User login
Did low amniotic fluid cause cerebral palsy?...and more

A BICORNUATE UTERUS and the infant’s breech position complicated a woman’s pregnancy. At her 39-week prenatal visit, testing showed a low amniotic fluid level, but the woman was sent home. Two days later, she went to the hospital in labor. Her ObGyn first allowed labor to proceed, then performed a cesarean delivery. The father recorded the birth on video camera. The baby was born “essentially lifeless” but with a weak heartbeat. The child was diagnosed with cerebral palsy.
PATIENT’S CLAIM A cesarean delivery should have been performed as soon as it was determined that the amniotic fluid level was low. During surgery, the ObGyn did not choose an incision location that would deliver the baby quickly. The recording evidenced that there was a delay in delivery.
PHYSICIAN’S DEFENSE Elective cesarean delivery was not necessary at the time of the patient’s last visit, as one is not performed before 40 weeks’ gestation. Cesarean delivery was appropriately performed. The baby had a good heart rate at birth. Brain damage was due to fetal inflammatory response syndrome.
VERDICT A $58 million Connecticut verdict was returned.
Death from meningitis after miscarriage
COMPLAINING OF VAGINAL BLEEDING, a woman in her 20s went to an emergency department. She was found to be about 12 weeks’ pregnant. An ObGyn diagnosed spontaneous abortion/miscarriage. Ultrasonography showed that fetal tissue had been expelled, and that no products of conception remained, only blood clots. The woman was given the option of 1) dilatation and curettage (D&C) or 2) letting the residual material expel without intervention. She chose the latter, and was discharged with instructions to return if her condition became worse. Three days later, the woman was admitted to another hospital with Group B streptococcal meningitis and a urinary tract infection. She died 2 days later.
ESTATE’S CLAIM A D&C should have been performed. Prophylactic antibiotics should have been prescribed, which would have stopped the infectious process and allowed the decedent to survive.
DEFENDANTS’ DEFENSE Prophylactic antibiotics were unnecessary because there were no signs or symptoms of infection when the woman was discharged. Prophylactic antibiotics would not have appropriately treated meningitis, and could have made the infection progress more rapidly by destroying the body’s infection-fighting process. There was no need for a D&C because ultrasonography identified no retained products of conception—indicating that there were no foreign substances to cause an infection.
VERDICT A Maryland defense verdict was returned.
Reduced fetal movement and severe brain damage
AT HER 39-WEEK PRENATAL VISIT, a woman reported that the baby wasn’t as active as usual. She was seen by a resident, who did not apply a fetal heart monitor or have the attending ObGyn examine the mother. She was sent home. Two days later, the mother realized the baby was not moving at all, and returned to the clinic. Emergency cesarean delivery was performed. The child has severe brain damage and cerebral palsy.
PATIENT’S CLAIM The resident failed to appropriately respond when the mother reported the baby was not active. The attending ObGyn should have been called, and the baby’s heart rate should have been monitored. It was later found that a clotting abnormality had developed, causing an inadequate supply of oxygen to the fetal brain. Proper response to the report of decreased movement would have resulted in the delivery of a healthy child.
PHYSICIANS’ DEFENSE Brain damage occurred prior to the mother’s 39th-week visit. This was apparent because of the child’s joint contractures, which, the defense argued, take a week or longer to develop. (The plaintiff countered that contractures were mild and that the infant was moving his arms and legs a short time after delivery.)
VERDICT A $4,821,000 Missouri verdict was returned.
Scalpel breaks during robotic surgery
ROBOT-ASSISTED LAPAROSCOPIC pelvic mass resection was performed on an obese 47-year-old woman. During surgery, the lower blade of an ultrasonic, vibrating scalpel dislodged. Dr. A spent 90 minutes searching for the blade, which he eventually found. The mass was removed and diagnosed as benign. During recovery, the patient became septic, went into acute renal failure, acute respiratory failure, and septic shock. A diagnosis of fecal peritonitis was made.
Dr. B assumed the care of the patient, and later found a colon perforation. Four days after the initial procedure, the patient underwent a colon resection. She was initially treated with a colostomy and then had a successful bowel reanastomosis 7 months after the injury.
PATIENT’S CLAIM Dr. A was negligent in applying too much pressure, dislodging the blade. Dr. A was also faulty in his search for the blade, which was the cause of bowel perforation. Both Drs. A and B were negligent in failing to discover the injury earlier.
PHYSICIAN’S DEFENSE The ultrasonic scalpel had a product defect that caused the lower blade to dislodge. The application of pressure wasn’t a factor; the 6-hour procedure had caused the robotic arm to overheat, weakening the metal and causing the blade to separate. Dr. A followed appropriate procedures when searching for the blade. The perforation did not occur until 3 days after surgery; it was diagnosed and treated in a timely manner. The removal of adhesions from the sigmoid colon weakened the bowel wall, leading to the perforation; this was a known risk of the procedure.
VERDICT A California defense verdict was reached.
Stroke during in vitro fertilization
DURING IN VITRO FERTILIZATION, a woman suffered a stroke to the right side of her brain, which initially paralyzed the left side of her body. She partially regained movement, but walks with a limp and has diminished dexterity in her right hand and diminished strength.
PATIENT’S CLAIM The ObGyn ignored warning signs of ovarian hyperstimulation syndrome (OHSS), and continued therapy. OHSS caused enlargement of the ovaries and leakage of fluid from the patient’s blood vessels into her abdomen. This leakage increased the viscosity of her blood, and enhanced the danger of blood clots. The ObGyn administered intravenous fluids, but did not prescribe an anticoagulant.
PHYSICIAN’S DEFENSE Stroke is a known complication of the surgery.
VERDICT A $1.5 million Virginia verdict was returned.
Umbilical cord in cervix; premature delivery
A WOMAN HAD AN ABNORMAL PAP smear during pregnancy. She was sent to a university hospital and placed on bed rest due to cervical incompetence. Tests indicated that the fetus was healthy. A month later, the baby was born 3 months’ premature. He weighed less than 2 lb at birth, and had brain damage and cerebral palsy.
PATIENT’S CLAIM A sonogram performed on the morning of the delivery showed the umbilical cord in the cervix and a low amniotic fluid level. An emergency cesarean delivery should have been performed. Delivery did not occur for another 12 hours; this delay caused oxygen deprivation and brain damage.
DEFENDANTS’ DEFENSE The hospital and physicians denied negligence.
VERDICT A $4,100,000 Maryland defense verdict was returned, but was reduced by the statutory cap on noneconomic damages to a net verdict of $3,605,000.
No ObGyn available for emergency cesarean
A WOMAN IN LABOR went to a hospital. When the fetal heart monitor indicated abnormalities, the only ObGyn on duty was busy in a scheduled elective procedure. The on-call resident was assisting with another surgery. After attempting to find another physician, the labor and delivery nurse waited 40 minutes before she put out a code that delivery was imminent. The resident then delivered the child, who was limp and discolored at birth. The child suffered physical and mental impairment, is confined to a wheelchair, and is unable to speak or to care for herself.
PATIENT’S CLAIM An ObGyn should have been available to perform emergency cesarean delivery. The resident was not skilled enough to attempt a high-risk birth. The nurse should not have waited so long to find a physician.
PHYSICIAN’S DEFENSE This is a teaching hospital; the resident was trained to perform delivery. The nurse attempted to find a physician, but all were occupied elsewhere.
VERDICT A $6,015,000 New Jersey verdict was returned against the resident’s university employer ($15,000), and the hospital, ObGyn, and nurse ($6 million).
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
A BICORNUATE UTERUS and the infant’s breech position complicated a woman’s pregnancy. At her 39-week prenatal visit, testing showed a low amniotic fluid level, but the woman was sent home. Two days later, she went to the hospital in labor. Her ObGyn first allowed labor to proceed, then performed a cesarean delivery. The father recorded the birth on video camera. The baby was born “essentially lifeless” but with a weak heartbeat. The child was diagnosed with cerebral palsy.
PATIENT’S CLAIM A cesarean delivery should have been performed as soon as it was determined that the amniotic fluid level was low. During surgery, the ObGyn did not choose an incision location that would deliver the baby quickly. The recording evidenced that there was a delay in delivery.
PHYSICIAN’S DEFENSE Elective cesarean delivery was not necessary at the time of the patient’s last visit, as one is not performed before 40 weeks’ gestation. Cesarean delivery was appropriately performed. The baby had a good heart rate at birth. Brain damage was due to fetal inflammatory response syndrome.
VERDICT A $58 million Connecticut verdict was returned.
Death from meningitis after miscarriage
COMPLAINING OF VAGINAL BLEEDING, a woman in her 20s went to an emergency department. She was found to be about 12 weeks’ pregnant. An ObGyn diagnosed spontaneous abortion/miscarriage. Ultrasonography showed that fetal tissue had been expelled, and that no products of conception remained, only blood clots. The woman was given the option of 1) dilatation and curettage (D&C) or 2) letting the residual material expel without intervention. She chose the latter, and was discharged with instructions to return if her condition became worse. Three days later, the woman was admitted to another hospital with Group B streptococcal meningitis and a urinary tract infection. She died 2 days later.
ESTATE’S CLAIM A D&C should have been performed. Prophylactic antibiotics should have been prescribed, which would have stopped the infectious process and allowed the decedent to survive.
DEFENDANTS’ DEFENSE Prophylactic antibiotics were unnecessary because there were no signs or symptoms of infection when the woman was discharged. Prophylactic antibiotics would not have appropriately treated meningitis, and could have made the infection progress more rapidly by destroying the body’s infection-fighting process. There was no need for a D&C because ultrasonography identified no retained products of conception—indicating that there were no foreign substances to cause an infection.
VERDICT A Maryland defense verdict was returned.
Reduced fetal movement and severe brain damage
AT HER 39-WEEK PRENATAL VISIT, a woman reported that the baby wasn’t as active as usual. She was seen by a resident, who did not apply a fetal heart monitor or have the attending ObGyn examine the mother. She was sent home. Two days later, the mother realized the baby was not moving at all, and returned to the clinic. Emergency cesarean delivery was performed. The child has severe brain damage and cerebral palsy.
PATIENT’S CLAIM The resident failed to appropriately respond when the mother reported the baby was not active. The attending ObGyn should have been called, and the baby’s heart rate should have been monitored. It was later found that a clotting abnormality had developed, causing an inadequate supply of oxygen to the fetal brain. Proper response to the report of decreased movement would have resulted in the delivery of a healthy child.
PHYSICIANS’ DEFENSE Brain damage occurred prior to the mother’s 39th-week visit. This was apparent because of the child’s joint contractures, which, the defense argued, take a week or longer to develop. (The plaintiff countered that contractures were mild and that the infant was moving his arms and legs a short time after delivery.)
VERDICT A $4,821,000 Missouri verdict was returned.
Scalpel breaks during robotic surgery
ROBOT-ASSISTED LAPAROSCOPIC pelvic mass resection was performed on an obese 47-year-old woman. During surgery, the lower blade of an ultrasonic, vibrating scalpel dislodged. Dr. A spent 90 minutes searching for the blade, which he eventually found. The mass was removed and diagnosed as benign. During recovery, the patient became septic, went into acute renal failure, acute respiratory failure, and septic shock. A diagnosis of fecal peritonitis was made.
Dr. B assumed the care of the patient, and later found a colon perforation. Four days after the initial procedure, the patient underwent a colon resection. She was initially treated with a colostomy and then had a successful bowel reanastomosis 7 months after the injury.
PATIENT’S CLAIM Dr. A was negligent in applying too much pressure, dislodging the blade. Dr. A was also faulty in his search for the blade, which was the cause of bowel perforation. Both Drs. A and B were negligent in failing to discover the injury earlier.
PHYSICIAN’S DEFENSE The ultrasonic scalpel had a product defect that caused the lower blade to dislodge. The application of pressure wasn’t a factor; the 6-hour procedure had caused the robotic arm to overheat, weakening the metal and causing the blade to separate. Dr. A followed appropriate procedures when searching for the blade. The perforation did not occur until 3 days after surgery; it was diagnosed and treated in a timely manner. The removal of adhesions from the sigmoid colon weakened the bowel wall, leading to the perforation; this was a known risk of the procedure.
VERDICT A California defense verdict was reached.
Stroke during in vitro fertilization
DURING IN VITRO FERTILIZATION, a woman suffered a stroke to the right side of her brain, which initially paralyzed the left side of her body. She partially regained movement, but walks with a limp and has diminished dexterity in her right hand and diminished strength.
PATIENT’S CLAIM The ObGyn ignored warning signs of ovarian hyperstimulation syndrome (OHSS), and continued therapy. OHSS caused enlargement of the ovaries and leakage of fluid from the patient’s blood vessels into her abdomen. This leakage increased the viscosity of her blood, and enhanced the danger of blood clots. The ObGyn administered intravenous fluids, but did not prescribe an anticoagulant.
PHYSICIAN’S DEFENSE Stroke is a known complication of the surgery.
VERDICT A $1.5 million Virginia verdict was returned.
Umbilical cord in cervix; premature delivery
A WOMAN HAD AN ABNORMAL PAP smear during pregnancy. She was sent to a university hospital and placed on bed rest due to cervical incompetence. Tests indicated that the fetus was healthy. A month later, the baby was born 3 months’ premature. He weighed less than 2 lb at birth, and had brain damage and cerebral palsy.
PATIENT’S CLAIM A sonogram performed on the morning of the delivery showed the umbilical cord in the cervix and a low amniotic fluid level. An emergency cesarean delivery should have been performed. Delivery did not occur for another 12 hours; this delay caused oxygen deprivation and brain damage.
DEFENDANTS’ DEFENSE The hospital and physicians denied negligence.
VERDICT A $4,100,000 Maryland defense verdict was returned, but was reduced by the statutory cap on noneconomic damages to a net verdict of $3,605,000.
No ObGyn available for emergency cesarean
A WOMAN IN LABOR went to a hospital. When the fetal heart monitor indicated abnormalities, the only ObGyn on duty was busy in a scheduled elective procedure. The on-call resident was assisting with another surgery. After attempting to find another physician, the labor and delivery nurse waited 40 minutes before she put out a code that delivery was imminent. The resident then delivered the child, who was limp and discolored at birth. The child suffered physical and mental impairment, is confined to a wheelchair, and is unable to speak or to care for herself.
PATIENT’S CLAIM An ObGyn should have been available to perform emergency cesarean delivery. The resident was not skilled enough to attempt a high-risk birth. The nurse should not have waited so long to find a physician.
PHYSICIAN’S DEFENSE This is a teaching hospital; the resident was trained to perform delivery. The nurse attempted to find a physician, but all were occupied elsewhere.
VERDICT A $6,015,000 New Jersey verdict was returned against the resident’s university employer ($15,000), and the hospital, ObGyn, and nurse ($6 million).
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A BICORNUATE UTERUS and the infant’s breech position complicated a woman’s pregnancy. At her 39-week prenatal visit, testing showed a low amniotic fluid level, but the woman was sent home. Two days later, she went to the hospital in labor. Her ObGyn first allowed labor to proceed, then performed a cesarean delivery. The father recorded the birth on video camera. The baby was born “essentially lifeless” but with a weak heartbeat. The child was diagnosed with cerebral palsy.
PATIENT’S CLAIM A cesarean delivery should have been performed as soon as it was determined that the amniotic fluid level was low. During surgery, the ObGyn did not choose an incision location that would deliver the baby quickly. The recording evidenced that there was a delay in delivery.
PHYSICIAN’S DEFENSE Elective cesarean delivery was not necessary at the time of the patient’s last visit, as one is not performed before 40 weeks’ gestation. Cesarean delivery was appropriately performed. The baby had a good heart rate at birth. Brain damage was due to fetal inflammatory response syndrome.
VERDICT A $58 million Connecticut verdict was returned.
Death from meningitis after miscarriage
COMPLAINING OF VAGINAL BLEEDING, a woman in her 20s went to an emergency department. She was found to be about 12 weeks’ pregnant. An ObGyn diagnosed spontaneous abortion/miscarriage. Ultrasonography showed that fetal tissue had been expelled, and that no products of conception remained, only blood clots. The woman was given the option of 1) dilatation and curettage (D&C) or 2) letting the residual material expel without intervention. She chose the latter, and was discharged with instructions to return if her condition became worse. Three days later, the woman was admitted to another hospital with Group B streptococcal meningitis and a urinary tract infection. She died 2 days later.
ESTATE’S CLAIM A D&C should have been performed. Prophylactic antibiotics should have been prescribed, which would have stopped the infectious process and allowed the decedent to survive.
DEFENDANTS’ DEFENSE Prophylactic antibiotics were unnecessary because there were no signs or symptoms of infection when the woman was discharged. Prophylactic antibiotics would not have appropriately treated meningitis, and could have made the infection progress more rapidly by destroying the body’s infection-fighting process. There was no need for a D&C because ultrasonography identified no retained products of conception—indicating that there were no foreign substances to cause an infection.
VERDICT A Maryland defense verdict was returned.
Reduced fetal movement and severe brain damage
AT HER 39-WEEK PRENATAL VISIT, a woman reported that the baby wasn’t as active as usual. She was seen by a resident, who did not apply a fetal heart monitor or have the attending ObGyn examine the mother. She was sent home. Two days later, the mother realized the baby was not moving at all, and returned to the clinic. Emergency cesarean delivery was performed. The child has severe brain damage and cerebral palsy.
PATIENT’S CLAIM The resident failed to appropriately respond when the mother reported the baby was not active. The attending ObGyn should have been called, and the baby’s heart rate should have been monitored. It was later found that a clotting abnormality had developed, causing an inadequate supply of oxygen to the fetal brain. Proper response to the report of decreased movement would have resulted in the delivery of a healthy child.
PHYSICIANS’ DEFENSE Brain damage occurred prior to the mother’s 39th-week visit. This was apparent because of the child’s joint contractures, which, the defense argued, take a week or longer to develop. (The plaintiff countered that contractures were mild and that the infant was moving his arms and legs a short time after delivery.)
VERDICT A $4,821,000 Missouri verdict was returned.
Scalpel breaks during robotic surgery
ROBOT-ASSISTED LAPAROSCOPIC pelvic mass resection was performed on an obese 47-year-old woman. During surgery, the lower blade of an ultrasonic, vibrating scalpel dislodged. Dr. A spent 90 minutes searching for the blade, which he eventually found. The mass was removed and diagnosed as benign. During recovery, the patient became septic, went into acute renal failure, acute respiratory failure, and septic shock. A diagnosis of fecal peritonitis was made.
Dr. B assumed the care of the patient, and later found a colon perforation. Four days after the initial procedure, the patient underwent a colon resection. She was initially treated with a colostomy and then had a successful bowel reanastomosis 7 months after the injury.
PATIENT’S CLAIM Dr. A was negligent in applying too much pressure, dislodging the blade. Dr. A was also faulty in his search for the blade, which was the cause of bowel perforation. Both Drs. A and B were negligent in failing to discover the injury earlier.
PHYSICIAN’S DEFENSE The ultrasonic scalpel had a product defect that caused the lower blade to dislodge. The application of pressure wasn’t a factor; the 6-hour procedure had caused the robotic arm to overheat, weakening the metal and causing the blade to separate. Dr. A followed appropriate procedures when searching for the blade. The perforation did not occur until 3 days after surgery; it was diagnosed and treated in a timely manner. The removal of adhesions from the sigmoid colon weakened the bowel wall, leading to the perforation; this was a known risk of the procedure.
VERDICT A California defense verdict was reached.
Stroke during in vitro fertilization
DURING IN VITRO FERTILIZATION, a woman suffered a stroke to the right side of her brain, which initially paralyzed the left side of her body. She partially regained movement, but walks with a limp and has diminished dexterity in her right hand and diminished strength.
PATIENT’S CLAIM The ObGyn ignored warning signs of ovarian hyperstimulation syndrome (OHSS), and continued therapy. OHSS caused enlargement of the ovaries and leakage of fluid from the patient’s blood vessels into her abdomen. This leakage increased the viscosity of her blood, and enhanced the danger of blood clots. The ObGyn administered intravenous fluids, but did not prescribe an anticoagulant.
PHYSICIAN’S DEFENSE Stroke is a known complication of the surgery.
VERDICT A $1.5 million Virginia verdict was returned.
Umbilical cord in cervix; premature delivery
A WOMAN HAD AN ABNORMAL PAP smear during pregnancy. She was sent to a university hospital and placed on bed rest due to cervical incompetence. Tests indicated that the fetus was healthy. A month later, the baby was born 3 months’ premature. He weighed less than 2 lb at birth, and had brain damage and cerebral palsy.
PATIENT’S CLAIM A sonogram performed on the morning of the delivery showed the umbilical cord in the cervix and a low amniotic fluid level. An emergency cesarean delivery should have been performed. Delivery did not occur for another 12 hours; this delay caused oxygen deprivation and brain damage.
DEFENDANTS’ DEFENSE The hospital and physicians denied negligence.
VERDICT A $4,100,000 Maryland defense verdict was returned, but was reduced by the statutory cap on noneconomic damages to a net verdict of $3,605,000.
No ObGyn available for emergency cesarean
A WOMAN IN LABOR went to a hospital. When the fetal heart monitor indicated abnormalities, the only ObGyn on duty was busy in a scheduled elective procedure. The on-call resident was assisting with another surgery. After attempting to find another physician, the labor and delivery nurse waited 40 minutes before she put out a code that delivery was imminent. The resident then delivered the child, who was limp and discolored at birth. The child suffered physical and mental impairment, is confined to a wheelchair, and is unable to speak or to care for herself.
PATIENT’S CLAIM An ObGyn should have been available to perform emergency cesarean delivery. The resident was not skilled enough to attempt a high-risk birth. The nurse should not have waited so long to find a physician.
PHYSICIAN’S DEFENSE This is a teaching hospital; the resident was trained to perform delivery. The nurse attempted to find a physician, but all were occupied elsewhere.
VERDICT A $6,015,000 New Jersey verdict was returned against the resident’s university employer ($15,000), and the hospital, ObGyn, and nurse ($6 million).
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: Fixing Health Care (Not)
My column on the potential impact of the 2010 health care legislation on private practitioners is now more than 6 months old; yet it continues to generate discussion.
Lately, many of the questions have become more fundamental in nature: What, exactly, is broken in our current system? And does the Affordable Care Act address any of the core problems?
There are no simple answers, of course, but in perusing the voluminous literature on this subject, there are a few basic truths on which most seem to agree. First, some kind of tort reform must be implemented. Second, the encroachment of third-party payers on the physician-patient relationship needs to be reined in. Yet neither of these basic issues was even on the table during the health care debate.
Most experts also agree that the present system of employer-financed health care is fundamentally flawed. Allowing employers to control health insurance has created thorny (and largely avoidable) problems. Think about it: What would happen, for example, if employers controlled food purchasing and employees could go to a grocery store, pay a $20 copay, and take as much food as they want? Clearly, food prices would increase enormously (and artificially) in a big hurry; but employees wouldn’t care, because they would never see the bill.
That is basically what has happened with health care: Costs have skyrocketed, but because most bills go from hospital or clinic to insurance company to employer, most patients are left completely out of the loop and have no idea of what their treatment costs.
The strange part is that nobody planned this nongovernmental, non–free market model. It was created through a series of historical accidents, beginning around World War II. During the war, a wage freeze was imposed to control inflation, but the war effort also created huge production demands and a worker shortage. Because businesses were unable to lure good employees with higher wages, they resorted to offering generous fringe benefits, especially health insurance. Before World War II, only 10% of American citizens had employer-based health insurance; by 1953, 60% did.
Ultimately, in response to lobbying by business and insurance interests, Congress enshrined this arbitrary system into the tax law. Tax incentives were created for employers to offer health insurance: For every dollar they contributed, employees would get about $1.30 in benefits. Businesses were given incentives to offer even more insurance than employees would normally buy for themselves. So most patients were – and are – overinsured, and health care is far more expensive than it needs to be.
Furthermore, insurers are competing for human resources departments rather than for the people they insure or for those who provide care. As a consequence, the plans they offer are generally good for employers, but bad for patients and doctors. Meanwhile, insurers continue to encroach on the practice of medicine through financial decisions that are driven by simplistic profit motives rather than by quality of care. Again, this situation is largely opaque to patients.
The fix seems pretty obvious, at least to me. A market-driven system in which individuals buy health insurance the way they buy anything else (cell phones, computers, cars, and yes, auto insurance) would eliminate most of the inefficiencies embedded in our current system. Yet Congress never considered this option during the reform debate.
In fact, many of the reform law’s provisions will only worsen the current situation. Small businesses will be given more tax-credit incentives to insure their workers. And the Small Business Health Options Program (SHOP) Exchange, which allows small businesses to pool their resources to buy health insurance, will only compound the problems of employer-based financing. On top of that, employers who do not offer coverage will face fines and other penalties.
So if employer-based insurance is a big part of the problem, why is Congress encouraging it rather than eliminating it? Obviously, there are big players (insurers, in particular) who have a lot more lobbying money than do either doctors or patients and who have a major interest in maintaining the status quo.
Basic economics and common sense tell us that staying the course will result only in a continuing exponential rise in costs; but until Congress understands that, there is little chance of any real reform.
My column on the potential impact of the 2010 health care legislation on private practitioners is now more than 6 months old; yet it continues to generate discussion.
Lately, many of the questions have become more fundamental in nature: What, exactly, is broken in our current system? And does the Affordable Care Act address any of the core problems?
There are no simple answers, of course, but in perusing the voluminous literature on this subject, there are a few basic truths on which most seem to agree. First, some kind of tort reform must be implemented. Second, the encroachment of third-party payers on the physician-patient relationship needs to be reined in. Yet neither of these basic issues was even on the table during the health care debate.
Most experts also agree that the present system of employer-financed health care is fundamentally flawed. Allowing employers to control health insurance has created thorny (and largely avoidable) problems. Think about it: What would happen, for example, if employers controlled food purchasing and employees could go to a grocery store, pay a $20 copay, and take as much food as they want? Clearly, food prices would increase enormously (and artificially) in a big hurry; but employees wouldn’t care, because they would never see the bill.
That is basically what has happened with health care: Costs have skyrocketed, but because most bills go from hospital or clinic to insurance company to employer, most patients are left completely out of the loop and have no idea of what their treatment costs.
The strange part is that nobody planned this nongovernmental, non–free market model. It was created through a series of historical accidents, beginning around World War II. During the war, a wage freeze was imposed to control inflation, but the war effort also created huge production demands and a worker shortage. Because businesses were unable to lure good employees with higher wages, they resorted to offering generous fringe benefits, especially health insurance. Before World War II, only 10% of American citizens had employer-based health insurance; by 1953, 60% did.
Ultimately, in response to lobbying by business and insurance interests, Congress enshrined this arbitrary system into the tax law. Tax incentives were created for employers to offer health insurance: For every dollar they contributed, employees would get about $1.30 in benefits. Businesses were given incentives to offer even more insurance than employees would normally buy for themselves. So most patients were – and are – overinsured, and health care is far more expensive than it needs to be.
Furthermore, insurers are competing for human resources departments rather than for the people they insure or for those who provide care. As a consequence, the plans they offer are generally good for employers, but bad for patients and doctors. Meanwhile, insurers continue to encroach on the practice of medicine through financial decisions that are driven by simplistic profit motives rather than by quality of care. Again, this situation is largely opaque to patients.
The fix seems pretty obvious, at least to me. A market-driven system in which individuals buy health insurance the way they buy anything else (cell phones, computers, cars, and yes, auto insurance) would eliminate most of the inefficiencies embedded in our current system. Yet Congress never considered this option during the reform debate.
In fact, many of the reform law’s provisions will only worsen the current situation. Small businesses will be given more tax-credit incentives to insure their workers. And the Small Business Health Options Program (SHOP) Exchange, which allows small businesses to pool their resources to buy health insurance, will only compound the problems of employer-based financing. On top of that, employers who do not offer coverage will face fines and other penalties.
So if employer-based insurance is a big part of the problem, why is Congress encouraging it rather than eliminating it? Obviously, there are big players (insurers, in particular) who have a lot more lobbying money than do either doctors or patients and who have a major interest in maintaining the status quo.
Basic economics and common sense tell us that staying the course will result only in a continuing exponential rise in costs; but until Congress understands that, there is little chance of any real reform.
My column on the potential impact of the 2010 health care legislation on private practitioners is now more than 6 months old; yet it continues to generate discussion.
Lately, many of the questions have become more fundamental in nature: What, exactly, is broken in our current system? And does the Affordable Care Act address any of the core problems?
There are no simple answers, of course, but in perusing the voluminous literature on this subject, there are a few basic truths on which most seem to agree. First, some kind of tort reform must be implemented. Second, the encroachment of third-party payers on the physician-patient relationship needs to be reined in. Yet neither of these basic issues was even on the table during the health care debate.
Most experts also agree that the present system of employer-financed health care is fundamentally flawed. Allowing employers to control health insurance has created thorny (and largely avoidable) problems. Think about it: What would happen, for example, if employers controlled food purchasing and employees could go to a grocery store, pay a $20 copay, and take as much food as they want? Clearly, food prices would increase enormously (and artificially) in a big hurry; but employees wouldn’t care, because they would never see the bill.
That is basically what has happened with health care: Costs have skyrocketed, but because most bills go from hospital or clinic to insurance company to employer, most patients are left completely out of the loop and have no idea of what their treatment costs.
The strange part is that nobody planned this nongovernmental, non–free market model. It was created through a series of historical accidents, beginning around World War II. During the war, a wage freeze was imposed to control inflation, but the war effort also created huge production demands and a worker shortage. Because businesses were unable to lure good employees with higher wages, they resorted to offering generous fringe benefits, especially health insurance. Before World War II, only 10% of American citizens had employer-based health insurance; by 1953, 60% did.
Ultimately, in response to lobbying by business and insurance interests, Congress enshrined this arbitrary system into the tax law. Tax incentives were created for employers to offer health insurance: For every dollar they contributed, employees would get about $1.30 in benefits. Businesses were given incentives to offer even more insurance than employees would normally buy for themselves. So most patients were – and are – overinsured, and health care is far more expensive than it needs to be.
Furthermore, insurers are competing for human resources departments rather than for the people they insure or for those who provide care. As a consequence, the plans they offer are generally good for employers, but bad for patients and doctors. Meanwhile, insurers continue to encroach on the practice of medicine through financial decisions that are driven by simplistic profit motives rather than by quality of care. Again, this situation is largely opaque to patients.
The fix seems pretty obvious, at least to me. A market-driven system in which individuals buy health insurance the way they buy anything else (cell phones, computers, cars, and yes, auto insurance) would eliminate most of the inefficiencies embedded in our current system. Yet Congress never considered this option during the reform debate.
In fact, many of the reform law’s provisions will only worsen the current situation. Small businesses will be given more tax-credit incentives to insure their workers. And the Small Business Health Options Program (SHOP) Exchange, which allows small businesses to pool their resources to buy health insurance, will only compound the problems of employer-based financing. On top of that, employers who do not offer coverage will face fines and other penalties.
So if employer-based insurance is a big part of the problem, why is Congress encouraging it rather than eliminating it? Obviously, there are big players (insurers, in particular) who have a lot more lobbying money than do either doctors or patients and who have a major interest in maintaining the status quo.
Basic economics and common sense tell us that staying the course will result only in a continuing exponential rise in costs; but until Congress understands that, there is little chance of any real reform.
ONLINE EXCLUSIVE: Scheduling Rules of Thumb
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
John Krisa, MD, medical director of the hospitalist group at Albany Memorial Hospital in New York, pictures his HM group as an organic whole when he draws up the schedule. He tries to avoid a strict 50-50 parceling out of night and day shifts. The hospitalist group makes liberal use of per-diem hospitalists and moonlighters, and has a few nocturnists.
“The vast majority of the work at night is processing new admissions, so these tend to be single encounters. You want your full-time people there multiple consecutive days for continuity and to represent the face of your program,” he says.
But for the required, ’round-the-clock coverage, he and other group members are expected to pull their share of nights as well. “I was always more of a nighttime person, in terms of my body clock,” Dr. Krisa says, “but now that I have more daytime nonclinical duties [as regional site director for Cogent HMG], it’s been more of a challenge to juggle home responsibilities, night shifts, and multiple administrative meetings.”
There are some basic principles of sleep hygiene and lessons learned from industrial settings that are good to keep in mind, says Christopher P. Landrigan, MD, SFHM, MPH, associate professor of medicine and pediatrics at Harvard Medical School and director of the Sleep and Patient Safety Program at Brigham and Women’s Hospital in Boston. “It’s really incumbent upon hospitalist group leaders to recognize the hazards of scheduling people for too many nights in a row, which conveys a risk both to the patients and to the hospitalists themselves,” Dr. Landrigan says. “We know that if hospitalists are driving home after night shifts, particularly multiple night shifts, that they’re at risk for motor vehicle crashes and at risk of sticking themselves with needles and scalpels toward the tail end of their shifts. None of us want that.”
Dr. Landrigan advises hospitalist groups to be cognizant of the hazards and think about the schedule “proactively.”
Power Struggles

Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Many hospitalist practices are started by “traditionalists”: primary-care physicians (PCPs) active in the outpatient and hospital settings. The practice typically grows due in large part to the leadership of the founders. Ultimately, the practice is made up of both the founders and a cadre of part- or full-time hospitalists who don’t work in the outpatient setting. And sometimes they have different incentives and ideas about how the practice should operate.
When these individuals disagree, which group should break the tie—the founding “hybrid” or “rotating” doctors who work part time on the hospitalist service or the doctors who work only as hospitalists?
This is a reasonably common issue for “medical” hospitalist groups, and in many cases is becoming an issue for groups in other specialties that adopt the hospitalist model, such as surgical hospitalists, laborists, etc.
A Common Scenario
Let me illustrate this issue with a composite of several former consulting clients. Let’s say this is a hospitalist practice that serves a 250-bed community hospital. One large private internal medicine group adopted a “rotating hospitalist” model there in the late 1990s. One of the internists provided the daytime hospital coverage for all the group’s patients one week out of every six. Their hospital volume grew quickly. They were asked to take on responsibility for admitting an increasing portion of the unassigned patients, provide care for patients referred by other PCPs who wanted to drop out of hospital work, and increasingly were asked to consult on patients admitted by surgeons.
When faced with this situation, many PCP groups decided to exit the hospital themselves and turn that work over to hospitalists. This group stuck it out. At first, the one doctor in the group covering the hospital each week kept up with the growing volume by simply working harder and longer every day. Eventually, the group sought financial help from the hospital to hire hospitalists who didn’t have outpatient responsibilities.
Years passed, and this PCP group transitioned to employment by the hospital, just like the full-time hospitalists. And by this time, the hospitalist practice was seen as distinct from the original PCP group. About 80% of the staffing was provided by hospitalists who didn’t work in the outpatient setting, the remainder by PCPs who essentially founded the practice. The PCPs chose to continue providing hospital care, both because they found it professionally satisfying and their compensation formula made it attractive for generating production in the hospital.
Tensions arose between the hospitalists and the “hybrids.” The hybrids refused to work night shifts and generally were unable to fill in for unplanned absences by the hospitalists. And because of the PCPs’ compensation formula, and possibly the work ethic of more senior doctors, they favored managing larger patient volumes and decreasing weekend staffing significantly to allow more weekends off in total for everyone. The hospitalists had other ideas about these things, and they were unhappy that the PCPs would have first say about when they could work hospital shifts, thereby decreasing the hospitalists’ scheduling flexibility.
The hospitalists were all within a few years of their residency training, and most of the PCPs were midcareer. This created a social divide, making it that much more difficult for the two groups to work through the issues. While the hybrid doctors saw the hospitalists as good clinicians, and vice versa, each group said: “The other guys are difficult to work with. They don’t understand what it is like for us.”
Need for Paradigm Shift
At many sites, the doctors and their administrative counterparts get stuck in a stalemate and have the same, unhappy conversations repeatedly. These conversations are really gripe sessions more than anything else.
I think the best solution is for everyone to acknowledge the valuable contribution of the hybrid doctors in founding and leading the hospitalist practice through years of growth, but also to begin seeing the hospitalist practice as being owned and governed primarily by the hospitalists who do most of the work. For most issues in which the two factions can’t agree, the hospitalists should have the tie-breaking vote.
While this approach reduces the autonomy of the hybrid doctors to make operational decisions, it doesn’t mean they have zero influence. In fact, the practice usually has a critical need for the hybrid doctors to continue providing some of the staffing. This usually means that the practice will need to ensure it puts together a package of compensation and available shifts on the schedule to ensure the hybrids want to remain active in the practice.
In most cases, all involved should ensure that those hybrid doctors who want to remain active in the hospital, and perform well in the hospitalist practice, should have the opportunity to do so indefinitely.
Compensation Methods for Hybrids
Even if the hybrids and hospitalists are able to harmoniously agree on things like work schedules, the hybrid doctors often have compensation schemes such that when working in the hospital, they have different financial incentives from the hospitalists. (I’m using “hybrid” to describe physicians who work in both inpatient and outpatient settings, usually more time in the office practice.) A common situation is that the production (i.e. wRVUs) generated in the hospital counts toward their office productivity. So the hybrids and the hospitalists will have different ideas about how hard they want to work.
The solution here is to divorce the office and hospital compensation schemes. There should be no connection between the compensation in the two settings, and both should be designed to ensure a competitive amount of money and performance incentives appropriate for that setting. Such methods usually mean that a day of work in the office will result in a different-sized paycheck than what comes with a day of work in the hospital.
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm. He is course codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Maternity Management
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.

The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."

—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.
The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."
—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
Editor's Note: Second in a two-part series
Lest anyone forget, it is essential to support workers having children for one reason—the continuation of the human species, says Rachel Lovins, MD, SFHM, who directs the hospitalist program at Waterbury Hospital in Waterbury, Conn. For HM program directors, that means following pregnancy labor laws. But it also should involve reasonably accommodating hospitalists who are balancing their new baby’s needs with the demands of their profession, says Dr. Lovins and other HM leaders.
"As there are more women in medicine, everybody needs to be more aware of this issue. We don’t want to make good talent feel uncomfortable with the process of taking maternity leave and reducing time," says Michelle Marks, DO, FAAP, SFHM, director of the Center for Pediatric Hospital Medicine at the Cleveland Clinic.
All HM program directors need to be aware of such federal laws as the Pregnancy Discrimination Act and the Family and Medical Leave Act (www.eeoc.gov/laws/types/pregnancy.cfm), as well as the corresponding laws of the state in which they work. Directors can contact their human resources (HR) department for assistance.
"Calling them upfront will save a lot of headaches later on," says Jasen Gundersen, MD, MBA, CPE, SFHM, chief medical officer of the hospital medicine division in Fort Lauderdale, Fla., for Knoxville, Tenn.-based TeamHealth.
Here are some other recommendations on how HM directors can best manage pregnancy issues affecting their team:
The "R" in Relationship
There are many reasons why the director of a hospitalist group should develop a good relationship with the providers in their group, but one of them is that a hospitalist is more likely to tell her director sooner rather than later that she is pregnant, Dr. Marks says.
"Knowing your staff well and knowing them personally helps a lot, too, because you can gauge where they are going personally, as far as marriage, children, that type of thing," she adds.
The earlier a group leader knows a staff member is pregnant, the more time they have to plan for maternity leave. And the better the plan, the easier the leave is on the entire group, says Dr. Gundersen.
Generally, finding out that a physician is pregnant within three to five months of conception provides enough time to make adequate arrangements for coverage, Drs. Marks and Lovins note.
The Conversation
Before scheduling a meeting to discuss maternity leave and plans for returning to work with the hospitalist, the group leader should call HR to see if such a conversation is permissible, says Dr. Marks. A better approach might be to wait until the hospitalist broaches the subject.
"So many times the hospitalist will ask for counseling as far as what are her options of coming back," Dr. Marks says. "That opens the door for an open discussion."
Once the conversation starts, the group leader should gauge the length of maternity leave, her plans for coming back full time or part time, and the anticipated scheduling limitations or childcare considerations, Dr. Gundersen says.
"That’s not to say the pregnant woman can really predict all the time what’s going to happen," says Kerry Weiner, MD, MPH, chief clinical officer for North Hollywood, Calif.-based IPC: The Hospitalist Company, Inc. "Obviously, it’s a medical condition that can change and everyone understands that. It’s getting a feel of what you can actually know at the time."
If it’s the HM director’s intent to call the physician while she is on leave to see how she and the baby are doing and how the maternity leave is going, that should be discussed during the conversation, Dr. Gundersen says.
"If you establish upfront that you are going to make that phone call, I think that’s fine to do," he explains. "If you’re calling constantly and pressuring the person, I don’t think that that’s kosher at all."
—Rachel Lovins, MD, SFHM, director, hospitalist program, Waterbury (Conn.) Hospital
The Coverage Plan
Most maternity leaves are from eight to 12 weeks, although the length varies by HM program and individual. It is essential to have your group’s coverage plan outlined well in advance of the maternity leave.
In a private-practice model in which hospitalists work weekdays and have a call-coverage schedule for nights and weekends, a group leader can spread the extra work among the other hospitalists in the group because there are more hospitalists working during the day when patient census is higher, Dr. Weiner says.
Shifting the workload in other schedule models isn’t always as easy. "In the seven-day-on, seven-day-off model, because of that maximum patient-to-doctor ratio, I don’t think there’s any way to do it without hiring help," Dr. Lovins says. "It’s important to recruit per diems all the time. When you’re in a bind is the worst time to do it."
To limit the disruption to patient care and operations quality, the goal when using outside hospitalists is to contract with physicians who have worked with the group before and who know the community, hospital, systems, and patients, Dr. Weiner says.
For HM groups that use a flexible schedule, maternity coverage plans aren’t really needed, says Reuben Tovar, MD, chairman of Hospital Internists of Austin, a physician-owned and -managed hospitalist practice in Texas.
"We’re not salary, so that changes the dynamic completely. People who work more make more, and people who work less make less," he explains. "We are much more liberal about time off, because if a person is taking off to do what is important to them, like taking care of a child, then the rest of us feel better about doing extra work."
—Michelle Marks, DO, FAAP, SFHM, director, Center for Pediatric Hospital Medicine, Cleveland Clinic
Things Change
Plans discussed at the outset with a pregnant hospitalist can change after the child is born, HM group directors caution.
"Particularly for the first child, people say, ‘I’ll come back full blast. Don’t worry about it.’ And they figure out how hard all that is in the first couple of weeks, and then I get a different answer," Dr. Tovar says. "I think the whole mom/wife/doctor thing is tough. I recognize how hard that is. Even though I am not in that role, I can see it."
Dr. Gundersen suggests group directors have a backup plan, in case the maternity leave lasts longer than expected or the transition back to work is delayed. "It really prevents you from putting pressure on the physician," he says.
If a hospitalist who had planned to come back full time decides that she wants to work less, a director should check with HR to see what the process would entail.
"Generally, we have to negotiate a time frame for when they can drop down" to part-time hours, Dr. Marks says. "It usually takes three to four months for me to be able to adjust staffing to make it work."
Back to Work
Physicians can return from maternity leave in a reduced role, but they very rarely drop out of medicine entirely, Dr. Marks says.
"[They] have put in a lot of time to get where they are," she says. "Plus, women in medicine are usually high achievers and very interested in their careers."
Yet hospitalist leaders should recognize that returning to work after having a baby is stressful. It will take some time for the returning hospitalist to develop a rhythm between her duties as a mother and a doctor.
Directors can review the hospitalist’s nonclinical roles, help with priorities, and perhaps reassign some of the responsibilities to colleagues, Dr. Marks says. With more women breastfeeding, it is important to provide a convenient space with a door that locks for women to breast-pump at work, she and the other directors say.
"The best thing in the world is to have colleagues that you trust and can rely on," Dr. Lovins says. "That way, people can help each other out in emergencies, like if someone has to take their kid to the doctor. That’s the kind of program I want to have and would want to be part of."
Lisa Ryan is a freelance writer based in New Jersey.
To blog or not to blog? What’s the answer for you and your practice?
CASE
Your gyn practice decides to publish an electronic newsletter for patients. You and your office manager spend a lot of time deciding on a format and writing content that you think is relevant to your patients. Everyone in the office agrees: It looks great.
But there’s a problem.
After your newsletter has been “live” for 6 months, fewer than 5% of your patients have signed up to receive it by e-mail (even though you’re sure that a lot more of them are on-line).
You’re perplexed: Why the poor response? The newsletter contains important information that your patients have told you they want—answers to the same questions that you get asked day in, day out.
Why does everyone seem so interested in getting answers to their questions when they’re in the office but not ahead of time and without a co-pay?
CASE: Resolved
The diagnosis: Newsletters are so 1990s.
Offering a Web-savvy patient a newsletter is like presenting her with a VHS tape of a surgical procedure you’re recommending. She will look at you and think, “Huh?”
It’s not that your patients don’t want health information—they are clearly eager for it: 80% of Americans who have Internet access look for health information on-line.1 The quest for health information is the third most popular on-line activity (behind e-mail and using a search engine), and women are more likely to search for health information on-line than men are.2 Nineteen percent of all Internet users search on-line for information about pregnancy and childbirth, and on WebMD (www.webmd.com, the second most popular Internet health site), hysterectomy was the fifth most commonly searched treatment in 2010.1
But getting health information from the Internet today does not mean another e-mail message in the in-box, where it sits waiting to be read or, more likely, deleted without having been opened. For most patients, looking for health information on-line entails 1) general searches (via Google, for example) for symptoms, specific diagnoses, or therapies or 2) searches on specific health-related Web sites (the top two for traffic in November 2010 were the National Institutes of Health and WebMD).1,3
More and more patients, however, are craving a dialogue about their health; 40% of on-line health-related activities involve interactive, user-generated content of social media, the most popular sources being Facebook, Twitter, and the Web-site tool known as blogs that I discuss in this article—with the aim of helping you determine whether placing your professional voice on the Web in a blog is workable, valuable, and respectable.1,3,4

Blog (noun, singular); blogs (plural)
What is it? A shortened form of “web log.” Has a different functional meaning for different people: A journal. A place to rant. A collaborative archive. A source of breaking news.
Whatever shape a blog takes, at its core it is an ongoing chronicle of information plus opinion. For a medical blog, that description typically refers to the perspective of the consumer/patient or the health-care professional who writes the “posts,” or entries.
The Web has thousands upon thousands of medical blogs. Some support an academic institution or a government agency (even the Centers for Disease Control and Prevention has a blog); many describe the experiences of an individual with one or another aspect of health care (from a patient’s or provider’s perspective). With one third of Americans reading blogs, they are an excellent way to disseminate information.1,3,4
Here are what I consider several good reasons to start a medical blog—reasons that, in part, motivated me to begin blogging (see “Why I blog,”):
- A blog is an ideal platform to deliver content to your patients and like-minded medical professionals. A blog allows your patients (and everyone else) to see information that you think is valuable and to hear your opinion on important health topics. Patients really like to know what their physician’s opinion is—how many times have you been asked, in the office, “What do you think I should do, doctor?”
- Blogging is good advertising for your practice. Your blog will appear in Web-search results, which may lead new patients to your doorstep. Reporters and other media workers troll the Web, fact-checking and looking for “angles” for news stories; you may be called to give your opinion about something you blogged about. Remember: Being mentioned in the local newspaper is free advertising (yes, people still read newspapers, though often on-line); ask the reporter to include a link to your blog in any story in which you’re quoted.
- Blogging helps you learn from your readers. Given the interactive nature of a blog (comments are encouraged), you might find feedback that is interesting at the least, possibly educational. Many people take commenting on blogs very seriously, and often post valuable links to other content.
- Contributing credible content drowns out garbage medical information that circulates widely on-line. The Internet is a powerhouse repository of medical knowledge, but it’s only as good as the content provided to it; in fact, 65% of Web pages contain inaccurate medical information.6 Regrettably, most people do not verify the medical information they find on-line.
- Blogging helps keep you relevant. Medicine is still trying to figure out how to best integrate itself with the user-centered operation and experience of Web 2.0. If you aren’t engaged here on some level, you risk being left behind.

I started blogging about prematurity 2 years ago, at my Web site, www.preemieprimer.com. I saw this as a way to support my book, The Preemie Primer, and to add content that I just didn’t have enough space for in the print edition.
Recently, I started a more general medical blog geared to women’s health (see an excerpt of a post below). I set up this blog myself, using WordPress (see the description in the main text), in under an hour (I’m of sub-average intelligence when it comes to computers, but I can follow directions). I paid a Web-savvy person to change the domain name to www.drjengunter.com.
Some days, my posts appeal to 20,000 people
Other days, I captivate, oh, a dozen. For me, the most important reasons for blogging are to use my voice (I really do write as I speak) and to add good content to the Web.
Like many of you, I was sick and tired of seeing page after page of what I can only describe as drivel that my unsuspecting patients were spending hours downloading and reading. I decided to stop just bemoaning this reality and to do something about it because—like most of my patients—I also research my own children’s medical conditions on the Web.
Let me tell you: If my son’s pediatric cardiologist had a blog, I’d be reading it every day.
—Jennifer Gunter, MD
Excerpt: “Are condoms with spermicide a good idea?”
“You are standing in the grocery store staring at the overwhelming selection of condoms. The last time you had sex, there was an unfortunate incident involving breakage and you are eager to avoid the pregnancy panic and STD scare that ensued. You look at the condoms with spermicide thinking that extra-protection sounds like a good idea right now.
After all, condoms without spermicide reduce your chance of getting gonorrhea and chlamydia by almost 100%, reduce your risk of catching HIV by 87%, reduce your chance of getting HPV (the virus that causes cervical cancer and genital warts) by 70%, and reduce your chance of getting herpes by 30%. Condoms with spermicide must be even better, right?
Wrong. Condoms with spermicide are no more effective than condoms with regular lube at preventing STDs. Condoms with spermicide are also more expensive and have a shorter shelf-life.
And here’s the big kicker. Spermicide damages the ecosystem and delicate skin of the vagina (it’s a secret garden in there, boys). Because of this, condoms with spermicide actually increase a woman’s risk of getting a bladder infection and can damage local defense mechanisms enough that the risk of catching an STD actually increases!
Source: Gunter J. Are condoms with spermicide a good idea? http://www.drjengunter.com. Accessed July 21, 2011.
The mechanics of starting a blog take little time and minimal technical knowledge. If you, or your practice, already have a Web site and a webmaster, he (she) can easily add a blog to the site for you. But you can also get a blog up and running yourself quite easily—at minimal or no cost to you (again, see “Why I blog”).
Two popular blog publishing platforms are WordPress (start at: https://en.wordpress.com/signup/) and Blogger (a service of Google; start at: https://www.blogger.com/signup.g). Both are free, although WordPress also sells a variety of upgrades that allow you to customize your site (if you have time and patience, you can navigate most of the upgrades on your own). Unless your blog needs a very specific look, however, you probably won’t need any of these options.
WordPress exacts an annual fee to keep third-party advertisements off your blog. Blogger does not charge to block advertising.
WordPress and Blogger both offer a variety of different templates so that you can trick out your blog to suit your style. You can delete the comments left by visitors with either platform. (Note: In 2 years of blogging, I’ve never had anyone post a comment that I thought needed deleting. But, you never know….)
So you’re not a writer. That’s OK—you aren’t chasing a Pulitzer.
People don’t linger on a blog. You want to make one or two points, not offer a dissertation. There is so much information on the Web that the only way to digest it is in small bites (think appetizers, not a four-course meal). Here are some pearls to consider for writing a blog successfully.
- Take the content that you might publish in a newsletter and simply cut it up into smaller pieces. Instead of a full page about the human papillomavirus (HPV) vaccine, divide what you’ve written into three or four discrete posts: for example, one post on the incidence of HPV; one on transmission; another on the vaccine schedule; and one on other means to prevent HPV (you can never have too many posts on the importance of using a condom, considering that almost 40% of sexually active high-school students did not use one the last time they had sexual intercourse).7
- Do some research. Read popular medical (and non-medical) blogs and decide what style suits you and your needs. A useful place to start is Dr. Kevin Pho’s blog at www.KevinMD.com" target="_blank">www.KevinMD.com. This is the most popular medical blog; in addition to his own writing, Dr. Pho posts content from an array of other physicians (including me), so you can find a number of different writing styles and viewpoints on a single blog.
- Post links to information from other blogs and traditional news sources (CNN, MSNBC, and so on) and add your brief comment to their reporting. This is an easy way to start a blog—just provide attribution and be careful not to infringe on your sources’ copyright.
- Answer the questions that you’re asked day in and day out in the office.
- Post on topics that are relevant to the moment. In autumn, for example, add information about the influenza vaccine in pregnancy, a link to the CDC Web page on influenza, and the date on which your office will begin offering shots.
- Add links to reputable sites; at the least, mention where you obtained specific information. This adds credibility, and people interested in learning more will appreciate knowing which sites are your sources.
- State that what you posted isn’t intended as individual medical advice. Given the medicolegal climate, I highly advise you to say this somewhere on your blog.
- End every post with a question. Doing so encourages comments.
- Stay true to your voice, whatever else you do. Insincerity is obvious. Painfully so.
Within your practice. Tell your patients that you have a blog. Consider listing the url of the blog on your business card.
And beyond. If you don’t want to promote your blog outside the practice, that’s fine. But if you like the idea of reaching more people, promote your posts on Twitter and Facebook and on information-sharing sites, such as reddit (http://www.reddit.com" target="_blank">http://www.reddit.com) and Digg (http://digg.com" target="_blank">http://digg.com). Note that Facebook and reddit are currently more popular among women; these two tools may be better suited to your needs if you’re looking to get the most promotion for a blog that’s geared to women’s health.
Promotion takes some work but, if what you write has value, you’ll be surprised at the viral life that a blog post can take on. Example: Recently, on my blog, I wrote a post that I titled “Oprah signs off and doctors everywhere rejoice.” The post went viral thanks to multiple re-postings on Twitter and Facebook and to views from reddit. In 3 days, the post was viewed more than 30,000 times.
This kind of traffic increases a blog’s ranking with search engines; it helped my blog stay at the top of the first “Results” page on various search engines for a while.
A blog can be a great tool for you and your practice
Blogging doesn’t have to take hours a day (although the public is fickle, and people will drift away if you don’t post at least three or four times a week); with only a little time and effort, you can have the satisfaction of self-expression. And, if you’re committed to good content, you will raise the quality of health information on the Web.
We want to hear from you! Tell us what you think.
1. Fox S. Health Topics. Pew Internet & American Life Project. http://pewinternet.org/Reports/2011/HealthTopics.aspx. Published February 1 2011. Accessed May 20, 2011.
2. Pew Research Center. Pew Internet & American Life Project Tracking Surveys: Trend data. http://www.pewinternet.org/Static-Pages/Trend-Data/Online-Activites-Total.aspx. Updated May 2011. Accessed June 1 2011.
3. McDaid D, Park A-la. Online health: Untangling the web. BUPA Health Pulse 2010. http://www.bupa.com/healthpulse. Published January 4 2011. Accessed June 1, 2010.
4. Pew Research Center. Generational differences in online activities. Pew Internet & American Life Project. http://www.pewinternet.org/Infographics/Generational-differences-in-online-activities.aspx. Published January 28 2009. Accessed June 1, 2011.
5. Gunter J. For better or maybe, worse, your patients are judging your care online. OBG Manage. 2011;23(3):47-51.
6. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
7. Eaton DK, Kann L, Kinchen S, et al. Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States 2009. MMWR Surveill Summ. 2010;59(5):1-142.
| Hear Dr. Gunter tally the benefits of blogging |
Jennifer Gunter, MD
Dr. Gunter, in ObGyn practice in San Francisco, Calif., blogs at www.preemieprimer.com/blog/ and www.drjengunter.com. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010).
Dr. Gunter reports no financial relationships relevant to this article.
| Hear Dr. Gunter tally the benefits of blogging |
Jennifer Gunter, MD
Dr. Gunter, in ObGyn practice in San Francisco, Calif., blogs at www.preemieprimer.com/blog/ and www.drjengunter.com. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010).
Dr. Gunter reports no financial relationships relevant to this article.
| Hear Dr. Gunter tally the benefits of blogging |
Jennifer Gunter, MD
Dr. Gunter, in ObGyn practice in San Francisco, Calif., blogs at www.preemieprimer.com/blog/ and www.drjengunter.com. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010).
Dr. Gunter reports no financial relationships relevant to this article.
CASE
Your gyn practice decides to publish an electronic newsletter for patients. You and your office manager spend a lot of time deciding on a format and writing content that you think is relevant to your patients. Everyone in the office agrees: It looks great.
But there’s a problem.
After your newsletter has been “live” for 6 months, fewer than 5% of your patients have signed up to receive it by e-mail (even though you’re sure that a lot more of them are on-line).
You’re perplexed: Why the poor response? The newsletter contains important information that your patients have told you they want—answers to the same questions that you get asked day in, day out.
Why does everyone seem so interested in getting answers to their questions when they’re in the office but not ahead of time and without a co-pay?
CASE: Resolved
The diagnosis: Newsletters are so 1990s.
Offering a Web-savvy patient a newsletter is like presenting her with a VHS tape of a surgical procedure you’re recommending. She will look at you and think, “Huh?”
It’s not that your patients don’t want health information—they are clearly eager for it: 80% of Americans who have Internet access look for health information on-line.1 The quest for health information is the third most popular on-line activity (behind e-mail and using a search engine), and women are more likely to search for health information on-line than men are.2 Nineteen percent of all Internet users search on-line for information about pregnancy and childbirth, and on WebMD (www.webmd.com, the second most popular Internet health site), hysterectomy was the fifth most commonly searched treatment in 2010.1
But getting health information from the Internet today does not mean another e-mail message in the in-box, where it sits waiting to be read or, more likely, deleted without having been opened. For most patients, looking for health information on-line entails 1) general searches (via Google, for example) for symptoms, specific diagnoses, or therapies or 2) searches on specific health-related Web sites (the top two for traffic in November 2010 were the National Institutes of Health and WebMD).1,3
More and more patients, however, are craving a dialogue about their health; 40% of on-line health-related activities involve interactive, user-generated content of social media, the most popular sources being Facebook, Twitter, and the Web-site tool known as blogs that I discuss in this article—with the aim of helping you determine whether placing your professional voice on the Web in a blog is workable, valuable, and respectable.1,3,4
Blog (noun, singular); blogs (plural)
What is it? A shortened form of “web log.” Has a different functional meaning for different people: A journal. A place to rant. A collaborative archive. A source of breaking news.
Whatever shape a blog takes, at its core it is an ongoing chronicle of information plus opinion. For a medical blog, that description typically refers to the perspective of the consumer/patient or the health-care professional who writes the “posts,” or entries.
The Web has thousands upon thousands of medical blogs. Some support an academic institution or a government agency (even the Centers for Disease Control and Prevention has a blog); many describe the experiences of an individual with one or another aspect of health care (from a patient’s or provider’s perspective). With one third of Americans reading blogs, they are an excellent way to disseminate information.1,3,4
Here are what I consider several good reasons to start a medical blog—reasons that, in part, motivated me to begin blogging (see “Why I blog,”):
- A blog is an ideal platform to deliver content to your patients and like-minded medical professionals. A blog allows your patients (and everyone else) to see information that you think is valuable and to hear your opinion on important health topics. Patients really like to know what their physician’s opinion is—how many times have you been asked, in the office, “What do you think I should do, doctor?”
- Blogging is good advertising for your practice. Your blog will appear in Web-search results, which may lead new patients to your doorstep. Reporters and other media workers troll the Web, fact-checking and looking for “angles” for news stories; you may be called to give your opinion about something you blogged about. Remember: Being mentioned in the local newspaper is free advertising (yes, people still read newspapers, though often on-line); ask the reporter to include a link to your blog in any story in which you’re quoted.
- Blogging helps you learn from your readers. Given the interactive nature of a blog (comments are encouraged), you might find feedback that is interesting at the least, possibly educational. Many people take commenting on blogs very seriously, and often post valuable links to other content.
- Contributing credible content drowns out garbage medical information that circulates widely on-line. The Internet is a powerhouse repository of medical knowledge, but it’s only as good as the content provided to it; in fact, 65% of Web pages contain inaccurate medical information.6 Regrettably, most people do not verify the medical information they find on-line.
- Blogging helps keep you relevant. Medicine is still trying to figure out how to best integrate itself with the user-centered operation and experience of Web 2.0. If you aren’t engaged here on some level, you risk being left behind.
I started blogging about prematurity 2 years ago, at my Web site, www.preemieprimer.com. I saw this as a way to support my book, The Preemie Primer, and to add content that I just didn’t have enough space for in the print edition.
Recently, I started a more general medical blog geared to women’s health (see an excerpt of a post below). I set up this blog myself, using WordPress (see the description in the main text), in under an hour (I’m of sub-average intelligence when it comes to computers, but I can follow directions). I paid a Web-savvy person to change the domain name to www.drjengunter.com.
Some days, my posts appeal to 20,000 people
Other days, I captivate, oh, a dozen. For me, the most important reasons for blogging are to use my voice (I really do write as I speak) and to add good content to the Web.
Like many of you, I was sick and tired of seeing page after page of what I can only describe as drivel that my unsuspecting patients were spending hours downloading and reading. I decided to stop just bemoaning this reality and to do something about it because—like most of my patients—I also research my own children’s medical conditions on the Web.
Let me tell you: If my son’s pediatric cardiologist had a blog, I’d be reading it every day.
—Jennifer Gunter, MD
Excerpt: “Are condoms with spermicide a good idea?”
“You are standing in the grocery store staring at the overwhelming selection of condoms. The last time you had sex, there was an unfortunate incident involving breakage and you are eager to avoid the pregnancy panic and STD scare that ensued. You look at the condoms with spermicide thinking that extra-protection sounds like a good idea right now.
After all, condoms without spermicide reduce your chance of getting gonorrhea and chlamydia by almost 100%, reduce your risk of catching HIV by 87%, reduce your chance of getting HPV (the virus that causes cervical cancer and genital warts) by 70%, and reduce your chance of getting herpes by 30%. Condoms with spermicide must be even better, right?
Wrong. Condoms with spermicide are no more effective than condoms with regular lube at preventing STDs. Condoms with spermicide are also more expensive and have a shorter shelf-life.
And here’s the big kicker. Spermicide damages the ecosystem and delicate skin of the vagina (it’s a secret garden in there, boys). Because of this, condoms with spermicide actually increase a woman’s risk of getting a bladder infection and can damage local defense mechanisms enough that the risk of catching an STD actually increases!
Source: Gunter J. Are condoms with spermicide a good idea? http://www.drjengunter.com. Accessed July 21, 2011.
The mechanics of starting a blog take little time and minimal technical knowledge. If you, or your practice, already have a Web site and a webmaster, he (she) can easily add a blog to the site for you. But you can also get a blog up and running yourself quite easily—at minimal or no cost to you (again, see “Why I blog”).
Two popular blog publishing platforms are WordPress (start at: https://en.wordpress.com/signup/) and Blogger (a service of Google; start at: https://www.blogger.com/signup.g). Both are free, although WordPress also sells a variety of upgrades that allow you to customize your site (if you have time and patience, you can navigate most of the upgrades on your own). Unless your blog needs a very specific look, however, you probably won’t need any of these options.
WordPress exacts an annual fee to keep third-party advertisements off your blog. Blogger does not charge to block advertising.
WordPress and Blogger both offer a variety of different templates so that you can trick out your blog to suit your style. You can delete the comments left by visitors with either platform. (Note: In 2 years of blogging, I’ve never had anyone post a comment that I thought needed deleting. But, you never know….)
So you’re not a writer. That’s OK—you aren’t chasing a Pulitzer.
People don’t linger on a blog. You want to make one or two points, not offer a dissertation. There is so much information on the Web that the only way to digest it is in small bites (think appetizers, not a four-course meal). Here are some pearls to consider for writing a blog successfully.
- Take the content that you might publish in a newsletter and simply cut it up into smaller pieces. Instead of a full page about the human papillomavirus (HPV) vaccine, divide what you’ve written into three or four discrete posts: for example, one post on the incidence of HPV; one on transmission; another on the vaccine schedule; and one on other means to prevent HPV (you can never have too many posts on the importance of using a condom, considering that almost 40% of sexually active high-school students did not use one the last time they had sexual intercourse).7
- Do some research. Read popular medical (and non-medical) blogs and decide what style suits you and your needs. A useful place to start is Dr. Kevin Pho’s blog at www.KevinMD.com" target="_blank">www.KevinMD.com. This is the most popular medical blog; in addition to his own writing, Dr. Pho posts content from an array of other physicians (including me), so you can find a number of different writing styles and viewpoints on a single blog.
- Post links to information from other blogs and traditional news sources (CNN, MSNBC, and so on) and add your brief comment to their reporting. This is an easy way to start a blog—just provide attribution and be careful not to infringe on your sources’ copyright.
- Answer the questions that you’re asked day in and day out in the office.
- Post on topics that are relevant to the moment. In autumn, for example, add information about the influenza vaccine in pregnancy, a link to the CDC Web page on influenza, and the date on which your office will begin offering shots.
- Add links to reputable sites; at the least, mention where you obtained specific information. This adds credibility, and people interested in learning more will appreciate knowing which sites are your sources.
- State that what you posted isn’t intended as individual medical advice. Given the medicolegal climate, I highly advise you to say this somewhere on your blog.
- End every post with a question. Doing so encourages comments.
- Stay true to your voice, whatever else you do. Insincerity is obvious. Painfully so.
Within your practice. Tell your patients that you have a blog. Consider listing the url of the blog on your business card.
And beyond. If you don’t want to promote your blog outside the practice, that’s fine. But if you like the idea of reaching more people, promote your posts on Twitter and Facebook and on information-sharing sites, such as reddit (http://www.reddit.com" target="_blank">http://www.reddit.com) and Digg (http://digg.com" target="_blank">http://digg.com). Note that Facebook and reddit are currently more popular among women; these two tools may be better suited to your needs if you’re looking to get the most promotion for a blog that’s geared to women’s health.
Promotion takes some work but, if what you write has value, you’ll be surprised at the viral life that a blog post can take on. Example: Recently, on my blog, I wrote a post that I titled “Oprah signs off and doctors everywhere rejoice.” The post went viral thanks to multiple re-postings on Twitter and Facebook and to views from reddit. In 3 days, the post was viewed more than 30,000 times.
This kind of traffic increases a blog’s ranking with search engines; it helped my blog stay at the top of the first “Results” page on various search engines for a while.
A blog can be a great tool for you and your practice
Blogging doesn’t have to take hours a day (although the public is fickle, and people will drift away if you don’t post at least three or four times a week); with only a little time and effort, you can have the satisfaction of self-expression. And, if you’re committed to good content, you will raise the quality of health information on the Web.
We want to hear from you! Tell us what you think.
CASE
Your gyn practice decides to publish an electronic newsletter for patients. You and your office manager spend a lot of time deciding on a format and writing content that you think is relevant to your patients. Everyone in the office agrees: It looks great.
But there’s a problem.
After your newsletter has been “live” for 6 months, fewer than 5% of your patients have signed up to receive it by e-mail (even though you’re sure that a lot more of them are on-line).
You’re perplexed: Why the poor response? The newsletter contains important information that your patients have told you they want—answers to the same questions that you get asked day in, day out.
Why does everyone seem so interested in getting answers to their questions when they’re in the office but not ahead of time and without a co-pay?
CASE: Resolved
The diagnosis: Newsletters are so 1990s.
Offering a Web-savvy patient a newsletter is like presenting her with a VHS tape of a surgical procedure you’re recommending. She will look at you and think, “Huh?”
It’s not that your patients don’t want health information—they are clearly eager for it: 80% of Americans who have Internet access look for health information on-line.1 The quest for health information is the third most popular on-line activity (behind e-mail and using a search engine), and women are more likely to search for health information on-line than men are.2 Nineteen percent of all Internet users search on-line for information about pregnancy and childbirth, and on WebMD (www.webmd.com, the second most popular Internet health site), hysterectomy was the fifth most commonly searched treatment in 2010.1
But getting health information from the Internet today does not mean another e-mail message in the in-box, where it sits waiting to be read or, more likely, deleted without having been opened. For most patients, looking for health information on-line entails 1) general searches (via Google, for example) for symptoms, specific diagnoses, or therapies or 2) searches on specific health-related Web sites (the top two for traffic in November 2010 were the National Institutes of Health and WebMD).1,3
More and more patients, however, are craving a dialogue about their health; 40% of on-line health-related activities involve interactive, user-generated content of social media, the most popular sources being Facebook, Twitter, and the Web-site tool known as blogs that I discuss in this article—with the aim of helping you determine whether placing your professional voice on the Web in a blog is workable, valuable, and respectable.1,3,4
Blog (noun, singular); blogs (plural)
What is it? A shortened form of “web log.” Has a different functional meaning for different people: A journal. A place to rant. A collaborative archive. A source of breaking news.
Whatever shape a blog takes, at its core it is an ongoing chronicle of information plus opinion. For a medical blog, that description typically refers to the perspective of the consumer/patient or the health-care professional who writes the “posts,” or entries.
The Web has thousands upon thousands of medical blogs. Some support an academic institution or a government agency (even the Centers for Disease Control and Prevention has a blog); many describe the experiences of an individual with one or another aspect of health care (from a patient’s or provider’s perspective). With one third of Americans reading blogs, they are an excellent way to disseminate information.1,3,4
Here are what I consider several good reasons to start a medical blog—reasons that, in part, motivated me to begin blogging (see “Why I blog,”):
- A blog is an ideal platform to deliver content to your patients and like-minded medical professionals. A blog allows your patients (and everyone else) to see information that you think is valuable and to hear your opinion on important health topics. Patients really like to know what their physician’s opinion is—how many times have you been asked, in the office, “What do you think I should do, doctor?”
- Blogging is good advertising for your practice. Your blog will appear in Web-search results, which may lead new patients to your doorstep. Reporters and other media workers troll the Web, fact-checking and looking for “angles” for news stories; you may be called to give your opinion about something you blogged about. Remember: Being mentioned in the local newspaper is free advertising (yes, people still read newspapers, though often on-line); ask the reporter to include a link to your blog in any story in which you’re quoted.
- Blogging helps you learn from your readers. Given the interactive nature of a blog (comments are encouraged), you might find feedback that is interesting at the least, possibly educational. Many people take commenting on blogs very seriously, and often post valuable links to other content.
- Contributing credible content drowns out garbage medical information that circulates widely on-line. The Internet is a powerhouse repository of medical knowledge, but it’s only as good as the content provided to it; in fact, 65% of Web pages contain inaccurate medical information.6 Regrettably, most people do not verify the medical information they find on-line.
- Blogging helps keep you relevant. Medicine is still trying to figure out how to best integrate itself with the user-centered operation and experience of Web 2.0. If you aren’t engaged here on some level, you risk being left behind.
I started blogging about prematurity 2 years ago, at my Web site, www.preemieprimer.com. I saw this as a way to support my book, The Preemie Primer, and to add content that I just didn’t have enough space for in the print edition.
Recently, I started a more general medical blog geared to women’s health (see an excerpt of a post below). I set up this blog myself, using WordPress (see the description in the main text), in under an hour (I’m of sub-average intelligence when it comes to computers, but I can follow directions). I paid a Web-savvy person to change the domain name to www.drjengunter.com.
Some days, my posts appeal to 20,000 people
Other days, I captivate, oh, a dozen. For me, the most important reasons for blogging are to use my voice (I really do write as I speak) and to add good content to the Web.
Like many of you, I was sick and tired of seeing page after page of what I can only describe as drivel that my unsuspecting patients were spending hours downloading and reading. I decided to stop just bemoaning this reality and to do something about it because—like most of my patients—I also research my own children’s medical conditions on the Web.
Let me tell you: If my son’s pediatric cardiologist had a blog, I’d be reading it every day.
—Jennifer Gunter, MD
Excerpt: “Are condoms with spermicide a good idea?”
“You are standing in the grocery store staring at the overwhelming selection of condoms. The last time you had sex, there was an unfortunate incident involving breakage and you are eager to avoid the pregnancy panic and STD scare that ensued. You look at the condoms with spermicide thinking that extra-protection sounds like a good idea right now.
After all, condoms without spermicide reduce your chance of getting gonorrhea and chlamydia by almost 100%, reduce your risk of catching HIV by 87%, reduce your chance of getting HPV (the virus that causes cervical cancer and genital warts) by 70%, and reduce your chance of getting herpes by 30%. Condoms with spermicide must be even better, right?
Wrong. Condoms with spermicide are no more effective than condoms with regular lube at preventing STDs. Condoms with spermicide are also more expensive and have a shorter shelf-life.
And here’s the big kicker. Spermicide damages the ecosystem and delicate skin of the vagina (it’s a secret garden in there, boys). Because of this, condoms with spermicide actually increase a woman’s risk of getting a bladder infection and can damage local defense mechanisms enough that the risk of catching an STD actually increases!
Source: Gunter J. Are condoms with spermicide a good idea? http://www.drjengunter.com. Accessed July 21, 2011.
The mechanics of starting a blog take little time and minimal technical knowledge. If you, or your practice, already have a Web site and a webmaster, he (she) can easily add a blog to the site for you. But you can also get a blog up and running yourself quite easily—at minimal or no cost to you (again, see “Why I blog”).
Two popular blog publishing platforms are WordPress (start at: https://en.wordpress.com/signup/) and Blogger (a service of Google; start at: https://www.blogger.com/signup.g). Both are free, although WordPress also sells a variety of upgrades that allow you to customize your site (if you have time and patience, you can navigate most of the upgrades on your own). Unless your blog needs a very specific look, however, you probably won’t need any of these options.
WordPress exacts an annual fee to keep third-party advertisements off your blog. Blogger does not charge to block advertising.
WordPress and Blogger both offer a variety of different templates so that you can trick out your blog to suit your style. You can delete the comments left by visitors with either platform. (Note: In 2 years of blogging, I’ve never had anyone post a comment that I thought needed deleting. But, you never know….)
So you’re not a writer. That’s OK—you aren’t chasing a Pulitzer.
People don’t linger on a blog. You want to make one or two points, not offer a dissertation. There is so much information on the Web that the only way to digest it is in small bites (think appetizers, not a four-course meal). Here are some pearls to consider for writing a blog successfully.
- Take the content that you might publish in a newsletter and simply cut it up into smaller pieces. Instead of a full page about the human papillomavirus (HPV) vaccine, divide what you’ve written into three or four discrete posts: for example, one post on the incidence of HPV; one on transmission; another on the vaccine schedule; and one on other means to prevent HPV (you can never have too many posts on the importance of using a condom, considering that almost 40% of sexually active high-school students did not use one the last time they had sexual intercourse).7
- Do some research. Read popular medical (and non-medical) blogs and decide what style suits you and your needs. A useful place to start is Dr. Kevin Pho’s blog at www.KevinMD.com" target="_blank">www.KevinMD.com. This is the most popular medical blog; in addition to his own writing, Dr. Pho posts content from an array of other physicians (including me), so you can find a number of different writing styles and viewpoints on a single blog.
- Post links to information from other blogs and traditional news sources (CNN, MSNBC, and so on) and add your brief comment to their reporting. This is an easy way to start a blog—just provide attribution and be careful not to infringe on your sources’ copyright.
- Answer the questions that you’re asked day in and day out in the office.
- Post on topics that are relevant to the moment. In autumn, for example, add information about the influenza vaccine in pregnancy, a link to the CDC Web page on influenza, and the date on which your office will begin offering shots.
- Add links to reputable sites; at the least, mention where you obtained specific information. This adds credibility, and people interested in learning more will appreciate knowing which sites are your sources.
- State that what you posted isn’t intended as individual medical advice. Given the medicolegal climate, I highly advise you to say this somewhere on your blog.
- End every post with a question. Doing so encourages comments.
- Stay true to your voice, whatever else you do. Insincerity is obvious. Painfully so.
Within your practice. Tell your patients that you have a blog. Consider listing the url of the blog on your business card.
And beyond. If you don’t want to promote your blog outside the practice, that’s fine. But if you like the idea of reaching more people, promote your posts on Twitter and Facebook and on information-sharing sites, such as reddit (http://www.reddit.com" target="_blank">http://www.reddit.com) and Digg (http://digg.com" target="_blank">http://digg.com). Note that Facebook and reddit are currently more popular among women; these two tools may be better suited to your needs if you’re looking to get the most promotion for a blog that’s geared to women’s health.
Promotion takes some work but, if what you write has value, you’ll be surprised at the viral life that a blog post can take on. Example: Recently, on my blog, I wrote a post that I titled “Oprah signs off and doctors everywhere rejoice.” The post went viral thanks to multiple re-postings on Twitter and Facebook and to views from reddit. In 3 days, the post was viewed more than 30,000 times.
This kind of traffic increases a blog’s ranking with search engines; it helped my blog stay at the top of the first “Results” page on various search engines for a while.
A blog can be a great tool for you and your practice
Blogging doesn’t have to take hours a day (although the public is fickle, and people will drift away if you don’t post at least three or four times a week); with only a little time and effort, you can have the satisfaction of self-expression. And, if you’re committed to good content, you will raise the quality of health information on the Web.
We want to hear from you! Tell us what you think.
1. Fox S. Health Topics. Pew Internet & American Life Project. http://pewinternet.org/Reports/2011/HealthTopics.aspx. Published February 1 2011. Accessed May 20, 2011.
2. Pew Research Center. Pew Internet & American Life Project Tracking Surveys: Trend data. http://www.pewinternet.org/Static-Pages/Trend-Data/Online-Activites-Total.aspx. Updated May 2011. Accessed June 1 2011.
3. McDaid D, Park A-la. Online health: Untangling the web. BUPA Health Pulse 2010. http://www.bupa.com/healthpulse. Published January 4 2011. Accessed June 1, 2010.
4. Pew Research Center. Generational differences in online activities. Pew Internet & American Life Project. http://www.pewinternet.org/Infographics/Generational-differences-in-online-activities.aspx. Published January 28 2009. Accessed June 1, 2011.
5. Gunter J. For better or maybe, worse, your patients are judging your care online. OBG Manage. 2011;23(3):47-51.
6. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
7. Eaton DK, Kann L, Kinchen S, et al. Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States 2009. MMWR Surveill Summ. 2010;59(5):1-142.
1. Fox S. Health Topics. Pew Internet & American Life Project. http://pewinternet.org/Reports/2011/HealthTopics.aspx. Published February 1 2011. Accessed May 20, 2011.
2. Pew Research Center. Pew Internet & American Life Project Tracking Surveys: Trend data. http://www.pewinternet.org/Static-Pages/Trend-Data/Online-Activites-Total.aspx. Updated May 2011. Accessed June 1 2011.
3. McDaid D, Park A-la. Online health: Untangling the web. BUPA Health Pulse 2010. http://www.bupa.com/healthpulse. Published January 4 2011. Accessed June 1, 2010.
4. Pew Research Center. Generational differences in online activities. Pew Internet & American Life Project. http://www.pewinternet.org/Infographics/Generational-differences-in-online-activities.aspx. Published January 28 2009. Accessed June 1, 2011.
5. Gunter J. For better or maybe, worse, your patients are judging your care online. OBG Manage. 2011;23(3):47-51.
6. Thompson LA, Dawson K, Ferdig R, et al. The intersection of online social networking with medical professionalism. J Gen Intern Med. 2008;23(7):954-957.
7. Eaton DK, Kann L, Kinchen S, et al. Centers for Disease Control and Prevention. Youth risk behavior surveillance—United States 2009. MMWR Surveill Summ. 2010;59(5):1-142.
Pelvic injury from the McRoberts maneuver?…and more

DURING PRENATAL CARE, a woman repeatedly complained of severe discomfort, and requested a cesarean delivery. The ObGyn’s charts did not note her complaints.
A first-year resident and nurse covered for the ObGyn because he did not arrive at the hospital for hours after the mother notified him she was in labor. When shoulder dystocia was encountered, the resident used the McRoberts maneuver. The ObGyn arrived a minute before the birth. The baby weighed 10 lbs. The mother suffered symphysis pubis diastasis, required several surgeries, and now uses a cane to walk.
PATIENT’S CLAIM The ObGyn was negligent in not arriving in time to deliver the baby. The mother’s pelvis was injured during the McRoberts maneuver. The baby’s size was not properly estimated.
PHYSICIAN’S DEFENSE The use of the resident’s care was appropriate, as this was a teaching hospital.
VERDICT A $5.5 million New York verdict was returned.
Cancer Dx “not timely”; additional tx required
IN JUNE 2000, AN OBGYN PALPATED a pelvic mass in a postmenopausal woman. After ultrasonography (US) in August 2000, the ObGyn told the woman that a uterine fibroid had been found but no further testing was needed. In December 2001, US revealed that the mass had enlarged, but no further testing was done. In May 2002, the patient reported fatigue, distention of her abdomen, and an increase in the frequency of urination.
In July 2002, the ObGyn removed a 3-lb malignant uterine tumor during hysterectomy. A second staging surgery was performed, and the patient underwent chemotherapy.
PATIENT’S CLAIM An earlier diagnosis would have reduced the amount of treatment required. The ObGyn should have reacted immediately when the mass was first palpated in June 2000 and found on US in August 2000, as postmenopausal women do not develop uterine fibroids. A gynecologic oncologist should have been present at the hysterectomy to perform concurrent staging.
PHYSICIAN’S DEFENSE The patient failed to report symptoms that suggested cancer for 10 months; a prompt response was made when symptoms were revealed. It was appropriate to accept the results of US regarding a uterine fibroid.
VERDICT A $1.25 million New York verdict was returned.
Abnormal thickness of fetal nuchal fold
WHEN A 31-YEAR-OLD WOMAN was 18 weeks’ pregnant, she underwent ultrasonography, which was reportedly normal. The child was born with Down syndrome.
PATIENT’S CLAIM The ObGyn and radiologist failed to detect an abnormal thickness in the fetal nuchal fold—often a sign of Down syndrome.
PHYSICIANS’ DEFENSE The sonogram was properly analyzed. A thickened fold is an unreliable indicator of Down syndrome.
VERDICT A $1.7 million New Jersey settlement was returned.
Ovary retained; cancer recurs; death
A WOMAN UNDERWENT SURGERY for ovarian cancer in July 2004. She died of ovarian cancer in 2008 at age 59.
ESTATE’S CLAIM The gynecologist did not tell the patient that only one ovary was removed, or that a pathologist had not found the second ovary in the specimen. Ovarian cancer developed in the retained ovary a few years later. She would have undergone additional surgery had she known the second ovary was still there.
PHYSICIAN’S DEFENSE Both ovaries were removed in July 2004. The left ovary was not found during an autopsy performed on the decedent.
VERDICT A $1.967 million Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
1. Severe birth asphyxia: cerebral palsy and seizures
AFTER A NORMAL PREGNANCY, a woman went to the hospital in labor. Her ObGyn, Dr. A, went off duty at 4 PM and was replaced by Dr. B, a practice partner who delivered five other babies between 11 PM and 2:15 AM.
At 9:40 PM, the fetus was occiput posterior. At 12:31 AM, Dr. B attempted manual rotation; no exam was recorded in the chart. By 2:30 AM, the fetus had returned to the occiput posterior position, and Dr. B again tried manual rotation. Then he left to take a nap while the mother’s epidural was reinforced. There was a delay in achieving a satisfactory epidural, and Dr. B was not called back to the bedside until 4 AM. He decided to perform a cesarean delivery when the fetal heart monitor showed an increased baseline with persistent variable decelerations.
Although Dr. B had called Dr. A earlier to elicit her help with the cesarean, she had gone back to bed and was not prepared to assist. During a 30-minute delay, the electronic fetal monitor was disconnected and never reconnected. A nurse checked the fetal heart rate with ultrasonography, and reported that it was normal; however, there was no copy in the chart.
The incision was made at 4:33 AM, and the baby was delivered at 5:06 AM. The infant was born without a heart rate or respiration (Apgar scores, all 0). A neonatologist was not available for resuscitation; a neonatal nurse practitioner arrived 7 minutes after delivery. The baby finally had a heart rate 24 minutes after delivery. The child suffered severe birth asphyxia, causing athetoid and spastic cerebral palsy and seizures.
PATIENT’S CLAIM The ObGyn failed to deliver the baby in a timely manner. The fetus was not continuously monitored with a fetal scalp electrode. The nurse violated several hospital policies.
DEFENDANTS’ DEFENSE The baby suffered an acute, total cord occlusion minutes before birth; this was unpredictable and the injuries could not have been prevented.
VERDICT At the end of the discovery period, the defendants’ attorney withdrew and new attorneys sought to name new experts. While these issues were pending, the matter was settled for a Washington total of $20 million. The mother settled with the hospital for $9.85 million. Although the doctors’ group had $5 million in insurance coverage, the plaintiff demanded that the insurance company pay in excess of limits due to potential bad-faith claims. The insurance company ultimately paid $10.15 million.
2. Profound metabolic acidosis after emergent delivery
WHEN A WOMAN WAS 2 CM DILATED and 99% effaced, she was given dinoprostone and oxytocin to begin induction and augment labor. Oxytocin was continued even though her pattern of contractions showed tachysystole. An intrauterine pressure catheter that had been placed to assess contractions was removed. Monitoring revealed an elevated fetal heart rate at 170 to 180 bpm. Ten minutes before birth, the fetal heart tracing ended; a sonogram showed fetal bradycardia and prompted an emergency vacuum extraction.
The baby was floppy at birth, did not cry, and was intubated and transferred to the NICU. Apgar scores were 1, 3, and 5 at 1, 5, and 10 minutes. The umbilical cord gas had a venous pH of 6.637, indicative of profound acidosis. Ongoing hypoxia and anoxia resulted in massive and irreversible brain injury. An EEG at 5 days confirmed the presence of encephalopathy due to perinatal asphyxia. The child will require specialized treatment and attendant care for life.
PATIENT’S CLAIM Oxytocin was never stopped or reduced throughout labor and delivery. The ObGyn failed to promptly deliver the baby. No internal scalp electrode was used to directly monitor the fetus; the intrauterine pressure catheter was never replaced.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence or causation, claiming that there was a sudden placental abruption 10 minutes before birth that caused perinatal asphyxia.
VERDICT A $6.95 million District of Columbia settlement was returned.
3. Breech 2nd twin has cerebral palsy
PREGNANT WITH TWINS and in early labor, a woman went to the hospital, where a nurse midwife administered dinoprostone. The labor and delivery nurses only monitored one fetal heart rate during most of the labor period. The mother’s contraction pattern was indicative of tachysystole, and the twin who was being monitored showed a decelerating heart rate. The ObGyn arrived minutes before the birth unprepared for delivery, and a nurse delivered a healthy first child.
The second child’s heart rate dropped to 90 bpm, and the baby shifted to a breech position; the ObGyn tried manual rotation but was unsuccessful. After 20 minutes, cesarean delivery was performed. The boy was born with signs of metabolic acidosis and suffered a seizure 2 hours later. He was given a diagnosis of cerebral palsy and is fed through a tube, cannot speak, and requires skilled nursing care.
PATIENT’S CLAIM The ObGyn and nurses were negligent in only monitoring one fetus, and for failing to perform cesarean delivery in a timely manner.
DEFENDANTS’ DEFENSE The ObGyn claimed he was not informed of the decelerations shown on the fetal monitor, nor of the mother’s rapidly progressing labor. The hospital maintained that the nurses had given the ObGyn proper information and that the injuries to the infant had occurred after the ObGyn’s arrival. The mother’s weight of 322 pounds made monitoring difficult during labor and delivery.
VERDICT A $21,573,993 Pennsylvania verdict was returned against the hospital; a defense verdict was returned for the physician.
4. Shoulder dystocia, uterine tachysystole complicate vaginal delivery
WITH MILD PRE-ECLAMPSIA and vaginal spotting, a woman was admitted to a hospital’s L&D unit. Dinoprostone was administered, but the fetus was unengaged. Oxytocin was added to induce labor. Labor was complicated by repeated tachysystole; prolonged dilation; prolonged descent; severe, prolonged decelerations; and tachycardia. Uterine tachysystole continued for extended periods. Vaginal delivery was complicated by shoulder dystocia, which took 2 minutes to resolve. The child was delivered without a heart rate or respirations. A heartbeat was obtained a minute after delivery, and Apgar scores were 0, 2, and 2. The child was given a diagnosis of hypoxic ischemic encephalopathy, cerebral palsy, and a seizure disorder.
PATIENT’S CLAIM The L&D nurses and physicians were negligent in failing to properly monitor labor progression, fetal heart rate, and oxytocin management. They failed to communicate with the woman’s ObGyn, and did not exercise the proper chain of command. The physicians failed to recommend a cesarean delivery when labor became complicated.
DEFENDANTS’ DEFENSE The patient’s treatment was appropriate. Brain damage did not occur during labor and delivery.
VERDICT A $3.55 million Idaho verdict was returned.
5. Fetus transverse; oxytocin given
A WOMAN ARRIVED AT THE HOSPITAL after her membranes ruptured. A first-year resident failed to realize that the fetus was in a transverse position, and, with the attending physician’s approval, ordered oxytocin. When vaginal bleeding began, it was suspected that the placenta had detached. An hour later, after vaginal bleeding increased and late decelerations were noted on the fetal heart monitor, cesarean delivery was performed. The child was given a diagnosis of cerebral palsy and other complications, and died at 16 months of age.
ESTATE’S CLAIM The use of oxytocin is contraindicated for a baby in a transverse position. The fetus’ position indicated a need for a cesarean delivery. Placental detachment was not promptly addressed, leading to fetal oxygen deprivation.
DEFENDANTS’ DEFENSE The fetus appeared to be fine under all objective criteria until a “softball-sized” clot emerged from the mother’s vagina. The attending physician came to the mother’s bedside at that time. Umbilical cord blood gases showed no evidence of acidosis. A fetal brain injury occurred prior to the mother’s arrival at the hospital.
VERDICT A $2.5 million Pennsylvania verdict was returned.
- Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
We want to hear from you! Tell us what you think.
DURING PRENATAL CARE, a woman repeatedly complained of severe discomfort, and requested a cesarean delivery. The ObGyn’s charts did not note her complaints.
A first-year resident and nurse covered for the ObGyn because he did not arrive at the hospital for hours after the mother notified him she was in labor. When shoulder dystocia was encountered, the resident used the McRoberts maneuver. The ObGyn arrived a minute before the birth. The baby weighed 10 lbs. The mother suffered symphysis pubis diastasis, required several surgeries, and now uses a cane to walk.
PATIENT’S CLAIM The ObGyn was negligent in not arriving in time to deliver the baby. The mother’s pelvis was injured during the McRoberts maneuver. The baby’s size was not properly estimated.
PHYSICIAN’S DEFENSE The use of the resident’s care was appropriate, as this was a teaching hospital.
VERDICT A $5.5 million New York verdict was returned.
Cancer Dx “not timely”; additional tx required
IN JUNE 2000, AN OBGYN PALPATED a pelvic mass in a postmenopausal woman. After ultrasonography (US) in August 2000, the ObGyn told the woman that a uterine fibroid had been found but no further testing was needed. In December 2001, US revealed that the mass had enlarged, but no further testing was done. In May 2002, the patient reported fatigue, distention of her abdomen, and an increase in the frequency of urination.
In July 2002, the ObGyn removed a 3-lb malignant uterine tumor during hysterectomy. A second staging surgery was performed, and the patient underwent chemotherapy.
PATIENT’S CLAIM An earlier diagnosis would have reduced the amount of treatment required. The ObGyn should have reacted immediately when the mass was first palpated in June 2000 and found on US in August 2000, as postmenopausal women do not develop uterine fibroids. A gynecologic oncologist should have been present at the hysterectomy to perform concurrent staging.
PHYSICIAN’S DEFENSE The patient failed to report symptoms that suggested cancer for 10 months; a prompt response was made when symptoms were revealed. It was appropriate to accept the results of US regarding a uterine fibroid.
VERDICT A $1.25 million New York verdict was returned.
Abnormal thickness of fetal nuchal fold
WHEN A 31-YEAR-OLD WOMAN was 18 weeks’ pregnant, she underwent ultrasonography, which was reportedly normal. The child was born with Down syndrome.
PATIENT’S CLAIM The ObGyn and radiologist failed to detect an abnormal thickness in the fetal nuchal fold—often a sign of Down syndrome.
PHYSICIANS’ DEFENSE The sonogram was properly analyzed. A thickened fold is an unreliable indicator of Down syndrome.
VERDICT A $1.7 million New Jersey settlement was returned.
Ovary retained; cancer recurs; death
A WOMAN UNDERWENT SURGERY for ovarian cancer in July 2004. She died of ovarian cancer in 2008 at age 59.
ESTATE’S CLAIM The gynecologist did not tell the patient that only one ovary was removed, or that a pathologist had not found the second ovary in the specimen. Ovarian cancer developed in the retained ovary a few years later. She would have undergone additional surgery had she known the second ovary was still there.
PHYSICIAN’S DEFENSE Both ovaries were removed in July 2004. The left ovary was not found during an autopsy performed on the decedent.
VERDICT A $1.967 million Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
1. Severe birth asphyxia: cerebral palsy and seizures
AFTER A NORMAL PREGNANCY, a woman went to the hospital in labor. Her ObGyn, Dr. A, went off duty at 4 PM and was replaced by Dr. B, a practice partner who delivered five other babies between 11 PM and 2:15 AM.
At 9:40 PM, the fetus was occiput posterior. At 12:31 AM, Dr. B attempted manual rotation; no exam was recorded in the chart. By 2:30 AM, the fetus had returned to the occiput posterior position, and Dr. B again tried manual rotation. Then he left to take a nap while the mother’s epidural was reinforced. There was a delay in achieving a satisfactory epidural, and Dr. B was not called back to the bedside until 4 AM. He decided to perform a cesarean delivery when the fetal heart monitor showed an increased baseline with persistent variable decelerations.
Although Dr. B had called Dr. A earlier to elicit her help with the cesarean, she had gone back to bed and was not prepared to assist. During a 30-minute delay, the electronic fetal monitor was disconnected and never reconnected. A nurse checked the fetal heart rate with ultrasonography, and reported that it was normal; however, there was no copy in the chart.
The incision was made at 4:33 AM, and the baby was delivered at 5:06 AM. The infant was born without a heart rate or respiration (Apgar scores, all 0). A neonatologist was not available for resuscitation; a neonatal nurse practitioner arrived 7 minutes after delivery. The baby finally had a heart rate 24 minutes after delivery. The child suffered severe birth asphyxia, causing athetoid and spastic cerebral palsy and seizures.
PATIENT’S CLAIM The ObGyn failed to deliver the baby in a timely manner. The fetus was not continuously monitored with a fetal scalp electrode. The nurse violated several hospital policies.
DEFENDANTS’ DEFENSE The baby suffered an acute, total cord occlusion minutes before birth; this was unpredictable and the injuries could not have been prevented.
VERDICT At the end of the discovery period, the defendants’ attorney withdrew and new attorneys sought to name new experts. While these issues were pending, the matter was settled for a Washington total of $20 million. The mother settled with the hospital for $9.85 million. Although the doctors’ group had $5 million in insurance coverage, the plaintiff demanded that the insurance company pay in excess of limits due to potential bad-faith claims. The insurance company ultimately paid $10.15 million.
2. Profound metabolic acidosis after emergent delivery
WHEN A WOMAN WAS 2 CM DILATED and 99% effaced, she was given dinoprostone and oxytocin to begin induction and augment labor. Oxytocin was continued even though her pattern of contractions showed tachysystole. An intrauterine pressure catheter that had been placed to assess contractions was removed. Monitoring revealed an elevated fetal heart rate at 170 to 180 bpm. Ten minutes before birth, the fetal heart tracing ended; a sonogram showed fetal bradycardia and prompted an emergency vacuum extraction.
The baby was floppy at birth, did not cry, and was intubated and transferred to the NICU. Apgar scores were 1, 3, and 5 at 1, 5, and 10 minutes. The umbilical cord gas had a venous pH of 6.637, indicative of profound acidosis. Ongoing hypoxia and anoxia resulted in massive and irreversible brain injury. An EEG at 5 days confirmed the presence of encephalopathy due to perinatal asphyxia. The child will require specialized treatment and attendant care for life.
PATIENT’S CLAIM Oxytocin was never stopped or reduced throughout labor and delivery. The ObGyn failed to promptly deliver the baby. No internal scalp electrode was used to directly monitor the fetus; the intrauterine pressure catheter was never replaced.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence or causation, claiming that there was a sudden placental abruption 10 minutes before birth that caused perinatal asphyxia.
VERDICT A $6.95 million District of Columbia settlement was returned.
3. Breech 2nd twin has cerebral palsy
PREGNANT WITH TWINS and in early labor, a woman went to the hospital, where a nurse midwife administered dinoprostone. The labor and delivery nurses only monitored one fetal heart rate during most of the labor period. The mother’s contraction pattern was indicative of tachysystole, and the twin who was being monitored showed a decelerating heart rate. The ObGyn arrived minutes before the birth unprepared for delivery, and a nurse delivered a healthy first child.
The second child’s heart rate dropped to 90 bpm, and the baby shifted to a breech position; the ObGyn tried manual rotation but was unsuccessful. After 20 minutes, cesarean delivery was performed. The boy was born with signs of metabolic acidosis and suffered a seizure 2 hours later. He was given a diagnosis of cerebral palsy and is fed through a tube, cannot speak, and requires skilled nursing care.
PATIENT’S CLAIM The ObGyn and nurses were negligent in only monitoring one fetus, and for failing to perform cesarean delivery in a timely manner.
DEFENDANTS’ DEFENSE The ObGyn claimed he was not informed of the decelerations shown on the fetal monitor, nor of the mother’s rapidly progressing labor. The hospital maintained that the nurses had given the ObGyn proper information and that the injuries to the infant had occurred after the ObGyn’s arrival. The mother’s weight of 322 pounds made monitoring difficult during labor and delivery.
VERDICT A $21,573,993 Pennsylvania verdict was returned against the hospital; a defense verdict was returned for the physician.
4. Shoulder dystocia, uterine tachysystole complicate vaginal delivery
WITH MILD PRE-ECLAMPSIA and vaginal spotting, a woman was admitted to a hospital’s L&D unit. Dinoprostone was administered, but the fetus was unengaged. Oxytocin was added to induce labor. Labor was complicated by repeated tachysystole; prolonged dilation; prolonged descent; severe, prolonged decelerations; and tachycardia. Uterine tachysystole continued for extended periods. Vaginal delivery was complicated by shoulder dystocia, which took 2 minutes to resolve. The child was delivered without a heart rate or respirations. A heartbeat was obtained a minute after delivery, and Apgar scores were 0, 2, and 2. The child was given a diagnosis of hypoxic ischemic encephalopathy, cerebral palsy, and a seizure disorder.
PATIENT’S CLAIM The L&D nurses and physicians were negligent in failing to properly monitor labor progression, fetal heart rate, and oxytocin management. They failed to communicate with the woman’s ObGyn, and did not exercise the proper chain of command. The physicians failed to recommend a cesarean delivery when labor became complicated.
DEFENDANTS’ DEFENSE The patient’s treatment was appropriate. Brain damage did not occur during labor and delivery.
VERDICT A $3.55 million Idaho verdict was returned.
5. Fetus transverse; oxytocin given
A WOMAN ARRIVED AT THE HOSPITAL after her membranes ruptured. A first-year resident failed to realize that the fetus was in a transverse position, and, with the attending physician’s approval, ordered oxytocin. When vaginal bleeding began, it was suspected that the placenta had detached. An hour later, after vaginal bleeding increased and late decelerations were noted on the fetal heart monitor, cesarean delivery was performed. The child was given a diagnosis of cerebral palsy and other complications, and died at 16 months of age.
ESTATE’S CLAIM The use of oxytocin is contraindicated for a baby in a transverse position. The fetus’ position indicated a need for a cesarean delivery. Placental detachment was not promptly addressed, leading to fetal oxygen deprivation.
DEFENDANTS’ DEFENSE The fetus appeared to be fine under all objective criteria until a “softball-sized” clot emerged from the mother’s vagina. The attending physician came to the mother’s bedside at that time. Umbilical cord blood gases showed no evidence of acidosis. A fetal brain injury occurred prior to the mother’s arrival at the hospital.
VERDICT A $2.5 million Pennsylvania verdict was returned.
- Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
DURING PRENATAL CARE, a woman repeatedly complained of severe discomfort, and requested a cesarean delivery. The ObGyn’s charts did not note her complaints.
A first-year resident and nurse covered for the ObGyn because he did not arrive at the hospital for hours after the mother notified him she was in labor. When shoulder dystocia was encountered, the resident used the McRoberts maneuver. The ObGyn arrived a minute before the birth. The baby weighed 10 lbs. The mother suffered symphysis pubis diastasis, required several surgeries, and now uses a cane to walk.
PATIENT’S CLAIM The ObGyn was negligent in not arriving in time to deliver the baby. The mother’s pelvis was injured during the McRoberts maneuver. The baby’s size was not properly estimated.
PHYSICIAN’S DEFENSE The use of the resident’s care was appropriate, as this was a teaching hospital.
VERDICT A $5.5 million New York verdict was returned.
Cancer Dx “not timely”; additional tx required
IN JUNE 2000, AN OBGYN PALPATED a pelvic mass in a postmenopausal woman. After ultrasonography (US) in August 2000, the ObGyn told the woman that a uterine fibroid had been found but no further testing was needed. In December 2001, US revealed that the mass had enlarged, but no further testing was done. In May 2002, the patient reported fatigue, distention of her abdomen, and an increase in the frequency of urination.
In July 2002, the ObGyn removed a 3-lb malignant uterine tumor during hysterectomy. A second staging surgery was performed, and the patient underwent chemotherapy.
PATIENT’S CLAIM An earlier diagnosis would have reduced the amount of treatment required. The ObGyn should have reacted immediately when the mass was first palpated in June 2000 and found on US in August 2000, as postmenopausal women do not develop uterine fibroids. A gynecologic oncologist should have been present at the hysterectomy to perform concurrent staging.
PHYSICIAN’S DEFENSE The patient failed to report symptoms that suggested cancer for 10 months; a prompt response was made when symptoms were revealed. It was appropriate to accept the results of US regarding a uterine fibroid.
VERDICT A $1.25 million New York verdict was returned.
Abnormal thickness of fetal nuchal fold
WHEN A 31-YEAR-OLD WOMAN was 18 weeks’ pregnant, she underwent ultrasonography, which was reportedly normal. The child was born with Down syndrome.
PATIENT’S CLAIM The ObGyn and radiologist failed to detect an abnormal thickness in the fetal nuchal fold—often a sign of Down syndrome.
PHYSICIANS’ DEFENSE The sonogram was properly analyzed. A thickened fold is an unreliable indicator of Down syndrome.
VERDICT A $1.7 million New Jersey settlement was returned.
Ovary retained; cancer recurs; death
A WOMAN UNDERWENT SURGERY for ovarian cancer in July 2004. She died of ovarian cancer in 2008 at age 59.
ESTATE’S CLAIM The gynecologist did not tell the patient that only one ovary was removed, or that a pathologist had not found the second ovary in the specimen. Ovarian cancer developed in the retained ovary a few years later. She would have undergone additional surgery had she known the second ovary was still there.
PHYSICIAN’S DEFENSE Both ovaries were removed in July 2004. The left ovary was not found during an autopsy performed on the decedent.
VERDICT A $1.967 million Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
1. Severe birth asphyxia: cerebral palsy and seizures
AFTER A NORMAL PREGNANCY, a woman went to the hospital in labor. Her ObGyn, Dr. A, went off duty at 4 PM and was replaced by Dr. B, a practice partner who delivered five other babies between 11 PM and 2:15 AM.
At 9:40 PM, the fetus was occiput posterior. At 12:31 AM, Dr. B attempted manual rotation; no exam was recorded in the chart. By 2:30 AM, the fetus had returned to the occiput posterior position, and Dr. B again tried manual rotation. Then he left to take a nap while the mother’s epidural was reinforced. There was a delay in achieving a satisfactory epidural, and Dr. B was not called back to the bedside until 4 AM. He decided to perform a cesarean delivery when the fetal heart monitor showed an increased baseline with persistent variable decelerations.
Although Dr. B had called Dr. A earlier to elicit her help with the cesarean, she had gone back to bed and was not prepared to assist. During a 30-minute delay, the electronic fetal monitor was disconnected and never reconnected. A nurse checked the fetal heart rate with ultrasonography, and reported that it was normal; however, there was no copy in the chart.
The incision was made at 4:33 AM, and the baby was delivered at 5:06 AM. The infant was born without a heart rate or respiration (Apgar scores, all 0). A neonatologist was not available for resuscitation; a neonatal nurse practitioner arrived 7 minutes after delivery. The baby finally had a heart rate 24 minutes after delivery. The child suffered severe birth asphyxia, causing athetoid and spastic cerebral palsy and seizures.
PATIENT’S CLAIM The ObGyn failed to deliver the baby in a timely manner. The fetus was not continuously monitored with a fetal scalp electrode. The nurse violated several hospital policies.
DEFENDANTS’ DEFENSE The baby suffered an acute, total cord occlusion minutes before birth; this was unpredictable and the injuries could not have been prevented.
VERDICT At the end of the discovery period, the defendants’ attorney withdrew and new attorneys sought to name new experts. While these issues were pending, the matter was settled for a Washington total of $20 million. The mother settled with the hospital for $9.85 million. Although the doctors’ group had $5 million in insurance coverage, the plaintiff demanded that the insurance company pay in excess of limits due to potential bad-faith claims. The insurance company ultimately paid $10.15 million.
2. Profound metabolic acidosis after emergent delivery
WHEN A WOMAN WAS 2 CM DILATED and 99% effaced, she was given dinoprostone and oxytocin to begin induction and augment labor. Oxytocin was continued even though her pattern of contractions showed tachysystole. An intrauterine pressure catheter that had been placed to assess contractions was removed. Monitoring revealed an elevated fetal heart rate at 170 to 180 bpm. Ten minutes before birth, the fetal heart tracing ended; a sonogram showed fetal bradycardia and prompted an emergency vacuum extraction.
The baby was floppy at birth, did not cry, and was intubated and transferred to the NICU. Apgar scores were 1, 3, and 5 at 1, 5, and 10 minutes. The umbilical cord gas had a venous pH of 6.637, indicative of profound acidosis. Ongoing hypoxia and anoxia resulted in massive and irreversible brain injury. An EEG at 5 days confirmed the presence of encephalopathy due to perinatal asphyxia. The child will require specialized treatment and attendant care for life.
PATIENT’S CLAIM Oxytocin was never stopped or reduced throughout labor and delivery. The ObGyn failed to promptly deliver the baby. No internal scalp electrode was used to directly monitor the fetus; the intrauterine pressure catheter was never replaced.
DEFENDANTS’ DEFENSE The ObGyn and hospital denied negligence or causation, claiming that there was a sudden placental abruption 10 minutes before birth that caused perinatal asphyxia.
VERDICT A $6.95 million District of Columbia settlement was returned.
3. Breech 2nd twin has cerebral palsy
PREGNANT WITH TWINS and in early labor, a woman went to the hospital, where a nurse midwife administered dinoprostone. The labor and delivery nurses only monitored one fetal heart rate during most of the labor period. The mother’s contraction pattern was indicative of tachysystole, and the twin who was being monitored showed a decelerating heart rate. The ObGyn arrived minutes before the birth unprepared for delivery, and a nurse delivered a healthy first child.
The second child’s heart rate dropped to 90 bpm, and the baby shifted to a breech position; the ObGyn tried manual rotation but was unsuccessful. After 20 minutes, cesarean delivery was performed. The boy was born with signs of metabolic acidosis and suffered a seizure 2 hours later. He was given a diagnosis of cerebral palsy and is fed through a tube, cannot speak, and requires skilled nursing care.
PATIENT’S CLAIM The ObGyn and nurses were negligent in only monitoring one fetus, and for failing to perform cesarean delivery in a timely manner.
DEFENDANTS’ DEFENSE The ObGyn claimed he was not informed of the decelerations shown on the fetal monitor, nor of the mother’s rapidly progressing labor. The hospital maintained that the nurses had given the ObGyn proper information and that the injuries to the infant had occurred after the ObGyn’s arrival. The mother’s weight of 322 pounds made monitoring difficult during labor and delivery.
VERDICT A $21,573,993 Pennsylvania verdict was returned against the hospital; a defense verdict was returned for the physician.
4. Shoulder dystocia, uterine tachysystole complicate vaginal delivery
WITH MILD PRE-ECLAMPSIA and vaginal spotting, a woman was admitted to a hospital’s L&D unit. Dinoprostone was administered, but the fetus was unengaged. Oxytocin was added to induce labor. Labor was complicated by repeated tachysystole; prolonged dilation; prolonged descent; severe, prolonged decelerations; and tachycardia. Uterine tachysystole continued for extended periods. Vaginal delivery was complicated by shoulder dystocia, which took 2 minutes to resolve. The child was delivered without a heart rate or respirations. A heartbeat was obtained a minute after delivery, and Apgar scores were 0, 2, and 2. The child was given a diagnosis of hypoxic ischemic encephalopathy, cerebral palsy, and a seizure disorder.
PATIENT’S CLAIM The L&D nurses and physicians were negligent in failing to properly monitor labor progression, fetal heart rate, and oxytocin management. They failed to communicate with the woman’s ObGyn, and did not exercise the proper chain of command. The physicians failed to recommend a cesarean delivery when labor became complicated.
DEFENDANTS’ DEFENSE The patient’s treatment was appropriate. Brain damage did not occur during labor and delivery.
VERDICT A $3.55 million Idaho verdict was returned.
5. Fetus transverse; oxytocin given
A WOMAN ARRIVED AT THE HOSPITAL after her membranes ruptured. A first-year resident failed to realize that the fetus was in a transverse position, and, with the attending physician’s approval, ordered oxytocin. When vaginal bleeding began, it was suspected that the placenta had detached. An hour later, after vaginal bleeding increased and late decelerations were noted on the fetal heart monitor, cesarean delivery was performed. The child was given a diagnosis of cerebral palsy and other complications, and died at 16 months of age.
ESTATE’S CLAIM The use of oxytocin is contraindicated for a baby in a transverse position. The fetus’ position indicated a need for a cesarean delivery. Placental detachment was not promptly addressed, leading to fetal oxygen deprivation.
DEFENDANTS’ DEFENSE The fetus appeared to be fine under all objective criteria until a “softball-sized” clot emerged from the mother’s vagina. The attending physician came to the mother’s bedside at that time. Umbilical cord blood gases showed no evidence of acidosis. A fetal brain injury occurred prior to the mother’s arrival at the hospital.
VERDICT A $2.5 million Pennsylvania verdict was returned.
- Does the use of multiple maneuvers in the management of shoulder dystocia increase the risk of neonatal injury?
Robert B. Gherman, MD (Examining the Evidence, August 2011)
We want to hear from you! Tell us what you think.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: Another E-Prescribing Update
You're probably tired of reading about electronic prescribing by now, and I really thought I was done writing about it for the year when I summarized the "final" 2011 rules.
Now, however, CMS has proposed further rule modifications in the spirit, they say, of working with physicians to encourage the wider use of e-prescribing technology.
In order to qualify for the 2011 incentive, the rules required you to send at least 10 electronic Medicare or Medicaid prescriptions by the end of June (and report them to CMS using the G8553 code by the end of July), followed by a minimum of 15 more by the end of the year.
So if you missed the June deadline, you are ineligible for the 2011 incentive no matter what you do in the second half of 2011. But you can use the remainder of the year to prepare for 2012, the first year that failing to e-prescribe will incur a 1% penalty against Medicare/Medicaid payments. (In 2013 the penalty increases to 1.5%, and then to 2% in 2014 and beyond.)
Practices in rural areas, those without high-speed Internet access, and those lacking a sufficient number of pharmacies equipped to accept electronic prescriptions may apply for exemptions.
Now, CMS has proposed additional exemption opportunities for practices that write very few prescriptions, and those that write large numbers of prescriptions for drugs that cannot, by law, be prescribed electronically (such as most narcotics).
Offices that see very few Medicare or Medicaid patients can still qualify for the incentive if at least 10% of their Medicare Part B claims involve an electronic prescription.
As I mentioned previously, many electronic health record systems do not satisfy e-prescribing requirements because the prescription software simply generates faxes that arrive, on paper, in the pharmacy's fax machine.
Under the proposed new rules, however, any certified electronic health records (EHR) system would be considered a "qualified" e-prescribing system, even those that don’t send prescriptions electronically. (The government's other major goal, after all, is to increase EHR usage.)
To be clear, manual faxing of prescriptions to pharmacies will still not qualify as e-prescribing, which remains, by definition, computer-to-computer (paperless) communication of prescriptions. If you don’t have a qualified EHR, you will still need to use a qualified stand-alone e-prescribing system.
Either way, the e-prescribing G-code must be submitted with a line-item charge of zero dollars ($0.00) at the time the associated covered service is billed. Those line items will be denied for payment, but are passed through the claims processing system to the National Claims History database (NCH), which will keep track of your e-prescribing usage.
Fortunately, a coalition of insurance and technology companies called the National e-Prescribing Patient Safety Initiative (NEPSI) has made it quite easy to acquire free qualified e-prescribing technology. Setup methods vary, but the concepts and requirements for each company are generally similar. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
NEPSI has also encouraged pharmacies to make themselves compatible, and about 75% of them can now handle electronic prescriptions.
Keep in mind that this will not be a complete transition; once you’re set up, you cannot throw away your paper prescription pads.
Beside the pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective websites, can be found at eprescribing.info.
Next year will be pivotal for electronic prescribing: If you are a Medicare or Medicaid participator you will either have to take the plunge or incur a penalty. However, with the free NEPSI program and only 25 e-prescriptions required over the course of an entire year, you can try out the technology with minimal cost and inconvenience.
You're probably tired of reading about electronic prescribing by now, and I really thought I was done writing about it for the year when I summarized the "final" 2011 rules.
Now, however, CMS has proposed further rule modifications in the spirit, they say, of working with physicians to encourage the wider use of e-prescribing technology.
In order to qualify for the 2011 incentive, the rules required you to send at least 10 electronic Medicare or Medicaid prescriptions by the end of June (and report them to CMS using the G8553 code by the end of July), followed by a minimum of 15 more by the end of the year.
So if you missed the June deadline, you are ineligible for the 2011 incentive no matter what you do in the second half of 2011. But you can use the remainder of the year to prepare for 2012, the first year that failing to e-prescribe will incur a 1% penalty against Medicare/Medicaid payments. (In 2013 the penalty increases to 1.5%, and then to 2% in 2014 and beyond.)
Practices in rural areas, those without high-speed Internet access, and those lacking a sufficient number of pharmacies equipped to accept electronic prescriptions may apply for exemptions.
Now, CMS has proposed additional exemption opportunities for practices that write very few prescriptions, and those that write large numbers of prescriptions for drugs that cannot, by law, be prescribed electronically (such as most narcotics).
Offices that see very few Medicare or Medicaid patients can still qualify for the incentive if at least 10% of their Medicare Part B claims involve an electronic prescription.
As I mentioned previously, many electronic health record systems do not satisfy e-prescribing requirements because the prescription software simply generates faxes that arrive, on paper, in the pharmacy's fax machine.
Under the proposed new rules, however, any certified electronic health records (EHR) system would be considered a "qualified" e-prescribing system, even those that don’t send prescriptions electronically. (The government's other major goal, after all, is to increase EHR usage.)
To be clear, manual faxing of prescriptions to pharmacies will still not qualify as e-prescribing, which remains, by definition, computer-to-computer (paperless) communication of prescriptions. If you don’t have a qualified EHR, you will still need to use a qualified stand-alone e-prescribing system.
Either way, the e-prescribing G-code must be submitted with a line-item charge of zero dollars ($0.00) at the time the associated covered service is billed. Those line items will be denied for payment, but are passed through the claims processing system to the National Claims History database (NCH), which will keep track of your e-prescribing usage.
Fortunately, a coalition of insurance and technology companies called the National e-Prescribing Patient Safety Initiative (NEPSI) has made it quite easy to acquire free qualified e-prescribing technology. Setup methods vary, but the concepts and requirements for each company are generally similar. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
NEPSI has also encouraged pharmacies to make themselves compatible, and about 75% of them can now handle electronic prescriptions.
Keep in mind that this will not be a complete transition; once you’re set up, you cannot throw away your paper prescription pads.
Beside the pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective websites, can be found at eprescribing.info.
Next year will be pivotal for electronic prescribing: If you are a Medicare or Medicaid participator you will either have to take the plunge or incur a penalty. However, with the free NEPSI program and only 25 e-prescriptions required over the course of an entire year, you can try out the technology with minimal cost and inconvenience.
You're probably tired of reading about electronic prescribing by now, and I really thought I was done writing about it for the year when I summarized the "final" 2011 rules.
Now, however, CMS has proposed further rule modifications in the spirit, they say, of working with physicians to encourage the wider use of e-prescribing technology.
In order to qualify for the 2011 incentive, the rules required you to send at least 10 electronic Medicare or Medicaid prescriptions by the end of June (and report them to CMS using the G8553 code by the end of July), followed by a minimum of 15 more by the end of the year.
So if you missed the June deadline, you are ineligible for the 2011 incentive no matter what you do in the second half of 2011. But you can use the remainder of the year to prepare for 2012, the first year that failing to e-prescribe will incur a 1% penalty against Medicare/Medicaid payments. (In 2013 the penalty increases to 1.5%, and then to 2% in 2014 and beyond.)
Practices in rural areas, those without high-speed Internet access, and those lacking a sufficient number of pharmacies equipped to accept electronic prescriptions may apply for exemptions.
Now, CMS has proposed additional exemption opportunities for practices that write very few prescriptions, and those that write large numbers of prescriptions for drugs that cannot, by law, be prescribed electronically (such as most narcotics).
Offices that see very few Medicare or Medicaid patients can still qualify for the incentive if at least 10% of their Medicare Part B claims involve an electronic prescription.
As I mentioned previously, many electronic health record systems do not satisfy e-prescribing requirements because the prescription software simply generates faxes that arrive, on paper, in the pharmacy's fax machine.
Under the proposed new rules, however, any certified electronic health records (EHR) system would be considered a "qualified" e-prescribing system, even those that don’t send prescriptions electronically. (The government's other major goal, after all, is to increase EHR usage.)
To be clear, manual faxing of prescriptions to pharmacies will still not qualify as e-prescribing, which remains, by definition, computer-to-computer (paperless) communication of prescriptions. If you don’t have a qualified EHR, you will still need to use a qualified stand-alone e-prescribing system.
Either way, the e-prescribing G-code must be submitted with a line-item charge of zero dollars ($0.00) at the time the associated covered service is billed. Those line items will be denied for payment, but are passed through the claims processing system to the National Claims History database (NCH), which will keep track of your e-prescribing usage.
Fortunately, a coalition of insurance and technology companies called the National e-Prescribing Patient Safety Initiative (NEPSI) has made it quite easy to acquire free qualified e-prescribing technology. Setup methods vary, but the concepts and requirements for each company are generally similar. In most cases, all you need to get started is an Internet-enabled computer with a high-speed connection and a database of patients.
NEPSI has also encouraged pharmacies to make themselves compatible, and about 75% of them can now handle electronic prescriptions.
Keep in mind that this will not be a complete transition; once you’re set up, you cannot throw away your paper prescription pads.
Beside the pharmacies not yet equipped for e-prescribing, the Drug Enforcement Administration strongly discourages sending controlled substance prescriptions electronically. (The DEA has, however, relaxed its rules somewhat on this issue in the past year.)
A nonprofit foundation called eHealth Initiative has released an excellent guide for physicians on e-prescribing.
A list of other companies currently offering e-prescribing software, along with links to their respective websites, can be found at eprescribing.info.
Next year will be pivotal for electronic prescribing: If you are a Medicare or Medicaid participator you will either have to take the plunge or incur a penalty. However, with the free NEPSI program and only 25 e-prescriptions required over the course of an entire year, you can try out the technology with minimal cost and inconvenience.
Managing Your Dermatology Practice: Payers Who Renege
My column on prior authorization seems to have struck a nerve. Almost a year later, I'm still getting notes and e-mails echoing my complaints, and favoring our strategy of assigning patients the task of obtaining prior authorization forms, since the dispute is between the patient and the insurer.
Several correspondents brought up the more serious issue of insurers who grant an authorization, then change their minds after the fact.
A colleague here on the East Coast described his own reductio ad absurdum experience, the worst-case scenario: Two insurers paid all of his claims for intense pulsed light (IPL) treatment for rosacea for more than a year. Then, without warning, they not only ceased paying for the procedure, but demanded that all payments already made for IPL be returned!
After a protracted exchange involving the AMA and the AAD Coding Task Force, the insurers backed down on their refund demands. However, they stood by their refusal to pay any IPL claims going forward.
Some third-party nightmares are unavoidable, but a little vigilance can prevent many of them. For one thing, don't cave to patients who insist that you submit a charge that you know (or strongly suspect) will not be covered in the first place.
I tell such patients they are welcome to submit the claim themselves, but I cannot tell their insurer that a treatment was medically necessary if it was not.
When a payer authorizes payment and then reneges, be ready with a solid counterattack.
First, check the laws in your state; many have statutes specifically forbidding such practices. In my state, for example, if a patient's benefits are subject to return or reduction, or if coverage is contingent on further investigation, providers must be informed of that in advance. Absent such prior warning, any reneging is unlawful.
In California, once an insurer authorizes treatment, it cannot be rescinded or modified "after the physician renders the service in good faith and pursuant to the authorization for any reason, including, but not limited to, the plan's subsequent determination that it did not make an accurate determination of the enrollee's or subscriber's eligibility" (Health and Safety Code 1371.8, Insurance Code 796.04).
Plainly stated, care that has been authorized must be paid, even if the payer made a mistake and the patient was not covered for the specific services provided. The California Code of Regulations has a nearly identical provision (28 CCR 1300.71 [a][8][T]).
There is precedent in federal law as well: In Meadows v. Employers Health Insurance, the court ruled that eligibility, once verified, cannot later be rescinded, as "plans are not insulated from the consequences of their own misrepresentations" to providers.
When a payer violates local or federal statutes, don't hesitate to call them on it. And don't hesitate to report them to appropriate government agencies if they won't comply.
Meanwhile, start looking ahead toward some long-range solutions to the burgeoning prior authorization problem.
If you have the ear of a state or federal legislator, discuss it with him or her. Explain how much time your staff wastes jumping through insurers' hoops to the detriment of your patients and at high cost to you, for the sole, undeserved benefit of payers.
Explain the predicament of patients on effective, stable treatment for a chronic condition that will never resolve, who are forced to repeat the entire preauthorization rigamarole every few months.
Obviously, there is no medical or common-sense justification for such rationing by inconvenience. A "one and done" law, stating that once a medication is authorized, it remains authorized unless or until the patient's medical status changes, would be a simple solution to a major problem.
And while you're at it, raise your voice against "step therapy" or "fail first" requirements, where patients must fail one or more cheap, ineffective medications before getting the one they need.
Such policies place the insurer's medical judgment ahead of the physician's, and some states are introducing laws to prohibit it. New Jersey now forbids step therapy for pain treatment, and California and other states are considering legislation that would outlaw it in any form.
My column on prior authorization seems to have struck a nerve. Almost a year later, I'm still getting notes and e-mails echoing my complaints, and favoring our strategy of assigning patients the task of obtaining prior authorization forms, since the dispute is between the patient and the insurer.
Several correspondents brought up the more serious issue of insurers who grant an authorization, then change their minds after the fact.
A colleague here on the East Coast described his own reductio ad absurdum experience, the worst-case scenario: Two insurers paid all of his claims for intense pulsed light (IPL) treatment for rosacea for more than a year. Then, without warning, they not only ceased paying for the procedure, but demanded that all payments already made for IPL be returned!
After a protracted exchange involving the AMA and the AAD Coding Task Force, the insurers backed down on their refund demands. However, they stood by their refusal to pay any IPL claims going forward.
Some third-party nightmares are unavoidable, but a little vigilance can prevent many of them. For one thing, don't cave to patients who insist that you submit a charge that you know (or strongly suspect) will not be covered in the first place.
I tell such patients they are welcome to submit the claim themselves, but I cannot tell their insurer that a treatment was medically necessary if it was not.
When a payer authorizes payment and then reneges, be ready with a solid counterattack.
First, check the laws in your state; many have statutes specifically forbidding such practices. In my state, for example, if a patient's benefits are subject to return or reduction, or if coverage is contingent on further investigation, providers must be informed of that in advance. Absent such prior warning, any reneging is unlawful.
In California, once an insurer authorizes treatment, it cannot be rescinded or modified "after the physician renders the service in good faith and pursuant to the authorization for any reason, including, but not limited to, the plan's subsequent determination that it did not make an accurate determination of the enrollee's or subscriber's eligibility" (Health and Safety Code 1371.8, Insurance Code 796.04).
Plainly stated, care that has been authorized must be paid, even if the payer made a mistake and the patient was not covered for the specific services provided. The California Code of Regulations has a nearly identical provision (28 CCR 1300.71 [a][8][T]).
There is precedent in federal law as well: In Meadows v. Employers Health Insurance, the court ruled that eligibility, once verified, cannot later be rescinded, as "plans are not insulated from the consequences of their own misrepresentations" to providers.
When a payer violates local or federal statutes, don't hesitate to call them on it. And don't hesitate to report them to appropriate government agencies if they won't comply.
Meanwhile, start looking ahead toward some long-range solutions to the burgeoning prior authorization problem.
If you have the ear of a state or federal legislator, discuss it with him or her. Explain how much time your staff wastes jumping through insurers' hoops to the detriment of your patients and at high cost to you, for the sole, undeserved benefit of payers.
Explain the predicament of patients on effective, stable treatment for a chronic condition that will never resolve, who are forced to repeat the entire preauthorization rigamarole every few months.
Obviously, there is no medical or common-sense justification for such rationing by inconvenience. A "one and done" law, stating that once a medication is authorized, it remains authorized unless or until the patient's medical status changes, would be a simple solution to a major problem.
And while you're at it, raise your voice against "step therapy" or "fail first" requirements, where patients must fail one or more cheap, ineffective medications before getting the one they need.
Such policies place the insurer's medical judgment ahead of the physician's, and some states are introducing laws to prohibit it. New Jersey now forbids step therapy for pain treatment, and California and other states are considering legislation that would outlaw it in any form.
My column on prior authorization seems to have struck a nerve. Almost a year later, I'm still getting notes and e-mails echoing my complaints, and favoring our strategy of assigning patients the task of obtaining prior authorization forms, since the dispute is between the patient and the insurer.
Several correspondents brought up the more serious issue of insurers who grant an authorization, then change their minds after the fact.
A colleague here on the East Coast described his own reductio ad absurdum experience, the worst-case scenario: Two insurers paid all of his claims for intense pulsed light (IPL) treatment for rosacea for more than a year. Then, without warning, they not only ceased paying for the procedure, but demanded that all payments already made for IPL be returned!
After a protracted exchange involving the AMA and the AAD Coding Task Force, the insurers backed down on their refund demands. However, they stood by their refusal to pay any IPL claims going forward.
Some third-party nightmares are unavoidable, but a little vigilance can prevent many of them. For one thing, don't cave to patients who insist that you submit a charge that you know (or strongly suspect) will not be covered in the first place.
I tell such patients they are welcome to submit the claim themselves, but I cannot tell their insurer that a treatment was medically necessary if it was not.
When a payer authorizes payment and then reneges, be ready with a solid counterattack.
First, check the laws in your state; many have statutes specifically forbidding such practices. In my state, for example, if a patient's benefits are subject to return or reduction, or if coverage is contingent on further investigation, providers must be informed of that in advance. Absent such prior warning, any reneging is unlawful.
In California, once an insurer authorizes treatment, it cannot be rescinded or modified "after the physician renders the service in good faith and pursuant to the authorization for any reason, including, but not limited to, the plan's subsequent determination that it did not make an accurate determination of the enrollee's or subscriber's eligibility" (Health and Safety Code 1371.8, Insurance Code 796.04).
Plainly stated, care that has been authorized must be paid, even if the payer made a mistake and the patient was not covered for the specific services provided. The California Code of Regulations has a nearly identical provision (28 CCR 1300.71 [a][8][T]).
There is precedent in federal law as well: In Meadows v. Employers Health Insurance, the court ruled that eligibility, once verified, cannot later be rescinded, as "plans are not insulated from the consequences of their own misrepresentations" to providers.
When a payer violates local or federal statutes, don't hesitate to call them on it. And don't hesitate to report them to appropriate government agencies if they won't comply.
Meanwhile, start looking ahead toward some long-range solutions to the burgeoning prior authorization problem.
If you have the ear of a state or federal legislator, discuss it with him or her. Explain how much time your staff wastes jumping through insurers' hoops to the detriment of your patients and at high cost to you, for the sole, undeserved benefit of payers.
Explain the predicament of patients on effective, stable treatment for a chronic condition that will never resolve, who are forced to repeat the entire preauthorization rigamarole every few months.
Obviously, there is no medical or common-sense justification for such rationing by inconvenience. A "one and done" law, stating that once a medication is authorized, it remains authorized unless or until the patient's medical status changes, would be a simple solution to a major problem.
And while you're at it, raise your voice against "step therapy" or "fail first" requirements, where patients must fail one or more cheap, ineffective medications before getting the one they need.
Such policies place the insurer's medical judgment ahead of the physician's, and some states are introducing laws to prohibit it. New Jersey now forbids step therapy for pain treatment, and California and other states are considering legislation that would outlaw it in any form.
How High Can Your Support Payments Go?
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
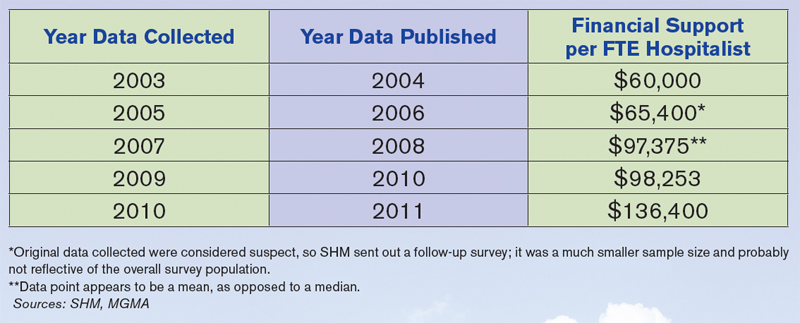
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.

—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”

—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?

When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.
—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”
—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?
When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ
Last December, St. Peter’s Hospital, a 122-bed acute-care facility in Helena, Mont., crossed a symbolic line in the decade-long evolution of the financial payments that hospitals have provided to HM groups to make up the gap that exists between the expenses of running a hospitalist service and the professional fees that generate its revenue.
Hospital administrators asked the outpatient providers at the Helena Physicians’ Clinic to pay nearly $400,000 per year to support the in-house HM service at St. Peter’s, according to a series of stories in the local paper, the Helena Independent Record. The fee was never instituted and, in fact, some Helena patients and physicians have questioned whether the high-stakes payment was part of a broader campaign for the hospital to take over the clinic, a process that culminated in March with the hospital’s purchase of the clinic’s building.
Still, the Montana case focused a spotlight on the doughnut hole of HM ledger sheets: hospital subsidies. More than 80% of HM groups took financial support from their host institutions in fiscal year 2010, according to new data from SHM and the Medical Group Management Association (MGMA), which will be released in September. And the amount of that support has more than doubled, from $60,000 per full-time equivalent (FTE) in 2003-2004 to $136,400 per FTE in the latest data, according to a presentation at HM11 in May.
HM leaders agree the growth is unsustainable, particularly in the new world of healthcare reform, but they also concur that satisfaction with the benefits a hospitalist service offers make it unlikely other institutions will implement a fee-for-service system similar to that of St. Peter’s (see “Pay to Play?,” p. 38). As hospital administrators struggle to dole out pieces of their ever-shrinking financial pie, hospitalists also agree that they will find it more and more difficult to ask their C-suite for continually larger payments (see Figure 1, “Growth in Hospitalist Financial Support,” p. 37). Even when portrayed as “investments” in physicians that provide more than clinical care (e.g. hospitalists assuming leadership roles on hospital committees and pushing quality-improvement initiatives), a hospital’s bottom line can only afford so much.
“It’s not sustainable,” says Burke Kealey, MD, SFHM, medical director of hospital specialties at HealthPartners in Minneapolis and an SHM board member. “I think hospitals are pretty much tapped out by and large.
“What we’ve been seeing is practices have been able to ramp up their productivity, but people have also found other revenue streams, be it perioperative clinics, be it trying to find direct subsidies from specialty practices, be it educational funds for teaching. … We’re kind of entering a time when payment reform of some sort is going to have to come into play.”
History Lesson
Support payments have been around since HM’s earliest days, Dr. Kealey says. From the outset, it was difficult for most practices to cover their own salaries and expenses with reimbursement to the charges that make up the bulk of the field’s billing opportunities. “The economics of the situation are such that it is pretty difficult for a hospitalist to cover their own salary with the standard E/M codes,” he adds.
Hospitals, though, quickly realized that hospitalist practices were a valuable presence and created a payment stream to help offset the difference.
John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn., says four main factors drive the need for the hospitalist subsidy:
- Physician productivity. How many patients can a practice see on a daily or a monthly basis? Most averages teeter between 15 and 20 patients per day, often less in academic models. There is a mathematical point at which a group can generate enough revenue to cover costs, but many HM leaders say that comes at the cost of quality care delivery and physician satisfaction.
- Nonclinical/non-revenue-generating activities performed by hospitalists. HM groups usually are involved in QI and patient-safety initiatives, which, while important, are not necessarily captured by billing codes. Some HM contracts call for compensation tied to those activities, but many still do not, leaving groups with a gap to cover.
- Payor mix. A particularly difficult mix with high charity care and uninsured patients can lower the average net collected revenue per visit. There also is the choice between being a Medicaid participating provider or a nonparticipating provider with managed-care payors. So-called “non-par” providers typically have the ability to negotiate higher rates.
- Expenses. “How rich is your benefit package for your physicians?” Laverty asks. “Do you provide a retirement plan? Health, dental and vision? … Do you pay for CME?”
Dr. Kealey says it’s not “impossible” to cover all of a hospitalist’s costs through professional fees; however, “it usually requires a hospitalist be in an area with a very good payor mix or a hospital of very high efficiency, where they can see lots of patients. And often, there might be a setup where they aren’t covering unproductive times or tasks.”
Another Point of View
Not everyone thinks the subsidy is a fait accompli. Jeff Taylor, president and chief operating officer of IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif., says subsidies do not need to be a factor in a practice’s bottom line. Taylor says that IPC generates just 5% of its revenues from subsidies, with the remaining 95% financed by professional fees.
He attributes much of that to the work schedule, particularly the popular model of seven days on clinical duty followed by seven days off. He says that model has led to increased practice costs that then require financial support from their hospital. The schedule’s popularity is fueled by the balance it offers physicians between their work and personal lives, Taylor says, but it also means that practitioners working under it lose two weeks a month of billing opportunities.
He’s right about the popularity, as more than 70% of hospitalist groups use a shift-based staffing model, according to the State of Hospital Medicine: 2010 Report Based on 2009 Data. The number of HM groups employing call-based and hybrid coverage (some shift, some call) is 30%.
—Todd Nelson, MBA, technical director, Healthcare Financial Management Association, Chicago
“There is nothing else inherent in hospital medicine that makes this expensive, other than scheduling,” Taylor says. “Absent a very difficult payor mix, it’s the scheduling and the number of days worked that drives the cost. … We have been saying that for years, but we haven’t seen much of a waver yet. Once hospitals realize—some of them are starting to get it—that it’s the underlying work schedule that drives cost, they’re not going to continue to do it.”
Todd Nelson, MBA, a technical director at the Healthcare Financial Management Association in Chicago, agrees that the upward trajectory of hospital support payments will have to end, likely in concert with the expected payment reform of the next five years. But, he adds, the mere fact that hospital administrators have allowed the payments to double suggests that they view the support as an investment. In return for that money, though, C-suite members should contract for and then demand adherence to performance measures, he notes.
“Many specialties say, ‘We’re valuable; help us out,’ ” says Nelson, a former chief financial officer at Grinnell Regional Medical Center in Iowa. “In the hospital world, you can’t just ‘help out.’ They need to be providing a service you’re paying them for.”
SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, could not agree more. “The way I view monies that are sent to a group for nonclinical work is exactly that,” he says. “It’s compensation for nonclinical work. Subsidy, to me, seems to mean that despite whatever you’re doing, you need some more to pay because you can’t make your ends meet. That’s not true. What that figure is, for my group and for the vast majority of groups in this country, is really compensation for nonclinical efforts.”
HM groups should take it upon themselves to discuss their value contribution with their chief financial officer, as many in that position view hospitalist services as a “cost center” rather than as a means to the end of better financial performance for the institution as a whole, says Beth Hawley, senior vice president with Brentwood, Tenn.-based Cogent HMG.
“You need to look at it from the viewpoint of your CFO,” she says. “It is really important to educate your CFO on the myriad ways that your hospitalist program can create value for the hospital.”
—Jeff Taylor, president, COO, IPC: The Hospitalist Co., North Hollywood, Calif.
Hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa., says such education should highlight the intangible values of HM services, but it also needs to include firm, eye-opening data points. Put another way: “Have true ROI [return on investment], not soft ROI,” he says.
Dr. Bulger suggests pointing out that what some call a subsidy, he views as simply a payment, no different from the lump-sum check a hospital or healthcare system might cut for the group running its ED, or the check it writes for a cardiology specialty.
“There’s a subsidy for all those groups, but it’s never been looked at as a subsidy,” he adds. “But from a business perspective, it’s the same thing.”
The Future of Support
The relative value, justification, and existence of the support aside, the question remains: What is its future?
“Subsidies are not going to go away, because you can’t recruit and retain physicians in this environment for the most part without them,” says Troy Ahlstrom, MD, SFHM, CFO of Hospitalists of Northern Michigan, a hospitalist-owned and -managed group based in Traverse City. “Especially not when physicians coming out of residency have a desire to maintain a reasonable work and personal life, with fewer shifts where possible, fewer patients per shift. And they also have income goals that they have to maintain with that because they’re coming out of training with larger debt loads than ever before. That’s the tricky part for CMS and the federal government moving forward.”
Nelson, however, says that the future of support will be tied to payment reform, as bundled payments, value-based purchasing (VBP), and other initiatives to reduce overall healthcare spending are implemented. He said HM and other specialties should keep in mind that the point of reform is less overall spending, which translates to less support for everyone.
“When the pie shrinks, the table manners change,” he adds. “People are going to have to figure out how to slice that pie.”
Accountable-care organizations (ACOs) could be one answer. An ACO is a type of healthcare delivery model being piloted by the Centers for Medicare & Medicaid Services (CMS), in which a group of providers band together to coordinate the care of beneficiaries (see “Quality over Quantity,” December 2009, p. 23). Reimbursement is shared by the group and is tied to the quality of care provided. Nelson says the model could significantly cut the need for support, as HM groups are allowed to share in the upside created by the ACO.
The program is set to go live Jan. 1, 2012, but a leading hospitalist already has questioned whether the proposed rules provide enough capitated risk and, therefore, whether the incentive is enough to spur adoption of the model and the potential support reductions it would bring.
“You can certainly start by taking a lower amount of risk, just upside risk,” Cogent HMG chief medical officer Ron Greeno, MD, FCCP, SFHM, told The Hospitalist eWire in April, when the proposed rules were issued. “But your plan should be not to stay there. Your plan should be to take more and more risk as soon as you can, as soon as you’re capable.”
Nelson says that the support can continue in some form or fashion in the new models as long as the hospital and its practitioners are integrated and looking to achieve the same goal.
“The reality is, from the hospital perspective, you need to make sure you’re getting some value,” he says. “What are they buying in exchange for that [payment]?” TH
Richard Quinn is a freelance writer based in New Jersey.
Pay to Play?
When St. Peter’s Hospital in Helena, Mont., proposed charging an outpatient clinic nearly $400,000 a year to use its in-house HM group, it prompted a new question from the hospitalist field: Will hospitals begin charging a fee for HM services?
The near-universal answer from hospitalists is no.
“At the end of the day, what the hospital wants is to keep peace in the valley and drive volume,” says John Laverty, DHA, vice president of hospital-based physicians at HCA Physician Services in Nashville, Tenn. “Any way that they encourage volume by going out and adding subscribing physicians, or docs that want to turn their patients over to hospitalists, I can’t see a hospital charging a fee for that service. Obviously, they’re cutting their nose off because they’re going to limit [referrals].”
Hospitalists have heard about institutions attempting to institute a fee, but pushback from stakeholders usually makes the paradigm unworkable.
Hospitals usually value their relationships with primary-care physicians (PCPs) too much to alienate them, says hospitalist John Bulger, DO, FACP, FHM, of Geisinger Medical Center in Danville, Pa. This is particularly so, he says, when PCPs point out that should they object to paying such a fee to use HM services, many of their patients would end up in a hospital regardless of referrals.
In that context, the attempt by St. Peter’s to charge a fee is the perfect example of the failed premise: The idea was raised but never executed.
“PCPs love hospitalists,” Dr. Bulger says. “But part of the reason they love HM is it’s free.”—RQ