User login
Basal cell cancer incidence higher than previously reported
ALBUQUERQUE – The incidence of basal cell carcinoma in northern California rose by about 13% during 1998 through 2012, according to an analysis of more than 147,000 insured patients.
The steepest rises occurred in whites, women, and adults aged 80 years and older, while rates remained relatively stable among individuals younger than 40, said Dr. Maryam Asgari, who conducted the analysis with colleagues at Kaiser Permanente Northern California in Oakland.

Estimated rates of basal cell carcinoma (BCC) have been increasing worldwide, Dr. Asgari noted. But the epidemiology of the disease in the United States "is tricky to study, because these are not reportable cancers, and they do not have unique ICD-9 identifiers," she said at the annual meeting of the Society for Investigational Dermatology
The investigators used a previously validated BCC registry of electronic pathology reports to estimate crude and standardized 15-year BCC incidence rates by age, sex, and race with year 2000 U.S. Census data, Dr. Asgari said. The registry included 147,093 patients from Kaiser Permanente Northern California, an integrated health care delivery system. Patients were included if they developed at least one incident BCC during the study period, but were not counted multiple times for developing additional BCCs in the same year, Dr. Asgari said. The researchers used Poisson regression to examine annual changes in incidence over time.
The overall incidence of BCC increased from 418 cases per 100,000 person-years in 1998 to 535 cases per 100,000 person-years in 2012, Dr. Asgari said. "The overall standardized incidence rate for BCCs in the U.S. population for 2012 was 448 per 100,000, much higher than previously reported estimates," she and her colleagues reported.
Patients with BCCs had a median age of 66 years, and most were aged 40-80 years, with a slight male predominance (55%) that was consistent with the literature, she said. Fully 92% of affected patients were non-Hispanic whites, she noted. Kaiser Permanente patients resembled the U.S. population in terms of age and sex, but were ethnically and racially more diverse, "so the fact that we’re seeing 92% of the cohort being non-Hispanic white means BCC is really a disease of non-Hispanic whites," she said.
In contrast, the incidence of BCC decreased slightly among Asians, African-Americans, and multiracial persons during the 15-year study period, Dr. Asgari added. Among Hispanics, the incidence increased slightly in males aged 65-80 years, but decreased overall in younger persons, she said.
Based on the data, "BCCs and their treatment pose an increasing burden to the health care system," Dr. Asgari and her associates concluded.
The National Institutes of Health funded the study. Dr. Asgari reported no conflicts of interest.
ALBUQUERQUE – The incidence of basal cell carcinoma in northern California rose by about 13% during 1998 through 2012, according to an analysis of more than 147,000 insured patients.
The steepest rises occurred in whites, women, and adults aged 80 years and older, while rates remained relatively stable among individuals younger than 40, said Dr. Maryam Asgari, who conducted the analysis with colleagues at Kaiser Permanente Northern California in Oakland.
Estimated rates of basal cell carcinoma (BCC) have been increasing worldwide, Dr. Asgari noted. But the epidemiology of the disease in the United States "is tricky to study, because these are not reportable cancers, and they do not have unique ICD-9 identifiers," she said at the annual meeting of the Society for Investigational Dermatology
The investigators used a previously validated BCC registry of electronic pathology reports to estimate crude and standardized 15-year BCC incidence rates by age, sex, and race with year 2000 U.S. Census data, Dr. Asgari said. The registry included 147,093 patients from Kaiser Permanente Northern California, an integrated health care delivery system. Patients were included if they developed at least one incident BCC during the study period, but were not counted multiple times for developing additional BCCs in the same year, Dr. Asgari said. The researchers used Poisson regression to examine annual changes in incidence over time.
The overall incidence of BCC increased from 418 cases per 100,000 person-years in 1998 to 535 cases per 100,000 person-years in 2012, Dr. Asgari said. "The overall standardized incidence rate for BCCs in the U.S. population for 2012 was 448 per 100,000, much higher than previously reported estimates," she and her colleagues reported.
Patients with BCCs had a median age of 66 years, and most were aged 40-80 years, with a slight male predominance (55%) that was consistent with the literature, she said. Fully 92% of affected patients were non-Hispanic whites, she noted. Kaiser Permanente patients resembled the U.S. population in terms of age and sex, but were ethnically and racially more diverse, "so the fact that we’re seeing 92% of the cohort being non-Hispanic white means BCC is really a disease of non-Hispanic whites," she said.
In contrast, the incidence of BCC decreased slightly among Asians, African-Americans, and multiracial persons during the 15-year study period, Dr. Asgari added. Among Hispanics, the incidence increased slightly in males aged 65-80 years, but decreased overall in younger persons, she said.
Based on the data, "BCCs and their treatment pose an increasing burden to the health care system," Dr. Asgari and her associates concluded.
The National Institutes of Health funded the study. Dr. Asgari reported no conflicts of interest.
ALBUQUERQUE – The incidence of basal cell carcinoma in northern California rose by about 13% during 1998 through 2012, according to an analysis of more than 147,000 insured patients.
The steepest rises occurred in whites, women, and adults aged 80 years and older, while rates remained relatively stable among individuals younger than 40, said Dr. Maryam Asgari, who conducted the analysis with colleagues at Kaiser Permanente Northern California in Oakland.
Estimated rates of basal cell carcinoma (BCC) have been increasing worldwide, Dr. Asgari noted. But the epidemiology of the disease in the United States "is tricky to study, because these are not reportable cancers, and they do not have unique ICD-9 identifiers," she said at the annual meeting of the Society for Investigational Dermatology
The investigators used a previously validated BCC registry of electronic pathology reports to estimate crude and standardized 15-year BCC incidence rates by age, sex, and race with year 2000 U.S. Census data, Dr. Asgari said. The registry included 147,093 patients from Kaiser Permanente Northern California, an integrated health care delivery system. Patients were included if they developed at least one incident BCC during the study period, but were not counted multiple times for developing additional BCCs in the same year, Dr. Asgari said. The researchers used Poisson regression to examine annual changes in incidence over time.
The overall incidence of BCC increased from 418 cases per 100,000 person-years in 1998 to 535 cases per 100,000 person-years in 2012, Dr. Asgari said. "The overall standardized incidence rate for BCCs in the U.S. population for 2012 was 448 per 100,000, much higher than previously reported estimates," she and her colleagues reported.
Patients with BCCs had a median age of 66 years, and most were aged 40-80 years, with a slight male predominance (55%) that was consistent with the literature, she said. Fully 92% of affected patients were non-Hispanic whites, she noted. Kaiser Permanente patients resembled the U.S. population in terms of age and sex, but were ethnically and racially more diverse, "so the fact that we’re seeing 92% of the cohort being non-Hispanic white means BCC is really a disease of non-Hispanic whites," she said.
In contrast, the incidence of BCC decreased slightly among Asians, African-Americans, and multiracial persons during the 15-year study period, Dr. Asgari added. Among Hispanics, the incidence increased slightly in males aged 65-80 years, but decreased overall in younger persons, she said.
Based on the data, "BCCs and their treatment pose an increasing burden to the health care system," Dr. Asgari and her associates concluded.
The National Institutes of Health funded the study. Dr. Asgari reported no conflicts of interest.
AT THE 2014 SID ANNUAL MEETING
Major finding: The incidence of basal cell carcinoma in northern California rose by about 13% from 1998 through 2012.
Data source: Registry of electronic pathology reports of basal cell carcinomas during 1998-2012 among 147,093 patients from the Kaiser Permanente Northern California health care system.
Disclosures: The National Institutes of Health funded the study. Dr. Asgari reported no conflicts of interest.

Nonmelanoma skin cancer linked to increased fracture risk in postmenopausal women
ALBUQUERQUE – Postmenopausal women who reported a history of nonmelanoma skin cancer were almost 16% more likely to sustain a lower arm fracture than were women without a skin cancer history, according to a large, prospective, longitudinal study.
Women with prior nonmelanoma skin cancers (NMSCs) also were more likely to suffer a subsequent hip fracture, although the association did not reach statistical significance, said Eric Anderson of the dermatology department at Stanford (Calif.) University School of Medicine.
"These results suggest that prior history of NMSC is associated with an increased risk of subsequent bone fracture, contrary to our hypothesis," noted Mr. Anderson. He presented the findings at the annual meeting of the Society for Investigational Dermatology.
Nonmelanoma skin cancer has been correlated with decreased fracture risk in at least one small cohort study, Mr. Anderson said (Osteoporos. Int. 2007;18:687-92). However, patients with NMSC also have been shown to wear more sunscreen and limit their sun exposure after diagnosis, which might lower their vitamin D levels and increase their fracture risk, Mr. Anderson noted (Cancer Causes Control 2012;23:133-40).
To better clarify the relationship between NMSC and fracture risk, Mr. Anderson and his associates compared prospective data from 4,289 women with self-reported NMSC and 67,470 women who did not report a history of NMSC at baseline. The participants were from the Womens Health Initiative, a prospective longitudinal cohort study of postmenopausal women aged 50-79 years who were enrolled at 40 centers in the United States. Participants were followed for more than 10 years, and new spine, hip, and lower arm fractures were recorded, Mr. Anderson said.
In age-adjusted Cox proportional hazards models, women with a history of NMSC were 1.55 times more likely to sustain a hip fracture (95% confidence interval, 1.31-1.85; P < 0.0001), 1.29 times more likely to suffer a spine fracture (95% CI, 1.10-1.51; P = 0.0018), and 1.28 times more likely to sustain a lower arm fracture (95% CI, 1.13-1.45; P < 0.0001) than were women who did not report a history of NMSC at baseline, Mr. Anderson and his associates reported.
After adjusting for sun exposure, sunscreen use, vitamin D intake, physical activity, and other risk factors for fracture, only lower arm fracture remained statistically significant (hazard ratio, 1.16; 95% CI, 1.31-1.85; P = 0.02), although hip fracture was borderline significant (HR, 1.18; 95% CI, 0.99-1.41; P = 0.06), the investigators reported. Baseline hip bone marrow density was not associated with risk of NMSC in a subgroup analysis of 4,267 women with available data, Mr. Anderson said.
"We’re inclined to believe that this increased fracture risk may be due to sun exposure avoidance after NMSC diagnosis," said Mr. Anderson. He added that, in future studies, the investigators would compare serum vitamin D levels between participants with and without a history of NMSC, and explore temporal relationships between diagnosis of NMSC and fracture occurrence.
The National Institutes of Health and the Medical Scholars Research Program at Stanford University funded the research. Mr. Anderson reported no conflicts of interest.
ALBUQUERQUE – Postmenopausal women who reported a history of nonmelanoma skin cancer were almost 16% more likely to sustain a lower arm fracture than were women without a skin cancer history, according to a large, prospective, longitudinal study.
Women with prior nonmelanoma skin cancers (NMSCs) also were more likely to suffer a subsequent hip fracture, although the association did not reach statistical significance, said Eric Anderson of the dermatology department at Stanford (Calif.) University School of Medicine.
"These results suggest that prior history of NMSC is associated with an increased risk of subsequent bone fracture, contrary to our hypothesis," noted Mr. Anderson. He presented the findings at the annual meeting of the Society for Investigational Dermatology.
Nonmelanoma skin cancer has been correlated with decreased fracture risk in at least one small cohort study, Mr. Anderson said (Osteoporos. Int. 2007;18:687-92). However, patients with NMSC also have been shown to wear more sunscreen and limit their sun exposure after diagnosis, which might lower their vitamin D levels and increase their fracture risk, Mr. Anderson noted (Cancer Causes Control 2012;23:133-40).
To better clarify the relationship between NMSC and fracture risk, Mr. Anderson and his associates compared prospective data from 4,289 women with self-reported NMSC and 67,470 women who did not report a history of NMSC at baseline. The participants were from the Womens Health Initiative, a prospective longitudinal cohort study of postmenopausal women aged 50-79 years who were enrolled at 40 centers in the United States. Participants were followed for more than 10 years, and new spine, hip, and lower arm fractures were recorded, Mr. Anderson said.
In age-adjusted Cox proportional hazards models, women with a history of NMSC were 1.55 times more likely to sustain a hip fracture (95% confidence interval, 1.31-1.85; P < 0.0001), 1.29 times more likely to suffer a spine fracture (95% CI, 1.10-1.51; P = 0.0018), and 1.28 times more likely to sustain a lower arm fracture (95% CI, 1.13-1.45; P < 0.0001) than were women who did not report a history of NMSC at baseline, Mr. Anderson and his associates reported.
After adjusting for sun exposure, sunscreen use, vitamin D intake, physical activity, and other risk factors for fracture, only lower arm fracture remained statistically significant (hazard ratio, 1.16; 95% CI, 1.31-1.85; P = 0.02), although hip fracture was borderline significant (HR, 1.18; 95% CI, 0.99-1.41; P = 0.06), the investigators reported. Baseline hip bone marrow density was not associated with risk of NMSC in a subgroup analysis of 4,267 women with available data, Mr. Anderson said.
"We’re inclined to believe that this increased fracture risk may be due to sun exposure avoidance after NMSC diagnosis," said Mr. Anderson. He added that, in future studies, the investigators would compare serum vitamin D levels between participants with and without a history of NMSC, and explore temporal relationships between diagnosis of NMSC and fracture occurrence.
The National Institutes of Health and the Medical Scholars Research Program at Stanford University funded the research. Mr. Anderson reported no conflicts of interest.
ALBUQUERQUE – Postmenopausal women who reported a history of nonmelanoma skin cancer were almost 16% more likely to sustain a lower arm fracture than were women without a skin cancer history, according to a large, prospective, longitudinal study.
Women with prior nonmelanoma skin cancers (NMSCs) also were more likely to suffer a subsequent hip fracture, although the association did not reach statistical significance, said Eric Anderson of the dermatology department at Stanford (Calif.) University School of Medicine.
"These results suggest that prior history of NMSC is associated with an increased risk of subsequent bone fracture, contrary to our hypothesis," noted Mr. Anderson. He presented the findings at the annual meeting of the Society for Investigational Dermatology.
Nonmelanoma skin cancer has been correlated with decreased fracture risk in at least one small cohort study, Mr. Anderson said (Osteoporos. Int. 2007;18:687-92). However, patients with NMSC also have been shown to wear more sunscreen and limit their sun exposure after diagnosis, which might lower their vitamin D levels and increase their fracture risk, Mr. Anderson noted (Cancer Causes Control 2012;23:133-40).
To better clarify the relationship between NMSC and fracture risk, Mr. Anderson and his associates compared prospective data from 4,289 women with self-reported NMSC and 67,470 women who did not report a history of NMSC at baseline. The participants were from the Womens Health Initiative, a prospective longitudinal cohort study of postmenopausal women aged 50-79 years who were enrolled at 40 centers in the United States. Participants were followed for more than 10 years, and new spine, hip, and lower arm fractures were recorded, Mr. Anderson said.
In age-adjusted Cox proportional hazards models, women with a history of NMSC were 1.55 times more likely to sustain a hip fracture (95% confidence interval, 1.31-1.85; P < 0.0001), 1.29 times more likely to suffer a spine fracture (95% CI, 1.10-1.51; P = 0.0018), and 1.28 times more likely to sustain a lower arm fracture (95% CI, 1.13-1.45; P < 0.0001) than were women who did not report a history of NMSC at baseline, Mr. Anderson and his associates reported.
After adjusting for sun exposure, sunscreen use, vitamin D intake, physical activity, and other risk factors for fracture, only lower arm fracture remained statistically significant (hazard ratio, 1.16; 95% CI, 1.31-1.85; P = 0.02), although hip fracture was borderline significant (HR, 1.18; 95% CI, 0.99-1.41; P = 0.06), the investigators reported. Baseline hip bone marrow density was not associated with risk of NMSC in a subgroup analysis of 4,267 women with available data, Mr. Anderson said.
"We’re inclined to believe that this increased fracture risk may be due to sun exposure avoidance after NMSC diagnosis," said Mr. Anderson. He added that, in future studies, the investigators would compare serum vitamin D levels between participants with and without a history of NMSC, and explore temporal relationships between diagnosis of NMSC and fracture occurrence.
The National Institutes of Health and the Medical Scholars Research Program at Stanford University funded the research. Mr. Anderson reported no conflicts of interest.
AT THE 2014 SID ANNUAL MEETING
Key clinical point: A history of nonmelanoma skin cancer may predispose patients to bone fractures.
Major finding: Incident lower arm fracture was significantly associated with a self-reported history of nonmelanoma skin cancer (hazard ratio, 1.16; P = 0.02).
Data source: Ten-year prospective cohort study of 4,289 women who self-reported a history of nonmelanoma skin cancer and 67,470 women who reported no history of NMSC.
Disclosures: The National Institutes of Health and the Medical Scholars Research Program at Stanford University funded the research. Mr. Anderson reported no conflicts of interest.
NSAID use linked to reduced risk for second nonmelanoma skin cancer
ALBUQUERQUE – Postmenopausal women who had a history of nonmelanoma skin cancer and regularly used nonsteroidal anti-inflammatory drugs had an 18% lower risk of developing subsequent skin cancers, based on a large prospective longitudinal study.
The effect was evident regardless of NSAID type and in women who had used NSAIDs regularly for less than 5 years, said Dr. Mina Ally at the annual meeting of the Society for Investigative Dermatology.
Data on how NSAID use affects the risk of nonmelanoma skin cancer (NMSC) have been inconsistent, noted Dr. Ally, who is a postdoctoral research fellow in dermatology at Stanford University in Redwood City, Calif.
Previously, a double-blind, placebo-controlled trial found that NSAID use reduced the risk of NMSC in patients with a skin cancer history, Dr. Ally said (J. Natl. Cancer Inst. 2010;102:1835-44). In contrast, the Nurses Health Study found no association, but excluded women with a history of skin cancer (Cancer Causes Control 2012;23:1451-61).
In the current study, self-reported skin cancer was not confirmed by reviewing medical records, and data on NMSC subtype was not collected, Dr. Ally said.
Dr. Ally and her associates analyzed data from standardized medication questionnaires given at baseline and 3 years later to postmenopausal women aged 50-79 years. Respondents were from the Women\'s Health Initiative, which began in 1991 and includes more than 161,000 women enrolled at 40 centers in the United States.
The analysis was limited to participants who were white, immunocompetent, and had no missing data, yielding a final cohort of 54,728 women. NSAID users were defined as those who reported using the medications at least twice in the past 2 weeks in the baseline and year-3 questionnaires. The researchers collected data on the type, strength, and duration of NSAID use, and validated participants’ responses with data from pill bottle labels and prescription records, although they did not examine dose-response associations, Dr. Ally said.
The women were followed for a median of 6.9 years, during which there were 7,652 incident cases of NMSC, Dr. Ally said. After adjusting for skin type, sun exposure history, reason for using NSAIDs, and other potential confounders, women who regularly used any type of NSAID had no significant difference in risk of NMSC compared with women who did not use NSAIDs or used them inconsistently, she added.
But in the subgroup of 5,488 women who reported a prior history of skin cancer, the odds of incident NMSC were significantly lower with regular NSAID use, whether for less than 5 years (odds ratio, 0.82; 95% confidence interval, 0.70-0.95) or 5 years or longer (OR, 0.82; 95% CI, 0.69-0.98), the researchers reported.
Cyclooxygenase-2 enzymes are unregulated in several cancers, including NMSC, Dr. Ally noted. High levels of ultraviolet exposure increase epidermal COX-2 expression, which might explain why women with a prior history of skin cancer appear to be more responsive to chemoprevention with NSAID treatment, she said.
The National Institutes of Health funded the study. Dr. Ally reported no conflicts of interest.
ALBUQUERQUE – Postmenopausal women who had a history of nonmelanoma skin cancer and regularly used nonsteroidal anti-inflammatory drugs had an 18% lower risk of developing subsequent skin cancers, based on a large prospective longitudinal study.
The effect was evident regardless of NSAID type and in women who had used NSAIDs regularly for less than 5 years, said Dr. Mina Ally at the annual meeting of the Society for Investigative Dermatology.
Data on how NSAID use affects the risk of nonmelanoma skin cancer (NMSC) have been inconsistent, noted Dr. Ally, who is a postdoctoral research fellow in dermatology at Stanford University in Redwood City, Calif.
Previously, a double-blind, placebo-controlled trial found that NSAID use reduced the risk of NMSC in patients with a skin cancer history, Dr. Ally said (J. Natl. Cancer Inst. 2010;102:1835-44). In contrast, the Nurses Health Study found no association, but excluded women with a history of skin cancer (Cancer Causes Control 2012;23:1451-61).
In the current study, self-reported skin cancer was not confirmed by reviewing medical records, and data on NMSC subtype was not collected, Dr. Ally said.
Dr. Ally and her associates analyzed data from standardized medication questionnaires given at baseline and 3 years later to postmenopausal women aged 50-79 years. Respondents were from the Women\'s Health Initiative, which began in 1991 and includes more than 161,000 women enrolled at 40 centers in the United States.
The analysis was limited to participants who were white, immunocompetent, and had no missing data, yielding a final cohort of 54,728 women. NSAID users were defined as those who reported using the medications at least twice in the past 2 weeks in the baseline and year-3 questionnaires. The researchers collected data on the type, strength, and duration of NSAID use, and validated participants’ responses with data from pill bottle labels and prescription records, although they did not examine dose-response associations, Dr. Ally said.
The women were followed for a median of 6.9 years, during which there were 7,652 incident cases of NMSC, Dr. Ally said. After adjusting for skin type, sun exposure history, reason for using NSAIDs, and other potential confounders, women who regularly used any type of NSAID had no significant difference in risk of NMSC compared with women who did not use NSAIDs or used them inconsistently, she added.
But in the subgroup of 5,488 women who reported a prior history of skin cancer, the odds of incident NMSC were significantly lower with regular NSAID use, whether for less than 5 years (odds ratio, 0.82; 95% confidence interval, 0.70-0.95) or 5 years or longer (OR, 0.82; 95% CI, 0.69-0.98), the researchers reported.
Cyclooxygenase-2 enzymes are unregulated in several cancers, including NMSC, Dr. Ally noted. High levels of ultraviolet exposure increase epidermal COX-2 expression, which might explain why women with a prior history of skin cancer appear to be more responsive to chemoprevention with NSAID treatment, she said.
The National Institutes of Health funded the study. Dr. Ally reported no conflicts of interest.
ALBUQUERQUE – Postmenopausal women who had a history of nonmelanoma skin cancer and regularly used nonsteroidal anti-inflammatory drugs had an 18% lower risk of developing subsequent skin cancers, based on a large prospective longitudinal study.
The effect was evident regardless of NSAID type and in women who had used NSAIDs regularly for less than 5 years, said Dr. Mina Ally at the annual meeting of the Society for Investigative Dermatology.
Data on how NSAID use affects the risk of nonmelanoma skin cancer (NMSC) have been inconsistent, noted Dr. Ally, who is a postdoctoral research fellow in dermatology at Stanford University in Redwood City, Calif.
Previously, a double-blind, placebo-controlled trial found that NSAID use reduced the risk of NMSC in patients with a skin cancer history, Dr. Ally said (J. Natl. Cancer Inst. 2010;102:1835-44). In contrast, the Nurses Health Study found no association, but excluded women with a history of skin cancer (Cancer Causes Control 2012;23:1451-61).
In the current study, self-reported skin cancer was not confirmed by reviewing medical records, and data on NMSC subtype was not collected, Dr. Ally said.
Dr. Ally and her associates analyzed data from standardized medication questionnaires given at baseline and 3 years later to postmenopausal women aged 50-79 years. Respondents were from the Women\'s Health Initiative, which began in 1991 and includes more than 161,000 women enrolled at 40 centers in the United States.
The analysis was limited to participants who were white, immunocompetent, and had no missing data, yielding a final cohort of 54,728 women. NSAID users were defined as those who reported using the medications at least twice in the past 2 weeks in the baseline and year-3 questionnaires. The researchers collected data on the type, strength, and duration of NSAID use, and validated participants’ responses with data from pill bottle labels and prescription records, although they did not examine dose-response associations, Dr. Ally said.
The women were followed for a median of 6.9 years, during which there were 7,652 incident cases of NMSC, Dr. Ally said. After adjusting for skin type, sun exposure history, reason for using NSAIDs, and other potential confounders, women who regularly used any type of NSAID had no significant difference in risk of NMSC compared with women who did not use NSAIDs or used them inconsistently, she added.
But in the subgroup of 5,488 women who reported a prior history of skin cancer, the odds of incident NMSC were significantly lower with regular NSAID use, whether for less than 5 years (odds ratio, 0.82; 95% confidence interval, 0.70-0.95) or 5 years or longer (OR, 0.82; 95% CI, 0.69-0.98), the researchers reported.
Cyclooxygenase-2 enzymes are unregulated in several cancers, including NMSC, Dr. Ally noted. High levels of ultraviolet exposure increase epidermal COX-2 expression, which might explain why women with a prior history of skin cancer appear to be more responsive to chemoprevention with NSAID treatment, she said.
The National Institutes of Health funded the study. Dr. Ally reported no conflicts of interest.
AT THE 2014 SID ANNUAL MEETING
Key clinical point: NSAID use is associated with a lower risk of a second nonmelanoma skin cancer in white women.
Major finding: In women with a history of skin cancer, the odds of incident non-melanoma skin cancer were significantly lower with regular use of NSAIDs, whether for less than 5 years (odds ratio, 0.82; 95% confidence interval, 0.70-0.95) or at least 5 years (OR 0.82; 95% CI, 0.69–0.98).
Data source: Subgroup analysis of 5,488 women from the Women’s Health Initiative who were aged 50-79 years had a history of skin cancer.
Disclosures: The National Institutes of Health funded the study. Dr. Ally reported no conflicts of interest.
Infrared detector distinguished malignant and benign skin lesions
ALBUQUERQUE – A long-wave infrared system distinguished malignant and benign skin lesions with a sensitivity of 96.97% and a specificity of 78.05%, with skin biopsies used as a benchmark, in a pilot study of 74 patients.
The results "suggest the technique is promising as a noninvasive screening tool" and merits continued research and development to improve sensitivity, specificity, and statistical confidence, reported Stephen Myers, Ph.D., of Skinfrared, and his associates.
Recent advances in infrared technology have led to the development of imaging devices that noninvasively detect tumors, based on differential thermal properties of malignant versus healthy tissue. The long-wave infrared detection device used in the pilot study was designed to identify thermal signatures of suspicious lesions and surrounding skin after the application of a temperature stimulus, Dr. Myers said at the annual conference of the Society for Investigative Dermatology.
In the United States skin cancers are diagnosed more often than all other cancers combined, noted Dr. Myers, but screening for them "requires the skill of a highly trained dermatologist," who must assess a range of morphologic characteristics. "This is a rather subjective approach that causes many biopsies to be performed on benign lesions," Dr. Myers added.
To test the device, investigators at the University of New Mexico, Albuquerque, Dermatology Clinic offered patients with suspicious skin lesions the option of being evaluated with the infrared device before undergoing biopsy.
The device has infrared and visible cameras, as well as a registration marker, a cold air source, and a computer and software to guide image acquisition and analysis, Dr. Myers said. Investigators placed the registration marker near the skin lesion of interest, captured a visible image of the lesion, and then took a 15-second baseline thermal image sequence. After cooling the lesions and surrounding skin to 10° C, they measured and compared 3-minute thermal recovery rates for the lesion and surrounding skin.
Participants averaged 55 years of age, and 53% were male. A total of 102 suspicious lesions were tested. Based on biopsy results, 55% were benign, 34% were basal cell carcinomas, 7% were squamous cell carcinomas, and 4% were melanomas, Dr. Myers reported. The receiver operating curve – calculated to assess the test’s ability to classify skin lesions – had an area under the curve of 95.3% (95% confidence interval, 90.0-99.0). Using biopsy results as a benchmark, the infrared device had a sensitivity of 96.97% and a specificity of 78.05%, Dr. Myers said.
The study was supported by the National Science Foundation and Skinfrared, which makes the device. Dr. Myers is an employee of Skinfrared.
ALBUQUERQUE – A long-wave infrared system distinguished malignant and benign skin lesions with a sensitivity of 96.97% and a specificity of 78.05%, with skin biopsies used as a benchmark, in a pilot study of 74 patients.
The results "suggest the technique is promising as a noninvasive screening tool" and merits continued research and development to improve sensitivity, specificity, and statistical confidence, reported Stephen Myers, Ph.D., of Skinfrared, and his associates.
Recent advances in infrared technology have led to the development of imaging devices that noninvasively detect tumors, based on differential thermal properties of malignant versus healthy tissue. The long-wave infrared detection device used in the pilot study was designed to identify thermal signatures of suspicious lesions and surrounding skin after the application of a temperature stimulus, Dr. Myers said at the annual conference of the Society for Investigative Dermatology.
In the United States skin cancers are diagnosed more often than all other cancers combined, noted Dr. Myers, but screening for them "requires the skill of a highly trained dermatologist," who must assess a range of morphologic characteristics. "This is a rather subjective approach that causes many biopsies to be performed on benign lesions," Dr. Myers added.
To test the device, investigators at the University of New Mexico, Albuquerque, Dermatology Clinic offered patients with suspicious skin lesions the option of being evaluated with the infrared device before undergoing biopsy.
The device has infrared and visible cameras, as well as a registration marker, a cold air source, and a computer and software to guide image acquisition and analysis, Dr. Myers said. Investigators placed the registration marker near the skin lesion of interest, captured a visible image of the lesion, and then took a 15-second baseline thermal image sequence. After cooling the lesions and surrounding skin to 10° C, they measured and compared 3-minute thermal recovery rates for the lesion and surrounding skin.
Participants averaged 55 years of age, and 53% were male. A total of 102 suspicious lesions were tested. Based on biopsy results, 55% were benign, 34% were basal cell carcinomas, 7% were squamous cell carcinomas, and 4% were melanomas, Dr. Myers reported. The receiver operating curve – calculated to assess the test’s ability to classify skin lesions – had an area under the curve of 95.3% (95% confidence interval, 90.0-99.0). Using biopsy results as a benchmark, the infrared device had a sensitivity of 96.97% and a specificity of 78.05%, Dr. Myers said.
The study was supported by the National Science Foundation and Skinfrared, which makes the device. Dr. Myers is an employee of Skinfrared.
ALBUQUERQUE – A long-wave infrared system distinguished malignant and benign skin lesions with a sensitivity of 96.97% and a specificity of 78.05%, with skin biopsies used as a benchmark, in a pilot study of 74 patients.
The results "suggest the technique is promising as a noninvasive screening tool" and merits continued research and development to improve sensitivity, specificity, and statistical confidence, reported Stephen Myers, Ph.D., of Skinfrared, and his associates.
Recent advances in infrared technology have led to the development of imaging devices that noninvasively detect tumors, based on differential thermal properties of malignant versus healthy tissue. The long-wave infrared detection device used in the pilot study was designed to identify thermal signatures of suspicious lesions and surrounding skin after the application of a temperature stimulus, Dr. Myers said at the annual conference of the Society for Investigative Dermatology.
In the United States skin cancers are diagnosed more often than all other cancers combined, noted Dr. Myers, but screening for them "requires the skill of a highly trained dermatologist," who must assess a range of morphologic characteristics. "This is a rather subjective approach that causes many biopsies to be performed on benign lesions," Dr. Myers added.
To test the device, investigators at the University of New Mexico, Albuquerque, Dermatology Clinic offered patients with suspicious skin lesions the option of being evaluated with the infrared device before undergoing biopsy.
The device has infrared and visible cameras, as well as a registration marker, a cold air source, and a computer and software to guide image acquisition and analysis, Dr. Myers said. Investigators placed the registration marker near the skin lesion of interest, captured a visible image of the lesion, and then took a 15-second baseline thermal image sequence. After cooling the lesions and surrounding skin to 10° C, they measured and compared 3-minute thermal recovery rates for the lesion and surrounding skin.
Participants averaged 55 years of age, and 53% were male. A total of 102 suspicious lesions were tested. Based on biopsy results, 55% were benign, 34% were basal cell carcinomas, 7% were squamous cell carcinomas, and 4% were melanomas, Dr. Myers reported. The receiver operating curve – calculated to assess the test’s ability to classify skin lesions – had an area under the curve of 95.3% (95% confidence interval, 90.0-99.0). Using biopsy results as a benchmark, the infrared device had a sensitivity of 96.97% and a specificity of 78.05%, Dr. Myers said.
The study was supported by the National Science Foundation and Skinfrared, which makes the device. Dr. Myers is an employee of Skinfrared.
AT THE 2014 SID ANNUAL MEETING
Major finding: Malignant skin lesions (basal cell carcinomas, squamous cell carcinomas, and malignant melanomas) were distinguished from benign lesions with a sensitivity of 96.97% and a specificity of 78.05%.
Data source: Observational pilot study of 74 patients with 102 suspicious skin lesions who underwent infrared imaging followed by biopsy.
Disclosures: The study was supported by the National Science Foundation and Skinfrared, which makes the device. Dr. Myers is an employee of Skinfrared.
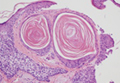
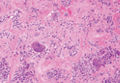
Cutaneous Metastasis of a Perivascular Epithelioid Cell Tumor
Cutaneous Metastasis From Primary Gastric Cancer: A Case Report and Review of the Literature

Giant Cell Tumor of the Tendon Sheath
Practice Question Answers: Chemotherapeutic Agents and Dermatologic Side Effects
1. Which of the following chemotherapy agents has demonstrated the ability to cause accelerated rheumatoid nodule formation?
a. cisplatin
b. methotrexate
c. paclitaxel
d. rituximab
e. tamoxifen
2. Which of the following chemotherapy agents can cause sticky skin syndrome when combined with ketoconazole?
a. doxorubicin
b. etoposide
c. imatinib
d. sorafenib
e. thalidomide
3. Which of the following agents is not a protein kinase inhibitor?
a. bortezomib
b. cetuximab
c. erlotinib
d. imatinib
e. sorafenib
4. Which of the following chemotherapy agents can be used off label in the treatment of dermatofibrosarcoma protuberans?
a. etoposide
b. imatinib
c. interferon alfa
d. lenalidomide
e. methotrexate
5. What chemotherapy agent has been shown to cause deep venous thromboembolism?
a. daunorubicin
b. doxorubicin
c. erlotinib
d. paclitaxel
e. thalidomide
1. Which of the following chemotherapy agents has demonstrated the ability to cause accelerated rheumatoid nodule formation?
a. cisplatin
b. methotrexate
c. paclitaxel
d. rituximab
e. tamoxifen
2. Which of the following chemotherapy agents can cause sticky skin syndrome when combined with ketoconazole?
a. doxorubicin
b. etoposide
c. imatinib
d. sorafenib
e. thalidomide
3. Which of the following agents is not a protein kinase inhibitor?
a. bortezomib
b. cetuximab
c. erlotinib
d. imatinib
e. sorafenib
4. Which of the following chemotherapy agents can be used off label in the treatment of dermatofibrosarcoma protuberans?
a. etoposide
b. imatinib
c. interferon alfa
d. lenalidomide
e. methotrexate
5. What chemotherapy agent has been shown to cause deep venous thromboembolism?
a. daunorubicin
b. doxorubicin
c. erlotinib
d. paclitaxel
e. thalidomide
1. Which of the following chemotherapy agents has demonstrated the ability to cause accelerated rheumatoid nodule formation?
a. cisplatin
b. methotrexate
c. paclitaxel
d. rituximab
e. tamoxifen
2. Which of the following chemotherapy agents can cause sticky skin syndrome when combined with ketoconazole?
a. doxorubicin
b. etoposide
c. imatinib
d. sorafenib
e. thalidomide
3. Which of the following agents is not a protein kinase inhibitor?
a. bortezomib
b. cetuximab
c. erlotinib
d. imatinib
e. sorafenib
4. Which of the following chemotherapy agents can be used off label in the treatment of dermatofibrosarcoma protuberans?
a. etoposide
b. imatinib
c. interferon alfa
d. lenalidomide
e. methotrexate
5. What chemotherapy agent has been shown to cause deep venous thromboembolism?
a. daunorubicin
b. doxorubicin
c. erlotinib
d. paclitaxel
e. thalidomide