User login
Thromboprophylaxis: Survey on Barriers
Each year in North America, over 7 million adults are hospitalized with a medical illness.1 Acute illness and decreased mobility in hospital places patients at increased risk for venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and life‐threatening pulmonary embolism (PE).2 Since VTE remains the most preventable cause of death in hospitalized patients, numerous studies have aimed at reducing the incidence of hospital‐acquired DVT. Aside from cost, the impact of VTE to the healthcare system is felt not only by those who diagnose and treat VTE, but also by those responsible for correcting the severe bleeding that can result from inappropriate use of thromboprophylaxis. Approximately 60% of symptomatic VTE occurs in medical patients, and recent hospitalization for medical illness accounts for 25% of all community‐diagnosed VTE. The Agency for Health Research and Quality ranks DVT prevention as the top priority out of 79 patient safety initiatives, and expert consensus groups provide a strong recommendation that DVT prophylaxis with a low‐dose anticoagulant should be administered to at‐risk hospitalized medical patients.2, 3
Despite the availability, efficacy, and safety of DVT prophylaxis,2 it is discouraging that only 21% to 62% of medical patients receive prophylaxis,49 and only 16% to 40% receive appropriate prophylaxis.46, 1012 However, 70% to 90% of patients in other at‐risk groups, such as surgical patients or critically ill patients, receive prophylaxis.1316 The reason why DVT prophylaxis is so underutilized in medical patients is unclear, as explanations for low rates of clinical practice guideline utilization are multifaceted,17 and few studies have investigated the barriers to optimal thromboprophylaxis.1820
To explore possible reasons for this disparity between evidence and practice, we conducted a cross‐sectional survey of 4 clinician groups involved in the care of hospitalized medical patients. Our objective was to identify barriers and potential solutions to the underutilization of DVT prophylaxis in hospitalized medical patients.
METHODS
Instrument Development
The survey focused on 3 domains: perceived importance, effectiveness, and safety of DVT prophylaxis; perceived barriers to implementation; and perceived potential success and feasibility of interventions to optimize DVT prophylaxis. The survey cover letter outlined background information, study design, and a statement on confidentiality. A prior survey of DVT prophylaxis administered to thrombosis experts was used to generate survey questions.21
Only survey respondents who answered yes to the first question, Are you involved in any aspect of the care of hospitalized general medical patients for whom DVT prophylaxis is considered? were asked to complete the remaining sections. Subsequent questions required respondents to check the box on a 7‐point Likert‐type scale that most accurately reflected their perception (Table 1). A successful intervention was defined as one that, if implemented, would yield the anticipated effect and a feasible intervention as one that was easy to implement without major logistical burden. Respondents were also asked which clinician group was best able to provide a daily assessment of patients' need for DVT prophylaxis, ensure DVT prophylaxis is prescribed, and ensure adherence.
|
| Section 1: Perceptions regarding DVT prophylaxis in hospitalized medical patients* |
| 1. How important an issue is the prevention of DVT in hospitalized general medical patients? |
| 2. To your knowledge, how effective are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 3. How safe are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 4. Current anticoagulant prophylaxis strategies are: 1 = underutilized, 4 = appropriately utilized, 7 = overutilized. |
| Section 2: Perceptions regarding barriers to the optimal use of DVT prophylaxis |
| 1. Lack of time to consider DVT prophylaxis in every patient |
| 2. Lack of clear indications for DVT prophylaxis (ie, who should get prophylaxis) |
| 3. Lack of clear contraindications for DVT prophylaxis (ie, who should not get prophylaxis) |
| 4. Lack of awareness about effectiveness of DVT prophylaxis |
| 5. Lack of physician agreement with current DVT prophylaxis guidelines |
| 6. Patient discomfort from subcutaneous injections of anticoagulants |
| 7. Clinician concerns about increased bleeding risk from anticoagulant administration |
| Section 3: Perceptions of interventions relating to DVT prophylaxis |
| 1. Yearly multidisciplinary educational meetings: to engage a wide spectrum of healthcare professionals to review DVT prophylaxis in hospitalized medical patients |
| 2. Posters on the wards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible or ineligible for this treatment |
| 3. Laminated pocket cards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 4. Preprinted order sheets: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 5. Periodic audit and feedback to healthcare providers: E‐mails to physicians containing reports on compliance with DVT prevention practice guidelines over recent years |
| 6. Computerized reminders (to the physicians): to prompt the physician to consider DVT prophylaxis upon opening a patient's electronic medical record |
| 7. Nurse reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 8. Pharmacist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 9. Physiotherapist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 10. Use of a local opinion leader (within the hospital) to promote evidence‐based use of DVT prophylaxis guidelines: to educate healthcare professionals on best practices for DVT prophylaxis |
Survey Administration
The survey was distributed between April and July 2007 in both paper‐based and web‐based formats using Survey Monkey software. Ontario members of the Canadian Society of Internal Medicine (n = 193) received a direct electronic invitation (from N.S.L., on behalf of J.D.D.) to participate, while members of the Canadian Society of Hospital Pharmacists (CSHP) (n = 1002) received an electronic invitation from an administrator for the CSHP to participate. The CSHP could not ensure that all members receiving the survey were hospital‐based pharmacists, so it was expected that the response rate from this group would be low. Nurse and physiotherapy managers at a convenience sample of 8 hospitals in Ontario, Canada, distributed paper‐based surveys to their staff using stamped, preaddressed envelopes. Nonresponders in all groups were sent reminders at 2 and 4 weeks.22 Data from all completed surveys were entered into an electronic database by a research coordinator (N.S.L.). A research assistant entered paper‐based survey data in duplicate, with discrepancies resolved by consensus and mediation by a third person (J.C.). The study was conducted with Institutional Ethics Review Board approval, and all respondents provided informed consent to participate. All responses were anonymous and confidential.
Statistical Considerations
Given the exploratory nature of this survey, there was no prespecified hypothesis‐driven respondent sample size. Proportions were used to describe response rates. Survey responses scored on the 7‐point Likert‐type scale were expressed as a mean and 95% confidence interval (CI). Important, highly potentially successful, and highly potentially feasible barriers were defined as those with a mean 5 points. Questions without responses, questions with multiple responses, and questions with illegible responses were treated as missing values. All statistical analyses were done using SAS version 9 (Cary, NC).
RESULTS
Survey Responses
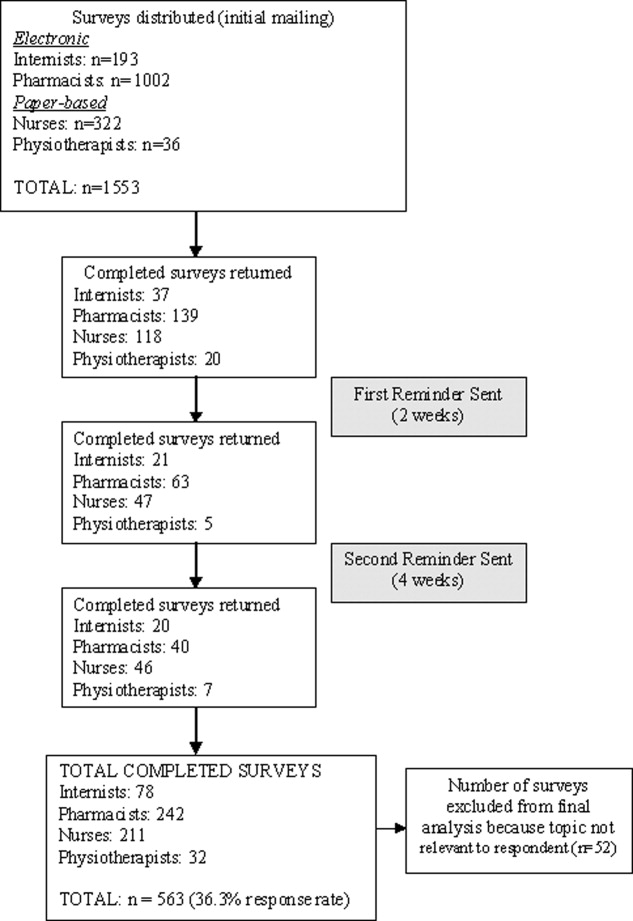
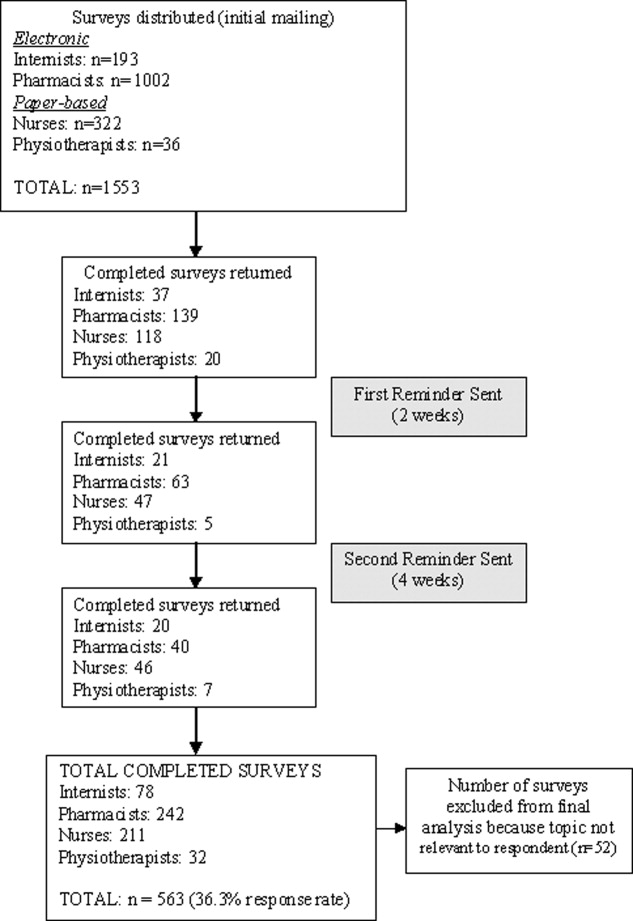
The overall response rate was 36.3% (563/1553), with 65.5% (211/322) of nurses, 40.4% (78/193) of physicians, 24.1% (242/1002) of pharmacists, and 88.8% (32/36) of physiotherapists completing surveys. When pharmacists were removed from the response rate calculation (since it was expected that many of those receiving the survey were not in a primarily hospital‐based practice), the overall response rate rose to 58.3% (321/551). Excluded were 9.2% (52/563) of returned surveys, as respondents indicated the topic was not relevant to their practice. Five hundred eleven surveys were included in the final analysis (Figure 1).
Importance, Effectiveness, Safety, and Appropriateness of DVT Prophylaxis Strategies
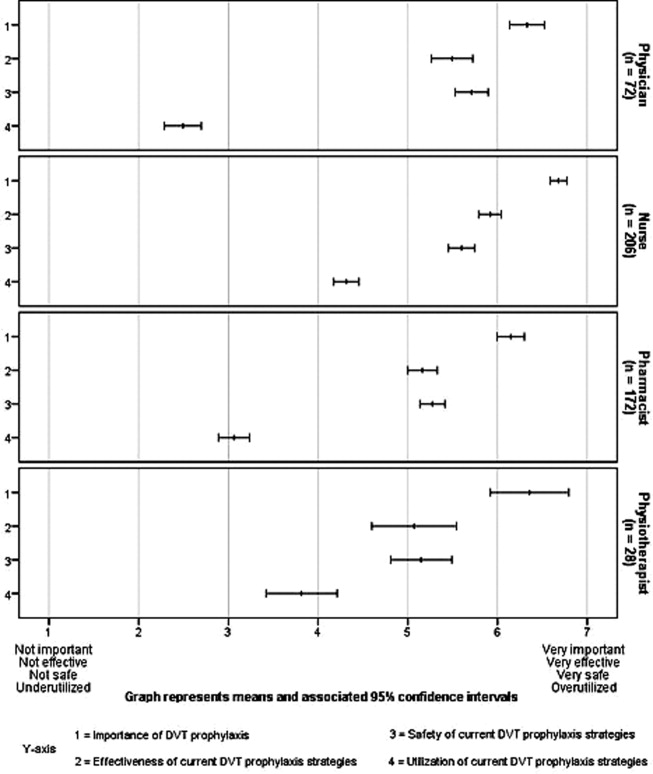
DVT prophylaxis was perceived across clinician groups as important (mean score 6.4; 95% CI 6.3 to 6.5), safe (mean 5.5; 95% CI 5.4 to 5.6), and effective (mean 5.5; 95% CI 5.4 to 6.6) (Figure 2). The mean score for the appropriateness of current DVT prophylaxis practices was 3.5 (95% CI 3.4 to 3.7), suggesting an overall perception of underutilization. However, by respondent groups, DVT prophylaxis was considered to be underutilized by physicians (mean 2.5; 95% CI 2.3 to 2.7) and pharmacists (mean 3.1; 95% CI 2.9 to 3.2), while nurses (mean 4.3; 95% CI 4.2 to 4.5) and physiotherapists (mean 3.8; 95% CI, 3.4 to 4.2) tended to consider current strategies as appropriate.
Potential Barriers to DVT Prophylaxis Utilization
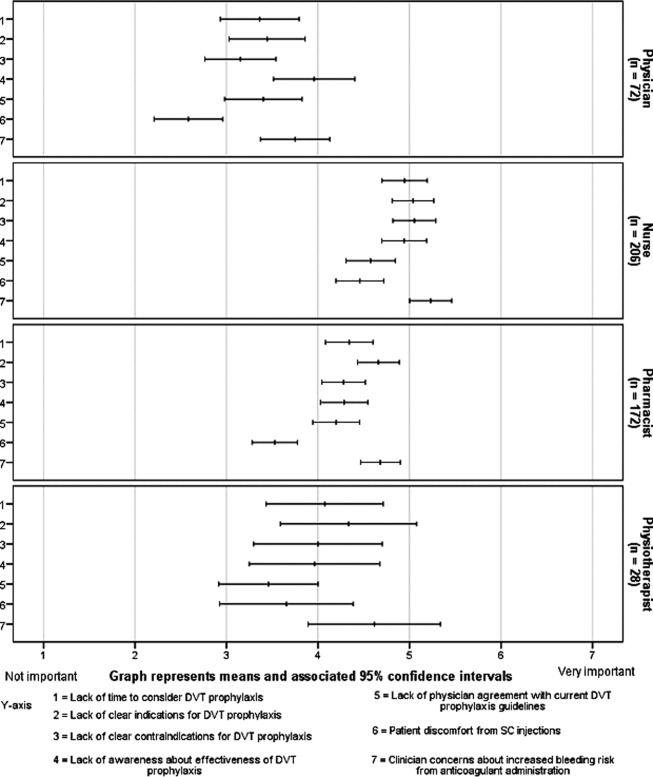
Figure 3 demonstrates that no single barrier to DVT prophylaxis utilization was dominant and no barriers were considered very important. Perceived barriers carrying comparable weight were: concerns about bleeding (mean 4.8; 95% CI 4.6 to 4.9); lack of clear indications (mean 4.6; 95% CI 4.5 to 4.8) and contraindications to DVT prophylaxis (mean 4.4; 95% CI 4.3 to 4.6); lack of awareness about effectiveness of DVT prophylaxis (mean 4.5; 95% CI 4.3 to 4.7); and lack of time to consider DVT prophylaxis in every patient (mean 4.4; 95% CI 4.3 to 4.6). Patient discomfort from subcutaneous injections was perceived as the least important barrier (mean 3.8; 95% CI 3.6 to 4.0). Physicians perceived lack of awareness about the effectiveness of DVT prophylaxis as the most important barrier (mean 4.0; 95% CI 3.5 to 4.4), whereas concern about bleeding was dominant among non‐physicians (nurses' mean 5.2; 95% CI 5.0 to 5.5; pharmacists' mean 4.7; 95% CI 4.5 to 4.9; physiotherapists' mean 4.6; 95% CI 3.9 to 5.3).
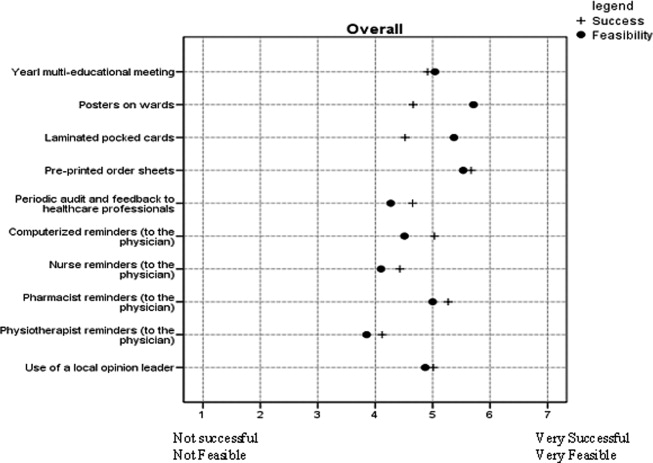
Potential Success and Feasibility of Interventions to Optimize DVT Prophylaxis Utilization
Interventions considered across clinician groups as highly potentially successful were: preprinted order sheets (5.7; 95% CI 5.6 to 5.8); pharmacist reminders to physicians (mean 5.3; 95% CI 5.1 to 5.4); computerized reminders to physicians (mean 5.0; 95% CI 4.9 to 5.2); and use of a local opinion leader (mean 5.0; 95% CI 4.9 to 5.2). Interventions considered highly potentially feasible were: posters (mean 5.7; CI 5.6 to 5.8); preprinted order sheets (mean 5.5; 95% CI 5.4 to 5.7); laminated pocket cards (mean 5.4; 95% CI 5.2 to 5.5); multidisciplinary educational meetings (mean 5.0; 95% CI 4.9 to 5.2); and pharmacist reminders to physicians (mean 5.0; 95% CI 4.9 to 5.1). Preprinted orders and pharmacist reminders were perceived by all clinician groups as having both high potential success and feasibility (Figure 4).
Perceptions on Which Clinician Group Is Best Able to Assess and Implement DVT Prophylaxis
Respondents were divided between considering the attending physician and the bedside nurse as best able to perform a daily assessment of patients' need for DVT prophylaxis (43.4% [204/470] vs 44.0% [207/470], respectively). Respondents from these groups each predominantly thought this responsibility was theirs, with 68.1% (49/72) of physicians and 61.5% (123/200) of nurses perceiving this as their responsibility (Figure 5).
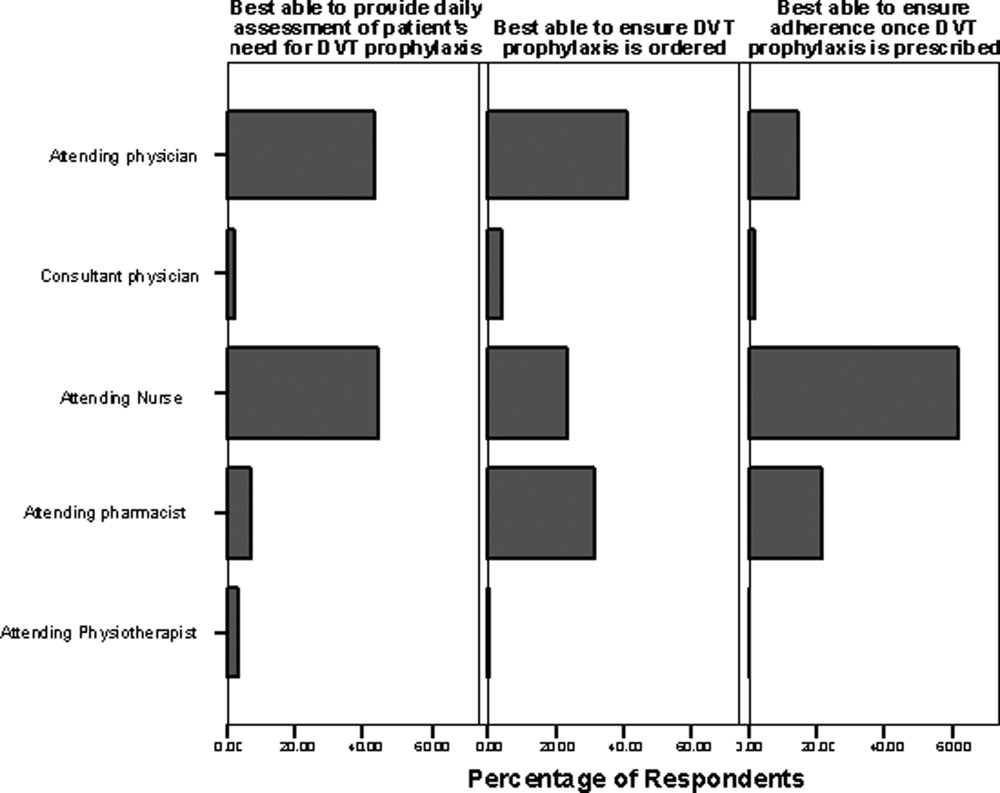
Forty‐one percent (193/471) of respondents perceived the attending physician as best able to ensure that DVT prophylaxis is ordered, while 31.2% (147/471) identified the pharmacist and 23.3% (110/471) identified the bedside nurse as best suited to this role. Among pharmacists, 66.3% (114/172) perceived that the attending pharmacist is best able to perform this task. Among respondents, 61.9% (296/478) felt the bedside nurse is best able to ensure adherence to DVT prophylaxis, with good agreement among all clinician groups.
DISCUSSION
Our survey identified several perceived barriers to optimizing DVT prophylaxis, consistent with those reported in the White Paper sponsored by the American Public Health Association.23 While no single barrier outlined in our survey was dominant, 2 novel barriers were identified: misperception of DVT prophylaxis underutilization, and confusion about roles and responsibilities in the area of DVT prophylaxis. Attention to these barriers may be helpful in developing an intervention aimed at bridging the gap between evidence and practice.
While our survey demonstrates agreement across clinician groups on the importance, efficacy, and safety of DVT prophylaxis, the discordant perceptions that exist about whether DVT prophylaxis is utilized appropriately is an important concern. Physician and pharmacist‐respondents demonstrated awareness that thromboprophylaxis is underutilized in medical patients. However, despite overwhelming published evidence to the contrary, nurses responding to our survey did not tend to recognize the problem of DVT prophylaxis underutilization in hospitalized medical patients. This knowledge deficit may be a significant barrier particularly since the pooled group of respondents indicated that nurses are among those caregivers best able to conduct a daily assessment of patients' need for DVT prophylaxis. A possible explanation for the finding that nurses and physiotherapists demonstrated a relative lack of awareness of the problem of DVT prophylaxis underutilization is ward‐specific healthcare priorities. Nursing and physiotherapy care on surgical wards is aimed at preventing postoperative complications, including DVT. However, its primary focus on medical wards is the management of acute medical problems. Prevention of hospital‐related complications, such as DVT, is often a secondary focus. Therefore, ensuring that all clinician groups are educated about the problem of DVT prophylaxis underutilization is necessary to drive quality improvement. A physician‐based survey on antithrombotic therapies demonstrated a similar need for education on guideline recommendations.20
A second important barrier identified in our survey is that both attending nurses and physicians feel that daily assessment of a patient's need for DVT prophylaxis is their responsibility. Confusion about roles and responsibilities in this area of patient care was reported by Cook et al., who identified that multidisciplinary care was perceived as a barrier to effective VTE prevention.18 Uncertainty as to which group should take ownership of DVT prophylaxis can lead to a diffusion of responsibility, a lack of accountability, and a gap in care. A resolution to whether DVT risk assessment is a nursing or a physician role could be reached through increased interdisciplinary communication and provision of clear definitions of roles to hospital staff.
Survey respondents felt that preprinted orders and pharmacist reminders to physicians were potentially successful and feasible strategies to optimize DVT prophylaxis. These components could be part of a simple tool to initiate prophylaxis. While electronic alerts have been shown to increase prophylaxis rates,24 we suspect that many respondents did not view these as highly important because of limited use of computerized order entry at their facilities. Interestingly, survey respondents did not perceive audit‐and‐feedback systems or local opinion leaders as potentially successful, though previous studies have demonstrated that they can change clinician behavior.25, 26 This may be because respondents may not be aware of the strength of technology‐based interventions (eg, electronic orders) and the role of opinion leaders, and the evidence in support of such interventions.24, 26 A systematic review of studies to improve DVT prophylaxis in hospitals reported that a combination of multiple active strategies is most effective, particularly those that link physician reminders with audit‐and‐feedback.27 For example, in the define study, a multicomponent intervention consisting of interactive educational sessions, verbal and computerized prompts, and individual performance feedback significantly improved adherence to DVT prophylaxis guidelines in critically ill patients.28 Whether a similar intervention could improve adherence to DVT prophylaxis guidelines in hospitalized medical patients merits further study. Any intervention must be paired with better education about which patients should, and should not, receive prophylaxis, as this may address many reported barriers in our survey (including concerns about bleeding). Respondents' uncertainty about these issues is not surprising, as studies of DVT prophylaxis in medical patients are not plentiful.2 However, recent guidelines do identify subgroups of medically ill patients in whom DVT prophylaxis is indicated.2 A clear and simple DVT risk assessment algorithm that identifies medical patients in whom DVT prophylaxis should (or should not) be administered may help to overcome respondents' concerns.
A limitation of our survey is the overall response rate of 36.3%, largely driven by the considerable number of nonresponding pharmacists (n = 760, reflecting 49% of the entire sample). However, the majority of the pharmacists were likely not hospital‐based, were thus not a target of this study, and their low response rate is not surprising. After excluding pharmacists, the response rate was 58.3% (321/551), which is consistent with response rates of other large‐sample surveys.29 The lower response rate for physicians and pharmacists may also reflect web‐based survey dissemination which, despite its feasibility, has lower response rates than paper‐based dissemination.3032 While the sample of physicians was relatively small compared to the other respondent groups surveyed, we aimed to identify barriers to actually implementing VTE prophylaxis, not just ordering prophylaxis, which is a multidisciplinary concern.
Although this survey was based on Canadian healthcare providers' perspectives, we believe the results are generalizable since both US and Canadian‐based studies have found that VTE prophylaxis is underutilized among hospitalized medical patients.4, 6 Furthermore, the American College of Chest Physicians (ACCP) guidelines on VTE prophylaxis, which are well‐recognized in both the United States and Canada, were developed with input from Canadian and American content experts.2 And while the US and Canadian healthcare systems are organized differently, at the patient‐care level, the roles of healthcare professionals are very similar. The generalizability of our findings is, however, limited by the institutional characteristics of respondents. We do not purport that the responses of any of the 4 clinician groups are generalizable to those groups as a whole. Although we surveyed clinicians in teaching and nonteaching, urban and rural practices, perceptions about DVT prophylaxis may be influenced by other factors, including the availability of local preprinted orders, electronic medical records, and quality improvement programs. Another potential limitation is that we did not assess all possible strategies to improve DVT prophylaxis, such as nurse practitioners and computerized decision support systems. These were purposely excluded, as they are not financially feasible in all centers, and thus not generalizable. Finally, like all self‐administered surveys, our findings reflect respondents' perceptions rather than objective observations about practice.
In conclusion, we identified novel and important barriers to optimal DVT prophylaxis utilization and potential interventions to address this important safety concern in hospitalized medical patients. To overcome some of these barriers, we propose an educational intervention prior to delivery of a top‐down, evidence‐based intervention to first increase healthcare providers' knowledge of the safety of DVT prophylaxis, system and team‐based approaches, and which interventions are most likely to be successful so as to encourage greater compliance with the intervention. A top‐down, system‐wide approach, involving the entire healthcare team and hospital administrators, can help drive this communication. As DVT prophylaxis becomes an increasingly important component in hospital accreditation, such solutions become appealing to facilitate change in practices. Results of this survey may inform future knowledge translation interventions by eliminating perceived barriers to DVT prophylaxis and by incorporating strategies that are perceived by healthcare professionals to be successful, feasible, and supported by evidence.
- ,.National hospital discharge survey: annual summary, 1996.Vital Health Stat.1999;13:1–46.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th ed).Chest.2008;133:381S–443S.
- ,,, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: No. 43. AHRQ Publication No. 01‐E058, July 2001. Rockville, MD: Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/ptsafety/. Accessed October 9,2007.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Hospitals' compliance with prophylaxis guidelines for venous thromboembolism.Am J Health Syst Pharm.2007;64:69–76.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- ,,.A retrospective evaluation of adherence to guidelines for prevention of thromboembolic events in general medical inpatients.Can J Hosp Pharm.2006;59:258–263.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of DVT prophylaxis guidelines.Chest2001;120:1964–1971.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,,,.The use of low molecular weight heparins for the prevention of postoperative venous thromboembolism in general surgery. A survey of practice in the United States.Int Angiol.2002;1:78–85.
- ,,, et al.Venous thromboembolic disease management patterns in total hip arthroplasty and total knee arthroplasty patients: a survey of the AAHKS membership.J Arthroplasty.2001;6:679–688.
- ,,.Thromboprophylaxis in medical‐surgical intensive care unit patients.J Crit Care.2005;20:320–323.
- ,.Utilization of venous thromboembolism prophylaxis in a medical‐surgical ICU.Chest.1998;113:162–164.
- ,,, et al.Why don't physicians follow clinical practice guidelines? A framework for improvement.JAMA.1999;282:1458–1465.
- ,,, et al.Thromboprophylaxis for hospitalized medical patients: a multicenter qualitative study.J Hosp Med.2009;4;269–275.
- ,,, et al.Definition of immobility in studies of thromboprophylaxis in hospitalized medical patients: a systematic review.J Vasc Nurs.2010;28:54–66.
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- .Mail and internet surveys: the tailored design method.New York, NY:John Wiley 2000.
- Deep‐vein thrombosis: advancing awareness to protect patient lives. Public Health Leadership Conference on Deep‐Vein Thrombosis. American Public Health Association. Available at: http://www.apha.org/NR/rdonlyres/A209F84A‐7C0E‐4761–9ECF‐61D22E1E11F7/0/DVT_White_Paper.pdf. Accessed May 28,2008.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Getting a validated guideline into local practice: implementation and audit of the SIGN guideline on the prevention of deep vein thrombosis in a district general hospital.Scott Med J.1998;43:23–25.
- ,,,.Local opinion leaders: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2007;24(1):CD000125.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE study.Crit Care Med.2006;34:694–699.
- ,,,.Using the Internet to conduct surveys of health professionals: a valid alternative?Fam Pract.2003;20:545–551.
- ,,,,,.Use of new technology in endourology and laparoscopy by American urologists: Internet and postal survey.Urology.2000;56:760–765.
- ,,,,.E‐mail versus conventional postal mail survey of geriatric chiefs.Gerontologist.2001;41:799–804.
- ,,, et al.Internet versus mailed questionnaires: a randomized comparison.J Med Internet Res.2004;6:e30.
Each year in North America, over 7 million adults are hospitalized with a medical illness.1 Acute illness and decreased mobility in hospital places patients at increased risk for venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and life‐threatening pulmonary embolism (PE).2 Since VTE remains the most preventable cause of death in hospitalized patients, numerous studies have aimed at reducing the incidence of hospital‐acquired DVT. Aside from cost, the impact of VTE to the healthcare system is felt not only by those who diagnose and treat VTE, but also by those responsible for correcting the severe bleeding that can result from inappropriate use of thromboprophylaxis. Approximately 60% of symptomatic VTE occurs in medical patients, and recent hospitalization for medical illness accounts for 25% of all community‐diagnosed VTE. The Agency for Health Research and Quality ranks DVT prevention as the top priority out of 79 patient safety initiatives, and expert consensus groups provide a strong recommendation that DVT prophylaxis with a low‐dose anticoagulant should be administered to at‐risk hospitalized medical patients.2, 3
Despite the availability, efficacy, and safety of DVT prophylaxis,2 it is discouraging that only 21% to 62% of medical patients receive prophylaxis,49 and only 16% to 40% receive appropriate prophylaxis.46, 1012 However, 70% to 90% of patients in other at‐risk groups, such as surgical patients or critically ill patients, receive prophylaxis.1316 The reason why DVT prophylaxis is so underutilized in medical patients is unclear, as explanations for low rates of clinical practice guideline utilization are multifaceted,17 and few studies have investigated the barriers to optimal thromboprophylaxis.1820
To explore possible reasons for this disparity between evidence and practice, we conducted a cross‐sectional survey of 4 clinician groups involved in the care of hospitalized medical patients. Our objective was to identify barriers and potential solutions to the underutilization of DVT prophylaxis in hospitalized medical patients.
METHODS
Instrument Development
The survey focused on 3 domains: perceived importance, effectiveness, and safety of DVT prophylaxis; perceived barriers to implementation; and perceived potential success and feasibility of interventions to optimize DVT prophylaxis. The survey cover letter outlined background information, study design, and a statement on confidentiality. A prior survey of DVT prophylaxis administered to thrombosis experts was used to generate survey questions.21
Only survey respondents who answered yes to the first question, Are you involved in any aspect of the care of hospitalized general medical patients for whom DVT prophylaxis is considered? were asked to complete the remaining sections. Subsequent questions required respondents to check the box on a 7‐point Likert‐type scale that most accurately reflected their perception (Table 1). A successful intervention was defined as one that, if implemented, would yield the anticipated effect and a feasible intervention as one that was easy to implement without major logistical burden. Respondents were also asked which clinician group was best able to provide a daily assessment of patients' need for DVT prophylaxis, ensure DVT prophylaxis is prescribed, and ensure adherence.
|
| Section 1: Perceptions regarding DVT prophylaxis in hospitalized medical patients* |
| 1. How important an issue is the prevention of DVT in hospitalized general medical patients? |
| 2. To your knowledge, how effective are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 3. How safe are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 4. Current anticoagulant prophylaxis strategies are: 1 = underutilized, 4 = appropriately utilized, 7 = overutilized. |
| Section 2: Perceptions regarding barriers to the optimal use of DVT prophylaxis |
| 1. Lack of time to consider DVT prophylaxis in every patient |
| 2. Lack of clear indications for DVT prophylaxis (ie, who should get prophylaxis) |
| 3. Lack of clear contraindications for DVT prophylaxis (ie, who should not get prophylaxis) |
| 4. Lack of awareness about effectiveness of DVT prophylaxis |
| 5. Lack of physician agreement with current DVT prophylaxis guidelines |
| 6. Patient discomfort from subcutaneous injections of anticoagulants |
| 7. Clinician concerns about increased bleeding risk from anticoagulant administration |
| Section 3: Perceptions of interventions relating to DVT prophylaxis |
| 1. Yearly multidisciplinary educational meetings: to engage a wide spectrum of healthcare professionals to review DVT prophylaxis in hospitalized medical patients |
| 2. Posters on the wards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible or ineligible for this treatment |
| 3. Laminated pocket cards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 4. Preprinted order sheets: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 5. Periodic audit and feedback to healthcare providers: E‐mails to physicians containing reports on compliance with DVT prevention practice guidelines over recent years |
| 6. Computerized reminders (to the physicians): to prompt the physician to consider DVT prophylaxis upon opening a patient's electronic medical record |
| 7. Nurse reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 8. Pharmacist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 9. Physiotherapist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 10. Use of a local opinion leader (within the hospital) to promote evidence‐based use of DVT prophylaxis guidelines: to educate healthcare professionals on best practices for DVT prophylaxis |
Survey Administration
The survey was distributed between April and July 2007 in both paper‐based and web‐based formats using Survey Monkey software. Ontario members of the Canadian Society of Internal Medicine (n = 193) received a direct electronic invitation (from N.S.L., on behalf of J.D.D.) to participate, while members of the Canadian Society of Hospital Pharmacists (CSHP) (n = 1002) received an electronic invitation from an administrator for the CSHP to participate. The CSHP could not ensure that all members receiving the survey were hospital‐based pharmacists, so it was expected that the response rate from this group would be low. Nurse and physiotherapy managers at a convenience sample of 8 hospitals in Ontario, Canada, distributed paper‐based surveys to their staff using stamped, preaddressed envelopes. Nonresponders in all groups were sent reminders at 2 and 4 weeks.22 Data from all completed surveys were entered into an electronic database by a research coordinator (N.S.L.). A research assistant entered paper‐based survey data in duplicate, with discrepancies resolved by consensus and mediation by a third person (J.C.). The study was conducted with Institutional Ethics Review Board approval, and all respondents provided informed consent to participate. All responses were anonymous and confidential.
Statistical Considerations
Given the exploratory nature of this survey, there was no prespecified hypothesis‐driven respondent sample size. Proportions were used to describe response rates. Survey responses scored on the 7‐point Likert‐type scale were expressed as a mean and 95% confidence interval (CI). Important, highly potentially successful, and highly potentially feasible barriers were defined as those with a mean 5 points. Questions without responses, questions with multiple responses, and questions with illegible responses were treated as missing values. All statistical analyses were done using SAS version 9 (Cary, NC).
RESULTS
Survey Responses
The overall response rate was 36.3% (563/1553), with 65.5% (211/322) of nurses, 40.4% (78/193) of physicians, 24.1% (242/1002) of pharmacists, and 88.8% (32/36) of physiotherapists completing surveys. When pharmacists were removed from the response rate calculation (since it was expected that many of those receiving the survey were not in a primarily hospital‐based practice), the overall response rate rose to 58.3% (321/551). Excluded were 9.2% (52/563) of returned surveys, as respondents indicated the topic was not relevant to their practice. Five hundred eleven surveys were included in the final analysis (Figure 1).
Importance, Effectiveness, Safety, and Appropriateness of DVT Prophylaxis Strategies
DVT prophylaxis was perceived across clinician groups as important (mean score 6.4; 95% CI 6.3 to 6.5), safe (mean 5.5; 95% CI 5.4 to 5.6), and effective (mean 5.5; 95% CI 5.4 to 6.6) (Figure 2). The mean score for the appropriateness of current DVT prophylaxis practices was 3.5 (95% CI 3.4 to 3.7), suggesting an overall perception of underutilization. However, by respondent groups, DVT prophylaxis was considered to be underutilized by physicians (mean 2.5; 95% CI 2.3 to 2.7) and pharmacists (mean 3.1; 95% CI 2.9 to 3.2), while nurses (mean 4.3; 95% CI 4.2 to 4.5) and physiotherapists (mean 3.8; 95% CI, 3.4 to 4.2) tended to consider current strategies as appropriate.
Potential Barriers to DVT Prophylaxis Utilization
Figure 3 demonstrates that no single barrier to DVT prophylaxis utilization was dominant and no barriers were considered very important. Perceived barriers carrying comparable weight were: concerns about bleeding (mean 4.8; 95% CI 4.6 to 4.9); lack of clear indications (mean 4.6; 95% CI 4.5 to 4.8) and contraindications to DVT prophylaxis (mean 4.4; 95% CI 4.3 to 4.6); lack of awareness about effectiveness of DVT prophylaxis (mean 4.5; 95% CI 4.3 to 4.7); and lack of time to consider DVT prophylaxis in every patient (mean 4.4; 95% CI 4.3 to 4.6). Patient discomfort from subcutaneous injections was perceived as the least important barrier (mean 3.8; 95% CI 3.6 to 4.0). Physicians perceived lack of awareness about the effectiveness of DVT prophylaxis as the most important barrier (mean 4.0; 95% CI 3.5 to 4.4), whereas concern about bleeding was dominant among non‐physicians (nurses' mean 5.2; 95% CI 5.0 to 5.5; pharmacists' mean 4.7; 95% CI 4.5 to 4.9; physiotherapists' mean 4.6; 95% CI 3.9 to 5.3).
Potential Success and Feasibility of Interventions to Optimize DVT Prophylaxis Utilization
Interventions considered across clinician groups as highly potentially successful were: preprinted order sheets (5.7; 95% CI 5.6 to 5.8); pharmacist reminders to physicians (mean 5.3; 95% CI 5.1 to 5.4); computerized reminders to physicians (mean 5.0; 95% CI 4.9 to 5.2); and use of a local opinion leader (mean 5.0; 95% CI 4.9 to 5.2). Interventions considered highly potentially feasible were: posters (mean 5.7; CI 5.6 to 5.8); preprinted order sheets (mean 5.5; 95% CI 5.4 to 5.7); laminated pocket cards (mean 5.4; 95% CI 5.2 to 5.5); multidisciplinary educational meetings (mean 5.0; 95% CI 4.9 to 5.2); and pharmacist reminders to physicians (mean 5.0; 95% CI 4.9 to 5.1). Preprinted orders and pharmacist reminders were perceived by all clinician groups as having both high potential success and feasibility (Figure 4).
Perceptions on Which Clinician Group Is Best Able to Assess and Implement DVT Prophylaxis
Respondents were divided between considering the attending physician and the bedside nurse as best able to perform a daily assessment of patients' need for DVT prophylaxis (43.4% [204/470] vs 44.0% [207/470], respectively). Respondents from these groups each predominantly thought this responsibility was theirs, with 68.1% (49/72) of physicians and 61.5% (123/200) of nurses perceiving this as their responsibility (Figure 5).
Forty‐one percent (193/471) of respondents perceived the attending physician as best able to ensure that DVT prophylaxis is ordered, while 31.2% (147/471) identified the pharmacist and 23.3% (110/471) identified the bedside nurse as best suited to this role. Among pharmacists, 66.3% (114/172) perceived that the attending pharmacist is best able to perform this task. Among respondents, 61.9% (296/478) felt the bedside nurse is best able to ensure adherence to DVT prophylaxis, with good agreement among all clinician groups.
DISCUSSION
Our survey identified several perceived barriers to optimizing DVT prophylaxis, consistent with those reported in the White Paper sponsored by the American Public Health Association.23 While no single barrier outlined in our survey was dominant, 2 novel barriers were identified: misperception of DVT prophylaxis underutilization, and confusion about roles and responsibilities in the area of DVT prophylaxis. Attention to these barriers may be helpful in developing an intervention aimed at bridging the gap between evidence and practice.
While our survey demonstrates agreement across clinician groups on the importance, efficacy, and safety of DVT prophylaxis, the discordant perceptions that exist about whether DVT prophylaxis is utilized appropriately is an important concern. Physician and pharmacist‐respondents demonstrated awareness that thromboprophylaxis is underutilized in medical patients. However, despite overwhelming published evidence to the contrary, nurses responding to our survey did not tend to recognize the problem of DVT prophylaxis underutilization in hospitalized medical patients. This knowledge deficit may be a significant barrier particularly since the pooled group of respondents indicated that nurses are among those caregivers best able to conduct a daily assessment of patients' need for DVT prophylaxis. A possible explanation for the finding that nurses and physiotherapists demonstrated a relative lack of awareness of the problem of DVT prophylaxis underutilization is ward‐specific healthcare priorities. Nursing and physiotherapy care on surgical wards is aimed at preventing postoperative complications, including DVT. However, its primary focus on medical wards is the management of acute medical problems. Prevention of hospital‐related complications, such as DVT, is often a secondary focus. Therefore, ensuring that all clinician groups are educated about the problem of DVT prophylaxis underutilization is necessary to drive quality improvement. A physician‐based survey on antithrombotic therapies demonstrated a similar need for education on guideline recommendations.20
A second important barrier identified in our survey is that both attending nurses and physicians feel that daily assessment of a patient's need for DVT prophylaxis is their responsibility. Confusion about roles and responsibilities in this area of patient care was reported by Cook et al., who identified that multidisciplinary care was perceived as a barrier to effective VTE prevention.18 Uncertainty as to which group should take ownership of DVT prophylaxis can lead to a diffusion of responsibility, a lack of accountability, and a gap in care. A resolution to whether DVT risk assessment is a nursing or a physician role could be reached through increased interdisciplinary communication and provision of clear definitions of roles to hospital staff.
Survey respondents felt that preprinted orders and pharmacist reminders to physicians were potentially successful and feasible strategies to optimize DVT prophylaxis. These components could be part of a simple tool to initiate prophylaxis. While electronic alerts have been shown to increase prophylaxis rates,24 we suspect that many respondents did not view these as highly important because of limited use of computerized order entry at their facilities. Interestingly, survey respondents did not perceive audit‐and‐feedback systems or local opinion leaders as potentially successful, though previous studies have demonstrated that they can change clinician behavior.25, 26 This may be because respondents may not be aware of the strength of technology‐based interventions (eg, electronic orders) and the role of opinion leaders, and the evidence in support of such interventions.24, 26 A systematic review of studies to improve DVT prophylaxis in hospitals reported that a combination of multiple active strategies is most effective, particularly those that link physician reminders with audit‐and‐feedback.27 For example, in the define study, a multicomponent intervention consisting of interactive educational sessions, verbal and computerized prompts, and individual performance feedback significantly improved adherence to DVT prophylaxis guidelines in critically ill patients.28 Whether a similar intervention could improve adherence to DVT prophylaxis guidelines in hospitalized medical patients merits further study. Any intervention must be paired with better education about which patients should, and should not, receive prophylaxis, as this may address many reported barriers in our survey (including concerns about bleeding). Respondents' uncertainty about these issues is not surprising, as studies of DVT prophylaxis in medical patients are not plentiful.2 However, recent guidelines do identify subgroups of medically ill patients in whom DVT prophylaxis is indicated.2 A clear and simple DVT risk assessment algorithm that identifies medical patients in whom DVT prophylaxis should (or should not) be administered may help to overcome respondents' concerns.
A limitation of our survey is the overall response rate of 36.3%, largely driven by the considerable number of nonresponding pharmacists (n = 760, reflecting 49% of the entire sample). However, the majority of the pharmacists were likely not hospital‐based, were thus not a target of this study, and their low response rate is not surprising. After excluding pharmacists, the response rate was 58.3% (321/551), which is consistent with response rates of other large‐sample surveys.29 The lower response rate for physicians and pharmacists may also reflect web‐based survey dissemination which, despite its feasibility, has lower response rates than paper‐based dissemination.3032 While the sample of physicians was relatively small compared to the other respondent groups surveyed, we aimed to identify barriers to actually implementing VTE prophylaxis, not just ordering prophylaxis, which is a multidisciplinary concern.
Although this survey was based on Canadian healthcare providers' perspectives, we believe the results are generalizable since both US and Canadian‐based studies have found that VTE prophylaxis is underutilized among hospitalized medical patients.4, 6 Furthermore, the American College of Chest Physicians (ACCP) guidelines on VTE prophylaxis, which are well‐recognized in both the United States and Canada, were developed with input from Canadian and American content experts.2 And while the US and Canadian healthcare systems are organized differently, at the patient‐care level, the roles of healthcare professionals are very similar. The generalizability of our findings is, however, limited by the institutional characteristics of respondents. We do not purport that the responses of any of the 4 clinician groups are generalizable to those groups as a whole. Although we surveyed clinicians in teaching and nonteaching, urban and rural practices, perceptions about DVT prophylaxis may be influenced by other factors, including the availability of local preprinted orders, electronic medical records, and quality improvement programs. Another potential limitation is that we did not assess all possible strategies to improve DVT prophylaxis, such as nurse practitioners and computerized decision support systems. These were purposely excluded, as they are not financially feasible in all centers, and thus not generalizable. Finally, like all self‐administered surveys, our findings reflect respondents' perceptions rather than objective observations about practice.
In conclusion, we identified novel and important barriers to optimal DVT prophylaxis utilization and potential interventions to address this important safety concern in hospitalized medical patients. To overcome some of these barriers, we propose an educational intervention prior to delivery of a top‐down, evidence‐based intervention to first increase healthcare providers' knowledge of the safety of DVT prophylaxis, system and team‐based approaches, and which interventions are most likely to be successful so as to encourage greater compliance with the intervention. A top‐down, system‐wide approach, involving the entire healthcare team and hospital administrators, can help drive this communication. As DVT prophylaxis becomes an increasingly important component in hospital accreditation, such solutions become appealing to facilitate change in practices. Results of this survey may inform future knowledge translation interventions by eliminating perceived barriers to DVT prophylaxis and by incorporating strategies that are perceived by healthcare professionals to be successful, feasible, and supported by evidence.
Each year in North America, over 7 million adults are hospitalized with a medical illness.1 Acute illness and decreased mobility in hospital places patients at increased risk for venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and life‐threatening pulmonary embolism (PE).2 Since VTE remains the most preventable cause of death in hospitalized patients, numerous studies have aimed at reducing the incidence of hospital‐acquired DVT. Aside from cost, the impact of VTE to the healthcare system is felt not only by those who diagnose and treat VTE, but also by those responsible for correcting the severe bleeding that can result from inappropriate use of thromboprophylaxis. Approximately 60% of symptomatic VTE occurs in medical patients, and recent hospitalization for medical illness accounts for 25% of all community‐diagnosed VTE. The Agency for Health Research and Quality ranks DVT prevention as the top priority out of 79 patient safety initiatives, and expert consensus groups provide a strong recommendation that DVT prophylaxis with a low‐dose anticoagulant should be administered to at‐risk hospitalized medical patients.2, 3
Despite the availability, efficacy, and safety of DVT prophylaxis,2 it is discouraging that only 21% to 62% of medical patients receive prophylaxis,49 and only 16% to 40% receive appropriate prophylaxis.46, 1012 However, 70% to 90% of patients in other at‐risk groups, such as surgical patients or critically ill patients, receive prophylaxis.1316 The reason why DVT prophylaxis is so underutilized in medical patients is unclear, as explanations for low rates of clinical practice guideline utilization are multifaceted,17 and few studies have investigated the barriers to optimal thromboprophylaxis.1820
To explore possible reasons for this disparity between evidence and practice, we conducted a cross‐sectional survey of 4 clinician groups involved in the care of hospitalized medical patients. Our objective was to identify barriers and potential solutions to the underutilization of DVT prophylaxis in hospitalized medical patients.
METHODS
Instrument Development
The survey focused on 3 domains: perceived importance, effectiveness, and safety of DVT prophylaxis; perceived barriers to implementation; and perceived potential success and feasibility of interventions to optimize DVT prophylaxis. The survey cover letter outlined background information, study design, and a statement on confidentiality. A prior survey of DVT prophylaxis administered to thrombosis experts was used to generate survey questions.21
Only survey respondents who answered yes to the first question, Are you involved in any aspect of the care of hospitalized general medical patients for whom DVT prophylaxis is considered? were asked to complete the remaining sections. Subsequent questions required respondents to check the box on a 7‐point Likert‐type scale that most accurately reflected their perception (Table 1). A successful intervention was defined as one that, if implemented, would yield the anticipated effect and a feasible intervention as one that was easy to implement without major logistical burden. Respondents were also asked which clinician group was best able to provide a daily assessment of patients' need for DVT prophylaxis, ensure DVT prophylaxis is prescribed, and ensure adherence.
|
| Section 1: Perceptions regarding DVT prophylaxis in hospitalized medical patients* |
| 1. How important an issue is the prevention of DVT in hospitalized general medical patients? |
| 2. To your knowledge, how effective are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 3. How safe are currently used anticoagulant strategies for the prevention of DVT in hospitalized medical patients? |
| 4. Current anticoagulant prophylaxis strategies are: 1 = underutilized, 4 = appropriately utilized, 7 = overutilized. |
| Section 2: Perceptions regarding barriers to the optimal use of DVT prophylaxis |
| 1. Lack of time to consider DVT prophylaxis in every patient |
| 2. Lack of clear indications for DVT prophylaxis (ie, who should get prophylaxis) |
| 3. Lack of clear contraindications for DVT prophylaxis (ie, who should not get prophylaxis) |
| 4. Lack of awareness about effectiveness of DVT prophylaxis |
| 5. Lack of physician agreement with current DVT prophylaxis guidelines |
| 6. Patient discomfort from subcutaneous injections of anticoagulants |
| 7. Clinician concerns about increased bleeding risk from anticoagulant administration |
| Section 3: Perceptions of interventions relating to DVT prophylaxis |
| 1. Yearly multidisciplinary educational meetings: to engage a wide spectrum of healthcare professionals to review DVT prophylaxis in hospitalized medical patients |
| 2. Posters on the wards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible or ineligible for this treatment |
| 3. Laminated pocket cards: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 4. Preprinted order sheets: to remind healthcare professionals about DVT prophylaxis and patients who are eligible and ineligible for this treatment |
| 5. Periodic audit and feedback to healthcare providers: E‐mails to physicians containing reports on compliance with DVT prevention practice guidelines over recent years |
| 6. Computerized reminders (to the physicians): to prompt the physician to consider DVT prophylaxis upon opening a patient's electronic medical record |
| 7. Nurse reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 8. Pharmacist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 9. Physiotherapist reminders (to the physician): to remind the physician about DVT prophylaxis using written or verbal reminders |
| 10. Use of a local opinion leader (within the hospital) to promote evidence‐based use of DVT prophylaxis guidelines: to educate healthcare professionals on best practices for DVT prophylaxis |
Survey Administration
The survey was distributed between April and July 2007 in both paper‐based and web‐based formats using Survey Monkey software. Ontario members of the Canadian Society of Internal Medicine (n = 193) received a direct electronic invitation (from N.S.L., on behalf of J.D.D.) to participate, while members of the Canadian Society of Hospital Pharmacists (CSHP) (n = 1002) received an electronic invitation from an administrator for the CSHP to participate. The CSHP could not ensure that all members receiving the survey were hospital‐based pharmacists, so it was expected that the response rate from this group would be low. Nurse and physiotherapy managers at a convenience sample of 8 hospitals in Ontario, Canada, distributed paper‐based surveys to their staff using stamped, preaddressed envelopes. Nonresponders in all groups were sent reminders at 2 and 4 weeks.22 Data from all completed surveys were entered into an electronic database by a research coordinator (N.S.L.). A research assistant entered paper‐based survey data in duplicate, with discrepancies resolved by consensus and mediation by a third person (J.C.). The study was conducted with Institutional Ethics Review Board approval, and all respondents provided informed consent to participate. All responses were anonymous and confidential.
Statistical Considerations
Given the exploratory nature of this survey, there was no prespecified hypothesis‐driven respondent sample size. Proportions were used to describe response rates. Survey responses scored on the 7‐point Likert‐type scale were expressed as a mean and 95% confidence interval (CI). Important, highly potentially successful, and highly potentially feasible barriers were defined as those with a mean 5 points. Questions without responses, questions with multiple responses, and questions with illegible responses were treated as missing values. All statistical analyses were done using SAS version 9 (Cary, NC).
RESULTS
Survey Responses
The overall response rate was 36.3% (563/1553), with 65.5% (211/322) of nurses, 40.4% (78/193) of physicians, 24.1% (242/1002) of pharmacists, and 88.8% (32/36) of physiotherapists completing surveys. When pharmacists were removed from the response rate calculation (since it was expected that many of those receiving the survey were not in a primarily hospital‐based practice), the overall response rate rose to 58.3% (321/551). Excluded were 9.2% (52/563) of returned surveys, as respondents indicated the topic was not relevant to their practice. Five hundred eleven surveys were included in the final analysis (Figure 1).
Importance, Effectiveness, Safety, and Appropriateness of DVT Prophylaxis Strategies
DVT prophylaxis was perceived across clinician groups as important (mean score 6.4; 95% CI 6.3 to 6.5), safe (mean 5.5; 95% CI 5.4 to 5.6), and effective (mean 5.5; 95% CI 5.4 to 6.6) (Figure 2). The mean score for the appropriateness of current DVT prophylaxis practices was 3.5 (95% CI 3.4 to 3.7), suggesting an overall perception of underutilization. However, by respondent groups, DVT prophylaxis was considered to be underutilized by physicians (mean 2.5; 95% CI 2.3 to 2.7) and pharmacists (mean 3.1; 95% CI 2.9 to 3.2), while nurses (mean 4.3; 95% CI 4.2 to 4.5) and physiotherapists (mean 3.8; 95% CI, 3.4 to 4.2) tended to consider current strategies as appropriate.
Potential Barriers to DVT Prophylaxis Utilization
Figure 3 demonstrates that no single barrier to DVT prophylaxis utilization was dominant and no barriers were considered very important. Perceived barriers carrying comparable weight were: concerns about bleeding (mean 4.8; 95% CI 4.6 to 4.9); lack of clear indications (mean 4.6; 95% CI 4.5 to 4.8) and contraindications to DVT prophylaxis (mean 4.4; 95% CI 4.3 to 4.6); lack of awareness about effectiveness of DVT prophylaxis (mean 4.5; 95% CI 4.3 to 4.7); and lack of time to consider DVT prophylaxis in every patient (mean 4.4; 95% CI 4.3 to 4.6). Patient discomfort from subcutaneous injections was perceived as the least important barrier (mean 3.8; 95% CI 3.6 to 4.0). Physicians perceived lack of awareness about the effectiveness of DVT prophylaxis as the most important barrier (mean 4.0; 95% CI 3.5 to 4.4), whereas concern about bleeding was dominant among non‐physicians (nurses' mean 5.2; 95% CI 5.0 to 5.5; pharmacists' mean 4.7; 95% CI 4.5 to 4.9; physiotherapists' mean 4.6; 95% CI 3.9 to 5.3).
Potential Success and Feasibility of Interventions to Optimize DVT Prophylaxis Utilization
Interventions considered across clinician groups as highly potentially successful were: preprinted order sheets (5.7; 95% CI 5.6 to 5.8); pharmacist reminders to physicians (mean 5.3; 95% CI 5.1 to 5.4); computerized reminders to physicians (mean 5.0; 95% CI 4.9 to 5.2); and use of a local opinion leader (mean 5.0; 95% CI 4.9 to 5.2). Interventions considered highly potentially feasible were: posters (mean 5.7; CI 5.6 to 5.8); preprinted order sheets (mean 5.5; 95% CI 5.4 to 5.7); laminated pocket cards (mean 5.4; 95% CI 5.2 to 5.5); multidisciplinary educational meetings (mean 5.0; 95% CI 4.9 to 5.2); and pharmacist reminders to physicians (mean 5.0; 95% CI 4.9 to 5.1). Preprinted orders and pharmacist reminders were perceived by all clinician groups as having both high potential success and feasibility (Figure 4).
Perceptions on Which Clinician Group Is Best Able to Assess and Implement DVT Prophylaxis
Respondents were divided between considering the attending physician and the bedside nurse as best able to perform a daily assessment of patients' need for DVT prophylaxis (43.4% [204/470] vs 44.0% [207/470], respectively). Respondents from these groups each predominantly thought this responsibility was theirs, with 68.1% (49/72) of physicians and 61.5% (123/200) of nurses perceiving this as their responsibility (Figure 5).
Forty‐one percent (193/471) of respondents perceived the attending physician as best able to ensure that DVT prophylaxis is ordered, while 31.2% (147/471) identified the pharmacist and 23.3% (110/471) identified the bedside nurse as best suited to this role. Among pharmacists, 66.3% (114/172) perceived that the attending pharmacist is best able to perform this task. Among respondents, 61.9% (296/478) felt the bedside nurse is best able to ensure adherence to DVT prophylaxis, with good agreement among all clinician groups.
DISCUSSION
Our survey identified several perceived barriers to optimizing DVT prophylaxis, consistent with those reported in the White Paper sponsored by the American Public Health Association.23 While no single barrier outlined in our survey was dominant, 2 novel barriers were identified: misperception of DVT prophylaxis underutilization, and confusion about roles and responsibilities in the area of DVT prophylaxis. Attention to these barriers may be helpful in developing an intervention aimed at bridging the gap between evidence and practice.
While our survey demonstrates agreement across clinician groups on the importance, efficacy, and safety of DVT prophylaxis, the discordant perceptions that exist about whether DVT prophylaxis is utilized appropriately is an important concern. Physician and pharmacist‐respondents demonstrated awareness that thromboprophylaxis is underutilized in medical patients. However, despite overwhelming published evidence to the contrary, nurses responding to our survey did not tend to recognize the problem of DVT prophylaxis underutilization in hospitalized medical patients. This knowledge deficit may be a significant barrier particularly since the pooled group of respondents indicated that nurses are among those caregivers best able to conduct a daily assessment of patients' need for DVT prophylaxis. A possible explanation for the finding that nurses and physiotherapists demonstrated a relative lack of awareness of the problem of DVT prophylaxis underutilization is ward‐specific healthcare priorities. Nursing and physiotherapy care on surgical wards is aimed at preventing postoperative complications, including DVT. However, its primary focus on medical wards is the management of acute medical problems. Prevention of hospital‐related complications, such as DVT, is often a secondary focus. Therefore, ensuring that all clinician groups are educated about the problem of DVT prophylaxis underutilization is necessary to drive quality improvement. A physician‐based survey on antithrombotic therapies demonstrated a similar need for education on guideline recommendations.20
A second important barrier identified in our survey is that both attending nurses and physicians feel that daily assessment of a patient's need for DVT prophylaxis is their responsibility. Confusion about roles and responsibilities in this area of patient care was reported by Cook et al., who identified that multidisciplinary care was perceived as a barrier to effective VTE prevention.18 Uncertainty as to which group should take ownership of DVT prophylaxis can lead to a diffusion of responsibility, a lack of accountability, and a gap in care. A resolution to whether DVT risk assessment is a nursing or a physician role could be reached through increased interdisciplinary communication and provision of clear definitions of roles to hospital staff.
Survey respondents felt that preprinted orders and pharmacist reminders to physicians were potentially successful and feasible strategies to optimize DVT prophylaxis. These components could be part of a simple tool to initiate prophylaxis. While electronic alerts have been shown to increase prophylaxis rates,24 we suspect that many respondents did not view these as highly important because of limited use of computerized order entry at their facilities. Interestingly, survey respondents did not perceive audit‐and‐feedback systems or local opinion leaders as potentially successful, though previous studies have demonstrated that they can change clinician behavior.25, 26 This may be because respondents may not be aware of the strength of technology‐based interventions (eg, electronic orders) and the role of opinion leaders, and the evidence in support of such interventions.24, 26 A systematic review of studies to improve DVT prophylaxis in hospitals reported that a combination of multiple active strategies is most effective, particularly those that link physician reminders with audit‐and‐feedback.27 For example, in the define study, a multicomponent intervention consisting of interactive educational sessions, verbal and computerized prompts, and individual performance feedback significantly improved adherence to DVT prophylaxis guidelines in critically ill patients.28 Whether a similar intervention could improve adherence to DVT prophylaxis guidelines in hospitalized medical patients merits further study. Any intervention must be paired with better education about which patients should, and should not, receive prophylaxis, as this may address many reported barriers in our survey (including concerns about bleeding). Respondents' uncertainty about these issues is not surprising, as studies of DVT prophylaxis in medical patients are not plentiful.2 However, recent guidelines do identify subgroups of medically ill patients in whom DVT prophylaxis is indicated.2 A clear and simple DVT risk assessment algorithm that identifies medical patients in whom DVT prophylaxis should (or should not) be administered may help to overcome respondents' concerns.
A limitation of our survey is the overall response rate of 36.3%, largely driven by the considerable number of nonresponding pharmacists (n = 760, reflecting 49% of the entire sample). However, the majority of the pharmacists were likely not hospital‐based, were thus not a target of this study, and their low response rate is not surprising. After excluding pharmacists, the response rate was 58.3% (321/551), which is consistent with response rates of other large‐sample surveys.29 The lower response rate for physicians and pharmacists may also reflect web‐based survey dissemination which, despite its feasibility, has lower response rates than paper‐based dissemination.3032 While the sample of physicians was relatively small compared to the other respondent groups surveyed, we aimed to identify barriers to actually implementing VTE prophylaxis, not just ordering prophylaxis, which is a multidisciplinary concern.
Although this survey was based on Canadian healthcare providers' perspectives, we believe the results are generalizable since both US and Canadian‐based studies have found that VTE prophylaxis is underutilized among hospitalized medical patients.4, 6 Furthermore, the American College of Chest Physicians (ACCP) guidelines on VTE prophylaxis, which are well‐recognized in both the United States and Canada, were developed with input from Canadian and American content experts.2 And while the US and Canadian healthcare systems are organized differently, at the patient‐care level, the roles of healthcare professionals are very similar. The generalizability of our findings is, however, limited by the institutional characteristics of respondents. We do not purport that the responses of any of the 4 clinician groups are generalizable to those groups as a whole. Although we surveyed clinicians in teaching and nonteaching, urban and rural practices, perceptions about DVT prophylaxis may be influenced by other factors, including the availability of local preprinted orders, electronic medical records, and quality improvement programs. Another potential limitation is that we did not assess all possible strategies to improve DVT prophylaxis, such as nurse practitioners and computerized decision support systems. These were purposely excluded, as they are not financially feasible in all centers, and thus not generalizable. Finally, like all self‐administered surveys, our findings reflect respondents' perceptions rather than objective observations about practice.
In conclusion, we identified novel and important barriers to optimal DVT prophylaxis utilization and potential interventions to address this important safety concern in hospitalized medical patients. To overcome some of these barriers, we propose an educational intervention prior to delivery of a top‐down, evidence‐based intervention to first increase healthcare providers' knowledge of the safety of DVT prophylaxis, system and team‐based approaches, and which interventions are most likely to be successful so as to encourage greater compliance with the intervention. A top‐down, system‐wide approach, involving the entire healthcare team and hospital administrators, can help drive this communication. As DVT prophylaxis becomes an increasingly important component in hospital accreditation, such solutions become appealing to facilitate change in practices. Results of this survey may inform future knowledge translation interventions by eliminating perceived barriers to DVT prophylaxis and by incorporating strategies that are perceived by healthcare professionals to be successful, feasible, and supported by evidence.
- ,.National hospital discharge survey: annual summary, 1996.Vital Health Stat.1999;13:1–46.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th ed).Chest.2008;133:381S–443S.
- ,,, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: No. 43. AHRQ Publication No. 01‐E058, July 2001. Rockville, MD: Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/ptsafety/. Accessed October 9,2007.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Hospitals' compliance with prophylaxis guidelines for venous thromboembolism.Am J Health Syst Pharm.2007;64:69–76.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- ,,.A retrospective evaluation of adherence to guidelines for prevention of thromboembolic events in general medical inpatients.Can J Hosp Pharm.2006;59:258–263.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of DVT prophylaxis guidelines.Chest2001;120:1964–1971.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,,,.The use of low molecular weight heparins for the prevention of postoperative venous thromboembolism in general surgery. A survey of practice in the United States.Int Angiol.2002;1:78–85.
- ,,, et al.Venous thromboembolic disease management patterns in total hip arthroplasty and total knee arthroplasty patients: a survey of the AAHKS membership.J Arthroplasty.2001;6:679–688.
- ,,.Thromboprophylaxis in medical‐surgical intensive care unit patients.J Crit Care.2005;20:320–323.
- ,.Utilization of venous thromboembolism prophylaxis in a medical‐surgical ICU.Chest.1998;113:162–164.
- ,,, et al.Why don't physicians follow clinical practice guidelines? A framework for improvement.JAMA.1999;282:1458–1465.
- ,,, et al.Thromboprophylaxis for hospitalized medical patients: a multicenter qualitative study.J Hosp Med.2009;4;269–275.
- ,,, et al.Definition of immobility in studies of thromboprophylaxis in hospitalized medical patients: a systematic review.J Vasc Nurs.2010;28:54–66.
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- .Mail and internet surveys: the tailored design method.New York, NY:John Wiley 2000.
- Deep‐vein thrombosis: advancing awareness to protect patient lives. Public Health Leadership Conference on Deep‐Vein Thrombosis. American Public Health Association. Available at: http://www.apha.org/NR/rdonlyres/A209F84A‐7C0E‐4761–9ECF‐61D22E1E11F7/0/DVT_White_Paper.pdf. Accessed May 28,2008.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Getting a validated guideline into local practice: implementation and audit of the SIGN guideline on the prevention of deep vein thrombosis in a district general hospital.Scott Med J.1998;43:23–25.
- ,,,.Local opinion leaders: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2007;24(1):CD000125.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE study.Crit Care Med.2006;34:694–699.
- ,,,.Using the Internet to conduct surveys of health professionals: a valid alternative?Fam Pract.2003;20:545–551.
- ,,,,,.Use of new technology in endourology and laparoscopy by American urologists: Internet and postal survey.Urology.2000;56:760–765.
- ,,,,.E‐mail versus conventional postal mail survey of geriatric chiefs.Gerontologist.2001;41:799–804.
- ,,, et al.Internet versus mailed questionnaires: a randomized comparison.J Med Internet Res.2004;6:e30.
- ,.National hospital discharge survey: annual summary, 1996.Vital Health Stat.1999;13:1–46.
- ,,, et al.Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th ed).Chest.2008;133:381S–443S.
- ,,, et al. Making health care safer: a critical analysis of patient safety practices. Evidence Report/Technology Assessment: No. 43. AHRQ Publication No. 01‐E058, July 2001. Rockville, MD: Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/ptsafety/. Accessed October 9,2007.
- ,,, et al.Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada.Thromb Res.2007;119:145–155.
- ,,,.Hospitals' compliance with prophylaxis guidelines for venous thromboembolism.Am J Health Syst Pharm.2007;64:69–76.
- ,,,.Thromboprophylaxis rates in US medical centers: success or failure?J Thromb Haemost.2007;5:1610–1616.
- ,,.A retrospective evaluation of adherence to guidelines for prevention of thromboembolic events in general medical inpatients.Can J Hosp Pharm.2006;59:258–263.
- ,,, et al.Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism.Chest.2007;132:936–945.
- ,,,.Venous thromboembolism prophylaxis in medical inpatients: a retrospective chart review.Thromb Res.2003;111:215–219.
- ,,.Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of DVT prophylaxis guidelines.Chest2001;120:1964–1971.
- ,,, et al.Thrombosis prophylaxis in medical patients: a retrospective review of clinical practice patterns.Haematologica.2002;87:746–750.
- ,,, et al.Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross‐sectional study.Lancet.2008;371:387–394.
- ,,,,.The use of low molecular weight heparins for the prevention of postoperative venous thromboembolism in general surgery. A survey of practice in the United States.Int Angiol.2002;1:78–85.
- ,,, et al.Venous thromboembolic disease management patterns in total hip arthroplasty and total knee arthroplasty patients: a survey of the AAHKS membership.J Arthroplasty.2001;6:679–688.
- ,,.Thromboprophylaxis in medical‐surgical intensive care unit patients.J Crit Care.2005;20:320–323.
- ,.Utilization of venous thromboembolism prophylaxis in a medical‐surgical ICU.Chest.1998;113:162–164.
- ,,, et al.Why don't physicians follow clinical practice guidelines? A framework for improvement.JAMA.1999;282:1458–1465.
- ,,, et al.Thromboprophylaxis for hospitalized medical patients: a multicenter qualitative study.J Hosp Med.2009;4;269–275.
- ,,, et al.Definition of immobility in studies of thromboprophylaxis in hospitalized medical patients: a systematic review.J Vasc Nurs.2010;28:54–66.
- ,,, et al.The use of antithrombotic therapies in the prevention and treatment of arterial and venous thrombosis: a survey of current knowledge and practice supporting the need for clinical education.Crit Pathw Cardiol.2010;9:41–48.
- ,,, et al.Antithrombotic and thrombolytic therapy: from evidence to application: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest.2004;126:688S–696S.
- .Mail and internet surveys: the tailored design method.New York, NY:John Wiley 2000.
- Deep‐vein thrombosis: advancing awareness to protect patient lives. Public Health Leadership Conference on Deep‐Vein Thrombosis. American Public Health Association. Available at: http://www.apha.org/NR/rdonlyres/A209F84A‐7C0E‐4761–9ECF‐61D22E1E11F7/0/DVT_White_Paper.pdf. Accessed May 28,2008.
- ,,, et al.Electronic alerts to prevent venous thromboembolism among hospitalized patients.N Engl J Med.2005;352:969–977.
- ,,, et al.Getting a validated guideline into local practice: implementation and audit of the SIGN guideline on the prevention of deep vein thrombosis in a district general hospital.Scott Med J.1998;43:23–25.
- ,,,.Local opinion leaders: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2007;24(1):CD000125.
- ,,, et al.A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals.Ann Surg.2005;241:397–415.
- ,,, et al.Minimizing errors of omission: behavioural reinforcement of heparin to avert venous emboli: the BEHAVE study.Crit Care Med.2006;34:694–699.
- ,,,.Using the Internet to conduct surveys of health professionals: a valid alternative?Fam Pract.2003;20:545–551.
- ,,,,,.Use of new technology in endourology and laparoscopy by American urologists: Internet and postal survey.Urology.2000;56:760–765.
- ,,,,.E‐mail versus conventional postal mail survey of geriatric chiefs.Gerontologist.2001;41:799–804.
- ,,, et al.Internet versus mailed questionnaires: a randomized comparison.J Med Internet Res.2004;6:e30.
Copyright © 2011 Society of Hospital Medicine