User login
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
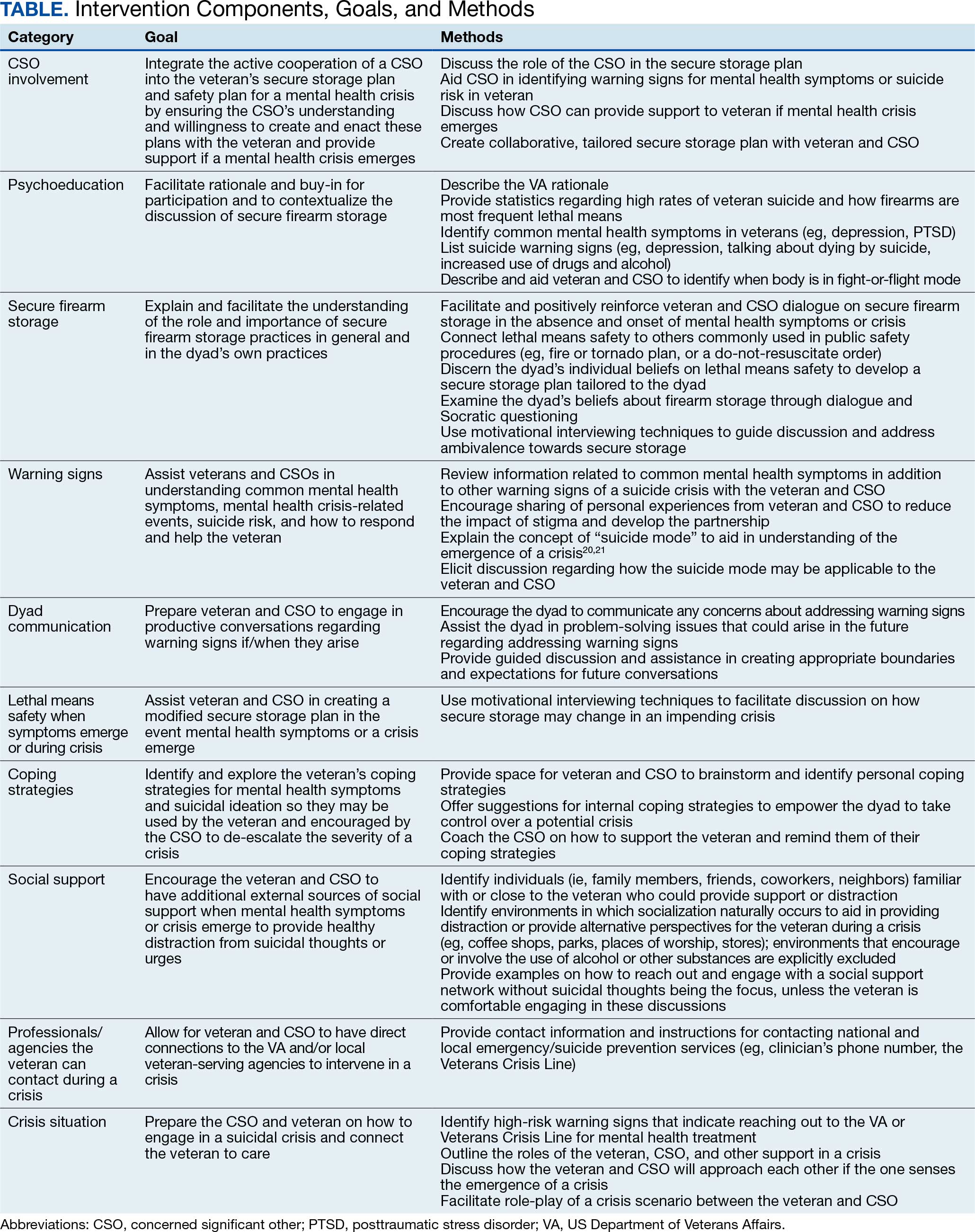
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
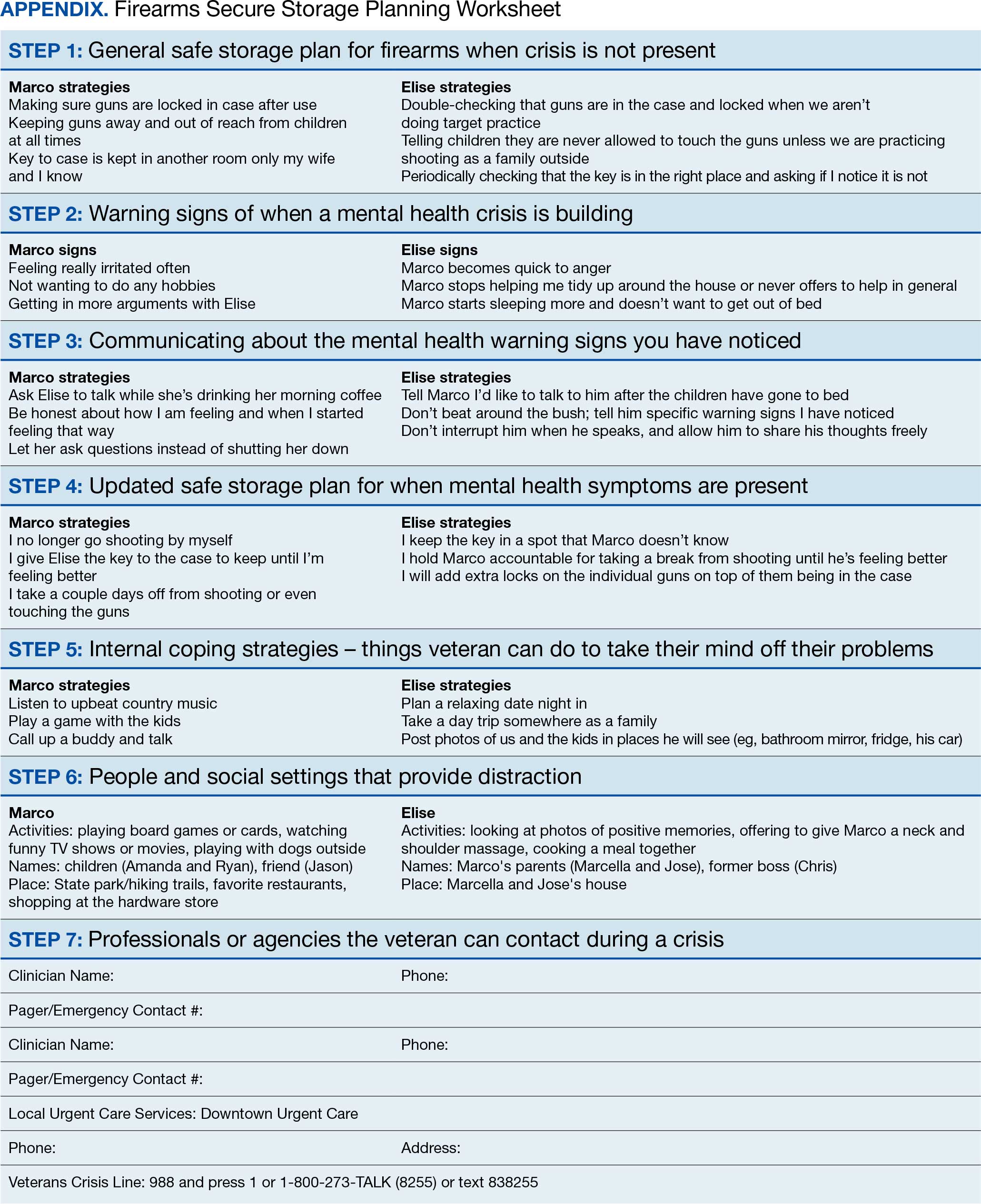
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention