User login
Teduglutide Trims Parenteral Support in Short Bowel Syndrome
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
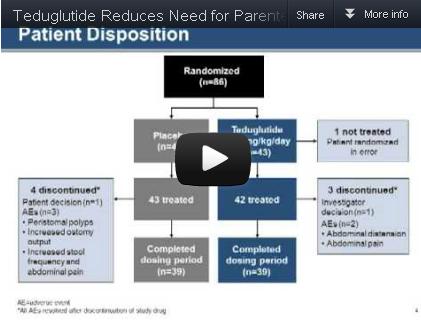
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.

|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Patients with short bowel syndrome whose absorption is insufficient to maintain nutritional or fluid autonomy have intestinal failure. These patients, particularly those with proximal jejunostomies, who may actually secrete more fluid than they ingest, are among the most complex and challenging to manage of patients with any gastrointestinal disease. Patients with short bowel syndrome and intestinal failure are dependent on parenteral nutrition and/or fluid support (PS) to maintain life. This therapy has substantial implications for employment, activities, sleep, and finances. Numerous, often life-threatening, complications develop.
|
|
|
A myriad of growth factors may be involved in the process of postresection intestinal adaptation, including glucagonlike peptide-2 (GLP-2), wherein intestinal epithelial growth is promoted. Teduglutide is a long-acting analog of native GLP-2 and is somewhat more resistant to enzymatic degradation in the enterocyte than is the native enzyme. Dr. Jeppesen and colleagues reported a sustained 20%-100% decrease in PS volume requirements during weeks 20-24 of treatment in 63% of patients who received teduglutide, compared with 30% of placebo-treated patients. The mean drop in weekly PS volume from baseline to week 24 totaled 4.4 L in patients who received teduglutide, which equates to a decrease of 1-2 nights of infusion weekly, a very profound improvement for individual patients. The PS weaning protocol used was similar to that used in most centers experienced in the care of these patients.
As would be expected in the SBS-IF patient population, there were many adverse events, although these were equally distributed across teduglutide and placebo groups. Stomal changes, primarily related to enlargement, were evident in a significant minority of patients in the teduglutide group, as would be expected given the hyperplastic effect of the medication on intestinal epithelial tissue.Concern has been raised about GLP-2’s potential to stimulate the development of colonic adenomas in rodent models. Although the risk for malignancy is hypothetical in humans, colonoscopy should be considered at baseline for those patients with residual colons and perhaps as frequently as annually while the patients are on therapy until more long-term safety data are available.
Is teduglutide a "game changer"? The only patients who will be able to discontinue PS completely will be those who are on the borderline between nutritional autonomy and PS dependence. It is important to realize that teduglutide should be used to augment, not replace conventional management. What happens when teduglutide is stopped? Preliminary evidence suggests the effects on adaptation may be persistent, although earlier study noted that histologic changes trended toward baseline within 4 weeks of discontinuation. Perhaps longer treatment or maintenance will be required. The real future is an artificially grown and harvested intestine; even intestinal transplantation represents a bridge at best.
Dr. Alan L. Buchman is a former professor of medicine and surgery at the Feinberg School of Medicine at Northwestern University, Chicago. Within the past 12 months he has consulted for Takeda Pharmaceuticals and NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Teduglutide significantly reduced the need for parenteral support in patients with short bowel syndrome and intestinal failure, based on data from 85 adults in a randomized, controlled multicenter trial. The findings were published in the December issue of Gastroenterology.
Patients with short bowel syndrome and intestinal failure (SBS-IF) have inadequate intestinal absorption and require parenteral support (PS) to maintain fluids, electrolytes, trace elements, vitamins, and nutrient balances, said Dr. Palle Bekker Jeppesen of Rigshospitalet in Copenhagen and colleagues.
Source: American Gastroenterological Association
Data from previous open-label studies suggest an association between teduglutide and clinically meaningful reductions in wet weight and energy, which may reduce the need for PS in these patients, the investigators noted.
The researchers randomized 86 adults with SBS-IF to either 0.05 mg/kg per day of teduglutide or a placebo. One patient was randomized in error; complete data were available for 42 teduglutide patients and 43 placebo patients.
Significantly more patients in the teduglutide group responded to treatment, compared with the placebo group (63% vs. 30%). This response was defined as sustaining a 20%-100% reduction from baseline in weekly PS volume during weeks 20-24. "Small bowel length did not appear to be a predictor of response," the researchers noted.
The high placebo response may be explained by examining the fluid composite effect, a measure of the combined effects of teduglutide on PS volume reduction as well as the ability to reduce oral fluid intake and increase urine output volume, the researchers noted.
"In the current study, where protocol modifications encouraged earlier and more aggressive PS reductions, significantly larger PS reductions were also achieved in patients receiving placebo, but subsequently these patients had to increase their oral fluid intake significantly to maintain urine production and hydration constant," they said.
After 24 weeks, overall PS volume was reduced by 32% from baseline in teduglutide patients, compared with 21% in placebo patients. Although no patients in either group were completely weaned from parenteral support at 24 weeks, the difference in PS volume reduction was significantly greater in the teduglutide group.
The average weekly PS volume in teduglutide patients decreased significantly from 12.5 L/wk at baseline to 8.1 L/wk at week 24. The placebo patients also had a significant decrease in average weekly PS volume, from 13.4 L/wk at baseline to 11.1 L/wk at week 24.
Treatment-ending adverse events were similar between the two groups; 5% of teduglutide patients and 7% of placebo patients discontinued treatment because of such events during the study period. The most frequently reported treatment-emergent adverse events included abdominal pain, abdominal distension, nausea, and gastrointestinal stoma complications.
Although the study did not specifically assess quality of life measures, significantly more teduglutide patients had at least 1 day off PS, compared with placebo patients, which could help to "liberate considerable time for unhindered daytime activities or undisturbed sleep," the researchers said.
The study did not address the possible benefit of teduglutide therapy earlier in the course of SBS, or the duration of effect after patients discontinued teduglutide, the researchers added.
However, the findings indicate that teduglutide was safe and well tolerated, and "could positively add to the limited treatment armamentarium" for patients with SBS-IF.
Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
FROM GASTROENTEROLOGY
Major Finding: Significantly more patients who received 0.05 mg/kg per day of teduglutide had a sustained response to treatment during weeks 20-24, compared with the placebo group (63% vs. 30%).
Data Source: The data come from a randomized, controlled multicenter trial of 85 adults with short bowel syndrome and intestinal failure.
Disclosures: Dr. Jeppesen and several coauthors have served on the advisory board of and as consultants to NPS Pharmaceuticals, the company that funded the study. One author is an employee of NPS Pharmaceuticals.
Factors Associated With Finding Capsule Endoscopy Lesions
Videocapsule endoscopy’s success at identifying the cause of obscure gastrointestinal bleeding was found to be associated with markedly different clinical factors in two separate studies published in the December issue of Clinical Gastroenterology and Hepatology.
Capsule endoscopy allows visualization of the entire small bowel. Knowing which factors are associated with positive findings on capsule endoscopy would allow more appropriate patient selection for the procedure. This in turn would improve its diagnostic yield and maximize resource utilization.
Unfortunately, no single factor was found to accurately predict the success of this form of endoscopy in patients who presented with obscure gastrointestinal bleeding (OGIB) and who had negative or ambiguous findings on upper and lower endoscopies. In fact, the two studies identified entirely different predictors.
In the first study, Dr. Neal C. Shahidi and his associates at the University of British Columbia, Vancouver, reviewed the records of all 698 capsule endoscopies performed at St. Paul’s Hospital in 2001-2011 for the indication of OGIB. Mean patient age was 63 years, and the cohort was equally composed of men and women.
Approximately 48% of these study subjects presented with overt bleeding: hematemesis, hematochezia, or melena. The other 52% presented with occult bleeding evidenced by a positive fecal occult blood test (28%), iron deficiency anemia (21%), or an acute drop in hemoglobin (3%). No causes for the bleeding were identified on conventional esophagogastroduodenoscopy, intraoperative enteroscopy, or colonoscopy.
In approximately 4% of cases, capsule endoscopy failed for technical reasons, including limited visualization because of excessive debris, failure of the videocapsule to enter the small bowel within the procedure time, or inadequate viewing of the small bowel.
Capsule endoscopy definitively identified the cause of the bleeding – ulcerations/erosions, masses, vascular lesions, or visible blood – in 42% of these cases. Most were localized to the small bowel, although 18% were found in the stomach or cecum.
Even though the investigators "rigorously assessed" symptoms, other clinical factors, and patient characteristics such as smoking status, alcohol consumption, and a variety of comorbid conditions, the only factors found to be significantly associated with positive findings on capsule endoscopy were a high number of esophagogastroduodenoscopies leading up to the procedure (odds ratio 1.17), an increase in the need for transfusions (3-9 transfusions, OR 1.70; 10 or more, OR 2.72), and the presence of comorbid connective-tissue disease (OR 2.24).
This is the first report in the literature linking connective-tissue disease with positive findings on capsule endoscopy. There were 41 patients with rheumatoid arthritis, polymyalgia rheumatica, scleroderma, or other connective-tissue disorders in this series.
The increased frequency of positive capsule endoscopy in this subgroup of patients may be due in part to their predisposition to vascular lesions. Alternatively, connective-tissue disease may simply be a marker for the regular use of NSAIDs, Dr. Shahidi and his associates said.
Regarding the association with an increasing need for transfusions, "it is acceptable to presume that a patient’s transfusion requirements may be a marker for ongoing or severe pathology within the gastrointestinal tract," they noted.
Similarly, more frequent esophagogastroduodenoscopies may be another marker for ongoing GI bleeding, "as patients who continue to experience significant bleeding may undergo more endoscopic assessment," they added.
In the second study, Dr. Lucie Lepileur of the University of Rouen (France) and her colleagues reviewed the records on 911 capsule endoscopies performed for OGIB at two university referral centers during 2004-2010.
All the study subjects had undergone upper and lower endoscopies that were deemed negative or insufficient to explain their symptoms. A total of 41% presented with overt bleeding, chiefly melena and hematochezia, and the remaining 59% had occult bleeding.
Capsule endoscopy failed for technical reasons in approximately 1% of the cohort. It permitted a definitive diagnosis in 56%, including 203 angioectasias, 88 ulcerations, 70 tumors, 24 varices, and 6 diverticula of the small bowel. The procedure also identified lesions in the esophagus or stomach and the colon.
In another 8% of patients, capsule endoscopy revealed signs of suspected recent bleeding such as residual blood, clots, or red spots, but didn’t identify a specific lesion. The procedure failed to reveal any possible source of bleeding in the remaining 35% of cases.
The only factors found to be significantly associated with positive findings on capsule endoscopy were a history of overt bleeding (OR 3.8), male gender (OR 1.4), age of more than 60 years (OR 1.4), and inpatient status (OR 1.3). Conversely, female gender was the only factor found to be predictive of a nondiagnostic procedure.
The link with advanced age "can easily be explained by the more frequent occurrence of angioectasia in the elderly, which was the main bleeding lesion found in our series," Dr. Lepileur and her colleagues wrote.
The link with inpatient status likely reflects the more fragile health or more critical bleeding among patients who are hospitalized than among outpatients.
The finding that capsule endoscopy is more fruitful in men and less so in women suggests that the cause of chronic blood loss among women may be gynecologic rather than gastrointestinal in nature, the researchers said.
Neither Dr. Shahidi nor Dr. Lepileur reported any potential financial conflicts of interest.
Obscure gastrointestinal hemorrhage (OGIB) is defined as the presence of overt or obscure gastrointestinal bleeding after standard upper and lower endoscopic examinations fail to detect a significant bleeding source. While only 5% of patients with OGIB ultimately are found to have a small bowel source, resources required in their management can be substantial. Videocapsule endoscopy (VCE) has been recommended as the third diagnostic test in patients with OGIB. The diagnostic yield has been enhanced by administration of a bowel preparation when the examination is performed within 2 weeks of a bleeding episode.
|
|
|
Dr. Lauren B. Gerson
|

The published diagnostic yield of VCE examinations for OGIB is approximately 40-50%. A prior study that included 707 VCE studies demonstrated that male inpatients had higher rates of VCE findings both inside and outside of the small bowel (Gastrointest. Endosc. 2011;74:1061-6). Two studies published in CGH have now further analyzed whether there are specific risk factors associated with positive VCE findings. The first article from Canada included 698 VCE studies (diagnostic yield 42%, 7% inpatients) and found that factors associated with positive findings included number of upper endoscopic examinations, high transfusional requirements, diabetes, and presence of connective tissue disorders. Ulcerations, vascular lesions, and AVMs were the most common findings, and 20% had lesions outside the small bowel. The second study that examined 911 patients in France (diagnostic rate 56%, 15% inpatients) found that risk factors associated with positive VCE findings included age over 60, male gender, history of overt bleeding, and current hospitalization. Similar to other series, small bowel AVMs were the most common finding and 15% had significant findings outside the small bowel. These studies, in addition to the prior literature, raise important concerns about performance of VCE if maximizing diagnostic yield is the ultimate goal. Factors associated with higher yields based on the literature include inpatient status, higher transfusional requirements, presence of comorbid conditions, male gender, and advanced age. Whether VCE should continue to be performed in populations at lower risk for small bowel pathology deserves ongoing evaluation.
Lauren B. Gerson, M.D., is an associate professor of medicine and gastroenterology at Stanford University, Redwood City, Calif. She reported receiving grant support from Capsovision Inc.
Obscure gastrointestinal hemorrhage (OGIB) is defined as the presence of overt or obscure gastrointestinal bleeding after standard upper and lower endoscopic examinations fail to detect a significant bleeding source. While only 5% of patients with OGIB ultimately are found to have a small bowel source, resources required in their management can be substantial. Videocapsule endoscopy (VCE) has been recommended as the third diagnostic test in patients with OGIB. The diagnostic yield has been enhanced by administration of a bowel preparation when the examination is performed within 2 weeks of a bleeding episode.
|
|
|
Dr. Lauren B. Gerson
|
The published diagnostic yield of VCE examinations for OGIB is approximately 40-50%. A prior study that included 707 VCE studies demonstrated that male inpatients had higher rates of VCE findings both inside and outside of the small bowel (Gastrointest. Endosc. 2011;74:1061-6). Two studies published in CGH have now further analyzed whether there are specific risk factors associated with positive VCE findings. The first article from Canada included 698 VCE studies (diagnostic yield 42%, 7% inpatients) and found that factors associated with positive findings included number of upper endoscopic examinations, high transfusional requirements, diabetes, and presence of connective tissue disorders. Ulcerations, vascular lesions, and AVMs were the most common findings, and 20% had lesions outside the small bowel. The second study that examined 911 patients in France (diagnostic rate 56%, 15% inpatients) found that risk factors associated with positive VCE findings included age over 60, male gender, history of overt bleeding, and current hospitalization. Similar to other series, small bowel AVMs were the most common finding and 15% had significant findings outside the small bowel. These studies, in addition to the prior literature, raise important concerns about performance of VCE if maximizing diagnostic yield is the ultimate goal. Factors associated with higher yields based on the literature include inpatient status, higher transfusional requirements, presence of comorbid conditions, male gender, and advanced age. Whether VCE should continue to be performed in populations at lower risk for small bowel pathology deserves ongoing evaluation.
Lauren B. Gerson, M.D., is an associate professor of medicine and gastroenterology at Stanford University, Redwood City, Calif. She reported receiving grant support from Capsovision Inc.
Obscure gastrointestinal hemorrhage (OGIB) is defined as the presence of overt or obscure gastrointestinal bleeding after standard upper and lower endoscopic examinations fail to detect a significant bleeding source. While only 5% of patients with OGIB ultimately are found to have a small bowel source, resources required in their management can be substantial. Videocapsule endoscopy (VCE) has been recommended as the third diagnostic test in patients with OGIB. The diagnostic yield has been enhanced by administration of a bowel preparation when the examination is performed within 2 weeks of a bleeding episode.
|
|
|
Dr. Lauren B. Gerson
|
The published diagnostic yield of VCE examinations for OGIB is approximately 40-50%. A prior study that included 707 VCE studies demonstrated that male inpatients had higher rates of VCE findings both inside and outside of the small bowel (Gastrointest. Endosc. 2011;74:1061-6). Two studies published in CGH have now further analyzed whether there are specific risk factors associated with positive VCE findings. The first article from Canada included 698 VCE studies (diagnostic yield 42%, 7% inpatients) and found that factors associated with positive findings included number of upper endoscopic examinations, high transfusional requirements, diabetes, and presence of connective tissue disorders. Ulcerations, vascular lesions, and AVMs were the most common findings, and 20% had lesions outside the small bowel. The second study that examined 911 patients in France (diagnostic rate 56%, 15% inpatients) found that risk factors associated with positive VCE findings included age over 60, male gender, history of overt bleeding, and current hospitalization. Similar to other series, small bowel AVMs were the most common finding and 15% had significant findings outside the small bowel. These studies, in addition to the prior literature, raise important concerns about performance of VCE if maximizing diagnostic yield is the ultimate goal. Factors associated with higher yields based on the literature include inpatient status, higher transfusional requirements, presence of comorbid conditions, male gender, and advanced age. Whether VCE should continue to be performed in populations at lower risk for small bowel pathology deserves ongoing evaluation.
Lauren B. Gerson, M.D., is an associate professor of medicine and gastroenterology at Stanford University, Redwood City, Calif. She reported receiving grant support from Capsovision Inc.
Videocapsule endoscopy’s success at identifying the cause of obscure gastrointestinal bleeding was found to be associated with markedly different clinical factors in two separate studies published in the December issue of Clinical Gastroenterology and Hepatology.
Capsule endoscopy allows visualization of the entire small bowel. Knowing which factors are associated with positive findings on capsule endoscopy would allow more appropriate patient selection for the procedure. This in turn would improve its diagnostic yield and maximize resource utilization.
Unfortunately, no single factor was found to accurately predict the success of this form of endoscopy in patients who presented with obscure gastrointestinal bleeding (OGIB) and who had negative or ambiguous findings on upper and lower endoscopies. In fact, the two studies identified entirely different predictors.
In the first study, Dr. Neal C. Shahidi and his associates at the University of British Columbia, Vancouver, reviewed the records of all 698 capsule endoscopies performed at St. Paul’s Hospital in 2001-2011 for the indication of OGIB. Mean patient age was 63 years, and the cohort was equally composed of men and women.
Approximately 48% of these study subjects presented with overt bleeding: hematemesis, hematochezia, or melena. The other 52% presented with occult bleeding evidenced by a positive fecal occult blood test (28%), iron deficiency anemia (21%), or an acute drop in hemoglobin (3%). No causes for the bleeding were identified on conventional esophagogastroduodenoscopy, intraoperative enteroscopy, or colonoscopy.
In approximately 4% of cases, capsule endoscopy failed for technical reasons, including limited visualization because of excessive debris, failure of the videocapsule to enter the small bowel within the procedure time, or inadequate viewing of the small bowel.
Capsule endoscopy definitively identified the cause of the bleeding – ulcerations/erosions, masses, vascular lesions, or visible blood – in 42% of these cases. Most were localized to the small bowel, although 18% were found in the stomach or cecum.
Even though the investigators "rigorously assessed" symptoms, other clinical factors, and patient characteristics such as smoking status, alcohol consumption, and a variety of comorbid conditions, the only factors found to be significantly associated with positive findings on capsule endoscopy were a high number of esophagogastroduodenoscopies leading up to the procedure (odds ratio 1.17), an increase in the need for transfusions (3-9 transfusions, OR 1.70; 10 or more, OR 2.72), and the presence of comorbid connective-tissue disease (OR 2.24).
This is the first report in the literature linking connective-tissue disease with positive findings on capsule endoscopy. There were 41 patients with rheumatoid arthritis, polymyalgia rheumatica, scleroderma, or other connective-tissue disorders in this series.
The increased frequency of positive capsule endoscopy in this subgroup of patients may be due in part to their predisposition to vascular lesions. Alternatively, connective-tissue disease may simply be a marker for the regular use of NSAIDs, Dr. Shahidi and his associates said.
Regarding the association with an increasing need for transfusions, "it is acceptable to presume that a patient’s transfusion requirements may be a marker for ongoing or severe pathology within the gastrointestinal tract," they noted.
Similarly, more frequent esophagogastroduodenoscopies may be another marker for ongoing GI bleeding, "as patients who continue to experience significant bleeding may undergo more endoscopic assessment," they added.
In the second study, Dr. Lucie Lepileur of the University of Rouen (France) and her colleagues reviewed the records on 911 capsule endoscopies performed for OGIB at two university referral centers during 2004-2010.
All the study subjects had undergone upper and lower endoscopies that were deemed negative or insufficient to explain their symptoms. A total of 41% presented with overt bleeding, chiefly melena and hematochezia, and the remaining 59% had occult bleeding.
Capsule endoscopy failed for technical reasons in approximately 1% of the cohort. It permitted a definitive diagnosis in 56%, including 203 angioectasias, 88 ulcerations, 70 tumors, 24 varices, and 6 diverticula of the small bowel. The procedure also identified lesions in the esophagus or stomach and the colon.
In another 8% of patients, capsule endoscopy revealed signs of suspected recent bleeding such as residual blood, clots, or red spots, but didn’t identify a specific lesion. The procedure failed to reveal any possible source of bleeding in the remaining 35% of cases.
The only factors found to be significantly associated with positive findings on capsule endoscopy were a history of overt bleeding (OR 3.8), male gender (OR 1.4), age of more than 60 years (OR 1.4), and inpatient status (OR 1.3). Conversely, female gender was the only factor found to be predictive of a nondiagnostic procedure.
The link with advanced age "can easily be explained by the more frequent occurrence of angioectasia in the elderly, which was the main bleeding lesion found in our series," Dr. Lepileur and her colleagues wrote.
The link with inpatient status likely reflects the more fragile health or more critical bleeding among patients who are hospitalized than among outpatients.
The finding that capsule endoscopy is more fruitful in men and less so in women suggests that the cause of chronic blood loss among women may be gynecologic rather than gastrointestinal in nature, the researchers said.
Neither Dr. Shahidi nor Dr. Lepileur reported any potential financial conflicts of interest.
Videocapsule endoscopy’s success at identifying the cause of obscure gastrointestinal bleeding was found to be associated with markedly different clinical factors in two separate studies published in the December issue of Clinical Gastroenterology and Hepatology.
Capsule endoscopy allows visualization of the entire small bowel. Knowing which factors are associated with positive findings on capsule endoscopy would allow more appropriate patient selection for the procedure. This in turn would improve its diagnostic yield and maximize resource utilization.
Unfortunately, no single factor was found to accurately predict the success of this form of endoscopy in patients who presented with obscure gastrointestinal bleeding (OGIB) and who had negative or ambiguous findings on upper and lower endoscopies. In fact, the two studies identified entirely different predictors.
In the first study, Dr. Neal C. Shahidi and his associates at the University of British Columbia, Vancouver, reviewed the records of all 698 capsule endoscopies performed at St. Paul’s Hospital in 2001-2011 for the indication of OGIB. Mean patient age was 63 years, and the cohort was equally composed of men and women.
Approximately 48% of these study subjects presented with overt bleeding: hematemesis, hematochezia, or melena. The other 52% presented with occult bleeding evidenced by a positive fecal occult blood test (28%), iron deficiency anemia (21%), or an acute drop in hemoglobin (3%). No causes for the bleeding were identified on conventional esophagogastroduodenoscopy, intraoperative enteroscopy, or colonoscopy.
In approximately 4% of cases, capsule endoscopy failed for technical reasons, including limited visualization because of excessive debris, failure of the videocapsule to enter the small bowel within the procedure time, or inadequate viewing of the small bowel.
Capsule endoscopy definitively identified the cause of the bleeding – ulcerations/erosions, masses, vascular lesions, or visible blood – in 42% of these cases. Most were localized to the small bowel, although 18% were found in the stomach or cecum.
Even though the investigators "rigorously assessed" symptoms, other clinical factors, and patient characteristics such as smoking status, alcohol consumption, and a variety of comorbid conditions, the only factors found to be significantly associated with positive findings on capsule endoscopy were a high number of esophagogastroduodenoscopies leading up to the procedure (odds ratio 1.17), an increase in the need for transfusions (3-9 transfusions, OR 1.70; 10 or more, OR 2.72), and the presence of comorbid connective-tissue disease (OR 2.24).
This is the first report in the literature linking connective-tissue disease with positive findings on capsule endoscopy. There were 41 patients with rheumatoid arthritis, polymyalgia rheumatica, scleroderma, or other connective-tissue disorders in this series.
The increased frequency of positive capsule endoscopy in this subgroup of patients may be due in part to their predisposition to vascular lesions. Alternatively, connective-tissue disease may simply be a marker for the regular use of NSAIDs, Dr. Shahidi and his associates said.
Regarding the association with an increasing need for transfusions, "it is acceptable to presume that a patient’s transfusion requirements may be a marker for ongoing or severe pathology within the gastrointestinal tract," they noted.
Similarly, more frequent esophagogastroduodenoscopies may be another marker for ongoing GI bleeding, "as patients who continue to experience significant bleeding may undergo more endoscopic assessment," they added.
In the second study, Dr. Lucie Lepileur of the University of Rouen (France) and her colleagues reviewed the records on 911 capsule endoscopies performed for OGIB at two university referral centers during 2004-2010.
All the study subjects had undergone upper and lower endoscopies that were deemed negative or insufficient to explain their symptoms. A total of 41% presented with overt bleeding, chiefly melena and hematochezia, and the remaining 59% had occult bleeding.
Capsule endoscopy failed for technical reasons in approximately 1% of the cohort. It permitted a definitive diagnosis in 56%, including 203 angioectasias, 88 ulcerations, 70 tumors, 24 varices, and 6 diverticula of the small bowel. The procedure also identified lesions in the esophagus or stomach and the colon.
In another 8% of patients, capsule endoscopy revealed signs of suspected recent bleeding such as residual blood, clots, or red spots, but didn’t identify a specific lesion. The procedure failed to reveal any possible source of bleeding in the remaining 35% of cases.
The only factors found to be significantly associated with positive findings on capsule endoscopy were a history of overt bleeding (OR 3.8), male gender (OR 1.4), age of more than 60 years (OR 1.4), and inpatient status (OR 1.3). Conversely, female gender was the only factor found to be predictive of a nondiagnostic procedure.
The link with advanced age "can easily be explained by the more frequent occurrence of angioectasia in the elderly, which was the main bleeding lesion found in our series," Dr. Lepileur and her colleagues wrote.
The link with inpatient status likely reflects the more fragile health or more critical bleeding among patients who are hospitalized than among outpatients.
The finding that capsule endoscopy is more fruitful in men and less so in women suggests that the cause of chronic blood loss among women may be gynecologic rather than gastrointestinal in nature, the researchers said.
Neither Dr. Shahidi nor Dr. Lepileur reported any potential financial conflicts of interest.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Major Finding: Videocapsule endoscopy’s ability to identify a causative lesion in cases of obscure gastrointestinal bleeding was associated with seven factors: a greater number of previous invasive endoscopies, an increased need for transfusions, comorbid connective-tissue disease, overt rather than occult bleeding, male gender, age over 60 years, and inpatient status.
Data Source: A retrospective review of 698 videocapsule endoscopies for OGIB performed at a single Canadian center during a 10-year period and another of 911 performed at two French centers over a 6-year period.
Disclosures: Neither Dr. Shahidi nor Dr. Lepileur reported any potential financial conflicts of interest.
Study Finds 'PPI Test' a Poor Predictor of GERD
Empiric acid suppression with the "PPI test," widely used to assess whether upper-GI symptoms are due to gastroesophageal reflux disease, actually performs poorly as a predictor of GERD, Dr. Peter Bytzer and his colleagues wrote in the December issue of Clinical Gastroenterology and Hepatology.
Typically, clinicians perform a PPI test to diagnose GERD without the need for endoscopy. They give patients a 2-week course of a proton pump inhibitor and then determine whether the brief treatment ameliorated upper GI symptoms. If so, the symptoms are assumed to be acid related, said Dr. Bytzer of Copenhagen University and his associates.
But in their study, such a PPI test "showed a disappointingly low validity" for diagnosing GERD, and couldn’t reliably distinguish between reflux esophagitis and nonerosive reflux disease. Even when combined with a clinical diagnosis made by a primary care physician, a clinical diagnosis made by a gastroenterologist, or the results of a detailed diagnostic questionnaire, the outcome of a PPI test didn’t add reliable information allowing clinicians to separate patients who had GERD from those who did not, the researchers said (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.06.030]).
Dr. Bytzer and his colleagues analyzed data originally collected in the DIAMOND clinical trial, an international study that found the Reflux Disease Questionnaire to be useful in diagnosing GERD among patients who consulted primary care physicians because of frequent upper GI symptoms. The DIAMOND study results indicated that unlike the Reflux Disease Questionnaire, PPI testing had very limited diagnostic value.
Dr. Bytzer and his associates performed more detailed analyses of the data, using different combinations of three main symptoms (heartburn, central chest pain, and dysphagia or regurgitation); different definitions of "PPI response"; and assessments of various subgroups of patients, all in the hope of improving the diagnostic yield of PPI testing. They compared the diagnostic usefulness of PPI testing against state-of-the-art comprehensive diagnostic work-ups for GERD in 299 of the DIAMOND study subjects.
"This large database provides the best platform so far to test whether there are better approaches for scoring a test of PPI therapy," the investigators noted.
All of the subjects underwent endoscopy with concomitant wireless esophageal pH monitoring and symptom assessment. They then completed the detailed Reflux Disease Questionnaire, and participated in a 2-week PPI test using esomeprazole (Nexium), during which they recorded GI symptoms in a diary.
A total of 69% of the patients who did have GERD showed a positive response to the PPI test. This means that 31% of the study participants with GERD were not identified by PPI testing.
Moreover, 51% of the patients who did not have GERD also showed a positive response to the PPI test, the investigators said.
Both patients who had GERD and patients who did not reported that their symptom response to acid suppression increased over the course of the first 5-6 days of treatment and then leveled off for the remaining 8-9 days.
The PPI test performed only marginally better across various subgroups of patients, such as those with GERD plus reflux esophagitis (as compared with patients who had GERD but no reflux esophagitis) or those whose physicians were certain of their GERD diagnosis (compared with patients whose physicians were uncertain about their GERD diagnosis).
For example, 48% of the study participants whose physicians predicted that they had GERD showed a positive response on PPI testing – a rate that was nearly identical to the 47% of study subjects whose physicians predicted that they had some disorder other than GERD.
Similarly, the PPI test performed only marginally better when different symptom combinations and different definitions of "PPI response" were assessed.
"In line with other researchers, we found that ... the clinical value of [the PPI test] is very limited," Dr. Bytzer and his colleagues said.
This study was funded by AstraZeneca. Dr. Bytzer reported ties to AstraZeneca, Boehringer Ingelheim, Eisai, Nycomed, Reckitt Benckiser, Takeda, and Wyeth, and his associates reported ties to numerous industry sources, including employment by AstraZeneca.
Empiric acid suppression with the "PPI test," widely used to assess whether upper-GI symptoms are due to gastroesophageal reflux disease, actually performs poorly as a predictor of GERD, Dr. Peter Bytzer and his colleagues wrote in the December issue of Clinical Gastroenterology and Hepatology.
Typically, clinicians perform a PPI test to diagnose GERD without the need for endoscopy. They give patients a 2-week course of a proton pump inhibitor and then determine whether the brief treatment ameliorated upper GI symptoms. If so, the symptoms are assumed to be acid related, said Dr. Bytzer of Copenhagen University and his associates.
But in their study, such a PPI test "showed a disappointingly low validity" for diagnosing GERD, and couldn’t reliably distinguish between reflux esophagitis and nonerosive reflux disease. Even when combined with a clinical diagnosis made by a primary care physician, a clinical diagnosis made by a gastroenterologist, or the results of a detailed diagnostic questionnaire, the outcome of a PPI test didn’t add reliable information allowing clinicians to separate patients who had GERD from those who did not, the researchers said (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.06.030]).
Dr. Bytzer and his colleagues analyzed data originally collected in the DIAMOND clinical trial, an international study that found the Reflux Disease Questionnaire to be useful in diagnosing GERD among patients who consulted primary care physicians because of frequent upper GI symptoms. The DIAMOND study results indicated that unlike the Reflux Disease Questionnaire, PPI testing had very limited diagnostic value.
Dr. Bytzer and his associates performed more detailed analyses of the data, using different combinations of three main symptoms (heartburn, central chest pain, and dysphagia or regurgitation); different definitions of "PPI response"; and assessments of various subgroups of patients, all in the hope of improving the diagnostic yield of PPI testing. They compared the diagnostic usefulness of PPI testing against state-of-the-art comprehensive diagnostic work-ups for GERD in 299 of the DIAMOND study subjects.
"This large database provides the best platform so far to test whether there are better approaches for scoring a test of PPI therapy," the investigators noted.
All of the subjects underwent endoscopy with concomitant wireless esophageal pH monitoring and symptom assessment. They then completed the detailed Reflux Disease Questionnaire, and participated in a 2-week PPI test using esomeprazole (Nexium), during which they recorded GI symptoms in a diary.
A total of 69% of the patients who did have GERD showed a positive response to the PPI test. This means that 31% of the study participants with GERD were not identified by PPI testing.
Moreover, 51% of the patients who did not have GERD also showed a positive response to the PPI test, the investigators said.
Both patients who had GERD and patients who did not reported that their symptom response to acid suppression increased over the course of the first 5-6 days of treatment and then leveled off for the remaining 8-9 days.
The PPI test performed only marginally better across various subgroups of patients, such as those with GERD plus reflux esophagitis (as compared with patients who had GERD but no reflux esophagitis) or those whose physicians were certain of their GERD diagnosis (compared with patients whose physicians were uncertain about their GERD diagnosis).
For example, 48% of the study participants whose physicians predicted that they had GERD showed a positive response on PPI testing – a rate that was nearly identical to the 47% of study subjects whose physicians predicted that they had some disorder other than GERD.
Similarly, the PPI test performed only marginally better when different symptom combinations and different definitions of "PPI response" were assessed.
"In line with other researchers, we found that ... the clinical value of [the PPI test] is very limited," Dr. Bytzer and his colleagues said.
This study was funded by AstraZeneca. Dr. Bytzer reported ties to AstraZeneca, Boehringer Ingelheim, Eisai, Nycomed, Reckitt Benckiser, Takeda, and Wyeth, and his associates reported ties to numerous industry sources, including employment by AstraZeneca.
Empiric acid suppression with the "PPI test," widely used to assess whether upper-GI symptoms are due to gastroesophageal reflux disease, actually performs poorly as a predictor of GERD, Dr. Peter Bytzer and his colleagues wrote in the December issue of Clinical Gastroenterology and Hepatology.
Typically, clinicians perform a PPI test to diagnose GERD without the need for endoscopy. They give patients a 2-week course of a proton pump inhibitor and then determine whether the brief treatment ameliorated upper GI symptoms. If so, the symptoms are assumed to be acid related, said Dr. Bytzer of Copenhagen University and his associates.
But in their study, such a PPI test "showed a disappointingly low validity" for diagnosing GERD, and couldn’t reliably distinguish between reflux esophagitis and nonerosive reflux disease. Even when combined with a clinical diagnosis made by a primary care physician, a clinical diagnosis made by a gastroenterologist, or the results of a detailed diagnostic questionnaire, the outcome of a PPI test didn’t add reliable information allowing clinicians to separate patients who had GERD from those who did not, the researchers said (Clin. Gastroenterol. Hepatol. 2012 [doi:10.1016/j.cgh.2012.06.030]).
Dr. Bytzer and his colleagues analyzed data originally collected in the DIAMOND clinical trial, an international study that found the Reflux Disease Questionnaire to be useful in diagnosing GERD among patients who consulted primary care physicians because of frequent upper GI symptoms. The DIAMOND study results indicated that unlike the Reflux Disease Questionnaire, PPI testing had very limited diagnostic value.
Dr. Bytzer and his associates performed more detailed analyses of the data, using different combinations of three main symptoms (heartburn, central chest pain, and dysphagia or regurgitation); different definitions of "PPI response"; and assessments of various subgroups of patients, all in the hope of improving the diagnostic yield of PPI testing. They compared the diagnostic usefulness of PPI testing against state-of-the-art comprehensive diagnostic work-ups for GERD in 299 of the DIAMOND study subjects.
"This large database provides the best platform so far to test whether there are better approaches for scoring a test of PPI therapy," the investigators noted.
All of the subjects underwent endoscopy with concomitant wireless esophageal pH monitoring and symptom assessment. They then completed the detailed Reflux Disease Questionnaire, and participated in a 2-week PPI test using esomeprazole (Nexium), during which they recorded GI symptoms in a diary.
A total of 69% of the patients who did have GERD showed a positive response to the PPI test. This means that 31% of the study participants with GERD were not identified by PPI testing.
Moreover, 51% of the patients who did not have GERD also showed a positive response to the PPI test, the investigators said.
Both patients who had GERD and patients who did not reported that their symptom response to acid suppression increased over the course of the first 5-6 days of treatment and then leveled off for the remaining 8-9 days.
The PPI test performed only marginally better across various subgroups of patients, such as those with GERD plus reflux esophagitis (as compared with patients who had GERD but no reflux esophagitis) or those whose physicians were certain of their GERD diagnosis (compared with patients whose physicians were uncertain about their GERD diagnosis).
For example, 48% of the study participants whose physicians predicted that they had GERD showed a positive response on PPI testing – a rate that was nearly identical to the 47% of study subjects whose physicians predicted that they had some disorder other than GERD.
Similarly, the PPI test performed only marginally better when different symptom combinations and different definitions of "PPI response" were assessed.
"In line with other researchers, we found that ... the clinical value of [the PPI test] is very limited," Dr. Bytzer and his colleagues said.
This study was funded by AstraZeneca. Dr. Bytzer reported ties to AstraZeneca, Boehringer Ingelheim, Eisai, Nycomed, Reckitt Benckiser, Takeda, and Wyeth, and his associates reported ties to numerous industry sources, including employment by AstraZeneca.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Major Finding: Thirty-one percent of study subjects who had GERD showed a negative response to the PPI test, indicating that they did not have the disorder, while 51% of those who did not have GERD showed a false-positive response.
Data Source: Investigators reported a secondary analysis of data from the international DIAMOND study, comparing the results of PPI testing to the actual diagnosis of GERD or other disorders.
Disclosures: This study was funded by AstraZeneca. Dr. Bytzer reported ties to AstraZeneca, Boehringer Ingelheim, Eisai, Nycomed, Reckitt Benckiser, Takeda, and Wyeth, and his associates reported ties to numerous industry sources, including employment by AstraZeneca.
Recurrent Acute Pancreatitis No Better After Dual Sphincterotomy
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
Performance of either biliary endoscopic sphincterotomy alone or dual biliary and pancreatic sphincterotomy similarly prevented approximately half of idiopathic recurrent acute pancreatitis cases in a trial in which 89 patients were randomized to treatments based on the presence or absence of sphincter of Oddi dysfunction.
The study is "the largest randomized clinical trial studying ERCP [endoscopic retrograde cholangiopancreatography] with SOM [sphincter of Oddi manometry] in this population" with long-term follow-up data, Dr. Gregory A. Coté of Indiana University in Indianapolis and his colleagues reported in the December issue of Gastroenterology (2012 [doi: 10.1053/j.gastro.2012.09.006]).
Source: American Gastroenterological Institute
Finding therapeutic equivalence between biliary endoscopic sphincterotomy (BES) and dual endoscopic sphincterotomy (DES) in preventing at least one episode of acute pancreatitis during follow-up is important, because the addition of pancreatic sphincterotomy to ERCP carries the risk of post-ERCP pancreatitis, bleeding, perforation, and sphincter restenosis, according to Dr. Coté and his associates.
To assess the therapeutic value of two types of sphincterotomy and the prognostic value of pancreatic SOD for patients with idiopathic recurrent acute pancreatitis (RAP), the researchers randomized 69 adults with SOD to BES or DES. The other 20 patients who did not have SOD were randomized to BES or a sham therapy. SOD was defined as basal pressure of 40 mm Hg or greater, "sustained for at least 30 seconds across two transducers," the researchers noted.
The patients were aged 18 years and older, and those with chronic pancreatitis or an identified cause of RAP were excluded from the study.
Of the 69 patients with SOD, RAP occurred in 49% of patients who underwent BES and 47% who underwent DES. There was no significant difference in rates of RAP between non-SOD patients who had BES and those who had a sham procedure (27% vs. 11%, respectively).
The risk of RAP was approximately four times higher in patients with SOD than in those without SOD, they added.
"Most RAP events occurred within 30 months of randomization in all subgroups," the researchers said.
Overall, chronic pancreatitis developed in 17% of all patients over a median of 78 months, and there was no difference in the probability of developing chronic pancreatitis in patients with and without SOD.
The study was limited by several factors, including its small sample size for the non-SOD population and the impact of environmental and genetic risk factors on idiopathic RAP, the researchers noted.
The small sample of patients with normal SOM meant that the researchers could draw no conclusions about the benefit of BES in these patients, but the results "represent preliminary data for estimating the sample size of a future definitive trial of ERCP with empiric biliary sphincterotomy," they noted.
In addition, the findings suggest that SOD "may be a secondary marker of more significant inflammation related to previous acute pancreatitis," and that pancreatic sphincterotomy "cannot be recommended as a curative treatment of unexplained RAP alone," they wrote.
None of the study authors had any financial conflicts to disclose.
FROM GASTROENTEROLOGY
Major Finding: Of 69 patients with sphincter of Oddi dysfunction, recurrent acute pancreatitis occurred in 49% of patients who underwent biliary endoscopic sphincterectomy and 47% who had dual biliary and pancreatic endoscopic sphincterectomy.
Data Source: The data come from a randomized trial of 89 adults with idiopathic recurrent acute pancreatitis.
Disclosures: None of the study authors had any financial conflicts to disclose.
Analysis Details the GI Disease Burden in U.S.
Clostridium difficile contributes mightily to the overall burden of gastrointestinal disease in the United States and was associated with a 237% increase in hospitalizations in the last decade.
Researchers who examined the latest data on the nationwide toll of GI and liver disease also found a 314% rise in hospitalizations related to morbid obesity and a continuing national health burden exacted by reflux symptoms, Barrett’s esophagus, and colorectal cancer.
Video from the American Gastroenterological Association (http://www.youtube.com/amergastroassn)
"We compiled the most recently available statistics on GI symptoms, quality of life, outpatient diagnoses, hospitalizations, costs, mortality, and endoscopic utilization from a variety of publicly and privately held databases," Dr. Anne F. Peery of the University of North Carolina, Chapel Hill, and her colleagues reported in the November issue of Gastroenterology (doi:10.1053/j.gastro.2012.08.002).
"Payers, policy makers, clinicians, and others interested in resource utilization may use these statistics to better understand evolving disease trends, and the best way to meet the challenge of these diseases."
The findings are based on data for 2009, the most recent year for which complete information was available, from the National Ambulatory Medical Care Survey, sponsored by the U.S. Centers for Disease Control and Prevention; the United States National Health and Wellness Survey, sponsored by the private company Kantar Health; the Nationwide Inpatient Sample, sponsored by the Agency for Healthcare Research and Quality; the Surveillance, Epidemiology, and End Results database of the National Cancer Institute; the National Vital Statistics System, sponsored by the National Center for Health Statistics and the CDC; and the Thomson Reuters MarketScan’s databases of commercial, Medicare, and Medicaid records.
Among the findings:
• C. difficile hospitalizations have increased 237% since 2000 and were associated with 4% in-hospital mortality. Now the ninth leading GI cause of mortality, with an absolute increase of 230% in the number of C. difficile–related deaths since 2002, the infection also markedly impairs quality of life and the capacity for work and other activities.
• Hospitalizations related to obesity remained relatively stable since 2000, but those associated with morbid obesity rose by 314%, and many were likely caused by the marked increase in bariatric surgery.
• Gastroesophageal reflux remains the most common GI-associated diagnosis in primary care, accounting for 9 million outpatient visits in 2009, and the most common GI-associated discharge diagnosis, with 4.4 million such diagnoses in 2009. Obesity was associated with 1.7 million discharge diagnoses and constipation with 1 million.
• Barrett’s esophagus accounted for almost half a million outpatient visits in 2009, when an estimated 3.3 million Americans had this diagnosis. Given that endoscopic surveillance is recommended every 3-5 years, Barrett’s contributes substantially to resource utilization.
• Colorectal cancer, with an estimated 147,000 patients diagnosed in 2008, accounts for more than half of all GI cancer diagnoses and continues to be the primary cause of GI-associated mortality. Pancreatic and hepatobiliary cancers are the next most frequently diagnosed GI cancers.
• Of the approximately 2.5 million deaths in the United States in 2009, 10% were attributed to an underlying GI cause. Chronic liver disease and cirrhosis are the 12th leading causes of death in the country.
• The total outpatient cost for GI endoscopy in 2009 was estimated to be $32.4 billion, which is higher than previously published estimates. An estimated 6.9 million upper endoscopies, 11.5 million lower endoscopies, and 228,000 biliary endoscopies were performed in the United States in 2009.
• Chronic liver disease and viral hepatitis were associated with 6% mortality and cost an estimated $1.8 billion per year in inpatient cost.
• Hospitalizations for nonalcoholic fatty liver disease increased 97% since 2000.
This study was supported in part by the National Institutes of Health. No financial conflicts of interest were reported.
Digestive (GI and liver) diseases constitute a substantial and growing burden in the United States. As detailed in the report by Dr. Peery and colleagues, there were over 46 million outpatient encounters associated with the top 20 digestive disease diagnoses in 2009, with approximately 10% of deaths nationwide with an underlying digestive disease cause. The observed increased prevalence of hospitalizations for many diagnoses (e.g., a 14% increase with principal discharge diagnosis of chronic liver disease with viral hepatitis) and procedures (e.g., a 17% increase in lower GI endoscopies among commercially insured patients) between 2000 and 2009 is expected given population growth and aging. In addition, dramatic increases in hospitalizations associated with C. difficile and morbid obesity were also noted.
The report provides crucial information for diverse constituencies, including healthcare planners, clinicians and researchers. However, as acknowledged by the authors, there are some important caveats with respect to coverage or quality for some data sources to bear in mind when interpreting these results. This is particularly relevant for non-alcoholic fatty liver disease, which is likely underestimated because of well-known problems in diagnostic code specificity and use.

Several factors suggest that the prevalence and costs of digestive diseases will increase substantially during the next decade. These include: an aging population with the number of people aged 65 years or older projected to be greater than 54 million by 2020;the estimated tens of millions of individuals with newly available healthcare coverage as of 2014 as part of the Affordable Care Act; continued increases in obesity rates; and the recent CDC recommendation that all baby-boomers be screened for hepatitis C. This report will facilitate timely planning and also serve as benchmark to help measure the impact of these forces on the scope and burden of digestive diseases and their clinical management.
DONNA L. WHITE, PH.D., MPH, is an investigator in the Clinical Epidemiology and Outcomes Program in the Houston VA Health Services Research and Development Center of Excellence at the Michael E. DeBakey VA Medical Center, Houston. She also is an assistant professor in the department of medicine at Baylor College of Medicine, Houston.
Digestive (GI and liver) diseases constitute a substantial and growing burden in the United States. As detailed in the report by Dr. Peery and colleagues, there were over 46 million outpatient encounters associated with the top 20 digestive disease diagnoses in 2009, with approximately 10% of deaths nationwide with an underlying digestive disease cause. The observed increased prevalence of hospitalizations for many diagnoses (e.g., a 14% increase with principal discharge diagnosis of chronic liver disease with viral hepatitis) and procedures (e.g., a 17% increase in lower GI endoscopies among commercially insured patients) between 2000 and 2009 is expected given population growth and aging. In addition, dramatic increases in hospitalizations associated with C. difficile and morbid obesity were also noted.
The report provides crucial information for diverse constituencies, including healthcare planners, clinicians and researchers. However, as acknowledged by the authors, there are some important caveats with respect to coverage or quality for some data sources to bear in mind when interpreting these results. This is particularly relevant for non-alcoholic fatty liver disease, which is likely underestimated because of well-known problems in diagnostic code specificity and use.
Several factors suggest that the prevalence and costs of digestive diseases will increase substantially during the next decade. These include: an aging population with the number of people aged 65 years or older projected to be greater than 54 million by 2020;the estimated tens of millions of individuals with newly available healthcare coverage as of 2014 as part of the Affordable Care Act; continued increases in obesity rates; and the recent CDC recommendation that all baby-boomers be screened for hepatitis C. This report will facilitate timely planning and also serve as benchmark to help measure the impact of these forces on the scope and burden of digestive diseases and their clinical management.
DONNA L. WHITE, PH.D., MPH, is an investigator in the Clinical Epidemiology and Outcomes Program in the Houston VA Health Services Research and Development Center of Excellence at the Michael E. DeBakey VA Medical Center, Houston. She also is an assistant professor in the department of medicine at Baylor College of Medicine, Houston.
Digestive (GI and liver) diseases constitute a substantial and growing burden in the United States. As detailed in the report by Dr. Peery and colleagues, there were over 46 million outpatient encounters associated with the top 20 digestive disease diagnoses in 2009, with approximately 10% of deaths nationwide with an underlying digestive disease cause. The observed increased prevalence of hospitalizations for many diagnoses (e.g., a 14% increase with principal discharge diagnosis of chronic liver disease with viral hepatitis) and procedures (e.g., a 17% increase in lower GI endoscopies among commercially insured patients) between 2000 and 2009 is expected given population growth and aging. In addition, dramatic increases in hospitalizations associated with C. difficile and morbid obesity were also noted.
The report provides crucial information for diverse constituencies, including healthcare planners, clinicians and researchers. However, as acknowledged by the authors, there are some important caveats with respect to coverage or quality for some data sources to bear in mind when interpreting these results. This is particularly relevant for non-alcoholic fatty liver disease, which is likely underestimated because of well-known problems in diagnostic code specificity and use.
Several factors suggest that the prevalence and costs of digestive diseases will increase substantially during the next decade. These include: an aging population with the number of people aged 65 years or older projected to be greater than 54 million by 2020;the estimated tens of millions of individuals with newly available healthcare coverage as of 2014 as part of the Affordable Care Act; continued increases in obesity rates; and the recent CDC recommendation that all baby-boomers be screened for hepatitis C. This report will facilitate timely planning and also serve as benchmark to help measure the impact of these forces on the scope and burden of digestive diseases and their clinical management.
DONNA L. WHITE, PH.D., MPH, is an investigator in the Clinical Epidemiology and Outcomes Program in the Houston VA Health Services Research and Development Center of Excellence at the Michael E. DeBakey VA Medical Center, Houston. She also is an assistant professor in the department of medicine at Baylor College of Medicine, Houston.
Clostridium difficile contributes mightily to the overall burden of gastrointestinal disease in the United States and was associated with a 237% increase in hospitalizations in the last decade.
Researchers who examined the latest data on the nationwide toll of GI and liver disease also found a 314% rise in hospitalizations related to morbid obesity and a continuing national health burden exacted by reflux symptoms, Barrett’s esophagus, and colorectal cancer.
Video from the American Gastroenterological Association (http://www.youtube.com/amergastroassn)
"We compiled the most recently available statistics on GI symptoms, quality of life, outpatient diagnoses, hospitalizations, costs, mortality, and endoscopic utilization from a variety of publicly and privately held databases," Dr. Anne F. Peery of the University of North Carolina, Chapel Hill, and her colleagues reported in the November issue of Gastroenterology (doi:10.1053/j.gastro.2012.08.002).
"Payers, policy makers, clinicians, and others interested in resource utilization may use these statistics to better understand evolving disease trends, and the best way to meet the challenge of these diseases."
The findings are based on data for 2009, the most recent year for which complete information was available, from the National Ambulatory Medical Care Survey, sponsored by the U.S. Centers for Disease Control and Prevention; the United States National Health and Wellness Survey, sponsored by the private company Kantar Health; the Nationwide Inpatient Sample, sponsored by the Agency for Healthcare Research and Quality; the Surveillance, Epidemiology, and End Results database of the National Cancer Institute; the National Vital Statistics System, sponsored by the National Center for Health Statistics and the CDC; and the Thomson Reuters MarketScan’s databases of commercial, Medicare, and Medicaid records.
Among the findings:
• C. difficile hospitalizations have increased 237% since 2000 and were associated with 4% in-hospital mortality. Now the ninth leading GI cause of mortality, with an absolute increase of 230% in the number of C. difficile–related deaths since 2002, the infection also markedly impairs quality of life and the capacity for work and other activities.
• Hospitalizations related to obesity remained relatively stable since 2000, but those associated with morbid obesity rose by 314%, and many were likely caused by the marked increase in bariatric surgery.
• Gastroesophageal reflux remains the most common GI-associated diagnosis in primary care, accounting for 9 million outpatient visits in 2009, and the most common GI-associated discharge diagnosis, with 4.4 million such diagnoses in 2009. Obesity was associated with 1.7 million discharge diagnoses and constipation with 1 million.
• Barrett’s esophagus accounted for almost half a million outpatient visits in 2009, when an estimated 3.3 million Americans had this diagnosis. Given that endoscopic surveillance is recommended every 3-5 years, Barrett’s contributes substantially to resource utilization.
• Colorectal cancer, with an estimated 147,000 patients diagnosed in 2008, accounts for more than half of all GI cancer diagnoses and continues to be the primary cause of GI-associated mortality. Pancreatic and hepatobiliary cancers are the next most frequently diagnosed GI cancers.
• Of the approximately 2.5 million deaths in the United States in 2009, 10% were attributed to an underlying GI cause. Chronic liver disease and cirrhosis are the 12th leading causes of death in the country.
• The total outpatient cost for GI endoscopy in 2009 was estimated to be $32.4 billion, which is higher than previously published estimates. An estimated 6.9 million upper endoscopies, 11.5 million lower endoscopies, and 228,000 biliary endoscopies were performed in the United States in 2009.
• Chronic liver disease and viral hepatitis were associated with 6% mortality and cost an estimated $1.8 billion per year in inpatient cost.
• Hospitalizations for nonalcoholic fatty liver disease increased 97% since 2000.
This study was supported in part by the National Institutes of Health. No financial conflicts of interest were reported.
Clostridium difficile contributes mightily to the overall burden of gastrointestinal disease in the United States and was associated with a 237% increase in hospitalizations in the last decade.
Researchers who examined the latest data on the nationwide toll of GI and liver disease also found a 314% rise in hospitalizations related to morbid obesity and a continuing national health burden exacted by reflux symptoms, Barrett’s esophagus, and colorectal cancer.
Video from the American Gastroenterological Association (http://www.youtube.com/amergastroassn)
"We compiled the most recently available statistics on GI symptoms, quality of life, outpatient diagnoses, hospitalizations, costs, mortality, and endoscopic utilization from a variety of publicly and privately held databases," Dr. Anne F. Peery of the University of North Carolina, Chapel Hill, and her colleagues reported in the November issue of Gastroenterology (doi:10.1053/j.gastro.2012.08.002).
"Payers, policy makers, clinicians, and others interested in resource utilization may use these statistics to better understand evolving disease trends, and the best way to meet the challenge of these diseases."
The findings are based on data for 2009, the most recent year for which complete information was available, from the National Ambulatory Medical Care Survey, sponsored by the U.S. Centers for Disease Control and Prevention; the United States National Health and Wellness Survey, sponsored by the private company Kantar Health; the Nationwide Inpatient Sample, sponsored by the Agency for Healthcare Research and Quality; the Surveillance, Epidemiology, and End Results database of the National Cancer Institute; the National Vital Statistics System, sponsored by the National Center for Health Statistics and the CDC; and the Thomson Reuters MarketScan’s databases of commercial, Medicare, and Medicaid records.
Among the findings:
• C. difficile hospitalizations have increased 237% since 2000 and were associated with 4% in-hospital mortality. Now the ninth leading GI cause of mortality, with an absolute increase of 230% in the number of C. difficile–related deaths since 2002, the infection also markedly impairs quality of life and the capacity for work and other activities.
• Hospitalizations related to obesity remained relatively stable since 2000, but those associated with morbid obesity rose by 314%, and many were likely caused by the marked increase in bariatric surgery.
• Gastroesophageal reflux remains the most common GI-associated diagnosis in primary care, accounting for 9 million outpatient visits in 2009, and the most common GI-associated discharge diagnosis, with 4.4 million such diagnoses in 2009. Obesity was associated with 1.7 million discharge diagnoses and constipation with 1 million.
• Barrett’s esophagus accounted for almost half a million outpatient visits in 2009, when an estimated 3.3 million Americans had this diagnosis. Given that endoscopic surveillance is recommended every 3-5 years, Barrett’s contributes substantially to resource utilization.
• Colorectal cancer, with an estimated 147,000 patients diagnosed in 2008, accounts for more than half of all GI cancer diagnoses and continues to be the primary cause of GI-associated mortality. Pancreatic and hepatobiliary cancers are the next most frequently diagnosed GI cancers.
• Of the approximately 2.5 million deaths in the United States in 2009, 10% were attributed to an underlying GI cause. Chronic liver disease and cirrhosis are the 12th leading causes of death in the country.
• The total outpatient cost for GI endoscopy in 2009 was estimated to be $32.4 billion, which is higher than previously published estimates. An estimated 6.9 million upper endoscopies, 11.5 million lower endoscopies, and 228,000 biliary endoscopies were performed in the United States in 2009.
• Chronic liver disease and viral hepatitis were associated with 6% mortality and cost an estimated $1.8 billion per year in inpatient cost.
• Hospitalizations for nonalcoholic fatty liver disease increased 97% since 2000.
This study was supported in part by the National Institutes of Health. No financial conflicts of interest were reported.
FROM GASTROENTEROLOGY
Management of Zollinger-Ellison May Depend on Presence of Tumors
Patients with Zollinger-Ellison syndrome who also have multiple endocrine neoplasia type 1 usually follow an indolent clinical course that rarely results in disease-related death, unlike those who have the sporadic form of the syndrome, Dr. Maneesh H. Singh and his colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
This finding, from a retrospective study of 49 patients treated at a single tertiary care center since 1994, argues against surgery for the estimated 25%-50% of Zollinger-Ellison syndrome (ZES) patients who have multiple endocrine neoplasia type 1 (MEN-1). "Given these results, we support a conservative approach to disease management ... focusing on symptom control with pharmacologic agents," the investigators wrote (Clin. Gastroenterol. Hepatol. 2012 Aug. 20 [doi:10.1016/j.cgh.2012.08.014]).
Early and aggressive surgery is recommended for sporadic ZES because it improves survival and can be curative. But surgery’s role in those with MEN-1 has been contentious because it doesn’t appear to improve survival in these patients. Only the most radical surgery, which carries a 40% complication rate, appears to be curative in those with MEN-1,reported Dr. Singh and his colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Because ZES is such a rare disorder, this follow-up study of 34 ZES patients who underwent surgery and 15 who did not "represents one of the largest long-term studies of surgical outcomes from a tertiary care hospital" conducted to date, they wrote.
The study subjects’ mean age at diagnosis was 47 years. The mean duration of follow-up from the time of diagnosis was 7 years, ranging from 0 to 5 years for 19 patients, from 5 to 10 years for 10, from 10 to 20 years for 15, and for more than 20 years for 5.
Of the 15 patients who did not undergo surgery, 5 declined after a discussion of the risks and benefits of the procedure, 2 because they had no lesions greater than 2 cm in diameter in imaging studies, 3 because of extensive liver involvement that was deemed unresectable, and 5 because they had unrelated comorbidities that made them poor surgical candidates.
A total of 33 subjects had sporadic ZES, while the other 16 had associated MEN-1. In the latter group, there was no significant difference between the median survival for the nine who underwent surgery (22.4 years) and for the seven who did not (25.5 years).
Standard gastrinoma resection with duodenotomy did not achieve a cure in any of the ZES patients with accompanying MEN-1.
In contrast, surgery improved both disease-related and all-cause mortality in the sporadic form of the disorder, and surgery was deemed curative in 6 (32%) of the patients with sporadic ZES.
None of the patients with MEN-1died of progressive ZES, compared with 28 (85%) of the patients with sporadic ZES. Thus, the form of the disease associated with MEN-1 appears to have a much more benign course than the sporadic form, Dr. Singh and his associates reported.
ZES associated with MEN-1 also tends to have an earlier symptom onset than does sporadic ZES, but because it is more indolent, the mean age at death was nearly identical between the two groups.
In this study, ZES patients with MEN-1had rates of liver involvement at diagnosis and rates of later liver metastases that were similar to those of patients with sporadic ZES. But again, this did not reduce their survival as it did with sporadic ZES.
This finding suggests that there may be a fundamental difference in the basic tumor biology between the two forms of the disease. It supports the theory that sporadic ZES is "a rapidly progressive, malignant form of gastrinoma that defies prediction and advocates for swift surgical intervention," the researchers wrote.
They reported no industry support for this study and no other financial conflicts.
Patients with Zollinger-Ellison syndrome who also have multiple endocrine neoplasia type 1 usually follow an indolent clinical course that rarely results in disease-related death, unlike those who have the sporadic form of the syndrome, Dr. Maneesh H. Singh and his colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
This finding, from a retrospective study of 49 patients treated at a single tertiary care center since 1994, argues against surgery for the estimated 25%-50% of Zollinger-Ellison syndrome (ZES) patients who have multiple endocrine neoplasia type 1 (MEN-1). "Given these results, we support a conservative approach to disease management ... focusing on symptom control with pharmacologic agents," the investigators wrote (Clin. Gastroenterol. Hepatol. 2012 Aug. 20 [doi:10.1016/j.cgh.2012.08.014]).
Early and aggressive surgery is recommended for sporadic ZES because it improves survival and can be curative. But surgery’s role in those with MEN-1 has been contentious because it doesn’t appear to improve survival in these patients. Only the most radical surgery, which carries a 40% complication rate, appears to be curative in those with MEN-1,reported Dr. Singh and his colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Because ZES is such a rare disorder, this follow-up study of 34 ZES patients who underwent surgery and 15 who did not "represents one of the largest long-term studies of surgical outcomes from a tertiary care hospital" conducted to date, they wrote.
The study subjects’ mean age at diagnosis was 47 years. The mean duration of follow-up from the time of diagnosis was 7 years, ranging from 0 to 5 years for 19 patients, from 5 to 10 years for 10, from 10 to 20 years for 15, and for more than 20 years for 5.
Of the 15 patients who did not undergo surgery, 5 declined after a discussion of the risks and benefits of the procedure, 2 because they had no lesions greater than 2 cm in diameter in imaging studies, 3 because of extensive liver involvement that was deemed unresectable, and 5 because they had unrelated comorbidities that made them poor surgical candidates.
A total of 33 subjects had sporadic ZES, while the other 16 had associated MEN-1. In the latter group, there was no significant difference between the median survival for the nine who underwent surgery (22.4 years) and for the seven who did not (25.5 years).
Standard gastrinoma resection with duodenotomy did not achieve a cure in any of the ZES patients with accompanying MEN-1.
In contrast, surgery improved both disease-related and all-cause mortality in the sporadic form of the disorder, and surgery was deemed curative in 6 (32%) of the patients with sporadic ZES.
None of the patients with MEN-1died of progressive ZES, compared with 28 (85%) of the patients with sporadic ZES. Thus, the form of the disease associated with MEN-1 appears to have a much more benign course than the sporadic form, Dr. Singh and his associates reported.
ZES associated with MEN-1 also tends to have an earlier symptom onset than does sporadic ZES, but because it is more indolent, the mean age at death was nearly identical between the two groups.
In this study, ZES patients with MEN-1had rates of liver involvement at diagnosis and rates of later liver metastases that were similar to those of patients with sporadic ZES. But again, this did not reduce their survival as it did with sporadic ZES.
This finding suggests that there may be a fundamental difference in the basic tumor biology between the two forms of the disease. It supports the theory that sporadic ZES is "a rapidly progressive, malignant form of gastrinoma that defies prediction and advocates for swift surgical intervention," the researchers wrote.
They reported no industry support for this study and no other financial conflicts.
Patients with Zollinger-Ellison syndrome who also have multiple endocrine neoplasia type 1 usually follow an indolent clinical course that rarely results in disease-related death, unlike those who have the sporadic form of the syndrome, Dr. Maneesh H. Singh and his colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
This finding, from a retrospective study of 49 patients treated at a single tertiary care center since 1994, argues against surgery for the estimated 25%-50% of Zollinger-Ellison syndrome (ZES) patients who have multiple endocrine neoplasia type 1 (MEN-1). "Given these results, we support a conservative approach to disease management ... focusing on symptom control with pharmacologic agents," the investigators wrote (Clin. Gastroenterol. Hepatol. 2012 Aug. 20 [doi:10.1016/j.cgh.2012.08.014]).
Early and aggressive surgery is recommended for sporadic ZES because it improves survival and can be curative. But surgery’s role in those with MEN-1 has been contentious because it doesn’t appear to improve survival in these patients. Only the most radical surgery, which carries a 40% complication rate, appears to be curative in those with MEN-1,reported Dr. Singh and his colleagues at the Hospital of the University of Pennsylvania, Philadelphia.
Because ZES is such a rare disorder, this follow-up study of 34 ZES patients who underwent surgery and 15 who did not "represents one of the largest long-term studies of surgical outcomes from a tertiary care hospital" conducted to date, they wrote.
The study subjects’ mean age at diagnosis was 47 years. The mean duration of follow-up from the time of diagnosis was 7 years, ranging from 0 to 5 years for 19 patients, from 5 to 10 years for 10, from 10 to 20 years for 15, and for more than 20 years for 5.
Of the 15 patients who did not undergo surgery, 5 declined after a discussion of the risks and benefits of the procedure, 2 because they had no lesions greater than 2 cm in diameter in imaging studies, 3 because of extensive liver involvement that was deemed unresectable, and 5 because they had unrelated comorbidities that made them poor surgical candidates.
A total of 33 subjects had sporadic ZES, while the other 16 had associated MEN-1. In the latter group, there was no significant difference between the median survival for the nine who underwent surgery (22.4 years) and for the seven who did not (25.5 years).
Standard gastrinoma resection with duodenotomy did not achieve a cure in any of the ZES patients with accompanying MEN-1.
In contrast, surgery improved both disease-related and all-cause mortality in the sporadic form of the disorder, and surgery was deemed curative in 6 (32%) of the patients with sporadic ZES.
None of the patients with MEN-1died of progressive ZES, compared with 28 (85%) of the patients with sporadic ZES. Thus, the form of the disease associated with MEN-1 appears to have a much more benign course than the sporadic form, Dr. Singh and his associates reported.
ZES associated with MEN-1 also tends to have an earlier symptom onset than does sporadic ZES, but because it is more indolent, the mean age at death was nearly identical between the two groups.
In this study, ZES patients with MEN-1had rates of liver involvement at diagnosis and rates of later liver metastases that were similar to those of patients with sporadic ZES. But again, this did not reduce their survival as it did with sporadic ZES.
This finding suggests that there may be a fundamental difference in the basic tumor biology between the two forms of the disease. It supports the theory that sporadic ZES is "a rapidly progressive, malignant form of gastrinoma that defies prediction and advocates for swift surgical intervention," the researchers wrote.
They reported no industry support for this study and no other financial conflicts.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Liver Candidates Decline Many Organ Offers
Eighty-four percent of candidates on the wait-list for liver transplant who either died or were removed from the list before they were able to undergo transplantation declined at least one offer of a donor liver, Dr. Jennifer Cindy Lai of the University of California, San Francisco, and her colleagues reported in the November issue of Gastroenterology.
Even more surprising, most of these candidates declined "not just one or two but a median of six liver offers during their time on the wait-list."
The "declined" donor organs were then successfully transplanted into lower-priority recipients.
These findings suggest that mortality among wait-listed patients "is not simply a result of not having the opportunity for transplantation, as many of us assume. Rather, wait-list mortality appears to result from opportunities for transplantation that were declined," Dr. Lai and her associates wrote.
The reasons that so many viable donor livers were initially declined are not yet clear. General, somewhat vague reasons were listed but not fully explained in the records the researchers analyzed for this study, which they obtained from the United Network for Organ Sharing/Organ Procurement Transplantation Network database.
The investigators assessed organ offers to 33,389 liver transplant candidates aged 18 years and older who were wait-listed across the United States between 2005 and 2010.
The reasons that proffered organs were declined, as listed in the medical records, fit into six broad categories: unfavorable donor age or quality of organ; unfavorable donor organ size/weight; other unfavorable donor factors, such as ABO blood transfusion incompatibility, "social history," "positive serologic tests," or "organ anatomical damage or defect"; unreadiness of the recipient, usually because he or she was ill, unavailable, refused the organ, or required multiple organ transplants at the same time; problems with the transplant program itself, such as a "heavy workload" or unavailability of a surgeon or operating room at the recipient’s medical center, failure to respond to the offer in a timely way, or excessive distance to ship the organ.
A total of 20% of the study population (6,737 patients) died or were removed from the wait-list because they became too sick before they could undergo transplantation. A total of 5,680 (84%) of those patients had been offered one or more donor livers before they died or were taken off the list.
Offers of donor livers were declined most often (68%) because of "unfavorable donor age or quality of organ," whereas 9% were declined because of unfavorable organ size, 15% because of "other donor factors," 4% because the recipient wasn’t ready, and 4% because of transplant program or miscellaneous other factors.
However, the dominant use of the "donor quality or age" refusal code in the database almost certainly "does not accurately or fully capture the true refusal reason," Dr. Lai and her associates said.
Even livers judged to be of high quality according to standard criteria were declined because of supposed "unfavorable donor age or quality of organ." But the investigators found no difference in the risk of graft failure between such high-quality livers that were declined and other high-quality livers that were accepted on the first offer.
Other reasons must be playing an important role in this high rate refusal, but "the nuances of these refusals cannot be determined" without more individualized data, they said.
Dr. Lai and her colleagues suggested that to cut down on refusals of apparently viable organs, the transplant community should "reduce the stigma associated with non–ideal livers, and set realistic expectations for wait-listed candidates" so that they’re less likely to pass up a suitable donation while assuming that a better offer will come along.
Patients also should be educated about the unpredictability of death or of sudden worsening of liver disease while on the wait-list. They should be advised that there is a survival benefit associated with the transplantation of any graft, compared with continuing on the wait-list.
In addition, the current regulatory environment focuses on transplant centers’ outcomes, which may influence some centers to discourage the acceptance of less than optimal donor organs. "This may be especially relevant for low-volume transplant centers, for whom even a small number of poor outcomes ... may make a relatively large difference in the centers’ perceived performance," the researchers wrote.
Finally, wait-list candidates should be encouraged to complete their transplant work-ups as expeditiously as possible to avoid having to refuse a donor offer simply because they have not yet undergone the necessary cardiac testing or cancer screening.
This study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases and the University of California, San Francisco. No financial conflicts of interest were reported.
Eighty-four percent of candidates on the wait-list for liver transplant who either died or were removed from the list before they were able to undergo transplantation declined at least one offer of a donor liver, Dr. Jennifer Cindy Lai of the University of California, San Francisco, and her colleagues reported in the November issue of Gastroenterology.
Even more surprising, most of these candidates declined "not just one or two but a median of six liver offers during their time on the wait-list."
The "declined" donor organs were then successfully transplanted into lower-priority recipients.
These findings suggest that mortality among wait-listed patients "is not simply a result of not having the opportunity for transplantation, as many of us assume. Rather, wait-list mortality appears to result from opportunities for transplantation that were declined," Dr. Lai and her associates wrote.
The reasons that so many viable donor livers were initially declined are not yet clear. General, somewhat vague reasons were listed but not fully explained in the records the researchers analyzed for this study, which they obtained from the United Network for Organ Sharing/Organ Procurement Transplantation Network database.
The investigators assessed organ offers to 33,389 liver transplant candidates aged 18 years and older who were wait-listed across the United States between 2005 and 2010.
The reasons that proffered organs were declined, as listed in the medical records, fit into six broad categories: unfavorable donor age or quality of organ; unfavorable donor organ size/weight; other unfavorable donor factors, such as ABO blood transfusion incompatibility, "social history," "positive serologic tests," or "organ anatomical damage or defect"; unreadiness of the recipient, usually because he or she was ill, unavailable, refused the organ, or required multiple organ transplants at the same time; problems with the transplant program itself, such as a "heavy workload" or unavailability of a surgeon or operating room at the recipient’s medical center, failure to respond to the offer in a timely way, or excessive distance to ship the organ.
A total of 20% of the study population (6,737 patients) died or were removed from the wait-list because they became too sick before they could undergo transplantation. A total of 5,680 (84%) of those patients had been offered one or more donor livers before they died or were taken off the list.
Offers of donor livers were declined most often (68%) because of "unfavorable donor age or quality of organ," whereas 9% were declined because of unfavorable organ size, 15% because of "other donor factors," 4% because the recipient wasn’t ready, and 4% because of transplant program or miscellaneous other factors.
However, the dominant use of the "donor quality or age" refusal code in the database almost certainly "does not accurately or fully capture the true refusal reason," Dr. Lai and her associates said.
Even livers judged to be of high quality according to standard criteria were declined because of supposed "unfavorable donor age or quality of organ." But the investigators found no difference in the risk of graft failure between such high-quality livers that were declined and other high-quality livers that were accepted on the first offer.
Other reasons must be playing an important role in this high rate refusal, but "the nuances of these refusals cannot be determined" without more individualized data, they said.
Dr. Lai and her colleagues suggested that to cut down on refusals of apparently viable organs, the transplant community should "reduce the stigma associated with non–ideal livers, and set realistic expectations for wait-listed candidates" so that they’re less likely to pass up a suitable donation while assuming that a better offer will come along.
Patients also should be educated about the unpredictability of death or of sudden worsening of liver disease while on the wait-list. They should be advised that there is a survival benefit associated with the transplantation of any graft, compared with continuing on the wait-list.
In addition, the current regulatory environment focuses on transplant centers’ outcomes, which may influence some centers to discourage the acceptance of less than optimal donor organs. "This may be especially relevant for low-volume transplant centers, for whom even a small number of poor outcomes ... may make a relatively large difference in the centers’ perceived performance," the researchers wrote.
Finally, wait-list candidates should be encouraged to complete their transplant work-ups as expeditiously as possible to avoid having to refuse a donor offer simply because they have not yet undergone the necessary cardiac testing or cancer screening.
This study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases and the University of California, San Francisco. No financial conflicts of interest were reported.
Eighty-four percent of candidates on the wait-list for liver transplant who either died or were removed from the list before they were able to undergo transplantation declined at least one offer of a donor liver, Dr. Jennifer Cindy Lai of the University of California, San Francisco, and her colleagues reported in the November issue of Gastroenterology.
Even more surprising, most of these candidates declined "not just one or two but a median of six liver offers during their time on the wait-list."
The "declined" donor organs were then successfully transplanted into lower-priority recipients.
These findings suggest that mortality among wait-listed patients "is not simply a result of not having the opportunity for transplantation, as many of us assume. Rather, wait-list mortality appears to result from opportunities for transplantation that were declined," Dr. Lai and her associates wrote.
The reasons that so many viable donor livers were initially declined are not yet clear. General, somewhat vague reasons were listed but not fully explained in the records the researchers analyzed for this study, which they obtained from the United Network for Organ Sharing/Organ Procurement Transplantation Network database.
The investigators assessed organ offers to 33,389 liver transplant candidates aged 18 years and older who were wait-listed across the United States between 2005 and 2010.
The reasons that proffered organs were declined, as listed in the medical records, fit into six broad categories: unfavorable donor age or quality of organ; unfavorable donor organ size/weight; other unfavorable donor factors, such as ABO blood transfusion incompatibility, "social history," "positive serologic tests," or "organ anatomical damage or defect"; unreadiness of the recipient, usually because he or she was ill, unavailable, refused the organ, or required multiple organ transplants at the same time; problems with the transplant program itself, such as a "heavy workload" or unavailability of a surgeon or operating room at the recipient’s medical center, failure to respond to the offer in a timely way, or excessive distance to ship the organ.
A total of 20% of the study population (6,737 patients) died or were removed from the wait-list because they became too sick before they could undergo transplantation. A total of 5,680 (84%) of those patients had been offered one or more donor livers before they died or were taken off the list.
Offers of donor livers were declined most often (68%) because of "unfavorable donor age or quality of organ," whereas 9% were declined because of unfavorable organ size, 15% because of "other donor factors," 4% because the recipient wasn’t ready, and 4% because of transplant program or miscellaneous other factors.
However, the dominant use of the "donor quality or age" refusal code in the database almost certainly "does not accurately or fully capture the true refusal reason," Dr. Lai and her associates said.
Even livers judged to be of high quality according to standard criteria were declined because of supposed "unfavorable donor age or quality of organ." But the investigators found no difference in the risk of graft failure between such high-quality livers that were declined and other high-quality livers that were accepted on the first offer.
Other reasons must be playing an important role in this high rate refusal, but "the nuances of these refusals cannot be determined" without more individualized data, they said.
Dr. Lai and her colleagues suggested that to cut down on refusals of apparently viable organs, the transplant community should "reduce the stigma associated with non–ideal livers, and set realistic expectations for wait-listed candidates" so that they’re less likely to pass up a suitable donation while assuming that a better offer will come along.
Patients also should be educated about the unpredictability of death or of sudden worsening of liver disease while on the wait-list. They should be advised that there is a survival benefit associated with the transplantation of any graft, compared with continuing on the wait-list.
In addition, the current regulatory environment focuses on transplant centers’ outcomes, which may influence some centers to discourage the acceptance of less than optimal donor organs. "This may be especially relevant for low-volume transplant centers, for whom even a small number of poor outcomes ... may make a relatively large difference in the centers’ perceived performance," the researchers wrote.
Finally, wait-list candidates should be encouraged to complete their transplant work-ups as expeditiously as possible to avoid having to refuse a donor offer simply because they have not yet undergone the necessary cardiac testing or cancer screening.
This study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases and the University of California, San Francisco. No financial conflicts of interest were reported.
FROM GASTROENTEROLOGY
Pretreatment Care Predicts HCV Outcomes
Patients with hepatitis C infections are more likely to initiate appropriate antiviral therapy and achieve a sustained virologic response if they receive high quality health care, Dr. Fasiha Kanwal of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and her colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
In their study of nearly 35,000 adults with HCV, the odds of initiating antiviral therapy were threefold higher in patients who received optimal care from the moment HCV infection was diagnosed than in those who did not. And among patients who initiated antiviral therapy, the quality of care they received before that therapy even began strongly predicted whether they would complete antiviral therapy and achieve a sustained virologic response, the investigators said.

The study showed, however, that only 11% of patients received all of the appropriate initial care.
Process-of-care measures are frequently used to assess the quality of care for HCV, but until now no study has assessed whether these measures actually correlate with better outcomes. To address this issue, Dr. Kanwal and her associates "evaluated the relationship between adherence to a broad set of process-based measures in HCV and 3 subsequent HCV-specific endpoints: receipt of antiviral treatment, completion of antiviral treatment, and the clinical outcome associated with improved survival: sustained virologic response."
The investigators used data from the VA registry on HCV clinical care, which covers patient demographics, lab tests, pharmacy information, and data on inpatient and outpatient care for approximately 300,000 patients across the country. For this study, they included data on 34,749 adults.
The mean subject age was 53 years, and 97% were men. Approximately half the study population was white and 26% was black; ethnicity was not reported for the others.
The researchers assessed seven process-of-care measures: confirmation of HCV viremia, evaluation by HCV specialists, HCV genotype testing, liver biopsy for those found to have genotype 1 HCV, and the ruling out of liver diseases related to hepatitis B, autoimmunity, or iron overload.
They also assessed seven process-of-care measures related to the prevention and management of comorbid conditions: HIV testing; hepatitis A and B serology testing, hepatitis A and B vaccination if serology results proved negative; treatment of depression; and treatment of substance abuse disorder.
Finally, they assessed six process-of-care measures related to monitoring of antiviral therapy’s effects: testing of viral load before antivirals were initiated and again at weeks 12, 24, and 48; reduction of ribavirin dose if anemia developed during treatment; and avoidance of prescribing growth-stimulating factors for leukopenia during antiviral therapy.
Overall, only 11% of the study subjects received all of the appropriate initial care, and 8% received all the appropriate care related to prevention and management of comorbid conditions. Moreover, of the study subjects who received antiviral therapy, just 37% received all the appropriate monitoring of treatment effects Dr. Kanwal and her associates said.
In patients who received optimal care before a definitive diagnosis was made, the odds of receiving antiviral therapy were 3.2 times higher than in patients who did not receive optimal care before diagnosis, they reported.
Similarly, patients who received optimal preventive and comorbid-condition care showed rates of antiviral therapy that were 36% higher than those of patients who received suboptimal preventive and comorbid-condition care.
The strong association between fulfillment of these process-of-care measures and appropriate antiviral therapy remained robust in a series of sensitivity analyses, which means it’s likely that meeting process-of-care goals directly leads to better HCV outcomes, Dr. Kanwal and her colleagues said.
The investigators could not, however, rule out the possibility that meeting these goals is simply a marker of more compliant patients, which in turn produces better outcomes.
The study findings imply that the effectiveness of the two new direct-acting antiviral agents that recently became available for HCV may hinge on the quality of care patients are receiving before they even start taking these drugs, rather than simply on the effectiveness of the drugs alone, Dr. Kanwal and her associates said.
This study was supported by the U.S. Department of Veterans Affairs Health Services Research and Development Service. No financial conflicts of interest were reported.
Financial reimbursement in medicine has long been driven by volume rather than quality. This incentive structure is changing, and in the near future practitioners will experience increased scrutiny of the quality of care we provide.

|
|
Quality can be divided into structure (having the proper equipment to clean endoscopes), process (testing for latent tuberculosis before beginning anti–tumor necrosis factor therapy), and outcomes (perforation rate during colonoscopy). The latter is, of course, the most important, but it is also the most difficult to measure because of low event rates and inadequate risk adjustment. Therefore, most quality measures are based on processes of care. For quality measurement to yield any true value to the patient, however, it is important that these processes are clearly linked to better patient outcomes.
Hepatitis C, which affects 1.3% of Americans, has recently been a target disease for measuring and improving quality of care. Dr. Kanwal and her colleagues found that patients receiving optimum process-related quality care were more likely to undergo antiviral therapy. Such patients also were more likely to complete treatment once started and to achieve sustained virologic response if treatment was completed. Since these findings persisted despite adjustment for numerous potential confounders such as comorbidities, it appears that higher quality of care (as measured by processes) may truly lead to better patient outcomes.
What does this mean for practitioners? Particularly in the era of triple therapy, hepatitis C virus (HCV) infection cannot be managed like any other disease. Protocols and tracking systems need to be developed to ensure that quality measures are met. Many practices find it helpful to funnel HCV patients to a single person for case management, such as a nurse or midlevel provider. Hopefully, these efforts, in conjunction with newer antivirals, will soon eradicate hepatitis C altogether.
Michael Volk, M.D., is assistant professor of hepatology at the University of Michigan, Ann Arbor.
Financial reimbursement in medicine has long been driven by volume rather than quality. This incentive structure is changing, and in the near future practitioners will experience increased scrutiny of the quality of care we provide.
|
|
|
Quality can be divided into structure (having the proper equipment to clean endoscopes), process (testing for latent tuberculosis before beginning anti–tumor necrosis factor therapy), and outcomes (perforation rate during colonoscopy). The latter is, of course, the most important, but it is also the most difficult to measure because of low event rates and inadequate risk adjustment. Therefore, most quality measures are based on processes of care. For quality measurement to yield any true value to the patient, however, it is important that these processes are clearly linked to better patient outcomes.
Hepatitis C, which affects 1.3% of Americans, has recently been a target disease for measuring and improving quality of care. Dr. Kanwal and her colleagues found that patients receiving optimum process-related quality care were more likely to undergo antiviral therapy. Such patients also were more likely to complete treatment once started and to achieve sustained virologic response if treatment was completed. Since these findings persisted despite adjustment for numerous potential confounders such as comorbidities, it appears that higher quality of care (as measured by processes) may truly lead to better patient outcomes.
What does this mean for practitioners? Particularly in the era of triple therapy, hepatitis C virus (HCV) infection cannot be managed like any other disease. Protocols and tracking systems need to be developed to ensure that quality measures are met. Many practices find it helpful to funnel HCV patients to a single person for case management, such as a nurse or midlevel provider. Hopefully, these efforts, in conjunction with newer antivirals, will soon eradicate hepatitis C altogether.
Michael Volk, M.D., is assistant professor of hepatology at the University of Michigan, Ann Arbor.
Financial reimbursement in medicine has long been driven by volume rather than quality. This incentive structure is changing, and in the near future practitioners will experience increased scrutiny of the quality of care we provide.
|
|
|
Quality can be divided into structure (having the proper equipment to clean endoscopes), process (testing for latent tuberculosis before beginning anti–tumor necrosis factor therapy), and outcomes (perforation rate during colonoscopy). The latter is, of course, the most important, but it is also the most difficult to measure because of low event rates and inadequate risk adjustment. Therefore, most quality measures are based on processes of care. For quality measurement to yield any true value to the patient, however, it is important that these processes are clearly linked to better patient outcomes.
Hepatitis C, which affects 1.3% of Americans, has recently been a target disease for measuring and improving quality of care. Dr. Kanwal and her colleagues found that patients receiving optimum process-related quality care were more likely to undergo antiviral therapy. Such patients also were more likely to complete treatment once started and to achieve sustained virologic response if treatment was completed. Since these findings persisted despite adjustment for numerous potential confounders such as comorbidities, it appears that higher quality of care (as measured by processes) may truly lead to better patient outcomes.
What does this mean for practitioners? Particularly in the era of triple therapy, hepatitis C virus (HCV) infection cannot be managed like any other disease. Protocols and tracking systems need to be developed to ensure that quality measures are met. Many practices find it helpful to funnel HCV patients to a single person for case management, such as a nurse or midlevel provider. Hopefully, these efforts, in conjunction with newer antivirals, will soon eradicate hepatitis C altogether.
Michael Volk, M.D., is assistant professor of hepatology at the University of Michigan, Ann Arbor.
Patients with hepatitis C infections are more likely to initiate appropriate antiviral therapy and achieve a sustained virologic response if they receive high quality health care, Dr. Fasiha Kanwal of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and her colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
In their study of nearly 35,000 adults with HCV, the odds of initiating antiviral therapy were threefold higher in patients who received optimal care from the moment HCV infection was diagnosed than in those who did not. And among patients who initiated antiviral therapy, the quality of care they received before that therapy even began strongly predicted whether they would complete antiviral therapy and achieve a sustained virologic response, the investigators said.
The study showed, however, that only 11% of patients received all of the appropriate initial care.
Process-of-care measures are frequently used to assess the quality of care for HCV, but until now no study has assessed whether these measures actually correlate with better outcomes. To address this issue, Dr. Kanwal and her associates "evaluated the relationship between adherence to a broad set of process-based measures in HCV and 3 subsequent HCV-specific endpoints: receipt of antiviral treatment, completion of antiviral treatment, and the clinical outcome associated with improved survival: sustained virologic response."
The investigators used data from the VA registry on HCV clinical care, which covers patient demographics, lab tests, pharmacy information, and data on inpatient and outpatient care for approximately 300,000 patients across the country. For this study, they included data on 34,749 adults.
The mean subject age was 53 years, and 97% were men. Approximately half the study population was white and 26% was black; ethnicity was not reported for the others.
The researchers assessed seven process-of-care measures: confirmation of HCV viremia, evaluation by HCV specialists, HCV genotype testing, liver biopsy for those found to have genotype 1 HCV, and the ruling out of liver diseases related to hepatitis B, autoimmunity, or iron overload.
They also assessed seven process-of-care measures related to the prevention and management of comorbid conditions: HIV testing; hepatitis A and B serology testing, hepatitis A and B vaccination if serology results proved negative; treatment of depression; and treatment of substance abuse disorder.
Finally, they assessed six process-of-care measures related to monitoring of antiviral therapy’s effects: testing of viral load before antivirals were initiated and again at weeks 12, 24, and 48; reduction of ribavirin dose if anemia developed during treatment; and avoidance of prescribing growth-stimulating factors for leukopenia during antiviral therapy.
Overall, only 11% of the study subjects received all of the appropriate initial care, and 8% received all the appropriate care related to prevention and management of comorbid conditions. Moreover, of the study subjects who received antiviral therapy, just 37% received all the appropriate monitoring of treatment effects Dr. Kanwal and her associates said.
In patients who received optimal care before a definitive diagnosis was made, the odds of receiving antiviral therapy were 3.2 times higher than in patients who did not receive optimal care before diagnosis, they reported.
Similarly, patients who received optimal preventive and comorbid-condition care showed rates of antiviral therapy that were 36% higher than those of patients who received suboptimal preventive and comorbid-condition care.
The strong association between fulfillment of these process-of-care measures and appropriate antiviral therapy remained robust in a series of sensitivity analyses, which means it’s likely that meeting process-of-care goals directly leads to better HCV outcomes, Dr. Kanwal and her colleagues said.
The investigators could not, however, rule out the possibility that meeting these goals is simply a marker of more compliant patients, which in turn produces better outcomes.
The study findings imply that the effectiveness of the two new direct-acting antiviral agents that recently became available for HCV may hinge on the quality of care patients are receiving before they even start taking these drugs, rather than simply on the effectiveness of the drugs alone, Dr. Kanwal and her associates said.
This study was supported by the U.S. Department of Veterans Affairs Health Services Research and Development Service. No financial conflicts of interest were reported.
Patients with hepatitis C infections are more likely to initiate appropriate antiviral therapy and achieve a sustained virologic response if they receive high quality health care, Dr. Fasiha Kanwal of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and her colleagues reported in the November issue of Clinical Gastroenterology and Hepatology.
In their study of nearly 35,000 adults with HCV, the odds of initiating antiviral therapy were threefold higher in patients who received optimal care from the moment HCV infection was diagnosed than in those who did not. And among patients who initiated antiviral therapy, the quality of care they received before that therapy even began strongly predicted whether they would complete antiviral therapy and achieve a sustained virologic response, the investigators said.
The study showed, however, that only 11% of patients received all of the appropriate initial care.
Process-of-care measures are frequently used to assess the quality of care for HCV, but until now no study has assessed whether these measures actually correlate with better outcomes. To address this issue, Dr. Kanwal and her associates "evaluated the relationship between adherence to a broad set of process-based measures in HCV and 3 subsequent HCV-specific endpoints: receipt of antiviral treatment, completion of antiviral treatment, and the clinical outcome associated with improved survival: sustained virologic response."
The investigators used data from the VA registry on HCV clinical care, which covers patient demographics, lab tests, pharmacy information, and data on inpatient and outpatient care for approximately 300,000 patients across the country. For this study, they included data on 34,749 adults.
The mean subject age was 53 years, and 97% were men. Approximately half the study population was white and 26% was black; ethnicity was not reported for the others.
The researchers assessed seven process-of-care measures: confirmation of HCV viremia, evaluation by HCV specialists, HCV genotype testing, liver biopsy for those found to have genotype 1 HCV, and the ruling out of liver diseases related to hepatitis B, autoimmunity, or iron overload.
They also assessed seven process-of-care measures related to the prevention and management of comorbid conditions: HIV testing; hepatitis A and B serology testing, hepatitis A and B vaccination if serology results proved negative; treatment of depression; and treatment of substance abuse disorder.
Finally, they assessed six process-of-care measures related to monitoring of antiviral therapy’s effects: testing of viral load before antivirals were initiated and again at weeks 12, 24, and 48; reduction of ribavirin dose if anemia developed during treatment; and avoidance of prescribing growth-stimulating factors for leukopenia during antiviral therapy.
Overall, only 11% of the study subjects received all of the appropriate initial care, and 8% received all the appropriate care related to prevention and management of comorbid conditions. Moreover, of the study subjects who received antiviral therapy, just 37% received all the appropriate monitoring of treatment effects Dr. Kanwal and her associates said.
In patients who received optimal care before a definitive diagnosis was made, the odds of receiving antiviral therapy were 3.2 times higher than in patients who did not receive optimal care before diagnosis, they reported.
Similarly, patients who received optimal preventive and comorbid-condition care showed rates of antiviral therapy that were 36% higher than those of patients who received suboptimal preventive and comorbid-condition care.
The strong association between fulfillment of these process-of-care measures and appropriate antiviral therapy remained robust in a series of sensitivity analyses, which means it’s likely that meeting process-of-care goals directly leads to better HCV outcomes, Dr. Kanwal and her colleagues said.
The investigators could not, however, rule out the possibility that meeting these goals is simply a marker of more compliant patients, which in turn produces better outcomes.
The study findings imply that the effectiveness of the two new direct-acting antiviral agents that recently became available for HCV may hinge on the quality of care patients are receiving before they even start taking these drugs, rather than simply on the effectiveness of the drugs alone, Dr. Kanwal and her associates said.
This study was supported by the U.S. Department of Veterans Affairs Health Services Research and Development Service. No financial conflicts of interest were reported.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Long-Term Follow-Up Warranted After Gastric MALT Lymphoma Remission
As many as 80% of gastric MALT lymphoma patients achieve remission after Helicobacter pylori eradication, yet these patients remain at a significantly increased risk for second gastric cancers and lymphomas, reported Dr. Thomas Wündisch and his colleagues in Gastroenterology.
"The clinical consequence of this should be yearly lifelong endoscopic follow-up in all patients with a history of GML [gastric MALT lymphoma] to detect gastric cancer as early as possible," they wrote.
Dr. Wündisch, of Heinrich-Heine-Universität in Düsseldorf, Germany, and his colleagues studied 120 patients (63 female, mean age 62 years) recruited between June 1993 and July 1999 with stage EI1 gastric mucosa–associated lymphoid tissue (MALT) lymphoma according to the Ann Arbor system, where lymphoma is limited to the mucosa and submucosa of the stomach with no lymph node involvement.
Patients in this multicenter study underwent H. pylori eradication therapy consisting of a 2-week course of amoxicillin (750 mg three times daily) and omeprazole (40 mg three times daily).
Endoscopy was performed monthly until complete histologic remission, defined as macroscopic disappearance of lymphoma and absence of lymphoma on biopsy in two consecutive analyses, and then every 6-12 months. Patients were followed for a median of 122 months after H. pylori eradication (range, 1-171 months).
Dr. Wündisch and his colleagues reported that 96 of the 120 patients with complete follow-up (80%) achieved complete GML remission between 1 and 28 months after eradication therapy began, and 80% of them (77/96) remained disease free (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.06.035]).
Histologic residual disease was seen in 16 out of 96 patients; indeed, it was likely "ongoing histological residual disease rather than complete remission, as the microscopic lesions were small and often found only upon examination of serial sections of one of multiple biopsies."
A "watch and wait" approach was used in these cases, and all but one patient showed complete remission again at the last time point, with a median second remission duration of 46 months. There was also no progression.
"We strongly support this strategy," the investigators wrote.
Overall, the 96 patients with complete GML remission had a 5-year survival rate of 94%, and a 10-year survival of 87%.
Nevertheless, the researchers observed a morbidity ratio of 8.567 for gastric cancer among these patients (95% confidence interval, 3.566-20.582; P less than .001) and 18.621 for non-Hodgkin’s lymphoma (95% CI, 8.365-41.448; P less than 10–6), compared with the general population. The morbidity rate for all cancers was also elevated, at 1.689, but this was not statistically significant.
According to the researchers, although treatment-related factors often contribute to the development of second cancers in patients with lymphoma, the 2-week-long H. pylori regimen employed was unlikely to cause long-term toxic effects.
"Patient-related factors, such as gene polymorphisms, might play a more important role in the development of GML and second cancers in our patients, but these factors have yet to be identified," they said.
In any case, "currently, follow-up of patients without significant comorbidities should extend beyond 5 years for detecting reinfection, relapse, second lymphoma, and early gastric cancer."
The authors stated that the study was funded by a grant from Deutsche Krebshilfe, and they had no personal disclosures.
As many as 80% of gastric MALT lymphoma patients achieve remission after Helicobacter pylori eradication, yet these patients remain at a significantly increased risk for second gastric cancers and lymphomas, reported Dr. Thomas Wündisch and his colleagues in Gastroenterology.
"The clinical consequence of this should be yearly lifelong endoscopic follow-up in all patients with a history of GML [gastric MALT lymphoma] to detect gastric cancer as early as possible," they wrote.
Dr. Wündisch, of Heinrich-Heine-Universität in Düsseldorf, Germany, and his colleagues studied 120 patients (63 female, mean age 62 years) recruited between June 1993 and July 1999 with stage EI1 gastric mucosa–associated lymphoid tissue (MALT) lymphoma according to the Ann Arbor system, where lymphoma is limited to the mucosa and submucosa of the stomach with no lymph node involvement.
Patients in this multicenter study underwent H. pylori eradication therapy consisting of a 2-week course of amoxicillin (750 mg three times daily) and omeprazole (40 mg three times daily).
Endoscopy was performed monthly until complete histologic remission, defined as macroscopic disappearance of lymphoma and absence of lymphoma on biopsy in two consecutive analyses, and then every 6-12 months. Patients were followed for a median of 122 months after H. pylori eradication (range, 1-171 months).
Dr. Wündisch and his colleagues reported that 96 of the 120 patients with complete follow-up (80%) achieved complete GML remission between 1 and 28 months after eradication therapy began, and 80% of them (77/96) remained disease free (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.06.035]).
Histologic residual disease was seen in 16 out of 96 patients; indeed, it was likely "ongoing histological residual disease rather than complete remission, as the microscopic lesions were small and often found only upon examination of serial sections of one of multiple biopsies."
A "watch and wait" approach was used in these cases, and all but one patient showed complete remission again at the last time point, with a median second remission duration of 46 months. There was also no progression.
"We strongly support this strategy," the investigators wrote.
Overall, the 96 patients with complete GML remission had a 5-year survival rate of 94%, and a 10-year survival of 87%.
Nevertheless, the researchers observed a morbidity ratio of 8.567 for gastric cancer among these patients (95% confidence interval, 3.566-20.582; P less than .001) and 18.621 for non-Hodgkin’s lymphoma (95% CI, 8.365-41.448; P less than 10–6), compared with the general population. The morbidity rate for all cancers was also elevated, at 1.689, but this was not statistically significant.
According to the researchers, although treatment-related factors often contribute to the development of second cancers in patients with lymphoma, the 2-week-long H. pylori regimen employed was unlikely to cause long-term toxic effects.
"Patient-related factors, such as gene polymorphisms, might play a more important role in the development of GML and second cancers in our patients, but these factors have yet to be identified," they said.
In any case, "currently, follow-up of patients without significant comorbidities should extend beyond 5 years for detecting reinfection, relapse, second lymphoma, and early gastric cancer."
The authors stated that the study was funded by a grant from Deutsche Krebshilfe, and they had no personal disclosures.
As many as 80% of gastric MALT lymphoma patients achieve remission after Helicobacter pylori eradication, yet these patients remain at a significantly increased risk for second gastric cancers and lymphomas, reported Dr. Thomas Wündisch and his colleagues in Gastroenterology.
"The clinical consequence of this should be yearly lifelong endoscopic follow-up in all patients with a history of GML [gastric MALT lymphoma] to detect gastric cancer as early as possible," they wrote.
Dr. Wündisch, of Heinrich-Heine-Universität in Düsseldorf, Germany, and his colleagues studied 120 patients (63 female, mean age 62 years) recruited between June 1993 and July 1999 with stage EI1 gastric mucosa–associated lymphoid tissue (MALT) lymphoma according to the Ann Arbor system, where lymphoma is limited to the mucosa and submucosa of the stomach with no lymph node involvement.
Patients in this multicenter study underwent H. pylori eradication therapy consisting of a 2-week course of amoxicillin (750 mg three times daily) and omeprazole (40 mg three times daily).
Endoscopy was performed monthly until complete histologic remission, defined as macroscopic disappearance of lymphoma and absence of lymphoma on biopsy in two consecutive analyses, and then every 6-12 months. Patients were followed for a median of 122 months after H. pylori eradication (range, 1-171 months).
Dr. Wündisch and his colleagues reported that 96 of the 120 patients with complete follow-up (80%) achieved complete GML remission between 1 and 28 months after eradication therapy began, and 80% of them (77/96) remained disease free (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.06.035]).
Histologic residual disease was seen in 16 out of 96 patients; indeed, it was likely "ongoing histological residual disease rather than complete remission, as the microscopic lesions were small and often found only upon examination of serial sections of one of multiple biopsies."
A "watch and wait" approach was used in these cases, and all but one patient showed complete remission again at the last time point, with a median second remission duration of 46 months. There was also no progression.
"We strongly support this strategy," the investigators wrote.
Overall, the 96 patients with complete GML remission had a 5-year survival rate of 94%, and a 10-year survival of 87%.
Nevertheless, the researchers observed a morbidity ratio of 8.567 for gastric cancer among these patients (95% confidence interval, 3.566-20.582; P less than .001) and 18.621 for non-Hodgkin’s lymphoma (95% CI, 8.365-41.448; P less than 10–6), compared with the general population. The morbidity rate for all cancers was also elevated, at 1.689, but this was not statistically significant.
According to the researchers, although treatment-related factors often contribute to the development of second cancers in patients with lymphoma, the 2-week-long H. pylori regimen employed was unlikely to cause long-term toxic effects.
"Patient-related factors, such as gene polymorphisms, might play a more important role in the development of GML and second cancers in our patients, but these factors have yet to be identified," they said.
In any case, "currently, follow-up of patients without significant comorbidities should extend beyond 5 years for detecting reinfection, relapse, second lymphoma, and early gastric cancer."
The authors stated that the study was funded by a grant from Deutsche Krebshilfe, and they had no personal disclosures.
FROM GASTROENTEROLOGY
Major Finding: Of 120 participants, 96 (80%) achieved complete remission of gastric MALT lymphoma, and 80% of them (77/96) remained disease free.
Data Source: A prospective, multicenter trial of 120 patients over a median 10 years of follow-up.
Disclosures: The authors stated that the study was funded by a grant from Deutsche Krebshilfe, and they had no personal disclosures.
Ablation Cost Effective for High-Grade Dysplasia in Barrett's Esophagus
Radiofrequency ablation for high-grade dysplasia in the setting of Barrett’s esophagus is more cost effective than endoscopic surveillance until progression to cancer, reported Dr. Chin Hur and his colleagues in the September issue of Gastroenterology.
Moreover, the use of radiofrequency ablation (RFA) for stable, confirmed low-grade dysplasia can also be cost effective, said the investigators.
Dr. Hur of Harvard University and Massachusetts General Hospital, both in Boston, and his colleagues conducted several analyses comparing three treatment strategies for each of three disease states: Barrett’s esophagus with high-grade dysplasia, Barrett’s esophagus with low-grade dysplasia, and Barrett’s esophagus with no dysplasia.
The treatment strategies consisted of surveillance followed by esophagectomy upon disease progression to cancer, RFA upon disease progression to a higher-grade dysplasia or cancer, or initial RFA before disease progression (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.05.010]).
Cost calculations were based on Medicare reimbursement rates for 2011. The cost estimate for RFA, for example, was $6,400, and the cost of esophagectomy was $25,882. Based on these values, the authors then conducted a base-case analysis.
They found that in high-grade dysplasia, the strategy of initial RFA resulted in 0.704 more quality-adjusted life-years (QALYs) and cost $25,609 less than the strategy of surveillance without RFA followed by esophagectomy upon disease progression to cancer, assuming a 1% disease progression rate.
Similarly, in low-grade dysplasia, RFA upon disease progression to high-grade dysplasia also bested the strategy of surveillance until cancer and esophagectomy, resulting in 0.17 more QALYs and costing $7,446 less, assuming a 0.5% progression rate.
However, in low-grade dysplasia, when comparing initial RFA versus surveillance until progression to high-grade dysplasia and then RFA, the authors found that the latter approach cost only $1,969 less than the former, and that the former was associated with a 0.108 gain in QALYs.
That amounted to an incremental cost-effectiveness ratio of $18,231 per QALY – "below our willingness-to-pay threshold of $100,000/QALY, making it the most plausible strategy in terms of cost-effectiveness."
Finally, in scenarios involving Barrett’s esophagus but no dysplasia, RFA upon progression of disease to high-grade dysplasia was still the most cost-effective strategy: It was associated with a savings of $7,709 as well as 0.194 additional QALYs, compared with esophagectomy upon disease progression to cancer, assuming a 0.33% progression rate.
The authors noted that their model relies on a stringent definition of low-grade dysplasia that assumes "review and agreement between more than one expert pathologist" as well as a consistent level of dysplasia found on more than one endoscopy spaced at least 6 months apart. In addition, the progression rates used in this analysis were based on the current literature, but were still estimates involving some uncertainty.
"We believe that a multicenter, randomized, controlled trial for initial RF ablation versus surveillance in patients with BE without dysplasia is needed to confirm our model results and to inform clinical decision making," they added.
Long-term follow-up data from such a study could "provide much needed data regarding cancer progression and the need for surveillance, which significantly impacts the cost-effectiveness and patients’ preferences for RFA."
The authors stated that they had no disclosures relevant to this study. The study was supported by grants from the National Institutes of Health.
Radiofrequency ablation for high-grade dysplasia in the setting of Barrett’s esophagus is more cost effective than endoscopic surveillance until progression to cancer, reported Dr. Chin Hur and his colleagues in the September issue of Gastroenterology.
Moreover, the use of radiofrequency ablation (RFA) for stable, confirmed low-grade dysplasia can also be cost effective, said the investigators.
Dr. Hur of Harvard University and Massachusetts General Hospital, both in Boston, and his colleagues conducted several analyses comparing three treatment strategies for each of three disease states: Barrett’s esophagus with high-grade dysplasia, Barrett’s esophagus with low-grade dysplasia, and Barrett’s esophagus with no dysplasia.
The treatment strategies consisted of surveillance followed by esophagectomy upon disease progression to cancer, RFA upon disease progression to a higher-grade dysplasia or cancer, or initial RFA before disease progression (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.05.010]).
Cost calculations were based on Medicare reimbursement rates for 2011. The cost estimate for RFA, for example, was $6,400, and the cost of esophagectomy was $25,882. Based on these values, the authors then conducted a base-case analysis.
They found that in high-grade dysplasia, the strategy of initial RFA resulted in 0.704 more quality-adjusted life-years (QALYs) and cost $25,609 less than the strategy of surveillance without RFA followed by esophagectomy upon disease progression to cancer, assuming a 1% disease progression rate.
Similarly, in low-grade dysplasia, RFA upon disease progression to high-grade dysplasia also bested the strategy of surveillance until cancer and esophagectomy, resulting in 0.17 more QALYs and costing $7,446 less, assuming a 0.5% progression rate.
However, in low-grade dysplasia, when comparing initial RFA versus surveillance until progression to high-grade dysplasia and then RFA, the authors found that the latter approach cost only $1,969 less than the former, and that the former was associated with a 0.108 gain in QALYs.
That amounted to an incremental cost-effectiveness ratio of $18,231 per QALY – "below our willingness-to-pay threshold of $100,000/QALY, making it the most plausible strategy in terms of cost-effectiveness."
Finally, in scenarios involving Barrett’s esophagus but no dysplasia, RFA upon progression of disease to high-grade dysplasia was still the most cost-effective strategy: It was associated with a savings of $7,709 as well as 0.194 additional QALYs, compared with esophagectomy upon disease progression to cancer, assuming a 0.33% progression rate.
The authors noted that their model relies on a stringent definition of low-grade dysplasia that assumes "review and agreement between more than one expert pathologist" as well as a consistent level of dysplasia found on more than one endoscopy spaced at least 6 months apart. In addition, the progression rates used in this analysis were based on the current literature, but were still estimates involving some uncertainty.
"We believe that a multicenter, randomized, controlled trial for initial RF ablation versus surveillance in patients with BE without dysplasia is needed to confirm our model results and to inform clinical decision making," they added.
Long-term follow-up data from such a study could "provide much needed data regarding cancer progression and the need for surveillance, which significantly impacts the cost-effectiveness and patients’ preferences for RFA."
The authors stated that they had no disclosures relevant to this study. The study was supported by grants from the National Institutes of Health.
Radiofrequency ablation for high-grade dysplasia in the setting of Barrett’s esophagus is more cost effective than endoscopic surveillance until progression to cancer, reported Dr. Chin Hur and his colleagues in the September issue of Gastroenterology.
Moreover, the use of radiofrequency ablation (RFA) for stable, confirmed low-grade dysplasia can also be cost effective, said the investigators.
Dr. Hur of Harvard University and Massachusetts General Hospital, both in Boston, and his colleagues conducted several analyses comparing three treatment strategies for each of three disease states: Barrett’s esophagus with high-grade dysplasia, Barrett’s esophagus with low-grade dysplasia, and Barrett’s esophagus with no dysplasia.
The treatment strategies consisted of surveillance followed by esophagectomy upon disease progression to cancer, RFA upon disease progression to a higher-grade dysplasia or cancer, or initial RFA before disease progression (Gastroenterology 2012 [doi: 10.1053/j.gastro.2012.05.010]).
Cost calculations were based on Medicare reimbursement rates for 2011. The cost estimate for RFA, for example, was $6,400, and the cost of esophagectomy was $25,882. Based on these values, the authors then conducted a base-case analysis.
They found that in high-grade dysplasia, the strategy of initial RFA resulted in 0.704 more quality-adjusted life-years (QALYs) and cost $25,609 less than the strategy of surveillance without RFA followed by esophagectomy upon disease progression to cancer, assuming a 1% disease progression rate.
Similarly, in low-grade dysplasia, RFA upon disease progression to high-grade dysplasia also bested the strategy of surveillance until cancer and esophagectomy, resulting in 0.17 more QALYs and costing $7,446 less, assuming a 0.5% progression rate.
However, in low-grade dysplasia, when comparing initial RFA versus surveillance until progression to high-grade dysplasia and then RFA, the authors found that the latter approach cost only $1,969 less than the former, and that the former was associated with a 0.108 gain in QALYs.
That amounted to an incremental cost-effectiveness ratio of $18,231 per QALY – "below our willingness-to-pay threshold of $100,000/QALY, making it the most plausible strategy in terms of cost-effectiveness."
Finally, in scenarios involving Barrett’s esophagus but no dysplasia, RFA upon progression of disease to high-grade dysplasia was still the most cost-effective strategy: It was associated with a savings of $7,709 as well as 0.194 additional QALYs, compared with esophagectomy upon disease progression to cancer, assuming a 0.33% progression rate.
The authors noted that their model relies on a stringent definition of low-grade dysplasia that assumes "review and agreement between more than one expert pathologist" as well as a consistent level of dysplasia found on more than one endoscopy spaced at least 6 months apart. In addition, the progression rates used in this analysis were based on the current literature, but were still estimates involving some uncertainty.
"We believe that a multicenter, randomized, controlled trial for initial RF ablation versus surveillance in patients with BE without dysplasia is needed to confirm our model results and to inform clinical decision making," they added.
Long-term follow-up data from such a study could "provide much needed data regarding cancer progression and the need for surveillance, which significantly impacts the cost-effectiveness and patients’ preferences for RFA."
The authors stated that they had no disclosures relevant to this study. The study was supported by grants from the National Institutes of Health.
FROM GASTROENTEROLOGY