User login
Limiting social media use in youths brings challenges, benefits
Amelia Kennedy, 19, of Royersford, Pa., a point guard on the Catholic University of America, Washington, basketball team who will begin her sophomore year in the fall, uses TikTok, Snapchat, Instagram, and YouTube regularly.
How regularly? She estimates 7 hours a day and about 9 on weekends. She’s aware of the time-wasting potential. “If my mom says, ‘Do dishes,’ and I say, ‘5 more minutes,’ it can be longer,’’ she said.
Now imagine the challenge of cutting that 7 or 9 hours a day of social media use down to 30 minutes.
A very tall order, considering a 2022 Pew Research Center survey of more than 1,300 teens found 35% are “nearly constantly” on at least one of the top five social media platforms: YouTube, TikTok, Instagram, Snapchat, and Facebook.
Researchers from Iowa State University, Ames, recently took on that daunting challenge, limiting a group of students to only 30 minutes of social media a day to see what happens. Two weeks into the study, the students reported improvement in psychological well-being and other important measures, including sleep quality, compared with a control group assigned to continue using social media as usual.
And the dreaded FOMO, or fear of missing out, didn’t happen, the researchers said. At the end, the students were rethinking their social media use and feeling positive about it.
As social media becomes more common and youth mental health more endangered, experts are sounding the alarm. In late May, U.S. Surgeon General Vivek Murthy, MD, issued an advisory on social media and youth mental health, calling for tech companies to do better, policymakers to strengthen safety, and researchers to get more information, among other actions.
After that, the Biden administration took actions including the launch of a task force on kids’ online health and safety. The American Psychological Association has issued recommendations on social media use in youths. And the Social Media Victims Law Center in Seattle has sued numerous social media companies for online activity resulting in death and other tragedies.
While experts acknowledge that much more research is needed to sort out how to balance social media’s risks and benefits to preserve youth mental health and prevent such disasters, the new Iowa State study, as well as other recent research, suggests that
Goal: 30 minutes a day
In the Iowa State study, 230 undergraduate students were assigned to one of two groups, with 99 in the 30-minute-a-day social media use group and 131 in the “usual” or control group, which made no changes. For those in the intervention group, “we sent a daily reminder email,” said Ella Faulhaber, a PhD candidate at Iowa State and the study’s lead author. It simply reminded them to limit social medial use to the 30-minute maximum.
At the study start and end, all participants provided a screenshot of their weekly social media usage time. The researchers gave both groups a battery of tests to assess anxiety, depression, loneliness, fear of missing out, and negative and positive feelings.
“By limiting their social media time, that resulted in less anxiety, less depression, less FOMO, fewer negative emotions, and greater positive emotions,” said Douglas Gentile, PhD, a distinguished professor of psychology at Iowa State and a study coauthor. “We know that it is the limiting [of] the social media that is causing that.”
Ms. Faulhaber recalled one participant who mentioned having trouble at first adjusting to the 30-minute time frame, but once sleep improved, it was easier to stick to that guidance. Another who gave up phone use at bedtime found: “Instead of looking at my phone, it was much easier to go straight to bed.”
Sleep improvements, of course, affect many parts of physical and mental health, Dr. Gentile said. And the study also showed that even with reduced screen time, “we can still get the benefit of being connected.” Those who didn’t make the 30-minute mark, but cut back, got benefits, too, the researchers said.
‘Youth are aware’
Self-monitoring works, agreed Jane Harness, DO, an adjunct clinical assistant professor of psychiatry at the University of Michigan, Ann Arbor, because “having that insight is often the first step.”
In a study she conducted, Dr. Harness aimed to gather youths’ insights about how their social media use affected them. With her colleagues, she asked more than 1,100 youths, aged 14-24, what advice they would give to those new to social media, if they ever felt they needed to change social media habits, and if they have deleted or considered deleting social media accounts.
From the 871 responses, Harness found that youths were especially concerned about safety online, that most had thought about deleting a social media app and some had, and that youths were more likely to say they wanted to change the amount of time spent on social media, compared with the content they view.
“Users responded with great advice for each other,” she said. “Safety was brought up,” with users reminding others to keep accounts private and to be aware of location tracking links and content that seems to promote eating disorders, suicide, and other harms.
In the study report, Dr. Harness concluded: “Youth are aware of ways in which social media could be negatively impacting them and they have employed methods to modulate their use because of this awareness.”
Less FOMO, less anxiety
In an earlier study, University of Pennsylvania, Philadelphia, researchers had 143 college students self-monitor social media for a week, then randomly assigned them either to a group told to limit Facebook, Instagram, and Snapchat use to 10 minutes per platform, per day, or to a group told to use social media as usual for 3 weeks.
At the end of the study, the researchers evaluated both groups and found “significant reductions in loneliness and depression over 3 weeks’’ in the limited-use group, compared with the usual-use group, according to study researcher Melissa G. Hunt, PhD, associate director of clinical training at the University of Pennsylvania.
And both groups showed declines in anxiety and fear of missing out, suggesting a benefit tied to self-monitoring itself, she said.
While Dr. Hunt’s study focused on 30 minutes a day, she said “about an hour a day seems to be the sweet spot for maximizing the positive effects of connecting, but limiting the negative effects of social media use.”
She also suggested that smartphones have no place in middle or high school classrooms. Instead, they should be on lockdown during classes.
“Parents need to set real limits of cellphone use during meals and in bedrooms,” Dr. Hunt said. At mealtime, for instance, all phones should be absent from the table. And after 10 p.m., “all family phones remain in the kitchen.”
Be ‘more mindful’
These recent study findings about self-monitoring and limiting social media time may not work the same for everyone, especially among those who aren’t as motivated, said psychiatrist Elizabeth Ortiz-Schwartz, MD, team lead for the adolescent inpatient unit at Silver Hill Hospital in New Canaan, Conn.
But “the bigger take-home piece is that being intentional and attempting to decrease the use in these individuals, even if they were not always successful, was clearly beneficial,” she said.
As we await clearer guidelines about what is the “right” amount of use in terms of social media content and time, Dr. Ortiz-Schwartz said, “becoming more mindful and aware of the risks and benefits can hopefully help individuals become more mindful and deliberate about its use.”
Real-world strategies
Max Schwandt, 23, is an outlier, but a happy one. He works as a sales clerk at a Los Angeles–area recreational gear shop, and he uses no social media. Why not? “It takes up too much time,” he explained. As simple as that.
But for many other teens and young adults, the struggle to stay off social media is real.
Amelia Kennedy, the Catholic University of America student, is trying to reduce her screen time. One way is to track it on her phone. These days, her summer job at a restaurant serving breakfast gets her up early. “If I have to work, I still go on my phone, but not that long.” And once at work, she only has time for quick checks between work responsibilities. “I definitely am more productive,” she said about days when she has work.
Last December, Lauren Young, 25, whose father was a researcher on the Iowa State study, was finishing law school at Georgetown University, Washington, and decided to take a break from social media for the entire month. “I can’t say I was always successful in avoiding it,” she said. But cutting down greatly “made me a lot more present in my day-to-day life, and it was easier to concentrate.”
She could even get through a meal, out with friends, without her phone, keeping it in her purse. That was a definite change from the norm. “I noticed I would go out to dinner and the standard for people my age is having the phone on the table. If you are being polite, you turn it over.”
During her social media “blackout,” Ms. Young had deleted TikTok, Instagram, and Facebook apps. Then, when she graduated, she had to reinstall to post a picture. But now, she is back to minimal social media use.
“I’m studying for the bar, so it’s kind of necessary, but it always makes me happier.” She figures she can always text family and friends if necessary, instead of posting. “I felt for a while I was missing out on things, but not now,” she said.
Others, including Sarah Goldstein, 22, of Chatsworth, Calif., a supermarket courtesy clerk who is thinking of returning to college, said she has developed a healthier attitude toward social media as she has gotten older.
“In middle and early high school, I would see parties, things I wasn’t invited to, on Snapchat and Instagram.” While she realized there could be legitimate reasons for not being included, she said it was easy to internalize those feelings of being left out.
These days, she said she doesn’t let it affect her mental health that way. She enjoys social media – especially TikTok and Instagram – for its benefits. “It kills time, gives you something to watch, can make you laugh and feel like you have a connection with other people.”
A version of this article first appeared on WebMD.com.
Amelia Kennedy, 19, of Royersford, Pa., a point guard on the Catholic University of America, Washington, basketball team who will begin her sophomore year in the fall, uses TikTok, Snapchat, Instagram, and YouTube regularly.
How regularly? She estimates 7 hours a day and about 9 on weekends. She’s aware of the time-wasting potential. “If my mom says, ‘Do dishes,’ and I say, ‘5 more minutes,’ it can be longer,’’ she said.
Now imagine the challenge of cutting that 7 or 9 hours a day of social media use down to 30 minutes.
A very tall order, considering a 2022 Pew Research Center survey of more than 1,300 teens found 35% are “nearly constantly” on at least one of the top five social media platforms: YouTube, TikTok, Instagram, Snapchat, and Facebook.
Researchers from Iowa State University, Ames, recently took on that daunting challenge, limiting a group of students to only 30 minutes of social media a day to see what happens. Two weeks into the study, the students reported improvement in psychological well-being and other important measures, including sleep quality, compared with a control group assigned to continue using social media as usual.
And the dreaded FOMO, or fear of missing out, didn’t happen, the researchers said. At the end, the students were rethinking their social media use and feeling positive about it.
As social media becomes more common and youth mental health more endangered, experts are sounding the alarm. In late May, U.S. Surgeon General Vivek Murthy, MD, issued an advisory on social media and youth mental health, calling for tech companies to do better, policymakers to strengthen safety, and researchers to get more information, among other actions.
After that, the Biden administration took actions including the launch of a task force on kids’ online health and safety. The American Psychological Association has issued recommendations on social media use in youths. And the Social Media Victims Law Center in Seattle has sued numerous social media companies for online activity resulting in death and other tragedies.
While experts acknowledge that much more research is needed to sort out how to balance social media’s risks and benefits to preserve youth mental health and prevent such disasters, the new Iowa State study, as well as other recent research, suggests that
Goal: 30 minutes a day
In the Iowa State study, 230 undergraduate students were assigned to one of two groups, with 99 in the 30-minute-a-day social media use group and 131 in the “usual” or control group, which made no changes. For those in the intervention group, “we sent a daily reminder email,” said Ella Faulhaber, a PhD candidate at Iowa State and the study’s lead author. It simply reminded them to limit social medial use to the 30-minute maximum.
At the study start and end, all participants provided a screenshot of their weekly social media usage time. The researchers gave both groups a battery of tests to assess anxiety, depression, loneliness, fear of missing out, and negative and positive feelings.
“By limiting their social media time, that resulted in less anxiety, less depression, less FOMO, fewer negative emotions, and greater positive emotions,” said Douglas Gentile, PhD, a distinguished professor of psychology at Iowa State and a study coauthor. “We know that it is the limiting [of] the social media that is causing that.”
Ms. Faulhaber recalled one participant who mentioned having trouble at first adjusting to the 30-minute time frame, but once sleep improved, it was easier to stick to that guidance. Another who gave up phone use at bedtime found: “Instead of looking at my phone, it was much easier to go straight to bed.”
Sleep improvements, of course, affect many parts of physical and mental health, Dr. Gentile said. And the study also showed that even with reduced screen time, “we can still get the benefit of being connected.” Those who didn’t make the 30-minute mark, but cut back, got benefits, too, the researchers said.
‘Youth are aware’
Self-monitoring works, agreed Jane Harness, DO, an adjunct clinical assistant professor of psychiatry at the University of Michigan, Ann Arbor, because “having that insight is often the first step.”
In a study she conducted, Dr. Harness aimed to gather youths’ insights about how their social media use affected them. With her colleagues, she asked more than 1,100 youths, aged 14-24, what advice they would give to those new to social media, if they ever felt they needed to change social media habits, and if they have deleted or considered deleting social media accounts.
From the 871 responses, Harness found that youths were especially concerned about safety online, that most had thought about deleting a social media app and some had, and that youths were more likely to say they wanted to change the amount of time spent on social media, compared with the content they view.
“Users responded with great advice for each other,” she said. “Safety was brought up,” with users reminding others to keep accounts private and to be aware of location tracking links and content that seems to promote eating disorders, suicide, and other harms.
In the study report, Dr. Harness concluded: “Youth are aware of ways in which social media could be negatively impacting them and they have employed methods to modulate their use because of this awareness.”
Less FOMO, less anxiety
In an earlier study, University of Pennsylvania, Philadelphia, researchers had 143 college students self-monitor social media for a week, then randomly assigned them either to a group told to limit Facebook, Instagram, and Snapchat use to 10 minutes per platform, per day, or to a group told to use social media as usual for 3 weeks.
At the end of the study, the researchers evaluated both groups and found “significant reductions in loneliness and depression over 3 weeks’’ in the limited-use group, compared with the usual-use group, according to study researcher Melissa G. Hunt, PhD, associate director of clinical training at the University of Pennsylvania.
And both groups showed declines in anxiety and fear of missing out, suggesting a benefit tied to self-monitoring itself, she said.
While Dr. Hunt’s study focused on 30 minutes a day, she said “about an hour a day seems to be the sweet spot for maximizing the positive effects of connecting, but limiting the negative effects of social media use.”
She also suggested that smartphones have no place in middle or high school classrooms. Instead, they should be on lockdown during classes.
“Parents need to set real limits of cellphone use during meals and in bedrooms,” Dr. Hunt said. At mealtime, for instance, all phones should be absent from the table. And after 10 p.m., “all family phones remain in the kitchen.”
Be ‘more mindful’
These recent study findings about self-monitoring and limiting social media time may not work the same for everyone, especially among those who aren’t as motivated, said psychiatrist Elizabeth Ortiz-Schwartz, MD, team lead for the adolescent inpatient unit at Silver Hill Hospital in New Canaan, Conn.
But “the bigger take-home piece is that being intentional and attempting to decrease the use in these individuals, even if they were not always successful, was clearly beneficial,” she said.
As we await clearer guidelines about what is the “right” amount of use in terms of social media content and time, Dr. Ortiz-Schwartz said, “becoming more mindful and aware of the risks and benefits can hopefully help individuals become more mindful and deliberate about its use.”
Real-world strategies
Max Schwandt, 23, is an outlier, but a happy one. He works as a sales clerk at a Los Angeles–area recreational gear shop, and he uses no social media. Why not? “It takes up too much time,” he explained. As simple as that.
But for many other teens and young adults, the struggle to stay off social media is real.
Amelia Kennedy, the Catholic University of America student, is trying to reduce her screen time. One way is to track it on her phone. These days, her summer job at a restaurant serving breakfast gets her up early. “If I have to work, I still go on my phone, but not that long.” And once at work, she only has time for quick checks between work responsibilities. “I definitely am more productive,” she said about days when she has work.
Last December, Lauren Young, 25, whose father was a researcher on the Iowa State study, was finishing law school at Georgetown University, Washington, and decided to take a break from social media for the entire month. “I can’t say I was always successful in avoiding it,” she said. But cutting down greatly “made me a lot more present in my day-to-day life, and it was easier to concentrate.”
She could even get through a meal, out with friends, without her phone, keeping it in her purse. That was a definite change from the norm. “I noticed I would go out to dinner and the standard for people my age is having the phone on the table. If you are being polite, you turn it over.”
During her social media “blackout,” Ms. Young had deleted TikTok, Instagram, and Facebook apps. Then, when she graduated, she had to reinstall to post a picture. But now, she is back to minimal social media use.
“I’m studying for the bar, so it’s kind of necessary, but it always makes me happier.” She figures she can always text family and friends if necessary, instead of posting. “I felt for a while I was missing out on things, but not now,” she said.
Others, including Sarah Goldstein, 22, of Chatsworth, Calif., a supermarket courtesy clerk who is thinking of returning to college, said she has developed a healthier attitude toward social media as she has gotten older.
“In middle and early high school, I would see parties, things I wasn’t invited to, on Snapchat and Instagram.” While she realized there could be legitimate reasons for not being included, she said it was easy to internalize those feelings of being left out.
These days, she said she doesn’t let it affect her mental health that way. She enjoys social media – especially TikTok and Instagram – for its benefits. “It kills time, gives you something to watch, can make you laugh and feel like you have a connection with other people.”
A version of this article first appeared on WebMD.com.
Amelia Kennedy, 19, of Royersford, Pa., a point guard on the Catholic University of America, Washington, basketball team who will begin her sophomore year in the fall, uses TikTok, Snapchat, Instagram, and YouTube regularly.
How regularly? She estimates 7 hours a day and about 9 on weekends. She’s aware of the time-wasting potential. “If my mom says, ‘Do dishes,’ and I say, ‘5 more minutes,’ it can be longer,’’ she said.
Now imagine the challenge of cutting that 7 or 9 hours a day of social media use down to 30 minutes.
A very tall order, considering a 2022 Pew Research Center survey of more than 1,300 teens found 35% are “nearly constantly” on at least one of the top five social media platforms: YouTube, TikTok, Instagram, Snapchat, and Facebook.
Researchers from Iowa State University, Ames, recently took on that daunting challenge, limiting a group of students to only 30 minutes of social media a day to see what happens. Two weeks into the study, the students reported improvement in psychological well-being and other important measures, including sleep quality, compared with a control group assigned to continue using social media as usual.
And the dreaded FOMO, or fear of missing out, didn’t happen, the researchers said. At the end, the students were rethinking their social media use and feeling positive about it.
As social media becomes more common and youth mental health more endangered, experts are sounding the alarm. In late May, U.S. Surgeon General Vivek Murthy, MD, issued an advisory on social media and youth mental health, calling for tech companies to do better, policymakers to strengthen safety, and researchers to get more information, among other actions.
After that, the Biden administration took actions including the launch of a task force on kids’ online health and safety. The American Psychological Association has issued recommendations on social media use in youths. And the Social Media Victims Law Center in Seattle has sued numerous social media companies for online activity resulting in death and other tragedies.
While experts acknowledge that much more research is needed to sort out how to balance social media’s risks and benefits to preserve youth mental health and prevent such disasters, the new Iowa State study, as well as other recent research, suggests that
Goal: 30 minutes a day
In the Iowa State study, 230 undergraduate students were assigned to one of two groups, with 99 in the 30-minute-a-day social media use group and 131 in the “usual” or control group, which made no changes. For those in the intervention group, “we sent a daily reminder email,” said Ella Faulhaber, a PhD candidate at Iowa State and the study’s lead author. It simply reminded them to limit social medial use to the 30-minute maximum.
At the study start and end, all participants provided a screenshot of their weekly social media usage time. The researchers gave both groups a battery of tests to assess anxiety, depression, loneliness, fear of missing out, and negative and positive feelings.
“By limiting their social media time, that resulted in less anxiety, less depression, less FOMO, fewer negative emotions, and greater positive emotions,” said Douglas Gentile, PhD, a distinguished professor of psychology at Iowa State and a study coauthor. “We know that it is the limiting [of] the social media that is causing that.”
Ms. Faulhaber recalled one participant who mentioned having trouble at first adjusting to the 30-minute time frame, but once sleep improved, it was easier to stick to that guidance. Another who gave up phone use at bedtime found: “Instead of looking at my phone, it was much easier to go straight to bed.”
Sleep improvements, of course, affect many parts of physical and mental health, Dr. Gentile said. And the study also showed that even with reduced screen time, “we can still get the benefit of being connected.” Those who didn’t make the 30-minute mark, but cut back, got benefits, too, the researchers said.
‘Youth are aware’
Self-monitoring works, agreed Jane Harness, DO, an adjunct clinical assistant professor of psychiatry at the University of Michigan, Ann Arbor, because “having that insight is often the first step.”
In a study she conducted, Dr. Harness aimed to gather youths’ insights about how their social media use affected them. With her colleagues, she asked more than 1,100 youths, aged 14-24, what advice they would give to those new to social media, if they ever felt they needed to change social media habits, and if they have deleted or considered deleting social media accounts.
From the 871 responses, Harness found that youths were especially concerned about safety online, that most had thought about deleting a social media app and some had, and that youths were more likely to say they wanted to change the amount of time spent on social media, compared with the content they view.
“Users responded with great advice for each other,” she said. “Safety was brought up,” with users reminding others to keep accounts private and to be aware of location tracking links and content that seems to promote eating disorders, suicide, and other harms.
In the study report, Dr. Harness concluded: “Youth are aware of ways in which social media could be negatively impacting them and they have employed methods to modulate their use because of this awareness.”
Less FOMO, less anxiety
In an earlier study, University of Pennsylvania, Philadelphia, researchers had 143 college students self-monitor social media for a week, then randomly assigned them either to a group told to limit Facebook, Instagram, and Snapchat use to 10 minutes per platform, per day, or to a group told to use social media as usual for 3 weeks.
At the end of the study, the researchers evaluated both groups and found “significant reductions in loneliness and depression over 3 weeks’’ in the limited-use group, compared with the usual-use group, according to study researcher Melissa G. Hunt, PhD, associate director of clinical training at the University of Pennsylvania.
And both groups showed declines in anxiety and fear of missing out, suggesting a benefit tied to self-monitoring itself, she said.
While Dr. Hunt’s study focused on 30 minutes a day, she said “about an hour a day seems to be the sweet spot for maximizing the positive effects of connecting, but limiting the negative effects of social media use.”
She also suggested that smartphones have no place in middle or high school classrooms. Instead, they should be on lockdown during classes.
“Parents need to set real limits of cellphone use during meals and in bedrooms,” Dr. Hunt said. At mealtime, for instance, all phones should be absent from the table. And after 10 p.m., “all family phones remain in the kitchen.”
Be ‘more mindful’
These recent study findings about self-monitoring and limiting social media time may not work the same for everyone, especially among those who aren’t as motivated, said psychiatrist Elizabeth Ortiz-Schwartz, MD, team lead for the adolescent inpatient unit at Silver Hill Hospital in New Canaan, Conn.
But “the bigger take-home piece is that being intentional and attempting to decrease the use in these individuals, even if they were not always successful, was clearly beneficial,” she said.
As we await clearer guidelines about what is the “right” amount of use in terms of social media content and time, Dr. Ortiz-Schwartz said, “becoming more mindful and aware of the risks and benefits can hopefully help individuals become more mindful and deliberate about its use.”
Real-world strategies
Max Schwandt, 23, is an outlier, but a happy one. He works as a sales clerk at a Los Angeles–area recreational gear shop, and he uses no social media. Why not? “It takes up too much time,” he explained. As simple as that.
But for many other teens and young adults, the struggle to stay off social media is real.
Amelia Kennedy, the Catholic University of America student, is trying to reduce her screen time. One way is to track it on her phone. These days, her summer job at a restaurant serving breakfast gets her up early. “If I have to work, I still go on my phone, but not that long.” And once at work, she only has time for quick checks between work responsibilities. “I definitely am more productive,” she said about days when she has work.
Last December, Lauren Young, 25, whose father was a researcher on the Iowa State study, was finishing law school at Georgetown University, Washington, and decided to take a break from social media for the entire month. “I can’t say I was always successful in avoiding it,” she said. But cutting down greatly “made me a lot more present in my day-to-day life, and it was easier to concentrate.”
She could even get through a meal, out with friends, without her phone, keeping it in her purse. That was a definite change from the norm. “I noticed I would go out to dinner and the standard for people my age is having the phone on the table. If you are being polite, you turn it over.”
During her social media “blackout,” Ms. Young had deleted TikTok, Instagram, and Facebook apps. Then, when she graduated, she had to reinstall to post a picture. But now, she is back to minimal social media use.
“I’m studying for the bar, so it’s kind of necessary, but it always makes me happier.” She figures she can always text family and friends if necessary, instead of posting. “I felt for a while I was missing out on things, but not now,” she said.
Others, including Sarah Goldstein, 22, of Chatsworth, Calif., a supermarket courtesy clerk who is thinking of returning to college, said she has developed a healthier attitude toward social media as she has gotten older.
“In middle and early high school, I would see parties, things I wasn’t invited to, on Snapchat and Instagram.” While she realized there could be legitimate reasons for not being included, she said it was easy to internalize those feelings of being left out.
These days, she said she doesn’t let it affect her mental health that way. She enjoys social media – especially TikTok and Instagram – for its benefits. “It kills time, gives you something to watch, can make you laugh and feel like you have a connection with other people.”
A version of this article first appeared on WebMD.com.
Agency issues advisory on mental health symptoms of long COVID
The nine mental health symptoms highlighted in the advisory are fatigue; cognitive impairment, including brain fog; anxiety; depression; obsessive-compulsive disorder; sleep disorders; PTSD; psychotic disorder; and start of a substance use disorder.
The advisory noted that social factors can contribute to the mental health problems for racial and ethnic minorities; people with limited access to health care; people who already have behavioral health conditions and physical disabilities; and people who are lesbian, gay, bisexual, transgender, queer, or intersex.
“Long COVID has a range of burdensome physical symptoms and can take a toll on a person’s mental health. It can be very challenging for a person, whether they are impacted themselves, or they are a caregiver for someone who is affected,” Health and Human Services Secretary Xavier Becerra said in a statement. “This advisory helps to raise awareness, especially among primary care practitioners and clinicians who are often the ones treating patients with long COVID.”
The department says about 10% of people infected with COVID have at least one long COVID symptom. Physical symptoms include dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements.
“We know that people living with long COVID need help today, and providers need help understanding what long COVID is and how to treat it,” Admiral Rachel Levine, MD, assistant secretary for health, said in the statement. “This advisory helps bridge that gap for the behavioral health impacts of long COVID.”
A version of this article first appeared on WebMD.com.
The nine mental health symptoms highlighted in the advisory are fatigue; cognitive impairment, including brain fog; anxiety; depression; obsessive-compulsive disorder; sleep disorders; PTSD; psychotic disorder; and start of a substance use disorder.
The advisory noted that social factors can contribute to the mental health problems for racial and ethnic minorities; people with limited access to health care; people who already have behavioral health conditions and physical disabilities; and people who are lesbian, gay, bisexual, transgender, queer, or intersex.
“Long COVID has a range of burdensome physical symptoms and can take a toll on a person’s mental health. It can be very challenging for a person, whether they are impacted themselves, or they are a caregiver for someone who is affected,” Health and Human Services Secretary Xavier Becerra said in a statement. “This advisory helps to raise awareness, especially among primary care practitioners and clinicians who are often the ones treating patients with long COVID.”
The department says about 10% of people infected with COVID have at least one long COVID symptom. Physical symptoms include dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements.
“We know that people living with long COVID need help today, and providers need help understanding what long COVID is and how to treat it,” Admiral Rachel Levine, MD, assistant secretary for health, said in the statement. “This advisory helps bridge that gap for the behavioral health impacts of long COVID.”
A version of this article first appeared on WebMD.com.
The nine mental health symptoms highlighted in the advisory are fatigue; cognitive impairment, including brain fog; anxiety; depression; obsessive-compulsive disorder; sleep disorders; PTSD; psychotic disorder; and start of a substance use disorder.
The advisory noted that social factors can contribute to the mental health problems for racial and ethnic minorities; people with limited access to health care; people who already have behavioral health conditions and physical disabilities; and people who are lesbian, gay, bisexual, transgender, queer, or intersex.
“Long COVID has a range of burdensome physical symptoms and can take a toll on a person’s mental health. It can be very challenging for a person, whether they are impacted themselves, or they are a caregiver for someone who is affected,” Health and Human Services Secretary Xavier Becerra said in a statement. “This advisory helps to raise awareness, especially among primary care practitioners and clinicians who are often the ones treating patients with long COVID.”
The department says about 10% of people infected with COVID have at least one long COVID symptom. Physical symptoms include dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements.
“We know that people living with long COVID need help today, and providers need help understanding what long COVID is and how to treat it,” Admiral Rachel Levine, MD, assistant secretary for health, said in the statement. “This advisory helps bridge that gap for the behavioral health impacts of long COVID.”
A version of this article first appeared on WebMD.com.
Myasthenia gravis drug gets FDA nod
, the drug’s manufacturer, UCB, has announced.

Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
, the drug’s manufacturer, UCB, has announced.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
, the drug’s manufacturer, UCB, has announced.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
FDA clears new biomarker assays for early Alzheimer’s detection
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
New DEA CME mandate affects 2 million prescribers
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.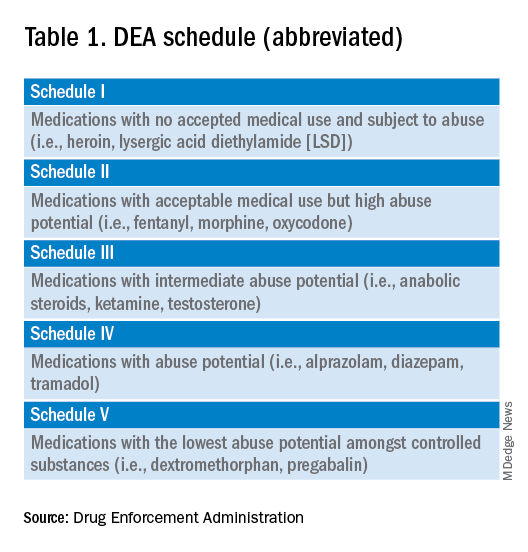
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements. 
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
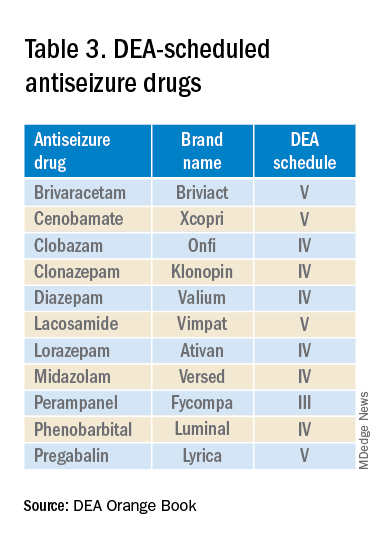
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
Fade haircut or something else?

The areas of hair loss and different length hairs in a patient with otherwise normal-density hair was consistent with a diagnosis of trichotillomania. The physician initially thought the patient had a “fade” hairstyle, but then observed him twirling his hair. Further queries confirmed a history of hair pulling (trichotillomania) and ingesting the hair (trichophagia).
In adulthood, trichotillomania affects females about 4 times more than males, although in childhood, the sex distribution appears about equal.1 The typical age of onset is between 10 to 13 years. Several mental health conditions are associated with trichotillomania, such as major depressive disorder, anxiety disorders, and substance use disorder, with trichotillomania generally preceding these comorbid disorders. It is important to rule out obsessive compulsive disorder and consider body dysmorphic disorder when making a diagnosis of trichotillomania.1
It is common to see androgenetic alopecia precipitated by hormone therapy in FTM individuals. This would usually cause thinning of the hair rather than the irregular hair lengths and pattern seen in this patient. Tinea capitis is also part of the differential diagnosis in a case such as this. It can be diagnosed by potassium hydroxide (KOH) preparations in the setting of friable and broken hair shafts (and sometimes erythema and inflammation).
Patients with trichotillomania may have hair with blunt or tapered ends; hair may also look like uneven stubble.2 The scalp is the most commonly involved site (72.8%), followed by eyebrows (50.7%), and the pubic region (50.7%).1 Useful diagnostic clues include an unusual shape of the affected area, accessible location, and a changing pattern from visit to visit.2 If trichotillomania is suspected, it might be useful to ask about hair-playing activities, such as twirling or twisting, or playing with the ends of eyelashes or eyebrows.2
Unwanted medical consequences of trichotillomania include skin damage (if sharp instruments are used for hair pulling), and the formation of gastrointestinal trichobezoars (hairballs) if trichophagia is present. Trichobezoars that cause bowel obstructions may need surgical intervention.1
Behavioral therapy is the first-line treatment for trichotillomania in all age groups.1,3 Treating any coexisting mental health disorders is also essential. There are currently no FDA-approved medications for treatment; however, there is evidence that N-acetylcysteine may be useful in treating adults with trichotillomania and other repetitive skin disorders.3 Antipsychotics and cannabinoid agonists also may be beneficial.1
This patient was continued on his current lithium, naltrexone, and bupropion regimen (rather than adding additional psychiatric medicines) as he was doing better than his previous baseline. He was advised to continue with his cognitive behavioral therapy. His hormone replacement therapy also was continued because it was not thought to be contributory. He was provided with education about symptoms of trichobezoar and red flag symptoms (eg, worsening nausea, vomiting, abdominal pain) that would necessitate emergency follow-up. His GERD symptoms were thought not to be related to his trichophagia. He was scheduled to follow up for routine primary care in 6 months.
Photo courtesy of Daniel Stulberg, MD. Text courtesy of Sarasawati Keeni, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, Western Michigan University Homer Stryker, MD School of Medicine, Kalamazoo.
1. Grant JE and Chamberlain SR. Trichotillomania. Am J Psychiatry. 2016;173:868-874. doi: 10.1176/appi.ajp.2016.15111432
2. Sah DE, Koo J, Price VH. Trichotillomania. Dermatol Ther. 2008;21:13-21. doi: 10.1111/j.1529-8019.2008.00165.x
3. Henkel ED, Jaquez SD, Diaz LZ. Pediatric trichotillomania: review of management. Pediatr Dermatol. 2019;36:803-807. doi: 10.1111/pde.13954
The areas of hair loss and different length hairs in a patient with otherwise normal-density hair was consistent with a diagnosis of trichotillomania. The physician initially thought the patient had a “fade” hairstyle, but then observed him twirling his hair. Further queries confirmed a history of hair pulling (trichotillomania) and ingesting the hair (trichophagia).
In adulthood, trichotillomania affects females about 4 times more than males, although in childhood, the sex distribution appears about equal.1 The typical age of onset is between 10 to 13 years. Several mental health conditions are associated with trichotillomania, such as major depressive disorder, anxiety disorders, and substance use disorder, with trichotillomania generally preceding these comorbid disorders. It is important to rule out obsessive compulsive disorder and consider body dysmorphic disorder when making a diagnosis of trichotillomania.1
It is common to see androgenetic alopecia precipitated by hormone therapy in FTM individuals. This would usually cause thinning of the hair rather than the irregular hair lengths and pattern seen in this patient. Tinea capitis is also part of the differential diagnosis in a case such as this. It can be diagnosed by potassium hydroxide (KOH) preparations in the setting of friable and broken hair shafts (and sometimes erythema and inflammation).
Patients with trichotillomania may have hair with blunt or tapered ends; hair may also look like uneven stubble.2 The scalp is the most commonly involved site (72.8%), followed by eyebrows (50.7%), and the pubic region (50.7%).1 Useful diagnostic clues include an unusual shape of the affected area, accessible location, and a changing pattern from visit to visit.2 If trichotillomania is suspected, it might be useful to ask about hair-playing activities, such as twirling or twisting, or playing with the ends of eyelashes or eyebrows.2
Unwanted medical consequences of trichotillomania include skin damage (if sharp instruments are used for hair pulling), and the formation of gastrointestinal trichobezoars (hairballs) if trichophagia is present. Trichobezoars that cause bowel obstructions may need surgical intervention.1
Behavioral therapy is the first-line treatment for trichotillomania in all age groups.1,3 Treating any coexisting mental health disorders is also essential. There are currently no FDA-approved medications for treatment; however, there is evidence that N-acetylcysteine may be useful in treating adults with trichotillomania and other repetitive skin disorders.3 Antipsychotics and cannabinoid agonists also may be beneficial.1
This patient was continued on his current lithium, naltrexone, and bupropion regimen (rather than adding additional psychiatric medicines) as he was doing better than his previous baseline. He was advised to continue with his cognitive behavioral therapy. His hormone replacement therapy also was continued because it was not thought to be contributory. He was provided with education about symptoms of trichobezoar and red flag symptoms (eg, worsening nausea, vomiting, abdominal pain) that would necessitate emergency follow-up. His GERD symptoms were thought not to be related to his trichophagia. He was scheduled to follow up for routine primary care in 6 months.
Photo courtesy of Daniel Stulberg, MD. Text courtesy of Sarasawati Keeni, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, Western Michigan University Homer Stryker, MD School of Medicine, Kalamazoo.
The areas of hair loss and different length hairs in a patient with otherwise normal-density hair was consistent with a diagnosis of trichotillomania. The physician initially thought the patient had a “fade” hairstyle, but then observed him twirling his hair. Further queries confirmed a history of hair pulling (trichotillomania) and ingesting the hair (trichophagia).
In adulthood, trichotillomania affects females about 4 times more than males, although in childhood, the sex distribution appears about equal.1 The typical age of onset is between 10 to 13 years. Several mental health conditions are associated with trichotillomania, such as major depressive disorder, anxiety disorders, and substance use disorder, with trichotillomania generally preceding these comorbid disorders. It is important to rule out obsessive compulsive disorder and consider body dysmorphic disorder when making a diagnosis of trichotillomania.1
It is common to see androgenetic alopecia precipitated by hormone therapy in FTM individuals. This would usually cause thinning of the hair rather than the irregular hair lengths and pattern seen in this patient. Tinea capitis is also part of the differential diagnosis in a case such as this. It can be diagnosed by potassium hydroxide (KOH) preparations in the setting of friable and broken hair shafts (and sometimes erythema and inflammation).
Patients with trichotillomania may have hair with blunt or tapered ends; hair may also look like uneven stubble.2 The scalp is the most commonly involved site (72.8%), followed by eyebrows (50.7%), and the pubic region (50.7%).1 Useful diagnostic clues include an unusual shape of the affected area, accessible location, and a changing pattern from visit to visit.2 If trichotillomania is suspected, it might be useful to ask about hair-playing activities, such as twirling or twisting, or playing with the ends of eyelashes or eyebrows.2
Unwanted medical consequences of trichotillomania include skin damage (if sharp instruments are used for hair pulling), and the formation of gastrointestinal trichobezoars (hairballs) if trichophagia is present. Trichobezoars that cause bowel obstructions may need surgical intervention.1
Behavioral therapy is the first-line treatment for trichotillomania in all age groups.1,3 Treating any coexisting mental health disorders is also essential. There are currently no FDA-approved medications for treatment; however, there is evidence that N-acetylcysteine may be useful in treating adults with trichotillomania and other repetitive skin disorders.3 Antipsychotics and cannabinoid agonists also may be beneficial.1
This patient was continued on his current lithium, naltrexone, and bupropion regimen (rather than adding additional psychiatric medicines) as he was doing better than his previous baseline. He was advised to continue with his cognitive behavioral therapy. His hormone replacement therapy also was continued because it was not thought to be contributory. He was provided with education about symptoms of trichobezoar and red flag symptoms (eg, worsening nausea, vomiting, abdominal pain) that would necessitate emergency follow-up. His GERD symptoms were thought not to be related to his trichophagia. He was scheduled to follow up for routine primary care in 6 months.
Photo courtesy of Daniel Stulberg, MD. Text courtesy of Sarasawati Keeni, MD, and Daniel Stulberg, MD, FAAFP, Department of Family and Community Medicine, Western Michigan University Homer Stryker, MD School of Medicine, Kalamazoo.
1. Grant JE and Chamberlain SR. Trichotillomania. Am J Psychiatry. 2016;173:868-874. doi: 10.1176/appi.ajp.2016.15111432
2. Sah DE, Koo J, Price VH. Trichotillomania. Dermatol Ther. 2008;21:13-21. doi: 10.1111/j.1529-8019.2008.00165.x
3. Henkel ED, Jaquez SD, Diaz LZ. Pediatric trichotillomania: review of management. Pediatr Dermatol. 2019;36:803-807. doi: 10.1111/pde.13954
1. Grant JE and Chamberlain SR. Trichotillomania. Am J Psychiatry. 2016;173:868-874. doi: 10.1176/appi.ajp.2016.15111432
2. Sah DE, Koo J, Price VH. Trichotillomania. Dermatol Ther. 2008;21:13-21. doi: 10.1111/j.1529-8019.2008.00165.x
3. Henkel ED, Jaquez SD, Diaz LZ. Pediatric trichotillomania: review of management. Pediatr Dermatol. 2019;36:803-807. doi: 10.1111/pde.13954

PsA Differential Diagnosis
HPV rates skyrocket despite safe, effective vaccine
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
Depression Treatment
Once-weekly basal insulin nears market for type 2 diabetes
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.

“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.
“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.
“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
AT ADA 2023