User login
Bariatric surgery should be considered as a treatment option for type 2 diabetes patients with body mass indexes between 30 and 35 kg/m2 and diabetes that can’t be controlled adequately by an optimal medical regimen – particularly in patients with other major cardiovascular disease risk factors, according to a statement from the International Diabetes Federation.
The position statement, "Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 Diabetes" is in response to the global epidemic of obesity-related diabetes and the failure of lifestyle and medical treatments to prevent dangerous and costly comorbidities. It goes further than does the American Diabetes Association’s guidance on bariatric surgery, which cautions that type 2 diabetes patients with a BMI between 30 and 35 should only undergo surgery in the context of a clinical research study.

However, "bariatric procedures are not a public health solution for ‘diabesity,’ " cautioned Dr. Paul Zimmet, cochair of the IDF Task Force on Epidemiology and Prevention, and research is needed to continue to define the persons most likely to benefit. It will require very strict criteria for patient selection and the availability of the best circumstances – high-volume centers with competent surgeons, the best procedures, adequate follow-up, and proper evaluation of outcomes, Dr. Zimmet said in an interview.
Results from lifestyle and medical methods for weight loss are "modest and rarely sustained, particularly in the severely obese," the IDF statement noted. Furthermore, pervasive attitudes toward obesity – as a personal failure rather than a complex condition influenced by strong physical, emotional, and societal issues – effectively erect barriers to care and equal treatment at work, according to the statement.
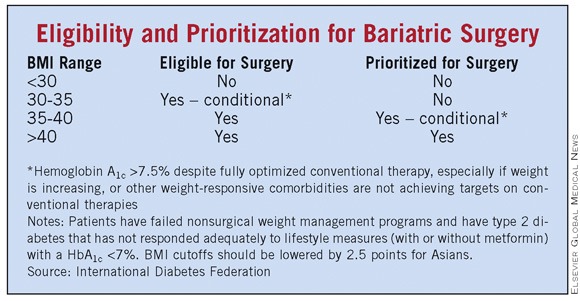
The metabolic benefits of gastrointestinal surgery go beyond that achieved by weight loss alone. Normalization not only of hyperglycemia but also of hyperlipidemia, blood pressure, and obstructive sleep apnea has been shown consistently. And long-term follow-up has shown reductions in mortality from coronary artery disease, diabetes, and cancer. Therefore, surgical intervention should be a part of diabetes treatment algorithms (see table), according to the IDF statement. In fact, because early intervention increases the likelihood of remission, and residual hyperglycemia is easier to manage after surgery, intervention for type 2 diabetes patients "should be considered early as an option for eligible patients, rather than being held back as a last resort," the IDF recommended.
Obesity and diabetes have such powerful effects on health and longevity that their surging worldwide prevalence constitutes a major global health issue that "demands urgent attention from governments, health care systems, and the medical community," said the group.
The IDF noted that the complication risks of surgery have gone down considerably over time, especially since laparoscopic procedures have been used. But the long-term risks are numerous and vary by procedure, ranging from the need for revision to nutritional deficiencies. Lifelong monitoring is required, and national registries should be established and funded.
The surgeries are cost effective for diabetes, according to the statement. Studies in the United States, Australia, and the United Kingdom have shown that an intervention leads to the rare outcome of generating "both cost savings and health benefits over the lifetime of the cohort" and "provides the most compelling evidence for funding based on economic criteria."
The IDF task force did not recommend any one type of surgery. "There is a need for well-designed, randomized, controlled trials to compare both efficacy and cost [of bariatric surgeries]. Those data do not exist," said Dr. Zimmet, director emeritus of the Baker IDI Heart and Diabetes Institute, Melbourne. But in the United States, the only procedure with Food and Drug Administration approval for patients with a BMI of 30 is adjustable gastric banding.
"This is the first time the International Diabetes Federation or any major international organization has made recommendations on this rapidly developing area of therapy," Dr. Francesco Rubino, chief of the gastrointestinal metabolic surgery at New York–Presbyterian Hospital/Weill Cornell Medical Center, New York, said in a statement. "It did so because of the urgent need for worldwide expert guidance on the use of bariatric surgery because of the increasing usage."
The announcement was made from the World Congress on Interventional Therapies for Type 2 Diabetes, held in New York and directed by Dr. Rubino.
The consensus meeting was supported with an unrestricted educational grant by Allergan Inc., Ethicon, Ethicon Endo-Surgery Inc., and MetaCure Inc. These companies played no role in the discussion or preparation of the position paper, according to the task force statement. Members of the writing group had no disclosures.
Bariatric surgery should be considered as a treatment option for type 2 diabetes patients with body mass indexes between 30 and 35 kg/m2 and diabetes that can’t be controlled adequately by an optimal medical regimen – particularly in patients with other major cardiovascular disease risk factors, according to a statement from the International Diabetes Federation.
The position statement, "Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 Diabetes" is in response to the global epidemic of obesity-related diabetes and the failure of lifestyle and medical treatments to prevent dangerous and costly comorbidities. It goes further than does the American Diabetes Association’s guidance on bariatric surgery, which cautions that type 2 diabetes patients with a BMI between 30 and 35 should only undergo surgery in the context of a clinical research study.
However, "bariatric procedures are not a public health solution for ‘diabesity,’ " cautioned Dr. Paul Zimmet, cochair of the IDF Task Force on Epidemiology and Prevention, and research is needed to continue to define the persons most likely to benefit. It will require very strict criteria for patient selection and the availability of the best circumstances – high-volume centers with competent surgeons, the best procedures, adequate follow-up, and proper evaluation of outcomes, Dr. Zimmet said in an interview.
Results from lifestyle and medical methods for weight loss are "modest and rarely sustained, particularly in the severely obese," the IDF statement noted. Furthermore, pervasive attitudes toward obesity – as a personal failure rather than a complex condition influenced by strong physical, emotional, and societal issues – effectively erect barriers to care and equal treatment at work, according to the statement.
The metabolic benefits of gastrointestinal surgery go beyond that achieved by weight loss alone. Normalization not only of hyperglycemia but also of hyperlipidemia, blood pressure, and obstructive sleep apnea has been shown consistently. And long-term follow-up has shown reductions in mortality from coronary artery disease, diabetes, and cancer. Therefore, surgical intervention should be a part of diabetes treatment algorithms (see table), according to the IDF statement. In fact, because early intervention increases the likelihood of remission, and residual hyperglycemia is easier to manage after surgery, intervention for type 2 diabetes patients "should be considered early as an option for eligible patients, rather than being held back as a last resort," the IDF recommended.
Obesity and diabetes have such powerful effects on health and longevity that their surging worldwide prevalence constitutes a major global health issue that "demands urgent attention from governments, health care systems, and the medical community," said the group.
The IDF noted that the complication risks of surgery have gone down considerably over time, especially since laparoscopic procedures have been used. But the long-term risks are numerous and vary by procedure, ranging from the need for revision to nutritional deficiencies. Lifelong monitoring is required, and national registries should be established and funded.
The surgeries are cost effective for diabetes, according to the statement. Studies in the United States, Australia, and the United Kingdom have shown that an intervention leads to the rare outcome of generating "both cost savings and health benefits over the lifetime of the cohort" and "provides the most compelling evidence for funding based on economic criteria."
The IDF task force did not recommend any one type of surgery. "There is a need for well-designed, randomized, controlled trials to compare both efficacy and cost [of bariatric surgeries]. Those data do not exist," said Dr. Zimmet, director emeritus of the Baker IDI Heart and Diabetes Institute, Melbourne. But in the United States, the only procedure with Food and Drug Administration approval for patients with a BMI of 30 is adjustable gastric banding.
"This is the first time the International Diabetes Federation or any major international organization has made recommendations on this rapidly developing area of therapy," Dr. Francesco Rubino, chief of the gastrointestinal metabolic surgery at New York–Presbyterian Hospital/Weill Cornell Medical Center, New York, said in a statement. "It did so because of the urgent need for worldwide expert guidance on the use of bariatric surgery because of the increasing usage."
The announcement was made from the World Congress on Interventional Therapies for Type 2 Diabetes, held in New York and directed by Dr. Rubino.
The consensus meeting was supported with an unrestricted educational grant by Allergan Inc., Ethicon, Ethicon Endo-Surgery Inc., and MetaCure Inc. These companies played no role in the discussion or preparation of the position paper, according to the task force statement. Members of the writing group had no disclosures.
Bariatric surgery should be considered as a treatment option for type 2 diabetes patients with body mass indexes between 30 and 35 kg/m2 and diabetes that can’t be controlled adequately by an optimal medical regimen – particularly in patients with other major cardiovascular disease risk factors, according to a statement from the International Diabetes Federation.
The position statement, "Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 Diabetes" is in response to the global epidemic of obesity-related diabetes and the failure of lifestyle and medical treatments to prevent dangerous and costly comorbidities. It goes further than does the American Diabetes Association’s guidance on bariatric surgery, which cautions that type 2 diabetes patients with a BMI between 30 and 35 should only undergo surgery in the context of a clinical research study.
However, "bariatric procedures are not a public health solution for ‘diabesity,’ " cautioned Dr. Paul Zimmet, cochair of the IDF Task Force on Epidemiology and Prevention, and research is needed to continue to define the persons most likely to benefit. It will require very strict criteria for patient selection and the availability of the best circumstances – high-volume centers with competent surgeons, the best procedures, adequate follow-up, and proper evaluation of outcomes, Dr. Zimmet said in an interview.
Results from lifestyle and medical methods for weight loss are "modest and rarely sustained, particularly in the severely obese," the IDF statement noted. Furthermore, pervasive attitudes toward obesity – as a personal failure rather than a complex condition influenced by strong physical, emotional, and societal issues – effectively erect barriers to care and equal treatment at work, according to the statement.
The metabolic benefits of gastrointestinal surgery go beyond that achieved by weight loss alone. Normalization not only of hyperglycemia but also of hyperlipidemia, blood pressure, and obstructive sleep apnea has been shown consistently. And long-term follow-up has shown reductions in mortality from coronary artery disease, diabetes, and cancer. Therefore, surgical intervention should be a part of diabetes treatment algorithms (see table), according to the IDF statement. In fact, because early intervention increases the likelihood of remission, and residual hyperglycemia is easier to manage after surgery, intervention for type 2 diabetes patients "should be considered early as an option for eligible patients, rather than being held back as a last resort," the IDF recommended.
Obesity and diabetes have such powerful effects on health and longevity that their surging worldwide prevalence constitutes a major global health issue that "demands urgent attention from governments, health care systems, and the medical community," said the group.
The IDF noted that the complication risks of surgery have gone down considerably over time, especially since laparoscopic procedures have been used. But the long-term risks are numerous and vary by procedure, ranging from the need for revision to nutritional deficiencies. Lifelong monitoring is required, and national registries should be established and funded.
The surgeries are cost effective for diabetes, according to the statement. Studies in the United States, Australia, and the United Kingdom have shown that an intervention leads to the rare outcome of generating "both cost savings and health benefits over the lifetime of the cohort" and "provides the most compelling evidence for funding based on economic criteria."
The IDF task force did not recommend any one type of surgery. "There is a need for well-designed, randomized, controlled trials to compare both efficacy and cost [of bariatric surgeries]. Those data do not exist," said Dr. Zimmet, director emeritus of the Baker IDI Heart and Diabetes Institute, Melbourne. But in the United States, the only procedure with Food and Drug Administration approval for patients with a BMI of 30 is adjustable gastric banding.
"This is the first time the International Diabetes Federation or any major international organization has made recommendations on this rapidly developing area of therapy," Dr. Francesco Rubino, chief of the gastrointestinal metabolic surgery at New York–Presbyterian Hospital/Weill Cornell Medical Center, New York, said in a statement. "It did so because of the urgent need for worldwide expert guidance on the use of bariatric surgery because of the increasing usage."
The announcement was made from the World Congress on Interventional Therapies for Type 2 Diabetes, held in New York and directed by Dr. Rubino.
The consensus meeting was supported with an unrestricted educational grant by Allergan Inc., Ethicon, Ethicon Endo-Surgery Inc., and MetaCure Inc. These companies played no role in the discussion or preparation of the position paper, according to the task force statement. Members of the writing group had no disclosures.
FROM A STATEMENT BY THE INTERNATIONAL DIABETES FEDERATION