User login
- Be concerned about brown recluse envenomation when a patient reports intensifying localized pain disproportionate to physical findings after a “bite” (C).
- Prescribe an oral antihistamine alone to control symptoms, even with a necrotic wound, and mark the patient’s progress over 24 hours (C).
- If the patient improves dramatically, continue the antihistamine; with little or no improvement, consider giving an antibiotic with the antihistamine (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
What is the best way to treat the bite of a brown recluse spider? Having treated more than 185 bite wounds on 150 patients over the past 30 years, I have found that an oral antihistamine works best and makes surgery unnecessary.
I did not arrive at this treatment protocol immediately but, rather, developed it in 4 phases, which I describe in this article. Not only does this conservative approach consistently heal confirmed brown recluse bite wounds, but should a bite be mistakenly attributed to the brown recluse (or one of its relatives in the Loxosceles genus of spider), there is no harm to the patient, nor any big expense.
Is a brown recluse to blame?
Due to limited experience among the wider medical community in identifying spider envenomation,1-4 bite recognition and selection of appropriate therapy can be difficult.
Early findings can be confusing. Brown recluse bites typically feel like a pin prick. A vasoconstrictive halo may surround the bite, but this sign is inconsistent. Usually there is nothing to see immediately and pain from the bite goes away, so most patients dismiss the incident.5 Soon, however, pain from the envenomation begins and, importantly, becomes disproportionate to physical findings—the patient shows you where it hurts, but there is nothing visible to support a diagnosis or suggest a course of action.
Progression of the wound usually tells more than a captured specimen. If you are fortunate enough to examine an intact spider caught by the patient, a “fiddle” mark on the spider’s back confirms it is a brown recluse (FIGURE 1). However, most specimens brought in for examination are so misshapen from the patient’s retribution as to make identification futile. I focus instead on the resultant wound.
Spider’s venom causes the wound. Spiders lack a mechanical digestive system; their so-called venom actually is a set of enzymes that liquefy a prey’s tissues.6 In the 48 hours after a bite, these digestive enzymes cause a progressive necrosis of fat under the skin. Eventually the overlying skin also turns necrotic. The venom does not penetrate underlying fascia planes, as many infectious processes do.
Necrosis can, rarely, cause disseminated intravascular coagulation and death. A more likely scenario, though still relatively uncommon, is that the necrotic sequence leads to an indolent wound that heals only with difficulty. Most patients recover without medical care and do not even seek it.7-9
Wounds can be categorized, as outlined by Auer et al,10 into groups 1 through 4, from least severe to most severe. However, this classification scheme has made no difference in my management decisions.
FIGURE 1
The distinctive “fiddle” mark
How my treatment protocol evolved
My protocol for treating necrotic bite wounds of the brown recluse, and similar wounds from other insects, progressed over 30 years through 4 phases of treatment concepts.
Phase 1: Surgical excision
From 1979 to 1980, I treated necrotic wounds with surgical excision and secondary closure or skin grafting.1 Many patients complained of severe itching around these wounds, which I treated empirically with the antihistamine Benadryl. All patients experienced symptom relief and had a reasonable cosmetic result (FIGURE 2).
In writing up the case results for a presentation to the Society of Air Force Clinical Surgeons, I conducted background research and found a postulate suggesting that antigen recognition was an important factor in wound progression and that it took approximately 7 days to achieve. That postulate drove the second phase of discovery.1
FIGURE 2
Bite wound treatment: Debridement and closure or skin grafting
From 1980 to 1981, I focused on the postulate, which also suggested that the antigen–antibody reaction following envenomation could make reactions to subsequent (“second set”) bites less severe.1 This made sense, though good clinical data were lacking.
I decided to simply observe patients’ wounds for 7 to 10 days before performing debridement, advising patients to use an antihistamine to control symptoms during the waiting period. I took photographs to document clinical progression of wounds. In reviewing these photographs, I noted that the necrotic wounds stabilized immediately on starting an antihistamine—specifically, Benadryl, 5 mg/kg or 50 mg qid. After 7 to 10 days, I debrided the wounds, using fluorescein and a Woods lamp to guide the procedure. I found that tissue of doubtful viability survived if debridement was conservative and the patient had used an antihistamine (FIGURE 3).
FIGURE 3
Bite wound treatment: Observation for 7 to 10 days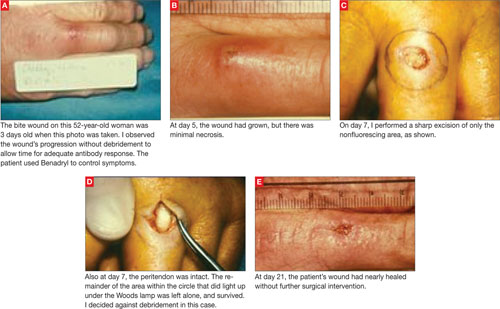
In reviewing phase 2 results in preparation for a presentation to the Southwestern Surgical Congress, I realized that debridement was rarely indicated. So, from 1981 to 1982, I relied less on surgery and more on conservative therapy. Patients got better simply with antihistamine therapy. Redness diminished very quickly once patients took the antihistamine, and pockets of purulent material drained on their own.
This approach also allowed antigen recognition to occur and seemed to prove the postulate of a less severe second bite. I saw 4 patients with proven “second set” spider bites (intact specimens were available) and all had an immediate inflammatory response and no subsequent necrosis. An 18-month-old patient with a bite below her right eye healed with Benadryl therapy alone (FIGURE 4).
FIGURE 4
Bite wound treatment: Antihistamine alone
Phase 4: Exclusive antihistamine therapy
Since 1982, I have treated more than 100 patients (myself included) with necrotic bite wounds from spiders and other insects. None have required operative debridement, and all have achieved much more acceptable cosmetic results using Benadryl therapy than with surgical therapy.
My encounter with a brown recluse. The bite I received was rather typical. I felt a sharp sting when outside working on the lawn. I looked down, saw nothing, and assumed I had run into a pin or small stick that was now not visible. For 3 days I noticed nothing unusual. On day 4, after showering I noticed a large amount of purulent material on the towel after drying my anterior left leg. On inspecting the area, I saw an area of necrosis approximately 6 × 6 cm with a central area oozing a purulent material. This appeared just like the necrotic insect bites I had treated with antihistamines, so I started myself on that regimen. The redness cleared up in 2 days and the wound healed completely in 10 days without antibiotics. A 3 × 3 mm circular scar remained; I lost none of the surrounding marginal skin.
Further evidence of less severe second bites. Another physician—my coauthor on the presentation to the Southwestern Surgical Congress—was bitten at age 12 by an unidentified insect, resulting in a large necrotic wound on his thigh. The lesion, reportedly 10 to 12 cm in diameter, healed with topical treatment only. After our joint report in 1982, a brown recluse spider bit him on the abdomen while he was working in the yard. He captured the spider and verified its genus and species. Guessing that the bite he received as a 12 year old was also from a brown recluse, he decided to wait and see if he had a “second set” reaction to the bite. He had an immediate inflammatory reaction, no skin necrosis, and the entire area returned to normal in 3 days. His experience became the fifth “second set” spider bite reaction in our series.
Another dramatic experience. One 22-year-old woman’s experience is worth a longer discussion. She visited her physician because 4 small areas of necrosis on her lower abdomen and chest had lasted several days and were getting worse. He assumed these were small abscesses and treated her with antibiotics. The lesions slowly enlarged to become 6 to 8 cm in diameter, and the physician hospitalized her for intravenous (IV) antibiotic therapy.
When the patient worsened after 2 days of IV antibiotics and incision and drainage, I was called to examine her for possible surgical debridement. I thought the lesions were necrotic insect bites and recommended starting Benadryl, 50 mg qid. She improved remarkably over the next 24 hours, her wounds decreasing in size by 50%. She was discharged from the hospital and, against my advice, the Benadryl was stopped. Within 48 hours the area of inflammation around the wounds had doubled in size. She was readmitted and given Benadryl. Again she improved remarkably in 24 hours. The purulent discharge was sent for culture, which grew an organism resistant to all of her previous antibiotics. She healed uneventfully in 10 days on antihistamines, and without antibiotics. This is typical in my experience. Antibiotics have seldom proved useful, and culture results are generally confusing.
Broader support for my observations
On January 27, 2006, on eMedicine (link is no longer active), dermatologist Adam S. Stibich, MD, published a physiology review of the brown recluse bite. He acknowledged that neutrophils accumulate in the wound at 24 to 72 hours, consistent with the antigen–antibody response postulated in my clinical review. Neutrophils are products of the histamine cascade that most likely brings about tissue necrosis.
Stibich’s plea for conservative management was well founded. He noted that only 10% of envenomation episodes result in large open wounds. The physical findings he described were in keeping with my observation that a subcutaneous necrotic process precedes surface changes.
His treatment of choice was dapsone. He pointed out that other clinicians, too, had reported success with dapsone, and with steroids, antibiotics, hyperbaric oxygen, electric shock therapy, and surgical therapy.3,4,11,12 Stibich commented extensively on these treatment modalities, except electrical shock. However, while the laboratory results achieved were good, clinical outcomes were mixed. Of these treatments, I have experience only with surgery, and I have found that it does not improve the healing process.
Antihistamine and observation: The ideal Tx
The ideal treatment for necrotic wounds from envenomation would account for an underlying antigen–antibody process, shorten the natural history of the illness, result in the least deformity, minimize cost, and allow for errors in diagnosis without harming patients.
The brown recluse spider is found primarily in the Mississippi River Valley and its tributaries. Its genus members can be found in Arizona, Texas, and South America. They are nocturnal creatures, typically living in woodpiles and secluded dark areas. Usually they are 8 to 9 mm in diameter, but they can reach several centimeters.
Unfortunately, the spider travels well hidden in clothing, so even if you don’t practice medicine in Arizona, Texas, or South America, you could still find yourself treating a patient with a brown recluse spider bite. I saw these wounds in Germany and Spain, on patients who had just arrived from the United States or whose family members had been there. Hite and others have also described this experience.5,12-14
Many people seek care in emergency departments for nasty looking spontaneous abscesses, some of which are in fact spider bites. Increasingly, though, lesions in this setting are colonized with methicillin-resistant Staphylococcus aureus (MRSA). One recent study showed that among patients who visited EDs because of skin infections, more than 58% were infected with MRSA.15 The difficulty is in determining whether MRSA has caused the nasty wound, is a secondary colonization of a spider bite, or if the wound is actually an uninfected spider bite.
Given the simplicity and low cost of antihistamine treatment, I recommend it for wound care in these instances. If the clinical response is good within 24 hours, you are probably dealing with an uninfected spider bite. If the response is slow or the wound worsens after 24 hours, consider adding an antibiotic or performing surgical debridement.
Based on my observations since 1982, I am convinced these necrotic wounds involve an antigen–antibody reaction, are histamine driven, and are adequately treated with oral antihistamines. I now treat presumed necrotic spider bite with antihistamines only. Laboratory or serum testing to confirm a diagnosis has not been useful. It takes too long, costs too much, and does not contribute to management decisions.
If the wound improves dramatically in 24 hours, which is the norm, I continue the antihistamines for 7 to 10 days. If the wound does not improve, I suspect a bacterial component and add an antibiotic. Not once in the last 26 years have I had to resort to surgery.
Correspondence
Paul K. Carlton, Jr, MD, FACS, The Texas A&M University Health Science Center, Office of Homeland Security, 301 Tarrow, 7th Floor, John Connally Building, College Station, TX 77840; [email protected]
1. Hershey FB, Aulenbacher CE. Surgical treatment of brown spider bites. Ann Surg. 1969;170:300-308.
2. Arnold RE. Brown recluse spider bites: five cases with a review of the literature. JACEP. 1976;5:262-264.
3. DeLozier JB, Reaves L, King LE, Jr, et al. Brown recluse spider bites of the upper extremity. South Med J. 1988;81:181-184.
4. Wright SW, Wrenn KD, Murray L, et al. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30:28-32.
5. Forks TP. Brown recluse spider bites. J Am Board Fam Pract. 2000;13:415-423.
6. Spiders: Digestive system. Available at: http://www.greensmiths.com/spiders.htm. Accessed November 20, 2007.
7. Nance WE. Hemolytic anemia of necrotic arachnidism. Am J Med. 1981;31:801-807.
8. Russell FE, Waldron WG, Madon MB. Bites by the brown spiders Loxosceles unicolor and Loxosceles arizonica in California and Arizona. Toxicon. 1969;17:109-117.
9. Atkins JA, Wingo CW, Sodeman WA, et al. Necrotic arachnidism. Am J Trop Med Hyg. 1958;7:165-184.
10. Auer A, Hershey FB. Proceedings: surgery for necrotic bites of the brown spider. Arch Surg. 1974;108:612-618.
11. Rees RS, Shack RB, Withers EH, et al. Management of the brown recluse spider bite. Plast Reconstr Surg. 1981;68:768-773.
12. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352:700-707.
13. Barnes JK. Brown recluse and Mediterranean recluse spiders. University of Arkansas Arthropod Museum Notes. Revised May 2003; #11. Available at: http://entomology.uark.edu/museum/browrec.html. Accessed January 16, 2009.
14. Hite JL, Gladney WJ, Lancaster JL, et al. Biology of the brown recluse spider. Arkansas Experiment Station Bulletin. 1966; #711.
15. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.
- Be concerned about brown recluse envenomation when a patient reports intensifying localized pain disproportionate to physical findings after a “bite” (C).
- Prescribe an oral antihistamine alone to control symptoms, even with a necrotic wound, and mark the patient’s progress over 24 hours (C).
- If the patient improves dramatically, continue the antihistamine; with little or no improvement, consider giving an antibiotic with the antihistamine (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
What is the best way to treat the bite of a brown recluse spider? Having treated more than 185 bite wounds on 150 patients over the past 30 years, I have found that an oral antihistamine works best and makes surgery unnecessary.
I did not arrive at this treatment protocol immediately but, rather, developed it in 4 phases, which I describe in this article. Not only does this conservative approach consistently heal confirmed brown recluse bite wounds, but should a bite be mistakenly attributed to the brown recluse (or one of its relatives in the Loxosceles genus of spider), there is no harm to the patient, nor any big expense.
Is a brown recluse to blame?
Due to limited experience among the wider medical community in identifying spider envenomation,1-4 bite recognition and selection of appropriate therapy can be difficult.
Early findings can be confusing. Brown recluse bites typically feel like a pin prick. A vasoconstrictive halo may surround the bite, but this sign is inconsistent. Usually there is nothing to see immediately and pain from the bite goes away, so most patients dismiss the incident.5 Soon, however, pain from the envenomation begins and, importantly, becomes disproportionate to physical findings—the patient shows you where it hurts, but there is nothing visible to support a diagnosis or suggest a course of action.
Progression of the wound usually tells more than a captured specimen. If you are fortunate enough to examine an intact spider caught by the patient, a “fiddle” mark on the spider’s back confirms it is a brown recluse (FIGURE 1). However, most specimens brought in for examination are so misshapen from the patient’s retribution as to make identification futile. I focus instead on the resultant wound.
Spider’s venom causes the wound. Spiders lack a mechanical digestive system; their so-called venom actually is a set of enzymes that liquefy a prey’s tissues.6 In the 48 hours after a bite, these digestive enzymes cause a progressive necrosis of fat under the skin. Eventually the overlying skin also turns necrotic. The venom does not penetrate underlying fascia planes, as many infectious processes do.
Necrosis can, rarely, cause disseminated intravascular coagulation and death. A more likely scenario, though still relatively uncommon, is that the necrotic sequence leads to an indolent wound that heals only with difficulty. Most patients recover without medical care and do not even seek it.7-9
Wounds can be categorized, as outlined by Auer et al,10 into groups 1 through 4, from least severe to most severe. However, this classification scheme has made no difference in my management decisions.
FIGURE 1
The distinctive “fiddle” mark
How my treatment protocol evolved
My protocol for treating necrotic bite wounds of the brown recluse, and similar wounds from other insects, progressed over 30 years through 4 phases of treatment concepts.
Phase 1: Surgical excision
From 1979 to 1980, I treated necrotic wounds with surgical excision and secondary closure or skin grafting.1 Many patients complained of severe itching around these wounds, which I treated empirically with the antihistamine Benadryl. All patients experienced symptom relief and had a reasonable cosmetic result (FIGURE 2).
In writing up the case results for a presentation to the Society of Air Force Clinical Surgeons, I conducted background research and found a postulate suggesting that antigen recognition was an important factor in wound progression and that it took approximately 7 days to achieve. That postulate drove the second phase of discovery.1
FIGURE 2
Bite wound treatment: Debridement and closure or skin grafting
From 1980 to 1981, I focused on the postulate, which also suggested that the antigen–antibody reaction following envenomation could make reactions to subsequent (“second set”) bites less severe.1 This made sense, though good clinical data were lacking.
I decided to simply observe patients’ wounds for 7 to 10 days before performing debridement, advising patients to use an antihistamine to control symptoms during the waiting period. I took photographs to document clinical progression of wounds. In reviewing these photographs, I noted that the necrotic wounds stabilized immediately on starting an antihistamine—specifically, Benadryl, 5 mg/kg or 50 mg qid. After 7 to 10 days, I debrided the wounds, using fluorescein and a Woods lamp to guide the procedure. I found that tissue of doubtful viability survived if debridement was conservative and the patient had used an antihistamine (FIGURE 3).
FIGURE 3
Bite wound treatment: Observation for 7 to 10 days
In reviewing phase 2 results in preparation for a presentation to the Southwestern Surgical Congress, I realized that debridement was rarely indicated. So, from 1981 to 1982, I relied less on surgery and more on conservative therapy. Patients got better simply with antihistamine therapy. Redness diminished very quickly once patients took the antihistamine, and pockets of purulent material drained on their own.
This approach also allowed antigen recognition to occur and seemed to prove the postulate of a less severe second bite. I saw 4 patients with proven “second set” spider bites (intact specimens were available) and all had an immediate inflammatory response and no subsequent necrosis. An 18-month-old patient with a bite below her right eye healed with Benadryl therapy alone (FIGURE 4).
FIGURE 4
Bite wound treatment: Antihistamine alone
Phase 4: Exclusive antihistamine therapy
Since 1982, I have treated more than 100 patients (myself included) with necrotic bite wounds from spiders and other insects. None have required operative debridement, and all have achieved much more acceptable cosmetic results using Benadryl therapy than with surgical therapy.
My encounter with a brown recluse. The bite I received was rather typical. I felt a sharp sting when outside working on the lawn. I looked down, saw nothing, and assumed I had run into a pin or small stick that was now not visible. For 3 days I noticed nothing unusual. On day 4, after showering I noticed a large amount of purulent material on the towel after drying my anterior left leg. On inspecting the area, I saw an area of necrosis approximately 6 × 6 cm with a central area oozing a purulent material. This appeared just like the necrotic insect bites I had treated with antihistamines, so I started myself on that regimen. The redness cleared up in 2 days and the wound healed completely in 10 days without antibiotics. A 3 × 3 mm circular scar remained; I lost none of the surrounding marginal skin.
Further evidence of less severe second bites. Another physician—my coauthor on the presentation to the Southwestern Surgical Congress—was bitten at age 12 by an unidentified insect, resulting in a large necrotic wound on his thigh. The lesion, reportedly 10 to 12 cm in diameter, healed with topical treatment only. After our joint report in 1982, a brown recluse spider bit him on the abdomen while he was working in the yard. He captured the spider and verified its genus and species. Guessing that the bite he received as a 12 year old was also from a brown recluse, he decided to wait and see if he had a “second set” reaction to the bite. He had an immediate inflammatory reaction, no skin necrosis, and the entire area returned to normal in 3 days. His experience became the fifth “second set” spider bite reaction in our series.
Another dramatic experience. One 22-year-old woman’s experience is worth a longer discussion. She visited her physician because 4 small areas of necrosis on her lower abdomen and chest had lasted several days and were getting worse. He assumed these were small abscesses and treated her with antibiotics. The lesions slowly enlarged to become 6 to 8 cm in diameter, and the physician hospitalized her for intravenous (IV) antibiotic therapy.
When the patient worsened after 2 days of IV antibiotics and incision and drainage, I was called to examine her for possible surgical debridement. I thought the lesions were necrotic insect bites and recommended starting Benadryl, 50 mg qid. She improved remarkably over the next 24 hours, her wounds decreasing in size by 50%. She was discharged from the hospital and, against my advice, the Benadryl was stopped. Within 48 hours the area of inflammation around the wounds had doubled in size. She was readmitted and given Benadryl. Again she improved remarkably in 24 hours. The purulent discharge was sent for culture, which grew an organism resistant to all of her previous antibiotics. She healed uneventfully in 10 days on antihistamines, and without antibiotics. This is typical in my experience. Antibiotics have seldom proved useful, and culture results are generally confusing.
Broader support for my observations
On January 27, 2006, on eMedicine (link is no longer active), dermatologist Adam S. Stibich, MD, published a physiology review of the brown recluse bite. He acknowledged that neutrophils accumulate in the wound at 24 to 72 hours, consistent with the antigen–antibody response postulated in my clinical review. Neutrophils are products of the histamine cascade that most likely brings about tissue necrosis.
Stibich’s plea for conservative management was well founded. He noted that only 10% of envenomation episodes result in large open wounds. The physical findings he described were in keeping with my observation that a subcutaneous necrotic process precedes surface changes.
His treatment of choice was dapsone. He pointed out that other clinicians, too, had reported success with dapsone, and with steroids, antibiotics, hyperbaric oxygen, electric shock therapy, and surgical therapy.3,4,11,12 Stibich commented extensively on these treatment modalities, except electrical shock. However, while the laboratory results achieved were good, clinical outcomes were mixed. Of these treatments, I have experience only with surgery, and I have found that it does not improve the healing process.
Antihistamine and observation: The ideal Tx
The ideal treatment for necrotic wounds from envenomation would account for an underlying antigen–antibody process, shorten the natural history of the illness, result in the least deformity, minimize cost, and allow for errors in diagnosis without harming patients.
The brown recluse spider is found primarily in the Mississippi River Valley and its tributaries. Its genus members can be found in Arizona, Texas, and South America. They are nocturnal creatures, typically living in woodpiles and secluded dark areas. Usually they are 8 to 9 mm in diameter, but they can reach several centimeters.
Unfortunately, the spider travels well hidden in clothing, so even if you don’t practice medicine in Arizona, Texas, or South America, you could still find yourself treating a patient with a brown recluse spider bite. I saw these wounds in Germany and Spain, on patients who had just arrived from the United States or whose family members had been there. Hite and others have also described this experience.5,12-14
Many people seek care in emergency departments for nasty looking spontaneous abscesses, some of which are in fact spider bites. Increasingly, though, lesions in this setting are colonized with methicillin-resistant Staphylococcus aureus (MRSA). One recent study showed that among patients who visited EDs because of skin infections, more than 58% were infected with MRSA.15 The difficulty is in determining whether MRSA has caused the nasty wound, is a secondary colonization of a spider bite, or if the wound is actually an uninfected spider bite.
Given the simplicity and low cost of antihistamine treatment, I recommend it for wound care in these instances. If the clinical response is good within 24 hours, you are probably dealing with an uninfected spider bite. If the response is slow or the wound worsens after 24 hours, consider adding an antibiotic or performing surgical debridement.
Based on my observations since 1982, I am convinced these necrotic wounds involve an antigen–antibody reaction, are histamine driven, and are adequately treated with oral antihistamines. I now treat presumed necrotic spider bite with antihistamines only. Laboratory or serum testing to confirm a diagnosis has not been useful. It takes too long, costs too much, and does not contribute to management decisions.
If the wound improves dramatically in 24 hours, which is the norm, I continue the antihistamines for 7 to 10 days. If the wound does not improve, I suspect a bacterial component and add an antibiotic. Not once in the last 26 years have I had to resort to surgery.
Correspondence
Paul K. Carlton, Jr, MD, FACS, The Texas A&M University Health Science Center, Office of Homeland Security, 301 Tarrow, 7th Floor, John Connally Building, College Station, TX 77840; [email protected]
- Be concerned about brown recluse envenomation when a patient reports intensifying localized pain disproportionate to physical findings after a “bite” (C).
- Prescribe an oral antihistamine alone to control symptoms, even with a necrotic wound, and mark the patient’s progress over 24 hours (C).
- If the patient improves dramatically, continue the antihistamine; with little or no improvement, consider giving an antibiotic with the antihistamine (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
What is the best way to treat the bite of a brown recluse spider? Having treated more than 185 bite wounds on 150 patients over the past 30 years, I have found that an oral antihistamine works best and makes surgery unnecessary.
I did not arrive at this treatment protocol immediately but, rather, developed it in 4 phases, which I describe in this article. Not only does this conservative approach consistently heal confirmed brown recluse bite wounds, but should a bite be mistakenly attributed to the brown recluse (or one of its relatives in the Loxosceles genus of spider), there is no harm to the patient, nor any big expense.
Is a brown recluse to blame?
Due to limited experience among the wider medical community in identifying spider envenomation,1-4 bite recognition and selection of appropriate therapy can be difficult.
Early findings can be confusing. Brown recluse bites typically feel like a pin prick. A vasoconstrictive halo may surround the bite, but this sign is inconsistent. Usually there is nothing to see immediately and pain from the bite goes away, so most patients dismiss the incident.5 Soon, however, pain from the envenomation begins and, importantly, becomes disproportionate to physical findings—the patient shows you where it hurts, but there is nothing visible to support a diagnosis or suggest a course of action.
Progression of the wound usually tells more than a captured specimen. If you are fortunate enough to examine an intact spider caught by the patient, a “fiddle” mark on the spider’s back confirms it is a brown recluse (FIGURE 1). However, most specimens brought in for examination are so misshapen from the patient’s retribution as to make identification futile. I focus instead on the resultant wound.
Spider’s venom causes the wound. Spiders lack a mechanical digestive system; their so-called venom actually is a set of enzymes that liquefy a prey’s tissues.6 In the 48 hours after a bite, these digestive enzymes cause a progressive necrosis of fat under the skin. Eventually the overlying skin also turns necrotic. The venom does not penetrate underlying fascia planes, as many infectious processes do.
Necrosis can, rarely, cause disseminated intravascular coagulation and death. A more likely scenario, though still relatively uncommon, is that the necrotic sequence leads to an indolent wound that heals only with difficulty. Most patients recover without medical care and do not even seek it.7-9
Wounds can be categorized, as outlined by Auer et al,10 into groups 1 through 4, from least severe to most severe. However, this classification scheme has made no difference in my management decisions.
FIGURE 1
The distinctive “fiddle” mark
How my treatment protocol evolved
My protocol for treating necrotic bite wounds of the brown recluse, and similar wounds from other insects, progressed over 30 years through 4 phases of treatment concepts.
Phase 1: Surgical excision
From 1979 to 1980, I treated necrotic wounds with surgical excision and secondary closure or skin grafting.1 Many patients complained of severe itching around these wounds, which I treated empirically with the antihistamine Benadryl. All patients experienced symptom relief and had a reasonable cosmetic result (FIGURE 2).
In writing up the case results for a presentation to the Society of Air Force Clinical Surgeons, I conducted background research and found a postulate suggesting that antigen recognition was an important factor in wound progression and that it took approximately 7 days to achieve. That postulate drove the second phase of discovery.1
FIGURE 2
Bite wound treatment: Debridement and closure or skin grafting
From 1980 to 1981, I focused on the postulate, which also suggested that the antigen–antibody reaction following envenomation could make reactions to subsequent (“second set”) bites less severe.1 This made sense, though good clinical data were lacking.
I decided to simply observe patients’ wounds for 7 to 10 days before performing debridement, advising patients to use an antihistamine to control symptoms during the waiting period. I took photographs to document clinical progression of wounds. In reviewing these photographs, I noted that the necrotic wounds stabilized immediately on starting an antihistamine—specifically, Benadryl, 5 mg/kg or 50 mg qid. After 7 to 10 days, I debrided the wounds, using fluorescein and a Woods lamp to guide the procedure. I found that tissue of doubtful viability survived if debridement was conservative and the patient had used an antihistamine (FIGURE 3).
FIGURE 3
Bite wound treatment: Observation for 7 to 10 days
In reviewing phase 2 results in preparation for a presentation to the Southwestern Surgical Congress, I realized that debridement was rarely indicated. So, from 1981 to 1982, I relied less on surgery and more on conservative therapy. Patients got better simply with antihistamine therapy. Redness diminished very quickly once patients took the antihistamine, and pockets of purulent material drained on their own.
This approach also allowed antigen recognition to occur and seemed to prove the postulate of a less severe second bite. I saw 4 patients with proven “second set” spider bites (intact specimens were available) and all had an immediate inflammatory response and no subsequent necrosis. An 18-month-old patient with a bite below her right eye healed with Benadryl therapy alone (FIGURE 4).
FIGURE 4
Bite wound treatment: Antihistamine alone
Phase 4: Exclusive antihistamine therapy
Since 1982, I have treated more than 100 patients (myself included) with necrotic bite wounds from spiders and other insects. None have required operative debridement, and all have achieved much more acceptable cosmetic results using Benadryl therapy than with surgical therapy.
My encounter with a brown recluse. The bite I received was rather typical. I felt a sharp sting when outside working on the lawn. I looked down, saw nothing, and assumed I had run into a pin or small stick that was now not visible. For 3 days I noticed nothing unusual. On day 4, after showering I noticed a large amount of purulent material on the towel after drying my anterior left leg. On inspecting the area, I saw an area of necrosis approximately 6 × 6 cm with a central area oozing a purulent material. This appeared just like the necrotic insect bites I had treated with antihistamines, so I started myself on that regimen. The redness cleared up in 2 days and the wound healed completely in 10 days without antibiotics. A 3 × 3 mm circular scar remained; I lost none of the surrounding marginal skin.
Further evidence of less severe second bites. Another physician—my coauthor on the presentation to the Southwestern Surgical Congress—was bitten at age 12 by an unidentified insect, resulting in a large necrotic wound on his thigh. The lesion, reportedly 10 to 12 cm in diameter, healed with topical treatment only. After our joint report in 1982, a brown recluse spider bit him on the abdomen while he was working in the yard. He captured the spider and verified its genus and species. Guessing that the bite he received as a 12 year old was also from a brown recluse, he decided to wait and see if he had a “second set” reaction to the bite. He had an immediate inflammatory reaction, no skin necrosis, and the entire area returned to normal in 3 days. His experience became the fifth “second set” spider bite reaction in our series.
Another dramatic experience. One 22-year-old woman’s experience is worth a longer discussion. She visited her physician because 4 small areas of necrosis on her lower abdomen and chest had lasted several days and were getting worse. He assumed these were small abscesses and treated her with antibiotics. The lesions slowly enlarged to become 6 to 8 cm in diameter, and the physician hospitalized her for intravenous (IV) antibiotic therapy.
When the patient worsened after 2 days of IV antibiotics and incision and drainage, I was called to examine her for possible surgical debridement. I thought the lesions were necrotic insect bites and recommended starting Benadryl, 50 mg qid. She improved remarkably over the next 24 hours, her wounds decreasing in size by 50%. She was discharged from the hospital and, against my advice, the Benadryl was stopped. Within 48 hours the area of inflammation around the wounds had doubled in size. She was readmitted and given Benadryl. Again she improved remarkably in 24 hours. The purulent discharge was sent for culture, which grew an organism resistant to all of her previous antibiotics. She healed uneventfully in 10 days on antihistamines, and without antibiotics. This is typical in my experience. Antibiotics have seldom proved useful, and culture results are generally confusing.
Broader support for my observations
On January 27, 2006, on eMedicine (link is no longer active), dermatologist Adam S. Stibich, MD, published a physiology review of the brown recluse bite. He acknowledged that neutrophils accumulate in the wound at 24 to 72 hours, consistent with the antigen–antibody response postulated in my clinical review. Neutrophils are products of the histamine cascade that most likely brings about tissue necrosis.
Stibich’s plea for conservative management was well founded. He noted that only 10% of envenomation episodes result in large open wounds. The physical findings he described were in keeping with my observation that a subcutaneous necrotic process precedes surface changes.
His treatment of choice was dapsone. He pointed out that other clinicians, too, had reported success with dapsone, and with steroids, antibiotics, hyperbaric oxygen, electric shock therapy, and surgical therapy.3,4,11,12 Stibich commented extensively on these treatment modalities, except electrical shock. However, while the laboratory results achieved were good, clinical outcomes were mixed. Of these treatments, I have experience only with surgery, and I have found that it does not improve the healing process.
Antihistamine and observation: The ideal Tx
The ideal treatment for necrotic wounds from envenomation would account for an underlying antigen–antibody process, shorten the natural history of the illness, result in the least deformity, minimize cost, and allow for errors in diagnosis without harming patients.
The brown recluse spider is found primarily in the Mississippi River Valley and its tributaries. Its genus members can be found in Arizona, Texas, and South America. They are nocturnal creatures, typically living in woodpiles and secluded dark areas. Usually they are 8 to 9 mm in diameter, but they can reach several centimeters.
Unfortunately, the spider travels well hidden in clothing, so even if you don’t practice medicine in Arizona, Texas, or South America, you could still find yourself treating a patient with a brown recluse spider bite. I saw these wounds in Germany and Spain, on patients who had just arrived from the United States or whose family members had been there. Hite and others have also described this experience.5,12-14
Many people seek care in emergency departments for nasty looking spontaneous abscesses, some of which are in fact spider bites. Increasingly, though, lesions in this setting are colonized with methicillin-resistant Staphylococcus aureus (MRSA). One recent study showed that among patients who visited EDs because of skin infections, more than 58% were infected with MRSA.15 The difficulty is in determining whether MRSA has caused the nasty wound, is a secondary colonization of a spider bite, or if the wound is actually an uninfected spider bite.
Given the simplicity and low cost of antihistamine treatment, I recommend it for wound care in these instances. If the clinical response is good within 24 hours, you are probably dealing with an uninfected spider bite. If the response is slow or the wound worsens after 24 hours, consider adding an antibiotic or performing surgical debridement.
Based on my observations since 1982, I am convinced these necrotic wounds involve an antigen–antibody reaction, are histamine driven, and are adequately treated with oral antihistamines. I now treat presumed necrotic spider bite with antihistamines only. Laboratory or serum testing to confirm a diagnosis has not been useful. It takes too long, costs too much, and does not contribute to management decisions.
If the wound improves dramatically in 24 hours, which is the norm, I continue the antihistamines for 7 to 10 days. If the wound does not improve, I suspect a bacterial component and add an antibiotic. Not once in the last 26 years have I had to resort to surgery.
Correspondence
Paul K. Carlton, Jr, MD, FACS, The Texas A&M University Health Science Center, Office of Homeland Security, 301 Tarrow, 7th Floor, John Connally Building, College Station, TX 77840; [email protected]
1. Hershey FB, Aulenbacher CE. Surgical treatment of brown spider bites. Ann Surg. 1969;170:300-308.
2. Arnold RE. Brown recluse spider bites: five cases with a review of the literature. JACEP. 1976;5:262-264.
3. DeLozier JB, Reaves L, King LE, Jr, et al. Brown recluse spider bites of the upper extremity. South Med J. 1988;81:181-184.
4. Wright SW, Wrenn KD, Murray L, et al. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30:28-32.
5. Forks TP. Brown recluse spider bites. J Am Board Fam Pract. 2000;13:415-423.
6. Spiders: Digestive system. Available at: http://www.greensmiths.com/spiders.htm. Accessed November 20, 2007.
7. Nance WE. Hemolytic anemia of necrotic arachnidism. Am J Med. 1981;31:801-807.
8. Russell FE, Waldron WG, Madon MB. Bites by the brown spiders Loxosceles unicolor and Loxosceles arizonica in California and Arizona. Toxicon. 1969;17:109-117.
9. Atkins JA, Wingo CW, Sodeman WA, et al. Necrotic arachnidism. Am J Trop Med Hyg. 1958;7:165-184.
10. Auer A, Hershey FB. Proceedings: surgery for necrotic bites of the brown spider. Arch Surg. 1974;108:612-618.
11. Rees RS, Shack RB, Withers EH, et al. Management of the brown recluse spider bite. Plast Reconstr Surg. 1981;68:768-773.
12. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352:700-707.
13. Barnes JK. Brown recluse and Mediterranean recluse spiders. University of Arkansas Arthropod Museum Notes. Revised May 2003; #11. Available at: http://entomology.uark.edu/museum/browrec.html. Accessed January 16, 2009.
14. Hite JL, Gladney WJ, Lancaster JL, et al. Biology of the brown recluse spider. Arkansas Experiment Station Bulletin. 1966; #711.
15. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.
1. Hershey FB, Aulenbacher CE. Surgical treatment of brown spider bites. Ann Surg. 1969;170:300-308.
2. Arnold RE. Brown recluse spider bites: five cases with a review of the literature. JACEP. 1976;5:262-264.
3. DeLozier JB, Reaves L, King LE, Jr, et al. Brown recluse spider bites of the upper extremity. South Med J. 1988;81:181-184.
4. Wright SW, Wrenn KD, Murray L, et al. Clinical presentation and outcome of brown recluse spider bite. Ann Emerg Med. 1997;30:28-32.
5. Forks TP. Brown recluse spider bites. J Am Board Fam Pract. 2000;13:415-423.
6. Spiders: Digestive system. Available at: http://www.greensmiths.com/spiders.htm. Accessed November 20, 2007.
7. Nance WE. Hemolytic anemia of necrotic arachnidism. Am J Med. 1981;31:801-807.
8. Russell FE, Waldron WG, Madon MB. Bites by the brown spiders Loxosceles unicolor and Loxosceles arizonica in California and Arizona. Toxicon. 1969;17:109-117.
9. Atkins JA, Wingo CW, Sodeman WA, et al. Necrotic arachnidism. Am J Trop Med Hyg. 1958;7:165-184.
10. Auer A, Hershey FB. Proceedings: surgery for necrotic bites of the brown spider. Arch Surg. 1974;108:612-618.
11. Rees RS, Shack RB, Withers EH, et al. Management of the brown recluse spider bite. Plast Reconstr Surg. 1981;68:768-773.
12. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352:700-707.
13. Barnes JK. Brown recluse and Mediterranean recluse spiders. University of Arkansas Arthropod Museum Notes. Revised May 2003; #11. Available at: http://entomology.uark.edu/museum/browrec.html. Accessed January 16, 2009.
14. Hite JL, Gladney WJ, Lancaster JL, et al. Biology of the brown recluse spider. Arkansas Experiment Station Bulletin. 1966; #711.
15. Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298:1763-1771.