User login
1.02 Common Clinical Diagnoses and Conditions: Acute Gastroenteritis
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1.01 Common Clinical Diagnoses and Conditions: Acute Abdominal Pain and Acute Abdomen
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Pediatric Hospital Medicine Core Competencies: 2020 Revision. Table of Contents
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
The Pediatric Hospital Medicine Core Competencies: 2020 Revision Dedication

Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
APPENDIX
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
The Pediatric Hospital Medicine Core Competencies: 2020 Revision. Authors, Editors, and Reviewers
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
The Pediatric Hospital Medicine Core Competencies: 2020 Revision. Introduction and Methodology
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14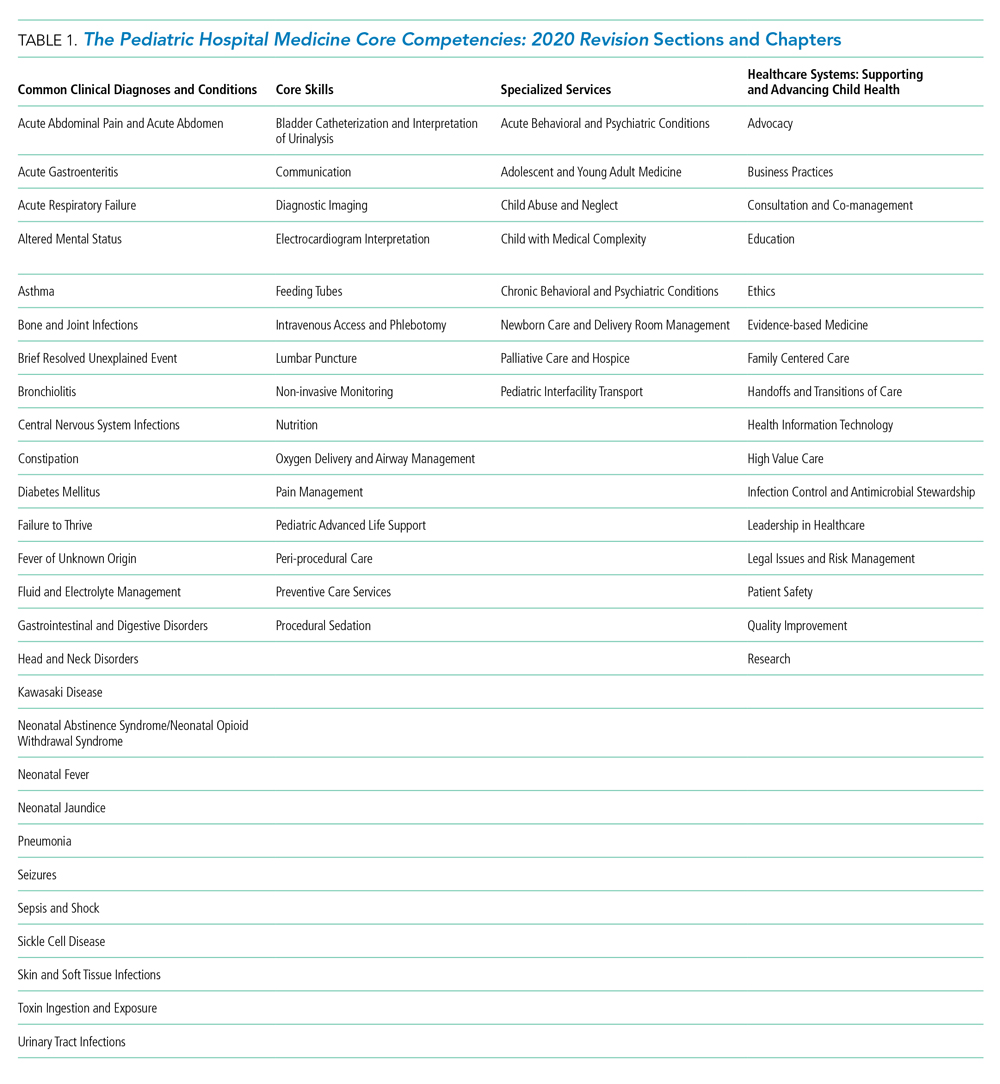
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.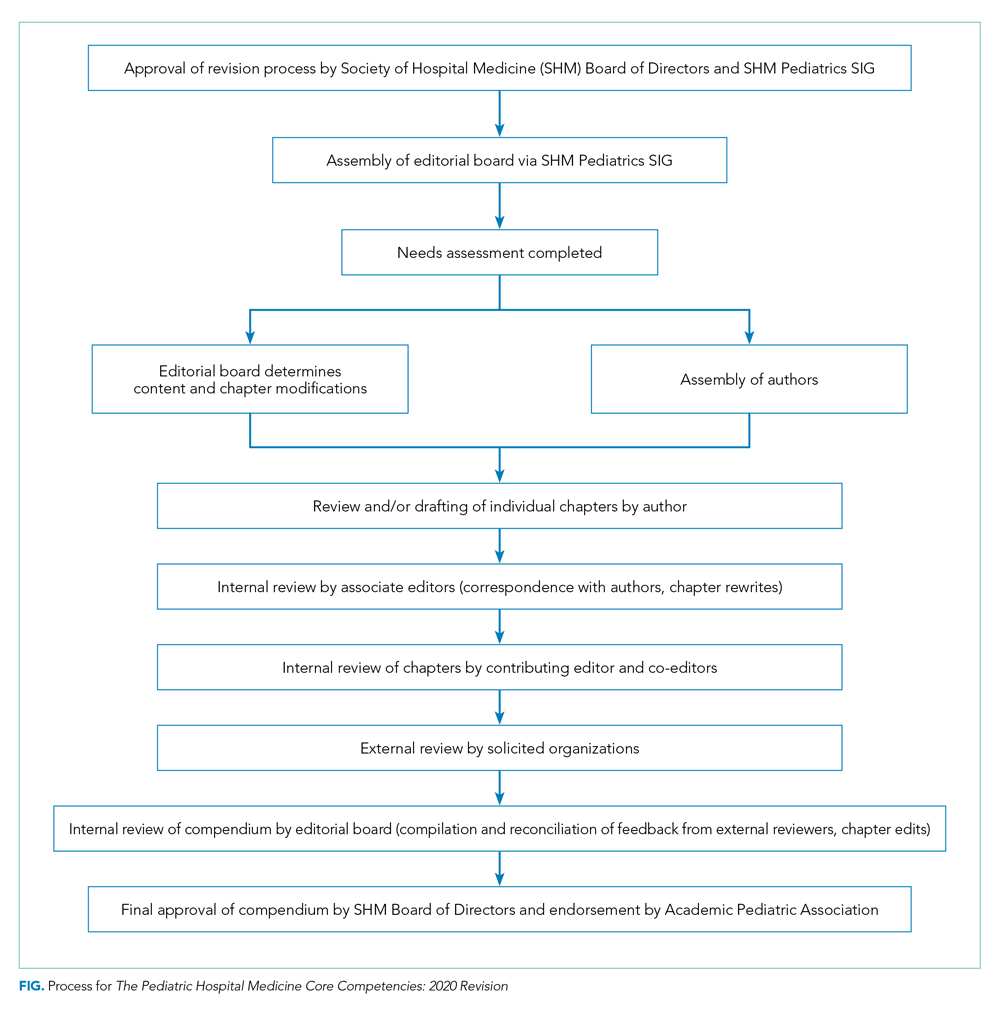
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.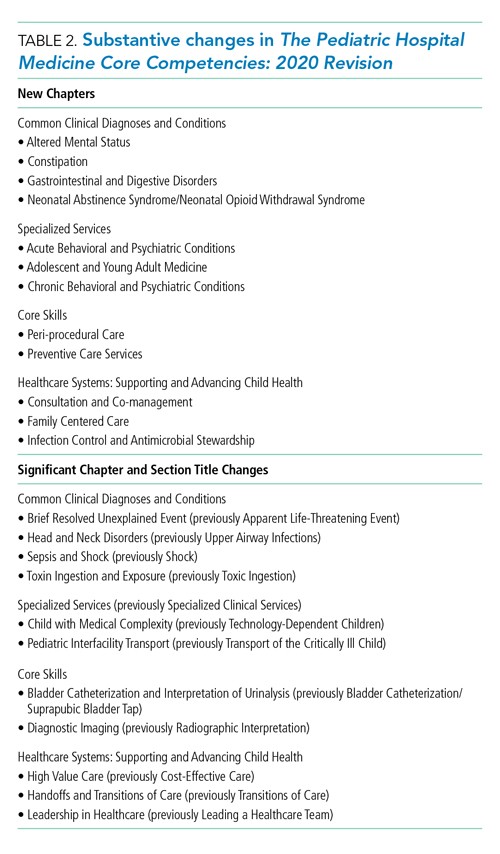
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
© 2020 Society of Hospital Medicine
Now Available: The 2017 JHM Core Competencies Compendium.
Want all 52 Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
Want all 52 Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
Want all 52 Core Competency articles in an easy-to-read compendium? Order your copy now from Amazon.com.
2017 Revision Editors
Core Competencies Table of Contents
2017 REVISION EDITORS
Satyen Nichani, MD, FHM
Director of Education, Hospital Medicine Program
Assistant Professor of Medicine
Department of Internal Medicine
Michigan Medicine
University of Michigan, Ann Arbor, MI
Nick Fitterman, MD, SFHM, FACP
Vice Chair, Hospital Medicine
Northwell Health
Associate Professor of Medicine
Hofstra Northwell School of Medicine
Long Island Jewish Medical Center
New Hyde Park, NY
Michel Lukela, MD, SFHM, FACP, FAAP
Director, Medicine-Pediatrics Residency Program
Clinical Associate Professor, Internal Medicine
Clinical Associate Professor, Pediatrics
Michigan Medicine
University of Michigan, Ann Arbor, MI
Jonathan Crocker, MD, FHM
Assistant Professor of Medicine
Harvard Medical School
Hospitalist, Department of Medicine
Assistant Program Director, Internal Medicine
Director Global Health Program, Internal Medicine
Director Global Health Fellowship in Medicine
Beth Israel Deaconess Medical Center
Boston, MA
CONTRIBUTING 2006 EDITORIAL TEAM
Daniel D. Dressler, MD, MSc, SFHM, FACP
Professor of Medicine
Associate Program Director, J. Willis Hurst Internal Medicine Residency Program
Co-Director, Simmelweis Society
Emory University School of Medicine
Atlanta, GA
Tina Budnitz, MPH, MHM
TLB Consulting
Senior Advisor
Society of Hospital Medicine
Peachtree Corners, GA
Alpesh Amin, MD, MBA, MACP, SFHM, FACC
Thomas and Mary Cesario Endowed Chair, Department of Medicine
Professor of Medicine, Business, Public Health, Nursing Science, & Biomedical Engineering
Executive Director, Hospitalist Program
University of California, Irvine
Orange, CA
Michael Pistoria, MEng, DO, FACP, SFHM
Chair, Hospital Medicine and Inpatient Services
Coordinated Health
Lehigh University
Allentown, PA
Sylvia C. McKean, MD, SFHM, FACP
Associate Professor of Medicine
Harvard Medical School
Brigham and Women’s Hospital
Boston, MA
Core Competencies Table of Contents
2017 REVISION EDITORS
Satyen Nichani, MD, FHM
Director of Education, Hospital Medicine Program
Assistant Professor of Medicine
Department of Internal Medicine
Michigan Medicine
University of Michigan, Ann Arbor, MI
Nick Fitterman, MD, SFHM, FACP
Vice Chair, Hospital Medicine
Northwell Health
Associate Professor of Medicine
Hofstra Northwell School of Medicine
Long Island Jewish Medical Center
New Hyde Park, NY
Michel Lukela, MD, SFHM, FACP, FAAP
Director, Medicine-Pediatrics Residency Program
Clinical Associate Professor, Internal Medicine
Clinical Associate Professor, Pediatrics
Michigan Medicine
University of Michigan, Ann Arbor, MI
Jonathan Crocker, MD, FHM
Assistant Professor of Medicine
Harvard Medical School
Hospitalist, Department of Medicine
Assistant Program Director, Internal Medicine
Director Global Health Program, Internal Medicine
Director Global Health Fellowship in Medicine
Beth Israel Deaconess Medical Center
Boston, MA
CONTRIBUTING 2006 EDITORIAL TEAM
Daniel D. Dressler, MD, MSc, SFHM, FACP
Professor of Medicine
Associate Program Director, J. Willis Hurst Internal Medicine Residency Program
Co-Director, Simmelweis Society
Emory University School of Medicine
Atlanta, GA
Tina Budnitz, MPH, MHM
TLB Consulting
Senior Advisor
Society of Hospital Medicine
Peachtree Corners, GA
Alpesh Amin, MD, MBA, MACP, SFHM, FACC
Thomas and Mary Cesario Endowed Chair, Department of Medicine
Professor of Medicine, Business, Public Health, Nursing Science, & Biomedical Engineering
Executive Director, Hospitalist Program
University of California, Irvine
Orange, CA
Michael Pistoria, MEng, DO, FACP, SFHM
Chair, Hospital Medicine and Inpatient Services
Coordinated Health
Lehigh University
Allentown, PA
Sylvia C. McKean, MD, SFHM, FACP
Associate Professor of Medicine
Harvard Medical School
Brigham and Women’s Hospital
Boston, MA
Core Competencies Table of Contents
2017 REVISION EDITORS
Satyen Nichani, MD, FHM
Director of Education, Hospital Medicine Program
Assistant Professor of Medicine
Department of Internal Medicine
Michigan Medicine
University of Michigan, Ann Arbor, MI
Nick Fitterman, MD, SFHM, FACP
Vice Chair, Hospital Medicine
Northwell Health
Associate Professor of Medicine
Hofstra Northwell School of Medicine
Long Island Jewish Medical Center
New Hyde Park, NY
Michel Lukela, MD, SFHM, FACP, FAAP
Director, Medicine-Pediatrics Residency Program
Clinical Associate Professor, Internal Medicine
Clinical Associate Professor, Pediatrics
Michigan Medicine
University of Michigan, Ann Arbor, MI
Jonathan Crocker, MD, FHM
Assistant Professor of Medicine
Harvard Medical School
Hospitalist, Department of Medicine
Assistant Program Director, Internal Medicine
Director Global Health Program, Internal Medicine
Director Global Health Fellowship in Medicine
Beth Israel Deaconess Medical Center
Boston, MA
CONTRIBUTING 2006 EDITORIAL TEAM
Daniel D. Dressler, MD, MSc, SFHM, FACP
Professor of Medicine
Associate Program Director, J. Willis Hurst Internal Medicine Residency Program
Co-Director, Simmelweis Society
Emory University School of Medicine
Atlanta, GA
Tina Budnitz, MPH, MHM
TLB Consulting
Senior Advisor
Society of Hospital Medicine
Peachtree Corners, GA
Alpesh Amin, MD, MBA, MACP, SFHM, FACC
Thomas and Mary Cesario Endowed Chair, Department of Medicine
Professor of Medicine, Business, Public Health, Nursing Science, & Biomedical Engineering
Executive Director, Hospitalist Program
University of California, Irvine
Orange, CA
Michael Pistoria, MEng, DO, FACP, SFHM
Chair, Hospital Medicine and Inpatient Services
Coordinated Health
Lehigh University
Allentown, PA
Sylvia C. McKean, MD, SFHM, FACP
Associate Professor of Medicine
Harvard Medical School
Brigham and Women’s Hospital
Boston, MA
© 2017 Society of Hospital Medicine