User login
Video study of physician selection: Preferences in the face of diversity
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors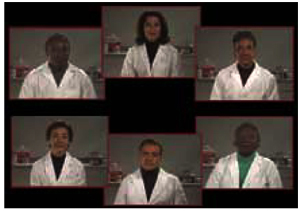
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
Objectives: To determine whether a diverse group of people would predominantly choose a white male physician regardless of group member’s sex and ethnicity when given a choice among 6 actor-portrayed video doctors (males and females of Latino, European, and African descent) and whether further exposure would alter initial selections.
Study Design: Participants selected a video doctor after viewing a brief introduction and again after viewing the delivery of a prevention message.
Population: Three hundred ninety-five participants recruited at a shopping mall in the San Francisco Bay Area (61% female, 39% male; 30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other).
Outcomes Measured: Initial and final video doctor selections; ratings of video doctors on interpersonal qualities.
Results: Most participants (85% of females and 63% of males) initially chose a female video doctor (P<.001) and even more did so at final selection. Approximately half initially chose a same-race video doctor (66% of European Americans, 51% of Latinos, and 50% of African Americans), but fewer did so at final selection (56% of European Americans, 44% of Latinos, and 52% of African Americans). In addition, at final selection 57% of Asian Americans and other-ethnicity participants chose a non–European American video doctor.
Conclusions: Many healthcare consumers will accept physicians of both sexes and of different races. After observing the video doctors demonstrate a professional and warm affect, participants became even more receptive to choosing a video doctor of a different race. Video doctor technology holds promise for increasing our understanding of patients’ preferences.
As the physician workforce diversifies,1,2 the question of patients’ preferences for physicians by sex and race becomes increasingly important. Early investigations suggested that many patients, especially males, prefer same-sex physicians across a variety of clinical complaints,3-5 but subsequent studies found these preferences to be more limited,6-9 except for sex-specific health problems (eg, gynecologic examinations and sexual health issues).10
A more recent study examining patients’ actual selections of physicians in a large health maintenance organization showed that most patients of both sexes chose a male physician.11 Whether these findings reflect actual patients’ preferences is debatable, however, because patients’ choices may have been influenced by the greater availability of male physicians on the panel.
Compared with sex, even less is known about preferences for physicians’ race, a topic that is complicated by patient and physician attributes such as language, religion, ethnicity, immigration status, acculturation, and multiracial identities. One recent survey on minority health care found that approximately one fourth of African American and Latino patients who had chosen same-race physicians reported explicitly considering the physician’s race or ethnicity in making their selection.12
In this study, we examined people’s choices when asked to select a male or female African American, Latino, or European American actor-portrayed “video doctor” to be their physician. Choices were examined at 2 time points: after viewing a brief introduction and after viewing the delivery of a brief health advice message. Our research questions were: After gaining a first impression, will patients choose a male of European descent regardless of their own sex and race? Will exposure to the video doctors’ deliveries of a brief health advice message alter these preferences? The video doctor methodology allowed us to offer participants a verisimilar experience of choosing a physician from a diverse panel and to avoid the limitations of availability and access inherent in real-life choices.
Methods
Video doctor filming and editing
We selected 6 actors of similar age (45 years) and attractiveness: 1 female and 1 male African American, Latino, and European American. We used the term Latino to represent a racial identity characterized by dark hair and a medium complexion. The fictitious surnames of the Latino and Latina video doctors also indicated their ethnicity.
When producing the video doctor presentations, we held constant the script, the setting (a doctor’s office), and the clothing. Two segments were produced for each video doctor: a brief introduction in which the doctor used a fictitious name assigned by the researchers to say, for example, “Hi, I’m Dr. Ann Johnson,” and a 45-second health advice message about eating 5 fruits and/or vegetables a day (chosen because of the neutral and universally relevant nature of this topic). The health message contained key elements known to enhance effectiveness of brief interventions.13 The actors’ deliveries of the message were standardized to include interpersonal elements associated with patient-centered health care and positive patient behavior change—for example, warmth, friendliness, empathy, and a nonjudgmental, respectful, and collaborative affect.14,15 (A full description of our procedures is available in Appendix A at www.jfponline.com.)
To balance the video doctors with respect to any possible order effect, we created 18 video presentations showing the video doctors in different orders. We obtained the sequences by creating 6 x 6 Latin squares containing all 720 possible orders and then randomly selecting 3 Latin squares and using the 18 orders contained therein. By delivering 1 of the 18 orders to each group of 22 to 24 participants, we obtained nearly perfect balance in the ordering of the video doctors.
Participants
Individuals at a shopping mall in the San Francisco Bay Area aged >18 years and able to read and write English were invited to watch a short video and rate doctors for a healthcare research project. Four hundred people participated; 395 completed questionnaires. Participants were told that their responses were anonymous, and each questionnaire was marked only with the group number. Study procedures were approved by the Committee on Human Research at the University of California at San Francisco.
FIGURE
Video doctors
Study design and procedures
After viewing brief introductions of each video doctor (Figure), participants were asked: “If you were to choose 1 of these doctors to be your doctor, which would you pick?” They were then instructed to write the number of their choice on the questionnaire.
Participants then viewed the message from each video doctor about eating 5 fruits and vegetables a day. After each presentation, participants rated the video doctor by circling a number on 7-point scales, where a response of 7 indicated the following qualities: very professional, very knowledgeable, excellent communication skills, respectfulness, genuine/authentic, warm/friendly, and pleasant facial expressions.14,15 Participants also rated each video doctor on a 7-point scale for how likely they would be to increase their fruit and vegetable consumption, how interested they might be in choosing this person as their doctor, and how comfortable they might be in talking with this person about personal health matters such as sexual, alcohol, and drug-using behaviors.
After viewing and rating all 6 video doctors, participants again viewed the 6 head shots together and answered the following question: “Now that you’ve heard each video doctor, which one would you pick to be your doctor?” To conclude, participants answered demographic questions, turned in their booklets, and received a $20 gift certificate.
Statistical analysis
Differences in the initial preferences for the sex and race of the video doctors by the sex and race of the participants were studied by using standard 2-way tables, with Fisher exact tests for 2 × 2 tables and χ2 tests for larger tables. Multivariable analysis of sex preferences for the video doctor was done with logistic regression to test the effect of participants’ demographic variables. Matched pair analysis, with an exact version of the McNemar test, was used to assess whether participants’ tendency to choose a same-sex or a same-race video doctor changed from their initial to their final selection.
From each participant’s ratings of the video doctors, an assessment score was generated by averaging the 10 scaled ratings. The clustered assessment scores were analyzed with a normal linear mixed model analysis with a random effect to represent participant scoring tendency and fixed effects to account for the differential mean score for the preferred vs nonpreferred video doctors and differences in mean score depending on the order in which the video doctor was scored. All analyses were performed in Stata 6.0. (More detailed on the methods is found in Appendix A at www.jfponline.com.)
Results
Demographics
Participants were diverse in sex (61% female, 39% male), ethnicity (30% Asian American, 29% European American, 26% Latino, 8% African American, and 7% other), age (11% were 18 to 19 years old, 24% were 20 to 29, 18% were 30 to 39, 17% were 40 to 49, 13% were 50 to 59, 8% were 60 to 69, and 9% were 70 to 87), and education (9% had less than a high school education, 34% had a high school diploma or graduation equivalency diploma, 26% had some college, 22% were college graduates, and 9% had graduate degrees).
Initial preferences for video doctors
Initial sex preference. The strong preference for a female video doctor was significantly different from the 50% preference for each sex that would be expected in the absence of any sex preference (P<.0001). Most females (85%) and males (63%) selected a female video doctor (difference between males and females significant at P<.001; Table 1). The percentages of sex preference by race were not significantly different from one another (P=.36).
Multivariable logistic regression confirmed the relation between participants’ sex and the sex preference of the video doctor but showed no convincing evidence of differences in sex preference related to race (P=.73), age (P=.15), schooling (P=.23), marital status (P=.13), or employment status (P=.19).
Initial race preference. For their initial video doctor selection, 53% of participants chose a European American, 29% chose a Latino, and 18% chose an African American. This pattern of preference was significantly different from the 33.3% for each race that would be expected in the absence of a racial preference (P<.001; Table 2).
Video doctor racial preferences differed significantly by race of the participant (P<.0001), with a preference for the same race. A substantial number of participants, however, chose a different-race video doctor. Racial preferences were similar across male and female participants (P=.98).
TABLE 1
Initial and final video doctor selections by sex
| Initial selection | Final selection | |||
|---|---|---|---|---|
| Participants | Female video doctor | Male doctor video | Female video doctor | Male video doctor |
| Female (n=240) | 85% | 15% | 88% | 12% |
| Male (n=155) | 63% | 37% | 71% | 29% |
| Overall (n=395) | 76% | 24% | 82% | 18% |
TABLE 2
Initial and final video doctor selections by race
| Initial selection | Final selection | |||||
|---|---|---|---|---|---|---|
| Participants | African American | Latino | European American | African American | Latino | European American |
| African American (n=30) | 50% | 17% | 33% | 52% | 19% | 29% |
| Latino (n=101) | 12% | 51% | 37% | 20% | 44% | 36% |
| European American (n=113) | 15% | 19% | 66% | 23% | 21% | 56% |
| Asian American or “other” (n=145) | 18% | 25% | 57% | 20% | 37% | 43% |
| Overall (n=389) | 18% | 29% | 53% | 23% | 32% | 44% |
Final preferences for video doctors
Final sex preference. The preference for a female video doctor increased across female and male participants (P<.001; Table 1). The net shift among males from male to female video doctor was significant (P=.014). More female participants shifted from male to female (9%) than from female to male (4%), although the difference was not statistically significant (P=.10).
Final race preference. Forty-eight percent of African American participants, 56% of Latino participants, and 44% of European Americans chose a different-race video doctor. Among Asian and other-race participants, a sizable shift occurred so that only 43% selected a European American video doctor (Table 2).
Between the initial and final selections, 3% of African American participants shifted to a video doctor of a different race, whereas 7% shifted to an African American video doctor. Eleven percent of Latino participants shifted to a different-race video doctor, whereas 6% shifted to a Latino video doctor. Among European American participants, 22% shifted to a different-race video doctor, whereas 12% shifted to a European American video doctor. With the exception of African American participants, there was a significant net shift from same- to different-race choice (P=.036). Many Asian and other-race participants shifted from a European American video doctor to a non–European American video doctor (14% net).
Assessment scores
The 3 female video doctors, who were chosen by more participants than were the 3 male video doctors at the initial and final selections, also received higher mean assessment scores (Table 3). On particular items, the highest score was 6.001 (of a possible 7), received by the European American female for the question: “How professional is this doctor?” The lowest score was 3.590 received by the European American male for the question: “If this person were your doctor, how comfortable might you be in talking with this person about personal health matters?”
TABLE 3
Selection of video doctor by sex and race
| Video doctor’s name* (ethnicity/sex) | Initial selection of video doctor | Mean assessment score | Final selection of video doctor† |
|---|---|---|---|
| Dr. Ann Johnson (European American/female) | 43% | 5.49 | 38% |
| Dr. Renee Garcia (Latina/female) | 22% | 5.32 | 26% |
| Dr. Terry Williams (African American/female) | 12% | 5.13 | 17% |
| Dr. Mark Benson (European American/male) | 10% | 4.31 | 6% |
| Dr. Glen Martinez (Latino/male) | 7% | 4.33 | 6% |
| Dr. Calvin Butler (African American/male) | 6% | 4.84 | 6% |
| *Fictitious names were assigned by the researchers. | |||
| †Figures do not add to 100% due to rounding. | |||
Association of preferences and ratings. Analysis of the mean assessment scores showed a substantial rating tendency among participants, by which they tended to give all 6 video doctors relatively high or low scores. Our analysis indicated that 34.9% (95% confidence interval [CI], 30.4–39.5) of the variance in assessment scores is explained by rating tendency.
We also found that participants tended to increase their scores as they proceeded through the sequence of doctors. Compared with the first video doctor, the second through the sixth video doctors received increases in mean scores of 0.15 (P=.016), 0.16 (P=.011), 0.29 (P<.001), 0.43 (P<.001), and 0.60 (P<.001), respectively. These results showed the importance of using multiple presentation orders to balance the order effect.
After adjusting for the order effect and the respondent rating tendency, the mean assessment scores given to video doctors selected at the initial stage were an average of 0.7 points higher than scores given to the other video doctors (P<.001, 95% CI, 0.56–0.81). At the final selection, the chosen video doctor scored on average 1.04 units higher on the assessment scores than did the other video doctors (P<.001, 95% CI, 0.94–1.1). Thus, the selection made based on the video doctors’ images and brief introductions alone was significantly associated with the subsequent assessment, and the final selection of video doctor was even more strongly associated with the assessment.
Discussion
More participants preferred same-race physicians at the initial selection (66% of European Americans, 51% of Latinos, and 50% of African Americans). This effect was not as large as one might expect, however, because a substantial minority of subjects in each racial category selected a different-race video doctor at the initial selection and a majority of Latinos selected a different-race video doctor at the final selection.
After viewing the delivery of the prevention message, more in each group, except for African Americans, chose a video doctor of a different race. In addition, at final selection, 57% of Asian and other-race participants chose a non– European American video doctor. With regard to sex, most males and females chose a female video doctor at the initial selection, and even more did so at the final selection. These data suggested that many healthcare consumers are in concordance with the recent shift toward a more diverse population of physicians and that the white male physician may no longer be viewed as the stereotypical medical professional.
The qualities patients seek in a doctor
The assessment scores for the video doctors indicated that participants were choosing, both on first impressions and after further exposure, video doctors who they perceived to possess the qualities associated with patient-centered care.21,22 Although the overall ranking of the 6 video doctors was unchanged from initial to final selection, after viewing the delivery of the prevention message, many participants altered their choices: more males and females chose a female video doctor; more European American and Latino participants shifted from same-race to different-race video doctors; and more Asian and other-race participants shifted from European American to non–European American video doctors.
These findings suggested that, even in brief meetings with physicians, patients respond to a combination of patient-centered qualities and that this combination may carry more weight than the physician’s sex and race. In other words, from the point of view of the public at large, physicians of both sexes and all races can possess the desired physician qualities, and people may be receptive to any physician who exhibits these qualities.
Preference for a female doctor
Our finding that men and women in our sample preferred a female video doctor contrasts with sex preference findings from previous studies,3,6,8,10,11 although in general studies on sex preference of physicians have shown inconsistent findings. The female preference finding in our study may represent evolving positive attitudes toward and increasing familiarity with female physicians. From 1971 to 1991, the percentage of women first-year medical school students rose from 13.7% to 39.8%.14
The strong female preference also may represent sex stereotyping. Patients reported that they desire physicians who are sensitive to their needs and circumstances, deliver a warm and empathic style of care,15 invite participation in decision making,16 engage in emotionally focused talk, and provide health information within patients’ social, emotional, and cultural contexts.17 Other studies found that women, when compared with men, provide a style of care that approximates these patient-centered characteristics.18-20
Our participants, many of whom preferred female video doctors even at first, may have strongly associated a patient-centered, empathic style with being female. The particular female actors we chose also may have been better able to exhibit, regardless of our efforts to standardize, the combination of professional and personal skills most desired in a doctor.
Racial preferences
The preference for a same-race video doctor may have several origins. People may feel more familiar and comfortable with race-concordant relationships in general and may believe that a physician of one’s own race can better attend to specific health concerns. Same-race preference also may arise from the desire to avoid a racially prejudiced physician. Racially concordant as opposed to discordant care has been associated with increased patient satisfaction and use of health care services and with higher ratings from patients regarding their level of participation during physician visits.16,23
As indicated in our study and others, African Americans express a stronger preference than do individuals from other racial groups for receiving care from physicians of their own race.23 To support patients in exercising their racial preferences, some health care professional organizations, such as the National Medical Association, have provided a toll-free number that patients can call to locate a local African American physician.
Limitations of the study
The study had several limitations. We may not have successfully held constant the actors’ personalities and acting abilities. Future video doctor studies about patients’ acceptance regarding physicians’ race and sex could address this drawback by including multiple video doctors in each sex and race category.
Because only English-speaking participants were included in the study, we do not know whether Latinos who spoke only Spanish would have chosen differently. Our study also used a convenience sample in a San Francisco Bay Area shopping mall, and our results may not be generalizable to other populations.
We were unable to study the same-race preferences of the Asian participants in our sample. Because more than 10% of physicians practicing in the United States are of Asian ancestry, patients’ receptivity to Asian physicians and Asian patients’ preference for a same-race physician would be important research topics. Diversity of language and culture among various Asian and other ethnicities also could be addressed with a well-designed video doctor study. The absence of an Asian video doctor, however, did allow us to examine the selections made by participants when no same-race video doctor was available.
Strengths of the study
A major strength of our study was that participants represented both sexes and a range of ages, races, and education levels. In addition, the video technology allowed participants to select a video doctor based on a verisimilar experience and without the constraints of availability and access found in real-life choices. All our study participants accepted the survey questions and responded to the video doctor as a “real” physician.
Video doctor technology does allow for holding constant certain variables such as age, appearance, message content, and style of delivery, an advantage that cannot be achieved in real encounters between patients and physicians.
Challenges for the future
Some of our most crucial health care challenges are providing access to quality care and equal career opportunities for those who seek to practice medicine. Our results supported the growing diversity of the population of physicians, and emphasized that many patients will choose physicians, regardless of their sex and race, who appear professional, competent, and caring. Medical schools need to continue the trend toward teaching patient-centered, empathic care and recruiting and retaining minority physicians to rectify current imbalances. In addition, practicing physicians can take note that providing quality care for patients of all cultural backgrounds may be an easier task than they think—the common language of compassion may transcend our differences.
Future studies could use video doctor technology to confirm our findings and to further investigate patients’ preferences and attitudes about various dimensions of the relationship between patient and physician. As the patient population and the physician workforce diversify, and as managed care organizations continue to strive to increase patient satisfaction and retention, information about patient preferences could inform the future of health care delivery.
Acknowledgments
We thank Scott Ludwig for his excellent casting of actors, directing, and video production; and Annabelle Ison for designing subject recruitment materials. We also thank our video doctors, the staff of Tanforan Park Shopping Center in San Bruno, CA, and the mall visitors who volunteered to participate in the study.
Corresponding author
Barbara Gerbert, PhD, University of California at San Francisco, 350 Parnassus Avenue, Suite 905, San Francisco, CA 94117. E-mail: [email protected].
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.
1. US Census Bureau Detailed occupation by race, Hispanic origin and sex: 1990. Available at: http://censtats.census.gov/ cgi-bin/eeo/eeojobs.pl. Accessed on June 9, 2003.
2. Johnson LMI ed. Minority Student Opportunities in United States Medical Schools. 15th ed. Washington, DC: Association of American Medical Colleges; 2000.
3. Ackerman-Ross SF, Sochat N. Close encounters of the medical kind: attitudes toward male and female physicians. Soc Sci Med 1980;14A:61-64.
4. Engleman E. Attitudes toward women physicians: a study of 500 clinic patients. West J Med 1974;120:95-100.
5. Challacombe C. Do women patients need women doctors? Practitioner 1983;227:848-850.
6. Fennema K, Meyer D, Owen N. Sex of physician: patients’ p and stereotypes. J Fam Pract 1990;30:441-446.
7. Weyrauch KF, Boiko PE, Alvin B. Patient sex role and preference for a male or female physician. J Fam Pract 1990;30:559-562.
8. Kerssens JJ, Bensing JM, Andela MG. Patient preference for genders of health professionals. Soc Sci Med 1997;44:1531-1540.
9. Graffy J. Patient choice in practice with men and women general practitioners. Br J Gen Pract 1990;40:13-15.
10. Elstad JI. Women’s priorities regarding physician behavior and their preference for a female physician. Women Health 1994;21(4):1-17.
11. Schmittdiel MA, Grumbach K, Selby JV, Quesenberry CP. Effect of physician and patient gender concordance on patient satisfaction and preventive care practices. J Gen Intern Med 2000;15:761-769.
12. Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? Health Aff (Millwood). 2000;19(4):76-83.
13. Miller W, Sanchez V. Motivating young adults for treatment and lifestyle change. In: Howard G, ed. Issues in Alcohol Use and Misuse by Young Adults. Notre Dame, Ind: University of Notre Dame Press; 1994;55-82.
14. Jonas H, Etzel S, Baransky B. Educational programs in the US medical schools. JAMA 1992;268:1083-1090.
15. Rollnick S, Mason P, Butler C. Health Behavior Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone; 1999.
16. Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. JAMA 1999;282:583-589.
17. Roter D, Hall J. Why physicians’ gender matters in the shaping of the patient-physician relationship. J Womens Health 1998;7:1093-1097.
18. Roter D, Lipkin M, Korsgaard A. Sex differences in patients’ and physicians’ communication during primary care medical visits. Med Care 1991;29:1083-1093.
19. Hall J, Irish J, Roter D, Ehrich C, Miller L. Gender in medical encounters: an analysis of physician and patient communication in a primary care setting. Health Psychol 1994;13:384-392.
20. Elderkin-Thompson V, Waitzkin H. Differences in clinical communication by gender. J Gen Intern Med 1999;14:112-121.
21. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behaviors. New York: Guilford Press; 1991.
22. Stewart M. Effective physician–patient communication and health outcomes. CMAJ 1995;152:1423-1433.
23. Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient–physician racial concordance and the perceived quality and use of health care. Arch Intern Med 1999;159:997-1004.
Interventions that Help Victims of Domestic Violence
METHODS: We conducted 6 focus groups with 45 San Francisco Bay Area physicians who had intervened with victims of domestic violence. The sessions were audiotaped and transcribed. We constructed, through constant comparison, a template of open codes to identify themes that emerged from the data.
RESULTS: Our analysis revealed that physicians viewed validation (ie, providing messages to the patients that they are worth caring about) as the foundation of intervention. Other interventions included labeling the abuse as abuse; listening and being nonjudgmental; documenting, referring, and safety planning; using a team approach; and prioritizing domestic violence in the health care environment. Physicians described a range of rewards for intervening with victims, from seeing a patient change her entire life to subtle shifts in the way a woman thinks of her relationship and herself.
CONCLUSIONS: Our study offers insight into how physicians can intervene to help victims of domestic violence. Recent interview and survey studies of battered women support the physician interventions described.
In response to the public health consequences of domestic violence and the number of battered women whom physicians see in their practices,1-4 medical organizations including the American Medical Association and the American College of Obstetricians and Gynecologists have called for physicians to act as agents of change in abused women’s lives.5,6 In the late 1980s and early 1990s these organizations and others issued guidelines and mandates based on information from domestic violence experts that outlined how physicians should intervene.6-8 Unfortunately, these recommendations are not specific enough and do not seem to have improved their responses to violence against women9-11; many physicians are simply not asking women about violence,12-17 and women whose health problems result from abuse are not receiving the health care they need.9,10,18-20
Physicians cite many barriers to intervening with victims, including patient evasiveness and failure to disclose information, lack of time and support resources, lack of education or training, fear of offending the patient, inability to “fix it,” and frustration with lack of change in the patient’s situation or the patient’s unresponsiveness to advice.16,18,21-28 Primary care physicians in the qualitative study by Sugg and Inui28 characterized talking about domestic violence with patients as opening Pandora’s box and associated the act of even asking about domestic violence with unleashing their own fears and discomforts.
Despite the barriers, some physicians are committed to addressing the underlying health problems of abused women. How do these physicians intervene, and what motivates them to continue in their commitment? In previous work,16 we described how physicians with expertise in domestic violence identify victims. With this study we explored how physicians with experience in identifying victims tried to help.
Methods
Participants
Qualitative research commonly uses purposive sampling, a method in which the participants best suited to provide a full description of the research topic are intentionally selected. We sought a sample of physicians in the San Francisco Bay Area who had experience in identifying and intervening with victims of domestic violence. To identify important common patterns that cut across different settings29,30 physicians from 3 medical specialties were sought: primary care (family practice and general internal medicine), obstetrics and gynecology, and emergency medicine.
We conducted our recruitment in consultation with a professional survey research organization. Thirteen physicians known to have domestic violence experience, and additional physicians selected from the yellow pages, were screened and asked to participate in a study exploring the most effective ways for the health care system to meet the needs of victims of domestic violence. Eligible participants were asked to identify other colleagues who are concerned about and treated victims of domestic violence, and these individuals were screened and asked to participate and to identify others. Physicians were eligible if they worked directly with patients 20 or more hours per week, had identified and intervened with victims of domestic violence, and were somewhat confident or very confident about addressing domestic violence issues with patients.
Recruitment ceased when the goal of 12 to 22 physicians in each medical specialty who had the relevant domestic violence experience was reached.
Focus Group Method and Data Collection
In comparison with survey or one-on-one interview formats, the focus group approach allows for a more extensive exploration of the area under discussion. Participants can collectively explore different experiences and perspectives, generate ideas, and debate and compare their ideas with those of others in the group.31 Six focus groups ranging in size from 6 to 11 individuals were conducted during a 3-week period in January and February 1998. Each group was facilitated by 2 moderators who were members of the research team. The sessions lasted approximately 90 minutes and were held in professional focus group settings that allowed hidden viewing. Several researchers viewed the groups from behind 2-way mirrors and completed field notes that were later compared with the observations of the moderators. Before each focus group session written informed consent was obtained from all participants and a written background survey was administered to gather demographic and practice information. Participants received a small stipend for participating. Study procedures were approved by the University of California San Francisco Committee on Human Research.
We used a semistructured guide that allowed the facilitators to follow certain topics and open new lines of inquiry when appropriate.32 Open-ended questions were formulated based on our previous interviews with survivors of domestic violence33 and a review of the literature ( Table 1 ). Audiotapes of the focus group sessions were transcribed by research staff; the principal investigator reviewed these transcripts for accuracy.
Coding and Analysis
For initial analysis we conducted multiple readings of transcripts to identify prominent themes. The investigators independently reviewed the transcripts and then met to review and discuss differences of opinion about interpretations and to further refine themes driven by the words and phrases of the participants. Through this process and the constant comparison of new data against emerging themes, a template of open codes was constructed. The transcripts were coded and specific themes within the narratives of the participants were identified in accordance with standard qualitative analytic convention.34 Coded data were organized using NUD*IST 4.0 software (Qualitative Solutions and Research; Victoria, Australia). This software helps ensure the consistency of study findings and creates an audit trail.35 The data were interpreted in the context of the original focus group sessions and the current literature. The final coding scheme and analysis of the findings were reviewed, and disagreements were discussed by the team until consensus was reached.
To further enhance the credibility of the findings, a qualitative technique called member check was used.36 Results were directed back to 3 research participants to confirm that their experiences and those of other participants in their focus group were reflected in the findings.
Results
Of the 80 physicians who were screened, 53 were eligible, and 45 were able to attend the focus group sessions. Their characteristics are presented in Table 2 . The participants reported that they had identified an average of 28 patients per year as having been physically abused by an intimate partner, and they thought they had helped approximately 60% of those patients.
Helpful Intervention Techniques
Even these physicians reported sometimes feeling overwhelmed, frustrated, and incompetent regarding their role in domestic violence cases. They believed, however, that addressing partner abuse was part of their job and reported various ways that they have tried to help battered women improve their situation and their health. Our data analyses revealed that the following themes were common across specialties.
Give Validating Messages. The most common aspect of intervention was validation. Whatever their approach to helping, these physicians gave compassionate messages that validated the woman’s worth as a human being and indicated that the abuse was undeserved. One participant put it this way: “Just my being there, caring about them consistently, giving another message [helped]: You are worth caring about, you are deserving, you are valuable.” Physicians tended to embed this kind of attitude and message into their interventions with abused patients, making validation the foundation of their interactions with them.
Break Through Denial and Plant Seeds for Change. Physicians reported that within the context of a trusting relationship they tried to break through the denial these women presented about the seriousness of their experiences. Some physicians reported labeling the abuse for what it is, blatantly wrong and criminal. They believed that over time they could help victims to begin to see this reality and change their situation. One participant said:
I let them know that what’s going on is outlandishly not right, that they don’t deserve to have that happen. It’s frankly illegal, and you can bring charges against someone for doing that. Sometimes people can be shocked by finding out that that’s the case. You can plant a seed about their self-esteem … and their ability over time to change that situation, but piecemeal.
Another physician reported showing women the photographs taken of past injuries to remind them of the partner’s pattern of abusive behavior: “We begin every session with: Do you remember that? Sometimes the reaction is: No, it didn’t happen that way. But the photograph just sits there.”
Listen Nonjudgmentally. Physicians described listening and attending to the whole person as central to providing good health care to all patients, especially victims of abuse. In the context of listening they reported on the need to maintain a healing attitude by banishing criticism, blame, and judgment, but agreed that achieving this was difficult and required letting go of the desire to fix it by treating the women as competent adults. One participant said:
I try to get across just from my tone of voice primarily, that I’m not judging them. Because I made that mistake quite a while ago—my judgment was right away: Well, this is terrible; you’ve got to get out. And I could watch the person psychologically fly away from me. So in order to maintain that [trusting] space, that connection with them, it’s really important for me to get clear that I’m going to listen and not judge them. And it’s all going to change on their time.
Document, Refer, and Help the Patient Plan for Safety. These physicians stated that they were careful to write down the specifics of what the woman said. In addition to medical charting, some took photographs of any injuries with color Polaroid cameras. One physician stated that for the photographs to be useful in court “you have to include their face so that a lawyer can’t argue that you’re taking a photograph of someone else.”
The most practicable example of documentation was the development of a domestic violence packet which included a body chart, an instruction list for documentation, a compartment for the color Polaroid photograph, a handy tear-out sheet for information services (resources, shelters), and a telephone number for the police.
In general when physicians knew or suspected abuse they offered information about domestic violence and referrals to local community resources, hot lines, and shelters. Some stated that patients often refused referrals and that they kept referral sheets in the waiting room so that individuals could decide on their own whether to take one.
Other physicians stated that on occasion women had made statements such as: “I can’t take that (handout) home … it’s like a flag in front of a bull.” To address this problem some physicians reported putting business-size cards with domestic violence hot line numbers (eg, local hot line numbers, shelter numbers, or community resource numbers) in all the bathrooms, sometimes the only place where the batterer could not easily follow a woman. Participants reported:
[The cards] are constantly replenished [by housekeeping] … and one of the things I tell people if they’re in an explosive situation is to put it in their shoe, in the insole.
I have a very small practice. I do only office gynecology, but I put about 10 cards a week [in the bathroom]. I would bet 2 disappear in a week. Isn’t that amazing? And this is a fairly affluent area.
Physicians described various ways they had tried to help women plan for their own immediate and ongoing safety. Some physicians talked about trying to stay aware and sensitive to the safety needs of women whose partners are controlling them through abuse, even when the partners are not currently threatening violence. One participant said:
I’ll try to role-play with them … how are they going to deal with telling their partner that they have this infection or that they really want to use this type of birth control. I’ll say, “Some people in your situation could have a fight with their significant other,” and go through predicting some possibilities. Sometimes you can see them start to close down because they know that could happen, or this is a repeated thing that they keep getting that they have no control over. So, I’ll say, “Well, I have other patients in this situation who sometimes need a safe place to go,” or I’ll talk about what somebody else did and at the same time give them some information.
Physicians also reported counseling victims to keep a suitcase packed and have 24-hour hot line numbers or contact numbers for safe places, and helping them to specify what circumstances should cause them to call the police.
Although physicians stated that acute cases were rare outside of the emergency department, they described attempts to ensure safety when the woman’s life was in immediate danger. These attempts included (1) working as a team to separate the partner from the woman (eg, the nurse talked with the abusive partner in the waiting room while the physician cared for the victim and, with the victim’s permission, called the police and a domestic violence advocate to remove her from the abusive home); (2) making excuses to separate the abuser from the victim in the immediate situation (eg, taking the woman for tests); and (3) admitting women who could not be placed in a shelter into the hospital under a false name. One physician reported that the hospital at which she had trained had a safe bed designated for victims of rape, domestic violence, and other assaults.
Using a Team Approach. In general, the physicians agreed that it takes a team approach to intervene successfully with victims of domestic violence. Some expressed frustration about accessing community referrals and discussed the benefits to victims of readily accessible resources on site. The on-site resources referred women directly to the nurse, rape crisis counselor, social worker, behavioral medicine counselor, or psychologist, who counseled the women and conducted follow-up. Some physicians without access to onsite counselors or social workers described making domestic violence part of every staff member’s educational process when they come on board.
Physicians described how intervention demanded a certain amount of flexibility of roles, with nurses and physicians playing off each other in tag-team fashion, as necessary. One physician said:
Sometimes when I finish with an exam, I’ll tell the nurse that I suspect something, so when the nurse is giving the discharge instructions, she’ll also re-approach certain kinds of issues and give the woman another opportunity to talk about [the abuse], once she has gotten dressed and composed herself. The door is closed. It’s one-on-one.
Some physicians described how their prenatal team takes advantage of a “window of opportunity” and has helped women get out of their situations and into counseling:
We have a prenatal team that really works together … our nurse, our social worker, our nutritionist, the receptionist, everybody.… It’s a real intense time. But I think once they get out of pregnancy, we really lose that ability to make a change in their lives. It’s a real window of opportunity.
Prioritize Domestic Violence. Even the committed physicians in our study expressed conflict about taking the time to intervene once they had identified abuse. Some physicians advocated dropping the medical procedure (even if that means the loss of reimbursement) to spend the rest of the patient’s time dealing with the abuse. Physicians also described prioritizing domestic violence by conducting continuing education courses and meetings for everyone in the department about rape, domestic violence, and child and elder abuse. One participant reported:
We try to create a culture of caring about domestic violence so that nurses who think they’ve recognized someone as being a nondeclared victim won’t be told, “I’m too busy” by a physician. And so when physicians say, “I think that might be a domestic violence victim, could you go talk to her?” the nurse will see that as a priority. And if anybody asks her, “How come you haven’t got that IV started?” she or he could say, “Because I was in talking to this person trying to determine whether they were a domestic violence victim.”
Small Victories Offer Positive Feedback
These physicians reported receiving little direct feedback about the effectiveness of their interventions with battered women. Yet, they also reported a range of rewards for intervening, from seeing a patient really change her life to glimpsing shifts in the way a woman thinks about herself and the relationship. One physician said:
And the rewarding piece for me comes when at some point she looks up and notices, and you can see this change of realizing that she’s cared about and then what that must mean to her, that she’s worth something. And then later on [there are] those little steps that you can see people make when they feel like they’re worth something. That’s the most ongoing and rewarding thing.
Discussion
The themes described by the purposive sample of physicians in our study offer insight into the process of intervention with victims of domestic violence and help delineate practicable examples of how to apply interventions ( Table 3 ). The behaviors described are supported by quantitative and qualitative data from battered women.33,37
These physicians described the foundation of intervention with victims as giving victims the message that they do not deserve abuse and that they are worth caring about. Battered women themselves report that validation is an important message. In a recent survey,37 battered women rated validating statements and compassion from physicians as among the most desirable interventions, equal to safety planning and offering referrals. In another study,33 survivors of domestic violence described how validation from a health care professional had not only provided relief and comfort, but also “started the wheels turning” toward realizing the seriousness of the situation. These women reported that validation helped them, regardless of whether they had disclosed the abuse or the health care professional had identified it.
Women who are being controlled through abuse by an intimate partner live with debilitating feelings of denial, shame, and humiliation that are sometimes reinforced in health care encounters and keep victims from seeking and receiving optimal care.33,38-41 The physicians in our study recognized these barriers and made efforts to help women break through their denial and plant seeds for change. They also made efforts—and learned through trial and error—to listen and be nonjudgmental. Both of these behaviors were rated as highly desirable by battered women.37 Physician statements made within the context of a trusting relationship can serve to remind women of the seriousness of their situation. Physician behaviors that convey respect through tone of voice and body language could lessen a victim’s shame and help her make small changes over time to improve her situation and her health.
The data we presented on documenting abuse, providing referrals, and planning for safety concur with the practices recommended by Physicians for a Violence-Free Society.42 We suggest that health care settings develop a domestic violence packet containing a body chart, documentation instructions, and referral sheets. We also suggest they provide Polaroid cameras to document specific injuries, since pictures offer an inviolable record of the abuse.42 Survivors report that the process of documenting abuse can serve to validate the individual if accompanied by genuine nonjudgmental statements of concern.33
Although the physicians in our study were aware of the need to provide victims with referrals to community resources and assess their safety needs,6,8,42,43 they had developed their own styles of intervention and admitted that victims sometimes refused referrals. One solution offered by participants in our study is to put easy-to-hide business-size cards with local domestic violence hot-line and shelter numbers in all of the bathrooms. We also suggest that physicians continue to offer referrals time after time: repetitive offering or availability of referrals may help survivors feel like they are not alone and may reassure them that support is available within and outside the health care system when they are ready to seek it. Physicians should remember that a woman may be able to talk about the abuse long before she can actualize any change. They should also be aware that ending the relationship does not necessarily end the abuse; it may escalate it.44 The study physicians were careful to consider safety from the battered woman’s point of view and to take preventive measures. We suggest that physicians review their options for facilitating safety (ie, availability of resources and time) and, when necessary, connect the victim by telephone to an agency trained in assessing and planning for their safety. Battered women report that they want physicians to offer referrals and help them plan for safety.37
Although current guidelines call for physicians to play a large role in identifying, intervening with, and following up on cases of partner abuse,6,45,46 the physicians in our study emphasized the need to work as a team to identify and provide optimal care to victims. This requires flexibility of roles within the health care team and ready access to on-site and community domestic violence resources. In an attempt to improve health care for victims of domestic violence, experts and researchers in the field have proposed simplifying and limiting the tasks of physicians in this area. One model uses the acronym AVDR: physicians should ask patients about abuse; provide validating messages that battering is wrong and the patient is a worthy individual; document presenting signs, symptoms, and disclosures; and refer victims to specialists in domestic violence.47 At that point specialists on site or on call from the community would assess the patient’s safety, make appropriate safety plans, and perform other in-depth interventions.
Physicians face ever-increasing demands on their limited time, yet these physicians committed to helping battered women found multiple ways to enable them to intervene. The holistic approaches described here—using a team approach, prioritizing domestic violence, developing a culture of caring—send a powerful message of prevention and intervention to victims: Battering is not a private, shameful issue, but a health care issue of great concern to physicians. These approaches also provide health care professionals with systematic support for helping battered women, perhaps allowing committed physicians to act as agents of change in battered women’s lives.5
Women who are being controlled by the abusive actions of their intimate partners report that even small signs of compassion from health care professionals have made a difference to them. As stated by physicians in this study and by survivors in our previous study,33 these acts of caring plant the seeds for change. In their efforts to help battered women, physicians must remember that incremental changes and small moments of recognition can eventually lead to major shifts in the lives of these women. Every time physicians successfully intervene with a person whose health problems are caused by abuse they have engendered a positive outcome.
Acknowledgments
Our project has been supported by the National Institute of Mental Health Grant #1 R01 MH51580. We thank the physicians who participated in the focus groups and those who participated in reviewing the study findings. We also thank Stephanie Greer and Survey Methods Group for their assistance in recruiting physician participants and organizing the focus groups; Candace Love, PhD, and Richard Carlton, MPH, for assisting the authors with moderating focus group sessions; Priscilla Abercrombie, NP, PhD, for assisting with coding the data; Karen Herzig, PhD, for assisting with the literature review; and Jennifer Fechner for transcribing the focus group session audiotapes and proofreading the manuscript.
1. Hamberger LK, Saunders DG, Hovey M. Prevalence of domestic violence in community practice and rate of physician inquiry. Fam Med 1992;24:283-87.
2. Rath GD, Jarratt LG, Leonardson G. Rates of domestic violence against adult women by men partners. J Am Board Fam Pract 1989;2:227-33.
3. Appleton W. The battered woman syndrome. Ann Emerg Med 1980;9:84-91.
4. Goldberg WG, Tomlanovich MC. Domestic violence in the emergency department: new findings. JAMA 1984;251:3259-64.
5. Chez R, Jones R. The battered woman. Am J Obstet Gynecol 1995;173:677-79.
6. American Medical Association Council on Scientific Affairs. Violence against women: relevance for medical practitioners. JAMA 1992;267:3184-89.
7. American College of Obstetricians and Gynecologists. The battered woman. Washington, DC: American College of Obstetricians and Gynecologists; 1989.
8. Sassetti MR. Domestic violence. Prim Care 1993;20:289-305.
9. Isaac NE, Sanchez RL. Emergency department response to battered women in Massachusetts. Ann Emerg Med 1994;23:855-58.
10. Waller AE, Hohenhaus SM, Shah PJ, Stern EA. Development and validation of an emergency department screening and referral protocol for victims of domestic violence. Ann Emerg Med 1996;27:754-60.
11. Tunis SR, Hayward RS, Wilson MC, et al. Internists’ attitudes about clinical practice guidelines. Ann Intern Med 1994;120:956-63.
12. Abbott J, Johnson R, Koziol-McLain J, Lowenstein SR. Domestic violence against women: incidence and prevalence in an emergency department population. JAMA 1995;273:1763-67.
13. Mazza D, Dennerstein L, Ryan V. Physical, sexual and emotional violence against women: a general practice-based prevalence study. Med J Aust 1996;164:14-17.
14. McGrath M, Hogan F, Peipert J. A prevalence survey of abuse and screening for abuse in urgent care patients. Obstet Gynecol 1998;91:511-14.
15. Caralis P, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997;90:1075-80.
16. Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999;131:578-84.
17. Sugg N, Thompson R, Thompson D, Maiuro R, Rivara F. Domestic violence and primary care. Arch Fam Med 1999;8:301-06.
18. Parsons LH, Zaccaro D, Wells B, Stovall TG. Methods of and attitudes toward screening obstetrics and gynecology patients for domestic violence. Am J Obstet Gynecol 1995;173:381-86; discussion386-87.
19. Olson L, Anctil C, Fullerton L, Brillman J, Arbuckle J, Sklar D. Increasing emergency physician recognition of domestic violence. Ann Emerg Med 1996;27:741-46.
20. Carbonell JL, Chez RA, Hassler RS. Florida physician and nurse education and practice related to domestic violence. Womens Health Issues 1995;5:203-07.
21. Lee D, Letellier P, McLoughlin E, Salber P. California hospital emergency departments response to domestic violence—survey report. San Francisco, Calif: Family Violence Prevention Fund; 1993.
22. Kurz D. Interventions with battered women in health care settings. Violence Vict 1990;5:243-56.
23. Kurz D. Emergency department responses to battered women: resistance to medicalization. Soc Probl 1987;34:69-81.
24. McGrath M, Bettacchi A, Duffy S, Peipert J, Becker B, St. Angelo L. Violence against women: provider barriers to intervention in emergency departments. Acad Emerg Med 1997;4:297-300.
25. Ferris LE. Canadian family physicians’ and general practitioners’ perceptions of their effectiveness in identifying and treating wife abuse. Med Care 1994;32:1163-72.
26. Ferris LE, Tudiver F. Family physicians’ approach to wife abuse: a study of Ontario, Canada, practices. Fam Med 1992;24:276-82.
27. Brown JB, Lent B, Sas G. Identifying and treating wife abuse. J Fam Pract 1993;36:185-91.
28. Sugg NK, Inui T. Primary care physicians’ response to domestic violence: opening Pandora’s box. JAMA 1992;267:3157-60.
29. Patton MQ. Qualitative evaluation and research methods. Newbury Park, Calif: Sage Publications; 1990.
30. Kuzel AJ. Sampling in qualitative inquiry. In: Crabtree BF, Miller WL, eds. Doing qualitative research. Newbury Park, Calif: Sage Publications; 1992;31-44.
31. Morgan DL. Focus groups as qualitative research. Beverly Hills, Calif: Sage Publications; 1988.
32. Stillman FA. Focus group research: an overview. In: Becker DM, Hill DR, Lackson JS, eds. Health behavior research in minority populations: access, design, and implementation. Bethesda, Md: US Department of Health and Human Services; 1992;168-75.
33. Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
34. Strauss AL, Corbin J. Basics of qualitative research: grounded theory procedures and techniques. Newbury Park, Calif: Sage Publications; 1990.
35. Sandelowski M. The problem of rigor in qualitative research. Adv Nurs Sci 1986;8:27-37.
36. Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills, Calif: Sage Publications; 1985.
37. Hamberger K, Ambuel B, Marbella A, Donze J. Physician interaction with battered women. Arch Fam Med 1998;7:575-82.
38. Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996;24:1-17.
39. Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996;5:153-58.
40. Martins R, Holzapfel S, Baker P. Wife abuse: are we detecting it? J Women Health 1992;1:77-80.
41. McCauley J, Yurk RA, Jenckes MW, Ford DE. Inside “Pandora’s box”: abused women’s experiences with clinicians and health services. J Gen Intern Med 1998;13:549-55.
42. Taliaferro E. Domestic violence: the need for good documentation. Action Notes: Physicians for a Violence-Free Society. 1997;23:1.-
43. American College of Obstetricians and Gynecologists. ACOG technical bulletin: domestic violence. Int J Gynecol Obstet 1995;51:161-70.
44. Salber PR, Taliaferro E. The physician’s guide to domestic violence: how to ask the right questions and recognize abuse. Volcano, Calif: Volcano Press, Inc; 1995.
45. Hyman A. Domestic violence: legal issues for health care practitioners and institutions. J Am Med Womens Assoc 1996;51:101-05.
46. Dutton MA, Mitchell B, Haywood Y. The emergency department as a violence prevention center. J Am Med Womens Assoc 1996;51:92-95, 117.
47. Gerbert B, Moe J, Caspers N, et al. Simplifying physicians’ response to domestic violence. West J Med 2000;172:329-31.
METHODS: We conducted 6 focus groups with 45 San Francisco Bay Area physicians who had intervened with victims of domestic violence. The sessions were audiotaped and transcribed. We constructed, through constant comparison, a template of open codes to identify themes that emerged from the data.
RESULTS: Our analysis revealed that physicians viewed validation (ie, providing messages to the patients that they are worth caring about) as the foundation of intervention. Other interventions included labeling the abuse as abuse; listening and being nonjudgmental; documenting, referring, and safety planning; using a team approach; and prioritizing domestic violence in the health care environment. Physicians described a range of rewards for intervening with victims, from seeing a patient change her entire life to subtle shifts in the way a woman thinks of her relationship and herself.
CONCLUSIONS: Our study offers insight into how physicians can intervene to help victims of domestic violence. Recent interview and survey studies of battered women support the physician interventions described.
In response to the public health consequences of domestic violence and the number of battered women whom physicians see in their practices,1-4 medical organizations including the American Medical Association and the American College of Obstetricians and Gynecologists have called for physicians to act as agents of change in abused women’s lives.5,6 In the late 1980s and early 1990s these organizations and others issued guidelines and mandates based on information from domestic violence experts that outlined how physicians should intervene.6-8 Unfortunately, these recommendations are not specific enough and do not seem to have improved their responses to violence against women9-11; many physicians are simply not asking women about violence,12-17 and women whose health problems result from abuse are not receiving the health care they need.9,10,18-20
Physicians cite many barriers to intervening with victims, including patient evasiveness and failure to disclose information, lack of time and support resources, lack of education or training, fear of offending the patient, inability to “fix it,” and frustration with lack of change in the patient’s situation or the patient’s unresponsiveness to advice.16,18,21-28 Primary care physicians in the qualitative study by Sugg and Inui28 characterized talking about domestic violence with patients as opening Pandora’s box and associated the act of even asking about domestic violence with unleashing their own fears and discomforts.
Despite the barriers, some physicians are committed to addressing the underlying health problems of abused women. How do these physicians intervene, and what motivates them to continue in their commitment? In previous work,16 we described how physicians with expertise in domestic violence identify victims. With this study we explored how physicians with experience in identifying victims tried to help.
Methods
Participants
Qualitative research commonly uses purposive sampling, a method in which the participants best suited to provide a full description of the research topic are intentionally selected. We sought a sample of physicians in the San Francisco Bay Area who had experience in identifying and intervening with victims of domestic violence. To identify important common patterns that cut across different settings29,30 physicians from 3 medical specialties were sought: primary care (family practice and general internal medicine), obstetrics and gynecology, and emergency medicine.
We conducted our recruitment in consultation with a professional survey research organization. Thirteen physicians known to have domestic violence experience, and additional physicians selected from the yellow pages, were screened and asked to participate in a study exploring the most effective ways for the health care system to meet the needs of victims of domestic violence. Eligible participants were asked to identify other colleagues who are concerned about and treated victims of domestic violence, and these individuals were screened and asked to participate and to identify others. Physicians were eligible if they worked directly with patients 20 or more hours per week, had identified and intervened with victims of domestic violence, and were somewhat confident or very confident about addressing domestic violence issues with patients.
Recruitment ceased when the goal of 12 to 22 physicians in each medical specialty who had the relevant domestic violence experience was reached.
Focus Group Method and Data Collection
In comparison with survey or one-on-one interview formats, the focus group approach allows for a more extensive exploration of the area under discussion. Participants can collectively explore different experiences and perspectives, generate ideas, and debate and compare their ideas with those of others in the group.31 Six focus groups ranging in size from 6 to 11 individuals were conducted during a 3-week period in January and February 1998. Each group was facilitated by 2 moderators who were members of the research team. The sessions lasted approximately 90 minutes and were held in professional focus group settings that allowed hidden viewing. Several researchers viewed the groups from behind 2-way mirrors and completed field notes that were later compared with the observations of the moderators. Before each focus group session written informed consent was obtained from all participants and a written background survey was administered to gather demographic and practice information. Participants received a small stipend for participating. Study procedures were approved by the University of California San Francisco Committee on Human Research.
We used a semistructured guide that allowed the facilitators to follow certain topics and open new lines of inquiry when appropriate.32 Open-ended questions were formulated based on our previous interviews with survivors of domestic violence33 and a review of the literature ( Table 1 ). Audiotapes of the focus group sessions were transcribed by research staff; the principal investigator reviewed these transcripts for accuracy.
Coding and Analysis
For initial analysis we conducted multiple readings of transcripts to identify prominent themes. The investigators independently reviewed the transcripts and then met to review and discuss differences of opinion about interpretations and to further refine themes driven by the words and phrases of the participants. Through this process and the constant comparison of new data against emerging themes, a template of open codes was constructed. The transcripts were coded and specific themes within the narratives of the participants were identified in accordance with standard qualitative analytic convention.34 Coded data were organized using NUD*IST 4.0 software (Qualitative Solutions and Research; Victoria, Australia). This software helps ensure the consistency of study findings and creates an audit trail.35 The data were interpreted in the context of the original focus group sessions and the current literature. The final coding scheme and analysis of the findings were reviewed, and disagreements were discussed by the team until consensus was reached.
To further enhance the credibility of the findings, a qualitative technique called member check was used.36 Results were directed back to 3 research participants to confirm that their experiences and those of other participants in their focus group were reflected in the findings.
Results
Of the 80 physicians who were screened, 53 were eligible, and 45 were able to attend the focus group sessions. Their characteristics are presented in Table 2 . The participants reported that they had identified an average of 28 patients per year as having been physically abused by an intimate partner, and they thought they had helped approximately 60% of those patients.
Helpful Intervention Techniques
Even these physicians reported sometimes feeling overwhelmed, frustrated, and incompetent regarding their role in domestic violence cases. They believed, however, that addressing partner abuse was part of their job and reported various ways that they have tried to help battered women improve their situation and their health. Our data analyses revealed that the following themes were common across specialties.
Give Validating Messages. The most common aspect of intervention was validation. Whatever their approach to helping, these physicians gave compassionate messages that validated the woman’s worth as a human being and indicated that the abuse was undeserved. One participant put it this way: “Just my being there, caring about them consistently, giving another message [helped]: You are worth caring about, you are deserving, you are valuable.” Physicians tended to embed this kind of attitude and message into their interventions with abused patients, making validation the foundation of their interactions with them.
Break Through Denial and Plant Seeds for Change. Physicians reported that within the context of a trusting relationship they tried to break through the denial these women presented about the seriousness of their experiences. Some physicians reported labeling the abuse for what it is, blatantly wrong and criminal. They believed that over time they could help victims to begin to see this reality and change their situation. One participant said:
I let them know that what’s going on is outlandishly not right, that they don’t deserve to have that happen. It’s frankly illegal, and you can bring charges against someone for doing that. Sometimes people can be shocked by finding out that that’s the case. You can plant a seed about their self-esteem … and their ability over time to change that situation, but piecemeal.
Another physician reported showing women the photographs taken of past injuries to remind them of the partner’s pattern of abusive behavior: “We begin every session with: Do you remember that? Sometimes the reaction is: No, it didn’t happen that way. But the photograph just sits there.”
Listen Nonjudgmentally. Physicians described listening and attending to the whole person as central to providing good health care to all patients, especially victims of abuse. In the context of listening they reported on the need to maintain a healing attitude by banishing criticism, blame, and judgment, but agreed that achieving this was difficult and required letting go of the desire to fix it by treating the women as competent adults. One participant said:
I try to get across just from my tone of voice primarily, that I’m not judging them. Because I made that mistake quite a while ago—my judgment was right away: Well, this is terrible; you’ve got to get out. And I could watch the person psychologically fly away from me. So in order to maintain that [trusting] space, that connection with them, it’s really important for me to get clear that I’m going to listen and not judge them. And it’s all going to change on their time.
Document, Refer, and Help the Patient Plan for Safety. These physicians stated that they were careful to write down the specifics of what the woman said. In addition to medical charting, some took photographs of any injuries with color Polaroid cameras. One physician stated that for the photographs to be useful in court “you have to include their face so that a lawyer can’t argue that you’re taking a photograph of someone else.”
The most practicable example of documentation was the development of a domestic violence packet which included a body chart, an instruction list for documentation, a compartment for the color Polaroid photograph, a handy tear-out sheet for information services (resources, shelters), and a telephone number for the police.
In general when physicians knew or suspected abuse they offered information about domestic violence and referrals to local community resources, hot lines, and shelters. Some stated that patients often refused referrals and that they kept referral sheets in the waiting room so that individuals could decide on their own whether to take one.
Other physicians stated that on occasion women had made statements such as: “I can’t take that (handout) home … it’s like a flag in front of a bull.” To address this problem some physicians reported putting business-size cards with domestic violence hot line numbers (eg, local hot line numbers, shelter numbers, or community resource numbers) in all the bathrooms, sometimes the only place where the batterer could not easily follow a woman. Participants reported:
[The cards] are constantly replenished [by housekeeping] … and one of the things I tell people if they’re in an explosive situation is to put it in their shoe, in the insole.
I have a very small practice. I do only office gynecology, but I put about 10 cards a week [in the bathroom]. I would bet 2 disappear in a week. Isn’t that amazing? And this is a fairly affluent area.
Physicians described various ways they had tried to help women plan for their own immediate and ongoing safety. Some physicians talked about trying to stay aware and sensitive to the safety needs of women whose partners are controlling them through abuse, even when the partners are not currently threatening violence. One participant said:
I’ll try to role-play with them … how are they going to deal with telling their partner that they have this infection or that they really want to use this type of birth control. I’ll say, “Some people in your situation could have a fight with their significant other,” and go through predicting some possibilities. Sometimes you can see them start to close down because they know that could happen, or this is a repeated thing that they keep getting that they have no control over. So, I’ll say, “Well, I have other patients in this situation who sometimes need a safe place to go,” or I’ll talk about what somebody else did and at the same time give them some information.
Physicians also reported counseling victims to keep a suitcase packed and have 24-hour hot line numbers or contact numbers for safe places, and helping them to specify what circumstances should cause them to call the police.
Although physicians stated that acute cases were rare outside of the emergency department, they described attempts to ensure safety when the woman’s life was in immediate danger. These attempts included (1) working as a team to separate the partner from the woman (eg, the nurse talked with the abusive partner in the waiting room while the physician cared for the victim and, with the victim’s permission, called the police and a domestic violence advocate to remove her from the abusive home); (2) making excuses to separate the abuser from the victim in the immediate situation (eg, taking the woman for tests); and (3) admitting women who could not be placed in a shelter into the hospital under a false name. One physician reported that the hospital at which she had trained had a safe bed designated for victims of rape, domestic violence, and other assaults.
Using a Team Approach. In general, the physicians agreed that it takes a team approach to intervene successfully with victims of domestic violence. Some expressed frustration about accessing community referrals and discussed the benefits to victims of readily accessible resources on site. The on-site resources referred women directly to the nurse, rape crisis counselor, social worker, behavioral medicine counselor, or psychologist, who counseled the women and conducted follow-up. Some physicians without access to onsite counselors or social workers described making domestic violence part of every staff member’s educational process when they come on board.
Physicians described how intervention demanded a certain amount of flexibility of roles, with nurses and physicians playing off each other in tag-team fashion, as necessary. One physician said:
Sometimes when I finish with an exam, I’ll tell the nurse that I suspect something, so when the nurse is giving the discharge instructions, she’ll also re-approach certain kinds of issues and give the woman another opportunity to talk about [the abuse], once she has gotten dressed and composed herself. The door is closed. It’s one-on-one.
Some physicians described how their prenatal team takes advantage of a “window of opportunity” and has helped women get out of their situations and into counseling:
We have a prenatal team that really works together … our nurse, our social worker, our nutritionist, the receptionist, everybody.… It’s a real intense time. But I think once they get out of pregnancy, we really lose that ability to make a change in their lives. It’s a real window of opportunity.
Prioritize Domestic Violence. Even the committed physicians in our study expressed conflict about taking the time to intervene once they had identified abuse. Some physicians advocated dropping the medical procedure (even if that means the loss of reimbursement) to spend the rest of the patient’s time dealing with the abuse. Physicians also described prioritizing domestic violence by conducting continuing education courses and meetings for everyone in the department about rape, domestic violence, and child and elder abuse. One participant reported:
We try to create a culture of caring about domestic violence so that nurses who think they’ve recognized someone as being a nondeclared victim won’t be told, “I’m too busy” by a physician. And so when physicians say, “I think that might be a domestic violence victim, could you go talk to her?” the nurse will see that as a priority. And if anybody asks her, “How come you haven’t got that IV started?” she or he could say, “Because I was in talking to this person trying to determine whether they were a domestic violence victim.”
Small Victories Offer Positive Feedback
These physicians reported receiving little direct feedback about the effectiveness of their interventions with battered women. Yet, they also reported a range of rewards for intervening, from seeing a patient really change her life to glimpsing shifts in the way a woman thinks about herself and the relationship. One physician said:
And the rewarding piece for me comes when at some point she looks up and notices, and you can see this change of realizing that she’s cared about and then what that must mean to her, that she’s worth something. And then later on [there are] those little steps that you can see people make when they feel like they’re worth something. That’s the most ongoing and rewarding thing.
Discussion
The themes described by the purposive sample of physicians in our study offer insight into the process of intervention with victims of domestic violence and help delineate practicable examples of how to apply interventions ( Table 3 ). The behaviors described are supported by quantitative and qualitative data from battered women.33,37
These physicians described the foundation of intervention with victims as giving victims the message that they do not deserve abuse and that they are worth caring about. Battered women themselves report that validation is an important message. In a recent survey,37 battered women rated validating statements and compassion from physicians as among the most desirable interventions, equal to safety planning and offering referrals. In another study,33 survivors of domestic violence described how validation from a health care professional had not only provided relief and comfort, but also “started the wheels turning” toward realizing the seriousness of the situation. These women reported that validation helped them, regardless of whether they had disclosed the abuse or the health care professional had identified it.
Women who are being controlled through abuse by an intimate partner live with debilitating feelings of denial, shame, and humiliation that are sometimes reinforced in health care encounters and keep victims from seeking and receiving optimal care.33,38-41 The physicians in our study recognized these barriers and made efforts to help women break through their denial and plant seeds for change. They also made efforts—and learned through trial and error—to listen and be nonjudgmental. Both of these behaviors were rated as highly desirable by battered women.37 Physician statements made within the context of a trusting relationship can serve to remind women of the seriousness of their situation. Physician behaviors that convey respect through tone of voice and body language could lessen a victim’s shame and help her make small changes over time to improve her situation and her health.
The data we presented on documenting abuse, providing referrals, and planning for safety concur with the practices recommended by Physicians for a Violence-Free Society.42 We suggest that health care settings develop a domestic violence packet containing a body chart, documentation instructions, and referral sheets. We also suggest they provide Polaroid cameras to document specific injuries, since pictures offer an inviolable record of the abuse.42 Survivors report that the process of documenting abuse can serve to validate the individual if accompanied by genuine nonjudgmental statements of concern.33
Although the physicians in our study were aware of the need to provide victims with referrals to community resources and assess their safety needs,6,8,42,43 they had developed their own styles of intervention and admitted that victims sometimes refused referrals. One solution offered by participants in our study is to put easy-to-hide business-size cards with local domestic violence hot-line and shelter numbers in all of the bathrooms. We also suggest that physicians continue to offer referrals time after time: repetitive offering or availability of referrals may help survivors feel like they are not alone and may reassure them that support is available within and outside the health care system when they are ready to seek it. Physicians should remember that a woman may be able to talk about the abuse long before she can actualize any change. They should also be aware that ending the relationship does not necessarily end the abuse; it may escalate it.44 The study physicians were careful to consider safety from the battered woman’s point of view and to take preventive measures. We suggest that physicians review their options for facilitating safety (ie, availability of resources and time) and, when necessary, connect the victim by telephone to an agency trained in assessing and planning for their safety. Battered women report that they want physicians to offer referrals and help them plan for safety.37
Although current guidelines call for physicians to play a large role in identifying, intervening with, and following up on cases of partner abuse,6,45,46 the physicians in our study emphasized the need to work as a team to identify and provide optimal care to victims. This requires flexibility of roles within the health care team and ready access to on-site and community domestic violence resources. In an attempt to improve health care for victims of domestic violence, experts and researchers in the field have proposed simplifying and limiting the tasks of physicians in this area. One model uses the acronym AVDR: physicians should ask patients about abuse; provide validating messages that battering is wrong and the patient is a worthy individual; document presenting signs, symptoms, and disclosures; and refer victims to specialists in domestic violence.47 At that point specialists on site or on call from the community would assess the patient’s safety, make appropriate safety plans, and perform other in-depth interventions.
Physicians face ever-increasing demands on their limited time, yet these physicians committed to helping battered women found multiple ways to enable them to intervene. The holistic approaches described here—using a team approach, prioritizing domestic violence, developing a culture of caring—send a powerful message of prevention and intervention to victims: Battering is not a private, shameful issue, but a health care issue of great concern to physicians. These approaches also provide health care professionals with systematic support for helping battered women, perhaps allowing committed physicians to act as agents of change in battered women’s lives.5
Women who are being controlled by the abusive actions of their intimate partners report that even small signs of compassion from health care professionals have made a difference to them. As stated by physicians in this study and by survivors in our previous study,33 these acts of caring plant the seeds for change. In their efforts to help battered women, physicians must remember that incremental changes and small moments of recognition can eventually lead to major shifts in the lives of these women. Every time physicians successfully intervene with a person whose health problems are caused by abuse they have engendered a positive outcome.
Acknowledgments
Our project has been supported by the National Institute of Mental Health Grant #1 R01 MH51580. We thank the physicians who participated in the focus groups and those who participated in reviewing the study findings. We also thank Stephanie Greer and Survey Methods Group for their assistance in recruiting physician participants and organizing the focus groups; Candace Love, PhD, and Richard Carlton, MPH, for assisting the authors with moderating focus group sessions; Priscilla Abercrombie, NP, PhD, for assisting with coding the data; Karen Herzig, PhD, for assisting with the literature review; and Jennifer Fechner for transcribing the focus group session audiotapes and proofreading the manuscript.
METHODS: We conducted 6 focus groups with 45 San Francisco Bay Area physicians who had intervened with victims of domestic violence. The sessions were audiotaped and transcribed. We constructed, through constant comparison, a template of open codes to identify themes that emerged from the data.
RESULTS: Our analysis revealed that physicians viewed validation (ie, providing messages to the patients that they are worth caring about) as the foundation of intervention. Other interventions included labeling the abuse as abuse; listening and being nonjudgmental; documenting, referring, and safety planning; using a team approach; and prioritizing domestic violence in the health care environment. Physicians described a range of rewards for intervening with victims, from seeing a patient change her entire life to subtle shifts in the way a woman thinks of her relationship and herself.
CONCLUSIONS: Our study offers insight into how physicians can intervene to help victims of domestic violence. Recent interview and survey studies of battered women support the physician interventions described.
In response to the public health consequences of domestic violence and the number of battered women whom physicians see in their practices,1-4 medical organizations including the American Medical Association and the American College of Obstetricians and Gynecologists have called for physicians to act as agents of change in abused women’s lives.5,6 In the late 1980s and early 1990s these organizations and others issued guidelines and mandates based on information from domestic violence experts that outlined how physicians should intervene.6-8 Unfortunately, these recommendations are not specific enough and do not seem to have improved their responses to violence against women9-11; many physicians are simply not asking women about violence,12-17 and women whose health problems result from abuse are not receiving the health care they need.9,10,18-20
Physicians cite many barriers to intervening with victims, including patient evasiveness and failure to disclose information, lack of time and support resources, lack of education or training, fear of offending the patient, inability to “fix it,” and frustration with lack of change in the patient’s situation or the patient’s unresponsiveness to advice.16,18,21-28 Primary care physicians in the qualitative study by Sugg and Inui28 characterized talking about domestic violence with patients as opening Pandora’s box and associated the act of even asking about domestic violence with unleashing their own fears and discomforts.
Despite the barriers, some physicians are committed to addressing the underlying health problems of abused women. How do these physicians intervene, and what motivates them to continue in their commitment? In previous work,16 we described how physicians with expertise in domestic violence identify victims. With this study we explored how physicians with experience in identifying victims tried to help.
Methods
Participants
Qualitative research commonly uses purposive sampling, a method in which the participants best suited to provide a full description of the research topic are intentionally selected. We sought a sample of physicians in the San Francisco Bay Area who had experience in identifying and intervening with victims of domestic violence. To identify important common patterns that cut across different settings29,30 physicians from 3 medical specialties were sought: primary care (family practice and general internal medicine), obstetrics and gynecology, and emergency medicine.
We conducted our recruitment in consultation with a professional survey research organization. Thirteen physicians known to have domestic violence experience, and additional physicians selected from the yellow pages, were screened and asked to participate in a study exploring the most effective ways for the health care system to meet the needs of victims of domestic violence. Eligible participants were asked to identify other colleagues who are concerned about and treated victims of domestic violence, and these individuals were screened and asked to participate and to identify others. Physicians were eligible if they worked directly with patients 20 or more hours per week, had identified and intervened with victims of domestic violence, and were somewhat confident or very confident about addressing domestic violence issues with patients.
Recruitment ceased when the goal of 12 to 22 physicians in each medical specialty who had the relevant domestic violence experience was reached.
Focus Group Method and Data Collection
In comparison with survey or one-on-one interview formats, the focus group approach allows for a more extensive exploration of the area under discussion. Participants can collectively explore different experiences and perspectives, generate ideas, and debate and compare their ideas with those of others in the group.31 Six focus groups ranging in size from 6 to 11 individuals were conducted during a 3-week period in January and February 1998. Each group was facilitated by 2 moderators who were members of the research team. The sessions lasted approximately 90 minutes and were held in professional focus group settings that allowed hidden viewing. Several researchers viewed the groups from behind 2-way mirrors and completed field notes that were later compared with the observations of the moderators. Before each focus group session written informed consent was obtained from all participants and a written background survey was administered to gather demographic and practice information. Participants received a small stipend for participating. Study procedures were approved by the University of California San Francisco Committee on Human Research.
We used a semistructured guide that allowed the facilitators to follow certain topics and open new lines of inquiry when appropriate.32 Open-ended questions were formulated based on our previous interviews with survivors of domestic violence33 and a review of the literature ( Table 1 ). Audiotapes of the focus group sessions were transcribed by research staff; the principal investigator reviewed these transcripts for accuracy.
Coding and Analysis
For initial analysis we conducted multiple readings of transcripts to identify prominent themes. The investigators independently reviewed the transcripts and then met to review and discuss differences of opinion about interpretations and to further refine themes driven by the words and phrases of the participants. Through this process and the constant comparison of new data against emerging themes, a template of open codes was constructed. The transcripts were coded and specific themes within the narratives of the participants were identified in accordance with standard qualitative analytic convention.34 Coded data were organized using NUD*IST 4.0 software (Qualitative Solutions and Research; Victoria, Australia). This software helps ensure the consistency of study findings and creates an audit trail.35 The data were interpreted in the context of the original focus group sessions and the current literature. The final coding scheme and analysis of the findings were reviewed, and disagreements were discussed by the team until consensus was reached.
To further enhance the credibility of the findings, a qualitative technique called member check was used.36 Results were directed back to 3 research participants to confirm that their experiences and those of other participants in their focus group were reflected in the findings.
Results
Of the 80 physicians who were screened, 53 were eligible, and 45 were able to attend the focus group sessions. Their characteristics are presented in Table 2 . The participants reported that they had identified an average of 28 patients per year as having been physically abused by an intimate partner, and they thought they had helped approximately 60% of those patients.
Helpful Intervention Techniques
Even these physicians reported sometimes feeling overwhelmed, frustrated, and incompetent regarding their role in domestic violence cases. They believed, however, that addressing partner abuse was part of their job and reported various ways that they have tried to help battered women improve their situation and their health. Our data analyses revealed that the following themes were common across specialties.
Give Validating Messages. The most common aspect of intervention was validation. Whatever their approach to helping, these physicians gave compassionate messages that validated the woman’s worth as a human being and indicated that the abuse was undeserved. One participant put it this way: “Just my being there, caring about them consistently, giving another message [helped]: You are worth caring about, you are deserving, you are valuable.” Physicians tended to embed this kind of attitude and message into their interventions with abused patients, making validation the foundation of their interactions with them.
Break Through Denial and Plant Seeds for Change. Physicians reported that within the context of a trusting relationship they tried to break through the denial these women presented about the seriousness of their experiences. Some physicians reported labeling the abuse for what it is, blatantly wrong and criminal. They believed that over time they could help victims to begin to see this reality and change their situation. One participant said:
I let them know that what’s going on is outlandishly not right, that they don’t deserve to have that happen. It’s frankly illegal, and you can bring charges against someone for doing that. Sometimes people can be shocked by finding out that that’s the case. You can plant a seed about their self-esteem … and their ability over time to change that situation, but piecemeal.
Another physician reported showing women the photographs taken of past injuries to remind them of the partner’s pattern of abusive behavior: “We begin every session with: Do you remember that? Sometimes the reaction is: No, it didn’t happen that way. But the photograph just sits there.”
Listen Nonjudgmentally. Physicians described listening and attending to the whole person as central to providing good health care to all patients, especially victims of abuse. In the context of listening they reported on the need to maintain a healing attitude by banishing criticism, blame, and judgment, but agreed that achieving this was difficult and required letting go of the desire to fix it by treating the women as competent adults. One participant said:
I try to get across just from my tone of voice primarily, that I’m not judging them. Because I made that mistake quite a while ago—my judgment was right away: Well, this is terrible; you’ve got to get out. And I could watch the person psychologically fly away from me. So in order to maintain that [trusting] space, that connection with them, it’s really important for me to get clear that I’m going to listen and not judge them. And it’s all going to change on their time.
Document, Refer, and Help the Patient Plan for Safety. These physicians stated that they were careful to write down the specifics of what the woman said. In addition to medical charting, some took photographs of any injuries with color Polaroid cameras. One physician stated that for the photographs to be useful in court “you have to include their face so that a lawyer can’t argue that you’re taking a photograph of someone else.”
The most practicable example of documentation was the development of a domestic violence packet which included a body chart, an instruction list for documentation, a compartment for the color Polaroid photograph, a handy tear-out sheet for information services (resources, shelters), and a telephone number for the police.
In general when physicians knew or suspected abuse they offered information about domestic violence and referrals to local community resources, hot lines, and shelters. Some stated that patients often refused referrals and that they kept referral sheets in the waiting room so that individuals could decide on their own whether to take one.
Other physicians stated that on occasion women had made statements such as: “I can’t take that (handout) home … it’s like a flag in front of a bull.” To address this problem some physicians reported putting business-size cards with domestic violence hot line numbers (eg, local hot line numbers, shelter numbers, or community resource numbers) in all the bathrooms, sometimes the only place where the batterer could not easily follow a woman. Participants reported:
[The cards] are constantly replenished [by housekeeping] … and one of the things I tell people if they’re in an explosive situation is to put it in their shoe, in the insole.
I have a very small practice. I do only office gynecology, but I put about 10 cards a week [in the bathroom]. I would bet 2 disappear in a week. Isn’t that amazing? And this is a fairly affluent area.
Physicians described various ways they had tried to help women plan for their own immediate and ongoing safety. Some physicians talked about trying to stay aware and sensitive to the safety needs of women whose partners are controlling them through abuse, even when the partners are not currently threatening violence. One participant said:
I’ll try to role-play with them … how are they going to deal with telling their partner that they have this infection or that they really want to use this type of birth control. I’ll say, “Some people in your situation could have a fight with their significant other,” and go through predicting some possibilities. Sometimes you can see them start to close down because they know that could happen, or this is a repeated thing that they keep getting that they have no control over. So, I’ll say, “Well, I have other patients in this situation who sometimes need a safe place to go,” or I’ll talk about what somebody else did and at the same time give them some information.
Physicians also reported counseling victims to keep a suitcase packed and have 24-hour hot line numbers or contact numbers for safe places, and helping them to specify what circumstances should cause them to call the police.
Although physicians stated that acute cases were rare outside of the emergency department, they described attempts to ensure safety when the woman’s life was in immediate danger. These attempts included (1) working as a team to separate the partner from the woman (eg, the nurse talked with the abusive partner in the waiting room while the physician cared for the victim and, with the victim’s permission, called the police and a domestic violence advocate to remove her from the abusive home); (2) making excuses to separate the abuser from the victim in the immediate situation (eg, taking the woman for tests); and (3) admitting women who could not be placed in a shelter into the hospital under a false name. One physician reported that the hospital at which she had trained had a safe bed designated for victims of rape, domestic violence, and other assaults.
Using a Team Approach. In general, the physicians agreed that it takes a team approach to intervene successfully with victims of domestic violence. Some expressed frustration about accessing community referrals and discussed the benefits to victims of readily accessible resources on site. The on-site resources referred women directly to the nurse, rape crisis counselor, social worker, behavioral medicine counselor, or psychologist, who counseled the women and conducted follow-up. Some physicians without access to onsite counselors or social workers described making domestic violence part of every staff member’s educational process when they come on board.
Physicians described how intervention demanded a certain amount of flexibility of roles, with nurses and physicians playing off each other in tag-team fashion, as necessary. One physician said:
Sometimes when I finish with an exam, I’ll tell the nurse that I suspect something, so when the nurse is giving the discharge instructions, she’ll also re-approach certain kinds of issues and give the woman another opportunity to talk about [the abuse], once she has gotten dressed and composed herself. The door is closed. It’s one-on-one.
Some physicians described how their prenatal team takes advantage of a “window of opportunity” and has helped women get out of their situations and into counseling:
We have a prenatal team that really works together … our nurse, our social worker, our nutritionist, the receptionist, everybody.… It’s a real intense time. But I think once they get out of pregnancy, we really lose that ability to make a change in their lives. It’s a real window of opportunity.
Prioritize Domestic Violence. Even the committed physicians in our study expressed conflict about taking the time to intervene once they had identified abuse. Some physicians advocated dropping the medical procedure (even if that means the loss of reimbursement) to spend the rest of the patient’s time dealing with the abuse. Physicians also described prioritizing domestic violence by conducting continuing education courses and meetings for everyone in the department about rape, domestic violence, and child and elder abuse. One participant reported:
We try to create a culture of caring about domestic violence so that nurses who think they’ve recognized someone as being a nondeclared victim won’t be told, “I’m too busy” by a physician. And so when physicians say, “I think that might be a domestic violence victim, could you go talk to her?” the nurse will see that as a priority. And if anybody asks her, “How come you haven’t got that IV started?” she or he could say, “Because I was in talking to this person trying to determine whether they were a domestic violence victim.”
Small Victories Offer Positive Feedback
These physicians reported receiving little direct feedback about the effectiveness of their interventions with battered women. Yet, they also reported a range of rewards for intervening, from seeing a patient really change her life to glimpsing shifts in the way a woman thinks about herself and the relationship. One physician said:
And the rewarding piece for me comes when at some point she looks up and notices, and you can see this change of realizing that she’s cared about and then what that must mean to her, that she’s worth something. And then later on [there are] those little steps that you can see people make when they feel like they’re worth something. That’s the most ongoing and rewarding thing.
Discussion
The themes described by the purposive sample of physicians in our study offer insight into the process of intervention with victims of domestic violence and help delineate practicable examples of how to apply interventions ( Table 3 ). The behaviors described are supported by quantitative and qualitative data from battered women.33,37
These physicians described the foundation of intervention with victims as giving victims the message that they do not deserve abuse and that they are worth caring about. Battered women themselves report that validation is an important message. In a recent survey,37 battered women rated validating statements and compassion from physicians as among the most desirable interventions, equal to safety planning and offering referrals. In another study,33 survivors of domestic violence described how validation from a health care professional had not only provided relief and comfort, but also “started the wheels turning” toward realizing the seriousness of the situation. These women reported that validation helped them, regardless of whether they had disclosed the abuse or the health care professional had identified it.
Women who are being controlled through abuse by an intimate partner live with debilitating feelings of denial, shame, and humiliation that are sometimes reinforced in health care encounters and keep victims from seeking and receiving optimal care.33,38-41 The physicians in our study recognized these barriers and made efforts to help women break through their denial and plant seeds for change. They also made efforts—and learned through trial and error—to listen and be nonjudgmental. Both of these behaviors were rated as highly desirable by battered women.37 Physician statements made within the context of a trusting relationship can serve to remind women of the seriousness of their situation. Physician behaviors that convey respect through tone of voice and body language could lessen a victim’s shame and help her make small changes over time to improve her situation and her health.
The data we presented on documenting abuse, providing referrals, and planning for safety concur with the practices recommended by Physicians for a Violence-Free Society.42 We suggest that health care settings develop a domestic violence packet containing a body chart, documentation instructions, and referral sheets. We also suggest they provide Polaroid cameras to document specific injuries, since pictures offer an inviolable record of the abuse.42 Survivors report that the process of documenting abuse can serve to validate the individual if accompanied by genuine nonjudgmental statements of concern.33
Although the physicians in our study were aware of the need to provide victims with referrals to community resources and assess their safety needs,6,8,42,43 they had developed their own styles of intervention and admitted that victims sometimes refused referrals. One solution offered by participants in our study is to put easy-to-hide business-size cards with local domestic violence hot-line and shelter numbers in all of the bathrooms. We also suggest that physicians continue to offer referrals time after time: repetitive offering or availability of referrals may help survivors feel like they are not alone and may reassure them that support is available within and outside the health care system when they are ready to seek it. Physicians should remember that a woman may be able to talk about the abuse long before she can actualize any change. They should also be aware that ending the relationship does not necessarily end the abuse; it may escalate it.44 The study physicians were careful to consider safety from the battered woman’s point of view and to take preventive measures. We suggest that physicians review their options for facilitating safety (ie, availability of resources and time) and, when necessary, connect the victim by telephone to an agency trained in assessing and planning for their safety. Battered women report that they want physicians to offer referrals and help them plan for safety.37
Although current guidelines call for physicians to play a large role in identifying, intervening with, and following up on cases of partner abuse,6,45,46 the physicians in our study emphasized the need to work as a team to identify and provide optimal care to victims. This requires flexibility of roles within the health care team and ready access to on-site and community domestic violence resources. In an attempt to improve health care for victims of domestic violence, experts and researchers in the field have proposed simplifying and limiting the tasks of physicians in this area. One model uses the acronym AVDR: physicians should ask patients about abuse; provide validating messages that battering is wrong and the patient is a worthy individual; document presenting signs, symptoms, and disclosures; and refer victims to specialists in domestic violence.47 At that point specialists on site or on call from the community would assess the patient’s safety, make appropriate safety plans, and perform other in-depth interventions.
Physicians face ever-increasing demands on their limited time, yet these physicians committed to helping battered women found multiple ways to enable them to intervene. The holistic approaches described here—using a team approach, prioritizing domestic violence, developing a culture of caring—send a powerful message of prevention and intervention to victims: Battering is not a private, shameful issue, but a health care issue of great concern to physicians. These approaches also provide health care professionals with systematic support for helping battered women, perhaps allowing committed physicians to act as agents of change in battered women’s lives.5
Women who are being controlled by the abusive actions of their intimate partners report that even small signs of compassion from health care professionals have made a difference to them. As stated by physicians in this study and by survivors in our previous study,33 these acts of caring plant the seeds for change. In their efforts to help battered women, physicians must remember that incremental changes and small moments of recognition can eventually lead to major shifts in the lives of these women. Every time physicians successfully intervene with a person whose health problems are caused by abuse they have engendered a positive outcome.
Acknowledgments
Our project has been supported by the National Institute of Mental Health Grant #1 R01 MH51580. We thank the physicians who participated in the focus groups and those who participated in reviewing the study findings. We also thank Stephanie Greer and Survey Methods Group for their assistance in recruiting physician participants and organizing the focus groups; Candace Love, PhD, and Richard Carlton, MPH, for assisting the authors with moderating focus group sessions; Priscilla Abercrombie, NP, PhD, for assisting with coding the data; Karen Herzig, PhD, for assisting with the literature review; and Jennifer Fechner for transcribing the focus group session audiotapes and proofreading the manuscript.
1. Hamberger LK, Saunders DG, Hovey M. Prevalence of domestic violence in community practice and rate of physician inquiry. Fam Med 1992;24:283-87.
2. Rath GD, Jarratt LG, Leonardson G. Rates of domestic violence against adult women by men partners. J Am Board Fam Pract 1989;2:227-33.
3. Appleton W. The battered woman syndrome. Ann Emerg Med 1980;9:84-91.
4. Goldberg WG, Tomlanovich MC. Domestic violence in the emergency department: new findings. JAMA 1984;251:3259-64.
5. Chez R, Jones R. The battered woman. Am J Obstet Gynecol 1995;173:677-79.
6. American Medical Association Council on Scientific Affairs. Violence against women: relevance for medical practitioners. JAMA 1992;267:3184-89.
7. American College of Obstetricians and Gynecologists. The battered woman. Washington, DC: American College of Obstetricians and Gynecologists; 1989.
8. Sassetti MR. Domestic violence. Prim Care 1993;20:289-305.
9. Isaac NE, Sanchez RL. Emergency department response to battered women in Massachusetts. Ann Emerg Med 1994;23:855-58.
10. Waller AE, Hohenhaus SM, Shah PJ, Stern EA. Development and validation of an emergency department screening and referral protocol for victims of domestic violence. Ann Emerg Med 1996;27:754-60.
11. Tunis SR, Hayward RS, Wilson MC, et al. Internists’ attitudes about clinical practice guidelines. Ann Intern Med 1994;120:956-63.
12. Abbott J, Johnson R, Koziol-McLain J, Lowenstein SR. Domestic violence against women: incidence and prevalence in an emergency department population. JAMA 1995;273:1763-67.
13. Mazza D, Dennerstein L, Ryan V. Physical, sexual and emotional violence against women: a general practice-based prevalence study. Med J Aust 1996;164:14-17.
14. McGrath M, Hogan F, Peipert J. A prevalence survey of abuse and screening for abuse in urgent care patients. Obstet Gynecol 1998;91:511-14.
15. Caralis P, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997;90:1075-80.
16. Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999;131:578-84.
17. Sugg N, Thompson R, Thompson D, Maiuro R, Rivara F. Domestic violence and primary care. Arch Fam Med 1999;8:301-06.
18. Parsons LH, Zaccaro D, Wells B, Stovall TG. Methods of and attitudes toward screening obstetrics and gynecology patients for domestic violence. Am J Obstet Gynecol 1995;173:381-86; discussion386-87.
19. Olson L, Anctil C, Fullerton L, Brillman J, Arbuckle J, Sklar D. Increasing emergency physician recognition of domestic violence. Ann Emerg Med 1996;27:741-46.
20. Carbonell JL, Chez RA, Hassler RS. Florida physician and nurse education and practice related to domestic violence. Womens Health Issues 1995;5:203-07.
21. Lee D, Letellier P, McLoughlin E, Salber P. California hospital emergency departments response to domestic violence—survey report. San Francisco, Calif: Family Violence Prevention Fund; 1993.
22. Kurz D. Interventions with battered women in health care settings. Violence Vict 1990;5:243-56.
23. Kurz D. Emergency department responses to battered women: resistance to medicalization. Soc Probl 1987;34:69-81.
24. McGrath M, Bettacchi A, Duffy S, Peipert J, Becker B, St. Angelo L. Violence against women: provider barriers to intervention in emergency departments. Acad Emerg Med 1997;4:297-300.
25. Ferris LE. Canadian family physicians’ and general practitioners’ perceptions of their effectiveness in identifying and treating wife abuse. Med Care 1994;32:1163-72.
26. Ferris LE, Tudiver F. Family physicians’ approach to wife abuse: a study of Ontario, Canada, practices. Fam Med 1992;24:276-82.
27. Brown JB, Lent B, Sas G. Identifying and treating wife abuse. J Fam Pract 1993;36:185-91.
28. Sugg NK, Inui T. Primary care physicians’ response to domestic violence: opening Pandora’s box. JAMA 1992;267:3157-60.
29. Patton MQ. Qualitative evaluation and research methods. Newbury Park, Calif: Sage Publications; 1990.
30. Kuzel AJ. Sampling in qualitative inquiry. In: Crabtree BF, Miller WL, eds. Doing qualitative research. Newbury Park, Calif: Sage Publications; 1992;31-44.
31. Morgan DL. Focus groups as qualitative research. Beverly Hills, Calif: Sage Publications; 1988.
32. Stillman FA. Focus group research: an overview. In: Becker DM, Hill DR, Lackson JS, eds. Health behavior research in minority populations: access, design, and implementation. Bethesda, Md: US Department of Health and Human Services; 1992;168-75.
33. Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
34. Strauss AL, Corbin J. Basics of qualitative research: grounded theory procedures and techniques. Newbury Park, Calif: Sage Publications; 1990.
35. Sandelowski M. The problem of rigor in qualitative research. Adv Nurs Sci 1986;8:27-37.
36. Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills, Calif: Sage Publications; 1985.
37. Hamberger K, Ambuel B, Marbella A, Donze J. Physician interaction with battered women. Arch Fam Med 1998;7:575-82.
38. Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996;24:1-17.
39. Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996;5:153-58.
40. Martins R, Holzapfel S, Baker P. Wife abuse: are we detecting it? J Women Health 1992;1:77-80.
41. McCauley J, Yurk RA, Jenckes MW, Ford DE. Inside “Pandora’s box”: abused women’s experiences with clinicians and health services. J Gen Intern Med 1998;13:549-55.
42. Taliaferro E. Domestic violence: the need for good documentation. Action Notes: Physicians for a Violence-Free Society. 1997;23:1.-
43. American College of Obstetricians and Gynecologists. ACOG technical bulletin: domestic violence. Int J Gynecol Obstet 1995;51:161-70.
44. Salber PR, Taliaferro E. The physician’s guide to domestic violence: how to ask the right questions and recognize abuse. Volcano, Calif: Volcano Press, Inc; 1995.
45. Hyman A. Domestic violence: legal issues for health care practitioners and institutions. J Am Med Womens Assoc 1996;51:101-05.
46. Dutton MA, Mitchell B, Haywood Y. The emergency department as a violence prevention center. J Am Med Womens Assoc 1996;51:92-95, 117.
47. Gerbert B, Moe J, Caspers N, et al. Simplifying physicians’ response to domestic violence. West J Med 2000;172:329-31.
1. Hamberger LK, Saunders DG, Hovey M. Prevalence of domestic violence in community practice and rate of physician inquiry. Fam Med 1992;24:283-87.
2. Rath GD, Jarratt LG, Leonardson G. Rates of domestic violence against adult women by men partners. J Am Board Fam Pract 1989;2:227-33.
3. Appleton W. The battered woman syndrome. Ann Emerg Med 1980;9:84-91.
4. Goldberg WG, Tomlanovich MC. Domestic violence in the emergency department: new findings. JAMA 1984;251:3259-64.
5. Chez R, Jones R. The battered woman. Am J Obstet Gynecol 1995;173:677-79.
6. American Medical Association Council on Scientific Affairs. Violence against women: relevance for medical practitioners. JAMA 1992;267:3184-89.
7. American College of Obstetricians and Gynecologists. The battered woman. Washington, DC: American College of Obstetricians and Gynecologists; 1989.
8. Sassetti MR. Domestic violence. Prim Care 1993;20:289-305.
9. Isaac NE, Sanchez RL. Emergency department response to battered women in Massachusetts. Ann Emerg Med 1994;23:855-58.
10. Waller AE, Hohenhaus SM, Shah PJ, Stern EA. Development and validation of an emergency department screening and referral protocol for victims of domestic violence. Ann Emerg Med 1996;27:754-60.
11. Tunis SR, Hayward RS, Wilson MC, et al. Internists’ attitudes about clinical practice guidelines. Ann Intern Med 1994;120:956-63.
12. Abbott J, Johnson R, Koziol-McLain J, Lowenstein SR. Domestic violence against women: incidence and prevalence in an emergency department population. JAMA 1995;273:1763-67.
13. Mazza D, Dennerstein L, Ryan V. Physical, sexual and emotional violence against women: a general practice-based prevalence study. Med J Aust 1996;164:14-17.
14. McGrath M, Hogan F, Peipert J. A prevalence survey of abuse and screening for abuse in urgent care patients. Obstet Gynecol 1998;91:511-14.
15. Caralis P, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997;90:1075-80.
16. Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999;131:578-84.
17. Sugg N, Thompson R, Thompson D, Maiuro R, Rivara F. Domestic violence and primary care. Arch Fam Med 1999;8:301-06.
18. Parsons LH, Zaccaro D, Wells B, Stovall TG. Methods of and attitudes toward screening obstetrics and gynecology patients for domestic violence. Am J Obstet Gynecol 1995;173:381-86; discussion386-87.
19. Olson L, Anctil C, Fullerton L, Brillman J, Arbuckle J, Sklar D. Increasing emergency physician recognition of domestic violence. Ann Emerg Med 1996;27:741-46.
20. Carbonell JL, Chez RA, Hassler RS. Florida physician and nurse education and practice related to domestic violence. Womens Health Issues 1995;5:203-07.
21. Lee D, Letellier P, McLoughlin E, Salber P. California hospital emergency departments response to domestic violence—survey report. San Francisco, Calif: Family Violence Prevention Fund; 1993.
22. Kurz D. Interventions with battered women in health care settings. Violence Vict 1990;5:243-56.
23. Kurz D. Emergency department responses to battered women: resistance to medicalization. Soc Probl 1987;34:69-81.
24. McGrath M, Bettacchi A, Duffy S, Peipert J, Becker B, St. Angelo L. Violence against women: provider barriers to intervention in emergency departments. Acad Emerg Med 1997;4:297-300.
25. Ferris LE. Canadian family physicians’ and general practitioners’ perceptions of their effectiveness in identifying and treating wife abuse. Med Care 1994;32:1163-72.
26. Ferris LE, Tudiver F. Family physicians’ approach to wife abuse: a study of Ontario, Canada, practices. Fam Med 1992;24:276-82.
27. Brown JB, Lent B, Sas G. Identifying and treating wife abuse. J Fam Pract 1993;36:185-91.
28. Sugg NK, Inui T. Primary care physicians’ response to domestic violence: opening Pandora’s box. JAMA 1992;267:3157-60.
29. Patton MQ. Qualitative evaluation and research methods. Newbury Park, Calif: Sage Publications; 1990.
30. Kuzel AJ. Sampling in qualitative inquiry. In: Crabtree BF, Miller WL, eds. Doing qualitative research. Newbury Park, Calif: Sage Publications; 1992;31-44.
31. Morgan DL. Focus groups as qualitative research. Beverly Hills, Calif: Sage Publications; 1988.
32. Stillman FA. Focus group research: an overview. In: Becker DM, Hill DR, Lackson JS, eds. Health behavior research in minority populations: access, design, and implementation. Bethesda, Md: US Department of Health and Human Services; 1992;168-75.
33. Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999;29:115-35.
34. Strauss AL, Corbin J. Basics of qualitative research: grounded theory procedures and techniques. Newbury Park, Calif: Sage Publications; 1990.
35. Sandelowski M. The problem of rigor in qualitative research. Adv Nurs Sci 1986;8:27-37.
36. Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills, Calif: Sage Publications; 1985.
37. Hamberger K, Ambuel B, Marbella A, Donze J. Physician interaction with battered women. Arch Fam Med 1998;7:575-82.
38. Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996;24:1-17.
39. Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996;5:153-58.
40. Martins R, Holzapfel S, Baker P. Wife abuse: are we detecting it? J Women Health 1992;1:77-80.
41. McCauley J, Yurk RA, Jenckes MW, Ford DE. Inside “Pandora’s box”: abused women’s experiences with clinicians and health services. J Gen Intern Med 1998;13:549-55.
42. Taliaferro E. Domestic violence: the need for good documentation. Action Notes: Physicians for a Violence-Free Society. 1997;23:1.-
43. American College of Obstetricians and Gynecologists. ACOG technical bulletin: domestic violence. Int J Gynecol Obstet 1995;51:161-70.
44. Salber PR, Taliaferro E. The physician’s guide to domestic violence: how to ask the right questions and recognize abuse. Volcano, Calif: Volcano Press, Inc; 1995.
45. Hyman A. Domestic violence: legal issues for health care practitioners and institutions. J Am Med Womens Assoc 1996;51:101-05.
46. Dutton MA, Mitchell B, Haywood Y. The emergency department as a violence prevention center. J Am Med Womens Assoc 1996;51:92-95, 117.
47. Gerbert B, Moe J, Caspers N, et al. Simplifying physicians’ response to domestic violence. West J Med 2000;172:329-31.