User login
Erectile dysfunction (ED) is a multifactorial disease that can lead to treatment nonadherence in men taking medications for chronic health problems. Despite the importance of adhering to medication protocols for disease management, several studies demonstrated that a lack of adherence to medication protocols may be a direct response to the development of ED.
The Health Belief Model (HBM) is a conceptual framework used to better understand the relationship between health behavior and adherence in men diagnosed with hypertension. The HBM consists of 3 components that help explain health care behaviors: (1) individual perceptions; (2) modifying factors; and (3) likelihood of action. These components align with the variables in this study, which include beliefs about medicines, illness perception, and erectile function.1 Thus, the research challenge was to determine the relationship between knowledge of hypertension and sexual satisfaction among men with hypertension by using instruments in the form of 2 questionnaires: (1) the Beliefs about Medicines Questionnaire (BMQ), and (2) the International Index of Erectile Functioning (IIEF).2
Methods
A descriptive correlational design was used to explore the relationship between male patients’ antihypertensive medication beliefs and erectile function.
A convenience sample of 47 eligible men (age range 18-75 years) was recruited for this pilot study. Inclusion criteria were hypertension diagnosed by a medical professional, current use of antihypertensive medication, ability to read and write in English, and a signed informed consent. Study participants were recruited from a nurse-managed center in Detroit, Michigan, and from 6 facilities identified through Project Healthy Living 2012. The mission of the nurse-managed center is to assist low-income and underinsured populations in Wayne County, Michigan. Project Healthy Living 2012 performs free and low-cost health screenings and provides general health information to the public at various locations in the Detroit metropolitan area. Written permission to collect data was obtained from the director of Project Healthy Living 2012. Recruitment began after institutional review board approval was obtained. Participants signed an informed consent form that fully explained the nature of the study and the benefits and potential risks of participation.
Instruments
This study used the BMQ and IIEF health-related questionnaires. In addition, demographic information (eg, age, race, marital status, education, length of time with hypertension diagnosis, and current antihypertensive medications) was collected.
The BMQ was originally developed to understand patients’ commonly held beliefs about medications and the factors influencing their adherence to prescribed medication regimens.3 This questionnaire has 2 scales, BMQ Specific and BMQ General (only BMQ Specific was relevant to this study).
The BMQ Specific scale consists of two 5-item subscales, specific-necessity and specific-concern, that are designed to assess respondents’ beliefs about prescribed medications they are taking for specific conditions, such as hypertension. According to Horne and colleagues, the specific-necessity construct represents the perceived role of medication in protecting against deterioration of present and future health status.4 Statement examples include “My current health depends on my medicines,” and “My medicines protect me from becoming worse.” The specific-concern construct has an emotional component (eg, “Having to take my medicines worries me”) and a cognitive component (eg, “My medicines are a mystery to me”).
Items are scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher BMQ scores signify stronger beliefs. Studies using the BMQ subscales have shown that respondents with stronger beliefs about the necessity of their medications and fewer concerns about their medications are more likely to be adherent.
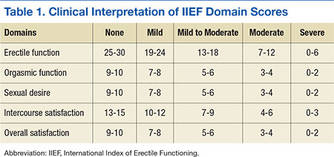
The self-administered IIEF is the instrument most widely used to assess sexual functioning and has been deployed in numerous clinical trials as the primary endpoint in evaluating the efficacy of phosphodiesterase 5-inhibitor therapy in the treatment of ED. The IIEF consists of 15 statements grouped into 5 domains assessing erectile function (6 items), orgasmic function (2 items), sexual desire (2 items), intercourse satisfaction (3 items), and overall satisfaction (2 items). Each domain is scored separately (Table 1).
Data Collection and Analysis
The researcher administered paper-and-pencil versions of the BMQ and the IIEF. Participants were allowed to complete these surveys in a semiprivate setting. No identifying information was collected—only general demographic information. IBM SPSS Version 16 statistical software was used to analyze the data. 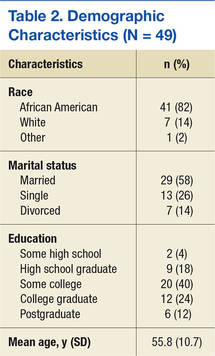
Results
Forty-five men who were taking antihypertensive medication prescribed by a primary care provider agreed to participate. Their mean age was 55.8 years. The majority were African American (82%), married (58%) with some post-high school education (76%) (Table 2). Mean length of time with a hypertension diagnosis was 9.2 years. All respondents reported taking at least 1 antihypertensive medication. The medication most often reported being used was amlodipine, followed by lisinopril and metoprolol.
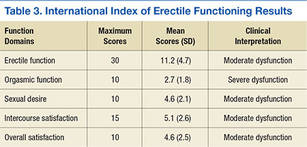
All of the respondents self-reported sexual dysfunction as indicated by the mean scores on the 5 domains of the IIEF (Table 3). Moreover, the vast majority of the total scores on the 5 domains fell within the moderate-to-severe dysfunction levels (Table 4).
BMQ Scores
The mean BMQ specific-necessity score was 16.7 (Table 5). More than half the respondents agreed or strongly agreed with 4 of the 5 statements regarding the necessity of their medications; the exception was “My life would be impossible without my medicines” (29.8%). The statement that generated the highest percentage of agreement was “My medicines protect me from becoming worse” (72.3%) (Table 6).
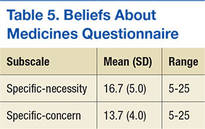
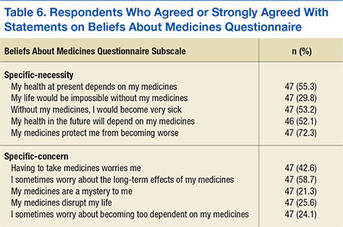
The mean BMQ specific-concern score was 13.7. Less than one-fourth of the respondents agreed or strongly agreed with 3 statements (of 4) regarding medication concerns: “My medicine is a mystery to me” (21.3%), “I sometimes worry about becoming too dependent on my medicine” (24.1%), and “My medicines disrupt my life” (25.6%). Regarding the fourth statement, “I sometimes worry about the long-term effects of my medicines,” 58.7% agreed or strongly agreed.
Spearman correlation analyses were performed to examine the relationships between BMQ specific-necessity, BMQ specific-concern, and the 5 IIEF sexual functioning domains. No statistically significant relationships were detected.
Time With Hypertension Diagnosis
The study also evaluated the results based on length of time the men had a hypertension diagnosis (≤ 10 years vs ≥ 11 years). An independent t test was used to compare mean BMQ specific-necessity and specific-concern scores. Crosstabs was used to compare length of time with diagnosis and the 5 IIEF domains. Mean specific-necessity score was 18.1 for the 20 respondents with a diagnosis of ≥ 11 years and 15.0 for the 22 respondents with a diagnosis of ≤ 10 years; this difference was statistically significant (P = .048). In addition, mean specific-concern score was 14.7 for respondents with a diagnosis of ≥ 11 years and 12.4 for those with a diagnosis of ≤ 10 years; this difference was not statistically significant but was trending in that direction (P = .076).
Length of time with a hypertension diagnosis did not necessarily relate to sexual function or satisfaction. Moderate-to-severe dysfunction in sexual desire was reported by 42% of the respondents with a diagnosis of ≥ 11 years compared with 57% of those with a diagnosis of ≤ 10 years. The same was found for overall satisfaction.
Discussion
Men with chronic health conditions, such as hypertension, are often prescribed medications that interfere with their sexual functioning.5 Patients who do not understand the importance of medication adherence in treating long-term chronic health conditions may discontinue taking these medications to improve their sexual functioning.5 Some men overestimate the control they have over chronic health conditions; others underestimate their control.
With a better understanding of men’s perceived ability to control chronic hypertension, practitioners can begin to provide appropriate educational interventions. These interventions must inform patients about the role of medication adherence in maintaining and enhancing sexual functioning and must impart a greater sense of control and empowerment over their condition, thereby increasing the likelihood of medication adherence.
To the authors’ knowledge, this is the first study to examine the potential associations of medication beliefs (using the BMQ) and erectile function in men with hypertension. There was no association between any of the demographic variables of age, race, marital status, and education, with respondents’ medication beliefs or erectile function. The IIEF domain that had the highest level of severe and moderate dysfunction combined was orgasmic function (n = 36; 80%), which suggests that antihypertensive medication may interfere with orgasmic function because achieving an orgasm is a physiologic process. This is consistent with the findings of Hellstrom and colleagues—that the vast majority of ED is related to orgasmic factors.6 Although 80% of respondents reported either moderate or severe dysfunction in this area, only 53% (n = 24) reported moderate or severe dysfunction in overall satisfaction. This might suggest that men taking antihypertensive medication, and their partners, have learned other methods or strategies for achieving sexual satisfaction.
The BMQ specific-necessity and specific-concern results offer insight into how men with hypertension view the need for antihypertensive medication. Mean (SD) specific-necessity score was 16.7 (5); the maximum was 25. Although no other studies have investigated men’s beliefs about antihypertensive medications, studies of other chronic illnesses have measured beliefs about the medications used in treatment. For example, Neame and Hammond reported a mean specific-necessity score of 19.9 and a mean specific-concern score of 15.9 in a sample of 108 men with arthritis.7 Of the respondents, 74.3% agreed or strongly agreed that their arthritis medication was necessary for health. However, 47.4% were concerned about potential adverse effects. Lennerling and Forsberg conducted a cross-sectional study of 250 renal transplant recipients.8 Respondents reported a mean specific-necessity score of 23 and a median specific-concern score of 11. In addition, length of time with hypertension diagnosis affected specific-necessity and specific-concern scores. For example, men with a hypertension diagnosis for 10 or fewer years had higher scores on both of these BMQ subscales.
The inability to detect a statistically significant correlation between BMQ specific-necessity and the 5 IIEF domains suggests that the sexual functioning of men with hypertension is not necessarily related to their antihypertensive medication beliefs. More than 50% agreed or strongly agreed that antihypertensive medications were necessary, but not that life would be impossible without them. Moreover, there was no statistically significant relationship between any of the 5 IIEF domains and the BMQ specific-concern subscale, which suggests that the sexual functioning of men with hypertension may not be related to their concern about their medications.
The findings of this study support HBM and provide a possible explanation for medication nonadherence in men diagnosed with hypertension. The HBM provides a conceptual framework that positions the study variables (eg, beliefs about medicines, illness perception, and erectile function) in terms of health care behaviors that can lead to increased medication adherence among men with hypertension. The HBM also allows the researcher to gain a better understanding about participants’ health behaviors, how these health behaviors are determined by personal beliefs or perceptions about a disease, and strategies available to decrease nonadherence.1
The HBM postulates that patients’ appraisals of disease risk (susceptibility) and severity influence their behavior.9 One study assessed respondents’ perceptions of the seriousness of their hypertension and its relationship to ED and of the consequences of failing to take prescribed blood pressure medications.9 When using the HBM, it is important to consider patients’ perceived barriers to and incentives for engaging in specific behaviors. The same study used the BMQ to address specific questions about respondents’ beliefs and feelings about their prescribed medications and medication adherence. The HBM suggests considering action cues that encourage patients to act by reminding them of the need to change their behavior.
Limitations
This study had several limitations. First, the sample size was small (47), which makes it difficult to generalize findings to a broader population of men with a hypertension diagnosis. In addition, because the study was underpowered, its ability to detect significant differences was compromised. Second, the study used a convenience sample of predominantly African American men. As always, there are concerns of self-selection and failure to represent the overall population. Third, the setting for completing the surveys was only semiprivate, and some respondents may have been uncomfortable, perhaps, working too quickly and not really thinking about the questions or their answers. Fourth, the ED survey was self-administered, so there is a concern about the truthfulness of responses. Fifth, failure to ask respondents whether they were taking a phosphodiesterase 5 inhibitor for ED could have significantly impacted study findings. Sixth, respondents were not asked about other medications, such as antidepressants and nonsteroidal anti-inflammatory drugs, which could have affected erectile function.
Clinical Implications
Despite the study limitations, several findings have important clinical implications. First, the vast majority of participants in this pilot study self-reported moderate or severe sexual dysfunction on all 5 IIEF domains. This finding is important because this was a convenience sample, and many of the IIEF statements are personal. The high rate of reported sexual dysfunction suggests that the incidence of ED may be underreported in the larger population. Second, mean BMQ scores were similar to those reported in other studies involving chronic illness: higher necessity and lower concern. Third, there was no statistically significant relationship between BMQ necessity and concern and IIEF sexual functioning. More research is needed to determine how to interpret these findings. Fourth, there was a significant relationship between length of time with hypertension diagnosis and BMQ specific-necessity score: The longer the diagnosis, the higher the score. However, this relationship did not hold for BMQ specific-concern, though it trended toward significance. Moreover, length of time with hypertension diagnosis did not necessarily predict or influence erectile function as measured with the IIEF. In fact, men with a hypertension diagnosis of ≥ 11 years reported less moderate-to-severe sexual dysfunction in overall satisfaction and sexual desire. Although there are several methodologic concerns about this study, its results offer direction for both clinical practice and future research.
Studies of erectile function and its relationship to hypertension have generated both cause for concern and reason for further research. The present study focused on gaining a better understanding of the relationship between antihypertensive medication beliefs and erectile function. Future clinical studies should explore the effects of antihypertensive medication on erectile function and men’s lack of knowledge and education about the importance of taking medication to prevent complications of hypertension. It is essential that this research be applied to improve the understanding of erectile function in men with hypertension. This will ultimately allow for better patient management and contribute to the overall sexual health and well-being of patients with hypertension.
Although it is important to identify men’s antihypertensive medication beliefs and the relationship of these beliefs to sexual satisfaction, most longitudinal studies suggest that the ED rate is high and that it increases with age.10 Therefore, it is crucial that men differentiate between how antihypertensive medications affect erectile function and changes associated with aging. The present study found no statistically significant relationships between the BMQ specific-necessity and specific-concern subscales and overall satisfaction with sexual functioning (IIEF). In addition, the study found no significant correlations between the BMQ specific and general scales and the 5 IIEF domains.
Conclusion
It was evident from this research that men with chronic health problems, such as hypertension, are often prescribed medications that affect sexual functioning. Unfortunately, the effect on sexual functioning often plays a significant role in the discontinuation of long-term therapy. Many of this study’s participants self-reported moderate or severe sexual dysfunction. Results showed no statistically significant relationships between either BMQ subscale or any of the 5 IIEF domains. Research is needed to further explore the association between ED and antihypertensive medication and men’s lack of knowledge and education about the importance of treatment adherence.
1. Hochbaum GM; U.S. Public Health Service, Division of Special Health Services. Public Participation in Medical Screening Programs: A Socio-Psychological Study. Public Health Service publication, no. 572 Washington, DC: U.S. Dept. of Health, Education, and Welfare, Public Health Service, Bureau of State Services, Division of Special Health Services, Tuberculosis Program; 1958.
2. International Index of Erectile Function (IIEF). Weill Cornell Medical College James Buchanan Brady Foundation Department of Urology website. https://www.cornellurology.com/images/uploads/IBPH-IIEF-Assessments.pdf. Accessed May 14, 2016.
3. Porteous T, Francis J, Bond C, Hannaford P. Temporal stability of beliefs about medicines: implications for optimizing adherence. Patient Educ Couns. 2010; 79(2):225-230.
4. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1-24.
5. Fogari R, Zoppi A, Corradi L, Mugellini A, Poletti L, Lusardi P. Sexual function in hypertensive males treated with lisinopril or atenolol: a cross-over study. Am J Hypertens. 1998;11(10):1244-1247.
6. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl. 2002;23(6):763-771.
7. Neame R, Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology (Oxford). 2005;44(6):762-767.
8. Lennerling A, Forsberg A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nurs J. 2012;6:41-46.
9. Kressin NR, Wang F, Long J, et al. Hypertensive patients' race, health beliefs, process of care, and medication adherence. J Gen Intern Med. 2007; 22(6):768-774.
10. Inman BA, Sauver JL, Jacobson DJ, et al. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009;84(2):108-113.
Erectile dysfunction (ED) is a multifactorial disease that can lead to treatment nonadherence in men taking medications for chronic health problems. Despite the importance of adhering to medication protocols for disease management, several studies demonstrated that a lack of adherence to medication protocols may be a direct response to the development of ED.
The Health Belief Model (HBM) is a conceptual framework used to better understand the relationship between health behavior and adherence in men diagnosed with hypertension. The HBM consists of 3 components that help explain health care behaviors: (1) individual perceptions; (2) modifying factors; and (3) likelihood of action. These components align with the variables in this study, which include beliefs about medicines, illness perception, and erectile function.1 Thus, the research challenge was to determine the relationship between knowledge of hypertension and sexual satisfaction among men with hypertension by using instruments in the form of 2 questionnaires: (1) the Beliefs about Medicines Questionnaire (BMQ), and (2) the International Index of Erectile Functioning (IIEF).2
Methods
A descriptive correlational design was used to explore the relationship between male patients’ antihypertensive medication beliefs and erectile function.
A convenience sample of 47 eligible men (age range 18-75 years) was recruited for this pilot study. Inclusion criteria were hypertension diagnosed by a medical professional, current use of antihypertensive medication, ability to read and write in English, and a signed informed consent. Study participants were recruited from a nurse-managed center in Detroit, Michigan, and from 6 facilities identified through Project Healthy Living 2012. The mission of the nurse-managed center is to assist low-income and underinsured populations in Wayne County, Michigan. Project Healthy Living 2012 performs free and low-cost health screenings and provides general health information to the public at various locations in the Detroit metropolitan area. Written permission to collect data was obtained from the director of Project Healthy Living 2012. Recruitment began after institutional review board approval was obtained. Participants signed an informed consent form that fully explained the nature of the study and the benefits and potential risks of participation.
Instruments
This study used the BMQ and IIEF health-related questionnaires. In addition, demographic information (eg, age, race, marital status, education, length of time with hypertension diagnosis, and current antihypertensive medications) was collected.
The BMQ was originally developed to understand patients’ commonly held beliefs about medications and the factors influencing their adherence to prescribed medication regimens.3 This questionnaire has 2 scales, BMQ Specific and BMQ General (only BMQ Specific was relevant to this study).
The BMQ Specific scale consists of two 5-item subscales, specific-necessity and specific-concern, that are designed to assess respondents’ beliefs about prescribed medications they are taking for specific conditions, such as hypertension. According to Horne and colleagues, the specific-necessity construct represents the perceived role of medication in protecting against deterioration of present and future health status.4 Statement examples include “My current health depends on my medicines,” and “My medicines protect me from becoming worse.” The specific-concern construct has an emotional component (eg, “Having to take my medicines worries me”) and a cognitive component (eg, “My medicines are a mystery to me”).
Items are scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher BMQ scores signify stronger beliefs. Studies using the BMQ subscales have shown that respondents with stronger beliefs about the necessity of their medications and fewer concerns about their medications are more likely to be adherent.
The self-administered IIEF is the instrument most widely used to assess sexual functioning and has been deployed in numerous clinical trials as the primary endpoint in evaluating the efficacy of phosphodiesterase 5-inhibitor therapy in the treatment of ED. The IIEF consists of 15 statements grouped into 5 domains assessing erectile function (6 items), orgasmic function (2 items), sexual desire (2 items), intercourse satisfaction (3 items), and overall satisfaction (2 items). Each domain is scored separately (Table 1).
Data Collection and Analysis
The researcher administered paper-and-pencil versions of the BMQ and the IIEF. Participants were allowed to complete these surveys in a semiprivate setting. No identifying information was collected—only general demographic information. IBM SPSS Version 16 statistical software was used to analyze the data.
Results
Forty-five men who were taking antihypertensive medication prescribed by a primary care provider agreed to participate. Their mean age was 55.8 years. The majority were African American (82%), married (58%) with some post-high school education (76%) (Table 2). Mean length of time with a hypertension diagnosis was 9.2 years. All respondents reported taking at least 1 antihypertensive medication. The medication most often reported being used was amlodipine, followed by lisinopril and metoprolol.
All of the respondents self-reported sexual dysfunction as indicated by the mean scores on the 5 domains of the IIEF (Table 3). Moreover, the vast majority of the total scores on the 5 domains fell within the moderate-to-severe dysfunction levels (Table 4).
BMQ Scores
The mean BMQ specific-necessity score was 16.7 (Table 5). More than half the respondents agreed or strongly agreed with 4 of the 5 statements regarding the necessity of their medications; the exception was “My life would be impossible without my medicines” (29.8%). The statement that generated the highest percentage of agreement was “My medicines protect me from becoming worse” (72.3%) (Table 6).
The mean BMQ specific-concern score was 13.7. Less than one-fourth of the respondents agreed or strongly agreed with 3 statements (of 4) regarding medication concerns: “My medicine is a mystery to me” (21.3%), “I sometimes worry about becoming too dependent on my medicine” (24.1%), and “My medicines disrupt my life” (25.6%). Regarding the fourth statement, “I sometimes worry about the long-term effects of my medicines,” 58.7% agreed or strongly agreed.
Spearman correlation analyses were performed to examine the relationships between BMQ specific-necessity, BMQ specific-concern, and the 5 IIEF sexual functioning domains. No statistically significant relationships were detected.
Time With Hypertension Diagnosis
The study also evaluated the results based on length of time the men had a hypertension diagnosis (≤ 10 years vs ≥ 11 years). An independent t test was used to compare mean BMQ specific-necessity and specific-concern scores. Crosstabs was used to compare length of time with diagnosis and the 5 IIEF domains. Mean specific-necessity score was 18.1 for the 20 respondents with a diagnosis of ≥ 11 years and 15.0 for the 22 respondents with a diagnosis of ≤ 10 years; this difference was statistically significant (P = .048). In addition, mean specific-concern score was 14.7 for respondents with a diagnosis of ≥ 11 years and 12.4 for those with a diagnosis of ≤ 10 years; this difference was not statistically significant but was trending in that direction (P = .076).
Length of time with a hypertension diagnosis did not necessarily relate to sexual function or satisfaction. Moderate-to-severe dysfunction in sexual desire was reported by 42% of the respondents with a diagnosis of ≥ 11 years compared with 57% of those with a diagnosis of ≤ 10 years. The same was found for overall satisfaction.
Discussion
Men with chronic health conditions, such as hypertension, are often prescribed medications that interfere with their sexual functioning.5 Patients who do not understand the importance of medication adherence in treating long-term chronic health conditions may discontinue taking these medications to improve their sexual functioning.5 Some men overestimate the control they have over chronic health conditions; others underestimate their control.
With a better understanding of men’s perceived ability to control chronic hypertension, practitioners can begin to provide appropriate educational interventions. These interventions must inform patients about the role of medication adherence in maintaining and enhancing sexual functioning and must impart a greater sense of control and empowerment over their condition, thereby increasing the likelihood of medication adherence.
To the authors’ knowledge, this is the first study to examine the potential associations of medication beliefs (using the BMQ) and erectile function in men with hypertension. There was no association between any of the demographic variables of age, race, marital status, and education, with respondents’ medication beliefs or erectile function. The IIEF domain that had the highest level of severe and moderate dysfunction combined was orgasmic function (n = 36; 80%), which suggests that antihypertensive medication may interfere with orgasmic function because achieving an orgasm is a physiologic process. This is consistent with the findings of Hellstrom and colleagues—that the vast majority of ED is related to orgasmic factors.6 Although 80% of respondents reported either moderate or severe dysfunction in this area, only 53% (n = 24) reported moderate or severe dysfunction in overall satisfaction. This might suggest that men taking antihypertensive medication, and their partners, have learned other methods or strategies for achieving sexual satisfaction.
The BMQ specific-necessity and specific-concern results offer insight into how men with hypertension view the need for antihypertensive medication. Mean (SD) specific-necessity score was 16.7 (5); the maximum was 25. Although no other studies have investigated men’s beliefs about antihypertensive medications, studies of other chronic illnesses have measured beliefs about the medications used in treatment. For example, Neame and Hammond reported a mean specific-necessity score of 19.9 and a mean specific-concern score of 15.9 in a sample of 108 men with arthritis.7 Of the respondents, 74.3% agreed or strongly agreed that their arthritis medication was necessary for health. However, 47.4% were concerned about potential adverse effects. Lennerling and Forsberg conducted a cross-sectional study of 250 renal transplant recipients.8 Respondents reported a mean specific-necessity score of 23 and a median specific-concern score of 11. In addition, length of time with hypertension diagnosis affected specific-necessity and specific-concern scores. For example, men with a hypertension diagnosis for 10 or fewer years had higher scores on both of these BMQ subscales.
The inability to detect a statistically significant correlation between BMQ specific-necessity and the 5 IIEF domains suggests that the sexual functioning of men with hypertension is not necessarily related to their antihypertensive medication beliefs. More than 50% agreed or strongly agreed that antihypertensive medications were necessary, but not that life would be impossible without them. Moreover, there was no statistically significant relationship between any of the 5 IIEF domains and the BMQ specific-concern subscale, which suggests that the sexual functioning of men with hypertension may not be related to their concern about their medications.
The findings of this study support HBM and provide a possible explanation for medication nonadherence in men diagnosed with hypertension. The HBM provides a conceptual framework that positions the study variables (eg, beliefs about medicines, illness perception, and erectile function) in terms of health care behaviors that can lead to increased medication adherence among men with hypertension. The HBM also allows the researcher to gain a better understanding about participants’ health behaviors, how these health behaviors are determined by personal beliefs or perceptions about a disease, and strategies available to decrease nonadherence.1
The HBM postulates that patients’ appraisals of disease risk (susceptibility) and severity influence their behavior.9 One study assessed respondents’ perceptions of the seriousness of their hypertension and its relationship to ED and of the consequences of failing to take prescribed blood pressure medications.9 When using the HBM, it is important to consider patients’ perceived barriers to and incentives for engaging in specific behaviors. The same study used the BMQ to address specific questions about respondents’ beliefs and feelings about their prescribed medications and medication adherence. The HBM suggests considering action cues that encourage patients to act by reminding them of the need to change their behavior.
Limitations
This study had several limitations. First, the sample size was small (47), which makes it difficult to generalize findings to a broader population of men with a hypertension diagnosis. In addition, because the study was underpowered, its ability to detect significant differences was compromised. Second, the study used a convenience sample of predominantly African American men. As always, there are concerns of self-selection and failure to represent the overall population. Third, the setting for completing the surveys was only semiprivate, and some respondents may have been uncomfortable, perhaps, working too quickly and not really thinking about the questions or their answers. Fourth, the ED survey was self-administered, so there is a concern about the truthfulness of responses. Fifth, failure to ask respondents whether they were taking a phosphodiesterase 5 inhibitor for ED could have significantly impacted study findings. Sixth, respondents were not asked about other medications, such as antidepressants and nonsteroidal anti-inflammatory drugs, which could have affected erectile function.
Clinical Implications
Despite the study limitations, several findings have important clinical implications. First, the vast majority of participants in this pilot study self-reported moderate or severe sexual dysfunction on all 5 IIEF domains. This finding is important because this was a convenience sample, and many of the IIEF statements are personal. The high rate of reported sexual dysfunction suggests that the incidence of ED may be underreported in the larger population. Second, mean BMQ scores were similar to those reported in other studies involving chronic illness: higher necessity and lower concern. Third, there was no statistically significant relationship between BMQ necessity and concern and IIEF sexual functioning. More research is needed to determine how to interpret these findings. Fourth, there was a significant relationship between length of time with hypertension diagnosis and BMQ specific-necessity score: The longer the diagnosis, the higher the score. However, this relationship did not hold for BMQ specific-concern, though it trended toward significance. Moreover, length of time with hypertension diagnosis did not necessarily predict or influence erectile function as measured with the IIEF. In fact, men with a hypertension diagnosis of ≥ 11 years reported less moderate-to-severe sexual dysfunction in overall satisfaction and sexual desire. Although there are several methodologic concerns about this study, its results offer direction for both clinical practice and future research.
Studies of erectile function and its relationship to hypertension have generated both cause for concern and reason for further research. The present study focused on gaining a better understanding of the relationship between antihypertensive medication beliefs and erectile function. Future clinical studies should explore the effects of antihypertensive medication on erectile function and men’s lack of knowledge and education about the importance of taking medication to prevent complications of hypertension. It is essential that this research be applied to improve the understanding of erectile function in men with hypertension. This will ultimately allow for better patient management and contribute to the overall sexual health and well-being of patients with hypertension.
Although it is important to identify men’s antihypertensive medication beliefs and the relationship of these beliefs to sexual satisfaction, most longitudinal studies suggest that the ED rate is high and that it increases with age.10 Therefore, it is crucial that men differentiate between how antihypertensive medications affect erectile function and changes associated with aging. The present study found no statistically significant relationships between the BMQ specific-necessity and specific-concern subscales and overall satisfaction with sexual functioning (IIEF). In addition, the study found no significant correlations between the BMQ specific and general scales and the 5 IIEF domains.
Conclusion
It was evident from this research that men with chronic health problems, such as hypertension, are often prescribed medications that affect sexual functioning. Unfortunately, the effect on sexual functioning often plays a significant role in the discontinuation of long-term therapy. Many of this study’s participants self-reported moderate or severe sexual dysfunction. Results showed no statistically significant relationships between either BMQ subscale or any of the 5 IIEF domains. Research is needed to further explore the association between ED and antihypertensive medication and men’s lack of knowledge and education about the importance of treatment adherence.
Erectile dysfunction (ED) is a multifactorial disease that can lead to treatment nonadherence in men taking medications for chronic health problems. Despite the importance of adhering to medication protocols for disease management, several studies demonstrated that a lack of adherence to medication protocols may be a direct response to the development of ED.
The Health Belief Model (HBM) is a conceptual framework used to better understand the relationship between health behavior and adherence in men diagnosed with hypertension. The HBM consists of 3 components that help explain health care behaviors: (1) individual perceptions; (2) modifying factors; and (3) likelihood of action. These components align with the variables in this study, which include beliefs about medicines, illness perception, and erectile function.1 Thus, the research challenge was to determine the relationship between knowledge of hypertension and sexual satisfaction among men with hypertension by using instruments in the form of 2 questionnaires: (1) the Beliefs about Medicines Questionnaire (BMQ), and (2) the International Index of Erectile Functioning (IIEF).2
Methods
A descriptive correlational design was used to explore the relationship between male patients’ antihypertensive medication beliefs and erectile function.
A convenience sample of 47 eligible men (age range 18-75 years) was recruited for this pilot study. Inclusion criteria were hypertension diagnosed by a medical professional, current use of antihypertensive medication, ability to read and write in English, and a signed informed consent. Study participants were recruited from a nurse-managed center in Detroit, Michigan, and from 6 facilities identified through Project Healthy Living 2012. The mission of the nurse-managed center is to assist low-income and underinsured populations in Wayne County, Michigan. Project Healthy Living 2012 performs free and low-cost health screenings and provides general health information to the public at various locations in the Detroit metropolitan area. Written permission to collect data was obtained from the director of Project Healthy Living 2012. Recruitment began after institutional review board approval was obtained. Participants signed an informed consent form that fully explained the nature of the study and the benefits and potential risks of participation.
Instruments
This study used the BMQ and IIEF health-related questionnaires. In addition, demographic information (eg, age, race, marital status, education, length of time with hypertension diagnosis, and current antihypertensive medications) was collected.
The BMQ was originally developed to understand patients’ commonly held beliefs about medications and the factors influencing their adherence to prescribed medication regimens.3 This questionnaire has 2 scales, BMQ Specific and BMQ General (only BMQ Specific was relevant to this study).
The BMQ Specific scale consists of two 5-item subscales, specific-necessity and specific-concern, that are designed to assess respondents’ beliefs about prescribed medications they are taking for specific conditions, such as hypertension. According to Horne and colleagues, the specific-necessity construct represents the perceived role of medication in protecting against deterioration of present and future health status.4 Statement examples include “My current health depends on my medicines,” and “My medicines protect me from becoming worse.” The specific-concern construct has an emotional component (eg, “Having to take my medicines worries me”) and a cognitive component (eg, “My medicines are a mystery to me”).
Items are scored on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher BMQ scores signify stronger beliefs. Studies using the BMQ subscales have shown that respondents with stronger beliefs about the necessity of their medications and fewer concerns about their medications are more likely to be adherent.
The self-administered IIEF is the instrument most widely used to assess sexual functioning and has been deployed in numerous clinical trials as the primary endpoint in evaluating the efficacy of phosphodiesterase 5-inhibitor therapy in the treatment of ED. The IIEF consists of 15 statements grouped into 5 domains assessing erectile function (6 items), orgasmic function (2 items), sexual desire (2 items), intercourse satisfaction (3 items), and overall satisfaction (2 items). Each domain is scored separately (Table 1).
Data Collection and Analysis
The researcher administered paper-and-pencil versions of the BMQ and the IIEF. Participants were allowed to complete these surveys in a semiprivate setting. No identifying information was collected—only general demographic information. IBM SPSS Version 16 statistical software was used to analyze the data.
Results
Forty-five men who were taking antihypertensive medication prescribed by a primary care provider agreed to participate. Their mean age was 55.8 years. The majority were African American (82%), married (58%) with some post-high school education (76%) (Table 2). Mean length of time with a hypertension diagnosis was 9.2 years. All respondents reported taking at least 1 antihypertensive medication. The medication most often reported being used was amlodipine, followed by lisinopril and metoprolol.
All of the respondents self-reported sexual dysfunction as indicated by the mean scores on the 5 domains of the IIEF (Table 3). Moreover, the vast majority of the total scores on the 5 domains fell within the moderate-to-severe dysfunction levels (Table 4).
BMQ Scores
The mean BMQ specific-necessity score was 16.7 (Table 5). More than half the respondents agreed or strongly agreed with 4 of the 5 statements regarding the necessity of their medications; the exception was “My life would be impossible without my medicines” (29.8%). The statement that generated the highest percentage of agreement was “My medicines protect me from becoming worse” (72.3%) (Table 6).
The mean BMQ specific-concern score was 13.7. Less than one-fourth of the respondents agreed or strongly agreed with 3 statements (of 4) regarding medication concerns: “My medicine is a mystery to me” (21.3%), “I sometimes worry about becoming too dependent on my medicine” (24.1%), and “My medicines disrupt my life” (25.6%). Regarding the fourth statement, “I sometimes worry about the long-term effects of my medicines,” 58.7% agreed or strongly agreed.
Spearman correlation analyses were performed to examine the relationships between BMQ specific-necessity, BMQ specific-concern, and the 5 IIEF sexual functioning domains. No statistically significant relationships were detected.
Time With Hypertension Diagnosis
The study also evaluated the results based on length of time the men had a hypertension diagnosis (≤ 10 years vs ≥ 11 years). An independent t test was used to compare mean BMQ specific-necessity and specific-concern scores. Crosstabs was used to compare length of time with diagnosis and the 5 IIEF domains. Mean specific-necessity score was 18.1 for the 20 respondents with a diagnosis of ≥ 11 years and 15.0 for the 22 respondents with a diagnosis of ≤ 10 years; this difference was statistically significant (P = .048). In addition, mean specific-concern score was 14.7 for respondents with a diagnosis of ≥ 11 years and 12.4 for those with a diagnosis of ≤ 10 years; this difference was not statistically significant but was trending in that direction (P = .076).
Length of time with a hypertension diagnosis did not necessarily relate to sexual function or satisfaction. Moderate-to-severe dysfunction in sexual desire was reported by 42% of the respondents with a diagnosis of ≥ 11 years compared with 57% of those with a diagnosis of ≤ 10 years. The same was found for overall satisfaction.
Discussion
Men with chronic health conditions, such as hypertension, are often prescribed medications that interfere with their sexual functioning.5 Patients who do not understand the importance of medication adherence in treating long-term chronic health conditions may discontinue taking these medications to improve their sexual functioning.5 Some men overestimate the control they have over chronic health conditions; others underestimate their control.
With a better understanding of men’s perceived ability to control chronic hypertension, practitioners can begin to provide appropriate educational interventions. These interventions must inform patients about the role of medication adherence in maintaining and enhancing sexual functioning and must impart a greater sense of control and empowerment over their condition, thereby increasing the likelihood of medication adherence.
To the authors’ knowledge, this is the first study to examine the potential associations of medication beliefs (using the BMQ) and erectile function in men with hypertension. There was no association between any of the demographic variables of age, race, marital status, and education, with respondents’ medication beliefs or erectile function. The IIEF domain that had the highest level of severe and moderate dysfunction combined was orgasmic function (n = 36; 80%), which suggests that antihypertensive medication may interfere with orgasmic function because achieving an orgasm is a physiologic process. This is consistent with the findings of Hellstrom and colleagues—that the vast majority of ED is related to orgasmic factors.6 Although 80% of respondents reported either moderate or severe dysfunction in this area, only 53% (n = 24) reported moderate or severe dysfunction in overall satisfaction. This might suggest that men taking antihypertensive medication, and their partners, have learned other methods or strategies for achieving sexual satisfaction.
The BMQ specific-necessity and specific-concern results offer insight into how men with hypertension view the need for antihypertensive medication. Mean (SD) specific-necessity score was 16.7 (5); the maximum was 25. Although no other studies have investigated men’s beliefs about antihypertensive medications, studies of other chronic illnesses have measured beliefs about the medications used in treatment. For example, Neame and Hammond reported a mean specific-necessity score of 19.9 and a mean specific-concern score of 15.9 in a sample of 108 men with arthritis.7 Of the respondents, 74.3% agreed or strongly agreed that their arthritis medication was necessary for health. However, 47.4% were concerned about potential adverse effects. Lennerling and Forsberg conducted a cross-sectional study of 250 renal transplant recipients.8 Respondents reported a mean specific-necessity score of 23 and a median specific-concern score of 11. In addition, length of time with hypertension diagnosis affected specific-necessity and specific-concern scores. For example, men with a hypertension diagnosis for 10 or fewer years had higher scores on both of these BMQ subscales.
The inability to detect a statistically significant correlation between BMQ specific-necessity and the 5 IIEF domains suggests that the sexual functioning of men with hypertension is not necessarily related to their antihypertensive medication beliefs. More than 50% agreed or strongly agreed that antihypertensive medications were necessary, but not that life would be impossible without them. Moreover, there was no statistically significant relationship between any of the 5 IIEF domains and the BMQ specific-concern subscale, which suggests that the sexual functioning of men with hypertension may not be related to their concern about their medications.
The findings of this study support HBM and provide a possible explanation for medication nonadherence in men diagnosed with hypertension. The HBM provides a conceptual framework that positions the study variables (eg, beliefs about medicines, illness perception, and erectile function) in terms of health care behaviors that can lead to increased medication adherence among men with hypertension. The HBM also allows the researcher to gain a better understanding about participants’ health behaviors, how these health behaviors are determined by personal beliefs or perceptions about a disease, and strategies available to decrease nonadherence.1
The HBM postulates that patients’ appraisals of disease risk (susceptibility) and severity influence their behavior.9 One study assessed respondents’ perceptions of the seriousness of their hypertension and its relationship to ED and of the consequences of failing to take prescribed blood pressure medications.9 When using the HBM, it is important to consider patients’ perceived barriers to and incentives for engaging in specific behaviors. The same study used the BMQ to address specific questions about respondents’ beliefs and feelings about their prescribed medications and medication adherence. The HBM suggests considering action cues that encourage patients to act by reminding them of the need to change their behavior.
Limitations
This study had several limitations. First, the sample size was small (47), which makes it difficult to generalize findings to a broader population of men with a hypertension diagnosis. In addition, because the study was underpowered, its ability to detect significant differences was compromised. Second, the study used a convenience sample of predominantly African American men. As always, there are concerns of self-selection and failure to represent the overall population. Third, the setting for completing the surveys was only semiprivate, and some respondents may have been uncomfortable, perhaps, working too quickly and not really thinking about the questions or their answers. Fourth, the ED survey was self-administered, so there is a concern about the truthfulness of responses. Fifth, failure to ask respondents whether they were taking a phosphodiesterase 5 inhibitor for ED could have significantly impacted study findings. Sixth, respondents were not asked about other medications, such as antidepressants and nonsteroidal anti-inflammatory drugs, which could have affected erectile function.
Clinical Implications
Despite the study limitations, several findings have important clinical implications. First, the vast majority of participants in this pilot study self-reported moderate or severe sexual dysfunction on all 5 IIEF domains. This finding is important because this was a convenience sample, and many of the IIEF statements are personal. The high rate of reported sexual dysfunction suggests that the incidence of ED may be underreported in the larger population. Second, mean BMQ scores were similar to those reported in other studies involving chronic illness: higher necessity and lower concern. Third, there was no statistically significant relationship between BMQ necessity and concern and IIEF sexual functioning. More research is needed to determine how to interpret these findings. Fourth, there was a significant relationship between length of time with hypertension diagnosis and BMQ specific-necessity score: The longer the diagnosis, the higher the score. However, this relationship did not hold for BMQ specific-concern, though it trended toward significance. Moreover, length of time with hypertension diagnosis did not necessarily predict or influence erectile function as measured with the IIEF. In fact, men with a hypertension diagnosis of ≥ 11 years reported less moderate-to-severe sexual dysfunction in overall satisfaction and sexual desire. Although there are several methodologic concerns about this study, its results offer direction for both clinical practice and future research.
Studies of erectile function and its relationship to hypertension have generated both cause for concern and reason for further research. The present study focused on gaining a better understanding of the relationship between antihypertensive medication beliefs and erectile function. Future clinical studies should explore the effects of antihypertensive medication on erectile function and men’s lack of knowledge and education about the importance of taking medication to prevent complications of hypertension. It is essential that this research be applied to improve the understanding of erectile function in men with hypertension. This will ultimately allow for better patient management and contribute to the overall sexual health and well-being of patients with hypertension.
Although it is important to identify men’s antihypertensive medication beliefs and the relationship of these beliefs to sexual satisfaction, most longitudinal studies suggest that the ED rate is high and that it increases with age.10 Therefore, it is crucial that men differentiate between how antihypertensive medications affect erectile function and changes associated with aging. The present study found no statistically significant relationships between the BMQ specific-necessity and specific-concern subscales and overall satisfaction with sexual functioning (IIEF). In addition, the study found no significant correlations between the BMQ specific and general scales and the 5 IIEF domains.
Conclusion
It was evident from this research that men with chronic health problems, such as hypertension, are often prescribed medications that affect sexual functioning. Unfortunately, the effect on sexual functioning often plays a significant role in the discontinuation of long-term therapy. Many of this study’s participants self-reported moderate or severe sexual dysfunction. Results showed no statistically significant relationships between either BMQ subscale or any of the 5 IIEF domains. Research is needed to further explore the association between ED and antihypertensive medication and men’s lack of knowledge and education about the importance of treatment adherence.
1. Hochbaum GM; U.S. Public Health Service, Division of Special Health Services. Public Participation in Medical Screening Programs: A Socio-Psychological Study. Public Health Service publication, no. 572 Washington, DC: U.S. Dept. of Health, Education, and Welfare, Public Health Service, Bureau of State Services, Division of Special Health Services, Tuberculosis Program; 1958.
2. International Index of Erectile Function (IIEF). Weill Cornell Medical College James Buchanan Brady Foundation Department of Urology website. https://www.cornellurology.com/images/uploads/IBPH-IIEF-Assessments.pdf. Accessed May 14, 2016.
3. Porteous T, Francis J, Bond C, Hannaford P. Temporal stability of beliefs about medicines: implications for optimizing adherence. Patient Educ Couns. 2010; 79(2):225-230.
4. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1-24.
5. Fogari R, Zoppi A, Corradi L, Mugellini A, Poletti L, Lusardi P. Sexual function in hypertensive males treated with lisinopril or atenolol: a cross-over study. Am J Hypertens. 1998;11(10):1244-1247.
6. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl. 2002;23(6):763-771.
7. Neame R, Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology (Oxford). 2005;44(6):762-767.
8. Lennerling A, Forsberg A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nurs J. 2012;6:41-46.
9. Kressin NR, Wang F, Long J, et al. Hypertensive patients' race, health beliefs, process of care, and medication adherence. J Gen Intern Med. 2007; 22(6):768-774.
10. Inman BA, Sauver JL, Jacobson DJ, et al. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009;84(2):108-113.
1. Hochbaum GM; U.S. Public Health Service, Division of Special Health Services. Public Participation in Medical Screening Programs: A Socio-Psychological Study. Public Health Service publication, no. 572 Washington, DC: U.S. Dept. of Health, Education, and Welfare, Public Health Service, Bureau of State Services, Division of Special Health Services, Tuberculosis Program; 1958.
2. International Index of Erectile Function (IIEF). Weill Cornell Medical College James Buchanan Brady Foundation Department of Urology website. https://www.cornellurology.com/images/uploads/IBPH-IIEF-Assessments.pdf. Accessed May 14, 2016.
3. Porteous T, Francis J, Bond C, Hannaford P. Temporal stability of beliefs about medicines: implications for optimizing adherence. Patient Educ Couns. 2010; 79(2):225-230.
4. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1-24.
5. Fogari R, Zoppi A, Corradi L, Mugellini A, Poletti L, Lusardi P. Sexual function in hypertensive males treated with lisinopril or atenolol: a cross-over study. Am J Hypertens. 1998;11(10):1244-1247.
6. Hellstrom WJ, Gittelman M, Karlin G, et al. Vardenafil for treatment of men with erectile dysfunction: efficacy and safety in a randomized, double-blind, placebo-controlled trial. J Androl. 2002;23(6):763-771.
7. Neame R, Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology (Oxford). 2005;44(6):762-767.
8. Lennerling A, Forsberg A. Self-reported non-adherence and beliefs about medication in a Swedish kidney transplant population. Open Nurs J. 2012;6:41-46.
9. Kressin NR, Wang F, Long J, et al. Hypertensive patients' race, health beliefs, process of care, and medication adherence. J Gen Intern Med. 2007; 22(6):768-774.
10. Inman BA, Sauver JL, Jacobson DJ, et al. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo Clin Proc. 2009;84(2):108-113.