User login
No, none of the 3—history, exam, or labs— is sufficiently accurate to diagnose acute appendicitis (strength of recommendation [SOR]: A, based on meta-analysis of high-quality studies). When combined, the following tests are helpful: an elevated C-reactive protein (CRP), elevated total white blood cell (WBC) count, elevated percentage of polymorphonuclear leukocyte (PMN) cells (left shift), and the presence of guarding or rebound on physical examination. The combination of any 2 of these tests yields a very high positive likelihood ratio (LR+), but the absence of these does not exclude appendicitis (SOR: A, based on meta-analysis of high-quality studies).
2 inexpensive tests can lower costs in low-probability presentations
Fereshteh Gerayli, MD
East Tennessee State University, Johnson City
Unlike physicians in other parts of the world, us physicians rely heavily on imaging studies to diagnose acute appendicitis. This has decreased the rate of negative appendectomies by 15% to 20%. However, the liberal and indiscriminate use of imaging studies increases medical costs while diminishing physicians’ clinical diagnostic skills.
The systematic review our authors cited demonstrated a high likelihood ratio for the presence of appendicitis by combining 2 inexpensive tests. Adding a thorough history and physical exam and a clinical scoring system can further enhance our clinical diagnosis. Considering the cost and the wide range of diagnostic accuracy of imaging studies (which depend on the experience of the reader), it is reasonable to skip CT scan in low probability presentations.
Evidence summary
Radiographic imaging to rule out appendicitis has become more commonplace, but it comes with an increased financial cost and additional delay in surgical intervention. Knowing the accuracy of common diagnostic tests may reduce the need for confirmatory imaging studies that increase both cost and time to surgery.
High levels of 2 or more inflammatory values are helpful
A meta-analysis of patients hospitalized for suspected acute appendicitis analyzed 28 different diagnostic variables in 24 studies.1 Variables included WBC, granulocyte count, PMN proportion, CRP level, and body temperature; histopathology was the gold standard. In no circumstance did an isolated elevation of any 1 factor result in a significant LR+. In addition, the absence of any 1 variable failed to yield a LR– <0.01 (low enough to exclude appendicitis).
Clinicians inherently combine multiple variables when evaluating patients, and when evaluating patients with abdominal pain, this technique can result in identification of adequate likelihood ratios (TABLE).1 In general, when 2 or more of the aforementioned inflammatory variables are present, the diagnosis of acute appendicitis is likely. When all markers of inflammation are normal, though acute appendicitis is less likely, the power is insufficient to exclude it as a possible diagnosis.
The value of CRP in the evaluation of suspected appendicitis was confirmed in a retrospective evaluation of 566 patients who underwent appendectomies.2 The sensitivity and specificity of the test improved depending on the duration of symptoms for both appendicitis and ruptured appendicitis. For appendicitis, CRP levels >1.4, 4.0, and 10.5 on Days 1, 2, and 3 had sensitivities/specificities of 0.38/0.81, 0.63/0.78, and 0.72/0.83, respectively. For ruptured appendicitis, levels of 3.3, 8.5, and 12.0 on Days 1, 2, and 3 had sensitivities/specificities of 0.77/0.89, 0.70/0.95, and 0.90/0.96, respectively.
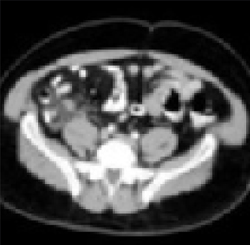
Enlarged appendix with inflammatory changes to mesenteric fatIn a series of 439 patients with symptoms suggestive of acute appendicitis, those with confirmed appendicitis (n=101) had a mean WBC count of 14.8 K/μL (95% CI, 13.9–15.8) and a mean neutrophil percentage of 82 (95% CI, 80–84).1 In contrast, those without appendicitis (n=338) had a mean WBC count of 9.2 K/μL (95% CI, 9.0–9.4) and a mean neutrophil percentage of 68 (95% CI, 66–70).
TABLE
How much do the inflammatory markers tell us? A look at likelihood ratios for appendicitis
| COMBINATION OF TESTS | LIKELIHOOD RATIOS | |
|---|---|---|
| POSITIVE (>10=STRONG EVIDENCE FOR DIAGNOSIS) | NEGATIVE (<0.1=EVIDENCE AGAINST DIAGNOSIS) | |
| WBC >10.0 × 109/L CRP >8 mg/L | 23.32 (95% CI, 6.87–84.79) | 0.03 (95% CI, 0.00–0.14) |
| WBC >10.0 × 109/L PMN cells >70% CRP >12 mg/L | 20.85 (95% CI, 5.47–80.27) | 0.03 (95% CI, 0.01–0.16) |
| Guarding/rebound tenderness WBC >10.0×109 | 11.34 (95% CI, 6.65–19.56) | 0.14 (95% CI, 0.08–0.24) |
| WBC, white blood cell count; CRP, C-reactive protein; PMN, polymorphonuclear leukocyte; CI, confidence interval. | ||
| Source: Andersson, Br J Surg 2004.1 | ||
Recommendations from others
A review of medical and professional associations revealed no official guidelines regarding the evaluation of suspected acute appendicitis. Surgical textbooks confirm that the diagnosis of acute appendicitis is made primarily by history and examination, with help from laboratory and radiographic studies.3
1. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg 2004;91:28-37.
2. Birkhahn R, Briggs M, Datillo PA, Van Deusen SK, Gaeta TJ. Classifying patient suspected of appendicitis with regard to likelihood. Am J Surgery 2006;191:497-502.
3. Townsend CM, Sabiston DC. Sabiston Textbook of Surgery. 17th ed. Philadelphia, Pa: Saunders, 2004:1381–1395.
No, none of the 3—history, exam, or labs— is sufficiently accurate to diagnose acute appendicitis (strength of recommendation [SOR]: A, based on meta-analysis of high-quality studies). When combined, the following tests are helpful: an elevated C-reactive protein (CRP), elevated total white blood cell (WBC) count, elevated percentage of polymorphonuclear leukocyte (PMN) cells (left shift), and the presence of guarding or rebound on physical examination. The combination of any 2 of these tests yields a very high positive likelihood ratio (LR+), but the absence of these does not exclude appendicitis (SOR: A, based on meta-analysis of high-quality studies).
2 inexpensive tests can lower costs in low-probability presentations
Fereshteh Gerayli, MD
East Tennessee State University, Johnson City
Unlike physicians in other parts of the world, us physicians rely heavily on imaging studies to diagnose acute appendicitis. This has decreased the rate of negative appendectomies by 15% to 20%. However, the liberal and indiscriminate use of imaging studies increases medical costs while diminishing physicians’ clinical diagnostic skills.
The systematic review our authors cited demonstrated a high likelihood ratio for the presence of appendicitis by combining 2 inexpensive tests. Adding a thorough history and physical exam and a clinical scoring system can further enhance our clinical diagnosis. Considering the cost and the wide range of diagnostic accuracy of imaging studies (which depend on the experience of the reader), it is reasonable to skip CT scan in low probability presentations.
Evidence summary
Radiographic imaging to rule out appendicitis has become more commonplace, but it comes with an increased financial cost and additional delay in surgical intervention. Knowing the accuracy of common diagnostic tests may reduce the need for confirmatory imaging studies that increase both cost and time to surgery.
High levels of 2 or more inflammatory values are helpful
A meta-analysis of patients hospitalized for suspected acute appendicitis analyzed 28 different diagnostic variables in 24 studies.1 Variables included WBC, granulocyte count, PMN proportion, CRP level, and body temperature; histopathology was the gold standard. In no circumstance did an isolated elevation of any 1 factor result in a significant LR+. In addition, the absence of any 1 variable failed to yield a LR– <0.01 (low enough to exclude appendicitis).
Clinicians inherently combine multiple variables when evaluating patients, and when evaluating patients with abdominal pain, this technique can result in identification of adequate likelihood ratios (TABLE).1 In general, when 2 or more of the aforementioned inflammatory variables are present, the diagnosis of acute appendicitis is likely. When all markers of inflammation are normal, though acute appendicitis is less likely, the power is insufficient to exclude it as a possible diagnosis.
The value of CRP in the evaluation of suspected appendicitis was confirmed in a retrospective evaluation of 566 patients who underwent appendectomies.2 The sensitivity and specificity of the test improved depending on the duration of symptoms for both appendicitis and ruptured appendicitis. For appendicitis, CRP levels >1.4, 4.0, and 10.5 on Days 1, 2, and 3 had sensitivities/specificities of 0.38/0.81, 0.63/0.78, and 0.72/0.83, respectively. For ruptured appendicitis, levels of 3.3, 8.5, and 12.0 on Days 1, 2, and 3 had sensitivities/specificities of 0.77/0.89, 0.70/0.95, and 0.90/0.96, respectively.
Enlarged appendix with inflammatory changes to mesenteric fatIn a series of 439 patients with symptoms suggestive of acute appendicitis, those with confirmed appendicitis (n=101) had a mean WBC count of 14.8 K/μL (95% CI, 13.9–15.8) and a mean neutrophil percentage of 82 (95% CI, 80–84).1 In contrast, those without appendicitis (n=338) had a mean WBC count of 9.2 K/μL (95% CI, 9.0–9.4) and a mean neutrophil percentage of 68 (95% CI, 66–70).
TABLE
How much do the inflammatory markers tell us? A look at likelihood ratios for appendicitis
| COMBINATION OF TESTS | LIKELIHOOD RATIOS | |
|---|---|---|
| POSITIVE (>10=STRONG EVIDENCE FOR DIAGNOSIS) | NEGATIVE (<0.1=EVIDENCE AGAINST DIAGNOSIS) | |
| WBC >10.0 × 109/L CRP >8 mg/L | 23.32 (95% CI, 6.87–84.79) | 0.03 (95% CI, 0.00–0.14) |
| WBC >10.0 × 109/L PMN cells >70% CRP >12 mg/L | 20.85 (95% CI, 5.47–80.27) | 0.03 (95% CI, 0.01–0.16) |
| Guarding/rebound tenderness WBC >10.0×109 | 11.34 (95% CI, 6.65–19.56) | 0.14 (95% CI, 0.08–0.24) |
| WBC, white blood cell count; CRP, C-reactive protein; PMN, polymorphonuclear leukocyte; CI, confidence interval. | ||
| Source: Andersson, Br J Surg 2004.1 | ||
Recommendations from others
A review of medical and professional associations revealed no official guidelines regarding the evaluation of suspected acute appendicitis. Surgical textbooks confirm that the diagnosis of acute appendicitis is made primarily by history and examination, with help from laboratory and radiographic studies.3
No, none of the 3—history, exam, or labs— is sufficiently accurate to diagnose acute appendicitis (strength of recommendation [SOR]: A, based on meta-analysis of high-quality studies). When combined, the following tests are helpful: an elevated C-reactive protein (CRP), elevated total white blood cell (WBC) count, elevated percentage of polymorphonuclear leukocyte (PMN) cells (left shift), and the presence of guarding or rebound on physical examination. The combination of any 2 of these tests yields a very high positive likelihood ratio (LR+), but the absence of these does not exclude appendicitis (SOR: A, based on meta-analysis of high-quality studies).
2 inexpensive tests can lower costs in low-probability presentations
Fereshteh Gerayli, MD
East Tennessee State University, Johnson City
Unlike physicians in other parts of the world, us physicians rely heavily on imaging studies to diagnose acute appendicitis. This has decreased the rate of negative appendectomies by 15% to 20%. However, the liberal and indiscriminate use of imaging studies increases medical costs while diminishing physicians’ clinical diagnostic skills.
The systematic review our authors cited demonstrated a high likelihood ratio for the presence of appendicitis by combining 2 inexpensive tests. Adding a thorough history and physical exam and a clinical scoring system can further enhance our clinical diagnosis. Considering the cost and the wide range of diagnostic accuracy of imaging studies (which depend on the experience of the reader), it is reasonable to skip CT scan in low probability presentations.
Evidence summary
Radiographic imaging to rule out appendicitis has become more commonplace, but it comes with an increased financial cost and additional delay in surgical intervention. Knowing the accuracy of common diagnostic tests may reduce the need for confirmatory imaging studies that increase both cost and time to surgery.
High levels of 2 or more inflammatory values are helpful
A meta-analysis of patients hospitalized for suspected acute appendicitis analyzed 28 different diagnostic variables in 24 studies.1 Variables included WBC, granulocyte count, PMN proportion, CRP level, and body temperature; histopathology was the gold standard. In no circumstance did an isolated elevation of any 1 factor result in a significant LR+. In addition, the absence of any 1 variable failed to yield a LR– <0.01 (low enough to exclude appendicitis).
Clinicians inherently combine multiple variables when evaluating patients, and when evaluating patients with abdominal pain, this technique can result in identification of adequate likelihood ratios (TABLE).1 In general, when 2 or more of the aforementioned inflammatory variables are present, the diagnosis of acute appendicitis is likely. When all markers of inflammation are normal, though acute appendicitis is less likely, the power is insufficient to exclude it as a possible diagnosis.
The value of CRP in the evaluation of suspected appendicitis was confirmed in a retrospective evaluation of 566 patients who underwent appendectomies.2 The sensitivity and specificity of the test improved depending on the duration of symptoms for both appendicitis and ruptured appendicitis. For appendicitis, CRP levels >1.4, 4.0, and 10.5 on Days 1, 2, and 3 had sensitivities/specificities of 0.38/0.81, 0.63/0.78, and 0.72/0.83, respectively. For ruptured appendicitis, levels of 3.3, 8.5, and 12.0 on Days 1, 2, and 3 had sensitivities/specificities of 0.77/0.89, 0.70/0.95, and 0.90/0.96, respectively.
Enlarged appendix with inflammatory changes to mesenteric fatIn a series of 439 patients with symptoms suggestive of acute appendicitis, those with confirmed appendicitis (n=101) had a mean WBC count of 14.8 K/μL (95% CI, 13.9–15.8) and a mean neutrophil percentage of 82 (95% CI, 80–84).1 In contrast, those without appendicitis (n=338) had a mean WBC count of 9.2 K/μL (95% CI, 9.0–9.4) and a mean neutrophil percentage of 68 (95% CI, 66–70).
TABLE
How much do the inflammatory markers tell us? A look at likelihood ratios for appendicitis
| COMBINATION OF TESTS | LIKELIHOOD RATIOS | |
|---|---|---|
| POSITIVE (>10=STRONG EVIDENCE FOR DIAGNOSIS) | NEGATIVE (<0.1=EVIDENCE AGAINST DIAGNOSIS) | |
| WBC >10.0 × 109/L CRP >8 mg/L | 23.32 (95% CI, 6.87–84.79) | 0.03 (95% CI, 0.00–0.14) |
| WBC >10.0 × 109/L PMN cells >70% CRP >12 mg/L | 20.85 (95% CI, 5.47–80.27) | 0.03 (95% CI, 0.01–0.16) |
| Guarding/rebound tenderness WBC >10.0×109 | 11.34 (95% CI, 6.65–19.56) | 0.14 (95% CI, 0.08–0.24) |
| WBC, white blood cell count; CRP, C-reactive protein; PMN, polymorphonuclear leukocyte; CI, confidence interval. | ||
| Source: Andersson, Br J Surg 2004.1 | ||
Recommendations from others
A review of medical and professional associations revealed no official guidelines regarding the evaluation of suspected acute appendicitis. Surgical textbooks confirm that the diagnosis of acute appendicitis is made primarily by history and examination, with help from laboratory and radiographic studies.3
1. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg 2004;91:28-37.
2. Birkhahn R, Briggs M, Datillo PA, Van Deusen SK, Gaeta TJ. Classifying patient suspected of appendicitis with regard to likelihood. Am J Surgery 2006;191:497-502.
3. Townsend CM, Sabiston DC. Sabiston Textbook of Surgery. 17th ed. Philadelphia, Pa: Saunders, 2004:1381–1395.
1. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg 2004;91:28-37.
2. Birkhahn R, Briggs M, Datillo PA, Van Deusen SK, Gaeta TJ. Classifying patient suspected of appendicitis with regard to likelihood. Am J Surgery 2006;191:497-502.
3. Townsend CM, Sabiston DC. Sabiston Textbook of Surgery. 17th ed. Philadelphia, Pa: Saunders, 2004:1381–1395.
Evidence-based answers from the Family Physicians Inquiries Network