User login
Record Number of Physicians Pass Hospice and Palliative Medicine Exam
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
VIDEO: Five Reasons You Should Attend Hospital Medicine 2013 in Washington, D.C.
New State Law Advances Malpractice Liability Reform
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
A new Oregon state law that creates a process to keep frivolous medical malpractice lawsuits out of the courts is a step in the right direction, says one hospitalist.
But uncertainty remains.
Jay Ham, MD, a hospitalist at Providence Newberg Medical Center in Newberg, Ore., says many hospitalists are still learning the ins and outs of the new law, which includes a definition for adverse healthcare incidents and establishes a procedure for providers and patients to discuss those incidents outside of court. The new law also provides for a mediation process.
The lawsuit mediation bill, signed into law earlier this month by Gov. John Kitzhaber, makes discussions between health care providers and patients "confidential and inadmissible with exception." The law does not preclude patients from later filing negligence claims.
"Allowing apologies and admission of guilt in this to be inadmissible at any later civil proceedings seems a nice touch," says Dr. Ham. "Deducting any awards given in the mediation process from civil court damages, while preventing knowledge of the initial award amount, also seems fair."
But there are areas of concern, he says. While most proceedings under the process "appear protected from disclosure if a civil case does go forward," there are caveats that might discourage some physicians from using the process, such as using discussions during the private process that contradict statements made in a court case. Also, there are questions about what types of cases will qualify for discussion outside the court system.
Still, the new law brings medical malpractice liability reform a bit closer, even if it doesn't reduce liability costs, Dr. Ham says. "Changing the cost of medicine doesn't need to be the defining impetus to implement reasonable [liability] reform," Dr. Ham says.
Read SHM's position statement on medical liability reform or visit our website for more information on medical malpractice liability.
In the Literature: Research You Need to Know
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does the use of steroids and/or antivirals improve recovery in patients with newly diagnosed Bell's palsy?
Background: The American Academy of Neurology's last recommendation in 2001 stated that steroids were probably effective and antivirals possibly effective. The current review and recommendations looked at additional studies published since 2000.
Study design: Systematic review of MEDLINE and Cochrane Database of Systematic Reviews data published since June 2000.
Setting: Prospective controlled studies from Germany, Sweden, Scotland, Italy, South Korea, Japan, and Bangladesh.
Synopsis: The authors identified nine studies that fulfilled inclusion criteria. Two of these studies examined treatment with steroids alone and were judged to have the lowest risk for bias. Both studies enrolled patients within three days of symptom onset, continued treatment for 10 days, and demonstrated a significant increase in the probability of complete recovery in patients randomized to steroids (NNT 6-8). Two high-quality studies were identified that looked at the addition of antivirals to steroids. Neither study showed a statistically significant benefit.
Of note, the studies did not quantify the risk of harm from steroid use in patients with comorbidities, such as diabetes. Thus, the authors concluded that in some patients, it would be reasonable to consider limiting steroid use.
Bottom line: For patients with new-onset Bell’s palsy, steroids increase the probability of recovery of facial nerve function. Patients offered antivirals should be counseled that a benefit from antivirals has not been established and, if there is a benefit, it is modest at best.
Citation: Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012;79(22):2209-2213.
Visit our website for more physician reviews of recent HM-relevant literature.
Hospitalists on Alert as CRE Infections Spike
Hospitalists should be on the lookout for carbapenem-resistant Enterobacteriaceae (CRE) infections, says one author of a CDC report that noted a three-fold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem within the past decade.
Earlier this month, the CDC's Morbidity and Mortality Weekly Report revealed that the percentage of CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
"It is a very serious public health threat," says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC's Division of Healthcare Quality Promotion. "Maybe it's not that common now, but with no action, it has the potential to become much more common, like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission."
Dr. Kallen says HM groups can help reduce the spread of CRE through antibiotic stewardship, the review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene. Hospitalists also play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions, such as skilled-nursing or assisted-living facilities, he says.
Dr. Kallen added that hospitalists should not dismiss CRE, even if they rarely encounter it.
"If you're a place that doesn't see this very often, and you see one, that's a big deal," he adds. "It needs to be acted on aggressively. Being proactive is much more effective than waiting until it's common and then trying to intervene."
Visit our website for more information on hospital-acquired infections.
Hospitalists should be on the lookout for carbapenem-resistant Enterobacteriaceae (CRE) infections, says one author of a CDC report that noted a three-fold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem within the past decade.
Earlier this month, the CDC's Morbidity and Mortality Weekly Report revealed that the percentage of CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
"It is a very serious public health threat," says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC's Division of Healthcare Quality Promotion. "Maybe it's not that common now, but with no action, it has the potential to become much more common, like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission."
Dr. Kallen says HM groups can help reduce the spread of CRE through antibiotic stewardship, the review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene. Hospitalists also play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions, such as skilled-nursing or assisted-living facilities, he says.
Dr. Kallen added that hospitalists should not dismiss CRE, even if they rarely encounter it.
"If you're a place that doesn't see this very often, and you see one, that's a big deal," he adds. "It needs to be acted on aggressively. Being proactive is much more effective than waiting until it's common and then trying to intervene."
Visit our website for more information on hospital-acquired infections.
Hospitalists should be on the lookout for carbapenem-resistant Enterobacteriaceae (CRE) infections, says one author of a CDC report that noted a three-fold increase in the proportion of Enterobacteriaceae bugs that proved resistant to carbapenem within the past decade.
Earlier this month, the CDC's Morbidity and Mortality Weekly Report revealed that the percentage of CRE infections jumped to 4.2% in 2011 from 1.2% in 2001, according to data from the National Nosocomial Infection Surveillance system.
"It is a very serious public health threat," says co-author Alex Kallen, MD, MPH, a medical epidemiologist and outbreak response coordinator in the CDC's Division of Healthcare Quality Promotion. "Maybe it's not that common now, but with no action, it has the potential to become much more common, like a lot of the other MDROs [multidrug-resistant organisms] that hospitalists see regularly. [Hospitalists] have a lot of control over some of the things that could potentially lead to increased transmission."
Dr. Kallen says HM groups can help reduce the spread of CRE through antibiotic stewardship, the review of detailed patient histories to ferret out risk factors, and dedication to contact precautions and hand hygiene. Hospitalists also play a leadership role in coordinating efforts for patients transferring between hospitals and other institutions, such as skilled-nursing or assisted-living facilities, he says.
Dr. Kallen added that hospitalists should not dismiss CRE, even if they rarely encounter it.
"If you're a place that doesn't see this very often, and you see one, that's a big deal," he adds. "It needs to be acted on aggressively. Being proactive is much more effective than waiting until it's common and then trying to intervene."
Visit our website for more information on hospital-acquired infections.
Foundation Chips in to Reduce 30-Day Readmissions
The Robert Wood Johnson Foundation of Princeton, N.J., the country’s largest healthcare-focused philanthropy, has undertaken a number of initiatives to improve care transitions and reduce preventable hospital readmissions.
One of the key conclusions from these initiatives, says Anne Weiss, MPP, director of the foundation's Quality/Equality Health Care Team, is that hospitals and hospitalists can't do it alone. "Hospitals are now being held financially accountable for something they can't possibly control," Weiss says, referring to whether or not the discharged patient returns to the hospital within 30 days.
The foundation has mobilized broad community coalitions through its Aligning Forces for Quality campaign, bringing together healthcare providers, purchasers, consumers, and other stakeholders to improve care transitions. One such coalition, Better Health Greater Cleveland of Ohio, announced a 10.7% reduction in avoidable hospitalizations for common cardiac conditions in 2011.
Successful care transitions also require healthcare providers to appreciate the need for patients and their families to engage in their plans for post-discharge care, Weiss says. "I have been stunned to learn the kinds of medical tasks patients and families are now expected to conduct when they go home," she adds. "I hear them say, 'Nobody told us we would have to flush IVs.'"
Through another initiative, the foundation produced an interactive map that displays the percentage of patients readmitted to hospitals within 30 days of discharge; it has supported research that found improvements in nurses' work environments helped to reduce avoidable hospital readmissions. It also has produced a "Transitions to Better Care" video contest for hospitals, as well as a national publicity campaign about these issues called "Care About Your Care."
Visit our website for more information about patient care transitions.
The Robert Wood Johnson Foundation of Princeton, N.J., the country’s largest healthcare-focused philanthropy, has undertaken a number of initiatives to improve care transitions and reduce preventable hospital readmissions.
One of the key conclusions from these initiatives, says Anne Weiss, MPP, director of the foundation's Quality/Equality Health Care Team, is that hospitals and hospitalists can't do it alone. "Hospitals are now being held financially accountable for something they can't possibly control," Weiss says, referring to whether or not the discharged patient returns to the hospital within 30 days.
The foundation has mobilized broad community coalitions through its Aligning Forces for Quality campaign, bringing together healthcare providers, purchasers, consumers, and other stakeholders to improve care transitions. One such coalition, Better Health Greater Cleveland of Ohio, announced a 10.7% reduction in avoidable hospitalizations for common cardiac conditions in 2011.
Successful care transitions also require healthcare providers to appreciate the need for patients and their families to engage in their plans for post-discharge care, Weiss says. "I have been stunned to learn the kinds of medical tasks patients and families are now expected to conduct when they go home," she adds. "I hear them say, 'Nobody told us we would have to flush IVs.'"
Through another initiative, the foundation produced an interactive map that displays the percentage of patients readmitted to hospitals within 30 days of discharge; it has supported research that found improvements in nurses' work environments helped to reduce avoidable hospital readmissions. It also has produced a "Transitions to Better Care" video contest for hospitals, as well as a national publicity campaign about these issues called "Care About Your Care."
Visit our website for more information about patient care transitions.
The Robert Wood Johnson Foundation of Princeton, N.J., the country’s largest healthcare-focused philanthropy, has undertaken a number of initiatives to improve care transitions and reduce preventable hospital readmissions.
One of the key conclusions from these initiatives, says Anne Weiss, MPP, director of the foundation's Quality/Equality Health Care Team, is that hospitals and hospitalists can't do it alone. "Hospitals are now being held financially accountable for something they can't possibly control," Weiss says, referring to whether or not the discharged patient returns to the hospital within 30 days.
The foundation has mobilized broad community coalitions through its Aligning Forces for Quality campaign, bringing together healthcare providers, purchasers, consumers, and other stakeholders to improve care transitions. One such coalition, Better Health Greater Cleveland of Ohio, announced a 10.7% reduction in avoidable hospitalizations for common cardiac conditions in 2011.
Successful care transitions also require healthcare providers to appreciate the need for patients and their families to engage in their plans for post-discharge care, Weiss says. "I have been stunned to learn the kinds of medical tasks patients and families are now expected to conduct when they go home," she adds. "I hear them say, 'Nobody told us we would have to flush IVs.'"
Through another initiative, the foundation produced an interactive map that displays the percentage of patients readmitted to hospitals within 30 days of discharge; it has supported research that found improvements in nurses' work environments helped to reduce avoidable hospital readmissions. It also has produced a "Transitions to Better Care" video contest for hospitals, as well as a national publicity campaign about these issues called "Care About Your Care."
Visit our website for more information about patient care transitions.
ONLINE EXCLUSIVE: Society of Physician Entrepreneurs Co-Founder Talks about MD Career Changes
Click here to listen to Dr. Hausfeld, managing director of FMS Financial Solutions, Greenbelt, Md., co-founder and treasurer of the Society of Physician Entrepreneurs.
Click here to listen to Dr. Hausfeld, managing director of FMS Financial Solutions, Greenbelt, Md., co-founder and treasurer of the Society of Physician Entrepreneurs.
Click here to listen to Dr. Hausfeld, managing director of FMS Financial Solutions, Greenbelt, Md., co-founder and treasurer of the Society of Physician Entrepreneurs.
Society of Hospital Medicine Launches Online Training Program for Hospitalists
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Hospitalists play an increasingly pivotal role in ensuring the highest quality and safety for patients in hospitals. The implementation of healthcare reform has only heightened the importance of hospital quality and patient safety for hospitalists. To enable education and advancement of quality improvement (QI), SHM has developed the Hospital Quality & Patient Safety (HQPS) Online Academy (http://www.hospitalmedicine.org/hqps).
The HQPS Online Academy consists of Internet-based modules that provide training not included in traditional medical education. These modules bridge the gap between the conceptualization and practice of quality in hospitals, helping hospitalists to prepare and lead quality initiatives to improve patient outcomes. The modules allow healthcare providers to explore and evaluate current quality initiatives and practices, as well as reflect on ways to improve core measures within their hospital.
Each module focuses on a core principle of QI and patient safety, and provides three AMA PRA Category 1 credits.
SHM members who are insured with The Doctors Company can earn a 5% risk-management credit by completing the first five HQPS modules (see below). Eligible members also enjoy premium savings through a 5% program discount and a claims-free credit of up to 25%.
HQPS Online Academy modules
- Quality measurement and stakeholder interests
- Teamwork and communication
- Organizational knowledge and leadership skills
- Patient safety principles
- Quality and safety improvement methods and skills (RCA and FMEA)
Survey Shows Five-Year Decrease in Employee Benefits, Paid Time Off for Hospitalists
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
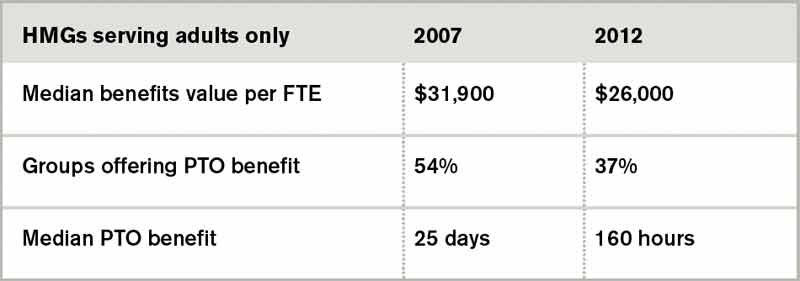
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
For the first time in several years, SHM included questions about employee benefits and paid time off in its 2012 State of Hospital Medicine survey. The median value of benefits per physician FTE reported by HM groups serving adults only was $26,000, according to the 2012 survey. But what a surprise it was when survey respondents in 2007 reported median benefits of $31,900.
I admit to being flummoxed by the decrease. The definition of “benefits” was identical in both surveys. The only difference is that in 2007, SHM collected actual benefit cost for each individual on the individual questionnaire; in 2012, we asked for the average benefits per FTE for the group. One possible explanation is that some respondents simply guessed about the average, because they didn’t have to report data for individual doctors. Of course, it’s also possible that groups are requiring physicians to pay a higher proportion of insurance premiums or are reducing retirement plan contributions due to the weak economy. But in the work I do with hospitalist groups around the country, I rarely see benefit costs below about $35,000.
Source: 2012 State of Hospital Medicine report
Another interesting finding from the 2012 survey is that 37% of adult medicine groups reported offering paid time off (PTO), down from 54% in 2007. Even among groups using a seven-on/seven-off schedule, the PTO rate was only 44%. Does this represent a survey design or respondent input error, differences in respondent populations, or an actual shift in the prevalence of PTO benefits? I suspect it’s the latter, because the median amount of PTO time awarded has also declined. In 2007, adult HMGs reported a median of 25 PTO days annually. In 2012, the median for those groups offering PTO was 160 hours of PTO, which represents somewhere around 13 to 20 days, depending on shift length.
Why might PTO benefits be declining? I suppose it could be belt-tightening associated with the poor economy. But I think many HM groups simply have found PTO benefits difficult to administer and fraught with unintended consequences. Many groups are so thinly staffed that for someone to take a PTO day, someone else must work extra to cover. Then, when the covering doctor takes PTO, the first doctor must work extra—effectively offsetting the value of PTO. And if a hospitalist takes PTO and also works extra shifts in the same pay period, do these two offset each other? Or does the doctor get paid for both the PTO days and the extra shift days?
For clinicians such as hospitalists, whose work is defined in highly variable, shift-based schedules that include a lot of night and weekend work, it becomes very difficult to determine which of the days not worked were PTO days versus just days the doctor wasn’t scheduled.
Personally, I don’t think it makes much sense for most hospitalists to have PTO. Don’t get me wrong—I think hospitalists should be paid well and have generous amounts of time off in exchange for long, challenging workdays and a disproportionate amount of night and weekend work. But arbitrarily assigning some of the days not worked as PTO while others are just unscheduled days seems unnecessarily complex.
Time will tell if the specialty as a whole agrees with me or not.
Leslie Flores is a principal in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Hospital Medicine Advocates Aid in Securing $10 Million for National Quality Forum
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.
Hospitalists on the Hill
WHEN: May 16, 2013
WHERE: Washington, D.C.
HOW: Register today at www.hospitalmedicine2013.org/onthehill Space is limited.
The American Taxpayer Relief Act, which was signed into law Jan. 3 to stave off the fiscal cliff, contained a little-mentioned provision that reauthorized $10 million in Medicare funding for the National Quality Forum (NQF). Hospitalists, taking on the role of policy advocates, helped secure this reauthorization and score a victory for national quality-improvement (QI) efforts.
The NQF is a nonprofit organization established to create consensus around national priorities and measures for performing reporting and improvement in healthcare. It receives funding through a variety of sources ranging from public funds, private organizations and membership dues. Since 2009, it has received $10 million annually from a U.S. Department of Health and Human Services contract. That contract, a significant portion of NQF funding, was set to end in 2012.
The Stand for Quality coalition, composed of healthcare organizations supportive of the NQF, helps ensure that Congress sustains funding and support of performance measurement reporting and QI. SHM historically has been a strong proponent of the NQF, pitching in at the start of Stand for Quality four years ago this month. As it became clear that the federal contract for the NQF was not likely to be renewed by Congress for the 2013 calendar year, the member organizations of Stand for Quality were asked to step up to the plate in any way they could.
Jumping at the opportunity to assist, SHM linked hospitalists to their members of Congress in support of the NQF. Through members of SHM's Public Policy and Performance Measurement and Reporting committees, SHM connected with congressional offices and urged them to join a sign-on letter from the office of U.S. Sen. Mark Begich (D-Alaska) office in support of continued NQF funding. Letters between members of Congress are a way that legislators internally lobby on behalf of a particular issue. Hearing from their constituents can help persuade a legislator to act.
Sharing professional expertise also can inform a legislator's decisions. SHM members have a wealth of specialized knowledge and experiences that greatly benefit health policy discussions. In December 2012, SHM was asked to join NQF staffers and several other organizations on Capitol Hill for visits with select members of Congress, including several physician-legislators. These meetings were designed to raise the profile of the important work NQF is doing for QI and to make sure that NQF funding was not forgotten in any debt deal.
Mangla Gulati, MD, FACP, FHM, a hospitalist and SHM member, participated in these visits on behalf of hospital medicine and provided much-needed physician input on the importance of NQF's work.
The benefits of in-person visits are mutual: Members of Congress learn more about the real-life effects of a particular policy and, according to Dr. Gulati, "the visits to the Hill were a very valuable experience and shed a whole new light on the challenges we face in medicine."
Taken together, these advocacy tactics—coalition-building, contacting congressional offices, and in-person visits in Washington—were crucial to securing NQF's funding reauthorization and are critical tools for the advocacy work at SHM. The most concrete and impactful advocacy includes positioning hospitalists on the front line and sharing their perspectives and experiences with policymakers and their staffs.
We hope you'll heed this call and join SHM in Washington, D.C., May 16 for Hospitalists on the Hill, part of SHM's annual meeting. For more information and to register, go to www.hospitalmedicine2013.org/onthehill.
Joshua Lapps is SHM's government relations specialist.