User login
E-Mail System Keeps Everyone on Same Page Surrounding Pending Test Results
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: More than 80% of physicians who tested an automatic e-mail system of test results pending at discharge were satisfied with its usefulness. Those who received the e-mails were six times more likely to be aware of final test results than were those who did not get them.
Data Source: A 1-month pilot and 6-month follow-up study of hospitalists and primary care physicians who are testing the program.
Disclosures: Dr. Dalal reported no financial disclosures.
E-Mail System Keeps Everyone on Same Page Surrounding Pending Test Results
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
E-Mail System Keeps Everyone on Same Page Surrounding Pending Test Results
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
GRAPEVINE, TEX. – E-mailing the results of tests still pending at patient discharge is a feasible solution to the "I never got this message" scenario.
Such a pilot project performed well for hospitalists and primary care doctors in the Partners HealthCare System’s "partners.org" database, Dr. Anuj K. Dalal said at the annual meeting of the Society of Hospital Medicine.
However, he warned, unless system bugs are hunted down and exterminated before deployment, one inaccurate discharge entry could set up a domino-effect deluge of e-mails to peeved primary care physicians.
"One unit clerk inadvertently ‘discharged’ a patient on day 4 of a 10-day hospital stay," he said. "The system then detected 510 pending tests at discharge, which resulted in nine e-mails to one very frustrated physician. I can’t tell you how important it is to have the process crisp before you jump into something like this. You have to remember the computer adage, ‘Garbage in, garbage out.’ "
He points to the not-uncommon scenario of patients who are discharged before all the lab results come back. Those results are returned to the physician who ordered them – most likely the hospitalist – and frequently stop there. "No one ever communicates the results to the PCP [primary care physician], and the attendings don’t review them," because the patient is no longer under their care, said Dr. Dalal, a hospitalist at Brigham and Women’s Hospital in Boston.
To address the problem, he conceived of and helped create a computer algorithm that automatically detects incoming test results and generates a single e-mail to the patient’s hospital attending and primary care physician. The system updates at midnight and keeps generating one e-mail a day to each provider until all results are finalized.
"Every e-mail has the date it was generated, the patient’s name, name of the discharging attending physician, the day of discharge, and the results of each test," Dr. Dalal said.
While the system is feasible in a large, interconnected health care system, it isn’t foolproof, he added. Sometimes, physicians outside the Partners e-mail system admit a patient; in that case only the hospitalist gets the e-mail. "But it always has the phone number of the primary care doc, so the hospitalist can call and relay the results."
The 1-month pilot period included chemistry/hematology, radiology/pathology, and microbiology results. It was tested on 83 discharges – including the one that caused the electronic mayhem. After excluding that one, Dr. Dalal said, the computer program found 405 pending tests, most of which (55%) were chemistry, while the remainder were hematology; 18% were abnormal. This generated 136 e-mails – about 1.7 per patient, although 34% of the patients had 2 or more e-mails sent. Aside from complaints about the inaccurate discharge, only three physicians (two PCPs and one hospitalist) said they received incorrect e-mails.
A survey of 70 physician users found that 84% were satisfied or very satisfied with the system, while 6% were neutral and 10% dissatisfied or very dissatisfied.
Comments from both sides of the issue included remarks such as "I found this extremely useful, knowing the final results of tests, both those that are positive as well as negative," and "Test was not needed and not ordered by me."
Dr. Dalal also presented a poster that examined the system’s 6-month outcomes among 36 discharging physicians who got the e-mails and 43 who did not. Physicians who got the e-mails were six times more likely to be aware of the results of any pending test, and five times more aware of any pending tests that required action on their part.
They were also significantly more likely to be satisfied with the automatic notification system than with the usual care system (84% vs. 21%).
In considering the impact of this novel collaboration on patient care, Dr. Dalal said, "I would challenge you on the thought that our responsibility as hospitalists ends when the patient is discharged. Does it really, especially as we are doing all this work on care transition and decreased readmission? We are going to become the care transition experts; we need to think of whether we are responsible for these results."
Dr. Dalal reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY OF HOSPITAL MEDICINE
Major Finding: More than 80% of physicians who tested an automatic e-mail system of test results pending at discharge were satisfied with its usefulness. Those who received the e-mails were six times more likely to be aware of final test results than were those who did not get them.
Data Source: A 1-month pilot and 6-month follow-up study of hospitalists and primary care physicians who are testing the program.
Disclosures: Dr. Dalal reported no financial disclosures.
Low Vitamin D Associated With Poor Prognostic Features in Breast Cancer
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
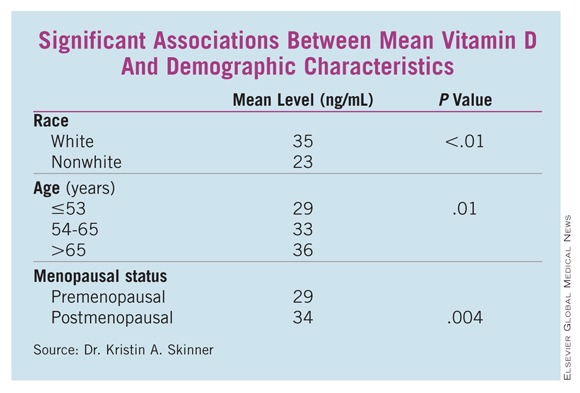
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Finding: Vitamin D deficiency was more than twice as common as normal levels in women undergoing surgery for breast cancer (OR, 2.4).
Data Source: A case-control study of vitamin D levels in 194 women with breast cancer matched 1:1 to a control population.
Disclosures: Dr. Skinner said she had no relevant disclosures.
Low Vitamin D Associated With Poor Prognostic Features in Breast Cancer
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Finding: Vitamin D deficiency was more than twice as common as normal levels in women undergoing surgery for breast cancer (OR, 2.4).
Data Source: A case-control study of vitamin D levels in 194 women with breast cancer matched 1:1 to a control population.
Disclosures: Dr. Skinner said she had no relevant disclosures.
Low Vitamin D Associated With Poor Prognostic Features in Breast Cancer
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
WASHINGTON – Vitamin D deficiency was not only twice as common in women undergoing breast cancer surgery, but it also was associated with poor-prognosis tumors in a case-control study that compared cancer patients with cancer-free women who had been tested for vitamin D.
The breast cancer patients had significantly lower mean vitamin D levels than did controls (33 ng/mL vs. 37 ng/mL), Dr. Kristin A. Skinner reported at the annual meeting of the American Association of Breast Surgeons. Patients were also more than twice as likely to have deficient levels (odds ratio, 2.4; P less than .01), she said.
Analyses presented by Dr. Skinner showed that mean vitamin D levels were significantly lower in the following subgroups of breast cancer patients:
• Those with estrogen receptornegative cancers vs. those with ER-positive cancers (28 ng/mL vs. 33 ng/mL; P = .04).
• Those with triple-negative cancers vs. those with cancers that were not triple negative (26 ng/mL vs.33 ng/mL; P -= .02).
• Those of the basal-like phenotype vs. those of the luminal A phenotype (24 ng/mL vs. 33 ng/mL; P = .04).
Some patient characteristics also carried significant associations with decreased vitamin D. White women, women aged 65 years and older, and those who were postmenopausal had significantly higher vitamin D levels than did nonwhite, younger, and premenopausal women, respectively. (See box.)
Although vitamin D levels were lower in patients with high Oncotype DX recurrence scores, progesterone receptornegative tumors, and invasive tumors, these differences were not statistically significant. Nor were family history or HER2, tumor, or nodal status significantly related to vitamin D levels, according to Dr. Skinner, a surgical oncologist and breast specialist at the cancer center of the University of Rochester (N.Y.).
In the case-control study, Dr. Skinner and her colleagues selected 194 women who were treated for breast cancer (stage 0-III) at the center and had total 25-hydroxy vitamin D levels drawn in the 3 months before or after their cancer surgery; the mean time of the blood draw was 30 days before surgery.
The patients were matched 1:1 with cancer-free controls who were drawn from a pool of more than 37,000 women who also underwent vitamin D testing in the university’s clinical labs in 2009-2010, the same time the cases were treated. The women were matched for age and the season of testing, since vitamin D levels can change as sun exposure varies.
The researchers divided vitamin D levels into tertiles: Optimal level was considered at least 32 ng/mL, suboptimal was 20-31 ng/mL, and deficient was less than 20 ng/mL.
The findings may argue for vitamin D testing and supplementation either in a primary care setting or in one devoted to breast health, Dr. Skinner said during a press briefing.
"At our institution, we routinely check vitamin D levels and replace them until they are well into the normal range," which is greater than 32 ng/mL, she said. "We really aim for a level of about 50 ng/mL, and titrate their replacement to those levels. In terms of taking supplements, we usually recommend starting at 1,000-2,000 IU daily, but the most effective way is to check levels, and replace accordingly."
Extant epidemiologic data have consistently found a link between more aggressive breast cancers and low vitamin D levels, she said, describing the relationship as biologically plausible. "The vitamin D receptor appears to modulate cell cycles, including the proliferation and differentiation of cells and the activation of apoptosis. Some studies have shown that vitamin D supplementation reduces the risk of breast cancer and improves survival outcomes, but very little is known about vitamin D levels and standard prognostic factors in breast cancer," she said.
"These findings may explain the associations seen in the epidemiologic studies, and may help explain why the black and other nonwhite populations tend to get more-aggressive breast cancer, and get breast cancer at a younger age," Dr. Skinner said.
She had no financial declarations with regard to the work.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Finding: Vitamin D deficiency was more than twice as common as normal levels in women undergoing surgery for breast cancer (OR, 2.4).
Data Source: A case-control study of vitamin D levels in 194 women with breast cancer matched 1:1 to a control population.
Disclosures: Dr. Skinner said she had no relevant disclosures.
Radioactive Seeds Guide Surgeons to Nonpalpable Breast Lesions
WASHINGTON – Radioactive seeds were a safe and effective method of pinpointing nonpalpable breast lesions for surgery, with an 85% rate of negative margins on the first excision and an ipsilateral recurrence rate of less than 2% over 33 months, according to a large retrospective study.
Close margins occurred in 12% of the 767 patients with nonpalpable breast lesions, and positive margins occurred in 3%. The overall re-excision rate was 15%, Dr. Lee McGhan of the Mayo Clinic, Scottsdale, Ariz., said at the annual meeting of the American Society of Breast Surgeons.
Performing the procedure is "almost intuitive," with a very low learning curve, he said. "It is now our method of choice when dealing with preoperative localization of nonpalpable breast lesions."
His retrospective review of 978 prospectively collected patient records comprised 1,000 radioactive in 2003-2010. Almost 1,150 seeds were deployed.
The patients’ mean age was 65 years; their mean lesion size was 1.2 cm. Most (550) had an invasive carcinoma; 217 had DCIS (ductal carcinoma in situ); 115 had atypical hyperplasia, and the remainder, uncertain or suspicious percutaneous biopsy results.
Dr. McGhan reported 33-month follow-up results on the 767 women with either invasive carcinoma or DCIS. Most patients (910) received just one seed; 84 received two seeds; 5 received three seeds; and 1 patient received four of the devices.
Most (76%) underwent the procedure at least 1 day before surgery. Typically, Dr. McGhan said, patients came to the clinic a few days before surgery for an evaluation. Many chose to have the localization on a Friday, stayed over the weekend, and had the seeds removed early on Monday morning.
The 4- to 5-mm seeds containing radioactive iodine-125 can be placed up to 5 days before surgery. They were deployed through an 18-gauge spinal needle under image guidance; post deployment, a mammogram or ultrasound confirmed their position near the lesion. "We used a handheld gamma probe to identify the area of greatest radioactivity at the skin surface, marking the optimal site of skin incision," Dr. McGhan said.
Intraoperative complications included 30 displaced seeds – including 3 suctioned up by operative tubing and 3 that were improperly deployed during radiology – as well as one instance of an incorrect incision site resulting from a miscommunication between the radiologist and the surgeon, Dr. McGhan said. All of these seeds were retrieved with no patient harm.
All of the localized lesions were successfully removed, along with their associated seeds; the specimens were sent to pathology. Among the 550 invasive cancers, margins were negative in 87%, close in 9%, and positive in 3%. Re-excision was required in 13% (69).
Among the 217 DCIS lesions, margins were negative in 77%, close in 19%, and positive in 3%. Re-excision was necessary in 23% (49).
Sentinel node biopsies occurred in 544 cases, and were successful in all but one, Dr. McGhan said. "There was no blue dye detected, which was determined to be due to tumor invasion of the lymphatics rather than a direct complication of the procedure."
The mean follow-up period was 33 months. Over this time, the overall ipsilateral recurrence rate was 1.6% (12 patients). The rate was slightly higher among patients with DCIS (3%; seven patients). The local recurrence rate was 1% (five patients) among those with invasive cancer. By the end of the follow-up period, there were six mastectomies secondary to recurrence: three (0.5%) in the invasive cancer group and three (1%) in the DCIS group.
Dr. McGhan had no financial declarations.
WASHINGTON – Radioactive seeds were a safe and effective method of pinpointing nonpalpable breast lesions for surgery, with an 85% rate of negative margins on the first excision and an ipsilateral recurrence rate of less than 2% over 33 months, according to a large retrospective study.
Close margins occurred in 12% of the 767 patients with nonpalpable breast lesions, and positive margins occurred in 3%. The overall re-excision rate was 15%, Dr. Lee McGhan of the Mayo Clinic, Scottsdale, Ariz., said at the annual meeting of the American Society of Breast Surgeons.
Performing the procedure is "almost intuitive," with a very low learning curve, he said. "It is now our method of choice when dealing with preoperative localization of nonpalpable breast lesions."
His retrospective review of 978 prospectively collected patient records comprised 1,000 radioactive in 2003-2010. Almost 1,150 seeds were deployed.
The patients’ mean age was 65 years; their mean lesion size was 1.2 cm. Most (550) had an invasive carcinoma; 217 had DCIS (ductal carcinoma in situ); 115 had atypical hyperplasia, and the remainder, uncertain or suspicious percutaneous biopsy results.
Dr. McGhan reported 33-month follow-up results on the 767 women with either invasive carcinoma or DCIS. Most patients (910) received just one seed; 84 received two seeds; 5 received three seeds; and 1 patient received four of the devices.
Most (76%) underwent the procedure at least 1 day before surgery. Typically, Dr. McGhan said, patients came to the clinic a few days before surgery for an evaluation. Many chose to have the localization on a Friday, stayed over the weekend, and had the seeds removed early on Monday morning.
The 4- to 5-mm seeds containing radioactive iodine-125 can be placed up to 5 days before surgery. They were deployed through an 18-gauge spinal needle under image guidance; post deployment, a mammogram or ultrasound confirmed their position near the lesion. "We used a handheld gamma probe to identify the area of greatest radioactivity at the skin surface, marking the optimal site of skin incision," Dr. McGhan said.
Intraoperative complications included 30 displaced seeds – including 3 suctioned up by operative tubing and 3 that were improperly deployed during radiology – as well as one instance of an incorrect incision site resulting from a miscommunication between the radiologist and the surgeon, Dr. McGhan said. All of these seeds were retrieved with no patient harm.
All of the localized lesions were successfully removed, along with their associated seeds; the specimens were sent to pathology. Among the 550 invasive cancers, margins were negative in 87%, close in 9%, and positive in 3%. Re-excision was required in 13% (69).
Among the 217 DCIS lesions, margins were negative in 77%, close in 19%, and positive in 3%. Re-excision was necessary in 23% (49).
Sentinel node biopsies occurred in 544 cases, and were successful in all but one, Dr. McGhan said. "There was no blue dye detected, which was determined to be due to tumor invasion of the lymphatics rather than a direct complication of the procedure."
The mean follow-up period was 33 months. Over this time, the overall ipsilateral recurrence rate was 1.6% (12 patients). The rate was slightly higher among patients with DCIS (3%; seven patients). The local recurrence rate was 1% (five patients) among those with invasive cancer. By the end of the follow-up period, there were six mastectomies secondary to recurrence: three (0.5%) in the invasive cancer group and three (1%) in the DCIS group.
Dr. McGhan had no financial declarations.
WASHINGTON – Radioactive seeds were a safe and effective method of pinpointing nonpalpable breast lesions for surgery, with an 85% rate of negative margins on the first excision and an ipsilateral recurrence rate of less than 2% over 33 months, according to a large retrospective study.
Close margins occurred in 12% of the 767 patients with nonpalpable breast lesions, and positive margins occurred in 3%. The overall re-excision rate was 15%, Dr. Lee McGhan of the Mayo Clinic, Scottsdale, Ariz., said at the annual meeting of the American Society of Breast Surgeons.
Performing the procedure is "almost intuitive," with a very low learning curve, he said. "It is now our method of choice when dealing with preoperative localization of nonpalpable breast lesions."
His retrospective review of 978 prospectively collected patient records comprised 1,000 radioactive in 2003-2010. Almost 1,150 seeds were deployed.
The patients’ mean age was 65 years; their mean lesion size was 1.2 cm. Most (550) had an invasive carcinoma; 217 had DCIS (ductal carcinoma in situ); 115 had atypical hyperplasia, and the remainder, uncertain or suspicious percutaneous biopsy results.
Dr. McGhan reported 33-month follow-up results on the 767 women with either invasive carcinoma or DCIS. Most patients (910) received just one seed; 84 received two seeds; 5 received three seeds; and 1 patient received four of the devices.
Most (76%) underwent the procedure at least 1 day before surgery. Typically, Dr. McGhan said, patients came to the clinic a few days before surgery for an evaluation. Many chose to have the localization on a Friday, stayed over the weekend, and had the seeds removed early on Monday morning.
The 4- to 5-mm seeds containing radioactive iodine-125 can be placed up to 5 days before surgery. They were deployed through an 18-gauge spinal needle under image guidance; post deployment, a mammogram or ultrasound confirmed their position near the lesion. "We used a handheld gamma probe to identify the area of greatest radioactivity at the skin surface, marking the optimal site of skin incision," Dr. McGhan said.
Intraoperative complications included 30 displaced seeds – including 3 suctioned up by operative tubing and 3 that were improperly deployed during radiology – as well as one instance of an incorrect incision site resulting from a miscommunication between the radiologist and the surgeon, Dr. McGhan said. All of these seeds were retrieved with no patient harm.
All of the localized lesions were successfully removed, along with their associated seeds; the specimens were sent to pathology. Among the 550 invasive cancers, margins were negative in 87%, close in 9%, and positive in 3%. Re-excision was required in 13% (69).
Among the 217 DCIS lesions, margins were negative in 77%, close in 19%, and positive in 3%. Re-excision was necessary in 23% (49).
Sentinel node biopsies occurred in 544 cases, and were successful in all but one, Dr. McGhan said. "There was no blue dye detected, which was determined to be due to tumor invasion of the lymphatics rather than a direct complication of the procedure."
The mean follow-up period was 33 months. Over this time, the overall ipsilateral recurrence rate was 1.6% (12 patients). The rate was slightly higher among patients with DCIS (3%; seven patients). The local recurrence rate was 1% (five patients) among those with invasive cancer. By the end of the follow-up period, there were six mastectomies secondary to recurrence: three (0.5%) in the invasive cancer group and three (1%) in the DCIS group.
Dr. McGhan had no financial declarations.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Major Finding: Radioactive seed localization resulted in initial negative margins in 85% of cases and an overall re-excision rate of 2%.
Data Source: A retrospective study of 767 women with invasive cancer or DCIS who were followed for a mean of 33 months.
Disclosures: Dr. McGhan had no financial declarations.
Mixed Outcomes When Radiation Is Added to Excision for DCIS
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Major Finding: Invasive cancer appeared in 57% of recurrences among women whose DCIS was treated with excision and radiation, compared with 37% of those in women treated with surgery alone.
Data Source: A prospective study of 1,014 women who were followed for up to 10 years.
Disclosures: Dr. Grumley had no financial conflicts to declare.
Mixed Outcomes When Radiation Is Added to Excision for DCIS
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
WASHINGTON – Five years might not be the magic number for a small group of women who are treated for the most curable form of breast cancer: ductal carcinoma in situ.
In a prospective study, women who underwent excision plus radiotherapy did have a significantly lower rate of local recurrence than did women who were treated with surgery alone. But among those who had a recurrence, it was almost twice as likely to be invasive. Additionally, these recurrences took almost twice as long to present: up to 105 months.
"This shows there is definitely an added benefit from radiation, but at the same time, we must be aware that patients who have radiation can still recur, and much later," Dr. Janie Weng Grumley said at a press briefing during the annual meeting of the American Society of Breast Surgeons.
"Many patients think, ‘after 5 years, I’m safe.’ This study really highlights the fact that there is a very different pattern of recurrence [in those who receive one of the two treatments]. We must be aware of this, and follow these women in a different way."
Dr. Grumley, a fellow at the University of Southern California in Los Angeles, presented a prospective study of 1,014 women with ductal carcinoma in situ (DCIS) who were treated with either excision alone (651) or excision plus radiotherapy (363). The average follow-up was significantly longer in the dual-therapy group (average, 109 months) than in the excision-only group (average, 72 months), reflecting the recent increase in lumpectomy-only treatment, Dr. Grumley said. The groups’ average age was 54 years.
The probability of any local recurrence was significantly lower in the dual-therapy group than in the lumpectomy group (18% vs. 30%; P = .0102). But invasive disease was significantly more common among those in the dual-therapy group who did recur (57% vs. 37%). The cancers also took significantly longer to recur, whether the study examined the mean time to any local recurrence (90 vs. 53 months; P less than or equal to .001), the mean time to DCIS recurrence (73 vs. 41 months; P = .002), or the mean time to invasive recurrence (105 vs. 72 months; P = .017).
Women who had surgery and radiation also experienced a significantly different pattern of recurrence, Dr. Grumley said. Among women treated only with surgery, 90% of recurrences were in the same quadrant, compared with 72% of recurrences in women who were treated with dual therapy (P = .0016). Conversely, 28% of recurrences after dual therapy occurred in a different quadrant, compared with 10% of those in the surgery-alone group. Lesions in different quadrants likely reflect new primary tumors, she said.
The increased rate of invasive, recurrent disease in the dual-therapy group was probably responsible for a small but statistically significant mortality difference (98% vs. 100%), Dr. Grumley said.
"This study shows that a small subgroup of irradiated DCIS patients may not be deriving maximum benefit from radiation therapy, or not benefiting from it at all," she said.
She was only able to speculate on the reason for the different recurrence patterns. "Radiation is a hypothesis, but we have nothing here that we can connect [as a] cause and effect. We do know that radiation does affect local recurrence, and we would never tell a patient not to get radiation. But this pattern is definitely something that should be further examined.
Dr. Grumley had no financial conflicts to declare.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF BREAST SURGEONS
Major Finding: Invasive cancer appeared in 57% of recurrences among women whose DCIS was treated with excision and radiation, compared with 37% of those in women treated with surgery alone.
Data Source: A prospective study of 1,014 women who were followed for up to 10 years.
Disclosures: Dr. Grumley had no financial conflicts to declare.
Confirm Celiac Diagnosis by Biopsy Before Advising Gluten-Free Diet
SAN DIEGO – An intestinal biopsy is almost always necessary to confirm celiac disease and is a must before committing a patient to the only effective treatment – a lifelong gluten-free diet.
Sticking to such a restricted diet is difficult and expensive, Dr. Sheila Crowe said at the annual meeting of the American College of Physicians. "A lifelong gluten-free diet sounds simple, unless you’re the patient. ... Eating out is very difficult, especially for children and teens who face a lot of peer pressure. And eating gluten free at home is expensive. Studies in the United States, Canada, and the United Kingdom confirm that a lifelong diet of gluten-free foods costs about three times more than a normal diet," said Dr. Crowe, professor in the division of gastroenterology and hepatology at the University of Virginia, Charlottesville.
Because treating celiac disease requires this lifelong commitment, a positive serologic test isn’t enough to rule it in, she said. Nor are any of the available immunologic tests, including the most widely used – tissue transglutaminase IgA (tTG IgA) – specific enough to replace intestinal biopsy as the sole method for reliably diagnosing celiac disease. "A positive tTG test is not enough to place a person on this lifelong treatment without confirmation from an intestinal biopsy," she said. "This is especially important for children, because of the higher likelihood of false positives in that group."
tTG IgA has a very high sensitivity and specificity, but it isn’t perfect, Dr. Crowe said. "If you have a patient with clinical symptoms and the tTG comes back negative, there is still a 10% chance that’s a false negative. Another scenario could be a patient who has an autoimmune disease or a relative with celiac, and is experiencing celiac symptoms. If the tTG came back negative on that person, I would still do an endoscopy."
The only possible exception might be a patient with celiac symptoms who already has biopsy-proven dermatitis herpetiformis, with the classic immunofluorescent deposits at the dermal-epidermal junction. "If you biopsy these patients, the intestine will show the changes associated with celiac disease every time," Dr. Crowe said.
Celiac disease is no longer considered a disorder of childhood. "The disease is there lifelong. It appears you cannot suppress the immune response," she said.
The intestine rapidly responds to a gluten-free diet, "But the tendency to have an immunologic response to gluten is always there," Dr. Crowe said.
Relapses are common. Patients are most likely to "fall off" the diet when symptoms begin to abate, she said. They may simply feel "cured" and resume old eating patterns, or they may drop the diet because of changes that can occur as the intestine heals. "If a patient had diarrhea and malabsorption of nutrients, they might find themselves getting constipated and gaining weight on the gluten-free diet, fall off, and get ill again. Even if the intestine is healed, the vast majority of data tell us that patient will relapse," at some point after abandoning the dietary restriction, Dr. Crowe said.
This can lead to the development of refractory celiac disease, in which the intestine fails to recover despite a gluten-free diet. Patients with refractory celiac disease may be unable to fully absorb nutrients and need supplemental feeding methods.
The goal of celiac management is to promote intestinal healing, optimize nutrition, and avoid long-term damage, Dr. Crowe said. "It’s key to bring in a knowledgeable dietitian to help. And I mean knowledgeable – not someone who is going to hand your patient a diet sheet and that’s all."
Many celiac patients are already nutritionally compromised at the time of diagnosis. "This is the time to measure their nutritional parameters," Dr. Crowe said. "They may need supplements. Many are deficient in vitamin D, iron, folate, zinc, or other trace elements."
The risks of untreated disease "are not inconsequential." Patients can develop problems related to nutrient malabsorption, including osteopenia, infertility, miscarriage, and intrauterine growth restriction, and are four times more likely than the general population to develop a malignancy.
Guidelines for managing nutritional status exist, but there are no evidence-based treatment guidelines for celiac disease, Dr. Crowe said. "Aside from nutrition, you have to just advise them to follow good health practices. I have several patients who still smoke, and yet they’re morose about their gluten-free diet. I say, ‘Why are you worried about that? You need to worry about quitting smoking!’ "
Dr. Crowe reported that she receives royalties from a book written for patients with celiac disease.
SAN DIEGO – An intestinal biopsy is almost always necessary to confirm celiac disease and is a must before committing a patient to the only effective treatment – a lifelong gluten-free diet.
Sticking to such a restricted diet is difficult and expensive, Dr. Sheila Crowe said at the annual meeting of the American College of Physicians. "A lifelong gluten-free diet sounds simple, unless you’re the patient. ... Eating out is very difficult, especially for children and teens who face a lot of peer pressure. And eating gluten free at home is expensive. Studies in the United States, Canada, and the United Kingdom confirm that a lifelong diet of gluten-free foods costs about three times more than a normal diet," said Dr. Crowe, professor in the division of gastroenterology and hepatology at the University of Virginia, Charlottesville.
Because treating celiac disease requires this lifelong commitment, a positive serologic test isn’t enough to rule it in, she said. Nor are any of the available immunologic tests, including the most widely used – tissue transglutaminase IgA (tTG IgA) – specific enough to replace intestinal biopsy as the sole method for reliably diagnosing celiac disease. "A positive tTG test is not enough to place a person on this lifelong treatment without confirmation from an intestinal biopsy," she said. "This is especially important for children, because of the higher likelihood of false positives in that group."
tTG IgA has a very high sensitivity and specificity, but it isn’t perfect, Dr. Crowe said. "If you have a patient with clinical symptoms and the tTG comes back negative, there is still a 10% chance that’s a false negative. Another scenario could be a patient who has an autoimmune disease or a relative with celiac, and is experiencing celiac symptoms. If the tTG came back negative on that person, I would still do an endoscopy."
The only possible exception might be a patient with celiac symptoms who already has biopsy-proven dermatitis herpetiformis, with the classic immunofluorescent deposits at the dermal-epidermal junction. "If you biopsy these patients, the intestine will show the changes associated with celiac disease every time," Dr. Crowe said.
Celiac disease is no longer considered a disorder of childhood. "The disease is there lifelong. It appears you cannot suppress the immune response," she said.
The intestine rapidly responds to a gluten-free diet, "But the tendency to have an immunologic response to gluten is always there," Dr. Crowe said.
Relapses are common. Patients are most likely to "fall off" the diet when symptoms begin to abate, she said. They may simply feel "cured" and resume old eating patterns, or they may drop the diet because of changes that can occur as the intestine heals. "If a patient had diarrhea and malabsorption of nutrients, they might find themselves getting constipated and gaining weight on the gluten-free diet, fall off, and get ill again. Even if the intestine is healed, the vast majority of data tell us that patient will relapse," at some point after abandoning the dietary restriction, Dr. Crowe said.
This can lead to the development of refractory celiac disease, in which the intestine fails to recover despite a gluten-free diet. Patients with refractory celiac disease may be unable to fully absorb nutrients and need supplemental feeding methods.
The goal of celiac management is to promote intestinal healing, optimize nutrition, and avoid long-term damage, Dr. Crowe said. "It’s key to bring in a knowledgeable dietitian to help. And I mean knowledgeable – not someone who is going to hand your patient a diet sheet and that’s all."
Many celiac patients are already nutritionally compromised at the time of diagnosis. "This is the time to measure their nutritional parameters," Dr. Crowe said. "They may need supplements. Many are deficient in vitamin D, iron, folate, zinc, or other trace elements."
The risks of untreated disease "are not inconsequential." Patients can develop problems related to nutrient malabsorption, including osteopenia, infertility, miscarriage, and intrauterine growth restriction, and are four times more likely than the general population to develop a malignancy.
Guidelines for managing nutritional status exist, but there are no evidence-based treatment guidelines for celiac disease, Dr. Crowe said. "Aside from nutrition, you have to just advise them to follow good health practices. I have several patients who still smoke, and yet they’re morose about their gluten-free diet. I say, ‘Why are you worried about that? You need to worry about quitting smoking!’ "
Dr. Crowe reported that she receives royalties from a book written for patients with celiac disease.
SAN DIEGO – An intestinal biopsy is almost always necessary to confirm celiac disease and is a must before committing a patient to the only effective treatment – a lifelong gluten-free diet.
Sticking to such a restricted diet is difficult and expensive, Dr. Sheila Crowe said at the annual meeting of the American College of Physicians. "A lifelong gluten-free diet sounds simple, unless you’re the patient. ... Eating out is very difficult, especially for children and teens who face a lot of peer pressure. And eating gluten free at home is expensive. Studies in the United States, Canada, and the United Kingdom confirm that a lifelong diet of gluten-free foods costs about three times more than a normal diet," said Dr. Crowe, professor in the division of gastroenterology and hepatology at the University of Virginia, Charlottesville.
Because treating celiac disease requires this lifelong commitment, a positive serologic test isn’t enough to rule it in, she said. Nor are any of the available immunologic tests, including the most widely used – tissue transglutaminase IgA (tTG IgA) – specific enough to replace intestinal biopsy as the sole method for reliably diagnosing celiac disease. "A positive tTG test is not enough to place a person on this lifelong treatment without confirmation from an intestinal biopsy," she said. "This is especially important for children, because of the higher likelihood of false positives in that group."
tTG IgA has a very high sensitivity and specificity, but it isn’t perfect, Dr. Crowe said. "If you have a patient with clinical symptoms and the tTG comes back negative, there is still a 10% chance that’s a false negative. Another scenario could be a patient who has an autoimmune disease or a relative with celiac, and is experiencing celiac symptoms. If the tTG came back negative on that person, I would still do an endoscopy."
The only possible exception might be a patient with celiac symptoms who already has biopsy-proven dermatitis herpetiformis, with the classic immunofluorescent deposits at the dermal-epidermal junction. "If you biopsy these patients, the intestine will show the changes associated with celiac disease every time," Dr. Crowe said.
Celiac disease is no longer considered a disorder of childhood. "The disease is there lifelong. It appears you cannot suppress the immune response," she said.
The intestine rapidly responds to a gluten-free diet, "But the tendency to have an immunologic response to gluten is always there," Dr. Crowe said.
Relapses are common. Patients are most likely to "fall off" the diet when symptoms begin to abate, she said. They may simply feel "cured" and resume old eating patterns, or they may drop the diet because of changes that can occur as the intestine heals. "If a patient had diarrhea and malabsorption of nutrients, they might find themselves getting constipated and gaining weight on the gluten-free diet, fall off, and get ill again. Even if the intestine is healed, the vast majority of data tell us that patient will relapse," at some point after abandoning the dietary restriction, Dr. Crowe said.
This can lead to the development of refractory celiac disease, in which the intestine fails to recover despite a gluten-free diet. Patients with refractory celiac disease may be unable to fully absorb nutrients and need supplemental feeding methods.
The goal of celiac management is to promote intestinal healing, optimize nutrition, and avoid long-term damage, Dr. Crowe said. "It’s key to bring in a knowledgeable dietitian to help. And I mean knowledgeable – not someone who is going to hand your patient a diet sheet and that’s all."
Many celiac patients are already nutritionally compromised at the time of diagnosis. "This is the time to measure their nutritional parameters," Dr. Crowe said. "They may need supplements. Many are deficient in vitamin D, iron, folate, zinc, or other trace elements."
The risks of untreated disease "are not inconsequential." Patients can develop problems related to nutrient malabsorption, including osteopenia, infertility, miscarriage, and intrauterine growth restriction, and are four times more likely than the general population to develop a malignancy.
Guidelines for managing nutritional status exist, but there are no evidence-based treatment guidelines for celiac disease, Dr. Crowe said. "Aside from nutrition, you have to just advise them to follow good health practices. I have several patients who still smoke, and yet they’re morose about their gluten-free diet. I say, ‘Why are you worried about that? You need to worry about quitting smoking!’ "
Dr. Crowe reported that she receives royalties from a book written for patients with celiac disease.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF PHYSICIANS