User login
Erythematous penile lesion
A 63-YEAR-OLD MAN came to our clinic complaining of a rash on his penis. He indicated that the rash had been there for almost 2 years and that he’d seen 2 other doctors about it, but they’d been unable to make a diagnosis.
The patient said the rash was mildly painful and tender. He denied pain on urination, discharge, fever, malaise, or arthralgias. He also denied any sexual contact outside of his marriage and indicated that he had not been able to have intimate contact with his wife because of the problem.
The patient was uncircumcised and when the foreskin was retracted, a bright red erythematous nonscaly circumferential plaque was visible on the glans penis, spreading to the foreskin (FIGURE 1).
FIGURE 1
A nonscaly, circumferential plaque on the glans penis
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Zoon’s balanitis
We ordered a biopsy because we suspected that the cause of the rash was either erythroplasia of Queyrat (a premalignant condition also known as Bowen’s disease of the glans penis) or Zoon’s balanitis (plasma cell balanitis or balanitis circumscripta plasmacellularis). The biopsy report confirmed the diagnosis of Zoon’s balanitis and showed no signs of malignancy. The features of Zoon’s balanitis include epidermal atrophy, loss of rete ridges, spongiosis, and subepidermal plasma cell infiltrate without evidence of malignancy (FIGURE 2).
FIGURE 2
Dense plasmacytic infiltration underlying the mucosal epidermis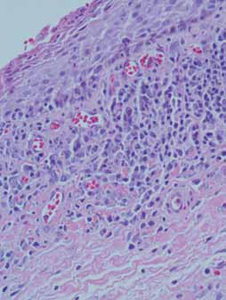
Condition affects older, uncircumcised men
Zoon’s balanitis is thought to be a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The differential for penile lesions is extensive, and includes psoriasis, nummular eczema, candidiasis, herpes simplex, scabies, lichen sclerosus et atrophicus or lichen planus, syphilis, balanitis, and erythroplasia of Queyrat.
The lesion associated with Zoon’s balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
Patients with erythroplasia of Queyrat have either a solitary or multiple nonhealing erythematous plaques on the glans penis. These lesions may also affect the adjacent mucosal epithelium. As is true with Zoon’s balanitis, the typical patient is uncircumcised and middle-aged to elderly.1,2
Presentations may be similar, but treatment differs
Because the treatments for Zoon’s balanitis and erythroplasia of Queyrat are different, a biopsy is imperative. Erythroplasia of Queyrat is a premalignant condition that is treated with topical fluorouracil or surgical excision.3 Treatment for Zoon’s balanitis consists of a topical corticosteroid with or without topical anticandidal agents and circumcision after the acute inflammation resolves.1,2 (If a skin biopsy cannot be obtained in the clinic, the foreskin [if affected] can be sent for biopsy after the circumcision.)
If resolution is not seen with topical steroid treatment, other treatments have demonstrated efficacy. These include topical tacrolimus, as well as YAG and carbon dioxide laser treatments.4-6
Although information is limited on rates of recurrence, circumcision is considered the treatment of choice and is usually curative.1
Ointment does the trick for our patient
Our patient was treated with a single combined topical ointment consisting of nystatin and triamcinolone cream with zinc oxide. The lesion resolved completely after 10 days. We requested a urology consult so that a circumcision could be performed.
CORRESPONDENCE Matthew R. Noss, DO, MSEd, Fort Belvoir Community Hospital Family Medicine Clinic, 1st Floor, Eagle Pavilion, 9300 Dewitt Loop, Ft. Belvoir, VA 22060; [email protected]
1. Scheinfeld NS, Keough GC, Lehman DS. Balanitis circumscripta plasmacellularis. Medscape. June 8, 2012. Available at: emedicine.medscape.com/article/1122283. Accessed October 26, 2012.
2. Barrisford GW. Balanitis and balanoposthitis in adults. UpToDate. December 19, 2011. Available at: www.uptodate.com/contents/balanitis-and-balanoposthitis-in-adults. Accessed October 26, 2012.
3. Egan KM, Maino KL. Erythroplasia of Queyrat (Bowen disease of the glans penis). Medscape. May 31, 2012. Available at: emedicine.medscape.com/article/1100317. Accessed October 26, 2012.
4. Santos-Juanes J, Sanchez del Rio J, Galache C, et al. Topical tacrolimus: an effective therapy for Zoon balanitis. Arch Dermatol. 2004;140:1538-1539.
5. Wollina U. Ablative erbium: YAG laser treatment of idiopathic chronic inflammatory non-cicatricial balanoposthitis (Zoon’s disease)—a series of 20 patients with long-term outcome. J Cosmet Laser Ther. 2010;12:120-123.
6. Retamar RA, Kien MC, Couela EN. Zoon’s balanitis: presentation of 15 patients, five treated with a carbon dioxide laser. Int J Dermatol. 2003;42:305-307.
A 63-YEAR-OLD MAN came to our clinic complaining of a rash on his penis. He indicated that the rash had been there for almost 2 years and that he’d seen 2 other doctors about it, but they’d been unable to make a diagnosis.
The patient said the rash was mildly painful and tender. He denied pain on urination, discharge, fever, malaise, or arthralgias. He also denied any sexual contact outside of his marriage and indicated that he had not been able to have intimate contact with his wife because of the problem.
The patient was uncircumcised and when the foreskin was retracted, a bright red erythematous nonscaly circumferential plaque was visible on the glans penis, spreading to the foreskin (FIGURE 1).
FIGURE 1
A nonscaly, circumferential plaque on the glans penis
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Zoon’s balanitis
We ordered a biopsy because we suspected that the cause of the rash was either erythroplasia of Queyrat (a premalignant condition also known as Bowen’s disease of the glans penis) or Zoon’s balanitis (plasma cell balanitis or balanitis circumscripta plasmacellularis). The biopsy report confirmed the diagnosis of Zoon’s balanitis and showed no signs of malignancy. The features of Zoon’s balanitis include epidermal atrophy, loss of rete ridges, spongiosis, and subepidermal plasma cell infiltrate without evidence of malignancy (FIGURE 2).
FIGURE 2
Dense plasmacytic infiltration underlying the mucosal epidermis
Condition affects older, uncircumcised men
Zoon’s balanitis is thought to be a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The differential for penile lesions is extensive, and includes psoriasis, nummular eczema, candidiasis, herpes simplex, scabies, lichen sclerosus et atrophicus or lichen planus, syphilis, balanitis, and erythroplasia of Queyrat.
The lesion associated with Zoon’s balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
Patients with erythroplasia of Queyrat have either a solitary or multiple nonhealing erythematous plaques on the glans penis. These lesions may also affect the adjacent mucosal epithelium. As is true with Zoon’s balanitis, the typical patient is uncircumcised and middle-aged to elderly.1,2
Presentations may be similar, but treatment differs
Because the treatments for Zoon’s balanitis and erythroplasia of Queyrat are different, a biopsy is imperative. Erythroplasia of Queyrat is a premalignant condition that is treated with topical fluorouracil or surgical excision.3 Treatment for Zoon’s balanitis consists of a topical corticosteroid with or without topical anticandidal agents and circumcision after the acute inflammation resolves.1,2 (If a skin biopsy cannot be obtained in the clinic, the foreskin [if affected] can be sent for biopsy after the circumcision.)
If resolution is not seen with topical steroid treatment, other treatments have demonstrated efficacy. These include topical tacrolimus, as well as YAG and carbon dioxide laser treatments.4-6
Although information is limited on rates of recurrence, circumcision is considered the treatment of choice and is usually curative.1
Ointment does the trick for our patient
Our patient was treated with a single combined topical ointment consisting of nystatin and triamcinolone cream with zinc oxide. The lesion resolved completely after 10 days. We requested a urology consult so that a circumcision could be performed.
CORRESPONDENCE Matthew R. Noss, DO, MSEd, Fort Belvoir Community Hospital Family Medicine Clinic, 1st Floor, Eagle Pavilion, 9300 Dewitt Loop, Ft. Belvoir, VA 22060; [email protected]
A 63-YEAR-OLD MAN came to our clinic complaining of a rash on his penis. He indicated that the rash had been there for almost 2 years and that he’d seen 2 other doctors about it, but they’d been unable to make a diagnosis.
The patient said the rash was mildly painful and tender. He denied pain on urination, discharge, fever, malaise, or arthralgias. He also denied any sexual contact outside of his marriage and indicated that he had not been able to have intimate contact with his wife because of the problem.
The patient was uncircumcised and when the foreskin was retracted, a bright red erythematous nonscaly circumferential plaque was visible on the glans penis, spreading to the foreskin (FIGURE 1).
FIGURE 1
A nonscaly, circumferential plaque on the glans penis
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Zoon’s balanitis
We ordered a biopsy because we suspected that the cause of the rash was either erythroplasia of Queyrat (a premalignant condition also known as Bowen’s disease of the glans penis) or Zoon’s balanitis (plasma cell balanitis or balanitis circumscripta plasmacellularis). The biopsy report confirmed the diagnosis of Zoon’s balanitis and showed no signs of malignancy. The features of Zoon’s balanitis include epidermal atrophy, loss of rete ridges, spongiosis, and subepidermal plasma cell infiltrate without evidence of malignancy (FIGURE 2).
FIGURE 2
Dense plasmacytic infiltration underlying the mucosal epidermis
Condition affects older, uncircumcised men
Zoon’s balanitis is thought to be a benign condition that typically affects uncircumcised middle-aged to elderly men.1,2 Worldwide prevalence among uncircumcised men is approximately 3%.2 The etiology is unknown; it’s thought that this condition may be caused by friction, trauma, heat, lack of hygiene, exogenous or infectious agents, an IgE hypersensitivity, or a chronic infection with Mycobacterium smegmatis.1,2
Typically, the appearance of the lesion precedes diagnosis by about one to 2 years.1 The patient usually complains of mild pruritus and tenderness. Undergarments may be bloodstained.
The differential for penile lesions is extensive, and includes psoriasis, nummular eczema, candidiasis, herpes simplex, scabies, lichen sclerosus et atrophicus or lichen planus, syphilis, balanitis, and erythroplasia of Queyrat.
The lesion associated with Zoon’s balanitis is a solitary, glistening, shiny, red-to-orange plaque of the glans penis or prepuce of an uncircumcised male. Pinpoint erythematous spots or “cayenne pepper spots” may also be associated with this condition.
Patients with erythroplasia of Queyrat have either a solitary or multiple nonhealing erythematous plaques on the glans penis. These lesions may also affect the adjacent mucosal epithelium. As is true with Zoon’s balanitis, the typical patient is uncircumcised and middle-aged to elderly.1,2
Presentations may be similar, but treatment differs
Because the treatments for Zoon’s balanitis and erythroplasia of Queyrat are different, a biopsy is imperative. Erythroplasia of Queyrat is a premalignant condition that is treated with topical fluorouracil or surgical excision.3 Treatment for Zoon’s balanitis consists of a topical corticosteroid with or without topical anticandidal agents and circumcision after the acute inflammation resolves.1,2 (If a skin biopsy cannot be obtained in the clinic, the foreskin [if affected] can be sent for biopsy after the circumcision.)
If resolution is not seen with topical steroid treatment, other treatments have demonstrated efficacy. These include topical tacrolimus, as well as YAG and carbon dioxide laser treatments.4-6
Although information is limited on rates of recurrence, circumcision is considered the treatment of choice and is usually curative.1
Ointment does the trick for our patient
Our patient was treated with a single combined topical ointment consisting of nystatin and triamcinolone cream with zinc oxide. The lesion resolved completely after 10 days. We requested a urology consult so that a circumcision could be performed.
CORRESPONDENCE Matthew R. Noss, DO, MSEd, Fort Belvoir Community Hospital Family Medicine Clinic, 1st Floor, Eagle Pavilion, 9300 Dewitt Loop, Ft. Belvoir, VA 22060; [email protected]
1. Scheinfeld NS, Keough GC, Lehman DS. Balanitis circumscripta plasmacellularis. Medscape. June 8, 2012. Available at: emedicine.medscape.com/article/1122283. Accessed October 26, 2012.
2. Barrisford GW. Balanitis and balanoposthitis in adults. UpToDate. December 19, 2011. Available at: www.uptodate.com/contents/balanitis-and-balanoposthitis-in-adults. Accessed October 26, 2012.
3. Egan KM, Maino KL. Erythroplasia of Queyrat (Bowen disease of the glans penis). Medscape. May 31, 2012. Available at: emedicine.medscape.com/article/1100317. Accessed October 26, 2012.
4. Santos-Juanes J, Sanchez del Rio J, Galache C, et al. Topical tacrolimus: an effective therapy for Zoon balanitis. Arch Dermatol. 2004;140:1538-1539.
5. Wollina U. Ablative erbium: YAG laser treatment of idiopathic chronic inflammatory non-cicatricial balanoposthitis (Zoon’s disease)—a series of 20 patients with long-term outcome. J Cosmet Laser Ther. 2010;12:120-123.
6. Retamar RA, Kien MC, Couela EN. Zoon’s balanitis: presentation of 15 patients, five treated with a carbon dioxide laser. Int J Dermatol. 2003;42:305-307.
1. Scheinfeld NS, Keough GC, Lehman DS. Balanitis circumscripta plasmacellularis. Medscape. June 8, 2012. Available at: emedicine.medscape.com/article/1122283. Accessed October 26, 2012.
2. Barrisford GW. Balanitis and balanoposthitis in adults. UpToDate. December 19, 2011. Available at: www.uptodate.com/contents/balanitis-and-balanoposthitis-in-adults. Accessed October 26, 2012.
3. Egan KM, Maino KL. Erythroplasia of Queyrat (Bowen disease of the glans penis). Medscape. May 31, 2012. Available at: emedicine.medscape.com/article/1100317. Accessed October 26, 2012.
4. Santos-Juanes J, Sanchez del Rio J, Galache C, et al. Topical tacrolimus: an effective therapy for Zoon balanitis. Arch Dermatol. 2004;140:1538-1539.
5. Wollina U. Ablative erbium: YAG laser treatment of idiopathic chronic inflammatory non-cicatricial balanoposthitis (Zoon’s disease)—a series of 20 patients with long-term outcome. J Cosmet Laser Ther. 2010;12:120-123.
6. Retamar RA, Kien MC, Couela EN. Zoon’s balanitis: presentation of 15 patients, five treated with a carbon dioxide laser. Int J Dermatol. 2003;42:305-307.