User login
If you are a solo orthopedic surgeon or practice in a small group and are 55 years or older, this article is for you. The answer to the question “When is the right time to begin planning for the transition out of practice?” is now. And planning is the most important word in that sentence.
Joining your peers who’ve quit, often rather quickly, because of Obamacare, electronic health records (EHRs), or the implementation of ICD-10 (International Classification of Diseases, Tenth Revision) may prove unsatisfying. As the saying goes, “act in haste, repent at leisure.” And as a gerontologist friend of mine liked to say, “Retiring from medicine without retiring to something is risky.” He often quipped that golf didn’t count.
Recent survey results help support his point. In the 2014 Medscape Orthopedist Compensation Report,1 respondents were asked:
What is the most rewarding part of your job?
- Gratitude/relationships with patients 43%
- Being very good at what I do/Finding answers, diagnoses 31%
- Making good money at a job that I like 10%
- Knowing that I’m making the world a better place 7%
- Being proud of being a doctor 4%
- Nothing 1%
- Let’s hope you are not part of the 1%!
In the often-quoted Deloitte 2013 Survey of U.S. Physicians,2 6 in 10 respondents predicted that many physicians will retire earlier than planned in the next 1 to 3 years. Yet even in that survey, 41% of surgical specialists said that patient relationships were the most satisfying factor about practicing medicine. Protecting and promoting individual health was second (33%), and intellectual stimulation was third (16%).2
As Steve Marsh, managing partner at The Medicus Firm, Dallas, was quoted as saying about this data, “For older doctors, being a physician is much more of a lifestyle than a job.”3 In my 40 years of working with physicians, I agree. And that’s why you, dear readers, must begin the transition planning process now, if you are 55 years or older, or soon, if you are approaching this age. Unraveling yourself from the patient relationships and the profession you have enjoyed for so long will feel like a big loss for the majority of you. There will be a grieving process. You’re not just leaving a “job,” you’re leaving your “life’s work,” and the sooner you begin planning for this shift, the less uncomfortable it will be.
Transition Planning Timeline
As the Chinese saying goes, “the longest journey begins with a single step.” The first, most challenging step in transition planning is deciding to address the issue head on—whether you see yourself practicing well into your late 60s or stepping aside 3 years from now.
Here are 7 questions to get you started. Discuss them with your spouse and a trusted advisor or mentor.
1. Have you done everything that you wanted to accomplish professionally? What’s left on your “to-do” list?
2. Are you satisfied with the legacy you are leaving to your community, partners, or employees?
3. What does your spouse think? His or her age and stage may dictate some choices. One wife said she believed in Henny Youngman’s advice: “Promise to take your wife for better or worse, but not for lunch.” Younger spouses in satisfying careers may not be ready to quit or slow down.
4. What could fill the void of, as the Medscape survey indicated, the “gratitude/patient relationships” and “being good at what you do” that you would be leaving behind? Could going on medical missions satisfy your need to keep your hands in? Or volunteering for the community clinic?
5. If you were to retire within the next 6 months, what would your routine look like? Because the first year is often filled with travel and long-postponed fun, think beyond that and describe year 3. (Assume good health and adequate finances.)
6. Are there options for part-time practice? Could you ease out instead of going basically full throttle until your retirement date?
7. Are challenges such as stress, fatigue, cognitive decline, or a feeling of burnout a reality for you? Be honest with yourself. These are real issues that not only impact your decision about when to transition, but also patient safety and care.
If you’ve reached 60 years of age and haven’t thought about questions like these, you aren’t alone. Many orthopedic surgeons delay this planning exercise for the same reasons other business owners do:
You are too busy spending all of your time putting out fires. Who has time to plan? Learning the new ICD-10 codes for local coverage determinations (LCDs), hiring a new physician assistant, firing the receptionist, and, oh by the way, taking care of a full schedule of patients, takes time and reduces the time to plan.
You think “it’s not time yet.” We often hear surgeons say, “Gosh, I don’t feel __ years old!” or “I plan to work until I’m 70.” Sound familiar?
You’re afraid to think about what life would be like without your profession. So you do nothing. Imagining a life without being needed on a daily basis can be daunting. Reread the survey results above. If you don’t have interesting and emotionally rewarding activities that will fill the void, that can cause anxiety. And the fact is, the demands on physicians, especially those in solo practice, haven’t left much time for outside interests.
Discussing personal goals and financial matters with others is messy or taboo. Transitioning out of practice is an awkward and uncomfortable topic. Plus, whom do you call for help with planning the next stage of your life?
These and others on a long list of excuses and anxieties result in fewer than 70% of all surgical specialists we talk with having a viable transition plan. Many, of course, have done a superb job of funding their retirement plans and have the assets set aside to fund a comfortable lifestyle. A lot has been written on the financial aspects of retirement. Your financial advisor, broker, or banker has formulas, tools, and advice that you’ve probably been following for decades. The 2014 Medscape Orthopedist Compensation Report shows the average salary is $413,000, with private practice doctors earning even more, $439,000 on average.1 Although such salaries should ensure the funding of retirement savings plans, undeniably, the financial crisis and stock market collapse of 2008 delayed many surgeons’ retirement. Even today, some surgeons who are considering their practice finish line are looking over their shoulder at market returns with a sense of insecurity.
Recruitment Is More Likely Than Cash Out
Thinking you can sell your practice for big bucks is a false hope. In the 1970s and early 1980s, before the onslaught of managed care, it was possible to sell your practice. A young surgeon would welcome having space, staff, and patients at the ready. This is no longer the case, since patient loyalty is now impacted by health insurance plan membership.
Pocketing a hefty sum from selling the office building may not be much of a windfall either. It depends on that all-important real estate formula: location, location, location. In addition, dividends from and investment in a surgery center rarely continue once you are no longer operating.
To maximize the profit potential that remains in this last phase of practice—which in turn can attract surgical talent as you transition—you’ve got to sharpen the sword and pay attention. One surgeon attributed a revenue decline of about 30% over the last 5 years to a combination of lesser insurance reimbursements, his taking more time off, and failing to pay attention to his staff’s write-off habits. Revenue cycle, management, coding, and practice operations must be finely tuned to optimize profitability, and failing to manage your practice effectively will make it less attractive when recruiting a younger surgeon to take your place or assume the patient base. Consider a practice evaluation regardless of where you are in your planning, which will help the practice prioritize improvements that deliver the best benefit and value within the context of your transition plan.
And if recruitment is part of that plan, be prepared to spend significant time on the search. Solo and small groups are finding it challenging to recruit just-out-of-training associates. This generation of new physicians values work-life balance and is more likely to prefer employment to entrepreneurship. Additionally, established physicians who have not invested in or adopted new technologies, such as EHR, will have a tough time attracting top talent. Having been trained using EHRs, few, if any, young doctors will find a reversion to paper records acceptable—and, in fact, most find it a turnoff. Thus, depending on your transition plan and your age and stage, updating technology may be a necessary investment.
Stepping Down But Not Out
If you’re thinking about slowing down but not ceasing practice completely just yet, 2 options are worth considering: practicing part-time and/or becoming a nonoperative orthopedist.
The 2014 Orthopaedic Practice in the United States (OPUS) report issued by the American Academy of Orthopaedic Surgeons shows that the average age of part-time surgeons is 69.14 years and that 48.6% are generalists.5 Part-time surgeons surveyed reported working an average of 23 hours per week and performing 5 procedures per month, compared with full-time surgeons who clock in at 56 hours per week and perform 31 procedures per month.5
Senior surgeons who want to pull back their hours or become nonoperative orthopedists may be quite marketable to group practices. There are several reasons for this. First, population growth will not be supported by the number of physicians graduating from Medicare-sponsored residency slots—which have not increased since 1997. Second, the physician workforce is growing older, and younger surgeons are harder to recruit. They tend to emphasize work-life balance over working the countless hours their senior counterparts did, and, thus, don’t treat as many patients as older colleagues did. And, third, a nonoperative or part-time physician may be more appealing to patients than nonphysician providers, yet accomplish the same purpose of keeping operating surgeons out of the office and in the operating room. So, that former competitor down the street may become a potential employer. You won’t be a voting partner, but that may be a low priority as you step into part-time practice.
We imagine an opportunity for nonoperative orthopedists similar to concierge internists, who go out of network and charge reasonable fees for longer appointments and less paperwork hassle. And this opportunity isn’t only for those practicing in groups. Solo orthopedists may see this change in practice attractive, as it offers reduced professional liability premiums, holds some clear attraction for patients not eager to go under the knife, and makes it easier to arrange time off for the doctor.
As I often tell clients about their business: “Plan your work, and work your plan.” This same maxim holds true of planning for retirement. The intangible aspects of leaving your livelihood require thought and contemplation. My hope is that you’ll put pen to paper and document the answers to the questions posed in this article, so they begin to become as important as the financial aspects of your retirement planning. Of course, the plan may be waylaid midstream owing to reimbursement challenges, an offer you can’t refuse from the hospital, or a change in your health or that of your spouse. However, taking that single step and starting your plan will give you the foundation necessary to move forward or pivot in the journey ahead.
1. Peckham C. Medscape Orthopedist Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/orthopedics#1. Published April 15, 2014. Accessed October 29, 2015.
2. Deloitte 2013 Survey of U.S. Physicians: Physician Perspectives About Health Care Reform and the Future of the Medical Profession. Deloitte Center for Health Solutions website. http://www2.deloitte.com/content/dam/Deloitte/us/Documents/life-sciences-health-care/us-lshc-deloitte-2013-physician-survey-10012014.pdf. Accessed October 29, 2015.
3. Hyden M. Are physicians retiring early? MGMA Connection Plus. Medical Group Management Association website. http://www.mgma.com/practice-resources/mgma-connection-plus/online-only/2015/august-(1)/are-physicians-retiring-early. Published July 28, 2015. Accessed November 10, 2015.
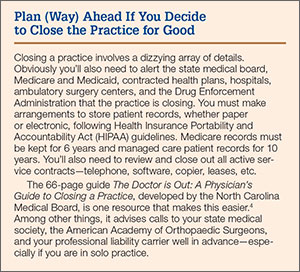
4. The Doctor is Out: A Physician’s Guide to Closing a Practice. North Carolina Medical Board website. http://www.ncmedboard.org/images/uploads/article_images/Physicians_Guide_to_Closing_a_Practice_05_12_2014.pdf. Published May 12, 2014. Accessed October 29, 2015.
5. Oreluk H, Cherf J. Practice settings and productivity. AAOS Now. 2015;9(10). http://www.aaos.org/news/aaosnow/oct15/managing1.asp. Accessed October 29, 2015.
If you are a solo orthopedic surgeon or practice in a small group and are 55 years or older, this article is for you. The answer to the question “When is the right time to begin planning for the transition out of practice?” is now. And planning is the most important word in that sentence.
Joining your peers who’ve quit, often rather quickly, because of Obamacare, electronic health records (EHRs), or the implementation of ICD-10 (International Classification of Diseases, Tenth Revision) may prove unsatisfying. As the saying goes, “act in haste, repent at leisure.” And as a gerontologist friend of mine liked to say, “Retiring from medicine without retiring to something is risky.” He often quipped that golf didn’t count.
Recent survey results help support his point. In the 2014 Medscape Orthopedist Compensation Report,1 respondents were asked:
What is the most rewarding part of your job?
- Gratitude/relationships with patients 43%
- Being very good at what I do/Finding answers, diagnoses 31%
- Making good money at a job that I like 10%
- Knowing that I’m making the world a better place 7%
- Being proud of being a doctor 4%
- Nothing 1%
- Let’s hope you are not part of the 1%!
In the often-quoted Deloitte 2013 Survey of U.S. Physicians,2 6 in 10 respondents predicted that many physicians will retire earlier than planned in the next 1 to 3 years. Yet even in that survey, 41% of surgical specialists said that patient relationships were the most satisfying factor about practicing medicine. Protecting and promoting individual health was second (33%), and intellectual stimulation was third (16%).2
As Steve Marsh, managing partner at The Medicus Firm, Dallas, was quoted as saying about this data, “For older doctors, being a physician is much more of a lifestyle than a job.”3 In my 40 years of working with physicians, I agree. And that’s why you, dear readers, must begin the transition planning process now, if you are 55 years or older, or soon, if you are approaching this age. Unraveling yourself from the patient relationships and the profession you have enjoyed for so long will feel like a big loss for the majority of you. There will be a grieving process. You’re not just leaving a “job,” you’re leaving your “life’s work,” and the sooner you begin planning for this shift, the less uncomfortable it will be.
Transition Planning Timeline
As the Chinese saying goes, “the longest journey begins with a single step.” The first, most challenging step in transition planning is deciding to address the issue head on—whether you see yourself practicing well into your late 60s or stepping aside 3 years from now.
Here are 7 questions to get you started. Discuss them with your spouse and a trusted advisor or mentor.
1. Have you done everything that you wanted to accomplish professionally? What’s left on your “to-do” list?
2. Are you satisfied with the legacy you are leaving to your community, partners, or employees?
3. What does your spouse think? His or her age and stage may dictate some choices. One wife said she believed in Henny Youngman’s advice: “Promise to take your wife for better or worse, but not for lunch.” Younger spouses in satisfying careers may not be ready to quit or slow down.
4. What could fill the void of, as the Medscape survey indicated, the “gratitude/patient relationships” and “being good at what you do” that you would be leaving behind? Could going on medical missions satisfy your need to keep your hands in? Or volunteering for the community clinic?
5. If you were to retire within the next 6 months, what would your routine look like? Because the first year is often filled with travel and long-postponed fun, think beyond that and describe year 3. (Assume good health and adequate finances.)
6. Are there options for part-time practice? Could you ease out instead of going basically full throttle until your retirement date?
7. Are challenges such as stress, fatigue, cognitive decline, or a feeling of burnout a reality for you? Be honest with yourself. These are real issues that not only impact your decision about when to transition, but also patient safety and care.
If you’ve reached 60 years of age and haven’t thought about questions like these, you aren’t alone. Many orthopedic surgeons delay this planning exercise for the same reasons other business owners do:
You are too busy spending all of your time putting out fires. Who has time to plan? Learning the new ICD-10 codes for local coverage determinations (LCDs), hiring a new physician assistant, firing the receptionist, and, oh by the way, taking care of a full schedule of patients, takes time and reduces the time to plan.
You think “it’s not time yet.” We often hear surgeons say, “Gosh, I don’t feel __ years old!” or “I plan to work until I’m 70.” Sound familiar?
You’re afraid to think about what life would be like without your profession. So you do nothing. Imagining a life without being needed on a daily basis can be daunting. Reread the survey results above. If you don’t have interesting and emotionally rewarding activities that will fill the void, that can cause anxiety. And the fact is, the demands on physicians, especially those in solo practice, haven’t left much time for outside interests.
Discussing personal goals and financial matters with others is messy or taboo. Transitioning out of practice is an awkward and uncomfortable topic. Plus, whom do you call for help with planning the next stage of your life?
These and others on a long list of excuses and anxieties result in fewer than 70% of all surgical specialists we talk with having a viable transition plan. Many, of course, have done a superb job of funding their retirement plans and have the assets set aside to fund a comfortable lifestyle. A lot has been written on the financial aspects of retirement. Your financial advisor, broker, or banker has formulas, tools, and advice that you’ve probably been following for decades. The 2014 Medscape Orthopedist Compensation Report shows the average salary is $413,000, with private practice doctors earning even more, $439,000 on average.1 Although such salaries should ensure the funding of retirement savings plans, undeniably, the financial crisis and stock market collapse of 2008 delayed many surgeons’ retirement. Even today, some surgeons who are considering their practice finish line are looking over their shoulder at market returns with a sense of insecurity.
Recruitment Is More Likely Than Cash Out
Thinking you can sell your practice for big bucks is a false hope. In the 1970s and early 1980s, before the onslaught of managed care, it was possible to sell your practice. A young surgeon would welcome having space, staff, and patients at the ready. This is no longer the case, since patient loyalty is now impacted by health insurance plan membership.
Pocketing a hefty sum from selling the office building may not be much of a windfall either. It depends on that all-important real estate formula: location, location, location. In addition, dividends from and investment in a surgery center rarely continue once you are no longer operating.
To maximize the profit potential that remains in this last phase of practice—which in turn can attract surgical talent as you transition—you’ve got to sharpen the sword and pay attention. One surgeon attributed a revenue decline of about 30% over the last 5 years to a combination of lesser insurance reimbursements, his taking more time off, and failing to pay attention to his staff’s write-off habits. Revenue cycle, management, coding, and practice operations must be finely tuned to optimize profitability, and failing to manage your practice effectively will make it less attractive when recruiting a younger surgeon to take your place or assume the patient base. Consider a practice evaluation regardless of where you are in your planning, which will help the practice prioritize improvements that deliver the best benefit and value within the context of your transition plan.
And if recruitment is part of that plan, be prepared to spend significant time on the search. Solo and small groups are finding it challenging to recruit just-out-of-training associates. This generation of new physicians values work-life balance and is more likely to prefer employment to entrepreneurship. Additionally, established physicians who have not invested in or adopted new technologies, such as EHR, will have a tough time attracting top talent. Having been trained using EHRs, few, if any, young doctors will find a reversion to paper records acceptable—and, in fact, most find it a turnoff. Thus, depending on your transition plan and your age and stage, updating technology may be a necessary investment.
Stepping Down But Not Out
If you’re thinking about slowing down but not ceasing practice completely just yet, 2 options are worth considering: practicing part-time and/or becoming a nonoperative orthopedist.
The 2014 Orthopaedic Practice in the United States (OPUS) report issued by the American Academy of Orthopaedic Surgeons shows that the average age of part-time surgeons is 69.14 years and that 48.6% are generalists.5 Part-time surgeons surveyed reported working an average of 23 hours per week and performing 5 procedures per month, compared with full-time surgeons who clock in at 56 hours per week and perform 31 procedures per month.5
Senior surgeons who want to pull back their hours or become nonoperative orthopedists may be quite marketable to group practices. There are several reasons for this. First, population growth will not be supported by the number of physicians graduating from Medicare-sponsored residency slots—which have not increased since 1997. Second, the physician workforce is growing older, and younger surgeons are harder to recruit. They tend to emphasize work-life balance over working the countless hours their senior counterparts did, and, thus, don’t treat as many patients as older colleagues did. And, third, a nonoperative or part-time physician may be more appealing to patients than nonphysician providers, yet accomplish the same purpose of keeping operating surgeons out of the office and in the operating room. So, that former competitor down the street may become a potential employer. You won’t be a voting partner, but that may be a low priority as you step into part-time practice.
We imagine an opportunity for nonoperative orthopedists similar to concierge internists, who go out of network and charge reasonable fees for longer appointments and less paperwork hassle. And this opportunity isn’t only for those practicing in groups. Solo orthopedists may see this change in practice attractive, as it offers reduced professional liability premiums, holds some clear attraction for patients not eager to go under the knife, and makes it easier to arrange time off for the doctor.
As I often tell clients about their business: “Plan your work, and work your plan.” This same maxim holds true of planning for retirement. The intangible aspects of leaving your livelihood require thought and contemplation. My hope is that you’ll put pen to paper and document the answers to the questions posed in this article, so they begin to become as important as the financial aspects of your retirement planning. Of course, the plan may be waylaid midstream owing to reimbursement challenges, an offer you can’t refuse from the hospital, or a change in your health or that of your spouse. However, taking that single step and starting your plan will give you the foundation necessary to move forward or pivot in the journey ahead.
If you are a solo orthopedic surgeon or practice in a small group and are 55 years or older, this article is for you. The answer to the question “When is the right time to begin planning for the transition out of practice?” is now. And planning is the most important word in that sentence.
Joining your peers who’ve quit, often rather quickly, because of Obamacare, electronic health records (EHRs), or the implementation of ICD-10 (International Classification of Diseases, Tenth Revision) may prove unsatisfying. As the saying goes, “act in haste, repent at leisure.” And as a gerontologist friend of mine liked to say, “Retiring from medicine without retiring to something is risky.” He often quipped that golf didn’t count.
Recent survey results help support his point. In the 2014 Medscape Orthopedist Compensation Report,1 respondents were asked:
What is the most rewarding part of your job?
- Gratitude/relationships with patients 43%
- Being very good at what I do/Finding answers, diagnoses 31%
- Making good money at a job that I like 10%
- Knowing that I’m making the world a better place 7%
- Being proud of being a doctor 4%
- Nothing 1%
- Let’s hope you are not part of the 1%!
In the often-quoted Deloitte 2013 Survey of U.S. Physicians,2 6 in 10 respondents predicted that many physicians will retire earlier than planned in the next 1 to 3 years. Yet even in that survey, 41% of surgical specialists said that patient relationships were the most satisfying factor about practicing medicine. Protecting and promoting individual health was second (33%), and intellectual stimulation was third (16%).2
As Steve Marsh, managing partner at The Medicus Firm, Dallas, was quoted as saying about this data, “For older doctors, being a physician is much more of a lifestyle than a job.”3 In my 40 years of working with physicians, I agree. And that’s why you, dear readers, must begin the transition planning process now, if you are 55 years or older, or soon, if you are approaching this age. Unraveling yourself from the patient relationships and the profession you have enjoyed for so long will feel like a big loss for the majority of you. There will be a grieving process. You’re not just leaving a “job,” you’re leaving your “life’s work,” and the sooner you begin planning for this shift, the less uncomfortable it will be.
Transition Planning Timeline
As the Chinese saying goes, “the longest journey begins with a single step.” The first, most challenging step in transition planning is deciding to address the issue head on—whether you see yourself practicing well into your late 60s or stepping aside 3 years from now.
Here are 7 questions to get you started. Discuss them with your spouse and a trusted advisor or mentor.
1. Have you done everything that you wanted to accomplish professionally? What’s left on your “to-do” list?
2. Are you satisfied with the legacy you are leaving to your community, partners, or employees?
3. What does your spouse think? His or her age and stage may dictate some choices. One wife said she believed in Henny Youngman’s advice: “Promise to take your wife for better or worse, but not for lunch.” Younger spouses in satisfying careers may not be ready to quit or slow down.
4. What could fill the void of, as the Medscape survey indicated, the “gratitude/patient relationships” and “being good at what you do” that you would be leaving behind? Could going on medical missions satisfy your need to keep your hands in? Or volunteering for the community clinic?
5. If you were to retire within the next 6 months, what would your routine look like? Because the first year is often filled with travel and long-postponed fun, think beyond that and describe year 3. (Assume good health and adequate finances.)
6. Are there options for part-time practice? Could you ease out instead of going basically full throttle until your retirement date?
7. Are challenges such as stress, fatigue, cognitive decline, or a feeling of burnout a reality for you? Be honest with yourself. These are real issues that not only impact your decision about when to transition, but also patient safety and care.
If you’ve reached 60 years of age and haven’t thought about questions like these, you aren’t alone. Many orthopedic surgeons delay this planning exercise for the same reasons other business owners do:
You are too busy spending all of your time putting out fires. Who has time to plan? Learning the new ICD-10 codes for local coverage determinations (LCDs), hiring a new physician assistant, firing the receptionist, and, oh by the way, taking care of a full schedule of patients, takes time and reduces the time to plan.
You think “it’s not time yet.” We often hear surgeons say, “Gosh, I don’t feel __ years old!” or “I plan to work until I’m 70.” Sound familiar?
You’re afraid to think about what life would be like without your profession. So you do nothing. Imagining a life without being needed on a daily basis can be daunting. Reread the survey results above. If you don’t have interesting and emotionally rewarding activities that will fill the void, that can cause anxiety. And the fact is, the demands on physicians, especially those in solo practice, haven’t left much time for outside interests.
Discussing personal goals and financial matters with others is messy or taboo. Transitioning out of practice is an awkward and uncomfortable topic. Plus, whom do you call for help with planning the next stage of your life?
These and others on a long list of excuses and anxieties result in fewer than 70% of all surgical specialists we talk with having a viable transition plan. Many, of course, have done a superb job of funding their retirement plans and have the assets set aside to fund a comfortable lifestyle. A lot has been written on the financial aspects of retirement. Your financial advisor, broker, or banker has formulas, tools, and advice that you’ve probably been following for decades. The 2014 Medscape Orthopedist Compensation Report shows the average salary is $413,000, with private practice doctors earning even more, $439,000 on average.1 Although such salaries should ensure the funding of retirement savings plans, undeniably, the financial crisis and stock market collapse of 2008 delayed many surgeons’ retirement. Even today, some surgeons who are considering their practice finish line are looking over their shoulder at market returns with a sense of insecurity.
Recruitment Is More Likely Than Cash Out
Thinking you can sell your practice for big bucks is a false hope. In the 1970s and early 1980s, before the onslaught of managed care, it was possible to sell your practice. A young surgeon would welcome having space, staff, and patients at the ready. This is no longer the case, since patient loyalty is now impacted by health insurance plan membership.
Pocketing a hefty sum from selling the office building may not be much of a windfall either. It depends on that all-important real estate formula: location, location, location. In addition, dividends from and investment in a surgery center rarely continue once you are no longer operating.
To maximize the profit potential that remains in this last phase of practice—which in turn can attract surgical talent as you transition—you’ve got to sharpen the sword and pay attention. One surgeon attributed a revenue decline of about 30% over the last 5 years to a combination of lesser insurance reimbursements, his taking more time off, and failing to pay attention to his staff’s write-off habits. Revenue cycle, management, coding, and practice operations must be finely tuned to optimize profitability, and failing to manage your practice effectively will make it less attractive when recruiting a younger surgeon to take your place or assume the patient base. Consider a practice evaluation regardless of where you are in your planning, which will help the practice prioritize improvements that deliver the best benefit and value within the context of your transition plan.
And if recruitment is part of that plan, be prepared to spend significant time on the search. Solo and small groups are finding it challenging to recruit just-out-of-training associates. This generation of new physicians values work-life balance and is more likely to prefer employment to entrepreneurship. Additionally, established physicians who have not invested in or adopted new technologies, such as EHR, will have a tough time attracting top talent. Having been trained using EHRs, few, if any, young doctors will find a reversion to paper records acceptable—and, in fact, most find it a turnoff. Thus, depending on your transition plan and your age and stage, updating technology may be a necessary investment.
Stepping Down But Not Out
If you’re thinking about slowing down but not ceasing practice completely just yet, 2 options are worth considering: practicing part-time and/or becoming a nonoperative orthopedist.
The 2014 Orthopaedic Practice in the United States (OPUS) report issued by the American Academy of Orthopaedic Surgeons shows that the average age of part-time surgeons is 69.14 years and that 48.6% are generalists.5 Part-time surgeons surveyed reported working an average of 23 hours per week and performing 5 procedures per month, compared with full-time surgeons who clock in at 56 hours per week and perform 31 procedures per month.5
Senior surgeons who want to pull back their hours or become nonoperative orthopedists may be quite marketable to group practices. There are several reasons for this. First, population growth will not be supported by the number of physicians graduating from Medicare-sponsored residency slots—which have not increased since 1997. Second, the physician workforce is growing older, and younger surgeons are harder to recruit. They tend to emphasize work-life balance over working the countless hours their senior counterparts did, and, thus, don’t treat as many patients as older colleagues did. And, third, a nonoperative or part-time physician may be more appealing to patients than nonphysician providers, yet accomplish the same purpose of keeping operating surgeons out of the office and in the operating room. So, that former competitor down the street may become a potential employer. You won’t be a voting partner, but that may be a low priority as you step into part-time practice.
We imagine an opportunity for nonoperative orthopedists similar to concierge internists, who go out of network and charge reasonable fees for longer appointments and less paperwork hassle. And this opportunity isn’t only for those practicing in groups. Solo orthopedists may see this change in practice attractive, as it offers reduced professional liability premiums, holds some clear attraction for patients not eager to go under the knife, and makes it easier to arrange time off for the doctor.
As I often tell clients about their business: “Plan your work, and work your plan.” This same maxim holds true of planning for retirement. The intangible aspects of leaving your livelihood require thought and contemplation. My hope is that you’ll put pen to paper and document the answers to the questions posed in this article, so they begin to become as important as the financial aspects of your retirement planning. Of course, the plan may be waylaid midstream owing to reimbursement challenges, an offer you can’t refuse from the hospital, or a change in your health or that of your spouse. However, taking that single step and starting your plan will give you the foundation necessary to move forward or pivot in the journey ahead.
1. Peckham C. Medscape Orthopedist Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/orthopedics#1. Published April 15, 2014. Accessed October 29, 2015.
2. Deloitte 2013 Survey of U.S. Physicians: Physician Perspectives About Health Care Reform and the Future of the Medical Profession. Deloitte Center for Health Solutions website. http://www2.deloitte.com/content/dam/Deloitte/us/Documents/life-sciences-health-care/us-lshc-deloitte-2013-physician-survey-10012014.pdf. Accessed October 29, 2015.
3. Hyden M. Are physicians retiring early? MGMA Connection Plus. Medical Group Management Association website. http://www.mgma.com/practice-resources/mgma-connection-plus/online-only/2015/august-(1)/are-physicians-retiring-early. Published July 28, 2015. Accessed November 10, 2015.
4. The Doctor is Out: A Physician’s Guide to Closing a Practice. North Carolina Medical Board website. http://www.ncmedboard.org/images/uploads/article_images/Physicians_Guide_to_Closing_a_Practice_05_12_2014.pdf. Published May 12, 2014. Accessed October 29, 2015.
5. Oreluk H, Cherf J. Practice settings and productivity. AAOS Now. 2015;9(10). http://www.aaos.org/news/aaosnow/oct15/managing1.asp. Accessed October 29, 2015.
1. Peckham C. Medscape Orthopedist Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/orthopedics#1. Published April 15, 2014. Accessed October 29, 2015.
2. Deloitte 2013 Survey of U.S. Physicians: Physician Perspectives About Health Care Reform and the Future of the Medical Profession. Deloitte Center for Health Solutions website. http://www2.deloitte.com/content/dam/Deloitte/us/Documents/life-sciences-health-care/us-lshc-deloitte-2013-physician-survey-10012014.pdf. Accessed October 29, 2015.
3. Hyden M. Are physicians retiring early? MGMA Connection Plus. Medical Group Management Association website. http://www.mgma.com/practice-resources/mgma-connection-plus/online-only/2015/august-(1)/are-physicians-retiring-early. Published July 28, 2015. Accessed November 10, 2015.
4. The Doctor is Out: A Physician’s Guide to Closing a Practice. North Carolina Medical Board website. http://www.ncmedboard.org/images/uploads/article_images/Physicians_Guide_to_Closing_a_Practice_05_12_2014.pdf. Published May 12, 2014. Accessed October 29, 2015.
5. Oreluk H, Cherf J. Practice settings and productivity. AAOS Now. 2015;9(10). http://www.aaos.org/news/aaosnow/oct15/managing1.asp. Accessed October 29, 2015.