User login
PRESsed for time
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
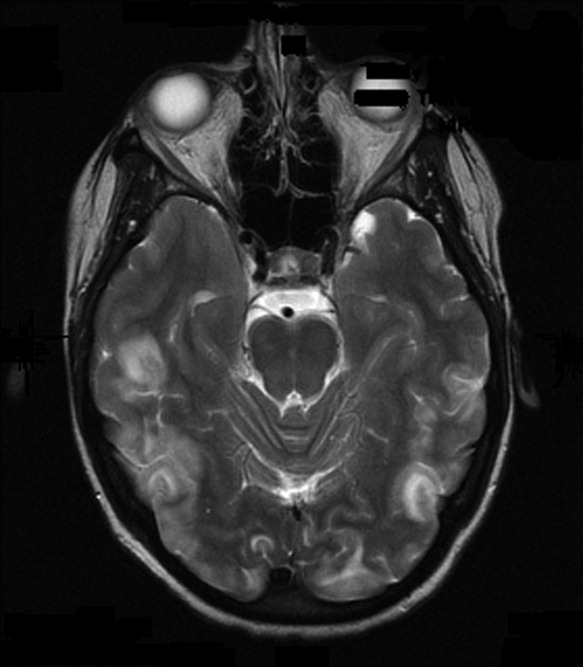
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).

Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).
Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
A 36‐year‐old woman was admitted after new‐onset Hseizures. She had been diagnosed with breast cancer 5 years prior to admission. At that time, she underwent left radical mastectomy and lymph node dissection. Lymph nodes were positive for metastatic disease with negative HER‐2‐Neu and positive estrogen and progesterone receptors. She was treated with docetaxel and tamoxifen but subsequently developed metastatic left hip lesions and was treated with letrozole and anastrozole. Three years later, scans revealed further metastatic disease to the liver, lung, and vertebral column. She was subsequently treated with capecitabine, until further disease progression led to the use of carboplatin and paclitaxel. Seven months prior to admission, her cancer was progressing and she was switched to doxorubicin, gemcitabine, and bevacizumab. Six weeks prior to admission, both positron emission tomography (PET) and computed tomography (CT) scan of her whole body and magnetic resonance imaging (MRI) of the brain illustrated significant improvement. Her last dose of bevacizumab was given 3 weeks prior to her admission.
Two weeks prior to admission, patient reported new‐onset daily headache. These were often localized in the occipital region. She reported some associated nausea and occasional emesis. Subsequently, she developed photophobia and phonophobia. On seeking outpatient treatment for her headache, it was noted that her systolic blood pressure had increased from a baseline of 100 mm Hg to 170 mm Hg. On the day prior to admission, she reported severe headache and several episodes of emesis and later that evening had a witnessed tonic‐clonic seizure.
The patient presented to an outside hospital and had an unremarkable noncontrast CT scan of her brain. An examination of her cerebrospinal fluid revealed negative gram stain, and a normal white blood cell count and protein level. She was treated with lorazepam, phenytoin, and decadron. On becoming more alert, she insisted on going home, where she later developed recurrent headache and presented to our emergency room.
On admission to our service, she was noted to be confused and irritable, and unable to provide any history. Her exam revealed a blood pressure of 143/102 mmHg. No localizing neurologic signs were noted and her laboratory values were normal. After sedation, MRI of the brain was obtained (Figure 1). This revealed diffuse and patchy gyriform hyperintensity of the white matter, most consistent with posterior reversible encephalopathy syndrome (PRES).
Upon reflection, the patient had new onset hypertension that coincided with the initiation and dosing of bevacizumab. Bevacizumab, an antineoplastic agent, is a recombinant humanized monoclonal antibody that binds to and neutralizes vascular endothelial growth factor, thereby preventing angiogenesis.1 It is known to cause grade 3 hypertension in a minority of patients. Therefore, it was postulated that the patient's persistent blood pressure elevation resulted in vasogenic brain edema, precipitating her seizure. Subsequent to the diagnosis, her blood pressure was aggressively controlled with oral enalapril, metoprolol, triamterene/hydrochlorothiazide, and hydralazine. By hospital day 7, her headache had subsided and her altered mental status had resolved. She had no further episodes of seizures and bevacizumab was discontinued.
PRES has a distinct constellation of clinical symptoms and radiologic findings. The name PRES is a misnomer, as this syndrome is not always reversible, nor is it restricted to the white matter or to the posterior areas of the brain.2 It is hypothesized that a sudden rise in blood pressure leads to elevations in intracranial pressure, which exceeds the brain's autoregulatory mechanisms. This subsequently leads to transudation of fluid into the brain parenchyma. Interestingly, it appears that it is not the absolute level of systolic blood pressure that is critical in the development of PRES, but the rate of change in blood pressure. Hence, patients with chronic hypertension have developed adaptive vascular changes that protect them from this type of parenchymal damage.
PRES has gained increasing recognition due to the use of immunosuppressive and chemotherapeutic medications in organ transplant and oncology patients. Drugs such as cyclosporine, tacrolimus, fludarabine, vincristine, cisplatin, cytarabine, interferon‐alpha, interleukin, antiretroviral therapy, erythropoietin, granulocyte stimulating factor, and intravenous immunoglobulin have all been implicated.3 In addition to increasing blood pressure, these agents likely cause direct toxic injury to the brain, disrupting the blood‐brain barrier and resulting in subsequent edema. Other conditions associated with PRES include renal disease, vasculitis, endocrine disorders, porphyria, cocaine or amphetamine abuse, and stimulant abuse.
Clinically, PRES can present as headache, altered mental status, confusion, drowsiness progressing to stupor, emesis, abnormal visual perceptions, visual neglect, cortical blindness, difficulty with memory and concentration, brisk deep tendon reflexes, weakness, ataxia, and seizure activity. PRES has a characteristic appearance on neuroimaging that differentiates it from other forms of hypertensive encephalopathy. Edema of the white or gray matter in the posterior cerebral hemispheres, particularly the bilateral parietooccipital regions, is seen. PRES can also diffusely involve the brain stem, cerebellum, basal ganglia, and the frontal lobes. Abnormalities on neuroimaging are often symmetric but clinical manifestations can be asymmetric. MRI and CT scans can both be utilized for characterization of PRES.4
There are currently no published guidelines for the management of PRES. Expert opinion suggests removing the underlying cause and aggressively treating the hypertension.5 Furthermore, initiation and duration of antiepileptics remains controversial. After aggressive blood pressure control, resolution of findings on neuroimaging studies are expected anywhere from 8 days to 17 months.
Timely recognition of PRES is critical for prevention of further neurologic compromise. Immediate discontinuation of offending agents, as well as aggressive treatment of blood pressure, is the cornerstone treatment for PRES. In the future, a better understanding of the pathophysiology of PRES can lead to improved diagnostic and management options.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
- ,,.Reversible posterior leukoencephalopathy syndrome and bevacizumab.N Engl J Med.2006;354(9):980–982.
- ,,, et al.A reversible posterior leukoencephalopathy syndrome.N Engl J Med.1996;334(8):494–500.
- ,,,,,.Reversible posterior leukoencephalopathy syndrome complicating cytotoxic chemotherapy for hematologic malignancies.Am J Hematol.2004;77(1):72–76.
- ,,, et al.Posterior leukoencephalopathy without severe hypertension: utility of diffusion‐weighted MRI.Neurology.1998;51(5):1369–1376.
- .Posterior leukoencephalopathy syndrome.Postgrad Med J.2001;77(903):24–28.
Pemetrexed
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Chandra P. Belani reports that maintenance therapy with pemetrexed significantly improves overall survival in advanced non-small cell lung cancer. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Elderly Patients & Pneumonia, Metoprolol after Vascular Surgery, and More

Elderly Pneumonia Patients after Antibiotic Switch
Nathan RV, Rhew DC, Bratzler DW, et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006 Jun;119(6):512.e1-7.
Community-acquired pneumonia (CAP) continues to be a common reason for hospital admission—especially among the elderly. As with many infectious diseases, the duration and route of antibiotic therapy is often based on expert recommendations rather than prospective randomized trials. The Patient Outcome Research Team (PORT) trials address the decision to admit a patient, but not other aspects of care. For hospitalists, the decision of when to discharge any patient with reasonable safety is often fraught with uncertainty. This study addresses the necessity of observing a patient for one day following the switch from IV to oral therapy. Two previous smaller retrospective studies have suggested this was unnecessary.
The current study is also retrospective but involves a large database derived from the U.S. Medicare National Pneumonia Project database. Ultimately 5,248 patients over 65 (mean age=80) were selected for analysis; 2,536 were not observed; and 2,712 were observed for one day.) Patients were excluded if their length of stay was greater than seven days or less than two days, suggesting complicated cases in the former instance and mild illness in the latter (i.e., perhaps not even requiring admission). Immunosupressed patients were also excluded. There was no significant difference in the observed 30-day mortality (5.1% in the “not observed” versus 4.4% in the “observed” cohort, respectively).
The obvious limitation of this study is that it was retrospective/observational and thus potentially subject to the bias inherent in this study design. It is possible that the sicker patients were logically watched longer. Propensity analysis was not a component of this study. The authors do present reasons why certain structural weaknesses would have favored the “observed “group.
Certainly there may be other reasons to observe a patient after the switch to oral therapy. A patient with associated gastrointestinal disturbance or a questionable history of GI or other intolerance to a class of antibiotics is an obvious example. Nevertheless, this study should convey a certain confidence to hospitalists when they assess the suitability for discharge for the type of patient covered in this analysis. Interestingly the recently published guidelines for treatment of community acquired pneumonia are concordant with this study.1
Reference
- Mandell L, Wundrelink A, Bartlett J. Guideline for the treatment of community acquired pneumonia. Clin Infect Dis. 2007;44: S27-72.
The Revised Geneva Score for PE
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department. Ann Intern Med. 2006 Feb 7:144(3):165-171. Comment in: ACP J Club. 2006 Jul-Aug;145(1):25 & Ann Intern Med. 2006 Feb 7;144(3):210-212.
Pulmonary embolism is a diagnosis frequently considered by the hospitalist—both as an explanation for the admitting clinical picture, as well as a complication arising during the course of a hospitalization for another condition.
My institutions’ ability to identify patients with this potentially lethal condition has greatly improved with the advent of multidetector CT angiography and various diagnostic schemata that include d-dimer testing and estimations of pre-test probability. It is a classic consideration whenever there is a onset of pleurisy, dyspnea, or aggravation thereof. Nevertheless multiple other situations arise in the hospital setting, such as unexplained tachycardia, hemoptysis, or vaguely possible but not clear-cut pleuritic chest pain, in which one feels obligated to at least consider the diagnosis. Further, to have to incorporate d-dimer testing into the diagnostic strategy is problematic as up to 80% of hospitalized patients are likely to be positive. Hospitalists need a reasonable strategy to avoid going down that proverbial pathway in certain low risk situations.
The Geneva scoring system and the Wells system are two methodologies that have been used in lieu of or as an adjunct to “clinical judgment.” The former requires arterial blood gases and the latter has as criteria “other diagnosis more likely than pulmonary embolus” that can be problematic and difficult to standardize.
This article presents a revised Geneva scoring system based solely on elements of the history and physical examination. The elements were derived retrospectively from a prior different study on diagnostic strategies for pulmonary thromboembolism (PTE). A different prospective study on PTE was utilized for the validation arm of this study. By logistical regression analysis the following eight elements were incorporated into the revised Geneva score: Age greater than 65 (1 point), previous deep venous thrombosis or pulmonary embolism (3 points), surgery or fracture within one month (2 points), active malignant condition (2 points), unilateral lower limb pain (3 points), hemoptysis (2 points), heart rate 75 to 94 beats/min (3 points) or heart rate 95 beats /minute or more (5 points), and pain on lower limb palpation and unilateral edema (4 points). The prevalence for pulmonary embolism was as follows: low probability or 8% (0 to 3 points), intermediate probability or 28% (4 to 10 points), and high probability or 74% (equal or greater than 11 points).
Significance for hospitalists: This scoring system is not validated a management system per se. However in the imperfect world of clinical reasoning it can help reinforce a thoughtful decision not to embark on the diagnostic path for pulmonary embolism, with its own inherent risks.
Metoprolol after Vascular Surgery
Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of metoprolol after vascular surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006 Nov;152(5):983-990. Comment in Am Heart J. 2006 Nov;152(5):815-818. McCullough PA. Failure of beta-blockers in the reduction of perioperative events: where did we go wrong? Am Heart J. 2006 Nov;152(5):815-818. Comment in: Am Heart J. 2006 Nov;152(5):983-990.
Hospitalists are frequently consulted regarding perioperative risk assessment and reduction for patients undergoing non-cardiac surgery. Over the last decade and supported by a few studies, the perioperative use of beta-blocker therapy has resolved the uncertainty frequently encountered. The McFalls study in 2004 showed no benefit to routine coronary revascularization for patients undergoing vascular surgery deemed at risk for myocardial ischemia.1 This provided further confidence for those of us supplying these preoperative assessments. However, the Lindenauer study in 2005 (a retrospective cohort analysis) was the first indication that perioperative beta blockade could be harmful.2 Lower-risk patients based on the revised cardiovascular index (RCRI) score actually did worse when treated. Still the ACC guidelines published in 2006 suggested perioperative beta blockers be considered for lower risk patients undergoing vascular surgery.3
This study is a randomized placebo-controlled trial of perioperative beta-blocker therapy in 500 treatment-naïve patients undergoing vascular surgery. Metoprolol was started two hours before surgery and continued for one week. Cardiovascular endpoints included cardiac death, arrhythmia requiring treatment, acute myocardial infarction or acute coronary syndrome, and congestive heart failure. No benefit was found for treatment with metoprolol regardless of the number of Revised Cardiac Risk Index (RCRI) factors present. No excess adverse outcomes were noted for therapy although intraoperative bradycardia and hypotension were significantly increased in the active treatment group.
In the accompanying editorial McCullough discusses possible reasons and implications of these findings. In fact, two other trials have reported similar findings. In contrast to the older trials suggesting a benefit to perioperative beta blockade these newer trials are larger and have a stronger design. He also notes that the patients in the more recent trials are more likely to have prior revascularization and hence are less prone to demand-type events, reflective of the type of insult beta blockade would most likely be helpful in preventing. These events may be more closely allied with plaque destabilization of subcritical lesions, with factors such as perioperative hypercoagulability and perhaps inflammation being more important. In this regard it is notable that recent trials on the perioperative use of statins have demonstrated favorable results, with these agents presumably acting to promote plaque stability, the so-called “pleiotropic” function of statins.
Significance for hospitalists: It is reasonable to be more circumspect in the recommendation of perioperative beta blockade. This practice is not likely the magic bullet, which is a common misconcpetion. An indicative situation is an 80-year-old patient undergoing total hip replacement. He has diabetes, COPD, and hypertension, a pulse of 65, a blood pressure of 110/50. There may also be concerns about bradycardia, hypotension, and bronchospasm. Given this analysis a clinician can be confident in withholding perioperative treatment.
The use of beta-blocker therapy in a patient with a single RCRI factor, which is not coronary artery disease, does not seem justified. On the other hand the use of perioperative statins should be more actively entertained. Emerging recommendations from various specialty organizations and other relevant professional entities should be anticipated and sought.
Bibliography
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Eng J Med. 2004Dec 30;351(27):2795-2804.
- Lindenauer PK, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Eng J Med. 2005 Jul 28;353(4):349-361.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery. J Am Coll Cardiol. 2006;47: 2343-2355
The New C. Diff Epidemic
Bartlett JG. Narrative review: the new epidemic of Clostridium difficile-associated enteric disease. Ann Intern Med. 2006 Nov 21;145(10):758-764.
C. difficile infection is emerging as one of the most important illnesses for hospitalists to be facile with. It not only occurs frequently, but is also often severe or life threatening, and most importantly iatrogenic and preventable. This review by Bartlett, who elucidated the cause of this disease in 1978, reviews important up-to-date information on C. difficile, focusing on the recent emergence of a more virulent form of the disease.
Infectious diarrhea that develops in the hospital is almost always due to C. difficile. The tissue culture cytotoxic assay (first described in 1978) remains the most sensitive and specific diagnostic tool. The toxin immunoassay used most routinely is only 75% sensitive.
An epidemic of unusually severe C. difficile was first described in Quebec in 2001. Important features include a higher tendency for toxic megacolon and a need for colectomy, protein-losing enteropathy, leukemoid reactions, refractoriness to treatment, a high rate of relapse and an astonishing 16.5% attributable mortality. Fluoroquinolones are the leading associated antibiotic causal factor, although extended spectrum cephalosporins remain important as well in this regard. The new strain is characterized by high levels of toxin production due to the deletion of a toxin production regulatory gene. The strain is also fluoroquinolone resistant, explaining the role of that antibiotic in its genesis.
Treatment of C. difficile colitis (especially the emergent strain) remains problematic. In particular the role of metronidazole versus vancomycin as initial therapy is often contentious. Bartlett cites some evidence suggesting vancomycin may be more effective and is especially recommended for severe disease, characteristics of which are often manifested by this new strain.
This review cites important considerations that hospitalist ought to vigilant and proactive in. Given the high risk of fluoroquinolone treatment we must be sure that these drugs are used appropriately. Nonchalantly stacking on levofloxacin therapy for the COPD flair without evidence for pneumonia should be discouraged. When possible antibiotics with a lower risk for C. difficile (sulfonamides, macrolides, tetracyclines) should be used for any infection. When disease is suspected, a negative toxin immunoassay should not discourage empiric treatment especially in a very ill patient. Isolation and barrier precautions are important in preventing the spread of this potentially lethal infection. C. difficile spores are not killed by alcohol-based detergents, and either soap and water or gloves are necessary to care for these patients. When your hospital experiences a clustering of severe C. difficile infection, alert appropriate infection control personnel. Administrative control of antibiotic use may be indicated.
Baclofen Versus Diazepam to Treat Alcohol Withdrawal
Addolorato G, Leggio L, Abenavoli L, et al. Baclofen in the treatment of alcohol withdrawal syndrome: a comparative study vs diazepam. Am J Med. 2006 Mar;119 (3):276.e13-18.
Alcohol withdrawal syndrome (AWS) is a frequent problem encountered in hospitalized patients; its management is considered one of SHM’s core competencies for hospitalists. Benzodiazepines are the gold standard of therapy for this problem given their established record for safety and efficacy; however, their use can be problematic in certain instances.
This study involved 37 outpatients, as inpatients may often be sicker and at higher risk of severe withdrawal.
There is a definite risk of oversedation—especially in patients with COPD or chronic liver disease. Some patients require inordinately high doses of benzodiazepines, thus setting the stage for a prolonged hospitalization. Occasional paradoxical or disinhibition reactions to benzodiazepines can also be problematic. Addiction and or diversion are also a concern in patients prone to substance abuse. An otherwise stable patient, ready for discharge, may still be on a relatively high dose of lorazepam, but it is generally not prudent to send the patient out with a supply of medication to finish the course given concerns over resumption of drinking while on the sedative. Conversely, the solution can be cold comfort for the attending physician if the patient resumes drinking, thus eliminating the need for additional medication.
Baclofen, a stereoselective gamma-aminobutyric acid agonist, has a long history of safety in the treatment of spasticity. As such it can counter balance the activation of the glutamate excitatory pathway that characterizes AWS. It has been proposed as an alternative treatment for AWS that would not share the above concerns cited for benzodiazepines.
This study is a randomized controlled trial of baclofen versus valium in the treatment for AWS. Thirty-seven subjects with a history of heavy alcohol use were randomized to either baclofen 30 mg per day or valium 0.5 to 0.75 mg/kg. All were outpatients treated for 10 days. Clinical Institute Withdrawal Assessment-Alcohol (CIWA) scores were assessed daily. Both regimens continuously decreased the baseline elevation of CIWA scores daily over the course of the study, without a significant difference in treatment efficacy. No adverse events or side effects were reported in either group.
Other than baseline CIWA and daily alcohol consumption, it is not clear that the two groups were at equal risk for severe withdrawal reactions. Relevant baseline characteristics such as history of seizures or delirium tremens, factors that raise this risk were not noted.
Significance for hospitalists: With a long history of safety and efficacy, benzodiazepines remain the drugs of choice for hospitalists treating patients with AWS. In certain instances it may be desirable to limit or even avoid their use. How effective and safe baclofen would be in filling this role remains to be fully established. In particular the relative risk for sedation and respiratory depression has not been defined. Nevertheless at least in my institutions, as guided by expert consultation, its use has been carefully considered and proven helpful in some of the situations noted above. TH
Elderly Pneumonia Patients after Antibiotic Switch
Nathan RV, Rhew DC, Bratzler DW, et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006 Jun;119(6):512.e1-7.
Community-acquired pneumonia (CAP) continues to be a common reason for hospital admission—especially among the elderly. As with many infectious diseases, the duration and route of antibiotic therapy is often based on expert recommendations rather than prospective randomized trials. The Patient Outcome Research Team (PORT) trials address the decision to admit a patient, but not other aspects of care. For hospitalists, the decision of when to discharge any patient with reasonable safety is often fraught with uncertainty. This study addresses the necessity of observing a patient for one day following the switch from IV to oral therapy. Two previous smaller retrospective studies have suggested this was unnecessary.
The current study is also retrospective but involves a large database derived from the U.S. Medicare National Pneumonia Project database. Ultimately 5,248 patients over 65 (mean age=80) were selected for analysis; 2,536 were not observed; and 2,712 were observed for one day.) Patients were excluded if their length of stay was greater than seven days or less than two days, suggesting complicated cases in the former instance and mild illness in the latter (i.e., perhaps not even requiring admission). Immunosupressed patients were also excluded. There was no significant difference in the observed 30-day mortality (5.1% in the “not observed” versus 4.4% in the “observed” cohort, respectively).
The obvious limitation of this study is that it was retrospective/observational and thus potentially subject to the bias inherent in this study design. It is possible that the sicker patients were logically watched longer. Propensity analysis was not a component of this study. The authors do present reasons why certain structural weaknesses would have favored the “observed “group.
Certainly there may be other reasons to observe a patient after the switch to oral therapy. A patient with associated gastrointestinal disturbance or a questionable history of GI or other intolerance to a class of antibiotics is an obvious example. Nevertheless, this study should convey a certain confidence to hospitalists when they assess the suitability for discharge for the type of patient covered in this analysis. Interestingly the recently published guidelines for treatment of community acquired pneumonia are concordant with this study.1
Reference
- Mandell L, Wundrelink A, Bartlett J. Guideline for the treatment of community acquired pneumonia. Clin Infect Dis. 2007;44: S27-72.
The Revised Geneva Score for PE
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department. Ann Intern Med. 2006 Feb 7:144(3):165-171. Comment in: ACP J Club. 2006 Jul-Aug;145(1):25 & Ann Intern Med. 2006 Feb 7;144(3):210-212.
Pulmonary embolism is a diagnosis frequently considered by the hospitalist—both as an explanation for the admitting clinical picture, as well as a complication arising during the course of a hospitalization for another condition.
My institutions’ ability to identify patients with this potentially lethal condition has greatly improved with the advent of multidetector CT angiography and various diagnostic schemata that include d-dimer testing and estimations of pre-test probability. It is a classic consideration whenever there is a onset of pleurisy, dyspnea, or aggravation thereof. Nevertheless multiple other situations arise in the hospital setting, such as unexplained tachycardia, hemoptysis, or vaguely possible but not clear-cut pleuritic chest pain, in which one feels obligated to at least consider the diagnosis. Further, to have to incorporate d-dimer testing into the diagnostic strategy is problematic as up to 80% of hospitalized patients are likely to be positive. Hospitalists need a reasonable strategy to avoid going down that proverbial pathway in certain low risk situations.
The Geneva scoring system and the Wells system are two methodologies that have been used in lieu of or as an adjunct to “clinical judgment.” The former requires arterial blood gases and the latter has as criteria “other diagnosis more likely than pulmonary embolus” that can be problematic and difficult to standardize.
This article presents a revised Geneva scoring system based solely on elements of the history and physical examination. The elements were derived retrospectively from a prior different study on diagnostic strategies for pulmonary thromboembolism (PTE). A different prospective study on PTE was utilized for the validation arm of this study. By logistical regression analysis the following eight elements were incorporated into the revised Geneva score: Age greater than 65 (1 point), previous deep venous thrombosis or pulmonary embolism (3 points), surgery or fracture within one month (2 points), active malignant condition (2 points), unilateral lower limb pain (3 points), hemoptysis (2 points), heart rate 75 to 94 beats/min (3 points) or heart rate 95 beats /minute or more (5 points), and pain on lower limb palpation and unilateral edema (4 points). The prevalence for pulmonary embolism was as follows: low probability or 8% (0 to 3 points), intermediate probability or 28% (4 to 10 points), and high probability or 74% (equal or greater than 11 points).
Significance for hospitalists: This scoring system is not validated a management system per se. However in the imperfect world of clinical reasoning it can help reinforce a thoughtful decision not to embark on the diagnostic path for pulmonary embolism, with its own inherent risks.
Metoprolol after Vascular Surgery
Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of metoprolol after vascular surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006 Nov;152(5):983-990. Comment in Am Heart J. 2006 Nov;152(5):815-818. McCullough PA. Failure of beta-blockers in the reduction of perioperative events: where did we go wrong? Am Heart J. 2006 Nov;152(5):815-818. Comment in: Am Heart J. 2006 Nov;152(5):983-990.
Hospitalists are frequently consulted regarding perioperative risk assessment and reduction for patients undergoing non-cardiac surgery. Over the last decade and supported by a few studies, the perioperative use of beta-blocker therapy has resolved the uncertainty frequently encountered. The McFalls study in 2004 showed no benefit to routine coronary revascularization for patients undergoing vascular surgery deemed at risk for myocardial ischemia.1 This provided further confidence for those of us supplying these preoperative assessments. However, the Lindenauer study in 2005 (a retrospective cohort analysis) was the first indication that perioperative beta blockade could be harmful.2 Lower-risk patients based on the revised cardiovascular index (RCRI) score actually did worse when treated. Still the ACC guidelines published in 2006 suggested perioperative beta blockers be considered for lower risk patients undergoing vascular surgery.3
This study is a randomized placebo-controlled trial of perioperative beta-blocker therapy in 500 treatment-naïve patients undergoing vascular surgery. Metoprolol was started two hours before surgery and continued for one week. Cardiovascular endpoints included cardiac death, arrhythmia requiring treatment, acute myocardial infarction or acute coronary syndrome, and congestive heart failure. No benefit was found for treatment with metoprolol regardless of the number of Revised Cardiac Risk Index (RCRI) factors present. No excess adverse outcomes were noted for therapy although intraoperative bradycardia and hypotension were significantly increased in the active treatment group.
In the accompanying editorial McCullough discusses possible reasons and implications of these findings. In fact, two other trials have reported similar findings. In contrast to the older trials suggesting a benefit to perioperative beta blockade these newer trials are larger and have a stronger design. He also notes that the patients in the more recent trials are more likely to have prior revascularization and hence are less prone to demand-type events, reflective of the type of insult beta blockade would most likely be helpful in preventing. These events may be more closely allied with plaque destabilization of subcritical lesions, with factors such as perioperative hypercoagulability and perhaps inflammation being more important. In this regard it is notable that recent trials on the perioperative use of statins have demonstrated favorable results, with these agents presumably acting to promote plaque stability, the so-called “pleiotropic” function of statins.
Significance for hospitalists: It is reasonable to be more circumspect in the recommendation of perioperative beta blockade. This practice is not likely the magic bullet, which is a common misconcpetion. An indicative situation is an 80-year-old patient undergoing total hip replacement. He has diabetes, COPD, and hypertension, a pulse of 65, a blood pressure of 110/50. There may also be concerns about bradycardia, hypotension, and bronchospasm. Given this analysis a clinician can be confident in withholding perioperative treatment.
The use of beta-blocker therapy in a patient with a single RCRI factor, which is not coronary artery disease, does not seem justified. On the other hand the use of perioperative statins should be more actively entertained. Emerging recommendations from various specialty organizations and other relevant professional entities should be anticipated and sought.
Bibliography
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Eng J Med. 2004Dec 30;351(27):2795-2804.
- Lindenauer PK, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Eng J Med. 2005 Jul 28;353(4):349-361.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery. J Am Coll Cardiol. 2006;47: 2343-2355
The New C. Diff Epidemic
Bartlett JG. Narrative review: the new epidemic of Clostridium difficile-associated enteric disease. Ann Intern Med. 2006 Nov 21;145(10):758-764.
C. difficile infection is emerging as one of the most important illnesses for hospitalists to be facile with. It not only occurs frequently, but is also often severe or life threatening, and most importantly iatrogenic and preventable. This review by Bartlett, who elucidated the cause of this disease in 1978, reviews important up-to-date information on C. difficile, focusing on the recent emergence of a more virulent form of the disease.
Infectious diarrhea that develops in the hospital is almost always due to C. difficile. The tissue culture cytotoxic assay (first described in 1978) remains the most sensitive and specific diagnostic tool. The toxin immunoassay used most routinely is only 75% sensitive.
An epidemic of unusually severe C. difficile was first described in Quebec in 2001. Important features include a higher tendency for toxic megacolon and a need for colectomy, protein-losing enteropathy, leukemoid reactions, refractoriness to treatment, a high rate of relapse and an astonishing 16.5% attributable mortality. Fluoroquinolones are the leading associated antibiotic causal factor, although extended spectrum cephalosporins remain important as well in this regard. The new strain is characterized by high levels of toxin production due to the deletion of a toxin production regulatory gene. The strain is also fluoroquinolone resistant, explaining the role of that antibiotic in its genesis.
Treatment of C. difficile colitis (especially the emergent strain) remains problematic. In particular the role of metronidazole versus vancomycin as initial therapy is often contentious. Bartlett cites some evidence suggesting vancomycin may be more effective and is especially recommended for severe disease, characteristics of which are often manifested by this new strain.
This review cites important considerations that hospitalist ought to vigilant and proactive in. Given the high risk of fluoroquinolone treatment we must be sure that these drugs are used appropriately. Nonchalantly stacking on levofloxacin therapy for the COPD flair without evidence for pneumonia should be discouraged. When possible antibiotics with a lower risk for C. difficile (sulfonamides, macrolides, tetracyclines) should be used for any infection. When disease is suspected, a negative toxin immunoassay should not discourage empiric treatment especially in a very ill patient. Isolation and barrier precautions are important in preventing the spread of this potentially lethal infection. C. difficile spores are not killed by alcohol-based detergents, and either soap and water or gloves are necessary to care for these patients. When your hospital experiences a clustering of severe C. difficile infection, alert appropriate infection control personnel. Administrative control of antibiotic use may be indicated.
Baclofen Versus Diazepam to Treat Alcohol Withdrawal
Addolorato G, Leggio L, Abenavoli L, et al. Baclofen in the treatment of alcohol withdrawal syndrome: a comparative study vs diazepam. Am J Med. 2006 Mar;119 (3):276.e13-18.
Alcohol withdrawal syndrome (AWS) is a frequent problem encountered in hospitalized patients; its management is considered one of SHM’s core competencies for hospitalists. Benzodiazepines are the gold standard of therapy for this problem given their established record for safety and efficacy; however, their use can be problematic in certain instances.
This study involved 37 outpatients, as inpatients may often be sicker and at higher risk of severe withdrawal.
There is a definite risk of oversedation—especially in patients with COPD or chronic liver disease. Some patients require inordinately high doses of benzodiazepines, thus setting the stage for a prolonged hospitalization. Occasional paradoxical or disinhibition reactions to benzodiazepines can also be problematic. Addiction and or diversion are also a concern in patients prone to substance abuse. An otherwise stable patient, ready for discharge, may still be on a relatively high dose of lorazepam, but it is generally not prudent to send the patient out with a supply of medication to finish the course given concerns over resumption of drinking while on the sedative. Conversely, the solution can be cold comfort for the attending physician if the patient resumes drinking, thus eliminating the need for additional medication.
Baclofen, a stereoselective gamma-aminobutyric acid agonist, has a long history of safety in the treatment of spasticity. As such it can counter balance the activation of the glutamate excitatory pathway that characterizes AWS. It has been proposed as an alternative treatment for AWS that would not share the above concerns cited for benzodiazepines.
This study is a randomized controlled trial of baclofen versus valium in the treatment for AWS. Thirty-seven subjects with a history of heavy alcohol use were randomized to either baclofen 30 mg per day or valium 0.5 to 0.75 mg/kg. All were outpatients treated for 10 days. Clinical Institute Withdrawal Assessment-Alcohol (CIWA) scores were assessed daily. Both regimens continuously decreased the baseline elevation of CIWA scores daily over the course of the study, without a significant difference in treatment efficacy. No adverse events or side effects were reported in either group.
Other than baseline CIWA and daily alcohol consumption, it is not clear that the two groups were at equal risk for severe withdrawal reactions. Relevant baseline characteristics such as history of seizures or delirium tremens, factors that raise this risk were not noted.
Significance for hospitalists: With a long history of safety and efficacy, benzodiazepines remain the drugs of choice for hospitalists treating patients with AWS. In certain instances it may be desirable to limit or even avoid their use. How effective and safe baclofen would be in filling this role remains to be fully established. In particular the relative risk for sedation and respiratory depression has not been defined. Nevertheless at least in my institutions, as guided by expert consultation, its use has been carefully considered and proven helpful in some of the situations noted above. TH
Elderly Pneumonia Patients after Antibiotic Switch
Nathan RV, Rhew DC, Bratzler DW, et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006 Jun;119(6):512.e1-7.
Community-acquired pneumonia (CAP) continues to be a common reason for hospital admission—especially among the elderly. As with many infectious diseases, the duration and route of antibiotic therapy is often based on expert recommendations rather than prospective randomized trials. The Patient Outcome Research Team (PORT) trials address the decision to admit a patient, but not other aspects of care. For hospitalists, the decision of when to discharge any patient with reasonable safety is often fraught with uncertainty. This study addresses the necessity of observing a patient for one day following the switch from IV to oral therapy. Two previous smaller retrospective studies have suggested this was unnecessary.
The current study is also retrospective but involves a large database derived from the U.S. Medicare National Pneumonia Project database. Ultimately 5,248 patients over 65 (mean age=80) were selected for analysis; 2,536 were not observed; and 2,712 were observed for one day.) Patients were excluded if their length of stay was greater than seven days or less than two days, suggesting complicated cases in the former instance and mild illness in the latter (i.e., perhaps not even requiring admission). Immunosupressed patients were also excluded. There was no significant difference in the observed 30-day mortality (5.1% in the “not observed” versus 4.4% in the “observed” cohort, respectively).
The obvious limitation of this study is that it was retrospective/observational and thus potentially subject to the bias inherent in this study design. It is possible that the sicker patients were logically watched longer. Propensity analysis was not a component of this study. The authors do present reasons why certain structural weaknesses would have favored the “observed “group.
Certainly there may be other reasons to observe a patient after the switch to oral therapy. A patient with associated gastrointestinal disturbance or a questionable history of GI or other intolerance to a class of antibiotics is an obvious example. Nevertheless, this study should convey a certain confidence to hospitalists when they assess the suitability for discharge for the type of patient covered in this analysis. Interestingly the recently published guidelines for treatment of community acquired pneumonia are concordant with this study.1
Reference
- Mandell L, Wundrelink A, Bartlett J. Guideline for the treatment of community acquired pneumonia. Clin Infect Dis. 2007;44: S27-72.
The Revised Geneva Score for PE
Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department. Ann Intern Med. 2006 Feb 7:144(3):165-171. Comment in: ACP J Club. 2006 Jul-Aug;145(1):25 & Ann Intern Med. 2006 Feb 7;144(3):210-212.
Pulmonary embolism is a diagnosis frequently considered by the hospitalist—both as an explanation for the admitting clinical picture, as well as a complication arising during the course of a hospitalization for another condition.
My institutions’ ability to identify patients with this potentially lethal condition has greatly improved with the advent of multidetector CT angiography and various diagnostic schemata that include d-dimer testing and estimations of pre-test probability. It is a classic consideration whenever there is a onset of pleurisy, dyspnea, or aggravation thereof. Nevertheless multiple other situations arise in the hospital setting, such as unexplained tachycardia, hemoptysis, or vaguely possible but not clear-cut pleuritic chest pain, in which one feels obligated to at least consider the diagnosis. Further, to have to incorporate d-dimer testing into the diagnostic strategy is problematic as up to 80% of hospitalized patients are likely to be positive. Hospitalists need a reasonable strategy to avoid going down that proverbial pathway in certain low risk situations.
The Geneva scoring system and the Wells system are two methodologies that have been used in lieu of or as an adjunct to “clinical judgment.” The former requires arterial blood gases and the latter has as criteria “other diagnosis more likely than pulmonary embolus” that can be problematic and difficult to standardize.
This article presents a revised Geneva scoring system based solely on elements of the history and physical examination. The elements were derived retrospectively from a prior different study on diagnostic strategies for pulmonary thromboembolism (PTE). A different prospective study on PTE was utilized for the validation arm of this study. By logistical regression analysis the following eight elements were incorporated into the revised Geneva score: Age greater than 65 (1 point), previous deep venous thrombosis or pulmonary embolism (3 points), surgery or fracture within one month (2 points), active malignant condition (2 points), unilateral lower limb pain (3 points), hemoptysis (2 points), heart rate 75 to 94 beats/min (3 points) or heart rate 95 beats /minute or more (5 points), and pain on lower limb palpation and unilateral edema (4 points). The prevalence for pulmonary embolism was as follows: low probability or 8% (0 to 3 points), intermediate probability or 28% (4 to 10 points), and high probability or 74% (equal or greater than 11 points).
Significance for hospitalists: This scoring system is not validated a management system per se. However in the imperfect world of clinical reasoning it can help reinforce a thoughtful decision not to embark on the diagnostic path for pulmonary embolism, with its own inherent risks.
Metoprolol after Vascular Surgery
Yang H, Raymer K, Butler R, et al. The effects of perioperative beta-blockade: results of metoprolol after vascular surgery (MaVS) study, a randomized controlled trial. Am Heart J. 2006 Nov;152(5):983-990. Comment in Am Heart J. 2006 Nov;152(5):815-818. McCullough PA. Failure of beta-blockers in the reduction of perioperative events: where did we go wrong? Am Heart J. 2006 Nov;152(5):815-818. Comment in: Am Heart J. 2006 Nov;152(5):983-990.
Hospitalists are frequently consulted regarding perioperative risk assessment and reduction for patients undergoing non-cardiac surgery. Over the last decade and supported by a few studies, the perioperative use of beta-blocker therapy has resolved the uncertainty frequently encountered. The McFalls study in 2004 showed no benefit to routine coronary revascularization for patients undergoing vascular surgery deemed at risk for myocardial ischemia.1 This provided further confidence for those of us supplying these preoperative assessments. However, the Lindenauer study in 2005 (a retrospective cohort analysis) was the first indication that perioperative beta blockade could be harmful.2 Lower-risk patients based on the revised cardiovascular index (RCRI) score actually did worse when treated. Still the ACC guidelines published in 2006 suggested perioperative beta blockers be considered for lower risk patients undergoing vascular surgery.3
This study is a randomized placebo-controlled trial of perioperative beta-blocker therapy in 500 treatment-naïve patients undergoing vascular surgery. Metoprolol was started two hours before surgery and continued for one week. Cardiovascular endpoints included cardiac death, arrhythmia requiring treatment, acute myocardial infarction or acute coronary syndrome, and congestive heart failure. No benefit was found for treatment with metoprolol regardless of the number of Revised Cardiac Risk Index (RCRI) factors present. No excess adverse outcomes were noted for therapy although intraoperative bradycardia and hypotension were significantly increased in the active treatment group.
In the accompanying editorial McCullough discusses possible reasons and implications of these findings. In fact, two other trials have reported similar findings. In contrast to the older trials suggesting a benefit to perioperative beta blockade these newer trials are larger and have a stronger design. He also notes that the patients in the more recent trials are more likely to have prior revascularization and hence are less prone to demand-type events, reflective of the type of insult beta blockade would most likely be helpful in preventing. These events may be more closely allied with plaque destabilization of subcritical lesions, with factors such as perioperative hypercoagulability and perhaps inflammation being more important. In this regard it is notable that recent trials on the perioperative use of statins have demonstrated favorable results, with these agents presumably acting to promote plaque stability, the so-called “pleiotropic” function of statins.
Significance for hospitalists: It is reasonable to be more circumspect in the recommendation of perioperative beta blockade. This practice is not likely the magic bullet, which is a common misconcpetion. An indicative situation is an 80-year-old patient undergoing total hip replacement. He has diabetes, COPD, and hypertension, a pulse of 65, a blood pressure of 110/50. There may also be concerns about bradycardia, hypotension, and bronchospasm. Given this analysis a clinician can be confident in withholding perioperative treatment.
The use of beta-blocker therapy in a patient with a single RCRI factor, which is not coronary artery disease, does not seem justified. On the other hand the use of perioperative statins should be more actively entertained. Emerging recommendations from various specialty organizations and other relevant professional entities should be anticipated and sought.
Bibliography
- McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery. N Eng J Med. 2004Dec 30;351(27):2795-2804.
- Lindenauer PK, Pekow P, Wang K, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Eng J Med. 2005 Jul 28;353(4):349-361.
- Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery. J Am Coll Cardiol. 2006;47: 2343-2355
The New C. Diff Epidemic
Bartlett JG. Narrative review: the new epidemic of Clostridium difficile-associated enteric disease. Ann Intern Med. 2006 Nov 21;145(10):758-764.
C. difficile infection is emerging as one of the most important illnesses for hospitalists to be facile with. It not only occurs frequently, but is also often severe or life threatening, and most importantly iatrogenic and preventable. This review by Bartlett, who elucidated the cause of this disease in 1978, reviews important up-to-date information on C. difficile, focusing on the recent emergence of a more virulent form of the disease.
Infectious diarrhea that develops in the hospital is almost always due to C. difficile. The tissue culture cytotoxic assay (first described in 1978) remains the most sensitive and specific diagnostic tool. The toxin immunoassay used most routinely is only 75% sensitive.
An epidemic of unusually severe C. difficile was first described in Quebec in 2001. Important features include a higher tendency for toxic megacolon and a need for colectomy, protein-losing enteropathy, leukemoid reactions, refractoriness to treatment, a high rate of relapse and an astonishing 16.5% attributable mortality. Fluoroquinolones are the leading associated antibiotic causal factor, although extended spectrum cephalosporins remain important as well in this regard. The new strain is characterized by high levels of toxin production due to the deletion of a toxin production regulatory gene. The strain is also fluoroquinolone resistant, explaining the role of that antibiotic in its genesis.
Treatment of C. difficile colitis (especially the emergent strain) remains problematic. In particular the role of metronidazole versus vancomycin as initial therapy is often contentious. Bartlett cites some evidence suggesting vancomycin may be more effective and is especially recommended for severe disease, characteristics of which are often manifested by this new strain.
This review cites important considerations that hospitalist ought to vigilant and proactive in. Given the high risk of fluoroquinolone treatment we must be sure that these drugs are used appropriately. Nonchalantly stacking on levofloxacin therapy for the COPD flair without evidence for pneumonia should be discouraged. When possible antibiotics with a lower risk for C. difficile (sulfonamides, macrolides, tetracyclines) should be used for any infection. When disease is suspected, a negative toxin immunoassay should not discourage empiric treatment especially in a very ill patient. Isolation and barrier precautions are important in preventing the spread of this potentially lethal infection. C. difficile spores are not killed by alcohol-based detergents, and either soap and water or gloves are necessary to care for these patients. When your hospital experiences a clustering of severe C. difficile infection, alert appropriate infection control personnel. Administrative control of antibiotic use may be indicated.
Baclofen Versus Diazepam to Treat Alcohol Withdrawal
Addolorato G, Leggio L, Abenavoli L, et al. Baclofen in the treatment of alcohol withdrawal syndrome: a comparative study vs diazepam. Am J Med. 2006 Mar;119 (3):276.e13-18.
Alcohol withdrawal syndrome (AWS) is a frequent problem encountered in hospitalized patients; its management is considered one of SHM’s core competencies for hospitalists. Benzodiazepines are the gold standard of therapy for this problem given their established record for safety and efficacy; however, their use can be problematic in certain instances.
This study involved 37 outpatients, as inpatients may often be sicker and at higher risk of severe withdrawal.
There is a definite risk of oversedation—especially in patients with COPD or chronic liver disease. Some patients require inordinately high doses of benzodiazepines, thus setting the stage for a prolonged hospitalization. Occasional paradoxical or disinhibition reactions to benzodiazepines can also be problematic. Addiction and or diversion are also a concern in patients prone to substance abuse. An otherwise stable patient, ready for discharge, may still be on a relatively high dose of lorazepam, but it is generally not prudent to send the patient out with a supply of medication to finish the course given concerns over resumption of drinking while on the sedative. Conversely, the solution can be cold comfort for the attending physician if the patient resumes drinking, thus eliminating the need for additional medication.
Baclofen, a stereoselective gamma-aminobutyric acid agonist, has a long history of safety in the treatment of spasticity. As such it can counter balance the activation of the glutamate excitatory pathway that characterizes AWS. It has been proposed as an alternative treatment for AWS that would not share the above concerns cited for benzodiazepines.
This study is a randomized controlled trial of baclofen versus valium in the treatment for AWS. Thirty-seven subjects with a history of heavy alcohol use were randomized to either baclofen 30 mg per day or valium 0.5 to 0.75 mg/kg. All were outpatients treated for 10 days. Clinical Institute Withdrawal Assessment-Alcohol (CIWA) scores were assessed daily. Both regimens continuously decreased the baseline elevation of CIWA scores daily over the course of the study, without a significant difference in treatment efficacy. No adverse events or side effects were reported in either group.
Other than baseline CIWA and daily alcohol consumption, it is not clear that the two groups were at equal risk for severe withdrawal reactions. Relevant baseline characteristics such as history of seizures or delirium tremens, factors that raise this risk were not noted.
Significance for hospitalists: With a long history of safety and efficacy, benzodiazepines remain the drugs of choice for hospitalists treating patients with AWS. In certain instances it may be desirable to limit or even avoid their use. How effective and safe baclofen would be in filling this role remains to be fully established. In particular the relative risk for sedation and respiratory depression has not been defined. Nevertheless at least in my institutions, as guided by expert consultation, its use has been carefully considered and proven helpful in some of the situations noted above. TH
New Path to Primary Care?
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."
A new bill that could steer more medical school students toward primary care is winding its way through Congress and will receive a careful look from SHM.
The Preserving Patient Access to Primary Care Act of 2009 (HR 2350) would provide financial assistance to medical students choosing a primary-care career, proposes changes to Medicare reimbursement, and suggests the development of measures to support and expand the patient-centered medical home (PCMH) model of care.
The bill, sponsored by U.S. Rep. Allyson Schwartz, D-Pa., has been endorsed by the American College of Physicians (ACP). In a press release, the ACP referred to the proposal as "the best medicine for curing the growing crisis in primary care."
SHM's Public Policy Committee will discuss HR 2350 during its June meeting. "SHM has been supportive of improving and expanding primary care because a strong primary-care base creates opportunities for a partnership with hospitalists," says Larry Wellikson, MD, FHM, CEO of SHM. "The committee also will look at HR 2350 from the hospitalist perspective and how it fits in with many of the other proposals that are part of healthcare reform."
In the Literature: The Latest Research You Need to Know
Clinical question: Are elevated fasting blood glucose levels independently associated with poor outcomes in all types of acute coronary syndromes (ACS)?
Background: Elevated admission blood glucose levels have been associated with poor outcomes in ACS patients; however, the role of fasting blood glucose levels in these settings, especially non-ST elevation myocardial infarction (NSTEMI), is unclear. It also is uncertain if one is a better predictor of outcomes than the other.
Study design: Prospective cohort of 57,406 patients in the Global Registry of Acute Coronary Events (GRACE).
Setting: 106 hospitals located in 14 countries in North and South America, Europe, Australia, and New Zealand.
Synopsis: 22,001 admission and 13,526 fasting blood glucose levels were extracted from GRACE and categorized into groups ranging from <100 mg/dL to =300 mg/dL. Multivariate logistic regression analysis of the association between these and the primary outcomes of in-hospital and six-month post-discharge all-cause mortality was carried out.
Fasting glucose levels higher than 100 mg/dL were associated with a linear increase in inpatient mortality (irrespective of diagnosis of diabetes) with an eightfold increase at levels =300mg/dL (17.22% vs. 1.71%). Increased six-month mortality, especially in patients with NSTEMI and STEMI, was also noted. However, this was a nonlinear relationship due to a lower mortality at 200-299 mg/dL, possibly reflecting the higher number of diabetics undergoing treatment in this group.
Admission glucose levels showed a linear increase in inpatient mortality at levels higher than 126 mg/dL. In contrast to fasting levels, admission levels were not associated with poor long-term outcome.
Study limitations included the use of registry data from a subgroup analysis and the possibility that fasting glucose levels in severely ill patients might not be representative of actual metabolic state.
Bottom line: Elevated fasting blood glucose in patients with acute coronary syndromes may portend a worse outcome and may be a better predictor than admission glucose levels.
Citation: Sinnaeve PR, Steg PG, Fox KA, et al. Association of elevated fasting glucose with increased short-term and 6-month mortality in ST-segment elevation and non-ST-segment elevation acute coronary syndromes: the Global Registry of Acute Coronary Events. Arch Intern Med. 2009;169(4):401-409.
— Reviewed for "TH eWire" by Mital Patel, MD, Alraies Chadi, MD, Saurabh Kandpal, MD, Iqbal Masood, MD, Anuradha Ramaswamy, MD, Department of Hospital Medicine, Cleveland Clinic
Clinical question: Are elevated fasting blood glucose levels independently associated with poor outcomes in all types of acute coronary syndromes (ACS)?
Background: Elevated admission blood glucose levels have been associated with poor outcomes in ACS patients; however, the role of fasting blood glucose levels in these settings, especially non-ST elevation myocardial infarction (NSTEMI), is unclear. It also is uncertain if one is a better predictor of outcomes than the other.
Study design: Prospective cohort of 57,406 patients in the Global Registry of Acute Coronary Events (GRACE).
Setting: 106 hospitals located in 14 countries in North and South America, Europe, Australia, and New Zealand.
Synopsis: 22,001 admission and 13,526 fasting blood glucose levels were extracted from GRACE and categorized into groups ranging from <100 mg/dL to =300 mg/dL. Multivariate logistic regression analysis of the association between these and the primary outcomes of in-hospital and six-month post-discharge all-cause mortality was carried out.
Fasting glucose levels higher than 100 mg/dL were associated with a linear increase in inpatient mortality (irrespective of diagnosis of diabetes) with an eightfold increase at levels =300mg/dL (17.22% vs. 1.71%). Increased six-month mortality, especially in patients with NSTEMI and STEMI, was also noted. However, this was a nonlinear relationship due to a lower mortality at 200-299 mg/dL, possibly reflecting the higher number of diabetics undergoing treatment in this group.
Admission glucose levels showed a linear increase in inpatient mortality at levels higher than 126 mg/dL. In contrast to fasting levels, admission levels were not associated with poor long-term outcome.
Study limitations included the use of registry data from a subgroup analysis and the possibility that fasting glucose levels in severely ill patients might not be representative of actual metabolic state.
Bottom line: Elevated fasting blood glucose in patients with acute coronary syndromes may portend a worse outcome and may be a better predictor than admission glucose levels.
Citation: Sinnaeve PR, Steg PG, Fox KA, et al. Association of elevated fasting glucose with increased short-term and 6-month mortality in ST-segment elevation and non-ST-segment elevation acute coronary syndromes: the Global Registry of Acute Coronary Events. Arch Intern Med. 2009;169(4):401-409.
— Reviewed for "TH eWire" by Mital Patel, MD, Alraies Chadi, MD, Saurabh Kandpal, MD, Iqbal Masood, MD, Anuradha Ramaswamy, MD, Department of Hospital Medicine, Cleveland Clinic
Clinical question: Are elevated fasting blood glucose levels independently associated with poor outcomes in all types of acute coronary syndromes (ACS)?
Background: Elevated admission blood glucose levels have been associated with poor outcomes in ACS patients; however, the role of fasting blood glucose levels in these settings, especially non-ST elevation myocardial infarction (NSTEMI), is unclear. It also is uncertain if one is a better predictor of outcomes than the other.
Study design: Prospective cohort of 57,406 patients in the Global Registry of Acute Coronary Events (GRACE).
Setting: 106 hospitals located in 14 countries in North and South America, Europe, Australia, and New Zealand.
Synopsis: 22,001 admission and 13,526 fasting blood glucose levels were extracted from GRACE and categorized into groups ranging from <100 mg/dL to =300 mg/dL. Multivariate logistic regression analysis of the association between these and the primary outcomes of in-hospital and six-month post-discharge all-cause mortality was carried out.
Fasting glucose levels higher than 100 mg/dL were associated with a linear increase in inpatient mortality (irrespective of diagnosis of diabetes) with an eightfold increase at levels =300mg/dL (17.22% vs. 1.71%). Increased six-month mortality, especially in patients with NSTEMI and STEMI, was also noted. However, this was a nonlinear relationship due to a lower mortality at 200-299 mg/dL, possibly reflecting the higher number of diabetics undergoing treatment in this group.
Admission glucose levels showed a linear increase in inpatient mortality at levels higher than 126 mg/dL. In contrast to fasting levels, admission levels were not associated with poor long-term outcome.
Study limitations included the use of registry data from a subgroup analysis and the possibility that fasting glucose levels in severely ill patients might not be representative of actual metabolic state.
Bottom line: Elevated fasting blood glucose in patients with acute coronary syndromes may portend a worse outcome and may be a better predictor than admission glucose levels.
Citation: Sinnaeve PR, Steg PG, Fox KA, et al. Association of elevated fasting glucose with increased short-term and 6-month mortality in ST-segment elevation and non-ST-segment elevation acute coronary syndromes: the Global Registry of Acute Coronary Events. Arch Intern Med. 2009;169(4):401-409.
— Reviewed for "TH eWire" by Mital Patel, MD, Alraies Chadi, MD, Saurabh Kandpal, MD, Iqbal Masood, MD, Anuradha Ramaswamy, MD, Department of Hospital Medicine, Cleveland Clinic
Back in the Saddle
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
Erlotinib in Lung Cancer
Dr. Vincent A. Miller describes study results that suggest the addition of erlotinib to bevacizumab treatment for advanced non-small cell lung cancer extends progression-free survival compared with bevacizumab alone. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Vincent A. Miller describes study results that suggest the addition of erlotinib to bevacizumab treatment for advanced non-small cell lung cancer extends progression-free survival compared with bevacizumab alone. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Vincent A. Miller describes study results that suggest the addition of erlotinib to bevacizumab treatment for advanced non-small cell lung cancer extends progression-free survival compared with bevacizumab alone. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
HRT and Lung Cancer
Dr. Rowan Chlebowski says his findings suggest an increased risk of non-small cell lung cancer associated with combination hormone therapy in a secondary analysis of data from the Women's Health Initiative study. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Rowan Chlebowski says his findings suggest an increased risk of non-small cell lung cancer associated with combination hormone therapy in a secondary analysis of data from the Women's Health Initiative study. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Dr. Rowan Chlebowski says his findings suggest an increased risk of non-small cell lung cancer associated with combination hormone therapy in a secondary analysis of data from the Women's Health Initiative study. Damian McNamara of the Global Medical News Network (GMNN) reports from the annual meeting of the American Society of Clinical Oncology in Orlando.
Go Green
How healthy is your hospital? When considering your answer, tally up latex gloves, sterilizing cleansers, disposable instruments, and gowns as pluses. However, these items and hundreds more can count against your facility—when you consider the effect your hospital has on its immediate (and not so immediate) environment.
Hospitals are tremendous producers of toxins, including mercury and excess pharmaceuticals, as well as solid and hazardous wastes.
“In healthcare, the footprint we’re leaving behind directly impacts our health,” points out Mary Daubach-Larsen, director of material operations and chairman of the Green LEEDers Task Force at Advocate Lutheran General Hospital in Park Ridge, Ill.
Many hospitals are taking steps to reduce that footprint.
It’s Easy Being Green
Hospitals that want to make a commitment to become more environmentally friendly can hire a full-time expert to guide their efforts, and/or they can appoint a task force—often called a green team. Lutheran General has had great success with the green team model.
A 617-bed teaching, research, and tertiary care hospital and Level 1 trauma center, Lutheran General is one of the largest hospitals in the Chicago area. Under the leadership of Daubach-Larsen, the hospital’s Green LEEDers Task Force has made great strides in several areas, earning Lutheran General a national 2006 Partners in Change award from Hospitals for a Healthy Environment (H2E).
“We’ve been recycling for more than five years,” says Daubach-Larsen. “We’ve stepped up and widened our efforts to include recycling glass, plastic, and aluminum, and we’re also reducing mercury in our environment. We’re close to being mercury free—that’s a goal of all [U.S.] hospitals.”
Lutheran General is now focusing on reducing toxins, examining their cleansers and their disposal of pharmaceuticals.
Like most hospitals that make an environmental commitment, Lutheran General began its efforts with guidance from H2E (www.h2e-online.org), a nonprofit group founded by the American Hospital Association, the U.S. Environmental Protection Agency, Health Care Without Harm, and the American Nurses Association.
“H2E’s mission is to green the entire healthcare sector,” says Laura Brannen, executive director of H2E. “We focus on reducing waste, toxic chemicals, and mercury.” Hospitals can join H2E for free, and nearly 25% of all U.S. hospitals currently belong to H2E.
About the Green Team
An effective hospital green team should include members from multiple departments, to ensure that new environmentally friendly practices, such as using recycling bins for specific waste materials or purchasing “green” cleansers, are taught to all applicable staff and followed by all necessary departments.
“A traditional green team brings together people from a variety of backgrounds,” says Brannen. “It’s best to have a balance between people who need to be [on the team] and those who are motivated to be there because they care.”
In addition to Daubach-Larsen, Lutheran General’s task force includes four nurses, a physician, a psychologist, and representatives from food/nutrition, infection control, pharmacy, public relations, physician relations, and guests from facilities.
Catholic Healthcare West (CHW), which made a commitment to environmentally friendly practices in 1996, has an environmental action committee at each of its 40 hospitals.
“Each of these committees is responsible for establishing goals, monitoring progress, overseeing implementation, and training staff at their hospital,” explains Sister Mary Ellen Leciejewski, OP, ecology program coordinator, CHW, Santa Cruz, Calif. “They also look for groups in their community that they should be partnering with.”
In addition to this overall team, Brannen recommends two other groups for a successful approach: recycling coordinators and an executive group. “Recycling coordinators are department liaisons for the staff in that area,” she explains. “They’re responsible for number and placement of recycling bins, labeling, and staff training in their area. This brings implementation down directly where it’s happening. You can have a coordinator for every shift.”
As for the executive level, Brannen recommends an “environmental leadership council” made up of the highest-level executives possible from a variety of departments. “This council would only meet twice a year, or maybe quarterly,” explains Brannen. “They make institutional decisions and commitments. They might sign off on an environmental mission statement, for example. They legitimize in a big way what the institution is doing.”
Talk Trash
An easy and obvious place to start an environmental effort is by reducing the amount of waste your hospital produces.
“It makes sense to start with waste and move on from there,” advises Daubach-Larsen of starting a Green Team effort. “H2E offers a waste management template to help you gather data on your waste streams. You can use that data to show management” how much more efficiently your hospital can work. She advises that hospitals audit their various waste outputs, including hazardous waste, recycling, and general trash, with the help of their waste vendor. “You can save money immediately, starting with a study of what’s going on,” she says.
With the data collected on waste and the buy-in of management, you can begin the work of shifting more waste toward recycling—or perhaps eliminating some waste altogether.
“Improve your relationship with your waste vendor,” advises Daubach-Larsen. “You can start to push them to accept more recyclables. When they realize there’s a demand, they’ll accept different materials.”
Address Toxins, Energy, and More
Beyond reducing waste, hospitals can make many environmental improvements—it’s simply a matter of choosing priorities. “The spectrum is large and can be overwhelming,” admits Daubach-Larsen.
In addition to waste and recycling, H2E helps hospitals address a wide variety of environmental issues. “We’ve moved on to environmentally friendly purchasing, green building, safer material choices, and energy efficiency,” says Brannen.
One area many green hospitals are beginning to watch closely is their purchasing, including their vendors. “We’re members of a group purchasing company that has green management strategies,” says Daubach-Larsen. “Most of the big groups are now on that bandwagon.” As part of their green purchasing habits, Lutheran General is trying to expand their use of products that are environmentally friendly. “We’ve also started sending out an RFP [request for proposal] asking vendors about their practices,” says Daubach-Larsen.
“Supply chain management is so important,” stresses Leciejewski. “If we watch what’s coming in our front door, we don’t have to worry so much about what we’re sending out our back door.”
CHW is currently working on multiple projects, including reprocessing surgical instruments, responsible disposal of their electronic waste (such as computers), reusable sharp’s containers, and a commitment to the healthiest food possible. “We’re looking at everything from working with organic vendors to the silverware and Styrofoam we use in our cafeterias,” says Leciejewski.
Another area of environmental consciousness is new construction. So-called green building is becoming a trend that reaches beyond healthcare. “If you’re not designing a green building before you break ground, you’re behind the times,” says Brannen. “This movement is really gaining steam, and the cost payback is pretty staggering over the life of the building.”
Daubach-Larsen adds, “Even if you’re not building, you can still incorporate new behaviors that will reduce your footprint on the environment.”
Save the Environment=Save Money
Are green practices too expensive for some hospitals? “The challenge is that people say they don’t have the money to spend [on better environmental practices], but they’re spending too much [now] and they’re tossing resources,” says Brannen.
Daubach-Larsen adds, “There are a lot of efficiencies” that can be realized through green practices. “Reducing solid waste and increasing recycling can save money,” she points out. “Our numbers of hazardous waste, or ‘red bag waste,’ are very low compared to other hospitals—it costs more to dispose of this waste.”
Green Hospitalists?
Where do hospitalists and other physicians fit into the green team picture? “There are hospitalists [who] get the relationships between their hospital[s] and the environment,” says Daubach-Larsen. “They can be ambassadors for that message.”
While green team leadership tends to fall on hospital operations staff, physicians can provide tremendous support simply by advocating with hospital leadership. “Executive sponsorship is key,” says Daubach-Larsen. “And physicians have a direct line to management. They can communicate that their satisfaction in the organization would be improved if that organization took an interest in the environment.”
Brannen says that physicians are “often the hardest community to reach” when spreading the message of environmentally friendly changes. “They can advocate or they can pitch in; having them in a leadership role is best, particularly if they have clout.”
Leciejewski recommends that hospitalists get involved in specific efforts. “We know that PVC (polyvinyl chloride )/DEHP (di[2-ethylhexyl]phthalate) IV bags are a known carcinogen, especially for preemies,” she says. “Doctors can support changing to different products or bring new products to our attention. They can write letters to [the companies we purchase from].”
Has your hospital made a commitment to reduce waste or otherwise reduce its footprint on the environment? If not, consider recommending a green team to start with some easy changes that can make a difference—and join the growing number of hospitals and healthcare workers committed to healing the environment.
“By collaborating, we can make a difference,” says Leciejewski. “Restoring the earth depends on us coming together as a community.” TH
Jane Jerrard is a frequent contributor to The Hospitalist.
How healthy is your hospital? When considering your answer, tally up latex gloves, sterilizing cleansers, disposable instruments, and gowns as pluses. However, these items and hundreds more can count against your facility—when you consider the effect your hospital has on its immediate (and not so immediate) environment.
Hospitals are tremendous producers of toxins, including mercury and excess pharmaceuticals, as well as solid and hazardous wastes.
“In healthcare, the footprint we’re leaving behind directly impacts our health,” points out Mary Daubach-Larsen, director of material operations and chairman of the Green LEEDers Task Force at Advocate Lutheran General Hospital in Park Ridge, Ill.
Many hospitals are taking steps to reduce that footprint.
It’s Easy Being Green
Hospitals that want to make a commitment to become more environmentally friendly can hire a full-time expert to guide their efforts, and/or they can appoint a task force—often called a green team. Lutheran General has had great success with the green team model.
A 617-bed teaching, research, and tertiary care hospital and Level 1 trauma center, Lutheran General is one of the largest hospitals in the Chicago area. Under the leadership of Daubach-Larsen, the hospital’s Green LEEDers Task Force has made great strides in several areas, earning Lutheran General a national 2006 Partners in Change award from Hospitals for a Healthy Environment (H2E).
“We’ve been recycling for more than five years,” says Daubach-Larsen. “We’ve stepped up and widened our efforts to include recycling glass, plastic, and aluminum, and we’re also reducing mercury in our environment. We’re close to being mercury free—that’s a goal of all [U.S.] hospitals.”
Lutheran General is now focusing on reducing toxins, examining their cleansers and their disposal of pharmaceuticals.
Like most hospitals that make an environmental commitment, Lutheran General began its efforts with guidance from H2E (www.h2e-online.org), a nonprofit group founded by the American Hospital Association, the U.S. Environmental Protection Agency, Health Care Without Harm, and the American Nurses Association.
“H2E’s mission is to green the entire healthcare sector,” says Laura Brannen, executive director of H2E. “We focus on reducing waste, toxic chemicals, and mercury.” Hospitals can join H2E for free, and nearly 25% of all U.S. hospitals currently belong to H2E.
About the Green Team
An effective hospital green team should include members from multiple departments, to ensure that new environmentally friendly practices, such as using recycling bins for specific waste materials or purchasing “green” cleansers, are taught to all applicable staff and followed by all necessary departments.
“A traditional green team brings together people from a variety of backgrounds,” says Brannen. “It’s best to have a balance between people who need to be [on the team] and those who are motivated to be there because they care.”
In addition to Daubach-Larsen, Lutheran General’s task force includes four nurses, a physician, a psychologist, and representatives from food/nutrition, infection control, pharmacy, public relations, physician relations, and guests from facilities.
Catholic Healthcare West (CHW), which made a commitment to environmentally friendly practices in 1996, has an environmental action committee at each of its 40 hospitals.
“Each of these committees is responsible for establishing goals, monitoring progress, overseeing implementation, and training staff at their hospital,” explains Sister Mary Ellen Leciejewski, OP, ecology program coordinator, CHW, Santa Cruz, Calif. “They also look for groups in their community that they should be partnering with.”
In addition to this overall team, Brannen recommends two other groups for a successful approach: recycling coordinators and an executive group. “Recycling coordinators are department liaisons for the staff in that area,” she explains. “They’re responsible for number and placement of recycling bins, labeling, and staff training in their area. This brings implementation down directly where it’s happening. You can have a coordinator for every shift.”
As for the executive level, Brannen recommends an “environmental leadership council” made up of the highest-level executives possible from a variety of departments. “This council would only meet twice a year, or maybe quarterly,” explains Brannen. “They make institutional decisions and commitments. They might sign off on an environmental mission statement, for example. They legitimize in a big way what the institution is doing.”
Talk Trash
An easy and obvious place to start an environmental effort is by reducing the amount of waste your hospital produces.
“It makes sense to start with waste and move on from there,” advises Daubach-Larsen of starting a Green Team effort. “H2E offers a waste management template to help you gather data on your waste streams. You can use that data to show management” how much more efficiently your hospital can work. She advises that hospitals audit their various waste outputs, including hazardous waste, recycling, and general trash, with the help of their waste vendor. “You can save money immediately, starting with a study of what’s going on,” she says.
With the data collected on waste and the buy-in of management, you can begin the work of shifting more waste toward recycling—or perhaps eliminating some waste altogether.
“Improve your relationship with your waste vendor,” advises Daubach-Larsen. “You can start to push them to accept more recyclables. When they realize there’s a demand, they’ll accept different materials.”
Address Toxins, Energy, and More
Beyond reducing waste, hospitals can make many environmental improvements—it’s simply a matter of choosing priorities. “The spectrum is large and can be overwhelming,” admits Daubach-Larsen.
In addition to waste and recycling, H2E helps hospitals address a wide variety of environmental issues. “We’ve moved on to environmentally friendly purchasing, green building, safer material choices, and energy efficiency,” says Brannen.
One area many green hospitals are beginning to watch closely is their purchasing, including their vendors. “We’re members of a group purchasing company that has green management strategies,” says Daubach-Larsen. “Most of the big groups are now on that bandwagon.” As part of their green purchasing habits, Lutheran General is trying to expand their use of products that are environmentally friendly. “We’ve also started sending out an RFP [request for proposal] asking vendors about their practices,” says Daubach-Larsen.
“Supply chain management is so important,” stresses Leciejewski. “If we watch what’s coming in our front door, we don’t have to worry so much about what we’re sending out our back door.”
CHW is currently working on multiple projects, including reprocessing surgical instruments, responsible disposal of their electronic waste (such as computers), reusable sharp’s containers, and a commitment to the healthiest food possible. “We’re looking at everything from working with organic vendors to the silverware and Styrofoam we use in our cafeterias,” says Leciejewski.
Another area of environmental consciousness is new construction. So-called green building is becoming a trend that reaches beyond healthcare. “If you’re not designing a green building before you break ground, you’re behind the times,” says Brannen. “This movement is really gaining steam, and the cost payback is pretty staggering over the life of the building.”
Daubach-Larsen adds, “Even if you’re not building, you can still incorporate new behaviors that will reduce your footprint on the environment.”
Save the Environment=Save Money
Are green practices too expensive for some hospitals? “The challenge is that people say they don’t have the money to spend [on better environmental practices], but they’re spending too much [now] and they’re tossing resources,” says Brannen.
Daubach-Larsen adds, “There are a lot of efficiencies” that can be realized through green practices. “Reducing solid waste and increasing recycling can save money,” she points out. “Our numbers of hazardous waste, or ‘red bag waste,’ are very low compared to other hospitals—it costs more to dispose of this waste.”
Green Hospitalists?
Where do hospitalists and other physicians fit into the green team picture? “There are hospitalists [who] get the relationships between their hospital[s] and the environment,” says Daubach-Larsen. “They can be ambassadors for that message.”
While green team leadership tends to fall on hospital operations staff, physicians can provide tremendous support simply by advocating with hospital leadership. “Executive sponsorship is key,” says Daubach-Larsen. “And physicians have a direct line to management. They can communicate that their satisfaction in the organization would be improved if that organization took an interest in the environment.”
Brannen says that physicians are “often the hardest community to reach” when spreading the message of environmentally friendly changes. “They can advocate or they can pitch in; having them in a leadership role is best, particularly if they have clout.”
Leciejewski recommends that hospitalists get involved in specific efforts. “We know that PVC (polyvinyl chloride )/DEHP (di[2-ethylhexyl]phthalate) IV bags are a known carcinogen, especially for preemies,” she says. “Doctors can support changing to different products or bring new products to our attention. They can write letters to [the companies we purchase from].”
Has your hospital made a commitment to reduce waste or otherwise reduce its footprint on the environment? If not, consider recommending a green team to start with some easy changes that can make a difference—and join the growing number of hospitals and healthcare workers committed to healing the environment.
“By collaborating, we can make a difference,” says Leciejewski. “Restoring the earth depends on us coming together as a community.” TH
Jane Jerrard is a frequent contributor to The Hospitalist.
How healthy is your hospital? When considering your answer, tally up latex gloves, sterilizing cleansers, disposable instruments, and gowns as pluses. However, these items and hundreds more can count against your facility—when you consider the effect your hospital has on its immediate (and not so immediate) environment.
Hospitals are tremendous producers of toxins, including mercury and excess pharmaceuticals, as well as solid and hazardous wastes.
“In healthcare, the footprint we’re leaving behind directly impacts our health,” points out Mary Daubach-Larsen, director of material operations and chairman of the Green LEEDers Task Force at Advocate Lutheran General Hospital in Park Ridge, Ill.
Many hospitals are taking steps to reduce that footprint.
It’s Easy Being Green
Hospitals that want to make a commitment to become more environmentally friendly can hire a full-time expert to guide their efforts, and/or they can appoint a task force—often called a green team. Lutheran General has had great success with the green team model.
A 617-bed teaching, research, and tertiary care hospital and Level 1 trauma center, Lutheran General is one of the largest hospitals in the Chicago area. Under the leadership of Daubach-Larsen, the hospital’s Green LEEDers Task Force has made great strides in several areas, earning Lutheran General a national 2006 Partners in Change award from Hospitals for a Healthy Environment (H2E).
“We’ve been recycling for more than five years,” says Daubach-Larsen. “We’ve stepped up and widened our efforts to include recycling glass, plastic, and aluminum, and we’re also reducing mercury in our environment. We’re close to being mercury free—that’s a goal of all [U.S.] hospitals.”
Lutheran General is now focusing on reducing toxins, examining their cleansers and their disposal of pharmaceuticals.
Like most hospitals that make an environmental commitment, Lutheran General began its efforts with guidance from H2E (www.h2e-online.org), a nonprofit group founded by the American Hospital Association, the U.S. Environmental Protection Agency, Health Care Without Harm, and the American Nurses Association.
“H2E’s mission is to green the entire healthcare sector,” says Laura Brannen, executive director of H2E. “We focus on reducing waste, toxic chemicals, and mercury.” Hospitals can join H2E for free, and nearly 25% of all U.S. hospitals currently belong to H2E.
About the Green Team
An effective hospital green team should include members from multiple departments, to ensure that new environmentally friendly practices, such as using recycling bins for specific waste materials or purchasing “green” cleansers, are taught to all applicable staff and followed by all necessary departments.
“A traditional green team brings together people from a variety of backgrounds,” says Brannen. “It’s best to have a balance between people who need to be [on the team] and those who are motivated to be there because they care.”
In addition to Daubach-Larsen, Lutheran General’s task force includes four nurses, a physician, a psychologist, and representatives from food/nutrition, infection control, pharmacy, public relations, physician relations, and guests from facilities.
Catholic Healthcare West (CHW), which made a commitment to environmentally friendly practices in 1996, has an environmental action committee at each of its 40 hospitals.
“Each of these committees is responsible for establishing goals, monitoring progress, overseeing implementation, and training staff at their hospital,” explains Sister Mary Ellen Leciejewski, OP, ecology program coordinator, CHW, Santa Cruz, Calif. “They also look for groups in their community that they should be partnering with.”
In addition to this overall team, Brannen recommends two other groups for a successful approach: recycling coordinators and an executive group. “Recycling coordinators are department liaisons for the staff in that area,” she explains. “They’re responsible for number and placement of recycling bins, labeling, and staff training in their area. This brings implementation down directly where it’s happening. You can have a coordinator for every shift.”
As for the executive level, Brannen recommends an “environmental leadership council” made up of the highest-level executives possible from a variety of departments. “This council would only meet twice a year, or maybe quarterly,” explains Brannen. “They make institutional decisions and commitments. They might sign off on an environmental mission statement, for example. They legitimize in a big way what the institution is doing.”
Talk Trash
An easy and obvious place to start an environmental effort is by reducing the amount of waste your hospital produces.
“It makes sense to start with waste and move on from there,” advises Daubach-Larsen of starting a Green Team effort. “H2E offers a waste management template to help you gather data on your waste streams. You can use that data to show management” how much more efficiently your hospital can work. She advises that hospitals audit their various waste outputs, including hazardous waste, recycling, and general trash, with the help of their waste vendor. “You can save money immediately, starting with a study of what’s going on,” she says.
With the data collected on waste and the buy-in of management, you can begin the work of shifting more waste toward recycling—or perhaps eliminating some waste altogether.
“Improve your relationship with your waste vendor,” advises Daubach-Larsen. “You can start to push them to accept more recyclables. When they realize there’s a demand, they’ll accept different materials.”
Address Toxins, Energy, and More
Beyond reducing waste, hospitals can make many environmental improvements—it’s simply a matter of choosing priorities. “The spectrum is large and can be overwhelming,” admits Daubach-Larsen.
In addition to waste and recycling, H2E helps hospitals address a wide variety of environmental issues. “We’ve moved on to environmentally friendly purchasing, green building, safer material choices, and energy efficiency,” says Brannen.
One area many green hospitals are beginning to watch closely is their purchasing, including their vendors. “We’re members of a group purchasing company that has green management strategies,” says Daubach-Larsen. “Most of the big groups are now on that bandwagon.” As part of their green purchasing habits, Lutheran General is trying to expand their use of products that are environmentally friendly. “We’ve also started sending out an RFP [request for proposal] asking vendors about their practices,” says Daubach-Larsen.
“Supply chain management is so important,” stresses Leciejewski. “If we watch what’s coming in our front door, we don’t have to worry so much about what we’re sending out our back door.”
CHW is currently working on multiple projects, including reprocessing surgical instruments, responsible disposal of their electronic waste (such as computers), reusable sharp’s containers, and a commitment to the healthiest food possible. “We’re looking at everything from working with organic vendors to the silverware and Styrofoam we use in our cafeterias,” says Leciejewski.
Another area of environmental consciousness is new construction. So-called green building is becoming a trend that reaches beyond healthcare. “If you’re not designing a green building before you break ground, you’re behind the times,” says Brannen. “This movement is really gaining steam, and the cost payback is pretty staggering over the life of the building.”
Daubach-Larsen adds, “Even if you’re not building, you can still incorporate new behaviors that will reduce your footprint on the environment.”
Save the Environment=Save Money
Are green practices too expensive for some hospitals? “The challenge is that people say they don’t have the money to spend [on better environmental practices], but they’re spending too much [now] and they’re tossing resources,” says Brannen.
Daubach-Larsen adds, “There are a lot of efficiencies” that can be realized through green practices. “Reducing solid waste and increasing recycling can save money,” she points out. “Our numbers of hazardous waste, or ‘red bag waste,’ are very low compared to other hospitals—it costs more to dispose of this waste.”
Green Hospitalists?
Where do hospitalists and other physicians fit into the green team picture? “There are hospitalists [who] get the relationships between their hospital[s] and the environment,” says Daubach-Larsen. “They can be ambassadors for that message.”
While green team leadership tends to fall on hospital operations staff, physicians can provide tremendous support simply by advocating with hospital leadership. “Executive sponsorship is key,” says Daubach-Larsen. “And physicians have a direct line to management. They can communicate that their satisfaction in the organization would be improved if that organization took an interest in the environment.”
Brannen says that physicians are “often the hardest community to reach” when spreading the message of environmentally friendly changes. “They can advocate or they can pitch in; having them in a leadership role is best, particularly if they have clout.”
Leciejewski recommends that hospitalists get involved in specific efforts. “We know that PVC (polyvinyl chloride )/DEHP (di[2-ethylhexyl]phthalate) IV bags are a known carcinogen, especially for preemies,” she says. “Doctors can support changing to different products or bring new products to our attention. They can write letters to [the companies we purchase from].”
Has your hospital made a commitment to reduce waste or otherwise reduce its footprint on the environment? If not, consider recommending a green team to start with some easy changes that can make a difference—and join the growing number of hospitals and healthcare workers committed to healing the environment.
“By collaborating, we can make a difference,” says Leciejewski. “Restoring the earth depends on us coming together as a community.” TH
Jane Jerrard is a frequent contributor to The Hospitalist.
Dr. Hospitalist

Resident Restrictions Might Be HM Game-Changer
I have heard regulators are thinking about further restricting resident work hours. Is this true? Do you think this has helped or hindered patient care? Is there any discussion about restriction of hospitalist work hours? I am working harder than I ever did during training. Have these rules affected the hospitalist field?
H. Jackson, MD, Dover, Del.
Dr. Hospitalist responds:
In 2003, the Accreditation Council for Graduate Medical Education (ACGME) established rules to limit the resident work schedule. The rules included an 80-hour limit on resident workweeks. Training programs around the country experienced difficulties in complying with the rules. Many hospitals established or expanded existing hospitalist programs to help their training programs comply with the rule change, which meant more jobs for hospitalists. From this perspective, the rules were a boon for hospitalists. But the rules also had some unintended consequences. Shorter resident shifts meant more handoffs, and this resulted in an increase in medical errors. Not only do we not do a good job of teaching patient handoffs to our trainees, but most attending physicians also do an inadequate job of communicating patient handoffs.
As you noted, a new report (www.nationalacademies.org/morenews/20081202.html) from the Institute of Medicine (IOM) called for changes to the ACGME rules. The IOM report does not call for a reduction in the 80-hour workweek, but it does recommend several changes to ACGME rules. The IOM calls for residents to work no more than 16 consecutive hours without sleep. It also calls for changes to the present ACGME rules regarding resident time off. Residents should:
- Have 12 hours off after every night shift, 10 hours off after every day shift, and 14 hours off after any shift of 30 hours;
- Not be on call in the hospital more frequently than every third night, with no averaging; and
- Have at least one day off per week, with no averaging.
The IOM report also calls for increased on-site supervision of residents, including immediate access to a supervisory physician for interns. For now, the IOM report is just that—a report. We’ll have to wait and see how ACGME reacts to these recommendations.
What is the potential impact for hospitalists? The work-schedule recommendations could mean residents will work fewer consecutive hours in the hospital. This has the potential to increase the demand for hospitalists to see patients, not only on the medical service, but on other clinical services as well. For example, we may see more hospitalists working with surgeons to manage surgical inpatients. Hospitalist programs will have to figure out a way to work with surgeons without feeling as though the surgeons are “dropping off” patients after surgeries.
With the current shortage of hospitalists, institutions and HM programs could hire more nonphysician clinical providers, such as nurse practitioners and physician assistants. Many hospitalist programs have struggled to incorporate these providers into their workflow in an efficient and cost-effective fashion. Such problems represent opportunities for HM.
The further fragmentation of the resident schedule could create additional patient handoffs. Early in the HM movement, the “voltage drop” issue was a hot topic. Since then, HM has not done enough to standardize the handoff and teach it to others. I encourage all HM programs to resolve the issue of patient handoffs. This is imperative to the safety of our patients.
Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is most easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. The first step is to determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the present and previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with other individuals in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH
Resident Restrictions Might Be HM Game-Changer
I have heard regulators are thinking about further restricting resident work hours. Is this true? Do you think this has helped or hindered patient care? Is there any discussion about restriction of hospitalist work hours? I am working harder than I ever did during training. Have these rules affected the hospitalist field?
H. Jackson, MD, Dover, Del.
Dr. Hospitalist responds:
In 2003, the Accreditation Council for Graduate Medical Education (ACGME) established rules to limit the resident work schedule. The rules included an 80-hour limit on resident workweeks. Training programs around the country experienced difficulties in complying with the rules. Many hospitals established or expanded existing hospitalist programs to help their training programs comply with the rule change, which meant more jobs for hospitalists. From this perspective, the rules were a boon for hospitalists. But the rules also had some unintended consequences. Shorter resident shifts meant more handoffs, and this resulted in an increase in medical errors. Not only do we not do a good job of teaching patient handoffs to our trainees, but most attending physicians also do an inadequate job of communicating patient handoffs.
As you noted, a new report (www.nationalacademies.org/morenews/20081202.html) from the Institute of Medicine (IOM) called for changes to the ACGME rules. The IOM report does not call for a reduction in the 80-hour workweek, but it does recommend several changes to ACGME rules. The IOM calls for residents to work no more than 16 consecutive hours without sleep. It also calls for changes to the present ACGME rules regarding resident time off. Residents should:
- Have 12 hours off after every night shift, 10 hours off after every day shift, and 14 hours off after any shift of 30 hours;
- Not be on call in the hospital more frequently than every third night, with no averaging; and
- Have at least one day off per week, with no averaging.
The IOM report also calls for increased on-site supervision of residents, including immediate access to a supervisory physician for interns. For now, the IOM report is just that—a report. We’ll have to wait and see how ACGME reacts to these recommendations.
What is the potential impact for hospitalists? The work-schedule recommendations could mean residents will work fewer consecutive hours in the hospital. This has the potential to increase the demand for hospitalists to see patients, not only on the medical service, but on other clinical services as well. For example, we may see more hospitalists working with surgeons to manage surgical inpatients. Hospitalist programs will have to figure out a way to work with surgeons without feeling as though the surgeons are “dropping off” patients after surgeries.
With the current shortage of hospitalists, institutions and HM programs could hire more nonphysician clinical providers, such as nurse practitioners and physician assistants. Many hospitalist programs have struggled to incorporate these providers into their workflow in an efficient and cost-effective fashion. Such problems represent opportunities for HM.
The further fragmentation of the resident schedule could create additional patient handoffs. Early in the HM movement, the “voltage drop” issue was a hot topic. Since then, HM has not done enough to standardize the handoff and teach it to others. I encourage all HM programs to resolve the issue of patient handoffs. This is imperative to the safety of our patients.
Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is most easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. The first step is to determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the present and previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with other individuals in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH
Resident Restrictions Might Be HM Game-Changer
I have heard regulators are thinking about further restricting resident work hours. Is this true? Do you think this has helped or hindered patient care? Is there any discussion about restriction of hospitalist work hours? I am working harder than I ever did during training. Have these rules affected the hospitalist field?
H. Jackson, MD, Dover, Del.
Dr. Hospitalist responds:
In 2003, the Accreditation Council for Graduate Medical Education (ACGME) established rules to limit the resident work schedule. The rules included an 80-hour limit on resident workweeks. Training programs around the country experienced difficulties in complying with the rules. Many hospitals established or expanded existing hospitalist programs to help their training programs comply with the rule change, which meant more jobs for hospitalists. From this perspective, the rules were a boon for hospitalists. But the rules also had some unintended consequences. Shorter resident shifts meant more handoffs, and this resulted in an increase in medical errors. Not only do we not do a good job of teaching patient handoffs to our trainees, but most attending physicians also do an inadequate job of communicating patient handoffs.
As you noted, a new report (www.nationalacademies.org/morenews/20081202.html) from the Institute of Medicine (IOM) called for changes to the ACGME rules. The IOM report does not call for a reduction in the 80-hour workweek, but it does recommend several changes to ACGME rules. The IOM calls for residents to work no more than 16 consecutive hours without sleep. It also calls for changes to the present ACGME rules regarding resident time off. Residents should:
- Have 12 hours off after every night shift, 10 hours off after every day shift, and 14 hours off after any shift of 30 hours;
- Not be on call in the hospital more frequently than every third night, with no averaging; and
- Have at least one day off per week, with no averaging.
The IOM report also calls for increased on-site supervision of residents, including immediate access to a supervisory physician for interns. For now, the IOM report is just that—a report. We’ll have to wait and see how ACGME reacts to these recommendations.
What is the potential impact for hospitalists? The work-schedule recommendations could mean residents will work fewer consecutive hours in the hospital. This has the potential to increase the demand for hospitalists to see patients, not only on the medical service, but on other clinical services as well. For example, we may see more hospitalists working with surgeons to manage surgical inpatients. Hospitalist programs will have to figure out a way to work with surgeons without feeling as though the surgeons are “dropping off” patients after surgeries.
With the current shortage of hospitalists, institutions and HM programs could hire more nonphysician clinical providers, such as nurse practitioners and physician assistants. Many hospitalist programs have struggled to incorporate these providers into their workflow in an efficient and cost-effective fashion. Such problems represent opportunities for HM.
The further fragmentation of the resident schedule could create additional patient handoffs. Early in the HM movement, the “voltage drop” issue was a hot topic. Since then, HM has not done enough to standardize the handoff and teach it to others. I encourage all HM programs to resolve the issue of patient handoffs. This is imperative to the safety of our patients.
Use Metrics to Identify Documentation and Coding Errors
I am the leader of a hospitalist group. We have a number of recent graduates in our group, and I have a feeling that not everyone is billing correctly. Do you have any suggestions on how I remedy this problem?
D. Perman, MD, Augusta, Ga.
Dr. Hospitalist responds:
I would not be surprised if your suspicions are correct. Unfortunately, many young physicians do not have a firm grasp on the rules and regulations surrounding coding and documentation. But before you set out to find a remedy, you need to identify and understand the problem.
I suggest you start by collecting data. This is most easily done by involving your administrative staff and billing service. Create individual and group dashboards to help you and the individual physicians examine the data. The first step is to determine whether the doctors in your group are submitting a bill with each clinical encounter. Measure the number of days between the date of service and the date they submit the bill. Create metrics and put them on the dashboard. For example, one could measure bills submitted divided by clinical encounters; another would calculate the percent of bills submitted within 72 hours of the service date.
Next, look at the individual and group code distributions. Assuming that all members of your group have a similar job description and see the same groups of patients, the code distribution should be similar. For example, the percentage of Level 3, Level 2, and Level 1 initial admission codes should be similar among all members of your group. A disparity would suggest that one or more physicians is not documenting and coding correctly.
Use your dashboard to compare individual and group distribution. In my group, I provide each physician with the metrics on their personal distribution of codes for the fiscal year, along with their distribution of codes from previous years. When I do this, I also provide each physician with our group’s distribution of codes for the present and previous years. This allows individual physicians to compare historical trends for themselves and the entire group. I do not share individual data with other individuals in the group.
Lastly, provide the distribution of codes for internal-medicine physicians from Medicare. This information is available at www.cms.hhs.gov/pqri/. It is important to note that I am not holding up the Medicare data or our group data as the standard; it is merely a reflection of how other internists in our group and across the country are billing.
This data is intended to supplement, not replace, our annual training on documentation, coding, and compliance. I have found that pushing this data to our physicians has helped them understand the importance of creating a system to ensure that all bills are submitted and coded appropriately to the level of service and documentation. TH