User login
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors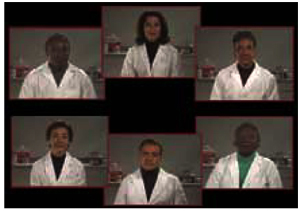
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.