User login
Is Anybody Out There?
In a tale all too familiar to HM group leaders, whether they head two- or three-physician services or the large, multistate hospitalist companies, Heather Bellow, MD, FAAP, is trying to recruit a pediatric hospitalist to her midsize Midwest town.
Her sales pitch, though, seems to focus more on the bounties of Lansing, Mich., rather than the work to be done as the fourth full-time member of Sparrow Hospital Inpatient Pediatric Services. Dr. Bellow often talks up the culture, lifestyle, and the vibrant atmosphere Michigan State University provides the community. And yet, she struggles to find new hires.
Her story is the new norm: Group directors outside the nation’s largest markets agree that they often work for months at a time to recruit hospitalists. Some relent and hire a steady string of residents from nearby institutions. Others throw money at the problem, only to lose those well-paid hospitalists to other groups that throw more money at the problem. The problem is particularly acute in secondary- and tertiary-population areas, where hiring managers often find themselves battling each other for the same hospitalists.
“That’s the million-dollar question,” Dr. Bellow says. “How do you find that outside person that’s willing to come to small-town USA? I really don’t know.”
One possible answer: A focused recruitment strategy should be considered its own subspecialty. Highlighting the growing importance of recruitment and retention issues, SHM offered its first recruitment course last month at HM09 in Chicago. More than 300 people attended the session, which looked at the hiring process from both perspectives. In anticipation of high demand, the presentation was one of only a handful of sessions that were held twice during the meeting, allowing those who missed the first-day session to attend the same session on the final day.
“It’s a crazy time in some ways,” says Kirk Mathews, co-founder and CEO of Inpatient Management Inc. in St. Louis. “In challenging times, people often abandon the fundamentals because they feel they’re in desperation mode. Just bring someone in, get a body in there—anything with an MD behind their name.”
Hospitalists looking to recruit to smaller markets say times are getting tougher. The job posting board at HM09—always a popular gathering site—was littered with fliers for practices in smaller markets: Albuquerque, N.M.; Coeur d’Alene, Idaho; Murphy, N.C. Most of the announcements focused on the natural beauty of an area, proximity to surf or sand, or the peaceful lifestyle a community affords. Few focused on compensation, rotation schedules, or whether malpractice insurance and continuing medical education would be reimbursed.
“These ads try to appeal to your life other than medicine,” says Cecelia Wong, MD, a hospitalist with Med One Hospitalist Physicians in Columbus, Ohio.
Rohit Uppal, MD, medical director of the hospitalist program at Grant Medical Center, also in Columbus, says job hopefuls now know they can be picky when it comes to looking at positions in markets struggling to maintain a job candidate pipeline. Dr. Uppal uses a fellowship program as a recruitment tool, but he concedes he’s not in a power position when it comes to negotiation. “We’re not saying ‘Here’s our great hospitalist group, move to Columbus,’ ” he says. “We’re hearing ‘I’m moving to Columbus ... looking to be a hospitalist.’ ”
Sweeten the Pot
Another potential recruiting tool some groups might overlook is physical office space. While many groups search for cost savings by moving to a “virtual office,” don’t underestimate the value a candidate might place in having a nice office to do their paperwork, says Joseph Ming-Wah Li, MD, FHM, SHM board member, director of the hospital medicine program at Harvard Medical School and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston. “What does that say to a hospitalist?” Dr. Li asks. “I take them to this nice suite with outside-looking windows—it sends a nice message of how you’re valued at your institution.”
Just don’t tilt too far toward fancy offices and big salaries. Mathews cautions clients not to focus solely on compensation, because it doesn’t solve long-term recruitment issues and might attract candidates only interested in short-term commitments. “It’s not wise to buy loyalty, because then you never know when it’s paid for,” Mathews says. “I’m going to throw a $40,000 signing bonus at this doctor. … Two years from now, somebody else can throw $50,000 at them and they’re gone. It’s not the candidate’s fault. They’re at the smorgasbord table.” TH
Richard Quinn is a freelance writer based in New Jersey.
In a tale all too familiar to HM group leaders, whether they head two- or three-physician services or the large, multistate hospitalist companies, Heather Bellow, MD, FAAP, is trying to recruit a pediatric hospitalist to her midsize Midwest town.
Her sales pitch, though, seems to focus more on the bounties of Lansing, Mich., rather than the work to be done as the fourth full-time member of Sparrow Hospital Inpatient Pediatric Services. Dr. Bellow often talks up the culture, lifestyle, and the vibrant atmosphere Michigan State University provides the community. And yet, she struggles to find new hires.
Her story is the new norm: Group directors outside the nation’s largest markets agree that they often work for months at a time to recruit hospitalists. Some relent and hire a steady string of residents from nearby institutions. Others throw money at the problem, only to lose those well-paid hospitalists to other groups that throw more money at the problem. The problem is particularly acute in secondary- and tertiary-population areas, where hiring managers often find themselves battling each other for the same hospitalists.
“That’s the million-dollar question,” Dr. Bellow says. “How do you find that outside person that’s willing to come to small-town USA? I really don’t know.”
One possible answer: A focused recruitment strategy should be considered its own subspecialty. Highlighting the growing importance of recruitment and retention issues, SHM offered its first recruitment course last month at HM09 in Chicago. More than 300 people attended the session, which looked at the hiring process from both perspectives. In anticipation of high demand, the presentation was one of only a handful of sessions that were held twice during the meeting, allowing those who missed the first-day session to attend the same session on the final day.
“It’s a crazy time in some ways,” says Kirk Mathews, co-founder and CEO of Inpatient Management Inc. in St. Louis. “In challenging times, people often abandon the fundamentals because they feel they’re in desperation mode. Just bring someone in, get a body in there—anything with an MD behind their name.”
Hospitalists looking to recruit to smaller markets say times are getting tougher. The job posting board at HM09—always a popular gathering site—was littered with fliers for practices in smaller markets: Albuquerque, N.M.; Coeur d’Alene, Idaho; Murphy, N.C. Most of the announcements focused on the natural beauty of an area, proximity to surf or sand, or the peaceful lifestyle a community affords. Few focused on compensation, rotation schedules, or whether malpractice insurance and continuing medical education would be reimbursed.
“These ads try to appeal to your life other than medicine,” says Cecelia Wong, MD, a hospitalist with Med One Hospitalist Physicians in Columbus, Ohio.
Rohit Uppal, MD, medical director of the hospitalist program at Grant Medical Center, also in Columbus, says job hopefuls now know they can be picky when it comes to looking at positions in markets struggling to maintain a job candidate pipeline. Dr. Uppal uses a fellowship program as a recruitment tool, but he concedes he’s not in a power position when it comes to negotiation. “We’re not saying ‘Here’s our great hospitalist group, move to Columbus,’ ” he says. “We’re hearing ‘I’m moving to Columbus ... looking to be a hospitalist.’ ”
Sweeten the Pot
Another potential recruiting tool some groups might overlook is physical office space. While many groups search for cost savings by moving to a “virtual office,” don’t underestimate the value a candidate might place in having a nice office to do their paperwork, says Joseph Ming-Wah Li, MD, FHM, SHM board member, director of the hospital medicine program at Harvard Medical School and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston. “What does that say to a hospitalist?” Dr. Li asks. “I take them to this nice suite with outside-looking windows—it sends a nice message of how you’re valued at your institution.”
Just don’t tilt too far toward fancy offices and big salaries. Mathews cautions clients not to focus solely on compensation, because it doesn’t solve long-term recruitment issues and might attract candidates only interested in short-term commitments. “It’s not wise to buy loyalty, because then you never know when it’s paid for,” Mathews says. “I’m going to throw a $40,000 signing bonus at this doctor. … Two years from now, somebody else can throw $50,000 at them and they’re gone. It’s not the candidate’s fault. They’re at the smorgasbord table.” TH
Richard Quinn is a freelance writer based in New Jersey.
In a tale all too familiar to HM group leaders, whether they head two- or three-physician services or the large, multistate hospitalist companies, Heather Bellow, MD, FAAP, is trying to recruit a pediatric hospitalist to her midsize Midwest town.
Her sales pitch, though, seems to focus more on the bounties of Lansing, Mich., rather than the work to be done as the fourth full-time member of Sparrow Hospital Inpatient Pediatric Services. Dr. Bellow often talks up the culture, lifestyle, and the vibrant atmosphere Michigan State University provides the community. And yet, she struggles to find new hires.
Her story is the new norm: Group directors outside the nation’s largest markets agree that they often work for months at a time to recruit hospitalists. Some relent and hire a steady string of residents from nearby institutions. Others throw money at the problem, only to lose those well-paid hospitalists to other groups that throw more money at the problem. The problem is particularly acute in secondary- and tertiary-population areas, where hiring managers often find themselves battling each other for the same hospitalists.
“That’s the million-dollar question,” Dr. Bellow says. “How do you find that outside person that’s willing to come to small-town USA? I really don’t know.”
One possible answer: A focused recruitment strategy should be considered its own subspecialty. Highlighting the growing importance of recruitment and retention issues, SHM offered its first recruitment course last month at HM09 in Chicago. More than 300 people attended the session, which looked at the hiring process from both perspectives. In anticipation of high demand, the presentation was one of only a handful of sessions that were held twice during the meeting, allowing those who missed the first-day session to attend the same session on the final day.
“It’s a crazy time in some ways,” says Kirk Mathews, co-founder and CEO of Inpatient Management Inc. in St. Louis. “In challenging times, people often abandon the fundamentals because they feel they’re in desperation mode. Just bring someone in, get a body in there—anything with an MD behind their name.”
Hospitalists looking to recruit to smaller markets say times are getting tougher. The job posting board at HM09—always a popular gathering site—was littered with fliers for practices in smaller markets: Albuquerque, N.M.; Coeur d’Alene, Idaho; Murphy, N.C. Most of the announcements focused on the natural beauty of an area, proximity to surf or sand, or the peaceful lifestyle a community affords. Few focused on compensation, rotation schedules, or whether malpractice insurance and continuing medical education would be reimbursed.
“These ads try to appeal to your life other than medicine,” says Cecelia Wong, MD, a hospitalist with Med One Hospitalist Physicians in Columbus, Ohio.
Rohit Uppal, MD, medical director of the hospitalist program at Grant Medical Center, also in Columbus, says job hopefuls now know they can be picky when it comes to looking at positions in markets struggling to maintain a job candidate pipeline. Dr. Uppal uses a fellowship program as a recruitment tool, but he concedes he’s not in a power position when it comes to negotiation. “We’re not saying ‘Here’s our great hospitalist group, move to Columbus,’ ” he says. “We’re hearing ‘I’m moving to Columbus ... looking to be a hospitalist.’ ”
Sweeten the Pot
Another potential recruiting tool some groups might overlook is physical office space. While many groups search for cost savings by moving to a “virtual office,” don’t underestimate the value a candidate might place in having a nice office to do their paperwork, says Joseph Ming-Wah Li, MD, FHM, SHM board member, director of the hospital medicine program at Harvard Medical School and associate chief of the division of general medicine and primary care at Beth Israel Deaconess Medical Center in Boston. “What does that say to a hospitalist?” Dr. Li asks. “I take them to this nice suite with outside-looking windows—it sends a nice message of how you’re valued at your institution.”
Just don’t tilt too far toward fancy offices and big salaries. Mathews cautions clients not to focus solely on compensation, because it doesn’t solve long-term recruitment issues and might attract candidates only interested in short-term commitments. “It’s not wise to buy loyalty, because then you never know when it’s paid for,” Mathews says. “I’m going to throw a $40,000 signing bonus at this doctor. … Two years from now, somebody else can throw $50,000 at them and they’re gone. It’s not the candidate’s fault. They’re at the smorgasbord table.” TH
Richard Quinn is a freelance writer based in New Jersey.
Communication King
When Kenneth Patrick, MD, joined Chestnut Hill Hospital in Philadelphia in 1982, he was known simply as a physician who practiced HM. It wasn’t until 14 years later that the term “hospitalist” appeared for the first time in a New England Journal of Medicine article.
As Dr. Patrick’s job title changed, so did his outlook on the future of the profession. “My practice was exceedingly unique and, for many years, people didn’t understand that a physician could practice exclusively in a hospital,” says Dr. Patrick, now the ICU director at Chestnut Hill. “But when I first heard the word ‘hospitalist,’ I was surprised. I remember thinking, ‘Hey, I’m one of them.’ ”
He also knew that if other physicians were recognizing the specialty, more and more physicians were going to jump on the HM bandwagon. “I knew it wasn’t just a short-lived thing,” he says.
With three decades of HM experience in the bank, Dr. Patrick offers his take on the evolution of HM, changes to the delivery of care, and the importance of communicating with patients.
Question: What drew you into the medical field?
Answer: I earned an undergraduate degree in mechanical engineering [from Drexel University]. The country was going through a recession and there weren’t many job offers, so when I was a junior, I decided to switch careers. I went into medicine.
Q: Have you found any similarities between engineering and HM?
A: Very much so, particularly in the intensive-care unit (ICU). That’s what drew me to critical care and HM. You have to be very detail-oriented. You have to go through your thinking process in a very organized fashion, and you have to be prepared to solve problems that aren’t apparent when you first start caring for a patient. That’s the basis of engineering.
—Kenneth Patrick, MD, Chestnut Hill Hospital, Philadelphia
Q: Did you face challenges in 1982 that new hospitalists won’t face today because the field is more established?
A: No, I would say it’s the other way around, particularly in terms of regulation and monitoring. The Joint Commission existed then, but the standards of hospital care, pressures from insurers, and things like length of stay were not so much of an issue. The challenge to get people evaluated and discharged exceedingly quickly did not exist back then.
Q: How has your role as a hospitalist changed in 26 years?
A: The most significant change is speed. I remember during residency caring for a patient with an infection of the heart valves. That patient stayed in the hospital for 28 days getting antibiotics, and I went to see the person every day to listen to the heart. … Today, that patient would be in the hospital two or, at most, three days. They’d be discharged either to home on IV antibiotics or to a skilled nursing facility. They’d no longer stay in the hospital for a prolonged period of time.
Q: How has that changed the delivery of care?
A: Our job as hospitalists is to see someone who is sick enough to be in the hospital, evaluate and diagnose them exceedingly quickly, get them started on treatment exceedingly quickly, and, as soon as they start improving, the regulators or insurers say they no longer need to be in the hospital. We don’t get to follow them through their entire illness.
I think that is something that is lacking for young hospitalists and residents during training. They don’t see the illness from start to finish. They see it from the start until the moment the patient begins to improve and is discharged.
Q: What is the consequence of that shift?
A: Less-experienced physicians, in terms of management of a patient from the beginning to end, unless there is good communication between hospital physicians and outpatient physicians. And I just think younger physicians are less well prepared for the complications that may ensue from a given illness because they only see the illness for such a short period of time.
Q: What’s the biggest reward of being a hospitalist?
A: Making patients better, if that can be done, and helping them through illnesses that can’t be made better. The outcome may be death, permanent disability, or something tragic, but patients and their families still feel thankful if they feel you’ve been a caring physician. Without the patient and the family being satisfied, I wouldn’t have many rewards.
Q: After 26 years as a hospitalist, what’s the best advice you could offer to someone new in the field?
A: Don’t cut corners. Be as complete and as thorough as you need to be. Communicate with patients and their families, which is crucial. Be open to suggestions, because you don’t know everything. I still feel that way after 26 years. Be optimistic and enjoy what you do. And it’s very important for busy, high-pressure physician specialists to keep their mind on their family and their outside-the-hospital relationships. Don’t forget your kids are going to grow up.
Q: You often emphasize the importance of physicians communicating with patients and their families. What’s the biggest barrier to communication?
A: First, reimbursement isn’t there for explanations and counseling. You get reimbursed for the evaluation, the diagnosis, and the management of the illness. No. 2, it takes time—sometimes an inordinate amount of time. If a patient is critically ill, I can spend 30 to 90 minutes with a family, not treating the patient, but explaining what’s the matter with the patient and what the treatment options are. During that time, you’re giving up other patient-care responsibilities.
And I don’t think physicians have been well trained to communicate with someone and explain the details of an illness and the treatment options nonmedically. I’ve seen doctors try to explain to families that a patient is dead and the family didn’t know what the doctor meant. I teach residents to speak English to patients and their families, not speak medical.
Q: Should there be a greater emphasis on communication during education and residency?
A: Absolutely. I tell residents they need this training as much as they need to know what antibiotic to use for pneumonia. … My experience over the years is patients think they’re getting better care from average doctors who communicate well than doctors who are brilliant and can’t communicate.
Q: What has kept you at Chestnut Hill Hospital for 26 years?
A: Some of it is inertia. When my children were young, it was the community in which I lived. And I like working in a small, community hospital because of the personal relationships I’ve developed with the other professionals, everyone from medical records to the secretarial staff.
Q: What’s next for you?
A: As I’ve gotten older, being woken up in the middle of the night gets harder and harder, so I’ve thought of doing something where the hours are more fixed and I have a little more time. I have thought about starting satellite practices in other community hospitals that are looking to start hospitalist programs, being more of an administrator and delivering less patient care. But I still like what I’m doing, and that’s why I keep doing it. TH
Mark Leiser is a freelance writer based in New Jersey.
When Kenneth Patrick, MD, joined Chestnut Hill Hospital in Philadelphia in 1982, he was known simply as a physician who practiced HM. It wasn’t until 14 years later that the term “hospitalist” appeared for the first time in a New England Journal of Medicine article.
As Dr. Patrick’s job title changed, so did his outlook on the future of the profession. “My practice was exceedingly unique and, for many years, people didn’t understand that a physician could practice exclusively in a hospital,” says Dr. Patrick, now the ICU director at Chestnut Hill. “But when I first heard the word ‘hospitalist,’ I was surprised. I remember thinking, ‘Hey, I’m one of them.’ ”
He also knew that if other physicians were recognizing the specialty, more and more physicians were going to jump on the HM bandwagon. “I knew it wasn’t just a short-lived thing,” he says.
With three decades of HM experience in the bank, Dr. Patrick offers his take on the evolution of HM, changes to the delivery of care, and the importance of communicating with patients.
Question: What drew you into the medical field?
Answer: I earned an undergraduate degree in mechanical engineering [from Drexel University]. The country was going through a recession and there weren’t many job offers, so when I was a junior, I decided to switch careers. I went into medicine.
Q: Have you found any similarities between engineering and HM?
A: Very much so, particularly in the intensive-care unit (ICU). That’s what drew me to critical care and HM. You have to be very detail-oriented. You have to go through your thinking process in a very organized fashion, and you have to be prepared to solve problems that aren’t apparent when you first start caring for a patient. That’s the basis of engineering.
—Kenneth Patrick, MD, Chestnut Hill Hospital, Philadelphia
Q: Did you face challenges in 1982 that new hospitalists won’t face today because the field is more established?
A: No, I would say it’s the other way around, particularly in terms of regulation and monitoring. The Joint Commission existed then, but the standards of hospital care, pressures from insurers, and things like length of stay were not so much of an issue. The challenge to get people evaluated and discharged exceedingly quickly did not exist back then.
Q: How has your role as a hospitalist changed in 26 years?
A: The most significant change is speed. I remember during residency caring for a patient with an infection of the heart valves. That patient stayed in the hospital for 28 days getting antibiotics, and I went to see the person every day to listen to the heart. … Today, that patient would be in the hospital two or, at most, three days. They’d be discharged either to home on IV antibiotics or to a skilled nursing facility. They’d no longer stay in the hospital for a prolonged period of time.
Q: How has that changed the delivery of care?
A: Our job as hospitalists is to see someone who is sick enough to be in the hospital, evaluate and diagnose them exceedingly quickly, get them started on treatment exceedingly quickly, and, as soon as they start improving, the regulators or insurers say they no longer need to be in the hospital. We don’t get to follow them through their entire illness.
I think that is something that is lacking for young hospitalists and residents during training. They don’t see the illness from start to finish. They see it from the start until the moment the patient begins to improve and is discharged.
Q: What is the consequence of that shift?
A: Less-experienced physicians, in terms of management of a patient from the beginning to end, unless there is good communication between hospital physicians and outpatient physicians. And I just think younger physicians are less well prepared for the complications that may ensue from a given illness because they only see the illness for such a short period of time.
Q: What’s the biggest reward of being a hospitalist?
A: Making patients better, if that can be done, and helping them through illnesses that can’t be made better. The outcome may be death, permanent disability, or something tragic, but patients and their families still feel thankful if they feel you’ve been a caring physician. Without the patient and the family being satisfied, I wouldn’t have many rewards.
Q: After 26 years as a hospitalist, what’s the best advice you could offer to someone new in the field?
A: Don’t cut corners. Be as complete and as thorough as you need to be. Communicate with patients and their families, which is crucial. Be open to suggestions, because you don’t know everything. I still feel that way after 26 years. Be optimistic and enjoy what you do. And it’s very important for busy, high-pressure physician specialists to keep their mind on their family and their outside-the-hospital relationships. Don’t forget your kids are going to grow up.
Q: You often emphasize the importance of physicians communicating with patients and their families. What’s the biggest barrier to communication?
A: First, reimbursement isn’t there for explanations and counseling. You get reimbursed for the evaluation, the diagnosis, and the management of the illness. No. 2, it takes time—sometimes an inordinate amount of time. If a patient is critically ill, I can spend 30 to 90 minutes with a family, not treating the patient, but explaining what’s the matter with the patient and what the treatment options are. During that time, you’re giving up other patient-care responsibilities.
And I don’t think physicians have been well trained to communicate with someone and explain the details of an illness and the treatment options nonmedically. I’ve seen doctors try to explain to families that a patient is dead and the family didn’t know what the doctor meant. I teach residents to speak English to patients and their families, not speak medical.
Q: Should there be a greater emphasis on communication during education and residency?
A: Absolutely. I tell residents they need this training as much as they need to know what antibiotic to use for pneumonia. … My experience over the years is patients think they’re getting better care from average doctors who communicate well than doctors who are brilliant and can’t communicate.
Q: What has kept you at Chestnut Hill Hospital for 26 years?
A: Some of it is inertia. When my children were young, it was the community in which I lived. And I like working in a small, community hospital because of the personal relationships I’ve developed with the other professionals, everyone from medical records to the secretarial staff.
Q: What’s next for you?
A: As I’ve gotten older, being woken up in the middle of the night gets harder and harder, so I’ve thought of doing something where the hours are more fixed and I have a little more time. I have thought about starting satellite practices in other community hospitals that are looking to start hospitalist programs, being more of an administrator and delivering less patient care. But I still like what I’m doing, and that’s why I keep doing it. TH
Mark Leiser is a freelance writer based in New Jersey.
When Kenneth Patrick, MD, joined Chestnut Hill Hospital in Philadelphia in 1982, he was known simply as a physician who practiced HM. It wasn’t until 14 years later that the term “hospitalist” appeared for the first time in a New England Journal of Medicine article.
As Dr. Patrick’s job title changed, so did his outlook on the future of the profession. “My practice was exceedingly unique and, for many years, people didn’t understand that a physician could practice exclusively in a hospital,” says Dr. Patrick, now the ICU director at Chestnut Hill. “But when I first heard the word ‘hospitalist,’ I was surprised. I remember thinking, ‘Hey, I’m one of them.’ ”
He also knew that if other physicians were recognizing the specialty, more and more physicians were going to jump on the HM bandwagon. “I knew it wasn’t just a short-lived thing,” he says.
With three decades of HM experience in the bank, Dr. Patrick offers his take on the evolution of HM, changes to the delivery of care, and the importance of communicating with patients.
Question: What drew you into the medical field?
Answer: I earned an undergraduate degree in mechanical engineering [from Drexel University]. The country was going through a recession and there weren’t many job offers, so when I was a junior, I decided to switch careers. I went into medicine.
Q: Have you found any similarities between engineering and HM?
A: Very much so, particularly in the intensive-care unit (ICU). That’s what drew me to critical care and HM. You have to be very detail-oriented. You have to go through your thinking process in a very organized fashion, and you have to be prepared to solve problems that aren’t apparent when you first start caring for a patient. That’s the basis of engineering.
—Kenneth Patrick, MD, Chestnut Hill Hospital, Philadelphia
Q: Did you face challenges in 1982 that new hospitalists won’t face today because the field is more established?
A: No, I would say it’s the other way around, particularly in terms of regulation and monitoring. The Joint Commission existed then, but the standards of hospital care, pressures from insurers, and things like length of stay were not so much of an issue. The challenge to get people evaluated and discharged exceedingly quickly did not exist back then.
Q: How has your role as a hospitalist changed in 26 years?
A: The most significant change is speed. I remember during residency caring for a patient with an infection of the heart valves. That patient stayed in the hospital for 28 days getting antibiotics, and I went to see the person every day to listen to the heart. … Today, that patient would be in the hospital two or, at most, three days. They’d be discharged either to home on IV antibiotics or to a skilled nursing facility. They’d no longer stay in the hospital for a prolonged period of time.
Q: How has that changed the delivery of care?
A: Our job as hospitalists is to see someone who is sick enough to be in the hospital, evaluate and diagnose them exceedingly quickly, get them started on treatment exceedingly quickly, and, as soon as they start improving, the regulators or insurers say they no longer need to be in the hospital. We don’t get to follow them through their entire illness.
I think that is something that is lacking for young hospitalists and residents during training. They don’t see the illness from start to finish. They see it from the start until the moment the patient begins to improve and is discharged.
Q: What is the consequence of that shift?
A: Less-experienced physicians, in terms of management of a patient from the beginning to end, unless there is good communication between hospital physicians and outpatient physicians. And I just think younger physicians are less well prepared for the complications that may ensue from a given illness because they only see the illness for such a short period of time.
Q: What’s the biggest reward of being a hospitalist?
A: Making patients better, if that can be done, and helping them through illnesses that can’t be made better. The outcome may be death, permanent disability, or something tragic, but patients and their families still feel thankful if they feel you’ve been a caring physician. Without the patient and the family being satisfied, I wouldn’t have many rewards.
Q: After 26 years as a hospitalist, what’s the best advice you could offer to someone new in the field?
A: Don’t cut corners. Be as complete and as thorough as you need to be. Communicate with patients and their families, which is crucial. Be open to suggestions, because you don’t know everything. I still feel that way after 26 years. Be optimistic and enjoy what you do. And it’s very important for busy, high-pressure physician specialists to keep their mind on their family and their outside-the-hospital relationships. Don’t forget your kids are going to grow up.
Q: You often emphasize the importance of physicians communicating with patients and their families. What’s the biggest barrier to communication?
A: First, reimbursement isn’t there for explanations and counseling. You get reimbursed for the evaluation, the diagnosis, and the management of the illness. No. 2, it takes time—sometimes an inordinate amount of time. If a patient is critically ill, I can spend 30 to 90 minutes with a family, not treating the patient, but explaining what’s the matter with the patient and what the treatment options are. During that time, you’re giving up other patient-care responsibilities.
And I don’t think physicians have been well trained to communicate with someone and explain the details of an illness and the treatment options nonmedically. I’ve seen doctors try to explain to families that a patient is dead and the family didn’t know what the doctor meant. I teach residents to speak English to patients and their families, not speak medical.
Q: Should there be a greater emphasis on communication during education and residency?
A: Absolutely. I tell residents they need this training as much as they need to know what antibiotic to use for pneumonia. … My experience over the years is patients think they’re getting better care from average doctors who communicate well than doctors who are brilliant and can’t communicate.
Q: What has kept you at Chestnut Hill Hospital for 26 years?
A: Some of it is inertia. When my children were young, it was the community in which I lived. And I like working in a small, community hospital because of the personal relationships I’ve developed with the other professionals, everyone from medical records to the secretarial staff.
Q: What’s next for you?
A: As I’ve gotten older, being woken up in the middle of the night gets harder and harder, so I’ve thought of doing something where the hours are more fixed and I have a little more time. I have thought about starting satellite practices in other community hospitals that are looking to start hospitalist programs, being more of an administrator and delivering less patient care. But I still like what I’m doing, and that’s why I keep doing it. TH
Mark Leiser is a freelance writer based in New Jersey.
Transition Time
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
The light at the end of the tunnel has arrived—finally. The long hours, scut work, and call nights have paid off; you’re an attending. The transition to the “real world” can be intimidating, especially when you’ve been in training for so long. Here are some tips to ease the transition.
1. Cultivate relationships. Your interactions with nurses, house staff, case managers, social workers, and your colleagues are even more important as an attending and will serve as the building blocks of your reputation. Diplomacy during times of conflict is invaluable. Your approach to resolving situations can further your career—or be a barrier to success.
In the beginning, you might be misidentified as a resident, so it’s important to introduce yourself and have regular conversations with colleagues and consultants until you are recognized and are on a first-name basis with them. Effective communication will go a long way with your patients, their families, and primary-care physicians (PCPs). The benefits of good communication include good Press Ganey patient satisfaction scores, less liability from lawsuits, safer hospital transitions and discharges, and a successful HM practice.
2. Learn the business of practice. The first year of practice will feature a steep learning curve in the areas of billing and documentation. Effective and appropriate billing is essential to maintaining the financial viability of a hospitalist group. Most HM groups provide formal training in billing and documentation as well as chart audits by billing experts. You may find it helpful to review “Billing and Coding” articles in The Hospitalist (also available at www.the-hospitalist.org).
Take time to learn business goals and areas in need of improvement, as this will allow you to improve individual and group performance. This may include maximizing pay for performance, improving hospital throughput by prioritizing discharges early in the morning, and reducing length of stay and readmission rates.
3. Seek work-life balance. Expect to be presented with multiple opportunities to get involved outside of your clinical duties. You could have the chance to participate in quality-improvement (QI) projects, teaching, hospital committees, and research. These activities will add to the depth of your curriculum vitae and give you a voice in hospital operations.
It’s important, however, to remember to pace yourself when you add duties outside the realm of your primary job responsibilities. Avoid spreading yourself too thin. As an attending, your work hours will be fewer and your salary will be better, but your responsibility will be greater. Be sure to set aside personal time and make job satisfaction a priority. More information is available in “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (www.hospitalmedicine.org/dashboard), which outlines the pillars of career satisfaction: autonomy/workflow, workload/schedule, reward/recognition, and community/ environment.
4. Stay current. In addition to reading prominent journals, such as the New England Journal of Medicine and the Journal of Hospital Medicine, look to newer resources that screen up-to-date literature for articles most relevant to hospitalists. American College of Physicians (ACP) members can sign up for ACP Journal Club Plus (acpjc.org), which provides periodic e-mail alerts when new articles meet customized quality and relevance filters. The Hospitalist has a monthly column, “In the Literature,” (see p. 9) that summarizes recent medical research. It also is important to understand how to find evidence-based information quickly. Familiarize yourself with Medline searches and pre-appraised literature resources, such as the Cochrane database, the print version of ACP Journal Club, and guidelines.gov.
5. Be efficient and thorough. Time-management skills are critical as an attending, especially when you’re being pulled in multiple directions. Develop a “to do” list to stay organized. When you are working with nurse practitioners, physician assistants, and residents, delegate certain duties to maximize your own efficiency. Their notes often can be used to assist with documentation, but remember to properly chart the clinical rationale for critical decisions and document medical stability on the day of patient discharge. Be sure you regularly review primary data, such as imaging, culture results, and consultant recommendations. Routinely communicate with PCPs—a prompt, real-time discharge summary is easiest when the information is fresh in your mind, and it ensures proper follow-up care.
6. Know help is available. Just because you’re not a trainee anymore doesn’t mean help isn’t available. Medicine is a constantly evolving field, and you will encounter novel disease states as well as changing diagnostics and therapeutics throughout your career. When you encounter a challenging case, use your colleagues as a sounding board for ideas. When you’re not sure what to do, consultants can be called to assist. Remember, you’re not there to impress others but to provide the best possible care for your patients. Sometimes that means obtaining the advice of a specialist.
If you practice with physician extenders or house staff, you’ll find it helpful to occasionally speak directly to the attending consultant. This helps promote collegial relationships, gives consultants a better understanding of your concerns, and improves your own base of knowledge.
7. Use supervisory skills. If you are practicing in an academic setting or one with physician extenders, you will want to be readily accessible to house staff, physician assistants, and nurse practitioners under your supervision. When you first greet a patient, be sure to clearly identify yourself as the attending physician. At the same time, afford trainees the opportunity to experience being the physician—allow them to actively participate in decision-making, reinforcing best-practice and evidence-based principles as you teach.
8. Understand licensing and certification. Understand your state’s policies and start the licensing process right away, especially if your first job is in a state other than where you completed residency. For most hospitalists, this means taking the medicine boards, then a recertification exam every 10 years, as well as regularly completing continuing medical education (CME). For those looking for a promotion down the line, familiarize yourself with the culture and selection criteria of your individual hospital or group. TH
Dr. Huang is assistant clinical professor in the department of hospital medicine at the University of California San Diego Department of Medicine. Dr. Patel is associate director of hospitalist services at Staten Island University Hospital and assistant clinical professor of medicine at SUNY-Brooklyn. Dr. Chacko is a member of SHM’s Young Physician Committee and medical director of the hospitalist program at Preferred Health Partners in New York City.
Congressional Adviser
A mystery. That’s what MedPAC is to many hospitalists. You might recognize the name from communications about Medicare’s physician fee schedule, but what is this entity, what power does it possess, and how does it affect the work you do and the pay you receive?
MedPAC is the Medicare Payment Advisory Commission, an independent agency established by the Balanced Budget Act of 1997. Its mission is to advise Congress on issues affecting Medicare, including payments to private health plans participating in Medicare as well as providers in Medicare’s traditional fee-for-service program. MedPAC also analyzes and advises legislators on two issues on HM’s radar: access to care and quality of care.
Ear of the Law
Why is MedPAC important to hospitalists? Money. The commission advises Congress on how Medicare is going to pay for healthcare services, and Medicare is a major payor for any hospitalist, says Ron Greeno, MD, FHM, chief medical officer of Cogent Healthcare in Irvine, Calif., and a member of SHM’s Public Policy Committee. “The majority of patients we’ll be taking care of in any hospital are Medicare patients,” he says, “and it’s not just how we get paid, but all the regulations around that. … MedPAC will weigh in on that and certainly shape the thinking of lawmakers.”
“MedPAC is about payment … but obviously there are other policy issues they weigh in on,” Dr. Greeno says. For example, MedPAC makes specific recommendations on the physician fee schedule and determines how hospitalists document and code.
How It Works
The commission is made up of 17 volunteer members from a diverse spectrum of healthcare backgrounds. Commissioners are appointed to three-year renewable terms. An executive director and staff of analysts with backgrounds in economics, health policy, public health, and medicine support the agency.
MedPAC holds monthly public meetings in Washington, D.C., to discuss Medicare issues and policy questions, and to formulate recommendations to Congress. Meetings include research presentations by MedPAC staff, policy experts, and interested parties. Each meeting allows time for public comment.
The commission provides its recommendations to Congress in biannual reports, issued in March and June. MedPAC also advises Congress through comment on reports and proposed regulations issued by the U.S. Department of Health and Human Services (HHS), testimony, and briefings for congressional staff.
A New Role
This year, as President Obama and his administration push for rapid and major healthcare changes, Dr. Greeno says MedPAC’s role will shift as Congress speeds toward new solutions. “How things are going to get done is already different than it was last year,” he says. “The pace of the government’s attempts to change how Medicare looks has picked up considerably.”
—Ron Greeno, MD, Cogent Healthcare, SHM Public Policy Committee
Citing SHM’s Public Policy Committee meetings with lawmakers in March, Dr. Greeno says healthcare reform is on the fast track. “Everything we were hearing from CMS [Centers for Medicare and Medicaid Services], the American Hospital Association, and MedPAC indicated that they’re looking to have a healthcare reform bill to Congress by summer,” he says. “When you have that kind of pace, things will come from a lot of different areas.”
Dr. Greeno uses pay for performance as one example of how government can be slow to change healthcare policy. “That process has taken years, but it’s still a small percentage of how we’re paid,” Dr. Greeno says, noting the current administration has expressed interest in changing course on the policy. “Now we may have complete reform of Medicare payments. In light of the rapidness of this pace, I’m not sure MedPAC’s role will be the same. They’ll continue to be a resource to Congress, but the commissioners are volunteers with full-time jobs; they meet once a month, while legislation is being worked on pretty much around the clock right now.”
MedPAC Sets the Tone
Even if the commission isn’t prepared to make direct recommendations for new legislation in the next few months, it still has significant influence. Since its inception, MedPac has routinely “set the tone” for policy reform, Dr. Greeno stresses. “For example, the healthcare reform legislation will likely include bundling payments to hospitals and physicians who work in hospitals,” he says. “MedPAC has already made recommendations to do this, as well as to start demonstration projects.” Earlier this year, sites were selected for Medicare’s Acute Care Episode (ACE) demonstration, under which a single global payment will be made for inpatient facility and professional services. “The same is true of the idea of paying based on quality, not patient volume,” Dr. Greeno says. “The commission has made recommendations on this.”
Then again, no one can say how the future of healthcare reform will unfold, or how quickly things will move this year. “The healthcare bill introduced this summer could completely do away with fee-for-service payments,” Dr. Greeno says. “Of course, nobody knows when—or if—that bill will get passed.” TH
Jane Jerrard is a medical writer based in Chicago.
A mystery. That’s what MedPAC is to many hospitalists. You might recognize the name from communications about Medicare’s physician fee schedule, but what is this entity, what power does it possess, and how does it affect the work you do and the pay you receive?
MedPAC is the Medicare Payment Advisory Commission, an independent agency established by the Balanced Budget Act of 1997. Its mission is to advise Congress on issues affecting Medicare, including payments to private health plans participating in Medicare as well as providers in Medicare’s traditional fee-for-service program. MedPAC also analyzes and advises legislators on two issues on HM’s radar: access to care and quality of care.
Ear of the Law
Why is MedPAC important to hospitalists? Money. The commission advises Congress on how Medicare is going to pay for healthcare services, and Medicare is a major payor for any hospitalist, says Ron Greeno, MD, FHM, chief medical officer of Cogent Healthcare in Irvine, Calif., and a member of SHM’s Public Policy Committee. “The majority of patients we’ll be taking care of in any hospital are Medicare patients,” he says, “and it’s not just how we get paid, but all the regulations around that. … MedPAC will weigh in on that and certainly shape the thinking of lawmakers.”
“MedPAC is about payment … but obviously there are other policy issues they weigh in on,” Dr. Greeno says. For example, MedPAC makes specific recommendations on the physician fee schedule and determines how hospitalists document and code.
How It Works
The commission is made up of 17 volunteer members from a diverse spectrum of healthcare backgrounds. Commissioners are appointed to three-year renewable terms. An executive director and staff of analysts with backgrounds in economics, health policy, public health, and medicine support the agency.
MedPAC holds monthly public meetings in Washington, D.C., to discuss Medicare issues and policy questions, and to formulate recommendations to Congress. Meetings include research presentations by MedPAC staff, policy experts, and interested parties. Each meeting allows time for public comment.
The commission provides its recommendations to Congress in biannual reports, issued in March and June. MedPAC also advises Congress through comment on reports and proposed regulations issued by the U.S. Department of Health and Human Services (HHS), testimony, and briefings for congressional staff.
A New Role
This year, as President Obama and his administration push for rapid and major healthcare changes, Dr. Greeno says MedPAC’s role will shift as Congress speeds toward new solutions. “How things are going to get done is already different than it was last year,” he says. “The pace of the government’s attempts to change how Medicare looks has picked up considerably.”
—Ron Greeno, MD, Cogent Healthcare, SHM Public Policy Committee
Citing SHM’s Public Policy Committee meetings with lawmakers in March, Dr. Greeno says healthcare reform is on the fast track. “Everything we were hearing from CMS [Centers for Medicare and Medicaid Services], the American Hospital Association, and MedPAC indicated that they’re looking to have a healthcare reform bill to Congress by summer,” he says. “When you have that kind of pace, things will come from a lot of different areas.”
Dr. Greeno uses pay for performance as one example of how government can be slow to change healthcare policy. “That process has taken years, but it’s still a small percentage of how we’re paid,” Dr. Greeno says, noting the current administration has expressed interest in changing course on the policy. “Now we may have complete reform of Medicare payments. In light of the rapidness of this pace, I’m not sure MedPAC’s role will be the same. They’ll continue to be a resource to Congress, but the commissioners are volunteers with full-time jobs; they meet once a month, while legislation is being worked on pretty much around the clock right now.”
MedPAC Sets the Tone
Even if the commission isn’t prepared to make direct recommendations for new legislation in the next few months, it still has significant influence. Since its inception, MedPac has routinely “set the tone” for policy reform, Dr. Greeno stresses. “For example, the healthcare reform legislation will likely include bundling payments to hospitals and physicians who work in hospitals,” he says. “MedPAC has already made recommendations to do this, as well as to start demonstration projects.” Earlier this year, sites were selected for Medicare’s Acute Care Episode (ACE) demonstration, under which a single global payment will be made for inpatient facility and professional services. “The same is true of the idea of paying based on quality, not patient volume,” Dr. Greeno says. “The commission has made recommendations on this.”
Then again, no one can say how the future of healthcare reform will unfold, or how quickly things will move this year. “The healthcare bill introduced this summer could completely do away with fee-for-service payments,” Dr. Greeno says. “Of course, nobody knows when—or if—that bill will get passed.” TH
Jane Jerrard is a medical writer based in Chicago.
A mystery. That’s what MedPAC is to many hospitalists. You might recognize the name from communications about Medicare’s physician fee schedule, but what is this entity, what power does it possess, and how does it affect the work you do and the pay you receive?
MedPAC is the Medicare Payment Advisory Commission, an independent agency established by the Balanced Budget Act of 1997. Its mission is to advise Congress on issues affecting Medicare, including payments to private health plans participating in Medicare as well as providers in Medicare’s traditional fee-for-service program. MedPAC also analyzes and advises legislators on two issues on HM’s radar: access to care and quality of care.
Ear of the Law
Why is MedPAC important to hospitalists? Money. The commission advises Congress on how Medicare is going to pay for healthcare services, and Medicare is a major payor for any hospitalist, says Ron Greeno, MD, FHM, chief medical officer of Cogent Healthcare in Irvine, Calif., and a member of SHM’s Public Policy Committee. “The majority of patients we’ll be taking care of in any hospital are Medicare patients,” he says, “and it’s not just how we get paid, but all the regulations around that. … MedPAC will weigh in on that and certainly shape the thinking of lawmakers.”
“MedPAC is about payment … but obviously there are other policy issues they weigh in on,” Dr. Greeno says. For example, MedPAC makes specific recommendations on the physician fee schedule and determines how hospitalists document and code.
How It Works
The commission is made up of 17 volunteer members from a diverse spectrum of healthcare backgrounds. Commissioners are appointed to three-year renewable terms. An executive director and staff of analysts with backgrounds in economics, health policy, public health, and medicine support the agency.
MedPAC holds monthly public meetings in Washington, D.C., to discuss Medicare issues and policy questions, and to formulate recommendations to Congress. Meetings include research presentations by MedPAC staff, policy experts, and interested parties. Each meeting allows time for public comment.
The commission provides its recommendations to Congress in biannual reports, issued in March and June. MedPAC also advises Congress through comment on reports and proposed regulations issued by the U.S. Department of Health and Human Services (HHS), testimony, and briefings for congressional staff.
A New Role
This year, as President Obama and his administration push for rapid and major healthcare changes, Dr. Greeno says MedPAC’s role will shift as Congress speeds toward new solutions. “How things are going to get done is already different than it was last year,” he says. “The pace of the government’s attempts to change how Medicare looks has picked up considerably.”
—Ron Greeno, MD, Cogent Healthcare, SHM Public Policy Committee
Citing SHM’s Public Policy Committee meetings with lawmakers in March, Dr. Greeno says healthcare reform is on the fast track. “Everything we were hearing from CMS [Centers for Medicare and Medicaid Services], the American Hospital Association, and MedPAC indicated that they’re looking to have a healthcare reform bill to Congress by summer,” he says. “When you have that kind of pace, things will come from a lot of different areas.”
Dr. Greeno uses pay for performance as one example of how government can be slow to change healthcare policy. “That process has taken years, but it’s still a small percentage of how we’re paid,” Dr. Greeno says, noting the current administration has expressed interest in changing course on the policy. “Now we may have complete reform of Medicare payments. In light of the rapidness of this pace, I’m not sure MedPAC’s role will be the same. They’ll continue to be a resource to Congress, but the commissioners are volunteers with full-time jobs; they meet once a month, while legislation is being worked on pretty much around the clock right now.”
MedPAC Sets the Tone
Even if the commission isn’t prepared to make direct recommendations for new legislation in the next few months, it still has significant influence. Since its inception, MedPac has routinely “set the tone” for policy reform, Dr. Greeno stresses. “For example, the healthcare reform legislation will likely include bundling payments to hospitals and physicians who work in hospitals,” he says. “MedPAC has already made recommendations to do this, as well as to start demonstration projects.” Earlier this year, sites were selected for Medicare’s Acute Care Episode (ACE) demonstration, under which a single global payment will be made for inpatient facility and professional services. “The same is true of the idea of paying based on quality, not patient volume,” Dr. Greeno says. “The commission has made recommendations on this.”
Then again, no one can say how the future of healthcare reform will unfold, or how quickly things will move this year. “The healthcare bill introduced this summer could completely do away with fee-for-service payments,” Dr. Greeno says. “Of course, nobody knows when—or if—that bill will get passed.” TH
Jane Jerrard is a medical writer based in Chicago.
Head Off Hypoglycemia
Let’s look at a case: A known diabetic patient has been in good control, with glycosylated hemoglobin (HbA1c) levels lower than 6.5 gm/dL the past two years. Her medication regimen has remained relatively stable during that time. Her daily medications include simvastatin, 40 mg; metformin extended release, 2,000 mg; sitagliptin, 100 mg; glimepiride, 8 mg; quinapril, 20 mg; a multivitamin; calcium carbonate, 1,500 mg; and an 81-mg aspirin.
Her lipid panel, liver and renal function tests, and blood pressure are all within normal limits. However, she was admitted to the hospital with a plasma glucose level of 38 mg/dL.
Upon physical examination, she appears diaphoretic, with weakness, confusion, tremulousness, and palpitations. She is treated with glucose to maintain a level of above 50 mg/dL, and she responds without long-term sequelae.
What precipitated this event?
Drug-Induced Hypoglycemia
Hypoglycemia may represent a lab error or artifactual hypoglycemia due to glycolysis in the collection sample. To determine a pathological cause of hypoglycemia, the triad of low plasma glucose, hypoglycemia symptoms, and symptom resolution with correction of the blood glucose level should be used.1 Hypoglycemia is most often seen in diabetic patients and is the most commonly noted endocrine emergency in the inpatient setting, as well as in the ambulatory setting. Some common causes of hypoglycemia in diabetes patients include alcohol consumption, skipping meals, too much exercise, and intentional or unintentional medication overdoses.2
Treatment is required when the blood glucose level is below 45 gm/dL. Symptoms include anxiety, tremulousness, nausea, sweating, palpitation, and hunger.3 More severe symptoms related to compromised central nervous system function include weakness, fatigue, confusion, seizures, focal neurologic deficits, and coma.
The most common causes of drug-induced hypoglycemia are insulin, ethanol, or sulfonylureas. Risk factors associated with unintentional overdose of sulfonylureas include advanced age, drug-to-drug interactions, and decreased renal or hepatic clearance. Other drugs have been reported to cause hypoglycemia. Some of these include high-dose salicylates, beta-blockers, haloperidol, monoamine oxidase inhibitors, other sulfonamides (particularly trimethoprim-sulfamethoxazole), pentamidine, quinine/quinidine, and quinolone antibiotics (e.g., gatifloxacin or levofloxacin).4
Diabetics use more than 120 natural medicines, either alone or in combination with their prescribed diabetes medications, to lower blood glucose and/or improve HbA1c.5 Some of the most commonly used products are banaba, bitter melon, fenugreek, and Gymnema (hypoglycemics), along with American or panax ginseng, cassia cinnamon, chromium, prickly pear cactus, soy, or vanadium (insulin sensitizers).
Diagnosis
Patient history aids in the clinical diagnosis of hypoglycemia and should be reviewed to determine a potential drug-induced cause. History also might identify a medication dispensing error (e.g., the onset of hypoglycemia following a recent medication refill). Hospitalists should question the patient or the patient’s family as to medication use, including over-the-counter drugs, vitamins, supplements, natural foods, and other related products.
Treatment
Glucose should be administered to maintain a plasma glucose level of at least 50 gm/dL. This may be achieved orally via frequent meals or snacks, or intravenously. The underlying cause should be addressed. In drug- or medication-induced cases, the causative agent should be removed or retitrated to an effective dose that does not cause hypoglycemia.
Upon further questioning, the patient admitted she’d been taking 3,000 mg of a bitter melon product per day. She took this in addition to all her prescribed medications. Because bitter melon has an insulin-like effect, its use in combination with glimepiride led to the clinically significant hypoglycemic reaction, which required hospitalization and treatment. Prior to discharge, the patient promised to discuss the use of alternative and natural products with her pharmacist or physician before trying anything new. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Guettier JM, Gorden P. Hypoglycemia. Endocrinol Metab Clin North Am. 2006;35:753-766.
- Holt HH. Drug-induced hypoglycemia: overview. The University of Maryland Medical Center Web site. Available at: www.umm.edu/ency/article/000310.htm. Accessed March 2, 2009.
- Hurd R. Drug-induced hypoglycemia. Drugs.com Web site. Available at: www.drugs.com/enc/drug-induced-hypoglycemia.html. Accessed March 2, 2009.
- Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother. 2007; 41:1859-1866.
- Natural medicines in the clinical management of diabetes. Natural Medicines Comprehensive Database Web site. Available at: www.naturaldatabase.com. Accessed March 3, 2009.
- Teva announces approval and launch of generic Imitrex tablets. Available at: finance.yahoo.com/news/Teva-Announces-Approval-and-bw-14308223.html/print. Accessed March 2, 2009.
- Additional strengths of Avinza available. Monthly Prescribing Reference Web site. Available at: www.empr.com/Additional-strengths-of-Avinza-available/article/126905/. Accessed March 2, 2009.
- Gelnique treatment for overactive bladder. Drugs.com Web site. Available at: www.drugs.com/gelnique.html. Accessed March 2, 2009.
- Reclast label. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2008/021817s002lbl.pdf. Accessed March 2, 2009.
- Clopidogrel bisulfate (marketed as Plavix). The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#plavix. Accessed March 2, 2009.
- PPI interactions with clopidogrel. Med Lett Drugs Ther. 2009;51 (1303):2-3.
- PPI interactions with clopidogrel revisited. Med Lett Drugs Ther. 2009;51(1306):13-4.
- Xigris (Drotrecogin alfa [activated]): early communication about an ongoing safety review. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#Xigris. Accessed March 2, 2009.
Let’s look at a case: A known diabetic patient has been in good control, with glycosylated hemoglobin (HbA1c) levels lower than 6.5 gm/dL the past two years. Her medication regimen has remained relatively stable during that time. Her daily medications include simvastatin, 40 mg; metformin extended release, 2,000 mg; sitagliptin, 100 mg; glimepiride, 8 mg; quinapril, 20 mg; a multivitamin; calcium carbonate, 1,500 mg; and an 81-mg aspirin.
Her lipid panel, liver and renal function tests, and blood pressure are all within normal limits. However, she was admitted to the hospital with a plasma glucose level of 38 mg/dL.
Upon physical examination, she appears diaphoretic, with weakness, confusion, tremulousness, and palpitations. She is treated with glucose to maintain a level of above 50 mg/dL, and she responds without long-term sequelae.
What precipitated this event?
Drug-Induced Hypoglycemia
Hypoglycemia may represent a lab error or artifactual hypoglycemia due to glycolysis in the collection sample. To determine a pathological cause of hypoglycemia, the triad of low plasma glucose, hypoglycemia symptoms, and symptom resolution with correction of the blood glucose level should be used.1 Hypoglycemia is most often seen in diabetic patients and is the most commonly noted endocrine emergency in the inpatient setting, as well as in the ambulatory setting. Some common causes of hypoglycemia in diabetes patients include alcohol consumption, skipping meals, too much exercise, and intentional or unintentional medication overdoses.2
Treatment is required when the blood glucose level is below 45 gm/dL. Symptoms include anxiety, tremulousness, nausea, sweating, palpitation, and hunger.3 More severe symptoms related to compromised central nervous system function include weakness, fatigue, confusion, seizures, focal neurologic deficits, and coma.
The most common causes of drug-induced hypoglycemia are insulin, ethanol, or sulfonylureas. Risk factors associated with unintentional overdose of sulfonylureas include advanced age, drug-to-drug interactions, and decreased renal or hepatic clearance. Other drugs have been reported to cause hypoglycemia. Some of these include high-dose salicylates, beta-blockers, haloperidol, monoamine oxidase inhibitors, other sulfonamides (particularly trimethoprim-sulfamethoxazole), pentamidine, quinine/quinidine, and quinolone antibiotics (e.g., gatifloxacin or levofloxacin).4
Diabetics use more than 120 natural medicines, either alone or in combination with their prescribed diabetes medications, to lower blood glucose and/or improve HbA1c.5 Some of the most commonly used products are banaba, bitter melon, fenugreek, and Gymnema (hypoglycemics), along with American or panax ginseng, cassia cinnamon, chromium, prickly pear cactus, soy, or vanadium (insulin sensitizers).
Diagnosis
Patient history aids in the clinical diagnosis of hypoglycemia and should be reviewed to determine a potential drug-induced cause. History also might identify a medication dispensing error (e.g., the onset of hypoglycemia following a recent medication refill). Hospitalists should question the patient or the patient’s family as to medication use, including over-the-counter drugs, vitamins, supplements, natural foods, and other related products.
Treatment
Glucose should be administered to maintain a plasma glucose level of at least 50 gm/dL. This may be achieved orally via frequent meals or snacks, or intravenously. The underlying cause should be addressed. In drug- or medication-induced cases, the causative agent should be removed or retitrated to an effective dose that does not cause hypoglycemia.
Upon further questioning, the patient admitted she’d been taking 3,000 mg of a bitter melon product per day. She took this in addition to all her prescribed medications. Because bitter melon has an insulin-like effect, its use in combination with glimepiride led to the clinically significant hypoglycemic reaction, which required hospitalization and treatment. Prior to discharge, the patient promised to discuss the use of alternative and natural products with her pharmacist or physician before trying anything new. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Guettier JM, Gorden P. Hypoglycemia. Endocrinol Metab Clin North Am. 2006;35:753-766.
- Holt HH. Drug-induced hypoglycemia: overview. The University of Maryland Medical Center Web site. Available at: www.umm.edu/ency/article/000310.htm. Accessed March 2, 2009.
- Hurd R. Drug-induced hypoglycemia. Drugs.com Web site. Available at: www.drugs.com/enc/drug-induced-hypoglycemia.html. Accessed March 2, 2009.
- Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother. 2007; 41:1859-1866.
- Natural medicines in the clinical management of diabetes. Natural Medicines Comprehensive Database Web site. Available at: www.naturaldatabase.com. Accessed March 3, 2009.
- Teva announces approval and launch of generic Imitrex tablets. Available at: finance.yahoo.com/news/Teva-Announces-Approval-and-bw-14308223.html/print. Accessed March 2, 2009.
- Additional strengths of Avinza available. Monthly Prescribing Reference Web site. Available at: www.empr.com/Additional-strengths-of-Avinza-available/article/126905/. Accessed March 2, 2009.
- Gelnique treatment for overactive bladder. Drugs.com Web site. Available at: www.drugs.com/gelnique.html. Accessed March 2, 2009.
- Reclast label. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2008/021817s002lbl.pdf. Accessed March 2, 2009.
- Clopidogrel bisulfate (marketed as Plavix). The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#plavix. Accessed March 2, 2009.
- PPI interactions with clopidogrel. Med Lett Drugs Ther. 2009;51 (1303):2-3.
- PPI interactions with clopidogrel revisited. Med Lett Drugs Ther. 2009;51(1306):13-4.
- Xigris (Drotrecogin alfa [activated]): early communication about an ongoing safety review. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#Xigris. Accessed March 2, 2009.
Let’s look at a case: A known diabetic patient has been in good control, with glycosylated hemoglobin (HbA1c) levels lower than 6.5 gm/dL the past two years. Her medication regimen has remained relatively stable during that time. Her daily medications include simvastatin, 40 mg; metformin extended release, 2,000 mg; sitagliptin, 100 mg; glimepiride, 8 mg; quinapril, 20 mg; a multivitamin; calcium carbonate, 1,500 mg; and an 81-mg aspirin.
Her lipid panel, liver and renal function tests, and blood pressure are all within normal limits. However, she was admitted to the hospital with a plasma glucose level of 38 mg/dL.
Upon physical examination, she appears diaphoretic, with weakness, confusion, tremulousness, and palpitations. She is treated with glucose to maintain a level of above 50 mg/dL, and she responds without long-term sequelae.
What precipitated this event?
Drug-Induced Hypoglycemia
Hypoglycemia may represent a lab error or artifactual hypoglycemia due to glycolysis in the collection sample. To determine a pathological cause of hypoglycemia, the triad of low plasma glucose, hypoglycemia symptoms, and symptom resolution with correction of the blood glucose level should be used.1 Hypoglycemia is most often seen in diabetic patients and is the most commonly noted endocrine emergency in the inpatient setting, as well as in the ambulatory setting. Some common causes of hypoglycemia in diabetes patients include alcohol consumption, skipping meals, too much exercise, and intentional or unintentional medication overdoses.2
Treatment is required when the blood glucose level is below 45 gm/dL. Symptoms include anxiety, tremulousness, nausea, sweating, palpitation, and hunger.3 More severe symptoms related to compromised central nervous system function include weakness, fatigue, confusion, seizures, focal neurologic deficits, and coma.
The most common causes of drug-induced hypoglycemia are insulin, ethanol, or sulfonylureas. Risk factors associated with unintentional overdose of sulfonylureas include advanced age, drug-to-drug interactions, and decreased renal or hepatic clearance. Other drugs have been reported to cause hypoglycemia. Some of these include high-dose salicylates, beta-blockers, haloperidol, monoamine oxidase inhibitors, other sulfonamides (particularly trimethoprim-sulfamethoxazole), pentamidine, quinine/quinidine, and quinolone antibiotics (e.g., gatifloxacin or levofloxacin).4
Diabetics use more than 120 natural medicines, either alone or in combination with their prescribed diabetes medications, to lower blood glucose and/or improve HbA1c.5 Some of the most commonly used products are banaba, bitter melon, fenugreek, and Gymnema (hypoglycemics), along with American or panax ginseng, cassia cinnamon, chromium, prickly pear cactus, soy, or vanadium (insulin sensitizers).
Diagnosis
Patient history aids in the clinical diagnosis of hypoglycemia and should be reviewed to determine a potential drug-induced cause. History also might identify a medication dispensing error (e.g., the onset of hypoglycemia following a recent medication refill). Hospitalists should question the patient or the patient’s family as to medication use, including over-the-counter drugs, vitamins, supplements, natural foods, and other related products.
Treatment
Glucose should be administered to maintain a plasma glucose level of at least 50 gm/dL. This may be achieved orally via frequent meals or snacks, or intravenously. The underlying cause should be addressed. In drug- or medication-induced cases, the causative agent should be removed or retitrated to an effective dose that does not cause hypoglycemia.
Upon further questioning, the patient admitted she’d been taking 3,000 mg of a bitter melon product per day. She took this in addition to all her prescribed medications. Because bitter melon has an insulin-like effect, its use in combination with glimepiride led to the clinically significant hypoglycemic reaction, which required hospitalization and treatment. Prior to discharge, the patient promised to discuss the use of alternative and natural products with her pharmacist or physician before trying anything new. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- Guettier JM, Gorden P. Hypoglycemia. Endocrinol Metab Clin North Am. 2006;35:753-766.
- Holt HH. Drug-induced hypoglycemia: overview. The University of Maryland Medical Center Web site. Available at: www.umm.edu/ency/article/000310.htm. Accessed March 2, 2009.
- Hurd R. Drug-induced hypoglycemia. Drugs.com Web site. Available at: www.drugs.com/enc/drug-induced-hypoglycemia.html. Accessed March 2, 2009.
- Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother. 2007; 41:1859-1866.
- Natural medicines in the clinical management of diabetes. Natural Medicines Comprehensive Database Web site. Available at: www.naturaldatabase.com. Accessed March 3, 2009.
- Teva announces approval and launch of generic Imitrex tablets. Available at: finance.yahoo.com/news/Teva-Announces-Approval-and-bw-14308223.html/print. Accessed March 2, 2009.
- Additional strengths of Avinza available. Monthly Prescribing Reference Web site. Available at: www.empr.com/Additional-strengths-of-Avinza-available/article/126905/. Accessed March 2, 2009.
- Gelnique treatment for overactive bladder. Drugs.com Web site. Available at: www.drugs.com/gelnique.html. Accessed March 2, 2009.
- Reclast label. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/cder/foi/label/2008/021817s002lbl.pdf. Accessed March 2, 2009.
- Clopidogrel bisulfate (marketed as Plavix). The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#plavix. Accessed March 2, 2009.
- PPI interactions with clopidogrel. Med Lett Drugs Ther. 2009;51 (1303):2-3.
- PPI interactions with clopidogrel revisited. Med Lett Drugs Ther. 2009;51(1306):13-4.
- Xigris (Drotrecogin alfa [activated]): early communication about an ongoing safety review. The U.S. Food and Drug Administration Web site. Available at: www.fda.gov/medwatch/safety/2009/safety09.htm#Xigris. Accessed March 2, 2009.
In the Literature
Literature at a Glance
A guide to this month’s studies
- Inhaled steroids and COPD.
- Communication about dietary supplement use.
- Glycemic control in stroke.
- Hospitalist-PCP communication and outcomes.
- Gentamicin nephrotoxicity in endocarditis.
- Outcomes after osteoporotic fractures.
- Predictors of readmission after pulmonary embolism.
- Provider awareness of hospital readmission.
Inhaled Corticosteroid Use in COPD Associated with Increased Pneumonia Risk
Clinical question: Does long-term use of inhaled corticosteroids in chronic obstructive pulmonary disease (COPD) increase the risk of developing pneumonia?
Background: Guidelines recommend a combination of inhaled corticosteroids and long-acting bronchodilators in patients with severe COPD. However, recent evidence has raised concerns about the increased risk of pneumonia in patients on inhaled steroids. The exact nature of this association and its specificity to the inhaled corticosteroid component is unclear.
Study design: Meta-analysis and systematic review of 18 randomized controlled trials (RCTs) evaluating inhaled corticosteroid use in COPD.
Setting: Medline, EMBASE, the Cochrane Database of Systematic Reviews, regulatory documents, and trial registries.
Synopsis: This study, which totaled 16,996 case reviews, focused on inhaled corticosteroid use in COPD (excluding asthma) with at least 24 weeks of followup. The study authors evaluated inhaled corticosteroid use—alone or in combination with long-acting beta-agonists (LABA)—against a control (placebo or LABA alone). Primary outcomes were any pneumonia and serious pneumonia leading to increased morbidity and mortality. Secondary outcomes included pneumonia-related mortality and all-cause mortality.
Inhaled corticosteroids—irrespective of associated LABA use—significantly increased the risk of pneumonia (7.4% vs. 4.7%) with a relative risk (RR) of 1.60; 95% CI, 1.33-1.92, P<0.001. Inhaled corticosteroids were strongly associated with an increase in serious pneumonia (RR 1.71; 95% CI, 1.46-1.99, P<0.001). However, inhaled corticosteroid use did not translate to significantly increased pneumonia-related or overall mortality, possibly due to the inadequate power of most of the individual trials.
The findings reflect those from other database studies, but lend specificity to the inhaled corticosteroid component. This can be cause for concern as studies of long-term inhaled corticosteroid use in patients with COPD have failed to show a benefit in mortality or decreased exacerbations.
Bottom line: Risk-benefit analysis for inhaled corticosteroid use in COPD patients should consider the increased risk of pneumonia, possibly related to local immunosuppression.
Citation: Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219-229.
Inadequate Physician Communication Regarding Dietary Supplement Usage
Clinical question: How frequently do hospital physicians communicate about the use of dietary supplements?
Background: About 20% of the U.S. population uses dietary supplements, products that have potential interactions with other prescription medications. Dietary supplement usage patterns, disclosure, and discussion with physicians have been studied in the outpatient setting. However, these metrics have not been evaluated in the inpatient setting.
Study design: A cross-sectional, observational pilot study.
Setting: Inpatients on a general medicine and geriatrics service at the University of North Carolina Medical Center.
Synopsis: Sixty inpatients were questioned regarding their use of dietary supplements in the past year. Patients were asked about their communication with the admitting resident physician regarding dietary supplements and their beliefs regarding continued use during hospitalization. Patient responses revealed prevalent dietary supplement use, with about 80% of patients using supplements and 52% using nonvitamin/nonmineral supplements.
The study revealed poor communication between residents and their patients. Only 20% of residents inquired about dietary supplement use during the admission process, while 74% of patients neglected to disclose their use of dietary supplements. Furthermore, 56% of patients thought communication was unimportant; they assumed that it was in their medical records (18%), or they expected the physician to ask them about it (20%). Though most patients agreed to stop using dietary supplements as inpatients, 13% did not think dietary supplement use was a problem, even if it went against medical advice.
Study limitations include the small sample size and recall bias inherent to the design. It also is likely that more patients using dietary supplements consented for the study, as evidenced by higher prevalence of use.
Bottom line: Use of dietary supplements in hospitalized patients is common, and communication about their use between patients and physicians is limited.
Citation: Young LA, Faurot KR, Gaylord SA. Use of and communication about dietary supplements among hospitalized patients. J Gen Intern Med. 2009;24(3):366-369.
Early Hyperglycemia Associated with Poor Outcomes After Acute Ischemic Stroke
Clinical question: Is there a threshold of hyperglycemia after an acute ischemic stroke (IS) that predicts a poor outcome?
Background: A growing body of evidence shows that admission hyperglycemia in an acute IS predicts a poor outcome. Current triggers to initiate glucose control measures are based on consensus data. However, capillary glucose is a continuous variable and could have a linear relationship with stroke outcomes. A particular glucose level may herald poor outcomes.
Study design: Prospective observational cohort study.
Setting: Seven university hospitals with dedicated stroke units in Spain.
Synopsis: 476 patients with acute IS had admission and maximum glucose levels recorded during the first 48 hours of admission. Stroke scales and brain imaging assessed the patients’ stroke severity. The primary endpoint of a poor outcome at three months was defined by a modified Rankin score of >2.
The primary endpoint was noted in 156 (38%) patients. Receiver operating characteristic curves for both capillary glucose at admission and maximal values within 48 hours pointed to 155mg/dL as a cutoff for the primary outcome. However, subsequent regression analysis confirmed only the maximal value as an independent predictor of poor outcome (OR 2.73; 95% CI, 1.42 to 5.24). Additionally, in contrast to patient age and infarct volume, the maximal glucose value of ≥155 mg/dL was associated with stroke severity on admission and a higher three-month mortality (HR 3.80; 95% CI, 1.79 to 8.10; P=0.001).
The observational nature of the study opens it to speculation: Does lowering the level to less than 155 mg/dl improve patient outcomes? However, it does offer a potential target for future interventional studies.
Bottom line: Hyperglycemia within the first 48 hours of an ischemic stroke offers a more robust predictor of poor outcomes compared with admission glucose levels. A glucose level less than 155 mg/dL could be a potential treatment goal in the future.
Citation: Fuentes B, Castillo J, San José B, et al. The prognostic value of capillary glucose levels in acute stroke: The GLycemia In Acute Stroke (GLIAS) study. Stroke. 2009;40(2):562-568.
Communication Between Inpatient Medical Teams and PCPs Does Not Improve Outcomes
Clinical question: Does communication between patients’ physicians in the hospital and their primary-care physicians (PCPs) improve outcomes after discharge?
Background: The increased use of the hospitalist model has resulted in concerns about discontinuity of patient care after discharge. This might hamper the quality of clinical care and increase adverse outcomes, including readmission or death. Effective communication could have the potential to improve clinical outcomes.
Study design: Survey based in a quasi-randomized cohort of medical inpatients.
Setting: Six academic medical centers throughout the U.S.
Synopsis: Of the initial 2,526 patients, only 1,078 were available for final analysis based on failure of patient followup and a 68% PCP response rate. PCP surveys were faxed two weeks after patient discharge. PCPs were asked about hospitalization awareness and communication methods. Patients were contacted post-discharge, and National Death Index data were reviewed to determine the primary composite outcomes of ED visits, hospital readmissions, or death at 30 days.
Four out of five PCPs surveyed were aware of their patients’ hospitalizations—23% via direct communication and 42% by discharge summary. The primary outcome occurred in 184 (22%) of 834 patients. In contrast, of the 244 PCPs unaware of their patients’ hospitalizations, the primary outcome occurred in 49 (20%) patients. After logistic regression, PCP awareness of hospitalization, irrespective of communication method, was not associated with risk of outcomes (adjusted OR 1.08, 95% CI, 0.73 to 1.59). Having a hospitalist as the hospital physician (34%) did not affect outcomes. These results could reflect the inclusion of patients with fewer comorbidities. Additionally, effect on adverse drug events, patient satisfaction, and quality of life were not evaluated.
Bottom line: Communication between inpatient physicians and PCPs needs improvement to affect clinical outcomes, especially in high-risk patients.
Citation: Bell CM, Schnipper JL, Auerbach AD, et al. Association of communication between hospital-based physicians and primary care providers with patient outcomes. J Gen Intern Med. 2008;24(3):381-386.
Gentamicin Use in Staphylococcal Bacteremia or Endocarditis Causes Nephrotoxicity
Clinical question: Does gentamicin synergism in Staphylococcal bacteremia and endocarditis achieve faster eradication at the cost of nephrotoxicity?
Background: Gentamicin has been used to help with sterilization of blood or cardiac vegetations in patients with Staphylococcal bacteremia or infective endocarditis (IE). However, historic data negate its role in decreasing morbidity or mortality. If its potential nephrotoxicity were better characterized, it could help assess the overall utility of this practice.
Study design: Retrospective analysis of a cohort from a published randomized control trial.
Setting: 44 hospitals in the U.S. and Europe.
Synopsis: Two hundred thirty-six patients with Staphylococcal bacteremia or native-valve IE (mostly right-sided) were randomized to receive standard therapy (vancomycin or antistaphylococcal penicillin) or daptomycin. Patients receiving standard therapy and those with left-side IE in the daptomycin arm also received low-dose gentamicin. Sequential creatinine levels were used to determine primary outcomes of renal impairment events and a decrease in creatinine clearance.
Renal impairment events, elevation of mean serum creatinine, and decrease in creatinine clearance were more prevalent with standard therapy, especially in the elderly and those with diabetes. Combination of gentamicin with penicillin caused an earlier creatinine elevation compared with that with vancomycin.
Patients on gentamicin had a modest decrease in creatinine clearance (22% vs. 8%; P= 0.005), especially if their baseline was 50 to 80 mL/min. The decrease was early and sustained with gentamicin exposure. Multivariate analysis revealed age (≥65 years) and gentamicin use (not dose and duration) to be independent predictors of renal impairment. The analysis fails to address use of gentamicin in prosthetic-valve IE and left-side IE.
Bottom line: Initial low-dose gentamicin use in Staphylococcal bacteremia or endocarditis increases nephrotoxicity with no clear mortality benefit.
Citation: Cosgrove SE, Vigliani GA, Fowler VG, et al. Initial low-dose gentamicin for Staphylococcus aureus bacteremia and endocarditis is nephrotoxic. Clin Infect Dis. 2009;48(6):713-721.
Osteoporotic Fractures Increase Five-Year Mortality, Especially in the Elderly
Clinical question: What is the effect of initial osteoporotic fractures and subsequent fractures on mortality?
Background: With an aging population, osteoporotic fractures are poised to escalate into a national healthcare problem. Studies have outlined the increase in premature and long-term mortality associated with hip or vertebral fractures. However, other appendicular fractures have not been studied, and little is known about the mortality risk with subsequent fracturing.
Study design: Prospective cohort from the Dubbo Osteoporosis Epidemiology Study, a longitudinal, population-based study.
Setting: Stable population of men and women 60 and older in Dubbo, Australia.
Synopsis: 1,300 people with at least one minimal-trauma fracture were selected. Fractures were grouped as hip, vertebral, major (long bones and ribs), and minor (any remaining). Mortality data were extracted from local media, along with state and national registries. Age- and sex-specific mortality rates in each group were compared with population mortality rates to provide standardized mortality ratios (SMRs) over five-year periods.
Osteoporotic fractures increased five-year mortality with SMRs of 1.38 to 2.53 for women and 1.64 to 3.52 for men. An exception was minor fractures in patients 60 to 75 years old with no increase in mortality. Only hip fractures influenced mortality adversely for up to 10 years.
Interestingly, the nonhip, nonvertebral group included 50% of the fractures and contributed to 29% of overall mortality. Another five-year increase in mortality was evident in 364 people with a subsequent fracture.
A subgroup analysis revealed independent predictors of mortality, including lower bone mineral density, weaker quadriceps, smoking history, and increased sway in female patients; weaker quadriceps and decreased activities were independent predictors in male patients. Apart from the limitation that most subjects were white, the study gives a robust mortality analysis on osteoporotic fractures.
Bottom line: Osteoporotic fractures, initial and subsequent, increase five-year mortality. This is true even for nonhip, nonvertebral fractures, especially in the elderly.
Citation: Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5): 513-521.
Early Rehospitalization After Pulmonary Embolism Dictated by Clinical Severity and Anticoagulation Practices
Clinical question: What factors portend readmission after acute pulmonary embolism (PE)?
Background: The significant clinical and economic burden of acute pulmonary embolism (PE) has fueled studies to define predictors of early mortality. However, the variables leading to readmission after PE remain uncharted. Knowledge of these factors can provide additional targets to improve the quality of care.
Study design: Prospective population-based cohort study.
Setting: 186 acute-care hospitals in Pennsylvania.
Synopsis: Using ICD-9-CM codes, 14,426 PE patients were selected for the study. Primary outcome was hospital readmission within 30 days; secondary outcomes were venous thromboembolism (VTE) and bleeding.
More than 2,000 patients (14.3%) experienced a 30-day readmission. The predominant reasons were VTE (21.9%) and bleeding (5%), with the rest related to comorbidities, such as cancer (10.8%), pneumonia (5.2%), and chest pain (5.0%).
The discrete proportional odds model showed a significant association of high PE Severity Index score (OR 2.04; 95% CI, 1.73-2.40) and previous home care provision (OR 1.40; 95% CI, 1.27-1.54) with readmission, indicating that sicker patients tend to be readmitted. Black patients and Medicaid recipients were more likely to be readmitted, especially for VTE, which reflects the possible socioeconomic bearing on outcomes. Surprisingly, the few patients leaving the hospital against medical advice (0.4%) had a high OR of 2.84 (95% CI, 1.80-4.48) for readmission. Academic centers were not associated with increased readmissions but had significantly more readmissions for bleeding.
Anticoagulation practices—initial choice of agents, intensity of treatment, and monitoring—were not evaluated, which could affect readmission after PE, especially due to VTE and bleeding.
Bottom line: Apart from severity of illness and demographics, high rates of readmission after PE, especially for bleeding and VTE, might be related to poor anticoagulation practices.
Citation: Aujesky D, Mor MK, Geng M, Stone RA, Fine MJ, Ibrahim SA. Predictors of early hospital readmission after acute pulmonary embolism. Arch Intern Med. 2009;169(3):287-293.
Need for Improved Awareness of Hospital Readmission
Clinical question: What is the frequency of readmission awareness in discharging physicians and the trends in their communications with readmitting physicians?
Background: Rotation-based schedules of inpatient physicians, especially at academic centers, increase the likelihood that patients with complex medical or psychosocial issues requiring readmission will be cared for by a different team.
Though gaps in communication between the successive teams have the potential to hamper the quality of care, these gaps have not been adequately characterized in the literature.
Study design: Prospective cohort study.
Setting: Inpatient general-medicine services at two academic medical centers.
Synopsis: Researchers selected 225 patients readmitted within two weeks. The discharge and readmission teams were surveyed by e-mail within 48 hours of readmission regarding frequency and content of communications.
On analysis, the discharging teams were aware of patient readmissions only 48.5% of the time. Most of the remaining teams acknowledged a desire to be notified.
Actual communication occurred in 43.7% of cases and included information on medical assessments (61.9%), psychosocial issues (52.9%), pending tests (34%), and discharge medications (30.9%).
As expected, physician perception of higher medical complexity increased the likelihood of communication. Surprisingly, though psychosocial issues did not predict communication, they were discussed in almost half the cases. Lapses in communication were attributed to lack of time, perceived necessity, and contact information.
The observational nature, nongeneralizable population, and effect of responder bias limit the study. Though an interventional study can better evaluate improvement in patient outcomes, communication at readmission can be used as an educational feedback tool for house staff and attendings.
Bottom line: Modest frequency of communication between discharge and readmission physicians is driven mostly by medical complexity. It bears the potential to improve patient outcomes and offer valuable feedback.
Citation: Roy CL, Kachalia A, Woolf S, Burdick E, Karson A, Gandhi TK. Hospital readmissions: physician awareness and communication practices. J Gen Intern Med. 2009;24(3):374–380. TH
Literature at a Glance
A guide to this month’s studies
- Inhaled steroids and COPD.
- Communication about dietary supplement use.
- Glycemic control in stroke.
- Hospitalist-PCP communication and outcomes.
- Gentamicin nephrotoxicity in endocarditis.
- Outcomes after osteoporotic fractures.
- Predictors of readmission after pulmonary embolism.
- Provider awareness of hospital readmission.
Inhaled Corticosteroid Use in COPD Associated with Increased Pneumonia Risk
Clinical question: Does long-term use of inhaled corticosteroids in chronic obstructive pulmonary disease (COPD) increase the risk of developing pneumonia?
Background: Guidelines recommend a combination of inhaled corticosteroids and long-acting bronchodilators in patients with severe COPD. However, recent evidence has raised concerns about the increased risk of pneumonia in patients on inhaled steroids. The exact nature of this association and its specificity to the inhaled corticosteroid component is unclear.
Study design: Meta-analysis and systematic review of 18 randomized controlled trials (RCTs) evaluating inhaled corticosteroid use in COPD.
Setting: Medline, EMBASE, the Cochrane Database of Systematic Reviews, regulatory documents, and trial registries.
Synopsis: This study, which totaled 16,996 case reviews, focused on inhaled corticosteroid use in COPD (excluding asthma) with at least 24 weeks of followup. The study authors evaluated inhaled corticosteroid use—alone or in combination with long-acting beta-agonists (LABA)—against a control (placebo or LABA alone). Primary outcomes were any pneumonia and serious pneumonia leading to increased morbidity and mortality. Secondary outcomes included pneumonia-related mortality and all-cause mortality.
Inhaled corticosteroids—irrespective of associated LABA use—significantly increased the risk of pneumonia (7.4% vs. 4.7%) with a relative risk (RR) of 1.60; 95% CI, 1.33-1.92, P<0.001. Inhaled corticosteroids were strongly associated with an increase in serious pneumonia (RR 1.71; 95% CI, 1.46-1.99, P<0.001). However, inhaled corticosteroid use did not translate to significantly increased pneumonia-related or overall mortality, possibly due to the inadequate power of most of the individual trials.
The findings reflect those from other database studies, but lend specificity to the inhaled corticosteroid component. This can be cause for concern as studies of long-term inhaled corticosteroid use in patients with COPD have failed to show a benefit in mortality or decreased exacerbations.
Bottom line: Risk-benefit analysis for inhaled corticosteroid use in COPD patients should consider the increased risk of pneumonia, possibly related to local immunosuppression.
Citation: Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219-229.
Inadequate Physician Communication Regarding Dietary Supplement Usage
Clinical question: How frequently do hospital physicians communicate about the use of dietary supplements?
Background: About 20% of the U.S. population uses dietary supplements, products that have potential interactions with other prescription medications. Dietary supplement usage patterns, disclosure, and discussion with physicians have been studied in the outpatient setting. However, these metrics have not been evaluated in the inpatient setting.
Study design: A cross-sectional, observational pilot study.
Setting: Inpatients on a general medicine and geriatrics service at the University of North Carolina Medical Center.
Synopsis: Sixty inpatients were questioned regarding their use of dietary supplements in the past year. Patients were asked about their communication with the admitting resident physician regarding dietary supplements and their beliefs regarding continued use during hospitalization. Patient responses revealed prevalent dietary supplement use, with about 80% of patients using supplements and 52% using nonvitamin/nonmineral supplements.
The study revealed poor communication between residents and their patients. Only 20% of residents inquired about dietary supplement use during the admission process, while 74% of patients neglected to disclose their use of dietary supplements. Furthermore, 56% of patients thought communication was unimportant; they assumed that it was in their medical records (18%), or they expected the physician to ask them about it (20%). Though most patients agreed to stop using dietary supplements as inpatients, 13% did not think dietary supplement use was a problem, even if it went against medical advice.
Study limitations include the small sample size and recall bias inherent to the design. It also is likely that more patients using dietary supplements consented for the study, as evidenced by higher prevalence of use.
Bottom line: Use of dietary supplements in hospitalized patients is common, and communication about their use between patients and physicians is limited.
Citation: Young LA, Faurot KR, Gaylord SA. Use of and communication about dietary supplements among hospitalized patients. J Gen Intern Med. 2009;24(3):366-369.
Early Hyperglycemia Associated with Poor Outcomes After Acute Ischemic Stroke
Clinical question: Is there a threshold of hyperglycemia after an acute ischemic stroke (IS) that predicts a poor outcome?
Background: A growing body of evidence shows that admission hyperglycemia in an acute IS predicts a poor outcome. Current triggers to initiate glucose control measures are based on consensus data. However, capillary glucose is a continuous variable and could have a linear relationship with stroke outcomes. A particular glucose level may herald poor outcomes.
Study design: Prospective observational cohort study.
Setting: Seven university hospitals with dedicated stroke units in Spain.
Synopsis: 476 patients with acute IS had admission and maximum glucose levels recorded during the first 48 hours of admission. Stroke scales and brain imaging assessed the patients’ stroke severity. The primary endpoint of a poor outcome at three months was defined by a modified Rankin score of >2.
The primary endpoint was noted in 156 (38%) patients. Receiver operating characteristic curves for both capillary glucose at admission and maximal values within 48 hours pointed to 155mg/dL as a cutoff for the primary outcome. However, subsequent regression analysis confirmed only the maximal value as an independent predictor of poor outcome (OR 2.73; 95% CI, 1.42 to 5.24). Additionally, in contrast to patient age and infarct volume, the maximal glucose value of ≥155 mg/dL was associated with stroke severity on admission and a higher three-month mortality (HR 3.80; 95% CI, 1.79 to 8.10; P=0.001).
The observational nature of the study opens it to speculation: Does lowering the level to less than 155 mg/dl improve patient outcomes? However, it does offer a potential target for future interventional studies.
Bottom line: Hyperglycemia within the first 48 hours of an ischemic stroke offers a more robust predictor of poor outcomes compared with admission glucose levels. A glucose level less than 155 mg/dL could be a potential treatment goal in the future.
Citation: Fuentes B, Castillo J, San José B, et al. The prognostic value of capillary glucose levels in acute stroke: The GLycemia In Acute Stroke (GLIAS) study. Stroke. 2009;40(2):562-568.
Communication Between Inpatient Medical Teams and PCPs Does Not Improve Outcomes
Clinical question: Does communication between patients’ physicians in the hospital and their primary-care physicians (PCPs) improve outcomes after discharge?
Background: The increased use of the hospitalist model has resulted in concerns about discontinuity of patient care after discharge. This might hamper the quality of clinical care and increase adverse outcomes, including readmission or death. Effective communication could have the potential to improve clinical outcomes.
Study design: Survey based in a quasi-randomized cohort of medical inpatients.
Setting: Six academic medical centers throughout the U.S.
Synopsis: Of the initial 2,526 patients, only 1,078 were available for final analysis based on failure of patient followup and a 68% PCP response rate. PCP surveys were faxed two weeks after patient discharge. PCPs were asked about hospitalization awareness and communication methods. Patients were contacted post-discharge, and National Death Index data were reviewed to determine the primary composite outcomes of ED visits, hospital readmissions, or death at 30 days.
Four out of five PCPs surveyed were aware of their patients’ hospitalizations—23% via direct communication and 42% by discharge summary. The primary outcome occurred in 184 (22%) of 834 patients. In contrast, of the 244 PCPs unaware of their patients’ hospitalizations, the primary outcome occurred in 49 (20%) patients. After logistic regression, PCP awareness of hospitalization, irrespective of communication method, was not associated with risk of outcomes (adjusted OR 1.08, 95% CI, 0.73 to 1.59). Having a hospitalist as the hospital physician (34%) did not affect outcomes. These results could reflect the inclusion of patients with fewer comorbidities. Additionally, effect on adverse drug events, patient satisfaction, and quality of life were not evaluated.
Bottom line: Communication between inpatient physicians and PCPs needs improvement to affect clinical outcomes, especially in high-risk patients.
Citation: Bell CM, Schnipper JL, Auerbach AD, et al. Association of communication between hospital-based physicians and primary care providers with patient outcomes. J Gen Intern Med. 2008;24(3):381-386.
Gentamicin Use in Staphylococcal Bacteremia or Endocarditis Causes Nephrotoxicity
Clinical question: Does gentamicin synergism in Staphylococcal bacteremia and endocarditis achieve faster eradication at the cost of nephrotoxicity?
Background: Gentamicin has been used to help with sterilization of blood or cardiac vegetations in patients with Staphylococcal bacteremia or infective endocarditis (IE). However, historic data negate its role in decreasing morbidity or mortality. If its potential nephrotoxicity were better characterized, it could help assess the overall utility of this practice.
Study design: Retrospective analysis of a cohort from a published randomized control trial.
Setting: 44 hospitals in the U.S. and Europe.
Synopsis: Two hundred thirty-six patients with Staphylococcal bacteremia or native-valve IE (mostly right-sided) were randomized to receive standard therapy (vancomycin or antistaphylococcal penicillin) or daptomycin. Patients receiving standard therapy and those with left-side IE in the daptomycin arm also received low-dose gentamicin. Sequential creatinine levels were used to determine primary outcomes of renal impairment events and a decrease in creatinine clearance.
Renal impairment events, elevation of mean serum creatinine, and decrease in creatinine clearance were more prevalent with standard therapy, especially in the elderly and those with diabetes. Combination of gentamicin with penicillin caused an earlier creatinine elevation compared with that with vancomycin.
Patients on gentamicin had a modest decrease in creatinine clearance (22% vs. 8%; P= 0.005), especially if their baseline was 50 to 80 mL/min. The decrease was early and sustained with gentamicin exposure. Multivariate analysis revealed age (≥65 years) and gentamicin use (not dose and duration) to be independent predictors of renal impairment. The analysis fails to address use of gentamicin in prosthetic-valve IE and left-side IE.
Bottom line: Initial low-dose gentamicin use in Staphylococcal bacteremia or endocarditis increases nephrotoxicity with no clear mortality benefit.
Citation: Cosgrove SE, Vigliani GA, Fowler VG, et al. Initial low-dose gentamicin for Staphylococcus aureus bacteremia and endocarditis is nephrotoxic. Clin Infect Dis. 2009;48(6):713-721.
Osteoporotic Fractures Increase Five-Year Mortality, Especially in the Elderly
Clinical question: What is the effect of initial osteoporotic fractures and subsequent fractures on mortality?
Background: With an aging population, osteoporotic fractures are poised to escalate into a national healthcare problem. Studies have outlined the increase in premature and long-term mortality associated with hip or vertebral fractures. However, other appendicular fractures have not been studied, and little is known about the mortality risk with subsequent fracturing.
Study design: Prospective cohort from the Dubbo Osteoporosis Epidemiology Study, a longitudinal, population-based study.
Setting: Stable population of men and women 60 and older in Dubbo, Australia.
Synopsis: 1,300 people with at least one minimal-trauma fracture were selected. Fractures were grouped as hip, vertebral, major (long bones and ribs), and minor (any remaining). Mortality data were extracted from local media, along with state and national registries. Age- and sex-specific mortality rates in each group were compared with population mortality rates to provide standardized mortality ratios (SMRs) over five-year periods.
Osteoporotic fractures increased five-year mortality with SMRs of 1.38 to 2.53 for women and 1.64 to 3.52 for men. An exception was minor fractures in patients 60 to 75 years old with no increase in mortality. Only hip fractures influenced mortality adversely for up to 10 years.
Interestingly, the nonhip, nonvertebral group included 50% of the fractures and contributed to 29% of overall mortality. Another five-year increase in mortality was evident in 364 people with a subsequent fracture.
A subgroup analysis revealed independent predictors of mortality, including lower bone mineral density, weaker quadriceps, smoking history, and increased sway in female patients; weaker quadriceps and decreased activities were independent predictors in male patients. Apart from the limitation that most subjects were white, the study gives a robust mortality analysis on osteoporotic fractures.
Bottom line: Osteoporotic fractures, initial and subsequent, increase five-year mortality. This is true even for nonhip, nonvertebral fractures, especially in the elderly.
Citation: Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5): 513-521.
Early Rehospitalization After Pulmonary Embolism Dictated by Clinical Severity and Anticoagulation Practices
Clinical question: What factors portend readmission after acute pulmonary embolism (PE)?
Background: The significant clinical and economic burden of acute pulmonary embolism (PE) has fueled studies to define predictors of early mortality. However, the variables leading to readmission after PE remain uncharted. Knowledge of these factors can provide additional targets to improve the quality of care.
Study design: Prospective population-based cohort study.
Setting: 186 acute-care hospitals in Pennsylvania.
Synopsis: Using ICD-9-CM codes, 14,426 PE patients were selected for the study. Primary outcome was hospital readmission within 30 days; secondary outcomes were venous thromboembolism (VTE) and bleeding.
More than 2,000 patients (14.3%) experienced a 30-day readmission. The predominant reasons were VTE (21.9%) and bleeding (5%), with the rest related to comorbidities, such as cancer (10.8%), pneumonia (5.2%), and chest pain (5.0%).
The discrete proportional odds model showed a significant association of high PE Severity Index score (OR 2.04; 95% CI, 1.73-2.40) and previous home care provision (OR 1.40; 95% CI, 1.27-1.54) with readmission, indicating that sicker patients tend to be readmitted. Black patients and Medicaid recipients were more likely to be readmitted, especially for VTE, which reflects the possible socioeconomic bearing on outcomes. Surprisingly, the few patients leaving the hospital against medical advice (0.4%) had a high OR of 2.84 (95% CI, 1.80-4.48) for readmission. Academic centers were not associated with increased readmissions but had significantly more readmissions for bleeding.
Anticoagulation practices—initial choice of agents, intensity of treatment, and monitoring—were not evaluated, which could affect readmission after PE, especially due to VTE and bleeding.
Bottom line: Apart from severity of illness and demographics, high rates of readmission after PE, especially for bleeding and VTE, might be related to poor anticoagulation practices.
Citation: Aujesky D, Mor MK, Geng M, Stone RA, Fine MJ, Ibrahim SA. Predictors of early hospital readmission after acute pulmonary embolism. Arch Intern Med. 2009;169(3):287-293.
Need for Improved Awareness of Hospital Readmission
Clinical question: What is the frequency of readmission awareness in discharging physicians and the trends in their communications with readmitting physicians?
Background: Rotation-based schedules of inpatient physicians, especially at academic centers, increase the likelihood that patients with complex medical or psychosocial issues requiring readmission will be cared for by a different team.
Though gaps in communication between the successive teams have the potential to hamper the quality of care, these gaps have not been adequately characterized in the literature.
Study design: Prospective cohort study.
Setting: Inpatient general-medicine services at two academic medical centers.
Synopsis: Researchers selected 225 patients readmitted within two weeks. The discharge and readmission teams were surveyed by e-mail within 48 hours of readmission regarding frequency and content of communications.
On analysis, the discharging teams were aware of patient readmissions only 48.5% of the time. Most of the remaining teams acknowledged a desire to be notified.
Actual communication occurred in 43.7% of cases and included information on medical assessments (61.9%), psychosocial issues (52.9%), pending tests (34%), and discharge medications (30.9%).
As expected, physician perception of higher medical complexity increased the likelihood of communication. Surprisingly, though psychosocial issues did not predict communication, they were discussed in almost half the cases. Lapses in communication were attributed to lack of time, perceived necessity, and contact information.
The observational nature, nongeneralizable population, and effect of responder bias limit the study. Though an interventional study can better evaluate improvement in patient outcomes, communication at readmission can be used as an educational feedback tool for house staff and attendings.
Bottom line: Modest frequency of communication between discharge and readmission physicians is driven mostly by medical complexity. It bears the potential to improve patient outcomes and offer valuable feedback.
Citation: Roy CL, Kachalia A, Woolf S, Burdick E, Karson A, Gandhi TK. Hospital readmissions: physician awareness and communication practices. J Gen Intern Med. 2009;24(3):374–380. TH
Literature at a Glance
A guide to this month’s studies
- Inhaled steroids and COPD.
- Communication about dietary supplement use.
- Glycemic control in stroke.
- Hospitalist-PCP communication and outcomes.
- Gentamicin nephrotoxicity in endocarditis.
- Outcomes after osteoporotic fractures.
- Predictors of readmission after pulmonary embolism.
- Provider awareness of hospital readmission.
Inhaled Corticosteroid Use in COPD Associated with Increased Pneumonia Risk
Clinical question: Does long-term use of inhaled corticosteroids in chronic obstructive pulmonary disease (COPD) increase the risk of developing pneumonia?
Background: Guidelines recommend a combination of inhaled corticosteroids and long-acting bronchodilators in patients with severe COPD. However, recent evidence has raised concerns about the increased risk of pneumonia in patients on inhaled steroids. The exact nature of this association and its specificity to the inhaled corticosteroid component is unclear.
Study design: Meta-analysis and systematic review of 18 randomized controlled trials (RCTs) evaluating inhaled corticosteroid use in COPD.
Setting: Medline, EMBASE, the Cochrane Database of Systematic Reviews, regulatory documents, and trial registries.
Synopsis: This study, which totaled 16,996 case reviews, focused on inhaled corticosteroid use in COPD (excluding asthma) with at least 24 weeks of followup. The study authors evaluated inhaled corticosteroid use—alone or in combination with long-acting beta-agonists (LABA)—against a control (placebo or LABA alone). Primary outcomes were any pneumonia and serious pneumonia leading to increased morbidity and mortality. Secondary outcomes included pneumonia-related mortality and all-cause mortality.
Inhaled corticosteroids—irrespective of associated LABA use—significantly increased the risk of pneumonia (7.4% vs. 4.7%) with a relative risk (RR) of 1.60; 95% CI, 1.33-1.92, P<0.001. Inhaled corticosteroids were strongly associated with an increase in serious pneumonia (RR 1.71; 95% CI, 1.46-1.99, P<0.001). However, inhaled corticosteroid use did not translate to significantly increased pneumonia-related or overall mortality, possibly due to the inadequate power of most of the individual trials.
The findings reflect those from other database studies, but lend specificity to the inhaled corticosteroid component. This can be cause for concern as studies of long-term inhaled corticosteroid use in patients with COPD have failed to show a benefit in mortality or decreased exacerbations.
Bottom line: Risk-benefit analysis for inhaled corticosteroid use in COPD patients should consider the increased risk of pneumonia, possibly related to local immunosuppression.
Citation: Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219-229.
Inadequate Physician Communication Regarding Dietary Supplement Usage
Clinical question: How frequently do hospital physicians communicate about the use of dietary supplements?
Background: About 20% of the U.S. population uses dietary supplements, products that have potential interactions with other prescription medications. Dietary supplement usage patterns, disclosure, and discussion with physicians have been studied in the outpatient setting. However, these metrics have not been evaluated in the inpatient setting.
Study design: A cross-sectional, observational pilot study.
Setting: Inpatients on a general medicine and geriatrics service at the University of North Carolina Medical Center.
Synopsis: Sixty inpatients were questioned regarding their use of dietary supplements in the past year. Patients were asked about their communication with the admitting resident physician regarding dietary supplements and their beliefs regarding continued use during hospitalization. Patient responses revealed prevalent dietary supplement use, with about 80% of patients using supplements and 52% using nonvitamin/nonmineral supplements.
The study revealed poor communication between residents and their patients. Only 20% of residents inquired about dietary supplement use during the admission process, while 74% of patients neglected to disclose their use of dietary supplements. Furthermore, 56% of patients thought communication was unimportant; they assumed that it was in their medical records (18%), or they expected the physician to ask them about it (20%). Though most patients agreed to stop using dietary supplements as inpatients, 13% did not think dietary supplement use was a problem, even if it went against medical advice.
Study limitations include the small sample size and recall bias inherent to the design. It also is likely that more patients using dietary supplements consented for the study, as evidenced by higher prevalence of use.
Bottom line: Use of dietary supplements in hospitalized patients is common, and communication about their use between patients and physicians is limited.
Citation: Young LA, Faurot KR, Gaylord SA. Use of and communication about dietary supplements among hospitalized patients. J Gen Intern Med. 2009;24(3):366-369.
Early Hyperglycemia Associated with Poor Outcomes After Acute Ischemic Stroke
Clinical question: Is there a threshold of hyperglycemia after an acute ischemic stroke (IS) that predicts a poor outcome?
Background: A growing body of evidence shows that admission hyperglycemia in an acute IS predicts a poor outcome. Current triggers to initiate glucose control measures are based on consensus data. However, capillary glucose is a continuous variable and could have a linear relationship with stroke outcomes. A particular glucose level may herald poor outcomes.
Study design: Prospective observational cohort study.
Setting: Seven university hospitals with dedicated stroke units in Spain.
Synopsis: 476 patients with acute IS had admission and maximum glucose levels recorded during the first 48 hours of admission. Stroke scales and brain imaging assessed the patients’ stroke severity. The primary endpoint of a poor outcome at three months was defined by a modified Rankin score of >2.
The primary endpoint was noted in 156 (38%) patients. Receiver operating characteristic curves for both capillary glucose at admission and maximal values within 48 hours pointed to 155mg/dL as a cutoff for the primary outcome. However, subsequent regression analysis confirmed only the maximal value as an independent predictor of poor outcome (OR 2.73; 95% CI, 1.42 to 5.24). Additionally, in contrast to patient age and infarct volume, the maximal glucose value of ≥155 mg/dL was associated with stroke severity on admission and a higher three-month mortality (HR 3.80; 95% CI, 1.79 to 8.10; P=0.001).
The observational nature of the study opens it to speculation: Does lowering the level to less than 155 mg/dl improve patient outcomes? However, it does offer a potential target for future interventional studies.
Bottom line: Hyperglycemia within the first 48 hours of an ischemic stroke offers a more robust predictor of poor outcomes compared with admission glucose levels. A glucose level less than 155 mg/dL could be a potential treatment goal in the future.
Citation: Fuentes B, Castillo J, San José B, et al. The prognostic value of capillary glucose levels in acute stroke: The GLycemia In Acute Stroke (GLIAS) study. Stroke. 2009;40(2):562-568.
Communication Between Inpatient Medical Teams and PCPs Does Not Improve Outcomes
Clinical question: Does communication between patients’ physicians in the hospital and their primary-care physicians (PCPs) improve outcomes after discharge?
Background: The increased use of the hospitalist model has resulted in concerns about discontinuity of patient care after discharge. This might hamper the quality of clinical care and increase adverse outcomes, including readmission or death. Effective communication could have the potential to improve clinical outcomes.
Study design: Survey based in a quasi-randomized cohort of medical inpatients.
Setting: Six academic medical centers throughout the U.S.
Synopsis: Of the initial 2,526 patients, only 1,078 were available for final analysis based on failure of patient followup and a 68% PCP response rate. PCP surveys were faxed two weeks after patient discharge. PCPs were asked about hospitalization awareness and communication methods. Patients were contacted post-discharge, and National Death Index data were reviewed to determine the primary composite outcomes of ED visits, hospital readmissions, or death at 30 days.
Four out of five PCPs surveyed were aware of their patients’ hospitalizations—23% via direct communication and 42% by discharge summary. The primary outcome occurred in 184 (22%) of 834 patients. In contrast, of the 244 PCPs unaware of their patients’ hospitalizations, the primary outcome occurred in 49 (20%) patients. After logistic regression, PCP awareness of hospitalization, irrespective of communication method, was not associated with risk of outcomes (adjusted OR 1.08, 95% CI, 0.73 to 1.59). Having a hospitalist as the hospital physician (34%) did not affect outcomes. These results could reflect the inclusion of patients with fewer comorbidities. Additionally, effect on adverse drug events, patient satisfaction, and quality of life were not evaluated.
Bottom line: Communication between inpatient physicians and PCPs needs improvement to affect clinical outcomes, especially in high-risk patients.
Citation: Bell CM, Schnipper JL, Auerbach AD, et al. Association of communication between hospital-based physicians and primary care providers with patient outcomes. J Gen Intern Med. 2008;24(3):381-386.
Gentamicin Use in Staphylococcal Bacteremia or Endocarditis Causes Nephrotoxicity
Clinical question: Does gentamicin synergism in Staphylococcal bacteremia and endocarditis achieve faster eradication at the cost of nephrotoxicity?
Background: Gentamicin has been used to help with sterilization of blood or cardiac vegetations in patients with Staphylococcal bacteremia or infective endocarditis (IE). However, historic data negate its role in decreasing morbidity or mortality. If its potential nephrotoxicity were better characterized, it could help assess the overall utility of this practice.
Study design: Retrospective analysis of a cohort from a published randomized control trial.
Setting: 44 hospitals in the U.S. and Europe.
Synopsis: Two hundred thirty-six patients with Staphylococcal bacteremia or native-valve IE (mostly right-sided) were randomized to receive standard therapy (vancomycin or antistaphylococcal penicillin) or daptomycin. Patients receiving standard therapy and those with left-side IE in the daptomycin arm also received low-dose gentamicin. Sequential creatinine levels were used to determine primary outcomes of renal impairment events and a decrease in creatinine clearance.
Renal impairment events, elevation of mean serum creatinine, and decrease in creatinine clearance were more prevalent with standard therapy, especially in the elderly and those with diabetes. Combination of gentamicin with penicillin caused an earlier creatinine elevation compared with that with vancomycin.
Patients on gentamicin had a modest decrease in creatinine clearance (22% vs. 8%; P= 0.005), especially if their baseline was 50 to 80 mL/min. The decrease was early and sustained with gentamicin exposure. Multivariate analysis revealed age (≥65 years) and gentamicin use (not dose and duration) to be independent predictors of renal impairment. The analysis fails to address use of gentamicin in prosthetic-valve IE and left-side IE.
Bottom line: Initial low-dose gentamicin use in Staphylococcal bacteremia or endocarditis increases nephrotoxicity with no clear mortality benefit.
Citation: Cosgrove SE, Vigliani GA, Fowler VG, et al. Initial low-dose gentamicin for Staphylococcus aureus bacteremia and endocarditis is nephrotoxic. Clin Infect Dis. 2009;48(6):713-721.
Osteoporotic Fractures Increase Five-Year Mortality, Especially in the Elderly
Clinical question: What is the effect of initial osteoporotic fractures and subsequent fractures on mortality?
Background: With an aging population, osteoporotic fractures are poised to escalate into a national healthcare problem. Studies have outlined the increase in premature and long-term mortality associated with hip or vertebral fractures. However, other appendicular fractures have not been studied, and little is known about the mortality risk with subsequent fracturing.
Study design: Prospective cohort from the Dubbo Osteoporosis Epidemiology Study, a longitudinal, population-based study.
Setting: Stable population of men and women 60 and older in Dubbo, Australia.
Synopsis: 1,300 people with at least one minimal-trauma fracture were selected. Fractures were grouped as hip, vertebral, major (long bones and ribs), and minor (any remaining). Mortality data were extracted from local media, along with state and national registries. Age- and sex-specific mortality rates in each group were compared with population mortality rates to provide standardized mortality ratios (SMRs) over five-year periods.
Osteoporotic fractures increased five-year mortality with SMRs of 1.38 to 2.53 for women and 1.64 to 3.52 for men. An exception was minor fractures in patients 60 to 75 years old with no increase in mortality. Only hip fractures influenced mortality adversely for up to 10 years.
Interestingly, the nonhip, nonvertebral group included 50% of the fractures and contributed to 29% of overall mortality. Another five-year increase in mortality was evident in 364 people with a subsequent fracture.
A subgroup analysis revealed independent predictors of mortality, including lower bone mineral density, weaker quadriceps, smoking history, and increased sway in female patients; weaker quadriceps and decreased activities were independent predictors in male patients. Apart from the limitation that most subjects were white, the study gives a robust mortality analysis on osteoporotic fractures.
Bottom line: Osteoporotic fractures, initial and subsequent, increase five-year mortality. This is true even for nonhip, nonvertebral fractures, especially in the elderly.
Citation: Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5): 513-521.
Early Rehospitalization After Pulmonary Embolism Dictated by Clinical Severity and Anticoagulation Practices
Clinical question: What factors portend readmission after acute pulmonary embolism (PE)?
Background: The significant clinical and economic burden of acute pulmonary embolism (PE) has fueled studies to define predictors of early mortality. However, the variables leading to readmission after PE remain uncharted. Knowledge of these factors can provide additional targets to improve the quality of care.
Study design: Prospective population-based cohort study.
Setting: 186 acute-care hospitals in Pennsylvania.
Synopsis: Using ICD-9-CM codes, 14,426 PE patients were selected for the study. Primary outcome was hospital readmission within 30 days; secondary outcomes were venous thromboembolism (VTE) and bleeding.
More than 2,000 patients (14.3%) experienced a 30-day readmission. The predominant reasons were VTE (21.9%) and bleeding (5%), with the rest related to comorbidities, such as cancer (10.8%), pneumonia (5.2%), and chest pain (5.0%).
The discrete proportional odds model showed a significant association of high PE Severity Index score (OR 2.04; 95% CI, 1.73-2.40) and previous home care provision (OR 1.40; 95% CI, 1.27-1.54) with readmission, indicating that sicker patients tend to be readmitted. Black patients and Medicaid recipients were more likely to be readmitted, especially for VTE, which reflects the possible socioeconomic bearing on outcomes. Surprisingly, the few patients leaving the hospital against medical advice (0.4%) had a high OR of 2.84 (95% CI, 1.80-4.48) for readmission. Academic centers were not associated with increased readmissions but had significantly more readmissions for bleeding.
Anticoagulation practices—initial choice of agents, intensity of treatment, and monitoring—were not evaluated, which could affect readmission after PE, especially due to VTE and bleeding.
Bottom line: Apart from severity of illness and demographics, high rates of readmission after PE, especially for bleeding and VTE, might be related to poor anticoagulation practices.
Citation: Aujesky D, Mor MK, Geng M, Stone RA, Fine MJ, Ibrahim SA. Predictors of early hospital readmission after acute pulmonary embolism. Arch Intern Med. 2009;169(3):287-293.
Need for Improved Awareness of Hospital Readmission
Clinical question: What is the frequency of readmission awareness in discharging physicians and the trends in their communications with readmitting physicians?
Background: Rotation-based schedules of inpatient physicians, especially at academic centers, increase the likelihood that patients with complex medical or psychosocial issues requiring readmission will be cared for by a different team.
Though gaps in communication between the successive teams have the potential to hamper the quality of care, these gaps have not been adequately characterized in the literature.
Study design: Prospective cohort study.
Setting: Inpatient general-medicine services at two academic medical centers.
Synopsis: Researchers selected 225 patients readmitted within two weeks. The discharge and readmission teams were surveyed by e-mail within 48 hours of readmission regarding frequency and content of communications.
On analysis, the discharging teams were aware of patient readmissions only 48.5% of the time. Most of the remaining teams acknowledged a desire to be notified.
Actual communication occurred in 43.7% of cases and included information on medical assessments (61.9%), psychosocial issues (52.9%), pending tests (34%), and discharge medications (30.9%).
As expected, physician perception of higher medical complexity increased the likelihood of communication. Surprisingly, though psychosocial issues did not predict communication, they were discussed in almost half the cases. Lapses in communication were attributed to lack of time, perceived necessity, and contact information.
The observational nature, nongeneralizable population, and effect of responder bias limit the study. Though an interventional study can better evaluate improvement in patient outcomes, communication at readmission can be used as an educational feedback tool for house staff and attendings.
Bottom line: Modest frequency of communication between discharge and readmission physicians is driven mostly by medical complexity. It bears the potential to improve patient outcomes and offer valuable feedback.
Citation: Roy CL, Kachalia A, Woolf S, Burdick E, Karson A, Gandhi TK. Hospital readmissions: physician awareness and communication practices. J Gen Intern Med. 2009;24(3):374–380. TH
Focused on the Practice
Most HM groups (HMGs) participate in quality initiatives in their hospitals, according to new SHM research. Moreover, 7 out of 10 HMGs participating in QI initiatives are leading those efforts at their hospitals.
The findings are part of SHM’s 2008-2009 Focused Survey, the latest in a series of reports commissioned by the Practice Analysis Committee. The survey and report concentrate on topics of interest from SHM’s comprehensive, biannual survey of its membership.
The survey compiled responses from 145 HMG leaders. In addition to QI initiatives, participants in the survey responded to a variety of questions, including quality-based incentives, hospitalist turnover, and the use of part-time hospitalists.

—Joe Miller, SHM’s executive advisor to the CEO
“This is certain to be a conversation starter for hospitalists, hospital executives, and others,” says Burke Kealey, MD, FHM, medical director for hospital medicine at St. Paul, Minn.-based HealthPartners and chair of SHM’s Practice Analysis Committee. “The Focused Survey is an opportunity for SHM to answer some of the pressing questions that healthcare executives and providers have about managing a hospitalist practice within the larger context of the hospital.”
Hospital executives and hospitalists use SHM survey findings to better understand what is going on in the specialty, says Joe Miller, SHM’s executive advisor to the CEO. “These surveys answer the kinds of questions that often come up when hospitalists and hospitals begin to evaluate their performance and plan for the future,” Miller says. “We use their questions as source material for this survey, so we can help them answer questions like, ‘How are most hospitalists participating in QI?’ or ‘How are other hospitalists using part-time staff members?’ ”
Hospitalists Lead the Way
Hospitalists continue to be at the forefront of QI initiatives within their hospitals, according to the latest survey. Almost all respondents (96.5%) reported that their HMG participated in QI programs; the average HMG has six hospitalists playing an active role in QI within the hospital.
The survey also found that 72.1% of respondents involved in QI activity reported that their hospitalists were “responsible for leading project(s)” on QI initiatives.
“The findings about the active role hospitalists play in QI initiatives may surprise even the most staunch advocate of QI within the hospital medicine specialty,” says Leslie Flores, MHA, SHM’s director of the Practice Management Institute and leader of the Focused Survey research. “In essence, it shows that nearly every hospitalist group is active in promoting QI, and that the vast majority of them are taking a leadership position to improve quality. … It is remarkable and extremely exciting that hospitalists are so deeply involved in QI in their organizations.”
The survey identified patient safety, clinical QI, and quality-related IT initiatives as most popular.
Quality Incentive Compensation
In order to track HMG quality incentive compensation, the 2008-2009 Focused Survey asked similar questions about the topic to questions in the 2006-2007 Focused Survey. Quality incentive compensation—paying bonuses or additional payments for meeting QI measures—not only increased markedly in the past two years, but a majority of HMGs also have adopted the practice. The number of HMGs that have quality incentive compensation plans has increased by 39% since 2006, according to the survey.
Nine out of 10 HMGs that receive performance-based compensation reported that the source of the compensation was the hospital or health system. In most cases, the compensation was paid to an individual hospitalist, which represents a shift from 2006, when more groups reported receiving the compensation directly.
The survey also shows that hospitals and HMGs use a number of process measures to evaluate QI incentives, including participation in quality or safety committees, transition of care measures, or core measures for heart failure, pneumonia, and acute myocardial infarction.
New Numbers Dispel High Turnover Myth
For years, the conventional wisdom throughout the healthcare community has been that HM suffers from a high turnover rate among its hospitalists. Focused Survey findings suggest otherwise. In fact, turnover rates for hospitalist groups have remained constant since 2005. Nearly a third (31.7%) of HMGs reported no turnover at all within the past 12 months.
“Getting an accurate idea about turnover in hospitalist groups has been an ongoing challenge in our research,” Flores says. “In this year’s Focused Survey, we provided clearer definitions and asked more specific questions to improve our measurement of turnover.”
The added specificity only served to reinforce findings from previous surveys that showed relatively low turnover rates. The most recent research revealed a 12.7% turnover rate, compared with 13% in 2007 and 12% in 2005.
The latest Focused Survey also includes detailed findings on turnover among full-time hospitalists compared with part-time hospitalists.
Part-Time vs. Full-Time
The new data challenge long-held assumptions about the role of part-time hospitalists. The survey queried HMGs about full-time and part-time hospitalist staff, and the proportion of time that each employee covers in the hospital.
Although there isn’t a consensus about what constitutes a full-time hospitalist, it is clear that they cover the vast majority (85%) of HMG staff hours. Part-time hospitalists are responsible for 10% of hospitalist staff hours, and “casual” hospitalists—temporary hospitalists or moonlighters—make up the remaining 5%.
Part-time hospitalists share the same responsibilities as their full-time colleagues, according to the report. More than 70% of HMG leaders said their part-time staff is deployed to cover the same shifts and responsibilities as full-time staff. Many HMGs use part-time staff to cover night and weekend shifts.
Trend Today, Initiative Tomorrow
Taken together, SHM’s bi-annual survey and Focused Survey have begun to reveal some of the most prevalent trends within the specialty, including low turnover and a specialty-wide QI emphasis. However, Flores sees room for additional research in the near future.
“There is a lot more to learn about the nature of hospitalists’ involvement in organizational quality initiatives and what benefits that involvement is delivering to their organizations,” she says. “The survey suggests some areas, particularly in the quality arena, where SHM can develop additional programs and services to support hospitalists and the work they do.”
The 10-page 2008-2009 Focused Survey report is available at www.hospitalmedicine.org/shmstore. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Philadelphia Tri-State Area

The Philadelphia Tri-State Area chapter kicked off its 2009 meeting March 26 with its new “pharma-free” format. The chapter’s decision to forgo an expensive meal and industry-sponsored lecture was the result of an agreement to create more open dialogue among its members.
Chapter co-presidents Jen Myers, assistant professor of clinical medicine and patient safety officer at the Hospital of the University of Pennsylvania, and Erik DeLue, MD, MBA, medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., kicked off the meeting, which focused on recruiting in a competitive market. Despite SHM’s collective recruiting challenges, most medical directors indicated that their groups were fully staffed.
Future meetings will be held at various medical institutions around the greater Philadelphia area. The next is to be held this month at Christiana Medical Center in Wilmington, Del. Future topics will be centered on pragmatic, nonclinical concerns for hospitalists, such as how to best utilize allied health providers.
Most HM groups (HMGs) participate in quality initiatives in their hospitals, according to new SHM research. Moreover, 7 out of 10 HMGs participating in QI initiatives are leading those efforts at their hospitals.
The findings are part of SHM’s 2008-2009 Focused Survey, the latest in a series of reports commissioned by the Practice Analysis Committee. The survey and report concentrate on topics of interest from SHM’s comprehensive, biannual survey of its membership.
The survey compiled responses from 145 HMG leaders. In addition to QI initiatives, participants in the survey responded to a variety of questions, including quality-based incentives, hospitalist turnover, and the use of part-time hospitalists.
—Joe Miller, SHM’s executive advisor to the CEO
“This is certain to be a conversation starter for hospitalists, hospital executives, and others,” says Burke Kealey, MD, FHM, medical director for hospital medicine at St. Paul, Minn.-based HealthPartners and chair of SHM’s Practice Analysis Committee. “The Focused Survey is an opportunity for SHM to answer some of the pressing questions that healthcare executives and providers have about managing a hospitalist practice within the larger context of the hospital.”
Hospital executives and hospitalists use SHM survey findings to better understand what is going on in the specialty, says Joe Miller, SHM’s executive advisor to the CEO. “These surveys answer the kinds of questions that often come up when hospitalists and hospitals begin to evaluate their performance and plan for the future,” Miller says. “We use their questions as source material for this survey, so we can help them answer questions like, ‘How are most hospitalists participating in QI?’ or ‘How are other hospitalists using part-time staff members?’ ”
Hospitalists Lead the Way
Hospitalists continue to be at the forefront of QI initiatives within their hospitals, according to the latest survey. Almost all respondents (96.5%) reported that their HMG participated in QI programs; the average HMG has six hospitalists playing an active role in QI within the hospital.
The survey also found that 72.1% of respondents involved in QI activity reported that their hospitalists were “responsible for leading project(s)” on QI initiatives.
“The findings about the active role hospitalists play in QI initiatives may surprise even the most staunch advocate of QI within the hospital medicine specialty,” says Leslie Flores, MHA, SHM’s director of the Practice Management Institute and leader of the Focused Survey research. “In essence, it shows that nearly every hospitalist group is active in promoting QI, and that the vast majority of them are taking a leadership position to improve quality. … It is remarkable and extremely exciting that hospitalists are so deeply involved in QI in their organizations.”
The survey identified patient safety, clinical QI, and quality-related IT initiatives as most popular.
Quality Incentive Compensation
In order to track HMG quality incentive compensation, the 2008-2009 Focused Survey asked similar questions about the topic to questions in the 2006-2007 Focused Survey. Quality incentive compensation—paying bonuses or additional payments for meeting QI measures—not only increased markedly in the past two years, but a majority of HMGs also have adopted the practice. The number of HMGs that have quality incentive compensation plans has increased by 39% since 2006, according to the survey.
Nine out of 10 HMGs that receive performance-based compensation reported that the source of the compensation was the hospital or health system. In most cases, the compensation was paid to an individual hospitalist, which represents a shift from 2006, when more groups reported receiving the compensation directly.
The survey also shows that hospitals and HMGs use a number of process measures to evaluate QI incentives, including participation in quality or safety committees, transition of care measures, or core measures for heart failure, pneumonia, and acute myocardial infarction.
New Numbers Dispel High Turnover Myth
For years, the conventional wisdom throughout the healthcare community has been that HM suffers from a high turnover rate among its hospitalists. Focused Survey findings suggest otherwise. In fact, turnover rates for hospitalist groups have remained constant since 2005. Nearly a third (31.7%) of HMGs reported no turnover at all within the past 12 months.
“Getting an accurate idea about turnover in hospitalist groups has been an ongoing challenge in our research,” Flores says. “In this year’s Focused Survey, we provided clearer definitions and asked more specific questions to improve our measurement of turnover.”
The added specificity only served to reinforce findings from previous surveys that showed relatively low turnover rates. The most recent research revealed a 12.7% turnover rate, compared with 13% in 2007 and 12% in 2005.
The latest Focused Survey also includes detailed findings on turnover among full-time hospitalists compared with part-time hospitalists.
Part-Time vs. Full-Time
The new data challenge long-held assumptions about the role of part-time hospitalists. The survey queried HMGs about full-time and part-time hospitalist staff, and the proportion of time that each employee covers in the hospital.
Although there isn’t a consensus about what constitutes a full-time hospitalist, it is clear that they cover the vast majority (85%) of HMG staff hours. Part-time hospitalists are responsible for 10% of hospitalist staff hours, and “casual” hospitalists—temporary hospitalists or moonlighters—make up the remaining 5%.
Part-time hospitalists share the same responsibilities as their full-time colleagues, according to the report. More than 70% of HMG leaders said their part-time staff is deployed to cover the same shifts and responsibilities as full-time staff. Many HMGs use part-time staff to cover night and weekend shifts.
Trend Today, Initiative Tomorrow
Taken together, SHM’s bi-annual survey and Focused Survey have begun to reveal some of the most prevalent trends within the specialty, including low turnover and a specialty-wide QI emphasis. However, Flores sees room for additional research in the near future.
“There is a lot more to learn about the nature of hospitalists’ involvement in organizational quality initiatives and what benefits that involvement is delivering to their organizations,” she says. “The survey suggests some areas, particularly in the quality arena, where SHM can develop additional programs and services to support hospitalists and the work they do.”
The 10-page 2008-2009 Focused Survey report is available at www.hospitalmedicine.org/shmstore. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Philadelphia Tri-State Area
The Philadelphia Tri-State Area chapter kicked off its 2009 meeting March 26 with its new “pharma-free” format. The chapter’s decision to forgo an expensive meal and industry-sponsored lecture was the result of an agreement to create more open dialogue among its members.
Chapter co-presidents Jen Myers, assistant professor of clinical medicine and patient safety officer at the Hospital of the University of Pennsylvania, and Erik DeLue, MD, MBA, medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., kicked off the meeting, which focused on recruiting in a competitive market. Despite SHM’s collective recruiting challenges, most medical directors indicated that their groups were fully staffed.
Future meetings will be held at various medical institutions around the greater Philadelphia area. The next is to be held this month at Christiana Medical Center in Wilmington, Del. Future topics will be centered on pragmatic, nonclinical concerns for hospitalists, such as how to best utilize allied health providers.
Most HM groups (HMGs) participate in quality initiatives in their hospitals, according to new SHM research. Moreover, 7 out of 10 HMGs participating in QI initiatives are leading those efforts at their hospitals.
The findings are part of SHM’s 2008-2009 Focused Survey, the latest in a series of reports commissioned by the Practice Analysis Committee. The survey and report concentrate on topics of interest from SHM’s comprehensive, biannual survey of its membership.
The survey compiled responses from 145 HMG leaders. In addition to QI initiatives, participants in the survey responded to a variety of questions, including quality-based incentives, hospitalist turnover, and the use of part-time hospitalists.
—Joe Miller, SHM’s executive advisor to the CEO
“This is certain to be a conversation starter for hospitalists, hospital executives, and others,” says Burke Kealey, MD, FHM, medical director for hospital medicine at St. Paul, Minn.-based HealthPartners and chair of SHM’s Practice Analysis Committee. “The Focused Survey is an opportunity for SHM to answer some of the pressing questions that healthcare executives and providers have about managing a hospitalist practice within the larger context of the hospital.”
Hospital executives and hospitalists use SHM survey findings to better understand what is going on in the specialty, says Joe Miller, SHM’s executive advisor to the CEO. “These surveys answer the kinds of questions that often come up when hospitalists and hospitals begin to evaluate their performance and plan for the future,” Miller says. “We use their questions as source material for this survey, so we can help them answer questions like, ‘How are most hospitalists participating in QI?’ or ‘How are other hospitalists using part-time staff members?’ ”
Hospitalists Lead the Way
Hospitalists continue to be at the forefront of QI initiatives within their hospitals, according to the latest survey. Almost all respondents (96.5%) reported that their HMG participated in QI programs; the average HMG has six hospitalists playing an active role in QI within the hospital.
The survey also found that 72.1% of respondents involved in QI activity reported that their hospitalists were “responsible for leading project(s)” on QI initiatives.
“The findings about the active role hospitalists play in QI initiatives may surprise even the most staunch advocate of QI within the hospital medicine specialty,” says Leslie Flores, MHA, SHM’s director of the Practice Management Institute and leader of the Focused Survey research. “In essence, it shows that nearly every hospitalist group is active in promoting QI, and that the vast majority of them are taking a leadership position to improve quality. … It is remarkable and extremely exciting that hospitalists are so deeply involved in QI in their organizations.”
The survey identified patient safety, clinical QI, and quality-related IT initiatives as most popular.
Quality Incentive Compensation
In order to track HMG quality incentive compensation, the 2008-2009 Focused Survey asked similar questions about the topic to questions in the 2006-2007 Focused Survey. Quality incentive compensation—paying bonuses or additional payments for meeting QI measures—not only increased markedly in the past two years, but a majority of HMGs also have adopted the practice. The number of HMGs that have quality incentive compensation plans has increased by 39% since 2006, according to the survey.
Nine out of 10 HMGs that receive performance-based compensation reported that the source of the compensation was the hospital or health system. In most cases, the compensation was paid to an individual hospitalist, which represents a shift from 2006, when more groups reported receiving the compensation directly.
The survey also shows that hospitals and HMGs use a number of process measures to evaluate QI incentives, including participation in quality or safety committees, transition of care measures, or core measures for heart failure, pneumonia, and acute myocardial infarction.
New Numbers Dispel High Turnover Myth
For years, the conventional wisdom throughout the healthcare community has been that HM suffers from a high turnover rate among its hospitalists. Focused Survey findings suggest otherwise. In fact, turnover rates for hospitalist groups have remained constant since 2005. Nearly a third (31.7%) of HMGs reported no turnover at all within the past 12 months.
“Getting an accurate idea about turnover in hospitalist groups has been an ongoing challenge in our research,” Flores says. “In this year’s Focused Survey, we provided clearer definitions and asked more specific questions to improve our measurement of turnover.”
The added specificity only served to reinforce findings from previous surveys that showed relatively low turnover rates. The most recent research revealed a 12.7% turnover rate, compared with 13% in 2007 and 12% in 2005.
The latest Focused Survey also includes detailed findings on turnover among full-time hospitalists compared with part-time hospitalists.
Part-Time vs. Full-Time
The new data challenge long-held assumptions about the role of part-time hospitalists. The survey queried HMGs about full-time and part-time hospitalist staff, and the proportion of time that each employee covers in the hospital.
Although there isn’t a consensus about what constitutes a full-time hospitalist, it is clear that they cover the vast majority (85%) of HMG staff hours. Part-time hospitalists are responsible for 10% of hospitalist staff hours, and “casual” hospitalists—temporary hospitalists or moonlighters—make up the remaining 5%.
Part-time hospitalists share the same responsibilities as their full-time colleagues, according to the report. More than 70% of HMG leaders said their part-time staff is deployed to cover the same shifts and responsibilities as full-time staff. Many HMGs use part-time staff to cover night and weekend shifts.
Trend Today, Initiative Tomorrow
Taken together, SHM’s bi-annual survey and Focused Survey have begun to reveal some of the most prevalent trends within the specialty, including low turnover and a specialty-wide QI emphasis. However, Flores sees room for additional research in the near future.
“There is a lot more to learn about the nature of hospitalists’ involvement in organizational quality initiatives and what benefits that involvement is delivering to their organizations,” she says. “The survey suggests some areas, particularly in the quality arena, where SHM can develop additional programs and services to support hospitalists and the work they do.”
The 10-page 2008-2009 Focused Survey report is available at www.hospitalmedicine.org/shmstore. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Philadelphia Tri-State Area
The Philadelphia Tri-State Area chapter kicked off its 2009 meeting March 26 with its new “pharma-free” format. The chapter’s decision to forgo an expensive meal and industry-sponsored lecture was the result of an agreement to create more open dialogue among its members.
Chapter co-presidents Jen Myers, assistant professor of clinical medicine and patient safety officer at the Hospital of the University of Pennsylvania, and Erik DeLue, MD, MBA, medical director of the hospitalist program at Virtua Memorial Hospital in Mount Holly, N.J., kicked off the meeting, which focused on recruiting in a competitive market. Despite SHM’s collective recruiting challenges, most medical directors indicated that their groups were fully staffed.
Future meetings will be held at various medical institutions around the greater Philadelphia area. The next is to be held this month at Christiana Medical Center in Wilmington, Del. Future topics will be centered on pragmatic, nonclinical concerns for hospitalists, such as how to best utilize allied health providers.
Family Comes First

I recently returned from a seminar where I sang “Kumbaya” (OK, maybe I hummed) and performed a skit in front of the 250 other participants. Having once been edited out of my own end-of-residency movie, you might think this was Acting 101 for the next Shen’s Anatomy. Rather, this was “Hospitals and Communities Moving Forward with Patient and Family-Centered Care.” Replete with experiential lessons in positive change, it transformed my vision of the future for patients, families, and our field.
Patient- and family-centered care (PFCC) is a movement rooted in the values at the core of our profession. As soon as the hunter-gatherers formed communities, a village healer emerged. Parents could turn to the healer for help when a child developed bronchiolitis. With similar amounts of hand-waving, these healers produced outcomes similar to current bronchiolitis care.
But what once was a simple relationship has become fractured through relentless de-evolutionary forces. Progressive specialization has exponentially increased the number of healers. The rapid, paternalistic injection of science and technology overwhelms even the most capable of Homo sapiens. The final product can be as cold and sterile as a modern-day operating room.
Amidst the labyrinthine tangle of providers, information, and facilities, there is a warm underglow of hope. Unless you’ve been hiding under the concrete foundation of the old part of your hospital, you’ve heard about family-centered rounds (FCR). It’s the new black, or the new steroids, of pediatric HM. And it carries with it the potential to be the bellwether of change.
A simplistic view entails moving teaching rounds from the conference room to the bedside. Throw in a multidisciplinary component and you have a theoretical therapeutic milieu from which all manner of positive education and patient outcomes might be measured.
But one must ask the question: Can creating patient- and family-centeredness really be this simple?
Work with Families
Let’s begin with definitions. At one end of the spectrum is system-centered care (SCC). In this system, family members are denied access to the recovery room because it’s easier for the post-operative staff to do their work. Children wake up terrified? Tough. SCC is what the system does to you.
The next step on the developmental continuum is patient- and family-focused care (PFFC). Providers work for the benefit of the patient and family. You transport your gaggle of learners to the bedside for each and every family. You do it for everyone because you believe it’s best for the patient. You do it … until Tyler, age 9, tells you that your intimidating team gives him ulcers, perhaps literally.
What I thought was PFCC really was PFF, at best. By imposing my form of rounds on each patient and family, I had left out a key tenet of PFCC: collaboration. PFCC is partnering with patients and families. A simple fix for rounds would be to ask each patient and family how they would like to be involved.
Then again, just as a family is not easily defined, FCR is not best viewed in light of its structural composition or mechanics, but in its ability to deliver what each individual patient and family desires. And given the alacrity with which research in our field has gravitated toward FCR as a clean, measurable intervention, the implications of an FCR-dominant agenda should be highlighted.
To date, we have focused on measuring the challenges and successes of FCR implementation in academic settings. The emphasis on traditional teaching rounds has been at the price of the exclusion of defining what is family-centered when consultants or nonteaching hospitalists provide care, let alone nonphysician staff and outpatient providers. The emphasis on measurable data has subdued the powerful voices of patient and family stories. We have, predictably, created a hospitalist-centered agenda.
PFCC’s broad umbrella involves working with families at every juncture, from the design of your unit to the format of rounds to the outcomes of your study. True PFCC is measured by culture change and is successful when patients and families are surrounded by continuous healing relationships. By focusing efforts squarely on the implementation of FCR, I fear we may lose sight of a tremendous opportunity.
Pediatric Calling
Adult HM has turned a focus on quality and safety into a building block for the growth and acceptance of the field. Pediatrics invented and advanced the medical home concept, now a core principle of healthcare reform. PFCC is a central yet underdeveloped component of both of these parent organization efforts. Meanwhile, federally mandated public reporting of patients’ and families’ experience of care is under way, and hospitals are at varying stages of funding relevant initiatives.
These winds of change have created a fertile climate from which pediatric HM should blossom and lead. We can build upon our strong start in FCR, but we also must expand our efforts to lead in all directions. We must align our goals with administrative leadership, extend our work laterally to all other physicians and healthcare personnel, and elevate patients and families from subjects to collaborators.
FCR becomes a speed bump only if it is seen as a distinct and removable piece of PFCC. FCR accelerates change when it is embedded in the continuum of PFCC. Translating this vision into the language of strategic planning, a mission statement for the future of pediatric HM might look something like this:
Our strategy is to demonstrate our value to healthcare by leveraging FCR knowledge and expertise to generate a strong leadership presence at the forefront of the PFCC movement.
- We will seek partnership with institutional, community, and national leaders to promote a unified and collective vision for change.
- We will continue to accumulate not only data, but also powerful stories with which to effect change.
- We will use our experience in interdisciplinary partnerships with families to engage early adopters from other domains of the healthcare system.
- We will maintain a central focus on relationships and communication to effectively model culture change. TH
Dr. Shen is pediatric editor of The Hospitalist and medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas.
I recently returned from a seminar where I sang “Kumbaya” (OK, maybe I hummed) and performed a skit in front of the 250 other participants. Having once been edited out of my own end-of-residency movie, you might think this was Acting 101 for the next Shen’s Anatomy. Rather, this was “Hospitals and Communities Moving Forward with Patient and Family-Centered Care.” Replete with experiential lessons in positive change, it transformed my vision of the future for patients, families, and our field.
Patient- and family-centered care (PFCC) is a movement rooted in the values at the core of our profession. As soon as the hunter-gatherers formed communities, a village healer emerged. Parents could turn to the healer for help when a child developed bronchiolitis. With similar amounts of hand-waving, these healers produced outcomes similar to current bronchiolitis care.
But what once was a simple relationship has become fractured through relentless de-evolutionary forces. Progressive specialization has exponentially increased the number of healers. The rapid, paternalistic injection of science and technology overwhelms even the most capable of Homo sapiens. The final product can be as cold and sterile as a modern-day operating room.
Amidst the labyrinthine tangle of providers, information, and facilities, there is a warm underglow of hope. Unless you’ve been hiding under the concrete foundation of the old part of your hospital, you’ve heard about family-centered rounds (FCR). It’s the new black, or the new steroids, of pediatric HM. And it carries with it the potential to be the bellwether of change.
A simplistic view entails moving teaching rounds from the conference room to the bedside. Throw in a multidisciplinary component and you have a theoretical therapeutic milieu from which all manner of positive education and patient outcomes might be measured.
But one must ask the question: Can creating patient- and family-centeredness really be this simple?
Work with Families
Let’s begin with definitions. At one end of the spectrum is system-centered care (SCC). In this system, family members are denied access to the recovery room because it’s easier for the post-operative staff to do their work. Children wake up terrified? Tough. SCC is what the system does to you.
The next step on the developmental continuum is patient- and family-focused care (PFFC). Providers work for the benefit of the patient and family. You transport your gaggle of learners to the bedside for each and every family. You do it for everyone because you believe it’s best for the patient. You do it … until Tyler, age 9, tells you that your intimidating team gives him ulcers, perhaps literally.
What I thought was PFCC really was PFF, at best. By imposing my form of rounds on each patient and family, I had left out a key tenet of PFCC: collaboration. PFCC is partnering with patients and families. A simple fix for rounds would be to ask each patient and family how they would like to be involved.
Then again, just as a family is not easily defined, FCR is not best viewed in light of its structural composition or mechanics, but in its ability to deliver what each individual patient and family desires. And given the alacrity with which research in our field has gravitated toward FCR as a clean, measurable intervention, the implications of an FCR-dominant agenda should be highlighted.
To date, we have focused on measuring the challenges and successes of FCR implementation in academic settings. The emphasis on traditional teaching rounds has been at the price of the exclusion of defining what is family-centered when consultants or nonteaching hospitalists provide care, let alone nonphysician staff and outpatient providers. The emphasis on measurable data has subdued the powerful voices of patient and family stories. We have, predictably, created a hospitalist-centered agenda.
PFCC’s broad umbrella involves working with families at every juncture, from the design of your unit to the format of rounds to the outcomes of your study. True PFCC is measured by culture change and is successful when patients and families are surrounded by continuous healing relationships. By focusing efforts squarely on the implementation of FCR, I fear we may lose sight of a tremendous opportunity.
Pediatric Calling
Adult HM has turned a focus on quality and safety into a building block for the growth and acceptance of the field. Pediatrics invented and advanced the medical home concept, now a core principle of healthcare reform. PFCC is a central yet underdeveloped component of both of these parent organization efforts. Meanwhile, federally mandated public reporting of patients’ and families’ experience of care is under way, and hospitals are at varying stages of funding relevant initiatives.
These winds of change have created a fertile climate from which pediatric HM should blossom and lead. We can build upon our strong start in FCR, but we also must expand our efforts to lead in all directions. We must align our goals with administrative leadership, extend our work laterally to all other physicians and healthcare personnel, and elevate patients and families from subjects to collaborators.
FCR becomes a speed bump only if it is seen as a distinct and removable piece of PFCC. FCR accelerates change when it is embedded in the continuum of PFCC. Translating this vision into the language of strategic planning, a mission statement for the future of pediatric HM might look something like this:
Our strategy is to demonstrate our value to healthcare by leveraging FCR knowledge and expertise to generate a strong leadership presence at the forefront of the PFCC movement.
- We will seek partnership with institutional, community, and national leaders to promote a unified and collective vision for change.
- We will continue to accumulate not only data, but also powerful stories with which to effect change.
- We will use our experience in interdisciplinary partnerships with families to engage early adopters from other domains of the healthcare system.
- We will maintain a central focus on relationships and communication to effectively model culture change. TH
Dr. Shen is pediatric editor of The Hospitalist and medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas.
I recently returned from a seminar where I sang “Kumbaya” (OK, maybe I hummed) and performed a skit in front of the 250 other participants. Having once been edited out of my own end-of-residency movie, you might think this was Acting 101 for the next Shen’s Anatomy. Rather, this was “Hospitals and Communities Moving Forward with Patient and Family-Centered Care.” Replete with experiential lessons in positive change, it transformed my vision of the future for patients, families, and our field.
Patient- and family-centered care (PFCC) is a movement rooted in the values at the core of our profession. As soon as the hunter-gatherers formed communities, a village healer emerged. Parents could turn to the healer for help when a child developed bronchiolitis. With similar amounts of hand-waving, these healers produced outcomes similar to current bronchiolitis care.
But what once was a simple relationship has become fractured through relentless de-evolutionary forces. Progressive specialization has exponentially increased the number of healers. The rapid, paternalistic injection of science and technology overwhelms even the most capable of Homo sapiens. The final product can be as cold and sterile as a modern-day operating room.
Amidst the labyrinthine tangle of providers, information, and facilities, there is a warm underglow of hope. Unless you’ve been hiding under the concrete foundation of the old part of your hospital, you’ve heard about family-centered rounds (FCR). It’s the new black, or the new steroids, of pediatric HM. And it carries with it the potential to be the bellwether of change.
A simplistic view entails moving teaching rounds from the conference room to the bedside. Throw in a multidisciplinary component and you have a theoretical therapeutic milieu from which all manner of positive education and patient outcomes might be measured.
But one must ask the question: Can creating patient- and family-centeredness really be this simple?
Work with Families
Let’s begin with definitions. At one end of the spectrum is system-centered care (SCC). In this system, family members are denied access to the recovery room because it’s easier for the post-operative staff to do their work. Children wake up terrified? Tough. SCC is what the system does to you.
The next step on the developmental continuum is patient- and family-focused care (PFFC). Providers work for the benefit of the patient and family. You transport your gaggle of learners to the bedside for each and every family. You do it for everyone because you believe it’s best for the patient. You do it … until Tyler, age 9, tells you that your intimidating team gives him ulcers, perhaps literally.
What I thought was PFCC really was PFF, at best. By imposing my form of rounds on each patient and family, I had left out a key tenet of PFCC: collaboration. PFCC is partnering with patients and families. A simple fix for rounds would be to ask each patient and family how they would like to be involved.
Then again, just as a family is not easily defined, FCR is not best viewed in light of its structural composition or mechanics, but in its ability to deliver what each individual patient and family desires. And given the alacrity with which research in our field has gravitated toward FCR as a clean, measurable intervention, the implications of an FCR-dominant agenda should be highlighted.
To date, we have focused on measuring the challenges and successes of FCR implementation in academic settings. The emphasis on traditional teaching rounds has been at the price of the exclusion of defining what is family-centered when consultants or nonteaching hospitalists provide care, let alone nonphysician staff and outpatient providers. The emphasis on measurable data has subdued the powerful voices of patient and family stories. We have, predictably, created a hospitalist-centered agenda.
PFCC’s broad umbrella involves working with families at every juncture, from the design of your unit to the format of rounds to the outcomes of your study. True PFCC is measured by culture change and is successful when patients and families are surrounded by continuous healing relationships. By focusing efforts squarely on the implementation of FCR, I fear we may lose sight of a tremendous opportunity.
Pediatric Calling
Adult HM has turned a focus on quality and safety into a building block for the growth and acceptance of the field. Pediatrics invented and advanced the medical home concept, now a core principle of healthcare reform. PFCC is a central yet underdeveloped component of both of these parent organization efforts. Meanwhile, federally mandated public reporting of patients’ and families’ experience of care is under way, and hospitals are at varying stages of funding relevant initiatives.
These winds of change have created a fertile climate from which pediatric HM should blossom and lead. We can build upon our strong start in FCR, but we also must expand our efforts to lead in all directions. We must align our goals with administrative leadership, extend our work laterally to all other physicians and healthcare personnel, and elevate patients and families from subjects to collaborators.
FCR becomes a speed bump only if it is seen as a distinct and removable piece of PFCC. FCR accelerates change when it is embedded in the continuum of PFCC. Translating this vision into the language of strategic planning, a mission statement for the future of pediatric HM might look something like this:
Our strategy is to demonstrate our value to healthcare by leveraging FCR knowledge and expertise to generate a strong leadership presence at the forefront of the PFCC movement.
- We will seek partnership with institutional, community, and national leaders to promote a unified and collective vision for change.
- We will continue to accumulate not only data, but also powerful stories with which to effect change.
- We will use our experience in interdisciplinary partnerships with families to engage early adopters from other domains of the healthcare system.
- We will maintain a central focus on relationships and communication to effectively model culture change. TH
Dr. Shen is pediatric editor of The Hospitalist and medical director of hospital medicine at Dell Children’s Medical Center in Austin, Texas.
Quality Commitment
Ehab Hanna, MD, MBBch, FHM, understands better than most why hospitalists are frustrated with all the grand plans to utilize information technology (IT) for streamlining admissions, medical reconciliations, and the discharge process. As assistant chief medical information officer at Eastern Maine Medical Center in Bangor, he spends half his time scouting and assessing the value of new IT platforms and the other half as a front-line hospitalist.
Dr. Hanna and his colleagues are frustrated that software systems promise to deliver electronic medical records (EMR) but freeze up too often, take too long to download files, or can’t handle the functions for which they were developed. But he also knows the future of healthcare hinges on IT as much as anything else—and that done correctly, and probably expensively, it can be a savior.
“Every time we want to come up with a quality-initiative project, we want to ask, ‘What can IT do for us?’ ” Dr. Hanna says. He also acknowledges that “it’s all types of money, whether it be resources, funding, or people to implement [the system]. And there’s physician resistance to it.”
The link between quality and cost is paramount to healthcare and HM. As evidence, the keynote theme of HM09 in Chicago was quality improvement (QI)—defining it, making it a priority, setting up analytical metrics to measure it, and the most difficult step: implementing it. QI projects vary in size, shape, and scope. On one end of the spectrum: hand-washing compliance systems and simple programs to increase the prescription of pneumococcal vaccines. On the laborious and expensive end: EMR system integration with ambulatory care and pharmacy.

Industry leaders agree QI projects must include measurable goals and incentives for success. The flip side is that failure to reach those goals has to include a level of accountability.
One thing is for sure: The choice to focus on patient safety no longer is a choice, it’s a mandate. Patient-safety advocates are barking louder than ever, and the public and politicians are taking note. Medicare reimbursements are increasingly tied to performance measures, a trend that is likely to accelerate in light of recent news that Medicare will sink into the red in just eight years. Many expect that threshold to keep moving closer, too. President Obama has pledged to push major healthcare reform legislation—including a focus on EMR—through Congress. He wants to sign it into law by Labor Day.
On the other hand, there still is a relatively small sample of data on the effectiveness of pay-for-performance contracting in relation to overall patient health. There is a recurring call from many outside the HM field for more independent, empirical data that can pinpoint the quantifiable value of hospitalists. Discussions based on those values could satisfy group leaders, hospital administrators, and government regulators who still use the tried-and-true HM formula: value equals quality divided by cost.
“I see about as many challenges in QI as I do opportunities,” says SHM President Scott Flanders, MD, FHM, director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “Is the horse before the cart? We have spent a lot of time and effort putting in place … programs before understanding the clinical effect.”

Can IT be EZ?
Dr. Hanna says hospitalists would embrace new IT initiatives immediately if they were easier to use. Many hospitalists are frustrated that in their pocket sits a handy, portable device that works in real time as a computer, a phone, a CD player, a GPS tracking device, and a scheduling secretary, yet they can’t use their E&M coding system without encountering constant hiccups, interruptions that take valuable time out of an already crowded 12-hour shift.
“Why isn’t it working like the iPhone?” is a complaint Dr. Hanna says he hears all the time.
One answer is that a number of medical software programs are limited in nature and don’t automatically network well with other systems already in place. User errors and other problems crop up regularly; plus, there isn’t a repository for people to measure different systems against each other. Some SHM leaders are considering a plan to create an online resource for IT vendors, but the society is leery of making recommendations because of potential conflicts of interest.
The Joint Commission, which accredits and certifies more than 15,000 healthcare organizations and programs, has been asked—by Dr. Hanna, among others—if it intends to regulate EMR vendors, which would let hospitalists know which systems are most reliable and useful. Commission President Mark Chassin, MD, MPP, MPH, said after his HM09 keynote address that his agency has no intention of doing so.
—Scott Flanders, MD, FHM, SHM president
“We don’t see [that] as a good message for us to give,” Dr. Chassin said.
IT also can be used in creative ways to spur patient-safety improvements. As hospitalists struggle to increase compliance with hand-hygiene standards, several hospitals have resorted to using video cameras above sinks to track whose hands are clean and whose hands are not clean, Robert Wachter, MD, FHM, said during his plenary address to conclude HM09. Real-time tracking runs through a software program and is displayed on a small, LED screen that hangs from the ceiling. Positive results are praised, while low rates of compliance result in pages to HM and hospital leaders to address hygiene issues. Dr. Wachter, professor and associate chairman of the department of medicine at the University of California at San Francisco Medical Center, chief of the division of hospital medicine, former SHM president and author of the blog “Wachter’s World” (www.wachtersworld), said UCSF hospital executives are considering the video system.
Dr. Wachter also says hospitalists can’t lament the rise of QI and the stricter standards that are attached. Nor can HM complain too loudly about the burdens QI places on them. As hospitalists argue that their value is partly defined by their contributions to hospital quality, they have to expect to be accountable to the claim. “We have positioned ourselves as being leaders in quality and safety,” he says. “This is not going out and being branded. We bring this in. We often say we have two sick patients; one is in front of us, the other is our organization.”
Pay for Performance?
Another largely unanswered question is how valuable pay-for-performance will be in improving patient care, safety, and satisfaction. While most HM contracts include additional compensation based on volume, bonus pay often ignores such measurable outcomes as readmission rates and length of stay.
“Does incentivizing healthcare quality actually improve health?” asks Susan Freeman, MD, chief medical officer at Temple University Hospital in Philadelphia. “It’s really hard to measure things that don’t happen—the myocardial infarction that didn’t happen, the stroke that didn’t happen.”
Active pay-for-performance programs numbered 160 in November 2007, four times the number of programs four years earlier.1 Yet as the concept catches on, the average physician incentive was 2% or less, and it seems to play a small role in how care was delivered.2
A more recent look at the issue concludes that if insurance companies and private employers worked with hospitals and physicians, attitudes toward pay for performance might change. “The amount of incentives available to physicians strongly affected their rate of participation,” say the authors of a May study in the American Journal of Managed Care. “Our analysis suggests that all stakeholders—health plans, physicians, and patients—would benefit from health plans collaborating on their pay-for-performance efforts to maximize physician participation.”3
Russell Holman, MD, FHM, chief operating officer of Cogent Healthcare, says another pay-for-performance concern is that improved quality is not always something that translates quickly into bottom-line savings. In today’s economic environment, in which every dollar spent has to be justified, it can actually be tougher to sell the upfront costs and long-term savings associated with investment in QI projects. “Improving quality is going to take a long time to see the advantages to the healthcare system,” says Dr. Holman, a former SHM president. “It is delayed gratification.”

Is HM Ready?
Dr. Holman says the pay-for-performance solution might end up as more of a hybrid of two reimbursement models, incentive-based pay and the controversial notion of billing bundling. Most hospitalists and HM groups are not entirely comfortable with the bundling idea, in which the hospital receives a lump-sum reimbursement for all services performed for a patient, then shells out payment to the surgeons, hospitalists, nurses, etc. The concept of hospitals as payment intermediaries adds an extra layer of bureaucracy, but the bundling concept appears to be gaining momentum.
While QI projects are the trendy way to measure value, Dr. Chassin points out that physicians need more detailed thresholds to exceed. Such measures as prescribing beta-blockers after myocardial infarction were good first-generation concepts, but better care requires better benchmarks, he says. Dr. Wachter echoes the sentiment, telling HM09 attendees that relying on past successes in QI won’t help hospitalists demonstrate their value or answer the “What have you done for me lately?” demand from hospital administrators.
Dr. Chassin compares healthcare to other high-pressure industries that do much better at controlling mistakes. Some estimates show nearly 100,000 people a year die from medical errors. Why? Many high-risk industries—airlines, nuclear energy, mining—have better quality and safety processes to protect against routine errors that continually plague healthcare (e.g., hospital-acquired infections, operations on the wrong patient).
The responsibility to get better doesn’t belong to one medical group, either. Dr. Chassin says researchers, the Centers for Medicare and Medicaid Services, and trade groups like SHM have to work collaboratively to design benchmarks that can be measured quantitatively. Once those measuring sticks are in place, though, Dr. Chassin believes hospitalists are the first responders who can best identify and solve problems.
“You have to understand the causes of the problems you’re trying to fix,” he says. “Hospitalists are on the front lines.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Baker G, Delbanco S. Pay for performance: national perspective. 2006 longitudinal survey results with 2007 market updates. MedVantage Web site. Available at www.medvantage.com/Pdf/2006 NationalP4PStudy.pdf. Accessed May 17, 2009.
- Pearson SD, Schneider EC, Kleinman KP, Colin KL, Singer JA. The impact of pay-for-performance on health care quality in Massachusetts, 2001-2003. Health Aff (Millwood). 2008;27(4):1167-1176.
- De Brantes FS, D’Andrea BG. Physicians respond to pay-for-performance incentives: larger incentives yield greater participation. Am J Manag Care. 2009;15(5):305-310.
Ehab Hanna, MD, MBBch, FHM, understands better than most why hospitalists are frustrated with all the grand plans to utilize information technology (IT) for streamlining admissions, medical reconciliations, and the discharge process. As assistant chief medical information officer at Eastern Maine Medical Center in Bangor, he spends half his time scouting and assessing the value of new IT platforms and the other half as a front-line hospitalist.
Dr. Hanna and his colleagues are frustrated that software systems promise to deliver electronic medical records (EMR) but freeze up too often, take too long to download files, or can’t handle the functions for which they were developed. But he also knows the future of healthcare hinges on IT as much as anything else—and that done correctly, and probably expensively, it can be a savior.
“Every time we want to come up with a quality-initiative project, we want to ask, ‘What can IT do for us?’ ” Dr. Hanna says. He also acknowledges that “it’s all types of money, whether it be resources, funding, or people to implement [the system]. And there’s physician resistance to it.”
The link between quality and cost is paramount to healthcare and HM. As evidence, the keynote theme of HM09 in Chicago was quality improvement (QI)—defining it, making it a priority, setting up analytical metrics to measure it, and the most difficult step: implementing it. QI projects vary in size, shape, and scope. On one end of the spectrum: hand-washing compliance systems and simple programs to increase the prescription of pneumococcal vaccines. On the laborious and expensive end: EMR system integration with ambulatory care and pharmacy.
Industry leaders agree QI projects must include measurable goals and incentives for success. The flip side is that failure to reach those goals has to include a level of accountability.
One thing is for sure: The choice to focus on patient safety no longer is a choice, it’s a mandate. Patient-safety advocates are barking louder than ever, and the public and politicians are taking note. Medicare reimbursements are increasingly tied to performance measures, a trend that is likely to accelerate in light of recent news that Medicare will sink into the red in just eight years. Many expect that threshold to keep moving closer, too. President Obama has pledged to push major healthcare reform legislation—including a focus on EMR—through Congress. He wants to sign it into law by Labor Day.
On the other hand, there still is a relatively small sample of data on the effectiveness of pay-for-performance contracting in relation to overall patient health. There is a recurring call from many outside the HM field for more independent, empirical data that can pinpoint the quantifiable value of hospitalists. Discussions based on those values could satisfy group leaders, hospital administrators, and government regulators who still use the tried-and-true HM formula: value equals quality divided by cost.
“I see about as many challenges in QI as I do opportunities,” says SHM President Scott Flanders, MD, FHM, director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “Is the horse before the cart? We have spent a lot of time and effort putting in place … programs before understanding the clinical effect.”
Can IT be EZ?
Dr. Hanna says hospitalists would embrace new IT initiatives immediately if they were easier to use. Many hospitalists are frustrated that in their pocket sits a handy, portable device that works in real time as a computer, a phone, a CD player, a GPS tracking device, and a scheduling secretary, yet they can’t use their E&M coding system without encountering constant hiccups, interruptions that take valuable time out of an already crowded 12-hour shift.
“Why isn’t it working like the iPhone?” is a complaint Dr. Hanna says he hears all the time.
One answer is that a number of medical software programs are limited in nature and don’t automatically network well with other systems already in place. User errors and other problems crop up regularly; plus, there isn’t a repository for people to measure different systems against each other. Some SHM leaders are considering a plan to create an online resource for IT vendors, but the society is leery of making recommendations because of potential conflicts of interest.
The Joint Commission, which accredits and certifies more than 15,000 healthcare organizations and programs, has been asked—by Dr. Hanna, among others—if it intends to regulate EMR vendors, which would let hospitalists know which systems are most reliable and useful. Commission President Mark Chassin, MD, MPP, MPH, said after his HM09 keynote address that his agency has no intention of doing so.
—Scott Flanders, MD, FHM, SHM president
“We don’t see [that] as a good message for us to give,” Dr. Chassin said.
IT also can be used in creative ways to spur patient-safety improvements. As hospitalists struggle to increase compliance with hand-hygiene standards, several hospitals have resorted to using video cameras above sinks to track whose hands are clean and whose hands are not clean, Robert Wachter, MD, FHM, said during his plenary address to conclude HM09. Real-time tracking runs through a software program and is displayed on a small, LED screen that hangs from the ceiling. Positive results are praised, while low rates of compliance result in pages to HM and hospital leaders to address hygiene issues. Dr. Wachter, professor and associate chairman of the department of medicine at the University of California at San Francisco Medical Center, chief of the division of hospital medicine, former SHM president and author of the blog “Wachter’s World” (www.wachtersworld), said UCSF hospital executives are considering the video system.
Dr. Wachter also says hospitalists can’t lament the rise of QI and the stricter standards that are attached. Nor can HM complain too loudly about the burdens QI places on them. As hospitalists argue that their value is partly defined by their contributions to hospital quality, they have to expect to be accountable to the claim. “We have positioned ourselves as being leaders in quality and safety,” he says. “This is not going out and being branded. We bring this in. We often say we have two sick patients; one is in front of us, the other is our organization.”
Pay for Performance?
Another largely unanswered question is how valuable pay-for-performance will be in improving patient care, safety, and satisfaction. While most HM contracts include additional compensation based on volume, bonus pay often ignores such measurable outcomes as readmission rates and length of stay.
“Does incentivizing healthcare quality actually improve health?” asks Susan Freeman, MD, chief medical officer at Temple University Hospital in Philadelphia. “It’s really hard to measure things that don’t happen—the myocardial infarction that didn’t happen, the stroke that didn’t happen.”
Active pay-for-performance programs numbered 160 in November 2007, four times the number of programs four years earlier.1 Yet as the concept catches on, the average physician incentive was 2% or less, and it seems to play a small role in how care was delivered.2
A more recent look at the issue concludes that if insurance companies and private employers worked with hospitals and physicians, attitudes toward pay for performance might change. “The amount of incentives available to physicians strongly affected their rate of participation,” say the authors of a May study in the American Journal of Managed Care. “Our analysis suggests that all stakeholders—health plans, physicians, and patients—would benefit from health plans collaborating on their pay-for-performance efforts to maximize physician participation.”3
Russell Holman, MD, FHM, chief operating officer of Cogent Healthcare, says another pay-for-performance concern is that improved quality is not always something that translates quickly into bottom-line savings. In today’s economic environment, in which every dollar spent has to be justified, it can actually be tougher to sell the upfront costs and long-term savings associated with investment in QI projects. “Improving quality is going to take a long time to see the advantages to the healthcare system,” says Dr. Holman, a former SHM president. “It is delayed gratification.”
Is HM Ready?
Dr. Holman says the pay-for-performance solution might end up as more of a hybrid of two reimbursement models, incentive-based pay and the controversial notion of billing bundling. Most hospitalists and HM groups are not entirely comfortable with the bundling idea, in which the hospital receives a lump-sum reimbursement for all services performed for a patient, then shells out payment to the surgeons, hospitalists, nurses, etc. The concept of hospitals as payment intermediaries adds an extra layer of bureaucracy, but the bundling concept appears to be gaining momentum.
While QI projects are the trendy way to measure value, Dr. Chassin points out that physicians need more detailed thresholds to exceed. Such measures as prescribing beta-blockers after myocardial infarction were good first-generation concepts, but better care requires better benchmarks, he says. Dr. Wachter echoes the sentiment, telling HM09 attendees that relying on past successes in QI won’t help hospitalists demonstrate their value or answer the “What have you done for me lately?” demand from hospital administrators.
Dr. Chassin compares healthcare to other high-pressure industries that do much better at controlling mistakes. Some estimates show nearly 100,000 people a year die from medical errors. Why? Many high-risk industries—airlines, nuclear energy, mining—have better quality and safety processes to protect against routine errors that continually plague healthcare (e.g., hospital-acquired infections, operations on the wrong patient).
The responsibility to get better doesn’t belong to one medical group, either. Dr. Chassin says researchers, the Centers for Medicare and Medicaid Services, and trade groups like SHM have to work collaboratively to design benchmarks that can be measured quantitatively. Once those measuring sticks are in place, though, Dr. Chassin believes hospitalists are the first responders who can best identify and solve problems.
“You have to understand the causes of the problems you’re trying to fix,” he says. “Hospitalists are on the front lines.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Baker G, Delbanco S. Pay for performance: national perspective. 2006 longitudinal survey results with 2007 market updates. MedVantage Web site. Available at www.medvantage.com/Pdf/2006 NationalP4PStudy.pdf. Accessed May 17, 2009.
- Pearson SD, Schneider EC, Kleinman KP, Colin KL, Singer JA. The impact of pay-for-performance on health care quality in Massachusetts, 2001-2003. Health Aff (Millwood). 2008;27(4):1167-1176.
- De Brantes FS, D’Andrea BG. Physicians respond to pay-for-performance incentives: larger incentives yield greater participation. Am J Manag Care. 2009;15(5):305-310.
Ehab Hanna, MD, MBBch, FHM, understands better than most why hospitalists are frustrated with all the grand plans to utilize information technology (IT) for streamlining admissions, medical reconciliations, and the discharge process. As assistant chief medical information officer at Eastern Maine Medical Center in Bangor, he spends half his time scouting and assessing the value of new IT platforms and the other half as a front-line hospitalist.
Dr. Hanna and his colleagues are frustrated that software systems promise to deliver electronic medical records (EMR) but freeze up too often, take too long to download files, or can’t handle the functions for which they were developed. But he also knows the future of healthcare hinges on IT as much as anything else—and that done correctly, and probably expensively, it can be a savior.
“Every time we want to come up with a quality-initiative project, we want to ask, ‘What can IT do for us?’ ” Dr. Hanna says. He also acknowledges that “it’s all types of money, whether it be resources, funding, or people to implement [the system]. And there’s physician resistance to it.”
The link between quality and cost is paramount to healthcare and HM. As evidence, the keynote theme of HM09 in Chicago was quality improvement (QI)—defining it, making it a priority, setting up analytical metrics to measure it, and the most difficult step: implementing it. QI projects vary in size, shape, and scope. On one end of the spectrum: hand-washing compliance systems and simple programs to increase the prescription of pneumococcal vaccines. On the laborious and expensive end: EMR system integration with ambulatory care and pharmacy.
Industry leaders agree QI projects must include measurable goals and incentives for success. The flip side is that failure to reach those goals has to include a level of accountability.
One thing is for sure: The choice to focus on patient safety no longer is a choice, it’s a mandate. Patient-safety advocates are barking louder than ever, and the public and politicians are taking note. Medicare reimbursements are increasingly tied to performance measures, a trend that is likely to accelerate in light of recent news that Medicare will sink into the red in just eight years. Many expect that threshold to keep moving closer, too. President Obama has pledged to push major healthcare reform legislation—including a focus on EMR—through Congress. He wants to sign it into law by Labor Day.
On the other hand, there still is a relatively small sample of data on the effectiveness of pay-for-performance contracting in relation to overall patient health. There is a recurring call from many outside the HM field for more independent, empirical data that can pinpoint the quantifiable value of hospitalists. Discussions based on those values could satisfy group leaders, hospital administrators, and government regulators who still use the tried-and-true HM formula: value equals quality divided by cost.
“I see about as many challenges in QI as I do opportunities,” says SHM President Scott Flanders, MD, FHM, director of the hospitalist program at the University of Michigan Health System in Ann Arbor. “Is the horse before the cart? We have spent a lot of time and effort putting in place … programs before understanding the clinical effect.”
Can IT be EZ?
Dr. Hanna says hospitalists would embrace new IT initiatives immediately if they were easier to use. Many hospitalists are frustrated that in their pocket sits a handy, portable device that works in real time as a computer, a phone, a CD player, a GPS tracking device, and a scheduling secretary, yet they can’t use their E&M coding system without encountering constant hiccups, interruptions that take valuable time out of an already crowded 12-hour shift.
“Why isn’t it working like the iPhone?” is a complaint Dr. Hanna says he hears all the time.
One answer is that a number of medical software programs are limited in nature and don’t automatically network well with other systems already in place. User errors and other problems crop up regularly; plus, there isn’t a repository for people to measure different systems against each other. Some SHM leaders are considering a plan to create an online resource for IT vendors, but the society is leery of making recommendations because of potential conflicts of interest.
The Joint Commission, which accredits and certifies more than 15,000 healthcare organizations and programs, has been asked—by Dr. Hanna, among others—if it intends to regulate EMR vendors, which would let hospitalists know which systems are most reliable and useful. Commission President Mark Chassin, MD, MPP, MPH, said after his HM09 keynote address that his agency has no intention of doing so.
—Scott Flanders, MD, FHM, SHM president
“We don’t see [that] as a good message for us to give,” Dr. Chassin said.
IT also can be used in creative ways to spur patient-safety improvements. As hospitalists struggle to increase compliance with hand-hygiene standards, several hospitals have resorted to using video cameras above sinks to track whose hands are clean and whose hands are not clean, Robert Wachter, MD, FHM, said during his plenary address to conclude HM09. Real-time tracking runs through a software program and is displayed on a small, LED screen that hangs from the ceiling. Positive results are praised, while low rates of compliance result in pages to HM and hospital leaders to address hygiene issues. Dr. Wachter, professor and associate chairman of the department of medicine at the University of California at San Francisco Medical Center, chief of the division of hospital medicine, former SHM president and author of the blog “Wachter’s World” (www.wachtersworld), said UCSF hospital executives are considering the video system.
Dr. Wachter also says hospitalists can’t lament the rise of QI and the stricter standards that are attached. Nor can HM complain too loudly about the burdens QI places on them. As hospitalists argue that their value is partly defined by their contributions to hospital quality, they have to expect to be accountable to the claim. “We have positioned ourselves as being leaders in quality and safety,” he says. “This is not going out and being branded. We bring this in. We often say we have two sick patients; one is in front of us, the other is our organization.”
Pay for Performance?
Another largely unanswered question is how valuable pay-for-performance will be in improving patient care, safety, and satisfaction. While most HM contracts include additional compensation based on volume, bonus pay often ignores such measurable outcomes as readmission rates and length of stay.
“Does incentivizing healthcare quality actually improve health?” asks Susan Freeman, MD, chief medical officer at Temple University Hospital in Philadelphia. “It’s really hard to measure things that don’t happen—the myocardial infarction that didn’t happen, the stroke that didn’t happen.”
Active pay-for-performance programs numbered 160 in November 2007, four times the number of programs four years earlier.1 Yet as the concept catches on, the average physician incentive was 2% or less, and it seems to play a small role in how care was delivered.2
A more recent look at the issue concludes that if insurance companies and private employers worked with hospitals and physicians, attitudes toward pay for performance might change. “The amount of incentives available to physicians strongly affected their rate of participation,” say the authors of a May study in the American Journal of Managed Care. “Our analysis suggests that all stakeholders—health plans, physicians, and patients—would benefit from health plans collaborating on their pay-for-performance efforts to maximize physician participation.”3
Russell Holman, MD, FHM, chief operating officer of Cogent Healthcare, says another pay-for-performance concern is that improved quality is not always something that translates quickly into bottom-line savings. In today’s economic environment, in which every dollar spent has to be justified, it can actually be tougher to sell the upfront costs and long-term savings associated with investment in QI projects. “Improving quality is going to take a long time to see the advantages to the healthcare system,” says Dr. Holman, a former SHM president. “It is delayed gratification.”
Is HM Ready?
Dr. Holman says the pay-for-performance solution might end up as more of a hybrid of two reimbursement models, incentive-based pay and the controversial notion of billing bundling. Most hospitalists and HM groups are not entirely comfortable with the bundling idea, in which the hospital receives a lump-sum reimbursement for all services performed for a patient, then shells out payment to the surgeons, hospitalists, nurses, etc. The concept of hospitals as payment intermediaries adds an extra layer of bureaucracy, but the bundling concept appears to be gaining momentum.
While QI projects are the trendy way to measure value, Dr. Chassin points out that physicians need more detailed thresholds to exceed. Such measures as prescribing beta-blockers after myocardial infarction were good first-generation concepts, but better care requires better benchmarks, he says. Dr. Wachter echoes the sentiment, telling HM09 attendees that relying on past successes in QI won’t help hospitalists demonstrate their value or answer the “What have you done for me lately?” demand from hospital administrators.
Dr. Chassin compares healthcare to other high-pressure industries that do much better at controlling mistakes. Some estimates show nearly 100,000 people a year die from medical errors. Why? Many high-risk industries—airlines, nuclear energy, mining—have better quality and safety processes to protect against routine errors that continually plague healthcare (e.g., hospital-acquired infections, operations on the wrong patient).
The responsibility to get better doesn’t belong to one medical group, either. Dr. Chassin says researchers, the Centers for Medicare and Medicaid Services, and trade groups like SHM have to work collaboratively to design benchmarks that can be measured quantitatively. Once those measuring sticks are in place, though, Dr. Chassin believes hospitalists are the first responders who can best identify and solve problems.
“You have to understand the causes of the problems you’re trying to fix,” he says. “Hospitalists are on the front lines.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Baker G, Delbanco S. Pay for performance: national perspective. 2006 longitudinal survey results with 2007 market updates. MedVantage Web site. Available at www.medvantage.com/Pdf/2006 NationalP4PStudy.pdf. Accessed May 17, 2009.
- Pearson SD, Schneider EC, Kleinman KP, Colin KL, Singer JA. The impact of pay-for-performance on health care quality in Massachusetts, 2001-2003. Health Aff (Millwood). 2008;27(4):1167-1176.
- De Brantes FS, D’Andrea BG. Physicians respond to pay-for-performance incentives: larger incentives yield greater participation. Am J Manag Care. 2009;15(5):305-310.
Beware the Doughnut Hole
Judy Zerzan, MD, MPH, was at a loss. A Health and Aging Policy Fellow and hospitalist at the University of Colorado Denver, Dr. Zerzan was examining a Medicare patient who was admitted to the hospital with an apparent urinary tract infection. But the same patient had been released from the hospital only five days earlier with an antibiotic prescription to treat an oddly similar infection.
The confusion only increased when lab cultures revealed an E. coli infection. It should have been sensitive to most antibiotics, especially to the brand-name moxifloxacin the patient said she had been taking since her last hospital stay.
Several days into the patient’s rehospitalization, a medical student finally cracked the case. “The medical student went in and started talking to her some more and learned that she didn’t fill the prescription because under her [insurance] plan, it was going to be something like $50, and she felt like she couldn’t afford it,” Dr. Zerzan recalls. “She felt really embarrassed about it, so she didn’t want to tell us that she didn’t fill it.”
The medical team sent the woman home with a $4 generic prescription. “She was much relieved,” Dr. Zerzan says. More importantly, the patient did not return to the hospital for a third stay.
Hospitalists might not see a $46 difference in drug pricing as a core consideration of patient care. But with many seniors enrolled in Medicare Part D’s prescription drug plan falling through holes in the partially privatized safety net, many agree that far more must be done to ensure that financial stress doesn’t lead to medical misfortune.
“It is an ethical issue,” says Stephen Soumerai, ScD, director of the Drug Policy Research Program and a professor in the Department of Ambulatory Care and Prevention at Harvard University. “ … It’s easy to target those people who are the most vulnerable in our society and, therefore, it is an opportunity to try to find ways for them to lower their problems of economic access to medicine.”
Soumerai calls cost-related medication nonadherence a matter of distributive justice. In a study published last year in the Journal of the American Medical Association, he and 10 co-authors found that even after enrolling in Medicare Part D, the sickest beneficiaries were just as likely to skip medications they couldn’t afford.1
Identify the Coverage Gap
Medicare’s prescription drug plan, initiated in 2006, has provided coverage for many beneficiaries who previously went without. But it has been widely criticized as unnecessarily confusing by both doctors and patients—and particularly expensive for beneficiaries unlucky enough to fall into its notorious gap in coverage, dubbed the “doughnut hole” (see “Medicare Part D: The Basics,” right).
That economic burden can be exacerbated by medical illiteracy, ignorance, and misinformation. Recent Consumer Reports polls suggest as few as 4% of patients discuss drug prices with their doctors; almost half of Americans have reservations or misgivings about lower-cost generic drugs.
As focal points in the coordination of patient care, hospitalists are better positioned than most to help steer the most vulnerable away from the douhgnut hole while helping hospitals equitably distribute limited resources. But hospitalists often are completely unaware of a patient’s plight. “My research interest is prescription drug coverage, so I think I’m more keyed into it, but certainly even I don’t generally think about, when discharging a patient, if something is going to be on their Part D formulary or not, or what sort of prior-authorization hoops their primary-care doc may have to go through,” Dr. Zerzan says. “And I think that’s generally true of my colleagues as well.”
With tight schedules, a limited personal history with patients, disparities in local resources, and a litany of cost-control measures established by insurers, even hospitalists in the know concede that helping Medicare patients manage drug costs can be an exercise in frustration. As a result, patients are often left with medications that require higher cost-sharing or aren’t even on a plan’s formulary, forcing them to pay out-of-pocket for a prescription. Adding insult to injury, any money spent on a medication not covered by a Part D plan doesn’t count toward getting a patient out of the doughnut hole.
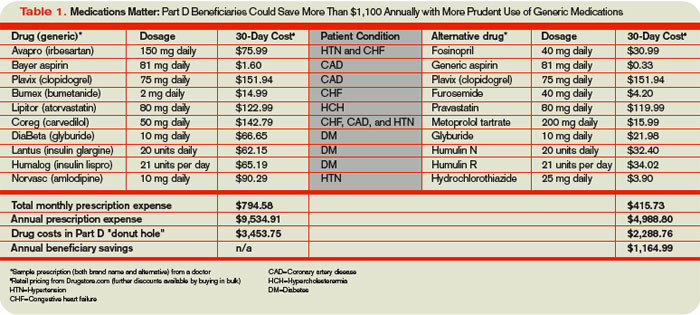
The Extra Mile
Jocelyne Watrous, a Medicare beneficiary consultant at the Willimantic, Conn.-based Center for Medicare Advocacy, says drug affordability while in the doughnut hole is a hardship for many. But so are specialty drug copays that range from 25% to 33% of the total price (see Table 1, below). For expensive prescriptions, Watrous says, hospitalists can get the name of a patient’s Part D formulary from the membership card and check for restrictions, such as prior authorization, quantity limits, or step therapy. “This is a terrible burden to place on physicians and their staffs, but nothing is worse than having the patient come back to the hospital via the ER because they could not get the drug prescribed by their doctor,” she says. “Best to square it all away before discharge, if possible.”
Brandon Koretz, MD, an associate clinical professor of geriatric medicine at the University of California at Los Angeles, says keeping track of differences among the dozens of Part D plans isn’t feasible. “Oftentimes, what happens is, you find yourself writing a prescription for what you think is a reasonable and cost-effective treatment, only to find out that drug A is not on insurance company B’s formulary, but drug C is,” Dr. Koretz says.
And if doctors are confused by the array of Part D formularies, hospitalists wonder, how can geriatric patients be expected to navigate the system, especially given the not-insignificant number with cognitive impairments?
Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C., compares the consumer paralysis created by the proliferation of prescription drug plans to walking by a store display featuring 20 brands of jam. “You’re kind of awed by it, but you don’t buy anything because you’re kind of intimidated,” he says. Only instead of 20 varieties, the typical local government agency offered 48 competing Part D plans in November 2006, with some boasting more than 70. In a new study sponsored by the Henry J. Kaiser Family Foundation, Massachusetts Institute of Technology economist Jonathan Gruber found that when seniors made a decision, only 6% to 9% chose the least expensive plan, while the remaining seniors paid an extra $360 to $520 annually (www.kff.org/medicare/7864.cfm).
All too often, economic problems are simply transferred to other providers. Nursing home pharmacists have complained to Dr. Zerzan about doctors switching seniors’ medications to hospital formulary drugs that aren’t covered under Part D, requiring pharmacists to switch the drugs back again. “From their standpoint, it takes a ton of work because hospitalists don’t know what’s on their formulary,” she says.
Miscommunication can wreak havoc in other ways. Dr. Zerzan recalls how her parents were hosting her grandmother in Oregon when she fell and broke her pelvis. At the hospital, she arrived with two overlapping medication lists from her primary-care physician, cardiologist, and rheumatologist in California. The lists contained several combination pills that essentially duplicated her cholesterol and blood pressure medications. Instead of conducting a medication review, the hospital left the lists intact and added its own, sending her grandmother home with a “fistful of prescriptions.” Unsurprisingly, her blood pressure dipped dangerously. “She actually ended up going back into the hospital briefly to sort out her medications because it was such a mess,” Dr. Zerzan says.
Two-Way Conversation
Hospitalists generally don’t have the benefit of a longstanding relationship with their patients, says Ashley Beard, MD, PhD, a pharmaceutical policy research fellow in the Department of Ambulatory Care and Prevention at Harvard University. “And they’re dealing with people who are at their most vulnerable and least able to communicate effectively about what is going on in their lives.”
The virtual impossibility of knowing Part D formularies for every patient, she says, only increases the importance of effective bedside discussions and open-ended questions. “I think that communicating about costs really has been, and continues to be, a taboo subject in direct patient encounters, even though it is widely talked about in the research and popular press,” she says.
Likewise, hospitalists can intervene during transition planning, Dr. Beard says, when “the goal of the hospitalist is to stabilize the patient to be able to go out into the community and then have community follow-up care, preferably by a primary-care physician.” For people who don’t seek care regularly, she says, part of that stabilization can be a medication review that eliminates nonessential or harmful drugs and alleviates a patient’s financial burden.
Christine Lum Lung, MD, medical director of the independent Northern Colorado Hospitalists group, says a proactive discharge-planning department can be a huge help in coordinating such transitions of care. Her privately run group, affiliated with two private nonprofit hospitals in Loveland and Fort Collins, works closely with a “very active and involved” department that regularly meets with patients to assess financial issues. “Then they will approach us oftentimes with any concerns or issues with the discharge plan and medication,” she says.
Real-Time Solutions
Patient advocates have proposed a combination of other incentives to encourage better coordination among healthcare providers, including penalties for preventable rehospitalizations and a faster rollout of e-prescribing and electronic databases. Many hospitalists are particularly enthusiastic about the potential of electronic health records to assist them and their patients, though researchers like Soumerai are far less convinced about the merits of such a billion-dollar investment.
In the meantime, Dr. Lum Lung points to other low-cost solutions. At every workstation, her hospitals have posted details of the $4-a-month generic prescription programs offered by retailers like Target and Walmart. “I think it is probably prudent for us to be cognizant of that for everybody,” she says, “regardless of their insurance or payor source.”
For a recently discharged patient, one hospital Dr. Lum Lung works with proactively asked a pharmacist to run a few antibiotics through the patient’s insurance formulary to help pick the most cost-effective one. If a patient can’t afford the drug, the discharge-planning department can look into local drug assistance programs or the hospital’s voucher system, which allows medications to be filled by an in-house pharmacy. “We don’t want to—especially right now—make somebody have to make a choice between making their mortgage or rent payment or paying for a very expensive medication,” she says.
With so much information coming at them at once, hospitalists say, patients may need to be monitored once they get home. And with limited medical resources, physicians must constantly ask themselves whether they’re using the most appropriate and least expensive medications for every patient. “The hospitalists, in particular, are the natural leaders for this kind of thinking,” Dr. Koretz says. “Thinking about medical problems not as isolated, patient-specific problems, but rather as problems of systems of care, and processes of care.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Madden JM, Graves AJ, Zhang F, et al. Cost-related medication nonadherence and spending on basic needs following implementation of Medicare Part D. JAMA. 2008;299(16):1922-1928.
Judy Zerzan, MD, MPH, was at a loss. A Health and Aging Policy Fellow and hospitalist at the University of Colorado Denver, Dr. Zerzan was examining a Medicare patient who was admitted to the hospital with an apparent urinary tract infection. But the same patient had been released from the hospital only five days earlier with an antibiotic prescription to treat an oddly similar infection.
The confusion only increased when lab cultures revealed an E. coli infection. It should have been sensitive to most antibiotics, especially to the brand-name moxifloxacin the patient said she had been taking since her last hospital stay.
Several days into the patient’s rehospitalization, a medical student finally cracked the case. “The medical student went in and started talking to her some more and learned that she didn’t fill the prescription because under her [insurance] plan, it was going to be something like $50, and she felt like she couldn’t afford it,” Dr. Zerzan recalls. “She felt really embarrassed about it, so she didn’t want to tell us that she didn’t fill it.”
The medical team sent the woman home with a $4 generic prescription. “She was much relieved,” Dr. Zerzan says. More importantly, the patient did not return to the hospital for a third stay.
Hospitalists might not see a $46 difference in drug pricing as a core consideration of patient care. But with many seniors enrolled in Medicare Part D’s prescription drug plan falling through holes in the partially privatized safety net, many agree that far more must be done to ensure that financial stress doesn’t lead to medical misfortune.
“It is an ethical issue,” says Stephen Soumerai, ScD, director of the Drug Policy Research Program and a professor in the Department of Ambulatory Care and Prevention at Harvard University. “ … It’s easy to target those people who are the most vulnerable in our society and, therefore, it is an opportunity to try to find ways for them to lower their problems of economic access to medicine.”
Soumerai calls cost-related medication nonadherence a matter of distributive justice. In a study published last year in the Journal of the American Medical Association, he and 10 co-authors found that even after enrolling in Medicare Part D, the sickest beneficiaries were just as likely to skip medications they couldn’t afford.1
Identify the Coverage Gap
Medicare’s prescription drug plan, initiated in 2006, has provided coverage for many beneficiaries who previously went without. But it has been widely criticized as unnecessarily confusing by both doctors and patients—and particularly expensive for beneficiaries unlucky enough to fall into its notorious gap in coverage, dubbed the “doughnut hole” (see “Medicare Part D: The Basics,” right).
That economic burden can be exacerbated by medical illiteracy, ignorance, and misinformation. Recent Consumer Reports polls suggest as few as 4% of patients discuss drug prices with their doctors; almost half of Americans have reservations or misgivings about lower-cost generic drugs.
As focal points in the coordination of patient care, hospitalists are better positioned than most to help steer the most vulnerable away from the douhgnut hole while helping hospitals equitably distribute limited resources. But hospitalists often are completely unaware of a patient’s plight. “My research interest is prescription drug coverage, so I think I’m more keyed into it, but certainly even I don’t generally think about, when discharging a patient, if something is going to be on their Part D formulary or not, or what sort of prior-authorization hoops their primary-care doc may have to go through,” Dr. Zerzan says. “And I think that’s generally true of my colleagues as well.”
With tight schedules, a limited personal history with patients, disparities in local resources, and a litany of cost-control measures established by insurers, even hospitalists in the know concede that helping Medicare patients manage drug costs can be an exercise in frustration. As a result, patients are often left with medications that require higher cost-sharing or aren’t even on a plan’s formulary, forcing them to pay out-of-pocket for a prescription. Adding insult to injury, any money spent on a medication not covered by a Part D plan doesn’t count toward getting a patient out of the doughnut hole.
The Extra Mile
Jocelyne Watrous, a Medicare beneficiary consultant at the Willimantic, Conn.-based Center for Medicare Advocacy, says drug affordability while in the doughnut hole is a hardship for many. But so are specialty drug copays that range from 25% to 33% of the total price (see Table 1, below). For expensive prescriptions, Watrous says, hospitalists can get the name of a patient’s Part D formulary from the membership card and check for restrictions, such as prior authorization, quantity limits, or step therapy. “This is a terrible burden to place on physicians and their staffs, but nothing is worse than having the patient come back to the hospital via the ER because they could not get the drug prescribed by their doctor,” she says. “Best to square it all away before discharge, if possible.”
Brandon Koretz, MD, an associate clinical professor of geriatric medicine at the University of California at Los Angeles, says keeping track of differences among the dozens of Part D plans isn’t feasible. “Oftentimes, what happens is, you find yourself writing a prescription for what you think is a reasonable and cost-effective treatment, only to find out that drug A is not on insurance company B’s formulary, but drug C is,” Dr. Koretz says.
And if doctors are confused by the array of Part D formularies, hospitalists wonder, how can geriatric patients be expected to navigate the system, especially given the not-insignificant number with cognitive impairments?
Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C., compares the consumer paralysis created by the proliferation of prescription drug plans to walking by a store display featuring 20 brands of jam. “You’re kind of awed by it, but you don’t buy anything because you’re kind of intimidated,” he says. Only instead of 20 varieties, the typical local government agency offered 48 competing Part D plans in November 2006, with some boasting more than 70. In a new study sponsored by the Henry J. Kaiser Family Foundation, Massachusetts Institute of Technology economist Jonathan Gruber found that when seniors made a decision, only 6% to 9% chose the least expensive plan, while the remaining seniors paid an extra $360 to $520 annually (www.kff.org/medicare/7864.cfm).
All too often, economic problems are simply transferred to other providers. Nursing home pharmacists have complained to Dr. Zerzan about doctors switching seniors’ medications to hospital formulary drugs that aren’t covered under Part D, requiring pharmacists to switch the drugs back again. “From their standpoint, it takes a ton of work because hospitalists don’t know what’s on their formulary,” she says.
Miscommunication can wreak havoc in other ways. Dr. Zerzan recalls how her parents were hosting her grandmother in Oregon when she fell and broke her pelvis. At the hospital, she arrived with two overlapping medication lists from her primary-care physician, cardiologist, and rheumatologist in California. The lists contained several combination pills that essentially duplicated her cholesterol and blood pressure medications. Instead of conducting a medication review, the hospital left the lists intact and added its own, sending her grandmother home with a “fistful of prescriptions.” Unsurprisingly, her blood pressure dipped dangerously. “She actually ended up going back into the hospital briefly to sort out her medications because it was such a mess,” Dr. Zerzan says.
Two-Way Conversation
Hospitalists generally don’t have the benefit of a longstanding relationship with their patients, says Ashley Beard, MD, PhD, a pharmaceutical policy research fellow in the Department of Ambulatory Care and Prevention at Harvard University. “And they’re dealing with people who are at their most vulnerable and least able to communicate effectively about what is going on in their lives.”
The virtual impossibility of knowing Part D formularies for every patient, she says, only increases the importance of effective bedside discussions and open-ended questions. “I think that communicating about costs really has been, and continues to be, a taboo subject in direct patient encounters, even though it is widely talked about in the research and popular press,” she says.
Likewise, hospitalists can intervene during transition planning, Dr. Beard says, when “the goal of the hospitalist is to stabilize the patient to be able to go out into the community and then have community follow-up care, preferably by a primary-care physician.” For people who don’t seek care regularly, she says, part of that stabilization can be a medication review that eliminates nonessential or harmful drugs and alleviates a patient’s financial burden.
Christine Lum Lung, MD, medical director of the independent Northern Colorado Hospitalists group, says a proactive discharge-planning department can be a huge help in coordinating such transitions of care. Her privately run group, affiliated with two private nonprofit hospitals in Loveland and Fort Collins, works closely with a “very active and involved” department that regularly meets with patients to assess financial issues. “Then they will approach us oftentimes with any concerns or issues with the discharge plan and medication,” she says.
Real-Time Solutions
Patient advocates have proposed a combination of other incentives to encourage better coordination among healthcare providers, including penalties for preventable rehospitalizations and a faster rollout of e-prescribing and electronic databases. Many hospitalists are particularly enthusiastic about the potential of electronic health records to assist them and their patients, though researchers like Soumerai are far less convinced about the merits of such a billion-dollar investment.
In the meantime, Dr. Lum Lung points to other low-cost solutions. At every workstation, her hospitals have posted details of the $4-a-month generic prescription programs offered by retailers like Target and Walmart. “I think it is probably prudent for us to be cognizant of that for everybody,” she says, “regardless of their insurance or payor source.”
For a recently discharged patient, one hospital Dr. Lum Lung works with proactively asked a pharmacist to run a few antibiotics through the patient’s insurance formulary to help pick the most cost-effective one. If a patient can’t afford the drug, the discharge-planning department can look into local drug assistance programs or the hospital’s voucher system, which allows medications to be filled by an in-house pharmacy. “We don’t want to—especially right now—make somebody have to make a choice between making their mortgage or rent payment or paying for a very expensive medication,” she says.
With so much information coming at them at once, hospitalists say, patients may need to be monitored once they get home. And with limited medical resources, physicians must constantly ask themselves whether they’re using the most appropriate and least expensive medications for every patient. “The hospitalists, in particular, are the natural leaders for this kind of thinking,” Dr. Koretz says. “Thinking about medical problems not as isolated, patient-specific problems, but rather as problems of systems of care, and processes of care.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Madden JM, Graves AJ, Zhang F, et al. Cost-related medication nonadherence and spending on basic needs following implementation of Medicare Part D. JAMA. 2008;299(16):1922-1928.
Judy Zerzan, MD, MPH, was at a loss. A Health and Aging Policy Fellow and hospitalist at the University of Colorado Denver, Dr. Zerzan was examining a Medicare patient who was admitted to the hospital with an apparent urinary tract infection. But the same patient had been released from the hospital only five days earlier with an antibiotic prescription to treat an oddly similar infection.
The confusion only increased when lab cultures revealed an E. coli infection. It should have been sensitive to most antibiotics, especially to the brand-name moxifloxacin the patient said she had been taking since her last hospital stay.
Several days into the patient’s rehospitalization, a medical student finally cracked the case. “The medical student went in and started talking to her some more and learned that she didn’t fill the prescription because under her [insurance] plan, it was going to be something like $50, and she felt like she couldn’t afford it,” Dr. Zerzan recalls. “She felt really embarrassed about it, so she didn’t want to tell us that she didn’t fill it.”
The medical team sent the woman home with a $4 generic prescription. “She was much relieved,” Dr. Zerzan says. More importantly, the patient did not return to the hospital for a third stay.
Hospitalists might not see a $46 difference in drug pricing as a core consideration of patient care. But with many seniors enrolled in Medicare Part D’s prescription drug plan falling through holes in the partially privatized safety net, many agree that far more must be done to ensure that financial stress doesn’t lead to medical misfortune.
“It is an ethical issue,” says Stephen Soumerai, ScD, director of the Drug Policy Research Program and a professor in the Department of Ambulatory Care and Prevention at Harvard University. “ … It’s easy to target those people who are the most vulnerable in our society and, therefore, it is an opportunity to try to find ways for them to lower their problems of economic access to medicine.”
Soumerai calls cost-related medication nonadherence a matter of distributive justice. In a study published last year in the Journal of the American Medical Association, he and 10 co-authors found that even after enrolling in Medicare Part D, the sickest beneficiaries were just as likely to skip medications they couldn’t afford.1
Identify the Coverage Gap
Medicare’s prescription drug plan, initiated in 2006, has provided coverage for many beneficiaries who previously went without. But it has been widely criticized as unnecessarily confusing by both doctors and patients—and particularly expensive for beneficiaries unlucky enough to fall into its notorious gap in coverage, dubbed the “doughnut hole” (see “Medicare Part D: The Basics,” right).
That economic burden can be exacerbated by medical illiteracy, ignorance, and misinformation. Recent Consumer Reports polls suggest as few as 4% of patients discuss drug prices with their doctors; almost half of Americans have reservations or misgivings about lower-cost generic drugs.
As focal points in the coordination of patient care, hospitalists are better positioned than most to help steer the most vulnerable away from the douhgnut hole while helping hospitals equitably distribute limited resources. But hospitalists often are completely unaware of a patient’s plight. “My research interest is prescription drug coverage, so I think I’m more keyed into it, but certainly even I don’t generally think about, when discharging a patient, if something is going to be on their Part D formulary or not, or what sort of prior-authorization hoops their primary-care doc may have to go through,” Dr. Zerzan says. “And I think that’s generally true of my colleagues as well.”
With tight schedules, a limited personal history with patients, disparities in local resources, and a litany of cost-control measures established by insurers, even hospitalists in the know concede that helping Medicare patients manage drug costs can be an exercise in frustration. As a result, patients are often left with medications that require higher cost-sharing or aren’t even on a plan’s formulary, forcing them to pay out-of-pocket for a prescription. Adding insult to injury, any money spent on a medication not covered by a Part D plan doesn’t count toward getting a patient out of the doughnut hole.
The Extra Mile
Jocelyne Watrous, a Medicare beneficiary consultant at the Willimantic, Conn.-based Center for Medicare Advocacy, says drug affordability while in the doughnut hole is a hardship for many. But so are specialty drug copays that range from 25% to 33% of the total price (see Table 1, below). For expensive prescriptions, Watrous says, hospitalists can get the name of a patient’s Part D formulary from the membership card and check for restrictions, such as prior authorization, quantity limits, or step therapy. “This is a terrible burden to place on physicians and their staffs, but nothing is worse than having the patient come back to the hospital via the ER because they could not get the drug prescribed by their doctor,” she says. “Best to square it all away before discharge, if possible.”
Brandon Koretz, MD, an associate clinical professor of geriatric medicine at the University of California at Los Angeles, says keeping track of differences among the dozens of Part D plans isn’t feasible. “Oftentimes, what happens is, you find yourself writing a prescription for what you think is a reasonable and cost-effective treatment, only to find out that drug A is not on insurance company B’s formulary, but drug C is,” Dr. Koretz says.
And if doctors are confused by the array of Part D formularies, hospitalists wonder, how can geriatric patients be expected to navigate the system, especially given the not-insignificant number with cognitive impairments?
Bill Vaughan, a health policy analyst for Consumers Union in Washington, D.C., compares the consumer paralysis created by the proliferation of prescription drug plans to walking by a store display featuring 20 brands of jam. “You’re kind of awed by it, but you don’t buy anything because you’re kind of intimidated,” he says. Only instead of 20 varieties, the typical local government agency offered 48 competing Part D plans in November 2006, with some boasting more than 70. In a new study sponsored by the Henry J. Kaiser Family Foundation, Massachusetts Institute of Technology economist Jonathan Gruber found that when seniors made a decision, only 6% to 9% chose the least expensive plan, while the remaining seniors paid an extra $360 to $520 annually (www.kff.org/medicare/7864.cfm).
All too often, economic problems are simply transferred to other providers. Nursing home pharmacists have complained to Dr. Zerzan about doctors switching seniors’ medications to hospital formulary drugs that aren’t covered under Part D, requiring pharmacists to switch the drugs back again. “From their standpoint, it takes a ton of work because hospitalists don’t know what’s on their formulary,” she says.
Miscommunication can wreak havoc in other ways. Dr. Zerzan recalls how her parents were hosting her grandmother in Oregon when she fell and broke her pelvis. At the hospital, she arrived with two overlapping medication lists from her primary-care physician, cardiologist, and rheumatologist in California. The lists contained several combination pills that essentially duplicated her cholesterol and blood pressure medications. Instead of conducting a medication review, the hospital left the lists intact and added its own, sending her grandmother home with a “fistful of prescriptions.” Unsurprisingly, her blood pressure dipped dangerously. “She actually ended up going back into the hospital briefly to sort out her medications because it was such a mess,” Dr. Zerzan says.
Two-Way Conversation
Hospitalists generally don’t have the benefit of a longstanding relationship with their patients, says Ashley Beard, MD, PhD, a pharmaceutical policy research fellow in the Department of Ambulatory Care and Prevention at Harvard University. “And they’re dealing with people who are at their most vulnerable and least able to communicate effectively about what is going on in their lives.”
The virtual impossibility of knowing Part D formularies for every patient, she says, only increases the importance of effective bedside discussions and open-ended questions. “I think that communicating about costs really has been, and continues to be, a taboo subject in direct patient encounters, even though it is widely talked about in the research and popular press,” she says.
Likewise, hospitalists can intervene during transition planning, Dr. Beard says, when “the goal of the hospitalist is to stabilize the patient to be able to go out into the community and then have community follow-up care, preferably by a primary-care physician.” For people who don’t seek care regularly, she says, part of that stabilization can be a medication review that eliminates nonessential or harmful drugs and alleviates a patient’s financial burden.
Christine Lum Lung, MD, medical director of the independent Northern Colorado Hospitalists group, says a proactive discharge-planning department can be a huge help in coordinating such transitions of care. Her privately run group, affiliated with two private nonprofit hospitals in Loveland and Fort Collins, works closely with a “very active and involved” department that regularly meets with patients to assess financial issues. “Then they will approach us oftentimes with any concerns or issues with the discharge plan and medication,” she says.
Real-Time Solutions
Patient advocates have proposed a combination of other incentives to encourage better coordination among healthcare providers, including penalties for preventable rehospitalizations and a faster rollout of e-prescribing and electronic databases. Many hospitalists are particularly enthusiastic about the potential of electronic health records to assist them and their patients, though researchers like Soumerai are far less convinced about the merits of such a billion-dollar investment.
In the meantime, Dr. Lum Lung points to other low-cost solutions. At every workstation, her hospitals have posted details of the $4-a-month generic prescription programs offered by retailers like Target and Walmart. “I think it is probably prudent for us to be cognizant of that for everybody,” she says, “regardless of their insurance or payor source.”
For a recently discharged patient, one hospital Dr. Lum Lung works with proactively asked a pharmacist to run a few antibiotics through the patient’s insurance formulary to help pick the most cost-effective one. If a patient can’t afford the drug, the discharge-planning department can look into local drug assistance programs or the hospital’s voucher system, which allows medications to be filled by an in-house pharmacy. “We don’t want to—especially right now—make somebody have to make a choice between making their mortgage or rent payment or paying for a very expensive medication,” she says.
With so much information coming at them at once, hospitalists say, patients may need to be monitored once they get home. And with limited medical resources, physicians must constantly ask themselves whether they’re using the most appropriate and least expensive medications for every patient. “The hospitalists, in particular, are the natural leaders for this kind of thinking,” Dr. Koretz says. “Thinking about medical problems not as isolated, patient-specific problems, but rather as problems of systems of care, and processes of care.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Madden JM, Graves AJ, Zhang F, et al. Cost-related medication nonadherence and spending on basic needs following implementation of Medicare Part D. JAMA. 2008;299(16):1922-1928.