User login
FDA Unveils Graphic Cigarette Packaging Intended to Deter Smoking
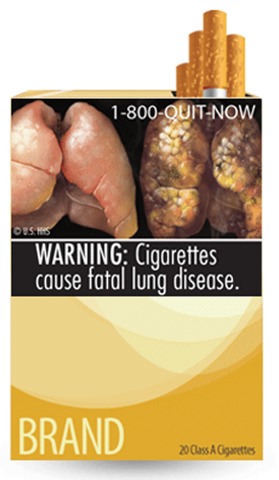
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
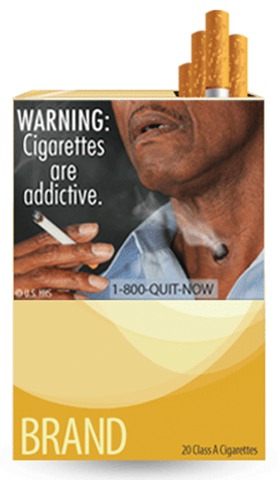
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
FDA Unveils Graphic Cigarette Packaging Intended to Deter Smoking
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
FDA Unveils Graphic Cigarette Packaging Intended to Deter Smoking
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
I give the FDA a
“B” on this action, but I don’t think it’s enough. Congress could have decided on
much stronger pictures. It could have made them larger, not just 20% of the
pack and located on the back . In other countries that use such warnings, the
pictures cover almost 80% of the packaging.
Plainly put, the United States is a Third
World country when it comes to warning about cigarettes. Similar
pictorial warnings have been used in Canada
for almost a decade; Australia,
almost all of the European Union countries, and even Uruguay have similar warnings.
Having said that, we do know
that pictures speak louder than words and may help motivate smokers to quit.
But here is the hard reality: Even though nearly everyone wants to quit smoking
and many are trying to do so every day, the ability to sustain that motivation
is not always present.
Two factors are highly
predictive of a successful quit: the clinical predictor of personal biology and
the financial predictor of cigarette engineering.
Biologically, some people
are more prone to developing addictions than others. If you have a patient who
reaches for a cigarette before their feet even hit the floor in the morning,
that patient is going to need more medical assistance to be successful.
The second factor is
cigarette engineering. Cigarettes are designed to get people hooked and keep
them hooked. This is what makes quitting so hard despite strong personal motivation.
If we look back in
history, around 1900 there were only a few hundred cases of lung cancer
diagnosed in the U.S.
each year. This year it will be around 160,000. What has happened since then?
People were indeed smoking
then – pipes, cigars, and roll-your-own cigarettes. But this was not a daily-use
situation, mostly because the pH of the smoke made it very hard to inhale.
Right around 1920, commercially available cigarette brands reformulated their
tobacco to make the smoke milder. This allowed people to smoke more, loading
their brains up with lots more nicotine, lots faster.
Around 1950, manufacturers
began adding chemicals to moderate the pH, facilitating deep inhalation. the
lungs. These ingredients – diammonium phosphate, urea, and hydrochloride among
them – are still on the packs’ ingredient list, although manufacturers call
them “flavorings.”
Filters were the next step
in developing an addictive product. Manufacturers presented filters as making
cigarettes safer. Their real purpose was both to break down the tar into
smaller particles and to force people to suck on the cigarette harder to get
the smoke. Filters actually make things worse by forcing rapid inhalation and
rapid absorption – delivering the nicotine to the brain within seconds.
These things were done
secretly and purposefully to promote tobacco addiction and maintain profits. Tobacco
companies deliberately suppressed this information until 2006, when a
racketeering lawsuit forced the disclosure of dozens of documents showing the
intention behind these decisions. U.S District Court Judge Gladys Kessler determined
that tobacco companies conspired to lie about the dangers of smoking and, in
her 1,600-page ruling, called the conspiracy “decades long.”
“In short, the defendants
have marketed and sold their lethal product with zeal, with deception, with a
single-minded focus on their financial success, and without regard for the
human tragedy or social costs that success exacted,” according to her ruling.
Despite lawsuits, public
information campaigns, and the current warnings on cigarette packs, Americans
continue to smoke and I continue to see the effects.
About a third of the
patients I see at the Roswell Park Cancer Institute have smoking-related
cancers. Imagine a vaccine that would prevent a third of cancers. The inventor would
be a Nobel Laureate, globally praised.
We already have this – but
it’s not a vaccine. It’s much simpler.
Just stop smoking.
K. Michael Cummings,
Ph.D, is the director of the New York State Smokers’ Quitline and a senior research
scientist at the Roswell Park cancer Institute, Buffalo.
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The Food and Drug Administration unveiled on June 21 the final nine warning images that will appear on every package of cigarettes by 2012 – graphic photos and drawings intended to educate and even deter consumers from buying cigarettes.
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings in 25 years. By Oct. 22, 2012, cigarette manufacturers will no longer be able to distribute cigarettes for sale in the United States unless they display these warnings.
The law required the warnings to cover the top half of the front and back of cigarette packs and 20% of cigarette advertisements, and they must contain color graphics depicting the negative health consequences of smoking.
"This is something Congress wanted to happen and mandated that the FDA carry out," Mr. Ventura said in an interview. Based on a study of 18,000 smokers conducted for the FDA by RTI International, federal officials said they firmly believe that visually communicating smoking’s harm will deter cigarette consumption over the long run.
The images include photos of tobacco-diseased lungs beside healthy lungs, a corpse in casket, a man exhaling smoke though a tracheostomy, and lip cancer. There are also several cartoons and photos of mothers blowing smoke into infants’ faces. One positive image shows a burly man exposing a T-shirt saying, "I Quit."
Blunt statements accompany each image, intended to drive home the messages that cigarette smoke not only directly harms the smoker, but the smokers’ children and people in close proximity.
"The introduction of these warnings is expected to have a significant public health impact by decreasing the number of smokers, resulting in lives saved, increased life expectancy, and improved health status," FDA officials said in a press statement.
Mr. Ventura said the images were selected after the consumer study involving smokers aged 15-50 years. After viewing each of the images, subjects rated their emotional and cognitive responses, their ability to recall the images, and their opinions on whether the pictures could alter their beliefs about the danger of smoking and the desire to buy tobacco products and quitting tobacco.
Young people responded most strongly to a cartoon image depicting tobacco addiction – a cigarette being injected into an arm vein as well as a puppet controlled by strings.
Adults, on the other hand, responded most strongly to photos showing the direct effects of cancer on their bodies – the man with the tracheostomy and a woman smoking in the pouring rain, trying to shield her cigarette with a folded newspaper. Adults also reacted more strongly than did young people to images depicting harm to young children.
The study did conclude, however, that none of the images were significantly related to an increased likelihood of quitting smoking within the next 30 days, or the likelihood of smoking a year after viewing the images. Thus, the report noted, the campaign is more likely to exert a long-term behavioral impact than any immediate effects.
"Eliciting strong emotional and cognitive reactions to the graphic cigarette warning label enhances recall and processing of the health warning, which helps ensure that the warning is better processed, understood, and remembered," the study said. "As attitudes and beliefs change, they eventually lead to changes in intentions to quit or start smoking and then later to lower smoking initiation and successful cessation. The time scale on which this behavior change process occurs is largely unknown in the context of the impact of exposure to graphic warning labels on smoking behaviors, but the effects on behavior change are unlikely to be immediate or short-term.
Nevertheless, groups promoting antitobacco messages – including the American Heart Association – strongly believe that the warnings will enhance consumer education and change behavior.
"Undoubtedly, the new graphic health warnings will heighten awareness about the dangers of smoking and, more importantly, encourage smokers to quit and discourage smoking initiation," an AHA press statement read. "We’re confident that the new labels will move us closer to our goal of making the nation 100% smoke free."
Tobacco-Free Kids, a group dedicated to educating children and teens about the dangers of smoking, also issued a statement of support, but with a moderated view on the campaign’s possible impact. The group also called on political leaders to financially commit to "waging war" against tobacco.
"The warnings and other FDA regulations are powerful tools, but they are a complement – not a replacement – to other federal and state strategies to reduce tobacco use," Matthew L. Meyers, the group’s president, said in the statement. "To win the fight against tobacco, elected leaders must also fund and implement public education campaigns, expand health care coverage for therapies to help smokers quit, increase tobacco taxes, and enact strong smoke-free laws in every state."
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
The images, set to debut in stores this September, are required by the 2009 Tobacco Control Act, according to FDA spokesman Jeffrey Ventura, who added that these are the first changes to cigarette pack warnings
Headache in Young Children Almost Never Dangerous
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Major Finding: Of 100 pediatric patients presenting with headache, only 2% were diagnosed with a life-threatening condition; 57% of the 49 with primary headaches had migraine.
Data Source: A retrospective chart study of 100 children who presented to a pediatric neurology clinic, pediatric hospital, or emergency department with a complaint of headache.
Disclosures: Dr. Taute said she had no relevant financial disclosures.
Headache in Young Children Almost Never Dangerous
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
WASHINGTON – The vast majority of headaches in children younger than 8 years old have no dangerous or life-threatening etiology, a retrospective study has shown.
Of 100 children who presented with headache, only 2 had a dangerous condition – brain tumor – and both of those patients also had concerning neurologic symptoms.
The findings should be reassuring not only to parents, but to physicians as well, Dr. Carey Taute said at the annual meeting of the American Headache Society.
"Headache is a very common complaint in the pediatric neurology clinic, emergency department, and pediatric hospital, and everyone is, of course, worried about a dangerous etiology," said Dr. Taute of the Cleveland Clinic. "But in young children, there is a poor ability to get descriptions like the time of onset, duration, location, and nature of pain.
"This can lead to physician uncertainty about how to manage," she added. "Sometimes, this leads to an extensive but unnecessary work-up in these children."
Dr. Taute presented the initial results of 100 patients included in a 300-patient retrospective chart study. The children’s median age was 5 years; gender was evenly split. Most (53%) presented to a pediatric neurology clinic; others presented at a pediatric hospital (27%) and the remainder, to an emergency department.
Of this initial group, nine were excluded from the review because of pre-existing medical conditions, including three with Chiari’s malformation – two of whom had undergone surgical decompression; three with ventriculoperitoneal shunt for hydrocephalus; and three with known brain tumors.
Of the remaining 91 children, 49 were determined to have primary headache. The most common finding was migraine (28), followed by nonclassifiable headache (18), chronic daily headache (2), and one child with tension-type headache.
Secondary headache occurred in 41 of the children. "Of these, the vast majority (37) were attributable to a viral or other illness, but not to any dangerous complications," Dr. Taute said. Physicians couldn’t determine one child’s headache as primary or secondary; that child was referred for brain imaging but did not undergo the test.
A life-threatening cause appeared in only 2 of the 91 children; both of those children had brain tumors. However, both children had concerning neurologic findings. One presented with progressively worse vomiting and falls over a period of a week, and the headache was worse when lying down. The other presented with a head tilt, unilateral increased tone, and unilateral dysmetria.
Overall, primary headache and headache caused by an illness are the most common types of headache in this age group, Dr. Taute said. "Fear of a life-threatening etiology is most often not supported without an abnormal neurologic exam or some concerning neurologic symptoms."
Dr. Taute said she had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN HEADACHE SOCIETY
Stave Off Damage From Status Epilepticus With Seizure Algorithm
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Stave Off Damage From Status Epilepticus With Seizure Algorithm
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Stave Off Damage From Status Epilepticus With Seizure Algorithm
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
GRAPEVINE, TEX. – Convulsive status epilepticus is a medical emergency that requires quick thinking and quick action to protect the patient from both acute and long-term damage.
Convulsive seizures can be strong enough to break bones, Dr. David Likosky said at the annual meeting of the Society of Hospital Medicine. They can acutely endanger the patient and, if not controlled, pave the way for more frequent episodes.
Experts now recognize that repeated seizures can cause brain injury that increases the risk of more seizures, "kindling is the idea that the more seizures you have, the more likely you are to have them," said Dr. Likosky, a neurohospitalist and director of the stroke program at Evergreen Medical Center in Kirkland, Wash. "There is even some evidence that patients who have repeated convulsive status can develop areas of gliosis over time."
The definition of status epilepticus has changed somewhat recently, he said. "It used to be a seizure lasting more than 20-30 minutes or frequent seizures without a return to a normal level of consciousness in between. Now most neurologists will call any seizure that lasts more than 5 minutes status and treat [as if it is] status," according to Dr. Likosky, who has developed an algorhithm for treating convulsive status epilepticus in the emergency department.
These events are not rare, with more than 152,000 cases presenting each year, resulting in about 42,000 deaths. "The odds are that you are going to see one of these at some time, and you need to be able to treat it."
Status doesn’t occur only in patients with a known epilepsy diagnosis. Infections, tumors, brain abscess, traumatic brain injury, metabolic derangement, and drug overdose can all precipitate an event. For patients with an epilepsy diagnosis, a frequent cause is medication noncompliance.
"Convulsive status is a medical emergency," Dr. Likosky said. "The repeated seizures cause a huge amount of metabolic stress, which can even lead to a mycoardial infarction."
The rapid cycling between convulsive and nonconvulsive states can cause hypotension. Strong muscle contractions can result in hypoxia and metabolic acidosis and actually put enough torque on the bones to crack them. Patients can go into shock, and all of these things complicate an already-dire situation.
Dr. Likosky’s treatment algorithm is similar to one published this year in the journal Neurohospitalist. Dr. Edward Manno, a neurointensivist at the Cerebrovascular Center in Cleveland, created a decision tree outlining the treatment process step by step (Neurohospitalist 2011;1:23-31).
As in most emergency situations, the first step is to maintain an open airway, using pulse oximetry and cardiac monitoring to measure vitals. A quick glucose test is necessary because hypoglycemia can be at the root of a seizure storm.
Intravenous benzodiazepines are the first level of treatment. Lorazepam, diazepam, and midazolam are frequently employed. Although all are effective, a 2001 study found that lorazepam was more effective than diazepam in treating status epilepticus (N. Engl. J. Med. 2001;345:631-7).
"A new study is looking at the effectiveness of intramuscular midazolam that can be given by medics, or even at home," Dr. Likosky said. The results should be available later this year.
Sometimes patients in status require a fairly large drug dose to stop the seizures. "Since the underlying point is to treat aggressively and quickly, underdosing really hurts these patients. People vary, for example, in how much lorazepam to give. Some give 2 mg and some give 4 mg, but don’t be shy about increasing it to 6 or even 8, Dr. Likosky said."
If the patient doesn’t respond to initial benzodiazepine treatment, the next step is to administer fosphenytoin intravenously. "The key here is that one size does not fit all. You can’t just give 1 g. What you want is 18-20 mg/kg. The most important thing is to get [the patient] to a good level, and you may even give an additional dose on top of that," increasing to 30 mg/kg if necessary.
If this doesn’t arrest the seizure, phenobarbital or pentobarbital are in order. "Keep in mind that they cause respiratory suppression, especially when given in high doses to someone who has already had a benzodiazepine. If you haven’t intubated the patient before this, you have to do it now, prophylactically, in case breathing stops."
Other antiepileptic medications should be tried next. An intravenous loading dose of valproic acid (20-25 mg/kg) or levetiracetam (500-1,000 mg) are two possible choices.
Refractory status occurs when a patient fails benzodiazepine, phenytoin, and antiseizure medications. "This is when you start thinking about anesthetics. You need to titrate these according to the EEG." Propofol, midazolam infusion, pentobarbital, or ketamine are possibilities here.
"Keep in mind you do not want a neuromuscular blockade," Dr. Likosky said. "It’s easy to stop convulsions [via paralysis] but it doesn’t really do what you want," which is normalizing the EEG.
The goal for the EEG changes is a transformation of the spike/wave epileptiform pattern to burst suppression – a pattern of flatter lines interrupted by bursts of electrical discharge. Motor symptoms are not a reliable indicator of ongoing seizure activity.
Several studies have shown that EEG status can persist after motor symptoms resolve, Dr. Likosky said. A 1996 study highlights this phenomenon. Of 164 patients treated for convulsive status epilepticus, 48% still showed persistent electrographic seizure activity after their motor seizures ceased (Epilepsia 1998;39:833-40).
These patients must be treated aggressively with regular lightening of sedating medications, accompanied by an assessment of their clinical picture and EEG findings.
Dr. Likosky reported having no financial disclosures relevant to his lecture.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Discharge Planning For Diabetics Should Begin at Admission
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Discharge Planning For Diabetics Should Begin at Admission
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
GRAPEVINE, TEX. – The time to start an effective diabetes discharge plan is the moment the hyperglycemic patient is admitted to the hospital.
"I’m making a plea for the idea that a successful transition from the hospital to home begins with patient admission," Dr. John MacIndoe said at the annual meeting of the Society of Hospital Medicine.
Getting a hemoglobin A1C on every hyperglycemic patient is a critical part of the plan. "With this information, we have a crystal ball in our hands. Almost all of the decisions we need to make about glycemic control are based on that very important thing we should do on admission: Get the HbA1c. That is a window into the 3 months prior to admission, telling you what the baseline glucose was before the patient became ill."
But even with the best clinical information, there’s no point in designing a diabetes discharge plan to which the patient can’t adhere because of financial or social barriers. "Identify patients with issues that will complicate their outpatient diabetes management, because what you send them home on has to work well for them."
Financial barriers (lack of health insurance or very high insurance deductibles) have become ever more common over the past few years, said Dr. MacIndoe of the HealthPartners Medical Group and Clinics in Minneapolis. Social barriers might include poor home support, difficulty with getting to the pharmacy or doctor’s office, and substance abuse problems that interfere with any kind of self-care.
"When you see these, it’s critical to get diabetes educators and social services involved [to] try to overcome those problems. Get the issues out on the table early and you have a much better shot at identifying the solution."
The baseline HbA1c is a key piece of information in determining a patient’s diabetes status during the hospitalization. "This allows you to identify the patient with a history of diabetes, the patient who has prediabetes or undiagnosed diabetes, and the one who develops temporary hyperglycemia simply from stress related to their illness, either before or during hospitalization. Regardless of the etiology, they all need to be treated aggressively to get the blood sugar in that target range."
But as the acute illness subsides, so may the need for insulin. "During recovery, patients almost always need less, and sometimes they need none at all. Use that admission HbA1c to predict predischarge and outpatient needs."
Dr. MacIndoe offered the following scenarios based on the admission HbA1c:
• Below 5.7%. These patients "don’t have diabetes and don’t need insulin. So take them off any insulin and monitor for 24 hours, and send them home with nothing to worry about."
• 5.8%-6.5%. "This person has a high risk for diabetes, but should be able to get off insulin entirely. You should recommend lifestyle changes [such as exercising and losing weight], because the data suggest that over time these patients are likely to develop diabetes, and lifestyle changes can prevent or postpone that." The American Diabetes Association now recommends adding metformin to the regimen of a prediabetic patient if the patient is younger than 60 years and overweight, he said.
• 6.6%-6.9%. "This is a person with well-controlled diabetes. If newly diagnosed, this patient needs to learn how to improve his lifestyle to maintain this control. And obviously, if it is a patient with established diabetes, you should send them home on whatever regimen they came in on, because it’s working."
• 7%-10%. "A level like this at admission means that diabetes is not well-controlled. If this is a new diagnosis, I usually send the patient home on an oral agent that won’t cause hypoglycemia. If it’s a known diabetic patient, you have an opportunely to make a difference here by increasing their regimen, either with orals or with insulin."
• 10% or higher. "This is urgently uncontrolled diabetes. Even though we’re loathe to start insulin on an inpatient before discharge, this is one time we would." This situation often requires repeat conversations and connection with diabetes educators, Dr. MacIndoe added. "People are not really in the frame of mind to comprehend what this all means," when they’re admitted. "Get them to see the educator as soon as they can understand what’s going on."
But even the best discharge plan won’t help if the patient doesn’t follow though because of financial or social issues. "Don’t forget, they have to be able to afford it. If they can’t, they are not likely to tell you so. They just won’t get it filled and will probably find themselves back" in the emergency department.
"Most of us really don’t have a clue about the real costs of medications, supplies, strips, lancets, lab tests, and medical office copays," he continued. "The average price of a blood glucose strip is $1.25. If you’re telling them to test four times a day, that’s $140 a month and almost $1,700 a year, if they test the way they should."
Going generic with medications can help patients save money and boost the chance of successful management. "This [name brand] stuff is not cheap. Patients can get a month of generic metformin and sulfonylurea options at a discount pharmacy for $4, or 3 months for $10."
Analog insulins are considerably more expensive than "good old NPH [isophane insulin] and regular insulin," Dr. MacIndoe said. "Given that fact, I would strongly suggest that you consider sending the patient with financial barriers home on NPH and regular because of its affordability. This combination will work if the patient remembers to eat regularly, particularly at lunch and snack time."
Finally, he said, get these patients back for a follow-up within 2 weeks of discharge. "It’s critical that they be seen 7-14 days afterward, particularly if they’re on a new regimen. It’s usually easier to get them to the diabetes educator, since most physicians are too busy, or too focused on the main reason they were in the hospital rather than [on] their diabetes."
Dr. MacIndoe disclosed that he is on the speakers bureau of Sanofi-Aventis.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE