User login
Acute Upper Abdominal Pain in Early Pregnancy
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
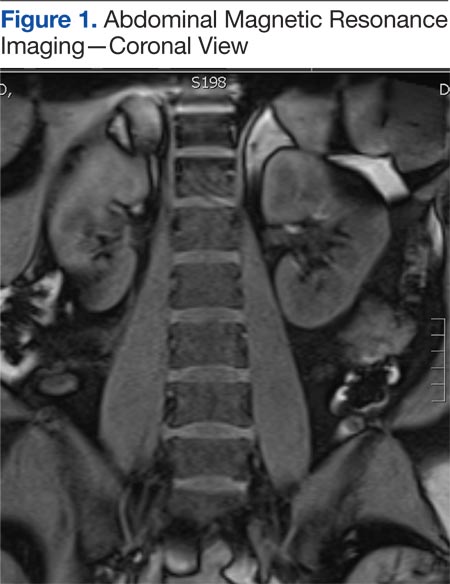
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
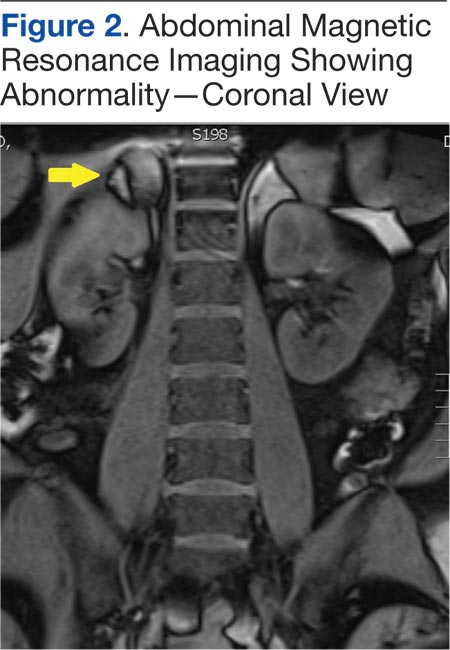
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
Discussion
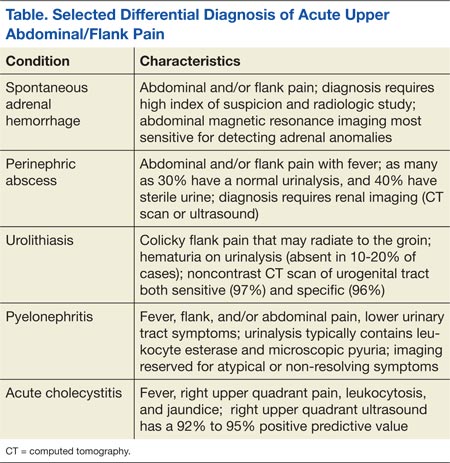
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
Discussion
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
A 32-year-old G1P0 woman at 7 4/7 weeks’ gestation (intrauterine pregnancy confirmed by ultrasound) with a history of hypertension and anxiety presented to the emergency department reporting right upper quadrant and right flank pain. The patient did not report taking any medications. Her symptoms had begun about 6 hours prior to presentation. She did not report fever, chills, nausea, vomiting, anorexia, or urinary or bowels symptoms. She was afebrile, and her initial blood pressure was 174/84 mm Hg, but within an hour of presentation had decreased to 137/82 mm Hg.
On exam she was in moderate-to-severe discomfort. She was tender to palpation in the right flank as well as the right upper quadrant and had a positive Murphy sign. Her white blood cell (WBC) count was 18,800/μL, hemoglobin and hematocrit were normal, liver function tests were within normal limits, and sodium was 133 mmol/L; otherwise, electrolytes were normal. The urinalysis showed a specific gravity of 1.022 with 3 red blood cells per high powered field, but was otherwise normal. A right upper quadrant ultrasound showed a normal gallbladder without cholelithiasis. Subsequently, a magnetic resonance imaging (MRI) of the abdomen was obtained (Figure 1).
- What is your diagnosis?
- How would you treat this patient?
[Click through to the next page to see the answer.]
Our Treatment
An MRI of the abdomen revealed a right adrenal hematoma (Figure 2). This diagnosis was made after common causes of the right upper quadrant and right flank pain were excluded and was confirmed with an MRI of the abdomen.
Discussion
Common causes of right flank and right upper quadrant pain include urolithiasis, pyelonephritis, and acute cholecystitis (Table). Patients with urolithiasis will typically present with sudden onset of colicky flank pain, which may radiate to the inguinal region, with or without nausea and vomiting.1,2 Microhematuria may be absent in as many as 10% to 20% of patients.2 Computed tomography is nearly 97% sensitive and 96% specific for urolithiasis.2 Although only 37% to 64% sensitive in detecting urolithiasis, abdominal ultrasound is 85% to 94% specific for detecting hydronephrosis.2
Symptoms of pyelonephritis range from mild to severe costovertebral angle pain with or without fever and/or lower urinary tract symptoms to sepsis.3 Urinalysis typically shows leukocyte esterase (72%-97% sensitive, 41%-86% specific for culture-confirmed urinary tract infection) and microscopic pyuria (90%-96% sensitive, 47%-50% specific for culture-confirmed urinary tract infection).3,4 Urine culture will reveal 105 colony-forming units in 95% of patients with acute uncomplicated pyelonephritis.3 Imaging is typically reserved for atypical presentations or in cases of nonresolution of symptoms despite treatment in order to rule out structural anomalies, an obstructive process, or abscess formation.3
Acute cholecystitis is suggested by right upper quadrant pain, often following a meal. Symptoms include fever, leukocytosis, and an elevated serum bilirubin level.5 Ultrasound findings of acute cholecystitis are gallbladder wall thickening, pericholecystic fluid, or sonographic Murphy sign.6 Ultrasound has a sensitivity of 81% and a specificity of 83% for detecting acute cholecystitis, whereas hepatobiliary iminodiacetic acid scan (cholescintigraphy) is 96% sensitive and 90% specific and is used in cases where ultrasound is indeterminate.6
Spontaneous adrenal hemorrhage (SAH) typically presents with symptoms of upper abdominal pain and/or flank pain. If hemorrhage is significant, hypotension and a drop in hematocrit may occur. Alternatively, if SAH is bilateral and results in a deficiency of adrenal hormones, hypotension may be secondary to adrenal insufficiency. Due to its ready availability, most SAHs are diagnosed by CT scan ordered for alternate reasons.7
In the pregnant patient, to avoid exposing the developing fetus to radiation, ultrasound is typically the first imaging modality to investigate right upper quadrant or flank pain. However, ultrasound is less sensitive for evaluating anomalies of the adrenal gland.8 An MRI is the most accurate imaging modality for diagnosing adrenal hemorrhage and avoids exposing the developing fetus to radiation.9 In this case, the absence of an etiology of the patient’s symptoms on right upper quadrant ultrasound led to further evaluation, with abdominal MRI revealing the diagnosis.
In a review of 141 cases of adrenal hemorrhage at the Mayo Clinic in Rochester, Minnesota, 16 patients had a spontaneous adrenal hemorrhage, which presented with severe abdominal and flank pain of sudden onset.7 Seven of these patients required surgery to control the bleeding.7 None of the 13 patients with a functioning contralateral adrenal gland required adrenal replacement therapy.7 Gavrilova-Jordan and colleagues reported a case of a spontaneous unilateral adrenal hemorrhage in the third trimester of pregnancy that was managed conservatively with favorable outcomes.10 Potential causes of spontaneous adrenal hemorrhage include:
• Antiphospholipid antibody syndrome
• Heparin-induced thrombocytopenia
• Trauma
• Physiologic stress (eg, sepsis)
• Adrenal mass (pheochromocytoma, angiomyolipoma, or metastatic cancer).6,11
Case Outcome
Initial right upper quadrant ultrasound in this patient revealed a normal gallbladder and a small amount of perinephric fluid surrounding the right kidney. On the night of admission she experienced an elevated temperature of 101.9°F. Due to the fever and leukocytosis, she was initiated on antibiotics (ampicillin-sulbactam 3 g IV every 6 hours) covering a urinary source. On hospital day 2, right lower quadrant and right upper quadrant ultrasounds were performed, revealing decreased fluid surrounding her right kidney and without evidence of appendicitis. Due to persistent leukocytosis (WBC count peaked at 26,400/μL), essentially normal urinalysis, and negative urine culture, an abdominal MRI was obtained to evaluate for a perinephric abscess. The MRI revealed the spontaneous adrenal hemorrhage.
The patient was observed as an inpatient for the following 48 hours. Her electrolytes remained normal and hemoglobin decreased to 9.5 g/dL. She remained hemodynamically stable. Serum cortisol and angiotensin levels were normal, antibiotics were discontinued, and the patient was discharged to outpatient follow-up.
A repeat MRI of the abdomen obtained 6 weeks later revealed a resolving right adrenal hematoma. At 39 weeks’ gestation, she delivered a vigorous female infant weighing 3,200 g (7 lb 1 oz) with an Apgar score at birth of 8/9.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
1. Wasserstein AG. Nephrolithiasis. Am J Kidney Dis. 2005;45(2):422-428.
2. Ban KM, Easter JS. Selected urologic problems. In: Marx JA, Hockberger RS, Walls, RM, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2010:1297-1324.
3. Colgan R, Williams M, Johnson JR. Diagnosis and treatment of acute pyelonephritis in women. Am Fam Physician. 2011;84(5):519-526.
4. Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A comprehensive review. Am Fam Physician. 2005;71(6):1153-1162.
5. Friedman LS. Liver, biliary tract & pancreas disorders. In: McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis and Treatment, 2012. 51st ed. New York, NY: Lange Medical Books/McGraw-Hill; 2012:644-698.
6. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708-720.
7. Vella A, Nippoldt TB, Morris JC 3rd. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76(2):161-168.
8. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4):949-963.
9. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-1651.
10. Gavrilova-Jordan L, Edmister WB, Farrell MA, Watson WJ. Spontaneous adrenal hemorrhage during pregnancy: A review of the literature and a case report of successful conservative management. Obstet Gynecol Surv. 2005;60(3):191-195.
11. Marti JL, Millet J, Sosa JA, Roman SA, Carling T, Udelsman R. Spontaneous adrenal hemorrhage with associated masses: Etiology and management in 6 cases and a review of 133 reported cases. World J Surg. 2012;36(1):75-82.
Intrauterine fetal demise: Care in the aftermath, and beyond
› Consider vaginal misoprostol for achieving delivery following intrauterine fetal demise (IUFD); it is as effective as other vaginal prostaglandin preparations and more effective than oral misoprostol. A
› Include in your postdelivery evaluation of IUFD autopsy, placental gross and histologic examination, fetal karyotype, and exam for fetomaternal hemorrhage. B
›Offer grieving parents early emotional support and counseling; research indicates it shortens the bereavement process. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Louise T, age 26, is pregnant with her first child. She attends all prenatal care visits with her health care team and appears to be doing well. However, at Ms. T’s 28-week visit, her physician is unable to detect a fetal heartbeat, or any movement of the fetus. He orders an ultrasound, which confirms his suspicions. Ms. T opts for immediate induction of labor. In his postdelivery evaluation, Ms. T’s physician does not determine a definitive cause for the intrauterine fetal demise.
Intrauterine fetal demise (IUFD) is fetal death that occurs after 20 weeks gestation but before birth.1 If the gestational age is unknown at the time of death, a fetus that weighs ≥350 g is considered an IUFD. In 2005, IUFD occurred at a rate of 6.22 per 1000 pregnancies, which amounted to 25,894 deaths.1
Family physicians who provide obstetric care are likely to care for women who have experienced an IUFD. This article describes what that care should include.
Keep these risk factors in mind
IUFD has been attributed to an extensive range of risk factors and possible causes, including various maternal medical conditions, obstetric complications, and pathologic fetal or placental conditions (TABLE 1).2-8 The 2 most common risk factors—obesity (body mass index [BMI] >30) and smoking—are modifiable and increase the odds of IUFD approximately three-fold.2 Though less common, 2 other notable risk factors are lupus and chronic renal disease; their impact on IUFD risk varies depending on the severity of the disease.2 However, keep in mind that these factors may not be causal and that most pregnant women with these conditions will deliver healthy infants.

Induce labor, or wait?
A woman experiencing an IUFD is likely to seek care when she notices that the fetus isn’t moving or when she experiences contractions, loss of fluid, or vaginal bleeding. Alternatively, she could be asymptomatic, and it may be the physician who suspects IUFD when he/she is unable to hear fetal heart tones. The diagnosis is confirmed by the absence of fetal cardiac activity on ultrasound; physicians may wish to obtain a second ultrasound for confirmation of the diagnosis.
Once IUFD is confirmed, most women choose to immediately undergo induction of labor. However, some elect to wait for spontaneous labor. Approximately 84% to 90% of women will go into spontaneous labor within 2 weeks of fetal death.9 Unless there is a compelling indication for immediate delivery (eg, coagulopathy, evidence of intrauterine infection, preeclampsia), expectant management may be permitted.
If a mother chooses expectant management, she should undergo periodic followup exams to assess for abdominal pain, fever, bleeding, bruising, labor, and emotional lability.10 Tell patients to seek immediate care if they develop a fever, abdominal pain, foul-smelling or purulent vaginal discharge, moderate bleeding, or bruising, or if they go into labor.
Vaginal prostaglandin effectively induces labor
Options for labor induction include oral or vaginal prostaglandins, continuous oxytocin infusion, or mechanical dilation (cervical placement of laminaria or a Foley bulb). Factors that affect which method to use include concomitant maternal illness, gestational age, Bishop score, or the presence of a uterine scar from a previous Cesarean section or other surgery. A Cochrane review found vaginal misoprostol was as effective as other vaginal prostaglandin preparations (E2 and F2-alpha) and more effective than oral misoprostol in achieving delivery for second- and third-trimester terminations and fetal deaths.11 Due to the risk of uterine rupture, most experts advise against use of misoprostol for a woman with a previously scarred uterus at >24 to 26 weeks gestation.10,12 In this circumstance, consider mechanical dilation followed by oxytocin infusion.
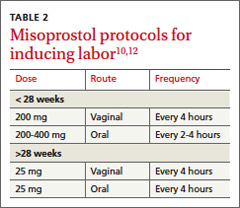
Beyond 28 weeks gestation, misoprostol can be used to induce labor by following the standard protocols utilized for term pregnancies (TABLE 2).10,12 Some patients may require additional doses of misoprostol to complete the third stage of labor. Pain can be managed via narcotic patient controlled analgesia, periodic use of intravenous narcotics, or continuous epidural.
A systematic approach to postdelivery evaluation
Although 25% to 60% of IUFDs are classified as “unexplained,” in up to 40% of cases the lack of explanation may be due to an incomplete evaluation.2-4 When performing an evaluation, it is important to be systematic and not confuse association with causality. Kortweg et al13 analyzed laboratory studies obtained in the evaluation of 1025 fetal deaths in the Netherlands from 2002 to 2008. The most useful tests were placental examination, fetal autopsy, and fetal karyotype, which aided in assigning the cause of death in 96%, 73%, and 29% of cases, respectively. Compared to fetal karyotyping from postpartum tissue sampling, samples obtained via amniocentesis or chorionic villus sampling before inducing labor are much more successful in identifying the cause of death (85% vs 28%).14
Testing for fetomaternal hemorrhage, which is the cause of IUFD about 12% of the time, needs to be performed when IUFD is diagnosed.13 Additional laboratory testing may be helpful depending on the mother’s history or symptoms at the time of IUFD. For example, a maternal history of drug use, thyroid disease, diabetes mellitus, hypertension, venous thromboembolism, or febrile illness should prompt further studies (TABLE 3).10,12-15
How to help grieving parents
Mothers may feel tremendous guilt upon suffering an IUFD. When addressing grief, mourning, and bereavement after an IUFD, the goal is to support the parents through the grieving process and properly identify when grief becomes pathologic. Grief is pathologic when there is a prolonged response—usually longer than 6 months—and when it interferes with daily activities.16 In a prospective study, patient characteristics that affected the intensity of grief were advanced gestational age at loss, lack of children in the home, relatively older age, pre-loss neurotic personality, and pre-loss psychiatric symptoms.17
Unlike the grief experienced by parents who lose an infant or child, the grief experienced by parents who experience an IUFD may not be socially validated. Therefore, it is important for physicians to acknowledge that patients’ feelings of loss are legitimate. Additionally, reassure mothers that there was very likely nothing that she could have done to change the outcome, unless there is compelling evidence to the contrary (eg, drug abuse causing abruption and fetal demise). Avoid using phrases such as “you can always try again.”
In a study of 769 women who experienced an IUFD, many reported receiving “support” or “great support” from family members (91.7%), nurses (90%), and physicians (53.4%).18 Adequate health care support is associated with lower levels of depression and anxiety, but family support appears to be the most important.18 Women who are single, divorced, or widowed experience higher levels of depression after IUFD than those who are married or cohabitating.18
In a different study of support for women who experienced IUFD or death of their child shortly after birth, mothers did not blame doctors or feel that the doctors should make them feel better.19 However, they did want an explanation in simple language of what had gone wrong and for physicians to listen and accept their distress.19 This study also found that early support and counseling shortened the bereavement process.19 Half of women had symptoms of depression and anxiety 6 months after the death of their fetus or child and 20% had these symptoms at 14 months. Fathers, however, recovered more quickly—14% were symptomatic at 6 months.19
Managing a subsequent therapy
A retrospective cohort study found that for women who had experienced an IUFD, the odds ratio of having a recurrent IUFD was 1.94 (99% confidence interval, 1.29-2.92) compared to women who had a previous live birth.20 The risk of recurrent IUFD in a specific patient is related to the underlying pathophysiologic cause of the initial IUFD, and how that cause was addressed. For example, a patient who experienced an IUFD believed to be the result of uncontrolled diabetes can expect to have an improved outcome if her diabetes is brought under control before conceiving and she maintains control throughout the pregnancy. On the contrary, a patient who experienced an IUFD that was believed to be secondary to a nonmodifiable risk factor, such as lupus-induced chronic kidney disease, will continue to have a significant risk of recurrence of IUFD in the subsequent pregnancy.
When managing a subsequent pregnancy of a woman who has experienced an IUFD, review all data from the prior pregnancy as well as the mother’s medical conditions. Order any studies in TABLE 3 that were not previously obtained and are clinically indicated. If applicable, encourage the woman to quite smoking and achieve a healthy BMI (<25).
In addition to routine obstetric care measures, these women should be offered antepartum fetal surveillance starting at 32 weeks gestation, or one to 2 weeks before the gestational age of the fetus at the time of the previous IUFD (whichever is earlier), as well as serial ultrasonography starting at 28 weeks to assess for fetal growth restriction.12,21 Most experts advise delivery at 39 weeks unless indicated earlier.12
Psychological risks. IUFD is associated with posttraumatic stress disorder (PTSD) and anxiety in a subsequent pregnancy.22,23 Approximately 21% of women in one study met criteria for PTSD in the third trimester of the first subsequent pregnancy; this decreased to 4% at one year postpartum.22 Risk factors for PTSD and anxiety were conceiving within one year of IUFD and a perceived lack of support at time of loss.22,23 Additionally, women who said they had poor partner support at the time of IUFD were more likely to have more severe PTSD symptoms, such as recurring, involuntary distressing memories of the IUFD, 6 to 8 years later.24 Because women who become pregnant after having an IUFD are likely to be anxious, physicians should be aware that there may be “false alarms” during the course of these pregnancies.
CASE › Two years after experiencing an IUFD , Ms. T becomes pregnant. Her physician carefully reviews her medical records and begins fetal surveillance at 26 weeks gestation, including serial ultrasounds. Ms. T’s pregnancy and labor proceed without complications, and at 38 weeks, she delivers a healthy 6.3-lb. boy.
CORRESPONDENCE
Richard Temple, MD, Naval Hospital Camp Lejeune Family Medicine Residency, 100 Brewster Blvd., Camp Lejeune, NC 28547; [email protected]
ACKNOWLEDGMENT
The authors thank Anthony Viera, MD for his assistance in the preparation of this manuscript.
1. MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep. 2009;57:1-19.
2. Goldstein DP, Johnson JP, Reid DE. Management of intrauterine fetal death. Obstet Gynecol. 1963;21:523-529.
3. Fretts RC. Etiology and prevention of stillbirth. Am J Obstet Gynecol. 2005;193:1923-1935.
4. Huang DY, Usher RH, Kramer MS, et al. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
5. Dudley DJ, Goldenberg R, Conway D, et al; Stillbirth Research Collaborative Network. A new system for determining the causes of stillbirth. Obstet Gynecol. 2010;116(2 pt 1):254-260.
6. Sims MA, Collins KA. Fetal death. A 10-year retrospective study. Am J Forensic Med Pathol. 2001;22:261-265.
7. Walsh CA, McMenamin MB, Foley ME, et al. Trends in intrapartum fetal death, 1979-2003. Am J Obstet Gynecol. 2008;198:47.e1-47.e7.
8. Smulian JC, Ananth CV, Vintzileos AM, et al. Fetal deaths in the United States. Influence of high-risk conditions and implications for management. Obstet Gynecol. 2002;100:1183-1189.
9. Silver RM. Fetal death. Obstet Gynecol. 2007;109:153-167.
10. Dodd JM, Crowther CA. Misoprostol for induction of labour to terminate pregnancy in the second or third trimester for women with a fetal anomaly or after intrauterine fetal death. Cochrane Database Syst Rev. 2010;(4):CD004901.
11. ACOG Practice Bulletin No. 102: management of stillbirth. Obstet Gynecol. 2009;113:748-761.
12. FrØen JF, Arnestad M, Frey K, et al. Risk factors for sudden intrauterine unexplained death: epidemiologic characteristics of singleton cases in Oslo, Norway, 1986-1995. Am J Obstet Gynecol. 2001;184:694-702.
13. Korteweg FJ, Erwich JJ, Timmer A, et al. Evaluation of 1025 fetal deaths: proposed diagnostic workup. Am J Obstet Gynecol. 2012;206:53.e1-53.e12.
14. Korteweg FJ, Bouman K, Erwich JJ, et al. Cytogenetic analysis after evaluation of 750 fetal deaths: proposal for diagnostic workup. Obstet Gynecol. 2008;111:865-874.
15. Silver RM, Varner MW, Reddy U, et al. Work-up of stillbirth: a review of the literature. Am J Obstet Gynecol. 2007;196:433-444.
16. Badenhorst W, Hughes P. Psychological aspects of perinatal loss. Best Pract Res Clin Obstet Gynaecol. 2007;21:249-259.
17. Janssen HJ, Cuisinier MC, de Graauw KP, et al. A prospective study of risk factors predicting grief intensity following pregnancy loss. Arch Gen Psychiatry. 1997;54:56-61.
18. Cacciatore J, Schnebly S, Froen JF. The effects of social support on maternal anxiety and depression after stillbirth. Health Soc Care Community. 2009;17:167-176.
19. Forrest GC, Standish E, Baum JD. Support after perinatal death: a study of support and counselling after perinatal bereavement. Br Med J (Clin Res Ed). 1982;285:1475-1479.
20. Bhattacharya S, Prescott GJ, Black M, et al. Recurrence risk of stillbirth in a second pregnancy. BJOG. 2010;117:1243-1247.
21. Reddy UM. Management of pregnancy after stillbirth. Clin Obstet Gynecol. 2010;53:700-709.
22. Turton P, Hughes P, Evans CD, et al. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry. 2001;178:556-560.
23. Hughes PM, Turton P, Evans CD. Stillbirth as risk factor for depression and anxiety in the subsequent pregnancy: cohort study. BMJ. 1999;318:1721-1724.
24. Turton P, Evans C, Hughes P. Long-term psychosocial sequelae of stillbirth: phase II of a nested case-control cohort study. Arch Womens Ment Health. 2009;12:35-41.
› Consider vaginal misoprostol for achieving delivery following intrauterine fetal demise (IUFD); it is as effective as other vaginal prostaglandin preparations and more effective than oral misoprostol. A
› Include in your postdelivery evaluation of IUFD autopsy, placental gross and histologic examination, fetal karyotype, and exam for fetomaternal hemorrhage. B
›Offer grieving parents early emotional support and counseling; research indicates it shortens the bereavement process. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Louise T, age 26, is pregnant with her first child. She attends all prenatal care visits with her health care team and appears to be doing well. However, at Ms. T’s 28-week visit, her physician is unable to detect a fetal heartbeat, or any movement of the fetus. He orders an ultrasound, which confirms his suspicions. Ms. T opts for immediate induction of labor. In his postdelivery evaluation, Ms. T’s physician does not determine a definitive cause for the intrauterine fetal demise.
Intrauterine fetal demise (IUFD) is fetal death that occurs after 20 weeks gestation but before birth.1 If the gestational age is unknown at the time of death, a fetus that weighs ≥350 g is considered an IUFD. In 2005, IUFD occurred at a rate of 6.22 per 1000 pregnancies, which amounted to 25,894 deaths.1
Family physicians who provide obstetric care are likely to care for women who have experienced an IUFD. This article describes what that care should include.
Keep these risk factors in mind
IUFD has been attributed to an extensive range of risk factors and possible causes, including various maternal medical conditions, obstetric complications, and pathologic fetal or placental conditions (TABLE 1).2-8 The 2 most common risk factors—obesity (body mass index [BMI] >30) and smoking—are modifiable and increase the odds of IUFD approximately three-fold.2 Though less common, 2 other notable risk factors are lupus and chronic renal disease; their impact on IUFD risk varies depending on the severity of the disease.2 However, keep in mind that these factors may not be causal and that most pregnant women with these conditions will deliver healthy infants.
Induce labor, or wait?
A woman experiencing an IUFD is likely to seek care when she notices that the fetus isn’t moving or when she experiences contractions, loss of fluid, or vaginal bleeding. Alternatively, she could be asymptomatic, and it may be the physician who suspects IUFD when he/she is unable to hear fetal heart tones. The diagnosis is confirmed by the absence of fetal cardiac activity on ultrasound; physicians may wish to obtain a second ultrasound for confirmation of the diagnosis.
Once IUFD is confirmed, most women choose to immediately undergo induction of labor. However, some elect to wait for spontaneous labor. Approximately 84% to 90% of women will go into spontaneous labor within 2 weeks of fetal death.9 Unless there is a compelling indication for immediate delivery (eg, coagulopathy, evidence of intrauterine infection, preeclampsia), expectant management may be permitted.
If a mother chooses expectant management, she should undergo periodic followup exams to assess for abdominal pain, fever, bleeding, bruising, labor, and emotional lability.10 Tell patients to seek immediate care if they develop a fever, abdominal pain, foul-smelling or purulent vaginal discharge, moderate bleeding, or bruising, or if they go into labor.
Vaginal prostaglandin effectively induces labor
Options for labor induction include oral or vaginal prostaglandins, continuous oxytocin infusion, or mechanical dilation (cervical placement of laminaria or a Foley bulb). Factors that affect which method to use include concomitant maternal illness, gestational age, Bishop score, or the presence of a uterine scar from a previous Cesarean section or other surgery. A Cochrane review found vaginal misoprostol was as effective as other vaginal prostaglandin preparations (E2 and F2-alpha) and more effective than oral misoprostol in achieving delivery for second- and third-trimester terminations and fetal deaths.11 Due to the risk of uterine rupture, most experts advise against use of misoprostol for a woman with a previously scarred uterus at >24 to 26 weeks gestation.10,12 In this circumstance, consider mechanical dilation followed by oxytocin infusion.
Beyond 28 weeks gestation, misoprostol can be used to induce labor by following the standard protocols utilized for term pregnancies (TABLE 2).10,12 Some patients may require additional doses of misoprostol to complete the third stage of labor. Pain can be managed via narcotic patient controlled analgesia, periodic use of intravenous narcotics, or continuous epidural.
A systematic approach to postdelivery evaluation
Although 25% to 60% of IUFDs are classified as “unexplained,” in up to 40% of cases the lack of explanation may be due to an incomplete evaluation.2-4 When performing an evaluation, it is important to be systematic and not confuse association with causality. Kortweg et al13 analyzed laboratory studies obtained in the evaluation of 1025 fetal deaths in the Netherlands from 2002 to 2008. The most useful tests were placental examination, fetal autopsy, and fetal karyotype, which aided in assigning the cause of death in 96%, 73%, and 29% of cases, respectively. Compared to fetal karyotyping from postpartum tissue sampling, samples obtained via amniocentesis or chorionic villus sampling before inducing labor are much more successful in identifying the cause of death (85% vs 28%).14
Testing for fetomaternal hemorrhage, which is the cause of IUFD about 12% of the time, needs to be performed when IUFD is diagnosed.13 Additional laboratory testing may be helpful depending on the mother’s history or symptoms at the time of IUFD. For example, a maternal history of drug use, thyroid disease, diabetes mellitus, hypertension, venous thromboembolism, or febrile illness should prompt further studies (TABLE 3).10,12-15
How to help grieving parents
Mothers may feel tremendous guilt upon suffering an IUFD. When addressing grief, mourning, and bereavement after an IUFD, the goal is to support the parents through the grieving process and properly identify when grief becomes pathologic. Grief is pathologic when there is a prolonged response—usually longer than 6 months—and when it interferes with daily activities.16 In a prospective study, patient characteristics that affected the intensity of grief were advanced gestational age at loss, lack of children in the home, relatively older age, pre-loss neurotic personality, and pre-loss psychiatric symptoms.17
Unlike the grief experienced by parents who lose an infant or child, the grief experienced by parents who experience an IUFD may not be socially validated. Therefore, it is important for physicians to acknowledge that patients’ feelings of loss are legitimate. Additionally, reassure mothers that there was very likely nothing that she could have done to change the outcome, unless there is compelling evidence to the contrary (eg, drug abuse causing abruption and fetal demise). Avoid using phrases such as “you can always try again.”
In a study of 769 women who experienced an IUFD, many reported receiving “support” or “great support” from family members (91.7%), nurses (90%), and physicians (53.4%).18 Adequate health care support is associated with lower levels of depression and anxiety, but family support appears to be the most important.18 Women who are single, divorced, or widowed experience higher levels of depression after IUFD than those who are married or cohabitating.18
In a different study of support for women who experienced IUFD or death of their child shortly after birth, mothers did not blame doctors or feel that the doctors should make them feel better.19 However, they did want an explanation in simple language of what had gone wrong and for physicians to listen and accept their distress.19 This study also found that early support and counseling shortened the bereavement process.19 Half of women had symptoms of depression and anxiety 6 months after the death of their fetus or child and 20% had these symptoms at 14 months. Fathers, however, recovered more quickly—14% were symptomatic at 6 months.19
Managing a subsequent therapy
A retrospective cohort study found that for women who had experienced an IUFD, the odds ratio of having a recurrent IUFD was 1.94 (99% confidence interval, 1.29-2.92) compared to women who had a previous live birth.20 The risk of recurrent IUFD in a specific patient is related to the underlying pathophysiologic cause of the initial IUFD, and how that cause was addressed. For example, a patient who experienced an IUFD believed to be the result of uncontrolled diabetes can expect to have an improved outcome if her diabetes is brought under control before conceiving and she maintains control throughout the pregnancy. On the contrary, a patient who experienced an IUFD that was believed to be secondary to a nonmodifiable risk factor, such as lupus-induced chronic kidney disease, will continue to have a significant risk of recurrence of IUFD in the subsequent pregnancy.
When managing a subsequent pregnancy of a woman who has experienced an IUFD, review all data from the prior pregnancy as well as the mother’s medical conditions. Order any studies in TABLE 3 that were not previously obtained and are clinically indicated. If applicable, encourage the woman to quite smoking and achieve a healthy BMI (<25).
In addition to routine obstetric care measures, these women should be offered antepartum fetal surveillance starting at 32 weeks gestation, or one to 2 weeks before the gestational age of the fetus at the time of the previous IUFD (whichever is earlier), as well as serial ultrasonography starting at 28 weeks to assess for fetal growth restriction.12,21 Most experts advise delivery at 39 weeks unless indicated earlier.12
Psychological risks. IUFD is associated with posttraumatic stress disorder (PTSD) and anxiety in a subsequent pregnancy.22,23 Approximately 21% of women in one study met criteria for PTSD in the third trimester of the first subsequent pregnancy; this decreased to 4% at one year postpartum.22 Risk factors for PTSD and anxiety were conceiving within one year of IUFD and a perceived lack of support at time of loss.22,23 Additionally, women who said they had poor partner support at the time of IUFD were more likely to have more severe PTSD symptoms, such as recurring, involuntary distressing memories of the IUFD, 6 to 8 years later.24 Because women who become pregnant after having an IUFD are likely to be anxious, physicians should be aware that there may be “false alarms” during the course of these pregnancies.
CASE › Two years after experiencing an IUFD , Ms. T becomes pregnant. Her physician carefully reviews her medical records and begins fetal surveillance at 26 weeks gestation, including serial ultrasounds. Ms. T’s pregnancy and labor proceed without complications, and at 38 weeks, she delivers a healthy 6.3-lb. boy.
CORRESPONDENCE
Richard Temple, MD, Naval Hospital Camp Lejeune Family Medicine Residency, 100 Brewster Blvd., Camp Lejeune, NC 28547; [email protected]
ACKNOWLEDGMENT
The authors thank Anthony Viera, MD for his assistance in the preparation of this manuscript.
› Consider vaginal misoprostol for achieving delivery following intrauterine fetal demise (IUFD); it is as effective as other vaginal prostaglandin preparations and more effective than oral misoprostol. A
› Include in your postdelivery evaluation of IUFD autopsy, placental gross and histologic examination, fetal karyotype, and exam for fetomaternal hemorrhage. B
›Offer grieving parents early emotional support and counseling; research indicates it shortens the bereavement process. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Louise T, age 26, is pregnant with her first child. She attends all prenatal care visits with her health care team and appears to be doing well. However, at Ms. T’s 28-week visit, her physician is unable to detect a fetal heartbeat, or any movement of the fetus. He orders an ultrasound, which confirms his suspicions. Ms. T opts for immediate induction of labor. In his postdelivery evaluation, Ms. T’s physician does not determine a definitive cause for the intrauterine fetal demise.
Intrauterine fetal demise (IUFD) is fetal death that occurs after 20 weeks gestation but before birth.1 If the gestational age is unknown at the time of death, a fetus that weighs ≥350 g is considered an IUFD. In 2005, IUFD occurred at a rate of 6.22 per 1000 pregnancies, which amounted to 25,894 deaths.1
Family physicians who provide obstetric care are likely to care for women who have experienced an IUFD. This article describes what that care should include.
Keep these risk factors in mind
IUFD has been attributed to an extensive range of risk factors and possible causes, including various maternal medical conditions, obstetric complications, and pathologic fetal or placental conditions (TABLE 1).2-8 The 2 most common risk factors—obesity (body mass index [BMI] >30) and smoking—are modifiable and increase the odds of IUFD approximately three-fold.2 Though less common, 2 other notable risk factors are lupus and chronic renal disease; their impact on IUFD risk varies depending on the severity of the disease.2 However, keep in mind that these factors may not be causal and that most pregnant women with these conditions will deliver healthy infants.
Induce labor, or wait?
A woman experiencing an IUFD is likely to seek care when she notices that the fetus isn’t moving or when she experiences contractions, loss of fluid, or vaginal bleeding. Alternatively, she could be asymptomatic, and it may be the physician who suspects IUFD when he/she is unable to hear fetal heart tones. The diagnosis is confirmed by the absence of fetal cardiac activity on ultrasound; physicians may wish to obtain a second ultrasound for confirmation of the diagnosis.
Once IUFD is confirmed, most women choose to immediately undergo induction of labor. However, some elect to wait for spontaneous labor. Approximately 84% to 90% of women will go into spontaneous labor within 2 weeks of fetal death.9 Unless there is a compelling indication for immediate delivery (eg, coagulopathy, evidence of intrauterine infection, preeclampsia), expectant management may be permitted.
If a mother chooses expectant management, she should undergo periodic followup exams to assess for abdominal pain, fever, bleeding, bruising, labor, and emotional lability.10 Tell patients to seek immediate care if they develop a fever, abdominal pain, foul-smelling or purulent vaginal discharge, moderate bleeding, or bruising, or if they go into labor.
Vaginal prostaglandin effectively induces labor
Options for labor induction include oral or vaginal prostaglandins, continuous oxytocin infusion, or mechanical dilation (cervical placement of laminaria or a Foley bulb). Factors that affect which method to use include concomitant maternal illness, gestational age, Bishop score, or the presence of a uterine scar from a previous Cesarean section or other surgery. A Cochrane review found vaginal misoprostol was as effective as other vaginal prostaglandin preparations (E2 and F2-alpha) and more effective than oral misoprostol in achieving delivery for second- and third-trimester terminations and fetal deaths.11 Due to the risk of uterine rupture, most experts advise against use of misoprostol for a woman with a previously scarred uterus at >24 to 26 weeks gestation.10,12 In this circumstance, consider mechanical dilation followed by oxytocin infusion.
Beyond 28 weeks gestation, misoprostol can be used to induce labor by following the standard protocols utilized for term pregnancies (TABLE 2).10,12 Some patients may require additional doses of misoprostol to complete the third stage of labor. Pain can be managed via narcotic patient controlled analgesia, periodic use of intravenous narcotics, or continuous epidural.
A systematic approach to postdelivery evaluation
Although 25% to 60% of IUFDs are classified as “unexplained,” in up to 40% of cases the lack of explanation may be due to an incomplete evaluation.2-4 When performing an evaluation, it is important to be systematic and not confuse association with causality. Kortweg et al13 analyzed laboratory studies obtained in the evaluation of 1025 fetal deaths in the Netherlands from 2002 to 2008. The most useful tests were placental examination, fetal autopsy, and fetal karyotype, which aided in assigning the cause of death in 96%, 73%, and 29% of cases, respectively. Compared to fetal karyotyping from postpartum tissue sampling, samples obtained via amniocentesis or chorionic villus sampling before inducing labor are much more successful in identifying the cause of death (85% vs 28%).14
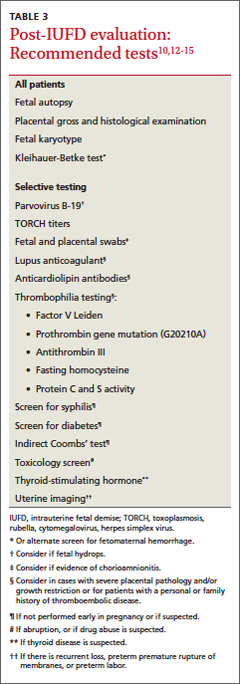
Testing for fetomaternal hemorrhage, which is the cause of IUFD about 12% of the time, needs to be performed when IUFD is diagnosed.13 Additional laboratory testing may be helpful depending on the mother’s history or symptoms at the time of IUFD. For example, a maternal history of drug use, thyroid disease, diabetes mellitus, hypertension, venous thromboembolism, or febrile illness should prompt further studies (TABLE 3).10,12-15
How to help grieving parents
Mothers may feel tremendous guilt upon suffering an IUFD. When addressing grief, mourning, and bereavement after an IUFD, the goal is to support the parents through the grieving process and properly identify when grief becomes pathologic. Grief is pathologic when there is a prolonged response—usually longer than 6 months—and when it interferes with daily activities.16 In a prospective study, patient characteristics that affected the intensity of grief were advanced gestational age at loss, lack of children in the home, relatively older age, pre-loss neurotic personality, and pre-loss psychiatric symptoms.17
Unlike the grief experienced by parents who lose an infant or child, the grief experienced by parents who experience an IUFD may not be socially validated. Therefore, it is important for physicians to acknowledge that patients’ feelings of loss are legitimate. Additionally, reassure mothers that there was very likely nothing that she could have done to change the outcome, unless there is compelling evidence to the contrary (eg, drug abuse causing abruption and fetal demise). Avoid using phrases such as “you can always try again.”
In a study of 769 women who experienced an IUFD, many reported receiving “support” or “great support” from family members (91.7%), nurses (90%), and physicians (53.4%).18 Adequate health care support is associated with lower levels of depression and anxiety, but family support appears to be the most important.18 Women who are single, divorced, or widowed experience higher levels of depression after IUFD than those who are married or cohabitating.18
In a different study of support for women who experienced IUFD or death of their child shortly after birth, mothers did not blame doctors or feel that the doctors should make them feel better.19 However, they did want an explanation in simple language of what had gone wrong and for physicians to listen and accept their distress.19 This study also found that early support and counseling shortened the bereavement process.19 Half of women had symptoms of depression and anxiety 6 months after the death of their fetus or child and 20% had these symptoms at 14 months. Fathers, however, recovered more quickly—14% were symptomatic at 6 months.19
Managing a subsequent therapy
A retrospective cohort study found that for women who had experienced an IUFD, the odds ratio of having a recurrent IUFD was 1.94 (99% confidence interval, 1.29-2.92) compared to women who had a previous live birth.20 The risk of recurrent IUFD in a specific patient is related to the underlying pathophysiologic cause of the initial IUFD, and how that cause was addressed. For example, a patient who experienced an IUFD believed to be the result of uncontrolled diabetes can expect to have an improved outcome if her diabetes is brought under control before conceiving and she maintains control throughout the pregnancy. On the contrary, a patient who experienced an IUFD that was believed to be secondary to a nonmodifiable risk factor, such as lupus-induced chronic kidney disease, will continue to have a significant risk of recurrence of IUFD in the subsequent pregnancy.
When managing a subsequent pregnancy of a woman who has experienced an IUFD, review all data from the prior pregnancy as well as the mother’s medical conditions. Order any studies in TABLE 3 that were not previously obtained and are clinically indicated. If applicable, encourage the woman to quite smoking and achieve a healthy BMI (<25).
In addition to routine obstetric care measures, these women should be offered antepartum fetal surveillance starting at 32 weeks gestation, or one to 2 weeks before the gestational age of the fetus at the time of the previous IUFD (whichever is earlier), as well as serial ultrasonography starting at 28 weeks to assess for fetal growth restriction.12,21 Most experts advise delivery at 39 weeks unless indicated earlier.12
Psychological risks. IUFD is associated with posttraumatic stress disorder (PTSD) and anxiety in a subsequent pregnancy.22,23 Approximately 21% of women in one study met criteria for PTSD in the third trimester of the first subsequent pregnancy; this decreased to 4% at one year postpartum.22 Risk factors for PTSD and anxiety were conceiving within one year of IUFD and a perceived lack of support at time of loss.22,23 Additionally, women who said they had poor partner support at the time of IUFD were more likely to have more severe PTSD symptoms, such as recurring, involuntary distressing memories of the IUFD, 6 to 8 years later.24 Because women who become pregnant after having an IUFD are likely to be anxious, physicians should be aware that there may be “false alarms” during the course of these pregnancies.
CASE › Two years after experiencing an IUFD , Ms. T becomes pregnant. Her physician carefully reviews her medical records and begins fetal surveillance at 26 weeks gestation, including serial ultrasounds. Ms. T’s pregnancy and labor proceed without complications, and at 38 weeks, she delivers a healthy 6.3-lb. boy.
CORRESPONDENCE
Richard Temple, MD, Naval Hospital Camp Lejeune Family Medicine Residency, 100 Brewster Blvd., Camp Lejeune, NC 28547; [email protected]
ACKNOWLEDGMENT
The authors thank Anthony Viera, MD for his assistance in the preparation of this manuscript.
1. MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep. 2009;57:1-19.
2. Goldstein DP, Johnson JP, Reid DE. Management of intrauterine fetal death. Obstet Gynecol. 1963;21:523-529.
3. Fretts RC. Etiology and prevention of stillbirth. Am J Obstet Gynecol. 2005;193:1923-1935.
4. Huang DY, Usher RH, Kramer MS, et al. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
5. Dudley DJ, Goldenberg R, Conway D, et al; Stillbirth Research Collaborative Network. A new system for determining the causes of stillbirth. Obstet Gynecol. 2010;116(2 pt 1):254-260.
6. Sims MA, Collins KA. Fetal death. A 10-year retrospective study. Am J Forensic Med Pathol. 2001;22:261-265.
7. Walsh CA, McMenamin MB, Foley ME, et al. Trends in intrapartum fetal death, 1979-2003. Am J Obstet Gynecol. 2008;198:47.e1-47.e7.
8. Smulian JC, Ananth CV, Vintzileos AM, et al. Fetal deaths in the United States. Influence of high-risk conditions and implications for management. Obstet Gynecol. 2002;100:1183-1189.
9. Silver RM. Fetal death. Obstet Gynecol. 2007;109:153-167.
10. Dodd JM, Crowther CA. Misoprostol for induction of labour to terminate pregnancy in the second or third trimester for women with a fetal anomaly or after intrauterine fetal death. Cochrane Database Syst Rev. 2010;(4):CD004901.
11. ACOG Practice Bulletin No. 102: management of stillbirth. Obstet Gynecol. 2009;113:748-761.
12. FrØen JF, Arnestad M, Frey K, et al. Risk factors for sudden intrauterine unexplained death: epidemiologic characteristics of singleton cases in Oslo, Norway, 1986-1995. Am J Obstet Gynecol. 2001;184:694-702.
13. Korteweg FJ, Erwich JJ, Timmer A, et al. Evaluation of 1025 fetal deaths: proposed diagnostic workup. Am J Obstet Gynecol. 2012;206:53.e1-53.e12.
14. Korteweg FJ, Bouman K, Erwich JJ, et al. Cytogenetic analysis after evaluation of 750 fetal deaths: proposal for diagnostic workup. Obstet Gynecol. 2008;111:865-874.
15. Silver RM, Varner MW, Reddy U, et al. Work-up of stillbirth: a review of the literature. Am J Obstet Gynecol. 2007;196:433-444.
16. Badenhorst W, Hughes P. Psychological aspects of perinatal loss. Best Pract Res Clin Obstet Gynaecol. 2007;21:249-259.
17. Janssen HJ, Cuisinier MC, de Graauw KP, et al. A prospective study of risk factors predicting grief intensity following pregnancy loss. Arch Gen Psychiatry. 1997;54:56-61.
18. Cacciatore J, Schnebly S, Froen JF. The effects of social support on maternal anxiety and depression after stillbirth. Health Soc Care Community. 2009;17:167-176.
19. Forrest GC, Standish E, Baum JD. Support after perinatal death: a study of support and counselling after perinatal bereavement. Br Med J (Clin Res Ed). 1982;285:1475-1479.
20. Bhattacharya S, Prescott GJ, Black M, et al. Recurrence risk of stillbirth in a second pregnancy. BJOG. 2010;117:1243-1247.
21. Reddy UM. Management of pregnancy after stillbirth. Clin Obstet Gynecol. 2010;53:700-709.
22. Turton P, Hughes P, Evans CD, et al. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry. 2001;178:556-560.
23. Hughes PM, Turton P, Evans CD. Stillbirth as risk factor for depression and anxiety in the subsequent pregnancy: cohort study. BMJ. 1999;318:1721-1724.
24. Turton P, Evans C, Hughes P. Long-term psychosocial sequelae of stillbirth: phase II of a nested case-control cohort study. Arch Womens Ment Health. 2009;12:35-41.
1. MacDorman MF, Kirmeyer S. Fetal and perinatal mortality, United States, 2005. Natl Vital Stat Rep. 2009;57:1-19.
2. Goldstein DP, Johnson JP, Reid DE. Management of intrauterine fetal death. Obstet Gynecol. 1963;21:523-529.
3. Fretts RC. Etiology and prevention of stillbirth. Am J Obstet Gynecol. 2005;193:1923-1935.
4. Huang DY, Usher RH, Kramer MS, et al. Determinants of unexplained antepartum fetal deaths. Obstet Gynecol. 2000;95:215-221.
5. Dudley DJ, Goldenberg R, Conway D, et al; Stillbirth Research Collaborative Network. A new system for determining the causes of stillbirth. Obstet Gynecol. 2010;116(2 pt 1):254-260.
6. Sims MA, Collins KA. Fetal death. A 10-year retrospective study. Am J Forensic Med Pathol. 2001;22:261-265.
7. Walsh CA, McMenamin MB, Foley ME, et al. Trends in intrapartum fetal death, 1979-2003. Am J Obstet Gynecol. 2008;198:47.e1-47.e7.
8. Smulian JC, Ananth CV, Vintzileos AM, et al. Fetal deaths in the United States. Influence of high-risk conditions and implications for management. Obstet Gynecol. 2002;100:1183-1189.
9. Silver RM. Fetal death. Obstet Gynecol. 2007;109:153-167.
10. Dodd JM, Crowther CA. Misoprostol for induction of labour to terminate pregnancy in the second or third trimester for women with a fetal anomaly or after intrauterine fetal death. Cochrane Database Syst Rev. 2010;(4):CD004901.
11. ACOG Practice Bulletin No. 102: management of stillbirth. Obstet Gynecol. 2009;113:748-761.
12. FrØen JF, Arnestad M, Frey K, et al. Risk factors for sudden intrauterine unexplained death: epidemiologic characteristics of singleton cases in Oslo, Norway, 1986-1995. Am J Obstet Gynecol. 2001;184:694-702.
13. Korteweg FJ, Erwich JJ, Timmer A, et al. Evaluation of 1025 fetal deaths: proposed diagnostic workup. Am J Obstet Gynecol. 2012;206:53.e1-53.e12.
14. Korteweg FJ, Bouman K, Erwich JJ, et al. Cytogenetic analysis after evaluation of 750 fetal deaths: proposal for diagnostic workup. Obstet Gynecol. 2008;111:865-874.
15. Silver RM, Varner MW, Reddy U, et al. Work-up of stillbirth: a review of the literature. Am J Obstet Gynecol. 2007;196:433-444.
16. Badenhorst W, Hughes P. Psychological aspects of perinatal loss. Best Pract Res Clin Obstet Gynaecol. 2007;21:249-259.
17. Janssen HJ, Cuisinier MC, de Graauw KP, et al. A prospective study of risk factors predicting grief intensity following pregnancy loss. Arch Gen Psychiatry. 1997;54:56-61.
18. Cacciatore J, Schnebly S, Froen JF. The effects of social support on maternal anxiety and depression after stillbirth. Health Soc Care Community. 2009;17:167-176.
19. Forrest GC, Standish E, Baum JD. Support after perinatal death: a study of support and counselling after perinatal bereavement. Br Med J (Clin Res Ed). 1982;285:1475-1479.
20. Bhattacharya S, Prescott GJ, Black M, et al. Recurrence risk of stillbirth in a second pregnancy. BJOG. 2010;117:1243-1247.
21. Reddy UM. Management of pregnancy after stillbirth. Clin Obstet Gynecol. 2010;53:700-709.
22. Turton P, Hughes P, Evans CD, et al. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry. 2001;178:556-560.
23. Hughes PM, Turton P, Evans CD. Stillbirth as risk factor for depression and anxiety in the subsequent pregnancy: cohort study. BMJ. 1999;318:1721-1724.
24. Turton P, Evans C, Hughes P. Long-term psychosocial sequelae of stillbirth: phase II of a nested case-control cohort study. Arch Womens Ment Health. 2009;12:35-41.