User login
Diagnosis at a Glance
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
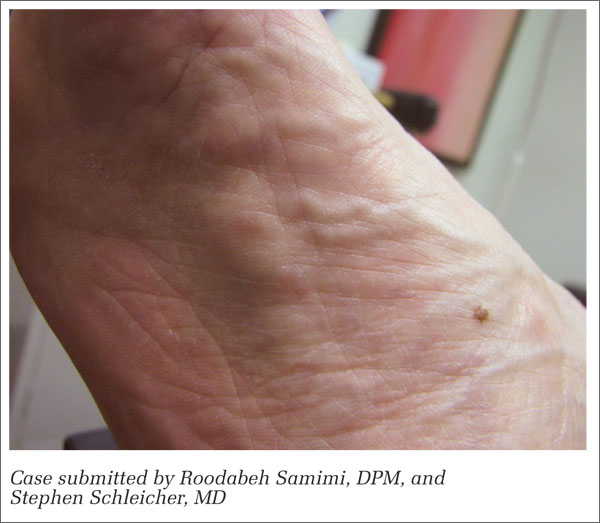
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2

A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2
A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.
Dr Samimi is a podiatric dermatology fellow at St Luke’s Hospital, Allentown, Pennsylvania. Dr Schleicher, editor of “Diagnosis at a Glance,” is director of the DermDOX Center in Hazleton, Pennsylvania; a clinical instructor of dermatology at King’s College in Wilkes-Barre, Pennsylvania; an associate professor of medicine at the Commonwealth Medical College in Scranton, Pennsylvania; and an adjunct assistant professor of dermatology at the University of Pennsylvania, Philadelphia. Ms Hammer is enrolled in the physician assistant program at Arcadia University, Glenside, Pennsylvania.
CASE 1
A 56-year-old woman presented to the urgent care center with a lump in the arch of her right foot which she stated had been slowly progressing in size over the past several months. She further noted experiencing pain on ambulation that had been unresponsive to over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs).
Physical examination of the affected foot revealed an ovoid-shaped lump on the medial band of the plantar fascia measuring approximately 1.5 cm x 0.8 cm. Moderate palpation elicited pain. There was no surrounding erythema or edema, and the lump was nonmobile, adherent to the fascia, and accentuated on dorsiflexion of the hallux.
What is your diagnosis?
CASE 2
A 77-year-old man presented to the urgent care center with a 3-week history of a blistering, intensely pruritic, and sometimes burning rash bilaterally on the extensor surfaces of his arms and legs, which he correlated to recent beer intake. His past medical history was positive for decades of similar outbreaks that had been controlled with oral dapsone, which he recently discontinued for unspecified reasons. He denied any gastrointestinal complaint. Physical examination revealed scattered vesicles and bullae of the affected areas; no similar lesions were noted elsewhere.
What is your diagnosis?
Answers
CASE 1
A plantar fibroma is a benign nodule of unknown etiology affecting the arch of the foot. Most cases are nontraumatic and originate in the deep fascia of the foot abutting the muscle. Lesions are firm and may be painful upon application of pressure. Most instances are solitary; multiple lesions may be hereditary and with variable penetrance. Initial management of symptomatic fibromas consists of off-loading with shoe padding or custom inserts, along with NSAID therapy to reduce inflammation. Intralesional steroid injections may also be beneficial in the initial stages. Due to the high incidence of recurrence, surgery is usually reserved for refractory cases.
CASE 2
Dermatitis herpetiformis (DH) is an autoimmune disorder linked to the ingestion of gluten and is associated with gluten-sensitive enteropathy (celiac disease). The condition is associated with human leukocyte antigens DQ2 and DQ8, the highest prevalence of which is seen in men of Northern European descent. Patients with DH develop intensely pruritic papules and vesicles of the extensor surfaces, scalp, and buttocks after ingesting gluten. Biopsy of these lesions reveals IgA deposits. A strict gluten-free diet is the cornerstone of therapy, though adherence often proves difficult for many patients. Dapsone provides rapid relief of pruritus and skin lesions.
