In 1984, a worker at a Pennsylvania nuclear power plant triggered the radiation detector as he was getting ready to go home. This would not be unusual for such a facility, but there was no nuclear fuel on site at the time. The alarm went off every time he left work.
One day, he triggered the alarm as he crossed the detector on arriving at the plant, leading him to suspect that he was bringing radiation from home. He eventually convinced the plant’s health physicists to check his home, although at first they were opposed to the idea. The results revealed high concentrations of radon everywhere, especially in his basement.
Radon was already known to be associated with health risks in underground miners at that time. This event revealed that a naturally occurring radioactive gas could be found in households at potentially hazardous concentrations.
The incident captured the public’s attention, and the Environmental Protection Agency (EPA) and the US Centers for Disease Control and Prevention (CDC) recommended that nearly all homes be tested.1,2 In 1988, the International Agency for Research on Cancer classified radon as a human carcinogen, and Congress passed the Indoor Radon Abatement Act in response to growing concern over health risks.3 This law funded state and federal measures to survey schools and federal buildings for radon levels, to educate citizens, and to develop programs for technical assistance. The long-term goal was to reduce indoor levels nationwide to no more than outdoor levels.
Radon is still considered an important public health hazard. From 15,000 to 21,000 people are estimated to die of lung cancer as a result of radon exposure each year in the United States, making it the second most common cause of lung cancer, behind smoking.4
Considering the relevance of this issue, this article will review the unique characteristics of radon as a risk factor for lung cancer.
WHAT IS RADON?
Figure 1.
Radon is a noble gas that occurs naturally as a decay product of uranium 238 and thorium 232. It is colorless, tasteless, and imperceptible to our senses. Its most common isotope is radon 222 (222Rn), which has a half-life of 3.8 days and decays by emitting an alpha particle to become polonium 218. The decay chain continues through several intermediate steps until the stable isotope lead 206 is formed (Figure 1). Two of the isotopes in this chain, polonium 218 and polonium 214, also emit alpha particles.5–7
Radon is primarily formed in soil. Its most important precursor, uranium 238, is ubiquitous, found in most soils and rocks in various concentrations. Radon can also be found in surface water, metal mines (uranium, phosphorus, silver, gold), residue of coal combustion, and natural gas.
Outdoor levels are usually much lower than indoor levels, as radon dissipates very quickly. Indoor radon mostly comes from the soil under the house or building, but it can also originate from coal combustion, gas appliances, and water (especially from private wells). In municipal water systems or surface reservoirs, most of the radon dissipates into the air or decays before the water reaches homes.8,9
Radon’s only commercial application in the United States is in calibrating measuring instruments. In the past, it was used in radiography and to treat cancer but was later replaced by other radiation sources that cost less and pose less hazard of alpha radiation.10
HOW RADON CAN HARM
Alpha particles, emitted by radon 222 and its progenies polonium 218 and polonium 214, are highly effective in damaging tissues. Although they do not travel far or fast, with their two protons and two neutrons, alpha particles are heavy and therefore can cause considerable damage at short range. Although alpha particles can be stopped by a thin barrier such as a piece of paper or the skin, if the source is inhaled or ingested and lodges against mucosal linings, the alpha particles emitted can destroy cells.11
The main route of radon exposure is by inhalation. Since radon is biologically inert, it is readily exhaled after it reaches the lungs. However, radon’s progenies can also be inhaled, either as free particles or attached to airborne particles such as dust, which they tend to attract as a result of their charged state. This attached fraction is believed to be more carcinogenic because it tends to deposit on the respiratory epithelium, notably in the carinae of bronchi. The smaller the dust particle, the deeper it can travel into the lung. The radiation emissions damage the genetic material of cells lining the airways, with the potential to result in lung cancer if the repair process is incomplete.5,8,9
Other routes of exposure include ingestion and dermal exposure. Radon and its progenies can be swallowed in drinking water, passing through the stomach walls and bowels and entering the blood.12 Dermal exposure is not considered a significant route unless the dermis is exposed, since in usual circumstances the skin protects the body from alpha radiation.13
Possible biologic mechanisms by which radon exposure might increase the risk of cancer include gene mutations, chromosome aberrations, generation of reactive oxygen species, up- or down-regulation of cytokines, and production of proteins associated with cell-cycle regulation.14–16
HOW IS RADON MEASURED?
Several devices are commercially available to measure radon levels at home. The most common ones are activated charcoal detectors, electret ion chambers, alpha-track detectors, electronic integrating devices, and continuous monitors. There is no evidence that one device is better than another, but devices that measure radon gas are usually preferred over those that measure decay products because they are simpler to use and more cost-effective. These devices are divided into those used for short-term testing (2–90 days) and long-term testing (Table 1).17
Radon levels can be expressed as follows:
Working levels. One working level (WL) is any combination of radon progeny in 1 L of air that ultimately releases 1.3 × 105 MeV of alpha energy during decay. In studies of miners, the radon progeny concentrations are generally expressed in WL. The cumulative exposure of an individual to this concentration over a “working month” of 170 hours is defined as a working level month (WLM).
Picocuries per liter. In the United States, the rate of decay is commonly reported in picocuries per liter (pCi/L): 1 pCi/L translates to 0.005 WL under usual conditions. The outdoor radon level is normally around 0.4 pCi/L.
Becquerel per cubic meter (Bq/m3) is an International System unit of measure: 1 WL corresponds to 3.7 × 103 Bq/m3, and 1 pCi/L is equivalent to 37 Bq/m3.
Different areas have different radon levels
The Indoor Radon Abatement Act of 1988 helped identify areas in the United States that have the potential for elevated indoor radon levels. An estimated 6 million homes have concentrations greater than 4 pCi/L.
Figure 2. Radon distribution in the United States with zone classification according to the predicted indoor level.From the US Environmental Protection Agency.
To assist in implementing radon-reducing strategies and allocation of resources, the EPA has created a map (Figure 2) that classifies counties according to the predicted indoor level.18
WHAT IS THE RELATIONSHIP BETWEEN RADON AND LUNG CANCER?
Determining the degree to which radon exposure contributes to lung cancer is a complex task. Radon can be found nearly everywhere, and there are diurnal, seasonal, and random year-to-year variations in the concentration of radon in indoor air.
A minority view
Not everyone agrees that radon is completely bad. For centuries, people have flocked to spas to “take the waters,” and the water at many of these spas has been found to contain radon. In the early 20th century, radiation was touted as having medicinal benefits, and people in many places in the world still go to “radon spas” (some of them in abandoned uranium mines) to help treat conditions such as arthritis and to feel invigorated and energized.
In 2006, a report by Zdrojewicz and Strzelczyk19 urged the medical community to keep an open mind about the possibility that radon exposure may be beneficial in very low doses, perhaps by stimulating repair mechanisms. This concept, called hormesis, differs from the mainstream view that cancer risk rises linearly with radiation dose, with no minimum threshold level (see below).
Risk in miners
As early as in the 16th century, metal miners in central Europe were noted to have a high rate of death from respiratory disease. Radon was discovered in 1900, and in the 20th century lung cancer was linked to high levels of radon detected in uranium mines.
Several small studies of underground miners exposed to high concentrations of radon consistently demonstrated an increased risk of lung cancer.
The Committee on the Biological Effects of Ionizing Radiation (BEIR VI 1999) reviewed 11 major cohort studies of miners. The studies included more than 60,000 miners in Europe, North America, Asia, and Australia, of whom 2,600 died of lung cancer. Lung cancer rates increased linearly with cumulative radon exposure, and the estimated average increase in the lung cancer death rate per WLM in the combined studies was 0.44% (95% confidence interval [CI] 0.20–1.00%). The percentage increase in the lung cancer death rate per WLM varied with time since exposure, with the highest increase in risk during the 5 to 14 years after exposure.4,17 Furthermore, the increase in risk was higher in younger miners, who were exposed to a relatively low radon concentration.
Risk in the general population
The magnitude of the risk in miners led to concern about radon exposure as a cause of lung cancer in the general population. Statistical models were generated that suggested a causal link between radon exposure and lung cancer. Although extrapolation of the results from miners caused controversy, the BEIR VI estimation of risk was validated by studies in the general population.7,20–23
Since the 1980s, several small case-control studies with limited power examined the relationship between indoor radon and lung cancer in the general population. In these studies, individuals who had developed lung cancer were compared with controls who had not developed the disease but who otherwise represented the population from which the cases of lung cancer came.
To improve the statistical power, the investigators of the major studies in Europe, North America, and China pooled the results in separate analyses (Table 2).7,20–23 The average radon concentration to which each individual had been exposed over the previous decades was estimated by measuring the radon concentration at their present and previous homes. On the basis of information from the uranium miners, these studies assumed that the period of exposure was the 30 years ending 5 years before the diagnosis or at death from lung cancer.
The results provided convincing evidence that radon exposure is a cause of lung cancer in the general population and substantiated the extrapolation from the studies of miners. Further, the results of all three pooled analyses were consistent with a linear dose-response relationship with no threshold, suggesting an increased risk of lung cancer even with a radon level below 4 pCi/L (200 Bq/m3), which is the concentration at which mitigation actions are recommended in many countries.17
The North American pooled analysis included 3,662 cases and 4,966 controls from seven studies in the United States and Canada. When data from all studies were combined, the risk of lung cancer was found to increase by 11% per 100-Bq/m3 (about 2.7-pCi/L) increase in measured radon concentration (95% CI 0%–28%). The estimated increase in lung cancer was independent of age, sex, or smoking history.7,20
The Chinese pooled data22 demonstrated a 13% (95% CI 1%–36%) increased risk per 100 Bq/m3.
In the European study, the risk of lung cancer increased by 8% per 100 Bq/m3 (95% CI 3%–16%). The European investigators repeated the analysis, taking into account the random year-to-year variability in measured radon concentration, finding the final estimated risk was an increase of 16% per 100 Bq/m3 using long-term average concentration.21
The combined estimate21,24 from the three pooling studies based on measured radon concentration is an increased risk of lung cancer of 10% per 100 Bq/m3.
Synergistic risk with smoking
Radon exposure was independently associated with lung cancer, and the relationship with cigarette smoking is believed to be synergistic. The radon progeny particles attach themselves to smoke and dust and are then deposited in the bronchial epithelium.25
In the pool of European case-control studies, the cancer risk for current smokers of 15 to 24 cigarettes per day relative to that in never-smokers was 25.8 (95% CI 21–31). Assuming that in the same analysis the lung cancer risk increased by 16% per 100 Bq/m3 of usual radon concentration regardless of smoking status, the cumulative absolute risk by age 75 would be 0.67% in those who never smoked and 16% in smokers at usual radon levels of 400 Bq/m3 (11 pCi/L).21
Rates of all lung cancer subtypes increased
Radon exposure is not associated with a specific histologic subtype of lung cancer. It has been speculated that the incidence of the small-cell subtype might be slightly increased because radon tends to deposit in the more central bronchial carinae.20,21 However, all subtypes have been described in association with radon, the most common being adenocarcinoma and squamous cell carcinoma.26–28
EFFECT OF MITIGATION MEASURES
The US Surgeon General and the EPA recommend that all homes be tested.18 Short-term tests should be used first, keeping in mind that diurnal and seasonal variations may occur.
The World Health Organization has proposed a reference level of 100 Bq/m3 (2.7 pCi/L) to minimize health hazards from indoor radon exposure.17 If this level cannot be reached under the country-specific conditions, the chosen reference level should not exceed 300 Bq/m3 (8 pCi/L).
In the United States, if the result of home testing is higher than 4 pCi/L, a follow-up measurement should be done using a different short-term test or a long-term test. If the follow-up result confirms a level of more than 4 pCi/L, mitigating actions are recommended. The goal is to reduce the indoor radon level as much as possible—down to zero or at least comparable to outdoor levels (national average 0.4 pCi/L).18
A variety of radon mitigation strategies have been used, with different rates of efficacy (Table 3). The optimal strategy depends on the likely source or cause, construction characteristics, soil, and climate.29Table 4 lists resources for the general public about testing and mitigation measures.
How beneficial is radon mitigation?
Although it is logical to try to reduce the indoor radon concentration, there is no strong evidence yet that this intervention decreases the incidence of lung cancer in the general population.
Using the BEIR VI risk model, Méndez et al30 estimated a 21% reduction in the annual radon-related lung cancer mortality rate by 2100 if all households were compliant with government recommendations (mitigation actions at levels of 4 pCi/L) and assuming that the percentage of cigarette smokers remained constant.
On the other hand, if the number of smokers continues to decline, the benefits from radon mitigation may be less. The expected benefit from mitigation in this scenario is a reduction of 12% in annual radon-related deaths by the year 2100.30 However, it will be challenging to determine whether the expected decline in the incidence of lung cancer and lung cancer deaths is truly attributable to mitigation measures.
MANAGING PATIENTS EXPOSED TO RADON
Screen for lung cancer in smokers only
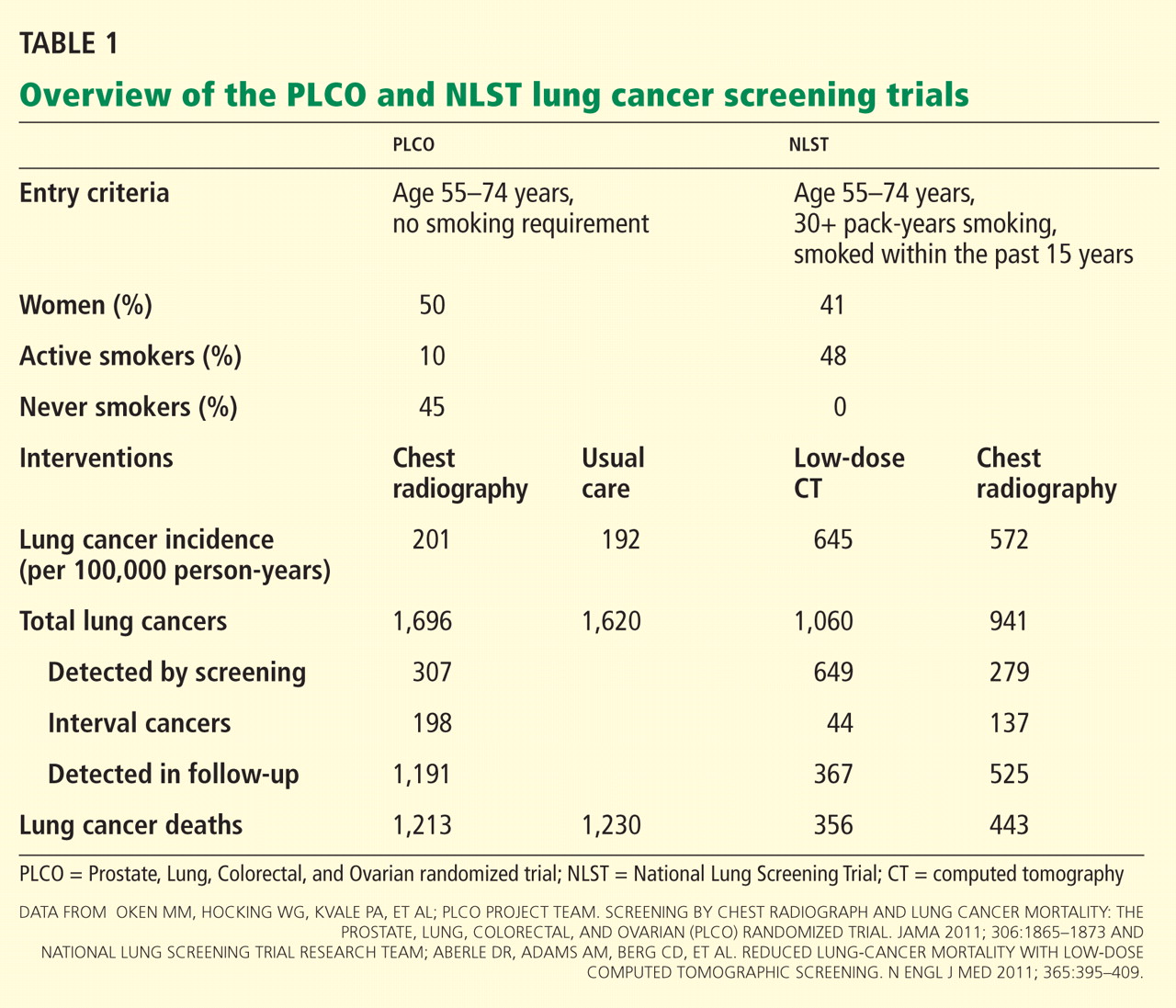
The National Lung Screening Study (NLST) was a large multicenter trial of annual low-dose computed tomography (CT) to screen for lung cancer in a cohort at high risk: age 55 to 74, at least a 30 pack-year history of smoking in a current smoker, or a former smoker who quit within the past 15 years. The trial demonstrated a 20% reduction in lung cancer deaths in the CT screening group.31
Since the publication of the NLST results, many societies have endorsed screening for lung cancer with low-dose CT using the study criteria. The National Comprehensive Cancer Network (NCCN) expanded these criteria and has recommended screening in patients over age 50 who have a history of smoking and one additional risk factor, such as radon exposure.
However, radon exposure has not been incorporated into a lung cancer risk-prediction model, and there is no empirical evidence suggesting that people who have such a history would benefit from screening.32,33 The joint guidelines of the American College of Chest Physicians and American Society of Clinical Oncology recommend annual low-dose CT screening only for patients who meet the NLST criteria.34
What to do about indeterminate lung nodules
The widely used guidelines from the Fleischner Society35 on how to manage small lung nodules stratify patients into groups at low and high risk of developing lung cancer on the basis of risk factors. The guidelines apply to adults age 35 and older in whom an indeterminate solid nodule was recently detected.
If a patient is at high risk, the recommended approach includes follow-up in shorter intervals depending on the nodule size. History of smoking is recognized as a major risk factor, and the statement also lists family history and exposure to asbestos, uranium, and radon.35
Although the association of radon with lung cancer has been shown in epidemiologic studies, radon exposure has not been included in validated statistical models that assess the probability that an indeterminate lung nodule is malignant. We would expect the risk to be higher in miners, who suffer a more intense exposure to higher levels of radon, than in the general population, which has a low and constantly variable residential exposure. Furthermore, there are no data to support a more aggressive follow-up approach in patients with indeterminate lung nodules and a history of radon exposure.
RADON AND OTHER CANCERS
When a person is exposed to radon, the bronchial epithelium receives the highest dose of ionizing radiation, but other organs such as the kidneys, stomach, and bone marrow may receive doses as well, although lower. Several studies have looked into possible associations, but there is no strong evidence to suggest an increased mortality rate related to radon from cancers other than lung.24,36 However, there seems to be a positive association between radon and the incidence of lymphoproliferative disorders in uranium miners.37,38
Radon can be measured in drinking water, and a few studies have looked at a possible association with gastrointestinal malignancies. The results did not reveal a consistent positive correlation.39,40 The risk of cancer from exposure to radon in the public water supply is likely small and mostly from the transfer of radon particles into the air and not from drinking the water. On the other hand, the risk could be higher with private wells, where radon levels are variable and are possibly higher than from public sources.41
DATA ARE INSUFFICIENT TO GUIDE MANAGEMENT
Radon is a naturally occurring and ubiquitous radioactive gas that can cause tissue damage. Cohort and case-control studies have demonstrated that radon exposure is associated with increased risk of lung cancer. It is recommended that radon levels be measured in every home in the United States and mitigation measures instituted if levels exceed 4 pCi/L.
There are insufficient data to help guide the management of patients with a history of radon exposure, and prospective studies are needed to better understand the individual risk of developing lung cancer and the appropriate management of such patients.
Smoking cessation is an integral part of lung cancer risk reduction from radon exposure.
World Health Organization (WHO). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Manmade mineral fibres and radon. Summary of data reported and evaluation. http://monographs.iarc.fr/ENG/Monographs/vol43/volume43.pdf. Accessed August 5, 2014.
Committee on Health Risks of Exposure to Radon (BEIR VI). Health effects of exposure to radon: BEIR VI. Washington, DC: National Academies Press; 1999.
Samet JM. Radon and lung cancer. J Natl Cancer Inst1989; 81:745–757.
Lewis RJ, Lewis Sr RJ.Hawley’s condensed chemical dictionary. 14thed. New York: Wiley-Interscience; 2001.
Krewski D, Lubin JH, Zielinski JM, et al. Residential radon and risk of lung cancer: a combined analysis of 7 North American case-control studies. Epidemiology2005; 16:137–145.
Darby S, Hill D, Doll R. Radon: a likely carcinogen at all exposures. Ann Oncol2001; 12:1341–1351.
Morrison A. Use of radon for industrial radiography. Can J Res1945; 23:413–419.
Narayanan PK, Goodwin EH, Lehnert BE. Alpha particles initiate biological production of superoxide anions and hydrogen peroxide in human cells. Cancer Res1997; 57:3963–3971.
Ishikawa T, Narazaki Y, Yasuoka Y, Tokonami S, Yamada Y. Bio-kinetics of radon ingested from drinking water. Radiat Prot Dosimetry2003; 105:65–70.
Ishikawa T, Yamada Y, Fukutsu K, Tokonami S. Deposition and clearance for radon progeny in the human respiratory tract. Radiat Prot Dosimetry2003; 105:143–148.
Farkas A, Hofmann W, Balásházy I, Szoke I, Madas BG, Moustafa M. Effect of site-specific bronchial radon progeny deposition on the spatial and temporal distributions of cellular responses. Radiat Environ Biophys2011; 50:281–297.
Robertson A, Allen J, Laney R, Curnow A. The cellular and molecular carcinogenic effects of radon exposure: a review. Int J Mol Sci2013; 14:14024–14063.
Chauhan V, Howland M, Wilkins R. Effects of alpha-particle radiation on microRNA responses in human cell-lines. Open Biochem J2012; 6:16–22.
Krewski D, Lubin JH, Zielinski JM, et al. A combined analysis of North American case-control studies of residential radon and lung cancer. J Toxicol Environ Health A2006; 69:533–597.
Darby S, Hill D, Auvinen A, et al. Radon in homes and risk of lung cancer: collaborative analysis of individual data from 13 European case-control studies. BMJ2005; 330:223.
Lubin JH, Wang ZY, Boice JD, et al. Risk of lung cancer and residential radon in China: pooled results of two studies. Int J Cancer2004; 109:132–137.
Darby S, Hill D, Deo H, et al. Residential radon and lung cancer—detailed results of a collaborative analysis of individual data on 7,148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand J Work Environ Health2006; 32(suppl 1):1–83.
Darby SC, Whitley E, Howe GR, et al. Radon and cancers other than lung cancer in underground miners: a collaborative analysis of 11 studies. J Natl Cancer Inst1995; 87:378–384.
Land CE, Shimosato Y, Saccomanno G, et al. Radiation-associated lung cancer: a comparison of the histology of lung cancers in uranium miners and survivors of the atomic bombings of Hiroshima and Nagasaki. Radiat Res1993; 134:234–243.
Kreuzer M, Müller KM, Brachner A, et al. Histopathologic findings of lung carcinoma in German uranium miners. Cancer2000; 89:2613–2621.
Saccomanno G, Auerbach O, Kuschner M, et al. A comparison between the localization of lung tumors in uranium miners and in nonminers from 1947 to 1991. Cancer1996; 77:1278–1283.
Rahman NM, Tracy BL. Radon control systems in existing and new construction: a review. Radiat Prot Dosimetry2009; 135:243–255.
Méndez D, Alshanqeety O, Warner KE, Lantz PM, Courant PN. The impact of declining smoking on radon-related lung cancer in the United States. Am J Public Health2011; 101:310–314.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Wood DE, Eapen GA, Ettinger DS, et al. Lung cancer screening. J Natl Compr Canc Netw2012; 10:240–265.
Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB. Screening for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest2013; 143(suppl 5):e78S–e92S.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Darby SC, Radford EP, Whitley E. Radon exposure and cancers other than lung cancer in Swedish iron miners. Environ Health Perspect1995; 103(suppl 2):45–47.
Laurier D, Tirmarche M, Mitton N, et al. An update of cancer mortality among the French cohort of uranium miners: extended follow-up and new source of data for causes of death. Eur J Epidemiol2004; 19:139–146.
Rericha V, Kulich M, Rericha R, Shore DL, Sandler DP. Incidence of leukemia, lymphoma, and multiple myeloma in Czech uranium miners: a case-cohort study. Environ Health Perspect2006; 114:818–822.
Auvinen A, Salonen L, Pekkanen J, Pukkala E, Ilus T, Kurttio P. Radon and other natural radionuclides in drinking water and risk of stomach cancer: a case-cohort study in Finland. Int J Cancer2005; 114:109–113.
Kjellberg S, Wiseman JS. The relationship of radon to gastrointestinal malignancies. Am Surg1995; 61:822–825.
Cappello MA, Ferraro A, Mendelsohn AB, Prehn AW. Radon-contaminated drinking water from private wells: an environmental health assessment examining a rural Colorado mountain community’s exposure. J Environ Health2013; 76:18–24.
Humberto Choi, MD Departments of Pulmonary Medicine and Critical Care Medicine, Respiratory Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Peter Mazzone, MD, MPH, FCCP Departments of Pulmonary Medicine, Critical Care Medicine, and Transplantation Center, Respiratory Institute, Cleveland Clinic
Humberto Choi, MD Departments of Pulmonary Medicine and Critical Care Medicine, Respiratory Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Peter Mazzone, MD, MPH, FCCP Departments of Pulmonary Medicine, Critical Care Medicine, and Transplantation Center, Respiratory Institute, Cleveland Clinic
Humberto Choi, MD Departments of Pulmonary Medicine and Critical Care Medicine, Respiratory Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Peter Mazzone, MD, MPH, FCCP Departments of Pulmonary Medicine, Critical Care Medicine, and Transplantation Center, Respiratory Institute, Cleveland Clinic
In 1984, a worker at a Pennsylvania nuclear power plant triggered the radiation detector as he was getting ready to go home. This would not be unusual for such a facility, but there was no nuclear fuel on site at the time. The alarm went off every time he left work.
One day, he triggered the alarm as he crossed the detector on arriving at the plant, leading him to suspect that he was bringing radiation from home. He eventually convinced the plant’s health physicists to check his home, although at first they were opposed to the idea. The results revealed high concentrations of radon everywhere, especially in his basement.
Radon was already known to be associated with health risks in underground miners at that time. This event revealed that a naturally occurring radioactive gas could be found in households at potentially hazardous concentrations.
The incident captured the public’s attention, and the Environmental Protection Agency (EPA) and the US Centers for Disease Control and Prevention (CDC) recommended that nearly all homes be tested.1,2 In 1988, the International Agency for Research on Cancer classified radon as a human carcinogen, and Congress passed the Indoor Radon Abatement Act in response to growing concern over health risks.3 This law funded state and federal measures to survey schools and federal buildings for radon levels, to educate citizens, and to develop programs for technical assistance. The long-term goal was to reduce indoor levels nationwide to no more than outdoor levels.
Radon is still considered an important public health hazard. From 15,000 to 21,000 people are estimated to die of lung cancer as a result of radon exposure each year in the United States, making it the second most common cause of lung cancer, behind smoking.4
Considering the relevance of this issue, this article will review the unique characteristics of radon as a risk factor for lung cancer.
WHAT IS RADON?
Figure 1.
Radon is a noble gas that occurs naturally as a decay product of uranium 238 and thorium 232. It is colorless, tasteless, and imperceptible to our senses. Its most common isotope is radon 222 (222Rn), which has a half-life of 3.8 days and decays by emitting an alpha particle to become polonium 218. The decay chain continues through several intermediate steps until the stable isotope lead 206 is formed (Figure 1). Two of the isotopes in this chain, polonium 218 and polonium 214, also emit alpha particles.5–7
Radon is primarily formed in soil. Its most important precursor, uranium 238, is ubiquitous, found in most soils and rocks in various concentrations. Radon can also be found in surface water, metal mines (uranium, phosphorus, silver, gold), residue of coal combustion, and natural gas.
Outdoor levels are usually much lower than indoor levels, as radon dissipates very quickly. Indoor radon mostly comes from the soil under the house or building, but it can also originate from coal combustion, gas appliances, and water (especially from private wells). In municipal water systems or surface reservoirs, most of the radon dissipates into the air or decays before the water reaches homes.8,9
Radon’s only commercial application in the United States is in calibrating measuring instruments. In the past, it was used in radiography and to treat cancer but was later replaced by other radiation sources that cost less and pose less hazard of alpha radiation.10
HOW RADON CAN HARM
Alpha particles, emitted by radon 222 and its progenies polonium 218 and polonium 214, are highly effective in damaging tissues. Although they do not travel far or fast, with their two protons and two neutrons, alpha particles are heavy and therefore can cause considerable damage at short range. Although alpha particles can be stopped by a thin barrier such as a piece of paper or the skin, if the source is inhaled or ingested and lodges against mucosal linings, the alpha particles emitted can destroy cells.11
The main route of radon exposure is by inhalation. Since radon is biologically inert, it is readily exhaled after it reaches the lungs. However, radon’s progenies can also be inhaled, either as free particles or attached to airborne particles such as dust, which they tend to attract as a result of their charged state. This attached fraction is believed to be more carcinogenic because it tends to deposit on the respiratory epithelium, notably in the carinae of bronchi. The smaller the dust particle, the deeper it can travel into the lung. The radiation emissions damage the genetic material of cells lining the airways, with the potential to result in lung cancer if the repair process is incomplete.5,8,9
Other routes of exposure include ingestion and dermal exposure. Radon and its progenies can be swallowed in drinking water, passing through the stomach walls and bowels and entering the blood.12 Dermal exposure is not considered a significant route unless the dermis is exposed, since in usual circumstances the skin protects the body from alpha radiation.13
Possible biologic mechanisms by which radon exposure might increase the risk of cancer include gene mutations, chromosome aberrations, generation of reactive oxygen species, up- or down-regulation of cytokines, and production of proteins associated with cell-cycle regulation.14–16
HOW IS RADON MEASURED?
Several devices are commercially available to measure radon levels at home. The most common ones are activated charcoal detectors, electret ion chambers, alpha-track detectors, electronic integrating devices, and continuous monitors. There is no evidence that one device is better than another, but devices that measure radon gas are usually preferred over those that measure decay products because they are simpler to use and more cost-effective. These devices are divided into those used for short-term testing (2–90 days) and long-term testing (Table 1).17
Radon levels can be expressed as follows:
Working levels. One working level (WL) is any combination of radon progeny in 1 L of air that ultimately releases 1.3 × 105 MeV of alpha energy during decay. In studies of miners, the radon progeny concentrations are generally expressed in WL. The cumulative exposure of an individual to this concentration over a “working month” of 170 hours is defined as a working level month (WLM).
Picocuries per liter. In the United States, the rate of decay is commonly reported in picocuries per liter (pCi/L): 1 pCi/L translates to 0.005 WL under usual conditions. The outdoor radon level is normally around 0.4 pCi/L.
Becquerel per cubic meter (Bq/m3) is an International System unit of measure: 1 WL corresponds to 3.7 × 103 Bq/m3, and 1 pCi/L is equivalent to 37 Bq/m3.
Different areas have different radon levels
The Indoor Radon Abatement Act of 1988 helped identify areas in the United States that have the potential for elevated indoor radon levels. An estimated 6 million homes have concentrations greater than 4 pCi/L.
Figure 2. Radon distribution in the United States with zone classification according to the predicted indoor level.From the US Environmental Protection Agency.
To assist in implementing radon-reducing strategies and allocation of resources, the EPA has created a map (Figure 2) that classifies counties according to the predicted indoor level.18
WHAT IS THE RELATIONSHIP BETWEEN RADON AND LUNG CANCER?
Determining the degree to which radon exposure contributes to lung cancer is a complex task. Radon can be found nearly everywhere, and there are diurnal, seasonal, and random year-to-year variations in the concentration of radon in indoor air.
A minority view
Not everyone agrees that radon is completely bad. For centuries, people have flocked to spas to “take the waters,” and the water at many of these spas has been found to contain radon. In the early 20th century, radiation was touted as having medicinal benefits, and people in many places in the world still go to “radon spas” (some of them in abandoned uranium mines) to help treat conditions such as arthritis and to feel invigorated and energized.
In 2006, a report by Zdrojewicz and Strzelczyk19 urged the medical community to keep an open mind about the possibility that radon exposure may be beneficial in very low doses, perhaps by stimulating repair mechanisms. This concept, called hormesis, differs from the mainstream view that cancer risk rises linearly with radiation dose, with no minimum threshold level (see below).
Risk in miners
As early as in the 16th century, metal miners in central Europe were noted to have a high rate of death from respiratory disease. Radon was discovered in 1900, and in the 20th century lung cancer was linked to high levels of radon detected in uranium mines.
Several small studies of underground miners exposed to high concentrations of radon consistently demonstrated an increased risk of lung cancer.
The Committee on the Biological Effects of Ionizing Radiation (BEIR VI 1999) reviewed 11 major cohort studies of miners. The studies included more than 60,000 miners in Europe, North America, Asia, and Australia, of whom 2,600 died of lung cancer. Lung cancer rates increased linearly with cumulative radon exposure, and the estimated average increase in the lung cancer death rate per WLM in the combined studies was 0.44% (95% confidence interval [CI] 0.20–1.00%). The percentage increase in the lung cancer death rate per WLM varied with time since exposure, with the highest increase in risk during the 5 to 14 years after exposure.4,17 Furthermore, the increase in risk was higher in younger miners, who were exposed to a relatively low radon concentration.
Risk in the general population
The magnitude of the risk in miners led to concern about radon exposure as a cause of lung cancer in the general population. Statistical models were generated that suggested a causal link between radon exposure and lung cancer. Although extrapolation of the results from miners caused controversy, the BEIR VI estimation of risk was validated by studies in the general population.7,20–23
Since the 1980s, several small case-control studies with limited power examined the relationship between indoor radon and lung cancer in the general population. In these studies, individuals who had developed lung cancer were compared with controls who had not developed the disease but who otherwise represented the population from which the cases of lung cancer came.
To improve the statistical power, the investigators of the major studies in Europe, North America, and China pooled the results in separate analyses (Table 2).7,20–23 The average radon concentration to which each individual had been exposed over the previous decades was estimated by measuring the radon concentration at their present and previous homes. On the basis of information from the uranium miners, these studies assumed that the period of exposure was the 30 years ending 5 years before the diagnosis or at death from lung cancer.
The results provided convincing evidence that radon exposure is a cause of lung cancer in the general population and substantiated the extrapolation from the studies of miners. Further, the results of all three pooled analyses were consistent with a linear dose-response relationship with no threshold, suggesting an increased risk of lung cancer even with a radon level below 4 pCi/L (200 Bq/m3), which is the concentration at which mitigation actions are recommended in many countries.17
The North American pooled analysis included 3,662 cases and 4,966 controls from seven studies in the United States and Canada. When data from all studies were combined, the risk of lung cancer was found to increase by 11% per 100-Bq/m3 (about 2.7-pCi/L) increase in measured radon concentration (95% CI 0%–28%). The estimated increase in lung cancer was independent of age, sex, or smoking history.7,20
The Chinese pooled data22 demonstrated a 13% (95% CI 1%–36%) increased risk per 100 Bq/m3.
In the European study, the risk of lung cancer increased by 8% per 100 Bq/m3 (95% CI 3%–16%). The European investigators repeated the analysis, taking into account the random year-to-year variability in measured radon concentration, finding the final estimated risk was an increase of 16% per 100 Bq/m3 using long-term average concentration.21
The combined estimate21,24 from the three pooling studies based on measured radon concentration is an increased risk of lung cancer of 10% per 100 Bq/m3.
Synergistic risk with smoking
Radon exposure was independently associated with lung cancer, and the relationship with cigarette smoking is believed to be synergistic. The radon progeny particles attach themselves to smoke and dust and are then deposited in the bronchial epithelium.25
In the pool of European case-control studies, the cancer risk for current smokers of 15 to 24 cigarettes per day relative to that in never-smokers was 25.8 (95% CI 21–31). Assuming that in the same analysis the lung cancer risk increased by 16% per 100 Bq/m3 of usual radon concentration regardless of smoking status, the cumulative absolute risk by age 75 would be 0.67% in those who never smoked and 16% in smokers at usual radon levels of 400 Bq/m3 (11 pCi/L).21
Rates of all lung cancer subtypes increased
Radon exposure is not associated with a specific histologic subtype of lung cancer. It has been speculated that the incidence of the small-cell subtype might be slightly increased because radon tends to deposit in the more central bronchial carinae.20,21 However, all subtypes have been described in association with radon, the most common being adenocarcinoma and squamous cell carcinoma.26–28
EFFECT OF MITIGATION MEASURES
The US Surgeon General and the EPA recommend that all homes be tested.18 Short-term tests should be used first, keeping in mind that diurnal and seasonal variations may occur.
The World Health Organization has proposed a reference level of 100 Bq/m3 (2.7 pCi/L) to minimize health hazards from indoor radon exposure.17 If this level cannot be reached under the country-specific conditions, the chosen reference level should not exceed 300 Bq/m3 (8 pCi/L).
In the United States, if the result of home testing is higher than 4 pCi/L, a follow-up measurement should be done using a different short-term test or a long-term test. If the follow-up result confirms a level of more than 4 pCi/L, mitigating actions are recommended. The goal is to reduce the indoor radon level as much as possible—down to zero or at least comparable to outdoor levels (national average 0.4 pCi/L).18
A variety of radon mitigation strategies have been used, with different rates of efficacy (Table 3). The optimal strategy depends on the likely source or cause, construction characteristics, soil, and climate.29Table 4 lists resources for the general public about testing and mitigation measures.
How beneficial is radon mitigation?
Although it is logical to try to reduce the indoor radon concentration, there is no strong evidence yet that this intervention decreases the incidence of lung cancer in the general population.
Using the BEIR VI risk model, Méndez et al30 estimated a 21% reduction in the annual radon-related lung cancer mortality rate by 2100 if all households were compliant with government recommendations (mitigation actions at levels of 4 pCi/L) and assuming that the percentage of cigarette smokers remained constant.
On the other hand, if the number of smokers continues to decline, the benefits from radon mitigation may be less. The expected benefit from mitigation in this scenario is a reduction of 12% in annual radon-related deaths by the year 2100.30 However, it will be challenging to determine whether the expected decline in the incidence of lung cancer and lung cancer deaths is truly attributable to mitigation measures.
MANAGING PATIENTS EXPOSED TO RADON
Screen for lung cancer in smokers only
The National Lung Screening Study (NLST) was a large multicenter trial of annual low-dose computed tomography (CT) to screen for lung cancer in a cohort at high risk: age 55 to 74, at least a 30 pack-year history of smoking in a current smoker, or a former smoker who quit within the past 15 years. The trial demonstrated a 20% reduction in lung cancer deaths in the CT screening group.31
Since the publication of the NLST results, many societies have endorsed screening for lung cancer with low-dose CT using the study criteria. The National Comprehensive Cancer Network (NCCN) expanded these criteria and has recommended screening in patients over age 50 who have a history of smoking and one additional risk factor, such as radon exposure.
However, radon exposure has not been incorporated into a lung cancer risk-prediction model, and there is no empirical evidence suggesting that people who have such a history would benefit from screening.32,33 The joint guidelines of the American College of Chest Physicians and American Society of Clinical Oncology recommend annual low-dose CT screening only for patients who meet the NLST criteria.34
What to do about indeterminate lung nodules
The widely used guidelines from the Fleischner Society35 on how to manage small lung nodules stratify patients into groups at low and high risk of developing lung cancer on the basis of risk factors. The guidelines apply to adults age 35 and older in whom an indeterminate solid nodule was recently detected.
If a patient is at high risk, the recommended approach includes follow-up in shorter intervals depending on the nodule size. History of smoking is recognized as a major risk factor, and the statement also lists family history and exposure to asbestos, uranium, and radon.35
Although the association of radon with lung cancer has been shown in epidemiologic studies, radon exposure has not been included in validated statistical models that assess the probability that an indeterminate lung nodule is malignant. We would expect the risk to be higher in miners, who suffer a more intense exposure to higher levels of radon, than in the general population, which has a low and constantly variable residential exposure. Furthermore, there are no data to support a more aggressive follow-up approach in patients with indeterminate lung nodules and a history of radon exposure.
RADON AND OTHER CANCERS
When a person is exposed to radon, the bronchial epithelium receives the highest dose of ionizing radiation, but other organs such as the kidneys, stomach, and bone marrow may receive doses as well, although lower. Several studies have looked into possible associations, but there is no strong evidence to suggest an increased mortality rate related to radon from cancers other than lung.24,36 However, there seems to be a positive association between radon and the incidence of lymphoproliferative disorders in uranium miners.37,38
Radon can be measured in drinking water, and a few studies have looked at a possible association with gastrointestinal malignancies. The results did not reveal a consistent positive correlation.39,40 The risk of cancer from exposure to radon in the public water supply is likely small and mostly from the transfer of radon particles into the air and not from drinking the water. On the other hand, the risk could be higher with private wells, where radon levels are variable and are possibly higher than from public sources.41
DATA ARE INSUFFICIENT TO GUIDE MANAGEMENT
Radon is a naturally occurring and ubiquitous radioactive gas that can cause tissue damage. Cohort and case-control studies have demonstrated that radon exposure is associated with increased risk of lung cancer. It is recommended that radon levels be measured in every home in the United States and mitigation measures instituted if levels exceed 4 pCi/L.
There are insufficient data to help guide the management of patients with a history of radon exposure, and prospective studies are needed to better understand the individual risk of developing lung cancer and the appropriate management of such patients.
Smoking cessation is an integral part of lung cancer risk reduction from radon exposure.
In 1984, a worker at a Pennsylvania nuclear power plant triggered the radiation detector as he was getting ready to go home. This would not be unusual for such a facility, but there was no nuclear fuel on site at the time. The alarm went off every time he left work.
One day, he triggered the alarm as he crossed the detector on arriving at the plant, leading him to suspect that he was bringing radiation from home. He eventually convinced the plant’s health physicists to check his home, although at first they were opposed to the idea. The results revealed high concentrations of radon everywhere, especially in his basement.
Radon was already known to be associated with health risks in underground miners at that time. This event revealed that a naturally occurring radioactive gas could be found in households at potentially hazardous concentrations.
The incident captured the public’s attention, and the Environmental Protection Agency (EPA) and the US Centers for Disease Control and Prevention (CDC) recommended that nearly all homes be tested.1,2 In 1988, the International Agency for Research on Cancer classified radon as a human carcinogen, and Congress passed the Indoor Radon Abatement Act in response to growing concern over health risks.3 This law funded state and federal measures to survey schools and federal buildings for radon levels, to educate citizens, and to develop programs for technical assistance. The long-term goal was to reduce indoor levels nationwide to no more than outdoor levels.
Radon is still considered an important public health hazard. From 15,000 to 21,000 people are estimated to die of lung cancer as a result of radon exposure each year in the United States, making it the second most common cause of lung cancer, behind smoking.4
Considering the relevance of this issue, this article will review the unique characteristics of radon as a risk factor for lung cancer.
WHAT IS RADON?
Figure 1.
Radon is a noble gas that occurs naturally as a decay product of uranium 238 and thorium 232. It is colorless, tasteless, and imperceptible to our senses. Its most common isotope is radon 222 (222Rn), which has a half-life of 3.8 days and decays by emitting an alpha particle to become polonium 218. The decay chain continues through several intermediate steps until the stable isotope lead 206 is formed (Figure 1). Two of the isotopes in this chain, polonium 218 and polonium 214, also emit alpha particles.5–7
Radon is primarily formed in soil. Its most important precursor, uranium 238, is ubiquitous, found in most soils and rocks in various concentrations. Radon can also be found in surface water, metal mines (uranium, phosphorus, silver, gold), residue of coal combustion, and natural gas.
Outdoor levels are usually much lower than indoor levels, as radon dissipates very quickly. Indoor radon mostly comes from the soil under the house or building, but it can also originate from coal combustion, gas appliances, and water (especially from private wells). In municipal water systems or surface reservoirs, most of the radon dissipates into the air or decays before the water reaches homes.8,9
Radon’s only commercial application in the United States is in calibrating measuring instruments. In the past, it was used in radiography and to treat cancer but was later replaced by other radiation sources that cost less and pose less hazard of alpha radiation.10
HOW RADON CAN HARM
Alpha particles, emitted by radon 222 and its progenies polonium 218 and polonium 214, are highly effective in damaging tissues. Although they do not travel far or fast, with their two protons and two neutrons, alpha particles are heavy and therefore can cause considerable damage at short range. Although alpha particles can be stopped by a thin barrier such as a piece of paper or the skin, if the source is inhaled or ingested and lodges against mucosal linings, the alpha particles emitted can destroy cells.11
The main route of radon exposure is by inhalation. Since radon is biologically inert, it is readily exhaled after it reaches the lungs. However, radon’s progenies can also be inhaled, either as free particles or attached to airborne particles such as dust, which they tend to attract as a result of their charged state. This attached fraction is believed to be more carcinogenic because it tends to deposit on the respiratory epithelium, notably in the carinae of bronchi. The smaller the dust particle, the deeper it can travel into the lung. The radiation emissions damage the genetic material of cells lining the airways, with the potential to result in lung cancer if the repair process is incomplete.5,8,9
Other routes of exposure include ingestion and dermal exposure. Radon and its progenies can be swallowed in drinking water, passing through the stomach walls and bowels and entering the blood.12 Dermal exposure is not considered a significant route unless the dermis is exposed, since in usual circumstances the skin protects the body from alpha radiation.13
Possible biologic mechanisms by which radon exposure might increase the risk of cancer include gene mutations, chromosome aberrations, generation of reactive oxygen species, up- or down-regulation of cytokines, and production of proteins associated with cell-cycle regulation.14–16
HOW IS RADON MEASURED?
Several devices are commercially available to measure radon levels at home. The most common ones are activated charcoal detectors, electret ion chambers, alpha-track detectors, electronic integrating devices, and continuous monitors. There is no evidence that one device is better than another, but devices that measure radon gas are usually preferred over those that measure decay products because they are simpler to use and more cost-effective. These devices are divided into those used for short-term testing (2–90 days) and long-term testing (Table 1).17
Radon levels can be expressed as follows:
Working levels. One working level (WL) is any combination of radon progeny in 1 L of air that ultimately releases 1.3 × 105 MeV of alpha energy during decay. In studies of miners, the radon progeny concentrations are generally expressed in WL. The cumulative exposure of an individual to this concentration over a “working month” of 170 hours is defined as a working level month (WLM).
Picocuries per liter. In the United States, the rate of decay is commonly reported in picocuries per liter (pCi/L): 1 pCi/L translates to 0.005 WL under usual conditions. The outdoor radon level is normally around 0.4 pCi/L.
Becquerel per cubic meter (Bq/m3) is an International System unit of measure: 1 WL corresponds to 3.7 × 103 Bq/m3, and 1 pCi/L is equivalent to 37 Bq/m3.
Different areas have different radon levels
The Indoor Radon Abatement Act of 1988 helped identify areas in the United States that have the potential for elevated indoor radon levels. An estimated 6 million homes have concentrations greater than 4 pCi/L.
Figure 2. Radon distribution in the United States with zone classification according to the predicted indoor level.From the US Environmental Protection Agency.
To assist in implementing radon-reducing strategies and allocation of resources, the EPA has created a map (Figure 2) that classifies counties according to the predicted indoor level.18
WHAT IS THE RELATIONSHIP BETWEEN RADON AND LUNG CANCER?
Determining the degree to which radon exposure contributes to lung cancer is a complex task. Radon can be found nearly everywhere, and there are diurnal, seasonal, and random year-to-year variations in the concentration of radon in indoor air.
A minority view
Not everyone agrees that radon is completely bad. For centuries, people have flocked to spas to “take the waters,” and the water at many of these spas has been found to contain radon. In the early 20th century, radiation was touted as having medicinal benefits, and people in many places in the world still go to “radon spas” (some of them in abandoned uranium mines) to help treat conditions such as arthritis and to feel invigorated and energized.
In 2006, a report by Zdrojewicz and Strzelczyk19 urged the medical community to keep an open mind about the possibility that radon exposure may be beneficial in very low doses, perhaps by stimulating repair mechanisms. This concept, called hormesis, differs from the mainstream view that cancer risk rises linearly with radiation dose, with no minimum threshold level (see below).
Risk in miners
As early as in the 16th century, metal miners in central Europe were noted to have a high rate of death from respiratory disease. Radon was discovered in 1900, and in the 20th century lung cancer was linked to high levels of radon detected in uranium mines.
Several small studies of underground miners exposed to high concentrations of radon consistently demonstrated an increased risk of lung cancer.
The Committee on the Biological Effects of Ionizing Radiation (BEIR VI 1999) reviewed 11 major cohort studies of miners. The studies included more than 60,000 miners in Europe, North America, Asia, and Australia, of whom 2,600 died of lung cancer. Lung cancer rates increased linearly with cumulative radon exposure, and the estimated average increase in the lung cancer death rate per WLM in the combined studies was 0.44% (95% confidence interval [CI] 0.20–1.00%). The percentage increase in the lung cancer death rate per WLM varied with time since exposure, with the highest increase in risk during the 5 to 14 years after exposure.4,17 Furthermore, the increase in risk was higher in younger miners, who were exposed to a relatively low radon concentration.
Risk in the general population
The magnitude of the risk in miners led to concern about radon exposure as a cause of lung cancer in the general population. Statistical models were generated that suggested a causal link between radon exposure and lung cancer. Although extrapolation of the results from miners caused controversy, the BEIR VI estimation of risk was validated by studies in the general population.7,20–23
Since the 1980s, several small case-control studies with limited power examined the relationship between indoor radon and lung cancer in the general population. In these studies, individuals who had developed lung cancer were compared with controls who had not developed the disease but who otherwise represented the population from which the cases of lung cancer came.
To improve the statistical power, the investigators of the major studies in Europe, North America, and China pooled the results in separate analyses (Table 2).7,20–23 The average radon concentration to which each individual had been exposed over the previous decades was estimated by measuring the radon concentration at their present and previous homes. On the basis of information from the uranium miners, these studies assumed that the period of exposure was the 30 years ending 5 years before the diagnosis or at death from lung cancer.
The results provided convincing evidence that radon exposure is a cause of lung cancer in the general population and substantiated the extrapolation from the studies of miners. Further, the results of all three pooled analyses were consistent with a linear dose-response relationship with no threshold, suggesting an increased risk of lung cancer even with a radon level below 4 pCi/L (200 Bq/m3), which is the concentration at which mitigation actions are recommended in many countries.17
The North American pooled analysis included 3,662 cases and 4,966 controls from seven studies in the United States and Canada. When data from all studies were combined, the risk of lung cancer was found to increase by 11% per 100-Bq/m3 (about 2.7-pCi/L) increase in measured radon concentration (95% CI 0%–28%). The estimated increase in lung cancer was independent of age, sex, or smoking history.7,20
The Chinese pooled data22 demonstrated a 13% (95% CI 1%–36%) increased risk per 100 Bq/m3.
In the European study, the risk of lung cancer increased by 8% per 100 Bq/m3 (95% CI 3%–16%). The European investigators repeated the analysis, taking into account the random year-to-year variability in measured radon concentration, finding the final estimated risk was an increase of 16% per 100 Bq/m3 using long-term average concentration.21
The combined estimate21,24 from the three pooling studies based on measured radon concentration is an increased risk of lung cancer of 10% per 100 Bq/m3.
Synergistic risk with smoking
Radon exposure was independently associated with lung cancer, and the relationship with cigarette smoking is believed to be synergistic. The radon progeny particles attach themselves to smoke and dust and are then deposited in the bronchial epithelium.25
In the pool of European case-control studies, the cancer risk for current smokers of 15 to 24 cigarettes per day relative to that in never-smokers was 25.8 (95% CI 21–31). Assuming that in the same analysis the lung cancer risk increased by 16% per 100 Bq/m3 of usual radon concentration regardless of smoking status, the cumulative absolute risk by age 75 would be 0.67% in those who never smoked and 16% in smokers at usual radon levels of 400 Bq/m3 (11 pCi/L).21
Rates of all lung cancer subtypes increased
Radon exposure is not associated with a specific histologic subtype of lung cancer. It has been speculated that the incidence of the small-cell subtype might be slightly increased because radon tends to deposit in the more central bronchial carinae.20,21 However, all subtypes have been described in association with radon, the most common being adenocarcinoma and squamous cell carcinoma.26–28
EFFECT OF MITIGATION MEASURES
The US Surgeon General and the EPA recommend that all homes be tested.18 Short-term tests should be used first, keeping in mind that diurnal and seasonal variations may occur.
The World Health Organization has proposed a reference level of 100 Bq/m3 (2.7 pCi/L) to minimize health hazards from indoor radon exposure.17 If this level cannot be reached under the country-specific conditions, the chosen reference level should not exceed 300 Bq/m3 (8 pCi/L).
In the United States, if the result of home testing is higher than 4 pCi/L, a follow-up measurement should be done using a different short-term test or a long-term test. If the follow-up result confirms a level of more than 4 pCi/L, mitigating actions are recommended. The goal is to reduce the indoor radon level as much as possible—down to zero or at least comparable to outdoor levels (national average 0.4 pCi/L).18
A variety of radon mitigation strategies have been used, with different rates of efficacy (Table 3). The optimal strategy depends on the likely source or cause, construction characteristics, soil, and climate.29Table 4 lists resources for the general public about testing and mitigation measures.
How beneficial is radon mitigation?
Although it is logical to try to reduce the indoor radon concentration, there is no strong evidence yet that this intervention decreases the incidence of lung cancer in the general population.
Using the BEIR VI risk model, Méndez et al30 estimated a 21% reduction in the annual radon-related lung cancer mortality rate by 2100 if all households were compliant with government recommendations (mitigation actions at levels of 4 pCi/L) and assuming that the percentage of cigarette smokers remained constant.
On the other hand, if the number of smokers continues to decline, the benefits from radon mitigation may be less. The expected benefit from mitigation in this scenario is a reduction of 12% in annual radon-related deaths by the year 2100.30 However, it will be challenging to determine whether the expected decline in the incidence of lung cancer and lung cancer deaths is truly attributable to mitigation measures.
MANAGING PATIENTS EXPOSED TO RADON
Screen for lung cancer in smokers only
The National Lung Screening Study (NLST) was a large multicenter trial of annual low-dose computed tomography (CT) to screen for lung cancer in a cohort at high risk: age 55 to 74, at least a 30 pack-year history of smoking in a current smoker, or a former smoker who quit within the past 15 years. The trial demonstrated a 20% reduction in lung cancer deaths in the CT screening group.31
Since the publication of the NLST results, many societies have endorsed screening for lung cancer with low-dose CT using the study criteria. The National Comprehensive Cancer Network (NCCN) expanded these criteria and has recommended screening in patients over age 50 who have a history of smoking and one additional risk factor, such as radon exposure.
However, radon exposure has not been incorporated into a lung cancer risk-prediction model, and there is no empirical evidence suggesting that people who have such a history would benefit from screening.32,33 The joint guidelines of the American College of Chest Physicians and American Society of Clinical Oncology recommend annual low-dose CT screening only for patients who meet the NLST criteria.34
What to do about indeterminate lung nodules
The widely used guidelines from the Fleischner Society35 on how to manage small lung nodules stratify patients into groups at low and high risk of developing lung cancer on the basis of risk factors. The guidelines apply to adults age 35 and older in whom an indeterminate solid nodule was recently detected.
If a patient is at high risk, the recommended approach includes follow-up in shorter intervals depending on the nodule size. History of smoking is recognized as a major risk factor, and the statement also lists family history and exposure to asbestos, uranium, and radon.35
Although the association of radon with lung cancer has been shown in epidemiologic studies, radon exposure has not been included in validated statistical models that assess the probability that an indeterminate lung nodule is malignant. We would expect the risk to be higher in miners, who suffer a more intense exposure to higher levels of radon, than in the general population, which has a low and constantly variable residential exposure. Furthermore, there are no data to support a more aggressive follow-up approach in patients with indeterminate lung nodules and a history of radon exposure.
RADON AND OTHER CANCERS
When a person is exposed to radon, the bronchial epithelium receives the highest dose of ionizing radiation, but other organs such as the kidneys, stomach, and bone marrow may receive doses as well, although lower. Several studies have looked into possible associations, but there is no strong evidence to suggest an increased mortality rate related to radon from cancers other than lung.24,36 However, there seems to be a positive association between radon and the incidence of lymphoproliferative disorders in uranium miners.37,38
Radon can be measured in drinking water, and a few studies have looked at a possible association with gastrointestinal malignancies. The results did not reveal a consistent positive correlation.39,40 The risk of cancer from exposure to radon in the public water supply is likely small and mostly from the transfer of radon particles into the air and not from drinking the water. On the other hand, the risk could be higher with private wells, where radon levels are variable and are possibly higher than from public sources.41
DATA ARE INSUFFICIENT TO GUIDE MANAGEMENT
Radon is a naturally occurring and ubiquitous radioactive gas that can cause tissue damage. Cohort and case-control studies have demonstrated that radon exposure is associated with increased risk of lung cancer. It is recommended that radon levels be measured in every home in the United States and mitigation measures instituted if levels exceed 4 pCi/L.
There are insufficient data to help guide the management of patients with a history of radon exposure, and prospective studies are needed to better understand the individual risk of developing lung cancer and the appropriate management of such patients.
Smoking cessation is an integral part of lung cancer risk reduction from radon exposure.
World Health Organization (WHO). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Manmade mineral fibres and radon. Summary of data reported and evaluation. http://monographs.iarc.fr/ENG/Monographs/vol43/volume43.pdf. Accessed August 5, 2014.
Committee on Health Risks of Exposure to Radon (BEIR VI). Health effects of exposure to radon: BEIR VI. Washington, DC: National Academies Press; 1999.
Samet JM. Radon and lung cancer. J Natl Cancer Inst1989; 81:745–757.
Lewis RJ, Lewis Sr RJ.Hawley’s condensed chemical dictionary. 14thed. New York: Wiley-Interscience; 2001.
Krewski D, Lubin JH, Zielinski JM, et al. Residential radon and risk of lung cancer: a combined analysis of 7 North American case-control studies. Epidemiology2005; 16:137–145.
Darby S, Hill D, Doll R. Radon: a likely carcinogen at all exposures. Ann Oncol2001; 12:1341–1351.
Morrison A. Use of radon for industrial radiography. Can J Res1945; 23:413–419.
Narayanan PK, Goodwin EH, Lehnert BE. Alpha particles initiate biological production of superoxide anions and hydrogen peroxide in human cells. Cancer Res1997; 57:3963–3971.
Ishikawa T, Narazaki Y, Yasuoka Y, Tokonami S, Yamada Y. Bio-kinetics of radon ingested from drinking water. Radiat Prot Dosimetry2003; 105:65–70.
Ishikawa T, Yamada Y, Fukutsu K, Tokonami S. Deposition and clearance for radon progeny in the human respiratory tract. Radiat Prot Dosimetry2003; 105:143–148.
Farkas A, Hofmann W, Balásházy I, Szoke I, Madas BG, Moustafa M. Effect of site-specific bronchial radon progeny deposition on the spatial and temporal distributions of cellular responses. Radiat Environ Biophys2011; 50:281–297.
Robertson A, Allen J, Laney R, Curnow A. The cellular and molecular carcinogenic effects of radon exposure: a review. Int J Mol Sci2013; 14:14024–14063.
Chauhan V, Howland M, Wilkins R. Effects of alpha-particle radiation on microRNA responses in human cell-lines. Open Biochem J2012; 6:16–22.
Krewski D, Lubin JH, Zielinski JM, et al. A combined analysis of North American case-control studies of residential radon and lung cancer. J Toxicol Environ Health A2006; 69:533–597.
Darby S, Hill D, Auvinen A, et al. Radon in homes and risk of lung cancer: collaborative analysis of individual data from 13 European case-control studies. BMJ2005; 330:223.
Lubin JH, Wang ZY, Boice JD, et al. Risk of lung cancer and residential radon in China: pooled results of two studies. Int J Cancer2004; 109:132–137.
Darby S, Hill D, Deo H, et al. Residential radon and lung cancer—detailed results of a collaborative analysis of individual data on 7,148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand J Work Environ Health2006; 32(suppl 1):1–83.
Darby SC, Whitley E, Howe GR, et al. Radon and cancers other than lung cancer in underground miners: a collaborative analysis of 11 studies. J Natl Cancer Inst1995; 87:378–384.
Land CE, Shimosato Y, Saccomanno G, et al. Radiation-associated lung cancer: a comparison of the histology of lung cancers in uranium miners and survivors of the atomic bombings of Hiroshima and Nagasaki. Radiat Res1993; 134:234–243.
Kreuzer M, Müller KM, Brachner A, et al. Histopathologic findings of lung carcinoma in German uranium miners. Cancer2000; 89:2613–2621.
Saccomanno G, Auerbach O, Kuschner M, et al. A comparison between the localization of lung tumors in uranium miners and in nonminers from 1947 to 1991. Cancer1996; 77:1278–1283.
Rahman NM, Tracy BL. Radon control systems in existing and new construction: a review. Radiat Prot Dosimetry2009; 135:243–255.
Méndez D, Alshanqeety O, Warner KE, Lantz PM, Courant PN. The impact of declining smoking on radon-related lung cancer in the United States. Am J Public Health2011; 101:310–314.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Wood DE, Eapen GA, Ettinger DS, et al. Lung cancer screening. J Natl Compr Canc Netw2012; 10:240–265.
Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB. Screening for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest2013; 143(suppl 5):e78S–e92S.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Darby SC, Radford EP, Whitley E. Radon exposure and cancers other than lung cancer in Swedish iron miners. Environ Health Perspect1995; 103(suppl 2):45–47.
Laurier D, Tirmarche M, Mitton N, et al. An update of cancer mortality among the French cohort of uranium miners: extended follow-up and new source of data for causes of death. Eur J Epidemiol2004; 19:139–146.
Rericha V, Kulich M, Rericha R, Shore DL, Sandler DP. Incidence of leukemia, lymphoma, and multiple myeloma in Czech uranium miners: a case-cohort study. Environ Health Perspect2006; 114:818–822.
Auvinen A, Salonen L, Pekkanen J, Pukkala E, Ilus T, Kurttio P. Radon and other natural radionuclides in drinking water and risk of stomach cancer: a case-cohort study in Finland. Int J Cancer2005; 114:109–113.
Kjellberg S, Wiseman JS. The relationship of radon to gastrointestinal malignancies. Am Surg1995; 61:822–825.
Cappello MA, Ferraro A, Mendelsohn AB, Prehn AW. Radon-contaminated drinking water from private wells: an environmental health assessment examining a rural Colorado mountain community’s exposure. J Environ Health2013; 76:18–24.
World Health Organization (WHO). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Manmade mineral fibres and radon. Summary of data reported and evaluation. http://monographs.iarc.fr/ENG/Monographs/vol43/volume43.pdf. Accessed August 5, 2014.
Committee on Health Risks of Exposure to Radon (BEIR VI). Health effects of exposure to radon: BEIR VI. Washington, DC: National Academies Press; 1999.
Samet JM. Radon and lung cancer. J Natl Cancer Inst1989; 81:745–757.
Lewis RJ, Lewis Sr RJ.Hawley’s condensed chemical dictionary. 14thed. New York: Wiley-Interscience; 2001.
Krewski D, Lubin JH, Zielinski JM, et al. Residential radon and risk of lung cancer: a combined analysis of 7 North American case-control studies. Epidemiology2005; 16:137–145.
Darby S, Hill D, Doll R. Radon: a likely carcinogen at all exposures. Ann Oncol2001; 12:1341–1351.
Morrison A. Use of radon for industrial radiography. Can J Res1945; 23:413–419.
Narayanan PK, Goodwin EH, Lehnert BE. Alpha particles initiate biological production of superoxide anions and hydrogen peroxide in human cells. Cancer Res1997; 57:3963–3971.
Ishikawa T, Narazaki Y, Yasuoka Y, Tokonami S, Yamada Y. Bio-kinetics of radon ingested from drinking water. Radiat Prot Dosimetry2003; 105:65–70.
Ishikawa T, Yamada Y, Fukutsu K, Tokonami S. Deposition and clearance for radon progeny in the human respiratory tract. Radiat Prot Dosimetry2003; 105:143–148.
Farkas A, Hofmann W, Balásházy I, Szoke I, Madas BG, Moustafa M. Effect of site-specific bronchial radon progeny deposition on the spatial and temporal distributions of cellular responses. Radiat Environ Biophys2011; 50:281–297.
Robertson A, Allen J, Laney R, Curnow A. The cellular and molecular carcinogenic effects of radon exposure: a review. Int J Mol Sci2013; 14:14024–14063.
Chauhan V, Howland M, Wilkins R. Effects of alpha-particle radiation on microRNA responses in human cell-lines. Open Biochem J2012; 6:16–22.
Krewski D, Lubin JH, Zielinski JM, et al. A combined analysis of North American case-control studies of residential radon and lung cancer. J Toxicol Environ Health A2006; 69:533–597.
Darby S, Hill D, Auvinen A, et al. Radon in homes and risk of lung cancer: collaborative analysis of individual data from 13 European case-control studies. BMJ2005; 330:223.
Lubin JH, Wang ZY, Boice JD, et al. Risk of lung cancer and residential radon in China: pooled results of two studies. Int J Cancer2004; 109:132–137.
Darby S, Hill D, Deo H, et al. Residential radon and lung cancer—detailed results of a collaborative analysis of individual data on 7,148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand J Work Environ Health2006; 32(suppl 1):1–83.
Darby SC, Whitley E, Howe GR, et al. Radon and cancers other than lung cancer in underground miners: a collaborative analysis of 11 studies. J Natl Cancer Inst1995; 87:378–384.
Land CE, Shimosato Y, Saccomanno G, et al. Radiation-associated lung cancer: a comparison of the histology of lung cancers in uranium miners and survivors of the atomic bombings of Hiroshima and Nagasaki. Radiat Res1993; 134:234–243.
Kreuzer M, Müller KM, Brachner A, et al. Histopathologic findings of lung carcinoma in German uranium miners. Cancer2000; 89:2613–2621.
Saccomanno G, Auerbach O, Kuschner M, et al. A comparison between the localization of lung tumors in uranium miners and in nonminers from 1947 to 1991. Cancer1996; 77:1278–1283.
Rahman NM, Tracy BL. Radon control systems in existing and new construction: a review. Radiat Prot Dosimetry2009; 135:243–255.
Méndez D, Alshanqeety O, Warner KE, Lantz PM, Courant PN. The impact of declining smoking on radon-related lung cancer in the United States. Am J Public Health2011; 101:310–314.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Wood DE, Eapen GA, Ettinger DS, et al. Lung cancer screening. J Natl Compr Canc Netw2012; 10:240–265.
Detterbeck FC, Mazzone PJ, Naidich DP, Bach PB. Screening for lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest2013; 143(suppl 5):e78S–e92S.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Darby SC, Radford EP, Whitley E. Radon exposure and cancers other than lung cancer in Swedish iron miners. Environ Health Perspect1995; 103(suppl 2):45–47.
Laurier D, Tirmarche M, Mitton N, et al. An update of cancer mortality among the French cohort of uranium miners: extended follow-up and new source of data for causes of death. Eur J Epidemiol2004; 19:139–146.
Rericha V, Kulich M, Rericha R, Shore DL, Sandler DP. Incidence of leukemia, lymphoma, and multiple myeloma in Czech uranium miners: a case-cohort study. Environ Health Perspect2006; 114:818–822.
Auvinen A, Salonen L, Pekkanen J, Pukkala E, Ilus T, Kurttio P. Radon and other natural radionuclides in drinking water and risk of stomach cancer: a case-cohort study in Finland. Int J Cancer2005; 114:109–113.
Kjellberg S, Wiseman JS. The relationship of radon to gastrointestinal malignancies. Am Surg1995; 61:822–825.
Cappello MA, Ferraro A, Mendelsohn AB, Prehn AW. Radon-contaminated drinking water from private wells: an environmental health assessment examining a rural Colorado mountain community’s exposure. J Environ Health2013; 76:18–24.
Radon is a noble gas that occurs naturally as a decay product of uranium 238 and thorium 232.
Radon 222 decays to polonium 218 and then, after several intermediate steps, to polonium 214, both of which emit alpha particles, which are highly effective in damaging tissues.
Radon exposure is associated with increased lung cancer incidence in underground miners. In the general population, it is estimated to be the second most common cause of lung cancer, after cigarette smoking.
There is no evidence yet of a benefit of lung cancer screening based on radon exposure.
Screening is the testing of an individual who is at risk for a disease, but who does not exhibit signs or symptoms of the disease. The goal of screening is to detect disease at a stage when cure or control is possible, and an effective screening program should reduce the number of disease-specific deaths in the screened population. Screening should focus on diseases that are associated with potentially serious consequences and that are detectable in the preclinical phase, yet it should avoid identifying “pseudodisease” (ie, positive test findings that would not be expected to affect the patient’s health) or causing morbidity due to the test procedure itself.1 Finally, screening is only worthwhile when treatment of the disease is more effective when administered early.
Since lung cancer screening began in the 1950s,2,3 many studies have attempted to define the medical benefits and economic impact of widespread screening. Many important unresolved issues remain, including the effectiveness of lung cancer screening for reducing disease-specific mortality, the potential harms of screening, its cost-effectiveness, and the potential impact of new research methods on the early identification of lung cancer.
DOES LUNG CANCER SCREENING REDUCE DISEASE-SPECIFIC MORTALITY?
Early studies examined the usefulness of large-scale chest radiograph programs, either with or without sputum cytology, for lung cancer screening. Although several studies reported that radiographic screening identified patients with early lung cancer and reported higher survival rates, reviews and meta-analyses of these reports concluded that screening did not significantly reduce disease-specific mortality.4,5
The utility of chest radiography for the detection of early lung cancer is limited by several factors, including poor sensitivity for the detection of small or subtle nodules and a relatively high false-positive rate.6–8 More recently, several cohort studies and randomized, controlled trials have shown that computed tomography (CT) screening is effective for the identification of early lung cancer in high-risk patients (eg, individuals with chronic, heavy tobacco use or asbestos exposure).9–11 A recent meta-analysis concluded that CT-based screening significantly increases the number of early lung cancers identified, but also increases the number of false-positive findings (nodules) and unnecessary thoracotomies for benign lesions.12
Lung cancer screening should increase the number of patients identified at early disease stages. Treatment of early-stage lung cancer should decrease the number of patients identified with late-stage cancer, resulting in a stage shift toward earlier disease for the population as a whole. Although lung cancer screening cohort studies and randomized, controlled trials have demonstrated that screening increases the number of early-stage lung cancer cases identified, these studies have generally not demonstrated decreased rates of late-stage lung cancers or stage shifting in the populations studied. In the 1970s, the National Cancer Institute began three large-scale screening trials at Mayo Clinic, Memorial Sloan-Kettering Cancer Institute, and The Johns Hopkins University, each enrolling approximately 10,000 patients. In the Mayo trial, the incidence of advanced-stage tumors was nearly identical for the screened versus unscreened patients, with 303 cancer cases detected in the screened group versus 304 cases in the control group.13 CT-based cohort studies have also reported increased rates of early recognition of lung cancer and accompanying large increases in the number of diagnostic procedures performed. However, early controlled trials of CT screening showed no differences between screened and unscreened groups in the numbers of patients with late-stage tumors or deaths due to lung cancer.14
Results such as these have led some researchers to argue that survival benefits of screening largely reflect observational biases. For example:
Figure 1. Lead-time bias. Patients identified by screening may live longer with disease than patients diagnosed clinically, although overall survival time is not improved.Lead-time bias occurs when screening results in earlier recognition of disease, but does not change the patient’s eventual lifespan, creating the appearance that the patient’s survival time with the disease is longer (Figure 1).15 Longer lead times should be observed in a successful screening program even if eventual mortality remains exactly the same, and lead time bias is therefore an expected outcome of screening.
Figure 2. Length-time bias. Indolent tumors move more gradually from the detectable stage to the onset of symptoms. These tumors are therefore more likely to be identified by intermittent screening.Length-time bias arises from the observation that any screening test that is applied intermittently is more likely to detect indolent tumors than aggressive, fast-growing tumors that would result in clinical symptoms(Figure 2).15 Indolent tumors move more gradually from the detectable state to the onset of clinical symptoms, and are therefore especially likely to be identified by screening.
Overdiagnosis bias occurs when a screening test identifies disease that never would have affected the patient’s life in the absence of screening. This type of bias might occur if screening identifies a lesion that is so indolent that it would never cause clinical disease, or if the population is otherwise in such poor health that successfully screened patients would die from other causes.
There is no question that these biases affect reports of survival in lung cancer screening, although it is unclear whether they explain the reported benefit of screening observed in cohort studies. Screening advocates have argued that the failure to screen high-risk patients for lung cancer has the potential for significant harm. In contrast, opponents of screening have argued that there was a lack of data showing a reduction in the number of patients diagnosed with late-stage cancers or in cancer-related mortality.
IS LUNG CANCER OVERDIAGNOSED IN SCREENED POPULATIONS?
Although the apparent benefit of lung cancer screening is susceptible to different sources of bias, overdiagnosis has received the greatest attention on the basis of both theoretical concerns and observations from screening studies. Estimates of lung cancer growth suggest that a typical 10-cm tumor, which is usually large enough to be fatal, has progressed through approximately 40 volume doublings during the course of its existence. In contrast, a more survivable—and clinically detectable—1-cm tumor has progressed through approximately 30 volume doublings.16,17 A lung tumor therefore spends most of its existence relatively undetectable. It has been estimated that the median doubling time is approximately 181 days, and that 22% of lung cancers have doubling times more than 465 days.18 The appearance of tumors on CT may suggest the growth rate, with 1 study showing that solid malignant nodules had a mean doubling time of 149 days, compared with 457 days for partial ground-glass–opacity nodules, and 813 days for pure ground-glass nodules.19
These estimates suggest that if a 1-cm tumor with a history of 30 volume doublings continues to grow at a typical rate (ie, a 181-day doubling time), the patient will die of cancer within 5 years. If the tumor is among the 22% of those with a 465-day doubling time, the survival time would be 12.7 years. For malignant pure ground-glass nodules, the projected time to death is 22 years. Individuals with lung cancer are often elderly, long-term cigarette smokers with emphysema or other chronic health problems—many of whom would die of other causes before their lung cancers progressed enough to cause significant health problems.
Reprinted with permission from the American College of Chest Physicians (Raz DJ, et al. Natural history of stage I non-small cell lung cancer: implications for early detection. Chest 2007; 132:193–199).
Figure 3. Survival is worse in untreated than in treated non–small cell lung cancer patients, arguing against overdiagnosis bias. Blue line: patients receiving surgery; green line: untreated patients who refused surgery.
As an argument against the significance of overdiagnosis in lung cancer screening, it has been noted that outcomes are worse for patients identified with early-stage lung cancer in screening studies who do not receive treatment. For example, the results of a study of 1,432 patients with stage I non–small cell lung cancer (NSCLC) are illustrated in Figure 3. Survival was much better in screened patients who were treated than in those who were untreated, with almost all the untreated patients dying within 10 years of diagnosis.20 However, the subjects in this study were atypical of those in most screening studies. Thirty-three percent of the patients had squamous cell carcinoma and 61% had relatively large T2 lesions, compared with a typical screening study comprised of patients with more than 50% T1 lesions and a smaller percentage of squamous cell carcinoma.
Another argument against overdiagnosis comes from gene profiling studies that have compared genetic tumor markers for tumors identified by screening with tumors identified clinically. One study found that the expression profile of 3,231 genes was similar for patients with lung cancer identified by screening or by symptoms.21 However, these investigators also found that nine genes known to be important in tumor growth differed between screened and nonscreened populations.
The significance of overdiagnosis is supported by a long-term follow-up study from the Mayo Clinic chest radiography screening trial, which found that the number of lung cancer cases remained higher in the screening group than the control group (585 vs 500 cases) for up to 28 years after screening, suggesting an overdiagnosis of lung cancer by approximately 85 cases per 500 patients screened (approximately 17%).22 Several studies have also demonstrated that screening populations may have tumors with more favorable histology or clinical characteristics, including higher levels of bronchioloalveolar carcinoma or well-differentiated adenocarcinoma.23–25 Finally, autopsy series have found undiagnosed lung tumors in as many as 1% of patients who died from natural causes, with fewer advanced tumors found in the 1970s than in the 1950s.26,27
These arguments led most to believe randomized controlled trials of CT-based screening were needed. The largest of these, the National Lung Screening Trial (NLST), has recently reported results that will clarify the impact of lung cancer screening on cancer-related mortality.28 This study enrolled 53,456 subjects between the ages of 55 and 74 years with a history of at least 30 pack-years of smoking. Patients were randomized to baseline screening followed by annual screening for 2 years using either low-dose helical CT or chest radiography and outcome follow-up 5 years after randomization. Data analysis after 6 to 8 years of follow-up found 442 lung cancer deaths in the chest radiograph arm versus 354 in the CT arm, representing a 20.3% reduction with CT.29 Screening of 320 patients using low-dose helical CT would be required to avoid each lung cancer death. Thus, after years of debate, it has been demonstrated that it is possible to reduce lung cancer-specific mortality with CT-based screening.
ARE THERE SIGNIFICANT RISKS WITH CT-BASED SCREENING?
Reprinted with kind permission from Springer Science+Business Media (Fischbach F, et al. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness. Eur Radiol 2003; 13:2378–2383).
Figure 4. Benign lung nodules visualized on computed tomography.
Lung cancer screening using chest CT may be associated with certain risks. The detailed high-resolution images produced by contemporary CT reveal small benign lung nodules in as many as 74% of patients(Figure 4).24,30 Although these nodules rarely represent a significant health problem, they require follow-up procedures and contribute to patient anxiety.31 In one study, every 1,000 individuals screened with CT imaging resulted in the identification of nine cases of stage I NSCLC, 235 false-positive nodules measuring at least 5 mm, and four thoracotomies for benign lesions.12
Radiation from CT tests is a potential concern, although it is difficult to quantify the importance of this risk. One estimate of CT-related radiation exposure found that annual CT screening of 50% of the eligible population between 50 and 75 years of age in the United States would result in approximately 36,000 new cancers, or a 1.8% increase in the rate of cancer over the expected rate.32 Many patients and health care professionals are already concerned about the degree of radiation exposure from medical diagnostics. A recent study that examined cumulative radiation exposure due to medical imaging in 952,420 adults aged 18 to 64 years found that approximately 57.9% of men and 78.7% of women receive at least some annual health care-related radiation exposure.33 Radiation exposure was considered moderate (> 3–20 mSv/yr) for 18.1% of men and 20.3% of women, and was considered high (> 20–50 mSv/yr) or very high (>50 mSv/hr) for 2.3% of men and 2.1% of women.
IS SCREENING COST-EFFECTIVE?
It is difficult to calculate the cost-effectiveness of CT screening because the impact of screening on mortality and the economic implications of false-positive findings are not well understood. A cost-effectiveness analysis of helical CT screening assumed that screening would result in a 50% stage shift and a 13% reduction in mortality.34 Under these assumptions, the cost-effectiveness was greater among current smokers ($116,300 per quality-adjusted life year saved by screening) than among currently quitting smokers ($558,600) or former smokers ($2,322,700). These investigators concluded that lung cancer screening is unlikely to be cost-effective, especially among those with the lowest levels of current tobacco exposure (quitting or former smokers).
Larger stage shifts or reductions in mortality would be expected to translate into greater cost-effectiveness, although the real-world effects of screening on these parameters are uncertain. Data from a US nationwide survey suggested that only about one-half of all current smokers would opt for surgery following a positive screening result, which might significantly decrease the cost-effectiveness of treatment.35
It is unclear how well the methods used in screening studies such as the NLST would translate to actual clinical practice at a national level, or how the health care system would manage the many small lung nodules that would be identified using this approach.
HOW WILL FUTURE DEVELOPMENTS AFFECT LUNG CANCER SCREENING?
Ongoing studies will continue to refine our understanding of the impact of lung cancer screening. For example, the randomized Prostate, Lung, Colorectal, and Ovarian Screening Trial is examining chest radiograph screening versus control in both smokers and never-smokers between 55 and 74 years of age.36 It is anticipated that this study will provide important information about how well chest radiographs perform for the identification of lung cancer in high- and lower-risk populations. Large randomized trials in Europe are comparing CT with no imaging for lung cancer screening.37 Efforts to better characterize specific patient populations who are at the greatest risk of lung cancer may help to improve the efficiency and cost-effectiveness of screening. Advances in molecular testing may help to identify molecular and genetic tumor biomarkers that herald increased lung cancer risk and greater need for screening. More research is needed to better understand the optimal management of patients with small lung nodules on screening tests. Professional societies are poised to publish revised screening recommendations as data from the NLST become available. Finally, insurers will need to evaluate the evidence and develop reimbursement policies.
SUMMARY AND CONCLUSIONS
Lung cancer screening efforts conducted over the last several decades have shown that it is possible to identify early lung cancer in high-risk patient populations. However, demonstrating a clear improvement in cancer-related mortality has been more difficult. Biases inherent to noncontrolled trials of screening may explain some of the beneficial effects on survival observed in some studies. Recent results from the NLST have for the first time demonstrated a significant reduction in lung cancer mortality in high-risk patients screened for lung cancer with chest CT, although there are continuing concerns about the cost of screening, the risks from radiation exposure, and the additional testing resulting from the identification of small benign lung nodules. Ongoing research will help to maximize the benefit of lung cancer screening and minimize the related risks.
References
Holin SM, Dwork RE, Glaser S, Rikli AE, Stocklen JB. Solitary pulmonary nodules found in a community-wide chest roentgenographic survey: a five-year follow-up study. Am Rev Tuberc1959; 79:427–439.
Nash FA, Morgan JM, Tomkins JG. South London Lung Cancer Study. Br Med J1968; 2:715–721.
Obuchowski NA, Graham RJ, Baker ME, Powell KA. Ten criteria for effective screening: their application to multislice CT screening for pulmonary and colorectal cancers. AJR Am J Roentgenol2001; 176:1357–1362.
Eddy DM. Screening for lung cancer. Ann Intern Med1989; 111:232–237.
Manser RL, Irving LB, Byrnes G, Abramson MJ, Stone CA, Campbell DA. Screening for lung cancer: a systematic review and meta-analysis of controlled trials. Thorax2003; 58:784–789.
Krupinski EA, Berger WG, Dallas WJ, Roehrig H. Searching for nodules: what features attract attention and influence detection?Acad Radiol2003; 10:861–868.
Yoshida H. Local contralateral subtraction based on bilateral symmetry of lung for reduction of false positives in computerized detection of pulmonary nodules. IEEE Trans Biomed Eng2004; 51:778–789.
Shiraishi J, Abe H.Engelmann R, Doi K. Effect of high sensitivity in a computerized scheme for detecting extremely subtle solitary pulmonary nodules in chest radiographs: observer performance study. Acad Radiol2003; 10:1302–1311.
Veronesi G, Bellomi M, Scanagatta P, et al. Difficulties encountered managing nodules detected during a computed tomography lung cancer screening program. J Thorac Cardiovasc Surg2008; 136:611–617.
Wilson DO, Weissfeld JL, Fuhrman CR, et al. The Pittsburgh Lung Screening Study (PLuSS): outcomes within 3 years of a first computed tomography scan [published online ahead of print July 17, 2008]. Am J Respir Crit Care Med2008; 178:956–961. doi: 10.1164/rccm.200802-336OC
Fasola G, Belvedere O, Aita M, et al. Low-dose computed tomography screening for lung cancer and pleural mesothelioma in an asbestos-exposed population: baseline results of a prospective, nonrandomized feasibility trial—an Alpe-adria Thoracic Oncology Multidisciplinary Group Study (ATOM 002). Oncologist2007; 12:1215–1224.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Fontana RS, Sanderson DR, Woolner LB, et al. Screening for lung cancer: a critique of the Mayo Lung Project. Cancer1991; 67( suppl 4):1155–1164.
Bach PB, Jett JR, Pastorino U, Tockman MS, Swensen SJ, Begg CB. Computed tomography screening and lung cancer outcomes. JAMA2007; 297:953–961.
Patz EF, Goodman PC, Bepler G. Screening for lung cancer. N Engl J Med2000; 343:1627–1633.
Weiss W. Implications of tumor growth rate for the natural history of lung cancer. J Occup Med1984; 26:345–352.
Reich JM. A critical appraisal of overdiagnosis: estimates of its magnitude and implications for lung cancer screening. Thorax2008; 63:377–383.
Winer-Muram HT, Jennings SG, Tarver RD, et al. Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology2002; 223:798–805.
Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol2000; 73:1252–1259.
Raz DJ, Zell JA, Ou SH, Gandara DR, Anton-Culver H, Jablons DM. Natural history of stage I non-small cell lung cancer: implications for early detection [published online ahead of print May 15, 2007]. Chest2007; 132:193–199. doi: 10.1378/chest.06-3096
Bianchi F, Hu J, Pelosi G, et al. Lung cancers detected by screening with spiral computed tomography have a malignant phenotype when analyzed by cDNA microarray. Clin Cancer Res2004; 10( 18 Pt 1):6023–6028.
Marcus PM, Bergstralh EJ, Zweig MH, Harris A, Offord KP, Fontana RS. Extended lung cancer incidence follow-up in the Mayo Lung Project and overdiagnosis. J Natl Cancer Inst2006; 98:748–756.
Sone S, Li F, Yang ZG, et al. Results of three-year mass screening programme for lung cancer using mobile low-dose spiral computed tomography scanner. Br J Cancer2001; 84:25–32.
Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience [published online ahead of print February 4, 2005]. Radiology2005; 235:259–265. doi: 10.1148/radiol.2351041662
International Early Lung Cancer Action Program Investigators, Henschke CI, Yankelevitz DF, Libby DM, et al. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med2006; 355:1763–1771.
Manser RL, Dodd M, Byrnes G, Irving LB, Campbell DA. Incidental lung cancers identified at coronial autopsy: implications for overdiagnosis of lung cancer by screening. Respir Med2005; 99:501–507.
Chan CK, Wells CK, McFarlane MJ, Feinstein AR. More lung cancer but better survival: implications of secular trends in “necropsy surprise” rates. Chest1989; 96:291–296.
National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, et al. Baseline characteristics of participants in the randomized national lung screening trial [published correction appears in J Natl Cancer Inst 2011; 103:1560]. J Natl Cancer Inst2010; 102:1771–1779.
Fischbach F, Knollmann F, Griesshaber V, Freund T, Akkol E, Felix R. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness [published online ahead of print May 13, 2003]. Eur Radiol2003; 13:2378–2383. doi: 10.1007/s00330-003-1915-7
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON) [published online ahead of pring November 24, 2009]. Br J Cancer2010; 102:27–34. doi: 10.1038/sj.bjc.6605459
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. [published online ahead of print November 13, 2006]Thorax2007; 62:126–130. doi: 10.1136/thx.2005.056036
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial models and validation [published online ahead of print May 23, 2011]. J Natl Cancer Inst2011; 103:1058–1068. doi: 10.1093/jnci/djr173
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
Author and Disclosure Information
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
Screening is the testing of an individual who is at risk for a disease, but who does not exhibit signs or symptoms of the disease. The goal of screening is to detect disease at a stage when cure or control is possible, and an effective screening program should reduce the number of disease-specific deaths in the screened population. Screening should focus on diseases that are associated with potentially serious consequences and that are detectable in the preclinical phase, yet it should avoid identifying “pseudodisease” (ie, positive test findings that would not be expected to affect the patient’s health) or causing morbidity due to the test procedure itself.1 Finally, screening is only worthwhile when treatment of the disease is more effective when administered early.
Since lung cancer screening began in the 1950s,2,3 many studies have attempted to define the medical benefits and economic impact of widespread screening. Many important unresolved issues remain, including the effectiveness of lung cancer screening for reducing disease-specific mortality, the potential harms of screening, its cost-effectiveness, and the potential impact of new research methods on the early identification of lung cancer.
DOES LUNG CANCER SCREENING REDUCE DISEASE-SPECIFIC MORTALITY?
Early studies examined the usefulness of large-scale chest radiograph programs, either with or without sputum cytology, for lung cancer screening. Although several studies reported that radiographic screening identified patients with early lung cancer and reported higher survival rates, reviews and meta-analyses of these reports concluded that screening did not significantly reduce disease-specific mortality.4,5
The utility of chest radiography for the detection of early lung cancer is limited by several factors, including poor sensitivity for the detection of small or subtle nodules and a relatively high false-positive rate.6–8 More recently, several cohort studies and randomized, controlled trials have shown that computed tomography (CT) screening is effective for the identification of early lung cancer in high-risk patients (eg, individuals with chronic, heavy tobacco use or asbestos exposure).9–11 A recent meta-analysis concluded that CT-based screening significantly increases the number of early lung cancers identified, but also increases the number of false-positive findings (nodules) and unnecessary thoracotomies for benign lesions.12
Lung cancer screening should increase the number of patients identified at early disease stages. Treatment of early-stage lung cancer should decrease the number of patients identified with late-stage cancer, resulting in a stage shift toward earlier disease for the population as a whole. Although lung cancer screening cohort studies and randomized, controlled trials have demonstrated that screening increases the number of early-stage lung cancer cases identified, these studies have generally not demonstrated decreased rates of late-stage lung cancers or stage shifting in the populations studied. In the 1970s, the National Cancer Institute began three large-scale screening trials at Mayo Clinic, Memorial Sloan-Kettering Cancer Institute, and The Johns Hopkins University, each enrolling approximately 10,000 patients. In the Mayo trial, the incidence of advanced-stage tumors was nearly identical for the screened versus unscreened patients, with 303 cancer cases detected in the screened group versus 304 cases in the control group.13 CT-based cohort studies have also reported increased rates of early recognition of lung cancer and accompanying large increases in the number of diagnostic procedures performed. However, early controlled trials of CT screening showed no differences between screened and unscreened groups in the numbers of patients with late-stage tumors or deaths due to lung cancer.14
Results such as these have led some researchers to argue that survival benefits of screening largely reflect observational biases. For example:
Figure 1. Lead-time bias. Patients identified by screening may live longer with disease than patients diagnosed clinically, although overall survival time is not improved.Lead-time bias occurs when screening results in earlier recognition of disease, but does not change the patient’s eventual lifespan, creating the appearance that the patient’s survival time with the disease is longer (Figure 1).15 Longer lead times should be observed in a successful screening program even if eventual mortality remains exactly the same, and lead time bias is therefore an expected outcome of screening.
Figure 2. Length-time bias. Indolent tumors move more gradually from the detectable stage to the onset of symptoms. These tumors are therefore more likely to be identified by intermittent screening.Length-time bias arises from the observation that any screening test that is applied intermittently is more likely to detect indolent tumors than aggressive, fast-growing tumors that would result in clinical symptoms(Figure 2).15 Indolent tumors move more gradually from the detectable state to the onset of clinical symptoms, and are therefore especially likely to be identified by screening.
Overdiagnosis bias occurs when a screening test identifies disease that never would have affected the patient’s life in the absence of screening. This type of bias might occur if screening identifies a lesion that is so indolent that it would never cause clinical disease, or if the population is otherwise in such poor health that successfully screened patients would die from other causes.
There is no question that these biases affect reports of survival in lung cancer screening, although it is unclear whether they explain the reported benefit of screening observed in cohort studies. Screening advocates have argued that the failure to screen high-risk patients for lung cancer has the potential for significant harm. In contrast, opponents of screening have argued that there was a lack of data showing a reduction in the number of patients diagnosed with late-stage cancers or in cancer-related mortality.
IS LUNG CANCER OVERDIAGNOSED IN SCREENED POPULATIONS?
Although the apparent benefit of lung cancer screening is susceptible to different sources of bias, overdiagnosis has received the greatest attention on the basis of both theoretical concerns and observations from screening studies. Estimates of lung cancer growth suggest that a typical 10-cm tumor, which is usually large enough to be fatal, has progressed through approximately 40 volume doublings during the course of its existence. In contrast, a more survivable—and clinically detectable—1-cm tumor has progressed through approximately 30 volume doublings.16,17 A lung tumor therefore spends most of its existence relatively undetectable. It has been estimated that the median doubling time is approximately 181 days, and that 22% of lung cancers have doubling times more than 465 days.18 The appearance of tumors on CT may suggest the growth rate, with 1 study showing that solid malignant nodules had a mean doubling time of 149 days, compared with 457 days for partial ground-glass–opacity nodules, and 813 days for pure ground-glass nodules.19
These estimates suggest that if a 1-cm tumor with a history of 30 volume doublings continues to grow at a typical rate (ie, a 181-day doubling time), the patient will die of cancer within 5 years. If the tumor is among the 22% of those with a 465-day doubling time, the survival time would be 12.7 years. For malignant pure ground-glass nodules, the projected time to death is 22 years. Individuals with lung cancer are often elderly, long-term cigarette smokers with emphysema or other chronic health problems—many of whom would die of other causes before their lung cancers progressed enough to cause significant health problems.
Reprinted with permission from the American College of Chest Physicians (Raz DJ, et al. Natural history of stage I non-small cell lung cancer: implications for early detection. Chest 2007; 132:193–199).
Figure 3. Survival is worse in untreated than in treated non–small cell lung cancer patients, arguing against overdiagnosis bias. Blue line: patients receiving surgery; green line: untreated patients who refused surgery.
As an argument against the significance of overdiagnosis in lung cancer screening, it has been noted that outcomes are worse for patients identified with early-stage lung cancer in screening studies who do not receive treatment. For example, the results of a study of 1,432 patients with stage I non–small cell lung cancer (NSCLC) are illustrated in Figure 3. Survival was much better in screened patients who were treated than in those who were untreated, with almost all the untreated patients dying within 10 years of diagnosis.20 However, the subjects in this study were atypical of those in most screening studies. Thirty-three percent of the patients had squamous cell carcinoma and 61% had relatively large T2 lesions, compared with a typical screening study comprised of patients with more than 50% T1 lesions and a smaller percentage of squamous cell carcinoma.
Another argument against overdiagnosis comes from gene profiling studies that have compared genetic tumor markers for tumors identified by screening with tumors identified clinically. One study found that the expression profile of 3,231 genes was similar for patients with lung cancer identified by screening or by symptoms.21 However, these investigators also found that nine genes known to be important in tumor growth differed between screened and nonscreened populations.
The significance of overdiagnosis is supported by a long-term follow-up study from the Mayo Clinic chest radiography screening trial, which found that the number of lung cancer cases remained higher in the screening group than the control group (585 vs 500 cases) for up to 28 years after screening, suggesting an overdiagnosis of lung cancer by approximately 85 cases per 500 patients screened (approximately 17%).22 Several studies have also demonstrated that screening populations may have tumors with more favorable histology or clinical characteristics, including higher levels of bronchioloalveolar carcinoma or well-differentiated adenocarcinoma.23–25 Finally, autopsy series have found undiagnosed lung tumors in as many as 1% of patients who died from natural causes, with fewer advanced tumors found in the 1970s than in the 1950s.26,27
These arguments led most to believe randomized controlled trials of CT-based screening were needed. The largest of these, the National Lung Screening Trial (NLST), has recently reported results that will clarify the impact of lung cancer screening on cancer-related mortality.28 This study enrolled 53,456 subjects between the ages of 55 and 74 years with a history of at least 30 pack-years of smoking. Patients were randomized to baseline screening followed by annual screening for 2 years using either low-dose helical CT or chest radiography and outcome follow-up 5 years after randomization. Data analysis after 6 to 8 years of follow-up found 442 lung cancer deaths in the chest radiograph arm versus 354 in the CT arm, representing a 20.3% reduction with CT.29 Screening of 320 patients using low-dose helical CT would be required to avoid each lung cancer death. Thus, after years of debate, it has been demonstrated that it is possible to reduce lung cancer-specific mortality with CT-based screening.
ARE THERE SIGNIFICANT RISKS WITH CT-BASED SCREENING?
Reprinted with kind permission from Springer Science+Business Media (Fischbach F, et al. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness. Eur Radiol 2003; 13:2378–2383).
Figure 4. Benign lung nodules visualized on computed tomography.
Lung cancer screening using chest CT may be associated with certain risks. The detailed high-resolution images produced by contemporary CT reveal small benign lung nodules in as many as 74% of patients(Figure 4).24,30 Although these nodules rarely represent a significant health problem, they require follow-up procedures and contribute to patient anxiety.31 In one study, every 1,000 individuals screened with CT imaging resulted in the identification of nine cases of stage I NSCLC, 235 false-positive nodules measuring at least 5 mm, and four thoracotomies for benign lesions.12
Radiation from CT tests is a potential concern, although it is difficult to quantify the importance of this risk. One estimate of CT-related radiation exposure found that annual CT screening of 50% of the eligible population between 50 and 75 years of age in the United States would result in approximately 36,000 new cancers, or a 1.8% increase in the rate of cancer over the expected rate.32 Many patients and health care professionals are already concerned about the degree of radiation exposure from medical diagnostics. A recent study that examined cumulative radiation exposure due to medical imaging in 952,420 adults aged 18 to 64 years found that approximately 57.9% of men and 78.7% of women receive at least some annual health care-related radiation exposure.33 Radiation exposure was considered moderate (> 3–20 mSv/yr) for 18.1% of men and 20.3% of women, and was considered high (> 20–50 mSv/yr) or very high (>50 mSv/hr) for 2.3% of men and 2.1% of women.
IS SCREENING COST-EFFECTIVE?
It is difficult to calculate the cost-effectiveness of CT screening because the impact of screening on mortality and the economic implications of false-positive findings are not well understood. A cost-effectiveness analysis of helical CT screening assumed that screening would result in a 50% stage shift and a 13% reduction in mortality.34 Under these assumptions, the cost-effectiveness was greater among current smokers ($116,300 per quality-adjusted life year saved by screening) than among currently quitting smokers ($558,600) or former smokers ($2,322,700). These investigators concluded that lung cancer screening is unlikely to be cost-effective, especially among those with the lowest levels of current tobacco exposure (quitting or former smokers).
Larger stage shifts or reductions in mortality would be expected to translate into greater cost-effectiveness, although the real-world effects of screening on these parameters are uncertain. Data from a US nationwide survey suggested that only about one-half of all current smokers would opt for surgery following a positive screening result, which might significantly decrease the cost-effectiveness of treatment.35
It is unclear how well the methods used in screening studies such as the NLST would translate to actual clinical practice at a national level, or how the health care system would manage the many small lung nodules that would be identified using this approach.
HOW WILL FUTURE DEVELOPMENTS AFFECT LUNG CANCER SCREENING?
Ongoing studies will continue to refine our understanding of the impact of lung cancer screening. For example, the randomized Prostate, Lung, Colorectal, and Ovarian Screening Trial is examining chest radiograph screening versus control in both smokers and never-smokers between 55 and 74 years of age.36 It is anticipated that this study will provide important information about how well chest radiographs perform for the identification of lung cancer in high- and lower-risk populations. Large randomized trials in Europe are comparing CT with no imaging for lung cancer screening.37 Efforts to better characterize specific patient populations who are at the greatest risk of lung cancer may help to improve the efficiency and cost-effectiveness of screening. Advances in molecular testing may help to identify molecular and genetic tumor biomarkers that herald increased lung cancer risk and greater need for screening. More research is needed to better understand the optimal management of patients with small lung nodules on screening tests. Professional societies are poised to publish revised screening recommendations as data from the NLST become available. Finally, insurers will need to evaluate the evidence and develop reimbursement policies.
SUMMARY AND CONCLUSIONS
Lung cancer screening efforts conducted over the last several decades have shown that it is possible to identify early lung cancer in high-risk patient populations. However, demonstrating a clear improvement in cancer-related mortality has been more difficult. Biases inherent to noncontrolled trials of screening may explain some of the beneficial effects on survival observed in some studies. Recent results from the NLST have for the first time demonstrated a significant reduction in lung cancer mortality in high-risk patients screened for lung cancer with chest CT, although there are continuing concerns about the cost of screening, the risks from radiation exposure, and the additional testing resulting from the identification of small benign lung nodules. Ongoing research will help to maximize the benefit of lung cancer screening and minimize the related risks.
Screening is the testing of an individual who is at risk for a disease, but who does not exhibit signs or symptoms of the disease. The goal of screening is to detect disease at a stage when cure or control is possible, and an effective screening program should reduce the number of disease-specific deaths in the screened population. Screening should focus on diseases that are associated with potentially serious consequences and that are detectable in the preclinical phase, yet it should avoid identifying “pseudodisease” (ie, positive test findings that would not be expected to affect the patient’s health) or causing morbidity due to the test procedure itself.1 Finally, screening is only worthwhile when treatment of the disease is more effective when administered early.
Since lung cancer screening began in the 1950s,2,3 many studies have attempted to define the medical benefits and economic impact of widespread screening. Many important unresolved issues remain, including the effectiveness of lung cancer screening for reducing disease-specific mortality, the potential harms of screening, its cost-effectiveness, and the potential impact of new research methods on the early identification of lung cancer.
DOES LUNG CANCER SCREENING REDUCE DISEASE-SPECIFIC MORTALITY?
Early studies examined the usefulness of large-scale chest radiograph programs, either with or without sputum cytology, for lung cancer screening. Although several studies reported that radiographic screening identified patients with early lung cancer and reported higher survival rates, reviews and meta-analyses of these reports concluded that screening did not significantly reduce disease-specific mortality.4,5
The utility of chest radiography for the detection of early lung cancer is limited by several factors, including poor sensitivity for the detection of small or subtle nodules and a relatively high false-positive rate.6–8 More recently, several cohort studies and randomized, controlled trials have shown that computed tomography (CT) screening is effective for the identification of early lung cancer in high-risk patients (eg, individuals with chronic, heavy tobacco use or asbestos exposure).9–11 A recent meta-analysis concluded that CT-based screening significantly increases the number of early lung cancers identified, but also increases the number of false-positive findings (nodules) and unnecessary thoracotomies for benign lesions.12
Lung cancer screening should increase the number of patients identified at early disease stages. Treatment of early-stage lung cancer should decrease the number of patients identified with late-stage cancer, resulting in a stage shift toward earlier disease for the population as a whole. Although lung cancer screening cohort studies and randomized, controlled trials have demonstrated that screening increases the number of early-stage lung cancer cases identified, these studies have generally not demonstrated decreased rates of late-stage lung cancers or stage shifting in the populations studied. In the 1970s, the National Cancer Institute began three large-scale screening trials at Mayo Clinic, Memorial Sloan-Kettering Cancer Institute, and The Johns Hopkins University, each enrolling approximately 10,000 patients. In the Mayo trial, the incidence of advanced-stage tumors was nearly identical for the screened versus unscreened patients, with 303 cancer cases detected in the screened group versus 304 cases in the control group.13 CT-based cohort studies have also reported increased rates of early recognition of lung cancer and accompanying large increases in the number of diagnostic procedures performed. However, early controlled trials of CT screening showed no differences between screened and unscreened groups in the numbers of patients with late-stage tumors or deaths due to lung cancer.14
Results such as these have led some researchers to argue that survival benefits of screening largely reflect observational biases. For example:
Figure 1. Lead-time bias. Patients identified by screening may live longer with disease than patients diagnosed clinically, although overall survival time is not improved.Lead-time bias occurs when screening results in earlier recognition of disease, but does not change the patient’s eventual lifespan, creating the appearance that the patient’s survival time with the disease is longer (Figure 1).15 Longer lead times should be observed in a successful screening program even if eventual mortality remains exactly the same, and lead time bias is therefore an expected outcome of screening.
Figure 2. Length-time bias. Indolent tumors move more gradually from the detectable stage to the onset of symptoms. These tumors are therefore more likely to be identified by intermittent screening.Length-time bias arises from the observation that any screening test that is applied intermittently is more likely to detect indolent tumors than aggressive, fast-growing tumors that would result in clinical symptoms(Figure 2).15 Indolent tumors move more gradually from the detectable state to the onset of clinical symptoms, and are therefore especially likely to be identified by screening.
Overdiagnosis bias occurs when a screening test identifies disease that never would have affected the patient’s life in the absence of screening. This type of bias might occur if screening identifies a lesion that is so indolent that it would never cause clinical disease, or if the population is otherwise in such poor health that successfully screened patients would die from other causes.
There is no question that these biases affect reports of survival in lung cancer screening, although it is unclear whether they explain the reported benefit of screening observed in cohort studies. Screening advocates have argued that the failure to screen high-risk patients for lung cancer has the potential for significant harm. In contrast, opponents of screening have argued that there was a lack of data showing a reduction in the number of patients diagnosed with late-stage cancers or in cancer-related mortality.
IS LUNG CANCER OVERDIAGNOSED IN SCREENED POPULATIONS?
Although the apparent benefit of lung cancer screening is susceptible to different sources of bias, overdiagnosis has received the greatest attention on the basis of both theoretical concerns and observations from screening studies. Estimates of lung cancer growth suggest that a typical 10-cm tumor, which is usually large enough to be fatal, has progressed through approximately 40 volume doublings during the course of its existence. In contrast, a more survivable—and clinically detectable—1-cm tumor has progressed through approximately 30 volume doublings.16,17 A lung tumor therefore spends most of its existence relatively undetectable. It has been estimated that the median doubling time is approximately 181 days, and that 22% of lung cancers have doubling times more than 465 days.18 The appearance of tumors on CT may suggest the growth rate, with 1 study showing that solid malignant nodules had a mean doubling time of 149 days, compared with 457 days for partial ground-glass–opacity nodules, and 813 days for pure ground-glass nodules.19
These estimates suggest that if a 1-cm tumor with a history of 30 volume doublings continues to grow at a typical rate (ie, a 181-day doubling time), the patient will die of cancer within 5 years. If the tumor is among the 22% of those with a 465-day doubling time, the survival time would be 12.7 years. For malignant pure ground-glass nodules, the projected time to death is 22 years. Individuals with lung cancer are often elderly, long-term cigarette smokers with emphysema or other chronic health problems—many of whom would die of other causes before their lung cancers progressed enough to cause significant health problems.
Reprinted with permission from the American College of Chest Physicians (Raz DJ, et al. Natural history of stage I non-small cell lung cancer: implications for early detection. Chest 2007; 132:193–199).
Figure 3. Survival is worse in untreated than in treated non–small cell lung cancer patients, arguing against overdiagnosis bias. Blue line: patients receiving surgery; green line: untreated patients who refused surgery.
As an argument against the significance of overdiagnosis in lung cancer screening, it has been noted that outcomes are worse for patients identified with early-stage lung cancer in screening studies who do not receive treatment. For example, the results of a study of 1,432 patients with stage I non–small cell lung cancer (NSCLC) are illustrated in Figure 3. Survival was much better in screened patients who were treated than in those who were untreated, with almost all the untreated patients dying within 10 years of diagnosis.20 However, the subjects in this study were atypical of those in most screening studies. Thirty-three percent of the patients had squamous cell carcinoma and 61% had relatively large T2 lesions, compared with a typical screening study comprised of patients with more than 50% T1 lesions and a smaller percentage of squamous cell carcinoma.
Another argument against overdiagnosis comes from gene profiling studies that have compared genetic tumor markers for tumors identified by screening with tumors identified clinically. One study found that the expression profile of 3,231 genes was similar for patients with lung cancer identified by screening or by symptoms.21 However, these investigators also found that nine genes known to be important in tumor growth differed between screened and nonscreened populations.
The significance of overdiagnosis is supported by a long-term follow-up study from the Mayo Clinic chest radiography screening trial, which found that the number of lung cancer cases remained higher in the screening group than the control group (585 vs 500 cases) for up to 28 years after screening, suggesting an overdiagnosis of lung cancer by approximately 85 cases per 500 patients screened (approximately 17%).22 Several studies have also demonstrated that screening populations may have tumors with more favorable histology or clinical characteristics, including higher levels of bronchioloalveolar carcinoma or well-differentiated adenocarcinoma.23–25 Finally, autopsy series have found undiagnosed lung tumors in as many as 1% of patients who died from natural causes, with fewer advanced tumors found in the 1970s than in the 1950s.26,27
These arguments led most to believe randomized controlled trials of CT-based screening were needed. The largest of these, the National Lung Screening Trial (NLST), has recently reported results that will clarify the impact of lung cancer screening on cancer-related mortality.28 This study enrolled 53,456 subjects between the ages of 55 and 74 years with a history of at least 30 pack-years of smoking. Patients were randomized to baseline screening followed by annual screening for 2 years using either low-dose helical CT or chest radiography and outcome follow-up 5 years after randomization. Data analysis after 6 to 8 years of follow-up found 442 lung cancer deaths in the chest radiograph arm versus 354 in the CT arm, representing a 20.3% reduction with CT.29 Screening of 320 patients using low-dose helical CT would be required to avoid each lung cancer death. Thus, after years of debate, it has been demonstrated that it is possible to reduce lung cancer-specific mortality with CT-based screening.
ARE THERE SIGNIFICANT RISKS WITH CT-BASED SCREENING?
Reprinted with kind permission from Springer Science+Business Media (Fischbach F, et al. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness. Eur Radiol 2003; 13:2378–2383).
Figure 4. Benign lung nodules visualized on computed tomography.
Lung cancer screening using chest CT may be associated with certain risks. The detailed high-resolution images produced by contemporary CT reveal small benign lung nodules in as many as 74% of patients(Figure 4).24,30 Although these nodules rarely represent a significant health problem, they require follow-up procedures and contribute to patient anxiety.31 In one study, every 1,000 individuals screened with CT imaging resulted in the identification of nine cases of stage I NSCLC, 235 false-positive nodules measuring at least 5 mm, and four thoracotomies for benign lesions.12
Radiation from CT tests is a potential concern, although it is difficult to quantify the importance of this risk. One estimate of CT-related radiation exposure found that annual CT screening of 50% of the eligible population between 50 and 75 years of age in the United States would result in approximately 36,000 new cancers, or a 1.8% increase in the rate of cancer over the expected rate.32 Many patients and health care professionals are already concerned about the degree of radiation exposure from medical diagnostics. A recent study that examined cumulative radiation exposure due to medical imaging in 952,420 adults aged 18 to 64 years found that approximately 57.9% of men and 78.7% of women receive at least some annual health care-related radiation exposure.33 Radiation exposure was considered moderate (> 3–20 mSv/yr) for 18.1% of men and 20.3% of women, and was considered high (> 20–50 mSv/yr) or very high (>50 mSv/hr) for 2.3% of men and 2.1% of women.
IS SCREENING COST-EFFECTIVE?
It is difficult to calculate the cost-effectiveness of CT screening because the impact of screening on mortality and the economic implications of false-positive findings are not well understood. A cost-effectiveness analysis of helical CT screening assumed that screening would result in a 50% stage shift and a 13% reduction in mortality.34 Under these assumptions, the cost-effectiveness was greater among current smokers ($116,300 per quality-adjusted life year saved by screening) than among currently quitting smokers ($558,600) or former smokers ($2,322,700). These investigators concluded that lung cancer screening is unlikely to be cost-effective, especially among those with the lowest levels of current tobacco exposure (quitting or former smokers).
Larger stage shifts or reductions in mortality would be expected to translate into greater cost-effectiveness, although the real-world effects of screening on these parameters are uncertain. Data from a US nationwide survey suggested that only about one-half of all current smokers would opt for surgery following a positive screening result, which might significantly decrease the cost-effectiveness of treatment.35
It is unclear how well the methods used in screening studies such as the NLST would translate to actual clinical practice at a national level, or how the health care system would manage the many small lung nodules that would be identified using this approach.
HOW WILL FUTURE DEVELOPMENTS AFFECT LUNG CANCER SCREENING?
Ongoing studies will continue to refine our understanding of the impact of lung cancer screening. For example, the randomized Prostate, Lung, Colorectal, and Ovarian Screening Trial is examining chest radiograph screening versus control in both smokers and never-smokers between 55 and 74 years of age.36 It is anticipated that this study will provide important information about how well chest radiographs perform for the identification of lung cancer in high- and lower-risk populations. Large randomized trials in Europe are comparing CT with no imaging for lung cancer screening.37 Efforts to better characterize specific patient populations who are at the greatest risk of lung cancer may help to improve the efficiency and cost-effectiveness of screening. Advances in molecular testing may help to identify molecular and genetic tumor biomarkers that herald increased lung cancer risk and greater need for screening. More research is needed to better understand the optimal management of patients with small lung nodules on screening tests. Professional societies are poised to publish revised screening recommendations as data from the NLST become available. Finally, insurers will need to evaluate the evidence and develop reimbursement policies.
SUMMARY AND CONCLUSIONS
Lung cancer screening efforts conducted over the last several decades have shown that it is possible to identify early lung cancer in high-risk patient populations. However, demonstrating a clear improvement in cancer-related mortality has been more difficult. Biases inherent to noncontrolled trials of screening may explain some of the beneficial effects on survival observed in some studies. Recent results from the NLST have for the first time demonstrated a significant reduction in lung cancer mortality in high-risk patients screened for lung cancer with chest CT, although there are continuing concerns about the cost of screening, the risks from radiation exposure, and the additional testing resulting from the identification of small benign lung nodules. Ongoing research will help to maximize the benefit of lung cancer screening and minimize the related risks.
References
Holin SM, Dwork RE, Glaser S, Rikli AE, Stocklen JB. Solitary pulmonary nodules found in a community-wide chest roentgenographic survey: a five-year follow-up study. Am Rev Tuberc1959; 79:427–439.
Nash FA, Morgan JM, Tomkins JG. South London Lung Cancer Study. Br Med J1968; 2:715–721.
Obuchowski NA, Graham RJ, Baker ME, Powell KA. Ten criteria for effective screening: their application to multislice CT screening for pulmonary and colorectal cancers. AJR Am J Roentgenol2001; 176:1357–1362.
Eddy DM. Screening for lung cancer. Ann Intern Med1989; 111:232–237.
Manser RL, Irving LB, Byrnes G, Abramson MJ, Stone CA, Campbell DA. Screening for lung cancer: a systematic review and meta-analysis of controlled trials. Thorax2003; 58:784–789.
Krupinski EA, Berger WG, Dallas WJ, Roehrig H. Searching for nodules: what features attract attention and influence detection?Acad Radiol2003; 10:861–868.
Yoshida H. Local contralateral subtraction based on bilateral symmetry of lung for reduction of false positives in computerized detection of pulmonary nodules. IEEE Trans Biomed Eng2004; 51:778–789.
Shiraishi J, Abe H.Engelmann R, Doi K. Effect of high sensitivity in a computerized scheme for detecting extremely subtle solitary pulmonary nodules in chest radiographs: observer performance study. Acad Radiol2003; 10:1302–1311.
Veronesi G, Bellomi M, Scanagatta P, et al. Difficulties encountered managing nodules detected during a computed tomography lung cancer screening program. J Thorac Cardiovasc Surg2008; 136:611–617.
Wilson DO, Weissfeld JL, Fuhrman CR, et al. The Pittsburgh Lung Screening Study (PLuSS): outcomes within 3 years of a first computed tomography scan [published online ahead of print July 17, 2008]. Am J Respir Crit Care Med2008; 178:956–961. doi: 10.1164/rccm.200802-336OC
Fasola G, Belvedere O, Aita M, et al. Low-dose computed tomography screening for lung cancer and pleural mesothelioma in an asbestos-exposed population: baseline results of a prospective, nonrandomized feasibility trial—an Alpe-adria Thoracic Oncology Multidisciplinary Group Study (ATOM 002). Oncologist2007; 12:1215–1224.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Fontana RS, Sanderson DR, Woolner LB, et al. Screening for lung cancer: a critique of the Mayo Lung Project. Cancer1991; 67( suppl 4):1155–1164.
Bach PB, Jett JR, Pastorino U, Tockman MS, Swensen SJ, Begg CB. Computed tomography screening and lung cancer outcomes. JAMA2007; 297:953–961.
Patz EF, Goodman PC, Bepler G. Screening for lung cancer. N Engl J Med2000; 343:1627–1633.
Weiss W. Implications of tumor growth rate for the natural history of lung cancer. J Occup Med1984; 26:345–352.
Reich JM. A critical appraisal of overdiagnosis: estimates of its magnitude and implications for lung cancer screening. Thorax2008; 63:377–383.
Winer-Muram HT, Jennings SG, Tarver RD, et al. Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology2002; 223:798–805.
Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol2000; 73:1252–1259.
Raz DJ, Zell JA, Ou SH, Gandara DR, Anton-Culver H, Jablons DM. Natural history of stage I non-small cell lung cancer: implications for early detection [published online ahead of print May 15, 2007]. Chest2007; 132:193–199. doi: 10.1378/chest.06-3096
Bianchi F, Hu J, Pelosi G, et al. Lung cancers detected by screening with spiral computed tomography have a malignant phenotype when analyzed by cDNA microarray. Clin Cancer Res2004; 10( 18 Pt 1):6023–6028.
Marcus PM, Bergstralh EJ, Zweig MH, Harris A, Offord KP, Fontana RS. Extended lung cancer incidence follow-up in the Mayo Lung Project and overdiagnosis. J Natl Cancer Inst2006; 98:748–756.
Sone S, Li F, Yang ZG, et al. Results of three-year mass screening programme for lung cancer using mobile low-dose spiral computed tomography scanner. Br J Cancer2001; 84:25–32.
Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience [published online ahead of print February 4, 2005]. Radiology2005; 235:259–265. doi: 10.1148/radiol.2351041662
International Early Lung Cancer Action Program Investigators, Henschke CI, Yankelevitz DF, Libby DM, et al. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med2006; 355:1763–1771.
Manser RL, Dodd M, Byrnes G, Irving LB, Campbell DA. Incidental lung cancers identified at coronial autopsy: implications for overdiagnosis of lung cancer by screening. Respir Med2005; 99:501–507.
Chan CK, Wells CK, McFarlane MJ, Feinstein AR. More lung cancer but better survival: implications of secular trends in “necropsy surprise” rates. Chest1989; 96:291–296.
National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, et al. Baseline characteristics of participants in the randomized national lung screening trial [published correction appears in J Natl Cancer Inst 2011; 103:1560]. J Natl Cancer Inst2010; 102:1771–1779.
Fischbach F, Knollmann F, Griesshaber V, Freund T, Akkol E, Felix R. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness [published online ahead of print May 13, 2003]. Eur Radiol2003; 13:2378–2383. doi: 10.1007/s00330-003-1915-7
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON) [published online ahead of pring November 24, 2009]. Br J Cancer2010; 102:27–34. doi: 10.1038/sj.bjc.6605459
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. [published online ahead of print November 13, 2006]Thorax2007; 62:126–130. doi: 10.1136/thx.2005.056036
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial models and validation [published online ahead of print May 23, 2011]. J Natl Cancer Inst2011; 103:1058–1068. doi: 10.1093/jnci/djr173
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
References
Holin SM, Dwork RE, Glaser S, Rikli AE, Stocklen JB. Solitary pulmonary nodules found in a community-wide chest roentgenographic survey: a five-year follow-up study. Am Rev Tuberc1959; 79:427–439.
Nash FA, Morgan JM, Tomkins JG. South London Lung Cancer Study. Br Med J1968; 2:715–721.
Obuchowski NA, Graham RJ, Baker ME, Powell KA. Ten criteria for effective screening: their application to multislice CT screening for pulmonary and colorectal cancers. AJR Am J Roentgenol2001; 176:1357–1362.
Eddy DM. Screening for lung cancer. Ann Intern Med1989; 111:232–237.
Manser RL, Irving LB, Byrnes G, Abramson MJ, Stone CA, Campbell DA. Screening for lung cancer: a systematic review and meta-analysis of controlled trials. Thorax2003; 58:784–789.
Krupinski EA, Berger WG, Dallas WJ, Roehrig H. Searching for nodules: what features attract attention and influence detection?Acad Radiol2003; 10:861–868.
Yoshida H. Local contralateral subtraction based on bilateral symmetry of lung for reduction of false positives in computerized detection of pulmonary nodules. IEEE Trans Biomed Eng2004; 51:778–789.
Shiraishi J, Abe H.Engelmann R, Doi K. Effect of high sensitivity in a computerized scheme for detecting extremely subtle solitary pulmonary nodules in chest radiographs: observer performance study. Acad Radiol2003; 10:1302–1311.
Veronesi G, Bellomi M, Scanagatta P, et al. Difficulties encountered managing nodules detected during a computed tomography lung cancer screening program. J Thorac Cardiovasc Surg2008; 136:611–617.
Wilson DO, Weissfeld JL, Fuhrman CR, et al. The Pittsburgh Lung Screening Study (PLuSS): outcomes within 3 years of a first computed tomography scan [published online ahead of print July 17, 2008]. Am J Respir Crit Care Med2008; 178:956–961. doi: 10.1164/rccm.200802-336OC
Fasola G, Belvedere O, Aita M, et al. Low-dose computed tomography screening for lung cancer and pleural mesothelioma in an asbestos-exposed population: baseline results of a prospective, nonrandomized feasibility trial—an Alpe-adria Thoracic Oncology Multidisciplinary Group Study (ATOM 002). Oncologist2007; 12:1215–1224.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Fontana RS, Sanderson DR, Woolner LB, et al. Screening for lung cancer: a critique of the Mayo Lung Project. Cancer1991; 67( suppl 4):1155–1164.
Bach PB, Jett JR, Pastorino U, Tockman MS, Swensen SJ, Begg CB. Computed tomography screening and lung cancer outcomes. JAMA2007; 297:953–961.
Patz EF, Goodman PC, Bepler G. Screening for lung cancer. N Engl J Med2000; 343:1627–1633.
Weiss W. Implications of tumor growth rate for the natural history of lung cancer. J Occup Med1984; 26:345–352.
Reich JM. A critical appraisal of overdiagnosis: estimates of its magnitude and implications for lung cancer screening. Thorax2008; 63:377–383.
Winer-Muram HT, Jennings SG, Tarver RD, et al. Volumetric growth rate of stage I lung cancer prior to treatment: serial CT scanning. Radiology2002; 223:798–805.
Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol2000; 73:1252–1259.
Raz DJ, Zell JA, Ou SH, Gandara DR, Anton-Culver H, Jablons DM. Natural history of stage I non-small cell lung cancer: implications for early detection [published online ahead of print May 15, 2007]. Chest2007; 132:193–199. doi: 10.1378/chest.06-3096
Bianchi F, Hu J, Pelosi G, et al. Lung cancers detected by screening with spiral computed tomography have a malignant phenotype when analyzed by cDNA microarray. Clin Cancer Res2004; 10( 18 Pt 1):6023–6028.
Marcus PM, Bergstralh EJ, Zweig MH, Harris A, Offord KP, Fontana RS. Extended lung cancer incidence follow-up in the Mayo Lung Project and overdiagnosis. J Natl Cancer Inst2006; 98:748–756.
Sone S, Li F, Yang ZG, et al. Results of three-year mass screening programme for lung cancer using mobile low-dose spiral computed tomography scanner. Br J Cancer2001; 84:25–32.
Swensen SJ, Jett JR, Hartman TE, et al. CT screening for lung cancer: five-year prospective experience [published online ahead of print February 4, 2005]. Radiology2005; 235:259–265. doi: 10.1148/radiol.2351041662
International Early Lung Cancer Action Program Investigators, Henschke CI, Yankelevitz DF, Libby DM, et al. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med2006; 355:1763–1771.
Manser RL, Dodd M, Byrnes G, Irving LB, Campbell DA. Incidental lung cancers identified at coronial autopsy: implications for overdiagnosis of lung cancer by screening. Respir Med2005; 99:501–507.
Chan CK, Wells CK, McFarlane MJ, Feinstein AR. More lung cancer but better survival: implications of secular trends in “necropsy surprise” rates. Chest1989; 96:291–296.
National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, et al. Baseline characteristics of participants in the randomized national lung screening trial [published correction appears in J Natl Cancer Inst 2011; 103:1560]. J Natl Cancer Inst2010; 102:1771–1779.
Fischbach F, Knollmann F, Griesshaber V, Freund T, Akkol E, Felix R. Detection of pulmonary nodules by multislice computed tomography: improved detection rate with reduced slice thickness [published online ahead of print May 13, 2003]. Eur Radiol2003; 13:2378–2383. doi: 10.1007/s00330-003-1915-7
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON) [published online ahead of pring November 24, 2009]. Br J Cancer2010; 102:27–34. doi: 10.1038/sj.bjc.6605459
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. [published online ahead of print November 13, 2006]Thorax2007; 62:126–130. doi: 10.1136/thx.2005.056036
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial models and validation [published online ahead of print May 23, 2011]. J Natl Cancer Inst2011; 103:1058–1068. doi: 10.1093/jnci/djr173
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
For patients with localized lung cancer, lung resection provides the highest likelihood of a cure. However, only about 20% to 30% of patients are potential candidates for surgical resection because of the stage at which the disease is diagnosed or because of comorbid conditions.1,2 In one study, poor lung function alone ruled out more than 37% of patients who presented with anatomically resectable disease.3 The poor prognosis for patients who do not undergo surgery, the likelihood of early mortality from lung resection, and the potential for loss of lung function following resection are all important considerations in the preoperative pulmonary evaluation of candidates for anatomical lung resection.
PROGNOSIS OF LUNG CANCER POOR WITHOUT SURGICAL RESECTION
Several studies support the poor prognosis of lung cancer patients who do not undergo resection. In one study of 1,297 screen- and symptom-detected patients, the median duration of survival without surgery was 25 months for patients with screen-detected stage I lung cancer (n = 42) and 13 months for those with symptom-detected stage I disease (n = 27).4 Another study of 799 patients with stage I lung cancer who were not treated surgically reported 5- and 10-year survival rates of 16.6% (n = 49) and 7.4% (n = 49), respectively.5 In a study of 251 patients with squamous cell carcinoma on sputum cytology, yet negative chest imaging, the 5-year and 10-year survival rates were 53.2% and 33.5%.6 Another study of 57 patients with potentially resectable disease who did not undergo surgery reported a median survival of 15.6 months, compared with 30.9 months for a group of 346 patients who underwent resection.7
PREDICTORS OF SURGICAL MORTALITY
Several large patient series describe perioperative mortality and the rate of complications for patients undergoing surgical resection for lung cancer. Reported surgical mortality rates in these studies vary from approximately 1% to 5%.2,8–10 The median age of patients in most of these studies was 65 to 70 years, and many patients had significant medical comorbidity. Predictors of increased surgical mortality include pneumonectomy, bilobectomy, American Society of Anesthesiologists (ASA) Physical Status Scale rating, Zubrod performance status score, renal dysfunction, induction chemoradiation therapy, steroid use, older age, urgent procedures, male gender, forced expiratory volume in 1 second (FEV1), and body mass index.11 In France, a thoracic surgery scoring system for in-hospital mortality (Thoracoscore) was developed using data obtained from more than 15,000 patients who were enrolled in a nationally representative thoracic surgery database. Mortality risk factors included in the model were patient age, sex, dyspnea score, ASA score, performance status, priority of surgery, diagnosis, procedure class, and comorbid disease.12 The model was highly accurate for the prediction of mortality, with a C statistic of 0.86. (1.00 corresponds to perfect outcome prediction.) The model was subsequently validated on 1,675 patients from the United States, where a similar accuracy was noted.13 The online version of the Thoracoscore risk assessment tool is available at: http://www.sfar.org/scores2/thoracoscore2.php.
REDUCED PULMONARY FUNCTION AFTER RESECTION
Several outcome measures have been used to assess the impact of resection on pulmonary function and quality of life after surgery. Across various studies, postoperative FEV1 values, diffusing capacity of the lung for carbon monoxide (Dlco) values, and peak oxygen consumption (VO2 peak) were assessed at various time intervals after lobectomy or pneumonectomy. FEV1 varied from 84% to 91% of preoperative values for lobectomy,14–16 and 64% to 66% for pneumonectomy.14–16 The Dlco was 89% to 96% of preoperative values after lobectomy and 72% to 80% after pneumonectomy.14,16 VO2 peak varied from 87% to 100% of preoperative values after lobectomy,14–16 and 71% to 89% after pneumonectomy.14–16
Patients with chronic obstructive pulmonary disease (COPD) typically experience smaller declines in FEV1 after lobectomy (0% to 8%) than those without COPD (16% to 20%). Declines in Dlco and VO2 peak are more variable, with reported decreases of 3% to 20% in those with COPD, and 0% to 21% for those without the disease.17–19
Lobectomy patients continue to recover pulmonary function for approximately 6 months after surgery. In patients who undergo pneumonectomy, improvement is generally limited after 3 months.14–16 Loss of lung function may vary significantly with the location of the resection. For example, resection of an emphysematous portion of the lung will probably result in less loss of function.
Few studies specifically examine quality of life after lung resection in patients with lung cancer. In general, patients who undergo resection have a lower quality of life before surgery than the general population.20 Postsurgical decline in physical measures of health-related quality of life has been reported during the month after surgery, with a return to baseline after 3 months. Mental quality of life scores did not decrease after surgery, and there was little correlation between quality of life outcomes and measures of pulmonary function.20
LUNG FUNCTION TESTING
Lung function testing helps predict the risk of postoperative complications, including mortality. The two most commonly used measures of pulmonary function are FEV1 and Dlco.
Both absolute FEV1 value and percent of predicted FEV1 strongly predict the risk of postoperative complications. It has been difficult to identify one cutoff value below which resection should not be considered. Studies have suggested preoperative absolute FEV1 values of 2 L for pneumonectomy and 1.5 L for lobectomy as cutoffs signifying increased short- and long-term surgical risk.21,22 Percent predicted FEV1, which incorporates patient age, sex, and height, is more commonly used to individualize treatment, since absolute values do not take into consideration other patient-related variables. An FEV1 of 80% predicted or higher has been proposed as a cutoff to proceed with resection without additional testing,23 but this decision must be individualized to each patient.
Similarly, it has been difficult to identify one cutoff value for the Dlco. As one might expect, the lower the value the higher the risk for a given patient. Patients with Dlco values less than 60% predicted normal24 had an increased mortality risk, longer hospital stay, and greater hospital costs in one report.
FEV1 and Dlco are only modestly correlated with one another.25 In one study, 43% of patients with FEV1 greater than 80% of predicted had Dlco less than 80% of predicted.26
According to guidelines developed by the American College of Chest Physicians (ACCP), spirometry is recommended for patients being considered for lung cancer resection.27 Patients with FEV1 that is greater than 80% predicted or greater than 2 L and without evidence of dyspnea or interstitial lung disease are considered suitable candidates for resection, including pneumonectomy, without further testing. Lobectomy without further evaluation may be performed if the FEV1 is greater than 1.5 L and there is no evidence of dyspnea or interstitial lung disease.
Although assessing FEV1 values alone may be adequate in patients being considered for lung cancer resection who have no evidence of either undue dyspnea on exertion or interstitial lung disease, the ACCP recommends also measuring Dlco when these signs are present. Guidelines from the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) recommend routinely measuring Dlco during preoperative evaluation regardless of whether the spirometric evaluation is abnormal.28 Similarly, the British Thoracic Society (BTS) recommends measuring transfer factor of the lung for carbon monoxide (Tlco) in all patients regardless of spirometric values.29
PREDICTING POSTOPERATIVE LUNG FUNCTION
Several methods have been used to predict postoperative lung function.
Segment method
The segment method estimates postoperative lung function by multiplying baseline function by the percentage of lung sections that will remain after resection.30 For example, if preoperative FEV1 is 1 L and surgery will result in the loss of 25% of lung segments, the predicted postoperative FEV1 is 750 mL. In a study using 19 lung segments in the calculation, the predicted postoperative lung function correlated well with actual postoperative lung function for patients undergoing lobectomy, but only modestly for patients undergoing pneumonectomy.30 Another method using 42 subsegments for the calculation, and correcting for segments that were obstructed by tumor, produced very similar results.31
Radionuclide scanning
In other studies, quantitative radionuclide scanning to identify the proportion of lung with poor perfusion produced fair to good correlations between predicted and actual postoperative FEV1.32–35 Techniques that are used less often include quantitative computed tomography (CT) and measurement of airway vibration during respiration.
Studies comparing different methods for predicting postoperative pulmonary function have found that perfusion imaging outperformed other approaches, and that the segment method is not a good predictor of outcome for patients undergoing pneumonectomy.17,36
Additional testing needed
For potential lung resection patients, the ACCP guidelines recommend that if either the FEV1 or Dlco is less than 80% of the predicted value, postoperative lung function should be predicted through additional testing.27 The ERS recommends that predicted postoperative FEV1 should not be used alone to select lung cancer patients for lung resection, especially those with moderate to severe COPD.28 These guidelines also recommend that the first estimate of residual lung function should be calculated based on segment counting, that only segments not totally obstructed should be counted, and that the patency of bronchus and segment structure should be preserved. In addition, patients with borderline function should undergo imaging-based calculation of residual lung function, including ventilation or perfusion scintigraphy before pneumonectomy, or quantitative CT scan before either lobectomy or pneumonectomy.28 The BTS recommends the use of segment counting to estimate postoperative lung function as part of risk assessment for postoperative dyspnea. Ventilation or perfusion scintigraphy should be considered to predict postoperative lung function if a ventilation or perfusion mismatch is suspected. Quantitative CT or MRI may be considered to predict postoperative lung function if the facility is available.29
Predicting mortality and complications: FEV1 and Dlco
The predicted postoperative FEV1 value is an independent predictor of postoperative mortality and other complications. Although there is no absolute cut-off value, studies identify an increased risk of complications below predicted postoperative FEV1 values ranging from 30%37 to 40%.38,39 Predicted postoperative Dlco is another outcome measure that can independently identify increased mortality risk in lung cancer resection patients. Dlco less than 40% has been associated with increased risk of postoperative respiratory complications even in those with predicted postoperative FEV1 values above 40%.26,39 One study stated that a combination of the two values, predicted postoperative FEV1 and predicted postoperative Dlco—called the predicted postoperative product (PPP)—is the best predictor of surgical mortality.40 Another study examined the utility of a prediction rule for pulmonary complications after lung surgery using a point system in which points were assigned based on predicted postoperative Dlco (1 point for each 5% decrement below 100%) plus 2 points for preoperative chemotherapy.41 The risk of complications was 9% for those with scores less than 11, 14% for those with scores of 11 to 13, and 26% for those with scores greater than 13.
When surgery is considered, ACCP guidelines state an increased risk of perioperative mortality in those lung cancer patients with either a PPP less than 1,650, or a predicted postoperative FEV1 less than 30%.27 These patients should be counseled about nonstandard surgery and nonsurgical treatment options. The ERS guidelines consider a predicted postoperative FEV1 value less than 30% to be a high-risk threshold when assessing pulmonary reserve before surgery.28
EXERCISE TESTING
In general, standardized cardiopulmonary exercise testing using VO2 peak has been shown to predict postoperative complications, including perioperative and long-term morbidity and mortality.42,43 Lower values are associated with a greater risk of poor outcome. Peak VO2 may not add significantly to the risk stratification of patients who have both FEV1 and Dlco values greater than 80%.44
According to ACCP recommendations for exercise testing in patients who are being evaluated for surgery, either an FEV1 or Dlco less than 40% of predicted postoperative (PPO) indicates increased risk for perioperative death and cardiopulmonary complications with standard lung resection. Preoperative exercise testing is recommended for these patients.27 Maximal oxygen consumption (VO2 max) less than 10 mL/kg/min, or the combination of VO2 max less than 15 mL/kg/min with both FEV1 and Dlco less than 40% PPO, also indicates increased risk for death and complications; these patients should be counseled about nonstandard surgery or nonsurgical treatment options. Guidelines from the ERS recommend exercise testing for all patients undergoing lung cancer surgery who have FEV1 or Dlco less than 80% of normal values.28 The VO2 peak measured during incremental exercise on a treadmill or cycle should be regarded as the most important parameter.
Figure. Distance walked during a shuttle walking test is strongly related to maximal oxygen consumption (VO2 max).
Several studies have found that distance traveled during walking tests predicts postoperative complications and can be related to VO2 max (Figure).45 According to ACCP guidelines, lung cancer patients who are potential candidates for standard lung resection are at increased risk for perioperative death and cardiopulmonary complications if they walk less than 25 shuttles on 2 shuttle walk tests or less than 1 flight of stairs. These patients should be counseled about nonstandard surgery and nonsurgical treatment options.27
Conversely, ERS/ESTS guidelines state that the shuttle walk test distance underestimates exercise capacity at the lower range, and does not discriminate between patients with and without complications.28 These guidelines state that shuttle walk test distance should not be used alone to select patients for resection. It may be used as a screening test, since patients walking less than 400 m are likely to also have VO2 peak less than 15 mL/kg/min. A standardized symptom-limited stair climbing test can be a cost-effective screening method to identify those who need more sophisticated exercise tests in order to optimize their perioperative management. The 6-minute walk test is not recommended.
British Thoracic Society guidelines recommend the use of the shuttle walk test as a functional assessment in patients with moderate to high risk of postoperative dyspnea.29 A distance walk of more than 400 m is recommended as a cutoff for acceptable pulmonary function. These guidelines recommend against using pulmonary function and exercise tests as the sole surrogates for a quality of life evaluation.
ALGORITHMS FOR TESTING
The ACCP, ERS/ESTS, and BTS guidelines all include algorithms for the preoperative evaluation of candidates for lung cancer resection.27–29 The guidelines differ from each other in many ways, including when to obtain a Dlco and cardiopulmonary exercise test, and in some of the cutoff values for various pulmonary function measures. ACCP guidelines begin with spirometry testing, supporting lobectomy in patients with spirometry results above the cutoff value of FEV1 greater than 1.5 L and pneumonectomy in those with a cutoff value of FEV1 greater than 2 L, and greater than 80% of predicted, unless the patient has dyspnea or evidence of interstitial lung disease. Measurement of the Dlco is recommended for those who do not meet the FEV1 cutoffs, or in those with unexplained dyspnea or diffuse parenchymal disease on chest radiograph or CT.27
A systematic review and set of treatment recommendations for high-risk patients with stage I lung cancer, developed by the Thoracic Oncology Network of the ACCP and the Workforce on Evidence-Based Surgery of the Society of Thoracic Surgeons, currently under review, will provide additional guidance regarding the use of lung function testing to evaluate risk of morbidity and mortality. These guidelines note that FEV1, Dlco, and peak VO2 all predict morbidity and mortality following major lung resection. Assessment of FEV1 and Dlco, including calculation of the estimated postoperative value, is strongly recommended before resection. The predictive value of peak VO2 is strongest in patients with impaired FEV1 or Dlco, and assessment of peak VO2 before major lung resection is recommended for these patients.
INTERVENTIONS TO DECREASE PERIOPERATIVE RISK
The impact of smoking cessation on perioperative outcome has been a matter of considerable debate. One large study found that the incidence of postoperative complications was actually greater when patients stopped smoking within 8 weeks before cardiac surgery.46 However, a recent meta-analysis including lung resection patients found no relationship between smoking cessation in the weeks before surgery and worse clinical outcomes.47 When a shorter duration of smoking cessation is examined, thoracotomy studies note that patients who continue to smoke within 1 month of pneumonectomy are at increased risk of major pulmonary events.48,49 An examination of perioperative mortality or major complications using data from the Society of Thoracic Surgeons found that smoking cessation within 1 month preceding surgery did not significantly affect perioperative morbidity or mortality, whereas longer abstention from tobacco use was associated with better surgical outcomes.50 The ACCP recommends that all patients with lung cancer be counseled regarding smoking cessation.27 ERS/ESTS guidelines recommend smoking cessation for at least 2 to 4 weeks before surgery, since this may change perioperative smoking behavior and decrease the risk of postoperative complications.28 Pulmonary rehabiliatation in the perioperative period has been shown to improve measures of activity tolerance, allowing resection of marginal candidates, and improving functional outcomes after resection.51 The ERS/ESTS guidelines state that early pre- and postoperative rehabilitation may produce functional benefits in resectable lung cancer patients.28
SUMMARY AND CONCLUSIONS
Lung function testing helps predict the risk of postoperative mortality, perioperative complications, and long-term dyspnea for patients with lung cancer undergoing surgical resection. Predicted postoperative FEV1 and Dlco should be evaluated in most resection candidates. Exercise testing adds to standard lung function testing in those with borderline values, discordance between standard measures, or discordance between subjective and objective lung function. Algorithms for preoperative assessment have been developed by the ACCP, the ERS/ESTS, and the BTS, which differ somewhat in the order of testing and specific testing cutoff values. Smoking cessation and pulmonary rehabilitation can help to reduce perioperative and long-term risks.
References
Damhuis RA, Schütte PR. Resection rates and postoperative mortality in 7,899 patients with lung cancer. Eur Respir J1996; 9:7–10.
Little AG, Rusch VW, Bonner JA, et al. Patterns of surgical care of lung cancer patients. Ann Thorac Surg2005; 80:2051–2056.
Baser S, Shannon VR, Eapen GA, et al. Pulmonary dysfunction as a major cause of inoperability among patients with non-small-cell lung cancer. Clin Lung Cancer2006; 7:344–349.
Sobue T, Suzuki T, Matsuda M, Kuroishi T, Ikeda S, Naruke T. Survival for clinical stage I lung cancer not surgically treated: comparison between screen-detected and symptom-detected cases. The Japanese Lung Cancer Screening Research Group. Cancer1992; 69:685–692.
Motohiro A, Ueda H, Komatsu H, Yanai N, Mori T; National Chest Hospital Study Group for Lung Cancer. Prognosis of nonsurgically treated, clinical stage I lung cancer patients in Japan. Lung Cancer2002; 36:65–69.
Sato M, Saito Y, Endo C, et al. The natural history of radiographically occult bronchogenic squamous cell carcinoma: a retrospective study of overdiagnosis bias. Chest2004; 126:108–113.
Loewen GM, Watson D, Kohman L, et al. Preoperative exercise Vo2 measurement for lung resection candidates: results of Cancer and Leukemia Group B Protocol 9238. J Thorac Oncol2007; 2:619–625.
Allen MS, Darling GE, Pechet TT, et al. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg2006; 81:1013–1020.
Meguid RA, Brooke BS, Chang DC, Sherwood JT, Brock MV, Yang SC. Are surgical outcomes for lung cancer resections improved at teaching hospitals?Ann Thorac Surg2008; 85:1015–1025.
Memtsoudis SG, Besculides MC, Zellos L, Patil N, Rogers SO. Trends in lung surgery: United States 1988 to 2002. Chest2006; 130:1462–1470.
Kozower BD, Sheng S, O’Brien SM, et al. STS database risk models: predictors of mortality and major morbidity for lung cancer resection. Ann Thorac Surg2010; 90:875–883.
Falcoz PE, Conti M, Brouchet L, et al. The Thoracic Surgery Scoring System (Thoracoscore): risk model for in-hospital death in 15,183 patients requiring thoracic surgery [published online ahead of print January 9, 2007]. J Thorac Cardiovasc Surg2007; 133:325–332. doi: 10.1016/j.jtcvs.2006.09.020
Bolliger CT, Jordan P, Solèr M, et al. Pulmonary function and exercise capacity after lung resection. Eur Respir J1996; 9:415–421.
Nezu K, Kushibe K, Tojo T, Takahama M, Kitamura S. Recovery and limitation of exercise capacity after lung resection for lung cancer. Chest1998; 113:1511–1516.
Brunelli A, Xiumé F, Refai M, et al. Evaluation of expiratory volume, diffusion capacity, and exercise tolerance following major lung resection: a prospective follow-up analysis. Chest2007; 131:141–147.
Smulders SA, Smeenk FW, Janssen-Heijnen ML, Postmus PE. Actual and predicted postoperative changes in lung function after pneumonectomy: a retrospective analysis. Chest2004; 125:1735–1741.
Edwards JG, Duthie DJ, Waller DA. Lobar volume reduction surgery: a method of increasing the lung cancer resection rate in patients with emphysema. Thorax2001; 56:791–795.
Bobbio A, Chetta A, Carbognani P, et al. Changes in pulmonary function test and cardiopulmonary exercise capacity in COPD patients after lobar pulmonary resection [published online ahead of print September 6, 2005]. Eur J Cardiothorac Surg2005; 28:754–758. doi: 10.1016/j.ejcts.2005.08.001
Brunelli A, Refai M, Salati M, Xiumé F, Sabbatini A. Predicted versus observed FEV1 and Dlco after major lung resection: a prospective evaluation at different postoperative periods. Ann Thorac Surg2007; 83:1134–1139.
Boushy SF, Billig DM, North LB, Helgason AH. Clinical course related to preoperative and postoperative pulmonary function in patients with bronchogenic carcinoma. Chest1971; 59:383–391.
Wernly JA, DeMeester TR, Kirchner PT, Myerowitz PD, Oxford DE, Golomb HM. Clinical value of quantitative ventilation-perfusion lung scans in the surgical management of bronchogenic carcinoma. J Thorac Cardiovasc Surg1980; 80:535–543.
Wyser C, Stulz P, Solèr M, et al. Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am J Respir Crit Care Med1999; 159:1450–1456.
Bousamra M, Presberg KW, Chammas JH, et al. Early and late morbidity in patients undergoing pulmonary resection with low diffusion capacity. Ann Thorac Surg1996; 62:968–975.
Ferguson MK, Little L, Rizzo L, et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg1988; 96:894–900.
Brunelli A, Refai MA, Salati M, Sabbatini A, Morgan-Hughes NJ, Rocco G. Carbon monoxide lung diffusion capacity improves risk stratification in patients without airflow limitation: evidence for systematic measurement before lung resection [published online ahead of print February 14, 2006]. Eur J Cardiothorac Surg2006; 29:567–570. doi: 10.1016/j.ejcts.2006.01.014
Colice GL, Shafazand S, Griffin JP, Keenan R, Bolliger CT; American College of Chest Physicians. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidenced-based clinical practice guidelines (2nd edition). Chest2007; 132( suppl 3):161S–177S.
Brunelli A, Charloux A, Bolliger CT, et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J2009; 34:17–41.
Lim E, Baldwin D, Beckles M, et al. Guidelines on the radical management of patients with lung cancer. Thorax2010; 65( suppl 3):iii1–iii27.
Nakahara K, Monden Y, Ohno K, Miyoshi S, Maeda H, Kawashima Y. A method for predicting postoperative lung function and its relation to postoperative complications in patients with lung cancer. Ann Thorac Surg1985; 39:260–265.
Kristersson S, Lindell SE, Svanberg L. Prediction of pulmonary function loss due to pneumonectomy using 133 Xe-radiospirometry. Chest1972; 62:694–698.
Bria WF, Kanarek DJ, Kazemi H. Prediction of postoperative pulmonary function following thoracic operations: value of ventilation-perfusion scanning. J Thorac Cardiovasc Surg1983; 86:186–192.
Ali MK, Mountain CF, Ewer MS, Johnston D, Haynie TP. Predicting loss of pulmonary function after pulmonary resection for bronchogenic carcinoma. Chest1980; 77:337–342.
Corris PA, Ellis DA, Hawkins T, Gibson GJ. Use of radionuclide scanning in the preoperative estimation of pulmonary function after pneumonectomy. Thorax1987; 42:285–291.
Bolliger CT, Gückel C, Engel H, et al. Prediction of functional reserves after lung resection: comparison between quantitative computed tomography, scintigraphy, and anatomy. Respiration2002; 69:482–489.
Nakahara K, Ohno K, Hashimoto J, et al. Prediction of postoperative respiratory failure in patients undergoing lung resection for lung cancer. Ann Thorac Surg1988; 46:549–552.
Markos J, Mullan BP, Hillman DR, et al. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis1989; 139:902–910.
Ribas J, Diaz O, Barberà JA, et al. Invasive exercise testing in the evaluation of patients at high-risk for lung resection. Eur Respir J1998; 12:1429–1435.
Pierce RJ, Copland JM, Sharpe K, Barter CE. Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med1994; 150:947–955.
Amar D, Munoz D, Shi W, Zhang H, Thaler HT. A clinical prediction rule for pulmonary complications after thoracic surgery for primary lung cancer [published online ahead of print October 27, 2009]. Anesth Analg2010; 110:1343–1348. doi: 10.1213/ANE.0b013e3181bf5c99
Benzo R, Kelley GA, Recchi L, Hofman A, Sciurba F. Complications of lung resection and exercise capacity: a meta-analysis [published online ahead of print April 3, 2007]. Respir Med2007; 101:1790–1797. doi: 10.1016/j.rmed.2007.02.012
Jones LW, Eves ND, Kraus WE, et al. The lung cancer exercise training study: a randomized trial of aerobic training, resistance training, or both in postsurgical lung cancer patients: rationale and design. BMC Cancer2010; 10:155.
Larsen KR, Svendsen UG, Milman N, Brenøe J, Petersen BN. Exercise testing in the preoperative evaluation of patients with bronchogenic carcinoma. Eur Respir J1997; 10:1559–1565.
Singh SJ, Morgan MDL, Hardman AE, Rowe C, Bardsley PA. Comparison of oxygen uptake during a conventional treadmill test and the shuttle walking test in chronic airflow limitation. Eur Respir J1994; 7:2016–2020.
Warner MA, Divertie MB, Tinker JH. Preoperative cessation of smoking and pulmonary complications in coronary artery bypass patients. Anesthesiology1984; 60:380–383.
Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis [published online ahead of print March 14, 2011]. Arch Intern Med2011; 171:983–989. doi: 10.1001/archinternmed.2011.97
Vaporciyan AA, Merriman KW, Ece F, et al. Incidence of major pulmonary morbidity after pneumonectomy: association with timing of smoking cessation. Ann Thorac Surg2002; 73:420–426.
Barrera R, Shi W, Amar D, et al. Smoking and timing of cessation: impact on pulmonary complications after thoracotomy. Chest2005; 127:1977–1983.
Mason DP, Subramanian S, Nowicki ER, et al. Impact of smoking cessation before resection of lung cancer. A Society of Thoracic Surgeons General Thoracic Surgery Database study. Ann Thorac Surg2009; 88:362–371.
Cesario A, Ferri L, Galetta D, et al. Pre-operative pulmonary rehabilitation and surgery for lung cancer. Lung Cancer2007; 57:118–119.
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
Author and Disclosure Information
Peter Mazzone, MD, MPH, FCCP Director of Education, Lung Cancer Program, and Pulmonary Rehabilitation Program; Respiratory Institute, Cleveland Clinic, Cleveland, OH
Correspondence: Peter Mazzone, MD, MPH, FCCP, Critical Care Medicine, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195; [email protected]
Dr. Mazzone reported that he has been a member of advisory committees for Boehringer Ingelheim and Oncimmune. He has research supported by Metabolomx.
This article was developed from an audio transcript of Dr. Mazzone’s presentation at the “Advances in Lung Cancer Evaluation and Management” symposium held in Cleveland, Ohio, on April 30, 2011. The transcript was formatted and edited by Cleveland Clinic Journal of Medicine staff for clarity and conciseness and was then reviewed, revised, and approved by Dr. Mazzone.
For patients with localized lung cancer, lung resection provides the highest likelihood of a cure. However, only about 20% to 30% of patients are potential candidates for surgical resection because of the stage at which the disease is diagnosed or because of comorbid conditions.1,2 In one study, poor lung function alone ruled out more than 37% of patients who presented with anatomically resectable disease.3 The poor prognosis for patients who do not undergo surgery, the likelihood of early mortality from lung resection, and the potential for loss of lung function following resection are all important considerations in the preoperative pulmonary evaluation of candidates for anatomical lung resection.
PROGNOSIS OF LUNG CANCER POOR WITHOUT SURGICAL RESECTION
Several studies support the poor prognosis of lung cancer patients who do not undergo resection. In one study of 1,297 screen- and symptom-detected patients, the median duration of survival without surgery was 25 months for patients with screen-detected stage I lung cancer (n = 42) and 13 months for those with symptom-detected stage I disease (n = 27).4 Another study of 799 patients with stage I lung cancer who were not treated surgically reported 5- and 10-year survival rates of 16.6% (n = 49) and 7.4% (n = 49), respectively.5 In a study of 251 patients with squamous cell carcinoma on sputum cytology, yet negative chest imaging, the 5-year and 10-year survival rates were 53.2% and 33.5%.6 Another study of 57 patients with potentially resectable disease who did not undergo surgery reported a median survival of 15.6 months, compared with 30.9 months for a group of 346 patients who underwent resection.7
PREDICTORS OF SURGICAL MORTALITY
Several large patient series describe perioperative mortality and the rate of complications for patients undergoing surgical resection for lung cancer. Reported surgical mortality rates in these studies vary from approximately 1% to 5%.2,8–10 The median age of patients in most of these studies was 65 to 70 years, and many patients had significant medical comorbidity. Predictors of increased surgical mortality include pneumonectomy, bilobectomy, American Society of Anesthesiologists (ASA) Physical Status Scale rating, Zubrod performance status score, renal dysfunction, induction chemoradiation therapy, steroid use, older age, urgent procedures, male gender, forced expiratory volume in 1 second (FEV1), and body mass index.11 In France, a thoracic surgery scoring system for in-hospital mortality (Thoracoscore) was developed using data obtained from more than 15,000 patients who were enrolled in a nationally representative thoracic surgery database. Mortality risk factors included in the model were patient age, sex, dyspnea score, ASA score, performance status, priority of surgery, diagnosis, procedure class, and comorbid disease.12 The model was highly accurate for the prediction of mortality, with a C statistic of 0.86. (1.00 corresponds to perfect outcome prediction.) The model was subsequently validated on 1,675 patients from the United States, where a similar accuracy was noted.13 The online version of the Thoracoscore risk assessment tool is available at: http://www.sfar.org/scores2/thoracoscore2.php.
REDUCED PULMONARY FUNCTION AFTER RESECTION
Several outcome measures have been used to assess the impact of resection on pulmonary function and quality of life after surgery. Across various studies, postoperative FEV1 values, diffusing capacity of the lung for carbon monoxide (Dlco) values, and peak oxygen consumption (VO2 peak) were assessed at various time intervals after lobectomy or pneumonectomy. FEV1 varied from 84% to 91% of preoperative values for lobectomy,14–16 and 64% to 66% for pneumonectomy.14–16 The Dlco was 89% to 96% of preoperative values after lobectomy and 72% to 80% after pneumonectomy.14,16 VO2 peak varied from 87% to 100% of preoperative values after lobectomy,14–16 and 71% to 89% after pneumonectomy.14–16
Patients with chronic obstructive pulmonary disease (COPD) typically experience smaller declines in FEV1 after lobectomy (0% to 8%) than those without COPD (16% to 20%). Declines in Dlco and VO2 peak are more variable, with reported decreases of 3% to 20% in those with COPD, and 0% to 21% for those without the disease.17–19
Lobectomy patients continue to recover pulmonary function for approximately 6 months after surgery. In patients who undergo pneumonectomy, improvement is generally limited after 3 months.14–16 Loss of lung function may vary significantly with the location of the resection. For example, resection of an emphysematous portion of the lung will probably result in less loss of function.
Few studies specifically examine quality of life after lung resection in patients with lung cancer. In general, patients who undergo resection have a lower quality of life before surgery than the general population.20 Postsurgical decline in physical measures of health-related quality of life has been reported during the month after surgery, with a return to baseline after 3 months. Mental quality of life scores did not decrease after surgery, and there was little correlation between quality of life outcomes and measures of pulmonary function.20
LUNG FUNCTION TESTING
Lung function testing helps predict the risk of postoperative complications, including mortality. The two most commonly used measures of pulmonary function are FEV1 and Dlco.
Both absolute FEV1 value and percent of predicted FEV1 strongly predict the risk of postoperative complications. It has been difficult to identify one cutoff value below which resection should not be considered. Studies have suggested preoperative absolute FEV1 values of 2 L for pneumonectomy and 1.5 L for lobectomy as cutoffs signifying increased short- and long-term surgical risk.21,22 Percent predicted FEV1, which incorporates patient age, sex, and height, is more commonly used to individualize treatment, since absolute values do not take into consideration other patient-related variables. An FEV1 of 80% predicted or higher has been proposed as a cutoff to proceed with resection without additional testing,23 but this decision must be individualized to each patient.
Similarly, it has been difficult to identify one cutoff value for the Dlco. As one might expect, the lower the value the higher the risk for a given patient. Patients with Dlco values less than 60% predicted normal24 had an increased mortality risk, longer hospital stay, and greater hospital costs in one report.
FEV1 and Dlco are only modestly correlated with one another.25 In one study, 43% of patients with FEV1 greater than 80% of predicted had Dlco less than 80% of predicted.26
According to guidelines developed by the American College of Chest Physicians (ACCP), spirometry is recommended for patients being considered for lung cancer resection.27 Patients with FEV1 that is greater than 80% predicted or greater than 2 L and without evidence of dyspnea or interstitial lung disease are considered suitable candidates for resection, including pneumonectomy, without further testing. Lobectomy without further evaluation may be performed if the FEV1 is greater than 1.5 L and there is no evidence of dyspnea or interstitial lung disease.
Although assessing FEV1 values alone may be adequate in patients being considered for lung cancer resection who have no evidence of either undue dyspnea on exertion or interstitial lung disease, the ACCP recommends also measuring Dlco when these signs are present. Guidelines from the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) recommend routinely measuring Dlco during preoperative evaluation regardless of whether the spirometric evaluation is abnormal.28 Similarly, the British Thoracic Society (BTS) recommends measuring transfer factor of the lung for carbon monoxide (Tlco) in all patients regardless of spirometric values.29
PREDICTING POSTOPERATIVE LUNG FUNCTION
Several methods have been used to predict postoperative lung function.
Segment method
The segment method estimates postoperative lung function by multiplying baseline function by the percentage of lung sections that will remain after resection.30 For example, if preoperative FEV1 is 1 L and surgery will result in the loss of 25% of lung segments, the predicted postoperative FEV1 is 750 mL. In a study using 19 lung segments in the calculation, the predicted postoperative lung function correlated well with actual postoperative lung function for patients undergoing lobectomy, but only modestly for patients undergoing pneumonectomy.30 Another method using 42 subsegments for the calculation, and correcting for segments that were obstructed by tumor, produced very similar results.31
Radionuclide scanning
In other studies, quantitative radionuclide scanning to identify the proportion of lung with poor perfusion produced fair to good correlations between predicted and actual postoperative FEV1.32–35 Techniques that are used less often include quantitative computed tomography (CT) and measurement of airway vibration during respiration.
Studies comparing different methods for predicting postoperative pulmonary function have found that perfusion imaging outperformed other approaches, and that the segment method is not a good predictor of outcome for patients undergoing pneumonectomy.17,36
Additional testing needed
For potential lung resection patients, the ACCP guidelines recommend that if either the FEV1 or Dlco is less than 80% of the predicted value, postoperative lung function should be predicted through additional testing.27 The ERS recommends that predicted postoperative FEV1 should not be used alone to select lung cancer patients for lung resection, especially those with moderate to severe COPD.28 These guidelines also recommend that the first estimate of residual lung function should be calculated based on segment counting, that only segments not totally obstructed should be counted, and that the patency of bronchus and segment structure should be preserved. In addition, patients with borderline function should undergo imaging-based calculation of residual lung function, including ventilation or perfusion scintigraphy before pneumonectomy, or quantitative CT scan before either lobectomy or pneumonectomy.28 The BTS recommends the use of segment counting to estimate postoperative lung function as part of risk assessment for postoperative dyspnea. Ventilation or perfusion scintigraphy should be considered to predict postoperative lung function if a ventilation or perfusion mismatch is suspected. Quantitative CT or MRI may be considered to predict postoperative lung function if the facility is available.29
Predicting mortality and complications: FEV1 and Dlco
The predicted postoperative FEV1 value is an independent predictor of postoperative mortality and other complications. Although there is no absolute cut-off value, studies identify an increased risk of complications below predicted postoperative FEV1 values ranging from 30%37 to 40%.38,39 Predicted postoperative Dlco is another outcome measure that can independently identify increased mortality risk in lung cancer resection patients. Dlco less than 40% has been associated with increased risk of postoperative respiratory complications even in those with predicted postoperative FEV1 values above 40%.26,39 One study stated that a combination of the two values, predicted postoperative FEV1 and predicted postoperative Dlco—called the predicted postoperative product (PPP)—is the best predictor of surgical mortality.40 Another study examined the utility of a prediction rule for pulmonary complications after lung surgery using a point system in which points were assigned based on predicted postoperative Dlco (1 point for each 5% decrement below 100%) plus 2 points for preoperative chemotherapy.41 The risk of complications was 9% for those with scores less than 11, 14% for those with scores of 11 to 13, and 26% for those with scores greater than 13.
When surgery is considered, ACCP guidelines state an increased risk of perioperative mortality in those lung cancer patients with either a PPP less than 1,650, or a predicted postoperative FEV1 less than 30%.27 These patients should be counseled about nonstandard surgery and nonsurgical treatment options. The ERS guidelines consider a predicted postoperative FEV1 value less than 30% to be a high-risk threshold when assessing pulmonary reserve before surgery.28
EXERCISE TESTING
In general, standardized cardiopulmonary exercise testing using VO2 peak has been shown to predict postoperative complications, including perioperative and long-term morbidity and mortality.42,43 Lower values are associated with a greater risk of poor outcome. Peak VO2 may not add significantly to the risk stratification of patients who have both FEV1 and Dlco values greater than 80%.44
According to ACCP recommendations for exercise testing in patients who are being evaluated for surgery, either an FEV1 or Dlco less than 40% of predicted postoperative (PPO) indicates increased risk for perioperative death and cardiopulmonary complications with standard lung resection. Preoperative exercise testing is recommended for these patients.27 Maximal oxygen consumption (VO2 max) less than 10 mL/kg/min, or the combination of VO2 max less than 15 mL/kg/min with both FEV1 and Dlco less than 40% PPO, also indicates increased risk for death and complications; these patients should be counseled about nonstandard surgery or nonsurgical treatment options. Guidelines from the ERS recommend exercise testing for all patients undergoing lung cancer surgery who have FEV1 or Dlco less than 80% of normal values.28 The VO2 peak measured during incremental exercise on a treadmill or cycle should be regarded as the most important parameter.
Figure. Distance walked during a shuttle walking test is strongly related to maximal oxygen consumption (VO2 max).
Several studies have found that distance traveled during walking tests predicts postoperative complications and can be related to VO2 max (Figure).45 According to ACCP guidelines, lung cancer patients who are potential candidates for standard lung resection are at increased risk for perioperative death and cardiopulmonary complications if they walk less than 25 shuttles on 2 shuttle walk tests or less than 1 flight of stairs. These patients should be counseled about nonstandard surgery and nonsurgical treatment options.27
Conversely, ERS/ESTS guidelines state that the shuttle walk test distance underestimates exercise capacity at the lower range, and does not discriminate between patients with and without complications.28 These guidelines state that shuttle walk test distance should not be used alone to select patients for resection. It may be used as a screening test, since patients walking less than 400 m are likely to also have VO2 peak less than 15 mL/kg/min. A standardized symptom-limited stair climbing test can be a cost-effective screening method to identify those who need more sophisticated exercise tests in order to optimize their perioperative management. The 6-minute walk test is not recommended.
British Thoracic Society guidelines recommend the use of the shuttle walk test as a functional assessment in patients with moderate to high risk of postoperative dyspnea.29 A distance walk of more than 400 m is recommended as a cutoff for acceptable pulmonary function. These guidelines recommend against using pulmonary function and exercise tests as the sole surrogates for a quality of life evaluation.
ALGORITHMS FOR TESTING
The ACCP, ERS/ESTS, and BTS guidelines all include algorithms for the preoperative evaluation of candidates for lung cancer resection.27–29 The guidelines differ from each other in many ways, including when to obtain a Dlco and cardiopulmonary exercise test, and in some of the cutoff values for various pulmonary function measures. ACCP guidelines begin with spirometry testing, supporting lobectomy in patients with spirometry results above the cutoff value of FEV1 greater than 1.5 L and pneumonectomy in those with a cutoff value of FEV1 greater than 2 L, and greater than 80% of predicted, unless the patient has dyspnea or evidence of interstitial lung disease. Measurement of the Dlco is recommended for those who do not meet the FEV1 cutoffs, or in those with unexplained dyspnea or diffuse parenchymal disease on chest radiograph or CT.27
A systematic review and set of treatment recommendations for high-risk patients with stage I lung cancer, developed by the Thoracic Oncology Network of the ACCP and the Workforce on Evidence-Based Surgery of the Society of Thoracic Surgeons, currently under review, will provide additional guidance regarding the use of lung function testing to evaluate risk of morbidity and mortality. These guidelines note that FEV1, Dlco, and peak VO2 all predict morbidity and mortality following major lung resection. Assessment of FEV1 and Dlco, including calculation of the estimated postoperative value, is strongly recommended before resection. The predictive value of peak VO2 is strongest in patients with impaired FEV1 or Dlco, and assessment of peak VO2 before major lung resection is recommended for these patients.
INTERVENTIONS TO DECREASE PERIOPERATIVE RISK
The impact of smoking cessation on perioperative outcome has been a matter of considerable debate. One large study found that the incidence of postoperative complications was actually greater when patients stopped smoking within 8 weeks before cardiac surgery.46 However, a recent meta-analysis including lung resection patients found no relationship between smoking cessation in the weeks before surgery and worse clinical outcomes.47 When a shorter duration of smoking cessation is examined, thoracotomy studies note that patients who continue to smoke within 1 month of pneumonectomy are at increased risk of major pulmonary events.48,49 An examination of perioperative mortality or major complications using data from the Society of Thoracic Surgeons found that smoking cessation within 1 month preceding surgery did not significantly affect perioperative morbidity or mortality, whereas longer abstention from tobacco use was associated with better surgical outcomes.50 The ACCP recommends that all patients with lung cancer be counseled regarding smoking cessation.27 ERS/ESTS guidelines recommend smoking cessation for at least 2 to 4 weeks before surgery, since this may change perioperative smoking behavior and decrease the risk of postoperative complications.28 Pulmonary rehabiliatation in the perioperative period has been shown to improve measures of activity tolerance, allowing resection of marginal candidates, and improving functional outcomes after resection.51 The ERS/ESTS guidelines state that early pre- and postoperative rehabilitation may produce functional benefits in resectable lung cancer patients.28
SUMMARY AND CONCLUSIONS
Lung function testing helps predict the risk of postoperative mortality, perioperative complications, and long-term dyspnea for patients with lung cancer undergoing surgical resection. Predicted postoperative FEV1 and Dlco should be evaluated in most resection candidates. Exercise testing adds to standard lung function testing in those with borderline values, discordance between standard measures, or discordance between subjective and objective lung function. Algorithms for preoperative assessment have been developed by the ACCP, the ERS/ESTS, and the BTS, which differ somewhat in the order of testing and specific testing cutoff values. Smoking cessation and pulmonary rehabilitation can help to reduce perioperative and long-term risks.
For patients with localized lung cancer, lung resection provides the highest likelihood of a cure. However, only about 20% to 30% of patients are potential candidates for surgical resection because of the stage at which the disease is diagnosed or because of comorbid conditions.1,2 In one study, poor lung function alone ruled out more than 37% of patients who presented with anatomically resectable disease.3 The poor prognosis for patients who do not undergo surgery, the likelihood of early mortality from lung resection, and the potential for loss of lung function following resection are all important considerations in the preoperative pulmonary evaluation of candidates for anatomical lung resection.
PROGNOSIS OF LUNG CANCER POOR WITHOUT SURGICAL RESECTION
Several studies support the poor prognosis of lung cancer patients who do not undergo resection. In one study of 1,297 screen- and symptom-detected patients, the median duration of survival without surgery was 25 months for patients with screen-detected stage I lung cancer (n = 42) and 13 months for those with symptom-detected stage I disease (n = 27).4 Another study of 799 patients with stage I lung cancer who were not treated surgically reported 5- and 10-year survival rates of 16.6% (n = 49) and 7.4% (n = 49), respectively.5 In a study of 251 patients with squamous cell carcinoma on sputum cytology, yet negative chest imaging, the 5-year and 10-year survival rates were 53.2% and 33.5%.6 Another study of 57 patients with potentially resectable disease who did not undergo surgery reported a median survival of 15.6 months, compared with 30.9 months for a group of 346 patients who underwent resection.7
PREDICTORS OF SURGICAL MORTALITY
Several large patient series describe perioperative mortality and the rate of complications for patients undergoing surgical resection for lung cancer. Reported surgical mortality rates in these studies vary from approximately 1% to 5%.2,8–10 The median age of patients in most of these studies was 65 to 70 years, and many patients had significant medical comorbidity. Predictors of increased surgical mortality include pneumonectomy, bilobectomy, American Society of Anesthesiologists (ASA) Physical Status Scale rating, Zubrod performance status score, renal dysfunction, induction chemoradiation therapy, steroid use, older age, urgent procedures, male gender, forced expiratory volume in 1 second (FEV1), and body mass index.11 In France, a thoracic surgery scoring system for in-hospital mortality (Thoracoscore) was developed using data obtained from more than 15,000 patients who were enrolled in a nationally representative thoracic surgery database. Mortality risk factors included in the model were patient age, sex, dyspnea score, ASA score, performance status, priority of surgery, diagnosis, procedure class, and comorbid disease.12 The model was highly accurate for the prediction of mortality, with a C statistic of 0.86. (1.00 corresponds to perfect outcome prediction.) The model was subsequently validated on 1,675 patients from the United States, where a similar accuracy was noted.13 The online version of the Thoracoscore risk assessment tool is available at: http://www.sfar.org/scores2/thoracoscore2.php.
REDUCED PULMONARY FUNCTION AFTER RESECTION
Several outcome measures have been used to assess the impact of resection on pulmonary function and quality of life after surgery. Across various studies, postoperative FEV1 values, diffusing capacity of the lung for carbon monoxide (Dlco) values, and peak oxygen consumption (VO2 peak) were assessed at various time intervals after lobectomy or pneumonectomy. FEV1 varied from 84% to 91% of preoperative values for lobectomy,14–16 and 64% to 66% for pneumonectomy.14–16 The Dlco was 89% to 96% of preoperative values after lobectomy and 72% to 80% after pneumonectomy.14,16 VO2 peak varied from 87% to 100% of preoperative values after lobectomy,14–16 and 71% to 89% after pneumonectomy.14–16
Patients with chronic obstructive pulmonary disease (COPD) typically experience smaller declines in FEV1 after lobectomy (0% to 8%) than those without COPD (16% to 20%). Declines in Dlco and VO2 peak are more variable, with reported decreases of 3% to 20% in those with COPD, and 0% to 21% for those without the disease.17–19
Lobectomy patients continue to recover pulmonary function for approximately 6 months after surgery. In patients who undergo pneumonectomy, improvement is generally limited after 3 months.14–16 Loss of lung function may vary significantly with the location of the resection. For example, resection of an emphysematous portion of the lung will probably result in less loss of function.
Few studies specifically examine quality of life after lung resection in patients with lung cancer. In general, patients who undergo resection have a lower quality of life before surgery than the general population.20 Postsurgical decline in physical measures of health-related quality of life has been reported during the month after surgery, with a return to baseline after 3 months. Mental quality of life scores did not decrease after surgery, and there was little correlation between quality of life outcomes and measures of pulmonary function.20
LUNG FUNCTION TESTING
Lung function testing helps predict the risk of postoperative complications, including mortality. The two most commonly used measures of pulmonary function are FEV1 and Dlco.
Both absolute FEV1 value and percent of predicted FEV1 strongly predict the risk of postoperative complications. It has been difficult to identify one cutoff value below which resection should not be considered. Studies have suggested preoperative absolute FEV1 values of 2 L for pneumonectomy and 1.5 L for lobectomy as cutoffs signifying increased short- and long-term surgical risk.21,22 Percent predicted FEV1, which incorporates patient age, sex, and height, is more commonly used to individualize treatment, since absolute values do not take into consideration other patient-related variables. An FEV1 of 80% predicted or higher has been proposed as a cutoff to proceed with resection without additional testing,23 but this decision must be individualized to each patient.
Similarly, it has been difficult to identify one cutoff value for the Dlco. As one might expect, the lower the value the higher the risk for a given patient. Patients with Dlco values less than 60% predicted normal24 had an increased mortality risk, longer hospital stay, and greater hospital costs in one report.
FEV1 and Dlco are only modestly correlated with one another.25 In one study, 43% of patients with FEV1 greater than 80% of predicted had Dlco less than 80% of predicted.26
According to guidelines developed by the American College of Chest Physicians (ACCP), spirometry is recommended for patients being considered for lung cancer resection.27 Patients with FEV1 that is greater than 80% predicted or greater than 2 L and without evidence of dyspnea or interstitial lung disease are considered suitable candidates for resection, including pneumonectomy, without further testing. Lobectomy without further evaluation may be performed if the FEV1 is greater than 1.5 L and there is no evidence of dyspnea or interstitial lung disease.
Although assessing FEV1 values alone may be adequate in patients being considered for lung cancer resection who have no evidence of either undue dyspnea on exertion or interstitial lung disease, the ACCP recommends also measuring Dlco when these signs are present. Guidelines from the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS) recommend routinely measuring Dlco during preoperative evaluation regardless of whether the spirometric evaluation is abnormal.28 Similarly, the British Thoracic Society (BTS) recommends measuring transfer factor of the lung for carbon monoxide (Tlco) in all patients regardless of spirometric values.29
PREDICTING POSTOPERATIVE LUNG FUNCTION
Several methods have been used to predict postoperative lung function.
Segment method
The segment method estimates postoperative lung function by multiplying baseline function by the percentage of lung sections that will remain after resection.30 For example, if preoperative FEV1 is 1 L and surgery will result in the loss of 25% of lung segments, the predicted postoperative FEV1 is 750 mL. In a study using 19 lung segments in the calculation, the predicted postoperative lung function correlated well with actual postoperative lung function for patients undergoing lobectomy, but only modestly for patients undergoing pneumonectomy.30 Another method using 42 subsegments for the calculation, and correcting for segments that were obstructed by tumor, produced very similar results.31
Radionuclide scanning
In other studies, quantitative radionuclide scanning to identify the proportion of lung with poor perfusion produced fair to good correlations between predicted and actual postoperative FEV1.32–35 Techniques that are used less often include quantitative computed tomography (CT) and measurement of airway vibration during respiration.
Studies comparing different methods for predicting postoperative pulmonary function have found that perfusion imaging outperformed other approaches, and that the segment method is not a good predictor of outcome for patients undergoing pneumonectomy.17,36
Additional testing needed
For potential lung resection patients, the ACCP guidelines recommend that if either the FEV1 or Dlco is less than 80% of the predicted value, postoperative lung function should be predicted through additional testing.27 The ERS recommends that predicted postoperative FEV1 should not be used alone to select lung cancer patients for lung resection, especially those with moderate to severe COPD.28 These guidelines also recommend that the first estimate of residual lung function should be calculated based on segment counting, that only segments not totally obstructed should be counted, and that the patency of bronchus and segment structure should be preserved. In addition, patients with borderline function should undergo imaging-based calculation of residual lung function, including ventilation or perfusion scintigraphy before pneumonectomy, or quantitative CT scan before either lobectomy or pneumonectomy.28 The BTS recommends the use of segment counting to estimate postoperative lung function as part of risk assessment for postoperative dyspnea. Ventilation or perfusion scintigraphy should be considered to predict postoperative lung function if a ventilation or perfusion mismatch is suspected. Quantitative CT or MRI may be considered to predict postoperative lung function if the facility is available.29
Predicting mortality and complications: FEV1 and Dlco
The predicted postoperative FEV1 value is an independent predictor of postoperative mortality and other complications. Although there is no absolute cut-off value, studies identify an increased risk of complications below predicted postoperative FEV1 values ranging from 30%37 to 40%.38,39 Predicted postoperative Dlco is another outcome measure that can independently identify increased mortality risk in lung cancer resection patients. Dlco less than 40% has been associated with increased risk of postoperative respiratory complications even in those with predicted postoperative FEV1 values above 40%.26,39 One study stated that a combination of the two values, predicted postoperative FEV1 and predicted postoperative Dlco—called the predicted postoperative product (PPP)—is the best predictor of surgical mortality.40 Another study examined the utility of a prediction rule for pulmonary complications after lung surgery using a point system in which points were assigned based on predicted postoperative Dlco (1 point for each 5% decrement below 100%) plus 2 points for preoperative chemotherapy.41 The risk of complications was 9% for those with scores less than 11, 14% for those with scores of 11 to 13, and 26% for those with scores greater than 13.
When surgery is considered, ACCP guidelines state an increased risk of perioperative mortality in those lung cancer patients with either a PPP less than 1,650, or a predicted postoperative FEV1 less than 30%.27 These patients should be counseled about nonstandard surgery and nonsurgical treatment options. The ERS guidelines consider a predicted postoperative FEV1 value less than 30% to be a high-risk threshold when assessing pulmonary reserve before surgery.28
EXERCISE TESTING
In general, standardized cardiopulmonary exercise testing using VO2 peak has been shown to predict postoperative complications, including perioperative and long-term morbidity and mortality.42,43 Lower values are associated with a greater risk of poor outcome. Peak VO2 may not add significantly to the risk stratification of patients who have both FEV1 and Dlco values greater than 80%.44
According to ACCP recommendations for exercise testing in patients who are being evaluated for surgery, either an FEV1 or Dlco less than 40% of predicted postoperative (PPO) indicates increased risk for perioperative death and cardiopulmonary complications with standard lung resection. Preoperative exercise testing is recommended for these patients.27 Maximal oxygen consumption (VO2 max) less than 10 mL/kg/min, or the combination of VO2 max less than 15 mL/kg/min with both FEV1 and Dlco less than 40% PPO, also indicates increased risk for death and complications; these patients should be counseled about nonstandard surgery or nonsurgical treatment options. Guidelines from the ERS recommend exercise testing for all patients undergoing lung cancer surgery who have FEV1 or Dlco less than 80% of normal values.28 The VO2 peak measured during incremental exercise on a treadmill or cycle should be regarded as the most important parameter.
Figure. Distance walked during a shuttle walking test is strongly related to maximal oxygen consumption (VO2 max).
Several studies have found that distance traveled during walking tests predicts postoperative complications and can be related to VO2 max (Figure).45 According to ACCP guidelines, lung cancer patients who are potential candidates for standard lung resection are at increased risk for perioperative death and cardiopulmonary complications if they walk less than 25 shuttles on 2 shuttle walk tests or less than 1 flight of stairs. These patients should be counseled about nonstandard surgery and nonsurgical treatment options.27
Conversely, ERS/ESTS guidelines state that the shuttle walk test distance underestimates exercise capacity at the lower range, and does not discriminate between patients with and without complications.28 These guidelines state that shuttle walk test distance should not be used alone to select patients for resection. It may be used as a screening test, since patients walking less than 400 m are likely to also have VO2 peak less than 15 mL/kg/min. A standardized symptom-limited stair climbing test can be a cost-effective screening method to identify those who need more sophisticated exercise tests in order to optimize their perioperative management. The 6-minute walk test is not recommended.
British Thoracic Society guidelines recommend the use of the shuttle walk test as a functional assessment in patients with moderate to high risk of postoperative dyspnea.29 A distance walk of more than 400 m is recommended as a cutoff for acceptable pulmonary function. These guidelines recommend against using pulmonary function and exercise tests as the sole surrogates for a quality of life evaluation.
ALGORITHMS FOR TESTING
The ACCP, ERS/ESTS, and BTS guidelines all include algorithms for the preoperative evaluation of candidates for lung cancer resection.27–29 The guidelines differ from each other in many ways, including when to obtain a Dlco and cardiopulmonary exercise test, and in some of the cutoff values for various pulmonary function measures. ACCP guidelines begin with spirometry testing, supporting lobectomy in patients with spirometry results above the cutoff value of FEV1 greater than 1.5 L and pneumonectomy in those with a cutoff value of FEV1 greater than 2 L, and greater than 80% of predicted, unless the patient has dyspnea or evidence of interstitial lung disease. Measurement of the Dlco is recommended for those who do not meet the FEV1 cutoffs, or in those with unexplained dyspnea or diffuse parenchymal disease on chest radiograph or CT.27
A systematic review and set of treatment recommendations for high-risk patients with stage I lung cancer, developed by the Thoracic Oncology Network of the ACCP and the Workforce on Evidence-Based Surgery of the Society of Thoracic Surgeons, currently under review, will provide additional guidance regarding the use of lung function testing to evaluate risk of morbidity and mortality. These guidelines note that FEV1, Dlco, and peak VO2 all predict morbidity and mortality following major lung resection. Assessment of FEV1 and Dlco, including calculation of the estimated postoperative value, is strongly recommended before resection. The predictive value of peak VO2 is strongest in patients with impaired FEV1 or Dlco, and assessment of peak VO2 before major lung resection is recommended for these patients.
INTERVENTIONS TO DECREASE PERIOPERATIVE RISK
The impact of smoking cessation on perioperative outcome has been a matter of considerable debate. One large study found that the incidence of postoperative complications was actually greater when patients stopped smoking within 8 weeks before cardiac surgery.46 However, a recent meta-analysis including lung resection patients found no relationship between smoking cessation in the weeks before surgery and worse clinical outcomes.47 When a shorter duration of smoking cessation is examined, thoracotomy studies note that patients who continue to smoke within 1 month of pneumonectomy are at increased risk of major pulmonary events.48,49 An examination of perioperative mortality or major complications using data from the Society of Thoracic Surgeons found that smoking cessation within 1 month preceding surgery did not significantly affect perioperative morbidity or mortality, whereas longer abstention from tobacco use was associated with better surgical outcomes.50 The ACCP recommends that all patients with lung cancer be counseled regarding smoking cessation.27 ERS/ESTS guidelines recommend smoking cessation for at least 2 to 4 weeks before surgery, since this may change perioperative smoking behavior and decrease the risk of postoperative complications.28 Pulmonary rehabiliatation in the perioperative period has been shown to improve measures of activity tolerance, allowing resection of marginal candidates, and improving functional outcomes after resection.51 The ERS/ESTS guidelines state that early pre- and postoperative rehabilitation may produce functional benefits in resectable lung cancer patients.28
SUMMARY AND CONCLUSIONS
Lung function testing helps predict the risk of postoperative mortality, perioperative complications, and long-term dyspnea for patients with lung cancer undergoing surgical resection. Predicted postoperative FEV1 and Dlco should be evaluated in most resection candidates. Exercise testing adds to standard lung function testing in those with borderline values, discordance between standard measures, or discordance between subjective and objective lung function. Algorithms for preoperative assessment have been developed by the ACCP, the ERS/ESTS, and the BTS, which differ somewhat in the order of testing and specific testing cutoff values. Smoking cessation and pulmonary rehabilitation can help to reduce perioperative and long-term risks.
References
Damhuis RA, Schütte PR. Resection rates and postoperative mortality in 7,899 patients with lung cancer. Eur Respir J1996; 9:7–10.
Little AG, Rusch VW, Bonner JA, et al. Patterns of surgical care of lung cancer patients. Ann Thorac Surg2005; 80:2051–2056.
Baser S, Shannon VR, Eapen GA, et al. Pulmonary dysfunction as a major cause of inoperability among patients with non-small-cell lung cancer. Clin Lung Cancer2006; 7:344–349.
Sobue T, Suzuki T, Matsuda M, Kuroishi T, Ikeda S, Naruke T. Survival for clinical stage I lung cancer not surgically treated: comparison between screen-detected and symptom-detected cases. The Japanese Lung Cancer Screening Research Group. Cancer1992; 69:685–692.
Motohiro A, Ueda H, Komatsu H, Yanai N, Mori T; National Chest Hospital Study Group for Lung Cancer. Prognosis of nonsurgically treated, clinical stage I lung cancer patients in Japan. Lung Cancer2002; 36:65–69.
Sato M, Saito Y, Endo C, et al. The natural history of radiographically occult bronchogenic squamous cell carcinoma: a retrospective study of overdiagnosis bias. Chest2004; 126:108–113.
Loewen GM, Watson D, Kohman L, et al. Preoperative exercise Vo2 measurement for lung resection candidates: results of Cancer and Leukemia Group B Protocol 9238. J Thorac Oncol2007; 2:619–625.
Allen MS, Darling GE, Pechet TT, et al. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg2006; 81:1013–1020.
Meguid RA, Brooke BS, Chang DC, Sherwood JT, Brock MV, Yang SC. Are surgical outcomes for lung cancer resections improved at teaching hospitals?Ann Thorac Surg2008; 85:1015–1025.
Memtsoudis SG, Besculides MC, Zellos L, Patil N, Rogers SO. Trends in lung surgery: United States 1988 to 2002. Chest2006; 130:1462–1470.
Kozower BD, Sheng S, O’Brien SM, et al. STS database risk models: predictors of mortality and major morbidity for lung cancer resection. Ann Thorac Surg2010; 90:875–883.
Falcoz PE, Conti M, Brouchet L, et al. The Thoracic Surgery Scoring System (Thoracoscore): risk model for in-hospital death in 15,183 patients requiring thoracic surgery [published online ahead of print January 9, 2007]. J Thorac Cardiovasc Surg2007; 133:325–332. doi: 10.1016/j.jtcvs.2006.09.020
Bolliger CT, Jordan P, Solèr M, et al. Pulmonary function and exercise capacity after lung resection. Eur Respir J1996; 9:415–421.
Nezu K, Kushibe K, Tojo T, Takahama M, Kitamura S. Recovery and limitation of exercise capacity after lung resection for lung cancer. Chest1998; 113:1511–1516.
Brunelli A, Xiumé F, Refai M, et al. Evaluation of expiratory volume, diffusion capacity, and exercise tolerance following major lung resection: a prospective follow-up analysis. Chest2007; 131:141–147.
Smulders SA, Smeenk FW, Janssen-Heijnen ML, Postmus PE. Actual and predicted postoperative changes in lung function after pneumonectomy: a retrospective analysis. Chest2004; 125:1735–1741.
Edwards JG, Duthie DJ, Waller DA. Lobar volume reduction surgery: a method of increasing the lung cancer resection rate in patients with emphysema. Thorax2001; 56:791–795.
Bobbio A, Chetta A, Carbognani P, et al. Changes in pulmonary function test and cardiopulmonary exercise capacity in COPD patients after lobar pulmonary resection [published online ahead of print September 6, 2005]. Eur J Cardiothorac Surg2005; 28:754–758. doi: 10.1016/j.ejcts.2005.08.001
Brunelli A, Refai M, Salati M, Xiumé F, Sabbatini A. Predicted versus observed FEV1 and Dlco after major lung resection: a prospective evaluation at different postoperative periods. Ann Thorac Surg2007; 83:1134–1139.
Boushy SF, Billig DM, North LB, Helgason AH. Clinical course related to preoperative and postoperative pulmonary function in patients with bronchogenic carcinoma. Chest1971; 59:383–391.
Wernly JA, DeMeester TR, Kirchner PT, Myerowitz PD, Oxford DE, Golomb HM. Clinical value of quantitative ventilation-perfusion lung scans in the surgical management of bronchogenic carcinoma. J Thorac Cardiovasc Surg1980; 80:535–543.
Wyser C, Stulz P, Solèr M, et al. Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am J Respir Crit Care Med1999; 159:1450–1456.
Bousamra M, Presberg KW, Chammas JH, et al. Early and late morbidity in patients undergoing pulmonary resection with low diffusion capacity. Ann Thorac Surg1996; 62:968–975.
Ferguson MK, Little L, Rizzo L, et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg1988; 96:894–900.
Brunelli A, Refai MA, Salati M, Sabbatini A, Morgan-Hughes NJ, Rocco G. Carbon monoxide lung diffusion capacity improves risk stratification in patients without airflow limitation: evidence for systematic measurement before lung resection [published online ahead of print February 14, 2006]. Eur J Cardiothorac Surg2006; 29:567–570. doi: 10.1016/j.ejcts.2006.01.014
Colice GL, Shafazand S, Griffin JP, Keenan R, Bolliger CT; American College of Chest Physicians. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidenced-based clinical practice guidelines (2nd edition). Chest2007; 132( suppl 3):161S–177S.
Brunelli A, Charloux A, Bolliger CT, et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J2009; 34:17–41.
Lim E, Baldwin D, Beckles M, et al. Guidelines on the radical management of patients with lung cancer. Thorax2010; 65( suppl 3):iii1–iii27.
Nakahara K, Monden Y, Ohno K, Miyoshi S, Maeda H, Kawashima Y. A method for predicting postoperative lung function and its relation to postoperative complications in patients with lung cancer. Ann Thorac Surg1985; 39:260–265.
Kristersson S, Lindell SE, Svanberg L. Prediction of pulmonary function loss due to pneumonectomy using 133 Xe-radiospirometry. Chest1972; 62:694–698.
Bria WF, Kanarek DJ, Kazemi H. Prediction of postoperative pulmonary function following thoracic operations: value of ventilation-perfusion scanning. J Thorac Cardiovasc Surg1983; 86:186–192.
Ali MK, Mountain CF, Ewer MS, Johnston D, Haynie TP. Predicting loss of pulmonary function after pulmonary resection for bronchogenic carcinoma. Chest1980; 77:337–342.
Corris PA, Ellis DA, Hawkins T, Gibson GJ. Use of radionuclide scanning in the preoperative estimation of pulmonary function after pneumonectomy. Thorax1987; 42:285–291.
Bolliger CT, Gückel C, Engel H, et al. Prediction of functional reserves after lung resection: comparison between quantitative computed tomography, scintigraphy, and anatomy. Respiration2002; 69:482–489.
Nakahara K, Ohno K, Hashimoto J, et al. Prediction of postoperative respiratory failure in patients undergoing lung resection for lung cancer. Ann Thorac Surg1988; 46:549–552.
Markos J, Mullan BP, Hillman DR, et al. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis1989; 139:902–910.
Ribas J, Diaz O, Barberà JA, et al. Invasive exercise testing in the evaluation of patients at high-risk for lung resection. Eur Respir J1998; 12:1429–1435.
Pierce RJ, Copland JM, Sharpe K, Barter CE. Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med1994; 150:947–955.
Amar D, Munoz D, Shi W, Zhang H, Thaler HT. A clinical prediction rule for pulmonary complications after thoracic surgery for primary lung cancer [published online ahead of print October 27, 2009]. Anesth Analg2010; 110:1343–1348. doi: 10.1213/ANE.0b013e3181bf5c99
Benzo R, Kelley GA, Recchi L, Hofman A, Sciurba F. Complications of lung resection and exercise capacity: a meta-analysis [published online ahead of print April 3, 2007]. Respir Med2007; 101:1790–1797. doi: 10.1016/j.rmed.2007.02.012
Jones LW, Eves ND, Kraus WE, et al. The lung cancer exercise training study: a randomized trial of aerobic training, resistance training, or both in postsurgical lung cancer patients: rationale and design. BMC Cancer2010; 10:155.
Larsen KR, Svendsen UG, Milman N, Brenøe J, Petersen BN. Exercise testing in the preoperative evaluation of patients with bronchogenic carcinoma. Eur Respir J1997; 10:1559–1565.
Singh SJ, Morgan MDL, Hardman AE, Rowe C, Bardsley PA. Comparison of oxygen uptake during a conventional treadmill test and the shuttle walking test in chronic airflow limitation. Eur Respir J1994; 7:2016–2020.
Warner MA, Divertie MB, Tinker JH. Preoperative cessation of smoking and pulmonary complications in coronary artery bypass patients. Anesthesiology1984; 60:380–383.
Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis [published online ahead of print March 14, 2011]. Arch Intern Med2011; 171:983–989. doi: 10.1001/archinternmed.2011.97
Vaporciyan AA, Merriman KW, Ece F, et al. Incidence of major pulmonary morbidity after pneumonectomy: association with timing of smoking cessation. Ann Thorac Surg2002; 73:420–426.
Barrera R, Shi W, Amar D, et al. Smoking and timing of cessation: impact on pulmonary complications after thoracotomy. Chest2005; 127:1977–1983.
Mason DP, Subramanian S, Nowicki ER, et al. Impact of smoking cessation before resection of lung cancer. A Society of Thoracic Surgeons General Thoracic Surgery Database study. Ann Thorac Surg2009; 88:362–371.
Cesario A, Ferri L, Galetta D, et al. Pre-operative pulmonary rehabilitation and surgery for lung cancer. Lung Cancer2007; 57:118–119.
References
Damhuis RA, Schütte PR. Resection rates and postoperative mortality in 7,899 patients with lung cancer. Eur Respir J1996; 9:7–10.
Little AG, Rusch VW, Bonner JA, et al. Patterns of surgical care of lung cancer patients. Ann Thorac Surg2005; 80:2051–2056.
Baser S, Shannon VR, Eapen GA, et al. Pulmonary dysfunction as a major cause of inoperability among patients with non-small-cell lung cancer. Clin Lung Cancer2006; 7:344–349.
Sobue T, Suzuki T, Matsuda M, Kuroishi T, Ikeda S, Naruke T. Survival for clinical stage I lung cancer not surgically treated: comparison between screen-detected and symptom-detected cases. The Japanese Lung Cancer Screening Research Group. Cancer1992; 69:685–692.
Motohiro A, Ueda H, Komatsu H, Yanai N, Mori T; National Chest Hospital Study Group for Lung Cancer. Prognosis of nonsurgically treated, clinical stage I lung cancer patients in Japan. Lung Cancer2002; 36:65–69.
Sato M, Saito Y, Endo C, et al. The natural history of radiographically occult bronchogenic squamous cell carcinoma: a retrospective study of overdiagnosis bias. Chest2004; 126:108–113.
Loewen GM, Watson D, Kohman L, et al. Preoperative exercise Vo2 measurement for lung resection candidates: results of Cancer and Leukemia Group B Protocol 9238. J Thorac Oncol2007; 2:619–625.
Allen MS, Darling GE, Pechet TT, et al. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg2006; 81:1013–1020.
Meguid RA, Brooke BS, Chang DC, Sherwood JT, Brock MV, Yang SC. Are surgical outcomes for lung cancer resections improved at teaching hospitals?Ann Thorac Surg2008; 85:1015–1025.
Memtsoudis SG, Besculides MC, Zellos L, Patil N, Rogers SO. Trends in lung surgery: United States 1988 to 2002. Chest2006; 130:1462–1470.
Kozower BD, Sheng S, O’Brien SM, et al. STS database risk models: predictors of mortality and major morbidity for lung cancer resection. Ann Thorac Surg2010; 90:875–883.
Falcoz PE, Conti M, Brouchet L, et al. The Thoracic Surgery Scoring System (Thoracoscore): risk model for in-hospital death in 15,183 patients requiring thoracic surgery [published online ahead of print January 9, 2007]. J Thorac Cardiovasc Surg2007; 133:325–332. doi: 10.1016/j.jtcvs.2006.09.020
Bolliger CT, Jordan P, Solèr M, et al. Pulmonary function and exercise capacity after lung resection. Eur Respir J1996; 9:415–421.
Nezu K, Kushibe K, Tojo T, Takahama M, Kitamura S. Recovery and limitation of exercise capacity after lung resection for lung cancer. Chest1998; 113:1511–1516.
Brunelli A, Xiumé F, Refai M, et al. Evaluation of expiratory volume, diffusion capacity, and exercise tolerance following major lung resection: a prospective follow-up analysis. Chest2007; 131:141–147.
Smulders SA, Smeenk FW, Janssen-Heijnen ML, Postmus PE. Actual and predicted postoperative changes in lung function after pneumonectomy: a retrospective analysis. Chest2004; 125:1735–1741.
Edwards JG, Duthie DJ, Waller DA. Lobar volume reduction surgery: a method of increasing the lung cancer resection rate in patients with emphysema. Thorax2001; 56:791–795.
Bobbio A, Chetta A, Carbognani P, et al. Changes in pulmonary function test and cardiopulmonary exercise capacity in COPD patients after lobar pulmonary resection [published online ahead of print September 6, 2005]. Eur J Cardiothorac Surg2005; 28:754–758. doi: 10.1016/j.ejcts.2005.08.001
Brunelli A, Refai M, Salati M, Xiumé F, Sabbatini A. Predicted versus observed FEV1 and Dlco after major lung resection: a prospective evaluation at different postoperative periods. Ann Thorac Surg2007; 83:1134–1139.
Boushy SF, Billig DM, North LB, Helgason AH. Clinical course related to preoperative and postoperative pulmonary function in patients with bronchogenic carcinoma. Chest1971; 59:383–391.
Wernly JA, DeMeester TR, Kirchner PT, Myerowitz PD, Oxford DE, Golomb HM. Clinical value of quantitative ventilation-perfusion lung scans in the surgical management of bronchogenic carcinoma. J Thorac Cardiovasc Surg1980; 80:535–543.
Wyser C, Stulz P, Solèr M, et al. Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am J Respir Crit Care Med1999; 159:1450–1456.
Bousamra M, Presberg KW, Chammas JH, et al. Early and late morbidity in patients undergoing pulmonary resection with low diffusion capacity. Ann Thorac Surg1996; 62:968–975.
Ferguson MK, Little L, Rizzo L, et al. Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg1988; 96:894–900.
Brunelli A, Refai MA, Salati M, Sabbatini A, Morgan-Hughes NJ, Rocco G. Carbon monoxide lung diffusion capacity improves risk stratification in patients without airflow limitation: evidence for systematic measurement before lung resection [published online ahead of print February 14, 2006]. Eur J Cardiothorac Surg2006; 29:567–570. doi: 10.1016/j.ejcts.2006.01.014
Colice GL, Shafazand S, Griffin JP, Keenan R, Bolliger CT; American College of Chest Physicians. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidenced-based clinical practice guidelines (2nd edition). Chest2007; 132( suppl 3):161S–177S.
Brunelli A, Charloux A, Bolliger CT, et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J2009; 34:17–41.
Lim E, Baldwin D, Beckles M, et al. Guidelines on the radical management of patients with lung cancer. Thorax2010; 65( suppl 3):iii1–iii27.
Nakahara K, Monden Y, Ohno K, Miyoshi S, Maeda H, Kawashima Y. A method for predicting postoperative lung function and its relation to postoperative complications in patients with lung cancer. Ann Thorac Surg1985; 39:260–265.
Kristersson S, Lindell SE, Svanberg L. Prediction of pulmonary function loss due to pneumonectomy using 133 Xe-radiospirometry. Chest1972; 62:694–698.
Bria WF, Kanarek DJ, Kazemi H. Prediction of postoperative pulmonary function following thoracic operations: value of ventilation-perfusion scanning. J Thorac Cardiovasc Surg1983; 86:186–192.
Ali MK, Mountain CF, Ewer MS, Johnston D, Haynie TP. Predicting loss of pulmonary function after pulmonary resection for bronchogenic carcinoma. Chest1980; 77:337–342.
Corris PA, Ellis DA, Hawkins T, Gibson GJ. Use of radionuclide scanning in the preoperative estimation of pulmonary function after pneumonectomy. Thorax1987; 42:285–291.
Bolliger CT, Gückel C, Engel H, et al. Prediction of functional reserves after lung resection: comparison between quantitative computed tomography, scintigraphy, and anatomy. Respiration2002; 69:482–489.
Nakahara K, Ohno K, Hashimoto J, et al. Prediction of postoperative respiratory failure in patients undergoing lung resection for lung cancer. Ann Thorac Surg1988; 46:549–552.
Markos J, Mullan BP, Hillman DR, et al. Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis1989; 139:902–910.
Ribas J, Diaz O, Barberà JA, et al. Invasive exercise testing in the evaluation of patients at high-risk for lung resection. Eur Respir J1998; 12:1429–1435.
Pierce RJ, Copland JM, Sharpe K, Barter CE. Preoperative risk evaluation for lung cancer resection: predicted postoperative product as a predictor of surgical mortality. Am J Respir Crit Care Med1994; 150:947–955.
Amar D, Munoz D, Shi W, Zhang H, Thaler HT. A clinical prediction rule for pulmonary complications after thoracic surgery for primary lung cancer [published online ahead of print October 27, 2009]. Anesth Analg2010; 110:1343–1348. doi: 10.1213/ANE.0b013e3181bf5c99
Benzo R, Kelley GA, Recchi L, Hofman A, Sciurba F. Complications of lung resection and exercise capacity: a meta-analysis [published online ahead of print April 3, 2007]. Respir Med2007; 101:1790–1797. doi: 10.1016/j.rmed.2007.02.012
Jones LW, Eves ND, Kraus WE, et al. The lung cancer exercise training study: a randomized trial of aerobic training, resistance training, or both in postsurgical lung cancer patients: rationale and design. BMC Cancer2010; 10:155.
Larsen KR, Svendsen UG, Milman N, Brenøe J, Petersen BN. Exercise testing in the preoperative evaluation of patients with bronchogenic carcinoma. Eur Respir J1997; 10:1559–1565.
Singh SJ, Morgan MDL, Hardman AE, Rowe C, Bardsley PA. Comparison of oxygen uptake during a conventional treadmill test and the shuttle walking test in chronic airflow limitation. Eur Respir J1994; 7:2016–2020.
Warner MA, Divertie MB, Tinker JH. Preoperative cessation of smoking and pulmonary complications in coronary artery bypass patients. Anesthesiology1984; 60:380–383.
Myers K, Hajek P, Hinds C, McRobbie H. Stopping smoking shortly before surgery and postoperative complications: a systematic review and meta-analysis [published online ahead of print March 14, 2011]. Arch Intern Med2011; 171:983–989. doi: 10.1001/archinternmed.2011.97
Vaporciyan AA, Merriman KW, Ece F, et al. Incidence of major pulmonary morbidity after pneumonectomy: association with timing of smoking cessation. Ann Thorac Surg2002; 73:420–426.
Barrera R, Shi W, Amar D, et al. Smoking and timing of cessation: impact on pulmonary complications after thoracotomy. Chest2005; 127:1977–1983.
Mason DP, Subramanian S, Nowicki ER, et al. Impact of smoking cessation before resection of lung cancer. A Society of Thoracic Surgeons General Thoracic Surgery Database study. Ann Thorac Surg2009; 88:362–371.
Cesario A, Ferri L, Galetta D, et al. Pre-operative pulmonary rehabilitation and surgery for lung cancer. Lung Cancer2007; 57:118–119.
In one, the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized controlled trial of chest radiography for lung cancer screening,1 researchers found that chest radiography was not an effective lung cancer screening tool. However, the National Lung Screening Trial (NLST)2 has transformed medicine by finding that screening with low-dose computed tomography (CT) reduced the lung cancer mortality rate (Table 1).
While the ability to screen for lung cancer is a major positive change, it also raises many thorny questions, such as who should be screened, how often should they be screened, and how should we respond when a nodule is detected.
To answer some of these questions, we will outline how Cleveland Clinic has structured its lung cancer screening program, and the rationale we used for making pragmatic patient-care decisions within this program. We will conclude with our thoughts about the potential evolution of lung cancer screening programs.
THE 40-YEAR QUEST FOR EFFECTIVE LUNG CANCER SCREENING
Lung cancer kills more people in the United States than the next four most lethal types of cancer combined.3 It is curable if found early in its course. Unfortunately, most people who develop lung cancer feel no symptoms when it is early in its course, and therefore it is too often diagnosed at a late stage. Treatment for late-stage lung cancer is effective, but it is rarely curative.
Screening refers to testing people at risk of developing a disease before its symptoms or signs have appeared. The goal of screening is to reduce the disease-specific mortality rate. For this to happen, the disease must be detectable in a preclinical form, and treatment must be more successful when applied early. Ideally, the screening test should pose little risk to the patient, be sensitive for detecting the disease early in its course, give few false-positive results, be acceptable to the patient, and be relatively inexpensive to the health system.
Over the past 4 decades, a large volume of research has been done in the hope of proving that conventional radiography or CT could be an effective screening test for lung cancer.4,5
Cohort studies (ie, in which all the patients were screened) of radiography or CT have shown a longer survival from the time of lung cancer diagnosis than would be expected without screening. These studies were not designed to prove a reduction in the lung cancer-specific mortality rate.
Controlled trials (in which half the patients received the screening and the other half did not) of chest radiography have been interpreted as not showing a reduction in lung cancer mortality rates, though debate about the interpretation of these trials persisted until this past year. Biases inherent in using duration of survival rather than the mortality rate as an end point have been suggested as the reason for the apparent benefit in survival without a reduction in the mortality rate.
Controlled trials of CT screening were started nearly a decade ago. Until 2011, the results of these trials were not mature enough to comment on.
THE PROSTATE, LUNG, COLORECTAL, AND OVARIAN TRIAL
The lung cancer screening portion of the PLCO trial aimed to determine the effect of screening chest radiography on lung cancer-specific mortality rates.1
In this trial, 154,901 people were randomized to undergo either posteroanterior chest radiography every year for 4 years or usual care, ie, no lung cancer screening. Participants were men and women age 55 to 74 with no history of prostate, lung, colorectal, or ovarian cancer. They did not need to be a smoker to participate. Those who had never smoked and who were randomized to the screening group received only 3 years of testing. All were followed for 13 years or until the conclusion of the study (8 years after the final participant was enrolled). About half were women, and nearly two-thirds were age 55 through 64. Only 10% were current smokers, while a full 45% had never smoked.
Results. Adherence to screening in the screening group ranged from 79% to 86.6% over the years of screening, and 11% of the usual-care group was estimated to have undergone screening chest radiography.
Cumulative lung cancer incidence rates were 201 per 100,000 person-years in the screening group and 192 in the usual-care group.
In the screening group, there were a total of 1,696 lung cancers during the entire study. Of these, 307 (18%) were detected by screening, 198 (12%) were interval cancers (diagnosed during the screening period but not by the screening test), and the remainder were diagnosed after the screening period during the years of follow-up. In the screening group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also in the screening group, the cancers detected by screening were more likely to be stage I (50%) than those not detected by screening.
The cumulative number of deaths from lung cancer was slightly but not significantly lower in the screening group from years 4 through 11. However, by the end of follow-up, the number of lung cancer deaths was equal between the groups (1,213 in the screening group vs 1,230 in the usual-care group). The cumulative overall mortality rate was also similar between the groups. For the subgroup who would have qualified for the NLST (see below), the lung cancer mortality rate was statistically similar between the two groups.
Comments. The results of the PLCO screening trial will be interpreted as the final word in lung cancer screening with standard chest radiography. The conclusion is that annual screening with chest radiography does not reduce lung cancer mortality rates and thus should not be performed in this context.
THE NATIONAL LUNG SCREENING TRIAL
The NLST aimed to determine if screening with low-dose chest CT could reduce lung cancer mortality rates.2
This controlled trial enrolled 53,454 people, who were randomized to undergo either low-dose chest CT or posteroanterior chest radiography at baseline and then yearly for 2 years.
Participants were men and women age 55 to 74 with at least 30 pack-years of cigarette smoking. If they had quit smoking, they had to have quit within the past 15 years. All were followed until study conclusion (median 6.5 years, maximum 7.4). About 41% were women, and nearly three-quarters were age 55 through 64. More than 48% were current smokers, with the rest being former smokers.
Results. Adherence to screening was 95% in the CT group and 93% in the radiography group, with a 4.3% annual rate of CT outside the study during the screening phase.
Cumulative lung cancer incidence rates were 645 per 100,000 person-years in the CT group and 572 in the radiography group.
In the CT group there were a total of 1,060 lung cancers during the entire study. Of these, 649 (61%) were detected by screening, 44 (4%) were interval cancers, and the rest were diagnosed after the screening period during follow-up.
In the chest radiography group, there were a total of 941 lung cancers during the entire study. Of these, 279 (30%) were detected by screening, 137 (15%) were interval cancers, and the rest were diagnosed after the screening period. Within the CT group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also within the CT group, the cancers detected by screening were more likely to be stage I (63%) than those not detected by screening.
The cumulative number of deaths from lung cancer was 443 in the radiography group, but only 356 in the CT group—20.0% lower (P =.004). The cumulative overall mortality rate was 6.7% lower in the CT group (P = .02).
Comments. The results of the NLST provide the first evidence that lung cancer mortality rates can be reduced by screening. Though many questions remain, the conclusions of this study are that screening a well-defined high-risk group with low-dose CT reduces the rate of death from lung cancer.
REMAINING CHALLENGES
The NLST showed that lung cancer screening with low-dose CT can meet the most important criterion for a successful screening program, ie, a reduction in the disease-specific mortality rate. Many challenges remain in meeting the other criteria for a successful or ideal screening program (low risk, few false-positive results, acceptability to the patient, and affordability). The issues with low-dose CT-based screening that challenge these ideals are outlined in this section.
Lung nodules: Benign or malignant?
Figure 1. Computed tomographic scan showing a small lung nodule (arrow). Although almost all small lung nodules are benign, there are no features to separate benign nodules from malignant ones.
Imaging-based lung cancer screening is designed to find lung nodules. CT has been more successful than radiography largely because it is more sensitive at finding lung nodules. Unfortunately, most lung nodules found by modern CT are not cancerous, but rather are benign. Distinguishing between a nodule that is an early malignancy and one that is benign remains challenging (Figure 1).
A meta-analysis of CT screening studies found that for every 1,000 people screened at baseline, 9 were found to have stage I non-small-cell lung cancer, 235 had false-positive nodules, and 4 underwent thoracotomy for benign lesions.6
The NLST results were similar. In this trial, only nodules that were 4 mm or greater in diameter were reported. Using these criteria, over 27% of all study participants were found to have a lung nodule on CT at baseline and at year 1. The rate fell to nearly 17% at year 2, as nodules present from baseline were not reported. Of all the lung nodules detected, only 3.6% were ultimately proven to represent lung cancer.2
Many issues with small lung nodules need to be considered. The nodules are difficult to find, with highly variable reporting even by expert radiologists.7 They are difficult to measure accurately and thus are difficult to assess for growth.8 Adjunctive imaging and nonsurgical biopsy have a low yield for small nodules.9–11 Follow-up of these lung nodules includes additional imaging and nonsurgical and surgical biopsy procedures, adding expense to the program and risk to the patient. Finally, knowing that they have a lung nodule makes patients feel anxious and thus negatively affects their quality of life.12,13
Radiation exposure: How great is the risk?
There is a great deal of concern about radiation exposure from medical imaging, as many people receive a substantial amount of radiation each year from medical testing.14 A single low-dose scan with chest CT delivers a whole-body effective dose of about 1.5 mSv—less than one-fifth of the radiation dose of a typical diagnostic CT scan.
Many have tried to estimate the consequences of radiation exposure from low-dose CT screening. All estimates are extrapolations from unrelated radiation exposures. The increase in risk of death ranged from 0.01% to a few percent,15 and the increase in cancers was as high as 1.8% over a 25-year screening period.16 In general, the risks are felt to be very low but not negligible.
Cost-effectiveness is unknown
The cost-effectiveness of lung cancer screening is also unknown. Many highly variable estimates have been published.17–20 The studies have differed in the perspective taken, the costs of testing assumed, and the rounds of screening included. The most cost-effective estimates are in populations with the highest risk of cancer, in programs that achieve the greatest reduction in mortality rate, and in programs that lead to high rates of smoking cessation.
Screening in the real world as opposed to a clinical trial may involve different risks, benefits, and costs. Compliance with screening and with nodule management algorithms may be lower outside of a study. One study suggested that those at highest risk of developing lung cancer would be the least likely to enroll in a screening program and the least likely to accept curative-intent surgery for screening-detected cancer.21
We expect that the NLST data will be analyzed for cost-effectiveness. This should provide the most accurate estimates for the group that was studied.
WE SET OUT TO DESIGN A SCREENING PROGRAM
With the evidence supporting a reduction in the rate of lung cancer mortality, and knowing the remaining challenges, we set out to provide a lung cancer screening program within Cleveland Clinic. In the design of our program, we considered several questions, outlined below.
Who should be offered low-dose CT screening?
The results of the NLST led to a great deal of excitement about lung cancer screening in both the medical community and the general public. The positive side of this publicity is that lung cancer is receiving attention that may lead to support for further advances. The negative side is that many patients who may seek out lung cancer screening are not at high enough risk of lung cancer to clearly benefit from it.
In the NLST, a very high-risk cohort was studied, as defined by clinical variables (age 55 to 74, at least 30 pack-years of smoking, and if a former smoker, had quit within the past 15 years). In this high-risk group, 320 patients needed to be screened (with three yearly chest CT scans) for one life to be saved from lung cancer, and only 3.6% of all lung nodules found (4 mm or larger) were actually lung cancer. In a group at lower risk, the number that needed to be screened to save one life would be higher, and the percentage of lung nodules that truly were lung cancer would be lower. This would lead to higher risks and costs related to screening, without a proven benefit to members of the lower-risk group.
The risk of the NLST cohort developing lung cancer was approximately 0.6% per year. Lung cancer risk-prediction models have been developed and published. Up to 2011, the three most commonly used models had only moderate accuracy at predicting risk.22–25 In 2011 a risk model based on the PLCO cohort was developed and published.26 This model seemed to be more accurate but perhaps a bit harder to apply in practice.
We discussed whether using a validated risk predictor with a target of 0.6% per year (ie, the risk in the NLST trial) would be an adequate means of deciding on candidacy for lung cancer screening or if we should strictly adhere to the inclusion criteria of the NLST cohort. We feel that the NLST cohort is the only group with true evidence of benefit (a reduction in the lung cancer-specific mortality rate). Thus, for our program’s entry criteria, we decided to use the same clinical predictors used for entry in the NLST.
How will the right patients get scheduled for low-dose screening CT?
Patients who enter the lung cancer screening program from our health system will require a physician’s order.
We are fortunate to have an electronic medical record in place. We have created an order set within the electronic record for low-dose chest CT. The order will eventually be able to be entered as “CT lung screening w/o” (ie, without contrast).
For patients from outside of our health system who would like to enter the lung cancer screening program, the entry criteria will be the same (see above). We will ask for the name of the patient’s primary care practitioner. If the patient does not have one, a member of our Respiratory Institute will see and enroll the patient.
How often should patients be screened, and for how many years?
Unfortunately, questions about the frequency of screening and how many years it should continue remain unanswered.
In the NLST, a similar number of early-stage lung cancers were detected during each of the three screening rounds. In both the NLST and PLCO trials, differences in the mortality rate curves began to narrow during the observation period, when active screening was no longer occurring. Thus, it is possible that a longer duration of screening could lead to a further reduction in mortality rates. Others have questioned whether a similar benefit, with less cost and risk, could be obtained by screening every 2 years.
The large amount of data obtained from the NLST and other CT-based studies is being reviewed so that models can be developed to help answer these questions. For now, we suggest at least three yearly CT screenings, with the hope that we will have clearer answers to these questions over time.
How will low-dose CT be performed and interpreted?
The parameters for low-dose CT were very tightly controlled and monitored during the NLST. This quality-control effort, designed to improve consistency across sites and to minimize risk to patients, should be carried into lung cancer screening programs.
Our program will closely mimic the CT performance criteria used in the NLST (tube current-time product 40 mAs for all patients, field of view lungs only, lung kernel images 3 mm at 1.5-mm intervals, and soft-tissue kernel images 5 mm at 2.5-mm intervals).27 In the initial phase of the program, all screening scans will be performed at Cleveland Clinic’s main imaging facility.
Small lung nodules remain quite challenging to detect and measure. To minimize variability in scan interpretation, the NLST readers were all expertly trained radiologists. Despite this, much variability was noted in the number of nodules detected, their measured size, and the follow-up recommendations. All of the screening CT images for our program will be interpreted by board-certified radiologists with expertise in chest imaging.
Other screening studies have included novel imaging assessment in their testing algorithms, particularly volumetric analysis of lung nodules.28 These tools may prove to assist in nodule detection, measurement, and management over time. At this point, we do not think they have been studied and standardized enough to include them in a standard-of-care screening program. We hope that they will evolve to the point of clinical utility in the near future.
Lung cancer screening is not currently covered by most insurers, including Medicare, although one major insurer has recently started to cover it. We expect decisions on coverage from other insurers in the next 12 months. In the meantime, we offer a low-dose screening chest CT to our patients for $125, which includes the radiologist’s fee for interpreting the scan.
Smoking cessation
The NLST showed that low-dose CT screening can reduce lung cancer mortality rates by 20% in a high-risk group. A 50-year-old active smoker who quits smoking reduces his or her risk of dying of lung cancer by more than 50%.29 Entry into a lung cancer screening program provides an opportunity for education and assistance with tobacco dependency.
At Cleveland Clinic, we have an active Tobacco Treatment Center within our Wellness Institute. All lung cancer screening participants who are identified as active smokers will be given a program brochure and will be offered a consult in the program.
What do we identify as a lung nodule, and how should they be managed?
Studies of CT-based screening have highlighted the tremendous number of lung nodules that are identified and the low likelihood of malignancy in those that are less than 1 cm in diameter. Many screening studies define a positive result as a lung nodule above a particular size. The NLST used 4 mm or greater as the cutoff. The lower the cutoff, the greater the number of nodules found, and the lower the overall likelihood of malignancy in the nodules.
Studies in which annual CT screening was the intervention are able to use size criteria in part because the study design ensures another CT will be performed 12 months later. Current nodule management guidelines suggest 12-month CT follow-up of incidentally discovered lung nodules, 4 mm or smaller, in at-risk patients.30 In a screening program, particularly one for which the patient must pay, the 12-month screening CT cannot be guaranteed. This makes it more difficult to ignore the smallest nodules identified on CT screening. Given this, we will be reporting all lung nodules identified, regardless of size on the initial screening.
Most studies of CT screening have reported any new nodule identified in subsequent screening rounds regardless of size. Though it is intuitive that a new nodule would have a high likelihood of malignancy in a high-risk cohort, malignancy rates have been reported to be as low as 1% for new nodules. As with the initial round of screening, we will report all new lung nodules identified in subsequent screening rounds.
All screening CT scans will be read and reported by board-certified radiologists with expertise in chest imaging. The report generated will be in a standard format and sent to the ordering physician (Table 2). The ordering physician will choose to manage the evaluation of any nodule that is detected or refer the patient to a specialty lung nodule clinic within the Respiratory Institute. A reminder of the availability of the lung nodule clinic will be present within the templated report. A consult to the lung nodule clinic is an order available within the electronic medical record.
The recommendations for the evaluation of lung nodules, both within the report and at the lung nodule clinic, are in keeping with currently available guidelines, such as those from the Fleischner Society30 and the American College of Chest Physicians.31 For incidentally discovered lung nodules in patients at high risk, the Fleischner Society recommendations are as follows30:
For nodules 4 mm or smaller, follow-up in 12 months; if no growth, then no further follow-up
For nodules 4 to 6 mm, follow-up at 6 to 12 months, then 18 to 24 months if no growth
For nodules 6 to 8 mm, follow-up at 3 to 6 months, then 9 to 12 months, then 24 months if no growth
For nodules 8 mm or larger, follow-up at 3, 9, and 24 months, or positron emission tomography, or biopsy, or both.
If the nodule is large enough or is deemed to be of high enough risk, adjuvant testing with diagnostic imaging, guided bronchoscopy, transthoracic needle aspiration, or minimally invasive resection will be offered. All patients with nodules believed to require biopsy will be discussed at our multidisciplinary lung cancer tumor board before biopsy.
How do we make practitioners and patients aware of the program and its indications, risks, and benefits?
Education will be the key to having lung cancer screening adopted as the standard of care, to lung cancer screening being provided within a well-designed and capable system, and to ensuring that patients have realistic expectations about screening. Articles such as this and grand rounds presentations within our health system will help provide education to our colleagues. Broader marketing campaigns will be considered in the future once demand and system capabilities are clearly identified. A patient information brochure will be provided at the time of the screening test (see the patient information sheet that accompanies this article).
How do we help to advance best practice?
As excited as we are that low-dose CT-based lung cancer screening has been proven to reduce lung cancer mortality rates, it is clear that there is a lot of room to improve the programs that are developed based on current data.
Advances in our ability to accurately predict an individual’s risk of developing lung cancer will allow us to offer screening to those it is most likely to benefit.
Advances in smoking cessation and chemoprevention will help to minimize the number of lung cancers that develop.
Advances in our ability to determine the nature of lung nodules will allow us to accelerate treatment of very early lung cancer while minimizing additional testing on benign nodules; advances in our ability to treat localized and advanced disease will improve the outcome for those identified as having lung cancer.
To help move the science of screening forward, we will develop a screening program registry that can be populated from the order set and the templated report. The registry can be used to ensure appropriate patient care, while studying relevant epidemiologic, quality, and cost-related questions.
We hope to assess novel imaging software capable of assisting with the detection and characterization of lung nodules.
We have an active biomarker development program to assess the ability of breath and blood-based biomarkers to identify those at risk of developing lung cancer; to assist with the management of screening-detected lung nodules; to assist with the diagnosis of early stage lung cancer; and to characterize the nature of the cancers identified. Accurate biomarkers could lead to further decreases in mortality rates while reducing the risks and costs of a screening program.
We have strong surgical, medical, and radiation oncology programs, actively pursuing advances in minimally invasive resection procedures and ablative and targeted therapies.
ENTERING A NEW ERA
We are entering a new era of lung cancer screening. The NLST has shown that lung cancer morality rates can be reduced through low-dose CT screening in a high-risk population. Many challenges remain, such as managing the nodules that are discovered, determining if the program is cost-effective, and minimizing radiation exposure. These need to be considered when designing a lung cancer screening program. Advances over time will help us optimize the programs that are developed.
References
Oken MM, Hocking WG, Kvale PA, et al; PLCO Project Team. Screening by chest radiograph and lung cancer mortality: the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized trial. JAMA2011; 306:1865–1873.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin2012; 62:10–29.
Mazzone PJ, Mekhail T. Lung cancer screening. Curr Oncol Rep2007; 9:265–274.
Mazzone PJ. Lung cancer screening: an update, discussion, and look ahead. Curr Oncol Rep2010; 12:226–234.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Gierada DS, Pilgram TK, Ford M, et al. Lung cancer: interobserver agreement on interpretation of pulmonary findings at low-dose CT screening. Radiology2008; 246:265–272.
Singh S, Pinsky P, Fineberg NS, et al. Evaluation of reader variability in the interpretation of follow-up CT scans at lung cancer screening. Radiology2011; 259:263–270.
Lindell RM, Hartman TE, Swensen SJ, et al. Lung cancer screening experience: a retrospective review of PET in 22 non-small cell lung carcinomas detected on screening chest CT in a high-risk population. AJR Am J Roentgenol2005; 185:126–131.
Baaklini WA, Reinoso MA, Gorin AB, Sharafkaneh A, Manian P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest2000; 117:1049–1054.
Kothary N, Lock L, Sze DY, Hofmann LV. Computed tomography-guided percutaneous needle biopsy of pulmonary nodules: impact of nodule size on diagnostic accuracy. Clin Lung Cancer2009; 10:360–363.
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON). Br J Cancer2010; 102:27–34.
Lemonnier I, Baumann C, Jolly D, et al. Solitary pulmonary nodules: consequences for patient quality of life. Qual Life Res2011; 20:101–109.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Buls N, de Mey J, Covens P, Stadnik T. Health screening with CT: prospective assessment of radiation dose and associated detriment. JBR-BTR2005; 88:12–16.
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Wisnivesky JP, Mushlin AI, Sicherman N, Henschke C. The cost-effectiveness of low-dose CT screening for lung cancer: preliminary results of baseline screening. Chest2003; 124:614–621.
Manser R, Dalton A, Carter R, Byrnes G, Elwood M, Campbell DA. Cost-effectiveness analysis of screening for lung cancer with low dose spiral CT (computed tomography) in the Australian setting. Lung Cancer2005; 48:171–185.
McMahon PM, Kong CY, Bouzan C, et al. Cost-effectiveness of computed tomography screening for lung cancer in the United States. J Thorac Oncol2011; 6:1841–1848.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. Thorax2007; 62:126–130.
Bach PB, Kattan MW, Thornquist MD, et al. Variations in lung cancer risk among smokers. J Natl Cancer Inst2003; 95:470–478.
Spitz MR, Hong WK, Amos CI, et al. A risk model for prediction of lung cancer. J Natl Cancer Inst2007; 99:715–726.
Cassidy A, Myles JP, van Tongeren M, et al. The LLP risk model: an individual risk prediction model for lung cancer. Br J Cancer2008; 98:270–276.
D’Amelio AM, Cassidy A, Asomaning K, et al. Comparison of discriminatory power and accuracy of three lung cancer risk models. Br J Cancer2010; 103:423–429.
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal And Ovarian Cancer Screening Trial models and validation. J Natl Cancer Inst2011; 103:1058–1068.
National Lung Screening Trial Research Team; Aberle DR, Berg CD, Black WC, et al. The National Lung Screening Trial: overview and study design. Radiology2011; 258:243–253.
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ2000; 321:323–329.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Gould MK, Fletcher J, Iannettoni MD, et al; American College of Chest Physicians. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest2007; 132(suppl 3):108S–130S.
In one, the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized controlled trial of chest radiography for lung cancer screening,1 researchers found that chest radiography was not an effective lung cancer screening tool. However, the National Lung Screening Trial (NLST)2 has transformed medicine by finding that screening with low-dose computed tomography (CT) reduced the lung cancer mortality rate (Table 1).
While the ability to screen for lung cancer is a major positive change, it also raises many thorny questions, such as who should be screened, how often should they be screened, and how should we respond when a nodule is detected.
To answer some of these questions, we will outline how Cleveland Clinic has structured its lung cancer screening program, and the rationale we used for making pragmatic patient-care decisions within this program. We will conclude with our thoughts about the potential evolution of lung cancer screening programs.
THE 40-YEAR QUEST FOR EFFECTIVE LUNG CANCER SCREENING
Lung cancer kills more people in the United States than the next four most lethal types of cancer combined.3 It is curable if found early in its course. Unfortunately, most people who develop lung cancer feel no symptoms when it is early in its course, and therefore it is too often diagnosed at a late stage. Treatment for late-stage lung cancer is effective, but it is rarely curative.
Screening refers to testing people at risk of developing a disease before its symptoms or signs have appeared. The goal of screening is to reduce the disease-specific mortality rate. For this to happen, the disease must be detectable in a preclinical form, and treatment must be more successful when applied early. Ideally, the screening test should pose little risk to the patient, be sensitive for detecting the disease early in its course, give few false-positive results, be acceptable to the patient, and be relatively inexpensive to the health system.
Over the past 4 decades, a large volume of research has been done in the hope of proving that conventional radiography or CT could be an effective screening test for lung cancer.4,5
Cohort studies (ie, in which all the patients were screened) of radiography or CT have shown a longer survival from the time of lung cancer diagnosis than would be expected without screening. These studies were not designed to prove a reduction in the lung cancer-specific mortality rate.
Controlled trials (in which half the patients received the screening and the other half did not) of chest radiography have been interpreted as not showing a reduction in lung cancer mortality rates, though debate about the interpretation of these trials persisted until this past year. Biases inherent in using duration of survival rather than the mortality rate as an end point have been suggested as the reason for the apparent benefit in survival without a reduction in the mortality rate.
Controlled trials of CT screening were started nearly a decade ago. Until 2011, the results of these trials were not mature enough to comment on.
THE PROSTATE, LUNG, COLORECTAL, AND OVARIAN TRIAL
The lung cancer screening portion of the PLCO trial aimed to determine the effect of screening chest radiography on lung cancer-specific mortality rates.1
In this trial, 154,901 people were randomized to undergo either posteroanterior chest radiography every year for 4 years or usual care, ie, no lung cancer screening. Participants were men and women age 55 to 74 with no history of prostate, lung, colorectal, or ovarian cancer. They did not need to be a smoker to participate. Those who had never smoked and who were randomized to the screening group received only 3 years of testing. All were followed for 13 years or until the conclusion of the study (8 years after the final participant was enrolled). About half were women, and nearly two-thirds were age 55 through 64. Only 10% were current smokers, while a full 45% had never smoked.
Results. Adherence to screening in the screening group ranged from 79% to 86.6% over the years of screening, and 11% of the usual-care group was estimated to have undergone screening chest radiography.
Cumulative lung cancer incidence rates were 201 per 100,000 person-years in the screening group and 192 in the usual-care group.
In the screening group, there were a total of 1,696 lung cancers during the entire study. Of these, 307 (18%) were detected by screening, 198 (12%) were interval cancers (diagnosed during the screening period but not by the screening test), and the remainder were diagnosed after the screening period during the years of follow-up. In the screening group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also in the screening group, the cancers detected by screening were more likely to be stage I (50%) than those not detected by screening.
The cumulative number of deaths from lung cancer was slightly but not significantly lower in the screening group from years 4 through 11. However, by the end of follow-up, the number of lung cancer deaths was equal between the groups (1,213 in the screening group vs 1,230 in the usual-care group). The cumulative overall mortality rate was also similar between the groups. For the subgroup who would have qualified for the NLST (see below), the lung cancer mortality rate was statistically similar between the two groups.
Comments. The results of the PLCO screening trial will be interpreted as the final word in lung cancer screening with standard chest radiography. The conclusion is that annual screening with chest radiography does not reduce lung cancer mortality rates and thus should not be performed in this context.
THE NATIONAL LUNG SCREENING TRIAL
The NLST aimed to determine if screening with low-dose chest CT could reduce lung cancer mortality rates.2
This controlled trial enrolled 53,454 people, who were randomized to undergo either low-dose chest CT or posteroanterior chest radiography at baseline and then yearly for 2 years.
Participants were men and women age 55 to 74 with at least 30 pack-years of cigarette smoking. If they had quit smoking, they had to have quit within the past 15 years. All were followed until study conclusion (median 6.5 years, maximum 7.4). About 41% were women, and nearly three-quarters were age 55 through 64. More than 48% were current smokers, with the rest being former smokers.
Results. Adherence to screening was 95% in the CT group and 93% in the radiography group, with a 4.3% annual rate of CT outside the study during the screening phase.
Cumulative lung cancer incidence rates were 645 per 100,000 person-years in the CT group and 572 in the radiography group.
In the CT group there were a total of 1,060 lung cancers during the entire study. Of these, 649 (61%) were detected by screening, 44 (4%) were interval cancers, and the rest were diagnosed after the screening period during follow-up.
In the chest radiography group, there were a total of 941 lung cancers during the entire study. Of these, 279 (30%) were detected by screening, 137 (15%) were interval cancers, and the rest were diagnosed after the screening period. Within the CT group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also within the CT group, the cancers detected by screening were more likely to be stage I (63%) than those not detected by screening.
The cumulative number of deaths from lung cancer was 443 in the radiography group, but only 356 in the CT group—20.0% lower (P =.004). The cumulative overall mortality rate was 6.7% lower in the CT group (P = .02).
Comments. The results of the NLST provide the first evidence that lung cancer mortality rates can be reduced by screening. Though many questions remain, the conclusions of this study are that screening a well-defined high-risk group with low-dose CT reduces the rate of death from lung cancer.
REMAINING CHALLENGES
The NLST showed that lung cancer screening with low-dose CT can meet the most important criterion for a successful screening program, ie, a reduction in the disease-specific mortality rate. Many challenges remain in meeting the other criteria for a successful or ideal screening program (low risk, few false-positive results, acceptability to the patient, and affordability). The issues with low-dose CT-based screening that challenge these ideals are outlined in this section.
Lung nodules: Benign or malignant?
Figure 1. Computed tomographic scan showing a small lung nodule (arrow). Although almost all small lung nodules are benign, there are no features to separate benign nodules from malignant ones.
Imaging-based lung cancer screening is designed to find lung nodules. CT has been more successful than radiography largely because it is more sensitive at finding lung nodules. Unfortunately, most lung nodules found by modern CT are not cancerous, but rather are benign. Distinguishing between a nodule that is an early malignancy and one that is benign remains challenging (Figure 1).
A meta-analysis of CT screening studies found that for every 1,000 people screened at baseline, 9 were found to have stage I non-small-cell lung cancer, 235 had false-positive nodules, and 4 underwent thoracotomy for benign lesions.6
The NLST results were similar. In this trial, only nodules that were 4 mm or greater in diameter were reported. Using these criteria, over 27% of all study participants were found to have a lung nodule on CT at baseline and at year 1. The rate fell to nearly 17% at year 2, as nodules present from baseline were not reported. Of all the lung nodules detected, only 3.6% were ultimately proven to represent lung cancer.2
Many issues with small lung nodules need to be considered. The nodules are difficult to find, with highly variable reporting even by expert radiologists.7 They are difficult to measure accurately and thus are difficult to assess for growth.8 Adjunctive imaging and nonsurgical biopsy have a low yield for small nodules.9–11 Follow-up of these lung nodules includes additional imaging and nonsurgical and surgical biopsy procedures, adding expense to the program and risk to the patient. Finally, knowing that they have a lung nodule makes patients feel anxious and thus negatively affects their quality of life.12,13
Radiation exposure: How great is the risk?
There is a great deal of concern about radiation exposure from medical imaging, as many people receive a substantial amount of radiation each year from medical testing.14 A single low-dose scan with chest CT delivers a whole-body effective dose of about 1.5 mSv—less than one-fifth of the radiation dose of a typical diagnostic CT scan.
Many have tried to estimate the consequences of radiation exposure from low-dose CT screening. All estimates are extrapolations from unrelated radiation exposures. The increase in risk of death ranged from 0.01% to a few percent,15 and the increase in cancers was as high as 1.8% over a 25-year screening period.16 In general, the risks are felt to be very low but not negligible.
Cost-effectiveness is unknown
The cost-effectiveness of lung cancer screening is also unknown. Many highly variable estimates have been published.17–20 The studies have differed in the perspective taken, the costs of testing assumed, and the rounds of screening included. The most cost-effective estimates are in populations with the highest risk of cancer, in programs that achieve the greatest reduction in mortality rate, and in programs that lead to high rates of smoking cessation.
Screening in the real world as opposed to a clinical trial may involve different risks, benefits, and costs. Compliance with screening and with nodule management algorithms may be lower outside of a study. One study suggested that those at highest risk of developing lung cancer would be the least likely to enroll in a screening program and the least likely to accept curative-intent surgery for screening-detected cancer.21
We expect that the NLST data will be analyzed for cost-effectiveness. This should provide the most accurate estimates for the group that was studied.
WE SET OUT TO DESIGN A SCREENING PROGRAM
With the evidence supporting a reduction in the rate of lung cancer mortality, and knowing the remaining challenges, we set out to provide a lung cancer screening program within Cleveland Clinic. In the design of our program, we considered several questions, outlined below.
Who should be offered low-dose CT screening?
The results of the NLST led to a great deal of excitement about lung cancer screening in both the medical community and the general public. The positive side of this publicity is that lung cancer is receiving attention that may lead to support for further advances. The negative side is that many patients who may seek out lung cancer screening are not at high enough risk of lung cancer to clearly benefit from it.
In the NLST, a very high-risk cohort was studied, as defined by clinical variables (age 55 to 74, at least 30 pack-years of smoking, and if a former smoker, had quit within the past 15 years). In this high-risk group, 320 patients needed to be screened (with three yearly chest CT scans) for one life to be saved from lung cancer, and only 3.6% of all lung nodules found (4 mm or larger) were actually lung cancer. In a group at lower risk, the number that needed to be screened to save one life would be higher, and the percentage of lung nodules that truly were lung cancer would be lower. This would lead to higher risks and costs related to screening, without a proven benefit to members of the lower-risk group.
The risk of the NLST cohort developing lung cancer was approximately 0.6% per year. Lung cancer risk-prediction models have been developed and published. Up to 2011, the three most commonly used models had only moderate accuracy at predicting risk.22–25 In 2011 a risk model based on the PLCO cohort was developed and published.26 This model seemed to be more accurate but perhaps a bit harder to apply in practice.
We discussed whether using a validated risk predictor with a target of 0.6% per year (ie, the risk in the NLST trial) would be an adequate means of deciding on candidacy for lung cancer screening or if we should strictly adhere to the inclusion criteria of the NLST cohort. We feel that the NLST cohort is the only group with true evidence of benefit (a reduction in the lung cancer-specific mortality rate). Thus, for our program’s entry criteria, we decided to use the same clinical predictors used for entry in the NLST.
How will the right patients get scheduled for low-dose screening CT?
Patients who enter the lung cancer screening program from our health system will require a physician’s order.
We are fortunate to have an electronic medical record in place. We have created an order set within the electronic record for low-dose chest CT. The order will eventually be able to be entered as “CT lung screening w/o” (ie, without contrast).
For patients from outside of our health system who would like to enter the lung cancer screening program, the entry criteria will be the same (see above). We will ask for the name of the patient’s primary care practitioner. If the patient does not have one, a member of our Respiratory Institute will see and enroll the patient.
How often should patients be screened, and for how many years?
Unfortunately, questions about the frequency of screening and how many years it should continue remain unanswered.
In the NLST, a similar number of early-stage lung cancers were detected during each of the three screening rounds. In both the NLST and PLCO trials, differences in the mortality rate curves began to narrow during the observation period, when active screening was no longer occurring. Thus, it is possible that a longer duration of screening could lead to a further reduction in mortality rates. Others have questioned whether a similar benefit, with less cost and risk, could be obtained by screening every 2 years.
The large amount of data obtained from the NLST and other CT-based studies is being reviewed so that models can be developed to help answer these questions. For now, we suggest at least three yearly CT screenings, with the hope that we will have clearer answers to these questions over time.
How will low-dose CT be performed and interpreted?
The parameters for low-dose CT were very tightly controlled and monitored during the NLST. This quality-control effort, designed to improve consistency across sites and to minimize risk to patients, should be carried into lung cancer screening programs.
Our program will closely mimic the CT performance criteria used in the NLST (tube current-time product 40 mAs for all patients, field of view lungs only, lung kernel images 3 mm at 1.5-mm intervals, and soft-tissue kernel images 5 mm at 2.5-mm intervals).27 In the initial phase of the program, all screening scans will be performed at Cleveland Clinic’s main imaging facility.
Small lung nodules remain quite challenging to detect and measure. To minimize variability in scan interpretation, the NLST readers were all expertly trained radiologists. Despite this, much variability was noted in the number of nodules detected, their measured size, and the follow-up recommendations. All of the screening CT images for our program will be interpreted by board-certified radiologists with expertise in chest imaging.
Other screening studies have included novel imaging assessment in their testing algorithms, particularly volumetric analysis of lung nodules.28 These tools may prove to assist in nodule detection, measurement, and management over time. At this point, we do not think they have been studied and standardized enough to include them in a standard-of-care screening program. We hope that they will evolve to the point of clinical utility in the near future.
Lung cancer screening is not currently covered by most insurers, including Medicare, although one major insurer has recently started to cover it. We expect decisions on coverage from other insurers in the next 12 months. In the meantime, we offer a low-dose screening chest CT to our patients for $125, which includes the radiologist’s fee for interpreting the scan.
Smoking cessation
The NLST showed that low-dose CT screening can reduce lung cancer mortality rates by 20% in a high-risk group. A 50-year-old active smoker who quits smoking reduces his or her risk of dying of lung cancer by more than 50%.29 Entry into a lung cancer screening program provides an opportunity for education and assistance with tobacco dependency.
At Cleveland Clinic, we have an active Tobacco Treatment Center within our Wellness Institute. All lung cancer screening participants who are identified as active smokers will be given a program brochure and will be offered a consult in the program.
What do we identify as a lung nodule, and how should they be managed?
Studies of CT-based screening have highlighted the tremendous number of lung nodules that are identified and the low likelihood of malignancy in those that are less than 1 cm in diameter. Many screening studies define a positive result as a lung nodule above a particular size. The NLST used 4 mm or greater as the cutoff. The lower the cutoff, the greater the number of nodules found, and the lower the overall likelihood of malignancy in the nodules.
Studies in which annual CT screening was the intervention are able to use size criteria in part because the study design ensures another CT will be performed 12 months later. Current nodule management guidelines suggest 12-month CT follow-up of incidentally discovered lung nodules, 4 mm or smaller, in at-risk patients.30 In a screening program, particularly one for which the patient must pay, the 12-month screening CT cannot be guaranteed. This makes it more difficult to ignore the smallest nodules identified on CT screening. Given this, we will be reporting all lung nodules identified, regardless of size on the initial screening.
Most studies of CT screening have reported any new nodule identified in subsequent screening rounds regardless of size. Though it is intuitive that a new nodule would have a high likelihood of malignancy in a high-risk cohort, malignancy rates have been reported to be as low as 1% for new nodules. As with the initial round of screening, we will report all new lung nodules identified in subsequent screening rounds.
All screening CT scans will be read and reported by board-certified radiologists with expertise in chest imaging. The report generated will be in a standard format and sent to the ordering physician (Table 2). The ordering physician will choose to manage the evaluation of any nodule that is detected or refer the patient to a specialty lung nodule clinic within the Respiratory Institute. A reminder of the availability of the lung nodule clinic will be present within the templated report. A consult to the lung nodule clinic is an order available within the electronic medical record.
The recommendations for the evaluation of lung nodules, both within the report and at the lung nodule clinic, are in keeping with currently available guidelines, such as those from the Fleischner Society30 and the American College of Chest Physicians.31 For incidentally discovered lung nodules in patients at high risk, the Fleischner Society recommendations are as follows30:
For nodules 4 mm or smaller, follow-up in 12 months; if no growth, then no further follow-up
For nodules 4 to 6 mm, follow-up at 6 to 12 months, then 18 to 24 months if no growth
For nodules 6 to 8 mm, follow-up at 3 to 6 months, then 9 to 12 months, then 24 months if no growth
For nodules 8 mm or larger, follow-up at 3, 9, and 24 months, or positron emission tomography, or biopsy, or both.
If the nodule is large enough or is deemed to be of high enough risk, adjuvant testing with diagnostic imaging, guided bronchoscopy, transthoracic needle aspiration, or minimally invasive resection will be offered. All patients with nodules believed to require biopsy will be discussed at our multidisciplinary lung cancer tumor board before biopsy.
How do we make practitioners and patients aware of the program and its indications, risks, and benefits?
Education will be the key to having lung cancer screening adopted as the standard of care, to lung cancer screening being provided within a well-designed and capable system, and to ensuring that patients have realistic expectations about screening. Articles such as this and grand rounds presentations within our health system will help provide education to our colleagues. Broader marketing campaigns will be considered in the future once demand and system capabilities are clearly identified. A patient information brochure will be provided at the time of the screening test (see the patient information sheet that accompanies this article).
How do we help to advance best practice?
As excited as we are that low-dose CT-based lung cancer screening has been proven to reduce lung cancer mortality rates, it is clear that there is a lot of room to improve the programs that are developed based on current data.
Advances in our ability to accurately predict an individual’s risk of developing lung cancer will allow us to offer screening to those it is most likely to benefit.
Advances in smoking cessation and chemoprevention will help to minimize the number of lung cancers that develop.
Advances in our ability to determine the nature of lung nodules will allow us to accelerate treatment of very early lung cancer while minimizing additional testing on benign nodules; advances in our ability to treat localized and advanced disease will improve the outcome for those identified as having lung cancer.
To help move the science of screening forward, we will develop a screening program registry that can be populated from the order set and the templated report. The registry can be used to ensure appropriate patient care, while studying relevant epidemiologic, quality, and cost-related questions.
We hope to assess novel imaging software capable of assisting with the detection and characterization of lung nodules.
We have an active biomarker development program to assess the ability of breath and blood-based biomarkers to identify those at risk of developing lung cancer; to assist with the management of screening-detected lung nodules; to assist with the diagnosis of early stage lung cancer; and to characterize the nature of the cancers identified. Accurate biomarkers could lead to further decreases in mortality rates while reducing the risks and costs of a screening program.
We have strong surgical, medical, and radiation oncology programs, actively pursuing advances in minimally invasive resection procedures and ablative and targeted therapies.
ENTERING A NEW ERA
We are entering a new era of lung cancer screening. The NLST has shown that lung cancer morality rates can be reduced through low-dose CT screening in a high-risk population. Many challenges remain, such as managing the nodules that are discovered, determining if the program is cost-effective, and minimizing radiation exposure. These need to be considered when designing a lung cancer screening program. Advances over time will help us optimize the programs that are developed.
In 2011, two papers were published that will shape the way we think about lung cancer screening for years to come.
In one, the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized controlled trial of chest radiography for lung cancer screening,1 researchers found that chest radiography was not an effective lung cancer screening tool. However, the National Lung Screening Trial (NLST)2 has transformed medicine by finding that screening with low-dose computed tomography (CT) reduced the lung cancer mortality rate (Table 1).
While the ability to screen for lung cancer is a major positive change, it also raises many thorny questions, such as who should be screened, how often should they be screened, and how should we respond when a nodule is detected.
To answer some of these questions, we will outline how Cleveland Clinic has structured its lung cancer screening program, and the rationale we used for making pragmatic patient-care decisions within this program. We will conclude with our thoughts about the potential evolution of lung cancer screening programs.
THE 40-YEAR QUEST FOR EFFECTIVE LUNG CANCER SCREENING
Lung cancer kills more people in the United States than the next four most lethal types of cancer combined.3 It is curable if found early in its course. Unfortunately, most people who develop lung cancer feel no symptoms when it is early in its course, and therefore it is too often diagnosed at a late stage. Treatment for late-stage lung cancer is effective, but it is rarely curative.
Screening refers to testing people at risk of developing a disease before its symptoms or signs have appeared. The goal of screening is to reduce the disease-specific mortality rate. For this to happen, the disease must be detectable in a preclinical form, and treatment must be more successful when applied early. Ideally, the screening test should pose little risk to the patient, be sensitive for detecting the disease early in its course, give few false-positive results, be acceptable to the patient, and be relatively inexpensive to the health system.
Over the past 4 decades, a large volume of research has been done in the hope of proving that conventional radiography or CT could be an effective screening test for lung cancer.4,5
Cohort studies (ie, in which all the patients were screened) of radiography or CT have shown a longer survival from the time of lung cancer diagnosis than would be expected without screening. These studies were not designed to prove a reduction in the lung cancer-specific mortality rate.
Controlled trials (in which half the patients received the screening and the other half did not) of chest radiography have been interpreted as not showing a reduction in lung cancer mortality rates, though debate about the interpretation of these trials persisted until this past year. Biases inherent in using duration of survival rather than the mortality rate as an end point have been suggested as the reason for the apparent benefit in survival without a reduction in the mortality rate.
Controlled trials of CT screening were started nearly a decade ago. Until 2011, the results of these trials were not mature enough to comment on.
THE PROSTATE, LUNG, COLORECTAL, AND OVARIAN TRIAL
The lung cancer screening portion of the PLCO trial aimed to determine the effect of screening chest radiography on lung cancer-specific mortality rates.1
In this trial, 154,901 people were randomized to undergo either posteroanterior chest radiography every year for 4 years or usual care, ie, no lung cancer screening. Participants were men and women age 55 to 74 with no history of prostate, lung, colorectal, or ovarian cancer. They did not need to be a smoker to participate. Those who had never smoked and who were randomized to the screening group received only 3 years of testing. All were followed for 13 years or until the conclusion of the study (8 years after the final participant was enrolled). About half were women, and nearly two-thirds were age 55 through 64. Only 10% were current smokers, while a full 45% had never smoked.
Results. Adherence to screening in the screening group ranged from 79% to 86.6% over the years of screening, and 11% of the usual-care group was estimated to have undergone screening chest radiography.
Cumulative lung cancer incidence rates were 201 per 100,000 person-years in the screening group and 192 in the usual-care group.
In the screening group, there were a total of 1,696 lung cancers during the entire study. Of these, 307 (18%) were detected by screening, 198 (12%) were interval cancers (diagnosed during the screening period but not by the screening test), and the remainder were diagnosed after the screening period during the years of follow-up. In the screening group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also in the screening group, the cancers detected by screening were more likely to be stage I (50%) than those not detected by screening.
The cumulative number of deaths from lung cancer was slightly but not significantly lower in the screening group from years 4 through 11. However, by the end of follow-up, the number of lung cancer deaths was equal between the groups (1,213 in the screening group vs 1,230 in the usual-care group). The cumulative overall mortality rate was also similar between the groups. For the subgroup who would have qualified for the NLST (see below), the lung cancer mortality rate was statistically similar between the two groups.
Comments. The results of the PLCO screening trial will be interpreted as the final word in lung cancer screening with standard chest radiography. The conclusion is that annual screening with chest radiography does not reduce lung cancer mortality rates and thus should not be performed in this context.
THE NATIONAL LUNG SCREENING TRIAL
The NLST aimed to determine if screening with low-dose chest CT could reduce lung cancer mortality rates.2
This controlled trial enrolled 53,454 people, who were randomized to undergo either low-dose chest CT or posteroanterior chest radiography at baseline and then yearly for 2 years.
Participants were men and women age 55 to 74 with at least 30 pack-years of cigarette smoking. If they had quit smoking, they had to have quit within the past 15 years. All were followed until study conclusion (median 6.5 years, maximum 7.4). About 41% were women, and nearly three-quarters were age 55 through 64. More than 48% were current smokers, with the rest being former smokers.
Results. Adherence to screening was 95% in the CT group and 93% in the radiography group, with a 4.3% annual rate of CT outside the study during the screening phase.
Cumulative lung cancer incidence rates were 645 per 100,000 person-years in the CT group and 572 in the radiography group.
In the CT group there were a total of 1,060 lung cancers during the entire study. Of these, 649 (61%) were detected by screening, 44 (4%) were interval cancers, and the rest were diagnosed after the screening period during follow-up.
In the chest radiography group, there were a total of 941 lung cancers during the entire study. Of these, 279 (30%) were detected by screening, 137 (15%) were interval cancers, and the rest were diagnosed after the screening period. Within the CT group, the cancers detected by screening were more likely to be adenocarcinomas and less likely to be small-cell carcinomas than those not detected by screening. Also within the CT group, the cancers detected by screening were more likely to be stage I (63%) than those not detected by screening.
The cumulative number of deaths from lung cancer was 443 in the radiography group, but only 356 in the CT group—20.0% lower (P =.004). The cumulative overall mortality rate was 6.7% lower in the CT group (P = .02).
Comments. The results of the NLST provide the first evidence that lung cancer mortality rates can be reduced by screening. Though many questions remain, the conclusions of this study are that screening a well-defined high-risk group with low-dose CT reduces the rate of death from lung cancer.
REMAINING CHALLENGES
The NLST showed that lung cancer screening with low-dose CT can meet the most important criterion for a successful screening program, ie, a reduction in the disease-specific mortality rate. Many challenges remain in meeting the other criteria for a successful or ideal screening program (low risk, few false-positive results, acceptability to the patient, and affordability). The issues with low-dose CT-based screening that challenge these ideals are outlined in this section.
Lung nodules: Benign or malignant?
Figure 1. Computed tomographic scan showing a small lung nodule (arrow). Although almost all small lung nodules are benign, there are no features to separate benign nodules from malignant ones.
Imaging-based lung cancer screening is designed to find lung nodules. CT has been more successful than radiography largely because it is more sensitive at finding lung nodules. Unfortunately, most lung nodules found by modern CT are not cancerous, but rather are benign. Distinguishing between a nodule that is an early malignancy and one that is benign remains challenging (Figure 1).
A meta-analysis of CT screening studies found that for every 1,000 people screened at baseline, 9 were found to have stage I non-small-cell lung cancer, 235 had false-positive nodules, and 4 underwent thoracotomy for benign lesions.6
The NLST results were similar. In this trial, only nodules that were 4 mm or greater in diameter were reported. Using these criteria, over 27% of all study participants were found to have a lung nodule on CT at baseline and at year 1. The rate fell to nearly 17% at year 2, as nodules present from baseline were not reported. Of all the lung nodules detected, only 3.6% were ultimately proven to represent lung cancer.2
Many issues with small lung nodules need to be considered. The nodules are difficult to find, with highly variable reporting even by expert radiologists.7 They are difficult to measure accurately and thus are difficult to assess for growth.8 Adjunctive imaging and nonsurgical biopsy have a low yield for small nodules.9–11 Follow-up of these lung nodules includes additional imaging and nonsurgical and surgical biopsy procedures, adding expense to the program and risk to the patient. Finally, knowing that they have a lung nodule makes patients feel anxious and thus negatively affects their quality of life.12,13
Radiation exposure: How great is the risk?
There is a great deal of concern about radiation exposure from medical imaging, as many people receive a substantial amount of radiation each year from medical testing.14 A single low-dose scan with chest CT delivers a whole-body effective dose of about 1.5 mSv—less than one-fifth of the radiation dose of a typical diagnostic CT scan.
Many have tried to estimate the consequences of radiation exposure from low-dose CT screening. All estimates are extrapolations from unrelated radiation exposures. The increase in risk of death ranged from 0.01% to a few percent,15 and the increase in cancers was as high as 1.8% over a 25-year screening period.16 In general, the risks are felt to be very low but not negligible.
Cost-effectiveness is unknown
The cost-effectiveness of lung cancer screening is also unknown. Many highly variable estimates have been published.17–20 The studies have differed in the perspective taken, the costs of testing assumed, and the rounds of screening included. The most cost-effective estimates are in populations with the highest risk of cancer, in programs that achieve the greatest reduction in mortality rate, and in programs that lead to high rates of smoking cessation.
Screening in the real world as opposed to a clinical trial may involve different risks, benefits, and costs. Compliance with screening and with nodule management algorithms may be lower outside of a study. One study suggested that those at highest risk of developing lung cancer would be the least likely to enroll in a screening program and the least likely to accept curative-intent surgery for screening-detected cancer.21
We expect that the NLST data will be analyzed for cost-effectiveness. This should provide the most accurate estimates for the group that was studied.
WE SET OUT TO DESIGN A SCREENING PROGRAM
With the evidence supporting a reduction in the rate of lung cancer mortality, and knowing the remaining challenges, we set out to provide a lung cancer screening program within Cleveland Clinic. In the design of our program, we considered several questions, outlined below.
Who should be offered low-dose CT screening?
The results of the NLST led to a great deal of excitement about lung cancer screening in both the medical community and the general public. The positive side of this publicity is that lung cancer is receiving attention that may lead to support for further advances. The negative side is that many patients who may seek out lung cancer screening are not at high enough risk of lung cancer to clearly benefit from it.
In the NLST, a very high-risk cohort was studied, as defined by clinical variables (age 55 to 74, at least 30 pack-years of smoking, and if a former smoker, had quit within the past 15 years). In this high-risk group, 320 patients needed to be screened (with three yearly chest CT scans) for one life to be saved from lung cancer, and only 3.6% of all lung nodules found (4 mm or larger) were actually lung cancer. In a group at lower risk, the number that needed to be screened to save one life would be higher, and the percentage of lung nodules that truly were lung cancer would be lower. This would lead to higher risks and costs related to screening, without a proven benefit to members of the lower-risk group.
The risk of the NLST cohort developing lung cancer was approximately 0.6% per year. Lung cancer risk-prediction models have been developed and published. Up to 2011, the three most commonly used models had only moderate accuracy at predicting risk.22–25 In 2011 a risk model based on the PLCO cohort was developed and published.26 This model seemed to be more accurate but perhaps a bit harder to apply in practice.
We discussed whether using a validated risk predictor with a target of 0.6% per year (ie, the risk in the NLST trial) would be an adequate means of deciding on candidacy for lung cancer screening or if we should strictly adhere to the inclusion criteria of the NLST cohort. We feel that the NLST cohort is the only group with true evidence of benefit (a reduction in the lung cancer-specific mortality rate). Thus, for our program’s entry criteria, we decided to use the same clinical predictors used for entry in the NLST.
How will the right patients get scheduled for low-dose screening CT?
Patients who enter the lung cancer screening program from our health system will require a physician’s order.
We are fortunate to have an electronic medical record in place. We have created an order set within the electronic record for low-dose chest CT. The order will eventually be able to be entered as “CT lung screening w/o” (ie, without contrast).
For patients from outside of our health system who would like to enter the lung cancer screening program, the entry criteria will be the same (see above). We will ask for the name of the patient’s primary care practitioner. If the patient does not have one, a member of our Respiratory Institute will see and enroll the patient.
How often should patients be screened, and for how many years?
Unfortunately, questions about the frequency of screening and how many years it should continue remain unanswered.
In the NLST, a similar number of early-stage lung cancers were detected during each of the three screening rounds. In both the NLST and PLCO trials, differences in the mortality rate curves began to narrow during the observation period, when active screening was no longer occurring. Thus, it is possible that a longer duration of screening could lead to a further reduction in mortality rates. Others have questioned whether a similar benefit, with less cost and risk, could be obtained by screening every 2 years.
The large amount of data obtained from the NLST and other CT-based studies is being reviewed so that models can be developed to help answer these questions. For now, we suggest at least three yearly CT screenings, with the hope that we will have clearer answers to these questions over time.
How will low-dose CT be performed and interpreted?
The parameters for low-dose CT were very tightly controlled and monitored during the NLST. This quality-control effort, designed to improve consistency across sites and to minimize risk to patients, should be carried into lung cancer screening programs.
Our program will closely mimic the CT performance criteria used in the NLST (tube current-time product 40 mAs for all patients, field of view lungs only, lung kernel images 3 mm at 1.5-mm intervals, and soft-tissue kernel images 5 mm at 2.5-mm intervals).27 In the initial phase of the program, all screening scans will be performed at Cleveland Clinic’s main imaging facility.
Small lung nodules remain quite challenging to detect and measure. To minimize variability in scan interpretation, the NLST readers were all expertly trained radiologists. Despite this, much variability was noted in the number of nodules detected, their measured size, and the follow-up recommendations. All of the screening CT images for our program will be interpreted by board-certified radiologists with expertise in chest imaging.
Other screening studies have included novel imaging assessment in their testing algorithms, particularly volumetric analysis of lung nodules.28 These tools may prove to assist in nodule detection, measurement, and management over time. At this point, we do not think they have been studied and standardized enough to include them in a standard-of-care screening program. We hope that they will evolve to the point of clinical utility in the near future.
Lung cancer screening is not currently covered by most insurers, including Medicare, although one major insurer has recently started to cover it. We expect decisions on coverage from other insurers in the next 12 months. In the meantime, we offer a low-dose screening chest CT to our patients for $125, which includes the radiologist’s fee for interpreting the scan.
Smoking cessation
The NLST showed that low-dose CT screening can reduce lung cancer mortality rates by 20% in a high-risk group. A 50-year-old active smoker who quits smoking reduces his or her risk of dying of lung cancer by more than 50%.29 Entry into a lung cancer screening program provides an opportunity for education and assistance with tobacco dependency.
At Cleveland Clinic, we have an active Tobacco Treatment Center within our Wellness Institute. All lung cancer screening participants who are identified as active smokers will be given a program brochure and will be offered a consult in the program.
What do we identify as a lung nodule, and how should they be managed?
Studies of CT-based screening have highlighted the tremendous number of lung nodules that are identified and the low likelihood of malignancy in those that are less than 1 cm in diameter. Many screening studies define a positive result as a lung nodule above a particular size. The NLST used 4 mm or greater as the cutoff. The lower the cutoff, the greater the number of nodules found, and the lower the overall likelihood of malignancy in the nodules.
Studies in which annual CT screening was the intervention are able to use size criteria in part because the study design ensures another CT will be performed 12 months later. Current nodule management guidelines suggest 12-month CT follow-up of incidentally discovered lung nodules, 4 mm or smaller, in at-risk patients.30 In a screening program, particularly one for which the patient must pay, the 12-month screening CT cannot be guaranteed. This makes it more difficult to ignore the smallest nodules identified on CT screening. Given this, we will be reporting all lung nodules identified, regardless of size on the initial screening.
Most studies of CT screening have reported any new nodule identified in subsequent screening rounds regardless of size. Though it is intuitive that a new nodule would have a high likelihood of malignancy in a high-risk cohort, malignancy rates have been reported to be as low as 1% for new nodules. As with the initial round of screening, we will report all new lung nodules identified in subsequent screening rounds.
All screening CT scans will be read and reported by board-certified radiologists with expertise in chest imaging. The report generated will be in a standard format and sent to the ordering physician (Table 2). The ordering physician will choose to manage the evaluation of any nodule that is detected or refer the patient to a specialty lung nodule clinic within the Respiratory Institute. A reminder of the availability of the lung nodule clinic will be present within the templated report. A consult to the lung nodule clinic is an order available within the electronic medical record.
The recommendations for the evaluation of lung nodules, both within the report and at the lung nodule clinic, are in keeping with currently available guidelines, such as those from the Fleischner Society30 and the American College of Chest Physicians.31 For incidentally discovered lung nodules in patients at high risk, the Fleischner Society recommendations are as follows30:
For nodules 4 mm or smaller, follow-up in 12 months; if no growth, then no further follow-up
For nodules 4 to 6 mm, follow-up at 6 to 12 months, then 18 to 24 months if no growth
For nodules 6 to 8 mm, follow-up at 3 to 6 months, then 9 to 12 months, then 24 months if no growth
For nodules 8 mm or larger, follow-up at 3, 9, and 24 months, or positron emission tomography, or biopsy, or both.
If the nodule is large enough or is deemed to be of high enough risk, adjuvant testing with diagnostic imaging, guided bronchoscopy, transthoracic needle aspiration, or minimally invasive resection will be offered. All patients with nodules believed to require biopsy will be discussed at our multidisciplinary lung cancer tumor board before biopsy.
How do we make practitioners and patients aware of the program and its indications, risks, and benefits?
Education will be the key to having lung cancer screening adopted as the standard of care, to lung cancer screening being provided within a well-designed and capable system, and to ensuring that patients have realistic expectations about screening. Articles such as this and grand rounds presentations within our health system will help provide education to our colleagues. Broader marketing campaigns will be considered in the future once demand and system capabilities are clearly identified. A patient information brochure will be provided at the time of the screening test (see the patient information sheet that accompanies this article).
How do we help to advance best practice?
As excited as we are that low-dose CT-based lung cancer screening has been proven to reduce lung cancer mortality rates, it is clear that there is a lot of room to improve the programs that are developed based on current data.
Advances in our ability to accurately predict an individual’s risk of developing lung cancer will allow us to offer screening to those it is most likely to benefit.
Advances in smoking cessation and chemoprevention will help to minimize the number of lung cancers that develop.
Advances in our ability to determine the nature of lung nodules will allow us to accelerate treatment of very early lung cancer while minimizing additional testing on benign nodules; advances in our ability to treat localized and advanced disease will improve the outcome for those identified as having lung cancer.
To help move the science of screening forward, we will develop a screening program registry that can be populated from the order set and the templated report. The registry can be used to ensure appropriate patient care, while studying relevant epidemiologic, quality, and cost-related questions.
We hope to assess novel imaging software capable of assisting with the detection and characterization of lung nodules.
We have an active biomarker development program to assess the ability of breath and blood-based biomarkers to identify those at risk of developing lung cancer; to assist with the management of screening-detected lung nodules; to assist with the diagnosis of early stage lung cancer; and to characterize the nature of the cancers identified. Accurate biomarkers could lead to further decreases in mortality rates while reducing the risks and costs of a screening program.
We have strong surgical, medical, and radiation oncology programs, actively pursuing advances in minimally invasive resection procedures and ablative and targeted therapies.
ENTERING A NEW ERA
We are entering a new era of lung cancer screening. The NLST has shown that lung cancer morality rates can be reduced through low-dose CT screening in a high-risk population. Many challenges remain, such as managing the nodules that are discovered, determining if the program is cost-effective, and minimizing radiation exposure. These need to be considered when designing a lung cancer screening program. Advances over time will help us optimize the programs that are developed.
References
Oken MM, Hocking WG, Kvale PA, et al; PLCO Project Team. Screening by chest radiograph and lung cancer mortality: the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized trial. JAMA2011; 306:1865–1873.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin2012; 62:10–29.
Mazzone PJ, Mekhail T. Lung cancer screening. Curr Oncol Rep2007; 9:265–274.
Mazzone PJ. Lung cancer screening: an update, discussion, and look ahead. Curr Oncol Rep2010; 12:226–234.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Gierada DS, Pilgram TK, Ford M, et al. Lung cancer: interobserver agreement on interpretation of pulmonary findings at low-dose CT screening. Radiology2008; 246:265–272.
Singh S, Pinsky P, Fineberg NS, et al. Evaluation of reader variability in the interpretation of follow-up CT scans at lung cancer screening. Radiology2011; 259:263–270.
Lindell RM, Hartman TE, Swensen SJ, et al. Lung cancer screening experience: a retrospective review of PET in 22 non-small cell lung carcinomas detected on screening chest CT in a high-risk population. AJR Am J Roentgenol2005; 185:126–131.
Baaklini WA, Reinoso MA, Gorin AB, Sharafkaneh A, Manian P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest2000; 117:1049–1054.
Kothary N, Lock L, Sze DY, Hofmann LV. Computed tomography-guided percutaneous needle biopsy of pulmonary nodules: impact of nodule size on diagnostic accuracy. Clin Lung Cancer2009; 10:360–363.
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON). Br J Cancer2010; 102:27–34.
Lemonnier I, Baumann C, Jolly D, et al. Solitary pulmonary nodules: consequences for patient quality of life. Qual Life Res2011; 20:101–109.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Buls N, de Mey J, Covens P, Stadnik T. Health screening with CT: prospective assessment of radiation dose and associated detriment. JBR-BTR2005; 88:12–16.
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Wisnivesky JP, Mushlin AI, Sicherman N, Henschke C. The cost-effectiveness of low-dose CT screening for lung cancer: preliminary results of baseline screening. Chest2003; 124:614–621.
Manser R, Dalton A, Carter R, Byrnes G, Elwood M, Campbell DA. Cost-effectiveness analysis of screening for lung cancer with low dose spiral CT (computed tomography) in the Australian setting. Lung Cancer2005; 48:171–185.
McMahon PM, Kong CY, Bouzan C, et al. Cost-effectiveness of computed tomography screening for lung cancer in the United States. J Thorac Oncol2011; 6:1841–1848.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. Thorax2007; 62:126–130.
Bach PB, Kattan MW, Thornquist MD, et al. Variations in lung cancer risk among smokers. J Natl Cancer Inst2003; 95:470–478.
Spitz MR, Hong WK, Amos CI, et al. A risk model for prediction of lung cancer. J Natl Cancer Inst2007; 99:715–726.
Cassidy A, Myles JP, van Tongeren M, et al. The LLP risk model: an individual risk prediction model for lung cancer. Br J Cancer2008; 98:270–276.
D’Amelio AM, Cassidy A, Asomaning K, et al. Comparison of discriminatory power and accuracy of three lung cancer risk models. Br J Cancer2010; 103:423–429.
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal And Ovarian Cancer Screening Trial models and validation. J Natl Cancer Inst2011; 103:1058–1068.
National Lung Screening Trial Research Team; Aberle DR, Berg CD, Black WC, et al. The National Lung Screening Trial: overview and study design. Radiology2011; 258:243–253.
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ2000; 321:323–329.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Gould MK, Fletcher J, Iannettoni MD, et al; American College of Chest Physicians. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest2007; 132(suppl 3):108S–130S.
References
Oken MM, Hocking WG, Kvale PA, et al; PLCO Project Team. Screening by chest radiograph and lung cancer mortality: the Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized trial. JAMA2011; 306:1865–1873.
National Lung Screening Trial Research Team; Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med2011; 365:395–409.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin2012; 62:10–29.
Mazzone PJ, Mekhail T. Lung cancer screening. Curr Oncol Rep2007; 9:265–274.
Mazzone PJ. Lung cancer screening: an update, discussion, and look ahead. Curr Oncol Rep2010; 12:226–234.
Gopal M, Abdullah SE, Grady JJ, Goodwin JS. Screening for lung cancer with low-dose computed tomography: a systematic review and meta-analysis of the baseline findings of randomized controlled trials. J Thorac Oncol2010; 5:1233–1239.
Gierada DS, Pilgram TK, Ford M, et al. Lung cancer: interobserver agreement on interpretation of pulmonary findings at low-dose CT screening. Radiology2008; 246:265–272.
Singh S, Pinsky P, Fineberg NS, et al. Evaluation of reader variability in the interpretation of follow-up CT scans at lung cancer screening. Radiology2011; 259:263–270.
Lindell RM, Hartman TE, Swensen SJ, et al. Lung cancer screening experience: a retrospective review of PET in 22 non-small cell lung carcinomas detected on screening chest CT in a high-risk population. AJR Am J Roentgenol2005; 185:126–131.
Baaklini WA, Reinoso MA, Gorin AB, Sharafkaneh A, Manian P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest2000; 117:1049–1054.
Kothary N, Lock L, Sze DY, Hofmann LV. Computed tomography-guided percutaneous needle biopsy of pulmonary nodules: impact of nodule size on diagnostic accuracy. Clin Lung Cancer2009; 10:360–363.
van den Bergh KA, Essink-Bot ML, Borsboom GJ, et al. Short-term health-related quality of life consequences in a lung cancer CT screening trial (NELSON). Br J Cancer2010; 102:27–34.
Lemonnier I, Baumann C, Jolly D, et al. Solitary pulmonary nodules: consequences for patient quality of life. Qual Life Res2011; 20:101–109.
Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med2009; 361:849–857.
Buls N, de Mey J, Covens P, Stadnik T. Health screening with CT: prospective assessment of radiation dose and associated detriment. JBR-BTR2005; 88:12–16.
Brenner DJ. Radiation risks potentially associated with low-dose CT screening of adult smokers for lung cancer. Radiology2004; 231:440–445.
Mahadevia PJ, Fleisher LA, Frick KD, Eng J, Goodman SN, Powe NR. Lung cancer screening with helical computed tomography in older adult smokers: a decision and cost-effectiveness analysis. JAMA2003; 289:313–322.
Wisnivesky JP, Mushlin AI, Sicherman N, Henschke C. The cost-effectiveness of low-dose CT screening for lung cancer: preliminary results of baseline screening. Chest2003; 124:614–621.
Manser R, Dalton A, Carter R, Byrnes G, Elwood M, Campbell DA. Cost-effectiveness analysis of screening for lung cancer with low dose spiral CT (computed tomography) in the Australian setting. Lung Cancer2005; 48:171–185.
McMahon PM, Kong CY, Bouzan C, et al. Cost-effectiveness of computed tomography screening for lung cancer in the United States. J Thorac Oncol2011; 6:1841–1848.
Silvestri GA, Nietert PJ, Zoller J, Carter C, Bradford D. Attitudes towards screening for lung cancer among smokers and their nonsmoking counterparts. Thorax2007; 62:126–130.
Bach PB, Kattan MW, Thornquist MD, et al. Variations in lung cancer risk among smokers. J Natl Cancer Inst2003; 95:470–478.
Spitz MR, Hong WK, Amos CI, et al. A risk model for prediction of lung cancer. J Natl Cancer Inst2007; 99:715–726.
Cassidy A, Myles JP, van Tongeren M, et al. The LLP risk model: an individual risk prediction model for lung cancer. Br J Cancer2008; 98:270–276.
D’Amelio AM, Cassidy A, Asomaning K, et al. Comparison of discriminatory power and accuracy of three lung cancer risk models. Br J Cancer2010; 103:423–429.
Tammemagi CM, Pinsky PF, Caporaso NE, et al. Lung cancer risk prediction: Prostate, Lung, Colorectal And Ovarian Cancer Screening Trial models and validation. J Natl Cancer Inst2011; 103:1058–1068.
National Lung Screening Trial Research Team; Aberle DR, Berg CD, Black WC, et al. The National Lung Screening Trial: overview and study design. Radiology2011; 258:243–253.
van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med2009; 361:2221–2229.
Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ2000; 321:323–329.
MacMahon H, Austin JH, Gamsu G, et al; Fleischner Society. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology2005; 237:395–400.
Gould MK, Fletcher J, Iannettoni MD, et al; American College of Chest Physicians. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest2007; 132(suppl 3):108S–130S.
The NLST documented a 20% reduction in the rate of death from lung cancer with low-dose CT screening compared with chest radiography screening (number needed to treat = 320). This was in a population at high risk (age 55–74 with a smoking history of at least 30 pack-years, at least some of it within the past 15 years).
CT screening detects many lung nodules, of which only a few (3.6% in the NLST) prove to be cancer.
In view of the positive results of the NLST, Cleveland Clinic has begun a lung cancer screening program, using the same entry criteria as those in the NLST.
Of possibly greater impact than detecting lung cancer will be the opportunity to promote smoking cessation.
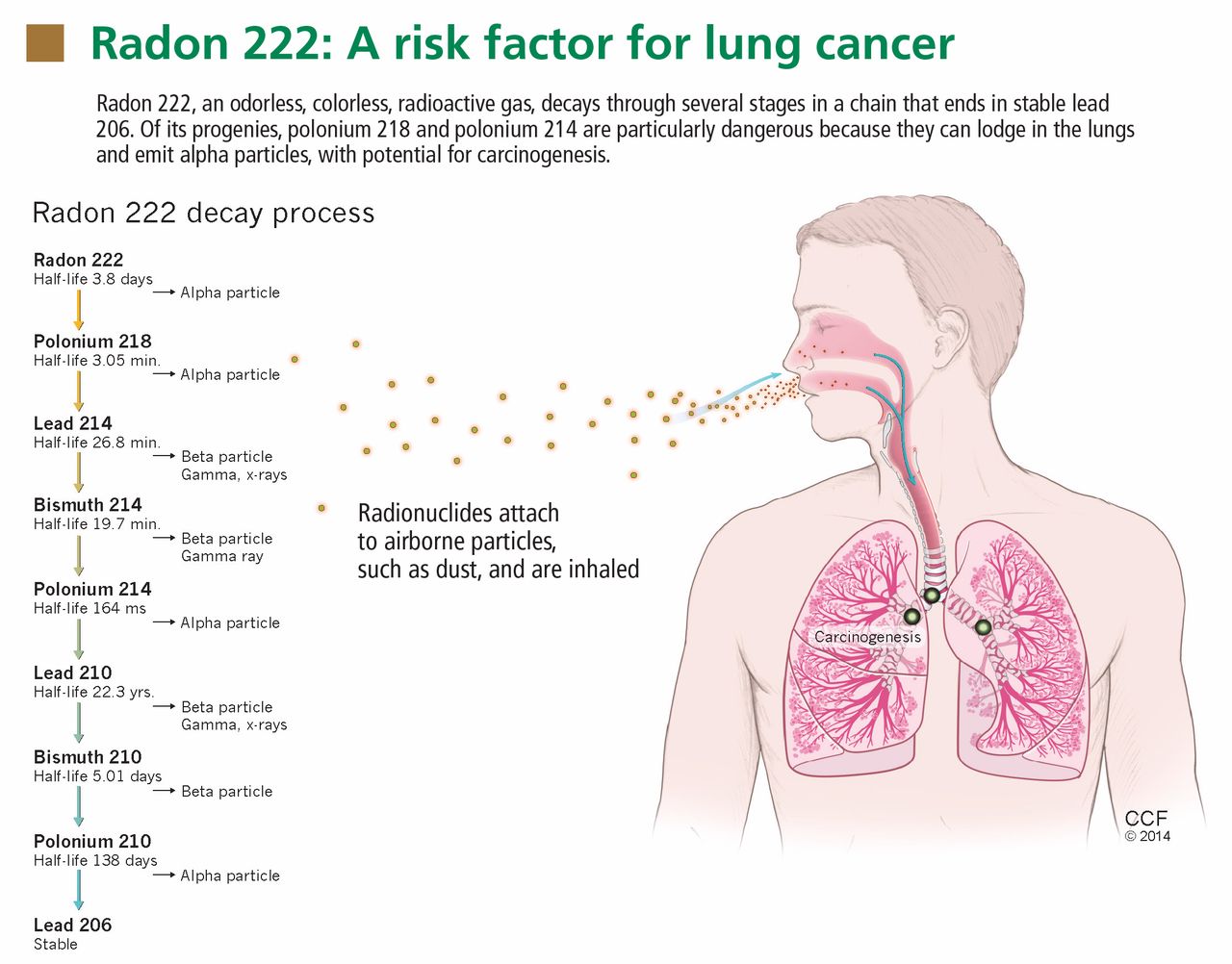
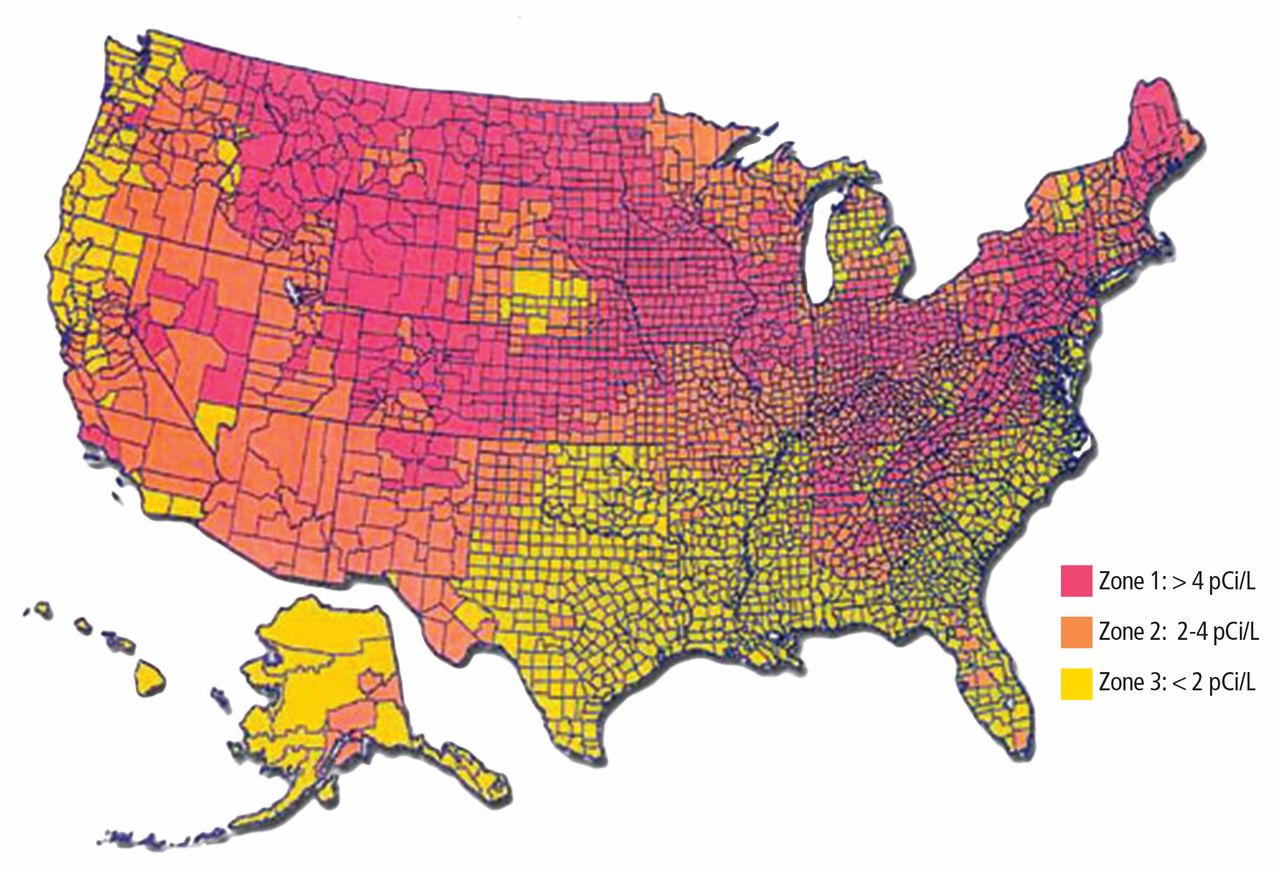
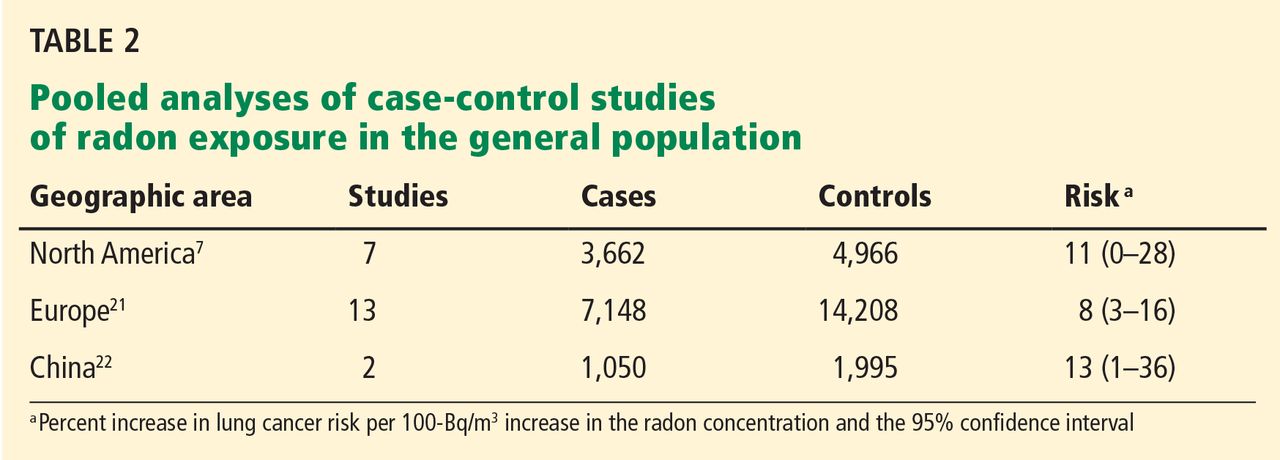
 Reprinted with permission from The New England Journal of Medicine (Patz EF, et al. Screening for lung cancer. N Engl J Med 2000; 343:1627–1633). Copyright © 2000 Massachusetts Medical Society. All rights reserved.
Reprinted with permission from The New England Journal of Medicine (Patz EF, et al. Screening for lung cancer. N Engl J Med 2000; 343:1627–1633). Copyright © 2000 Massachusetts Medical Society. All rights reserved. Reprinted with permission from The New England Journal of Medicine (Patz EF, et al. Screening for lung cancer. N Engl J Med 2000; 343:1627–1633). Copyright © 2000 Massachusetts Medical Society. All rights reserved.
Reprinted with permission from The New England Journal of Medicine (Patz EF, et al. Screening for lung cancer. N Engl J Med 2000; 343:1627–1633). Copyright © 2000 Massachusetts Medical Society. All rights reserved.