User login
Hospitals are complex adaptive systems within which practitioners, technology, physical resources, and other components adapt interdependently to attempt to best meet the needs of patients.1 Hospitals must provide a stable, dependable level of care while also surging to respond to times of high demand, such as patient emergencies or swells in patient volume. Given the critical and resource-intensive nature of this work, optimizing the system is essential; however, because of the complexity of the system, making changes can result in unexpected and possibly deleterious effects. We need to approach change in hospital processes carefully and thoughtfully.
The Institute of Medicine, the National Academy of Engineering, and the President’s Council of Advisors on Science and Technology have recommended the application of systems engineering approaches to improve health care delivery.2,3 Systems engineering seeks to coordinate, synchronize, and integrate complex systems of people, information, materials, technology, and financial resources.4,5 To determine how complex systems can be improved, engineers apply analytic methods to describe how such systems operate and what the impact of changes might be. These methodologies have improved patient care and reduced costs at several hospitals.6 For example, a decision support system that combined simulation, optimization, and machine learning methods in an emergency department (ED) resulted in a 33% reduction in length of stay (LOS) and a 28% decrease in ED readmissions.7 Other strategies to improve patient flow include shaping demand (decreasing variation in surgical scheduling, relocating low acuity care ED visit to primary care, etc.), redesigning systems (early discharges, improving efficiency, and coordination of hospital discharge process, decreasing care variation, etc.), or aligning capacity and demand. Another approach, real-time demand capacity (RTDC), is based on management principles and queuing and constraint theory and has been implemented successfully in a variety of health care organizations. RTDC represents a promising approach to improve hospitalwide patient flow and can be integrated into current bed management processes.8 Unfortunately, many of these approaches are not well known to clinicians and would benefit from greater awareness and input from healthcare practitioners.
One systems engineering tool that can be used to describe, analyze, and evaluate proposed changes in care is simulation.9 Simulation creates a model within which what-if scenarios (ie, adjusting various inputs into the simulation) allow researchers to define the likelihood of consequences from various courses of action and determine the optimal change to a system. Such analyses can predict the impact of a proposed change on patients and healthcare practitioners.10-13
A critical concern for hospitals that simulation may help address is managing the volume of inpatients. A high inpatient census is necessary for financial solvency, yet too high a census of inpatients or an unexpected surge in acuity can overwhelm hospital resources. Many hospitals, pressured by growing numbers of increasingly complex patients, have seen medical inpatients spread across multiple nonmedical nursing units (NUs) of their institution such that a particular medical team may have only a couple patients assigned to each nursing unit.14 This dispersion may hinder communication between physicians and nurses and limits the time physicians have to interact with patients.15 Additionally, coordination of care may become more challenging for discharge planning.16 Aligning medical teams with NUs may benefit the quality and efficiency of care or may create a barrier to patient flow, which worsens these problems.15,17 Alternatively, hospitals might meet the increasing demands for care by choosing to add capacity by opening new NUs or hiring additional healthcare providers.
This article describes the application of simulation to model the interconnected variables and subsequent future states created by several possible
METHODS
Setting and Present State
Virginia Commonwealth University (VCU) is a 865-bed tertiary academic medical center, with inpatient care activities spread between four connected buildings and 50 different NUs. The occupancy rate had been over 92% during the time period of this project with admission volume limited primarily by the capacity of the facility. Three of the NUs were primarily allocated to general medicine (GIM) patients. However, over the years, GIM inpatients grew to over 7500 admissions annually, resulting in nearly 50% of GIM patients being admitted to a non-GIM nursing unit.
Additionally, patients on each medical team had a high degree of spread across NUs due to several factors. Admissions and discharges from the hospital did not align across the day. While discharges clumped in the late afternoon, admission occurred throughout the day with a surge in the later afternoon. This mismatch frequently led to patients waiting in the ED for a bed, medical team, or both, and patients were typically assigned to the first available bed and team. For medical team assignments, newly admitted patients were distributed relatively equally across five hospitalist teams and five housestaff teams (that include residents, interns, and medical students). This steady distribution of patients through the day supported meeting housestaff work-hour restrictions of 80 hours each week.18 Yet, as a result of the high occupancy rate, the patterns of patient admissions and discharges, and the distribution of patients among medical teams and across NUs, medical teams and NUs rarely shared more than a few patients.
Leaders at our institution outlined several possible options to address these challenges, including aligning medical teams with NU, adding an additional hospitalist team, or adding an additional nursing unit. In addition, institutional leaders were concerned about the impact of continued growth in admission volume and the impact of patient dispersion on trainees and students. The overall goal of creating a simulation model was to determine the impact of an increased volume of patients and these possible strategic decisions on operational metrics, including number of patients waiting in the ED, ED boarding time per patient, time in system per patient (ED boarding time plus inpatient LOS), team utilization, and rounding travel time.
Simulation Modeling
To model the impact of some possible system changes on patient care, we applied Kelton and Law’s simulation study framework,19 including data collection; model building and validation; and what-if scenario testing (Figure 1).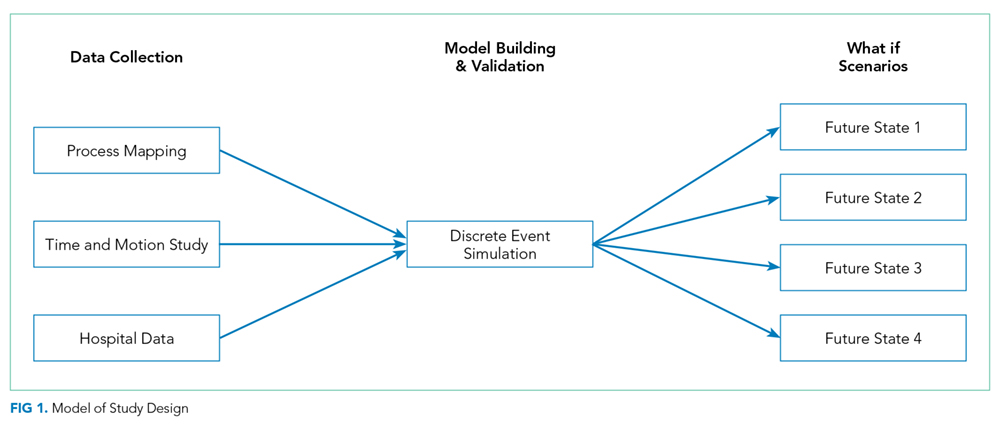
Data Collection
Process Flow Map
We created a complex process flow map of patient care activities on medical teams. The map was developed by four general medicine physicians (R.C., H.M., V.M., and S.P.T.) who all provided medical care on the hospital-based services and ensured expert input on the patient care activities captured by the simulation modeling.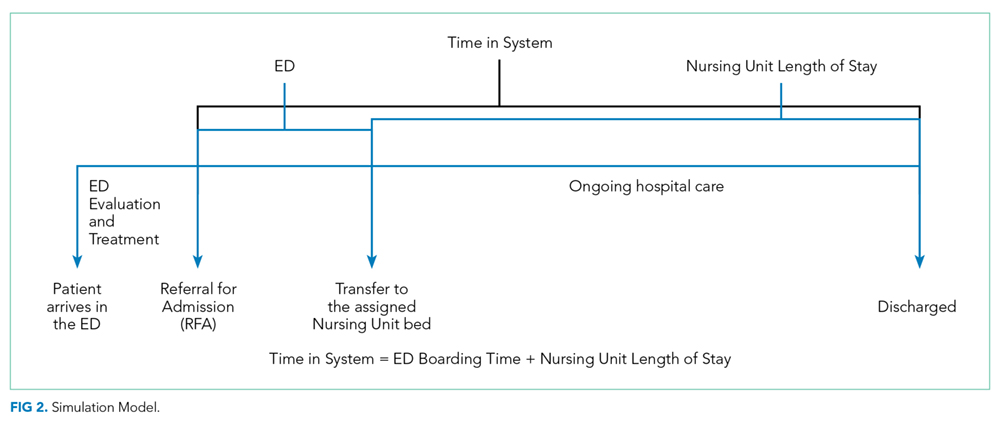
Time and Motion Studies
Time and motion study is a well-established technique used to evaluate the efficiency of work processes.20,21 Originally applied to increase productivity in manufacturing, this technique uses first-hand observations to measure the time allotted to different work tasks to systematically analyze workflow.22 Workflow in healthcare, like manufacturing tasks, tends to have a repetitive pattern, making time and motion studies a highly applicable tool.
A research assistant observed a total of 30 hospitalist work cycles to describe the work of our inpatient clinicians. A work cycle, defined as one complete process flow,23 began when the hospitalist started a daytime shift of patient care and concluded after the physician “signed out” to the physician who was assuming responsibility for ongoing medical care of the patients (ie, cross-coverage). Time spent on different activities identified by the process flow map was captured throughout the cycle. These activities included time spent traveling to evaluate patients located on different NUs. To minimize disruptions in patient care and adhere to privacy standards, no observations were conducted in patient rooms, and details of computer work were not recorded. To ensure stable estimates of the mean and standard deviation of the time spent at each step, at least 30 cycles of observation are recommended. Thus, 300 hours of observations over the course of 30 separate days were collected.
Hospital Data
We extracted admission and discharge data from the electronic health records (EHR) for general medicine patients admitted from the ED for the calendar year 2013. These records were used to establish means and standard deviations for admission date and time, distribution of patients across NUs, and LOS.
Model Building and Internal Validation
On the basis of these data inputs and using SIMIO® Simulation Software version 7, we constructed a discrete event simulation (DES) model representing the patient care activities of general medicine teams. Each patient was assigned a bed on a nursing unit through a probability distribution based on prior EHR data and then randomly assigned to a general medicine team. We replicated the model 200 times, and each model ran for 365 days. Each team was limited to 16 assigned patients, the maximum number of patients per housestaff team allowed by VCU protocol; henceforth, this number is referred to as team-patient capacity. The model assumed patients remained on the assigned nursing unit and medical team for the entirety of their hospital stay and that each patient was seen by their assigned medical team every day. The results of the present state model, including mean number of patients on each nursing unit, mean team census, patient dispersion (ie, the number of NUs on which each medical team had patients), and team utilization (ie, mean team census divided by team patient capacity), were compared with actual data from 2013 to internally validate the model.
What-If Scenario Testing
We constructed four what-if scenarios based on possible strategic directions identified by leadership. These models evaluated:
- constraining patients on housestaff (but not hospitalist) teams to the three general medicine NUs (Future State 1),
- increasing bed capacity for general medicine patients by adding one additional nursing unit of 26 beds (Future State 2),
- increasing the number of general medicine teams by adding one additional hospitalist team of up to 16 patients (Future State 3),
- modeling the impact of increased patient admissions from 21 per day to 25 per day while also adding a nursing unit and an additional medical team (Future State 4).
For Future States 1-3, admission volume was held constant. The model generated nursing unit LOS using a random continuous exponential probability distribution with a mean of 133 hours to match the LOS distribution derived from health system data. As patients entered the system for admission, the model assigned a bed to the patient, but the patient could not move to the assigned bed until a bed and care team were both available. We were only interested in the steady-state behavior of the system, so collecting performance statistics only after the model had been populated and steady state had been achieved was important.
Table 1 summarizes the input data, fixed, and dynamic variable for each future state model.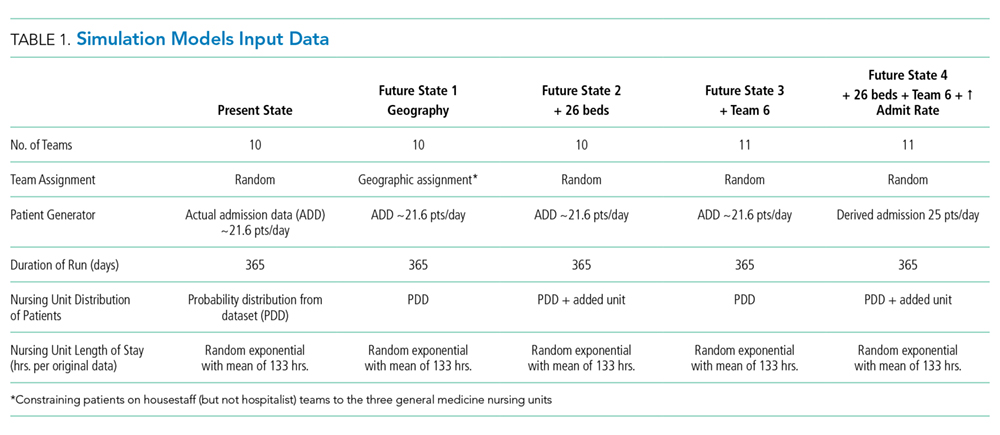
We examined the impact of these scenarios on the following variables (Table 2): (1) average time in system; (2) average number of patients waiting for a bed; (3) average ED boarding time; (4) total daily general medicine census; (5) average housestaff team census per team; (6) average hospitalist team census per team; (7) average combined housestaff and hospitalist team census per team; (8) average housestaff team utilization (ie, mean team census divided by team patient capacity of 16); (9) average hospitalist team utilization (ie, mean team census divided by team patient capacity of 16); (10) average nursing unit utilization (ie, mean nursing unit census divided by maximum number of patients that can be cared for on each nursing unit); (11) patient dispersion to NUs (ie, average number of NUs on which each general medicine team has patients); 12) estimated average rounding time per general medicine team.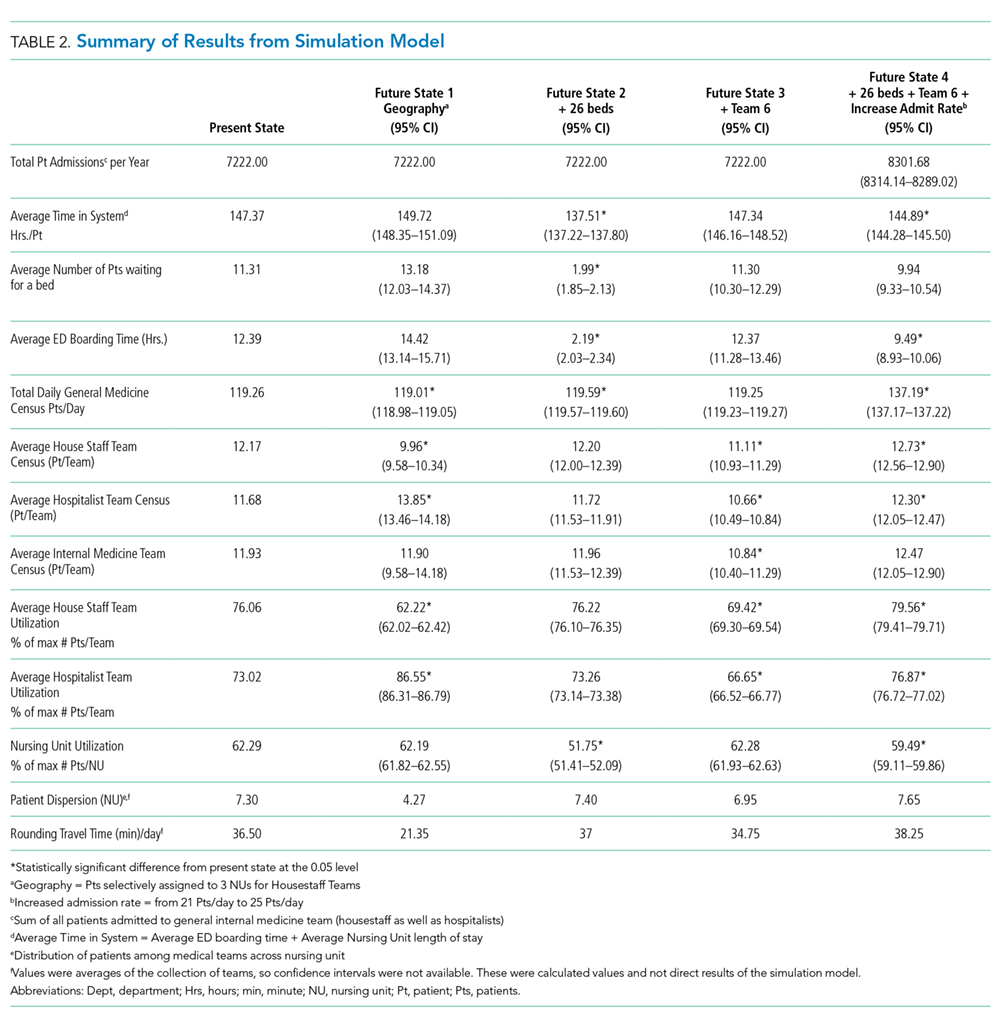
Of note, the average time in the system included time patients spent waiting for bed and team assignments (ED boarding time) in addition to the time they spent in the assigned nursing unit (nursing LOS). The difference between the nursing LOS (ie, time on the nursing unit) and total time in the system is one indicator of system efficiency around hospital admission.
The Institutional Review Board of Virginia Commonwealth University approved this study.
RESULTS
Time and Motion Data
The mean time spent with each patient was nine minutes. The mean time traveling between NUs Healthcare Quality for Children and Adolescents with Suicidality Admitted to Acute Care Hospitals in the United States was five minutes. Average rounding time was noted to be two hours, 53 minutes. Thirty-seven minutes, about ~21% of the time, was wasted in traveling. Each team, on average, traveled to seven different NUs to round on their daily census, averaging 1.6 patients in each nursing unit.
Hospital Data
Between January 1, 2011 to December 31, 2013, a total of 7,902 patients were admitted to the general medicine teams, spanning 23 NU. The average number of admissions per day was 21.6, and the average nursing unit LOS was 133 hours. Average team census was derived from historical data across all GIM team for 2013 and was noted to be 11.5 patients per team, and these patients were spread over seven NU.
Model Validation
The mean number of patients admitted to different NUs was estimated from the simulation model then compared with the EHR data from 2013. None were statistically different (P > .05), which signified that the validated simulation model is similar to the EHR data from 2013 despite the underlying assumptions.
Model Outputs
Analysis of the models indicated that steady-state (based upon hospital census) was realized at approximately 800 hours or after 680 patients were admitted to the GIM teams. Statistics collection, therefore, was started after 800 hours of simulated time and reflected the admission of the remaining 7222 patients in the model validation sample (Table 2).
In the model, the total daily general medicine patient census was 119.26. Average time in the system per patient was noted to be 147.37 hours, which was 14.37 hours more than the average nursing unit LOS of 133 hours. Average number of patients waiting for a bed was noted to be 11.31, while the average wait time for a patient to get a bed was 12.39 hours.
Average housestaff team and hospitalist team utilization were 76.06% and 73.02%, respectively, with average team utilization of 74.54% (range: 72.88%-76.19%). Housestaff team and hospitalist team averaged 12.17 and 11.68 patients per care team, respectively. General medicine teams had patients on 7.30 NUs on average. GIM teams rounding travel time was 36.5 minutes.
What-If Scenario Testing
Simulation outputs for the four future states are summarized in Table 2. With Future State 1, through which patients were selectively assigned to housestaff teams aligned with three NUs, the average time in the system per patient increased by 2.35 hours, with 1.87 more patients waiting for a bed and waiting for 2.03 more hours as compared with the present state. A marked disparity was observed in hospitalist and housestaff team utilization of 62.22% and 86.55% respectively. Patient dispersion to various NUs significantly decreased, and rounding time correspondingly decreased by approximately 41%.
Future State 2, adding a nursing unit, decreased average time in the system per patient by 9.86 hours, with 9.32 fewer patients waiting for a bed as compared with the present state. A slight increase in patient dispersion and rounding time was observed. Overall, patients spent 137.51 hours in the system, which demonstrated improved efficiency of the system.
Future State 3, adding an additional medical team, interestingly did not have a significant effect on patients’ average time in system or the number of patients waiting for a bed even though a decrease occurred in average team census, team utilization, and patient dispersion.
Finally, Future State 4, increasing admissions while also adding a nursing unit and a hospitalist team, resulted in an increase in admission volume while maintaining similar utilization rates for teams and NU. Patients spent about 2.48 hours less in the system, while only 9.94 patients were noted to be waiting for a bed as compared with 11.21 patients in the present state model. The total daily general medicine patient census was noted to be 137.19. Average team census and average team utilization were noted to be similar to those of the present state model, while admissions were up by approximately 1,080 per year. Both patient dispersion and rounding were slightly worsened.
Sensitivity Analysis
Overall, average time in system was most affected by the number of patient arrivals. This became particularly significant as the volume of patient arrivals approached and exceeded the capacity of the rounding teams. Adding a nursing unit had more impact on decreasing average time in the system than adding a medical team or aligning teams with NUs under the conditions defined by the model. However, under different conditions, such as increasing admission volume, the relative benefit of different approaches may vary.
DISCUSSION
Given that hospitals are large, complex systems,2 the impact of system-level changes can have unpredictable and potentially deleterious effects. Simulation provides a technique for modeling the impact of changes to understand the ramifications of these interventions more thoroughly.3 In this study, we describe the process of building a simulation model for the admission and discharge of patients from general medicine services in a tertiary care hospital, internally validating this model, and examining the outcomes from several potential changes to the system.
The outcomes for these what-if scenarios provided some important insights about the secondary effect of system changes and the need for multiple, simultaneous interventions. Given that hospitals often function at near capacity, adding a hospitalist team or nursing unit might be seen as a reasonable strategy to improve the system metrics, number of patient discharges, or average LOS. On the basis of our analysis, adding a nursing unit would have more benefit than adding a hospitalist team. Leaders who want to increase capacity may need to consider both adding a hospitalist team and a nursing unit, and model the impact of each choice as described with a simulation.
Additionally, assigning patients to medical teams aligned with NUs seems theoretically appealing to improve interprofessional communication and decrease the time spent in transit between patients by physicians. While our findings supported a decrease in rounding time and patient dispersion, the teams not aligned with a nursing unit (ie, the hospitalists) exceeded 80% utilization, the threshold at which efficiency is known to decrease.24 Potentially, benefits resulting from teams being aligned with NUs were offset by decrements in performance of the teams not aligned with NU. If medical teams and NUs become aligned, then a higher number of teams may be necessary to maintain patient throughput.
Simulation models identify these unexpected consequences prior to investing resources in a significant change; however, modeling is not simple. Simulation models depend on the characteristics of the model and the quality of the input data. For example, we used an expert approach to map physician workflow as an underpinning of the model, but we may have missed an important variation in physician workflow. Understanding this variation could strengthen the model and provide some testable variables for future study. Likewise, understanding nursing workflow and how variation in physician workflow shapes nursing workflow, and vice versa, is worth exploring.
Other data could also be added to, and help interpret, the outputs of this model. For example, the impact of various levels of team and unit utilization on diversion time for the hospital ED may help determine whether adding team capacity or unit capacity is more beneficial for the system. Likewise, aligning medical teams with NUs seems to hinder patient throughput on this analysis, but benefits in patient satisfaction or decreased readmissions might improve reimbursement and outweigh the revenue lost from throughput. Underpinning each of these types of decisions is a need to model the system well and thoughtfully choose the inputs, processes, and outputs. Pursuing a new strategic decision usually involves cost; simulation modeling provides data to help leaders weigh the benefits in terms of the needed investment.
The major limitations of the study stem from these choices. Our study focused on matching capacity and demand while limiting other changes in the system, such as changes in nursing unit LOS. Future work to quantify the relationship of other variables on parameters, such as the impact of decreased team dispersion on LOS, early discharges, and decreasing care variation, would make future models more robust. This model does not consider other strategies to improve patient flow, such as shaping demand, adaptive team assignment algorithms, or creating surge capacity. We also used only hospitalist time and motion data in our model; housestaff workflow is likely different. In addition, we modeled all patients as having a general level of nursing care and did not account for admissions or transfers to intensive care units or other services. These parameters could be added in future iterations. Finally, the biggest limitation in any simulation is the underlying assumptions made to construct the model. While we validated the model retrospectively, prospective validation and refinement should also be performed with attention to how the model functions under extreme conditions, such as a very high patient load.
CONCLUSION
Major system changes are expensive and must be made carefully. Systems engineering techniques, such as DES, provide techniques to estimate the impact of changes on pertinent care delivery variables. Results from this study underscore the complexity of patient care delivery and how simulation models can integrate multiple system components to provide a data-driven approach to inform decision making in a complex system.
Acknowledgments
The simulation software used in this study was awarded as an educational software grant from SIMIO®. We would like to acknowledge support from the Department of Internal Medicine at Virginia Commonwealth University for this project and thank Lena Rivera for her assistance with the manuscript preparation.
Dislosures
Dr. Heim recived a consulting fee for programming guidance from Virginia Commonwealth University. All other authors have nothing to disclose.
1. James BC. Learning opportunities for health care. In: Grossmann C, Goolsby WA, Olsen LA, McGinnis JM, eds. Engineering a Learning Healthcare System: A Look at the Future: Workshop Summary. Washington, DC: National Academies Press; 2011:31-46. PubMed
2. Reid PP, Compton WD, Grossman J, Fanjiang G. Building a Better Delivery System: A New Engineering/Health Care Partnership. Washington, DC: National Academy of Engineering and Institute of Medicine, National Academies Press; 2005. PubMed
3. President’s Council of Advisors on Science and Technology (US). Report to the President, better health care and lower costs: accelerating improvement through systems engineering. Washington, DC; 2014.
4. Kossiakoff A, Sweet W. Systems Engineering Principles and Practice. New York: Wiley; 2003.
5. Kopach-Konrad R, Lawley M, Criswell M, et al. Applying systems engineering principles in improving health care delivery. J Gen Intern Med. 2007;22(Suppl 3):431-437. doi: 10.1007/s11606-007-0292-3. PubMed
6. Weed J. Factory efficiency comes to the hospital. The New York Times; July 9, 2010.
7. Lee EK, Atallah HY, Wright MD, et al. Transforming hospital emergency department workflow and patient care. Interfaces. 2015;45(1):58-82. doi: 10.1287/inte.2014.0788.
8. Resar R, Nolan K, Kaczynski D, Jensen K. Using real-time demand capacity management to improve hospitalwide patient flow. Joint Comm J Qual Patient Saf. 2011;37(5):217-227. doi: 10.1016/S1553-7250(11)37029-8. PubMed
9. McJoynt TA, Hirzallah MA, Satele DV et al. Building a protocol expressway: the case of Mayo Clinic Cancer Center. J Clin Oncol. 2009;27(23):3855-3860. doi: 10.1200/JCO.2008.21.4338. PubMed
10. Blanchard BS, Fabrycky WJ. Systems Engineering and Analysis. 5th ed. Englewood Cliffs: Prentice Hall; 2010.
11. Segev D, Levi R, Dunn PF, Sandberg WS. Modeling the impact of changing patient transportation systems on peri-operative process performance in a large hospital: insights from a computer simulation study. Health Care Manag Sci. 2012;15(2):155-169. doi: 10.1007/s10729-012-9191-1. PubMed
12. Schoenmeyr T, Dunn PF, Gamarnik D, et al. A model for understanding the impacts of demand and capacity on waiting time to enter a congested recovery room. Anesthesiology. 2009;110(6):1293-1304. doi: 10.1097/ALN.0b013e3181a16983 PubMed
13. Levin SR, Dittus R, Aronsky D, et al. Optimizing cardiology capacity to reduce emergency department boarding: a systems engineering approach. Am Heart J. 2008;156(6):1202-1209. doi: 10.1016/j.ahj.2008.07.007. PubMed
14. Bryson C, Boynton G, Stepczynski A, et al. Geographical assignment of hospitalists in an urban teaching hospital: feasibility and impact on efficiency and provider satisfaction. Hosp Pract. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884. PubMed
15. Artenstein AW, Higgins TL, Seiler A, et al. Promoting high value inpatient care via a coaching model of structured, interdisciplinary team rounds. Br J Hosp Med (Lond). 2015;76(1):41-45. doi: 10.12968/hmed.2015.76.1.41. PubMed
PubMed
16. O’Leary KJ, Wayne DB, Landler MP, et al. Impact of localizing physicians to hospital units on nurse-physician communication and agreement on the plan of care. J Gen Intern Med. 2009;24(11):1223-1227. doi: 10.1007/s11606-009-1113-7. PubMed
17. Dunn AS, Reyna M, Radbill B, et al. The impact of bedside interdisciplinary rounds on length of stay and complications. J Hosp Med. 2017;12(3):137-142. doi: 10.12788/jhm.2695. PubMed
18. Accreditation Council for Graduate Medical Education. Common program requirements. Chicago, IL; 2011.
19. Eldabi T, Irani Z, Paul RJ. A proposed approach for modelling health-care systems for understanding. J Manag Med. 2002;16(2-3):170-187. PubMed
20. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. doi: 10.1007/s11606-013-2376-6. PubMed
21. Tipping MD, Forth VE, Magill DB, Englert K, Williams MV. Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353-359. doi: 10.1002/jhm.647. PubMed
22. Cady R, Finkelstein S, Lindgren B, et al. Exploring the translational impact of a home telemonitoring intervention using time-motion study. Telemed J e Health. 2010;16(5):576-584. doi: 10.1089/tmj.2009.0148. PubMed
23. Rother M, Shook J. Learning to See: Value Stream Mapping to Add Value and Eliminate Muda. Cambridge, MA: Lean Enterprise Institute, Inc; 2009.
24. Terwiesch C, Diwas KC, Kahn JM. Working with capacity limitations: operations management in critical care. Crit Care. 2011;15(4):308. doi: 10.1186/cc10217. PubMed
Hospitals are complex adaptive systems within which practitioners, technology, physical resources, and other components adapt interdependently to attempt to best meet the needs of patients.1 Hospitals must provide a stable, dependable level of care while also surging to respond to times of high demand, such as patient emergencies or swells in patient volume. Given the critical and resource-intensive nature of this work, optimizing the system is essential; however, because of the complexity of the system, making changes can result in unexpected and possibly deleterious effects. We need to approach change in hospital processes carefully and thoughtfully.
The Institute of Medicine, the National Academy of Engineering, and the President’s Council of Advisors on Science and Technology have recommended the application of systems engineering approaches to improve health care delivery.2,3 Systems engineering seeks to coordinate, synchronize, and integrate complex systems of people, information, materials, technology, and financial resources.4,5 To determine how complex systems can be improved, engineers apply analytic methods to describe how such systems operate and what the impact of changes might be. These methodologies have improved patient care and reduced costs at several hospitals.6 For example, a decision support system that combined simulation, optimization, and machine learning methods in an emergency department (ED) resulted in a 33% reduction in length of stay (LOS) and a 28% decrease in ED readmissions.7 Other strategies to improve patient flow include shaping demand (decreasing variation in surgical scheduling, relocating low acuity care ED visit to primary care, etc.), redesigning systems (early discharges, improving efficiency, and coordination of hospital discharge process, decreasing care variation, etc.), or aligning capacity and demand. Another approach, real-time demand capacity (RTDC), is based on management principles and queuing and constraint theory and has been implemented successfully in a variety of health care organizations. RTDC represents a promising approach to improve hospitalwide patient flow and can be integrated into current bed management processes.8 Unfortunately, many of these approaches are not well known to clinicians and would benefit from greater awareness and input from healthcare practitioners.
One systems engineering tool that can be used to describe, analyze, and evaluate proposed changes in care is simulation.9 Simulation creates a model within which what-if scenarios (ie, adjusting various inputs into the simulation) allow researchers to define the likelihood of consequences from various courses of action and determine the optimal change to a system. Such analyses can predict the impact of a proposed change on patients and healthcare practitioners.10-13
A critical concern for hospitals that simulation may help address is managing the volume of inpatients. A high inpatient census is necessary for financial solvency, yet too high a census of inpatients or an unexpected surge in acuity can overwhelm hospital resources. Many hospitals, pressured by growing numbers of increasingly complex patients, have seen medical inpatients spread across multiple nonmedical nursing units (NUs) of their institution such that a particular medical team may have only a couple patients assigned to each nursing unit.14 This dispersion may hinder communication between physicians and nurses and limits the time physicians have to interact with patients.15 Additionally, coordination of care may become more challenging for discharge planning.16 Aligning medical teams with NUs may benefit the quality and efficiency of care or may create a barrier to patient flow, which worsens these problems.15,17 Alternatively, hospitals might meet the increasing demands for care by choosing to add capacity by opening new NUs or hiring additional healthcare providers.
This article describes the application of simulation to model the interconnected variables and subsequent future states created by several possible
METHODS
Setting and Present State
Virginia Commonwealth University (VCU) is a 865-bed tertiary academic medical center, with inpatient care activities spread between four connected buildings and 50 different NUs. The occupancy rate had been over 92% during the time period of this project with admission volume limited primarily by the capacity of the facility. Three of the NUs were primarily allocated to general medicine (GIM) patients. However, over the years, GIM inpatients grew to over 7500 admissions annually, resulting in nearly 50% of GIM patients being admitted to a non-GIM nursing unit.
Additionally, patients on each medical team had a high degree of spread across NUs due to several factors. Admissions and discharges from the hospital did not align across the day. While discharges clumped in the late afternoon, admission occurred throughout the day with a surge in the later afternoon. This mismatch frequently led to patients waiting in the ED for a bed, medical team, or both, and patients were typically assigned to the first available bed and team. For medical team assignments, newly admitted patients were distributed relatively equally across five hospitalist teams and five housestaff teams (that include residents, interns, and medical students). This steady distribution of patients through the day supported meeting housestaff work-hour restrictions of 80 hours each week.18 Yet, as a result of the high occupancy rate, the patterns of patient admissions and discharges, and the distribution of patients among medical teams and across NUs, medical teams and NUs rarely shared more than a few patients.
Leaders at our institution outlined several possible options to address these challenges, including aligning medical teams with NU, adding an additional hospitalist team, or adding an additional nursing unit. In addition, institutional leaders were concerned about the impact of continued growth in admission volume and the impact of patient dispersion on trainees and students. The overall goal of creating a simulation model was to determine the impact of an increased volume of patients and these possible strategic decisions on operational metrics, including number of patients waiting in the ED, ED boarding time per patient, time in system per patient (ED boarding time plus inpatient LOS), team utilization, and rounding travel time.
Simulation Modeling
To model the impact of some possible system changes on patient care, we applied Kelton and Law’s simulation study framework,19 including data collection; model building and validation; and what-if scenario testing (Figure 1).
Data Collection
Process Flow Map
We created a complex process flow map of patient care activities on medical teams. The map was developed by four general medicine physicians (R.C., H.M., V.M., and S.P.T.) who all provided medical care on the hospital-based services and ensured expert input on the patient care activities captured by the simulation modeling.
Time and Motion Studies
Time and motion study is a well-established technique used to evaluate the efficiency of work processes.20,21 Originally applied to increase productivity in manufacturing, this technique uses first-hand observations to measure the time allotted to different work tasks to systematically analyze workflow.22 Workflow in healthcare, like manufacturing tasks, tends to have a repetitive pattern, making time and motion studies a highly applicable tool.
A research assistant observed a total of 30 hospitalist work cycles to describe the work of our inpatient clinicians. A work cycle, defined as one complete process flow,23 began when the hospitalist started a daytime shift of patient care and concluded after the physician “signed out” to the physician who was assuming responsibility for ongoing medical care of the patients (ie, cross-coverage). Time spent on different activities identified by the process flow map was captured throughout the cycle. These activities included time spent traveling to evaluate patients located on different NUs. To minimize disruptions in patient care and adhere to privacy standards, no observations were conducted in patient rooms, and details of computer work were not recorded. To ensure stable estimates of the mean and standard deviation of the time spent at each step, at least 30 cycles of observation are recommended. Thus, 300 hours of observations over the course of 30 separate days were collected.
Hospital Data
We extracted admission and discharge data from the electronic health records (EHR) for general medicine patients admitted from the ED for the calendar year 2013. These records were used to establish means and standard deviations for admission date and time, distribution of patients across NUs, and LOS.
Model Building and Internal Validation
On the basis of these data inputs and using SIMIO® Simulation Software version 7, we constructed a discrete event simulation (DES) model representing the patient care activities of general medicine teams. Each patient was assigned a bed on a nursing unit through a probability distribution based on prior EHR data and then randomly assigned to a general medicine team. We replicated the model 200 times, and each model ran for 365 days. Each team was limited to 16 assigned patients, the maximum number of patients per housestaff team allowed by VCU protocol; henceforth, this number is referred to as team-patient capacity. The model assumed patients remained on the assigned nursing unit and medical team for the entirety of their hospital stay and that each patient was seen by their assigned medical team every day. The results of the present state model, including mean number of patients on each nursing unit, mean team census, patient dispersion (ie, the number of NUs on which each medical team had patients), and team utilization (ie, mean team census divided by team patient capacity), were compared with actual data from 2013 to internally validate the model.
What-If Scenario Testing
We constructed four what-if scenarios based on possible strategic directions identified by leadership. These models evaluated:
- constraining patients on housestaff (but not hospitalist) teams to the three general medicine NUs (Future State 1),
- increasing bed capacity for general medicine patients by adding one additional nursing unit of 26 beds (Future State 2),
- increasing the number of general medicine teams by adding one additional hospitalist team of up to 16 patients (Future State 3),
- modeling the impact of increased patient admissions from 21 per day to 25 per day while also adding a nursing unit and an additional medical team (Future State 4).
For Future States 1-3, admission volume was held constant. The model generated nursing unit LOS using a random continuous exponential probability distribution with a mean of 133 hours to match the LOS distribution derived from health system data. As patients entered the system for admission, the model assigned a bed to the patient, but the patient could not move to the assigned bed until a bed and care team were both available. We were only interested in the steady-state behavior of the system, so collecting performance statistics only after the model had been populated and steady state had been achieved was important.
Table 1 summarizes the input data, fixed, and dynamic variable for each future state model.
We examined the impact of these scenarios on the following variables (Table 2): (1) average time in system; (2) average number of patients waiting for a bed; (3) average ED boarding time; (4) total daily general medicine census; (5) average housestaff team census per team; (6) average hospitalist team census per team; (7) average combined housestaff and hospitalist team census per team; (8) average housestaff team utilization (ie, mean team census divided by team patient capacity of 16); (9) average hospitalist team utilization (ie, mean team census divided by team patient capacity of 16); (10) average nursing unit utilization (ie, mean nursing unit census divided by maximum number of patients that can be cared for on each nursing unit); (11) patient dispersion to NUs (ie, average number of NUs on which each general medicine team has patients); 12) estimated average rounding time per general medicine team.
Of note, the average time in the system included time patients spent waiting for bed and team assignments (ED boarding time) in addition to the time they spent in the assigned nursing unit (nursing LOS). The difference between the nursing LOS (ie, time on the nursing unit) and total time in the system is one indicator of system efficiency around hospital admission.
The Institutional Review Board of Virginia Commonwealth University approved this study.
RESULTS
Time and Motion Data
The mean time spent with each patient was nine minutes. The mean time traveling between NUs Healthcare Quality for Children and Adolescents with Suicidality Admitted to Acute Care Hospitals in the United States was five minutes. Average rounding time was noted to be two hours, 53 minutes. Thirty-seven minutes, about ~21% of the time, was wasted in traveling. Each team, on average, traveled to seven different NUs to round on their daily census, averaging 1.6 patients in each nursing unit.
Hospital Data
Between January 1, 2011 to December 31, 2013, a total of 7,902 patients were admitted to the general medicine teams, spanning 23 NU. The average number of admissions per day was 21.6, and the average nursing unit LOS was 133 hours. Average team census was derived from historical data across all GIM team for 2013 and was noted to be 11.5 patients per team, and these patients were spread over seven NU.
Model Validation
The mean number of patients admitted to different NUs was estimated from the simulation model then compared with the EHR data from 2013. None were statistically different (P > .05), which signified that the validated simulation model is similar to the EHR data from 2013 despite the underlying assumptions.
Model Outputs
Analysis of the models indicated that steady-state (based upon hospital census) was realized at approximately 800 hours or after 680 patients were admitted to the GIM teams. Statistics collection, therefore, was started after 800 hours of simulated time and reflected the admission of the remaining 7222 patients in the model validation sample (Table 2).
In the model, the total daily general medicine patient census was 119.26. Average time in the system per patient was noted to be 147.37 hours, which was 14.37 hours more than the average nursing unit LOS of 133 hours. Average number of patients waiting for a bed was noted to be 11.31, while the average wait time for a patient to get a bed was 12.39 hours.
Average housestaff team and hospitalist team utilization were 76.06% and 73.02%, respectively, with average team utilization of 74.54% (range: 72.88%-76.19%). Housestaff team and hospitalist team averaged 12.17 and 11.68 patients per care team, respectively. General medicine teams had patients on 7.30 NUs on average. GIM teams rounding travel time was 36.5 minutes.
What-If Scenario Testing
Simulation outputs for the four future states are summarized in Table 2. With Future State 1, through which patients were selectively assigned to housestaff teams aligned with three NUs, the average time in the system per patient increased by 2.35 hours, with 1.87 more patients waiting for a bed and waiting for 2.03 more hours as compared with the present state. A marked disparity was observed in hospitalist and housestaff team utilization of 62.22% and 86.55% respectively. Patient dispersion to various NUs significantly decreased, and rounding time correspondingly decreased by approximately 41%.
Future State 2, adding a nursing unit, decreased average time in the system per patient by 9.86 hours, with 9.32 fewer patients waiting for a bed as compared with the present state. A slight increase in patient dispersion and rounding time was observed. Overall, patients spent 137.51 hours in the system, which demonstrated improved efficiency of the system.
Future State 3, adding an additional medical team, interestingly did not have a significant effect on patients’ average time in system or the number of patients waiting for a bed even though a decrease occurred in average team census, team utilization, and patient dispersion.
Finally, Future State 4, increasing admissions while also adding a nursing unit and a hospitalist team, resulted in an increase in admission volume while maintaining similar utilization rates for teams and NU. Patients spent about 2.48 hours less in the system, while only 9.94 patients were noted to be waiting for a bed as compared with 11.21 patients in the present state model. The total daily general medicine patient census was noted to be 137.19. Average team census and average team utilization were noted to be similar to those of the present state model, while admissions were up by approximately 1,080 per year. Both patient dispersion and rounding were slightly worsened.
Sensitivity Analysis
Overall, average time in system was most affected by the number of patient arrivals. This became particularly significant as the volume of patient arrivals approached and exceeded the capacity of the rounding teams. Adding a nursing unit had more impact on decreasing average time in the system than adding a medical team or aligning teams with NUs under the conditions defined by the model. However, under different conditions, such as increasing admission volume, the relative benefit of different approaches may vary.
DISCUSSION
Given that hospitals are large, complex systems,2 the impact of system-level changes can have unpredictable and potentially deleterious effects. Simulation provides a technique for modeling the impact of changes to understand the ramifications of these interventions more thoroughly.3 In this study, we describe the process of building a simulation model for the admission and discharge of patients from general medicine services in a tertiary care hospital, internally validating this model, and examining the outcomes from several potential changes to the system.
The outcomes for these what-if scenarios provided some important insights about the secondary effect of system changes and the need for multiple, simultaneous interventions. Given that hospitals often function at near capacity, adding a hospitalist team or nursing unit might be seen as a reasonable strategy to improve the system metrics, number of patient discharges, or average LOS. On the basis of our analysis, adding a nursing unit would have more benefit than adding a hospitalist team. Leaders who want to increase capacity may need to consider both adding a hospitalist team and a nursing unit, and model the impact of each choice as described with a simulation.
Additionally, assigning patients to medical teams aligned with NUs seems theoretically appealing to improve interprofessional communication and decrease the time spent in transit between patients by physicians. While our findings supported a decrease in rounding time and patient dispersion, the teams not aligned with a nursing unit (ie, the hospitalists) exceeded 80% utilization, the threshold at which efficiency is known to decrease.24 Potentially, benefits resulting from teams being aligned with NUs were offset by decrements in performance of the teams not aligned with NU. If medical teams and NUs become aligned, then a higher number of teams may be necessary to maintain patient throughput.
Simulation models identify these unexpected consequences prior to investing resources in a significant change; however, modeling is not simple. Simulation models depend on the characteristics of the model and the quality of the input data. For example, we used an expert approach to map physician workflow as an underpinning of the model, but we may have missed an important variation in physician workflow. Understanding this variation could strengthen the model and provide some testable variables for future study. Likewise, understanding nursing workflow and how variation in physician workflow shapes nursing workflow, and vice versa, is worth exploring.
Other data could also be added to, and help interpret, the outputs of this model. For example, the impact of various levels of team and unit utilization on diversion time for the hospital ED may help determine whether adding team capacity or unit capacity is more beneficial for the system. Likewise, aligning medical teams with NUs seems to hinder patient throughput on this analysis, but benefits in patient satisfaction or decreased readmissions might improve reimbursement and outweigh the revenue lost from throughput. Underpinning each of these types of decisions is a need to model the system well and thoughtfully choose the inputs, processes, and outputs. Pursuing a new strategic decision usually involves cost; simulation modeling provides data to help leaders weigh the benefits in terms of the needed investment.
The major limitations of the study stem from these choices. Our study focused on matching capacity and demand while limiting other changes in the system, such as changes in nursing unit LOS. Future work to quantify the relationship of other variables on parameters, such as the impact of decreased team dispersion on LOS, early discharges, and decreasing care variation, would make future models more robust. This model does not consider other strategies to improve patient flow, such as shaping demand, adaptive team assignment algorithms, or creating surge capacity. We also used only hospitalist time and motion data in our model; housestaff workflow is likely different. In addition, we modeled all patients as having a general level of nursing care and did not account for admissions or transfers to intensive care units or other services. These parameters could be added in future iterations. Finally, the biggest limitation in any simulation is the underlying assumptions made to construct the model. While we validated the model retrospectively, prospective validation and refinement should also be performed with attention to how the model functions under extreme conditions, such as a very high patient load.
CONCLUSION
Major system changes are expensive and must be made carefully. Systems engineering techniques, such as DES, provide techniques to estimate the impact of changes on pertinent care delivery variables. Results from this study underscore the complexity of patient care delivery and how simulation models can integrate multiple system components to provide a data-driven approach to inform decision making in a complex system.
Acknowledgments
The simulation software used in this study was awarded as an educational software grant from SIMIO®. We would like to acknowledge support from the Department of Internal Medicine at Virginia Commonwealth University for this project and thank Lena Rivera for her assistance with the manuscript preparation.
Dislosures
Dr. Heim recived a consulting fee for programming guidance from Virginia Commonwealth University. All other authors have nothing to disclose.
Hospitals are complex adaptive systems within which practitioners, technology, physical resources, and other components adapt interdependently to attempt to best meet the needs of patients.1 Hospitals must provide a stable, dependable level of care while also surging to respond to times of high demand, such as patient emergencies or swells in patient volume. Given the critical and resource-intensive nature of this work, optimizing the system is essential; however, because of the complexity of the system, making changes can result in unexpected and possibly deleterious effects. We need to approach change in hospital processes carefully and thoughtfully.
The Institute of Medicine, the National Academy of Engineering, and the President’s Council of Advisors on Science and Technology have recommended the application of systems engineering approaches to improve health care delivery.2,3 Systems engineering seeks to coordinate, synchronize, and integrate complex systems of people, information, materials, technology, and financial resources.4,5 To determine how complex systems can be improved, engineers apply analytic methods to describe how such systems operate and what the impact of changes might be. These methodologies have improved patient care and reduced costs at several hospitals.6 For example, a decision support system that combined simulation, optimization, and machine learning methods in an emergency department (ED) resulted in a 33% reduction in length of stay (LOS) and a 28% decrease in ED readmissions.7 Other strategies to improve patient flow include shaping demand (decreasing variation in surgical scheduling, relocating low acuity care ED visit to primary care, etc.), redesigning systems (early discharges, improving efficiency, and coordination of hospital discharge process, decreasing care variation, etc.), or aligning capacity and demand. Another approach, real-time demand capacity (RTDC), is based on management principles and queuing and constraint theory and has been implemented successfully in a variety of health care organizations. RTDC represents a promising approach to improve hospitalwide patient flow and can be integrated into current bed management processes.8 Unfortunately, many of these approaches are not well known to clinicians and would benefit from greater awareness and input from healthcare practitioners.
One systems engineering tool that can be used to describe, analyze, and evaluate proposed changes in care is simulation.9 Simulation creates a model within which what-if scenarios (ie, adjusting various inputs into the simulation) allow researchers to define the likelihood of consequences from various courses of action and determine the optimal change to a system. Such analyses can predict the impact of a proposed change on patients and healthcare practitioners.10-13
A critical concern for hospitals that simulation may help address is managing the volume of inpatients. A high inpatient census is necessary for financial solvency, yet too high a census of inpatients or an unexpected surge in acuity can overwhelm hospital resources. Many hospitals, pressured by growing numbers of increasingly complex patients, have seen medical inpatients spread across multiple nonmedical nursing units (NUs) of their institution such that a particular medical team may have only a couple patients assigned to each nursing unit.14 This dispersion may hinder communication between physicians and nurses and limits the time physicians have to interact with patients.15 Additionally, coordination of care may become more challenging for discharge planning.16 Aligning medical teams with NUs may benefit the quality and efficiency of care or may create a barrier to patient flow, which worsens these problems.15,17 Alternatively, hospitals might meet the increasing demands for care by choosing to add capacity by opening new NUs or hiring additional healthcare providers.
This article describes the application of simulation to model the interconnected variables and subsequent future states created by several possible
METHODS
Setting and Present State
Virginia Commonwealth University (VCU) is a 865-bed tertiary academic medical center, with inpatient care activities spread between four connected buildings and 50 different NUs. The occupancy rate had been over 92% during the time period of this project with admission volume limited primarily by the capacity of the facility. Three of the NUs were primarily allocated to general medicine (GIM) patients. However, over the years, GIM inpatients grew to over 7500 admissions annually, resulting in nearly 50% of GIM patients being admitted to a non-GIM nursing unit.
Additionally, patients on each medical team had a high degree of spread across NUs due to several factors. Admissions and discharges from the hospital did not align across the day. While discharges clumped in the late afternoon, admission occurred throughout the day with a surge in the later afternoon. This mismatch frequently led to patients waiting in the ED for a bed, medical team, or both, and patients were typically assigned to the first available bed and team. For medical team assignments, newly admitted patients were distributed relatively equally across five hospitalist teams and five housestaff teams (that include residents, interns, and medical students). This steady distribution of patients through the day supported meeting housestaff work-hour restrictions of 80 hours each week.18 Yet, as a result of the high occupancy rate, the patterns of patient admissions and discharges, and the distribution of patients among medical teams and across NUs, medical teams and NUs rarely shared more than a few patients.
Leaders at our institution outlined several possible options to address these challenges, including aligning medical teams with NU, adding an additional hospitalist team, or adding an additional nursing unit. In addition, institutional leaders were concerned about the impact of continued growth in admission volume and the impact of patient dispersion on trainees and students. The overall goal of creating a simulation model was to determine the impact of an increased volume of patients and these possible strategic decisions on operational metrics, including number of patients waiting in the ED, ED boarding time per patient, time in system per patient (ED boarding time plus inpatient LOS), team utilization, and rounding travel time.
Simulation Modeling
To model the impact of some possible system changes on patient care, we applied Kelton and Law’s simulation study framework,19 including data collection; model building and validation; and what-if scenario testing (Figure 1).
Data Collection
Process Flow Map
We created a complex process flow map of patient care activities on medical teams. The map was developed by four general medicine physicians (R.C., H.M., V.M., and S.P.T.) who all provided medical care on the hospital-based services and ensured expert input on the patient care activities captured by the simulation modeling.
Time and Motion Studies
Time and motion study is a well-established technique used to evaluate the efficiency of work processes.20,21 Originally applied to increase productivity in manufacturing, this technique uses first-hand observations to measure the time allotted to different work tasks to systematically analyze workflow.22 Workflow in healthcare, like manufacturing tasks, tends to have a repetitive pattern, making time and motion studies a highly applicable tool.
A research assistant observed a total of 30 hospitalist work cycles to describe the work of our inpatient clinicians. A work cycle, defined as one complete process flow,23 began when the hospitalist started a daytime shift of patient care and concluded after the physician “signed out” to the physician who was assuming responsibility for ongoing medical care of the patients (ie, cross-coverage). Time spent on different activities identified by the process flow map was captured throughout the cycle. These activities included time spent traveling to evaluate patients located on different NUs. To minimize disruptions in patient care and adhere to privacy standards, no observations were conducted in patient rooms, and details of computer work were not recorded. To ensure stable estimates of the mean and standard deviation of the time spent at each step, at least 30 cycles of observation are recommended. Thus, 300 hours of observations over the course of 30 separate days were collected.
Hospital Data
We extracted admission and discharge data from the electronic health records (EHR) for general medicine patients admitted from the ED for the calendar year 2013. These records were used to establish means and standard deviations for admission date and time, distribution of patients across NUs, and LOS.
Model Building and Internal Validation
On the basis of these data inputs and using SIMIO® Simulation Software version 7, we constructed a discrete event simulation (DES) model representing the patient care activities of general medicine teams. Each patient was assigned a bed on a nursing unit through a probability distribution based on prior EHR data and then randomly assigned to a general medicine team. We replicated the model 200 times, and each model ran for 365 days. Each team was limited to 16 assigned patients, the maximum number of patients per housestaff team allowed by VCU protocol; henceforth, this number is referred to as team-patient capacity. The model assumed patients remained on the assigned nursing unit and medical team for the entirety of their hospital stay and that each patient was seen by their assigned medical team every day. The results of the present state model, including mean number of patients on each nursing unit, mean team census, patient dispersion (ie, the number of NUs on which each medical team had patients), and team utilization (ie, mean team census divided by team patient capacity), were compared with actual data from 2013 to internally validate the model.
What-If Scenario Testing
We constructed four what-if scenarios based on possible strategic directions identified by leadership. These models evaluated:
- constraining patients on housestaff (but not hospitalist) teams to the three general medicine NUs (Future State 1),
- increasing bed capacity for general medicine patients by adding one additional nursing unit of 26 beds (Future State 2),
- increasing the number of general medicine teams by adding one additional hospitalist team of up to 16 patients (Future State 3),
- modeling the impact of increased patient admissions from 21 per day to 25 per day while also adding a nursing unit and an additional medical team (Future State 4).
For Future States 1-3, admission volume was held constant. The model generated nursing unit LOS using a random continuous exponential probability distribution with a mean of 133 hours to match the LOS distribution derived from health system data. As patients entered the system for admission, the model assigned a bed to the patient, but the patient could not move to the assigned bed until a bed and care team were both available. We were only interested in the steady-state behavior of the system, so collecting performance statistics only after the model had been populated and steady state had been achieved was important.
Table 1 summarizes the input data, fixed, and dynamic variable for each future state model.
We examined the impact of these scenarios on the following variables (Table 2): (1) average time in system; (2) average number of patients waiting for a bed; (3) average ED boarding time; (4) total daily general medicine census; (5) average housestaff team census per team; (6) average hospitalist team census per team; (7) average combined housestaff and hospitalist team census per team; (8) average housestaff team utilization (ie, mean team census divided by team patient capacity of 16); (9) average hospitalist team utilization (ie, mean team census divided by team patient capacity of 16); (10) average nursing unit utilization (ie, mean nursing unit census divided by maximum number of patients that can be cared for on each nursing unit); (11) patient dispersion to NUs (ie, average number of NUs on which each general medicine team has patients); 12) estimated average rounding time per general medicine team.
Of note, the average time in the system included time patients spent waiting for bed and team assignments (ED boarding time) in addition to the time they spent in the assigned nursing unit (nursing LOS). The difference between the nursing LOS (ie, time on the nursing unit) and total time in the system is one indicator of system efficiency around hospital admission.
The Institutional Review Board of Virginia Commonwealth University approved this study.
RESULTS
Time and Motion Data
The mean time spent with each patient was nine minutes. The mean time traveling between NUs Healthcare Quality for Children and Adolescents with Suicidality Admitted to Acute Care Hospitals in the United States was five minutes. Average rounding time was noted to be two hours, 53 minutes. Thirty-seven minutes, about ~21% of the time, was wasted in traveling. Each team, on average, traveled to seven different NUs to round on their daily census, averaging 1.6 patients in each nursing unit.
Hospital Data
Between January 1, 2011 to December 31, 2013, a total of 7,902 patients were admitted to the general medicine teams, spanning 23 NU. The average number of admissions per day was 21.6, and the average nursing unit LOS was 133 hours. Average team census was derived from historical data across all GIM team for 2013 and was noted to be 11.5 patients per team, and these patients were spread over seven NU.
Model Validation
The mean number of patients admitted to different NUs was estimated from the simulation model then compared with the EHR data from 2013. None were statistically different (P > .05), which signified that the validated simulation model is similar to the EHR data from 2013 despite the underlying assumptions.
Model Outputs
Analysis of the models indicated that steady-state (based upon hospital census) was realized at approximately 800 hours or after 680 patients were admitted to the GIM teams. Statistics collection, therefore, was started after 800 hours of simulated time and reflected the admission of the remaining 7222 patients in the model validation sample (Table 2).
In the model, the total daily general medicine patient census was 119.26. Average time in the system per patient was noted to be 147.37 hours, which was 14.37 hours more than the average nursing unit LOS of 133 hours. Average number of patients waiting for a bed was noted to be 11.31, while the average wait time for a patient to get a bed was 12.39 hours.
Average housestaff team and hospitalist team utilization were 76.06% and 73.02%, respectively, with average team utilization of 74.54% (range: 72.88%-76.19%). Housestaff team and hospitalist team averaged 12.17 and 11.68 patients per care team, respectively. General medicine teams had patients on 7.30 NUs on average. GIM teams rounding travel time was 36.5 minutes.
What-If Scenario Testing
Simulation outputs for the four future states are summarized in Table 2. With Future State 1, through which patients were selectively assigned to housestaff teams aligned with three NUs, the average time in the system per patient increased by 2.35 hours, with 1.87 more patients waiting for a bed and waiting for 2.03 more hours as compared with the present state. A marked disparity was observed in hospitalist and housestaff team utilization of 62.22% and 86.55% respectively. Patient dispersion to various NUs significantly decreased, and rounding time correspondingly decreased by approximately 41%.
Future State 2, adding a nursing unit, decreased average time in the system per patient by 9.86 hours, with 9.32 fewer patients waiting for a bed as compared with the present state. A slight increase in patient dispersion and rounding time was observed. Overall, patients spent 137.51 hours in the system, which demonstrated improved efficiency of the system.
Future State 3, adding an additional medical team, interestingly did not have a significant effect on patients’ average time in system or the number of patients waiting for a bed even though a decrease occurred in average team census, team utilization, and patient dispersion.
Finally, Future State 4, increasing admissions while also adding a nursing unit and a hospitalist team, resulted in an increase in admission volume while maintaining similar utilization rates for teams and NU. Patients spent about 2.48 hours less in the system, while only 9.94 patients were noted to be waiting for a bed as compared with 11.21 patients in the present state model. The total daily general medicine patient census was noted to be 137.19. Average team census and average team utilization were noted to be similar to those of the present state model, while admissions were up by approximately 1,080 per year. Both patient dispersion and rounding were slightly worsened.
Sensitivity Analysis
Overall, average time in system was most affected by the number of patient arrivals. This became particularly significant as the volume of patient arrivals approached and exceeded the capacity of the rounding teams. Adding a nursing unit had more impact on decreasing average time in the system than adding a medical team or aligning teams with NUs under the conditions defined by the model. However, under different conditions, such as increasing admission volume, the relative benefit of different approaches may vary.
DISCUSSION
Given that hospitals are large, complex systems,2 the impact of system-level changes can have unpredictable and potentially deleterious effects. Simulation provides a technique for modeling the impact of changes to understand the ramifications of these interventions more thoroughly.3 In this study, we describe the process of building a simulation model for the admission and discharge of patients from general medicine services in a tertiary care hospital, internally validating this model, and examining the outcomes from several potential changes to the system.
The outcomes for these what-if scenarios provided some important insights about the secondary effect of system changes and the need for multiple, simultaneous interventions. Given that hospitals often function at near capacity, adding a hospitalist team or nursing unit might be seen as a reasonable strategy to improve the system metrics, number of patient discharges, or average LOS. On the basis of our analysis, adding a nursing unit would have more benefit than adding a hospitalist team. Leaders who want to increase capacity may need to consider both adding a hospitalist team and a nursing unit, and model the impact of each choice as described with a simulation.
Additionally, assigning patients to medical teams aligned with NUs seems theoretically appealing to improve interprofessional communication and decrease the time spent in transit between patients by physicians. While our findings supported a decrease in rounding time and patient dispersion, the teams not aligned with a nursing unit (ie, the hospitalists) exceeded 80% utilization, the threshold at which efficiency is known to decrease.24 Potentially, benefits resulting from teams being aligned with NUs were offset by decrements in performance of the teams not aligned with NU. If medical teams and NUs become aligned, then a higher number of teams may be necessary to maintain patient throughput.
Simulation models identify these unexpected consequences prior to investing resources in a significant change; however, modeling is not simple. Simulation models depend on the characteristics of the model and the quality of the input data. For example, we used an expert approach to map physician workflow as an underpinning of the model, but we may have missed an important variation in physician workflow. Understanding this variation could strengthen the model and provide some testable variables for future study. Likewise, understanding nursing workflow and how variation in physician workflow shapes nursing workflow, and vice versa, is worth exploring.
Other data could also be added to, and help interpret, the outputs of this model. For example, the impact of various levels of team and unit utilization on diversion time for the hospital ED may help determine whether adding team capacity or unit capacity is more beneficial for the system. Likewise, aligning medical teams with NUs seems to hinder patient throughput on this analysis, but benefits in patient satisfaction or decreased readmissions might improve reimbursement and outweigh the revenue lost from throughput. Underpinning each of these types of decisions is a need to model the system well and thoughtfully choose the inputs, processes, and outputs. Pursuing a new strategic decision usually involves cost; simulation modeling provides data to help leaders weigh the benefits in terms of the needed investment.
The major limitations of the study stem from these choices. Our study focused on matching capacity and demand while limiting other changes in the system, such as changes in nursing unit LOS. Future work to quantify the relationship of other variables on parameters, such as the impact of decreased team dispersion on LOS, early discharges, and decreasing care variation, would make future models more robust. This model does not consider other strategies to improve patient flow, such as shaping demand, adaptive team assignment algorithms, or creating surge capacity. We also used only hospitalist time and motion data in our model; housestaff workflow is likely different. In addition, we modeled all patients as having a general level of nursing care and did not account for admissions or transfers to intensive care units or other services. These parameters could be added in future iterations. Finally, the biggest limitation in any simulation is the underlying assumptions made to construct the model. While we validated the model retrospectively, prospective validation and refinement should also be performed with attention to how the model functions under extreme conditions, such as a very high patient load.
CONCLUSION
Major system changes are expensive and must be made carefully. Systems engineering techniques, such as DES, provide techniques to estimate the impact of changes on pertinent care delivery variables. Results from this study underscore the complexity of patient care delivery and how simulation models can integrate multiple system components to provide a data-driven approach to inform decision making in a complex system.
Acknowledgments
The simulation software used in this study was awarded as an educational software grant from SIMIO®. We would like to acknowledge support from the Department of Internal Medicine at Virginia Commonwealth University for this project and thank Lena Rivera for her assistance with the manuscript preparation.
Dislosures
Dr. Heim recived a consulting fee for programming guidance from Virginia Commonwealth University. All other authors have nothing to disclose.
1. James BC. Learning opportunities for health care. In: Grossmann C, Goolsby WA, Olsen LA, McGinnis JM, eds. Engineering a Learning Healthcare System: A Look at the Future: Workshop Summary. Washington, DC: National Academies Press; 2011:31-46. PubMed
2. Reid PP, Compton WD, Grossman J, Fanjiang G. Building a Better Delivery System: A New Engineering/Health Care Partnership. Washington, DC: National Academy of Engineering and Institute of Medicine, National Academies Press; 2005. PubMed
3. President’s Council of Advisors on Science and Technology (US). Report to the President, better health care and lower costs: accelerating improvement through systems engineering. Washington, DC; 2014.
4. Kossiakoff A, Sweet W. Systems Engineering Principles and Practice. New York: Wiley; 2003.
5. Kopach-Konrad R, Lawley M, Criswell M, et al. Applying systems engineering principles in improving health care delivery. J Gen Intern Med. 2007;22(Suppl 3):431-437. doi: 10.1007/s11606-007-0292-3. PubMed
6. Weed J. Factory efficiency comes to the hospital. The New York Times; July 9, 2010.
7. Lee EK, Atallah HY, Wright MD, et al. Transforming hospital emergency department workflow and patient care. Interfaces. 2015;45(1):58-82. doi: 10.1287/inte.2014.0788.
8. Resar R, Nolan K, Kaczynski D, Jensen K. Using real-time demand capacity management to improve hospitalwide patient flow. Joint Comm J Qual Patient Saf. 2011;37(5):217-227. doi: 10.1016/S1553-7250(11)37029-8. PubMed
9. McJoynt TA, Hirzallah MA, Satele DV et al. Building a protocol expressway: the case of Mayo Clinic Cancer Center. J Clin Oncol. 2009;27(23):3855-3860. doi: 10.1200/JCO.2008.21.4338. PubMed
10. Blanchard BS, Fabrycky WJ. Systems Engineering and Analysis. 5th ed. Englewood Cliffs: Prentice Hall; 2010.
11. Segev D, Levi R, Dunn PF, Sandberg WS. Modeling the impact of changing patient transportation systems on peri-operative process performance in a large hospital: insights from a computer simulation study. Health Care Manag Sci. 2012;15(2):155-169. doi: 10.1007/s10729-012-9191-1. PubMed
12. Schoenmeyr T, Dunn PF, Gamarnik D, et al. A model for understanding the impacts of demand and capacity on waiting time to enter a congested recovery room. Anesthesiology. 2009;110(6):1293-1304. doi: 10.1097/ALN.0b013e3181a16983 PubMed
13. Levin SR, Dittus R, Aronsky D, et al. Optimizing cardiology capacity to reduce emergency department boarding: a systems engineering approach. Am Heart J. 2008;156(6):1202-1209. doi: 10.1016/j.ahj.2008.07.007. PubMed
14. Bryson C, Boynton G, Stepczynski A, et al. Geographical assignment of hospitalists in an urban teaching hospital: feasibility and impact on efficiency and provider satisfaction. Hosp Pract. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884. PubMed
15. Artenstein AW, Higgins TL, Seiler A, et al. Promoting high value inpatient care via a coaching model of structured, interdisciplinary team rounds. Br J Hosp Med (Lond). 2015;76(1):41-45. doi: 10.12968/hmed.2015.76.1.41. PubMed
16. O’Leary KJ, Wayne DB, Landler MP, et al. Impact of localizing physicians to hospital units on nurse-physician communication and agreement on the plan of care. J Gen Intern Med. 2009;24(11):1223-1227. doi: 10.1007/s11606-009-1113-7. PubMed
17. Dunn AS, Reyna M, Radbill B, et al. The impact of bedside interdisciplinary rounds on length of stay and complications. J Hosp Med. 2017;12(3):137-142. doi: 10.12788/jhm.2695. PubMed
18. Accreditation Council for Graduate Medical Education. Common program requirements. Chicago, IL; 2011.
19. Eldabi T, Irani Z, Paul RJ. A proposed approach for modelling health-care systems for understanding. J Manag Med. 2002;16(2-3):170-187. PubMed
20. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. doi: 10.1007/s11606-013-2376-6. PubMed
21. Tipping MD, Forth VE, Magill DB, Englert K, Williams MV. Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353-359. doi: 10.1002/jhm.647. PubMed
22. Cady R, Finkelstein S, Lindgren B, et al. Exploring the translational impact of a home telemonitoring intervention using time-motion study. Telemed J e Health. 2010;16(5):576-584. doi: 10.1089/tmj.2009.0148. PubMed
23. Rother M, Shook J. Learning to See: Value Stream Mapping to Add Value and Eliminate Muda. Cambridge, MA: Lean Enterprise Institute, Inc; 2009.
24. Terwiesch C, Diwas KC, Kahn JM. Working with capacity limitations: operations management in critical care. Crit Care. 2011;15(4):308. doi: 10.1186/cc10217. PubMed
1. James BC. Learning opportunities for health care. In: Grossmann C, Goolsby WA, Olsen LA, McGinnis JM, eds. Engineering a Learning Healthcare System: A Look at the Future: Workshop Summary. Washington, DC: National Academies Press; 2011:31-46. PubMed
2. Reid PP, Compton WD, Grossman J, Fanjiang G. Building a Better Delivery System: A New Engineering/Health Care Partnership. Washington, DC: National Academy of Engineering and Institute of Medicine, National Academies Press; 2005. PubMed
3. President’s Council of Advisors on Science and Technology (US). Report to the President, better health care and lower costs: accelerating improvement through systems engineering. Washington, DC; 2014.
4. Kossiakoff A, Sweet W. Systems Engineering Principles and Practice. New York: Wiley; 2003.
5. Kopach-Konrad R, Lawley M, Criswell M, et al. Applying systems engineering principles in improving health care delivery. J Gen Intern Med. 2007;22(Suppl 3):431-437. doi: 10.1007/s11606-007-0292-3. PubMed
6. Weed J. Factory efficiency comes to the hospital. The New York Times; July 9, 2010.
7. Lee EK, Atallah HY, Wright MD, et al. Transforming hospital emergency department workflow and patient care. Interfaces. 2015;45(1):58-82. doi: 10.1287/inte.2014.0788.
8. Resar R, Nolan K, Kaczynski D, Jensen K. Using real-time demand capacity management to improve hospitalwide patient flow. Joint Comm J Qual Patient Saf. 2011;37(5):217-227. doi: 10.1016/S1553-7250(11)37029-8. PubMed
9. McJoynt TA, Hirzallah MA, Satele DV et al. Building a protocol expressway: the case of Mayo Clinic Cancer Center. J Clin Oncol. 2009;27(23):3855-3860. doi: 10.1200/JCO.2008.21.4338. PubMed
10. Blanchard BS, Fabrycky WJ. Systems Engineering and Analysis. 5th ed. Englewood Cliffs: Prentice Hall; 2010.
11. Segev D, Levi R, Dunn PF, Sandberg WS. Modeling the impact of changing patient transportation systems on peri-operative process performance in a large hospital: insights from a computer simulation study. Health Care Manag Sci. 2012;15(2):155-169. doi: 10.1007/s10729-012-9191-1. PubMed
12. Schoenmeyr T, Dunn PF, Gamarnik D, et al. A model for understanding the impacts of demand and capacity on waiting time to enter a congested recovery room. Anesthesiology. 2009;110(6):1293-1304. doi: 10.1097/ALN.0b013e3181a16983 PubMed
13. Levin SR, Dittus R, Aronsky D, et al. Optimizing cardiology capacity to reduce emergency department boarding: a systems engineering approach. Am Heart J. 2008;156(6):1202-1209. doi: 10.1016/j.ahj.2008.07.007. PubMed
14. Bryson C, Boynton G, Stepczynski A, et al. Geographical assignment of hospitalists in an urban teaching hospital: feasibility and impact on efficiency and provider satisfaction. Hosp Pract. 2017;45(4):135-142. doi: 10.1080/21548331.2017.1353884. PubMed
15. Artenstein AW, Higgins TL, Seiler A, et al. Promoting high value inpatient care via a coaching model of structured, interdisciplinary team rounds. Br J Hosp Med (Lond). 2015;76(1):41-45. doi: 10.12968/hmed.2015.76.1.41. PubMed
16. O’Leary KJ, Wayne DB, Landler MP, et al. Impact of localizing physicians to hospital units on nurse-physician communication and agreement on the plan of care. J Gen Intern Med. 2009;24(11):1223-1227. doi: 10.1007/s11606-009-1113-7. PubMed
17. Dunn AS, Reyna M, Radbill B, et al. The impact of bedside interdisciplinary rounds on length of stay and complications. J Hosp Med. 2017;12(3):137-142. doi: 10.12788/jhm.2695. PubMed
18. Accreditation Council for Graduate Medical Education. Common program requirements. Chicago, IL; 2011.
19. Eldabi T, Irani Z, Paul RJ. A proposed approach for modelling health-care systems for understanding. J Manag Med. 2002;16(2-3):170-187. PubMed
20. Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hours regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013;28(8):1042-1047. doi: 10.1007/s11606-013-2376-6. PubMed
21. Tipping MD, Forth VE, Magill DB, Englert K, Williams MV. Systematic review of time studies evaluating physicians in the hospital setting. J Hosp Med. 2010;5(6):353-359. doi: 10.1002/jhm.647. PubMed
22. Cady R, Finkelstein S, Lindgren B, et al. Exploring the translational impact of a home telemonitoring intervention using time-motion study. Telemed J e Health. 2010;16(5):576-584. doi: 10.1089/tmj.2009.0148. PubMed
23. Rother M, Shook J. Learning to See: Value Stream Mapping to Add Value and Eliminate Muda. Cambridge, MA: Lean Enterprise Institute, Inc; 2009.
24. Terwiesch C, Diwas KC, Kahn JM. Working with capacity limitations: operations management in critical care. Crit Care. 2011;15(4):308. doi: 10.1186/cc10217. PubMed
© 2019 Society of Hospital Medicine