User login
Letters to the Editor
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
When Should a Patient with Ascites Receive Spontaneous Bacterial Peritonitis (SBP) Prophylaxis?
Case
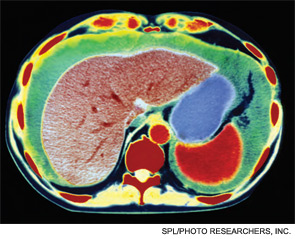
A 54-year-old man with end-stage liver disease (ESLD) and no prior history of spontaneous bacterial peritonitis (SBP) presents with increasing shortness of breath and abdominal distention. He is admitted for worsening volume overload. The patient reveals that he has not been compliant with his diuretics. On the day of admission, a large-volume paracentesis is performed. Results are significant for a white blood cell count of 150 cells/mm3 and a total protein of 0.9 g/ul. The patient is started on furosemide and spironolactone, and his symptoms significantly improve throughout his hospitalization. His medications are reconciled on the day of discharge. He is not on any antibiotics for SBP prophylaxis; should he be? In general, which patients with ascites should receive SBP prophylaxis?
Overview
Spontaneous bacterial peritonitis is an infection of ascitic fluid that occurs in the absence of an indentified intra-abdominal source of infection or inflammation, i.e., perforation or abscess.1 It is diagnosed when the polymorphonuclear cell (PMN) count in the ascitic fluid is equal to or greater than 250 cells/mm3, with or without positive cultures.
SBP is a significant cause of morbidity and mortality in patients with cirrhosis, with the mortality rate approaching 20% to 40%.2 Of the 32% to 34% of cirrhotic patients who present with, or develop, a bacterial infection during their hospitalization, 25% are due to SBP.1 Changes in gut motility, mucosal defense, and microflora allow for translocation of bacteria into enteric lymph nodes and the bloodstream, resulting in seeding of the peritoneal fluid and SBP.1 Alterations in both systemic and localized immune defenses, both of which are reduced in patients with liver disease, also play a role in SBP pathogenesis (see Table 1, p. 41).
Current evidence supports the use of a third-generation cephalosporin or amoxicillin/clavulanate for initial treatment of SBP, as most infections are caused by gram-negative bacilli, in particular E. coli (see Table 2 on p. 41 and Table 3 on p. 42).1 Alternatively, an oral or intravenous fluoroquinolone could be used if the prevalence of fluoroquinolone-resistant organisms is low.1
Due to the frequency and morbidity associated with SBP, there is great interest in preventing it. However, the use of prophylactic antibiotics needs to be restricted to patients who are at highest risk of developing SBP. According to numerous studies, patients at high risk for SBP include:
- Patients with a prior SBP history;
- Patients admitted with a gastrointestinal bleed; and
- Patients with low total protein content in their ascitic fluid (defined as <1.5 g/ul).1
SBP History
Spontaneous bacterial peritonitis portends bad outcomes. The one-year mortality rate after an episode of SBP is 30% to 50%.1 Furthermore, patients who have recovered from a previous episode of SBP have a 70% chance of developing another episode of SBP in that year.1,2 In one study, norfloxacin was shown to decrease the one-year risk of SBP to 20% from 68% in patients with a history of SBP.3 Additionally, the likelihood of developing SBP from gram-negative bacilli was reduced to 3% from 60%. In order to be efficacious, norfloxacin must be given daily. When fluoroquinolones are prescribed less than once daily, there is a higher rate of fluoroquinolone resistant organisms in the stool.1
Though once-daily dosing of norfloxacin is recommended to decrease the promotion of resistant organisms in prophylaxis against SBP, ciprofloxacin once weekly is acceptable. In a group of patients with low ascitic protein content, with or without a history of SBP, weekly ciprofloxacin has been shown to decrease SBP incidence to 4% from 22% at six months.4 In regard to length of treatment, recommendations are to continue prophylactic antibiotics until resolution of ascites, the patient receives a transplant, or the patient passes away.1
Saab et al studied the impact of oral antibiotic prophylaxis in patients with advanced liver disease on morbidity and mortality.5 The authors examined prospective, randomized, controlled trials that compared high-risk cirrhotic patients receiving oral antibiotic prophylaxis for SBP with groups receiving placebo or no intervention. Eight studies totaling 647 patients were included in the analysis.
The overall mortality rate for patients treated with SBP prophylaxis was 16%, compared with 25% for the control group. Groups treated with prophylactic antibiotics also had a lower incidence of all infections (6.2% vs. 22.2% in the control groups). Additionally, a survival benefit was seen at three months in the group that received prophylactic antibiotics.
The absolute risk reduction with prophylactic antibiotics for primary prevention of SBP was 8% with a number needed to treat of 13. The incidence of gastrointestinal (GI) bleeding, renal failure, and hepatic failure did not significantly differ between treatment and control groups. Thus, survival benefit is thought to be related to the reduced incidence of infections in the group receiving prophylactic antibiotics.5
History of GI Bleeding
The incidence of developing SBP in cirrhotics with an active GI bleed is anywhere from 20% to 45%.1,2 For those with ascites of any etiology and a GI bleed, the incidence can be as high as 60%.5 In general, bacterial infections are frequently diagnosed in patients with cirrhosis and GI bleeding, and have been documented in 22% of these patients within the first 48 hours after admission. According to several studies, that percentage can reach as high as 35% to 66% within seven to 14 days of admission.6 A seven-day course of antibiotics, or antibiotics until discharge, is generally acceptable for SBP prophylaxis in the setting of ascites and GI bleeding (see Table 2, right).1
Bernard et al performed a meta-analysis of five trials to assess the efficacy of antibiotic prophylaxis in the prevention of infections and effect on survival in patients with cirrhosis and GI bleeding. Out of 534 patients, 264 were treated with antibiotics between four and 10 days, and 270 did not receive any antibiotics.
The endpoints of the study were infection, bacteremia and/or SBP; incidence of SBP; and death. Antibiotic prophylaxis not only increased the mean survival rate by 9.1%, but also increased the mean percentage of patients free of infection (32% improvement); bacteremia and/or SBP (19% improvement); and SBP (7% improvement).7
Low Ascitic Fluid Protein
Of the three major risk factors for SBP, ascitic fluid protein content is the most debated. Guarner et al studied the risk of first community-acquired SBP in cirrhotics with low ascitic fluid protein.2 Patients were seen immediately after discharge from the hospital and at two- to three-month intervals. Of the 109 hospitalized patients, 23 (21%) developed SBP, nine of which developed SBP during their hospitalization. The one-year cumulative probability of SBP in these patients with low ascitic fluid protein levels was 35%.
During this study, the authors also looked at 20 different patient variables on admission and found that two parameters—high bilirubin (>3.2mg/dL) and low platelet count (<98,000 cells/ul)—were associated with an increased risk of SBP. This is consistent with studies showing that patients with higher Model for End-Stage Liver Disease (MELD) or Child-Pugh scores, indicating more severe liver disease, are at increased risk for SBP. This likely is the reason SBP prophylaxis is recommended for patients with an elevated bilirubin, and higher Child-Pugh scores, by the American Association for the Study of Liver Disease (see Table 2, p. 41).
Runyon et al showed that 15% of patients with low ascitic fluid protein developed SBP during their hospitalization, as compared with 2% of patients with ascitic fluid levels greater than 1 g/dl.8 A randomized, non-placebo-controlled trial by Navasa et al evaluating 70 cirrhotic patients with low ascitic ascitic protein levels showed a lower probability of developing SBP in the group placed on SBP prophylaxis with norfloxacin (5% vs. 31%).9 Six-month mortality rate was also lower (19% vs. 36%).
In contrast to the previous studies, Grothe et al found that the presence of SBP was not related to ascitic protein content.10 Given conflicting studies, controversy still remains on whether patients with low ascitic protein should receive long-term prophylactic antibiotics.
Antibiotic Drawbacks
The consensus in the literature is that patients with ascites who are admitted with a GI bleed, or those with a history of SBP, should be placed on SBP prophylaxis. However, patients placed on long-term antibiotics are at risk for developing bacterial resistance. Bacterial resistance in cultures taken from cirrhotic patients with SBP has increased over the last decade, particularly in gram-negative bacteria.5 Patients who receive antibiotics in the pre-transplant setting also are at risk for post-transplant fungal infections.
Additionally, the antibiotic of choice for SBP prophylaxis is typically a fluoroquinolone, which can be expensive. However, numerous studies have shown that the cost of initiating prophylactic therapy for SBP in patients with a prior episode of SBP can be cheaper than treating SBP after diagnosis.2
Back to the Case
Our patient’s paracentesis was negative for SBP. Additionally, he does not have a history of SBP, nor does he have an active GI bleed. His only possible indication for SBP prophylaxis is low ascitic protein concentration. His electrolytes were all within normal limits. Additionally, total bilirubin was only slightly elevated at 2.3 mg/dL.
Based on the American Association for the Study of Liver Diseases guidelines, the patient was not started on SBP prophylaxis. Additionally, given his history of medication noncompliance, there is concern that he might not take the antibiotics as prescribed, thus leading to the development of bacterial resistance and more serious infections in the future.
Bottom Line
Patients with ascites and a prior episode of SBP, and those admitted to the hospital for GI bleeding, should be placed on SBP prophylaxis. SBP prophylaxis for low protein ascitic fluid remains controversial but is recommended by the American Association for the Study of Liver Diseases. TH
Dr. del Pino Jones is a hospitalist at the University of Colorado Denver.
References
- Ghassemi S, Garcia-Tsao G. Prevention and treatment of infections in patients with cirrhosis. Best Pract Res Clin Gastroenterol. 2007;21(1):77-93.
- Guarner C, Solà R, Soriono G, et al. Risk of a first community-acquired spontaneous bacterial peritonitis in cirrhotics with low ascitic fluid protein levels. Gastroenterology. 1999;117(2):414-419.
- Ginés P, Rimola A, Planas R, et al. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo-controlled trial. Hepatology. 1990;12(4 Pt 1):716-724.
- Rolachon A, Cordier L, Bacq Y, et al. Ciprofloxacin and long-term prevention of spontaneous bacterial peritonitis: results of a prospective controlled trial. Hepatology. 1995;22(4 Pt 1):1171-1174.
- Saab S, Hernandez J, Chi AC, Tong MJ. Oral antibiotic prophylaxis reduces spontaneous bacterial peritonitis occurrence and improves short-term survival in cirrhosis: a meta-analysis. Am J Gastroenterol. 2009;104(4):993-1001.
- Deschênes M, Villeneuve J. Risk factors for the development of bacterial infections in hospitalized patients with cirrhosis. Am J Gastroenterol. 1999;94(8):2193-2197.
- Bernard B, Grangé J, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology. 1999;29(6):1655-1661.
- Runyon B. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology. 1986;91(6):1343-1346.
- Navasa M, Fernandez J, Montoliu S, et al. Randomized, double-blind, placebo-controlled trial evaluating norfloxacin in the primary prophylaxis of spontaneous bacterial peritonitis in cirrhotics with renal impairment, hyponatremia or severe liver failure. J Hepatol. 2006;44(Supp2):S51.
- Grothe W, Lottere E, Fleig W. Factors predictive for spontaneous bacterial peritonitis (SBP) under routine inpatient conditions in patients with cirrhosis: a prospective multicenter trial. J Hepatol. 1990;34(4):547.
Case
A 54-year-old man with end-stage liver disease (ESLD) and no prior history of spontaneous bacterial peritonitis (SBP) presents with increasing shortness of breath and abdominal distention. He is admitted for worsening volume overload. The patient reveals that he has not been compliant with his diuretics. On the day of admission, a large-volume paracentesis is performed. Results are significant for a white blood cell count of 150 cells/mm3 and a total protein of 0.9 g/ul. The patient is started on furosemide and spironolactone, and his symptoms significantly improve throughout his hospitalization. His medications are reconciled on the day of discharge. He is not on any antibiotics for SBP prophylaxis; should he be? In general, which patients with ascites should receive SBP prophylaxis?
Overview
Spontaneous bacterial peritonitis is an infection of ascitic fluid that occurs in the absence of an indentified intra-abdominal source of infection or inflammation, i.e., perforation or abscess.1 It is diagnosed when the polymorphonuclear cell (PMN) count in the ascitic fluid is equal to or greater than 250 cells/mm3, with or without positive cultures.
SBP is a significant cause of morbidity and mortality in patients with cirrhosis, with the mortality rate approaching 20% to 40%.2 Of the 32% to 34% of cirrhotic patients who present with, or develop, a bacterial infection during their hospitalization, 25% are due to SBP.1 Changes in gut motility, mucosal defense, and microflora allow for translocation of bacteria into enteric lymph nodes and the bloodstream, resulting in seeding of the peritoneal fluid and SBP.1 Alterations in both systemic and localized immune defenses, both of which are reduced in patients with liver disease, also play a role in SBP pathogenesis (see Table 1, p. 41).
Current evidence supports the use of a third-generation cephalosporin or amoxicillin/clavulanate for initial treatment of SBP, as most infections are caused by gram-negative bacilli, in particular E. coli (see Table 2 on p. 41 and Table 3 on p. 42).1 Alternatively, an oral or intravenous fluoroquinolone could be used if the prevalence of fluoroquinolone-resistant organisms is low.1
Due to the frequency and morbidity associated with SBP, there is great interest in preventing it. However, the use of prophylactic antibiotics needs to be restricted to patients who are at highest risk of developing SBP. According to numerous studies, patients at high risk for SBP include:
- Patients with a prior SBP history;
- Patients admitted with a gastrointestinal bleed; and
- Patients with low total protein content in their ascitic fluid (defined as <1.5 g/ul).1
SBP History
Spontaneous bacterial peritonitis portends bad outcomes. The one-year mortality rate after an episode of SBP is 30% to 50%.1 Furthermore, patients who have recovered from a previous episode of SBP have a 70% chance of developing another episode of SBP in that year.1,2 In one study, norfloxacin was shown to decrease the one-year risk of SBP to 20% from 68% in patients with a history of SBP.3 Additionally, the likelihood of developing SBP from gram-negative bacilli was reduced to 3% from 60%. In order to be efficacious, norfloxacin must be given daily. When fluoroquinolones are prescribed less than once daily, there is a higher rate of fluoroquinolone resistant organisms in the stool.1
Though once-daily dosing of norfloxacin is recommended to decrease the promotion of resistant organisms in prophylaxis against SBP, ciprofloxacin once weekly is acceptable. In a group of patients with low ascitic protein content, with or without a history of SBP, weekly ciprofloxacin has been shown to decrease SBP incidence to 4% from 22% at six months.4 In regard to length of treatment, recommendations are to continue prophylactic antibiotics until resolution of ascites, the patient receives a transplant, or the patient passes away.1
Saab et al studied the impact of oral antibiotic prophylaxis in patients with advanced liver disease on morbidity and mortality.5 The authors examined prospective, randomized, controlled trials that compared high-risk cirrhotic patients receiving oral antibiotic prophylaxis for SBP with groups receiving placebo or no intervention. Eight studies totaling 647 patients were included in the analysis.
The overall mortality rate for patients treated with SBP prophylaxis was 16%, compared with 25% for the control group. Groups treated with prophylactic antibiotics also had a lower incidence of all infections (6.2% vs. 22.2% in the control groups). Additionally, a survival benefit was seen at three months in the group that received prophylactic antibiotics.
The absolute risk reduction with prophylactic antibiotics for primary prevention of SBP was 8% with a number needed to treat of 13. The incidence of gastrointestinal (GI) bleeding, renal failure, and hepatic failure did not significantly differ between treatment and control groups. Thus, survival benefit is thought to be related to the reduced incidence of infections in the group receiving prophylactic antibiotics.5
History of GI Bleeding
The incidence of developing SBP in cirrhotics with an active GI bleed is anywhere from 20% to 45%.1,2 For those with ascites of any etiology and a GI bleed, the incidence can be as high as 60%.5 In general, bacterial infections are frequently diagnosed in patients with cirrhosis and GI bleeding, and have been documented in 22% of these patients within the first 48 hours after admission. According to several studies, that percentage can reach as high as 35% to 66% within seven to 14 days of admission.6 A seven-day course of antibiotics, or antibiotics until discharge, is generally acceptable for SBP prophylaxis in the setting of ascites and GI bleeding (see Table 2, right).1
Bernard et al performed a meta-analysis of five trials to assess the efficacy of antibiotic prophylaxis in the prevention of infections and effect on survival in patients with cirrhosis and GI bleeding. Out of 534 patients, 264 were treated with antibiotics between four and 10 days, and 270 did not receive any antibiotics.
The endpoints of the study were infection, bacteremia and/or SBP; incidence of SBP; and death. Antibiotic prophylaxis not only increased the mean survival rate by 9.1%, but also increased the mean percentage of patients free of infection (32% improvement); bacteremia and/or SBP (19% improvement); and SBP (7% improvement).7
Low Ascitic Fluid Protein
Of the three major risk factors for SBP, ascitic fluid protein content is the most debated. Guarner et al studied the risk of first community-acquired SBP in cirrhotics with low ascitic fluid protein.2 Patients were seen immediately after discharge from the hospital and at two- to three-month intervals. Of the 109 hospitalized patients, 23 (21%) developed SBP, nine of which developed SBP during their hospitalization. The one-year cumulative probability of SBP in these patients with low ascitic fluid protein levels was 35%.
During this study, the authors also looked at 20 different patient variables on admission and found that two parameters—high bilirubin (>3.2mg/dL) and low platelet count (<98,000 cells/ul)—were associated with an increased risk of SBP. This is consistent with studies showing that patients with higher Model for End-Stage Liver Disease (MELD) or Child-Pugh scores, indicating more severe liver disease, are at increased risk for SBP. This likely is the reason SBP prophylaxis is recommended for patients with an elevated bilirubin, and higher Child-Pugh scores, by the American Association for the Study of Liver Disease (see Table 2, p. 41).
Runyon et al showed that 15% of patients with low ascitic fluid protein developed SBP during their hospitalization, as compared with 2% of patients with ascitic fluid levels greater than 1 g/dl.8 A randomized, non-placebo-controlled trial by Navasa et al evaluating 70 cirrhotic patients with low ascitic ascitic protein levels showed a lower probability of developing SBP in the group placed on SBP prophylaxis with norfloxacin (5% vs. 31%).9 Six-month mortality rate was also lower (19% vs. 36%).
In contrast to the previous studies, Grothe et al found that the presence of SBP was not related to ascitic protein content.10 Given conflicting studies, controversy still remains on whether patients with low ascitic protein should receive long-term prophylactic antibiotics.
Antibiotic Drawbacks
The consensus in the literature is that patients with ascites who are admitted with a GI bleed, or those with a history of SBP, should be placed on SBP prophylaxis. However, patients placed on long-term antibiotics are at risk for developing bacterial resistance. Bacterial resistance in cultures taken from cirrhotic patients with SBP has increased over the last decade, particularly in gram-negative bacteria.5 Patients who receive antibiotics in the pre-transplant setting also are at risk for post-transplant fungal infections.
Additionally, the antibiotic of choice for SBP prophylaxis is typically a fluoroquinolone, which can be expensive. However, numerous studies have shown that the cost of initiating prophylactic therapy for SBP in patients with a prior episode of SBP can be cheaper than treating SBP after diagnosis.2
Back to the Case
Our patient’s paracentesis was negative for SBP. Additionally, he does not have a history of SBP, nor does he have an active GI bleed. His only possible indication for SBP prophylaxis is low ascitic protein concentration. His electrolytes were all within normal limits. Additionally, total bilirubin was only slightly elevated at 2.3 mg/dL.
Based on the American Association for the Study of Liver Diseases guidelines, the patient was not started on SBP prophylaxis. Additionally, given his history of medication noncompliance, there is concern that he might not take the antibiotics as prescribed, thus leading to the development of bacterial resistance and more serious infections in the future.
Bottom Line
Patients with ascites and a prior episode of SBP, and those admitted to the hospital for GI bleeding, should be placed on SBP prophylaxis. SBP prophylaxis for low protein ascitic fluid remains controversial but is recommended by the American Association for the Study of Liver Diseases. TH
Dr. del Pino Jones is a hospitalist at the University of Colorado Denver.
References
- Ghassemi S, Garcia-Tsao G. Prevention and treatment of infections in patients with cirrhosis. Best Pract Res Clin Gastroenterol. 2007;21(1):77-93.
- Guarner C, Solà R, Soriono G, et al. Risk of a first community-acquired spontaneous bacterial peritonitis in cirrhotics with low ascitic fluid protein levels. Gastroenterology. 1999;117(2):414-419.
- Ginés P, Rimola A, Planas R, et al. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo-controlled trial. Hepatology. 1990;12(4 Pt 1):716-724.
- Rolachon A, Cordier L, Bacq Y, et al. Ciprofloxacin and long-term prevention of spontaneous bacterial peritonitis: results of a prospective controlled trial. Hepatology. 1995;22(4 Pt 1):1171-1174.
- Saab S, Hernandez J, Chi AC, Tong MJ. Oral antibiotic prophylaxis reduces spontaneous bacterial peritonitis occurrence and improves short-term survival in cirrhosis: a meta-analysis. Am J Gastroenterol. 2009;104(4):993-1001.
- Deschênes M, Villeneuve J. Risk factors for the development of bacterial infections in hospitalized patients with cirrhosis. Am J Gastroenterol. 1999;94(8):2193-2197.
- Bernard B, Grangé J, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology. 1999;29(6):1655-1661.
- Runyon B. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology. 1986;91(6):1343-1346.
- Navasa M, Fernandez J, Montoliu S, et al. Randomized, double-blind, placebo-controlled trial evaluating norfloxacin in the primary prophylaxis of spontaneous bacterial peritonitis in cirrhotics with renal impairment, hyponatremia or severe liver failure. J Hepatol. 2006;44(Supp2):S51.
- Grothe W, Lottere E, Fleig W. Factors predictive for spontaneous bacterial peritonitis (SBP) under routine inpatient conditions in patients with cirrhosis: a prospective multicenter trial. J Hepatol. 1990;34(4):547.
Case
A 54-year-old man with end-stage liver disease (ESLD) and no prior history of spontaneous bacterial peritonitis (SBP) presents with increasing shortness of breath and abdominal distention. He is admitted for worsening volume overload. The patient reveals that he has not been compliant with his diuretics. On the day of admission, a large-volume paracentesis is performed. Results are significant for a white blood cell count of 150 cells/mm3 and a total protein of 0.9 g/ul. The patient is started on furosemide and spironolactone, and his symptoms significantly improve throughout his hospitalization. His medications are reconciled on the day of discharge. He is not on any antibiotics for SBP prophylaxis; should he be? In general, which patients with ascites should receive SBP prophylaxis?
Overview
Spontaneous bacterial peritonitis is an infection of ascitic fluid that occurs in the absence of an indentified intra-abdominal source of infection or inflammation, i.e., perforation or abscess.1 It is diagnosed when the polymorphonuclear cell (PMN) count in the ascitic fluid is equal to or greater than 250 cells/mm3, with or without positive cultures.
SBP is a significant cause of morbidity and mortality in patients with cirrhosis, with the mortality rate approaching 20% to 40%.2 Of the 32% to 34% of cirrhotic patients who present with, or develop, a bacterial infection during their hospitalization, 25% are due to SBP.1 Changes in gut motility, mucosal defense, and microflora allow for translocation of bacteria into enteric lymph nodes and the bloodstream, resulting in seeding of the peritoneal fluid and SBP.1 Alterations in both systemic and localized immune defenses, both of which are reduced in patients with liver disease, also play a role in SBP pathogenesis (see Table 1, p. 41).
Current evidence supports the use of a third-generation cephalosporin or amoxicillin/clavulanate for initial treatment of SBP, as most infections are caused by gram-negative bacilli, in particular E. coli (see Table 2 on p. 41 and Table 3 on p. 42).1 Alternatively, an oral or intravenous fluoroquinolone could be used if the prevalence of fluoroquinolone-resistant organisms is low.1
Due to the frequency and morbidity associated with SBP, there is great interest in preventing it. However, the use of prophylactic antibiotics needs to be restricted to patients who are at highest risk of developing SBP. According to numerous studies, patients at high risk for SBP include:
- Patients with a prior SBP history;
- Patients admitted with a gastrointestinal bleed; and
- Patients with low total protein content in their ascitic fluid (defined as <1.5 g/ul).1
SBP History
Spontaneous bacterial peritonitis portends bad outcomes. The one-year mortality rate after an episode of SBP is 30% to 50%.1 Furthermore, patients who have recovered from a previous episode of SBP have a 70% chance of developing another episode of SBP in that year.1,2 In one study, norfloxacin was shown to decrease the one-year risk of SBP to 20% from 68% in patients with a history of SBP.3 Additionally, the likelihood of developing SBP from gram-negative bacilli was reduced to 3% from 60%. In order to be efficacious, norfloxacin must be given daily. When fluoroquinolones are prescribed less than once daily, there is a higher rate of fluoroquinolone resistant organisms in the stool.1
Though once-daily dosing of norfloxacin is recommended to decrease the promotion of resistant organisms in prophylaxis against SBP, ciprofloxacin once weekly is acceptable. In a group of patients with low ascitic protein content, with or without a history of SBP, weekly ciprofloxacin has been shown to decrease SBP incidence to 4% from 22% at six months.4 In regard to length of treatment, recommendations are to continue prophylactic antibiotics until resolution of ascites, the patient receives a transplant, or the patient passes away.1
Saab et al studied the impact of oral antibiotic prophylaxis in patients with advanced liver disease on morbidity and mortality.5 The authors examined prospective, randomized, controlled trials that compared high-risk cirrhotic patients receiving oral antibiotic prophylaxis for SBP with groups receiving placebo or no intervention. Eight studies totaling 647 patients were included in the analysis.
The overall mortality rate for patients treated with SBP prophylaxis was 16%, compared with 25% for the control group. Groups treated with prophylactic antibiotics also had a lower incidence of all infections (6.2% vs. 22.2% in the control groups). Additionally, a survival benefit was seen at three months in the group that received prophylactic antibiotics.
The absolute risk reduction with prophylactic antibiotics for primary prevention of SBP was 8% with a number needed to treat of 13. The incidence of gastrointestinal (GI) bleeding, renal failure, and hepatic failure did not significantly differ between treatment and control groups. Thus, survival benefit is thought to be related to the reduced incidence of infections in the group receiving prophylactic antibiotics.5
History of GI Bleeding
The incidence of developing SBP in cirrhotics with an active GI bleed is anywhere from 20% to 45%.1,2 For those with ascites of any etiology and a GI bleed, the incidence can be as high as 60%.5 In general, bacterial infections are frequently diagnosed in patients with cirrhosis and GI bleeding, and have been documented in 22% of these patients within the first 48 hours after admission. According to several studies, that percentage can reach as high as 35% to 66% within seven to 14 days of admission.6 A seven-day course of antibiotics, or antibiotics until discharge, is generally acceptable for SBP prophylaxis in the setting of ascites and GI bleeding (see Table 2, right).1
Bernard et al performed a meta-analysis of five trials to assess the efficacy of antibiotic prophylaxis in the prevention of infections and effect on survival in patients with cirrhosis and GI bleeding. Out of 534 patients, 264 were treated with antibiotics between four and 10 days, and 270 did not receive any antibiotics.
The endpoints of the study were infection, bacteremia and/or SBP; incidence of SBP; and death. Antibiotic prophylaxis not only increased the mean survival rate by 9.1%, but also increased the mean percentage of patients free of infection (32% improvement); bacteremia and/or SBP (19% improvement); and SBP (7% improvement).7
Low Ascitic Fluid Protein
Of the three major risk factors for SBP, ascitic fluid protein content is the most debated. Guarner et al studied the risk of first community-acquired SBP in cirrhotics with low ascitic fluid protein.2 Patients were seen immediately after discharge from the hospital and at two- to three-month intervals. Of the 109 hospitalized patients, 23 (21%) developed SBP, nine of which developed SBP during their hospitalization. The one-year cumulative probability of SBP in these patients with low ascitic fluid protein levels was 35%.
During this study, the authors also looked at 20 different patient variables on admission and found that two parameters—high bilirubin (>3.2mg/dL) and low platelet count (<98,000 cells/ul)—were associated with an increased risk of SBP. This is consistent with studies showing that patients with higher Model for End-Stage Liver Disease (MELD) or Child-Pugh scores, indicating more severe liver disease, are at increased risk for SBP. This likely is the reason SBP prophylaxis is recommended for patients with an elevated bilirubin, and higher Child-Pugh scores, by the American Association for the Study of Liver Disease (see Table 2, p. 41).
Runyon et al showed that 15% of patients with low ascitic fluid protein developed SBP during their hospitalization, as compared with 2% of patients with ascitic fluid levels greater than 1 g/dl.8 A randomized, non-placebo-controlled trial by Navasa et al evaluating 70 cirrhotic patients with low ascitic ascitic protein levels showed a lower probability of developing SBP in the group placed on SBP prophylaxis with norfloxacin (5% vs. 31%).9 Six-month mortality rate was also lower (19% vs. 36%).
In contrast to the previous studies, Grothe et al found that the presence of SBP was not related to ascitic protein content.10 Given conflicting studies, controversy still remains on whether patients with low ascitic protein should receive long-term prophylactic antibiotics.
Antibiotic Drawbacks
The consensus in the literature is that patients with ascites who are admitted with a GI bleed, or those with a history of SBP, should be placed on SBP prophylaxis. However, patients placed on long-term antibiotics are at risk for developing bacterial resistance. Bacterial resistance in cultures taken from cirrhotic patients with SBP has increased over the last decade, particularly in gram-negative bacteria.5 Patients who receive antibiotics in the pre-transplant setting also are at risk for post-transplant fungal infections.
Additionally, the antibiotic of choice for SBP prophylaxis is typically a fluoroquinolone, which can be expensive. However, numerous studies have shown that the cost of initiating prophylactic therapy for SBP in patients with a prior episode of SBP can be cheaper than treating SBP after diagnosis.2
Back to the Case
Our patient’s paracentesis was negative for SBP. Additionally, he does not have a history of SBP, nor does he have an active GI bleed. His only possible indication for SBP prophylaxis is low ascitic protein concentration. His electrolytes were all within normal limits. Additionally, total bilirubin was only slightly elevated at 2.3 mg/dL.
Based on the American Association for the Study of Liver Diseases guidelines, the patient was not started on SBP prophylaxis. Additionally, given his history of medication noncompliance, there is concern that he might not take the antibiotics as prescribed, thus leading to the development of bacterial resistance and more serious infections in the future.
Bottom Line
Patients with ascites and a prior episode of SBP, and those admitted to the hospital for GI bleeding, should be placed on SBP prophylaxis. SBP prophylaxis for low protein ascitic fluid remains controversial but is recommended by the American Association for the Study of Liver Diseases. TH
Dr. del Pino Jones is a hospitalist at the University of Colorado Denver.
References
- Ghassemi S, Garcia-Tsao G. Prevention and treatment of infections in patients with cirrhosis. Best Pract Res Clin Gastroenterol. 2007;21(1):77-93.
- Guarner C, Solà R, Soriono G, et al. Risk of a first community-acquired spontaneous bacterial peritonitis in cirrhotics with low ascitic fluid protein levels. Gastroenterology. 1999;117(2):414-419.
- Ginés P, Rimola A, Planas R, et al. Norfloxacin prevents spontaneous bacterial peritonitis recurrence in cirrhosis: results of a double-blind, placebo-controlled trial. Hepatology. 1990;12(4 Pt 1):716-724.
- Rolachon A, Cordier L, Bacq Y, et al. Ciprofloxacin and long-term prevention of spontaneous bacterial peritonitis: results of a prospective controlled trial. Hepatology. 1995;22(4 Pt 1):1171-1174.
- Saab S, Hernandez J, Chi AC, Tong MJ. Oral antibiotic prophylaxis reduces spontaneous bacterial peritonitis occurrence and improves short-term survival in cirrhosis: a meta-analysis. Am J Gastroenterol. 2009;104(4):993-1001.
- Deschênes M, Villeneuve J. Risk factors for the development of bacterial infections in hospitalized patients with cirrhosis. Am J Gastroenterol. 1999;94(8):2193-2197.
- Bernard B, Grangé J, Khac EN, Amiot X, Opolon P, Poynard T. Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis. Hepatology. 1999;29(6):1655-1661.
- Runyon B. Low-protein-concentration ascitic fluid is predisposed to spontaneous bacterial peritonitis. Gastroenterology. 1986;91(6):1343-1346.
- Navasa M, Fernandez J, Montoliu S, et al. Randomized, double-blind, placebo-controlled trial evaluating norfloxacin in the primary prophylaxis of spontaneous bacterial peritonitis in cirrhotics with renal impairment, hyponatremia or severe liver failure. J Hepatol. 2006;44(Supp2):S51.
- Grothe W, Lottere E, Fleig W. Factors predictive for spontaneous bacterial peritonitis (SBP) under routine inpatient conditions in patients with cirrhosis: a prospective multicenter trial. J Hepatol. 1990;34(4):547.
ONLINE EXCLUSIVE: Listen to HM experts discuss comanagement opportunities
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
ONLINE EXCLUSIVE: Listen to former Obama healthcare advisor Bob Kocher, MD
Click here to listen to Dr. Kocher
Click here to listen to Dr. Kocher
Click here to listen to Dr. Kocher
ONLINE EXCLUSIVE: Comanagement Business Models
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
ONLINE EXCLUSIVE: Wachter Relishes Opportunity to Guide Hospitalists
Robert Wachter, MD, MHM, has spoken at SHM’s annual meeting every year since 2003.
The opportunity to address 2,500 physician leaders in clinical work, education, and quality improvement—and the chance to suggest where they should be placing their emphasis—is incredibly special, Dr. Wachter says.
“It’s an amazing chance to try to influence the fastest-growing specialty in history,” says the professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center.
“I like to think I have some small impact on the work they go out and do the next day, so it feels like a way of extending my own influence on this extraordinary field,” adds Dr. Wachter, a former SHM president and author of the blog Wachter’s World (www.wachtersworld.com). “That’s a great privilege.”
Dr. Wachter will speak at HM11 on Friday, May 13. The Hospitalist caught up with him to discuss some of his presentation.
Question: Why would you encourage hospitalists to attend HM11?
Answer: The content is great, and it is broad enough that it doesn’t matter whether you are coming to learn the latest ways to manage sepsis or the best ways to organize your program. We are able to attract the best leaders in the world to come speak, so the talent pool is unmatched. And the collegial exchange is fantastic. There’s as much important work that happens in the hallways as happens in the conference room.
Q: Bob Kocher, MD, a former special assistant to the president for healthcare and economic policy, will be a featured speaker this year. Why is it important for hospitalists to hear from him?
A: He was as important as any architect of the healthcare reform legislation. Because he left the White House, he can be open and honest about what’s working and not working. I think we need to understand what reform means, why it was organized the way it was, and where someone who was in the middle of that thinks it will go over time.
Q: What do you see as the legislation’s most significant impact on HM?
A: The dominant issue is, how do we create an environment, and a set of policy and payment initiatives, that incent and promote the delivery of the highest quality, safest, most satisfying care at the lowest cost? That’s not just within the silo we call a hospital but across the continuum of care. The bill takes that concept and puts it on steroids.
Robert Wachter, MD, MHM, has spoken at SHM’s annual meeting every year since 2003.
The opportunity to address 2,500 physician leaders in clinical work, education, and quality improvement—and the chance to suggest where they should be placing their emphasis—is incredibly special, Dr. Wachter says.
“It’s an amazing chance to try to influence the fastest-growing specialty in history,” says the professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center.
“I like to think I have some small impact on the work they go out and do the next day, so it feels like a way of extending my own influence on this extraordinary field,” adds Dr. Wachter, a former SHM president and author of the blog Wachter’s World (www.wachtersworld.com). “That’s a great privilege.”
Dr. Wachter will speak at HM11 on Friday, May 13. The Hospitalist caught up with him to discuss some of his presentation.
Question: Why would you encourage hospitalists to attend HM11?
Answer: The content is great, and it is broad enough that it doesn’t matter whether you are coming to learn the latest ways to manage sepsis or the best ways to organize your program. We are able to attract the best leaders in the world to come speak, so the talent pool is unmatched. And the collegial exchange is fantastic. There’s as much important work that happens in the hallways as happens in the conference room.
Q: Bob Kocher, MD, a former special assistant to the president for healthcare and economic policy, will be a featured speaker this year. Why is it important for hospitalists to hear from him?
A: He was as important as any architect of the healthcare reform legislation. Because he left the White House, he can be open and honest about what’s working and not working. I think we need to understand what reform means, why it was organized the way it was, and where someone who was in the middle of that thinks it will go over time.
Q: What do you see as the legislation’s most significant impact on HM?
A: The dominant issue is, how do we create an environment, and a set of policy and payment initiatives, that incent and promote the delivery of the highest quality, safest, most satisfying care at the lowest cost? That’s not just within the silo we call a hospital but across the continuum of care. The bill takes that concept and puts it on steroids.
Robert Wachter, MD, MHM, has spoken at SHM’s annual meeting every year since 2003.
The opportunity to address 2,500 physician leaders in clinical work, education, and quality improvement—and the chance to suggest where they should be placing their emphasis—is incredibly special, Dr. Wachter says.
“It’s an amazing chance to try to influence the fastest-growing specialty in history,” says the professor, chief of the Division of Hospital Medicine, and chief of the medical service at the University of California at San Francisco Medical Center.
“I like to think I have some small impact on the work they go out and do the next day, so it feels like a way of extending my own influence on this extraordinary field,” adds Dr. Wachter, a former SHM president and author of the blog Wachter’s World (www.wachtersworld.com). “That’s a great privilege.”
Dr. Wachter will speak at HM11 on Friday, May 13. The Hospitalist caught up with him to discuss some of his presentation.
Question: Why would you encourage hospitalists to attend HM11?
Answer: The content is great, and it is broad enough that it doesn’t matter whether you are coming to learn the latest ways to manage sepsis or the best ways to organize your program. We are able to attract the best leaders in the world to come speak, so the talent pool is unmatched. And the collegial exchange is fantastic. There’s as much important work that happens in the hallways as happens in the conference room.
Q: Bob Kocher, MD, a former special assistant to the president for healthcare and economic policy, will be a featured speaker this year. Why is it important for hospitalists to hear from him?
A: He was as important as any architect of the healthcare reform legislation. Because he left the White House, he can be open and honest about what’s working and not working. I think we need to understand what reform means, why it was organized the way it was, and where someone who was in the middle of that thinks it will go over time.
Q: What do you see as the legislation’s most significant impact on HM?
A: The dominant issue is, how do we create an environment, and a set of policy and payment initiatives, that incent and promote the delivery of the highest quality, safest, most satisfying care at the lowest cost? That’s not just within the silo we call a hospital but across the continuum of care. The bill takes that concept and puts it on steroids.
HM11 PREVIEW: Insider’s Viewpoint
Robert Kocher, MD, is not a household name for hospitalists who aren’t policy wonks. That’s not to say he shouldn’t be.
Dr. Kocher, a former special assistant to President Obama on healthcare and economic policy who is now the director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., was a behind-the-scenes player in the landmark healthcare reform legislation signed into law last year. After a two-year stint in the White House, he transitioned back to the private sector late in 2010, landing at McKinsey & Co., a powerhouse consulting firm in the nation’s capital.
On May 11, Dr. Kocher will give HM11’s first keynote speech, “Coming to Your Hospital: Healthcare Reform. What Does This Mean for Hospitalists.” His talk will be an inside look at how the reform package came together and point out how hospitalists can be “the solution that hospitals will want to deploy to allow them to capitalize” on reform.
“Instead of hospitalists being a de facto link [between different departments of a given hospital], I think hospitalists will be a value-creating link,” Dr. Kocher says. “There’s going to be much more information that’s going to have to flow between the inpatient side and the outpatient side if you’re going to manage population health and lower per capita costs. … It’s going to require more specialization, which hospitalists are in the right position to really take on and to deliver.”
Dr. Kocher (pronounced “coacher”) joined the reform fight in January 2009, taking a post at the National Economic Council as special assistant to the president for healthcare. He left that job last fall and rejoined McKinsey, the firm he had been with for seven years before joining the Obama administration. His career began with a medical degree from George Washington University and internal-medicine residency at Beth Israel Deaconess Medical Center in Boston.

He followed that with a stint as a clinical fellow and instructor at Harvard Medical School. In addition to his role as a principal at McKinsey, Dr. Kocher is a nonresident senior fellow at the Brookings Institution Engleberg Center for Health Reform.
He is a well-known speaker on healthcare topics and a frequent writer who has authored pieces for major outlets, including the New England Journal of Medicine, the Washington Post and The New York Times. The White House last year filmed him as part of its “Reality Check” Web series (www.whitehouse.gov/realitycheck/31), which is aimed at “debunking the myths” swirling around reform.
Dr. Kocher says all of his career stops pale in comparison to being part of once-in-a-generation talks that shaped the future of U.S. healthcare.
“Certainly, [it was] the most impactful thing I’ll ever get to actually do, because we were able to shape the lasting policies that will change the way healthcare is delivered for years to come,” he says. “It was an incredible privilege to get to observe and take part in that policy-making process and understand that some compromises have to happen to make successful legislation.”
Brendon Shank, SHM’s assistant vice president of communications, says that having a White House participant in the reform negotiations as a featured speaker is a treat for hospitalists.
“This is exciting because it’s someone who helped define policy,” Shank says. “This is someone who knows the inside of it. He’s been in the room for discussions that will affect hospitalists for years down the road.”
Exactly what those effects will be will take time to understand. But Dr. Kocher sees reform as a chance for HM to make itself indispensable to hospitals looking to improve quality, efficiency, and transitional-care outcomes.
More HM11 Preview
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The responsibility will, of course, come with the challenge of actually proving that HM can deliver on the pledge of better care at better prices.
“For hospitals, as the payment system evolves and matures, we’re going to be paying more often for outcomes,” Dr. Kocher says. “That change is going to require hospitalists to become much more reliable.
“It’s a more specialized skill that doctors who are part-time hospital doctors are going to have a hard time developing. It clearly makes the system more dependent on hospitalists. … That said, I think that it’s the responsibility of hospitalists to prove they can deliver.”
Dr. Kocher is optimistic that the political squabbling the reform process has sparked will have little lasting impact. He understands HM leaders might be nervous about the potential for political upheaval to translate into medical upheaval, but he doubts that will happen.
“The political rhetoric and scuffling going on in Washington has almost no bearing on the fundamental underlying trend which will drive the market to near-universal use of hospitalists,” he says. “Whether you’re a Republican or Democrat, you share the perspective that the current health system is wildly too expensive.” HM11
Richard Quinn is a freelance writer based in New Jersey.
Robert Kocher, MD, is not a household name for hospitalists who aren’t policy wonks. That’s not to say he shouldn’t be.
Dr. Kocher, a former special assistant to President Obama on healthcare and economic policy who is now the director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., was a behind-the-scenes player in the landmark healthcare reform legislation signed into law last year. After a two-year stint in the White House, he transitioned back to the private sector late in 2010, landing at McKinsey & Co., a powerhouse consulting firm in the nation’s capital.
On May 11, Dr. Kocher will give HM11’s first keynote speech, “Coming to Your Hospital: Healthcare Reform. What Does This Mean for Hospitalists.” His talk will be an inside look at how the reform package came together and point out how hospitalists can be “the solution that hospitals will want to deploy to allow them to capitalize” on reform.
“Instead of hospitalists being a de facto link [between different departments of a given hospital], I think hospitalists will be a value-creating link,” Dr. Kocher says. “There’s going to be much more information that’s going to have to flow between the inpatient side and the outpatient side if you’re going to manage population health and lower per capita costs. … It’s going to require more specialization, which hospitalists are in the right position to really take on and to deliver.”
Dr. Kocher (pronounced “coacher”) joined the reform fight in January 2009, taking a post at the National Economic Council as special assistant to the president for healthcare. He left that job last fall and rejoined McKinsey, the firm he had been with for seven years before joining the Obama administration. His career began with a medical degree from George Washington University and internal-medicine residency at Beth Israel Deaconess Medical Center in Boston.
He followed that with a stint as a clinical fellow and instructor at Harvard Medical School. In addition to his role as a principal at McKinsey, Dr. Kocher is a nonresident senior fellow at the Brookings Institution Engleberg Center for Health Reform.
He is a well-known speaker on healthcare topics and a frequent writer who has authored pieces for major outlets, including the New England Journal of Medicine, the Washington Post and The New York Times. The White House last year filmed him as part of its “Reality Check” Web series (www.whitehouse.gov/realitycheck/31), which is aimed at “debunking the myths” swirling around reform.
Dr. Kocher says all of his career stops pale in comparison to being part of once-in-a-generation talks that shaped the future of U.S. healthcare.
“Certainly, [it was] the most impactful thing I’ll ever get to actually do, because we were able to shape the lasting policies that will change the way healthcare is delivered for years to come,” he says. “It was an incredible privilege to get to observe and take part in that policy-making process and understand that some compromises have to happen to make successful legislation.”
Brendon Shank, SHM’s assistant vice president of communications, says that having a White House participant in the reform negotiations as a featured speaker is a treat for hospitalists.
“This is exciting because it’s someone who helped define policy,” Shank says. “This is someone who knows the inside of it. He’s been in the room for discussions that will affect hospitalists for years down the road.”
Exactly what those effects will be will take time to understand. But Dr. Kocher sees reform as a chance for HM to make itself indispensable to hospitals looking to improve quality, efficiency, and transitional-care outcomes.
More HM11 Preview
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The responsibility will, of course, come with the challenge of actually proving that HM can deliver on the pledge of better care at better prices.
“For hospitals, as the payment system evolves and matures, we’re going to be paying more often for outcomes,” Dr. Kocher says. “That change is going to require hospitalists to become much more reliable.
“It’s a more specialized skill that doctors who are part-time hospital doctors are going to have a hard time developing. It clearly makes the system more dependent on hospitalists. … That said, I think that it’s the responsibility of hospitalists to prove they can deliver.”
Dr. Kocher is optimistic that the political squabbling the reform process has sparked will have little lasting impact. He understands HM leaders might be nervous about the potential for political upheaval to translate into medical upheaval, but he doubts that will happen.
“The political rhetoric and scuffling going on in Washington has almost no bearing on the fundamental underlying trend which will drive the market to near-universal use of hospitalists,” he says. “Whether you’re a Republican or Democrat, you share the perspective that the current health system is wildly too expensive.” HM11
Richard Quinn is a freelance writer based in New Jersey.
Robert Kocher, MD, is not a household name for hospitalists who aren’t policy wonks. That’s not to say he shouldn’t be.
Dr. Kocher, a former special assistant to President Obama on healthcare and economic policy who is now the director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., was a behind-the-scenes player in the landmark healthcare reform legislation signed into law last year. After a two-year stint in the White House, he transitioned back to the private sector late in 2010, landing at McKinsey & Co., a powerhouse consulting firm in the nation’s capital.
On May 11, Dr. Kocher will give HM11’s first keynote speech, “Coming to Your Hospital: Healthcare Reform. What Does This Mean for Hospitalists.” His talk will be an inside look at how the reform package came together and point out how hospitalists can be “the solution that hospitals will want to deploy to allow them to capitalize” on reform.
“Instead of hospitalists being a de facto link [between different departments of a given hospital], I think hospitalists will be a value-creating link,” Dr. Kocher says. “There’s going to be much more information that’s going to have to flow between the inpatient side and the outpatient side if you’re going to manage population health and lower per capita costs. … It’s going to require more specialization, which hospitalists are in the right position to really take on and to deliver.”
Dr. Kocher (pronounced “coacher”) joined the reform fight in January 2009, taking a post at the National Economic Council as special assistant to the president for healthcare. He left that job last fall and rejoined McKinsey, the firm he had been with for seven years before joining the Obama administration. His career began with a medical degree from George Washington University and internal-medicine residency at Beth Israel Deaconess Medical Center in Boston.
He followed that with a stint as a clinical fellow and instructor at Harvard Medical School. In addition to his role as a principal at McKinsey, Dr. Kocher is a nonresident senior fellow at the Brookings Institution Engleberg Center for Health Reform.
He is a well-known speaker on healthcare topics and a frequent writer who has authored pieces for major outlets, including the New England Journal of Medicine, the Washington Post and The New York Times. The White House last year filmed him as part of its “Reality Check” Web series (www.whitehouse.gov/realitycheck/31), which is aimed at “debunking the myths” swirling around reform.
Dr. Kocher says all of his career stops pale in comparison to being part of once-in-a-generation talks that shaped the future of U.S. healthcare.
“Certainly, [it was] the most impactful thing I’ll ever get to actually do, because we were able to shape the lasting policies that will change the way healthcare is delivered for years to come,” he says. “It was an incredible privilege to get to observe and take part in that policy-making process and understand that some compromises have to happen to make successful legislation.”
Brendon Shank, SHM’s assistant vice president of communications, says that having a White House participant in the reform negotiations as a featured speaker is a treat for hospitalists.
“This is exciting because it’s someone who helped define policy,” Shank says. “This is someone who knows the inside of it. He’s been in the room for discussions that will affect hospitalists for years down the road.”
Exactly what those effects will be will take time to understand. But Dr. Kocher sees reform as a chance for HM to make itself indispensable to hospitals looking to improve quality, efficiency, and transitional-care outcomes.
More HM11 Preview
HM11’s visiting professor to serve as mentor, stimulate discussion
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The responsibility will, of course, come with the challenge of actually proving that HM can deliver on the pledge of better care at better prices.
“For hospitals, as the payment system evolves and matures, we’re going to be paying more often for outcomes,” Dr. Kocher says. “That change is going to require hospitalists to become much more reliable.
“It’s a more specialized skill that doctors who are part-time hospital doctors are going to have a hard time developing. It clearly makes the system more dependent on hospitalists. … That said, I think that it’s the responsibility of hospitalists to prove they can deliver.”
Dr. Kocher is optimistic that the political squabbling the reform process has sparked will have little lasting impact. He understands HM leaders might be nervous about the potential for political upheaval to translate into medical upheaval, but he doubts that will happen.
“The political rhetoric and scuffling going on in Washington has almost no bearing on the fundamental underlying trend which will drive the market to near-universal use of hospitalists,” he says. “Whether you’re a Republican or Democrat, you share the perspective that the current health system is wildly too expensive.” HM11
Richard Quinn is a freelance writer based in New Jersey.
HM11 PREVIEW: Teacher As Student

More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The position of visiting professor is a bit amorphous at the SHM annual meeting. The honoree presides over the best of the Research, Innovations, and Clinical Vignettes (RIV) presentations and leads rounds of the RIV poster sessions. They can serve as an informal mentor to early-career physicians and be a sounding board for seasoned practitioners.
This year, the visiting professor will be as much a student as a teacher.
“I always think when I go to educate others … the best way of doing that is to have a bidirectional kind of interchange,” says Malcolm Cox, MD, chief academic affiliations officer for the U.S. Department of Veterans Affairs in Washington, D.C., and an adjunct professor of medicine at the University of Pennsylvania in Philadelphia. “I inevitably learn more from my ‘students’ than I think I ever provide to my students, in any teaching opportunity. That’s just a philosophy I’ve had for 40 years.”
Dr. Cox, a kidney specialist and career academician, was invited to be the visiting professor by SHM President Jeff Wiese, MD, FACP, SFHM. Dr. Cox views his role as that of an “interrogative fly on the wall,” and he hopes to stimulate discussions about HM’s role in the broader medical landscape.
“How hospitalists can work with their other colleagues to enhance continuity,” he says, “and, in particular, within that more narrow frame, an even more narrow frame is how they would relate to and work with primary-care folks in the aftercare environment to enhance continuity of care.” HM11
Richard Quinn is a freelance writer based in New Jersey.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The position of visiting professor is a bit amorphous at the SHM annual meeting. The honoree presides over the best of the Research, Innovations, and Clinical Vignettes (RIV) presentations and leads rounds of the RIV poster sessions. They can serve as an informal mentor to early-career physicians and be a sounding board for seasoned practitioners.
This year, the visiting professor will be as much a student as a teacher.
“I always think when I go to educate others … the best way of doing that is to have a bidirectional kind of interchange,” says Malcolm Cox, MD, chief academic affiliations officer for the U.S. Department of Veterans Affairs in Washington, D.C., and an adjunct professor of medicine at the University of Pennsylvania in Philadelphia. “I inevitably learn more from my ‘students’ than I think I ever provide to my students, in any teaching opportunity. That’s just a philosophy I’ve had for 40 years.”
Dr. Cox, a kidney specialist and career academician, was invited to be the visiting professor by SHM President Jeff Wiese, MD, FACP, SFHM. Dr. Cox views his role as that of an “interrogative fly on the wall,” and he hopes to stimulate discussions about HM’s role in the broader medical landscape.
“How hospitalists can work with their other colleagues to enhance continuity,” he says, “and, in particular, within that more narrow frame, an even more narrow frame is how they would relate to and work with primary-care folks in the aftercare environment to enhance continuity of care.” HM11
Richard Quinn is a freelance writer based in New Jersey.
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
Hospitalists come from all walks; HM11 has a place for all of them
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The position of visiting professor is a bit amorphous at the SHM annual meeting. The honoree presides over the best of the Research, Innovations, and Clinical Vignettes (RIV) presentations and leads rounds of the RIV poster sessions. They can serve as an informal mentor to early-career physicians and be a sounding board for seasoned practitioners.
This year, the visiting professor will be as much a student as a teacher.
“I always think when I go to educate others … the best way of doing that is to have a bidirectional kind of interchange,” says Malcolm Cox, MD, chief academic affiliations officer for the U.S. Department of Veterans Affairs in Washington, D.C., and an adjunct professor of medicine at the University of Pennsylvania in Philadelphia. “I inevitably learn more from my ‘students’ than I think I ever provide to my students, in any teaching opportunity. That’s just a philosophy I’ve had for 40 years.”
Dr. Cox, a kidney specialist and career academician, was invited to be the visiting professor by SHM President Jeff Wiese, MD, FACP, SFHM. Dr. Cox views his role as that of an “interrogative fly on the wall,” and he hopes to stimulate discussions about HM’s role in the broader medical landscape.
“How hospitalists can work with their other colleagues to enhance continuity,” he says, “and, in particular, within that more narrow frame, an even more narrow frame is how they would relate to and work with primary-care folks in the aftercare environment to enhance continuity of care.” HM11
Richard Quinn is a freelance writer based in New Jersey.
HM11 PREVIEW: Different Strokes

Ron Greeno, MD, SFHM, chief medical officer for Brentwood, Tenn.-based Cogent Healthcare, will arrive at HM11 and embark on a whirlwind of meet-and-greets, dinners, drinks, and introductions. At the same time, first-year attendee Amaka Nweke, assistant site director for Hospitalists Management Group at Kenosha Medical Center in Wisconsin, will focus on sessions that will help her learn the management skills she can use to further her career.
To be sure, Dr. Greeno will attend a few classes to brush up on specific topics. And Dr. Nweke will ask for business cards as she builds a professional network. But each has to pick a strategy to navigate the four-day annual meeting in Grapevine, Texas.
“You can’t do everything,” says Daniel Dressler, MD, MSc, SFHM, associate professor and director of internal-medicine teaching services at Emory University Hospital in Atlanta, SHM board member, and HM11’s course director. “You have to plan and ask, ‘What do I want to get out of this meeting this year?’ ”
The Hospitalist talked to more than a half-dozen providers in various HM roles to determine just what they expect out of their annual meeting. The physicians fall into broad categories that capture most of the roughly 2,500 attendees at the annual meeting: first-timer, veteran, academic, rural hospitalist, up-and-comer, socialite. And while each says plenary sessions and keynote addresses are must-sees, the tack they take for the rest of the week is custom-made.
The First-Timer
Dr. Nweke, who finished her residency in 2009, wasn’t sure how to map out her meeting schedule until she decided to attend two medical conferences this year. She plans to get her clinical refreshers at the annual meeting of the American College of Physicians (ACP), and use SHM’s affair to teach her the managerial and administrative skills she needs to eventually become an HM group leader. Her particular focuses include process improvement and length-of-stay (LOS) reduction methods.
“Originally, when I wasn’t sure what I wanted to get out of SHM, it was very daunting,” she says. “For meetings like this, you have to figure out what you want out of the course. Once you figure that out, it makes it easy to register for a course. If you don’t know and you’re just going, it’s definitely extremely daunting.”
The Veteran

Jeffrey Dichter, MD, FACP, SFHM, medical director for the cardiovascular ICU at Regions Hospital in St. Paul, Minn., only missed two of the first 14 annual meetings. He picks a topic area each year that he wants to focus on, then tailors his schedule to that idea. This year, it’s quality improvement. An academician at heart, he also attends the abstract poster sessions to get “a real flavor for the researchers and what people are thinking about for HM.”
“You’re not going to get to everything every year,” he says knowingly. “You just try to mix and match. Early on, you could see everything. Since it’s grown, you realize you can’t see everything. You learn to adapt.”
The Academic
Danielle Scheurer, MD, MSc, SFHM, medical director of quality and safety at the Medical University of South Carolina in Charleston, uses the meeting as a sounding board to solve problems. Community HM groups don’t have the sort of turnover issues that academic medical centers do, so meeting with like-minded colleagues provides the chance to find the “little pearls from any medical center that you can take back.”
“Since I do a lot of quality improvement, I just like the opportunity to see how other people are doing things that we are struggling with,” says Dr. Scheurer, SHM’s physician advisor. “It amazes me the ubiquity of how we all struggle around the same types of things.”
The Rural Hospitalist
Martin Johns, MD, a hospitalist at Gifford Medical Center in Randolph, Vt., (pop. 4,853) could use an entire focused track on rural medicine. In particular, rural hospitalists often perform multiple roles—administrative or clinical—and best-practice recommendations would be valuable. Networking has its place at the meeting, but given that many rural physicians have long tenures, the real goal is bring useful information back to the group. “What is good about the SHM [meeting] is you are exposed to know what’s happening regionally,” Dr. Johns says. “You get a flavor for the national tenor. That’s important, because in a small place, you only have a certain allotment for CME funds.”
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The Up-and-Comer
Christina Payne, MD, an academic hospitalist at Emory University Hospital in Atlanta who finished her residency in June, sees herself as a potential future leader in the field. She presented a poster at last year’s meeting and works on a SHM committee for early-career hospitalists.
A quality-minded academician, Dr. Payne plans to take advantage of meeting the leading minds in HM and use them as mentors to help her help the field.
“It’s learning to walk the walk and talk the talk,” she says. “I’m still new at that, but I’m ready to put myself out there. … My excitement for hospital medicine puts me in an ideal spot. In 20 years, hopefully, we’ll be the ones for other people to come to for mentorship.”
The Socialite
Dr. Dressler refers to Dr. Greeno, a cofounder of Cogent, as the “ultimate socialite.” Dr. Greeno is often a panelist at the annual meeting and spends much of his time catching up with colleagues around the country he does not often see in person. He makes sure to catch three or four handpicked sessions but typically looks most forward to being approached by younger physicians as he sees the young field of HM take hold with a new generation.
“The entire time I’m there, I’m talking to someone, whether it’s planned or I run into someone,” he says. “It’s the one time I usually end up having dinner and end up having drinks with folks and talking with people well into the night. It really does give you a chance to recharge your battery and get excited about what we’re doing again.” HM11
Richard Quinn is a freelance writer based in New Jersey.
Ron Greeno, MD, SFHM, chief medical officer for Brentwood, Tenn.-based Cogent Healthcare, will arrive at HM11 and embark on a whirlwind of meet-and-greets, dinners, drinks, and introductions. At the same time, first-year attendee Amaka Nweke, assistant site director for Hospitalists Management Group at Kenosha Medical Center in Wisconsin, will focus on sessions that will help her learn the management skills she can use to further her career.
To be sure, Dr. Greeno will attend a few classes to brush up on specific topics. And Dr. Nweke will ask for business cards as she builds a professional network. But each has to pick a strategy to navigate the four-day annual meeting in Grapevine, Texas.
“You can’t do everything,” says Daniel Dressler, MD, MSc, SFHM, associate professor and director of internal-medicine teaching services at Emory University Hospital in Atlanta, SHM board member, and HM11’s course director. “You have to plan and ask, ‘What do I want to get out of this meeting this year?’ ”
The Hospitalist talked to more than a half-dozen providers in various HM roles to determine just what they expect out of their annual meeting. The physicians fall into broad categories that capture most of the roughly 2,500 attendees at the annual meeting: first-timer, veteran, academic, rural hospitalist, up-and-comer, socialite. And while each says plenary sessions and keynote addresses are must-sees, the tack they take for the rest of the week is custom-made.
The First-Timer
Dr. Nweke, who finished her residency in 2009, wasn’t sure how to map out her meeting schedule until she decided to attend two medical conferences this year. She plans to get her clinical refreshers at the annual meeting of the American College of Physicians (ACP), and use SHM’s affair to teach her the managerial and administrative skills she needs to eventually become an HM group leader. Her particular focuses include process improvement and length-of-stay (LOS) reduction methods.
“Originally, when I wasn’t sure what I wanted to get out of SHM, it was very daunting,” she says. “For meetings like this, you have to figure out what you want out of the course. Once you figure that out, it makes it easy to register for a course. If you don’t know and you’re just going, it’s definitely extremely daunting.”
The Veteran
Jeffrey Dichter, MD, FACP, SFHM, medical director for the cardiovascular ICU at Regions Hospital in St. Paul, Minn., only missed two of the first 14 annual meetings. He picks a topic area each year that he wants to focus on, then tailors his schedule to that idea. This year, it’s quality improvement. An academician at heart, he also attends the abstract poster sessions to get “a real flavor for the researchers and what people are thinking about for HM.”
“You’re not going to get to everything every year,” he says knowingly. “You just try to mix and match. Early on, you could see everything. Since it’s grown, you realize you can’t see everything. You learn to adapt.”
The Academic
Danielle Scheurer, MD, MSc, SFHM, medical director of quality and safety at the Medical University of South Carolina in Charleston, uses the meeting as a sounding board to solve problems. Community HM groups don’t have the sort of turnover issues that academic medical centers do, so meeting with like-minded colleagues provides the chance to find the “little pearls from any medical center that you can take back.”
“Since I do a lot of quality improvement, I just like the opportunity to see how other people are doing things that we are struggling with,” says Dr. Scheurer, SHM’s physician advisor. “It amazes me the ubiquity of how we all struggle around the same types of things.”
The Rural Hospitalist
Martin Johns, MD, a hospitalist at Gifford Medical Center in Randolph, Vt., (pop. 4,853) could use an entire focused track on rural medicine. In particular, rural hospitalists often perform multiple roles—administrative or clinical—and best-practice recommendations would be valuable. Networking has its place at the meeting, but given that many rural physicians have long tenures, the real goal is bring useful information back to the group. “What is good about the SHM [meeting] is you are exposed to know what’s happening regionally,” Dr. Johns says. “You get a flavor for the national tenor. That’s important, because in a small place, you only have a certain allotment for CME funds.”
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The Up-and-Comer
Christina Payne, MD, an academic hospitalist at Emory University Hospital in Atlanta who finished her residency in June, sees herself as a potential future leader in the field. She presented a poster at last year’s meeting and works on a SHM committee for early-career hospitalists.
A quality-minded academician, Dr. Payne plans to take advantage of meeting the leading minds in HM and use them as mentors to help her help the field.
“It’s learning to walk the walk and talk the talk,” she says. “I’m still new at that, but I’m ready to put myself out there. … My excitement for hospital medicine puts me in an ideal spot. In 20 years, hopefully, we’ll be the ones for other people to come to for mentorship.”
The Socialite
Dr. Dressler refers to Dr. Greeno, a cofounder of Cogent, as the “ultimate socialite.” Dr. Greeno is often a panelist at the annual meeting and spends much of his time catching up with colleagues around the country he does not often see in person. He makes sure to catch three or four handpicked sessions but typically looks most forward to being approached by younger physicians as he sees the young field of HM take hold with a new generation.
“The entire time I’m there, I’m talking to someone, whether it’s planned or I run into someone,” he says. “It’s the one time I usually end up having dinner and end up having drinks with folks and talking with people well into the night. It really does give you a chance to recharge your battery and get excited about what we’re doing again.” HM11
Richard Quinn is a freelance writer based in New Jersey.
Ron Greeno, MD, SFHM, chief medical officer for Brentwood, Tenn.-based Cogent Healthcare, will arrive at HM11 and embark on a whirlwind of meet-and-greets, dinners, drinks, and introductions. At the same time, first-year attendee Amaka Nweke, assistant site director for Hospitalists Management Group at Kenosha Medical Center in Wisconsin, will focus on sessions that will help her learn the management skills she can use to further her career.
To be sure, Dr. Greeno will attend a few classes to brush up on specific topics. And Dr. Nweke will ask for business cards as she builds a professional network. But each has to pick a strategy to navigate the four-day annual meeting in Grapevine, Texas.
“You can’t do everything,” says Daniel Dressler, MD, MSc, SFHM, associate professor and director of internal-medicine teaching services at Emory University Hospital in Atlanta, SHM board member, and HM11’s course director. “You have to plan and ask, ‘What do I want to get out of this meeting this year?’ ”
The Hospitalist talked to more than a half-dozen providers in various HM roles to determine just what they expect out of their annual meeting. The physicians fall into broad categories that capture most of the roughly 2,500 attendees at the annual meeting: first-timer, veteran, academic, rural hospitalist, up-and-comer, socialite. And while each says plenary sessions and keynote addresses are must-sees, the tack they take for the rest of the week is custom-made.
The First-Timer
Dr. Nweke, who finished her residency in 2009, wasn’t sure how to map out her meeting schedule until she decided to attend two medical conferences this year. She plans to get her clinical refreshers at the annual meeting of the American College of Physicians (ACP), and use SHM’s affair to teach her the managerial and administrative skills she needs to eventually become an HM group leader. Her particular focuses include process improvement and length-of-stay (LOS) reduction methods.
“Originally, when I wasn’t sure what I wanted to get out of SHM, it was very daunting,” she says. “For meetings like this, you have to figure out what you want out of the course. Once you figure that out, it makes it easy to register for a course. If you don’t know and you’re just going, it’s definitely extremely daunting.”
The Veteran
Jeffrey Dichter, MD, FACP, SFHM, medical director for the cardiovascular ICU at Regions Hospital in St. Paul, Minn., only missed two of the first 14 annual meetings. He picks a topic area each year that he wants to focus on, then tailors his schedule to that idea. This year, it’s quality improvement. An academician at heart, he also attends the abstract poster sessions to get “a real flavor for the researchers and what people are thinking about for HM.”
“You’re not going to get to everything every year,” he says knowingly. “You just try to mix and match. Early on, you could see everything. Since it’s grown, you realize you can’t see everything. You learn to adapt.”
The Academic
Danielle Scheurer, MD, MSc, SFHM, medical director of quality and safety at the Medical University of South Carolina in Charleston, uses the meeting as a sounding board to solve problems. Community HM groups don’t have the sort of turnover issues that academic medical centers do, so meeting with like-minded colleagues provides the chance to find the “little pearls from any medical center that you can take back.”
“Since I do a lot of quality improvement, I just like the opportunity to see how other people are doing things that we are struggling with,” says Dr. Scheurer, SHM’s physician advisor. “It amazes me the ubiquity of how we all struggle around the same types of things.”
The Rural Hospitalist
Martin Johns, MD, a hospitalist at Gifford Medical Center in Randolph, Vt., (pop. 4,853) could use an entire focused track on rural medicine. In particular, rural hospitalists often perform multiple roles—administrative or clinical—and best-practice recommendations would be valuable. Networking has its place at the meeting, but given that many rural physicians have long tenures, the real goal is bring useful information back to the group. “What is good about the SHM [meeting] is you are exposed to know what’s happening regionally,” Dr. Johns says. “You get a flavor for the national tenor. That’s important, because in a small place, you only have a certain allotment for CME funds.”
More HM11 Preview
Former Obama advisor will speak to hospitalists about health reform
HM11’s visiting professor to serve as mentor, stimulate discussion
HM11 attendees can earn as many as 18.75 CME credits
Industry pioneer recounts HM’s meteoric rise, sees bright future for hospitalists
Lots to See, Lots to Do in ‘Big D’
From sports to culture to Tex-Mex, Dallas metroplex has something for every visitor
You may also
HM11 PREVIEW SUPPLEMENT
in pdf format.
The Up-and-Comer
Christina Payne, MD, an academic hospitalist at Emory University Hospital in Atlanta who finished her residency in June, sees herself as a potential future leader in the field. She presented a poster at last year’s meeting and works on a SHM committee for early-career hospitalists.
A quality-minded academician, Dr. Payne plans to take advantage of meeting the leading minds in HM and use them as mentors to help her help the field.
“It’s learning to walk the walk and talk the talk,” she says. “I’m still new at that, but I’m ready to put myself out there. … My excitement for hospital medicine puts me in an ideal spot. In 20 years, hopefully, we’ll be the ones for other people to come to for mentorship.”
The Socialite
Dr. Dressler refers to Dr. Greeno, a cofounder of Cogent, as the “ultimate socialite.” Dr. Greeno is often a panelist at the annual meeting and spends much of his time catching up with colleagues around the country he does not often see in person. He makes sure to catch three or four handpicked sessions but typically looks most forward to being approached by younger physicians as he sees the young field of HM take hold with a new generation.
“The entire time I’m there, I’m talking to someone, whether it’s planned or I run into someone,” he says. “It’s the one time I usually end up having dinner and end up having drinks with folks and talking with people well into the night. It really does give you a chance to recharge your battery and get excited about what we’re doing again.” HM11
Richard Quinn is a freelance writer based in New Jersey.
HM11 PREVIEW: HM11 Day-by-Day Schedule
Enter text here
Enter text here
Enter text here