User login
Screening accuracy for late-life depression in primary care: A systematic review
Objective: To determine the accuracy of depression screening instruments for older adults in primary care.
Study Design: Systematic review
Data Sources: MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety and neurosis. We also searched the second Guide to Clinical Preventive Services, the 1993 Agency for Health Care Policy and Research Clinical Practice Guideline on Depression, and recent systematic reviews. Hand-checking of bibliographies and extensive peer review were also used to identify potential articles.
Outcomes Measured: A predefined search strategy targeted only studies of adults aged 65 years or older in primary care or community settings, including long-term care. Articles were included in this review if they reported original data and tested depression screening instruments against a criterion standard, yielding sensitivity and specificity.
Results: Eighteen articles met criteria and are included in this review, representing 9 different screening instruments. The most commonly evaluated were the Geriatric Depression Scale (30-and 15-item versions), the Center for Epidemiologic Studies Depression Scale, and the SelfCARE(D). Differences in the performance of these 3 instruments were minimal; sensitivities ranged from 74% to 100% and specificities ranged from 53% to 98%.
Conclusions: Accurate and feasible screening instruments are available for detecting late-life depression in primary care. More research is needed to determine the accuracy of depression screening instruments for demented individuals, and for those with subthreshold depressive disorders.
When depression is detected and treated in older patients, not only do symptoms subside, but behavior, cognitive functioning, and overall quality of life improve.1 We conducted a systematic review to determine the accuracy of instruments for detecting unrecognized late-life depression in the primary care setting. Several instruments are comparable in sensitivity and specificity, though the 15-item Geriatric Depression Scale is particularly useful in the primary care setting.
Search methods
As a part of a broader review for the US Preventive Services Task Force and the Research Triangle Institute–University of North Carolina at Chapel Hill Evidence-Based Practice Center, we prepared a strategy to identify articles relevant to the accuracy of depression screening instruments for older adults in the primary care setting. We searched for articles in MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety, and neurosis. We also searched the second Guide to Clinical Preventive Services,2 the 1993 Agency for Health Care Policy and Research (AHCPR) Clinical Practice Guideline on Depression, and recent systematic reviews.3 We also hand-checked bibliographies and used extensive peer review to identify potential articles.
We used the search terms depression, depressive disorder, mass screening, sensitivity and specificity, reproducibility of results, primary health care, ambulatory care, family practice, and the names of common screening and diagnostic instruments used to detect depression. Our search was limited to English-language texts and to ages greater than 65 years.
Inclusion and exclusion criteria
For inclusion, articles must have reported on depression screening in a primary care population of adults aged greater than 65 years. They must have used a criterion standard as comparison and provided information on diagnostic accuracy (usually sensitivity and specificity). Studies performed in the community and in long-term care settings, but not in psychiatric facilities or clinics, were included.
We excluded studies that extracted briefer instruments from the parent version retrospectively; for example, if an investigator evaluated a 5-item version of the Geriatric Depression Scale (GDS), he or she must have defined the specific questions prior to administering the instrument, rather than extracting the 5 items based on posthoc analyses.
The criterion standards must have been commonly accepted, structured or semistructured diagnostic interviews or independent evaluations performed by psychiatrists based on Diagnostic and Statistic Manual of Mental Disorders, revised 3rd or 4th editions (DSM-IIIR, DSM-IV), International Classification of Diseases, 10th ed (ICD-10), or Research Diagnostic Criteria. Our selection criteria are consistent with recognized standards for reviewing diagnostic tests, specifically in eliminating spectrum bias and requiring a criterion standard.4
Review standards
Both authors independently reviewed the abstracts and full articles generated from the searches. Discrepancies about eligibility were resolved by consensus after review of the entire article. For each included study, we extracted information about the screening instrument, the criterion standard, sensitivity and specificity, average age of participants, their dementia status, and the study setting. To further estimate accuracy, we calculated 95% confidence intervals around each measure of sensitivity and specificity. Multiple screening instruments precluded a meaningful meta-analysis of these results.
Results
Our initial search strategy yielded 1325 potential articles, 1269 of which could be eliminated by title review. Of the 56 articles remaining, 38 were eliminated after identifying exclusion criteria in the abstract or the manuscript: 17 because there was no criterion standard, 7 because the setting was not appropriate, 8 because the population was not geriatric, and 6 with varying methodologic exclusions. Eighteen articles met our inclusion criteria and specifically examined the performance of depression screening instruments for older adults in primary care ( Table 1 ).
The included studies were carried out among a wide spectrum of patients mostly in general practice settings, with the exception of 1 in a nursing home and 1 receiving home care. Two studies specifically included patients with dementia. Nine different instruments were used; most had 20 or fewer questions and were relatively easy to administer.
Overall test performance in detecting major depression was similarly favorable among the instruments, with sensitivities ranging from 67% to 100% and specificities ranging from 53% to 98%. All but 2 studies5,6 reported sensitivity and specificity based on optimal cutpoints determined by post-hoc receiving-operating characteristic (ROC) curve analyses, possibly exaggerating test performance in comparison with the studies testing predetermined cutpoints.
Five studies6,11,19,22,23 explicitly stated that interviewers performing the criterion standard exam were blinded to the results of the screening test; the remainder did not report on blinding, although in most cases blinding was implied by the use of a second “independent” rater.
Geriatric Depression Scale. The GDS, the Center for Epidemiologic Studies Depression scale (CES-D), and the SelfCARE(D) were the most-evaluated screening instruments. The GDS has both a 30- and 15-item version and was designed in a yes/no format for self- or caregiver administration, making it easy to use. It minimizes questions about somatic and vegetative symptoms, which can overlap with symptoms of concurrent medical illness.
The GDS has been validated repeatedly in psychiatric settings.23-27 Nine studies5-10,12 evaluated its use in primary care elderly, most using the 15-item version and a cutpoint of 3 to 5. Sensitivity and specificity ranged from 79%–100% and 67%–80%, respectively.
Center for Epidemiological Studies Depression Scale. The CES-D can be self-administered. It lists 20 statements addressing depressive symptoms over the last week, asking the participant to rank the frequency of these feelings from “rarely” to “most of the time.” Its psychometric properties have been consistently strong in younger adults in the community.
In the 5 studies13-16 that evaluated this instrument, cutpoints varied from 9 to 21. The resultant sensitivities were 75%–93%, with specificities ranging from 73%–87%. One study16 also specifically evaluated the performance of the CES-D in mildly demented subjects with an average Mini-Mental State Examination (MMSE) of 19, and showed similar test characteristics to the patients without dementia. This instrument was perceived as generally easy to administer, except in a nursing-home population where the questions had to be repeated multiple times.
Papassotiropoulos et al17 used the CES-D and the General Health Questionnaire (GHQ) to identify subthreshold depression in a community sample in Greece. They defined subthreshold depression as fewer than 5 depressive symptoms in a 2-week period; brief, monthly depressive symptoms not occurring for a 2-week duration; and, any significant single depressive symptom not specified by duration or frequency. Accuracy was poor for delineating these syndromes, with sensitivities below 50% and specificities of 75% and 72%, respectively.
Lyness and colleagues15 used the CES-D, as well as the GDS-15, to identify minor depression in their cohort. They defined minor depression as having sad mood or loss of interest and at least 2, but fewer than 5, additional depressive symptoms within a 2-week period. The CES-D revealed a sensitivity of 40% and specificity of 82% for detecting minor depression, while the GDS-15 had a sensitivity and specificity of 70% and 80%, respectively.
SelfCARE(D). The SelfCARE(D) is a self-administered instrument that requests responses to 12 items on a Likert scale, reflecting depressive symptoms over the last month. It was derived from a larger, previously validated instrument used in England.18
In 1 of 3 included studies, Bird and colleagues18 reported the original results in a 1987 outpatient sample, showing a sensitivity of 77% and specificity of 98%, with a cutpoint of 5. Since then it has been validated again in general practice and in home care.19,20 Both studies revealed sensitivities in the 90% range, but the specificity in home care was 53% vs 86% in general practice.
Caribbean Culture–Specific Screen. In an effort to address the potential cultural limitations of common instruments, Rait and colleagues11 tested the Caribbean Culture–Specific Screen (CCSS) in the growing contingent of Caribbeans of African descent in the United Kingdom. They found that it performed well, but not better than the Brief Assessment Schedule Depression Cards or the GDS-15. Each had a sensitivity of 92%, with specificities ranging from 71%–84%.
Similarly, Abas et al12 tested the CCSS and the GDS-15 in an African-Caribbean population, reporting sensitivities of 82% for both instruments, and specificities of 68% for the CCSS and 82% for the GDS-15.
Cornell Scale for Depression in Dementia. Dementia poses barriers to effective screening for depression given the obvious limitations in self report due to cognitive impairment. The Cornell Scale for Depression in Dementia (CSDD) was specifically designed for this population and calls for the clinician to use both patient and caregiver information to complete the screen.
The CSDD is categorized by questions on mood, behavior, physical signs, diurnal patterns, and ideational disturbances. Each item is on a 3-point scale for a possible total score of 38, with higher scores indicating more depression. Most data generated about the CSDD have come from hospitalized patients, in whom it has demonstrated acceptable validity and reliability in demented and nondemented patients.29-31
We identified 1 study evaluating the CSDD that met our criteria. Vida et al22 screened outpatients from a family medicine clinic and found a sensitivity of 90% and specificity of 75% for detecting major depression.
Other instruments. Several very brief instruments have been validated in psychiatric or hospital settings where the prevalence of depressive symptoms is often high,32,33 but few have been tested in older primary care patients. Howe et al34 attempted to validate a 1-question screen (MHI-1) derived from the mental health component of the SF-36, asking elderly participants, “in the past month, how much of the time have you felt downhearted or sad?” (1=none, 6=all the time). They showed that as a “stand alone” screen, the MHI-1 did not perform well in the primary care setting, with a sensitivity of 67% and a specificity of 60%.
TABLE 1
Articles relevant to late-life depression screening
| Author | Test/cutpoint | Criterion standard | Avg. age | Dementia | Sn (%) (95% CI) | Sp (%) (95% CI) |
|---|---|---|---|---|---|---|
| D’Ath et al5 | GDS-15/5 | GMS/AGECAT | 74 | Not tested | 91 (86–96) | 72 (66–78) |
| Gerety et al6 | GDS/11 | SCID* | 79 | Avg MMSE 23 (SD4.7) | 89 (72–96) | 68 (58–77) |
| CES-D/16 | 74 (55–86) | 70 (60–79) | ||||
| Neal and Baldwin7 | GDS/11 | GMS/AGECAT | 77 | Not tested | 83 (72–94) | 80 (68–92) |
| Van Marjwick et al8 | GDS/7 | DIS | 74 | Mild/none | 79 (76–82) | 67 (63–71) |
| Arthur et al9 | GDS-15/3 | ICD-10 | 80 | None | 100 (98–102) | 72 (67–77) |
| Hoyl et al10 | GDS-15/5 | SCID | 75 | Avg MMSE 27 (SD 2.6) | 94 (89–99) | 82 (73–91) |
| Rait et al11 | GDS-15/4 | GMS/AGECAT* | >60 | Not tested | 92 (64–100) | 71 (63–79) |
| BASEDEC/6 | 92 (64–100) | 84 (78–91) | ||||
| CCSS/6 | 92 (64–100) | 79 (71–86) | ||||
| Abas et al12 | GDS-15/5 | GMS/AGECAT | >60 | Avg. MMSE 24 (SD 4.6) | 82 (62–92) | 82 (62–92) |
| CCSS/5 | 82 (62–92) | 68 (54–79) | ||||
| Beekman et al13 | CES-D/20 | DIS | 55-82 | None | 93 (91–95) | 73 (69–77) |
| Lewisohn et al14 | CES-D/12 | RDC, DSM-IIIR | 64 | Not reported | 76 (73–79) | 77 (74–80) |
| Lyness et al15 | CES-D/21 | SCID | 71 | Not tested | – | – |
| – Major depression | 92 (87–97) | 87 (81–93) | ||||
| – Minor depression | 40 (32–48) | 82 (75–89) | ||||
| GDS/10 | ||||||
| – Major depression | 100 (98–102) | 84 (78–90) | ||||
| – Minor depression | 70 (62–78) | 80 (73–87) | ||||
| Papassotiropoulos et al16 | CES-D/8 (demented excluded) | CIDI | >60 | Avg MMSE 27 (SD 6.0) | 75 (70–80) | 74 (67–81) |
| CES-D/9 (demented excluded) | CIDI | >60 | Avg MMSE 19 (SD 5.5)n demented sample | 75 (70–80) | 72 (67–77) | |
| 75 (70–80) | 72 (67–77) | |||||
| Papassotiropoulos et al17 | GHQ-12/0 Subthreshold depression | CIDI, DSM-IIIR; not reported | >60 | Avg. MMSE 28 (SD 2.0) | 46 (40-52) | 72 (67–77) |
| CES-D/9 Subthreshold depression | 39 (33-45) | 75 (70-80) | ||||
| Bird et al18 | SelfCARE(D)/5 | Independent psychiatric assessment* | 73 | Not tested | 77 (67–87) | 98 (95–101) |
| Upadhyaya and Stanley19 | SelfCARE(D)/5 | GMS/AGECAT* | 71 | Not tested | 95 (90–100) | 86 (78–94) |
| 74 (55–86) | 70 (60–79) | |||||
| Banerjee et al20 | SelfCARE(D)/8 | GMS/AGECAT | >65 | Not tested | 90 (86–94 | 53 (46–60) |
| Howe et al21 | MHI-1/2 | GMS/AGECAT | 81 | Excluded “organic mpairment” | 67 (58–76) | 60 (50–70) |
| Vida et al22 | Cornell Screen/7 | RDC* | 72 | Avg MMSE 19 (SD 7.8) | 90 (80–100) | 75 (60–90) |
| *These studies were blinded; all others were not reported. | ||||||
| GDS, Geriatric Depression Scale, 30-item; GDS-15, Geriatric Depression Scale, 15-item; GHQ, General Health Questionnaire; DIS, Diagnostic Interview Schedule; BASEDEC, Brief Assessment Schedule Depression Cards; CES-D, Center for Epidemiologic Study-Depression; MHI-1, single question from the Mental Health Inventory [“in the past month, how much have you felt downhearted or sad (1: none-6: all the time)”]; GMS, Geriatric Mental State/AGECAT computer program; CIDI, Composite International Diagnostic Interview; SCID, Structured Clinical Interview for DSM IIIR; CCSS, Caribbean Culture Specific Screen; RDC, Research Diagnostic Criteria; DSM IIIR, Diagnostic and Statistical Manual of Mental Disorders,3rd ed rev; MMSE, Mini Mental State Examination; ICD-10, International Classification of Diseases, 10th ed | ||||||
Discussion: late-life depression can be diagnosed accurately
Our systematic review shows that several instruments demonstrate good accuracy for detecting late-life major depression in primary care. The GDS, CES-D and SelfCARE(D) have comparable sensitivities and specificities. The CES-D and CCSD have similarly favorable accuracy in demented patients with an average MMSE score of 19.
A 1-question screen shows poor results, as do studies using the GHQ, CES-D, and GDS-15 to detect nonmajor depression. Finally, 2 studies demonstrate that a culturally specific screen in African-Caribbeans performs well, but no better than, the GDS.
The GDS has longstanding success in identifying major depression in psychiatric and hospital settings and now demonstrates accuracy in primary care, where the 15-item version in its yes/no self-administered format represents a realistic tool for use in the community or the clinic.
With a record of successful use in general adult research, the CES-D also has the benefit of a known track record and relative ease of administration. Evidence from this review suggests that it can be extended to the older primary care population. The SelfCARE(D) is comparably accurate in general practice, but has lower specificity in home care.
Our review highlights the need to further investigate the accuracy of screening tools for depression in patients with dementia, specifically where cognitive impairment may be severe. Using the CSDD, an instrument specifically designed for patients with dementia, Vida et al22 found good accuracy for detecting depression; however, they studied patients with relatively mild dementia. The prevalence of depression in dementia is 15% to 40%.35 Given the increasing incidence of dementia in our aging population, the availability of accurate screening tools that specifically account for the coexistence of these 2 common disorders is important.
This review also reveals a lack of screening accuracy for nonmajor depressive disorders using 3 common instruments. Lyness and colleagues36 showed that there is considerable functional disability in subsyndromal depression, which is more prevalent than major depression. Others show similar findings, supporting the significant morbidity caused by depressive symptoms not severe enough to cross threshold for a major disorder.37,38 As the characterization of nonmajor depressive disorders evolves, screening instruments should be developed and validated specifically for these syndromes.39
Late-life depressive disorders have a convincing burden of suffering, often go undetected, and have known effective treatments.40 Our systematic review reveals that accurate screening instruments are available to detect major depression in older primary care patients. Based on format and length ( Table 2 ), several could easily be self-administered or administered by nonclinicians in the waiting room. We recommend the 15-item GDS ( Figure ) because of its yes/no format and ease of scoring. Future work should include tests of depression screening accuracy for demented populations, and for nonmajor depressive disorders. Investigators should also evaluate the accuracy of very short instruments, such as the 5-item version of the GDS10 in the primary care setting. Acceptable administration times and ease of use is likely to determine the realistic application of proven instruments.
TABLE 2
Selected screening instruments and their characteristics
| Instrument | Format | Item | Time to administer | Sn (%) | Sp (%) |
|---|---|---|---|---|---|
| GDS-15 | Yes/no questions about current symptoms | 15 | 2–3 minutes | 82–100 | 72–82 |
| CES-D | Rates frequency of selected symptoms over last week | 20 | 2–3 minutes | 74–93 | 70–87 |
| SelfCareD | Multiple choice responses regarding symptoms over last month | 12 | 2–3 minutes | 77–95 | 53–98 |
| GDS-15: Geriatric Depression Scale, 15-item; CES-D: Center for Epidemiologic Study-Depression; Sn, sensitivity; Sp, specificity. Sensitivity and specificity values represent the range reported from the eligible studies in our review. | |||||
FIGURE
Geriatric Depression Scale, 15-item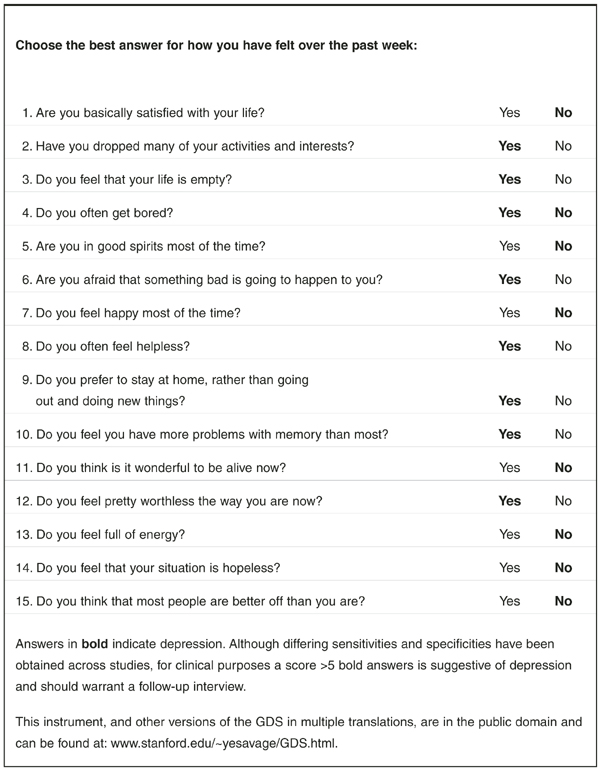
Acknowledgments
The authors would like to thank Dr. Carmen Lewis for her thoughtful review of this manuscript. The authors report no competing interests. Funding sources: Robert Wood Johnson Clinical Scholars Program; Agency for Healthcare Research and Quality contract # 290-97-0011.
Corresponding author
Lea C. Watson MD, MPH, Geriatric Psychiatry, Box 3903, Duke University Medical Center, Durham, NC 27710. E-mail: [email protected].
1. Mulsant BH, Ganguli M. Epidemiology and diagnosis of depression in late life. J Clin Psychiatry 1999;60(suppl 20):9-15.
2. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Alexandria, Va: International Medical Publishing; 1996.
3. Pignone MP, Gaynes BN, Rushton JL, et al. Screening for depression in adults: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002;136:765-776.
4. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1066.
5. D’Ath P, Katona P, Mullan E, Evans S, Katona C. Screening, detection and management of depression in elderly primary care attenders. I: The acceptability and performance of the 15 item Geriatric Depression Scale (GDS15) and the development of short versions. Fam Pract 1994;11:260-266.
6. Gerety MB, Williams JW, Jr, Mulrow CD, et al. Performance of case-finding tools for depression in the nursing home: influence of clinical and functional characteristics and selection of optimal threshold scores. J Am Geriatr Soc 1994;42:1103-1109.
7. Neal R, Baldwin R. Screening for anxiety and depression in elderly medical outpatients. Age and Ageing 1994;23:461-464.
8. van Marwijk HV, Wallace P, de Bock GD, Hermans J, Kapteinaa Mulder JD. Evaluation of the feasibility, reliability and diagnostic value of shortened versions of the geriatric depression scale. Br J Gen Prac 1995;45:195-199.
9. Arthur A, Jagger C, Lindesay J, Graham C, Clarke M. Using an annual over-75 health check to screen for depression: validation of the short Geriatric Depression Scale (GDS15) within general practice. Int J Geriatr Psychiatry 1999;14:431-439.
10. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the Geriatric Depression Scale. J Am Geriatr Soc 1999;47:873-878.
11. Rait G, Burns A, Baldwin R, et al. Screening for depression in African-Caribbean elders. Fam Pract 1999;16:591-595.
12. Abas MA, Phillips C, Carter J, Walter S, Banerjee S, Levy R. Culturally sensitive validation of screening questionnaires for depression in older African-Caribbean people living in south London. Br J Psychiatry 1998;173:249-254.
13. Beekman AT, Deeg DJ, Van Limbeek J, Braam AW, de Vries MR, Van Tillburg W. Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): results from a community-based sample of older subjects in The Netherlands. Psychol Med 1997;27:231-235.
14. Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol Aging 1997;12:277-287.
15. Lyness JM, Noel TK, Cox C, et al. Screening for depression in elderly primary care patients. A comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch Intern Med 1997;157:449-454.
16. Papassotiropoulos A, Heun R, Maier W. The impact of dementia on the detection of depression in elderly subjects from the general population. Psychol Med 1999;29:113-120.
17. Papassotiropoulos A, Heun R. Detection of subthreshold depression and subthreshold anxiety in the elderly. Int J Geriatr Psychiatry 1999;14:643-650.
18. Bird A, Macdonald A, Mann A, et al. Preliminary experience with the SelfCARE(D): a self-rating depression questionnaire for use in elderly, non-institutionalized subjects. Int J Geriatr Psychiatry 1987;2.
19. Upadhyaya AK, Stanley I. Detection of depression in primary care comparison of two self. administered scales. Int J Geriatr Psychiatry 1997;12:35-37.
20. Banerjee S, Shamash K, MacDonald AJ, et al. The use of the SelfCARE(D) as a screening tool for depression in the clients of local authority home care services-a preliminary study. Int J Geriatr Psychiatry 1998;13:695-699.
21. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
22. Vida S, Des Rosiers P, Carrier L, Gauthier S. Depression in Alzheimer’s disease: receiver operating characteristic analysis of the Cornell Scale for Depression in Dementia and the Hamilton Depression Scale. J Geriatr Psychiatry Neur 1994;7:159-162.
23. Sheik J, Yesavage J. Geriatric Depression Scale (GDS): recent findings and development of a shorter version. New York, NY: Howarth Press; 1986.
24. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982;17:37-49.
25. Fountoulakis KN, Tsolaki M, Iacovides A, et al. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging (Milano) 1999;11:367-372.
26. Lim PP, Ng LL, Chiam PC, Ong PS, Ngui FT, Sahadevan S. Validation and comparison of three brief depression scales in an elderly Chinese population. Int J Geriatr Psychiatry 2000;15:824-830.
27. Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 1999;14:858-865.
28. Mulrow CD, Williams JW, Jr, Gerety MB, Ramirez G, Montiel OM, Kerber C. Case-finding instruments for depression in primary care settings. Ann Intern Med 1995;122:913-921.
29. Alexopoulos G, Abrams R, Young R, Shamoian CA. Use of the Cornell Scale in Nondemented Patients. J Am Geriatr Soc 1988;36:230-236.
30. Alexopoulos G, Abrams R, Young R, Shamoian CA. Cornell Scale for Depression in Dementia. Biol Psychiatry 1988;23:271-284.
31. Harwood D, Ownby R, Barker W, Duara R. The factor structure of the Cornell Scale for Depression in Dementia among probable Alzheimer’s disease patients. Am J Geriatr Psychiatry 1998;6:212-220.
32. Weyerer S, Killmann U, Ames D, Allen N. The Even Briefer Assessment Scale for Depression (EBAS DEP): its suitability for the elderly in geriatric care in English-and German- speaking countries. Int J Geriatr Psychiatry 1999;14:473-480.
33. Pomeroy IM, Clark CR, Philp I. The effectiveness of very short scales for depression screening in elderly medical patients. Int J Geriatr Psychiatry 2001;16:321-326.
34. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
35. Lyketsos G, Baker L, Warren A, et al. Major and minor depression in Alzheimer’s disease: prevalence and impact. J Neuropsychiatry Clin Neurosci 1997;9:556-561.
36. Lyness JM, King DA, Cox C, Yoediono Z, Caine ED. The importance of subsyndromal depression in older primary care patients: prevalence and associated functional disability. J Am Geriatr Soc 1999;47:647-652.
37. Hendrie H, Callahan C, Levitt E. Prevalence rates of major depressive disorders: the effect of varying diagnostic criteria in an older primary care population. Am J Geriatr Psychiatry 1995;3:119-131.
38. Unutzer J, Patrick D, Simon G, et al. Depressive symptoms and the cost of health services in HMO patients aged 65 years and older. JAMA 1997;277:1618-1623.
39. Lavretsky H, Kumar A. Clinically significant non-major depression: old concepts, new insights. Am J Geriatr Psychiatry 2002;10:239-255.
40. Lebowitz BD, Pearson JL, Schneider LS, et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA 1997;278:1186-1190.
Objective: To determine the accuracy of depression screening instruments for older adults in primary care.
Study Design: Systematic review
Data Sources: MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety and neurosis. We also searched the second Guide to Clinical Preventive Services, the 1993 Agency for Health Care Policy and Research Clinical Practice Guideline on Depression, and recent systematic reviews. Hand-checking of bibliographies and extensive peer review were also used to identify potential articles.
Outcomes Measured: A predefined search strategy targeted only studies of adults aged 65 years or older in primary care or community settings, including long-term care. Articles were included in this review if they reported original data and tested depression screening instruments against a criterion standard, yielding sensitivity and specificity.
Results: Eighteen articles met criteria and are included in this review, representing 9 different screening instruments. The most commonly evaluated were the Geriatric Depression Scale (30-and 15-item versions), the Center for Epidemiologic Studies Depression Scale, and the SelfCARE(D). Differences in the performance of these 3 instruments were minimal; sensitivities ranged from 74% to 100% and specificities ranged from 53% to 98%.
Conclusions: Accurate and feasible screening instruments are available for detecting late-life depression in primary care. More research is needed to determine the accuracy of depression screening instruments for demented individuals, and for those with subthreshold depressive disorders.
When depression is detected and treated in older patients, not only do symptoms subside, but behavior, cognitive functioning, and overall quality of life improve.1 We conducted a systematic review to determine the accuracy of instruments for detecting unrecognized late-life depression in the primary care setting. Several instruments are comparable in sensitivity and specificity, though the 15-item Geriatric Depression Scale is particularly useful in the primary care setting.
Search methods
As a part of a broader review for the US Preventive Services Task Force and the Research Triangle Institute–University of North Carolina at Chapel Hill Evidence-Based Practice Center, we prepared a strategy to identify articles relevant to the accuracy of depression screening instruments for older adults in the primary care setting. We searched for articles in MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety, and neurosis. We also searched the second Guide to Clinical Preventive Services,2 the 1993 Agency for Health Care Policy and Research (AHCPR) Clinical Practice Guideline on Depression, and recent systematic reviews.3 We also hand-checked bibliographies and used extensive peer review to identify potential articles.
We used the search terms depression, depressive disorder, mass screening, sensitivity and specificity, reproducibility of results, primary health care, ambulatory care, family practice, and the names of common screening and diagnostic instruments used to detect depression. Our search was limited to English-language texts and to ages greater than 65 years.
Inclusion and exclusion criteria
For inclusion, articles must have reported on depression screening in a primary care population of adults aged greater than 65 years. They must have used a criterion standard as comparison and provided information on diagnostic accuracy (usually sensitivity and specificity). Studies performed in the community and in long-term care settings, but not in psychiatric facilities or clinics, were included.
We excluded studies that extracted briefer instruments from the parent version retrospectively; for example, if an investigator evaluated a 5-item version of the Geriatric Depression Scale (GDS), he or she must have defined the specific questions prior to administering the instrument, rather than extracting the 5 items based on posthoc analyses.
The criterion standards must have been commonly accepted, structured or semistructured diagnostic interviews or independent evaluations performed by psychiatrists based on Diagnostic and Statistic Manual of Mental Disorders, revised 3rd or 4th editions (DSM-IIIR, DSM-IV), International Classification of Diseases, 10th ed (ICD-10), or Research Diagnostic Criteria. Our selection criteria are consistent with recognized standards for reviewing diagnostic tests, specifically in eliminating spectrum bias and requiring a criterion standard.4
Review standards
Both authors independently reviewed the abstracts and full articles generated from the searches. Discrepancies about eligibility were resolved by consensus after review of the entire article. For each included study, we extracted information about the screening instrument, the criterion standard, sensitivity and specificity, average age of participants, their dementia status, and the study setting. To further estimate accuracy, we calculated 95% confidence intervals around each measure of sensitivity and specificity. Multiple screening instruments precluded a meaningful meta-analysis of these results.
Results
Our initial search strategy yielded 1325 potential articles, 1269 of which could be eliminated by title review. Of the 56 articles remaining, 38 were eliminated after identifying exclusion criteria in the abstract or the manuscript: 17 because there was no criterion standard, 7 because the setting was not appropriate, 8 because the population was not geriatric, and 6 with varying methodologic exclusions. Eighteen articles met our inclusion criteria and specifically examined the performance of depression screening instruments for older adults in primary care ( Table 1 ).
The included studies were carried out among a wide spectrum of patients mostly in general practice settings, with the exception of 1 in a nursing home and 1 receiving home care. Two studies specifically included patients with dementia. Nine different instruments were used; most had 20 or fewer questions and were relatively easy to administer.
Overall test performance in detecting major depression was similarly favorable among the instruments, with sensitivities ranging from 67% to 100% and specificities ranging from 53% to 98%. All but 2 studies5,6 reported sensitivity and specificity based on optimal cutpoints determined by post-hoc receiving-operating characteristic (ROC) curve analyses, possibly exaggerating test performance in comparison with the studies testing predetermined cutpoints.
Five studies6,11,19,22,23 explicitly stated that interviewers performing the criterion standard exam were blinded to the results of the screening test; the remainder did not report on blinding, although in most cases blinding was implied by the use of a second “independent” rater.
Geriatric Depression Scale. The GDS, the Center for Epidemiologic Studies Depression scale (CES-D), and the SelfCARE(D) were the most-evaluated screening instruments. The GDS has both a 30- and 15-item version and was designed in a yes/no format for self- or caregiver administration, making it easy to use. It minimizes questions about somatic and vegetative symptoms, which can overlap with symptoms of concurrent medical illness.
The GDS has been validated repeatedly in psychiatric settings.23-27 Nine studies5-10,12 evaluated its use in primary care elderly, most using the 15-item version and a cutpoint of 3 to 5. Sensitivity and specificity ranged from 79%–100% and 67%–80%, respectively.
Center for Epidemiological Studies Depression Scale. The CES-D can be self-administered. It lists 20 statements addressing depressive symptoms over the last week, asking the participant to rank the frequency of these feelings from “rarely” to “most of the time.” Its psychometric properties have been consistently strong in younger adults in the community.
In the 5 studies13-16 that evaluated this instrument, cutpoints varied from 9 to 21. The resultant sensitivities were 75%–93%, with specificities ranging from 73%–87%. One study16 also specifically evaluated the performance of the CES-D in mildly demented subjects with an average Mini-Mental State Examination (MMSE) of 19, and showed similar test characteristics to the patients without dementia. This instrument was perceived as generally easy to administer, except in a nursing-home population where the questions had to be repeated multiple times.
Papassotiropoulos et al17 used the CES-D and the General Health Questionnaire (GHQ) to identify subthreshold depression in a community sample in Greece. They defined subthreshold depression as fewer than 5 depressive symptoms in a 2-week period; brief, monthly depressive symptoms not occurring for a 2-week duration; and, any significant single depressive symptom not specified by duration or frequency. Accuracy was poor for delineating these syndromes, with sensitivities below 50% and specificities of 75% and 72%, respectively.
Lyness and colleagues15 used the CES-D, as well as the GDS-15, to identify minor depression in their cohort. They defined minor depression as having sad mood or loss of interest and at least 2, but fewer than 5, additional depressive symptoms within a 2-week period. The CES-D revealed a sensitivity of 40% and specificity of 82% for detecting minor depression, while the GDS-15 had a sensitivity and specificity of 70% and 80%, respectively.
SelfCARE(D). The SelfCARE(D) is a self-administered instrument that requests responses to 12 items on a Likert scale, reflecting depressive symptoms over the last month. It was derived from a larger, previously validated instrument used in England.18
In 1 of 3 included studies, Bird and colleagues18 reported the original results in a 1987 outpatient sample, showing a sensitivity of 77% and specificity of 98%, with a cutpoint of 5. Since then it has been validated again in general practice and in home care.19,20 Both studies revealed sensitivities in the 90% range, but the specificity in home care was 53% vs 86% in general practice.
Caribbean Culture–Specific Screen. In an effort to address the potential cultural limitations of common instruments, Rait and colleagues11 tested the Caribbean Culture–Specific Screen (CCSS) in the growing contingent of Caribbeans of African descent in the United Kingdom. They found that it performed well, but not better than the Brief Assessment Schedule Depression Cards or the GDS-15. Each had a sensitivity of 92%, with specificities ranging from 71%–84%.
Similarly, Abas et al12 tested the CCSS and the GDS-15 in an African-Caribbean population, reporting sensitivities of 82% for both instruments, and specificities of 68% for the CCSS and 82% for the GDS-15.
Cornell Scale for Depression in Dementia. Dementia poses barriers to effective screening for depression given the obvious limitations in self report due to cognitive impairment. The Cornell Scale for Depression in Dementia (CSDD) was specifically designed for this population and calls for the clinician to use both patient and caregiver information to complete the screen.
The CSDD is categorized by questions on mood, behavior, physical signs, diurnal patterns, and ideational disturbances. Each item is on a 3-point scale for a possible total score of 38, with higher scores indicating more depression. Most data generated about the CSDD have come from hospitalized patients, in whom it has demonstrated acceptable validity and reliability in demented and nondemented patients.29-31
We identified 1 study evaluating the CSDD that met our criteria. Vida et al22 screened outpatients from a family medicine clinic and found a sensitivity of 90% and specificity of 75% for detecting major depression.
Other instruments. Several very brief instruments have been validated in psychiatric or hospital settings where the prevalence of depressive symptoms is often high,32,33 but few have been tested in older primary care patients. Howe et al34 attempted to validate a 1-question screen (MHI-1) derived from the mental health component of the SF-36, asking elderly participants, “in the past month, how much of the time have you felt downhearted or sad?” (1=none, 6=all the time). They showed that as a “stand alone” screen, the MHI-1 did not perform well in the primary care setting, with a sensitivity of 67% and a specificity of 60%.
TABLE 1
Articles relevant to late-life depression screening
| Author | Test/cutpoint | Criterion standard | Avg. age | Dementia | Sn (%) (95% CI) | Sp (%) (95% CI) |
|---|---|---|---|---|---|---|
| D’Ath et al5 | GDS-15/5 | GMS/AGECAT | 74 | Not tested | 91 (86–96) | 72 (66–78) |
| Gerety et al6 | GDS/11 | SCID* | 79 | Avg MMSE 23 (SD4.7) | 89 (72–96) | 68 (58–77) |
| CES-D/16 | 74 (55–86) | 70 (60–79) | ||||
| Neal and Baldwin7 | GDS/11 | GMS/AGECAT | 77 | Not tested | 83 (72–94) | 80 (68–92) |
| Van Marjwick et al8 | GDS/7 | DIS | 74 | Mild/none | 79 (76–82) | 67 (63–71) |
| Arthur et al9 | GDS-15/3 | ICD-10 | 80 | None | 100 (98–102) | 72 (67–77) |
| Hoyl et al10 | GDS-15/5 | SCID | 75 | Avg MMSE 27 (SD 2.6) | 94 (89–99) | 82 (73–91) |
| Rait et al11 | GDS-15/4 | GMS/AGECAT* | >60 | Not tested | 92 (64–100) | 71 (63–79) |
| BASEDEC/6 | 92 (64–100) | 84 (78–91) | ||||
| CCSS/6 | 92 (64–100) | 79 (71–86) | ||||
| Abas et al12 | GDS-15/5 | GMS/AGECAT | >60 | Avg. MMSE 24 (SD 4.6) | 82 (62–92) | 82 (62–92) |
| CCSS/5 | 82 (62–92) | 68 (54–79) | ||||
| Beekman et al13 | CES-D/20 | DIS | 55-82 | None | 93 (91–95) | 73 (69–77) |
| Lewisohn et al14 | CES-D/12 | RDC, DSM-IIIR | 64 | Not reported | 76 (73–79) | 77 (74–80) |
| Lyness et al15 | CES-D/21 | SCID | 71 | Not tested | – | – |
| – Major depression | 92 (87–97) | 87 (81–93) | ||||
| – Minor depression | 40 (32–48) | 82 (75–89) | ||||
| GDS/10 | ||||||
| – Major depression | 100 (98–102) | 84 (78–90) | ||||
| – Minor depression | 70 (62–78) | 80 (73–87) | ||||
| Papassotiropoulos et al16 | CES-D/8 (demented excluded) | CIDI | >60 | Avg MMSE 27 (SD 6.0) | 75 (70–80) | 74 (67–81) |
| CES-D/9 (demented excluded) | CIDI | >60 | Avg MMSE 19 (SD 5.5)n demented sample | 75 (70–80) | 72 (67–77) | |
| 75 (70–80) | 72 (67–77) | |||||
| Papassotiropoulos et al17 | GHQ-12/0 Subthreshold depression | CIDI, DSM-IIIR; not reported | >60 | Avg. MMSE 28 (SD 2.0) | 46 (40-52) | 72 (67–77) |
| CES-D/9 Subthreshold depression | 39 (33-45) | 75 (70-80) | ||||
| Bird et al18 | SelfCARE(D)/5 | Independent psychiatric assessment* | 73 | Not tested | 77 (67–87) | 98 (95–101) |
| Upadhyaya and Stanley19 | SelfCARE(D)/5 | GMS/AGECAT* | 71 | Not tested | 95 (90–100) | 86 (78–94) |
| 74 (55–86) | 70 (60–79) | |||||
| Banerjee et al20 | SelfCARE(D)/8 | GMS/AGECAT | >65 | Not tested | 90 (86–94 | 53 (46–60) |
| Howe et al21 | MHI-1/2 | GMS/AGECAT | 81 | Excluded “organic mpairment” | 67 (58–76) | 60 (50–70) |
| Vida et al22 | Cornell Screen/7 | RDC* | 72 | Avg MMSE 19 (SD 7.8) | 90 (80–100) | 75 (60–90) |
| *These studies were blinded; all others were not reported. | ||||||
| GDS, Geriatric Depression Scale, 30-item; GDS-15, Geriatric Depression Scale, 15-item; GHQ, General Health Questionnaire; DIS, Diagnostic Interview Schedule; BASEDEC, Brief Assessment Schedule Depression Cards; CES-D, Center for Epidemiologic Study-Depression; MHI-1, single question from the Mental Health Inventory [“in the past month, how much have you felt downhearted or sad (1: none-6: all the time)”]; GMS, Geriatric Mental State/AGECAT computer program; CIDI, Composite International Diagnostic Interview; SCID, Structured Clinical Interview for DSM IIIR; CCSS, Caribbean Culture Specific Screen; RDC, Research Diagnostic Criteria; DSM IIIR, Diagnostic and Statistical Manual of Mental Disorders,3rd ed rev; MMSE, Mini Mental State Examination; ICD-10, International Classification of Diseases, 10th ed | ||||||
Discussion: late-life depression can be diagnosed accurately
Our systematic review shows that several instruments demonstrate good accuracy for detecting late-life major depression in primary care. The GDS, CES-D and SelfCARE(D) have comparable sensitivities and specificities. The CES-D and CCSD have similarly favorable accuracy in demented patients with an average MMSE score of 19.
A 1-question screen shows poor results, as do studies using the GHQ, CES-D, and GDS-15 to detect nonmajor depression. Finally, 2 studies demonstrate that a culturally specific screen in African-Caribbeans performs well, but no better than, the GDS.
The GDS has longstanding success in identifying major depression in psychiatric and hospital settings and now demonstrates accuracy in primary care, where the 15-item version in its yes/no self-administered format represents a realistic tool for use in the community or the clinic.
With a record of successful use in general adult research, the CES-D also has the benefit of a known track record and relative ease of administration. Evidence from this review suggests that it can be extended to the older primary care population. The SelfCARE(D) is comparably accurate in general practice, but has lower specificity in home care.
Our review highlights the need to further investigate the accuracy of screening tools for depression in patients with dementia, specifically where cognitive impairment may be severe. Using the CSDD, an instrument specifically designed for patients with dementia, Vida et al22 found good accuracy for detecting depression; however, they studied patients with relatively mild dementia. The prevalence of depression in dementia is 15% to 40%.35 Given the increasing incidence of dementia in our aging population, the availability of accurate screening tools that specifically account for the coexistence of these 2 common disorders is important.
This review also reveals a lack of screening accuracy for nonmajor depressive disorders using 3 common instruments. Lyness and colleagues36 showed that there is considerable functional disability in subsyndromal depression, which is more prevalent than major depression. Others show similar findings, supporting the significant morbidity caused by depressive symptoms not severe enough to cross threshold for a major disorder.37,38 As the characterization of nonmajor depressive disorders evolves, screening instruments should be developed and validated specifically for these syndromes.39
Late-life depressive disorders have a convincing burden of suffering, often go undetected, and have known effective treatments.40 Our systematic review reveals that accurate screening instruments are available to detect major depression in older primary care patients. Based on format and length ( Table 2 ), several could easily be self-administered or administered by nonclinicians in the waiting room. We recommend the 15-item GDS ( Figure ) because of its yes/no format and ease of scoring. Future work should include tests of depression screening accuracy for demented populations, and for nonmajor depressive disorders. Investigators should also evaluate the accuracy of very short instruments, such as the 5-item version of the GDS10 in the primary care setting. Acceptable administration times and ease of use is likely to determine the realistic application of proven instruments.
TABLE 2
Selected screening instruments and their characteristics
| Instrument | Format | Item | Time to administer | Sn (%) | Sp (%) |
|---|---|---|---|---|---|
| GDS-15 | Yes/no questions about current symptoms | 15 | 2–3 minutes | 82–100 | 72–82 |
| CES-D | Rates frequency of selected symptoms over last week | 20 | 2–3 minutes | 74–93 | 70–87 |
| SelfCareD | Multiple choice responses regarding symptoms over last month | 12 | 2–3 minutes | 77–95 | 53–98 |
| GDS-15: Geriatric Depression Scale, 15-item; CES-D: Center for Epidemiologic Study-Depression; Sn, sensitivity; Sp, specificity. Sensitivity and specificity values represent the range reported from the eligible studies in our review. | |||||
FIGURE
Geriatric Depression Scale, 15-item
Acknowledgments
The authors would like to thank Dr. Carmen Lewis for her thoughtful review of this manuscript. The authors report no competing interests. Funding sources: Robert Wood Johnson Clinical Scholars Program; Agency for Healthcare Research and Quality contract # 290-97-0011.
Corresponding author
Lea C. Watson MD, MPH, Geriatric Psychiatry, Box 3903, Duke University Medical Center, Durham, NC 27710. E-mail: [email protected].
Objective: To determine the accuracy of depression screening instruments for older adults in primary care.
Study Design: Systematic review
Data Sources: MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety and neurosis. We also searched the second Guide to Clinical Preventive Services, the 1993 Agency for Health Care Policy and Research Clinical Practice Guideline on Depression, and recent systematic reviews. Hand-checking of bibliographies and extensive peer review were also used to identify potential articles.
Outcomes Measured: A predefined search strategy targeted only studies of adults aged 65 years or older in primary care or community settings, including long-term care. Articles were included in this review if they reported original data and tested depression screening instruments against a criterion standard, yielding sensitivity and specificity.
Results: Eighteen articles met criteria and are included in this review, representing 9 different screening instruments. The most commonly evaluated were the Geriatric Depression Scale (30-and 15-item versions), the Center for Epidemiologic Studies Depression Scale, and the SelfCARE(D). Differences in the performance of these 3 instruments were minimal; sensitivities ranged from 74% to 100% and specificities ranged from 53% to 98%.
Conclusions: Accurate and feasible screening instruments are available for detecting late-life depression in primary care. More research is needed to determine the accuracy of depression screening instruments for demented individuals, and for those with subthreshold depressive disorders.
When depression is detected and treated in older patients, not only do symptoms subside, but behavior, cognitive functioning, and overall quality of life improve.1 We conducted a systematic review to determine the accuracy of instruments for detecting unrecognized late-life depression in the primary care setting. Several instruments are comparable in sensitivity and specificity, though the 15-item Geriatric Depression Scale is particularly useful in the primary care setting.
Search methods
As a part of a broader review for the US Preventive Services Task Force and the Research Triangle Institute–University of North Carolina at Chapel Hill Evidence-Based Practice Center, we prepared a strategy to identify articles relevant to the accuracy of depression screening instruments for older adults in the primary care setting. We searched for articles in MEDLINE, PsycINFO (search dates 1966 to January 2002), and the Cochrane database on depression, anxiety, and neurosis. We also searched the second Guide to Clinical Preventive Services,2 the 1993 Agency for Health Care Policy and Research (AHCPR) Clinical Practice Guideline on Depression, and recent systematic reviews.3 We also hand-checked bibliographies and used extensive peer review to identify potential articles.
We used the search terms depression, depressive disorder, mass screening, sensitivity and specificity, reproducibility of results, primary health care, ambulatory care, family practice, and the names of common screening and diagnostic instruments used to detect depression. Our search was limited to English-language texts and to ages greater than 65 years.
Inclusion and exclusion criteria
For inclusion, articles must have reported on depression screening in a primary care population of adults aged greater than 65 years. They must have used a criterion standard as comparison and provided information on diagnostic accuracy (usually sensitivity and specificity). Studies performed in the community and in long-term care settings, but not in psychiatric facilities or clinics, were included.
We excluded studies that extracted briefer instruments from the parent version retrospectively; for example, if an investigator evaluated a 5-item version of the Geriatric Depression Scale (GDS), he or she must have defined the specific questions prior to administering the instrument, rather than extracting the 5 items based on posthoc analyses.
The criterion standards must have been commonly accepted, structured or semistructured diagnostic interviews or independent evaluations performed by psychiatrists based on Diagnostic and Statistic Manual of Mental Disorders, revised 3rd or 4th editions (DSM-IIIR, DSM-IV), International Classification of Diseases, 10th ed (ICD-10), or Research Diagnostic Criteria. Our selection criteria are consistent with recognized standards for reviewing diagnostic tests, specifically in eliminating spectrum bias and requiring a criterion standard.4
Review standards
Both authors independently reviewed the abstracts and full articles generated from the searches. Discrepancies about eligibility were resolved by consensus after review of the entire article. For each included study, we extracted information about the screening instrument, the criterion standard, sensitivity and specificity, average age of participants, their dementia status, and the study setting. To further estimate accuracy, we calculated 95% confidence intervals around each measure of sensitivity and specificity. Multiple screening instruments precluded a meaningful meta-analysis of these results.
Results
Our initial search strategy yielded 1325 potential articles, 1269 of which could be eliminated by title review. Of the 56 articles remaining, 38 were eliminated after identifying exclusion criteria in the abstract or the manuscript: 17 because there was no criterion standard, 7 because the setting was not appropriate, 8 because the population was not geriatric, and 6 with varying methodologic exclusions. Eighteen articles met our inclusion criteria and specifically examined the performance of depression screening instruments for older adults in primary care ( Table 1 ).
The included studies were carried out among a wide spectrum of patients mostly in general practice settings, with the exception of 1 in a nursing home and 1 receiving home care. Two studies specifically included patients with dementia. Nine different instruments were used; most had 20 or fewer questions and were relatively easy to administer.
Overall test performance in detecting major depression was similarly favorable among the instruments, with sensitivities ranging from 67% to 100% and specificities ranging from 53% to 98%. All but 2 studies5,6 reported sensitivity and specificity based on optimal cutpoints determined by post-hoc receiving-operating characteristic (ROC) curve analyses, possibly exaggerating test performance in comparison with the studies testing predetermined cutpoints.
Five studies6,11,19,22,23 explicitly stated that interviewers performing the criterion standard exam were blinded to the results of the screening test; the remainder did not report on blinding, although in most cases blinding was implied by the use of a second “independent” rater.
Geriatric Depression Scale. The GDS, the Center for Epidemiologic Studies Depression scale (CES-D), and the SelfCARE(D) were the most-evaluated screening instruments. The GDS has both a 30- and 15-item version and was designed in a yes/no format for self- or caregiver administration, making it easy to use. It minimizes questions about somatic and vegetative symptoms, which can overlap with symptoms of concurrent medical illness.
The GDS has been validated repeatedly in psychiatric settings.23-27 Nine studies5-10,12 evaluated its use in primary care elderly, most using the 15-item version and a cutpoint of 3 to 5. Sensitivity and specificity ranged from 79%–100% and 67%–80%, respectively.
Center for Epidemiological Studies Depression Scale. The CES-D can be self-administered. It lists 20 statements addressing depressive symptoms over the last week, asking the participant to rank the frequency of these feelings from “rarely” to “most of the time.” Its psychometric properties have been consistently strong in younger adults in the community.
In the 5 studies13-16 that evaluated this instrument, cutpoints varied from 9 to 21. The resultant sensitivities were 75%–93%, with specificities ranging from 73%–87%. One study16 also specifically evaluated the performance of the CES-D in mildly demented subjects with an average Mini-Mental State Examination (MMSE) of 19, and showed similar test characteristics to the patients without dementia. This instrument was perceived as generally easy to administer, except in a nursing-home population where the questions had to be repeated multiple times.
Papassotiropoulos et al17 used the CES-D and the General Health Questionnaire (GHQ) to identify subthreshold depression in a community sample in Greece. They defined subthreshold depression as fewer than 5 depressive symptoms in a 2-week period; brief, monthly depressive symptoms not occurring for a 2-week duration; and, any significant single depressive symptom not specified by duration or frequency. Accuracy was poor for delineating these syndromes, with sensitivities below 50% and specificities of 75% and 72%, respectively.
Lyness and colleagues15 used the CES-D, as well as the GDS-15, to identify minor depression in their cohort. They defined minor depression as having sad mood or loss of interest and at least 2, but fewer than 5, additional depressive symptoms within a 2-week period. The CES-D revealed a sensitivity of 40% and specificity of 82% for detecting minor depression, while the GDS-15 had a sensitivity and specificity of 70% and 80%, respectively.
SelfCARE(D). The SelfCARE(D) is a self-administered instrument that requests responses to 12 items on a Likert scale, reflecting depressive symptoms over the last month. It was derived from a larger, previously validated instrument used in England.18
In 1 of 3 included studies, Bird and colleagues18 reported the original results in a 1987 outpatient sample, showing a sensitivity of 77% and specificity of 98%, with a cutpoint of 5. Since then it has been validated again in general practice and in home care.19,20 Both studies revealed sensitivities in the 90% range, but the specificity in home care was 53% vs 86% in general practice.
Caribbean Culture–Specific Screen. In an effort to address the potential cultural limitations of common instruments, Rait and colleagues11 tested the Caribbean Culture–Specific Screen (CCSS) in the growing contingent of Caribbeans of African descent in the United Kingdom. They found that it performed well, but not better than the Brief Assessment Schedule Depression Cards or the GDS-15. Each had a sensitivity of 92%, with specificities ranging from 71%–84%.
Similarly, Abas et al12 tested the CCSS and the GDS-15 in an African-Caribbean population, reporting sensitivities of 82% for both instruments, and specificities of 68% for the CCSS and 82% for the GDS-15.
Cornell Scale for Depression in Dementia. Dementia poses barriers to effective screening for depression given the obvious limitations in self report due to cognitive impairment. The Cornell Scale for Depression in Dementia (CSDD) was specifically designed for this population and calls for the clinician to use both patient and caregiver information to complete the screen.
The CSDD is categorized by questions on mood, behavior, physical signs, diurnal patterns, and ideational disturbances. Each item is on a 3-point scale for a possible total score of 38, with higher scores indicating more depression. Most data generated about the CSDD have come from hospitalized patients, in whom it has demonstrated acceptable validity and reliability in demented and nondemented patients.29-31
We identified 1 study evaluating the CSDD that met our criteria. Vida et al22 screened outpatients from a family medicine clinic and found a sensitivity of 90% and specificity of 75% for detecting major depression.
Other instruments. Several very brief instruments have been validated in psychiatric or hospital settings where the prevalence of depressive symptoms is often high,32,33 but few have been tested in older primary care patients. Howe et al34 attempted to validate a 1-question screen (MHI-1) derived from the mental health component of the SF-36, asking elderly participants, “in the past month, how much of the time have you felt downhearted or sad?” (1=none, 6=all the time). They showed that as a “stand alone” screen, the MHI-1 did not perform well in the primary care setting, with a sensitivity of 67% and a specificity of 60%.
TABLE 1
Articles relevant to late-life depression screening
| Author | Test/cutpoint | Criterion standard | Avg. age | Dementia | Sn (%) (95% CI) | Sp (%) (95% CI) |
|---|---|---|---|---|---|---|
| D’Ath et al5 | GDS-15/5 | GMS/AGECAT | 74 | Not tested | 91 (86–96) | 72 (66–78) |
| Gerety et al6 | GDS/11 | SCID* | 79 | Avg MMSE 23 (SD4.7) | 89 (72–96) | 68 (58–77) |
| CES-D/16 | 74 (55–86) | 70 (60–79) | ||||
| Neal and Baldwin7 | GDS/11 | GMS/AGECAT | 77 | Not tested | 83 (72–94) | 80 (68–92) |
| Van Marjwick et al8 | GDS/7 | DIS | 74 | Mild/none | 79 (76–82) | 67 (63–71) |
| Arthur et al9 | GDS-15/3 | ICD-10 | 80 | None | 100 (98–102) | 72 (67–77) |
| Hoyl et al10 | GDS-15/5 | SCID | 75 | Avg MMSE 27 (SD 2.6) | 94 (89–99) | 82 (73–91) |
| Rait et al11 | GDS-15/4 | GMS/AGECAT* | >60 | Not tested | 92 (64–100) | 71 (63–79) |
| BASEDEC/6 | 92 (64–100) | 84 (78–91) | ||||
| CCSS/6 | 92 (64–100) | 79 (71–86) | ||||
| Abas et al12 | GDS-15/5 | GMS/AGECAT | >60 | Avg. MMSE 24 (SD 4.6) | 82 (62–92) | 82 (62–92) |
| CCSS/5 | 82 (62–92) | 68 (54–79) | ||||
| Beekman et al13 | CES-D/20 | DIS | 55-82 | None | 93 (91–95) | 73 (69–77) |
| Lewisohn et al14 | CES-D/12 | RDC, DSM-IIIR | 64 | Not reported | 76 (73–79) | 77 (74–80) |
| Lyness et al15 | CES-D/21 | SCID | 71 | Not tested | – | – |
| – Major depression | 92 (87–97) | 87 (81–93) | ||||
| – Minor depression | 40 (32–48) | 82 (75–89) | ||||
| GDS/10 | ||||||
| – Major depression | 100 (98–102) | 84 (78–90) | ||||
| – Minor depression | 70 (62–78) | 80 (73–87) | ||||
| Papassotiropoulos et al16 | CES-D/8 (demented excluded) | CIDI | >60 | Avg MMSE 27 (SD 6.0) | 75 (70–80) | 74 (67–81) |
| CES-D/9 (demented excluded) | CIDI | >60 | Avg MMSE 19 (SD 5.5)n demented sample | 75 (70–80) | 72 (67–77) | |
| 75 (70–80) | 72 (67–77) | |||||
| Papassotiropoulos et al17 | GHQ-12/0 Subthreshold depression | CIDI, DSM-IIIR; not reported | >60 | Avg. MMSE 28 (SD 2.0) | 46 (40-52) | 72 (67–77) |
| CES-D/9 Subthreshold depression | 39 (33-45) | 75 (70-80) | ||||
| Bird et al18 | SelfCARE(D)/5 | Independent psychiatric assessment* | 73 | Not tested | 77 (67–87) | 98 (95–101) |
| Upadhyaya and Stanley19 | SelfCARE(D)/5 | GMS/AGECAT* | 71 | Not tested | 95 (90–100) | 86 (78–94) |
| 74 (55–86) | 70 (60–79) | |||||
| Banerjee et al20 | SelfCARE(D)/8 | GMS/AGECAT | >65 | Not tested | 90 (86–94 | 53 (46–60) |
| Howe et al21 | MHI-1/2 | GMS/AGECAT | 81 | Excluded “organic mpairment” | 67 (58–76) | 60 (50–70) |
| Vida et al22 | Cornell Screen/7 | RDC* | 72 | Avg MMSE 19 (SD 7.8) | 90 (80–100) | 75 (60–90) |
| *These studies were blinded; all others were not reported. | ||||||
| GDS, Geriatric Depression Scale, 30-item; GDS-15, Geriatric Depression Scale, 15-item; GHQ, General Health Questionnaire; DIS, Diagnostic Interview Schedule; BASEDEC, Brief Assessment Schedule Depression Cards; CES-D, Center for Epidemiologic Study-Depression; MHI-1, single question from the Mental Health Inventory [“in the past month, how much have you felt downhearted or sad (1: none-6: all the time)”]; GMS, Geriatric Mental State/AGECAT computer program; CIDI, Composite International Diagnostic Interview; SCID, Structured Clinical Interview for DSM IIIR; CCSS, Caribbean Culture Specific Screen; RDC, Research Diagnostic Criteria; DSM IIIR, Diagnostic and Statistical Manual of Mental Disorders,3rd ed rev; MMSE, Mini Mental State Examination; ICD-10, International Classification of Diseases, 10th ed | ||||||
Discussion: late-life depression can be diagnosed accurately
Our systematic review shows that several instruments demonstrate good accuracy for detecting late-life major depression in primary care. The GDS, CES-D and SelfCARE(D) have comparable sensitivities and specificities. The CES-D and CCSD have similarly favorable accuracy in demented patients with an average MMSE score of 19.
A 1-question screen shows poor results, as do studies using the GHQ, CES-D, and GDS-15 to detect nonmajor depression. Finally, 2 studies demonstrate that a culturally specific screen in African-Caribbeans performs well, but no better than, the GDS.
The GDS has longstanding success in identifying major depression in psychiatric and hospital settings and now demonstrates accuracy in primary care, where the 15-item version in its yes/no self-administered format represents a realistic tool for use in the community or the clinic.
With a record of successful use in general adult research, the CES-D also has the benefit of a known track record and relative ease of administration. Evidence from this review suggests that it can be extended to the older primary care population. The SelfCARE(D) is comparably accurate in general practice, but has lower specificity in home care.
Our review highlights the need to further investigate the accuracy of screening tools for depression in patients with dementia, specifically where cognitive impairment may be severe. Using the CSDD, an instrument specifically designed for patients with dementia, Vida et al22 found good accuracy for detecting depression; however, they studied patients with relatively mild dementia. The prevalence of depression in dementia is 15% to 40%.35 Given the increasing incidence of dementia in our aging population, the availability of accurate screening tools that specifically account for the coexistence of these 2 common disorders is important.
This review also reveals a lack of screening accuracy for nonmajor depressive disorders using 3 common instruments. Lyness and colleagues36 showed that there is considerable functional disability in subsyndromal depression, which is more prevalent than major depression. Others show similar findings, supporting the significant morbidity caused by depressive symptoms not severe enough to cross threshold for a major disorder.37,38 As the characterization of nonmajor depressive disorders evolves, screening instruments should be developed and validated specifically for these syndromes.39
Late-life depressive disorders have a convincing burden of suffering, often go undetected, and have known effective treatments.40 Our systematic review reveals that accurate screening instruments are available to detect major depression in older primary care patients. Based on format and length ( Table 2 ), several could easily be self-administered or administered by nonclinicians in the waiting room. We recommend the 15-item GDS ( Figure ) because of its yes/no format and ease of scoring. Future work should include tests of depression screening accuracy for demented populations, and for nonmajor depressive disorders. Investigators should also evaluate the accuracy of very short instruments, such as the 5-item version of the GDS10 in the primary care setting. Acceptable administration times and ease of use is likely to determine the realistic application of proven instruments.
TABLE 2
Selected screening instruments and their characteristics
| Instrument | Format | Item | Time to administer | Sn (%) | Sp (%) |
|---|---|---|---|---|---|
| GDS-15 | Yes/no questions about current symptoms | 15 | 2–3 minutes | 82–100 | 72–82 |
| CES-D | Rates frequency of selected symptoms over last week | 20 | 2–3 minutes | 74–93 | 70–87 |
| SelfCareD | Multiple choice responses regarding symptoms over last month | 12 | 2–3 minutes | 77–95 | 53–98 |
| GDS-15: Geriatric Depression Scale, 15-item; CES-D: Center for Epidemiologic Study-Depression; Sn, sensitivity; Sp, specificity. Sensitivity and specificity values represent the range reported from the eligible studies in our review. | |||||
FIGURE
Geriatric Depression Scale, 15-item
Acknowledgments
The authors would like to thank Dr. Carmen Lewis for her thoughtful review of this manuscript. The authors report no competing interests. Funding sources: Robert Wood Johnson Clinical Scholars Program; Agency for Healthcare Research and Quality contract # 290-97-0011.
Corresponding author
Lea C. Watson MD, MPH, Geriatric Psychiatry, Box 3903, Duke University Medical Center, Durham, NC 27710. E-mail: [email protected].
1. Mulsant BH, Ganguli M. Epidemiology and diagnosis of depression in late life. J Clin Psychiatry 1999;60(suppl 20):9-15.
2. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Alexandria, Va: International Medical Publishing; 1996.
3. Pignone MP, Gaynes BN, Rushton JL, et al. Screening for depression in adults: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002;136:765-776.
4. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1066.
5. D’Ath P, Katona P, Mullan E, Evans S, Katona C. Screening, detection and management of depression in elderly primary care attenders. I: The acceptability and performance of the 15 item Geriatric Depression Scale (GDS15) and the development of short versions. Fam Pract 1994;11:260-266.
6. Gerety MB, Williams JW, Jr, Mulrow CD, et al. Performance of case-finding tools for depression in the nursing home: influence of clinical and functional characteristics and selection of optimal threshold scores. J Am Geriatr Soc 1994;42:1103-1109.
7. Neal R, Baldwin R. Screening for anxiety and depression in elderly medical outpatients. Age and Ageing 1994;23:461-464.
8. van Marwijk HV, Wallace P, de Bock GD, Hermans J, Kapteinaa Mulder JD. Evaluation of the feasibility, reliability and diagnostic value of shortened versions of the geriatric depression scale. Br J Gen Prac 1995;45:195-199.
9. Arthur A, Jagger C, Lindesay J, Graham C, Clarke M. Using an annual over-75 health check to screen for depression: validation of the short Geriatric Depression Scale (GDS15) within general practice. Int J Geriatr Psychiatry 1999;14:431-439.
10. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the Geriatric Depression Scale. J Am Geriatr Soc 1999;47:873-878.
11. Rait G, Burns A, Baldwin R, et al. Screening for depression in African-Caribbean elders. Fam Pract 1999;16:591-595.
12. Abas MA, Phillips C, Carter J, Walter S, Banerjee S, Levy R. Culturally sensitive validation of screening questionnaires for depression in older African-Caribbean people living in south London. Br J Psychiatry 1998;173:249-254.
13. Beekman AT, Deeg DJ, Van Limbeek J, Braam AW, de Vries MR, Van Tillburg W. Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): results from a community-based sample of older subjects in The Netherlands. Psychol Med 1997;27:231-235.
14. Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol Aging 1997;12:277-287.
15. Lyness JM, Noel TK, Cox C, et al. Screening for depression in elderly primary care patients. A comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch Intern Med 1997;157:449-454.
16. Papassotiropoulos A, Heun R, Maier W. The impact of dementia on the detection of depression in elderly subjects from the general population. Psychol Med 1999;29:113-120.
17. Papassotiropoulos A, Heun R. Detection of subthreshold depression and subthreshold anxiety in the elderly. Int J Geriatr Psychiatry 1999;14:643-650.
18. Bird A, Macdonald A, Mann A, et al. Preliminary experience with the SelfCARE(D): a self-rating depression questionnaire for use in elderly, non-institutionalized subjects. Int J Geriatr Psychiatry 1987;2.
19. Upadhyaya AK, Stanley I. Detection of depression in primary care comparison of two self. administered scales. Int J Geriatr Psychiatry 1997;12:35-37.
20. Banerjee S, Shamash K, MacDonald AJ, et al. The use of the SelfCARE(D) as a screening tool for depression in the clients of local authority home care services-a preliminary study. Int J Geriatr Psychiatry 1998;13:695-699.
21. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
22. Vida S, Des Rosiers P, Carrier L, Gauthier S. Depression in Alzheimer’s disease: receiver operating characteristic analysis of the Cornell Scale for Depression in Dementia and the Hamilton Depression Scale. J Geriatr Psychiatry Neur 1994;7:159-162.
23. Sheik J, Yesavage J. Geriatric Depression Scale (GDS): recent findings and development of a shorter version. New York, NY: Howarth Press; 1986.
24. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982;17:37-49.
25. Fountoulakis KN, Tsolaki M, Iacovides A, et al. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging (Milano) 1999;11:367-372.
26. Lim PP, Ng LL, Chiam PC, Ong PS, Ngui FT, Sahadevan S. Validation and comparison of three brief depression scales in an elderly Chinese population. Int J Geriatr Psychiatry 2000;15:824-830.
27. Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 1999;14:858-865.
28. Mulrow CD, Williams JW, Jr, Gerety MB, Ramirez G, Montiel OM, Kerber C. Case-finding instruments for depression in primary care settings. Ann Intern Med 1995;122:913-921.
29. Alexopoulos G, Abrams R, Young R, Shamoian CA. Use of the Cornell Scale in Nondemented Patients. J Am Geriatr Soc 1988;36:230-236.
30. Alexopoulos G, Abrams R, Young R, Shamoian CA. Cornell Scale for Depression in Dementia. Biol Psychiatry 1988;23:271-284.
31. Harwood D, Ownby R, Barker W, Duara R. The factor structure of the Cornell Scale for Depression in Dementia among probable Alzheimer’s disease patients. Am J Geriatr Psychiatry 1998;6:212-220.
32. Weyerer S, Killmann U, Ames D, Allen N. The Even Briefer Assessment Scale for Depression (EBAS DEP): its suitability for the elderly in geriatric care in English-and German- speaking countries. Int J Geriatr Psychiatry 1999;14:473-480.
33. Pomeroy IM, Clark CR, Philp I. The effectiveness of very short scales for depression screening in elderly medical patients. Int J Geriatr Psychiatry 2001;16:321-326.
34. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
35. Lyketsos G, Baker L, Warren A, et al. Major and minor depression in Alzheimer’s disease: prevalence and impact. J Neuropsychiatry Clin Neurosci 1997;9:556-561.
36. Lyness JM, King DA, Cox C, Yoediono Z, Caine ED. The importance of subsyndromal depression in older primary care patients: prevalence and associated functional disability. J Am Geriatr Soc 1999;47:647-652.
37. Hendrie H, Callahan C, Levitt E. Prevalence rates of major depressive disorders: the effect of varying diagnostic criteria in an older primary care population. Am J Geriatr Psychiatry 1995;3:119-131.
38. Unutzer J, Patrick D, Simon G, et al. Depressive symptoms and the cost of health services in HMO patients aged 65 years and older. JAMA 1997;277:1618-1623.
39. Lavretsky H, Kumar A. Clinically significant non-major depression: old concepts, new insights. Am J Geriatr Psychiatry 2002;10:239-255.
40. Lebowitz BD, Pearson JL, Schneider LS, et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA 1997;278:1186-1190.
1. Mulsant BH, Ganguli M. Epidemiology and diagnosis of depression in late life. J Clin Psychiatry 1999;60(suppl 20):9-15.
2. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Alexandria, Va: International Medical Publishing; 1996.
3. Pignone MP, Gaynes BN, Rushton JL, et al. Screening for depression in adults: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002;136:765-776.
4. Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061-1066.
5. D’Ath P, Katona P, Mullan E, Evans S, Katona C. Screening, detection and management of depression in elderly primary care attenders. I: The acceptability and performance of the 15 item Geriatric Depression Scale (GDS15) and the development of short versions. Fam Pract 1994;11:260-266.
6. Gerety MB, Williams JW, Jr, Mulrow CD, et al. Performance of case-finding tools for depression in the nursing home: influence of clinical and functional characteristics and selection of optimal threshold scores. J Am Geriatr Soc 1994;42:1103-1109.
7. Neal R, Baldwin R. Screening for anxiety and depression in elderly medical outpatients. Age and Ageing 1994;23:461-464.
8. van Marwijk HV, Wallace P, de Bock GD, Hermans J, Kapteinaa Mulder JD. Evaluation of the feasibility, reliability and diagnostic value of shortened versions of the geriatric depression scale. Br J Gen Prac 1995;45:195-199.
9. Arthur A, Jagger C, Lindesay J, Graham C, Clarke M. Using an annual over-75 health check to screen for depression: validation of the short Geriatric Depression Scale (GDS15) within general practice. Int J Geriatr Psychiatry 1999;14:431-439.
10. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the Geriatric Depression Scale. J Am Geriatr Soc 1999;47:873-878.
11. Rait G, Burns A, Baldwin R, et al. Screening for depression in African-Caribbean elders. Fam Pract 1999;16:591-595.
12. Abas MA, Phillips C, Carter J, Walter S, Banerjee S, Levy R. Culturally sensitive validation of screening questionnaires for depression in older African-Caribbean people living in south London. Br J Psychiatry 1998;173:249-254.
13. Beekman AT, Deeg DJ, Van Limbeek J, Braam AW, de Vries MR, Van Tillburg W. Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): results from a community-based sample of older subjects in The Netherlands. Psychol Med 1997;27:231-235.
14. Lewinsohn PM, Seeley JR, Roberts RE, Allen NB. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol Aging 1997;12:277-287.
15. Lyness JM, Noel TK, Cox C, et al. Screening for depression in elderly primary care patients. A comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch Intern Med 1997;157:449-454.
16. Papassotiropoulos A, Heun R, Maier W. The impact of dementia on the detection of depression in elderly subjects from the general population. Psychol Med 1999;29:113-120.
17. Papassotiropoulos A, Heun R. Detection of subthreshold depression and subthreshold anxiety in the elderly. Int J Geriatr Psychiatry 1999;14:643-650.
18. Bird A, Macdonald A, Mann A, et al. Preliminary experience with the SelfCARE(D): a self-rating depression questionnaire for use in elderly, non-institutionalized subjects. Int J Geriatr Psychiatry 1987;2.
19. Upadhyaya AK, Stanley I. Detection of depression in primary care comparison of two self. administered scales. Int J Geriatr Psychiatry 1997;12:35-37.
20. Banerjee S, Shamash K, MacDonald AJ, et al. The use of the SelfCARE(D) as a screening tool for depression in the clients of local authority home care services-a preliminary study. Int J Geriatr Psychiatry 1998;13:695-699.
21. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
22. Vida S, Des Rosiers P, Carrier L, Gauthier S. Depression in Alzheimer’s disease: receiver operating characteristic analysis of the Cornell Scale for Depression in Dementia and the Hamilton Depression Scale. J Geriatr Psychiatry Neur 1994;7:159-162.
23. Sheik J, Yesavage J. Geriatric Depression Scale (GDS): recent findings and development of a shorter version. New York, NY: Howarth Press; 1986.
24. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 1982;17:37-49.
25. Fountoulakis KN, Tsolaki M, Iacovides A, et al. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging (Milano) 1999;11:367-372.
26. Lim PP, Ng LL, Chiam PC, Ong PS, Ngui FT, Sahadevan S. Validation and comparison of three brief depression scales in an elderly Chinese population. Int J Geriatr Psychiatry 2000;15:824-830.
27. Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 1999;14:858-865.
28. Mulrow CD, Williams JW, Jr, Gerety MB, Ramirez G, Montiel OM, Kerber C. Case-finding instruments for depression in primary care settings. Ann Intern Med 1995;122:913-921.
29. Alexopoulos G, Abrams R, Young R, Shamoian CA. Use of the Cornell Scale in Nondemented Patients. J Am Geriatr Soc 1988;36:230-236.
30. Alexopoulos G, Abrams R, Young R, Shamoian CA. Cornell Scale for Depression in Dementia. Biol Psychiatry 1988;23:271-284.
31. Harwood D, Ownby R, Barker W, Duara R. The factor structure of the Cornell Scale for Depression in Dementia among probable Alzheimer’s disease patients. Am J Geriatr Psychiatry 1998;6:212-220.
32. Weyerer S, Killmann U, Ames D, Allen N. The Even Briefer Assessment Scale for Depression (EBAS DEP): its suitability for the elderly in geriatric care in English-and German- speaking countries. Int J Geriatr Psychiatry 1999;14:473-480.
33. Pomeroy IM, Clark CR, Philp I. The effectiveness of very short scales for depression screening in elderly medical patients. Int J Geriatr Psychiatry 2001;16:321-326.
34. Howe A, Bath P, Goudie F, et al. Getting the questions right: an example of loss of validity during transfer of a brief screening approach for depression in the elderly. Int J Geriatr Psychiatry 2000;15:650-655.
35. Lyketsos G, Baker L, Warren A, et al. Major and minor depression in Alzheimer’s disease: prevalence and impact. J Neuropsychiatry Clin Neurosci 1997;9:556-561.
36. Lyness JM, King DA, Cox C, Yoediono Z, Caine ED. The importance of subsyndromal depression in older primary care patients: prevalence and associated functional disability. J Am Geriatr Soc 1999;47:647-652.
37. Hendrie H, Callahan C, Levitt E. Prevalence rates of major depressive disorders: the effect of varying diagnostic criteria in an older primary care population. Am J Geriatr Psychiatry 1995;3:119-131.
38. Unutzer J, Patrick D, Simon G, et al. Depressive symptoms and the cost of health services in HMO patients aged 65 years and older. JAMA 1997;277:1618-1623.
39. Lavretsky H, Kumar A. Clinically significant non-major depression: old concepts, new insights. Am J Geriatr Psychiatry 2002;10:239-255.
40. Lebowitz BD, Pearson JL, Schneider LS, et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA 1997;278:1186-1190.