User login
Depression and suicide among physicians
Discuss this article at www.facebook.com/CurrentPsychiatry
Dr. G, a second-year surgical resident, becomes depressed when his girlfriend abruptly ends their relationship. His phone calls and e-mails seeking an explanation go unanswered. Having long struggled with his self-esteem, Dr. G interprets this rejection as confirmation of his self-criticism.
Because of his work schedule, Dr. G feels that there is no way to see a therapist or psychiatrist and believes that asking for time off to do so would adversely affect his evaluations. He feels too embarrassed and “weak” to disclose his breakup and depression to his colleagues and attending physicians and senses that fellow residents would resent having to “carry his load.” Dr. G has spent the past 2 years moonlighting at the local emergency room and thinks it would be humiliating to go there for psychiatric help. His work performance and attendance decline until eventually his residency director forces him to take a medical leave of absence.
Dr. G feels that his pain will never end. He writes goodbye letters to his family, makes arrangements for his possessions and funeral, and hangs himself from the balcony outside his apartment.
Although the rate of depression among physicians is comparable to that of the general population, physicians’ risk of suicide is markedly higher.1 Depression and other mood disorders may be under-recognized and inadequately treated in physicians because physicians might:
- be reluctant to seek treatment
- attempt to diagnose and treat themselves
- seek and receive “VIP treatment” from other health care providers.
This article examines physicians’ risk for depression and suicide, licensing concerns and other barriers to effective treatment, and what can be done to overcome such obstacles.
Not immune to depression
Rates of depression are higher in medical students and residents (15% to 30%) than in the general population.2-4 A longitudinal study of medical students at the University of California, San Francisco showed that students’ rates of depression when they enter medical school are similar to those of the general population, but students’ depression scores rise over time; approximately one-fourth of first- and second-year students were depressed.3 Fahrenkopf et al5 reported that 20% of 123 pediatric residents at 3 U.S. children’s hospitals were depressed. These depressed residents made 6.2 times more medication errors than did their non-depressed peers.5 For more information on physicians-in-training, see “Treating depression in medical residents“.
After completing residency, the risk of depression persists. The lifetime prevalence of depression among physicians is 13% in men and 20% in women6; these rates are comparable to those of the general population. Firth-Cozens7 found a range of factors that predict depression among general practitioners; relationships with senior doctors and patients were the main stressors (Table 1).7 Although these stressors increase depression risk, Vaillant et al8 showed that they did not increase suicide risk in physicians who did not have underlying psychological difficulties when they entered college. Certain personality traits common among physicians, such as self-criticism and perfectionism, may increase risk for depression and substance abuse.8
A depressed physician might enter a downward spiral. Feelings of hopelessness and worthlessness frequently lead to declining professional performance. Professional and personal relationships are strained as internal dysphoria manifests as irritability and anger. Spouses and partners can feel overwhelmed and bewildered by changes in the depressed person’s behavior, which may lead to separation or divorce. Patient care and the physician’s professional standing can be endangered. Signs that suggest a physician may be suffering from depression or another mental illness appear in Table 2.9
Table 1
Predictors of depression in physicians
| Difficult relationships with senior doctors, staff, and/or patients |
| Lack of sleep |
| Dealing with death |
| Making mistakes |
| Loneliness |
| 24-hour responsibility |
| Self-criticism |
| Source: Reference 7 |
Table 2
Manifestations of mental illness in physicians
| Severe irritability and anger, resulting in interpersonal conflict |
| Marked vacillations in energy, creativity, enthusiasm, confidence, and productivity |
| Erratic behavior at the office or hospital (ie, performing rounds at 3 am or not showing up until noon) |
| Inappropriate boundaries with patients, staff, or peers |
| Isolation and withdrawal |
| Increased errors in or inattention to chart work and patient calls |
| Personality change, mood swings |
| Impulsivity or irrationality in decision making or action |
| Inappropriate dress, change in hygiene |
| Sexually inappropriate comments or behavior |
| Diminished or heightened need for sleep |
| Frequent job changes and/or moves |
| Inconsistency in performance, absenteeism |
| Source: Adapted from reference 9 |
Increased suicide risk
A review of 14 studies found that the relative risk of suicide in physicians compared with the general population is between 1.1 and 3.4 for men and 2.5 to 5.7 for women.1 A retrospective study of English and Welsh doctors showed elevated suicide rates in female but not male physicians compared with the general population.10 There are no recent studies of suicide rates among U.S. physicians. A 1984-1995 study showed that white male physicians have a higher risk for suicide than other white male professionals.11 A survey of 4,500 women physicians found that female doctors are less likely to attempt suicide than the general female population6; however, their attempts more often are lethal, perhaps because they have greater knowledge of toxicology and access to lethal drugs.12
The relative rate of suicide among medical specialties is unknown. Studies had indicated higher rates of suicide among psychiatrists and anesthesiologists, but these trials were methodologically flawed.12
Silverman12 developed a profile of the physician at high risk for suicide: a workaholic white male age ≥50 or female age ≥45 who is divorced, single, or currently experiencing marital disruption and is suffering from depression. He or she has a substance abuse problem and a history of risk-taking (high-stakes gambling, etc.). Physicians with chronic pain or illness or with a recent change in occupational or financial status also are at risk. Recent increased work demands, personal losses, diminished autonomy, and access to lethal means (medications, firearms) complete the profile.
Protective factors that lower the risk of completed suicide include effective treatment, social and family support, resilience and coping skills, religious faith, and restricted access to lethal means.13,14
Barriers to treatment
Physicians often are hesitant to seek mental health treatment.15 They may fear social stigma and could have trouble finding a local provider who they trust but is not a colleague. Physicians might be concerned about confidentiality and fear recrimination by colleagues, facilities where they work, or licensing boards.16 Givens and Tjia3 found that only 22% of medical students who screened positive for depression sought help and only 42% of students with suicidal ideation received treatment. These students reported that time constraints, confidentiality concerns, stigma, cost, and fear that their illness will be documented on their academic record were major barriers to seeking mental health care.
Licensing concerns. Physicians may be required to disclose a mental health diagnosis or treatment history when applying for or renewing their medical license. Increasingly, medical boards are asking applicants if they have been treated for bipolar disorder, schizophrenia, paranoia, or other disorders.17 Credentialing bodies, clinics, and hospitals may make similar queries.
In an analysis of 51 medical licensing applications (50 states and the District of Columbia), Schroeder et al17 determined that 69% contained at least 1 question that was “likely impermissible” or “impermissible” in terms of compliance with the Americans with Disabilities Act (ADA). In 1993, a U.S. District Court found that the New Jersey State Board of Medical Examiners was in violation of the ADA because licensure application questions did not focus on current fitness to practice medicine but rather on information about a candidate’s status as a person with a disability (illness or diagnosis).18
In Alexander v Margolis,19 however, the court found that because patient safety is in question, medical licensing boards and credentialing bodies can solicit information about serious mental illness that could lead to impaired performance. Courts have ruled that questions regarding a history of treatment or hospitalization for bipolar disorder or schizophrenia and other psychotic disorders are permissible because they are considered “serious disorders” likely to interfere with a physician’s current ability to practice.20 In a 2008 review of all U.S. -affiliated medical licensing boards (N=54), Polfliet21 found that 7 specifically asked applicants about a history of bipolar disorder or schizophrenia, paranoia, and other psychotic disorders. Polfliet21 also found that state medical boards’ compliance with ADA guidelines was not uniform and some questions were “just as broad, and potentially discriminatory, as they were before enactment of the ADA.”
Worley22 reported a successful appeal to the Arkansas State Medical Board to revise its licensure questions following a cluster of medical student and physician suicides. The Board changed the question “Have you ever, or are you presently, being treated for a mental health condition?” to “Have you ever been advised or required by any licensing or privileging body to seek treatment for a physical or mental health condition?”
Providing inaccurate information on a medical licensure application may result in denial or revocation,23 but acknowledging a history of mental health or substance abuse treatment triggers a more in-depth inquiry by the medical board. The lack of distinction between diagnosis and impairment further stigmatizes physicians who seek care and impedes treatment.
Bipolar disorder. The trend in psychiatry toward diagnosing bipolar II disorder and “soft bipolarity” in patients previously diagnosed with and treated for major depression presents a new challenge. Despite no change in their history or functioning, a physician whose diagnosis is changed from depression to bipolar II disorder might be moved from a non-reportable to a board-reportable diagnostic category. With the evolving understanding of bipolar spectrum disorders, medical boards may need to revise their screening questions to ensure that they are seeking information about impairment, not simply the presence of a medical disorder.
Seeking special treatment
Self-treatment. Physicians may attempt to treat their mood disorder with self-prescribed medications before seeking consultation from a psychiatrist. Others use alcohol or illicit drugs to try to alleviate mood disorder symptoms. Self-diagnosis and treatment are not advisable because it is impossible to be objective. Professional boards and state medical boards discourage or prohibit self-prescribing because of the need for ongoing evaluation and monitoring for adverse reactions.
‘VIP’ treatment. When a physician comes to a colleague for help with a mental health issue, both parties might underestimate the severity of the crisis.24 Weintraub25 reported a case series of 12 “VIP” psychiatric inpatients, 10 of whom he described as “therapeutic failures, “including 2 who committed suicide and 3 who left the hospital against medical advice. He observed that improvement occurred only after patients lost their VIP status/treatment.
In a literature review, Groves et al26 found delays in pursuing diagnostic evaluation and treatment for physician patients. He described risks of VIP treatment (Table 3),26 including the physician’s ability to circumscribe the care regimen to obtain “special treatment, “which can create conflict among care providers and other patients. The ailing physician might have trouble relinquishing control. Care providers might not give physician patients necessary information about the illness or treatment because they make assumptions about the physician’s knowledge or fear causing narcissistic injury. Providers’ identification with their peers, deference to their background, and desire to preserve these patients’ autonomy may lead to interventions that are different from those they would provide to other patients.
Treating physicians might underestimate the patient’s suicide risk and tend to not hospitalize a physician patient who faces an imminent risk of self-harm. Similarly, a physician patient might know what key words to use to deny suicidal ideation or avoid hospitalization. Providers assessing physician patients should provide the same interventions they would give to nonphysician patients with the same history and suicide risk factors. To do otherwise is to risk a fatal outcome.
Physician health programs provide confidential treatment and assistance to physicians with mental illness and/or substance abuse problems. Some programs are affiliated with licensing boards, some are branches of the state medical societies, and others are independent of the licensing agencies. Directories of these programs are available from the Federation of State Physician Health Programs and the Federation of State Medical Boards (see Related Resources). Physician health programs aim to help impaired physicians receive treatment and rehabilitation without censure or licensure revocation, provided they comply with treatment and monitoring requirements.
Table 3
Risks of caring for ‘VIP’ patients
| Caregivers, family, and the patient may deny the possibility of alcohol or substance abuse |
| Caregivers may avoid or poorly handle discussions of death and ‘do not resuscitate’ orders |
| The patient may suffer from emotional isolation when protected from the normal hospital culture |
| The patient’s feelings of shame and fear in the sick role can go uncomforted |
| Caregivers may overlook neuropsychiatric symptoms because they do not wish to ‘insult’ the patient |
| Staff may neglect or poorly handle the patient’s toileting and hygiene |
| Ordinary clinical routine may be short-circuited |
| Caregivers may avoid discussing issues related to the patient’s sexuality |
| Source: Reference 26 |
- American Foundation for Suicide Prevention. www.afsp.org. 24-hour crisis line: 1-800-273-TALK (8255).
- Center for Patient and Professional Advocacy. www.mc.vanderbilt.edu/root/vumc.php?site=CPPA.
- Depression and Bipolar Support Alliance. www.dbsalliance.org.
- Federation of State Physician Health Programs, Inc. www.fsphp.org.
- National Alliance on Mental Illness. www.nami.org.
- Vanderbilt Center for Professional Health. www.mc.vanderbilt.edu/cph.
- Vanderbilt Comprehensive Assessment Program. www.mc.vanderbilt.edu/root/vcap.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Lindeman S, Laara E, Hakko H, et al. A systematic review on gender-specific suicide mortality in medical doctors. Br J Psychiatry. 1996;168:274-279.
2. Zoccolillo M, Murphy GE, Wetzel RD. Depression among medical students. J Affect Disord. 1986;11(1):91-96.
3. Givens JL, Tjia J. Depressed medical students’ use of mental health services and barriers to use. Acad Med. 2002;77(9):918-921.
4. Shanafelt TD, Bradley KA, Wipf JE, et al. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358-367.
5. Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
6. Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. Am J Psychiatry. 1999;156:1887-94.
7. Firth-Cozens J. Individual and organizational predictors of depression in general practitioners. Br J Gen Practice. 1998;48:1647-1651.
8. Vaillant GE, Sobowale NC, McArthur C. Some psychological vulnerabilities of physicians. N Engl J Med. 1972;287:372-375.
9. Michalak EE, Yatham LN, Maxwell V, et al. The impact of bipolar disorder upon work functioning: a qualitative analysis. Bipolar Disord. 2007;9:126-143.
10. Hawton K, Clements A, Sakarovitch C, et al. Suicide in doctors: a study of risk according to gender, seniority and specialty in medical practitioners in England and Wales, 1979-1995. J Epidemiol Community Health. 2001;55:296-300.
11. Frank E, Biola H, Burnett CA. Mortality rates and causes among U.S. physicians. Am J Prev Med. 2000;19:155-159.
12. Silverman M. Physicians and suicide. In: The handbook of physician health: essential guide to understanding the health care needs of physicians. Goldman LS Myers M, Dickstein LJ, eds. Chicago, IL: American Medical Association; 2000:95–117.
13. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: National Academies Press; 2002.
14. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med. 2002;136:358-367.
15. Center CD, Davis M, Detre T, et al. Confronting depression and suicide in physicians: a consensus statement. JAMA. 2003;289(23):3161-3166.
16. Baldisseri MR. Impaired healthcare professional. Crit Care Med. 2007;35(2):S106-116.
17. Schroeder R, Brazeau CM, Zackin F, et al. Do state medical board applications violate the Americans with Disabilities Act? Acad Med. 2009;84(6):776-781.
18. The Medical Society of New Jersey v Jacobs, No, 93-3670 (DNJ 1993)
19. Alexander v Margolis. 921 F Supp 482, 488 (WD Mich 1995).
20. Applicants v Texas State Board of Law examiners, WL 923404 (WD Tex 1994)
21. Polfliet SJ. A national analysis of medical licensure applications. J Am Acad Psychiatry Law. 2008;36(3):369-374.
22. Worley LL. Our fallen peers: a mandate for change. Acad Psychiatry. 2008;32(1):8-12.
23. Sansone RA, Wiederman MW, Sansone LA. Physician mental health and substance abuse. What are state medical licensure applications asking? Arch Fam Med. 1999;8(5):448-451.
24. Robbins GF, Macdonald MC, Pack GT. Delay in the diagnosis and treatment of physicians with cancer. Cancer. 1953;6(3):624-626.
25. Weintraub W. The VIP syndrome: a clinical study in hospital psychiatry. J Nerv Ment Dis. 1964;138:181-193.
26. Groves JE, Dunderdale BA, Stern TA. Celebrity patients VIPs, and potentates. Prim Care Companion J Clin Psychiatry. 2002;4(6):215-223.
Discuss this article at www.facebook.com/CurrentPsychiatry
Dr. G, a second-year surgical resident, becomes depressed when his girlfriend abruptly ends their relationship. His phone calls and e-mails seeking an explanation go unanswered. Having long struggled with his self-esteem, Dr. G interprets this rejection as confirmation of his self-criticism.
Because of his work schedule, Dr. G feels that there is no way to see a therapist or psychiatrist and believes that asking for time off to do so would adversely affect his evaluations. He feels too embarrassed and “weak” to disclose his breakup and depression to his colleagues and attending physicians and senses that fellow residents would resent having to “carry his load.” Dr. G has spent the past 2 years moonlighting at the local emergency room and thinks it would be humiliating to go there for psychiatric help. His work performance and attendance decline until eventually his residency director forces him to take a medical leave of absence.
Dr. G feels that his pain will never end. He writes goodbye letters to his family, makes arrangements for his possessions and funeral, and hangs himself from the balcony outside his apartment.
Although the rate of depression among physicians is comparable to that of the general population, physicians’ risk of suicide is markedly higher.1 Depression and other mood disorders may be under-recognized and inadequately treated in physicians because physicians might:
- be reluctant to seek treatment
- attempt to diagnose and treat themselves
- seek and receive “VIP treatment” from other health care providers.
This article examines physicians’ risk for depression and suicide, licensing concerns and other barriers to effective treatment, and what can be done to overcome such obstacles.
Not immune to depression
Rates of depression are higher in medical students and residents (15% to 30%) than in the general population.2-4 A longitudinal study of medical students at the University of California, San Francisco showed that students’ rates of depression when they enter medical school are similar to those of the general population, but students’ depression scores rise over time; approximately one-fourth of first- and second-year students were depressed.3 Fahrenkopf et al5 reported that 20% of 123 pediatric residents at 3 U.S. children’s hospitals were depressed. These depressed residents made 6.2 times more medication errors than did their non-depressed peers.5 For more information on physicians-in-training, see “Treating depression in medical residents“.
After completing residency, the risk of depression persists. The lifetime prevalence of depression among physicians is 13% in men and 20% in women6; these rates are comparable to those of the general population. Firth-Cozens7 found a range of factors that predict depression among general practitioners; relationships with senior doctors and patients were the main stressors (Table 1).7 Although these stressors increase depression risk, Vaillant et al8 showed that they did not increase suicide risk in physicians who did not have underlying psychological difficulties when they entered college. Certain personality traits common among physicians, such as self-criticism and perfectionism, may increase risk for depression and substance abuse.8
A depressed physician might enter a downward spiral. Feelings of hopelessness and worthlessness frequently lead to declining professional performance. Professional and personal relationships are strained as internal dysphoria manifests as irritability and anger. Spouses and partners can feel overwhelmed and bewildered by changes in the depressed person’s behavior, which may lead to separation or divorce. Patient care and the physician’s professional standing can be endangered. Signs that suggest a physician may be suffering from depression or another mental illness appear in Table 2.9
Table 1
Predictors of depression in physicians
| Difficult relationships with senior doctors, staff, and/or patients |
| Lack of sleep |
| Dealing with death |
| Making mistakes |
| Loneliness |
| 24-hour responsibility |
| Self-criticism |
| Source: Reference 7 |
Table 2
Manifestations of mental illness in physicians
| Severe irritability and anger, resulting in interpersonal conflict |
| Marked vacillations in energy, creativity, enthusiasm, confidence, and productivity |
| Erratic behavior at the office or hospital (ie, performing rounds at 3 am or not showing up until noon) |
| Inappropriate boundaries with patients, staff, or peers |
| Isolation and withdrawal |
| Increased errors in or inattention to chart work and patient calls |
| Personality change, mood swings |
| Impulsivity or irrationality in decision making or action |
| Inappropriate dress, change in hygiene |
| Sexually inappropriate comments or behavior |
| Diminished or heightened need for sleep |
| Frequent job changes and/or moves |
| Inconsistency in performance, absenteeism |
| Source: Adapted from reference 9 |
Increased suicide risk
A review of 14 studies found that the relative risk of suicide in physicians compared with the general population is between 1.1 and 3.4 for men and 2.5 to 5.7 for women.1 A retrospective study of English and Welsh doctors showed elevated suicide rates in female but not male physicians compared with the general population.10 There are no recent studies of suicide rates among U.S. physicians. A 1984-1995 study showed that white male physicians have a higher risk for suicide than other white male professionals.11 A survey of 4,500 women physicians found that female doctors are less likely to attempt suicide than the general female population6; however, their attempts more often are lethal, perhaps because they have greater knowledge of toxicology and access to lethal drugs.12
The relative rate of suicide among medical specialties is unknown. Studies had indicated higher rates of suicide among psychiatrists and anesthesiologists, but these trials were methodologically flawed.12
Silverman12 developed a profile of the physician at high risk for suicide: a workaholic white male age ≥50 or female age ≥45 who is divorced, single, or currently experiencing marital disruption and is suffering from depression. He or she has a substance abuse problem and a history of risk-taking (high-stakes gambling, etc.). Physicians with chronic pain or illness or with a recent change in occupational or financial status also are at risk. Recent increased work demands, personal losses, diminished autonomy, and access to lethal means (medications, firearms) complete the profile.
Protective factors that lower the risk of completed suicide include effective treatment, social and family support, resilience and coping skills, religious faith, and restricted access to lethal means.13,14
Barriers to treatment
Physicians often are hesitant to seek mental health treatment.15 They may fear social stigma and could have trouble finding a local provider who they trust but is not a colleague. Physicians might be concerned about confidentiality and fear recrimination by colleagues, facilities where they work, or licensing boards.16 Givens and Tjia3 found that only 22% of medical students who screened positive for depression sought help and only 42% of students with suicidal ideation received treatment. These students reported that time constraints, confidentiality concerns, stigma, cost, and fear that their illness will be documented on their academic record were major barriers to seeking mental health care.
Licensing concerns. Physicians may be required to disclose a mental health diagnosis or treatment history when applying for or renewing their medical license. Increasingly, medical boards are asking applicants if they have been treated for bipolar disorder, schizophrenia, paranoia, or other disorders.17 Credentialing bodies, clinics, and hospitals may make similar queries.
In an analysis of 51 medical licensing applications (50 states and the District of Columbia), Schroeder et al17 determined that 69% contained at least 1 question that was “likely impermissible” or “impermissible” in terms of compliance with the Americans with Disabilities Act (ADA). In 1993, a U.S. District Court found that the New Jersey State Board of Medical Examiners was in violation of the ADA because licensure application questions did not focus on current fitness to practice medicine but rather on information about a candidate’s status as a person with a disability (illness or diagnosis).18
In Alexander v Margolis,19 however, the court found that because patient safety is in question, medical licensing boards and credentialing bodies can solicit information about serious mental illness that could lead to impaired performance. Courts have ruled that questions regarding a history of treatment or hospitalization for bipolar disorder or schizophrenia and other psychotic disorders are permissible because they are considered “serious disorders” likely to interfere with a physician’s current ability to practice.20 In a 2008 review of all U.S. -affiliated medical licensing boards (N=54), Polfliet21 found that 7 specifically asked applicants about a history of bipolar disorder or schizophrenia, paranoia, and other psychotic disorders. Polfliet21 also found that state medical boards’ compliance with ADA guidelines was not uniform and some questions were “just as broad, and potentially discriminatory, as they were before enactment of the ADA.”
Worley22 reported a successful appeal to the Arkansas State Medical Board to revise its licensure questions following a cluster of medical student and physician suicides. The Board changed the question “Have you ever, or are you presently, being treated for a mental health condition?” to “Have you ever been advised or required by any licensing or privileging body to seek treatment for a physical or mental health condition?”
Providing inaccurate information on a medical licensure application may result in denial or revocation,23 but acknowledging a history of mental health or substance abuse treatment triggers a more in-depth inquiry by the medical board. The lack of distinction between diagnosis and impairment further stigmatizes physicians who seek care and impedes treatment.
Bipolar disorder. The trend in psychiatry toward diagnosing bipolar II disorder and “soft bipolarity” in patients previously diagnosed with and treated for major depression presents a new challenge. Despite no change in their history or functioning, a physician whose diagnosis is changed from depression to bipolar II disorder might be moved from a non-reportable to a board-reportable diagnostic category. With the evolving understanding of bipolar spectrum disorders, medical boards may need to revise their screening questions to ensure that they are seeking information about impairment, not simply the presence of a medical disorder.
Seeking special treatment
Self-treatment. Physicians may attempt to treat their mood disorder with self-prescribed medications before seeking consultation from a psychiatrist. Others use alcohol or illicit drugs to try to alleviate mood disorder symptoms. Self-diagnosis and treatment are not advisable because it is impossible to be objective. Professional boards and state medical boards discourage or prohibit self-prescribing because of the need for ongoing evaluation and monitoring for adverse reactions.
‘VIP’ treatment. When a physician comes to a colleague for help with a mental health issue, both parties might underestimate the severity of the crisis.24 Weintraub25 reported a case series of 12 “VIP” psychiatric inpatients, 10 of whom he described as “therapeutic failures, “including 2 who committed suicide and 3 who left the hospital against medical advice. He observed that improvement occurred only after patients lost their VIP status/treatment.
In a literature review, Groves et al26 found delays in pursuing diagnostic evaluation and treatment for physician patients. He described risks of VIP treatment (Table 3),26 including the physician’s ability to circumscribe the care regimen to obtain “special treatment, “which can create conflict among care providers and other patients. The ailing physician might have trouble relinquishing control. Care providers might not give physician patients necessary information about the illness or treatment because they make assumptions about the physician’s knowledge or fear causing narcissistic injury. Providers’ identification with their peers, deference to their background, and desire to preserve these patients’ autonomy may lead to interventions that are different from those they would provide to other patients.
Treating physicians might underestimate the patient’s suicide risk and tend to not hospitalize a physician patient who faces an imminent risk of self-harm. Similarly, a physician patient might know what key words to use to deny suicidal ideation or avoid hospitalization. Providers assessing physician patients should provide the same interventions they would give to nonphysician patients with the same history and suicide risk factors. To do otherwise is to risk a fatal outcome.
Physician health programs provide confidential treatment and assistance to physicians with mental illness and/or substance abuse problems. Some programs are affiliated with licensing boards, some are branches of the state medical societies, and others are independent of the licensing agencies. Directories of these programs are available from the Federation of State Physician Health Programs and the Federation of State Medical Boards (see Related Resources). Physician health programs aim to help impaired physicians receive treatment and rehabilitation without censure or licensure revocation, provided they comply with treatment and monitoring requirements.
Table 3
Risks of caring for ‘VIP’ patients
| Caregivers, family, and the patient may deny the possibility of alcohol or substance abuse |
| Caregivers may avoid or poorly handle discussions of death and ‘do not resuscitate’ orders |
| The patient may suffer from emotional isolation when protected from the normal hospital culture |
| The patient’s feelings of shame and fear in the sick role can go uncomforted |
| Caregivers may overlook neuropsychiatric symptoms because they do not wish to ‘insult’ the patient |
| Staff may neglect or poorly handle the patient’s toileting and hygiene |
| Ordinary clinical routine may be short-circuited |
| Caregivers may avoid discussing issues related to the patient’s sexuality |
| Source: Reference 26 |
- American Foundation for Suicide Prevention. www.afsp.org. 24-hour crisis line: 1-800-273-TALK (8255).
- Center for Patient and Professional Advocacy. www.mc.vanderbilt.edu/root/vumc.php?site=CPPA.
- Depression and Bipolar Support Alliance. www.dbsalliance.org.
- Federation of State Physician Health Programs, Inc. www.fsphp.org.
- National Alliance on Mental Illness. www.nami.org.
- Vanderbilt Center for Professional Health. www.mc.vanderbilt.edu/cph.
- Vanderbilt Comprehensive Assessment Program. www.mc.vanderbilt.edu/root/vcap.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Dr. G, a second-year surgical resident, becomes depressed when his girlfriend abruptly ends their relationship. His phone calls and e-mails seeking an explanation go unanswered. Having long struggled with his self-esteem, Dr. G interprets this rejection as confirmation of his self-criticism.
Because of his work schedule, Dr. G feels that there is no way to see a therapist or psychiatrist and believes that asking for time off to do so would adversely affect his evaluations. He feels too embarrassed and “weak” to disclose his breakup and depression to his colleagues and attending physicians and senses that fellow residents would resent having to “carry his load.” Dr. G has spent the past 2 years moonlighting at the local emergency room and thinks it would be humiliating to go there for psychiatric help. His work performance and attendance decline until eventually his residency director forces him to take a medical leave of absence.
Dr. G feels that his pain will never end. He writes goodbye letters to his family, makes arrangements for his possessions and funeral, and hangs himself from the balcony outside his apartment.
Although the rate of depression among physicians is comparable to that of the general population, physicians’ risk of suicide is markedly higher.1 Depression and other mood disorders may be under-recognized and inadequately treated in physicians because physicians might:
- be reluctant to seek treatment
- attempt to diagnose and treat themselves
- seek and receive “VIP treatment” from other health care providers.
This article examines physicians’ risk for depression and suicide, licensing concerns and other barriers to effective treatment, and what can be done to overcome such obstacles.
Not immune to depression
Rates of depression are higher in medical students and residents (15% to 30%) than in the general population.2-4 A longitudinal study of medical students at the University of California, San Francisco showed that students’ rates of depression when they enter medical school are similar to those of the general population, but students’ depression scores rise over time; approximately one-fourth of first- and second-year students were depressed.3 Fahrenkopf et al5 reported that 20% of 123 pediatric residents at 3 U.S. children’s hospitals were depressed. These depressed residents made 6.2 times more medication errors than did their non-depressed peers.5 For more information on physicians-in-training, see “Treating depression in medical residents“.
After completing residency, the risk of depression persists. The lifetime prevalence of depression among physicians is 13% in men and 20% in women6; these rates are comparable to those of the general population. Firth-Cozens7 found a range of factors that predict depression among general practitioners; relationships with senior doctors and patients were the main stressors (Table 1).7 Although these stressors increase depression risk, Vaillant et al8 showed that they did not increase suicide risk in physicians who did not have underlying psychological difficulties when they entered college. Certain personality traits common among physicians, such as self-criticism and perfectionism, may increase risk for depression and substance abuse.8
A depressed physician might enter a downward spiral. Feelings of hopelessness and worthlessness frequently lead to declining professional performance. Professional and personal relationships are strained as internal dysphoria manifests as irritability and anger. Spouses and partners can feel overwhelmed and bewildered by changes in the depressed person’s behavior, which may lead to separation or divorce. Patient care and the physician’s professional standing can be endangered. Signs that suggest a physician may be suffering from depression or another mental illness appear in Table 2.9
Table 1
Predictors of depression in physicians
| Difficult relationships with senior doctors, staff, and/or patients |
| Lack of sleep |
| Dealing with death |
| Making mistakes |
| Loneliness |
| 24-hour responsibility |
| Self-criticism |
| Source: Reference 7 |
Table 2
Manifestations of mental illness in physicians
| Severe irritability and anger, resulting in interpersonal conflict |
| Marked vacillations in energy, creativity, enthusiasm, confidence, and productivity |
| Erratic behavior at the office or hospital (ie, performing rounds at 3 am or not showing up until noon) |
| Inappropriate boundaries with patients, staff, or peers |
| Isolation and withdrawal |
| Increased errors in or inattention to chart work and patient calls |
| Personality change, mood swings |
| Impulsivity or irrationality in decision making or action |
| Inappropriate dress, change in hygiene |
| Sexually inappropriate comments or behavior |
| Diminished or heightened need for sleep |
| Frequent job changes and/or moves |
| Inconsistency in performance, absenteeism |
| Source: Adapted from reference 9 |
Increased suicide risk
A review of 14 studies found that the relative risk of suicide in physicians compared with the general population is between 1.1 and 3.4 for men and 2.5 to 5.7 for women.1 A retrospective study of English and Welsh doctors showed elevated suicide rates in female but not male physicians compared with the general population.10 There are no recent studies of suicide rates among U.S. physicians. A 1984-1995 study showed that white male physicians have a higher risk for suicide than other white male professionals.11 A survey of 4,500 women physicians found that female doctors are less likely to attempt suicide than the general female population6; however, their attempts more often are lethal, perhaps because they have greater knowledge of toxicology and access to lethal drugs.12
The relative rate of suicide among medical specialties is unknown. Studies had indicated higher rates of suicide among psychiatrists and anesthesiologists, but these trials were methodologically flawed.12
Silverman12 developed a profile of the physician at high risk for suicide: a workaholic white male age ≥50 or female age ≥45 who is divorced, single, or currently experiencing marital disruption and is suffering from depression. He or she has a substance abuse problem and a history of risk-taking (high-stakes gambling, etc.). Physicians with chronic pain or illness or with a recent change in occupational or financial status also are at risk. Recent increased work demands, personal losses, diminished autonomy, and access to lethal means (medications, firearms) complete the profile.
Protective factors that lower the risk of completed suicide include effective treatment, social and family support, resilience and coping skills, religious faith, and restricted access to lethal means.13,14
Barriers to treatment
Physicians often are hesitant to seek mental health treatment.15 They may fear social stigma and could have trouble finding a local provider who they trust but is not a colleague. Physicians might be concerned about confidentiality and fear recrimination by colleagues, facilities where they work, or licensing boards.16 Givens and Tjia3 found that only 22% of medical students who screened positive for depression sought help and only 42% of students with suicidal ideation received treatment. These students reported that time constraints, confidentiality concerns, stigma, cost, and fear that their illness will be documented on their academic record were major barriers to seeking mental health care.
Licensing concerns. Physicians may be required to disclose a mental health diagnosis or treatment history when applying for or renewing their medical license. Increasingly, medical boards are asking applicants if they have been treated for bipolar disorder, schizophrenia, paranoia, or other disorders.17 Credentialing bodies, clinics, and hospitals may make similar queries.
In an analysis of 51 medical licensing applications (50 states and the District of Columbia), Schroeder et al17 determined that 69% contained at least 1 question that was “likely impermissible” or “impermissible” in terms of compliance with the Americans with Disabilities Act (ADA). In 1993, a U.S. District Court found that the New Jersey State Board of Medical Examiners was in violation of the ADA because licensure application questions did not focus on current fitness to practice medicine but rather on information about a candidate’s status as a person with a disability (illness or diagnosis).18
In Alexander v Margolis,19 however, the court found that because patient safety is in question, medical licensing boards and credentialing bodies can solicit information about serious mental illness that could lead to impaired performance. Courts have ruled that questions regarding a history of treatment or hospitalization for bipolar disorder or schizophrenia and other psychotic disorders are permissible because they are considered “serious disorders” likely to interfere with a physician’s current ability to practice.20 In a 2008 review of all U.S. -affiliated medical licensing boards (N=54), Polfliet21 found that 7 specifically asked applicants about a history of bipolar disorder or schizophrenia, paranoia, and other psychotic disorders. Polfliet21 also found that state medical boards’ compliance with ADA guidelines was not uniform and some questions were “just as broad, and potentially discriminatory, as they were before enactment of the ADA.”
Worley22 reported a successful appeal to the Arkansas State Medical Board to revise its licensure questions following a cluster of medical student and physician suicides. The Board changed the question “Have you ever, or are you presently, being treated for a mental health condition?” to “Have you ever been advised or required by any licensing or privileging body to seek treatment for a physical or mental health condition?”
Providing inaccurate information on a medical licensure application may result in denial or revocation,23 but acknowledging a history of mental health or substance abuse treatment triggers a more in-depth inquiry by the medical board. The lack of distinction between diagnosis and impairment further stigmatizes physicians who seek care and impedes treatment.
Bipolar disorder. The trend in psychiatry toward diagnosing bipolar II disorder and “soft bipolarity” in patients previously diagnosed with and treated for major depression presents a new challenge. Despite no change in their history or functioning, a physician whose diagnosis is changed from depression to bipolar II disorder might be moved from a non-reportable to a board-reportable diagnostic category. With the evolving understanding of bipolar spectrum disorders, medical boards may need to revise their screening questions to ensure that they are seeking information about impairment, not simply the presence of a medical disorder.
Seeking special treatment
Self-treatment. Physicians may attempt to treat their mood disorder with self-prescribed medications before seeking consultation from a psychiatrist. Others use alcohol or illicit drugs to try to alleviate mood disorder symptoms. Self-diagnosis and treatment are not advisable because it is impossible to be objective. Professional boards and state medical boards discourage or prohibit self-prescribing because of the need for ongoing evaluation and monitoring for adverse reactions.
‘VIP’ treatment. When a physician comes to a colleague for help with a mental health issue, both parties might underestimate the severity of the crisis.24 Weintraub25 reported a case series of 12 “VIP” psychiatric inpatients, 10 of whom he described as “therapeutic failures, “including 2 who committed suicide and 3 who left the hospital against medical advice. He observed that improvement occurred only after patients lost their VIP status/treatment.
In a literature review, Groves et al26 found delays in pursuing diagnostic evaluation and treatment for physician patients. He described risks of VIP treatment (Table 3),26 including the physician’s ability to circumscribe the care regimen to obtain “special treatment, “which can create conflict among care providers and other patients. The ailing physician might have trouble relinquishing control. Care providers might not give physician patients necessary information about the illness or treatment because they make assumptions about the physician’s knowledge or fear causing narcissistic injury. Providers’ identification with their peers, deference to their background, and desire to preserve these patients’ autonomy may lead to interventions that are different from those they would provide to other patients.
Treating physicians might underestimate the patient’s suicide risk and tend to not hospitalize a physician patient who faces an imminent risk of self-harm. Similarly, a physician patient might know what key words to use to deny suicidal ideation or avoid hospitalization. Providers assessing physician patients should provide the same interventions they would give to nonphysician patients with the same history and suicide risk factors. To do otherwise is to risk a fatal outcome.
Physician health programs provide confidential treatment and assistance to physicians with mental illness and/or substance abuse problems. Some programs are affiliated with licensing boards, some are branches of the state medical societies, and others are independent of the licensing agencies. Directories of these programs are available from the Federation of State Physician Health Programs and the Federation of State Medical Boards (see Related Resources). Physician health programs aim to help impaired physicians receive treatment and rehabilitation without censure or licensure revocation, provided they comply with treatment and monitoring requirements.
Table 3
Risks of caring for ‘VIP’ patients
| Caregivers, family, and the patient may deny the possibility of alcohol or substance abuse |
| Caregivers may avoid or poorly handle discussions of death and ‘do not resuscitate’ orders |
| The patient may suffer from emotional isolation when protected from the normal hospital culture |
| The patient’s feelings of shame and fear in the sick role can go uncomforted |
| Caregivers may overlook neuropsychiatric symptoms because they do not wish to ‘insult’ the patient |
| Staff may neglect or poorly handle the patient’s toileting and hygiene |
| Ordinary clinical routine may be short-circuited |
| Caregivers may avoid discussing issues related to the patient’s sexuality |
| Source: Reference 26 |
- American Foundation for Suicide Prevention. www.afsp.org. 24-hour crisis line: 1-800-273-TALK (8255).
- Center for Patient and Professional Advocacy. www.mc.vanderbilt.edu/root/vumc.php?site=CPPA.
- Depression and Bipolar Support Alliance. www.dbsalliance.org.
- Federation of State Physician Health Programs, Inc. www.fsphp.org.
- National Alliance on Mental Illness. www.nami.org.
- Vanderbilt Center for Professional Health. www.mc.vanderbilt.edu/cph.
- Vanderbilt Comprehensive Assessment Program. www.mc.vanderbilt.edu/root/vcap.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Lindeman S, Laara E, Hakko H, et al. A systematic review on gender-specific suicide mortality in medical doctors. Br J Psychiatry. 1996;168:274-279.
2. Zoccolillo M, Murphy GE, Wetzel RD. Depression among medical students. J Affect Disord. 1986;11(1):91-96.
3. Givens JL, Tjia J. Depressed medical students’ use of mental health services and barriers to use. Acad Med. 2002;77(9):918-921.
4. Shanafelt TD, Bradley KA, Wipf JE, et al. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358-367.
5. Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
6. Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. Am J Psychiatry. 1999;156:1887-94.
7. Firth-Cozens J. Individual and organizational predictors of depression in general practitioners. Br J Gen Practice. 1998;48:1647-1651.
8. Vaillant GE, Sobowale NC, McArthur C. Some psychological vulnerabilities of physicians. N Engl J Med. 1972;287:372-375.
9. Michalak EE, Yatham LN, Maxwell V, et al. The impact of bipolar disorder upon work functioning: a qualitative analysis. Bipolar Disord. 2007;9:126-143.
10. Hawton K, Clements A, Sakarovitch C, et al. Suicide in doctors: a study of risk according to gender, seniority and specialty in medical practitioners in England and Wales, 1979-1995. J Epidemiol Community Health. 2001;55:296-300.
11. Frank E, Biola H, Burnett CA. Mortality rates and causes among U.S. physicians. Am J Prev Med. 2000;19:155-159.
12. Silverman M. Physicians and suicide. In: The handbook of physician health: essential guide to understanding the health care needs of physicians. Goldman LS Myers M, Dickstein LJ, eds. Chicago, IL: American Medical Association; 2000:95–117.
13. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: National Academies Press; 2002.
14. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med. 2002;136:358-367.
15. Center CD, Davis M, Detre T, et al. Confronting depression and suicide in physicians: a consensus statement. JAMA. 2003;289(23):3161-3166.
16. Baldisseri MR. Impaired healthcare professional. Crit Care Med. 2007;35(2):S106-116.
17. Schroeder R, Brazeau CM, Zackin F, et al. Do state medical board applications violate the Americans with Disabilities Act? Acad Med. 2009;84(6):776-781.
18. The Medical Society of New Jersey v Jacobs, No, 93-3670 (DNJ 1993)
19. Alexander v Margolis. 921 F Supp 482, 488 (WD Mich 1995).
20. Applicants v Texas State Board of Law examiners, WL 923404 (WD Tex 1994)
21. Polfliet SJ. A national analysis of medical licensure applications. J Am Acad Psychiatry Law. 2008;36(3):369-374.
22. Worley LL. Our fallen peers: a mandate for change. Acad Psychiatry. 2008;32(1):8-12.
23. Sansone RA, Wiederman MW, Sansone LA. Physician mental health and substance abuse. What are state medical licensure applications asking? Arch Fam Med. 1999;8(5):448-451.
24. Robbins GF, Macdonald MC, Pack GT. Delay in the diagnosis and treatment of physicians with cancer. Cancer. 1953;6(3):624-626.
25. Weintraub W. The VIP syndrome: a clinical study in hospital psychiatry. J Nerv Ment Dis. 1964;138:181-193.
26. Groves JE, Dunderdale BA, Stern TA. Celebrity patients VIPs, and potentates. Prim Care Companion J Clin Psychiatry. 2002;4(6):215-223.
1. Lindeman S, Laara E, Hakko H, et al. A systematic review on gender-specific suicide mortality in medical doctors. Br J Psychiatry. 1996;168:274-279.
2. Zoccolillo M, Murphy GE, Wetzel RD. Depression among medical students. J Affect Disord. 1986;11(1):91-96.
3. Givens JL, Tjia J. Depressed medical students’ use of mental health services and barriers to use. Acad Med. 2002;77(9):918-921.
4. Shanafelt TD, Bradley KA, Wipf JE, et al. Burnout and self-reported patient care in an internal medicine residency program. Ann Intern Med. 2002;136(5):358-367.
5. Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
6. Frank E, Dingle AD. Self-reported depression and suicide attempts among U.S. women physicians. Am J Psychiatry. 1999;156:1887-94.
7. Firth-Cozens J. Individual and organizational predictors of depression in general practitioners. Br J Gen Practice. 1998;48:1647-1651.
8. Vaillant GE, Sobowale NC, McArthur C. Some psychological vulnerabilities of physicians. N Engl J Med. 1972;287:372-375.
9. Michalak EE, Yatham LN, Maxwell V, et al. The impact of bipolar disorder upon work functioning: a qualitative analysis. Bipolar Disord. 2007;9:126-143.
10. Hawton K, Clements A, Sakarovitch C, et al. Suicide in doctors: a study of risk according to gender, seniority and specialty in medical practitioners in England and Wales, 1979-1995. J Epidemiol Community Health. 2001;55:296-300.
11. Frank E, Biola H, Burnett CA. Mortality rates and causes among U.S. physicians. Am J Prev Med. 2000;19:155-159.
12. Silverman M. Physicians and suicide. In: The handbook of physician health: essential guide to understanding the health care needs of physicians. Goldman LS Myers M, Dickstein LJ, eds. Chicago, IL: American Medical Association; 2000:95–117.
13. Goldsmith SK, Pellmar TC, Kleinman AM, et al. eds. Reducing suicide: a national imperative. Washington, DC: National Academies Press; 2002.
14. Mann JJ. A current perspective of suicide and attempted suicide. Ann Intern Med. 2002;136:358-367.
15. Center CD, Davis M, Detre T, et al. Confronting depression and suicide in physicians: a consensus statement. JAMA. 2003;289(23):3161-3166.
16. Baldisseri MR. Impaired healthcare professional. Crit Care Med. 2007;35(2):S106-116.
17. Schroeder R, Brazeau CM, Zackin F, et al. Do state medical board applications violate the Americans with Disabilities Act? Acad Med. 2009;84(6):776-781.
18. The Medical Society of New Jersey v Jacobs, No, 93-3670 (DNJ 1993)
19. Alexander v Margolis. 921 F Supp 482, 488 (WD Mich 1995).
20. Applicants v Texas State Board of Law examiners, WL 923404 (WD Tex 1994)
21. Polfliet SJ. A national analysis of medical licensure applications. J Am Acad Psychiatry Law. 2008;36(3):369-374.
22. Worley LL. Our fallen peers: a mandate for change. Acad Psychiatry. 2008;32(1):8-12.
23. Sansone RA, Wiederman MW, Sansone LA. Physician mental health and substance abuse. What are state medical licensure applications asking? Arch Fam Med. 1999;8(5):448-451.
24. Robbins GF, Macdonald MC, Pack GT. Delay in the diagnosis and treatment of physicians with cancer. Cancer. 1953;6(3):624-626.
25. Weintraub W. The VIP syndrome: a clinical study in hospital psychiatry. J Nerv Ment Dis. 1964;138:181-193.
26. Groves JE, Dunderdale BA, Stern TA. Celebrity patients VIPs, and potentates. Prim Care Companion J Clin Psychiatry. 2002;4(6):215-223.
How anxiety presents differently in older adults
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/how-anxiety-presents-differently-in.html#comments
Although anxiety disorders are common at all ages, there is a misconception that their prevalence drastically declines with age. For this reason anxiety disorders often are underdiagnosed and undertreated in geriatric patients, especially when the clinical presentation of these disorders in older patients differs from that seen in younger adults.
In older persons, anxiety symptoms often overlap with medical conditions such as hyperthyroidism and geriatric patients tend to express anxiety symptoms as medical or somatic problems such as pain rather than as psychological distress.1 As a result, older adults often seek treatment for depressive or anxiety symptoms from their primary care physician instead of a psychiatrist. Unfortunately, primary care physicians often miss psychiatric illness, including anxiety disorders, in geriatric patients.
Anxiety may be a symptom of an underlying psychiatric disturbance, secondary to a general medical condition, or induced by dietary substances, substances of abuse, or medications. Late-life anxiety often is comorbid with major depressive disorder (MDD) ( Box ) and other psychological stressors as older adults recognize declining cognitive and physical functioning.2 Anxiety disorders commonly begin in early adulthood, tend to be chronic and interspersed with remissions and relapses, and usually continue into old age.3 In generalized anxiety disorder (GAD), there is a bimodal distribution of onset; approximately two-thirds of patients experience onset between the late teens and late 20s and one-third develop the disorder for the first time after age 50.3
Prevalence rates for anxiety disorders among older adults (age ≥55) range from 3. 5% to 10. 2%.4 These rates are slightly lower than those for younger adults.5 Among older adults, presence of a 12-month anxiety disorder was associated with female sex, lower education, being unmarried, and having ≥3 or more chronic conditions.6
The Longitudinal Aging Study Amsterdam study—one of the largest epidemiologic studies to examine comorbidity of anxiety disorders and depression in patients age 55 to 85—found that 48% of older persons with primary major depressive disorder (MDD) also had a comorbid anxiety disorder, whereas approximately one-fourth of those with anxiety disorders also had MDD.a Pre-existing anxiety disorders, such as social phobia, obsessive-compulsive disorder, specific phobia, agoraphobia, and panic disorder, increase the risk of developing depression.b Rates of comorbid anxiety and depression increase with age.c
Late-life MDD comorbid with generalized anxiety disorder or panic disorder is associated with greater memory decline than MDD alone.d In addition, comorbid anxiety and depression is associated with greater symptom severity and persistence, greater functional impairment, substance dependence, poorer compliance and response to treatment, worse overall prognosis and outcome than patients with either disorder alone,e and greater likelihood of suicidal ideation in older men.f
References
a. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry. 2000; 157(1): 89-95.
b. Goodwin RD. Anxiety disorders and the onset of depression among adults in the community. Psychol Med. 2002; 32: 1121-1124.
c. Merikangas KR, Zhang H, Avenevoli S, et al. Longitudinal trajectories of depression and anxiety in a prospective community study: the Zurich Cohort Study. Arch Gen Psychiatry. 2003; 60: 993-1000.
d. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry. 2005; 20(9): 848-854.
e. Merikangas KR, Kalaydjian A. Magnitude and impact of comorbidity of mental disorders from epidemiologic surveys. Curr Opin Psychiatry. 2007; 20: 353-358.
f. Lenze E, Mulsant BH, Shear MK, et al. Comorbid anxiety disorders in depressed elderly patients. Am J Psychiatry. 2000; 157: 722-728.
Anxiety and disability risk
Anxiety disorders affect geriatric patients more profoundly than their younger counterparts. Persons age ≥65 who have an anxiety disorder are 3 to 10 times more likely to be hospitalized than younger individuals.1 Anxiety is associated with high rates of medically unexplained symptoms, increased use of health care resources, chronic medical illness, low levels of physical health-related quality of life, and physical disability.7,8
Anxiety symptoms may predict progressing physical disability among older women and reduced ability to perform activities of daily living over 1 year.9 Anxious geriatric patients are less independent and increase the burden on family and caregivers.10 Anxiety disorders are associated with lower compliance with medical treatment, which could worsen chronic medical conditions and increase the risk for nursing home admission.11 Anxious older adults report decreased life satisfaction, memory impairment, poorer self perception of health, and increased loneliness.12
Generalized anxiety disorder
Although GAD is the most common anxiety disorder among geriatric patients, with a prevalence of 0. 7% to 9%,13 it remains underdiagnosed and undertreated.14 In a cross-sectional observational study of 439 adults age ≥55 with lifetime GAD, approximately one-half experienced onset after age 50.15 Late onset is associated with more frequent hypertension and a poorer health-related quality of life than early onset.15
Compared with younger individuals, older persons with GAD have a greater variety of worry topics, including memory loss, medical illnesses, and fear of falls,16 but worry less about the future and work than younger patients. This type of anxiety is largely situational and temporary, and often accompanies comorbid medical problems (Table 1) .
Obsessive-compulsive disorder
A study comparing older (age ≥60) and younger obsessive-compulsive disorder (OCD) patients found that the clinical presentation of the disorder does not substantially differ between age groups; however, geriatric patients had fewer concerns about symmetry, needing to know, and counting rituals. Handwashing and fear of having sinned were more common.17
OCD is fairly uncommon in geriatric patients. Prevalence rates decrease with age, ranging between 0% and 0. 8% among persons age ≥60.18 OCD seldom begins in late life; most geriatric patients with OCD have had symptoms for decades. By late life, most individuals with OCD improve, although they may continue to experience clinical or subclinical symptoms.19 However, 1 report found a second peak of incidence of OCD in women age ≥65.20 Case reports of late-onset OCD have found evidence of cerebral lesions, often in the basal ganglia, which suggests a possible neurodegenerative pathophysiology.21
Table 1
DSM-IV-TR criteria for generalized anxiety disorder
| A. | Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance) |
| B. | The person finds it difficult to control the worry |
| C. | The anxiety and worry are associated with 3 or more of the following symptoms with at least some symptoms present for more days than not for the past 6 months:
|
| D. | The focus of the anxiety and worry is not confined to features of an axis I disorder |
| E. | The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| F. | The disturbance is not due to the direct physiological effects of a substance or a general medical condition and does not occur exclusively during a mood disorder, a psychotic disorder, or a pervasive developmental disorder |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | |
Posttraumatic stress disorder
Untreated posttraumatic stress disorder (PTSD) often is assumed to be a chronic disorder. Recollections of past trauma may lead to new PTSD symptoms in older patients. Neurodegeneration of memory pathways and cognitive impairment associated with Alzheimer‘s disease or vascular or alcohol-related dementia may disinhibit PTSD symptoms in patients whose PTSD was fairly well controlled.22
Life events associated with aging—death of a spouse, financial and physical decline, chronic pain, or diminished cognitive coping resources—may precipitate or revive PTSD symptoms associated with earlier exposure to severe psychological trauma.23 These life changes also may precipitate socalled delayed PTSD, when symptoms relating to past traumatic experiences present for the first time. Geriatric patients may be more likely than younger persons to deny their PTSD symptoms if their cultural background emphasizes stoicism and fortitude.24
Phobias
Specific phobias. The prevalence of specific phobias drops dramatically in late life, although older patients might underreport symptoms. Many older persons are afraid of falling. Approximately 60% of older adults with a history of falling—and 30% of older individuals with no such history— report this fear. Fear of falling is more prevalent in women and increases with age.25,26 This fear may be a protective response to a real threat that prevents older persons from attempting high-risk activities, but it also can cause patients to restrict their activities, which can result in decreased social, physical, or cognitive functioning and loss of in-dependence.25
Social phobias (social anxiety disorder).
Among older adults, common social phobias include eating food around strangers, and—especially in men—being unable to urinate in public bathrooms. In a cross-sectional observational study, social anxiety disorder (SAD) was more common among older persons who reported stressful life events, such as death of a spouse.27 MDD, specific phobia, and personality disorder are associated with SAD in geriatric patients.27 Prevalence rates of SAD appear to slightly decrease with age, although the condition remains common in geriatric patients—5% of older adults report lifetime prevalence—and its presentation is similar to that seen in younger adults.27
Agoraphobia. In older persons the prevalence of agoraphobia is 0. 6%.28 Most cases are of early onset but the condition can present de novo following a stroke or other medical event and can inhibit activities needed for successful rehabilitation. Agoraphobia can present within the context of panic attacks as is seen in younger adults but most geriatric patients with agoraphobia do not have concurrent panic disorder. This phobia is more common in women, widowed or divorced individuals, patients with chronic health conditions, and those with comorbid psychiatric disorders.29
Panic disorder
Panic disorder (PD) rarely starts for the first time after age 60, and most late-onset panic attacks are associated with medical and psychiatric comorbidities. PD tends to be less severe in older individuals than in younger adults.30 Recent stressful life events or losses can predict onset and maintenance of PD. Older patients may present with panic symptoms, such as shortness of breath, dizziness, or trembling, that overlap with age-related medical conditions. PD may be prevalent in older patients with chest pain and no evidence of coronary artery disease.31 Panic symptoms that are secondary to underlying medical conditions, such as chronic obstructive pulmonary disease exacerbation, usually wax and wane.32
Treatment
Treatment for anxiety disorders in geriatric patients may involve a combination of psychotherapy, pharmacotherapy, and complementary and alternative therapies. Treatment may be complicated if patients have ≥1 anxiety disorder or suffer from comorbid depression, substance abuse, or medical problems. As is seen with younger adults, the course of anxiety disorders in older patients waxes and wanes, but most disorders are unlikely to remit completely.33 Aging may influence the effects of psychotropic medications in older patients. Increased distribution and decreased metabolism and clearance of medications results in higher medication plasma levels and longer elimination half-lives. Medication compliance in older patients may be complicated by:
- older patients’ sensitivity to anticho-linergic side effects
- coexisting medical illnesses
- polypharmacy, particularly in institutionalized settings
- sensory and cognitive deficits.34
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) generally are safe and produce fewer side effects compared with tricyclic antidepressants (TCAs), especially in geriatric patients. SSRIs and SNRIs may be useful for GAD, PD, OCD, and PTSD in older patients.35 TCAs can effectively treat anxiety symptoms but may be cardiotoxic and their anticholinergic properties can lead to serious side effects. Benzodiazepines often are used for acute or short-term anxiety management, but chronic use in geriatric patients can cause cognitive impairment, falls, and other serious side effects. Buspirone may be beneficial for GAD but is not effective for PD.36 The drug is well tolerated in older persons, but may take 2 to 4 weeks to be effective ( Table 2 ).35
Pharmacotherapy for anxiety disorders in geriatric patients often is used in conjunction with psychotherapy. Psychotherapeutic approaches include cognitive-behavioral therapy (CBT), exposure therapy, dialectical behavioral therapy, and interpersonal therapy. Increasing evidence supports the effectiveness of psychotherapy in treating anxiety disorders in younger adults as well as in older patients, often in combination with pharmacotherapy.37 In older patients with GAD, CBT is associated with a greater improvement in worry severity, depressive symptoms, and overall mental health compared with usual care.38
In addition to traditional pharmacotherapy, complementary and alternative therapies often are used for late-life anxiety. These therapies include biofeedback, progressive relaxation, acupuncture, yoga, massage therapy, art, music, or dance therapy, meditation, prayer, and spiritual counseling.
Table 2
Pharmacotherapy for anxiety disorders in older adults
| Medication | Comments |
|---|---|
| Selective serotonin reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Serotonin-norepinephrine reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Tricyclic antidepressants | Potential for cardiotoxicity and overdose, anticholinergic properties |
| Benzodiazepines | Chronic use can lead to cognitive impairment, falls |
| Buspirone | Effective for GAD, but not panic disorder; may take 2 to 4 weeks to be effective |
| GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PTSD: posttraumatic stress disorder | |
| Source: Reference 35 | |
Related Resources
- Wetherell JL, Lenze EJ, Stanley MA. Evidence-based treatment of geriatric anxiety disorders. Psychiatr Clin North Am. 2005; 28(4): 871-896, ix.
- Lenze EJ, Wetherell JL. Anxiety disorders. In: Blazer DG, Steffens DC, eds. The American Psychiatric Publishing textbook of geriatric psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 2009: 333-345.
Drug Brand Name
- Buspirone • BuSpar
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Fuentes K, Cox BJ. Prevalence of anxiety disorders in elderly adults: a critical analysis. J Behav Ther Exp Psychiatry. 1997;28:269-279.
2. Préville M, Hérbert R, Bravo G, et al. Predisposing and facilitating factors of severe psychological distress among frail elderly. Can J Aging. 2002;21:195-204.
3. Le Roux H, Gatz M, Wetherell JL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2005;13:23-30.
4. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry. 1998;13:717-726.
5. Regier DA, Rae DS, Narrow WE, et al. Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. Br J Psychiatry Suppl. 1998;34:24-28.
6. Gum AM, King-Kallimanis B, Kohn R. Prevalence of mood anxiety, and substance-abuse disorders for older Americans in the national comorbidity survey-replication. Am J Geriatr Psychiatry. 2009;17(9):769-781.
7. Sareen J, Jacobi F, Cox BJ, et al. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med. 2006;166:2109-2116.
8. Porensky EK, Dew MA, Karp JF, et al. The burden of late-life generalized anxiety disorder: effects on disability, health-related quality of life, and healthcare utilization. Am J Geriatr Psychiatry. 2009;17(6):473-482.
9. Tinetti ME, Inouye SK, Gill TM, et al. Shared risk-factors for falls, incontinence, and functional dependence: unifying the approach to geriatric syndromes. JAMA. 1995;273:1348-1353.
10. Lenze EJ, Karp JF, Mulsant BH, et al. Somatic symptoms in late-life anxiety: treatment issues. J Geriatr Psychiatry Neurol. 2005;18:89-96.
11. Gibbons LE, Teri L, Logsdon R, et al. Anxiety symptoms as predictors of nursing home placement in patients with Alzheimer’s disease. Journal of Clinical Geropsychology. 2002;4:335-342.
12. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being and use of health services. Psychol Med. 1999;29(3):583-593.
13. Schoevers RA, Beekman AT, Deeg DJ, et al. Comorbidity and risk-patterns of depression, generalised anxiety disorder and mixed anxiety-depression in later life: results from the AMSTEL study. Int J Geriatr Psychiatry. 2003;18:944-1001.
14. Wilk J, West J, Narrow W, et al. Are anxiety disorders underdiagnosed and undertreated in routine psychiatric practice? Poster presented at: AcademyHealth Annual Meeting; June 8, 2004; San Diego, CA.
15. Chou KL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2009;17(6):455-464.
16. Howland J, Peterson EW, Levin WC, et al. Fear of falling among the community-dwelling elderly. J Aging Health. 1993;5(2):229-243.
17. Kohn R, Westlake RJ, Rasmussen SA, et al. Clinical features of obsessive-compulsive disorder in elderly patients. Am J Geriatr Psychiatry. 1997;5(3):211-215.
18. Flint AJ. Epidemiology and comorbidity of anxiety disorders in the elderly. Am J Psychiatry. 1994;151:640-649.
19. Skoog G, Skoog I. A 40-year follow-up of patients with obsessive-compulsive disorder. Arch Gen Psychiatry. 1999;56(2):121-127.
20. Nestadt G, Bienvenu OJ, Cai G, et al. Incidence of obsessive-compulsive disorder in adults. J Nerv Ment Dis. 1998;186:401-406.
21. Chacko RC, Corbin MA, Harper RG. Acquired obsessive-compulsive disorder associated with basal ganglia lesions. J Neuropsychiatry Clin Neurosci. 2000;12:269-272.
22. Mittal D, Torres R, Abashidze A, et al. Worsening of post-traumatic stress disorder symptoms with cognitive decline: case series. J Geriatr Psychiatry Neurol. 2001;14(1):17-20.
23. Tedstone JE, Tarrier N. Posttraumatic stress disorder following medical illness and treatment. Clin Psychol Rev. 2003;23(3):409-448.
24. Creamer M, Parslow R. Trauma exposure and posttraumatic stress disorder in the elderly: a community prevalence study. Am J Ger Psychiatry. 2008;16:853-856.
25. Alcalde Tirado P. Fear of falling. Rev Esp Geriatr Gerontol. 2010;45(1):38-44.
26. Boyd R, Stevens JA. Falls and fear of falling: burden beliefs and behaviours. Age Ageing. 2009;38(4):423-428.
27. Cairney J, McCabe L, Veldhuizen S, et al. Epidemiology of social phobia in later life. Am J Geriatr Psychiatry. 2007;15(3):224-233.
28. Pontillo DC, Lang AJ, Stein MB. Management and treatment of anxiety disorders in the older patient. Clinical Geriatrics. 2002;10(10):38-49.
29. McCabe L, Cairney J, Veldhuizen S, et al. Prevalence and correlates of agoraphobia in older adults. Am J Geriatr Psychiatry. 2006;14(6):515-522.
30. Hassan R, Pollard CA. Late-life-onset panic disorder: clinical and demographic characteristics of a patient sample. J Geriatr Psychiatry Neurol. 1994;7:86-90.
31. Beitman BD, Kushner M, Grossberg GT. Late onset panic disorder: evidence from a study of patients with chest pain and normal cardiac evaluations. Int J Psychiatry Med. 1991;21(1):29-35.
32. Garvey MJ. Panic disorder: guidelines to safe use of benzodiazepines. Geriatrics. 1993;48(7):49-58.
33. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at six-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand. 2005;111:420-428.
34. Von Moltke LL, Abernethy DR, Greenblatt DJ. Kinetics and dynamics of psychotropic drugs in the elderly. In: Salzman C ed. Clinical geriatric psychopharmacology. 3rd ed. Baltimore, MD: Williams and Wilkins; 1998:70-93.
35. Baldwin DS, Anderson IM, Nutt DJ, et al and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological treatment of anxiety disorders: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2005;19(6):567-596.
36. Sheehan DV, Raj AB, Sheehan KH, et al. Is buspirone effective for panic disorder? J Clin Psychopharmacol. 1990;10(1):3-11.
37. Black DW. Efficacy of combined pharmacotherapy and psychotherapy versus monotherapy in the treatment of anxiety disorders. CNS Spectr. 2006;11(10 suppl 12):29-33.
38. Stanley MA, Wilson NL, Novy DM, et al. Cognitive behavior therapy for generalized anxiety disorder among older adults in primary care: a randomized clinical trial. JAMA. 2009;301(14):1460-1467.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/how-anxiety-presents-differently-in.html#comments
Although anxiety disorders are common at all ages, there is a misconception that their prevalence drastically declines with age. For this reason anxiety disorders often are underdiagnosed and undertreated in geriatric patients, especially when the clinical presentation of these disorders in older patients differs from that seen in younger adults.
In older persons, anxiety symptoms often overlap with medical conditions such as hyperthyroidism and geriatric patients tend to express anxiety symptoms as medical or somatic problems such as pain rather than as psychological distress.1 As a result, older adults often seek treatment for depressive or anxiety symptoms from their primary care physician instead of a psychiatrist. Unfortunately, primary care physicians often miss psychiatric illness, including anxiety disorders, in geriatric patients.
Anxiety may be a symptom of an underlying psychiatric disturbance, secondary to a general medical condition, or induced by dietary substances, substances of abuse, or medications. Late-life anxiety often is comorbid with major depressive disorder (MDD) ( Box ) and other psychological stressors as older adults recognize declining cognitive and physical functioning.2 Anxiety disorders commonly begin in early adulthood, tend to be chronic and interspersed with remissions and relapses, and usually continue into old age.3 In generalized anxiety disorder (GAD), there is a bimodal distribution of onset; approximately two-thirds of patients experience onset between the late teens and late 20s and one-third develop the disorder for the first time after age 50.3
Prevalence rates for anxiety disorders among older adults (age ≥55) range from 3. 5% to 10. 2%.4 These rates are slightly lower than those for younger adults.5 Among older adults, presence of a 12-month anxiety disorder was associated with female sex, lower education, being unmarried, and having ≥3 or more chronic conditions.6
The Longitudinal Aging Study Amsterdam study—one of the largest epidemiologic studies to examine comorbidity of anxiety disorders and depression in patients age 55 to 85—found that 48% of older persons with primary major depressive disorder (MDD) also had a comorbid anxiety disorder, whereas approximately one-fourth of those with anxiety disorders also had MDD.a Pre-existing anxiety disorders, such as social phobia, obsessive-compulsive disorder, specific phobia, agoraphobia, and panic disorder, increase the risk of developing depression.b Rates of comorbid anxiety and depression increase with age.c
Late-life MDD comorbid with generalized anxiety disorder or panic disorder is associated with greater memory decline than MDD alone.d In addition, comorbid anxiety and depression is associated with greater symptom severity and persistence, greater functional impairment, substance dependence, poorer compliance and response to treatment, worse overall prognosis and outcome than patients with either disorder alone,e and greater likelihood of suicidal ideation in older men.f
References
a. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry. 2000; 157(1): 89-95.
b. Goodwin RD. Anxiety disorders and the onset of depression among adults in the community. Psychol Med. 2002; 32: 1121-1124.
c. Merikangas KR, Zhang H, Avenevoli S, et al. Longitudinal trajectories of depression and anxiety in a prospective community study: the Zurich Cohort Study. Arch Gen Psychiatry. 2003; 60: 993-1000.
d. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry. 2005; 20(9): 848-854.
e. Merikangas KR, Kalaydjian A. Magnitude and impact of comorbidity of mental disorders from epidemiologic surveys. Curr Opin Psychiatry. 2007; 20: 353-358.
f. Lenze E, Mulsant BH, Shear MK, et al. Comorbid anxiety disorders in depressed elderly patients. Am J Psychiatry. 2000; 157: 722-728.
Anxiety and disability risk
Anxiety disorders affect geriatric patients more profoundly than their younger counterparts. Persons age ≥65 who have an anxiety disorder are 3 to 10 times more likely to be hospitalized than younger individuals.1 Anxiety is associated with high rates of medically unexplained symptoms, increased use of health care resources, chronic medical illness, low levels of physical health-related quality of life, and physical disability.7,8
Anxiety symptoms may predict progressing physical disability among older women and reduced ability to perform activities of daily living over 1 year.9 Anxious geriatric patients are less independent and increase the burden on family and caregivers.10 Anxiety disorders are associated with lower compliance with medical treatment, which could worsen chronic medical conditions and increase the risk for nursing home admission.11 Anxious older adults report decreased life satisfaction, memory impairment, poorer self perception of health, and increased loneliness.12
Generalized anxiety disorder
Although GAD is the most common anxiety disorder among geriatric patients, with a prevalence of 0. 7% to 9%,13 it remains underdiagnosed and undertreated.14 In a cross-sectional observational study of 439 adults age ≥55 with lifetime GAD, approximately one-half experienced onset after age 50.15 Late onset is associated with more frequent hypertension and a poorer health-related quality of life than early onset.15
Compared with younger individuals, older persons with GAD have a greater variety of worry topics, including memory loss, medical illnesses, and fear of falls,16 but worry less about the future and work than younger patients. This type of anxiety is largely situational and temporary, and often accompanies comorbid medical problems (Table 1) .
Obsessive-compulsive disorder
A study comparing older (age ≥60) and younger obsessive-compulsive disorder (OCD) patients found that the clinical presentation of the disorder does not substantially differ between age groups; however, geriatric patients had fewer concerns about symmetry, needing to know, and counting rituals. Handwashing and fear of having sinned were more common.17
OCD is fairly uncommon in geriatric patients. Prevalence rates decrease with age, ranging between 0% and 0. 8% among persons age ≥60.18 OCD seldom begins in late life; most geriatric patients with OCD have had symptoms for decades. By late life, most individuals with OCD improve, although they may continue to experience clinical or subclinical symptoms.19 However, 1 report found a second peak of incidence of OCD in women age ≥65.20 Case reports of late-onset OCD have found evidence of cerebral lesions, often in the basal ganglia, which suggests a possible neurodegenerative pathophysiology.21
Table 1
DSM-IV-TR criteria for generalized anxiety disorder
| A. | Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance) |
| B. | The person finds it difficult to control the worry |
| C. | The anxiety and worry are associated with 3 or more of the following symptoms with at least some symptoms present for more days than not for the past 6 months:
|
| D. | The focus of the anxiety and worry is not confined to features of an axis I disorder |
| E. | The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| F. | The disturbance is not due to the direct physiological effects of a substance or a general medical condition and does not occur exclusively during a mood disorder, a psychotic disorder, or a pervasive developmental disorder |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | |
Posttraumatic stress disorder
Untreated posttraumatic stress disorder (PTSD) often is assumed to be a chronic disorder. Recollections of past trauma may lead to new PTSD symptoms in older patients. Neurodegeneration of memory pathways and cognitive impairment associated with Alzheimer‘s disease or vascular or alcohol-related dementia may disinhibit PTSD symptoms in patients whose PTSD was fairly well controlled.22
Life events associated with aging—death of a spouse, financial and physical decline, chronic pain, or diminished cognitive coping resources—may precipitate or revive PTSD symptoms associated with earlier exposure to severe psychological trauma.23 These life changes also may precipitate socalled delayed PTSD, when symptoms relating to past traumatic experiences present for the first time. Geriatric patients may be more likely than younger persons to deny their PTSD symptoms if their cultural background emphasizes stoicism and fortitude.24
Phobias
Specific phobias. The prevalence of specific phobias drops dramatically in late life, although older patients might underreport symptoms. Many older persons are afraid of falling. Approximately 60% of older adults with a history of falling—and 30% of older individuals with no such history— report this fear. Fear of falling is more prevalent in women and increases with age.25,26 This fear may be a protective response to a real threat that prevents older persons from attempting high-risk activities, but it also can cause patients to restrict their activities, which can result in decreased social, physical, or cognitive functioning and loss of in-dependence.25
Social phobias (social anxiety disorder).
Among older adults, common social phobias include eating food around strangers, and—especially in men—being unable to urinate in public bathrooms. In a cross-sectional observational study, social anxiety disorder (SAD) was more common among older persons who reported stressful life events, such as death of a spouse.27 MDD, specific phobia, and personality disorder are associated with SAD in geriatric patients.27 Prevalence rates of SAD appear to slightly decrease with age, although the condition remains common in geriatric patients—5% of older adults report lifetime prevalence—and its presentation is similar to that seen in younger adults.27
Agoraphobia. In older persons the prevalence of agoraphobia is 0. 6%.28 Most cases are of early onset but the condition can present de novo following a stroke or other medical event and can inhibit activities needed for successful rehabilitation. Agoraphobia can present within the context of panic attacks as is seen in younger adults but most geriatric patients with agoraphobia do not have concurrent panic disorder. This phobia is more common in women, widowed or divorced individuals, patients with chronic health conditions, and those with comorbid psychiatric disorders.29
Panic disorder
Panic disorder (PD) rarely starts for the first time after age 60, and most late-onset panic attacks are associated with medical and psychiatric comorbidities. PD tends to be less severe in older individuals than in younger adults.30 Recent stressful life events or losses can predict onset and maintenance of PD. Older patients may present with panic symptoms, such as shortness of breath, dizziness, or trembling, that overlap with age-related medical conditions. PD may be prevalent in older patients with chest pain and no evidence of coronary artery disease.31 Panic symptoms that are secondary to underlying medical conditions, such as chronic obstructive pulmonary disease exacerbation, usually wax and wane.32
Treatment
Treatment for anxiety disorders in geriatric patients may involve a combination of psychotherapy, pharmacotherapy, and complementary and alternative therapies. Treatment may be complicated if patients have ≥1 anxiety disorder or suffer from comorbid depression, substance abuse, or medical problems. As is seen with younger adults, the course of anxiety disorders in older patients waxes and wanes, but most disorders are unlikely to remit completely.33 Aging may influence the effects of psychotropic medications in older patients. Increased distribution and decreased metabolism and clearance of medications results in higher medication plasma levels and longer elimination half-lives. Medication compliance in older patients may be complicated by:
- older patients’ sensitivity to anticho-linergic side effects
- coexisting medical illnesses
- polypharmacy, particularly in institutionalized settings
- sensory and cognitive deficits.34
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) generally are safe and produce fewer side effects compared with tricyclic antidepressants (TCAs), especially in geriatric patients. SSRIs and SNRIs may be useful for GAD, PD, OCD, and PTSD in older patients.35 TCAs can effectively treat anxiety symptoms but may be cardiotoxic and their anticholinergic properties can lead to serious side effects. Benzodiazepines often are used for acute or short-term anxiety management, but chronic use in geriatric patients can cause cognitive impairment, falls, and other serious side effects. Buspirone may be beneficial for GAD but is not effective for PD.36 The drug is well tolerated in older persons, but may take 2 to 4 weeks to be effective ( Table 2 ).35
Pharmacotherapy for anxiety disorders in geriatric patients often is used in conjunction with psychotherapy. Psychotherapeutic approaches include cognitive-behavioral therapy (CBT), exposure therapy, dialectical behavioral therapy, and interpersonal therapy. Increasing evidence supports the effectiveness of psychotherapy in treating anxiety disorders in younger adults as well as in older patients, often in combination with pharmacotherapy.37 In older patients with GAD, CBT is associated with a greater improvement in worry severity, depressive symptoms, and overall mental health compared with usual care.38
In addition to traditional pharmacotherapy, complementary and alternative therapies often are used for late-life anxiety. These therapies include biofeedback, progressive relaxation, acupuncture, yoga, massage therapy, art, music, or dance therapy, meditation, prayer, and spiritual counseling.
Table 2
Pharmacotherapy for anxiety disorders in older adults
| Medication | Comments |
|---|---|
| Selective serotonin reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Serotonin-norepinephrine reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Tricyclic antidepressants | Potential for cardiotoxicity and overdose, anticholinergic properties |
| Benzodiazepines | Chronic use can lead to cognitive impairment, falls |
| Buspirone | Effective for GAD, but not panic disorder; may take 2 to 4 weeks to be effective |
| GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PTSD: posttraumatic stress disorder | |
| Source: Reference 35 | |
Related Resources
- Wetherell JL, Lenze EJ, Stanley MA. Evidence-based treatment of geriatric anxiety disorders. Psychiatr Clin North Am. 2005; 28(4): 871-896, ix.
- Lenze EJ, Wetherell JL. Anxiety disorders. In: Blazer DG, Steffens DC, eds. The American Psychiatric Publishing textbook of geriatric psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 2009: 333-345.
Drug Brand Name
- Buspirone • BuSpar
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/how-anxiety-presents-differently-in.html#comments
Although anxiety disorders are common at all ages, there is a misconception that their prevalence drastically declines with age. For this reason anxiety disorders often are underdiagnosed and undertreated in geriatric patients, especially when the clinical presentation of these disorders in older patients differs from that seen in younger adults.
In older persons, anxiety symptoms often overlap with medical conditions such as hyperthyroidism and geriatric patients tend to express anxiety symptoms as medical or somatic problems such as pain rather than as psychological distress.1 As a result, older adults often seek treatment for depressive or anxiety symptoms from their primary care physician instead of a psychiatrist. Unfortunately, primary care physicians often miss psychiatric illness, including anxiety disorders, in geriatric patients.
Anxiety may be a symptom of an underlying psychiatric disturbance, secondary to a general medical condition, or induced by dietary substances, substances of abuse, or medications. Late-life anxiety often is comorbid with major depressive disorder (MDD) ( Box ) and other psychological stressors as older adults recognize declining cognitive and physical functioning.2 Anxiety disorders commonly begin in early adulthood, tend to be chronic and interspersed with remissions and relapses, and usually continue into old age.3 In generalized anxiety disorder (GAD), there is a bimodal distribution of onset; approximately two-thirds of patients experience onset between the late teens and late 20s and one-third develop the disorder for the first time after age 50.3
Prevalence rates for anxiety disorders among older adults (age ≥55) range from 3. 5% to 10. 2%.4 These rates are slightly lower than those for younger adults.5 Among older adults, presence of a 12-month anxiety disorder was associated with female sex, lower education, being unmarried, and having ≥3 or more chronic conditions.6
The Longitudinal Aging Study Amsterdam study—one of the largest epidemiologic studies to examine comorbidity of anxiety disorders and depression in patients age 55 to 85—found that 48% of older persons with primary major depressive disorder (MDD) also had a comorbid anxiety disorder, whereas approximately one-fourth of those with anxiety disorders also had MDD.a Pre-existing anxiety disorders, such as social phobia, obsessive-compulsive disorder, specific phobia, agoraphobia, and panic disorder, increase the risk of developing depression.b Rates of comorbid anxiety and depression increase with age.c
Late-life MDD comorbid with generalized anxiety disorder or panic disorder is associated with greater memory decline than MDD alone.d In addition, comorbid anxiety and depression is associated with greater symptom severity and persistence, greater functional impairment, substance dependence, poorer compliance and response to treatment, worse overall prognosis and outcome than patients with either disorder alone,e and greater likelihood of suicidal ideation in older men.f
References
a. Beekman AT, de Beurs E, van Balkom AJ, et al. Anxiety and depression in later life: co-occurrence and communality of risk factors. Am J Psychiatry. 2000; 157(1): 89-95.
b. Goodwin RD. Anxiety disorders and the onset of depression among adults in the community. Psychol Med. 2002; 32: 1121-1124.
c. Merikangas KR, Zhang H, Avenevoli S, et al. Longitudinal trajectories of depression and anxiety in a prospective community study: the Zurich Cohort Study. Arch Gen Psychiatry. 2003; 60: 993-1000.
d. DeLuca AK, Lenze EJ, Mulsant BH, et al. Comorbid anxiety disorder in late life depression: association with memory decline over four years. Int J Geriatr Psychiatry. 2005; 20(9): 848-854.
e. Merikangas KR, Kalaydjian A. Magnitude and impact of comorbidity of mental disorders from epidemiologic surveys. Curr Opin Psychiatry. 2007; 20: 353-358.
f. Lenze E, Mulsant BH, Shear MK, et al. Comorbid anxiety disorders in depressed elderly patients. Am J Psychiatry. 2000; 157: 722-728.
Anxiety and disability risk
Anxiety disorders affect geriatric patients more profoundly than their younger counterparts. Persons age ≥65 who have an anxiety disorder are 3 to 10 times more likely to be hospitalized than younger individuals.1 Anxiety is associated with high rates of medically unexplained symptoms, increased use of health care resources, chronic medical illness, low levels of physical health-related quality of life, and physical disability.7,8
Anxiety symptoms may predict progressing physical disability among older women and reduced ability to perform activities of daily living over 1 year.9 Anxious geriatric patients are less independent and increase the burden on family and caregivers.10 Anxiety disorders are associated with lower compliance with medical treatment, which could worsen chronic medical conditions and increase the risk for nursing home admission.11 Anxious older adults report decreased life satisfaction, memory impairment, poorer self perception of health, and increased loneliness.12
Generalized anxiety disorder
Although GAD is the most common anxiety disorder among geriatric patients, with a prevalence of 0. 7% to 9%,13 it remains underdiagnosed and undertreated.14 In a cross-sectional observational study of 439 adults age ≥55 with lifetime GAD, approximately one-half experienced onset after age 50.15 Late onset is associated with more frequent hypertension and a poorer health-related quality of life than early onset.15
Compared with younger individuals, older persons with GAD have a greater variety of worry topics, including memory loss, medical illnesses, and fear of falls,16 but worry less about the future and work than younger patients. This type of anxiety is largely situational and temporary, and often accompanies comorbid medical problems (Table 1) .
Obsessive-compulsive disorder
A study comparing older (age ≥60) and younger obsessive-compulsive disorder (OCD) patients found that the clinical presentation of the disorder does not substantially differ between age groups; however, geriatric patients had fewer concerns about symmetry, needing to know, and counting rituals. Handwashing and fear of having sinned were more common.17
OCD is fairly uncommon in geriatric patients. Prevalence rates decrease with age, ranging between 0% and 0. 8% among persons age ≥60.18 OCD seldom begins in late life; most geriatric patients with OCD have had symptoms for decades. By late life, most individuals with OCD improve, although they may continue to experience clinical or subclinical symptoms.19 However, 1 report found a second peak of incidence of OCD in women age ≥65.20 Case reports of late-onset OCD have found evidence of cerebral lesions, often in the basal ganglia, which suggests a possible neurodegenerative pathophysiology.21
Table 1
DSM-IV-TR criteria for generalized anxiety disorder
| A. | Excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance) |
| B. | The person finds it difficult to control the worry |
| C. | The anxiety and worry are associated with 3 or more of the following symptoms with at least some symptoms present for more days than not for the past 6 months:
|
| D. | The focus of the anxiety and worry is not confined to features of an axis I disorder |
| E. | The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| F. | The disturbance is not due to the direct physiological effects of a substance or a general medical condition and does not occur exclusively during a mood disorder, a psychotic disorder, or a pervasive developmental disorder |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 | |
Posttraumatic stress disorder
Untreated posttraumatic stress disorder (PTSD) often is assumed to be a chronic disorder. Recollections of past trauma may lead to new PTSD symptoms in older patients. Neurodegeneration of memory pathways and cognitive impairment associated with Alzheimer‘s disease or vascular or alcohol-related dementia may disinhibit PTSD symptoms in patients whose PTSD was fairly well controlled.22
Life events associated with aging—death of a spouse, financial and physical decline, chronic pain, or diminished cognitive coping resources—may precipitate or revive PTSD symptoms associated with earlier exposure to severe psychological trauma.23 These life changes also may precipitate socalled delayed PTSD, when symptoms relating to past traumatic experiences present for the first time. Geriatric patients may be more likely than younger persons to deny their PTSD symptoms if their cultural background emphasizes stoicism and fortitude.24
Phobias
Specific phobias. The prevalence of specific phobias drops dramatically in late life, although older patients might underreport symptoms. Many older persons are afraid of falling. Approximately 60% of older adults with a history of falling—and 30% of older individuals with no such history— report this fear. Fear of falling is more prevalent in women and increases with age.25,26 This fear may be a protective response to a real threat that prevents older persons from attempting high-risk activities, but it also can cause patients to restrict their activities, which can result in decreased social, physical, or cognitive functioning and loss of in-dependence.25
Social phobias (social anxiety disorder).
Among older adults, common social phobias include eating food around strangers, and—especially in men—being unable to urinate in public bathrooms. In a cross-sectional observational study, social anxiety disorder (SAD) was more common among older persons who reported stressful life events, such as death of a spouse.27 MDD, specific phobia, and personality disorder are associated with SAD in geriatric patients.27 Prevalence rates of SAD appear to slightly decrease with age, although the condition remains common in geriatric patients—5% of older adults report lifetime prevalence—and its presentation is similar to that seen in younger adults.27
Agoraphobia. In older persons the prevalence of agoraphobia is 0. 6%.28 Most cases are of early onset but the condition can present de novo following a stroke or other medical event and can inhibit activities needed for successful rehabilitation. Agoraphobia can present within the context of panic attacks as is seen in younger adults but most geriatric patients with agoraphobia do not have concurrent panic disorder. This phobia is more common in women, widowed or divorced individuals, patients with chronic health conditions, and those with comorbid psychiatric disorders.29
Panic disorder
Panic disorder (PD) rarely starts for the first time after age 60, and most late-onset panic attacks are associated with medical and psychiatric comorbidities. PD tends to be less severe in older individuals than in younger adults.30 Recent stressful life events or losses can predict onset and maintenance of PD. Older patients may present with panic symptoms, such as shortness of breath, dizziness, or trembling, that overlap with age-related medical conditions. PD may be prevalent in older patients with chest pain and no evidence of coronary artery disease.31 Panic symptoms that are secondary to underlying medical conditions, such as chronic obstructive pulmonary disease exacerbation, usually wax and wane.32
Treatment
Treatment for anxiety disorders in geriatric patients may involve a combination of psychotherapy, pharmacotherapy, and complementary and alternative therapies. Treatment may be complicated if patients have ≥1 anxiety disorder or suffer from comorbid depression, substance abuse, or medical problems. As is seen with younger adults, the course of anxiety disorders in older patients waxes and wanes, but most disorders are unlikely to remit completely.33 Aging may influence the effects of psychotropic medications in older patients. Increased distribution and decreased metabolism and clearance of medications results in higher medication plasma levels and longer elimination half-lives. Medication compliance in older patients may be complicated by:
- older patients’ sensitivity to anticho-linergic side effects
- coexisting medical illnesses
- polypharmacy, particularly in institutionalized settings
- sensory and cognitive deficits.34
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) generally are safe and produce fewer side effects compared with tricyclic antidepressants (TCAs), especially in geriatric patients. SSRIs and SNRIs may be useful for GAD, PD, OCD, and PTSD in older patients.35 TCAs can effectively treat anxiety symptoms but may be cardiotoxic and their anticholinergic properties can lead to serious side effects. Benzodiazepines often are used for acute or short-term anxiety management, but chronic use in geriatric patients can cause cognitive impairment, falls, and other serious side effects. Buspirone may be beneficial for GAD but is not effective for PD.36 The drug is well tolerated in older persons, but may take 2 to 4 weeks to be effective ( Table 2 ).35
Pharmacotherapy for anxiety disorders in geriatric patients often is used in conjunction with psychotherapy. Psychotherapeutic approaches include cognitive-behavioral therapy (CBT), exposure therapy, dialectical behavioral therapy, and interpersonal therapy. Increasing evidence supports the effectiveness of psychotherapy in treating anxiety disorders in younger adults as well as in older patients, often in combination with pharmacotherapy.37 In older patients with GAD, CBT is associated with a greater improvement in worry severity, depressive symptoms, and overall mental health compared with usual care.38
In addition to traditional pharmacotherapy, complementary and alternative therapies often are used for late-life anxiety. These therapies include biofeedback, progressive relaxation, acupuncture, yoga, massage therapy, art, music, or dance therapy, meditation, prayer, and spiritual counseling.
Table 2
Pharmacotherapy for anxiety disorders in older adults
| Medication | Comments |
|---|---|
| Selective serotonin reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Serotonin-norepinephrine reuptake inhibitors | May be useful for GAD, panic disorder, OCD, and PTSD |
| Tricyclic antidepressants | Potential for cardiotoxicity and overdose, anticholinergic properties |
| Benzodiazepines | Chronic use can lead to cognitive impairment, falls |
| Buspirone | Effective for GAD, but not panic disorder; may take 2 to 4 weeks to be effective |
| GAD: generalized anxiety disorder; OCD: obsessive-compulsive disorder; PTSD: posttraumatic stress disorder | |
| Source: Reference 35 | |
Related Resources
- Wetherell JL, Lenze EJ, Stanley MA. Evidence-based treatment of geriatric anxiety disorders. Psychiatr Clin North Am. 2005; 28(4): 871-896, ix.
- Lenze EJ, Wetherell JL. Anxiety disorders. In: Blazer DG, Steffens DC, eds. The American Psychiatric Publishing textbook of geriatric psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 2009: 333-345.
Drug Brand Name
- Buspirone • BuSpar
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
1. Fuentes K, Cox BJ. Prevalence of anxiety disorders in elderly adults: a critical analysis. J Behav Ther Exp Psychiatry. 1997;28:269-279.
2. Préville M, Hérbert R, Bravo G, et al. Predisposing and facilitating factors of severe psychological distress among frail elderly. Can J Aging. 2002;21:195-204.
3. Le Roux H, Gatz M, Wetherell JL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2005;13:23-30.
4. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry. 1998;13:717-726.
5. Regier DA, Rae DS, Narrow WE, et al. Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. Br J Psychiatry Suppl. 1998;34:24-28.
6. Gum AM, King-Kallimanis B, Kohn R. Prevalence of mood anxiety, and substance-abuse disorders for older Americans in the national comorbidity survey-replication. Am J Geriatr Psychiatry. 2009;17(9):769-781.
7. Sareen J, Jacobi F, Cox BJ, et al. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med. 2006;166:2109-2116.
8. Porensky EK, Dew MA, Karp JF, et al. The burden of late-life generalized anxiety disorder: effects on disability, health-related quality of life, and healthcare utilization. Am J Geriatr Psychiatry. 2009;17(6):473-482.
9. Tinetti ME, Inouye SK, Gill TM, et al. Shared risk-factors for falls, incontinence, and functional dependence: unifying the approach to geriatric syndromes. JAMA. 1995;273:1348-1353.
10. Lenze EJ, Karp JF, Mulsant BH, et al. Somatic symptoms in late-life anxiety: treatment issues. J Geriatr Psychiatry Neurol. 2005;18:89-96.
11. Gibbons LE, Teri L, Logsdon R, et al. Anxiety symptoms as predictors of nursing home placement in patients with Alzheimer’s disease. Journal of Clinical Geropsychology. 2002;4:335-342.
12. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being and use of health services. Psychol Med. 1999;29(3):583-593.
13. Schoevers RA, Beekman AT, Deeg DJ, et al. Comorbidity and risk-patterns of depression, generalised anxiety disorder and mixed anxiety-depression in later life: results from the AMSTEL study. Int J Geriatr Psychiatry. 2003;18:944-1001.
14. Wilk J, West J, Narrow W, et al. Are anxiety disorders underdiagnosed and undertreated in routine psychiatric practice? Poster presented at: AcademyHealth Annual Meeting; June 8, 2004; San Diego, CA.
15. Chou KL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2009;17(6):455-464.
16. Howland J, Peterson EW, Levin WC, et al. Fear of falling among the community-dwelling elderly. J Aging Health. 1993;5(2):229-243.
17. Kohn R, Westlake RJ, Rasmussen SA, et al. Clinical features of obsessive-compulsive disorder in elderly patients. Am J Geriatr Psychiatry. 1997;5(3):211-215.
18. Flint AJ. Epidemiology and comorbidity of anxiety disorders in the elderly. Am J Psychiatry. 1994;151:640-649.
19. Skoog G, Skoog I. A 40-year follow-up of patients with obsessive-compulsive disorder. Arch Gen Psychiatry. 1999;56(2):121-127.
20. Nestadt G, Bienvenu OJ, Cai G, et al. Incidence of obsessive-compulsive disorder in adults. J Nerv Ment Dis. 1998;186:401-406.
21. Chacko RC, Corbin MA, Harper RG. Acquired obsessive-compulsive disorder associated with basal ganglia lesions. J Neuropsychiatry Clin Neurosci. 2000;12:269-272.
22. Mittal D, Torres R, Abashidze A, et al. Worsening of post-traumatic stress disorder symptoms with cognitive decline: case series. J Geriatr Psychiatry Neurol. 2001;14(1):17-20.
23. Tedstone JE, Tarrier N. Posttraumatic stress disorder following medical illness and treatment. Clin Psychol Rev. 2003;23(3):409-448.
24. Creamer M, Parslow R. Trauma exposure and posttraumatic stress disorder in the elderly: a community prevalence study. Am J Ger Psychiatry. 2008;16:853-856.
25. Alcalde Tirado P. Fear of falling. Rev Esp Geriatr Gerontol. 2010;45(1):38-44.
26. Boyd R, Stevens JA. Falls and fear of falling: burden beliefs and behaviours. Age Ageing. 2009;38(4):423-428.
27. Cairney J, McCabe L, Veldhuizen S, et al. Epidemiology of social phobia in later life. Am J Geriatr Psychiatry. 2007;15(3):224-233.
28. Pontillo DC, Lang AJ, Stein MB. Management and treatment of anxiety disorders in the older patient. Clinical Geriatrics. 2002;10(10):38-49.
29. McCabe L, Cairney J, Veldhuizen S, et al. Prevalence and correlates of agoraphobia in older adults. Am J Geriatr Psychiatry. 2006;14(6):515-522.
30. Hassan R, Pollard CA. Late-life-onset panic disorder: clinical and demographic characteristics of a patient sample. J Geriatr Psychiatry Neurol. 1994;7:86-90.
31. Beitman BD, Kushner M, Grossberg GT. Late onset panic disorder: evidence from a study of patients with chest pain and normal cardiac evaluations. Int J Psychiatry Med. 1991;21(1):29-35.
32. Garvey MJ. Panic disorder: guidelines to safe use of benzodiazepines. Geriatrics. 1993;48(7):49-58.
33. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at six-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand. 2005;111:420-428.
34. Von Moltke LL, Abernethy DR, Greenblatt DJ. Kinetics and dynamics of psychotropic drugs in the elderly. In: Salzman C ed. Clinical geriatric psychopharmacology. 3rd ed. Baltimore, MD: Williams and Wilkins; 1998:70-93.
35. Baldwin DS, Anderson IM, Nutt DJ, et al and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological treatment of anxiety disorders: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2005;19(6):567-596.
36. Sheehan DV, Raj AB, Sheehan KH, et al. Is buspirone effective for panic disorder? J Clin Psychopharmacol. 1990;10(1):3-11.
37. Black DW. Efficacy of combined pharmacotherapy and psychotherapy versus monotherapy in the treatment of anxiety disorders. CNS Spectr. 2006;11(10 suppl 12):29-33.
38. Stanley MA, Wilson NL, Novy DM, et al. Cognitive behavior therapy for generalized anxiety disorder among older adults in primary care: a randomized clinical trial. JAMA. 2009;301(14):1460-1467.
1. Fuentes K, Cox BJ. Prevalence of anxiety disorders in elderly adults: a critical analysis. J Behav Ther Exp Psychiatry. 1997;28:269-279.
2. Préville M, Hérbert R, Bravo G, et al. Predisposing and facilitating factors of severe psychological distress among frail elderly. Can J Aging. 2002;21:195-204.
3. Le Roux H, Gatz M, Wetherell JL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2005;13:23-30.
4. Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int J Geriatr Psychiatry. 1998;13:717-726.
5. Regier DA, Rae DS, Narrow WE, et al. Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. Br J Psychiatry Suppl. 1998;34:24-28.
6. Gum AM, King-Kallimanis B, Kohn R. Prevalence of mood anxiety, and substance-abuse disorders for older Americans in the national comorbidity survey-replication. Am J Geriatr Psychiatry. 2009;17(9):769-781.
7. Sareen J, Jacobi F, Cox BJ, et al. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med. 2006;166:2109-2116.
8. Porensky EK, Dew MA, Karp JF, et al. The burden of late-life generalized anxiety disorder: effects on disability, health-related quality of life, and healthcare utilization. Am J Geriatr Psychiatry. 2009;17(6):473-482.
9. Tinetti ME, Inouye SK, Gill TM, et al. Shared risk-factors for falls, incontinence, and functional dependence: unifying the approach to geriatric syndromes. JAMA. 1995;273:1348-1353.
10. Lenze EJ, Karp JF, Mulsant BH, et al. Somatic symptoms in late-life anxiety: treatment issues. J Geriatr Psychiatry Neurol. 2005;18:89-96.
11. Gibbons LE, Teri L, Logsdon R, et al. Anxiety symptoms as predictors of nursing home placement in patients with Alzheimer’s disease. Journal of Clinical Geropsychology. 2002;4:335-342.
12. de Beurs E, Beekman AT, van Balkom AJ, et al. Consequences of anxiety in older persons: its effect on disability, well-being and use of health services. Psychol Med. 1999;29(3):583-593.
13. Schoevers RA, Beekman AT, Deeg DJ, et al. Comorbidity and risk-patterns of depression, generalised anxiety disorder and mixed anxiety-depression in later life: results from the AMSTEL study. Int J Geriatr Psychiatry. 2003;18:944-1001.
14. Wilk J, West J, Narrow W, et al. Are anxiety disorders underdiagnosed and undertreated in routine psychiatric practice? Poster presented at: AcademyHealth Annual Meeting; June 8, 2004; San Diego, CA.
15. Chou KL. Age at onset of generalized anxiety disorder in older adults. Am J Geriatr Psychiatry. 2009;17(6):455-464.
16. Howland J, Peterson EW, Levin WC, et al. Fear of falling among the community-dwelling elderly. J Aging Health. 1993;5(2):229-243.
17. Kohn R, Westlake RJ, Rasmussen SA, et al. Clinical features of obsessive-compulsive disorder in elderly patients. Am J Geriatr Psychiatry. 1997;5(3):211-215.
18. Flint AJ. Epidemiology and comorbidity of anxiety disorders in the elderly. Am J Psychiatry. 1994;151:640-649.
19. Skoog G, Skoog I. A 40-year follow-up of patients with obsessive-compulsive disorder. Arch Gen Psychiatry. 1999;56(2):121-127.
20. Nestadt G, Bienvenu OJ, Cai G, et al. Incidence of obsessive-compulsive disorder in adults. J Nerv Ment Dis. 1998;186:401-406.
21. Chacko RC, Corbin MA, Harper RG. Acquired obsessive-compulsive disorder associated with basal ganglia lesions. J Neuropsychiatry Clin Neurosci. 2000;12:269-272.
22. Mittal D, Torres R, Abashidze A, et al. Worsening of post-traumatic stress disorder symptoms with cognitive decline: case series. J Geriatr Psychiatry Neurol. 2001;14(1):17-20.
23. Tedstone JE, Tarrier N. Posttraumatic stress disorder following medical illness and treatment. Clin Psychol Rev. 2003;23(3):409-448.
24. Creamer M, Parslow R. Trauma exposure and posttraumatic stress disorder in the elderly: a community prevalence study. Am J Ger Psychiatry. 2008;16:853-856.
25. Alcalde Tirado P. Fear of falling. Rev Esp Geriatr Gerontol. 2010;45(1):38-44.
26. Boyd R, Stevens JA. Falls and fear of falling: burden beliefs and behaviours. Age Ageing. 2009;38(4):423-428.
27. Cairney J, McCabe L, Veldhuizen S, et al. Epidemiology of social phobia in later life. Am J Geriatr Psychiatry. 2007;15(3):224-233.
28. Pontillo DC, Lang AJ, Stein MB. Management and treatment of anxiety disorders in the older patient. Clinical Geriatrics. 2002;10(10):38-49.
29. McCabe L, Cairney J, Veldhuizen S, et al. Prevalence and correlates of agoraphobia in older adults. Am J Geriatr Psychiatry. 2006;14(6):515-522.
30. Hassan R, Pollard CA. Late-life-onset panic disorder: clinical and demographic characteristics of a patient sample. J Geriatr Psychiatry Neurol. 1994;7:86-90.
31. Beitman BD, Kushner M, Grossberg GT. Late onset panic disorder: evidence from a study of patients with chest pain and normal cardiac evaluations. Int J Psychiatry Med. 1991;21(1):29-35.
32. Garvey MJ. Panic disorder: guidelines to safe use of benzodiazepines. Geriatrics. 1993;48(7):49-58.
33. Schuurmans J, Comijs HC, Beekman AT, et al. The outcome of anxiety disorders in older people at six-year follow-up: results from the Longitudinal Aging Study Amsterdam. Acta Psychiatr Scand. 2005;111:420-428.
34. Von Moltke LL, Abernethy DR, Greenblatt DJ. Kinetics and dynamics of psychotropic drugs in the elderly. In: Salzman C ed. Clinical geriatric psychopharmacology. 3rd ed. Baltimore, MD: Williams and Wilkins; 1998:70-93.
35. Baldwin DS, Anderson IM, Nutt DJ, et al and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological treatment of anxiety disorders: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2005;19(6):567-596.
36. Sheehan DV, Raj AB, Sheehan KH, et al. Is buspirone effective for panic disorder? J Clin Psychopharmacol. 1990;10(1):3-11.
37. Black DW. Efficacy of combined pharmacotherapy and psychotherapy versus monotherapy in the treatment of anxiety disorders. CNS Spectr. 2006;11(10 suppl 12):29-33.
38. Stanley MA, Wilson NL, Novy DM, et al. Cognitive behavior therapy for generalized anxiety disorder among older adults in primary care: a randomized clinical trial. JAMA. 2009;301(14):1460-1467.
Adapting dialectical behavior therapy to help suicidal adolescents
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/adapting-dialectical-behavior-therapy.html#comments

Treating suicidal adolescents is fraught with challenges. Antidepressants may be associated with increased suicidal ideation in adolescents,1-3 although some data suggest that increased adolescent suicide rates are correlated with decreases in antidepressant prescribing.4 Adolescents hospitalized after a suicide attempt are likely to attempt suicide again after they are discharged.5,6 Such patients might not attend outpatient psychotherapy; a study of 167 adolescents discharged after a suicide attempt found that 26% never attended follow-up appointments and 11% went once.7
Emerging research supports the effectiveness of dialectical behavior therapy (DBT) for suicidal adolescents. DBT is a form of cognitive-behavioral therapy that combines individual therapy, skills training, and telephone coaching and is implemented by a therapist consultation team that meets weekly. This article reviews evidence supporting the efficacy of DBT for suicidal adolescents and describes principles of outpatient DBT for these patients as developed by Miller et al.8
Evidence of DBT’s effectiveness
A review of DBT research found strong evidence for DBT’s effectiveness for suicidal adults.9 Recently, DBT has been adapted to treat adolescents with suicidal behavior and nonsuicidal self-injury (NSSI).10-15
In a nonrandomized trial, Rathus and Miller10 compared 29 suicidal adolescent outpatients receiving DBT with 82 participants receiving treatment as usual (TAU). Patients were assigned to DBT if they had a suicide attempt in the previous 16 weeks and ≥3 borderline personality disorder (BPD) features or to TAU if they met only 1 of those conditions. Patients in the DBT group had more axis I disorders and pretreatment hospitalizations than the TAU group. Compared with those receiving TAU, patients treated with DBT had fewer hospitalizations (13% in TAU vs 0% in DBT) and a lower dropout rate (60% in TAU vs 38% in DBT). The DBT group experienced significant reductions in suicidal ideation, BPD symptoms, and general psychiatric symptoms. There was 1 suicide attempt in the DBT group vs 7 attempts in the TAU group; however, this difference was not statistically significant.
Woodberry and Popenoe11 examined the use of DBT for suicidal adolescents and their families in a community outpatient clinic. Adolescents reported reductions in overall symptoms, depression, anger, dissociative symptoms, and urges for intentional self-injury. Parents reported reductions in their children’s problem behaviors and in their own depressive symptoms. In a study of DBT in 16 adolescent females with chronic intentional self-injury, patients reported significant reductions in incidents of intentional self-injury, depression, and hopelessness, and increases in overall functioning.12
Three studies have examined using DBT for suicidal adolescents in residential facilities. In a pilot study, Katz et al13 compared DBT with TAU for 62 suicidal adolescent inpatients. At 1-year follow-up, both groups experienced significant reductions in suicidal ideation, NSSI, and depression. However, compared with those who received TAU, DBT patients had fewer behavioral problems during hospitalization. Sunseri14 used DBT to treat adolescent females in residential treatment. After DBT was implemented, residents were hospitalized because of NSSI and suicidality for fewer days than before DBT. Trupin et al15 taught DBT to staff who worked with female adolescent offenders at a juvenile rehabilitation facility. After the staff implemented DBT, the rates of problem behaviors and punishment by staff decreased on 1 unit; there were no behavior or punishment changes on another unit.
Theoretical foundations
Biosocial theory. The problems DBT treats in suicidal adolescents include emotion dysregulation, interpersonal conflict, impulsivity, cognitive dysregulation, and self-dysregulation.8 The biosocial theory postulates that these problems are the result of the transaction, or reciprocal relationship, between biologic predispositions and an invalidating environment. The biosocial theory suggests 3 biologic characteristics often are found among suicidal adolescents:
- high emotional sensitivity
- high extremity in reactions
- a slow return to baseline after experiencing a surge in affect.8
Although these characteristics indicate higher emotionality, they are not sufficient to account for suicidal adolescents’ difficulties. Problems arise when individuals with these biologic characteristics are raised in an invalidating environment, where the adolescent does not learn how to regulate emotions. Common characteristics of invalidating environments and their effects on adolescents are described in Table 1 .8
Treatment theory. DBT for suicidal adolescents focuses on a synthesis between 2 seemingly opposite treatment strategies: change and acceptance. The change focus is derived from behavioral science, and treatment incorporates standard behavior therapy practices, including chain analysis (described below), skills training, contingency management, and exposure.
The acceptance focus draws upon principles of Zen and other Eastern spiritual traditions. Therapists teach patients to accept reality as it is in this moment, without judgment. A key extension of this acceptance is the use of validation—radical acceptance and acknowledgement that all behavior has validity and understandability. DBT therapists strive to use 6 levels of validation with their patients ( Table 2 ),16 which often is a critical strategy for adolescents who reside in an invalidating environment.
DBT attempts to synthesize the acceptance-based Zen tradition with the change-based strategies of behavioral science through a dialectical philosophy. A fundamental postulate of dialectical philosophy is that a tension occurs when an initial truth or thesis is opposed by an apparently contradictory truth or antithesis.8 DBT therapists work with adolescents to find a synthesis that is the “middle path, “ which includes the truth in both positions as well as what is left out of both. For an example of how this might work for an adolescent patient with NSSI, visit this article at CurrentPsychiatry.com.
Table 1
Characteristics of an invalidating environment
| Characteristic | Result |
|---|---|
| Indiscriminately rejects communications of private experiences | Adolescents learn to actively self-invalidate and do not learn to validate themselves, label their emotions, or effectively regulate their emotions |
| Actively punishes displays of emotions, interspersed with intermittent reinforcement of emotional outbursts | Adolescents develop problematic emotion regulation strategies that oscillate between suppression and extreme outbursts |
| Oversimplifies problem solving | Adolescents develop high perfectionism and sensitivity to perceived failure, form unrealistic goals, and experience intense negative arousal in response to challenging feedback |
| Source: Reference 8 | |
Table 2
6 levels of validation employed by DBT therapists
| Level | Validation practices |
|---|---|
| Accurate reflection | Paraphrase what an adolescent says; communicate that you accurately understand what the adolescent has said |
| Mindreading | Communicate that you understand the adolescent’s private experiences or that which is unsaid. Articulate private experiences of the adolescent based on your knowledge of him or her |
| Observing and listening | Use nonverbal and paralinguistic cues to indicate interest. Communicate that you wish to know the adolescent’s emotions, thoughts, and behaviors |
| Validating in terms of causes | Make sense of behavior based on the adolescent’s learning history or biology. Describe how a behavior is effective for short-term but not long-term goals |
| Validating in terms of the present | Search for and reflect the wisdom and truth in the adolescent’s behavior by saying things such as ‘Of course you feel this way! Anyone would feel the same in your situation’ |
| Radical genuineness | Act natural, like a real person, rather than a ‘therapist. ‘ Communicate belief and confidence in the adolescent |
| DBT: dialectical behavior therapy | |
| Source: Reference 16 | |
How DBT works
DBT serves 5 functions. It enhances patient capabilities, increases patient motivation, structures the environment to increase the likelihood of success, works to assure generalization from therapy to the natural environment, and enhances therapists’ capabilities and motivation to treat patients effectively.8 Outpatient DBT for suicidal adolescents uses 4 modes of treatment:
- weekly individual therapy
- weekly skills training
- telephone coaching
- weekly therapist consultation team meetings.8
Although Linehan’s original research with adults was based on a 1-year treatment model,17 treatment lasts 12 to 16 weeks in the adolescent DBT model designed and studied by Miller et al.8 Treatment for adolescents is shorter because research indicates that suicidal adolescents frequently fail to complete longer courses of therapy.18
Individual therapy. The rank-ordered targets of individual therapy in the first stage of DBT are to:
- eliminate life-threatening behavior, including NSSI
- stop therapy-interfering behaviors (eg, not showing up to sessions)
- change behaviors that interfere with the adolescent’s quality of life (eg, substance abuse)
- enhance the adolescent’s use of skills.8
The individual therapist sets treatment goals in accord with these targets, monitors progress, integrates all modes of therapy, and balances acceptance and validation of the patient with being a catalyst for change. Family members may be included in therapy sessions when family problems emerge as the highest priority.
DBT therapists use chain analysis—which is a process of assessing the series of events, link by link, that lead from a prompting event to a problem behavior (eg, suicide attempt)—to assess problematic behavior and identify methods of change.8 The therapist and patient use this process to develop alternative behaviors for the patient to use to reach a more effective outcome.
DBT therapists also ask adolescents to fill out a daily diary card that tracks targeted behaviors, including NSSI, suicidal urges, and important emotions. The diary card helps the therapist determine what needs to be targeted in therapy, increases mindfulness and understanding of problem behaviors, and helps change targeted behavior.
Skills training addresses skills deficits believed to be causing the suicidal adolescent’s problems. DBT systematically teaches 5 skill sets:
- emotional regulation
- mindfulness
- interpersonal effectiveness
- distress tolerance
- “walking the middle path. “8
These skills are designed to treat specific problems common among suicidal adolescents and their families. For example, suicidal adolescents often experience a spike in emotions that leads to urges for ineffective behavior, such as attempting suicide or attacking another person. Table 3 provides steps that teach “opposite action, “ which can reduce ineffective emotions and problematic urges associated with these emotions. Table 4 provides mindfulness practices that can help patients address problems such as mindlessness and avoiding the present moment. Although adolescent DBT skills training is similar to that in adults, Table 5 describes key differences.
Table 3
Teaching adolescents ‘opposite action’
| Ask, what emotion am I experiencing? (eg, anger) |
| Ask, is it effective for me to experience this emotion? Does this emotion fit the facts of the situation? (If the answer to either of these questions is no, then proceed) |
| Ask, what is the action urge associated with this emotion? (eg, to attack) |
| Do actions that are opposite to the action urge (eg, gently avoid the person with whom you are angry) |
| Act opposite to the action all the way and completely (eg, have empathy and understanding for the other person, change your body posture by unclenching hands and relaxing facial muscles) |
| Keep repeating the opposite action until the emotion decreases |
| Source: Reference 8 |
Table 4
Mindfulness practices: Teach adolescents to live in the present moment
| Practice | Description |
|---|---|
| Mindful eating | Provide patients with a piece of food such as a carrot slice, raisin, saltine, candy, etc. Instruct them to eat the food using all of their senses. Tell them to observe it visually, notice the smells and textures, the taste, etc. Encourage patients to notice all that goes into the process and mechanics of chewing and swallowing. Observe the taste, changes in texture, and even sounds |
| Observing different body parts | Ask patients to get in a comfortable, relaxed, and still position. Provide verbal instructions to attend to a body part. For example, ‘Focus your attention on your left knee. If you notice your mind wandering, bring your attention back to your left knee. ‘ Spend about 30 seconds attending to the body part and then switch to another body part (eg, upper lip, right ear lobe, third toe on your left foot, etc. ) |
| Mindful blowing bubbles | Provide patients with bubbles and ask them to blow bubbles. Pay attention to the activity and the bubbles themselves. If patients get distracted or have judgments about the activities, instruct them to notice these thoughts and bring themselves back to participating |
| Source: Reference 8 | |
Table 5
Adapting DBT skills training for adolescents
| Alteration | Reason |
|---|---|
| Added ‘walking the middle path’ skills | This skill set was added to elaborate on topics including validation, polarities in behavioral patterns in the family, and how to apply learning principles to the self and others. The goals of these skills are to decrease parent and teen conflict, increase understanding of typical vs pathological teen behavior, and effectively change behavior through contingency management |
| Parents and family members of the suicidal adolescent attend weekly skills training | Generalization of the skills outside of therapy is more likely to occur with families’ help. Additionally, having family members practice the skills will decrease the likelihood that the home environment invalidates the adolescent, reinforces problematic behaviors, and/or persists in familial dysfunction |
| Duration of skills training decreased to 16 weeks | Increases the likelihood that adolescents complete therapy by reducing the number of skills taught |
| Some handouts have been modified | The forms are more appropriate for adolescents and family members |
| Source: Reference 8 | |
Telephone consultation. The purpose of brief (5 to 15 minutes) telephone consultations between a patient and therapist is to:
- enhance the likelihood of effective behavior
- coach the use of skills
- decrease the likelihood of problematic behaviors.
DBT telephone consultation for adults differs from that for suicidal adolescents. In DBT for adults, if a patient engages in NSSI or suicidal behavior, there is no telephone contact for 24 hours. This rule aims to avoid reinforcing the behavior with additional contact. However, this rule does not apply to adolescents because restricting adolescents’ access to resources for managing the aftereffects of self-harm could increase their risk of injury or death. Nonetheless, adolescents are strongly encouraged to use telephone coaching before rather than after self-harm. A second difference is that in DBT for adolescents, telephone coaching is offered to parents to help them use skills in the home. To avoid complications with dual relationships, the parents’ telephone coach should not be the adolescent’s individual therapist.
Consultation team meetings. The consultation team meets weekly to increase therapists’ capabilities and motivation.
Therapists who treat suicidal adolescents often have a high degree of burnout, which leads to ineffective treatment and/or quitting.8 The team provides support, engages in problem-solving, and helps therapists adhere to the treatment model to improve effectiveness. Clinicians interested in participating a consultation team may review http://behavioraltech.org/resources/crd.cfm for a directory of existing DBT programs. Those interested in starting a consultation team may explore training programs such as those offered at www.behavioraltech.org.
Related Resources
- Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. Annu Rev Clin Psychol. 2007; 3: 181-205.
- Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: The Guilford Press; 2007.
- Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002; 32(2): 146-157.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Many adolescents who receive dialectical behavior therapy (DBT) find that nonsuicidal self-injury (NSSI) leads to physiological, affective, and/or cognitive relief from suffering. Research indicates that persons who engage in NSSI have significant improvement in mood and reductions in dissociation after NSSIa and significantly higher analgesic response to pain than healthy controls.b The antithesis of this is that NSSI causes long-term suffering by, for example, alienating friends and family.c
One resolves this dialectical tension—ie, the validity in 2 opposing truths—by seeking a synthesis that maintains the truth in both sides and looks for what is being left out from both. In this case the DBT therapist must accept that NSSI provides benefits and validate the adolescent’s attempts to ease his or her emotional suffering. The therapist and patient also must recognize the harm and exacerbation of suffering that results from NSSI. The therapist and adolescent work to create a “middle path” to replace the NSSI with more skillful means that provide short-term relief, don’t exacerbate long-term suffering, and help the adolescent reach goals.
References
a. Kemperman I, Russ M, Shearin E. Self-injurious behavior and mood regulation in borderline patients. J Pers Disord. 1997; 11: 146-157.
b. Bohus M, Limberger M, Ebner U, et al. Pain perception during self-reported distress and calmness in patients with borderline personality disorder and self-mutilating behavior. Psychiatry Res. 2000; 95: 251-260.
c. Klonsky E, Oltmanns T, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003; 160: 1501-1508.
1. Barbui C, Esposito E, Cipriani A. Selective serotonin reuptake inhibitors and risk of suicide: a systematic review of observational studies. CMAJ. 2009;180:291-297.
2. Dubicka B, Hadley S, Roberts C. Suicidal behavior in youths with depression treated with new-generation antidepressants: meta-analysis. Br J Psychiatry. 2006;189:393-398.
3. Hammad TA, Laughren TP, Racoosin JA. Suicidality in pediatric patients treated with antidepressant drugs. Arch Gen Psychiatry. 2006;63:332-339.
4. Katz LY, Kozyrskyi AL, Prior HJ, et al. Effect of regulatory warnings on antidepressant prescription rates, use of health services and outcomes among children, adolescents and young adults. CMAJ. 2008;178:1005-1011.
5. Brent DA, Kolko DJ, Wartella ME, et al. Adolescent psychiatric inpatients’ risk of suicide attempt at 6-month follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:95-105.
6. Pfeffer CR, Klerman GL, Hurt SW, et al. Suicidal children grow up: rates and psychosocial risk factors for suicide attempts during follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:106-113.
7. Granboulan V, Roudot-Thoraval F, Lemerle S, et al. Predictive factors of post-discharge follow-up care among adolescent suicide attempters. Acta Psychiatr Scand. 2001;104:31-36.
8. Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York NY: The Guilford Press; 2007.
9. Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. In: Nolen-Hoeksema S, Cannon TD, Widiger T, eds. Annual review of clinical psychology. Vol 3. Palo Alto, CA: Annual Reviews; 2007:181-205.
10. Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002;32(2):146-157.
11. Woodberry KA, Popenoe EJ. Implementing dialectical behavior therapy with adolescents and their families in a community outpatient clinic. Cogn Behav Pract. 2008;15:277-286.
12. James AC, Taylor A, Winmill L, et al. A preliminary community study of dialectical behaviour therapy (DBT) with adolescent females demonstrating persistent, deliberate self-harm (DSH). Child Adolesc Ment Health. 2008;13:148-152.
13. Katz LY, Cox BJ, Gunasekara S, et al. Feasibility of dialectical behavior therapy for suicidal adolescents inpatients. J Am Acad Child Adolesc Psychiatry. 2004;45:276-282.
14. Sunseri PA. Preliminary outcomes on the use of dialectical behavior therapy to reduce hospitalization among adolescents in residential care. Resid Treat Child Youth. 2004;21:59-76.
15. Trupin EW, Stewart DG, Beach B, et al. Effectiveness of a dialectical behaviour therapy program for incarcerated female juvenile offenders. Child Adolesc Ment Health. 2002;7:121-127.
16. Linehan MM. Validation and psychotherapy. In: Bohart AC Greenberg LS, eds. Empathy reconsidered: new directions in psychotherapy. Washington, DC: American Psychological Association; 1997:353-392.
17. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48:1060-1064.
18. Trautman PD, Stewart N, Morishima A. Are adolescent suicide attempters noncompliant with outpatient care? J Am Acad Child Adolesc Psychiatry. 1993;32:89-94.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/adapting-dialectical-behavior-therapy.html#comments
Treating suicidal adolescents is fraught with challenges. Antidepressants may be associated with increased suicidal ideation in adolescents,1-3 although some data suggest that increased adolescent suicide rates are correlated with decreases in antidepressant prescribing.4 Adolescents hospitalized after a suicide attempt are likely to attempt suicide again after they are discharged.5,6 Such patients might not attend outpatient psychotherapy; a study of 167 adolescents discharged after a suicide attempt found that 26% never attended follow-up appointments and 11% went once.7
Emerging research supports the effectiveness of dialectical behavior therapy (DBT) for suicidal adolescents. DBT is a form of cognitive-behavioral therapy that combines individual therapy, skills training, and telephone coaching and is implemented by a therapist consultation team that meets weekly. This article reviews evidence supporting the efficacy of DBT for suicidal adolescents and describes principles of outpatient DBT for these patients as developed by Miller et al.8
Evidence of DBT’s effectiveness
A review of DBT research found strong evidence for DBT’s effectiveness for suicidal adults.9 Recently, DBT has been adapted to treat adolescents with suicidal behavior and nonsuicidal self-injury (NSSI).10-15
In a nonrandomized trial, Rathus and Miller10 compared 29 suicidal adolescent outpatients receiving DBT with 82 participants receiving treatment as usual (TAU). Patients were assigned to DBT if they had a suicide attempt in the previous 16 weeks and ≥3 borderline personality disorder (BPD) features or to TAU if they met only 1 of those conditions. Patients in the DBT group had more axis I disorders and pretreatment hospitalizations than the TAU group. Compared with those receiving TAU, patients treated with DBT had fewer hospitalizations (13% in TAU vs 0% in DBT) and a lower dropout rate (60% in TAU vs 38% in DBT). The DBT group experienced significant reductions in suicidal ideation, BPD symptoms, and general psychiatric symptoms. There was 1 suicide attempt in the DBT group vs 7 attempts in the TAU group; however, this difference was not statistically significant.
Woodberry and Popenoe11 examined the use of DBT for suicidal adolescents and their families in a community outpatient clinic. Adolescents reported reductions in overall symptoms, depression, anger, dissociative symptoms, and urges for intentional self-injury. Parents reported reductions in their children’s problem behaviors and in their own depressive symptoms. In a study of DBT in 16 adolescent females with chronic intentional self-injury, patients reported significant reductions in incidents of intentional self-injury, depression, and hopelessness, and increases in overall functioning.12
Three studies have examined using DBT for suicidal adolescents in residential facilities. In a pilot study, Katz et al13 compared DBT with TAU for 62 suicidal adolescent inpatients. At 1-year follow-up, both groups experienced significant reductions in suicidal ideation, NSSI, and depression. However, compared with those who received TAU, DBT patients had fewer behavioral problems during hospitalization. Sunseri14 used DBT to treat adolescent females in residential treatment. After DBT was implemented, residents were hospitalized because of NSSI and suicidality for fewer days than before DBT. Trupin et al15 taught DBT to staff who worked with female adolescent offenders at a juvenile rehabilitation facility. After the staff implemented DBT, the rates of problem behaviors and punishment by staff decreased on 1 unit; there were no behavior or punishment changes on another unit.
Theoretical foundations
Biosocial theory. The problems DBT treats in suicidal adolescents include emotion dysregulation, interpersonal conflict, impulsivity, cognitive dysregulation, and self-dysregulation.8 The biosocial theory postulates that these problems are the result of the transaction, or reciprocal relationship, between biologic predispositions and an invalidating environment. The biosocial theory suggests 3 biologic characteristics often are found among suicidal adolescents:
- high emotional sensitivity
- high extremity in reactions
- a slow return to baseline after experiencing a surge in affect.8
Although these characteristics indicate higher emotionality, they are not sufficient to account for suicidal adolescents’ difficulties. Problems arise when individuals with these biologic characteristics are raised in an invalidating environment, where the adolescent does not learn how to regulate emotions. Common characteristics of invalidating environments and their effects on adolescents are described in Table 1 .8
Treatment theory. DBT for suicidal adolescents focuses on a synthesis between 2 seemingly opposite treatment strategies: change and acceptance. The change focus is derived from behavioral science, and treatment incorporates standard behavior therapy practices, including chain analysis (described below), skills training, contingency management, and exposure.
The acceptance focus draws upon principles of Zen and other Eastern spiritual traditions. Therapists teach patients to accept reality as it is in this moment, without judgment. A key extension of this acceptance is the use of validation—radical acceptance and acknowledgement that all behavior has validity and understandability. DBT therapists strive to use 6 levels of validation with their patients ( Table 2 ),16 which often is a critical strategy for adolescents who reside in an invalidating environment.
DBT attempts to synthesize the acceptance-based Zen tradition with the change-based strategies of behavioral science through a dialectical philosophy. A fundamental postulate of dialectical philosophy is that a tension occurs when an initial truth or thesis is opposed by an apparently contradictory truth or antithesis.8 DBT therapists work with adolescents to find a synthesis that is the “middle path, “ which includes the truth in both positions as well as what is left out of both. For an example of how this might work for an adolescent patient with NSSI, visit this article at CurrentPsychiatry.com.
Table 1
Characteristics of an invalidating environment
| Characteristic | Result |
|---|---|
| Indiscriminately rejects communications of private experiences | Adolescents learn to actively self-invalidate and do not learn to validate themselves, label their emotions, or effectively regulate their emotions |
| Actively punishes displays of emotions, interspersed with intermittent reinforcement of emotional outbursts | Adolescents develop problematic emotion regulation strategies that oscillate between suppression and extreme outbursts |
| Oversimplifies problem solving | Adolescents develop high perfectionism and sensitivity to perceived failure, form unrealistic goals, and experience intense negative arousal in response to challenging feedback |
| Source: Reference 8 | |
Table 2
6 levels of validation employed by DBT therapists
| Level | Validation practices |
|---|---|
| Accurate reflection | Paraphrase what an adolescent says; communicate that you accurately understand what the adolescent has said |
| Mindreading | Communicate that you understand the adolescent’s private experiences or that which is unsaid. Articulate private experiences of the adolescent based on your knowledge of him or her |
| Observing and listening | Use nonverbal and paralinguistic cues to indicate interest. Communicate that you wish to know the adolescent’s emotions, thoughts, and behaviors |
| Validating in terms of causes | Make sense of behavior based on the adolescent’s learning history or biology. Describe how a behavior is effective for short-term but not long-term goals |
| Validating in terms of the present | Search for and reflect the wisdom and truth in the adolescent’s behavior by saying things such as ‘Of course you feel this way! Anyone would feel the same in your situation’ |
| Radical genuineness | Act natural, like a real person, rather than a ‘therapist. ‘ Communicate belief and confidence in the adolescent |
| DBT: dialectical behavior therapy | |
| Source: Reference 16 | |
How DBT works
DBT serves 5 functions. It enhances patient capabilities, increases patient motivation, structures the environment to increase the likelihood of success, works to assure generalization from therapy to the natural environment, and enhances therapists’ capabilities and motivation to treat patients effectively.8 Outpatient DBT for suicidal adolescents uses 4 modes of treatment:
- weekly individual therapy
- weekly skills training
- telephone coaching
- weekly therapist consultation team meetings.8
Although Linehan’s original research with adults was based on a 1-year treatment model,17 treatment lasts 12 to 16 weeks in the adolescent DBT model designed and studied by Miller et al.8 Treatment for adolescents is shorter because research indicates that suicidal adolescents frequently fail to complete longer courses of therapy.18
Individual therapy. The rank-ordered targets of individual therapy in the first stage of DBT are to:
- eliminate life-threatening behavior, including NSSI
- stop therapy-interfering behaviors (eg, not showing up to sessions)
- change behaviors that interfere with the adolescent’s quality of life (eg, substance abuse)
- enhance the adolescent’s use of skills.8
The individual therapist sets treatment goals in accord with these targets, monitors progress, integrates all modes of therapy, and balances acceptance and validation of the patient with being a catalyst for change. Family members may be included in therapy sessions when family problems emerge as the highest priority.
DBT therapists use chain analysis—which is a process of assessing the series of events, link by link, that lead from a prompting event to a problem behavior (eg, suicide attempt)—to assess problematic behavior and identify methods of change.8 The therapist and patient use this process to develop alternative behaviors for the patient to use to reach a more effective outcome.
DBT therapists also ask adolescents to fill out a daily diary card that tracks targeted behaviors, including NSSI, suicidal urges, and important emotions. The diary card helps the therapist determine what needs to be targeted in therapy, increases mindfulness and understanding of problem behaviors, and helps change targeted behavior.
Skills training addresses skills deficits believed to be causing the suicidal adolescent’s problems. DBT systematically teaches 5 skill sets:
- emotional regulation
- mindfulness
- interpersonal effectiveness
- distress tolerance
- “walking the middle path. “8
These skills are designed to treat specific problems common among suicidal adolescents and their families. For example, suicidal adolescents often experience a spike in emotions that leads to urges for ineffective behavior, such as attempting suicide or attacking another person. Table 3 provides steps that teach “opposite action, “ which can reduce ineffective emotions and problematic urges associated with these emotions. Table 4 provides mindfulness practices that can help patients address problems such as mindlessness and avoiding the present moment. Although adolescent DBT skills training is similar to that in adults, Table 5 describes key differences.
Table 3
Teaching adolescents ‘opposite action’
| Ask, what emotion am I experiencing? (eg, anger) |
| Ask, is it effective for me to experience this emotion? Does this emotion fit the facts of the situation? (If the answer to either of these questions is no, then proceed) |
| Ask, what is the action urge associated with this emotion? (eg, to attack) |
| Do actions that are opposite to the action urge (eg, gently avoid the person with whom you are angry) |
| Act opposite to the action all the way and completely (eg, have empathy and understanding for the other person, change your body posture by unclenching hands and relaxing facial muscles) |
| Keep repeating the opposite action until the emotion decreases |
| Source: Reference 8 |
Table 4
Mindfulness practices: Teach adolescents to live in the present moment
| Practice | Description |
|---|---|
| Mindful eating | Provide patients with a piece of food such as a carrot slice, raisin, saltine, candy, etc. Instruct them to eat the food using all of their senses. Tell them to observe it visually, notice the smells and textures, the taste, etc. Encourage patients to notice all that goes into the process and mechanics of chewing and swallowing. Observe the taste, changes in texture, and even sounds |
| Observing different body parts | Ask patients to get in a comfortable, relaxed, and still position. Provide verbal instructions to attend to a body part. For example, ‘Focus your attention on your left knee. If you notice your mind wandering, bring your attention back to your left knee. ‘ Spend about 30 seconds attending to the body part and then switch to another body part (eg, upper lip, right ear lobe, third toe on your left foot, etc. ) |
| Mindful blowing bubbles | Provide patients with bubbles and ask them to blow bubbles. Pay attention to the activity and the bubbles themselves. If patients get distracted or have judgments about the activities, instruct them to notice these thoughts and bring themselves back to participating |
| Source: Reference 8 | |
Table 5
Adapting DBT skills training for adolescents
| Alteration | Reason |
|---|---|
| Added ‘walking the middle path’ skills | This skill set was added to elaborate on topics including validation, polarities in behavioral patterns in the family, and how to apply learning principles to the self and others. The goals of these skills are to decrease parent and teen conflict, increase understanding of typical vs pathological teen behavior, and effectively change behavior through contingency management |
| Parents and family members of the suicidal adolescent attend weekly skills training | Generalization of the skills outside of therapy is more likely to occur with families’ help. Additionally, having family members practice the skills will decrease the likelihood that the home environment invalidates the adolescent, reinforces problematic behaviors, and/or persists in familial dysfunction |
| Duration of skills training decreased to 16 weeks | Increases the likelihood that adolescents complete therapy by reducing the number of skills taught |
| Some handouts have been modified | The forms are more appropriate for adolescents and family members |
| Source: Reference 8 | |
Telephone consultation. The purpose of brief (5 to 15 minutes) telephone consultations between a patient and therapist is to:
- enhance the likelihood of effective behavior
- coach the use of skills
- decrease the likelihood of problematic behaviors.
DBT telephone consultation for adults differs from that for suicidal adolescents. In DBT for adults, if a patient engages in NSSI or suicidal behavior, there is no telephone contact for 24 hours. This rule aims to avoid reinforcing the behavior with additional contact. However, this rule does not apply to adolescents because restricting adolescents’ access to resources for managing the aftereffects of self-harm could increase their risk of injury or death. Nonetheless, adolescents are strongly encouraged to use telephone coaching before rather than after self-harm. A second difference is that in DBT for adolescents, telephone coaching is offered to parents to help them use skills in the home. To avoid complications with dual relationships, the parents’ telephone coach should not be the adolescent’s individual therapist.
Consultation team meetings. The consultation team meets weekly to increase therapists’ capabilities and motivation.
Therapists who treat suicidal adolescents often have a high degree of burnout, which leads to ineffective treatment and/or quitting.8 The team provides support, engages in problem-solving, and helps therapists adhere to the treatment model to improve effectiveness. Clinicians interested in participating a consultation team may review http://behavioraltech.org/resources/crd.cfm for a directory of existing DBT programs. Those interested in starting a consultation team may explore training programs such as those offered at www.behavioraltech.org.
Related Resources
- Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. Annu Rev Clin Psychol. 2007; 3: 181-205.
- Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: The Guilford Press; 2007.
- Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002; 32(2): 146-157.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Many adolescents who receive dialectical behavior therapy (DBT) find that nonsuicidal self-injury (NSSI) leads to physiological, affective, and/or cognitive relief from suffering. Research indicates that persons who engage in NSSI have significant improvement in mood and reductions in dissociation after NSSIa and significantly higher analgesic response to pain than healthy controls.b The antithesis of this is that NSSI causes long-term suffering by, for example, alienating friends and family.c
One resolves this dialectical tension—ie, the validity in 2 opposing truths—by seeking a synthesis that maintains the truth in both sides and looks for what is being left out from both. In this case the DBT therapist must accept that NSSI provides benefits and validate the adolescent’s attempts to ease his or her emotional suffering. The therapist and patient also must recognize the harm and exacerbation of suffering that results from NSSI. The therapist and adolescent work to create a “middle path” to replace the NSSI with more skillful means that provide short-term relief, don’t exacerbate long-term suffering, and help the adolescent reach goals.
References
a. Kemperman I, Russ M, Shearin E. Self-injurious behavior and mood regulation in borderline patients. J Pers Disord. 1997; 11: 146-157.
b. Bohus M, Limberger M, Ebner U, et al. Pain perception during self-reported distress and calmness in patients with borderline personality disorder and self-mutilating behavior. Psychiatry Res. 2000; 95: 251-260.
c. Klonsky E, Oltmanns T, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003; 160: 1501-1508.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/adapting-dialectical-behavior-therapy.html#comments
Treating suicidal adolescents is fraught with challenges. Antidepressants may be associated with increased suicidal ideation in adolescents,1-3 although some data suggest that increased adolescent suicide rates are correlated with decreases in antidepressant prescribing.4 Adolescents hospitalized after a suicide attempt are likely to attempt suicide again after they are discharged.5,6 Such patients might not attend outpatient psychotherapy; a study of 167 adolescents discharged after a suicide attempt found that 26% never attended follow-up appointments and 11% went once.7
Emerging research supports the effectiveness of dialectical behavior therapy (DBT) for suicidal adolescents. DBT is a form of cognitive-behavioral therapy that combines individual therapy, skills training, and telephone coaching and is implemented by a therapist consultation team that meets weekly. This article reviews evidence supporting the efficacy of DBT for suicidal adolescents and describes principles of outpatient DBT for these patients as developed by Miller et al.8
Evidence of DBT’s effectiveness
A review of DBT research found strong evidence for DBT’s effectiveness for suicidal adults.9 Recently, DBT has been adapted to treat adolescents with suicidal behavior and nonsuicidal self-injury (NSSI).10-15
In a nonrandomized trial, Rathus and Miller10 compared 29 suicidal adolescent outpatients receiving DBT with 82 participants receiving treatment as usual (TAU). Patients were assigned to DBT if they had a suicide attempt in the previous 16 weeks and ≥3 borderline personality disorder (BPD) features or to TAU if they met only 1 of those conditions. Patients in the DBT group had more axis I disorders and pretreatment hospitalizations than the TAU group. Compared with those receiving TAU, patients treated with DBT had fewer hospitalizations (13% in TAU vs 0% in DBT) and a lower dropout rate (60% in TAU vs 38% in DBT). The DBT group experienced significant reductions in suicidal ideation, BPD symptoms, and general psychiatric symptoms. There was 1 suicide attempt in the DBT group vs 7 attempts in the TAU group; however, this difference was not statistically significant.
Woodberry and Popenoe11 examined the use of DBT for suicidal adolescents and their families in a community outpatient clinic. Adolescents reported reductions in overall symptoms, depression, anger, dissociative symptoms, and urges for intentional self-injury. Parents reported reductions in their children’s problem behaviors and in their own depressive symptoms. In a study of DBT in 16 adolescent females with chronic intentional self-injury, patients reported significant reductions in incidents of intentional self-injury, depression, and hopelessness, and increases in overall functioning.12
Three studies have examined using DBT for suicidal adolescents in residential facilities. In a pilot study, Katz et al13 compared DBT with TAU for 62 suicidal adolescent inpatients. At 1-year follow-up, both groups experienced significant reductions in suicidal ideation, NSSI, and depression. However, compared with those who received TAU, DBT patients had fewer behavioral problems during hospitalization. Sunseri14 used DBT to treat adolescent females in residential treatment. After DBT was implemented, residents were hospitalized because of NSSI and suicidality for fewer days than before DBT. Trupin et al15 taught DBT to staff who worked with female adolescent offenders at a juvenile rehabilitation facility. After the staff implemented DBT, the rates of problem behaviors and punishment by staff decreased on 1 unit; there were no behavior or punishment changes on another unit.
Theoretical foundations
Biosocial theory. The problems DBT treats in suicidal adolescents include emotion dysregulation, interpersonal conflict, impulsivity, cognitive dysregulation, and self-dysregulation.8 The biosocial theory postulates that these problems are the result of the transaction, or reciprocal relationship, between biologic predispositions and an invalidating environment. The biosocial theory suggests 3 biologic characteristics often are found among suicidal adolescents:
- high emotional sensitivity
- high extremity in reactions
- a slow return to baseline after experiencing a surge in affect.8
Although these characteristics indicate higher emotionality, they are not sufficient to account for suicidal adolescents’ difficulties. Problems arise when individuals with these biologic characteristics are raised in an invalidating environment, where the adolescent does not learn how to regulate emotions. Common characteristics of invalidating environments and their effects on adolescents are described in Table 1 .8
Treatment theory. DBT for suicidal adolescents focuses on a synthesis between 2 seemingly opposite treatment strategies: change and acceptance. The change focus is derived from behavioral science, and treatment incorporates standard behavior therapy practices, including chain analysis (described below), skills training, contingency management, and exposure.
The acceptance focus draws upon principles of Zen and other Eastern spiritual traditions. Therapists teach patients to accept reality as it is in this moment, without judgment. A key extension of this acceptance is the use of validation—radical acceptance and acknowledgement that all behavior has validity and understandability. DBT therapists strive to use 6 levels of validation with their patients ( Table 2 ),16 which often is a critical strategy for adolescents who reside in an invalidating environment.
DBT attempts to synthesize the acceptance-based Zen tradition with the change-based strategies of behavioral science through a dialectical philosophy. A fundamental postulate of dialectical philosophy is that a tension occurs when an initial truth or thesis is opposed by an apparently contradictory truth or antithesis.8 DBT therapists work with adolescents to find a synthesis that is the “middle path, “ which includes the truth in both positions as well as what is left out of both. For an example of how this might work for an adolescent patient with NSSI, visit this article at CurrentPsychiatry.com.
Table 1
Characteristics of an invalidating environment
| Characteristic | Result |
|---|---|
| Indiscriminately rejects communications of private experiences | Adolescents learn to actively self-invalidate and do not learn to validate themselves, label their emotions, or effectively regulate their emotions |
| Actively punishes displays of emotions, interspersed with intermittent reinforcement of emotional outbursts | Adolescents develop problematic emotion regulation strategies that oscillate between suppression and extreme outbursts |
| Oversimplifies problem solving | Adolescents develop high perfectionism and sensitivity to perceived failure, form unrealistic goals, and experience intense negative arousal in response to challenging feedback |
| Source: Reference 8 | |
Table 2
6 levels of validation employed by DBT therapists
| Level | Validation practices |
|---|---|
| Accurate reflection | Paraphrase what an adolescent says; communicate that you accurately understand what the adolescent has said |
| Mindreading | Communicate that you understand the adolescent’s private experiences or that which is unsaid. Articulate private experiences of the adolescent based on your knowledge of him or her |
| Observing and listening | Use nonverbal and paralinguistic cues to indicate interest. Communicate that you wish to know the adolescent’s emotions, thoughts, and behaviors |
| Validating in terms of causes | Make sense of behavior based on the adolescent’s learning history or biology. Describe how a behavior is effective for short-term but not long-term goals |
| Validating in terms of the present | Search for and reflect the wisdom and truth in the adolescent’s behavior by saying things such as ‘Of course you feel this way! Anyone would feel the same in your situation’ |
| Radical genuineness | Act natural, like a real person, rather than a ‘therapist. ‘ Communicate belief and confidence in the adolescent |
| DBT: dialectical behavior therapy | |
| Source: Reference 16 | |
How DBT works
DBT serves 5 functions. It enhances patient capabilities, increases patient motivation, structures the environment to increase the likelihood of success, works to assure generalization from therapy to the natural environment, and enhances therapists’ capabilities and motivation to treat patients effectively.8 Outpatient DBT for suicidal adolescents uses 4 modes of treatment:
- weekly individual therapy
- weekly skills training
- telephone coaching
- weekly therapist consultation team meetings.8
Although Linehan’s original research with adults was based on a 1-year treatment model,17 treatment lasts 12 to 16 weeks in the adolescent DBT model designed and studied by Miller et al.8 Treatment for adolescents is shorter because research indicates that suicidal adolescents frequently fail to complete longer courses of therapy.18
Individual therapy. The rank-ordered targets of individual therapy in the first stage of DBT are to:
- eliminate life-threatening behavior, including NSSI
- stop therapy-interfering behaviors (eg, not showing up to sessions)
- change behaviors that interfere with the adolescent’s quality of life (eg, substance abuse)
- enhance the adolescent’s use of skills.8
The individual therapist sets treatment goals in accord with these targets, monitors progress, integrates all modes of therapy, and balances acceptance and validation of the patient with being a catalyst for change. Family members may be included in therapy sessions when family problems emerge as the highest priority.
DBT therapists use chain analysis—which is a process of assessing the series of events, link by link, that lead from a prompting event to a problem behavior (eg, suicide attempt)—to assess problematic behavior and identify methods of change.8 The therapist and patient use this process to develop alternative behaviors for the patient to use to reach a more effective outcome.
DBT therapists also ask adolescents to fill out a daily diary card that tracks targeted behaviors, including NSSI, suicidal urges, and important emotions. The diary card helps the therapist determine what needs to be targeted in therapy, increases mindfulness and understanding of problem behaviors, and helps change targeted behavior.
Skills training addresses skills deficits believed to be causing the suicidal adolescent’s problems. DBT systematically teaches 5 skill sets:
- emotional regulation
- mindfulness
- interpersonal effectiveness
- distress tolerance
- “walking the middle path. “8
These skills are designed to treat specific problems common among suicidal adolescents and their families. For example, suicidal adolescents often experience a spike in emotions that leads to urges for ineffective behavior, such as attempting suicide or attacking another person. Table 3 provides steps that teach “opposite action, “ which can reduce ineffective emotions and problematic urges associated with these emotions. Table 4 provides mindfulness practices that can help patients address problems such as mindlessness and avoiding the present moment. Although adolescent DBT skills training is similar to that in adults, Table 5 describes key differences.
Table 3
Teaching adolescents ‘opposite action’
| Ask, what emotion am I experiencing? (eg, anger) |
| Ask, is it effective for me to experience this emotion? Does this emotion fit the facts of the situation? (If the answer to either of these questions is no, then proceed) |
| Ask, what is the action urge associated with this emotion? (eg, to attack) |
| Do actions that are opposite to the action urge (eg, gently avoid the person with whom you are angry) |
| Act opposite to the action all the way and completely (eg, have empathy and understanding for the other person, change your body posture by unclenching hands and relaxing facial muscles) |
| Keep repeating the opposite action until the emotion decreases |
| Source: Reference 8 |
Table 4
Mindfulness practices: Teach adolescents to live in the present moment
| Practice | Description |
|---|---|
| Mindful eating | Provide patients with a piece of food such as a carrot slice, raisin, saltine, candy, etc. Instruct them to eat the food using all of their senses. Tell them to observe it visually, notice the smells and textures, the taste, etc. Encourage patients to notice all that goes into the process and mechanics of chewing and swallowing. Observe the taste, changes in texture, and even sounds |
| Observing different body parts | Ask patients to get in a comfortable, relaxed, and still position. Provide verbal instructions to attend to a body part. For example, ‘Focus your attention on your left knee. If you notice your mind wandering, bring your attention back to your left knee. ‘ Spend about 30 seconds attending to the body part and then switch to another body part (eg, upper lip, right ear lobe, third toe on your left foot, etc. ) |
| Mindful blowing bubbles | Provide patients with bubbles and ask them to blow bubbles. Pay attention to the activity and the bubbles themselves. If patients get distracted or have judgments about the activities, instruct them to notice these thoughts and bring themselves back to participating |
| Source: Reference 8 | |
Table 5
Adapting DBT skills training for adolescents
| Alteration | Reason |
|---|---|
| Added ‘walking the middle path’ skills | This skill set was added to elaborate on topics including validation, polarities in behavioral patterns in the family, and how to apply learning principles to the self and others. The goals of these skills are to decrease parent and teen conflict, increase understanding of typical vs pathological teen behavior, and effectively change behavior through contingency management |
| Parents and family members of the suicidal adolescent attend weekly skills training | Generalization of the skills outside of therapy is more likely to occur with families’ help. Additionally, having family members practice the skills will decrease the likelihood that the home environment invalidates the adolescent, reinforces problematic behaviors, and/or persists in familial dysfunction |
| Duration of skills training decreased to 16 weeks | Increases the likelihood that adolescents complete therapy by reducing the number of skills taught |
| Some handouts have been modified | The forms are more appropriate for adolescents and family members |
| Source: Reference 8 | |
Telephone consultation. The purpose of brief (5 to 15 minutes) telephone consultations between a patient and therapist is to:
- enhance the likelihood of effective behavior
- coach the use of skills
- decrease the likelihood of problematic behaviors.
DBT telephone consultation for adults differs from that for suicidal adolescents. In DBT for adults, if a patient engages in NSSI or suicidal behavior, there is no telephone contact for 24 hours. This rule aims to avoid reinforcing the behavior with additional contact. However, this rule does not apply to adolescents because restricting adolescents’ access to resources for managing the aftereffects of self-harm could increase their risk of injury or death. Nonetheless, adolescents are strongly encouraged to use telephone coaching before rather than after self-harm. A second difference is that in DBT for adolescents, telephone coaching is offered to parents to help them use skills in the home. To avoid complications with dual relationships, the parents’ telephone coach should not be the adolescent’s individual therapist.
Consultation team meetings. The consultation team meets weekly to increase therapists’ capabilities and motivation.
Therapists who treat suicidal adolescents often have a high degree of burnout, which leads to ineffective treatment and/or quitting.8 The team provides support, engages in problem-solving, and helps therapists adhere to the treatment model to improve effectiveness. Clinicians interested in participating a consultation team may review http://behavioraltech.org/resources/crd.cfm for a directory of existing DBT programs. Those interested in starting a consultation team may explore training programs such as those offered at www.behavioraltech.org.
Related Resources
- Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. Annu Rev Clin Psychol. 2007; 3: 181-205.
- Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: The Guilford Press; 2007.
- Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002; 32(2): 146-157.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Many adolescents who receive dialectical behavior therapy (DBT) find that nonsuicidal self-injury (NSSI) leads to physiological, affective, and/or cognitive relief from suffering. Research indicates that persons who engage in NSSI have significant improvement in mood and reductions in dissociation after NSSIa and significantly higher analgesic response to pain than healthy controls.b The antithesis of this is that NSSI causes long-term suffering by, for example, alienating friends and family.c
One resolves this dialectical tension—ie, the validity in 2 opposing truths—by seeking a synthesis that maintains the truth in both sides and looks for what is being left out from both. In this case the DBT therapist must accept that NSSI provides benefits and validate the adolescent’s attempts to ease his or her emotional suffering. The therapist and patient also must recognize the harm and exacerbation of suffering that results from NSSI. The therapist and adolescent work to create a “middle path” to replace the NSSI with more skillful means that provide short-term relief, don’t exacerbate long-term suffering, and help the adolescent reach goals.
References
a. Kemperman I, Russ M, Shearin E. Self-injurious behavior and mood regulation in borderline patients. J Pers Disord. 1997; 11: 146-157.
b. Bohus M, Limberger M, Ebner U, et al. Pain perception during self-reported distress and calmness in patients with borderline personality disorder and self-mutilating behavior. Psychiatry Res. 2000; 95: 251-260.
c. Klonsky E, Oltmanns T, Turkheimer E. Deliberate self-harm in a nonclinical population: prevalence and psychological correlates. Am J Psychiatry. 2003; 160: 1501-1508.
1. Barbui C, Esposito E, Cipriani A. Selective serotonin reuptake inhibitors and risk of suicide: a systematic review of observational studies. CMAJ. 2009;180:291-297.
2. Dubicka B, Hadley S, Roberts C. Suicidal behavior in youths with depression treated with new-generation antidepressants: meta-analysis. Br J Psychiatry. 2006;189:393-398.
3. Hammad TA, Laughren TP, Racoosin JA. Suicidality in pediatric patients treated with antidepressant drugs. Arch Gen Psychiatry. 2006;63:332-339.
4. Katz LY, Kozyrskyi AL, Prior HJ, et al. Effect of regulatory warnings on antidepressant prescription rates, use of health services and outcomes among children, adolescents and young adults. CMAJ. 2008;178:1005-1011.
5. Brent DA, Kolko DJ, Wartella ME, et al. Adolescent psychiatric inpatients’ risk of suicide attempt at 6-month follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:95-105.
6. Pfeffer CR, Klerman GL, Hurt SW, et al. Suicidal children grow up: rates and psychosocial risk factors for suicide attempts during follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:106-113.
7. Granboulan V, Roudot-Thoraval F, Lemerle S, et al. Predictive factors of post-discharge follow-up care among adolescent suicide attempters. Acta Psychiatr Scand. 2001;104:31-36.
8. Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York NY: The Guilford Press; 2007.
9. Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. In: Nolen-Hoeksema S, Cannon TD, Widiger T, eds. Annual review of clinical psychology. Vol 3. Palo Alto, CA: Annual Reviews; 2007:181-205.
10. Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002;32(2):146-157.
11. Woodberry KA, Popenoe EJ. Implementing dialectical behavior therapy with adolescents and their families in a community outpatient clinic. Cogn Behav Pract. 2008;15:277-286.
12. James AC, Taylor A, Winmill L, et al. A preliminary community study of dialectical behaviour therapy (DBT) with adolescent females demonstrating persistent, deliberate self-harm (DSH). Child Adolesc Ment Health. 2008;13:148-152.
13. Katz LY, Cox BJ, Gunasekara S, et al. Feasibility of dialectical behavior therapy for suicidal adolescents inpatients. J Am Acad Child Adolesc Psychiatry. 2004;45:276-282.
14. Sunseri PA. Preliminary outcomes on the use of dialectical behavior therapy to reduce hospitalization among adolescents in residential care. Resid Treat Child Youth. 2004;21:59-76.
15. Trupin EW, Stewart DG, Beach B, et al. Effectiveness of a dialectical behaviour therapy program for incarcerated female juvenile offenders. Child Adolesc Ment Health. 2002;7:121-127.
16. Linehan MM. Validation and psychotherapy. In: Bohart AC Greenberg LS, eds. Empathy reconsidered: new directions in psychotherapy. Washington, DC: American Psychological Association; 1997:353-392.
17. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48:1060-1064.
18. Trautman PD, Stewart N, Morishima A. Are adolescent suicide attempters noncompliant with outpatient care? J Am Acad Child Adolesc Psychiatry. 1993;32:89-94.
1. Barbui C, Esposito E, Cipriani A. Selective serotonin reuptake inhibitors and risk of suicide: a systematic review of observational studies. CMAJ. 2009;180:291-297.
2. Dubicka B, Hadley S, Roberts C. Suicidal behavior in youths with depression treated with new-generation antidepressants: meta-analysis. Br J Psychiatry. 2006;189:393-398.
3. Hammad TA, Laughren TP, Racoosin JA. Suicidality in pediatric patients treated with antidepressant drugs. Arch Gen Psychiatry. 2006;63:332-339.
4. Katz LY, Kozyrskyi AL, Prior HJ, et al. Effect of regulatory warnings on antidepressant prescription rates, use of health services and outcomes among children, adolescents and young adults. CMAJ. 2008;178:1005-1011.
5. Brent DA, Kolko DJ, Wartella ME, et al. Adolescent psychiatric inpatients’ risk of suicide attempt at 6-month follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:95-105.
6. Pfeffer CR, Klerman GL, Hurt SW, et al. Suicidal children grow up: rates and psychosocial risk factors for suicide attempts during follow-up. J Am Acad Child Adolesc Psychiatry. 1993;32:106-113.
7. Granboulan V, Roudot-Thoraval F, Lemerle S, et al. Predictive factors of post-discharge follow-up care among adolescent suicide attempters. Acta Psychiatr Scand. 2001;104:31-36.
8. Miller A, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York NY: The Guilford Press; 2007.
9. Lynch TR, Trost WT, Salsman N, et al. Dialectical behavior therapy for borderline personality disorder. In: Nolen-Hoeksema S, Cannon TD, Widiger T, eds. Annual review of clinical psychology. Vol 3. Palo Alto, CA: Annual Reviews; 2007:181-205.
10. Rathus JH, Miller AL. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat Behav. 2002;32(2):146-157.
11. Woodberry KA, Popenoe EJ. Implementing dialectical behavior therapy with adolescents and their families in a community outpatient clinic. Cogn Behav Pract. 2008;15:277-286.
12. James AC, Taylor A, Winmill L, et al. A preliminary community study of dialectical behaviour therapy (DBT) with adolescent females demonstrating persistent, deliberate self-harm (DSH). Child Adolesc Ment Health. 2008;13:148-152.
13. Katz LY, Cox BJ, Gunasekara S, et al. Feasibility of dialectical behavior therapy for suicidal adolescents inpatients. J Am Acad Child Adolesc Psychiatry. 2004;45:276-282.
14. Sunseri PA. Preliminary outcomes on the use of dialectical behavior therapy to reduce hospitalization among adolescents in residential care. Resid Treat Child Youth. 2004;21:59-76.
15. Trupin EW, Stewart DG, Beach B, et al. Effectiveness of a dialectical behaviour therapy program for incarcerated female juvenile offenders. Child Adolesc Ment Health. 2002;7:121-127.
16. Linehan MM. Validation and psychotherapy. In: Bohart AC Greenberg LS, eds. Empathy reconsidered: new directions in psychotherapy. Washington, DC: American Psychological Association; 1997:353-392.
17. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48:1060-1064.
18. Trautman PD, Stewart N, Morishima A. Are adolescent suicide attempters noncompliant with outpatient care? J Am Acad Child Adolesc Psychiatry. 1993;32:89-94.
Opioid use disorder during pregnancy
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/opioid-use-disorder-during-pregnancy.html#comments
For 3 years, your mental health clinic has been treating Ms. J, age 23, for bipolar disorder. She is single, unemployed, lives alone, and receives Social Security disability assistance and financial support from her parents. She has been successfully maintained on aripiprazole, 15 mg/d, and citalopram, 20 mg/d, for 18 months. Six months ago she began to miss therapy sessions and physician visits.
Her parents inform Ms. J’s therapist that she is “snorting oxycontin” with her new boyfriend. At her next visit Ms. J confirms she has been struggling to manage an opioid use disorder for more than 1 year, and requests help.
After you educate her about the diagnosis, pathophysiology, and treatment of opioid addiction, she chooses to include pharmacotherapy as part of her treatment. After informed consent, Ms. J agrees to take buprenorphine and naloxone, meet with her therapist weekly, and attend twice-weekly Narcotics Anonymous (NA) meetings. Over the ensuing months she is gradually inducted onto buprenorphine and naloxone, 12 mg, shows improved insight and motivation, provides negative urine drug screens, and demonstrates increased ability to manage her recovery. Two weeks later Ms. J tells you she may be pregnant but wants to continue buprenorphine and naloxone.
Opioid use disorder (OUD) during pregnancy is among the most difficult clinical scenarios to manage. The prevalence of OUD during pregnancy is largely unknown. However, stigma against pregnant patients with OUD is substantial.1 This article briefly summarizes identification, assessment, and treatment of OUD during pregnancy. To avoid confusion with the term “physical dependence, “ we will use “opioid use disorder” instead of “opioid dependence. “ The DSM-5 Substance Use Disorders Workgroup recommends combining abuse and dependence into a single disorder of graded clinical severity; however, this has not been finalized.2
Early identification is crucial
Early identification of OUD in pregnant women can be challenging. Self-reports underestimate use3 and shame, fear of prosecution or involvement of child welfare services, and guilt can further erode self-report. Women with OUD may have irregular menses and might not be aware of their pregnancy until several months after conception.4 Also, women with OUD who are maintained on opioid agonist therapies may misinterpret early signs of pregnancy—such as fatigue, nausea, vomiting, headaches, and cramps—as withdrawal symptoms and may respond by increasing their opioid dosing, thus exposing their fetus to increased drug levels. Finally, many women with OUD experience amenorrhea as a result of their stressful, unhealthy lifestyle, which may preclude pregnancy despite sexual activity. When these women later enroll in an opioid maintenance program, their endocrine function may return to normal, leading to unexpected pregnancy.5
Screening for OUD in pregnant patients has not been well studied. An interviewer’s nonjudgmental, empathic attitude may be more important than the specific questions he or she asks. It may be best to begin with less threatening questions and proceed to more specific questions after developing a therapeutic alliance.6
Chasnoff et al7 studied >2, 000 Medicaid-eligible pregnant patients from 9 prenatal clinics to identify risk factors for substance use during pregnancy. Alcohol or tobacco use in the month before pregnancy most differentiated current drug or alcohol use from nonuse while pregnant; however, a wide variation in use rates among patients in this study limits the generalizability of these findings. Consider OUD in women with:
- physical examination findings or history that suggests substance use or withdrawal symptoms
- positive drug test results for illicit or nonprescribed opioids
- aberrant medication-taking behaviors in those receiving prescribed opioids
- nicotine or alcohol use in the month before they knew they were pregnant
- a history of addiction-related disorders
- evidence of diseases associated with drug use, such as human immunodeficiency virus or hepatitis C
- poor prenatal care attendance
- unexplained fetal growth abnormalities.
9 OUD-specific screening approaches are lacking; screening for general substance use is discussed elsewhere in the literature.10
A combination of interviewing and biologic drug screening may be more effective than either approach alone.11 Drug screening should include opioids typically screened for (morphine, codeine, heroin metabolite) and those for which additional tests may be required (eg, semi-synthetics such as oxycodone and synthetics such as fentanyl). Learn your state’s civil mandates regarding drug-using pregnant women, guidelines for addiction treatment, and confidentiality provisions, especially as they relate to drug testing and mandatory reporting. Ideally, patients should be informed of these issues before they undergo drug testing or other procedures. These requirements may vary according to physician specialty or role in providing care.
Diagnosis of opioid dependence is based on DSM-IV-TR criteria; however, the proposed DSM-5 criteria for OUD may better emphasize cautions about including tolerance or withdrawal when diagnosing OUD in the setting of medically supervised and appropriate opioid use.2
Table 1
The ‘4P’s Plus’ screen for substance use during pregnancy
| Parents: Did either of your parents ever have a problem with alcohol or drugs? |
| Partner: Does your partner have a problem with alcohol or drugs? |
| Past: Have you ever drunk beer, wine, or liquor? |
| Pregnancy: In the month before you knew you were pregnant, how many cigarettes did you smoke? |
| In the month before you knew you were pregnant, how many beers/how much wine/ how much liquor did you drink? |
| A positive screen results when a patient answers either of the 2 questions relating to pregnancy, indicating any alcohol or tobacco use in the month before she knew she was pregnant |
| Source: Reference 8 |
Office management
OUD-specific treatment decreases opioid use and improves birth outcomes14 ; however, retaining these patients in treatment can be difficult. Addressing social issues— including financial burdens, unstable living conditions, intimate partner violence, transportation difficulties, and limited access to medical and child care—can facilitate treatment.5 The Addiction Severity Index version tailored to women and pregnancy15 examines 7 domains of functioning (drugs, alcohol, psychological, social, medical, legal, and employment), informs treatment planning, quantifies treatment progress, and has predictive validity.16 Services are more likely to be effective if started during pregnancy as opposed to after delivery. Although detoxification is possible under carefully monitored conditions, many women relapse after detoxifying, and neonatal abstinence syndrome (NAS)—a disorder in which an addicted newborn experiences drug withdrawal—is common. Therefore, the risks of detoxification often outweigh benefits.5,17,18
Rehabilitation services for the mother can be provided at various levels of care, including outpatient, intensive outpatient, day hospital, residential, and inpatient. Although pregnancy-specific OUD treatment is ideal, it may not be available. Clinicians should attempt to locate services that can incorporate resources for pregnant women. Providing a means for child care during treatment is paramount to compliance. Develop a plan for nonconfrontational counseling, job skills training/education, and ongoing care after delivery (including child care and transportation resources) at the onset of treatment. The length of time maintained in treatment is one of the strongest predictors of abstinence.5
Increased education and screening for substance use as the pregnancy approaches term is necessary because patients may mistake early labor for symptoms of opioid withdrawal or worry that delivery room pain management will be inadequate and therefore relapse. Among pregnant women with addiction, preterm labor may be most common in those with OUD.12
Table 2
Medical complications common to pregnancy and substance abuse
| Anemia |
| Bacteremia/sepsis |
| Endocarditis |
| Cellulitis |
| Depression/anxiety |
| Gestational diabetes |
| Hepatitis (chronic and acute) |
| Hypertension/tachycardia |
| Phlebitis |
| Pneumonia |
| Gingivitis/poor oral hygiene |
| Sexually transmitted diseases |
|
| Tetanus |
| Cystitis |
| Pyelonephritis |
| AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus |
| Source: Reference 6 |
Table 3
Obstetric complications in women with addiction disorders
| Placental abruption |
| Chorioamnionitis |
| Placental insufficiency |
| Intrauterine growth restriction |
| Hypoxic/ischemic brain injury |
| Meconium passage |
| Neonatal abstinence syndrome |
| Spontaneous abortion |
| Intrauterine fetal death |
| Premature labor and delivery |
| Preterm, premature rupture of membranes |
| Postpartum hemorrhage |
| Hypertensive emergencies/preeclampsia |
| Source: Reference 6 |
Opioid agonist therapy
Obstetric complications in women with OUD may be related to rapid, frequent fluctuations of opioid blood levels during intoxication and withdrawal. Therefore, the first goal of pharmacotherapy is to reduce physical stress associated with cycling opioid blood levels. Opioid agonist medications can be extremely effective. Opioid agonist treatment for pregnant patients is similar to that of nonpregnant patients but includes pregnancy-specific objectives ( Table 4 ).20
Few anti-relapse medications have been studied in pregnant patients. Pharmacotherapies for OUD include methadone and buprenorphine. In our experience, opioid antagonists such as naltrexone typically would not be considered for pregnant patients because:
- their expected efficacy in reducing relapse in pregnant patients is lower than that of other medications
- their expected risk for inducing withdrawal is higher compared with methadone or buprenorphine
- research on the use of naltrexone during pregnancy is lacking.
Fluctuating blood opioid levels are minimized when methadone dosage is individually determined. Dosages should be based on a woman’s stage of pregnancy, relapse risk, pre-pregnancy methadone dose, experience with methadone, and clinical history. Some women experience lowered methadone blood levels during pregnancy because of increased fluid space, a larger tissue reservoir that can store methadone, and increased drug metabolism by both placenta and fetus. As a result, increased or split (twice daily) dosing may be indicated.22-24
The few randomized clinical trials comparing methadone with buprenorphine during pregnancy suggest that buprenorphine is not inferior to methadone in safety and discomfort of induction from a short-acting opioid, nor in outcome measures assessing NAS and maternal and neonatal safety.26,27 Results from the recent Maternal Opioid Treatment: Human Experimental Research project suggest that buprenorphine may have some advantages over methadone in pregnancy. Buprenorphine-maintained neonates may need less morphine, have shorter hospital stays, and require shorter treatment for NAS.28 However, treatment retention may be lower for buprenorphine-maintained mothers; any resultant long-term consequences on maternal and child health are as yet unexplored. These findings require replication.
Methadone and buprenorphine are not interchangeable. Many patients maintained on methadone do not respond optimally to buprenorphine. Clinics that dispense maintenance methadone are required to provide counseling services and random drug testing; these requirements do not apply to physicians who prescribe buprenorphine. Moreover, in our experience buprenorphine at times has been prescribed without close regard to psychosocial issues, adequate random drug testing, or coordination of care with other providers.
In pregnant patients, buprenorphine is preferred over buprenorphine and naloxone to avoid fetal exposure to naloxone, which may cause intrauterine withdrawal and maternal-fetal hormonal changes. To reduce abuse or diversion, patients should undergo drug testing to ensure buprenorphine is present, smaller prescriptions may be provided, and tablets can be counted. Limited data suggests buprenorphine is not teratogenic. Some data show low placental transfer of buprenorphine, thereby limiting fetal exposure and lowering risk for intrauterine growth restriction.29
Table 4
Opioid agonist treatment objectives for addicted patients who are pregnant
| General objectives |
| Prevent opioid withdrawal signs and symptoms |
| Provide a comfortable induction onto the medication |
| Block the euphoric and reinforcing effects of illicit opioids while also attenuating the motivation (craving, social interactions) to use illicit opioids and other drugs |
| Enhance treatment retention |
| Create a more optimal environment for behavioral and psychosocial interventions |
| Pregnancy-specific objectives |
| Eliminate or reduce fetal exposure to illicit opioids and other illicit drugs |
| Stabilize the intrauterine environment |
| Enhance involvement in prenatal care |
| Create an optimal environment to address pregnancy-specific problems |
| Source: Reference 20 |
Delivery and postnatal care
Compared with those not in treatment, women who are engaged in a multidisciplinary treatment program at the time of delivery demonstrated higher gestational age, increased birth weights, and lower rates of neonatal ICU admissions. They also realized a cost savings of $4, 644 per mother-infant pair.30
During delivery, pain medication should not be withheld solely because a pregnant woman has a history of addiction-related disorders; these women are subject to pain during delivery as much as other women. Avoid using mixed agonists/antagonists such as nalbuphine or butorphanol in women receiving opioid maintenance medication. Labor and delivery pain management for a pregnant patient maintained on opioid agonist therapies is discussed elsewhere in the literature.31 Every effort should be made to ensure that the mother remains in treatment through delivery and beyond.
To read about advising women with OUD on the benefits and risks of breastfeeding while receiving opioid agonist maintenance treatment, see the Box below.
CASE CONTINUED: Medication change
Ms. J’s boyfriend has left her and her parents have not readily accepted her pregnancy and need for support. She continues to attend NA meetings and weekly therapy. After educating her about the differences between buprenorphine and buprenorphine and naloxone in relation to risk, benefits, and side effects, you switch Ms. J to buprenorphine, 12 mg/d, while maintaining her on aripiprazole and citalopram. She consents to exchanging information about her medical, mental health, and addiction-related treatment with her primary care provider, who helps locate an obstetrician/gynecologist comfortable with her OUD and buprenorphine. Ms. J’s therapist helps link her with social services agencies to ensure prenatal care, assist with removing barriers to care, and plan for her needs as a parent.
After checking your state’s mandates, you determine you are not required to report Ms. J’s drug testing results. Ms. J’s ongoing drug testing shows the presence of buprenorphine and the absence of other opioids and all drugs of abuse.
Ms. J’s delivery is uncomplicated medically; however, family, financial, and parental role issues remain problematic. Encouraging her involvement in therapy and social services as part of her continued buprenorphine prescribing proves beneficial.
- Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008; 35(3): 245-259.
- Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003; 70(suppl 1 ): S87-S101.
- Velez M, Jansson LM. The opioid dependent mother and the newborn dyad: nonpharmacologic care. J Addict Med. 2008; 2(3): 113-120.
- Aripiprazole • Abilify
- Buprenorphine and naloxone •Suboxone
- Buprenorphine • Subutex
- Butorphanol • Stadol
- Citalopram • Celexa
- Fentanyl • Duragesic, Sublimaze, others
- Methadone • Dolophine
- Naloxone • Narcan
- Naltrexone • ReVia
- Nalbuphine • Nubain
- Oxycodone • Oxycontin
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Fernandez’ time toward this project was funded by the University Hospital/University of Cincinnati Addiction Psychiatry Fellowship Training Program operated by the Center for Treatment, Research, and Education in Addictive Disorders (CeTREAD), Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati and by the Veterans Affairs Medical Center, Cincinnati, OH.
The statements in this publication do not necessarily reflect the views or opinions of the Department of Veterans Affairs, the United States Government, or Opiate Addiction Recovery Services.
Acknowledgments
The authors wish to thank Kathleen Peak for her administrative assistance and Paul Horn, Professor, Department of Mathematical Sciences and Cincinnati VA, for statistical assistance.
Methadone is compatible with breast-feedinga and the American Academy of Pediatricsb and World Health Organizationc recommend breast-feeding for women receiving methadone unless there are contraindications such as human immunodeficiency virus infection.a Instruct mothers to seek medical advice if their breast-fed infant appears sedated.b Because the amount of methadone in breast milk is very small and depends on the methadone dose, the breast milk of mothers receiving methadone may be insufficient to prevent neonatal abstinence syndrome (NAS) and infants still may require opioid agonist treatment.d
Although breast-feeding by mothers receiving buprenorphine is not recommended by the drug’s manufacturer, there is consensus that buprenorphine is found in low levels in breast milke, f and is compatible with breast-feeding.g Because of partial agonism and low oral bioavailability, buprenorphine may not suppress NAS from methadone withdrawal. Always obtain appropriate informed consent.
References
a. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
b. Committee on Drugs, American Academy of Pediatrics. The transfer of drugs and other chemicals into human breast milk. Pediatrics. 2001;108:776-789.
c. The WHO Working Group, Bennet PN, ed. Monographs on individual drugs (WHO Working Group). In: Drugs and human lactation. Amsterdam, The Netherlands: Elsevier; 1988:319-320.
d. Jansson LM, Velez M, Harrow C. Methadone maintenance and lactation: a review of the literature and current management guidelines. J Hum Lact. 2004;20(1):62-71.
e. Grimm D, Pauly E, Pöschl J, et al. Buprenorphine and norbuprenorphine concentrations in human breast milk samples determined by liquid chromotography-tandem mass spectrometry. Ther Drug Monit. 2005;27(4):526-530.
f. Lindemalm S, Nydert P, Svensson JO, et al. Transfer of buprenorphine into breast milk and calculation of infant drug dose. J Hum Lact. 2009;25(2):199-205.
g. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP)) Series 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
1. Flavin J, Paltrow LM. Punishing pregnant drug-using women: defying law medicine, and common sense. J Addict Dis. 2010;29(2):231-244.
2. American Psychiatric Association. Opioid use disorder. DSM-5 development. Available at: http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=460#. Accessed January 26 2011.
3. Pichini S, Puig C, Zuccaro P, et al. Assessment of exposure to opiates and cocaine during pregnancy in a Mediterranean city: preliminary results of the “Meconium Project. “ Forensic Sci Int. 2005;153:59-65.
4. Mitchell JL, Brown G. Physiological effects of cocaine heroin, and methadone. In: Engs RC, ed. Women: alcohol and other drugs. Dubuque, IA: Kendall/Hunt Publishing Co; 1990:53-60.
5. Center for Substance Abuse Treatment. Medication-assisted treatment for opioid addiction during pregnancy. In: Medication-assisted treatment for opioid addiction in opioid treatment programs. Treatment Improvement Protocol (TIP) Series 43. Rockville MD: Substance Abuse and Mental Health Services Administration; 2005, reprinted 2006. DHHS Publication No. (SMA) 06-4212.
6. Helmbrecht GD, Thiagarajah S. Management of addiction disorders in pregnancy. J Addict Med. 2008;2(1):1-16.
7. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
8. Chasnoff IJ, Wells AM, McGourty RF, et al. Validation of the 4P’s Plus screen for substance use in pregnancy validation of the 4P’s Plus. J Perinatol. 2007;27:744-748.
9. Jones HE. The challenges of screening for substance use in pregnant women: commentary on the 4P’s Plus tool. J Perinatol. 2005;25:365-367.
10. Center for Substance Abuse Treatment. Substance abuse treatment: addressing the specific needs of women. Treatment Improvement Protocol (TIP) Series 51. Rockville MD: Substance Abuse and Mental Health Services Administration; 2009. HHS Publication No. (SMA) 09-4426.
11. Christmas JT, Knisely JS, Dawson KS, et al. Comparison of questionnaire screening and urine toxicology for detection of pregnancy complicated by substance use. Obstet Gynecol. 1992;80:750-754.
12. Wunsch MJ, Weaver MF. Alcohol and other drug use during pregnancy: management of the mother and child. In: Ries RK Fiellin DA, Miller SC, et al, eds. Principles of addiction medicine, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2009:1111-1124.
13. Ondersma SJ, Winhusen T, Erickson SJ, et al. Motivation enhancement therapy with pregnant substance-abusing women: does baseline motivation moderate efficacy? Drug Alcohol Depend. 2009;101(1-2):74-79.
14. Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy: effects and management. Obstet Gynecol Clin North Am. 1998;25:139-151.
15. Comfort M, Zanis DA, Whiteley MJ, et al. Assessing the needs of substance abusing women. Psychometric data on the psychosocial history. J Subst Abuse Treat. 1999;17:79-83.
16. Kissin WB, Svikis DS, Moylan P, et al. Identifying pregnant women at risk for early attrition from substance abuse treatment. J Subst Abuse Treat. 2004;27:31-38.
17. Jones HE, O’Grady KE, Malfi D, et al. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict. 2008;17(5):372-386.
18. Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? J Subst Abuse Treat. 2003;24(4):363-367.
19. Vesga-Lopez O, Blanco C, Keyes K, et al. Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry. 2008;65(7):805-815.
20. Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008;35(3):245-259.
21. NIDA International Program. National Institute on Drug Abuse. Methadone research web guide. Available at: http://international.drugabuse.gov/collaboration/guide_methadone/index.html. Accessed December 2, 2010.
22. Wittmann BK, Segal S. A comparison of the effects of single- and split-dose methadone administration on the fetus: ultrasound evaluation. Int J Addict. 1991;26:213-218.
23. DePetrillo PB, Rice JM. Methadone dosing and pregnancy: impact on program compliance. Int J Addict. 1995;30:207-217.
24. Jansson LM, Dipietro JA, Velez M, et al. Maternal methadone dosing schedule and fetal neurobehaviour. J Matern Fetal Neonatal Med. 2009;22(1):29-35.
25. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP) Series 40. Rockville MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
26. Jones HE, Johnson RE, Jasinski DR, et al. Randomized controlled study transitioning opioid-dependent pregnant women from short-acting morphine to buprenorphine or methadone. Drug Alcohol Depend. 2005;78(1):33-38.
27. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients; effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79(1):1-10.
28. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363(24):2320-2331.
29. Nanovskaya T, Deshmukh S, Brooks M, et al. Transplacental transfer and metabolism of buprenorphine. J Pharmacol Exp Ther. 2002;300(1):26-33.
30. Svikis DS, Golden AS, Huggins GR, et al. Cost-effectiveness of treatment for drug-abusing pregnant women. Drug Alcohol Depend. 1997;45:105-113.
31. Jones HE, O’Grady K, Dahne J, et al. Management of acute postpartum pain in patients maintained on methadone or buprenorphine during pregnancy. Am J Drug Alcohol Abuse. 2009;35(3):151-156.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/opioid-use-disorder-during-pregnancy.html#comments
For 3 years, your mental health clinic has been treating Ms. J, age 23, for bipolar disorder. She is single, unemployed, lives alone, and receives Social Security disability assistance and financial support from her parents. She has been successfully maintained on aripiprazole, 15 mg/d, and citalopram, 20 mg/d, for 18 months. Six months ago she began to miss therapy sessions and physician visits.
Her parents inform Ms. J’s therapist that she is “snorting oxycontin” with her new boyfriend. At her next visit Ms. J confirms she has been struggling to manage an opioid use disorder for more than 1 year, and requests help.
After you educate her about the diagnosis, pathophysiology, and treatment of opioid addiction, she chooses to include pharmacotherapy as part of her treatment. After informed consent, Ms. J agrees to take buprenorphine and naloxone, meet with her therapist weekly, and attend twice-weekly Narcotics Anonymous (NA) meetings. Over the ensuing months she is gradually inducted onto buprenorphine and naloxone, 12 mg, shows improved insight and motivation, provides negative urine drug screens, and demonstrates increased ability to manage her recovery. Two weeks later Ms. J tells you she may be pregnant but wants to continue buprenorphine and naloxone.
Opioid use disorder (OUD) during pregnancy is among the most difficult clinical scenarios to manage. The prevalence of OUD during pregnancy is largely unknown. However, stigma against pregnant patients with OUD is substantial.1 This article briefly summarizes identification, assessment, and treatment of OUD during pregnancy. To avoid confusion with the term “physical dependence, “ we will use “opioid use disorder” instead of “opioid dependence. “ The DSM-5 Substance Use Disorders Workgroup recommends combining abuse and dependence into a single disorder of graded clinical severity; however, this has not been finalized.2
Early identification is crucial
Early identification of OUD in pregnant women can be challenging. Self-reports underestimate use3 and shame, fear of prosecution or involvement of child welfare services, and guilt can further erode self-report. Women with OUD may have irregular menses and might not be aware of their pregnancy until several months after conception.4 Also, women with OUD who are maintained on opioid agonist therapies may misinterpret early signs of pregnancy—such as fatigue, nausea, vomiting, headaches, and cramps—as withdrawal symptoms and may respond by increasing their opioid dosing, thus exposing their fetus to increased drug levels. Finally, many women with OUD experience amenorrhea as a result of their stressful, unhealthy lifestyle, which may preclude pregnancy despite sexual activity. When these women later enroll in an opioid maintenance program, their endocrine function may return to normal, leading to unexpected pregnancy.5
Screening for OUD in pregnant patients has not been well studied. An interviewer’s nonjudgmental, empathic attitude may be more important than the specific questions he or she asks. It may be best to begin with less threatening questions and proceed to more specific questions after developing a therapeutic alliance.6
Chasnoff et al7 studied >2, 000 Medicaid-eligible pregnant patients from 9 prenatal clinics to identify risk factors for substance use during pregnancy. Alcohol or tobacco use in the month before pregnancy most differentiated current drug or alcohol use from nonuse while pregnant; however, a wide variation in use rates among patients in this study limits the generalizability of these findings. Consider OUD in women with:
- physical examination findings or history that suggests substance use or withdrawal symptoms
- positive drug test results for illicit or nonprescribed opioids
- aberrant medication-taking behaviors in those receiving prescribed opioids
- nicotine or alcohol use in the month before they knew they were pregnant
- a history of addiction-related disorders
- evidence of diseases associated with drug use, such as human immunodeficiency virus or hepatitis C
- poor prenatal care attendance
- unexplained fetal growth abnormalities.
9 OUD-specific screening approaches are lacking; screening for general substance use is discussed elsewhere in the literature.10
A combination of interviewing and biologic drug screening may be more effective than either approach alone.11 Drug screening should include opioids typically screened for (morphine, codeine, heroin metabolite) and those for which additional tests may be required (eg, semi-synthetics such as oxycodone and synthetics such as fentanyl). Learn your state’s civil mandates regarding drug-using pregnant women, guidelines for addiction treatment, and confidentiality provisions, especially as they relate to drug testing and mandatory reporting. Ideally, patients should be informed of these issues before they undergo drug testing or other procedures. These requirements may vary according to physician specialty or role in providing care.
Diagnosis of opioid dependence is based on DSM-IV-TR criteria; however, the proposed DSM-5 criteria for OUD may better emphasize cautions about including tolerance or withdrawal when diagnosing OUD in the setting of medically supervised and appropriate opioid use.2
Table 1
The ‘4P’s Plus’ screen for substance use during pregnancy
| Parents: Did either of your parents ever have a problem with alcohol or drugs? |
| Partner: Does your partner have a problem with alcohol or drugs? |
| Past: Have you ever drunk beer, wine, or liquor? |
| Pregnancy: In the month before you knew you were pregnant, how many cigarettes did you smoke? |
| In the month before you knew you were pregnant, how many beers/how much wine/ how much liquor did you drink? |
| A positive screen results when a patient answers either of the 2 questions relating to pregnancy, indicating any alcohol or tobacco use in the month before she knew she was pregnant |
| Source: Reference 8 |
Office management
OUD-specific treatment decreases opioid use and improves birth outcomes14 ; however, retaining these patients in treatment can be difficult. Addressing social issues— including financial burdens, unstable living conditions, intimate partner violence, transportation difficulties, and limited access to medical and child care—can facilitate treatment.5 The Addiction Severity Index version tailored to women and pregnancy15 examines 7 domains of functioning (drugs, alcohol, psychological, social, medical, legal, and employment), informs treatment planning, quantifies treatment progress, and has predictive validity.16 Services are more likely to be effective if started during pregnancy as opposed to after delivery. Although detoxification is possible under carefully monitored conditions, many women relapse after detoxifying, and neonatal abstinence syndrome (NAS)—a disorder in which an addicted newborn experiences drug withdrawal—is common. Therefore, the risks of detoxification often outweigh benefits.5,17,18
Rehabilitation services for the mother can be provided at various levels of care, including outpatient, intensive outpatient, day hospital, residential, and inpatient. Although pregnancy-specific OUD treatment is ideal, it may not be available. Clinicians should attempt to locate services that can incorporate resources for pregnant women. Providing a means for child care during treatment is paramount to compliance. Develop a plan for nonconfrontational counseling, job skills training/education, and ongoing care after delivery (including child care and transportation resources) at the onset of treatment. The length of time maintained in treatment is one of the strongest predictors of abstinence.5
Increased education and screening for substance use as the pregnancy approaches term is necessary because patients may mistake early labor for symptoms of opioid withdrawal or worry that delivery room pain management will be inadequate and therefore relapse. Among pregnant women with addiction, preterm labor may be most common in those with OUD.12
Table 2
Medical complications common to pregnancy and substance abuse
| Anemia |
| Bacteremia/sepsis |
| Endocarditis |
| Cellulitis |
| Depression/anxiety |
| Gestational diabetes |
| Hepatitis (chronic and acute) |
| Hypertension/tachycardia |
| Phlebitis |
| Pneumonia |
| Gingivitis/poor oral hygiene |
| Sexually transmitted diseases |
|
| Tetanus |
| Cystitis |
| Pyelonephritis |
| AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus |
| Source: Reference 6 |
Table 3
Obstetric complications in women with addiction disorders
| Placental abruption |
| Chorioamnionitis |
| Placental insufficiency |
| Intrauterine growth restriction |
| Hypoxic/ischemic brain injury |
| Meconium passage |
| Neonatal abstinence syndrome |
| Spontaneous abortion |
| Intrauterine fetal death |
| Premature labor and delivery |
| Preterm, premature rupture of membranes |
| Postpartum hemorrhage |
| Hypertensive emergencies/preeclampsia |
| Source: Reference 6 |
Opioid agonist therapy
Obstetric complications in women with OUD may be related to rapid, frequent fluctuations of opioid blood levels during intoxication and withdrawal. Therefore, the first goal of pharmacotherapy is to reduce physical stress associated with cycling opioid blood levels. Opioid agonist medications can be extremely effective. Opioid agonist treatment for pregnant patients is similar to that of nonpregnant patients but includes pregnancy-specific objectives ( Table 4 ).20
Few anti-relapse medications have been studied in pregnant patients. Pharmacotherapies for OUD include methadone and buprenorphine. In our experience, opioid antagonists such as naltrexone typically would not be considered for pregnant patients because:
- their expected efficacy in reducing relapse in pregnant patients is lower than that of other medications
- their expected risk for inducing withdrawal is higher compared with methadone or buprenorphine
- research on the use of naltrexone during pregnancy is lacking.
Fluctuating blood opioid levels are minimized when methadone dosage is individually determined. Dosages should be based on a woman’s stage of pregnancy, relapse risk, pre-pregnancy methadone dose, experience with methadone, and clinical history. Some women experience lowered methadone blood levels during pregnancy because of increased fluid space, a larger tissue reservoir that can store methadone, and increased drug metabolism by both placenta and fetus. As a result, increased or split (twice daily) dosing may be indicated.22-24
The few randomized clinical trials comparing methadone with buprenorphine during pregnancy suggest that buprenorphine is not inferior to methadone in safety and discomfort of induction from a short-acting opioid, nor in outcome measures assessing NAS and maternal and neonatal safety.26,27 Results from the recent Maternal Opioid Treatment: Human Experimental Research project suggest that buprenorphine may have some advantages over methadone in pregnancy. Buprenorphine-maintained neonates may need less morphine, have shorter hospital stays, and require shorter treatment for NAS.28 However, treatment retention may be lower for buprenorphine-maintained mothers; any resultant long-term consequences on maternal and child health are as yet unexplored. These findings require replication.
Methadone and buprenorphine are not interchangeable. Many patients maintained on methadone do not respond optimally to buprenorphine. Clinics that dispense maintenance methadone are required to provide counseling services and random drug testing; these requirements do not apply to physicians who prescribe buprenorphine. Moreover, in our experience buprenorphine at times has been prescribed without close regard to psychosocial issues, adequate random drug testing, or coordination of care with other providers.
In pregnant patients, buprenorphine is preferred over buprenorphine and naloxone to avoid fetal exposure to naloxone, which may cause intrauterine withdrawal and maternal-fetal hormonal changes. To reduce abuse or diversion, patients should undergo drug testing to ensure buprenorphine is present, smaller prescriptions may be provided, and tablets can be counted. Limited data suggests buprenorphine is not teratogenic. Some data show low placental transfer of buprenorphine, thereby limiting fetal exposure and lowering risk for intrauterine growth restriction.29
Table 4
Opioid agonist treatment objectives for addicted patients who are pregnant
| General objectives |
| Prevent opioid withdrawal signs and symptoms |
| Provide a comfortable induction onto the medication |
| Block the euphoric and reinforcing effects of illicit opioids while also attenuating the motivation (craving, social interactions) to use illicit opioids and other drugs |
| Enhance treatment retention |
| Create a more optimal environment for behavioral and psychosocial interventions |
| Pregnancy-specific objectives |
| Eliminate or reduce fetal exposure to illicit opioids and other illicit drugs |
| Stabilize the intrauterine environment |
| Enhance involvement in prenatal care |
| Create an optimal environment to address pregnancy-specific problems |
| Source: Reference 20 |
Delivery and postnatal care
Compared with those not in treatment, women who are engaged in a multidisciplinary treatment program at the time of delivery demonstrated higher gestational age, increased birth weights, and lower rates of neonatal ICU admissions. They also realized a cost savings of $4, 644 per mother-infant pair.30
During delivery, pain medication should not be withheld solely because a pregnant woman has a history of addiction-related disorders; these women are subject to pain during delivery as much as other women. Avoid using mixed agonists/antagonists such as nalbuphine or butorphanol in women receiving opioid maintenance medication. Labor and delivery pain management for a pregnant patient maintained on opioid agonist therapies is discussed elsewhere in the literature.31 Every effort should be made to ensure that the mother remains in treatment through delivery and beyond.
To read about advising women with OUD on the benefits and risks of breastfeeding while receiving opioid agonist maintenance treatment, see the Box below.
CASE CONTINUED: Medication change
Ms. J’s boyfriend has left her and her parents have not readily accepted her pregnancy and need for support. She continues to attend NA meetings and weekly therapy. After educating her about the differences between buprenorphine and buprenorphine and naloxone in relation to risk, benefits, and side effects, you switch Ms. J to buprenorphine, 12 mg/d, while maintaining her on aripiprazole and citalopram. She consents to exchanging information about her medical, mental health, and addiction-related treatment with her primary care provider, who helps locate an obstetrician/gynecologist comfortable with her OUD and buprenorphine. Ms. J’s therapist helps link her with social services agencies to ensure prenatal care, assist with removing barriers to care, and plan for her needs as a parent.
After checking your state’s mandates, you determine you are not required to report Ms. J’s drug testing results. Ms. J’s ongoing drug testing shows the presence of buprenorphine and the absence of other opioids and all drugs of abuse.
Ms. J’s delivery is uncomplicated medically; however, family, financial, and parental role issues remain problematic. Encouraging her involvement in therapy and social services as part of her continued buprenorphine prescribing proves beneficial.
- Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008; 35(3): 245-259.
- Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003; 70(suppl 1 ): S87-S101.
- Velez M, Jansson LM. The opioid dependent mother and the newborn dyad: nonpharmacologic care. J Addict Med. 2008; 2(3): 113-120.
- Aripiprazole • Abilify
- Buprenorphine and naloxone •Suboxone
- Buprenorphine • Subutex
- Butorphanol • Stadol
- Citalopram • Celexa
- Fentanyl • Duragesic, Sublimaze, others
- Methadone • Dolophine
- Naloxone • Narcan
- Naltrexone • ReVia
- Nalbuphine • Nubain
- Oxycodone • Oxycontin
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Fernandez’ time toward this project was funded by the University Hospital/University of Cincinnati Addiction Psychiatry Fellowship Training Program operated by the Center for Treatment, Research, and Education in Addictive Disorders (CeTREAD), Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati and by the Veterans Affairs Medical Center, Cincinnati, OH.
The statements in this publication do not necessarily reflect the views or opinions of the Department of Veterans Affairs, the United States Government, or Opiate Addiction Recovery Services.
Acknowledgments
The authors wish to thank Kathleen Peak for her administrative assistance and Paul Horn, Professor, Department of Mathematical Sciences and Cincinnati VA, for statistical assistance.
Methadone is compatible with breast-feedinga and the American Academy of Pediatricsb and World Health Organizationc recommend breast-feeding for women receiving methadone unless there are contraindications such as human immunodeficiency virus infection.a Instruct mothers to seek medical advice if their breast-fed infant appears sedated.b Because the amount of methadone in breast milk is very small and depends on the methadone dose, the breast milk of mothers receiving methadone may be insufficient to prevent neonatal abstinence syndrome (NAS) and infants still may require opioid agonist treatment.d
Although breast-feeding by mothers receiving buprenorphine is not recommended by the drug’s manufacturer, there is consensus that buprenorphine is found in low levels in breast milke, f and is compatible with breast-feeding.g Because of partial agonism and low oral bioavailability, buprenorphine may not suppress NAS from methadone withdrawal. Always obtain appropriate informed consent.
References
a. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
b. Committee on Drugs, American Academy of Pediatrics. The transfer of drugs and other chemicals into human breast milk. Pediatrics. 2001;108:776-789.
c. The WHO Working Group, Bennet PN, ed. Monographs on individual drugs (WHO Working Group). In: Drugs and human lactation. Amsterdam, The Netherlands: Elsevier; 1988:319-320.
d. Jansson LM, Velez M, Harrow C. Methadone maintenance and lactation: a review of the literature and current management guidelines. J Hum Lact. 2004;20(1):62-71.
e. Grimm D, Pauly E, Pöschl J, et al. Buprenorphine and norbuprenorphine concentrations in human breast milk samples determined by liquid chromotography-tandem mass spectrometry. Ther Drug Monit. 2005;27(4):526-530.
f. Lindemalm S, Nydert P, Svensson JO, et al. Transfer of buprenorphine into breast milk and calculation of infant drug dose. J Hum Lact. 2009;25(2):199-205.
g. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP)) Series 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/03/opioid-use-disorder-during-pregnancy.html#comments
For 3 years, your mental health clinic has been treating Ms. J, age 23, for bipolar disorder. She is single, unemployed, lives alone, and receives Social Security disability assistance and financial support from her parents. She has been successfully maintained on aripiprazole, 15 mg/d, and citalopram, 20 mg/d, for 18 months. Six months ago she began to miss therapy sessions and physician visits.
Her parents inform Ms. J’s therapist that she is “snorting oxycontin” with her new boyfriend. At her next visit Ms. J confirms she has been struggling to manage an opioid use disorder for more than 1 year, and requests help.
After you educate her about the diagnosis, pathophysiology, and treatment of opioid addiction, she chooses to include pharmacotherapy as part of her treatment. After informed consent, Ms. J agrees to take buprenorphine and naloxone, meet with her therapist weekly, and attend twice-weekly Narcotics Anonymous (NA) meetings. Over the ensuing months she is gradually inducted onto buprenorphine and naloxone, 12 mg, shows improved insight and motivation, provides negative urine drug screens, and demonstrates increased ability to manage her recovery. Two weeks later Ms. J tells you she may be pregnant but wants to continue buprenorphine and naloxone.
Opioid use disorder (OUD) during pregnancy is among the most difficult clinical scenarios to manage. The prevalence of OUD during pregnancy is largely unknown. However, stigma against pregnant patients with OUD is substantial.1 This article briefly summarizes identification, assessment, and treatment of OUD during pregnancy. To avoid confusion with the term “physical dependence, “ we will use “opioid use disorder” instead of “opioid dependence. “ The DSM-5 Substance Use Disorders Workgroup recommends combining abuse and dependence into a single disorder of graded clinical severity; however, this has not been finalized.2
Early identification is crucial
Early identification of OUD in pregnant women can be challenging. Self-reports underestimate use3 and shame, fear of prosecution or involvement of child welfare services, and guilt can further erode self-report. Women with OUD may have irregular menses and might not be aware of their pregnancy until several months after conception.4 Also, women with OUD who are maintained on opioid agonist therapies may misinterpret early signs of pregnancy—such as fatigue, nausea, vomiting, headaches, and cramps—as withdrawal symptoms and may respond by increasing their opioid dosing, thus exposing their fetus to increased drug levels. Finally, many women with OUD experience amenorrhea as a result of their stressful, unhealthy lifestyle, which may preclude pregnancy despite sexual activity. When these women later enroll in an opioid maintenance program, their endocrine function may return to normal, leading to unexpected pregnancy.5
Screening for OUD in pregnant patients has not been well studied. An interviewer’s nonjudgmental, empathic attitude may be more important than the specific questions he or she asks. It may be best to begin with less threatening questions and proceed to more specific questions after developing a therapeutic alliance.6
Chasnoff et al7 studied >2, 000 Medicaid-eligible pregnant patients from 9 prenatal clinics to identify risk factors for substance use during pregnancy. Alcohol or tobacco use in the month before pregnancy most differentiated current drug or alcohol use from nonuse while pregnant; however, a wide variation in use rates among patients in this study limits the generalizability of these findings. Consider OUD in women with:
- physical examination findings or history that suggests substance use or withdrawal symptoms
- positive drug test results for illicit or nonprescribed opioids
- aberrant medication-taking behaviors in those receiving prescribed opioids
- nicotine or alcohol use in the month before they knew they were pregnant
- a history of addiction-related disorders
- evidence of diseases associated with drug use, such as human immunodeficiency virus or hepatitis C
- poor prenatal care attendance
- unexplained fetal growth abnormalities.
9 OUD-specific screening approaches are lacking; screening for general substance use is discussed elsewhere in the literature.10
A combination of interviewing and biologic drug screening may be more effective than either approach alone.11 Drug screening should include opioids typically screened for (morphine, codeine, heroin metabolite) and those for which additional tests may be required (eg, semi-synthetics such as oxycodone and synthetics such as fentanyl). Learn your state’s civil mandates regarding drug-using pregnant women, guidelines for addiction treatment, and confidentiality provisions, especially as they relate to drug testing and mandatory reporting. Ideally, patients should be informed of these issues before they undergo drug testing or other procedures. These requirements may vary according to physician specialty or role in providing care.
Diagnosis of opioid dependence is based on DSM-IV-TR criteria; however, the proposed DSM-5 criteria for OUD may better emphasize cautions about including tolerance or withdrawal when diagnosing OUD in the setting of medically supervised and appropriate opioid use.2
Table 1
The ‘4P’s Plus’ screen for substance use during pregnancy
| Parents: Did either of your parents ever have a problem with alcohol or drugs? |
| Partner: Does your partner have a problem with alcohol or drugs? |
| Past: Have you ever drunk beer, wine, or liquor? |
| Pregnancy: In the month before you knew you were pregnant, how many cigarettes did you smoke? |
| In the month before you knew you were pregnant, how many beers/how much wine/ how much liquor did you drink? |
| A positive screen results when a patient answers either of the 2 questions relating to pregnancy, indicating any alcohol or tobacco use in the month before she knew she was pregnant |
| Source: Reference 8 |
Office management
OUD-specific treatment decreases opioid use and improves birth outcomes14 ; however, retaining these patients in treatment can be difficult. Addressing social issues— including financial burdens, unstable living conditions, intimate partner violence, transportation difficulties, and limited access to medical and child care—can facilitate treatment.5 The Addiction Severity Index version tailored to women and pregnancy15 examines 7 domains of functioning (drugs, alcohol, psychological, social, medical, legal, and employment), informs treatment planning, quantifies treatment progress, and has predictive validity.16 Services are more likely to be effective if started during pregnancy as opposed to after delivery. Although detoxification is possible under carefully monitored conditions, many women relapse after detoxifying, and neonatal abstinence syndrome (NAS)—a disorder in which an addicted newborn experiences drug withdrawal—is common. Therefore, the risks of detoxification often outweigh benefits.5,17,18
Rehabilitation services for the mother can be provided at various levels of care, including outpatient, intensive outpatient, day hospital, residential, and inpatient. Although pregnancy-specific OUD treatment is ideal, it may not be available. Clinicians should attempt to locate services that can incorporate resources for pregnant women. Providing a means for child care during treatment is paramount to compliance. Develop a plan for nonconfrontational counseling, job skills training/education, and ongoing care after delivery (including child care and transportation resources) at the onset of treatment. The length of time maintained in treatment is one of the strongest predictors of abstinence.5
Increased education and screening for substance use as the pregnancy approaches term is necessary because patients may mistake early labor for symptoms of opioid withdrawal or worry that delivery room pain management will be inadequate and therefore relapse. Among pregnant women with addiction, preterm labor may be most common in those with OUD.12
Table 2
Medical complications common to pregnancy and substance abuse
| Anemia |
| Bacteremia/sepsis |
| Endocarditis |
| Cellulitis |
| Depression/anxiety |
| Gestational diabetes |
| Hepatitis (chronic and acute) |
| Hypertension/tachycardia |
| Phlebitis |
| Pneumonia |
| Gingivitis/poor oral hygiene |
| Sexually transmitted diseases |
|
| Tetanus |
| Cystitis |
| Pyelonephritis |
| AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus |
| Source: Reference 6 |
Table 3
Obstetric complications in women with addiction disorders
| Placental abruption |
| Chorioamnionitis |
| Placental insufficiency |
| Intrauterine growth restriction |
| Hypoxic/ischemic brain injury |
| Meconium passage |
| Neonatal abstinence syndrome |
| Spontaneous abortion |
| Intrauterine fetal death |
| Premature labor and delivery |
| Preterm, premature rupture of membranes |
| Postpartum hemorrhage |
| Hypertensive emergencies/preeclampsia |
| Source: Reference 6 |
Opioid agonist therapy
Obstetric complications in women with OUD may be related to rapid, frequent fluctuations of opioid blood levels during intoxication and withdrawal. Therefore, the first goal of pharmacotherapy is to reduce physical stress associated with cycling opioid blood levels. Opioid agonist medications can be extremely effective. Opioid agonist treatment for pregnant patients is similar to that of nonpregnant patients but includes pregnancy-specific objectives ( Table 4 ).20
Few anti-relapse medications have been studied in pregnant patients. Pharmacotherapies for OUD include methadone and buprenorphine. In our experience, opioid antagonists such as naltrexone typically would not be considered for pregnant patients because:
- their expected efficacy in reducing relapse in pregnant patients is lower than that of other medications
- their expected risk for inducing withdrawal is higher compared with methadone or buprenorphine
- research on the use of naltrexone during pregnancy is lacking.
Fluctuating blood opioid levels are minimized when methadone dosage is individually determined. Dosages should be based on a woman’s stage of pregnancy, relapse risk, pre-pregnancy methadone dose, experience with methadone, and clinical history. Some women experience lowered methadone blood levels during pregnancy because of increased fluid space, a larger tissue reservoir that can store methadone, and increased drug metabolism by both placenta and fetus. As a result, increased or split (twice daily) dosing may be indicated.22-24
The few randomized clinical trials comparing methadone with buprenorphine during pregnancy suggest that buprenorphine is not inferior to methadone in safety and discomfort of induction from a short-acting opioid, nor in outcome measures assessing NAS and maternal and neonatal safety.26,27 Results from the recent Maternal Opioid Treatment: Human Experimental Research project suggest that buprenorphine may have some advantages over methadone in pregnancy. Buprenorphine-maintained neonates may need less morphine, have shorter hospital stays, and require shorter treatment for NAS.28 However, treatment retention may be lower for buprenorphine-maintained mothers; any resultant long-term consequences on maternal and child health are as yet unexplored. These findings require replication.
Methadone and buprenorphine are not interchangeable. Many patients maintained on methadone do not respond optimally to buprenorphine. Clinics that dispense maintenance methadone are required to provide counseling services and random drug testing; these requirements do not apply to physicians who prescribe buprenorphine. Moreover, in our experience buprenorphine at times has been prescribed without close regard to psychosocial issues, adequate random drug testing, or coordination of care with other providers.
In pregnant patients, buprenorphine is preferred over buprenorphine and naloxone to avoid fetal exposure to naloxone, which may cause intrauterine withdrawal and maternal-fetal hormonal changes. To reduce abuse or diversion, patients should undergo drug testing to ensure buprenorphine is present, smaller prescriptions may be provided, and tablets can be counted. Limited data suggests buprenorphine is not teratogenic. Some data show low placental transfer of buprenorphine, thereby limiting fetal exposure and lowering risk for intrauterine growth restriction.29
Table 4
Opioid agonist treatment objectives for addicted patients who are pregnant
| General objectives |
| Prevent opioid withdrawal signs and symptoms |
| Provide a comfortable induction onto the medication |
| Block the euphoric and reinforcing effects of illicit opioids while also attenuating the motivation (craving, social interactions) to use illicit opioids and other drugs |
| Enhance treatment retention |
| Create a more optimal environment for behavioral and psychosocial interventions |
| Pregnancy-specific objectives |
| Eliminate or reduce fetal exposure to illicit opioids and other illicit drugs |
| Stabilize the intrauterine environment |
| Enhance involvement in prenatal care |
| Create an optimal environment to address pregnancy-specific problems |
| Source: Reference 20 |
Delivery and postnatal care
Compared with those not in treatment, women who are engaged in a multidisciplinary treatment program at the time of delivery demonstrated higher gestational age, increased birth weights, and lower rates of neonatal ICU admissions. They also realized a cost savings of $4, 644 per mother-infant pair.30
During delivery, pain medication should not be withheld solely because a pregnant woman has a history of addiction-related disorders; these women are subject to pain during delivery as much as other women. Avoid using mixed agonists/antagonists such as nalbuphine or butorphanol in women receiving opioid maintenance medication. Labor and delivery pain management for a pregnant patient maintained on opioid agonist therapies is discussed elsewhere in the literature.31 Every effort should be made to ensure that the mother remains in treatment through delivery and beyond.
To read about advising women with OUD on the benefits and risks of breastfeeding while receiving opioid agonist maintenance treatment, see the Box below.
CASE CONTINUED: Medication change
Ms. J’s boyfriend has left her and her parents have not readily accepted her pregnancy and need for support. She continues to attend NA meetings and weekly therapy. After educating her about the differences between buprenorphine and buprenorphine and naloxone in relation to risk, benefits, and side effects, you switch Ms. J to buprenorphine, 12 mg/d, while maintaining her on aripiprazole and citalopram. She consents to exchanging information about her medical, mental health, and addiction-related treatment with her primary care provider, who helps locate an obstetrician/gynecologist comfortable with her OUD and buprenorphine. Ms. J’s therapist helps link her with social services agencies to ensure prenatal care, assist with removing barriers to care, and plan for her needs as a parent.
After checking your state’s mandates, you determine you are not required to report Ms. J’s drug testing results. Ms. J’s ongoing drug testing shows the presence of buprenorphine and the absence of other opioids and all drugs of abuse.
Ms. J’s delivery is uncomplicated medically; however, family, financial, and parental role issues remain problematic. Encouraging her involvement in therapy and social services as part of her continued buprenorphine prescribing proves beneficial.
- Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008; 35(3): 245-259.
- Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend. 2003; 70(suppl 1 ): S87-S101.
- Velez M, Jansson LM. The opioid dependent mother and the newborn dyad: nonpharmacologic care. J Addict Med. 2008; 2(3): 113-120.
- Aripiprazole • Abilify
- Buprenorphine and naloxone •Suboxone
- Buprenorphine • Subutex
- Butorphanol • Stadol
- Citalopram • Celexa
- Fentanyl • Duragesic, Sublimaze, others
- Methadone • Dolophine
- Naloxone • Narcan
- Naltrexone • ReVia
- Nalbuphine • Nubain
- Oxycodone • Oxycontin
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Fernandez’ time toward this project was funded by the University Hospital/University of Cincinnati Addiction Psychiatry Fellowship Training Program operated by the Center for Treatment, Research, and Education in Addictive Disorders (CeTREAD), Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati and by the Veterans Affairs Medical Center, Cincinnati, OH.
The statements in this publication do not necessarily reflect the views or opinions of the Department of Veterans Affairs, the United States Government, or Opiate Addiction Recovery Services.
Acknowledgments
The authors wish to thank Kathleen Peak for her administrative assistance and Paul Horn, Professor, Department of Mathematical Sciences and Cincinnati VA, for statistical assistance.
Methadone is compatible with breast-feedinga and the American Academy of Pediatricsb and World Health Organizationc recommend breast-feeding for women receiving methadone unless there are contraindications such as human immunodeficiency virus infection.a Instruct mothers to seek medical advice if their breast-fed infant appears sedated.b Because the amount of methadone in breast milk is very small and depends on the methadone dose, the breast milk of mothers receiving methadone may be insufficient to prevent neonatal abstinence syndrome (NAS) and infants still may require opioid agonist treatment.d
Although breast-feeding by mothers receiving buprenorphine is not recommended by the drug’s manufacturer, there is consensus that buprenorphine is found in low levels in breast milke, f and is compatible with breast-feeding.g Because of partial agonism and low oral bioavailability, buprenorphine may not suppress NAS from methadone withdrawal. Always obtain appropriate informed consent.
References
a. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
b. Committee on Drugs, American Academy of Pediatrics. The transfer of drugs and other chemicals into human breast milk. Pediatrics. 2001;108:776-789.
c. The WHO Working Group, Bennet PN, ed. Monographs on individual drugs (WHO Working Group). In: Drugs and human lactation. Amsterdam, The Netherlands: Elsevier; 1988:319-320.
d. Jansson LM, Velez M, Harrow C. Methadone maintenance and lactation: a review of the literature and current management guidelines. J Hum Lact. 2004;20(1):62-71.
e. Grimm D, Pauly E, Pöschl J, et al. Buprenorphine and norbuprenorphine concentrations in human breast milk samples determined by liquid chromotography-tandem mass spectrometry. Ther Drug Monit. 2005;27(4):526-530.
f. Lindemalm S, Nydert P, Svensson JO, et al. Transfer of buprenorphine into breast milk and calculation of infant drug dose. J Hum Lact. 2009;25(2):199-205.
g. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP)) Series 40. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
1. Flavin J, Paltrow LM. Punishing pregnant drug-using women: defying law medicine, and common sense. J Addict Dis. 2010;29(2):231-244.
2. American Psychiatric Association. Opioid use disorder. DSM-5 development. Available at: http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=460#. Accessed January 26 2011.
3. Pichini S, Puig C, Zuccaro P, et al. Assessment of exposure to opiates and cocaine during pregnancy in a Mediterranean city: preliminary results of the “Meconium Project. “ Forensic Sci Int. 2005;153:59-65.
4. Mitchell JL, Brown G. Physiological effects of cocaine heroin, and methadone. In: Engs RC, ed. Women: alcohol and other drugs. Dubuque, IA: Kendall/Hunt Publishing Co; 1990:53-60.
5. Center for Substance Abuse Treatment. Medication-assisted treatment for opioid addiction during pregnancy. In: Medication-assisted treatment for opioid addiction in opioid treatment programs. Treatment Improvement Protocol (TIP) Series 43. Rockville MD: Substance Abuse and Mental Health Services Administration; 2005, reprinted 2006. DHHS Publication No. (SMA) 06-4212.
6. Helmbrecht GD, Thiagarajah S. Management of addiction disorders in pregnancy. J Addict Med. 2008;2(1):1-16.
7. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
8. Chasnoff IJ, Wells AM, McGourty RF, et al. Validation of the 4P’s Plus screen for substance use in pregnancy validation of the 4P’s Plus. J Perinatol. 2007;27:744-748.
9. Jones HE. The challenges of screening for substance use in pregnant women: commentary on the 4P’s Plus tool. J Perinatol. 2005;25:365-367.
10. Center for Substance Abuse Treatment. Substance abuse treatment: addressing the specific needs of women. Treatment Improvement Protocol (TIP) Series 51. Rockville MD: Substance Abuse and Mental Health Services Administration; 2009. HHS Publication No. (SMA) 09-4426.
11. Christmas JT, Knisely JS, Dawson KS, et al. Comparison of questionnaire screening and urine toxicology for detection of pregnancy complicated by substance use. Obstet Gynecol. 1992;80:750-754.
12. Wunsch MJ, Weaver MF. Alcohol and other drug use during pregnancy: management of the mother and child. In: Ries RK Fiellin DA, Miller SC, et al, eds. Principles of addiction medicine, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2009:1111-1124.
13. Ondersma SJ, Winhusen T, Erickson SJ, et al. Motivation enhancement therapy with pregnant substance-abusing women: does baseline motivation moderate efficacy? Drug Alcohol Depend. 2009;101(1-2):74-79.
14. Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy: effects and management. Obstet Gynecol Clin North Am. 1998;25:139-151.
15. Comfort M, Zanis DA, Whiteley MJ, et al. Assessing the needs of substance abusing women. Psychometric data on the psychosocial history. J Subst Abuse Treat. 1999;17:79-83.
16. Kissin WB, Svikis DS, Moylan P, et al. Identifying pregnant women at risk for early attrition from substance abuse treatment. J Subst Abuse Treat. 2004;27:31-38.
17. Jones HE, O’Grady KE, Malfi D, et al. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict. 2008;17(5):372-386.
18. Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? J Subst Abuse Treat. 2003;24(4):363-367.
19. Vesga-Lopez O, Blanco C, Keyes K, et al. Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry. 2008;65(7):805-815.
20. Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008;35(3):245-259.
21. NIDA International Program. National Institute on Drug Abuse. Methadone research web guide. Available at: http://international.drugabuse.gov/collaboration/guide_methadone/index.html. Accessed December 2, 2010.
22. Wittmann BK, Segal S. A comparison of the effects of single- and split-dose methadone administration on the fetus: ultrasound evaluation. Int J Addict. 1991;26:213-218.
23. DePetrillo PB, Rice JM. Methadone dosing and pregnancy: impact on program compliance. Int J Addict. 1995;30:207-217.
24. Jansson LM, Dipietro JA, Velez M, et al. Maternal methadone dosing schedule and fetal neurobehaviour. J Matern Fetal Neonatal Med. 2009;22(1):29-35.
25. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP) Series 40. Rockville MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
26. Jones HE, Johnson RE, Jasinski DR, et al. Randomized controlled study transitioning opioid-dependent pregnant women from short-acting morphine to buprenorphine or methadone. Drug Alcohol Depend. 2005;78(1):33-38.
27. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients; effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79(1):1-10.
28. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363(24):2320-2331.
29. Nanovskaya T, Deshmukh S, Brooks M, et al. Transplacental transfer and metabolism of buprenorphine. J Pharmacol Exp Ther. 2002;300(1):26-33.
30. Svikis DS, Golden AS, Huggins GR, et al. Cost-effectiveness of treatment for drug-abusing pregnant women. Drug Alcohol Depend. 1997;45:105-113.
31. Jones HE, O’Grady K, Dahne J, et al. Management of acute postpartum pain in patients maintained on methadone or buprenorphine during pregnancy. Am J Drug Alcohol Abuse. 2009;35(3):151-156.
1. Flavin J, Paltrow LM. Punishing pregnant drug-using women: defying law medicine, and common sense. J Addict Dis. 2010;29(2):231-244.
2. American Psychiatric Association. Opioid use disorder. DSM-5 development. Available at: http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=460#. Accessed January 26 2011.
3. Pichini S, Puig C, Zuccaro P, et al. Assessment of exposure to opiates and cocaine during pregnancy in a Mediterranean city: preliminary results of the “Meconium Project. “ Forensic Sci Int. 2005;153:59-65.
4. Mitchell JL, Brown G. Physiological effects of cocaine heroin, and methadone. In: Engs RC, ed. Women: alcohol and other drugs. Dubuque, IA: Kendall/Hunt Publishing Co; 1990:53-60.
5. Center for Substance Abuse Treatment. Medication-assisted treatment for opioid addiction during pregnancy. In: Medication-assisted treatment for opioid addiction in opioid treatment programs. Treatment Improvement Protocol (TIP) Series 43. Rockville MD: Substance Abuse and Mental Health Services Administration; 2005, reprinted 2006. DHHS Publication No. (SMA) 06-4212.
6. Helmbrecht GD, Thiagarajah S. Management of addiction disorders in pregnancy. J Addict Med. 2008;2(1):1-16.
7. Chasnoff If, Neuman MA, Thornton C, et al. Screening for substance abuse in pregnancy: a practical approach for the primary care physician. Am J Obstet Gynecol. 2001;184(4):752-758.
8. Chasnoff IJ, Wells AM, McGourty RF, et al. Validation of the 4P’s Plus screen for substance use in pregnancy validation of the 4P’s Plus. J Perinatol. 2007;27:744-748.
9. Jones HE. The challenges of screening for substance use in pregnant women: commentary on the 4P’s Plus tool. J Perinatol. 2005;25:365-367.
10. Center for Substance Abuse Treatment. Substance abuse treatment: addressing the specific needs of women. Treatment Improvement Protocol (TIP) Series 51. Rockville MD: Substance Abuse and Mental Health Services Administration; 2009. HHS Publication No. (SMA) 09-4426.
11. Christmas JT, Knisely JS, Dawson KS, et al. Comparison of questionnaire screening and urine toxicology for detection of pregnancy complicated by substance use. Obstet Gynecol. 1992;80:750-754.
12. Wunsch MJ, Weaver MF. Alcohol and other drug use during pregnancy: management of the mother and child. In: Ries RK Fiellin DA, Miller SC, et al, eds. Principles of addiction medicine, 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2009:1111-1124.
13. Ondersma SJ, Winhusen T, Erickson SJ, et al. Motivation enhancement therapy with pregnant substance-abusing women: does baseline motivation moderate efficacy? Drug Alcohol Depend. 2009;101(1-2):74-79.
14. Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy: effects and management. Obstet Gynecol Clin North Am. 1998;25:139-151.
15. Comfort M, Zanis DA, Whiteley MJ, et al. Assessing the needs of substance abusing women. Psychometric data on the psychosocial history. J Subst Abuse Treat. 1999;17:79-83.
16. Kissin WB, Svikis DS, Moylan P, et al. Identifying pregnant women at risk for early attrition from substance abuse treatment. J Subst Abuse Treat. 2004;27:31-38.
17. Jones HE, O’Grady KE, Malfi D, et al. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict. 2008;17(5):372-386.
18. Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? J Subst Abuse Treat. 2003;24(4):363-367.
19. Vesga-Lopez O, Blanco C, Keyes K, et al. Psychiatric disorders in pregnant and postpartum women in the United States. Arch Gen Psychiatry. 2008;65(7):805-815.
20. Jones HE, Martin PR, Heil SH, et al. Treatment of opioid dependent pregnant women: clinical and research issues. J Subst Abuse Treat. 2008;35(3):245-259.
21. NIDA International Program. National Institute on Drug Abuse. Methadone research web guide. Available at: http://international.drugabuse.gov/collaboration/guide_methadone/index.html. Accessed December 2, 2010.
22. Wittmann BK, Segal S. A comparison of the effects of single- and split-dose methadone administration on the fetus: ultrasound evaluation. Int J Addict. 1991;26:213-218.
23. DePetrillo PB, Rice JM. Methadone dosing and pregnancy: impact on program compliance. Int J Addict. 1995;30:207-217.
24. Jansson LM, Dipietro JA, Velez M, et al. Maternal methadone dosing schedule and fetal neurobehaviour. J Matern Fetal Neonatal Med. 2009;22(1):29-35.
25. Center for Substance Abuse Treatment. Special populations: pregnant women and neonates. In: Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol (TIP) Series 40. Rockville MD: Substance Abuse and Mental Health Services Administration; 2004. DHHS Publication No. (SMA) 04-3939.
26. Jones HE, Johnson RE, Jasinski DR, et al. Randomized controlled study transitioning opioid-dependent pregnant women from short-acting morphine to buprenorphine or methadone. Drug Alcohol Depend. 2005;78(1):33-38.
27. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients; effects on the neonatal abstinence syndrome. Drug Alcohol Depend. 2005;79(1):1-10.
28. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363(24):2320-2331.
29. Nanovskaya T, Deshmukh S, Brooks M, et al. Transplacental transfer and metabolism of buprenorphine. J Pharmacol Exp Ther. 2002;300(1):26-33.
30. Svikis DS, Golden AS, Huggins GR, et al. Cost-effectiveness of treatment for drug-abusing pregnant women. Drug Alcohol Depend. 1997;45:105-113.
31. Jones HE, O’Grady K, Dahne J, et al. Management of acute postpartum pain in patients maintained on methadone or buprenorphine during pregnancy. Am J Drug Alcohol Abuse. 2009;35(3):151-156.
Traumatic brain injury: Pharmacotherapy options for cognitive deficits
Mr. A, age 45, presents to the psychiatry clinic complaining of “ADHD.” He says he is not able to sit through movies and often gets distracted while on his computer at work. He also is having problems in his relationship with his wife; she says having a conversation with him is difficult. He has seen a psychiatrist for depression, which is currently managed by his primary care physician (PCP), who prescribed sertraline, 100 mg/d. Mr. A feels that although his depression is now under control, the medication has had limited effect on improving his concentration.
With further discussion, Mr. A reveals that 6 months ago he was involved in a car accident and suffered a mild traumatic brain injury (TBI). He was hospitalized overnight and was encouraged to follow up with his PCP. During his only follow-up visit, Mr. A told his PCP that he was having difficulty concentrating since the accident. However, because Mr. A has a remote history of alcohol abuse, his physician was reluctant to give him additional medication and referred him to a psychiatrist.
TBI is increasingly common but often overlooked or not treated in the emergency room (ER). Each year at least 1.7 million people experience a TBI; 275,000 are hospitalized and 52,000 die.1 The true incidence likely is greater because patients who do not present to the ER or hospital are not included in most studies, and the often-subtle psychiatric sequelae may preclude patients from seeking mental health treatment.
Psychiatric disorders are common among those who sustain a TBI (Table 1).2 One prospective cohort study found that patients with mild TBI are 2.8 times more likely than other patients to develop a psychiatric disorder.3 Statistics regarding TBI and psychiatric illness often are limited because they rely on self-reports, chart review, or retrospective studies.4
TBI severity can be classified on the basis of Glasgow Coma Scale score and other factors (Table 2).5 The correlation between severity of injury and resulting psychiatric illness or post-concussive symptoms is unclear.6 There is evidence that cognitive defects are associated with decreased function. Cognitive dysfunction also has been associated with disability 10 years after moderate to severe TBI.7 The association between cognitive dysfunction and outcome is more strongly correlated with moderate to severe TBI; there is no clear association in mild TBI.7 Additionally, compared with patients with severe TBI, those with mild TBI were more likely to be employed. At all severity levels, function improves over time. Mild, moderate, and severe TBI have a similar recovery curve.7
Table 1
Psychiatric symptoms: Common among TBI patients
| Psychiatric symptom | Incidence |
|---|---|
| Aggression | 30% |
| Anxiety | 10% to 70% |
| Apathy | 10% |
| Cognitive impairment | 25% to 70% |
| Depression | 25% to 50% |
| Mania | 1% to 10% |
| Psychosis | 3% to 8% |
| TBI: traumatic brain injury | |
| Source: Adapted from reference 2 | |
Table 2
Classifying severity of traumatic brain injury
| Severity | GCS score | LOC duration | PTA* |
|---|---|---|---|
| Mild | 13 to 15 | <30 minutes | <1 hour |
| Moderate | 9 to 12 | 1 to 24 hours | 1 to 24 hours |
| Severe | <8 | >24 hours | >24 hours |
| *Includes loss of memory immediately before or after the accident | |||
| GCS: Glasgow Coma Scale; LOC: loss of consciousness; PTA: posttraumatic amnesia | |||
| Source: Reference 5 | |||
Cognitive dysfunction and TBI
Cognitive dysfunction can be split into 3 categories:
- executive function
- memory
- processing speed.
The incidence of cognitive dysfunction after TBI is unclear. Several methods are used to quantify cognitive dysfunction in TBI patients; it is widely regarded that the Mini-Mental State Exam is not adequate to screen for subtle cognitive deficits.6 However, there is no clear consensus on which tool should be used.5
Off-label pharmacotherapy
There are no FDA-approved medications for treating neuropsychiatric sequelae of TBI. Treatment should be symptom-based and employ the “start low, go slow” approach. Compared with patients without brain injury, TBI patients may experience increased adverse effects from psychotropics but may require standard doses. These patients also may have comorbidities such as seizure disorders, substance abuse, and depression that will affect treatment.2 Different areas of cognitive function respond to different medication classes. Suggested medications include stimulant and nonstimulant catecholaminergic agents and cholinesterase inhibitors (Table 3).8
Executive function responds to non-stimulant catecholaminergics. In a review, Writer and Schillerstrom5 found that TBI patients who received catecholaminergic augmentation showed improved function in 6 of 7 studies. In 2 randomized controlled trials (RCTs) and 4 nonrandomized, placebo-controlled trials, patients with mild to severe TBI showed improved executive function, attention, global cognitive function, memory, language, and/ or arousal with use of bromocriptine, pramipexole, carbidopa/levodopa, or amantadine.5 The greatest improvements were found in executive function. In 1 RCT, 10 patients with mild to severe TBI showed no functional improvement after 2 weeks of treatment.
Amantadine, 200 to 400 mg/d, has been shown to safely improve arousal and cognitive function in patients with moderate to severe TBI when started 3 days to 5 months after injury.9 Amantadine, 400 mg/d, also improves executive function measures without significant benefit in attention or memory in patients with mild to severe TBI 6 months post-injury.10
Memory responds to cholinesterase inhibitors. Memory deficits secondary to TBI affect immediate and delayed memory. The cholinesterase inhibitor donepezil is approved for treating Alzheimer’s disease (AD) in the United States and Canada, and research suggests memory deficits after TBI may be similar to those seen in AD.11 This includes deficits in long-term memory storage, which likely is associated with the cholinergic system.11 Post-mortem studies have found similarities in traumatically injured brains and those of AD patients.11
Three small prospective studies of done-pezil have shown improved memory and attention in TBI patients when cognition is the primary outcome, with 1 small negative open-label trial.7 In a study of 53 patients, Whelan et al12 found that donepezil improved patients’ intelligence quotient and clinician-based assessment of cognition over 2 years. Taverni et al13 found memory improvement in 2 TBI patients within 3 weeks of starting donepezil. These results suggest that donepezil may be used in acute and late phases of memory deficits following mild, moderate, or severe TBI.6 All studies titrated donepezil from 5 to 10 mg/d over several weeks. Dosing guidelines for donepezil in AD suggest 5 mg/d for 4 to 6 weeks, which may be increased to 10 mg/d if needed.8
Rivastigmine (3 to 6 mg/d) has been shown to be effective in mild TBI when started 1 year after injury and safe for 12 to 38 weeks of treatment.14,15 One retrospective cohort study of 111 patients with chronic TBI found no difference among donepezil, rivastigmine, or galantamine, with mean doses of 7.2 mg/d, 10 mg/d, and 2.3 mg/d, respectively.16 Sixty-one percent of patients showed improvement and the remainder had modest or no response. This study suggests that positive response on cognition may be similar among cholinesterase inhibitors. In case reports, physostigmine has offered some benefit17,18; however, cardiovascular and autonomic side effects restrict its use.11 Tacrine is associated with problematic gastrointestinal and hepatic side effects.11
Processing speed responds to stimulant catecholaminergics. Although the incidence of psychiatric illness is not correlated with TBI severity, evidence suggests that speed of processing mediates the relationship between injury severity and functional decline.19 Therefore, aggressively treating these deficits may help improve function.
Methylphenidate improves attention and processing speed after TBI. A review of 7 randomized trials and 2 nonrandomized trials indicated that patients with mild to severe, chronic TBI experienced significantly improved cognitive function after methylphenidate treatment.5 Willmott and Ponsford20 found significant enhancement in information processing speed within 2 weeks of methylphenidate treatment in 40 patients with moderate or severe TBI. Methylphenidate increased the rate of recovery and led to improvement in acute21 and post-acute phases.22 In addition, methylphenidate may improve processing speed even in the absence of significant changes in attention.23
The standard methylphenidate dose used in most studies, 0.3 mg/kg twice daily, is safe and effective. Dosing usually is started at 5 mg/d and titrated to symptomatic relief. Because methylphenidate does not lower the seizure threshold, it is safe for patients at high risk for seizure.24 Methylphenidate also significantly improves attention and speed of processing in pediatric head trauma.25,26
Dextroamphetamine also is used to treat speed of processing dysfunction after TBI, but is less studied than methylphenidate. Dextroamphetamine, 5 to 30 mg/d, was found to effectively treat attention problems that interfered with rehabilitation in patients with severe TBI.27
Table 3
Recommended treatments for mild TBI-related cognitive deficits
| Deficit | First-line medication | Side effects | Contraindications | Other treatments |
|---|---|---|---|---|
| Memory | Donepezil (5 to 10 mg/d) | Diarrhea, nausea, vomiting, muscle cramps, fatigue, anorexia | Hypersensitivity to donepezil or piperidine derivatives | Rivastigmine, galantamine, physostigmine, CDP-choline |
| Speed of processing | Methylphenidate (0.3 mg/kg twice daily) | Headache, insomnia, decreased appetite, nausea, vomiting, anxiety, irritability | Hypersensitivity to methylphenidate, glaucoma, history of Tourette syndrome or tics, use of MAOI within 14 days | Dextroamphetamine |
| Executive function | Amantadine (200 to 400 mg/d) | CNS depression, orthostatic hypotension, peripheral edema, agitation, nausea, anorexia | Hypersensitivity to amantadine | Bromocriptine, pramipexole, carbidopa/levodopa |
| CDP-choline: cytidinediphosphocholine; MAOI: monoamine oxidase inhibitor | ||||
| Source: Reference 8 | ||||
Nonpharmacologic treatments
In addition to pharmacotherapy, nonpharmacologic interventions also should be a mainstay of treatment. Compensatory training and cognitive exercise may improve patients’ cognitive deficits and return some sense of control. Individual and family psychotherapy, including cognitive-behavioral therapy, also may be beneficial.2 Review sources have identified the importance of validating patients’ symptoms and developing a goal-based treatment plan.6
CASE CONTINUED: Improvement with stimulants
Unlike many TBI patients who do not recognize the often-subtle psychiatric sequelae of their injury, Mr. A is aware of his difficulty concentrating, which is temporally linked with his accident. After exploring the association between Mr. A’s symptoms and his injury, his psychiatrist concludes that Mr. A’s cognitive deficits likely are associated with his TBI. Mr. A’s history of alcohol abuse raises concerns about prescribing stimulants. However, after assuring that Mr. A’s depression is well controlled and addressing his risk of substance abuse, his psychiatrist prescribes methylphenidate titrated to 30 mg/d. When he returns to the clinic several weeks later, Mr. A reports improved attention and functioning at work, and continues to follow up with the psychiatrist without requiring changes to his medication regimen.
Related Resource
- Konrad C, Geburek AJ, Rist F, et al. Long-term cognitive and emotional consequences of mild traumatic brain injury. Psychol Med. 2010;22:1-15.
Drug Brand Names
- Amantadine • Symadine, Symmetrel
- Bromocriptine • Parlodel
- Carbidopa/levodopa • Sinemet
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Galantamine • Razadyne
- Methylphenidate • Ritalin, Methylin, others
- Physostigmine • Antilirium
- Pramipexole • Mirapex
- Rivastigmine • Exelon
- Sertraline • Zoloft
- Tacrine • Cognex
Disclosures
Dr. Scher and Ms. Loomis report no financial relationship with any company whose products mentioned in this article or with the manufacturers of competing products.
Dr. McCarron is a speaker for Eli Lilly and Company.
1. Faul M, Xu L, Wald MM, et al. Traumatic brain injury in the United States; emergency department visits, hospitalizations, and deaths, 2002-2006. Atlanta, GA: Centers for Disease Control and Prevention; 2010. Available at: http://www.cdc.gov/traumaticbraininjury/tbi_ed.html. Accessed December 1, 2010.
2. Vaishnavi S, Rao V, Fann JR. Neuropsychiatric problems after traumatic brain injury: unraveling the silent epidemic. Psychosomatics. 2009;50(3):198-205.
3. Fann JR, Burington B, Leonetti A, et al. Psychiatric illness following traumatic brain injury in an adult health maintenance organization population. Arch Gen Psychiatry. 2004;61(1):53-61.
4. Bryant RA, O’Donnell ML, Creamer M, et al. The psychiatric sequelae of traumatic injury. Am J Psychiatry. 2010;167(3):312-320.
5. Writer BW, Schillerstrom JE. Psychopharmacological treatment for cognitive impairment in survivors of traumatic brain injury: a critical review. J Neuropsychiatry Clin Neurosci. 2009;21(4):362-370.
6. Arciniegas DB, Anderson CA, Topkoff J, et al. Mild traumatic brain injury: a neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr Dis Treat. 2005;1(4):311-327.
7. Sigurdardottir S, Andelic N, Roe C, et al. Cognitive recovery and predictors of functional outcome 1 year after traumatic brain injury. J Int Neuropsychol Soc. 2009;15(5):740-750.
8. Physicians’ desk reference 64th ed. Montvale, NJ: Thomson Reuters; 2010.
9. Sawyer E Mauro LS, Mauro LS, Ohlinger MJ. Amantadine enhancement of arousal and cognition after traumatic brain injury. Ann Pharmacother. 2008;42(2):247-252.
10. Kraus MF, Smith GS, Butters M, et al. Effects of the dopaminergic agent and NMDA receptor antagonist amantadine on cognitive function, cerebral glucose metabolism and D2 receptor availability in chronic traumatic brain injury: a study using positron emission tomography (PET). Brain Inj. 2005;19(7):471-479.
11. Griffin SL, van Reekum R, Masanic C. A review of cholinergic agents in the treatment of neurobehavioral deficits following traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2003;15(1):17-26.
12. Whelan FJ, Walker MS, Schultz SK. Donepezil in the treatment of cognitive dysfunction associated with traumatic brain injury. Ann Clin Psychiatry. 2000;12(3):131-135.
13. Taverni JP, Seliger G, Lichtman SW. Donepezil medicated memory improvement in traumatic brain injury during post acute rehabilitation. Brain Inj. 1998;12(1):77-80.
14. Silver JM, McAllister TW, Arciniegas DB. Depression and cognitive complaints following mild traumatic brain injury. Am J Psychiatry. 2009;166(6):653-661.
15. Silver JM, Koumaras B, Chen M, et al. Effects of rivastigmine on cognitive function in patients with traumatic brain injury. Neurology. 2006;67(5):748-755.
16. Tenovuo O. Central acetylcholinesterase inhibitors in the treatment of chronic traumatic brain injury—clinical experience in 111 patients. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):61-67.
17. Goldberg E, Gerstman LJ, Mattis S, et al. Selective effects of cholinergic treatment on verbal memory in posttraumatic amnesia. J Clin Neuropsychol. 1982;4(3):219-234.
18. Eames P, Sutton A. Protracted post-traumatic confusional state treated with physostigmine. Brain Inj. 1995;9(7):729-734.
19. Rassovsky Y, Satz P, Alfano MS, et al. Functional outcome in TBI II: verbal memory and information processing speed mediators. J Clin Exp Neuropsychol. 2006;28(4):581-591.
20. Willmott C, Ponsford J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: a randomised, crossover, double blind, placebo controlled inpatient trial. J Neurol Neurosurg Psychiatry. 2009;80(5):552-557.
20. Kaelin DL, Cifu DX, Matthies B. Methylphenidate effect on attention deficit in the acutely brain-injured adult. Arch Phys Med Rehabil. 1996;77(1):6-9.
22. Whyte J, Hart T, Vaccaro M, et al. Effects of methylphenidate on attention deficits after traumatic brain injury: a multidimensional, randomized, controlled trial. Am J Phys Med Rehabil. 2004;83(6):401-420.
23. Whyte J, Hart T, Schuster K, et al. Effects of methylphenidate on attentional function after traumatic brain injury. A randomized, placebo-controlled trial. Am J Phys Med Rehabil. 1997;76(6):440-450.
24. Wroblewski BA, Leary JM, Phelan AM, et al. Methylphenidate and seizure frequency in brain injured patients with seizure disorders. J Clin Psychiatry. 1992;53(3):86-89.
25. Mahalick DM, Carmel PW, Greenberg JP, et al. Psychopharmacologic treatment of acquired attention disorders in children with brain injury. Pediatr Neurosurg. 1998;29(3):121-126.
26. Hornyak JE, Nelson VS, Hurvitz EA. The use of methylphenidate in paediatric traumatic brain injury. Pediatr Rehabil. 1997;1(1):15-17.
27. Hornstein A, Lennihan L, Seliger G. Amphetamine in recovery from brain injury. Brain Inj. 1996;10(2):145-148.
Mr. A, age 45, presents to the psychiatry clinic complaining of “ADHD.” He says he is not able to sit through movies and often gets distracted while on his computer at work. He also is having problems in his relationship with his wife; she says having a conversation with him is difficult. He has seen a psychiatrist for depression, which is currently managed by his primary care physician (PCP), who prescribed sertraline, 100 mg/d. Mr. A feels that although his depression is now under control, the medication has had limited effect on improving his concentration.
With further discussion, Mr. A reveals that 6 months ago he was involved in a car accident and suffered a mild traumatic brain injury (TBI). He was hospitalized overnight and was encouraged to follow up with his PCP. During his only follow-up visit, Mr. A told his PCP that he was having difficulty concentrating since the accident. However, because Mr. A has a remote history of alcohol abuse, his physician was reluctant to give him additional medication and referred him to a psychiatrist.
TBI is increasingly common but often overlooked or not treated in the emergency room (ER). Each year at least 1.7 million people experience a TBI; 275,000 are hospitalized and 52,000 die.1 The true incidence likely is greater because patients who do not present to the ER or hospital are not included in most studies, and the often-subtle psychiatric sequelae may preclude patients from seeking mental health treatment.
Psychiatric disorders are common among those who sustain a TBI (Table 1).2 One prospective cohort study found that patients with mild TBI are 2.8 times more likely than other patients to develop a psychiatric disorder.3 Statistics regarding TBI and psychiatric illness often are limited because they rely on self-reports, chart review, or retrospective studies.4
TBI severity can be classified on the basis of Glasgow Coma Scale score and other factors (Table 2).5 The correlation between severity of injury and resulting psychiatric illness or post-concussive symptoms is unclear.6 There is evidence that cognitive defects are associated with decreased function. Cognitive dysfunction also has been associated with disability 10 years after moderate to severe TBI.7 The association between cognitive dysfunction and outcome is more strongly correlated with moderate to severe TBI; there is no clear association in mild TBI.7 Additionally, compared with patients with severe TBI, those with mild TBI were more likely to be employed. At all severity levels, function improves over time. Mild, moderate, and severe TBI have a similar recovery curve.7
Table 1
Psychiatric symptoms: Common among TBI patients
| Psychiatric symptom | Incidence |
|---|---|
| Aggression | 30% |
| Anxiety | 10% to 70% |
| Apathy | 10% |
| Cognitive impairment | 25% to 70% |
| Depression | 25% to 50% |
| Mania | 1% to 10% |
| Psychosis | 3% to 8% |
| TBI: traumatic brain injury | |
| Source: Adapted from reference 2 | |
Table 2
Classifying severity of traumatic brain injury
| Severity | GCS score | LOC duration | PTA* |
|---|---|---|---|
| Mild | 13 to 15 | <30 minutes | <1 hour |
| Moderate | 9 to 12 | 1 to 24 hours | 1 to 24 hours |
| Severe | <8 | >24 hours | >24 hours |
| *Includes loss of memory immediately before or after the accident | |||
| GCS: Glasgow Coma Scale; LOC: loss of consciousness; PTA: posttraumatic amnesia | |||
| Source: Reference 5 | |||
Cognitive dysfunction and TBI
Cognitive dysfunction can be split into 3 categories:
- executive function
- memory
- processing speed.
The incidence of cognitive dysfunction after TBI is unclear. Several methods are used to quantify cognitive dysfunction in TBI patients; it is widely regarded that the Mini-Mental State Exam is not adequate to screen for subtle cognitive deficits.6 However, there is no clear consensus on which tool should be used.5
Off-label pharmacotherapy
There are no FDA-approved medications for treating neuropsychiatric sequelae of TBI. Treatment should be symptom-based and employ the “start low, go slow” approach. Compared with patients without brain injury, TBI patients may experience increased adverse effects from psychotropics but may require standard doses. These patients also may have comorbidities such as seizure disorders, substance abuse, and depression that will affect treatment.2 Different areas of cognitive function respond to different medication classes. Suggested medications include stimulant and nonstimulant catecholaminergic agents and cholinesterase inhibitors (Table 3).8
Executive function responds to non-stimulant catecholaminergics. In a review, Writer and Schillerstrom5 found that TBI patients who received catecholaminergic augmentation showed improved function in 6 of 7 studies. In 2 randomized controlled trials (RCTs) and 4 nonrandomized, placebo-controlled trials, patients with mild to severe TBI showed improved executive function, attention, global cognitive function, memory, language, and/ or arousal with use of bromocriptine, pramipexole, carbidopa/levodopa, or amantadine.5 The greatest improvements were found in executive function. In 1 RCT, 10 patients with mild to severe TBI showed no functional improvement after 2 weeks of treatment.
Amantadine, 200 to 400 mg/d, has been shown to safely improve arousal and cognitive function in patients with moderate to severe TBI when started 3 days to 5 months after injury.9 Amantadine, 400 mg/d, also improves executive function measures without significant benefit in attention or memory in patients with mild to severe TBI 6 months post-injury.10
Memory responds to cholinesterase inhibitors. Memory deficits secondary to TBI affect immediate and delayed memory. The cholinesterase inhibitor donepezil is approved for treating Alzheimer’s disease (AD) in the United States and Canada, and research suggests memory deficits after TBI may be similar to those seen in AD.11 This includes deficits in long-term memory storage, which likely is associated with the cholinergic system.11 Post-mortem studies have found similarities in traumatically injured brains and those of AD patients.11
Three small prospective studies of done-pezil have shown improved memory and attention in TBI patients when cognition is the primary outcome, with 1 small negative open-label trial.7 In a study of 53 patients, Whelan et al12 found that donepezil improved patients’ intelligence quotient and clinician-based assessment of cognition over 2 years. Taverni et al13 found memory improvement in 2 TBI patients within 3 weeks of starting donepezil. These results suggest that donepezil may be used in acute and late phases of memory deficits following mild, moderate, or severe TBI.6 All studies titrated donepezil from 5 to 10 mg/d over several weeks. Dosing guidelines for donepezil in AD suggest 5 mg/d for 4 to 6 weeks, which may be increased to 10 mg/d if needed.8
Rivastigmine (3 to 6 mg/d) has been shown to be effective in mild TBI when started 1 year after injury and safe for 12 to 38 weeks of treatment.14,15 One retrospective cohort study of 111 patients with chronic TBI found no difference among donepezil, rivastigmine, or galantamine, with mean doses of 7.2 mg/d, 10 mg/d, and 2.3 mg/d, respectively.16 Sixty-one percent of patients showed improvement and the remainder had modest or no response. This study suggests that positive response on cognition may be similar among cholinesterase inhibitors. In case reports, physostigmine has offered some benefit17,18; however, cardiovascular and autonomic side effects restrict its use.11 Tacrine is associated with problematic gastrointestinal and hepatic side effects.11
Processing speed responds to stimulant catecholaminergics. Although the incidence of psychiatric illness is not correlated with TBI severity, evidence suggests that speed of processing mediates the relationship between injury severity and functional decline.19 Therefore, aggressively treating these deficits may help improve function.
Methylphenidate improves attention and processing speed after TBI. A review of 7 randomized trials and 2 nonrandomized trials indicated that patients with mild to severe, chronic TBI experienced significantly improved cognitive function after methylphenidate treatment.5 Willmott and Ponsford20 found significant enhancement in information processing speed within 2 weeks of methylphenidate treatment in 40 patients with moderate or severe TBI. Methylphenidate increased the rate of recovery and led to improvement in acute21 and post-acute phases.22 In addition, methylphenidate may improve processing speed even in the absence of significant changes in attention.23
The standard methylphenidate dose used in most studies, 0.3 mg/kg twice daily, is safe and effective. Dosing usually is started at 5 mg/d and titrated to symptomatic relief. Because methylphenidate does not lower the seizure threshold, it is safe for patients at high risk for seizure.24 Methylphenidate also significantly improves attention and speed of processing in pediatric head trauma.25,26
Dextroamphetamine also is used to treat speed of processing dysfunction after TBI, but is less studied than methylphenidate. Dextroamphetamine, 5 to 30 mg/d, was found to effectively treat attention problems that interfered with rehabilitation in patients with severe TBI.27
Table 3
Recommended treatments for mild TBI-related cognitive deficits
| Deficit | First-line medication | Side effects | Contraindications | Other treatments |
|---|---|---|---|---|
| Memory | Donepezil (5 to 10 mg/d) | Diarrhea, nausea, vomiting, muscle cramps, fatigue, anorexia | Hypersensitivity to donepezil or piperidine derivatives | Rivastigmine, galantamine, physostigmine, CDP-choline |
| Speed of processing | Methylphenidate (0.3 mg/kg twice daily) | Headache, insomnia, decreased appetite, nausea, vomiting, anxiety, irritability | Hypersensitivity to methylphenidate, glaucoma, history of Tourette syndrome or tics, use of MAOI within 14 days | Dextroamphetamine |
| Executive function | Amantadine (200 to 400 mg/d) | CNS depression, orthostatic hypotension, peripheral edema, agitation, nausea, anorexia | Hypersensitivity to amantadine | Bromocriptine, pramipexole, carbidopa/levodopa |
| CDP-choline: cytidinediphosphocholine; MAOI: monoamine oxidase inhibitor | ||||
| Source: Reference 8 | ||||
Nonpharmacologic treatments
In addition to pharmacotherapy, nonpharmacologic interventions also should be a mainstay of treatment. Compensatory training and cognitive exercise may improve patients’ cognitive deficits and return some sense of control. Individual and family psychotherapy, including cognitive-behavioral therapy, also may be beneficial.2 Review sources have identified the importance of validating patients’ symptoms and developing a goal-based treatment plan.6
CASE CONTINUED: Improvement with stimulants
Unlike many TBI patients who do not recognize the often-subtle psychiatric sequelae of their injury, Mr. A is aware of his difficulty concentrating, which is temporally linked with his accident. After exploring the association between Mr. A’s symptoms and his injury, his psychiatrist concludes that Mr. A’s cognitive deficits likely are associated with his TBI. Mr. A’s history of alcohol abuse raises concerns about prescribing stimulants. However, after assuring that Mr. A’s depression is well controlled and addressing his risk of substance abuse, his psychiatrist prescribes methylphenidate titrated to 30 mg/d. When he returns to the clinic several weeks later, Mr. A reports improved attention and functioning at work, and continues to follow up with the psychiatrist without requiring changes to his medication regimen.
Related Resource
- Konrad C, Geburek AJ, Rist F, et al. Long-term cognitive and emotional consequences of mild traumatic brain injury. Psychol Med. 2010;22:1-15.
Drug Brand Names
- Amantadine • Symadine, Symmetrel
- Bromocriptine • Parlodel
- Carbidopa/levodopa • Sinemet
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Galantamine • Razadyne
- Methylphenidate • Ritalin, Methylin, others
- Physostigmine • Antilirium
- Pramipexole • Mirapex
- Rivastigmine • Exelon
- Sertraline • Zoloft
- Tacrine • Cognex
Disclosures
Dr. Scher and Ms. Loomis report no financial relationship with any company whose products mentioned in this article or with the manufacturers of competing products.
Dr. McCarron is a speaker for Eli Lilly and Company.
Mr. A, age 45, presents to the psychiatry clinic complaining of “ADHD.” He says he is not able to sit through movies and often gets distracted while on his computer at work. He also is having problems in his relationship with his wife; she says having a conversation with him is difficult. He has seen a psychiatrist for depression, which is currently managed by his primary care physician (PCP), who prescribed sertraline, 100 mg/d. Mr. A feels that although his depression is now under control, the medication has had limited effect on improving his concentration.
With further discussion, Mr. A reveals that 6 months ago he was involved in a car accident and suffered a mild traumatic brain injury (TBI). He was hospitalized overnight and was encouraged to follow up with his PCP. During his only follow-up visit, Mr. A told his PCP that he was having difficulty concentrating since the accident. However, because Mr. A has a remote history of alcohol abuse, his physician was reluctant to give him additional medication and referred him to a psychiatrist.
TBI is increasingly common but often overlooked or not treated in the emergency room (ER). Each year at least 1.7 million people experience a TBI; 275,000 are hospitalized and 52,000 die.1 The true incidence likely is greater because patients who do not present to the ER or hospital are not included in most studies, and the often-subtle psychiatric sequelae may preclude patients from seeking mental health treatment.
Psychiatric disorders are common among those who sustain a TBI (Table 1).2 One prospective cohort study found that patients with mild TBI are 2.8 times more likely than other patients to develop a psychiatric disorder.3 Statistics regarding TBI and psychiatric illness often are limited because they rely on self-reports, chart review, or retrospective studies.4
TBI severity can be classified on the basis of Glasgow Coma Scale score and other factors (Table 2).5 The correlation between severity of injury and resulting psychiatric illness or post-concussive symptoms is unclear.6 There is evidence that cognitive defects are associated with decreased function. Cognitive dysfunction also has been associated with disability 10 years after moderate to severe TBI.7 The association between cognitive dysfunction and outcome is more strongly correlated with moderate to severe TBI; there is no clear association in mild TBI.7 Additionally, compared with patients with severe TBI, those with mild TBI were more likely to be employed. At all severity levels, function improves over time. Mild, moderate, and severe TBI have a similar recovery curve.7
Table 1
Psychiatric symptoms: Common among TBI patients
| Psychiatric symptom | Incidence |
|---|---|
| Aggression | 30% |
| Anxiety | 10% to 70% |
| Apathy | 10% |
| Cognitive impairment | 25% to 70% |
| Depression | 25% to 50% |
| Mania | 1% to 10% |
| Psychosis | 3% to 8% |
| TBI: traumatic brain injury | |
| Source: Adapted from reference 2 | |
Table 2
Classifying severity of traumatic brain injury
| Severity | GCS score | LOC duration | PTA* |
|---|---|---|---|
| Mild | 13 to 15 | <30 minutes | <1 hour |
| Moderate | 9 to 12 | 1 to 24 hours | 1 to 24 hours |
| Severe | <8 | >24 hours | >24 hours |
| *Includes loss of memory immediately before or after the accident | |||
| GCS: Glasgow Coma Scale; LOC: loss of consciousness; PTA: posttraumatic amnesia | |||
| Source: Reference 5 | |||
Cognitive dysfunction and TBI
Cognitive dysfunction can be split into 3 categories:
- executive function
- memory
- processing speed.
The incidence of cognitive dysfunction after TBI is unclear. Several methods are used to quantify cognitive dysfunction in TBI patients; it is widely regarded that the Mini-Mental State Exam is not adequate to screen for subtle cognitive deficits.6 However, there is no clear consensus on which tool should be used.5
Off-label pharmacotherapy
There are no FDA-approved medications for treating neuropsychiatric sequelae of TBI. Treatment should be symptom-based and employ the “start low, go slow” approach. Compared with patients without brain injury, TBI patients may experience increased adverse effects from psychotropics but may require standard doses. These patients also may have comorbidities such as seizure disorders, substance abuse, and depression that will affect treatment.2 Different areas of cognitive function respond to different medication classes. Suggested medications include stimulant and nonstimulant catecholaminergic agents and cholinesterase inhibitors (Table 3).8
Executive function responds to non-stimulant catecholaminergics. In a review, Writer and Schillerstrom5 found that TBI patients who received catecholaminergic augmentation showed improved function in 6 of 7 studies. In 2 randomized controlled trials (RCTs) and 4 nonrandomized, placebo-controlled trials, patients with mild to severe TBI showed improved executive function, attention, global cognitive function, memory, language, and/ or arousal with use of bromocriptine, pramipexole, carbidopa/levodopa, or amantadine.5 The greatest improvements were found in executive function. In 1 RCT, 10 patients with mild to severe TBI showed no functional improvement after 2 weeks of treatment.
Amantadine, 200 to 400 mg/d, has been shown to safely improve arousal and cognitive function in patients with moderate to severe TBI when started 3 days to 5 months after injury.9 Amantadine, 400 mg/d, also improves executive function measures without significant benefit in attention or memory in patients with mild to severe TBI 6 months post-injury.10
Memory responds to cholinesterase inhibitors. Memory deficits secondary to TBI affect immediate and delayed memory. The cholinesterase inhibitor donepezil is approved for treating Alzheimer’s disease (AD) in the United States and Canada, and research suggests memory deficits after TBI may be similar to those seen in AD.11 This includes deficits in long-term memory storage, which likely is associated with the cholinergic system.11 Post-mortem studies have found similarities in traumatically injured brains and those of AD patients.11
Three small prospective studies of done-pezil have shown improved memory and attention in TBI patients when cognition is the primary outcome, with 1 small negative open-label trial.7 In a study of 53 patients, Whelan et al12 found that donepezil improved patients’ intelligence quotient and clinician-based assessment of cognition over 2 years. Taverni et al13 found memory improvement in 2 TBI patients within 3 weeks of starting donepezil. These results suggest that donepezil may be used in acute and late phases of memory deficits following mild, moderate, or severe TBI.6 All studies titrated donepezil from 5 to 10 mg/d over several weeks. Dosing guidelines for donepezil in AD suggest 5 mg/d for 4 to 6 weeks, which may be increased to 10 mg/d if needed.8
Rivastigmine (3 to 6 mg/d) has been shown to be effective in mild TBI when started 1 year after injury and safe for 12 to 38 weeks of treatment.14,15 One retrospective cohort study of 111 patients with chronic TBI found no difference among donepezil, rivastigmine, or galantamine, with mean doses of 7.2 mg/d, 10 mg/d, and 2.3 mg/d, respectively.16 Sixty-one percent of patients showed improvement and the remainder had modest or no response. This study suggests that positive response on cognition may be similar among cholinesterase inhibitors. In case reports, physostigmine has offered some benefit17,18; however, cardiovascular and autonomic side effects restrict its use.11 Tacrine is associated with problematic gastrointestinal and hepatic side effects.11
Processing speed responds to stimulant catecholaminergics. Although the incidence of psychiatric illness is not correlated with TBI severity, evidence suggests that speed of processing mediates the relationship between injury severity and functional decline.19 Therefore, aggressively treating these deficits may help improve function.
Methylphenidate improves attention and processing speed after TBI. A review of 7 randomized trials and 2 nonrandomized trials indicated that patients with mild to severe, chronic TBI experienced significantly improved cognitive function after methylphenidate treatment.5 Willmott and Ponsford20 found significant enhancement in information processing speed within 2 weeks of methylphenidate treatment in 40 patients with moderate or severe TBI. Methylphenidate increased the rate of recovery and led to improvement in acute21 and post-acute phases.22 In addition, methylphenidate may improve processing speed even in the absence of significant changes in attention.23
The standard methylphenidate dose used in most studies, 0.3 mg/kg twice daily, is safe and effective. Dosing usually is started at 5 mg/d and titrated to symptomatic relief. Because methylphenidate does not lower the seizure threshold, it is safe for patients at high risk for seizure.24 Methylphenidate also significantly improves attention and speed of processing in pediatric head trauma.25,26
Dextroamphetamine also is used to treat speed of processing dysfunction after TBI, but is less studied than methylphenidate. Dextroamphetamine, 5 to 30 mg/d, was found to effectively treat attention problems that interfered with rehabilitation in patients with severe TBI.27
Table 3
Recommended treatments for mild TBI-related cognitive deficits
| Deficit | First-line medication | Side effects | Contraindications | Other treatments |
|---|---|---|---|---|
| Memory | Donepezil (5 to 10 mg/d) | Diarrhea, nausea, vomiting, muscle cramps, fatigue, anorexia | Hypersensitivity to donepezil or piperidine derivatives | Rivastigmine, galantamine, physostigmine, CDP-choline |
| Speed of processing | Methylphenidate (0.3 mg/kg twice daily) | Headache, insomnia, decreased appetite, nausea, vomiting, anxiety, irritability | Hypersensitivity to methylphenidate, glaucoma, history of Tourette syndrome or tics, use of MAOI within 14 days | Dextroamphetamine |
| Executive function | Amantadine (200 to 400 mg/d) | CNS depression, orthostatic hypotension, peripheral edema, agitation, nausea, anorexia | Hypersensitivity to amantadine | Bromocriptine, pramipexole, carbidopa/levodopa |
| CDP-choline: cytidinediphosphocholine; MAOI: monoamine oxidase inhibitor | ||||
| Source: Reference 8 | ||||
Nonpharmacologic treatments
In addition to pharmacotherapy, nonpharmacologic interventions also should be a mainstay of treatment. Compensatory training and cognitive exercise may improve patients’ cognitive deficits and return some sense of control. Individual and family psychotherapy, including cognitive-behavioral therapy, also may be beneficial.2 Review sources have identified the importance of validating patients’ symptoms and developing a goal-based treatment plan.6
CASE CONTINUED: Improvement with stimulants
Unlike many TBI patients who do not recognize the often-subtle psychiatric sequelae of their injury, Mr. A is aware of his difficulty concentrating, which is temporally linked with his accident. After exploring the association between Mr. A’s symptoms and his injury, his psychiatrist concludes that Mr. A’s cognitive deficits likely are associated with his TBI. Mr. A’s history of alcohol abuse raises concerns about prescribing stimulants. However, after assuring that Mr. A’s depression is well controlled and addressing his risk of substance abuse, his psychiatrist prescribes methylphenidate titrated to 30 mg/d. When he returns to the clinic several weeks later, Mr. A reports improved attention and functioning at work, and continues to follow up with the psychiatrist without requiring changes to his medication regimen.
Related Resource
- Konrad C, Geburek AJ, Rist F, et al. Long-term cognitive and emotional consequences of mild traumatic brain injury. Psychol Med. 2010;22:1-15.
Drug Brand Names
- Amantadine • Symadine, Symmetrel
- Bromocriptine • Parlodel
- Carbidopa/levodopa • Sinemet
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Galantamine • Razadyne
- Methylphenidate • Ritalin, Methylin, others
- Physostigmine • Antilirium
- Pramipexole • Mirapex
- Rivastigmine • Exelon
- Sertraline • Zoloft
- Tacrine • Cognex
Disclosures
Dr. Scher and Ms. Loomis report no financial relationship with any company whose products mentioned in this article or with the manufacturers of competing products.
Dr. McCarron is a speaker for Eli Lilly and Company.
1. Faul M, Xu L, Wald MM, et al. Traumatic brain injury in the United States; emergency department visits, hospitalizations, and deaths, 2002-2006. Atlanta, GA: Centers for Disease Control and Prevention; 2010. Available at: http://www.cdc.gov/traumaticbraininjury/tbi_ed.html. Accessed December 1, 2010.
2. Vaishnavi S, Rao V, Fann JR. Neuropsychiatric problems after traumatic brain injury: unraveling the silent epidemic. Psychosomatics. 2009;50(3):198-205.
3. Fann JR, Burington B, Leonetti A, et al. Psychiatric illness following traumatic brain injury in an adult health maintenance organization population. Arch Gen Psychiatry. 2004;61(1):53-61.
4. Bryant RA, O’Donnell ML, Creamer M, et al. The psychiatric sequelae of traumatic injury. Am J Psychiatry. 2010;167(3):312-320.
5. Writer BW, Schillerstrom JE. Psychopharmacological treatment for cognitive impairment in survivors of traumatic brain injury: a critical review. J Neuropsychiatry Clin Neurosci. 2009;21(4):362-370.
6. Arciniegas DB, Anderson CA, Topkoff J, et al. Mild traumatic brain injury: a neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr Dis Treat. 2005;1(4):311-327.
7. Sigurdardottir S, Andelic N, Roe C, et al. Cognitive recovery and predictors of functional outcome 1 year after traumatic brain injury. J Int Neuropsychol Soc. 2009;15(5):740-750.
8. Physicians’ desk reference 64th ed. Montvale, NJ: Thomson Reuters; 2010.
9. Sawyer E Mauro LS, Mauro LS, Ohlinger MJ. Amantadine enhancement of arousal and cognition after traumatic brain injury. Ann Pharmacother. 2008;42(2):247-252.
10. Kraus MF, Smith GS, Butters M, et al. Effects of the dopaminergic agent and NMDA receptor antagonist amantadine on cognitive function, cerebral glucose metabolism and D2 receptor availability in chronic traumatic brain injury: a study using positron emission tomography (PET). Brain Inj. 2005;19(7):471-479.
11. Griffin SL, van Reekum R, Masanic C. A review of cholinergic agents in the treatment of neurobehavioral deficits following traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2003;15(1):17-26.
12. Whelan FJ, Walker MS, Schultz SK. Donepezil in the treatment of cognitive dysfunction associated with traumatic brain injury. Ann Clin Psychiatry. 2000;12(3):131-135.
13. Taverni JP, Seliger G, Lichtman SW. Donepezil medicated memory improvement in traumatic brain injury during post acute rehabilitation. Brain Inj. 1998;12(1):77-80.
14. Silver JM, McAllister TW, Arciniegas DB. Depression and cognitive complaints following mild traumatic brain injury. Am J Psychiatry. 2009;166(6):653-661.
15. Silver JM, Koumaras B, Chen M, et al. Effects of rivastigmine on cognitive function in patients with traumatic brain injury. Neurology. 2006;67(5):748-755.
16. Tenovuo O. Central acetylcholinesterase inhibitors in the treatment of chronic traumatic brain injury—clinical experience in 111 patients. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):61-67.
17. Goldberg E, Gerstman LJ, Mattis S, et al. Selective effects of cholinergic treatment on verbal memory in posttraumatic amnesia. J Clin Neuropsychol. 1982;4(3):219-234.
18. Eames P, Sutton A. Protracted post-traumatic confusional state treated with physostigmine. Brain Inj. 1995;9(7):729-734.
19. Rassovsky Y, Satz P, Alfano MS, et al. Functional outcome in TBI II: verbal memory and information processing speed mediators. J Clin Exp Neuropsychol. 2006;28(4):581-591.
20. Willmott C, Ponsford J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: a randomised, crossover, double blind, placebo controlled inpatient trial. J Neurol Neurosurg Psychiatry. 2009;80(5):552-557.
20. Kaelin DL, Cifu DX, Matthies B. Methylphenidate effect on attention deficit in the acutely brain-injured adult. Arch Phys Med Rehabil. 1996;77(1):6-9.
22. Whyte J, Hart T, Vaccaro M, et al. Effects of methylphenidate on attention deficits after traumatic brain injury: a multidimensional, randomized, controlled trial. Am J Phys Med Rehabil. 2004;83(6):401-420.
23. Whyte J, Hart T, Schuster K, et al. Effects of methylphenidate on attentional function after traumatic brain injury. A randomized, placebo-controlled trial. Am J Phys Med Rehabil. 1997;76(6):440-450.
24. Wroblewski BA, Leary JM, Phelan AM, et al. Methylphenidate and seizure frequency in brain injured patients with seizure disorders. J Clin Psychiatry. 1992;53(3):86-89.
25. Mahalick DM, Carmel PW, Greenberg JP, et al. Psychopharmacologic treatment of acquired attention disorders in children with brain injury. Pediatr Neurosurg. 1998;29(3):121-126.
26. Hornyak JE, Nelson VS, Hurvitz EA. The use of methylphenidate in paediatric traumatic brain injury. Pediatr Rehabil. 1997;1(1):15-17.
27. Hornstein A, Lennihan L, Seliger G. Amphetamine in recovery from brain injury. Brain Inj. 1996;10(2):145-148.
1. Faul M, Xu L, Wald MM, et al. Traumatic brain injury in the United States; emergency department visits, hospitalizations, and deaths, 2002-2006. Atlanta, GA: Centers for Disease Control and Prevention; 2010. Available at: http://www.cdc.gov/traumaticbraininjury/tbi_ed.html. Accessed December 1, 2010.
2. Vaishnavi S, Rao V, Fann JR. Neuropsychiatric problems after traumatic brain injury: unraveling the silent epidemic. Psychosomatics. 2009;50(3):198-205.
3. Fann JR, Burington B, Leonetti A, et al. Psychiatric illness following traumatic brain injury in an adult health maintenance organization population. Arch Gen Psychiatry. 2004;61(1):53-61.
4. Bryant RA, O’Donnell ML, Creamer M, et al. The psychiatric sequelae of traumatic injury. Am J Psychiatry. 2010;167(3):312-320.
5. Writer BW, Schillerstrom JE. Psychopharmacological treatment for cognitive impairment in survivors of traumatic brain injury: a critical review. J Neuropsychiatry Clin Neurosci. 2009;21(4):362-370.
6. Arciniegas DB, Anderson CA, Topkoff J, et al. Mild traumatic brain injury: a neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr Dis Treat. 2005;1(4):311-327.
7. Sigurdardottir S, Andelic N, Roe C, et al. Cognitive recovery and predictors of functional outcome 1 year after traumatic brain injury. J Int Neuropsychol Soc. 2009;15(5):740-750.
8. Physicians’ desk reference 64th ed. Montvale, NJ: Thomson Reuters; 2010.
9. Sawyer E Mauro LS, Mauro LS, Ohlinger MJ. Amantadine enhancement of arousal and cognition after traumatic brain injury. Ann Pharmacother. 2008;42(2):247-252.
10. Kraus MF, Smith GS, Butters M, et al. Effects of the dopaminergic agent and NMDA receptor antagonist amantadine on cognitive function, cerebral glucose metabolism and D2 receptor availability in chronic traumatic brain injury: a study using positron emission tomography (PET). Brain Inj. 2005;19(7):471-479.
11. Griffin SL, van Reekum R, Masanic C. A review of cholinergic agents in the treatment of neurobehavioral deficits following traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2003;15(1):17-26.
12. Whelan FJ, Walker MS, Schultz SK. Donepezil in the treatment of cognitive dysfunction associated with traumatic brain injury. Ann Clin Psychiatry. 2000;12(3):131-135.
13. Taverni JP, Seliger G, Lichtman SW. Donepezil medicated memory improvement in traumatic brain injury during post acute rehabilitation. Brain Inj. 1998;12(1):77-80.
14. Silver JM, McAllister TW, Arciniegas DB. Depression and cognitive complaints following mild traumatic brain injury. Am J Psychiatry. 2009;166(6):653-661.
15. Silver JM, Koumaras B, Chen M, et al. Effects of rivastigmine on cognitive function in patients with traumatic brain injury. Neurology. 2006;67(5):748-755.
16. Tenovuo O. Central acetylcholinesterase inhibitors in the treatment of chronic traumatic brain injury—clinical experience in 111 patients. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):61-67.
17. Goldberg E, Gerstman LJ, Mattis S, et al. Selective effects of cholinergic treatment on verbal memory in posttraumatic amnesia. J Clin Neuropsychol. 1982;4(3):219-234.
18. Eames P, Sutton A. Protracted post-traumatic confusional state treated with physostigmine. Brain Inj. 1995;9(7):729-734.
19. Rassovsky Y, Satz P, Alfano MS, et al. Functional outcome in TBI II: verbal memory and information processing speed mediators. J Clin Exp Neuropsychol. 2006;28(4):581-591.
20. Willmott C, Ponsford J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: a randomised, crossover, double blind, placebo controlled inpatient trial. J Neurol Neurosurg Psychiatry. 2009;80(5):552-557.
20. Kaelin DL, Cifu DX, Matthies B. Methylphenidate effect on attention deficit in the acutely brain-injured adult. Arch Phys Med Rehabil. 1996;77(1):6-9.
22. Whyte J, Hart T, Vaccaro M, et al. Effects of methylphenidate on attention deficits after traumatic brain injury: a multidimensional, randomized, controlled trial. Am J Phys Med Rehabil. 2004;83(6):401-420.
23. Whyte J, Hart T, Schuster K, et al. Effects of methylphenidate on attentional function after traumatic brain injury. A randomized, placebo-controlled trial. Am J Phys Med Rehabil. 1997;76(6):440-450.
24. Wroblewski BA, Leary JM, Phelan AM, et al. Methylphenidate and seizure frequency in brain injured patients with seizure disorders. J Clin Psychiatry. 1992;53(3):86-89.
25. Mahalick DM, Carmel PW, Greenberg JP, et al. Psychopharmacologic treatment of acquired attention disorders in children with brain injury. Pediatr Neurosurg. 1998;29(3):121-126.
26. Hornyak JE, Nelson VS, Hurvitz EA. The use of methylphenidate in paediatric traumatic brain injury. Pediatr Rehabil. 1997;1(1):15-17.
27. Hornstein A, Lennihan L, Seliger G. Amphetamine in recovery from brain injury. Brain Inj. 1996;10(2):145-148.
Not all mood swings are bipolar disorder
M, age 13, is referred by her pediatrician with the chief complaint of “severe mood swings, rule out bipolar disorder (BD).” In the past she was treated for attention-deficit/hyperactivity disorder (ADHD) with stimulants with mixed results. M’s parents are concerned about her “flipping out” whenever she is asked to do something she does not want to do. Her mother has a history of depression and anxiety; her father had a “drinking problem.” There is no history of BD in her first- or second-degree relatives. Are M’s rapid mood swings a sign of BD or another disorder?
The differential diagnosis of “mood swings” is important because they are a common presenting symptom of many children and adolescents with mood and behavioral disorders. Mood swings often occur in children and adolescents with ADHD, oppositional defiant disorder (ODD), developmental disorders, depressive disorders, BD, anxiety disorders, and conduct disorders. Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but are not diagnostic as an isolated symptom.
Mood swings in children are common, nonspecific symptoms that more often are a sign of anxiety or behavioral disorders than BD. This article discusses the differential diagnosis of mood swings in children and adolescents and how to best screen and diagnose these patients.
What are ‘mood swings’?
Mood swings is a popular term that is nonspecific and not part of DSM-IV-TR diagnostic criteria for BD. The complaint of “mood swings” may reflect severe mood lability of pediatric patients with BD. This mood lability is best described by the Kiddie-Mania Rating Scale (K-MRS) developed by Axelson and colleagues as “rapid mood variation with several mood states within a brief period of time which appears internally driven without regard to the circumstance.”1 On K-MRS mood lability items, children with mania typically score:
- Moderate—many mood changes throughout the day, can vary from elevated mood to anger to sadness within a few hours; changes in mood are clearly out of proportion to circumstances and cause impairment in functioning
- Severe—rapid mood swings nearly all of the time, with mood intensity greatly out of proportion to circumstances
- Extreme—constant, explosive variability in mood, several mood changes occurring within minutes, difficult to identify a particular mood, changes in mood radically out of proportion to circumstances.
Patients with BD typically exhibit what is best described as a “mood cycle”—a pronounced shift in mood and energy from 1 extreme to another.2 An example of this would be a child who wakes up with extreme silliness, high energy, and intrusive behavior that persists for several hours and then later in the day becomes sad, depressed, and suicidal with no precipitant for either mood cycle. BD patients also will exhibit other symptoms of mania during these mood cycling periods.
Rapid cycling is a DSM-IV course specifier that indicates ≥4 mood episodes per year in patients with BD with a typical course of mania or hypomania followed by depression, or vice versa.3 The episodes must be demarcated by full or partial remission that lasts ≥2 months or by a switch to a mood state of opposite polarity. In the past, children with frequent mood swings were described incorrectly as “rapid cycling,” but this term has been dropped because it engenders confusion between adult and pediatric BD phenomenology.2
A more precise method of describing mood symptoms in a child or adolescent is to use the FIND criteria, which include:4
- Frequency of symptoms per week
- Intensity of mood symptoms
- Number of mood cycles per day
- Duration of symptoms per day.
Visit this article at CurrentPsychiatry.com to view a table that outlines what to look for when using the FIND criteria to evaluate common pediatric psychiatric disorders that include mood swings. Table 1
describes clinical characteristics and tools and resources used to differentiate these and other disorders.4
Table 1
Clinical characteristics of psychiatric disorders that often feature mood swings
| Disorder | Clinical description | Useful tools/resources |
|---|---|---|
| ADHD | Chronic symptoms of hyperactivity, distractibility, impulsivity, poor attentional skills, disorganization | Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L) |
| ODD | Chronic symptoms of oppositionality, negativity; short, frequent mood swings in response to being asked to do something they do not want to do | CPRS-R:L |
| Anxiety disorders | Excessive ‘worry,’ difficulty with transitions, increased mood swings during stressful periods, psychosomatic symptoms | Self-Report for Childhood Anxiety Related Disorders |
| ARND | History of exposure to alcohol in-utero; mild dysmorphia, attentional, mood, and executive functioning problems | National Organization on Fetal Alcohol Syndrome |
| Bipolar disorder | In children: clustering together of episodes or ‘mini-episodes’ (several days) of increased energy, decreased need for sleep, increased mood cycling, pressured speech, etc. In adolescents: depressive episodes with episodes of hypomania or mania | Mood Disorders Questionnaire Kiddie Schedule for Affective Disorders and Schizophrenia Mania Rating Scale |
| ADHD: attention-deficit/hyperactivity disorder; ARND: alcohol-related neurodevelopmental disorder; ODD: oppositional defiant disorder | ||
| Source: Reference 4 | ||
Mood swings: A chart review
We recently completed a retrospective chart review of 100 patients consecutively referred to our pediatric mood disorders clinic for evaluation of “mood swings, rule out BD.” These patients were self-referred, referred by a psychiatrist for a second opinion, or referred by their primary care physician. The mean age of these patients was 8±2.8 years and 68% were male.
Two experienced clinicians (RAK and EM) interviewed each patient and their caregivers and reviewed results of the Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L)5 and other outside information.
Figure 1 illustrates these patients’ diagnoses. Diagnoses for each of these disorders were made using DSM-IV-TR criteria.3
The most common diagnoses among patients with the chief complaint of mood swings were ADHD (39%); ODD with ADHD (15%); an anxiety disorder, usually generalized anxiety disorder (GAD) (15%); BD (12%); and a secondary mood disorder, usually fetal alcohol spectrum disorder (10%). We were surprised at how often ADHD, ODD, and anxiety disorders were found to be responsible for these patients’ mood swings and how frequently the referring clinician did not recognize these disorders. In the following sections, we discuss each of these disorders and how they differ from BD.
Figure 1 Underlying diagnoses of 100 children/adolescents referred for ‘mood swings’
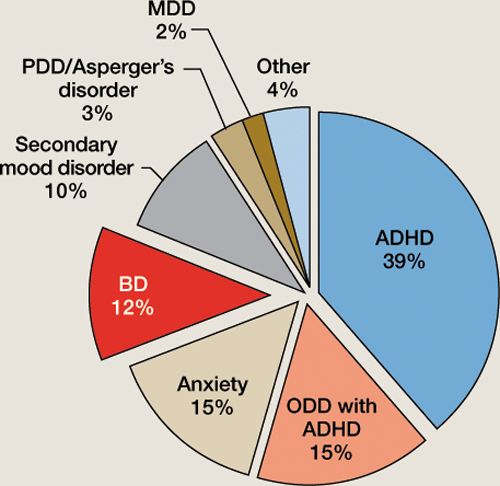
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder; MDD: major depressive disorder; ODD: oppositional defiant disorder; PDD: pervasive developmental disorder
ADHD and ODD
In our sample, patients with undiagnosed ADHD made up the largest group of those with frequent mood swings. ADHD inattentive type was missed frequently in adolescent girls who still had behavioral aspects of ADHD, including impulsivity and aggression.6
The CPRS-R:L is useful for screening and diagnosing children and adolescents with ADHD and ODD. It contains 80 items, can be used in males and females and patients age 3 to 17, and has validated norms by age and sex.5 It takes parents approximately 10 minutes to fill out this questionnaire and the results can be scored by hand. The CPRS-R:L includes the following scales: oppositional; cognitive problems/inattention; hyperactivity; anxious-shy; perfectionism; social problems; psychosomatic; Connors’ global index; DSM-IV symptom subscales; and an ADHD index. Patients with mood swings and ADHD combined typically score >2 standard deviations above their age/sex mean on the CPRS-R:L hyperactivity scale, Connors’ Global Index, and ADHD index.5
A common childhood disorder, ODD has multiple etiologies.7 The first DSM-IV criteria for ODD is “often loses temper”3—essentially mood swings that often are expressed behaviorally as anger and at times as aggressive outbursts.
Dodge and Cole8 categorized aggression as reactive (impulsivity with a high affective valence) or proactive (characterized by low arousal and premeditation, ie, predatory conduct disorder). Reactive aggression typically is an angry defensive response to frustration, threat, or provocation, whereas proactive aggression is deliberate, coercive behavior often used to obtain a goal.9 Reactive aggression is common among children with ADHD and ODD and typically begins as a mood swing that escalates into reactive aggressive behavior. In a study of 268 consecutively referred children and adolescents with ADHD and 100 community controls, Connor et al10 found significantly more reactive than proactive forms of aggression in ADHD patients.
It can be difficult to differentiate the moods swings and symptoms of ODD from those of pediatric BD. Mick et al11 found that severe irritability may be a diagnostic indicator of BD in children with ADHD. Using the Kiddie Schedule for Affective Disorders and Schizophrenia (epidemiologic version) structured diagnostic interview,12 they evaluated 274 children (mean age 10.8±3.2) with ADHD; 37% had no comorbid mood disorder, 36% had ADHD with depression, and 11% had ADHD with BD. Researchers characterized 3 types of irritability in these patients:
- ODD-type irritability characterized by a low frustration tolerance that is seen in ODD
- Mad/cranky irritability found in depressive disorders
- Super-angry/grouchy/cranky irritability with frequent, prolonged, and largely unprovoked anger episodes and characteristics of mania.
ODD-type irritability was common among all ADHD patients, was the least impairing type of irritability, and did not increase the risk of a mood disorder. Mad/cranky irritability was common only in children with ADHD and a mood disorder (depression or BD), was more impairing than ODD-type irritability, and was most predictive of unipolar depression. Super-angry/grouchy/cranky irritability was common only among children with ADHD and BD (77%), was the most impairing, and was predictive of both unipolar depression and BD. The type of irritability and clustering of DSM-IV manic symptoms best differentiated ADHD subjects from those with ADHD and BD. Figure 2 illustrates symptoms that differentiated patients with ADHD from those with ADHD and comorbid BD.11
A review of pharmacotherapy for aggression in children found the largest effects for methylphenidate for aggression in ADHD (mean effect size=0.9, combined N=844).13 Our clinical experience has been that pediatric patients with ADHD or ODD with ADHD often have high levels of reactive aggression that presents as mood swings, and aggressively treating ADHD often results in improved mood and other ADHD symptoms.
Figure 2 Symptoms that differentiate BD from BD with comorbid ADHD
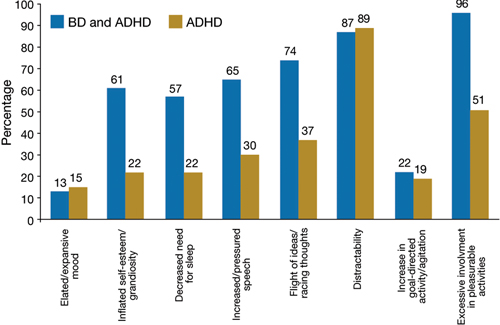
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder
Source: Reference 11
Anxiety disorders
The estimated prevalence of child and adolescent anxiety disorders is 10% to 20%14; in our sample the prevalence was 15%. These disorders include GAD, separation anxiety disorder, social phobias, posttraumatic stress disorder (PTSD), and obsessive-compulsive disorder. Often, children with GAD worry excessively and become upset during transitions when things don’t proceed as they expect, with resultant angry outbursts and mood swings. Mood swings and difficulty sleeping are common in children with anxiety disorders or BD. Anxiety disorders often will be missed unless specific triggers of the mood swings or angry outbursts—as well as differentiating symptoms such as excessive fear, worry, and psychosomatic symptoms—are assessed.
In our clinical experience, simply asking a child if he or she is anxious is not sufficient to uncover an anxiety disorder. Although the CPRS-L:R will screen for anxiety disorders, we have found that the Self-Report for Childhood Anxiety Related Disorders (SCARED) developed by Birmaher et al15 is more specific. This tool can be used in patients age ≥8. The parent and child versions of the SCARED contain 41 items that measure 5 factors:
- general anxiety
- separation anxiety
- social phobia
- school phobia
- physical symptoms of anxiety.
The SCARED takes 5 minutes to fill out and is available in parent and child versions.
Secondary mood disorders
Many patients in our sample had a mood disorder secondary to the neurologic effects of alcohol on the developing brain. For more about maternal alcohol use, fetal alcohol spectrum disorders, and mood swings, visit this article at CurrentPsychiatry.com.
What BD looks like in children
In our sample, 12% of patients referred for mood swings were diagnosed with bipolar I disorder (BDI), bipolar II disorder (BDII), or bipolar disorder, not otherwise specified (BD-NOS). In the United States, lifetime prevalence of BDI and BDII in adolescents age 13 to 17 is 2.9%.16 No large epidemiologic studies have looked at the lifetime prevalence of BD in children age <13.
How often a clinician sees BD in children and adolescents largely depends on the type of setting in which he or she practices. Although in the general population BD is relatively rare compared with other childhood psychiatric disorders, on child/adolescent inpatient units it is common to find that 30% to 40% of patients have BD.17
The best longitudinal study to date of the phenomenology, comorbidity, and outcome of BD in children and adolescents is the National Institute of Mental Health-funded Course and Outcome of Bipolar Youth study (COBY).18 In this ongoing, longitudinal study, 413 youths (age 7 to 17) with BDI (N=244), BDII (N=28), or BD-NOS (N=141) were rigorously diagnosed using state-of-the-art measures, including the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present version19 and re-evaluated every 9.4 months for 4 years. When organizing this study, investigators found that DSM-IV criteria for BD-NOS were too vague to be useful and developed their own criteria (Table 2).18
For BDI patients in the COBY study, the mean age of onset for bipolar symptoms was 9.0±4.1 years and the mean duration of illness was 4.4±3.1 years. Researchers reported that at the 4-year assessment approximately 70% of patients with BD recovered from their index episode, and 50% had at least 1 syndromal recurrence, particularly depressive episodes.20 Analyses of these patients’ weekly mood symptoms showed that they had syndromal or subsyndromal symptoms with numerous changes in symptoms and shifts of mood polarity 60% of the time, and psychosis 3% of the time. During this study, 20% of BDII patients progressed to BDI, and 25% of BD-NOS patients converted to BDI or BDII.
Further analysis of the COBY data revealed that onset of mood symptoms preceded onset of clear bipolar episodes by an average of 1.0±1.7 years. Depression was the most common initial and most frequent episode for adolescents; mood lability was seen more often in childhood-onset and adolescents with early-onset BD. Depressed children had more severe irritability than depressed adolescents, and older age was associated with more severe and typical mood symptomatology.21
The clinical picture of a child with BD that emerges from the COBY study is:
- a fairly young child with the onset of mood symptoms between age 5 to 12
- subsyndromal and less frequently clear syndromal episodes
- primarily mixed and depressed symptoms with rapid mood cycles during these episodes.22
It is clear that there is a spectrum of bipolar disorders in children and adolescents with varying degrees of symptom expression and children differ from adolescents and adults in their initial presentation of BD.
Table 2
COBY criteria for bipolar disorder, not otherwise specified
| Presence of clinically relevant bipolar symptoms that do not fulfill DSM-IV criteria for BDI or BDII |
| In addition, patients are required to have elevated mood plus 2 associated DSM-IV symptoms or irritable mood plus 3 DSM-IV associated symptoms, along with a change in level of functioning |
| Duration of a minimum of 4 hours within a 24-hour period |
| At least 4 cumulative lifetime days meeting the criteria |
| BDI: bipolar I disorder; BDII: bipolar II disorder; COBY: Course and Outcome of Bipolar Youth study |
| Source: Reference 18 |
Related Resources
- Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Goodwin FK, Jamison KR. Manic-depressive illness. 2nd ed. Oxford, United Kingdom: Oxford University Press; 2007.
- Miklowitz DJ, Cicchetti D, eds. Understanding bipolar disorder: a developmental perspective. New York, NY: Guilford Press; 2010.
Drug Brand Name
- Methylphenidate • Ritalin, Concerta, others
Disclosures
Dr. Kowatch receives grant/research support from the National Institute of Child Health and Human Development and the National Institute of Mental Health and is a consultant to AstraZeneca, Forest Pharmaceuticals, Merck, and the REACH Foundation.
Dr. Delgado and Ms. Monroe report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table
FIND criteria of disorders found to cause mood swings
| Criteria | BDI | BP-NOS | ODD | GAD | ARND |
|---|---|---|---|---|---|
| Frequency of symptoms/week | 7 days (more days than not in an average week) | 2 to 3 days/week | Daily (chronic) irritability and mood swings precipitated by ‘not getting their way’ | Greatest during times of change/stress | Daily |
| Intensity of symptoms | Severe—parents often are afraid to take the child out in public because of mood symptoms | Moderate | Mild/moderate | Mild/moderate when stressed | Mild/moderate |
| Number of mood cycles/day | Daily cycles of euphoria and depression | 3 to 4 | 5 to 10 | 2 to 3 | 8 to 10 |
| Duration of symptoms/day | Euphoria: 30 to 60 minutes Depression: 30 minutes to 6 hours | 4 hours total/day of mood symptoms | Short; 5 to 10 minutes | Short; 5 to 10 minutes | Short; 5 to 10 minutes |
| ARND: alcohol-related neurodevelopmental disorder; BDI: bipolar I disorder; BD-NOS: bipolar disorder, not otherwise specified; GAD: generalized anxiety disorder; ODD: oppositional defiant disorder | |||||
| Source: Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008 | |||||
Even small amounts of alcohol use by a pregnant woman can impact her child’s development. In a controlled study examining drinking behavior of 12,678 pregnant women and the effect this had on their children, Sayel et ala found that <1 drink per week during the first trimester was clinically significant for mental health problems in girls, measured at age 4 and 8, when using parent or teacher report.
Fetal alcohol spectrum disorder describes the range of effects that can occur in an individual whose mother drank alcohol during pregnancy. These disorders include fetal alcohol syndrome (FAS), alcohol-related neurodevelopmental disorder (ARND), and alcohol-related birth defects (ARBD).
FAS. Individuals with FAS have a distinct pattern of facial abnormalities, growth deficiency, and evidence of CNS dysfunction. Characteristic facial abnormalities may include a smooth philtrum, thin upper lip, upturned nose, flat nasal bridge and midface, epicanthal folds, small palpebral fissures, and small head circumference. Growth deficiency begins in-utero and continues throughout childhood and into adulthood. CNS abnormalities can include impaired brain growth or abnormal structure, manifested differently depending on age.
ARND. Many individuals affected by alcohol exposure before birth do not have the characteristic facial abnormalities and growth retardation identified with full FAS, yet have significant brain and behavioral impairments. Individuals with ARND have either the facial anomalies, growth retardation, and other physical abnormalities, or a complex pattern of behavioral or cognitive abnormalities inconsistent with developmental level and unexplained by genetic background or environmental conditions (ie, poor impulse control, language deficits, problems with abstraction, mathematical and social perception deficits, learning problems, and impairment in attention, memory, or judgment).b
ARBD. Persons with ARBD have malformations of the skeletal and major organ systems, such as cardiac or renal abnormalities.
Comorbid psychiatric conditions in children with prenatal alcohol exposure are 5 to 16 times more prevalent than in the general population; these children are 38% more likely to have an anger disorder.c O’Connor and Paleyd found that “…mood disorder symptoms were significantly higher for children with parental alcohol exposure compared to children without exposure.” Children with ARND are treated symptomatically depending upon which deficits and behaviors they exhibit.e
References
a. Sayal K, Heron J, Golding J, et al. Binge pattern of alcohol consumption during pregnancy and childhood mental health outcomes: longitudinal population-based study. Pediatrics. 2009;123(2):e289-296.
b. Warren KR, Foudin LL. Alcohol-related birth defects—the past, present, and future. Alcohol Res Health. 2001;25(3):153-158.
c. Burd L, Klug MG, Martsolf JT, et al. Fetal alcohol syndrome: neuropsychiatric phenomics. Neurotoxicol Teratol. 2003;25(6):697-705.
d. O’Connor MJ, Paley B. Psychiatric conditions associated with prenatal alcohol exposure. Dev Disabil Res Rev. 2009;15(3):225-234.
e. Paley B, O’Connor MJ. Intervention for individuals with fetal alcohol spectrum disorders: treatment approaches and case management. Dev Disabil Res Rev. 2009;15(3):258-267.
1. Axelson D, Birmaher BJ, Brent D, et al. A preliminary study of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children mania rating scale for children and adolescents. J Child Adolesc Psychopharmacol. 2003;13(4):463-470.
2. Youngstrom EA, Birmaher B, Findling RL. Pediatric bipolar disorder: validity, phenomenology, and recommendations for diagnosis. Bipolar Disord. 2008;10(1 Pt 2):194-214.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
4. Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008.
5. Conners CK. Conners’ Parent Rating Scale Long Form (CPRS-R:L) North Tonawanda, NY: Multi-Health Systems, Inc.; 1997.
6. Martel MM. Research review: a new perspective on attention-deficit/hyperactivity disorder: emotion dysregulation and trait models. J Child Psychol Psychiatry. 2009;50(9):1042-1051.
7. Steiner H, Remsing L. and the Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(1):126-141.
8. Dodge KA, Cole JD. Social-information-processing factors in reactive and proactive aggression in children’s peer groups. J Pers Soc Psychol. 1987;53(6):1146-1158.
9. Connor DF, Steingard RJ, Cunningham JA, et al. Proactive and reactive aggression in referred children and adolescents. Am J Orthopsychiatry. 2004;74(2):129-136.
10. Connor DF, Chartier KG, Preen EC, et al. Impulsive aggression in attention-deficit/hyperactivity disorder: symptom severity, co-morbidity, and attention-deficit/hyperactivity disorder subtype. J Child Adolesc Psychopharmacol. 2010;20(2):119-126.
11. Mick E, Spencer T, Wozniak J, et al. Heterogeneity of irritability in attention-deficit/hyperactivity disorder subjects with and without mood disorders. Biol Psychiatry. 2005;58(7):576-582.
12. Orvaschel H. Schizophrenia and Affective Disorders Schedule for children—Epidemiological Version (KSADS-E). Fort Lauderdale, FL: Nova Southeastern University; 1995.
13. Pappadopulos E, Woolston S, Chait A, et al. Pharmacotherapy of aggression in children and adolescents: efficacy and effect size. J Can Acad Child Adolesc Psychiatry. 2006;15(1):27-39.
14. Achenbach TM, Howell CT, McConaughy SH, et al. Six-year predictors of problems in a national sample: IV. Young adult signs of disturbance. J Am Acad Child Adolesc Psychiatry. 1998;37(7):718-727.
15. Birmaher B, Khetarpal S, Brent D, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36:545-553.
16. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980-989.
17. Youngstrom EA, Duax J. Evidence-based assessment of pediatric bipolar disorder, part I: base rate and family history. J Am Acad Child Adolesc Psychiatry. 2005;44(7):712-717.
18. Birmaher B, Axelson D, Strober M, et al. Clinical course of children and adolescents with bipolar spectrum disorders. Arch Gen Psychiatry. 2006;63(2):175-183.
19. Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980-988.
20. Birmaher B, Axelson D. Course and outcome of bipolar spectrum disorder in children and adolescents: a review of the existing literature. Dev Psychopathol. 2006;18(4):1023-1035.
21. Birmaher B, Axelson D, Strober M, et al. Comparison of manic and depressive symptoms between children and adolescents with bipolar spectrum disorders. Bipolar Disord. 2009;11(1):52-62.
22. Birmaher B, Axelson D, Goldstein B, et al. Four-year longitudinal course of children and adolescents with bipolar spectrum disorders: the Course and Outcome of Bipolar Youth (COBY) study. Am J Psychiatry. 2009;166(7):795-804.
M, age 13, is referred by her pediatrician with the chief complaint of “severe mood swings, rule out bipolar disorder (BD).” In the past she was treated for attention-deficit/hyperactivity disorder (ADHD) with stimulants with mixed results. M’s parents are concerned about her “flipping out” whenever she is asked to do something she does not want to do. Her mother has a history of depression and anxiety; her father had a “drinking problem.” There is no history of BD in her first- or second-degree relatives. Are M’s rapid mood swings a sign of BD or another disorder?
The differential diagnosis of “mood swings” is important because they are a common presenting symptom of many children and adolescents with mood and behavioral disorders. Mood swings often occur in children and adolescents with ADHD, oppositional defiant disorder (ODD), developmental disorders, depressive disorders, BD, anxiety disorders, and conduct disorders. Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but are not diagnostic as an isolated symptom.
Mood swings in children are common, nonspecific symptoms that more often are a sign of anxiety or behavioral disorders than BD. This article discusses the differential diagnosis of mood swings in children and adolescents and how to best screen and diagnose these patients.
What are ‘mood swings’?
Mood swings is a popular term that is nonspecific and not part of DSM-IV-TR diagnostic criteria for BD. The complaint of “mood swings” may reflect severe mood lability of pediatric patients with BD. This mood lability is best described by the Kiddie-Mania Rating Scale (K-MRS) developed by Axelson and colleagues as “rapid mood variation with several mood states within a brief period of time which appears internally driven without regard to the circumstance.”1 On K-MRS mood lability items, children with mania typically score:
- Moderate—many mood changes throughout the day, can vary from elevated mood to anger to sadness within a few hours; changes in mood are clearly out of proportion to circumstances and cause impairment in functioning
- Severe—rapid mood swings nearly all of the time, with mood intensity greatly out of proportion to circumstances
- Extreme—constant, explosive variability in mood, several mood changes occurring within minutes, difficult to identify a particular mood, changes in mood radically out of proportion to circumstances.
Patients with BD typically exhibit what is best described as a “mood cycle”—a pronounced shift in mood and energy from 1 extreme to another.2 An example of this would be a child who wakes up with extreme silliness, high energy, and intrusive behavior that persists for several hours and then later in the day becomes sad, depressed, and suicidal with no precipitant for either mood cycle. BD patients also will exhibit other symptoms of mania during these mood cycling periods.
Rapid cycling is a DSM-IV course specifier that indicates ≥4 mood episodes per year in patients with BD with a typical course of mania or hypomania followed by depression, or vice versa.3 The episodes must be demarcated by full or partial remission that lasts ≥2 months or by a switch to a mood state of opposite polarity. In the past, children with frequent mood swings were described incorrectly as “rapid cycling,” but this term has been dropped because it engenders confusion between adult and pediatric BD phenomenology.2
A more precise method of describing mood symptoms in a child or adolescent is to use the FIND criteria, which include:4
- Frequency of symptoms per week
- Intensity of mood symptoms
- Number of mood cycles per day
- Duration of symptoms per day.
Visit this article at CurrentPsychiatry.com to view a table that outlines what to look for when using the FIND criteria to evaluate common pediatric psychiatric disorders that include mood swings. Table 1
describes clinical characteristics and tools and resources used to differentiate these and other disorders.4
Table 1
Clinical characteristics of psychiatric disorders that often feature mood swings
| Disorder | Clinical description | Useful tools/resources |
|---|---|---|
| ADHD | Chronic symptoms of hyperactivity, distractibility, impulsivity, poor attentional skills, disorganization | Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L) |
| ODD | Chronic symptoms of oppositionality, negativity; short, frequent mood swings in response to being asked to do something they do not want to do | CPRS-R:L |
| Anxiety disorders | Excessive ‘worry,’ difficulty with transitions, increased mood swings during stressful periods, psychosomatic symptoms | Self-Report for Childhood Anxiety Related Disorders |
| ARND | History of exposure to alcohol in-utero; mild dysmorphia, attentional, mood, and executive functioning problems | National Organization on Fetal Alcohol Syndrome |
| Bipolar disorder | In children: clustering together of episodes or ‘mini-episodes’ (several days) of increased energy, decreased need for sleep, increased mood cycling, pressured speech, etc. In adolescents: depressive episodes with episodes of hypomania or mania | Mood Disorders Questionnaire Kiddie Schedule for Affective Disorders and Schizophrenia Mania Rating Scale |
| ADHD: attention-deficit/hyperactivity disorder; ARND: alcohol-related neurodevelopmental disorder; ODD: oppositional defiant disorder | ||
| Source: Reference 4 | ||
Mood swings: A chart review
We recently completed a retrospective chart review of 100 patients consecutively referred to our pediatric mood disorders clinic for evaluation of “mood swings, rule out BD.” These patients were self-referred, referred by a psychiatrist for a second opinion, or referred by their primary care physician. The mean age of these patients was 8±2.8 years and 68% were male.
Two experienced clinicians (RAK and EM) interviewed each patient and their caregivers and reviewed results of the Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L)5 and other outside information.
Figure 1 illustrates these patients’ diagnoses. Diagnoses for each of these disorders were made using DSM-IV-TR criteria.3
The most common diagnoses among patients with the chief complaint of mood swings were ADHD (39%); ODD with ADHD (15%); an anxiety disorder, usually generalized anxiety disorder (GAD) (15%); BD (12%); and a secondary mood disorder, usually fetal alcohol spectrum disorder (10%). We were surprised at how often ADHD, ODD, and anxiety disorders were found to be responsible for these patients’ mood swings and how frequently the referring clinician did not recognize these disorders. In the following sections, we discuss each of these disorders and how they differ from BD.
Figure 1 Underlying diagnoses of 100 children/adolescents referred for ‘mood swings’
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder; MDD: major depressive disorder; ODD: oppositional defiant disorder; PDD: pervasive developmental disorder
ADHD and ODD
In our sample, patients with undiagnosed ADHD made up the largest group of those with frequent mood swings. ADHD inattentive type was missed frequently in adolescent girls who still had behavioral aspects of ADHD, including impulsivity and aggression.6
The CPRS-R:L is useful for screening and diagnosing children and adolescents with ADHD and ODD. It contains 80 items, can be used in males and females and patients age 3 to 17, and has validated norms by age and sex.5 It takes parents approximately 10 minutes to fill out this questionnaire and the results can be scored by hand. The CPRS-R:L includes the following scales: oppositional; cognitive problems/inattention; hyperactivity; anxious-shy; perfectionism; social problems; psychosomatic; Connors’ global index; DSM-IV symptom subscales; and an ADHD index. Patients with mood swings and ADHD combined typically score >2 standard deviations above their age/sex mean on the CPRS-R:L hyperactivity scale, Connors’ Global Index, and ADHD index.5
A common childhood disorder, ODD has multiple etiologies.7 The first DSM-IV criteria for ODD is “often loses temper”3—essentially mood swings that often are expressed behaviorally as anger and at times as aggressive outbursts.
Dodge and Cole8 categorized aggression as reactive (impulsivity with a high affective valence) or proactive (characterized by low arousal and premeditation, ie, predatory conduct disorder). Reactive aggression typically is an angry defensive response to frustration, threat, or provocation, whereas proactive aggression is deliberate, coercive behavior often used to obtain a goal.9 Reactive aggression is common among children with ADHD and ODD and typically begins as a mood swing that escalates into reactive aggressive behavior. In a study of 268 consecutively referred children and adolescents with ADHD and 100 community controls, Connor et al10 found significantly more reactive than proactive forms of aggression in ADHD patients.
It can be difficult to differentiate the moods swings and symptoms of ODD from those of pediatric BD. Mick et al11 found that severe irritability may be a diagnostic indicator of BD in children with ADHD. Using the Kiddie Schedule for Affective Disorders and Schizophrenia (epidemiologic version) structured diagnostic interview,12 they evaluated 274 children (mean age 10.8±3.2) with ADHD; 37% had no comorbid mood disorder, 36% had ADHD with depression, and 11% had ADHD with BD. Researchers characterized 3 types of irritability in these patients:
- ODD-type irritability characterized by a low frustration tolerance that is seen in ODD
- Mad/cranky irritability found in depressive disorders
- Super-angry/grouchy/cranky irritability with frequent, prolonged, and largely unprovoked anger episodes and characteristics of mania.
ODD-type irritability was common among all ADHD patients, was the least impairing type of irritability, and did not increase the risk of a mood disorder. Mad/cranky irritability was common only in children with ADHD and a mood disorder (depression or BD), was more impairing than ODD-type irritability, and was most predictive of unipolar depression. Super-angry/grouchy/cranky irritability was common only among children with ADHD and BD (77%), was the most impairing, and was predictive of both unipolar depression and BD. The type of irritability and clustering of DSM-IV manic symptoms best differentiated ADHD subjects from those with ADHD and BD. Figure 2 illustrates symptoms that differentiated patients with ADHD from those with ADHD and comorbid BD.11
A review of pharmacotherapy for aggression in children found the largest effects for methylphenidate for aggression in ADHD (mean effect size=0.9, combined N=844).13 Our clinical experience has been that pediatric patients with ADHD or ODD with ADHD often have high levels of reactive aggression that presents as mood swings, and aggressively treating ADHD often results in improved mood and other ADHD symptoms.
Figure 2 Symptoms that differentiate BD from BD with comorbid ADHD
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder
Source: Reference 11
Anxiety disorders
The estimated prevalence of child and adolescent anxiety disorders is 10% to 20%14; in our sample the prevalence was 15%. These disorders include GAD, separation anxiety disorder, social phobias, posttraumatic stress disorder (PTSD), and obsessive-compulsive disorder. Often, children with GAD worry excessively and become upset during transitions when things don’t proceed as they expect, with resultant angry outbursts and mood swings. Mood swings and difficulty sleeping are common in children with anxiety disorders or BD. Anxiety disorders often will be missed unless specific triggers of the mood swings or angry outbursts—as well as differentiating symptoms such as excessive fear, worry, and psychosomatic symptoms—are assessed.
In our clinical experience, simply asking a child if he or she is anxious is not sufficient to uncover an anxiety disorder. Although the CPRS-L:R will screen for anxiety disorders, we have found that the Self-Report for Childhood Anxiety Related Disorders (SCARED) developed by Birmaher et al15 is more specific. This tool can be used in patients age ≥8. The parent and child versions of the SCARED contain 41 items that measure 5 factors:
- general anxiety
- separation anxiety
- social phobia
- school phobia
- physical symptoms of anxiety.
The SCARED takes 5 minutes to fill out and is available in parent and child versions.
Secondary mood disorders
Many patients in our sample had a mood disorder secondary to the neurologic effects of alcohol on the developing brain. For more about maternal alcohol use, fetal alcohol spectrum disorders, and mood swings, visit this article at CurrentPsychiatry.com.
What BD looks like in children
In our sample, 12% of patients referred for mood swings were diagnosed with bipolar I disorder (BDI), bipolar II disorder (BDII), or bipolar disorder, not otherwise specified (BD-NOS). In the United States, lifetime prevalence of BDI and BDII in adolescents age 13 to 17 is 2.9%.16 No large epidemiologic studies have looked at the lifetime prevalence of BD in children age <13.
How often a clinician sees BD in children and adolescents largely depends on the type of setting in which he or she practices. Although in the general population BD is relatively rare compared with other childhood psychiatric disorders, on child/adolescent inpatient units it is common to find that 30% to 40% of patients have BD.17
The best longitudinal study to date of the phenomenology, comorbidity, and outcome of BD in children and adolescents is the National Institute of Mental Health-funded Course and Outcome of Bipolar Youth study (COBY).18 In this ongoing, longitudinal study, 413 youths (age 7 to 17) with BDI (N=244), BDII (N=28), or BD-NOS (N=141) were rigorously diagnosed using state-of-the-art measures, including the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present version19 and re-evaluated every 9.4 months for 4 years. When organizing this study, investigators found that DSM-IV criteria for BD-NOS were too vague to be useful and developed their own criteria (Table 2).18
For BDI patients in the COBY study, the mean age of onset for bipolar symptoms was 9.0±4.1 years and the mean duration of illness was 4.4±3.1 years. Researchers reported that at the 4-year assessment approximately 70% of patients with BD recovered from their index episode, and 50% had at least 1 syndromal recurrence, particularly depressive episodes.20 Analyses of these patients’ weekly mood symptoms showed that they had syndromal or subsyndromal symptoms with numerous changes in symptoms and shifts of mood polarity 60% of the time, and psychosis 3% of the time. During this study, 20% of BDII patients progressed to BDI, and 25% of BD-NOS patients converted to BDI or BDII.
Further analysis of the COBY data revealed that onset of mood symptoms preceded onset of clear bipolar episodes by an average of 1.0±1.7 years. Depression was the most common initial and most frequent episode for adolescents; mood lability was seen more often in childhood-onset and adolescents with early-onset BD. Depressed children had more severe irritability than depressed adolescents, and older age was associated with more severe and typical mood symptomatology.21
The clinical picture of a child with BD that emerges from the COBY study is:
- a fairly young child with the onset of mood symptoms between age 5 to 12
- subsyndromal and less frequently clear syndromal episodes
- primarily mixed and depressed symptoms with rapid mood cycles during these episodes.22
It is clear that there is a spectrum of bipolar disorders in children and adolescents with varying degrees of symptom expression and children differ from adolescents and adults in their initial presentation of BD.
Table 2
COBY criteria for bipolar disorder, not otherwise specified
| Presence of clinically relevant bipolar symptoms that do not fulfill DSM-IV criteria for BDI or BDII |
| In addition, patients are required to have elevated mood plus 2 associated DSM-IV symptoms or irritable mood plus 3 DSM-IV associated symptoms, along with a change in level of functioning |
| Duration of a minimum of 4 hours within a 24-hour period |
| At least 4 cumulative lifetime days meeting the criteria |
| BDI: bipolar I disorder; BDII: bipolar II disorder; COBY: Course and Outcome of Bipolar Youth study |
| Source: Reference 18 |
Related Resources
- Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Goodwin FK, Jamison KR. Manic-depressive illness. 2nd ed. Oxford, United Kingdom: Oxford University Press; 2007.
- Miklowitz DJ, Cicchetti D, eds. Understanding bipolar disorder: a developmental perspective. New York, NY: Guilford Press; 2010.
Drug Brand Name
- Methylphenidate • Ritalin, Concerta, others
Disclosures
Dr. Kowatch receives grant/research support from the National Institute of Child Health and Human Development and the National Institute of Mental Health and is a consultant to AstraZeneca, Forest Pharmaceuticals, Merck, and the REACH Foundation.
Dr. Delgado and Ms. Monroe report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table
FIND criteria of disorders found to cause mood swings
| Criteria | BDI | BP-NOS | ODD | GAD | ARND |
|---|---|---|---|---|---|
| Frequency of symptoms/week | 7 days (more days than not in an average week) | 2 to 3 days/week | Daily (chronic) irritability and mood swings precipitated by ‘not getting their way’ | Greatest during times of change/stress | Daily |
| Intensity of symptoms | Severe—parents often are afraid to take the child out in public because of mood symptoms | Moderate | Mild/moderate | Mild/moderate when stressed | Mild/moderate |
| Number of mood cycles/day | Daily cycles of euphoria and depression | 3 to 4 | 5 to 10 | 2 to 3 | 8 to 10 |
| Duration of symptoms/day | Euphoria: 30 to 60 minutes Depression: 30 minutes to 6 hours | 4 hours total/day of mood symptoms | Short; 5 to 10 minutes | Short; 5 to 10 minutes | Short; 5 to 10 minutes |
| ARND: alcohol-related neurodevelopmental disorder; BDI: bipolar I disorder; BD-NOS: bipolar disorder, not otherwise specified; GAD: generalized anxiety disorder; ODD: oppositional defiant disorder | |||||
| Source: Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008 | |||||
Even small amounts of alcohol use by a pregnant woman can impact her child’s development. In a controlled study examining drinking behavior of 12,678 pregnant women and the effect this had on their children, Sayel et ala found that <1 drink per week during the first trimester was clinically significant for mental health problems in girls, measured at age 4 and 8, when using parent or teacher report.
Fetal alcohol spectrum disorder describes the range of effects that can occur in an individual whose mother drank alcohol during pregnancy. These disorders include fetal alcohol syndrome (FAS), alcohol-related neurodevelopmental disorder (ARND), and alcohol-related birth defects (ARBD).
FAS. Individuals with FAS have a distinct pattern of facial abnormalities, growth deficiency, and evidence of CNS dysfunction. Characteristic facial abnormalities may include a smooth philtrum, thin upper lip, upturned nose, flat nasal bridge and midface, epicanthal folds, small palpebral fissures, and small head circumference. Growth deficiency begins in-utero and continues throughout childhood and into adulthood. CNS abnormalities can include impaired brain growth or abnormal structure, manifested differently depending on age.
ARND. Many individuals affected by alcohol exposure before birth do not have the characteristic facial abnormalities and growth retardation identified with full FAS, yet have significant brain and behavioral impairments. Individuals with ARND have either the facial anomalies, growth retardation, and other physical abnormalities, or a complex pattern of behavioral or cognitive abnormalities inconsistent with developmental level and unexplained by genetic background or environmental conditions (ie, poor impulse control, language deficits, problems with abstraction, mathematical and social perception deficits, learning problems, and impairment in attention, memory, or judgment).b
ARBD. Persons with ARBD have malformations of the skeletal and major organ systems, such as cardiac or renal abnormalities.
Comorbid psychiatric conditions in children with prenatal alcohol exposure are 5 to 16 times more prevalent than in the general population; these children are 38% more likely to have an anger disorder.c O’Connor and Paleyd found that “…mood disorder symptoms were significantly higher for children with parental alcohol exposure compared to children without exposure.” Children with ARND are treated symptomatically depending upon which deficits and behaviors they exhibit.e
References
a. Sayal K, Heron J, Golding J, et al. Binge pattern of alcohol consumption during pregnancy and childhood mental health outcomes: longitudinal population-based study. Pediatrics. 2009;123(2):e289-296.
b. Warren KR, Foudin LL. Alcohol-related birth defects—the past, present, and future. Alcohol Res Health. 2001;25(3):153-158.
c. Burd L, Klug MG, Martsolf JT, et al. Fetal alcohol syndrome: neuropsychiatric phenomics. Neurotoxicol Teratol. 2003;25(6):697-705.
d. O’Connor MJ, Paley B. Psychiatric conditions associated with prenatal alcohol exposure. Dev Disabil Res Rev. 2009;15(3):225-234.
e. Paley B, O’Connor MJ. Intervention for individuals with fetal alcohol spectrum disorders: treatment approaches and case management. Dev Disabil Res Rev. 2009;15(3):258-267.
M, age 13, is referred by her pediatrician with the chief complaint of “severe mood swings, rule out bipolar disorder (BD).” In the past she was treated for attention-deficit/hyperactivity disorder (ADHD) with stimulants with mixed results. M’s parents are concerned about her “flipping out” whenever she is asked to do something she does not want to do. Her mother has a history of depression and anxiety; her father had a “drinking problem.” There is no history of BD in her first- or second-degree relatives. Are M’s rapid mood swings a sign of BD or another disorder?
The differential diagnosis of “mood swings” is important because they are a common presenting symptom of many children and adolescents with mood and behavioral disorders. Mood swings often occur in children and adolescents with ADHD, oppositional defiant disorder (ODD), developmental disorders, depressive disorders, BD, anxiety disorders, and conduct disorders. Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but are not diagnostic as an isolated symptom.
Mood swings in children are common, nonspecific symptoms that more often are a sign of anxiety or behavioral disorders than BD. This article discusses the differential diagnosis of mood swings in children and adolescents and how to best screen and diagnose these patients.
What are ‘mood swings’?
Mood swings is a popular term that is nonspecific and not part of DSM-IV-TR diagnostic criteria for BD. The complaint of “mood swings” may reflect severe mood lability of pediatric patients with BD. This mood lability is best described by the Kiddie-Mania Rating Scale (K-MRS) developed by Axelson and colleagues as “rapid mood variation with several mood states within a brief period of time which appears internally driven without regard to the circumstance.”1 On K-MRS mood lability items, children with mania typically score:
- Moderate—many mood changes throughout the day, can vary from elevated mood to anger to sadness within a few hours; changes in mood are clearly out of proportion to circumstances and cause impairment in functioning
- Severe—rapid mood swings nearly all of the time, with mood intensity greatly out of proportion to circumstances
- Extreme—constant, explosive variability in mood, several mood changes occurring within minutes, difficult to identify a particular mood, changes in mood radically out of proportion to circumstances.
Patients with BD typically exhibit what is best described as a “mood cycle”—a pronounced shift in mood and energy from 1 extreme to another.2 An example of this would be a child who wakes up with extreme silliness, high energy, and intrusive behavior that persists for several hours and then later in the day becomes sad, depressed, and suicidal with no precipitant for either mood cycle. BD patients also will exhibit other symptoms of mania during these mood cycling periods.
Rapid cycling is a DSM-IV course specifier that indicates ≥4 mood episodes per year in patients with BD with a typical course of mania or hypomania followed by depression, or vice versa.3 The episodes must be demarcated by full or partial remission that lasts ≥2 months or by a switch to a mood state of opposite polarity. In the past, children with frequent mood swings were described incorrectly as “rapid cycling,” but this term has been dropped because it engenders confusion between adult and pediatric BD phenomenology.2
A more precise method of describing mood symptoms in a child or adolescent is to use the FIND criteria, which include:4
- Frequency of symptoms per week
- Intensity of mood symptoms
- Number of mood cycles per day
- Duration of symptoms per day.
Visit this article at CurrentPsychiatry.com to view a table that outlines what to look for when using the FIND criteria to evaluate common pediatric psychiatric disorders that include mood swings. Table 1
describes clinical characteristics and tools and resources used to differentiate these and other disorders.4
Table 1
Clinical characteristics of psychiatric disorders that often feature mood swings
| Disorder | Clinical description | Useful tools/resources |
|---|---|---|
| ADHD | Chronic symptoms of hyperactivity, distractibility, impulsivity, poor attentional skills, disorganization | Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L) |
| ODD | Chronic symptoms of oppositionality, negativity; short, frequent mood swings in response to being asked to do something they do not want to do | CPRS-R:L |
| Anxiety disorders | Excessive ‘worry,’ difficulty with transitions, increased mood swings during stressful periods, psychosomatic symptoms | Self-Report for Childhood Anxiety Related Disorders |
| ARND | History of exposure to alcohol in-utero; mild dysmorphia, attentional, mood, and executive functioning problems | National Organization on Fetal Alcohol Syndrome |
| Bipolar disorder | In children: clustering together of episodes or ‘mini-episodes’ (several days) of increased energy, decreased need for sleep, increased mood cycling, pressured speech, etc. In adolescents: depressive episodes with episodes of hypomania or mania | Mood Disorders Questionnaire Kiddie Schedule for Affective Disorders and Schizophrenia Mania Rating Scale |
| ADHD: attention-deficit/hyperactivity disorder; ARND: alcohol-related neurodevelopmental disorder; ODD: oppositional defiant disorder | ||
| Source: Reference 4 | ||
Mood swings: A chart review
We recently completed a retrospective chart review of 100 patients consecutively referred to our pediatric mood disorders clinic for evaluation of “mood swings, rule out BD.” These patients were self-referred, referred by a psychiatrist for a second opinion, or referred by their primary care physician. The mean age of these patients was 8±2.8 years and 68% were male.
Two experienced clinicians (RAK and EM) interviewed each patient and their caregivers and reviewed results of the Conners’ Parent Rating Scale-Revised: Long Form (CPRS-R:L)5 and other outside information.
Figure 1 illustrates these patients’ diagnoses. Diagnoses for each of these disorders were made using DSM-IV-TR criteria.3
The most common diagnoses among patients with the chief complaint of mood swings were ADHD (39%); ODD with ADHD (15%); an anxiety disorder, usually generalized anxiety disorder (GAD) (15%); BD (12%); and a secondary mood disorder, usually fetal alcohol spectrum disorder (10%). We were surprised at how often ADHD, ODD, and anxiety disorders were found to be responsible for these patients’ mood swings and how frequently the referring clinician did not recognize these disorders. In the following sections, we discuss each of these disorders and how they differ from BD.
Figure 1 Underlying diagnoses of 100 children/adolescents referred for ‘mood swings’
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder; MDD: major depressive disorder; ODD: oppositional defiant disorder; PDD: pervasive developmental disorder
ADHD and ODD
In our sample, patients with undiagnosed ADHD made up the largest group of those with frequent mood swings. ADHD inattentive type was missed frequently in adolescent girls who still had behavioral aspects of ADHD, including impulsivity and aggression.6
The CPRS-R:L is useful for screening and diagnosing children and adolescents with ADHD and ODD. It contains 80 items, can be used in males and females and patients age 3 to 17, and has validated norms by age and sex.5 It takes parents approximately 10 minutes to fill out this questionnaire and the results can be scored by hand. The CPRS-R:L includes the following scales: oppositional; cognitive problems/inattention; hyperactivity; anxious-shy; perfectionism; social problems; psychosomatic; Connors’ global index; DSM-IV symptom subscales; and an ADHD index. Patients with mood swings and ADHD combined typically score >2 standard deviations above their age/sex mean on the CPRS-R:L hyperactivity scale, Connors’ Global Index, and ADHD index.5
A common childhood disorder, ODD has multiple etiologies.7 The first DSM-IV criteria for ODD is “often loses temper”3—essentially mood swings that often are expressed behaviorally as anger and at times as aggressive outbursts.
Dodge and Cole8 categorized aggression as reactive (impulsivity with a high affective valence) or proactive (characterized by low arousal and premeditation, ie, predatory conduct disorder). Reactive aggression typically is an angry defensive response to frustration, threat, or provocation, whereas proactive aggression is deliberate, coercive behavior often used to obtain a goal.9 Reactive aggression is common among children with ADHD and ODD and typically begins as a mood swing that escalates into reactive aggressive behavior. In a study of 268 consecutively referred children and adolescents with ADHD and 100 community controls, Connor et al10 found significantly more reactive than proactive forms of aggression in ADHD patients.
It can be difficult to differentiate the moods swings and symptoms of ODD from those of pediatric BD. Mick et al11 found that severe irritability may be a diagnostic indicator of BD in children with ADHD. Using the Kiddie Schedule for Affective Disorders and Schizophrenia (epidemiologic version) structured diagnostic interview,12 they evaluated 274 children (mean age 10.8±3.2) with ADHD; 37% had no comorbid mood disorder, 36% had ADHD with depression, and 11% had ADHD with BD. Researchers characterized 3 types of irritability in these patients:
- ODD-type irritability characterized by a low frustration tolerance that is seen in ODD
- Mad/cranky irritability found in depressive disorders
- Super-angry/grouchy/cranky irritability with frequent, prolonged, and largely unprovoked anger episodes and characteristics of mania.
ODD-type irritability was common among all ADHD patients, was the least impairing type of irritability, and did not increase the risk of a mood disorder. Mad/cranky irritability was common only in children with ADHD and a mood disorder (depression or BD), was more impairing than ODD-type irritability, and was most predictive of unipolar depression. Super-angry/grouchy/cranky irritability was common only among children with ADHD and BD (77%), was the most impairing, and was predictive of both unipolar depression and BD. The type of irritability and clustering of DSM-IV manic symptoms best differentiated ADHD subjects from those with ADHD and BD. Figure 2 illustrates symptoms that differentiated patients with ADHD from those with ADHD and comorbid BD.11
A review of pharmacotherapy for aggression in children found the largest effects for methylphenidate for aggression in ADHD (mean effect size=0.9, combined N=844).13 Our clinical experience has been that pediatric patients with ADHD or ODD with ADHD often have high levels of reactive aggression that presents as mood swings, and aggressively treating ADHD often results in improved mood and other ADHD symptoms.
Figure 2 Symptoms that differentiate BD from BD with comorbid ADHD
ADHD: attention-deficit/hyperactivity disorder; BD: bipolar disorder
Source: Reference 11
Anxiety disorders
The estimated prevalence of child and adolescent anxiety disorders is 10% to 20%14; in our sample the prevalence was 15%. These disorders include GAD, separation anxiety disorder, social phobias, posttraumatic stress disorder (PTSD), and obsessive-compulsive disorder. Often, children with GAD worry excessively and become upset during transitions when things don’t proceed as they expect, with resultant angry outbursts and mood swings. Mood swings and difficulty sleeping are common in children with anxiety disorders or BD. Anxiety disorders often will be missed unless specific triggers of the mood swings or angry outbursts—as well as differentiating symptoms such as excessive fear, worry, and psychosomatic symptoms—are assessed.
In our clinical experience, simply asking a child if he or she is anxious is not sufficient to uncover an anxiety disorder. Although the CPRS-L:R will screen for anxiety disorders, we have found that the Self-Report for Childhood Anxiety Related Disorders (SCARED) developed by Birmaher et al15 is more specific. This tool can be used in patients age ≥8. The parent and child versions of the SCARED contain 41 items that measure 5 factors:
- general anxiety
- separation anxiety
- social phobia
- school phobia
- physical symptoms of anxiety.
The SCARED takes 5 minutes to fill out and is available in parent and child versions.
Secondary mood disorders
Many patients in our sample had a mood disorder secondary to the neurologic effects of alcohol on the developing brain. For more about maternal alcohol use, fetal alcohol spectrum disorders, and mood swings, visit this article at CurrentPsychiatry.com.
What BD looks like in children
In our sample, 12% of patients referred for mood swings were diagnosed with bipolar I disorder (BDI), bipolar II disorder (BDII), or bipolar disorder, not otherwise specified (BD-NOS). In the United States, lifetime prevalence of BDI and BDII in adolescents age 13 to 17 is 2.9%.16 No large epidemiologic studies have looked at the lifetime prevalence of BD in children age <13.
How often a clinician sees BD in children and adolescents largely depends on the type of setting in which he or she practices. Although in the general population BD is relatively rare compared with other childhood psychiatric disorders, on child/adolescent inpatient units it is common to find that 30% to 40% of patients have BD.17
The best longitudinal study to date of the phenomenology, comorbidity, and outcome of BD in children and adolescents is the National Institute of Mental Health-funded Course and Outcome of Bipolar Youth study (COBY).18 In this ongoing, longitudinal study, 413 youths (age 7 to 17) with BDI (N=244), BDII (N=28), or BD-NOS (N=141) were rigorously diagnosed using state-of-the-art measures, including the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present version19 and re-evaluated every 9.4 months for 4 years. When organizing this study, investigators found that DSM-IV criteria for BD-NOS were too vague to be useful and developed their own criteria (Table 2).18
For BDI patients in the COBY study, the mean age of onset for bipolar symptoms was 9.0±4.1 years and the mean duration of illness was 4.4±3.1 years. Researchers reported that at the 4-year assessment approximately 70% of patients with BD recovered from their index episode, and 50% had at least 1 syndromal recurrence, particularly depressive episodes.20 Analyses of these patients’ weekly mood symptoms showed that they had syndromal or subsyndromal symptoms with numerous changes in symptoms and shifts of mood polarity 60% of the time, and psychosis 3% of the time. During this study, 20% of BDII patients progressed to BDI, and 25% of BD-NOS patients converted to BDI or BDII.
Further analysis of the COBY data revealed that onset of mood symptoms preceded onset of clear bipolar episodes by an average of 1.0±1.7 years. Depression was the most common initial and most frequent episode for adolescents; mood lability was seen more often in childhood-onset and adolescents with early-onset BD. Depressed children had more severe irritability than depressed adolescents, and older age was associated with more severe and typical mood symptomatology.21
The clinical picture of a child with BD that emerges from the COBY study is:
- a fairly young child with the onset of mood symptoms between age 5 to 12
- subsyndromal and less frequently clear syndromal episodes
- primarily mixed and depressed symptoms with rapid mood cycles during these episodes.22
It is clear that there is a spectrum of bipolar disorders in children and adolescents with varying degrees of symptom expression and children differ from adolescents and adults in their initial presentation of BD.
Table 2
COBY criteria for bipolar disorder, not otherwise specified
| Presence of clinically relevant bipolar symptoms that do not fulfill DSM-IV criteria for BDI or BDII |
| In addition, patients are required to have elevated mood plus 2 associated DSM-IV symptoms or irritable mood plus 3 DSM-IV associated symptoms, along with a change in level of functioning |
| Duration of a minimum of 4 hours within a 24-hour period |
| At least 4 cumulative lifetime days meeting the criteria |
| BDI: bipolar I disorder; BDII: bipolar II disorder; COBY: Course and Outcome of Bipolar Youth study |
| Source: Reference 18 |
Related Resources
- Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Goodwin FK, Jamison KR. Manic-depressive illness. 2nd ed. Oxford, United Kingdom: Oxford University Press; 2007.
- Miklowitz DJ, Cicchetti D, eds. Understanding bipolar disorder: a developmental perspective. New York, NY: Guilford Press; 2010.
Drug Brand Name
- Methylphenidate • Ritalin, Concerta, others
Disclosures
Dr. Kowatch receives grant/research support from the National Institute of Child Health and Human Development and the National Institute of Mental Health and is a consultant to AstraZeneca, Forest Pharmaceuticals, Merck, and the REACH Foundation.
Dr. Delgado and Ms. Monroe report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Table
FIND criteria of disorders found to cause mood swings
| Criteria | BDI | BP-NOS | ODD | GAD | ARND |
|---|---|---|---|---|---|
| Frequency of symptoms/week | 7 days (more days than not in an average week) | 2 to 3 days/week | Daily (chronic) irritability and mood swings precipitated by ‘not getting their way’ | Greatest during times of change/stress | Daily |
| Intensity of symptoms | Severe—parents often are afraid to take the child out in public because of mood symptoms | Moderate | Mild/moderate | Mild/moderate when stressed | Mild/moderate |
| Number of mood cycles/day | Daily cycles of euphoria and depression | 3 to 4 | 5 to 10 | 2 to 3 | 8 to 10 |
| Duration of symptoms/day | Euphoria: 30 to 60 minutes Depression: 30 minutes to 6 hours | 4 hours total/day of mood symptoms | Short; 5 to 10 minutes | Short; 5 to 10 minutes | Short; 5 to 10 minutes |
| ARND: alcohol-related neurodevelopmental disorder; BDI: bipolar I disorder; BD-NOS: bipolar disorder, not otherwise specified; GAD: generalized anxiety disorder; ODD: oppositional defiant disorder | |||||
| Source: Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008 | |||||
Even small amounts of alcohol use by a pregnant woman can impact her child’s development. In a controlled study examining drinking behavior of 12,678 pregnant women and the effect this had on their children, Sayel et ala found that <1 drink per week during the first trimester was clinically significant for mental health problems in girls, measured at age 4 and 8, when using parent or teacher report.
Fetal alcohol spectrum disorder describes the range of effects that can occur in an individual whose mother drank alcohol during pregnancy. These disorders include fetal alcohol syndrome (FAS), alcohol-related neurodevelopmental disorder (ARND), and alcohol-related birth defects (ARBD).
FAS. Individuals with FAS have a distinct pattern of facial abnormalities, growth deficiency, and evidence of CNS dysfunction. Characteristic facial abnormalities may include a smooth philtrum, thin upper lip, upturned nose, flat nasal bridge and midface, epicanthal folds, small palpebral fissures, and small head circumference. Growth deficiency begins in-utero and continues throughout childhood and into adulthood. CNS abnormalities can include impaired brain growth or abnormal structure, manifested differently depending on age.
ARND. Many individuals affected by alcohol exposure before birth do not have the characteristic facial abnormalities and growth retardation identified with full FAS, yet have significant brain and behavioral impairments. Individuals with ARND have either the facial anomalies, growth retardation, and other physical abnormalities, or a complex pattern of behavioral or cognitive abnormalities inconsistent with developmental level and unexplained by genetic background or environmental conditions (ie, poor impulse control, language deficits, problems with abstraction, mathematical and social perception deficits, learning problems, and impairment in attention, memory, or judgment).b
ARBD. Persons with ARBD have malformations of the skeletal and major organ systems, such as cardiac or renal abnormalities.
Comorbid psychiatric conditions in children with prenatal alcohol exposure are 5 to 16 times more prevalent than in the general population; these children are 38% more likely to have an anger disorder.c O’Connor and Paleyd found that “…mood disorder symptoms were significantly higher for children with parental alcohol exposure compared to children without exposure.” Children with ARND are treated symptomatically depending upon which deficits and behaviors they exhibit.e
References
a. Sayal K, Heron J, Golding J, et al. Binge pattern of alcohol consumption during pregnancy and childhood mental health outcomes: longitudinal population-based study. Pediatrics. 2009;123(2):e289-296.
b. Warren KR, Foudin LL. Alcohol-related birth defects—the past, present, and future. Alcohol Res Health. 2001;25(3):153-158.
c. Burd L, Klug MG, Martsolf JT, et al. Fetal alcohol syndrome: neuropsychiatric phenomics. Neurotoxicol Teratol. 2003;25(6):697-705.
d. O’Connor MJ, Paley B. Psychiatric conditions associated with prenatal alcohol exposure. Dev Disabil Res Rev. 2009;15(3):225-234.
e. Paley B, O’Connor MJ. Intervention for individuals with fetal alcohol spectrum disorders: treatment approaches and case management. Dev Disabil Res Rev. 2009;15(3):258-267.
1. Axelson D, Birmaher BJ, Brent D, et al. A preliminary study of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children mania rating scale for children and adolescents. J Child Adolesc Psychopharmacol. 2003;13(4):463-470.
2. Youngstrom EA, Birmaher B, Findling RL. Pediatric bipolar disorder: validity, phenomenology, and recommendations for diagnosis. Bipolar Disord. 2008;10(1 Pt 2):194-214.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
4. Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008.
5. Conners CK. Conners’ Parent Rating Scale Long Form (CPRS-R:L) North Tonawanda, NY: Multi-Health Systems, Inc.; 1997.
6. Martel MM. Research review: a new perspective on attention-deficit/hyperactivity disorder: emotion dysregulation and trait models. J Child Psychol Psychiatry. 2009;50(9):1042-1051.
7. Steiner H, Remsing L. and the Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(1):126-141.
8. Dodge KA, Cole JD. Social-information-processing factors in reactive and proactive aggression in children’s peer groups. J Pers Soc Psychol. 1987;53(6):1146-1158.
9. Connor DF, Steingard RJ, Cunningham JA, et al. Proactive and reactive aggression in referred children and adolescents. Am J Orthopsychiatry. 2004;74(2):129-136.
10. Connor DF, Chartier KG, Preen EC, et al. Impulsive aggression in attention-deficit/hyperactivity disorder: symptom severity, co-morbidity, and attention-deficit/hyperactivity disorder subtype. J Child Adolesc Psychopharmacol. 2010;20(2):119-126.
11. Mick E, Spencer T, Wozniak J, et al. Heterogeneity of irritability in attention-deficit/hyperactivity disorder subjects with and without mood disorders. Biol Psychiatry. 2005;58(7):576-582.
12. Orvaschel H. Schizophrenia and Affective Disorders Schedule for children—Epidemiological Version (KSADS-E). Fort Lauderdale, FL: Nova Southeastern University; 1995.
13. Pappadopulos E, Woolston S, Chait A, et al. Pharmacotherapy of aggression in children and adolescents: efficacy and effect size. J Can Acad Child Adolesc Psychiatry. 2006;15(1):27-39.
14. Achenbach TM, Howell CT, McConaughy SH, et al. Six-year predictors of problems in a national sample: IV. Young adult signs of disturbance. J Am Acad Child Adolesc Psychiatry. 1998;37(7):718-727.
15. Birmaher B, Khetarpal S, Brent D, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36:545-553.
16. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980-989.
17. Youngstrom EA, Duax J. Evidence-based assessment of pediatric bipolar disorder, part I: base rate and family history. J Am Acad Child Adolesc Psychiatry. 2005;44(7):712-717.
18. Birmaher B, Axelson D, Strober M, et al. Clinical course of children and adolescents with bipolar spectrum disorders. Arch Gen Psychiatry. 2006;63(2):175-183.
19. Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980-988.
20. Birmaher B, Axelson D. Course and outcome of bipolar spectrum disorder in children and adolescents: a review of the existing literature. Dev Psychopathol. 2006;18(4):1023-1035.
21. Birmaher B, Axelson D, Strober M, et al. Comparison of manic and depressive symptoms between children and adolescents with bipolar spectrum disorders. Bipolar Disord. 2009;11(1):52-62.
22. Birmaher B, Axelson D, Goldstein B, et al. Four-year longitudinal course of children and adolescents with bipolar spectrum disorders: the Course and Outcome of Bipolar Youth (COBY) study. Am J Psychiatry. 2009;166(7):795-804.
1. Axelson D, Birmaher BJ, Brent D, et al. A preliminary study of the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children mania rating scale for children and adolescents. J Child Adolesc Psychopharmacol. 2003;13(4):463-470.
2. Youngstrom EA, Birmaher B, Findling RL. Pediatric bipolar disorder: validity, phenomenology, and recommendations for diagnosis. Bipolar Disord. 2008;10(1 Pt 2):194-214.
3. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
4. Kowatch RA, Fristad MA, Findling RL, et al. Clinical manual for the management of bipolar disorder in children and adolescents. Arlington, VA: American Psychiatric Publishing, Inc.; 2008.
5. Conners CK. Conners’ Parent Rating Scale Long Form (CPRS-R:L) North Tonawanda, NY: Multi-Health Systems, Inc.; 1997.
6. Martel MM. Research review: a new perspective on attention-deficit/hyperactivity disorder: emotion dysregulation and trait models. J Child Psychol Psychiatry. 2009;50(9):1042-1051.
7. Steiner H, Remsing L. and the Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(1):126-141.
8. Dodge KA, Cole JD. Social-information-processing factors in reactive and proactive aggression in children’s peer groups. J Pers Soc Psychol. 1987;53(6):1146-1158.
9. Connor DF, Steingard RJ, Cunningham JA, et al. Proactive and reactive aggression in referred children and adolescents. Am J Orthopsychiatry. 2004;74(2):129-136.
10. Connor DF, Chartier KG, Preen EC, et al. Impulsive aggression in attention-deficit/hyperactivity disorder: symptom severity, co-morbidity, and attention-deficit/hyperactivity disorder subtype. J Child Adolesc Psychopharmacol. 2010;20(2):119-126.
11. Mick E, Spencer T, Wozniak J, et al. Heterogeneity of irritability in attention-deficit/hyperactivity disorder subjects with and without mood disorders. Biol Psychiatry. 2005;58(7):576-582.
12. Orvaschel H. Schizophrenia and Affective Disorders Schedule for children—Epidemiological Version (KSADS-E). Fort Lauderdale, FL: Nova Southeastern University; 1995.
13. Pappadopulos E, Woolston S, Chait A, et al. Pharmacotherapy of aggression in children and adolescents: efficacy and effect size. J Can Acad Child Adolesc Psychiatry. 2006;15(1):27-39.
14. Achenbach TM, Howell CT, McConaughy SH, et al. Six-year predictors of problems in a national sample: IV. Young adult signs of disturbance. J Am Acad Child Adolesc Psychiatry. 1998;37(7):718-727.
15. Birmaher B, Khetarpal S, Brent D, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997;36:545-553.
16. Merikangas KR, He JP, Burstein M, et al. Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980-989.
17. Youngstrom EA, Duax J. Evidence-based assessment of pediatric bipolar disorder, part I: base rate and family history. J Am Acad Child Adolesc Psychiatry. 2005;44(7):712-717.
18. Birmaher B, Axelson D, Strober M, et al. Clinical course of children and adolescents with bipolar spectrum disorders. Arch Gen Psychiatry. 2006;63(2):175-183.
19. Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980-988.
20. Birmaher B, Axelson D. Course and outcome of bipolar spectrum disorder in children and adolescents: a review of the existing literature. Dev Psychopathol. 2006;18(4):1023-1035.
21. Birmaher B, Axelson D, Strober M, et al. Comparison of manic and depressive symptoms between children and adolescents with bipolar spectrum disorders. Bipolar Disord. 2009;11(1):52-62.
22. Birmaher B, Axelson D, Goldstein B, et al. Four-year longitudinal course of children and adolescents with bipolar spectrum disorders: the Course and Outcome of Bipolar Youth (COBY) study. Am J Psychiatry. 2009;166(7):795-804.
Psychiatry behind bars: Practicing in jails and prisons
Discuss this article at http://currentpsychiatry.blogspot.com/2011/02/psychiatry-behind-bars-practicing-in.html#comments
Over the last 2 decades mandatory prison sentences, longer prison terms, and more restrictive release policies have lead to a dramatic increase in the number of persons in jails and prisons. Currently, more than 2 million individuals are incarcerated in the United States.1 Psychiatric illness is over-represented in correctional populations compared with the general population—more than half of all inmates have a mental health diagnosis.2 Correctional facilities are legally obligated to address the medical and mental health needs of the persons committed to them. As a result, more psychiatrists are practicing in jails and prisons.
This article explains correctional facilities’ obligation to provide for inmates’ mental health needs and describes correctional mental health processes and how psychiatrists can play a role in screening, evaluation, and suicide prevention.
Lack of training
Despite the increasing number of psychiatrists working in correctional institutions, most have had little or no training, education, or even orientation to these settings. Forensic psychiatry fellowship requirements include experience in treating acutely and chronically ill patients in correctional systems.3 Although general psychiatric training doesn’t preclude correctional experience, it is not required. The forensic component of general psychiatric residency is limited to evaluation of forensic issues, report writing, and testimony.
Professional organizations—including the American Psychiatric Association,4 the American Public Health Association,5 the National Commission on Correctional Health Care,6 and the American Correctional Health Services Association7—have developed standards and position statements on providing medical and mental health care in correctional facilities. Although psychiatrists’ work in correctional settings generally has been reserved for consultation and medication management, it is important for these clinicians to understand and appreciate the wider landscape and environment in which they practice. Psychiatrists can help develop and implement mental health processes that lead to better services and improved clinical outcomes.
Right to treatment
Convicted persons have a constitutional right to medical and mental health treatment under extension of the Eighth Amendment of the U.S. Constitution, which prohibits cruel and unusual punishment.8 In 1976, the U.S. Supreme Court concluded that “deliberate indifference to serious medical needs of prisoners constitutes the ‘unnecessary and wanton infliction of pain’… proscribed by the Eighth Amendment.”9 This coverage was expanded to mental health needs when the court found “…no underlying distinction between the right to medical care for physical ills and its psychological or psychiatric counterpart.”10 Correctional facilities also are obligated to provide medical and mental health treatment for persons in custody who are not yet convicted of an offense.8 In subsequent litigation, the court formulated 6 components of a minimally adequate correctional mental health treatment program; these are described in Table 1.11
Table 1
Components of minimally adequate mental health system in correctional facilities
| A systematic screening and evaluation program to identify inmates requiring mental health treatment |
| Treatment that encompasses more than simply segregating the mentally ill inmate and increasing correctional supervision |
| Treatment by trained mental health professionals in sufficient numbers to identify and treat inmates suffering from serious mental disorders |
| Maintenance of accurate, complete, and confidential records of the mental health treatment process |
| A suicide prevention program |
| Appropriate use of psychotropic medication (prescription and monitoring by appropriately trained and licensed staff to treat bona fide mental disorders rather than solely as a means of behavioral management) |
| Source: Reference 11 |
Jails vs prisons
The type of psychiatric treatment provided differs based on whether the facility is a jail or a prison, how long inmates are confined, and whether the facility serves a special mission or population, such as serving as a reception center for a prison system or housing only juveniles. Jails generally house inmates for short periods—often <1 year—experience rapid population turnover, and receive admissions day and night. Jails vary in size from a few holding cells to several thousand beds. These factors have implications for screening and evaluation processes, suicide prevention, and coordination of care with community treatment providers. In jails, clinicians’ work focuses on rapid identification of psychiatric illness, assessment, stabilization, and re-linkage to treatment providers in the community. Access to inpatient and ongoing psychiatric care also should be available.
In contrast, prisons house people who have been convicted and sentenced to serve time, generally for >1 year. Turnover is less rapid, admissions and discharges are more predictable, and there is greater opportunity and obligation to develop a continuum of mental health care. Prison systems generally provide or make arrangements for crisis intervention, residential treatment services, and inpatient and outpatient psychiatric care. These services may be provided on the prison grounds, or the inmate may be transferred to another prison within the system that offers specialized treatment or to a community hospital, where the inmate is under the constant supervision of corrections officers. Residential treatment includes intensive, coordinated, and structured mental health services and consists of group and individual therapies, psychoeducation, and therapeutic activities; these services are analogous to intensive day treatment or partial hospitalization programs in the community. In prisons mental health care emphasizes ongoing treatment. As in the community, treatment teams in correctional settings often include mental health professionals such as psychiatric nurses, psychotherapists, and psychology staff in addition to psychiatrists.
Screening and evaluation
Correctional facilities need a systematic screening process that is conducted on all inmates. This preliminary entry or “receiving screening” is intended to identify urgent medical and mental health concerns and persons in need of immediate treatment. A nurse or corrections staff officer who has been trained by medical staff could conduct this screening. Screening consists of observing the inmate’s current condition and conducting a structured inquiry into medical and psychiatric symptoms, psychotropic medications, drug and alcohol use history, and suicide risk. A positive screen leads to immediate action such as instituting drug or alcohol detoxification or initiating suicide precautions or an emergency medical referral and assessment.4,6
Within a few days of an inmate’s arrival, a mental health professional should conduct a more detailed mental health screening to identify non-emergent psychiatric needs. The mental health screening includes:
- a review of accompanying mental health information received from the county jail or arresting/transporting officer
- a self-reported history of psychiatric treatment, such as hospitalization, pharmacotherapy, or outpatient counseling
- current or prior suicidal thoughts or attempts
- intellectual functioning
- history of violence and/or victimization
- a brief mental status examination.4
Records from previous incarcerations should be reviewed. Also, if relevant, obtain the inmate’s consent to collect outside treatment records and/or speak with family or significant others. The results of this brief mental health assessment could prompt a referral for further evaluation and determine the need for psychotropic therapy.
Although usually not directly involved in this systematic screening and evaluation, psychiatrists should be familiar with how and why referrals are made to be sure that they are appropriate and to reduce unnecessary evaluations, leaving more time for medication follow-up, treatment planning, and suicide risk assessment. An efficient and effective mental health screening and assessment process helps ensure that limited psychiatric resources are used to maximal benefit.
Suicide prevention
Suicide prevention programs often include teaching corrections staff to identify suicide risk factors and instructing them to screen at-risk inmates at any time during incarceration. These programs should implement steps to keep inmates safe, such as increasing intensity and frequency of monitoring by corrections staff, removing or limiting access to items that could be used to harm oneself, and moving inmates to a housing area where the means and opportunity for self harm are reduced.4,6 Suicide prevention programs also should include delivery of appropriate mental health interventions to improve the inmate’s clinical condition, resolve the crisis, or otherwise lower suicide risk. These interventions include:
- increased frequency of interaction with mental health staff (more than a brief daily interaction conducted at the cell front)
- treatment of drug and/or alcohol withdrawal
- referral for evaluation and assessment of the need for psychotropic medication or dosage adjustment (Table 2).6
A correctional facility’s policy should allow a low threshold for corrections staff to initiate a suicide prevention watch—it is better to err on the side of caution and institute a watch than to expect non-mental health professionals to conduct clinical risk level assessments. Full assessment of an inmate’s clinical condition and the decision to reduce or discontinue the watch should be left to a trained mental health professional. This function may fall within the psychiatrist’s duties and it is important to be aware of the ramifications of watch discontinuation, such as:
- what type of property is returned
- where the inmate will be housed
- how often the inmate will be monitored by custody staff
- when the next mental health follow-up will occur.
Failure to articulate your expectations to staff members can lead to catastrophic consequences if watches are discontinued without an appropriate plan for monitoring and follow-up.
Psychiatrists can help train corrections staff on signs of suicide risk and also should review suicide attempts and/or completed suicides. This often can be a challenge because a psychiatrist’s time at a facility may be limited, but is an important consideration for quality improvement efforts.
Table 2
Components of a correctional suicide prevention program
| Training for staff on verbal and behavior cues indicating suicide risk and appropriate response |
| Identification of potentially suicidal inmates |
| Referral to mental health providers or facilities |
| Evaluation by qualified mental health professional |
| Housing in safe area of the institution |
| Treatment to address the cause of or reasons for suicidal thoughts |
| Monitoring procedures that permit regular, documented supervision |
| Communication procedures between health care and corrections personnel |
| Intervention procedures addressing how to handle a suicide attempt in progress |
| Notification procedures to ensure appropriate correctional authorities, outside authorities, and family are contacted |
| Reporting procedures for documenting attempted or completed suicides |
| Review of suicides and serious attempts by health care and administrative staff |
| Critical incident debriefing offered to affected personnel and inmates in event of completed suicide |
| Source: Reference 6 |
Pharmacotherapy
Traditionally, the primary role of psychiatrists working in correctional facilities has been psychotropic medication management. Understanding the correctional context and procedures permits more informed prescription choices and recommendations for psychotropics to be included in the formulary.
Antipsychotics, antidepressants, and mood stabilizers should be included in a facility’s formulary. Considerations concerning types of psychotropic medication within a formulary depend on the facility’s size and mission, psychiatric illnesses encountered in the population, and lengths of inmates’ stay.12 A mechanism should be in place to prescribe off-formulary and access other types of psychotropic medication on a case-by-case basis to ensure inmates are not denied appropriate treatment. A psychiatrist may have to advocate strongly for these principles.
Most correctional facilities require that staff administer every dose of psychotropic medication directly to the inmate for whom it is prescribed. In some facilities, only nursing personnel can administer medication, while others use trained corrections staff to deliver medication. Psychiatrists who prescribe psychotropics in correctional institutions must be familiar with the facility’s medication administration procedures, which may impact medication choice and form, dosing frequency, timing of laboratory studies, and inmate medication compliance. Prescribers’ capacity to order emergency or “as needed” medications may be limited or nonexistent if nursing staff is unavailable.
Appropriate use of psychotropic medication for treating psychiatric illness is the standard of care, but is only 1 component of an effective treatment plan for inmates with serious mental illness. Others include group and individual therapy, psychoeducation, and therapeutic activities such as recreational therapy, activity therapy, and opportunities for education and work within the correctional system.
Related Resources
- Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Thienhaus OJ, Piasecki M, eds. Correctional psychiatry practice guidelines and strategies. Kingston, NJ: Civic Research Institute, Inc.; 2007.
- National Commission on Correctional Healthcare. www.ncchc.org.
- Society of Correctional Physicians. www.CorrDocs.org.
Disclosure
Dr. Burns reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Glaze LE. Correctional populations in the United States, 2009. Washington, DC: Bureau of Justice Statistics. December 2010. NCJ 231681.
2. James DJ, Glaze LE. Mental health problems of prison and jail inmates. Washington, DC: Bureau of Justice Statistics. September 2006. NCJ 213600.
3. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in forensic psychiatry. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/406pr703_u105.pdf. Accessed December 30, 2010.
4. American Psychiatric Association. Psychiatric services in jails and prisons. 2nd ed. Washington, DC: American Psychiatric Association; 2000.
5. Standards for health services in correctional institutions. 3rd ed. Washington, DC: American Public Health Association; 2003.
6. National Commission on Correctional Health Care. Standards for mental health services in correctional facilities. Chicago, IL: National Commission on Correctional Health Care; 2008.
7. American Correctional Health Services Association. Position statement on forced and involuntary psychotropic medication. Available at: http://www.achsa.org/displaycommon.cfm?an=12. Accessed December 30, 2010.
8. Cohen F. Overview of legal issues. In: Cohen F. The mentally disordered inmate and the law. Kingston, NJ: Civic Research Institute, Inc.; 1998:2-1-2-20.
9. Estelle v Gamble. 429 U.S. 97 (1976).
10. Bowring v Godwin. 551 F2d 44, 47 (4th Cir 1977).
11. Ruiz v Estelle. 503 F Supp 1265 (SD Tex 1980).
12. Burns K. Pharmacotherapy in correctional settings. In: Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010:321-344.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/02/psychiatry-behind-bars-practicing-in.html#comments
Over the last 2 decades mandatory prison sentences, longer prison terms, and more restrictive release policies have lead to a dramatic increase in the number of persons in jails and prisons. Currently, more than 2 million individuals are incarcerated in the United States.1 Psychiatric illness is over-represented in correctional populations compared with the general population—more than half of all inmates have a mental health diagnosis.2 Correctional facilities are legally obligated to address the medical and mental health needs of the persons committed to them. As a result, more psychiatrists are practicing in jails and prisons.
This article explains correctional facilities’ obligation to provide for inmates’ mental health needs and describes correctional mental health processes and how psychiatrists can play a role in screening, evaluation, and suicide prevention.
Lack of training
Despite the increasing number of psychiatrists working in correctional institutions, most have had little or no training, education, or even orientation to these settings. Forensic psychiatry fellowship requirements include experience in treating acutely and chronically ill patients in correctional systems.3 Although general psychiatric training doesn’t preclude correctional experience, it is not required. The forensic component of general psychiatric residency is limited to evaluation of forensic issues, report writing, and testimony.
Professional organizations—including the American Psychiatric Association,4 the American Public Health Association,5 the National Commission on Correctional Health Care,6 and the American Correctional Health Services Association7—have developed standards and position statements on providing medical and mental health care in correctional facilities. Although psychiatrists’ work in correctional settings generally has been reserved for consultation and medication management, it is important for these clinicians to understand and appreciate the wider landscape and environment in which they practice. Psychiatrists can help develop and implement mental health processes that lead to better services and improved clinical outcomes.
Right to treatment
Convicted persons have a constitutional right to medical and mental health treatment under extension of the Eighth Amendment of the U.S. Constitution, which prohibits cruel and unusual punishment.8 In 1976, the U.S. Supreme Court concluded that “deliberate indifference to serious medical needs of prisoners constitutes the ‘unnecessary and wanton infliction of pain’… proscribed by the Eighth Amendment.”9 This coverage was expanded to mental health needs when the court found “…no underlying distinction between the right to medical care for physical ills and its psychological or psychiatric counterpart.”10 Correctional facilities also are obligated to provide medical and mental health treatment for persons in custody who are not yet convicted of an offense.8 In subsequent litigation, the court formulated 6 components of a minimally adequate correctional mental health treatment program; these are described in Table 1.11
Table 1
Components of minimally adequate mental health system in correctional facilities
| A systematic screening and evaluation program to identify inmates requiring mental health treatment |
| Treatment that encompasses more than simply segregating the mentally ill inmate and increasing correctional supervision |
| Treatment by trained mental health professionals in sufficient numbers to identify and treat inmates suffering from serious mental disorders |
| Maintenance of accurate, complete, and confidential records of the mental health treatment process |
| A suicide prevention program |
| Appropriate use of psychotropic medication (prescription and monitoring by appropriately trained and licensed staff to treat bona fide mental disorders rather than solely as a means of behavioral management) |
| Source: Reference 11 |
Jails vs prisons
The type of psychiatric treatment provided differs based on whether the facility is a jail or a prison, how long inmates are confined, and whether the facility serves a special mission or population, such as serving as a reception center for a prison system or housing only juveniles. Jails generally house inmates for short periods—often <1 year—experience rapid population turnover, and receive admissions day and night. Jails vary in size from a few holding cells to several thousand beds. These factors have implications for screening and evaluation processes, suicide prevention, and coordination of care with community treatment providers. In jails, clinicians’ work focuses on rapid identification of psychiatric illness, assessment, stabilization, and re-linkage to treatment providers in the community. Access to inpatient and ongoing psychiatric care also should be available.
In contrast, prisons house people who have been convicted and sentenced to serve time, generally for >1 year. Turnover is less rapid, admissions and discharges are more predictable, and there is greater opportunity and obligation to develop a continuum of mental health care. Prison systems generally provide or make arrangements for crisis intervention, residential treatment services, and inpatient and outpatient psychiatric care. These services may be provided on the prison grounds, or the inmate may be transferred to another prison within the system that offers specialized treatment or to a community hospital, where the inmate is under the constant supervision of corrections officers. Residential treatment includes intensive, coordinated, and structured mental health services and consists of group and individual therapies, psychoeducation, and therapeutic activities; these services are analogous to intensive day treatment or partial hospitalization programs in the community. In prisons mental health care emphasizes ongoing treatment. As in the community, treatment teams in correctional settings often include mental health professionals such as psychiatric nurses, psychotherapists, and psychology staff in addition to psychiatrists.
Screening and evaluation
Correctional facilities need a systematic screening process that is conducted on all inmates. This preliminary entry or “receiving screening” is intended to identify urgent medical and mental health concerns and persons in need of immediate treatment. A nurse or corrections staff officer who has been trained by medical staff could conduct this screening. Screening consists of observing the inmate’s current condition and conducting a structured inquiry into medical and psychiatric symptoms, psychotropic medications, drug and alcohol use history, and suicide risk. A positive screen leads to immediate action such as instituting drug or alcohol detoxification or initiating suicide precautions or an emergency medical referral and assessment.4,6
Within a few days of an inmate’s arrival, a mental health professional should conduct a more detailed mental health screening to identify non-emergent psychiatric needs. The mental health screening includes:
- a review of accompanying mental health information received from the county jail or arresting/transporting officer
- a self-reported history of psychiatric treatment, such as hospitalization, pharmacotherapy, or outpatient counseling
- current or prior suicidal thoughts or attempts
- intellectual functioning
- history of violence and/or victimization
- a brief mental status examination.4
Records from previous incarcerations should be reviewed. Also, if relevant, obtain the inmate’s consent to collect outside treatment records and/or speak with family or significant others. The results of this brief mental health assessment could prompt a referral for further evaluation and determine the need for psychotropic therapy.
Although usually not directly involved in this systematic screening and evaluation, psychiatrists should be familiar with how and why referrals are made to be sure that they are appropriate and to reduce unnecessary evaluations, leaving more time for medication follow-up, treatment planning, and suicide risk assessment. An efficient and effective mental health screening and assessment process helps ensure that limited psychiatric resources are used to maximal benefit.
Suicide prevention
Suicide prevention programs often include teaching corrections staff to identify suicide risk factors and instructing them to screen at-risk inmates at any time during incarceration. These programs should implement steps to keep inmates safe, such as increasing intensity and frequency of monitoring by corrections staff, removing or limiting access to items that could be used to harm oneself, and moving inmates to a housing area where the means and opportunity for self harm are reduced.4,6 Suicide prevention programs also should include delivery of appropriate mental health interventions to improve the inmate’s clinical condition, resolve the crisis, or otherwise lower suicide risk. These interventions include:
- increased frequency of interaction with mental health staff (more than a brief daily interaction conducted at the cell front)
- treatment of drug and/or alcohol withdrawal
- referral for evaluation and assessment of the need for psychotropic medication or dosage adjustment (Table 2).6
A correctional facility’s policy should allow a low threshold for corrections staff to initiate a suicide prevention watch—it is better to err on the side of caution and institute a watch than to expect non-mental health professionals to conduct clinical risk level assessments. Full assessment of an inmate’s clinical condition and the decision to reduce or discontinue the watch should be left to a trained mental health professional. This function may fall within the psychiatrist’s duties and it is important to be aware of the ramifications of watch discontinuation, such as:
- what type of property is returned
- where the inmate will be housed
- how often the inmate will be monitored by custody staff
- when the next mental health follow-up will occur.
Failure to articulate your expectations to staff members can lead to catastrophic consequences if watches are discontinued without an appropriate plan for monitoring and follow-up.
Psychiatrists can help train corrections staff on signs of suicide risk and also should review suicide attempts and/or completed suicides. This often can be a challenge because a psychiatrist’s time at a facility may be limited, but is an important consideration for quality improvement efforts.
Table 2
Components of a correctional suicide prevention program
| Training for staff on verbal and behavior cues indicating suicide risk and appropriate response |
| Identification of potentially suicidal inmates |
| Referral to mental health providers or facilities |
| Evaluation by qualified mental health professional |
| Housing in safe area of the institution |
| Treatment to address the cause of or reasons for suicidal thoughts |
| Monitoring procedures that permit regular, documented supervision |
| Communication procedures between health care and corrections personnel |
| Intervention procedures addressing how to handle a suicide attempt in progress |
| Notification procedures to ensure appropriate correctional authorities, outside authorities, and family are contacted |
| Reporting procedures for documenting attempted or completed suicides |
| Review of suicides and serious attempts by health care and administrative staff |
| Critical incident debriefing offered to affected personnel and inmates in event of completed suicide |
| Source: Reference 6 |
Pharmacotherapy
Traditionally, the primary role of psychiatrists working in correctional facilities has been psychotropic medication management. Understanding the correctional context and procedures permits more informed prescription choices and recommendations for psychotropics to be included in the formulary.
Antipsychotics, antidepressants, and mood stabilizers should be included in a facility’s formulary. Considerations concerning types of psychotropic medication within a formulary depend on the facility’s size and mission, psychiatric illnesses encountered in the population, and lengths of inmates’ stay.12 A mechanism should be in place to prescribe off-formulary and access other types of psychotropic medication on a case-by-case basis to ensure inmates are not denied appropriate treatment. A psychiatrist may have to advocate strongly for these principles.
Most correctional facilities require that staff administer every dose of psychotropic medication directly to the inmate for whom it is prescribed. In some facilities, only nursing personnel can administer medication, while others use trained corrections staff to deliver medication. Psychiatrists who prescribe psychotropics in correctional institutions must be familiar with the facility’s medication administration procedures, which may impact medication choice and form, dosing frequency, timing of laboratory studies, and inmate medication compliance. Prescribers’ capacity to order emergency or “as needed” medications may be limited or nonexistent if nursing staff is unavailable.
Appropriate use of psychotropic medication for treating psychiatric illness is the standard of care, but is only 1 component of an effective treatment plan for inmates with serious mental illness. Others include group and individual therapy, psychoeducation, and therapeutic activities such as recreational therapy, activity therapy, and opportunities for education and work within the correctional system.
Related Resources
- Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Thienhaus OJ, Piasecki M, eds. Correctional psychiatry practice guidelines and strategies. Kingston, NJ: Civic Research Institute, Inc.; 2007.
- National Commission on Correctional Healthcare. www.ncchc.org.
- Society of Correctional Physicians. www.CorrDocs.org.
Disclosure
Dr. Burns reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/02/psychiatry-behind-bars-practicing-in.html#comments
Over the last 2 decades mandatory prison sentences, longer prison terms, and more restrictive release policies have lead to a dramatic increase in the number of persons in jails and prisons. Currently, more than 2 million individuals are incarcerated in the United States.1 Psychiatric illness is over-represented in correctional populations compared with the general population—more than half of all inmates have a mental health diagnosis.2 Correctional facilities are legally obligated to address the medical and mental health needs of the persons committed to them. As a result, more psychiatrists are practicing in jails and prisons.
This article explains correctional facilities’ obligation to provide for inmates’ mental health needs and describes correctional mental health processes and how psychiatrists can play a role in screening, evaluation, and suicide prevention.
Lack of training
Despite the increasing number of psychiatrists working in correctional institutions, most have had little or no training, education, or even orientation to these settings. Forensic psychiatry fellowship requirements include experience in treating acutely and chronically ill patients in correctional systems.3 Although general psychiatric training doesn’t preclude correctional experience, it is not required. The forensic component of general psychiatric residency is limited to evaluation of forensic issues, report writing, and testimony.
Professional organizations—including the American Psychiatric Association,4 the American Public Health Association,5 the National Commission on Correctional Health Care,6 and the American Correctional Health Services Association7—have developed standards and position statements on providing medical and mental health care in correctional facilities. Although psychiatrists’ work in correctional settings generally has been reserved for consultation and medication management, it is important for these clinicians to understand and appreciate the wider landscape and environment in which they practice. Psychiatrists can help develop and implement mental health processes that lead to better services and improved clinical outcomes.
Right to treatment
Convicted persons have a constitutional right to medical and mental health treatment under extension of the Eighth Amendment of the U.S. Constitution, which prohibits cruel and unusual punishment.8 In 1976, the U.S. Supreme Court concluded that “deliberate indifference to serious medical needs of prisoners constitutes the ‘unnecessary and wanton infliction of pain’… proscribed by the Eighth Amendment.”9 This coverage was expanded to mental health needs when the court found “…no underlying distinction between the right to medical care for physical ills and its psychological or psychiatric counterpart.”10 Correctional facilities also are obligated to provide medical and mental health treatment for persons in custody who are not yet convicted of an offense.8 In subsequent litigation, the court formulated 6 components of a minimally adequate correctional mental health treatment program; these are described in Table 1.11
Table 1
Components of minimally adequate mental health system in correctional facilities
| A systematic screening and evaluation program to identify inmates requiring mental health treatment |
| Treatment that encompasses more than simply segregating the mentally ill inmate and increasing correctional supervision |
| Treatment by trained mental health professionals in sufficient numbers to identify and treat inmates suffering from serious mental disorders |
| Maintenance of accurate, complete, and confidential records of the mental health treatment process |
| A suicide prevention program |
| Appropriate use of psychotropic medication (prescription and monitoring by appropriately trained and licensed staff to treat bona fide mental disorders rather than solely as a means of behavioral management) |
| Source: Reference 11 |
Jails vs prisons
The type of psychiatric treatment provided differs based on whether the facility is a jail or a prison, how long inmates are confined, and whether the facility serves a special mission or population, such as serving as a reception center for a prison system or housing only juveniles. Jails generally house inmates for short periods—often <1 year—experience rapid population turnover, and receive admissions day and night. Jails vary in size from a few holding cells to several thousand beds. These factors have implications for screening and evaluation processes, suicide prevention, and coordination of care with community treatment providers. In jails, clinicians’ work focuses on rapid identification of psychiatric illness, assessment, stabilization, and re-linkage to treatment providers in the community. Access to inpatient and ongoing psychiatric care also should be available.
In contrast, prisons house people who have been convicted and sentenced to serve time, generally for >1 year. Turnover is less rapid, admissions and discharges are more predictable, and there is greater opportunity and obligation to develop a continuum of mental health care. Prison systems generally provide or make arrangements for crisis intervention, residential treatment services, and inpatient and outpatient psychiatric care. These services may be provided on the prison grounds, or the inmate may be transferred to another prison within the system that offers specialized treatment or to a community hospital, where the inmate is under the constant supervision of corrections officers. Residential treatment includes intensive, coordinated, and structured mental health services and consists of group and individual therapies, psychoeducation, and therapeutic activities; these services are analogous to intensive day treatment or partial hospitalization programs in the community. In prisons mental health care emphasizes ongoing treatment. As in the community, treatment teams in correctional settings often include mental health professionals such as psychiatric nurses, psychotherapists, and psychology staff in addition to psychiatrists.
Screening and evaluation
Correctional facilities need a systematic screening process that is conducted on all inmates. This preliminary entry or “receiving screening” is intended to identify urgent medical and mental health concerns and persons in need of immediate treatment. A nurse or corrections staff officer who has been trained by medical staff could conduct this screening. Screening consists of observing the inmate’s current condition and conducting a structured inquiry into medical and psychiatric symptoms, psychotropic medications, drug and alcohol use history, and suicide risk. A positive screen leads to immediate action such as instituting drug or alcohol detoxification or initiating suicide precautions or an emergency medical referral and assessment.4,6
Within a few days of an inmate’s arrival, a mental health professional should conduct a more detailed mental health screening to identify non-emergent psychiatric needs. The mental health screening includes:
- a review of accompanying mental health information received from the county jail or arresting/transporting officer
- a self-reported history of psychiatric treatment, such as hospitalization, pharmacotherapy, or outpatient counseling
- current or prior suicidal thoughts or attempts
- intellectual functioning
- history of violence and/or victimization
- a brief mental status examination.4
Records from previous incarcerations should be reviewed. Also, if relevant, obtain the inmate’s consent to collect outside treatment records and/or speak with family or significant others. The results of this brief mental health assessment could prompt a referral for further evaluation and determine the need for psychotropic therapy.
Although usually not directly involved in this systematic screening and evaluation, psychiatrists should be familiar with how and why referrals are made to be sure that they are appropriate and to reduce unnecessary evaluations, leaving more time for medication follow-up, treatment planning, and suicide risk assessment. An efficient and effective mental health screening and assessment process helps ensure that limited psychiatric resources are used to maximal benefit.
Suicide prevention
Suicide prevention programs often include teaching corrections staff to identify suicide risk factors and instructing them to screen at-risk inmates at any time during incarceration. These programs should implement steps to keep inmates safe, such as increasing intensity and frequency of monitoring by corrections staff, removing or limiting access to items that could be used to harm oneself, and moving inmates to a housing area where the means and opportunity for self harm are reduced.4,6 Suicide prevention programs also should include delivery of appropriate mental health interventions to improve the inmate’s clinical condition, resolve the crisis, or otherwise lower suicide risk. These interventions include:
- increased frequency of interaction with mental health staff (more than a brief daily interaction conducted at the cell front)
- treatment of drug and/or alcohol withdrawal
- referral for evaluation and assessment of the need for psychotropic medication or dosage adjustment (Table 2).6
A correctional facility’s policy should allow a low threshold for corrections staff to initiate a suicide prevention watch—it is better to err on the side of caution and institute a watch than to expect non-mental health professionals to conduct clinical risk level assessments. Full assessment of an inmate’s clinical condition and the decision to reduce or discontinue the watch should be left to a trained mental health professional. This function may fall within the psychiatrist’s duties and it is important to be aware of the ramifications of watch discontinuation, such as:
- what type of property is returned
- where the inmate will be housed
- how often the inmate will be monitored by custody staff
- when the next mental health follow-up will occur.
Failure to articulate your expectations to staff members can lead to catastrophic consequences if watches are discontinued without an appropriate plan for monitoring and follow-up.
Psychiatrists can help train corrections staff on signs of suicide risk and also should review suicide attempts and/or completed suicides. This often can be a challenge because a psychiatrist’s time at a facility may be limited, but is an important consideration for quality improvement efforts.
Table 2
Components of a correctional suicide prevention program
| Training for staff on verbal and behavior cues indicating suicide risk and appropriate response |
| Identification of potentially suicidal inmates |
| Referral to mental health providers or facilities |
| Evaluation by qualified mental health professional |
| Housing in safe area of the institution |
| Treatment to address the cause of or reasons for suicidal thoughts |
| Monitoring procedures that permit regular, documented supervision |
| Communication procedures between health care and corrections personnel |
| Intervention procedures addressing how to handle a suicide attempt in progress |
| Notification procedures to ensure appropriate correctional authorities, outside authorities, and family are contacted |
| Reporting procedures for documenting attempted or completed suicides |
| Review of suicides and serious attempts by health care and administrative staff |
| Critical incident debriefing offered to affected personnel and inmates in event of completed suicide |
| Source: Reference 6 |
Pharmacotherapy
Traditionally, the primary role of psychiatrists working in correctional facilities has been psychotropic medication management. Understanding the correctional context and procedures permits more informed prescription choices and recommendations for psychotropics to be included in the formulary.
Antipsychotics, antidepressants, and mood stabilizers should be included in a facility’s formulary. Considerations concerning types of psychotropic medication within a formulary depend on the facility’s size and mission, psychiatric illnesses encountered in the population, and lengths of inmates’ stay.12 A mechanism should be in place to prescribe off-formulary and access other types of psychotropic medication on a case-by-case basis to ensure inmates are not denied appropriate treatment. A psychiatrist may have to advocate strongly for these principles.
Most correctional facilities require that staff administer every dose of psychotropic medication directly to the inmate for whom it is prescribed. In some facilities, only nursing personnel can administer medication, while others use trained corrections staff to deliver medication. Psychiatrists who prescribe psychotropics in correctional institutions must be familiar with the facility’s medication administration procedures, which may impact medication choice and form, dosing frequency, timing of laboratory studies, and inmate medication compliance. Prescribers’ capacity to order emergency or “as needed” medications may be limited or nonexistent if nursing staff is unavailable.
Appropriate use of psychotropic medication for treating psychiatric illness is the standard of care, but is only 1 component of an effective treatment plan for inmates with serious mental illness. Others include group and individual therapy, psychoeducation, and therapeutic activities such as recreational therapy, activity therapy, and opportunities for education and work within the correctional system.
Related Resources
- Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2009.
- Thienhaus OJ, Piasecki M, eds. Correctional psychiatry practice guidelines and strategies. Kingston, NJ: Civic Research Institute, Inc.; 2007.
- National Commission on Correctional Healthcare. www.ncchc.org.
- Society of Correctional Physicians. www.CorrDocs.org.
Disclosure
Dr. Burns reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Glaze LE. Correctional populations in the United States, 2009. Washington, DC: Bureau of Justice Statistics. December 2010. NCJ 231681.
2. James DJ, Glaze LE. Mental health problems of prison and jail inmates. Washington, DC: Bureau of Justice Statistics. September 2006. NCJ 213600.
3. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in forensic psychiatry. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/406pr703_u105.pdf. Accessed December 30, 2010.
4. American Psychiatric Association. Psychiatric services in jails and prisons. 2nd ed. Washington, DC: American Psychiatric Association; 2000.
5. Standards for health services in correctional institutions. 3rd ed. Washington, DC: American Public Health Association; 2003.
6. National Commission on Correctional Health Care. Standards for mental health services in correctional facilities. Chicago, IL: National Commission on Correctional Health Care; 2008.
7. American Correctional Health Services Association. Position statement on forced and involuntary psychotropic medication. Available at: http://www.achsa.org/displaycommon.cfm?an=12. Accessed December 30, 2010.
8. Cohen F. Overview of legal issues. In: Cohen F. The mentally disordered inmate and the law. Kingston, NJ: Civic Research Institute, Inc.; 1998:2-1-2-20.
9. Estelle v Gamble. 429 U.S. 97 (1976).
10. Bowring v Godwin. 551 F2d 44, 47 (4th Cir 1977).
11. Ruiz v Estelle. 503 F Supp 1265 (SD Tex 1980).
12. Burns K. Pharmacotherapy in correctional settings. In: Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010:321-344.
1. Glaze LE. Correctional populations in the United States, 2009. Washington, DC: Bureau of Justice Statistics. December 2010. NCJ 231681.
2. James DJ, Glaze LE. Mental health problems of prison and jail inmates. Washington, DC: Bureau of Justice Statistics. September 2006. NCJ 213600.
3. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in forensic psychiatry. Available at: http://www.acgme.org/acWebsite/downloads/RRC_progReq/406pr703_u105.pdf. Accessed December 30, 2010.
4. American Psychiatric Association. Psychiatric services in jails and prisons. 2nd ed. Washington, DC: American Psychiatric Association; 2000.
5. Standards for health services in correctional institutions. 3rd ed. Washington, DC: American Public Health Association; 2003.
6. National Commission on Correctional Health Care. Standards for mental health services in correctional facilities. Chicago, IL: National Commission on Correctional Health Care; 2008.
7. American Correctional Health Services Association. Position statement on forced and involuntary psychotropic medication. Available at: http://www.achsa.org/displaycommon.cfm?an=12. Accessed December 30, 2010.
8. Cohen F. Overview of legal issues. In: Cohen F. The mentally disordered inmate and the law. Kingston, NJ: Civic Research Institute, Inc.; 1998:2-1-2-20.
9. Estelle v Gamble. 429 U.S. 97 (1976).
10. Bowring v Godwin. 551 F2d 44, 47 (4th Cir 1977).
11. Ruiz v Estelle. 503 F Supp 1265 (SD Tex 1980).
12. Burns K. Pharmacotherapy in correctional settings. In: Scott CL, ed. Handbook of correctional mental health. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010:321-344.
Atypical antipsychotics for delirium: A reasonable alternative to haloperidol?
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/atypical-antipsychotics-for-delirium.html#comments
Ms. B, age 48, is admitted to our hospital after overdosing on unknown amounts of amitriptyline, diphenhydramine, and laxatives. Three days after admission, the psychiatry service is consulted to assess her for “bipolar disorder.” Although Ms. B does not have a psychiatric history, her internist believes her pressured speech and psychomotor agitation warrant investigation.
During the initial psychiatric interview, Ms. B is disoriented, with fluctuating alertness and cognition. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU)1 is positive for delirium. We perform a delirium workup while we start Ms. B on olanzapine, 5 mg/d orally and 5 mg intramuscular (IM) every 8 hours as needed.
Ms. B’s laboratory results (complete blood count, complete metabolic profile, urinalysis, chest roentgenogram, vitamin B12 level, blood alcohol level, urine drug screen, arterial blood gas, and head CT) are unremarkable except for her amitriptyline/nortriptyline level, which is in the toxic range. On physical examination, Ms. B’s heart rate and temperature are elevated, her pupils are dilated and sluggish, and her skin is hot and dry. Based on these findings, we determine that Ms. B’s delirium most likely is an anticholinergic syndrome from amitriptyline/diphenhydramine toxicity.2 We discontinue olanzapine after only 2 doses because of its potential anticholinergic effects.3
In hospitalized patients, delirium is one of the most frequently encountered mental disorders, but because of its variable presentation the condition often is underrecognized and undertreated, which leads to longer hospitalizations and increased mortality.4,5 Ms. B’s case illustrates the classical delirium presentation (Table 1),6 highlighting 2 hallmark features of the disorder: inattention and an acute fluctuating course.4 Unfortunately, delirium is a diverse disorder that may present with numerous nonclassical symptoms—including lethargy, emotionality, sleep irregularities, and neurologic abnormalities—in lieu of more commonly recognized symptoms.4,5
In addition to recommending identifying and addressing the underlying acute illness, American Psychiatric Association guidelines suggest prescribing psychotropic medications to treat delirium symptoms.5,7 Antipsychotics are considered first-line pharmacotherapy because they have been shown to lower hospital mortality rates8 and improve delirium symptoms even before underlying medical etiologies are treated.5 Haloperidol is the mainstay of delirium treatment.8 Compared with atypical antipsychotics in delirium treatment, haloperidol doses <3.5 mg/d have not been associated with an increase in extrapyramidal symptoms (EPS).9
Although not devoid of side effects, atypical antipsychotics are an alternative to haloperidol.8,10 This article briefly summarizes the current evidence on the use of atypicals for treating delirium.
Table 1
Delirium: Diagnostic criteria
| Delirium describes a group of related disorders with variable clinical presentations and differing causation. Regardless of the etiology, all types of delirium share a set of common symptoms that include: |
| Disturbances of consciousness and attention |
| Changes in cognition such as memory deficit, language disturbance, or disorientation |
| Perceptual disturbances not better accounted for by dementia |
| Abrupt onset (usually hours to days) |
| Fluctuating symptoms throughout the course of the day |
| Source: Adapted from reference 6 |
CASE CONTINUED: IM ziprasidone
After reassessing our treatment options, we prescribe ziprasidone, 10 mg IM twice a day, and an additional 10 mg IM every 12 hours as needed. Ziprasidone’s minimal anticholinergic and sedative effects3 seem favorable for Ms. B’s delirium; however, this medication has several drawbacks, including IM administration, greater expense compared with intravenous haloperidol, and risk of adverse cardiac affects, specifically prolonged corrected QT (QTc) interval.11 Bioavailability of oral ziprasidone is markedly less than the IM preparation (~60% vs 100%, respectively), and oral bioavailability decreases to approximately 30% when taken without food.12 Given Ms. B’s her current mental state, we feel that IM ziprasidone is a more reliable means to achieve therapeutic efficacy.13
With respect to cardiac concerns, we evaluate Ms. B’s predisposing and precipitating risk factors.11 Family members confirm that she had no cardiac history. We obtain baseline ECGs and continually monitor her QTc interval, which remained at <500 msec during ziprasidone treatment.
Ms. B tolerates ziprasidone and we note modest improvement in her mental status after 2 days of treatment; her vigilant-A portion of the CAM-ICU improves, but she still screens positive for delirium. During the next week Ms. B develops several medical comorbidities, including ileus, urinary tract infection, and methicillin-resistant Staphylococcus aureus infection. Despite these complications her mental status continues to improve. Within 6 days, Ms. B’s attention and cognition improve dramatically. She is oriented and able to engage in medical decision-making, and she screens negative for delirium on the CAM-ICU. We begin to assess her for psychiatric disorders that may have contributed to her hospitalization.
Evidence for antipsychotics
Haloperidol has been the antipsychotic of choice for treating delirium symptoms. It is recommended by the Society of Critical Care Medicine7 and is regarded as safe, cost-effective, and efficacious for delirium5 despite a risk of dose-related EPS and potential cardiac conduction alterations.5,14
Risperidone is not indicated for treating delirium but is one of the most extensively studied atypical antipsychotic alternatives to haloperidol. Evidence consisting primarily of case reports has illustrated the potential efficacy of risperidone in treating delirium (Table 2).10,15-19
In 2004, Parellada et al17 observed significant mean improvements in all measures (Delirium Rating Scale [DRS], Mini-Mental State Exam [MMSE], positive subscale of the Positive and Negative Syndrome Scale [PANSS-P], and Clinical Global Impressions scale [CGI]) in 64 delirium patients treated with risperidone. In a 2004 double-blind trial of 28 delirium patients randomly assigned to risperidone or haloperidol, risperidone was effective but not significantly more efficacious than low-dose haloperidol for acute delirium treatment.18
Advantages of using risperidone include its lack of anticholinergic effects. Potential side effects include dose-related EPS and weight gain, which were observed in patients with schizophrenia and other psychotic disorders and dementia-related behavioral disorders.20,21
Olanzapine. Much like risperidone, olanzapine’s use in delirium is relatively well described in the literature (Table 3).22-24 In a randomized, placebo-controlled study comparing olanzapine with haloperidol, 175 patients were treated for 7 days with olanzapine, haloperidol, or placebo. Olanzapine and haloperidol showed significantly greater DRS score improvement than placebo.24 There was no difference between olanzapine and haloperidol outcomes; however, olanzapine showed significant improvement by days 2 and 3 compared with haloperidol. Haloperidol was associated with a significantly higher rate of dystonia compared with olanzapine.
Olanzapine carries a risk of anticholinergic effects. This can be a drawback, especially in patients such as Ms. B whose delirium has an anticholinergic component. Olanzapine is available in an IM formulation, which can be an advantage when addressing agitation and medical comorbidities of delirium.
Quetiapine. Case reports have suggested quetiapine is effective for delirium (Table 4).10,25-27 In a prospective, open-label trial, Sasaki et al26 treated 12 delirium patients with a single bedtime dose of quetiapine. All patients achieved remission within several days of beginning quetiapine, and the drug was well tolerated with no detected EPS or excessive sedation.
In 2010 Devlin et al27 reported on the efficacy and safety of quetiapine in a prospective double-blind, placebo-controlled study of 36 adult ICU patients. Compared with those receiving placebo, patients taking quetiapine had a statistically significant shorter time to first resolution of delirium, reduced duration of delirium, and less agitation as measured by the Sedation-Agitation Scale. Mortality, ICU length of stay, and incidence of QTc prolongation did not differ, but patients treated with quetiapine were more likely to be discharged home or to rehabilitation and to have more somnolence. Quetiapine’s side effect profile includes a low occurrence of EPS, sedation, and dose-related anticholinergic effects.25
Ziprasidone. The literature on ziprasidone for delirium so far is limited to a few anecdotal case reports (Table 5).28-31 In 2002, Leso and Schwartz28 successfully used ziprasidone to treat delirium in a patient with human immunodeficiency virus and cryptococcal meningitis. Ziprasidone was chosen for its lack of sedating effects and low EPS risk. The patient experienced significant clearing of his delirium and lowering of his DRS score. Ziprasidone eventually was discontinued because a fluctuating QTc interval associated with comorbid electrolyte imbalances—a potential drawback to ziprasidone.
In the case of Ms. B, ziprasidone appeared to be efficacious; however, improvement in her medical condition, rather than ziprasidone treatment, is the most likely explanation for the resolution of her delirium symptoms.
Aripiprazole. Alao et al30 reported on 2 delirium patients treated with 30 mg and 15 mg aripiprazole; improvement was monitored using the MMSE and DRS (Table 5).28-31 In both cases, confusion, disorientation, and agitation improved within 7 days of treatment. In the first case, the patient’s MMSE score improved from 5 to 28 and his DRS score decreased from 28 to 6. The second patient’s MMSE score improved from 7 to 27 and her DRS score went from 18 to 6.
Straker et al31 reported on 14 delirium patients treated with aripiprazole. Twelve patients had a ≥50% reduction in DRS, Revised-98 scores, and 13 showed improvement on CGI scores. The rate of adverse side effects was low. Three patients had prolonged QTc interval, but no patients developed arrhythmia or discontinued aripiprazole.
Table 2
Risperidone for delirium: What the evidence says
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199715 | N=2 (age 14 and 60). Initial dose: 1 mg/d; maintenance dose: 2 mg/d | 10 to 14 days | MMSE score increased. AEs: extrapyramidal symptoms (dystonia and cogwheeling) |
| Schwartz et al, 200210 | N=11 (age range 14 to 74). Mean dose: 1.59 ± 0.8 mg/d | 5.1 ± 4.3 days | CGI score decreased. No reported AEs |
| Horikawa et al, 200316 | N=10 (mean age: 56.8; range: 22 to 81). Mean dose: 1.7 mg/d | 7.1 days | DRS score decreased significantly in 80% of patients (P=.03) AEs: sleepiness (30%), mild drug-induced parkinsonism (10%) |
| Parellada et al, 200417 | N=64 (mean age: 67.3 ± 11.4 years). Mean dose: 2.6 ± 1.7 mg/d | 3 to 7 days | Effective in 90.6% of patients with significant decreases in DRS, PANSS-P, and CGI and increase in MMSE (P < .001). AEs: drowsiness (3.1%), nausea (1.6%) |
| Hans et al, 200418 | N=12 (mean age: 65.6). Mean dose: 1.02 mg/d | 4 to 7 days | MDAS scores decreased significantly (P < .05). No reported AEs |
| Bourgeois et al, 200519 | N=1 (age 57). Initial dose: 8 mg/d; maintenance dose: 2 mg/d | 9 days | MMSE score increased. No reported AEs |
| CGI: Clinical Global Impressions scale; DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale; MMSE: Mini-Mental State Exam; PANSS-P: positive subscale of the Positive and Negative Syndrome Scale | |||
Table 3
Olanzapine may have a role in treating delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Sipahimalani et al, 199822 | N=11 (mean age: 63.5 ± 23.2 years). Mean dose: 8.2 ± 3.4 mg/d | 6.8 ± 3.5 days | Marked decrease (>50%) in DRS score for 5 patients. No reported AEs |
| Breitbart et al, 200223 | N=79 (mean age: 60.6 ± 17.3 years; range: 19 to 89). Initial dose: 3 ± 0.14 mg/d; mean dose: 4.6 to 6.3 mg/d | 2 to 7 days | MDAS decreased significantly (P < .001), with 76% of patients’ delirium reaching resolution (MDAS ≤10). AEs: sedation (30%) |
| Hu et al, 200424 | N=74 (mean age: 74). Mean dose: 1.25 to 2 mg/d | 2.78 ± 1.85 days | DRS score decreased significantly (P < .01) in 72.2% of patients. AEs: drowsiness (18.9%), dystonia (2.7%), dry mouth (2.7%) |
| DRS: Delirium Rating Scale; MDAS: Memorial Delirium Assessment Scale | |||
Table 4
Evidence suggests quetiapine could reduce delirium symptoms
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Schwartz et al, 200210 | N=11 (age range: 19 to 91). Mean dose: 211.4 mg/d | 6.5 days | Decrease in DRS score (>50% reduction in global delirium symptoms) for 10 patients. AEs: sedation |
| Al-Samarrai et al, 200325 | N=2 (age 50 and 52). Mean dose: 200 to 400 mg/d | 2 to 4 days | No specific rating scale used but clinical reduction in agitation and improvement in cognition were reported. AEs: drowsiness |
| Sasaki et al, 200326 | N=12 (mean age: 67.3 ± 14.8 years). Mean dose: 44.9 ± 31.0 mg/d | 4.8 ± 3.5 days | Decrease in DRS score and remission of delirium for all patients. Significant increase in MMSE (P=.0256). No reported AEs |
| Devlin et al, 201027 | N=18 (adult ICU patients). Initial dose: 100 mg/d | 36 to 87 hours | Significantly shorter time to first resolution of delirium and duration of delirium compared with placebo. AEs: somnolence |
| DRS: Delirium Rating Scale; ICU: intensive care unit; MMSE: Mini-Mental State Exam | |||
Table 5
Limited data support ziprasidone and aripiprazole for treating delirium
| Study | Patients/dosage | Peak clinical response | Results/adverse effects (AEs) |
|---|---|---|---|
| Ziprasidone | |||
| Leso et al, 200228 | N=1 (age 34). Initial dose: 40 mg/d; maintenance dose: 100 mg/d | 21 days | DRS score decreased from 26 to 14. AEs: 8.4% increase in QTc interval |
| Young et al, 200429 | N=1 (age 47). Initial dose: 20 mg IV bolus, followed by an oral taper over 7 days. | 7 days | No specific rating scale was used but dramatic improvement in patient’s restlessness was reported. No AEs reported |
| Aripiprazole | |||
| Alao et al, 200630 | N=2 (age 62 and 37). Mean dose: 15 and 30 mg/d | 2 to 7 days | Patient 1: DRS score decreased from 28 to 6 and MMSE score increased from 5 to 28. Patient 2: DRS score decreased from 18 to 6 and MMSE score increased from 7 to 27. No AEs reported |
| Straker et al, 200631 | N=14 (age range: 18 to 85). Mean dose: 8.9 mg/d | 2 to 14 days | 12 of 14 patients had a ≥50% decrease in DRS-R-98. AEs: 3 patients had prolonged QTc interval |
| DRS: Delirium Rating Scale; DRS-R-98: Delirium Rating Scale–Revised-98; MMSE: Mini-Mental State Exam | |||
Anticholinergic activity
Decreased acetylcholine activity (AA) is suspected in delirium pathogenesis.32 By extension of this theory, medications that block muscarinic receptors could worsen delirium. Haloperidol, risperidone, and ziprasidone have negligible or no AA, as reported in atropine equivalents. Quetiapine and olanzapine have mild (0.5 to 5 pmol/ mL) and moderate (5 to 15 pmol/mL) dose-related AA, respectively. For example, olanzapine, 5 mg/d, has roughly the same AA as quetiapine, 300 mg/d, whereas olanzapine, 10 mg/d, has about the same AA as quetiapine, 600 mg/d.32,33
Although we used this evidence, in part, to select an atypical antipsychotic for Ms. B, this model should be used only to estimate the possible anticholinergic burden associated with a specific medication or combination. The risk of anticholinergic burden needs to be considered along with a medication’s potential nonanticholinergic adverse effects and the patient’s overall clinical history (eg, past sensitivity to anticholinergic agents, memory complaints, effectiveness of an agent, concomitant medications, disease state, adherence concerns). For example, an atypical antipsychotic that is potently anti-histaminergic and therefore sedating could be beneficial when treating an agitated delirium patient. Establishing the presence of a risk of anticholinergic burden cannot be equated with the presence of anticholinergic toxicity, because the exact relationship between AA and cognitive performance is still unknown.32,33
Cardiovascular safety
The most common cardiovascular effects of atypical antipsychotics are tachycardia, hypotension (usually mild), and prolongation of QTc interval.34 For example, haloperidol, 15 mg/d, was found to increase mean QTc by 7 msec, with a reported odds ratio ranging from 2.2 to 6.1 for ventricular dysrhythmia and sudden cardiac death,35 although risk may be more strongly associated with high-dose, IV haloperidol.36
QTc interval prolongation warrants concern because it suggests that patients may be predisposed to torsades de pointes (TdP). Conventional antipsychotics— especially phenothiazines—have the highest risk of inducing TdP. One review concluded that compared with other antipsychotics, chlorpromazine, pimozide, thioridazine, and the atypical clozapine have a higher risk of cardiac arrhythmias and sudden cardiac death.11 Another review found cases of TdP with haloperidol, ziprasidone, olanzapine, and thioridazine.37 When prescribing an antipsychotic, consider both pharmacologic and nonpharmacologic risks factors, including preexisting cardiovascular disease, female sex, hepatic insufficiency, electrolyte abnormalities, stimulant drug abuse,36 and genetic predisposition (Table 6).11,35-37
Table 6
Risk factors for antipsychotic-induced QT interval prolongation and torsades de pointes*
| Pharmacologic |
|---|
| Antipsychotic selection |
| Drug interaction (QT-prolonging agents) |
| Drug interaction (slow metabolism by cytochrome P450 inhibitors of 2D6, 3A4, 1A2) |
| Nonpharmacologic |
| Advanced age (>65) |
| Bradycardia |
| Hypokalemia |
| Hypomagnesemia |
| Hepatic/renal dysfunction |
| Genetic predisposition |
| Female sex |
| Screening (major risk factors) |
| Structural cardiac disease |
| Congenital long QT syndrome |
| Family history of sudden cardiac death |
| Previous episodes of drug-induced QT prolongation or torsades de pointes |
| * Serial electrocardiograms are recommended for patients with a major risk factor or multiple pharmacologic/ nonpharmacologic risk factors Source: References 11,35-37 |
Related Resource
- Stern TA, Celano CM, Gross AF, et al. The assessment and management of agitation and delirium in the general hospital. Prim Care Companion J Clin Psychiatry 2010;12(1):e1–e11. www.psychiatrist.com/private/pccpdf/article_wrapper.asp?art=2010/09r00938yel/09r00938yel.htm.
Drug Brand Names
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Atropine • Sal-Tropine
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Diphenhydramine • Benadryl
- Haloperidol • Haldol
- Nortriptyline • Aventyl
- Olanzapine • Zyprexa
- Pimozide • Orap
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thioridazine • Mellaril
- Ziprasidone • Geodon
Disclosures
Dr. Spiegel is a speaker for AstraZeneca, Pfizer, Inc., and Janssen Pharmaceuticals.
Drs. Ahlers, Yoder, and Qureshi report no financial relationship with any company whose products are mention in this article or with manufacturers of competing products.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
1. Ely EW, Inouye SK, Bernard GR, et al. Delirium in the mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. 2001;286:2703-2710.
2. Rudolph JL, Salow MJ, Angelini MC, et al. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508-513.
3. Albers LJ, Hahn RK, Reist C. Handbook of psychiatric drugs 2008. Blue Jay, CA: Current Clinical Strategies Publishing; 2007.
4. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-1165.
5. American Psychiatric Association. Practice guideline for the treatment of patients with delirium. Am J Psychiatry. 1999;156(suppl 5):1-20.
6. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
7. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry. 2007;68(1):11-21.
8. Lacasse H, Perreault MM, Williamson DR. Systematic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Ann Pharmacother. 2006;40(11):1966-1973.
9. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.-
10. Schwartz TL, Masand PS. The role of atypical antipsychotics in the treatment of delirium. Psychosomatics. 2002;43(3):171-174.
11. Sicouri S, Antzelevitch C. Sudden cardiac death secondary to antidepressant and antipsychotic drugs. Expert Opin Drug Saf. 2008;7(2):181-194.
12. Citrome L. Using oral ziprasidone effectively: the food effect and dose-response. Adv Ther. 2009;26(8):739-748.
13. Preskorn SH. Pharmacokinetics and therapeutics of acute intramuscular ziprasidone. Clin Pharmacokinet. 2005;44(11):1117-1133.
14. Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428-437.
15. Sipahimalani A, Masand PS. Use of risperidone in delirium: case reports. Ann Clin Psychiatry. 1997;9(2):105-107.
16. Horikawa N, Yamazaki T, Miyamoto K, et al. Treatment for delirium with risperidone: results of a prospective open trial with 10 patients. Gen Hosp Psychiatry. 2003;25(4):289-292.
17. Parellada E, Baeza I, de Pablo J, et al. Risperidone in the treatment of patients with delirium. J Clin Psychiatry. 2004;65(3):348-353.
18. Hans CS, Kim YK. A double-blind trial of risperidone and haloperidol for the treatment of delirium. Psychosomatics. 2004;45(4):297-301.
19. Bourgeois JA, Hilty DM. Prolonged delirium managed with risperidone. Psychosomatics. 2005;46(1):90-91.
20. Naber D, Lambert M. The CATIE and CUtLASS studies in schizophrenia: results and implications for clinicians. CNS Drugs. 2009;23(8):649-659.
21. Zheng L, Mack WJ, Dagerman KS, et al. Metabolic changes associated with second-generation antipsychotic use in Alzheimer’s disease patients: the CATIE-AD study. Am J Psychiatry. 2009;166(5):583-590.
22. Sipahimalani A, Masand PS. Olanzapine in the treatment of delirium. Psychosomatics. 1998;39(5):422-430.
23. Breitbart W, Tremblay A, Gibson C. An open trial of olanzapine for the treatment of delirium in hospitalized cancer patients. Psychosomatics. 2002;43(3):175-182.
24. Hu H, Deng W, Yang H. A prospective random control study comparison of olanzapine and haloperidol in senile dementia. Chongqing Medical Journal. 2004;8:1234-1237.
25. Al-Samarrai S, Dunn J, Newmark T, et al. Quetiapine for treatment-resistant delirium. Psychosomatics. 2003;44(4):350-351.
26. Sasaki Y, Matsuyama T, Inoue S, et al. A prospective, open-label, flexible-dose study of quetiapine in the treatment of delirium. J Clin Psychiatry. 2003;64(11):1316-1321.
27. Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419-427.
28. Leso L, Schwartz TL. Ziprasidone treatment of delirium. Psychosomatics. 2002;43(1):61-62.
29. Young CC, Lujan E. Intravenous ziprasidone for treatment of delirium in the intensive care unit. Anesthesiology. 2004;101(3):794-795.
30. Alao AO, Moskowitz L. Aripiprazole and delirium. Ann Clin Psychiatry. 2006;18(4):267-269.
31. Straker DA, Shapiro PA, Muskin PR. Aripiprazole in the treatment of delirium. Psychosomatics. 2006;47(5):385-391.
32. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
33. Chew ML, Mulsant BH, Pollock BG, et al. A model of anticholinergic activity of atypical antipsychotic medications. Schizophr Res. 2006;88(1-3):63-72.
34. Buckley NA, Sanders P. Cardiovascular adverse effects of antipsychotic drugs. Drug Saf. 2000;23:215-228.
35. Stöllberger C, Huber JO, Finsterer J. Antipsychotic drugs and QT prolongation. Int Clin Psychopharmacol. 2005;20(5):243-251.
36. Zemrak WR, Kenna GA. Association of antipsychotic and antidepressant drugs with Q-T interval prolongation. Am J Health Syst Pharm. 2008;65(11):1029-1038.
37. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104.
Bariatric procedures: Managing patients after surgery
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments

Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
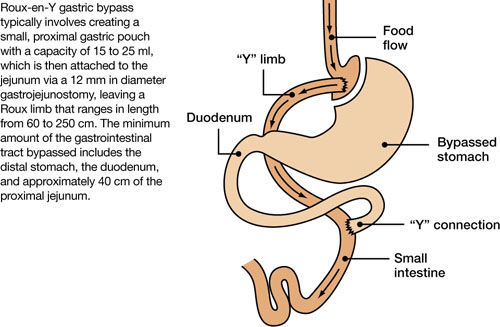
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments
Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2011/01/bariatric-procedures-managing-patients.html#comments
Bariatric surgery is the most effective treatment for obesity (defined as a body mass index [BMI] >30 kg/m2) and is recommended for extremely obese individuals (BMI >40 kg/m2) age >18.1,2 Most patients experience significant weight loss accompanied by improvements in mood, physical comorbidities, and quality of life (Box).3-8 Despite these favorable outcomes, several aspects of postoperative care—such as management of mental health issues—remain unclear. Bariatric surgery candidates show high rates of preoperative psychopathology, particularly depression and dysphoria. Little is known about how bariatric surgery affects absorption of psychiatric medications, leaving prescribing clinicians with minimal guidance when a postoperative patient reports changes in mood symptoms.
This article discusses the psychosocial status of bariatric surgery candidates and presents a rationale for increased medication monitoring after surgery.
Weight loss after bariatric surgery is associated with significant improvements in obesity-related comorbidities, including diabetes and cardiovascular disease, and decreased mortality.3,4
Many patients are able to reduce or discontinue many of their nonpsychiatric preoperative medications as their comorbid conditions improve.5 Symptoms of depression and anxiety, health-related quality of life, self-esteem, and body image often improve dramatically in the first year after surgery and endure for several years.6,7
Psychosocial improvements, however, may not translate into changes in psychotropic use. In a sample of 114 bariatric surgery patients, 43% were taking a selective serotonin reuptake inhibitor before surgery, 40% at 12 months postsurgery, and 31% at 24 months.8 These percentages do not account for patients who were taking other types of antidepressants.
Surgical treatment of obesity
The most common surgical procedures for weight loss are adjustable gastric banding (AGB) and Roux-en-Y gastric bypass (RYGB); each can be performed laparoscopically. With both procedures, food intake is restricted by creating a gastric pouch at the base of the esophagus. RYGB (Figure)9,10 also is thought to induce weight loss through selective malabsorption and favorable effects on gut peptides11,12 and currently is the procedure of choice in the United States.13
Figure Roux-en-Y: Bariatric procedure of choice
Source: References 9,10Bariatric surgery patients typically lose 25% to 35% of their initial body weight within 12 to 18 months of surgery.3,4 However, 20% to 30% of patients fail to achieve typical postoperative weight loss or regain large amounts of weight within a few years.14-16 Suboptimal results have been attributed to multiple factors, including problematic dietary intake, disordered eating, low levels of physical activity, preoperative psychopathology, and poor follow-up.6,17,18
Preop psychopathology
Twenty percent to 60% of extremely obese persons who pursue bariatric surgery have a psychiatric illness.6,7 In a study of 288 bariatric surgery candidates assessed with the Structured Clinical Interview for DSMIV, 38% received a current axis I diagnosis and 66% were given a lifetime diagnosis.19 In a separate study of 174 individuals seeking bariatric surgery, 24% met criteria for a current axis I or axis II disorder and 37% were found to have ≥1 lifetime diagnoses.20 The most common lifetime diagnoses were affective disorders (22%), anxiety disorders (16%), and eating disorders (14%).20
Psychopathology could negatively impact postoperative outcome. In an observational study, patients with a lifetime diagnosis of any axis I disorder—particularly mood and anxiety disorders—experienced less weight loss 6 months after RYGB compared with those who never received an axis I diagnosis.21 Bariatric surgery patients with ≥2 psychiatric diagnoses were more likely to stop losing weight or regain weight after 1 year compared with those with 1 or no diagnosis.22 Psychiatric illness also appears to impact longer term weight loss.23
Most bariatric surgery programs in the United States require a mental health evaluation as part of the patient selection process.24 These assessments may include evaluating a patient’s behavior patterns, motivation, expectations, and cognitive and emotional functioning, and performing psychological testing (see Related Resources). Psychiatric problems such as substance abuse, active psychosis, bulimia nervosa, and severe, uncontrolled depression1,9,25 are widely considered contraindications to bariatric surgery.24,26
Postsurgery considerations
At the time of bariatric surgery 16% to 40% of patients are receiving mental health treatment, which often includes antidepressants.27-29 Unfortunately, little is known about how medications interact with these surgical procedures. Dramatic changes in medication absorption may occur because of reduced gastrointestinal (GI) surface area. Rapid reduction in body weight and fat mass and postoperative complications also may impact the efficacy and tolerability of antidepressants.
Pharmacokinetics. Anatomic and physiologic changes with bariatric surgery may lead to changes in the pharmacokinetic (PK) parameters of certain medications, particularly after RYGB. PK studies typically are conducted by collecting a series of plasma samples at predetermined intervals after a patient takes a medication. The blood levels of the medication and its active metabolites are used to compute multiple PK parameters that illustrate drug absorption, distribution, and metabolism. Theoretically, a bariatric surgery patient may experience changes in the rate and/or extent of:
- medication absorption from the GI tract into systemic circulation
- distribution throughout the body as fat mass and total body water change after surgery
- drug metabolism.
The effects of bariatric surgery on medication PK appears to be drug-specific.30-33
The bypassed portion of the GI tract is the primary absorption site for most medications; therefore, the length of the Roux limb may affect the extent of drug absorption impairment. However, the duodenum wall is one of many locations of the cytochrome P450 (CYP) isoenzymes CYP3A4 and CYP3A5,34 which are the primary metabolic enzymes for drugs such as atorvastatin. Eliminating this portion of the bowel could increase rather than decrease bioavailability.35 Alterations in drug absorption also may result from changes in gastric emptying rate, reduced exposure to absorptive mucosal surfaces, and alterations in gastric pH that can impair drug dissolution and solubility.30 These changes could reduce medication bioavailability.33 The impact of such changes may differ according to the characteristics of the specific drug. It has been theorized that drugs that are intrinsically poorly absorbed, are highly lipophilic, and undergo enterohepatic circulation carry the highest risk of malabsorption.30 Antidepressants vary in the extent to which they demonstrate these characteristics. Progressive changes in the volume of distribution as weight is lost also could affect the blood levels of some antidepressants.
A series of small studies and case reports of PK changes in medications such as digoxin, oral contraceptives, cyclosporine, sulfisoxazole, and tacrolimus after jejunoileal bypass—an older, obsolete bariatric procedure—reveal variability in the surgery’s effect on PK parameters, although most reported reduced absorption. Data specific to RYGB consist of small studies and case series that show reduced absorption after surgery with significant variability among agents (see our bibliography of studies describing PK changes in nonpsychiatric medications after bariatric surgery). In a systematic literature review, Padwal et al found evidence for a decreased magnitude of absorption in 15 of 22 studies of jejunoileal bypass patients, 1 of 3 studies of gastric bypass/gastroplasty, and no studies examining biliopancreatic diversion.30
It is unclear if antidepressant absorption is impaired after RYGB because currently only 1 case report presents in-vivo data. Hamad et al describe an obese patient (BMI 46 kg/m2) taking sertraline, 100 mg/d, for depression.36 Researchers measured sertraline levels before and 1 month after RYGB, at which time the patient’s depression worsened. After surgery, sertraline maximum concentration was lower (14.4 ng/ml vs 41.6 ng/ml), trough concentration was lower (11.1 ng/ml vs 17.5 ng/ml), and time to maximum concentration was shorter (240 vs 300 minutes). This suggests that a shift in sertraline absorption after surgery may have contributed to the patient’s worsened mood symptoms.
An in-vitro study that simulated preand post-RYGB GI environments found that 12 of 22 psychotropic drugs tested dissolved differently between the models.37 Whereas the dissolved fractions of amitriptyline, fluoxetine, paroxetine, and sertraline were significantly less in the post-RYGB environment, bupropion dissolved to a greater extent in the pre-RYGB environment, and venlafaxine and citalopram were not different between the 2 conditions (Table).37 Although several limitations prevent translating these data into clinical recommendations, this study suggests that there may be significant variability among medications with regard to the implications of an altered GI environment.
Blouin RA, Bauer LA, Miller DD, et al. Vancomycin pharmacokinetics in normal and morbidly obese subjects. Antimicrob Agents Chemother. 1982;21(4):575-580.
Blouin RA, Brouwer KL, Record KE, et al. Amikacin pharmacokinetics in morbidly obese patients undergoing gastric-bypass surgery. Clin Pharm. 1985;4:70-72.
Chenhsu RY, Wu Y, Katz D, et al. Dose-adjusted cyclosporine c2 in a patient with jejunoileal bypass as compared to seven other liver transplant recipients. Ther Drug Monit. 2003;25(6):665-670.
Fuller AK, Tingle D, DeVane CL, et al. Haloperidol pharmacokinetics following gastric bypass surgery. J Clin Psychopharmacol. 1986;6:376-378.
Garrett ER, Süverkrup RS, Eberst K, et al. Surgically affected sulfisoxazole pharmacokinetics in the morbidly obese. Biopharm Drug Dispos. 1981;2:329-365.
Gerson CD, Lowe EH, Lindenbaum J. Bioavailability of digoxin tablets in patients with gastrointestinal dysfunction. Am J Med. 1980;69:43-49.
Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25th Annual Meeting; June 15-20, 2008; Washington, DC.
Kelley M, Jain A, Kashyap R, et al. Change in oral absorption of tacrolimus in a liver transplant recipient after reversal of jejunoileal bypass: case report. Transplant Proc. 2005; 37:3165-3167.
Knight GC, Macris MP, Peric M, et al. Cyclosporine A pharmacokinetics in a cardiac allograft recipient with a jejunoileal bypass. Transplant Proc. 1988;20:351-355.
Marcus FI, Quinn EJ, Horton H, et al. The effect of jejunoileal bypass on the pharmacokinetics of digoxin in man. Circulation. 1977;55:537-541.
Magee SR, Shih G, Hume A. Malabsorption of oral antibiotics in pregnancy after gastric bypass surgery. J Am Board Fam Med. 2007;20:310-313.
Marterre WF, Hariharan S, First MR, et al. Gastric bypass in morbidly obese kidney transplant recipients. Clin Transplant. 1996;10:414-419.
Prince RA, Pincheira JC, Mason EE, et al. Influence of bariatric surgery on erythromycin absorption. J Clin Pharmacol. 1984;24:523-527.
Rogers CC, Alloway RR, Alexander JW, et al. Pharmacokinetics of mycophenolic acid, tacrolimus and sirolimus after gastric bypass surgery in end-stage renal disease and transplant patients: a pilot study. Clin Transplant. 2008;22:281-291.
Shepherd MF, Rosborough TK, Schwartz ML. Heparin thrombophylaxis in gastric bypass surgery. Obes Surg. 2003;13(2):249-253.
Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
Victor A, Odlind V, Kral JG. Oral contraceptive absorption and sex hormone binding globulins in obese women: effects of jejunoileal bypass. Gastroenterol Clin North Am. 1987;16(3):483-491.
PK: pharmacokinetic
Table
Weights of dissolved portions of antidepressants before and after simulated RYGB
| Simulated pre-RYGB environment | Simulated post-RYGB environment | ||||
|---|---|---|---|---|---|
| Drug | Median weight of dissolved portion (mg) | Percentage* | Median weight of dissolved portion (mg) | Percentage* | P† |
| Amitriptyline, 75 mg/d | 80 | 28% | 60 | 21% | <.04 |
| Fluoxetine, 20 mg/d | 110 | 30% | 40 | 11% | <.04 |
| Paroxetine, 20 mg/d | 30 | 9% | 10 | 3% | <.04 |
| Sertraline, 100 mg/d | 50 | 16% | 30 | 10% | <.04 |
| Bupropion, 100 mg/d | 320 | 52% | 450 | 73% | <.05 |
| Venlafaxine, 75 mg/d | 180 | 59% | 180 | 59% | Not significant |
| Citalopram, 20 mg/d | 70 | 27% | 80 | 31% | Not significant |
| *Relative to original pill weight †Mann-Whitney U test RYGB: Roux-en-Y gastric bypass Source: Adapted from reference 37 | |||||
Altering antidepressant doses
Current PK data are insufficient to make clinical recommendations regarding appropriate postsurgical adjustment of dose or alternate dosage formulations (liquid, extended-release, etc.). However, based on theoretical considerations, Miller and Smith suggest that patients avoid extended-release preparations whenever possible after bariatric surgery, citing the rationale that decreased intestinal length and surface area leads to reduced absorption.33 No data are available to advise clinicians regarding the appropriateness of switching patients from extended-release products to immediate-release or liquid preparations following surgery.
Presently, increased medication monitoring may be the most appropriate clinical approach. If appropriate doses have little or no effect, consider the possibility of decreased medication absorption.33 Monitoring plasma levels of medications that have therapeutic ranges also is advisable.
Areas for future research
Before specific clinical recommendations for managing antidepressants following RYGB can be proposed, the extent to which the absorption, volume of distribution, drug metabolism, and other measures change after surgery need to be quantified. It is also unclear whether changes in medication absorption are subject to inter-patient variability, whether predictive characteristics can be identified, and whether any observed changes remain stable over time. Similarly, the extent to which variability in surgical procedures (eg, surgeon preference regarding remnant intestinal length) affects medication absorption is unknown. Data regarding medication absorption following AGB and other bariatric procedures also will be needed.
- American Society for Metabolic and Bariatric Surgery. Fact sheet: Metabolic and bariatric surgery. www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf.
- American Society for Metabolic and Bariatric Surgery. Suggestions for the pre-surgical psychological assessment of bariatric surgery candidates. www.asmbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
Drug Brand Names
- Amitriptyline • Elavil
- Atorvastatin • Lipitor
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Digoxin • Lanoxin
- Fluoxetine • Prozac
- Paroxetine • Paxil
- Sertraline • Zoloft
- Sulfisoxazole • Truxazole
- Tacrolimus • Prograf
- Venlafaxine • Effexor
Disclosures
Dr. Sarwer receives grant/research support from the National Institutes of Health, the American Society for Metabolic and Bariatric Surgery, and Ethicon Endo-Surgery, Inc., is consultant to Allergan, BAROnova, Inc., EnteroMedics, and Ethocon Endo-Surgery, Inc., and is on the board of directors of Surgical Review Corporation.
Dr. Roerig receives grant/research support from Eli Lilly and Company.
Drs. Faulconbridge, Steffen, and Mitchell report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
1. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic and Bariatric Surgery Medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:318-336.
2. NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med. 1991;115:956-961.
3. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724-1737.
4. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547-559.
5. Hodo DM, Waller JL, Martindale RG, et al. Medication use after bariatric surgery in a managed care cohort. Surg Obes Rel Dis. 2008;4:601-607.
6. Sarwer DB, Wadden TA, Fabricatore AN. Psychosocial and behavioral aspects of bariatric surgery. Obes Res. 2005;13:639-648.
7. Mitchell JE, de Zwaan M. Bariatric surgery: a guide for mental health professionals. New York, NY: Routledge; 2005.
8. Malone M, Alger-Mayer SA. Medication use patterns after gastric bypass surgery for weight management. Ann Pharmacopher. 2005;39:637-642.
9. Buchwald H. and the Consensus Conference Panel. Consensus conference statement: bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Rel Dis. 2005;1:371-381.
10. Needleman BJ, Happel LC. Bariatric surgery: choosing the optimal procedure. Surg Clin North Am. 2008;88:991-1007.
11. Albrecht RJ, Pories WJ. Surgical intervention for the severely obese. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13:149-172.
12. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002;288:2793-2796.
13. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909-1917.
14. Brolin RE, Kenler HA, Gorman RC, et al. The dilemma of outcome assessment after operations for morbid obesity. Surgery. 1989;105:337-346.
15. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-2693.
16. Sjöström L, Narbro K, Sjöström CD, et al. and the Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741-752.
17. Bocchieri LE, Meana M, Fisher BL. A review of psychosocial outcomes of surgery for morbid obesity. J Psychosom Res. 2002;52:155-165.
18. Herpertz S, Kielmann R, Wolf AM, et al. Do psychosocial variables predict weight loss or mental health after obesity surgery? A systematic review. Obes Res. 2004;12:1554-1569.
19. Kalarchian MA, Marcus MD, Levine MD, et al. Psychiatric disorders among bariatric surgery candidates: relationship to obesity and functional health status. Am J Psychiatry. 2007;164:328-334.
20. Rosenberger PH, Henderson KE, Grilo CM. Psychiatric disorder comorbidity and association with eating disorders in bariatric surgery patients: a cross-sectional study using structured interview based diagnosis. J Clin Psychiatry. 2006;67:1080-1085.
21. Kalarchian MA, Marcus MD, Levine MD, et al. Relationship of psychiatric disorders to 6-month outcomes after gastric bypass. Surg Obes Relat Dis. 2008;4:544-549.
22. Rutledge T, Groesz LM, Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes Surg. 2009;[Epub ahead of print].
23. Kinzl JF, Schrattenecker M, Traweger C, et al. Psychosocial predictors of weight loss after bariatric surgery. Obes Surg. 2006;16:1609-1614.
24. Bauchowitz AU, Gonder-Frederick LA, Olbrisch ME, et al. Psychosocial evaluation of bariatric surgery candidates: a survey of present practices. Psychosom Med. 2005;67(5):825-832.
25. Wadden TA, Sarwer DB, Womble LG, et al. Psychosocial aspects of obesity and obesity surgery. Surg Clin North Am. 2001;81:1001-1024.
26. Fabricatore AN, Crerand CE, Wadden TA, et al. How do mental health professionals evaluate candidates for bariatric surgery? Survey results. Obes Surg. 2006;16:567-573.
27. Sarwer DB, Cohn NI, Gibbons LM, et al. Psychiatric diagnoses and psychiatric treatment among bariatric surgery candidates. Obes Surg. 2004;14(9):1148-1156.
28. Larsen JK, Greenen R, van Ramshorst B, et al. Psychosocial functioning before and after laparoscopic adjustable gastric banding: a cross-sectional study. Obes Surg. 2003;13(4):629-636.
29. Clark MM, Balsiger BM, Sletten CD, et al. Psychosocial factors and 2-year outcome following bariatric surgery for weight loss. Obes Surg. 2003;13(5):739-745.
30. Padwal R, Brocks D, Sharma AM. A systematic review of drug absorption following bariatric surgery and its theoretical implications. Obes Rev. 2010;11(1):41-50.
31. Macgreggor AMC, Boggs L. Drug distribution in obesity and following bariatric surgery: a literature review. Obes Surg. 1996;6:17-27.
32. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract. 2003;18:131-135.
33. Miller AD, Smith KM. Medication and nutrient administration considerations after bariatric surgery. Am J Health Syst Pharm. 2006;63:1852-1857.
34. Paine MF, Khalighi M, Fisher JM, et al. Characterization of interintestinal and intraintestinal variations in human CYP3A-dependent metabolism. J Pharmacol Exp Ther. 1997;283:1552-1562.
35. Skottheim IB, Stormark K, Christensen H, et al. Significantly altered systemic exposure to atorvastatin acid following gastric bypass surgery in morbidly obese patients. Clin Pharmacol Ther. 2009;86(3):311-318.
36. Hamad GG, Kozak GM, Wisner KL, et al. The effect of gastric bypass on SSRI pharmacokinetics and pharmacodynamics. Abstract presented at: American Society for Metabolic and Bariatric Surgery 25 Annual Meeting; June 15-20, 2008; Washington, DC.
37. Seaman JS, Bowers SP, Dixon P, et al. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics. 2005;46:250-253.
Antiepileptics for psychiatric illness: Find the right match
Discuss this article at http://currentpsychiatry.blogspot.com/2010/12/antiepileptics-for-psychiatric-illness.html#comments
Although antiepileptic drugs (AEDs) are used to treat a spectrum of psychiatric disorders, in some instances they are prescribed without clear evidence of clinical benefit or safety. When considering prescribing an AED, ask yourself:
- Does the evidence show the drug is efficacious for my patient’s disorder or symptoms?
- Which adverse effects are associated with this medication?
- What are the advantages of monitoring the patient’s serum drug concentration?
This review provides an evidence-based framework regarding the safe and effective use of AEDs in psychiatric patients.
For which disorders are AEDs effective?
Bipolar disorder. Multiple studies have found that AEDs are efficacious for treating bipolar disorder. Carbamazepine, valproate (divalproex), and lamotrigine have the most evidence supporting their use (Table 1). For an extensive bibliography of studies supporting AEDs for bipolar disorder and other psychiatric illnesses, see this article at CurrentPsychiatry.com. Carbamazepine and valproate are FDA-approved for treating acute manic or mixed episodes associated with bipolar I disorder in adults, and may be beneficial for maintenance treatment. Lamotrigine is FDA- approved for maintenance treatment of bipolar I disorder in adults; however, it lacks efficacy for mania and acute bipolar depression.1 The use of newer AEDs—including gabapentin, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—for bipolar disorder is not recommended because evidence is limited or inconclusive.
Major depressive disorder (MDD). Most studies of AEDs in MDD feature open-label designs with small samples. AEDs might have a role as an augmentation strategy, perhaps for patients with agitation or irritability or who partially respond to antidepressants.2
Schizophrenia. Although limited data support the practice, AEDs commonly are combined with antipsychotics to treat patients with schizophrenia.3,4 Clinicians who prescribe carbamazepine should recognize the potential for drug-drug interactions with antipsychotics (ie, increased metabolism of antipsychotics caused by cytochrome P450 [CYP450] 3A4 induction).
Anxiety disorders. AEDs have a limited role in treating anxiety disorders. These agents may be used as augmentation for patients who exhibit partial response or treatment resistance to recommended agents for anxiety disorders, such as selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines. For patients who cannot tolerate SSRIs or benzodiazepines, AEDs may be alternatives.5
Other disorders. AEDs could be used to treat other psychiatric conditions and disorders, including alcohol withdrawal and relapse prevention, benzodiazepine withdrawal, drug dependence and abstinence, obesity, and eating disorders.4,6,7 A list of suggested AEDs for some of these disorders appears in Table 2. However, these recommendations are based on findings from small randomized controlled trials, open-label trials, or case reports.
Table 1
Evidence supporting antiepileptics for mood disorders and schizophrenia
| Medication | Bipolar disorder | Major depressive disorder | Schizophrenia | ||
|---|---|---|---|---|---|
| Mania | Depression | Maintenance | |||
| Carbamazepine | |||||
| Lamotrigine | |||||
| Valproate | |||||
| Gabapentin | |||||
| Levetiracetam | |||||
| Oxcarbazepine | |||||
| Tiagabine | |||||
| Topiramate | |||||
| Zonisamide | |||||
| : strong evidence supporting efficacy; | |||||
| : moderate evidence supporting efficacy; | |||||
| : weak evidence supporting efficacy | |||||
| Source: For an extensive bibliography of studies that support these recommendations, see this article at CurrentPsychiatry.com | |||||
Table 2
Off-label use of antiepileptics for various psychiatric disorders
| Condition/disorder | Possible medication(s)* |
|---|---|
| Alcohol withdrawal/relapse prevention | Carbamazepine, topiramate, valproate |
| Benzodiazepine withdrawal | Carbamazepine, valproate |
| Binge eating disorder | Topiramate, zonisamide |
| Bulimia nervosa | Topiramate |
| Drug dependence/abstinence | Carbamazepine, lamotrigine, topiramate, tiagabine |
| Generalized anxiety disorder | Pregabalin, tiagabine |
| Obesity | Lamotrigine, topiramate, zonisamide |
| Panic disorder | Valproate |
| Posttraumatic stress disorder | Lamotrigine |
| Social phobia | Gabapentin, pregabalin |
| * Based on small randomized controlled trials, open-label trials, or case reports. Further investigation in large systematic trials is needed | |
What about adverse effects?
A thorough understanding of each AED’s adverse effect profile is critical to determine which agent is most suitable for your patient. Factors that may affect the risk of adverse effects include:
- rate of dose escalation
- length of early tolerance development
- rate of increase in and magnitude of peak serum concentrations
- dosing frequency
- pharmacodynamic/pharmacokinetic interactions
- pharmacogenomics.
Cardiovascular effects. Although many AED clinical trials reported “edema” as an adverse effect, peripheral edema specifically has been reported with gabapentin, lamotrigine, tiagabine, and valproate.8 Peripheral edema with these agents generally has not been linked to cardiovascular complications in healthy adults. Carbamazepine and pregabalin may cause conduction abnormalities and should be used with caution in patients with underlying electrocardiogram abnormalities.8
Chronic carbamazepine use results in elevated plasma homocysteine and serum lipoprotein concentrations, which are biomarkers of cardiovascular disease.9 If clinically appropriate, switching from carbamazepine to a non-inducing AED (ie, lamotrigine) may ameliorate such effects. Chronic valproate use has been associated with increased plasma homocysteine levels; increases in serum lipoproteins may parallel valproate-induced weight gain.9
CNS effects. Common acute neurologic effects of AEDs include somnolence, dizziness, and ataxia. The incidence of these effects vary by agent; gabapentin and zonisamide appear to be the most sedating.8 However, in general these effects occur at the start of treatment and abate within a few days with continued treatment or dosage reduction. Starting at a low dose and slowly titrating may help prevent neurologic adverse effects.8 Peripheral neurologic effects—specifically paresthesias—are primarily associated with topiramate and zonisamide and may be attributed to carbonic anhydrase inhibition.8
AEDs’ primary cognitive effects include impaired attention/vigilance, psychomotor speed, and secondary involvement of other cognitive functions (eg, memory). Whereas carbamazepine and valproate have similar cognitive effects (ie, negative effects on attention, learning, memory, and psychomotor speed), newer AEDs except topiramate may produce fewer cognitive adverse effects (Table 3).10 Topiramate is associated with the highest rate of cognitive dysfunction, with frequent complaints of decreased concentration and attention, word-finding problems, and/or impaired memory.8,10
The FDA recently announced a warning of a risk of aseptic meningitis with lamotrigine.11 In 40 reported cases, symptoms—headache, fever, nausea, vomiting, nuchal rigidity, rash, photophobia, and myalgias—occurred between 1 and 42 days of treatment and typically resolved after lamotrigine was withdrawn. In 15 patients in whom lamotrigine was re-initiated, meningitis symptoms returned quickly and with greater severity.11
Dermatologic effects. Skin rashes have been reported with all AEDs; the highest risk is associated with carbamazepine and lamotrigine.12 Predictors of cutaneous reactions to lamotrigine include:
- high initial dose and rapid escalation
- concomitant valproate use without lamotrigine dosage adjustment
- young age.12
A history of AED-induced rash also increases risk. For example, patients with a history of rash with carbamazepine are at risk for rash with oxcarbazepine because of cross-reactivity.
Any AED-induced skin rash may progress to a fatal reaction, such as toxic epidermal necrolysis or Stevens-Johnson syndrome. Carbamazepine and lamotrigine are most strongly associated with these severe reactions.12 Patients who exhibit painful rash, fever, enlarged lymph nodes, malaise, and mucosal involvement may be at risk for a more severe disease course.12 If a patient taking an AED develops a rash, immediately stop the drug and perform a thorough risk-benefit analysis before considering re-initiation.
Hematologic effects. Thrombocytopenia has been reported with carbamazepine, lamotrigine, pregabalin, and valproate. The highest risk is for valproate at doses >50 mg/kg/d or serum concentrations >110 μg/mL in women or >135 μg/mL in men.13,14 Decreased platelet count is common with valproate, but coagulation dysfunction may not be present until counts fall below 50,000/mL. Carbamazepine is associated with leukopenia, which usually occurs in early treatment and resolves without dosage adjustments; however, this agent carries a black-box warning for risks of agranulocytosis and aplastic anemia. Similar postmarketing findings have been reported with lamotrigine.8 Baseline hematologic testing and monitoring is recommended.
Hepatic effects. Transient abnormalities in liver function test (LFT) results often have been reported with carbamazepine, valproate, and zonisamide. Valproate has the highest risk of hepatotoxicity, which generally begins within the first 6 months of therapy and does not correlate with serum concentrations.8 Valproate-induced hepatotoxicity may have acute onset, and hepatic dysfunction may progress despite discontinuing the drug. LFTs are recommended at baseline and regular intervals.8
Metabolic effects. AEDs may increase appetite and body weight. Weight gain is common with valproate and pregabalin, but may occur with carbamazepine and gabapentin as well.8 Weight gain does not appear to be dose-related and may be minimized by diet and exercise. Lamotrigine and levetiracetam do not appear to affect weight, whereas weight loss and anorexia have been reported with topiramate and zonisamide.8
Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion have been reported with both carbamaze-pine and oxcarbazepine; the incidence is higher for oxcarbazepine. For both agents, hyponatremia risk is highest in elderly patients.12 Valproate—alone and concomitant with topiramate—may elevate ammonia levels, but monitoring generally is necessary only in symptomatic patients. Topira-mate and zonisamide increase the risks of hyperchloremic, nonanion gap metabolic acidosis and hypohidrosis; serum bicarbonate should be monitored at baseline and as clinically indicated.12,15
Psychiatric effects. Levetiracetam is associated with aggressive behavior, irritability, and increased anxiety and depression, which usually occur soon after drug initiation.8 Similarly, topiramate use is associated with affective and psychotic symptoms. Carbamazepine, gabapentin, lamotrigine, oxcarbazepine, and valproate have been associated with a decreased risk of psychiatric adverse effects compared with the overall incidence among AEDs.8
An FDA analysis suggested patients receiving AEDs have an elevated risk of suicidal ideation or behaviors, regardless of the indication.16 However, the data for increased suicidality are better supported for epilepsy patients than for those with a psychiatric diagnosis. The increased risk was noted as early as 1 week after initiating an AED and extended up to 6 months. The findings generally were consistent across demographic subgroups and AEDs.16 However, a recent study suggests the risk of suicidal acts or violent death is lowest with topiramate compared with gabapentin, lamotrigine, oxcarbazepine, and tiagabine.17 In patients with bipolar disorder, AEDs might not be associated with increased risk of suicidality and may be protective.18 All patients treated with AEDs should be closely monitored for emergence of or worsening depression, suicidality, and other behavior changes.16
Other effects. Valproate-induced pancreatitis is a rare, life-threatening adverse effect that generally occurs in the first 12 months of treatment and with dose increases.8 Amylase levels are not strong predictors of valproate-induced pancreatitis because elevations occur in asymptomatic users and normal levels have been reported in affected patients. Valproate also is linked to polycystic ovaries; evidence of this association is stronger in women with seizures than in those with mood disorders.19
Secondary to developing metabolic acidosis, both topiramate and zonisamide elevate the risk of developing calcium phosphate kidney stones with long-term use (>1 year).12,20 The risk appears higher in patients who are male, elderly, or have a personal or family history of kidney stones. Encourage patients taking topiramate or zonisamide to increase their fluid intake because this significantly reduces kidney stone risk.
Rare but potentially fatal angioedema has been reported with oxcarbazepine and pregabalin.12 History of angioedema or concurrent use of medications associated with angioedema (eg, angiotensin-converting enzyme inhibitors) may confer additional risk.12
Pregnancy and lactation. Carbamazepine and valproate have been associated with neural tube, craniofacial, and cardiac defects in the developing fetus.21 If possible, these agents should be avoided during pregnancy.21 Despite being teratogenic, carbamaze-pine and valproate are thought to be safe for women who are breast-feeding.8 Lamotrigine is associated with mid-facial clefts with first trimester exposure, but is still believed to be a relatively safe option during pregnancy.2 Because lamotrigine clearance increases as pregnancy progresses, the dosage may need to be increased during pregnancy and decreased after delivery to maintain therapeutic levels. Data are inadequate to assess the safety of gabapentin, levetiracetam, oxcarbaze-pine, tiagabine, topiramate, and zonisamide use during pregnancy and lactation.8,21
Table 422 provides additional clinical pearls regarding AED adverse effects.
Table 3
Comparison of antiepileptics’ effects on cognition
| Medication | Comparative effect on cognition | Compared with |
|---|---|---|
| Carbamazepine | ↑ | Topiramate |
| ↔ | Oxcarbazepine, tiagabine, valproate | |
| ↓ | Gabapentin, lamotrigine, levetiracetam, oxcarbazepine | |
| Lamotrigine | ↑ | Carbamazepine, topiramate |
| ↔ | Gabapentin | |
| Valproate | ↑ | Topiramate |
| ↔ | Carbamazepine, oxcarbazepine | |
| Gabapentin | ↑ | Carbamazepine, topiramate |
| ↔ | Lamotrigine | |
| Levetiracetam | ↑ | Carbamazepine, pregabalin, topiramate |
| Oxcarbazepine | ↔ | Carbamazepine, valproate |
| Pregabalin | ↓ | Levetiracetam |
| Tiagabine | ↑ | Topiramate |
| ↔ | Carbamazepine | |
| Topiramate | ↓ | Carbamazepine, gabapentin, lamotrigine, levetiracetam, tiagabine, valproate |
| ↑: positive profile; ↔: similar profile; ↓: negative profile Source: Reference 10 | ||
Table 4
Managing adverse effects of antiepileptics
| Medication | Comment(s) |
|---|---|
| Carbamazepine | Patients screening positive for the variant HLA-B1502 allele are at an elevated risk of developing Stevens-Johnson syndrome or toxic epidermal necrolysis. All patients of Asian descent should be screened22 |
| Gabapentin | Associated with weight gain, edema, and sedation; no reported effects on liver function tests |
| Lamotrigine | If therapy has been interrupted for ≥5 to 7 days (≥5 half-lives), restart according to initial dosing recommendations to significantly reduce the risk of rash |
| Levetiracetam | Appears to have the highest risk of psychiatric adverse effects |
| Oxcarbazepine | Higher risk of hyponatremia than carbamazepine |
| Pregabalin | Cases of angioedema have been reported (rare); may cause PR prolongation |
| Tiagabine | Elevated risk of seizures and status epilepticus when used in non-seizure patients |
| Topiramate | Increased fluid intake reduces the risk of developing kidney stones |
| Valproate | Tremor, thrombocytopenia, alopecia, and elevated liver enzymes have been associated with higher valproate doses/serum concentrations |
| Zonisamide | Avoid use in patients with severe sulfonamide allergy |
Therapeutic monitoring
Therapeutic serum drug concentration monitoring can help evaluate toxicity, medication adherence, and effects of potential drug-drug interactions. Individual variances in drug metabolism and distribution may affect the correlation between serum concentrations and clinical benefit or toxicity. Therapeutic monitoring can help establish target drug concentrations specific to your patient. The best time to obtain a drug concentration is when your patient is stable or free of most symptoms; this concentration may serve as the patient’s “therapeutic” concentration. Although laboratories have set therapeutic concentration ranges for each medication, treatment should focus on addressing your patient’s clinical presentation, rather than achieving the laboratory-suggested range.
Carbamazepine and valproate require therapeutic monitoring to prevent adverse effects from supratherapeutic concentrations (see this article at CurrentPsychiatry.com for a Table listing suggested ranges). The foundation for the therapeutic concentrations of these agents stems from neurology; however, these concentration ranges have been applicable in psychiatry.23
Carbamazepine generally requires more frequent monitoring because it has a narrow therapeutic index and relatively high potential for drug-drug interactions. Compared with lower doses, carbamazepine dosing associated with levels >12 μg/mL is more likely to induce toxicity.23 Carbamazepine autoinduction begins approximately 3 to 5 days after initiation and peaks between 3 to 4 weeks. Therefore, a drop in carbamazepine level from week 1 to week 4 of treatment likely is a pharmacokinetic indicator rather than a sign of nonadherence.
Some acute mania and maintenance bipolar studies have shown a correlation between clinical efficacy and valproate levels.24 A range of 50 to 125 μg/mL is well-accepted in clinical practice.24 For some patients, however, symptoms might not resolve until they are above the therapeutic range, but adverse effects are more likely at higher levels.24
Because concentrations of newer AEDs—including gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—have not been shown to correlate with therapeutic response, monitoring of serum concentrations is not necessary. However, routine laboratory tests to monitor for adverse effects are recommended.
Table
Therapeutic concentration monitoring for carbamazepine and valproate
| Medication | Suggested therapeutic range (trough level)* | Supratherapeutic presentation |
|---|---|---|
| Carbamazepine | 4 to 12 μg/mL | Ataxia, gastrointestinal upset, drowsiness, dizziness, diplopia, rash |
| Valproate (divalproex) | 50 to 125 μ/mL | Ataxia, nystagmus, tremor, hallucinations |
| *Values may vary among laboratories Source: Reference 23 | ||
Related Resources
- McElroy SL, Keck PE, Post RM, eds. Antiepileptic drugs to treat psychiatric disorders. New York, NY: Informa Health-care USA, Inc.; 2008.
- U.S. Food and Drug Administration. Suicidal behavior and ideation and antiepileptic drugs. www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM100190.
Drug Brand Names
- Carbamazepine • Carbatrol, Equetro, others
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Lamotrigine • Lamictal, Lamictal XR
- Levetiracetam • Keppra, Keppra XR
- Oxcarbazepine • Trileptal
- Pregabalin • Lyrica
- Tiagabine • Gabitril
- Topiramate • Topamax
- Valproate (Divalproex) • Depakote, Depakote ER
- Zonisamide • Zonegram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bowden CL. Anticonvulsants in bipolar disorders: current research and practice and future directions. Bipolar Disord. 2009;11(suppl 2):20-33.
2. Vigo DV, Baldessarini RJ. Anticonvulsants in the treatment of major depressive disorder: an overview. Harv Rev Psychiatry. 2009;17(4):231-241.
3. Citrome L. Adjunctive lithium and anticonvulsants for the treatment of schizophrenia: what is the evidence? Expert Rev Neurother. 2009;9(1):55-71.
4. Grunze HC. The effectiveness of anticonvulsants in psychiatric disorders. Dialogues Clin Neurosci. 2008;10(1):77-89.
5. Hoffman EJ, Mathew SJ. Anxiety disorders: a comprehensive review of pharmacotherapies. Mt Sinai J Med. 2008;75(3):248-262.
6. Rosenberg JM, Salzman C. Update: new uses for lithium and anticonvulsants. CNS Spectr. 2007;12(11):831-841.
7. McElroy SL, Guerdjikova AI, Martens B, et al. Role of antiepileptic drugs in the management of eating disorders. CNS Drugs. 2009;23(2):139-156.
8. Wilby J, Kainth A, Hawkins N, et al. Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation. Health Technol Assess. 2005;9(15):1-157.
9. Cheng LS, Prasad AN, Rieder MJ. Relationship between antiepileptic drugs and biological markers affecting long-term cardiovascular function in children and adolescents. Can J Clin Pharmacol. 2010;17(1):e5-46.
10. Park SP, Kwon SH. Cognitive effects of antiepileptic drugs. J Clin Neurol. 2008;4(3):99-106.
11. U.S. Food and Drug Administration. FDA drug safety communication: aseptic meningitis associated with use of lamictal (lamotrigine). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm221847.htm. Accessed October 29, 2010.
12. Wade JF, Dang CV, Nelson L, et al. Emergent complications of the newer anticonvulsants. J Emerg Med. 2010;38(2):231-237.
13. Beydoun A, Sackellares JC, Shu V, et al. Safety and efficacy of divalproex sodium monotherapy in partial epilepsy: a double-blind, concentration-response design clinical trial. Neurology. 1997;48(1):182-188.
14. Depakote [package inset]. North Chicago, IL: Abbott Laboratories; 2009.
15. Cerminara C, Seri S, Bombardieri R, et al. Hypohidrosis during topiramate treatment: a rare and reversible side effect. Pediatr Neurol. 2006;34(5):392-394.
16. U.S. Food and Drug Administration. Information for healthcare professionals: suicidal behavior and ideation and antiepileptic drugs. 2008. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm100192.htm. Accessed May 10, 2010.
17. Patorno E, Bohn RL, Wahl PM, et al. Anticonvulsant medications and the risk of suicide, attempted suicide, or violent death. JAMA. 2010;303(14):1401-1409.
18. Gibbons RD, Hur K, Brown CH, et al. Relationship between antiepileptic drugs and suicide attempts in patients with bipolar disorder. Arch Gen Psychiatry. 2009;66(12):1354-1360.
19. Bilo L, Meo R. Polycystic ovary syndrome in women using valproate: a review. Gynecol Endocrinol. 2008;24(10):562-570.
20. Welch BJ, Graybeal D, Moe OW, et al. Biochemical and stone-risk profiles with topiramate treatment. Am J Kidney Dis. 2006;48(4):555-563.
21. Harden CL, Meador KJ, Pennell PB, et al. Practice parameter update: management issues for women with epilepsy—focus on pregnancy (an evidence-based review): teratogenesis and perinatal outcomes: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology. 2009;73(2):133-141.
22. Chung WH, Hung SI, Chen YT. Genetic predisposition of life-threatening antiepileptic-induced skin reactions. Expert Opin Drug Saf. 2010;9(1):15-21.
23. Warner A, Privitera M, Bates D. Standards of laboratory practice: antiepileptic drug monitoring. Clin Chem. 1998;44(5):1085-1095.
24. Kaneria KM, Patel NC, Keck PE, Jr. Bipolar disorder: new strategy for checking serum valproate. Current Psychiatry. 2005;4(12):31-44.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/12/antiepileptics-for-psychiatric-illness.html#comments
Although antiepileptic drugs (AEDs) are used to treat a spectrum of psychiatric disorders, in some instances they are prescribed without clear evidence of clinical benefit or safety. When considering prescribing an AED, ask yourself:
- Does the evidence show the drug is efficacious for my patient’s disorder or symptoms?
- Which adverse effects are associated with this medication?
- What are the advantages of monitoring the patient’s serum drug concentration?
This review provides an evidence-based framework regarding the safe and effective use of AEDs in psychiatric patients.
For which disorders are AEDs effective?
Bipolar disorder. Multiple studies have found that AEDs are efficacious for treating bipolar disorder. Carbamazepine, valproate (divalproex), and lamotrigine have the most evidence supporting their use (Table 1). For an extensive bibliography of studies supporting AEDs for bipolar disorder and other psychiatric illnesses, see this article at CurrentPsychiatry.com. Carbamazepine and valproate are FDA-approved for treating acute manic or mixed episodes associated with bipolar I disorder in adults, and may be beneficial for maintenance treatment. Lamotrigine is FDA- approved for maintenance treatment of bipolar I disorder in adults; however, it lacks efficacy for mania and acute bipolar depression.1 The use of newer AEDs—including gabapentin, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—for bipolar disorder is not recommended because evidence is limited or inconclusive.
Major depressive disorder (MDD). Most studies of AEDs in MDD feature open-label designs with small samples. AEDs might have a role as an augmentation strategy, perhaps for patients with agitation or irritability or who partially respond to antidepressants.2
Schizophrenia. Although limited data support the practice, AEDs commonly are combined with antipsychotics to treat patients with schizophrenia.3,4 Clinicians who prescribe carbamazepine should recognize the potential for drug-drug interactions with antipsychotics (ie, increased metabolism of antipsychotics caused by cytochrome P450 [CYP450] 3A4 induction).
Anxiety disorders. AEDs have a limited role in treating anxiety disorders. These agents may be used as augmentation for patients who exhibit partial response or treatment resistance to recommended agents for anxiety disorders, such as selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines. For patients who cannot tolerate SSRIs or benzodiazepines, AEDs may be alternatives.5
Other disorders. AEDs could be used to treat other psychiatric conditions and disorders, including alcohol withdrawal and relapse prevention, benzodiazepine withdrawal, drug dependence and abstinence, obesity, and eating disorders.4,6,7 A list of suggested AEDs for some of these disorders appears in Table 2. However, these recommendations are based on findings from small randomized controlled trials, open-label trials, or case reports.
Table 1
Evidence supporting antiepileptics for mood disorders and schizophrenia
| Medication | Bipolar disorder | Major depressive disorder | Schizophrenia | ||
|---|---|---|---|---|---|
| Mania | Depression | Maintenance | |||
| Carbamazepine | (aggression, impulsivity) | ||||
| Lamotrigine | |||||
| Valproate | (aggression, impulsivity) | ||||
| Gabapentin | |||||
| Levetiracetam | |||||
| Oxcarbazepine | |||||
| Tiagabine | |||||
| Topiramate | |||||
| Zonisamide | |||||
| : strong evidence supporting efficacy; | |||||
| : moderate evidence supporting efficacy; | |||||
| : weak evidence supporting efficacy | |||||
| Source: For an extensive bibliography of studies that support these recommendations, see this article at CurrentPsychiatry.com | |||||
Table 2
Off-label use of antiepileptics for various psychiatric disorders
| Condition/disorder | Possible medication(s)* |
|---|---|
| Alcohol withdrawal/relapse prevention | Carbamazepine, topiramate, valproate |
| Benzodiazepine withdrawal | Carbamazepine, valproate |
| Binge eating disorder | Topiramate, zonisamide |
| Bulimia nervosa | Topiramate |
| Drug dependence/abstinence | Carbamazepine, lamotrigine, topiramate, tiagabine |
| Generalized anxiety disorder | Pregabalin, tiagabine |
| Obesity | Lamotrigine, topiramate, zonisamide |
| Panic disorder | Valproate |
| Posttraumatic stress disorder | Lamotrigine |
| Social phobia | Gabapentin, pregabalin |
| * Based on small randomized controlled trials, open-label trials, or case reports. Further investigation in large systematic trials is needed | |
What about adverse effects?
A thorough understanding of each AED’s adverse effect profile is critical to determine which agent is most suitable for your patient. Factors that may affect the risk of adverse effects include:
- rate of dose escalation
- length of early tolerance development
- rate of increase in and magnitude of peak serum concentrations
- dosing frequency
- pharmacodynamic/pharmacokinetic interactions
- pharmacogenomics.
Cardiovascular effects. Although many AED clinical trials reported “edema” as an adverse effect, peripheral edema specifically has been reported with gabapentin, lamotrigine, tiagabine, and valproate.8 Peripheral edema with these agents generally has not been linked to cardiovascular complications in healthy adults. Carbamazepine and pregabalin may cause conduction abnormalities and should be used with caution in patients with underlying electrocardiogram abnormalities.8
Chronic carbamazepine use results in elevated plasma homocysteine and serum lipoprotein concentrations, which are biomarkers of cardiovascular disease.9 If clinically appropriate, switching from carbamazepine to a non-inducing AED (ie, lamotrigine) may ameliorate such effects. Chronic valproate use has been associated with increased plasma homocysteine levels; increases in serum lipoproteins may parallel valproate-induced weight gain.9
CNS effects. Common acute neurologic effects of AEDs include somnolence, dizziness, and ataxia. The incidence of these effects vary by agent; gabapentin and zonisamide appear to be the most sedating.8 However, in general these effects occur at the start of treatment and abate within a few days with continued treatment or dosage reduction. Starting at a low dose and slowly titrating may help prevent neurologic adverse effects.8 Peripheral neurologic effects—specifically paresthesias—are primarily associated with topiramate and zonisamide and may be attributed to carbonic anhydrase inhibition.8
AEDs’ primary cognitive effects include impaired attention/vigilance, psychomotor speed, and secondary involvement of other cognitive functions (eg, memory). Whereas carbamazepine and valproate have similar cognitive effects (ie, negative effects on attention, learning, memory, and psychomotor speed), newer AEDs except topiramate may produce fewer cognitive adverse effects (Table 3).10 Topiramate is associated with the highest rate of cognitive dysfunction, with frequent complaints of decreased concentration and attention, word-finding problems, and/or impaired memory.8,10
The FDA recently announced a warning of a risk of aseptic meningitis with lamotrigine.11 In 40 reported cases, symptoms—headache, fever, nausea, vomiting, nuchal rigidity, rash, photophobia, and myalgias—occurred between 1 and 42 days of treatment and typically resolved after lamotrigine was withdrawn. In 15 patients in whom lamotrigine was re-initiated, meningitis symptoms returned quickly and with greater severity.11
Dermatologic effects. Skin rashes have been reported with all AEDs; the highest risk is associated with carbamazepine and lamotrigine.12 Predictors of cutaneous reactions to lamotrigine include:
- high initial dose and rapid escalation
- concomitant valproate use without lamotrigine dosage adjustment
- young age.12
A history of AED-induced rash also increases risk. For example, patients with a history of rash with carbamazepine are at risk for rash with oxcarbazepine because of cross-reactivity.
Any AED-induced skin rash may progress to a fatal reaction, such as toxic epidermal necrolysis or Stevens-Johnson syndrome. Carbamazepine and lamotrigine are most strongly associated with these severe reactions.12 Patients who exhibit painful rash, fever, enlarged lymph nodes, malaise, and mucosal involvement may be at risk for a more severe disease course.12 If a patient taking an AED develops a rash, immediately stop the drug and perform a thorough risk-benefit analysis before considering re-initiation.
Hematologic effects. Thrombocytopenia has been reported with carbamazepine, lamotrigine, pregabalin, and valproate. The highest risk is for valproate at doses >50 mg/kg/d or serum concentrations >110 μg/mL in women or >135 μg/mL in men.13,14 Decreased platelet count is common with valproate, but coagulation dysfunction may not be present until counts fall below 50,000/mL. Carbamazepine is associated with leukopenia, which usually occurs in early treatment and resolves without dosage adjustments; however, this agent carries a black-box warning for risks of agranulocytosis and aplastic anemia. Similar postmarketing findings have been reported with lamotrigine.8 Baseline hematologic testing and monitoring is recommended.
Hepatic effects. Transient abnormalities in liver function test (LFT) results often have been reported with carbamazepine, valproate, and zonisamide. Valproate has the highest risk of hepatotoxicity, which generally begins within the first 6 months of therapy and does not correlate with serum concentrations.8 Valproate-induced hepatotoxicity may have acute onset, and hepatic dysfunction may progress despite discontinuing the drug. LFTs are recommended at baseline and regular intervals.8
Metabolic effects. AEDs may increase appetite and body weight. Weight gain is common with valproate and pregabalin, but may occur with carbamazepine and gabapentin as well.8 Weight gain does not appear to be dose-related and may be minimized by diet and exercise. Lamotrigine and levetiracetam do not appear to affect weight, whereas weight loss and anorexia have been reported with topiramate and zonisamide.8
Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion have been reported with both carbamaze-pine and oxcarbazepine; the incidence is higher for oxcarbazepine. For both agents, hyponatremia risk is highest in elderly patients.12 Valproate—alone and concomitant with topiramate—may elevate ammonia levels, but monitoring generally is necessary only in symptomatic patients. Topira-mate and zonisamide increase the risks of hyperchloremic, nonanion gap metabolic acidosis and hypohidrosis; serum bicarbonate should be monitored at baseline and as clinically indicated.12,15
Psychiatric effects. Levetiracetam is associated with aggressive behavior, irritability, and increased anxiety and depression, which usually occur soon after drug initiation.8 Similarly, topiramate use is associated with affective and psychotic symptoms. Carbamazepine, gabapentin, lamotrigine, oxcarbazepine, and valproate have been associated with a decreased risk of psychiatric adverse effects compared with the overall incidence among AEDs.8
An FDA analysis suggested patients receiving AEDs have an elevated risk of suicidal ideation or behaviors, regardless of the indication.16 However, the data for increased suicidality are better supported for epilepsy patients than for those with a psychiatric diagnosis. The increased risk was noted as early as 1 week after initiating an AED and extended up to 6 months. The findings generally were consistent across demographic subgroups and AEDs.16 However, a recent study suggests the risk of suicidal acts or violent death is lowest with topiramate compared with gabapentin, lamotrigine, oxcarbazepine, and tiagabine.17 In patients with bipolar disorder, AEDs might not be associated with increased risk of suicidality and may be protective.18 All patients treated with AEDs should be closely monitored for emergence of or worsening depression, suicidality, and other behavior changes.16
Other effects. Valproate-induced pancreatitis is a rare, life-threatening adverse effect that generally occurs in the first 12 months of treatment and with dose increases.8 Amylase levels are not strong predictors of valproate-induced pancreatitis because elevations occur in asymptomatic users and normal levels have been reported in affected patients. Valproate also is linked to polycystic ovaries; evidence of this association is stronger in women with seizures than in those with mood disorders.19
Secondary to developing metabolic acidosis, both topiramate and zonisamide elevate the risk of developing calcium phosphate kidney stones with long-term use (>1 year).12,20 The risk appears higher in patients who are male, elderly, or have a personal or family history of kidney stones. Encourage patients taking topiramate or zonisamide to increase their fluid intake because this significantly reduces kidney stone risk.
Rare but potentially fatal angioedema has been reported with oxcarbazepine and pregabalin.12 History of angioedema or concurrent use of medications associated with angioedema (eg, angiotensin-converting enzyme inhibitors) may confer additional risk.12
Pregnancy and lactation. Carbamazepine and valproate have been associated with neural tube, craniofacial, and cardiac defects in the developing fetus.21 If possible, these agents should be avoided during pregnancy.21 Despite being teratogenic, carbamaze-pine and valproate are thought to be safe for women who are breast-feeding.8 Lamotrigine is associated with mid-facial clefts with first trimester exposure, but is still believed to be a relatively safe option during pregnancy.2 Because lamotrigine clearance increases as pregnancy progresses, the dosage may need to be increased during pregnancy and decreased after delivery to maintain therapeutic levels. Data are inadequate to assess the safety of gabapentin, levetiracetam, oxcarbaze-pine, tiagabine, topiramate, and zonisamide use during pregnancy and lactation.8,21
Table 422 provides additional clinical pearls regarding AED adverse effects.
Table 3
Comparison of antiepileptics’ effects on cognition
| Medication | Comparative effect on cognition | Compared with |
|---|---|---|
| Carbamazepine | ↑ | Topiramate |
| ↔ | Oxcarbazepine, tiagabine, valproate | |
| ↓ | Gabapentin, lamotrigine, levetiracetam, oxcarbazepine | |
| Lamotrigine | ↑ | Carbamazepine, topiramate |
| ↔ | Gabapentin | |
| Valproate | ↑ | Topiramate |
| ↔ | Carbamazepine, oxcarbazepine | |
| Gabapentin | ↑ | Carbamazepine, topiramate |
| ↔ | Lamotrigine | |
| Levetiracetam | ↑ | Carbamazepine, pregabalin, topiramate |
| Oxcarbazepine | ↔ | Carbamazepine, valproate |
| Pregabalin | ↓ | Levetiracetam |
| Tiagabine | ↑ | Topiramate |
| ↔ | Carbamazepine | |
| Topiramate | ↓ | Carbamazepine, gabapentin, lamotrigine, levetiracetam, tiagabine, valproate |
| ↑: positive profile; ↔: similar profile; ↓: negative profile Source: Reference 10 | ||
Table 4
Managing adverse effects of antiepileptics
| Medication | Comment(s) |
|---|---|
| Carbamazepine | Patients screening positive for the variant HLA-B1502 allele are at an elevated risk of developing Stevens-Johnson syndrome or toxic epidermal necrolysis. All patients of Asian descent should be screened22 |
| Gabapentin | Associated with weight gain, edema, and sedation; no reported effects on liver function tests |
| Lamotrigine | If therapy has been interrupted for ≥5 to 7 days (≥5 half-lives), restart according to initial dosing recommendations to significantly reduce the risk of rash |
| Levetiracetam | Appears to have the highest risk of psychiatric adverse effects |
| Oxcarbazepine | Higher risk of hyponatremia than carbamazepine |
| Pregabalin | Cases of angioedema have been reported (rare); may cause PR prolongation |
| Tiagabine | Elevated risk of seizures and status epilepticus when used in non-seizure patients |
| Topiramate | Increased fluid intake reduces the risk of developing kidney stones |
| Valproate | Tremor, thrombocytopenia, alopecia, and elevated liver enzymes have been associated with higher valproate doses/serum concentrations |
| Zonisamide | Avoid use in patients with severe sulfonamide allergy |
Therapeutic monitoring
Therapeutic serum drug concentration monitoring can help evaluate toxicity, medication adherence, and effects of potential drug-drug interactions. Individual variances in drug metabolism and distribution may affect the correlation between serum concentrations and clinical benefit or toxicity. Therapeutic monitoring can help establish target drug concentrations specific to your patient. The best time to obtain a drug concentration is when your patient is stable or free of most symptoms; this concentration may serve as the patient’s “therapeutic” concentration. Although laboratories have set therapeutic concentration ranges for each medication, treatment should focus on addressing your patient’s clinical presentation, rather than achieving the laboratory-suggested range.
Carbamazepine and valproate require therapeutic monitoring to prevent adverse effects from supratherapeutic concentrations (see this article at CurrentPsychiatry.com for a Table listing suggested ranges). The foundation for the therapeutic concentrations of these agents stems from neurology; however, these concentration ranges have been applicable in psychiatry.23
Carbamazepine generally requires more frequent monitoring because it has a narrow therapeutic index and relatively high potential for drug-drug interactions. Compared with lower doses, carbamazepine dosing associated with levels >12 μg/mL is more likely to induce toxicity.23 Carbamazepine autoinduction begins approximately 3 to 5 days after initiation and peaks between 3 to 4 weeks. Therefore, a drop in carbamazepine level from week 1 to week 4 of treatment likely is a pharmacokinetic indicator rather than a sign of nonadherence.
Some acute mania and maintenance bipolar studies have shown a correlation between clinical efficacy and valproate levels.24 A range of 50 to 125 μg/mL is well-accepted in clinical practice.24 For some patients, however, symptoms might not resolve until they are above the therapeutic range, but adverse effects are more likely at higher levels.24
Because concentrations of newer AEDs—including gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—have not been shown to correlate with therapeutic response, monitoring of serum concentrations is not necessary. However, routine laboratory tests to monitor for adverse effects are recommended.
Table
Therapeutic concentration monitoring for carbamazepine and valproate
| Medication | Suggested therapeutic range (trough level)* | Supratherapeutic presentation |
|---|---|---|
| Carbamazepine | 4 to 12 μg/mL | Ataxia, gastrointestinal upset, drowsiness, dizziness, diplopia, rash |
| Valproate (divalproex) | 50 to 125 μ/mL | Ataxia, nystagmus, tremor, hallucinations |
| *Values may vary among laboratories Source: Reference 23 | ||
Related Resources
- McElroy SL, Keck PE, Post RM, eds. Antiepileptic drugs to treat psychiatric disorders. New York, NY: Informa Health-care USA, Inc.; 2008.
- U.S. Food and Drug Administration. Suicidal behavior and ideation and antiepileptic drugs. www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM100190.
Drug Brand Names
- Carbamazepine • Carbatrol, Equetro, others
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Lamotrigine • Lamictal, Lamictal XR
- Levetiracetam • Keppra, Keppra XR
- Oxcarbazepine • Trileptal
- Pregabalin • Lyrica
- Tiagabine • Gabitril
- Topiramate • Topamax
- Valproate (Divalproex) • Depakote, Depakote ER
- Zonisamide • Zonegram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at http://currentpsychiatry.blogspot.com/2010/12/antiepileptics-for-psychiatric-illness.html#comments
Although antiepileptic drugs (AEDs) are used to treat a spectrum of psychiatric disorders, in some instances they are prescribed without clear evidence of clinical benefit or safety. When considering prescribing an AED, ask yourself:
- Does the evidence show the drug is efficacious for my patient’s disorder or symptoms?
- Which adverse effects are associated with this medication?
- What are the advantages of monitoring the patient’s serum drug concentration?
This review provides an evidence-based framework regarding the safe and effective use of AEDs in psychiatric patients.
For which disorders are AEDs effective?
Bipolar disorder. Multiple studies have found that AEDs are efficacious for treating bipolar disorder. Carbamazepine, valproate (divalproex), and lamotrigine have the most evidence supporting their use (Table 1). For an extensive bibliography of studies supporting AEDs for bipolar disorder and other psychiatric illnesses, see this article at CurrentPsychiatry.com. Carbamazepine and valproate are FDA-approved for treating acute manic or mixed episodes associated with bipolar I disorder in adults, and may be beneficial for maintenance treatment. Lamotrigine is FDA- approved for maintenance treatment of bipolar I disorder in adults; however, it lacks efficacy for mania and acute bipolar depression.1 The use of newer AEDs—including gabapentin, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—for bipolar disorder is not recommended because evidence is limited or inconclusive.
Major depressive disorder (MDD). Most studies of AEDs in MDD feature open-label designs with small samples. AEDs might have a role as an augmentation strategy, perhaps for patients with agitation or irritability or who partially respond to antidepressants.2
Schizophrenia. Although limited data support the practice, AEDs commonly are combined with antipsychotics to treat patients with schizophrenia.3,4 Clinicians who prescribe carbamazepine should recognize the potential for drug-drug interactions with antipsychotics (ie, increased metabolism of antipsychotics caused by cytochrome P450 [CYP450] 3A4 induction).
Anxiety disorders. AEDs have a limited role in treating anxiety disorders. These agents may be used as augmentation for patients who exhibit partial response or treatment resistance to recommended agents for anxiety disorders, such as selective serotonin reuptake inhibitors (SSRIs) or benzodiazepines. For patients who cannot tolerate SSRIs or benzodiazepines, AEDs may be alternatives.5
Other disorders. AEDs could be used to treat other psychiatric conditions and disorders, including alcohol withdrawal and relapse prevention, benzodiazepine withdrawal, drug dependence and abstinence, obesity, and eating disorders.4,6,7 A list of suggested AEDs for some of these disorders appears in Table 2. However, these recommendations are based on findings from small randomized controlled trials, open-label trials, or case reports.
Table 1
Evidence supporting antiepileptics for mood disorders and schizophrenia
| Medication | Bipolar disorder | Major depressive disorder | Schizophrenia | ||
|---|---|---|---|---|---|
| Mania | Depression | Maintenance | |||
| Carbamazepine | (aggression, impulsivity) | ||||
| Lamotrigine | |||||
| Valproate | (aggression, impulsivity) | ||||
| Gabapentin | |||||
| Levetiracetam | |||||
| Oxcarbazepine | |||||
| Tiagabine | |||||
| Topiramate | |||||
| Zonisamide | |||||
| : strong evidence supporting efficacy; | |||||
| : moderate evidence supporting efficacy; | |||||
| : weak evidence supporting efficacy | |||||
| Source: For an extensive bibliography of studies that support these recommendations, see this article at CurrentPsychiatry.com | |||||
Table 2
Off-label use of antiepileptics for various psychiatric disorders
| Condition/disorder | Possible medication(s)* |
|---|---|
| Alcohol withdrawal/relapse prevention | Carbamazepine, topiramate, valproate |
| Benzodiazepine withdrawal | Carbamazepine, valproate |
| Binge eating disorder | Topiramate, zonisamide |
| Bulimia nervosa | Topiramate |
| Drug dependence/abstinence | Carbamazepine, lamotrigine, topiramate, tiagabine |
| Generalized anxiety disorder | Pregabalin, tiagabine |
| Obesity | Lamotrigine, topiramate, zonisamide |
| Panic disorder | Valproate |
| Posttraumatic stress disorder | Lamotrigine |
| Social phobia | Gabapentin, pregabalin |
| * Based on small randomized controlled trials, open-label trials, or case reports. Further investigation in large systematic trials is needed | |
What about adverse effects?
A thorough understanding of each AED’s adverse effect profile is critical to determine which agent is most suitable for your patient. Factors that may affect the risk of adverse effects include:
- rate of dose escalation
- length of early tolerance development
- rate of increase in and magnitude of peak serum concentrations
- dosing frequency
- pharmacodynamic/pharmacokinetic interactions
- pharmacogenomics.
Cardiovascular effects. Although many AED clinical trials reported “edema” as an adverse effect, peripheral edema specifically has been reported with gabapentin, lamotrigine, tiagabine, and valproate.8 Peripheral edema with these agents generally has not been linked to cardiovascular complications in healthy adults. Carbamazepine and pregabalin may cause conduction abnormalities and should be used with caution in patients with underlying electrocardiogram abnormalities.8
Chronic carbamazepine use results in elevated plasma homocysteine and serum lipoprotein concentrations, which are biomarkers of cardiovascular disease.9 If clinically appropriate, switching from carbamazepine to a non-inducing AED (ie, lamotrigine) may ameliorate such effects. Chronic valproate use has been associated with increased plasma homocysteine levels; increases in serum lipoproteins may parallel valproate-induced weight gain.9
CNS effects. Common acute neurologic effects of AEDs include somnolence, dizziness, and ataxia. The incidence of these effects vary by agent; gabapentin and zonisamide appear to be the most sedating.8 However, in general these effects occur at the start of treatment and abate within a few days with continued treatment or dosage reduction. Starting at a low dose and slowly titrating may help prevent neurologic adverse effects.8 Peripheral neurologic effects—specifically paresthesias—are primarily associated with topiramate and zonisamide and may be attributed to carbonic anhydrase inhibition.8
AEDs’ primary cognitive effects include impaired attention/vigilance, psychomotor speed, and secondary involvement of other cognitive functions (eg, memory). Whereas carbamazepine and valproate have similar cognitive effects (ie, negative effects on attention, learning, memory, and psychomotor speed), newer AEDs except topiramate may produce fewer cognitive adverse effects (Table 3).10 Topiramate is associated with the highest rate of cognitive dysfunction, with frequent complaints of decreased concentration and attention, word-finding problems, and/or impaired memory.8,10
The FDA recently announced a warning of a risk of aseptic meningitis with lamotrigine.11 In 40 reported cases, symptoms—headache, fever, nausea, vomiting, nuchal rigidity, rash, photophobia, and myalgias—occurred between 1 and 42 days of treatment and typically resolved after lamotrigine was withdrawn. In 15 patients in whom lamotrigine was re-initiated, meningitis symptoms returned quickly and with greater severity.11
Dermatologic effects. Skin rashes have been reported with all AEDs; the highest risk is associated with carbamazepine and lamotrigine.12 Predictors of cutaneous reactions to lamotrigine include:
- high initial dose and rapid escalation
- concomitant valproate use without lamotrigine dosage adjustment
- young age.12
A history of AED-induced rash also increases risk. For example, patients with a history of rash with carbamazepine are at risk for rash with oxcarbazepine because of cross-reactivity.
Any AED-induced skin rash may progress to a fatal reaction, such as toxic epidermal necrolysis or Stevens-Johnson syndrome. Carbamazepine and lamotrigine are most strongly associated with these severe reactions.12 Patients who exhibit painful rash, fever, enlarged lymph nodes, malaise, and mucosal involvement may be at risk for a more severe disease course.12 If a patient taking an AED develops a rash, immediately stop the drug and perform a thorough risk-benefit analysis before considering re-initiation.
Hematologic effects. Thrombocytopenia has been reported with carbamazepine, lamotrigine, pregabalin, and valproate. The highest risk is for valproate at doses >50 mg/kg/d or serum concentrations >110 μg/mL in women or >135 μg/mL in men.13,14 Decreased platelet count is common with valproate, but coagulation dysfunction may not be present until counts fall below 50,000/mL. Carbamazepine is associated with leukopenia, which usually occurs in early treatment and resolves without dosage adjustments; however, this agent carries a black-box warning for risks of agranulocytosis and aplastic anemia. Similar postmarketing findings have been reported with lamotrigine.8 Baseline hematologic testing and monitoring is recommended.
Hepatic effects. Transient abnormalities in liver function test (LFT) results often have been reported with carbamazepine, valproate, and zonisamide. Valproate has the highest risk of hepatotoxicity, which generally begins within the first 6 months of therapy and does not correlate with serum concentrations.8 Valproate-induced hepatotoxicity may have acute onset, and hepatic dysfunction may progress despite discontinuing the drug. LFTs are recommended at baseline and regular intervals.8
Metabolic effects. AEDs may increase appetite and body weight. Weight gain is common with valproate and pregabalin, but may occur with carbamazepine and gabapentin as well.8 Weight gain does not appear to be dose-related and may be minimized by diet and exercise. Lamotrigine and levetiracetam do not appear to affect weight, whereas weight loss and anorexia have been reported with topiramate and zonisamide.8
Hyponatremia and syndrome of inappropriate antidiuretic hormone secretion have been reported with both carbamaze-pine and oxcarbazepine; the incidence is higher for oxcarbazepine. For both agents, hyponatremia risk is highest in elderly patients.12 Valproate—alone and concomitant with topiramate—may elevate ammonia levels, but monitoring generally is necessary only in symptomatic patients. Topira-mate and zonisamide increase the risks of hyperchloremic, nonanion gap metabolic acidosis and hypohidrosis; serum bicarbonate should be monitored at baseline and as clinically indicated.12,15
Psychiatric effects. Levetiracetam is associated with aggressive behavior, irritability, and increased anxiety and depression, which usually occur soon after drug initiation.8 Similarly, topiramate use is associated with affective and psychotic symptoms. Carbamazepine, gabapentin, lamotrigine, oxcarbazepine, and valproate have been associated with a decreased risk of psychiatric adverse effects compared with the overall incidence among AEDs.8
An FDA analysis suggested patients receiving AEDs have an elevated risk of suicidal ideation or behaviors, regardless of the indication.16 However, the data for increased suicidality are better supported for epilepsy patients than for those with a psychiatric diagnosis. The increased risk was noted as early as 1 week after initiating an AED and extended up to 6 months. The findings generally were consistent across demographic subgroups and AEDs.16 However, a recent study suggests the risk of suicidal acts or violent death is lowest with topiramate compared with gabapentin, lamotrigine, oxcarbazepine, and tiagabine.17 In patients with bipolar disorder, AEDs might not be associated with increased risk of suicidality and may be protective.18 All patients treated with AEDs should be closely monitored for emergence of or worsening depression, suicidality, and other behavior changes.16
Other effects. Valproate-induced pancreatitis is a rare, life-threatening adverse effect that generally occurs in the first 12 months of treatment and with dose increases.8 Amylase levels are not strong predictors of valproate-induced pancreatitis because elevations occur in asymptomatic users and normal levels have been reported in affected patients. Valproate also is linked to polycystic ovaries; evidence of this association is stronger in women with seizures than in those with mood disorders.19
Secondary to developing metabolic acidosis, both topiramate and zonisamide elevate the risk of developing calcium phosphate kidney stones with long-term use (>1 year).12,20 The risk appears higher in patients who are male, elderly, or have a personal or family history of kidney stones. Encourage patients taking topiramate or zonisamide to increase their fluid intake because this significantly reduces kidney stone risk.
Rare but potentially fatal angioedema has been reported with oxcarbazepine and pregabalin.12 History of angioedema or concurrent use of medications associated with angioedema (eg, angiotensin-converting enzyme inhibitors) may confer additional risk.12
Pregnancy and lactation. Carbamazepine and valproate have been associated with neural tube, craniofacial, and cardiac defects in the developing fetus.21 If possible, these agents should be avoided during pregnancy.21 Despite being teratogenic, carbamaze-pine and valproate are thought to be safe for women who are breast-feeding.8 Lamotrigine is associated with mid-facial clefts with first trimester exposure, but is still believed to be a relatively safe option during pregnancy.2 Because lamotrigine clearance increases as pregnancy progresses, the dosage may need to be increased during pregnancy and decreased after delivery to maintain therapeutic levels. Data are inadequate to assess the safety of gabapentin, levetiracetam, oxcarbaze-pine, tiagabine, topiramate, and zonisamide use during pregnancy and lactation.8,21
Table 422 provides additional clinical pearls regarding AED adverse effects.
Table 3
Comparison of antiepileptics’ effects on cognition
| Medication | Comparative effect on cognition | Compared with |
|---|---|---|
| Carbamazepine | ↑ | Topiramate |
| ↔ | Oxcarbazepine, tiagabine, valproate | |
| ↓ | Gabapentin, lamotrigine, levetiracetam, oxcarbazepine | |
| Lamotrigine | ↑ | Carbamazepine, topiramate |
| ↔ | Gabapentin | |
| Valproate | ↑ | Topiramate |
| ↔ | Carbamazepine, oxcarbazepine | |
| Gabapentin | ↑ | Carbamazepine, topiramate |
| ↔ | Lamotrigine | |
| Levetiracetam | ↑ | Carbamazepine, pregabalin, topiramate |
| Oxcarbazepine | ↔ | Carbamazepine, valproate |
| Pregabalin | ↓ | Levetiracetam |
| Tiagabine | ↑ | Topiramate |
| ↔ | Carbamazepine | |
| Topiramate | ↓ | Carbamazepine, gabapentin, lamotrigine, levetiracetam, tiagabine, valproate |
| ↑: positive profile; ↔: similar profile; ↓: negative profile Source: Reference 10 | ||
Table 4
Managing adverse effects of antiepileptics
| Medication | Comment(s) |
|---|---|
| Carbamazepine | Patients screening positive for the variant HLA-B1502 allele are at an elevated risk of developing Stevens-Johnson syndrome or toxic epidermal necrolysis. All patients of Asian descent should be screened22 |
| Gabapentin | Associated with weight gain, edema, and sedation; no reported effects on liver function tests |
| Lamotrigine | If therapy has been interrupted for ≥5 to 7 days (≥5 half-lives), restart according to initial dosing recommendations to significantly reduce the risk of rash |
| Levetiracetam | Appears to have the highest risk of psychiatric adverse effects |
| Oxcarbazepine | Higher risk of hyponatremia than carbamazepine |
| Pregabalin | Cases of angioedema have been reported (rare); may cause PR prolongation |
| Tiagabine | Elevated risk of seizures and status epilepticus when used in non-seizure patients |
| Topiramate | Increased fluid intake reduces the risk of developing kidney stones |
| Valproate | Tremor, thrombocytopenia, alopecia, and elevated liver enzymes have been associated with higher valproate doses/serum concentrations |
| Zonisamide | Avoid use in patients with severe sulfonamide allergy |
Therapeutic monitoring
Therapeutic serum drug concentration monitoring can help evaluate toxicity, medication adherence, and effects of potential drug-drug interactions. Individual variances in drug metabolism and distribution may affect the correlation between serum concentrations and clinical benefit or toxicity. Therapeutic monitoring can help establish target drug concentrations specific to your patient. The best time to obtain a drug concentration is when your patient is stable or free of most symptoms; this concentration may serve as the patient’s “therapeutic” concentration. Although laboratories have set therapeutic concentration ranges for each medication, treatment should focus on addressing your patient’s clinical presentation, rather than achieving the laboratory-suggested range.
Carbamazepine and valproate require therapeutic monitoring to prevent adverse effects from supratherapeutic concentrations (see this article at CurrentPsychiatry.com for a Table listing suggested ranges). The foundation for the therapeutic concentrations of these agents stems from neurology; however, these concentration ranges have been applicable in psychiatry.23
Carbamazepine generally requires more frequent monitoring because it has a narrow therapeutic index and relatively high potential for drug-drug interactions. Compared with lower doses, carbamazepine dosing associated with levels >12 μg/mL is more likely to induce toxicity.23 Carbamazepine autoinduction begins approximately 3 to 5 days after initiation and peaks between 3 to 4 weeks. Therefore, a drop in carbamazepine level from week 1 to week 4 of treatment likely is a pharmacokinetic indicator rather than a sign of nonadherence.
Some acute mania and maintenance bipolar studies have shown a correlation between clinical efficacy and valproate levels.24 A range of 50 to 125 μg/mL is well-accepted in clinical practice.24 For some patients, however, symptoms might not resolve until they are above the therapeutic range, but adverse effects are more likely at higher levels.24
Because concentrations of newer AEDs—including gabapentin, lamotrigine, levetiracetam, oxcarbazepine, tiagabine, topiramate, and zonisamide—have not been shown to correlate with therapeutic response, monitoring of serum concentrations is not necessary. However, routine laboratory tests to monitor for adverse effects are recommended.
Table
Therapeutic concentration monitoring for carbamazepine and valproate
| Medication | Suggested therapeutic range (trough level)* | Supratherapeutic presentation |
|---|---|---|
| Carbamazepine | 4 to 12 μg/mL | Ataxia, gastrointestinal upset, drowsiness, dizziness, diplopia, rash |
| Valproate (divalproex) | 50 to 125 μ/mL | Ataxia, nystagmus, tremor, hallucinations |
| *Values may vary among laboratories Source: Reference 23 | ||
Related Resources
- McElroy SL, Keck PE, Post RM, eds. Antiepileptic drugs to treat psychiatric disorders. New York, NY: Informa Health-care USA, Inc.; 2008.
- U.S. Food and Drug Administration. Suicidal behavior and ideation and antiepileptic drugs. www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM100190.
Drug Brand Names
- Carbamazepine • Carbatrol, Equetro, others
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Lamotrigine • Lamictal, Lamictal XR
- Levetiracetam • Keppra, Keppra XR
- Oxcarbazepine • Trileptal
- Pregabalin • Lyrica
- Tiagabine • Gabitril
- Topiramate • Topamax
- Valproate (Divalproex) • Depakote, Depakote ER
- Zonisamide • Zonegram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bowden CL. Anticonvulsants in bipolar disorders: current research and practice and future directions. Bipolar Disord. 2009;11(suppl 2):20-33.
2. Vigo DV, Baldessarini RJ. Anticonvulsants in the treatment of major depressive disorder: an overview. Harv Rev Psychiatry. 2009;17(4):231-241.
3. Citrome L. Adjunctive lithium and anticonvulsants for the treatment of schizophrenia: what is the evidence? Expert Rev Neurother. 2009;9(1):55-71.
4. Grunze HC. The effectiveness of anticonvulsants in psychiatric disorders. Dialogues Clin Neurosci. 2008;10(1):77-89.
5. Hoffman EJ, Mathew SJ. Anxiety disorders: a comprehensive review of pharmacotherapies. Mt Sinai J Med. 2008;75(3):248-262.
6. Rosenberg JM, Salzman C. Update: new uses for lithium and anticonvulsants. CNS Spectr. 2007;12(11):831-841.
7. McElroy SL, Guerdjikova AI, Martens B, et al. Role of antiepileptic drugs in the management of eating disorders. CNS Drugs. 2009;23(2):139-156.
8. Wilby J, Kainth A, Hawkins N, et al. Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation. Health Technol Assess. 2005;9(15):1-157.
9. Cheng LS, Prasad AN, Rieder MJ. Relationship between antiepileptic drugs and biological markers affecting long-term cardiovascular function in children and adolescents. Can J Clin Pharmacol. 2010;17(1):e5-46.
10. Park SP, Kwon SH. Cognitive effects of antiepileptic drugs. J Clin Neurol. 2008;4(3):99-106.
11. U.S. Food and Drug Administration. FDA drug safety communication: aseptic meningitis associated with use of lamictal (lamotrigine). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm221847.htm. Accessed October 29, 2010.
12. Wade JF, Dang CV, Nelson L, et al. Emergent complications of the newer anticonvulsants. J Emerg Med. 2010;38(2):231-237.
13. Beydoun A, Sackellares JC, Shu V, et al. Safety and efficacy of divalproex sodium monotherapy in partial epilepsy: a double-blind, concentration-response design clinical trial. Neurology. 1997;48(1):182-188.
14. Depakote [package inset]. North Chicago, IL: Abbott Laboratories; 2009.
15. Cerminara C, Seri S, Bombardieri R, et al. Hypohidrosis during topiramate treatment: a rare and reversible side effect. Pediatr Neurol. 2006;34(5):392-394.
16. U.S. Food and Drug Administration. Information for healthcare professionals: suicidal behavior and ideation and antiepileptic drugs. 2008. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm100192.htm. Accessed May 10, 2010.
17. Patorno E, Bohn RL, Wahl PM, et al. Anticonvulsant medications and the risk of suicide, attempted suicide, or violent death. JAMA. 2010;303(14):1401-1409.
18. Gibbons RD, Hur K, Brown CH, et al. Relationship between antiepileptic drugs and suicide attempts in patients with bipolar disorder. Arch Gen Psychiatry. 2009;66(12):1354-1360.
19. Bilo L, Meo R. Polycystic ovary syndrome in women using valproate: a review. Gynecol Endocrinol. 2008;24(10):562-570.
20. Welch BJ, Graybeal D, Moe OW, et al. Biochemical and stone-risk profiles with topiramate treatment. Am J Kidney Dis. 2006;48(4):555-563.
21. Harden CL, Meador KJ, Pennell PB, et al. Practice parameter update: management issues for women with epilepsy—focus on pregnancy (an evidence-based review): teratogenesis and perinatal outcomes: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology. 2009;73(2):133-141.
22. Chung WH, Hung SI, Chen YT. Genetic predisposition of life-threatening antiepileptic-induced skin reactions. Expert Opin Drug Saf. 2010;9(1):15-21.
23. Warner A, Privitera M, Bates D. Standards of laboratory practice: antiepileptic drug monitoring. Clin Chem. 1998;44(5):1085-1095.
24. Kaneria KM, Patel NC, Keck PE, Jr. Bipolar disorder: new strategy for checking serum valproate. Current Psychiatry. 2005;4(12):31-44.
1. Bowden CL. Anticonvulsants in bipolar disorders: current research and practice and future directions. Bipolar Disord. 2009;11(suppl 2):20-33.
2. Vigo DV, Baldessarini RJ. Anticonvulsants in the treatment of major depressive disorder: an overview. Harv Rev Psychiatry. 2009;17(4):231-241.
3. Citrome L. Adjunctive lithium and anticonvulsants for the treatment of schizophrenia: what is the evidence? Expert Rev Neurother. 2009;9(1):55-71.
4. Grunze HC. The effectiveness of anticonvulsants in psychiatric disorders. Dialogues Clin Neurosci. 2008;10(1):77-89.
5. Hoffman EJ, Mathew SJ. Anxiety disorders: a comprehensive review of pharmacotherapies. Mt Sinai J Med. 2008;75(3):248-262.
6. Rosenberg JM, Salzman C. Update: new uses for lithium and anticonvulsants. CNS Spectr. 2007;12(11):831-841.
7. McElroy SL, Guerdjikova AI, Martens B, et al. Role of antiepileptic drugs in the management of eating disorders. CNS Drugs. 2009;23(2):139-156.
8. Wilby J, Kainth A, Hawkins N, et al. Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation. Health Technol Assess. 2005;9(15):1-157.
9. Cheng LS, Prasad AN, Rieder MJ. Relationship between antiepileptic drugs and biological markers affecting long-term cardiovascular function in children and adolescents. Can J Clin Pharmacol. 2010;17(1):e5-46.
10. Park SP, Kwon SH. Cognitive effects of antiepileptic drugs. J Clin Neurol. 2008;4(3):99-106.
11. U.S. Food and Drug Administration. FDA drug safety communication: aseptic meningitis associated with use of lamictal (lamotrigine). Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm221847.htm. Accessed October 29, 2010.
12. Wade JF, Dang CV, Nelson L, et al. Emergent complications of the newer anticonvulsants. J Emerg Med. 2010;38(2):231-237.
13. Beydoun A, Sackellares JC, Shu V, et al. Safety and efficacy of divalproex sodium monotherapy in partial epilepsy: a double-blind, concentration-response design clinical trial. Neurology. 1997;48(1):182-188.
14. Depakote [package inset]. North Chicago, IL: Abbott Laboratories; 2009.
15. Cerminara C, Seri S, Bombardieri R, et al. Hypohidrosis during topiramate treatment: a rare and reversible side effect. Pediatr Neurol. 2006;34(5):392-394.
16. U.S. Food and Drug Administration. Information for healthcare professionals: suicidal behavior and ideation and antiepileptic drugs. 2008. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm100192.htm. Accessed May 10, 2010.
17. Patorno E, Bohn RL, Wahl PM, et al. Anticonvulsant medications and the risk of suicide, attempted suicide, or violent death. JAMA. 2010;303(14):1401-1409.
18. Gibbons RD, Hur K, Brown CH, et al. Relationship between antiepileptic drugs and suicide attempts in patients with bipolar disorder. Arch Gen Psychiatry. 2009;66(12):1354-1360.
19. Bilo L, Meo R. Polycystic ovary syndrome in women using valproate: a review. Gynecol Endocrinol. 2008;24(10):562-570.
20. Welch BJ, Graybeal D, Moe OW, et al. Biochemical and stone-risk profiles with topiramate treatment. Am J Kidney Dis. 2006;48(4):555-563.
21. Harden CL, Meador KJ, Pennell PB, et al. Practice parameter update: management issues for women with epilepsy—focus on pregnancy (an evidence-based review): teratogenesis and perinatal outcomes: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology. 2009;73(2):133-141.
22. Chung WH, Hung SI, Chen YT. Genetic predisposition of life-threatening antiepileptic-induced skin reactions. Expert Opin Drug Saf. 2010;9(1):15-21.
23. Warner A, Privitera M, Bates D. Standards of laboratory practice: antiepileptic drug monitoring. Clin Chem. 1998;44(5):1085-1095.
24. Kaneria KM, Patel NC, Keck PE, Jr. Bipolar disorder: new strategy for checking serum valproate. Current Psychiatry. 2005;4(12):31-44.