User login
CE/CME No: CR-1510
PROGRAM OVERVIEW
Earn credit by reading this article and successfully completing the posttest and evaluation. Successful completion is defined as a cumulative score of at least 70% correct.
EDUCATIONAL OBJECTIVES
• Explain the pathophysiology of and risk factors for diabetes.
• Identify the current diagnostic criteria for prediabetes.
• Discuss health risks associated with metabolic syndrome.
• Describe the management of prediabetes and metabolic syndrome.
FACULTY
Annie Abraham is an Assistant Clinical Professor at Texas Woman's University, Dallas and Doctor of Nursing Practice candidate at Texas Christian University, Fort Worth, Texas. Susan Chaney is a Professor, Allison Huffman is an Assistant Clinical Professor, and Kathryn Kremer is an Associate Clinical Professor, at Texas Woman’s University, Dallas.
The authors have no financial relationships to disclose.
ACCREDITATION STATEMENT
![]()
This program has been reviewed and is approved for a maximum of 1.0 hour of American Academy of Physician Assistants (AAPA) Category 1 CME credit by the Physician Assistant Review Panel. [NPs: Both ANCC and the AANP Certification Program recognize AAPA as an approved provider of Category 1 credit.] Approval is valid for one year from the issue date of October 2015.
Article begins on next page >>
Prediabetes and metabolic syndrome are growing health concerns in the United States and around the world. Lack of awareness of current recommendations may lead to delays in treatment and subsequent increases in diabetes and cardiovascular disease. Evidence-based recommendations for the management of prediabetes and metabolic syndrome focus on lifestyle changes. The most effective strategies for the prevention of type 2 diabetes and management of metabolic syndrome are reviewed here.
The global prevalence of type 2 diabetes mellitus (T2DM) in adults has reached epidemic proportions. Approximately 285 million adults (ages 20-79), or 6.4% of the adult population, around the world are affected, and these numbers are expected to rise to 439 million (7.7%) by 2030.1 In the United States, however, the prevalence is even higher, at 8.3% of the adult population.2
T2DM is a chronic disease that can cause significant morbidity and mortality. Diabetes is associated with macrovascular (eg, heart disease and stroke) as well as microvascular (eg, retinopathy, neuropathy, and microalbuminuria) complications.3 The economic cost of diagnosed diabetes in the US was approximately $245 billion in 2012.4 Early identification and management of prediabetes by nurse practitioners and physician assistants is essential to minimize disease prevalence and progression and to reduce the tremendous economic burden associated with T2DM.
PATHOPHYSIOLOGY AND RISK FACTORS FOR DIABETES
Diabetes is a complex disorder characterized by hyperglycemia resulting from insufficient insulin secretion and/or decreased tissue response to insulin.5 The progression of normal glucose tolerance to diabetes is a continuous process involving many organ systems. The disease develops primarily as a result of impaired insulin action in muscle, impaired insulin secretion from the pancreatic β-cells, and increased hepatic glucose production.6
In addition, defects in other organs, including increased free fatty acid production in the adipose tissue, decreased incretin effect in the digestive tract, increased glucagon secretion from the pancreatic α-cells, increased glucose reabsorption from the kidneys, and neurotransmitter dysfunction, lead to progression of diabetes.6 This phenomenon is called the ominous octet.6 Gradual increases in glucose levels have been detected as early as 13 years prior to diagnosis of diabetes, with an abrupt increase occurring in the final two to six years before diagnosis.7
Modifiable risk factors such as obesity, poor dietary intake, and a sedentary lifestyle have been associated with increased risk for T2DM.2 Certain antipsychotic medications may also play a part in disease progression.3
According to the American Diabetes Association (ADA), screening for diabetes should begin at age 45 and be repeated every three years.8 For adults younger than 45, screening should be done in those with a BMI of 25 or higher and at least one of the following additional risk factors:
• Family history (first-degree relative with diabetes)
• Ethnicity (high-risk populations include African American, Latino, Native American, Asian American, Pacific Islander)
• History of polycystic ovary syndrome
• History of gestational diabetes (GDM) or delivering a baby weighing more than 9 lb
• Physical inactivity
• Hypertension and/or hyperlipidemia
• History of cardiovascular disease (CVD)
• Insulin resistance.8
IDENTIFICATION/DIAGNOSIS OF PREDIABETES
Diabetes is preceded by an asymptomatic phase known as prediabetes. In prediabetes, blood glucose levels are higher than normal but do not meet the criteria for diabetes.8 According to the American Association of Clinical Endocrinologists (AACE) and the ADA, prediabetes is defined as impaired fasting glucose (fasting plasma glucose level of 100-125 mg/dL) and/or impaired glucose tolerance (two-hour plasma glucose value of 140-199 mg/dL after a 75-g oral glucose tolerance test).8,9 The ADA also considers a hemoglobin A1C value of 5.7% to 6.4% to be indicative of prediabetes.8
In the US, it is estimated that more than 79 million adults have prediabetes.2 Approximately 70% of individuals with prediabetes will progress to T2DM.7 Prediabetes not only increases the risk for T2DM but is also associated with an increased risk for microvascular and macrovascular complications and end-organ damage.3 Impaired fasting glucose and impaired glucose tolerance are linked with obesity, lipid abnormalities, and hypertension.8 Early identification and treatment of prediabetes is therefore important to prevent or delay the onset of diabetes as well as its complications.3
Continue for health risks and the metabolic syndrome >>
HEALTH RISKS AND THE METABOLIC SYNDROME
It is estimated that up to 25% of the general nonobese, nondiabetic population has insulin resistance patterns similar to those seen in T2DM.10 These persons are at much higher risk for T2DM than are insulin-sensitive persons and also often have elevated plasma triglycerides, low levels of high-density lipoproteins (HDLs), and higher blood pressure. This clustering of metabolic risk factors is termed metabolic syndrome. The five criteria for metabolic syndrome are
• Large waistline or abdominal obesity
• High triglyceride level
• Low HDL cholesterol level High blood pressure
• High fasting blood sugar.11
Over time, the list of factors associated with the metabolic syndrome has been expanded to include small, dense, low-density lipoproteins (LDLs);12 hyperuricemia;13 prothrombotic state with increased levels of plasminogen activator inhibitor type 1;14 and proinflammatory states.14 These metabolic abnormalities significantly increase the risk for atherosclerotic disease.10
A number of health risks are associated with metabolic syndrome, including low-grade inflammation leading to bone loss in men, hypertension, hypertriglyceridemia, low LDL, abdominal obesity, xanthomas, heart disease, diabetes, fatty liver, cancers (including breast cancer), obstructive sleep apnea, and recurrent preeclampsia.11 Importantly, the risk for heart disease, diabetes, and stroke increases; patients with metabolic syndrome are two times more likely to develop heart disease and five times more likely to develop diabetes than those without it.15
A combination of factors contributes to the propensity for certain individuals to develop metabolic abnormalities. Nonmodifiable risk factors for metabolic syndrome include age, gender, ethnicity, and family history or genetic predisposition. Mexican Americans have the highest overall prevalence of metabolic syndrome at 31.9%.11 In general, the incidence is slightly higher in females; Hispanic and African American women are 1.5 times more likely to be affected than non-Hispanic Caucasian women.11
Some research suggests that criteria parameters should be adjusted for the nonmodifiable risk factors. For example, BMI, often used as a marker for obesity and a tool for predicting cardiometabolic risk, is much lower among Asian Americans compared with other ethnic groups, yet Asian Americans have a significantly higher prevalence of metabolic syndrome in all BMI categories compared with non-Hispanic Caucasians.16 This finding suggests that lower BMIs should be used for defining overweight/obesity in Asian Americans.16
Hypertension
Metabolic syndrome has been associated with an increased risk for hypertension as well as an increase in adverse cardiovascular events.10 The relationship between obesity and hypertension is also well established. With obesity, factors such as an increase in intravascular volume, elevated cardiac output, activation of the renin-angiotensin system, and elevated sympathetic outflow all can contribute to the development of hypertension. Weight control/reduction measures can result in lowered blood pressure.10
Obesity/overweight
Weight gain and abdominal adiposity have been associated with increased prevalence and incidence of metabolic syndrome. While as much as a quarter of the general population meets the criteria for metabolic syndrome, the distribution in relation to weight reflects a prevalence of 4.6% in normal-weight individuals (BMI < 25), 22.4% in those who are overweight (BMI 25-29.9), and nearly 60% in those who are obese (BMI > 30).17
A longitudinal study of mean risk factors for metabolic syndrome demonstrated that young adults whose BMI increased over a 15-year period had steadily worsening levels of all metabolic components, regardless of their baseline BMI.18 Conversely, those with a stable or decreased BMI had no or only minimal worsening of risk factor levels, also independent from baseline.18 Thus, young adults who can maintain a stable BMI into middle age (when the incidence of metabolic syndrome peaks) may prevent the progression of other cardiovascular risk factors and the development of metabolic syndrome and T2DM, even if they are already overweight.
Screening for risk for macrovascular events
The original Framingham Heart Study (FHS) gave rise to a screening tool for identifying persons at risk for atherosclerotic cardiovascular disease (ASCVD) based on risk factors. These risk factors include hypertension, smoking, hyperlipidemia, and postmenopausal status. Nonmodifiable factors include male gender, increasing age, family history, and African American ethnicity. Contributing factors include obesity, T2DM, and stress.19 Although the risk assessment tool based on the FHS data was widely used for many years, cardiovascular events that were unexpected for given risk stratifications highlighted inconsistencies in the tool’s risk identification process.
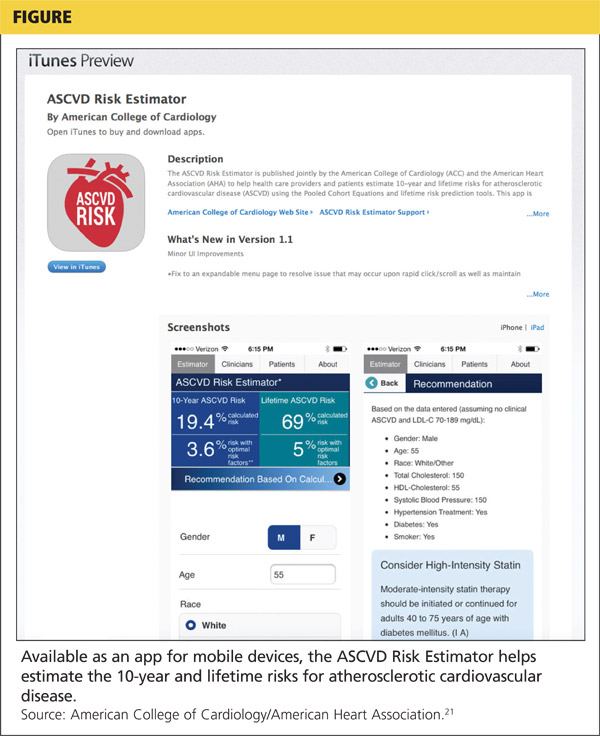
To more accurately identify patients at risk for ASCVD and suggest preventive strategies, the American College of Cardiology (ACC) and American Heart Association (AHA) convened an expert panel in 2013 to develop new guidelines for screening and treatment of high cholesterol.20 These guidelines introduced a new screening tool for estimating risk for a cardiovascular event based on gender, age, race, total cholesterol, HDL cholesterol, systolic blood pressure, need for treatment for hypertension, presence of diabetes, and smoking status. The lifetime risk estimate tool is only appropriate for individuals ages 20 to 59 but can serve as an educational guideline for demonstrating how lifestyle factors can positively or negatively affect risk for a cardiovascular event. Based on the risk stratification generated by the ASCVD screening tool, clinicians can recommend and implement treatment strategies to lower the risk for a future event (see Figure).21
Continue for management of prediabetes and metabolic syndrome >>
MANAGEMENT OF PREDIABETES AND METABOLIC SYNDROME
Lifestyle interventions
Early intervention in prediabetes will delay and even prevent diabetes. Only 11.1% of American adults with prediabetes are aware of their diagnosis.22 Therefore, the initial step in the management of prediabetes is increasing patient awareness.23 Lifestyle changes improve insulin sensitivity and preserve β-cell function and therefore must be the cornerstone of any diabetes prevention program.6,24
According to AACE, weight loss is essential for the management of prediabetes.9 Intensive lifestyle interventions such as dietary changes, exercise, and weight loss can reduce the rate of conversion to T2DM by approximately 58% after three years.8 In addition, lifestyle modification is recommended as a firstline measure before pharmacologic therapies are started and should be continued throughout the process of any hypertension treatment plan.25
Activity level. Physical inactivity is a major risk factor for metabolic syndrome. As such, physical activity can become a therapeutic strategy to reduce body weight and increase fitness in adults with metabolic syndrome.26 Obesity incidence has increased globally, largely due to a combination of poor dietary habits and a sedentary lifestyle.
The clinical benefits of physical activity and exercise programs include weight loss, increased insulin sensitivity, improved glycemic control, and a reduction in all-cause mortality risk.26 When an exercise intervention is maintained, there is also an improvement in the lipid profile and a decrease in mean arterial blood pressure.26 Even when not combined with dietary restrictions, endurance-type exercise reduces body weight, waist circumference, and visceral adipose tissue mass in obese individuals, although the reductions are less than those seen with diet–exercise interventions.26
There is a strong relationship between visceral obesity and risk for CVD, but individuals with visceral obesity who are physically active have a 24% lower mortality risk than their sedentary counterparts.27 Exercise interventions for metabolic syndrome also improve insulin sensitivity and decrease blood A1C, which in turn leads to a reduced risk for microvascular and macrovascular disease and premature death.26
The goals for individuals with prediabetes should include a 7% weight loss and at least 30 min/d of walking at least five times per week, or participation in other moderate-intensity exercise for a minimum of 150 min/wk.8,28 Many guidelines recommend exercising three to five times per week, but few studies demonstrate the level of activity necessary to generate adventitious effects. Hansen and colleagues conducted a literature review focusing on the effects of exercise interventions on metabolic syndrome and related conditions and found that prolonged low-intensity exercise sessions are at least as effective as high-intensity exercise performed for a shorter duration in persons with known metabolic syndrome.26
Dietary considerations. Dietary education should include instruction regarding portion control and use of the glycemic index.29 Maintenance of a food and exercise diary, with regular review by an educator or primary care provider, may encourage compliance in at-risk individuals. Many different diet types have been studied, and the therapeutic efficacy of certain diets has been demonstrated for multiple components of metabolic syndrome.
The Dietary Approaches to Stop Hypertension (DASH) diet has been shown to be the most effective diet for lowering blood pressure. The DASH recommendations include consuming a diet that emphasizes high intake of vegetables, fruits, whole grains, low-fat dairy products, poultry, nontropical vegetable oils, nuts, fish, and legumes.30 The DASH diet limits the intake of sweets, sugar-sweetened beverages, and red meats and also limits sodium intake to a desirable level of 1,500 mg/d.
Numerous studies have demonstrated the effects of “heart healthy” diets in reducing metabolic risk factors, with recommendations for low-fat, low-carbohydrate, and low-sugar meals, but relatively few studies have evaluated specific dietary alterations. Dhingra and colleagues examined the link between the obesity epidemic and the rising consumption of soft drinks and found a more than 50% higher incidence of metabolic syndrome among persons who drank at least one regular or diet soft drink per day as compared with those who drank less than one soft drink per week.31 High-fructose corn syrup, the primary added sweetener in soft drinks, contains approximately 55% fructose and can lead to weight gain, increased insulin resistance, a decrease in HDL cholesterol, and an increase in triglycerides.31 In this study, however, both regular and diet soft drinks led to similar metabolic derangements, suggesting that additional factors may be involved.31
Geographic studies of metabolic syndrome have given rise to research in regional diets and their beneficial effects. The low incidence of coronary heart disease in Mediterranean countries drove the research for the PREDIMED trial, which compared the effects of two Mediterranean-style diets with a typical low-fat diet. The term “low fat” is often misleading, because it suggests that all fats are bad for the body. While the general principles of Mediterranean-type diets include eating more fruits, vegetables, whole grains, legumes, and nuts, their main component is the use of olive oil in place of butter. Olive oil is a rich source of monounsaturated fatty acids, which have proven beneficial effects on cardiovascular risk factors, obesity, and diabetes.32
In the PREDIMED trial, the participating high-risk individuals on all three diet interventions experienced a decrease in body weight and adiposity measurements, with no observed differences in outcomes for subgroups defined by age, sex, ethnicity, baseline weight, or activity level.32 Compared with the low-fat diet group, participants in the Mediterranean diet groups had decreased systolic and diastolic blood pressures, improved lipid profiles, decreased insulin resistance, and reduced concentrations of inflammatory molecules.32 Since low-fat diets tend to lower both LDL and HDL cholesterol, a fat-rich Mediterranean diet may be more appropriate for high-risk individuals because it decreases LDL cholesterol, triglycerides, and total cholesterol while increasing HDL cholesterol.32 These findings challenge the efficacy of low-fat diets centered on carbohydrate intake by demonstrating greater benefits through carbohydrate replacement with dietary fats.
Pharmacologic interventions
Diabetes. Many studies have shown that pharmacologic intervention can delay the onset of T2DM in those at high risk. Several classes of medications have been studied to evaluate their effectiveness in diabetes prevention. In the Diabetes Prevention Program study, metformin reduced the incidence of T2DM by 31% when compared with placebo; lifestyle intervention reduced the incidence by 58%.24 Metformin reduces the risk for diabetes by inhibiting glucose production in the liver while improving peripheral muscle tissue sensitivity to insulin.6
Other oral agents, such as thiazolidinediones, α-glucosidase inhibitors, and the lipase inhibitor orlistat, have been shown to decrease the incidence of T2DM. However, because studies have demonstrated that medications such as metformin are not as effective as diet and exercise in delaying the onset of diabetes, their use must be limited to high-risk individuals, such as those with a history of GDM, those who are extremely obese, and/or those with uncontrolled hyperglycemia.8
Dyslipidemia. Persons with prediabetes are prone to progression to T2DM and experience cardiovascular events.33 Dyslipidemias—or abnormal blood cholesterol levels—commonly occur in persons with prediabetes and are strongly associated with macrovascular events such as MI or CVD.
The 2013 ACC/AHA guidelines for lowering cholesterol to reduce ASCVD risk in adults are unlike previous guidelines in that they do not provide hard and fast rules about reducing the LDL cholesterol (LDL-C) level to a specific number.20 Instead, the guidelines focus on using statins to reduce the risk for primary and secondary cardiovascular events in those most likely to benefit.20 The panel described four groups who would most likely benefit from statin therapy:
• Persons who have clinical ASCVD
• Persons with LDL-C levels ≥ 190 mg/dL
• Persons ages 40 to 75 with diabetes and LDL-C levels of 70-189 mg/dL
• And (most pertinent to those with prediabetes) persons ages 40 to 75 who do not have clinical ASCVD or diabetes but have LDL-C levels of 70-189 mg/dL and an estimated 10-year ASCVD risk of 7.5% or higher.20
Based on risk stratification, treatment strategies such as statins are recommended to lower an individual’s risk for a future event. High-intensity statin therapy should be initiated in persons with a lifetime risk of 7.5% or higher.20
Hypertension. Metabolic syndrome has a strong relationship with the development of hypertension.10 Pharmacologic intervention for hypertension may be appropriate if lifestyle changes alone do not provide adequate control of blood pressure. Evidence-based guidelines for hypertension management were released in 2014 by the panel members appointed to the Eighth Joint National Committee (JNC 8).25 The JNC 8 guidelines include new, specific recommendations aimed at managing high blood pressure in adults.
For individuals ages 60 and older, pharmacologic therapy should be initiated at a blood pressure of 150/90 mm Hg or higher. For adults younger than 60 or those with comorbidities such as diabetes and chronic kidney disease, the guidelines recommend initiating pharmacologic therapy at a blood pressure of 140/90 mm Hg or higher.
Firstline drug recommendations vary among individuals. For nonblack adults, even those with diabetes, the recommended initial medications include a thiazide-type diuretic, calcium channel blocker, ACE inhibitor, or angiotensin receptor blocker. For the general black population, including those with diabetes, initial treatment with either a thiazide-type diuretic or calcium channel blocker is preferred.25
Continue for other interventions >>
Other interventions
Group-based educational interventions. Innovative methods are needed to successfully implement diabetes prevention measures in the general population. The ADA recommends diabetes self-management education to help those with prediabetes make behavioral changes.8
Education provided in a group setting using a patient-centered approach has been shown to be effective in improving health care outcomes and increasing self-management.8,29,34 Group-based diabetes education programs have also been found to be cost-effective over the long term.8,29 The ultimate goal of a group-based educational program is to improve the lifestyle practices of the participants through healthier eating and higher activity levels, thus preventing or delaying the onset of T2DM.
Culture-specific interventions. Health care providers should consider cultural variations when formulating treatment plans to improve disease outcomes.35 Patients often find it difficult to adopt a new lifestyle that they see as irrelevant to their cultural practices. For example, in one study, low-income Latina women did not consider cervical cancer screenings necessary due to absence of symptoms such as pain.35
Cultural influences are present in patients’ values and beliefs about disease processes, symptoms, prevention, treatment, self-management, and patient-provider relationships.35 Primary care providers must consider these values and beliefs, as well as their own, to avoid bias.
A culturally oriented approach to the management of prediabetes ensures that care is tailored to individual patients’ needs.36 Measures aimed at fostering culturally competent care include programs that provide culture-specific training for health care providers, use of language-appropriate patient education materials, recruitment of bicultural health care providers, and use of interpreter services.35 Culturally relevant care improves the success rate of sustained lifestyle changes in individuals at risk for chronic conditions such as diabetes.36
Surgical intervention. Bariatric surgery, reserved for high-risk individuals (BMI ≥ 35), has been shown to significantly decrease the incidence of T2DM in morbidly obese individuals.8 These benefits are probably related to the immediate metabolic changes that occur following the surgery, as well as the long-term sustained weight loss. For patients who undergo bariatric surgery, it is important to maintain regular follow-up to promote and maintain behavioral changes and identify barriers to a healthy lifestyle.
CONCLUSION
Clinicians must be able to effectively diagnose and treat prediabetes and metabolic syndrome. Due to its chronic nature and the resources needed to manage the disease and its complications, diabetes places an enormous burden on society. Efforts to prevent or delay the onset of diabetes are therefore essential to curb the costs and burden associated with this chronic disease.
While lifestyle changes are considered the mainstay of prediabetes and metabolic syndrome management, pharmacologic treatment may be considered in high-risk individuals. Patient education, though important, will not improve glycemic control or modify learned behaviors on its own. Health care providers should use a patient-centered approach to guide implementation of evidence-based guidelines in individuals with prediabetes and/or metabolic syndrome.8
Furthermore, innovative methods are needed to successfully implement diabetes and CVD prevention measures in the general population. Health care policies must be put in place to proactively encourage disease prevention rather than just focusing on acute care.37 It is important for NPs and PAs to devise viable strategies for the management of prediabetes and metabolic syndrome.
Environmental change must be made at the population level, incorporating lifestyle changes outside the health care system. There must be collaboration among various governmental and social organizations to ensure a society that promotes a healthy lifestyle.
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4-14.
2. American Association of Diabetes Educators. AADE position statement: primary prevention of type 2 diabetes. Diabetes Educ. 2012;38(1):147-150.
3. Garber AJ, Handelsman Y, Einhorn D, et al. Diagnosis and management of prediabetes in the continuum of hyperglycemia—when do the risks of diabetes begin? A consensus statement from the American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE). Endocr Pract. 2008;14(7):933-946.
4. American Diabetes Association. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013;36(4):1033-1046.
5. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):S81-S90.
6. DeFronzo RA, Triplitt CL, Abdul-Ghani M, Cersosimo E. Novel agents for the treatment of type 2 diabetes. Diabetes Spectr. 2014;27(2):100-112.
7. Tabák AG, Herder C, Rathmann W, et al. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279-2290.
8. American Diabetes Association. Standards of medical care in diabetes—2015. Diabetes Care. 2015;38(1):S1-S94.
9. Garber AJ, Abrahamson MJ, Barzilay JI, et al. American Association of Clinical Endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr Pract. 2013;19(suppl 2):1-48. www.aace.com/files/algorithm-07-11-2013.pdf. Accessed September 18, 2015.
10. Masharani U. Diabetes mellitus & hypoglycemia. In: Papadakis MA, McPhee SJ, eds. Current Medical Diagnosis & Treatment 2014. 53rd ed. New York, NY: McGraw-Hill Education; 2014:1154-1159.
11. Cash JC, Hall M. Endocrine guidelines. In: Cash JC, Glass CA. Family Practice Guidelines. 3rd ed. New York, NY: Springer Publishing Company; 2014:649-651.
12. Reaven GM, Chen Y-DI, Jeppesen J, et al. Insulin resistance and hyperinsulinemia in individuals with small, dense, low density lipoprotein particles. J Clin Invest. 1993;92:141-146.
13. Facchini F, Chen YD, Hollenbeck CB, Reaven GM. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA. 1991;266(21):3008-3011.
14. Grundy SM, Brewer HB, Cleemen JI, et al; for the Conference Participants. Definition of metabolic syndrome. Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation. 2004;109:433-438.
15. National Heart, Lung, and Blood Institute. What is metabolic syndrome? www.nhlbi.nih.gov/health/health-topics/topics/ms. Accessed September 18, 2015.
16. Palaniappan LP, Wong EC, Shin JJ, et al. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int J Obes (Lond). 2011;35(3):393-400.
17. Park Y, Zhu S, Palaniappan L, et al. The metabolic syndrome: prevalence and associated risk factor findings in the US population from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Intern Med. 2003;163(4):427-436.
18. Lloyd-Jones DM, Liu K, Colangelo LA, et al. Consistently stable or decreased body mass index in young adulthood and longitudinal changes in metabolic syndrome components: the Coronary Artery Risk Development in Young Adults Study. Circulation. 2007;115:1004-1011.
19. Boudi FB, Ahsan CH. Risk factors for coronary artery disease. MedScape. http://emedicine.medscape.com/article/164163-overview#a4. Accessed September 18, 2015.
20. Stone NJ, Robinson J, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S1-S45.
21. American College of Cardiology/American Heart Association. ASCVD risk estimator. http://tools.cardiosource.org/ASCVD-Risk-Estimator/. Accessed July 19, 2015.
22. CDC. Awareness of prediabetes—United States, 2005-2010. MMWR Morb Mortal Wkly Rep. 2013;62(11):209-212.
23. Geiss LS, James C, Gregg EW, et al. Diabetes risk reduction behaviors among U.S. adults with prediabetes. Am J Prev Med. 2010;38:403-409.
24. Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6): 393-403.
25. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
26. Hansen D, Dendale P, van Loon LJC, Meeusen R. The impact of training modalities on the clinical benefits of exercise intervention in patients with cardiovascular disease risk or type 2 diabetes mellitus. Sports Med. 2010;40(11):921-940.
27. Tjonna AE, Nilsen TIL, Slordahl SA, et al. The association of metabolic clustering and physical activity with cardiovascular mortality: the HUNT study in Norway. J Epidemiol Community Health. 2010;64(8):690-695.
28. Kawahara T, Takahashi K, Inazu T, et al. Reduced progression to type 2 diabetes from impaired glucose tolerance after a 2-day in-hospital diabetes educational program: the Joetsu Diabetes Prevention Trial. Diabetes Care. 2008;31(10):1949-1954.
29. Imai S, Kozai H, Naruse Y, et al. Randomized controlled trial of two forms of self-management group education in Japanese people with impaired glucose tolerance. J Clin Biochem Nutr. 2008;43(2):82-87.
30. Eckel RH, Jakicic JM, Ard JD, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S76-S99.
31. Dhingra R, Sullivan L, Jacques PF, et al. Soft drink consumption and risk of developing cardiometabolic risk factors and the metabolic syndrome in middle-aged adults in the community. Circulation. 2007;116(5):480-488.
32. Estruch R, Martínez-González MA, Corella D, et al; PREDIMED Study Investigators. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med. 2006;145(1):1-11.
33. Grundy SM. Pre-diabetes, metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol. 2012;59(7):635-643.
34. Davis AM, Sawyer DR, Vinci LM. The potential of group visits in diabetes care. Clin Diabetes. 2008;26(2):58-62.
35. Shaw SJ, Huebner C, Armin J, et al. The role of culture in health literacy and chronic disease screening and management. J Immigr Minor Health. 2009;11(6):460-467.
36. Orzech KM, Vivian J, Huebner Torres C, et al. Diet and exercise adherence and practices among medically underserved patients with chronic disease: variation across four ethnic groups. Health Educ Behav. 2013;40(1): 56-66.
37. Narayan KM, Echouffo-Tcheugui J, Mohan V, Ali MK. Analysis & commentary: Global prevention and control of type 2 diabetes will require paradigm shifts in policies within and among countries. Health Aff. 2012;31(1):84-92.
CE/CME No: CR-1510
PROGRAM OVERVIEW
Earn credit by reading this article and successfully completing the posttest and evaluation. Successful completion is defined as a cumulative score of at least 70% correct.
EDUCATIONAL OBJECTIVES
• Explain the pathophysiology of and risk factors for diabetes.
• Identify the current diagnostic criteria for prediabetes.
• Discuss health risks associated with metabolic syndrome.
• Describe the management of prediabetes and metabolic syndrome.
FACULTY
Annie Abraham is an Assistant Clinical Professor at Texas Woman's University, Dallas and Doctor of Nursing Practice candidate at Texas Christian University, Fort Worth, Texas. Susan Chaney is a Professor, Allison Huffman is an Assistant Clinical Professor, and Kathryn Kremer is an Associate Clinical Professor, at Texas Woman’s University, Dallas.
The authors have no financial relationships to disclose.
ACCREDITATION STATEMENT
![]()
This program has been reviewed and is approved for a maximum of 1.0 hour of American Academy of Physician Assistants (AAPA) Category 1 CME credit by the Physician Assistant Review Panel. [NPs: Both ANCC and the AANP Certification Program recognize AAPA as an approved provider of Category 1 credit.] Approval is valid for one year from the issue date of October 2015.
Article begins on next page >>
Prediabetes and metabolic syndrome are growing health concerns in the United States and around the world. Lack of awareness of current recommendations may lead to delays in treatment and subsequent increases in diabetes and cardiovascular disease. Evidence-based recommendations for the management of prediabetes and metabolic syndrome focus on lifestyle changes. The most effective strategies for the prevention of type 2 diabetes and management of metabolic syndrome are reviewed here.
The global prevalence of type 2 diabetes mellitus (T2DM) in adults has reached epidemic proportions. Approximately 285 million adults (ages 20-79), or 6.4% of the adult population, around the world are affected, and these numbers are expected to rise to 439 million (7.7%) by 2030.1 In the United States, however, the prevalence is even higher, at 8.3% of the adult population.2
T2DM is a chronic disease that can cause significant morbidity and mortality. Diabetes is associated with macrovascular (eg, heart disease and stroke) as well as microvascular (eg, retinopathy, neuropathy, and microalbuminuria) complications.3 The economic cost of diagnosed diabetes in the US was approximately $245 billion in 2012.4 Early identification and management of prediabetes by nurse practitioners and physician assistants is essential to minimize disease prevalence and progression and to reduce the tremendous economic burden associated with T2DM.
PATHOPHYSIOLOGY AND RISK FACTORS FOR DIABETES
Diabetes is a complex disorder characterized by hyperglycemia resulting from insufficient insulin secretion and/or decreased tissue response to insulin.5 The progression of normal glucose tolerance to diabetes is a continuous process involving many organ systems. The disease develops primarily as a result of impaired insulin action in muscle, impaired insulin secretion from the pancreatic β-cells, and increased hepatic glucose production.6
In addition, defects in other organs, including increased free fatty acid production in the adipose tissue, decreased incretin effect in the digestive tract, increased glucagon secretion from the pancreatic α-cells, increased glucose reabsorption from the kidneys, and neurotransmitter dysfunction, lead to progression of diabetes.6 This phenomenon is called the ominous octet.6 Gradual increases in glucose levels have been detected as early as 13 years prior to diagnosis of diabetes, with an abrupt increase occurring in the final two to six years before diagnosis.7
Modifiable risk factors such as obesity, poor dietary intake, and a sedentary lifestyle have been associated with increased risk for T2DM.2 Certain antipsychotic medications may also play a part in disease progression.3
According to the American Diabetes Association (ADA), screening for diabetes should begin at age 45 and be repeated every three years.8 For adults younger than 45, screening should be done in those with a BMI of 25 or higher and at least one of the following additional risk factors:
• Family history (first-degree relative with diabetes)
• Ethnicity (high-risk populations include African American, Latino, Native American, Asian American, Pacific Islander)
• History of polycystic ovary syndrome
• History of gestational diabetes (GDM) or delivering a baby weighing more than 9 lb
• Physical inactivity
• Hypertension and/or hyperlipidemia
• History of cardiovascular disease (CVD)
• Insulin resistance.8
IDENTIFICATION/DIAGNOSIS OF PREDIABETES
Diabetes is preceded by an asymptomatic phase known as prediabetes. In prediabetes, blood glucose levels are higher than normal but do not meet the criteria for diabetes.8 According to the American Association of Clinical Endocrinologists (AACE) and the ADA, prediabetes is defined as impaired fasting glucose (fasting plasma glucose level of 100-125 mg/dL) and/or impaired glucose tolerance (two-hour plasma glucose value of 140-199 mg/dL after a 75-g oral glucose tolerance test).8,9 The ADA also considers a hemoglobin A1C value of 5.7% to 6.4% to be indicative of prediabetes.8
In the US, it is estimated that more than 79 million adults have prediabetes.2 Approximately 70% of individuals with prediabetes will progress to T2DM.7 Prediabetes not only increases the risk for T2DM but is also associated with an increased risk for microvascular and macrovascular complications and end-organ damage.3 Impaired fasting glucose and impaired glucose tolerance are linked with obesity, lipid abnormalities, and hypertension.8 Early identification and treatment of prediabetes is therefore important to prevent or delay the onset of diabetes as well as its complications.3
Continue for health risks and the metabolic syndrome >>
HEALTH RISKS AND THE METABOLIC SYNDROME
It is estimated that up to 25% of the general nonobese, nondiabetic population has insulin resistance patterns similar to those seen in T2DM.10 These persons are at much higher risk for T2DM than are insulin-sensitive persons and also often have elevated plasma triglycerides, low levels of high-density lipoproteins (HDLs), and higher blood pressure. This clustering of metabolic risk factors is termed metabolic syndrome. The five criteria for metabolic syndrome are
• Large waistline or abdominal obesity
• High triglyceride level
• Low HDL cholesterol level High blood pressure
• High fasting blood sugar.11
Over time, the list of factors associated with the metabolic syndrome has been expanded to include small, dense, low-density lipoproteins (LDLs);12 hyperuricemia;13 prothrombotic state with increased levels of plasminogen activator inhibitor type 1;14 and proinflammatory states.14 These metabolic abnormalities significantly increase the risk for atherosclerotic disease.10
A number of health risks are associated with metabolic syndrome, including low-grade inflammation leading to bone loss in men, hypertension, hypertriglyceridemia, low LDL, abdominal obesity, xanthomas, heart disease, diabetes, fatty liver, cancers (including breast cancer), obstructive sleep apnea, and recurrent preeclampsia.11 Importantly, the risk for heart disease, diabetes, and stroke increases; patients with metabolic syndrome are two times more likely to develop heart disease and five times more likely to develop diabetes than those without it.15
A combination of factors contributes to the propensity for certain individuals to develop metabolic abnormalities. Nonmodifiable risk factors for metabolic syndrome include age, gender, ethnicity, and family history or genetic predisposition. Mexican Americans have the highest overall prevalence of metabolic syndrome at 31.9%.11 In general, the incidence is slightly higher in females; Hispanic and African American women are 1.5 times more likely to be affected than non-Hispanic Caucasian women.11
Some research suggests that criteria parameters should be adjusted for the nonmodifiable risk factors. For example, BMI, often used as a marker for obesity and a tool for predicting cardiometabolic risk, is much lower among Asian Americans compared with other ethnic groups, yet Asian Americans have a significantly higher prevalence of metabolic syndrome in all BMI categories compared with non-Hispanic Caucasians.16 This finding suggests that lower BMIs should be used for defining overweight/obesity in Asian Americans.16
Hypertension
Metabolic syndrome has been associated with an increased risk for hypertension as well as an increase in adverse cardiovascular events.10 The relationship between obesity and hypertension is also well established. With obesity, factors such as an increase in intravascular volume, elevated cardiac output, activation of the renin-angiotensin system, and elevated sympathetic outflow all can contribute to the development of hypertension. Weight control/reduction measures can result in lowered blood pressure.10
Obesity/overweight
Weight gain and abdominal adiposity have been associated with increased prevalence and incidence of metabolic syndrome. While as much as a quarter of the general population meets the criteria for metabolic syndrome, the distribution in relation to weight reflects a prevalence of 4.6% in normal-weight individuals (BMI < 25), 22.4% in those who are overweight (BMI 25-29.9), and nearly 60% in those who are obese (BMI > 30).17
A longitudinal study of mean risk factors for metabolic syndrome demonstrated that young adults whose BMI increased over a 15-year period had steadily worsening levels of all metabolic components, regardless of their baseline BMI.18 Conversely, those with a stable or decreased BMI had no or only minimal worsening of risk factor levels, also independent from baseline.18 Thus, young adults who can maintain a stable BMI into middle age (when the incidence of metabolic syndrome peaks) may prevent the progression of other cardiovascular risk factors and the development of metabolic syndrome and T2DM, even if they are already overweight.
Screening for risk for macrovascular events
The original Framingham Heart Study (FHS) gave rise to a screening tool for identifying persons at risk for atherosclerotic cardiovascular disease (ASCVD) based on risk factors. These risk factors include hypertension, smoking, hyperlipidemia, and postmenopausal status. Nonmodifiable factors include male gender, increasing age, family history, and African American ethnicity. Contributing factors include obesity, T2DM, and stress.19 Although the risk assessment tool based on the FHS data was widely used for many years, cardiovascular events that were unexpected for given risk stratifications highlighted inconsistencies in the tool’s risk identification process.
To more accurately identify patients at risk for ASCVD and suggest preventive strategies, the American College of Cardiology (ACC) and American Heart Association (AHA) convened an expert panel in 2013 to develop new guidelines for screening and treatment of high cholesterol.20 These guidelines introduced a new screening tool for estimating risk for a cardiovascular event based on gender, age, race, total cholesterol, HDL cholesterol, systolic blood pressure, need for treatment for hypertension, presence of diabetes, and smoking status. The lifetime risk estimate tool is only appropriate for individuals ages 20 to 59 but can serve as an educational guideline for demonstrating how lifestyle factors can positively or negatively affect risk for a cardiovascular event. Based on the risk stratification generated by the ASCVD screening tool, clinicians can recommend and implement treatment strategies to lower the risk for a future event (see Figure).21
Continue for management of prediabetes and metabolic syndrome >>
MANAGEMENT OF PREDIABETES AND METABOLIC SYNDROME
Lifestyle interventions
Early intervention in prediabetes will delay and even prevent diabetes. Only 11.1% of American adults with prediabetes are aware of their diagnosis.22 Therefore, the initial step in the management of prediabetes is increasing patient awareness.23 Lifestyle changes improve insulin sensitivity and preserve β-cell function and therefore must be the cornerstone of any diabetes prevention program.6,24
According to AACE, weight loss is essential for the management of prediabetes.9 Intensive lifestyle interventions such as dietary changes, exercise, and weight loss can reduce the rate of conversion to T2DM by approximately 58% after three years.8 In addition, lifestyle modification is recommended as a firstline measure before pharmacologic therapies are started and should be continued throughout the process of any hypertension treatment plan.25
Activity level. Physical inactivity is a major risk factor for metabolic syndrome. As such, physical activity can become a therapeutic strategy to reduce body weight and increase fitness in adults with metabolic syndrome.26 Obesity incidence has increased globally, largely due to a combination of poor dietary habits and a sedentary lifestyle.
The clinical benefits of physical activity and exercise programs include weight loss, increased insulin sensitivity, improved glycemic control, and a reduction in all-cause mortality risk.26 When an exercise intervention is maintained, there is also an improvement in the lipid profile and a decrease in mean arterial blood pressure.26 Even when not combined with dietary restrictions, endurance-type exercise reduces body weight, waist circumference, and visceral adipose tissue mass in obese individuals, although the reductions are less than those seen with diet–exercise interventions.26
There is a strong relationship between visceral obesity and risk for CVD, but individuals with visceral obesity who are physically active have a 24% lower mortality risk than their sedentary counterparts.27 Exercise interventions for metabolic syndrome also improve insulin sensitivity and decrease blood A1C, which in turn leads to a reduced risk for microvascular and macrovascular disease and premature death.26
The goals for individuals with prediabetes should include a 7% weight loss and at least 30 min/d of walking at least five times per week, or participation in other moderate-intensity exercise for a minimum of 150 min/wk.8,28 Many guidelines recommend exercising three to five times per week, but few studies demonstrate the level of activity necessary to generate adventitious effects. Hansen and colleagues conducted a literature review focusing on the effects of exercise interventions on metabolic syndrome and related conditions and found that prolonged low-intensity exercise sessions are at least as effective as high-intensity exercise performed for a shorter duration in persons with known metabolic syndrome.26
Dietary considerations. Dietary education should include instruction regarding portion control and use of the glycemic index.29 Maintenance of a food and exercise diary, with regular review by an educator or primary care provider, may encourage compliance in at-risk individuals. Many different diet types have been studied, and the therapeutic efficacy of certain diets has been demonstrated for multiple components of metabolic syndrome.
The Dietary Approaches to Stop Hypertension (DASH) diet has been shown to be the most effective diet for lowering blood pressure. The DASH recommendations include consuming a diet that emphasizes high intake of vegetables, fruits, whole grains, low-fat dairy products, poultry, nontropical vegetable oils, nuts, fish, and legumes.30 The DASH diet limits the intake of sweets, sugar-sweetened beverages, and red meats and also limits sodium intake to a desirable level of 1,500 mg/d.
Numerous studies have demonstrated the effects of “heart healthy” diets in reducing metabolic risk factors, with recommendations for low-fat, low-carbohydrate, and low-sugar meals, but relatively few studies have evaluated specific dietary alterations. Dhingra and colleagues examined the link between the obesity epidemic and the rising consumption of soft drinks and found a more than 50% higher incidence of metabolic syndrome among persons who drank at least one regular or diet soft drink per day as compared with those who drank less than one soft drink per week.31 High-fructose corn syrup, the primary added sweetener in soft drinks, contains approximately 55% fructose and can lead to weight gain, increased insulin resistance, a decrease in HDL cholesterol, and an increase in triglycerides.31 In this study, however, both regular and diet soft drinks led to similar metabolic derangements, suggesting that additional factors may be involved.31
Geographic studies of metabolic syndrome have given rise to research in regional diets and their beneficial effects. The low incidence of coronary heart disease in Mediterranean countries drove the research for the PREDIMED trial, which compared the effects of two Mediterranean-style diets with a typical low-fat diet. The term “low fat” is often misleading, because it suggests that all fats are bad for the body. While the general principles of Mediterranean-type diets include eating more fruits, vegetables, whole grains, legumes, and nuts, their main component is the use of olive oil in place of butter. Olive oil is a rich source of monounsaturated fatty acids, which have proven beneficial effects on cardiovascular risk factors, obesity, and diabetes.32
In the PREDIMED trial, the participating high-risk individuals on all three diet interventions experienced a decrease in body weight and adiposity measurements, with no observed differences in outcomes for subgroups defined by age, sex, ethnicity, baseline weight, or activity level.32 Compared with the low-fat diet group, participants in the Mediterranean diet groups had decreased systolic and diastolic blood pressures, improved lipid profiles, decreased insulin resistance, and reduced concentrations of inflammatory molecules.32 Since low-fat diets tend to lower both LDL and HDL cholesterol, a fat-rich Mediterranean diet may be more appropriate for high-risk individuals because it decreases LDL cholesterol, triglycerides, and total cholesterol while increasing HDL cholesterol.32 These findings challenge the efficacy of low-fat diets centered on carbohydrate intake by demonstrating greater benefits through carbohydrate replacement with dietary fats.
Pharmacologic interventions
Diabetes. Many studies have shown that pharmacologic intervention can delay the onset of T2DM in those at high risk. Several classes of medications have been studied to evaluate their effectiveness in diabetes prevention. In the Diabetes Prevention Program study, metformin reduced the incidence of T2DM by 31% when compared with placebo; lifestyle intervention reduced the incidence by 58%.24 Metformin reduces the risk for diabetes by inhibiting glucose production in the liver while improving peripheral muscle tissue sensitivity to insulin.6
Other oral agents, such as thiazolidinediones, α-glucosidase inhibitors, and the lipase inhibitor orlistat, have been shown to decrease the incidence of T2DM. However, because studies have demonstrated that medications such as metformin are not as effective as diet and exercise in delaying the onset of diabetes, their use must be limited to high-risk individuals, such as those with a history of GDM, those who are extremely obese, and/or those with uncontrolled hyperglycemia.8
Dyslipidemia. Persons with prediabetes are prone to progression to T2DM and experience cardiovascular events.33 Dyslipidemias—or abnormal blood cholesterol levels—commonly occur in persons with prediabetes and are strongly associated with macrovascular events such as MI or CVD.
The 2013 ACC/AHA guidelines for lowering cholesterol to reduce ASCVD risk in adults are unlike previous guidelines in that they do not provide hard and fast rules about reducing the LDL cholesterol (LDL-C) level to a specific number.20 Instead, the guidelines focus on using statins to reduce the risk for primary and secondary cardiovascular events in those most likely to benefit.20 The panel described four groups who would most likely benefit from statin therapy:
• Persons who have clinical ASCVD
• Persons with LDL-C levels ≥ 190 mg/dL
• Persons ages 40 to 75 with diabetes and LDL-C levels of 70-189 mg/dL
• And (most pertinent to those with prediabetes) persons ages 40 to 75 who do not have clinical ASCVD or diabetes but have LDL-C levels of 70-189 mg/dL and an estimated 10-year ASCVD risk of 7.5% or higher.20
Based on risk stratification, treatment strategies such as statins are recommended to lower an individual’s risk for a future event. High-intensity statin therapy should be initiated in persons with a lifetime risk of 7.5% or higher.20
Hypertension. Metabolic syndrome has a strong relationship with the development of hypertension.10 Pharmacologic intervention for hypertension may be appropriate if lifestyle changes alone do not provide adequate control of blood pressure. Evidence-based guidelines for hypertension management were released in 2014 by the panel members appointed to the Eighth Joint National Committee (JNC 8).25 The JNC 8 guidelines include new, specific recommendations aimed at managing high blood pressure in adults.
For individuals ages 60 and older, pharmacologic therapy should be initiated at a blood pressure of 150/90 mm Hg or higher. For adults younger than 60 or those with comorbidities such as diabetes and chronic kidney disease, the guidelines recommend initiating pharmacologic therapy at a blood pressure of 140/90 mm Hg or higher.
Firstline drug recommendations vary among individuals. For nonblack adults, even those with diabetes, the recommended initial medications include a thiazide-type diuretic, calcium channel blocker, ACE inhibitor, or angiotensin receptor blocker. For the general black population, including those with diabetes, initial treatment with either a thiazide-type diuretic or calcium channel blocker is preferred.25
Continue for other interventions >>
Other interventions
Group-based educational interventions. Innovative methods are needed to successfully implement diabetes prevention measures in the general population. The ADA recommends diabetes self-management education to help those with prediabetes make behavioral changes.8
Education provided in a group setting using a patient-centered approach has been shown to be effective in improving health care outcomes and increasing self-management.8,29,34 Group-based diabetes education programs have also been found to be cost-effective over the long term.8,29 The ultimate goal of a group-based educational program is to improve the lifestyle practices of the participants through healthier eating and higher activity levels, thus preventing or delaying the onset of T2DM.
Culture-specific interventions. Health care providers should consider cultural variations when formulating treatment plans to improve disease outcomes.35 Patients often find it difficult to adopt a new lifestyle that they see as irrelevant to their cultural practices. For example, in one study, low-income Latina women did not consider cervical cancer screenings necessary due to absence of symptoms such as pain.35
Cultural influences are present in patients’ values and beliefs about disease processes, symptoms, prevention, treatment, self-management, and patient-provider relationships.35 Primary care providers must consider these values and beliefs, as well as their own, to avoid bias.
A culturally oriented approach to the management of prediabetes ensures that care is tailored to individual patients’ needs.36 Measures aimed at fostering culturally competent care include programs that provide culture-specific training for health care providers, use of language-appropriate patient education materials, recruitment of bicultural health care providers, and use of interpreter services.35 Culturally relevant care improves the success rate of sustained lifestyle changes in individuals at risk for chronic conditions such as diabetes.36
Surgical intervention. Bariatric surgery, reserved for high-risk individuals (BMI ≥ 35), has been shown to significantly decrease the incidence of T2DM in morbidly obese individuals.8 These benefits are probably related to the immediate metabolic changes that occur following the surgery, as well as the long-term sustained weight loss. For patients who undergo bariatric surgery, it is important to maintain regular follow-up to promote and maintain behavioral changes and identify barriers to a healthy lifestyle.
CONCLUSION
Clinicians must be able to effectively diagnose and treat prediabetes and metabolic syndrome. Due to its chronic nature and the resources needed to manage the disease and its complications, diabetes places an enormous burden on society. Efforts to prevent or delay the onset of diabetes are therefore essential to curb the costs and burden associated with this chronic disease.
While lifestyle changes are considered the mainstay of prediabetes and metabolic syndrome management, pharmacologic treatment may be considered in high-risk individuals. Patient education, though important, will not improve glycemic control or modify learned behaviors on its own. Health care providers should use a patient-centered approach to guide implementation of evidence-based guidelines in individuals with prediabetes and/or metabolic syndrome.8
Furthermore, innovative methods are needed to successfully implement diabetes and CVD prevention measures in the general population. Health care policies must be put in place to proactively encourage disease prevention rather than just focusing on acute care.37 It is important for NPs and PAs to devise viable strategies for the management of prediabetes and metabolic syndrome.
Environmental change must be made at the population level, incorporating lifestyle changes outside the health care system. There must be collaboration among various governmental and social organizations to ensure a society that promotes a healthy lifestyle.
CE/CME No: CR-1510
PROGRAM OVERVIEW
Earn credit by reading this article and successfully completing the posttest and evaluation. Successful completion is defined as a cumulative score of at least 70% correct.
EDUCATIONAL OBJECTIVES
• Explain the pathophysiology of and risk factors for diabetes.
• Identify the current diagnostic criteria for prediabetes.
• Discuss health risks associated with metabolic syndrome.
• Describe the management of prediabetes and metabolic syndrome.
FACULTY
Annie Abraham is an Assistant Clinical Professor at Texas Woman's University, Dallas and Doctor of Nursing Practice candidate at Texas Christian University, Fort Worth, Texas. Susan Chaney is a Professor, Allison Huffman is an Assistant Clinical Professor, and Kathryn Kremer is an Associate Clinical Professor, at Texas Woman’s University, Dallas.
The authors have no financial relationships to disclose.
ACCREDITATION STATEMENT
![]()
This program has been reviewed and is approved for a maximum of 1.0 hour of American Academy of Physician Assistants (AAPA) Category 1 CME credit by the Physician Assistant Review Panel. [NPs: Both ANCC and the AANP Certification Program recognize AAPA as an approved provider of Category 1 credit.] Approval is valid for one year from the issue date of October 2015.
Article begins on next page >>
Prediabetes and metabolic syndrome are growing health concerns in the United States and around the world. Lack of awareness of current recommendations may lead to delays in treatment and subsequent increases in diabetes and cardiovascular disease. Evidence-based recommendations for the management of prediabetes and metabolic syndrome focus on lifestyle changes. The most effective strategies for the prevention of type 2 diabetes and management of metabolic syndrome are reviewed here.
The global prevalence of type 2 diabetes mellitus (T2DM) in adults has reached epidemic proportions. Approximately 285 million adults (ages 20-79), or 6.4% of the adult population, around the world are affected, and these numbers are expected to rise to 439 million (7.7%) by 2030.1 In the United States, however, the prevalence is even higher, at 8.3% of the adult population.2
T2DM is a chronic disease that can cause significant morbidity and mortality. Diabetes is associated with macrovascular (eg, heart disease and stroke) as well as microvascular (eg, retinopathy, neuropathy, and microalbuminuria) complications.3 The economic cost of diagnosed diabetes in the US was approximately $245 billion in 2012.4 Early identification and management of prediabetes by nurse practitioners and physician assistants is essential to minimize disease prevalence and progression and to reduce the tremendous economic burden associated with T2DM.
PATHOPHYSIOLOGY AND RISK FACTORS FOR DIABETES
Diabetes is a complex disorder characterized by hyperglycemia resulting from insufficient insulin secretion and/or decreased tissue response to insulin.5 The progression of normal glucose tolerance to diabetes is a continuous process involving many organ systems. The disease develops primarily as a result of impaired insulin action in muscle, impaired insulin secretion from the pancreatic β-cells, and increased hepatic glucose production.6
In addition, defects in other organs, including increased free fatty acid production in the adipose tissue, decreased incretin effect in the digestive tract, increased glucagon secretion from the pancreatic α-cells, increased glucose reabsorption from the kidneys, and neurotransmitter dysfunction, lead to progression of diabetes.6 This phenomenon is called the ominous octet.6 Gradual increases in glucose levels have been detected as early as 13 years prior to diagnosis of diabetes, with an abrupt increase occurring in the final two to six years before diagnosis.7
Modifiable risk factors such as obesity, poor dietary intake, and a sedentary lifestyle have been associated with increased risk for T2DM.2 Certain antipsychotic medications may also play a part in disease progression.3
According to the American Diabetes Association (ADA), screening for diabetes should begin at age 45 and be repeated every three years.8 For adults younger than 45, screening should be done in those with a BMI of 25 or higher and at least one of the following additional risk factors:
• Family history (first-degree relative with diabetes)
• Ethnicity (high-risk populations include African American, Latino, Native American, Asian American, Pacific Islander)
• History of polycystic ovary syndrome
• History of gestational diabetes (GDM) or delivering a baby weighing more than 9 lb
• Physical inactivity
• Hypertension and/or hyperlipidemia
• History of cardiovascular disease (CVD)
• Insulin resistance.8
IDENTIFICATION/DIAGNOSIS OF PREDIABETES
Diabetes is preceded by an asymptomatic phase known as prediabetes. In prediabetes, blood glucose levels are higher than normal but do not meet the criteria for diabetes.8 According to the American Association of Clinical Endocrinologists (AACE) and the ADA, prediabetes is defined as impaired fasting glucose (fasting plasma glucose level of 100-125 mg/dL) and/or impaired glucose tolerance (two-hour plasma glucose value of 140-199 mg/dL after a 75-g oral glucose tolerance test).8,9 The ADA also considers a hemoglobin A1C value of 5.7% to 6.4% to be indicative of prediabetes.8
In the US, it is estimated that more than 79 million adults have prediabetes.2 Approximately 70% of individuals with prediabetes will progress to T2DM.7 Prediabetes not only increases the risk for T2DM but is also associated with an increased risk for microvascular and macrovascular complications and end-organ damage.3 Impaired fasting glucose and impaired glucose tolerance are linked with obesity, lipid abnormalities, and hypertension.8 Early identification and treatment of prediabetes is therefore important to prevent or delay the onset of diabetes as well as its complications.3
Continue for health risks and the metabolic syndrome >>
HEALTH RISKS AND THE METABOLIC SYNDROME
It is estimated that up to 25% of the general nonobese, nondiabetic population has insulin resistance patterns similar to those seen in T2DM.10 These persons are at much higher risk for T2DM than are insulin-sensitive persons and also often have elevated plasma triglycerides, low levels of high-density lipoproteins (HDLs), and higher blood pressure. This clustering of metabolic risk factors is termed metabolic syndrome. The five criteria for metabolic syndrome are
• Large waistline or abdominal obesity
• High triglyceride level
• Low HDL cholesterol level High blood pressure
• High fasting blood sugar.11
Over time, the list of factors associated with the metabolic syndrome has been expanded to include small, dense, low-density lipoproteins (LDLs);12 hyperuricemia;13 prothrombotic state with increased levels of plasminogen activator inhibitor type 1;14 and proinflammatory states.14 These metabolic abnormalities significantly increase the risk for atherosclerotic disease.10
A number of health risks are associated with metabolic syndrome, including low-grade inflammation leading to bone loss in men, hypertension, hypertriglyceridemia, low LDL, abdominal obesity, xanthomas, heart disease, diabetes, fatty liver, cancers (including breast cancer), obstructive sleep apnea, and recurrent preeclampsia.11 Importantly, the risk for heart disease, diabetes, and stroke increases; patients with metabolic syndrome are two times more likely to develop heart disease and five times more likely to develop diabetes than those without it.15
A combination of factors contributes to the propensity for certain individuals to develop metabolic abnormalities. Nonmodifiable risk factors for metabolic syndrome include age, gender, ethnicity, and family history or genetic predisposition. Mexican Americans have the highest overall prevalence of metabolic syndrome at 31.9%.11 In general, the incidence is slightly higher in females; Hispanic and African American women are 1.5 times more likely to be affected than non-Hispanic Caucasian women.11
Some research suggests that criteria parameters should be adjusted for the nonmodifiable risk factors. For example, BMI, often used as a marker for obesity and a tool for predicting cardiometabolic risk, is much lower among Asian Americans compared with other ethnic groups, yet Asian Americans have a significantly higher prevalence of metabolic syndrome in all BMI categories compared with non-Hispanic Caucasians.16 This finding suggests that lower BMIs should be used for defining overweight/obesity in Asian Americans.16
Hypertension
Metabolic syndrome has been associated with an increased risk for hypertension as well as an increase in adverse cardiovascular events.10 The relationship between obesity and hypertension is also well established. With obesity, factors such as an increase in intravascular volume, elevated cardiac output, activation of the renin-angiotensin system, and elevated sympathetic outflow all can contribute to the development of hypertension. Weight control/reduction measures can result in lowered blood pressure.10
Obesity/overweight
Weight gain and abdominal adiposity have been associated with increased prevalence and incidence of metabolic syndrome. While as much as a quarter of the general population meets the criteria for metabolic syndrome, the distribution in relation to weight reflects a prevalence of 4.6% in normal-weight individuals (BMI < 25), 22.4% in those who are overweight (BMI 25-29.9), and nearly 60% in those who are obese (BMI > 30).17
A longitudinal study of mean risk factors for metabolic syndrome demonstrated that young adults whose BMI increased over a 15-year period had steadily worsening levels of all metabolic components, regardless of their baseline BMI.18 Conversely, those with a stable or decreased BMI had no or only minimal worsening of risk factor levels, also independent from baseline.18 Thus, young adults who can maintain a stable BMI into middle age (when the incidence of metabolic syndrome peaks) may prevent the progression of other cardiovascular risk factors and the development of metabolic syndrome and T2DM, even if they are already overweight.
Screening for risk for macrovascular events
The original Framingham Heart Study (FHS) gave rise to a screening tool for identifying persons at risk for atherosclerotic cardiovascular disease (ASCVD) based on risk factors. These risk factors include hypertension, smoking, hyperlipidemia, and postmenopausal status. Nonmodifiable factors include male gender, increasing age, family history, and African American ethnicity. Contributing factors include obesity, T2DM, and stress.19 Although the risk assessment tool based on the FHS data was widely used for many years, cardiovascular events that were unexpected for given risk stratifications highlighted inconsistencies in the tool’s risk identification process.
To more accurately identify patients at risk for ASCVD and suggest preventive strategies, the American College of Cardiology (ACC) and American Heart Association (AHA) convened an expert panel in 2013 to develop new guidelines for screening and treatment of high cholesterol.20 These guidelines introduced a new screening tool for estimating risk for a cardiovascular event based on gender, age, race, total cholesterol, HDL cholesterol, systolic blood pressure, need for treatment for hypertension, presence of diabetes, and smoking status. The lifetime risk estimate tool is only appropriate for individuals ages 20 to 59 but can serve as an educational guideline for demonstrating how lifestyle factors can positively or negatively affect risk for a cardiovascular event. Based on the risk stratification generated by the ASCVD screening tool, clinicians can recommend and implement treatment strategies to lower the risk for a future event (see Figure).21
Continue for management of prediabetes and metabolic syndrome >>
MANAGEMENT OF PREDIABETES AND METABOLIC SYNDROME
Lifestyle interventions
Early intervention in prediabetes will delay and even prevent diabetes. Only 11.1% of American adults with prediabetes are aware of their diagnosis.22 Therefore, the initial step in the management of prediabetes is increasing patient awareness.23 Lifestyle changes improve insulin sensitivity and preserve β-cell function and therefore must be the cornerstone of any diabetes prevention program.6,24
According to AACE, weight loss is essential for the management of prediabetes.9 Intensive lifestyle interventions such as dietary changes, exercise, and weight loss can reduce the rate of conversion to T2DM by approximately 58% after three years.8 In addition, lifestyle modification is recommended as a firstline measure before pharmacologic therapies are started and should be continued throughout the process of any hypertension treatment plan.25
Activity level. Physical inactivity is a major risk factor for metabolic syndrome. As such, physical activity can become a therapeutic strategy to reduce body weight and increase fitness in adults with metabolic syndrome.26 Obesity incidence has increased globally, largely due to a combination of poor dietary habits and a sedentary lifestyle.
The clinical benefits of physical activity and exercise programs include weight loss, increased insulin sensitivity, improved glycemic control, and a reduction in all-cause mortality risk.26 When an exercise intervention is maintained, there is also an improvement in the lipid profile and a decrease in mean arterial blood pressure.26 Even when not combined with dietary restrictions, endurance-type exercise reduces body weight, waist circumference, and visceral adipose tissue mass in obese individuals, although the reductions are less than those seen with diet–exercise interventions.26
There is a strong relationship between visceral obesity and risk for CVD, but individuals with visceral obesity who are physically active have a 24% lower mortality risk than their sedentary counterparts.27 Exercise interventions for metabolic syndrome also improve insulin sensitivity and decrease blood A1C, which in turn leads to a reduced risk for microvascular and macrovascular disease and premature death.26
The goals for individuals with prediabetes should include a 7% weight loss and at least 30 min/d of walking at least five times per week, or participation in other moderate-intensity exercise for a minimum of 150 min/wk.8,28 Many guidelines recommend exercising three to five times per week, but few studies demonstrate the level of activity necessary to generate adventitious effects. Hansen and colleagues conducted a literature review focusing on the effects of exercise interventions on metabolic syndrome and related conditions and found that prolonged low-intensity exercise sessions are at least as effective as high-intensity exercise performed for a shorter duration in persons with known metabolic syndrome.26
Dietary considerations. Dietary education should include instruction regarding portion control and use of the glycemic index.29 Maintenance of a food and exercise diary, with regular review by an educator or primary care provider, may encourage compliance in at-risk individuals. Many different diet types have been studied, and the therapeutic efficacy of certain diets has been demonstrated for multiple components of metabolic syndrome.
The Dietary Approaches to Stop Hypertension (DASH) diet has been shown to be the most effective diet for lowering blood pressure. The DASH recommendations include consuming a diet that emphasizes high intake of vegetables, fruits, whole grains, low-fat dairy products, poultry, nontropical vegetable oils, nuts, fish, and legumes.30 The DASH diet limits the intake of sweets, sugar-sweetened beverages, and red meats and also limits sodium intake to a desirable level of 1,500 mg/d.
Numerous studies have demonstrated the effects of “heart healthy” diets in reducing metabolic risk factors, with recommendations for low-fat, low-carbohydrate, and low-sugar meals, but relatively few studies have evaluated specific dietary alterations. Dhingra and colleagues examined the link between the obesity epidemic and the rising consumption of soft drinks and found a more than 50% higher incidence of metabolic syndrome among persons who drank at least one regular or diet soft drink per day as compared with those who drank less than one soft drink per week.31 High-fructose corn syrup, the primary added sweetener in soft drinks, contains approximately 55% fructose and can lead to weight gain, increased insulin resistance, a decrease in HDL cholesterol, and an increase in triglycerides.31 In this study, however, both regular and diet soft drinks led to similar metabolic derangements, suggesting that additional factors may be involved.31
Geographic studies of metabolic syndrome have given rise to research in regional diets and their beneficial effects. The low incidence of coronary heart disease in Mediterranean countries drove the research for the PREDIMED trial, which compared the effects of two Mediterranean-style diets with a typical low-fat diet. The term “low fat” is often misleading, because it suggests that all fats are bad for the body. While the general principles of Mediterranean-type diets include eating more fruits, vegetables, whole grains, legumes, and nuts, their main component is the use of olive oil in place of butter. Olive oil is a rich source of monounsaturated fatty acids, which have proven beneficial effects on cardiovascular risk factors, obesity, and diabetes.32
In the PREDIMED trial, the participating high-risk individuals on all three diet interventions experienced a decrease in body weight and adiposity measurements, with no observed differences in outcomes for subgroups defined by age, sex, ethnicity, baseline weight, or activity level.32 Compared with the low-fat diet group, participants in the Mediterranean diet groups had decreased systolic and diastolic blood pressures, improved lipid profiles, decreased insulin resistance, and reduced concentrations of inflammatory molecules.32 Since low-fat diets tend to lower both LDL and HDL cholesterol, a fat-rich Mediterranean diet may be more appropriate for high-risk individuals because it decreases LDL cholesterol, triglycerides, and total cholesterol while increasing HDL cholesterol.32 These findings challenge the efficacy of low-fat diets centered on carbohydrate intake by demonstrating greater benefits through carbohydrate replacement with dietary fats.
Pharmacologic interventions
Diabetes. Many studies have shown that pharmacologic intervention can delay the onset of T2DM in those at high risk. Several classes of medications have been studied to evaluate their effectiveness in diabetes prevention. In the Diabetes Prevention Program study, metformin reduced the incidence of T2DM by 31% when compared with placebo; lifestyle intervention reduced the incidence by 58%.24 Metformin reduces the risk for diabetes by inhibiting glucose production in the liver while improving peripheral muscle tissue sensitivity to insulin.6
Other oral agents, such as thiazolidinediones, α-glucosidase inhibitors, and the lipase inhibitor orlistat, have been shown to decrease the incidence of T2DM. However, because studies have demonstrated that medications such as metformin are not as effective as diet and exercise in delaying the onset of diabetes, their use must be limited to high-risk individuals, such as those with a history of GDM, those who are extremely obese, and/or those with uncontrolled hyperglycemia.8
Dyslipidemia. Persons with prediabetes are prone to progression to T2DM and experience cardiovascular events.33 Dyslipidemias—or abnormal blood cholesterol levels—commonly occur in persons with prediabetes and are strongly associated with macrovascular events such as MI or CVD.
The 2013 ACC/AHA guidelines for lowering cholesterol to reduce ASCVD risk in adults are unlike previous guidelines in that they do not provide hard and fast rules about reducing the LDL cholesterol (LDL-C) level to a specific number.20 Instead, the guidelines focus on using statins to reduce the risk for primary and secondary cardiovascular events in those most likely to benefit.20 The panel described four groups who would most likely benefit from statin therapy:
• Persons who have clinical ASCVD
• Persons with LDL-C levels ≥ 190 mg/dL
• Persons ages 40 to 75 with diabetes and LDL-C levels of 70-189 mg/dL
• And (most pertinent to those with prediabetes) persons ages 40 to 75 who do not have clinical ASCVD or diabetes but have LDL-C levels of 70-189 mg/dL and an estimated 10-year ASCVD risk of 7.5% or higher.20
Based on risk stratification, treatment strategies such as statins are recommended to lower an individual’s risk for a future event. High-intensity statin therapy should be initiated in persons with a lifetime risk of 7.5% or higher.20
Hypertension. Metabolic syndrome has a strong relationship with the development of hypertension.10 Pharmacologic intervention for hypertension may be appropriate if lifestyle changes alone do not provide adequate control of blood pressure. Evidence-based guidelines for hypertension management were released in 2014 by the panel members appointed to the Eighth Joint National Committee (JNC 8).25 The JNC 8 guidelines include new, specific recommendations aimed at managing high blood pressure in adults.
For individuals ages 60 and older, pharmacologic therapy should be initiated at a blood pressure of 150/90 mm Hg or higher. For adults younger than 60 or those with comorbidities such as diabetes and chronic kidney disease, the guidelines recommend initiating pharmacologic therapy at a blood pressure of 140/90 mm Hg or higher.
Firstline drug recommendations vary among individuals. For nonblack adults, even those with diabetes, the recommended initial medications include a thiazide-type diuretic, calcium channel blocker, ACE inhibitor, or angiotensin receptor blocker. For the general black population, including those with diabetes, initial treatment with either a thiazide-type diuretic or calcium channel blocker is preferred.25
Continue for other interventions >>
Other interventions
Group-based educational interventions. Innovative methods are needed to successfully implement diabetes prevention measures in the general population. The ADA recommends diabetes self-management education to help those with prediabetes make behavioral changes.8
Education provided in a group setting using a patient-centered approach has been shown to be effective in improving health care outcomes and increasing self-management.8,29,34 Group-based diabetes education programs have also been found to be cost-effective over the long term.8,29 The ultimate goal of a group-based educational program is to improve the lifestyle practices of the participants through healthier eating and higher activity levels, thus preventing or delaying the onset of T2DM.
Culture-specific interventions. Health care providers should consider cultural variations when formulating treatment plans to improve disease outcomes.35 Patients often find it difficult to adopt a new lifestyle that they see as irrelevant to their cultural practices. For example, in one study, low-income Latina women did not consider cervical cancer screenings necessary due to absence of symptoms such as pain.35
Cultural influences are present in patients’ values and beliefs about disease processes, symptoms, prevention, treatment, self-management, and patient-provider relationships.35 Primary care providers must consider these values and beliefs, as well as their own, to avoid bias.
A culturally oriented approach to the management of prediabetes ensures that care is tailored to individual patients’ needs.36 Measures aimed at fostering culturally competent care include programs that provide culture-specific training for health care providers, use of language-appropriate patient education materials, recruitment of bicultural health care providers, and use of interpreter services.35 Culturally relevant care improves the success rate of sustained lifestyle changes in individuals at risk for chronic conditions such as diabetes.36
Surgical intervention. Bariatric surgery, reserved for high-risk individuals (BMI ≥ 35), has been shown to significantly decrease the incidence of T2DM in morbidly obese individuals.8 These benefits are probably related to the immediate metabolic changes that occur following the surgery, as well as the long-term sustained weight loss. For patients who undergo bariatric surgery, it is important to maintain regular follow-up to promote and maintain behavioral changes and identify barriers to a healthy lifestyle.
CONCLUSION
Clinicians must be able to effectively diagnose and treat prediabetes and metabolic syndrome. Due to its chronic nature and the resources needed to manage the disease and its complications, diabetes places an enormous burden on society. Efforts to prevent or delay the onset of diabetes are therefore essential to curb the costs and burden associated with this chronic disease.
While lifestyle changes are considered the mainstay of prediabetes and metabolic syndrome management, pharmacologic treatment may be considered in high-risk individuals. Patient education, though important, will not improve glycemic control or modify learned behaviors on its own. Health care providers should use a patient-centered approach to guide implementation of evidence-based guidelines in individuals with prediabetes and/or metabolic syndrome.8
Furthermore, innovative methods are needed to successfully implement diabetes and CVD prevention measures in the general population. Health care policies must be put in place to proactively encourage disease prevention rather than just focusing on acute care.37 It is important for NPs and PAs to devise viable strategies for the management of prediabetes and metabolic syndrome.
Environmental change must be made at the population level, incorporating lifestyle changes outside the health care system. There must be collaboration among various governmental and social organizations to ensure a society that promotes a healthy lifestyle.
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4-14.
2. American Association of Diabetes Educators. AADE position statement: primary prevention of type 2 diabetes. Diabetes Educ. 2012;38(1):147-150.
3. Garber AJ, Handelsman Y, Einhorn D, et al. Diagnosis and management of prediabetes in the continuum of hyperglycemia—when do the risks of diabetes begin? A consensus statement from the American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE). Endocr Pract. 2008;14(7):933-946.
4. American Diabetes Association. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013;36(4):1033-1046.
5. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):S81-S90.
6. DeFronzo RA, Triplitt CL, Abdul-Ghani M, Cersosimo E. Novel agents for the treatment of type 2 diabetes. Diabetes Spectr. 2014;27(2):100-112.
7. Tabák AG, Herder C, Rathmann W, et al. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279-2290.
8. American Diabetes Association. Standards of medical care in diabetes—2015. Diabetes Care. 2015;38(1):S1-S94.
9. Garber AJ, Abrahamson MJ, Barzilay JI, et al. American Association of Clinical Endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr Pract. 2013;19(suppl 2):1-48. www.aace.com/files/algorithm-07-11-2013.pdf. Accessed September 18, 2015.
10. Masharani U. Diabetes mellitus & hypoglycemia. In: Papadakis MA, McPhee SJ, eds. Current Medical Diagnosis & Treatment 2014. 53rd ed. New York, NY: McGraw-Hill Education; 2014:1154-1159.
11. Cash JC, Hall M. Endocrine guidelines. In: Cash JC, Glass CA. Family Practice Guidelines. 3rd ed. New York, NY: Springer Publishing Company; 2014:649-651.
12. Reaven GM, Chen Y-DI, Jeppesen J, et al. Insulin resistance and hyperinsulinemia in individuals with small, dense, low density lipoprotein particles. J Clin Invest. 1993;92:141-146.
13. Facchini F, Chen YD, Hollenbeck CB, Reaven GM. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA. 1991;266(21):3008-3011.
14. Grundy SM, Brewer HB, Cleemen JI, et al; for the Conference Participants. Definition of metabolic syndrome. Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation. 2004;109:433-438.
15. National Heart, Lung, and Blood Institute. What is metabolic syndrome? www.nhlbi.nih.gov/health/health-topics/topics/ms. Accessed September 18, 2015.
16. Palaniappan LP, Wong EC, Shin JJ, et al. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int J Obes (Lond). 2011;35(3):393-400.
17. Park Y, Zhu S, Palaniappan L, et al. The metabolic syndrome: prevalence and associated risk factor findings in the US population from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Intern Med. 2003;163(4):427-436.
18. Lloyd-Jones DM, Liu K, Colangelo LA, et al. Consistently stable or decreased body mass index in young adulthood and longitudinal changes in metabolic syndrome components: the Coronary Artery Risk Development in Young Adults Study. Circulation. 2007;115:1004-1011.
19. Boudi FB, Ahsan CH. Risk factors for coronary artery disease. MedScape. http://emedicine.medscape.com/article/164163-overview#a4. Accessed September 18, 2015.
20. Stone NJ, Robinson J, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S1-S45.
21. American College of Cardiology/American Heart Association. ASCVD risk estimator. http://tools.cardiosource.org/ASCVD-Risk-Estimator/. Accessed July 19, 2015.
22. CDC. Awareness of prediabetes—United States, 2005-2010. MMWR Morb Mortal Wkly Rep. 2013;62(11):209-212.
23. Geiss LS, James C, Gregg EW, et al. Diabetes risk reduction behaviors among U.S. adults with prediabetes. Am J Prev Med. 2010;38:403-409.
24. Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6): 393-403.
25. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
26. Hansen D, Dendale P, van Loon LJC, Meeusen R. The impact of training modalities on the clinical benefits of exercise intervention in patients with cardiovascular disease risk or type 2 diabetes mellitus. Sports Med. 2010;40(11):921-940.
27. Tjonna AE, Nilsen TIL, Slordahl SA, et al. The association of metabolic clustering and physical activity with cardiovascular mortality: the HUNT study in Norway. J Epidemiol Community Health. 2010;64(8):690-695.
28. Kawahara T, Takahashi K, Inazu T, et al. Reduced progression to type 2 diabetes from impaired glucose tolerance after a 2-day in-hospital diabetes educational program: the Joetsu Diabetes Prevention Trial. Diabetes Care. 2008;31(10):1949-1954.
29. Imai S, Kozai H, Naruse Y, et al. Randomized controlled trial of two forms of self-management group education in Japanese people with impaired glucose tolerance. J Clin Biochem Nutr. 2008;43(2):82-87.
30. Eckel RH, Jakicic JM, Ard JD, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S76-S99.
31. Dhingra R, Sullivan L, Jacques PF, et al. Soft drink consumption and risk of developing cardiometabolic risk factors and the metabolic syndrome in middle-aged adults in the community. Circulation. 2007;116(5):480-488.
32. Estruch R, Martínez-González MA, Corella D, et al; PREDIMED Study Investigators. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med. 2006;145(1):1-11.
33. Grundy SM. Pre-diabetes, metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol. 2012;59(7):635-643.
34. Davis AM, Sawyer DR, Vinci LM. The potential of group visits in diabetes care. Clin Diabetes. 2008;26(2):58-62.
35. Shaw SJ, Huebner C, Armin J, et al. The role of culture in health literacy and chronic disease screening and management. J Immigr Minor Health. 2009;11(6):460-467.
36. Orzech KM, Vivian J, Huebner Torres C, et al. Diet and exercise adherence and practices among medically underserved patients with chronic disease: variation across four ethnic groups. Health Educ Behav. 2013;40(1): 56-66.
37. Narayan KM, Echouffo-Tcheugui J, Mohan V, Ali MK. Analysis & commentary: Global prevention and control of type 2 diabetes will require paradigm shifts in policies within and among countries. Health Aff. 2012;31(1):84-92.
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4-14.
2. American Association of Diabetes Educators. AADE position statement: primary prevention of type 2 diabetes. Diabetes Educ. 2012;38(1):147-150.
3. Garber AJ, Handelsman Y, Einhorn D, et al. Diagnosis and management of prediabetes in the continuum of hyperglycemia—when do the risks of diabetes begin? A consensus statement from the American College of Endocrinology (ACE) and the American Association of Clinical Endocrinologists (AACE). Endocr Pract. 2008;14(7):933-946.
4. American Diabetes Association. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013;36(4):1033-1046.
5. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(1):S81-S90.
6. DeFronzo RA, Triplitt CL, Abdul-Ghani M, Cersosimo E. Novel agents for the treatment of type 2 diabetes. Diabetes Spectr. 2014;27(2):100-112.
7. Tabák AG, Herder C, Rathmann W, et al. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279-2290.
8. American Diabetes Association. Standards of medical care in diabetes—2015. Diabetes Care. 2015;38(1):S1-S94.
9. Garber AJ, Abrahamson MJ, Barzilay JI, et al. American Association of Clinical Endocrinologists’ comprehensive diabetes management algorithm 2013 consensus statement. Endocr Pract. 2013;19(suppl 2):1-48. www.aace.com/files/algorithm-07-11-2013.pdf. Accessed September 18, 2015.
10. Masharani U. Diabetes mellitus & hypoglycemia. In: Papadakis MA, McPhee SJ, eds. Current Medical Diagnosis & Treatment 2014. 53rd ed. New York, NY: McGraw-Hill Education; 2014:1154-1159.
11. Cash JC, Hall M. Endocrine guidelines. In: Cash JC, Glass CA. Family Practice Guidelines. 3rd ed. New York, NY: Springer Publishing Company; 2014:649-651.
12. Reaven GM, Chen Y-DI, Jeppesen J, et al. Insulin resistance and hyperinsulinemia in individuals with small, dense, low density lipoprotein particles. J Clin Invest. 1993;92:141-146.
13. Facchini F, Chen YD, Hollenbeck CB, Reaven GM. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration. JAMA. 1991;266(21):3008-3011.
14. Grundy SM, Brewer HB, Cleemen JI, et al; for the Conference Participants. Definition of metabolic syndrome. Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation. 2004;109:433-438.
15. National Heart, Lung, and Blood Institute. What is metabolic syndrome? www.nhlbi.nih.gov/health/health-topics/topics/ms. Accessed September 18, 2015.
16. Palaniappan LP, Wong EC, Shin JJ, et al. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int J Obes (Lond). 2011;35(3):393-400.
17. Park Y, Zhu S, Palaniappan L, et al. The metabolic syndrome: prevalence and associated risk factor findings in the US population from the third National Health and Nutrition Examination Survey, 1988-1994. Arch Intern Med. 2003;163(4):427-436.
18. Lloyd-Jones DM, Liu K, Colangelo LA, et al. Consistently stable or decreased body mass index in young adulthood and longitudinal changes in metabolic syndrome components: the Coronary Artery Risk Development in Young Adults Study. Circulation. 2007;115:1004-1011.
19. Boudi FB, Ahsan CH. Risk factors for coronary artery disease. MedScape. http://emedicine.medscape.com/article/164163-overview#a4. Accessed September 18, 2015.
20. Stone NJ, Robinson J, Lichtenstein AH, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S1-S45.
21. American College of Cardiology/American Heart Association. ASCVD risk estimator. http://tools.cardiosource.org/ASCVD-Risk-Estimator/. Accessed July 19, 2015.
22. CDC. Awareness of prediabetes—United States, 2005-2010. MMWR Morb Mortal Wkly Rep. 2013;62(11):209-212.
23. Geiss LS, James C, Gregg EW, et al. Diabetes risk reduction behaviors among U.S. adults with prediabetes. Am J Prev Med. 2010;38:403-409.
24. Knowler WC, Barrett-Connor E, Fowler SE, et al; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6): 393-403.
25. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
26. Hansen D, Dendale P, van Loon LJC, Meeusen R. The impact of training modalities on the clinical benefits of exercise intervention in patients with cardiovascular disease risk or type 2 diabetes mellitus. Sports Med. 2010;40(11):921-940.
27. Tjonna AE, Nilsen TIL, Slordahl SA, et al. The association of metabolic clustering and physical activity with cardiovascular mortality: the HUNT study in Norway. J Epidemiol Community Health. 2010;64(8):690-695.
28. Kawahara T, Takahashi K, Inazu T, et al. Reduced progression to type 2 diabetes from impaired glucose tolerance after a 2-day in-hospital diabetes educational program: the Joetsu Diabetes Prevention Trial. Diabetes Care. 2008;31(10):1949-1954.
29. Imai S, Kozai H, Naruse Y, et al. Randomized controlled trial of two forms of self-management group education in Japanese people with impaired glucose tolerance. J Clin Biochem Nutr. 2008;43(2):82-87.
30. Eckel RH, Jakicic JM, Ard JD, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 suppl 2):S76-S99.
31. Dhingra R, Sullivan L, Jacques PF, et al. Soft drink consumption and risk of developing cardiometabolic risk factors and the metabolic syndrome in middle-aged adults in the community. Circulation. 2007;116(5):480-488.
32. Estruch R, Martínez-González MA, Corella D, et al; PREDIMED Study Investigators. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med. 2006;145(1):1-11.
33. Grundy SM. Pre-diabetes, metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol. 2012;59(7):635-643.
34. Davis AM, Sawyer DR, Vinci LM. The potential of group visits in diabetes care. Clin Diabetes. 2008;26(2):58-62.
35. Shaw SJ, Huebner C, Armin J, et al. The role of culture in health literacy and chronic disease screening and management. J Immigr Minor Health. 2009;11(6):460-467.
36. Orzech KM, Vivian J, Huebner Torres C, et al. Diet and exercise adherence and practices among medically underserved patients with chronic disease: variation across four ethnic groups. Health Educ Behav. 2013;40(1): 56-66.
37. Narayan KM, Echouffo-Tcheugui J, Mohan V, Ali MK. Analysis & commentary: Global prevention and control of type 2 diabetes will require paradigm shifts in policies within and among countries. Health Aff. 2012;31(1):84-92.