User login
HM11 PREVIEW: Wachter’s Vision

When Robert Wachter, MD, MHM, delivers his keynote address to unofficially close HM11, he’ll toast the field he helped define. His remarks will coincide with the 15th anniversary of the article he and Lee Goldman, MD, coauthored in The New England Journal of Medicine that coined the term “hospitalist” and fostered an understanding that the HM movement was a true phenomenon.
The milestone presents the perfect opportunity to examine the specialty’s meteoric growth and celebrate the successes of its pioneers, says Dr. Wachter, a professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center. He also considers it an ideal time to examine the unforeseen developments of the past decade and a half, believing a critical analysis of a few key case studies can help lay the groundwork for an even brighter future.
“At 15, you’re in mid- to late adolescence,” Dr. Wachter says. “We can no longer say we’re this new kid on the block and, ‘Gee, whiz, isn’t this neat?’
“This is a good chance to reflect on things that went as we expected,” he adds. “It’s an even better chance to take a second look at things that were surprising but provide valuable lessons as we think about what the next 15 years are going to be like.”
Question: Fifteen years ago, did you envision HM would grow so quickly?
Answer: I had a sense this was a trend that was starting to emerge and could fill an important niche. At the same time, when Sergey (Brin) and Larry (Page) founded Google, I doubt they believed it would become a $200 billion company. In the beginning, I couldn’t have predicted what this would become.
Q: What surprised you most in the past 15 years?
A: I didn’t fully appreciate how quickly the push toward value would become a dominant theme. Once we discovered quality was important and there was a set of skills we needed to learn to improve it, we tackled it aggressively. It has been harder to tackle the cost part of the equation.
This goes beyond making sure patients don’t stay in the hospital longer than they need to. It means looking hard at the cost of care and the way we spend money, such as our patterns of ordering X-rays, consultants, and lab tests. I’m going to focus a fair amount on that.
Q: Why do you want to emphasize that point?
A: The cost of healthcare is going to bankrupt the country unless we get a handle on it. Our field needs to lead the way to show how a good, ethical physician not only focuses on improving quality of care, but also focuses on ridding the system of waste and of care that adds no real value to our patients. We’ve been a little sluggish in that area.
Q: What other surprises do you intend to discuss?
A: I didn’t anticipate the emergence of two different versions of the hospitalist field. One is the role of comanagement. The other is what I call the hyphenated hospitalist—these OB hospitalists and surgery hospitalists. This concept we came up with for general patients has been embraced by a variety of specialties. How do those people fit into our society and our field? Are they really part of us or are they fundamentally different? I think we need to think carefully about it.
Q: Why are the unexpected developments so important to consider?
A: Leaders in the field need to get really good at reading tea leaves. One of the ways you do that is to figure out, when you didn’t read them correctly the first time, why didn’t you? Could you have read them better if you were more clever or more thoughtful?
Q: What is the biggest challenge facing HM?
A: When we have been given new tasks and new opportunities, our members have stepped up to the plate and done what they’ve been asked to do as well, if not better, than expected. I’m a little fearful of the flip side. How we will meet the demand for our services? How do we ensure the job stays attractive and we don’t burn out? We have to demonstrate our value, but we have to make sure the jobs are truly sustainable and that we don’t shoot ourselves in the foot.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
Q:What do you see as the solution?
A: I don’t think we’ll be able to meet all of the demand. There will be hospitals that can only partly staff the needs they have with hospitalists. I don’t want them to go too far down the quality curve. We need to be sure people entering the field are good and have the skills they need.
I think we’ll begin to ask important questions like, “Do I really need a hospitalist for this, or can I leverage fewer hospitalists with other nonphysician providers?” Or, “Can some of the work our hospitalists are doing be done as well and more cheaply by computers?” It opens a pathway to think more creatively about people and tasks and technologies.
Q: Despite the challenges associated with growth pressure, is HM better positioned for the future because of it?
A: Definitely. We will see a further extension of our reach into other areas of the hospital and healthcare system. We will continue to see our people begin as leaders in our world of hospital medicine but rapidly graduate to become hospital CEOs, chairs of departments of medicine, and major leaders in healthcare. There is a recognition that there’s no better training ground to be a leader in healthcare than to be a leader in our field. So I can’t help but be optimistic that our place in the world of healthcare is extraordinarily secure. HM11
Mark Leiser is a freelance writer based in New Jersey.
When Robert Wachter, MD, MHM, delivers his keynote address to unofficially close HM11, he’ll toast the field he helped define. His remarks will coincide with the 15th anniversary of the article he and Lee Goldman, MD, coauthored in The New England Journal of Medicine that coined the term “hospitalist” and fostered an understanding that the HM movement was a true phenomenon.
The milestone presents the perfect opportunity to examine the specialty’s meteoric growth and celebrate the successes of its pioneers, says Dr. Wachter, a professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center. He also considers it an ideal time to examine the unforeseen developments of the past decade and a half, believing a critical analysis of a few key case studies can help lay the groundwork for an even brighter future.
“At 15, you’re in mid- to late adolescence,” Dr. Wachter says. “We can no longer say we’re this new kid on the block and, ‘Gee, whiz, isn’t this neat?’
“This is a good chance to reflect on things that went as we expected,” he adds. “It’s an even better chance to take a second look at things that were surprising but provide valuable lessons as we think about what the next 15 years are going to be like.”
Question: Fifteen years ago, did you envision HM would grow so quickly?
Answer: I had a sense this was a trend that was starting to emerge and could fill an important niche. At the same time, when Sergey (Brin) and Larry (Page) founded Google, I doubt they believed it would become a $200 billion company. In the beginning, I couldn’t have predicted what this would become.
Q: What surprised you most in the past 15 years?
A: I didn’t fully appreciate how quickly the push toward value would become a dominant theme. Once we discovered quality was important and there was a set of skills we needed to learn to improve it, we tackled it aggressively. It has been harder to tackle the cost part of the equation.
This goes beyond making sure patients don’t stay in the hospital longer than they need to. It means looking hard at the cost of care and the way we spend money, such as our patterns of ordering X-rays, consultants, and lab tests. I’m going to focus a fair amount on that.
Q: Why do you want to emphasize that point?
A: The cost of healthcare is going to bankrupt the country unless we get a handle on it. Our field needs to lead the way to show how a good, ethical physician not only focuses on improving quality of care, but also focuses on ridding the system of waste and of care that adds no real value to our patients. We’ve been a little sluggish in that area.
Q: What other surprises do you intend to discuss?
A: I didn’t anticipate the emergence of two different versions of the hospitalist field. One is the role of comanagement. The other is what I call the hyphenated hospitalist—these OB hospitalists and surgery hospitalists. This concept we came up with for general patients has been embraced by a variety of specialties. How do those people fit into our society and our field? Are they really part of us or are they fundamentally different? I think we need to think carefully about it.
Q: Why are the unexpected developments so important to consider?
A: Leaders in the field need to get really good at reading tea leaves. One of the ways you do that is to figure out, when you didn’t read them correctly the first time, why didn’t you? Could you have read them better if you were more clever or more thoughtful?
Q: What is the biggest challenge facing HM?
A: When we have been given new tasks and new opportunities, our members have stepped up to the plate and done what they’ve been asked to do as well, if not better, than expected. I’m a little fearful of the flip side. How we will meet the demand for our services? How do we ensure the job stays attractive and we don’t burn out? We have to demonstrate our value, but we have to make sure the jobs are truly sustainable and that we don’t shoot ourselves in the foot.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
Q:What do you see as the solution?
A: I don’t think we’ll be able to meet all of the demand. There will be hospitals that can only partly staff the needs they have with hospitalists. I don’t want them to go too far down the quality curve. We need to be sure people entering the field are good and have the skills they need.
I think we’ll begin to ask important questions like, “Do I really need a hospitalist for this, or can I leverage fewer hospitalists with other nonphysician providers?” Or, “Can some of the work our hospitalists are doing be done as well and more cheaply by computers?” It opens a pathway to think more creatively about people and tasks and technologies.
Q: Despite the challenges associated with growth pressure, is HM better positioned for the future because of it?
A: Definitely. We will see a further extension of our reach into other areas of the hospital and healthcare system. We will continue to see our people begin as leaders in our world of hospital medicine but rapidly graduate to become hospital CEOs, chairs of departments of medicine, and major leaders in healthcare. There is a recognition that there’s no better training ground to be a leader in healthcare than to be a leader in our field. So I can’t help but be optimistic that our place in the world of healthcare is extraordinarily secure. HM11
Mark Leiser is a freelance writer based in New Jersey.
When Robert Wachter, MD, MHM, delivers his keynote address to unofficially close HM11, he’ll toast the field he helped define. His remarks will coincide with the 15th anniversary of the article he and Lee Goldman, MD, coauthored in The New England Journal of Medicine that coined the term “hospitalist” and fostered an understanding that the HM movement was a true phenomenon.
The milestone presents the perfect opportunity to examine the specialty’s meteoric growth and celebrate the successes of its pioneers, says Dr. Wachter, a professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center. He also considers it an ideal time to examine the unforeseen developments of the past decade and a half, believing a critical analysis of a few key case studies can help lay the groundwork for an even brighter future.
“At 15, you’re in mid- to late adolescence,” Dr. Wachter says. “We can no longer say we’re this new kid on the block and, ‘Gee, whiz, isn’t this neat?’
“This is a good chance to reflect on things that went as we expected,” he adds. “It’s an even better chance to take a second look at things that were surprising but provide valuable lessons as we think about what the next 15 years are going to be like.”
Question: Fifteen years ago, did you envision HM would grow so quickly?
Answer: I had a sense this was a trend that was starting to emerge and could fill an important niche. At the same time, when Sergey (Brin) and Larry (Page) founded Google, I doubt they believed it would become a $200 billion company. In the beginning, I couldn’t have predicted what this would become.
Q: What surprised you most in the past 15 years?
A: I didn’t fully appreciate how quickly the push toward value would become a dominant theme. Once we discovered quality was important and there was a set of skills we needed to learn to improve it, we tackled it aggressively. It has been harder to tackle the cost part of the equation.
This goes beyond making sure patients don’t stay in the hospital longer than they need to. It means looking hard at the cost of care and the way we spend money, such as our patterns of ordering X-rays, consultants, and lab tests. I’m going to focus a fair amount on that.
Q: Why do you want to emphasize that point?
A: The cost of healthcare is going to bankrupt the country unless we get a handle on it. Our field needs to lead the way to show how a good, ethical physician not only focuses on improving quality of care, but also focuses on ridding the system of waste and of care that adds no real value to our patients. We’ve been a little sluggish in that area.
Q: What other surprises do you intend to discuss?
A: I didn’t anticipate the emergence of two different versions of the hospitalist field. One is the role of comanagement. The other is what I call the hyphenated hospitalist—these OB hospitalists and surgery hospitalists. This concept we came up with for general patients has been embraced by a variety of specialties. How do those people fit into our society and our field? Are they really part of us or are they fundamentally different? I think we need to think carefully about it.
Q: Why are the unexpected developments so important to consider?
A: Leaders in the field need to get really good at reading tea leaves. One of the ways you do that is to figure out, when you didn’t read them correctly the first time, why didn’t you? Could you have read them better if you were more clever or more thoughtful?
Q: What is the biggest challenge facing HM?
A: When we have been given new tasks and new opportunities, our members have stepped up to the plate and done what they’ve been asked to do as well, if not better, than expected. I’m a little fearful of the flip side. How we will meet the demand for our services? How do we ensure the job stays attractive and we don’t burn out? We have to demonstrate our value, but we have to make sure the jobs are truly sustainable and that we don’t shoot ourselves in the foot.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
Q:What do you see as the solution?
A: I don’t think we’ll be able to meet all of the demand. There will be hospitals that can only partly staff the needs they have with hospitalists. I don’t want them to go too far down the quality curve. We need to be sure people entering the field are good and have the skills they need.
I think we’ll begin to ask important questions like, “Do I really need a hospitalist for this, or can I leverage fewer hospitalists with other nonphysician providers?” Or, “Can some of the work our hospitalists are doing be done as well and more cheaply by computers?” It opens a pathway to think more creatively about people and tasks and technologies.
Q: Despite the challenges associated with growth pressure, is HM better positioned for the future because of it?
A: Definitely. We will see a further extension of our reach into other areas of the hospital and healthcare system. We will continue to see our people begin as leaders in our world of hospital medicine but rapidly graduate to become hospital CEOs, chairs of departments of medicine, and major leaders in healthcare. There is a recognition that there’s no better training ground to be a leader in healthcare than to be a leader in our field. So I can’t help but be optimistic that our place in the world of healthcare is extraordinarily secure. HM11
Mark Leiser is a freelance writer based in New Jersey.
HM11 PREVIEW: Lots to See, Lots to Do in ‘Big D’
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.

A billion-dollar football stadium that offers on-field tours. A real-life cattle ride. A chance to honor the country’s last assassinated president. And don’t overlook the museums, art galleries, and restaurants.
Hospitalists from across the country will have the opportunity to experience all of it during HM11 at the Gaylord Texan Hotel & Convention Center in Grapevine, Texas, situated between Dallas and Fort Worth.
“I think it’s a nice blend of both sides,” says Ben Lee, MD, a hospitalist at Children’s Medical Center of Dallas and assistant professor of pediatrics at University of Texas Southwestern. “You can get the modern amenities, but you also have a capturing of, ‘Hey, this is stuff that’s occurred in the past that’s still available.’ ”
For the sports-minded, Dallas is a veritable Mecca. Cowboys Stadium, which hosted Super Bowl XV in February, offers VIP and self-guided tours. For more information, call 800-745-3000. The Texas Rangers baseball team will be playing at home in Arlington the week of HM11, while NBA fans might be able to catch a Dallas Mavericks playoff game. The same could be true of the NHL’s Dallas Stars.
The art-minded and culturists should not fret, though. Dallas offers both the eponymous Dallas Museum of Art and the outdoor Nasher Sculpture Center. Meanwhile, Fort Worth offers the Modern Art Museum of Forth Worth and a half-dozen other arts institutions in its downtown cultural district.
History buffs can try the Fort Worth Stockyards National Historic District, a nod to Texas’ frontier history that includes twice-daily cattle drives, or the Sixth Floor Museum at Dealey Plaza to learn about the assassination of President Kennedy.
When you’re hungry, steak and Tex-Mex are the specialties. If you aren’t able to leave the Gaylord, try the Old Hickory Steakhouse (just make sure to reserve a table early). Away from the hotel, look for local Tex-Mex chains like Uncle Julio’s or Gloria’s.
One last tip, if we may. “I would definitely rent a car,” Dr. Lee says. “Texas is wide open.” HM11
Richard Quinn is a freelance writer based in New Jersey.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
A billion-dollar football stadium that offers on-field tours. A real-life cattle ride. A chance to honor the country’s last assassinated president. And don’t overlook the museums, art galleries, and restaurants.
Hospitalists from across the country will have the opportunity to experience all of it during HM11 at the Gaylord Texan Hotel & Convention Center in Grapevine, Texas, situated between Dallas and Fort Worth.
“I think it’s a nice blend of both sides,” says Ben Lee, MD, a hospitalist at Children’s Medical Center of Dallas and assistant professor of pediatrics at University of Texas Southwestern. “You can get the modern amenities, but you also have a capturing of, ‘Hey, this is stuff that’s occurred in the past that’s still available.’ ”
For the sports-minded, Dallas is a veritable Mecca. Cowboys Stadium, which hosted Super Bowl XV in February, offers VIP and self-guided tours. For more information, call 800-745-3000. The Texas Rangers baseball team will be playing at home in Arlington the week of HM11, while NBA fans might be able to catch a Dallas Mavericks playoff game. The same could be true of the NHL’s Dallas Stars.
The art-minded and culturists should not fret, though. Dallas offers both the eponymous Dallas Museum of Art and the outdoor Nasher Sculpture Center. Meanwhile, Fort Worth offers the Modern Art Museum of Forth Worth and a half-dozen other arts institutions in its downtown cultural district.
History buffs can try the Fort Worth Stockyards National Historic District, a nod to Texas’ frontier history that includes twice-daily cattle drives, or the Sixth Floor Museum at Dealey Plaza to learn about the assassination of President Kennedy.
When you’re hungry, steak and Tex-Mex are the specialties. If you aren’t able to leave the Gaylord, try the Old Hickory Steakhouse (just make sure to reserve a table early). Away from the hotel, look for local Tex-Mex chains like Uncle Julio’s or Gloria’s.
One last tip, if we may. “I would definitely rent a car,” Dr. Lee says. “Texas is wide open.” HM11
Richard Quinn is a freelance writer based in New Jersey.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
A billion-dollar football stadium that offers on-field tours. A real-life cattle ride. A chance to honor the country’s last assassinated president. And don’t overlook the museums, art galleries, and restaurants.
Hospitalists from across the country will have the opportunity to experience all of it during HM11 at the Gaylord Texan Hotel & Convention Center in Grapevine, Texas, situated between Dallas and Fort Worth.
“I think it’s a nice blend of both sides,” says Ben Lee, MD, a hospitalist at Children’s Medical Center of Dallas and assistant professor of pediatrics at University of Texas Southwestern. “You can get the modern amenities, but you also have a capturing of, ‘Hey, this is stuff that’s occurred in the past that’s still available.’ ”
For the sports-minded, Dallas is a veritable Mecca. Cowboys Stadium, which hosted Super Bowl XV in February, offers VIP and self-guided tours. For more information, call 800-745-3000. The Texas Rangers baseball team will be playing at home in Arlington the week of HM11, while NBA fans might be able to catch a Dallas Mavericks playoff game. The same could be true of the NHL’s Dallas Stars.
The art-minded and culturists should not fret, though. Dallas offers both the eponymous Dallas Museum of Art and the outdoor Nasher Sculpture Center. Meanwhile, Fort Worth offers the Modern Art Museum of Forth Worth and a half-dozen other arts institutions in its downtown cultural district.
History buffs can try the Fort Worth Stockyards National Historic District, a nod to Texas’ frontier history that includes twice-daily cattle drives, or the Sixth Floor Museum at Dealey Plaza to learn about the assassination of President Kennedy.
When you’re hungry, steak and Tex-Mex are the specialties. If you aren’t able to leave the Gaylord, try the Old Hickory Steakhouse (just make sure to reserve a table early). Away from the hotel, look for local Tex-Mex chains like Uncle Julio’s or Gloria’s.
One last tip, if we may. “I would definitely rent a car,” Dr. Lee says. “Texas is wide open.” HM11
Richard Quinn is a freelance writer based in New Jersey.
Top Leaders, Hot Topics
Since its inception, SHM’s annual meeting has grown every year, attracting more hospitalists, bringing influential leaders to presentations, and creating a welcome environment for some of the most innovative ideas in healthcare. That growth in influence—and influencers—will be evident at HM11 next month.
This year, HM11 will bring hospitalists closer than ever to the decision-makers. Featured presenters Robert Wachter, MD, MHM, professor, chief of the division of hospital medicine at the University of California at San Francisco, and former White House advisor Robert Kocher, MD, will be joined by Cecil B. Wilson, MD, president of the American Medical Association.
“The Society of Hospital Medicine is a dynamic, growing organization that is very responsive to the interests and needs of hospitalists,” Dr. Wilson told SHM. “So when the SHM leadership offered me the opportunity to speak at Hospital Medicine 2011, I was pleased and honored. … I am hopeful that the AMA and the SHM can continue to work together productively to advance the interests of physicians and our patients.”

In addition to hosting the country’s most influential figures in healthcare, HM11 will present some of its most cutting-edge ideas in improving care. The continued focus on reducing unplanned readmissions in hospitals across the country has turned to a search for solutions. A new session will put the spotlight on SHM’s own program, Project BOOST (Boosting Outcomes for Older Adults through Safe Transitions).
“Healthcare Reform and Optimizing Care Transitions to Reduce Readmissions” will be presented by Mark V. Williams, MD, FACP, FHM, principal investigator of Project BOOST; Jeffrey Greenwald, MD, SFHM; and Linda Magno, the director of the Medicare Demonstrations Group in the Office of Research, Development, and Information at the Centers for Medicare & Medicaid Services.
The presentation will bring the audience to the very crossroads of healthcare policy reform and quality improvement (QI) by illustrating the impact of readmissions on healthcare costs and patient safety, coupled with the innovative and individualized approaches that Project BOOST hospitalists are implementing.
Development of and pilot testing of Project BOOST was supported through grant funding from the John A. Hartford Foundation. Today, Project BOOST has been implemented in more than 60 sites and the program is now recruiting for its fall cohort.
For more information about HM11, visit www.hospitalmedicine2011.org.
For information about Project BOOST, visit www.hospitalmedicine.org/boost. TH
Brendon Shank is SHM’s assistant vice president of communications.
Since its inception, SHM’s annual meeting has grown every year, attracting more hospitalists, bringing influential leaders to presentations, and creating a welcome environment for some of the most innovative ideas in healthcare. That growth in influence—and influencers—will be evident at HM11 next month.
This year, HM11 will bring hospitalists closer than ever to the decision-makers. Featured presenters Robert Wachter, MD, MHM, professor, chief of the division of hospital medicine at the University of California at San Francisco, and former White House advisor Robert Kocher, MD, will be joined by Cecil B. Wilson, MD, president of the American Medical Association.
“The Society of Hospital Medicine is a dynamic, growing organization that is very responsive to the interests and needs of hospitalists,” Dr. Wilson told SHM. “So when the SHM leadership offered me the opportunity to speak at Hospital Medicine 2011, I was pleased and honored. … I am hopeful that the AMA and the SHM can continue to work together productively to advance the interests of physicians and our patients.”
In addition to hosting the country’s most influential figures in healthcare, HM11 will present some of its most cutting-edge ideas in improving care. The continued focus on reducing unplanned readmissions in hospitals across the country has turned to a search for solutions. A new session will put the spotlight on SHM’s own program, Project BOOST (Boosting Outcomes for Older Adults through Safe Transitions).
“Healthcare Reform and Optimizing Care Transitions to Reduce Readmissions” will be presented by Mark V. Williams, MD, FACP, FHM, principal investigator of Project BOOST; Jeffrey Greenwald, MD, SFHM; and Linda Magno, the director of the Medicare Demonstrations Group in the Office of Research, Development, and Information at the Centers for Medicare & Medicaid Services.
The presentation will bring the audience to the very crossroads of healthcare policy reform and quality improvement (QI) by illustrating the impact of readmissions on healthcare costs and patient safety, coupled with the innovative and individualized approaches that Project BOOST hospitalists are implementing.
Development of and pilot testing of Project BOOST was supported through grant funding from the John A. Hartford Foundation. Today, Project BOOST has been implemented in more than 60 sites and the program is now recruiting for its fall cohort.
For more information about HM11, visit www.hospitalmedicine2011.org.
For information about Project BOOST, visit www.hospitalmedicine.org/boost. TH
Brendon Shank is SHM’s assistant vice president of communications.
Since its inception, SHM’s annual meeting has grown every year, attracting more hospitalists, bringing influential leaders to presentations, and creating a welcome environment for some of the most innovative ideas in healthcare. That growth in influence—and influencers—will be evident at HM11 next month.
This year, HM11 will bring hospitalists closer than ever to the decision-makers. Featured presenters Robert Wachter, MD, MHM, professor, chief of the division of hospital medicine at the University of California at San Francisco, and former White House advisor Robert Kocher, MD, will be joined by Cecil B. Wilson, MD, president of the American Medical Association.
“The Society of Hospital Medicine is a dynamic, growing organization that is very responsive to the interests and needs of hospitalists,” Dr. Wilson told SHM. “So when the SHM leadership offered me the opportunity to speak at Hospital Medicine 2011, I was pleased and honored. … I am hopeful that the AMA and the SHM can continue to work together productively to advance the interests of physicians and our patients.”
In addition to hosting the country’s most influential figures in healthcare, HM11 will present some of its most cutting-edge ideas in improving care. The continued focus on reducing unplanned readmissions in hospitals across the country has turned to a search for solutions. A new session will put the spotlight on SHM’s own program, Project BOOST (Boosting Outcomes for Older Adults through Safe Transitions).
“Healthcare Reform and Optimizing Care Transitions to Reduce Readmissions” will be presented by Mark V. Williams, MD, FACP, FHM, principal investigator of Project BOOST; Jeffrey Greenwald, MD, SFHM; and Linda Magno, the director of the Medicare Demonstrations Group in the Office of Research, Development, and Information at the Centers for Medicare & Medicaid Services.
The presentation will bring the audience to the very crossroads of healthcare policy reform and quality improvement (QI) by illustrating the impact of readmissions on healthcare costs and patient safety, coupled with the innovative and individualized approaches that Project BOOST hospitalists are implementing.
Development of and pilot testing of Project BOOST was supported through grant funding from the John A. Hartford Foundation. Today, Project BOOST has been implemented in more than 60 sites and the program is now recruiting for its fall cohort.
For more information about HM11, visit www.hospitalmedicine2011.org.
For information about Project BOOST, visit www.hospitalmedicine.org/boost. TH
Brendon Shank is SHM’s assistant vice president of communications.
Q&A with Hospitalist Administrator Amit Prachand

Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Q&A with Hospitalist Administrator Kristi Gylten

Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
POLICY CORNER: Despite significant QI, disparities among poor Americans persist.
The Agency for Healthcare Research and Quality (AHRQ) recently released the annual National Healthcare Quality & Disparities Reports. The reports provide in-depth quality information on the overall population and divide this information along such subgroups as race, ethnicity, and education level. The report is more than 200 pages long, but it can be summarized in one sentence: If you are poor, the quality of your healthcare is likely to be poor.
Despite significant quality improvement (QI) in a number of areas, disparities among poor Americans persist. For example, the percentage of heart-attack patients who underwent procedures to unblock heart arteries within 90 minutes improved to 81% in 2008 from 42% in 2005. This is very positive news, but unfortunately, these and many other gains in quality only apply to higher-income populations.
A new section of the report focused on care coordination and transitions of care contains some statistics of particular interest to hospitalists. One statistic shows that the percentage of hospitalized adult patients with heart failure who were given complete written discharge instructions improved to 82.0% in 2008, up from 57.5% in 2005.
It is important to note that this number remains more or less constant across all racial/ethnic divisions. Could part of this improvement be attributed to the growth and success of the hospitalist movement?
Hospitalists know that despite the numbers, a successful transition does not simply include discharge instructions; it is the combination of those instructions, along with coordination with primary care, that prevents avoidable readmissions.
Unfortunately, 15% to 20% of low-income patients have no regular primary-care physician (PCP). If a condition begins to deteriorate, this group often has little choice but to return to the hospital.
In the absence of a PCP, it is the hospitalist who can provide patients with the tools they need to stay healthy after leaving the hospital.
Such assistance can range from ensuring that patients truly understand their discharge instructions to being a resource for future questions. Hospitalists are ahead of the game when it comes to quality and reducing disparities; it is just a matter of the other facets of healthcare catching up.
The National Healthcare Quality & Disparities reports are available at www.ahrq.gov/qual/qrdr10.htm. TH
The Agency for Healthcare Research and Quality (AHRQ) recently released the annual National Healthcare Quality & Disparities Reports. The reports provide in-depth quality information on the overall population and divide this information along such subgroups as race, ethnicity, and education level. The report is more than 200 pages long, but it can be summarized in one sentence: If you are poor, the quality of your healthcare is likely to be poor.
Despite significant quality improvement (QI) in a number of areas, disparities among poor Americans persist. For example, the percentage of heart-attack patients who underwent procedures to unblock heart arteries within 90 minutes improved to 81% in 2008 from 42% in 2005. This is very positive news, but unfortunately, these and many other gains in quality only apply to higher-income populations.
A new section of the report focused on care coordination and transitions of care contains some statistics of particular interest to hospitalists. One statistic shows that the percentage of hospitalized adult patients with heart failure who were given complete written discharge instructions improved to 82.0% in 2008, up from 57.5% in 2005.
It is important to note that this number remains more or less constant across all racial/ethnic divisions. Could part of this improvement be attributed to the growth and success of the hospitalist movement?
Hospitalists know that despite the numbers, a successful transition does not simply include discharge instructions; it is the combination of those instructions, along with coordination with primary care, that prevents avoidable readmissions.
Unfortunately, 15% to 20% of low-income patients have no regular primary-care physician (PCP). If a condition begins to deteriorate, this group often has little choice but to return to the hospital.
In the absence of a PCP, it is the hospitalist who can provide patients with the tools they need to stay healthy after leaving the hospital.
Such assistance can range from ensuring that patients truly understand their discharge instructions to being a resource for future questions. Hospitalists are ahead of the game when it comes to quality and reducing disparities; it is just a matter of the other facets of healthcare catching up.
The National Healthcare Quality & Disparities reports are available at www.ahrq.gov/qual/qrdr10.htm. TH
The Agency for Healthcare Research and Quality (AHRQ) recently released the annual National Healthcare Quality & Disparities Reports. The reports provide in-depth quality information on the overall population and divide this information along such subgroups as race, ethnicity, and education level. The report is more than 200 pages long, but it can be summarized in one sentence: If you are poor, the quality of your healthcare is likely to be poor.
Despite significant quality improvement (QI) in a number of areas, disparities among poor Americans persist. For example, the percentage of heart-attack patients who underwent procedures to unblock heart arteries within 90 minutes improved to 81% in 2008 from 42% in 2005. This is very positive news, but unfortunately, these and many other gains in quality only apply to higher-income populations.
A new section of the report focused on care coordination and transitions of care contains some statistics of particular interest to hospitalists. One statistic shows that the percentage of hospitalized adult patients with heart failure who were given complete written discharge instructions improved to 82.0% in 2008, up from 57.5% in 2005.
It is important to note that this number remains more or less constant across all racial/ethnic divisions. Could part of this improvement be attributed to the growth and success of the hospitalist movement?
Hospitalists know that despite the numbers, a successful transition does not simply include discharge instructions; it is the combination of those instructions, along with coordination with primary care, that prevents avoidable readmissions.
Unfortunately, 15% to 20% of low-income patients have no regular primary-care physician (PCP). If a condition begins to deteriorate, this group often has little choice but to return to the hospital.
In the absence of a PCP, it is the hospitalist who can provide patients with the tools they need to stay healthy after leaving the hospital.
Such assistance can range from ensuring that patients truly understand their discharge instructions to being a resource for future questions. Hospitalists are ahead of the game when it comes to quality and reducing disparities; it is just a matter of the other facets of healthcare catching up.
The National Healthcare Quality & Disparities reports are available at www.ahrq.gov/qual/qrdr10.htm. TH
FPHM Toolkit: Medical Knowledge Modules

FPHM Toolkit: Medical Knowledge Modules
How well do you know quality improvement (QI) and patient safety? Are you ready to prove it?
A new online assessment tool developed by SHM and approved by the American Board of Internal Medicine (ABIM) lets hospitalists put their knowledge to the test—and earn CME and MOC credits at the same time.
SHM’s Quality Improvement and Patient Safety Medical Knowledge Module, now available at www.hospitalmedicine.org, is a 25-question, multiple-choice test that assesses knowledge of topics that increasingly are assigned to hospitalists. The test is geared toward the general hospitalist and not intended exclusively for hospitalists who focus on QI issues, according to Danielle Scheurer, MD, SFHM, physician advisor to SHM and one of the test’s authors. In fact, the content applies to care providers in a hospital-based system, she says.
In addition to assessing the test-taker’s knowledge, the interactive test also educates. Correct answers are followed up with a rationale explaining the answer. If the test-taker chooses an incorrect answer, they are invited to try again; if the second try is also incorrect, the correct answer is highlighted and explained.
The module was developed as an “open book” test, so test-takers are encouraged to use any QI or patient-safety educational resources to verify their answers before submitting them. “The questions in the Medical Knowledge Module were extensively vetted for content and pilot tested for difficulty,” Dr. Scheurer says. “Each question includes a comprehensive discussion of the rationale for the correct and incorrect answers and accompanying references for more information.”
The Medical Knowledge Module costs $65 for SHM members and $100 for nonmembers.
Hospitalists receiving a score of 76% or higher are eligible for MOC credit from ABIM and three AMA PRA Category 1 credits, as designated by Blackwell Futura Media Services.
This is the first in a series of Medical Knowledge Modules. The next is scheduled to be available by midsummer.—BS
FPHM Toolkit: Medical Knowledge Modules
How well do you know quality improvement (QI) and patient safety? Are you ready to prove it?
A new online assessment tool developed by SHM and approved by the American Board of Internal Medicine (ABIM) lets hospitalists put their knowledge to the test—and earn CME and MOC credits at the same time.
SHM’s Quality Improvement and Patient Safety Medical Knowledge Module, now available at www.hospitalmedicine.org, is a 25-question, multiple-choice test that assesses knowledge of topics that increasingly are assigned to hospitalists. The test is geared toward the general hospitalist and not intended exclusively for hospitalists who focus on QI issues, according to Danielle Scheurer, MD, SFHM, physician advisor to SHM and one of the test’s authors. In fact, the content applies to care providers in a hospital-based system, she says.
In addition to assessing the test-taker’s knowledge, the interactive test also educates. Correct answers are followed up with a rationale explaining the answer. If the test-taker chooses an incorrect answer, they are invited to try again; if the second try is also incorrect, the correct answer is highlighted and explained.
The module was developed as an “open book” test, so test-takers are encouraged to use any QI or patient-safety educational resources to verify their answers before submitting them. “The questions in the Medical Knowledge Module were extensively vetted for content and pilot tested for difficulty,” Dr. Scheurer says. “Each question includes a comprehensive discussion of the rationale for the correct and incorrect answers and accompanying references for more information.”
The Medical Knowledge Module costs $65 for SHM members and $100 for nonmembers.
Hospitalists receiving a score of 76% or higher are eligible for MOC credit from ABIM and three AMA PRA Category 1 credits, as designated by Blackwell Futura Media Services.
This is the first in a series of Medical Knowledge Modules. The next is scheduled to be available by midsummer.—BS
FPHM Toolkit: Medical Knowledge Modules
How well do you know quality improvement (QI) and patient safety? Are you ready to prove it?
A new online assessment tool developed by SHM and approved by the American Board of Internal Medicine (ABIM) lets hospitalists put their knowledge to the test—and earn CME and MOC credits at the same time.
SHM’s Quality Improvement and Patient Safety Medical Knowledge Module, now available at www.hospitalmedicine.org, is a 25-question, multiple-choice test that assesses knowledge of topics that increasingly are assigned to hospitalists. The test is geared toward the general hospitalist and not intended exclusively for hospitalists who focus on QI issues, according to Danielle Scheurer, MD, SFHM, physician advisor to SHM and one of the test’s authors. In fact, the content applies to care providers in a hospital-based system, she says.
In addition to assessing the test-taker’s knowledge, the interactive test also educates. Correct answers are followed up with a rationale explaining the answer. If the test-taker chooses an incorrect answer, they are invited to try again; if the second try is also incorrect, the correct answer is highlighted and explained.
The module was developed as an “open book” test, so test-takers are encouraged to use any QI or patient-safety educational resources to verify their answers before submitting them. “The questions in the Medical Knowledge Module were extensively vetted for content and pilot tested for difficulty,” Dr. Scheurer says. “Each question includes a comprehensive discussion of the rationale for the correct and incorrect answers and accompanying references for more information.”
The Medical Knowledge Module costs $65 for SHM members and $100 for nonmembers.
Hospitalists receiving a score of 76% or higher are eligible for MOC credit from ABIM and three AMA PRA Category 1 credits, as designated by Blackwell Futura Media Services.
This is the first in a series of Medical Knowledge Modules. The next is scheduled to be available by midsummer.—BS
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children

Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
The GOP Viewpoint
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
HM DEBATE CON: Should Internal-Medicine Residency Training Be Extended?
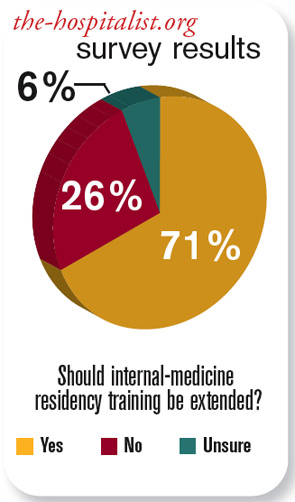

In the 25 years since I completed my internal-medicine residency, 16 of those as a hospitalist, I’ve begun to look at the recent Accreditation Council for Graduate Medical Education (ACGME) program requirements with some concern. It is true that the training I received as a medical resident is vastly different from the training today. I also would not suggest returning to the hours I worked as a resident, either! After all, there are only so many night shifts in a hospitalist, and if not properly managed, those hours can be used up before age 50.
The present 36-month training program covers the clinical conditions and procedures outlined in SHM’s core competency recommendations.1 It is the section of training concerning competency in health systems that I believe requires additional time in training.
What I did as a hospitalist 16 years ago is vastly different from what I do now. In 1995, the focus was more clinically oriented. Fast-forward to the present, and we all are aware of what we are being asked to do. In addition to clinical expertise in care of patients, our hospital administrators rely on hospitalists to be the stewards of patient safety, quality, throughput, information technology, and comanagement. I think we all would agree that nowhere in our training did we learn the skill set to perform these additional duties.
Working as an HM chief and being responsible for five programs and more than 50 hospitalists, I would have difficulty trying to structure additional training in early employment. Community hospitalist programs usually are understaffed and overworked, and many lack the structure to offer on-the-job training. Certainly, academic hospitalist programs and the larger hospitalist companies would have such infrastructure in place to achieve these additional competencies.
What is being asked of HM today raises the question of whether we are entering a stage for serious consideration of fellowship programs. There are few HM-specific fellowship programs out there. Perhaps we are reaching that crucial junction where our academic colleagues need to think about this.
Historically, when we look at emergency medicine, the early ED doctors came from other disciplines. Our trajectory and acceleration in growth of our field will require us to think about this sooner rather than later.
I consider the American Board of Internal Medicine’s (ABIM) Focused Practice in Hospital Medicine (FPHM) the starting point for vigorous debate about movement towards HM fellowship programs. I would suggest that the time is right for SHM to consider developing a task force to address fellowship programs. TH
Dr. Atchley is chief of the division of hospital medicine at Sentara Medical Group in Norfolk, Va. He is a former SHM board member and is a Team Hospitalist member.
Reference
- Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1 Suppl 1:48-56.
In the 25 years since I completed my internal-medicine residency, 16 of those as a hospitalist, I’ve begun to look at the recent Accreditation Council for Graduate Medical Education (ACGME) program requirements with some concern. It is true that the training I received as a medical resident is vastly different from the training today. I also would not suggest returning to the hours I worked as a resident, either! After all, there are only so many night shifts in a hospitalist, and if not properly managed, those hours can be used up before age 50.
The present 36-month training program covers the clinical conditions and procedures outlined in SHM’s core competency recommendations.1 It is the section of training concerning competency in health systems that I believe requires additional time in training.
What I did as a hospitalist 16 years ago is vastly different from what I do now. In 1995, the focus was more clinically oriented. Fast-forward to the present, and we all are aware of what we are being asked to do. In addition to clinical expertise in care of patients, our hospital administrators rely on hospitalists to be the stewards of patient safety, quality, throughput, information technology, and comanagement. I think we all would agree that nowhere in our training did we learn the skill set to perform these additional duties.
Working as an HM chief and being responsible for five programs and more than 50 hospitalists, I would have difficulty trying to structure additional training in early employment. Community hospitalist programs usually are understaffed and overworked, and many lack the structure to offer on-the-job training. Certainly, academic hospitalist programs and the larger hospitalist companies would have such infrastructure in place to achieve these additional competencies.
What is being asked of HM today raises the question of whether we are entering a stage for serious consideration of fellowship programs. There are few HM-specific fellowship programs out there. Perhaps we are reaching that crucial junction where our academic colleagues need to think about this.
Historically, when we look at emergency medicine, the early ED doctors came from other disciplines. Our trajectory and acceleration in growth of our field will require us to think about this sooner rather than later.
I consider the American Board of Internal Medicine’s (ABIM) Focused Practice in Hospital Medicine (FPHM) the starting point for vigorous debate about movement towards HM fellowship programs. I would suggest that the time is right for SHM to consider developing a task force to address fellowship programs. TH
Dr. Atchley is chief of the division of hospital medicine at Sentara Medical Group in Norfolk, Va. He is a former SHM board member and is a Team Hospitalist member.
Reference
- Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1 Suppl 1:48-56.
In the 25 years since I completed my internal-medicine residency, 16 of those as a hospitalist, I’ve begun to look at the recent Accreditation Council for Graduate Medical Education (ACGME) program requirements with some concern. It is true that the training I received as a medical resident is vastly different from the training today. I also would not suggest returning to the hours I worked as a resident, either! After all, there are only so many night shifts in a hospitalist, and if not properly managed, those hours can be used up before age 50.
The present 36-month training program covers the clinical conditions and procedures outlined in SHM’s core competency recommendations.1 It is the section of training concerning competency in health systems that I believe requires additional time in training.
What I did as a hospitalist 16 years ago is vastly different from what I do now. In 1995, the focus was more clinically oriented. Fast-forward to the present, and we all are aware of what we are being asked to do. In addition to clinical expertise in care of patients, our hospital administrators rely on hospitalists to be the stewards of patient safety, quality, throughput, information technology, and comanagement. I think we all would agree that nowhere in our training did we learn the skill set to perform these additional duties.
Working as an HM chief and being responsible for five programs and more than 50 hospitalists, I would have difficulty trying to structure additional training in early employment. Community hospitalist programs usually are understaffed and overworked, and many lack the structure to offer on-the-job training. Certainly, academic hospitalist programs and the larger hospitalist companies would have such infrastructure in place to achieve these additional competencies.
What is being asked of HM today raises the question of whether we are entering a stage for serious consideration of fellowship programs. There are few HM-specific fellowship programs out there. Perhaps we are reaching that crucial junction where our academic colleagues need to think about this.
Historically, when we look at emergency medicine, the early ED doctors came from other disciplines. Our trajectory and acceleration in growth of our field will require us to think about this sooner rather than later.
I consider the American Board of Internal Medicine’s (ABIM) Focused Practice in Hospital Medicine (FPHM) the starting point for vigorous debate about movement towards HM fellowship programs. I would suggest that the time is right for SHM to consider developing a task force to address fellowship programs. TH
Dr. Atchley is chief of the division of hospital medicine at Sentara Medical Group in Norfolk, Va. He is a former SHM board member and is a Team Hospitalist member.
Reference
- Dressler DD, Pistoria MJ, Budnitz TL, McKean SC, Amin AN. Core competencies in hospital medicine: development and methodology. J Hosp Med. 2006;1 Suppl 1:48-56.