User login
Are ObGyns offering the range of treatment options for early pregnancy failure?
One in every four women experiences EPF. Although office uterine evacuation and misoprostol administration are less invasive and less expensive alternatives to traditional OR evacuation, it is not clear how extensively clinicians employ these options in the United States.1,2
In 2008, Dalton and colleagues surveyed ObGyns, certified nurse midwives (CNMs), and family physicians (FPs) in the United States who had evaluated or treated, or both, a woman for EPF in the preceding 6 months. They achieved response rates of 51.0%, 70.9%, and 53.5%, respectively. Evaluable respondents had a mean age of 49 to 50 years and included 309 ObGyns (46.9% of whom were female), 368 CNMs (97.8% female), and 299 FPs (43.6% female).
Overall, approximately one third of respondents believe that office evacuation is riskier than OR evacuation. In addition, 65.7% of ObGyns believe that most patients prefer OR evacuation, compared with 46.2% and 43.1% of CNMs and FPs, respectively (P < .001). Among ObGyns, an adjusted analysis estimated the likelihood of providing office evacuation to be five times higher among those who have undergone training in induced abortion (P < .05). As for misoprostol for EPF, about two thirds of respondents overall believe that it is safe.
Dalton and associates posit that providers “perceive that their personal treatment preferences are different than their patients’. Whether this discordance results in women undergoing operating room uterine evacuation more often than is necessary or preferred could not be assessed by this study.” However, the authors also assert that, “given that providers affect treatment choice greatly, it is plausible that provider treatment preferences are an important influence on current treatment patterns.”
Certainly, women have diverse preferences for how EPF is managed, but many do find office evacuation and misoprostol to be acceptable methods. Accordingly, we should offer all options to them. As the investigators in this study suggest, we may need to focus on correcting inaccurate beliefs about these modalities among providers to increase their willingness to offer them.
The findings of this survey also underscore the fact that training programs that do not teach induced abortion—or that allow trainees to opt out of such training—can compromise the care provided to women who have EPF.—ANDREW M. KAUNITZ, MD
We want to hear from you! Tell us what you think.
1. Zhang J, Gilles JM, Barnhart K, et al. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353(8):761-769.
2. Harris LH, Dalton VK, Johnson TR. Surgical management of early pregnancy failure: history, politics, and safe, cost-effective care. Am J Obstet Gynecol. 2007;196(5):445.e1–e5.-
One in every four women experiences EPF. Although office uterine evacuation and misoprostol administration are less invasive and less expensive alternatives to traditional OR evacuation, it is not clear how extensively clinicians employ these options in the United States.1,2
In 2008, Dalton and colleagues surveyed ObGyns, certified nurse midwives (CNMs), and family physicians (FPs) in the United States who had evaluated or treated, or both, a woman for EPF in the preceding 6 months. They achieved response rates of 51.0%, 70.9%, and 53.5%, respectively. Evaluable respondents had a mean age of 49 to 50 years and included 309 ObGyns (46.9% of whom were female), 368 CNMs (97.8% female), and 299 FPs (43.6% female).
Overall, approximately one third of respondents believe that office evacuation is riskier than OR evacuation. In addition, 65.7% of ObGyns believe that most patients prefer OR evacuation, compared with 46.2% and 43.1% of CNMs and FPs, respectively (P < .001). Among ObGyns, an adjusted analysis estimated the likelihood of providing office evacuation to be five times higher among those who have undergone training in induced abortion (P < .05). As for misoprostol for EPF, about two thirds of respondents overall believe that it is safe.
Dalton and associates posit that providers “perceive that their personal treatment preferences are different than their patients’. Whether this discordance results in women undergoing operating room uterine evacuation more often than is necessary or preferred could not be assessed by this study.” However, the authors also assert that, “given that providers affect treatment choice greatly, it is plausible that provider treatment preferences are an important influence on current treatment patterns.”
Certainly, women have diverse preferences for how EPF is managed, but many do find office evacuation and misoprostol to be acceptable methods. Accordingly, we should offer all options to them. As the investigators in this study suggest, we may need to focus on correcting inaccurate beliefs about these modalities among providers to increase their willingness to offer them.
The findings of this survey also underscore the fact that training programs that do not teach induced abortion—or that allow trainees to opt out of such training—can compromise the care provided to women who have EPF.—ANDREW M. KAUNITZ, MD
We want to hear from you! Tell us what you think.
One in every four women experiences EPF. Although office uterine evacuation and misoprostol administration are less invasive and less expensive alternatives to traditional OR evacuation, it is not clear how extensively clinicians employ these options in the United States.1,2
In 2008, Dalton and colleagues surveyed ObGyns, certified nurse midwives (CNMs), and family physicians (FPs) in the United States who had evaluated or treated, or both, a woman for EPF in the preceding 6 months. They achieved response rates of 51.0%, 70.9%, and 53.5%, respectively. Evaluable respondents had a mean age of 49 to 50 years and included 309 ObGyns (46.9% of whom were female), 368 CNMs (97.8% female), and 299 FPs (43.6% female).
Overall, approximately one third of respondents believe that office evacuation is riskier than OR evacuation. In addition, 65.7% of ObGyns believe that most patients prefer OR evacuation, compared with 46.2% and 43.1% of CNMs and FPs, respectively (P < .001). Among ObGyns, an adjusted analysis estimated the likelihood of providing office evacuation to be five times higher among those who have undergone training in induced abortion (P < .05). As for misoprostol for EPF, about two thirds of respondents overall believe that it is safe.
Dalton and associates posit that providers “perceive that their personal treatment preferences are different than their patients’. Whether this discordance results in women undergoing operating room uterine evacuation more often than is necessary or preferred could not be assessed by this study.” However, the authors also assert that, “given that providers affect treatment choice greatly, it is plausible that provider treatment preferences are an important influence on current treatment patterns.”
Certainly, women have diverse preferences for how EPF is managed, but many do find office evacuation and misoprostol to be acceptable methods. Accordingly, we should offer all options to them. As the investigators in this study suggest, we may need to focus on correcting inaccurate beliefs about these modalities among providers to increase their willingness to offer them.
The findings of this survey also underscore the fact that training programs that do not teach induced abortion—or that allow trainees to opt out of such training—can compromise the care provided to women who have EPF.—ANDREW M. KAUNITZ, MD
We want to hear from you! Tell us what you think.
1. Zhang J, Gilles JM, Barnhart K, et al. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353(8):761-769.
2. Harris LH, Dalton VK, Johnson TR. Surgical management of early pregnancy failure: history, politics, and safe, cost-effective care. Am J Obstet Gynecol. 2007;196(5):445.e1–e5.-
1. Zhang J, Gilles JM, Barnhart K, et al. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. N Engl J Med. 2005;353(8):761-769.
2. Harris LH, Dalton VK, Johnson TR. Surgical management of early pregnancy failure: history, politics, and safe, cost-effective care. Am J Obstet Gynecol. 2007;196(5):445.e1–e5.-
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Anti-emetics and drug-induced parkinsonism in a gyn-onc patient
The anti-emetics prochlorperazine (Compazine) and metoclopramide (Reglan) are commonly used in obstetric and gynecologic care. Extrapyramidal reactions are rare side effects of these drugs, and have been described with metoclopramide since 1978. Such reactions vary—from acute dystonic reaction, akathisia, and tardive dyskinesia all the way up to full-blown parkinsonism.
Drug-induced parkinsonism (DIP) can be difficult to diagnose; it is often missed by clinicians (even by neurologists).1 This is regrettable, because DIP is usually reversible once the offending agent is withdrawn.
In this brief report, we discuss the case of a gynecologic oncology patient who developed DIP after receiving anti-emetics to alleviate side effects of chemoradiation.
CASE: Late postop complaints
A 43-year-old G0 gyn-onc patient came to the emergency department of our hospital several weeks after radical abdominal hysterectomy, bilateral salpingo-oophorectomy, and bilateral pelvic lymph node dissection for Stage IB1 squamous cell carcinoma of the cervix. Her primary complaints in the ED were “throbbing” in the thighs bilaterally and leg pain.
The woman’s postop course had otherwise been uncomplicated. Because she had one pelvic lymph node positive for disease, however, she had received:
- a total dose of 240 mg/m2 of external-beam pelvic radiation
- concurrent weekly doses of 40 mg/m2 of cisplatin.
Before this ED visit, chemoradiation was complicated by persistent nausea that, eventually, responded to a combination of metoclopramide and prochlorperazine.
Deep-vein thrombosis was ruled out in the ED. No diagnosis or treatment was offered. 1 week later. The patient returned, complaining of generalized weakness. The ED workup this time, comprising laboratory testing and computed tomography of the abdomen and pelvis, was negative. She was given a diagnosis of “cisplatin neurotoxicity.” No treatment was provided.
CASE: Continued Off in the wrong direction?
Cisplatin neurotoxicity has a variety of presentations, including peripheral neuropathy, gait disturbance, autonomic neuropathy, seizures, and Lhermitte’s sign (inducible tingling or a sensation like electrical shock in the arms and legs, upon flexion of the neck). Peripheral neuropathy, most common, begins in the hands or feet and ascends proximally.
Neurotoxicity following cisplatin is usually observed after a total dosage of 300 mg/m2; symptoms are irreversible in 30% to 50% of patients.2
Our patient had received a total cisplatin dosage of just 240 mg/m2, however, and never exhibited classic signs of cisplatin neurotoxicity. Was the ED diagnosis off the mark? 10 days later. Now, approximately one month after chemoradiation, the patient visited our outpatient facility, complaining that her original symptoms (“throbbing” leg pain, restlessness in the extremities, generalized weakness) had become worse and that she had developed a generalized tremor. She had also become severely de-conditioned and required assistance with activities of daily living.
On physical exam, the patient displayed a bilateral upper-extremity resting tremor that was exacerbated by intentional movement. She drooled, and had dysarthria, a shuffling gait, and cogwheel rigidity.
Medications included metoclopramide, three times daily; prochlorperazine, every 6 hours; omeprazole; and dexamethasone.
The medical history and family history were negative for neurodegenerative disease.
A neurology consult was requested. The neurologist diagnosed drug-induced parkinsonism (DIP) secondary to metoclopramide and prochlorperazine.
Parkinsonism encompasses a spectrum of disease. It is characterized by resting tremor, bradykinesia, rigidity, and postural instability. Secondary parkinsonism, such as DIP, has an identifiable cause and can, potentially, be reversed.
Distinguishing primary and secondary parkinsonism can be a challenge. In DIP, rigidity and bradykinesia typically dominate; DIP also:
- tends to be more common with increasing age
- occurs more often in women (2:1 prevalence)
- has a bimodal age distribution
- is characterized by a symmetric resting tremor that affects primarily the upper extremities.3
Any medication that decreases dopaminergic activity in the nigrostriatal pathway can cause parkinsonism. These include a number of medications commonly administered to OB and gynecology patients:
- disulfiram
- some calcium channel blockers
- methyldopa
- meperidine
- some selective serotonin reuptake inhibitors
- antiepileptics
- estrogen and oral contraceptives (although estrogen can have an anti-dopaminergic effect).4
DIP is reported most often after neuroleptic therapy and after exposure to certain anti-emetics, such as the metoclopramide and prochlorperazine given to this patient, that block dopamine receptors.
Whether the manifestations of DIP are reversible depends on the dosage and duration of exposure to the medication. Subtle side effects, such as masked facies and difficulty swallowing, may occur within minutes, or hours, after the patient is exposed to the drug.
Most symptoms of DIP are misdiagnosed
In a series of patients reported by Miller and colleagues,5 131 who had a drug-induced movement disorder continued on the offending medication for, on average, 6 months after onset of symptoms. In a study by Esper and coworkers of DIP patients at movement disorder clinics, average time to correct diagnosis after symptoms were reported was 1.8 years.1
Our patient exhibited symptoms for 1 month before the correct diagnosis was made, at her third visit for those symptoms.
CASE: Resolved
The patient was hospitalized and the anti-emetics discontinued upon the neurologist’s diagnosis. Diphenhydramine and benztropine were started to counteract extrapyramidal symptoms.
Within 24 hours, neurologic symptoms improved strikingly.
At discharge, the patient was able to walk without assistance and had normal facial expressions. The tremor had ceased.
At 6-week follow-up, neurologic symptoms had not returned.
Our patient’s complaints encompassed the full range of extrapyramidal side effects—akathisia (leg restlessness), trouble swallowing and drooling (acute dystonic reaction), tremor, cogwheel rigidity, and dysarthria (parkinsonism).
Of new cases of parkinsonism among a series of 95 patients seen at a geriatric clinic, 51% were given a diagnosis of DIP.6 In a large, prospective study by Bateman and colleagues in northern Great Britain, the incidence of metoclopramide-induced dystonia was 1 in 213; akathisia, 1 in 320; and DIP, 1 in 512.7 The incidence of prochlorperazine-induced dystonia was 1 in 702, akathisia 1 in 937, and parkinsonism 1 in 312. Most retrospective cases of metoclopramide-induced parkinsonism occur in the elderly (older than 60 years).5,8,9
Parkinsonism develops when the striatal dopamine levels fall below 80% of expected (normal) values. This may explain why certain populations in whom the dopamine level is already low, such as the elderly, may be more susceptible to DIP.9
It is difficult to discern which anti-emetic was responsible for our patient’s symptoms; both may be guilty. In the time-line of the case, symptoms manifested when prochlorperazine was started and appeared to have been compounded by addition of metoclopramide. The literature shows that both medications can produce extrapyramidal reactions and parkinsonism.
Symptoms of DIP usually resolve within weeks or months in most patients. In fact, problems that persist beyond 6 months after the medication is withdrawn should raise suspicion of primary Parkinson’s disease or a permanent sequela, such as tardive dyskinesia.3,5
In short, failure to diagnose and treat DIP prolongs the patient’s suffering, which could be relieved by doing something as simple as stopping the agents in question.
1. Esper CD, Factor SA. Failure of recognition of drug-induced parkinsonism in the elderly. Mov Disord. 2008;23(3):401-404.
2. Cersosimo RJ. Cisplatin neurotoxicity. Cancer Treat Rev. 1989;16(4):195-211.
3. Susatia F, Fernandez HH. Drug-induced parkinsonism. Curr Treat Options Neurol. 2009;11(3):162-169.
4. Van Gerpen JA. Drug-induced parkinsonism. Neurologist. 2002;8(6):363-370.
5. Miller LG, Jankovic J. Metoclopramide-induced movement disorders. Clinical findings with a review of the literature. Arch Intern Med. 1989;149(11):2486-2492.
6. Stephen PJ, Williamson J. Drug-induced parkinsonism in the elderly. Lancet. 1984;2(8411):1082-1083.
7. Bateman DN, Darling WM, Boys R, Rawlins MD. Extrapyramidal reactions to metoclopramide and prochlorperazine. Q J Med. 1989;71(264):307-311.
8. Grimes JD, Hassan MN, Preston DN. Adverse neurologic effects of metoclopramide. Can Med Assoc J. 1982;126(1):23-25.
9. Bateman DN, Rawlins MD, Simpson JM. Extrapyramidal reactions with metoclopramide. Br Med J (Clin Res Ed). 1985;291(6500):930-932.
The anti-emetics prochlorperazine (Compazine) and metoclopramide (Reglan) are commonly used in obstetric and gynecologic care. Extrapyramidal reactions are rare side effects of these drugs, and have been described with metoclopramide since 1978. Such reactions vary—from acute dystonic reaction, akathisia, and tardive dyskinesia all the way up to full-blown parkinsonism.
Drug-induced parkinsonism (DIP) can be difficult to diagnose; it is often missed by clinicians (even by neurologists).1 This is regrettable, because DIP is usually reversible once the offending agent is withdrawn.
In this brief report, we discuss the case of a gynecologic oncology patient who developed DIP after receiving anti-emetics to alleviate side effects of chemoradiation.
CASE: Late postop complaints
A 43-year-old G0 gyn-onc patient came to the emergency department of our hospital several weeks after radical abdominal hysterectomy, bilateral salpingo-oophorectomy, and bilateral pelvic lymph node dissection for Stage IB1 squamous cell carcinoma of the cervix. Her primary complaints in the ED were “throbbing” in the thighs bilaterally and leg pain.
The woman’s postop course had otherwise been uncomplicated. Because she had one pelvic lymph node positive for disease, however, she had received:
- a total dose of 240 mg/m2 of external-beam pelvic radiation
- concurrent weekly doses of 40 mg/m2 of cisplatin.
Before this ED visit, chemoradiation was complicated by persistent nausea that, eventually, responded to a combination of metoclopramide and prochlorperazine.
Deep-vein thrombosis was ruled out in the ED. No diagnosis or treatment was offered. 1 week later. The patient returned, complaining of generalized weakness. The ED workup this time, comprising laboratory testing and computed tomography of the abdomen and pelvis, was negative. She was given a diagnosis of “cisplatin neurotoxicity.” No treatment was provided.
CASE: Continued Off in the wrong direction?
Cisplatin neurotoxicity has a variety of presentations, including peripheral neuropathy, gait disturbance, autonomic neuropathy, seizures, and Lhermitte’s sign (inducible tingling or a sensation like electrical shock in the arms and legs, upon flexion of the neck). Peripheral neuropathy, most common, begins in the hands or feet and ascends proximally.
Neurotoxicity following cisplatin is usually observed after a total dosage of 300 mg/m2; symptoms are irreversible in 30% to 50% of patients.2
Our patient had received a total cisplatin dosage of just 240 mg/m2, however, and never exhibited classic signs of cisplatin neurotoxicity. Was the ED diagnosis off the mark? 10 days later. Now, approximately one month after chemoradiation, the patient visited our outpatient facility, complaining that her original symptoms (“throbbing” leg pain, restlessness in the extremities, generalized weakness) had become worse and that she had developed a generalized tremor. She had also become severely de-conditioned and required assistance with activities of daily living.
On physical exam, the patient displayed a bilateral upper-extremity resting tremor that was exacerbated by intentional movement. She drooled, and had dysarthria, a shuffling gait, and cogwheel rigidity.
Medications included metoclopramide, three times daily; prochlorperazine, every 6 hours; omeprazole; and dexamethasone.
The medical history and family history were negative for neurodegenerative disease.
A neurology consult was requested. The neurologist diagnosed drug-induced parkinsonism (DIP) secondary to metoclopramide and prochlorperazine.
Parkinsonism encompasses a spectrum of disease. It is characterized by resting tremor, bradykinesia, rigidity, and postural instability. Secondary parkinsonism, such as DIP, has an identifiable cause and can, potentially, be reversed.
Distinguishing primary and secondary parkinsonism can be a challenge. In DIP, rigidity and bradykinesia typically dominate; DIP also:
- tends to be more common with increasing age
- occurs more often in women (2:1 prevalence)
- has a bimodal age distribution
- is characterized by a symmetric resting tremor that affects primarily the upper extremities.3
Any medication that decreases dopaminergic activity in the nigrostriatal pathway can cause parkinsonism. These include a number of medications commonly administered to OB and gynecology patients:
- disulfiram
- some calcium channel blockers
- methyldopa
- meperidine
- some selective serotonin reuptake inhibitors
- antiepileptics
- estrogen and oral contraceptives (although estrogen can have an anti-dopaminergic effect).4
DIP is reported most often after neuroleptic therapy and after exposure to certain anti-emetics, such as the metoclopramide and prochlorperazine given to this patient, that block dopamine receptors.
Whether the manifestations of DIP are reversible depends on the dosage and duration of exposure to the medication. Subtle side effects, such as masked facies and difficulty swallowing, may occur within minutes, or hours, after the patient is exposed to the drug.
Most symptoms of DIP are misdiagnosed
In a series of patients reported by Miller and colleagues,5 131 who had a drug-induced movement disorder continued on the offending medication for, on average, 6 months after onset of symptoms. In a study by Esper and coworkers of DIP patients at movement disorder clinics, average time to correct diagnosis after symptoms were reported was 1.8 years.1
Our patient exhibited symptoms for 1 month before the correct diagnosis was made, at her third visit for those symptoms.
CASE: Resolved
The patient was hospitalized and the anti-emetics discontinued upon the neurologist’s diagnosis. Diphenhydramine and benztropine were started to counteract extrapyramidal symptoms.
Within 24 hours, neurologic symptoms improved strikingly.
At discharge, the patient was able to walk without assistance and had normal facial expressions. The tremor had ceased.
At 6-week follow-up, neurologic symptoms had not returned.
Our patient’s complaints encompassed the full range of extrapyramidal side effects—akathisia (leg restlessness), trouble swallowing and drooling (acute dystonic reaction), tremor, cogwheel rigidity, and dysarthria (parkinsonism).
Of new cases of parkinsonism among a series of 95 patients seen at a geriatric clinic, 51% were given a diagnosis of DIP.6 In a large, prospective study by Bateman and colleagues in northern Great Britain, the incidence of metoclopramide-induced dystonia was 1 in 213; akathisia, 1 in 320; and DIP, 1 in 512.7 The incidence of prochlorperazine-induced dystonia was 1 in 702, akathisia 1 in 937, and parkinsonism 1 in 312. Most retrospective cases of metoclopramide-induced parkinsonism occur in the elderly (older than 60 years).5,8,9
Parkinsonism develops when the striatal dopamine levels fall below 80% of expected (normal) values. This may explain why certain populations in whom the dopamine level is already low, such as the elderly, may be more susceptible to DIP.9
It is difficult to discern which anti-emetic was responsible for our patient’s symptoms; both may be guilty. In the time-line of the case, symptoms manifested when prochlorperazine was started and appeared to have been compounded by addition of metoclopramide. The literature shows that both medications can produce extrapyramidal reactions and parkinsonism.
Symptoms of DIP usually resolve within weeks or months in most patients. In fact, problems that persist beyond 6 months after the medication is withdrawn should raise suspicion of primary Parkinson’s disease or a permanent sequela, such as tardive dyskinesia.3,5
In short, failure to diagnose and treat DIP prolongs the patient’s suffering, which could be relieved by doing something as simple as stopping the agents in question.
The anti-emetics prochlorperazine (Compazine) and metoclopramide (Reglan) are commonly used in obstetric and gynecologic care. Extrapyramidal reactions are rare side effects of these drugs, and have been described with metoclopramide since 1978. Such reactions vary—from acute dystonic reaction, akathisia, and tardive dyskinesia all the way up to full-blown parkinsonism.
Drug-induced parkinsonism (DIP) can be difficult to diagnose; it is often missed by clinicians (even by neurologists).1 This is regrettable, because DIP is usually reversible once the offending agent is withdrawn.
In this brief report, we discuss the case of a gynecologic oncology patient who developed DIP after receiving anti-emetics to alleviate side effects of chemoradiation.
CASE: Late postop complaints
A 43-year-old G0 gyn-onc patient came to the emergency department of our hospital several weeks after radical abdominal hysterectomy, bilateral salpingo-oophorectomy, and bilateral pelvic lymph node dissection for Stage IB1 squamous cell carcinoma of the cervix. Her primary complaints in the ED were “throbbing” in the thighs bilaterally and leg pain.
The woman’s postop course had otherwise been uncomplicated. Because she had one pelvic lymph node positive for disease, however, she had received:
- a total dose of 240 mg/m2 of external-beam pelvic radiation
- concurrent weekly doses of 40 mg/m2 of cisplatin.
Before this ED visit, chemoradiation was complicated by persistent nausea that, eventually, responded to a combination of metoclopramide and prochlorperazine.
Deep-vein thrombosis was ruled out in the ED. No diagnosis or treatment was offered. 1 week later. The patient returned, complaining of generalized weakness. The ED workup this time, comprising laboratory testing and computed tomography of the abdomen and pelvis, was negative. She was given a diagnosis of “cisplatin neurotoxicity.” No treatment was provided.
CASE: Continued Off in the wrong direction?
Cisplatin neurotoxicity has a variety of presentations, including peripheral neuropathy, gait disturbance, autonomic neuropathy, seizures, and Lhermitte’s sign (inducible tingling or a sensation like electrical shock in the arms and legs, upon flexion of the neck). Peripheral neuropathy, most common, begins in the hands or feet and ascends proximally.
Neurotoxicity following cisplatin is usually observed after a total dosage of 300 mg/m2; symptoms are irreversible in 30% to 50% of patients.2
Our patient had received a total cisplatin dosage of just 240 mg/m2, however, and never exhibited classic signs of cisplatin neurotoxicity. Was the ED diagnosis off the mark? 10 days later. Now, approximately one month after chemoradiation, the patient visited our outpatient facility, complaining that her original symptoms (“throbbing” leg pain, restlessness in the extremities, generalized weakness) had become worse and that she had developed a generalized tremor. She had also become severely de-conditioned and required assistance with activities of daily living.
On physical exam, the patient displayed a bilateral upper-extremity resting tremor that was exacerbated by intentional movement. She drooled, and had dysarthria, a shuffling gait, and cogwheel rigidity.
Medications included metoclopramide, three times daily; prochlorperazine, every 6 hours; omeprazole; and dexamethasone.
The medical history and family history were negative for neurodegenerative disease.
A neurology consult was requested. The neurologist diagnosed drug-induced parkinsonism (DIP) secondary to metoclopramide and prochlorperazine.
Parkinsonism encompasses a spectrum of disease. It is characterized by resting tremor, bradykinesia, rigidity, and postural instability. Secondary parkinsonism, such as DIP, has an identifiable cause and can, potentially, be reversed.
Distinguishing primary and secondary parkinsonism can be a challenge. In DIP, rigidity and bradykinesia typically dominate; DIP also:
- tends to be more common with increasing age
- occurs more often in women (2:1 prevalence)
- has a bimodal age distribution
- is characterized by a symmetric resting tremor that affects primarily the upper extremities.3
Any medication that decreases dopaminergic activity in the nigrostriatal pathway can cause parkinsonism. These include a number of medications commonly administered to OB and gynecology patients:
- disulfiram
- some calcium channel blockers
- methyldopa
- meperidine
- some selective serotonin reuptake inhibitors
- antiepileptics
- estrogen and oral contraceptives (although estrogen can have an anti-dopaminergic effect).4
DIP is reported most often after neuroleptic therapy and after exposure to certain anti-emetics, such as the metoclopramide and prochlorperazine given to this patient, that block dopamine receptors.
Whether the manifestations of DIP are reversible depends on the dosage and duration of exposure to the medication. Subtle side effects, such as masked facies and difficulty swallowing, may occur within minutes, or hours, after the patient is exposed to the drug.
Most symptoms of DIP are misdiagnosed
In a series of patients reported by Miller and colleagues,5 131 who had a drug-induced movement disorder continued on the offending medication for, on average, 6 months after onset of symptoms. In a study by Esper and coworkers of DIP patients at movement disorder clinics, average time to correct diagnosis after symptoms were reported was 1.8 years.1
Our patient exhibited symptoms for 1 month before the correct diagnosis was made, at her third visit for those symptoms.
CASE: Resolved
The patient was hospitalized and the anti-emetics discontinued upon the neurologist’s diagnosis. Diphenhydramine and benztropine were started to counteract extrapyramidal symptoms.
Within 24 hours, neurologic symptoms improved strikingly.
At discharge, the patient was able to walk without assistance and had normal facial expressions. The tremor had ceased.
At 6-week follow-up, neurologic symptoms had not returned.
Our patient’s complaints encompassed the full range of extrapyramidal side effects—akathisia (leg restlessness), trouble swallowing and drooling (acute dystonic reaction), tremor, cogwheel rigidity, and dysarthria (parkinsonism).
Of new cases of parkinsonism among a series of 95 patients seen at a geriatric clinic, 51% were given a diagnosis of DIP.6 In a large, prospective study by Bateman and colleagues in northern Great Britain, the incidence of metoclopramide-induced dystonia was 1 in 213; akathisia, 1 in 320; and DIP, 1 in 512.7 The incidence of prochlorperazine-induced dystonia was 1 in 702, akathisia 1 in 937, and parkinsonism 1 in 312. Most retrospective cases of metoclopramide-induced parkinsonism occur in the elderly (older than 60 years).5,8,9
Parkinsonism develops when the striatal dopamine levels fall below 80% of expected (normal) values. This may explain why certain populations in whom the dopamine level is already low, such as the elderly, may be more susceptible to DIP.9
It is difficult to discern which anti-emetic was responsible for our patient’s symptoms; both may be guilty. In the time-line of the case, symptoms manifested when prochlorperazine was started and appeared to have been compounded by addition of metoclopramide. The literature shows that both medications can produce extrapyramidal reactions and parkinsonism.
Symptoms of DIP usually resolve within weeks or months in most patients. In fact, problems that persist beyond 6 months after the medication is withdrawn should raise suspicion of primary Parkinson’s disease or a permanent sequela, such as tardive dyskinesia.3,5
In short, failure to diagnose and treat DIP prolongs the patient’s suffering, which could be relieved by doing something as simple as stopping the agents in question.
1. Esper CD, Factor SA. Failure of recognition of drug-induced parkinsonism in the elderly. Mov Disord. 2008;23(3):401-404.
2. Cersosimo RJ. Cisplatin neurotoxicity. Cancer Treat Rev. 1989;16(4):195-211.
3. Susatia F, Fernandez HH. Drug-induced parkinsonism. Curr Treat Options Neurol. 2009;11(3):162-169.
4. Van Gerpen JA. Drug-induced parkinsonism. Neurologist. 2002;8(6):363-370.
5. Miller LG, Jankovic J. Metoclopramide-induced movement disorders. Clinical findings with a review of the literature. Arch Intern Med. 1989;149(11):2486-2492.
6. Stephen PJ, Williamson J. Drug-induced parkinsonism in the elderly. Lancet. 1984;2(8411):1082-1083.
7. Bateman DN, Darling WM, Boys R, Rawlins MD. Extrapyramidal reactions to metoclopramide and prochlorperazine. Q J Med. 1989;71(264):307-311.
8. Grimes JD, Hassan MN, Preston DN. Adverse neurologic effects of metoclopramide. Can Med Assoc J. 1982;126(1):23-25.
9. Bateman DN, Rawlins MD, Simpson JM. Extrapyramidal reactions with metoclopramide. Br Med J (Clin Res Ed). 1985;291(6500):930-932.
1. Esper CD, Factor SA. Failure of recognition of drug-induced parkinsonism in the elderly. Mov Disord. 2008;23(3):401-404.
2. Cersosimo RJ. Cisplatin neurotoxicity. Cancer Treat Rev. 1989;16(4):195-211.
3. Susatia F, Fernandez HH. Drug-induced parkinsonism. Curr Treat Options Neurol. 2009;11(3):162-169.
4. Van Gerpen JA. Drug-induced parkinsonism. Neurologist. 2002;8(6):363-370.
5. Miller LG, Jankovic J. Metoclopramide-induced movement disorders. Clinical findings with a review of the literature. Arch Intern Med. 1989;149(11):2486-2492.
6. Stephen PJ, Williamson J. Drug-induced parkinsonism in the elderly. Lancet. 1984;2(8411):1082-1083.
7. Bateman DN, Darling WM, Boys R, Rawlins MD. Extrapyramidal reactions to metoclopramide and prochlorperazine. Q J Med. 1989;71(264):307-311.
8. Grimes JD, Hassan MN, Preston DN. Adverse neurologic effects of metoclopramide. Can Med Assoc J. 1982;126(1):23-25.
9. Bateman DN, Rawlins MD, Simpson JM. Extrapyramidal reactions with metoclopramide. Br Med J (Clin Res Ed). 1985;291(6500):930-932.
Thoughts about ObGyn after practicing in Tanzania
Two years ago, our family moved to Tanzania to help build a women’s health collaboration between Duke University and the Kilimanjaro Christian Medical Center (KCMC) in the town of Moshi, one of four tertiary referral centers in Tanzania that serves a population of nearly 14 million people. The goal of the collaboration was to expand the successful Duke-KCMC HIV/AIDS program that had been in operation at KCMC for 10 years to a broader women’s health service. Here is a synopsis of what we found in Tanzania and what we learned in those 2 years working alongside excellent local consultants and medical residents. (For ease of narration here, the word “we” expresses our individual and in-common experiences and thoughts.)
Welcoming party: Fire ants
Introductions. We are faculty members at Duke, in obstetrics and gynecology (Jeff) and family medicine (Sumera). In 2007, after we rented out our house for the coming 2 years, sold both cars, and packed 20 suitcases with our clothes and medical supplies, we left for Tanzania with our children in tow.
In Moshi. We arrived late at night, after the airline lost at least 30% of our baggage, to a house near the hospital that was in disrepair and infested with fire ants. There were (passing) thoughts of turning around and heading home.
Jeff had done a good deal of OB and gynecology in under-resourced settings—India and West Africa. But the work had always been brief surgical excursions, mostly to care for women who had obstetric fistula.
Now, however, broadening the Duke-KCMC HIV/AIDS to general women’s health presented great challenges and great opportunity. Yes, the Tanzanian ground was fertile for sowing seeds of collaboration in women’s health, but opportunities for federal funding for global women’s health projects, apart from HIV/AIDS, were limited. Duke’s goal was to build a research platform that cultivated awards from the National Institutes of Health, which, ultimately, are essential to the sustainability of most East-West and North-South research collaborations.
Priorities are everywhere. The fact that, every year, worldwide, more than 500,000 women die in childbirth and there are more than 6 million stillbirths and early neonatal deaths has, for a long time, eluded the conscience of the world’s major funding organizations. Devastating related problems, such as obstetric fistula, have been so neglected that some expert voices have labeled obstetric fistula “an orphan initiative.” United Nations Millennium Development Goal #5—a 75% reduction in maternal mortality by 2015—is far off target, with minimal progress made in sub-Saharan Africa.
Every week at KCMC presents interesting challenges to our intellect, our surgical skills, and our resolve to press on to the next happy outcome—or tragedy. We admire our Tanzanian colleagues who confront these challenges every day of their professional lives.
- A woman with massive labial elephantiasis with a 40-cm labial mass
- Multiple abdominal pregnancies of advanced gestation (testing the surgical skills and resolve of anyone who dares enter the abdomen)
- A 40 week-size molar pregnancy
- Many cases of uterine rupture and associated complications
- Countless women with complications of HIV infection and AIDS, in and out of pregnancy
- More cesarean hysterectomies than we can count
- A woman with a 18 week-size fetus in the right broad ligament, inside a huge retroperitoneal abscess that developed as a result of a botched abortion, performed in her village, that perforated the cervix.
Our strengths had been in clinical care, teaching, and program development. Based on the priority areas of the KCMC department of ObGyn and our professional experience, we chose to focus on four areas of care in expanding the Duke-KCMC program:
- emergency OB care and neonatal resuscitation
- OB fistula repair and recovery
- cervical cancer screening and prevention
- laparoscopic surgery.
In Moshi, any one of these areas could have consumed all our time. (See “Some interesting [often medically devastating] cases that we encountered in Tanzania.”)
We then determined that instruction in emergency OB care and neonatal resuscitation was needed most urgently at KCMC.
In most of sub-Saharan Africa, medical education focuses on learning theory. If we were to put medical students in Tanzania up against their US counterparts in an examination of the theoretical aspects of medicine, the Tanzanian students would perform as well or better.
Regrettably, however, the structure of clinical education here does not afford the same opportunities for students to learn a systematic approach to managing clinical problems. For example, at Duke, there are upwards of 50 ObGyn faculty members; at KCMC, there are only four—yet they handle similar numbers of deliveries, outpatient visits, and surgeries. Such a level of staffing is inadequate to manage the clinical load and to teach residents and medical students.
Consequently, students often learn “on the fly,” independently, and without the benefit of a systematic approach to OB emergencies.
We teach a systematic, evidence-based approach to the management of OB emergencies with the Advanced Life Support in Obstetrics (ALSO) program. We modified the course for an under-resourced setting and to meet the specific needs of this place. So far, we have taught the course to more than 250 OB providers in the region, with help from our colleague from Denmark, Dr. Bjarke Sørenson. We have watched the nurses and physicians grasp this knowledge and apply it with great success and satisfaction.
Postpartum hemorrhage. PPH remains the leading cause of death of pregnant women in under-resourced countries—even though it is often one of the easiest complications to prevent. By teaching active management of the third stage of labor and a progressive, staged approach to managing PPH at KCMC, the rate of maternal mortality from PPH has dropped substantially: Of 26 maternal deaths at KCMC in 2008, 25 % were related to PPH; after emergency OB instruction, not a single maternal death in 2009 was attributable to PPH. We think this is at least in part related to the teaching of ALSO and the rapid uptake of the methodology by the doctors and midwives there.
Pre-eclampsia. This condition, on the other hand, remains stubbornly resistant to quick change. The ALSO course teaches management of pre-eclampsia, but we often encounter patients too late in their course to intervene meaningfully. After KCMC’s success managing PPH, complications of hypertensive disorders rapidly became the #1 cause of maternal death here in 2009. Few drugs to control hypertension (we have hydralazine most of the time; labetalol, never; and no other IV options) and a frequent lack of magnesium sulfate make management of women with severe preeclampsia difficult, almost impossible.
Lack of sophisticated life support systems and trained personnel make the very sick patient much more likely to succumb to her illness. Some of the most tragic cases we’ve seen here are adolescent mothers with preeclampsia who died from a cerebral accident or renal failure, either of which could have been prevented with timely access to OB care, proper medication, trained personnel, and at times, advanced imaging modalities and hemodialysis.
Stillbirth. Even more common are the staggeringly high numbers of stillbirths that we encounter, either as referrals from smaller hospitals or on site during labor.
Use of continuous electronic fetal monitoring (CEFM) in resource-rich settings has been analyzed and scrutinized at length, mostly because of the high rate of unnecessary cesarean deliveries that false-positive interpretations of the fetal heart rate inspire in the cautious obstetrician. Every OB, we would guess, has intervened surgically because of what seemed to be an ominous fetal heart rate tracing—only to have the newborn nearly jump out of your delivering hands with its vigor.
Where there is no electronic fetal monitoring—and there is certainly none in Moshi—one must rely on a fetoscope (we still can’t hear the fetal heart with one of those) or a hand-held Doppler device to divine the fate of the fetus.
Intermittent auscultation has been shown to be as reliable as CEFM in low-risk patients, but the technique requires a high nurse-to-patient ratio to be effective. This is nearly impossible in many under-resourced settings. The nurse-to-patient ratio at KCMC may be as high as 30 to 1 (it’s higher still in other hospitals in the surrounding areas), and patients sleep, even labor, two or three to a bed. That makes true intermittent auscultation impossible.
Intrapartum stillbirths are a tragedy wherever they occur; the reality is that 95% occur in under-resourced countries. Concern over preventing stillbirth often leads to a quicker decision to perform a cesarean delivery where this service is available. Audible decelerations or meconium may be benign findings if one has the luxury of CEFM, but may prompt a cesarean when the outcome is less certain. Paradoxically, therefore, both the availability of CEFM in resource-rich settings leads—and the absence of CEFM in under-resourced settings—lead to unnecessary cesareans.
Finding a means of reliably monitoring the fetus during labor is critical in both settings, but is needed most acutely where resources are scarce. As the capacity for performing cesarean deliveries increases in these settings, so does the rate of cesarean deliveries—to a point at which the rate exceeds 50% in some centers. This situation will, ultimately, lead to its own set of complications, including future placentation abnormalities and their potentially life-threatening consequences.
Neonatal resuscitation. Before we moved to Africa, neither of us had resuscitated a newborn suffering the stress of difficult labor and delivery. Here, however, mastering this skill has proved invaluable. In fact, applying simple neonatal resuscitation efforts and witnessing remarkable results must count as one of the most satisfying moments in a physician’s career.
Here is what we have often seen: A baby, blue and appearing lifeless, is born after a long labor inside a sick mother. It isn’t breathing, and the pulse is very slow or undetectable.
In many under-resourced settings, such babies are put aside to, almost always, die.
But we have also seen how warming, drying, stimulation, and a few breaths with bag-mask ventilation are easily the difference between life and death for these babies. Those techniques can be learned in a course lasting less than 1 day, and the nurses at KCMC have embraced them with great enthusiasm—with dramatic results.
Devastating problem: OB fistula
The problem of OB fistula recently gained widespread attention in the international media; as a result, some effort is being made to address the problem. But, with as many as 3 million women suffering from this devastating condition, that effort has only scratched the surface of the problem.
The typical fistula patient in Tanzania. Consider an impoverished 17-year-old new mother, of short stature, who lives in a rural area and has no access to OB care. It’s likely that she delivered at home; perhaps she had the assistance of a lay midwife.
After labor that lasted for as long as 5 or 6 days, the woman delivered a dead, macerated fetus. Despite the risk, she did not die of PPH or infection, but she is left with a vesicovaginal or (less commonly) rectovaginal fistula. She leaks waste constantly.
More often than not, her husband then divorces her.
Her family and community shun her because of her constant wetness, her odor, and her status as a mother bereft of child. Associated problems, such as foot drop, infertility, amenorrhea, and debilitating skin excoriations, worsen her status as a pariah.
An especially horrifying case. One patient—she was in our care for longer than 16 months—was brought in by her family and abandoned at the casualty department. She was emaciated and near death. The skin on the buttocks had huge ulcerations down to muscle from pressure necrosis and chronic wetness. She had long ago given up hope of living. She had both a vesicovaginal fistula and a rectovaginal fistula, with extensive scarring and no identifiable urethra or cervix.
This woman underwent resuscitation and, once she was stable, diverting colostomy. After months of wound care and nutritional supplementation, she was able to undergo repair of the rectovaginal fistula. She is now ready for a urinary diversion procedure.
Many of our fistula patients are not as sick as this woman was upon presentation; their problem can be addressed with a 1- or 2-hour vaginal surgical procedure. Their equanimity and humility belie their suffering. They are, we think, the most beautiful and thankful of all patients. They deserve any attention that the world can give to them.
How we’ve been reimbursed
What we’ve described here establishes a context for the work we do, but our words give only a glimpse of the challenges of providing care in such a setting. Gaps in language and culture; corruption; apathy; and a shortage of nearly everything that we have come to consider necessary in the United States to practice medicine—all these make life in Moshi challenging and interesting.
After 2 years managing the women’s health collaboration program, we’ve barely scratched the surface of understanding what it means to work and live in this setting. What we hope is that our understanding, compassion, and usefulness will continue to grow as we experience more and more in this and similar settings.
We close by observing that the most important personal characteristics needed for a successful venture into global women’s health are, we believe, humility, patience, honesty, and courage. These qualities are slow to come by; for us, acquiring them will be a life’s work—they are not a welcoming party that greets you when you step off a plane in a distant land.
Editors note: Questions about the Duke-KCMC women’s health collaboration can be directed to Dr. Wilkinson at [email protected].
Two years ago, our family moved to Tanzania to help build a women’s health collaboration between Duke University and the Kilimanjaro Christian Medical Center (KCMC) in the town of Moshi, one of four tertiary referral centers in Tanzania that serves a population of nearly 14 million people. The goal of the collaboration was to expand the successful Duke-KCMC HIV/AIDS program that had been in operation at KCMC for 10 years to a broader women’s health service. Here is a synopsis of what we found in Tanzania and what we learned in those 2 years working alongside excellent local consultants and medical residents. (For ease of narration here, the word “we” expresses our individual and in-common experiences and thoughts.)
Welcoming party: Fire ants
Introductions. We are faculty members at Duke, in obstetrics and gynecology (Jeff) and family medicine (Sumera). In 2007, after we rented out our house for the coming 2 years, sold both cars, and packed 20 suitcases with our clothes and medical supplies, we left for Tanzania with our children in tow.
In Moshi. We arrived late at night, after the airline lost at least 30% of our baggage, to a house near the hospital that was in disrepair and infested with fire ants. There were (passing) thoughts of turning around and heading home.
Jeff had done a good deal of OB and gynecology in under-resourced settings—India and West Africa. But the work had always been brief surgical excursions, mostly to care for women who had obstetric fistula.
Now, however, broadening the Duke-KCMC HIV/AIDS to general women’s health presented great challenges and great opportunity. Yes, the Tanzanian ground was fertile for sowing seeds of collaboration in women’s health, but opportunities for federal funding for global women’s health projects, apart from HIV/AIDS, were limited. Duke’s goal was to build a research platform that cultivated awards from the National Institutes of Health, which, ultimately, are essential to the sustainability of most East-West and North-South research collaborations.
Priorities are everywhere. The fact that, every year, worldwide, more than 500,000 women die in childbirth and there are more than 6 million stillbirths and early neonatal deaths has, for a long time, eluded the conscience of the world’s major funding organizations. Devastating related problems, such as obstetric fistula, have been so neglected that some expert voices have labeled obstetric fistula “an orphan initiative.” United Nations Millennium Development Goal #5—a 75% reduction in maternal mortality by 2015—is far off target, with minimal progress made in sub-Saharan Africa.
Every week at KCMC presents interesting challenges to our intellect, our surgical skills, and our resolve to press on to the next happy outcome—or tragedy. We admire our Tanzanian colleagues who confront these challenges every day of their professional lives.
- A woman with massive labial elephantiasis with a 40-cm labial mass
- Multiple abdominal pregnancies of advanced gestation (testing the surgical skills and resolve of anyone who dares enter the abdomen)
- A 40 week-size molar pregnancy
- Many cases of uterine rupture and associated complications
- Countless women with complications of HIV infection and AIDS, in and out of pregnancy
- More cesarean hysterectomies than we can count
- A woman with a 18 week-size fetus in the right broad ligament, inside a huge retroperitoneal abscess that developed as a result of a botched abortion, performed in her village, that perforated the cervix.
Our strengths had been in clinical care, teaching, and program development. Based on the priority areas of the KCMC department of ObGyn and our professional experience, we chose to focus on four areas of care in expanding the Duke-KCMC program:
- emergency OB care and neonatal resuscitation
- OB fistula repair and recovery
- cervical cancer screening and prevention
- laparoscopic surgery.
In Moshi, any one of these areas could have consumed all our time. (See “Some interesting [often medically devastating] cases that we encountered in Tanzania.”)
We then determined that instruction in emergency OB care and neonatal resuscitation was needed most urgently at KCMC.
In most of sub-Saharan Africa, medical education focuses on learning theory. If we were to put medical students in Tanzania up against their US counterparts in an examination of the theoretical aspects of medicine, the Tanzanian students would perform as well or better.
Regrettably, however, the structure of clinical education here does not afford the same opportunities for students to learn a systematic approach to managing clinical problems. For example, at Duke, there are upwards of 50 ObGyn faculty members; at KCMC, there are only four—yet they handle similar numbers of deliveries, outpatient visits, and surgeries. Such a level of staffing is inadequate to manage the clinical load and to teach residents and medical students.
Consequently, students often learn “on the fly,” independently, and without the benefit of a systematic approach to OB emergencies.
We teach a systematic, evidence-based approach to the management of OB emergencies with the Advanced Life Support in Obstetrics (ALSO) program. We modified the course for an under-resourced setting and to meet the specific needs of this place. So far, we have taught the course to more than 250 OB providers in the region, with help from our colleague from Denmark, Dr. Bjarke Sørenson. We have watched the nurses and physicians grasp this knowledge and apply it with great success and satisfaction.
Postpartum hemorrhage. PPH remains the leading cause of death of pregnant women in under-resourced countries—even though it is often one of the easiest complications to prevent. By teaching active management of the third stage of labor and a progressive, staged approach to managing PPH at KCMC, the rate of maternal mortality from PPH has dropped substantially: Of 26 maternal deaths at KCMC in 2008, 25 % were related to PPH; after emergency OB instruction, not a single maternal death in 2009 was attributable to PPH. We think this is at least in part related to the teaching of ALSO and the rapid uptake of the methodology by the doctors and midwives there.
Pre-eclampsia. This condition, on the other hand, remains stubbornly resistant to quick change. The ALSO course teaches management of pre-eclampsia, but we often encounter patients too late in their course to intervene meaningfully. After KCMC’s success managing PPH, complications of hypertensive disorders rapidly became the #1 cause of maternal death here in 2009. Few drugs to control hypertension (we have hydralazine most of the time; labetalol, never; and no other IV options) and a frequent lack of magnesium sulfate make management of women with severe preeclampsia difficult, almost impossible.
Lack of sophisticated life support systems and trained personnel make the very sick patient much more likely to succumb to her illness. Some of the most tragic cases we’ve seen here are adolescent mothers with preeclampsia who died from a cerebral accident or renal failure, either of which could have been prevented with timely access to OB care, proper medication, trained personnel, and at times, advanced imaging modalities and hemodialysis.
Stillbirth. Even more common are the staggeringly high numbers of stillbirths that we encounter, either as referrals from smaller hospitals or on site during labor.
Use of continuous electronic fetal monitoring (CEFM) in resource-rich settings has been analyzed and scrutinized at length, mostly because of the high rate of unnecessary cesarean deliveries that false-positive interpretations of the fetal heart rate inspire in the cautious obstetrician. Every OB, we would guess, has intervened surgically because of what seemed to be an ominous fetal heart rate tracing—only to have the newborn nearly jump out of your delivering hands with its vigor.
Where there is no electronic fetal monitoring—and there is certainly none in Moshi—one must rely on a fetoscope (we still can’t hear the fetal heart with one of those) or a hand-held Doppler device to divine the fate of the fetus.
Intermittent auscultation has been shown to be as reliable as CEFM in low-risk patients, but the technique requires a high nurse-to-patient ratio to be effective. This is nearly impossible in many under-resourced settings. The nurse-to-patient ratio at KCMC may be as high as 30 to 1 (it’s higher still in other hospitals in the surrounding areas), and patients sleep, even labor, two or three to a bed. That makes true intermittent auscultation impossible.
Intrapartum stillbirths are a tragedy wherever they occur; the reality is that 95% occur in under-resourced countries. Concern over preventing stillbirth often leads to a quicker decision to perform a cesarean delivery where this service is available. Audible decelerations or meconium may be benign findings if one has the luxury of CEFM, but may prompt a cesarean when the outcome is less certain. Paradoxically, therefore, both the availability of CEFM in resource-rich settings leads—and the absence of CEFM in under-resourced settings—lead to unnecessary cesareans.
Finding a means of reliably monitoring the fetus during labor is critical in both settings, but is needed most acutely where resources are scarce. As the capacity for performing cesarean deliveries increases in these settings, so does the rate of cesarean deliveries—to a point at which the rate exceeds 50% in some centers. This situation will, ultimately, lead to its own set of complications, including future placentation abnormalities and their potentially life-threatening consequences.
Neonatal resuscitation. Before we moved to Africa, neither of us had resuscitated a newborn suffering the stress of difficult labor and delivery. Here, however, mastering this skill has proved invaluable. In fact, applying simple neonatal resuscitation efforts and witnessing remarkable results must count as one of the most satisfying moments in a physician’s career.
Here is what we have often seen: A baby, blue and appearing lifeless, is born after a long labor inside a sick mother. It isn’t breathing, and the pulse is very slow or undetectable.
In many under-resourced settings, such babies are put aside to, almost always, die.
But we have also seen how warming, drying, stimulation, and a few breaths with bag-mask ventilation are easily the difference between life and death for these babies. Those techniques can be learned in a course lasting less than 1 day, and the nurses at KCMC have embraced them with great enthusiasm—with dramatic results.
Devastating problem: OB fistula
The problem of OB fistula recently gained widespread attention in the international media; as a result, some effort is being made to address the problem. But, with as many as 3 million women suffering from this devastating condition, that effort has only scratched the surface of the problem.
The typical fistula patient in Tanzania. Consider an impoverished 17-year-old new mother, of short stature, who lives in a rural area and has no access to OB care. It’s likely that she delivered at home; perhaps she had the assistance of a lay midwife.
After labor that lasted for as long as 5 or 6 days, the woman delivered a dead, macerated fetus. Despite the risk, she did not die of PPH or infection, but she is left with a vesicovaginal or (less commonly) rectovaginal fistula. She leaks waste constantly.
More often than not, her husband then divorces her.
Her family and community shun her because of her constant wetness, her odor, and her status as a mother bereft of child. Associated problems, such as foot drop, infertility, amenorrhea, and debilitating skin excoriations, worsen her status as a pariah.
An especially horrifying case. One patient—she was in our care for longer than 16 months—was brought in by her family and abandoned at the casualty department. She was emaciated and near death. The skin on the buttocks had huge ulcerations down to muscle from pressure necrosis and chronic wetness. She had long ago given up hope of living. She had both a vesicovaginal fistula and a rectovaginal fistula, with extensive scarring and no identifiable urethra or cervix.
This woman underwent resuscitation and, once she was stable, diverting colostomy. After months of wound care and nutritional supplementation, she was able to undergo repair of the rectovaginal fistula. She is now ready for a urinary diversion procedure.
Many of our fistula patients are not as sick as this woman was upon presentation; their problem can be addressed with a 1- or 2-hour vaginal surgical procedure. Their equanimity and humility belie their suffering. They are, we think, the most beautiful and thankful of all patients. They deserve any attention that the world can give to them.
How we’ve been reimbursed
What we’ve described here establishes a context for the work we do, but our words give only a glimpse of the challenges of providing care in such a setting. Gaps in language and culture; corruption; apathy; and a shortage of nearly everything that we have come to consider necessary in the United States to practice medicine—all these make life in Moshi challenging and interesting.
After 2 years managing the women’s health collaboration program, we’ve barely scratched the surface of understanding what it means to work and live in this setting. What we hope is that our understanding, compassion, and usefulness will continue to grow as we experience more and more in this and similar settings.
We close by observing that the most important personal characteristics needed for a successful venture into global women’s health are, we believe, humility, patience, honesty, and courage. These qualities are slow to come by; for us, acquiring them will be a life’s work—they are not a welcoming party that greets you when you step off a plane in a distant land.
Two years ago, our family moved to Tanzania to help build a women’s health collaboration between Duke University and the Kilimanjaro Christian Medical Center (KCMC) in the town of Moshi, one of four tertiary referral centers in Tanzania that serves a population of nearly 14 million people. The goal of the collaboration was to expand the successful Duke-KCMC HIV/AIDS program that had been in operation at KCMC for 10 years to a broader women’s health service. Here is a synopsis of what we found in Tanzania and what we learned in those 2 years working alongside excellent local consultants and medical residents. (For ease of narration here, the word “we” expresses our individual and in-common experiences and thoughts.)
Welcoming party: Fire ants
Introductions. We are faculty members at Duke, in obstetrics and gynecology (Jeff) and family medicine (Sumera). In 2007, after we rented out our house for the coming 2 years, sold both cars, and packed 20 suitcases with our clothes and medical supplies, we left for Tanzania with our children in tow.
In Moshi. We arrived late at night, after the airline lost at least 30% of our baggage, to a house near the hospital that was in disrepair and infested with fire ants. There were (passing) thoughts of turning around and heading home.
Jeff had done a good deal of OB and gynecology in under-resourced settings—India and West Africa. But the work had always been brief surgical excursions, mostly to care for women who had obstetric fistula.
Now, however, broadening the Duke-KCMC HIV/AIDS to general women’s health presented great challenges and great opportunity. Yes, the Tanzanian ground was fertile for sowing seeds of collaboration in women’s health, but opportunities for federal funding for global women’s health projects, apart from HIV/AIDS, were limited. Duke’s goal was to build a research platform that cultivated awards from the National Institutes of Health, which, ultimately, are essential to the sustainability of most East-West and North-South research collaborations.
Priorities are everywhere. The fact that, every year, worldwide, more than 500,000 women die in childbirth and there are more than 6 million stillbirths and early neonatal deaths has, for a long time, eluded the conscience of the world’s major funding organizations. Devastating related problems, such as obstetric fistula, have been so neglected that some expert voices have labeled obstetric fistula “an orphan initiative.” United Nations Millennium Development Goal #5—a 75% reduction in maternal mortality by 2015—is far off target, with minimal progress made in sub-Saharan Africa.
Every week at KCMC presents interesting challenges to our intellect, our surgical skills, and our resolve to press on to the next happy outcome—or tragedy. We admire our Tanzanian colleagues who confront these challenges every day of their professional lives.
- A woman with massive labial elephantiasis with a 40-cm labial mass
- Multiple abdominal pregnancies of advanced gestation (testing the surgical skills and resolve of anyone who dares enter the abdomen)
- A 40 week-size molar pregnancy
- Many cases of uterine rupture and associated complications
- Countless women with complications of HIV infection and AIDS, in and out of pregnancy
- More cesarean hysterectomies than we can count
- A woman with a 18 week-size fetus in the right broad ligament, inside a huge retroperitoneal abscess that developed as a result of a botched abortion, performed in her village, that perforated the cervix.
Our strengths had been in clinical care, teaching, and program development. Based on the priority areas of the KCMC department of ObGyn and our professional experience, we chose to focus on four areas of care in expanding the Duke-KCMC program:
- emergency OB care and neonatal resuscitation
- OB fistula repair and recovery
- cervical cancer screening and prevention
- laparoscopic surgery.
In Moshi, any one of these areas could have consumed all our time. (See “Some interesting [often medically devastating] cases that we encountered in Tanzania.”)
We then determined that instruction in emergency OB care and neonatal resuscitation was needed most urgently at KCMC.
In most of sub-Saharan Africa, medical education focuses on learning theory. If we were to put medical students in Tanzania up against their US counterparts in an examination of the theoretical aspects of medicine, the Tanzanian students would perform as well or better.
Regrettably, however, the structure of clinical education here does not afford the same opportunities for students to learn a systematic approach to managing clinical problems. For example, at Duke, there are upwards of 50 ObGyn faculty members; at KCMC, there are only four—yet they handle similar numbers of deliveries, outpatient visits, and surgeries. Such a level of staffing is inadequate to manage the clinical load and to teach residents and medical students.
Consequently, students often learn “on the fly,” independently, and without the benefit of a systematic approach to OB emergencies.
We teach a systematic, evidence-based approach to the management of OB emergencies with the Advanced Life Support in Obstetrics (ALSO) program. We modified the course for an under-resourced setting and to meet the specific needs of this place. So far, we have taught the course to more than 250 OB providers in the region, with help from our colleague from Denmark, Dr. Bjarke Sørenson. We have watched the nurses and physicians grasp this knowledge and apply it with great success and satisfaction.
Postpartum hemorrhage. PPH remains the leading cause of death of pregnant women in under-resourced countries—even though it is often one of the easiest complications to prevent. By teaching active management of the third stage of labor and a progressive, staged approach to managing PPH at KCMC, the rate of maternal mortality from PPH has dropped substantially: Of 26 maternal deaths at KCMC in 2008, 25 % were related to PPH; after emergency OB instruction, not a single maternal death in 2009 was attributable to PPH. We think this is at least in part related to the teaching of ALSO and the rapid uptake of the methodology by the doctors and midwives there.
Pre-eclampsia. This condition, on the other hand, remains stubbornly resistant to quick change. The ALSO course teaches management of pre-eclampsia, but we often encounter patients too late in their course to intervene meaningfully. After KCMC’s success managing PPH, complications of hypertensive disorders rapidly became the #1 cause of maternal death here in 2009. Few drugs to control hypertension (we have hydralazine most of the time; labetalol, never; and no other IV options) and a frequent lack of magnesium sulfate make management of women with severe preeclampsia difficult, almost impossible.
Lack of sophisticated life support systems and trained personnel make the very sick patient much more likely to succumb to her illness. Some of the most tragic cases we’ve seen here are adolescent mothers with preeclampsia who died from a cerebral accident or renal failure, either of which could have been prevented with timely access to OB care, proper medication, trained personnel, and at times, advanced imaging modalities and hemodialysis.
Stillbirth. Even more common are the staggeringly high numbers of stillbirths that we encounter, either as referrals from smaller hospitals or on site during labor.
Use of continuous electronic fetal monitoring (CEFM) in resource-rich settings has been analyzed and scrutinized at length, mostly because of the high rate of unnecessary cesarean deliveries that false-positive interpretations of the fetal heart rate inspire in the cautious obstetrician. Every OB, we would guess, has intervened surgically because of what seemed to be an ominous fetal heart rate tracing—only to have the newborn nearly jump out of your delivering hands with its vigor.
Where there is no electronic fetal monitoring—and there is certainly none in Moshi—one must rely on a fetoscope (we still can’t hear the fetal heart with one of those) or a hand-held Doppler device to divine the fate of the fetus.
Intermittent auscultation has been shown to be as reliable as CEFM in low-risk patients, but the technique requires a high nurse-to-patient ratio to be effective. This is nearly impossible in many under-resourced settings. The nurse-to-patient ratio at KCMC may be as high as 30 to 1 (it’s higher still in other hospitals in the surrounding areas), and patients sleep, even labor, two or three to a bed. That makes true intermittent auscultation impossible.
Intrapartum stillbirths are a tragedy wherever they occur; the reality is that 95% occur in under-resourced countries. Concern over preventing stillbirth often leads to a quicker decision to perform a cesarean delivery where this service is available. Audible decelerations or meconium may be benign findings if one has the luxury of CEFM, but may prompt a cesarean when the outcome is less certain. Paradoxically, therefore, both the availability of CEFM in resource-rich settings leads—and the absence of CEFM in under-resourced settings—lead to unnecessary cesareans.
Finding a means of reliably monitoring the fetus during labor is critical in both settings, but is needed most acutely where resources are scarce. As the capacity for performing cesarean deliveries increases in these settings, so does the rate of cesarean deliveries—to a point at which the rate exceeds 50% in some centers. This situation will, ultimately, lead to its own set of complications, including future placentation abnormalities and their potentially life-threatening consequences.
Neonatal resuscitation. Before we moved to Africa, neither of us had resuscitated a newborn suffering the stress of difficult labor and delivery. Here, however, mastering this skill has proved invaluable. In fact, applying simple neonatal resuscitation efforts and witnessing remarkable results must count as one of the most satisfying moments in a physician’s career.
Here is what we have often seen: A baby, blue and appearing lifeless, is born after a long labor inside a sick mother. It isn’t breathing, and the pulse is very slow or undetectable.
In many under-resourced settings, such babies are put aside to, almost always, die.
But we have also seen how warming, drying, stimulation, and a few breaths with bag-mask ventilation are easily the difference between life and death for these babies. Those techniques can be learned in a course lasting less than 1 day, and the nurses at KCMC have embraced them with great enthusiasm—with dramatic results.
Devastating problem: OB fistula
The problem of OB fistula recently gained widespread attention in the international media; as a result, some effort is being made to address the problem. But, with as many as 3 million women suffering from this devastating condition, that effort has only scratched the surface of the problem.
The typical fistula patient in Tanzania. Consider an impoverished 17-year-old new mother, of short stature, who lives in a rural area and has no access to OB care. It’s likely that she delivered at home; perhaps she had the assistance of a lay midwife.
After labor that lasted for as long as 5 or 6 days, the woman delivered a dead, macerated fetus. Despite the risk, she did not die of PPH or infection, but she is left with a vesicovaginal or (less commonly) rectovaginal fistula. She leaks waste constantly.
More often than not, her husband then divorces her.
Her family and community shun her because of her constant wetness, her odor, and her status as a mother bereft of child. Associated problems, such as foot drop, infertility, amenorrhea, and debilitating skin excoriations, worsen her status as a pariah.
An especially horrifying case. One patient—she was in our care for longer than 16 months—was brought in by her family and abandoned at the casualty department. She was emaciated and near death. The skin on the buttocks had huge ulcerations down to muscle from pressure necrosis and chronic wetness. She had long ago given up hope of living. She had both a vesicovaginal fistula and a rectovaginal fistula, with extensive scarring and no identifiable urethra or cervix.
This woman underwent resuscitation and, once she was stable, diverting colostomy. After months of wound care and nutritional supplementation, she was able to undergo repair of the rectovaginal fistula. She is now ready for a urinary diversion procedure.
Many of our fistula patients are not as sick as this woman was upon presentation; their problem can be addressed with a 1- or 2-hour vaginal surgical procedure. Their equanimity and humility belie their suffering. They are, we think, the most beautiful and thankful of all patients. They deserve any attention that the world can give to them.
How we’ve been reimbursed
What we’ve described here establishes a context for the work we do, but our words give only a glimpse of the challenges of providing care in such a setting. Gaps in language and culture; corruption; apathy; and a shortage of nearly everything that we have come to consider necessary in the United States to practice medicine—all these make life in Moshi challenging and interesting.
After 2 years managing the women’s health collaboration program, we’ve barely scratched the surface of understanding what it means to work and live in this setting. What we hope is that our understanding, compassion, and usefulness will continue to grow as we experience more and more in this and similar settings.
We close by observing that the most important personal characteristics needed for a successful venture into global women’s health are, we believe, humility, patience, honesty, and courage. These qualities are slow to come by; for us, acquiring them will be a life’s work—they are not a welcoming party that greets you when you step off a plane in a distant land.
Editors note: Questions about the Duke-KCMC women’s health collaboration can be directed to Dr. Wilkinson at [email protected].
Editors note: Questions about the Duke-KCMC women’s health collaboration can be directed to Dr. Wilkinson at [email protected].
Is the incidence of amniotic fluid embolism rising?
From February 2005 to February 2009, Knight and associates identified a total of 60 cases of AFE in the UK Obstetric Surveillance System. Their analysis of these cases, along with the cases of 1,227 women in the control group, is a valuable contribution to our understanding of AFE—an entity that few obstetricians will have the occasion to manage in their professional careers. One of the strengths of the study is the use of a comprehensive database, which made it possible to exclude 26 additional cases originally diagnosed as AFE but determined to be another entity. Scrutiny of these cases suggests that AFE may be over-reported.
Although the findings of this study are interesting—particularly the association between AFE and induction of labor, twin gestation, cesarean delivery, and the combination of older age and ethnic-minority status—they must be interpreted with caution. The study was an elegant mathematical exercise, but I would hesitate to join the authors in sounding too many alarms. For example, without a biological explanation, I would be reluctant to tell clinicians to look for any increased risk of AFE among ethnic minorities.
I would be just as hesitant to “warn” obstetricians about induction of labor. If the risk of AFE attributable to induction is 35%, as the authors maintain, the elimination of induction altogether would only lower the rate of AFE from 2 cases to 1.3 cases for every 100,000 deliveries. Moreover, some of the variables that contribute to the need for induction could also contribute to an increased risk of AFE.
Postpartum cases that occur after cesarean delivery could actually be air embolism misclassified as AFE, especially if the uterus was exteriorized for repair—a phenomenon that has been reported.2
Recognition of amniotic fluid embolism (AFE) is exceedingly rare. In general, unless maternal hemorrhage is the presenting feature (without coagulopathy or cardiorespiratory compromise), suspect AFE when the mother experiences acute collapse along with one of the following features:
- acute fetal compromise
- cardiac arrest or arrhythmia
- coagulopathy
- hypotension
- hemorrhage
- premonitory symptoms (e.g., agitation)
- seizure.
When AFE is suspected, prompt intervention and initiation of supportive care are essential.
Although there are some risk factors for AFE, most cases of this phenomenon will remain sporadic and unpredictable.—JOHN T. REPKE, MD
We want to hear from you! Tell us what you think.
1. Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid emoblism: a population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–e8.-
2. Younker D, Rodriguez V, Kavanagh J. Massive air embolism during cesarean section. Anesthesiology. 1986;65(1):77-79.
From February 2005 to February 2009, Knight and associates identified a total of 60 cases of AFE in the UK Obstetric Surveillance System. Their analysis of these cases, along with the cases of 1,227 women in the control group, is a valuable contribution to our understanding of AFE—an entity that few obstetricians will have the occasion to manage in their professional careers. One of the strengths of the study is the use of a comprehensive database, which made it possible to exclude 26 additional cases originally diagnosed as AFE but determined to be another entity. Scrutiny of these cases suggests that AFE may be over-reported.
Although the findings of this study are interesting—particularly the association between AFE and induction of labor, twin gestation, cesarean delivery, and the combination of older age and ethnic-minority status—they must be interpreted with caution. The study was an elegant mathematical exercise, but I would hesitate to join the authors in sounding too many alarms. For example, without a biological explanation, I would be reluctant to tell clinicians to look for any increased risk of AFE among ethnic minorities.
I would be just as hesitant to “warn” obstetricians about induction of labor. If the risk of AFE attributable to induction is 35%, as the authors maintain, the elimination of induction altogether would only lower the rate of AFE from 2 cases to 1.3 cases for every 100,000 deliveries. Moreover, some of the variables that contribute to the need for induction could also contribute to an increased risk of AFE.
Postpartum cases that occur after cesarean delivery could actually be air embolism misclassified as AFE, especially if the uterus was exteriorized for repair—a phenomenon that has been reported.2
Recognition of amniotic fluid embolism (AFE) is exceedingly rare. In general, unless maternal hemorrhage is the presenting feature (without coagulopathy or cardiorespiratory compromise), suspect AFE when the mother experiences acute collapse along with one of the following features:
- acute fetal compromise
- cardiac arrest or arrhythmia
- coagulopathy
- hypotension
- hemorrhage
- premonitory symptoms (e.g., agitation)
- seizure.
When AFE is suspected, prompt intervention and initiation of supportive care are essential.
Although there are some risk factors for AFE, most cases of this phenomenon will remain sporadic and unpredictable.—JOHN T. REPKE, MD
We want to hear from you! Tell us what you think.
From February 2005 to February 2009, Knight and associates identified a total of 60 cases of AFE in the UK Obstetric Surveillance System. Their analysis of these cases, along with the cases of 1,227 women in the control group, is a valuable contribution to our understanding of AFE—an entity that few obstetricians will have the occasion to manage in their professional careers. One of the strengths of the study is the use of a comprehensive database, which made it possible to exclude 26 additional cases originally diagnosed as AFE but determined to be another entity. Scrutiny of these cases suggests that AFE may be over-reported.
Although the findings of this study are interesting—particularly the association between AFE and induction of labor, twin gestation, cesarean delivery, and the combination of older age and ethnic-minority status—they must be interpreted with caution. The study was an elegant mathematical exercise, but I would hesitate to join the authors in sounding too many alarms. For example, without a biological explanation, I would be reluctant to tell clinicians to look for any increased risk of AFE among ethnic minorities.
I would be just as hesitant to “warn” obstetricians about induction of labor. If the risk of AFE attributable to induction is 35%, as the authors maintain, the elimination of induction altogether would only lower the rate of AFE from 2 cases to 1.3 cases for every 100,000 deliveries. Moreover, some of the variables that contribute to the need for induction could also contribute to an increased risk of AFE.
Postpartum cases that occur after cesarean delivery could actually be air embolism misclassified as AFE, especially if the uterus was exteriorized for repair—a phenomenon that has been reported.2
Recognition of amniotic fluid embolism (AFE) is exceedingly rare. In general, unless maternal hemorrhage is the presenting feature (without coagulopathy or cardiorespiratory compromise), suspect AFE when the mother experiences acute collapse along with one of the following features:
- acute fetal compromise
- cardiac arrest or arrhythmia
- coagulopathy
- hypotension
- hemorrhage
- premonitory symptoms (e.g., agitation)
- seizure.
When AFE is suspected, prompt intervention and initiation of supportive care are essential.
Although there are some risk factors for AFE, most cases of this phenomenon will remain sporadic and unpredictable.—JOHN T. REPKE, MD
We want to hear from you! Tell us what you think.
1. Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid emoblism: a population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–e8.-
2. Younker D, Rodriguez V, Kavanagh J. Massive air embolism during cesarean section. Anesthesiology. 1986;65(1):77-79.
1. Abenhaim HA, Azoulay L, Kramer MS, Leduc L. Incidence and risk factors of amniotic fluid emoblism: a population-based study on 3 million births in the United States. Am J Obstet Gynecol. 2008;199(1):49.e1–e8.-
2. Younker D, Rodriguez V, Kavanagh J. Massive air embolism during cesarean section. Anesthesiology. 1986;65(1):77-79.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
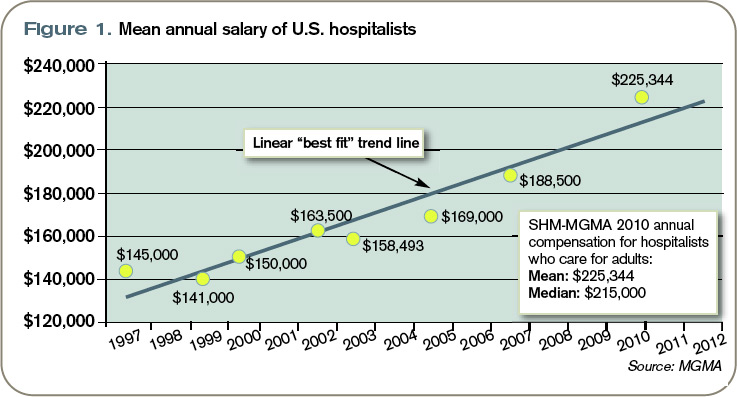
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Is the HPV test effective as the primary screen for cervical cancer?
Until now, the HPV test has been evaluated primarily as an adjunct to the Pap test and not as the primary screen for cervical cancer. In this randomized trial from Finland, 58,076 women 30 to 60 years old were invited to participate in a routine, population-based screening program for cervical cancer. Participants were randomized to primary screening with the HPV DNA test (hybrid capture 2) or to conventional cytology. In the group undergoing HPV testing, women who had a positive result were triaged to conventional cytology.
The HPV and conventional-cytology arms involved 95,600 and 95,700 woman-years of follow-up, respectively, and detected 76 and 53 cases of CIN 3 or higher. Six and eight cases, respectively, involved cancer.
The relative risk (RR) of CIN 3 or higher in the HPV arm versus conventional cytology was 1.44 (95% confidence interval [CI], 1.01–2.05) among all women invited for screening and 1.77 (95% CI, 1.16–2.74) among those who attended. Among women who had a normal or negative HPV test, the RR of subsequent CIN 3 or greater was 0.28 (95% CI, 0.04–1.17).
The greatest strengths of this study are the 1:1 randomization of just over 58,000 women and the ability to link study participants to outcomes, over a 5-year period, using the comprehensive Finnish population database and cancer registry.
One concern that clinicians may have is whether the findings are applicable to a US population that is now rarely screened using conventional cytology (liquid-based cytology is the norm). That concern should be allayed by a large meta-analysis that found no difference in the sensitivity of liquid-based cytology versus conventional Pap testing.1
Although nearly one third of women invited to participate in screening did not do so, the two groups had comparable numbers of women deciding not to participate (9,588 in the HPV arm versus 9,818 in the conventional-cytology arm).
One variable limiting applicability to a US population is the lack of an organized screening program like the one in Finland.
Despite its large size, the study had limited statistical power to show the impact of the two screening modalities on the rate of cervical cancer, primarily because that rate is so low in the population screened. To determine that impact, the screening options need to be repeated for another round, with follow-up extended to 10 years.
I recommend that you follow current US guidelines and screen women 30 years and older with both the Pap and HPV tests and extend the screening interval to 3 years for women who have a negative result on both tests. Numerous studies support the overwhelming conclusion that HPV testing in primary cervical cancer screening significantly increases detection of CIN 3 or higher and should reduce the woman’s subsequent risk of developing cervical cancer.—J. THOMAS COX, MD
Co-testing is the standard
US guidelines from the American Cancer Society (2002) and ACOG (2003, 2009) offer clinicians the option of screening women 30 years and older using both cytology and HPV testing—an approach known as “co-testing.” However, even though about 90% of the women who have a negative response to both tests can safely forgo further screening for at least 3 years, many clinicians screen them more frequently with co-testing, decreasing the cost-effectiveness of this option.2
The findings of Antilla and coworkers are in line with those of other authors. For example, Naucler and colleagues found that using the most sensitive test first (the HPV test), followed by reflex testing of positive HPV findings using the most specific test (the Pap), increased the sensitivity of screening for CIN 3 or greater by 30%, compared with screening with the Pap test alone.3 Other authors, including Ronco and coworkers and Sankaranarayanan and colleagues, have pointed to the superiority of either co-testing or HPV testing to use of the Pap test alone.4,5
1. Arbyn M, Bergeron C, Klinkhamer P, Martin-Hirsch P, Siebers Ag, Bulten J. Liquid compared with conventional cervical cytology: a systematic review and meta-analysis. Obstet Gynecol. 2008;111(1):167-177.
2. Saraiya M, Berkotwitz Z, Yabroff KR, Wideroff L, Kobrin S, Benard V. Cervical cancer screening with both human papillomavirus and Papanicolaou testing vs Papanicolaou testing alone: what screening intervals are physicians recommending? Arch Intern Med. 2010;170(11):977-985.
3. Naucler P, Ryd W, Törnberg S, et al. Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in primary cervical cancer screening. J Natl Cancer Inst. 2009;101(2):88-99.
4. Ronco G, Giorgi-Rossi P, Carozzi F, et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial. Lancet Oncol. 2010;11(3):249-257.
5. Sankaranarayanan R, Nene BM, Shastri SS, et al. HPV screening for cervical cancer in rural India. N Engl J Med. 2009;360(14):1385-1394.
Until now, the HPV test has been evaluated primarily as an adjunct to the Pap test and not as the primary screen for cervical cancer. In this randomized trial from Finland, 58,076 women 30 to 60 years old were invited to participate in a routine, population-based screening program for cervical cancer. Participants were randomized to primary screening with the HPV DNA test (hybrid capture 2) or to conventional cytology. In the group undergoing HPV testing, women who had a positive result were triaged to conventional cytology.
The HPV and conventional-cytology arms involved 95,600 and 95,700 woman-years of follow-up, respectively, and detected 76 and 53 cases of CIN 3 or higher. Six and eight cases, respectively, involved cancer.
The relative risk (RR) of CIN 3 or higher in the HPV arm versus conventional cytology was 1.44 (95% confidence interval [CI], 1.01–2.05) among all women invited for screening and 1.77 (95% CI, 1.16–2.74) among those who attended. Among women who had a normal or negative HPV test, the RR of subsequent CIN 3 or greater was 0.28 (95% CI, 0.04–1.17).
The greatest strengths of this study are the 1:1 randomization of just over 58,000 women and the ability to link study participants to outcomes, over a 5-year period, using the comprehensive Finnish population database and cancer registry.
One concern that clinicians may have is whether the findings are applicable to a US population that is now rarely screened using conventional cytology (liquid-based cytology is the norm). That concern should be allayed by a large meta-analysis that found no difference in the sensitivity of liquid-based cytology versus conventional Pap testing.1
Although nearly one third of women invited to participate in screening did not do so, the two groups had comparable numbers of women deciding not to participate (9,588 in the HPV arm versus 9,818 in the conventional-cytology arm).
One variable limiting applicability to a US population is the lack of an organized screening program like the one in Finland.
Despite its large size, the study had limited statistical power to show the impact of the two screening modalities on the rate of cervical cancer, primarily because that rate is so low in the population screened. To determine that impact, the screening options need to be repeated for another round, with follow-up extended to 10 years.
I recommend that you follow current US guidelines and screen women 30 years and older with both the Pap and HPV tests and extend the screening interval to 3 years for women who have a negative result on both tests. Numerous studies support the overwhelming conclusion that HPV testing in primary cervical cancer screening significantly increases detection of CIN 3 or higher and should reduce the woman’s subsequent risk of developing cervical cancer.—J. THOMAS COX, MD
Co-testing is the standard
US guidelines from the American Cancer Society (2002) and ACOG (2003, 2009) offer clinicians the option of screening women 30 years and older using both cytology and HPV testing—an approach known as “co-testing.” However, even though about 90% of the women who have a negative response to both tests can safely forgo further screening for at least 3 years, many clinicians screen them more frequently with co-testing, decreasing the cost-effectiveness of this option.2
The findings of Antilla and coworkers are in line with those of other authors. For example, Naucler and colleagues found that using the most sensitive test first (the HPV test), followed by reflex testing of positive HPV findings using the most specific test (the Pap), increased the sensitivity of screening for CIN 3 or greater by 30%, compared with screening with the Pap test alone.3 Other authors, including Ronco and coworkers and Sankaranarayanan and colleagues, have pointed to the superiority of either co-testing or HPV testing to use of the Pap test alone.4,5
Until now, the HPV test has been evaluated primarily as an adjunct to the Pap test and not as the primary screen for cervical cancer. In this randomized trial from Finland, 58,076 women 30 to 60 years old were invited to participate in a routine, population-based screening program for cervical cancer. Participants were randomized to primary screening with the HPV DNA test (hybrid capture 2) or to conventional cytology. In the group undergoing HPV testing, women who had a positive result were triaged to conventional cytology.
The HPV and conventional-cytology arms involved 95,600 and 95,700 woman-years of follow-up, respectively, and detected 76 and 53 cases of CIN 3 or higher. Six and eight cases, respectively, involved cancer.
The relative risk (RR) of CIN 3 or higher in the HPV arm versus conventional cytology was 1.44 (95% confidence interval [CI], 1.01–2.05) among all women invited for screening and 1.77 (95% CI, 1.16–2.74) among those who attended. Among women who had a normal or negative HPV test, the RR of subsequent CIN 3 or greater was 0.28 (95% CI, 0.04–1.17).
The greatest strengths of this study are the 1:1 randomization of just over 58,000 women and the ability to link study participants to outcomes, over a 5-year period, using the comprehensive Finnish population database and cancer registry.
One concern that clinicians may have is whether the findings are applicable to a US population that is now rarely screened using conventional cytology (liquid-based cytology is the norm). That concern should be allayed by a large meta-analysis that found no difference in the sensitivity of liquid-based cytology versus conventional Pap testing.1
Although nearly one third of women invited to participate in screening did not do so, the two groups had comparable numbers of women deciding not to participate (9,588 in the HPV arm versus 9,818 in the conventional-cytology arm).
One variable limiting applicability to a US population is the lack of an organized screening program like the one in Finland.
Despite its large size, the study had limited statistical power to show the impact of the two screening modalities on the rate of cervical cancer, primarily because that rate is so low in the population screened. To determine that impact, the screening options need to be repeated for another round, with follow-up extended to 10 years.
I recommend that you follow current US guidelines and screen women 30 years and older with both the Pap and HPV tests and extend the screening interval to 3 years for women who have a negative result on both tests. Numerous studies support the overwhelming conclusion that HPV testing in primary cervical cancer screening significantly increases detection of CIN 3 or higher and should reduce the woman’s subsequent risk of developing cervical cancer.—J. THOMAS COX, MD
Co-testing is the standard
US guidelines from the American Cancer Society (2002) and ACOG (2003, 2009) offer clinicians the option of screening women 30 years and older using both cytology and HPV testing—an approach known as “co-testing.” However, even though about 90% of the women who have a negative response to both tests can safely forgo further screening for at least 3 years, many clinicians screen them more frequently with co-testing, decreasing the cost-effectiveness of this option.2
The findings of Antilla and coworkers are in line with those of other authors. For example, Naucler and colleagues found that using the most sensitive test first (the HPV test), followed by reflex testing of positive HPV findings using the most specific test (the Pap), increased the sensitivity of screening for CIN 3 or greater by 30%, compared with screening with the Pap test alone.3 Other authors, including Ronco and coworkers and Sankaranarayanan and colleagues, have pointed to the superiority of either co-testing or HPV testing to use of the Pap test alone.4,5
1. Arbyn M, Bergeron C, Klinkhamer P, Martin-Hirsch P, Siebers Ag, Bulten J. Liquid compared with conventional cervical cytology: a systematic review and meta-analysis. Obstet Gynecol. 2008;111(1):167-177.
2. Saraiya M, Berkotwitz Z, Yabroff KR, Wideroff L, Kobrin S, Benard V. Cervical cancer screening with both human papillomavirus and Papanicolaou testing vs Papanicolaou testing alone: what screening intervals are physicians recommending? Arch Intern Med. 2010;170(11):977-985.
3. Naucler P, Ryd W, Törnberg S, et al. Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in primary cervical cancer screening. J Natl Cancer Inst. 2009;101(2):88-99.
4. Ronco G, Giorgi-Rossi P, Carozzi F, et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial. Lancet Oncol. 2010;11(3):249-257.
5. Sankaranarayanan R, Nene BM, Shastri SS, et al. HPV screening for cervical cancer in rural India. N Engl J Med. 2009;360(14):1385-1394.
1. Arbyn M, Bergeron C, Klinkhamer P, Martin-Hirsch P, Siebers Ag, Bulten J. Liquid compared with conventional cervical cytology: a systematic review and meta-analysis. Obstet Gynecol. 2008;111(1):167-177.
2. Saraiya M, Berkotwitz Z, Yabroff KR, Wideroff L, Kobrin S, Benard V. Cervical cancer screening with both human papillomavirus and Papanicolaou testing vs Papanicolaou testing alone: what screening intervals are physicians recommending? Arch Intern Med. 2010;170(11):977-985.
3. Naucler P, Ryd W, Törnberg S, et al. Efficacy of HPV DNA testing with cytology triage and/or repeat HPV DNA testing in primary cervical cancer screening. J Natl Cancer Inst. 2009;101(2):88-99.
4. Ronco G, Giorgi-Rossi P, Carozzi F, et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial. Lancet Oncol. 2010;11(3):249-257.
5. Sankaranarayanan R, Nene BM, Shastri SS, et al. HPV screening for cervical cancer in rural India. N Engl J Med. 2009;360(14):1385-1394.
“You say you want a revolution. Well….”
You say you want a revolution
Well, you know
We all want to change the world
—John Lennon
Gynecology was once a revolutionary specialty. Innovative and enterprising, its members were pioneers in operative laparoscopy, and they educated other surgical services on the merits and techniques of endoscopy.
Today the specialty lags behind others in both innovation and adoption of minimally invasive surgical techniques (FIGURE). By 2007, 95% of cholecystectomies were performed laparoscopically, as well as 90% of bariatric procedures and 70% of appendectomies. In contrast, only 20% of hysterectomies were performed using the laparoscopic approach. One reason for this discrepancy may be the extraordinary confidence that patients have in their gynecologist.
Consider the two sides of a coin that were revealed by the findings of an Internet survey of 526 women conducted by Russell Research and commissioned by the Patient Awareness Program of the AAGL. On one hand, investigators found that survey participants shared a steadfast opinion that their gynecologist would describe all available treatment choices, including the least traumatic and safest surgical procedures. Ninety-eight percent expected their physician to describe minimally invasive treatment options even if he or she was not proficient in them at the time—and to mention options that entail the least amount of pain. In addition, 94% of respondents expected their gynecologist to promote options with the lowest impact on lifestyle.1 Yet, on the other hand, although 517 of 528 (98%) respondents who were 18 years or older had experienced stress urinary incontinence, fibroids, or uterine prolapse, fewer than 40% were aware that a number of minimally invasive techniques could greatly reduce the need for hysterectomy. Fewer than 50% of respondents who suffered from menorrhagia were aware of endometrial ablation as a treatment, and only 21% realized that it could be performed in an office. Only 45% of women who had leiomyomata had heard of myomectomy. And one of every three women who had stress urinary incontinence was unaware of sling procedures. Fewer than 20% knew that sterilization could be performed in an office.1 Although these women expected to be thoroughly informed by their physician, their lack of awareness suggests the opposite.
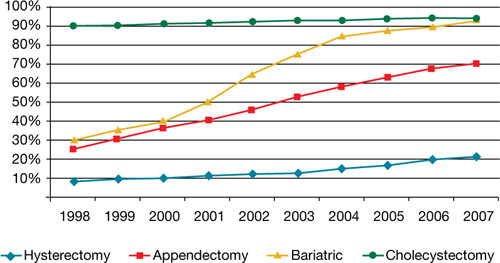
Use of minimally invasive options for 4 common surgeries
Resident physicians need more hands-on experience
A barrier to adoption of minimally invasive surgical approaches is the limited access many residents have to training and experience. This barrier could become especially problematic as third-party payers gain awareness of the advantages of minimally invasive surgery and shift reimbursement accordingly. In association with the American Society of Reproductive Medicine (ASRM), AAGL is actively engaged in enhancing surgical education through its Fellowship in Minimally Invasive Gynecology and is designing programs to supplement resident education. It is also establishing centers of excellence through its professional interest partner, the Council on Gynecologic Endoscopy (CGE).
Although the solution to our problem seems simple—increase the number of gynecologists who perform minimally invasive gynecologic surgery—that is easier said than done. According to data from the Accreditation Council for Graduate Medical Education ( ACGME), one of every three graduating residents has limited experience in minimally invasive procedures, and 30% of residents perform an average of only 12 laparoscopic operations a year as the primary surgeon. The average is even lower for hysteroscopic procedures!2

In an article published earlier this year in the Journal of Minimally Invasive Gynecology, Jon I. Einarsson, MD, MPH, and colleagues explore attitudes toward hysterectomy among gynecologists in the United States.3 Although nearly three quarters of hysterectomies are performed using an open abdominal approach, only 8% of respondents said they would choose the abdominal approach for themselves or their spouse. Among respondents who reported the highest surgical volumes, the percentage likely to choose a laparoscopic approach was significantly higher. The main barriers to laparoscopic hysterectomy? Limited opportunity for training during residency, technical difficulty, personal surgical experience, and operating time.3
We need an advanced curriculum
We have made tremendous progress in postgraduate education, thanks to the efforts of AAGL and ASRM. Nevertheless, we lack a specific, unified curriculum to train and ultimately credential gynecology residents and fellows in minimally invasive surgery.
Once again, our specialty lags behind general surgery. As of July 2009, all residents performing general surgery are required to complete and pass a course, “Fundamentals of laparoscopic surgery” (FLS). This joint undertaking of the American College of Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons has established minimum standards for basic cognitive and technical skills required for laparoscopic surgery.
Using the FLS course as a model, AAGL is designing a structured core curriculum to educate not only residents and fellows, but practicing gynecologists as well. Like the FLS course, the AAGL curriculum will emphasize both didactic teaching and lab skills, but it will be even more extensive because it will include hysteroscopy.
What we are doing now
After analyzing the needs of patients and providers around the world and acknowledging the lack of national standards to improve outcomes, AAGL and CGE have launched two other ambitious programs:
- a registry of physicians that includes operative experience and complication rate, as reviewed by their peers. This system lists physicians by level of practice, according to complexity of procedures, and by proactive experience and specialization
- a center of excellence in minimally invasive gynecology. The CGE recognizes that the achievement of best-in-class surgical outcomes requires not only an expert minimally invasive gynecologic surgeon but also an integrated, multidisciplinary surgical facility with systems and procedures to maximize quality, cost-effectiveness, and safety. For example, it is the vision of AAGL President C. Y. Liu that complex endometriosis surgery will one day be performed only by competent and experienced laparoscopic surgeons in endometriosis surgery centers.
Another initiative, launched in 2009, is the American Institute of Minimally Invasive Surgery (AIMIS). This not-for-profit organization offers member surgeons and hospitals not only accreditation and recognition, but also a number of useful products and programs, including:
- education
- guidance on technology
- business development
- insurance
- marketing strategies
- financial services
- consultation in practice management.
AIMIS is not a medical society but a national institute of which surgeons and hospitals become affiliated members.
Minimally invasive approach reduces costs, too
Rising health care costs have focused attention on ways to improve quality of care and contain costs at the same time, and minimally invasive surgery has emerged as a means of doing both. A recent study of 15,404 patients compared total abdominal hysterectomy with the minimally invasive alternatives (vaginal and laparoscopic hysterectomy) and found that the latter shortened hospitalization, reduced infection, and decreased the cost by $4,000 for the vaginal approach and $2,000 for laparoscopy.4 A study of more than 11,000 patients demonstrated a 52% reduction in the rate of hospital-acquired infection when a minimally invasive approach was utilized rather than open abdominal surgery.4
Some initiatives focus on the patient as a way of increasing utilization of minimally invasive approaches. For example, in Colorado, a 6,000-member self-funded medical plan launched a value-based program for patients undergoing colectomy, cholecystectomy, hysterectomy, appendectomy, and bariatric surgery. The program educated patients about minimally invasive options and encouraged them to seek consultation with a minimally invasive surgeon. Members who chose a minimally invasive procedure saw their copayment go down significantly. In addition, any surgeon who decided to perform one of these five procedures using an open approach was required to obtain preauthorization. Referral physicians were notified of the initiative, and minimally invasive surgeons were identified on the plan’s Web site.4
After 2 years, the plan saved nearly $1 million in direct hospital and surgeon claim costs. (Indirect savings from reduced need for prescription drugs and fewer complications were not included in this estimate. Nor were the economic advantages gained from the patient’s faster return to work and increased productivity.) After only 1 year, the utilization of minimally invasive hysterectomy rose from 28% to 80%!4
In New England, a 167-store grocery chain with 9,000 employees enrolled in the company’s self-funded health plan was able to reduce costs by identifying minimally invasive surgeons and steering members to them. The company covered 80% of surgical costs if minimally invasive surgery was performed, versus 70% for open surgery. Ultimately, the company’s per capita cost was 40% lower than all available benchmarks.4
We’re at a tipping point
The time has come for gynecologic surgeons to rejoin the revolution. Although we face many challenges, from limited experience and restricted access to training opportunities to lack of patient awareness of the benefits of minimally invasive surgery, it is imperative that we utilize minimally invasive approaches as often as possible. Educational opportunities are available, and third-party payers are beginning to demand it.
I believe it is only a matter of time before minimally invasive gynecologic procedures are the norm, not the exception.
You tell me that it’s evolution…
1. AAGL study finds women still in the dark about minimally invasive treatments for pelvic health disorders [press release]. Cypress, Calif: AAGL; 2008.
2. Accreditation Council for Graduate Medical Education. Obstetrics and gynecology case logs. National data report. 2008–2009. http://www.acgme.org/acWebsite/RRC_220/ObGynNatData0809.pdf. Accessed May 6, 2010.
3. Einarsson JI, Matteson KA, Schulkin J, Chavan NR, Sangi-Haghpeykar H. Minimally invasive hysterectomies—a survey on attitudes and barriers among practicing gynecologists. JMIG. 2010;17(2):167-175
4. Detweiler K, Hayes P, Cardinal A. Targeting surgery to reduce costs for employers. Employee Benefit Adviser. 2009. http://eba.benefitnews.com/news/targeting-surgery-to-reduce-costs-for-employers-2682543-1.html. Accessed May 6, 2010.
This commentary is based on the author’s 2008 presidential address to the 37th World Congress and Annual Meeting of the AAGL, which took place October 30 in Las Vegas, Nevada.

Charles E. Miller, MD
Dr. Miller is Director of Minimally Invasive Gynecologic Surgery at Lutheran General Hospital and the Advanced Gynecologic Surgery Institute in Naperville, Ill, and Clinical Associate Professor at the University of Chicago in Chicago, Ill. He is a past president of AAGL and the current vice president of the International Society for Gynecologic Endoscopy.
Dr. Miller has received research or grant support from Baxter Healthcare, Covidien, Duramed Research, Genzyme, Femasys, and Ferring Pharmaceuticals. He is a consultant to Boston Scientific, Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, Interlace Medical, and V. Mueller/Cardinal Health Medical Products. He is on the speakers’ bureau at Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, and Merck/Schering Plough.
Charles E. Miller, MD
Dr. Miller is Director of Minimally Invasive Gynecologic Surgery at Lutheran General Hospital and the Advanced Gynecologic Surgery Institute in Naperville, Ill, and Clinical Associate Professor at the University of Chicago in Chicago, Ill. He is a past president of AAGL and the current vice president of the International Society for Gynecologic Endoscopy.
Dr. Miller has received research or grant support from Baxter Healthcare, Covidien, Duramed Research, Genzyme, Femasys, and Ferring Pharmaceuticals. He is a consultant to Boston Scientific, Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, Interlace Medical, and V. Mueller/Cardinal Health Medical Products. He is on the speakers’ bureau at Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, and Merck/Schering Plough.
Charles E. Miller, MD
Dr. Miller is Director of Minimally Invasive Gynecologic Surgery at Lutheran General Hospital and the Advanced Gynecologic Surgery Institute in Naperville, Ill, and Clinical Associate Professor at the University of Chicago in Chicago, Ill. He is a past president of AAGL and the current vice president of the International Society for Gynecologic Endoscopy.
Dr. Miller has received research or grant support from Baxter Healthcare, Covidien, Duramed Research, Genzyme, Femasys, and Ferring Pharmaceuticals. He is a consultant to Boston Scientific, Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, Interlace Medical, and V. Mueller/Cardinal Health Medical Products. He is on the speakers’ bureau at Ethicon Endo Surgery, Ethicon Women’s Health and Urology, Ferring Pharmaceuticals, and Merck/Schering Plough.
You say you want a revolution
Well, you know
We all want to change the world
—John Lennon
Gynecology was once a revolutionary specialty. Innovative and enterprising, its members were pioneers in operative laparoscopy, and they educated other surgical services on the merits and techniques of endoscopy.
Today the specialty lags behind others in both innovation and adoption of minimally invasive surgical techniques (FIGURE). By 2007, 95% of cholecystectomies were performed laparoscopically, as well as 90% of bariatric procedures and 70% of appendectomies. In contrast, only 20% of hysterectomies were performed using the laparoscopic approach. One reason for this discrepancy may be the extraordinary confidence that patients have in their gynecologist.
Consider the two sides of a coin that were revealed by the findings of an Internet survey of 526 women conducted by Russell Research and commissioned by the Patient Awareness Program of the AAGL. On one hand, investigators found that survey participants shared a steadfast opinion that their gynecologist would describe all available treatment choices, including the least traumatic and safest surgical procedures. Ninety-eight percent expected their physician to describe minimally invasive treatment options even if he or she was not proficient in them at the time—and to mention options that entail the least amount of pain. In addition, 94% of respondents expected their gynecologist to promote options with the lowest impact on lifestyle.1 Yet, on the other hand, although 517 of 528 (98%) respondents who were 18 years or older had experienced stress urinary incontinence, fibroids, or uterine prolapse, fewer than 40% were aware that a number of minimally invasive techniques could greatly reduce the need for hysterectomy. Fewer than 50% of respondents who suffered from menorrhagia were aware of endometrial ablation as a treatment, and only 21% realized that it could be performed in an office. Only 45% of women who had leiomyomata had heard of myomectomy. And one of every three women who had stress urinary incontinence was unaware of sling procedures. Fewer than 20% knew that sterilization could be performed in an office.1 Although these women expected to be thoroughly informed by their physician, their lack of awareness suggests the opposite.
Use of minimally invasive options for 4 common surgeries
Resident physicians need more hands-on experience
A barrier to adoption of minimally invasive surgical approaches is the limited access many residents have to training and experience. This barrier could become especially problematic as third-party payers gain awareness of the advantages of minimally invasive surgery and shift reimbursement accordingly. In association with the American Society of Reproductive Medicine (ASRM), AAGL is actively engaged in enhancing surgical education through its Fellowship in Minimally Invasive Gynecology and is designing programs to supplement resident education. It is also establishing centers of excellence through its professional interest partner, the Council on Gynecologic Endoscopy (CGE).
Although the solution to our problem seems simple—increase the number of gynecologists who perform minimally invasive gynecologic surgery—that is easier said than done. According to data from the Accreditation Council for Graduate Medical Education ( ACGME), one of every three graduating residents has limited experience in minimally invasive procedures, and 30% of residents perform an average of only 12 laparoscopic operations a year as the primary surgeon. The average is even lower for hysteroscopic procedures!2
In an article published earlier this year in the Journal of Minimally Invasive Gynecology, Jon I. Einarsson, MD, MPH, and colleagues explore attitudes toward hysterectomy among gynecologists in the United States.3 Although nearly three quarters of hysterectomies are performed using an open abdominal approach, only 8% of respondents said they would choose the abdominal approach for themselves or their spouse. Among respondents who reported the highest surgical volumes, the percentage likely to choose a laparoscopic approach was significantly higher. The main barriers to laparoscopic hysterectomy? Limited opportunity for training during residency, technical difficulty, personal surgical experience, and operating time.3
We need an advanced curriculum
We have made tremendous progress in postgraduate education, thanks to the efforts of AAGL and ASRM. Nevertheless, we lack a specific, unified curriculum to train and ultimately credential gynecology residents and fellows in minimally invasive surgery.
Once again, our specialty lags behind general surgery. As of July 2009, all residents performing general surgery are required to complete and pass a course, “Fundamentals of laparoscopic surgery” (FLS). This joint undertaking of the American College of Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons has established minimum standards for basic cognitive and technical skills required for laparoscopic surgery.
Using the FLS course as a model, AAGL is designing a structured core curriculum to educate not only residents and fellows, but practicing gynecologists as well. Like the FLS course, the AAGL curriculum will emphasize both didactic teaching and lab skills, but it will be even more extensive because it will include hysteroscopy.
What we are doing now
After analyzing the needs of patients and providers around the world and acknowledging the lack of national standards to improve outcomes, AAGL and CGE have launched two other ambitious programs:
- a registry of physicians that includes operative experience and complication rate, as reviewed by their peers. This system lists physicians by level of practice, according to complexity of procedures, and by proactive experience and specialization
- a center of excellence in minimally invasive gynecology. The CGE recognizes that the achievement of best-in-class surgical outcomes requires not only an expert minimally invasive gynecologic surgeon but also an integrated, multidisciplinary surgical facility with systems and procedures to maximize quality, cost-effectiveness, and safety. For example, it is the vision of AAGL President C. Y. Liu that complex endometriosis surgery will one day be performed only by competent and experienced laparoscopic surgeons in endometriosis surgery centers.
Another initiative, launched in 2009, is the American Institute of Minimally Invasive Surgery (AIMIS). This not-for-profit organization offers member surgeons and hospitals not only accreditation and recognition, but also a number of useful products and programs, including:
- education
- guidance on technology
- business development
- insurance
- marketing strategies
- financial services
- consultation in practice management.
AIMIS is not a medical society but a national institute of which surgeons and hospitals become affiliated members.
Minimally invasive approach reduces costs, too
Rising health care costs have focused attention on ways to improve quality of care and contain costs at the same time, and minimally invasive surgery has emerged as a means of doing both. A recent study of 15,404 patients compared total abdominal hysterectomy with the minimally invasive alternatives (vaginal and laparoscopic hysterectomy) and found that the latter shortened hospitalization, reduced infection, and decreased the cost by $4,000 for the vaginal approach and $2,000 for laparoscopy.4 A study of more than 11,000 patients demonstrated a 52% reduction in the rate of hospital-acquired infection when a minimally invasive approach was utilized rather than open abdominal surgery.4
Some initiatives focus on the patient as a way of increasing utilization of minimally invasive approaches. For example, in Colorado, a 6,000-member self-funded medical plan launched a value-based program for patients undergoing colectomy, cholecystectomy, hysterectomy, appendectomy, and bariatric surgery. The program educated patients about minimally invasive options and encouraged them to seek consultation with a minimally invasive surgeon. Members who chose a minimally invasive procedure saw their copayment go down significantly. In addition, any surgeon who decided to perform one of these five procedures using an open approach was required to obtain preauthorization. Referral physicians were notified of the initiative, and minimally invasive surgeons were identified on the plan’s Web site.4
After 2 years, the plan saved nearly $1 million in direct hospital and surgeon claim costs. (Indirect savings from reduced need for prescription drugs and fewer complications were not included in this estimate. Nor were the economic advantages gained from the patient’s faster return to work and increased productivity.) After only 1 year, the utilization of minimally invasive hysterectomy rose from 28% to 80%!4
In New England, a 167-store grocery chain with 9,000 employees enrolled in the company’s self-funded health plan was able to reduce costs by identifying minimally invasive surgeons and steering members to them. The company covered 80% of surgical costs if minimally invasive surgery was performed, versus 70% for open surgery. Ultimately, the company’s per capita cost was 40% lower than all available benchmarks.4
We’re at a tipping point
The time has come for gynecologic surgeons to rejoin the revolution. Although we face many challenges, from limited experience and restricted access to training opportunities to lack of patient awareness of the benefits of minimally invasive surgery, it is imperative that we utilize minimally invasive approaches as often as possible. Educational opportunities are available, and third-party payers are beginning to demand it.
I believe it is only a matter of time before minimally invasive gynecologic procedures are the norm, not the exception.
You tell me that it’s evolution…
You say you want a revolution
Well, you know
We all want to change the world
—John Lennon
Gynecology was once a revolutionary specialty. Innovative and enterprising, its members were pioneers in operative laparoscopy, and they educated other surgical services on the merits and techniques of endoscopy.
Today the specialty lags behind others in both innovation and adoption of minimally invasive surgical techniques (FIGURE). By 2007, 95% of cholecystectomies were performed laparoscopically, as well as 90% of bariatric procedures and 70% of appendectomies. In contrast, only 20% of hysterectomies were performed using the laparoscopic approach. One reason for this discrepancy may be the extraordinary confidence that patients have in their gynecologist.
Consider the two sides of a coin that were revealed by the findings of an Internet survey of 526 women conducted by Russell Research and commissioned by the Patient Awareness Program of the AAGL. On one hand, investigators found that survey participants shared a steadfast opinion that their gynecologist would describe all available treatment choices, including the least traumatic and safest surgical procedures. Ninety-eight percent expected their physician to describe minimally invasive treatment options even if he or she was not proficient in them at the time—and to mention options that entail the least amount of pain. In addition, 94% of respondents expected their gynecologist to promote options with the lowest impact on lifestyle.1 Yet, on the other hand, although 517 of 528 (98%) respondents who were 18 years or older had experienced stress urinary incontinence, fibroids, or uterine prolapse, fewer than 40% were aware that a number of minimally invasive techniques could greatly reduce the need for hysterectomy. Fewer than 50% of respondents who suffered from menorrhagia were aware of endometrial ablation as a treatment, and only 21% realized that it could be performed in an office. Only 45% of women who had leiomyomata had heard of myomectomy. And one of every three women who had stress urinary incontinence was unaware of sling procedures. Fewer than 20% knew that sterilization could be performed in an office.1 Although these women expected to be thoroughly informed by their physician, their lack of awareness suggests the opposite.
Use of minimally invasive options for 4 common surgeries
Resident physicians need more hands-on experience
A barrier to adoption of minimally invasive surgical approaches is the limited access many residents have to training and experience. This barrier could become especially problematic as third-party payers gain awareness of the advantages of minimally invasive surgery and shift reimbursement accordingly. In association with the American Society of Reproductive Medicine (ASRM), AAGL is actively engaged in enhancing surgical education through its Fellowship in Minimally Invasive Gynecology and is designing programs to supplement resident education. It is also establishing centers of excellence through its professional interest partner, the Council on Gynecologic Endoscopy (CGE).
Although the solution to our problem seems simple—increase the number of gynecologists who perform minimally invasive gynecologic surgery—that is easier said than done. According to data from the Accreditation Council for Graduate Medical Education ( ACGME), one of every three graduating residents has limited experience in minimally invasive procedures, and 30% of residents perform an average of only 12 laparoscopic operations a year as the primary surgeon. The average is even lower for hysteroscopic procedures!2
In an article published earlier this year in the Journal of Minimally Invasive Gynecology, Jon I. Einarsson, MD, MPH, and colleagues explore attitudes toward hysterectomy among gynecologists in the United States.3 Although nearly three quarters of hysterectomies are performed using an open abdominal approach, only 8% of respondents said they would choose the abdominal approach for themselves or their spouse. Among respondents who reported the highest surgical volumes, the percentage likely to choose a laparoscopic approach was significantly higher. The main barriers to laparoscopic hysterectomy? Limited opportunity for training during residency, technical difficulty, personal surgical experience, and operating time.3
We need an advanced curriculum
We have made tremendous progress in postgraduate education, thanks to the efforts of AAGL and ASRM. Nevertheless, we lack a specific, unified curriculum to train and ultimately credential gynecology residents and fellows in minimally invasive surgery.
Once again, our specialty lags behind general surgery. As of July 2009, all residents performing general surgery are required to complete and pass a course, “Fundamentals of laparoscopic surgery” (FLS). This joint undertaking of the American College of Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons has established minimum standards for basic cognitive and technical skills required for laparoscopic surgery.
Using the FLS course as a model, AAGL is designing a structured core curriculum to educate not only residents and fellows, but practicing gynecologists as well. Like the FLS course, the AAGL curriculum will emphasize both didactic teaching and lab skills, but it will be even more extensive because it will include hysteroscopy.
What we are doing now
After analyzing the needs of patients and providers around the world and acknowledging the lack of national standards to improve outcomes, AAGL and CGE have launched two other ambitious programs:
- a registry of physicians that includes operative experience and complication rate, as reviewed by their peers. This system lists physicians by level of practice, according to complexity of procedures, and by proactive experience and specialization
- a center of excellence in minimally invasive gynecology. The CGE recognizes that the achievement of best-in-class surgical outcomes requires not only an expert minimally invasive gynecologic surgeon but also an integrated, multidisciplinary surgical facility with systems and procedures to maximize quality, cost-effectiveness, and safety. For example, it is the vision of AAGL President C. Y. Liu that complex endometriosis surgery will one day be performed only by competent and experienced laparoscopic surgeons in endometriosis surgery centers.
Another initiative, launched in 2009, is the American Institute of Minimally Invasive Surgery (AIMIS). This not-for-profit organization offers member surgeons and hospitals not only accreditation and recognition, but also a number of useful products and programs, including:
- education
- guidance on technology
- business development
- insurance
- marketing strategies
- financial services
- consultation in practice management.
AIMIS is not a medical society but a national institute of which surgeons and hospitals become affiliated members.
Minimally invasive approach reduces costs, too
Rising health care costs have focused attention on ways to improve quality of care and contain costs at the same time, and minimally invasive surgery has emerged as a means of doing both. A recent study of 15,404 patients compared total abdominal hysterectomy with the minimally invasive alternatives (vaginal and laparoscopic hysterectomy) and found that the latter shortened hospitalization, reduced infection, and decreased the cost by $4,000 for the vaginal approach and $2,000 for laparoscopy.4 A study of more than 11,000 patients demonstrated a 52% reduction in the rate of hospital-acquired infection when a minimally invasive approach was utilized rather than open abdominal surgery.4
Some initiatives focus on the patient as a way of increasing utilization of minimally invasive approaches. For example, in Colorado, a 6,000-member self-funded medical plan launched a value-based program for patients undergoing colectomy, cholecystectomy, hysterectomy, appendectomy, and bariatric surgery. The program educated patients about minimally invasive options and encouraged them to seek consultation with a minimally invasive surgeon. Members who chose a minimally invasive procedure saw their copayment go down significantly. In addition, any surgeon who decided to perform one of these five procedures using an open approach was required to obtain preauthorization. Referral physicians were notified of the initiative, and minimally invasive surgeons were identified on the plan’s Web site.4
After 2 years, the plan saved nearly $1 million in direct hospital and surgeon claim costs. (Indirect savings from reduced need for prescription drugs and fewer complications were not included in this estimate. Nor were the economic advantages gained from the patient’s faster return to work and increased productivity.) After only 1 year, the utilization of minimally invasive hysterectomy rose from 28% to 80%!4
In New England, a 167-store grocery chain with 9,000 employees enrolled in the company’s self-funded health plan was able to reduce costs by identifying minimally invasive surgeons and steering members to them. The company covered 80% of surgical costs if minimally invasive surgery was performed, versus 70% for open surgery. Ultimately, the company’s per capita cost was 40% lower than all available benchmarks.4
We’re at a tipping point
The time has come for gynecologic surgeons to rejoin the revolution. Although we face many challenges, from limited experience and restricted access to training opportunities to lack of patient awareness of the benefits of minimally invasive surgery, it is imperative that we utilize minimally invasive approaches as often as possible. Educational opportunities are available, and third-party payers are beginning to demand it.
I believe it is only a matter of time before minimally invasive gynecologic procedures are the norm, not the exception.
You tell me that it’s evolution…
1. AAGL study finds women still in the dark about minimally invasive treatments for pelvic health disorders [press release]. Cypress, Calif: AAGL; 2008.
2. Accreditation Council for Graduate Medical Education. Obstetrics and gynecology case logs. National data report. 2008–2009. http://www.acgme.org/acWebsite/RRC_220/ObGynNatData0809.pdf. Accessed May 6, 2010.
3. Einarsson JI, Matteson KA, Schulkin J, Chavan NR, Sangi-Haghpeykar H. Minimally invasive hysterectomies—a survey on attitudes and barriers among practicing gynecologists. JMIG. 2010;17(2):167-175
4. Detweiler K, Hayes P, Cardinal A. Targeting surgery to reduce costs for employers. Employee Benefit Adviser. 2009. http://eba.benefitnews.com/news/targeting-surgery-to-reduce-costs-for-employers-2682543-1.html. Accessed May 6, 2010.
This commentary is based on the author’s 2008 presidential address to the 37th World Congress and Annual Meeting of the AAGL, which took place October 30 in Las Vegas, Nevada.
1. AAGL study finds women still in the dark about minimally invasive treatments for pelvic health disorders [press release]. Cypress, Calif: AAGL; 2008.
2. Accreditation Council for Graduate Medical Education. Obstetrics and gynecology case logs. National data report. 2008–2009. http://www.acgme.org/acWebsite/RRC_220/ObGynNatData0809.pdf. Accessed May 6, 2010.
3. Einarsson JI, Matteson KA, Schulkin J, Chavan NR, Sangi-Haghpeykar H. Minimally invasive hysterectomies—a survey on attitudes and barriers among practicing gynecologists. JMIG. 2010;17(2):167-175
4. Detweiler K, Hayes P, Cardinal A. Targeting surgery to reduce costs for employers. Employee Benefit Adviser. 2009. http://eba.benefitnews.com/news/targeting-surgery-to-reduce-costs-for-employers-2682543-1.html. Accessed May 6, 2010.
This commentary is based on the author’s 2008 presidential address to the 37th World Congress and Annual Meeting of the AAGL, which took place October 30 in Las Vegas, Nevada.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
14 questions (and answers) about health reform and you
With passage of the Patient Protection and Affordable Care Act earlier this year, big changes are afoot in the way Americans practice medicine. In a plethora of articles, blogs, and broadcast spots, the media have focused on what the new law portends for the average employee, employers, and the uninsured—but what, exactly, does it entail for ObGyns and their patients?
To find an answer to that overarching question—and 13 others—we invited Lucia DiVenere, director of government relations at the American Congress of Obstetricians and Gynecologists, to join us in an extended discussion of the law and its ramifications. She offered insight into ACOG’s extensive lobbying efforts on behalf of women and the specialty and described the many ways ObGyn care will change in the near and proximal future, focusing on questions that you might find yourself asking, including:
- Will I see a lot more patients?
- What reforms are woman-specific?
- How will my practice change?
- Which of my services will be fully covered?
- Will expanded coverage improve birth outcomes?
- Is “femaleness” a preexisting condition?
- What happened to tort reform?
- Is the system repairable?
1 Will ObGyns see a lot more patients?
OBG Management: The most talked about change the new law heralds is the addition of roughly 32 million people to the insurance rolls. Is the most significant impact of the legislation for ObGyns likely to be an increase in the number of patients they will be seeing?
Lucia DiVenere: Congress wanted to increase the ranks of the insured and expand access to health care, and it addressed these goals with individual and employer mandates, state exchanges, Medicaid expansion, and insurance reforms.
But that isn’t the most significant change in store for us. Congress also wanted to reform our health care system in a number of fundamental ways, some of which are designed to change the way physicians provide care to their patients.
For example, Congress wanted to “bend the cost curve”—to reduce the expected rate of growth in health care spending over the long term. That doesn’t mean that health care costs in 2020 will be less than they were in 2018, but it does mean that annual and long-term growth rates should level off and become sustainable. To accomplish this goal, Congress created an Independent Payment Advisory Commission, which may prove to be extremely powerful in reducing health care costs and is likely to significantly affect all physicians. Greater protections against fraud and abuse, experiments with new kinds of payment and delivery systems, including “medical homes,” and increased reliance on nonphysician practitioners—all included in the law—are also expected to reduce costs.
OBG Management: What other changes are coming?
DiVenere: Congress was determined to alter the practice of health care, ensuring higher quality for each dollar spent and consistent delivery of care. It also sought to kick-start our health care system—especially in the physician arena—into greater and, theoretically, more efficient reliance on electronic health records (EHR). Medicare and Medicaid physician payments will be juggled to increase reimbursement for E&M services and for physicians who provide greater value in relation to cost. Physicians will be required to participate in the Physician Quality Reporting Initiative (PQRI) program in 2015 and beyond to avoid stiff penalties. And EHR systems are required to adopt uniform standards for electronic transactions.
2 What reforms are woman-specific?
OBG Management: What initiatives are planned for the care of women, in particular?
DiVenere: Congress recognized the importance of reforming women’s health and included many provisions advocated by ACOG in our “Health care for women, health care for all” campaign.
Probably the most important of these provisions is the guarantee of direct access to ObGyn care without need of a referral or pre-authorization from a primary care provider or insurance company. Nor can an insurance company restrict a patient’s direct access to her ObGyn to a certain number of visits or types of services.
This was a major ACOG victory. For 20 years, ObGyns have been waging battles in the states for direct access for patients. Last year, nine states did not require insurers to grant women direct access to ObGyns, and 16 states allowed insurers to restrict ObGyn visits and services. This part of the law, which is effective this year, provides national direct access to all women in all states, and is not tied to an ObGyn’s primary care designation.
Another area of reform concerns maternity care. In 2009, 13% of all pregnant women in the United States were uninsured, as were 20.4% of all women between the ages of 15 and 44, the childbearing years. The uninsured rate for nonelderly women in 2007 ranged from a high of 28% in New Mexico and Texas to a low of 8% in Massachusetts. Today, 42% of all pregnancies are covered by Medicaid. Women have been able, usually, to gain access to some kind of care—sometimes in emergency departments at the time of labor—but the nation clearly needs to do better.
Medicaid and new insurance plans will be required to offer maternity care and women’s preventive services, including mammography screening. The exact parameters of maternity care and other types of care in the essential benefits package will be determined by the Secretary of Health and Human Services (HHS), based on the typical package offered to employees in group health plans. The idea behind the law is that many women who are now covered by Medicaid will transfer to private insurance in their states’ exchanges.
3 How will ObGyn practice change?
OBG Management: What are some of the opportunities and challenges ObGyns will encounter?
DiVenere: There are three key areas of challenge and opportunity:
- Development of the “medical home.” A medical home is a practice designed to provide and coordinate comprehensive patient care. State Medicaid agencies are authorized to require certain beneficiaries, including those who have two or more chronic conditions, to join a medical home. Medicare will also experiment with medical homes, and both Medicaid and Medicare medical home practices will receive additional payments. Most medical homes are expected to be family practice, internal medicine, or pediatric care providers, but ObGyn practices can participate, too. ObGyns should look carefully at the opportunities this paradigm provides and consider having their practice designated as a medical home.
- Increased use of nonphysician providers. The new law strongly encourages this practice, including in the ObGyn specialty. Congress is determined to experiment with non-ObGyn deliveries in response to patient demand and midlevel assurances that nonphysicians can deliver babies with better outcomes at significantly lower cost. Our specialty’s cesarean delivery rate is under intense scrutiny. Skewed studies “prove” happier and healthier deliveries in homes and other out-of-hospital locations without an ObGyn in attendance. And midlevel practitioners are offering vaginal birth after cesarean delivery in many cases where ObGyns are restricted by hospital rules.
- The law extends Medicaid payments to free-standing birth centers and birth attendants and does not specify which kinds of practitioners can qualify as birth attendants. Free-standing birth centers can provide high-quality care if they are appropriately accredited and have an established transfer relationship with a nearby hospital. The law does not specify these criteria, either.
- Increasing payments to nonphysicians. Medicare payments to certified nurse midwives (CNMs) will reach the rate paid to physicians for the same services in January 2011, up from 65% of the physician rate. Medicare will also pay CNMs a 10% bonus if primary care services account for at least 60% of their allowed charges. And the law requires health plans in the state exchanges to pay for covered health services provided by any practitioner recognized under state law, whether or not the plan contracts with that individual or type of provider. Certified professional midwives (lay midwives) are licensed in 21 states, and this provision may give them significant new entry.
ObGyns stop delivering babies at increasingly early points in their career, and only 13% of family physicians deliver babies today. So we need to find ways to extend our care—and increasing collaborative practice between ObGyns and CNMs and certified midwives may help close this gap. The increased focus on midlevel providers in the law may present us with both a challenge and an important opportunity.
4 What services will be fully covered now?
OBG Management: Beginning this year, health plans will be required to provide a minimum level of coverage without cost-sharing for preventive care and screenings for women, among others. What will this requirement encompass?
DiVenere: Congress emphasized prevention in the reform law as part of its strategy to bend the cost curve, investing in prevention in order to reduce higher spending on illness.
Beginning in September 2010, all plans—including those that existed before this law was passed—must cover preventive health services without any patient cost sharing, whether copayments or deductibles. These services include women’s preventive care and screening included in comprehensive guidelines supported by the Health Resources and Services Administration (HRSA), even if they are more extensive than services recommended by the Centers for Disease Control and Prevention (CDC) and US Preventive Services Task Force (USPSTF). Breast cancer screening, mammography, and prevention services are covered as though the November 2009 USPSTF recommendations suggesting limits on mammography screening for certain age groups did not exist.
The mammography screening coverage was a big win for ACOG. We worked closely with Senator Barbara Mikulski (D-Md.) on this amendment, and it was the first Democratic amendment offered. It passed on the Senate floor during a contentious floor fight.
ACOG continues to recommend screening mammography every 1 to 2 years for women 40 to 49 years old; annual screening for women 50 and older; clinical breast examination every year for women 19 years and older; and regular breast self-examination.
The Senate bill that was brought to the floor would have limited women’s preventive care to USPSTF recommendations only. Working with Senator Mikulski, we made sure that women younger than 50 will be covered for mammography every 1 to 2 years.
OBG Management: Are there other important benefits for women included in the law?
DiVenere: Yes. One provision will improve research, screening, and treatment for postpartum depression, a signature issue of ACOG President Gerald F. Joseph Jr., MD, during his presidential year. ACOG and Dr. Joseph worked closely with Senator Bob Menendez (D-NJ) to introduce the Moms Act and win its inclusion in the health reform law.
Under this section, HHS will:
- conduct research into the causes of, and treatments for, postpartum conditions
- create a national public awareness campaign to increase knowledge of postpartum depression and postpartum psychosis
- provide grants to study the benefits of screening for postpartum depression and postpartum psychosis
- establish grants to deliver or enhance outpatient, inpatient, and home-based health and support services, including case management and comprehensive treatment services for women with or at risk of postpartum conditions.
5 Will expanded coverage improve birth outcomes?
OBG Management: Do you expect that guaranteed coverage of pregnancy will increase the number of women who seek prenatal care—as opposed to waiting until labor begins—to see a doctor? Will guaranteed coverage of pregnancy improve birth outcomes over the long term?
DiVenere: Those are certainly the goals. And guaranteed coverage of pregnancy was one of ACOG’s essential elements in health care reform. Prenatal care has been shown to save $3 for every $1 spent in the Medicaid program and continues to be the primary way to identify problems during pregnancy, giving ObGyns the opportunity to assess and manage the risk of preterm labor and other threats to the health of the mother and baby.
The health reform law recognizes that better prenatal care can lead to healthier babies—both in its coverage of maternity and preventive care, and by new Medicaid coverage of smoking-cessation counseling and family planning, both beginning this year.
Medicaid will now cover the costs of diagnostic, therapeutic, and counseling services, as well as pharmacotherapy for pregnant women covered by Medicaid, at no cost to the patient. Before health reform passed, only 24 states reimbursed ObGyns and other physicians for smoking-cessation counseling for pregnant women. Five states didn’t cover any smoking-cessation services at all.
Also beginning this year, states can provide family planning services to nonpregnant women up to the same eligibility levels to which they cover pregnant women, without the need to apply for federal waivers or permission. Forty-five states extend Medicaid coverage to pregnant women who have incomes above the regular Medicaid eligibility levels, from a low of 150% to a high of 300% of the federal poverty levels.
Before this new law, 27 states had federal waivers to provide family planning to women who had an income above the Medicaid eligibility levels, most of them at or near 200% of the federal poverty level. Eleven of these waivers expire this year.
6 Is femaleness a “preexisting condition”?
OBG Management: During the debate on health reform, many people claimed, somewhat facetiously, that female sex has been a preexisting condition. The new law will ensure that patients can’t be dropped by their insurance company—or denied coverage—for arbitrary or unfair reasons, such as preexisting conditions. How are these changes likely to affect women and their ObGyns?
DiVenere: The insurance reforms in the new law are very important to women and to ObGyn practices. In fact, the prohibition on preexisting conditions was a top priority of ACOG’s “Health care for women, health care for all” campaign, and Congress included this provision with women’s health in mind.
Many members of Congress were shocked to learn that it was not unusual for insurers to deny coverage to women who were pregnant, who had had a previous cesarean delivery, or who had been the victim of domestic violence at some point in their history. In fact, almost any medical history, genetic information, disability, or current health condition was grounds for denial of coverage.
Women were also often charged higher premiums than men for the same coverage. And insurance companies would sometimes require waiting periods for coverage—sometimes as long as 9 months.
All of these practices are outlawed by the health reform law, which prohibits plans from using preexisting condition exclusions to deny children coverage as of September 1, 2010 and adults as of January 1, 2014. Beginning on January 1, 2014, women cannot be denied coverage due to pregnancy, previous cesarean delivery, or domestic violence, or medical history, among many other reasons.
Effective March 23, 2010 and ending January 1, 2014, a high-risk pool insurance program has been created for people who have been uninsured for 6 months and who have a preexisting condition. Funding for the temporary risk pool is capped at $5 billion.
Insurers in the small and individual markets and in the exchanges cannot discriminate on the basis of medical history or other variables; may only charge limited premium differentials for age, family size, and smoking, but not for gender; and cannot mandate a waiting period longer than 90 days.
Insurance plans that were in existence before enactment must comply with reforms on waiting periods; lifetime limits; rescission; extension of dependent coverage; uniform explanation of coverage; and loss ratio reporting and premium rebates. Group grandfather plans must also comply with restrictions on annual limits and preexisting conditions.
All these protections should benefit ObGyn practices by ensuring coverage and continuity of care for their patients.
7 What happened to tort reform?
OBG Management: No tort reform was included in the law. Why not?
DiVenere: The law authorizes HHS to award $50 million over 5 years, up to $500,000 per state, to develop, implement, and evaluate alternative medical liability reform initiatives that meet several specific criteria. Medical liability protections under the Federal Tort Claims Act are extended to officers, governing board members, employees, and contractors of free clinics.
We at ACOG were very disappointed that Congress didn’t take a serious step toward medical liability reform in this bill. Liability reform was one of ACOG’s five essential elements of health reform, and its absence from the final bill was a prominent reason why we ultimately “reluctantly opposed” passage. We, and the rest of the House of Medicine, were clear that health reform wouldn’t work without meaningful medical liability reform.
ACOG supports caps on noneconomic damages and other reforms in California and Texas law. We also support testing alternatives, including health courts, alternative dispute resolution, “Sorry Works!” programs, and birth injury compensation funds. But this part of the health reform law requires that tests be linked to patient safety, an association that is impossible to establish in cases of neonatal encephalopathy. The law also requires that patients be allowed to opt out of a system if they choose to go to court. Both of these requirements hamper the development of meaningful alternatives for the ObGyn specialty.
8 Is the system repairable?
OBG Management: Can the US health care system be fixed in one fell swoop?
DiVenere: ACOG pursued two integral missions in reform efforts: improving women’s health and advocating for practicing ObGyns. Our mission in women’s health included guaranteed maternity care, important insurance reforms, and direct access to ObGyns. Our mission in regard to practicing ObGyns included the protection of ultrasonography, the reform of medical liability laws, and repeal of the Medicare sustainable growth rate, along with an array of other issues, all of which were shared by the entire House of Medicine.
We see these missions as integral; Congress saw them as separable. We were largely successful on the women’s health side of the ledger. But Congress responded to the House of Medicine issues with little interest.
We believe that we can fulfill our mission to women’s health only if the issues of practicing ObGyns are addressed in the process. You can’t build a new health care system on a broken medical liability system or a broken Medicare physician payment system, and we still have both. We have a lot more work to do on these issues and the myriad of other issues that need to be addressed. This is really just the beginning of health reform.
9 Has PQRI regained the limelight?
OBG Management: The Medicare quality reporting incentive payments under the Physician Quality Reporting Initiative (PQRI) have been extended. In fact, physicians will be penalized, beginning in 2015, if they do not participate. Are the incentive payments a good thing for ObGyns?
DiVenere: Yes, a big change is coming in this program. ObGyns who participate in PQRI will be eligible to receive bonus payments of 1% in 2011 and 0.5% from 2012 to 2014. Payments will be reduced by 1.5% in 2015 and by 2.0% in 2016 for physicians who don’t participate in the PQRI program.
Beginning in 2012, PQRI participation becomes a meaningful use qualifier for EHR grants.
In 2011 to 2014, physicians who complete Maintenance of Certification (MOC) are eligible for an additional 1% bonus in 2011 and 0.5% bonus in 2012 to 2014. Data on a physician’s quality measures must be submitted on the physician’s behalf by the MOC program. After 2014, the Secretary of HHS can add MOC completion to the quality measures used for the value-based payment modifier. The American Board of Obstetrics and Gynecology hasn’t yet qualified its MOC for this part of the program.
ObGyn participation in the PQRI program is very limited (less than 10%). While only about 25 of the 215 PQRI quality measures apply to ObGyn care, most are easily applicable, and a physician needs to report on only three to five measures to qualify for the program.
The very low participation rate is likely because many ObGyn practices just didn’t think the incentive payment was worth the trouble. They may need to rethink that math once they’re faced with payment cuts in 2015.
ObGyns should also be aware that the Secretary of HHS, with input from stakeholders, will set up a Physician Compare Web site (modeled after the program that already exists for hospitals) using PQRI data. Data will be made public on January 1, 2013, comparing physicians in terms of quality of care and patient experience.
The Secretary must ensure that the data are statistically valid and risk-adjusted. In addition, the physician must be given time to review the information before it becomes public, and data must ensure appropriate attribution of care when multiple physicians and other providers are involved. The Secretary must also give physicians timely performance feedback.
For all these reasons, ACOG is working with the physician community to make a number of improvements to the PQRI program, doing our best to make it as easy as possible for our members to participate and benefit.
10 What effect will the expansion of Medicaid have on ObGyn practice?
DiVenere: Starting in 2014, the same year that state exchanges are expected to be established, Medicaid eligibility will be broadened to cover all individuals younger than 65 years who have incomes up to 133% of the federal poverty level. All newly eligible adults will be guaranteed a benchmark benefit package that provides the essential health benefits.
States that have already expanded eligibility to adults who have incomes up to 100% of the federal poverty level will receive a phased-in increase in the federal medical assistance percentage so that, by 2019, they will receive the same federal financing as other states (93% in 2019 and 90% in 2020 and later). And states have the option to expand Medicaid eligibility to childless adults as of April 1, 2010, but will receive their regular federal medical assistance percentage until 2014.
Although these changes will broaden the range and increase the number of individuals who will be eligible for Medicaid, the effect on ObGyn practice remains to be seen, especially as pregnant women who were covered by Medicaid at income levels above 133% of the federal poverty level transition off of Medicaid and into private health insurance offered in the exchanges.
Today, about 38% of all ObGyns accept Medicaid gynecologic patients, and 44% accept Medicaid obstetric patients. Medicaid accounts for 18% of revenues of the average ObGyn practice.
11 Will the extension of benefits to young adults have a measurable impact on ObGyn practice?
DiVenere: Congress included two provisions to target “young immortals,” young adults who don’t think they need health insurance because they’re young and healthy and never need to see a doctor. Many young adults are not offered employer-based health insurance, and many see no advantage in buying coverage that they don’t expect to use. But we all know that someone pays when any uninsured person falls sick or has an accident that necessitates medical care.
Beginning this year, adult children as old as 26 years can go onto their parents’ health insurance plan. In addition, catastrophic plans will soon be available to individuals younger than 30 who want to purchase a higher deductible plan through their state exchange or on the individual and small group markets. These catastrophic plans are not required to include the essential benefits package, including maternity care. Nevertheless, both of these provisions should be helpful to ObGyn practices.
12 Will the mandate for employers to provide health insurance affect many ObGyns?
DiVenere: The employer mandate takes effect in 2014, when employers with more than 50 employees, at least one of whom receives a premium tax credit, are required to offer health insurance coverage to employees or be assessed a range of fees. Employers that have 50 or fewer employees are exempt from this requirement.
In 2007, 75% of ObGyn practices had fewer than 42 full-time employees, with an average number of full-time employees, including physicians, of 34.4. So this mandate should not apply to the average ObGyn practice.
A range of small business tax credits for employers that contribute at least 50% of the cost of coverage for their employees will also be available, with credits phasing out as the size of the firm and the average employee wage increase.
13 Who will benefit from the Medicare geographic payment adjustments?
DiVenere: The increased Medicare geographic practice cost index (GPCI) payments and new Frontier payments won’t affect many ObGyns nationally, but they are likely to affect most ObGyns in the related rural locations.
The law reestablishes the national average floor on Medicare’s GPCI for physician work. In 2010 and 2011, Medicare makes a separate adjustment for the practice expense portion of physician payments that will benefit physicians in rural and low-cost areas.
Beginning in 2011, a third adjustment will increase the practice expense GPCI for physicians in frontier states. A frontier state is one in which at least half of its counties have populations smaller than six people per square mile. Frontier states are expected to be Montana, North Dakota, South Dakota, Utah, and Wyoming.
Physicians in 51 localities in 42 states, Puerto Rico, and the Virgin Islands will benefit from the two practice expense adjustments.
ObGyns should also know about two other payment changes:
- The HHS Secretary will create and apply to Medicare provider payments a value-based modifier that will result in higher Medicare payments for high-quality, low-cost physicians and lower payments for high-cost, low-quality physicians. The modifier is to be based on a composite quality score and a composite cost score determined by measures selected by the HHS Secretary and endorsed by a consensus organization. This change begins with 2015 Medicare payments and applies only to physicians in 2015. In 2017, it will also apply to other health professionals.
- Effective immediately, the HHS Secretary has the authority to increase or decrease Medicare relative values, and payments for services, with special attention focused on:
- – services that have high growth rates
- – services that have seen substantial changes in the practice expense or work components
- – services for which new technology has reduced costs
- – instances in which multiple codes are frequently billed for a single service
- – codes that have not been reviewed since implementation of the resource-based relative value scale (RBRVS).
ObGyns who participate in Medicare will start receiving individual physician resource use reports in 2012. These reports will compare per capita utilization of physicians (or physician groups) with the utilization rate of physicians who see similar patients. Reports are required to be risk-adjusted and standardized to take into account local health-care costs.
14 Do you expect the law’s requirements for “administrative simplification” to reduce overhead and increase efficiency?
DiVenere: Don’t we all hope so.
The bill contains several requirements such as:
- establishment of a standardized claim form
- streamlining of claims processing
- improvement of interoperability to allow for more electronic information sharing. These changes will not be implemented until 2013 at the earliest.
Today, about 34% of all ObGyn practices use electronic health records. The systemwide benefits of health information technology (HIT) can be many. Insurers can save by reducing unnecessary tests. Patients can benefit from better coordination of care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices.
Instead, physicians face Medicare and private insurance payment cuts. Little assistance is available for the investment in HIT. And uncertain interoperability standards and rapid technological changes can very quickly make this year’s investment obsolete. Many physicians in solo and small practices are understandably reluctant to take the HIT plunge.
The initial cost of purchasing HIT for a small practice is typically at least $50,000 per physician. Physicians face additional, ongoing costs in staff training and hardware and software updates as well. And many physicians see significant efficiency losses for months and sometimes years after upgrading to an electronic health record system.
Still, with interoperable, shareable electronic records, all physicians treating a particular patient can have the full story. A patient’s paper record kept in her physician’s office shows only a slice of her medical history, potentially missing important information from the patient’s other physicians, including allergies to medication, test results, and the results of particular therapies.
Without a shared electronic record, a physician relies on the recollection of each patient, which is often unintentionally incomplete. A patient may be uncertain about the name or dosage of a medication, fail to remember the date of a screening examination, or lack results of lab tests ordered by another physician.
A physician’s access to the full story with shareable electronic records is important to the care of all patients and can be particularly relevant for patients who have inconsistent contact with health care providers. Often, these patients get care in various settings, including physician offices, community clinics, and emergency departments. Because these patients tend to have a higher incidence of chronic disease, they may greatly benefit from the sharing of medical information.
Clearly, Congress wants to move us to full adoption of HIT. Beginning in 2013, all plans must comply with a uniform standard for electronic transactions, including eligibility verification and health claims status.
In 2014, uniform standards must allow automatic reconciliation of electronic funds transfers and HIPAA payment and remittance; use standardized and consistent methods of health plan enrollment and claim edits; use unique health plan identifiers to simplify and improve routing of health care transactions; and use standard electronic claims attachments.
Uniformity and standardization can help address one of the major roadblocks to physician adoption of health information technology.
Janelle Yates,
Senior Editor, OBG Management
Lucia DiVenere
Janelle Yates,
Senior Editor, OBG Management
Lucia DiVenere
Janelle Yates,
Senior Editor, OBG Management
Lucia DiVenere
With passage of the Patient Protection and Affordable Care Act earlier this year, big changes are afoot in the way Americans practice medicine. In a plethora of articles, blogs, and broadcast spots, the media have focused on what the new law portends for the average employee, employers, and the uninsured—but what, exactly, does it entail for ObGyns and their patients?
To find an answer to that overarching question—and 13 others—we invited Lucia DiVenere, director of government relations at the American Congress of Obstetricians and Gynecologists, to join us in an extended discussion of the law and its ramifications. She offered insight into ACOG’s extensive lobbying efforts on behalf of women and the specialty and described the many ways ObGyn care will change in the near and proximal future, focusing on questions that you might find yourself asking, including:
- Will I see a lot more patients?
- What reforms are woman-specific?
- How will my practice change?
- Which of my services will be fully covered?
- Will expanded coverage improve birth outcomes?
- Is “femaleness” a preexisting condition?
- What happened to tort reform?
- Is the system repairable?
1 Will ObGyns see a lot more patients?
OBG Management: The most talked about change the new law heralds is the addition of roughly 32 million people to the insurance rolls. Is the most significant impact of the legislation for ObGyns likely to be an increase in the number of patients they will be seeing?
Lucia DiVenere: Congress wanted to increase the ranks of the insured and expand access to health care, and it addressed these goals with individual and employer mandates, state exchanges, Medicaid expansion, and insurance reforms.
But that isn’t the most significant change in store for us. Congress also wanted to reform our health care system in a number of fundamental ways, some of which are designed to change the way physicians provide care to their patients.
For example, Congress wanted to “bend the cost curve”—to reduce the expected rate of growth in health care spending over the long term. That doesn’t mean that health care costs in 2020 will be less than they were in 2018, but it does mean that annual and long-term growth rates should level off and become sustainable. To accomplish this goal, Congress created an Independent Payment Advisory Commission, which may prove to be extremely powerful in reducing health care costs and is likely to significantly affect all physicians. Greater protections against fraud and abuse, experiments with new kinds of payment and delivery systems, including “medical homes,” and increased reliance on nonphysician practitioners—all included in the law—are also expected to reduce costs.
OBG Management: What other changes are coming?
DiVenere: Congress was determined to alter the practice of health care, ensuring higher quality for each dollar spent and consistent delivery of care. It also sought to kick-start our health care system—especially in the physician arena—into greater and, theoretically, more efficient reliance on electronic health records (EHR). Medicare and Medicaid physician payments will be juggled to increase reimbursement for E&M services and for physicians who provide greater value in relation to cost. Physicians will be required to participate in the Physician Quality Reporting Initiative (PQRI) program in 2015 and beyond to avoid stiff penalties. And EHR systems are required to adopt uniform standards for electronic transactions.
2 What reforms are woman-specific?
OBG Management: What initiatives are planned for the care of women, in particular?
DiVenere: Congress recognized the importance of reforming women’s health and included many provisions advocated by ACOG in our “Health care for women, health care for all” campaign.
Probably the most important of these provisions is the guarantee of direct access to ObGyn care without need of a referral or pre-authorization from a primary care provider or insurance company. Nor can an insurance company restrict a patient’s direct access to her ObGyn to a certain number of visits or types of services.
This was a major ACOG victory. For 20 years, ObGyns have been waging battles in the states for direct access for patients. Last year, nine states did not require insurers to grant women direct access to ObGyns, and 16 states allowed insurers to restrict ObGyn visits and services. This part of the law, which is effective this year, provides national direct access to all women in all states, and is not tied to an ObGyn’s primary care designation.
Another area of reform concerns maternity care. In 2009, 13% of all pregnant women in the United States were uninsured, as were 20.4% of all women between the ages of 15 and 44, the childbearing years. The uninsured rate for nonelderly women in 2007 ranged from a high of 28% in New Mexico and Texas to a low of 8% in Massachusetts. Today, 42% of all pregnancies are covered by Medicaid. Women have been able, usually, to gain access to some kind of care—sometimes in emergency departments at the time of labor—but the nation clearly needs to do better.
Medicaid and new insurance plans will be required to offer maternity care and women’s preventive services, including mammography screening. The exact parameters of maternity care and other types of care in the essential benefits package will be determined by the Secretary of Health and Human Services (HHS), based on the typical package offered to employees in group health plans. The idea behind the law is that many women who are now covered by Medicaid will transfer to private insurance in their states’ exchanges.
3 How will ObGyn practice change?
OBG Management: What are some of the opportunities and challenges ObGyns will encounter?
DiVenere: There are three key areas of challenge and opportunity:
- Development of the “medical home.” A medical home is a practice designed to provide and coordinate comprehensive patient care. State Medicaid agencies are authorized to require certain beneficiaries, including those who have two or more chronic conditions, to join a medical home. Medicare will also experiment with medical homes, and both Medicaid and Medicare medical home practices will receive additional payments. Most medical homes are expected to be family practice, internal medicine, or pediatric care providers, but ObGyn practices can participate, too. ObGyns should look carefully at the opportunities this paradigm provides and consider having their practice designated as a medical home.
- Increased use of nonphysician providers. The new law strongly encourages this practice, including in the ObGyn specialty. Congress is determined to experiment with non-ObGyn deliveries in response to patient demand and midlevel assurances that nonphysicians can deliver babies with better outcomes at significantly lower cost. Our specialty’s cesarean delivery rate is under intense scrutiny. Skewed studies “prove” happier and healthier deliveries in homes and other out-of-hospital locations without an ObGyn in attendance. And midlevel practitioners are offering vaginal birth after cesarean delivery in many cases where ObGyns are restricted by hospital rules.
- The law extends Medicaid payments to free-standing birth centers and birth attendants and does not specify which kinds of practitioners can qualify as birth attendants. Free-standing birth centers can provide high-quality care if they are appropriately accredited and have an established transfer relationship with a nearby hospital. The law does not specify these criteria, either.
- Increasing payments to nonphysicians. Medicare payments to certified nurse midwives (CNMs) will reach the rate paid to physicians for the same services in January 2011, up from 65% of the physician rate. Medicare will also pay CNMs a 10% bonus if primary care services account for at least 60% of their allowed charges. And the law requires health plans in the state exchanges to pay for covered health services provided by any practitioner recognized under state law, whether or not the plan contracts with that individual or type of provider. Certified professional midwives (lay midwives) are licensed in 21 states, and this provision may give them significant new entry.
ObGyns stop delivering babies at increasingly early points in their career, and only 13% of family physicians deliver babies today. So we need to find ways to extend our care—and increasing collaborative practice between ObGyns and CNMs and certified midwives may help close this gap. The increased focus on midlevel providers in the law may present us with both a challenge and an important opportunity.
4 What services will be fully covered now?
OBG Management: Beginning this year, health plans will be required to provide a minimum level of coverage without cost-sharing for preventive care and screenings for women, among others. What will this requirement encompass?
DiVenere: Congress emphasized prevention in the reform law as part of its strategy to bend the cost curve, investing in prevention in order to reduce higher spending on illness.
Beginning in September 2010, all plans—including those that existed before this law was passed—must cover preventive health services without any patient cost sharing, whether copayments or deductibles. These services include women’s preventive care and screening included in comprehensive guidelines supported by the Health Resources and Services Administration (HRSA), even if they are more extensive than services recommended by the Centers for Disease Control and Prevention (CDC) and US Preventive Services Task Force (USPSTF). Breast cancer screening, mammography, and prevention services are covered as though the November 2009 USPSTF recommendations suggesting limits on mammography screening for certain age groups did not exist.
The mammography screening coverage was a big win for ACOG. We worked closely with Senator Barbara Mikulski (D-Md.) on this amendment, and it was the first Democratic amendment offered. It passed on the Senate floor during a contentious floor fight.
ACOG continues to recommend screening mammography every 1 to 2 years for women 40 to 49 years old; annual screening for women 50 and older; clinical breast examination every year for women 19 years and older; and regular breast self-examination.
The Senate bill that was brought to the floor would have limited women’s preventive care to USPSTF recommendations only. Working with Senator Mikulski, we made sure that women younger than 50 will be covered for mammography every 1 to 2 years.
OBG Management: Are there other important benefits for women included in the law?
DiVenere: Yes. One provision will improve research, screening, and treatment for postpartum depression, a signature issue of ACOG President Gerald F. Joseph Jr., MD, during his presidential year. ACOG and Dr. Joseph worked closely with Senator Bob Menendez (D-NJ) to introduce the Moms Act and win its inclusion in the health reform law.
Under this section, HHS will:
- conduct research into the causes of, and treatments for, postpartum conditions
- create a national public awareness campaign to increase knowledge of postpartum depression and postpartum psychosis
- provide grants to study the benefits of screening for postpartum depression and postpartum psychosis
- establish grants to deliver or enhance outpatient, inpatient, and home-based health and support services, including case management and comprehensive treatment services for women with or at risk of postpartum conditions.
5 Will expanded coverage improve birth outcomes?
OBG Management: Do you expect that guaranteed coverage of pregnancy will increase the number of women who seek prenatal care—as opposed to waiting until labor begins—to see a doctor? Will guaranteed coverage of pregnancy improve birth outcomes over the long term?
DiVenere: Those are certainly the goals. And guaranteed coverage of pregnancy was one of ACOG’s essential elements in health care reform. Prenatal care has been shown to save $3 for every $1 spent in the Medicaid program and continues to be the primary way to identify problems during pregnancy, giving ObGyns the opportunity to assess and manage the risk of preterm labor and other threats to the health of the mother and baby.
The health reform law recognizes that better prenatal care can lead to healthier babies—both in its coverage of maternity and preventive care, and by new Medicaid coverage of smoking-cessation counseling and family planning, both beginning this year.
Medicaid will now cover the costs of diagnostic, therapeutic, and counseling services, as well as pharmacotherapy for pregnant women covered by Medicaid, at no cost to the patient. Before health reform passed, only 24 states reimbursed ObGyns and other physicians for smoking-cessation counseling for pregnant women. Five states didn’t cover any smoking-cessation services at all.
Also beginning this year, states can provide family planning services to nonpregnant women up to the same eligibility levels to which they cover pregnant women, without the need to apply for federal waivers or permission. Forty-five states extend Medicaid coverage to pregnant women who have incomes above the regular Medicaid eligibility levels, from a low of 150% to a high of 300% of the federal poverty levels.
Before this new law, 27 states had federal waivers to provide family planning to women who had an income above the Medicaid eligibility levels, most of them at or near 200% of the federal poverty level. Eleven of these waivers expire this year.
6 Is femaleness a “preexisting condition”?
OBG Management: During the debate on health reform, many people claimed, somewhat facetiously, that female sex has been a preexisting condition. The new law will ensure that patients can’t be dropped by their insurance company—or denied coverage—for arbitrary or unfair reasons, such as preexisting conditions. How are these changes likely to affect women and their ObGyns?
DiVenere: The insurance reforms in the new law are very important to women and to ObGyn practices. In fact, the prohibition on preexisting conditions was a top priority of ACOG’s “Health care for women, health care for all” campaign, and Congress included this provision with women’s health in mind.
Many members of Congress were shocked to learn that it was not unusual for insurers to deny coverage to women who were pregnant, who had had a previous cesarean delivery, or who had been the victim of domestic violence at some point in their history. In fact, almost any medical history, genetic information, disability, or current health condition was grounds for denial of coverage.
Women were also often charged higher premiums than men for the same coverage. And insurance companies would sometimes require waiting periods for coverage—sometimes as long as 9 months.
All of these practices are outlawed by the health reform law, which prohibits plans from using preexisting condition exclusions to deny children coverage as of September 1, 2010 and adults as of January 1, 2014. Beginning on January 1, 2014, women cannot be denied coverage due to pregnancy, previous cesarean delivery, or domestic violence, or medical history, among many other reasons.
Effective March 23, 2010 and ending January 1, 2014, a high-risk pool insurance program has been created for people who have been uninsured for 6 months and who have a preexisting condition. Funding for the temporary risk pool is capped at $5 billion.
Insurers in the small and individual markets and in the exchanges cannot discriminate on the basis of medical history or other variables; may only charge limited premium differentials for age, family size, and smoking, but not for gender; and cannot mandate a waiting period longer than 90 days.
Insurance plans that were in existence before enactment must comply with reforms on waiting periods; lifetime limits; rescission; extension of dependent coverage; uniform explanation of coverage; and loss ratio reporting and premium rebates. Group grandfather plans must also comply with restrictions on annual limits and preexisting conditions.
All these protections should benefit ObGyn practices by ensuring coverage and continuity of care for their patients.
7 What happened to tort reform?
OBG Management: No tort reform was included in the law. Why not?
DiVenere: The law authorizes HHS to award $50 million over 5 years, up to $500,000 per state, to develop, implement, and evaluate alternative medical liability reform initiatives that meet several specific criteria. Medical liability protections under the Federal Tort Claims Act are extended to officers, governing board members, employees, and contractors of free clinics.
We at ACOG were very disappointed that Congress didn’t take a serious step toward medical liability reform in this bill. Liability reform was one of ACOG’s five essential elements of health reform, and its absence from the final bill was a prominent reason why we ultimately “reluctantly opposed” passage. We, and the rest of the House of Medicine, were clear that health reform wouldn’t work without meaningful medical liability reform.
ACOG supports caps on noneconomic damages and other reforms in California and Texas law. We also support testing alternatives, including health courts, alternative dispute resolution, “Sorry Works!” programs, and birth injury compensation funds. But this part of the health reform law requires that tests be linked to patient safety, an association that is impossible to establish in cases of neonatal encephalopathy. The law also requires that patients be allowed to opt out of a system if they choose to go to court. Both of these requirements hamper the development of meaningful alternatives for the ObGyn specialty.
8 Is the system repairable?
OBG Management: Can the US health care system be fixed in one fell swoop?
DiVenere: ACOG pursued two integral missions in reform efforts: improving women’s health and advocating for practicing ObGyns. Our mission in women’s health included guaranteed maternity care, important insurance reforms, and direct access to ObGyns. Our mission in regard to practicing ObGyns included the protection of ultrasonography, the reform of medical liability laws, and repeal of the Medicare sustainable growth rate, along with an array of other issues, all of which were shared by the entire House of Medicine.
We see these missions as integral; Congress saw them as separable. We were largely successful on the women’s health side of the ledger. But Congress responded to the House of Medicine issues with little interest.
We believe that we can fulfill our mission to women’s health only if the issues of practicing ObGyns are addressed in the process. You can’t build a new health care system on a broken medical liability system or a broken Medicare physician payment system, and we still have both. We have a lot more work to do on these issues and the myriad of other issues that need to be addressed. This is really just the beginning of health reform.
9 Has PQRI regained the limelight?
OBG Management: The Medicare quality reporting incentive payments under the Physician Quality Reporting Initiative (PQRI) have been extended. In fact, physicians will be penalized, beginning in 2015, if they do not participate. Are the incentive payments a good thing for ObGyns?
DiVenere: Yes, a big change is coming in this program. ObGyns who participate in PQRI will be eligible to receive bonus payments of 1% in 2011 and 0.5% from 2012 to 2014. Payments will be reduced by 1.5% in 2015 and by 2.0% in 2016 for physicians who don’t participate in the PQRI program.
Beginning in 2012, PQRI participation becomes a meaningful use qualifier for EHR grants.
In 2011 to 2014, physicians who complete Maintenance of Certification (MOC) are eligible for an additional 1% bonus in 2011 and 0.5% bonus in 2012 to 2014. Data on a physician’s quality measures must be submitted on the physician’s behalf by the MOC program. After 2014, the Secretary of HHS can add MOC completion to the quality measures used for the value-based payment modifier. The American Board of Obstetrics and Gynecology hasn’t yet qualified its MOC for this part of the program.
ObGyn participation in the PQRI program is very limited (less than 10%). While only about 25 of the 215 PQRI quality measures apply to ObGyn care, most are easily applicable, and a physician needs to report on only three to five measures to qualify for the program.
The very low participation rate is likely because many ObGyn practices just didn’t think the incentive payment was worth the trouble. They may need to rethink that math once they’re faced with payment cuts in 2015.
ObGyns should also be aware that the Secretary of HHS, with input from stakeholders, will set up a Physician Compare Web site (modeled after the program that already exists for hospitals) using PQRI data. Data will be made public on January 1, 2013, comparing physicians in terms of quality of care and patient experience.
The Secretary must ensure that the data are statistically valid and risk-adjusted. In addition, the physician must be given time to review the information before it becomes public, and data must ensure appropriate attribution of care when multiple physicians and other providers are involved. The Secretary must also give physicians timely performance feedback.
For all these reasons, ACOG is working with the physician community to make a number of improvements to the PQRI program, doing our best to make it as easy as possible for our members to participate and benefit.
10 What effect will the expansion of Medicaid have on ObGyn practice?
DiVenere: Starting in 2014, the same year that state exchanges are expected to be established, Medicaid eligibility will be broadened to cover all individuals younger than 65 years who have incomes up to 133% of the federal poverty level. All newly eligible adults will be guaranteed a benchmark benefit package that provides the essential health benefits.
States that have already expanded eligibility to adults who have incomes up to 100% of the federal poverty level will receive a phased-in increase in the federal medical assistance percentage so that, by 2019, they will receive the same federal financing as other states (93% in 2019 and 90% in 2020 and later). And states have the option to expand Medicaid eligibility to childless adults as of April 1, 2010, but will receive their regular federal medical assistance percentage until 2014.
Although these changes will broaden the range and increase the number of individuals who will be eligible for Medicaid, the effect on ObGyn practice remains to be seen, especially as pregnant women who were covered by Medicaid at income levels above 133% of the federal poverty level transition off of Medicaid and into private health insurance offered in the exchanges.
Today, about 38% of all ObGyns accept Medicaid gynecologic patients, and 44% accept Medicaid obstetric patients. Medicaid accounts for 18% of revenues of the average ObGyn practice.
11 Will the extension of benefits to young adults have a measurable impact on ObGyn practice?
DiVenere: Congress included two provisions to target “young immortals,” young adults who don’t think they need health insurance because they’re young and healthy and never need to see a doctor. Many young adults are not offered employer-based health insurance, and many see no advantage in buying coverage that they don’t expect to use. But we all know that someone pays when any uninsured person falls sick or has an accident that necessitates medical care.
Beginning this year, adult children as old as 26 years can go onto their parents’ health insurance plan. In addition, catastrophic plans will soon be available to individuals younger than 30 who want to purchase a higher deductible plan through their state exchange or on the individual and small group markets. These catastrophic plans are not required to include the essential benefits package, including maternity care. Nevertheless, both of these provisions should be helpful to ObGyn practices.
12 Will the mandate for employers to provide health insurance affect many ObGyns?
DiVenere: The employer mandate takes effect in 2014, when employers with more than 50 employees, at least one of whom receives a premium tax credit, are required to offer health insurance coverage to employees or be assessed a range of fees. Employers that have 50 or fewer employees are exempt from this requirement.
In 2007, 75% of ObGyn practices had fewer than 42 full-time employees, with an average number of full-time employees, including physicians, of 34.4. So this mandate should not apply to the average ObGyn practice.
A range of small business tax credits for employers that contribute at least 50% of the cost of coverage for their employees will also be available, with credits phasing out as the size of the firm and the average employee wage increase.
13 Who will benefit from the Medicare geographic payment adjustments?
DiVenere: The increased Medicare geographic practice cost index (GPCI) payments and new Frontier payments won’t affect many ObGyns nationally, but they are likely to affect most ObGyns in the related rural locations.
The law reestablishes the national average floor on Medicare’s GPCI for physician work. In 2010 and 2011, Medicare makes a separate adjustment for the practice expense portion of physician payments that will benefit physicians in rural and low-cost areas.
Beginning in 2011, a third adjustment will increase the practice expense GPCI for physicians in frontier states. A frontier state is one in which at least half of its counties have populations smaller than six people per square mile. Frontier states are expected to be Montana, North Dakota, South Dakota, Utah, and Wyoming.
Physicians in 51 localities in 42 states, Puerto Rico, and the Virgin Islands will benefit from the two practice expense adjustments.
ObGyns should also know about two other payment changes:
- The HHS Secretary will create and apply to Medicare provider payments a value-based modifier that will result in higher Medicare payments for high-quality, low-cost physicians and lower payments for high-cost, low-quality physicians. The modifier is to be based on a composite quality score and a composite cost score determined by measures selected by the HHS Secretary and endorsed by a consensus organization. This change begins with 2015 Medicare payments and applies only to physicians in 2015. In 2017, it will also apply to other health professionals.
- Effective immediately, the HHS Secretary has the authority to increase or decrease Medicare relative values, and payments for services, with special attention focused on:
- – services that have high growth rates
- – services that have seen substantial changes in the practice expense or work components
- – services for which new technology has reduced costs
- – instances in which multiple codes are frequently billed for a single service
- – codes that have not been reviewed since implementation of the resource-based relative value scale (RBRVS).
ObGyns who participate in Medicare will start receiving individual physician resource use reports in 2012. These reports will compare per capita utilization of physicians (or physician groups) with the utilization rate of physicians who see similar patients. Reports are required to be risk-adjusted and standardized to take into account local health-care costs.
14 Do you expect the law’s requirements for “administrative simplification” to reduce overhead and increase efficiency?
DiVenere: Don’t we all hope so.
The bill contains several requirements such as:
- establishment of a standardized claim form
- streamlining of claims processing
- improvement of interoperability to allow for more electronic information sharing. These changes will not be implemented until 2013 at the earliest.
Today, about 34% of all ObGyn practices use electronic health records. The systemwide benefits of health information technology (HIT) can be many. Insurers can save by reducing unnecessary tests. Patients can benefit from better coordination of care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices.
Instead, physicians face Medicare and private insurance payment cuts. Little assistance is available for the investment in HIT. And uncertain interoperability standards and rapid technological changes can very quickly make this year’s investment obsolete. Many physicians in solo and small practices are understandably reluctant to take the HIT plunge.
The initial cost of purchasing HIT for a small practice is typically at least $50,000 per physician. Physicians face additional, ongoing costs in staff training and hardware and software updates as well. And many physicians see significant efficiency losses for months and sometimes years after upgrading to an electronic health record system.
Still, with interoperable, shareable electronic records, all physicians treating a particular patient can have the full story. A patient’s paper record kept in her physician’s office shows only a slice of her medical history, potentially missing important information from the patient’s other physicians, including allergies to medication, test results, and the results of particular therapies.
Without a shared electronic record, a physician relies on the recollection of each patient, which is often unintentionally incomplete. A patient may be uncertain about the name or dosage of a medication, fail to remember the date of a screening examination, or lack results of lab tests ordered by another physician.
A physician’s access to the full story with shareable electronic records is important to the care of all patients and can be particularly relevant for patients who have inconsistent contact with health care providers. Often, these patients get care in various settings, including physician offices, community clinics, and emergency departments. Because these patients tend to have a higher incidence of chronic disease, they may greatly benefit from the sharing of medical information.
Clearly, Congress wants to move us to full adoption of HIT. Beginning in 2013, all plans must comply with a uniform standard for electronic transactions, including eligibility verification and health claims status.
In 2014, uniform standards must allow automatic reconciliation of electronic funds transfers and HIPAA payment and remittance; use standardized and consistent methods of health plan enrollment and claim edits; use unique health plan identifiers to simplify and improve routing of health care transactions; and use standard electronic claims attachments.
Uniformity and standardization can help address one of the major roadblocks to physician adoption of health information technology.
With passage of the Patient Protection and Affordable Care Act earlier this year, big changes are afoot in the way Americans practice medicine. In a plethora of articles, blogs, and broadcast spots, the media have focused on what the new law portends for the average employee, employers, and the uninsured—but what, exactly, does it entail for ObGyns and their patients?
To find an answer to that overarching question—and 13 others—we invited Lucia DiVenere, director of government relations at the American Congress of Obstetricians and Gynecologists, to join us in an extended discussion of the law and its ramifications. She offered insight into ACOG’s extensive lobbying efforts on behalf of women and the specialty and described the many ways ObGyn care will change in the near and proximal future, focusing on questions that you might find yourself asking, including:
- Will I see a lot more patients?
- What reforms are woman-specific?
- How will my practice change?
- Which of my services will be fully covered?
- Will expanded coverage improve birth outcomes?
- Is “femaleness” a preexisting condition?
- What happened to tort reform?
- Is the system repairable?
1 Will ObGyns see a lot more patients?
OBG Management: The most talked about change the new law heralds is the addition of roughly 32 million people to the insurance rolls. Is the most significant impact of the legislation for ObGyns likely to be an increase in the number of patients they will be seeing?
Lucia DiVenere: Congress wanted to increase the ranks of the insured and expand access to health care, and it addressed these goals with individual and employer mandates, state exchanges, Medicaid expansion, and insurance reforms.
But that isn’t the most significant change in store for us. Congress also wanted to reform our health care system in a number of fundamental ways, some of which are designed to change the way physicians provide care to their patients.
For example, Congress wanted to “bend the cost curve”—to reduce the expected rate of growth in health care spending over the long term. That doesn’t mean that health care costs in 2020 will be less than they were in 2018, but it does mean that annual and long-term growth rates should level off and become sustainable. To accomplish this goal, Congress created an Independent Payment Advisory Commission, which may prove to be extremely powerful in reducing health care costs and is likely to significantly affect all physicians. Greater protections against fraud and abuse, experiments with new kinds of payment and delivery systems, including “medical homes,” and increased reliance on nonphysician practitioners—all included in the law—are also expected to reduce costs.
OBG Management: What other changes are coming?
DiVenere: Congress was determined to alter the practice of health care, ensuring higher quality for each dollar spent and consistent delivery of care. It also sought to kick-start our health care system—especially in the physician arena—into greater and, theoretically, more efficient reliance on electronic health records (EHR). Medicare and Medicaid physician payments will be juggled to increase reimbursement for E&M services and for physicians who provide greater value in relation to cost. Physicians will be required to participate in the Physician Quality Reporting Initiative (PQRI) program in 2015 and beyond to avoid stiff penalties. And EHR systems are required to adopt uniform standards for electronic transactions.
2 What reforms are woman-specific?
OBG Management: What initiatives are planned for the care of women, in particular?
DiVenere: Congress recognized the importance of reforming women’s health and included many provisions advocated by ACOG in our “Health care for women, health care for all” campaign.
Probably the most important of these provisions is the guarantee of direct access to ObGyn care without need of a referral or pre-authorization from a primary care provider or insurance company. Nor can an insurance company restrict a patient’s direct access to her ObGyn to a certain number of visits or types of services.
This was a major ACOG victory. For 20 years, ObGyns have been waging battles in the states for direct access for patients. Last year, nine states did not require insurers to grant women direct access to ObGyns, and 16 states allowed insurers to restrict ObGyn visits and services. This part of the law, which is effective this year, provides national direct access to all women in all states, and is not tied to an ObGyn’s primary care designation.
Another area of reform concerns maternity care. In 2009, 13% of all pregnant women in the United States were uninsured, as were 20.4% of all women between the ages of 15 and 44, the childbearing years. The uninsured rate for nonelderly women in 2007 ranged from a high of 28% in New Mexico and Texas to a low of 8% in Massachusetts. Today, 42% of all pregnancies are covered by Medicaid. Women have been able, usually, to gain access to some kind of care—sometimes in emergency departments at the time of labor—but the nation clearly needs to do better.
Medicaid and new insurance plans will be required to offer maternity care and women’s preventive services, including mammography screening. The exact parameters of maternity care and other types of care in the essential benefits package will be determined by the Secretary of Health and Human Services (HHS), based on the typical package offered to employees in group health plans. The idea behind the law is that many women who are now covered by Medicaid will transfer to private insurance in their states’ exchanges.
3 How will ObGyn practice change?
OBG Management: What are some of the opportunities and challenges ObGyns will encounter?
DiVenere: There are three key areas of challenge and opportunity:
- Development of the “medical home.” A medical home is a practice designed to provide and coordinate comprehensive patient care. State Medicaid agencies are authorized to require certain beneficiaries, including those who have two or more chronic conditions, to join a medical home. Medicare will also experiment with medical homes, and both Medicaid and Medicare medical home practices will receive additional payments. Most medical homes are expected to be family practice, internal medicine, or pediatric care providers, but ObGyn practices can participate, too. ObGyns should look carefully at the opportunities this paradigm provides and consider having their practice designated as a medical home.
- Increased use of nonphysician providers. The new law strongly encourages this practice, including in the ObGyn specialty. Congress is determined to experiment with non-ObGyn deliveries in response to patient demand and midlevel assurances that nonphysicians can deliver babies with better outcomes at significantly lower cost. Our specialty’s cesarean delivery rate is under intense scrutiny. Skewed studies “prove” happier and healthier deliveries in homes and other out-of-hospital locations without an ObGyn in attendance. And midlevel practitioners are offering vaginal birth after cesarean delivery in many cases where ObGyns are restricted by hospital rules.
- The law extends Medicaid payments to free-standing birth centers and birth attendants and does not specify which kinds of practitioners can qualify as birth attendants. Free-standing birth centers can provide high-quality care if they are appropriately accredited and have an established transfer relationship with a nearby hospital. The law does not specify these criteria, either.
- Increasing payments to nonphysicians. Medicare payments to certified nurse midwives (CNMs) will reach the rate paid to physicians for the same services in January 2011, up from 65% of the physician rate. Medicare will also pay CNMs a 10% bonus if primary care services account for at least 60% of their allowed charges. And the law requires health plans in the state exchanges to pay for covered health services provided by any practitioner recognized under state law, whether or not the plan contracts with that individual or type of provider. Certified professional midwives (lay midwives) are licensed in 21 states, and this provision may give them significant new entry.
ObGyns stop delivering babies at increasingly early points in their career, and only 13% of family physicians deliver babies today. So we need to find ways to extend our care—and increasing collaborative practice between ObGyns and CNMs and certified midwives may help close this gap. The increased focus on midlevel providers in the law may present us with both a challenge and an important opportunity.
4 What services will be fully covered now?
OBG Management: Beginning this year, health plans will be required to provide a minimum level of coverage without cost-sharing for preventive care and screenings for women, among others. What will this requirement encompass?
DiVenere: Congress emphasized prevention in the reform law as part of its strategy to bend the cost curve, investing in prevention in order to reduce higher spending on illness.
Beginning in September 2010, all plans—including those that existed before this law was passed—must cover preventive health services without any patient cost sharing, whether copayments or deductibles. These services include women’s preventive care and screening included in comprehensive guidelines supported by the Health Resources and Services Administration (HRSA), even if they are more extensive than services recommended by the Centers for Disease Control and Prevention (CDC) and US Preventive Services Task Force (USPSTF). Breast cancer screening, mammography, and prevention services are covered as though the November 2009 USPSTF recommendations suggesting limits on mammography screening for certain age groups did not exist.
The mammography screening coverage was a big win for ACOG. We worked closely with Senator Barbara Mikulski (D-Md.) on this amendment, and it was the first Democratic amendment offered. It passed on the Senate floor during a contentious floor fight.
ACOG continues to recommend screening mammography every 1 to 2 years for women 40 to 49 years old; annual screening for women 50 and older; clinical breast examination every year for women 19 years and older; and regular breast self-examination.
The Senate bill that was brought to the floor would have limited women’s preventive care to USPSTF recommendations only. Working with Senator Mikulski, we made sure that women younger than 50 will be covered for mammography every 1 to 2 years.
OBG Management: Are there other important benefits for women included in the law?
DiVenere: Yes. One provision will improve research, screening, and treatment for postpartum depression, a signature issue of ACOG President Gerald F. Joseph Jr., MD, during his presidential year. ACOG and Dr. Joseph worked closely with Senator Bob Menendez (D-NJ) to introduce the Moms Act and win its inclusion in the health reform law.
Under this section, HHS will:
- conduct research into the causes of, and treatments for, postpartum conditions
- create a national public awareness campaign to increase knowledge of postpartum depression and postpartum psychosis
- provide grants to study the benefits of screening for postpartum depression and postpartum psychosis
- establish grants to deliver or enhance outpatient, inpatient, and home-based health and support services, including case management and comprehensive treatment services for women with or at risk of postpartum conditions.
5 Will expanded coverage improve birth outcomes?
OBG Management: Do you expect that guaranteed coverage of pregnancy will increase the number of women who seek prenatal care—as opposed to waiting until labor begins—to see a doctor? Will guaranteed coverage of pregnancy improve birth outcomes over the long term?
DiVenere: Those are certainly the goals. And guaranteed coverage of pregnancy was one of ACOG’s essential elements in health care reform. Prenatal care has been shown to save $3 for every $1 spent in the Medicaid program and continues to be the primary way to identify problems during pregnancy, giving ObGyns the opportunity to assess and manage the risk of preterm labor and other threats to the health of the mother and baby.
The health reform law recognizes that better prenatal care can lead to healthier babies—both in its coverage of maternity and preventive care, and by new Medicaid coverage of smoking-cessation counseling and family planning, both beginning this year.
Medicaid will now cover the costs of diagnostic, therapeutic, and counseling services, as well as pharmacotherapy for pregnant women covered by Medicaid, at no cost to the patient. Before health reform passed, only 24 states reimbursed ObGyns and other physicians for smoking-cessation counseling for pregnant women. Five states didn’t cover any smoking-cessation services at all.
Also beginning this year, states can provide family planning services to nonpregnant women up to the same eligibility levels to which they cover pregnant women, without the need to apply for federal waivers or permission. Forty-five states extend Medicaid coverage to pregnant women who have incomes above the regular Medicaid eligibility levels, from a low of 150% to a high of 300% of the federal poverty levels.
Before this new law, 27 states had federal waivers to provide family planning to women who had an income above the Medicaid eligibility levels, most of them at or near 200% of the federal poverty level. Eleven of these waivers expire this year.
6 Is femaleness a “preexisting condition”?
OBG Management: During the debate on health reform, many people claimed, somewhat facetiously, that female sex has been a preexisting condition. The new law will ensure that patients can’t be dropped by their insurance company—or denied coverage—for arbitrary or unfair reasons, such as preexisting conditions. How are these changes likely to affect women and their ObGyns?
DiVenere: The insurance reforms in the new law are very important to women and to ObGyn practices. In fact, the prohibition on preexisting conditions was a top priority of ACOG’s “Health care for women, health care for all” campaign, and Congress included this provision with women’s health in mind.
Many members of Congress were shocked to learn that it was not unusual for insurers to deny coverage to women who were pregnant, who had had a previous cesarean delivery, or who had been the victim of domestic violence at some point in their history. In fact, almost any medical history, genetic information, disability, or current health condition was grounds for denial of coverage.
Women were also often charged higher premiums than men for the same coverage. And insurance companies would sometimes require waiting periods for coverage—sometimes as long as 9 months.
All of these practices are outlawed by the health reform law, which prohibits plans from using preexisting condition exclusions to deny children coverage as of September 1, 2010 and adults as of January 1, 2014. Beginning on January 1, 2014, women cannot be denied coverage due to pregnancy, previous cesarean delivery, or domestic violence, or medical history, among many other reasons.
Effective March 23, 2010 and ending January 1, 2014, a high-risk pool insurance program has been created for people who have been uninsured for 6 months and who have a preexisting condition. Funding for the temporary risk pool is capped at $5 billion.
Insurers in the small and individual markets and in the exchanges cannot discriminate on the basis of medical history or other variables; may only charge limited premium differentials for age, family size, and smoking, but not for gender; and cannot mandate a waiting period longer than 90 days.
Insurance plans that were in existence before enactment must comply with reforms on waiting periods; lifetime limits; rescission; extension of dependent coverage; uniform explanation of coverage; and loss ratio reporting and premium rebates. Group grandfather plans must also comply with restrictions on annual limits and preexisting conditions.
All these protections should benefit ObGyn practices by ensuring coverage and continuity of care for their patients.
7 What happened to tort reform?
OBG Management: No tort reform was included in the law. Why not?
DiVenere: The law authorizes HHS to award $50 million over 5 years, up to $500,000 per state, to develop, implement, and evaluate alternative medical liability reform initiatives that meet several specific criteria. Medical liability protections under the Federal Tort Claims Act are extended to officers, governing board members, employees, and contractors of free clinics.
We at ACOG were very disappointed that Congress didn’t take a serious step toward medical liability reform in this bill. Liability reform was one of ACOG’s five essential elements of health reform, and its absence from the final bill was a prominent reason why we ultimately “reluctantly opposed” passage. We, and the rest of the House of Medicine, were clear that health reform wouldn’t work without meaningful medical liability reform.
ACOG supports caps on noneconomic damages and other reforms in California and Texas law. We also support testing alternatives, including health courts, alternative dispute resolution, “Sorry Works!” programs, and birth injury compensation funds. But this part of the health reform law requires that tests be linked to patient safety, an association that is impossible to establish in cases of neonatal encephalopathy. The law also requires that patients be allowed to opt out of a system if they choose to go to court. Both of these requirements hamper the development of meaningful alternatives for the ObGyn specialty.
8 Is the system repairable?
OBG Management: Can the US health care system be fixed in one fell swoop?
DiVenere: ACOG pursued two integral missions in reform efforts: improving women’s health and advocating for practicing ObGyns. Our mission in women’s health included guaranteed maternity care, important insurance reforms, and direct access to ObGyns. Our mission in regard to practicing ObGyns included the protection of ultrasonography, the reform of medical liability laws, and repeal of the Medicare sustainable growth rate, along with an array of other issues, all of which were shared by the entire House of Medicine.
We see these missions as integral; Congress saw them as separable. We were largely successful on the women’s health side of the ledger. But Congress responded to the House of Medicine issues with little interest.
We believe that we can fulfill our mission to women’s health only if the issues of practicing ObGyns are addressed in the process. You can’t build a new health care system on a broken medical liability system or a broken Medicare physician payment system, and we still have both. We have a lot more work to do on these issues and the myriad of other issues that need to be addressed. This is really just the beginning of health reform.
9 Has PQRI regained the limelight?
OBG Management: The Medicare quality reporting incentive payments under the Physician Quality Reporting Initiative (PQRI) have been extended. In fact, physicians will be penalized, beginning in 2015, if they do not participate. Are the incentive payments a good thing for ObGyns?
DiVenere: Yes, a big change is coming in this program. ObGyns who participate in PQRI will be eligible to receive bonus payments of 1% in 2011 and 0.5% from 2012 to 2014. Payments will be reduced by 1.5% in 2015 and by 2.0% in 2016 for physicians who don’t participate in the PQRI program.
Beginning in 2012, PQRI participation becomes a meaningful use qualifier for EHR grants.
In 2011 to 2014, physicians who complete Maintenance of Certification (MOC) are eligible for an additional 1% bonus in 2011 and 0.5% bonus in 2012 to 2014. Data on a physician’s quality measures must be submitted on the physician’s behalf by the MOC program. After 2014, the Secretary of HHS can add MOC completion to the quality measures used for the value-based payment modifier. The American Board of Obstetrics and Gynecology hasn’t yet qualified its MOC for this part of the program.
ObGyn participation in the PQRI program is very limited (less than 10%). While only about 25 of the 215 PQRI quality measures apply to ObGyn care, most are easily applicable, and a physician needs to report on only three to five measures to qualify for the program.
The very low participation rate is likely because many ObGyn practices just didn’t think the incentive payment was worth the trouble. They may need to rethink that math once they’re faced with payment cuts in 2015.
ObGyns should also be aware that the Secretary of HHS, with input from stakeholders, will set up a Physician Compare Web site (modeled after the program that already exists for hospitals) using PQRI data. Data will be made public on January 1, 2013, comparing physicians in terms of quality of care and patient experience.
The Secretary must ensure that the data are statistically valid and risk-adjusted. In addition, the physician must be given time to review the information before it becomes public, and data must ensure appropriate attribution of care when multiple physicians and other providers are involved. The Secretary must also give physicians timely performance feedback.
For all these reasons, ACOG is working with the physician community to make a number of improvements to the PQRI program, doing our best to make it as easy as possible for our members to participate and benefit.
10 What effect will the expansion of Medicaid have on ObGyn practice?
DiVenere: Starting in 2014, the same year that state exchanges are expected to be established, Medicaid eligibility will be broadened to cover all individuals younger than 65 years who have incomes up to 133% of the federal poverty level. All newly eligible adults will be guaranteed a benchmark benefit package that provides the essential health benefits.
States that have already expanded eligibility to adults who have incomes up to 100% of the federal poverty level will receive a phased-in increase in the federal medical assistance percentage so that, by 2019, they will receive the same federal financing as other states (93% in 2019 and 90% in 2020 and later). And states have the option to expand Medicaid eligibility to childless adults as of April 1, 2010, but will receive their regular federal medical assistance percentage until 2014.
Although these changes will broaden the range and increase the number of individuals who will be eligible for Medicaid, the effect on ObGyn practice remains to be seen, especially as pregnant women who were covered by Medicaid at income levels above 133% of the federal poverty level transition off of Medicaid and into private health insurance offered in the exchanges.
Today, about 38% of all ObGyns accept Medicaid gynecologic patients, and 44% accept Medicaid obstetric patients. Medicaid accounts for 18% of revenues of the average ObGyn practice.
11 Will the extension of benefits to young adults have a measurable impact on ObGyn practice?
DiVenere: Congress included two provisions to target “young immortals,” young adults who don’t think they need health insurance because they’re young and healthy and never need to see a doctor. Many young adults are not offered employer-based health insurance, and many see no advantage in buying coverage that they don’t expect to use. But we all know that someone pays when any uninsured person falls sick or has an accident that necessitates medical care.
Beginning this year, adult children as old as 26 years can go onto their parents’ health insurance plan. In addition, catastrophic plans will soon be available to individuals younger than 30 who want to purchase a higher deductible plan through their state exchange or on the individual and small group markets. These catastrophic plans are not required to include the essential benefits package, including maternity care. Nevertheless, both of these provisions should be helpful to ObGyn practices.
12 Will the mandate for employers to provide health insurance affect many ObGyns?
DiVenere: The employer mandate takes effect in 2014, when employers with more than 50 employees, at least one of whom receives a premium tax credit, are required to offer health insurance coverage to employees or be assessed a range of fees. Employers that have 50 or fewer employees are exempt from this requirement.
In 2007, 75% of ObGyn practices had fewer than 42 full-time employees, with an average number of full-time employees, including physicians, of 34.4. So this mandate should not apply to the average ObGyn practice.
A range of small business tax credits for employers that contribute at least 50% of the cost of coverage for their employees will also be available, with credits phasing out as the size of the firm and the average employee wage increase.
13 Who will benefit from the Medicare geographic payment adjustments?
DiVenere: The increased Medicare geographic practice cost index (GPCI) payments and new Frontier payments won’t affect many ObGyns nationally, but they are likely to affect most ObGyns in the related rural locations.
The law reestablishes the national average floor on Medicare’s GPCI for physician work. In 2010 and 2011, Medicare makes a separate adjustment for the practice expense portion of physician payments that will benefit physicians in rural and low-cost areas.
Beginning in 2011, a third adjustment will increase the practice expense GPCI for physicians in frontier states. A frontier state is one in which at least half of its counties have populations smaller than six people per square mile. Frontier states are expected to be Montana, North Dakota, South Dakota, Utah, and Wyoming.
Physicians in 51 localities in 42 states, Puerto Rico, and the Virgin Islands will benefit from the two practice expense adjustments.
ObGyns should also know about two other payment changes:
- The HHS Secretary will create and apply to Medicare provider payments a value-based modifier that will result in higher Medicare payments for high-quality, low-cost physicians and lower payments for high-cost, low-quality physicians. The modifier is to be based on a composite quality score and a composite cost score determined by measures selected by the HHS Secretary and endorsed by a consensus organization. This change begins with 2015 Medicare payments and applies only to physicians in 2015. In 2017, it will also apply to other health professionals.
- Effective immediately, the HHS Secretary has the authority to increase or decrease Medicare relative values, and payments for services, with special attention focused on:
- – services that have high growth rates
- – services that have seen substantial changes in the practice expense or work components
- – services for which new technology has reduced costs
- – instances in which multiple codes are frequently billed for a single service
- – codes that have not been reviewed since implementation of the resource-based relative value scale (RBRVS).
ObGyns who participate in Medicare will start receiving individual physician resource use reports in 2012. These reports will compare per capita utilization of physicians (or physician groups) with the utilization rate of physicians who see similar patients. Reports are required to be risk-adjusted and standardized to take into account local health-care costs.
14 Do you expect the law’s requirements for “administrative simplification” to reduce overhead and increase efficiency?
DiVenere: Don’t we all hope so.
The bill contains several requirements such as:
- establishment of a standardized claim form
- streamlining of claims processing
- improvement of interoperability to allow for more electronic information sharing. These changes will not be implemented until 2013 at the earliest.
Today, about 34% of all ObGyn practices use electronic health records. The systemwide benefits of health information technology (HIT) can be many. Insurers can save by reducing unnecessary tests. Patients can benefit from better coordination of care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices.
Instead, physicians face Medicare and private insurance payment cuts. Little assistance is available for the investment in HIT. And uncertain interoperability standards and rapid technological changes can very quickly make this year’s investment obsolete. Many physicians in solo and small practices are understandably reluctant to take the HIT plunge.
The initial cost of purchasing HIT for a small practice is typically at least $50,000 per physician. Physicians face additional, ongoing costs in staff training and hardware and software updates as well. And many physicians see significant efficiency losses for months and sometimes years after upgrading to an electronic health record system.
Still, with interoperable, shareable electronic records, all physicians treating a particular patient can have the full story. A patient’s paper record kept in her physician’s office shows only a slice of her medical history, potentially missing important information from the patient’s other physicians, including allergies to medication, test results, and the results of particular therapies.
Without a shared electronic record, a physician relies on the recollection of each patient, which is often unintentionally incomplete. A patient may be uncertain about the name or dosage of a medication, fail to remember the date of a screening examination, or lack results of lab tests ordered by another physician.
A physician’s access to the full story with shareable electronic records is important to the care of all patients and can be particularly relevant for patients who have inconsistent contact with health care providers. Often, these patients get care in various settings, including physician offices, community clinics, and emergency departments. Because these patients tend to have a higher incidence of chronic disease, they may greatly benefit from the sharing of medical information.
Clearly, Congress wants to move us to full adoption of HIT. Beginning in 2013, all plans must comply with a uniform standard for electronic transactions, including eligibility verification and health claims status.
In 2014, uniform standards must allow automatic reconciliation of electronic funds transfers and HIPAA payment and remittance; use standardized and consistent methods of health plan enrollment and claim edits; use unique health plan identifiers to simplify and improve routing of health care transactions; and use standard electronic claims attachments.
Uniformity and standardization can help address one of the major roadblocks to physician adoption of health information technology.