User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Mainstreaming psychiatry
I commend Dr. Henry A. Nasrallah on his editorial, “Integrating psychiatry with other medical specialties” (From the Editor, Current Psychiatry, September 2010, p. 14-15). I could not agree more with the importance of fully integrating psychiatry into mainstream medical practice, and can attest that this can be accomplished. For the past year I have been part of a family practice where I work closely with the primary care physicians, nurse practitioners, and physician assistants. This practice has electronic medical records, and I have complete access to patients’ entire medical records, allowing other practitioners to read my psychiatric evaluations and progress notes. Being in the same location facilitates easy and frequent clinical exchange. The benefits to our patients are real and substantial.
Ralph G. Walton, MD
Family Health Medical Services
Mayville, NY
I commend Dr. Henry A. Nasrallah on his editorial, “Integrating psychiatry with other medical specialties” (From the Editor, Current Psychiatry, September 2010, p. 14-15). I could not agree more with the importance of fully integrating psychiatry into mainstream medical practice, and can attest that this can be accomplished. For the past year I have been part of a family practice where I work closely with the primary care physicians, nurse practitioners, and physician assistants. This practice has electronic medical records, and I have complete access to patients’ entire medical records, allowing other practitioners to read my psychiatric evaluations and progress notes. Being in the same location facilitates easy and frequent clinical exchange. The benefits to our patients are real and substantial.
Ralph G. Walton, MD
Family Health Medical Services
Mayville, NY
I commend Dr. Henry A. Nasrallah on his editorial, “Integrating psychiatry with other medical specialties” (From the Editor, Current Psychiatry, September 2010, p. 14-15). I could not agree more with the importance of fully integrating psychiatry into mainstream medical practice, and can attest that this can be accomplished. For the past year I have been part of a family practice where I work closely with the primary care physicians, nurse practitioners, and physician assistants. This practice has electronic medical records, and I have complete access to patients’ entire medical records, allowing other practitioners to read my psychiatric evaluations and progress notes. Being in the same location facilitates easy and frequent clinical exchange. The benefits to our patients are real and substantial.
Ralph G. Walton, MD
Family Health Medical Services
Mayville, NY
Med check distress
We read with distress “Successfully navigating the 15-minute ‘med check,’” (Malpractice Rx, Current Psychiatry, June 2010, p. 40-43). Even if 15-minute med checks have become “standard care,” they should not be. Unless a patient is stably medicated, 15 minutes is insufficient to evaluate the situation and make treatment decisions. Psychiatric diagnoses cannot be made by drawing blood or doing physical exams, so information beyond superficial questions must be elicited.
Does it make sense, as Table 2 suggests, that a psychiatrist should “have a psychotherapist or case manager present to facilitate communication?” Clearly not. Although theoretically possible, these therapists—apart from the question of their level of competency and training—are overworked and lack time to join psychiatric sessions.
Again, in Table 2, is apologizing sufficient “when a patient truly needs more time”? Clearly not. Although the author notes that intakes should warrant extra time, there is little awareness of the “real-life” difficulty involved in seeing patients who are not new to the clinic but new to a particular psychiatrist. Patients often arrive with as many as a dozen medications and multiple conflicting diagnoses. Charts are voluminous. To become thoroughly familiar with what has transpired takes a competent psychiatrist a minimum of 30 minutes to review. Rapid staff turnover and disconnected care exacerbate this problem.
Having worked in academic settings and in the field, we can state with certainty that dangerous shortcuts are now the norm. Who, if not the psychiatrist, will be addressing the fact that many of these patients have no teeth, out-of-control diabetes, no primary care physician, etc.? This raises more than malpractice issues, this raises quality-of-care issues.
Some days there are “no-shows” and some days every patient comes. In practice, the need for more than 15 minutes per patient exceeds the time gained when a patient does not keep an appointment.
Psychiatrists should serve as purveyors of quality care, not merely signers of prescriptions.
Elizabeth H. Levin, MD
Former director of residency training
Trenton Psychiatric Hospital
Former clinical associate professor
Robert Wood Johnson Medical School
Camden, NJ
Arthur H. Schwartz, MD
Retired professor of psychiatry
Robert Wood Johnson Medical School
Piscataway, NJ
Dr. Mossman responds
Unlike Drs. Levin and Schwartz, I am unwilling to declare that colleagues who conduct 15-minute med checks are, by that fact itself, doing something psychiatrists should not do. That does not mean 15-minute med checks are ideal. But several psychiatrists feel that despite severe time constraints, they can do many patients much good in 15 minutes—certainly more good than if those patients had no time with a psychiatrist at all. No scientific evidence that I know of contradicts this position.
Drs. Levin and Schwartz and I agree that certain types of patient visits require more than 15 minutes, which is why my column contained suggestions about negotiating for “seeing no more than 3 patients an hour, scheduling longer appointments for new patients, and having some built-in time to return phone calls, do paperwork, review charts, and complete progress notes.” The “strategies” listed in Table 2 are ideas about improving care and efficiency that come from psychiatrists with a lot of med check experience. Like most clinical suggestions, the strategies may make sense in some settings, but certainly not all.
Douglas Mossman, MD
Director
Glenn M. Weaver Institute of Law and Psychiatry
University of Cincinnati College of Medicine
Adjunct professor of clinical psychiatry
University of Cincinnati College of Medicine
Cincinnati, OH
We read with distress “Successfully navigating the 15-minute ‘med check,’” (Malpractice Rx, Current Psychiatry, June 2010, p. 40-43). Even if 15-minute med checks have become “standard care,” they should not be. Unless a patient is stably medicated, 15 minutes is insufficient to evaluate the situation and make treatment decisions. Psychiatric diagnoses cannot be made by drawing blood or doing physical exams, so information beyond superficial questions must be elicited.
Does it make sense, as Table 2 suggests, that a psychiatrist should “have a psychotherapist or case manager present to facilitate communication?” Clearly not. Although theoretically possible, these therapists—apart from the question of their level of competency and training—are overworked and lack time to join psychiatric sessions.
Again, in Table 2, is apologizing sufficient “when a patient truly needs more time”? Clearly not. Although the author notes that intakes should warrant extra time, there is little awareness of the “real-life” difficulty involved in seeing patients who are not new to the clinic but new to a particular psychiatrist. Patients often arrive with as many as a dozen medications and multiple conflicting diagnoses. Charts are voluminous. To become thoroughly familiar with what has transpired takes a competent psychiatrist a minimum of 30 minutes to review. Rapid staff turnover and disconnected care exacerbate this problem.
Having worked in academic settings and in the field, we can state with certainty that dangerous shortcuts are now the norm. Who, if not the psychiatrist, will be addressing the fact that many of these patients have no teeth, out-of-control diabetes, no primary care physician, etc.? This raises more than malpractice issues, this raises quality-of-care issues.
Some days there are “no-shows” and some days every patient comes. In practice, the need for more than 15 minutes per patient exceeds the time gained when a patient does not keep an appointment.
Psychiatrists should serve as purveyors of quality care, not merely signers of prescriptions.
Elizabeth H. Levin, MD
Former director of residency training
Trenton Psychiatric Hospital
Former clinical associate professor
Robert Wood Johnson Medical School
Camden, NJ
Arthur H. Schwartz, MD
Retired professor of psychiatry
Robert Wood Johnson Medical School
Piscataway, NJ
Dr. Mossman responds
Unlike Drs. Levin and Schwartz, I am unwilling to declare that colleagues who conduct 15-minute med checks are, by that fact itself, doing something psychiatrists should not do. That does not mean 15-minute med checks are ideal. But several psychiatrists feel that despite severe time constraints, they can do many patients much good in 15 minutes—certainly more good than if those patients had no time with a psychiatrist at all. No scientific evidence that I know of contradicts this position.
Drs. Levin and Schwartz and I agree that certain types of patient visits require more than 15 minutes, which is why my column contained suggestions about negotiating for “seeing no more than 3 patients an hour, scheduling longer appointments for new patients, and having some built-in time to return phone calls, do paperwork, review charts, and complete progress notes.” The “strategies” listed in Table 2 are ideas about improving care and efficiency that come from psychiatrists with a lot of med check experience. Like most clinical suggestions, the strategies may make sense in some settings, but certainly not all.
Douglas Mossman, MD
Director
Glenn M. Weaver Institute of Law and Psychiatry
University of Cincinnati College of Medicine
Adjunct professor of clinical psychiatry
University of Cincinnati College of Medicine
Cincinnati, OH
We read with distress “Successfully navigating the 15-minute ‘med check,’” (Malpractice Rx, Current Psychiatry, June 2010, p. 40-43). Even if 15-minute med checks have become “standard care,” they should not be. Unless a patient is stably medicated, 15 minutes is insufficient to evaluate the situation and make treatment decisions. Psychiatric diagnoses cannot be made by drawing blood or doing physical exams, so information beyond superficial questions must be elicited.
Does it make sense, as Table 2 suggests, that a psychiatrist should “have a psychotherapist or case manager present to facilitate communication?” Clearly not. Although theoretically possible, these therapists—apart from the question of their level of competency and training—are overworked and lack time to join psychiatric sessions.
Again, in Table 2, is apologizing sufficient “when a patient truly needs more time”? Clearly not. Although the author notes that intakes should warrant extra time, there is little awareness of the “real-life” difficulty involved in seeing patients who are not new to the clinic but new to a particular psychiatrist. Patients often arrive with as many as a dozen medications and multiple conflicting diagnoses. Charts are voluminous. To become thoroughly familiar with what has transpired takes a competent psychiatrist a minimum of 30 minutes to review. Rapid staff turnover and disconnected care exacerbate this problem.
Having worked in academic settings and in the field, we can state with certainty that dangerous shortcuts are now the norm. Who, if not the psychiatrist, will be addressing the fact that many of these patients have no teeth, out-of-control diabetes, no primary care physician, etc.? This raises more than malpractice issues, this raises quality-of-care issues.
Some days there are “no-shows” and some days every patient comes. In practice, the need for more than 15 minutes per patient exceeds the time gained when a patient does not keep an appointment.
Psychiatrists should serve as purveyors of quality care, not merely signers of prescriptions.
Elizabeth H. Levin, MD
Former director of residency training
Trenton Psychiatric Hospital
Former clinical associate professor
Robert Wood Johnson Medical School
Camden, NJ
Arthur H. Schwartz, MD
Retired professor of psychiatry
Robert Wood Johnson Medical School
Piscataway, NJ
Dr. Mossman responds
Unlike Drs. Levin and Schwartz, I am unwilling to declare that colleagues who conduct 15-minute med checks are, by that fact itself, doing something psychiatrists should not do. That does not mean 15-minute med checks are ideal. But several psychiatrists feel that despite severe time constraints, they can do many patients much good in 15 minutes—certainly more good than if those patients had no time with a psychiatrist at all. No scientific evidence that I know of contradicts this position.
Drs. Levin and Schwartz and I agree that certain types of patient visits require more than 15 minutes, which is why my column contained suggestions about negotiating for “seeing no more than 3 patients an hour, scheduling longer appointments for new patients, and having some built-in time to return phone calls, do paperwork, review charts, and complete progress notes.” The “strategies” listed in Table 2 are ideas about improving care and efficiency that come from psychiatrists with a lot of med check experience. Like most clinical suggestions, the strategies may make sense in some settings, but certainly not all.
Douglas Mossman, MD
Director
Glenn M. Weaver Institute of Law and Psychiatry
University of Cincinnati College of Medicine
Adjunct professor of clinical psychiatry
University of Cincinnati College of Medicine
Cincinnati, OH
Question BPD outcomes
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
In Drs. Ali M. Hashmi and Dennis Vowell’s article “The manipulative self-harmer” (Cases That Test Your Skills, Current Psychiatry, June 2010, p. 44-48), the authors regard the patient’s outcome (“Recently she was placed in a more restrictive setting because her hostile and self-destructive behavior escalated”) as characteristic of borderline personality disorder (BPD) (“Ms. L is no different from most axis II Cluster B disordered patients.”). In my view, this is the greatest risk of calling a patient borderline—it tends to justify poor outcomes by thinking that it is just characteristic of the illness. Instead, shouldn’t we worry that our treatment may be suboptimal? Maybe we are missing something?
For example, Ms. L may have some degree of bipolarity (see the Harvard Bipolarity Index as a characterization of that concept, incorporating but going beyond the DSM-IV-TR) that could account for their observation, “Her mood and behavior continue to oscillate; she is relatively calm and satisfied 1 week, angry and assaultive the next.” Instead of concluding, “this stormy course is expected…” the authors should be wondering whether they might be contributing to it by restarting venlafaxine despite simultaneous carbamazepine initiation. Granted, the possibilities of bipolarity and antidepressant-induced rapid cycling are complex considerations, because we lack solid footing for differentiating BPD and bipolar disorder and for determining causality when a patient experiences rapid mood changes while taking an antidepressant. These are controversial issues, but why present the case as though it’s illustrative of accepted principles? I find it perfectly illustrative of how badly we’re floundering as a field.
Jim Phelps, MD
PsychEducation.org
Corvallis, OR
The authors respond
Dr. Phelps’ contention is that our observation that Ms. L’s “hostile and self-destructive behavior” makes her “no different from most axis II Cluster B disordered patients” somehow understates the extent of her illness, perhaps leading to poorer outcomes. Negative countertransference toward such patients is the norm and handling it empathically is an integral part of the treatment relationship. This is true even though the severity of Ms. L’s personality pathology, as evidenced by her placement in the “911 program,” may not be representative of all patients with BPD.
We agree that “the possibilities of…antidepressant-induced rapid cycling are complex considerations.” Even experts disagree on this. In fact, as we pointed out, Ms. L resisted medication tapers, at one point insisting that high doses of fluoxetine and venafaxine be used together for depression, a request we denied specifically for fear of worsening her mood lability. Fluoxetine was discontinued and venlafaxine restarted at a lower dose to treat her persistent depression as well as to help with her chronic back pain. Because by this time she was taking carbamazepine as well, we felt the risk was acceptable. Her positive long-term outcome has validated our approach.
We disagree that psychiatry is “floundering” as a field. In fact, exchanges like this are a core component of placing our specialty on a more solid, scientific basis to position it for future challenges.
Ali M. Hashmi, MD
Medical director
Mid-South Health Systems
Jonesboro, AR
Clinical instructor
Department of psychiatry
University of Arkansas for Medical Science
College of Medicine
Little Rock, AR
Dennis Vowell, PsyD
Clinical psychologist
Mid-South Health Systems
Paragould, AR
Out-of-the-box questions about psychotherapy
As a National Institutes of Health-trained psychopharmacologist who also received substantial psychotherapy training during residency, I value both as pillars of psychiatric practice.
However, often I think about the evidence-based conduct of psychotherapy, which I regard as a neurobiologic treatment similar to drug therapy, and then I ask research questions that remain unanswered, such as:
- What is the therapeutic “dose” of psychotherapy? Does it differ by type of therapy or the patient’s diagnosis?
- Is the dose measured in the number of sessions or the time the patient is in a therapy session? Is there a loading dose? What is the maintenance dose?
- What is the optimal schedule for psychotherapy? By what established criteria does a therapist determine how often to administer psychotherapy? Why weekly and not daily? Why not 2 or 3 times a day intensive psychotherapy for acutely ill patients? Is the scheduling based on the cost to the patient, the therapist’s availability, or insurance coverage rather than the patient’s needs?
- How long should a session be? How was the weekly 50-minute session determined? Why not 10, 20, 30, or 40 minutes? Is 15 minutes 3 times a week more or less effective than 50 minutes once a week?
- What is the primary indication for a given psychotherapy? Why do therapists use the same psychotherapy for many different psychiatric disorders? Isn’t that like giving the same drug to everyone with any psychiatric illness? Is there such a thing as using a psychotherapeutic technique “off-label”? Why don’t therapy techniques come with a label like drug therapy?
- What is the best time of day to conduct psychotherapy to achieve maximum benefit? Patients are assigned a slot almost randomly between 8 am and 5 pm, but is early morning psychotherapy more effective than, say, mid-afternoon? Could going to sleep immediately after a session help consolidate memories, insights, learning, and emotional processing more than returning to one’s work setting or home, where many distractions may disrupt or erase the salutary neurobiologic effects of psychotherapy? If this could be proven with controlled studies then perhaps patients could schedule a nap right after a session in a dark cubicle adjacent to the therapist’s suite? This could result in a boom of “psychotherapy motels!”
- What effect does food have on psychotherapy efficacy? Is an empty stomach and hunger better or worse for patients? Would the borborygmi be distracting to some therapists? Is there a possible benefit for a postprandial session when serum glucose levels are higher? Could cognition be sharper for assimilating psychotherapy after eating vs before?
- Does ambient light intensity impact psychotherapy? Could ultra-bright light that is used for seasonal depression (10,000 lux vs the usual 100 lux fluorescent bulbs) placed in a patient’s field of vision during a session accentuate psychotherapy’s beneficial effects?
- What are the side effects of psychotherapy? Why is it assumed that psychotherapy exerts efficacy without any tolerability or safety problems? Can certain types of psychotherapy cause somatic adverse effects—such as headache, nausea, dizziness, or appetite and sleep changes—that are unwittingly attributed to the psychiatric illness rather than the treatment?
- Is there such a thing as psychotherapy overdose? What is it and what are its symptoms? Is it initiated by the patient, the therapist, or both?
- Could co-administration of modest doses of neurogenesis-enhancing drugs such as a selective serotonin reuptake inhibitor or lithium potentiate the effects of psychotherapy, because learning and memory are improved with neurogenesis-associated hippocampal growth?
- Does psychotherapy work differently in different age groups (adolescent vs adult vs middle age vs elderly) because of ongoing brain circuitry and neuroplastic changes throughout the life cycle?
- Are there “me too” psychotherapies similar to “me too” drugs?
- Can a combination of 2 or 3 different psychotherapies work better than a single psychotherapy? Could cognitive-behavioral therapy combined with psychodynamic psychotherapy exert higher efficacy then either alone?
- Assuming that ongoing psychotherapy costs about $100 per session and a patient receives 40 to 50 sessions a year for a total of $4,000 to $5,000 a year, why the outcry about medications that cost a similar amount?
- Is the adherence rate to psychotherapy similar to that of pharmacotherapy? Do some patients “intellectually cheek” an occasional psychotherapeutic dose?
- Is there a generic psychotherapy? Is it cheaper? Is it as good as “brand-name” psychotherapy?
I am sure readers realize that some of my questions are serious while others are tongue-in-cheek, but I hope my musings prompt you to join me in thinking outside the box about psychotherapy and the many gaps of knowledge that persist. Rigorous research is needed to substantiate or negate some current assumptions about the use of psychotherapy.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com, or go to our Web site at CurrentPsychiatry.com and click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com, or go to our Web site at CurrentPsychiatry.com and click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://CurrentPsychiatry.blogspot.com, or go to our Web site at CurrentPsychiatry.com and click on the “Send Letters” link.
As a National Institutes of Health-trained psychopharmacologist who also received substantial psychotherapy training during residency, I value both as pillars of psychiatric practice.
However, often I think about the evidence-based conduct of psychotherapy, which I regard as a neurobiologic treatment similar to drug therapy, and then I ask research questions that remain unanswered, such as:
- What is the therapeutic “dose” of psychotherapy? Does it differ by type of therapy or the patient’s diagnosis?
- Is the dose measured in the number of sessions or the time the patient is in a therapy session? Is there a loading dose? What is the maintenance dose?
- What is the optimal schedule for psychotherapy? By what established criteria does a therapist determine how often to administer psychotherapy? Why weekly and not daily? Why not 2 or 3 times a day intensive psychotherapy for acutely ill patients? Is the scheduling based on the cost to the patient, the therapist’s availability, or insurance coverage rather than the patient’s needs?
- How long should a session be? How was the weekly 50-minute session determined? Why not 10, 20, 30, or 40 minutes? Is 15 minutes 3 times a week more or less effective than 50 minutes once a week?
- What is the primary indication for a given psychotherapy? Why do therapists use the same psychotherapy for many different psychiatric disorders? Isn’t that like giving the same drug to everyone with any psychiatric illness? Is there such a thing as using a psychotherapeutic technique “off-label”? Why don’t therapy techniques come with a label like drug therapy?
- What is the best time of day to conduct psychotherapy to achieve maximum benefit? Patients are assigned a slot almost randomly between 8 am and 5 pm, but is early morning psychotherapy more effective than, say, mid-afternoon? Could going to sleep immediately after a session help consolidate memories, insights, learning, and emotional processing more than returning to one’s work setting or home, where many distractions may disrupt or erase the salutary neurobiologic effects of psychotherapy? If this could be proven with controlled studies then perhaps patients could schedule a nap right after a session in a dark cubicle adjacent to the therapist’s suite? This could result in a boom of “psychotherapy motels!”
- What effect does food have on psychotherapy efficacy? Is an empty stomach and hunger better or worse for patients? Would the borborygmi be distracting to some therapists? Is there a possible benefit for a postprandial session when serum glucose levels are higher? Could cognition be sharper for assimilating psychotherapy after eating vs before?
- Does ambient light intensity impact psychotherapy? Could ultra-bright light that is used for seasonal depression (10,000 lux vs the usual 100 lux fluorescent bulbs) placed in a patient’s field of vision during a session accentuate psychotherapy’s beneficial effects?
- What are the side effects of psychotherapy? Why is it assumed that psychotherapy exerts efficacy without any tolerability or safety problems? Can certain types of psychotherapy cause somatic adverse effects—such as headache, nausea, dizziness, or appetite and sleep changes—that are unwittingly attributed to the psychiatric illness rather than the treatment?
- Is there such a thing as psychotherapy overdose? What is it and what are its symptoms? Is it initiated by the patient, the therapist, or both?
- Could co-administration of modest doses of neurogenesis-enhancing drugs such as a selective serotonin reuptake inhibitor or lithium potentiate the effects of psychotherapy, because learning and memory are improved with neurogenesis-associated hippocampal growth?
- Does psychotherapy work differently in different age groups (adolescent vs adult vs middle age vs elderly) because of ongoing brain circuitry and neuroplastic changes throughout the life cycle?
- Are there “me too” psychotherapies similar to “me too” drugs?
- Can a combination of 2 or 3 different psychotherapies work better than a single psychotherapy? Could cognitive-behavioral therapy combined with psychodynamic psychotherapy exert higher efficacy then either alone?
- Assuming that ongoing psychotherapy costs about $100 per session and a patient receives 40 to 50 sessions a year for a total of $4,000 to $5,000 a year, why the outcry about medications that cost a similar amount?
- Is the adherence rate to psychotherapy similar to that of pharmacotherapy? Do some patients “intellectually cheek” an occasional psychotherapeutic dose?
- Is there a generic psychotherapy? Is it cheaper? Is it as good as “brand-name” psychotherapy?
I am sure readers realize that some of my questions are serious while others are tongue-in-cheek, but I hope my musings prompt you to join me in thinking outside the box about psychotherapy and the many gaps of knowledge that persist. Rigorous research is needed to substantiate or negate some current assumptions about the use of psychotherapy.
As a National Institutes of Health-trained psychopharmacologist who also received substantial psychotherapy training during residency, I value both as pillars of psychiatric practice.
However, often I think about the evidence-based conduct of psychotherapy, which I regard as a neurobiologic treatment similar to drug therapy, and then I ask research questions that remain unanswered, such as:
- What is the therapeutic “dose” of psychotherapy? Does it differ by type of therapy or the patient’s diagnosis?
- Is the dose measured in the number of sessions or the time the patient is in a therapy session? Is there a loading dose? What is the maintenance dose?
- What is the optimal schedule for psychotherapy? By what established criteria does a therapist determine how often to administer psychotherapy? Why weekly and not daily? Why not 2 or 3 times a day intensive psychotherapy for acutely ill patients? Is the scheduling based on the cost to the patient, the therapist’s availability, or insurance coverage rather than the patient’s needs?
- How long should a session be? How was the weekly 50-minute session determined? Why not 10, 20, 30, or 40 minutes? Is 15 minutes 3 times a week more or less effective than 50 minutes once a week?
- What is the primary indication for a given psychotherapy? Why do therapists use the same psychotherapy for many different psychiatric disorders? Isn’t that like giving the same drug to everyone with any psychiatric illness? Is there such a thing as using a psychotherapeutic technique “off-label”? Why don’t therapy techniques come with a label like drug therapy?
- What is the best time of day to conduct psychotherapy to achieve maximum benefit? Patients are assigned a slot almost randomly between 8 am and 5 pm, but is early morning psychotherapy more effective than, say, mid-afternoon? Could going to sleep immediately after a session help consolidate memories, insights, learning, and emotional processing more than returning to one’s work setting or home, where many distractions may disrupt or erase the salutary neurobiologic effects of psychotherapy? If this could be proven with controlled studies then perhaps patients could schedule a nap right after a session in a dark cubicle adjacent to the therapist’s suite? This could result in a boom of “psychotherapy motels!”
- What effect does food have on psychotherapy efficacy? Is an empty stomach and hunger better or worse for patients? Would the borborygmi be distracting to some therapists? Is there a possible benefit for a postprandial session when serum glucose levels are higher? Could cognition be sharper for assimilating psychotherapy after eating vs before?
- Does ambient light intensity impact psychotherapy? Could ultra-bright light that is used for seasonal depression (10,000 lux vs the usual 100 lux fluorescent bulbs) placed in a patient’s field of vision during a session accentuate psychotherapy’s beneficial effects?
- What are the side effects of psychotherapy? Why is it assumed that psychotherapy exerts efficacy without any tolerability or safety problems? Can certain types of psychotherapy cause somatic adverse effects—such as headache, nausea, dizziness, or appetite and sleep changes—that are unwittingly attributed to the psychiatric illness rather than the treatment?
- Is there such a thing as psychotherapy overdose? What is it and what are its symptoms? Is it initiated by the patient, the therapist, or both?
- Could co-administration of modest doses of neurogenesis-enhancing drugs such as a selective serotonin reuptake inhibitor or lithium potentiate the effects of psychotherapy, because learning and memory are improved with neurogenesis-associated hippocampal growth?
- Does psychotherapy work differently in different age groups (adolescent vs adult vs middle age vs elderly) because of ongoing brain circuitry and neuroplastic changes throughout the life cycle?
- Are there “me too” psychotherapies similar to “me too” drugs?
- Can a combination of 2 or 3 different psychotherapies work better than a single psychotherapy? Could cognitive-behavioral therapy combined with psychodynamic psychotherapy exert higher efficacy then either alone?
- Assuming that ongoing psychotherapy costs about $100 per session and a patient receives 40 to 50 sessions a year for a total of $4,000 to $5,000 a year, why the outcry about medications that cost a similar amount?
- Is the adherence rate to psychotherapy similar to that of pharmacotherapy? Do some patients “intellectually cheek” an occasional psychotherapeutic dose?
- Is there a generic psychotherapy? Is it cheaper? Is it as good as “brand-name” psychotherapy?
I am sure readers realize that some of my questions are serious while others are tongue-in-cheek, but I hope my musings prompt you to join me in thinking outside the box about psychotherapy and the many gaps of knowledge that persist. Rigorous research is needed to substantiate or negate some current assumptions about the use of psychotherapy.
Hallucinations in children: Diagnostic and treatment strategies
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/hallucinations-in-children-diagnostic.html#comments
Hallucinations in children are of grave concern to parents and clinicians, but aren’t necessarily a symptom of mental illness. In adults, hallucinations usually are linked to serious psychopathology; however, in children they are not uncommon and may be part of normal development (Box).
A hallucination is a false auditory, visual, gustatory, tactile, or olfactory perception not associated with real external stimuli.1 It must be differentiated from similar phenomenon such as illusions (misperception of actual stimuli), elaborate fantasies, imaginary companions, and eidetic images (visual images stored in memory).
Although hallucinations frequently are considered synonymous with psychotic disorders, in children this rare. Neurobiologic studies (fMRI) of adults show activation of Broca’s area (left inferior frontal gyrus) seconds before patients perceive auditory verbal hallucinations, which suggests that auditory hallucinations may be misidentified self-talk.a,b According to Piaget,c children age <7 may have difficulty distinguishing between events occurring while dreaming and awake. He further theorized that nonpathologic hallucinations could become pathologic when combined with trauma such as abuse. Straussd suggested that psychosis might lie on a continuum with normal phenomenon. In a case series, Wilking and Paulie described how developmental difficulties, deprivation, sociocultural conditions, and family relationships could contribute to impaired reality testing.
Imaginary friends or companions are common among all children. Children who have imaginary friends are more likely to report hearing “voices.”f Imaginary friends:
- appear, function, and disappear at the wish of the child
- pose no threat and often are a source of comfort
- often can be described in detail
- are not ego-dystonic.g
Also, children with imaginary friends will not show evidence of a thought disorder.
Source:
a. Shergill SS, Brammer MJ, Amaro E, et al. Temporal course of auditory hallucinations. Br J Psychiatry. 2004;185:516-517.
b. Shergill SS, Brammer JJ, Williams SC, et al. Mapping auditory hallucinations in schizophrenia; using functional magnetic resonance imaging. Arch Gen Psychiatry. 2000;57;1033-1038.
c. Piaget J. The child’s conception of the world. London, United Kingdom: Routledge and Kegan Paul; 1929.
d. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21:581-586.
e. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
f. Pearson D, Burrow A, FitzGerald C, et al. Auditory hallucinations in normal child populations. Pers Individ Dif. 2001;31:401-407.
g. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002.
Common, yet a cause for concern
Epidemiologic studies show 2.8% of adults report hallucinations before age 21.2 Nonpsychotic children as young as age 5 have reported hallucinations.3 Hallucinatory phenomenon may be present in 8% to 21% of all 11-year-old children; two-thirds of these patients have no DSM-IV-TR diagnosis.4,5 However, 1 evaluation of 62 nonpsychotic hallucinating children treated in a psychiatric emergency department (ED):
- 34% had depression
- 22% had attention-deficit/hyperactivity disorder (ADHD)
- 21% had disruptive behavior disorders
- 23% had other diagnoses.6
Studies suggest that children who have hallucinations but no other psychotic symptoms have a better long-term prognosis than those with additional psychotic symptoms.7 A 17-year longitudinal study of children with hallucinations and concurrent emotional and conduct problems found:
- up to 50% of patients still experience hallucinations at age 30
- hallucinations did not significantly predict clinical outcome at age 30
- childhood hallucinations did not increase the risk for psychosis, depression, organic brain disorder, or other psychiatric illnesses.7
In a study of children with psychosis and disruptive disorders, at 2- to 8-years follow-up 50% met criteria for major depressive disorder, bipolar disorder, or schizophreniform disorders.8 In a 15-year longitudinal study of 11-year-olds, self-reported psychotic symptoms—such as delusional beliefs and hallucinatory experiences—predicted a high risk of schizophreniform disorder at age 26.9 These studies suggest that experiencing significant disruptions in thoughts and perceptions during childhood may be related to later development of prominent mood and thought disorders.
Differential diagnosis
Table 1 lists possible causes of hallucination in children.6,10-13 Hallucinations during childhood can occur in the context of several psychiatric disorders, including:
They can also manifest as comorbid or associated symptoms of disorders not commonly associated with hallucinations, such as ADHD, disruptive disorders, anxiety disorders, and prodromal clinical states. Medications, substance use, and organic and metabolic disorders also must be considered in the differential diagnosis (Table 3).
Hallucinations may occur in low-functioning or anxious children, in the context of psychosocial adversity or abuse, and during bereavement of a deceased parent when the surviving parent is emotionally unavailable.11-13,15-17 Rule out hypnagogic and hypnopompic hallucinations, which are predominantly visual hallucinations that occur immediately before falling asleep and during the transition from sleep to wakefulness, respectively.18 Rarely, a child who has had hallucinations for some time may learn to complain of them when he or she is not hallucinating in order to obtain a primary or secondary gain, such as getting attention from caregivers.
Little is known about psychosis and hallucinations in preschoolers (age ≤5); therefore, their language use may help assessment. Because of cognitive immaturity, children often use illogical thinking and loose association and may describe their thoughts as “voices.” This is common in children with language disorders—and sometimes in healthy patients—who may talk about voices because they cannot describe their own thoughts.
Children with ADHD and/or oppositional defiant disorder often are impulsive and show poor judgment and may blame voices for telling them to do bad things. These “hallucinations” may represent internal thoughts battling with the child’s conscience.6 Auditory and visual hallucinations have been reported in children with Tourette syndrome, especially when associated with ADHD or obsessive-compulsive disorder.19
Medical causes. Electrolyte disturbances, metabolic disorders, fever, and serious infections are common nonpsychiatric causes of hallucinations.20 Brain neoplasm—particularly in visual association areas, the temporal lobe, or portions of the optic nerve or retina—also may produce hallucinations, which can be complex with full images.21
Medications such as steroids and anticholinergics may cause hallucinations. Case studies report visual and tactile hallucinations with methylphenidate therapy that resolve after discontinuing the medication.22 Illicit substances, including cannabis, lysergic acid diethylamide (LSD), cocaine, amphetamines, 3,4-methylenedioxymeth-amphetamine (ecstasy), opiates, and barbiturates, can induce hallucinations.
Suspect substance-induced hallucinations if your patient shows:
- acute onset of hallucinations
- dilated pupils
- extreme agitation or drowsiness
- other signs of intoxication.
Hallucinations caused by seizure disorders are rare but can be somatosensory, visual (occipital lobe focus), auditory, olfactory (uncinate, complex partial), or gustatory. The hallucinations may be unformed (flashing lights or rushing noises) or formed (images, spoken words, or music) and could be part of the aura arising from the temporal lobe (dreamlike, flashbacks). Command hallucinations are rare and adult and pediatric patients usually sense they are not real.23
Migraines occur in approximately 5% of prepubertal children and often are comorbid with affective and anxiety disorders.24 Hallucinations associated with migraine commonly are visual, but gustatory, olfactory, and auditory hallucinations also can occur, with or without headaches.3 Any hallucination associated with headaches should be investigated neurologically. Other diagnostic aspects of hallucinations to consider while interviewing children are listed in Table 4.25-28
Table 1
Possible causes of hallucinations in children and adolescents
| Normal development |
| Nonpsychotic psychopathology |
| Psychosocial adversity |
| Psychotic illness |
| Stress |
| Family dysfunction |
| Deprivation |
| Developmental difficulties |
| Sociocultural interaction (immigration) |
| Poorly differentiated male and female family roles |
| Presence or absence of different mother figures |
| Cultural factors (witches, ghosts, spiritualism) |
| Hallucination of deceased parent, when unresolved mourning persists in the surviving parent |
| Source: References 6,10-13 |
Table 2
Content of hallucinations may point to their cause
| Schizophrenia or other psychotic disorders | May hear several voices making a critical commentary Command hallucinations telling patients to harm themselves or others Bizarre voices like ‘a computer in my head’ or aliens Voices of someone familiar or a ‘relative’ Visual hallucinations of devils, scary faces, space creatures, and skeletons |
| Depressive disorders | Usually a single voice speaking from outside the patient’s head with derogatory or suicidal content |
| Bipolar disorder | Usually involves grandiose ideas about power, worth, knowledge, family, or relationship |
| Bereavement | Usually a transient (visual or auditory) perception of the deceased person |
| Posttraumatic stress disorder | Transient visual hallucinations, usually with phobic content |
| Source: Reference 11 | |
Table 3
Hallucinations in young patients: Differential diagnoses
Psychiatric disorders that are usually defined by psychotic features, including:
|
Psychiatric disorders that commonly do not include hallucinations but in which hallucinations can occur as comorbid or associated symptoms, such as:
|
| Prodromal and at-risk clinical states of psychiatric disorders (psychotic and mood disorders) |
| Medications (steroids, anticholinergics, stimulants) |
Drug intoxication and abuse
|
Organic or nonpsychiatric disorders
|
Metabolic disorders
|
| Source: a. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625. b. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380. c. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581. d. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002. e. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34. f. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785. g. Sosland MD, Edelsohn GA. Hallucinations in children and adolescents. Curr Psychiatry Rep. 2005;7:180-188. |
Table 4
Diagnostic considerations when assessing a hallucinating child
| General: |
| Hallucinations are a symptom, not a diagnosis |
| They can have a developmental, neurologic, metabolic, or psychiatric basis |
| Visual, gustatory, and olfactory hallucinations suggest a medical- or substance-related origin |
| Schizophrenia is rare before age 11 |
| In pervasive developmental disorders, schizophrenia is diagnosed only if prominent delusions and hallucinations are present for at least 1 month |
| Hallucinations are not uncommon in major depressive disorder but may be associated with higher risk of bipolar disorder |
| During interviewing, remember that children: |
| are highly suggestible |
| may answer questions in the affirmative to get attention or to please the interviewer |
| may not fully or partially understand what is being asked |
| may blame their misbehavior on voices to escape punishment |
| may not distinguish between night terrors and illusions |
| Source:References 25-28 |
Psychotic disorder not otherwise specified
(NOS) in children often is overused and misused. One reason could be that DSM-IV-TR does not have a category for hallucinations in nonpsychotic children or for children who are at risk for psychosis. However, recommendations regarding the diagnosis of psychotic disorder NOS note it:
- may be used if uncertainty persists after ruling out all other diagnoses
- should be avoided when hallucinations occur in nonpsychotic children
- should not be used longitudinally if a clinician later determines a specific disorder accounts for the hallucinations.29
Treatment
Addressing underlying medical or psychiatric illness, including substance use, is primary. Some adolescents or children may think that cannabis use is relatively benign. Discuss the risks of cannabis use in an age-appropriate manner.
In the ED. Children or adolescents who present with hallucinations in the ED should undergo a thorough evaluation that explores the differential diagnoses. Suggestions for evaluating patients in this setting appear in Table 5.21
Prodromal or at-risk children. There is no consensus on how early to initiate treatment for children in the prodromal stages of psychosis. Early identification and treatment is imperative because duration of untreated psychosis (DUP) is a primary predictor of treatment response in first-admission patients, and longer DUP corresponds to poorer prognosis in children.30
Assessment scales for early identification of psychosis have limitations because most are not standardized for use in children age <14. To assess symptoms and predict future psychosis in children consider using:
- Scale of Prodromal Symptoms
- Structured Interview for Prodromal Symptoms
- Comprehensive Assessment of At-Risk Mental States
- Bonn Scale for the Assessment of Basic Symptoms.
A hallucinating child may be considered prodromal if he or she has:
- 30% drop in Global Assessment Functioning score in the past month
- a first-degree relative with affective or nonaffective psychotic disorder or schizotypal personality disorder.31
Antipsychotics. When treating children, use antipsychotics with caution and consider short- and long-term risks and benefits. Early treatment is indicated when hallucinations are among a patient’s psychotic symptoms; however, antipsychotic use for children in the prodromal phase lacks consensus. McGlashan et al32 showed that in 60 high-risk patients (mean age 16), olanzapine, 5 to 15 mg/d, reduced conversion to psychosis by 50% over 6 months. McGorry et al33 observed that in 59 ultra-high risk patients (mean age 20), adding low-dose risperidone (1 to 2 mg/d) and cognitive-behavioral therapy (CBT) was superior to case management and supportive psychotherapy in preventing psychosis after 6 months of treatment, but this difference was not maintained at 6 months of follow-up.
CBT slows progression to psychosis in ultra-high risk patients and reduces positive symptoms more specifically than it improves emotional dysfunction.34 CBT for psychosis is based on the concept that auditory hallucinations have an underlying personalized meaning or cognitive schema.35 The initial goal of treatment is to engage the child and understand:
- What do the hallucinations mean to the patient?
- How did they start?
- Can the child start or stop them?
- What does the patient think they are?
The clinician then strives to help the child identify alternative explanations for these hallucinations and develop coping strategies.36 “Normalizing” the voices helps the child attribute these voices to a less anxiety-provoking cause.37 Consider suggesting common reasons for the hallucinations, such as:
- lack of sleep
- isolation
- dehydration
- extreme stress
- strong thoughts (obsessions)
- fever and illness
- lack of food
- drugs and alcohol.
If your patient learns that any of these reasons could explain the hallucinations, he or she may start to have a less delusional understanding of them. Suggest that the voices are “real” only if your patient believes it.
Help children develop coping strategies to control auditory hallucinations such as:
- humming
- listening to music
- reading (forwards and backwards)
- talking to others
- exercising
- singing
- medication
- ignoring the voices.
With normalization and other coping strategies, children with visual hallucinations can learn to transform in their mind the frightful image to a funnier one, which is less anxiety-provoking and gives them a sense of control.
Table 5
Suggestions for evaluating hallucinating children in the ED
| Evaluate risk factors for suicidality |
| Rule out medical and neurologic causes, including substance abuse/intoxication |
| Identify underlying psychopathological, psychosocial, and cultural factors |
| Contact key adult informants for collateral information |
| Decide if hallucinations are psychotic or nonpsychotic |
| Reassure your patients that hearing voices does not mean that they are ‘crazy’ |
| Evaluate hallucinations in the context of other features of psychoses (onset, frequency, severity, and chronicity) |
| Initiate psychotherapy and antidepressants if needed for patients with underlying depression, anxiety, or PTSD |
| ED: emergency department; PTSD: posttraumatic stress disorder Source: Reference 21 |
Related Resources
- Bartels-Velthuis AA, Jenner JA, van de Willige G, et al. Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
- Cepeda C. Psychotic symptoms in children and adolescents: assessment, differential diagnosis, and treatment. New York, NY: Routledge; 2007.
Drug Brand Names
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sadock BJ, Sadock VA. Kaplan and Sadock’s concise textbook of clinical psychiatry. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:26.
2. Fenning S, Susser ES, Pilowsky DJ, et al. Childhood hallucinations preceding the first psychotic episode. J Nerv Ment Dis. 1997;185:115-117.
3. Schreier HA. Auditory hallucinations in nonpsychotic children with affective syndromes and migraines: report of 13 cases. J Child Neurol. 1998;13:377-382.
4. McGee R, Williams S, Poulton R. Hallucinations in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 2000;39:12-13.
5. Yoshizumi T, Murase S, Honjo S, et al. Hallucinatory experiences in a community sample of Japanese children. J Am Acad Child Adolesc Psychiatry. 2004;43:1030-1036.
6. Edelsohn GA, Rabinovich H, Portnoy R. Hallucinations in nonpsychotic children: findings from a psychiatric emergency service. Ann N Y Acad Sciences. 2003;1008:261-264.
7. Rothstein A. Hallucinatory phenomenon in childhood: a critique of the literature. J Am Acad Child Psychiatry. 1981;20:623-635.
8. Nicholson R, Lenane M, Brookner F, et al. Children and adolescents with psychotic disorder not otherwise specified: a 2- to 8-year follow-up study. Compr Psychiatry. 2001;42:319-325.
9. Poulton R, Caspi A, Moffitt TE, et al. Children’s self reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57:1053-1058.
10. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
11. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625.
12. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380.
13. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581.
14. Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. 9th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2003:1276-1277,1283.
15. Famularo R, Kinscherff R, Fenton T. Psychiatric diagnosis of maltreated children: preliminary findings. J Am Acad Child Adolesc Psychiatry. 1992;31:863-867.
16. Putnam FW, Peterson G. Further validation of the child dissociative checklist. Dissociation. 1994;7:204-211.
17. Kaufman J, Birmaher B, Clayton S, et al. Case study: trauma-related hallucinations. J Am Acad Child Adolesc Psychiatry. 1997;36(11):1602-1605.
18. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005.
19. Kerbeshian J, Burd L. Are schizophreniform symptoms present in attenuated form in children with Tourette Disorder and other developmental disorders? Can J Psychiatry. 1987;32(2):123-135.
20. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34.
21. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785.
22. Gross-Tsur V, Joseph A, Shalev RS. Hallucinations during methylphenidate therapy. Neurology. 2004;63:753-754.
23. Wyllie E. The treatment of epilepsy: principles and practices, Philadelphia, PA: Lippincott Williams and Wilkins; 1993.
24. Saeed MA, Pumariega AJ, Cinciripini PM. Psychopharmacological management of migraine in children in children and adolescents. J Child Adolesc Psychopharmacol. 1992;2:199-211.
25. Chambers WJ, Puig-Antich J, Tabrizi MA, et al. Psychotic symptoms in prepubertal major depressive disorder. Arch Gen Psychiatry. 1982;39:921-927.
26. Volkmar FR. Childhood and adolescent psychosis: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. 1996;35:843-851.
27. First MB, Frances A, Pincus HA. DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press; 1995.
28. Birmaher B, Ryan ND, Williamson DE, et al. Childhood and adolescent depression: a review of the past 10 years. Part I. J Am Acad Child Adolesc Psychiatry. 1996;35:1427-1439.
29. Meyer SE, Bearden CE, Lux CR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
30. Drake RJ, Haley CJ, Akhtar S, et al. Causes and consequences of duration of untreated psychosis in schizophrenia. Br J Psychiatry. 2000;177:511-515.
31. McGorry PD, Yung AR, Phillips LJ. The “close-in” or ultra high-risk model: a safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr Bull. 2003;29(4):771-790.
32. McGlashan TH, Zipursky RB, Perkins DO, et al. Olanzapine versus placebo treatment of schizophrenia prodrome: one year results. Poster presented at: International Congress of Schizophrenia Research, Colorado Springs, CO, April-May 2003.
33. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry. 2002;59:921-928.
34. French P, Shryane N, Bentall RP, et al. Effects of cognitive therapy on the longitudinal development of psychotic experiences in people at high risk of developing psychosis. Br J Psychiatry Suppl. 2007;51:s82-87.
35. Turkington D, Siddle R. Cognitive therapy for the treatment of delusions. Advances in Psychiatric Treatment. 1998;4:235-242.
36. Sosland MD, Pinninti N. Five ways to quiet auditory hallucinations. Current Psychiatry. 2005;4:40.-
37. Kingdon DG, Turkington D. Cognitive behavioral therapy of schizophrenia, New York, NY: Guilford Press; 1994.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/hallucinations-in-children-diagnostic.html#comments
Hallucinations in children are of grave concern to parents and clinicians, but aren’t necessarily a symptom of mental illness. In adults, hallucinations usually are linked to serious psychopathology; however, in children they are not uncommon and may be part of normal development (Box).
A hallucination is a false auditory, visual, gustatory, tactile, or olfactory perception not associated with real external stimuli.1 It must be differentiated from similar phenomenon such as illusions (misperception of actual stimuli), elaborate fantasies, imaginary companions, and eidetic images (visual images stored in memory).
Although hallucinations frequently are considered synonymous with psychotic disorders, in children this rare. Neurobiologic studies (fMRI) of adults show activation of Broca’s area (left inferior frontal gyrus) seconds before patients perceive auditory verbal hallucinations, which suggests that auditory hallucinations may be misidentified self-talk.a,b According to Piaget,c children age <7 may have difficulty distinguishing between events occurring while dreaming and awake. He further theorized that nonpathologic hallucinations could become pathologic when combined with trauma such as abuse. Straussd suggested that psychosis might lie on a continuum with normal phenomenon. In a case series, Wilking and Paulie described how developmental difficulties, deprivation, sociocultural conditions, and family relationships could contribute to impaired reality testing.
Imaginary friends or companions are common among all children. Children who have imaginary friends are more likely to report hearing “voices.”f Imaginary friends:
- appear, function, and disappear at the wish of the child
- pose no threat and often are a source of comfort
- often can be described in detail
- are not ego-dystonic.g
Also, children with imaginary friends will not show evidence of a thought disorder.
Source:
a. Shergill SS, Brammer MJ, Amaro E, et al. Temporal course of auditory hallucinations. Br J Psychiatry. 2004;185:516-517.
b. Shergill SS, Brammer JJ, Williams SC, et al. Mapping auditory hallucinations in schizophrenia; using functional magnetic resonance imaging. Arch Gen Psychiatry. 2000;57;1033-1038.
c. Piaget J. The child’s conception of the world. London, United Kingdom: Routledge and Kegan Paul; 1929.
d. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21:581-586.
e. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
f. Pearson D, Burrow A, FitzGerald C, et al. Auditory hallucinations in normal child populations. Pers Individ Dif. 2001;31:401-407.
g. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002.
Common, yet a cause for concern
Epidemiologic studies show 2.8% of adults report hallucinations before age 21.2 Nonpsychotic children as young as age 5 have reported hallucinations.3 Hallucinatory phenomenon may be present in 8% to 21% of all 11-year-old children; two-thirds of these patients have no DSM-IV-TR diagnosis.4,5 However, 1 evaluation of 62 nonpsychotic hallucinating children treated in a psychiatric emergency department (ED):
- 34% had depression
- 22% had attention-deficit/hyperactivity disorder (ADHD)
- 21% had disruptive behavior disorders
- 23% had other diagnoses.6
Studies suggest that children who have hallucinations but no other psychotic symptoms have a better long-term prognosis than those with additional psychotic symptoms.7 A 17-year longitudinal study of children with hallucinations and concurrent emotional and conduct problems found:
- up to 50% of patients still experience hallucinations at age 30
- hallucinations did not significantly predict clinical outcome at age 30
- childhood hallucinations did not increase the risk for psychosis, depression, organic brain disorder, or other psychiatric illnesses.7
In a study of children with psychosis and disruptive disorders, at 2- to 8-years follow-up 50% met criteria for major depressive disorder, bipolar disorder, or schizophreniform disorders.8 In a 15-year longitudinal study of 11-year-olds, self-reported psychotic symptoms—such as delusional beliefs and hallucinatory experiences—predicted a high risk of schizophreniform disorder at age 26.9 These studies suggest that experiencing significant disruptions in thoughts and perceptions during childhood may be related to later development of prominent mood and thought disorders.
Differential diagnosis
Table 1 lists possible causes of hallucination in children.6,10-13 Hallucinations during childhood can occur in the context of several psychiatric disorders, including:
They can also manifest as comorbid or associated symptoms of disorders not commonly associated with hallucinations, such as ADHD, disruptive disorders, anxiety disorders, and prodromal clinical states. Medications, substance use, and organic and metabolic disorders also must be considered in the differential diagnosis (Table 3).
Hallucinations may occur in low-functioning or anxious children, in the context of psychosocial adversity or abuse, and during bereavement of a deceased parent when the surviving parent is emotionally unavailable.11-13,15-17 Rule out hypnagogic and hypnopompic hallucinations, which are predominantly visual hallucinations that occur immediately before falling asleep and during the transition from sleep to wakefulness, respectively.18 Rarely, a child who has had hallucinations for some time may learn to complain of them when he or she is not hallucinating in order to obtain a primary or secondary gain, such as getting attention from caregivers.
Little is known about psychosis and hallucinations in preschoolers (age ≤5); therefore, their language use may help assessment. Because of cognitive immaturity, children often use illogical thinking and loose association and may describe their thoughts as “voices.” This is common in children with language disorders—and sometimes in healthy patients—who may talk about voices because they cannot describe their own thoughts.
Children with ADHD and/or oppositional defiant disorder often are impulsive and show poor judgment and may blame voices for telling them to do bad things. These “hallucinations” may represent internal thoughts battling with the child’s conscience.6 Auditory and visual hallucinations have been reported in children with Tourette syndrome, especially when associated with ADHD or obsessive-compulsive disorder.19
Medical causes. Electrolyte disturbances, metabolic disorders, fever, and serious infections are common nonpsychiatric causes of hallucinations.20 Brain neoplasm—particularly in visual association areas, the temporal lobe, or portions of the optic nerve or retina—also may produce hallucinations, which can be complex with full images.21
Medications such as steroids and anticholinergics may cause hallucinations. Case studies report visual and tactile hallucinations with methylphenidate therapy that resolve after discontinuing the medication.22 Illicit substances, including cannabis, lysergic acid diethylamide (LSD), cocaine, amphetamines, 3,4-methylenedioxymeth-amphetamine (ecstasy), opiates, and barbiturates, can induce hallucinations.
Suspect substance-induced hallucinations if your patient shows:
- acute onset of hallucinations
- dilated pupils
- extreme agitation or drowsiness
- other signs of intoxication.
Hallucinations caused by seizure disorders are rare but can be somatosensory, visual (occipital lobe focus), auditory, olfactory (uncinate, complex partial), or gustatory. The hallucinations may be unformed (flashing lights or rushing noises) or formed (images, spoken words, or music) and could be part of the aura arising from the temporal lobe (dreamlike, flashbacks). Command hallucinations are rare and adult and pediatric patients usually sense they are not real.23
Migraines occur in approximately 5% of prepubertal children and often are comorbid with affective and anxiety disorders.24 Hallucinations associated with migraine commonly are visual, but gustatory, olfactory, and auditory hallucinations also can occur, with or without headaches.3 Any hallucination associated with headaches should be investigated neurologically. Other diagnostic aspects of hallucinations to consider while interviewing children are listed in Table 4.25-28
Table 1
Possible causes of hallucinations in children and adolescents
| Normal development |
| Nonpsychotic psychopathology |
| Psychosocial adversity |
| Psychotic illness |
| Stress |
| Family dysfunction |
| Deprivation |
| Developmental difficulties |
| Sociocultural interaction (immigration) |
| Poorly differentiated male and female family roles |
| Presence or absence of different mother figures |
| Cultural factors (witches, ghosts, spiritualism) |
| Hallucination of deceased parent, when unresolved mourning persists in the surviving parent |
| Source: References 6,10-13 |
Table 2
Content of hallucinations may point to their cause
| Schizophrenia or other psychotic disorders | May hear several voices making a critical commentary Command hallucinations telling patients to harm themselves or others Bizarre voices like ‘a computer in my head’ or aliens Voices of someone familiar or a ‘relative’ Visual hallucinations of devils, scary faces, space creatures, and skeletons |
| Depressive disorders | Usually a single voice speaking from outside the patient’s head with derogatory or suicidal content |
| Bipolar disorder | Usually involves grandiose ideas about power, worth, knowledge, family, or relationship |
| Bereavement | Usually a transient (visual or auditory) perception of the deceased person |
| Posttraumatic stress disorder | Transient visual hallucinations, usually with phobic content |
| Source: Reference 11 | |
Table 3
Hallucinations in young patients: Differential diagnoses
Psychiatric disorders that are usually defined by psychotic features, including:
|
Psychiatric disorders that commonly do not include hallucinations but in which hallucinations can occur as comorbid or associated symptoms, such as:
|
| Prodromal and at-risk clinical states of psychiatric disorders (psychotic and mood disorders) |
| Medications (steroids, anticholinergics, stimulants) |
Drug intoxication and abuse
|
Organic or nonpsychiatric disorders
|
Metabolic disorders
|
| Source: a. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625. b. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380. c. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581. d. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002. e. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34. f. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785. g. Sosland MD, Edelsohn GA. Hallucinations in children and adolescents. Curr Psychiatry Rep. 2005;7:180-188. |
Table 4
Diagnostic considerations when assessing a hallucinating child
| General: |
| Hallucinations are a symptom, not a diagnosis |
| They can have a developmental, neurologic, metabolic, or psychiatric basis |
| Visual, gustatory, and olfactory hallucinations suggest a medical- or substance-related origin |
| Schizophrenia is rare before age 11 |
| In pervasive developmental disorders, schizophrenia is diagnosed only if prominent delusions and hallucinations are present for at least 1 month |
| Hallucinations are not uncommon in major depressive disorder but may be associated with higher risk of bipolar disorder |
| During interviewing, remember that children: |
| are highly suggestible |
| may answer questions in the affirmative to get attention or to please the interviewer |
| may not fully or partially understand what is being asked |
| may blame their misbehavior on voices to escape punishment |
| may not distinguish between night terrors and illusions |
| Source:References 25-28 |
Psychotic disorder not otherwise specified
(NOS) in children often is overused and misused. One reason could be that DSM-IV-TR does not have a category for hallucinations in nonpsychotic children or for children who are at risk for psychosis. However, recommendations regarding the diagnosis of psychotic disorder NOS note it:
- may be used if uncertainty persists after ruling out all other diagnoses
- should be avoided when hallucinations occur in nonpsychotic children
- should not be used longitudinally if a clinician later determines a specific disorder accounts for the hallucinations.29
Treatment
Addressing underlying medical or psychiatric illness, including substance use, is primary. Some adolescents or children may think that cannabis use is relatively benign. Discuss the risks of cannabis use in an age-appropriate manner.
In the ED. Children or adolescents who present with hallucinations in the ED should undergo a thorough evaluation that explores the differential diagnoses. Suggestions for evaluating patients in this setting appear in Table 5.21
Prodromal or at-risk children. There is no consensus on how early to initiate treatment for children in the prodromal stages of psychosis. Early identification and treatment is imperative because duration of untreated psychosis (DUP) is a primary predictor of treatment response in first-admission patients, and longer DUP corresponds to poorer prognosis in children.30
Assessment scales for early identification of psychosis have limitations because most are not standardized for use in children age <14. To assess symptoms and predict future psychosis in children consider using:
- Scale of Prodromal Symptoms
- Structured Interview for Prodromal Symptoms
- Comprehensive Assessment of At-Risk Mental States
- Bonn Scale for the Assessment of Basic Symptoms.
A hallucinating child may be considered prodromal if he or she has:
- 30% drop in Global Assessment Functioning score in the past month
- a first-degree relative with affective or nonaffective psychotic disorder or schizotypal personality disorder.31
Antipsychotics. When treating children, use antipsychotics with caution and consider short- and long-term risks and benefits. Early treatment is indicated when hallucinations are among a patient’s psychotic symptoms; however, antipsychotic use for children in the prodromal phase lacks consensus. McGlashan et al32 showed that in 60 high-risk patients (mean age 16), olanzapine, 5 to 15 mg/d, reduced conversion to psychosis by 50% over 6 months. McGorry et al33 observed that in 59 ultra-high risk patients (mean age 20), adding low-dose risperidone (1 to 2 mg/d) and cognitive-behavioral therapy (CBT) was superior to case management and supportive psychotherapy in preventing psychosis after 6 months of treatment, but this difference was not maintained at 6 months of follow-up.
CBT slows progression to psychosis in ultra-high risk patients and reduces positive symptoms more specifically than it improves emotional dysfunction.34 CBT for psychosis is based on the concept that auditory hallucinations have an underlying personalized meaning or cognitive schema.35 The initial goal of treatment is to engage the child and understand:
- What do the hallucinations mean to the patient?
- How did they start?
- Can the child start or stop them?
- What does the patient think they are?
The clinician then strives to help the child identify alternative explanations for these hallucinations and develop coping strategies.36 “Normalizing” the voices helps the child attribute these voices to a less anxiety-provoking cause.37 Consider suggesting common reasons for the hallucinations, such as:
- lack of sleep
- isolation
- dehydration
- extreme stress
- strong thoughts (obsessions)
- fever and illness
- lack of food
- drugs and alcohol.
If your patient learns that any of these reasons could explain the hallucinations, he or she may start to have a less delusional understanding of them. Suggest that the voices are “real” only if your patient believes it.
Help children develop coping strategies to control auditory hallucinations such as:
- humming
- listening to music
- reading (forwards and backwards)
- talking to others
- exercising
- singing
- medication
- ignoring the voices.
With normalization and other coping strategies, children with visual hallucinations can learn to transform in their mind the frightful image to a funnier one, which is less anxiety-provoking and gives them a sense of control.
Table 5
Suggestions for evaluating hallucinating children in the ED
| Evaluate risk factors for suicidality |
| Rule out medical and neurologic causes, including substance abuse/intoxication |
| Identify underlying psychopathological, psychosocial, and cultural factors |
| Contact key adult informants for collateral information |
| Decide if hallucinations are psychotic or nonpsychotic |
| Reassure your patients that hearing voices does not mean that they are ‘crazy’ |
| Evaluate hallucinations in the context of other features of psychoses (onset, frequency, severity, and chronicity) |
| Initiate psychotherapy and antidepressants if needed for patients with underlying depression, anxiety, or PTSD |
| ED: emergency department; PTSD: posttraumatic stress disorder Source: Reference 21 |
Related Resources
- Bartels-Velthuis AA, Jenner JA, van de Willige G, et al. Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
- Cepeda C. Psychotic symptoms in children and adolescents: assessment, differential diagnosis, and treatment. New York, NY: Routledge; 2007.
Drug Brand Names
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/hallucinations-in-children-diagnostic.html#comments
Hallucinations in children are of grave concern to parents and clinicians, but aren’t necessarily a symptom of mental illness. In adults, hallucinations usually are linked to serious psychopathology; however, in children they are not uncommon and may be part of normal development (Box).
A hallucination is a false auditory, visual, gustatory, tactile, or olfactory perception not associated with real external stimuli.1 It must be differentiated from similar phenomenon such as illusions (misperception of actual stimuli), elaborate fantasies, imaginary companions, and eidetic images (visual images stored in memory).
Although hallucinations frequently are considered synonymous with psychotic disorders, in children this rare. Neurobiologic studies (fMRI) of adults show activation of Broca’s area (left inferior frontal gyrus) seconds before patients perceive auditory verbal hallucinations, which suggests that auditory hallucinations may be misidentified self-talk.a,b According to Piaget,c children age <7 may have difficulty distinguishing between events occurring while dreaming and awake. He further theorized that nonpathologic hallucinations could become pathologic when combined with trauma such as abuse. Straussd suggested that psychosis might lie on a continuum with normal phenomenon. In a case series, Wilking and Paulie described how developmental difficulties, deprivation, sociocultural conditions, and family relationships could contribute to impaired reality testing.
Imaginary friends or companions are common among all children. Children who have imaginary friends are more likely to report hearing “voices.”f Imaginary friends:
- appear, function, and disappear at the wish of the child
- pose no threat and often are a source of comfort
- often can be described in detail
- are not ego-dystonic.g
Also, children with imaginary friends will not show evidence of a thought disorder.
Source:
a. Shergill SS, Brammer MJ, Amaro E, et al. Temporal course of auditory hallucinations. Br J Psychiatry. 2004;185:516-517.
b. Shergill SS, Brammer JJ, Williams SC, et al. Mapping auditory hallucinations in schizophrenia; using functional magnetic resonance imaging. Arch Gen Psychiatry. 2000;57;1033-1038.
c. Piaget J. The child’s conception of the world. London, United Kingdom: Routledge and Kegan Paul; 1929.
d. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21:581-586.
e. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
f. Pearson D, Burrow A, FitzGerald C, et al. Auditory hallucinations in normal child populations. Pers Individ Dif. 2001;31:401-407.
g. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002.
Common, yet a cause for concern
Epidemiologic studies show 2.8% of adults report hallucinations before age 21.2 Nonpsychotic children as young as age 5 have reported hallucinations.3 Hallucinatory phenomenon may be present in 8% to 21% of all 11-year-old children; two-thirds of these patients have no DSM-IV-TR diagnosis.4,5 However, 1 evaluation of 62 nonpsychotic hallucinating children treated in a psychiatric emergency department (ED):
- 34% had depression
- 22% had attention-deficit/hyperactivity disorder (ADHD)
- 21% had disruptive behavior disorders
- 23% had other diagnoses.6
Studies suggest that children who have hallucinations but no other psychotic symptoms have a better long-term prognosis than those with additional psychotic symptoms.7 A 17-year longitudinal study of children with hallucinations and concurrent emotional and conduct problems found:
- up to 50% of patients still experience hallucinations at age 30
- hallucinations did not significantly predict clinical outcome at age 30
- childhood hallucinations did not increase the risk for psychosis, depression, organic brain disorder, or other psychiatric illnesses.7
In a study of children with psychosis and disruptive disorders, at 2- to 8-years follow-up 50% met criteria for major depressive disorder, bipolar disorder, or schizophreniform disorders.8 In a 15-year longitudinal study of 11-year-olds, self-reported psychotic symptoms—such as delusional beliefs and hallucinatory experiences—predicted a high risk of schizophreniform disorder at age 26.9 These studies suggest that experiencing significant disruptions in thoughts and perceptions during childhood may be related to later development of prominent mood and thought disorders.
Differential diagnosis
Table 1 lists possible causes of hallucination in children.6,10-13 Hallucinations during childhood can occur in the context of several psychiatric disorders, including:
They can also manifest as comorbid or associated symptoms of disorders not commonly associated with hallucinations, such as ADHD, disruptive disorders, anxiety disorders, and prodromal clinical states. Medications, substance use, and organic and metabolic disorders also must be considered in the differential diagnosis (Table 3).
Hallucinations may occur in low-functioning or anxious children, in the context of psychosocial adversity or abuse, and during bereavement of a deceased parent when the surviving parent is emotionally unavailable.11-13,15-17 Rule out hypnagogic and hypnopompic hallucinations, which are predominantly visual hallucinations that occur immediately before falling asleep and during the transition from sleep to wakefulness, respectively.18 Rarely, a child who has had hallucinations for some time may learn to complain of them when he or she is not hallucinating in order to obtain a primary or secondary gain, such as getting attention from caregivers.
Little is known about psychosis and hallucinations in preschoolers (age ≤5); therefore, their language use may help assessment. Because of cognitive immaturity, children often use illogical thinking and loose association and may describe their thoughts as “voices.” This is common in children with language disorders—and sometimes in healthy patients—who may talk about voices because they cannot describe their own thoughts.
Children with ADHD and/or oppositional defiant disorder often are impulsive and show poor judgment and may blame voices for telling them to do bad things. These “hallucinations” may represent internal thoughts battling with the child’s conscience.6 Auditory and visual hallucinations have been reported in children with Tourette syndrome, especially when associated with ADHD or obsessive-compulsive disorder.19
Medical causes. Electrolyte disturbances, metabolic disorders, fever, and serious infections are common nonpsychiatric causes of hallucinations.20 Brain neoplasm—particularly in visual association areas, the temporal lobe, or portions of the optic nerve or retina—also may produce hallucinations, which can be complex with full images.21
Medications such as steroids and anticholinergics may cause hallucinations. Case studies report visual and tactile hallucinations with methylphenidate therapy that resolve after discontinuing the medication.22 Illicit substances, including cannabis, lysergic acid diethylamide (LSD), cocaine, amphetamines, 3,4-methylenedioxymeth-amphetamine (ecstasy), opiates, and barbiturates, can induce hallucinations.
Suspect substance-induced hallucinations if your patient shows:
- acute onset of hallucinations
- dilated pupils
- extreme agitation or drowsiness
- other signs of intoxication.
Hallucinations caused by seizure disorders are rare but can be somatosensory, visual (occipital lobe focus), auditory, olfactory (uncinate, complex partial), or gustatory. The hallucinations may be unformed (flashing lights or rushing noises) or formed (images, spoken words, or music) and could be part of the aura arising from the temporal lobe (dreamlike, flashbacks). Command hallucinations are rare and adult and pediatric patients usually sense they are not real.23
Migraines occur in approximately 5% of prepubertal children and often are comorbid with affective and anxiety disorders.24 Hallucinations associated with migraine commonly are visual, but gustatory, olfactory, and auditory hallucinations also can occur, with or without headaches.3 Any hallucination associated with headaches should be investigated neurologically. Other diagnostic aspects of hallucinations to consider while interviewing children are listed in Table 4.25-28
Table 1
Possible causes of hallucinations in children and adolescents
| Normal development |
| Nonpsychotic psychopathology |
| Psychosocial adversity |
| Psychotic illness |
| Stress |
| Family dysfunction |
| Deprivation |
| Developmental difficulties |
| Sociocultural interaction (immigration) |
| Poorly differentiated male and female family roles |
| Presence or absence of different mother figures |
| Cultural factors (witches, ghosts, spiritualism) |
| Hallucination of deceased parent, when unresolved mourning persists in the surviving parent |
| Source: References 6,10-13 |
Table 2
Content of hallucinations may point to their cause
| Schizophrenia or other psychotic disorders | May hear several voices making a critical commentary Command hallucinations telling patients to harm themselves or others Bizarre voices like ‘a computer in my head’ or aliens Voices of someone familiar or a ‘relative’ Visual hallucinations of devils, scary faces, space creatures, and skeletons |
| Depressive disorders | Usually a single voice speaking from outside the patient’s head with derogatory or suicidal content |
| Bipolar disorder | Usually involves grandiose ideas about power, worth, knowledge, family, or relationship |
| Bereavement | Usually a transient (visual or auditory) perception of the deceased person |
| Posttraumatic stress disorder | Transient visual hallucinations, usually with phobic content |
| Source: Reference 11 | |
Table 3
Hallucinations in young patients: Differential diagnoses
Psychiatric disorders that are usually defined by psychotic features, including:
|
Psychiatric disorders that commonly do not include hallucinations but in which hallucinations can occur as comorbid or associated symptoms, such as:
|
| Prodromal and at-risk clinical states of psychiatric disorders (psychotic and mood disorders) |
| Medications (steroids, anticholinergics, stimulants) |
Drug intoxication and abuse
|
Organic or nonpsychiatric disorders
|
Metabolic disorders
|
| Source: a. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625. b. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380. c. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581. d. Lewis M. Child and adolescent psychiatry: a comprehensive textbook. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2002. e. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34. f. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785. g. Sosland MD, Edelsohn GA. Hallucinations in children and adolescents. Curr Psychiatry Rep. 2005;7:180-188. |
Table 4
Diagnostic considerations when assessing a hallucinating child
| General: |
| Hallucinations are a symptom, not a diagnosis |
| They can have a developmental, neurologic, metabolic, or psychiatric basis |
| Visual, gustatory, and olfactory hallucinations suggest a medical- or substance-related origin |
| Schizophrenia is rare before age 11 |
| In pervasive developmental disorders, schizophrenia is diagnosed only if prominent delusions and hallucinations are present for at least 1 month |
| Hallucinations are not uncommon in major depressive disorder but may be associated with higher risk of bipolar disorder |
| During interviewing, remember that children: |
| are highly suggestible |
| may answer questions in the affirmative to get attention or to please the interviewer |
| may not fully or partially understand what is being asked |
| may blame their misbehavior on voices to escape punishment |
| may not distinguish between night terrors and illusions |
| Source:References 25-28 |
Psychotic disorder not otherwise specified
(NOS) in children often is overused and misused. One reason could be that DSM-IV-TR does not have a category for hallucinations in nonpsychotic children or for children who are at risk for psychosis. However, recommendations regarding the diagnosis of psychotic disorder NOS note it:
- may be used if uncertainty persists after ruling out all other diagnoses
- should be avoided when hallucinations occur in nonpsychotic children
- should not be used longitudinally if a clinician later determines a specific disorder accounts for the hallucinations.29
Treatment
Addressing underlying medical or psychiatric illness, including substance use, is primary. Some adolescents or children may think that cannabis use is relatively benign. Discuss the risks of cannabis use in an age-appropriate manner.
In the ED. Children or adolescents who present with hallucinations in the ED should undergo a thorough evaluation that explores the differential diagnoses. Suggestions for evaluating patients in this setting appear in Table 5.21
Prodromal or at-risk children. There is no consensus on how early to initiate treatment for children in the prodromal stages of psychosis. Early identification and treatment is imperative because duration of untreated psychosis (DUP) is a primary predictor of treatment response in first-admission patients, and longer DUP corresponds to poorer prognosis in children.30
Assessment scales for early identification of psychosis have limitations because most are not standardized for use in children age <14. To assess symptoms and predict future psychosis in children consider using:
- Scale of Prodromal Symptoms
- Structured Interview for Prodromal Symptoms
- Comprehensive Assessment of At-Risk Mental States
- Bonn Scale for the Assessment of Basic Symptoms.
A hallucinating child may be considered prodromal if he or she has:
- 30% drop in Global Assessment Functioning score in the past month
- a first-degree relative with affective or nonaffective psychotic disorder or schizotypal personality disorder.31
Antipsychotics. When treating children, use antipsychotics with caution and consider short- and long-term risks and benefits. Early treatment is indicated when hallucinations are among a patient’s psychotic symptoms; however, antipsychotic use for children in the prodromal phase lacks consensus. McGlashan et al32 showed that in 60 high-risk patients (mean age 16), olanzapine, 5 to 15 mg/d, reduced conversion to psychosis by 50% over 6 months. McGorry et al33 observed that in 59 ultra-high risk patients (mean age 20), adding low-dose risperidone (1 to 2 mg/d) and cognitive-behavioral therapy (CBT) was superior to case management and supportive psychotherapy in preventing psychosis after 6 months of treatment, but this difference was not maintained at 6 months of follow-up.
CBT slows progression to psychosis in ultra-high risk patients and reduces positive symptoms more specifically than it improves emotional dysfunction.34 CBT for psychosis is based on the concept that auditory hallucinations have an underlying personalized meaning or cognitive schema.35 The initial goal of treatment is to engage the child and understand:
- What do the hallucinations mean to the patient?
- How did they start?
- Can the child start or stop them?
- What does the patient think they are?
The clinician then strives to help the child identify alternative explanations for these hallucinations and develop coping strategies.36 “Normalizing” the voices helps the child attribute these voices to a less anxiety-provoking cause.37 Consider suggesting common reasons for the hallucinations, such as:
- lack of sleep
- isolation
- dehydration
- extreme stress
- strong thoughts (obsessions)
- fever and illness
- lack of food
- drugs and alcohol.
If your patient learns that any of these reasons could explain the hallucinations, he or she may start to have a less delusional understanding of them. Suggest that the voices are “real” only if your patient believes it.
Help children develop coping strategies to control auditory hallucinations such as:
- humming
- listening to music
- reading (forwards and backwards)
- talking to others
- exercising
- singing
- medication
- ignoring the voices.
With normalization and other coping strategies, children with visual hallucinations can learn to transform in their mind the frightful image to a funnier one, which is less anxiety-provoking and gives them a sense of control.
Table 5
Suggestions for evaluating hallucinating children in the ED
| Evaluate risk factors for suicidality |
| Rule out medical and neurologic causes, including substance abuse/intoxication |
| Identify underlying psychopathological, psychosocial, and cultural factors |
| Contact key adult informants for collateral information |
| Decide if hallucinations are psychotic or nonpsychotic |
| Reassure your patients that hearing voices does not mean that they are ‘crazy’ |
| Evaluate hallucinations in the context of other features of psychoses (onset, frequency, severity, and chronicity) |
| Initiate psychotherapy and antidepressants if needed for patients with underlying depression, anxiety, or PTSD |
| ED: emergency department; PTSD: posttraumatic stress disorder Source: Reference 21 |
Related Resources
- Bartels-Velthuis AA, Jenner JA, van de Willige G, et al. Prevalence and correlates of auditory vocal hallucinations in middle childhood. Br J Psychiatry. 2010;196(1):41-46.
- Cepeda C. Psychotic symptoms in children and adolescents: assessment, differential diagnosis, and treatment. New York, NY: Routledge; 2007.
Drug Brand Names
- Methylphenidate • Ritalin
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sadock BJ, Sadock VA. Kaplan and Sadock’s concise textbook of clinical psychiatry. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:26.
2. Fenning S, Susser ES, Pilowsky DJ, et al. Childhood hallucinations preceding the first psychotic episode. J Nerv Ment Dis. 1997;185:115-117.
3. Schreier HA. Auditory hallucinations in nonpsychotic children with affective syndromes and migraines: report of 13 cases. J Child Neurol. 1998;13:377-382.
4. McGee R, Williams S, Poulton R. Hallucinations in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 2000;39:12-13.
5. Yoshizumi T, Murase S, Honjo S, et al. Hallucinatory experiences in a community sample of Japanese children. J Am Acad Child Adolesc Psychiatry. 2004;43:1030-1036.
6. Edelsohn GA, Rabinovich H, Portnoy R. Hallucinations in nonpsychotic children: findings from a psychiatric emergency service. Ann N Y Acad Sciences. 2003;1008:261-264.
7. Rothstein A. Hallucinatory phenomenon in childhood: a critique of the literature. J Am Acad Child Psychiatry. 1981;20:623-635.
8. Nicholson R, Lenane M, Brookner F, et al. Children and adolescents with psychotic disorder not otherwise specified: a 2- to 8-year follow-up study. Compr Psychiatry. 2001;42:319-325.
9. Poulton R, Caspi A, Moffitt TE, et al. Children’s self reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57:1053-1058.
10. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
11. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625.
12. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380.
13. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581.
14. Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. 9th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2003:1276-1277,1283.
15. Famularo R, Kinscherff R, Fenton T. Psychiatric diagnosis of maltreated children: preliminary findings. J Am Acad Child Adolesc Psychiatry. 1992;31:863-867.
16. Putnam FW, Peterson G. Further validation of the child dissociative checklist. Dissociation. 1994;7:204-211.
17. Kaufman J, Birmaher B, Clayton S, et al. Case study: trauma-related hallucinations. J Am Acad Child Adolesc Psychiatry. 1997;36(11):1602-1605.
18. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005.
19. Kerbeshian J, Burd L. Are schizophreniform symptoms present in attenuated form in children with Tourette Disorder and other developmental disorders? Can J Psychiatry. 1987;32(2):123-135.
20. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34.
21. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785.
22. Gross-Tsur V, Joseph A, Shalev RS. Hallucinations during methylphenidate therapy. Neurology. 2004;63:753-754.
23. Wyllie E. The treatment of epilepsy: principles and practices, Philadelphia, PA: Lippincott Williams and Wilkins; 1993.
24. Saeed MA, Pumariega AJ, Cinciripini PM. Psychopharmacological management of migraine in children in children and adolescents. J Child Adolesc Psychopharmacol. 1992;2:199-211.
25. Chambers WJ, Puig-Antich J, Tabrizi MA, et al. Psychotic symptoms in prepubertal major depressive disorder. Arch Gen Psychiatry. 1982;39:921-927.
26. Volkmar FR. Childhood and adolescent psychosis: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. 1996;35:843-851.
27. First MB, Frances A, Pincus HA. DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press; 1995.
28. Birmaher B, Ryan ND, Williamson DE, et al. Childhood and adolescent depression: a review of the past 10 years. Part I. J Am Acad Child Adolesc Psychiatry. 1996;35:1427-1439.
29. Meyer SE, Bearden CE, Lux CR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
30. Drake RJ, Haley CJ, Akhtar S, et al. Causes and consequences of duration of untreated psychosis in schizophrenia. Br J Psychiatry. 2000;177:511-515.
31. McGorry PD, Yung AR, Phillips LJ. The “close-in” or ultra high-risk model: a safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr Bull. 2003;29(4):771-790.
32. McGlashan TH, Zipursky RB, Perkins DO, et al. Olanzapine versus placebo treatment of schizophrenia prodrome: one year results. Poster presented at: International Congress of Schizophrenia Research, Colorado Springs, CO, April-May 2003.
33. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry. 2002;59:921-928.
34. French P, Shryane N, Bentall RP, et al. Effects of cognitive therapy on the longitudinal development of psychotic experiences in people at high risk of developing psychosis. Br J Psychiatry Suppl. 2007;51:s82-87.
35. Turkington D, Siddle R. Cognitive therapy for the treatment of delusions. Advances in Psychiatric Treatment. 1998;4:235-242.
36. Sosland MD, Pinninti N. Five ways to quiet auditory hallucinations. Current Psychiatry. 2005;4:40.-
37. Kingdon DG, Turkington D. Cognitive behavioral therapy of schizophrenia, New York, NY: Guilford Press; 1994.
1. Sadock BJ, Sadock VA. Kaplan and Sadock’s concise textbook of clinical psychiatry. 3rd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:26.
2. Fenning S, Susser ES, Pilowsky DJ, et al. Childhood hallucinations preceding the first psychotic episode. J Nerv Ment Dis. 1997;185:115-117.
3. Schreier HA. Auditory hallucinations in nonpsychotic children with affective syndromes and migraines: report of 13 cases. J Child Neurol. 1998;13:377-382.
4. McGee R, Williams S, Poulton R. Hallucinations in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 2000;39:12-13.
5. Yoshizumi T, Murase S, Honjo S, et al. Hallucinatory experiences in a community sample of Japanese children. J Am Acad Child Adolesc Psychiatry. 2004;43:1030-1036.
6. Edelsohn GA, Rabinovich H, Portnoy R. Hallucinations in nonpsychotic children: findings from a psychiatric emergency service. Ann N Y Acad Sciences. 2003;1008:261-264.
7. Rothstein A. Hallucinatory phenomenon in childhood: a critique of the literature. J Am Acad Child Psychiatry. 1981;20:623-635.
8. Nicholson R, Lenane M, Brookner F, et al. Children and adolescents with psychotic disorder not otherwise specified: a 2- to 8-year follow-up study. Compr Psychiatry. 2001;42:319-325.
9. Poulton R, Caspi A, Moffitt TE, et al. Children’s self reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57:1053-1058.
10. Wilking VN, Paoli C. The hallucinatory experience: an attempt at a psychodynamic classification and reconsideration of its diagnostic significance. J Am Acad Child Psychiatry. 1966;5:431-440.
11. Schreier HA. Hallucinations in nonpsychotic children: more common than we think? J Am Acad Child Adolesc Psychiatry. 1999;38(5):623-625.
12. Kotsopoulos S, Konigsberg J, Cote A, et al. Hallucinatory experiences in nonpsychotic children. J Am Acad Child Adolesc Psychiatry. 1987;26:375-380.
13. Yates TT, Bannard JR. The “haunted” child: grief, hallucinations and family dynamics. J Am Acad Child Adolesc Psychiatry. 1988;27:573-581.
14. Sadock BJ, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry. 9th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2003:1276-1277,1283.
15. Famularo R, Kinscherff R, Fenton T. Psychiatric diagnosis of maltreated children: preliminary findings. J Am Acad Child Adolesc Psychiatry. 1992;31:863-867.
16. Putnam FW, Peterson G. Further validation of the child dissociative checklist. Dissociation. 1994;7:204-211.
17. Kaufman J, Birmaher B, Clayton S, et al. Case study: trauma-related hallucinations. J Am Acad Child Adolesc Psychiatry. 1997;36(11):1602-1605.
18. Sadock BJ, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry. 8th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2005.
19. Kerbeshian J, Burd L. Are schizophreniform symptoms present in attenuated form in children with Tourette Disorder and other developmental disorders? Can J Psychiatry. 1987;32(2):123-135.
20. Pao M, Lohman C, Gracey D, et al. Visual, tactile, and phobic hallucinations: recognition and management in the emergency department. Pediatr Emerg Care. 2004;20:30-34.
21. Edelsohn GA. Hallucinations in children and adolescents: considerations in the emergency setting. Am J Psychiatry. 2006;163(5):781-785.
22. Gross-Tsur V, Joseph A, Shalev RS. Hallucinations during methylphenidate therapy. Neurology. 2004;63:753-754.
23. Wyllie E. The treatment of epilepsy: principles and practices, Philadelphia, PA: Lippincott Williams and Wilkins; 1993.
24. Saeed MA, Pumariega AJ, Cinciripini PM. Psychopharmacological management of migraine in children in children and adolescents. J Child Adolesc Psychopharmacol. 1992;2:199-211.
25. Chambers WJ, Puig-Antich J, Tabrizi MA, et al. Psychotic symptoms in prepubertal major depressive disorder. Arch Gen Psychiatry. 1982;39:921-927.
26. Volkmar FR. Childhood and adolescent psychosis: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. 1996;35:843-851.
27. First MB, Frances A, Pincus HA. DSM-IV handbook of differential diagnosis. Washington, DC: American Psychiatric Press; 1995.
28. Birmaher B, Ryan ND, Williamson DE, et al. Childhood and adolescent depression: a review of the past 10 years. Part I. J Am Acad Child Adolesc Psychiatry. 1996;35:1427-1439.
29. Meyer SE, Bearden CE, Lux CR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
30. Drake RJ, Haley CJ, Akhtar S, et al. Causes and consequences of duration of untreated psychosis in schizophrenia. Br J Psychiatry. 2000;177:511-515.
31. McGorry PD, Yung AR, Phillips LJ. The “close-in” or ultra high-risk model: a safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr Bull. 2003;29(4):771-790.
32. McGlashan TH, Zipursky RB, Perkins DO, et al. Olanzapine versus placebo treatment of schizophrenia prodrome: one year results. Poster presented at: International Congress of Schizophrenia Research, Colorado Springs, CO, April-May 2003.
33. McGorry PD, Yung AR, Phillips LJ, et al. Randomized controlled trial of interventions designed to reduce the risk of progression to first episode psychosis in a clinical sample with subthreshold symptoms. Arch Gen Psychiatry. 2002;59:921-928.
34. French P, Shryane N, Bentall RP, et al. Effects of cognitive therapy on the longitudinal development of psychotic experiences in people at high risk of developing psychosis. Br J Psychiatry Suppl. 2007;51:s82-87.
35. Turkington D, Siddle R. Cognitive therapy for the treatment of delusions. Advances in Psychiatric Treatment. 1998;4:235-242.
36. Sosland MD, Pinninti N. Five ways to quiet auditory hallucinations. Current Psychiatry. 2005;4:40.-
37. Kingdon DG, Turkington D. Cognitive behavioral therapy of schizophrenia, New York, NY: Guilford Press; 1994.
CAM for your anxious patient: What the evidence says

The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
The number of people with psychiatric disorders who use complementary and alternative medicine (CAM) is on the rise. In surveys of patients seeking psychiatric care, estimates of CAM use range from 8% to 57%; the most frequent uses are for depression and anxiety disorders. A population-based study in the United States found that 9% of respondents had anxiety attacks and 57% of these individuals had used CAM.1 Similarly, in a Finnish population-based study (N=5,987) 35% of subjects reported some form of CAM use in the previous year; those with comorbid anxiety and depressive disorders used CAM most frequently.2
Unfortunately, a MEDLINE search shows that the number of studies examining psychotropic medications dwarfs the number of studies on even the most common CAM treatments used for psychiatric disorders. Far more patients with diagnosed mental disorders are studied in trials of standard treatments than CAM treatments. Because very few studies evaluate the cost-effectiveness of CAM treatments for psychiatric disorders, the risk-to-benefit ratio is difficult to calculate. Although several CAM treatments for depressive disorders have enough support to be considered options,3 CAM options for anxiety disorders are fewer and have less evidence of efficacy.
For these reasons, it is hard to recommend any CAM treatment as first line. Despite the relative lack of high quality research on CAM treatment outcomes, high rates of CAM use make it critical for clinicians to understand what treatments are available—or at least which treatments should be favored if patients are intent on trying them. We review the current research for yoga, exercise, bibliotherapy, and the dietary supplements kava and inositol for treating anxiety disorders and suggest those that warrant consideration for patients who do not respond, respond partially, or suffer from side effects from selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines.
Limitations of CAM research
There are several limitations to the research literature on CAM approaches for anxiety disorders.4 First, there is a wide diversity of practices considered alternative or complementary and various ways in which these methods are applied across cultures. Some authors consider complementary medicines to be only herbal remedies, whereas others include individual therapies such as acupuncture, aromatherapy, herbal therapy, homeopathy, iridology, naturopathy, and reflexology.5 This article defines “alternative” treatments as those other than a form of psychotherapy or an FDA-approved medication that substitute for standard psychiatric treatment, and “complementary” approaches as those used to augment standard psychiatric treatments.
Anxiety and stress are ubiquitous, perhaps motivating interest in CAM options and prompting research on heterogeneous groups of individuals with poorly defined clinical syndromes or with isolated symptoms of anxiety or subjective distress. Few studies examine well-defined patient groups with diagnosed anxiety disorders. There are also multiple research design problems, including poorly specified treatments, poorly chosen placebos, and interpreting nonsignificant differences from established treatments as equivalence in underpowered studies.
The CAM treatments reviewed in this article have ≥2 randomized controlled trials (RCTs) that support their use for patients with diagnosed anxiety disorders, and ≥1 study that shows that the treatment can induce remission.
Yoga
In 2005 Kirkwood et al carried out the first systematic review of research evidence for the effectiveness of yoga in anxiety treatment.6 Of 19 studies identified, 4 RCTs and 1 nonrandomized trial met their inclusion criteria, which were an anxiety disorder diagnosis, use of yoga or yoga-based exercises alone, and anxiety rating scales used as outcome measures. Most found significant improvement in anxiety symptoms with yoga compared with placebo. Details of the 5 trials evaluated in Kirkwood’s review are summarized in Table 1.7-11
Since the 2005 review, 3 additional studies of yoga and anxiety have been published, but none would meet Kirkwood’s inclusion criteria. One that evaluated a heterogeneous group of patients using an intervention with multiple components—only 1 of which was yoga—found the intervention significantly reduced anxiety scores.12 A second study comparing yoga with relaxation in 131 patients with mild-to-moderate stress but no anxiety disorder diagnosis showed yoga was as effective as relaxation in improving anxiety symptoms as measured by the anxiety subscale of the State Trait Personality Inventory.13 In a study of 183 nonrandomized survivors of the 2004 southeast Asia tsunami with posttraumatic stress disorder (PTSD) symptoms, yoga-based breathing either alone or paired with trauma reduction exposure techniques significantly reduced PTSD symptoms compared with wait-list controls.14
Conclusion. Few controlled studies evaluated yoga for anxiety disorders, and all have significant methodologic limitations and/or poor methodology reporting. The diagnostic conditions treated and both yoga interventions and control conditions varied. However, these limited results are encouraging, particularly for treatment of obsessive-compulsive disorder (OCD). There is little information regarding safety or contraindications of yoga. Reported attrition rates were high in most studies, which may raise concerns about patient motivation and compliance.
Table 1
Evidence on the effectiveness of yoga for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Vahia et al, 19737 | 36 patients with psychoneurosis randomly assigned to yoga (N=15) or a control intervention of relaxation, postures, breathing, and writing (N=12) | Significant difference between groups in TAS scores after but not before treatment. Reduction in mean TAS score for yoga group but not control group |
| Vahia et al,19738 | 39 patients received 6 weeks of yoga (N=21) or medication (amitriptyline and chlordiazepoxide on a variable dosage schedule) (N=18) | Yoga showed significantly greater reductions in TAS in this non-randomized sample |
| Sahasi et al, 19899 | 91 patients randomly assigned to yoga practiced daily for 40 minutes (N=38) or diazepam at unspecified frequency or doses (N=53) for 3 months | Mean reduction in IPAT with yoga (3.39, P < .05) vs control group (0.36, P > .05). Attrition rate was 21.1% in yoga group and 66% in controls |
| Sharma et al, 199110 | 71 patients with anxiety neurosis randomly assigned to 1-week yoga training, then daily practice (N=41) or control (N=30, placebo capsule) | HAM-A measured at 3 weekly intervals for 12 weeks. Significant between group mean difference at 3 weeks (greater improvement in yoga group compared with controls). Significant improvement in yoga group between 3 and 6 weeks but not for controls |
| Shannahoff-Khalsa et al, 199911 | 21 OCD patients randomly assigned to kundalini yoga (N=11) or relaxation and mindfulness meditation (N=10). Multiple outcome measures; Y-BOCS was primary | Seven in each group completed 3 months; patients who practiced yoga demonstrated greater improvements on Y-BOCS. Intent-to-treat analysis (Y-BOCS) for the baseline and 3-month tests showed that only the yoga group improved. Groups were merged for an additional year of yoga; at 15 months, the final group (N=11) improved 71% on the Y-BOCS |
| HAM-A: Hamilton Anxiety Rating scale; IPAT: Institute for Personality and Ability Testing, Anxiety Scale; OCD: obsessive-compulsive disorder; TAS: Taylor’s Anxiety Scale; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Exercise
The literature examining the relationship between exercise and depression is extensive, but much less has been published about exercise in patients with anxiety disorders (Table 2).15-17 In a 10-week trial, Broocks and colleagues compared clomipramine, exercise (running), and placebo in 46 outpatients with panic disorder.15 Both exercise and clomipramine, 112.5 mg/d, significantly reduced panic symptoms compared with placebo, but clomipramine was more effective and faster-acting.
A more recent RCT compared group cognitive-behavioral therapy (GCBT) plus a home-based walking program vs GCBT and in 21 patients with panic disorder, generalized anxiety disorder (GAD), or social phobia.16 Compared with GCBT plus educational sessions, GCBT plus walking had a significant effect on self-reported depression, anxiety, and stress. Results differed by diagnosis; the most marked effects occurred in individuals with social phobia, whereas benefits for those with panic disorder or GAD were questionable.
Fifteen patients with OCD were recruited to participate in a 12-week, moderate-intensity aerobic exercise program added to their standard behavioral and/or pharmacologic treatment.17 Subjects demonstrated improvement in negative mood, anxiety, obsessions, and compulsions after each exercise session. Changes after each session persisted over the 12-week intervention, although the magnitude attenuated over the duration of the intervention.
Conclusion. Although initial results from small trials suggest exercise may help improve anxiety symptoms, further studies are needed to determine how to best use exercise training to treat anxious patients, specifically regarding dose-response relationship, differences in effectiveness between aerobic and resistance training, and the mechanisms by which exercise improves psychiatric symptoms.
Table 2
Exercise for anxiety: More research is needed
| Study | Design | Results |
|---|---|---|
| Broocks et al, 199915 | 46 patients with panic disorder randomly assigned to 10 weeks of running, clomipramine, or wplacebo pills | Both exercise and clomipramine resulted in significant decreases in symptoms but clomipramine improved symptoms earlier and more effectively |
| Merom et al, 200816 | 21 patients with panic disorder, GAD, or social phobia randomly assigned to GCBT and either a home-based walking program or educational sessions | GCBT plus walking had a significant effect on depression, anxiety, and stress compared with GCBT plus educational sessions |
| Abrantes et al, 200917 | 15 patients with OCD assigned to a 12-week exercise intervention that was added to their standard behavioral and/or pharmacologic treatment | Subjects reported improved mood, anxiety, obsessions, and compulsions after each exercise session |
| GAD: generalized anxiety disorder; GCBT: group cognitive-behavioral therapy | ||
Bibliotherapy
Investigation of bibliotherapy for treatment of anxiety disorders has been limited (Table 3).18-20 A 2009 RCT demonstrated that for 21 patients with mild-to-moderate social phobia, bibliotherapy—in the form of an 8-week self-directed CBT program with minimal therapist involvement—was superior to a wait-list control and induced clinically significant change in approximately one-third of patients.20
Rapee et al randomly assigned 267 children age 6 to 12 with anxiety disorders to bibliotherapy that consisted of parents treating their children in the home with written materials, 9 sessions of GCBT, or a wait-list control condition.19 Bibliotherapy provided by parents demonstrated benefit compared with wait-listing but was not as efficacious as GCBT at post-treatment and 3-month follow-up.
Lidren and colleagues randomly assigned 36 adult patients with panic disorder to bibliotherapy, group therapy combined with bibliotherapy, or a waitlist.18 Both treatments were more effective than wait-listing in reducing the frequency of panic attacks, severity of physical panic symptoms, catastrophic cognitions, agoraphobic avoidance, and depression. Both interventions maintained their effects at 3-and 6-month follow-up and produced clinically significant change in most patients.
Conclusion. Some preliminary evidence supports the effectiveness of bibliotherapy for social anxiety disorder, childhood anxiety disorders, and panic disorder.
Table 3
Preliminary evidence supports bibliotherapy for select anxiety disorders
| Study | Design | Results |
|---|---|---|
| Lidren et al, 199418 | 36 adults with panic disorder randomly assigned to bibliotherapy, bibliotherapy plus group therapy, or wait-list control | Both bibliotherapy and bibliotherapy plus group therapy were more effective than wait-listing in reducing the frequency of panic attacks and severity of physical panic symptoms |
| Rapee et al, 200619 | 267 children with anxiety disorders randomly assigned to bibliotherapy (parents treating their children in the home with written materials with no therapist contact), 9 sessions of group CBT, or wait-list control | Parent-delivered bibliotherapy was beneficial compared with wait-listing but was not as efficacious as group CBT |
| Abramowitz et al, 200920 | 21 patients with mild-to-moderate social phobia underwent an 8-week self-directed CBT program with minimal therapist involvement | Bibliotherapy was superior to wait-listing. One-third of patients experienced clinically significant change |
| CBT: cognitive-behavioral therapy | ||
Dietary supplements
Many dietary and herbal supplements are purported to have therapeutic efficacy for anxiety symptoms. Because of inadequate FDA regulation of manufacturing and marketing of these agents, most of these supplements have not been tested on patients with anxiety disorders.21 Limited evidence supports the use of kava for GAD and inositol for panic disorder (Table 4).22-28
Kava. Multiple double-blind RCTs found kava (Piper methysticum)—a plant indigenous to South Pacific islands—has effects greater than placebo and comparable to standard treatments for mild to moderately severe GAD. A Cochrane meta-analysis22 of 11 trials with 645 participants concluded that kava is effective for reducing GAD symptoms, with risks comparable to standard treatments for up to 6 months of use.
Case reports of kava-associated liver toxicity led to a marketing ban in Canada in 2000, followed shortly by Germany, Australia, and the United Kingdom. In 2002 the FDA issued a Consumer Advisory29 discouraging kava use. Since then a flurry of research has looked for sources of possible toxicity, including individual sensitivities,29 excessive dosing, use of toxic parts of the kava plant instead of the roots,30,31 interactions with other hepatoactive substances, and non-water based extraction methods. RCTs demonstrating kava’s efficacy and safety were characterized by careful dosing supervision, use of standardized kava extracts, and avoidance of interactions with other hepatoactive medications or CAM treatments. Doses ≤300 mg/d are recommended.22
RCTs that used the standardized acetone extract WS149023 found that women and younger adults show more positive effects from kava, and showed no liver toxicity when used for 1 to 24 weeks. A recent RCT that used kava extracts obtained via water-based methods showed kava had significant anxiolytic effects.24 However, a study of liver toxicity reports found that water-based extractions, acetonic extractions, and ethanol extractions all have been associated with toxic hepatic reactions.32 Aqueous extraction does not guarantee safety, and the extraction solvent does not cause toxicity. A recent report of a severe liver reaction to the native drink by a tourist in Samoa33 suggests that aqueous extractions from the root stock— the type of kava used by South Pacific islanders—also can be unsafe.
Conclusion. Multiple RCTs have found kava relatively safe and effective for treating anxiety symptoms. Caution is necessary, however, because of reports of liver toxicity associated with its use. Physician oversight and monitoring of kava use are appropriate.
Inositol. Evidence from RCTs suggests inositol, a natural isomer of glucose and a precursor in the phosphatidylinositol cycle, can significantly improve panic disorder symptoms.25-28 In 1 trial, efficacy and side effects were comparable to fluvoxamine.28 Effective doses ranged from 12 g/d to 18 g/d. Researchers tested inositol as monotherapy or augmentation to SSRIs for patients with mild-to-moderate OCD. In small double-blind crossover RCTs, inositol monotherapy significantly reduced Yale-Brown Obsessive Compulsive Scale scores compared with placebo26 but inositol augmentation added nothing to the effects of SSRIs.27
Conclusion. Inositol appears to be effective in improving symptoms of panic disorder. Its use for other anxiety disorders is unproven.
Table 4
Dietary supplements for anxiety disorders
| Study | Design | Results |
|---|---|---|
| Kava | ||
| Pittler et al, 200322 | Meta-analysis of 11 RCTs with a total of 645 GAD patients | Compared with placebo, kava significantly reduced anxiety as measured by total HAM-A score |
| Witte et al, 200523 | Meta-analysis of 6 RCTs using kava extract WS1490 in patients with nonpsychotic anxiety disorders | Kava reduced HAM-A score more than placebo and seemed to be more effective in women and younger adults |
| Sarris et al, 200924 | 60 adults with ≥1 month of elevated generalized anxiety randomly assigned to an aqueous extract of kava | Aqueous-extract kava was significantly more effective than placebo in reducing HAM-A score |
| Inositol | ||
| Benjamin et al, 199525 | 21 patients with panic disorder with or without agoraphobia randomly assigned to inositol, 12 g/d, or placebo | Inositol significantly reduced frequency and severity of panic attacks and severity of agoraphobia compared with placebo |
| Fux et al, 199626 | 13 OCD patients randomly assigned to inositol,18 g/d, or placebo for 6 weeks | Patients taking inositol had significantly lower Y-BOCS scores compared with those receiving placebo |
| Fux et al, 199927 | 10 OCD patients receiving an SSRI randomly assigned to augmentation with inositol, 18 g/d, or placebo for 6 weeks | No significant differences between treatments |
| Palatnik et al, 200128 | In a crossover trial, 20 panic disorder patients completed 1 month of inositol, up to 18 g/d, and 1 month of fluvoxamine, up to 150 mg/d | Improvements in HAM-A, CGI, and agoraphobia scores were similar for both treatments |
| CGI: Clinical Global Impression scale; GAD: generalized anxiety disorder; HAM-A: Hamilton Anxiety Rating scale; OCD: obsessive-compulsive disorder; RCTs: randomized controlled trials; SSRI: selective serotonin reuptake inhibitor; Y-BOCS: Yale-Brown Obsessive Compulsive Scale | ||
Supervision is recommended
The evidence base for most CAM interventions commonly used for anxiety is relatively poor and recent systematic reviews found few methodologically rigorous studies. This has not, however, diminished CAM treatments’ popularity. Despite a paucity of high-quality studies regarding CAM for anxiety disorders, there is enough data supporting yoga, exercise, bibliotherapy, kava, and inositol to allow psychiatrists to collaborate with patients who wish to try these treatments. Advise patients that they may need physician supervision similar to that used with standard psychiatric treatments.
Related Resources
- National Center for Complementary and Alternative Medicine. http://nccam.nih.gov.
- The Journal of Alternative and Complementary Medicine. www.liebertonline.com/loi/acm.
- MedlinePlus: Complementary and Alternative Medicine. www.nlm.nih.gov/medlineplus/complementaryandalternativemedicine.html.
Drug Brand Names
- Amitriptyline • Elavil
- Chlordiazepoxide • Librium
- Clomipramine • Anafranil
- Diazepam • Valium
- Fluvoxamine • Luvox
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
1. Kessler RC, Soukup J, Davis RB, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. Am J Psychiatry. 2001;158(2):289-294.
2. Wahlström M, Sihvo S, Haukkala A, et al. Use of mental health services and complementary and alternative medicine in persons with common mental disorders. Acta Psychiatr Scand. 2008;118(1):73-80.
3. Saeed SA, Bloch RM, Antonacci DJ, et al. CAM for your depressed patient: 6 recommended options. Current Psychiatry. 2009;8(10):39-47.
4. Pilkington K. Searching for CAM evidence: an evaluation of therapy-specific search strategies. J Altern Complement Med. 2007;13(4):451-459.
5. van der Watt G, Laugharne J, Janca A. Complementary and alternative medicine in the treatment of anxiety and depression. Curr Opin Psychiatry. 2008;21(1):37-42.
6. Kirkwood G, Rampes H, Tuffrey V, et al. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-891.
7. Vahia NS, Doongaji DR, Jeste DV, et al. Psychophysiologic therapy based on the concepts of Patanjali. A new approach to the treatment of neurotic and psychosomatic disorders. Am J Psychother. 1973;27(4):557-565.
8. Vahia NS, Doongaji DR, Jeste DV, et al. Further experience with the therapy based upon concepts of Patanjali in the treatment of psychiatric disorders. Indian J Psychiatry. 1973;15(1):32-37.
9. Sahasi G, Mohan D, Kacker C. Effectiveness of yogic techniques in the management of anxiety. J Pers Clin Stud. 1989;5(1):51-55.
10. Sharma I, Azmi SA, Settiwar RM. Evaluation of the effect of pranayama in anxiety state. Alternative Medicine. 1991;3:227-235.
11. Shannahoff-Khalsa DS, Ray LE, Levine S, et al. Randomized controlled trial of yogic meditation techniques for patients with obsessive-compulsive disorder. CNS Spectr. 1999;4(12):34-47.
12. Gupta N, Khera S, Vempati RP, et al. Effect of yoga based lifestyle intervention on state and trait anxiety. Indian J Physiol Pharmacol. 2006;50(1):41-47.
13. Smith C, Hancock H, Blake-Mortimer J, et al. A randomised comparative trial of yoga and relaxation to reduce stress and anxiety. Complement Ther Med. 2007;15(2):77-83.
14. Descilo T, Vedamurtachar A, Gerbarg PL, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121(4):289-300.
15. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603-609.
16. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—a pilot group randomized trial. J Anxiety Disord. 2008;22(6):959-968.
17. Abrantes AM, Strong DR, Cohn A, et al. Acute changes in obsessions and compulsions following moderate-intensity aerobic exercise among patients with obsessive-compulsive disorder. J Anxiety Disord. 2009;23(7):923-927.
18. Lidren DM, Watkins PL, Gould RA, et al. A comparison of bibliotherapy and group therapy in the treatment of panic disorder. J Consult Clin Psychol. 1994;62(4):865-869.
19. Rapee RM, Abbott MJ, Lyneham HJ. Bibliotherapy for children with anxiety disorders using written materials for parents: a randomized controlled trial. J Consult Clin Psychol. 2006;74(3):436-444.
20. Abramowitz JS, Moore EL, Braddock AE, et al. Self-help cognitive-behavioral therapy with minimal therapist contact for social phobia: a controlled trial. J Behav Ther Exp Psychiatry. 2009;40(1):98-105.
21. Saeed SA, Bloch RM, Antonacci DJ. Herbal and dietary supplements for treatment of anxiety disorders. Am Fam Physician. 2007;76(4):549-556.
22. Pittler MH, Ernst E. Kava extract for treating anxiety. Cochrane Database Syst Rev. 2003;(1):CD003383.-
23. Witte S, Loew D, Gaus W. Meta-analysis of the efficacy of the acetonic kava-kava extract WS1490 in patients with non-psychotic anxiety disorders. Phytother Res. 2005;19(3):183-188.
24. Sarris J, Kavanagh DJ, Byrne G, et al. The Kava Anxiety Depression Spectrum Study (KADSS): a randomized, placebo-controlled crossover trial using an aqueous extract of piper methysticum. Psychopharmacology (Berl). 2009;205:399-407.
25. Benjamin J, Levine J, Fux M, et al. Double-blind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
26. Fux M, Levine J, Aviv A, et al. Inositol treatment of obsessive-compulsive disorder. Am J Psychiatry. 1996;153(9):1219-1221.
27. Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessive-compulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmcol. 1999;2(3):193-195.
28. Palatnik A, Frolov K, Fux M, et al. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
29. US Food and Drug Administration. Consumer advisory: kava-containing dietary supplements may be associated with severe injury. Available at: http://www.fda.gov/Food/ResourcesForYou/Consumers/ucm085482.htm. Accessed August 25, 2010.
30. Dragull K, Yoshida WY, Tang CS. Piperidine alkaloids from piper methysticum. Phytochemistry. 2003;63(2):193-198.
31. Simkins A, Thurston D, Colyar M, et al. Nature’s wrath? A closer look at complications with five popular herbs. Adv Nurse Pract. 2005;13(6):55-56.
32. Teschke R, Genthner A, Wolff A. Kava hepatotoxicity: comparison of aqueous, ethanolic, acetonic kava extracts and kava-herbs mixtures. J Ethnopharmacol. 2009;123(3):378-384.
33. Christl SU, Seifert A, Seeler D. Toxic hepatitis after consumption of traditional kava preparation. J Travel Med. 2009;16(1):55-56.
Re-envisioning psychosis: A new language for clinical practice
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/re-envisioning-psychosis-new-language.html#comments
“I haven’t wanted to call it psychosis yet…”
“I’m not sure if this is psychosis or neurosis.”
“I wonder if there’s a psychotic process underneath all of this?”
“Psychotherapy won’t help psychosis.”
In our experience as practitioners in an early psychosis program, the above statements are common among mental health care providers. In our opinion, they are examples of vestiges of an archaic, overly simplistic clinical language that is not representative of current conceptions of psychosis as being on a continuum with normal experience.1,2
The above quotes speak of psychosis as an all-or-none distinction: a “switch,” something fundamentally different from other psychological processes. In this article, we highlight common “all-or-none” myths about psychosis and argue for a more fluid, normalized psychosis language, where impairment is defined not by the absolute presence or absence of “weirdness” but instead by distress, conviction, preoccupation, and behavioral disturbance. We challenge the notion that the presence of psychosis mandates a “fast track” diagnosis that ignores the complexity of human experience.
Power of language
The word “psychosis” has enormous power for patients, families, clinicians, and the public. It often is used interchangeably with “craziness,” “insanity,” or “madness.” Mental health clinicians use psychosis to describe many phenomena, including:
- breaks with reality testing
- odd or delusional beliefs
- abnormal sensations
- catatonia
- bizarre behaviors
- so-called formal thought disorders.
It is likely one of the most heterogeneous symptom terms in psychiatry. DSM-IV-TR notes “the term psychotic has historically received a number of different definitions, none of which has achieved universal acceptance.”3
Psychosis myths. In addition to its phenomenological usage, the word psychosis also has various theoretical interpretations and often is used to demonstrate a fundamental pivot point for making qualitative distinctions. For example, clinicians and theorists have used “psychotic” to assume that someone experiencing psychosis:
- is operating on a core or primitive mode of thought, the so-called “primary process”4
- has a belief that is beyond understanding, one for which empathy is meaningless and misplaced5
- has clear convictions that violate social norms and refuses to accept society’s “proper” rules for logic and emotion6
- is in a state of “brain toxicity” with an “organic” cause (this comes from discussing psychosis with other clinicians, not from the literature).
Such seemingly disparate definitions share the assumption that psychosis represents a shift in categorical status, whether the category is developmental (advanced vs primitive), interpersonal judgment (able to be empathized with or not), sociopolitical status (conformist or not), or functional brain state (organic or non-organic).
Even the etymological basis for schizophrenia (its Greek roots signify “split mind,” which arguably spawned the long-held erroneous view that schizophrenia is a “split personality”) exemplifies this stance and reinforces the notion of discrete “all-or-none” categories of experience. In our view, such assumptions do not adequately reflect the reality of psychosis as a continuum of human experience, and could lead to serious, if unintended, stigmatization and oversimplification of persons who have psychotic symptoms. We argue that such all-or-none thinking reifies 2 clinical “myths” about what psychosis represents:
- Psychosis represents a fundamentally different type of cognitive process.
- Psychosis is so different from normal human experience that mood and anxiety symptoms become “subsumed” by it and treated as “secondary.”
Our goal is not to redefine psychosis or present an argument for diagnostically recategorizing schizophrenia, schizoaffective disorder, and bipolar disorder, which others have already done well.7-10 Instead we want to reinforce the evidence-based and clinically relevant concept that psychosis exists on a definable continuum of human experience and to offer practitioners a clinical language of psychosis for assessing and treating psychotic symptoms that avoids unsupported all-or-none distinctions.
Defining ‘the schizophrenic’
In our experience, an unintended consequence of assuming psychosis is an all-or-none state is the clinician’s perpetual search for “real psychosis” as separate from “psychosis for which I have a good explanation.” Although this distinction is reminiscent of earlier arguments regarding “neurotic” vs “endogenous” depression, we feel that in this case “real or not” acts at a more basic level: the characterization of person types.
We assume that every clinician—ourselves included—who has worked with seriously mentally ill patients has heard an individual with schizophrenia referred to as “a schizophrenic.” Although the problem of defining a person as an illness is not unique to psychosis, we think that you will agree that the phrases “a depressive,” “a bipolar,” or “a generalized anxiotic” [sic] are rare.
DSM-IV-TR specifically avoids using expressions such as “a schizophrenic…and [instead uses]…an individual with schizophrenia.”11 But we believe that DSM-IV-TR accidentally encourages the distinction of a “psychotic person type” by making schizoaffective disorder—a disorder that suggests a continuum—use Criterion A for schizophrenia as its defining feature. The implicit assumption is that “something categorical”—in this case defined by Criterion A—identifies a “psychotic person type,” as opposed to a person who simply has psychotic symptoms. If we see evidence of Criterion A, then the person is naturally moved into the realm of “schizophrenia and other psychotic disorders.” In other words, Criterion A subsumes other types of symptoms. In contrast, the presence of 1 month of social anxiety or obsessions and compulsions does not subsume other symptoms into primary anxiety disorders. To make this example explicit, we have developed a set of criteria for hypothetical disorders that overlap major categories of DSM-IV-TR (Table 1).
Table 1
The ‘logic’ of schizoaffective disorder applied to anxiety and OCD
| Symptom course | ‘Primary’ feature | ‘Secondary’ feature | Diagnosis |
|---|---|---|---|
| 2 weeks of ≥2 psychotic symptoms outside of a major mood episode plus a manic or depressed episode | 2 weeks of psychotic and negative symptoms | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | Schizoaffective disorder |
| 1 month of social anxiety and avoidance outside of a major mood episode plus a manic or depressed episode | 1 month of social anxiety and avoidance | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Socio-anxious-affective disorder’* |
| 1 month of obsessions and compulsions outside of a major mood episode plus a manic or depressed episode | 1 month of obsessions and compulsions | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Obsessocompulso-affective disorder’* |
| OCD: obsessive-compulsive disorder | |||
| * These diagnoses are hypothetical disorders used to illustrate how the criteria used to define schizoaffective disorder subsume other types of symptoms | |||
A continuum approach
As a way out of this inductive logic trap, we suggest the following statements as evidence-based and clinically realistic ways of approaching psychosis assessment.
‘Normal sadness’ and ‘normal psychosis’ are equivalent. The DSM-IV-TR description of major depressive disorder, states that “periods of sadness are inherent aspects of the human experience.”12 However, descriptions of psychosis rarely reflect that psychotic-like experiences are quite common13-19 and easily induced in otherwise healthy people.20 Psychotic symptoms are widely described as being genetically linked to normally distributed personality traits.21-24 Finally, research on risk for developing chronic psychosis has identified that most patients who develop attenuated psychotic symptoms do not experience them chronically.25-28 Together, these data argue strongly for a concept of psychosis as common and continuously distributed across large groups.
A psychosis screen can be much more than ‘+/- AH/VH/PI.’ We reject the idea that psychotic phenomena are fundamentally different from “normal” occurrences such as imagined or inner speech, perceptual fluctuations, distorted or rigid beliefs, or inability to accurately express one’s emotional state. Yet abnormal perception, affect flattening, and delusions often are viewed as “really weird,” which suggests most people never experience these phenomena, only “affected” people. This easily can lead to cognitive errors that associate psychosis as a state of mind that is fundamentally different from non-psychosis. In fact, DSMIV-TR categorizes the presence of persistent psychotic symptoms as evidence of disorder until proven otherwise.3
We feel that this simplistic language describing psychosis as inherently pathological ignores the clinical richness of psychotic experience. In our experience, many individuals who have been diagnosed with chronic psychosis have never been asked:
- about the timing, intensity, and character of their abnormal sensory experiences29
- how their beliefs and schemas affect day-to-day behavior and choices
- if their psychotic symptoms are bothersome or troubling.
We worry that a person experiencing impairing psychotic symptoms could become overshadowed by all-or-none assumptions about the symptoms themselves.
We propose Table 2 as a guideline for approaching psychotic symptoms as expressions along a continuum of experience, one that shares much in common with recent well-developed biopsychosocial models of psychotic phenomena.30 In our view, this allows for a therapeutic alliance that focuses on patient recovery, as opposed to seeing psychotic symptoms as the only treatment targets. By moving beyond all-or-none myths and approaching psychosis as a continuum with normal experience, we believe that patient recovery can become a realistic goal.
Table 2
Revising the clinical language of psychosis to separate presence from pathology
| Symptom | Continuum | Attenuated experience | Pathological experience (‘disorder’) | Psychotherapeutic intervention |
|---|---|---|---|---|
| Paranoid ideation/delusions | Schematization and testing of environmental information |
|
|
|
| Hallucination | Higher order sensory processing and self/other discrimination |
|
|
|
| Disorganized speech / ‘thought disorder’ | Social pragmatics and conceptual linking |
|
|
|
| Source: Bechdolf A, Phillips LJ, Francey SM, et al. Recent approaches to psychological interventions for people at risk of psychosis. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):159-173. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020. French P, Morrison AP. Early detection and cognitive therapy for people at high risk of developing psychosis: a treatment approach. West Sussex, United Kingdom: John Wiley and Sons; 2004. Christodoulides T, Dudley R, Brown S, et al. Cognitive behaviour therapy in patients with schizophrenia who are not prescribed antipsychotic medication: a case series. Psychol Psychother. 2008;81(Pt 2):199-207. Davis LW, Ringer JM, Strasburger AM, et al. Participant evaluation of a CBT program for enhancing work function in schizophrenia. Psychiatr Rehabil J. 2008;32(1):55-58. Jackson HJ, McGorry PD, Killackey E, et al. Acute-phase and 1-year follow-up results of a randomized controlled trial of CBT versus befriending for first-episode psychosis: the ACE project. Psychol Med. 2008;38(5):725-735. Lecomte T, Leclerc C, Corbiere M, et al. Group cognitive behavior therapy or social skills training for individuals with a recent onset of psychosis? Results of a randomized controlled trial. J Nerv Ment Dis. 2008;196(12):866-875. Loewy RL, Johnson JK, Cannon TD. Self-report of attenuated psychotic experiences in a college population. Schizophr Res. 2007; 93(1-3):144-151. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715. Mitchell AJ. CBT for psychosis. Br J Psychiatry. 2004;185:438; author reply 438. Rathod S, Kingdon D, Weiden P, et al. Cognitive-behavioral therapy for medication-resistant schizophrenia: a review. J Psychiatr Pract. 2008;14(1):22-33. Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc.; 2008. | ||||
Re-envisioning psychosis
We conclude with a reiteration of recovery in the language of the US Surgeon General almost 10 years ago: “…hope and restoration of a meaningful life are possible, despite serious mental illness… Instead of focusing primarily on symptom relief…recovery casts a much wider spotlight on restoration of self-esteem and identity and on attaining meaningful roles in society.”31 We see no reason why people cannot live meaningful lives while also having symptoms of psychosis. Data from well-designed studies32 and accounts from individuals who have experienced or continue to experience psychosis33 suggest that this is realistic.
By dispelling all-or-none myths, revealing the flawed logic of psychosis as “subsumer” of mood and anxiety, and describing the continuum of psychotic symptoms, we hope to encourage clinicians to be more positive and proactive in their approach to people experiencing impairing psychotic symptoms. Through assertive alliance and informed clinical technique, we envision a landscape in which psychosis is seen as a “normal” part of outpatient psychiatric practice.
Related resources
- Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
- Gleeson JFM, McGorry PD, eds. Psychological interventions in early psychosis: a treatment handbook. West Sussex, United Kingdom: John Wiley & Sons; 2004.
- Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Disclosure
The authors report no financial relationship with any manufacturer of products mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors wish to acknowledge Dr. Carol Mathews for her comments on this manuscript.
1. Stefanis NC, Hanssen M, Smirnis NK, et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med. 2002;32(2):347-358.
2. Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and the continuum of psychosis. Schizophr Res. 2002;54(1-2):59-65.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:297–343.
4. Tyson P, Tyson RL. Psychoanalytic theories of development: an integration. New Haven, CT: Yale University Press; 1990.
5. Schilpp PA. Philosophy of Karl Jaspers. Chicago, IL: Open Court Publishing Company; 1981.
6. Szasz TS. The second sin. Garden City, NY: Anchor Press; 1974.
7. Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
8. van Os J. ‘Salience syndrome’ replaces ‘schizophrenia’ in DSM-V and ICD-11: psychiatry’s evidence-based entry into the 21st century? Acta Psychiatr Scand. 2009;120(5):363-372.
9. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res. 2006;143(2-3):255-287.
10. Craddock N, Owen MJ. The Kraepelinian dichotomy—going, going…but still not gone. Br J Psychiatry. 2010;196(2):92-95.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:xxxi.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:345–428.
13. Yung AR, Buckby JA, Cotton SM, et al. Psychotic-like experiences in nonpsychotic help-seekers: associations with distress, depression, and disability. Schizophr Bull. 2006;32(2):352-359.
14. Tien AY. Distributions of hallucinations in the population. Soc Psychiatry Psychiatr Epidemiol. 1991;26(6):287-292.
15. Eaton WW, Romanoski A, Anthony JC, et al. Screening for psychosis in the general population with a self-report interview. J Nerv Ment Dis. 1991;179(11):689-693.
16. Poulton R, Caspi A, Moffitt TE, et al. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57(11):1053-1058.
17. van Os J, Hanssen M, Bijl RV, et al. Prevalence of psychotic disorder and community level of psychotic symptoms: an urban-rural comparison. Arch Gen Psychiatry. 2001;58(7):663-668.
18. Sommer IE, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
19. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21(5):581-586.
20. Merabet LB, Maguire D, Warde A, et al. Visual hallucinations during prolonged blindfolding in sighted subjects. J Neuroophthalmol. 2004;24(2):109-113.
21. Fanous AH, Neale MC, Gardner CO, et al. Significant correlation in linkage signals from genome-wide scans of schizophrenia and schizotypy. Mol Psychiatry. 2007;12(10):958-965.
22. Fanous A, Gardner C, Walsh D, et al. Relationship between positive and negative symptoms of schizophrenia and schizotypal symptoms in nonpsychotic relatives. Arch Gen Psychiatry. 2001;58(7):669-673.
23. Webb CT, Levinson DF. Schizotypal and paranoid personality disorder in the relatives of patients with schizophrenia and affective disorders: a review. Schizophr Res. 1993;11(1):81-92.
24. Asai T, Sugimori E, Bando N, et al. The hierarchic structure in schizotypy and the five-factor model of personality. Psychiatry Res. 2010 May 26. [Epub ahead of print].
25. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715.
26. Meyer SE, Bearden CE, Lux SR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
27. Cannon TD, Cadenhead K, Cornblatt B, et al. Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America. Arch Gen Psychiatry. 2008;65(1):28-37.
28. Yung AR, McGorry PD. The prodromal phase of first-episode psychosis: past and current conceptualizations. Schizophr Bull. 1996;22(2):353-370.
29. Nasrallah HA. The hallucination portrait of psychosis. Current Psychiatry. 2009;8(5):10-12.
30. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020.
31. US Department of Health and Human Services. Mental health: a report of the surgeon general—executive summary. Washington, DC: US Department of Health and Human Services; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/summary.html. Accessed September 10, 2010.
32. Kane JM. An evidence-based strategy for remission in schizophrenia. J Clin Psychiatry. 2008;69(suppl 3):25-30.
33. Wagner PS. First person account: a voice from another closet. Schizophr Bull. 1996;22(2):399-401.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/re-envisioning-psychosis-new-language.html#comments
“I haven’t wanted to call it psychosis yet…”
“I’m not sure if this is psychosis or neurosis.”
“I wonder if there’s a psychotic process underneath all of this?”
“Psychotherapy won’t help psychosis.”
In our experience as practitioners in an early psychosis program, the above statements are common among mental health care providers. In our opinion, they are examples of vestiges of an archaic, overly simplistic clinical language that is not representative of current conceptions of psychosis as being on a continuum with normal experience.1,2
The above quotes speak of psychosis as an all-or-none distinction: a “switch,” something fundamentally different from other psychological processes. In this article, we highlight common “all-or-none” myths about psychosis and argue for a more fluid, normalized psychosis language, where impairment is defined not by the absolute presence or absence of “weirdness” but instead by distress, conviction, preoccupation, and behavioral disturbance. We challenge the notion that the presence of psychosis mandates a “fast track” diagnosis that ignores the complexity of human experience.
Power of language
The word “psychosis” has enormous power for patients, families, clinicians, and the public. It often is used interchangeably with “craziness,” “insanity,” or “madness.” Mental health clinicians use psychosis to describe many phenomena, including:
- breaks with reality testing
- odd or delusional beliefs
- abnormal sensations
- catatonia
- bizarre behaviors
- so-called formal thought disorders.
It is likely one of the most heterogeneous symptom terms in psychiatry. DSM-IV-TR notes “the term psychotic has historically received a number of different definitions, none of which has achieved universal acceptance.”3
Psychosis myths. In addition to its phenomenological usage, the word psychosis also has various theoretical interpretations and often is used to demonstrate a fundamental pivot point for making qualitative distinctions. For example, clinicians and theorists have used “psychotic” to assume that someone experiencing psychosis:
- is operating on a core or primitive mode of thought, the so-called “primary process”4
- has a belief that is beyond understanding, one for which empathy is meaningless and misplaced5
- has clear convictions that violate social norms and refuses to accept society’s “proper” rules for logic and emotion6
- is in a state of “brain toxicity” with an “organic” cause (this comes from discussing psychosis with other clinicians, not from the literature).
Such seemingly disparate definitions share the assumption that psychosis represents a shift in categorical status, whether the category is developmental (advanced vs primitive), interpersonal judgment (able to be empathized with or not), sociopolitical status (conformist or not), or functional brain state (organic or non-organic).
Even the etymological basis for schizophrenia (its Greek roots signify “split mind,” which arguably spawned the long-held erroneous view that schizophrenia is a “split personality”) exemplifies this stance and reinforces the notion of discrete “all-or-none” categories of experience. In our view, such assumptions do not adequately reflect the reality of psychosis as a continuum of human experience, and could lead to serious, if unintended, stigmatization and oversimplification of persons who have psychotic symptoms. We argue that such all-or-none thinking reifies 2 clinical “myths” about what psychosis represents:
- Psychosis represents a fundamentally different type of cognitive process.
- Psychosis is so different from normal human experience that mood and anxiety symptoms become “subsumed” by it and treated as “secondary.”
Our goal is not to redefine psychosis or present an argument for diagnostically recategorizing schizophrenia, schizoaffective disorder, and bipolar disorder, which others have already done well.7-10 Instead we want to reinforce the evidence-based and clinically relevant concept that psychosis exists on a definable continuum of human experience and to offer practitioners a clinical language of psychosis for assessing and treating psychotic symptoms that avoids unsupported all-or-none distinctions.
Defining ‘the schizophrenic’
In our experience, an unintended consequence of assuming psychosis is an all-or-none state is the clinician’s perpetual search for “real psychosis” as separate from “psychosis for which I have a good explanation.” Although this distinction is reminiscent of earlier arguments regarding “neurotic” vs “endogenous” depression, we feel that in this case “real or not” acts at a more basic level: the characterization of person types.
We assume that every clinician—ourselves included—who has worked with seriously mentally ill patients has heard an individual with schizophrenia referred to as “a schizophrenic.” Although the problem of defining a person as an illness is not unique to psychosis, we think that you will agree that the phrases “a depressive,” “a bipolar,” or “a generalized anxiotic” [sic] are rare.
DSM-IV-TR specifically avoids using expressions such as “a schizophrenic…and [instead uses]…an individual with schizophrenia.”11 But we believe that DSM-IV-TR accidentally encourages the distinction of a “psychotic person type” by making schizoaffective disorder—a disorder that suggests a continuum—use Criterion A for schizophrenia as its defining feature. The implicit assumption is that “something categorical”—in this case defined by Criterion A—identifies a “psychotic person type,” as opposed to a person who simply has psychotic symptoms. If we see evidence of Criterion A, then the person is naturally moved into the realm of “schizophrenia and other psychotic disorders.” In other words, Criterion A subsumes other types of symptoms. In contrast, the presence of 1 month of social anxiety or obsessions and compulsions does not subsume other symptoms into primary anxiety disorders. To make this example explicit, we have developed a set of criteria for hypothetical disorders that overlap major categories of DSM-IV-TR (Table 1).
Table 1
The ‘logic’ of schizoaffective disorder applied to anxiety and OCD
| Symptom course | ‘Primary’ feature | ‘Secondary’ feature | Diagnosis |
|---|---|---|---|
| 2 weeks of ≥2 psychotic symptoms outside of a major mood episode plus a manic or depressed episode | 2 weeks of psychotic and negative symptoms | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | Schizoaffective disorder |
| 1 month of social anxiety and avoidance outside of a major mood episode plus a manic or depressed episode | 1 month of social anxiety and avoidance | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Socio-anxious-affective disorder’* |
| 1 month of obsessions and compulsions outside of a major mood episode plus a manic or depressed episode | 1 month of obsessions and compulsions | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Obsessocompulso-affective disorder’* |
| OCD: obsessive-compulsive disorder | |||
| * These diagnoses are hypothetical disorders used to illustrate how the criteria used to define schizoaffective disorder subsume other types of symptoms | |||
A continuum approach
As a way out of this inductive logic trap, we suggest the following statements as evidence-based and clinically realistic ways of approaching psychosis assessment.
‘Normal sadness’ and ‘normal psychosis’ are equivalent. The DSM-IV-TR description of major depressive disorder, states that “periods of sadness are inherent aspects of the human experience.”12 However, descriptions of psychosis rarely reflect that psychotic-like experiences are quite common13-19 and easily induced in otherwise healthy people.20 Psychotic symptoms are widely described as being genetically linked to normally distributed personality traits.21-24 Finally, research on risk for developing chronic psychosis has identified that most patients who develop attenuated psychotic symptoms do not experience them chronically.25-28 Together, these data argue strongly for a concept of psychosis as common and continuously distributed across large groups.
A psychosis screen can be much more than ‘+/- AH/VH/PI.’ We reject the idea that psychotic phenomena are fundamentally different from “normal” occurrences such as imagined or inner speech, perceptual fluctuations, distorted or rigid beliefs, or inability to accurately express one’s emotional state. Yet abnormal perception, affect flattening, and delusions often are viewed as “really weird,” which suggests most people never experience these phenomena, only “affected” people. This easily can lead to cognitive errors that associate psychosis as a state of mind that is fundamentally different from non-psychosis. In fact, DSMIV-TR categorizes the presence of persistent psychotic symptoms as evidence of disorder until proven otherwise.3
We feel that this simplistic language describing psychosis as inherently pathological ignores the clinical richness of psychotic experience. In our experience, many individuals who have been diagnosed with chronic psychosis have never been asked:
- about the timing, intensity, and character of their abnormal sensory experiences29
- how their beliefs and schemas affect day-to-day behavior and choices
- if their psychotic symptoms are bothersome or troubling.
We worry that a person experiencing impairing psychotic symptoms could become overshadowed by all-or-none assumptions about the symptoms themselves.
We propose Table 2 as a guideline for approaching psychotic symptoms as expressions along a continuum of experience, one that shares much in common with recent well-developed biopsychosocial models of psychotic phenomena.30 In our view, this allows for a therapeutic alliance that focuses on patient recovery, as opposed to seeing psychotic symptoms as the only treatment targets. By moving beyond all-or-none myths and approaching psychosis as a continuum with normal experience, we believe that patient recovery can become a realistic goal.
Table 2
Revising the clinical language of psychosis to separate presence from pathology
| Symptom | Continuum | Attenuated experience | Pathological experience (‘disorder’) | Psychotherapeutic intervention |
|---|---|---|---|---|
| Paranoid ideation/delusions | Schematization and testing of environmental information |
|
|
|
| Hallucination | Higher order sensory processing and self/other discrimination |
|
|
|
| Disorganized speech / ‘thought disorder’ | Social pragmatics and conceptual linking |
|
|
|
| Source: Bechdolf A, Phillips LJ, Francey SM, et al. Recent approaches to psychological interventions for people at risk of psychosis. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):159-173. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020. French P, Morrison AP. Early detection and cognitive therapy for people at high risk of developing psychosis: a treatment approach. West Sussex, United Kingdom: John Wiley and Sons; 2004. Christodoulides T, Dudley R, Brown S, et al. Cognitive behaviour therapy in patients with schizophrenia who are not prescribed antipsychotic medication: a case series. Psychol Psychother. 2008;81(Pt 2):199-207. Davis LW, Ringer JM, Strasburger AM, et al. Participant evaluation of a CBT program for enhancing work function in schizophrenia. Psychiatr Rehabil J. 2008;32(1):55-58. Jackson HJ, McGorry PD, Killackey E, et al. Acute-phase and 1-year follow-up results of a randomized controlled trial of CBT versus befriending for first-episode psychosis: the ACE project. Psychol Med. 2008;38(5):725-735. Lecomte T, Leclerc C, Corbiere M, et al. Group cognitive behavior therapy or social skills training for individuals with a recent onset of psychosis? Results of a randomized controlled trial. J Nerv Ment Dis. 2008;196(12):866-875. Loewy RL, Johnson JK, Cannon TD. Self-report of attenuated psychotic experiences in a college population. Schizophr Res. 2007; 93(1-3):144-151. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715. Mitchell AJ. CBT for psychosis. Br J Psychiatry. 2004;185:438; author reply 438. Rathod S, Kingdon D, Weiden P, et al. Cognitive-behavioral therapy for medication-resistant schizophrenia: a review. J Psychiatr Pract. 2008;14(1):22-33. Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc.; 2008. | ||||
Re-envisioning psychosis
We conclude with a reiteration of recovery in the language of the US Surgeon General almost 10 years ago: “…hope and restoration of a meaningful life are possible, despite serious mental illness… Instead of focusing primarily on symptom relief…recovery casts a much wider spotlight on restoration of self-esteem and identity and on attaining meaningful roles in society.”31 We see no reason why people cannot live meaningful lives while also having symptoms of psychosis. Data from well-designed studies32 and accounts from individuals who have experienced or continue to experience psychosis33 suggest that this is realistic.
By dispelling all-or-none myths, revealing the flawed logic of psychosis as “subsumer” of mood and anxiety, and describing the continuum of psychotic symptoms, we hope to encourage clinicians to be more positive and proactive in their approach to people experiencing impairing psychotic symptoms. Through assertive alliance and informed clinical technique, we envision a landscape in which psychosis is seen as a “normal” part of outpatient psychiatric practice.
Related resources
- Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
- Gleeson JFM, McGorry PD, eds. Psychological interventions in early psychosis: a treatment handbook. West Sussex, United Kingdom: John Wiley & Sons; 2004.
- Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Disclosure
The authors report no financial relationship with any manufacturer of products mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors wish to acknowledge Dr. Carol Mathews for her comments on this manuscript.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/10/re-envisioning-psychosis-new-language.html#comments
“I haven’t wanted to call it psychosis yet…”
“I’m not sure if this is psychosis or neurosis.”
“I wonder if there’s a psychotic process underneath all of this?”
“Psychotherapy won’t help psychosis.”
In our experience as practitioners in an early psychosis program, the above statements are common among mental health care providers. In our opinion, they are examples of vestiges of an archaic, overly simplistic clinical language that is not representative of current conceptions of psychosis as being on a continuum with normal experience.1,2
The above quotes speak of psychosis as an all-or-none distinction: a “switch,” something fundamentally different from other psychological processes. In this article, we highlight common “all-or-none” myths about psychosis and argue for a more fluid, normalized psychosis language, where impairment is defined not by the absolute presence or absence of “weirdness” but instead by distress, conviction, preoccupation, and behavioral disturbance. We challenge the notion that the presence of psychosis mandates a “fast track” diagnosis that ignores the complexity of human experience.
Power of language
The word “psychosis” has enormous power for patients, families, clinicians, and the public. It often is used interchangeably with “craziness,” “insanity,” or “madness.” Mental health clinicians use psychosis to describe many phenomena, including:
- breaks with reality testing
- odd or delusional beliefs
- abnormal sensations
- catatonia
- bizarre behaviors
- so-called formal thought disorders.
It is likely one of the most heterogeneous symptom terms in psychiatry. DSM-IV-TR notes “the term psychotic has historically received a number of different definitions, none of which has achieved universal acceptance.”3
Psychosis myths. In addition to its phenomenological usage, the word psychosis also has various theoretical interpretations and often is used to demonstrate a fundamental pivot point for making qualitative distinctions. For example, clinicians and theorists have used “psychotic” to assume that someone experiencing psychosis:
- is operating on a core or primitive mode of thought, the so-called “primary process”4
- has a belief that is beyond understanding, one for which empathy is meaningless and misplaced5
- has clear convictions that violate social norms and refuses to accept society’s “proper” rules for logic and emotion6
- is in a state of “brain toxicity” with an “organic” cause (this comes from discussing psychosis with other clinicians, not from the literature).
Such seemingly disparate definitions share the assumption that psychosis represents a shift in categorical status, whether the category is developmental (advanced vs primitive), interpersonal judgment (able to be empathized with or not), sociopolitical status (conformist or not), or functional brain state (organic or non-organic).
Even the etymological basis for schizophrenia (its Greek roots signify “split mind,” which arguably spawned the long-held erroneous view that schizophrenia is a “split personality”) exemplifies this stance and reinforces the notion of discrete “all-or-none” categories of experience. In our view, such assumptions do not adequately reflect the reality of psychosis as a continuum of human experience, and could lead to serious, if unintended, stigmatization and oversimplification of persons who have psychotic symptoms. We argue that such all-or-none thinking reifies 2 clinical “myths” about what psychosis represents:
- Psychosis represents a fundamentally different type of cognitive process.
- Psychosis is so different from normal human experience that mood and anxiety symptoms become “subsumed” by it and treated as “secondary.”
Our goal is not to redefine psychosis or present an argument for diagnostically recategorizing schizophrenia, schizoaffective disorder, and bipolar disorder, which others have already done well.7-10 Instead we want to reinforce the evidence-based and clinically relevant concept that psychosis exists on a definable continuum of human experience and to offer practitioners a clinical language of psychosis for assessing and treating psychotic symptoms that avoids unsupported all-or-none distinctions.
Defining ‘the schizophrenic’
In our experience, an unintended consequence of assuming psychosis is an all-or-none state is the clinician’s perpetual search for “real psychosis” as separate from “psychosis for which I have a good explanation.” Although this distinction is reminiscent of earlier arguments regarding “neurotic” vs “endogenous” depression, we feel that in this case “real or not” acts at a more basic level: the characterization of person types.
We assume that every clinician—ourselves included—who has worked with seriously mentally ill patients has heard an individual with schizophrenia referred to as “a schizophrenic.” Although the problem of defining a person as an illness is not unique to psychosis, we think that you will agree that the phrases “a depressive,” “a bipolar,” or “a generalized anxiotic” [sic] are rare.
DSM-IV-TR specifically avoids using expressions such as “a schizophrenic…and [instead uses]…an individual with schizophrenia.”11 But we believe that DSM-IV-TR accidentally encourages the distinction of a “psychotic person type” by making schizoaffective disorder—a disorder that suggests a continuum—use Criterion A for schizophrenia as its defining feature. The implicit assumption is that “something categorical”—in this case defined by Criterion A—identifies a “psychotic person type,” as opposed to a person who simply has psychotic symptoms. If we see evidence of Criterion A, then the person is naturally moved into the realm of “schizophrenia and other psychotic disorders.” In other words, Criterion A subsumes other types of symptoms. In contrast, the presence of 1 month of social anxiety or obsessions and compulsions does not subsume other symptoms into primary anxiety disorders. To make this example explicit, we have developed a set of criteria for hypothetical disorders that overlap major categories of DSM-IV-TR (Table 1).
Table 1
The ‘logic’ of schizoaffective disorder applied to anxiety and OCD
| Symptom course | ‘Primary’ feature | ‘Secondary’ feature | Diagnosis |
|---|---|---|---|
| 2 weeks of ≥2 psychotic symptoms outside of a major mood episode plus a manic or depressed episode | 2 weeks of psychotic and negative symptoms | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | Schizoaffective disorder |
| 1 month of social anxiety and avoidance outside of a major mood episode plus a manic or depressed episode | 1 month of social anxiety and avoidance | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Socio-anxious-affective disorder’* |
| 1 month of obsessions and compulsions outside of a major mood episode plus a manic or depressed episode | 1 month of obsessions and compulsions | 2 weeks of low mood or anhedonia or 1 week of elevated or expansive mood | ‘Obsessocompulso-affective disorder’* |
| OCD: obsessive-compulsive disorder | |||
| * These diagnoses are hypothetical disorders used to illustrate how the criteria used to define schizoaffective disorder subsume other types of symptoms | |||
A continuum approach
As a way out of this inductive logic trap, we suggest the following statements as evidence-based and clinically realistic ways of approaching psychosis assessment.
‘Normal sadness’ and ‘normal psychosis’ are equivalent. The DSM-IV-TR description of major depressive disorder, states that “periods of sadness are inherent aspects of the human experience.”12 However, descriptions of psychosis rarely reflect that psychotic-like experiences are quite common13-19 and easily induced in otherwise healthy people.20 Psychotic symptoms are widely described as being genetically linked to normally distributed personality traits.21-24 Finally, research on risk for developing chronic psychosis has identified that most patients who develop attenuated psychotic symptoms do not experience them chronically.25-28 Together, these data argue strongly for a concept of psychosis as common and continuously distributed across large groups.
A psychosis screen can be much more than ‘+/- AH/VH/PI.’ We reject the idea that psychotic phenomena are fundamentally different from “normal” occurrences such as imagined or inner speech, perceptual fluctuations, distorted or rigid beliefs, or inability to accurately express one’s emotional state. Yet abnormal perception, affect flattening, and delusions often are viewed as “really weird,” which suggests most people never experience these phenomena, only “affected” people. This easily can lead to cognitive errors that associate psychosis as a state of mind that is fundamentally different from non-psychosis. In fact, DSMIV-TR categorizes the presence of persistent psychotic symptoms as evidence of disorder until proven otherwise.3
We feel that this simplistic language describing psychosis as inherently pathological ignores the clinical richness of psychotic experience. In our experience, many individuals who have been diagnosed with chronic psychosis have never been asked:
- about the timing, intensity, and character of their abnormal sensory experiences29
- how their beliefs and schemas affect day-to-day behavior and choices
- if their psychotic symptoms are bothersome or troubling.
We worry that a person experiencing impairing psychotic symptoms could become overshadowed by all-or-none assumptions about the symptoms themselves.
We propose Table 2 as a guideline for approaching psychotic symptoms as expressions along a continuum of experience, one that shares much in common with recent well-developed biopsychosocial models of psychotic phenomena.30 In our view, this allows for a therapeutic alliance that focuses on patient recovery, as opposed to seeing psychotic symptoms as the only treatment targets. By moving beyond all-or-none myths and approaching psychosis as a continuum with normal experience, we believe that patient recovery can become a realistic goal.
Table 2
Revising the clinical language of psychosis to separate presence from pathology
| Symptom | Continuum | Attenuated experience | Pathological experience (‘disorder’) | Psychotherapeutic intervention |
|---|---|---|---|---|
| Paranoid ideation/delusions | Schematization and testing of environmental information |
|
|
|
| Hallucination | Higher order sensory processing and self/other discrimination |
|
|
|
| Disorganized speech / ‘thought disorder’ | Social pragmatics and conceptual linking |
|
|
|
| Source: Bechdolf A, Phillips LJ, Francey SM, et al. Recent approaches to psychological interventions for people at risk of psychosis. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):159-173. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020. French P, Morrison AP. Early detection and cognitive therapy for people at high risk of developing psychosis: a treatment approach. West Sussex, United Kingdom: John Wiley and Sons; 2004. Christodoulides T, Dudley R, Brown S, et al. Cognitive behaviour therapy in patients with schizophrenia who are not prescribed antipsychotic medication: a case series. Psychol Psychother. 2008;81(Pt 2):199-207. Davis LW, Ringer JM, Strasburger AM, et al. Participant evaluation of a CBT program for enhancing work function in schizophrenia. Psychiatr Rehabil J. 2008;32(1):55-58. Jackson HJ, McGorry PD, Killackey E, et al. Acute-phase and 1-year follow-up results of a randomized controlled trial of CBT versus befriending for first-episode psychosis: the ACE project. Psychol Med. 2008;38(5):725-735. Lecomte T, Leclerc C, Corbiere M, et al. Group cognitive behavior therapy or social skills training for individuals with a recent onset of psychosis? Results of a randomized controlled trial. J Nerv Ment Dis. 2008;196(12):866-875. Loewy RL, Johnson JK, Cannon TD. Self-report of attenuated psychotic experiences in a college population. Schizophr Res. 2007; 93(1-3):144-151. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715. Mitchell AJ. CBT for psychosis. Br J Psychiatry. 2004;185:438; author reply 438. Rathod S, Kingdon D, Weiden P, et al. Cognitive-behavioral therapy for medication-resistant schizophrenia: a review. J Psychiatr Pract. 2008;14(1):22-33. Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc.; 2008. | ||||
Re-envisioning psychosis
We conclude with a reiteration of recovery in the language of the US Surgeon General almost 10 years ago: “…hope and restoration of a meaningful life are possible, despite serious mental illness… Instead of focusing primarily on symptom relief…recovery casts a much wider spotlight on restoration of self-esteem and identity and on attaining meaningful roles in society.”31 We see no reason why people cannot live meaningful lives while also having symptoms of psychosis. Data from well-designed studies32 and accounts from individuals who have experienced or continue to experience psychosis33 suggest that this is realistic.
By dispelling all-or-none myths, revealing the flawed logic of psychosis as “subsumer” of mood and anxiety, and describing the continuum of psychotic symptoms, we hope to encourage clinicians to be more positive and proactive in their approach to people experiencing impairing psychotic symptoms. Through assertive alliance and informed clinical technique, we envision a landscape in which psychosis is seen as a “normal” part of outpatient psychiatric practice.
Related resources
- Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
- Gleeson JFM, McGorry PD, eds. Psychological interventions in early psychosis: a treatment handbook. West Sussex, United Kingdom: John Wiley & Sons; 2004.
- Wright JH, Kingdon D, Turkington D, et al. Cognitive-behavior therapy for severe mental illness. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Disclosure
The authors report no financial relationship with any manufacturer of products mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors wish to acknowledge Dr. Carol Mathews for her comments on this manuscript.
1. Stefanis NC, Hanssen M, Smirnis NK, et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med. 2002;32(2):347-358.
2. Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and the continuum of psychosis. Schizophr Res. 2002;54(1-2):59-65.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:297–343.
4. Tyson P, Tyson RL. Psychoanalytic theories of development: an integration. New Haven, CT: Yale University Press; 1990.
5. Schilpp PA. Philosophy of Karl Jaspers. Chicago, IL: Open Court Publishing Company; 1981.
6. Szasz TS. The second sin. Garden City, NY: Anchor Press; 1974.
7. Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
8. van Os J. ‘Salience syndrome’ replaces ‘schizophrenia’ in DSM-V and ICD-11: psychiatry’s evidence-based entry into the 21st century? Acta Psychiatr Scand. 2009;120(5):363-372.
9. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res. 2006;143(2-3):255-287.
10. Craddock N, Owen MJ. The Kraepelinian dichotomy—going, going…but still not gone. Br J Psychiatry. 2010;196(2):92-95.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:xxxi.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:345–428.
13. Yung AR, Buckby JA, Cotton SM, et al. Psychotic-like experiences in nonpsychotic help-seekers: associations with distress, depression, and disability. Schizophr Bull. 2006;32(2):352-359.
14. Tien AY. Distributions of hallucinations in the population. Soc Psychiatry Psychiatr Epidemiol. 1991;26(6):287-292.
15. Eaton WW, Romanoski A, Anthony JC, et al. Screening for psychosis in the general population with a self-report interview. J Nerv Ment Dis. 1991;179(11):689-693.
16. Poulton R, Caspi A, Moffitt TE, et al. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57(11):1053-1058.
17. van Os J, Hanssen M, Bijl RV, et al. Prevalence of psychotic disorder and community level of psychotic symptoms: an urban-rural comparison. Arch Gen Psychiatry. 2001;58(7):663-668.
18. Sommer IE, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
19. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21(5):581-586.
20. Merabet LB, Maguire D, Warde A, et al. Visual hallucinations during prolonged blindfolding in sighted subjects. J Neuroophthalmol. 2004;24(2):109-113.
21. Fanous AH, Neale MC, Gardner CO, et al. Significant correlation in linkage signals from genome-wide scans of schizophrenia and schizotypy. Mol Psychiatry. 2007;12(10):958-965.
22. Fanous A, Gardner C, Walsh D, et al. Relationship between positive and negative symptoms of schizophrenia and schizotypal symptoms in nonpsychotic relatives. Arch Gen Psychiatry. 2001;58(7):669-673.
23. Webb CT, Levinson DF. Schizotypal and paranoid personality disorder in the relatives of patients with schizophrenia and affective disorders: a review. Schizophr Res. 1993;11(1):81-92.
24. Asai T, Sugimori E, Bando N, et al. The hierarchic structure in schizotypy and the five-factor model of personality. Psychiatry Res. 2010 May 26. [Epub ahead of print].
25. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715.
26. Meyer SE, Bearden CE, Lux SR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
27. Cannon TD, Cadenhead K, Cornblatt B, et al. Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America. Arch Gen Psychiatry. 2008;65(1):28-37.
28. Yung AR, McGorry PD. The prodromal phase of first-episode psychosis: past and current conceptualizations. Schizophr Bull. 1996;22(2):353-370.
29. Nasrallah HA. The hallucination portrait of psychosis. Current Psychiatry. 2009;8(5):10-12.
30. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020.
31. US Department of Health and Human Services. Mental health: a report of the surgeon general—executive summary. Washington, DC: US Department of Health and Human Services; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/summary.html. Accessed September 10, 2010.
32. Kane JM. An evidence-based strategy for remission in schizophrenia. J Clin Psychiatry. 2008;69(suppl 3):25-30.
33. Wagner PS. First person account: a voice from another closet. Schizophr Bull. 1996;22(2):399-401.
1. Stefanis NC, Hanssen M, Smirnis NK, et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med. 2002;32(2):347-358.
2. Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and the continuum of psychosis. Schizophr Res. 2002;54(1-2):59-65.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:297–343.
4. Tyson P, Tyson RL. Psychoanalytic theories of development: an integration. New Haven, CT: Yale University Press; 1990.
5. Schilpp PA. Philosophy of Karl Jaspers. Chicago, IL: Open Court Publishing Company; 1981.
6. Szasz TS. The second sin. Garden City, NY: Anchor Press; 1974.
7. Bentall R. Madness explained: psychosis and human nature. London, United Kingdom: Penguin Books; 2003.
8. van Os J. ‘Salience syndrome’ replaces ‘schizophrenia’ in DSM-V and ICD-11: psychiatry’s evidence-based entry into the 21st century? Acta Psychiatr Scand. 2009;120(5):363-372.
9. Lake CR, Hurwitz N. Schizoaffective disorders are psychotic mood disorders; there are no schizoaffective disorders. Psychiatry Res. 2006;143(2-3):255-287.
10. Craddock N, Owen MJ. The Kraepelinian dichotomy—going, going…but still not gone. Br J Psychiatry. 2010;196(2):92-95.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:xxxi.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000:345–428.
13. Yung AR, Buckby JA, Cotton SM, et al. Psychotic-like experiences in nonpsychotic help-seekers: associations with distress, depression, and disability. Schizophr Bull. 2006;32(2):352-359.
14. Tien AY. Distributions of hallucinations in the population. Soc Psychiatry Psychiatr Epidemiol. 1991;26(6):287-292.
15. Eaton WW, Romanoski A, Anthony JC, et al. Screening for psychosis in the general population with a self-report interview. J Nerv Ment Dis. 1991;179(11):689-693.
16. Poulton R, Caspi A, Moffitt TE, et al. Children’s self-reported psychotic symptoms and adult schizophreniform disorder: a 15-year longitudinal study. Arch Gen Psychiatry. 2000;57(11):1053-1058.
17. van Os J, Hanssen M, Bijl RV, et al. Prevalence of psychotic disorder and community level of psychotic symptoms: an urban-rural comparison. Arch Gen Psychiatry. 2001;58(7):663-668.
18. Sommer IE, Daalman K, Rietkerk T, et al. Healthy individuals with auditory verbal hallucinations; who are they? Psychiatric assessments of a selected sample of 103 subjects. Schizophr Bull. 2010;36(3):633-641.
19. Strauss JS. Hallucinations and delusions as points on continua function. Rating scale evidence. Arch Gen Psychiatry. 1969;21(5):581-586.
20. Merabet LB, Maguire D, Warde A, et al. Visual hallucinations during prolonged blindfolding in sighted subjects. J Neuroophthalmol. 2004;24(2):109-113.
21. Fanous AH, Neale MC, Gardner CO, et al. Significant correlation in linkage signals from genome-wide scans of schizophrenia and schizotypy. Mol Psychiatry. 2007;12(10):958-965.
22. Fanous A, Gardner C, Walsh D, et al. Relationship between positive and negative symptoms of schizophrenia and schizotypal symptoms in nonpsychotic relatives. Arch Gen Psychiatry. 2001;58(7):669-673.
23. Webb CT, Levinson DF. Schizotypal and paranoid personality disorder in the relatives of patients with schizophrenia and affective disorders: a review. Schizophr Res. 1993;11(1):81-92.
24. Asai T, Sugimori E, Bando N, et al. The hierarchic structure in schizotypy and the five-factor model of personality. Psychiatry Res. 2010 May 26. [Epub ahead of print].
25. Miller TJ, McGlashan TH, Rosen JL, et al. Prodromal assessment with the structured interview for prodromal syndromes and the scale of prodromal symptoms: predictive validity, interrater reliability, and training to reliability. Schizophr Bull. 2003;29(4):703-715.
26. Meyer SE, Bearden CE, Lux SR, et al. The psychosis prodrome in adolescent patients viewed through the lens of DSM-IV. J Child Adolesc Psychopharmacol. 2005;15(3):434-451.
27. Cannon TD, Cadenhead K, Cornblatt B, et al. Prediction of psychosis in youth at high clinical risk: a multisite longitudinal study in North America. Arch Gen Psychiatry. 2008;65(1):28-37.
28. Yung AR, McGorry PD. The prodromal phase of first-episode psychosis: past and current conceptualizations. Schizophr Bull. 1996;22(2):353-370.
29. Nasrallah HA. The hallucination portrait of psychosis. Current Psychiatry. 2009;8(5):10-12.
30. Bentall RP, Fernyhough C. Social predictors of psychotic experiences: specificity and psychological mechanisms. Schizophr Bull. 2008;34(6):1012-1020.
31. US Department of Health and Human Services. Mental health: a report of the surgeon general—executive summary. Washington, DC: US Department of Health and Human Services; 1999. Available at: http://www.surgeongeneral.gov/library/mentalhealth/summary.html. Accessed September 10, 2010.
32. Kane JM. An evidence-based strategy for remission in schizophrenia. J Clin Psychiatry. 2008;69(suppl 3):25-30.
33. Wagner PS. First person account: a voice from another closet. Schizophr Bull. 1996;22(2):399-401.
Adherence to the vaccine
The psychotic pot smoker
CASE: Scared and confused
Mr. C, age 28, presents to the emergency department (ED) in police custody with agitation and altered mental status. Earlier that evening, Mr. C’s girlfriend noticed he was talking to himself while watching television. A few hours later, Mr. C thought someone was breaking into his house. Mr. C ran out of the house screaming for help, broke his neighbor’s window, and eventually called the police. When the police arrived Mr. C was wearing only his underwear, shaking, and bleeding from his hands. He said he was afraid and refused to respond to police instructions. Police officers used an electronic stun gun to facilitate transport to the hospital.
Mr. C admits to smoking 3 to 4 marijuana joints daily for the past 16 years. His last drug use was 2 hours before his symptoms began. Mr. C suggests that someone may have adulterated his marijuana joint but he has no factual basis for this accusation. He denies using alcohol and other illicit drugs and has no personal or family psychiatric history. He denies recent fever, loss of consciousness, chest pain, weakness, myalgia, or headache. Medically stable, his only complaint is mild hand pain.
Mr. C is alert, awake, and oriented to his name, and he responds properly to questions. He is tachycardic (101 bpm), his blood pressure is 149/57 mm Hg with normal S1 and S2 sounds, and he has no meningismus or nystagmus. Glasgow Coma Scale score is 15. He has increased deep tendon reflexes on the right upper and lower limb with good hand-grip and multiple abrasions and lacerations on his hands.
The authors’ observations
New-onset psychosis can have a wide differential diagnosis, particularly when reliable history is not available. Mr. C’s allegation that someone tampered with his marijuana raises 2 possibilities: embalming fluid (form-aldehyde) toxicity or PCP intoxication.
Embalming fluid toxicity can cause:
- agitation and sudden unpredictable behavior
- confusion or toxic delirium
- coma or seizure
- cerebral and pulmonary edema or death in severe cases.
The terms “wet,” “sherm,” “fly,” “amp,” or “illy” are used to describe a marijuana cigarette that has been dipped into embalming fluid, dried, and then smoked.1 The effect is similar to that of PCP and causes extreme hallucinations. Reported highs last 30 minutes to 1 hour.2
Symptomatology of PCP intoxication may be indistinguishable from functional psychosis (Table 1).3 Visual, auditory, and tactile misperceptions are common and highly changeable disorientation often is accompanied by alternating periods of lethargy and fearful agitation. These patients typically show catatonic posturing and/or stereotyped movement. Somatic sensations appear to be disassociated; patients may misperceive pain, distance, and time. Patients taking PCP rarely admit to true hallucinations; however their thinking usually is grossly disoriented.4 Symptoms of delirium may last from 30 minutes to 6 hours in 80% of cases; 12% of patients may remain symptomatic for 12 hours. Violent behavior and agitation usually lasts only a few hours.5
Long-term marijuana abuse can lead to psychosis6 but acute onset is not typical, and recent prospective trials raised doubts that cannabis would be a sole factor.7 Instead, cannabis may be 1 of several factors that contribute to psychosis, particularly in patients who are predisposed.
Table 1
Phencyclidine (PCP) intoxication: What to look for
| Findings | Percentage of cases |
|---|---|
| Nystagmus | 57.4% |
| Hypertension | 57.0% |
| Delirium | 36.9% |
| Violent behavior | 35.4% |
| Agitation | 34.0% |
| Tachycardia | 30.0% |
| Bizarre behavior | 28.5% |
| Hallucinations/delusions | 18.5% |
| Unconsciousness | 10.6% |
| Lethargy/stupor | 6.6% |
| Hypothermia | 6.4% |
| Generalized rigidity | 5.2% |
| Profuse sweating | 3.9% |
| No behavior effect | 3.5% |
| Grand mal seizure | 3.1% |
| Source: Reference 3 | |
Possible neurologic causes
Complex partial seizures—also known as psychomotor epilepsy—are caused by a surge of electrical activity in the brain. Seizures often involve 1 of the brain’s temporal lobes but can affect any brain region. Symptoms include:
- impaired social interaction
- inability to control one’s movements
- alogia
- amnesia.
Episodes typically start with a blank stare followed by automatisms. The actions and movements often are unorganized or confused. Motor symptoms typically last for 1 to 2 minutes and confusion persists for another 1 to 2 minutes.8 In rare cases, a patient may become agitated or engage in behaviors such as undressing. Complex partial seizures may cause a person to run in apparent fear, cry out, or repeat a phrase.9 Electroencephalogram, CT, MRI, or positron-emission tomography scan could reveal any intracranial focus of complex partial seizures.
We suspect PCP or embalming fluid intoxication and initiate supportive therapy.
EVALUATION: Still confused
Initial baseline labs include a urine drug screen (UDS), chest radiography, ECG, and head CT. Mr. C’s UDS is positive for cannabis. A specific PCP assay is negative. White blood cell count (WBC) is 22,000/μL with high neutrophil count (88%), creatine kinase (CK) is 458 U/L, and urinalyis reveals protein 75 mg/dL and ketone 50 mg/dL. Head CT is negative for any acute process (click here for detailed description of Mr. C�s hospital course while in the ED).
During psychiatric evaluation 7 hours after presentation, Mr. C’s speech is loose and somewhat pressured, but intelligible. He cannot follow commands. Mr. C is delusional and appears to be hallucinating. He can repeat 3 words immediately but not after 3 minutes. We start Mr. C on divalproex, 1,500 mg/d, haloperidol, 6 mg/d, and IV lorazepam, 2 mg as needed for agitation. Although mildly disoriented, he gradually becomes less agitated.
The authors’ observations
At this point further evaluation is needed. Mr. C’s elevated WBC count could explain his fluctuating symptoms. He cannot provide further history and his family denies any past psychiatric episodes. Thyroid-stimulating hormone, B12, and folate levels are within normal limits. A negative LP rules out meningitic infection. We give Mr. C a diagnosis of psychosis NOS (Table 2).10
Table 2
DSM-IV-TR criteria for psychotic disorder, not otherwise specified
| This category includes psychotic symptomatology (ie, delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior) about which there is inadequate information to make a specific diagnosis or about which there is contradictory information, or disorders with psychotic symptoms that do not meet the criteria for any specific psychotic disorder. Examples include: |
|
| Source: Reference 10 |
TREATMENT: Medication choices
After 8 hours in the ED, Mr. C is transferred to the medical unit, where he becomes agitated and complains of auditory and visual hallucinations. He receives divalproex, 750 mg, haloperidol, 3 mg, and IM diphenhydramine, 50 mg, to calm him. He remains agitated but not violent until bedtime. At midnight he is agitated and violent and receives another dose of haloperidol and IM diphenhydramine with IV lorazepam, 2 mg. These medications calm him and he is able to sleep until morning.
Morning labs reveal CK is 674 U/L and WBC decreased to 13,200/μL. Mr. C denies any distress but after the fourth dose of haloperidol, he develops dystonia of his arms so we discontinue this medication. We start aripiprazole, 10 mg/d gradually increased to 30 mg/d, and Mr. C receives 1 injection of diphenhydramine. He responds well to the treatment.
The next few hours are uneventful but then Mr. C becomes verbally abusive to his relatives and sitter; physical restraints are ordered and he receives IM ziprasidone, 20 mg, and IV lorazepam, 2 mg. He remains awake and babbling. His perception continues to wax and wane and his words are jumbled. He remains calm until the next morning (click here for detailed description of Mr. C�s hospital course while on the medical unit).
After 4 days on the medical unit Mr. C is transferred to the psychiatry unit, where he is angry, belligerent, and hostile, but not placed in restraints. His symptoms resolve in 2 days without any further episodes of violent behavior.
OUTCOME: Solving the puzzle
When Mr. C becomes cooperative, he gives a detailed history. He repeats his suspicion of smoking adulterated marijuana, but during detailed questioning, he admits to using alprazolam, which he purchased illegally, to sleep for the past 6 to 7 months. He started with 1 or 2 “footballs” (1 to 2 mg) and gradually increased to 3 or 4 “bars” (6 to 8 mg) each day. Mr. C could no longer afford the drug and last took alprazolam 6 days before his symptoms began. He says that after stopping alprazolam he felt anxious and could not sleep. His girlfriend adds that he was irritable and “he had not been acting himself” several days before admission. She says he complained of hearing the voice of God, particularly when he was not taking alprazolam.
Mr. C’s hand wounds heal and his vitals are normal during his 1-week stay on the psychiatric unit. His interactions with staff and peers improve. Aripiprazole is tapered and discontinued; divalproex is reduced to 1,000 mg/d. Mr. C is discharged 11 days after presentation and prescribed divalproex, 1,000 mg/d, with instructions to taper the drug over several days to prevent withdrawal seizures before stopping it in 1 week.
Mr. C does not return for his follow-up appointment; however, in a telephone follow-up 6 months later, he denies experiencing withdrawal symptoms after discharge. Mr. C is now undergoing drug rehabilitation.
The authors’ observations
Benzodiazepine withdrawal symptoms occur 7 to 10 days after abrupt cessation (Table 3).10 Symptoms are similar to those of alcohol withdrawal and include tachycardia, hypertension, clouding of consciousness, and auditory and visual hallucinations.11 Serious reactions to benzodiazepine withdrawal include seizures and death.12
Because of the high prevalence of poly-substance misuse, obtain a detailed substance use history in patients undergoing benzodiazepine withdrawal to determine the likelihood of polysubstance withdrawal.13 A cross-tolerant sedative such as clonazepam could prevent withdrawal symptoms as the dose is gradually decreased. Long-acting benzodiazepines such as clonazepam or diazepam are recommended.14
In Mr. C’s case, minor withdrawal symptoms, such as disturbed sleep and irritability, began 3 to 4 days after discontinuing benzodiazepines15 and preceded development of psychosis. Withdrawal symptoms usually resolve after 2 weeks.16 Mr. C responded only partially to IV lorazepam because he did not receive the total replacement dose. Had we known he was experiencing benzodiazepine withdrawal, Mr. C could have been managed with detoxi"cation of the primary drug, alprazolam, with diazepam substitution and tapering over 3 weeks.17
Table 3
Criteria for sedative, hypnotic, or anxiolytic withdrawal
| A. Cessation of (or reduction in) sedative, hypnotic, or anxiolytic use that has been heavy and prolonged |
B. Two (or more) of the following, developing within several hours to a few days after Criterion A:
|
| C. The symptoms in Criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 10 |
Related Resource
- Vikander B, Koechling UM, Borg S, et al. Benzodiazepine tapering: a prospective study. Nord J Psychiatry. 2010; 64(4):273-282.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Chlordiazepoxide • Librium
- Diazepam • Valium
- Diphenhydramine • Diphenhydramine injection
- Divalproex • Depakote
- Haloperidol • Haldol
- Lorazepam • Ativan
- Ziprasidone • Geodon
Acknowledgements
The authors wish to thank Reena Kumar, MD, and Sonja Gennuso, fourth-year medical student at Louisiana State University Health Sciences Center, Shreveport, for their help in preparing this manuscript.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 1
Mr. C’s hospital course in the emergency department
| Time after presentation | Description |
|---|---|
| 2 hours | Mr. C is alert and oriented to his name and place. He rests comfortably but asks questions about his girlfriend and uncle, falsely believing they are in the emergency department |
| 4 hours | Hand lacerations are repaired, but Mr. C continues to dig in his wounds with the opposite hand and place it over his mouth despite constant redirection. He reports hearing his uncle’s voice behind the curtain. He then uses the pulse oximeter as a telephone and holds a conversation with his uncle on the other side of the curtain. On redirection, Mr. C replies that the pulse oximeter looks like a telephone and begins mumbling to himself |
| 5 hours | Mr. C continues to mumble but responds when directly questioned. He keeps insisting that the pulse oximeter is a telephone and that he can tell his uncle to come over from the other side of the curtain. He continues to act inappropriately despite the presence of family members but he is aware of their identities |
| 6 hours | Mr. C becomes disoriented and agitated and pulls out his IV line. Because of the high WBC count, we order blood cultures and a urine culture and give him IV antibiotics |
| WBC: white blood cell count | |
Table 2
Mr. C’s hospital course on the medical unit
| Time after presentation | Description |
|---|---|
| 54 hours | He is oriented to person and place. Staff notices he is talking to someone in the room but no one is present. Mr. C appears to be responding to visual hallucinations, but upon questioning he denies any symptoms. Restraints are discontinued. Divalproex is increased to 2,000 mg/d |
| 62 hours | Mr. C remains calm for several hours but later begins hallucinating and calls to his mother and others when no one is in the room. He receives IV lorazepam, 2 mg, without much response. Again he is placed in restraints and receives another dose of IV lorazepam, 3 mg, and IM ziprasidone, 20 mg. He becomes calmer. Restraints are continued as a precautionary measure. Mr. C calms down after several hours but cannot sleep |
| 78 hours | The next morning, Mr. C remains agitated and aggressive with loud speech. He denies any further hallucinations but talks to an invisible person. He remains in restraints and receives his routine medications. His blood pressure is 141/99 mm Hg and pulse is 110. Pulse rate normalizes during the day and he becomes calmer but seclusive |
1. Office of National Drug Control Policy. Street terms: drugs and the drug trade. Available at:http://www.whitehousedrugpolicy.gov/streetterms/ByType.asp?intTypeID=1. Accessed July 26, 2010.
2. Elwood WN. TCADA research brief: “Fry:” a study of adolescents’ use of embalming fluid with marijuana and tobacco. Texas Commission on Alcohol and Drug Abuse. 1998. Available at:http://www.dshs.state.tx.us/sa/research/populations/fry.pdf. Accessed August 9, 2010.
3. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: incidence of clinical findings in 1,000 cases. Ann Emerg Med. 1981;10(5):237-242.
4. Aniline O, Pitts FN, Jr. Phencyclidine (PCP): a review and perspectives. Crit Rev Toxicol. 1982;10(2):145-177.
5. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: clinical patterns, complications, and treatment. Ann Emerg Med. 1981;10(6):290-297.
6. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194.
7. Degenhardt L, Hall W. Cannabis and psychosis. Curr Psychiatry Rep. 2002;4(3):191-196.
8. Carroll E, Benbadis SR. Complex partial seizures. eMedicine. April 21, 2010. Available at:http://emedicine.medscape.com/article/1183962-overview. Accessed July 20, 2010.
9. Epilepsy.com. Complex partial seizures. Available at: http://www.epilepsy.com/epilepsy/seizure_complexpartial. Accessed July 20, 2010.
10. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
11. Mellor CS, Jain VK. Diazepam withdrawal syndrome: its prolonged and changing nature. Can Med Assoc J. 1982;127(11):1093-1096.
12. Lann MA, Molina DK. A fatal case of benzodiazepine withdrawal. Am J Forensic Med Pathol. 2009;30(2):177-179.
13. Busto UE, Romach MK, Sellers EM. Multiple drug use and psychiatric comorbidity in patients admitted to the hospital with severe benzodiazepine dependence. J Clin Psychopharmacol. 1996;16(1):51-57.
14. Franklin JE, Jr., Levenson JL, McCance-Katz EF. Substance-related disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:400–401.
15. Preskorn SH, Denner LJ. Benzodiazepines and withdrawal psychosis. Report of three cases. JAMA. 1977;237(1):36-38.
16. Miller F, Nulsen J. Single case study. Diazepam (valium) detoxification. J Nerv Ment Dis. 1979;167:637-638.
17. Seivewright N, Dougal W. Withdrawal symptoms from high dose benzodiazepines in poly drug users. Drug Alcohol Depend. 1993;32(1):15-23.
CASE: Scared and confused
Mr. C, age 28, presents to the emergency department (ED) in police custody with agitation and altered mental status. Earlier that evening, Mr. C’s girlfriend noticed he was talking to himself while watching television. A few hours later, Mr. C thought someone was breaking into his house. Mr. C ran out of the house screaming for help, broke his neighbor’s window, and eventually called the police. When the police arrived Mr. C was wearing only his underwear, shaking, and bleeding from his hands. He said he was afraid and refused to respond to police instructions. Police officers used an electronic stun gun to facilitate transport to the hospital.
Mr. C admits to smoking 3 to 4 marijuana joints daily for the past 16 years. His last drug use was 2 hours before his symptoms began. Mr. C suggests that someone may have adulterated his marijuana joint but he has no factual basis for this accusation. He denies using alcohol and other illicit drugs and has no personal or family psychiatric history. He denies recent fever, loss of consciousness, chest pain, weakness, myalgia, or headache. Medically stable, his only complaint is mild hand pain.
Mr. C is alert, awake, and oriented to his name, and he responds properly to questions. He is tachycardic (101 bpm), his blood pressure is 149/57 mm Hg with normal S1 and S2 sounds, and he has no meningismus or nystagmus. Glasgow Coma Scale score is 15. He has increased deep tendon reflexes on the right upper and lower limb with good hand-grip and multiple abrasions and lacerations on his hands.
The authors’ observations
New-onset psychosis can have a wide differential diagnosis, particularly when reliable history is not available. Mr. C’s allegation that someone tampered with his marijuana raises 2 possibilities: embalming fluid (form-aldehyde) toxicity or PCP intoxication.
Embalming fluid toxicity can cause:
- agitation and sudden unpredictable behavior
- confusion or toxic delirium
- coma or seizure
- cerebral and pulmonary edema or death in severe cases.
The terms “wet,” “sherm,” “fly,” “amp,” or “illy” are used to describe a marijuana cigarette that has been dipped into embalming fluid, dried, and then smoked.1 The effect is similar to that of PCP and causes extreme hallucinations. Reported highs last 30 minutes to 1 hour.2
Symptomatology of PCP intoxication may be indistinguishable from functional psychosis (Table 1).3 Visual, auditory, and tactile misperceptions are common and highly changeable disorientation often is accompanied by alternating periods of lethargy and fearful agitation. These patients typically show catatonic posturing and/or stereotyped movement. Somatic sensations appear to be disassociated; patients may misperceive pain, distance, and time. Patients taking PCP rarely admit to true hallucinations; however their thinking usually is grossly disoriented.4 Symptoms of delirium may last from 30 minutes to 6 hours in 80% of cases; 12% of patients may remain symptomatic for 12 hours. Violent behavior and agitation usually lasts only a few hours.5
Long-term marijuana abuse can lead to psychosis6 but acute onset is not typical, and recent prospective trials raised doubts that cannabis would be a sole factor.7 Instead, cannabis may be 1 of several factors that contribute to psychosis, particularly in patients who are predisposed.
Table 1
Phencyclidine (PCP) intoxication: What to look for
| Findings | Percentage of cases |
|---|---|
| Nystagmus | 57.4% |
| Hypertension | 57.0% |
| Delirium | 36.9% |
| Violent behavior | 35.4% |
| Agitation | 34.0% |
| Tachycardia | 30.0% |
| Bizarre behavior | 28.5% |
| Hallucinations/delusions | 18.5% |
| Unconsciousness | 10.6% |
| Lethargy/stupor | 6.6% |
| Hypothermia | 6.4% |
| Generalized rigidity | 5.2% |
| Profuse sweating | 3.9% |
| No behavior effect | 3.5% |
| Grand mal seizure | 3.1% |
| Source: Reference 3 | |
Possible neurologic causes
Complex partial seizures—also known as psychomotor epilepsy—are caused by a surge of electrical activity in the brain. Seizures often involve 1 of the brain’s temporal lobes but can affect any brain region. Symptoms include:
- impaired social interaction
- inability to control one’s movements
- alogia
- amnesia.
Episodes typically start with a blank stare followed by automatisms. The actions and movements often are unorganized or confused. Motor symptoms typically last for 1 to 2 minutes and confusion persists for another 1 to 2 minutes.8 In rare cases, a patient may become agitated or engage in behaviors such as undressing. Complex partial seizures may cause a person to run in apparent fear, cry out, or repeat a phrase.9 Electroencephalogram, CT, MRI, or positron-emission tomography scan could reveal any intracranial focus of complex partial seizures.
We suspect PCP or embalming fluid intoxication and initiate supportive therapy.
EVALUATION: Still confused
Initial baseline labs include a urine drug screen (UDS), chest radiography, ECG, and head CT. Mr. C’s UDS is positive for cannabis. A specific PCP assay is negative. White blood cell count (WBC) is 22,000/μL with high neutrophil count (88%), creatine kinase (CK) is 458 U/L, and urinalyis reveals protein 75 mg/dL and ketone 50 mg/dL. Head CT is negative for any acute process (click here for detailed description of Mr. C�s hospital course while in the ED).
During psychiatric evaluation 7 hours after presentation, Mr. C’s speech is loose and somewhat pressured, but intelligible. He cannot follow commands. Mr. C is delusional and appears to be hallucinating. He can repeat 3 words immediately but not after 3 minutes. We start Mr. C on divalproex, 1,500 mg/d, haloperidol, 6 mg/d, and IV lorazepam, 2 mg as needed for agitation. Although mildly disoriented, he gradually becomes less agitated.
The authors’ observations
At this point further evaluation is needed. Mr. C’s elevated WBC count could explain his fluctuating symptoms. He cannot provide further history and his family denies any past psychiatric episodes. Thyroid-stimulating hormone, B12, and folate levels are within normal limits. A negative LP rules out meningitic infection. We give Mr. C a diagnosis of psychosis NOS (Table 2).10
Table 2
DSM-IV-TR criteria for psychotic disorder, not otherwise specified
| This category includes psychotic symptomatology (ie, delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior) about which there is inadequate information to make a specific diagnosis or about which there is contradictory information, or disorders with psychotic symptoms that do not meet the criteria for any specific psychotic disorder. Examples include: |
|
| Source: Reference 10 |
TREATMENT: Medication choices
After 8 hours in the ED, Mr. C is transferred to the medical unit, where he becomes agitated and complains of auditory and visual hallucinations. He receives divalproex, 750 mg, haloperidol, 3 mg, and IM diphenhydramine, 50 mg, to calm him. He remains agitated but not violent until bedtime. At midnight he is agitated and violent and receives another dose of haloperidol and IM diphenhydramine with IV lorazepam, 2 mg. These medications calm him and he is able to sleep until morning.
Morning labs reveal CK is 674 U/L and WBC decreased to 13,200/μL. Mr. C denies any distress but after the fourth dose of haloperidol, he develops dystonia of his arms so we discontinue this medication. We start aripiprazole, 10 mg/d gradually increased to 30 mg/d, and Mr. C receives 1 injection of diphenhydramine. He responds well to the treatment.
The next few hours are uneventful but then Mr. C becomes verbally abusive to his relatives and sitter; physical restraints are ordered and he receives IM ziprasidone, 20 mg, and IV lorazepam, 2 mg. He remains awake and babbling. His perception continues to wax and wane and his words are jumbled. He remains calm until the next morning (click here for detailed description of Mr. C�s hospital course while on the medical unit).
After 4 days on the medical unit Mr. C is transferred to the psychiatry unit, where he is angry, belligerent, and hostile, but not placed in restraints. His symptoms resolve in 2 days without any further episodes of violent behavior.
OUTCOME: Solving the puzzle
When Mr. C becomes cooperative, he gives a detailed history. He repeats his suspicion of smoking adulterated marijuana, but during detailed questioning, he admits to using alprazolam, which he purchased illegally, to sleep for the past 6 to 7 months. He started with 1 or 2 “footballs” (1 to 2 mg) and gradually increased to 3 or 4 “bars” (6 to 8 mg) each day. Mr. C could no longer afford the drug and last took alprazolam 6 days before his symptoms began. He says that after stopping alprazolam he felt anxious and could not sleep. His girlfriend adds that he was irritable and “he had not been acting himself” several days before admission. She says he complained of hearing the voice of God, particularly when he was not taking alprazolam.
Mr. C’s hand wounds heal and his vitals are normal during his 1-week stay on the psychiatric unit. His interactions with staff and peers improve. Aripiprazole is tapered and discontinued; divalproex is reduced to 1,000 mg/d. Mr. C is discharged 11 days after presentation and prescribed divalproex, 1,000 mg/d, with instructions to taper the drug over several days to prevent withdrawal seizures before stopping it in 1 week.
Mr. C does not return for his follow-up appointment; however, in a telephone follow-up 6 months later, he denies experiencing withdrawal symptoms after discharge. Mr. C is now undergoing drug rehabilitation.
The authors’ observations
Benzodiazepine withdrawal symptoms occur 7 to 10 days after abrupt cessation (Table 3).10 Symptoms are similar to those of alcohol withdrawal and include tachycardia, hypertension, clouding of consciousness, and auditory and visual hallucinations.11 Serious reactions to benzodiazepine withdrawal include seizures and death.12
Because of the high prevalence of poly-substance misuse, obtain a detailed substance use history in patients undergoing benzodiazepine withdrawal to determine the likelihood of polysubstance withdrawal.13 A cross-tolerant sedative such as clonazepam could prevent withdrawal symptoms as the dose is gradually decreased. Long-acting benzodiazepines such as clonazepam or diazepam are recommended.14
In Mr. C’s case, minor withdrawal symptoms, such as disturbed sleep and irritability, began 3 to 4 days after discontinuing benzodiazepines15 and preceded development of psychosis. Withdrawal symptoms usually resolve after 2 weeks.16 Mr. C responded only partially to IV lorazepam because he did not receive the total replacement dose. Had we known he was experiencing benzodiazepine withdrawal, Mr. C could have been managed with detoxi"cation of the primary drug, alprazolam, with diazepam substitution and tapering over 3 weeks.17
Table 3
Criteria for sedative, hypnotic, or anxiolytic withdrawal
| A. Cessation of (or reduction in) sedative, hypnotic, or anxiolytic use that has been heavy and prolonged |
B. Two (or more) of the following, developing within several hours to a few days after Criterion A:
|
| C. The symptoms in Criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 10 |
Related Resource
- Vikander B, Koechling UM, Borg S, et al. Benzodiazepine tapering: a prospective study. Nord J Psychiatry. 2010; 64(4):273-282.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Chlordiazepoxide • Librium
- Diazepam • Valium
- Diphenhydramine • Diphenhydramine injection
- Divalproex • Depakote
- Haloperidol • Haldol
- Lorazepam • Ativan
- Ziprasidone • Geodon
Acknowledgements
The authors wish to thank Reena Kumar, MD, and Sonja Gennuso, fourth-year medical student at Louisiana State University Health Sciences Center, Shreveport, for their help in preparing this manuscript.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 1
Mr. C’s hospital course in the emergency department
| Time after presentation | Description |
|---|---|
| 2 hours | Mr. C is alert and oriented to his name and place. He rests comfortably but asks questions about his girlfriend and uncle, falsely believing they are in the emergency department |
| 4 hours | Hand lacerations are repaired, but Mr. C continues to dig in his wounds with the opposite hand and place it over his mouth despite constant redirection. He reports hearing his uncle’s voice behind the curtain. He then uses the pulse oximeter as a telephone and holds a conversation with his uncle on the other side of the curtain. On redirection, Mr. C replies that the pulse oximeter looks like a telephone and begins mumbling to himself |
| 5 hours | Mr. C continues to mumble but responds when directly questioned. He keeps insisting that the pulse oximeter is a telephone and that he can tell his uncle to come over from the other side of the curtain. He continues to act inappropriately despite the presence of family members but he is aware of their identities |
| 6 hours | Mr. C becomes disoriented and agitated and pulls out his IV line. Because of the high WBC count, we order blood cultures and a urine culture and give him IV antibiotics |
| WBC: white blood cell count | |
Table 2
Mr. C’s hospital course on the medical unit
| Time after presentation | Description |
|---|---|
| 54 hours | He is oriented to person and place. Staff notices he is talking to someone in the room but no one is present. Mr. C appears to be responding to visual hallucinations, but upon questioning he denies any symptoms. Restraints are discontinued. Divalproex is increased to 2,000 mg/d |
| 62 hours | Mr. C remains calm for several hours but later begins hallucinating and calls to his mother and others when no one is in the room. He receives IV lorazepam, 2 mg, without much response. Again he is placed in restraints and receives another dose of IV lorazepam, 3 mg, and IM ziprasidone, 20 mg. He becomes calmer. Restraints are continued as a precautionary measure. Mr. C calms down after several hours but cannot sleep |
| 78 hours | The next morning, Mr. C remains agitated and aggressive with loud speech. He denies any further hallucinations but talks to an invisible person. He remains in restraints and receives his routine medications. His blood pressure is 141/99 mm Hg and pulse is 110. Pulse rate normalizes during the day and he becomes calmer but seclusive |
CASE: Scared and confused
Mr. C, age 28, presents to the emergency department (ED) in police custody with agitation and altered mental status. Earlier that evening, Mr. C’s girlfriend noticed he was talking to himself while watching television. A few hours later, Mr. C thought someone was breaking into his house. Mr. C ran out of the house screaming for help, broke his neighbor’s window, and eventually called the police. When the police arrived Mr. C was wearing only his underwear, shaking, and bleeding from his hands. He said he was afraid and refused to respond to police instructions. Police officers used an electronic stun gun to facilitate transport to the hospital.
Mr. C admits to smoking 3 to 4 marijuana joints daily for the past 16 years. His last drug use was 2 hours before his symptoms began. Mr. C suggests that someone may have adulterated his marijuana joint but he has no factual basis for this accusation. He denies using alcohol and other illicit drugs and has no personal or family psychiatric history. He denies recent fever, loss of consciousness, chest pain, weakness, myalgia, or headache. Medically stable, his only complaint is mild hand pain.
Mr. C is alert, awake, and oriented to his name, and he responds properly to questions. He is tachycardic (101 bpm), his blood pressure is 149/57 mm Hg with normal S1 and S2 sounds, and he has no meningismus or nystagmus. Glasgow Coma Scale score is 15. He has increased deep tendon reflexes on the right upper and lower limb with good hand-grip and multiple abrasions and lacerations on his hands.
The authors’ observations
New-onset psychosis can have a wide differential diagnosis, particularly when reliable history is not available. Mr. C’s allegation that someone tampered with his marijuana raises 2 possibilities: embalming fluid (form-aldehyde) toxicity or PCP intoxication.
Embalming fluid toxicity can cause:
- agitation and sudden unpredictable behavior
- confusion or toxic delirium
- coma or seizure
- cerebral and pulmonary edema or death in severe cases.
The terms “wet,” “sherm,” “fly,” “amp,” or “illy” are used to describe a marijuana cigarette that has been dipped into embalming fluid, dried, and then smoked.1 The effect is similar to that of PCP and causes extreme hallucinations. Reported highs last 30 minutes to 1 hour.2
Symptomatology of PCP intoxication may be indistinguishable from functional psychosis (Table 1).3 Visual, auditory, and tactile misperceptions are common and highly changeable disorientation often is accompanied by alternating periods of lethargy and fearful agitation. These patients typically show catatonic posturing and/or stereotyped movement. Somatic sensations appear to be disassociated; patients may misperceive pain, distance, and time. Patients taking PCP rarely admit to true hallucinations; however their thinking usually is grossly disoriented.4 Symptoms of delirium may last from 30 minutes to 6 hours in 80% of cases; 12% of patients may remain symptomatic for 12 hours. Violent behavior and agitation usually lasts only a few hours.5
Long-term marijuana abuse can lead to psychosis6 but acute onset is not typical, and recent prospective trials raised doubts that cannabis would be a sole factor.7 Instead, cannabis may be 1 of several factors that contribute to psychosis, particularly in patients who are predisposed.
Table 1
Phencyclidine (PCP) intoxication: What to look for
| Findings | Percentage of cases |
|---|---|
| Nystagmus | 57.4% |
| Hypertension | 57.0% |
| Delirium | 36.9% |
| Violent behavior | 35.4% |
| Agitation | 34.0% |
| Tachycardia | 30.0% |
| Bizarre behavior | 28.5% |
| Hallucinations/delusions | 18.5% |
| Unconsciousness | 10.6% |
| Lethargy/stupor | 6.6% |
| Hypothermia | 6.4% |
| Generalized rigidity | 5.2% |
| Profuse sweating | 3.9% |
| No behavior effect | 3.5% |
| Grand mal seizure | 3.1% |
| Source: Reference 3 | |
Possible neurologic causes
Complex partial seizures—also known as psychomotor epilepsy—are caused by a surge of electrical activity in the brain. Seizures often involve 1 of the brain’s temporal lobes but can affect any brain region. Symptoms include:
- impaired social interaction
- inability to control one’s movements
- alogia
- amnesia.
Episodes typically start with a blank stare followed by automatisms. The actions and movements often are unorganized or confused. Motor symptoms typically last for 1 to 2 minutes and confusion persists for another 1 to 2 minutes.8 In rare cases, a patient may become agitated or engage in behaviors such as undressing. Complex partial seizures may cause a person to run in apparent fear, cry out, or repeat a phrase.9 Electroencephalogram, CT, MRI, or positron-emission tomography scan could reveal any intracranial focus of complex partial seizures.
We suspect PCP or embalming fluid intoxication and initiate supportive therapy.
EVALUATION: Still confused
Initial baseline labs include a urine drug screen (UDS), chest radiography, ECG, and head CT. Mr. C’s UDS is positive for cannabis. A specific PCP assay is negative. White blood cell count (WBC) is 22,000/μL with high neutrophil count (88%), creatine kinase (CK) is 458 U/L, and urinalyis reveals protein 75 mg/dL and ketone 50 mg/dL. Head CT is negative for any acute process (click here for detailed description of Mr. C�s hospital course while in the ED).
During psychiatric evaluation 7 hours after presentation, Mr. C’s speech is loose and somewhat pressured, but intelligible. He cannot follow commands. Mr. C is delusional and appears to be hallucinating. He can repeat 3 words immediately but not after 3 minutes. We start Mr. C on divalproex, 1,500 mg/d, haloperidol, 6 mg/d, and IV lorazepam, 2 mg as needed for agitation. Although mildly disoriented, he gradually becomes less agitated.
The authors’ observations
At this point further evaluation is needed. Mr. C’s elevated WBC count could explain his fluctuating symptoms. He cannot provide further history and his family denies any past psychiatric episodes. Thyroid-stimulating hormone, B12, and folate levels are within normal limits. A negative LP rules out meningitic infection. We give Mr. C a diagnosis of psychosis NOS (Table 2).10
Table 2
DSM-IV-TR criteria for psychotic disorder, not otherwise specified
| This category includes psychotic symptomatology (ie, delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior) about which there is inadequate information to make a specific diagnosis or about which there is contradictory information, or disorders with psychotic symptoms that do not meet the criteria for any specific psychotic disorder. Examples include: |
|
| Source: Reference 10 |
TREATMENT: Medication choices
After 8 hours in the ED, Mr. C is transferred to the medical unit, where he becomes agitated and complains of auditory and visual hallucinations. He receives divalproex, 750 mg, haloperidol, 3 mg, and IM diphenhydramine, 50 mg, to calm him. He remains agitated but not violent until bedtime. At midnight he is agitated and violent and receives another dose of haloperidol and IM diphenhydramine with IV lorazepam, 2 mg. These medications calm him and he is able to sleep until morning.
Morning labs reveal CK is 674 U/L and WBC decreased to 13,200/μL. Mr. C denies any distress but after the fourth dose of haloperidol, he develops dystonia of his arms so we discontinue this medication. We start aripiprazole, 10 mg/d gradually increased to 30 mg/d, and Mr. C receives 1 injection of diphenhydramine. He responds well to the treatment.
The next few hours are uneventful but then Mr. C becomes verbally abusive to his relatives and sitter; physical restraints are ordered and he receives IM ziprasidone, 20 mg, and IV lorazepam, 2 mg. He remains awake and babbling. His perception continues to wax and wane and his words are jumbled. He remains calm until the next morning (click here for detailed description of Mr. C�s hospital course while on the medical unit).
After 4 days on the medical unit Mr. C is transferred to the psychiatry unit, where he is angry, belligerent, and hostile, but not placed in restraints. His symptoms resolve in 2 days without any further episodes of violent behavior.
OUTCOME: Solving the puzzle
When Mr. C becomes cooperative, he gives a detailed history. He repeats his suspicion of smoking adulterated marijuana, but during detailed questioning, he admits to using alprazolam, which he purchased illegally, to sleep for the past 6 to 7 months. He started with 1 or 2 “footballs” (1 to 2 mg) and gradually increased to 3 or 4 “bars” (6 to 8 mg) each day. Mr. C could no longer afford the drug and last took alprazolam 6 days before his symptoms began. He says that after stopping alprazolam he felt anxious and could not sleep. His girlfriend adds that he was irritable and “he had not been acting himself” several days before admission. She says he complained of hearing the voice of God, particularly when he was not taking alprazolam.
Mr. C’s hand wounds heal and his vitals are normal during his 1-week stay on the psychiatric unit. His interactions with staff and peers improve. Aripiprazole is tapered and discontinued; divalproex is reduced to 1,000 mg/d. Mr. C is discharged 11 days after presentation and prescribed divalproex, 1,000 mg/d, with instructions to taper the drug over several days to prevent withdrawal seizures before stopping it in 1 week.
Mr. C does not return for his follow-up appointment; however, in a telephone follow-up 6 months later, he denies experiencing withdrawal symptoms after discharge. Mr. C is now undergoing drug rehabilitation.
The authors’ observations
Benzodiazepine withdrawal symptoms occur 7 to 10 days after abrupt cessation (Table 3).10 Symptoms are similar to those of alcohol withdrawal and include tachycardia, hypertension, clouding of consciousness, and auditory and visual hallucinations.11 Serious reactions to benzodiazepine withdrawal include seizures and death.12
Because of the high prevalence of poly-substance misuse, obtain a detailed substance use history in patients undergoing benzodiazepine withdrawal to determine the likelihood of polysubstance withdrawal.13 A cross-tolerant sedative such as clonazepam could prevent withdrawal symptoms as the dose is gradually decreased. Long-acting benzodiazepines such as clonazepam or diazepam are recommended.14
In Mr. C’s case, minor withdrawal symptoms, such as disturbed sleep and irritability, began 3 to 4 days after discontinuing benzodiazepines15 and preceded development of psychosis. Withdrawal symptoms usually resolve after 2 weeks.16 Mr. C responded only partially to IV lorazepam because he did not receive the total replacement dose. Had we known he was experiencing benzodiazepine withdrawal, Mr. C could have been managed with detoxi"cation of the primary drug, alprazolam, with diazepam substitution and tapering over 3 weeks.17
Table 3
Criteria for sedative, hypnotic, or anxiolytic withdrawal
| A. Cessation of (or reduction in) sedative, hypnotic, or anxiolytic use that has been heavy and prolonged |
B. Two (or more) of the following, developing within several hours to a few days after Criterion A:
|
| C. The symptoms in Criterion B cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| D. The symptoms are not due to a general medical condition and are not better accounted for by another mental disorder |
| Source: Reference 10 |
Related Resource
- Vikander B, Koechling UM, Borg S, et al. Benzodiazepine tapering: a prospective study. Nord J Psychiatry. 2010; 64(4):273-282.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Chlordiazepoxide • Librium
- Diazepam • Valium
- Diphenhydramine • Diphenhydramine injection
- Divalproex • Depakote
- Haloperidol • Haldol
- Lorazepam • Ativan
- Ziprasidone • Geodon
Acknowledgements
The authors wish to thank Reena Kumar, MD, and Sonja Gennuso, fourth-year medical student at Louisiana State University Health Sciences Center, Shreveport, for their help in preparing this manuscript.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table 1
Mr. C’s hospital course in the emergency department
| Time after presentation | Description |
|---|---|
| 2 hours | Mr. C is alert and oriented to his name and place. He rests comfortably but asks questions about his girlfriend and uncle, falsely believing they are in the emergency department |
| 4 hours | Hand lacerations are repaired, but Mr. C continues to dig in his wounds with the opposite hand and place it over his mouth despite constant redirection. He reports hearing his uncle’s voice behind the curtain. He then uses the pulse oximeter as a telephone and holds a conversation with his uncle on the other side of the curtain. On redirection, Mr. C replies that the pulse oximeter looks like a telephone and begins mumbling to himself |
| 5 hours | Mr. C continues to mumble but responds when directly questioned. He keeps insisting that the pulse oximeter is a telephone and that he can tell his uncle to come over from the other side of the curtain. He continues to act inappropriately despite the presence of family members but he is aware of their identities |
| 6 hours | Mr. C becomes disoriented and agitated and pulls out his IV line. Because of the high WBC count, we order blood cultures and a urine culture and give him IV antibiotics |
| WBC: white blood cell count | |
Table 2
Mr. C’s hospital course on the medical unit
| Time after presentation | Description |
|---|---|
| 54 hours | He is oriented to person and place. Staff notices he is talking to someone in the room but no one is present. Mr. C appears to be responding to visual hallucinations, but upon questioning he denies any symptoms. Restraints are discontinued. Divalproex is increased to 2,000 mg/d |
| 62 hours | Mr. C remains calm for several hours but later begins hallucinating and calls to his mother and others when no one is in the room. He receives IV lorazepam, 2 mg, without much response. Again he is placed in restraints and receives another dose of IV lorazepam, 3 mg, and IM ziprasidone, 20 mg. He becomes calmer. Restraints are continued as a precautionary measure. Mr. C calms down after several hours but cannot sleep |
| 78 hours | The next morning, Mr. C remains agitated and aggressive with loud speech. He denies any further hallucinations but talks to an invisible person. He remains in restraints and receives his routine medications. His blood pressure is 141/99 mm Hg and pulse is 110. Pulse rate normalizes during the day and he becomes calmer but seclusive |
1. Office of National Drug Control Policy. Street terms: drugs and the drug trade. Available at:http://www.whitehousedrugpolicy.gov/streetterms/ByType.asp?intTypeID=1. Accessed July 26, 2010.
2. Elwood WN. TCADA research brief: “Fry:” a study of adolescents’ use of embalming fluid with marijuana and tobacco. Texas Commission on Alcohol and Drug Abuse. 1998. Available at:http://www.dshs.state.tx.us/sa/research/populations/fry.pdf. Accessed August 9, 2010.
3. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: incidence of clinical findings in 1,000 cases. Ann Emerg Med. 1981;10(5):237-242.
4. Aniline O, Pitts FN, Jr. Phencyclidine (PCP): a review and perspectives. Crit Rev Toxicol. 1982;10(2):145-177.
5. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: clinical patterns, complications, and treatment. Ann Emerg Med. 1981;10(6):290-297.
6. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194.
7. Degenhardt L, Hall W. Cannabis and psychosis. Curr Psychiatry Rep. 2002;4(3):191-196.
8. Carroll E, Benbadis SR. Complex partial seizures. eMedicine. April 21, 2010. Available at:http://emedicine.medscape.com/article/1183962-overview. Accessed July 20, 2010.
9. Epilepsy.com. Complex partial seizures. Available at: http://www.epilepsy.com/epilepsy/seizure_complexpartial. Accessed July 20, 2010.
10. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
11. Mellor CS, Jain VK. Diazepam withdrawal syndrome: its prolonged and changing nature. Can Med Assoc J. 1982;127(11):1093-1096.
12. Lann MA, Molina DK. A fatal case of benzodiazepine withdrawal. Am J Forensic Med Pathol. 2009;30(2):177-179.
13. Busto UE, Romach MK, Sellers EM. Multiple drug use and psychiatric comorbidity in patients admitted to the hospital with severe benzodiazepine dependence. J Clin Psychopharmacol. 1996;16(1):51-57.
14. Franklin JE, Jr., Levenson JL, McCance-Katz EF. Substance-related disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:400–401.
15. Preskorn SH, Denner LJ. Benzodiazepines and withdrawal psychosis. Report of three cases. JAMA. 1977;237(1):36-38.
16. Miller F, Nulsen J. Single case study. Diazepam (valium) detoxification. J Nerv Ment Dis. 1979;167:637-638.
17. Seivewright N, Dougal W. Withdrawal symptoms from high dose benzodiazepines in poly drug users. Drug Alcohol Depend. 1993;32(1):15-23.
1. Office of National Drug Control Policy. Street terms: drugs and the drug trade. Available at:http://www.whitehousedrugpolicy.gov/streetterms/ByType.asp?intTypeID=1. Accessed July 26, 2010.
2. Elwood WN. TCADA research brief: “Fry:” a study of adolescents’ use of embalming fluid with marijuana and tobacco. Texas Commission on Alcohol and Drug Abuse. 1998. Available at:http://www.dshs.state.tx.us/sa/research/populations/fry.pdf. Accessed August 9, 2010.
3. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: incidence of clinical findings in 1,000 cases. Ann Emerg Med. 1981;10(5):237-242.
4. Aniline O, Pitts FN, Jr. Phencyclidine (PCP): a review and perspectives. Crit Rev Toxicol. 1982;10(2):145-177.
5. McCarron MM, Schulze BW, Thomson GA, et al. Acute phencyclidine intoxication: clinical patterns, complications, and treatment. Ann Emerg Med. 1981;10(6):290-297.
6. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194.
7. Degenhardt L, Hall W. Cannabis and psychosis. Curr Psychiatry Rep. 2002;4(3):191-196.
8. Carroll E, Benbadis SR. Complex partial seizures. eMedicine. April 21, 2010. Available at:http://emedicine.medscape.com/article/1183962-overview. Accessed July 20, 2010.
9. Epilepsy.com. Complex partial seizures. Available at: http://www.epilepsy.com/epilepsy/seizure_complexpartial. Accessed July 20, 2010.
10. Diagnostic and statistical manual of mental disorders 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
11. Mellor CS, Jain VK. Diazepam withdrawal syndrome: its prolonged and changing nature. Can Med Assoc J. 1982;127(11):1093-1096.
12. Lann MA, Molina DK. A fatal case of benzodiazepine withdrawal. Am J Forensic Med Pathol. 2009;30(2):177-179.
13. Busto UE, Romach MK, Sellers EM. Multiple drug use and psychiatric comorbidity in patients admitted to the hospital with severe benzodiazepine dependence. J Clin Psychopharmacol. 1996;16(1):51-57.
14. Franklin JE, Jr., Levenson JL, McCance-Katz EF. Substance-related disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Arlington, VA: American Psychiatric Publishing, Inc.; 2005:400–401.
15. Preskorn SH, Denner LJ. Benzodiazepines and withdrawal psychosis. Report of three cases. JAMA. 1977;237(1):36-38.
16. Miller F, Nulsen J. Single case study. Diazepam (valium) detoxification. J Nerv Ment Dis. 1979;167:637-638.
17. Seivewright N, Dougal W. Withdrawal symptoms from high dose benzodiazepines in poly drug users. Drug Alcohol Depend. 1993;32(1):15-23.
Should you order genetic testing to identify how patients metabolize antipsychotics?
Two months ago, Mr. P, age 20, experienced paranoid thoughts, anxiety, agitation, and auditory hallucinations. During a brief hospitalization 1 month later, he received IM haloperidol, 2 mg, which he said “made his neck stiff.” After he was discharged, Mr. P, who is White, stopped taking his antipsychotics. During a recent outpatient evaluation, the clinician gives Mr. P a working diagnosis of schizophrenia and prescribes risperidone, 2 mg/d, with plans to titrate to 4 mg/d in the next 2 weeks. However, a week later, Mr. P complains of extreme sedation and feeling “knocked out” and does not want to continue taking the medication. Physical exam reveals slight cogwheel rigidity. His delusional thought content is not improved. The treating physician considers ordering a genetic test to determine Mr. P’s cytochrome P450 (CYP) 2D6 metabolizer status.
Studies investigating relationships among genetic variants thought to impact pharmacokinetics and pharmacodynamics of psychotropic medications have had mixed results.1 Metabolism of most antipsychotics depends on the CYP450 enzyme system, which is expressed predominantly in the liver (Table 1). CYP2D6 is one of these enzymes and may be responsible for metabolizing approximately 20% to 50% of all medications, including a number of antipsychotics.2 Genetic variations of CYP2D6 are common and the frequencies of these variants differ among racial groups.3
The half-life and other pharmacokinetic parameters of an antipsychotic metabolized by CYP2D6 may differ based on whether someone is a poor metabolizer (PM), intermediate metabolizer (IM), extensive metabolizer (EM), or ultrarapid metabolizer (UM).4 Regarding CYP2D6 metabolism among Whites, 3% to 5% are UMs, 70% to 80% are EMs, 10% to 17% are IMs, and 5% to 10% are PMs.5 By contrast, the percentage of PMs and UMs in the Asian population is low—about 1% for each phenotype; the IM phenotype is more common (65% to 70% in the Chinese population).5,6 The percentage of PMs in African Americans is roughly 2% to 6%.2
- Genetic variants of CYP2D6 may result in decreased or increased metabolism of some drugs, including risperidone, iloperidone, perphenazine, haloperidol, and thioridazine.
- The effect of reduced CYP2D6 activity may increase a patient’s risk for dose-related adverse effects.
- It is currently unknown if clinical genotyping for CYP2D6 variants and using this information to guide drug selection or dosing improves patient outcomes.
The clinical effect of altered metabolizer status depends on the extent the metabolism of a given agent is dependent on CYP2D6. PM status results in an approximately 2- to 6-fold increase in elimination half-life and overall exposure of aripiprazole,7 risperidone,8 and iloperidone9 (Figure). On the other end of the spectrum are UMs. Because of gene duplication, patients who fall into this category have enhanced metabolic activity. As a result, the therapeutic effect of several medications may be decreased because of faster clearance from the body, leading some physicians to label them as treatment-resistant.
Because side effects of many antipsychotics are dose-dependent, genotyping may be valuable for patients taking agents that are primarily metabolized by CYP2D6.10 Clinicians now have access to laboratory resources and FDA-approved methods for assessing CYP2D6 gene variants.11 It is debatable, however, whether this testing—which is expensive (≥$400) and may not be covered by health insurance—improves patient outcomes. In Mr. P’s case, if he had been genotyped as a CYP2D6 PM before treatment, his physicians might not have prescribed haloperidol and could have prevented a mild dystonic reaction. Also, they could have lowered the initial risperidone dose or chosen an antipsychotic such as ziprasidone, paliperidone, or quetiapine where the pharmacokinetic consequences of 2D6 poor metabolism are not as severe. Theoretically, one may argue that this could have reduced the risk for antipsychotic-associated side effects that now are a barrier to Mr. P’s desire to continue antipsychotics. On the other hand one may also reasonably argue that there may be other/additional reasons (genetic or non-genetic) that make some patients more sensitive to the side effects of antipsychotics and that simply assessing CYP2D6 status is not enough to guide drug selection and dosing.
Table 1
Cytochrome P450 (CYP) metabolism of commonly used antipsychotics*
| Drug | CYP1A2 | CYP2C9 | CYP2C19 | CYP2D6 | CYP3A4/5 |
|---|---|---|---|---|---|
| Aripiprazole | X | X | |||
| Asenapine | X | X | X | ||
| Chlorpromazine | X | X | X | ||
| Clozapine | X | X | X | X | X |
| Fluphenazine | X | ||||
| Haloperidol | X | X | X | ||
| Iloperidone | X | X | |||
| Olanzapine | X | X | |||
| Paliperidone | X† | X† | |||
| Perphenazine | X | X | X | X | X |
| Quetiapine | X | X | |||
| Risperidone | X | X | |||
| Thioridazine | X | X | |||
| Ziprasidone | X | X | |||
| *Information obtained from the most recent prescribing information available from each drug’s manufacturer †According to paliperidone’s prescribing information, in vitro studies identify that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, but in vivo studies indicate that their role in eliminating paliperidone is minimal | |||||
Figure: Effects of CYP2D6 poor metabolizer status on the half-life of risperidone, aripiprazole, and iloperidone
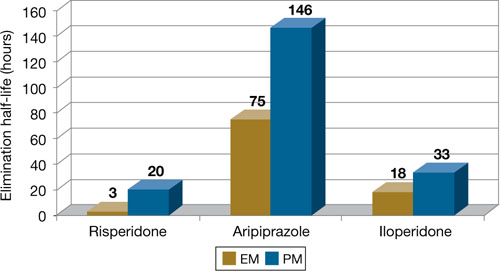
EM: extensive metabolizer; PM: poor metabolizer
Source: References 7-9
Use in clinical practice
Proposed expert guidelines recommend halving the normal target dose of risperidone and avoiding haloperidol and phenothiazine antipsychotics in CYP2D6 PMs.12 These guidelines are based on expert review of the pharmacokinetic effects of CYP2D6 PM status as well as case reports and studies associating CYP2D6 with poor outcomes, usually side effects. Although these studies suggest that determining metabolizer status may be clinically important, many other studies—some very large—have not found evidence for associations between drug metabolizing enzyme variants and clinical outcomes from antipsychotics.13
There are 2 clinical scenarios in which one may consider obtaining CYP2D6 genotype information:
- before initiating treatment (Table 2)
- after trying ≥1 agent primarily dependent on CYP2D6 with evidence of dose-related side effect (Table 3).
Identifying PMs could influence drug selection and dosing if this information is available before antipsychotic exposure. Studies have found evidence that CYP2D6 PMs may be at greater risk of experiencing adverse reactions to risperidone compared with other metabolizer groups.14 Also, prescribing information for aripiprazole and iloperidone recommends halving the dose of these drugs in the presence of CYP2D6 inhibitors, a condition that pharmacokinetically mimics PM status.
Knowing genotype information after ≥1 drugs have been tried may not be as useful. Clinicians often base drug switches or dose titrations on a patient’s experience with present or past doses of the antipsychotic. Examples include slowing titrations or reducing a target dose when a patient, such as Mr. P, experiences side effects, or selecting non-2D6 substrate agents after detecting a pattern of drug sensitivity.
Table 2
CYP2D6 testing before initiating antipsychotics: Benefits vs drawbacks
| Benefits | Drawbacks |
|---|---|
| Clinicians could avoid 2D6 substrate drugs with high likelihood for ADEs or increased risk of 2D6-based interactions in PMs | No empiric evidence shows that routine genotyping produces better clinical outcomes (eg, fewer side effects and better treatment adherence) |
| May lower initial dose, slow titration, and lower initial target dose to minimize risk of side effects in PMs | Many clinicians titrate slowly or adjust titration schedule and target doses based on initial tolerability as part of routine practice |
| The test would need to be done only once and the information may be useful for other therapy decisions | Patients who need immediate drug therapy may not be able to wait for test results |
| Testing may not be covered by a patient’s health insurance | |
| ADEs: adverse drug events; PMs: poor metabolizers | |
Table 3
Genotype testing after a patient experiences side effects
| Benefits |
| Identifying a biologic reason for side effect sensitivity may aid choice and dosing of subsequent antipsychotics and other medications |
| Drawbacks |
| In clinical practice, antipsychotic switching because of tolerability (and response) often is guided by outcomes experienced from previously used agents. In general, patients with a history of experiencing side effects at lower doses of antipsychotics are likely to be initiated at lower doses and titrated more cautiously during subsequent therapy choices regardless of whether side effects were caused by metabolizer status or other factor(s) |
Better patient outcomes?
It is not known if obtaining genotype information will provide better outcomes than a “trial and error” approach. Currently, obtaining genotype information before antipsychotic treatment is not standard clinical practice. Because this testing is expensive and requires prior approval from third party payers or out-of-pocket financial resources, testing is not recommended for all patients at this time.
However, a growing body of evidence suggests that knowing metabolizer status could be useful in drug selection or dosing for antipsychotics. This scientific knowledge continues to accumulate, and CYP2D6 genotyping may some day be integrated into routine clinical care. Currently, for patients and physicians with the resources to obtain and the ability to appropriately interpret the test results, this information may prove useful on an individual basis. However, additional studies are needed to support better outcomes from dosing and drug selection based on CYP2D6 genotype information.
Related Resources
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP). www.egappreviews.org.
- Pharmacogenomics Knowledge Base. www.pharmgkb.org.
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Iloperidone • Fanapt
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Bishop receives grant/research support from the National Institute of Mental Health, NARSAD, and Ortho-McNeil-Janssen and has received honoraria from Eli Lilly and Company.
Ms. Chae reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Leckband SG, Bishop JR, Ellingrod VL. Pharmacogenomics in psychiatry. J Pharm Pract. 2007;20:252-264.
2. Neafsey P, Ginsberg G, Hattis D, et al. Genetic polymorphism in cytochrome P450 2D6 (CYP2D6): population distribution of CYP2D6 activity. J Toxicol Environ Health B Crit Rev. 2009;12(5-6):334-361.
3. Bradford LD, Gaedigk A, Leeder JS. High frequency of CYP2D6 poor and “intermediate” metabolizers in black populations: a review and preliminary data. Psychopharmacol Bull. 1998;34:797-804.
4. Gaedigk A, Simon SD, Pearce RE, et al. The CYP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin Pharmacol Ther. 2008;83:234-242.
5. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: part II. Clin Pharmacokinet. 2009;48(12):761-804.
6. Cascorbi I. Pharmacogenetics of cytochrome P4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17-22.
7. Risperdal [package insert]. Titusville, NJ: Janssen; 2010.
8. Abilify [package insert]. Tokyo, Japan: Otsuka Pharmaceutical Co.; 2009.
9. Fanapt [package insert]. Rockville, MD: Vanda Pharmaceuticals, Inc.; 2009.
10. Kirchheiner J, Rodriguez-Antona C. Cytochrome P450 2D6 genotyping: potential role in improving treatment outcomes in psychiatric disorders. CNS Drugs. 2009;23:181-191.
11. de Leon J, Susce MT, Murray-Carmichael E. The AmpliChip CYP450 genotyping test: integrating a new clinical tool. Mol Diagn Ther. 2006;10:135-151.
12. de Leon J, Armstrong SC, Cozza KL. Clinical guidelines for psychiatrists for the use of pharmacogenetic testing for CYP450 2D6 and CYP450 2C19. Psychosomatics. 2006;47:75-85.
13. Grossman I, Sullivan PF, Walley N, et al. Genetic determinants of variable metabolism have little impact on the clinical use of leading antipsychotics in the CATIE study. Genet Med. 2008;10:720-729.
14. Rodriguez-Antona C, Gurwitz D, de Leon J, et al. CYP2D6 genotyping for psychiatric patients treated with risperidone: considerations for cost-effectiveness studies. Pharmacogenomics. 2009;10:685-699.
Jeffrey R. Bishop, PharmD, BCPP
Sharon Chae, BS
Dr. Bishop is assistant professor, department of pharmacy practice, center for cognitive medicine, department of psychiatry, University of Illinois at Chicago College of Pharmacy; Ms. Chae is a PharmD candidate, department of pharmacy practice, University of Illinois at Chicago College of Pharmacy, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jeffrey R. Bishop, PharmD, BCPP
Sharon Chae, BS
Dr. Bishop is assistant professor, department of pharmacy practice, center for cognitive medicine, department of psychiatry, University of Illinois at Chicago College of Pharmacy; Ms. Chae is a PharmD candidate, department of pharmacy practice, University of Illinois at Chicago College of Pharmacy, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Jeffrey R. Bishop, PharmD, BCPP
Sharon Chae, BS
Dr. Bishop is assistant professor, department of pharmacy practice, center for cognitive medicine, department of psychiatry, University of Illinois at Chicago College of Pharmacy; Ms. Chae is a PharmD candidate, department of pharmacy practice, University of Illinois at Chicago College of Pharmacy, Chicago, IL.
Vicki L. Ellingrod, PharmD, BCPP, FCCP
Series Editor
Two months ago, Mr. P, age 20, experienced paranoid thoughts, anxiety, agitation, and auditory hallucinations. During a brief hospitalization 1 month later, he received IM haloperidol, 2 mg, which he said “made his neck stiff.” After he was discharged, Mr. P, who is White, stopped taking his antipsychotics. During a recent outpatient evaluation, the clinician gives Mr. P a working diagnosis of schizophrenia and prescribes risperidone, 2 mg/d, with plans to titrate to 4 mg/d in the next 2 weeks. However, a week later, Mr. P complains of extreme sedation and feeling “knocked out” and does not want to continue taking the medication. Physical exam reveals slight cogwheel rigidity. His delusional thought content is not improved. The treating physician considers ordering a genetic test to determine Mr. P’s cytochrome P450 (CYP) 2D6 metabolizer status.
Studies investigating relationships among genetic variants thought to impact pharmacokinetics and pharmacodynamics of psychotropic medications have had mixed results.1 Metabolism of most antipsychotics depends on the CYP450 enzyme system, which is expressed predominantly in the liver (Table 1). CYP2D6 is one of these enzymes and may be responsible for metabolizing approximately 20% to 50% of all medications, including a number of antipsychotics.2 Genetic variations of CYP2D6 are common and the frequencies of these variants differ among racial groups.3
The half-life and other pharmacokinetic parameters of an antipsychotic metabolized by CYP2D6 may differ based on whether someone is a poor metabolizer (PM), intermediate metabolizer (IM), extensive metabolizer (EM), or ultrarapid metabolizer (UM).4 Regarding CYP2D6 metabolism among Whites, 3% to 5% are UMs, 70% to 80% are EMs, 10% to 17% are IMs, and 5% to 10% are PMs.5 By contrast, the percentage of PMs and UMs in the Asian population is low—about 1% for each phenotype; the IM phenotype is more common (65% to 70% in the Chinese population).5,6 The percentage of PMs in African Americans is roughly 2% to 6%.2
- Genetic variants of CYP2D6 may result in decreased or increased metabolism of some drugs, including risperidone, iloperidone, perphenazine, haloperidol, and thioridazine.
- The effect of reduced CYP2D6 activity may increase a patient’s risk for dose-related adverse effects.
- It is currently unknown if clinical genotyping for CYP2D6 variants and using this information to guide drug selection or dosing improves patient outcomes.
The clinical effect of altered metabolizer status depends on the extent the metabolism of a given agent is dependent on CYP2D6. PM status results in an approximately 2- to 6-fold increase in elimination half-life and overall exposure of aripiprazole,7 risperidone,8 and iloperidone9 (Figure). On the other end of the spectrum are UMs. Because of gene duplication, patients who fall into this category have enhanced metabolic activity. As a result, the therapeutic effect of several medications may be decreased because of faster clearance from the body, leading some physicians to label them as treatment-resistant.
Because side effects of many antipsychotics are dose-dependent, genotyping may be valuable for patients taking agents that are primarily metabolized by CYP2D6.10 Clinicians now have access to laboratory resources and FDA-approved methods for assessing CYP2D6 gene variants.11 It is debatable, however, whether this testing—which is expensive (≥$400) and may not be covered by health insurance—improves patient outcomes. In Mr. P’s case, if he had been genotyped as a CYP2D6 PM before treatment, his physicians might not have prescribed haloperidol and could have prevented a mild dystonic reaction. Also, they could have lowered the initial risperidone dose or chosen an antipsychotic such as ziprasidone, paliperidone, or quetiapine where the pharmacokinetic consequences of 2D6 poor metabolism are not as severe. Theoretically, one may argue that this could have reduced the risk for antipsychotic-associated side effects that now are a barrier to Mr. P’s desire to continue antipsychotics. On the other hand one may also reasonably argue that there may be other/additional reasons (genetic or non-genetic) that make some patients more sensitive to the side effects of antipsychotics and that simply assessing CYP2D6 status is not enough to guide drug selection and dosing.
Table 1
Cytochrome P450 (CYP) metabolism of commonly used antipsychotics*
| Drug | CYP1A2 | CYP2C9 | CYP2C19 | CYP2D6 | CYP3A4/5 |
|---|---|---|---|---|---|
| Aripiprazole | X | X | |||
| Asenapine | X | X | X | ||
| Chlorpromazine | X | X | X | ||
| Clozapine | X | X | X | X | X |
| Fluphenazine | X | ||||
| Haloperidol | X | X | X | ||
| Iloperidone | X | X | |||
| Olanzapine | X | X | |||
| Paliperidone | X† | X† | |||
| Perphenazine | X | X | X | X | X |
| Quetiapine | X | X | |||
| Risperidone | X | X | |||
| Thioridazine | X | X | |||
| Ziprasidone | X | X | |||
| *Information obtained from the most recent prescribing information available from each drug’s manufacturer †According to paliperidone’s prescribing information, in vitro studies identify that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, but in vivo studies indicate that their role in eliminating paliperidone is minimal | |||||
Figure: Effects of CYP2D6 poor metabolizer status on the half-life of risperidone, aripiprazole, and iloperidone
EM: extensive metabolizer; PM: poor metabolizer
Source: References 7-9
Use in clinical practice
Proposed expert guidelines recommend halving the normal target dose of risperidone and avoiding haloperidol and phenothiazine antipsychotics in CYP2D6 PMs.12 These guidelines are based on expert review of the pharmacokinetic effects of CYP2D6 PM status as well as case reports and studies associating CYP2D6 with poor outcomes, usually side effects. Although these studies suggest that determining metabolizer status may be clinically important, many other studies—some very large—have not found evidence for associations between drug metabolizing enzyme variants and clinical outcomes from antipsychotics.13
There are 2 clinical scenarios in which one may consider obtaining CYP2D6 genotype information:
- before initiating treatment (Table 2)
- after trying ≥1 agent primarily dependent on CYP2D6 with evidence of dose-related side effect (Table 3).
Identifying PMs could influence drug selection and dosing if this information is available before antipsychotic exposure. Studies have found evidence that CYP2D6 PMs may be at greater risk of experiencing adverse reactions to risperidone compared with other metabolizer groups.14 Also, prescribing information for aripiprazole and iloperidone recommends halving the dose of these drugs in the presence of CYP2D6 inhibitors, a condition that pharmacokinetically mimics PM status.
Knowing genotype information after ≥1 drugs have been tried may not be as useful. Clinicians often base drug switches or dose titrations on a patient’s experience with present or past doses of the antipsychotic. Examples include slowing titrations or reducing a target dose when a patient, such as Mr. P, experiences side effects, or selecting non-2D6 substrate agents after detecting a pattern of drug sensitivity.
Table 2
CYP2D6 testing before initiating antipsychotics: Benefits vs drawbacks
| Benefits | Drawbacks |
|---|---|
| Clinicians could avoid 2D6 substrate drugs with high likelihood for ADEs or increased risk of 2D6-based interactions in PMs | No empiric evidence shows that routine genotyping produces better clinical outcomes (eg, fewer side effects and better treatment adherence) |
| May lower initial dose, slow titration, and lower initial target dose to minimize risk of side effects in PMs | Many clinicians titrate slowly or adjust titration schedule and target doses based on initial tolerability as part of routine practice |
| The test would need to be done only once and the information may be useful for other therapy decisions | Patients who need immediate drug therapy may not be able to wait for test results |
| Testing may not be covered by a patient’s health insurance | |
| ADEs: adverse drug events; PMs: poor metabolizers | |
Table 3
Genotype testing after a patient experiences side effects
| Benefits |
| Identifying a biologic reason for side effect sensitivity may aid choice and dosing of subsequent antipsychotics and other medications |
| Drawbacks |
| In clinical practice, antipsychotic switching because of tolerability (and response) often is guided by outcomes experienced from previously used agents. In general, patients with a history of experiencing side effects at lower doses of antipsychotics are likely to be initiated at lower doses and titrated more cautiously during subsequent therapy choices regardless of whether side effects were caused by metabolizer status or other factor(s) |
Better patient outcomes?
It is not known if obtaining genotype information will provide better outcomes than a “trial and error” approach. Currently, obtaining genotype information before antipsychotic treatment is not standard clinical practice. Because this testing is expensive and requires prior approval from third party payers or out-of-pocket financial resources, testing is not recommended for all patients at this time.
However, a growing body of evidence suggests that knowing metabolizer status could be useful in drug selection or dosing for antipsychotics. This scientific knowledge continues to accumulate, and CYP2D6 genotyping may some day be integrated into routine clinical care. Currently, for patients and physicians with the resources to obtain and the ability to appropriately interpret the test results, this information may prove useful on an individual basis. However, additional studies are needed to support better outcomes from dosing and drug selection based on CYP2D6 genotype information.
Related Resources
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP). www.egappreviews.org.
- Pharmacogenomics Knowledge Base. www.pharmgkb.org.
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Iloperidone • Fanapt
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Bishop receives grant/research support from the National Institute of Mental Health, NARSAD, and Ortho-McNeil-Janssen and has received honoraria from Eli Lilly and Company.
Ms. Chae reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Two months ago, Mr. P, age 20, experienced paranoid thoughts, anxiety, agitation, and auditory hallucinations. During a brief hospitalization 1 month later, he received IM haloperidol, 2 mg, which he said “made his neck stiff.” After he was discharged, Mr. P, who is White, stopped taking his antipsychotics. During a recent outpatient evaluation, the clinician gives Mr. P a working diagnosis of schizophrenia and prescribes risperidone, 2 mg/d, with plans to titrate to 4 mg/d in the next 2 weeks. However, a week later, Mr. P complains of extreme sedation and feeling “knocked out” and does not want to continue taking the medication. Physical exam reveals slight cogwheel rigidity. His delusional thought content is not improved. The treating physician considers ordering a genetic test to determine Mr. P’s cytochrome P450 (CYP) 2D6 metabolizer status.
Studies investigating relationships among genetic variants thought to impact pharmacokinetics and pharmacodynamics of psychotropic medications have had mixed results.1 Metabolism of most antipsychotics depends on the CYP450 enzyme system, which is expressed predominantly in the liver (Table 1). CYP2D6 is one of these enzymes and may be responsible for metabolizing approximately 20% to 50% of all medications, including a number of antipsychotics.2 Genetic variations of CYP2D6 are common and the frequencies of these variants differ among racial groups.3
The half-life and other pharmacokinetic parameters of an antipsychotic metabolized by CYP2D6 may differ based on whether someone is a poor metabolizer (PM), intermediate metabolizer (IM), extensive metabolizer (EM), or ultrarapid metabolizer (UM).4 Regarding CYP2D6 metabolism among Whites, 3% to 5% are UMs, 70% to 80% are EMs, 10% to 17% are IMs, and 5% to 10% are PMs.5 By contrast, the percentage of PMs and UMs in the Asian population is low—about 1% for each phenotype; the IM phenotype is more common (65% to 70% in the Chinese population).5,6 The percentage of PMs in African Americans is roughly 2% to 6%.2
- Genetic variants of CYP2D6 may result in decreased or increased metabolism of some drugs, including risperidone, iloperidone, perphenazine, haloperidol, and thioridazine.
- The effect of reduced CYP2D6 activity may increase a patient’s risk for dose-related adverse effects.
- It is currently unknown if clinical genotyping for CYP2D6 variants and using this information to guide drug selection or dosing improves patient outcomes.
The clinical effect of altered metabolizer status depends on the extent the metabolism of a given agent is dependent on CYP2D6. PM status results in an approximately 2- to 6-fold increase in elimination half-life and overall exposure of aripiprazole,7 risperidone,8 and iloperidone9 (Figure). On the other end of the spectrum are UMs. Because of gene duplication, patients who fall into this category have enhanced metabolic activity. As a result, the therapeutic effect of several medications may be decreased because of faster clearance from the body, leading some physicians to label them as treatment-resistant.
Because side effects of many antipsychotics are dose-dependent, genotyping may be valuable for patients taking agents that are primarily metabolized by CYP2D6.10 Clinicians now have access to laboratory resources and FDA-approved methods for assessing CYP2D6 gene variants.11 It is debatable, however, whether this testing—which is expensive (≥$400) and may not be covered by health insurance—improves patient outcomes. In Mr. P’s case, if he had been genotyped as a CYP2D6 PM before treatment, his physicians might not have prescribed haloperidol and could have prevented a mild dystonic reaction. Also, they could have lowered the initial risperidone dose or chosen an antipsychotic such as ziprasidone, paliperidone, or quetiapine where the pharmacokinetic consequences of 2D6 poor metabolism are not as severe. Theoretically, one may argue that this could have reduced the risk for antipsychotic-associated side effects that now are a barrier to Mr. P’s desire to continue antipsychotics. On the other hand one may also reasonably argue that there may be other/additional reasons (genetic or non-genetic) that make some patients more sensitive to the side effects of antipsychotics and that simply assessing CYP2D6 status is not enough to guide drug selection and dosing.
Table 1
Cytochrome P450 (CYP) metabolism of commonly used antipsychotics*
| Drug | CYP1A2 | CYP2C9 | CYP2C19 | CYP2D6 | CYP3A4/5 |
|---|---|---|---|---|---|
| Aripiprazole | X | X | |||
| Asenapine | X | X | X | ||
| Chlorpromazine | X | X | X | ||
| Clozapine | X | X | X | X | X |
| Fluphenazine | X | ||||
| Haloperidol | X | X | X | ||
| Iloperidone | X | X | |||
| Olanzapine | X | X | |||
| Paliperidone | X† | X† | |||
| Perphenazine | X | X | X | X | X |
| Quetiapine | X | X | |||
| Risperidone | X | X | |||
| Thioridazine | X | X | |||
| Ziprasidone | X | X | |||
| *Information obtained from the most recent prescribing information available from each drug’s manufacturer †According to paliperidone’s prescribing information, in vitro studies identify that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, but in vivo studies indicate that their role in eliminating paliperidone is minimal | |||||
Figure: Effects of CYP2D6 poor metabolizer status on the half-life of risperidone, aripiprazole, and iloperidone
EM: extensive metabolizer; PM: poor metabolizer
Source: References 7-9
Use in clinical practice
Proposed expert guidelines recommend halving the normal target dose of risperidone and avoiding haloperidol and phenothiazine antipsychotics in CYP2D6 PMs.12 These guidelines are based on expert review of the pharmacokinetic effects of CYP2D6 PM status as well as case reports and studies associating CYP2D6 with poor outcomes, usually side effects. Although these studies suggest that determining metabolizer status may be clinically important, many other studies—some very large—have not found evidence for associations between drug metabolizing enzyme variants and clinical outcomes from antipsychotics.13
There are 2 clinical scenarios in which one may consider obtaining CYP2D6 genotype information:
- before initiating treatment (Table 2)
- after trying ≥1 agent primarily dependent on CYP2D6 with evidence of dose-related side effect (Table 3).
Identifying PMs could influence drug selection and dosing if this information is available before antipsychotic exposure. Studies have found evidence that CYP2D6 PMs may be at greater risk of experiencing adverse reactions to risperidone compared with other metabolizer groups.14 Also, prescribing information for aripiprazole and iloperidone recommends halving the dose of these drugs in the presence of CYP2D6 inhibitors, a condition that pharmacokinetically mimics PM status.
Knowing genotype information after ≥1 drugs have been tried may not be as useful. Clinicians often base drug switches or dose titrations on a patient’s experience with present or past doses of the antipsychotic. Examples include slowing titrations or reducing a target dose when a patient, such as Mr. P, experiences side effects, or selecting non-2D6 substrate agents after detecting a pattern of drug sensitivity.
Table 2
CYP2D6 testing before initiating antipsychotics: Benefits vs drawbacks
| Benefits | Drawbacks |
|---|---|
| Clinicians could avoid 2D6 substrate drugs with high likelihood for ADEs or increased risk of 2D6-based interactions in PMs | No empiric evidence shows that routine genotyping produces better clinical outcomes (eg, fewer side effects and better treatment adherence) |
| May lower initial dose, slow titration, and lower initial target dose to minimize risk of side effects in PMs | Many clinicians titrate slowly or adjust titration schedule and target doses based on initial tolerability as part of routine practice |
| The test would need to be done only once and the information may be useful for other therapy decisions | Patients who need immediate drug therapy may not be able to wait for test results |
| Testing may not be covered by a patient’s health insurance | |
| ADEs: adverse drug events; PMs: poor metabolizers | |
Table 3
Genotype testing after a patient experiences side effects
| Benefits |
| Identifying a biologic reason for side effect sensitivity may aid choice and dosing of subsequent antipsychotics and other medications |
| Drawbacks |
| In clinical practice, antipsychotic switching because of tolerability (and response) often is guided by outcomes experienced from previously used agents. In general, patients with a history of experiencing side effects at lower doses of antipsychotics are likely to be initiated at lower doses and titrated more cautiously during subsequent therapy choices regardless of whether side effects were caused by metabolizer status or other factor(s) |
Better patient outcomes?
It is not known if obtaining genotype information will provide better outcomes than a “trial and error” approach. Currently, obtaining genotype information before antipsychotic treatment is not standard clinical practice. Because this testing is expensive and requires prior approval from third party payers or out-of-pocket financial resources, testing is not recommended for all patients at this time.
However, a growing body of evidence suggests that knowing metabolizer status could be useful in drug selection or dosing for antipsychotics. This scientific knowledge continues to accumulate, and CYP2D6 genotyping may some day be integrated into routine clinical care. Currently, for patients and physicians with the resources to obtain and the ability to appropriately interpret the test results, this information may prove useful on an individual basis. However, additional studies are needed to support better outcomes from dosing and drug selection based on CYP2D6 genotype information.
Related Resources
- Evaluation of Genomic Applications in Practice and Prevention (EGAPP). www.egappreviews.org.
- Pharmacogenomics Knowledge Base. www.pharmgkb.org.
- Indiana University School of Medicine. P450 drug interaction table. http://medicine.iupui.edu/clinpharm/ddis/table.asp.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Iloperidone • Fanapt
- Olanzapine • Zyprexa
- Paliperidone • Invega
- Perphenazine • Trilafon
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Bishop receives grant/research support from the National Institute of Mental Health, NARSAD, and Ortho-McNeil-Janssen and has received honoraria from Eli Lilly and Company.
Ms. Chae reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Leckband SG, Bishop JR, Ellingrod VL. Pharmacogenomics in psychiatry. J Pharm Pract. 2007;20:252-264.
2. Neafsey P, Ginsberg G, Hattis D, et al. Genetic polymorphism in cytochrome P450 2D6 (CYP2D6): population distribution of CYP2D6 activity. J Toxicol Environ Health B Crit Rev. 2009;12(5-6):334-361.
3. Bradford LD, Gaedigk A, Leeder JS. High frequency of CYP2D6 poor and “intermediate” metabolizers in black populations: a review and preliminary data. Psychopharmacol Bull. 1998;34:797-804.
4. Gaedigk A, Simon SD, Pearce RE, et al. The CYP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin Pharmacol Ther. 2008;83:234-242.
5. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: part II. Clin Pharmacokinet. 2009;48(12):761-804.
6. Cascorbi I. Pharmacogenetics of cytochrome P4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17-22.
7. Risperdal [package insert]. Titusville, NJ: Janssen; 2010.
8. Abilify [package insert]. Tokyo, Japan: Otsuka Pharmaceutical Co.; 2009.
9. Fanapt [package insert]. Rockville, MD: Vanda Pharmaceuticals, Inc.; 2009.
10. Kirchheiner J, Rodriguez-Antona C. Cytochrome P450 2D6 genotyping: potential role in improving treatment outcomes in psychiatric disorders. CNS Drugs. 2009;23:181-191.
11. de Leon J, Susce MT, Murray-Carmichael E. The AmpliChip CYP450 genotyping test: integrating a new clinical tool. Mol Diagn Ther. 2006;10:135-151.
12. de Leon J, Armstrong SC, Cozza KL. Clinical guidelines for psychiatrists for the use of pharmacogenetic testing for CYP450 2D6 and CYP450 2C19. Psychosomatics. 2006;47:75-85.
13. Grossman I, Sullivan PF, Walley N, et al. Genetic determinants of variable metabolism have little impact on the clinical use of leading antipsychotics in the CATIE study. Genet Med. 2008;10:720-729.
14. Rodriguez-Antona C, Gurwitz D, de Leon J, et al. CYP2D6 genotyping for psychiatric patients treated with risperidone: considerations for cost-effectiveness studies. Pharmacogenomics. 2009;10:685-699.
1. Leckband SG, Bishop JR, Ellingrod VL. Pharmacogenomics in psychiatry. J Pharm Pract. 2007;20:252-264.
2. Neafsey P, Ginsberg G, Hattis D, et al. Genetic polymorphism in cytochrome P450 2D6 (CYP2D6): population distribution of CYP2D6 activity. J Toxicol Environ Health B Crit Rev. 2009;12(5-6):334-361.
3. Bradford LD, Gaedigk A, Leeder JS. High frequency of CYP2D6 poor and “intermediate” metabolizers in black populations: a review and preliminary data. Psychopharmacol Bull. 1998;34:797-804.
4. Gaedigk A, Simon SD, Pearce RE, et al. The CYP2D6 activity score: translating genotype information into a qualitative measure of phenotype. Clin Pharmacol Ther. 2008;83:234-242.
5. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: part II. Clin Pharmacokinet. 2009;48(12):761-804.
6. Cascorbi I. Pharmacogenetics of cytochrome P4502D6: genetic background and clinical implication. Eur J Clin Invest. 2003;33(suppl 2):17-22.
7. Risperdal [package insert]. Titusville, NJ: Janssen; 2010.
8. Abilify [package insert]. Tokyo, Japan: Otsuka Pharmaceutical Co.; 2009.
9. Fanapt [package insert]. Rockville, MD: Vanda Pharmaceuticals, Inc.; 2009.
10. Kirchheiner J, Rodriguez-Antona C. Cytochrome P450 2D6 genotyping: potential role in improving treatment outcomes in psychiatric disorders. CNS Drugs. 2009;23:181-191.
11. de Leon J, Susce MT, Murray-Carmichael E. The AmpliChip CYP450 genotyping test: integrating a new clinical tool. Mol Diagn Ther. 2006;10:135-151.
12. de Leon J, Armstrong SC, Cozza KL. Clinical guidelines for psychiatrists for the use of pharmacogenetic testing for CYP450 2D6 and CYP450 2C19. Psychosomatics. 2006;47:75-85.
13. Grossman I, Sullivan PF, Walley N, et al. Genetic determinants of variable metabolism have little impact on the clinical use of leading antipsychotics in the CATIE study. Genet Med. 2008;10:720-729.
14. Rodriguez-Antona C, Gurwitz D, de Leon J, et al. CYP2D6 genotyping for psychiatric patients treated with risperidone: considerations for cost-effectiveness studies. Pharmacogenomics. 2009;10:685-699.