User login
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
Render unto Caesar the things that are Caesar’s, and to God the things that are God’s.
Matthew 22:21
While in my 20s, I taught religious education at a church on the Army base where I was born and had the honor of working with military chaplains. During my US Department of Veterans Affairs career, I closely collaborated with chaplains—many of whom were veterans—on patient care and ethics consultations. Some were quite proud of their rank and interested in climbing the ladder of promotion. A few made sure you knew what they wore or had worn on their uniform, while most were incredibly humble and sheepish when soldiers saluted them. Those visible responses to rank may be hidden if chaplains will no longer be permitted to wear insignia indicating their grade.
Department of War Secretary Peter Hegseth, a combat veteran who has championed a “combative” form of Christianity, announced in April 2026 that chaplains would no longer wear their rank on their uniform.1 Details of how this shift will be translated into regulation, policy, and actions were not provided. Secretary Hegseth did not remove the actual rank of members of the chaplain corps and they would retain their rank, attendant pay, benefits, responsibilities, and privileges. However, instead of bearing the insignia of their military station, under this new policy only the symbol of their religious profession would identify them. Currently, both a military officer’s rank and religious symbol are displayed.2
Useful insight can be gained from an historical perspective, which demonstrates that the concerns and contention about the issue of chaplain’s wearing rank are not new. There have been chaplains in the US Army since 1775.3 Army chaplains initially wore only a religious symbol on their clothing. In April 1914, chaplain leaders successful argued that chaplains deserved the privileges, respect, and prospect for promotion that rank symbolized and where authorized to display their position. Four years later, General Jack Pershing cabled the then Secretary of War opposing the new policy: “Believe the work of chaplains would be facilitated if they were not given military rank ... Many of our principal ministers believe that their relations would be closer if they did not have military titles and did not wear insignia.”4 Interestingly, Secretary Hegseth articulated the same concern: “A chaplain is first and foremost a chaplain and an officer second. This change is a visual representation of that fact.”5
Hegseth has stated that in recent years the military chaplain corps had drifted too far in the direction of providing spiritual counseling and psychological support. This contravenes the current competencies especially for company-grade military chaplains who primarily minister to the moral distress and spiritual needs of service members.4 The removal of rank is thus best understood as part of Secretary Hegseth’s broader plan to remake the chaplain corps into his vision of religious ministry in the military.5
Secretary Hegseth proffered several arguments for the necessity of removing rank in part to reorient the chaplain corps to what he calls a more fundamental mission. The first was theological: chaplains need to prioritize their “divine calling” rather than any human distinction. Chaplain theologians and ethicists have expressed similar concerns that in wearing rank, military chaplains become servants of the state and not of God. Adam Tietje articulates the corruptive influence this shift in the source of legitimacy has on the military chaplain’s spiritual mission:
This undermines the ability of chaplains to provide care and counsel to both soldiers and leaders that is not muddied with the interests of the military. Chaplains without rank are better positioned to hear and advocate for their soldier’s matters of conscience as well as bear witness to the moral claims of their respective religious communities especially about war itself.3
The second argument is pastoral. Hegseth contends that service members of lower rank would feel more comfortable and secure approaching chaplains with no outward sign of their higher position. Chaplain interactions with military personnel carry a degree of confidentiality higher than that of either doctors or lawyers. Chaplains, as they were in the past, remain divided on this important consideration.4,5
The third argument is ethical in nature. Secretary Hegseth contends that excluding any manifestation of military rank, “speaks to the difficult balance of the duality” of the role.6 It seems he is proposing that chaplains displaying only the image of their faith commitment symbolically resolves the inherent moral conflict between serving human masters as a military officer, and the divine as a minister.7 Military chaplains and health care professionals are all too familiar with the dilemma of having 2 masters and the challenge of negotiating legally and ethically overlapping roles.8-10
This may seem to some like a minor change in chaplain etiquette to some, but to others it signals a significant ethical and political change with potential import beyond chaplaincy. One military commentator has suggested the move sets a dangerous precedent that could eventually be applied to both health care professionals and the judge advocate corps.11 At this point this is only speculation and its slippery slope arguments are logically suspect without evidence. Yet at least 1 study suggests that the influence of military physician’s rank on patient care may lead to inequities in the care delivered to patients with lower grade.12
It is commanders who are the decision-makers in the military. Chaplains who are field grade officers serve as trusted staff advisors in moral, ethical, and spiritual matters.4 Some chaplains fear that without rank leaders at all levels will not have adequate trust and sufficient respect to heed their crucial counsel especially regarding high-stakes strategic decisions in wartime.8 The more serious concern is with a major shift in the locus of authority to determine the professional identity of chaplains, that could in theory be expanded to impact military health care practitioners, and attorneys. The independent expert judgment of these professionals regarding what is necessary to fulfil their respective roles in providing spiritual ministry, medical care, and legal is critical to uphold the highest values of the US military.11 Chaplains have long struggled with what they owe to the Caesar and to God: how the Secretary’s recent decision will shape that rendering is uncertain. What is certain is that military chaplains of all faiths and in every branch of the armed services will continue to minister to their brothers and sisters in arms with courage and compassion.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
- Baker R, Graham R. Pete Hegseth and his ‘battle cry’ for a new christian crusade. The New York Times. December 6, 2024. Accessed April 24, 2026. https://www.nytimes.com/2024/12/05/us/hegseth-church-crusades.html
- Sampson E. Hegseth removes rank insignia from military chaplains. Military Times. March 25, 2026. Accessed April 24, 2026. https://www.militarytimes.com/news/pentagon-congress/2026/03/25/hegseth-removes-rank-insignia-from-military-chaplains/
- Tietje A. A seductive confusion of authority: military chaplains and the wearing of rank. J Church State. 2020;62:506-524.
- Morris JT. Military chaplaincy in the USA: an unfolding of roles and functions. In: Weiss H, Federschmidt KH, Louw DJ, et al, eds. Care, Healing, and Human Well-Being Within Interreligious Discourses. African Sun Media; 2021:319-333.
- Cox M. Hegseth’s push for chaplain’s to shed remove rank sparks debate. Air and Space Forces Magazine. March 27, 2026. Accessed April 29, 2026. https://www.airandspaceforces.com/chaplains-ordered-to-shed-rank-ret-af-leaders-question-move/
- Mitchell E. Hegseth: Military chaplains will no longer display rank. The Hill. March 25, 2026. Accessed April 24, 2026. https://thehill.com/policy/defense/5800026-pete-hegseth-military-chaplains-faith-insignia/
- Banks AM. Hegseth’s removal of the top Army chaplain raises ‘troubling questions’ from Black denomination. Religious News Service. April 9, 2026. Accessed April 24, 2026. https://religionnews.com/2026/04/09/army-chaplains-chiefs-firing-prompts-serious-concern-from-black-baptist-denomination/
- Burchard WW. Role conflicts of military chaplains. Amer Sociolog Rev. 1954;19:528-535 https://www.jstor.org/stable/2087790
- Sturtz DL. Commitment. Mil Med. 2001;166:741-744.
- Carver D. New Department of War policy: military chaplains no longer wear rank insignia. North American Mission Board. April 8, 2026. Accessed April 24, 2026. https://www.namb.net/resource/new-department-of-war-policy-military-chaplains-no-longer-wear-rank-insignia/
- Petri D. If chaplains are ‘officers second,’ which staff corps officers are next? Military Times. April 1, 2026. Accessed April 24, 2026. https://www.militarytimes.com/opinion/2026/04/01/if-chaplains-are-officers-second-which-staff-corps-officers-are-next/
- Schwab SD, Singh M. How power shapes behavior: evidence from physicians. Science. 2024; 384:802-807.
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains
Divine Calling and Human Rank: The Locus of Authority for Military Chaplains

AI Scribes or VHA Docs: Which Created Better Clinical Notes?
Artificial intelligence (AI) scribes produced lower-quality documentation of clinical notes than human clinicians, and especially struggled in settings with background noise or clinicians wearing masks, a new Veterans Health Administration (VHA) study finds.
In 5 simulated clinical cases, notes written by various AI programs scored lower than reports produced by humans on the modified Physician Documentation Quality Instrument (PDQI-9), a measurement of note quality scale, reported Ashok Reddy, MD, MSc, of the University of Washington and Veterans Affairs Puget Sound Health Care System, Seattle, et al in the April issue of Annals of Internal Medicine.
AI scribes scored lower compared with humans across all domains, including accuracy, thoroughness, and usefulness. There was an especially large gap in scores on the 50-point PDQI-9 in an acute low back pain case (human, 43.8 points; AI, 20.3 points; difference, 23.5 points).
“For clinicians, AI scribes should be regarded as tools for generating draft documentation that requires review and editing, rather than as a substitute for clinician-authored notes,” the authors wrote. “Although ambient AI scribes hold promise for reducing clinician burden, rigorous and ongoing evaluation of their quality is essential to ensure that these tools enhance rather than compromise the quality of clinical care.”
AI Scribe Use is Widespread
Taylor N. Anderson, MD, a clinical informatics fellow at Oregon Health & Science University, Portland, is familiar with the study findings and noted that the use of AI scribes in medicine has grown rapidly. All major health organizations are either using it or facing “enormous pressure” from clinicians to do so, she told Federal Practitioner.
Previous research has linked the use of AI scribes for clinical notes to less electronic health record usage and documentation time for clinicians, leading to more time for patient visits. Still, the quality of clinical notes written by AI is “quite variable across vendors,” Anderson said.
Anderson led a 2025 study that examined 5 AI scribe platforms and found an average of 3.0 errors per case with “potential for moderate-to-severe harm.”
For the new study on the simulated cases, part of a VHA-sponsored “technology sprint” via Challenge.gov, researchers developed audio descriptions of 5 clinical cases reflecting common patient encounters in primary care: acute low back pain, chest pain, a new diagnosis of diabetes, a pharmacy consultation, and a follow-up with a nurse case manager for heart failure.
Two cases included non-English accents, 1 included background noise, and 1 featured speech through a medical mask. All the “patients” were played by what the authors described as “trained standardized patient actors.”
For each case, 3 humans and 11 AI scribe programs produced clinical notes. The clinical notes were then evaluated by 6 raters.
Researchers found that AI scribe-generated notes scored worse than human-generated notes across all 10 domains of the modified PDQI-9 (accuracy, thoroughness, usefulness, organization, comprehensiveness, succinctness, synthesization, internal consistency, and freedom from hallucination and bias).
There were especially large gaps between the AI and human notes in the domains of thoroughness, organization, and usefulness. Even wider gaps were observed for the encounters with noise and mask usage.
“These findings highlight that although ambient AI scribes can generate complete notes, the overall quality remains broadly below that of human-authored documentation,” the authors wrote.
No Comparison Between AI Scribes
The researchers noted that “given contractual limitations, we cannot interpret the results for specific vendors.” They also noted that the study did not use professional scribes, who may produce even higher-quality results, and the humans were not producing notes in a real-world clinical environment.
Anderson, the clinical informatics fellow, pointed out that the study does not examine the common scenario in which a clinician edits notes produced by an AI scribe. In fact, she said, there is no current research on this, failing to examine “the postediting note that would actually go into the chart.”
In an accompanying commentary, collaborative scientist Aaron Tierney, PhD, and Kristine Lee, MD, an associate executive director, both with the Permanente Medical Group, California, called for future research to focus on “real-world performance, promote the development of documentation policies that prioritize patient care over billing requirements, and systematically incorporate patient perspectives into assessments of quality.”
Why AI Misses the Mark
In an interview with Federal Practitioner, AI researcher Maxim Topaz, PhD, RN, MA, an associate professor of Nursing and Data Science at Columbia University School of Nursing, New York City, who is familiar with the study but did not participate in it, praised the research.
He pointed out that AI has trouble accurately representing clinical encounters because they “tend to fill gaps with plausible-sounding language, which can mask omissions and make errors harder to catch.” Also, “ambient scribes can only document what is verbalized aloud. Physical exam findings the clinician notices but does not narrate, nonverbal cues, and patient-initiated concerns that drift past in conversation are systematically underrepresented.”
Moving forward, Topaz advised clinicians to “treat AI-generated notes as a first draft, not a finished product. Read them carefully, especially for omissions, which the current evidence suggests are by far the most common error type and which are harder to spot than fabrications because the surrounding note still reads coherently.”
Two study authors disclosed employment by the US Department of Veterans Affairs. Other authors had no disclosures. The commentary authors have no disclosures. Anderson has no disclosures. Topaz discloses relationships with the National Institutes of Health and other federal sources.
Artificial intelligence (AI) scribes produced lower-quality documentation of clinical notes than human clinicians, and especially struggled in settings with background noise or clinicians wearing masks, a new Veterans Health Administration (VHA) study finds.
In 5 simulated clinical cases, notes written by various AI programs scored lower than reports produced by humans on the modified Physician Documentation Quality Instrument (PDQI-9), a measurement of note quality scale, reported Ashok Reddy, MD, MSc, of the University of Washington and Veterans Affairs Puget Sound Health Care System, Seattle, et al in the April issue of Annals of Internal Medicine.
AI scribes scored lower compared with humans across all domains, including accuracy, thoroughness, and usefulness. There was an especially large gap in scores on the 50-point PDQI-9 in an acute low back pain case (human, 43.8 points; AI, 20.3 points; difference, 23.5 points).
“For clinicians, AI scribes should be regarded as tools for generating draft documentation that requires review and editing, rather than as a substitute for clinician-authored notes,” the authors wrote. “Although ambient AI scribes hold promise for reducing clinician burden, rigorous and ongoing evaluation of their quality is essential to ensure that these tools enhance rather than compromise the quality of clinical care.”
AI Scribe Use is Widespread
Taylor N. Anderson, MD, a clinical informatics fellow at Oregon Health & Science University, Portland, is familiar with the study findings and noted that the use of AI scribes in medicine has grown rapidly. All major health organizations are either using it or facing “enormous pressure” from clinicians to do so, she told Federal Practitioner.
Previous research has linked the use of AI scribes for clinical notes to less electronic health record usage and documentation time for clinicians, leading to more time for patient visits. Still, the quality of clinical notes written by AI is “quite variable across vendors,” Anderson said.
Anderson led a 2025 study that examined 5 AI scribe platforms and found an average of 3.0 errors per case with “potential for moderate-to-severe harm.”
For the new study on the simulated cases, part of a VHA-sponsored “technology sprint” via Challenge.gov, researchers developed audio descriptions of 5 clinical cases reflecting common patient encounters in primary care: acute low back pain, chest pain, a new diagnosis of diabetes, a pharmacy consultation, and a follow-up with a nurse case manager for heart failure.
Two cases included non-English accents, 1 included background noise, and 1 featured speech through a medical mask. All the “patients” were played by what the authors described as “trained standardized patient actors.”
For each case, 3 humans and 11 AI scribe programs produced clinical notes. The clinical notes were then evaluated by 6 raters.
Researchers found that AI scribe-generated notes scored worse than human-generated notes across all 10 domains of the modified PDQI-9 (accuracy, thoroughness, usefulness, organization, comprehensiveness, succinctness, synthesization, internal consistency, and freedom from hallucination and bias).
There were especially large gaps between the AI and human notes in the domains of thoroughness, organization, and usefulness. Even wider gaps were observed for the encounters with noise and mask usage.
“These findings highlight that although ambient AI scribes can generate complete notes, the overall quality remains broadly below that of human-authored documentation,” the authors wrote.
No Comparison Between AI Scribes
The researchers noted that “given contractual limitations, we cannot interpret the results for specific vendors.” They also noted that the study did not use professional scribes, who may produce even higher-quality results, and the humans were not producing notes in a real-world clinical environment.
Anderson, the clinical informatics fellow, pointed out that the study does not examine the common scenario in which a clinician edits notes produced by an AI scribe. In fact, she said, there is no current research on this, failing to examine “the postediting note that would actually go into the chart.”
In an accompanying commentary, collaborative scientist Aaron Tierney, PhD, and Kristine Lee, MD, an associate executive director, both with the Permanente Medical Group, California, called for future research to focus on “real-world performance, promote the development of documentation policies that prioritize patient care over billing requirements, and systematically incorporate patient perspectives into assessments of quality.”
Why AI Misses the Mark
In an interview with Federal Practitioner, AI researcher Maxim Topaz, PhD, RN, MA, an associate professor of Nursing and Data Science at Columbia University School of Nursing, New York City, who is familiar with the study but did not participate in it, praised the research.
He pointed out that AI has trouble accurately representing clinical encounters because they “tend to fill gaps with plausible-sounding language, which can mask omissions and make errors harder to catch.” Also, “ambient scribes can only document what is verbalized aloud. Physical exam findings the clinician notices but does not narrate, nonverbal cues, and patient-initiated concerns that drift past in conversation are systematically underrepresented.”
Moving forward, Topaz advised clinicians to “treat AI-generated notes as a first draft, not a finished product. Read them carefully, especially for omissions, which the current evidence suggests are by far the most common error type and which are harder to spot than fabrications because the surrounding note still reads coherently.”
Two study authors disclosed employment by the US Department of Veterans Affairs. Other authors had no disclosures. The commentary authors have no disclosures. Anderson has no disclosures. Topaz discloses relationships with the National Institutes of Health and other federal sources.
Artificial intelligence (AI) scribes produced lower-quality documentation of clinical notes than human clinicians, and especially struggled in settings with background noise or clinicians wearing masks, a new Veterans Health Administration (VHA) study finds.
In 5 simulated clinical cases, notes written by various AI programs scored lower than reports produced by humans on the modified Physician Documentation Quality Instrument (PDQI-9), a measurement of note quality scale, reported Ashok Reddy, MD, MSc, of the University of Washington and Veterans Affairs Puget Sound Health Care System, Seattle, et al in the April issue of Annals of Internal Medicine.
AI scribes scored lower compared with humans across all domains, including accuracy, thoroughness, and usefulness. There was an especially large gap in scores on the 50-point PDQI-9 in an acute low back pain case (human, 43.8 points; AI, 20.3 points; difference, 23.5 points).
“For clinicians, AI scribes should be regarded as tools for generating draft documentation that requires review and editing, rather than as a substitute for clinician-authored notes,” the authors wrote. “Although ambient AI scribes hold promise for reducing clinician burden, rigorous and ongoing evaluation of their quality is essential to ensure that these tools enhance rather than compromise the quality of clinical care.”
AI Scribe Use is Widespread
Taylor N. Anderson, MD, a clinical informatics fellow at Oregon Health & Science University, Portland, is familiar with the study findings and noted that the use of AI scribes in medicine has grown rapidly. All major health organizations are either using it or facing “enormous pressure” from clinicians to do so, she told Federal Practitioner.
Previous research has linked the use of AI scribes for clinical notes to less electronic health record usage and documentation time for clinicians, leading to more time for patient visits. Still, the quality of clinical notes written by AI is “quite variable across vendors,” Anderson said.
Anderson led a 2025 study that examined 5 AI scribe platforms and found an average of 3.0 errors per case with “potential for moderate-to-severe harm.”
For the new study on the simulated cases, part of a VHA-sponsored “technology sprint” via Challenge.gov, researchers developed audio descriptions of 5 clinical cases reflecting common patient encounters in primary care: acute low back pain, chest pain, a new diagnosis of diabetes, a pharmacy consultation, and a follow-up with a nurse case manager for heart failure.
Two cases included non-English accents, 1 included background noise, and 1 featured speech through a medical mask. All the “patients” were played by what the authors described as “trained standardized patient actors.”
For each case, 3 humans and 11 AI scribe programs produced clinical notes. The clinical notes were then evaluated by 6 raters.
Researchers found that AI scribe-generated notes scored worse than human-generated notes across all 10 domains of the modified PDQI-9 (accuracy, thoroughness, usefulness, organization, comprehensiveness, succinctness, synthesization, internal consistency, and freedom from hallucination and bias).
There were especially large gaps between the AI and human notes in the domains of thoroughness, organization, and usefulness. Even wider gaps were observed for the encounters with noise and mask usage.
“These findings highlight that although ambient AI scribes can generate complete notes, the overall quality remains broadly below that of human-authored documentation,” the authors wrote.
No Comparison Between AI Scribes
The researchers noted that “given contractual limitations, we cannot interpret the results for specific vendors.” They also noted that the study did not use professional scribes, who may produce even higher-quality results, and the humans were not producing notes in a real-world clinical environment.
Anderson, the clinical informatics fellow, pointed out that the study does not examine the common scenario in which a clinician edits notes produced by an AI scribe. In fact, she said, there is no current research on this, failing to examine “the postediting note that would actually go into the chart.”
In an accompanying commentary, collaborative scientist Aaron Tierney, PhD, and Kristine Lee, MD, an associate executive director, both with the Permanente Medical Group, California, called for future research to focus on “real-world performance, promote the development of documentation policies that prioritize patient care over billing requirements, and systematically incorporate patient perspectives into assessments of quality.”
Why AI Misses the Mark
In an interview with Federal Practitioner, AI researcher Maxim Topaz, PhD, RN, MA, an associate professor of Nursing and Data Science at Columbia University School of Nursing, New York City, who is familiar with the study but did not participate in it, praised the research.
He pointed out that AI has trouble accurately representing clinical encounters because they “tend to fill gaps with plausible-sounding language, which can mask omissions and make errors harder to catch.” Also, “ambient scribes can only document what is verbalized aloud. Physical exam findings the clinician notices but does not narrate, nonverbal cues, and patient-initiated concerns that drift past in conversation are systematically underrepresented.”
Moving forward, Topaz advised clinicians to “treat AI-generated notes as a first draft, not a finished product. Read them carefully, especially for omissions, which the current evidence suggests are by far the most common error type and which are harder to spot than fabrications because the surrounding note still reads coherently.”
Two study authors disclosed employment by the US Department of Veterans Affairs. Other authors had no disclosures. The commentary authors have no disclosures. Anderson has no disclosures. Topaz discloses relationships with the National Institutes of Health and other federal sources.
State Firearm Laws Linked to Veteran Suicide Rates
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
TOPLINE: Among veterans and demographically matched nonveterans from 2002 to 2019, higher state household firearm ownership was associated with higher rates of deaths by suicide, while greater state firearm law restrictiveness was associated with lower rates of deaths by suicide. In 2017 to 2019 models, these associations were seen for both veterans and matched nonveterans and driven primarily by firearm deaths by suicide rates.
METHODOLOGY:
US state-level data across 6 consecutive 3-year periods from 2002-2019, stratified suicide rates by veteran status (veteran vs matched nonveterans) and method (firearm vs nonfirearm).
Data sources included US Department of Veterans Affairs (VA) Office of Mental Health and Suicide Prevention counts matched to the National Death Index, plus Centers for Disease Control suicide counts and population estimates by sex and age.
Participants included veterans with state- and period-specific death suicide counts and population denominators from the VetPop model, and a matched nonveteran comparison created by comparing state deaths by suicide data to veterans’ age and gender distributions.
Exposure measures included annual state household firearm ownership rate estimates carried forward to 2017-2019, and a 7-item state firearm policy restrictiveness index derived from the RAND Corporation state firearm law database.
TAKEAWAY:
Average death by suicide rates from 2002-2019 were 28.2 per 100,000 for veterans and 27.5 per 100,000 for matched nonveterans, with most deaths involving a firearm.
Across states, the maximum average death by suicide rate was about 3 times the minimum over the study period, and veteran and matched nonveteran state patterns aligned closely.
Higher household firearm ownership was associated with higher firearm death by suicide rates for veterans and matched nonveterans from 2017-2019.
Greater firearm law restrictiveness, equivalent to 3 additional restrictive laws, was associated with fewer firearm deaths by suicide for veterans and matched nonveterans from 2017-2019.
IN PRACTICE: “The results suggest that changes to state firearm laws and policies should be investigated as a possibly cost-effective primary prevention strategy for reducing suicide rates among veterans and nonveterans,” the authors wrote.
SOURCE:The study was led by Andrew R. Morral, PhD, RAND Corporation in Arlington, Virginia, and Terry L. Schell, PhD, and Adam Scherling, RAND Corporation in Santa Monica, California and published online in Injury Prevention.
LIMITATIONS: The estimates are correlational and should not be interpreted as causal effect estimates, as most interstate variation in gun ownership and firearm laws predates the beginning of the available VA death by suicide data, limiting the analytical approach to identify causal effects. VA does not share microdata on veteran suicide, requiring construction of a matched comparison sample of nonveterans by estimating veteran decedent removal from general population suicide totals within cells of a 5-way table based on publicly released 3-way tables, introducing imprecision. Veteran suicide counts are known to undercount suicides among veterans who separated from the military prior to 1974, likely resulting in a slight underestimate of veteran suicide rates for the oldest cohort of veterans, particularly in earlier study periods. Restricting analysis to identify modeled effects solely through limited changes in state firearm ownership and policies during the study period yields imprecise effect estimates.
DISCLOSURES: This work received support from a grant provided by The RAND Epstein Family Veterans Policy Research Institute, established through a contribution from Daniel J. Epstein via the Epstein Family Foundation. Neither the Institute, the Foundation, nor Mr. Epstein participated in the design, conduct, analysis, or drafting of this report. The authors disclosed no relevant conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
New Scheduler Connects Veterans to Community Care Faster
New Scheduler Connects Veterans to Community Care Faster
The US Department of Veterans Affairs (VA) has adopted new technology designed to make it easier and faster for veterans to schedule appointments with community care health care practitioners (HCPs).
Through the External Provider Scheduling (EPS) system, VA employees can access the scheduling systems of participating community care HCPs. As of March 2026, 27,000 community care HCPs were participating in EPS across 78 medical specialties.
Without this system, VA employees have to call multiple community care HCPs and relay that information back to veterans before booking an appointment. As a result, a single VA employee could only schedule a handful of community care appointments per day, and it could take days or even weeks to book an appointment for a veteran.
Now, the new system—implemented in all VA facilities starting in late 2025—enables VA employees to schedule as many as 25 appointments daily.
“We are making it easier and more convenient than ever for those who have worn the uniform to choose the care that best fits their lifestyle,” VA Secretary Doug Collins said in a news release.
The VA goal is to sign up thousands of additional community care HCPs in 2026 as part of its continuing efforts to deliver timely, veteran-centered care. There is no cost for institutions to participate in the program.
Select Medical, an outpatient rehabilitation organization with > 1900 centers in 39 states and the District of Columbia, became aware of this opportunity in the first half of 2025: “At that time, we met with key VA stakeholders to learn more about the new program, the challenges it would address, and how it worked to evaluate our ability to participate,” said Chad Smith, president of the company’s outpatient division, headquartered in Mechanicsburg, Pennsylvania.
“We immediately saw the value in what the VA was seeking to accomplish and wanted to be part of providing increased access to exceptional care for our nation’s veterans,” Smith said.
In July 2025, Smith noted, Select Medical piloted the program in 2 states. After successful deployment, the organization broadened its participation to 15 states, offering “seamless access to care” to > 3000 veterans. They receive outpatient rehabilitative care, including physical and occupational therapy.
“The External Provider Scheduling system creates a more streamlined way for veterans and VA administrators to manage the appointment process,” Smith said.
Northwell Health in Lake Success, New York, expressed interest in the program last summer when approached by the VA and “jumped at it,” said Juan Serrano, MBA, MS, vice president of military liaison services at Northwell Health.
The Long Island-based system, which already had a long-standing relationship with the VA, rolled out the program to give veterans the ability to see community care HCPs, Serrano said.
The program started in November, with the first appointment booked in December. From then until the end of April, the program booked 69 appointments for almost 80 veterans, with gastroenterology and otolaryngology representing the highest volume specialties.
Veterans also have gained entry to several other specialty clinics, including imaging services. The program has decreased waiting times for veterans’ appointments and helped them establish rapport with community care HCPs, Serrano said.
“One of the biggest setbacks and difficulties veterans experience is timely access to care outside of the VA,” he said, adding, “as an organization, we made a pledge to create a pathway for veterans to complement the work of the VA and give veterans access to our network.”
The US Department of Veterans Affairs (VA) has adopted new technology designed to make it easier and faster for veterans to schedule appointments with community care health care practitioners (HCPs).
Through the External Provider Scheduling (EPS) system, VA employees can access the scheduling systems of participating community care HCPs. As of March 2026, 27,000 community care HCPs were participating in EPS across 78 medical specialties.
Without this system, VA employees have to call multiple community care HCPs and relay that information back to veterans before booking an appointment. As a result, a single VA employee could only schedule a handful of community care appointments per day, and it could take days or even weeks to book an appointment for a veteran.
Now, the new system—implemented in all VA facilities starting in late 2025—enables VA employees to schedule as many as 25 appointments daily.
“We are making it easier and more convenient than ever for those who have worn the uniform to choose the care that best fits their lifestyle,” VA Secretary Doug Collins said in a news release.
The VA goal is to sign up thousands of additional community care HCPs in 2026 as part of its continuing efforts to deliver timely, veteran-centered care. There is no cost for institutions to participate in the program.
Select Medical, an outpatient rehabilitation organization with > 1900 centers in 39 states and the District of Columbia, became aware of this opportunity in the first half of 2025: “At that time, we met with key VA stakeholders to learn more about the new program, the challenges it would address, and how it worked to evaluate our ability to participate,” said Chad Smith, president of the company’s outpatient division, headquartered in Mechanicsburg, Pennsylvania.
“We immediately saw the value in what the VA was seeking to accomplish and wanted to be part of providing increased access to exceptional care for our nation’s veterans,” Smith said.
In July 2025, Smith noted, Select Medical piloted the program in 2 states. After successful deployment, the organization broadened its participation to 15 states, offering “seamless access to care” to > 3000 veterans. They receive outpatient rehabilitative care, including physical and occupational therapy.
“The External Provider Scheduling system creates a more streamlined way for veterans and VA administrators to manage the appointment process,” Smith said.
Northwell Health in Lake Success, New York, expressed interest in the program last summer when approached by the VA and “jumped at it,” said Juan Serrano, MBA, MS, vice president of military liaison services at Northwell Health.
The Long Island-based system, which already had a long-standing relationship with the VA, rolled out the program to give veterans the ability to see community care HCPs, Serrano said.
The program started in November, with the first appointment booked in December. From then until the end of April, the program booked 69 appointments for almost 80 veterans, with gastroenterology and otolaryngology representing the highest volume specialties.
Veterans also have gained entry to several other specialty clinics, including imaging services. The program has decreased waiting times for veterans’ appointments and helped them establish rapport with community care HCPs, Serrano said.
“One of the biggest setbacks and difficulties veterans experience is timely access to care outside of the VA,” he said, adding, “as an organization, we made a pledge to create a pathway for veterans to complement the work of the VA and give veterans access to our network.”
The US Department of Veterans Affairs (VA) has adopted new technology designed to make it easier and faster for veterans to schedule appointments with community care health care practitioners (HCPs).
Through the External Provider Scheduling (EPS) system, VA employees can access the scheduling systems of participating community care HCPs. As of March 2026, 27,000 community care HCPs were participating in EPS across 78 medical specialties.
Without this system, VA employees have to call multiple community care HCPs and relay that information back to veterans before booking an appointment. As a result, a single VA employee could only schedule a handful of community care appointments per day, and it could take days or even weeks to book an appointment for a veteran.
Now, the new system—implemented in all VA facilities starting in late 2025—enables VA employees to schedule as many as 25 appointments daily.
“We are making it easier and more convenient than ever for those who have worn the uniform to choose the care that best fits their lifestyle,” VA Secretary Doug Collins said in a news release.
The VA goal is to sign up thousands of additional community care HCPs in 2026 as part of its continuing efforts to deliver timely, veteran-centered care. There is no cost for institutions to participate in the program.
Select Medical, an outpatient rehabilitation organization with > 1900 centers in 39 states and the District of Columbia, became aware of this opportunity in the first half of 2025: “At that time, we met with key VA stakeholders to learn more about the new program, the challenges it would address, and how it worked to evaluate our ability to participate,” said Chad Smith, president of the company’s outpatient division, headquartered in Mechanicsburg, Pennsylvania.
“We immediately saw the value in what the VA was seeking to accomplish and wanted to be part of providing increased access to exceptional care for our nation’s veterans,” Smith said.
In July 2025, Smith noted, Select Medical piloted the program in 2 states. After successful deployment, the organization broadened its participation to 15 states, offering “seamless access to care” to > 3000 veterans. They receive outpatient rehabilitative care, including physical and occupational therapy.
“The External Provider Scheduling system creates a more streamlined way for veterans and VA administrators to manage the appointment process,” Smith said.
Northwell Health in Lake Success, New York, expressed interest in the program last summer when approached by the VA and “jumped at it,” said Juan Serrano, MBA, MS, vice president of military liaison services at Northwell Health.
The Long Island-based system, which already had a long-standing relationship with the VA, rolled out the program to give veterans the ability to see community care HCPs, Serrano said.
The program started in November, with the first appointment booked in December. From then until the end of April, the program booked 69 appointments for almost 80 veterans, with gastroenterology and otolaryngology representing the highest volume specialties.
Veterans also have gained entry to several other specialty clinics, including imaging services. The program has decreased waiting times for veterans’ appointments and helped them establish rapport with community care HCPs, Serrano said.
“One of the biggest setbacks and difficulties veterans experience is timely access to care outside of the VA,” he said, adding, “as an organization, we made a pledge to create a pathway for veterans to complement the work of the VA and give veterans access to our network.”
New Scheduler Connects Veterans to Community Care Faster
New Scheduler Connects Veterans to Community Care Faster
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
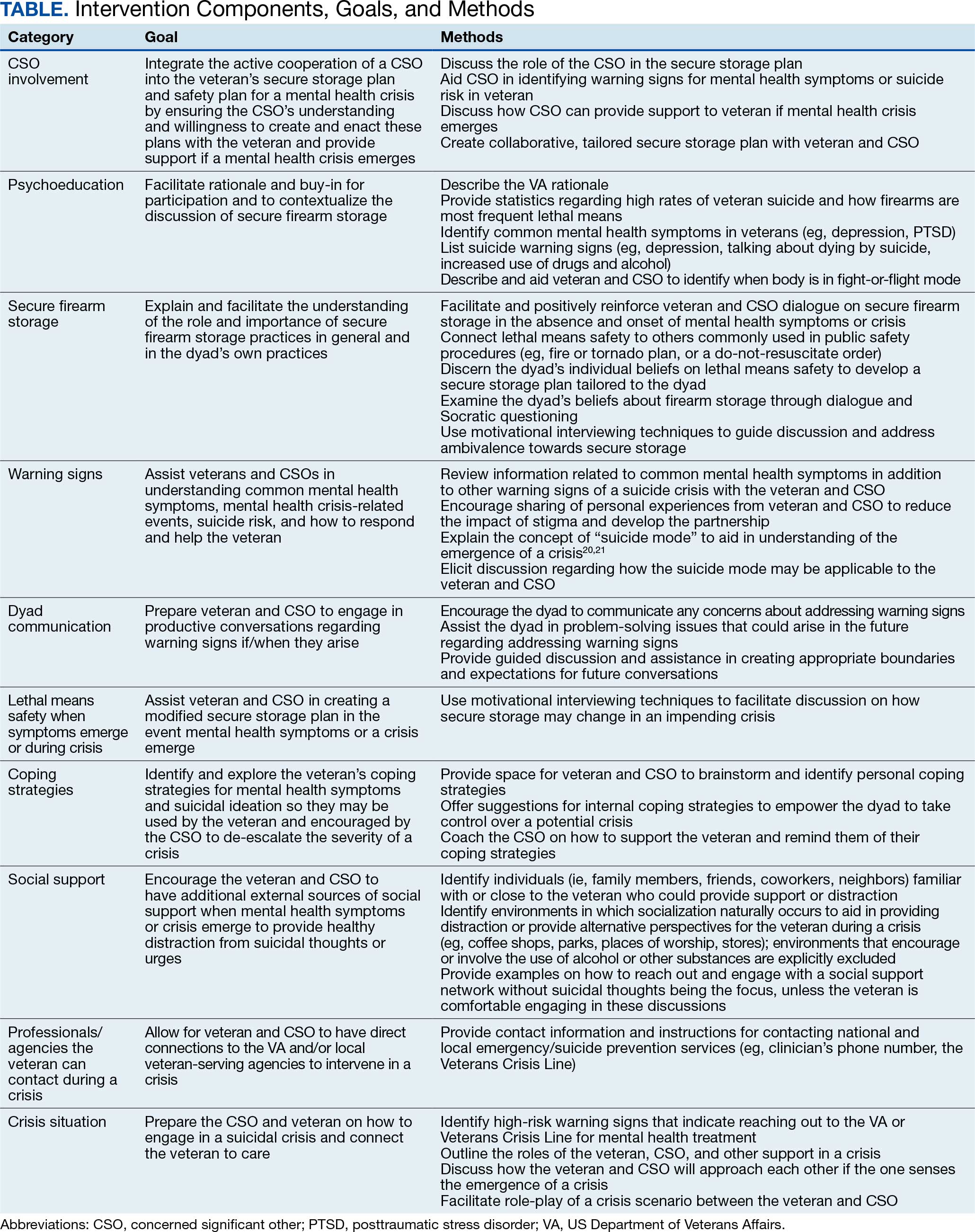
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
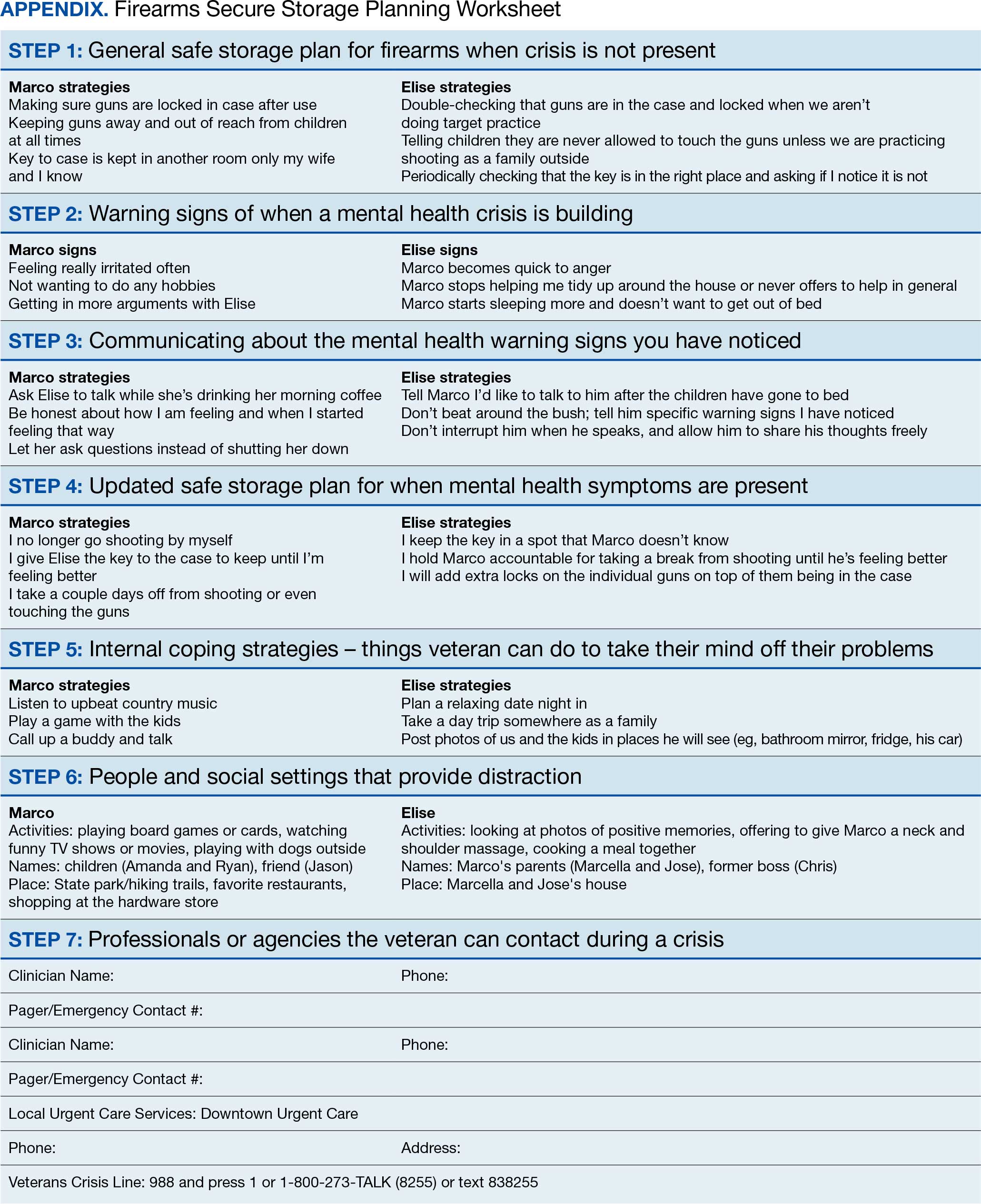
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
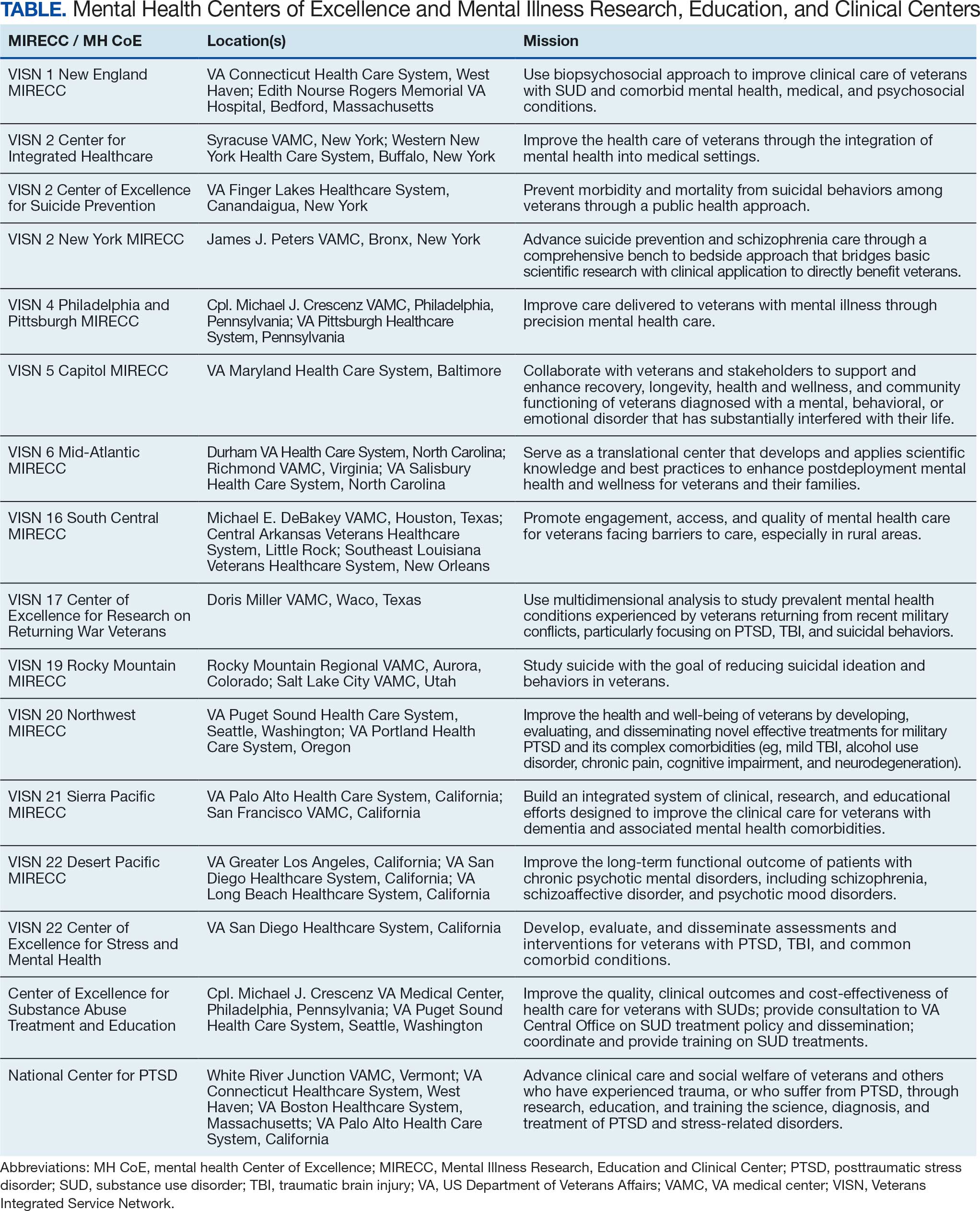
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
Accessible and effective mental health services are a vital component of the Veterans Health Administration (VHA) mission to provide exceptional care that improves veterans’ health and well-being. Veterans are seeking mental health care at the VHA at significantly higher rates than in previous years. From 2009 through 2024, the number of veterans who received direct mental health care from the VHA increased 78%.1 The proportion of veterans enrolled in the VHA who also received direct mental health care expanded from 23% of total enrollees in 2009 to 33% in 2024. The increase in VHA mental health care delivery is also reflected in the number of outpatient mental health care and treatment visits at the VHA, which increased from 12.7 million to 21.5 million over the same period.
The Sergeant First Class (SFC) Heath Robinson Honoring Our Promise to Address Comprehensive Toxics (PACT) Act of 2022 expanded eligibility for VHA services, including mental health care and counseling, to new cohorts of toxic-exposed veterans. From 2022 to 2024, > 680,000 veterans enrolled in VHA care, and 45% of those were PACT Act-eligible cohorts.2 Research highlighted the high prevalence of physical and psychiatric comorbidities in toxic-exposed veterans.3 As such, the VHA may face greater demand for direct mental health care with these newly eligible cohorts of veterans.
Veterans often have mental health conditions (eg, depression, posttraumatic stress disorder [PTSD]), substance use disorders (SUDs), unique military experiences (eg, deployments), and injuries and illnesses (eg, traumatic brain injury [TBI]) that increase the complexity of their clinical presentation. The varied nature of these mental health conditions, as well as veterans’ unique military-related experiences, necessitates specialized centers focused on distinct high-priority areas of mental health in the VHA.
A series of public laws charged the US Department of Veterans Affairs (VA) with developing specialized mental health Centers of Excellence (CoEs) focused on high-priority areas of veteran mental health. The first of these laws, Public Law 98- 528, established the National Center for PTSD (NCPTSD), which opened in 1989.4 In 1996, Congress established specialized mental health CoEs known as Mental Illness Research, Education, and Clinical Centers (MIRECCs) across the VHA.5 To address the unique needs of post-9/11 veterans, 3 additional specialized centers were established in 2005.6 Finally, under the authority of the Secretary of the VA, specialized mental health CoEs were established to focus on SUD and integrated health care.
There are 17 geographically diverse mental health CoEs and MIRECCs across the VA (Table). CoEs are embedded in VA medical centers (VAMCs) with strong medical school academic affiliations. Organizational oversight of the CoEs is provided by the VA Office of Mental Health and Office of Suicide Prevention, respectively. As part of the oversight process, CoEs submit annual reports detailing their advancements in research, education and training, and clinical activities, as well as participate in a peer-reviewed renewal process.
These specialized centers are united in a shared tripartite mission to generate new knowledge about the causes and treatments of mental health conditions, to educate and train VHA clinicians and personnel, and to develop and implement innovative clinical programs within the VHA. This combined focus on research, education, and improved clinical care reduces the time from discovery to implementation and improves the health and well-being of veterans.
Examples of this acceleration translation from scientific discovery to clinical practice are evident throughout mental health CoEs. The NCPTSD is a leader in research on PTSD and traumatic stress. Its work led to the development of national training programs for VHA clinicians, facilitating the broad dissemination of efficacious PTSD treatments across the enterprise.7 Researchers at the Veterans Integrated Service Network (VISN) 21 Sierra Pacific MIRECC identified depression as a significant risk factor for dementia and subsequently launched the first multisite trial of repetitive transcranial magnetic stimulation (rTMS) in the VHA in 2012 (CSP #556: the effectiveness of rTMS in depressed VA patients).8 This project laid the groundwork for the national clinical rTMS program launched in 2017, which is now clinically available at 60 VAMCs. In the largest pragmatic randomized clinical trial of its kind, the VISN 4 Philadelphia and Pittsburgh MIRECC found that pharmacogenomic testing significantly reduced the number of prescription medications with predicted drug-gene interactions and improved clinical outcomes among veterans with depression.9
Mental health CoEs are also leaders in suicide prevention, a top clinical priority for the VHA. The VISN 2 New York MIRECC developed Project Life Force, a safety planning skills group for veterans with suicidal ideation, now implemented across 10 VAMCs, including telehealth hubs, outpatient settings, and veteran peer programs.10 The VISN 2 CoE for Suicide Prevention and VISN 19 Rocky Mountain MIRECC coordinate key suicide prevention services for VA, including the analysis of suicide surveillance data; evaluation of national VA suicide prevention initiatives; the support of veterans, families, and clinicians; and enhanced access to evidence-based treatments for at-risk veterans.
Mental health CoEs are a key operational partner in VHA treatment of SUDs. The CoEs in Substance Addiction Treatment and Education (CESATEs) are national resources dedicated to improving the quality, clinical outcomes, and cost-effectiveness of VHA SUD treatment. CESATEs developed and implemented a national rollout of an effective treatment for stimulant use disorders, training staff at > 120 VA programs. The VISN 1 Mid-Atlantic MIRECC’s focus on SUD and comorbid/co-occurring mental health conditions has highlighted the significant prevalence of these conditions and the impact they have on treatment response.11
Serious mental illness (SMI) (eg, schizophrenia, schizoaffective disorder) impacts up to 5% of veterans.12 VISN 22 Desert Pacific MIRECC has developed interventions to improve the lives of veterans with SMI. Its research established supported employment as an effective intervention to improve outcomes in veterans with psychotic disorders and supported its implementation in the VHA.13 Peer specialists are a cornerstone in the VHA commitment to recovery-oriented services for veterans with SMI. VISN 5 Capitol MIRECC has long championed research, clinical training, and educational activities that contributed to the effective deployment of peer specialists across the VHA enterprise.
Veterans have unique military-related experiences (eg, deployment, traumatic stress, transition to civilian status) and injuries and illnesses (eg, TBI, posttraumatic headaches) that significantly impact their mental health and quality of life.
The period between active duty and transition to civilian status is a critical time in a veteran’s life. The VISN 17 CoE Veteran Sponsorship Initiative connects veterans with VA care within 30 days postdischarge, with the option of additional support in the community. The VISN 22 CoE for Stress and Mental Health (CESAMH) develops, evaluates, and disseminates diagnostics and treatments for veterans affected by traumatic events and brain injuries, with a unique focus on supporting their whole health needs. The VISN 6 Mid-Atlantic MIRECC leads the ongoing VISN-6 Post-Deployment Mental Health (PDMH) study, the largest biorepository of post-9/11 veterans. PDMH has greatly expanded the understanding of the unique needs of post-9/11 veterans, with > 100 peer-reviewed publications to date. Veterans with mild TBI frequently experience chronic posttraumatic headaches that can be disabling and nonresponsive to treatment. The VISN 20 Northwest MIRECC demonstrated that prazosin, a repurposed, low-cost, widely available, nonaddictive medication, can safely and effectively reduce the frequency of these headaches and improve functional impairment in veterans and active-duty service members.14
Increased and enhanced access to effective mental health treatment is a priority for VA. In 2007, the VA launched the National Primary Care Mental Health Integration program, which integrated mental health services into primary care settings. The Center for Integrated Healthcare (CIH) has supported the VA in these efforts. In 2024, CIH trained > 5000 health care staff on high-fidelity integration of behavioral health and medical care. VA has also focused on increasing access to mental health services via expanded telehealth offerings. The VISN 16 MIRECC, with its unique focus on increasing access to care for rural veterans via distance-based and digital health technology, supported the VA Offices of Mental Health and Connected Care to virtualize mental health care and promote adoption and sustained use of VA Video Connect across the enterprise.
Specialized MH CoEs are uniquely equipped to support the VHA in providing training and education to VA clinicians, veterans, care partners and family members, and the community on high-priority mental health topics. Education is a core component of the MH CoEs tripartite mission. As such, MH CoEs offer national trainings, conferences, consultation services, clinical demonstration projects, development of clinical dashboards and toolkits, and public awareness campaigns. Researchers, educators, and clinicians at the CoEs frequently serve as subject matter experts on topics aligned with their respective missions. Several national rollout programs that disseminated evidence-based treatments for mental health conditions to the field (eg, cognitive behavioral therapy for depression, cognitive behavioral therapy for insomnia, and prolonged exposure) were developed at specialized CoEs.
The VHA provides advanced training, residencies, and fellowships to > 120,000 trainees annually. Many of these trainees choose to remain at the VA. Seven of 10 VHA psychologists and 6 of 10 VHA physicians trained within the VHA prior to their employment.15 The MH CoEs and MIRECCs play an important role in preparing these trainees for VHA mental health careers. These centers are funded to provide advanced postdoctoral training to physicians as well as allied health professionals in clinical and counseling psychology, social work, pharmacy, and nursing. Training is not limited to postdoctoral fellows: graduate students, residents, and interns from affiliated accredited training programs may rotate through mental health CoEs each academic year.
Conclusions
For > 30 years, mental health CoEs have brought thousands of veterans advanced treatments for their mental health needs and helped reduce death by suicide. The centers have a bright future ahead, harnessing advances in artificial intelligence and genomics to permit the matching of the individual veterans to the treatment most likely to benefit them. Precision medicine, as espoused by the Hannon Act, will not only encourage the efficient use of health care resources but also rapidly reduce pain in veterans with mental health and SUDs.
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
- Congressionally Mandated Report: Report on Transparency in Mental Health Care Services. US Dept of Veterans Affairs; December 2022. Accessed December 5, 2025. https://www.govinfo.gov/content/pkg/CMR-VA1-00181657/pdf/CMR-VA1-00181657.pdf
- Beckman AL, Jacobs J, Elnahal SM. The PACT Act—expanding coverage and access for veterans. JAMA. 2024;332:1423-1424. doi:10.1001/jama.2024.16013
- Morse JL, Acheson DT, Almklov E, et al. Associations among environmental exposures and physical and psychiatric symptoms in a care-seeking sample of U.S. military veterans. Mil Med. 2024;189:e1397-e1402. doi:10.1093/milmed/usae035
- Veterans’ Health Care Act of 1984, 38 USC §98-528 (1984). Accessed March 27, 2026. https://www.congress.gov/bill/98th-congress/house-bill/5618/text
- Veterans’ Health Care Eligibility Reform Act of 1996, 38 USC §104-262 (1996). Accessed March 27, 2026. https://www.congress.gov/bill/104th-congress/house-bill/3118/text
- Military Quality of Life and Veterans Affairs Appropriations Act, 2006. Pub L No. 109-114, 119 Stat. 2372. Accessed March 27, 2026. https://www.congress.gov/bill/109th-congress/house-bill/2528/text
- Karlin BE, Ruzek JI, Chard KM, et al. Dissemination of evidence‐based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration. J Trauma Stress. 2010;23:663-673. doi:10.1002/jts.20588
- Byers AL, Covinsky KE, Barnes DE, et al. Dysthymia and depression increase risk of dementia and mortality among older veterans. Am J Geriatr Psychiatry. 2012;20:664-672. doi:10.1097/JGP.0b013e31822001c1
- Oslin DW, Lynch KG, Shih MC, et al. Effect of pharmacogenomic testing for drug-gene interactions on medication selection and remission of symptoms in major depressive disorder: the PRIME Care randomized clinical trial. JAMA. 2022;328:151-161. doi:10.1001/jama.2022.9805
- Goodman M, Brown GK, Galfalvy HC, et al. Group (“Project Life Force”) versus individual suicide safety planning: a randomized clinical trial. Contemp Clin Trials Commun. 2020;17:100520. doi:10.1016/j.conctc.2020.100520
- Na PJ, Ralevski E, Jegede O, et al. Depression and/or PTSD comorbidity affects response to antidepressants in those with alcohol use disorder. Front Psychiatry. 2022;12:768318. doi:10.3389/fpsyt.2021.768318
- McCarthy JF, Blow FC, Valenstein M, et al. Veterans Affairs Health System and mental health treatment retention among patients with serious mental illness: evaluating accessibility and availability barriers. Health Serv Res. 2007;42:1042-1060. doi:10.1111/j.1475-6773.2006.00642.x
- Glynn SM, Marder SR, Noordsy DL, et al. An RCT evaluating the effects of skills training and medication type on work outcomes among patients with schizophrenia. Psychiatr Serv. 2016;67:500-506. doi:10.1176/appips201500171
- Mayer CL, Savage PJ, Engle CK, et al. Randomized controlled pilot trial of prazosin for prophylaxis of posttraumatic headaches in active-duty service members and veterans. Headache. 2023;63:751-762. doi:10.1111/head.14529
- Hill C. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed December 5, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
Meeting the Needs of Those Who Have Served: The Role of VHA Specialized Mental Health Centers of Excellence
VA Restarts EHR Rollout After Addressing Issues
After a nearly 3-year pause, the US Department of Veterans Affairs (VA) is again ramping up the rollout of its new federal electronic health records (EHR) system from Oracle-Cerner, which previously experienced various issues and led to numerous setbacks. On April 11, 2026, the federal EHR went live at 4 Michigan sites: VA Ann Arbor Healthcare System, VA Battle Creek Medical Center, VA Detroit Healthcare System, and VA Saginaw Healthcare System.
VA officials have promised that things will be different this time, claiming it has fixed “hundreds of problems related to the initial rollout of the EHR system at the [6] original VA sites” and eliminated “the bureaucracy that was holding the project back.” At a press conference announcing the relaunch of the EHR rollout, VA Secretary Doug Collins said the old system cost the department hundreds of millions of dollars each year. He also said the VA has been too resistant to change at the expense of proper veteran health care.
“We’re all going to stay close to ensure that this is a smooth transition,” Collins said. “This needs to be a win for the VA patients.”
A VA Office of Inspector General (OIG) investigation found 360 major performance incidents—outages, performance degradations, and incomplete functionality—that occurred between October 24, 2020, and August 31, 2022. Additionally, an investigation by The Spokesman-Review and The Washington Post found that the EHR “played a role” in > 4400 cases of patient harm and 6 deaths.
VA Deputy Secretary Paul Lawrence said that the VA plans to stagger the release of the system, unlike in previous deployments. The agency intends to implement the EHR at 13 sites in 2026 and 26 in 2027, anticipating a pace of about 28 to 30 sites each year after that.
The VA said it is also boosting staffing to ensure the transition goes smoothly and is in the process of hiring 400 employees. Other problems may arise, though. At the end of March laid off between 20,000 and 30,000. This prompted concerns that resources could be redirected from the VA EHR at a critical stage.
After a nearly 3-year pause, the US Department of Veterans Affairs (VA) is again ramping up the rollout of its new federal electronic health records (EHR) system from Oracle-Cerner, which previously experienced various issues and led to numerous setbacks. On April 11, 2026, the federal EHR went live at 4 Michigan sites: VA Ann Arbor Healthcare System, VA Battle Creek Medical Center, VA Detroit Healthcare System, and VA Saginaw Healthcare System.
VA officials have promised that things will be different this time, claiming it has fixed “hundreds of problems related to the initial rollout of the EHR system at the [6] original VA sites” and eliminated “the bureaucracy that was holding the project back.” At a press conference announcing the relaunch of the EHR rollout, VA Secretary Doug Collins said the old system cost the department hundreds of millions of dollars each year. He also said the VA has been too resistant to change at the expense of proper veteran health care.
“We’re all going to stay close to ensure that this is a smooth transition,” Collins said. “This needs to be a win for the VA patients.”
A VA Office of Inspector General (OIG) investigation found 360 major performance incidents—outages, performance degradations, and incomplete functionality—that occurred between October 24, 2020, and August 31, 2022. Additionally, an investigation by The Spokesman-Review and The Washington Post found that the EHR “played a role” in > 4400 cases of patient harm and 6 deaths.
VA Deputy Secretary Paul Lawrence said that the VA plans to stagger the release of the system, unlike in previous deployments. The agency intends to implement the EHR at 13 sites in 2026 and 26 in 2027, anticipating a pace of about 28 to 30 sites each year after that.
The VA said it is also boosting staffing to ensure the transition goes smoothly and is in the process of hiring 400 employees. Other problems may arise, though. At the end of March laid off between 20,000 and 30,000. This prompted concerns that resources could be redirected from the VA EHR at a critical stage.
After a nearly 3-year pause, the US Department of Veterans Affairs (VA) is again ramping up the rollout of its new federal electronic health records (EHR) system from Oracle-Cerner, which previously experienced various issues and led to numerous setbacks. On April 11, 2026, the federal EHR went live at 4 Michigan sites: VA Ann Arbor Healthcare System, VA Battle Creek Medical Center, VA Detroit Healthcare System, and VA Saginaw Healthcare System.
VA officials have promised that things will be different this time, claiming it has fixed “hundreds of problems related to the initial rollout of the EHR system at the [6] original VA sites” and eliminated “the bureaucracy that was holding the project back.” At a press conference announcing the relaunch of the EHR rollout, VA Secretary Doug Collins said the old system cost the department hundreds of millions of dollars each year. He also said the VA has been too resistant to change at the expense of proper veteran health care.
“We’re all going to stay close to ensure that this is a smooth transition,” Collins said. “This needs to be a win for the VA patients.”
A VA Office of Inspector General (OIG) investigation found 360 major performance incidents—outages, performance degradations, and incomplete functionality—that occurred between October 24, 2020, and August 31, 2022. Additionally, an investigation by The Spokesman-Review and The Washington Post found that the EHR “played a role” in > 4400 cases of patient harm and 6 deaths.
VA Deputy Secretary Paul Lawrence said that the VA plans to stagger the release of the system, unlike in previous deployments. The agency intends to implement the EHR at 13 sites in 2026 and 26 in 2027, anticipating a pace of about 28 to 30 sites each year after that.
The VA said it is also boosting staffing to ensure the transition goes smoothly and is in the process of hiring 400 employees. Other problems may arise, though. At the end of March laid off between 20,000 and 30,000. This prompted concerns that resources could be redirected from the VA EHR at a critical stage.
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
Mostly it is loss that teaches us about the worth of things.
Arthur Schopenhauer1
One of the leaders I most respected in my US Department of Veterans Affairs (VA) career was a man who had worked his way up through the ranks to become a medical center director. Usually calm, cool, and collected, he would wax poetic when discussing the hero of the VA Health Care System revolution, Ken Kizer, MD, MPH.
In this issue of Federal Practitioner, journalist Randy Dotinga interviews Kizer about the current challenges facing the VA. Though many readers will have participated in or at least know about Kizer’s unprecedented overhaul of the agency, many others, especially those new to VA, may not. It seemed a fitting time to offer an outline of the immense and positive accomplishments that occurred in the agency during his tenure, especially as, under the current administration, many of his most forward-thinking initiatives seem to be moving backward.2
When President Clinton nominated Kizer to serve as the Under Secretary for Health for the Veterans Health Administration in 1994, the poor quality care the agency delivered was castigated in popular movies like Born on the Fourth of July. Veterans who were seen in that era, and who eventually returned to a far better, kinder VA thanks to Kizer, would often tell me, “Doc, the VA was really bad then, and I was afraid to come back.” The critique of VA health care in the mid-1990s sounds like a bureaucratic déjà vu of many of the concerns Kizer raised in his interview, including fragmentation of care, access barriers, and poor coordination of treatment.3
If anyone was prepared and qualified to take on this seeming mission impossible, it was Kizer. A US Navy veteran with 6 board certifications, he came to the VA following a brave and innovative stint as the top health official in California, where he successfully took on the tobacco lobby and dramatically reduced the state’s rates of smoking and related diseases.4
Long before it was the subject of reality TV shows, Kizer dubbed his major renovation of the VA’s antiquated structure an “extreme makeover.”3 Though this description is an oversimplification of Kizer’s monumental efforts, the makeover can be considered in 4 to 6 buckets, depending on how various health policy experts parse the re-engineering efforts.5-7
Decentralization. Kizer instituted the Veterans Integrated Service Network (VISN) system to coordinate the management and operations of all the hospitals, clinics, and other VA health care entities in what is roughly a region. The locus of decision-making shifted from the VA Central Office to the VISNs, intended to promote more efficient, economical, and streamlined health care delivery.
Capitation. Accompanying this restructuring was a shift to a capitated system focused on preventive care. The Veterans Equitable Resource Allocation system was designed to logically link workload and funding. This was a major shift away from VA’s previous emphasis on inpatient and specialty care and resulted in the closing of multiple hospitals.4
Information Systems. I can still remember the first time I sat down at a prehistoric computer to use the Computerized Patient Record System (CPRS). Though now much maligned, then it was like something out of Star Trek, at a time when almost every other health care institution was buried in paper charts. With CPRS, VA suddenly had a pioneering and much-envied electronic medical record that facilitated continuity of care, communication between professionals, and accuracy and completeness of documentation.
Data Driven Performance Improvement. The VISNs and information systems inaugurated a new era of data-driven quality improvement. The assembly and analysis of data enabled VISNs to have real-time input about comparative facility performance.
Performance Measures. The data enabled evidence-based performance measures to be developed and monitored. Though these have now become the bane of many Federal Practitioner readers’ existence, they were originally intended for VISN directors and members of the senior executive service at VA central office. These were tied to incentives that, though recently the subject of watchdog investigation, were intended to motivate and reward high-quality care.6
Even this cursory look at Kizer’s accomplishments is more than enough to demonstrate the magnitude of the makeover, and when the time frame of the achievements is factored in, the transformation is the equivalent of a planet changing its orbit at light speed. Rhetoric aside, there are now hundreds of research articles published in top medical and health policy journals, many of them authored by Kizer,7,8 that have amply demonstrated that when he departed the VA in 1999, it had become “the best care anywhere.” 9 For example, a 2000 New England Journal of Medicine article found that from 1994 to 2000, the percentage of veterans whose care met ≥ 90% of 9 of 17 quality standards was > 70% for 13 of the measures, outperforming fee-for-service Medicare.10
There had been uncertainty about whether Kizer would seek a second term as Under Secretary when he announced that he was leaving. With concise modesty, Kizer said he had met his charge to, “re-engineer the veterans’ health care system so that it could effectively function in the 21st century.”11
Despite openly and critically discussing the many difficulties the VA currently confronts, Kizer ends his interview on a note of hope. Since he likely knows more about VA than any person alive, we need to trust his judgment that his legacy, which currently seems more in jeopardy than ever before, will somehow prevail. Perhaps I am too melancholic, but I believe it will take a professional of the stature of Dr. Kizer to take us back to that future, and I fear we will not see his likes again.
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
- Schopenhaur A, translated by Saunders TB. Parerga and Paralipomena: A Collection of Philosophical Essays. Cosimo Classics: 2007.
- Spotswood, S. Massive VA restructuring would cut number of VISNS, reduce high-level leadership. U.S. Medicine. January 15, 2026. Accessed March 23, 2026. https://www .usmedicine.com/non-clinical-topics/policy/massive -va-restructuring-would-cut-number-of-visns-reduce-high -level-leadership/
- Kizer KW, Dudley RA. Extreme makeover: transformation of the veterans health ca re system. Annu Rev Public Health. 2009;30:313-339. doi:10.1146/annurev.publhealth.29.020907.090940
- Payne D. How Kizer healed the VA. BMJ. 2012;344:e3324. doi:10.1136/bmj.e3324
- Jha AK. What can the rest of the health care system learn from VA’s quality and safety transformation? Agency for Healthcare Research and Quality. Patient Safety Network. September 1, 2006. Accessed March 23, 2026. https://psnet .ahrq.gov/perspective/what-can-rest-health-care-system -learn-vas-quality-and-safety-transformation
- US Department of Veterans Affairs, Office of Inspector General. VA improperly awarded 10.8 million in incentives to central office senior executives. Report # 23-03773-169. May 9, 2024. Accessed March 23, 2026. https://www.vaoig.gov /reports/administrative-investigation/va-improperly-awarded -108-million-incentives-central-office
- Kizer KW. The “new VA”: a national laboratory for health care quality management. Am J Med Qual. 1999;14:3-20. doi:10.1177/106286069901400103
- Kizer KW, Pane GA. The “new VA”: delivering health care value through integrated service networks. Ann Emerg Med. 1997;30:804-807. doi:10.1016/s0196-0644(97)70053-2
- Longman P. Best Care Anywhere: Why VA Health Care is Better than Yours. 3rd ed. Berrett-Koehler Publishers; 2012.
- Jha AK, Perlin JB, Kizer KW, Dudley RA. Effect of the transformation of the Veterans Affairs Health Care System on the quality of care. N Engl J Med. 2003;348:2218-2227. doi:10.1056/NEJMsa021899
- US Department of Veterans Affairs. Kizer withdraws name from consideration for second term as VA Under Secretary for Health. Vanguard. June/July 1999. Accessed March 23, 2026. https://www.va.gov/opa/publications/archives /vanguard/99junjulvg.pdf
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
Is Ken Kizer’s Legacy at Risk? The Future of the Veterans Health Administration
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
For there was never yet philosopher that could endure the toothache patiently
Much Ado About Nothing by William Shakespeare
Almost anyone who has worked for a long time in a US Department of Veterans Affairs (VA) clinic or hospital has had patients in dire need of dental services who could neither access nor pay for them. I have seen dental problems ranging from older veterans who were nearly edentulous and needed expensive dentures or implants to younger veterans who never had regular dental care and needed a periodontist to save their teeth, to individuals with terrible toothaches that antibiotics could not cure. As Shakespeare quips in Much Ado About Nothing, almost nothing is worse than a toothache.
Many VA primary care practitioners and social workers kept lists of local sliding-scale dentists or arranged for veterans to visit dental and hygiene school clinics for reduced fees. Even when VA dentists were not permitted to see a veteran, many would assist in finding them affordable care in the community. However, that was never enough to meet the oral health needs of veterans. One of the most common complaints of patients who otherwise were pleased with their VA health care was that it did not cover dental services.1
Most veterans qualify for health care and other VA benefits. Dental care is an exception, with only about a quarter (26%) of the > 9 million veterans active in the Veterans Health Administration (VHA) eligible for care. Even under this restricted eligibility, about 888,000 veterans have received dental services either through the VHA or in the community. In 2025, the VA paid community-based dentists for > 3.5 million procedures for veterans, which underscores the magnitude of the demand.2
Given the gap in dental care, many veterans and their caregivers both personal and professional will likely be encouraged that in February the VA announced plans to improve access to dental care through expanding community care dental services. “Dental health is a critical component of overall well-being,” VA Secretary Doug Collins noted. VA issued a request for proposals (RFP) for a new dental administrator who would oversee the operations of a new network of dental practitioners. The new vendor contract would operationalize general dental services, like tooth extractions, as well as specialized services such as periodontics, dentures, and pharmacy support for dental medications. Most importantly, the new program would cover preventive care to help avoid many of the dental problems veterans now experience. Proposals are due March 16.2
Yet, there is a catch. The community care program will only be available to eligible veterans just like previous dental services both in the VA and the community. I was always somewhat ashamed that despite my working decades at the VHA, I never had a satisfactory answer for veterans who asked me why they were not eligible for dental care. The regulatory response is that eligibility for dental services is a complex determination depending on service-connected military service, and specialized clinical indices. Dental coverage is provided for veterans who have 100% service-connected or total disability, prisoners of war, and veterans whose dental disease exacerbates a comorbid medical condition. Those not eligible for VA dental coverage may still get treatment if they, for example, have a cancer diagnosis and without dental work the chemotherapy treatment would place them at a higher risk of an oral infection. Veterans participating in a rehabilitation program who have poor dentition that prevents them from reaching their rehabilitative goals also may receive VA dental care. In addition, some veterans who are experiencing homelessness and others who did not receive a dental examination prior to discharge from active duty may be eligible for dental benefits.3 VA also offers lower-priced dental insurance for ineligible veterans.4
The new RFP does little to expand eligibility of veterans to receive VA dental care, and it is hard to not see the announcement as another step in the privatization of VHA. Medically and ethically, it seems to perpetuate a double standard between physical and oral health that makes no scientific sense.5-7 I sometimes joke that in medical school we had maybe 2 days of teaching about teeth and even that limited exposure to dental pathology was sufficient for us to learn that chronic conditions like respiratory disease and lifestyle choices like poor diet cause and contribute to dental problems.
Like so many areas of veteran care, dental health in veterans is worse compared with those who never served, making it harder to justify the exclusion of dental services from veteran health benefits. A study in Military Medicine looked at 11,539 former service members and found a higher prevalence of individuals with tooth decay, missing teeth, tooth fillings, caries, and periodontitis. While military service per se was not associated with the findings, higher rates of hypertension, hyperlipidemia, depression, and diabetes in veterans compared with nonveterans, which are related to serving in uniform, were covariates.8
That depression is an indirect factor in dental disease may seem surprising. However, this is more evidence that human health is truly holistic, with mutual interactions between the body (including the teeth) and mind. Oral care needs to be incorporated into the VA whole health approach for all veterans. In a series of articles in Psychiatric News, VA psychiatrist Antoinette Shappell and VA dentist Pierre Cartier identify several links between dental and mental health.9,10 Veterans with anxiety disorders may fear going to the dentist even when care is needed. Serious mental illness may result in poor diet, and difficulty performing preventive care. Many psychotropic medications may cause xerostomia that worsens tooth decay and veterans with posttraumatic stress disorder may suffer from bruxism. I regularly saw these conditions when I worked in a primary care psychiatry clinic. Being able to coordinate with VA dentists and staff to provide integrated care would have benefited these already burdened veterans.
An estimated $5.4 billion has been spent on 3.6 million veterans who were seen in emergency departments for dental problems. That cost alone should convince policy makers that the deficit in VA dental care needs to be filled with efficacious high-quality comprehensive dental services for as many veterans as possible. And there are signs that is exactly what is happening in Congress. A bill in the House of Representatives proposes to expand dental care benefits to all veterans eligible for other VA health benefits.11 There are also other legislative initiatives in the works.4 Together with the VA’s plans for a new community care dental network, that does give veterans and federal practitioners something to smile about.
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
- Shane L III. A dental debacle: why veterans struggle to navigate VA’s oral care. Military Times. June 17, 2024. Accessed February 25, 2026. https://www.militarytimes.com/news/your-military/2024/06/17/a-dental-debacle-why-veterans-struggle-to-navigate-vas-oral-care/
- US Dept of Veterans Affairs Office of Media Relations. VA moves to improve dental care access to eligible veterans. VA News. February 18, 2026. Accessed February 23, 2026. https://news.va.gov/145117/va-improve-dental-care-access-eligible-veterans/
- Wile B. VA launches plans to expand dental care access for veterans. Military.com. February 16, 2026. Accessed February 23, 2026. https://www.military.com/benefits/veterans-healthcare/va-launches-plan-expand-dental-care-access-veterans.html
- US Department of Veterans Affairs. VA Dental Insurance Program (VADIP). Updated May 1, 2024. Accessed February 23, 2026. https://www.va.gov/health-care/about-va-health-benefits/dental-care/dental-insurance/
- McMains V. Healthy mouth, healthy body. National Institutes of Health, National Institute of Dental and Craniofacial Research. May 8, 2024. Accessed February 23, 2026. https:// www.nidcr.nih.gov/news-events/nidcr-news/2024/healthy-mouth-healthy-body
- Seymour GJ. Good oral health is essential for good general health: the oral–systemic connection. Clin Microbiol Infect. 2007;13:1-2. doi:10.1111/j.1469-0691.2007.01797.x
- Martin SA, Simon L. Oral health and medicine integration: overcoming historical artifact to relieve suffering. Am J Public Health. 2017;107:S30-S31. doi:10.2105/AJPH.2017.303683
- Schindler DK, Lopez Mitnik GV, Solivan-Ortiz DC, et al. Oral health status among adults with and without prior active duty service in the US Armed Forces, NHANES 2011-2014. Mil Med. 2021;186:e149-e159. doi:10.1093/milmed/usaa355
- Shappell AV, Cartier PM. Understanding the mental-dental health connection said to be integral to patient care. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.07.6.15
- Shappell AV, Cartier PM. Good ‘mental-dental’ health important in preventing, slowing dementia. Psychiatr News. 2023;58. doi:10.1176/appi.pn.2023.08.8.64
- Dental Care for Veterans Act, HR 210, 119th Cong (2025- 2026). Accessed February 23, 2026. https://www.congress.gov/bill/119th-congress/house-bill/210
The Gap in VA Dental Care is Nothing to Smile About
The Gap in VA Dental Care is Nothing to Smile About
Indian Affairs Staffing Fell 11% in 2025
The US Department of the Interior Bureau of Indian Affairs (BIA) workforce shrunk 11% through the first 6 months of 2025, a result of executive orders, hiring freezes, a voluntary deferred resignation program (DRP), and terminations of probationary employees, according to a recently US Government Accountability Office (GAO) report. Though these reductions are complete, GAO said it has not yet analyzed projected cost savings or operational impacts from these staff reductions, and the department has shown signs of growth so far in 2026.
The reduction in force (RIF) from 7470 to 6624 employees aligns with the February 2025 executive order aimed at “restoring accountability, eliminating waste, bloat, and insularity” and reforming the federal workforce to maximize efficiency and productivity. The directives also instructed agencies to develop plans for large-scale RIFs and reorganizations. GAO auditors reviewed workforce data from January 25, 2025, through July 31, 2025, interviewed BIA officials, and reviewed comments from Native American tribal representatives to compose the report.
All BIA regions experienced a reduction in staff: 10% in the Western and Rocky Mountain regions, 29% in the Pacific region, and > 20% each in the Alaska, Midwest, and Southern Plains regions. Positions within law enforcement and social work agencies were excluded from the May program due to job functions and responsibilities.
A small portion of separations included resignations and retirements outside of the DRPs; of the staff separating from BIA after January 25, 2025, while 24% left for other reasons. Although the downsizing was not unexpected and some staff were already planning to retire, repercussions were felt immediately.
“Some remaining staff took on additional responsibilities to mitigate the effects of reductions,” the GAO report said. “Some Indian Affairs staff said the reductions would exacerbate preexisting staffing limitations in their offices and make it more difficult to carry out their responsibilities serving Tribes.”
Tribal leaders voiced concerns, claiming BIA already was understaffed to effectively carry out its responsibilities and that service delivery was impaired. Some BIA staff reported that departures forced them to take on duties beyond their main area of responsibility, compromising their primary work. Regional BIA staff also described confusion about which employees were leaving, which limited their ability to effectively plan for impending departures, and reported receiving limited guidance from superiors about how to cover the responsibilities of those departing, particularly those in leadership positions. As of June 2, 2025, 6 of 12 BIA regional directors were serving in an acting capacity, and 12 of the 24 deputy regional director positions were either vacant or acting.
BIA officials have said there are no plans to reorganize or enact additional RIFs, but existing functions “might need to be restructured or realigned to achieve administration priorities.”
As of 2024, the Indiana Health Service (IHS) had a near 30% vacancy rate. In 2025, it awarded > 1800 scholarships and loan repayments under programs aimed at educating and training health professionals for careers at IHS facilities. And in January 2026, IHS announced it was launching the “largest hiring effort in agency history.”
“[O]ur top priority is filling vacancies for positions essential to keeping our health care facilities operating smoothly, especially in some of the more rural and remote locations,” said IHS Chief of Staff Clayton Fulton.
The US Department of the Interior Bureau of Indian Affairs (BIA) workforce shrunk 11% through the first 6 months of 2025, a result of executive orders, hiring freezes, a voluntary deferred resignation program (DRP), and terminations of probationary employees, according to a recently US Government Accountability Office (GAO) report. Though these reductions are complete, GAO said it has not yet analyzed projected cost savings or operational impacts from these staff reductions, and the department has shown signs of growth so far in 2026.
The reduction in force (RIF) from 7470 to 6624 employees aligns with the February 2025 executive order aimed at “restoring accountability, eliminating waste, bloat, and insularity” and reforming the federal workforce to maximize efficiency and productivity. The directives also instructed agencies to develop plans for large-scale RIFs and reorganizations. GAO auditors reviewed workforce data from January 25, 2025, through July 31, 2025, interviewed BIA officials, and reviewed comments from Native American tribal representatives to compose the report.
All BIA regions experienced a reduction in staff: 10% in the Western and Rocky Mountain regions, 29% in the Pacific region, and > 20% each in the Alaska, Midwest, and Southern Plains regions. Positions within law enforcement and social work agencies were excluded from the May program due to job functions and responsibilities.
A small portion of separations included resignations and retirements outside of the DRPs; of the staff separating from BIA after January 25, 2025, while 24% left for other reasons. Although the downsizing was not unexpected and some staff were already planning to retire, repercussions were felt immediately.
“Some remaining staff took on additional responsibilities to mitigate the effects of reductions,” the GAO report said. “Some Indian Affairs staff said the reductions would exacerbate preexisting staffing limitations in their offices and make it more difficult to carry out their responsibilities serving Tribes.”
Tribal leaders voiced concerns, claiming BIA already was understaffed to effectively carry out its responsibilities and that service delivery was impaired. Some BIA staff reported that departures forced them to take on duties beyond their main area of responsibility, compromising their primary work. Regional BIA staff also described confusion about which employees were leaving, which limited their ability to effectively plan for impending departures, and reported receiving limited guidance from superiors about how to cover the responsibilities of those departing, particularly those in leadership positions. As of June 2, 2025, 6 of 12 BIA regional directors were serving in an acting capacity, and 12 of the 24 deputy regional director positions were either vacant or acting.
BIA officials have said there are no plans to reorganize or enact additional RIFs, but existing functions “might need to be restructured or realigned to achieve administration priorities.”
As of 2024, the Indiana Health Service (IHS) had a near 30% vacancy rate. In 2025, it awarded > 1800 scholarships and loan repayments under programs aimed at educating and training health professionals for careers at IHS facilities. And in January 2026, IHS announced it was launching the “largest hiring effort in agency history.”
“[O]ur top priority is filling vacancies for positions essential to keeping our health care facilities operating smoothly, especially in some of the more rural and remote locations,” said IHS Chief of Staff Clayton Fulton.
The US Department of the Interior Bureau of Indian Affairs (BIA) workforce shrunk 11% through the first 6 months of 2025, a result of executive orders, hiring freezes, a voluntary deferred resignation program (DRP), and terminations of probationary employees, according to a recently US Government Accountability Office (GAO) report. Though these reductions are complete, GAO said it has not yet analyzed projected cost savings or operational impacts from these staff reductions, and the department has shown signs of growth so far in 2026.
The reduction in force (RIF) from 7470 to 6624 employees aligns with the February 2025 executive order aimed at “restoring accountability, eliminating waste, bloat, and insularity” and reforming the federal workforce to maximize efficiency and productivity. The directives also instructed agencies to develop plans for large-scale RIFs and reorganizations. GAO auditors reviewed workforce data from January 25, 2025, through July 31, 2025, interviewed BIA officials, and reviewed comments from Native American tribal representatives to compose the report.
All BIA regions experienced a reduction in staff: 10% in the Western and Rocky Mountain regions, 29% in the Pacific region, and > 20% each in the Alaska, Midwest, and Southern Plains regions. Positions within law enforcement and social work agencies were excluded from the May program due to job functions and responsibilities.
A small portion of separations included resignations and retirements outside of the DRPs; of the staff separating from BIA after January 25, 2025, while 24% left for other reasons. Although the downsizing was not unexpected and some staff were already planning to retire, repercussions were felt immediately.
“Some remaining staff took on additional responsibilities to mitigate the effects of reductions,” the GAO report said. “Some Indian Affairs staff said the reductions would exacerbate preexisting staffing limitations in their offices and make it more difficult to carry out their responsibilities serving Tribes.”
Tribal leaders voiced concerns, claiming BIA already was understaffed to effectively carry out its responsibilities and that service delivery was impaired. Some BIA staff reported that departures forced them to take on duties beyond their main area of responsibility, compromising their primary work. Regional BIA staff also described confusion about which employees were leaving, which limited their ability to effectively plan for impending departures, and reported receiving limited guidance from superiors about how to cover the responsibilities of those departing, particularly those in leadership positions. As of June 2, 2025, 6 of 12 BIA regional directors were serving in an acting capacity, and 12 of the 24 deputy regional director positions were either vacant or acting.
BIA officials have said there are no plans to reorganize or enact additional RIFs, but existing functions “might need to be restructured or realigned to achieve administration priorities.”
As of 2024, the Indiana Health Service (IHS) had a near 30% vacancy rate. In 2025, it awarded > 1800 scholarships and loan repayments under programs aimed at educating and training health professionals for careers at IHS facilities. And in January 2026, IHS announced it was launching the “largest hiring effort in agency history.”
“[O]ur top priority is filling vacancies for positions essential to keeping our health care facilities operating smoothly, especially in some of the more rural and remote locations,” said IHS Chief of Staff Clayton Fulton.