User login
Soft bipolarity: How to recognize and treat bipolar II disorder
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
WEB AUDIO
At least 25% and possibly up to 50% of patients with recurrent major depressive disorder (MDD) have features of mild hypomania (the “soft end” of the bipolar spectrum1) and might be better conceptualized as suffering from a broadly defined bipolar (BP) II disorder.2 The challenge is to differentiate MDD from BP II so that we make treatment decisions—such as antidepressants vs mood stabilizers—shown to improve the long-term course of patients’ depressive symptoms.
Diagnosis of BP II often is not straightforward and unfortunately may be delayed several years after patients first present for evaluation. To help clinicians make correct diagnostic decisions, this article:
- describes diagnostic criteria outside of DSM-IV-TR that can assist in identifying BP II disorder
- identifies subgroups of recurrently depressed patients whose primary disorder is more likely to be bipolar than unipolar
- provides a screening tool validated for identifying “soft” bipolarity
- offers a pragmatic clinical perspective on the treatment of BP II disorder.
How common is BP II disorder?
As with all psychiatric diagnoses, the prevalence of BP II disorder is a function of the diagnostic criteria used to define it.3 BP II—1 or more depressive episodes with at least 1 hypomanic episode—affects 1% to 2% of the population, based on DSM-IV-TR criteria for hypomania (Box 1). However, the DSM definition of BP II might be too restrictive. Regarding the diagnosis of hypomania, in particular:
- the symptom of “overactivity” should be given as much weight as the stem criteria of “euphoria” and “irritability”
- the 4-day threshold for a hypomanic episode probably is too long.
These deficiencies in DSM-IV-TR exclude many patients who experience brief but clinically significant periods of hypomania. A more realistic definition of hypomania within BP II disorder would:
- include overactivity as an additional stem criterion
- specify a threshold duration for hypomanic symptoms of at least 1 day rather than 4 days
- stipulate the experience of negative consequences of the episode as necessary for the diagnosis (Table 1).
- A distinct period of persistently elevated, expansive, or irritable mood, lasting at least 4 days, that is clearly different from the usual nondepressed mood
- During the period of mood disturbance, 3 or more of the following symptoms have persisted (4 if the mood is only irritable) and have been present to a significant degree:
- The episode is associated with an unequivocal change in functioning that is uncharacteristic of the person when not symptomatic
- The disturbance in mood and the change in functioning are observable by others
- The episode is not severe enough to cause marked impairment in social or occupational functioning, or to necessitate hospitalization, and there are no psychotic features
- The symptoms are not due to the direct physiological effects of a substance (a drug of abuse, a medication, or other treatment) or a general medical condition (such as hyperthyroidism)
Note: Hypomanic-like episodes that are clearly caused by somatic antidepressant treatment (such as medication, electroconvulsive therapy, or light therapy) should not count toward a diagnosis of bipolar II disorder
Proposed hypomania criteria in broadly defined BP II
| A. Euphoria, irritability, or overactivity |
| B. At least 3 of the 7 DSM-IV-TR symptoms of hypomania |
| C. Hypomanic symptoms of at least 1 day’s duration |
| D. Experience of negative consequences of hypomanic periods |
| BP II: bipolar II disorder |
| Source: Reference 4 |
Depression’s subgroups
Recurrent MDD is an extremely heterogeneous diagnosis. It includes many clinical presentations of depressive illness that may share little in terms of etiology, pathophysiology, and response to treatment. When carefully assessed, 2 subgroups of recurrently depressed patients in particular appear to be more likely to have a primary bipolar disorder:
- young patients with early-onset severe depression
- older adults with difficult-to-treat or treatment-resistant depression.
6 Other reports have indicated that at least 40% of young adults with recurrent MDD satisfy broad diagnostic criteria for bipolar disorder.7
Higher rates of unrecognized bipolar disorder have been identified in patients with treatment-resistant depression. In a prospective study of 61 consecutive MDD patients referred to a mood disorders clinic, 59% satisfied DSM-IV-TR criteria for bipolar disorder.8
Consequences. Undiagnosed BP II disorder is an important clinical issue because bipolar features in patients presumed to have recurrent MDD can adversely affect long-term outcomes. Many of these patients will be treated exclusively with antidepressants despite evidence that antidepressant monotherapy for bipolar depression—at least for some patients—can cause more frequent mood episodes, mood destabilization, and possibly an increase in suicidal behaviors.9,10
This point is highlighted in the United Kingdom’s National Institute of Health and Clinical Excellence (NICE) guidelines for bipolar disorder, which recommended that antidepressants be prescribed for bipolar depression only in combination with mood stabilizer treatment and withdrawn within 2 to 3 months of recovery.11
The American Psychiatric Association’s (APA) practice guideline for treating bipolar disorder, published in 2002, advises against antidepressants as monotherapy for bipolar depression, recommending instead that lithium or lamotrigine be used first-line. A revised APA guideline is scheduled for publication this year.12
Why is BP II underdiagnosed?
Notwithstanding the limitations of DSMIV-TR criteria for hypomania, additional factors contribute to under-recognition of BP II in clinical practice.
Dominant depressive symptoms. The clinical course of bipolar disorders is dominated by low-grade depressive symptoms and recurrent depressive episodes rather than mania or hypomania. This is especially true for BP II disorder, where the ratio of time spent with depressive symptoms relative to time with hypomanic symptoms is approximately 30:1.13 The fact that BP II patients in general seek help only during depressive periods means that consultations inevitably focus on the diagnosis and treatment of depression, rather than long-term prophylaxis of both depressive and hypomanic episodes.
Indistinguishable symptoms? Bipolar depressions are generally thought to be clinically indistinguishable from unipolar depressions, but this might not be clear-cut. Although differentiating symptoms of unipolar and bipolar depression can be difficult in clinical practice, evidence suggests that certain symptoms may be more common in bipolar than unipolar depression:
- atypical depressive features such as mood reactivity, overeating, oversleeping, and excessive fatigue14
- depressive psychotic symptoms, especially in younger patients15
- “mixed” depressive episodes (depressive episodes with concurrent manic symptoms).16
How to recognize BP II disorder
To detect and diagnose BP II disorder, systematically assess hypomanic features in all patients who present with recurrent MDD, especially those who have an early age of onset or don’t seem to be responding well to antidepressant monotherapy. As noted, a corroborative history from a close relative is essential. Within a full clinical assessment, use the features listed in Table 2 to help differentiate bipolar depression from unipolar depression.
Screening instruments for hypomania are no substitute for a careful psychiatric history but can be very helpful in everyday clinical practice. The most well-known is the Mood Disorder Questionnaire (MDQ);17 other options include the Hypomania Checklist (HCL-32)18 and the Bipolar Spectrum Diagnostic Scale (BSDS).19 In general, the MDQ performs better at detecting BP I in psychiatric practice settings, whereas the HCL-32 and BSDS may be more useful in primary care and general population settings.20
The BSDS has a particular focus on the softer end of the bipolar spectrum,19 and in my experience patients like its narrative structure. It can help prompt discussions about previous hypomania symptoms and mood instability. In this sense, the BSDS is a useful adjunct to the routine clinical assessment of patients with recurrent depressive disorders. Click here to view the BSDS.
Table 2
Possible indicators of bipolarity in apparently unipolar depression
| Atypical features |
| First-degree relative with bipolar disorder |
| Antidepressant-induced mania or hypomania |
| Multiple family members with major depression |
| Early onset of depression (age |
| Lack of response to ≥3 antidepressant trials |
| Psychotic features (before age 35) |
| Mixed depressive episodes |
| Brief but frequent episodes of depression |
| Complex comorbidity (anxiety disorders, drug and alcohol misuse, previous diagnosis of borderline personality disorder) |
| Source: References 2,13,14 |
Treatment strategies for BP II
As with all psychiatric disorders, treatment needs to multimodal and tailored to the individual. For a detailed assessment of pharmacologic and psychological options, see Goodwin and Jamison’s authoritative text, chapters 17 to 20.21
Pharmacologic options. Because few clinical trials have focused exclusively on BP II patients, much psychiatric practice has been extrapolated from trials involving BP I patients. Obviously, trials with BP II samples are needed, but these may be limited by the restrictive DSM-IV-TR definition of hypomania.
Lithium has the most supporting evidence, showing efficacy for all 3 phases of BP II—treatment of hypomania, treatment of bipolar depression, and prophylaxis against hypomanic and depressive relapses.22 Different medications used in bipolar disorder appear to have different efficacy profiles, however. For example, a systematic review of 14 randomized controlled trials with 2,526 patients found that although lithium, lamotrigine, olanzapine, and valproate were more effective than placebo at preventing relapse due to any mood episode:
- only lithium and olanzapine significantly reduced manic relapses
- only lamotrigine and valproate significantly reduced depressive relapses.23
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) trial did not find any therapeutic benefit or increased risk of switching to mania for anti depressants plus mood stabilizer vs mood stabilizer alone.26 Many trials of bipolar depression have recruited such heterogeneous groups of patients (including BP I, BP II, and BP NOS; schizoaffective disorder, bipolar type; and even recurrent MDD) that it is difficult to make firm recommendations about pharmacologic options for the depressive phase of BP II disorder.
In my experience, approximately one-third of BP II patients have a history of poor response to antidepressants or adverse effects from antidepressants (extreme irritability, activation, and antidepressant-induced hypomania). In the long term, these patients often do much better on mood stabilizer monotherapy or a combination of mood stabilizers such as lithium plus lamotrigine. The key is to be flexible with treatment options within recommended guidelines and to tailor treatment choices to the individual’s pattern of illness and treatment preferences.
Psychological interventions. Some evidence supports cognitive-behavioral therapy (CBT) and interpersonal and social rhythm therapy (IPSRT) in long-term treatment of bipolar disorders, although—as with medication trials—we need to be careful about extrapolating these findings to BP II disorder.29 For example, a recent large-scale randomized controlled trial of CBT for bipolar disorder was largely negative.30 Psychoeducation given in families and groups can be effective long-term options when used as adjuncts to medications.31
Table 3
Recommendations for treating patients with BP II disorder
| Most BP II patients require a multimodal team approach |
| Look for and treat psychiatric comorbidities, such as alcohol abuse |
| Lithium remains a gold standard treatment for BP II disorder |
| Quetiapine or lamotrigine may be helpful for acute bipolar II depression |
| Avoid antidepressant monotherapy for bipolar depression; some patients should avoid antidepressants altogether |
| CBT and IPSRT are useful psychological interventions |
| Family-focused and group psychoeducation are helpful in the long term |
| Always tailor treatments to the individual |
| BP II: bipolar II disorder; CBT: cognitive-behavioral therapy; IPSRT: interpersonal and social rhythm therapy |
Related Resources
- Goodwin GM and the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition—recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346-388. www.bap.org.uk/pdfs/Bipolar_guidelines.pdf.
- Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
- Phelps J. Bipolar psychoeducation. www.psycheducation.org.
- Mood Disorders Treatment Team, Cardiff University. Interactive online psychoeducational treatment for bipolar disorder. www.BeatingBipolar.org.
- Goodwin GM, Geddes JR. What is the heartland of psychiatry? Br J Psychiatry. 2007;191(3):189-191.
- Lamotrigine • Lamictal
- Lithium • Various
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Valproate • Depakon
Dr. Smith receives research funding from the National Institute of Health Research UK, the MRC/Welsh Assembly Government, NARSAD, and the American Psychiatric Institute for Research and Education. He is a speaker for Eli Lilly and Company, AstraZeneca, and Bristol-Myers Squibb and is a consultant to Shire Pharmaceuticals.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
1. Pies R. The “softer” end of the bipolar spectrum. J Psychiatr Pract. 2002;8(4):189-195.
2. Angst J. The bipolar spectrum. Br J Psychiatry. 2007;190(3):189-191.
3. Smith DJ, Ghaemi SN, Craddock N. The broad clinical spectrum of bipolar disorder: implications for research and practice. J Psychopharmacol. 2008;22(4):397-400.
4. Angst J, Gamma A, Bennazzi F, et al. Toward a re-definition of subthreshold bipolarity: epidemiology and proposed criteria for bipolar-II, minor bipolar disorders and hypomania. J Affect Disord. 2003;73:133-146.
5. Judd LJ, Akiskal HS. The prevalence and disability of bipolar spectrum disorders in the US population: re-analysis of the ECA database taking into account subthreshold cases. J Affect Disord. 2003;73:123-131.
6. Goldberg JF, Harrow M, Whiteside JE. Risk for bipolar illness in patients initially hospitalized for unipolar depression. Am J Psychiatry. 2001;58:1265-1270.
7. Smith DJ, Harrison N, Muir W, et al. The high prevalence of bipolar spectrum disorders in young adults with recurrent depression: toward an innovative diagnostic framework. J Affect Disord. 2005;84(2-3):167-178.
8. Sharma V, Khan M, Smith A. A closer look at treatment resistant depression: is it due to a bipolar diathesis? J Affect Disord. 2005;84(2-3):251-257.
9. Akiskal HS, Benazzi F, Perugi G. Agitated “unipolar” depression re-conceptualized as a depressive mixed state: implications for the antidepressant-suicide controversy. J Affect Disord. 2005;85(3):245-258.
10. Ghaemi SN, Wingo AP, Filkowski MA, et al. Long-term antidepressant treatment in bipolar disorder: meta-analyses of benefits and risks. Acta Psychiatr Scand. 2008;118(5):347-356.
11. National Institute of Health and Clinical Excellence. Bipolar disorder: the management of bipolar disorder in adults, children and adolescents, in primary and secondary care. Issued July 2006. Available at: http://www.nice.org.uk/CG038. Accessed June 3, 2009.
12. American Psychiatric Association practice guidelines. Treatment of patients with bipolar disorder, 2nd ed. Issued April 2002. Available at: http://www.psychiatryonline.com/pracGuide/pracGuideTopic_8.aspx. Accessed June 3, 2009.
13. Judd LL, Akiskal HS, Schletter PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261-269.
14. Forty L, Smith D, Jones L, et al. Clinical differences between bipolar and unipolar depression. Br J Psychiatry. 2008;192(5):388-389.
15. Mitchell PB, Wilhelm K, Parker G, et al. The clinical features of bipolar depression: a comparison with matched major depressive disorder patients. J Clin Psychiatry. 2001;62:212-216.
16. Akiskal HS, Benazzi F. Family history validation of the bipolar nature of depressive mixed states. J Affect Disord. 2003;73(1-2):113-122.
17. Hirschfeld RMA, Williams JB, Spitzer RL, et al. Development and validation of a screening instrument for bipolar spectrum disorder: The Mood Disorder Questionnaire. Am J Psychiatry. 2000;157:1873-1875.
18. Angst J, Adolfsson R, Benazzi F, et al. The HCL-32: towards a self-assessment tool for hypomanic symptoms in outpatients. J Affect Disord. 2005;88(2):217-233.
19. Ghaemi SN, Millar C, Berv DA, et al. Sensitivity and specificity of a new bipolar spectrum diagnostic scale. J Affect Disord. 2005;84:273-277.
20. Allen R, Smith DJ. Screening for bipolar disorder: strengths and limitations of currently available instruments. Primary Care and Community Psychiatry. 2008;13(2):47-51.
21. Goodwin FK, Jamison KR. Manic-depressive illness: bipolar disorders and recurrent depression. 2nd ed. New York, NY: Oxford University Press; 2007.
22. Young AH, Hammond JM. Lithium in mood disorders: increasing evidence base, declining use? Br J Psychiatry. 2007;191(6):474-476.
23. Smith LA, Cornelius V, Warnock A, et al. Effectiveness of mood stabilizers and antipsychotics in the maintenance phase of bipolar disorder: a systematic review of randomized controlled trials. Bipolar Disord. 2007;9(4):394-412.
24. Licht RW, Gijsman H, Nolen WA, et al. Are antidepressants safe in the treatment of bipolar depression? A critical evaluation of their potential risk to induce switch into mania or cycle acceleration. Acta Psychiatr Scand. 2008;118(5):337-346.
25. Smith DJ, Forty L, Russell E, et al. Sub-threshold manic symptoms in recurrent major depressive disorder are a marker for poor outcome. Acta Psychiatr Scand. 2009;119(4):325-329.Epub 2008 Dec 16.
26. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med. 2007;356(17):1711-1722.
27. Thase ME, Madfadden W, Weisler RH, et al. Efficacy of quetiapine monotherapy in bipolar I and II depression: a double-blind, placebo-controlled study (the BOLDER II study). J Clin Psychopharmacology. 2006;26(6):600-609.
28. Geddes JR, Calabrese JR, Goodwin GM. Lamotrigine for treatment of bipolar depression: independent meta-analysis and meta-regression of individual patient data from five randomised trials. Br J Psychiatry. 2009;194:4-9.
29. Beynon S, Soares-Weiser K, Woolacott N, et al. Psychosocial interventions for the prevention of relapse in bipolar disorder: systematic review of controlled trials. Br J Psychiatry. 2008;192(1):5-11.
30. Scott J, Paykel E, Morriss R, et al. Cognitive-behavioural therapy for severe and recurrent bipolar disorders: randomised controlled trial. Br J Psychiatry. 2006;188(4):313-320.
31. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.Epub 2008 Sep 15.
Assessing potential for harm: Would your patient injure himself or others?
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Police take Ms. L, age 23, to the emergency room (ER) after her fiancé called them. He told the police that after a “night of drinking” they argued about a girl he had flirted with. Ms. L took out a loaded gun and threatened to shoot herself. She eventually handed the gun over to the police.
In the ER, Ms. L’s blood alcohol level is 0.20%. She tells the admitting emergency room nurse, “I would never hurt myself. I drank too much and was acting stupid. I just want to go home and sleep it off. I promise not to harm myself.” Emergency room staff observe Ms. L smile and giggle while waiting for a psychiatric evaluation.
What would you do? Hospitalize Ms. L for safety, or accept her promise not to hurt herself and send her home? What criteria would you use?
Knowing how to assess patients such as Ms. L is an essential psychiatric skill, whether or not you trained in forensic psychiatry. This article includes case reports that illustrate techniques for evaluating patients who may harbor suicidal or homicidal thoughts.
Evaluating danger to self
Your role is to weigh an individual’s risk factors for suicide against potential protective factors and to make a judgment call. Potential risk factors for suicide include (but are not limited to):
- current suicidal thoughts
- prior suicide attempts
- presence of a comorbid psychiatric disorder (particularly depression)
- intoxication or ongoing substance use
- feelings of hopelessness
- marked anxiety
- recent stressors
- family history of suicide
- lack of psychosocial support.1
Also review information that is reasonably available. In the ER, records from other facilities or private psychiatric treatment notes may not be accessed easily. However, in addition to conducting a suicide risk assessment and mental status examination, consider reviewing the collateral information outlined in Table 2.
Furthermore, do not rely on “no-suicide” contracts. They do not guarantee that a person won’t attempt suicide, and they will not provide legal protection if the patient commits suicide after being released from your care.2
What to document. After completing your evaluation, specifically document:
- that a suicide risk assessment was conducted
- what risk factors were present
- interventions to address those risk factors
- the level of risk determined (minimal, moderate, or high)
- factors that may protect the patient against suicide.
Table 1
Evaluating suicidality: Sample questions to ask
| Do you wish you were dead? |
| Do you have thoughts about harming yourself? |
| Do you have an actual plan as to how you would harm yourself? If yes: Have you taken any steps to enact that plan? If so, what were they? |
| Have you ever attempted suicide before? If yes: What stopped you from enacting this plan? What do you think would keep you from acting on this plan in the future? |
| Has anyone in your family or close to you committed suicide? |
| How close have you come to killing yourself? |
Table 2
Sources of information to assess suicidality in the ER
| Police reports on circumstances that led the patient to come to the ER |
| ER nursing/physician notes |
| Family members’/friends’ statements regarding reasons for the patient’s visit |
| Observations by anyone assigned to monitor the patient while awaiting your consult |
| Laboratory and physical exam findings, particularly related to substance use and/or self-injurious behavior |
| Psychiatric records at that facility |
| Concerns expressed by anyone responsible for the patient if he/she is released from the hospital |
| ER: emergency room |
CASE REPORT: Paranoid and armed
Mr. J, age 21, is brought involuntarily to the psychiatric ER by police. His mother reports he was locked in his room with a gun, claiming “the FBI is going to kill me.”
Mr. J’s mother tells the ER psychiatrist that her son has schizophrenia, paranoid type, and stopped taking risperidone, 3 mg/d, 4 weeks ago. She explains that Mr. J sometimes “hears voices” whispering to him that his medications are poison and to not trust his family. She states that Mr. J also abuses alcohol and methamphetamine and has 2 prior arrests for assault with a deadly weapon.
She adds that Mr. J now believes his family is working with the FBI to have him placed in a “secret detention camp.” Mr. J’s mother found a loaded pistol in his room and is “scared of what might happen.” During your psychiatric interview, Mr. J appears frightened and paranoid and provides only minimal answers to your questions. He clenches his teeth while staring intently at you.
Evaluating danger to others
There is good reason to be concerned that Mr. J might behave violently, and you likely have sufficient information to hospitalize him. When creating a long-term violence risk prevention plan, divide the concept of dangerousness into 5 components:
- magnitude of potential harm
- likelihood that harm will occur
- imminence of harm
- frequency of dangerous behavior
- situational variables that promote or protect against aggressive behavior.
A person who has used weapons against others may pose a serious risk of future violence. Ask patients whether they own or have ever owned a weapon. In our experience, the recent movement of a weapon—such as transferring a gun from a closet to a nightstand—is particularly ominous in a paranoid person. The greater the psychotic fear, the more likely a paranoid person is to kill someone he misperceives as a persecutor.
Drugs and alcohol are strongly associated with violent behavior.5 Most persons involved in violent crimes are under the influence of alcohol or drugs at the time of their aggression.6 Stimulants such as cocaine, crack, amphetamines, and phencyclidine are of special concern. These drugs often are associated with feelings of disinhibition, a sense of power, and paranoia. The violence linked with cocaine use differs by gender: men are more likely to perpetrate violent crimes, whereas women are more likely to be the victims of violence.7
Table 3
10 questions to ask patients about a history of violence
| What is the most violent thing you have ever done? |
| What types of violent behavior have you engaged in? |
| What is your understanding of why this violence occurred? |
| Who was involved in prior violent incidents? |
| Have you ever been arrested for any type of violent act? |
| Have you ever been intoxicated at the time you were violent? |
| Were you experiencing mental health symptoms when violent? |
| What is the greatest degree of injury you inflicted on someone else? |
| What weapons have you used when violent? |
| Have you ever been a victim of violence? |
Mental illness and violence
Studies examining whether individuals with mental illness are more violent than the non-mentally ill have yielded mixed results.8,9 In a study of civilly committed psychiatric patients released into the community, most mentally ill individuals were not violent.10 Although researchers noted a weak relationship between mental illness and violence, violent conduct was greater only when the person was experiencing acute psychiatric symptoms. Subsequent research suggests that individuals with schizophrenia may have increased rates of violence even when not experiencing active signs of their illness.11
Psychosis. In paranoid psychotic patients, violence often is well planned and in line with their false beliefs.12 These patients usually direct the violence at a specific person they perceive as a persecutor. Paranoid individuals often target relatives or friends. In addition, community-dwelling paranoid persons are more likely to be dangerous because they have greater access to weapons than institutionalized patients.12
Carefully inquire about hallucinations—particularly auditory ones—to determine whether their presence increases the person’s risk to commit a violent act. Patients with schizophrenia are more likely to be violent if their auditory hallucinations generate negative emotions (anger, anxiety, or sadness) and if the patients have not developed successful coping strategies.13 Although most patients ignore violent command hallucinations to harm others, the presence of command hallucinations may increase the likelihood of behaving violently,14 particularly if:
- the voice is familiar to the person,15 and
- the person has delusional beliefs associated with the hallucinations.16
18
Antisocial personality disorder (APD). Violence by those with APD often is motivated by revenge or occurs during a period of heavy drinking. Violent behavior by these persons frequently is cold, calculated, and lacks emotionality.19
In addition to DSM-IV-TR personality disorders, be familiar with the psychological construct known as psychopathy. Cleckley20 used the term psychopath to describe a person who is superficially charming, lacks close relationships, is impulsive, and is primarily concerned with self-gratification. Hare et al21 developed the Psychopathy Checklist-Revised as a validated measure of psychopathy in adults. Psychopathy is a strong predictor of criminal behavior and violence among adults.22
Affect. Individuals who are angry and lack empathy for others are at increased risk for violent behavior.23 Also observe the patient for physical signs and symptoms of changes indicating incipient violence. Berg et al24 noted that signs of imminent violence can include:
- chanting
- clenched jaw
- flared nostrils
- flushed face
- darting eyes
- close proximity to the clinician
- clenched or gripping hands.
Static vs dynamic factors. When organizing strategies to decrease risk factors for violence, distinguish static from dynamic factors. Static factors include demographic information and history of violence. Dynamic factors, which are subject to change with intervention, include access to weapons, psychotic symptoms, active substance use, and a person’s living situation.
Table 4
Sample violence risk management chart for Mr. J
| Risk factor | Intervention | Status |
|---|---|---|
| Paranoia | Antipsychotic medication | Admitted to inpatient psychiatric facility; antipsychotic medications ordered with continued assessments of mental status |
| Antipsychotic medication nonadherence | Depot form of antipsychotic | Mr. J agreed to depot medication |
| Gun at home | Remove guns | His mother removed all guns from home |
| Alcohol and methamphetamine abuse | Evaluate for potential alcohol detox; urine drug screen on admission | Mr. J refused group substance treatment in the hospital; substance use treatment in the community to be arranged prior to discharge |
Related resource
- Simon RI, Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2006.
- Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
- Risperidone • Risperdal
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.
1. El-Mallakh RS, Roberts RJ, El-Mallakh RL. Mood disorders. In: Simon RI, Tardiff K, eds. Textbook of violence assessment and management. Arlington, VA: American Psychiatric Publishing, Inc; 2008:86–92.
2. Resnick PJ. Recognizing that the suicidal patient views you as an “adversary.” Current Psychiatry. 2002;1:8.-
3. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. 2nd ed. In: Practice guidelines for the treatment of psychiatric disorders compendium. Arlington, VA: American Psychiatric Publishing, Inc; 2004:835–1027.
4. Klassen D, O’Connor WA. A prospective study of predictors of violence in adult male mental health admissions. Law Hum Behav. 1988;12(3):143-158.
5. Tardiff K. Violence. In: Hales R, Yudofsky S, Talbott A, eds. American Psychiatric Press textbook of psychiatry. Arlington, VA: American Psychiatric Publishing, Inc; 1999:1405–1428.
6. Murdoch D, Phil RO, Ross D. Alcohol and crimes of violence: present issues. Int J Addict. 1990;25:1065-1081.
7. Goldstein PJ, Bellucci PA, Spunt BJ, et al. Frequency of cocaine use and violence: a comparison between men and women. In: Scholber S, Schade C, eds. The epidemiology of cocaine use and abuse. Research monograph 110. Rockville, MD: National Institute on Drug Abuse; 1991:113–138.
8. Link BG, Stueve A. Evidence bearing on mental illness as a possible cause of violent behavior. Epidemiol Rev. 1995;17:172-181.
9. Torrey EF. Violent behavior by individuals with serious mental illness. Hosp Community Psychiatry. 1994;45:653-662.
10. Monahan J. Actuarial support for the clinical assessment of violence risk. Int Rev Psychiatry. 1997;9:167-170.
11. Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161:716-727.
12. Krakowski M, Volavka J, Brizer D. Psychopathology and violence: a review of literature. Compr Psychiatry. 1986;27:131-148.
13. Cheung P, Schweitzer I, Crowley K, et al. Violence in schizophrenia: role of hallucinations and delusions. Schizophr Res. 1997;26:181-190.
14. McNiel DE, Eisner JP, Binder RL. The relationship between command hallucinations and violence. Psychiatr Serv. 2000;51:1288-1292.
15. Rudnick A. Relation between command hallucinations and dangerous behavior. J Am Acad Psychiatry Law. 1999;27:253-257.
16. Junginger J. Predicting compliance with command hallucinations. Am J Psychiatry. 1990;147:245-247.
17. Marjuk PM, Tardiff K, Hirsh CS. The epidemiology of murder-suicide. JAMA. 1992;267:3179-3183.
18. Tardiff K, Sweillam A. Assaultive behavior among inpatients. Am J Psychiatry. 1982;139:212-215.
19. Williamson S, Hare R, Wong S. Violence: criminal psychopaths and their victims. Canadian Journal of Behavioral Sciences. 1987;19:454-462.
20. Cleckley HM. The mask of sanity. St. Louis, MO: Mosby; 1976.
21. Hare RD. The Hare Psychopathy Checklist-Revised. Toronto, ON, Canada: Multi-Health Systems; 1991.
22. Salekin RT, Rogers R, Sewell KW. A review of meta-analysis of the Psychopathy Checklist and Psychopathy Checklist-Revised: predictive validity of dangerousness. Clinical Psychology Science and Practice. 1996;3:203-213.
23. Menzies RJ, Webster CD, Sepejak DS. The dimensions of dangerousness: evaluating the accuracy of psychometric predictions of violence among forensic patients. Law Hum Behav. 1985;9:49-70.
24. Berg AZ, Bell CC, Tupin J. Clinician safety: assessing and managing the violent patient. New Dir Ment Health Serv. 2000;(86):9-29.
Alcohol dependence in women: Comorbidities can complicate treatment
Ms. F, a 53-year-old high school English teacher, is referred to you by her family physician after she was suspended from work for suspected intoxication. She was divorced 2 years ago from her husband of 20 years, and she says her drinking has escalated to 2 bottles of wine every night. She wants to reduce her alcohol use but experiences shakiness, nausea, and diaphoresis when she tries to cut back.
Ms. F began drinking at age 16 “to feel more comfortable in social situations” and has experienced binge drinking with intermittent blackouts. She denies illicit drug use and legal consequences from drinking. Her father died from cirrhosis at age 58. Her mother suffers from depression but is in remission with medication.
Ms. F is hesitant to date or establish intimate relationships. She has stopped attending church, a book club, and her 15-year-old daughter’s booster club activities.
For years, little was known about alcohol use and alcohol-related problems in women such as Ms. F.1 Alcohol dependence studies rarely included women, so findings and treatment outcomes observed in men were assumed to apply to both genders.
Awareness of gender differences in addiction has grown (Box 1).2-5 Biological and psychosocial differences between alcohol-dependent women and men now are understood to influence etiology, epidemiology, psychiatric and medical comorbidity, course of illness, and treatment outcomes. This article discusses recent insights into planning treatment to address specific needs of alcohol-dependent women.
Epidemiologic surveys consistently show higher rates of alcohol use disorders in men than women, but recent data suggest a narrowing of the gender gap. Studies from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) from 1991 to 1992 and 2001 to 2002, found:
- a significant increase in the 12-month prevalence of alcohol abuse among men (4.7% to 6.9%) and women (1.5% to 2.6%).
- a significant decrease in alcohol dependence among men (6.3% to 5.4%) but not women (from 2.6% to 2.3%).
- a significant increase in rate of alcohol dependence among African-American women age 18 to 29 (from 2.1% to 3.8%).
- the gender differential in alcohol dependence narrowed from 3.8% to 3.1%.2,3
Similarly, studies conducted 60 years ago showed that boys were more likely than girls to report first alcohol use between ages 10 and 14 (4:1 ratio). Now the age of first alcohol use is relatively equivalent in boys and girls.3 This convergence is disconcerting and suggests that screening and prevention initiatives for adolescents need to increase their focus on girls.
Overall, these observations support the ‘convergence hypothesis,’ which holds that the gap between men’s and women’s alcohol consumption has narrowed as women’s use of alcohol has increased.4,5
Accelerated consequences
As a group, women may consume less alcohol than men but progress more rapidly to alcohol-related illnesses and negative consequences. Specifically, alcohol-dependent women develop liver disease, hypertension, and gastrointestinal hemorrhage more rapidly than alcohol-dependent men.3 Cognitive deficits and brain atrophy also develop sooner in alcohol-dependent women than men.6 Causes of this accelerated progression—”telescoping”—include gender-specific biological differences:
- Women have lower levels of gastric alcohol dehydrogenase—the enzyme that initiates alcohol metabolism—and therefore experience a higher blood alcohol concentration than men drinking the same amount of alcohol.
- Women have less total body water and less capacity to dilute alcohol than men.
‘At-risk’ drinking. Gender-related physiologic differences have led to different thresholds for defining “at-risk drinking” and binge drinking for men and women (Table 1).7 Alcohol use also has negative effects on women’s reproductive system and menstrual cycle. Women with alcohol dependence have higher rates of sexual dysfunction, irregular menstrual cycles, early menopause, and amenorrhea as compared with nonalcohol-dependent women.8
Table 1
Different thresholds: Number of drinks* that increases risk for alcohol-related problems
| Drinks/week | Drinks/day | |
|---|---|---|
| Men | >14 | >4 |
| Women | >7 | >3 |
| *A standard drink is 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits | ||
| Source: Reference 7 | ||
Motives for drinking
Research suggests different motives for alcohol use in girls and women vs boys and men. Women appear more likely to use alcohol to “self-medicate” negative affect or emotional pain (Box 2).9-12 Men are more likely to use alcohol to enhance pleasurable emotional states, “feel high” or because of social pressures to conform.5
Drinking partners. Compared with men’s motives for alcohol use, women’s drinking motives are more strongly influenced by their spouse’s or partner’s drinking patterns. In a large twin study (N = 5,974), 13% of alcohol-dependent women vs 3% of alcohol-dependent men reported that their spouse had a history of alcohol problems.9 Thus, consider the addiction status and drinking patterns of a woman’s partner when developing a treatment plan and relapse prevention strategies.
Trauma and alcohol use. Converging lines of evidence suggest that a relationship among trauma, posttraumatic stress disorder, and substance use disorders is particularly important for women. Early life stress—particularly sexual abuse—is more common in girls than in boys and is associated with the risk of developing substance use disorders.10
Women in alcohol treatment programs report more moderate (87%) and severe (40%) intimate partner violence than women in community samples (28% and 8%, respectively), as well as higher rates of childhood physical abuse (37% vs 11%, respectively).11 Moreover, alcohol abuse places women at risk for repeated victimization and serves to perpetuate a cycle of victimization and addiction.12 These are critical issues to assess and address when treating women with alcohol dependence.
In a study of >1,200 adolescents, girls age 13 With age, drinking for social and enhancement motives increases more among male than female adolescents. Drinking to reduce or manage negative affect is associated with an increased risk of heavy drinking (particularly for adolescent girls), more frequent intoxication, and alcohol dependence.14 These findings suggest:
- Young women with alcohol use problems may benefit from learning strategies to regulate negative emotions and alleviate depression or anxiety symptoms that may be contributing to their drinking.
- Young men with alcohol use problems may benefit from learning to manage peer pressure and from finding alternate sources of pleasure enhancement.5
CASE CONTINUED: Depressed and anxious
Ms. F admits to depressed mood, crying episodes, isolation from others, anhedonia, feelings of guilt, low motivation, difficulty concentrating at work, restless sleep, and weight loss. These symptoms recurred soon after she and her husband separated 4 years ago. She denies suicidal thoughts or suicide attempts.
She suffered similar episodes in the past, including when she was breastfeeding and abstinent from alcohol after the birth of her daughter. Her obstetrician treated her depression with fluoxetine. Problems with anxiety began in high school, especially associated with parties and dating. In college, she often would drink beer before class presentations.
You diagnose alcohol dependence, major depressive disorder, and social phobia. You also ask Ms. F about a history of trauma. She reports that her father was “real harsh” when he was drinking and often hit her and her sister. She also relates being struck by her ex-husband during arguments. Screening with the Clinician-Administered PTSD Scale is negative for posttraumatic stress disorder (PTSD), however.
Comorbid psychiatric disorders
Gender differences in reasons for alcohol use may be related to women’s higher rate of medical and psychiatric comorbidity (Table 2).6,8,15,16 Vital signs, physical examination, and lab work are helpful for diagnosis and monitoring of medical comorbidities and complications. The gamma-glutamyl transferase (GGT) test for liver disease and carbohydrate deficient transferrin (CDT) test for chronic heavy alcohol consumption are less sensitive and specific in women than in men.17 Even so, monitoring GGT and CDT results over time may serve as a valuable marker of continued drinking by women.
Mood and anxiety disorders are significantly more common in women than in men among individuals with alcohol use disorders.15,16 This pattern is not unique to alcohol-dependent persons, however. In the general population:
- women are more likely than men to meet diagnostic criteria for anxiety, depression, bulimia nervosa, and borderline personality disorder
- men are more likely than women to meet diagnostic criteria for antisocial personality disorder.18
Comorbid disorders in women with alcohol dependence
| Psychiatric Posttraumatic stress disorder Other anxiety disorders (such as panic disorder without agoraphobia, simple phobia, or social phobia) Major depressive disorder Cognitive impairment |
| Medical Hypertension Fatty liver disease Gastrointestinal hemorrhage Brain atrophy Reproductive system irregularities |
| Source: References 6,8,15,16 |
Suicide risk. A recent study by Connor et al20 examined suicidal ideation, planning, and attempts in 3,729 alcohol dependent subjects (35% female) and found an association between female gender and both planned (odds ratio [OR] = 3.4) and unplanned suicide attempts (OR = 3.8). Further research is needed to clarify the relationship between female gender, alcohol dependence, and suicide risk, behaviors, and attempts.
Anxiety disorders are the most common psychiatric disorders in women,21 and social anxiety and social phobia may play a predisposing role in alcohol dependence.22 Individuals with social anxiety may self-medicate with alcohol as a social lubricant. Some research suggests that anxiety disorders are more severe in alcohol-dependent women than in men with similarly severe alcohol dependence.22
23
Therefore, when assessing and treating alcohol-dependent women, screen for trauma history as well as mood and anxiety disorders. To optimize outcomes, treat these disorders simultaneously with the alcohol use disorder.24
Treatment planning
Underuse of treatment programs. Women with alcohol dependence are more likely to seek treatment in primary care or mental health settings, rather than in alcohol treatment settings.25,26 Women’s underuse of alcohol treatment programs is likely related to:
- greater stigma associated with alcohol use for women as compared with men
- socioeconomic factors, including pregnancy, child care, and concerns about child custody issues.25
Gender-specific treatment? Women-only treatment programs have been studied because of observed differences in men’s and women’s interaction styles and the hypothesis that men’s traditional societal dominance could negatively affect women in mixed-gender groups.25 Better treatment outcomes have been hypothesized if treatment is tailored to address women’s unique issues: risk factors for alcohol dependence, course of disease progression, medical problems associated with alcohol dependence, and reasons for relapse.
Gender-specific treatment may provide an environment where women—particularly those with a history of trauma from a male perpetrator—feel safe discussing issues related to their alcohol problems. For practical purposes, these programs also may be more likely to address women’s needs for on-site child care, prenatal care, and mental health programming.
A recent study compared a manual-based 12-session women’s recovery group with mixed-gender, manualized group drug counseling (GDC). The women’s recovery group focused on gender-specific topics such as relationships, the caregiver role, trauma, comorbid psychiatric conditions (including eating, mood, and anxiety disorders), and the effects of drug and alcohol use on women’s health. The women’s recovery group was:
- as effective as mixed-gender GDC in reducing substance use during the 12-week treatment
- significantly more effective during the 6-month post-treatment phase.28
CASE CONTINUED: Developing a treatment plan
Ms. F identifies 3 triggers for her alcohol use: a stressful day at school, arguments with her ex-husband, and feeling lonely. Because these are high-risk situations for relapse, you incorporate strategies to deal with them into her treatment plan. Other factors to consider:
- whether she requires detoxification
- an FDA-approved medication for alcohol dependence (acamprosate, oral or injectable naltrexone, or disulfiram)
- cognitive-behavioral therapy and medication for major depression and social phobia
- referral to psychosocial support groups (such as Alcoholics Anonymous).
Three factors determine the need for detoxification: the course of previous alcohol withdrawals (alcoholic hallucinosis, seizures, or delirium tremens), elevated vital signs or other evidence of autonomic hyperactivity such as diaphoresis or tremors, and the patient’s general medical condition. During early recovery, monitor patients closely to assess mood and anxiety symptoms. Blood alcohol tests or GGT and CDT are useful to monitor self-reported abstinence.
Related resources
- National Clearing House for Alcohol and Drug Information. Publications and materials on women and substance abuse. Substance Abuse and Mental Health Services Administration. http://ncadistore.samhsa.gov/catalogresults.aspx?h=drugs&topic=11.
- National Institute on Drug Abuse (www.nida.nih.gov). Articles that address women’s health and gender differences. www.drugabuse.gov/NIDA_Notes/NN0013.html.
- Acamprosate • Campral
- Disulfiram • Antabuse
- Fluoxetine • Prozac
- Naltrexone • Vivitrol, ReVia
Drs. Payne, Back, Wright, and Hartwell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Brady receives research support from Abbott Laboratories, GlaxoSmithKline, Forest Pharmaceuticals, and Wyeth. She is a consultant and speaker for Pfizer Inc., Eli Lilly and Company, Abbott Laboratories, GlaxoSmithKline, and Forest Pharmaceuticals.
1. Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
2. Grant BF, Dawson DA, Stinson FS, et al. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991-1992 and 2001-2002. Drug Alcohol Depend. 2004;74(3):223-234.
3. Greenfield SH. Women and alcohol use disorders. Harv Rev Psychiatry. 2002;10(2):76-85.
4. Greenfield TK, Room R. Situational norms for drinking and drunkenness: trends in the US adult population, 1979-1990. Addiction. 1997;92:33-47.
5. Stewart SH, Gavric D, Collins P. Women, girls, and alcohol. In: Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
6. Mann K, Ackermann K, Croissant B, et al. Neuroimaging of gender differences in alcohol dependence: are women more vulnerable? Alcohol Clin Exp Res. 2005;29(5):896-901.
7. National Institute of Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Bethesda, MD: National Institute of Alcohol Abuse and Alcoholism; 2005. NIH Publication No. 07-3769.
8. Blume SB, Zilberman ML. Addiction in women. In: Galanter M, Kleber H, eds. Textbook of substance abuse treatment. 3rd ed. Washington, DC: American Psychiatric Publishing, Inc; 2004:539-546.
9. Grant JD, Heath AC, Bucholz KK, et al. Spousal concordance for alcohol dependence: evidence for assortative mating or spousal interaction effect? Alcohol Clin Exp Res. 2007;31(5):717-728.
10. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women: an epidemiological and co-twin control analysis. Arch Gen Psychiatry. 2000;57:953-959.
11. Miller BA, Wilsnack SC, Cunradi CB. Family violence and victimization: treatment issues for women with alcohol problems. Alcohol Clin Exp Res. 2000;24(8):1287-1297.
12. Kilpatrick DG, Resnick HS, Saunders BE, et al. Victimization, posttraumatic stress disorder, and substance use and abuse among women. In: Wetherington CL, Roman AB, eds. Drug addiction research and the health of women. Rockville, MD: U.S. Department of Health and Human Services; 1998. NIH 98-4290:285-307.
13. Cooper ML. Motivations for alcohol use among adolescents: development and validation of a four-factor model. Psychol Assess. 1994;6(2):117-128.
14. Prescott CA, Cross RJ, Kuhn JW, et al. Is risk for alcoholism mediated by individual differences in drinking motivations? Alcohol Clin Exp Res. 2004;28(1):29-39.
15. Brady KT, Grice DE, Dustan L, et al. Gender differences in substance use disorders. Am J Psychiatry. 1993;150:1707-1711.
16. Helzer JE, Pryzbeck TR. The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. J Stud Alcohol. 1988;49(3):219-224.
17. Center for Substance Abuse Treatment. Detoxification and substance abuse treatment. Treatment Improvement Protocol (TIP) Series 45. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2006. DHHS (SMA) 06-4131.
18. Sinha R, Rounsaville BJ. Sex differences in depressed substance abusers. J Clin Psychiatry. 2002;63(7):616-627.
19. Gilman SE, Abraham HD. A longitudinal study of the order of onset of alcohol dependence and major depression. Drug Alcohol Depend. 2001;63(3):277-286.
20. Connor KR, Hesselbrock VM, Meldrum SC, et al. Transitions to, and correlates of, suicidal ideations, plans, and unplanned and planned suicide attempts among 3,728 men and women with alcohol dependence. J Stud Alcohol Drugs. 2007;68:654-662.
21. Pigott TA. Anxiety disorders in women. Psychiatr Clin North Am. 2003;26(3):621-672.
22. Randall CL, Thomas SE, Thevos AK. Gender comparison in alcoholics with concurrent social phobia: implications for alcoholism treatment. Am J Addict. 2000;9(3):202-215.
23. Logan TK, Walker R, Cole J, et al. Victimization and substance abuse among women: contributing factors, interventions, and implications. Review of General Psychology. 2002;6:325-397.
24. Volkow N. Comorbidity: addiction and other mental illnesses. Rockville, MD: U.S. Department of Health and Human Services; 2009. NIH 08-5771.
25. Greenfield SF, Brooks AJ, Gordon SM, et al. Substance abuse treatment entry, retention, and outcome in women: a review of the literature. Drug Alcohol Depend. 2007;86(1):1-21.
26. Green CA. Gender and use of substance abuse treatment services. Alcohol Res Health. 2006;29(1):55-62.
27. Brady TM, Ashley OS. Women in substance abuse treatment: results from the alcohol and drug services study (ADSS). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2005. DHHS Publication No. SMA 04-3968, Analytic Series A-26. Available at: http://www.oas.samhsa.gov/womenTX/womenTX.pdf. Accessed July 22, 2007.
28. Greenfield SF, Trucco EM, McHugh RK, et al. The Women’s Recovery Group Study: a stage I trial of women-focused group therapy for substance use disorders versus mixedgender group drug counseling. Drug Alcohol Depend. 2007;90:39-47.
29. Garbutt JC, Kranzler HR, O’Malley SS, et al. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a randomized controlled trial. JAMA. 2005;293(13):1617-1625.
30. O’Malley SS, Sinha R, Grilo CM, et al. Naltrexone and cognitive behavioral coping skills therapy for the treatment of alcohol drinking and eating disorder features in alcoholdependent women: a randomized controlled trial. Alcohol Clin Exp Res. 2007;31(4):625-634.
Ms. F, a 53-year-old high school English teacher, is referred to you by her family physician after she was suspended from work for suspected intoxication. She was divorced 2 years ago from her husband of 20 years, and she says her drinking has escalated to 2 bottles of wine every night. She wants to reduce her alcohol use but experiences shakiness, nausea, and diaphoresis when she tries to cut back.
Ms. F began drinking at age 16 “to feel more comfortable in social situations” and has experienced binge drinking with intermittent blackouts. She denies illicit drug use and legal consequences from drinking. Her father died from cirrhosis at age 58. Her mother suffers from depression but is in remission with medication.
Ms. F is hesitant to date or establish intimate relationships. She has stopped attending church, a book club, and her 15-year-old daughter’s booster club activities.
For years, little was known about alcohol use and alcohol-related problems in women such as Ms. F.1 Alcohol dependence studies rarely included women, so findings and treatment outcomes observed in men were assumed to apply to both genders.
Awareness of gender differences in addiction has grown (Box 1).2-5 Biological and psychosocial differences between alcohol-dependent women and men now are understood to influence etiology, epidemiology, psychiatric and medical comorbidity, course of illness, and treatment outcomes. This article discusses recent insights into planning treatment to address specific needs of alcohol-dependent women.
Epidemiologic surveys consistently show higher rates of alcohol use disorders in men than women, but recent data suggest a narrowing of the gender gap. Studies from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) from 1991 to 1992 and 2001 to 2002, found:
- a significant increase in the 12-month prevalence of alcohol abuse among men (4.7% to 6.9%) and women (1.5% to 2.6%).
- a significant decrease in alcohol dependence among men (6.3% to 5.4%) but not women (from 2.6% to 2.3%).
- a significant increase in rate of alcohol dependence among African-American women age 18 to 29 (from 2.1% to 3.8%).
- the gender differential in alcohol dependence narrowed from 3.8% to 3.1%.2,3
Similarly, studies conducted 60 years ago showed that boys were more likely than girls to report first alcohol use between ages 10 and 14 (4:1 ratio). Now the age of first alcohol use is relatively equivalent in boys and girls.3 This convergence is disconcerting and suggests that screening and prevention initiatives for adolescents need to increase their focus on girls.
Overall, these observations support the ‘convergence hypothesis,’ which holds that the gap between men’s and women’s alcohol consumption has narrowed as women’s use of alcohol has increased.4,5
Accelerated consequences
As a group, women may consume less alcohol than men but progress more rapidly to alcohol-related illnesses and negative consequences. Specifically, alcohol-dependent women develop liver disease, hypertension, and gastrointestinal hemorrhage more rapidly than alcohol-dependent men.3 Cognitive deficits and brain atrophy also develop sooner in alcohol-dependent women than men.6 Causes of this accelerated progression—”telescoping”—include gender-specific biological differences:
- Women have lower levels of gastric alcohol dehydrogenase—the enzyme that initiates alcohol metabolism—and therefore experience a higher blood alcohol concentration than men drinking the same amount of alcohol.
- Women have less total body water and less capacity to dilute alcohol than men.
‘At-risk’ drinking. Gender-related physiologic differences have led to different thresholds for defining “at-risk drinking” and binge drinking for men and women (Table 1).7 Alcohol use also has negative effects on women’s reproductive system and menstrual cycle. Women with alcohol dependence have higher rates of sexual dysfunction, irregular menstrual cycles, early menopause, and amenorrhea as compared with nonalcohol-dependent women.8
Table 1
Different thresholds: Number of drinks* that increases risk for alcohol-related problems
| Drinks/week | Drinks/day | |
|---|---|---|
| Men | >14 | >4 |
| Women | >7 | >3 |
| *A standard drink is 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits | ||
| Source: Reference 7 | ||
Motives for drinking
Research suggests different motives for alcohol use in girls and women vs boys and men. Women appear more likely to use alcohol to “self-medicate” negative affect or emotional pain (Box 2).9-12 Men are more likely to use alcohol to enhance pleasurable emotional states, “feel high” or because of social pressures to conform.5
Drinking partners. Compared with men’s motives for alcohol use, women’s drinking motives are more strongly influenced by their spouse’s or partner’s drinking patterns. In a large twin study (N = 5,974), 13% of alcohol-dependent women vs 3% of alcohol-dependent men reported that their spouse had a history of alcohol problems.9 Thus, consider the addiction status and drinking patterns of a woman’s partner when developing a treatment plan and relapse prevention strategies.
Trauma and alcohol use. Converging lines of evidence suggest that a relationship among trauma, posttraumatic stress disorder, and substance use disorders is particularly important for women. Early life stress—particularly sexual abuse—is more common in girls than in boys and is associated with the risk of developing substance use disorders.10
Women in alcohol treatment programs report more moderate (87%) and severe (40%) intimate partner violence than women in community samples (28% and 8%, respectively), as well as higher rates of childhood physical abuse (37% vs 11%, respectively).11 Moreover, alcohol abuse places women at risk for repeated victimization and serves to perpetuate a cycle of victimization and addiction.12 These are critical issues to assess and address when treating women with alcohol dependence.
In a study of >1,200 adolescents, girls age 13 With age, drinking for social and enhancement motives increases more among male than female adolescents. Drinking to reduce or manage negative affect is associated with an increased risk of heavy drinking (particularly for adolescent girls), more frequent intoxication, and alcohol dependence.14 These findings suggest:
- Young women with alcohol use problems may benefit from learning strategies to regulate negative emotions and alleviate depression or anxiety symptoms that may be contributing to their drinking.
- Young men with alcohol use problems may benefit from learning to manage peer pressure and from finding alternate sources of pleasure enhancement.5
CASE CONTINUED: Depressed and anxious
Ms. F admits to depressed mood, crying episodes, isolation from others, anhedonia, feelings of guilt, low motivation, difficulty concentrating at work, restless sleep, and weight loss. These symptoms recurred soon after she and her husband separated 4 years ago. She denies suicidal thoughts or suicide attempts.
She suffered similar episodes in the past, including when she was breastfeeding and abstinent from alcohol after the birth of her daughter. Her obstetrician treated her depression with fluoxetine. Problems with anxiety began in high school, especially associated with parties and dating. In college, she often would drink beer before class presentations.
You diagnose alcohol dependence, major depressive disorder, and social phobia. You also ask Ms. F about a history of trauma. She reports that her father was “real harsh” when he was drinking and often hit her and her sister. She also relates being struck by her ex-husband during arguments. Screening with the Clinician-Administered PTSD Scale is negative for posttraumatic stress disorder (PTSD), however.
Comorbid psychiatric disorders
Gender differences in reasons for alcohol use may be related to women’s higher rate of medical and psychiatric comorbidity (Table 2).6,8,15,16 Vital signs, physical examination, and lab work are helpful for diagnosis and monitoring of medical comorbidities and complications. The gamma-glutamyl transferase (GGT) test for liver disease and carbohydrate deficient transferrin (CDT) test for chronic heavy alcohol consumption are less sensitive and specific in women than in men.17 Even so, monitoring GGT and CDT results over time may serve as a valuable marker of continued drinking by women.
Mood and anxiety disorders are significantly more common in women than in men among individuals with alcohol use disorders.15,16 This pattern is not unique to alcohol-dependent persons, however. In the general population:
- women are more likely than men to meet diagnostic criteria for anxiety, depression, bulimia nervosa, and borderline personality disorder
- men are more likely than women to meet diagnostic criteria for antisocial personality disorder.18
Comorbid disorders in women with alcohol dependence
| Psychiatric Posttraumatic stress disorder Other anxiety disorders (such as panic disorder without agoraphobia, simple phobia, or social phobia) Major depressive disorder Cognitive impairment |
| Medical Hypertension Fatty liver disease Gastrointestinal hemorrhage Brain atrophy Reproductive system irregularities |
| Source: References 6,8,15,16 |
Suicide risk. A recent study by Connor et al20 examined suicidal ideation, planning, and attempts in 3,729 alcohol dependent subjects (35% female) and found an association between female gender and both planned (odds ratio [OR] = 3.4) and unplanned suicide attempts (OR = 3.8). Further research is needed to clarify the relationship between female gender, alcohol dependence, and suicide risk, behaviors, and attempts.
Anxiety disorders are the most common psychiatric disorders in women,21 and social anxiety and social phobia may play a predisposing role in alcohol dependence.22 Individuals with social anxiety may self-medicate with alcohol as a social lubricant. Some research suggests that anxiety disorders are more severe in alcohol-dependent women than in men with similarly severe alcohol dependence.22
23
Therefore, when assessing and treating alcohol-dependent women, screen for trauma history as well as mood and anxiety disorders. To optimize outcomes, treat these disorders simultaneously with the alcohol use disorder.24
Treatment planning
Underuse of treatment programs. Women with alcohol dependence are more likely to seek treatment in primary care or mental health settings, rather than in alcohol treatment settings.25,26 Women’s underuse of alcohol treatment programs is likely related to:
- greater stigma associated with alcohol use for women as compared with men
- socioeconomic factors, including pregnancy, child care, and concerns about child custody issues.25
Gender-specific treatment? Women-only treatment programs have been studied because of observed differences in men’s and women’s interaction styles and the hypothesis that men’s traditional societal dominance could negatively affect women in mixed-gender groups.25 Better treatment outcomes have been hypothesized if treatment is tailored to address women’s unique issues: risk factors for alcohol dependence, course of disease progression, medical problems associated with alcohol dependence, and reasons for relapse.
Gender-specific treatment may provide an environment where women—particularly those with a history of trauma from a male perpetrator—feel safe discussing issues related to their alcohol problems. For practical purposes, these programs also may be more likely to address women’s needs for on-site child care, prenatal care, and mental health programming.
A recent study compared a manual-based 12-session women’s recovery group with mixed-gender, manualized group drug counseling (GDC). The women’s recovery group focused on gender-specific topics such as relationships, the caregiver role, trauma, comorbid psychiatric conditions (including eating, mood, and anxiety disorders), and the effects of drug and alcohol use on women’s health. The women’s recovery group was:
- as effective as mixed-gender GDC in reducing substance use during the 12-week treatment
- significantly more effective during the 6-month post-treatment phase.28
CASE CONTINUED: Developing a treatment plan
Ms. F identifies 3 triggers for her alcohol use: a stressful day at school, arguments with her ex-husband, and feeling lonely. Because these are high-risk situations for relapse, you incorporate strategies to deal with them into her treatment plan. Other factors to consider:
- whether she requires detoxification
- an FDA-approved medication for alcohol dependence (acamprosate, oral or injectable naltrexone, or disulfiram)
- cognitive-behavioral therapy and medication for major depression and social phobia
- referral to psychosocial support groups (such as Alcoholics Anonymous).
Three factors determine the need for detoxification: the course of previous alcohol withdrawals (alcoholic hallucinosis, seizures, or delirium tremens), elevated vital signs or other evidence of autonomic hyperactivity such as diaphoresis or tremors, and the patient’s general medical condition. During early recovery, monitor patients closely to assess mood and anxiety symptoms. Blood alcohol tests or GGT and CDT are useful to monitor self-reported abstinence.
Related resources
- National Clearing House for Alcohol and Drug Information. Publications and materials on women and substance abuse. Substance Abuse and Mental Health Services Administration. http://ncadistore.samhsa.gov/catalogresults.aspx?h=drugs&topic=11.
- National Institute on Drug Abuse (www.nida.nih.gov). Articles that address women’s health and gender differences. www.drugabuse.gov/NIDA_Notes/NN0013.html.
- Acamprosate • Campral
- Disulfiram • Antabuse
- Fluoxetine • Prozac
- Naltrexone • Vivitrol, ReVia
Drs. Payne, Back, Wright, and Hartwell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Brady receives research support from Abbott Laboratories, GlaxoSmithKline, Forest Pharmaceuticals, and Wyeth. She is a consultant and speaker for Pfizer Inc., Eli Lilly and Company, Abbott Laboratories, GlaxoSmithKline, and Forest Pharmaceuticals.
Ms. F, a 53-year-old high school English teacher, is referred to you by her family physician after she was suspended from work for suspected intoxication. She was divorced 2 years ago from her husband of 20 years, and she says her drinking has escalated to 2 bottles of wine every night. She wants to reduce her alcohol use but experiences shakiness, nausea, and diaphoresis when she tries to cut back.
Ms. F began drinking at age 16 “to feel more comfortable in social situations” and has experienced binge drinking with intermittent blackouts. She denies illicit drug use and legal consequences from drinking. Her father died from cirrhosis at age 58. Her mother suffers from depression but is in remission with medication.
Ms. F is hesitant to date or establish intimate relationships. She has stopped attending church, a book club, and her 15-year-old daughter’s booster club activities.
For years, little was known about alcohol use and alcohol-related problems in women such as Ms. F.1 Alcohol dependence studies rarely included women, so findings and treatment outcomes observed in men were assumed to apply to both genders.
Awareness of gender differences in addiction has grown (Box 1).2-5 Biological and psychosocial differences between alcohol-dependent women and men now are understood to influence etiology, epidemiology, psychiatric and medical comorbidity, course of illness, and treatment outcomes. This article discusses recent insights into planning treatment to address specific needs of alcohol-dependent women.
Epidemiologic surveys consistently show higher rates of alcohol use disorders in men than women, but recent data suggest a narrowing of the gender gap. Studies from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) from 1991 to 1992 and 2001 to 2002, found:
- a significant increase in the 12-month prevalence of alcohol abuse among men (4.7% to 6.9%) and women (1.5% to 2.6%).
- a significant decrease in alcohol dependence among men (6.3% to 5.4%) but not women (from 2.6% to 2.3%).
- a significant increase in rate of alcohol dependence among African-American women age 18 to 29 (from 2.1% to 3.8%).
- the gender differential in alcohol dependence narrowed from 3.8% to 3.1%.2,3
Similarly, studies conducted 60 years ago showed that boys were more likely than girls to report first alcohol use between ages 10 and 14 (4:1 ratio). Now the age of first alcohol use is relatively equivalent in boys and girls.3 This convergence is disconcerting and suggests that screening and prevention initiatives for adolescents need to increase their focus on girls.
Overall, these observations support the ‘convergence hypothesis,’ which holds that the gap between men’s and women’s alcohol consumption has narrowed as women’s use of alcohol has increased.4,5
Accelerated consequences
As a group, women may consume less alcohol than men but progress more rapidly to alcohol-related illnesses and negative consequences. Specifically, alcohol-dependent women develop liver disease, hypertension, and gastrointestinal hemorrhage more rapidly than alcohol-dependent men.3 Cognitive deficits and brain atrophy also develop sooner in alcohol-dependent women than men.6 Causes of this accelerated progression—”telescoping”—include gender-specific biological differences:
- Women have lower levels of gastric alcohol dehydrogenase—the enzyme that initiates alcohol metabolism—and therefore experience a higher blood alcohol concentration than men drinking the same amount of alcohol.
- Women have less total body water and less capacity to dilute alcohol than men.
‘At-risk’ drinking. Gender-related physiologic differences have led to different thresholds for defining “at-risk drinking” and binge drinking for men and women (Table 1).7 Alcohol use also has negative effects on women’s reproductive system and menstrual cycle. Women with alcohol dependence have higher rates of sexual dysfunction, irregular menstrual cycles, early menopause, and amenorrhea as compared with nonalcohol-dependent women.8
Table 1
Different thresholds: Number of drinks* that increases risk for alcohol-related problems
| Drinks/week | Drinks/day | |
|---|---|---|
| Men | >14 | >4 |
| Women | >7 | >3 |
| *A standard drink is 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits | ||
| Source: Reference 7 | ||
Motives for drinking
Research suggests different motives for alcohol use in girls and women vs boys and men. Women appear more likely to use alcohol to “self-medicate” negative affect or emotional pain (Box 2).9-12 Men are more likely to use alcohol to enhance pleasurable emotional states, “feel high” or because of social pressures to conform.5
Drinking partners. Compared with men’s motives for alcohol use, women’s drinking motives are more strongly influenced by their spouse’s or partner’s drinking patterns. In a large twin study (N = 5,974), 13% of alcohol-dependent women vs 3% of alcohol-dependent men reported that their spouse had a history of alcohol problems.9 Thus, consider the addiction status and drinking patterns of a woman’s partner when developing a treatment plan and relapse prevention strategies.
Trauma and alcohol use. Converging lines of evidence suggest that a relationship among trauma, posttraumatic stress disorder, and substance use disorders is particularly important for women. Early life stress—particularly sexual abuse—is more common in girls than in boys and is associated with the risk of developing substance use disorders.10
Women in alcohol treatment programs report more moderate (87%) and severe (40%) intimate partner violence than women in community samples (28% and 8%, respectively), as well as higher rates of childhood physical abuse (37% vs 11%, respectively).11 Moreover, alcohol abuse places women at risk for repeated victimization and serves to perpetuate a cycle of victimization and addiction.12 These are critical issues to assess and address when treating women with alcohol dependence.
In a study of >1,200 adolescents, girls age 13 With age, drinking for social and enhancement motives increases more among male than female adolescents. Drinking to reduce or manage negative affect is associated with an increased risk of heavy drinking (particularly for adolescent girls), more frequent intoxication, and alcohol dependence.14 These findings suggest:
- Young women with alcohol use problems may benefit from learning strategies to regulate negative emotions and alleviate depression or anxiety symptoms that may be contributing to their drinking.
- Young men with alcohol use problems may benefit from learning to manage peer pressure and from finding alternate sources of pleasure enhancement.5
CASE CONTINUED: Depressed and anxious
Ms. F admits to depressed mood, crying episodes, isolation from others, anhedonia, feelings of guilt, low motivation, difficulty concentrating at work, restless sleep, and weight loss. These symptoms recurred soon after she and her husband separated 4 years ago. She denies suicidal thoughts or suicide attempts.
She suffered similar episodes in the past, including when she was breastfeeding and abstinent from alcohol after the birth of her daughter. Her obstetrician treated her depression with fluoxetine. Problems with anxiety began in high school, especially associated with parties and dating. In college, she often would drink beer before class presentations.
You diagnose alcohol dependence, major depressive disorder, and social phobia. You also ask Ms. F about a history of trauma. She reports that her father was “real harsh” when he was drinking and often hit her and her sister. She also relates being struck by her ex-husband during arguments. Screening with the Clinician-Administered PTSD Scale is negative for posttraumatic stress disorder (PTSD), however.
Comorbid psychiatric disorders
Gender differences in reasons for alcohol use may be related to women’s higher rate of medical and psychiatric comorbidity (Table 2).6,8,15,16 Vital signs, physical examination, and lab work are helpful for diagnosis and monitoring of medical comorbidities and complications. The gamma-glutamyl transferase (GGT) test for liver disease and carbohydrate deficient transferrin (CDT) test for chronic heavy alcohol consumption are less sensitive and specific in women than in men.17 Even so, monitoring GGT and CDT results over time may serve as a valuable marker of continued drinking by women.
Mood and anxiety disorders are significantly more common in women than in men among individuals with alcohol use disorders.15,16 This pattern is not unique to alcohol-dependent persons, however. In the general population:
- women are more likely than men to meet diagnostic criteria for anxiety, depression, bulimia nervosa, and borderline personality disorder
- men are more likely than women to meet diagnostic criteria for antisocial personality disorder.18
Comorbid disorders in women with alcohol dependence
| Psychiatric Posttraumatic stress disorder Other anxiety disorders (such as panic disorder without agoraphobia, simple phobia, or social phobia) Major depressive disorder Cognitive impairment |
| Medical Hypertension Fatty liver disease Gastrointestinal hemorrhage Brain atrophy Reproductive system irregularities |
| Source: References 6,8,15,16 |
Suicide risk. A recent study by Connor et al20 examined suicidal ideation, planning, and attempts in 3,729 alcohol dependent subjects (35% female) and found an association between female gender and both planned (odds ratio [OR] = 3.4) and unplanned suicide attempts (OR = 3.8). Further research is needed to clarify the relationship between female gender, alcohol dependence, and suicide risk, behaviors, and attempts.
Anxiety disorders are the most common psychiatric disorders in women,21 and social anxiety and social phobia may play a predisposing role in alcohol dependence.22 Individuals with social anxiety may self-medicate with alcohol as a social lubricant. Some research suggests that anxiety disorders are more severe in alcohol-dependent women than in men with similarly severe alcohol dependence.22
23
Therefore, when assessing and treating alcohol-dependent women, screen for trauma history as well as mood and anxiety disorders. To optimize outcomes, treat these disorders simultaneously with the alcohol use disorder.24
Treatment planning
Underuse of treatment programs. Women with alcohol dependence are more likely to seek treatment in primary care or mental health settings, rather than in alcohol treatment settings.25,26 Women’s underuse of alcohol treatment programs is likely related to:
- greater stigma associated with alcohol use for women as compared with men
- socioeconomic factors, including pregnancy, child care, and concerns about child custody issues.25
Gender-specific treatment? Women-only treatment programs have been studied because of observed differences in men’s and women’s interaction styles and the hypothesis that men’s traditional societal dominance could negatively affect women in mixed-gender groups.25 Better treatment outcomes have been hypothesized if treatment is tailored to address women’s unique issues: risk factors for alcohol dependence, course of disease progression, medical problems associated with alcohol dependence, and reasons for relapse.
Gender-specific treatment may provide an environment where women—particularly those with a history of trauma from a male perpetrator—feel safe discussing issues related to their alcohol problems. For practical purposes, these programs also may be more likely to address women’s needs for on-site child care, prenatal care, and mental health programming.
A recent study compared a manual-based 12-session women’s recovery group with mixed-gender, manualized group drug counseling (GDC). The women’s recovery group focused on gender-specific topics such as relationships, the caregiver role, trauma, comorbid psychiatric conditions (including eating, mood, and anxiety disorders), and the effects of drug and alcohol use on women’s health. The women’s recovery group was:
- as effective as mixed-gender GDC in reducing substance use during the 12-week treatment
- significantly more effective during the 6-month post-treatment phase.28
CASE CONTINUED: Developing a treatment plan
Ms. F identifies 3 triggers for her alcohol use: a stressful day at school, arguments with her ex-husband, and feeling lonely. Because these are high-risk situations for relapse, you incorporate strategies to deal with them into her treatment plan. Other factors to consider:
- whether she requires detoxification
- an FDA-approved medication for alcohol dependence (acamprosate, oral or injectable naltrexone, or disulfiram)
- cognitive-behavioral therapy and medication for major depression and social phobia
- referral to psychosocial support groups (such as Alcoholics Anonymous).
Three factors determine the need for detoxification: the course of previous alcohol withdrawals (alcoholic hallucinosis, seizures, or delirium tremens), elevated vital signs or other evidence of autonomic hyperactivity such as diaphoresis or tremors, and the patient’s general medical condition. During early recovery, monitor patients closely to assess mood and anxiety symptoms. Blood alcohol tests or GGT and CDT are useful to monitor self-reported abstinence.
Related resources
- National Clearing House for Alcohol and Drug Information. Publications and materials on women and substance abuse. Substance Abuse and Mental Health Services Administration. http://ncadistore.samhsa.gov/catalogresults.aspx?h=drugs&topic=11.
- National Institute on Drug Abuse (www.nida.nih.gov). Articles that address women’s health and gender differences. www.drugabuse.gov/NIDA_Notes/NN0013.html.
- Acamprosate • Campral
- Disulfiram • Antabuse
- Fluoxetine • Prozac
- Naltrexone • Vivitrol, ReVia
Drs. Payne, Back, Wright, and Hartwell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Brady receives research support from Abbott Laboratories, GlaxoSmithKline, Forest Pharmaceuticals, and Wyeth. She is a consultant and speaker for Pfizer Inc., Eli Lilly and Company, Abbott Laboratories, GlaxoSmithKline, and Forest Pharmaceuticals.
1. Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
2. Grant BF, Dawson DA, Stinson FS, et al. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991-1992 and 2001-2002. Drug Alcohol Depend. 2004;74(3):223-234.
3. Greenfield SH. Women and alcohol use disorders. Harv Rev Psychiatry. 2002;10(2):76-85.
4. Greenfield TK, Room R. Situational norms for drinking and drunkenness: trends in the US adult population, 1979-1990. Addiction. 1997;92:33-47.
5. Stewart SH, Gavric D, Collins P. Women, girls, and alcohol. In: Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
6. Mann K, Ackermann K, Croissant B, et al. Neuroimaging of gender differences in alcohol dependence: are women more vulnerable? Alcohol Clin Exp Res. 2005;29(5):896-901.
7. National Institute of Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Bethesda, MD: National Institute of Alcohol Abuse and Alcoholism; 2005. NIH Publication No. 07-3769.
8. Blume SB, Zilberman ML. Addiction in women. In: Galanter M, Kleber H, eds. Textbook of substance abuse treatment. 3rd ed. Washington, DC: American Psychiatric Publishing, Inc; 2004:539-546.
9. Grant JD, Heath AC, Bucholz KK, et al. Spousal concordance for alcohol dependence: evidence for assortative mating or spousal interaction effect? Alcohol Clin Exp Res. 2007;31(5):717-728.
10. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women: an epidemiological and co-twin control analysis. Arch Gen Psychiatry. 2000;57:953-959.
11. Miller BA, Wilsnack SC, Cunradi CB. Family violence and victimization: treatment issues for women with alcohol problems. Alcohol Clin Exp Res. 2000;24(8):1287-1297.
12. Kilpatrick DG, Resnick HS, Saunders BE, et al. Victimization, posttraumatic stress disorder, and substance use and abuse among women. In: Wetherington CL, Roman AB, eds. Drug addiction research and the health of women. Rockville, MD: U.S. Department of Health and Human Services; 1998. NIH 98-4290:285-307.
13. Cooper ML. Motivations for alcohol use among adolescents: development and validation of a four-factor model. Psychol Assess. 1994;6(2):117-128.
14. Prescott CA, Cross RJ, Kuhn JW, et al. Is risk for alcoholism mediated by individual differences in drinking motivations? Alcohol Clin Exp Res. 2004;28(1):29-39.
15. Brady KT, Grice DE, Dustan L, et al. Gender differences in substance use disorders. Am J Psychiatry. 1993;150:1707-1711.
16. Helzer JE, Pryzbeck TR. The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. J Stud Alcohol. 1988;49(3):219-224.
17. Center for Substance Abuse Treatment. Detoxification and substance abuse treatment. Treatment Improvement Protocol (TIP) Series 45. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2006. DHHS (SMA) 06-4131.
18. Sinha R, Rounsaville BJ. Sex differences in depressed substance abusers. J Clin Psychiatry. 2002;63(7):616-627.
19. Gilman SE, Abraham HD. A longitudinal study of the order of onset of alcohol dependence and major depression. Drug Alcohol Depend. 2001;63(3):277-286.
20. Connor KR, Hesselbrock VM, Meldrum SC, et al. Transitions to, and correlates of, suicidal ideations, plans, and unplanned and planned suicide attempts among 3,728 men and women with alcohol dependence. J Stud Alcohol Drugs. 2007;68:654-662.
21. Pigott TA. Anxiety disorders in women. Psychiatr Clin North Am. 2003;26(3):621-672.
22. Randall CL, Thomas SE, Thevos AK. Gender comparison in alcoholics with concurrent social phobia: implications for alcoholism treatment. Am J Addict. 2000;9(3):202-215.
23. Logan TK, Walker R, Cole J, et al. Victimization and substance abuse among women: contributing factors, interventions, and implications. Review of General Psychology. 2002;6:325-397.
24. Volkow N. Comorbidity: addiction and other mental illnesses. Rockville, MD: U.S. Department of Health and Human Services; 2009. NIH 08-5771.
25. Greenfield SF, Brooks AJ, Gordon SM, et al. Substance abuse treatment entry, retention, and outcome in women: a review of the literature. Drug Alcohol Depend. 2007;86(1):1-21.
26. Green CA. Gender and use of substance abuse treatment services. Alcohol Res Health. 2006;29(1):55-62.
27. Brady TM, Ashley OS. Women in substance abuse treatment: results from the alcohol and drug services study (ADSS). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2005. DHHS Publication No. SMA 04-3968, Analytic Series A-26. Available at: http://www.oas.samhsa.gov/womenTX/womenTX.pdf. Accessed July 22, 2007.
28. Greenfield SF, Trucco EM, McHugh RK, et al. The Women’s Recovery Group Study: a stage I trial of women-focused group therapy for substance use disorders versus mixedgender group drug counseling. Drug Alcohol Depend. 2007;90:39-47.
29. Garbutt JC, Kranzler HR, O’Malley SS, et al. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a randomized controlled trial. JAMA. 2005;293(13):1617-1625.
30. O’Malley SS, Sinha R, Grilo CM, et al. Naltrexone and cognitive behavioral coping skills therapy for the treatment of alcohol drinking and eating disorder features in alcoholdependent women: a randomized controlled trial. Alcohol Clin Exp Res. 2007;31(4):625-634.
1. Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
2. Grant BF, Dawson DA, Stinson FS, et al. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991-1992 and 2001-2002. Drug Alcohol Depend. 2004;74(3):223-234.
3. Greenfield SH. Women and alcohol use disorders. Harv Rev Psychiatry. 2002;10(2):76-85.
4. Greenfield TK, Room R. Situational norms for drinking and drunkenness: trends in the US adult population, 1979-1990. Addiction. 1997;92:33-47.
5. Stewart SH, Gavric D, Collins P. Women, girls, and alcohol. In: Brady KT, Back SE, Greenfield S, eds. Women and addiction: a comprehensive handbook. New York, NY: Guilford Press; 2009.
6. Mann K, Ackermann K, Croissant B, et al. Neuroimaging of gender differences in alcohol dependence: are women more vulnerable? Alcohol Clin Exp Res. 2005;29(5):896-901.
7. National Institute of Alcohol Abuse and Alcoholism. Helping patients who drink too much: a clinician’s guide. Bethesda, MD: National Institute of Alcohol Abuse and Alcoholism; 2005. NIH Publication No. 07-3769.
8. Blume SB, Zilberman ML. Addiction in women. In: Galanter M, Kleber H, eds. Textbook of substance abuse treatment. 3rd ed. Washington, DC: American Psychiatric Publishing, Inc; 2004:539-546.
9. Grant JD, Heath AC, Bucholz KK, et al. Spousal concordance for alcohol dependence: evidence for assortative mating or spousal interaction effect? Alcohol Clin Exp Res. 2007;31(5):717-728.
10. Kendler KS, Bulik CM, Silberg J, et al. Childhood sexual abuse and adult psychiatric and substance use disorders in women: an epidemiological and co-twin control analysis. Arch Gen Psychiatry. 2000;57:953-959.
11. Miller BA, Wilsnack SC, Cunradi CB. Family violence and victimization: treatment issues for women with alcohol problems. Alcohol Clin Exp Res. 2000;24(8):1287-1297.
12. Kilpatrick DG, Resnick HS, Saunders BE, et al. Victimization, posttraumatic stress disorder, and substance use and abuse among women. In: Wetherington CL, Roman AB, eds. Drug addiction research and the health of women. Rockville, MD: U.S. Department of Health and Human Services; 1998. NIH 98-4290:285-307.
13. Cooper ML. Motivations for alcohol use among adolescents: development and validation of a four-factor model. Psychol Assess. 1994;6(2):117-128.
14. Prescott CA, Cross RJ, Kuhn JW, et al. Is risk for alcoholism mediated by individual differences in drinking motivations? Alcohol Clin Exp Res. 2004;28(1):29-39.
15. Brady KT, Grice DE, Dustan L, et al. Gender differences in substance use disorders. Am J Psychiatry. 1993;150:1707-1711.
16. Helzer JE, Pryzbeck TR. The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. J Stud Alcohol. 1988;49(3):219-224.
17. Center for Substance Abuse Treatment. Detoxification and substance abuse treatment. Treatment Improvement Protocol (TIP) Series 45. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2006. DHHS (SMA) 06-4131.
18. Sinha R, Rounsaville BJ. Sex differences in depressed substance abusers. J Clin Psychiatry. 2002;63(7):616-627.
19. Gilman SE, Abraham HD. A longitudinal study of the order of onset of alcohol dependence and major depression. Drug Alcohol Depend. 2001;63(3):277-286.
20. Connor KR, Hesselbrock VM, Meldrum SC, et al. Transitions to, and correlates of, suicidal ideations, plans, and unplanned and planned suicide attempts among 3,728 men and women with alcohol dependence. J Stud Alcohol Drugs. 2007;68:654-662.
21. Pigott TA. Anxiety disorders in women. Psychiatr Clin North Am. 2003;26(3):621-672.
22. Randall CL, Thomas SE, Thevos AK. Gender comparison in alcoholics with concurrent social phobia: implications for alcoholism treatment. Am J Addict. 2000;9(3):202-215.
23. Logan TK, Walker R, Cole J, et al. Victimization and substance abuse among women: contributing factors, interventions, and implications. Review of General Psychology. 2002;6:325-397.
24. Volkow N. Comorbidity: addiction and other mental illnesses. Rockville, MD: U.S. Department of Health and Human Services; 2009. NIH 08-5771.
25. Greenfield SF, Brooks AJ, Gordon SM, et al. Substance abuse treatment entry, retention, and outcome in women: a review of the literature. Drug Alcohol Depend. 2007;86(1):1-21.
26. Green CA. Gender and use of substance abuse treatment services. Alcohol Res Health. 2006;29(1):55-62.
27. Brady TM, Ashley OS. Women in substance abuse treatment: results from the alcohol and drug services study (ADSS). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2005. DHHS Publication No. SMA 04-3968, Analytic Series A-26. Available at: http://www.oas.samhsa.gov/womenTX/womenTX.pdf. Accessed July 22, 2007.
28. Greenfield SF, Trucco EM, McHugh RK, et al. The Women’s Recovery Group Study: a stage I trial of women-focused group therapy for substance use disorders versus mixedgender group drug counseling. Drug Alcohol Depend. 2007;90:39-47.
29. Garbutt JC, Kranzler HR, O’Malley SS, et al. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a randomized controlled trial. JAMA. 2005;293(13):1617-1625.
30. O’Malley SS, Sinha R, Grilo CM, et al. Naltrexone and cognitive behavioral coping skills therapy for the treatment of alcohol drinking and eating disorder features in alcoholdependent women: a randomized controlled trial. Alcohol Clin Exp Res. 2007;31(4):625-634.
Exercise prescription: A practical, effective therapy for depression
Mrs. S, age 44, is on leave from her job as a bank cashier because depressive symptoms interfered with her performance. At a university-based psychiatric clinic she reports feeling depressed, reduced interest in daily activities, problems with sleep onset and maintenance, inconsistent appetite, low energy, hopelessness, and decreased memory and concentration.
The resident psychiatrist diagnoses major depressive disorder (MDD) and starts Mrs. S on sertraline, 50 mg/d. The dosage is gradually titrated to 200 mg/d, and after 8 weeks she reports substantial improvement.
Mrs. S returns to her job but experiences residual low energy, lethargy, and inconsistent sleep. Her work schedule and caring for her 2 children at home prevent her from continuing weekly cognitive-behavioral therapy (CBT), but she soon notices that she feels more energetic. She reports that because of high gasoline prices she has been walking several miles daily to commute by train to work. The resident psychiatrist sees this as an opportunity to reinforce the benefits of exercise for depression.
Antidepressants alone do not adequately treat many patients with depression. In the STAR*D Project—which compared long-term outcomes of various depression treatments—only 28% to 33% of outpatients achieved remission with selective serotonin reuptake inhibitor (SSRI) monotherapy. Rates were somewhat higher with bupropion or serotonin norepinephrine reuptake inhibitor (SNRI) monotherapy, but greater benefit was obtained from augmenting SSRIs.1
Combining antidepressants with psychotherapy2 and lifestyle changes—particularly exercise—makes sense intuitively and is supported by well-designed studies:
- The 60% of adults in the National Comorbidity Survey who said they exercised regularly reported lower rates of depression and anxiety, compared with less active adults.3
- A meta-analysis of 11 randomized, controlled trials supports the use of exercise as an effective intervention for clinical depression.4
Elevation of endorphins in the CNS
Changes in neurotransmitters such as serotonin and norepinephrine
Increased levels of brain-derived neurotrophic factor
Reduction of serum cortisol
Elevation of body temperature
Improved self-esteem
Distraction from daily stress
Induction of a relaxed state via biofeedback
This article examines the evidence supporting exercise for treating and preventing clinical depression. We begin by addressing clinicians’ concerns about motivating depressed patients to exercise.
Overcoming barriers
Physician issues. Busy physicians often omit discussions about exercise during brief office visits. Only 34% of 9,299 patients in a population-based survey5 reported that their doctors counseled them about exercise during their most recent visits. Counseling patients does not have to be time-intensive, however. A study of the Physician-based Assessment and Counseling for Exercise (PACE) project showed that 70% of physicians could provide exercise counseling in 3 to 5 minutes, and most patients reported following their physicians’ advice.6
Highly depressed individuals are at risk to quit when they encounter barriers to exercise and to respond to difficulties with frustration and self-disappointment. Thus, depressed patients may need support and encouragement to initiate and maintain regular exercise routines.7 Set small, realistic goals for them, and discuss how to solve problems and remove barriers to increase their likelihood to exercise.
Interventions are most likely to be effective when you counsel patients about exercise as prescription and discuss exercise at each visit.8 Previously sedentary patients have shown short-term moderate increases in physical activity in response to physician counseling. In a study of 212 adults (mean age 39, 84% female), the PACE project significantly increased minutes of weekly walking.9 More than one-half (52%) of patients increased their physical activity, compared with 12% of controls whose physicians did not provide the PACE intervention.
Patient issues. Lack of time and no appropriate space to exercise are common complaints, particularly among residents of regions with long, cold winters. Some patients perceive regular exercise as monotonous or boring, and others may lack the necessary initiative because of poor physical health, fear, negative experiences, or lack of knowledge about exercising. These barriers can be pronounced in older depressed persons. In a cross-sectional study of 645 residents of Jyväskylä, Finland, those age >75 with depressive symptoms were more than twice as likely to be physically inactive as nondepressed residents.10
An intensive exercise program is not the optimal starting point for many patients. Even walking or light jogging can be an effective exercise for depressed individuals with physical limitations. For these patients, a consultation with their primary physician may be necessary if a more intensive program has to be recommended.
Exercise as monotherapy
A dose-response relationship? Various mechanisms have been suggested for the benefits of exercise in depression (Box 1). Exercise alone—without medication—may be an effective treatment for mild and in some cases moderate MDD, and aerobic exercise may reduce depressive symptoms in a dose-response relationship.11
A study of exercise in a supervised laboratory setting demonstrated this relationship in 80 adults age 20 to 45 with mild-to-moderate depressive symptoms. Subjects were randomly assigned to an exercise control group (3 days/week of flexibility exercise) or 1 of 4 aerobic exercise groups that varied in total energy expenditure (a “low dose” of 7.0 kcal/kg/week or a “public health dose” of 17.5 kcal/kg/week). The 17-item Hamilton Rating Scale for Depression (HRSD) was the primary outcome measure.
After 12 weeks, HRSD scores declined from baseline by 47% in subjects engaged in the public health dose of aerobic exercise—a significant reduction. Depressive symptoms declined by 30% in the low-dose exercisers, but this was comparable to the 29% reduction in the control group.
Comment. The effective exercise dose in this study is similar to the public health recommendation of 30 minutes of moderate-to-vigorous activity on all or most days per week (see Related Resources). Antidepressant effects have been associated with more modest physical activity, however, which may be easier to initiate and maintain for individuals with depression. The study did not find significant differences in outcomes based on the subjects’ age, gender, or exercise frequency. Nevertheless, the exercise dose may be important to produce an antidepressant effect.
An inverse relationship? Compared with occasional exercise, habitual physical activity usually is associated with greater cardiorespiratory fitness. Whether habitual activity also results in fewer depressive symptoms and greater emotional well-being remains to be seen.
A large, cross-sectional, National Institutes of Health-funded study of 5,451 men and 1,277 women12 suggests an inverse relationship between physical activity and depressive symptoms. Subjects underwent a treadmill exercise test to evaluate physical fitness. A 20-point self-report scale assessed depressive symptoms, and the General Well-Being Schedule13 was used to assess emotional well-being. Depressive symptoms were more severe in “inactive” and “insufficiently active” subjects compared with “sufficiently active” and “highly active” subjects.
On the other hand, although regular exercise may be associated with reduced depressive symptoms in the population at large, no cause-effect relationship was found in a population-based, longitudinal study of 5,952 twins.14
A prospective, randomized, controlled trial15 suggests that exercise could be an important treatment tool in patients diagnosed with MDD. The 202 adult subjects (153 women, 49 men) were randomly assigned to 1 of 4 treatments:
- supervised exercise in a group setting
- home-based exercise
- antidepressant medication (sertraline, 50 to 200 mg/d)
- placebo pills.
Patients underwent the structured clinical interview for depression and completed the HRSD. After 16 weeks, 41% of participants achieved remission, defined as no longer meeting MDD criteria and a HRSD score <8. Compared with placebo controls, patients receiving active treatments tended to have higher remission rates:
- 45% with supervised exercise
- 40% with home-based exercise
- 47% with medication
- 31% with placebo.
Comment. The placebo response rate was relatively high in this study, and antidepressant dosages might not have been optimal. These factors could explain why remission rates with supervised exercise and antidepressant medication were comparable. The study might have been more reliable if it had included a medication plus exercise arm. Patients treated in an office setting might not fare as well as these study subjects whose exercise was supervised.
Postpartum depression occurs in an estimated 13% of new mothers.16 In a controlled trial, 80 women with depression at 4 weeks postpartum were assigned to either:
- an exercise support program (1 hour supervised exercise and 2 sessions at home each week for 3 months)
- standard care.
Most depressed patients can benefit from aerobic exercise or high-intensity progressive resistance training (PRT). Consult with your patient’s primary care physician before designing an exercise regimen. Incorporate warm-up and cool-down periods during each exercise session.
Aerobics. A 30- to 45-minute daily regimen of running, walking, swimming, biking, dancing, or elliptical training is recommended for most people. An optimum regimen achieves a target heart rate of 70% to 85% of the individual’s maximum heart rate. A goal of 40% to 50% of maximum heart rate is an appropriate goal for patients starting an exercise program. At least 10 minutes of aerobic activity is necessary to produce the desired benefit.
PRT. High-intensity progressive resistance training may be recommended in consultation with a physical therapist or certified trainer. This usually consists of 30 to 45 minutes of systematic training of various muscle groups 3 days a week. An optimal resistance of 80% of maximal load is desirable, but this may be adjusted for individual patients. Lifting weights, push-ups, sit-ups, using resistance bands, and heavy gardening may be part of this regimen.
No subjects received medication. Women in the exercise support program were less likely to have high scores on the Edinburgh Postnatal Depression Scale, compared with controls. Women who exercised also reported a greater sense of well-being. Differences between the 2 groups were not statistically significant at 4 weeks post partum but achieved significance at 5 months.17
Depressive symptoms may exacerbate fatigue in postpartum women.18 A study of 88 women with postpartum depression showed the benefits of a home-based exercise program on physical and mental fatigue.19 This finding may be important because fatigue often is associated with treatment-resistant depression and may increase the likelihood of relapse in women with postpartum depression.20
Late-life depression. Exercise can benefit the depressed elderly as well. In a 10-week randomized, controlled trial21 of volunteers age ≥60 with major or minor depression or dysthymia, progressive resistance training (PRT) significantly reduced depression, as measured by the Beck Depression Inventory (BDI) and HRSD. PRT also improved quality of life, vitality, social functioning, and emotional well-being when compared with a control group (Box 2).
A dose-response relationship of exercise for treating late-life depression was shown in a blinded, controlled trial22 of 60 community-dwelling, depressed subjects age >60. These patients were randomly assigned to high-intensity PRT, low-intensity PRT, or standard care by a general practitioner (GP). A ≥50% reduction in HRSD score was achieved by:
- 61% of the high-intensity PRT group
- 29% of the low-intensity PRT group
- 21% of the GP care group.
Sleep quality improved in all participants, with the greatest relative change in the high-intensity PRT group.
Exercise vs psychotherapy. The benefits of exercise may be comparable or superior to those of cognitive or group psychotherapy.23,24 This may be good news for patients such as Mrs. S who lack time or financial resources for regular psychotherapy.
Adjunctive exercise
In depressed patients, exercise may increase the perceived quality of life when combined with medication. This was demonstrated in a randomized, 32-week naturalistic study of 30 women, age 40 to 60, with treatment-resistant MDD.25 The 10 women who received various antidepressants plus physical exercise showed significantly greater long-term improvement in depression symptoms, as measured by the HRSD and Global Assessment of Functioning (GAF) scores, compared with 20 women who received pharmacotherapy alone.26 Study limitations included the absence of a placebo arm, small sample size, and inclusion of subjects with comorbid anxiety disorders.
Group aerobic exercise programs can be an effective and feasible treatment for depression, particularly for older adults. In a controlled trial,27 156 men and women age >50 with MDD were randomly assigned to 3 groups: a program of aerobic exercise; sertraline, ≤200 mg/d; or exercise plus sertraline. HRSD and BDI scores before and after treatment were the primary outcome measures. Secondary measures included aerobic capacity, life satisfaction, self-esteem, anxiety, and dysfunctional cognitions. After 16 weeks of treatment, similar percentages of patients in each group no longer met DSM-IV-TR criteria for MDD:
- 60.4% of patients in the exercise-only group
- 68.8% of patients in the medication-only group
- 65.5% of patients receiving exercise plus medication.
Depression severity appeared to predict the rate of response to the different treatments. Patients who received medication alone seemed to have the most rapid response to treatment. Patients with less severe depression appeared to respond more quickly to exercise plus medication than those with more severe depression.
Long-term benefits
Because depression is a chronic, relapsing illness, any treatment will be widely accepted only if its benefits are long-term. A study of aerobic exercise in 156 adults age ≥50 with MDD28 found that benefits were sustained for >6 months.
Participants were randomly assigned to 4 months of aerobic exercise; sertraline, ≤200 mg/d; or a combination of exercise and sertraline. Aerobic exercise consisted of 30 minutes of brisk walking and jogging on a treadmill, with training ranges equivalent to 70% to 85% of individuals’ maximum heart rate. Appropriate warm-up and cool-down sessions of 5 to 10 minutes were included.
Depressive symptoms improved significantly from baseline in all 3 groups—as assessed by clinical interview, HRSD, and BDI—and after 4 months a comparable number in each group no longer met diagnostic criteria for MDD. When subjects were reassessed 6 months later, the exercisers had significantly lower relapse rates than those receiving medication (P=.01). Those who continued to exercise also were less likely to meet MDD criteria at the end of the 10-month study.
Ask about physical activity at every visit to gauge motivation to exercise
Discuss benefits of exercise for depression and other ailments, and use motivational interviewing techniques when appropriate
Screen for barriers to an exercise routine, and discuss strategies to overcome barriers
Recommend exercise as a prescription, rather than simply advice, because adherence may be greater
Encourage patients to increase physical activity each day, participate in exercise support groups, and seek support from coworkers, family, and friends
Even when unsupervised, exercise can have long-term benefits—as was shown in a randomized, blinded, controlled study of 32 elderly subjects.29 An active treatment group underwent 10 weeks of supervised weight lifting, followed by 10 weeks of unsupervised exercise. Controls received no active treatment. Depression scores as measured by BDI were significantly lower at 20 weeks and 26 months in exercisers compared with controls. An antidepressant effect was seen in 73% of exercisers vs 36% of controls at 20 weeks of treatment.
Comment. These studies show that exercise can maintain an anti depressant effect for 10 to 26 months, but additional randomized controlled studies are needed.
Preventing depression? Inactive nondepressed individuals may be at greater risk to develop depression compared with active individuals, according to a 29-year longitudinal study of Californians age 17 to 94. This association was somewhat diminished when findings were adjusted for the Alameda County residents’ physical health, socioeconomic status, social supports, life events, and other health habits.30 The authors recommended that exercise programs be offered in community mental health programs.
Box 4
Simple steps to build physical activity into daily life
| The American Heart Association offers helpful tips for increasing daily exercise at home, at work, and at play. For additional suggestions, go to www.americanheart.org. | ||
|---|---|---|
| At home | At the office | At play |
| Do housework yourself instead of hiring someone else to do it | Brainstorm project ideas with a coworker while taking a walk | Plan family outings and vacations that include physical |
| Work in the garden or mow the grass (using a riding mower doesn’t count); rake leaves, prune, dig, and pick up trash | Stand while talking on the telephone | activity (hiking, backpacking, swimming, etc.) |
| Go out for a short walk before breakfast, after dinner or both; start with 5 to 10 minutes and work up to 30 minutes | Walk down the hall to speak with someone rather than using the telephone | See the sights in new cities by walking, jogging, or bicycling |
| Walk or bike to the corner store instead of driving | Take the stairs instead of the elevator, or get off a few floors early and take the stairs the rest of the way | Make a date with a friend to enjoy your favorite physical activities, and do them regularly |
| When walking, increase the pace from leisurely to brisk; choose a hilly route | Schedule exercise time on your business calendar, and treat it as any other important appointment | Play your favorite music while exercising, something that motivates you |
| Dance with someone or by yourself; take dancing lessons | ||
| Join a recreational club that emphasizes physical activity | ||
| When golfing, walk the course instead of using a cart | ||
CASE CONTINUED: Removing barriers to exercise
The resident psychiatrist treating Mrs. S encourages her to join an aerobic exercise class at the nearby fitness facility. Because cost is a potential barrier, he helps her negotiate a discount for the first 6 months of membership. Her husband agrees in a joint counseling session to help more with the care of their children so that she can attend the classes.
With continued sertraline, 200 mg/d, and aerobic exercise, Mrs. S’s residual depressive symptoms gradually improve. She still has days when she is unable to attend the exercise classes, but she benefits from the program and is functioning better at work and home.
Getting started
We recommend that psychiatrists inquire about physical activity at every visit to gauge patients’ perception and motivation to exercise. Find ways to overcome patients’ fears and negative experiences with exercise. Provide information to help increase physical activity among patients with depressive symptoms10 (see Related Resources).
Encourage patients to take steps each day to increase their physical activity (Box 3). Depending on the severity of the individual’s depression and inactivity, a realistic starting point may be to take the stairs instead of an elevator, play with children and pets, or take short brisk walks in the yard or neighborhood (Box 4). Consider stationary bikes or swimming as alternatives for physically handicapped individuals and patients who have undergone knee replacements.
- 2008 physical activity guidelines for Americans. U.S. Department of Health and Human Services; 2008:vi-viii. www.health.gov/paguidelines.
- American College of Sports Medicine/American Health Association physical activity guidelines and keys to exercise success. www.acsm.org.
- American Heart Association. www.americanheart.org.
- U.S. Department of Health and Human Services. Quick Guide for Healthy Living. Get Active. www.healthfinder.gov/prevention/ViewTopic.aspx?topicID=22.
Drug brand names
- Bupropion • Wellbutrin
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Warden D, Rush AJ, Trivedi MH, et al. The STAR*D Project results: a comprehensive review of findings. Curr Psychiatry Rep. 2007;9(6):449-459.
2. Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry. 2007;164(5):739-752.
3. Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. 2003;36(6):698-703.
4. Stathopoulou G, Powers MB, Berry AC, et al. Exercise interventions for mental health: a quantitative and qualitative review. Clinical Psychology Science and Practice. 2006;13(2):179-193.
5. Wee CC, McCarthy EP, Davis RB, et al. Physician counseling about exercise. JAMA. 1999;282(16):1583-1588.
6. Long BJ, Calfas KJ, Wooten W, et al. A multisite field test of the acceptability of physical activity counseling in primary care: project PACE. Am J Prev Med. 1996;12(2):73-81.
7. Vickers KS, Nies MA, Patten CA, et al. Patients with diabetes and depression may need additional support for exercise. Am J Health Behav. 2006;30(4):353-362.
8. Weidinger KA, Lovegreen SL, Elliott MB, et al. How to make exercise counseling more effective: lessons from rural America. J Fam Pract. 2008;57(6):394-402.
9. Calfas KJ, Long BJ, Sallis JF, et al. A controlled trial of physician counseling to promote the adoption of physical activity. Prev Med. 1996;25(3):225-233.
10. Rosqvist E, Heikkinen E, Lyyra TM, et al. Factors affecting the increased risk of physical inactivity among older people with depressive symptoms. Scand J Med Sci Sports. 2008 May 22 [Epub ahead of print].
11. Dunn AL, Trivedi MH, Kampert JB, et al. Exercise treatment for depression: efficacy and dose response. Am J Prev Med. 2005;28(1):1-8.
12. Galper DI, Trivedi MH, Barlow CE, et al. Inverse association between physical inactivity and mental health in men and women. Med Sci Sports Exerc. 2006;38(1):173-178.
Fazio AF. A concurrent validation study of the NCHS General Well-Being Schedule. Vital and Health Statistics. Hyattsville, MD: National Center for Health Statistics, US Public Health Service; September 1977. Series 2, No. 73, DHEW Publication No. (HRA) 78-1347:1-13.
14. De Moor MH, Boomsma DI, Stubbe JH, et al. Testing causality in the association between regular exercise and symptoms of anxiety and depression. Arch Gen Psychiatry. 2008;65(8):897-905.
15. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69(7):587-596.
16. O’Hara MW, Swain AM. Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry. 1996;8(1):37-54.
17. Heh SS, Huang LH, Ho SM, et al. Effectiveness of an exercise support program in reducing the severity of postnatal depression in Taiwanese women. Birth. 2008;35(1):60-65.
18. Saurel-Cubizolles MJ, Romito P, Lelong N, et al. Women’s health after childbirth: a longitudinal study in France and Italy. BJOG. 2000;107(10):1202-1209.
19. Dritsa M, Da Costa D, Dupuis G, et al. Effects of a home-based exercise intervention on fatigue in postpartum depressed women: results of a randomized controlled trial. Ann Behav Med. 2008;35(2):179-187.
20. Corwin EJ, Brownstead J, Barton N, et al. The impact of fatigue on the development of postpartum depression. J Obstet Gynecol Neonatal Nurs. 2005;34(5):577-586.
21. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. J Gerontol A Biol Sci Med Sci. 1997;52(1):M27-35.
22. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high versus low intensity weight training versus general practitioner care for clinical depression in older adults. J Gerontol A Biol Sci Med Sci. 2005;60(6):768-776.
23. Fremont J, Wilcoxon Craighead L. Aerobic exercise and cognitive therapy in the treatment of dysphoric moods. Cognit Ther Res. 1987;11(2):241-251.
24. Klein MH, Greist JH, Gurman RA, et al. A comparative outcome study of group psychotherapy vs. exercise treatments for depression. Int J Ment Health. 1985;13:148-177.
25. Carta MG, Hardoy MC, Pilu A, et al. Improving physical quality of life with group physical activity in the adjunctive treatment of major depressive disorder. Clin Pract Epidemiol Ment Health. 2008;4:1.
26. Pilu A, Sorba M, Hardoy MC, et al. Efficacy of physical activity in the adjunctive treatment of major depressive disorders: preliminary results. Clin Pract Epidemiol Ment Health. 2007;3:8.
27. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159(19):2349-2356.
28. Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med. 2000;62(5):633-638.
29. Singh NA, Clements KM, Singh MA. The efficacy of exercise as a long-term antidepressant in elderly subjects: a randomized, controlled trial. J Gerontol A Biol Sci Med Sci. 2001;56(8):M497-504.
30. Camacho TC, Roberts RE, Lazarus NB, et al. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol. 1991;134(2):220-231.
Mrs. S, age 44, is on leave from her job as a bank cashier because depressive symptoms interfered with her performance. At a university-based psychiatric clinic she reports feeling depressed, reduced interest in daily activities, problems with sleep onset and maintenance, inconsistent appetite, low energy, hopelessness, and decreased memory and concentration.
The resident psychiatrist diagnoses major depressive disorder (MDD) and starts Mrs. S on sertraline, 50 mg/d. The dosage is gradually titrated to 200 mg/d, and after 8 weeks she reports substantial improvement.
Mrs. S returns to her job but experiences residual low energy, lethargy, and inconsistent sleep. Her work schedule and caring for her 2 children at home prevent her from continuing weekly cognitive-behavioral therapy (CBT), but she soon notices that she feels more energetic. She reports that because of high gasoline prices she has been walking several miles daily to commute by train to work. The resident psychiatrist sees this as an opportunity to reinforce the benefits of exercise for depression.
Antidepressants alone do not adequately treat many patients with depression. In the STAR*D Project—which compared long-term outcomes of various depression treatments—only 28% to 33% of outpatients achieved remission with selective serotonin reuptake inhibitor (SSRI) monotherapy. Rates were somewhat higher with bupropion or serotonin norepinephrine reuptake inhibitor (SNRI) monotherapy, but greater benefit was obtained from augmenting SSRIs.1
Combining antidepressants with psychotherapy2 and lifestyle changes—particularly exercise—makes sense intuitively and is supported by well-designed studies:
- The 60% of adults in the National Comorbidity Survey who said they exercised regularly reported lower rates of depression and anxiety, compared with less active adults.3
- A meta-analysis of 11 randomized, controlled trials supports the use of exercise as an effective intervention for clinical depression.4
Elevation of endorphins in the CNS
Changes in neurotransmitters such as serotonin and norepinephrine
Increased levels of brain-derived neurotrophic factor
Reduction of serum cortisol
Elevation of body temperature
Improved self-esteem
Distraction from daily stress
Induction of a relaxed state via biofeedback
This article examines the evidence supporting exercise for treating and preventing clinical depression. We begin by addressing clinicians’ concerns about motivating depressed patients to exercise.
Overcoming barriers
Physician issues. Busy physicians often omit discussions about exercise during brief office visits. Only 34% of 9,299 patients in a population-based survey5 reported that their doctors counseled them about exercise during their most recent visits. Counseling patients does not have to be time-intensive, however. A study of the Physician-based Assessment and Counseling for Exercise (PACE) project showed that 70% of physicians could provide exercise counseling in 3 to 5 minutes, and most patients reported following their physicians’ advice.6
Highly depressed individuals are at risk to quit when they encounter barriers to exercise and to respond to difficulties with frustration and self-disappointment. Thus, depressed patients may need support and encouragement to initiate and maintain regular exercise routines.7 Set small, realistic goals for them, and discuss how to solve problems and remove barriers to increase their likelihood to exercise.
Interventions are most likely to be effective when you counsel patients about exercise as prescription and discuss exercise at each visit.8 Previously sedentary patients have shown short-term moderate increases in physical activity in response to physician counseling. In a study of 212 adults (mean age 39, 84% female), the PACE project significantly increased minutes of weekly walking.9 More than one-half (52%) of patients increased their physical activity, compared with 12% of controls whose physicians did not provide the PACE intervention.
Patient issues. Lack of time and no appropriate space to exercise are common complaints, particularly among residents of regions with long, cold winters. Some patients perceive regular exercise as monotonous or boring, and others may lack the necessary initiative because of poor physical health, fear, negative experiences, or lack of knowledge about exercising. These barriers can be pronounced in older depressed persons. In a cross-sectional study of 645 residents of Jyväskylä, Finland, those age >75 with depressive symptoms were more than twice as likely to be physically inactive as nondepressed residents.10
An intensive exercise program is not the optimal starting point for many patients. Even walking or light jogging can be an effective exercise for depressed individuals with physical limitations. For these patients, a consultation with their primary physician may be necessary if a more intensive program has to be recommended.
Exercise as monotherapy
A dose-response relationship? Various mechanisms have been suggested for the benefits of exercise in depression (Box 1). Exercise alone—without medication—may be an effective treatment for mild and in some cases moderate MDD, and aerobic exercise may reduce depressive symptoms in a dose-response relationship.11
A study of exercise in a supervised laboratory setting demonstrated this relationship in 80 adults age 20 to 45 with mild-to-moderate depressive symptoms. Subjects were randomly assigned to an exercise control group (3 days/week of flexibility exercise) or 1 of 4 aerobic exercise groups that varied in total energy expenditure (a “low dose” of 7.0 kcal/kg/week or a “public health dose” of 17.5 kcal/kg/week). The 17-item Hamilton Rating Scale for Depression (HRSD) was the primary outcome measure.
After 12 weeks, HRSD scores declined from baseline by 47% in subjects engaged in the public health dose of aerobic exercise—a significant reduction. Depressive symptoms declined by 30% in the low-dose exercisers, but this was comparable to the 29% reduction in the control group.
Comment. The effective exercise dose in this study is similar to the public health recommendation of 30 minutes of moderate-to-vigorous activity on all or most days per week (see Related Resources). Antidepressant effects have been associated with more modest physical activity, however, which may be easier to initiate and maintain for individuals with depression. The study did not find significant differences in outcomes based on the subjects’ age, gender, or exercise frequency. Nevertheless, the exercise dose may be important to produce an antidepressant effect.
An inverse relationship? Compared with occasional exercise, habitual physical activity usually is associated with greater cardiorespiratory fitness. Whether habitual activity also results in fewer depressive symptoms and greater emotional well-being remains to be seen.
A large, cross-sectional, National Institutes of Health-funded study of 5,451 men and 1,277 women12 suggests an inverse relationship between physical activity and depressive symptoms. Subjects underwent a treadmill exercise test to evaluate physical fitness. A 20-point self-report scale assessed depressive symptoms, and the General Well-Being Schedule13 was used to assess emotional well-being. Depressive symptoms were more severe in “inactive” and “insufficiently active” subjects compared with “sufficiently active” and “highly active” subjects.
On the other hand, although regular exercise may be associated with reduced depressive symptoms in the population at large, no cause-effect relationship was found in a population-based, longitudinal study of 5,952 twins.14
A prospective, randomized, controlled trial15 suggests that exercise could be an important treatment tool in patients diagnosed with MDD. The 202 adult subjects (153 women, 49 men) were randomly assigned to 1 of 4 treatments:
- supervised exercise in a group setting
- home-based exercise
- antidepressant medication (sertraline, 50 to 200 mg/d)
- placebo pills.
Patients underwent the structured clinical interview for depression and completed the HRSD. After 16 weeks, 41% of participants achieved remission, defined as no longer meeting MDD criteria and a HRSD score <8. Compared with placebo controls, patients receiving active treatments tended to have higher remission rates:
- 45% with supervised exercise
- 40% with home-based exercise
- 47% with medication
- 31% with placebo.
Comment. The placebo response rate was relatively high in this study, and antidepressant dosages might not have been optimal. These factors could explain why remission rates with supervised exercise and antidepressant medication were comparable. The study might have been more reliable if it had included a medication plus exercise arm. Patients treated in an office setting might not fare as well as these study subjects whose exercise was supervised.
Postpartum depression occurs in an estimated 13% of new mothers.16 In a controlled trial, 80 women with depression at 4 weeks postpartum were assigned to either:
- an exercise support program (1 hour supervised exercise and 2 sessions at home each week for 3 months)
- standard care.
Most depressed patients can benefit from aerobic exercise or high-intensity progressive resistance training (PRT). Consult with your patient’s primary care physician before designing an exercise regimen. Incorporate warm-up and cool-down periods during each exercise session.
Aerobics. A 30- to 45-minute daily regimen of running, walking, swimming, biking, dancing, or elliptical training is recommended for most people. An optimum regimen achieves a target heart rate of 70% to 85% of the individual’s maximum heart rate. A goal of 40% to 50% of maximum heart rate is an appropriate goal for patients starting an exercise program. At least 10 minutes of aerobic activity is necessary to produce the desired benefit.
PRT. High-intensity progressive resistance training may be recommended in consultation with a physical therapist or certified trainer. This usually consists of 30 to 45 minutes of systematic training of various muscle groups 3 days a week. An optimal resistance of 80% of maximal load is desirable, but this may be adjusted for individual patients. Lifting weights, push-ups, sit-ups, using resistance bands, and heavy gardening may be part of this regimen.
No subjects received medication. Women in the exercise support program were less likely to have high scores on the Edinburgh Postnatal Depression Scale, compared with controls. Women who exercised also reported a greater sense of well-being. Differences between the 2 groups were not statistically significant at 4 weeks post partum but achieved significance at 5 months.17
Depressive symptoms may exacerbate fatigue in postpartum women.18 A study of 88 women with postpartum depression showed the benefits of a home-based exercise program on physical and mental fatigue.19 This finding may be important because fatigue often is associated with treatment-resistant depression and may increase the likelihood of relapse in women with postpartum depression.20
Late-life depression. Exercise can benefit the depressed elderly as well. In a 10-week randomized, controlled trial21 of volunteers age ≥60 with major or minor depression or dysthymia, progressive resistance training (PRT) significantly reduced depression, as measured by the Beck Depression Inventory (BDI) and HRSD. PRT also improved quality of life, vitality, social functioning, and emotional well-being when compared with a control group (Box 2).
A dose-response relationship of exercise for treating late-life depression was shown in a blinded, controlled trial22 of 60 community-dwelling, depressed subjects age >60. These patients were randomly assigned to high-intensity PRT, low-intensity PRT, or standard care by a general practitioner (GP). A ≥50% reduction in HRSD score was achieved by:
- 61% of the high-intensity PRT group
- 29% of the low-intensity PRT group
- 21% of the GP care group.
Sleep quality improved in all participants, with the greatest relative change in the high-intensity PRT group.
Exercise vs psychotherapy. The benefits of exercise may be comparable or superior to those of cognitive or group psychotherapy.23,24 This may be good news for patients such as Mrs. S who lack time or financial resources for regular psychotherapy.
Adjunctive exercise
In depressed patients, exercise may increase the perceived quality of life when combined with medication. This was demonstrated in a randomized, 32-week naturalistic study of 30 women, age 40 to 60, with treatment-resistant MDD.25 The 10 women who received various antidepressants plus physical exercise showed significantly greater long-term improvement in depression symptoms, as measured by the HRSD and Global Assessment of Functioning (GAF) scores, compared with 20 women who received pharmacotherapy alone.26 Study limitations included the absence of a placebo arm, small sample size, and inclusion of subjects with comorbid anxiety disorders.
Group aerobic exercise programs can be an effective and feasible treatment for depression, particularly for older adults. In a controlled trial,27 156 men and women age >50 with MDD were randomly assigned to 3 groups: a program of aerobic exercise; sertraline, ≤200 mg/d; or exercise plus sertraline. HRSD and BDI scores before and after treatment were the primary outcome measures. Secondary measures included aerobic capacity, life satisfaction, self-esteem, anxiety, and dysfunctional cognitions. After 16 weeks of treatment, similar percentages of patients in each group no longer met DSM-IV-TR criteria for MDD:
- 60.4% of patients in the exercise-only group
- 68.8% of patients in the medication-only group
- 65.5% of patients receiving exercise plus medication.
Depression severity appeared to predict the rate of response to the different treatments. Patients who received medication alone seemed to have the most rapid response to treatment. Patients with less severe depression appeared to respond more quickly to exercise plus medication than those with more severe depression.
Long-term benefits
Because depression is a chronic, relapsing illness, any treatment will be widely accepted only if its benefits are long-term. A study of aerobic exercise in 156 adults age ≥50 with MDD28 found that benefits were sustained for >6 months.
Participants were randomly assigned to 4 months of aerobic exercise; sertraline, ≤200 mg/d; or a combination of exercise and sertraline. Aerobic exercise consisted of 30 minutes of brisk walking and jogging on a treadmill, with training ranges equivalent to 70% to 85% of individuals’ maximum heart rate. Appropriate warm-up and cool-down sessions of 5 to 10 minutes were included.
Depressive symptoms improved significantly from baseline in all 3 groups—as assessed by clinical interview, HRSD, and BDI—and after 4 months a comparable number in each group no longer met diagnostic criteria for MDD. When subjects were reassessed 6 months later, the exercisers had significantly lower relapse rates than those receiving medication (P=.01). Those who continued to exercise also were less likely to meet MDD criteria at the end of the 10-month study.
Ask about physical activity at every visit to gauge motivation to exercise
Discuss benefits of exercise for depression and other ailments, and use motivational interviewing techniques when appropriate
Screen for barriers to an exercise routine, and discuss strategies to overcome barriers
Recommend exercise as a prescription, rather than simply advice, because adherence may be greater
Encourage patients to increase physical activity each day, participate in exercise support groups, and seek support from coworkers, family, and friends
Even when unsupervised, exercise can have long-term benefits—as was shown in a randomized, blinded, controlled study of 32 elderly subjects.29 An active treatment group underwent 10 weeks of supervised weight lifting, followed by 10 weeks of unsupervised exercise. Controls received no active treatment. Depression scores as measured by BDI were significantly lower at 20 weeks and 26 months in exercisers compared with controls. An antidepressant effect was seen in 73% of exercisers vs 36% of controls at 20 weeks of treatment.
Comment. These studies show that exercise can maintain an anti depressant effect for 10 to 26 months, but additional randomized controlled studies are needed.
Preventing depression? Inactive nondepressed individuals may be at greater risk to develop depression compared with active individuals, according to a 29-year longitudinal study of Californians age 17 to 94. This association was somewhat diminished when findings were adjusted for the Alameda County residents’ physical health, socioeconomic status, social supports, life events, and other health habits.30 The authors recommended that exercise programs be offered in community mental health programs.
Box 4
Simple steps to build physical activity into daily life
| The American Heart Association offers helpful tips for increasing daily exercise at home, at work, and at play. For additional suggestions, go to www.americanheart.org. | ||
|---|---|---|
| At home | At the office | At play |
| Do housework yourself instead of hiring someone else to do it | Brainstorm project ideas with a coworker while taking a walk | Plan family outings and vacations that include physical |
| Work in the garden or mow the grass (using a riding mower doesn’t count); rake leaves, prune, dig, and pick up trash | Stand while talking on the telephone | activity (hiking, backpacking, swimming, etc.) |
| Go out for a short walk before breakfast, after dinner or both; start with 5 to 10 minutes and work up to 30 minutes | Walk down the hall to speak with someone rather than using the telephone | See the sights in new cities by walking, jogging, or bicycling |
| Walk or bike to the corner store instead of driving | Take the stairs instead of the elevator, or get off a few floors early and take the stairs the rest of the way | Make a date with a friend to enjoy your favorite physical activities, and do them regularly |
| When walking, increase the pace from leisurely to brisk; choose a hilly route | Schedule exercise time on your business calendar, and treat it as any other important appointment | Play your favorite music while exercising, something that motivates you |
| Dance with someone or by yourself; take dancing lessons | ||
| Join a recreational club that emphasizes physical activity | ||
| When golfing, walk the course instead of using a cart | ||
CASE CONTINUED: Removing barriers to exercise
The resident psychiatrist treating Mrs. S encourages her to join an aerobic exercise class at the nearby fitness facility. Because cost is a potential barrier, he helps her negotiate a discount for the first 6 months of membership. Her husband agrees in a joint counseling session to help more with the care of their children so that she can attend the classes.
With continued sertraline, 200 mg/d, and aerobic exercise, Mrs. S’s residual depressive symptoms gradually improve. She still has days when she is unable to attend the exercise classes, but she benefits from the program and is functioning better at work and home.
Getting started
We recommend that psychiatrists inquire about physical activity at every visit to gauge patients’ perception and motivation to exercise. Find ways to overcome patients’ fears and negative experiences with exercise. Provide information to help increase physical activity among patients with depressive symptoms10 (see Related Resources).
Encourage patients to take steps each day to increase their physical activity (Box 3). Depending on the severity of the individual’s depression and inactivity, a realistic starting point may be to take the stairs instead of an elevator, play with children and pets, or take short brisk walks in the yard or neighborhood (Box 4). Consider stationary bikes or swimming as alternatives for physically handicapped individuals and patients who have undergone knee replacements.
- 2008 physical activity guidelines for Americans. U.S. Department of Health and Human Services; 2008:vi-viii. www.health.gov/paguidelines.
- American College of Sports Medicine/American Health Association physical activity guidelines and keys to exercise success. www.acsm.org.
- American Heart Association. www.americanheart.org.
- U.S. Department of Health and Human Services. Quick Guide for Healthy Living. Get Active. www.healthfinder.gov/prevention/ViewTopic.aspx?topicID=22.
Drug brand names
- Bupropion • Wellbutrin
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. S, age 44, is on leave from her job as a bank cashier because depressive symptoms interfered with her performance. At a university-based psychiatric clinic she reports feeling depressed, reduced interest in daily activities, problems with sleep onset and maintenance, inconsistent appetite, low energy, hopelessness, and decreased memory and concentration.
The resident psychiatrist diagnoses major depressive disorder (MDD) and starts Mrs. S on sertraline, 50 mg/d. The dosage is gradually titrated to 200 mg/d, and after 8 weeks she reports substantial improvement.
Mrs. S returns to her job but experiences residual low energy, lethargy, and inconsistent sleep. Her work schedule and caring for her 2 children at home prevent her from continuing weekly cognitive-behavioral therapy (CBT), but she soon notices that she feels more energetic. She reports that because of high gasoline prices she has been walking several miles daily to commute by train to work. The resident psychiatrist sees this as an opportunity to reinforce the benefits of exercise for depression.
Antidepressants alone do not adequately treat many patients with depression. In the STAR*D Project—which compared long-term outcomes of various depression treatments—only 28% to 33% of outpatients achieved remission with selective serotonin reuptake inhibitor (SSRI) monotherapy. Rates were somewhat higher with bupropion or serotonin norepinephrine reuptake inhibitor (SNRI) monotherapy, but greater benefit was obtained from augmenting SSRIs.1
Combining antidepressants with psychotherapy2 and lifestyle changes—particularly exercise—makes sense intuitively and is supported by well-designed studies:
- The 60% of adults in the National Comorbidity Survey who said they exercised regularly reported lower rates of depression and anxiety, compared with less active adults.3
- A meta-analysis of 11 randomized, controlled trials supports the use of exercise as an effective intervention for clinical depression.4
Elevation of endorphins in the CNS
Changes in neurotransmitters such as serotonin and norepinephrine
Increased levels of brain-derived neurotrophic factor
Reduction of serum cortisol
Elevation of body temperature
Improved self-esteem
Distraction from daily stress
Induction of a relaxed state via biofeedback
This article examines the evidence supporting exercise for treating and preventing clinical depression. We begin by addressing clinicians’ concerns about motivating depressed patients to exercise.
Overcoming barriers
Physician issues. Busy physicians often omit discussions about exercise during brief office visits. Only 34% of 9,299 patients in a population-based survey5 reported that their doctors counseled them about exercise during their most recent visits. Counseling patients does not have to be time-intensive, however. A study of the Physician-based Assessment and Counseling for Exercise (PACE) project showed that 70% of physicians could provide exercise counseling in 3 to 5 minutes, and most patients reported following their physicians’ advice.6
Highly depressed individuals are at risk to quit when they encounter barriers to exercise and to respond to difficulties with frustration and self-disappointment. Thus, depressed patients may need support and encouragement to initiate and maintain regular exercise routines.7 Set small, realistic goals for them, and discuss how to solve problems and remove barriers to increase their likelihood to exercise.
Interventions are most likely to be effective when you counsel patients about exercise as prescription and discuss exercise at each visit.8 Previously sedentary patients have shown short-term moderate increases in physical activity in response to physician counseling. In a study of 212 adults (mean age 39, 84% female), the PACE project significantly increased minutes of weekly walking.9 More than one-half (52%) of patients increased their physical activity, compared with 12% of controls whose physicians did not provide the PACE intervention.
Patient issues. Lack of time and no appropriate space to exercise are common complaints, particularly among residents of regions with long, cold winters. Some patients perceive regular exercise as monotonous or boring, and others may lack the necessary initiative because of poor physical health, fear, negative experiences, or lack of knowledge about exercising. These barriers can be pronounced in older depressed persons. In a cross-sectional study of 645 residents of Jyväskylä, Finland, those age >75 with depressive symptoms were more than twice as likely to be physically inactive as nondepressed residents.10
An intensive exercise program is not the optimal starting point for many patients. Even walking or light jogging can be an effective exercise for depressed individuals with physical limitations. For these patients, a consultation with their primary physician may be necessary if a more intensive program has to be recommended.
Exercise as monotherapy
A dose-response relationship? Various mechanisms have been suggested for the benefits of exercise in depression (Box 1). Exercise alone—without medication—may be an effective treatment for mild and in some cases moderate MDD, and aerobic exercise may reduce depressive symptoms in a dose-response relationship.11
A study of exercise in a supervised laboratory setting demonstrated this relationship in 80 adults age 20 to 45 with mild-to-moderate depressive symptoms. Subjects were randomly assigned to an exercise control group (3 days/week of flexibility exercise) or 1 of 4 aerobic exercise groups that varied in total energy expenditure (a “low dose” of 7.0 kcal/kg/week or a “public health dose” of 17.5 kcal/kg/week). The 17-item Hamilton Rating Scale for Depression (HRSD) was the primary outcome measure.
After 12 weeks, HRSD scores declined from baseline by 47% in subjects engaged in the public health dose of aerobic exercise—a significant reduction. Depressive symptoms declined by 30% in the low-dose exercisers, but this was comparable to the 29% reduction in the control group.
Comment. The effective exercise dose in this study is similar to the public health recommendation of 30 minutes of moderate-to-vigorous activity on all or most days per week (see Related Resources). Antidepressant effects have been associated with more modest physical activity, however, which may be easier to initiate and maintain for individuals with depression. The study did not find significant differences in outcomes based on the subjects’ age, gender, or exercise frequency. Nevertheless, the exercise dose may be important to produce an antidepressant effect.
An inverse relationship? Compared with occasional exercise, habitual physical activity usually is associated with greater cardiorespiratory fitness. Whether habitual activity also results in fewer depressive symptoms and greater emotional well-being remains to be seen.
A large, cross-sectional, National Institutes of Health-funded study of 5,451 men and 1,277 women12 suggests an inverse relationship between physical activity and depressive symptoms. Subjects underwent a treadmill exercise test to evaluate physical fitness. A 20-point self-report scale assessed depressive symptoms, and the General Well-Being Schedule13 was used to assess emotional well-being. Depressive symptoms were more severe in “inactive” and “insufficiently active” subjects compared with “sufficiently active” and “highly active” subjects.
On the other hand, although regular exercise may be associated with reduced depressive symptoms in the population at large, no cause-effect relationship was found in a population-based, longitudinal study of 5,952 twins.14
A prospective, randomized, controlled trial15 suggests that exercise could be an important treatment tool in patients diagnosed with MDD. The 202 adult subjects (153 women, 49 men) were randomly assigned to 1 of 4 treatments:
- supervised exercise in a group setting
- home-based exercise
- antidepressant medication (sertraline, 50 to 200 mg/d)
- placebo pills.
Patients underwent the structured clinical interview for depression and completed the HRSD. After 16 weeks, 41% of participants achieved remission, defined as no longer meeting MDD criteria and a HRSD score <8. Compared with placebo controls, patients receiving active treatments tended to have higher remission rates:
- 45% with supervised exercise
- 40% with home-based exercise
- 47% with medication
- 31% with placebo.
Comment. The placebo response rate was relatively high in this study, and antidepressant dosages might not have been optimal. These factors could explain why remission rates with supervised exercise and antidepressant medication were comparable. The study might have been more reliable if it had included a medication plus exercise arm. Patients treated in an office setting might not fare as well as these study subjects whose exercise was supervised.
Postpartum depression occurs in an estimated 13% of new mothers.16 In a controlled trial, 80 women with depression at 4 weeks postpartum were assigned to either:
- an exercise support program (1 hour supervised exercise and 2 sessions at home each week for 3 months)
- standard care.
Most depressed patients can benefit from aerobic exercise or high-intensity progressive resistance training (PRT). Consult with your patient’s primary care physician before designing an exercise regimen. Incorporate warm-up and cool-down periods during each exercise session.
Aerobics. A 30- to 45-minute daily regimen of running, walking, swimming, biking, dancing, or elliptical training is recommended for most people. An optimum regimen achieves a target heart rate of 70% to 85% of the individual’s maximum heart rate. A goal of 40% to 50% of maximum heart rate is an appropriate goal for patients starting an exercise program. At least 10 minutes of aerobic activity is necessary to produce the desired benefit.
PRT. High-intensity progressive resistance training may be recommended in consultation with a physical therapist or certified trainer. This usually consists of 30 to 45 minutes of systematic training of various muscle groups 3 days a week. An optimal resistance of 80% of maximal load is desirable, but this may be adjusted for individual patients. Lifting weights, push-ups, sit-ups, using resistance bands, and heavy gardening may be part of this regimen.
No subjects received medication. Women in the exercise support program were less likely to have high scores on the Edinburgh Postnatal Depression Scale, compared with controls. Women who exercised also reported a greater sense of well-being. Differences between the 2 groups were not statistically significant at 4 weeks post partum but achieved significance at 5 months.17
Depressive symptoms may exacerbate fatigue in postpartum women.18 A study of 88 women with postpartum depression showed the benefits of a home-based exercise program on physical and mental fatigue.19 This finding may be important because fatigue often is associated with treatment-resistant depression and may increase the likelihood of relapse in women with postpartum depression.20
Late-life depression. Exercise can benefit the depressed elderly as well. In a 10-week randomized, controlled trial21 of volunteers age ≥60 with major or minor depression or dysthymia, progressive resistance training (PRT) significantly reduced depression, as measured by the Beck Depression Inventory (BDI) and HRSD. PRT also improved quality of life, vitality, social functioning, and emotional well-being when compared with a control group (Box 2).
A dose-response relationship of exercise for treating late-life depression was shown in a blinded, controlled trial22 of 60 community-dwelling, depressed subjects age >60. These patients were randomly assigned to high-intensity PRT, low-intensity PRT, or standard care by a general practitioner (GP). A ≥50% reduction in HRSD score was achieved by:
- 61% of the high-intensity PRT group
- 29% of the low-intensity PRT group
- 21% of the GP care group.
Sleep quality improved in all participants, with the greatest relative change in the high-intensity PRT group.
Exercise vs psychotherapy. The benefits of exercise may be comparable or superior to those of cognitive or group psychotherapy.23,24 This may be good news for patients such as Mrs. S who lack time or financial resources for regular psychotherapy.
Adjunctive exercise
In depressed patients, exercise may increase the perceived quality of life when combined with medication. This was demonstrated in a randomized, 32-week naturalistic study of 30 women, age 40 to 60, with treatment-resistant MDD.25 The 10 women who received various antidepressants plus physical exercise showed significantly greater long-term improvement in depression symptoms, as measured by the HRSD and Global Assessment of Functioning (GAF) scores, compared with 20 women who received pharmacotherapy alone.26 Study limitations included the absence of a placebo arm, small sample size, and inclusion of subjects with comorbid anxiety disorders.
Group aerobic exercise programs can be an effective and feasible treatment for depression, particularly for older adults. In a controlled trial,27 156 men and women age >50 with MDD were randomly assigned to 3 groups: a program of aerobic exercise; sertraline, ≤200 mg/d; or exercise plus sertraline. HRSD and BDI scores before and after treatment were the primary outcome measures. Secondary measures included aerobic capacity, life satisfaction, self-esteem, anxiety, and dysfunctional cognitions. After 16 weeks of treatment, similar percentages of patients in each group no longer met DSM-IV-TR criteria for MDD:
- 60.4% of patients in the exercise-only group
- 68.8% of patients in the medication-only group
- 65.5% of patients receiving exercise plus medication.
Depression severity appeared to predict the rate of response to the different treatments. Patients who received medication alone seemed to have the most rapid response to treatment. Patients with less severe depression appeared to respond more quickly to exercise plus medication than those with more severe depression.
Long-term benefits
Because depression is a chronic, relapsing illness, any treatment will be widely accepted only if its benefits are long-term. A study of aerobic exercise in 156 adults age ≥50 with MDD28 found that benefits were sustained for >6 months.
Participants were randomly assigned to 4 months of aerobic exercise; sertraline, ≤200 mg/d; or a combination of exercise and sertraline. Aerobic exercise consisted of 30 minutes of brisk walking and jogging on a treadmill, with training ranges equivalent to 70% to 85% of individuals’ maximum heart rate. Appropriate warm-up and cool-down sessions of 5 to 10 minutes were included.
Depressive symptoms improved significantly from baseline in all 3 groups—as assessed by clinical interview, HRSD, and BDI—and after 4 months a comparable number in each group no longer met diagnostic criteria for MDD. When subjects were reassessed 6 months later, the exercisers had significantly lower relapse rates than those receiving medication (P=.01). Those who continued to exercise also were less likely to meet MDD criteria at the end of the 10-month study.
Ask about physical activity at every visit to gauge motivation to exercise
Discuss benefits of exercise for depression and other ailments, and use motivational interviewing techniques when appropriate
Screen for barriers to an exercise routine, and discuss strategies to overcome barriers
Recommend exercise as a prescription, rather than simply advice, because adherence may be greater
Encourage patients to increase physical activity each day, participate in exercise support groups, and seek support from coworkers, family, and friends
Even when unsupervised, exercise can have long-term benefits—as was shown in a randomized, blinded, controlled study of 32 elderly subjects.29 An active treatment group underwent 10 weeks of supervised weight lifting, followed by 10 weeks of unsupervised exercise. Controls received no active treatment. Depression scores as measured by BDI were significantly lower at 20 weeks and 26 months in exercisers compared with controls. An antidepressant effect was seen in 73% of exercisers vs 36% of controls at 20 weeks of treatment.
Comment. These studies show that exercise can maintain an anti depressant effect for 10 to 26 months, but additional randomized controlled studies are needed.
Preventing depression? Inactive nondepressed individuals may be at greater risk to develop depression compared with active individuals, according to a 29-year longitudinal study of Californians age 17 to 94. This association was somewhat diminished when findings were adjusted for the Alameda County residents’ physical health, socioeconomic status, social supports, life events, and other health habits.30 The authors recommended that exercise programs be offered in community mental health programs.
Box 4
Simple steps to build physical activity into daily life
| The American Heart Association offers helpful tips for increasing daily exercise at home, at work, and at play. For additional suggestions, go to www.americanheart.org. | ||
|---|---|---|
| At home | At the office | At play |
| Do housework yourself instead of hiring someone else to do it | Brainstorm project ideas with a coworker while taking a walk | Plan family outings and vacations that include physical |
| Work in the garden or mow the grass (using a riding mower doesn’t count); rake leaves, prune, dig, and pick up trash | Stand while talking on the telephone | activity (hiking, backpacking, swimming, etc.) |
| Go out for a short walk before breakfast, after dinner or both; start with 5 to 10 minutes and work up to 30 minutes | Walk down the hall to speak with someone rather than using the telephone | See the sights in new cities by walking, jogging, or bicycling |
| Walk or bike to the corner store instead of driving | Take the stairs instead of the elevator, or get off a few floors early and take the stairs the rest of the way | Make a date with a friend to enjoy your favorite physical activities, and do them regularly |
| When walking, increase the pace from leisurely to brisk; choose a hilly route | Schedule exercise time on your business calendar, and treat it as any other important appointment | Play your favorite music while exercising, something that motivates you |
| Dance with someone or by yourself; take dancing lessons | ||
| Join a recreational club that emphasizes physical activity | ||
| When golfing, walk the course instead of using a cart | ||
CASE CONTINUED: Removing barriers to exercise
The resident psychiatrist treating Mrs. S encourages her to join an aerobic exercise class at the nearby fitness facility. Because cost is a potential barrier, he helps her negotiate a discount for the first 6 months of membership. Her husband agrees in a joint counseling session to help more with the care of their children so that she can attend the classes.
With continued sertraline, 200 mg/d, and aerobic exercise, Mrs. S’s residual depressive symptoms gradually improve. She still has days when she is unable to attend the exercise classes, but she benefits from the program and is functioning better at work and home.
Getting started
We recommend that psychiatrists inquire about physical activity at every visit to gauge patients’ perception and motivation to exercise. Find ways to overcome patients’ fears and negative experiences with exercise. Provide information to help increase physical activity among patients with depressive symptoms10 (see Related Resources).
Encourage patients to take steps each day to increase their physical activity (Box 3). Depending on the severity of the individual’s depression and inactivity, a realistic starting point may be to take the stairs instead of an elevator, play with children and pets, or take short brisk walks in the yard or neighborhood (Box 4). Consider stationary bikes or swimming as alternatives for physically handicapped individuals and patients who have undergone knee replacements.
- 2008 physical activity guidelines for Americans. U.S. Department of Health and Human Services; 2008:vi-viii. www.health.gov/paguidelines.
- American College of Sports Medicine/American Health Association physical activity guidelines and keys to exercise success. www.acsm.org.
- American Heart Association. www.americanheart.org.
- U.S. Department of Health and Human Services. Quick Guide for Healthy Living. Get Active. www.healthfinder.gov/prevention/ViewTopic.aspx?topicID=22.
Drug brand names
- Bupropion • Wellbutrin
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Warden D, Rush AJ, Trivedi MH, et al. The STAR*D Project results: a comprehensive review of findings. Curr Psychiatry Rep. 2007;9(6):449-459.
2. Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry. 2007;164(5):739-752.
3. Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. 2003;36(6):698-703.
4. Stathopoulou G, Powers MB, Berry AC, et al. Exercise interventions for mental health: a quantitative and qualitative review. Clinical Psychology Science and Practice. 2006;13(2):179-193.
5. Wee CC, McCarthy EP, Davis RB, et al. Physician counseling about exercise. JAMA. 1999;282(16):1583-1588.
6. Long BJ, Calfas KJ, Wooten W, et al. A multisite field test of the acceptability of physical activity counseling in primary care: project PACE. Am J Prev Med. 1996;12(2):73-81.
7. Vickers KS, Nies MA, Patten CA, et al. Patients with diabetes and depression may need additional support for exercise. Am J Health Behav. 2006;30(4):353-362.
8. Weidinger KA, Lovegreen SL, Elliott MB, et al. How to make exercise counseling more effective: lessons from rural America. J Fam Pract. 2008;57(6):394-402.
9. Calfas KJ, Long BJ, Sallis JF, et al. A controlled trial of physician counseling to promote the adoption of physical activity. Prev Med. 1996;25(3):225-233.
10. Rosqvist E, Heikkinen E, Lyyra TM, et al. Factors affecting the increased risk of physical inactivity among older people with depressive symptoms. Scand J Med Sci Sports. 2008 May 22 [Epub ahead of print].
11. Dunn AL, Trivedi MH, Kampert JB, et al. Exercise treatment for depression: efficacy and dose response. Am J Prev Med. 2005;28(1):1-8.
12. Galper DI, Trivedi MH, Barlow CE, et al. Inverse association between physical inactivity and mental health in men and women. Med Sci Sports Exerc. 2006;38(1):173-178.
Fazio AF. A concurrent validation study of the NCHS General Well-Being Schedule. Vital and Health Statistics. Hyattsville, MD: National Center for Health Statistics, US Public Health Service; September 1977. Series 2, No. 73, DHEW Publication No. (HRA) 78-1347:1-13.
14. De Moor MH, Boomsma DI, Stubbe JH, et al. Testing causality in the association between regular exercise and symptoms of anxiety and depression. Arch Gen Psychiatry. 2008;65(8):897-905.
15. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69(7):587-596.
16. O’Hara MW, Swain AM. Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry. 1996;8(1):37-54.
17. Heh SS, Huang LH, Ho SM, et al. Effectiveness of an exercise support program in reducing the severity of postnatal depression in Taiwanese women. Birth. 2008;35(1):60-65.
18. Saurel-Cubizolles MJ, Romito P, Lelong N, et al. Women’s health after childbirth: a longitudinal study in France and Italy. BJOG. 2000;107(10):1202-1209.
19. Dritsa M, Da Costa D, Dupuis G, et al. Effects of a home-based exercise intervention on fatigue in postpartum depressed women: results of a randomized controlled trial. Ann Behav Med. 2008;35(2):179-187.
20. Corwin EJ, Brownstead J, Barton N, et al. The impact of fatigue on the development of postpartum depression. J Obstet Gynecol Neonatal Nurs. 2005;34(5):577-586.
21. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. J Gerontol A Biol Sci Med Sci. 1997;52(1):M27-35.
22. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high versus low intensity weight training versus general practitioner care for clinical depression in older adults. J Gerontol A Biol Sci Med Sci. 2005;60(6):768-776.
23. Fremont J, Wilcoxon Craighead L. Aerobic exercise and cognitive therapy in the treatment of dysphoric moods. Cognit Ther Res. 1987;11(2):241-251.
24. Klein MH, Greist JH, Gurman RA, et al. A comparative outcome study of group psychotherapy vs. exercise treatments for depression. Int J Ment Health. 1985;13:148-177.
25. Carta MG, Hardoy MC, Pilu A, et al. Improving physical quality of life with group physical activity in the adjunctive treatment of major depressive disorder. Clin Pract Epidemiol Ment Health. 2008;4:1.
26. Pilu A, Sorba M, Hardoy MC, et al. Efficacy of physical activity in the adjunctive treatment of major depressive disorders: preliminary results. Clin Pract Epidemiol Ment Health. 2007;3:8.
27. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159(19):2349-2356.
28. Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med. 2000;62(5):633-638.
29. Singh NA, Clements KM, Singh MA. The efficacy of exercise as a long-term antidepressant in elderly subjects: a randomized, controlled trial. J Gerontol A Biol Sci Med Sci. 2001;56(8):M497-504.
30. Camacho TC, Roberts RE, Lazarus NB, et al. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol. 1991;134(2):220-231.
1. Warden D, Rush AJ, Trivedi MH, et al. The STAR*D Project results: a comprehensive review of findings. Curr Psychiatry Rep. 2007;9(6):449-459.
2. Thase ME, Friedman ES, Biggs MM, et al. Cognitive therapy versus medication in augmentation and switch strategies as second-step treatments: a STAR*D report. Am J Psychiatry. 2007;164(5):739-752.
3. Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. 2003;36(6):698-703.
4. Stathopoulou G, Powers MB, Berry AC, et al. Exercise interventions for mental health: a quantitative and qualitative review. Clinical Psychology Science and Practice. 2006;13(2):179-193.
5. Wee CC, McCarthy EP, Davis RB, et al. Physician counseling about exercise. JAMA. 1999;282(16):1583-1588.
6. Long BJ, Calfas KJ, Wooten W, et al. A multisite field test of the acceptability of physical activity counseling in primary care: project PACE. Am J Prev Med. 1996;12(2):73-81.
7. Vickers KS, Nies MA, Patten CA, et al. Patients with diabetes and depression may need additional support for exercise. Am J Health Behav. 2006;30(4):353-362.
8. Weidinger KA, Lovegreen SL, Elliott MB, et al. How to make exercise counseling more effective: lessons from rural America. J Fam Pract. 2008;57(6):394-402.
9. Calfas KJ, Long BJ, Sallis JF, et al. A controlled trial of physician counseling to promote the adoption of physical activity. Prev Med. 1996;25(3):225-233.
10. Rosqvist E, Heikkinen E, Lyyra TM, et al. Factors affecting the increased risk of physical inactivity among older people with depressive symptoms. Scand J Med Sci Sports. 2008 May 22 [Epub ahead of print].
11. Dunn AL, Trivedi MH, Kampert JB, et al. Exercise treatment for depression: efficacy and dose response. Am J Prev Med. 2005;28(1):1-8.
12. Galper DI, Trivedi MH, Barlow CE, et al. Inverse association between physical inactivity and mental health in men and women. Med Sci Sports Exerc. 2006;38(1):173-178.
Fazio AF. A concurrent validation study of the NCHS General Well-Being Schedule. Vital and Health Statistics. Hyattsville, MD: National Center for Health Statistics, US Public Health Service; September 1977. Series 2, No. 73, DHEW Publication No. (HRA) 78-1347:1-13.
14. De Moor MH, Boomsma DI, Stubbe JH, et al. Testing causality in the association between regular exercise and symptoms of anxiety and depression. Arch Gen Psychiatry. 2008;65(8):897-905.
15. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69(7):587-596.
16. O’Hara MW, Swain AM. Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry. 1996;8(1):37-54.
17. Heh SS, Huang LH, Ho SM, et al. Effectiveness of an exercise support program in reducing the severity of postnatal depression in Taiwanese women. Birth. 2008;35(1):60-65.
18. Saurel-Cubizolles MJ, Romito P, Lelong N, et al. Women’s health after childbirth: a longitudinal study in France and Italy. BJOG. 2000;107(10):1202-1209.
19. Dritsa M, Da Costa D, Dupuis G, et al. Effects of a home-based exercise intervention on fatigue in postpartum depressed women: results of a randomized controlled trial. Ann Behav Med. 2008;35(2):179-187.
20. Corwin EJ, Brownstead J, Barton N, et al. The impact of fatigue on the development of postpartum depression. J Obstet Gynecol Neonatal Nurs. 2005;34(5):577-586.
21. Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. J Gerontol A Biol Sci Med Sci. 1997;52(1):M27-35.
22. Singh NA, Stavrinos TM, Scarbek Y, et al. A randomized controlled trial of high versus low intensity weight training versus general practitioner care for clinical depression in older adults. J Gerontol A Biol Sci Med Sci. 2005;60(6):768-776.
23. Fremont J, Wilcoxon Craighead L. Aerobic exercise and cognitive therapy in the treatment of dysphoric moods. Cognit Ther Res. 1987;11(2):241-251.
24. Klein MH, Greist JH, Gurman RA, et al. A comparative outcome study of group psychotherapy vs. exercise treatments for depression. Int J Ment Health. 1985;13:148-177.
25. Carta MG, Hardoy MC, Pilu A, et al. Improving physical quality of life with group physical activity in the adjunctive treatment of major depressive disorder. Clin Pract Epidemiol Ment Health. 2008;4:1.
26. Pilu A, Sorba M, Hardoy MC, et al. Efficacy of physical activity in the adjunctive treatment of major depressive disorders: preliminary results. Clin Pract Epidemiol Ment Health. 2007;3:8.
27. Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med. 1999;159(19):2349-2356.
28. Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med. 2000;62(5):633-638.
29. Singh NA, Clements KM, Singh MA. The efficacy of exercise as a long-term antidepressant in elderly subjects: a randomized, controlled trial. J Gerontol A Biol Sci Med Sci. 2001;56(8):M497-504.
30. Camacho TC, Roberts RE, Lazarus NB, et al. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol. 1991;134(2):220-231.
Weight gain with antipsychotics: What role does leptin play?
Clinical studies indicate that clozapine and olanzapine carry a high risk of treatment-related metabolic dysfunction—including weight gain, hyperlipidemia, and glucose intolerance—but certain patients with high metabolic liabilities who take atypical antipsychotics do not necessarily develop these adverse effects. Though the underlying mechanism for atypical antipsychotic-related weight gain is strongly associated with central histamine H1 antagonism and increased appetite, the pharmacologic basis for other metabolic changes is not fully understood and may involve weight-independent mechanisms.
One potentially relevant research area is peptide hormones’ impact on the regulation of food intake, body weight, and other metabolic parameters. As research has elucidated the properties of 1 of these hormones—leptin—investigators have started to examine possible correlations between changes in serum levels of leptin and weight gain during atypical anti-psychotic treatment.
This article summarizes available clinical data on the interaction of atypical antipsychotics with leptin and indicates directions for future research on interactions between psychotropic medications and metabolic hormones.
Leptin’s function
Since its initial sequencing as the product of the obese (ob) gene in 1994, leptin has garnered substantial attention as a metabolic regulatory hormone.1 Leptin is produced primarily by fat cells as part of a long-term central feedback mechanism involving central control of appetite and peripheral metabolic activity regulation. Leptin is a 167 amino acid, 16-kilodalton protein that binds to cell surface receptors (the product of the diabetes [db] gene) at both central (ventromedial hypothalamic) and peripheral sites (liver, skeletal muscle, and pancreatic β-cells).2
Evidence for leptin’s activity is seen in ob/ob mice, whose genetic inability to produce leptin is manifested phenotypically in overeating and obesity. Administering recombinant leptin to these mice results in reduced appetite and weight loss.3
On average, women have greater fat mass and higher serum leptin levels than men. Humans rarely have mutations in both copies of the ob gene, but those who do are severely obese and respond to exogenous leptin. Heterozygotes are not quite as heavy.
Leptin circulates in a free form but in humans is predominantly bound to the soluble leptin receptor (sOB-R). Levels of sOB-R increase with weight loss—with concomitant decreases in leptin levels—and these effects can be seen even during 72-hour fasts.4 Leptin levels are positively correlated with fat mass, but the fact that obese individuals have chronically elevated leptin levels argues for some level of leptin insensitivity or resistance to the hormone’s appetite-suppressing effects.2
Drug effects
Clozapine and olanzapine. Literature on leptin and antipsychotic-related obesity is relatively well developed. The first papers focused on the association between clozapine and olanzapine and increases in serum leptin levels.5,6 As patients gained substantial weight on clozapine and olanzapine, serum leptin also rose, but neither weight nor leptin changes were seen in patients exposed to haloperidol or those who did not receive antipsychotics.6
Numerous subsequent prospective trials of patients treated with olanzapine4,7,8 and clozapine9-11 confirmed previousl established associations among use of these medications, weight gain, and increased serum leptin levels. Olanzapine- and clozapine-exposed subjects experienced marked increases in adiposity, weight, and serum leptin (Box 1). 5,9,12-16
Other agents. For agents associated with less weight gain liability—such as high-potency typical antipsychotics,12,17,18 sulpiride,19 quetiapine,18 or risperidone20,21—comparative trials noted modest weight gain and leptin increases. Prospective trials of weight-modifying strategies using adjunctive amantadine8 or nizatidine22 found positive effects of the adjunctive medication, with proportional decreases in leptin levels compared with antipsychotics alone.
Because the other 2 atypical antipsychotics—ziprasidone and aripiprazole—were found to be weight-neutral or have the lowest weight-gain burden, few studies have examined the relationship between leptin with weight gain in patients taking these drugs. One study reported no significant body weight or leptin level change in patients after 4-week trial of ziprasidone.23
Most of the weight gain associated with olanzapine and clozapine therapy occurs over the first 6 months of treatment and then plateaus between months 6 and 12. Leptin changes, however, do not parallel weight changes during extended antipsychotic treatment.
A prospective 10-week clozapine trial by Bromel5 found that leptin levels peaked early in treatment—at week 2—followed by a subsequent decrease and then a steady rise, though not to the peak levels seen earlier. This pattern was replicated in Monteleone’s 32-week prospective clozapine study, again with the initial peak in serum leptin levels occurring at week 2.9
Despite these fluctuations, overall leptin levels during longer-term antipsychotic treatment are highly correlated with weight and body mass index changes. Cross-sectional studies with patients on various medications generally found that those exposed to olanzapine and clozapine were heavier and had higher serum leptin levels.12-14 Younger and thinner patients—regardless of medication—have lower serum leptin levels15 and the association between the medication and leptin levels disappears when adjustments are made for differences in body mass index (BMI).16 Once BMI is accounted for, antipsychotics appear to have no effects on leptin physiology independent of their effects on adiposity.
Other metabolic parameters
In humans, elevated serum leptin levels are associated with adverse metabolic markers, particularly those associated with insulin activity (including insulin itself) and serum triglycerides.24 Several antipsychotic studies measured metabolic outcomes along with serum leptin levels but did not specifically calculate correlation coefficients between leptin and other parameters.7,8,11,16,17,19
Nonetheless, in many instances leptin levels increased significantly without significant changes in serum insulin or other glycemic or lipid measures.11,25 One cross-sectional study in bipolar subjects also found no correlation between any glucose or lipid parameter and leptin levels.26 A few studies reported significant correlations among leptin and serum insulin,13,27 glucose,15 and serum triglycerides,18 although most did not control for body mass index (BMI).
Diagnosis effects
As the association was established between antipsychotic-induced weight gain and changes in serum leptin, investigators sought to understand whether disease influences modified the drug effects.
Schizophrenia. One early cross-sectional analysis of 14 olanzapine-treated schizophrenia patients noted that 57% had elevated serum leptin when compared with normal levels adjusted for BMI and gender,27 but the absence of a weight-matched control group limits interpretation of these findings.
To separate diagnosis and treatment effects, Arranz28 performed a cross-sectional study of 50 drug-naïve schizophrenia patients, 50 drug-free schizophrenia patients, and 50 unmatched healthy controls. Leptin levels across all cohorts were positively correlated with age and BMI, and—as found in several other studies (Box 2)9,12,13,20,25,28-30—women had higher levels than men in all 3 cohorts. The antipsychotic-free patients were older and heavier than the other 2 cohorts and had higher serum leptin levels, but neuroleptic-naïve schizophrenia subjects did not differ from controls. The absence of BMI matching between the drug-free patients and other cohorts limits the ability to make definitive statements about the treatment’s impact on leptin levels.
Other studies removed these limitations by matching schizophrenia patients with controls on the basis of gender, BMI, and—in some cases—age. These studies indicate conclusively that—when matched appropriately with nonpsychiatric subjects—patients with schizophrenia do not exhibit greater-than-expected serum leptin levels, regardless of antipsychotic drug exposure.7,11,12,19,26,28-31
Other diagnoses. The only controlled comparative study of medication-treated bipolar patients vs matched controls also reported no significant difference in leptin levels.26 Interestingly, a 6-month prospective study of risperidone in autistic children noted no increase in serum leptin despite a 5.6-kg mean weight gain.21
Lastly, a single 12-week prospective trial compared the effects of antipsychotics on levodopa psychosis in Parkinson’s disease subjects treated with olanzapine (n=10), risperidone (n=10), quetiapine (n=10), or solely with antiparkinsonian medications (n=10); an unmedicated, healthy cohort (n=8) served as controls.32 Only olanzapine was associated with significant weight gain, but BMI changes were positively correlated with changes in leptin levels across all cohorts.
Most—but not all—cross-sectional studies of patients receiving antipsychotic treatment have found higher serum leptin levels in women than men, even when men had greater body mass index (BMI).13,28,29 In several prospective trials, this gender discrepancy gradually disappeared as men’s serum leptin increased.12,30 Data from 1 long-term study of patients treated with clozapine indicate that leptin changes were independent of gender and proportional to weight gain,9 but other analyses that examined both weight and fat depots continued to find significant gender effects.25 One notable exception was McIntyre’s 6-month randomized adjunctive study of risperidone vs olanzapine in symptomatic bipolar patients on mood stabilizers, in which women had greater increases in serum leptin with either antipsychotic.20
Clinical implications
Driven by obesity’s public health impact, researchers have achieved a basic understanding of the regulation of appetite and body weight, including identifying genetic polymorphisms and other obesity risk markers. Evidence exploring the association between peptide metabolic regulatory hormones and antipsychotic-induced weight gain and metabolic dysfunction is accumulating.
Overall, evidence strongly suggests that leptin levels increase during long-term antipsychotic treatment and are highly correlated with weight and BMI changes. Although the increase in serum leptin often parallels substantial weight gain, these changes appear to be more the result of weight gain than a direct effect of the anti-psychotic on the leptin feedback pathway.29 Virtually none of the papers we reviewed examined the association between leptin and glucose-insulin measures independent of the effect of weight changes.
Predicting weight gain? Because increased serum leptin is likely the result of weight gain in patients taking antipsychotics, measuring leptin for clinical prediction or monitoring of weight gain may not be very useful. Measuring weight or BMI will be more feasible in most clinical settings. However, leptin level changes may help us understand the potential mechanism of hormonal feedback and its physiologic effect in weight gain.
Medications such as olanzapine and clozapine carry substantial metabolic burdens but are effective treatments for some patients who do not respond to other antipsychotics. Elucidating mechanisms by which antipsychotic medications affect metabolic parameters remains important for:
- quantifying patient risk
- informing the frequency and targets of metabolic monitoring during antipsychotic therapy
- permitting the development of novel agents without these limitations.
Related resource
- Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31-41.
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Jin receives grant/research support from the National Institutes of Health, the National Institute of Mental Health, Otsuka Pharmaceuticals, and the Stanley Medical Research Foundation. He is a consultant to the Stanley Medical Research Foundation.
Dr. Meyer receives grant/research support from Bristol-Myers Squibb, the National Institutes of Health, the National Institute of Mental Health, and Pfizer Inc. He is a consultant to Bristol-Myers Squibb, Janssen Pharmaceutica, Organon USA (now Merck), Pfizer Inc., Vanda Pharmaceuticals, and Wyeth Pharmaceuticals (now Pfizer Inc.) and a speaker for AstraZeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, and Pfizer Inc.
1. Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue[erratum appears in Nature 1995;374(6521):479]. Nature. 1994;372:425-432.
2. Friedman JM. The function of leptin in nutrition, weight, and physiology. Nutr Rev. 2002;60:S1-14.discussion S68-S84.
3. Halaas JL, Gajiwala KS, Maffei M, et al. Weight reducing effects of the plasma protein encoded by the obese gene. Science. 1995;269:543-546.
4. Ebenbichler C, Laimer M, Kranebitter M, et al. The soluble leptin receptor in olanzapine-induced weight gain: results from a prospective study. Schizophr Res. 2005;75:143-146.
5. Bromel T, Blum WF, Ziegler A. Serum leptin levels increase rapidly after initiation of clozapine therapy. Mol Psychiatry. 1998;3:76-80.
6. Kraus T, Haack M, Schuld A, et al. Body weight and leptin plasma levels during treatment with antipsychotic drugs. Am J Psychiatry. 1999;156:312-314.
7. Eder U, Mangweth B, Ebenbichler C, et al. Association of olanzapine-induced weight gain with an increase in body fat. Am J Psychiatry. 2001;158:1719-1722.
8. Graham KA, Gu H, Lieberman JA. Double-blind, placebo-controlled investigation of amantadine for weight loss in subjects who gained weight with olanzapine. Am J Psychiatry. 2005;162:1744-1746.
9. Monteleone P, Fabrazzo M, Tortorella A, et al. Pronounced early increase in circulating leptin predicts a lower weight gain during clozapine treatment. J Clin Psychopharmacol. 2002;22:424-426.
10. Kivircik BB, Alptekin K, Caliskan S, et al. Effect of clozapine on serum leptin, insulin levels, and body weight and composition in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2003;27:795-799.
11. Sporn AL, Bobb AJ, Gogtay N, et al. Hormonal correlates of clozapine-induced weight gain in psychotic children: an exploratory study. J Am Acad Child Adolesc Psychiatry. 2005;44:925-933.
12. Hagg S, Soderberg S, Ahren B, et al. Leptin concentrations are increased in subjects treated with clozapine or conventional antipsychotics. J Clin Psychiatry. 2001;62:843-848.
13. Melkersson KI, Hulting AL. Insulin and leptin levels in patients with schizophrenia or related psychoses—a comparison between different antipsychotic agents. Psychopharmacology (Berl). 2001;154:205-212.
14. Melkersson KI, Dahl ML. Relationship between levels of insulin or triglycerides and serum concentrations of the atypical antipsychotics clozapine and olanzapine in patients on treatment with therapeutic doses. Psychopharmacology. 2003;70:157-166.
15. Wang CJ, Zhang ZJ, Sun J. Serum free fatty acids and glucose metabolism, insulin resistance in schizophrenia with chronic antipsychotics. Biol Psychiatry. 2006;60:1309-1313.
16. Smith RC, Lindenmayer JP, Bark N, et al. Clozapine, risperidone, olanzapine, and conventional antipsychotic drug effects on glucose, lipids, and leptin in schizophrenic patients. Int J Neuropsychopharmacol. 2005;8:183-194.
17. Atmaca M, Kuloglu M, Tezcan E, et al. Weight gain, serum leptin and triglyceride levels in patients with schizophrenia on antipsychotic treatment with quetiapine, olanzapine and haloperidol. Schizophr Res. 2003;60:99-100.
18. Atmaca M, Kuloglu M, Tezcan E, et al. Serum leptin and triglyceride levels in patients on treatment with atypical antipsychotics. J Clin Psychiatry. 2003;64:598-604.
19. Baptista T, Lacruz A, Angeles F, et al. Endocrine and metabolic abnormalities involved in obesity associated with typical antipsychotic drug administration. Pharmacopsychiatry. 2001;34:223-231.
20. McIntyre RS, Mancini DA, Basile VS, et al. Antipsychotic-induced weight gain: bipolar disorder and leptin. J Clin Psychopharmacol. 2003;23:323-327.
21. Martin A, Scahill L, Anderson GM, et al. Weight and leptin changes among risperidone-treated youths with autism: 6-month prospective data. Am J Psychiatry. 2004;161:1125-1127.
22. Atmaca M, Kuloglu M, Tezcan E, et al. Nizatidine treatment and its relationship with leptin levels in patients with olanzapine-induced weight gain. Hum Psychopharmacol. 2003;18:457-461.
23. Tschoner A, Engl J, Rettenbacher M, et al. Effects of six second generation antipsychotics on body weight and metabolism—risk assessment and results from a prospective study. Pharmacopsychiatry. 2009;42(1):29-34.
24. Franks PW, Brage S, Luan J, et al. Leptin predicts a worsening of the features of the metabolic syndrome independently of obesity. Obes Res. 2005;13:1476-1484.
25. Zhang ZJ, Yao ZJ, Liu W, et al. Effects of antipsychotics on fat deposition and changes in leptin and insulin levels. Magnetic resonance imaging study of previously untreated people with schizophrenia. Br J Psychiatry. 2004;184:58-62.
26. Gergerlioglu HZ, Savas HA, Celik A, et al. Atypical antipsychotic usage-related higher serum leptin levels and disabled lipid profiles in euthymic bipolar patients. Neuropsychobiology. 2006;53:108-112.
27. Melkersson KI, Hulting AL, Brismar KE. Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychoses. J Clin Psychiatry. 2000;61:742-749.
28. Arranz B, Rosel P, Ramirez N, et al. Insulin resistance and increased leptin concentrations in noncompliant schizophrenia patients but not in antipsychotic-naive first-episode schizophrenia patients. J Clin Psychiatry. 2004;65:1335-1342.
29. Haupt DW, Luber A, Maeda J, et al. Plasma leptin and adiposity during antipsychotic treatment of schizophrenia. Neuropsychopharmacology. 2005;30:184-191.
30. Zhang ZJ, Yao ZJ, Mou XD, et al. Association of -2548G/A functional polymorphism in the promoter region of leptin gene with antipsychotic agent-induced weight gain. Zhonghua Yi Xue Za Zhi. 2003;83:2119-2123.
31. Herran A, Garcia-Unzueta MT, Amado JA, et al. Effects of long-term treatment with antipsychotics on serum leptin levels. Br J Psychiatry. 2001;179:59-62.
32. Rustembegovic A, Sofic E, Wichart I. Serum prolactin, leptin, lipids and lipoproteins levels during antipsychotics treatment in Parkinson’s disease and related psychosis. Med Arh. 2006;60:211-212.
Clinical studies indicate that clozapine and olanzapine carry a high risk of treatment-related metabolic dysfunction—including weight gain, hyperlipidemia, and glucose intolerance—but certain patients with high metabolic liabilities who take atypical antipsychotics do not necessarily develop these adverse effects. Though the underlying mechanism for atypical antipsychotic-related weight gain is strongly associated with central histamine H1 antagonism and increased appetite, the pharmacologic basis for other metabolic changes is not fully understood and may involve weight-independent mechanisms.
One potentially relevant research area is peptide hormones’ impact on the regulation of food intake, body weight, and other metabolic parameters. As research has elucidated the properties of 1 of these hormones—leptin—investigators have started to examine possible correlations between changes in serum levels of leptin and weight gain during atypical anti-psychotic treatment.
This article summarizes available clinical data on the interaction of atypical antipsychotics with leptin and indicates directions for future research on interactions between psychotropic medications and metabolic hormones.
Leptin’s function
Since its initial sequencing as the product of the obese (ob) gene in 1994, leptin has garnered substantial attention as a metabolic regulatory hormone.1 Leptin is produced primarily by fat cells as part of a long-term central feedback mechanism involving central control of appetite and peripheral metabolic activity regulation. Leptin is a 167 amino acid, 16-kilodalton protein that binds to cell surface receptors (the product of the diabetes [db] gene) at both central (ventromedial hypothalamic) and peripheral sites (liver, skeletal muscle, and pancreatic β-cells).2
Evidence for leptin’s activity is seen in ob/ob mice, whose genetic inability to produce leptin is manifested phenotypically in overeating and obesity. Administering recombinant leptin to these mice results in reduced appetite and weight loss.3
On average, women have greater fat mass and higher serum leptin levels than men. Humans rarely have mutations in both copies of the ob gene, but those who do are severely obese and respond to exogenous leptin. Heterozygotes are not quite as heavy.
Leptin circulates in a free form but in humans is predominantly bound to the soluble leptin receptor (sOB-R). Levels of sOB-R increase with weight loss—with concomitant decreases in leptin levels—and these effects can be seen even during 72-hour fasts.4 Leptin levels are positively correlated with fat mass, but the fact that obese individuals have chronically elevated leptin levels argues for some level of leptin insensitivity or resistance to the hormone’s appetite-suppressing effects.2
Drug effects
Clozapine and olanzapine. Literature on leptin and antipsychotic-related obesity is relatively well developed. The first papers focused on the association between clozapine and olanzapine and increases in serum leptin levels.5,6 As patients gained substantial weight on clozapine and olanzapine, serum leptin also rose, but neither weight nor leptin changes were seen in patients exposed to haloperidol or those who did not receive antipsychotics.6
Numerous subsequent prospective trials of patients treated with olanzapine4,7,8 and clozapine9-11 confirmed previousl established associations among use of these medications, weight gain, and increased serum leptin levels. Olanzapine- and clozapine-exposed subjects experienced marked increases in adiposity, weight, and serum leptin (Box 1). 5,9,12-16
Other agents. For agents associated with less weight gain liability—such as high-potency typical antipsychotics,12,17,18 sulpiride,19 quetiapine,18 or risperidone20,21—comparative trials noted modest weight gain and leptin increases. Prospective trials of weight-modifying strategies using adjunctive amantadine8 or nizatidine22 found positive effects of the adjunctive medication, with proportional decreases in leptin levels compared with antipsychotics alone.
Because the other 2 atypical antipsychotics—ziprasidone and aripiprazole—were found to be weight-neutral or have the lowest weight-gain burden, few studies have examined the relationship between leptin with weight gain in patients taking these drugs. One study reported no significant body weight or leptin level change in patients after 4-week trial of ziprasidone.23
Most of the weight gain associated with olanzapine and clozapine therapy occurs over the first 6 months of treatment and then plateaus between months 6 and 12. Leptin changes, however, do not parallel weight changes during extended antipsychotic treatment.
A prospective 10-week clozapine trial by Bromel5 found that leptin levels peaked early in treatment—at week 2—followed by a subsequent decrease and then a steady rise, though not to the peak levels seen earlier. This pattern was replicated in Monteleone’s 32-week prospective clozapine study, again with the initial peak in serum leptin levels occurring at week 2.9
Despite these fluctuations, overall leptin levels during longer-term antipsychotic treatment are highly correlated with weight and body mass index changes. Cross-sectional studies with patients on various medications generally found that those exposed to olanzapine and clozapine were heavier and had higher serum leptin levels.12-14 Younger and thinner patients—regardless of medication—have lower serum leptin levels15 and the association between the medication and leptin levels disappears when adjustments are made for differences in body mass index (BMI).16 Once BMI is accounted for, antipsychotics appear to have no effects on leptin physiology independent of their effects on adiposity.
Other metabolic parameters
In humans, elevated serum leptin levels are associated with adverse metabolic markers, particularly those associated with insulin activity (including insulin itself) and serum triglycerides.24 Several antipsychotic studies measured metabolic outcomes along with serum leptin levels but did not specifically calculate correlation coefficients between leptin and other parameters.7,8,11,16,17,19
Nonetheless, in many instances leptin levels increased significantly without significant changes in serum insulin or other glycemic or lipid measures.11,25 One cross-sectional study in bipolar subjects also found no correlation between any glucose or lipid parameter and leptin levels.26 A few studies reported significant correlations among leptin and serum insulin,13,27 glucose,15 and serum triglycerides,18 although most did not control for body mass index (BMI).
Diagnosis effects
As the association was established between antipsychotic-induced weight gain and changes in serum leptin, investigators sought to understand whether disease influences modified the drug effects.
Schizophrenia. One early cross-sectional analysis of 14 olanzapine-treated schizophrenia patients noted that 57% had elevated serum leptin when compared with normal levels adjusted for BMI and gender,27 but the absence of a weight-matched control group limits interpretation of these findings.
To separate diagnosis and treatment effects, Arranz28 performed a cross-sectional study of 50 drug-naïve schizophrenia patients, 50 drug-free schizophrenia patients, and 50 unmatched healthy controls. Leptin levels across all cohorts were positively correlated with age and BMI, and—as found in several other studies (Box 2)9,12,13,20,25,28-30—women had higher levels than men in all 3 cohorts. The antipsychotic-free patients were older and heavier than the other 2 cohorts and had higher serum leptin levels, but neuroleptic-naïve schizophrenia subjects did not differ from controls. The absence of BMI matching between the drug-free patients and other cohorts limits the ability to make definitive statements about the treatment’s impact on leptin levels.
Other studies removed these limitations by matching schizophrenia patients with controls on the basis of gender, BMI, and—in some cases—age. These studies indicate conclusively that—when matched appropriately with nonpsychiatric subjects—patients with schizophrenia do not exhibit greater-than-expected serum leptin levels, regardless of antipsychotic drug exposure.7,11,12,19,26,28-31
Other diagnoses. The only controlled comparative study of medication-treated bipolar patients vs matched controls also reported no significant difference in leptin levels.26 Interestingly, a 6-month prospective study of risperidone in autistic children noted no increase in serum leptin despite a 5.6-kg mean weight gain.21
Lastly, a single 12-week prospective trial compared the effects of antipsychotics on levodopa psychosis in Parkinson’s disease subjects treated with olanzapine (n=10), risperidone (n=10), quetiapine (n=10), or solely with antiparkinsonian medications (n=10); an unmedicated, healthy cohort (n=8) served as controls.32 Only olanzapine was associated with significant weight gain, but BMI changes were positively correlated with changes in leptin levels across all cohorts.
Most—but not all—cross-sectional studies of patients receiving antipsychotic treatment have found higher serum leptin levels in women than men, even when men had greater body mass index (BMI).13,28,29 In several prospective trials, this gender discrepancy gradually disappeared as men’s serum leptin increased.12,30 Data from 1 long-term study of patients treated with clozapine indicate that leptin changes were independent of gender and proportional to weight gain,9 but other analyses that examined both weight and fat depots continued to find significant gender effects.25 One notable exception was McIntyre’s 6-month randomized adjunctive study of risperidone vs olanzapine in symptomatic bipolar patients on mood stabilizers, in which women had greater increases in serum leptin with either antipsychotic.20
Clinical implications
Driven by obesity’s public health impact, researchers have achieved a basic understanding of the regulation of appetite and body weight, including identifying genetic polymorphisms and other obesity risk markers. Evidence exploring the association between peptide metabolic regulatory hormones and antipsychotic-induced weight gain and metabolic dysfunction is accumulating.
Overall, evidence strongly suggests that leptin levels increase during long-term antipsychotic treatment and are highly correlated with weight and BMI changes. Although the increase in serum leptin often parallels substantial weight gain, these changes appear to be more the result of weight gain than a direct effect of the anti-psychotic on the leptin feedback pathway.29 Virtually none of the papers we reviewed examined the association between leptin and glucose-insulin measures independent of the effect of weight changes.
Predicting weight gain? Because increased serum leptin is likely the result of weight gain in patients taking antipsychotics, measuring leptin for clinical prediction or monitoring of weight gain may not be very useful. Measuring weight or BMI will be more feasible in most clinical settings. However, leptin level changes may help us understand the potential mechanism of hormonal feedback and its physiologic effect in weight gain.
Medications such as olanzapine and clozapine carry substantial metabolic burdens but are effective treatments for some patients who do not respond to other antipsychotics. Elucidating mechanisms by which antipsychotic medications affect metabolic parameters remains important for:
- quantifying patient risk
- informing the frequency and targets of metabolic monitoring during antipsychotic therapy
- permitting the development of novel agents without these limitations.
Related resource
- Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31-41.
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Jin receives grant/research support from the National Institutes of Health, the National Institute of Mental Health, Otsuka Pharmaceuticals, and the Stanley Medical Research Foundation. He is a consultant to the Stanley Medical Research Foundation.
Dr. Meyer receives grant/research support from Bristol-Myers Squibb, the National Institutes of Health, the National Institute of Mental Health, and Pfizer Inc. He is a consultant to Bristol-Myers Squibb, Janssen Pharmaceutica, Organon USA (now Merck), Pfizer Inc., Vanda Pharmaceuticals, and Wyeth Pharmaceuticals (now Pfizer Inc.) and a speaker for AstraZeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, and Pfizer Inc.
Clinical studies indicate that clozapine and olanzapine carry a high risk of treatment-related metabolic dysfunction—including weight gain, hyperlipidemia, and glucose intolerance—but certain patients with high metabolic liabilities who take atypical antipsychotics do not necessarily develop these adverse effects. Though the underlying mechanism for atypical antipsychotic-related weight gain is strongly associated with central histamine H1 antagonism and increased appetite, the pharmacologic basis for other metabolic changes is not fully understood and may involve weight-independent mechanisms.
One potentially relevant research area is peptide hormones’ impact on the regulation of food intake, body weight, and other metabolic parameters. As research has elucidated the properties of 1 of these hormones—leptin—investigators have started to examine possible correlations between changes in serum levels of leptin and weight gain during atypical anti-psychotic treatment.
This article summarizes available clinical data on the interaction of atypical antipsychotics with leptin and indicates directions for future research on interactions between psychotropic medications and metabolic hormones.
Leptin’s function
Since its initial sequencing as the product of the obese (ob) gene in 1994, leptin has garnered substantial attention as a metabolic regulatory hormone.1 Leptin is produced primarily by fat cells as part of a long-term central feedback mechanism involving central control of appetite and peripheral metabolic activity regulation. Leptin is a 167 amino acid, 16-kilodalton protein that binds to cell surface receptors (the product of the diabetes [db] gene) at both central (ventromedial hypothalamic) and peripheral sites (liver, skeletal muscle, and pancreatic β-cells).2
Evidence for leptin’s activity is seen in ob/ob mice, whose genetic inability to produce leptin is manifested phenotypically in overeating and obesity. Administering recombinant leptin to these mice results in reduced appetite and weight loss.3
On average, women have greater fat mass and higher serum leptin levels than men. Humans rarely have mutations in both copies of the ob gene, but those who do are severely obese and respond to exogenous leptin. Heterozygotes are not quite as heavy.
Leptin circulates in a free form but in humans is predominantly bound to the soluble leptin receptor (sOB-R). Levels of sOB-R increase with weight loss—with concomitant decreases in leptin levels—and these effects can be seen even during 72-hour fasts.4 Leptin levels are positively correlated with fat mass, but the fact that obese individuals have chronically elevated leptin levels argues for some level of leptin insensitivity or resistance to the hormone’s appetite-suppressing effects.2
Drug effects
Clozapine and olanzapine. Literature on leptin and antipsychotic-related obesity is relatively well developed. The first papers focused on the association between clozapine and olanzapine and increases in serum leptin levels.5,6 As patients gained substantial weight on clozapine and olanzapine, serum leptin also rose, but neither weight nor leptin changes were seen in patients exposed to haloperidol or those who did not receive antipsychotics.6
Numerous subsequent prospective trials of patients treated with olanzapine4,7,8 and clozapine9-11 confirmed previousl established associations among use of these medications, weight gain, and increased serum leptin levels. Olanzapine- and clozapine-exposed subjects experienced marked increases in adiposity, weight, and serum leptin (Box 1). 5,9,12-16
Other agents. For agents associated with less weight gain liability—such as high-potency typical antipsychotics,12,17,18 sulpiride,19 quetiapine,18 or risperidone20,21—comparative trials noted modest weight gain and leptin increases. Prospective trials of weight-modifying strategies using adjunctive amantadine8 or nizatidine22 found positive effects of the adjunctive medication, with proportional decreases in leptin levels compared with antipsychotics alone.
Because the other 2 atypical antipsychotics—ziprasidone and aripiprazole—were found to be weight-neutral or have the lowest weight-gain burden, few studies have examined the relationship between leptin with weight gain in patients taking these drugs. One study reported no significant body weight or leptin level change in patients after 4-week trial of ziprasidone.23
Most of the weight gain associated with olanzapine and clozapine therapy occurs over the first 6 months of treatment and then plateaus between months 6 and 12. Leptin changes, however, do not parallel weight changes during extended antipsychotic treatment.
A prospective 10-week clozapine trial by Bromel5 found that leptin levels peaked early in treatment—at week 2—followed by a subsequent decrease and then a steady rise, though not to the peak levels seen earlier. This pattern was replicated in Monteleone’s 32-week prospective clozapine study, again with the initial peak in serum leptin levels occurring at week 2.9
Despite these fluctuations, overall leptin levels during longer-term antipsychotic treatment are highly correlated with weight and body mass index changes. Cross-sectional studies with patients on various medications generally found that those exposed to olanzapine and clozapine were heavier and had higher serum leptin levels.12-14 Younger and thinner patients—regardless of medication—have lower serum leptin levels15 and the association between the medication and leptin levels disappears when adjustments are made for differences in body mass index (BMI).16 Once BMI is accounted for, antipsychotics appear to have no effects on leptin physiology independent of their effects on adiposity.
Other metabolic parameters
In humans, elevated serum leptin levels are associated with adverse metabolic markers, particularly those associated with insulin activity (including insulin itself) and serum triglycerides.24 Several antipsychotic studies measured metabolic outcomes along with serum leptin levels but did not specifically calculate correlation coefficients between leptin and other parameters.7,8,11,16,17,19
Nonetheless, in many instances leptin levels increased significantly without significant changes in serum insulin or other glycemic or lipid measures.11,25 One cross-sectional study in bipolar subjects also found no correlation between any glucose or lipid parameter and leptin levels.26 A few studies reported significant correlations among leptin and serum insulin,13,27 glucose,15 and serum triglycerides,18 although most did not control for body mass index (BMI).
Diagnosis effects
As the association was established between antipsychotic-induced weight gain and changes in serum leptin, investigators sought to understand whether disease influences modified the drug effects.
Schizophrenia. One early cross-sectional analysis of 14 olanzapine-treated schizophrenia patients noted that 57% had elevated serum leptin when compared with normal levels adjusted for BMI and gender,27 but the absence of a weight-matched control group limits interpretation of these findings.
To separate diagnosis and treatment effects, Arranz28 performed a cross-sectional study of 50 drug-naïve schizophrenia patients, 50 drug-free schizophrenia patients, and 50 unmatched healthy controls. Leptin levels across all cohorts were positively correlated with age and BMI, and—as found in several other studies (Box 2)9,12,13,20,25,28-30—women had higher levels than men in all 3 cohorts. The antipsychotic-free patients were older and heavier than the other 2 cohorts and had higher serum leptin levels, but neuroleptic-naïve schizophrenia subjects did not differ from controls. The absence of BMI matching between the drug-free patients and other cohorts limits the ability to make definitive statements about the treatment’s impact on leptin levels.
Other studies removed these limitations by matching schizophrenia patients with controls on the basis of gender, BMI, and—in some cases—age. These studies indicate conclusively that—when matched appropriately with nonpsychiatric subjects—patients with schizophrenia do not exhibit greater-than-expected serum leptin levels, regardless of antipsychotic drug exposure.7,11,12,19,26,28-31
Other diagnoses. The only controlled comparative study of medication-treated bipolar patients vs matched controls also reported no significant difference in leptin levels.26 Interestingly, a 6-month prospective study of risperidone in autistic children noted no increase in serum leptin despite a 5.6-kg mean weight gain.21
Lastly, a single 12-week prospective trial compared the effects of antipsychotics on levodopa psychosis in Parkinson’s disease subjects treated with olanzapine (n=10), risperidone (n=10), quetiapine (n=10), or solely with antiparkinsonian medications (n=10); an unmedicated, healthy cohort (n=8) served as controls.32 Only olanzapine was associated with significant weight gain, but BMI changes were positively correlated with changes in leptin levels across all cohorts.
Most—but not all—cross-sectional studies of patients receiving antipsychotic treatment have found higher serum leptin levels in women than men, even when men had greater body mass index (BMI).13,28,29 In several prospective trials, this gender discrepancy gradually disappeared as men’s serum leptin increased.12,30 Data from 1 long-term study of patients treated with clozapine indicate that leptin changes were independent of gender and proportional to weight gain,9 but other analyses that examined both weight and fat depots continued to find significant gender effects.25 One notable exception was McIntyre’s 6-month randomized adjunctive study of risperidone vs olanzapine in symptomatic bipolar patients on mood stabilizers, in which women had greater increases in serum leptin with either antipsychotic.20
Clinical implications
Driven by obesity’s public health impact, researchers have achieved a basic understanding of the regulation of appetite and body weight, including identifying genetic polymorphisms and other obesity risk markers. Evidence exploring the association between peptide metabolic regulatory hormones and antipsychotic-induced weight gain and metabolic dysfunction is accumulating.
Overall, evidence strongly suggests that leptin levels increase during long-term antipsychotic treatment and are highly correlated with weight and BMI changes. Although the increase in serum leptin often parallels substantial weight gain, these changes appear to be more the result of weight gain than a direct effect of the anti-psychotic on the leptin feedback pathway.29 Virtually none of the papers we reviewed examined the association between leptin and glucose-insulin measures independent of the effect of weight changes.
Predicting weight gain? Because increased serum leptin is likely the result of weight gain in patients taking antipsychotics, measuring leptin for clinical prediction or monitoring of weight gain may not be very useful. Measuring weight or BMI will be more feasible in most clinical settings. However, leptin level changes may help us understand the potential mechanism of hormonal feedback and its physiologic effect in weight gain.
Medications such as olanzapine and clozapine carry substantial metabolic burdens but are effective treatments for some patients who do not respond to other antipsychotics. Elucidating mechanisms by which antipsychotic medications affect metabolic parameters remains important for:
- quantifying patient risk
- informing the frequency and targets of metabolic monitoring during antipsychotic therapy
- permitting the development of novel agents without these limitations.
Related resource
- Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31-41.
Drug brand names
- Amantadine • Symmetrel
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Haloperidol • Haldol
- Nizatidine • Axid
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Ziprasidone • Geodon
Disclosures
Dr. Jin receives grant/research support from the National Institutes of Health, the National Institute of Mental Health, Otsuka Pharmaceuticals, and the Stanley Medical Research Foundation. He is a consultant to the Stanley Medical Research Foundation.
Dr. Meyer receives grant/research support from Bristol-Myers Squibb, the National Institutes of Health, the National Institute of Mental Health, and Pfizer Inc. He is a consultant to Bristol-Myers Squibb, Janssen Pharmaceutica, Organon USA (now Merck), Pfizer Inc., Vanda Pharmaceuticals, and Wyeth Pharmaceuticals (now Pfizer Inc.) and a speaker for AstraZeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, and Pfizer Inc.
1. Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue[erratum appears in Nature 1995;374(6521):479]. Nature. 1994;372:425-432.
2. Friedman JM. The function of leptin in nutrition, weight, and physiology. Nutr Rev. 2002;60:S1-14.discussion S68-S84.
3. Halaas JL, Gajiwala KS, Maffei M, et al. Weight reducing effects of the plasma protein encoded by the obese gene. Science. 1995;269:543-546.
4. Ebenbichler C, Laimer M, Kranebitter M, et al. The soluble leptin receptor in olanzapine-induced weight gain: results from a prospective study. Schizophr Res. 2005;75:143-146.
5. Bromel T, Blum WF, Ziegler A. Serum leptin levels increase rapidly after initiation of clozapine therapy. Mol Psychiatry. 1998;3:76-80.
6. Kraus T, Haack M, Schuld A, et al. Body weight and leptin plasma levels during treatment with antipsychotic drugs. Am J Psychiatry. 1999;156:312-314.
7. Eder U, Mangweth B, Ebenbichler C, et al. Association of olanzapine-induced weight gain with an increase in body fat. Am J Psychiatry. 2001;158:1719-1722.
8. Graham KA, Gu H, Lieberman JA. Double-blind, placebo-controlled investigation of amantadine for weight loss in subjects who gained weight with olanzapine. Am J Psychiatry. 2005;162:1744-1746.
9. Monteleone P, Fabrazzo M, Tortorella A, et al. Pronounced early increase in circulating leptin predicts a lower weight gain during clozapine treatment. J Clin Psychopharmacol. 2002;22:424-426.
10. Kivircik BB, Alptekin K, Caliskan S, et al. Effect of clozapine on serum leptin, insulin levels, and body weight and composition in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2003;27:795-799.
11. Sporn AL, Bobb AJ, Gogtay N, et al. Hormonal correlates of clozapine-induced weight gain in psychotic children: an exploratory study. J Am Acad Child Adolesc Psychiatry. 2005;44:925-933.
12. Hagg S, Soderberg S, Ahren B, et al. Leptin concentrations are increased in subjects treated with clozapine or conventional antipsychotics. J Clin Psychiatry. 2001;62:843-848.
13. Melkersson KI, Hulting AL. Insulin and leptin levels in patients with schizophrenia or related psychoses—a comparison between different antipsychotic agents. Psychopharmacology (Berl). 2001;154:205-212.
14. Melkersson KI, Dahl ML. Relationship between levels of insulin or triglycerides and serum concentrations of the atypical antipsychotics clozapine and olanzapine in patients on treatment with therapeutic doses. Psychopharmacology. 2003;70:157-166.
15. Wang CJ, Zhang ZJ, Sun J. Serum free fatty acids and glucose metabolism, insulin resistance in schizophrenia with chronic antipsychotics. Biol Psychiatry. 2006;60:1309-1313.
16. Smith RC, Lindenmayer JP, Bark N, et al. Clozapine, risperidone, olanzapine, and conventional antipsychotic drug effects on glucose, lipids, and leptin in schizophrenic patients. Int J Neuropsychopharmacol. 2005;8:183-194.
17. Atmaca M, Kuloglu M, Tezcan E, et al. Weight gain, serum leptin and triglyceride levels in patients with schizophrenia on antipsychotic treatment with quetiapine, olanzapine and haloperidol. Schizophr Res. 2003;60:99-100.
18. Atmaca M, Kuloglu M, Tezcan E, et al. Serum leptin and triglyceride levels in patients on treatment with atypical antipsychotics. J Clin Psychiatry. 2003;64:598-604.
19. Baptista T, Lacruz A, Angeles F, et al. Endocrine and metabolic abnormalities involved in obesity associated with typical antipsychotic drug administration. Pharmacopsychiatry. 2001;34:223-231.
20. McIntyre RS, Mancini DA, Basile VS, et al. Antipsychotic-induced weight gain: bipolar disorder and leptin. J Clin Psychopharmacol. 2003;23:323-327.
21. Martin A, Scahill L, Anderson GM, et al. Weight and leptin changes among risperidone-treated youths with autism: 6-month prospective data. Am J Psychiatry. 2004;161:1125-1127.
22. Atmaca M, Kuloglu M, Tezcan E, et al. Nizatidine treatment and its relationship with leptin levels in patients with olanzapine-induced weight gain. Hum Psychopharmacol. 2003;18:457-461.
23. Tschoner A, Engl J, Rettenbacher M, et al. Effects of six second generation antipsychotics on body weight and metabolism—risk assessment and results from a prospective study. Pharmacopsychiatry. 2009;42(1):29-34.
24. Franks PW, Brage S, Luan J, et al. Leptin predicts a worsening of the features of the metabolic syndrome independently of obesity. Obes Res. 2005;13:1476-1484.
25. Zhang ZJ, Yao ZJ, Liu W, et al. Effects of antipsychotics on fat deposition and changes in leptin and insulin levels. Magnetic resonance imaging study of previously untreated people with schizophrenia. Br J Psychiatry. 2004;184:58-62.
26. Gergerlioglu HZ, Savas HA, Celik A, et al. Atypical antipsychotic usage-related higher serum leptin levels and disabled lipid profiles in euthymic bipolar patients. Neuropsychobiology. 2006;53:108-112.
27. Melkersson KI, Hulting AL, Brismar KE. Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychoses. J Clin Psychiatry. 2000;61:742-749.
28. Arranz B, Rosel P, Ramirez N, et al. Insulin resistance and increased leptin concentrations in noncompliant schizophrenia patients but not in antipsychotic-naive first-episode schizophrenia patients. J Clin Psychiatry. 2004;65:1335-1342.
29. Haupt DW, Luber A, Maeda J, et al. Plasma leptin and adiposity during antipsychotic treatment of schizophrenia. Neuropsychopharmacology. 2005;30:184-191.
30. Zhang ZJ, Yao ZJ, Mou XD, et al. Association of -2548G/A functional polymorphism in the promoter region of leptin gene with antipsychotic agent-induced weight gain. Zhonghua Yi Xue Za Zhi. 2003;83:2119-2123.
31. Herran A, Garcia-Unzueta MT, Amado JA, et al. Effects of long-term treatment with antipsychotics on serum leptin levels. Br J Psychiatry. 2001;179:59-62.
32. Rustembegovic A, Sofic E, Wichart I. Serum prolactin, leptin, lipids and lipoproteins levels during antipsychotics treatment in Parkinson’s disease and related psychosis. Med Arh. 2006;60:211-212.
1. Zhang Y, Proenca R, Maffei M, et al. Positional cloning of the mouse obese gene and its human homologue[erratum appears in Nature 1995;374(6521):479]. Nature. 1994;372:425-432.
2. Friedman JM. The function of leptin in nutrition, weight, and physiology. Nutr Rev. 2002;60:S1-14.discussion S68-S84.
3. Halaas JL, Gajiwala KS, Maffei M, et al. Weight reducing effects of the plasma protein encoded by the obese gene. Science. 1995;269:543-546.
4. Ebenbichler C, Laimer M, Kranebitter M, et al. The soluble leptin receptor in olanzapine-induced weight gain: results from a prospective study. Schizophr Res. 2005;75:143-146.
5. Bromel T, Blum WF, Ziegler A. Serum leptin levels increase rapidly after initiation of clozapine therapy. Mol Psychiatry. 1998;3:76-80.
6. Kraus T, Haack M, Schuld A, et al. Body weight and leptin plasma levels during treatment with antipsychotic drugs. Am J Psychiatry. 1999;156:312-314.
7. Eder U, Mangweth B, Ebenbichler C, et al. Association of olanzapine-induced weight gain with an increase in body fat. Am J Psychiatry. 2001;158:1719-1722.
8. Graham KA, Gu H, Lieberman JA. Double-blind, placebo-controlled investigation of amantadine for weight loss in subjects who gained weight with olanzapine. Am J Psychiatry. 2005;162:1744-1746.
9. Monteleone P, Fabrazzo M, Tortorella A, et al. Pronounced early increase in circulating leptin predicts a lower weight gain during clozapine treatment. J Clin Psychopharmacol. 2002;22:424-426.
10. Kivircik BB, Alptekin K, Caliskan S, et al. Effect of clozapine on serum leptin, insulin levels, and body weight and composition in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2003;27:795-799.
11. Sporn AL, Bobb AJ, Gogtay N, et al. Hormonal correlates of clozapine-induced weight gain in psychotic children: an exploratory study. J Am Acad Child Adolesc Psychiatry. 2005;44:925-933.
12. Hagg S, Soderberg S, Ahren B, et al. Leptin concentrations are increased in subjects treated with clozapine or conventional antipsychotics. J Clin Psychiatry. 2001;62:843-848.
13. Melkersson KI, Hulting AL. Insulin and leptin levels in patients with schizophrenia or related psychoses—a comparison between different antipsychotic agents. Psychopharmacology (Berl). 2001;154:205-212.
14. Melkersson KI, Dahl ML. Relationship between levels of insulin or triglycerides and serum concentrations of the atypical antipsychotics clozapine and olanzapine in patients on treatment with therapeutic doses. Psychopharmacology. 2003;70:157-166.
15. Wang CJ, Zhang ZJ, Sun J. Serum free fatty acids and glucose metabolism, insulin resistance in schizophrenia with chronic antipsychotics. Biol Psychiatry. 2006;60:1309-1313.
16. Smith RC, Lindenmayer JP, Bark N, et al. Clozapine, risperidone, olanzapine, and conventional antipsychotic drug effects on glucose, lipids, and leptin in schizophrenic patients. Int J Neuropsychopharmacol. 2005;8:183-194.
17. Atmaca M, Kuloglu M, Tezcan E, et al. Weight gain, serum leptin and triglyceride levels in patients with schizophrenia on antipsychotic treatment with quetiapine, olanzapine and haloperidol. Schizophr Res. 2003;60:99-100.
18. Atmaca M, Kuloglu M, Tezcan E, et al. Serum leptin and triglyceride levels in patients on treatment with atypical antipsychotics. J Clin Psychiatry. 2003;64:598-604.
19. Baptista T, Lacruz A, Angeles F, et al. Endocrine and metabolic abnormalities involved in obesity associated with typical antipsychotic drug administration. Pharmacopsychiatry. 2001;34:223-231.
20. McIntyre RS, Mancini DA, Basile VS, et al. Antipsychotic-induced weight gain: bipolar disorder and leptin. J Clin Psychopharmacol. 2003;23:323-327.
21. Martin A, Scahill L, Anderson GM, et al. Weight and leptin changes among risperidone-treated youths with autism: 6-month prospective data. Am J Psychiatry. 2004;161:1125-1127.
22. Atmaca M, Kuloglu M, Tezcan E, et al. Nizatidine treatment and its relationship with leptin levels in patients with olanzapine-induced weight gain. Hum Psychopharmacol. 2003;18:457-461.
23. Tschoner A, Engl J, Rettenbacher M, et al. Effects of six second generation antipsychotics on body weight and metabolism—risk assessment and results from a prospective study. Pharmacopsychiatry. 2009;42(1):29-34.
24. Franks PW, Brage S, Luan J, et al. Leptin predicts a worsening of the features of the metabolic syndrome independently of obesity. Obes Res. 2005;13:1476-1484.
25. Zhang ZJ, Yao ZJ, Liu W, et al. Effects of antipsychotics on fat deposition and changes in leptin and insulin levels. Magnetic resonance imaging study of previously untreated people with schizophrenia. Br J Psychiatry. 2004;184:58-62.
26. Gergerlioglu HZ, Savas HA, Celik A, et al. Atypical antipsychotic usage-related higher serum leptin levels and disabled lipid profiles in euthymic bipolar patients. Neuropsychobiology. 2006;53:108-112.
27. Melkersson KI, Hulting AL, Brismar KE. Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychoses. J Clin Psychiatry. 2000;61:742-749.
28. Arranz B, Rosel P, Ramirez N, et al. Insulin resistance and increased leptin concentrations in noncompliant schizophrenia patients but not in antipsychotic-naive first-episode schizophrenia patients. J Clin Psychiatry. 2004;65:1335-1342.
29. Haupt DW, Luber A, Maeda J, et al. Plasma leptin and adiposity during antipsychotic treatment of schizophrenia. Neuropsychopharmacology. 2005;30:184-191.
30. Zhang ZJ, Yao ZJ, Mou XD, et al. Association of -2548G/A functional polymorphism in the promoter region of leptin gene with antipsychotic agent-induced weight gain. Zhonghua Yi Xue Za Zhi. 2003;83:2119-2123.
31. Herran A, Garcia-Unzueta MT, Amado JA, et al. Effects of long-term treatment with antipsychotics on serum leptin levels. Br J Psychiatry. 2001;179:59-62.
32. Rustembegovic A, Sofic E, Wichart I. Serum prolactin, leptin, lipids and lipoproteins levels during antipsychotics treatment in Parkinson’s disease and related psychosis. Med Arh. 2006;60:211-212.
Economic anxiety: First aid for the recession’s casualties
Mr. R, age 45, developed severe depression 4 years ago after his mother died. He had suffered previous major depressive episodes and was treated effiectively with fluoxetine for 15 years. This time he took a medical leave from his job as an engineer and received disability. After numerous medication trials and psychotherapy, his symptoms improved.
Mr. R is ready to think about returning to work, but he will need to refresh his skills and consider starting at a lower level than before. Headlines remind him daily about increasing unemployment and decreasing prospects of finding a job.
During his illness, Mr. R and his family depleted their savings and incurred substantial debt. His wife has not worked outside the home while caring for him and their 4 children. She is increasingly anxious and depressed. The couple argue often about money but share a common hope: that Mr. R will find a job in the next few months.
How is the recession affecting psychiatric practice? Christopher Palmer, MD, the psychiatrist who treated Mr. R, says, “We in psychiatry and psychology are well-equipped to help people who are unemployed, underemployed, and financially ruined. We do it all the time. The difference in this economy is that we’re going to be seeing a lot more people.”
Psychiatrists who read Current Psychiatry and were polled in March 2009 agree. Most were seeing an increase in patients experiencing psychological stress because of the recession, which by then had persisted 16 months. “All my patients are reporting increased stress as a result of the economic situation. The more successful my patient is, the more distress they seem to be feeling,” says a psychiatrist from Melbourne, FL.
This article on the psychological effects of the recession discusses the results of an online survey of Current Psychiatry readers, with analysis and recommendations from an interview with Dr. Palmer and colleagues Jeffrey Rediger, MD, MDiv, and Carol Kauffman, PhD, ABPP, PCC, from McLean Hospital, Belmont, MA, and the department of psychiatry, Harvard Medical School.
 | Carol Kauffman, PhD, ABPP, PCC, is director of the Institute of Coaching, McLean Hospital, Belmont, MA, and assistant clinical professor, department of psychiatry, Harvard Medical School. A veteran psychologist, she maintains an executive coaching practice in the United States and Europe. |
 | Christopher Palmer, MD, is medical director of continuing medical education, McLean Hospital. His outpatient practice focuses on substance abuse, sleep disorders, mood and anxiety disorders, psychotic disorders, and individual and family psychotherapy. |
 | Jeffrey Rediger, MD, MDiv, is medical director, adult psychiatric program, McLean Hospital SouthEast. He also is an instructor, department of psychiatry, Harvard Medical School and has a master of divinity degree. He publishes in the fields of medicine, psychiatry, and spirituality. |
Survey results
Methods. Using an e-mail questionnaire (Box), Current Psychiatry contacted 45 Reader Reactors—clinical psychiatrists who provide feedback to our editorial staff about topics being considered for publication. The 15 readers who responded practice psychiatry in the Northeast (New York and New Jersey), the South (Florida and Georgia), the West (California, Washington, and Oregon), and the Midwest (Pennsylvania, Illinois, and Missouri).
Nine of 11 readers who answered all questions in the survey said they have seen an increase in patients describing psychological reactions to the effects of the economic recession. A reader from Red Bank, NJ, reported, “I see a pattern of issues: ‘I was just laid off.’ ‘I am afraid I will be laid off.’ ‘Others have been laid off, and I’m overwhelmed with their work as well as my own.’ ‘I was planning to retire in a couple years, but now I will have to work longer than I was planning.’” Two psychiatrists reported no increase in patients with economic worries—in a prison and a state hospital with geriatric patients with cognitive impairment.
Timeline. For some survey respondents, the increase in patients with economy-related problems emerged in mid-to-late 2008—particularly in October—but others report seeing symptoms sooner. A reader from Harrisburg, PA, said, “I’ve noticed this increase for the past 4 to 5 months (dramatic), but there has been a general increase for 1 to 2 years.”
These observations mirror the rise in unemployment in the 16 months since the recession officially began in December 2007. In March 2009, the U.S. Bureau of Labor Statistics reported a national unemployment rate of 8.5% (13.2 million unemployed), which was a 25-year high. That same month, employers eliminated 663,000 jobs, for a total of 5.1 million layoffs since the recession began. Two-thirds of all layoffs occurred between November 2008 and March 2009.1
Symptoms. Depression, anxiety, or both are the most common symptoms associated with patients’ financial difficulties, survey respondents say. Other symptoms include insomnia, hopelessness, helplessness, loss of trust, anger, bitterness, resentment, suicidal ideation or attempts, numbness, desires for retaliation, increased alcohol/drug use, fear of being unable to afford medications or of losing a job, paranoia, and marital problems. Readers’ comments include:
- Augusta, GA: “Patients with depression and anxiety symptoms have increased in the emergency department.”
- Portland, OR: “I see people giving up and planning to live on unemployment as long as possible.”
- Fresno, CA: “Some married people are wishing they were single and did not have children.”
- Red Bank, NJ: “Some who have adapted are doing well, often with a low-overhead business, meeting a specialty need, or entering into a business that meets an emerging need.”
Who is affected? Overall, readers estimated that 70% to 100% of affected patients had pre-existing psychiatric disorders, whereas 20% to 30% had not sought treatment in the past. “Individuals with preexisting problems are having considerable difficulty,” one psychiatrist said.
Similarly, Dr. Jeffrey Rediger, medical director of the adult psychiatric inpatient service at McLean SouthEast, Brockton, MA, told Current Psychiatry, “For some people who were functioning marginally before the recession, this stress has pushed them over the edge. But we’re also seeing a number of young to middle-aged adults who are seeking treatment and hospitalization for the first time.”
The Current Psychiatry editorial staff conducted the survey reported in this article. The following questions were emailed to 45 Current Psychiatry Reader Reactors March 20, 2009. Fifteen responded by March 30 (response rate 33%).
Current Psychiatry is preparing an article on the psychological effects of the economic recession. We would like to know about the experiences of practicing psychiatrists. Would you please take a few minutes and answer the following questions?
- Are you seeing an increase in patients describing psychological reactions to the effects of the economic recession?
- If so, when did you notice this increase?
- What symptoms are you seeing in your patients?
- What event or events seem to be causing your patients the greatest psychological distress (loss of a job, worry about losing a job, mortgage foreclosure, loss of value in retirement savings, other)?
- What proportion of these patients has pre-existing psychiatric disorders versus persons who have not sought psychological/psychiatric treatment in the past?
- In what area of the country do you practice (city and state)?
Feel free to provide additional comments you may have.
Interview: Emerging patterns
When interviewed March 17, 2009, Dr. Rediger, Dr. Palmer, and Dr. Kauffman discussed their experiences, provided case examples, and suggested treatments they have found useful for recession-stressed psychiatric patients.
DR. PALMER: People went into panic mode in September/October. Losing a job, a retirement plan, or a home is about who we are and our worth as human beings. My sense is that most people are resilient and adaptive and will be fine despite the recession, but a portion of the population is impaired in adaptability.
DR. REDIGER: Would you explain what you mean?
DR. PALMER: A lot of people become so defiant, so angry, that they withdraw instead of adapting to a new way of life that they consider inferior. They’re humiliated; they feel complete and utter failure. For example, the contractor who owns his own business and says there’s no way he’s going to work for somebody else. He may have to go work for somebody else, get his personal finances in order for a year or two, and then start up a business again. But he has to survive in the meantime.
DR. REDIGER: People are walking around with a lot fear and self-blame. They don’t talk about this very easily; they may say things are fine, but they feel terrible. I wonder how much people are blaming themselves, perhaps for overextending their credit.
DR. PALMER: I think most of these people sensed their finances were marginal before the recession hit. They felt out of control, but their options were limited as housing prices rose beyond affordability. Clinically, I’m seeing increased rates of depression, anxiety, hopelessness. Denial is a big one; there’s a mindset that this can’t be happening.
Helplessness and dread
DR. KAUFFMAN: I resonate with the hopelessness. A lot of people tell me they are experiencing a sense of free fall, and I’ve been working with them to recalibrate a sense of empowerment. First I try some reality testing. I’ll say, “Maybe you’re feeling anxious, helpless, a little denial, fear. Is your survival in danger? Yes or no?” If the answer is no, then I’ll say, “So what can you do so you’re not living as if your survival is in danger?”
DR. REDIGER: Some people—such as the patient in the case report I submitted (Case Report 1)—are paralyzed by dread and anxiety. Two years ago their house was like an ATM machine, but now they feel trapped and worry that they can’t meet the mortgage payments.
DR. REDIGER: An economic recession is stressful because money represents power, control, and survival. The recession is not just about money. It’s about security, identity, and loss of face.
DR. KAUFFMAN: The evidence is pretty clear that financial losses are a risk factor for suicide, especially among men.2,3 You can go up and down Maslow’s hierarchy of needs and see what money means to people. I’ve also noticed that economic stress is a trigger for my clients with posttraumatic stress disorder. They feel out of control of a situation they thought they controlled.
DR. PALMER: An economic downturn can trigger learned helplessness. A construction worker has applied to 50 different construction companies, and none are hiring. He concludes, “I have to wait until the economy turns around, and then I’ll get another job in construction because that’s what I do.” He thinks he doesn’t have enough money or isn’t smart enough to get a degree, or whatever.
DR. REDIGER: And that’s another reason why someone with a history of trauma might experience a reactivation. Learned helplessness can be an aspect of chronic, repeated trauma. A person learns not to try any longer.
DR. PALMER: An inflexible perfectionist would probably have the most difficult time. A person who feels “there are rights and wrongs in the world, and the right thing is that I should be working. My family has grown accustomed to a certain lifestyle, and it’s my job to keep that up.”
DR. REDIGER: “If I work hard, this should be given to me.”
DR. PALMER: Right. A person with more flexibility might think in terms of problem-solving. “I worked in construction (or whatever), and now I can’t get a job. Therefore, I’ll go into a different field and take a lesser salary. The family will have to cut the budget, and the kids will go to a public college instead of a fancy private college.”
Mr. D, age 38, was admitted to our inpatient service in October 2008 with no psychiatric history but worsening depression and anxiety. He was thinking seriously about suicide by carbon monoxide poisoning. A paternal uncle and 2 paternal cousins died by suicide.
Mr. D reported GI complaints and chronic headaches. He had been married 11 years and had 3-year-old twins. He talked about financial problems and increasing debt at his construction business of 15 years. Instead of asking for help, Mr. D had ignored his accountant’s warnings and buried himself in work.
At admission, he was experiencing crying spells, insomnia, and hopelessness. That day he took 16 aspirins, 5 hydrocodone/acetaminophen tablets, and 4 lorazepam tablets to treat an intractable headache. He denied this was a suicide attempt but admitted to poor judgment.
During hospitalization, he received fluoxetine for depression and lorazepam for anxiety and insomnia. Prominent themes in psychotherapy included self-blame and isolation.
As his financial problems increased, Mr. D had borrowed money without completely disclosing his difficulties to the bank. He also felt ashamed because his 2 brothers were not facing financial problems. Creditors were knocking on the door of his home, demanding payment. He felt angry and humiliated that his wife and children were subjected to this. He felt certain his home would soon be in foreclosure.
After 3 weeks, Mr D was discharged to a partial hospital program with prescriptions for fluoxetine and short-term use of lorazepam. After 5 days he was re-admitted with suicidal thoughts. He had filed for personal and professional bankruptcy, but he could not imagine working for someone else after so many years of running his own business.
As treatment for his depression progressed, he began to develop greater insight into how his avoidant and isolative style of problem-solving contributed to a situation that left him vulnerable. He became more interested in cognitive-behavioral techniques for dealing with self-destructive thoughts and began to allow his stepfather (a retired corporate chief executive officer) and his wife to help him solve some of the practical problems facing him.—JEFFREY REDIGER, MD
Putting losses into perspective
DR. KAUFFMAN: Here’s where a cognitive-behavioral intervention with a goal to increase the flexibility—not just content—of thinking can help. You can ask patients, “What is most important to you? Is it money? Or is it your relationship with your family?” Or you could ask questions such as, “In the challenges you’re facing, what opportunities are there for you to do things that matter to you?”
For people who feel hopeless, I often describe this true story. A pilot was flying a jet cross-country when his engines flamed out and the plane began spinning downward. He tried everything, but nothing worked until he lowered the landing gear. This changed the vortex of forces, so that when the pilot went through his emergency procedures again he was able to pull the plane out of the death spiral.
When people become paralyzed by their problems, you can say the equivalent of “what’s your landing gear?” What small thing you could do that might create a different experience for you?
DR. REDIGER: So you’re saying, “If the big picture is too overwhelming, what’s something small you can do today?”
DR. KAUFFMAN: Yes, but not that the small thing is insignificant. As in the case report I submitted (Case Report 2), doing a small thing that makes a difference in a huge problem increases one’s internal locus of control. Feeling more empowered may lead the person to take on another thing.
DR. REDIGER: People have enormous resources that they don’t always know how to tap into. We may be experiencing a material recession but also an opportunity to recover what truly matters to us.
DR. KAUFFMAN: We’re talking about challenging people’s values and encouraging flexibility of thinking. This is a low-cost, powerful strategy that anyone can use to cope with the economic recession.
DR. PALMER: So you begin by challenging assumptions, cognitive-behavioral therapy (CBT), adaptive mechanisms, coming up with a plan, and implementing the plan, then being flexible, assessing if it’s working, and—if it’s not—coming up with another plan or revising it. That process has to be done first, before things I would recommend that are unrelated to the person’s immediate problem. If somebody tells you, “I just got laid off from work,” and you say, “Exercise could help,” he’s going to say, “Did you not hear me? I just got laid off from work.”
DR. KAUFFMAN: Evidence supports the positive psychology that 2 factors are key to sustaining hope:
- a sense of agency that you can achieve a goal
- multiple pathways planned out to reach the goal.4
Together, these 2 factors—which Snyder called “the will and the way5—are the highest predictors of performance, health, and ability to withstand adversity.
DR. PALMER: Along with CBT, I remind patients to stay connected, to see and talk to people every day. This doesn’t mean getting together to watch television; it means having real conversations. Other people can help you get unstuck. Evidence also indicates that a social network mitigates against depression and anxiety. The happier your friends are, the happier you are.6
Mr. A, age 45, is receiving executive coaching after being fired from his $1.5 million job as head of a consulting firm. He has half-time custody of his 2 children and pays hundreds of thousands of dollars per year in alimony and child support. He has a history of depression and anxiety and has been treated in the past with escitalopram.
During initial coaching sessions, Mr. A identifies himself as a victim and ruminates about how to get back at “the evil empire,” as he defines his former employer and his ex-wife. Mr. A says it seems odd not be at the top anymore. He feels stuck, depressed, and lost. We examine his role in his job and marital difficulties and identify skills he needs for a successful job search, career, and future relationships.
Early goals include becoming less chaotic and avoidant and building self-esteem. Stress management therapy is useful for his anxiety and avoidance. Cognitive-behavioral therapy and acceptance and commitment therapy help him access his strengths in new ways.
He transitions from a verbal avalanche of complaints to dialogue and self-exploration. He moves from avoiding a job search to trying to find what would “float my boat,” even if it means far lower income. He also becomes sanguine about work opportunities during the economic recession.
He creates lists of networking opportunities and reports on his successes and failures. Eventually, he works on his search at least 4 hours a day. After disappointments, we examine how he can keep himself going, increase awareness of how he is communicating, and engage in self-care to keep up motivation.
He continues to pursue opportunities and focus on the process rather than the outcome of his job search. He now sees himself as challenged by his circumstances and not as much a victim of them.—CAROL KAUFFMAN, PhD, ABPP, PCC
Addressing depression
DR. KAUFFMAN: Medication also can play a useful role for some patients.
DR. PALMER: Patients who meet criteria for major depression—in particular if they’re having suicidal thoughts—absolutely need psychotropics. Mr. R, my case patient, benefited greatly from CBT and medication. We also worked on financial planning and handling financial conflicts with his wife and children. He is exercising, doing volunteer work, and staying connected with friends and family. He is hoping to find a job in the next few months.
DR. REDIGER: For a person who’s going though a stressful period, I try to keep medication time-limited. We talk about treating symptoms, but it’s important to look at what’s causing the patient’s problems and address it.
DR. PALMER: During this recession, a lot of people are going to be down but not clinically depressed. If the depression is mild to moderate, I sometimes recommend exercise instead of medication (such as when a patient is refusing medication or has had serious side effects from medications). I recommend exercise for all my outpatients—even if they’re taking psychotropics—because exercise has been shown to be as effective as antidepressants for moderate depression.7,8
DR. REDIGER: We’ve also been encouraging people who’ve lost jobs to volunteer in the community. Having a reason to get out of the house takes the mind off one’s worries.
DR. KAUFFMAN: The “3 good things in life” exercise studied by psychologist Martin E.P. Seligman, PhD, has been shown in a 6-month, randomized, placebo-controlled study to increase happiness and decrease depressive symptoms.9 In this exercise, you look back at the end of each day and write down 3 things that went well, their causes, and an explanation for each good thing. Ask yourself, “When was I at my best today? What happened today that I feel grateful for? What did I do to make that good thing happen?”
DR. REDIGER: Remind people to talk to their children about the recession, too. If they have to move to a different home or to a different school, let their children know things are going on and how to think about that. This can help kids understand how to deal with their anxiety.
Related resources
- Getting through tough economic times. A SAMHSA guide. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. www.samhsa.gov/economy.
- Seligman MEP. Authentic happiness: using the new positive psychology to realize your potential for lasting fulfillment. New York, NY: Simon & Schuster; 2002.
- Positive Psychology Center. University of Pennsylvania, Philadelphia. www.ppc.sas.upenn.edu.
Drug brand names
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Lorazepam • Ativan
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This article was researched and written by Current Psychiatry Editor Alice V. Luddington, ELS, and Senior Associate Editor Erica Vonderheid.
1. Employment situation summary: March 2009. Bureau of Labor Statistics. Washington, DC: U.S. Department of Labor; April 3, 2009. Available at: http://www.bls.gov/news.release/empsit.nr0.htm. Accessed April 14, 2009.
2. Stack S, Wasserman I. Economic strain and suicide risk: a qualitative analysis. Suicide Life Threat Behav. 2007;37:103-112.
3. Heikkinen M, Aro H, Lonngvist J. Recent life events, social support, and suicide. Acta Psychiatr Scand Suppl. 1994;377:65-72.
4. Snyder CR. Hope theory: rainbows of the mind. Psychological Inquiry. 2002;13:249-275.
5. Snyder CR, Harris C, Anderson JR, et al. The will and the ways: development and validation of an individual-differences measure of hope. J Pers Soc Psychol. 1991;60:570-585.
6. Fowler JH, Christakis NA. Dynamic spread of happiness in a large social network: longitudinal analysis over 20 years in the Framingham Heart Study. BMJ. 2008;337:a2338.-
7. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69:587-596.
8. Craft LL, Landers DM. The effects of exercise on clinical depression and depression resulting from mental illness: a meta-analysis. JSEP. 1998;20:339-357.
9. Seligman MEP, Steen TA, Park N, et al. Positive psychology progress: empirical validation of interventions. Am Psychol. 2005;60:410-421.
Mr. R, age 45, developed severe depression 4 years ago after his mother died. He had suffered previous major depressive episodes and was treated effiectively with fluoxetine for 15 years. This time he took a medical leave from his job as an engineer and received disability. After numerous medication trials and psychotherapy, his symptoms improved.
Mr. R is ready to think about returning to work, but he will need to refresh his skills and consider starting at a lower level than before. Headlines remind him daily about increasing unemployment and decreasing prospects of finding a job.
During his illness, Mr. R and his family depleted their savings and incurred substantial debt. His wife has not worked outside the home while caring for him and their 4 children. She is increasingly anxious and depressed. The couple argue often about money but share a common hope: that Mr. R will find a job in the next few months.
How is the recession affecting psychiatric practice? Christopher Palmer, MD, the psychiatrist who treated Mr. R, says, “We in psychiatry and psychology are well-equipped to help people who are unemployed, underemployed, and financially ruined. We do it all the time. The difference in this economy is that we’re going to be seeing a lot more people.”
Psychiatrists who read Current Psychiatry and were polled in March 2009 agree. Most were seeing an increase in patients experiencing psychological stress because of the recession, which by then had persisted 16 months. “All my patients are reporting increased stress as a result of the economic situation. The more successful my patient is, the more distress they seem to be feeling,” says a psychiatrist from Melbourne, FL.
This article on the psychological effects of the recession discusses the results of an online survey of Current Psychiatry readers, with analysis and recommendations from an interview with Dr. Palmer and colleagues Jeffrey Rediger, MD, MDiv, and Carol Kauffman, PhD, ABPP, PCC, from McLean Hospital, Belmont, MA, and the department of psychiatry, Harvard Medical School.
| Carol Kauffman, PhD, ABPP, PCC, is director of the Institute of Coaching, McLean Hospital, Belmont, MA, and assistant clinical professor, department of psychiatry, Harvard Medical School. A veteran psychologist, she maintains an executive coaching practice in the United States and Europe. |
| Christopher Palmer, MD, is medical director of continuing medical education, McLean Hospital. His outpatient practice focuses on substance abuse, sleep disorders, mood and anxiety disorders, psychotic disorders, and individual and family psychotherapy. |
| Jeffrey Rediger, MD, MDiv, is medical director, adult psychiatric program, McLean Hospital SouthEast. He also is an instructor, department of psychiatry, Harvard Medical School and has a master of divinity degree. He publishes in the fields of medicine, psychiatry, and spirituality. |
Survey results
Methods. Using an e-mail questionnaire (Box), Current Psychiatry contacted 45 Reader Reactors—clinical psychiatrists who provide feedback to our editorial staff about topics being considered for publication. The 15 readers who responded practice psychiatry in the Northeast (New York and New Jersey), the South (Florida and Georgia), the West (California, Washington, and Oregon), and the Midwest (Pennsylvania, Illinois, and Missouri).
Nine of 11 readers who answered all questions in the survey said they have seen an increase in patients describing psychological reactions to the effects of the economic recession. A reader from Red Bank, NJ, reported, “I see a pattern of issues: ‘I was just laid off.’ ‘I am afraid I will be laid off.’ ‘Others have been laid off, and I’m overwhelmed with their work as well as my own.’ ‘I was planning to retire in a couple years, but now I will have to work longer than I was planning.’” Two psychiatrists reported no increase in patients with economic worries—in a prison and a state hospital with geriatric patients with cognitive impairment.
Timeline. For some survey respondents, the increase in patients with economy-related problems emerged in mid-to-late 2008—particularly in October—but others report seeing symptoms sooner. A reader from Harrisburg, PA, said, “I’ve noticed this increase for the past 4 to 5 months (dramatic), but there has been a general increase for 1 to 2 years.”
These observations mirror the rise in unemployment in the 16 months since the recession officially began in December 2007. In March 2009, the U.S. Bureau of Labor Statistics reported a national unemployment rate of 8.5% (13.2 million unemployed), which was a 25-year high. That same month, employers eliminated 663,000 jobs, for a total of 5.1 million layoffs since the recession began. Two-thirds of all layoffs occurred between November 2008 and March 2009.1
Symptoms. Depression, anxiety, or both are the most common symptoms associated with patients’ financial difficulties, survey respondents say. Other symptoms include insomnia, hopelessness, helplessness, loss of trust, anger, bitterness, resentment, suicidal ideation or attempts, numbness, desires for retaliation, increased alcohol/drug use, fear of being unable to afford medications or of losing a job, paranoia, and marital problems. Readers’ comments include:
- Augusta, GA: “Patients with depression and anxiety symptoms have increased in the emergency department.”
- Portland, OR: “I see people giving up and planning to live on unemployment as long as possible.”
- Fresno, CA: “Some married people are wishing they were single and did not have children.”
- Red Bank, NJ: “Some who have adapted are doing well, often with a low-overhead business, meeting a specialty need, or entering into a business that meets an emerging need.”
Who is affected? Overall, readers estimated that 70% to 100% of affected patients had pre-existing psychiatric disorders, whereas 20% to 30% had not sought treatment in the past. “Individuals with preexisting problems are having considerable difficulty,” one psychiatrist said.
Similarly, Dr. Jeffrey Rediger, medical director of the adult psychiatric inpatient service at McLean SouthEast, Brockton, MA, told Current Psychiatry, “For some people who were functioning marginally before the recession, this stress has pushed them over the edge. But we’re also seeing a number of young to middle-aged adults who are seeking treatment and hospitalization for the first time.”
The Current Psychiatry editorial staff conducted the survey reported in this article. The following questions were emailed to 45 Current Psychiatry Reader Reactors March 20, 2009. Fifteen responded by March 30 (response rate 33%).
Current Psychiatry is preparing an article on the psychological effects of the economic recession. We would like to know about the experiences of practicing psychiatrists. Would you please take a few minutes and answer the following questions?
- Are you seeing an increase in patients describing psychological reactions to the effects of the economic recession?
- If so, when did you notice this increase?
- What symptoms are you seeing in your patients?
- What event or events seem to be causing your patients the greatest psychological distress (loss of a job, worry about losing a job, mortgage foreclosure, loss of value in retirement savings, other)?
- What proportion of these patients has pre-existing psychiatric disorders versus persons who have not sought psychological/psychiatric treatment in the past?
- In what area of the country do you practice (city and state)?
Feel free to provide additional comments you may have.
Interview: Emerging patterns
When interviewed March 17, 2009, Dr. Rediger, Dr. Palmer, and Dr. Kauffman discussed their experiences, provided case examples, and suggested treatments they have found useful for recession-stressed psychiatric patients.
DR. PALMER: People went into panic mode in September/October. Losing a job, a retirement plan, or a home is about who we are and our worth as human beings. My sense is that most people are resilient and adaptive and will be fine despite the recession, but a portion of the population is impaired in adaptability.
DR. REDIGER: Would you explain what you mean?
DR. PALMER: A lot of people become so defiant, so angry, that they withdraw instead of adapting to a new way of life that they consider inferior. They’re humiliated; they feel complete and utter failure. For example, the contractor who owns his own business and says there’s no way he’s going to work for somebody else. He may have to go work for somebody else, get his personal finances in order for a year or two, and then start up a business again. But he has to survive in the meantime.
DR. REDIGER: People are walking around with a lot fear and self-blame. They don’t talk about this very easily; they may say things are fine, but they feel terrible. I wonder how much people are blaming themselves, perhaps for overextending their credit.
DR. PALMER: I think most of these people sensed their finances were marginal before the recession hit. They felt out of control, but their options were limited as housing prices rose beyond affordability. Clinically, I’m seeing increased rates of depression, anxiety, hopelessness. Denial is a big one; there’s a mindset that this can’t be happening.
Helplessness and dread
DR. KAUFFMAN: I resonate with the hopelessness. A lot of people tell me they are experiencing a sense of free fall, and I’ve been working with them to recalibrate a sense of empowerment. First I try some reality testing. I’ll say, “Maybe you’re feeling anxious, helpless, a little denial, fear. Is your survival in danger? Yes or no?” If the answer is no, then I’ll say, “So what can you do so you’re not living as if your survival is in danger?”
DR. REDIGER: Some people—such as the patient in the case report I submitted (Case Report 1)—are paralyzed by dread and anxiety. Two years ago their house was like an ATM machine, but now they feel trapped and worry that they can’t meet the mortgage payments.
DR. REDIGER: An economic recession is stressful because money represents power, control, and survival. The recession is not just about money. It’s about security, identity, and loss of face.
DR. KAUFFMAN: The evidence is pretty clear that financial losses are a risk factor for suicide, especially among men.2,3 You can go up and down Maslow’s hierarchy of needs and see what money means to people. I’ve also noticed that economic stress is a trigger for my clients with posttraumatic stress disorder. They feel out of control of a situation they thought they controlled.
DR. PALMER: An economic downturn can trigger learned helplessness. A construction worker has applied to 50 different construction companies, and none are hiring. He concludes, “I have to wait until the economy turns around, and then I’ll get another job in construction because that’s what I do.” He thinks he doesn’t have enough money or isn’t smart enough to get a degree, or whatever.
DR. REDIGER: And that’s another reason why someone with a history of trauma might experience a reactivation. Learned helplessness can be an aspect of chronic, repeated trauma. A person learns not to try any longer.
DR. PALMER: An inflexible perfectionist would probably have the most difficult time. A person who feels “there are rights and wrongs in the world, and the right thing is that I should be working. My family has grown accustomed to a certain lifestyle, and it’s my job to keep that up.”
DR. REDIGER: “If I work hard, this should be given to me.”
DR. PALMER: Right. A person with more flexibility might think in terms of problem-solving. “I worked in construction (or whatever), and now I can’t get a job. Therefore, I’ll go into a different field and take a lesser salary. The family will have to cut the budget, and the kids will go to a public college instead of a fancy private college.”
Mr. D, age 38, was admitted to our inpatient service in October 2008 with no psychiatric history but worsening depression and anxiety. He was thinking seriously about suicide by carbon monoxide poisoning. A paternal uncle and 2 paternal cousins died by suicide.
Mr. D reported GI complaints and chronic headaches. He had been married 11 years and had 3-year-old twins. He talked about financial problems and increasing debt at his construction business of 15 years. Instead of asking for help, Mr. D had ignored his accountant’s warnings and buried himself in work.
At admission, he was experiencing crying spells, insomnia, and hopelessness. That day he took 16 aspirins, 5 hydrocodone/acetaminophen tablets, and 4 lorazepam tablets to treat an intractable headache. He denied this was a suicide attempt but admitted to poor judgment.
During hospitalization, he received fluoxetine for depression and lorazepam for anxiety and insomnia. Prominent themes in psychotherapy included self-blame and isolation.
As his financial problems increased, Mr. D had borrowed money without completely disclosing his difficulties to the bank. He also felt ashamed because his 2 brothers were not facing financial problems. Creditors were knocking on the door of his home, demanding payment. He felt angry and humiliated that his wife and children were subjected to this. He felt certain his home would soon be in foreclosure.
After 3 weeks, Mr D was discharged to a partial hospital program with prescriptions for fluoxetine and short-term use of lorazepam. After 5 days he was re-admitted with suicidal thoughts. He had filed for personal and professional bankruptcy, but he could not imagine working for someone else after so many years of running his own business.
As treatment for his depression progressed, he began to develop greater insight into how his avoidant and isolative style of problem-solving contributed to a situation that left him vulnerable. He became more interested in cognitive-behavioral techniques for dealing with self-destructive thoughts and began to allow his stepfather (a retired corporate chief executive officer) and his wife to help him solve some of the practical problems facing him.—JEFFREY REDIGER, MD
Putting losses into perspective
DR. KAUFFMAN: Here’s where a cognitive-behavioral intervention with a goal to increase the flexibility—not just content—of thinking can help. You can ask patients, “What is most important to you? Is it money? Or is it your relationship with your family?” Or you could ask questions such as, “In the challenges you’re facing, what opportunities are there for you to do things that matter to you?”
For people who feel hopeless, I often describe this true story. A pilot was flying a jet cross-country when his engines flamed out and the plane began spinning downward. He tried everything, but nothing worked until he lowered the landing gear. This changed the vortex of forces, so that when the pilot went through his emergency procedures again he was able to pull the plane out of the death spiral.
When people become paralyzed by their problems, you can say the equivalent of “what’s your landing gear?” What small thing you could do that might create a different experience for you?
DR. REDIGER: So you’re saying, “If the big picture is too overwhelming, what’s something small you can do today?”
DR. KAUFFMAN: Yes, but not that the small thing is insignificant. As in the case report I submitted (Case Report 2), doing a small thing that makes a difference in a huge problem increases one’s internal locus of control. Feeling more empowered may lead the person to take on another thing.
DR. REDIGER: People have enormous resources that they don’t always know how to tap into. We may be experiencing a material recession but also an opportunity to recover what truly matters to us.
DR. KAUFFMAN: We’re talking about challenging people’s values and encouraging flexibility of thinking. This is a low-cost, powerful strategy that anyone can use to cope with the economic recession.
DR. PALMER: So you begin by challenging assumptions, cognitive-behavioral therapy (CBT), adaptive mechanisms, coming up with a plan, and implementing the plan, then being flexible, assessing if it’s working, and—if it’s not—coming up with another plan or revising it. That process has to be done first, before things I would recommend that are unrelated to the person’s immediate problem. If somebody tells you, “I just got laid off from work,” and you say, “Exercise could help,” he’s going to say, “Did you not hear me? I just got laid off from work.”
DR. KAUFFMAN: Evidence supports the positive psychology that 2 factors are key to sustaining hope:
- a sense of agency that you can achieve a goal
- multiple pathways planned out to reach the goal.4
Together, these 2 factors—which Snyder called “the will and the way5—are the highest predictors of performance, health, and ability to withstand adversity.
DR. PALMER: Along with CBT, I remind patients to stay connected, to see and talk to people every day. This doesn’t mean getting together to watch television; it means having real conversations. Other people can help you get unstuck. Evidence also indicates that a social network mitigates against depression and anxiety. The happier your friends are, the happier you are.6
Mr. A, age 45, is receiving executive coaching after being fired from his $1.5 million job as head of a consulting firm. He has half-time custody of his 2 children and pays hundreds of thousands of dollars per year in alimony and child support. He has a history of depression and anxiety and has been treated in the past with escitalopram.
During initial coaching sessions, Mr. A identifies himself as a victim and ruminates about how to get back at “the evil empire,” as he defines his former employer and his ex-wife. Mr. A says it seems odd not be at the top anymore. He feels stuck, depressed, and lost. We examine his role in his job and marital difficulties and identify skills he needs for a successful job search, career, and future relationships.
Early goals include becoming less chaotic and avoidant and building self-esteem. Stress management therapy is useful for his anxiety and avoidance. Cognitive-behavioral therapy and acceptance and commitment therapy help him access his strengths in new ways.
He transitions from a verbal avalanche of complaints to dialogue and self-exploration. He moves from avoiding a job search to trying to find what would “float my boat,” even if it means far lower income. He also becomes sanguine about work opportunities during the economic recession.
He creates lists of networking opportunities and reports on his successes and failures. Eventually, he works on his search at least 4 hours a day. After disappointments, we examine how he can keep himself going, increase awareness of how he is communicating, and engage in self-care to keep up motivation.
He continues to pursue opportunities and focus on the process rather than the outcome of his job search. He now sees himself as challenged by his circumstances and not as much a victim of them.—CAROL KAUFFMAN, PhD, ABPP, PCC
Addressing depression
DR. KAUFFMAN: Medication also can play a useful role for some patients.
DR. PALMER: Patients who meet criteria for major depression—in particular if they’re having suicidal thoughts—absolutely need psychotropics. Mr. R, my case patient, benefited greatly from CBT and medication. We also worked on financial planning and handling financial conflicts with his wife and children. He is exercising, doing volunteer work, and staying connected with friends and family. He is hoping to find a job in the next few months.
DR. REDIGER: For a person who’s going though a stressful period, I try to keep medication time-limited. We talk about treating symptoms, but it’s important to look at what’s causing the patient’s problems and address it.
DR. PALMER: During this recession, a lot of people are going to be down but not clinically depressed. If the depression is mild to moderate, I sometimes recommend exercise instead of medication (such as when a patient is refusing medication or has had serious side effects from medications). I recommend exercise for all my outpatients—even if they’re taking psychotropics—because exercise has been shown to be as effective as antidepressants for moderate depression.7,8
DR. REDIGER: We’ve also been encouraging people who’ve lost jobs to volunteer in the community. Having a reason to get out of the house takes the mind off one’s worries.
DR. KAUFFMAN: The “3 good things in life” exercise studied by psychologist Martin E.P. Seligman, PhD, has been shown in a 6-month, randomized, placebo-controlled study to increase happiness and decrease depressive symptoms.9 In this exercise, you look back at the end of each day and write down 3 things that went well, their causes, and an explanation for each good thing. Ask yourself, “When was I at my best today? What happened today that I feel grateful for? What did I do to make that good thing happen?”
DR. REDIGER: Remind people to talk to their children about the recession, too. If they have to move to a different home or to a different school, let their children know things are going on and how to think about that. This can help kids understand how to deal with their anxiety.
Related resources
- Getting through tough economic times. A SAMHSA guide. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. www.samhsa.gov/economy.
- Seligman MEP. Authentic happiness: using the new positive psychology to realize your potential for lasting fulfillment. New York, NY: Simon & Schuster; 2002.
- Positive Psychology Center. University of Pennsylvania, Philadelphia. www.ppc.sas.upenn.edu.
Drug brand names
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Lorazepam • Ativan
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This article was researched and written by Current Psychiatry Editor Alice V. Luddington, ELS, and Senior Associate Editor Erica Vonderheid.
Mr. R, age 45, developed severe depression 4 years ago after his mother died. He had suffered previous major depressive episodes and was treated effiectively with fluoxetine for 15 years. This time he took a medical leave from his job as an engineer and received disability. After numerous medication trials and psychotherapy, his symptoms improved.
Mr. R is ready to think about returning to work, but he will need to refresh his skills and consider starting at a lower level than before. Headlines remind him daily about increasing unemployment and decreasing prospects of finding a job.
During his illness, Mr. R and his family depleted their savings and incurred substantial debt. His wife has not worked outside the home while caring for him and their 4 children. She is increasingly anxious and depressed. The couple argue often about money but share a common hope: that Mr. R will find a job in the next few months.
How is the recession affecting psychiatric practice? Christopher Palmer, MD, the psychiatrist who treated Mr. R, says, “We in psychiatry and psychology are well-equipped to help people who are unemployed, underemployed, and financially ruined. We do it all the time. The difference in this economy is that we’re going to be seeing a lot more people.”
Psychiatrists who read Current Psychiatry and were polled in March 2009 agree. Most were seeing an increase in patients experiencing psychological stress because of the recession, which by then had persisted 16 months. “All my patients are reporting increased stress as a result of the economic situation. The more successful my patient is, the more distress they seem to be feeling,” says a psychiatrist from Melbourne, FL.
This article on the psychological effects of the recession discusses the results of an online survey of Current Psychiatry readers, with analysis and recommendations from an interview with Dr. Palmer and colleagues Jeffrey Rediger, MD, MDiv, and Carol Kauffman, PhD, ABPP, PCC, from McLean Hospital, Belmont, MA, and the department of psychiatry, Harvard Medical School.
| Carol Kauffman, PhD, ABPP, PCC, is director of the Institute of Coaching, McLean Hospital, Belmont, MA, and assistant clinical professor, department of psychiatry, Harvard Medical School. A veteran psychologist, she maintains an executive coaching practice in the United States and Europe. |
| Christopher Palmer, MD, is medical director of continuing medical education, McLean Hospital. His outpatient practice focuses on substance abuse, sleep disorders, mood and anxiety disorders, psychotic disorders, and individual and family psychotherapy. |
| Jeffrey Rediger, MD, MDiv, is medical director, adult psychiatric program, McLean Hospital SouthEast. He also is an instructor, department of psychiatry, Harvard Medical School and has a master of divinity degree. He publishes in the fields of medicine, psychiatry, and spirituality. |
Survey results
Methods. Using an e-mail questionnaire (Box), Current Psychiatry contacted 45 Reader Reactors—clinical psychiatrists who provide feedback to our editorial staff about topics being considered for publication. The 15 readers who responded practice psychiatry in the Northeast (New York and New Jersey), the South (Florida and Georgia), the West (California, Washington, and Oregon), and the Midwest (Pennsylvania, Illinois, and Missouri).
Nine of 11 readers who answered all questions in the survey said they have seen an increase in patients describing psychological reactions to the effects of the economic recession. A reader from Red Bank, NJ, reported, “I see a pattern of issues: ‘I was just laid off.’ ‘I am afraid I will be laid off.’ ‘Others have been laid off, and I’m overwhelmed with their work as well as my own.’ ‘I was planning to retire in a couple years, but now I will have to work longer than I was planning.’” Two psychiatrists reported no increase in patients with economic worries—in a prison and a state hospital with geriatric patients with cognitive impairment.
Timeline. For some survey respondents, the increase in patients with economy-related problems emerged in mid-to-late 2008—particularly in October—but others report seeing symptoms sooner. A reader from Harrisburg, PA, said, “I’ve noticed this increase for the past 4 to 5 months (dramatic), but there has been a general increase for 1 to 2 years.”
These observations mirror the rise in unemployment in the 16 months since the recession officially began in December 2007. In March 2009, the U.S. Bureau of Labor Statistics reported a national unemployment rate of 8.5% (13.2 million unemployed), which was a 25-year high. That same month, employers eliminated 663,000 jobs, for a total of 5.1 million layoffs since the recession began. Two-thirds of all layoffs occurred between November 2008 and March 2009.1
Symptoms. Depression, anxiety, or both are the most common symptoms associated with patients’ financial difficulties, survey respondents say. Other symptoms include insomnia, hopelessness, helplessness, loss of trust, anger, bitterness, resentment, suicidal ideation or attempts, numbness, desires for retaliation, increased alcohol/drug use, fear of being unable to afford medications or of losing a job, paranoia, and marital problems. Readers’ comments include:
- Augusta, GA: “Patients with depression and anxiety symptoms have increased in the emergency department.”
- Portland, OR: “I see people giving up and planning to live on unemployment as long as possible.”
- Fresno, CA: “Some married people are wishing they were single and did not have children.”
- Red Bank, NJ: “Some who have adapted are doing well, often with a low-overhead business, meeting a specialty need, or entering into a business that meets an emerging need.”
Who is affected? Overall, readers estimated that 70% to 100% of affected patients had pre-existing psychiatric disorders, whereas 20% to 30% had not sought treatment in the past. “Individuals with preexisting problems are having considerable difficulty,” one psychiatrist said.
Similarly, Dr. Jeffrey Rediger, medical director of the adult psychiatric inpatient service at McLean SouthEast, Brockton, MA, told Current Psychiatry, “For some people who were functioning marginally before the recession, this stress has pushed them over the edge. But we’re also seeing a number of young to middle-aged adults who are seeking treatment and hospitalization for the first time.”
The Current Psychiatry editorial staff conducted the survey reported in this article. The following questions were emailed to 45 Current Psychiatry Reader Reactors March 20, 2009. Fifteen responded by March 30 (response rate 33%).
Current Psychiatry is preparing an article on the psychological effects of the economic recession. We would like to know about the experiences of practicing psychiatrists. Would you please take a few minutes and answer the following questions?
- Are you seeing an increase in patients describing psychological reactions to the effects of the economic recession?
- If so, when did you notice this increase?
- What symptoms are you seeing in your patients?
- What event or events seem to be causing your patients the greatest psychological distress (loss of a job, worry about losing a job, mortgage foreclosure, loss of value in retirement savings, other)?
- What proportion of these patients has pre-existing psychiatric disorders versus persons who have not sought psychological/psychiatric treatment in the past?
- In what area of the country do you practice (city and state)?
Feel free to provide additional comments you may have.
Interview: Emerging patterns
When interviewed March 17, 2009, Dr. Rediger, Dr. Palmer, and Dr. Kauffman discussed their experiences, provided case examples, and suggested treatments they have found useful for recession-stressed psychiatric patients.
DR. PALMER: People went into panic mode in September/October. Losing a job, a retirement plan, or a home is about who we are and our worth as human beings. My sense is that most people are resilient and adaptive and will be fine despite the recession, but a portion of the population is impaired in adaptability.
DR. REDIGER: Would you explain what you mean?
DR. PALMER: A lot of people become so defiant, so angry, that they withdraw instead of adapting to a new way of life that they consider inferior. They’re humiliated; they feel complete and utter failure. For example, the contractor who owns his own business and says there’s no way he’s going to work for somebody else. He may have to go work for somebody else, get his personal finances in order for a year or two, and then start up a business again. But he has to survive in the meantime.
DR. REDIGER: People are walking around with a lot fear and self-blame. They don’t talk about this very easily; they may say things are fine, but they feel terrible. I wonder how much people are blaming themselves, perhaps for overextending their credit.
DR. PALMER: I think most of these people sensed their finances were marginal before the recession hit. They felt out of control, but their options were limited as housing prices rose beyond affordability. Clinically, I’m seeing increased rates of depression, anxiety, hopelessness. Denial is a big one; there’s a mindset that this can’t be happening.
Helplessness and dread
DR. KAUFFMAN: I resonate with the hopelessness. A lot of people tell me they are experiencing a sense of free fall, and I’ve been working with them to recalibrate a sense of empowerment. First I try some reality testing. I’ll say, “Maybe you’re feeling anxious, helpless, a little denial, fear. Is your survival in danger? Yes or no?” If the answer is no, then I’ll say, “So what can you do so you’re not living as if your survival is in danger?”
DR. REDIGER: Some people—such as the patient in the case report I submitted (Case Report 1)—are paralyzed by dread and anxiety. Two years ago their house was like an ATM machine, but now they feel trapped and worry that they can’t meet the mortgage payments.
DR. REDIGER: An economic recession is stressful because money represents power, control, and survival. The recession is not just about money. It’s about security, identity, and loss of face.
DR. KAUFFMAN: The evidence is pretty clear that financial losses are a risk factor for suicide, especially among men.2,3 You can go up and down Maslow’s hierarchy of needs and see what money means to people. I’ve also noticed that economic stress is a trigger for my clients with posttraumatic stress disorder. They feel out of control of a situation they thought they controlled.
DR. PALMER: An economic downturn can trigger learned helplessness. A construction worker has applied to 50 different construction companies, and none are hiring. He concludes, “I have to wait until the economy turns around, and then I’ll get another job in construction because that’s what I do.” He thinks he doesn’t have enough money or isn’t smart enough to get a degree, or whatever.
DR. REDIGER: And that’s another reason why someone with a history of trauma might experience a reactivation. Learned helplessness can be an aspect of chronic, repeated trauma. A person learns not to try any longer.
DR. PALMER: An inflexible perfectionist would probably have the most difficult time. A person who feels “there are rights and wrongs in the world, and the right thing is that I should be working. My family has grown accustomed to a certain lifestyle, and it’s my job to keep that up.”
DR. REDIGER: “If I work hard, this should be given to me.”
DR. PALMER: Right. A person with more flexibility might think in terms of problem-solving. “I worked in construction (or whatever), and now I can’t get a job. Therefore, I’ll go into a different field and take a lesser salary. The family will have to cut the budget, and the kids will go to a public college instead of a fancy private college.”
Mr. D, age 38, was admitted to our inpatient service in October 2008 with no psychiatric history but worsening depression and anxiety. He was thinking seriously about suicide by carbon monoxide poisoning. A paternal uncle and 2 paternal cousins died by suicide.
Mr. D reported GI complaints and chronic headaches. He had been married 11 years and had 3-year-old twins. He talked about financial problems and increasing debt at his construction business of 15 years. Instead of asking for help, Mr. D had ignored his accountant’s warnings and buried himself in work.
At admission, he was experiencing crying spells, insomnia, and hopelessness. That day he took 16 aspirins, 5 hydrocodone/acetaminophen tablets, and 4 lorazepam tablets to treat an intractable headache. He denied this was a suicide attempt but admitted to poor judgment.
During hospitalization, he received fluoxetine for depression and lorazepam for anxiety and insomnia. Prominent themes in psychotherapy included self-blame and isolation.
As his financial problems increased, Mr. D had borrowed money without completely disclosing his difficulties to the bank. He also felt ashamed because his 2 brothers were not facing financial problems. Creditors were knocking on the door of his home, demanding payment. He felt angry and humiliated that his wife and children were subjected to this. He felt certain his home would soon be in foreclosure.
After 3 weeks, Mr D was discharged to a partial hospital program with prescriptions for fluoxetine and short-term use of lorazepam. After 5 days he was re-admitted with suicidal thoughts. He had filed for personal and professional bankruptcy, but he could not imagine working for someone else after so many years of running his own business.
As treatment for his depression progressed, he began to develop greater insight into how his avoidant and isolative style of problem-solving contributed to a situation that left him vulnerable. He became more interested in cognitive-behavioral techniques for dealing with self-destructive thoughts and began to allow his stepfather (a retired corporate chief executive officer) and his wife to help him solve some of the practical problems facing him.—JEFFREY REDIGER, MD
Putting losses into perspective
DR. KAUFFMAN: Here’s where a cognitive-behavioral intervention with a goal to increase the flexibility—not just content—of thinking can help. You can ask patients, “What is most important to you? Is it money? Or is it your relationship with your family?” Or you could ask questions such as, “In the challenges you’re facing, what opportunities are there for you to do things that matter to you?”
For people who feel hopeless, I often describe this true story. A pilot was flying a jet cross-country when his engines flamed out and the plane began spinning downward. He tried everything, but nothing worked until he lowered the landing gear. This changed the vortex of forces, so that when the pilot went through his emergency procedures again he was able to pull the plane out of the death spiral.
When people become paralyzed by their problems, you can say the equivalent of “what’s your landing gear?” What small thing you could do that might create a different experience for you?
DR. REDIGER: So you’re saying, “If the big picture is too overwhelming, what’s something small you can do today?”
DR. KAUFFMAN: Yes, but not that the small thing is insignificant. As in the case report I submitted (Case Report 2), doing a small thing that makes a difference in a huge problem increases one’s internal locus of control. Feeling more empowered may lead the person to take on another thing.
DR. REDIGER: People have enormous resources that they don’t always know how to tap into. We may be experiencing a material recession but also an opportunity to recover what truly matters to us.
DR. KAUFFMAN: We’re talking about challenging people’s values and encouraging flexibility of thinking. This is a low-cost, powerful strategy that anyone can use to cope with the economic recession.
DR. PALMER: So you begin by challenging assumptions, cognitive-behavioral therapy (CBT), adaptive mechanisms, coming up with a plan, and implementing the plan, then being flexible, assessing if it’s working, and—if it’s not—coming up with another plan or revising it. That process has to be done first, before things I would recommend that are unrelated to the person’s immediate problem. If somebody tells you, “I just got laid off from work,” and you say, “Exercise could help,” he’s going to say, “Did you not hear me? I just got laid off from work.”
DR. KAUFFMAN: Evidence supports the positive psychology that 2 factors are key to sustaining hope:
- a sense of agency that you can achieve a goal
- multiple pathways planned out to reach the goal.4
Together, these 2 factors—which Snyder called “the will and the way5—are the highest predictors of performance, health, and ability to withstand adversity.
DR. PALMER: Along with CBT, I remind patients to stay connected, to see and talk to people every day. This doesn’t mean getting together to watch television; it means having real conversations. Other people can help you get unstuck. Evidence also indicates that a social network mitigates against depression and anxiety. The happier your friends are, the happier you are.6
Mr. A, age 45, is receiving executive coaching after being fired from his $1.5 million job as head of a consulting firm. He has half-time custody of his 2 children and pays hundreds of thousands of dollars per year in alimony and child support. He has a history of depression and anxiety and has been treated in the past with escitalopram.
During initial coaching sessions, Mr. A identifies himself as a victim and ruminates about how to get back at “the evil empire,” as he defines his former employer and his ex-wife. Mr. A says it seems odd not be at the top anymore. He feels stuck, depressed, and lost. We examine his role in his job and marital difficulties and identify skills he needs for a successful job search, career, and future relationships.
Early goals include becoming less chaotic and avoidant and building self-esteem. Stress management therapy is useful for his anxiety and avoidance. Cognitive-behavioral therapy and acceptance and commitment therapy help him access his strengths in new ways.
He transitions from a verbal avalanche of complaints to dialogue and self-exploration. He moves from avoiding a job search to trying to find what would “float my boat,” even if it means far lower income. He also becomes sanguine about work opportunities during the economic recession.
He creates lists of networking opportunities and reports on his successes and failures. Eventually, he works on his search at least 4 hours a day. After disappointments, we examine how he can keep himself going, increase awareness of how he is communicating, and engage in self-care to keep up motivation.
He continues to pursue opportunities and focus on the process rather than the outcome of his job search. He now sees himself as challenged by his circumstances and not as much a victim of them.—CAROL KAUFFMAN, PhD, ABPP, PCC
Addressing depression
DR. KAUFFMAN: Medication also can play a useful role for some patients.
DR. PALMER: Patients who meet criteria for major depression—in particular if they’re having suicidal thoughts—absolutely need psychotropics. Mr. R, my case patient, benefited greatly from CBT and medication. We also worked on financial planning and handling financial conflicts with his wife and children. He is exercising, doing volunteer work, and staying connected with friends and family. He is hoping to find a job in the next few months.
DR. REDIGER: For a person who’s going though a stressful period, I try to keep medication time-limited. We talk about treating symptoms, but it’s important to look at what’s causing the patient’s problems and address it.
DR. PALMER: During this recession, a lot of people are going to be down but not clinically depressed. If the depression is mild to moderate, I sometimes recommend exercise instead of medication (such as when a patient is refusing medication or has had serious side effects from medications). I recommend exercise for all my outpatients—even if they’re taking psychotropics—because exercise has been shown to be as effective as antidepressants for moderate depression.7,8
DR. REDIGER: We’ve also been encouraging people who’ve lost jobs to volunteer in the community. Having a reason to get out of the house takes the mind off one’s worries.
DR. KAUFFMAN: The “3 good things in life” exercise studied by psychologist Martin E.P. Seligman, PhD, has been shown in a 6-month, randomized, placebo-controlled study to increase happiness and decrease depressive symptoms.9 In this exercise, you look back at the end of each day and write down 3 things that went well, their causes, and an explanation for each good thing. Ask yourself, “When was I at my best today? What happened today that I feel grateful for? What did I do to make that good thing happen?”
DR. REDIGER: Remind people to talk to their children about the recession, too. If they have to move to a different home or to a different school, let their children know things are going on and how to think about that. This can help kids understand how to deal with their anxiety.
Related resources
- Getting through tough economic times. A SAMHSA guide. Substance Abuse and Mental Health Services Administration. U.S. Department of Health and Human Services. www.samhsa.gov/economy.
- Seligman MEP. Authentic happiness: using the new positive psychology to realize your potential for lasting fulfillment. New York, NY: Simon & Schuster; 2002.
- Positive Psychology Center. University of Pennsylvania, Philadelphia. www.ppc.sas.upenn.edu.
Drug brand names
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Lorazepam • Ativan
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
This article was researched and written by Current Psychiatry Editor Alice V. Luddington, ELS, and Senior Associate Editor Erica Vonderheid.
1. Employment situation summary: March 2009. Bureau of Labor Statistics. Washington, DC: U.S. Department of Labor; April 3, 2009. Available at: http://www.bls.gov/news.release/empsit.nr0.htm. Accessed April 14, 2009.
2. Stack S, Wasserman I. Economic strain and suicide risk: a qualitative analysis. Suicide Life Threat Behav. 2007;37:103-112.
3. Heikkinen M, Aro H, Lonngvist J. Recent life events, social support, and suicide. Acta Psychiatr Scand Suppl. 1994;377:65-72.
4. Snyder CR. Hope theory: rainbows of the mind. Psychological Inquiry. 2002;13:249-275.
5. Snyder CR, Harris C, Anderson JR, et al. The will and the ways: development and validation of an individual-differences measure of hope. J Pers Soc Psychol. 1991;60:570-585.
6. Fowler JH, Christakis NA. Dynamic spread of happiness in a large social network: longitudinal analysis over 20 years in the Framingham Heart Study. BMJ. 2008;337:a2338.-
7. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69:587-596.
8. Craft LL, Landers DM. The effects of exercise on clinical depression and depression resulting from mental illness: a meta-analysis. JSEP. 1998;20:339-357.
9. Seligman MEP, Steen TA, Park N, et al. Positive psychology progress: empirical validation of interventions. Am Psychol. 2005;60:410-421.
1. Employment situation summary: March 2009. Bureau of Labor Statistics. Washington, DC: U.S. Department of Labor; April 3, 2009. Available at: http://www.bls.gov/news.release/empsit.nr0.htm. Accessed April 14, 2009.
2. Stack S, Wasserman I. Economic strain and suicide risk: a qualitative analysis. Suicide Life Threat Behav. 2007;37:103-112.
3. Heikkinen M, Aro H, Lonngvist J. Recent life events, social support, and suicide. Acta Psychiatr Scand Suppl. 1994;377:65-72.
4. Snyder CR. Hope theory: rainbows of the mind. Psychological Inquiry. 2002;13:249-275.
5. Snyder CR, Harris C, Anderson JR, et al. The will and the ways: development and validation of an individual-differences measure of hope. J Pers Soc Psychol. 1991;60:570-585.
6. Fowler JH, Christakis NA. Dynamic spread of happiness in a large social network: longitudinal analysis over 20 years in the Framingham Heart Study. BMJ. 2008;337:a2338.-
7. Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. 2007;69:587-596.
8. Craft LL, Landers DM. The effects of exercise on clinical depression and depression resulting from mental illness: a meta-analysis. JSEP. 1998;20:339-357.
9. Seligman MEP, Steen TA, Park N, et al. Positive psychology progress: empirical validation of interventions. Am Psychol. 2005;60:410-421.
Beyond threats: Risk factors for suicide in borderline personality disorder
Manipulative, “just threats,” or suicide gestures are terms you may have heard or used to label suicidal thoughts and behavior in individuals with borderline personality disorder (BPD). These terms imply that the risk of injury or death is low, but evidence shows that BPD patients are at high risk for completed suicide1-3 —and clinicians who use these labels may underestimate this risk and respond inadequately.
BPD is the only personality disorder to have suicidal or self-injurious behavior among its diagnostic criteria.2 A prospective study showed a 3.8% completed suicide rate in a sample of borderline patients at 6-year follow-up.2 Earlier studies reported rates from 8% to 10%—approximately 50 times greater than the general population.1
Recent suicide attempts by individuals with BPD have shown:
- the same degree of lethality and intent to die ( Box 1 )5-7 as recent suicide attempts by individuals without BPD8
- no differences in degree of intent to die compared with attempts by persons experiencing a major depressive episode or persons with both BPD and depression.9
Moreover, patients with BPD (including those with comorbid depression) have reported greater lethality for their most serious life-time suicide attempt than those with depression alone.9
Based on the literature and our clinical experience, this article offers recommendations for assessing and treating suicidal behavior in BPD patients. We review risk factors for suicide and suicide attempts and suggest strategies for safety management, psychotherapy, and pharmacotherapy. Because of the high-risk nature of this population, we recommend that all clinicians working with suicidal BPD patients obtain consultation and supervision as needed when using these strategies.
Self-injurious behavior in borderline personality disorder (BPD) patients can be divided into 2 categories: suicide attempts and nonsuicidal self-injury.
- Suicide attempts are performed with some evidence of intent to die.5
- Nonsuicidal self-injury behaviors (NSIB) are performed without intent to die.6
How can clinicians respond effectively when suicidal behaviors are repetitive and performed both with and without the intent to die? Although patients may perform NSIB for reasons other than intent to die (such as to express anger, punish oneself, or relieve distress),7 these behaviors require active intervention because of the possibility of serious injury (intentional or accidental). Also, the intent of a self-injurious behavior may change as the patient performs the behavior; what started as a nonsuicidal act may turn into a suicide attempt.6 Therefore, address all potentially harmful behaviors.
Risk factors for suicidal behavior
Several risk factors for suicide attempts and completed suicide among individuals diagnosed with BPD have been identified. Previous suicide attempts are one of the strongest predictors of completed suicide and suicide attempts in individuals with BPD.10-12 In general, clinicians cannot accurately predict which individuals will die by suicide.10,13 Suicide risk factors identified in BPD ( Table 1 )12-16 are similar to those in persons without the BPD diagnosis. In BPD patients, risk factors for attempted and completed suicide largely overlap.
Individuals with BPD may be distinguished by elevated risk factors for suicidal behavior as compared with suicide attempters without the BPD diagnosis. In a study comparing recent suicide attempters with and without BPD, those with BPD showed greater severity across a number of risk factors, including overall psychopathology, depression, hopelessness, suicide ideation, past suicide attempts, and social problem solving skills.8
Table 1
Common risk factors for suicidal behavior in BPD
| Behavioral factors Previous suicide attempts Impulsivity Aggression Poor social problem-solving skills Poor social adjustment |
| Cognitive/emotional factors Affective instability Hopelessness |
| Comorbid diagnoses Major depressive disorder Antisocial personality disorder Substance abuse disorders |
| Psychosocial/psychiatric history Childhood physical abuse Childhood sexual abuse Psychiatric hospitalizations |
| BPD: borderline personality disorder |
| Source: References 12-16 |
Remove lethal means
When working with patients with a history of suicidal behavior, it is critical to ensure the safety of the patient’s environment. Restricting access to lethal means has been shown to be an effective form of suicide prevention.17 Direct all patients with a history of recent suicidality or nonsuicidal self-injurious behavior (NSIB) to remove lethal means and means of self-harm from their homes and possession ( Table 2 ). Continue to monitor access to lethal means throughout treatment, as patients may acquire new means or reveal possession of items they had previously concealed.
We have found the following metaphor useful in discussing with patients the rationale for removing lethal means: “If you were on a diet, would it make sense to have a chocolate cake in the house?” Objections to removing lethal means often reveal important therapeutic issues. For example, those unwilling to relinquish lethal means may not be fully committed to giving up suicide or NSIB as an option. This would become a critical treatment goal.18
Tell patients to remove or discard fire-arms, knives, razors, and pills, as well as other items used in past suicide attempts/NSIB. Although patients can acquire new lethal means, removing immediate access lowers the possibility of an impulsive suicide attempt or NSIB and may give the patient time to reconsider.
Address overdose risk. Some physicians are reluctant or refuse to prescribe medication to BPD patients out of fear that it will be used to attempt suicide. A more productive approach is to ensure through informed choice of medications and strict management of their distribution that the patient safely and consistently receives necessary treatment.
Avoid prescribing psychiatric medications in quantities that could be lethal in overdose. Also determine whether the patient has other potentially lethal medications. If possible, have a friend or family member keep and administer the patient’s medications. If this is not possible, consider prescribing medications 1 week at a time.
Monitor as needed. If a patient continues to refuse to part with lethal means:
- involve family members or friends in removing and monitoring the patient’s lethal means
- assess the degree of imminent danger and if the individual can be safely managed as an outpatient.
Create a safety plan. Every BPD patient with a history of suicidality needs a detailed safety plan for what to do when suicidal ( Table 3 ).19,20 Inform family members (and friends, when appropriate) of the safety plan, and involve them as needed to monitor a patient at risk. Give your BPD patients clear instructions about when you will be available by phone and emergency contacts for when you are not available.
Table 2
7 clinical tips for managing safety in BPD patients
| Work with the patient in every session to remove all potentially lethal means (guns, knives, razors, pills) from his or her home and possession |
| Create a detailed safety plan to use during a suicidal crisis |
| Assess suicide risk in every session |
| Involve family and friends if possible to help monitor the patient and to call you or 911 if the patient appears to be in imminent danger of suicidal behavior |
| Create a ‘hope kit’ ( Box 2 ) as a companion to the safety plan |
| Consider hospitalization if the patient is in imminent danger of suicidal behavior or has engaged in suicidal behavior requiring medical attention |
| Consult with other clinicians about crucial safety management decisions, such as whether or not to hospitalize a patient |
| BPD: borderline personality disorder |
Lifeline for suicidal patients: What to include in a safety plan
| Warning signs of a suicidal crisis for that individual (such as increased depression or negative thinking) |
| Coping skills the patient can perform on his or her own |
| Family members and friends the patient can contact in an emergency |
| Therapist’s contact information |
| Phone numbers of emergency services available 24 hours daily (such as 911, suicide hotlines) |
| Source: References 19,20 |
Assess suicide risk
In every session, assess suicidal ideation, plans, intent, and urges to engage in NSIB. Consider using:
- self-monitoring forms, such as a dialectical behavior therapy (DBT) “diary card,” on which the patient each day records urges to self-harm or attempt suicide18
- Beck Depression Inventory (which contains a question about suicidal ideation).28
Risk assessment is not always straightforward. We have found that patients do not always provide consistent and/or accurate information about their degree of suicidality, making it difficult to know how to intervene. Reasons may include:
- fear of hospitalization
- uncertainty about whether or not they will attempt suicide
- desire to conceal a planned suicide attempt.
Hospitalize for suicidality?
If possible, consult with other professionals when making difficult decisions about hospitalizing a patient. These decisions often are subjective and open to influence by therapists’ emotional reactions. Psychotherapies for BPD emphasize the importance of consulting with other clinicians when working with this population. DBT requires a therapist consultation meeting, and cognitive therapies also have recommended consultation.18-20
If you work alone in private practice, consider consulting by phone with colleagues experienced with working with BPD patients. Document this consultation to help protect yourself from liability should an adverse outcome occur.
Little evidence supports hospitalization as an effective treatment for suicidality in BPD.24 It has been argued that hospitalization might increase future suicidal behavior when the patient perceives it as a positive experience or a means of escaping problems.18 The patient’s safety must remain a top priority, however, and we recommend admission if the patient is in imminent danger or has engaged in self-injurious behavior requiring medical attention.
The length of a hospital stay should be determined on a case-by-case basis. In general, it has been recommended that hospitalization for BPD patients be crisis-oriented and brief to avoid reinforcing suicidal behavior and to promote coping with suicidality in the natural environment.18,24 Also take into account acute exacerbation of comorbid Axis I diagnoses when determining the duration of hospitalization.
‘No-suicide’ contracts. Be careful not to rely on “no-suicide” contracts. They have no legal standing and may give you a false sense of security. Clearly, a patient may attempt suicide despite promising not to do so.
Asking if the patient can commit to staying safe for a specified time can be useful in assessing his/her level of suicidality and motivation to behave safely, but this is no substitute for a thorough clinical evaluation. Consider increasing the level of care and degree of monitoring or hospitalization if other suicide risk factors are elevated, even if the patient has “contracted for safety.”
Validated psychotherapies
Psychotherapy is the primary treatment for BPD, according to American Psychiatric Association (APA) guidelines.1 DBT,21-22 transference-focused therapy,25 and mentalization-based therapy26 are 3 validated psychotherapeutic approaches for BPD that have been shown to reduce suicide attempt rates in randomized clinical trials (RCTs). DBT has the greatest number of RCTs supporting its efficacy. We advise clinicians who work frequently with BPD patients to become familiar with these effective, empirical treatments.
A recent open trial of cognitive therapy for BPD demonstrated a decrease in self-harm behaviors.27 Cognitive therapy for recent suicide attempters—including those with BPD—decreased subsequent suicide attempts by approximately 50% over 18 months of follow-up in a RCT.28
Target suicidality. For all patients with a recent suicide attempt, make suicidal behavior the primary treatment target.18-20 Work with the patient on skills to reduce suicidal behavior, rather than assuming the behavior will resolve after you treat the psychiatric disorder (such as depression or BPD).
Throughout treatment, make suicidality or NSIB the priority in sessions whenever it occurs.18 This ensures that self-harm behavior is adequately addressed and provides an aversive consequence for this behavior. The patient cannot talk about other topics he/she might want to discuss until the suicidal behavior is addressed.18
Also target risk factors for suicidal behavior, such as depression, hopelessness, substance abuse, impulsivity, affective instability, social adjustment, and social problem-solving skills.
Teach coping skills. Because suicide attempts and NSIB in BPD often occur as maladaptive means of coping with distress, teach your patient alternatives such as distraction and self-soothing techniques, relaxation, positive self-statements, problem-solving skills, and how to use social support.18-20 The patient is likely to be flooded with affect when suicidal, so teach simple, easy-to-perform coping skills. Because self-harm behaviors in BPD patients often occur impulsively, create a written safety plan in advance. A “hope kit” can be an extremely useful part of the safety plan ( Box 2 ).18,18,27
A ‘hope kit’ can be an extremely useful intervention with recent suicide attempters.18,19 In a randomized, controlled trial, use of a hope kit as part of cognitive therapy for recent suicide attempters decreased suicide attempt rates by approximately 50%, compared with treatment as usual plus case management.27
Instruct the patient to fill a box or container with tangible reminders of reasons to live (such as photos of loved ones) and cues to use coping skills (a relaxation tape, a comic book, music, positive written self-statements). Tell the patient to keep the hope kit easily accessible and use it to guide positive coping during a suicidal crisis.
Symptom-guided medication
Use pharmacotherapy to complement psychotherapy for BPD and to address comorbid Axis I conditions. The BPD symptom domains targeted by medications may be sorted into 3 categories: ( Table 4 ):1
- affective dysregulation
- impulsive behavioral dyscontrol
- cognitive and perceptual problems.
Recommendations for pharmacologic management in BPD are based on a relatively small number of studies. Medication can decrease symptoms and increase the patient’s ability and willingness to engage in therapy. However, no drug has been proven effective or received FDA approval to treat BPD. Thus, our prescribing recommendations—though based on available evidence—are off-label uses.
In our experience, BPD patients often are prescribed multiple medications, probably because no single medication targets all symptoms of the disorder. To avoid the accumulation of medications that have lost or have not demonstrated therapeutic effect, we recommend caution when addressing BPD pathology with polypharmacy.
Table 4
Symptom-guided approach to medication for BPD patients
| Symptom domain | Medication(s) |
|---|---|
| Affective dysregulation | SSRI (first-line) or mood stabilizer (second-line) |
| Impulsive behavioral dyscontrol | SSRI and/or low-dose atypical antipsychotic |
| Cognitive and perceptual problems, acute dissociation/psychotic symptoms | Low-dose atypical antipsychotic |
| Acute anxiety (severe) | Low-dose atypical antipsychotic |
| Chronic anxiety | SSRI |
| BPD: borderline personality disorder; SSRI: selective serotonin reuptake inhibitor | |
| Source: Reference 1 | |
Antidepressants. APA guidelines suggest a selective serotonin reuptake inhibitor (SSRI) as the first-line initial treatment for affective dysregulation and impulsive behavioral dyscontrol.1,35-37 Because reports have shown increased risk of suicidal thoughts and behaviors with SSRI use in children, adolescents, and young adults,38 follow FDA guidelines for monitoring these populations during the first 12 weeks of therapy.39
Dosages typically are lower than those used to treat Axis I psychotic disorders. Because of clozapine’s complex maintenance and potential for side effects, consider using it only after trials of other antipsychotics have failed. Also consider short-term antipsychotic use to manage acute symptoms such as dissociation, intense paranoia, hostility, or severe anxiety.
Agents to consider with caution. Because of the potential for abuse, tolerance, overdose, and behavioral disinhibition, be very cautious when using benzodiazepines to treat chronic and acute anxiety in BPD patients.1
Tricyclic antidepressants and monoamine oxidase inhibitors are at times recommended for medication-resistant patients. Avoid these drugs in highly suicidal BPD patients because of the potential for lethal overdose.
Related resources
- Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
- Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cognit Behav Pract. 2004;11:265-277.
- Behavioral Tech, LLC. Training courses in dialectical behavior therapy. www.behavioraltech.org.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Ira Lesser, MD, for reviewing and providing feedback on this article.
1. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
2. Zanarini MC, Frankenburg FR, Hennen J, et al. The McLean study of adult development: overview and implications of the first six years of prospective follow-up. J Personal Disord. 2005;19(5):505-523.
3. Paris J. Chronic suicidality among patients with borderline personality disorder. Psychiatr Serv. 2002;53(6):738-742.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. O’Carroll PW, Berman AL, Maris RW, et al. Beyond the Tower of Babel: a nomenclature for suicidology. Suicide Life Threat Behav. 1996;26(3):237-252.
6. Miller AL, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: Guilford; 2007.
7. Brown MZ, Comtois KA, Linehan MM. Reasons for suicide attempts and nonsuicidal self-injury in women with borderline personality disorder. J Abnorm Psychol. 2002;111(1):198-202.
8. Berk MS, Jeglic E, Brown GK, et al. Characteristics of recent suicide attempters with and without borderline personality disorder. Arch Suicide Res. 2007;11(1):91-104.
9. Soloff PH, Lynch KG, Kelly TM, et al. Characteristics of suicide attempts of patients with major depressive episode and borderline personality disorder: a comparative study. Am J Psychiatry. 2000;157(4):601-608.
10. Paris J, Nowlis D, Brown R. Predictors of suicide in borderline personality disorder. Can J Psychiatry. 1989;34(1):8-9.
11. Paris J. Completed suicide in borderline personality disorder. Psychiatr Ann. 1990;20:19-21.
12. Soloff PH, Fabio A. Prospective predictors of suicide attempts in borderline personality disorder at one, two, and two-to-five year follow-up. J Personal Disord. 2008;22(2):123-134.
13. Oldham JM. Borderline personality disorder and suicidality. Am J Psychiatry. 2006;163(1):20-26.
14. Black DW, Blum N, Pfohl B, et al. Suicidal behavior in borderline personality disorder: prevalence, risk factors, prediction, and prevention. J Personal Disord. 2004;18(3):226-239.
15. Kolla NJ, Eisenberg H, Links PS. Epidemiology, risk factors, and psychopharmacological management of suicidal behavior in borderline personality disorder. Arch Suicide Res. 2008;12(1):1-19.
16. McGirr A, Paris J, Lesage A. Risk factors for suicide completion in borderline personality disorder: a case control study of cluster B comorbidity and impulsive aggression. J Clin Psychiatry. 2007;68:721-729.
17. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
18. Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
19. Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cogn Behav Pract. 2004;11:265-277.
20. Wenzel A, Brown GK, Beck AT. Cognitive therapy for suicidal patients: scientific and clinical applications. Washington, DC: APA Books; 2008.
21. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48(12):1060-1064.
22. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
23. Beck AT, Steer RA, Brown GK. The Beck Depression Inventory, 2nd ed. San Antonio, TX: Psychological Corporation; 1996.
24. Paris J. Is hospitalization useful for suicidal patients with borderline personality disorder? J Personal Disord. 2004;18(3):240-247.
25. Clarkin JF, Levy KN, Lenzenweger MF, et al. Evaluating three treatments for borderline personality disorder: a multiwave study. Am J Psychiatry. 2007;164(6):1-7.
26. Bateman A, Fonagy P. Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial. Am J Psychiatry. 1999;156(10):1563-1569.
27. Brown GK, Newman CF, Charlesworth SE, et al. An open clinical trial of cognitive therapy for borderline personality disorder. J Personal Disord. 2004;18(3):257-271.
28. Brown GK, Tenhave T, Henriques GR, et al. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial. JAMA. 2005;294(5):563-570.
29. Benedetti F, Sforzini L, Colombo C, et al. Low-dose clozapine in acute and continuation treatment of severe borderline personality disorder. J Clin Psychiatry. 1998;59(3):103-107.
30. Chengappa KN, Ebeling T, Kang JS, et al. Clozapine reduces severe self-mutilation and aggression in psychotic patients with borderline personality disorder. J Clin Psychiatry. 1999;60(7):477-484.
31. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;15;46(10):1429-1435.
32. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
33. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
34. Nickel MK, Loew TH, Pedrosa Gil F. Aripiprazole in treatment of borderline patients, part II: an 18-month follow-up. Psychopharmacology (Berl). 2007;191(4):1023-1026.
35. Coccaro E, Kavoussi R. Fluoxetine and impulsive aggressive behavior in personality disordered subjects. Arch Gen Psychiatry. 1997;54:1081-1088.
36. Kallioniemi H, Syvalahti E. Citalopram, a specific inhibitor of serotonin reuptake, in treatment of psychotic and borderline patients. Nord J Psychiatry. 1993;47(suppl 28):79-84.
37. Kavoussi R, Liu J, Coccaro E. An open trial of sertraline in borderline personality disordered patients with impulsive aggression. J Clin Psychiatry. 1994;55:137-141.
38. FDA public health advisory: suicidality in children and adolescents being treated with antidepressant medications. Silver Spring, MD: U.S. Food and Drug Administration; October 15, 2004. Available at: http://www.fda.gov/cder/drug/antidepressants/SSRIPHA200410.htm. Accessed March 18, 2009.
39. Medication guide: about using antidepressants in children and teenagers. Silver Spring, MD: U.S. Food and Drug Administration; 2005. Available at: http://www.fda.gov/cder/drug/antidepressants/MG_template.pdf. Accessed March 18, 2009.
Manipulative, “just threats,” or suicide gestures are terms you may have heard or used to label suicidal thoughts and behavior in individuals with borderline personality disorder (BPD). These terms imply that the risk of injury or death is low, but evidence shows that BPD patients are at high risk for completed suicide1-3 —and clinicians who use these labels may underestimate this risk and respond inadequately.
BPD is the only personality disorder to have suicidal or self-injurious behavior among its diagnostic criteria.2 A prospective study showed a 3.8% completed suicide rate in a sample of borderline patients at 6-year follow-up.2 Earlier studies reported rates from 8% to 10%—approximately 50 times greater than the general population.1
Recent suicide attempts by individuals with BPD have shown:
- the same degree of lethality and intent to die ( Box 1 )5-7 as recent suicide attempts by individuals without BPD8
- no differences in degree of intent to die compared with attempts by persons experiencing a major depressive episode or persons with both BPD and depression.9
Moreover, patients with BPD (including those with comorbid depression) have reported greater lethality for their most serious life-time suicide attempt than those with depression alone.9
Based on the literature and our clinical experience, this article offers recommendations for assessing and treating suicidal behavior in BPD patients. We review risk factors for suicide and suicide attempts and suggest strategies for safety management, psychotherapy, and pharmacotherapy. Because of the high-risk nature of this population, we recommend that all clinicians working with suicidal BPD patients obtain consultation and supervision as needed when using these strategies.
Self-injurious behavior in borderline personality disorder (BPD) patients can be divided into 2 categories: suicide attempts and nonsuicidal self-injury.
- Suicide attempts are performed with some evidence of intent to die.5
- Nonsuicidal self-injury behaviors (NSIB) are performed without intent to die.6
How can clinicians respond effectively when suicidal behaviors are repetitive and performed both with and without the intent to die? Although patients may perform NSIB for reasons other than intent to die (such as to express anger, punish oneself, or relieve distress),7 these behaviors require active intervention because of the possibility of serious injury (intentional or accidental). Also, the intent of a self-injurious behavior may change as the patient performs the behavior; what started as a nonsuicidal act may turn into a suicide attempt.6 Therefore, address all potentially harmful behaviors.
Risk factors for suicidal behavior
Several risk factors for suicide attempts and completed suicide among individuals diagnosed with BPD have been identified. Previous suicide attempts are one of the strongest predictors of completed suicide and suicide attempts in individuals with BPD.10-12 In general, clinicians cannot accurately predict which individuals will die by suicide.10,13 Suicide risk factors identified in BPD ( Table 1 )12-16 are similar to those in persons without the BPD diagnosis. In BPD patients, risk factors for attempted and completed suicide largely overlap.
Individuals with BPD may be distinguished by elevated risk factors for suicidal behavior as compared with suicide attempters without the BPD diagnosis. In a study comparing recent suicide attempters with and without BPD, those with BPD showed greater severity across a number of risk factors, including overall psychopathology, depression, hopelessness, suicide ideation, past suicide attempts, and social problem solving skills.8
Table 1
Common risk factors for suicidal behavior in BPD
| Behavioral factors Previous suicide attempts Impulsivity Aggression Poor social problem-solving skills Poor social adjustment |
| Cognitive/emotional factors Affective instability Hopelessness |
| Comorbid diagnoses Major depressive disorder Antisocial personality disorder Substance abuse disorders |
| Psychosocial/psychiatric history Childhood physical abuse Childhood sexual abuse Psychiatric hospitalizations |
| BPD: borderline personality disorder |
| Source: References 12-16 |
Remove lethal means
When working with patients with a history of suicidal behavior, it is critical to ensure the safety of the patient’s environment. Restricting access to lethal means has been shown to be an effective form of suicide prevention.17 Direct all patients with a history of recent suicidality or nonsuicidal self-injurious behavior (NSIB) to remove lethal means and means of self-harm from their homes and possession ( Table 2 ). Continue to monitor access to lethal means throughout treatment, as patients may acquire new means or reveal possession of items they had previously concealed.
We have found the following metaphor useful in discussing with patients the rationale for removing lethal means: “If you were on a diet, would it make sense to have a chocolate cake in the house?” Objections to removing lethal means often reveal important therapeutic issues. For example, those unwilling to relinquish lethal means may not be fully committed to giving up suicide or NSIB as an option. This would become a critical treatment goal.18
Tell patients to remove or discard fire-arms, knives, razors, and pills, as well as other items used in past suicide attempts/NSIB. Although patients can acquire new lethal means, removing immediate access lowers the possibility of an impulsive suicide attempt or NSIB and may give the patient time to reconsider.
Address overdose risk. Some physicians are reluctant or refuse to prescribe medication to BPD patients out of fear that it will be used to attempt suicide. A more productive approach is to ensure through informed choice of medications and strict management of their distribution that the patient safely and consistently receives necessary treatment.
Avoid prescribing psychiatric medications in quantities that could be lethal in overdose. Also determine whether the patient has other potentially lethal medications. If possible, have a friend or family member keep and administer the patient’s medications. If this is not possible, consider prescribing medications 1 week at a time.
Monitor as needed. If a patient continues to refuse to part with lethal means:
- involve family members or friends in removing and monitoring the patient’s lethal means
- assess the degree of imminent danger and if the individual can be safely managed as an outpatient.
Create a safety plan. Every BPD patient with a history of suicidality needs a detailed safety plan for what to do when suicidal ( Table 3 ).19,20 Inform family members (and friends, when appropriate) of the safety plan, and involve them as needed to monitor a patient at risk. Give your BPD patients clear instructions about when you will be available by phone and emergency contacts for when you are not available.
Table 2
7 clinical tips for managing safety in BPD patients
| Work with the patient in every session to remove all potentially lethal means (guns, knives, razors, pills) from his or her home and possession |
| Create a detailed safety plan to use during a suicidal crisis |
| Assess suicide risk in every session |
| Involve family and friends if possible to help monitor the patient and to call you or 911 if the patient appears to be in imminent danger of suicidal behavior |
| Create a ‘hope kit’ ( Box 2 ) as a companion to the safety plan |
| Consider hospitalization if the patient is in imminent danger of suicidal behavior or has engaged in suicidal behavior requiring medical attention |
| Consult with other clinicians about crucial safety management decisions, such as whether or not to hospitalize a patient |
| BPD: borderline personality disorder |
Lifeline for suicidal patients: What to include in a safety plan
| Warning signs of a suicidal crisis for that individual (such as increased depression or negative thinking) |
| Coping skills the patient can perform on his or her own |
| Family members and friends the patient can contact in an emergency |
| Therapist’s contact information |
| Phone numbers of emergency services available 24 hours daily (such as 911, suicide hotlines) |
| Source: References 19,20 |
Assess suicide risk
In every session, assess suicidal ideation, plans, intent, and urges to engage in NSIB. Consider using:
- self-monitoring forms, such as a dialectical behavior therapy (DBT) “diary card,” on which the patient each day records urges to self-harm or attempt suicide18
- Beck Depression Inventory (which contains a question about suicidal ideation).28
Risk assessment is not always straightforward. We have found that patients do not always provide consistent and/or accurate information about their degree of suicidality, making it difficult to know how to intervene. Reasons may include:
- fear of hospitalization
- uncertainty about whether or not they will attempt suicide
- desire to conceal a planned suicide attempt.
Hospitalize for suicidality?
If possible, consult with other professionals when making difficult decisions about hospitalizing a patient. These decisions often are subjective and open to influence by therapists’ emotional reactions. Psychotherapies for BPD emphasize the importance of consulting with other clinicians when working with this population. DBT requires a therapist consultation meeting, and cognitive therapies also have recommended consultation.18-20
If you work alone in private practice, consider consulting by phone with colleagues experienced with working with BPD patients. Document this consultation to help protect yourself from liability should an adverse outcome occur.
Little evidence supports hospitalization as an effective treatment for suicidality in BPD.24 It has been argued that hospitalization might increase future suicidal behavior when the patient perceives it as a positive experience or a means of escaping problems.18 The patient’s safety must remain a top priority, however, and we recommend admission if the patient is in imminent danger or has engaged in self-injurious behavior requiring medical attention.
The length of a hospital stay should be determined on a case-by-case basis. In general, it has been recommended that hospitalization for BPD patients be crisis-oriented and brief to avoid reinforcing suicidal behavior and to promote coping with suicidality in the natural environment.18,24 Also take into account acute exacerbation of comorbid Axis I diagnoses when determining the duration of hospitalization.
‘No-suicide’ contracts. Be careful not to rely on “no-suicide” contracts. They have no legal standing and may give you a false sense of security. Clearly, a patient may attempt suicide despite promising not to do so.
Asking if the patient can commit to staying safe for a specified time can be useful in assessing his/her level of suicidality and motivation to behave safely, but this is no substitute for a thorough clinical evaluation. Consider increasing the level of care and degree of monitoring or hospitalization if other suicide risk factors are elevated, even if the patient has “contracted for safety.”
Validated psychotherapies
Psychotherapy is the primary treatment for BPD, according to American Psychiatric Association (APA) guidelines.1 DBT,21-22 transference-focused therapy,25 and mentalization-based therapy26 are 3 validated psychotherapeutic approaches for BPD that have been shown to reduce suicide attempt rates in randomized clinical trials (RCTs). DBT has the greatest number of RCTs supporting its efficacy. We advise clinicians who work frequently with BPD patients to become familiar with these effective, empirical treatments.
A recent open trial of cognitive therapy for BPD demonstrated a decrease in self-harm behaviors.27 Cognitive therapy for recent suicide attempters—including those with BPD—decreased subsequent suicide attempts by approximately 50% over 18 months of follow-up in a RCT.28
Target suicidality. For all patients with a recent suicide attempt, make suicidal behavior the primary treatment target.18-20 Work with the patient on skills to reduce suicidal behavior, rather than assuming the behavior will resolve after you treat the psychiatric disorder (such as depression or BPD).
Throughout treatment, make suicidality or NSIB the priority in sessions whenever it occurs.18 This ensures that self-harm behavior is adequately addressed and provides an aversive consequence for this behavior. The patient cannot talk about other topics he/she might want to discuss until the suicidal behavior is addressed.18
Also target risk factors for suicidal behavior, such as depression, hopelessness, substance abuse, impulsivity, affective instability, social adjustment, and social problem-solving skills.
Teach coping skills. Because suicide attempts and NSIB in BPD often occur as maladaptive means of coping with distress, teach your patient alternatives such as distraction and self-soothing techniques, relaxation, positive self-statements, problem-solving skills, and how to use social support.18-20 The patient is likely to be flooded with affect when suicidal, so teach simple, easy-to-perform coping skills. Because self-harm behaviors in BPD patients often occur impulsively, create a written safety plan in advance. A “hope kit” can be an extremely useful part of the safety plan ( Box 2 ).18,18,27
A ‘hope kit’ can be an extremely useful intervention with recent suicide attempters.18,19 In a randomized, controlled trial, use of a hope kit as part of cognitive therapy for recent suicide attempters decreased suicide attempt rates by approximately 50%, compared with treatment as usual plus case management.27
Instruct the patient to fill a box or container with tangible reminders of reasons to live (such as photos of loved ones) and cues to use coping skills (a relaxation tape, a comic book, music, positive written self-statements). Tell the patient to keep the hope kit easily accessible and use it to guide positive coping during a suicidal crisis.
Symptom-guided medication
Use pharmacotherapy to complement psychotherapy for BPD and to address comorbid Axis I conditions. The BPD symptom domains targeted by medications may be sorted into 3 categories: ( Table 4 ):1
- affective dysregulation
- impulsive behavioral dyscontrol
- cognitive and perceptual problems.
Recommendations for pharmacologic management in BPD are based on a relatively small number of studies. Medication can decrease symptoms and increase the patient’s ability and willingness to engage in therapy. However, no drug has been proven effective or received FDA approval to treat BPD. Thus, our prescribing recommendations—though based on available evidence—are off-label uses.
In our experience, BPD patients often are prescribed multiple medications, probably because no single medication targets all symptoms of the disorder. To avoid the accumulation of medications that have lost or have not demonstrated therapeutic effect, we recommend caution when addressing BPD pathology with polypharmacy.
Table 4
Symptom-guided approach to medication for BPD patients
| Symptom domain | Medication(s) |
|---|---|
| Affective dysregulation | SSRI (first-line) or mood stabilizer (second-line) |
| Impulsive behavioral dyscontrol | SSRI and/or low-dose atypical antipsychotic |
| Cognitive and perceptual problems, acute dissociation/psychotic symptoms | Low-dose atypical antipsychotic |
| Acute anxiety (severe) | Low-dose atypical antipsychotic |
| Chronic anxiety | SSRI |
| BPD: borderline personality disorder; SSRI: selective serotonin reuptake inhibitor | |
| Source: Reference 1 | |
Antidepressants. APA guidelines suggest a selective serotonin reuptake inhibitor (SSRI) as the first-line initial treatment for affective dysregulation and impulsive behavioral dyscontrol.1,35-37 Because reports have shown increased risk of suicidal thoughts and behaviors with SSRI use in children, adolescents, and young adults,38 follow FDA guidelines for monitoring these populations during the first 12 weeks of therapy.39
Dosages typically are lower than those used to treat Axis I psychotic disorders. Because of clozapine’s complex maintenance and potential for side effects, consider using it only after trials of other antipsychotics have failed. Also consider short-term antipsychotic use to manage acute symptoms such as dissociation, intense paranoia, hostility, or severe anxiety.
Agents to consider with caution. Because of the potential for abuse, tolerance, overdose, and behavioral disinhibition, be very cautious when using benzodiazepines to treat chronic and acute anxiety in BPD patients.1
Tricyclic antidepressants and monoamine oxidase inhibitors are at times recommended for medication-resistant patients. Avoid these drugs in highly suicidal BPD patients because of the potential for lethal overdose.
Related resources
- Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
- Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cognit Behav Pract. 2004;11:265-277.
- Behavioral Tech, LLC. Training courses in dialectical behavior therapy. www.behavioraltech.org.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Ira Lesser, MD, for reviewing and providing feedback on this article.
Manipulative, “just threats,” or suicide gestures are terms you may have heard or used to label suicidal thoughts and behavior in individuals with borderline personality disorder (BPD). These terms imply that the risk of injury or death is low, but evidence shows that BPD patients are at high risk for completed suicide1-3 —and clinicians who use these labels may underestimate this risk and respond inadequately.
BPD is the only personality disorder to have suicidal or self-injurious behavior among its diagnostic criteria.2 A prospective study showed a 3.8% completed suicide rate in a sample of borderline patients at 6-year follow-up.2 Earlier studies reported rates from 8% to 10%—approximately 50 times greater than the general population.1
Recent suicide attempts by individuals with BPD have shown:
- the same degree of lethality and intent to die ( Box 1 )5-7 as recent suicide attempts by individuals without BPD8
- no differences in degree of intent to die compared with attempts by persons experiencing a major depressive episode or persons with both BPD and depression.9
Moreover, patients with BPD (including those with comorbid depression) have reported greater lethality for their most serious life-time suicide attempt than those with depression alone.9
Based on the literature and our clinical experience, this article offers recommendations for assessing and treating suicidal behavior in BPD patients. We review risk factors for suicide and suicide attempts and suggest strategies for safety management, psychotherapy, and pharmacotherapy. Because of the high-risk nature of this population, we recommend that all clinicians working with suicidal BPD patients obtain consultation and supervision as needed when using these strategies.
Self-injurious behavior in borderline personality disorder (BPD) patients can be divided into 2 categories: suicide attempts and nonsuicidal self-injury.
- Suicide attempts are performed with some evidence of intent to die.5
- Nonsuicidal self-injury behaviors (NSIB) are performed without intent to die.6
How can clinicians respond effectively when suicidal behaviors are repetitive and performed both with and without the intent to die? Although patients may perform NSIB for reasons other than intent to die (such as to express anger, punish oneself, or relieve distress),7 these behaviors require active intervention because of the possibility of serious injury (intentional or accidental). Also, the intent of a self-injurious behavior may change as the patient performs the behavior; what started as a nonsuicidal act may turn into a suicide attempt.6 Therefore, address all potentially harmful behaviors.
Risk factors for suicidal behavior
Several risk factors for suicide attempts and completed suicide among individuals diagnosed with BPD have been identified. Previous suicide attempts are one of the strongest predictors of completed suicide and suicide attempts in individuals with BPD.10-12 In general, clinicians cannot accurately predict which individuals will die by suicide.10,13 Suicide risk factors identified in BPD ( Table 1 )12-16 are similar to those in persons without the BPD diagnosis. In BPD patients, risk factors for attempted and completed suicide largely overlap.
Individuals with BPD may be distinguished by elevated risk factors for suicidal behavior as compared with suicide attempters without the BPD diagnosis. In a study comparing recent suicide attempters with and without BPD, those with BPD showed greater severity across a number of risk factors, including overall psychopathology, depression, hopelessness, suicide ideation, past suicide attempts, and social problem solving skills.8
Table 1
Common risk factors for suicidal behavior in BPD
| Behavioral factors Previous suicide attempts Impulsivity Aggression Poor social problem-solving skills Poor social adjustment |
| Cognitive/emotional factors Affective instability Hopelessness |
| Comorbid diagnoses Major depressive disorder Antisocial personality disorder Substance abuse disorders |
| Psychosocial/psychiatric history Childhood physical abuse Childhood sexual abuse Psychiatric hospitalizations |
| BPD: borderline personality disorder |
| Source: References 12-16 |
Remove lethal means
When working with patients with a history of suicidal behavior, it is critical to ensure the safety of the patient’s environment. Restricting access to lethal means has been shown to be an effective form of suicide prevention.17 Direct all patients with a history of recent suicidality or nonsuicidal self-injurious behavior (NSIB) to remove lethal means and means of self-harm from their homes and possession ( Table 2 ). Continue to monitor access to lethal means throughout treatment, as patients may acquire new means or reveal possession of items they had previously concealed.
We have found the following metaphor useful in discussing with patients the rationale for removing lethal means: “If you were on a diet, would it make sense to have a chocolate cake in the house?” Objections to removing lethal means often reveal important therapeutic issues. For example, those unwilling to relinquish lethal means may not be fully committed to giving up suicide or NSIB as an option. This would become a critical treatment goal.18
Tell patients to remove or discard fire-arms, knives, razors, and pills, as well as other items used in past suicide attempts/NSIB. Although patients can acquire new lethal means, removing immediate access lowers the possibility of an impulsive suicide attempt or NSIB and may give the patient time to reconsider.
Address overdose risk. Some physicians are reluctant or refuse to prescribe medication to BPD patients out of fear that it will be used to attempt suicide. A more productive approach is to ensure through informed choice of medications and strict management of their distribution that the patient safely and consistently receives necessary treatment.
Avoid prescribing psychiatric medications in quantities that could be lethal in overdose. Also determine whether the patient has other potentially lethal medications. If possible, have a friend or family member keep and administer the patient’s medications. If this is not possible, consider prescribing medications 1 week at a time.
Monitor as needed. If a patient continues to refuse to part with lethal means:
- involve family members or friends in removing and monitoring the patient’s lethal means
- assess the degree of imminent danger and if the individual can be safely managed as an outpatient.
Create a safety plan. Every BPD patient with a history of suicidality needs a detailed safety plan for what to do when suicidal ( Table 3 ).19,20 Inform family members (and friends, when appropriate) of the safety plan, and involve them as needed to monitor a patient at risk. Give your BPD patients clear instructions about when you will be available by phone and emergency contacts for when you are not available.
Table 2
7 clinical tips for managing safety in BPD patients
| Work with the patient in every session to remove all potentially lethal means (guns, knives, razors, pills) from his or her home and possession |
| Create a detailed safety plan to use during a suicidal crisis |
| Assess suicide risk in every session |
| Involve family and friends if possible to help monitor the patient and to call you or 911 if the patient appears to be in imminent danger of suicidal behavior |
| Create a ‘hope kit’ ( Box 2 ) as a companion to the safety plan |
| Consider hospitalization if the patient is in imminent danger of suicidal behavior or has engaged in suicidal behavior requiring medical attention |
| Consult with other clinicians about crucial safety management decisions, such as whether or not to hospitalize a patient |
| BPD: borderline personality disorder |
Lifeline for suicidal patients: What to include in a safety plan
| Warning signs of a suicidal crisis for that individual (such as increased depression or negative thinking) |
| Coping skills the patient can perform on his or her own |
| Family members and friends the patient can contact in an emergency |
| Therapist’s contact information |
| Phone numbers of emergency services available 24 hours daily (such as 911, suicide hotlines) |
| Source: References 19,20 |
Assess suicide risk
In every session, assess suicidal ideation, plans, intent, and urges to engage in NSIB. Consider using:
- self-monitoring forms, such as a dialectical behavior therapy (DBT) “diary card,” on which the patient each day records urges to self-harm or attempt suicide18
- Beck Depression Inventory (which contains a question about suicidal ideation).28
Risk assessment is not always straightforward. We have found that patients do not always provide consistent and/or accurate information about their degree of suicidality, making it difficult to know how to intervene. Reasons may include:
- fear of hospitalization
- uncertainty about whether or not they will attempt suicide
- desire to conceal a planned suicide attempt.
Hospitalize for suicidality?
If possible, consult with other professionals when making difficult decisions about hospitalizing a patient. These decisions often are subjective and open to influence by therapists’ emotional reactions. Psychotherapies for BPD emphasize the importance of consulting with other clinicians when working with this population. DBT requires a therapist consultation meeting, and cognitive therapies also have recommended consultation.18-20
If you work alone in private practice, consider consulting by phone with colleagues experienced with working with BPD patients. Document this consultation to help protect yourself from liability should an adverse outcome occur.
Little evidence supports hospitalization as an effective treatment for suicidality in BPD.24 It has been argued that hospitalization might increase future suicidal behavior when the patient perceives it as a positive experience or a means of escaping problems.18 The patient’s safety must remain a top priority, however, and we recommend admission if the patient is in imminent danger or has engaged in self-injurious behavior requiring medical attention.
The length of a hospital stay should be determined on a case-by-case basis. In general, it has been recommended that hospitalization for BPD patients be crisis-oriented and brief to avoid reinforcing suicidal behavior and to promote coping with suicidality in the natural environment.18,24 Also take into account acute exacerbation of comorbid Axis I diagnoses when determining the duration of hospitalization.
‘No-suicide’ contracts. Be careful not to rely on “no-suicide” contracts. They have no legal standing and may give you a false sense of security. Clearly, a patient may attempt suicide despite promising not to do so.
Asking if the patient can commit to staying safe for a specified time can be useful in assessing his/her level of suicidality and motivation to behave safely, but this is no substitute for a thorough clinical evaluation. Consider increasing the level of care and degree of monitoring or hospitalization if other suicide risk factors are elevated, even if the patient has “contracted for safety.”
Validated psychotherapies
Psychotherapy is the primary treatment for BPD, according to American Psychiatric Association (APA) guidelines.1 DBT,21-22 transference-focused therapy,25 and mentalization-based therapy26 are 3 validated psychotherapeutic approaches for BPD that have been shown to reduce suicide attempt rates in randomized clinical trials (RCTs). DBT has the greatest number of RCTs supporting its efficacy. We advise clinicians who work frequently with BPD patients to become familiar with these effective, empirical treatments.
A recent open trial of cognitive therapy for BPD demonstrated a decrease in self-harm behaviors.27 Cognitive therapy for recent suicide attempters—including those with BPD—decreased subsequent suicide attempts by approximately 50% over 18 months of follow-up in a RCT.28
Target suicidality. For all patients with a recent suicide attempt, make suicidal behavior the primary treatment target.18-20 Work with the patient on skills to reduce suicidal behavior, rather than assuming the behavior will resolve after you treat the psychiatric disorder (such as depression or BPD).
Throughout treatment, make suicidality or NSIB the priority in sessions whenever it occurs.18 This ensures that self-harm behavior is adequately addressed and provides an aversive consequence for this behavior. The patient cannot talk about other topics he/she might want to discuss until the suicidal behavior is addressed.18
Also target risk factors for suicidal behavior, such as depression, hopelessness, substance abuse, impulsivity, affective instability, social adjustment, and social problem-solving skills.
Teach coping skills. Because suicide attempts and NSIB in BPD often occur as maladaptive means of coping with distress, teach your patient alternatives such as distraction and self-soothing techniques, relaxation, positive self-statements, problem-solving skills, and how to use social support.18-20 The patient is likely to be flooded with affect when suicidal, so teach simple, easy-to-perform coping skills. Because self-harm behaviors in BPD patients often occur impulsively, create a written safety plan in advance. A “hope kit” can be an extremely useful part of the safety plan ( Box 2 ).18,18,27
A ‘hope kit’ can be an extremely useful intervention with recent suicide attempters.18,19 In a randomized, controlled trial, use of a hope kit as part of cognitive therapy for recent suicide attempters decreased suicide attempt rates by approximately 50%, compared with treatment as usual plus case management.27
Instruct the patient to fill a box or container with tangible reminders of reasons to live (such as photos of loved ones) and cues to use coping skills (a relaxation tape, a comic book, music, positive written self-statements). Tell the patient to keep the hope kit easily accessible and use it to guide positive coping during a suicidal crisis.
Symptom-guided medication
Use pharmacotherapy to complement psychotherapy for BPD and to address comorbid Axis I conditions. The BPD symptom domains targeted by medications may be sorted into 3 categories: ( Table 4 ):1
- affective dysregulation
- impulsive behavioral dyscontrol
- cognitive and perceptual problems.
Recommendations for pharmacologic management in BPD are based on a relatively small number of studies. Medication can decrease symptoms and increase the patient’s ability and willingness to engage in therapy. However, no drug has been proven effective or received FDA approval to treat BPD. Thus, our prescribing recommendations—though based on available evidence—are off-label uses.
In our experience, BPD patients often are prescribed multiple medications, probably because no single medication targets all symptoms of the disorder. To avoid the accumulation of medications that have lost or have not demonstrated therapeutic effect, we recommend caution when addressing BPD pathology with polypharmacy.
Table 4
Symptom-guided approach to medication for BPD patients
| Symptom domain | Medication(s) |
|---|---|
| Affective dysregulation | SSRI (first-line) or mood stabilizer (second-line) |
| Impulsive behavioral dyscontrol | SSRI and/or low-dose atypical antipsychotic |
| Cognitive and perceptual problems, acute dissociation/psychotic symptoms | Low-dose atypical antipsychotic |
| Acute anxiety (severe) | Low-dose atypical antipsychotic |
| Chronic anxiety | SSRI |
| BPD: borderline personality disorder; SSRI: selective serotonin reuptake inhibitor | |
| Source: Reference 1 | |
Antidepressants. APA guidelines suggest a selective serotonin reuptake inhibitor (SSRI) as the first-line initial treatment for affective dysregulation and impulsive behavioral dyscontrol.1,35-37 Because reports have shown increased risk of suicidal thoughts and behaviors with SSRI use in children, adolescents, and young adults,38 follow FDA guidelines for monitoring these populations during the first 12 weeks of therapy.39
Dosages typically are lower than those used to treat Axis I psychotic disorders. Because of clozapine’s complex maintenance and potential for side effects, consider using it only after trials of other antipsychotics have failed. Also consider short-term antipsychotic use to manage acute symptoms such as dissociation, intense paranoia, hostility, or severe anxiety.
Agents to consider with caution. Because of the potential for abuse, tolerance, overdose, and behavioral disinhibition, be very cautious when using benzodiazepines to treat chronic and acute anxiety in BPD patients.1
Tricyclic antidepressants and monoamine oxidase inhibitors are at times recommended for medication-resistant patients. Avoid these drugs in highly suicidal BPD patients because of the potential for lethal overdose.
Related resources
- Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
- Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cognit Behav Pract. 2004;11:265-277.
- Behavioral Tech, LLC. Training courses in dialectical behavior therapy. www.behavioraltech.org.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The authors thank Ira Lesser, MD, for reviewing and providing feedback on this article.
1. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
2. Zanarini MC, Frankenburg FR, Hennen J, et al. The McLean study of adult development: overview and implications of the first six years of prospective follow-up. J Personal Disord. 2005;19(5):505-523.
3. Paris J. Chronic suicidality among patients with borderline personality disorder. Psychiatr Serv. 2002;53(6):738-742.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. O’Carroll PW, Berman AL, Maris RW, et al. Beyond the Tower of Babel: a nomenclature for suicidology. Suicide Life Threat Behav. 1996;26(3):237-252.
6. Miller AL, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: Guilford; 2007.
7. Brown MZ, Comtois KA, Linehan MM. Reasons for suicide attempts and nonsuicidal self-injury in women with borderline personality disorder. J Abnorm Psychol. 2002;111(1):198-202.
8. Berk MS, Jeglic E, Brown GK, et al. Characteristics of recent suicide attempters with and without borderline personality disorder. Arch Suicide Res. 2007;11(1):91-104.
9. Soloff PH, Lynch KG, Kelly TM, et al. Characteristics of suicide attempts of patients with major depressive episode and borderline personality disorder: a comparative study. Am J Psychiatry. 2000;157(4):601-608.
10. Paris J, Nowlis D, Brown R. Predictors of suicide in borderline personality disorder. Can J Psychiatry. 1989;34(1):8-9.
11. Paris J. Completed suicide in borderline personality disorder. Psychiatr Ann. 1990;20:19-21.
12. Soloff PH, Fabio A. Prospective predictors of suicide attempts in borderline personality disorder at one, two, and two-to-five year follow-up. J Personal Disord. 2008;22(2):123-134.
13. Oldham JM. Borderline personality disorder and suicidality. Am J Psychiatry. 2006;163(1):20-26.
14. Black DW, Blum N, Pfohl B, et al. Suicidal behavior in borderline personality disorder: prevalence, risk factors, prediction, and prevention. J Personal Disord. 2004;18(3):226-239.
15. Kolla NJ, Eisenberg H, Links PS. Epidemiology, risk factors, and psychopharmacological management of suicidal behavior in borderline personality disorder. Arch Suicide Res. 2008;12(1):1-19.
16. McGirr A, Paris J, Lesage A. Risk factors for suicide completion in borderline personality disorder: a case control study of cluster B comorbidity and impulsive aggression. J Clin Psychiatry. 2007;68:721-729.
17. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
18. Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
19. Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cogn Behav Pract. 2004;11:265-277.
20. Wenzel A, Brown GK, Beck AT. Cognitive therapy for suicidal patients: scientific and clinical applications. Washington, DC: APA Books; 2008.
21. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48(12):1060-1064.
22. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
23. Beck AT, Steer RA, Brown GK. The Beck Depression Inventory, 2nd ed. San Antonio, TX: Psychological Corporation; 1996.
24. Paris J. Is hospitalization useful for suicidal patients with borderline personality disorder? J Personal Disord. 2004;18(3):240-247.
25. Clarkin JF, Levy KN, Lenzenweger MF, et al. Evaluating three treatments for borderline personality disorder: a multiwave study. Am J Psychiatry. 2007;164(6):1-7.
26. Bateman A, Fonagy P. Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial. Am J Psychiatry. 1999;156(10):1563-1569.
27. Brown GK, Newman CF, Charlesworth SE, et al. An open clinical trial of cognitive therapy for borderline personality disorder. J Personal Disord. 2004;18(3):257-271.
28. Brown GK, Tenhave T, Henriques GR, et al. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial. JAMA. 2005;294(5):563-570.
29. Benedetti F, Sforzini L, Colombo C, et al. Low-dose clozapine in acute and continuation treatment of severe borderline personality disorder. J Clin Psychiatry. 1998;59(3):103-107.
30. Chengappa KN, Ebeling T, Kang JS, et al. Clozapine reduces severe self-mutilation and aggression in psychotic patients with borderline personality disorder. J Clin Psychiatry. 1999;60(7):477-484.
31. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;15;46(10):1429-1435.
32. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
33. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
34. Nickel MK, Loew TH, Pedrosa Gil F. Aripiprazole in treatment of borderline patients, part II: an 18-month follow-up. Psychopharmacology (Berl). 2007;191(4):1023-1026.
35. Coccaro E, Kavoussi R. Fluoxetine and impulsive aggressive behavior in personality disordered subjects. Arch Gen Psychiatry. 1997;54:1081-1088.
36. Kallioniemi H, Syvalahti E. Citalopram, a specific inhibitor of serotonin reuptake, in treatment of psychotic and borderline patients. Nord J Psychiatry. 1993;47(suppl 28):79-84.
37. Kavoussi R, Liu J, Coccaro E. An open trial of sertraline in borderline personality disordered patients with impulsive aggression. J Clin Psychiatry. 1994;55:137-141.
38. FDA public health advisory: suicidality in children and adolescents being treated with antidepressant medications. Silver Spring, MD: U.S. Food and Drug Administration; October 15, 2004. Available at: http://www.fda.gov/cder/drug/antidepressants/SSRIPHA200410.htm. Accessed March 18, 2009.
39. Medication guide: about using antidepressants in children and teenagers. Silver Spring, MD: U.S. Food and Drug Administration; 2005. Available at: http://www.fda.gov/cder/drug/antidepressants/MG_template.pdf. Accessed March 18, 2009.
1. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
2. Zanarini MC, Frankenburg FR, Hennen J, et al. The McLean study of adult development: overview and implications of the first six years of prospective follow-up. J Personal Disord. 2005;19(5):505-523.
3. Paris J. Chronic suicidality among patients with borderline personality disorder. Psychiatr Serv. 2002;53(6):738-742.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. O’Carroll PW, Berman AL, Maris RW, et al. Beyond the Tower of Babel: a nomenclature for suicidology. Suicide Life Threat Behav. 1996;26(3):237-252.
6. Miller AL, Rathus JH, Linehan MM. Dialectical behavior therapy with suicidal adolescents. New York, NY: Guilford; 2007.
7. Brown MZ, Comtois KA, Linehan MM. Reasons for suicide attempts and nonsuicidal self-injury in women with borderline personality disorder. J Abnorm Psychol. 2002;111(1):198-202.
8. Berk MS, Jeglic E, Brown GK, et al. Characteristics of recent suicide attempters with and without borderline personality disorder. Arch Suicide Res. 2007;11(1):91-104.
9. Soloff PH, Lynch KG, Kelly TM, et al. Characteristics of suicide attempts of patients with major depressive episode and borderline personality disorder: a comparative study. Am J Psychiatry. 2000;157(4):601-608.
10. Paris J, Nowlis D, Brown R. Predictors of suicide in borderline personality disorder. Can J Psychiatry. 1989;34(1):8-9.
11. Paris J. Completed suicide in borderline personality disorder. Psychiatr Ann. 1990;20:19-21.
12. Soloff PH, Fabio A. Prospective predictors of suicide attempts in borderline personality disorder at one, two, and two-to-five year follow-up. J Personal Disord. 2008;22(2):123-134.
13. Oldham JM. Borderline personality disorder and suicidality. Am J Psychiatry. 2006;163(1):20-26.
14. Black DW, Blum N, Pfohl B, et al. Suicidal behavior in borderline personality disorder: prevalence, risk factors, prediction, and prevention. J Personal Disord. 2004;18(3):226-239.
15. Kolla NJ, Eisenberg H, Links PS. Epidemiology, risk factors, and psychopharmacological management of suicidal behavior in borderline personality disorder. Arch Suicide Res. 2008;12(1):1-19.
16. McGirr A, Paris J, Lesage A. Risk factors for suicide completion in borderline personality disorder: a case control study of cluster B comorbidity and impulsive aggression. J Clin Psychiatry. 2007;68:721-729.
17. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
18. Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York, NY: Guilford Press; 1993.
19. Berk MS, Henriques GR, Warman DM, et al. Cognitive therapy for suicide attempters: overview of the treatment and case examples. Cogn Behav Pract. 2004;11:265-277.
20. Wenzel A, Brown GK, Beck AT. Cognitive therapy for suicidal patients: scientific and clinical applications. Washington, DC: APA Books; 2008.
21. Linehan MM, Armstrong HE, Suarez A, et al. Cognitive behavioral treatment of chronically parasuicidal borderline patients. Arch Gen Psychiatry. 1991;48(12):1060-1064.
22. Linehan MM, Comtois KA, Murray AM, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. 2006;63(7):757-766.
23. Beck AT, Steer RA, Brown GK. The Beck Depression Inventory, 2nd ed. San Antonio, TX: Psychological Corporation; 1996.
24. Paris J. Is hospitalization useful for suicidal patients with borderline personality disorder? J Personal Disord. 2004;18(3):240-247.
25. Clarkin JF, Levy KN, Lenzenweger MF, et al. Evaluating three treatments for borderline personality disorder: a multiwave study. Am J Psychiatry. 2007;164(6):1-7.
26. Bateman A, Fonagy P. Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial. Am J Psychiatry. 1999;156(10):1563-1569.
27. Brown GK, Newman CF, Charlesworth SE, et al. An open clinical trial of cognitive therapy for borderline personality disorder. J Personal Disord. 2004;18(3):257-271.
28. Brown GK, Tenhave T, Henriques GR, et al. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial. JAMA. 2005;294(5):563-570.
29. Benedetti F, Sforzini L, Colombo C, et al. Low-dose clozapine in acute and continuation treatment of severe borderline personality disorder. J Clin Psychiatry. 1998;59(3):103-107.
30. Chengappa KN, Ebeling T, Kang JS, et al. Clozapine reduces severe self-mutilation and aggression in psychotic patients with borderline personality disorder. J Clin Psychiatry. 1999;60(7):477-484.
31. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;15;46(10):1429-1435.
32. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
33. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
34. Nickel MK, Loew TH, Pedrosa Gil F. Aripiprazole in treatment of borderline patients, part II: an 18-month follow-up. Psychopharmacology (Berl). 2007;191(4):1023-1026.
35. Coccaro E, Kavoussi R. Fluoxetine and impulsive aggressive behavior in personality disordered subjects. Arch Gen Psychiatry. 1997;54:1081-1088.
36. Kallioniemi H, Syvalahti E. Citalopram, a specific inhibitor of serotonin reuptake, in treatment of psychotic and borderline patients. Nord J Psychiatry. 1993;47(suppl 28):79-84.
37. Kavoussi R, Liu J, Coccaro E. An open trial of sertraline in borderline personality disordered patients with impulsive aggression. J Clin Psychiatry. 1994;55:137-141.
38. FDA public health advisory: suicidality in children and adolescents being treated with antidepressant medications. Silver Spring, MD: U.S. Food and Drug Administration; October 15, 2004. Available at: http://www.fda.gov/cder/drug/antidepressants/SSRIPHA200410.htm. Accessed March 18, 2009.
39. Medication guide: about using antidepressants in children and teenagers. Silver Spring, MD: U.S. Food and Drug Administration; 2005. Available at: http://www.fda.gov/cder/drug/antidepressants/MG_template.pdf. Accessed March 18, 2009.
What is your patient’s predicament? Knowing can inform clinical care
Eight weeks after his wife died from an unexpected illness, Mr. M, age 55, remains overwhelmed, disconsolate, and virtually incapacitated. Previously in good health and a successful accountant, he struggles with low mood, guilt, anxiety, and anhedonia and is troubled by feelings of helplessness and hopelessness. “My life has been turned upside down,” he says.
His primary care physician’s support and encouragement—along with hypnotics, an anxiolytic, and antidepressants—have done little to improve his sleep and mood or relieve his emotional suffering. Mr. M has resumed work for financial reasons but returns home exhausted and demoralized, shunning the few friends who call. He has no history of a mood disorder or substance abuse. He has never expressed suicidal or homicidal ideation and shows no evidence of psychotic symptoms. He is referred to a psychiatrist for what his physician regards as a treatment-resistant depression.
When a patient’s symptoms seem disproportionate to apparent stressors, I call this presentation a patient’s predicament: a unique, profoundly unsettling, but poorly understood misgiving that something is wrong—perhaps terribly so—and that life may never be the same again (Table). Emotional flooding typically overwhelms these patients, and they are unable to express what they are experiencing.
For mental health professionals, the concept of a predicament is useful when working with patients who are moderately to severely ill or facing a life-diminishing or life-threatening illness.
Table
Patient in a predicament? Look for these 6 clues
| Shows an unusual, disproportionate, or prolonged response to a distressing experience |
| Is incapacitated by persistent suffering and misery |
| Expresses feelings of drastic personal change, turmoil, life disruption, or hopelessness |
| Describes feeling lost, bewildered, and helpless or shows behavioral equivalents (such as aimlessness, loss of purpose) |
| Experiences difficulty achieving or maintaining an expected response to conventional and evidence-based treatment in the absence of psychosis |
| Demonstrates a clinical course punctuated by noncompliance with treatment that suggests the patient may have given up or feels unworthy of relief |
Affected by a ‘field of forces’
I conceptualize Mr. M’s unrelieved suffering as resulting from 1 or more threats—typically not fully appreciated by the patient—to important elements that undergird and sustain his sense of self. A predicament can be related to:
- Eric Cassell’s conception of suffering that accompanies threats to an individual’s sense of “personhood” in terms of its many domains1
- Thomas Merton’s concept of emotional destabilization caused by threats to a person’s “false self”2
- William Shaver’s concept of a person’s fragile “illusory self” and threats to “safety zones” that protect it.3
Patients experience a predicament as an emotional perturbation caused by something that has happened to them or is evolving from an acute loss, trauma, acute or chronic illness, unpleasant occurrence, or a recommended medical intervention. A predicament may embody multiple dimensions (biological, psychological, interpersonal, familial, occupational, spiritual, existential, economic, ethnic, and cultural).
Extrapolating from a social science concept, these dimensions comprise a “field of forces”—the interplay of internal and external, proximate, and global factors—that act on an individual (Figure). These forces:
- contribute to a person’s sense of self and shape the manner in which that self is manifested to others—including the attending physician
- do not invalidate or discount the importance of the patient’s transference but may cloud it and render it less “transparent.”
Treatment resistance? A biomedical intervention focused on symptoms or a prominent symptom complex may be partially effective but result in a lowered threshold for recurrences. Although both patient and psychiatrist feel relief when symptoms abate, the individual is not necessarily healed. The disorder may continue to affect the patient, his family, his work performance, or other aspects of life.
One might conclude that this is a “treatment-resistant” depression or a “difficult patient” who has somehow not responded as anticipated. Yet, as author Norman Cousins observed from his experience with life-threatening illness, “patients are a vast collection of emotional needs, and understanding how patients are affected by serious illness as well as the illness itself paves the way for communicating without crippling the patient.”4
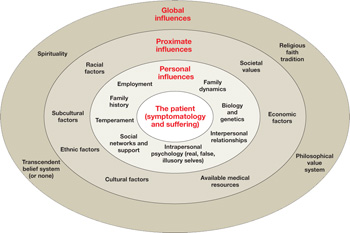
Figure A predicament comprises an interactive ‘field of forces’
The patient resides at the epicenter of inborn and external factors that make up his or her interactive, multidimensional environment. Concentric rings convey the interplay of personal, proximate, and global influences with which the patient must cope, whether or not he or she is aware of these influences.
Exploring the predicament
By sensitively exploring the personal story behind the patient’s presenting symptoms (the predicament the patient is in), you become a nonjudgmental, affirming witness to that story. Simultaneously, you can urge the patient to consider how he or she might have arrived at the state of feeling overwhelmed (a process of demystification and early insight aptly described by psychotherapist Anthony Storr as “making the incomprehensible comprehensible”5).
This conceptualization of a patient’s predicament regards the presenting problem as best understood and treated using a biopsychosocial model of causation (an amplification by George L. Engel of Adolf Meyer’s concept of psychobiology) combined with a systemic view of how these dimensions interact with each other, both within and upon the patient at any point in time.6–8
Dimensions of a predicament. A person functions and experiences his or her sense of self within a multidimensional environment. Mr. M’s predicament embodies numerous dimensions:
- Biological. Pharmacologic interventions intended to contain Mr. M’s distress have helped, but his acute grief and bereavement have merged into a severe major depressive episode.
- Psychological, with counter-dependency. Further exploration reveals that the abrupt loss of his wife unmasked a repressed, lifelong passive-dependency. Until she died, Mr. M had been able to compensate by the sense of control afforded by his profession and his pride in being self-reliant.
- Spiritual. The loss—and anger associated with it—seriously undermined Mr. M’s faith because he felt that “God let my wife die.”
- Interpersonal and social. Mr. M is aware that his wife’s death severed his few connections with her friends and community activities.
- Existential. He feels distressingly alone in an unfriendly world in which he had never felt comfortable.
- Ethnic, familial, economic, cultural, and societal. Mr. M is struggling with the emergence of a life-long sense of inferiority, insecurity, guilt, and self-consciousness related to his immigrant parents’ low socioeconomic status.
I do not believe that medicine and skillful manipulation of central nervous system neurotransmitters can cure this kind of multidimensional, cumulative misery. One is reminded of neo-Freudian Harry Stack Sullivan’s view that “it takes people to make people sick, and it takes people to make people well.”9
CASE CONTINUED: The ‘real work’ begins
Mr. M begins to improve as these factors are elicited and introduced in therapy as dynamic elements of the “field of forces” in which he finds himself struggling. This process essentially detoxifies Mr. M’s misery. He says, “I guess it’s not surprising that I have felt as bad as I have, despite my doctor’s help.”
Insights gained—as well as medication and the psychiatrist’s support and encouragement—are synergistic, and his mood slowly lifts. Mr. M now can begin the difficult work of achieving a more stable sense of security and a closer approximation to his undiscovered “real self” that has eluded him.6 He also is beginning to perceive how his wife’s death has revealed a pre-existing dependency—with persistent fears of abandonment—that left him vulnerable to losses.
Exploring a patient’s predicament is not symptom-focused per se. Some psychiatrists may feel they don’t have time to explore the nature of a patient’s predicament because of managed care constraints or lack of training and experience in using explorative and interpretive psychodynamic techniques. Psychiatrists who employ cognitive-behavioral therapy and related approaches may be uncomfortable or unfamiliar with a biopsychosocial and systems orientation to patient evaluation and treatment that considers the entire context—past and present—in which symptoms emerge.
One could argue, however, that not exploring a patient’s predicament would correspond biomedically to identifying the presence of symptoms (such as anemia, hypertension, a phobia, or orthopnea) but not basing treatment on comprehending their pathophysiology.
Serving the patient’s interests. In psychiatric practice, patients’ interests usually are best served by treatment that is based on understanding their predicaments while refraining from being too distracted by vivid symptoms the components of their predicaments can produce. A biopsychosocial and systemic orientation is clinically useful because:
- The clinician develops a greater connectedness, empathy, and therapeutic leverage from apprehending the field of forces affecting the patient and fashions a treatment plan that takes these forces into consideration. Mr. M’s plan, for example, might include spiritual and financial counseling in addition to conventional treatment for a mood disorder.
- The patient feels the psychiatrist is interested, skilled, and attentive enough to inquire about troublesome areas the patient might or might not have thought were related to his condition.
- The psychiatrist is gratified to see the clinical benefit that can come from recognizing and understanding the patient’s plight when developing a comprehensive treatment plan.
As you gain experience in using this concept, the uniqueness of each person’s predicament will become clear more quickly, even as you encourage the patient to “connect the dots” of his suffering in terms of his personal biopsychosocial history. In doing so, patients will gain a measure of control over situations they had considered overwhelming and mystifying.
I do not consider my assessment of a new patient adequate until I have at least sketched out as many of the elements contributing to his or her distress as I can.
What about a patient’s symptoms?
An objection to a biopsychosocial/systemic approach is that some patients will resist attempts to redirect attention away from their presenting complaints. This very objection explains why you need to understand what forces underlie a patient’s “death grip” on his or her symptoms, while refraining from concluding that the patient has a treatment-resistant depression, requires ever more sophisticated polypharmacy, or is “untreatable.”
Finally, patients with a serious illness almost invariably experience a predicament—whether recognized or not—and it may render the clinical outcome less than satisfactory if you do not identify its elements and bring them into therapy when appropriate. Regardless of presenting symptoms or diagnosis—and independent of your theoretical orientation—experience suggests the usefulness of assuming every new patient is in a predicament. If you cannot address the predicament early in therapy, it is usually possible to do so after you and the patient develop a therapeutic relationship and you have used other interventions to lower the intensity of the target symptoms.
By helping patients understand more fully their unique predicaments, you can reduce their burdens, foster realistic hopefulness, and be gratified by having truly connected with what patients experience as serious threats to their sense of self.
Related resource
- Reiser D, Rosen D. Medicine as a human experience. Baltimore, MD: University Park Press; 1984 (an excellent reference on George L. Engel’s biopsychosocial concept, the care of patients, and the doctor-patient relationship).
Disclosure
Dr. Cowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassell E. The nature of suffering and the goals of medicine. N Engl J Med. 1982;306:639.-
2. Merton T. Real and false selves. In: Inchausti R, ed. Seeds. Boston, MA: Shambala Publications, Inc.; 2002:3-24.
3. Shaver W. Suffering and the role of abandonment of self. Journal of Hospice and Palliative Nursing. 2002;4(1):46-53.
4. Cousins N. Foreword. In: Reiser D, Rosen D, eds. Medicine as a human experience. Baltimore, MD: University Park Press; 1984:IX-XVI.
5. Storr A. The art of psychotherapy. New York, NY: Methuen, Inc; 1980.
6. Meyer A. Psychobiology: a science of man. Springfield, IL: Charles C. Thomas; 1957.
7. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-36.
8. Von Bertalanffy L. General systems theory. New York, NY: George Braziller, Inc; 1968.
9. Sullivan HS. Interpersonal theory of psychiatry. New York, NY: W.W. Norton & Company; 1953.
Eight weeks after his wife died from an unexpected illness, Mr. M, age 55, remains overwhelmed, disconsolate, and virtually incapacitated. Previously in good health and a successful accountant, he struggles with low mood, guilt, anxiety, and anhedonia and is troubled by feelings of helplessness and hopelessness. “My life has been turned upside down,” he says.
His primary care physician’s support and encouragement—along with hypnotics, an anxiolytic, and antidepressants—have done little to improve his sleep and mood or relieve his emotional suffering. Mr. M has resumed work for financial reasons but returns home exhausted and demoralized, shunning the few friends who call. He has no history of a mood disorder or substance abuse. He has never expressed suicidal or homicidal ideation and shows no evidence of psychotic symptoms. He is referred to a psychiatrist for what his physician regards as a treatment-resistant depression.
When a patient’s symptoms seem disproportionate to apparent stressors, I call this presentation a patient’s predicament: a unique, profoundly unsettling, but poorly understood misgiving that something is wrong—perhaps terribly so—and that life may never be the same again (Table). Emotional flooding typically overwhelms these patients, and they are unable to express what they are experiencing.
For mental health professionals, the concept of a predicament is useful when working with patients who are moderately to severely ill or facing a life-diminishing or life-threatening illness.
Table
Patient in a predicament? Look for these 6 clues
| Shows an unusual, disproportionate, or prolonged response to a distressing experience |
| Is incapacitated by persistent suffering and misery |
| Expresses feelings of drastic personal change, turmoil, life disruption, or hopelessness |
| Describes feeling lost, bewildered, and helpless or shows behavioral equivalents (such as aimlessness, loss of purpose) |
| Experiences difficulty achieving or maintaining an expected response to conventional and evidence-based treatment in the absence of psychosis |
| Demonstrates a clinical course punctuated by noncompliance with treatment that suggests the patient may have given up or feels unworthy of relief |
Affected by a ‘field of forces’
I conceptualize Mr. M’s unrelieved suffering as resulting from 1 or more threats—typically not fully appreciated by the patient—to important elements that undergird and sustain his sense of self. A predicament can be related to:
- Eric Cassell’s conception of suffering that accompanies threats to an individual’s sense of “personhood” in terms of its many domains1
- Thomas Merton’s concept of emotional destabilization caused by threats to a person’s “false self”2
- William Shaver’s concept of a person’s fragile “illusory self” and threats to “safety zones” that protect it.3
Patients experience a predicament as an emotional perturbation caused by something that has happened to them or is evolving from an acute loss, trauma, acute or chronic illness, unpleasant occurrence, or a recommended medical intervention. A predicament may embody multiple dimensions (biological, psychological, interpersonal, familial, occupational, spiritual, existential, economic, ethnic, and cultural).
Extrapolating from a social science concept, these dimensions comprise a “field of forces”—the interplay of internal and external, proximate, and global factors—that act on an individual (Figure). These forces:
- contribute to a person’s sense of self and shape the manner in which that self is manifested to others—including the attending physician
- do not invalidate or discount the importance of the patient’s transference but may cloud it and render it less “transparent.”
Treatment resistance? A biomedical intervention focused on symptoms or a prominent symptom complex may be partially effective but result in a lowered threshold for recurrences. Although both patient and psychiatrist feel relief when symptoms abate, the individual is not necessarily healed. The disorder may continue to affect the patient, his family, his work performance, or other aspects of life.
One might conclude that this is a “treatment-resistant” depression or a “difficult patient” who has somehow not responded as anticipated. Yet, as author Norman Cousins observed from his experience with life-threatening illness, “patients are a vast collection of emotional needs, and understanding how patients are affected by serious illness as well as the illness itself paves the way for communicating without crippling the patient.”4
Figure A predicament comprises an interactive ‘field of forces’
The patient resides at the epicenter of inborn and external factors that make up his or her interactive, multidimensional environment. Concentric rings convey the interplay of personal, proximate, and global influences with which the patient must cope, whether or not he or she is aware of these influences.
Exploring the predicament
By sensitively exploring the personal story behind the patient’s presenting symptoms (the predicament the patient is in), you become a nonjudgmental, affirming witness to that story. Simultaneously, you can urge the patient to consider how he or she might have arrived at the state of feeling overwhelmed (a process of demystification and early insight aptly described by psychotherapist Anthony Storr as “making the incomprehensible comprehensible”5).
This conceptualization of a patient’s predicament regards the presenting problem as best understood and treated using a biopsychosocial model of causation (an amplification by George L. Engel of Adolf Meyer’s concept of psychobiology) combined with a systemic view of how these dimensions interact with each other, both within and upon the patient at any point in time.6–8
Dimensions of a predicament. A person functions and experiences his or her sense of self within a multidimensional environment. Mr. M’s predicament embodies numerous dimensions:
- Biological. Pharmacologic interventions intended to contain Mr. M’s distress have helped, but his acute grief and bereavement have merged into a severe major depressive episode.
- Psychological, with counter-dependency. Further exploration reveals that the abrupt loss of his wife unmasked a repressed, lifelong passive-dependency. Until she died, Mr. M had been able to compensate by the sense of control afforded by his profession and his pride in being self-reliant.
- Spiritual. The loss—and anger associated with it—seriously undermined Mr. M’s faith because he felt that “God let my wife die.”
- Interpersonal and social. Mr. M is aware that his wife’s death severed his few connections with her friends and community activities.
- Existential. He feels distressingly alone in an unfriendly world in which he had never felt comfortable.
- Ethnic, familial, economic, cultural, and societal. Mr. M is struggling with the emergence of a life-long sense of inferiority, insecurity, guilt, and self-consciousness related to his immigrant parents’ low socioeconomic status.
I do not believe that medicine and skillful manipulation of central nervous system neurotransmitters can cure this kind of multidimensional, cumulative misery. One is reminded of neo-Freudian Harry Stack Sullivan’s view that “it takes people to make people sick, and it takes people to make people well.”9
CASE CONTINUED: The ‘real work’ begins
Mr. M begins to improve as these factors are elicited and introduced in therapy as dynamic elements of the “field of forces” in which he finds himself struggling. This process essentially detoxifies Mr. M’s misery. He says, “I guess it’s not surprising that I have felt as bad as I have, despite my doctor’s help.”
Insights gained—as well as medication and the psychiatrist’s support and encouragement—are synergistic, and his mood slowly lifts. Mr. M now can begin the difficult work of achieving a more stable sense of security and a closer approximation to his undiscovered “real self” that has eluded him.6 He also is beginning to perceive how his wife’s death has revealed a pre-existing dependency—with persistent fears of abandonment—that left him vulnerable to losses.
Exploring a patient’s predicament is not symptom-focused per se. Some psychiatrists may feel they don’t have time to explore the nature of a patient’s predicament because of managed care constraints or lack of training and experience in using explorative and interpretive psychodynamic techniques. Psychiatrists who employ cognitive-behavioral therapy and related approaches may be uncomfortable or unfamiliar with a biopsychosocial and systems orientation to patient evaluation and treatment that considers the entire context—past and present—in which symptoms emerge.
One could argue, however, that not exploring a patient’s predicament would correspond biomedically to identifying the presence of symptoms (such as anemia, hypertension, a phobia, or orthopnea) but not basing treatment on comprehending their pathophysiology.
Serving the patient’s interests. In psychiatric practice, patients’ interests usually are best served by treatment that is based on understanding their predicaments while refraining from being too distracted by vivid symptoms the components of their predicaments can produce. A biopsychosocial and systemic orientation is clinically useful because:
- The clinician develops a greater connectedness, empathy, and therapeutic leverage from apprehending the field of forces affecting the patient and fashions a treatment plan that takes these forces into consideration. Mr. M’s plan, for example, might include spiritual and financial counseling in addition to conventional treatment for a mood disorder.
- The patient feels the psychiatrist is interested, skilled, and attentive enough to inquire about troublesome areas the patient might or might not have thought were related to his condition.
- The psychiatrist is gratified to see the clinical benefit that can come from recognizing and understanding the patient’s plight when developing a comprehensive treatment plan.
As you gain experience in using this concept, the uniqueness of each person’s predicament will become clear more quickly, even as you encourage the patient to “connect the dots” of his suffering in terms of his personal biopsychosocial history. In doing so, patients will gain a measure of control over situations they had considered overwhelming and mystifying.
I do not consider my assessment of a new patient adequate until I have at least sketched out as many of the elements contributing to his or her distress as I can.
What about a patient’s symptoms?
An objection to a biopsychosocial/systemic approach is that some patients will resist attempts to redirect attention away from their presenting complaints. This very objection explains why you need to understand what forces underlie a patient’s “death grip” on his or her symptoms, while refraining from concluding that the patient has a treatment-resistant depression, requires ever more sophisticated polypharmacy, or is “untreatable.”
Finally, patients with a serious illness almost invariably experience a predicament—whether recognized or not—and it may render the clinical outcome less than satisfactory if you do not identify its elements and bring them into therapy when appropriate. Regardless of presenting symptoms or diagnosis—and independent of your theoretical orientation—experience suggests the usefulness of assuming every new patient is in a predicament. If you cannot address the predicament early in therapy, it is usually possible to do so after you and the patient develop a therapeutic relationship and you have used other interventions to lower the intensity of the target symptoms.
By helping patients understand more fully their unique predicaments, you can reduce their burdens, foster realistic hopefulness, and be gratified by having truly connected with what patients experience as serious threats to their sense of self.
Related resource
- Reiser D, Rosen D. Medicine as a human experience. Baltimore, MD: University Park Press; 1984 (an excellent reference on George L. Engel’s biopsychosocial concept, the care of patients, and the doctor-patient relationship).
Disclosure
Dr. Cowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Eight weeks after his wife died from an unexpected illness, Mr. M, age 55, remains overwhelmed, disconsolate, and virtually incapacitated. Previously in good health and a successful accountant, he struggles with low mood, guilt, anxiety, and anhedonia and is troubled by feelings of helplessness and hopelessness. “My life has been turned upside down,” he says.
His primary care physician’s support and encouragement—along with hypnotics, an anxiolytic, and antidepressants—have done little to improve his sleep and mood or relieve his emotional suffering. Mr. M has resumed work for financial reasons but returns home exhausted and demoralized, shunning the few friends who call. He has no history of a mood disorder or substance abuse. He has never expressed suicidal or homicidal ideation and shows no evidence of psychotic symptoms. He is referred to a psychiatrist for what his physician regards as a treatment-resistant depression.
When a patient’s symptoms seem disproportionate to apparent stressors, I call this presentation a patient’s predicament: a unique, profoundly unsettling, but poorly understood misgiving that something is wrong—perhaps terribly so—and that life may never be the same again (Table). Emotional flooding typically overwhelms these patients, and they are unable to express what they are experiencing.
For mental health professionals, the concept of a predicament is useful when working with patients who are moderately to severely ill or facing a life-diminishing or life-threatening illness.
Table
Patient in a predicament? Look for these 6 clues
| Shows an unusual, disproportionate, or prolonged response to a distressing experience |
| Is incapacitated by persistent suffering and misery |
| Expresses feelings of drastic personal change, turmoil, life disruption, or hopelessness |
| Describes feeling lost, bewildered, and helpless or shows behavioral equivalents (such as aimlessness, loss of purpose) |
| Experiences difficulty achieving or maintaining an expected response to conventional and evidence-based treatment in the absence of psychosis |
| Demonstrates a clinical course punctuated by noncompliance with treatment that suggests the patient may have given up or feels unworthy of relief |
Affected by a ‘field of forces’
I conceptualize Mr. M’s unrelieved suffering as resulting from 1 or more threats—typically not fully appreciated by the patient—to important elements that undergird and sustain his sense of self. A predicament can be related to:
- Eric Cassell’s conception of suffering that accompanies threats to an individual’s sense of “personhood” in terms of its many domains1
- Thomas Merton’s concept of emotional destabilization caused by threats to a person’s “false self”2
- William Shaver’s concept of a person’s fragile “illusory self” and threats to “safety zones” that protect it.3
Patients experience a predicament as an emotional perturbation caused by something that has happened to them or is evolving from an acute loss, trauma, acute or chronic illness, unpleasant occurrence, or a recommended medical intervention. A predicament may embody multiple dimensions (biological, psychological, interpersonal, familial, occupational, spiritual, existential, economic, ethnic, and cultural).
Extrapolating from a social science concept, these dimensions comprise a “field of forces”—the interplay of internal and external, proximate, and global factors—that act on an individual (Figure). These forces:
- contribute to a person’s sense of self and shape the manner in which that self is manifested to others—including the attending physician
- do not invalidate or discount the importance of the patient’s transference but may cloud it and render it less “transparent.”
Treatment resistance? A biomedical intervention focused on symptoms or a prominent symptom complex may be partially effective but result in a lowered threshold for recurrences. Although both patient and psychiatrist feel relief when symptoms abate, the individual is not necessarily healed. The disorder may continue to affect the patient, his family, his work performance, or other aspects of life.
One might conclude that this is a “treatment-resistant” depression or a “difficult patient” who has somehow not responded as anticipated. Yet, as author Norman Cousins observed from his experience with life-threatening illness, “patients are a vast collection of emotional needs, and understanding how patients are affected by serious illness as well as the illness itself paves the way for communicating without crippling the patient.”4
Figure A predicament comprises an interactive ‘field of forces’
The patient resides at the epicenter of inborn and external factors that make up his or her interactive, multidimensional environment. Concentric rings convey the interplay of personal, proximate, and global influences with which the patient must cope, whether or not he or she is aware of these influences.
Exploring the predicament
By sensitively exploring the personal story behind the patient’s presenting symptoms (the predicament the patient is in), you become a nonjudgmental, affirming witness to that story. Simultaneously, you can urge the patient to consider how he or she might have arrived at the state of feeling overwhelmed (a process of demystification and early insight aptly described by psychotherapist Anthony Storr as “making the incomprehensible comprehensible”5).
This conceptualization of a patient’s predicament regards the presenting problem as best understood and treated using a biopsychosocial model of causation (an amplification by George L. Engel of Adolf Meyer’s concept of psychobiology) combined with a systemic view of how these dimensions interact with each other, both within and upon the patient at any point in time.6–8
Dimensions of a predicament. A person functions and experiences his or her sense of self within a multidimensional environment. Mr. M’s predicament embodies numerous dimensions:
- Biological. Pharmacologic interventions intended to contain Mr. M’s distress have helped, but his acute grief and bereavement have merged into a severe major depressive episode.
- Psychological, with counter-dependency. Further exploration reveals that the abrupt loss of his wife unmasked a repressed, lifelong passive-dependency. Until she died, Mr. M had been able to compensate by the sense of control afforded by his profession and his pride in being self-reliant.
- Spiritual. The loss—and anger associated with it—seriously undermined Mr. M’s faith because he felt that “God let my wife die.”
- Interpersonal and social. Mr. M is aware that his wife’s death severed his few connections with her friends and community activities.
- Existential. He feels distressingly alone in an unfriendly world in which he had never felt comfortable.
- Ethnic, familial, economic, cultural, and societal. Mr. M is struggling with the emergence of a life-long sense of inferiority, insecurity, guilt, and self-consciousness related to his immigrant parents’ low socioeconomic status.
I do not believe that medicine and skillful manipulation of central nervous system neurotransmitters can cure this kind of multidimensional, cumulative misery. One is reminded of neo-Freudian Harry Stack Sullivan’s view that “it takes people to make people sick, and it takes people to make people well.”9
CASE CONTINUED: The ‘real work’ begins
Mr. M begins to improve as these factors are elicited and introduced in therapy as dynamic elements of the “field of forces” in which he finds himself struggling. This process essentially detoxifies Mr. M’s misery. He says, “I guess it’s not surprising that I have felt as bad as I have, despite my doctor’s help.”
Insights gained—as well as medication and the psychiatrist’s support and encouragement—are synergistic, and his mood slowly lifts. Mr. M now can begin the difficult work of achieving a more stable sense of security and a closer approximation to his undiscovered “real self” that has eluded him.6 He also is beginning to perceive how his wife’s death has revealed a pre-existing dependency—with persistent fears of abandonment—that left him vulnerable to losses.
Exploring a patient’s predicament is not symptom-focused per se. Some psychiatrists may feel they don’t have time to explore the nature of a patient’s predicament because of managed care constraints or lack of training and experience in using explorative and interpretive psychodynamic techniques. Psychiatrists who employ cognitive-behavioral therapy and related approaches may be uncomfortable or unfamiliar with a biopsychosocial and systems orientation to patient evaluation and treatment that considers the entire context—past and present—in which symptoms emerge.
One could argue, however, that not exploring a patient’s predicament would correspond biomedically to identifying the presence of symptoms (such as anemia, hypertension, a phobia, or orthopnea) but not basing treatment on comprehending their pathophysiology.
Serving the patient’s interests. In psychiatric practice, patients’ interests usually are best served by treatment that is based on understanding their predicaments while refraining from being too distracted by vivid symptoms the components of their predicaments can produce. A biopsychosocial and systemic orientation is clinically useful because:
- The clinician develops a greater connectedness, empathy, and therapeutic leverage from apprehending the field of forces affecting the patient and fashions a treatment plan that takes these forces into consideration. Mr. M’s plan, for example, might include spiritual and financial counseling in addition to conventional treatment for a mood disorder.
- The patient feels the psychiatrist is interested, skilled, and attentive enough to inquire about troublesome areas the patient might or might not have thought were related to his condition.
- The psychiatrist is gratified to see the clinical benefit that can come from recognizing and understanding the patient’s plight when developing a comprehensive treatment plan.
As you gain experience in using this concept, the uniqueness of each person’s predicament will become clear more quickly, even as you encourage the patient to “connect the dots” of his suffering in terms of his personal biopsychosocial history. In doing so, patients will gain a measure of control over situations they had considered overwhelming and mystifying.
I do not consider my assessment of a new patient adequate until I have at least sketched out as many of the elements contributing to his or her distress as I can.
What about a patient’s symptoms?
An objection to a biopsychosocial/systemic approach is that some patients will resist attempts to redirect attention away from their presenting complaints. This very objection explains why you need to understand what forces underlie a patient’s “death grip” on his or her symptoms, while refraining from concluding that the patient has a treatment-resistant depression, requires ever more sophisticated polypharmacy, or is “untreatable.”
Finally, patients with a serious illness almost invariably experience a predicament—whether recognized or not—and it may render the clinical outcome less than satisfactory if you do not identify its elements and bring them into therapy when appropriate. Regardless of presenting symptoms or diagnosis—and independent of your theoretical orientation—experience suggests the usefulness of assuming every new patient is in a predicament. If you cannot address the predicament early in therapy, it is usually possible to do so after you and the patient develop a therapeutic relationship and you have used other interventions to lower the intensity of the target symptoms.
By helping patients understand more fully their unique predicaments, you can reduce their burdens, foster realistic hopefulness, and be gratified by having truly connected with what patients experience as serious threats to their sense of self.
Related resource
- Reiser D, Rosen D. Medicine as a human experience. Baltimore, MD: University Park Press; 1984 (an excellent reference on George L. Engel’s biopsychosocial concept, the care of patients, and the doctor-patient relationship).
Disclosure
Dr. Cowell reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Cassell E. The nature of suffering and the goals of medicine. N Engl J Med. 1982;306:639.-
2. Merton T. Real and false selves. In: Inchausti R, ed. Seeds. Boston, MA: Shambala Publications, Inc.; 2002:3-24.
3. Shaver W. Suffering and the role of abandonment of self. Journal of Hospice and Palliative Nursing. 2002;4(1):46-53.
4. Cousins N. Foreword. In: Reiser D, Rosen D, eds. Medicine as a human experience. Baltimore, MD: University Park Press; 1984:IX-XVI.
5. Storr A. The art of psychotherapy. New York, NY: Methuen, Inc; 1980.
6. Meyer A. Psychobiology: a science of man. Springfield, IL: Charles C. Thomas; 1957.
7. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-36.
8. Von Bertalanffy L. General systems theory. New York, NY: George Braziller, Inc; 1968.
9. Sullivan HS. Interpersonal theory of psychiatry. New York, NY: W.W. Norton & Company; 1953.
1. Cassell E. The nature of suffering and the goals of medicine. N Engl J Med. 1982;306:639.-
2. Merton T. Real and false selves. In: Inchausti R, ed. Seeds. Boston, MA: Shambala Publications, Inc.; 2002:3-24.
3. Shaver W. Suffering and the role of abandonment of self. Journal of Hospice and Palliative Nursing. 2002;4(1):46-53.
4. Cousins N. Foreword. In: Reiser D, Rosen D, eds. Medicine as a human experience. Baltimore, MD: University Park Press; 1984:IX-XVI.
5. Storr A. The art of psychotherapy. New York, NY: Methuen, Inc; 1980.
6. Meyer A. Psychobiology: a science of man. Springfield, IL: Charles C. Thomas; 1957.
7. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196:129-36.
8. Von Bertalanffy L. General systems theory. New York, NY: George Braziller, Inc; 1968.
9. Sullivan HS. Interpersonal theory of psychiatry. New York, NY: W.W. Norton & Company; 1953.
Workplace mobbing: Are they really out to get your patient?
Mr. G, age 46, works for a large federal government agency in a middle-management position. He presents seeking treatment for insomnia. He says, “I just need a sleeping pill. I haven’t been able to sleep for the last 3 months because everybody at work is talking behind my back and spreading rumors about how I’m crazy. My boss is in on it, too. She is always trying to undermine me and makes a big deal out of every little mistake I make.”
Mr. G is suspicious, asking questions about the confidentiality of medical records. His speech is rapid, and he is anxious but exhibits a full range of affect and no pressured speech or flight of ideas. Mr. G describes early, middle, and late insomnia, decreased energy and interest, and gaining 10 pounds over the past 3 months.
He admits owning a gun and having frequent thoughts of suicide and fantasies of killing his boss, although Mr. G repeatedly affirms he would never act on these thoughts. A week ago, his wife moved in with her parents because, he says, “she just couldn’t stand to be around me any longer.”
I consider involuntary hospitalization for Mr. G. Ultimately I contact his wife, who agrees to pick him up, stay with him overnight, and return with him the next morning. Because the only medication Mr. G is willing to consider is sleeping pills, I prescribe flurazepam, 30 mg qhs.
Mr. G was apparently paranoid, thinking of killing his boss, and had a gun. If his wife had not answered the phone and been willing to stay with him, he might have been involuntarily committed. As it was, further interviews with him revealed that Mr. G had been a target of workplace “mobbing,” and that his insomnia and paranoia developed because of a deliberate campaign by coworkers.
This article discusses how to recognize symptoms of workplace mobbing, using Mr. G’s experience to illustrate the dynamics of this group behavior. An informed mental health professional can be of enormous help to a mobbing victim, but an uninformed professional can unwittingly make the situation much worse.
What is ‘mobbing’?
Initiated most often by a person in a position of power or influence, mobbing has been described as “a desperate urge to crush and eliminate the target…. As the campaign proceeds, a steadily larger range of hostile ploys and communications comes to be seen as legitimate.”1 This behavior pattern has been recognized in Europe since the 1980s but is not well recognized in the United States.
Davenport et al2 brought the phenomenon and its consequences to the U.S. public’s attention in 1999 with the publication of Mobbing: emotional abuse in the American workplace. Otherwise, little professional literature on workplace mobbing has been produced in the United States.
A PubMed search on the term “mobbing” limited to 1982 through October 2008 returned 95 listings, excluding those dealing purely with ethology, but only 1 report from the United States. Studies from outside the United States indicate that mobbing is relatively common (Box).
Mobbing, bullying, and harassment. The term “workplace mobbing” was coined by Leymann,3 an occupational psychologist who investigated the psychology of workers who had suffered severe trauma. He observed that some of the most severe reactions were among workers who had been the target of “an impassioned collective campaign by coworkers to exclude, punish, or humiliate” them.
Many researchers use the term mobbing to describe a negative work environment created by several individuals working together.1–3 However, some researchers such as Namie et al4 use the term workplace bullying to describe the creation of a hostile work environment by either a single individual—usually a boss—or a number of individuals.
In 1990 Leymann3 estimated that 3.5% of the Swedish workforce had been victims of significant mobbing. Studies from various other European countries have estimated prevalence of mobbing at 4% to 15% of the total workforce.10
Studies from Europe have shown that all age groups can be affected, but that posttraumatic stress disorder among mobbing victims is more common in patients age >40. Both genders are equally at risk.6
CASE CONTINUED: Why I first thought ‘paranoia’
During our first interview, Mr. G said that 6 months before he sought treatment he had reported misuse of government property by his supervisor’s boss. The case was investigated and dismissed. Mr. G’s supervisor never confronted him about the complaint, but shortly afterwards Mr. G started to notice disturbing changes in the workplace.
His supervisor avoided Mr. G’s phone calls and e-mails and stopped meeting with him. Instead, she met with Mr. G’s subordinates. The subordinates started to ignore Mr. G’s instructions and would roll their eyes or be inattentive when he spoke. Coworkers stopped talking when Mr. G approached, and he started receiving anonymous e-mails questioning his ability and sanity. He was reprimanded in writing for having made a $9 mathematical error in an expense reimbursement request.
Mr. G said when he approached his superior about the work environment, she stated that he was “just paranoid” and needed to see a psychiatrist.
When Mr. G’s wife accompanies him to the second interview, she confirms his impressions of ostracism and gossip at work. She also relates her experiences with people from Mr. G’s office who previously had been friendly but now were distant or hostile. Mr. G shows me copies of harassing work e-mails and memos. I tell Mr. G I believe his story and diagnose him as suffering from posttraumatic stress disorder (PTSD). He begins supportive/cognitive therapy and continues flurazepam.
Mobbing syndrome
As it turns out, Mr. G was not paranoid; his coworkers really were trying to get him. Leymann5 divided 45 types of mobbing behaviors into 5 categories. These were organized as attacks on:
- self-expression and ability to communicate (victim is silenced, given no opportunity to communicate, subject to verbal attacks)
- social relationships (colleagues do not talk to the victim, victim is physically isolated from others)
- reputation (victim is the target of gossip and ridicule)
- occupational situation (victim is given meaningless tasks or no work at all)
- physical health (victim is assigned dangerous tasks, threatened with bodily harm, or physically attacked).
Table 1
Mobbing syndrome: 10 factors
| Assaults on dignity, integrity, credibility, and competence |
| Negative, humiliating, intimidating, abusive, malevolent, and controlling communication |
| Committed directly or indirectly in subtle or obvious ways |
| Perpetrated by ≥1 staff members* |
| Occurring in a continual, multiple, and systematic fashion over time |
| Portraying the victim as being at fault |
| Engineered to discredit, confuse, intimidate, isolate, and force the person into submission |
| Committed with the intent to force the person out |
| Representing the removal as the victim’s choice |
| Unrecognized, misinterpreted, ignored, tolerated, encouraged, or even instigated by management |
| *Some researchers limit their definition of mobbing to acts committed by >1 person |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:41 |
- different ethnicity
- an “odd” personality
- high achievement.
Phases of mobbing
| Conflict, often characterized by a ‘critical incident’ |
| Aggressive acts, such as those in Table 1 |
| Management involvement |
| Branding as difficult or mentally ill |
| Expulsion or resignation from the workplace |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:38 |
Secondary morbidity. Victims of workplace mobbing frequently suffer from:
- adjustment disorders
- somatic symptoms (eg, headaches or irritable bowel syndrome)
- PTSD6,7
- major depression.8
Leymann3 estimated that 15% of suicides in Sweden could be directly attributed to workplace mobbing. Although no other researcher has reported such a dramatic proportion, others have reported increased risk of suicidal behavior among mobbing victims.10
Table 3
Degrees of mobbing
| First degree: Victim manages to resist, escapes at an early stage, or is fully rehabilitated in the original workplace or elsewhere |
| Second degree: Victim cannot resist or escape immediately and suffers temporary or prolonged mental and/or physical disability and has difficulty reentering the workforce |
| Third degree: Victim is unable to reenter the workforce and suffers serious, long-lasting mental or physical disability |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:39 |
CASE CONTINUED: Redirecting energy into a job search
As I met with Mr. G over the next 3 months, the pattern of malicious communication and actions continued at his office. For example, he received a written reprimand for being 10 minutes late after having overslept when starting flurazepam, which he continued to take for about 6 weeks without further tardiness. I encouraged Mr. G to withdraw energy from work by keeping a low profile and trying not to react to provocations. Instead, I counseled him to put energy into family activities and try to find a new job.
Mr. G experienced relatively mild, first-degree workplace mobbing, but it had a substantial effect on his quality of life and that of his wife for almost 1 year. If I had followed my first impulse and had Mr. G involuntarily hospitalized after our first interview, it would have confirmed rumors at his office and probably would have escalated the mobbing behavior.
Diagnostic recommendations
Consider the possibility that seemingly paranoid individuals could be the target of mobbing at work, and don’t underestimate the psychological stress of being mobbed. Other forms of workplace harassment can be extremely stressful but do not have the “paranoidogenic” potential of mobbing. Patients may be so distressed that it is difficult to figure out what is going on in their work environment.
Ask patients to present physical evidence of conspiracy or harassment. Mobbing patients usually are willing to bring in large quantities of material. Keep in mind that when subjected to mobbing behavior over time, a person who is not initially paranoid is likely to develop some secondary suspiciousness and even frank paranoia.
Also consider the possibility of “pseudomobbing,” in which an individual falsely believes he or she is a mobbing victim. Cases of pseudomobbing have been reported in European literature11 and may represent a negative side effect of greater public awareness of the mobbing phenomenon (and of legal remedies to mobbing available in various European countries).
Mobbing is a serious stressor that can lead to psychiatric and medical morbidity and even suicide. Major depressive disorder—often with suicidal ideation—is frequently associated with being mobbed.12
A diagnosis of PTSD can be missed if the mobbing victim does not seem to have been subjected to a severe enough stress to meet PTSD criteria.
Treatment recommendations
First, do no harm: Do not allow yourself to be used by the mob. This process can be direct—as in the Mr. G’s case, where the patient was almost involuntarily committed—or subtle. For example, a person you know may describe the behavior of “someone at work,” and you may be tempted to respond, “Well, I have not examined this person, but from what you say, it sounds like maybe…” You could then be quoted as a psychiatrist who agrees that the person is paranoid.
Giving your patient a name for what is happening to him or her may be the most therapeutic intervention. Generally, patients have not heard of mobbing. They typically are confused about what is happening and may blame themselves.
Treat secondary symptoms of depression, anxiety, PTSD, or other sequelae with pharmacotherapy, psychotherapy, or a combination as appropriate. Refer patients with somatic symptoms to primary care if you feel that they need further evaluation.
Encourage your patient to visualize choices and ways to escape the situation. Frequently, patients will be locked into “fighting for justice” or putting up with the situation because they see no options.
Encourage your patient to withdraw energy from work and invest it in family, social life, or anything else. At the appropriate time, encourage him or her to grieve losses experienced as a result of the mobbing.
Related resources
- Leymann H. The Mobbing Encyclopaedia. www.leymann.se.
- Westhues K. Workplace mobbing in academe. http://arts.uwaterloo.ca/~kwesthue/mobbing.htm.
- Namie R, Namie G. The Workplace Bullying Institute. www.bullyinginstitute.org.
- Flurazepam • Dalmane
Dr. Hillard reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Westhues K. At the mercy of the mob: a summary of research on workplace mobbing. Canada’s Occupational Health and Safety Magazine. 2002;18:30-36.
2. Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999.
3. Leymann H. Mobbing and psychological terror at workplaces. Violence Vict. 1990;5:119-125.
4. Namie G, Namie R. The bully at work: what you can do to stop the hurt and reclaim your dignity on the job. Naperville, IL: Sourcebooks, Inc; 2003.
5. Leymann H. The content and development of mobbing at work. European Journal of Work and Organizational Psychology. 1996;5:165-184.
6. Leymann H, Gustafsson A. Mobbing at work and the development of post-traumatic stress disorders. European Journal of Work and Organizational Psychology. 1996;5:251-275.
7. Bonafons C, Jehel L, Coroller-Bequet A. Specificity of the links between workplace harassment and PTSD: primary results using court decisions, a pilot study in France. Int Arch Occup Environ Health. 2008 Oct 25 (Epub ahead of print).
8. Girardi P, Monaco C, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22:172-188.
9. Duffy M. Workplace mobbing: individual and family health consequences. The Family Journal. 2007;15:398-404.
10. Pompili M, Lester D, Innamorati M, et al. Suicide risk and exposure to mobbing. Work. 2008;31:237-243.
11. Jarreta BM. Medico-legal implications of mobbing. A false accusation of psychological harassment at the workplace. Forensic Sci Int. 2004;146(suppl):S17-S18.
12. Girardi P, Monaco E, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22(2):172-188.
Mr. G, age 46, works for a large federal government agency in a middle-management position. He presents seeking treatment for insomnia. He says, “I just need a sleeping pill. I haven’t been able to sleep for the last 3 months because everybody at work is talking behind my back and spreading rumors about how I’m crazy. My boss is in on it, too. She is always trying to undermine me and makes a big deal out of every little mistake I make.”
Mr. G is suspicious, asking questions about the confidentiality of medical records. His speech is rapid, and he is anxious but exhibits a full range of affect and no pressured speech or flight of ideas. Mr. G describes early, middle, and late insomnia, decreased energy and interest, and gaining 10 pounds over the past 3 months.
He admits owning a gun and having frequent thoughts of suicide and fantasies of killing his boss, although Mr. G repeatedly affirms he would never act on these thoughts. A week ago, his wife moved in with her parents because, he says, “she just couldn’t stand to be around me any longer.”
I consider involuntary hospitalization for Mr. G. Ultimately I contact his wife, who agrees to pick him up, stay with him overnight, and return with him the next morning. Because the only medication Mr. G is willing to consider is sleeping pills, I prescribe flurazepam, 30 mg qhs.
Mr. G was apparently paranoid, thinking of killing his boss, and had a gun. If his wife had not answered the phone and been willing to stay with him, he might have been involuntarily committed. As it was, further interviews with him revealed that Mr. G had been a target of workplace “mobbing,” and that his insomnia and paranoia developed because of a deliberate campaign by coworkers.
This article discusses how to recognize symptoms of workplace mobbing, using Mr. G’s experience to illustrate the dynamics of this group behavior. An informed mental health professional can be of enormous help to a mobbing victim, but an uninformed professional can unwittingly make the situation much worse.
What is ‘mobbing’?
Initiated most often by a person in a position of power or influence, mobbing has been described as “a desperate urge to crush and eliminate the target…. As the campaign proceeds, a steadily larger range of hostile ploys and communications comes to be seen as legitimate.”1 This behavior pattern has been recognized in Europe since the 1980s but is not well recognized in the United States.
Davenport et al2 brought the phenomenon and its consequences to the U.S. public’s attention in 1999 with the publication of Mobbing: emotional abuse in the American workplace. Otherwise, little professional literature on workplace mobbing has been produced in the United States.
A PubMed search on the term “mobbing” limited to 1982 through October 2008 returned 95 listings, excluding those dealing purely with ethology, but only 1 report from the United States. Studies from outside the United States indicate that mobbing is relatively common (Box).
Mobbing, bullying, and harassment. The term “workplace mobbing” was coined by Leymann,3 an occupational psychologist who investigated the psychology of workers who had suffered severe trauma. He observed that some of the most severe reactions were among workers who had been the target of “an impassioned collective campaign by coworkers to exclude, punish, or humiliate” them.
Many researchers use the term mobbing to describe a negative work environment created by several individuals working together.1–3 However, some researchers such as Namie et al4 use the term workplace bullying to describe the creation of a hostile work environment by either a single individual—usually a boss—or a number of individuals.
In 1990 Leymann3 estimated that 3.5% of the Swedish workforce had been victims of significant mobbing. Studies from various other European countries have estimated prevalence of mobbing at 4% to 15% of the total workforce.10
Studies from Europe have shown that all age groups can be affected, but that posttraumatic stress disorder among mobbing victims is more common in patients age >40. Both genders are equally at risk.6
CASE CONTINUED: Why I first thought ‘paranoia’
During our first interview, Mr. G said that 6 months before he sought treatment he had reported misuse of government property by his supervisor’s boss. The case was investigated and dismissed. Mr. G’s supervisor never confronted him about the complaint, but shortly afterwards Mr. G started to notice disturbing changes in the workplace.
His supervisor avoided Mr. G’s phone calls and e-mails and stopped meeting with him. Instead, she met with Mr. G’s subordinates. The subordinates started to ignore Mr. G’s instructions and would roll their eyes or be inattentive when he spoke. Coworkers stopped talking when Mr. G approached, and he started receiving anonymous e-mails questioning his ability and sanity. He was reprimanded in writing for having made a $9 mathematical error in an expense reimbursement request.
Mr. G said when he approached his superior about the work environment, she stated that he was “just paranoid” and needed to see a psychiatrist.
When Mr. G’s wife accompanies him to the second interview, she confirms his impressions of ostracism and gossip at work. She also relates her experiences with people from Mr. G’s office who previously had been friendly but now were distant or hostile. Mr. G shows me copies of harassing work e-mails and memos. I tell Mr. G I believe his story and diagnose him as suffering from posttraumatic stress disorder (PTSD). He begins supportive/cognitive therapy and continues flurazepam.
Mobbing syndrome
As it turns out, Mr. G was not paranoid; his coworkers really were trying to get him. Leymann5 divided 45 types of mobbing behaviors into 5 categories. These were organized as attacks on:
- self-expression and ability to communicate (victim is silenced, given no opportunity to communicate, subject to verbal attacks)
- social relationships (colleagues do not talk to the victim, victim is physically isolated from others)
- reputation (victim is the target of gossip and ridicule)
- occupational situation (victim is given meaningless tasks or no work at all)
- physical health (victim is assigned dangerous tasks, threatened with bodily harm, or physically attacked).
Table 1
Mobbing syndrome: 10 factors
| Assaults on dignity, integrity, credibility, and competence |
| Negative, humiliating, intimidating, abusive, malevolent, and controlling communication |
| Committed directly or indirectly in subtle or obvious ways |
| Perpetrated by ≥1 staff members* |
| Occurring in a continual, multiple, and systematic fashion over time |
| Portraying the victim as being at fault |
| Engineered to discredit, confuse, intimidate, isolate, and force the person into submission |
| Committed with the intent to force the person out |
| Representing the removal as the victim’s choice |
| Unrecognized, misinterpreted, ignored, tolerated, encouraged, or even instigated by management |
| *Some researchers limit their definition of mobbing to acts committed by >1 person |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:41 |
- different ethnicity
- an “odd” personality
- high achievement.
Phases of mobbing
| Conflict, often characterized by a ‘critical incident’ |
| Aggressive acts, such as those in Table 1 |
| Management involvement |
| Branding as difficult or mentally ill |
| Expulsion or resignation from the workplace |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:38 |
Secondary morbidity. Victims of workplace mobbing frequently suffer from:
- adjustment disorders
- somatic symptoms (eg, headaches or irritable bowel syndrome)
- PTSD6,7
- major depression.8
Leymann3 estimated that 15% of suicides in Sweden could be directly attributed to workplace mobbing. Although no other researcher has reported such a dramatic proportion, others have reported increased risk of suicidal behavior among mobbing victims.10
Table 3
Degrees of mobbing
| First degree: Victim manages to resist, escapes at an early stage, or is fully rehabilitated in the original workplace or elsewhere |
| Second degree: Victim cannot resist or escape immediately and suffers temporary or prolonged mental and/or physical disability and has difficulty reentering the workforce |
| Third degree: Victim is unable to reenter the workforce and suffers serious, long-lasting mental or physical disability |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:39 |
CASE CONTINUED: Redirecting energy into a job search
As I met with Mr. G over the next 3 months, the pattern of malicious communication and actions continued at his office. For example, he received a written reprimand for being 10 minutes late after having overslept when starting flurazepam, which he continued to take for about 6 weeks without further tardiness. I encouraged Mr. G to withdraw energy from work by keeping a low profile and trying not to react to provocations. Instead, I counseled him to put energy into family activities and try to find a new job.
Mr. G experienced relatively mild, first-degree workplace mobbing, but it had a substantial effect on his quality of life and that of his wife for almost 1 year. If I had followed my first impulse and had Mr. G involuntarily hospitalized after our first interview, it would have confirmed rumors at his office and probably would have escalated the mobbing behavior.
Diagnostic recommendations
Consider the possibility that seemingly paranoid individuals could be the target of mobbing at work, and don’t underestimate the psychological stress of being mobbed. Other forms of workplace harassment can be extremely stressful but do not have the “paranoidogenic” potential of mobbing. Patients may be so distressed that it is difficult to figure out what is going on in their work environment.
Ask patients to present physical evidence of conspiracy or harassment. Mobbing patients usually are willing to bring in large quantities of material. Keep in mind that when subjected to mobbing behavior over time, a person who is not initially paranoid is likely to develop some secondary suspiciousness and even frank paranoia.
Also consider the possibility of “pseudomobbing,” in which an individual falsely believes he or she is a mobbing victim. Cases of pseudomobbing have been reported in European literature11 and may represent a negative side effect of greater public awareness of the mobbing phenomenon (and of legal remedies to mobbing available in various European countries).
Mobbing is a serious stressor that can lead to psychiatric and medical morbidity and even suicide. Major depressive disorder—often with suicidal ideation—is frequently associated with being mobbed.12
A diagnosis of PTSD can be missed if the mobbing victim does not seem to have been subjected to a severe enough stress to meet PTSD criteria.
Treatment recommendations
First, do no harm: Do not allow yourself to be used by the mob. This process can be direct—as in the Mr. G’s case, where the patient was almost involuntarily committed—or subtle. For example, a person you know may describe the behavior of “someone at work,” and you may be tempted to respond, “Well, I have not examined this person, but from what you say, it sounds like maybe…” You could then be quoted as a psychiatrist who agrees that the person is paranoid.
Giving your patient a name for what is happening to him or her may be the most therapeutic intervention. Generally, patients have not heard of mobbing. They typically are confused about what is happening and may blame themselves.
Treat secondary symptoms of depression, anxiety, PTSD, or other sequelae with pharmacotherapy, psychotherapy, or a combination as appropriate. Refer patients with somatic symptoms to primary care if you feel that they need further evaluation.
Encourage your patient to visualize choices and ways to escape the situation. Frequently, patients will be locked into “fighting for justice” or putting up with the situation because they see no options.
Encourage your patient to withdraw energy from work and invest it in family, social life, or anything else. At the appropriate time, encourage him or her to grieve losses experienced as a result of the mobbing.
Related resources
- Leymann H. The Mobbing Encyclopaedia. www.leymann.se.
- Westhues K. Workplace mobbing in academe. http://arts.uwaterloo.ca/~kwesthue/mobbing.htm.
- Namie R, Namie G. The Workplace Bullying Institute. www.bullyinginstitute.org.
- Flurazepam • Dalmane
Dr. Hillard reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. G, age 46, works for a large federal government agency in a middle-management position. He presents seeking treatment for insomnia. He says, “I just need a sleeping pill. I haven’t been able to sleep for the last 3 months because everybody at work is talking behind my back and spreading rumors about how I’m crazy. My boss is in on it, too. She is always trying to undermine me and makes a big deal out of every little mistake I make.”
Mr. G is suspicious, asking questions about the confidentiality of medical records. His speech is rapid, and he is anxious but exhibits a full range of affect and no pressured speech or flight of ideas. Mr. G describes early, middle, and late insomnia, decreased energy and interest, and gaining 10 pounds over the past 3 months.
He admits owning a gun and having frequent thoughts of suicide and fantasies of killing his boss, although Mr. G repeatedly affirms he would never act on these thoughts. A week ago, his wife moved in with her parents because, he says, “she just couldn’t stand to be around me any longer.”
I consider involuntary hospitalization for Mr. G. Ultimately I contact his wife, who agrees to pick him up, stay with him overnight, and return with him the next morning. Because the only medication Mr. G is willing to consider is sleeping pills, I prescribe flurazepam, 30 mg qhs.
Mr. G was apparently paranoid, thinking of killing his boss, and had a gun. If his wife had not answered the phone and been willing to stay with him, he might have been involuntarily committed. As it was, further interviews with him revealed that Mr. G had been a target of workplace “mobbing,” and that his insomnia and paranoia developed because of a deliberate campaign by coworkers.
This article discusses how to recognize symptoms of workplace mobbing, using Mr. G’s experience to illustrate the dynamics of this group behavior. An informed mental health professional can be of enormous help to a mobbing victim, but an uninformed professional can unwittingly make the situation much worse.
What is ‘mobbing’?
Initiated most often by a person in a position of power or influence, mobbing has been described as “a desperate urge to crush and eliminate the target…. As the campaign proceeds, a steadily larger range of hostile ploys and communications comes to be seen as legitimate.”1 This behavior pattern has been recognized in Europe since the 1980s but is not well recognized in the United States.
Davenport et al2 brought the phenomenon and its consequences to the U.S. public’s attention in 1999 with the publication of Mobbing: emotional abuse in the American workplace. Otherwise, little professional literature on workplace mobbing has been produced in the United States.
A PubMed search on the term “mobbing” limited to 1982 through October 2008 returned 95 listings, excluding those dealing purely with ethology, but only 1 report from the United States. Studies from outside the United States indicate that mobbing is relatively common (Box).
Mobbing, bullying, and harassment. The term “workplace mobbing” was coined by Leymann,3 an occupational psychologist who investigated the psychology of workers who had suffered severe trauma. He observed that some of the most severe reactions were among workers who had been the target of “an impassioned collective campaign by coworkers to exclude, punish, or humiliate” them.
Many researchers use the term mobbing to describe a negative work environment created by several individuals working together.1–3 However, some researchers such as Namie et al4 use the term workplace bullying to describe the creation of a hostile work environment by either a single individual—usually a boss—or a number of individuals.
In 1990 Leymann3 estimated that 3.5% of the Swedish workforce had been victims of significant mobbing. Studies from various other European countries have estimated prevalence of mobbing at 4% to 15% of the total workforce.10
Studies from Europe have shown that all age groups can be affected, but that posttraumatic stress disorder among mobbing victims is more common in patients age >40. Both genders are equally at risk.6
CASE CONTINUED: Why I first thought ‘paranoia’
During our first interview, Mr. G said that 6 months before he sought treatment he had reported misuse of government property by his supervisor’s boss. The case was investigated and dismissed. Mr. G’s supervisor never confronted him about the complaint, but shortly afterwards Mr. G started to notice disturbing changes in the workplace.
His supervisor avoided Mr. G’s phone calls and e-mails and stopped meeting with him. Instead, she met with Mr. G’s subordinates. The subordinates started to ignore Mr. G’s instructions and would roll their eyes or be inattentive when he spoke. Coworkers stopped talking when Mr. G approached, and he started receiving anonymous e-mails questioning his ability and sanity. He was reprimanded in writing for having made a $9 mathematical error in an expense reimbursement request.
Mr. G said when he approached his superior about the work environment, she stated that he was “just paranoid” and needed to see a psychiatrist.
When Mr. G’s wife accompanies him to the second interview, she confirms his impressions of ostracism and gossip at work. She also relates her experiences with people from Mr. G’s office who previously had been friendly but now were distant or hostile. Mr. G shows me copies of harassing work e-mails and memos. I tell Mr. G I believe his story and diagnose him as suffering from posttraumatic stress disorder (PTSD). He begins supportive/cognitive therapy and continues flurazepam.
Mobbing syndrome
As it turns out, Mr. G was not paranoid; his coworkers really were trying to get him. Leymann5 divided 45 types of mobbing behaviors into 5 categories. These were organized as attacks on:
- self-expression and ability to communicate (victim is silenced, given no opportunity to communicate, subject to verbal attacks)
- social relationships (colleagues do not talk to the victim, victim is physically isolated from others)
- reputation (victim is the target of gossip and ridicule)
- occupational situation (victim is given meaningless tasks or no work at all)
- physical health (victim is assigned dangerous tasks, threatened with bodily harm, or physically attacked).
Table 1
Mobbing syndrome: 10 factors
| Assaults on dignity, integrity, credibility, and competence |
| Negative, humiliating, intimidating, abusive, malevolent, and controlling communication |
| Committed directly or indirectly in subtle or obvious ways |
| Perpetrated by ≥1 staff members* |
| Occurring in a continual, multiple, and systematic fashion over time |
| Portraying the victim as being at fault |
| Engineered to discredit, confuse, intimidate, isolate, and force the person into submission |
| Committed with the intent to force the person out |
| Representing the removal as the victim’s choice |
| Unrecognized, misinterpreted, ignored, tolerated, encouraged, or even instigated by management |
| *Some researchers limit their definition of mobbing to acts committed by >1 person |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:41 |
- different ethnicity
- an “odd” personality
- high achievement.
Phases of mobbing
| Conflict, often characterized by a ‘critical incident’ |
| Aggressive acts, such as those in Table 1 |
| Management involvement |
| Branding as difficult or mentally ill |
| Expulsion or resignation from the workplace |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:38 |
Secondary morbidity. Victims of workplace mobbing frequently suffer from:
- adjustment disorders
- somatic symptoms (eg, headaches or irritable bowel syndrome)
- PTSD6,7
- major depression.8
Leymann3 estimated that 15% of suicides in Sweden could be directly attributed to workplace mobbing. Although no other researcher has reported such a dramatic proportion, others have reported increased risk of suicidal behavior among mobbing victims.10
Table 3
Degrees of mobbing
| First degree: Victim manages to resist, escapes at an early stage, or is fully rehabilitated in the original workplace or elsewhere |
| Second degree: Victim cannot resist or escape immediately and suffers temporary or prolonged mental and/or physical disability and has difficulty reentering the workforce |
| Third degree: Victim is unable to reenter the workforce and suffers serious, long-lasting mental or physical disability |
| Source: Adapted with permission from Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999:39 |
CASE CONTINUED: Redirecting energy into a job search
As I met with Mr. G over the next 3 months, the pattern of malicious communication and actions continued at his office. For example, he received a written reprimand for being 10 minutes late after having overslept when starting flurazepam, which he continued to take for about 6 weeks without further tardiness. I encouraged Mr. G to withdraw energy from work by keeping a low profile and trying not to react to provocations. Instead, I counseled him to put energy into family activities and try to find a new job.
Mr. G experienced relatively mild, first-degree workplace mobbing, but it had a substantial effect on his quality of life and that of his wife for almost 1 year. If I had followed my first impulse and had Mr. G involuntarily hospitalized after our first interview, it would have confirmed rumors at his office and probably would have escalated the mobbing behavior.
Diagnostic recommendations
Consider the possibility that seemingly paranoid individuals could be the target of mobbing at work, and don’t underestimate the psychological stress of being mobbed. Other forms of workplace harassment can be extremely stressful but do not have the “paranoidogenic” potential of mobbing. Patients may be so distressed that it is difficult to figure out what is going on in their work environment.
Ask patients to present physical evidence of conspiracy or harassment. Mobbing patients usually are willing to bring in large quantities of material. Keep in mind that when subjected to mobbing behavior over time, a person who is not initially paranoid is likely to develop some secondary suspiciousness and even frank paranoia.
Also consider the possibility of “pseudomobbing,” in which an individual falsely believes he or she is a mobbing victim. Cases of pseudomobbing have been reported in European literature11 and may represent a negative side effect of greater public awareness of the mobbing phenomenon (and of legal remedies to mobbing available in various European countries).
Mobbing is a serious stressor that can lead to psychiatric and medical morbidity and even suicide. Major depressive disorder—often with suicidal ideation—is frequently associated with being mobbed.12
A diagnosis of PTSD can be missed if the mobbing victim does not seem to have been subjected to a severe enough stress to meet PTSD criteria.
Treatment recommendations
First, do no harm: Do not allow yourself to be used by the mob. This process can be direct—as in the Mr. G’s case, where the patient was almost involuntarily committed—or subtle. For example, a person you know may describe the behavior of “someone at work,” and you may be tempted to respond, “Well, I have not examined this person, but from what you say, it sounds like maybe…” You could then be quoted as a psychiatrist who agrees that the person is paranoid.
Giving your patient a name for what is happening to him or her may be the most therapeutic intervention. Generally, patients have not heard of mobbing. They typically are confused about what is happening and may blame themselves.
Treat secondary symptoms of depression, anxiety, PTSD, or other sequelae with pharmacotherapy, psychotherapy, or a combination as appropriate. Refer patients with somatic symptoms to primary care if you feel that they need further evaluation.
Encourage your patient to visualize choices and ways to escape the situation. Frequently, patients will be locked into “fighting for justice” or putting up with the situation because they see no options.
Encourage your patient to withdraw energy from work and invest it in family, social life, or anything else. At the appropriate time, encourage him or her to grieve losses experienced as a result of the mobbing.
Related resources
- Leymann H. The Mobbing Encyclopaedia. www.leymann.se.
- Westhues K. Workplace mobbing in academe. http://arts.uwaterloo.ca/~kwesthue/mobbing.htm.
- Namie R, Namie G. The Workplace Bullying Institute. www.bullyinginstitute.org.
- Flurazepam • Dalmane
Dr. Hillard reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Westhues K. At the mercy of the mob: a summary of research on workplace mobbing. Canada’s Occupational Health and Safety Magazine. 2002;18:30-36.
2. Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999.
3. Leymann H. Mobbing and psychological terror at workplaces. Violence Vict. 1990;5:119-125.
4. Namie G, Namie R. The bully at work: what you can do to stop the hurt and reclaim your dignity on the job. Naperville, IL: Sourcebooks, Inc; 2003.
5. Leymann H. The content and development of mobbing at work. European Journal of Work and Organizational Psychology. 1996;5:165-184.
6. Leymann H, Gustafsson A. Mobbing at work and the development of post-traumatic stress disorders. European Journal of Work and Organizational Psychology. 1996;5:251-275.
7. Bonafons C, Jehel L, Coroller-Bequet A. Specificity of the links between workplace harassment and PTSD: primary results using court decisions, a pilot study in France. Int Arch Occup Environ Health. 2008 Oct 25 (Epub ahead of print).
8. Girardi P, Monaco C, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22:172-188.
9. Duffy M. Workplace mobbing: individual and family health consequences. The Family Journal. 2007;15:398-404.
10. Pompili M, Lester D, Innamorati M, et al. Suicide risk and exposure to mobbing. Work. 2008;31:237-243.
11. Jarreta BM. Medico-legal implications of mobbing. A false accusation of psychological harassment at the workplace. Forensic Sci Int. 2004;146(suppl):S17-S18.
12. Girardi P, Monaco E, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22(2):172-188.
1. Westhues K. At the mercy of the mob: a summary of research on workplace mobbing. Canada’s Occupational Health and Safety Magazine. 2002;18:30-36.
2. Davenport N, Schwartz RD, Elliott GP. Mobbing: emotional abuse in the American workplace. Ames, IA: Civil Society Publishing; 1999.
3. Leymann H. Mobbing and psychological terror at workplaces. Violence Vict. 1990;5:119-125.
4. Namie G, Namie R. The bully at work: what you can do to stop the hurt and reclaim your dignity on the job. Naperville, IL: Sourcebooks, Inc; 2003.
5. Leymann H. The content and development of mobbing at work. European Journal of Work and Organizational Psychology. 1996;5:165-184.
6. Leymann H, Gustafsson A. Mobbing at work and the development of post-traumatic stress disorders. European Journal of Work and Organizational Psychology. 1996;5:251-275.
7. Bonafons C, Jehel L, Coroller-Bequet A. Specificity of the links between workplace harassment and PTSD: primary results using court decisions, a pilot study in France. Int Arch Occup Environ Health. 2008 Oct 25 (Epub ahead of print).
8. Girardi P, Monaco C, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22:172-188.
9. Duffy M. Workplace mobbing: individual and family health consequences. The Family Journal. 2007;15:398-404.
10. Pompili M, Lester D, Innamorati M, et al. Suicide risk and exposure to mobbing. Work. 2008;31:237-243.
11. Jarreta BM. Medico-legal implications of mobbing. A false accusation of psychological harassment at the workplace. Forensic Sci Int. 2004;146(suppl):S17-S18.
12. Girardi P, Monaco E, Prestigiacomo C, et al. Personality and psychopathological profiles in individuals exposed to mobbing. Violence Vict. 2007;22(2):172-188.
Informed consent: Is your patient competent to refuse treatment?
Mr. D, age 45 with a history of schizophrenia, is admitted to an inpatient psychiatric unit. The psychiatrist recommends an antipsychotic to help Mr. D with fears that the FBI has implanted a radio signal device into his tooth filling. She explains the risks and benefits of the proposed drug and alternate medications, as well as the risks of no treatment.
Mr. D calmly but consistently declines the treatment. He states that he recognizes the antipsychotic is used to treat psychotic symptoms, can help people who hear voices, and can have side effects such as tardive dyskinesia. His thoughts become disorganized and difficult to follow, however, as he explains that he does not believe the medication is needed for his situation because the FBI is involved in tracking his behavior.
Informed consent in clinical settings is designed to allow patients to make rational choices about their treatment before it begins. When a psychiatric patient such as Mr. D declines a treatment you recommend, how can you balance the 2 ethical principles in medicine: beneficence toward the patient and respect for individual autonomy?1
Some authors have raised concerns that informed consent in physician-patient interactions are at times an empty exercise undertaken solely to satisfy a legal expectation.2 If executed properly, however, informed consent can enhance the therapeutic alliance and help improve treatment adherence.
Patient-centered treatment
As patients have become more informed consumers, the “doctor knows best” model of care has given way to an expectation that patients know best what they would want done regarding their health. Lawsuits related to informed consent generally allege that physicians failed to provide appropriate informed consent for treatment the plaintiffs received. These complaints suggest that had the patient been more appropriately informed, he or she might have made a different choice and would not have suffered harm related to treatment.
In a patient-centered approach to treatment, informed consent allows the patient to make an autonomous decision with the appropriate information. Providing treatment without the patient’s expressed consent could be viewed more seriously, potentially even as battery.3 Recent informed consent cases tend to rely on negligence theories, however, rather than on claims of battery. Negligence cases helped set the stage of evolving expectations—first seen with surgical procedures, then medical interventions, then medication treatment, and now even with psychotherapy (Box 1)—that informed consent should be obtained in clinical settings.4
Because failure to provide informed consent can be grounds for a negligence claim, consider strategies to reduce the chance of successful litigation.
Although a written form can provide some proof that informed consent occurred, it may not prove that you conveyed adequate information or that your patient understood the information. Overly simplistic or complex forms can pose other difficulties in malpractice claims. Documenting aspects of the informed consent dialogue often provides the best “proof” that such a conversation occurred.
In retrospect, helpful evidence that adequate informed consent was obtained may include information related to the disclosed information and the patient’s response to the information (such as might be seen in a quote that indicated his or her understanding of a particular side effect). Although a full accounting of the conversation would not be a reasonable expectation for documentation, you might wish to consider the risks and benefits inherent to the particular treatment and tailor the note related to the informed consent accordingly.
3 components of informed consent
Informed consent includes 3 components: voluntariness, disclosure, and competence.5
Voluntariness implies that the patient must make treatment-related choices of his or her own free will and without coercion. In Kaimowitz v Michigan Department of Mental Health,6 the court ruled that involuntarily committed persons living in what was considered an inherently coercive institutional environment were not capable of providing voluntary consent to a high-risk experimental procedure. This case had a major impact on prison research.
In treatment settings as well, a patient’s circumstances might be considered coercive. Historically, civilly committed patients did not have the right to refuse treatment. A movement in the 1980s helped to separate civil commitment and the right to refuse treatment, which is well-established in most jurisdictions today.7 In psychiatric inpatient settings, even an involuntarily committed patient generally has a right to refuse recommended medications unless a legally permissible mechanism overrides the refusal.
Disclosure means that a person requires certain information to make a rational decision to accept or reject treatment. The question is: How much information needs to be disclosed for a patient to be adequately informed?
Disclosure requirements vary across jurisdictions. In 1960, Natanson v Kline supported the standard that disclosure required that which a “reasonable practitioner” might disclose to patients about their treatment in similar circumstances.8 Although some jurisdictions have maintained that standard,5 subsequent cases identified a more patient-centered approach to disclosure called the “reasonable person” standard (Box 2).5,9
Competence. In many settings, clinicians use the construct of “capacity” rather than “competence” because competence is a legal term that can be determined only by a judge. When an individual is deemed incompetent, his or her right to make autonomous decisions can be overridden. Children are not competent by virtue of their status as minors, although exceptions may be made for certain older youth. Adults are presumed competent unless adjudicated otherwise.
The “reasonable person” standard endorses the obligation of the professional to disclose information that a reasonable person would want to know about a proposed treatment. This standard evolved in part from Canterbury v Spence,9 in which a plaintiff who had become paralyzed alleged that he was not informed of the risks of a laminectomy. The court found that the patient must be able to rely on information that the physician holds that would be material to the patient in making an informed treatment decision in his or her best interest.
The typically required elements of disclosure include:
- diagnosis, if known
- nature and purpose of proposed treatment
- risks and benefits of proposed treatment
- alternatives to treatment and their risks and benefits
- risks and benefits of no treatment.
Disclosing information that is uniquely relevant to an individual’s situation and would be generally unknown to the clinician might not be required. For example, a clinician might not realize that it is important for a particular patient to be able to make small art objects as a hobby, so the clinician might not reveal that a medication very rarely causes a tremor. Nevertheless, when you are aware of a need for such nuanced information, the usual general disclosure can be modified to include whatever details are relevant to that patient.5
Competence can be broken down into 4 component capacities (Box 3).11 The degree of incapacity required for a finding of incompetence is complicated and difficult to codify. Instruments designed to standardize competence assessment are available12 but not routinely used in clinical settings. Even with these instruments, no threshold of capacity clearly defines competence. Some authors have argued for a sliding scale of competence, with standards becoming more stringent as the degree of risk related to the treatment decision increases.13,14
Express and sustain a choice. To be considered competent to give informed consent, a person must be able to evidence a choice regarding the decision at hand. The choice need not be expressed verbally, but a patient must be able to communicate in some fashion (such as eye blinking or handwritten communication). The patient also must be able to maintain that choice over time, long enough for treatment to be implemented.
Understand presented information. A person must have a factual understanding of the information presented about the treatment. A full scientific understanding of diagnosis and subtleties of treatment likely would be an excessive expectation. For example, a patient would not be expected to understand the nuances of the serotonin neurotransmitter system. A physician should, however, assess whether the patient understands—in the patient’s words—that a selective serotonin reuptake inhibitor could induce manic-type symptoms and that the patient should bring these symptoms to the prescribing physician’s attention if they occur.
Appreciate one’s situation. Individuals who are competent must have a realistic appreciation of their situation. Though a patient may understand the facts you have presented, he may fail to fully integrate why the information is relevant to him. Persons with schizophrenia who do not believe they are ill—such as Mr. D—might have a limited appreciation of why an antipsychotic would help them.
Rationally manipulate information. A person also must be able to rationally manipulate the information in a way that is not impaired by symptoms of illness. Patients faced with a treatment decision should be able to use reason to reach a logical and rational decision that they see as being in their best interest. This might not be the same decision you would make. For example, a patient with thought disorganization or one who psychotically believes that the color of a recommended medication signals that someone tampered with the pills might not be able to rationally manipulate information presented about treatment options.
Source: Reference 11
Exceptions to informed consent
Emergencies. Informed consent is not required under some circumstances.5 Consider the patient who is brought to the emergency room unconscious after a fall, with no family contact information. A neurosurgeon might need to intervene immediately to save the patient’s life, using the emergency exception to informed consent.
In an emergency, when a person is unable to give informed consent or time does not allow for a full informed consent process, the clinician generally follows the principle of doing no harm. Treatment may be started in an emergency without full informed consent on the assumption that most competent people would consent to treatment, especially where life or limb was at risk. If time and circumstances permit in an emergency, obtaining the consent of available family members may be prudent.
Incompetence. If a judge determines that a patient is incompetent to make his or her own treatment decisions, a substitute decision-maker—such as a guardian—could be appointed. In these cases, respect would suggest that to the extent possible and appropriate you would inform the incompetent ward about treatment in a way that he or she may understand.
In other circumstances, such as when a healthcare proxy has been invoked, previously designated surrogate decision-makers provide informed consent on behalf of the patient who clinically is found to lack the capacity to make healthcare decisions.
Waivers. Sometimes a competent patient decides to waive the right to further information and may turn the decision over to the clinician. To rely upon this exception, some documented assessment—even if brief—of the patient’s capacity to waive information may be important.
As noted, informing patients of their health situations is expected and accepted. Even in psychiatric settings, receiving information about potentially serious medication side effects has not necessarily led to patient harm or refusal of treatment.15 Therefore, use of this exception is only for very narrowly tailored circumstances, if used at all, and not simply because you believe a patient will refuse to consent if informed about a proposed treatment.
Some case law exists on the need to establish why the therapeutic privilege was justified as a rationale to not provide informed consent in a particular situation.16 Therefore, though it should be rarely invoked, if you use therapeutic privilege, document why you invoked this exception for that particular patient and in that particular circumstance.
Building the therapeutic alliance
Although it may meet policy or legal informed consent requirements, simply providing the patient with a form to sign before treatment begins does little to enhance patient-clinician communication.2 Providing detailed written information also might not be adequate to ensure that the patient understands the complexity of a treatment you have asked him to consider.17 Instead, an informed consent model that relies on active, ongoing dialogue about treatment can maximize patient autonomy while working for the good of the patient (Table).
- the patient’s role is understood as that of an inquisitive consumer who may challenge the physician’s authority in the quest for information
- the clinician challenges the patient’s preconceived beliefs about his or her illness and educates the patient so that both parties approach the medical issue from common ground.
1 In this model of shared decision-making, the clinician reveals information material to the decision, and the patient helps the clinician understand the circumstances that make him or her prefer 1 treatment over another.1,18
By engaging in ongoing informed consent, you may achieve greater gains within the therapeutic alliance and reduce the risk of liability.19 Where uncertainties are related to treatment, share these ambiguities as an aspect of informed consent, especially when the patient plays an active role in treatment.4 Similarly, an expanded informed consent process may be needed when:
- proposed treatments are particularly risky
- several treatment alternatives could be acceptable and effective
- evidence supports opposing views of a treatment’s effectiveness.4,20
Using informed consent to build a therapeutic alliance
|
CASE CONTINUED: A question of competence
Mr. D is calm in his discussions with the psychiatrist, and the information she presents does not seem to cause him further harm. Thus, the emergency and therapeutic privilege exceptions do not eliminate the need for an ongoing informed consent process at this time.
Mr. D has a factual understanding of the risks and benefits of the recommended antipsychotic and is able to express a consistent choice about starting this treatment. He lacks, however, an ability to appreciate his situation and has difficulty manipulating information rationally. Overall, he has deficits in aspects of his decision-making competence, which could signal the need for an exception to obtaining informed consent.
Related resources
- Pinals DA, Appelbaum PS. The history and current status of competence and informed consent in psychiatric research. Isr J Psychiatry Relat Sci. 2000;37(2):82-94.
- American Medical Association. Legal issues/patient physician relationship topics. www.ama-assn.org/ama/pub/physician-resources/legal-topics.shtml.
Dr. Pinals reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. King JS, Moulton BW. Rethinking informed consent: the case for shared medical decision-making. Am J Law Med. 2006;32(4):429-501.
2. Lidz CW, Appelbaum PS, Meisel A. Two models of implementing informed consent. Arch Intern Med. 1988;148(6):1385-1389.
3. Schloendorff v Society of New York Hospital, 105 NE 92 (1914).
4. Beahrs JO, Gutheil TG. Informed consent in psychotherapy. Am J Psychiatry. 2001;158(1):4-10.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. Philadelphia, PA: Wolters Kluwer and Lippincott Williams & Wilkins; 2007.
6. Kaimowitz v Michigan, DMH 1 MDLR 147 (1976).
7. Pinals DA, Hoge SK. Treatment refusal in psychiatric practice. In: Rosner R, ed. Principles and practice of forensic psychiatry, 2nd ed. London, UK: Arnold Press; 2003:129-136.
8. Natanson v Kline, 350 P.2D 1093 (1960).
9. Canterbury v Spence, 464 F.2d 772 (1972).
10. Grisso T, Appelbaum PS. The MacArthur Treatment Competence Study: III. Abilities of patients to consent to psychiatric and medical treatment. Law Human Behav. 1995;19(2):149-174.
11. Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
12. Dunn LB, Nowrangi MA, Palmer BW, et al. Assessing decisional capacity for clinical research or treatment: a review of instruments. Am J Psychiatry. 2006;163(8):1323-1334.
13. Drane JF. Competency to give an informed consent: a model for making clinical assessments. JAMA. 1984;252(7):925-927.
14. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
15. Munetz MR, Roth LH. Informing patients about tardive dyskinesia. Arch Gen Psychiatry. 1985;42(9):866-871.
16. Barcai v Betwee MD, 50 P3d 946 (2002).
17. Hafeez A, Wiseman O, Hill JT. Informed consent: are we deluding ourselves? A randomized controlled study. BJU International. 2007;99(1):4-5.
18. Kaplan RM. Shared medical decision making: a new tool for preventative medicine. Am J Prev Med. 2004;26(1):81-83.
19. Gutheil TG, Bursztajn H, Brodsky A. Malpractice prevention through the sharing of uncertainty. Informed consent and the therapeutic alliance. N Engl J Med. 1984;311(1):49-51.
20. Packman WL, Cabot MG, Bongar B. Malpractice arising from negligent psychotherapy: ethical, legal, and clinical implications of Osheroff v Chestnut Lodge. Ethics Behav. 1994;4(3):175-197.
Mr. D, age 45 with a history of schizophrenia, is admitted to an inpatient psychiatric unit. The psychiatrist recommends an antipsychotic to help Mr. D with fears that the FBI has implanted a radio signal device into his tooth filling. She explains the risks and benefits of the proposed drug and alternate medications, as well as the risks of no treatment.
Mr. D calmly but consistently declines the treatment. He states that he recognizes the antipsychotic is used to treat psychotic symptoms, can help people who hear voices, and can have side effects such as tardive dyskinesia. His thoughts become disorganized and difficult to follow, however, as he explains that he does not believe the medication is needed for his situation because the FBI is involved in tracking his behavior.
Informed consent in clinical settings is designed to allow patients to make rational choices about their treatment before it begins. When a psychiatric patient such as Mr. D declines a treatment you recommend, how can you balance the 2 ethical principles in medicine: beneficence toward the patient and respect for individual autonomy?1
Some authors have raised concerns that informed consent in physician-patient interactions are at times an empty exercise undertaken solely to satisfy a legal expectation.2 If executed properly, however, informed consent can enhance the therapeutic alliance and help improve treatment adherence.
Patient-centered treatment
As patients have become more informed consumers, the “doctor knows best” model of care has given way to an expectation that patients know best what they would want done regarding their health. Lawsuits related to informed consent generally allege that physicians failed to provide appropriate informed consent for treatment the plaintiffs received. These complaints suggest that had the patient been more appropriately informed, he or she might have made a different choice and would not have suffered harm related to treatment.
In a patient-centered approach to treatment, informed consent allows the patient to make an autonomous decision with the appropriate information. Providing treatment without the patient’s expressed consent could be viewed more seriously, potentially even as battery.3 Recent informed consent cases tend to rely on negligence theories, however, rather than on claims of battery. Negligence cases helped set the stage of evolving expectations—first seen with surgical procedures, then medical interventions, then medication treatment, and now even with psychotherapy (Box 1)—that informed consent should be obtained in clinical settings.4
Because failure to provide informed consent can be grounds for a negligence claim, consider strategies to reduce the chance of successful litigation.
Although a written form can provide some proof that informed consent occurred, it may not prove that you conveyed adequate information or that your patient understood the information. Overly simplistic or complex forms can pose other difficulties in malpractice claims. Documenting aspects of the informed consent dialogue often provides the best “proof” that such a conversation occurred.
In retrospect, helpful evidence that adequate informed consent was obtained may include information related to the disclosed information and the patient’s response to the information (such as might be seen in a quote that indicated his or her understanding of a particular side effect). Although a full accounting of the conversation would not be a reasonable expectation for documentation, you might wish to consider the risks and benefits inherent to the particular treatment and tailor the note related to the informed consent accordingly.
3 components of informed consent
Informed consent includes 3 components: voluntariness, disclosure, and competence.5
Voluntariness implies that the patient must make treatment-related choices of his or her own free will and without coercion. In Kaimowitz v Michigan Department of Mental Health,6 the court ruled that involuntarily committed persons living in what was considered an inherently coercive institutional environment were not capable of providing voluntary consent to a high-risk experimental procedure. This case had a major impact on prison research.
In treatment settings as well, a patient’s circumstances might be considered coercive. Historically, civilly committed patients did not have the right to refuse treatment. A movement in the 1980s helped to separate civil commitment and the right to refuse treatment, which is well-established in most jurisdictions today.7 In psychiatric inpatient settings, even an involuntarily committed patient generally has a right to refuse recommended medications unless a legally permissible mechanism overrides the refusal.
Disclosure means that a person requires certain information to make a rational decision to accept or reject treatment. The question is: How much information needs to be disclosed for a patient to be adequately informed?
Disclosure requirements vary across jurisdictions. In 1960, Natanson v Kline supported the standard that disclosure required that which a “reasonable practitioner” might disclose to patients about their treatment in similar circumstances.8 Although some jurisdictions have maintained that standard,5 subsequent cases identified a more patient-centered approach to disclosure called the “reasonable person” standard (Box 2).5,9
Competence. In many settings, clinicians use the construct of “capacity” rather than “competence” because competence is a legal term that can be determined only by a judge. When an individual is deemed incompetent, his or her right to make autonomous decisions can be overridden. Children are not competent by virtue of their status as minors, although exceptions may be made for certain older youth. Adults are presumed competent unless adjudicated otherwise.
The “reasonable person” standard endorses the obligation of the professional to disclose information that a reasonable person would want to know about a proposed treatment. This standard evolved in part from Canterbury v Spence,9 in which a plaintiff who had become paralyzed alleged that he was not informed of the risks of a laminectomy. The court found that the patient must be able to rely on information that the physician holds that would be material to the patient in making an informed treatment decision in his or her best interest.
The typically required elements of disclosure include:
- diagnosis, if known
- nature and purpose of proposed treatment
- risks and benefits of proposed treatment
- alternatives to treatment and their risks and benefits
- risks and benefits of no treatment.
Disclosing information that is uniquely relevant to an individual’s situation and would be generally unknown to the clinician might not be required. For example, a clinician might not realize that it is important for a particular patient to be able to make small art objects as a hobby, so the clinician might not reveal that a medication very rarely causes a tremor. Nevertheless, when you are aware of a need for such nuanced information, the usual general disclosure can be modified to include whatever details are relevant to that patient.5
Competence can be broken down into 4 component capacities (Box 3).11 The degree of incapacity required for a finding of incompetence is complicated and difficult to codify. Instruments designed to standardize competence assessment are available12 but not routinely used in clinical settings. Even with these instruments, no threshold of capacity clearly defines competence. Some authors have argued for a sliding scale of competence, with standards becoming more stringent as the degree of risk related to the treatment decision increases.13,14
Express and sustain a choice. To be considered competent to give informed consent, a person must be able to evidence a choice regarding the decision at hand. The choice need not be expressed verbally, but a patient must be able to communicate in some fashion (such as eye blinking or handwritten communication). The patient also must be able to maintain that choice over time, long enough for treatment to be implemented.
Understand presented information. A person must have a factual understanding of the information presented about the treatment. A full scientific understanding of diagnosis and subtleties of treatment likely would be an excessive expectation. For example, a patient would not be expected to understand the nuances of the serotonin neurotransmitter system. A physician should, however, assess whether the patient understands—in the patient’s words—that a selective serotonin reuptake inhibitor could induce manic-type symptoms and that the patient should bring these symptoms to the prescribing physician’s attention if they occur.
Appreciate one’s situation. Individuals who are competent must have a realistic appreciation of their situation. Though a patient may understand the facts you have presented, he may fail to fully integrate why the information is relevant to him. Persons with schizophrenia who do not believe they are ill—such as Mr. D—might have a limited appreciation of why an antipsychotic would help them.
Rationally manipulate information. A person also must be able to rationally manipulate the information in a way that is not impaired by symptoms of illness. Patients faced with a treatment decision should be able to use reason to reach a logical and rational decision that they see as being in their best interest. This might not be the same decision you would make. For example, a patient with thought disorganization or one who psychotically believes that the color of a recommended medication signals that someone tampered with the pills might not be able to rationally manipulate information presented about treatment options.
Source: Reference 11
Exceptions to informed consent
Emergencies. Informed consent is not required under some circumstances.5 Consider the patient who is brought to the emergency room unconscious after a fall, with no family contact information. A neurosurgeon might need to intervene immediately to save the patient’s life, using the emergency exception to informed consent.
In an emergency, when a person is unable to give informed consent or time does not allow for a full informed consent process, the clinician generally follows the principle of doing no harm. Treatment may be started in an emergency without full informed consent on the assumption that most competent people would consent to treatment, especially where life or limb was at risk. If time and circumstances permit in an emergency, obtaining the consent of available family members may be prudent.
Incompetence. If a judge determines that a patient is incompetent to make his or her own treatment decisions, a substitute decision-maker—such as a guardian—could be appointed. In these cases, respect would suggest that to the extent possible and appropriate you would inform the incompetent ward about treatment in a way that he or she may understand.
In other circumstances, such as when a healthcare proxy has been invoked, previously designated surrogate decision-makers provide informed consent on behalf of the patient who clinically is found to lack the capacity to make healthcare decisions.
Waivers. Sometimes a competent patient decides to waive the right to further information and may turn the decision over to the clinician. To rely upon this exception, some documented assessment—even if brief—of the patient’s capacity to waive information may be important.
As noted, informing patients of their health situations is expected and accepted. Even in psychiatric settings, receiving information about potentially serious medication side effects has not necessarily led to patient harm or refusal of treatment.15 Therefore, use of this exception is only for very narrowly tailored circumstances, if used at all, and not simply because you believe a patient will refuse to consent if informed about a proposed treatment.
Some case law exists on the need to establish why the therapeutic privilege was justified as a rationale to not provide informed consent in a particular situation.16 Therefore, though it should be rarely invoked, if you use therapeutic privilege, document why you invoked this exception for that particular patient and in that particular circumstance.
Building the therapeutic alliance
Although it may meet policy or legal informed consent requirements, simply providing the patient with a form to sign before treatment begins does little to enhance patient-clinician communication.2 Providing detailed written information also might not be adequate to ensure that the patient understands the complexity of a treatment you have asked him to consider.17 Instead, an informed consent model that relies on active, ongoing dialogue about treatment can maximize patient autonomy while working for the good of the patient (Table).
- the patient’s role is understood as that of an inquisitive consumer who may challenge the physician’s authority in the quest for information
- the clinician challenges the patient’s preconceived beliefs about his or her illness and educates the patient so that both parties approach the medical issue from common ground.
1 In this model of shared decision-making, the clinician reveals information material to the decision, and the patient helps the clinician understand the circumstances that make him or her prefer 1 treatment over another.1,18
By engaging in ongoing informed consent, you may achieve greater gains within the therapeutic alliance and reduce the risk of liability.19 Where uncertainties are related to treatment, share these ambiguities as an aspect of informed consent, especially when the patient plays an active role in treatment.4 Similarly, an expanded informed consent process may be needed when:
- proposed treatments are particularly risky
- several treatment alternatives could be acceptable and effective
- evidence supports opposing views of a treatment’s effectiveness.4,20
Using informed consent to build a therapeutic alliance
|
CASE CONTINUED: A question of competence
Mr. D is calm in his discussions with the psychiatrist, and the information she presents does not seem to cause him further harm. Thus, the emergency and therapeutic privilege exceptions do not eliminate the need for an ongoing informed consent process at this time.
Mr. D has a factual understanding of the risks and benefits of the recommended antipsychotic and is able to express a consistent choice about starting this treatment. He lacks, however, an ability to appreciate his situation and has difficulty manipulating information rationally. Overall, he has deficits in aspects of his decision-making competence, which could signal the need for an exception to obtaining informed consent.
Related resources
- Pinals DA, Appelbaum PS. The history and current status of competence and informed consent in psychiatric research. Isr J Psychiatry Relat Sci. 2000;37(2):82-94.
- American Medical Association. Legal issues/patient physician relationship topics. www.ama-assn.org/ama/pub/physician-resources/legal-topics.shtml.
Dr. Pinals reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mr. D, age 45 with a history of schizophrenia, is admitted to an inpatient psychiatric unit. The psychiatrist recommends an antipsychotic to help Mr. D with fears that the FBI has implanted a radio signal device into his tooth filling. She explains the risks and benefits of the proposed drug and alternate medications, as well as the risks of no treatment.
Mr. D calmly but consistently declines the treatment. He states that he recognizes the antipsychotic is used to treat psychotic symptoms, can help people who hear voices, and can have side effects such as tardive dyskinesia. His thoughts become disorganized and difficult to follow, however, as he explains that he does not believe the medication is needed for his situation because the FBI is involved in tracking his behavior.
Informed consent in clinical settings is designed to allow patients to make rational choices about their treatment before it begins. When a psychiatric patient such as Mr. D declines a treatment you recommend, how can you balance the 2 ethical principles in medicine: beneficence toward the patient and respect for individual autonomy?1
Some authors have raised concerns that informed consent in physician-patient interactions are at times an empty exercise undertaken solely to satisfy a legal expectation.2 If executed properly, however, informed consent can enhance the therapeutic alliance and help improve treatment adherence.
Patient-centered treatment
As patients have become more informed consumers, the “doctor knows best” model of care has given way to an expectation that patients know best what they would want done regarding their health. Lawsuits related to informed consent generally allege that physicians failed to provide appropriate informed consent for treatment the plaintiffs received. These complaints suggest that had the patient been more appropriately informed, he or she might have made a different choice and would not have suffered harm related to treatment.
In a patient-centered approach to treatment, informed consent allows the patient to make an autonomous decision with the appropriate information. Providing treatment without the patient’s expressed consent could be viewed more seriously, potentially even as battery.3 Recent informed consent cases tend to rely on negligence theories, however, rather than on claims of battery. Negligence cases helped set the stage of evolving expectations—first seen with surgical procedures, then medical interventions, then medication treatment, and now even with psychotherapy (Box 1)—that informed consent should be obtained in clinical settings.4
Because failure to provide informed consent can be grounds for a negligence claim, consider strategies to reduce the chance of successful litigation.
Although a written form can provide some proof that informed consent occurred, it may not prove that you conveyed adequate information or that your patient understood the information. Overly simplistic or complex forms can pose other difficulties in malpractice claims. Documenting aspects of the informed consent dialogue often provides the best “proof” that such a conversation occurred.
In retrospect, helpful evidence that adequate informed consent was obtained may include information related to the disclosed information and the patient’s response to the information (such as might be seen in a quote that indicated his or her understanding of a particular side effect). Although a full accounting of the conversation would not be a reasonable expectation for documentation, you might wish to consider the risks and benefits inherent to the particular treatment and tailor the note related to the informed consent accordingly.
3 components of informed consent
Informed consent includes 3 components: voluntariness, disclosure, and competence.5
Voluntariness implies that the patient must make treatment-related choices of his or her own free will and without coercion. In Kaimowitz v Michigan Department of Mental Health,6 the court ruled that involuntarily committed persons living in what was considered an inherently coercive institutional environment were not capable of providing voluntary consent to a high-risk experimental procedure. This case had a major impact on prison research.
In treatment settings as well, a patient’s circumstances might be considered coercive. Historically, civilly committed patients did not have the right to refuse treatment. A movement in the 1980s helped to separate civil commitment and the right to refuse treatment, which is well-established in most jurisdictions today.7 In psychiatric inpatient settings, even an involuntarily committed patient generally has a right to refuse recommended medications unless a legally permissible mechanism overrides the refusal.
Disclosure means that a person requires certain information to make a rational decision to accept or reject treatment. The question is: How much information needs to be disclosed for a patient to be adequately informed?
Disclosure requirements vary across jurisdictions. In 1960, Natanson v Kline supported the standard that disclosure required that which a “reasonable practitioner” might disclose to patients about their treatment in similar circumstances.8 Although some jurisdictions have maintained that standard,5 subsequent cases identified a more patient-centered approach to disclosure called the “reasonable person” standard (Box 2).5,9
Competence. In many settings, clinicians use the construct of “capacity” rather than “competence” because competence is a legal term that can be determined only by a judge. When an individual is deemed incompetent, his or her right to make autonomous decisions can be overridden. Children are not competent by virtue of their status as minors, although exceptions may be made for certain older youth. Adults are presumed competent unless adjudicated otherwise.
The “reasonable person” standard endorses the obligation of the professional to disclose information that a reasonable person would want to know about a proposed treatment. This standard evolved in part from Canterbury v Spence,9 in which a plaintiff who had become paralyzed alleged that he was not informed of the risks of a laminectomy. The court found that the patient must be able to rely on information that the physician holds that would be material to the patient in making an informed treatment decision in his or her best interest.
The typically required elements of disclosure include:
- diagnosis, if known
- nature and purpose of proposed treatment
- risks and benefits of proposed treatment
- alternatives to treatment and their risks and benefits
- risks and benefits of no treatment.
Disclosing information that is uniquely relevant to an individual’s situation and would be generally unknown to the clinician might not be required. For example, a clinician might not realize that it is important for a particular patient to be able to make small art objects as a hobby, so the clinician might not reveal that a medication very rarely causes a tremor. Nevertheless, when you are aware of a need for such nuanced information, the usual general disclosure can be modified to include whatever details are relevant to that patient.5
Competence can be broken down into 4 component capacities (Box 3).11 The degree of incapacity required for a finding of incompetence is complicated and difficult to codify. Instruments designed to standardize competence assessment are available12 but not routinely used in clinical settings. Even with these instruments, no threshold of capacity clearly defines competence. Some authors have argued for a sliding scale of competence, with standards becoming more stringent as the degree of risk related to the treatment decision increases.13,14
Express and sustain a choice. To be considered competent to give informed consent, a person must be able to evidence a choice regarding the decision at hand. The choice need not be expressed verbally, but a patient must be able to communicate in some fashion (such as eye blinking or handwritten communication). The patient also must be able to maintain that choice over time, long enough for treatment to be implemented.
Understand presented information. A person must have a factual understanding of the information presented about the treatment. A full scientific understanding of diagnosis and subtleties of treatment likely would be an excessive expectation. For example, a patient would not be expected to understand the nuances of the serotonin neurotransmitter system. A physician should, however, assess whether the patient understands—in the patient’s words—that a selective serotonin reuptake inhibitor could induce manic-type symptoms and that the patient should bring these symptoms to the prescribing physician’s attention if they occur.
Appreciate one’s situation. Individuals who are competent must have a realistic appreciation of their situation. Though a patient may understand the facts you have presented, he may fail to fully integrate why the information is relevant to him. Persons with schizophrenia who do not believe they are ill—such as Mr. D—might have a limited appreciation of why an antipsychotic would help them.
Rationally manipulate information. A person also must be able to rationally manipulate the information in a way that is not impaired by symptoms of illness. Patients faced with a treatment decision should be able to use reason to reach a logical and rational decision that they see as being in their best interest. This might not be the same decision you would make. For example, a patient with thought disorganization or one who psychotically believes that the color of a recommended medication signals that someone tampered with the pills might not be able to rationally manipulate information presented about treatment options.
Source: Reference 11
Exceptions to informed consent
Emergencies. Informed consent is not required under some circumstances.5 Consider the patient who is brought to the emergency room unconscious after a fall, with no family contact information. A neurosurgeon might need to intervene immediately to save the patient’s life, using the emergency exception to informed consent.
In an emergency, when a person is unable to give informed consent or time does not allow for a full informed consent process, the clinician generally follows the principle of doing no harm. Treatment may be started in an emergency without full informed consent on the assumption that most competent people would consent to treatment, especially where life or limb was at risk. If time and circumstances permit in an emergency, obtaining the consent of available family members may be prudent.
Incompetence. If a judge determines that a patient is incompetent to make his or her own treatment decisions, a substitute decision-maker—such as a guardian—could be appointed. In these cases, respect would suggest that to the extent possible and appropriate you would inform the incompetent ward about treatment in a way that he or she may understand.
In other circumstances, such as when a healthcare proxy has been invoked, previously designated surrogate decision-makers provide informed consent on behalf of the patient who clinically is found to lack the capacity to make healthcare decisions.
Waivers. Sometimes a competent patient decides to waive the right to further information and may turn the decision over to the clinician. To rely upon this exception, some documented assessment—even if brief—of the patient’s capacity to waive information may be important.
As noted, informing patients of their health situations is expected and accepted. Even in psychiatric settings, receiving information about potentially serious medication side effects has not necessarily led to patient harm or refusal of treatment.15 Therefore, use of this exception is only for very narrowly tailored circumstances, if used at all, and not simply because you believe a patient will refuse to consent if informed about a proposed treatment.
Some case law exists on the need to establish why the therapeutic privilege was justified as a rationale to not provide informed consent in a particular situation.16 Therefore, though it should be rarely invoked, if you use therapeutic privilege, document why you invoked this exception for that particular patient and in that particular circumstance.
Building the therapeutic alliance
Although it may meet policy or legal informed consent requirements, simply providing the patient with a form to sign before treatment begins does little to enhance patient-clinician communication.2 Providing detailed written information also might not be adequate to ensure that the patient understands the complexity of a treatment you have asked him to consider.17 Instead, an informed consent model that relies on active, ongoing dialogue about treatment can maximize patient autonomy while working for the good of the patient (Table).
- the patient’s role is understood as that of an inquisitive consumer who may challenge the physician’s authority in the quest for information
- the clinician challenges the patient’s preconceived beliefs about his or her illness and educates the patient so that both parties approach the medical issue from common ground.
1 In this model of shared decision-making, the clinician reveals information material to the decision, and the patient helps the clinician understand the circumstances that make him or her prefer 1 treatment over another.1,18
By engaging in ongoing informed consent, you may achieve greater gains within the therapeutic alliance and reduce the risk of liability.19 Where uncertainties are related to treatment, share these ambiguities as an aspect of informed consent, especially when the patient plays an active role in treatment.4 Similarly, an expanded informed consent process may be needed when:
- proposed treatments are particularly risky
- several treatment alternatives could be acceptable and effective
- evidence supports opposing views of a treatment’s effectiveness.4,20
Using informed consent to build a therapeutic alliance
|
CASE CONTINUED: A question of competence
Mr. D is calm in his discussions with the psychiatrist, and the information she presents does not seem to cause him further harm. Thus, the emergency and therapeutic privilege exceptions do not eliminate the need for an ongoing informed consent process at this time.
Mr. D has a factual understanding of the risks and benefits of the recommended antipsychotic and is able to express a consistent choice about starting this treatment. He lacks, however, an ability to appreciate his situation and has difficulty manipulating information rationally. Overall, he has deficits in aspects of his decision-making competence, which could signal the need for an exception to obtaining informed consent.
Related resources
- Pinals DA, Appelbaum PS. The history and current status of competence and informed consent in psychiatric research. Isr J Psychiatry Relat Sci. 2000;37(2):82-94.
- American Medical Association. Legal issues/patient physician relationship topics. www.ama-assn.org/ama/pub/physician-resources/legal-topics.shtml.
Dr. Pinals reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. King JS, Moulton BW. Rethinking informed consent: the case for shared medical decision-making. Am J Law Med. 2006;32(4):429-501.
2. Lidz CW, Appelbaum PS, Meisel A. Two models of implementing informed consent. Arch Intern Med. 1988;148(6):1385-1389.
3. Schloendorff v Society of New York Hospital, 105 NE 92 (1914).
4. Beahrs JO, Gutheil TG. Informed consent in psychotherapy. Am J Psychiatry. 2001;158(1):4-10.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. Philadelphia, PA: Wolters Kluwer and Lippincott Williams & Wilkins; 2007.
6. Kaimowitz v Michigan, DMH 1 MDLR 147 (1976).
7. Pinals DA, Hoge SK. Treatment refusal in psychiatric practice. In: Rosner R, ed. Principles and practice of forensic psychiatry, 2nd ed. London, UK: Arnold Press; 2003:129-136.
8. Natanson v Kline, 350 P.2D 1093 (1960).
9. Canterbury v Spence, 464 F.2d 772 (1972).
10. Grisso T, Appelbaum PS. The MacArthur Treatment Competence Study: III. Abilities of patients to consent to psychiatric and medical treatment. Law Human Behav. 1995;19(2):149-174.
11. Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
12. Dunn LB, Nowrangi MA, Palmer BW, et al. Assessing decisional capacity for clinical research or treatment: a review of instruments. Am J Psychiatry. 2006;163(8):1323-1334.
13. Drane JF. Competency to give an informed consent: a model for making clinical assessments. JAMA. 1984;252(7):925-927.
14. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
15. Munetz MR, Roth LH. Informing patients about tardive dyskinesia. Arch Gen Psychiatry. 1985;42(9):866-871.
16. Barcai v Betwee MD, 50 P3d 946 (2002).
17. Hafeez A, Wiseman O, Hill JT. Informed consent: are we deluding ourselves? A randomized controlled study. BJU International. 2007;99(1):4-5.
18. Kaplan RM. Shared medical decision making: a new tool for preventative medicine. Am J Prev Med. 2004;26(1):81-83.
19. Gutheil TG, Bursztajn H, Brodsky A. Malpractice prevention through the sharing of uncertainty. Informed consent and the therapeutic alliance. N Engl J Med. 1984;311(1):49-51.
20. Packman WL, Cabot MG, Bongar B. Malpractice arising from negligent psychotherapy: ethical, legal, and clinical implications of Osheroff v Chestnut Lodge. Ethics Behav. 1994;4(3):175-197.
1. King JS, Moulton BW. Rethinking informed consent: the case for shared medical decision-making. Am J Law Med. 2006;32(4):429-501.
2. Lidz CW, Appelbaum PS, Meisel A. Two models of implementing informed consent. Arch Intern Med. 1988;148(6):1385-1389.
3. Schloendorff v Society of New York Hospital, 105 NE 92 (1914).
4. Beahrs JO, Gutheil TG. Informed consent in psychotherapy. Am J Psychiatry. 2001;158(1):4-10.
5. Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. Philadelphia, PA: Wolters Kluwer and Lippincott Williams & Wilkins; 2007.
6. Kaimowitz v Michigan, DMH 1 MDLR 147 (1976).
7. Pinals DA, Hoge SK. Treatment refusal in psychiatric practice. In: Rosner R, ed. Principles and practice of forensic psychiatry, 2nd ed. London, UK: Arnold Press; 2003:129-136.
8. Natanson v Kline, 350 P.2D 1093 (1960).
9. Canterbury v Spence, 464 F.2d 772 (1972).
10. Grisso T, Appelbaum PS. The MacArthur Treatment Competence Study: III. Abilities of patients to consent to psychiatric and medical treatment. Law Human Behav. 1995;19(2):149-174.
11. Appelbaum PS, Grisso T. Assessing patients’ capacities to consent to treatment. N Engl J Med. 1988;319(25):1635-1638.
12. Dunn LB, Nowrangi MA, Palmer BW, et al. Assessing decisional capacity for clinical research or treatment: a review of instruments. Am J Psychiatry. 2006;163(8):1323-1334.
13. Drane JF. Competency to give an informed consent: a model for making clinical assessments. JAMA. 1984;252(7):925-927.
14. Appelbaum PS. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
15. Munetz MR, Roth LH. Informing patients about tardive dyskinesia. Arch Gen Psychiatry. 1985;42(9):866-871.
16. Barcai v Betwee MD, 50 P3d 946 (2002).
17. Hafeez A, Wiseman O, Hill JT. Informed consent: are we deluding ourselves? A randomized controlled study. BJU International. 2007;99(1):4-5.
18. Kaplan RM. Shared medical decision making: a new tool for preventative medicine. Am J Prev Med. 2004;26(1):81-83.
19. Gutheil TG, Bursztajn H, Brodsky A. Malpractice prevention through the sharing of uncertainty. Informed consent and the therapeutic alliance. N Engl J Med. 1984;311(1):49-51.
20. Packman WL, Cabot MG, Bongar B. Malpractice arising from negligent psychotherapy: ethical, legal, and clinical implications of Osheroff v Chestnut Lodge. Ethics Behav. 1994;4(3):175-197.