the work of breathing, and may decrease the need for intubation.2
Patient Disposition
One of the most challenging tasks for emergency physicians (EPs) is determining the appropriate disposition of infants with bronchiolitis. The variable presentation and dynamic nature of the disease make this particularly difficult. Patients at high risk for apnea should be admitted to the hospital for observation and further care as needed. Admission also should be strongly considered for those with significantly increased work of breathing and tachypnea that does not improve with suctioning—especially when these interfere with feeding. Infants with poor feeding or evidence of dehydration should be admitted to the hospital for intravenous (IV) fluid hydration or nasogastric feedings. Patients with hypoxia (SpO2 saturations <90%) should also be admitted for supplemental oxygen therapy. It should be noted, however, the AAP recommends “spot-checks” over continuous pulse oximetry in patients who do not require oxygen therapy.2
Another important factor affecting patient disposition is the ability of the caregiver to provide basic patient care and ensure close outpatient follow-up. Prior to discharge, caregivers should be educated on the highly dynamic nature of bronchiolitis and the signs and symptoms that would require prompt return to the ED—especially if the infant has risk factors for the development of severe disease.
Case Conclusion
Based on the patient’s symptoms, history (most notably, the recent incident of sleep apnea at home), and physical examination, the EP quickly identified this infant was at a high risk for both severe bronchiolitis and apnea and required aggressive management. Nasal suctioning was immediately performed to help clear the patient’s secretions; this, however, only slightly improved his RR and work of breathing. Although the infant’s SpO2 was greater than 90% on room air, the EP administered oxygen via HHHFNC at 6 L per minute, which produced a significant improvement in both RR and effort.
Given the patient’s age and the presence of a fever, a urinalysis was also obtained, the results of which showed no evidence of infection. Since the patient was only able to bottle-feed for a few minutes at a time, the EP initiated IV fluid hydration and contacted the hospitalist team for inpatient admission.
The infant was gradually weaned from HHHFNC on hospital day 2 but remained with suboptimal oral intake for another 24 hours. By hospital day 4, his work of breathing had improved significantly, and he was feeding well with through the assistance of pre-feeding nasal syringe suctioning. The patient was discharged home in the care of his parents later that same day with only mild tachypnea over baseline. At discharge, the EP emphasized the importance of providing close follow-up with their son’s pediatrician. The infant continued to gradually improve as an outpatient, with resolution of nasal congestion by day 12 of his illness; he returned to his baseline breathing and feeding pattern on day 14.
Dr Schneider is a pediatric emergency medicine fellow, Eastern Virginia Medical School, Children’s Hospital of The King’s Daughters, Norfolk. Dr Clingenpeel is a fellowship director of pediatric emergency medicine, and an associate professor of pediatrics, Eastern Virginia Medical School, Norfolk.
Case
An 8-week-old male infant was brought to the ED by his parents after an episode in which it appeared the baby had stopped breathing. The parents stated that while lying on his mother’s lap at home, the patient stopped breathing for approximately 10 to 15 seconds, during which time his face exhibited a bluish color. They further noted that the patient began breathing again after gentle stimulation and had been acting normally since.
The patient was born at 39 weeks gestation via normal vaginal delivery and without any complications. His parents further stated that prior to the cessation of breathing incident, his symptoms of nasal congestion, decreased energy level, and fast breathing had gradually worsened over the past 2 days. The parents also noted that the infant had not been feeding as well over the past 2 days.
Upon arrival, the patient’s vital signs were: heart rate, 140 beats/minute; respiratory rate (RR), 72 beats/minute; and temperature 101.3°F. Oxygen saturation was 92% on room air. On physical examination, the infant had significant rhinorrhea, moderate intercostal and supraclavicular retractions, ausculatory wheezes, and transmitted upper airway noises throughout.
Overview
Bronchiolitis, a disorder caused by a viral lower respiratory tract infection, is the most common lower respiratory infection in children younger than age 2 years.1 In 2014, the American Academy of Pediatrics (AAP) characterized bronchiolitis as “rhinitis, cough, tachypnea, wheezing, rales, use of accessory muscles, and/or nasal flaring in children under 24 months of age.”2 This condition is the most common cause of hospitalization in the first 12 months of life. It is responsible for over 100,000 admissions annually at an estimated cost to the healthcare system of $1.73 billion.3
Etiology and Pathophysiology
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis. In the United States, the highest incidence of infection occurs during the months of December through March, with some degree of regional variability.4 A number of other viruses that can cause bronchiolitis include human metapneumovirus, parainfluenza virus, and influenza virus.1 Infection with RSV does not grant permanent immunity, and reinfection is common throughout life.2
Pathophysiologically, bronchiolitis is characterized by an invasion of bronchial epithelial cells that lead to to cell death and sloughing into the bronchial lumen. This, coupled with increased mucous production and submucosal edema, leads to a narrowing of the bronchial lumen and obstruction of airflow.5
Clinical Manifestations
Bronchiolitis represents a constellation of signs and symptoms beginning with those of an upper respiratory tract infection, including nasal congestion and rhinorrhea with mild cough. On days 3 to 5, the following symptoms develop: tachypnea, wheezing, rales, and signs of respiratory distress (eg, grunting, nasal flaring, inter-/subcostal retractions). Approximately two-thirds of patients will develop a fever.2 Recovery tends to begin around days 5 to 7, with the median duration of illness being 12 days.1 It should be noted that bronchiolitis represents a highly variable and dynamic disease state. Transient episodes of improvement and worsening are common, emphasizing the importance of serial examinations and assessments. Though rare, progression to respiratory failure and death do occur.2
History and Risk Stratification
The focus of the initial history by the clinician should serve two primary purposes. First, it is important to differentiate infants with probable bronchiolitis from those with other disease states having similar clinical manifestations. One of the most challenging diseases to differentiate from bronchiolitis is that of reactive airway disease (RAD). Eliciting a history of allergic rhinitis, eczema, or a family history of asthma may be helpful in determining the precise etiology of the patient’s symptoms. Although no longer recommended for children with bronchiolitis (as will be later discussed), a trial of a bronchodilation may be beneficial in the setting of familial atopy.
The second—and perhaps most important—aspect of patient history is to determine the presence of risk factors for both apnea and the development of severe bronchiolitis. Regarding the risk factors for apnea, Willwerth et al6 developed a set of criteria to identify patients at high risk for apnea in the inpatient setting. Patients were considered high risk if they were born at full term and were younger than 1 month of age; if they were born preterm (<37 weeks gestation) and were younger than 48 weeks postconception; and/or if the infant’s parents or a clinician had already witnessed an episode of apnea during the patient’s illness. In this study, all patients who developed apnea were correctly identified by the risk criteria.6 Risk factors for severe bronchiolitis include the following: patient age younger than 12 weeks; patient prematurity younger than 37 weeks gestation; and an underlying hemodynamically significant congenital heart disease, chronic lung disease/bronchopulmonary dysplasia, or an immunocompromised state.1
Diagnosis
In 2014, the AAP updated its guidelines on the diagnosis, management, and prevention of bronchiolitis. One of the strongest statements in these guidelines emphasize that the diagnosis of bronchiolitis should be based almost exclusively on the history and physical examination.2 In children younger than age 2 years, historical features such as a viral prodrome, followed by progressively worsening increased respiratory effort and signs and symptoms of lower respiratory-tract disease (eg, wheezing), should guide clinicians to the diagnosis of bronchiolitis. Although nonspecific, physical examination findings such as rhinorrhea, cough, tachypnea, wheezing, rales, and increased respiratory effort—when coupled with a good history—can be beneficial in the diagnosis of bronchiolitis.
Pulse Oximetry
Pulse oximetry has become a standard part of the clinical assessment of patients with bronchiolitis. This is based on data suggesting that pulse oximetry detects hypoxia in cases where it was not suspected on physical examination alone.7 However, the effectiveness of pulse oximetry in predicting clinical outcomes is limited. Pulse oximetry should not be used as a proxy for respiratory distress, as studies have shown poor correlation between respiratory distress and oxygen saturations in infants with lower respiratory tract infection.8
Radiographic Evaluation
Regarding the diagnosis of bronchiolitis, the AAP notes, “radiographic and laboratory studies should not be obtained routinely.”2 While many children with bronchiolitis may have abnormalities on radiographs, there is insufficient data to suggest that chest radiographs correlate with disease severity. In addition, several studies, including a prospective cohort study by Schuh et al,9 have shown that infants with suspected lower respiratory tract infections who undergo radiography are more likely to receive antibiotics without any difference in outcomes.
Laboratory Studies
As stated in the AAP guidelines, routine laboratory testing, particularly virologic studies for RSV, have little role in the diagnosis of bronchiolitis. Since numerous viruses can cause bronchiolitis and have similar clinical presentations, the absence of identification of a particular virologic agent does not exclude the diagnosis of bronchiolitis and is moreover unlikely to alter management.
Although routine laboratory evaluation is not recommended in infants with bronchiolitis, one subgroup in which it may be beneficial is in the assessment of serious bacterial infections (SBIs) in febrile infants with bronchiolitis who are younger than 60 days old. Levine et al10 conducted a large, multicenter, prospective, cross-sectional study of young, febrile infants to determine the risk of SBI in those with RSV bronchiolitis versus those without RSV bronchiolitis. They found that overall febrile infants younger than age 60 days with RSV bronchiolitis have a lower rate of SBI than those without RSV (7% v 12.5%, respectively).10 In infants between age 28 and 60 days with RSV bronchiolitis, the origin of all SBIs in the study were urinary tract infections. In patients younger than 28 days of age, the risk of developing an SBI was found to be no different between the RSV-positive and RSV-negative groups.10
Based on the findings in this study, it is recommended that, at the very least, urinalysis for bacterial infection be performed in all infants with RSV bronchiolitis who are younger than age 60 days. Furthermore, since there was no difference in the rates of SBI in patients younger than age 28 days, infants in this age range should undergo a full septic work-up (blood, urine, and cerebrospinal fluid)—regardless of RSV infection status. For infants between ages 28 and 60 days, there is not enough evidence to recommend for or against further laboratory evaluation other than urinalysis.
Treatment
Nasal Suctioning
Nasal suctioning has become the first-line treatment for infants with bronchiolitis. It is used to clear secretions from the nasal passages to aid in respiration, which is particularly important in younger infants—who are obligate nose breathers. Current recommendations are to perform suctioning with increasing respiratory effort, before feeding and before laying the infant down to sleep.1
Bronchodilators
In the past, bronchodilators such as the β-agonist albuterol have been used to treat bronchiolitis with the idea that bronchial smooth muscle relaxation would improve clinical symptoms. In its 2006 guidelines, the AAP had recommended a trial of albuterol and continuation only if there was a documented objective response. In the 2014 updated guidelines, however, the AAP no longer recommends the use of albuterol in any capacity.
Although several meta-analyses and systematic reviews have demonstrated that bronchodilators may improve clinical symptoms scores, they did not affect disease resolution, need for hospitalization, or length of hospital stay.2 In addition, a recent Cochrane systematic review noted no benefit in the clinical course of infants with bronchiolitis treated with bronchodilators, and cited the potential adverse events (tachycardia and tremors) as outweighing any potential benefit.11 In addition to albuterol, the AAP no longer recommends the use of nebulized epinephrine in the treatment of bronchiolitis.2
Hypertonic Saline
Although hypertonic saline (HTS) has been increasingly studied for the treatment of bronchiolitis, the AAP does not recommend its use in the ED. Despite evidence that HTS may reduce hospital length of stay after 24 hours of use in settings where the typical duration of hospitalization exceeds 3 days, it has not been shown to reduce the rate of hospitalization when used in an emergency setting.2
Corticosteroids
While there is good evidence that corticosteroids are beneficial in treating some respiratory diseases, such as asthma and croup, numerous studies have repeatedly failed to show a benefit in treating bronchiolitis. One of the largest studies, a multicenter, randomized, controlled trial of dexamethasone for bronchiolitis by the Pediatric Emergency Care Applied Research Network, did not show any alteration in admission rates, respiratory status after 4 hours of observation, or length of hospital stay.12 Accordingly, the AAP strongly recommends against the administration of corticosteroids for bronchiolitis in any setting.2
Oxygen Therapy
Oxygen therapy is often necessary in patients with bronchiolitis who demonstrate hypoxia. The definition of hypoxia in this patient population has remained variable. The AAP has established a threshold of oxyhemoglobin saturation (SpO2) of less than 90% to define hypoxia and has empowered clinicians to not administer oxygen if the SpO2 exceeds 90%. Based on the oxyhemoglobin dissociation curve, the authors of the AAP guidelines note that when the SpO2 is less than 90%, small decreases in the arterial partial pressure of oxygen (PaO2) result in large decreases in the SpO2. When SpO2 is greater than 90%, however, large increases in PaO2 are associated with only small increased in SpO2. The AAP guidelines note, “In infants and children with bronchiolitis, no data exist to suggest that such increases [in PaO2 and SpO2] result in any clinically significant differences in physiologic function, patient symptoms, or clinical outcomes.”2
A relatively new method of administration of oxygen to infants with bronchiolitis is via a humidified, heated, high-flow nasal cannula (HHHFNC). This therapy has been shown to generate continuous positive airway pressure, which improves respiratory effort, reduces the work of breathing, and may decrease the need for intubation.2
Patient Disposition
One of the most challenging tasks for emergency physicians (EPs) is determining the appropriate disposition of infants with bronchiolitis. The variable presentation and dynamic nature of the disease make this particularly difficult. Patients at high risk for apnea should be admitted to the hospital for observation and further care as needed. Admission also should be strongly considered for those with significantly increased work of breathing and tachypnea that does not improve with suctioning—especially when these interfere with feeding. Infants with poor feeding or evidence of dehydration should be admitted to the hospital for intravenous (IV) fluid hydration or nasogastric feedings. Patients with hypoxia (SpO2 saturations <90%) should also be admitted for supplemental oxygen therapy. It should be noted, however, the AAP recommends “spot-checks” over continuous pulse oximetry in patients who do not require oxygen therapy.2
Another important factor affecting patient disposition is the ability of the caregiver to provide basic patient care and ensure close outpatient follow-up. Prior to discharge, caregivers should be educated on the highly dynamic nature of bronchiolitis and the signs and symptoms that would require prompt return to the ED—especially if the infant has risk factors for the development of severe disease.
Case Conclusion
Based on the patient’s symptoms, history (most notably, the recent incident of sleep apnea at home), and physical examination, the EP quickly identified this infant was at a high risk for both severe bronchiolitis and apnea and required aggressive management. Nasal suctioning was immediately performed to help clear the patient’s secretions; this, however, only slightly improved his RR and work of breathing. Although the infant’s SpO2 was greater than 90% on room air, the EP administered oxygen via HHHFNC at 6 L per minute, which produced a significant improvement in both RR and effort.
Given the patient’s age and the presence of a fever, a urinalysis was also obtained, the results of which showed no evidence of infection. Since the patient was only able to bottle-feed for a few minutes at a time, the EP initiated IV fluid hydration and contacted the hospitalist team for inpatient admission.
The infant was gradually weaned from HHHFNC on hospital day 2 but remained with suboptimal oral intake for another 24 hours. By hospital day 4, his work of breathing had improved significantly, and he was feeding well with through the assistance of pre-feeding nasal syringe suctioning. The patient was discharged home in the care of his parents later that same day with only mild tachypnea over baseline. At discharge, the EP emphasized the importance of providing close follow-up with their son’s pediatrician. The infant continued to gradually improve as an outpatient, with resolution of nasal congestion by day 12 of his illness; he returned to his baseline breathing and feeding pattern on day 14.
Dr Schneider is a pediatric emergency medicine fellow, Eastern Virginia Medical School, Children’s Hospital of The King’s Daughters, Norfolk. Dr Clingenpeel is a fellowship director of pediatric emergency medicine, and an associate professor of pediatrics, Eastern Virginia Medical School, Norfolk.
- Joseph M. Evidence-based assessment and management of acute bronchiolitis in the emergency department. Pediatr Emerg Med Pract. 2011;8(3):1-20.
- Ralston SL, Lieberthal AS, Meissner HC, et al; American Academy of Pediatrics. Clinical practice guidelines: the diagnosis, management, and prevention of bronchiolitis [Published correction appears in Pediatrics. 2014;134(5):e1474-e1502]. Pediatrics. 2014;134:5 e1474-e1502.
- Hasegawa K, Tsugawa Y, Brown DF, Mansbach JM, Camargo CA Jr. Trends in bronchiolitis hospitalizations in the United States, 2000-20009. Pediatrics. 2013;32(1):28-36.
- Centers for Disease Control and Prevention (CDC). Respiratory syncytial virus activity—United States, July 2011-January 2013. MMWR Morb Mortal Wkly Rep. 2013;62(8):141-144.
- Harper MB, Fleisher GR. Infectious emergencies. In: Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2010:916-917.
- Willwerth BM, Harper MB, Greenes DS. Identifying hospitalized infants who have bronchiolitis and are at high risk for apnea. Ann Emerg Med. 2006;48(4):441-447.
- Shaw KN, Bell LM, Sherman NH. Outpatient assessment of infants with bronchiolitis. Am J Dis Child. 1991;145(2):151-155.
- Wang EE, Milner RA, Navas L, Maj H. Observer agreement for respiratory signs and oximetry in infants hospitalized with lower respiratory infections. Am Rev Respir Dis. 1992;145(1):106-109.
- Schuh S, Lalani A, Allen U, et al. Evaluation of the utility of radiography in acute bronchiolitis. J Pediatr. 2007;150(4):429-433.
- Levine DA, Platt SL, Dayan PS, et al; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infection. Pediatrics. 2004;113(6):1728-1734.
- Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;(6):CD001266.
- Corneli HM, Zorc JJ, Majahan P, et al; Bronchiolitis Study Group of the Pediatric Emergency Care Applied Research Network (PECARN). A multicenter, randomized, controlled trial of dexamethasone for bronchiolitis. N Engl J Med. 2007;357(4):331-339.
- Joseph M. Evidence-based assessment and management of acute bronchiolitis in the emergency department. Pediatr Emerg Med Pract. 2011;8(3):1-20.
- Ralston SL, Lieberthal AS, Meissner HC, et al; American Academy of Pediatrics. Clinical practice guidelines: the diagnosis, management, and prevention of bronchiolitis [Published correction appears in Pediatrics. 2014;134(5):e1474-e1502]. Pediatrics. 2014;134:5 e1474-e1502.
- Hasegawa K, Tsugawa Y, Brown DF, Mansbach JM, Camargo CA Jr. Trends in bronchiolitis hospitalizations in the United States, 2000-20009. Pediatrics. 2013;32(1):28-36.
- Centers for Disease Control and Prevention (CDC). Respiratory syncytial virus activity—United States, July 2011-January 2013. MMWR Morb Mortal Wkly Rep. 2013;62(8):141-144.
- Harper MB, Fleisher GR. Infectious emergencies. In: Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2010:916-917.
- Willwerth BM, Harper MB, Greenes DS. Identifying hospitalized infants who have bronchiolitis and are at high risk for apnea. Ann Emerg Med. 2006;48(4):441-447.
- Shaw KN, Bell LM, Sherman NH. Outpatient assessment of infants with bronchiolitis. Am J Dis Child. 1991;145(2):151-155.
- Wang EE, Milner RA, Navas L, Maj H. Observer agreement for respiratory signs and oximetry in infants hospitalized with lower respiratory infections. Am Rev Respir Dis. 1992;145(1):106-109.
- Schuh S, Lalani A, Allen U, et al. Evaluation of the utility of radiography in acute bronchiolitis. J Pediatr. 2007;150(4):429-433.
- Levine DA, Platt SL, Dayan PS, et al; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Risk of serious bacterial infection in young febrile infants with respiratory syncytial virus infection. Pediatrics. 2004;113(6):1728-1734.
- Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;(6):CD001266.
- Corneli HM, Zorc JJ, Majahan P, et al; Bronchiolitis Study Group of the Pediatric Emergency Care Applied Research Network (PECARN). A multicenter, randomized, controlled trial of dexamethasone for bronchiolitis. N Engl J Med. 2007;357(4):331-339.
