User login
› Consider using age-specific published milestones, such as those found online at the American Speech-Language-Hearing Association’s site, to evaluate children’s developmental progress. C
› Consult your state’s early intervention agency (cited in this article) for assistance in referring children for further evaluation and possible treatment. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice arrives with her 2-year-old son for a well-child visit. She remarks that, although her son uses a few single words to indicate hunger and other needs, her sister’s child at the same age had begun using multiple words to ask questions and express her wishes. She’s concerned about whether her son’s behavior is normal. As you start to engage the child, you note that he responds only after you repeat his name a few times. Are these observations indicative of a typical delay in development, or are they clues to a serious medical issue or communication disability? Given the absence of any known medical problem or evident physical or intellectual disability, how would you proceed in this case and in counseling the mother?
Developmental screening minimizes adverse long-term consequences
Speech, language, and hearing delays and disorders in children can lead to learning and socialization problems that may persist into adulthood. Health care providers who monitor speech, language, and hearing development in children can guide parents, as needed, to appropriate services for further assessment or treatment1 and direct them to advocacy programs such as the Center for Parent Information and Resources (formerly the National Dissemination Center for Children with Disabilities).2
A useful tool at well-child visits is the Denver II, a quick developmental screening test to help identify a variety of disorders of intelligence, language, mental health, and motor and self-help skills.3
Suspicion of a developmental delay not likely due to a medical issue or congenital abnormality requiring examination by an otorhinolaryngologist could warrant referral of the child for early intervention (EI).
Communication disorders and their manifestations
Communication—the ability to receive, process, comprehend, and transmit information—is essential for a successful life.4 Speech, language, and hearing impairments affect a child’s ability to send (speak, write, or gesture) and receive (hear, interpret, or decipher) messages.
Speech impairments
Beginning at birth, we systematically develop speech sounds and an ability to use these sounds to convey meaning by forming words and using language.5 Speech and language pathologists make a distinction between speech and language impairments.6
Speech disorders may involve problems of articulation, fluency, voice, or resonance. About 8% to 9% of preschool children have speech disorders, and approximately 5% of school-age children have speech or language impairments.7
Problems of articulation are heard in such instances as substituting a “w” for an “r” (“wabbit” for “rabbit”) or in distorting or omitting sounds or syllables (“tato” for “potato”). Considering that articulation involves the precise coordination of about 70 muscles (tongue, lips, velum, vocal folds, etc), development of this skill normally goes through phases of inaccurate sound productions. Concerns arise when these phases persist or are atypical.
Speech fluency/stuttering is the uncontrollable blocking of speech, sound prolongation (“wwwwater”), or repetition of a sound, syllable, or word during speaking (“pu-pu-pu-puppy”).
Problems of voice include symptoms such as hoarseness, an exceptionally weak voice or one that is too high or too low, or abnormal resonance (hyper- or hyponasality, which gives the impression the child is talking “through the nose” or is constantly congested).
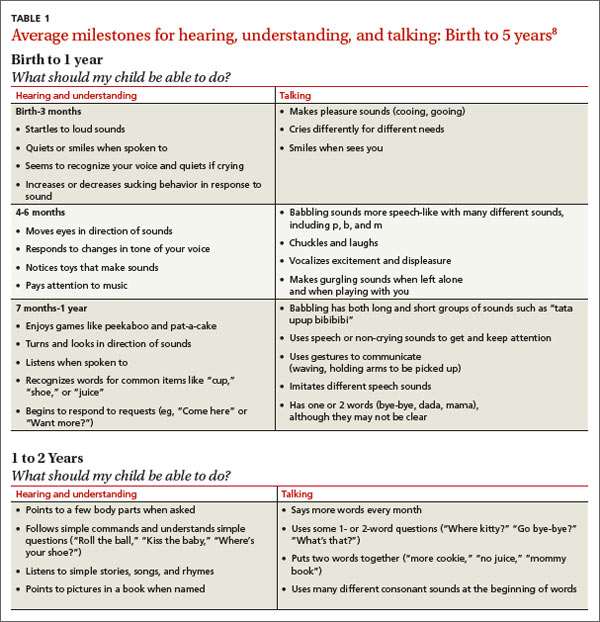
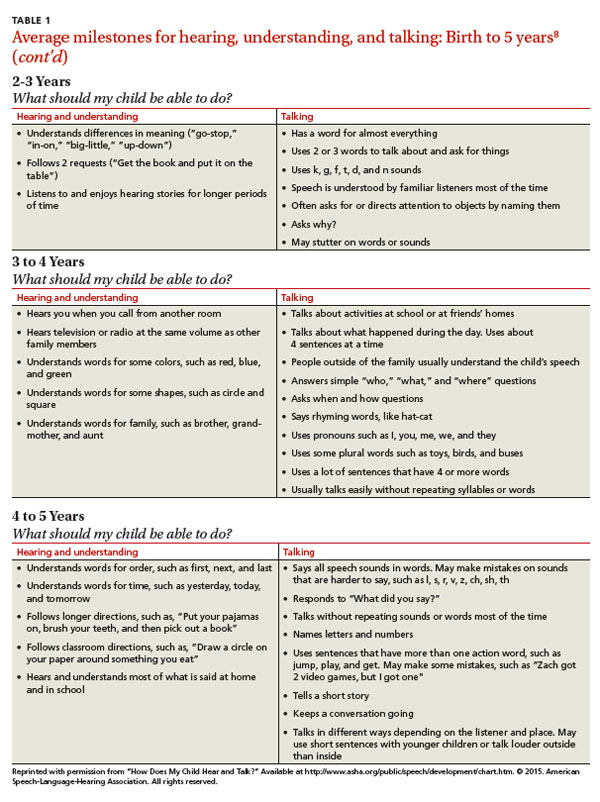
Using common milestones as reference points. The American Speech-Language-Hearing Association (ASHA)8 lists the milestones for speech development (English and Spanish) at http://www.asha.org/public/speech/development/chart.htm. For example, between 12 and 24 months of age, a child should be learning vocabulary (“doggie, nana”), combining 2 words (“mommy car”), asking 2-word questions (“where daddy?”), and producing a variety of speech sounds. These milestones represent an average and some children may not master all the items in a category until they reach the upper limit of the age range (TABLE 1).8 Roth et al9 found that intervention benefited preschoolers with speech and language disabilities when applied earlier than previously recommended. In other words, avoid the “wait-and-see” option. Busari and Weggelaar,10 studying referral recommendations for children who are “slow to speak,” concluded that EI may diminish further consequences later in the child’s life.
ASHA launched a campaign to increase awareness of communication disorders across the lifespan and to encourage early identification (http://identifythesigns.org/).11 The site has basic lists of signs of common speech and language disorders and hearing loss in children from birth to 4 years of age. This period in a child’s life is “an important stage in early detection of communication disorders.”
Language impairments
Language impairments affect 3 domains of language: form (grammar/syntax), content, or use. These domains are governed by rules specific to the language spoken in the home. Language impairment can interfere with comprehension and formulation of messages. About 2% to 3% of preschoolers have language disorders.12
Language impairments may be observed in one or more of the language components, including phonology (rules of the sounds in the language), lexicon (vocabulary), morphology (word markers—eg, final “s” to make the plural of “cat”), syntax (word order) and pragmatics (socially appropriate speech, gesture, eye contact, and language use).
While there is great variability in typical development, atypical language development can be a secondary characteristic of other physical or developmental problems attributed to other conditions such as autism spectrum disorder (ASD), cerebral palsy, childhood apraxia of speech, dysarthria, intellectual disability, or selective mutism.13
Verbal communication difficulties may appear in expressive and receptive language.14Receptive language is the ability to comprehend language communicated by another person.6 Receptive language (processing) skills can be demonstrated as follows. If a child is asked “Do you like cats?” she must first decide to whom the question is directed (to her and not someone else). She must then search her long-term memory for the word/concept “cat” (compared with dog, a similar concept; or with mat, a similar-sounding word), and process the word “like” (compared with “dislike”). Now the child understands the question and can decide on an answer.
Expressive language is a child’s ability to speak; the mental process used to produce speech and communicate a message.6 To answer, “Yes, I like cats,” the child retrieves the concept “cat” from memory (cognition and semantics: the meanings of words, their relationships and usage), finds the right words (vocabulary), puts them in the right order (syntax), uses the right verb tense (grammar/morphology), assembles the right sounds in order, initiates the neuromotor acts (phonology/speech production), and communicates that she understands what cats are and that she likes them (pragmatics; socially/contextually appropriate responses).
Resources on language development. Typical language development, the length of which varies among children, must be practiced in a rich linguistic environment. Some children are adventurous with language. They babble, talk, and communicate in a carefree manner. Others are cautious. They may wait until they are sure of their skills before attempting a new word. Usually, concern about a child’s speech and language development arises if there is no speech, if speech is not clear, or if speech or language is different from that of peers.
The Centers for Disease Control and Prevention, under their “Learn the signs. Act early” campaign (www.cdc.gov/actearly), has published checklists of children’s developmental milestones from 2 months to 5 years of age on social, communication, cognitive, and motor skills. Health care providers helping parents determine if their child’s communication is developing normally can find information and materials at http://www.cdc.gov/ncbddd/actearly/hcp/index.html.15
Hearing impairments
Moeller et al16 surveyed 1968 primary care physicians on their attitude, practices, and knowledge of universal hearing screenings for newborns. They noted limitations in awareness of EI options for infants with hearing loss: proper times and places for referrals, available communication modalities, cochlear implant candidacy, and professionals in their locale with expertise on hearing loss. These knowledge gaps involved some medical issues, such as hearing loss genetics and later-onset hearing loss in infants and children. They also found low confidence in providing information to families about how to proceed with EI and in discussing intervention needs and resources.
Adverse effects of hearing loss. Hearing loss can be unilateral or bilateral, conductive or sensorineural, and can range in severity from mild to profound. According to the National Institute on Deafness and Communication Disorders (NIDCD), one in every 350 infants is born with a significant hearing loss, and others become deaf due to childhood illness or injury.17 According to ASHA,18 hearing loss can affect children in 4 major ways:19 delays in the development of receptive (comprehension) and expressive communication skills; a language deficit that causes learning problems and reduces academic achievement; communication difficulties that often lead to social isolation and poor self-concept; and impact on vocational choices and options.20 NIDCD provides a checklist to determine a child’s hearing status at http://www.nidcd.nih.gov/health/hearing/silence.asp.17
Timing of intervention is significant. EI is critical in minimizing the deleterious effects of hearing loss and in optimizing speech and language development. Severity of hearing loss influences EI outcome, and treatment options depend on the hearing loss having occurred either before language development (prelingually) or after (postlingually). Early management of hearing impairment can improve language, especially for children with a severe or profound hearing loss.21
Devices and methods that promote communication development for students who are deaf or hard of hearing include the use of hearing aids to amplify residual hearing for oral or auditory-oral approaches; the manual approach stressing sign-language (American Sign Language or Signed English); or Total Communication using both the oral and sign-language methods.
With an infant, suspicion of a hearing problem warrants referral to an otorhinolaryngologist or an audiologist for thorough evaluation. In New Jersey, an EI referral typically triggers a referral to one of these specialists. TABLE 2 lists resources for early identification and intervention in communication disorders.
TABLE 2
| Resources for early identification and intervention in communication disorders | |
| Resource | Information |
| American Speech-Language-Hearing Association (ASHA) | Communication skills, milestones, disorders, and treatment resources across the lifespan; for parents and professionals |
| CDC’s “Learn the signs. Act early” campaign
| Children’s developmental milestones from 2 months to 5 years; checklists for parents |
| Children’s developmental milestones and Early Intervention for health care providers | |
| National Institute on Deafness and Other Communication Disorders | Speech and language development checklists |
| National Institute on Deafness and Other Communication Disorders | Hearing loss and its effects on communication; identification and management options |
| Center for Parent Information and Resources | Early Intervention: overview and process |
| National Institute of Mental Health | Autism spectrum disorder; a guide for parents |
| First Signs, Inc | Early warning signs of autism spectrum disorder; for parents and professionals |
| The Autism Screening Test | Autism screening test to identify children 16-30 months who should receive a more thorough assessment for possible early signs of autism spectrum disorder or developmental delay |
Autism spectrum disorder
The fifth edition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-5)22 has revised its diagnostic codes for ASD. An in-depth analysis of the new diagnosis is beyond the purview of this article, but it deserves a few comments.
The revised diagnosis of ASD consolidates the previously separate diagnoses of autistic disorder, Asperger’s disorder, childhood disintegrative disorder, and pervasive developmental disorder/not otherwise specified.22-24 According to DSM-5, an individual with ASD must have 1) persistent deficits in social communication and social interactions, 2) restricted, repetitive patterns of behavior, interests or activities, 3) symptoms present in early childhood (but may not become fully manifest until social demands exceed limited capacities), and 4) symptoms that limit and impair everyday functioning.22,24
Onset of the disorder must be obvious before age 3 for a child to be eligible for EI. Children who do not qualify for an ASD diagnosis under the new DSM-5 definition may be included in a new category called social communication disorder (SCD) under “Communication Disorders” in DSM-5. SCD is defined as impairment in pragmatics that impacts development of social relationships and comprehension of social conversations. ASD must be ruled out before a diagnosis of SCD can be made.23,24
Early intervention services
Individual states offer EI services to families to facilitate detection of developmental delays in children and to provide a comprehensive system of support designed to reduce the effects of disabilities (or to prevent learning and developmental problems later in life).5 The rationale for EI is that the earlier interventions are started, the less likely later interventions will be needed.25 EI services are provided to children from birth through their third birthday; services are free of charge to eligible families or on a sliding payment scale determined by a family’s income.
Resources for information and referrals. To access EI services on behalf of a family, contact a local hospital or point them to the CPIR (http://www.parentcenterhub.org/repository/disability-landing/).2 For families with disabled children older than 3, consider suggesting that parents contact the local school district (even if the child isn’t enrolled there) to arrange an evaluation under the Individuals with Disabilities Education Act (http://idea.ed.gov/).26 Because individual states’ EI organizations may have slightly different procedures, it is best to consult one’s own state EI site for specific information regarding referrals (TABLE 3).
Efficacy of treatment
The prevalence of specific communication disorders varies widely, as do prognoses, possibly due to the variability of underlying causes (physical/biological/medical or environmental/educational).27 Also, as described earlier, “communication disorder” is an umbrella term inclusive of problems as diverse as resonance (eg, hypernasality due to a submucous palatal cleft), severe language delay (eg, due to Down syndrome), or lisp (misarticulation of the “s” sound).
Is therapy effective? Speech and language pathologists use the National Outcomes Measurement System (NOMS) as an index of the outcomes of treatment on functional communication along 6 scales. The most frequent types of communication problems seen in the prekindergarten children’s NOMS were “articulation” (75% of children), “spoken language production” (61%), and “spoken language comprehension” (42%). Problems in the remaining 3 scales (“pragmatics,” “cognitive orientation,” and “swallowing”) were seen in fewer than 15% of the preschool-age students.28
Articulation therapy yielded improvement in 69.3% of cases, spoken language comprehension therapy in 65.3%, and spoken language production therapy in 65.2%.28 Such outcomes support regular screening of children’s communication development and, as needed, referral for EI.
TABLE 3
CORRESPONDENCE
Christopher Mulrine, EdD; William Paterson University, 1600 Valley Road 3003 Wayne, NJ 07474-0920; [email protected]
1. Wankoff LS. Warning signs in the development of speech, language, and communication: when to refer to a speech-language pathologist. J Child Adolesc Psychiatr Nurs. 2011;24:175-184.
2. Center for Parent Information and Resources. Disabilities. Center for Parent Information and Resources Web site. Available at: http://www.parentcenterhub.org/repository/disability-landing/. Updated June 2014. Accessed January 24, 2015.
3. Denver Developmental Materials, Inc. Denver II Online. Denver Developmental Materials, Inc Web site. Available at: http://denverii.com/denverii/. Accessed January 24, 2015.
4. Guralnick MJ. The Effectiveness of Early Intervention. Baltimore, MD: Brookes Publishing; 2013.
5. Schwartz HD. A Primer on Communication and Communicative Disorders. Boston, MA: Pearson Education; 2012.
6. Heward WL. Exceptional Children: An Introduction to Special Education. 10th ed. Boston, Mass: Pearson Education; 2013.
7. Hallahan DP, Kauffman J M, Pullen PC. Exceptional Learners: An Introduction to Special Education. 13th ed. Upper Saddle River, NJ: Pearson Education; 2015.
8. American Speech-Language-Hearing Association. How does your child hear and talk? American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/development/chart.htm. Accessed January 24, 2015.
9. Roth FP, Troia GA, Worthington CK, et al. Promoting awareness of sounds in speech: An initial report of an early intervention program for children with speech and language impairments. Appl Psycholinguistics. 2002;23:535-565.
10. Busari JO, Weggelaar NM. How to investigate and manage the child who is slow to speak. BMJ. 2004;328:272-276.
11. American Speech-Language-Hearing Association. Identify the Signs of Communication Disorders. Identify the Signs of Communication Disorders Web site. Available at: http://identifythesigns.org/. Accessed January 24, 2015.
12. McLaughlin MR. Speech and language delay in children. Am Fam Physician. 2011;83:1183-1188.
13. American Speech-Language-Hearing Association. Child speech and language. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/disorders/ChildSandL.htm. Accessed January 24, 2015.
14. Bondurant-Utz JA. Practical Guide to Assessing Infants and Preschoolers with Special Needs. Upper Saddle River, NJ: Pearson Education; 2002.
15. Centers for Disease Control and Prevention. Learn the Signs: Act Early. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/actearly/hcp/index.html. Accessed January 24, 2015.
16. Moeller MP, White KR, Shisler L. Primary care physicians’ knowledge, attitudes, and practices related to newborn hearing screening. Pediatrics. 2006;118:1357-1370.
17. National Institute on Deafness and Other Communication Disorders. Your baby’s hearing and communicative checklist. National Institute on Deafness and Other Communication Disorders Web site. Available at: http://www.nidcd.nih.gov/health/hearing/silence.asp. Accessed January 24, 2015.
18. American Speech-Language-Hearing Association. Effects of hearing loss on development. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/hearing/Effects-of-Hearing-Loss-on-Development/. Accessed January 24, 2015.
19. American Speech-Language-Hearing Association. Facts about pediatric hearing loss. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/aud/Facts-about-Pediatric-Hearing-Loss/. Accessed January 24, 2015.
20. Tang BG, Feldman HM, Padden C, et al. Delayed recognition of profound hearing loss in a 7-year-old girl with a neurological condition. J Dev Behav Pediatr. 2010;31(3 suppl):S42-S45.
21. Watkin P, McCann D, Law C, et al. Language ability in children with permanent hearing impairment: the influence of early management and family participation. Pediatrics. 2007;120:e694-e701.
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
23. Autism Match. 5 things to know about autism and DSM-5. Austism Match Web site. Available at: https://autismmatch.org/info/news/2012/05/02/5-things-to-know-about-autism-and-dsm-5. Accessed January 24, 2015.
24. American Psychiatric Publishing. Autism Spectrum Disorder. American Psychiatric Association Web site. Available at: http://www.dsm5.org/Documents/Autism%20Spectrum%20Disorder%20Fact%20Sheet.pdf. Accessed January 24, 2015.
25. Law J, Garrett Z, Nye C. Speech and language therapy interventions for children with primary speech and language delay or disorder. Cochrane Database Syst Rev. 2003;(3):CD004110.
26. U.S. Department of Education. Building the legacy: IDEA 2004. Individuals with Disabilities Education Act Web site. Available at: http://idea.ed.gov/. Accessed January 24, 2015.
27. Friend MP. Special Education: Contemporary Perspectives for School Professionals. Boston, MA: Pearson; 2005.
28. Mullen R, Schooling T. The National Outcomes Measurement System for Pediatric Speech-Language Pathology. Lang Speech Hearing Services Schools. 2010;41:44-60.
› Consider using age-specific published milestones, such as those found online at the American Speech-Language-Hearing Association’s site, to evaluate children’s developmental progress. C
› Consult your state’s early intervention agency (cited in this article) for assistance in referring children for further evaluation and possible treatment. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice arrives with her 2-year-old son for a well-child visit. She remarks that, although her son uses a few single words to indicate hunger and other needs, her sister’s child at the same age had begun using multiple words to ask questions and express her wishes. She’s concerned about whether her son’s behavior is normal. As you start to engage the child, you note that he responds only after you repeat his name a few times. Are these observations indicative of a typical delay in development, or are they clues to a serious medical issue or communication disability? Given the absence of any known medical problem or evident physical or intellectual disability, how would you proceed in this case and in counseling the mother?
Developmental screening minimizes adverse long-term consequences
Speech, language, and hearing delays and disorders in children can lead to learning and socialization problems that may persist into adulthood. Health care providers who monitor speech, language, and hearing development in children can guide parents, as needed, to appropriate services for further assessment or treatment1 and direct them to advocacy programs such as the Center for Parent Information and Resources (formerly the National Dissemination Center for Children with Disabilities).2
A useful tool at well-child visits is the Denver II, a quick developmental screening test to help identify a variety of disorders of intelligence, language, mental health, and motor and self-help skills.3
Suspicion of a developmental delay not likely due to a medical issue or congenital abnormality requiring examination by an otorhinolaryngologist could warrant referral of the child for early intervention (EI).
Communication disorders and their manifestations
Communication—the ability to receive, process, comprehend, and transmit information—is essential for a successful life.4 Speech, language, and hearing impairments affect a child’s ability to send (speak, write, or gesture) and receive (hear, interpret, or decipher) messages.
Speech impairments
Beginning at birth, we systematically develop speech sounds and an ability to use these sounds to convey meaning by forming words and using language.5 Speech and language pathologists make a distinction between speech and language impairments.6
Speech disorders may involve problems of articulation, fluency, voice, or resonance. About 8% to 9% of preschool children have speech disorders, and approximately 5% of school-age children have speech or language impairments.7
Problems of articulation are heard in such instances as substituting a “w” for an “r” (“wabbit” for “rabbit”) or in distorting or omitting sounds or syllables (“tato” for “potato”). Considering that articulation involves the precise coordination of about 70 muscles (tongue, lips, velum, vocal folds, etc), development of this skill normally goes through phases of inaccurate sound productions. Concerns arise when these phases persist or are atypical.
Speech fluency/stuttering is the uncontrollable blocking of speech, sound prolongation (“wwwwater”), or repetition of a sound, syllable, or word during speaking (“pu-pu-pu-puppy”).
Problems of voice include symptoms such as hoarseness, an exceptionally weak voice or one that is too high or too low, or abnormal resonance (hyper- or hyponasality, which gives the impression the child is talking “through the nose” or is constantly congested).
Using common milestones as reference points. The American Speech-Language-Hearing Association (ASHA)8 lists the milestones for speech development (English and Spanish) at http://www.asha.org/public/speech/development/chart.htm. For example, between 12 and 24 months of age, a child should be learning vocabulary (“doggie, nana”), combining 2 words (“mommy car”), asking 2-word questions (“where daddy?”), and producing a variety of speech sounds. These milestones represent an average and some children may not master all the items in a category until they reach the upper limit of the age range (TABLE 1).8 Roth et al9 found that intervention benefited preschoolers with speech and language disabilities when applied earlier than previously recommended. In other words, avoid the “wait-and-see” option. Busari and Weggelaar,10 studying referral recommendations for children who are “slow to speak,” concluded that EI may diminish further consequences later in the child’s life.
ASHA launched a campaign to increase awareness of communication disorders across the lifespan and to encourage early identification (http://identifythesigns.org/).11 The site has basic lists of signs of common speech and language disorders and hearing loss in children from birth to 4 years of age. This period in a child’s life is “an important stage in early detection of communication disorders.”
Language impairments
Language impairments affect 3 domains of language: form (grammar/syntax), content, or use. These domains are governed by rules specific to the language spoken in the home. Language impairment can interfere with comprehension and formulation of messages. About 2% to 3% of preschoolers have language disorders.12
Language impairments may be observed in one or more of the language components, including phonology (rules of the sounds in the language), lexicon (vocabulary), morphology (word markers—eg, final “s” to make the plural of “cat”), syntax (word order) and pragmatics (socially appropriate speech, gesture, eye contact, and language use).
While there is great variability in typical development, atypical language development can be a secondary characteristic of other physical or developmental problems attributed to other conditions such as autism spectrum disorder (ASD), cerebral palsy, childhood apraxia of speech, dysarthria, intellectual disability, or selective mutism.13
Verbal communication difficulties may appear in expressive and receptive language.14Receptive language is the ability to comprehend language communicated by another person.6 Receptive language (processing) skills can be demonstrated as follows. If a child is asked “Do you like cats?” she must first decide to whom the question is directed (to her and not someone else). She must then search her long-term memory for the word/concept “cat” (compared with dog, a similar concept; or with mat, a similar-sounding word), and process the word “like” (compared with “dislike”). Now the child understands the question and can decide on an answer.
Expressive language is a child’s ability to speak; the mental process used to produce speech and communicate a message.6 To answer, “Yes, I like cats,” the child retrieves the concept “cat” from memory (cognition and semantics: the meanings of words, their relationships and usage), finds the right words (vocabulary), puts them in the right order (syntax), uses the right verb tense (grammar/morphology), assembles the right sounds in order, initiates the neuromotor acts (phonology/speech production), and communicates that she understands what cats are and that she likes them (pragmatics; socially/contextually appropriate responses).
Resources on language development. Typical language development, the length of which varies among children, must be practiced in a rich linguistic environment. Some children are adventurous with language. They babble, talk, and communicate in a carefree manner. Others are cautious. They may wait until they are sure of their skills before attempting a new word. Usually, concern about a child’s speech and language development arises if there is no speech, if speech is not clear, or if speech or language is different from that of peers.
The Centers for Disease Control and Prevention, under their “Learn the signs. Act early” campaign (www.cdc.gov/actearly), has published checklists of children’s developmental milestones from 2 months to 5 years of age on social, communication, cognitive, and motor skills. Health care providers helping parents determine if their child’s communication is developing normally can find information and materials at http://www.cdc.gov/ncbddd/actearly/hcp/index.html.15
Hearing impairments
Moeller et al16 surveyed 1968 primary care physicians on their attitude, practices, and knowledge of universal hearing screenings for newborns. They noted limitations in awareness of EI options for infants with hearing loss: proper times and places for referrals, available communication modalities, cochlear implant candidacy, and professionals in their locale with expertise on hearing loss. These knowledge gaps involved some medical issues, such as hearing loss genetics and later-onset hearing loss in infants and children. They also found low confidence in providing information to families about how to proceed with EI and in discussing intervention needs and resources.
Adverse effects of hearing loss. Hearing loss can be unilateral or bilateral, conductive or sensorineural, and can range in severity from mild to profound. According to the National Institute on Deafness and Communication Disorders (NIDCD), one in every 350 infants is born with a significant hearing loss, and others become deaf due to childhood illness or injury.17 According to ASHA,18 hearing loss can affect children in 4 major ways:19 delays in the development of receptive (comprehension) and expressive communication skills; a language deficit that causes learning problems and reduces academic achievement; communication difficulties that often lead to social isolation and poor self-concept; and impact on vocational choices and options.20 NIDCD provides a checklist to determine a child’s hearing status at http://www.nidcd.nih.gov/health/hearing/silence.asp.17
Timing of intervention is significant. EI is critical in minimizing the deleterious effects of hearing loss and in optimizing speech and language development. Severity of hearing loss influences EI outcome, and treatment options depend on the hearing loss having occurred either before language development (prelingually) or after (postlingually). Early management of hearing impairment can improve language, especially for children with a severe or profound hearing loss.21
Devices and methods that promote communication development for students who are deaf or hard of hearing include the use of hearing aids to amplify residual hearing for oral or auditory-oral approaches; the manual approach stressing sign-language (American Sign Language or Signed English); or Total Communication using both the oral and sign-language methods.
With an infant, suspicion of a hearing problem warrants referral to an otorhinolaryngologist or an audiologist for thorough evaluation. In New Jersey, an EI referral typically triggers a referral to one of these specialists. TABLE 2 lists resources for early identification and intervention in communication disorders.
TABLE 2
| Resources for early identification and intervention in communication disorders | |
| Resource | Information |
| American Speech-Language-Hearing Association (ASHA) | Communication skills, milestones, disorders, and treatment resources across the lifespan; for parents and professionals |
| CDC’s “Learn the signs. Act early” campaign
| Children’s developmental milestones from 2 months to 5 years; checklists for parents |
| Children’s developmental milestones and Early Intervention for health care providers | |
| National Institute on Deafness and Other Communication Disorders | Speech and language development checklists |
| National Institute on Deafness and Other Communication Disorders | Hearing loss and its effects on communication; identification and management options |
| Center for Parent Information and Resources | Early Intervention: overview and process |
| National Institute of Mental Health | Autism spectrum disorder; a guide for parents |
| First Signs, Inc | Early warning signs of autism spectrum disorder; for parents and professionals |
| The Autism Screening Test | Autism screening test to identify children 16-30 months who should receive a more thorough assessment for possible early signs of autism spectrum disorder or developmental delay |
Autism spectrum disorder
The fifth edition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-5)22 has revised its diagnostic codes for ASD. An in-depth analysis of the new diagnosis is beyond the purview of this article, but it deserves a few comments.
The revised diagnosis of ASD consolidates the previously separate diagnoses of autistic disorder, Asperger’s disorder, childhood disintegrative disorder, and pervasive developmental disorder/not otherwise specified.22-24 According to DSM-5, an individual with ASD must have 1) persistent deficits in social communication and social interactions, 2) restricted, repetitive patterns of behavior, interests or activities, 3) symptoms present in early childhood (but may not become fully manifest until social demands exceed limited capacities), and 4) symptoms that limit and impair everyday functioning.22,24
Onset of the disorder must be obvious before age 3 for a child to be eligible for EI. Children who do not qualify for an ASD diagnosis under the new DSM-5 definition may be included in a new category called social communication disorder (SCD) under “Communication Disorders” in DSM-5. SCD is defined as impairment in pragmatics that impacts development of social relationships and comprehension of social conversations. ASD must be ruled out before a diagnosis of SCD can be made.23,24
Early intervention services
Individual states offer EI services to families to facilitate detection of developmental delays in children and to provide a comprehensive system of support designed to reduce the effects of disabilities (or to prevent learning and developmental problems later in life).5 The rationale for EI is that the earlier interventions are started, the less likely later interventions will be needed.25 EI services are provided to children from birth through their third birthday; services are free of charge to eligible families or on a sliding payment scale determined by a family’s income.
Resources for information and referrals. To access EI services on behalf of a family, contact a local hospital or point them to the CPIR (http://www.parentcenterhub.org/repository/disability-landing/).2 For families with disabled children older than 3, consider suggesting that parents contact the local school district (even if the child isn’t enrolled there) to arrange an evaluation under the Individuals with Disabilities Education Act (http://idea.ed.gov/).26 Because individual states’ EI organizations may have slightly different procedures, it is best to consult one’s own state EI site for specific information regarding referrals (TABLE 3).
Efficacy of treatment
The prevalence of specific communication disorders varies widely, as do prognoses, possibly due to the variability of underlying causes (physical/biological/medical or environmental/educational).27 Also, as described earlier, “communication disorder” is an umbrella term inclusive of problems as diverse as resonance (eg, hypernasality due to a submucous palatal cleft), severe language delay (eg, due to Down syndrome), or lisp (misarticulation of the “s” sound).
Is therapy effective? Speech and language pathologists use the National Outcomes Measurement System (NOMS) as an index of the outcomes of treatment on functional communication along 6 scales. The most frequent types of communication problems seen in the prekindergarten children’s NOMS were “articulation” (75% of children), “spoken language production” (61%), and “spoken language comprehension” (42%). Problems in the remaining 3 scales (“pragmatics,” “cognitive orientation,” and “swallowing”) were seen in fewer than 15% of the preschool-age students.28
Articulation therapy yielded improvement in 69.3% of cases, spoken language comprehension therapy in 65.3%, and spoken language production therapy in 65.2%.28 Such outcomes support regular screening of children’s communication development and, as needed, referral for EI.
TABLE 3
CORRESPONDENCE
Christopher Mulrine, EdD; William Paterson University, 1600 Valley Road 3003 Wayne, NJ 07474-0920; [email protected]
› Consider using age-specific published milestones, such as those found online at the American Speech-Language-Hearing Association’s site, to evaluate children’s developmental progress. C
› Consult your state’s early intervention agency (cited in this article) for assistance in referring children for further evaluation and possible treatment. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice arrives with her 2-year-old son for a well-child visit. She remarks that, although her son uses a few single words to indicate hunger and other needs, her sister’s child at the same age had begun using multiple words to ask questions and express her wishes. She’s concerned about whether her son’s behavior is normal. As you start to engage the child, you note that he responds only after you repeat his name a few times. Are these observations indicative of a typical delay in development, or are they clues to a serious medical issue or communication disability? Given the absence of any known medical problem or evident physical or intellectual disability, how would you proceed in this case and in counseling the mother?
Developmental screening minimizes adverse long-term consequences
Speech, language, and hearing delays and disorders in children can lead to learning and socialization problems that may persist into adulthood. Health care providers who monitor speech, language, and hearing development in children can guide parents, as needed, to appropriate services for further assessment or treatment1 and direct them to advocacy programs such as the Center for Parent Information and Resources (formerly the National Dissemination Center for Children with Disabilities).2
A useful tool at well-child visits is the Denver II, a quick developmental screening test to help identify a variety of disorders of intelligence, language, mental health, and motor and self-help skills.3
Suspicion of a developmental delay not likely due to a medical issue or congenital abnormality requiring examination by an otorhinolaryngologist could warrant referral of the child for early intervention (EI).
Communication disorders and their manifestations
Communication—the ability to receive, process, comprehend, and transmit information—is essential for a successful life.4 Speech, language, and hearing impairments affect a child’s ability to send (speak, write, or gesture) and receive (hear, interpret, or decipher) messages.
Speech impairments
Beginning at birth, we systematically develop speech sounds and an ability to use these sounds to convey meaning by forming words and using language.5 Speech and language pathologists make a distinction between speech and language impairments.6
Speech disorders may involve problems of articulation, fluency, voice, or resonance. About 8% to 9% of preschool children have speech disorders, and approximately 5% of school-age children have speech or language impairments.7
Problems of articulation are heard in such instances as substituting a “w” for an “r” (“wabbit” for “rabbit”) or in distorting or omitting sounds or syllables (“tato” for “potato”). Considering that articulation involves the precise coordination of about 70 muscles (tongue, lips, velum, vocal folds, etc), development of this skill normally goes through phases of inaccurate sound productions. Concerns arise when these phases persist or are atypical.
Speech fluency/stuttering is the uncontrollable blocking of speech, sound prolongation (“wwwwater”), or repetition of a sound, syllable, or word during speaking (“pu-pu-pu-puppy”).
Problems of voice include symptoms such as hoarseness, an exceptionally weak voice or one that is too high or too low, or abnormal resonance (hyper- or hyponasality, which gives the impression the child is talking “through the nose” or is constantly congested).
Using common milestones as reference points. The American Speech-Language-Hearing Association (ASHA)8 lists the milestones for speech development (English and Spanish) at http://www.asha.org/public/speech/development/chart.htm. For example, between 12 and 24 months of age, a child should be learning vocabulary (“doggie, nana”), combining 2 words (“mommy car”), asking 2-word questions (“where daddy?”), and producing a variety of speech sounds. These milestones represent an average and some children may not master all the items in a category until they reach the upper limit of the age range (TABLE 1).8 Roth et al9 found that intervention benefited preschoolers with speech and language disabilities when applied earlier than previously recommended. In other words, avoid the “wait-and-see” option. Busari and Weggelaar,10 studying referral recommendations for children who are “slow to speak,” concluded that EI may diminish further consequences later in the child’s life.
ASHA launched a campaign to increase awareness of communication disorders across the lifespan and to encourage early identification (http://identifythesigns.org/).11 The site has basic lists of signs of common speech and language disorders and hearing loss in children from birth to 4 years of age. This period in a child’s life is “an important stage in early detection of communication disorders.”
Language impairments
Language impairments affect 3 domains of language: form (grammar/syntax), content, or use. These domains are governed by rules specific to the language spoken in the home. Language impairment can interfere with comprehension and formulation of messages. About 2% to 3% of preschoolers have language disorders.12
Language impairments may be observed in one or more of the language components, including phonology (rules of the sounds in the language), lexicon (vocabulary), morphology (word markers—eg, final “s” to make the plural of “cat”), syntax (word order) and pragmatics (socially appropriate speech, gesture, eye contact, and language use).
While there is great variability in typical development, atypical language development can be a secondary characteristic of other physical or developmental problems attributed to other conditions such as autism spectrum disorder (ASD), cerebral palsy, childhood apraxia of speech, dysarthria, intellectual disability, or selective mutism.13
Verbal communication difficulties may appear in expressive and receptive language.14Receptive language is the ability to comprehend language communicated by another person.6 Receptive language (processing) skills can be demonstrated as follows. If a child is asked “Do you like cats?” she must first decide to whom the question is directed (to her and not someone else). She must then search her long-term memory for the word/concept “cat” (compared with dog, a similar concept; or with mat, a similar-sounding word), and process the word “like” (compared with “dislike”). Now the child understands the question and can decide on an answer.
Expressive language is a child’s ability to speak; the mental process used to produce speech and communicate a message.6 To answer, “Yes, I like cats,” the child retrieves the concept “cat” from memory (cognition and semantics: the meanings of words, their relationships and usage), finds the right words (vocabulary), puts them in the right order (syntax), uses the right verb tense (grammar/morphology), assembles the right sounds in order, initiates the neuromotor acts (phonology/speech production), and communicates that she understands what cats are and that she likes them (pragmatics; socially/contextually appropriate responses).
Resources on language development. Typical language development, the length of which varies among children, must be practiced in a rich linguistic environment. Some children are adventurous with language. They babble, talk, and communicate in a carefree manner. Others are cautious. They may wait until they are sure of their skills before attempting a new word. Usually, concern about a child’s speech and language development arises if there is no speech, if speech is not clear, or if speech or language is different from that of peers.
The Centers for Disease Control and Prevention, under their “Learn the signs. Act early” campaign (www.cdc.gov/actearly), has published checklists of children’s developmental milestones from 2 months to 5 years of age on social, communication, cognitive, and motor skills. Health care providers helping parents determine if their child’s communication is developing normally can find information and materials at http://www.cdc.gov/ncbddd/actearly/hcp/index.html.15
Hearing impairments
Moeller et al16 surveyed 1968 primary care physicians on their attitude, practices, and knowledge of universal hearing screenings for newborns. They noted limitations in awareness of EI options for infants with hearing loss: proper times and places for referrals, available communication modalities, cochlear implant candidacy, and professionals in their locale with expertise on hearing loss. These knowledge gaps involved some medical issues, such as hearing loss genetics and later-onset hearing loss in infants and children. They also found low confidence in providing information to families about how to proceed with EI and in discussing intervention needs and resources.
Adverse effects of hearing loss. Hearing loss can be unilateral or bilateral, conductive or sensorineural, and can range in severity from mild to profound. According to the National Institute on Deafness and Communication Disorders (NIDCD), one in every 350 infants is born with a significant hearing loss, and others become deaf due to childhood illness or injury.17 According to ASHA,18 hearing loss can affect children in 4 major ways:19 delays in the development of receptive (comprehension) and expressive communication skills; a language deficit that causes learning problems and reduces academic achievement; communication difficulties that often lead to social isolation and poor self-concept; and impact on vocational choices and options.20 NIDCD provides a checklist to determine a child’s hearing status at http://www.nidcd.nih.gov/health/hearing/silence.asp.17
Timing of intervention is significant. EI is critical in minimizing the deleterious effects of hearing loss and in optimizing speech and language development. Severity of hearing loss influences EI outcome, and treatment options depend on the hearing loss having occurred either before language development (prelingually) or after (postlingually). Early management of hearing impairment can improve language, especially for children with a severe or profound hearing loss.21
Devices and methods that promote communication development for students who are deaf or hard of hearing include the use of hearing aids to amplify residual hearing for oral or auditory-oral approaches; the manual approach stressing sign-language (American Sign Language or Signed English); or Total Communication using both the oral and sign-language methods.
With an infant, suspicion of a hearing problem warrants referral to an otorhinolaryngologist or an audiologist for thorough evaluation. In New Jersey, an EI referral typically triggers a referral to one of these specialists. TABLE 2 lists resources for early identification and intervention in communication disorders.
TABLE 2
| Resources for early identification and intervention in communication disorders | |
| Resource | Information |
| American Speech-Language-Hearing Association (ASHA) | Communication skills, milestones, disorders, and treatment resources across the lifespan; for parents and professionals |
| CDC’s “Learn the signs. Act early” campaign
| Children’s developmental milestones from 2 months to 5 years; checklists for parents |
| Children’s developmental milestones and Early Intervention for health care providers | |
| National Institute on Deafness and Other Communication Disorders | Speech and language development checklists |
| National Institute on Deafness and Other Communication Disorders | Hearing loss and its effects on communication; identification and management options |
| Center for Parent Information and Resources | Early Intervention: overview and process |
| National Institute of Mental Health | Autism spectrum disorder; a guide for parents |
| First Signs, Inc | Early warning signs of autism spectrum disorder; for parents and professionals |
| The Autism Screening Test | Autism screening test to identify children 16-30 months who should receive a more thorough assessment for possible early signs of autism spectrum disorder or developmental delay |
Autism spectrum disorder
The fifth edition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM-5)22 has revised its diagnostic codes for ASD. An in-depth analysis of the new diagnosis is beyond the purview of this article, but it deserves a few comments.
The revised diagnosis of ASD consolidates the previously separate diagnoses of autistic disorder, Asperger’s disorder, childhood disintegrative disorder, and pervasive developmental disorder/not otherwise specified.22-24 According to DSM-5, an individual with ASD must have 1) persistent deficits in social communication and social interactions, 2) restricted, repetitive patterns of behavior, interests or activities, 3) symptoms present in early childhood (but may not become fully manifest until social demands exceed limited capacities), and 4) symptoms that limit and impair everyday functioning.22,24
Onset of the disorder must be obvious before age 3 for a child to be eligible for EI. Children who do not qualify for an ASD diagnosis under the new DSM-5 definition may be included in a new category called social communication disorder (SCD) under “Communication Disorders” in DSM-5. SCD is defined as impairment in pragmatics that impacts development of social relationships and comprehension of social conversations. ASD must be ruled out before a diagnosis of SCD can be made.23,24
Early intervention services
Individual states offer EI services to families to facilitate detection of developmental delays in children and to provide a comprehensive system of support designed to reduce the effects of disabilities (or to prevent learning and developmental problems later in life).5 The rationale for EI is that the earlier interventions are started, the less likely later interventions will be needed.25 EI services are provided to children from birth through their third birthday; services are free of charge to eligible families or on a sliding payment scale determined by a family’s income.
Resources for information and referrals. To access EI services on behalf of a family, contact a local hospital or point them to the CPIR (http://www.parentcenterhub.org/repository/disability-landing/).2 For families with disabled children older than 3, consider suggesting that parents contact the local school district (even if the child isn’t enrolled there) to arrange an evaluation under the Individuals with Disabilities Education Act (http://idea.ed.gov/).26 Because individual states’ EI organizations may have slightly different procedures, it is best to consult one’s own state EI site for specific information regarding referrals (TABLE 3).
Efficacy of treatment
The prevalence of specific communication disorders varies widely, as do prognoses, possibly due to the variability of underlying causes (physical/biological/medical or environmental/educational).27 Also, as described earlier, “communication disorder” is an umbrella term inclusive of problems as diverse as resonance (eg, hypernasality due to a submucous palatal cleft), severe language delay (eg, due to Down syndrome), or lisp (misarticulation of the “s” sound).
Is therapy effective? Speech and language pathologists use the National Outcomes Measurement System (NOMS) as an index of the outcomes of treatment on functional communication along 6 scales. The most frequent types of communication problems seen in the prekindergarten children’s NOMS were “articulation” (75% of children), “spoken language production” (61%), and “spoken language comprehension” (42%). Problems in the remaining 3 scales (“pragmatics,” “cognitive orientation,” and “swallowing”) were seen in fewer than 15% of the preschool-age students.28
Articulation therapy yielded improvement in 69.3% of cases, spoken language comprehension therapy in 65.3%, and spoken language production therapy in 65.2%.28 Such outcomes support regular screening of children’s communication development and, as needed, referral for EI.
TABLE 3
CORRESPONDENCE
Christopher Mulrine, EdD; William Paterson University, 1600 Valley Road 3003 Wayne, NJ 07474-0920; [email protected]
1. Wankoff LS. Warning signs in the development of speech, language, and communication: when to refer to a speech-language pathologist. J Child Adolesc Psychiatr Nurs. 2011;24:175-184.
2. Center for Parent Information and Resources. Disabilities. Center for Parent Information and Resources Web site. Available at: http://www.parentcenterhub.org/repository/disability-landing/. Updated June 2014. Accessed January 24, 2015.
3. Denver Developmental Materials, Inc. Denver II Online. Denver Developmental Materials, Inc Web site. Available at: http://denverii.com/denverii/. Accessed January 24, 2015.
4. Guralnick MJ. The Effectiveness of Early Intervention. Baltimore, MD: Brookes Publishing; 2013.
5. Schwartz HD. A Primer on Communication and Communicative Disorders. Boston, MA: Pearson Education; 2012.
6. Heward WL. Exceptional Children: An Introduction to Special Education. 10th ed. Boston, Mass: Pearson Education; 2013.
7. Hallahan DP, Kauffman J M, Pullen PC. Exceptional Learners: An Introduction to Special Education. 13th ed. Upper Saddle River, NJ: Pearson Education; 2015.
8. American Speech-Language-Hearing Association. How does your child hear and talk? American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/development/chart.htm. Accessed January 24, 2015.
9. Roth FP, Troia GA, Worthington CK, et al. Promoting awareness of sounds in speech: An initial report of an early intervention program for children with speech and language impairments. Appl Psycholinguistics. 2002;23:535-565.
10. Busari JO, Weggelaar NM. How to investigate and manage the child who is slow to speak. BMJ. 2004;328:272-276.
11. American Speech-Language-Hearing Association. Identify the Signs of Communication Disorders. Identify the Signs of Communication Disorders Web site. Available at: http://identifythesigns.org/. Accessed January 24, 2015.
12. McLaughlin MR. Speech and language delay in children. Am Fam Physician. 2011;83:1183-1188.
13. American Speech-Language-Hearing Association. Child speech and language. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/disorders/ChildSandL.htm. Accessed January 24, 2015.
14. Bondurant-Utz JA. Practical Guide to Assessing Infants and Preschoolers with Special Needs. Upper Saddle River, NJ: Pearson Education; 2002.
15. Centers for Disease Control and Prevention. Learn the Signs: Act Early. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/actearly/hcp/index.html. Accessed January 24, 2015.
16. Moeller MP, White KR, Shisler L. Primary care physicians’ knowledge, attitudes, and practices related to newborn hearing screening. Pediatrics. 2006;118:1357-1370.
17. National Institute on Deafness and Other Communication Disorders. Your baby’s hearing and communicative checklist. National Institute on Deafness and Other Communication Disorders Web site. Available at: http://www.nidcd.nih.gov/health/hearing/silence.asp. Accessed January 24, 2015.
18. American Speech-Language-Hearing Association. Effects of hearing loss on development. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/hearing/Effects-of-Hearing-Loss-on-Development/. Accessed January 24, 2015.
19. American Speech-Language-Hearing Association. Facts about pediatric hearing loss. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/aud/Facts-about-Pediatric-Hearing-Loss/. Accessed January 24, 2015.
20. Tang BG, Feldman HM, Padden C, et al. Delayed recognition of profound hearing loss in a 7-year-old girl with a neurological condition. J Dev Behav Pediatr. 2010;31(3 suppl):S42-S45.
21. Watkin P, McCann D, Law C, et al. Language ability in children with permanent hearing impairment: the influence of early management and family participation. Pediatrics. 2007;120:e694-e701.
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
23. Autism Match. 5 things to know about autism and DSM-5. Austism Match Web site. Available at: https://autismmatch.org/info/news/2012/05/02/5-things-to-know-about-autism-and-dsm-5. Accessed January 24, 2015.
24. American Psychiatric Publishing. Autism Spectrum Disorder. American Psychiatric Association Web site. Available at: http://www.dsm5.org/Documents/Autism%20Spectrum%20Disorder%20Fact%20Sheet.pdf. Accessed January 24, 2015.
25. Law J, Garrett Z, Nye C. Speech and language therapy interventions for children with primary speech and language delay or disorder. Cochrane Database Syst Rev. 2003;(3):CD004110.
26. U.S. Department of Education. Building the legacy: IDEA 2004. Individuals with Disabilities Education Act Web site. Available at: http://idea.ed.gov/. Accessed January 24, 2015.
27. Friend MP. Special Education: Contemporary Perspectives for School Professionals. Boston, MA: Pearson; 2005.
28. Mullen R, Schooling T. The National Outcomes Measurement System for Pediatric Speech-Language Pathology. Lang Speech Hearing Services Schools. 2010;41:44-60.
1. Wankoff LS. Warning signs in the development of speech, language, and communication: when to refer to a speech-language pathologist. J Child Adolesc Psychiatr Nurs. 2011;24:175-184.
2. Center for Parent Information and Resources. Disabilities. Center for Parent Information and Resources Web site. Available at: http://www.parentcenterhub.org/repository/disability-landing/. Updated June 2014. Accessed January 24, 2015.
3. Denver Developmental Materials, Inc. Denver II Online. Denver Developmental Materials, Inc Web site. Available at: http://denverii.com/denverii/. Accessed January 24, 2015.
4. Guralnick MJ. The Effectiveness of Early Intervention. Baltimore, MD: Brookes Publishing; 2013.
5. Schwartz HD. A Primer on Communication and Communicative Disorders. Boston, MA: Pearson Education; 2012.
6. Heward WL. Exceptional Children: An Introduction to Special Education. 10th ed. Boston, Mass: Pearson Education; 2013.
7. Hallahan DP, Kauffman J M, Pullen PC. Exceptional Learners: An Introduction to Special Education. 13th ed. Upper Saddle River, NJ: Pearson Education; 2015.
8. American Speech-Language-Hearing Association. How does your child hear and talk? American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/development/chart.htm. Accessed January 24, 2015.
9. Roth FP, Troia GA, Worthington CK, et al. Promoting awareness of sounds in speech: An initial report of an early intervention program for children with speech and language impairments. Appl Psycholinguistics. 2002;23:535-565.
10. Busari JO, Weggelaar NM. How to investigate and manage the child who is slow to speak. BMJ. 2004;328:272-276.
11. American Speech-Language-Hearing Association. Identify the Signs of Communication Disorders. Identify the Signs of Communication Disorders Web site. Available at: http://identifythesigns.org/. Accessed January 24, 2015.
12. McLaughlin MR. Speech and language delay in children. Am Fam Physician. 2011;83:1183-1188.
13. American Speech-Language-Hearing Association. Child speech and language. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/speech/disorders/ChildSandL.htm. Accessed January 24, 2015.
14. Bondurant-Utz JA. Practical Guide to Assessing Infants and Preschoolers with Special Needs. Upper Saddle River, NJ: Pearson Education; 2002.
15. Centers for Disease Control and Prevention. Learn the Signs: Act Early. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/ncbddd/actearly/hcp/index.html. Accessed January 24, 2015.
16. Moeller MP, White KR, Shisler L. Primary care physicians’ knowledge, attitudes, and practices related to newborn hearing screening. Pediatrics. 2006;118:1357-1370.
17. National Institute on Deafness and Other Communication Disorders. Your baby’s hearing and communicative checklist. National Institute on Deafness and Other Communication Disorders Web site. Available at: http://www.nidcd.nih.gov/health/hearing/silence.asp. Accessed January 24, 2015.
18. American Speech-Language-Hearing Association. Effects of hearing loss on development. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/public/hearing/Effects-of-Hearing-Loss-on-Development/. Accessed January 24, 2015.
19. American Speech-Language-Hearing Association. Facts about pediatric hearing loss. American Speech-Language-Hearing Association Web site. Available at: http://www.asha.org/aud/Facts-about-Pediatric-Hearing-Loss/. Accessed January 24, 2015.
20. Tang BG, Feldman HM, Padden C, et al. Delayed recognition of profound hearing loss in a 7-year-old girl with a neurological condition. J Dev Behav Pediatr. 2010;31(3 suppl):S42-S45.
21. Watkin P, McCann D, Law C, et al. Language ability in children with permanent hearing impairment: the influence of early management and family participation. Pediatrics. 2007;120:e694-e701.
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing; 2013.
23. Autism Match. 5 things to know about autism and DSM-5. Austism Match Web site. Available at: https://autismmatch.org/info/news/2012/05/02/5-things-to-know-about-autism-and-dsm-5. Accessed January 24, 2015.
24. American Psychiatric Publishing. Autism Spectrum Disorder. American Psychiatric Association Web site. Available at: http://www.dsm5.org/Documents/Autism%20Spectrum%20Disorder%20Fact%20Sheet.pdf. Accessed January 24, 2015.
25. Law J, Garrett Z, Nye C. Speech and language therapy interventions for children with primary speech and language delay or disorder. Cochrane Database Syst Rev. 2003;(3):CD004110.
26. U.S. Department of Education. Building the legacy: IDEA 2004. Individuals with Disabilities Education Act Web site. Available at: http://idea.ed.gov/. Accessed January 24, 2015.
27. Friend MP. Special Education: Contemporary Perspectives for School Professionals. Boston, MA: Pearson; 2005.
28. Mullen R, Schooling T. The National Outcomes Measurement System for Pediatric Speech-Language Pathology. Lang Speech Hearing Services Schools. 2010;41:44-60.
