User login
A Brief History
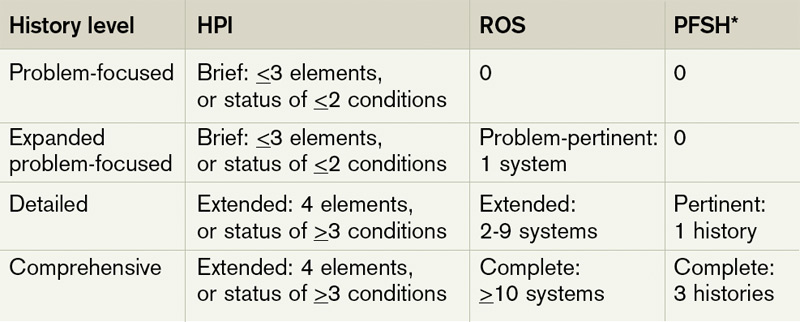
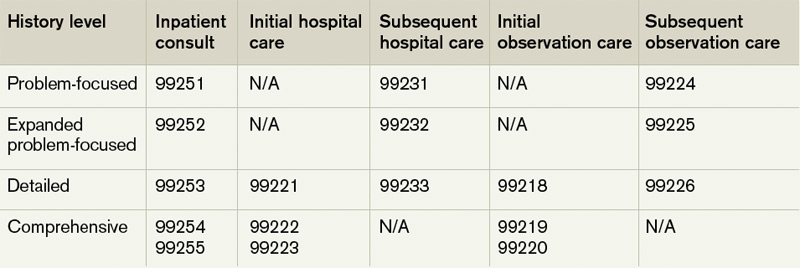
Each visit category and level of service has corresponding documentation requirements.1 Selecting an evaluation and management (E/M) level is based upon 1) the content of the three “key” components: history, exam, and decision-making, or 2) time, but only when counseling or coordination of care dominates more than 50% of the physician’s total visit time. Failure to document any essential element in a given visit level (e.g. family history required but missing for 99222 and 99223) could result in downcoding or service denial. Be aware of what an auditor expects when reviewing the key component of “history.”
Documentation Options
Auditors recognize two sets of documentation guidelines: “1995” and “1997” guidelines.2,3,4 Each set of guidelines has received valid criticism. The 1995 guidelines undoubtedly are vague and subjective in some areas, whereas the 1997 guidelines are known for arduous specificity.
However, to benefit all physicians and specialties, both sets of guidelines apply to visit-level selection. In other words, physicians can utilize either set when documenting their services, and auditors must review provider records against both styles. The final audited outcome reflects the highest visit level supported upon comparison.
Elements of History2,3,4
Chief complaint. The chief complaint (CC) is the reason for the visit, as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
History of present illness (HPI). The HPI is a description of the patient’s present illness as it developed. It characteristically is referenced as location, quality, severity, timing, context, modifying factors, and associated signs/symptoms, as related to the chief complaint. The 1997 guidelines allow physicians to receive HPI credit for providing the status of the patient’s chronic or inactive conditions, such as “extrinsic asthma without acute exacerbation in past six months.” An auditor will not assign HPI credit to a chronic or inactive condition that does not have a corresponding status (e.g. “asthma”). This will be considered “past medical history.”
The HPI is classified as brief (a comment on <3 HPI elements, or the status of <2 conditions) or extended (a comment on >4 HPI elements, or the status of >3 conditions). Consider these examples of an extended HPI:
- “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90.” (Status of three chronic conditions.)
Physicians receive credit for confirming and personally documenting the HPI, or linking to documentation recorded by residents (residents, fellows, interns) or nonphysician providers (NPPs) when performing services according to the Teaching Physician Rules or Split-Shared Billing Rules, respectively. An auditor will not assign physician credit for HPI elements documented by ancillary staff (registered nurses, medical assistants) or students.
Review of systems (ROS). The ROS is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient: constitutional; eyes, ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/ lymphatic; and allergic/immunologic. Auditors classify the ROS as brief (a comment on one system), extended (a comment on two to nine systems), or complete (a comment on >10 systems). Physicians can document a complete ROS by noting individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal); and occasional runny nose (ears, nose, mouth, throat),” or by eliciting a complete system review but documenting only the positive and pertinent negative findings related to the chief complaint, along with an additional comment that “all other systems are negative.”
Although the latter method is formally included in Medicare’s documentation guidelines and accepted by some Medicare contractors (e.g. Highmark, WPS), be aware that it is not universally accepted.5,6
Documentation involving the ROS can be provided by anyone, including the patient. The physician should reference ROS information that is completed by individuals other than residents or NPPs during services provided under the Teaching Physician Rules or Split-Shared Billing Rules. Physician duplication of ROS information is unnecessary unless an update or revision is required.
Past, family, and social history (PFSH). The PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH could be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). The physician merely needs a single comment associated with each history for the PFSH to be regarded as complete. Refrain from using “noncontributory” to describe any of the histories, as previous misuse of this term has resulted in its prohibition. An example of a complete PFSH documentation includes: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
Similar to the ROS, PFSH documentation can be provided by anyone, including the patient, and the physician should reference the documented PFSH in his own progress note. Redocumentation of the PFSH is not necessary unless a revision is required.
PFSH documentation is only required for initial care services (i.e. initial hospital care, initial observation care, consultations). It is not warranted in subsequent care services unless additional, pertinent information is obtained during the hospital stay that impacts care.
Considerations
When a physician cannot elicit historical information from the patient directly, and no other source is available, they should document “unable to obtain” the history. A comment regarding the circumstances surrounding this problem (e.g. patient confused, no caregiver present) should be provided, along with the available information from the limited resources (e.g. emergency medical technicians, previous hospitalizations at the same facility). Some contractors will not penalize the physician for the inability to ascertain complete historical information, as long as a proven attempt to obtain the information is evident.
Never document any item for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed July 7, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed July 7, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
- History of E/M (Q&As). WPS Health Insurance website. Available at: http://www.wpsmedicare.com/j5macpartb/resources/provider_types/2009_0526_emqahistory.shtml. Accessed July 11, 2011.
- Frequently Asked Questions: Evaluation and Management Services (Part B). Highmark Medicare Services website. Available at: www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed on July 11, 2011.
Each visit category and level of service has corresponding documentation requirements.1 Selecting an evaluation and management (E/M) level is based upon 1) the content of the three “key” components: history, exam, and decision-making, or 2) time, but only when counseling or coordination of care dominates more than 50% of the physician’s total visit time. Failure to document any essential element in a given visit level (e.g. family history required but missing for 99222 and 99223) could result in downcoding or service denial. Be aware of what an auditor expects when reviewing the key component of “history.”
Documentation Options
Auditors recognize two sets of documentation guidelines: “1995” and “1997” guidelines.2,3,4 Each set of guidelines has received valid criticism. The 1995 guidelines undoubtedly are vague and subjective in some areas, whereas the 1997 guidelines are known for arduous specificity.
However, to benefit all physicians and specialties, both sets of guidelines apply to visit-level selection. In other words, physicians can utilize either set when documenting their services, and auditors must review provider records against both styles. The final audited outcome reflects the highest visit level supported upon comparison.
Elements of History2,3,4
Chief complaint. The chief complaint (CC) is the reason for the visit, as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
History of present illness (HPI). The HPI is a description of the patient’s present illness as it developed. It characteristically is referenced as location, quality, severity, timing, context, modifying factors, and associated signs/symptoms, as related to the chief complaint. The 1997 guidelines allow physicians to receive HPI credit for providing the status of the patient’s chronic or inactive conditions, such as “extrinsic asthma without acute exacerbation in past six months.” An auditor will not assign HPI credit to a chronic or inactive condition that does not have a corresponding status (e.g. “asthma”). This will be considered “past medical history.”
The HPI is classified as brief (a comment on <3 HPI elements, or the status of <2 conditions) or extended (a comment on >4 HPI elements, or the status of >3 conditions). Consider these examples of an extended HPI:
- “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90.” (Status of three chronic conditions.)
Physicians receive credit for confirming and personally documenting the HPI, or linking to documentation recorded by residents (residents, fellows, interns) or nonphysician providers (NPPs) when performing services according to the Teaching Physician Rules or Split-Shared Billing Rules, respectively. An auditor will not assign physician credit for HPI elements documented by ancillary staff (registered nurses, medical assistants) or students.
Review of systems (ROS). The ROS is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient: constitutional; eyes, ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/ lymphatic; and allergic/immunologic. Auditors classify the ROS as brief (a comment on one system), extended (a comment on two to nine systems), or complete (a comment on >10 systems). Physicians can document a complete ROS by noting individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal); and occasional runny nose (ears, nose, mouth, throat),” or by eliciting a complete system review but documenting only the positive and pertinent negative findings related to the chief complaint, along with an additional comment that “all other systems are negative.”
Although the latter method is formally included in Medicare’s documentation guidelines and accepted by some Medicare contractors (e.g. Highmark, WPS), be aware that it is not universally accepted.5,6
Documentation involving the ROS can be provided by anyone, including the patient. The physician should reference ROS information that is completed by individuals other than residents or NPPs during services provided under the Teaching Physician Rules or Split-Shared Billing Rules. Physician duplication of ROS information is unnecessary unless an update or revision is required.
Past, family, and social history (PFSH). The PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH could be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). The physician merely needs a single comment associated with each history for the PFSH to be regarded as complete. Refrain from using “noncontributory” to describe any of the histories, as previous misuse of this term has resulted in its prohibition. An example of a complete PFSH documentation includes: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
Similar to the ROS, PFSH documentation can be provided by anyone, including the patient, and the physician should reference the documented PFSH in his own progress note. Redocumentation of the PFSH is not necessary unless a revision is required.
PFSH documentation is only required for initial care services (i.e. initial hospital care, initial observation care, consultations). It is not warranted in subsequent care services unless additional, pertinent information is obtained during the hospital stay that impacts care.
Considerations
When a physician cannot elicit historical information from the patient directly, and no other source is available, they should document “unable to obtain” the history. A comment regarding the circumstances surrounding this problem (e.g. patient confused, no caregiver present) should be provided, along with the available information from the limited resources (e.g. emergency medical technicians, previous hospitalizations at the same facility). Some contractors will not penalize the physician for the inability to ascertain complete historical information, as long as a proven attempt to obtain the information is evident.
Never document any item for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed July 7, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed July 7, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
- History of E/M (Q&As). WPS Health Insurance website. Available at: http://www.wpsmedicare.com/j5macpartb/resources/provider_types/2009_0526_emqahistory.shtml. Accessed July 11, 2011.
- Frequently Asked Questions: Evaluation and Management Services (Part B). Highmark Medicare Services website. Available at: www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed on July 11, 2011.
Each visit category and level of service has corresponding documentation requirements.1 Selecting an evaluation and management (E/M) level is based upon 1) the content of the three “key” components: history, exam, and decision-making, or 2) time, but only when counseling or coordination of care dominates more than 50% of the physician’s total visit time. Failure to document any essential element in a given visit level (e.g. family history required but missing for 99222 and 99223) could result in downcoding or service denial. Be aware of what an auditor expects when reviewing the key component of “history.”
Documentation Options
Auditors recognize two sets of documentation guidelines: “1995” and “1997” guidelines.2,3,4 Each set of guidelines has received valid criticism. The 1995 guidelines undoubtedly are vague and subjective in some areas, whereas the 1997 guidelines are known for arduous specificity.
However, to benefit all physicians and specialties, both sets of guidelines apply to visit-level selection. In other words, physicians can utilize either set when documenting their services, and auditors must review provider records against both styles. The final audited outcome reflects the highest visit level supported upon comparison.
Elements of History2,3,4
Chief complaint. The chief complaint (CC) is the reason for the visit, as stated in the patient’s own words. Every encounter, regardless of visit type, must include a CC. The physician must personally document and/or validate the CC with reference to a specific condition or symptom (e.g. patient complains of abdominal pain).
History of present illness (HPI). The HPI is a description of the patient’s present illness as it developed. It characteristically is referenced as location, quality, severity, timing, context, modifying factors, and associated signs/symptoms, as related to the chief complaint. The 1997 guidelines allow physicians to receive HPI credit for providing the status of the patient’s chronic or inactive conditions, such as “extrinsic asthma without acute exacerbation in past six months.” An auditor will not assign HPI credit to a chronic or inactive condition that does not have a corresponding status (e.g. “asthma”). This will be considered “past medical history.”
The HPI is classified as brief (a comment on <3 HPI elements, or the status of <2 conditions) or extended (a comment on >4 HPI elements, or the status of >3 conditions). Consider these examples of an extended HPI:
- “The patient has intermittent (duration), sharp (quality) pain in the right upper quadrant (location) without associated nausea, vomiting, or diarrhea (associated signs/symptoms).”
- “Diabetes controlled by oral medication; hyperlipidemia stable on simvastatin with increased dietary efforts; hypertension stable with pressures ranging from 130-140/80-90.” (Status of three chronic conditions.)
Physicians receive credit for confirming and personally documenting the HPI, or linking to documentation recorded by residents (residents, fellows, interns) or nonphysician providers (NPPs) when performing services according to the Teaching Physician Rules or Split-Shared Billing Rules, respectively. An auditor will not assign physician credit for HPI elements documented by ancillary staff (registered nurses, medical assistants) or students.
Review of systems (ROS). The ROS is a series of questions used to elicit information about additional signs, symptoms, or problems currently or previously experienced by the patient: constitutional; eyes, ears, nose, mouth, throat; cardiovascular; respiratory; gastrointestinal; genitourinary; musculoskeletal; integumentary (including skin and/or breast); neurological; psychiatric; endocrine; hematologic/ lymphatic; and allergic/immunologic. Auditors classify the ROS as brief (a comment on one system), extended (a comment on two to nine systems), or complete (a comment on >10 systems). Physicians can document a complete ROS by noting individual systems: “no fever/chills (constitutional) or blurred vision (eyes); no chest pain (cardiovascular) or shortness of breath (respiratory); intermittent nausea (gastrointestinal); and occasional runny nose (ears, nose, mouth, throat),” or by eliciting a complete system review but documenting only the positive and pertinent negative findings related to the chief complaint, along with an additional comment that “all other systems are negative.”
Although the latter method is formally included in Medicare’s documentation guidelines and accepted by some Medicare contractors (e.g. Highmark, WPS), be aware that it is not universally accepted.5,6
Documentation involving the ROS can be provided by anyone, including the patient. The physician should reference ROS information that is completed by individuals other than residents or NPPs during services provided under the Teaching Physician Rules or Split-Shared Billing Rules. Physician duplication of ROS information is unnecessary unless an update or revision is required.
Past, family, and social history (PFSH). The PFSH involves data obtained about the patient’s previous illness or medical conditions/therapies, family occurrences with illness, and relevant patient activities. The PFSH could be classified as pertinent (a comment on one history) or complete (a comment in each of the three histories). The physician merely needs a single comment associated with each history for the PFSH to be regarded as complete. Refrain from using “noncontributory” to describe any of the histories, as previous misuse of this term has resulted in its prohibition. An example of a complete PFSH documentation includes: “Patient currently on Prilosec 20 mg daily; family history of Barrett’s esophagus; no tobacco or alcohol use.”
Similar to the ROS, PFSH documentation can be provided by anyone, including the patient, and the physician should reference the documented PFSH in his own progress note. Redocumentation of the PFSH is not necessary unless a revision is required.
PFSH documentation is only required for initial care services (i.e. initial hospital care, initial observation care, consultations). It is not warranted in subsequent care services unless additional, pertinent information is obtained during the hospital stay that impacts care.
Considerations
When a physician cannot elicit historical information from the patient directly, and no other source is available, they should document “unable to obtain” the history. A comment regarding the circumstances surrounding this problem (e.g. patient confused, no caregiver present) should be provided, along with the available information from the limited resources (e.g. emergency medical technicians, previous hospitalizations at the same facility). Some contractors will not penalize the physician for the inability to ascertain complete historical information, as long as a proven attempt to obtain the information is evident.
Never document any item for the purpose of “getting paid.” Only document information that is clinically relevant, lends to the quality of care provided, or demonstrates the delivery of healthcare services. This prevents accusations of fraud and abuse, promotes billing compliance, and supports medical necessity for the services provided.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is faculty for SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, IL: American College of Chest Physicians, 2009; 87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf. Accessed July 7, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. CMS website. Available at: http://www.cms.hhs.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed July 7, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011.
- History of E/M (Q&As). WPS Health Insurance website. Available at: http://www.wpsmedicare.com/j5macpartb/resources/provider_types/2009_0526_emqahistory.shtml. Accessed July 11, 2011.
- Frequently Asked Questions: Evaluation and Management Services (Part B). Highmark Medicare Services website. Available at: www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html. Accessed on July 11, 2011.
ONLINE EXCLUSIVE: The Pros and Cons of a Super-Commuter Lifestyle
Wrongful birth claim: Child has a chromosomal disorder...and more

A WOMAN’S HUSBAND AND AN INTERPRETER came to her first prenatal appointment at 10 weeks’ gestation, as she spoke only Mandarin and the father’s English was limited. The ObGyn offered maternal serum sequential screening. At subsequent visits, with the husband and interpreter present, the mother saw a geneticist, genetic counselor, and nurse practitioner. At no time was additional genetic testing offered. At the 23-week visit, the husband was present, but the interpreter had not yet arrived; the ObGyn attempted to communicate through the husband.
The baby was born at term with cri-du-chat syndrome. The child is severely physically and mentally handicapped, and will require constant medical and attendant care for life.
PATIENT’S CLAIM The ObGyn did not offer amniocentesis or chorionic villus sampling (CVS), and failed to inform the parents that the chance of a 37-year-old woman having a child with a chromosomal aberration was 1.5%. The ObGyn did not obtain the woman’s signature waiving the presence of an interpreter at the 23-week visit. If the physician offered amniocentesis then, the parents did not understand. She would have terminated the pregnancy if she had been told the fetus had a severe chromosomal defect.
PHYSICIAN’S DEFENSE The ObGyn claimed to have offered amniocentesis at the 23-week visit, but it was declined. Proper care and treatment was provided.
VERDICT A $7 million Massachusetts settlement was reached.
Hematoma after biopsy; death
A 77-YEAR -OLD WOMAN underwent percutaneous biopsy of three right axillary lymph nodes. She developed a hematoma. She was sent to the hospital from the physician’s office because of the increasing size of the hematoma, low blood pressure, and pain, then admitted to the ICU for monitoring. She declined exploratory surgery to discover and repair the bleeding source. When her blood pressure and hemoglobin level dropped overnight, the physician again tried to persuade the woman to have surgery; she refused. The physician then undertook surgery on another patient.
An ICU resident and nurse subsequently obtained consent from the woman’s family. The surgeon was not told this for 4 hours, at which time the woman was taken immediately to the operating room. The surgeon repaired a severed axillary vein and punctured axillary artery.
The woman suffered two episodes of asystole during surgery. She later died of multiple organ failure.
ESTATE’S CLAIM The surgeon failed to take adequate measures to obtain surgical consent to repair the hematoma, and failed to perform surgery in a timely manner once consent was given.
PHYSICIAN’S DEFENSE The woman was awake, alert, and oriented both times she refused consent; her family could not be contacted without her authorization. Proper actions were taken when consent was obtained.
VERDICT An Illinois defense verdict was returned.
Epidural pump stolen—while in use
A WOMAN WAS GIVEN AN EPIDURAL during labor. While she slept, a newly hired physician assistant (PA) entered her room, disconnected the epidural pump, and stole it. The woman awoke but the PA assured her that everything was fine. Soon, she experienced significant labor pains and called the nurses, who paged an anesthesiologist to administer another epidural. Security personnel questioned the woman.
She gave birth to a healthy child.
PATIENT’S CLAIM The hospital failed to provide adequate security. Security personnel unduly questioned the woman before the second epidural was administered, delaying the procedure and increasing the length of time she was in pain.
DEFENDANTS’ DEFENSE The hospital claimed no responsibility for the theft; the PA’s actions were outside the scope of his employment, and his criminal behavior was unforeseeable.
VERDICT A Connecticut defense verdict was returned for the hospital. (The PA pleaded guilty to stealing the epidural pump, received 3 years’ probation, and lost his license.)
Ectopic pregnancy didn’t miscarry despite methotrexate
THINKING SHE WAS PREGNANT, a woman saw her ObGyn, Dr. A, who found no evidence of pregnancy, and suspected that she had miscarried. The next day, Dr. A’s office called the woman to return because of an elevated hCG level. A sonogram performed at the second visit did not reveal any signs of pregnancy.
Eleven days later, she went to the emergency department (ED) in excruciating pain. A sonogram revealed an ectopic pregnancy. Methotrexate was administered to terminate the pregnancy. The woman was advised to follow up with her ObGyn. Ten days later, blood tests continued to show an elevated hCG level, but Dr. A did not order further testing or follow up.
Two weeks later, the woman went to Dr. B, a different ObGyn, who ordered blood work to monitor her hCG. The next day, she went to the ED in great pain. The ED physician contacted Dr. B, who advised that the woman should be discharged with instructions to follow up with him. Nine days later, the woman saw Dr. B, who diagnosed and surgically removed a ruptured fallopian tube.
PATIENT’S CLAIM Neither physician properly monitored the patient after administration of methotrexate. The ectopic pregnancy continued, and caused rupture of the fallopian tube. Dr. B failed to respond properly to the call from the ED physician.
PHYSICIANS’ DEFENSE Dr. A admitted that the patient had not been properly monitored, but claimed that the lack of monitoring caused no harm. Dr. B denied any negligence.
VERDICT A Georgia defense verdict was returned for both physicians.
Uterine laceration during cesarean
A WOMAN BEGAN TO BLEED excessively in the recovery room after a nonemergent cesarean delivery. Blood pressure and blood oxygen saturation decreased, heart rate increased, and she passed large clots. The recovery room nurse notified the woman’s ObGyn, who ordered medication to constrict the uterus and diminish blood flow, but treatment was unsuccessful.
She was returned to the operating room, where the ObGyn repaired a low-segment uterine laceration. Blood was administered with additional uterotonics. After surgery, the woman was sent to the labor and delivery recovery room. When tests indicated that her hematocrit and hemoglobin level had decreased and she showed signs of a clotting difficulty, the ObGyn ordered additional blood products and fundal massage. Two hours later, the woman suffered cardiac arrest and was revived, but suffered significant brain damage. After six months, mechanical ventilation was withdrawn and she died.
ESTATE’S CLAIM The patient’s vital signs never returned to normal after uterine repair surgery. The ObGyn and anesthesiologist did not stabilize the patient, and failed to perform a hysterectomy to save her life. The nurses did not notify the ObGyn and anesthesiologist of unstable vital signs that signaled blood loss.
DEFENDANTS’ DEFENSE The anesthesiologist found the patient’s vital signs normal after repair of the laceration and left the woman in the care of the nursing staff and ObGyn. The ObGyn was not notified of unstable vital signs. The nurses asserted that they did not tell the ObGyn of the changes because they expected him to look at, review, and interpret the monitor. The physicians claimed that the arrest and death were due to an amniotic fluid embolism or amniotic fluid syndrome that was sudden, unpredictable, and difficult to treat.
VERDICT A $1,350,000 Virginia settlement was reached.
Was she discharged too early?
AN OBGYN PERFORMED total transvaginal hysterectomy on a 54-year-old patient, and discharged her the next day. Several hours later, she began to have severe abdominal pain, and was readmitted. The ObGyn prescribed IV antibiotics and ordered fluid management. When she continued to deteriorate, she was transferred to the ICU.
The next day, the ICU physician ordered diagnostic laparoscopy. A perforation of the sigmoid colon was found and repaired, but the woman continued to deteriorate. Nine days later, she was transferred to another hospital, where she died.
ESTATE’S CLAIM The ObGyn failed to find the perforation during hysterectomy. He did not properly follow-up with the patient after surgery, and improperly discharged her despite abnormal blood work and vital signs; elevated temperature and pulse rate; and an increase in her white blood cell count. Both physicians failed to diagnose and treat the perforation in a timely manner. Delay in diagnosis and treatment led to the woman’s death.
PHYSICIANS’ DEFENSE The physicians denied negligence.
VERDICT A $7 million North Carolina verdict was returned against the ObGyn. A defense verdict was returned for the ICU physician.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
A WOMAN’S HUSBAND AND AN INTERPRETER came to her first prenatal appointment at 10 weeks’ gestation, as she spoke only Mandarin and the father’s English was limited. The ObGyn offered maternal serum sequential screening. At subsequent visits, with the husband and interpreter present, the mother saw a geneticist, genetic counselor, and nurse practitioner. At no time was additional genetic testing offered. At the 23-week visit, the husband was present, but the interpreter had not yet arrived; the ObGyn attempted to communicate through the husband.
The baby was born at term with cri-du-chat syndrome. The child is severely physically and mentally handicapped, and will require constant medical and attendant care for life.
PATIENT’S CLAIM The ObGyn did not offer amniocentesis or chorionic villus sampling (CVS), and failed to inform the parents that the chance of a 37-year-old woman having a child with a chromosomal aberration was 1.5%. The ObGyn did not obtain the woman’s signature waiving the presence of an interpreter at the 23-week visit. If the physician offered amniocentesis then, the parents did not understand. She would have terminated the pregnancy if she had been told the fetus had a severe chromosomal defect.
PHYSICIAN’S DEFENSE The ObGyn claimed to have offered amniocentesis at the 23-week visit, but it was declined. Proper care and treatment was provided.
VERDICT A $7 million Massachusetts settlement was reached.
Hematoma after biopsy; death
A 77-YEAR -OLD WOMAN underwent percutaneous biopsy of three right axillary lymph nodes. She developed a hematoma. She was sent to the hospital from the physician’s office because of the increasing size of the hematoma, low blood pressure, and pain, then admitted to the ICU for monitoring. She declined exploratory surgery to discover and repair the bleeding source. When her blood pressure and hemoglobin level dropped overnight, the physician again tried to persuade the woman to have surgery; she refused. The physician then undertook surgery on another patient.
An ICU resident and nurse subsequently obtained consent from the woman’s family. The surgeon was not told this for 4 hours, at which time the woman was taken immediately to the operating room. The surgeon repaired a severed axillary vein and punctured axillary artery.
The woman suffered two episodes of asystole during surgery. She later died of multiple organ failure.
ESTATE’S CLAIM The surgeon failed to take adequate measures to obtain surgical consent to repair the hematoma, and failed to perform surgery in a timely manner once consent was given.
PHYSICIAN’S DEFENSE The woman was awake, alert, and oriented both times she refused consent; her family could not be contacted without her authorization. Proper actions were taken when consent was obtained.
VERDICT An Illinois defense verdict was returned.
Epidural pump stolen—while in use
A WOMAN WAS GIVEN AN EPIDURAL during labor. While she slept, a newly hired physician assistant (PA) entered her room, disconnected the epidural pump, and stole it. The woman awoke but the PA assured her that everything was fine. Soon, she experienced significant labor pains and called the nurses, who paged an anesthesiologist to administer another epidural. Security personnel questioned the woman.
She gave birth to a healthy child.
PATIENT’S CLAIM The hospital failed to provide adequate security. Security personnel unduly questioned the woman before the second epidural was administered, delaying the procedure and increasing the length of time she was in pain.
DEFENDANTS’ DEFENSE The hospital claimed no responsibility for the theft; the PA’s actions were outside the scope of his employment, and his criminal behavior was unforeseeable.
VERDICT A Connecticut defense verdict was returned for the hospital. (The PA pleaded guilty to stealing the epidural pump, received 3 years’ probation, and lost his license.)
Ectopic pregnancy didn’t miscarry despite methotrexate
THINKING SHE WAS PREGNANT, a woman saw her ObGyn, Dr. A, who found no evidence of pregnancy, and suspected that she had miscarried. The next day, Dr. A’s office called the woman to return because of an elevated hCG level. A sonogram performed at the second visit did not reveal any signs of pregnancy.
Eleven days later, she went to the emergency department (ED) in excruciating pain. A sonogram revealed an ectopic pregnancy. Methotrexate was administered to terminate the pregnancy. The woman was advised to follow up with her ObGyn. Ten days later, blood tests continued to show an elevated hCG level, but Dr. A did not order further testing or follow up.
Two weeks later, the woman went to Dr. B, a different ObGyn, who ordered blood work to monitor her hCG. The next day, she went to the ED in great pain. The ED physician contacted Dr. B, who advised that the woman should be discharged with instructions to follow up with him. Nine days later, the woman saw Dr. B, who diagnosed and surgically removed a ruptured fallopian tube.
PATIENT’S CLAIM Neither physician properly monitored the patient after administration of methotrexate. The ectopic pregnancy continued, and caused rupture of the fallopian tube. Dr. B failed to respond properly to the call from the ED physician.
PHYSICIANS’ DEFENSE Dr. A admitted that the patient had not been properly monitored, but claimed that the lack of monitoring caused no harm. Dr. B denied any negligence.
VERDICT A Georgia defense verdict was returned for both physicians.
Uterine laceration during cesarean
A WOMAN BEGAN TO BLEED excessively in the recovery room after a nonemergent cesarean delivery. Blood pressure and blood oxygen saturation decreased, heart rate increased, and she passed large clots. The recovery room nurse notified the woman’s ObGyn, who ordered medication to constrict the uterus and diminish blood flow, but treatment was unsuccessful.
She was returned to the operating room, where the ObGyn repaired a low-segment uterine laceration. Blood was administered with additional uterotonics. After surgery, the woman was sent to the labor and delivery recovery room. When tests indicated that her hematocrit and hemoglobin level had decreased and she showed signs of a clotting difficulty, the ObGyn ordered additional blood products and fundal massage. Two hours later, the woman suffered cardiac arrest and was revived, but suffered significant brain damage. After six months, mechanical ventilation was withdrawn and she died.
ESTATE’S CLAIM The patient’s vital signs never returned to normal after uterine repair surgery. The ObGyn and anesthesiologist did not stabilize the patient, and failed to perform a hysterectomy to save her life. The nurses did not notify the ObGyn and anesthesiologist of unstable vital signs that signaled blood loss.
DEFENDANTS’ DEFENSE The anesthesiologist found the patient’s vital signs normal after repair of the laceration and left the woman in the care of the nursing staff and ObGyn. The ObGyn was not notified of unstable vital signs. The nurses asserted that they did not tell the ObGyn of the changes because they expected him to look at, review, and interpret the monitor. The physicians claimed that the arrest and death were due to an amniotic fluid embolism or amniotic fluid syndrome that was sudden, unpredictable, and difficult to treat.
VERDICT A $1,350,000 Virginia settlement was reached.
Was she discharged too early?
AN OBGYN PERFORMED total transvaginal hysterectomy on a 54-year-old patient, and discharged her the next day. Several hours later, she began to have severe abdominal pain, and was readmitted. The ObGyn prescribed IV antibiotics and ordered fluid management. When she continued to deteriorate, she was transferred to the ICU.
The next day, the ICU physician ordered diagnostic laparoscopy. A perforation of the sigmoid colon was found and repaired, but the woman continued to deteriorate. Nine days later, she was transferred to another hospital, where she died.
ESTATE’S CLAIM The ObGyn failed to find the perforation during hysterectomy. He did not properly follow-up with the patient after surgery, and improperly discharged her despite abnormal blood work and vital signs; elevated temperature and pulse rate; and an increase in her white blood cell count. Both physicians failed to diagnose and treat the perforation in a timely manner. Delay in diagnosis and treatment led to the woman’s death.
PHYSICIANS’ DEFENSE The physicians denied negligence.
VERDICT A $7 million North Carolina verdict was returned against the ObGyn. A defense verdict was returned for the ICU physician.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A WOMAN’S HUSBAND AND AN INTERPRETER came to her first prenatal appointment at 10 weeks’ gestation, as she spoke only Mandarin and the father’s English was limited. The ObGyn offered maternal serum sequential screening. At subsequent visits, with the husband and interpreter present, the mother saw a geneticist, genetic counselor, and nurse practitioner. At no time was additional genetic testing offered. At the 23-week visit, the husband was present, but the interpreter had not yet arrived; the ObGyn attempted to communicate through the husband.
The baby was born at term with cri-du-chat syndrome. The child is severely physically and mentally handicapped, and will require constant medical and attendant care for life.
PATIENT’S CLAIM The ObGyn did not offer amniocentesis or chorionic villus sampling (CVS), and failed to inform the parents that the chance of a 37-year-old woman having a child with a chromosomal aberration was 1.5%. The ObGyn did not obtain the woman’s signature waiving the presence of an interpreter at the 23-week visit. If the physician offered amniocentesis then, the parents did not understand. She would have terminated the pregnancy if she had been told the fetus had a severe chromosomal defect.
PHYSICIAN’S DEFENSE The ObGyn claimed to have offered amniocentesis at the 23-week visit, but it was declined. Proper care and treatment was provided.
VERDICT A $7 million Massachusetts settlement was reached.
Hematoma after biopsy; death
A 77-YEAR -OLD WOMAN underwent percutaneous biopsy of three right axillary lymph nodes. She developed a hematoma. She was sent to the hospital from the physician’s office because of the increasing size of the hematoma, low blood pressure, and pain, then admitted to the ICU for monitoring. She declined exploratory surgery to discover and repair the bleeding source. When her blood pressure and hemoglobin level dropped overnight, the physician again tried to persuade the woman to have surgery; she refused. The physician then undertook surgery on another patient.
An ICU resident and nurse subsequently obtained consent from the woman’s family. The surgeon was not told this for 4 hours, at which time the woman was taken immediately to the operating room. The surgeon repaired a severed axillary vein and punctured axillary artery.
The woman suffered two episodes of asystole during surgery. She later died of multiple organ failure.
ESTATE’S CLAIM The surgeon failed to take adequate measures to obtain surgical consent to repair the hematoma, and failed to perform surgery in a timely manner once consent was given.
PHYSICIAN’S DEFENSE The woman was awake, alert, and oriented both times she refused consent; her family could not be contacted without her authorization. Proper actions were taken when consent was obtained.
VERDICT An Illinois defense verdict was returned.
Epidural pump stolen—while in use
A WOMAN WAS GIVEN AN EPIDURAL during labor. While she slept, a newly hired physician assistant (PA) entered her room, disconnected the epidural pump, and stole it. The woman awoke but the PA assured her that everything was fine. Soon, she experienced significant labor pains and called the nurses, who paged an anesthesiologist to administer another epidural. Security personnel questioned the woman.
She gave birth to a healthy child.
PATIENT’S CLAIM The hospital failed to provide adequate security. Security personnel unduly questioned the woman before the second epidural was administered, delaying the procedure and increasing the length of time she was in pain.
DEFENDANTS’ DEFENSE The hospital claimed no responsibility for the theft; the PA’s actions were outside the scope of his employment, and his criminal behavior was unforeseeable.
VERDICT A Connecticut defense verdict was returned for the hospital. (The PA pleaded guilty to stealing the epidural pump, received 3 years’ probation, and lost his license.)
Ectopic pregnancy didn’t miscarry despite methotrexate
THINKING SHE WAS PREGNANT, a woman saw her ObGyn, Dr. A, who found no evidence of pregnancy, and suspected that she had miscarried. The next day, Dr. A’s office called the woman to return because of an elevated hCG level. A sonogram performed at the second visit did not reveal any signs of pregnancy.
Eleven days later, she went to the emergency department (ED) in excruciating pain. A sonogram revealed an ectopic pregnancy. Methotrexate was administered to terminate the pregnancy. The woman was advised to follow up with her ObGyn. Ten days later, blood tests continued to show an elevated hCG level, but Dr. A did not order further testing or follow up.
Two weeks later, the woman went to Dr. B, a different ObGyn, who ordered blood work to monitor her hCG. The next day, she went to the ED in great pain. The ED physician contacted Dr. B, who advised that the woman should be discharged with instructions to follow up with him. Nine days later, the woman saw Dr. B, who diagnosed and surgically removed a ruptured fallopian tube.
PATIENT’S CLAIM Neither physician properly monitored the patient after administration of methotrexate. The ectopic pregnancy continued, and caused rupture of the fallopian tube. Dr. B failed to respond properly to the call from the ED physician.
PHYSICIANS’ DEFENSE Dr. A admitted that the patient had not been properly monitored, but claimed that the lack of monitoring caused no harm. Dr. B denied any negligence.
VERDICT A Georgia defense verdict was returned for both physicians.
Uterine laceration during cesarean
A WOMAN BEGAN TO BLEED excessively in the recovery room after a nonemergent cesarean delivery. Blood pressure and blood oxygen saturation decreased, heart rate increased, and she passed large clots. The recovery room nurse notified the woman’s ObGyn, who ordered medication to constrict the uterus and diminish blood flow, but treatment was unsuccessful.
She was returned to the operating room, where the ObGyn repaired a low-segment uterine laceration. Blood was administered with additional uterotonics. After surgery, the woman was sent to the labor and delivery recovery room. When tests indicated that her hematocrit and hemoglobin level had decreased and she showed signs of a clotting difficulty, the ObGyn ordered additional blood products and fundal massage. Two hours later, the woman suffered cardiac arrest and was revived, but suffered significant brain damage. After six months, mechanical ventilation was withdrawn and she died.
ESTATE’S CLAIM The patient’s vital signs never returned to normal after uterine repair surgery. The ObGyn and anesthesiologist did not stabilize the patient, and failed to perform a hysterectomy to save her life. The nurses did not notify the ObGyn and anesthesiologist of unstable vital signs that signaled blood loss.
DEFENDANTS’ DEFENSE The anesthesiologist found the patient’s vital signs normal after repair of the laceration and left the woman in the care of the nursing staff and ObGyn. The ObGyn was not notified of unstable vital signs. The nurses asserted that they did not tell the ObGyn of the changes because they expected him to look at, review, and interpret the monitor. The physicians claimed that the arrest and death were due to an amniotic fluid embolism or amniotic fluid syndrome that was sudden, unpredictable, and difficult to treat.
VERDICT A $1,350,000 Virginia settlement was reached.
Was she discharged too early?
AN OBGYN PERFORMED total transvaginal hysterectomy on a 54-year-old patient, and discharged her the next day. Several hours later, she began to have severe abdominal pain, and was readmitted. The ObGyn prescribed IV antibiotics and ordered fluid management. When she continued to deteriorate, she was transferred to the ICU.
The next day, the ICU physician ordered diagnostic laparoscopy. A perforation of the sigmoid colon was found and repaired, but the woman continued to deteriorate. Nine days later, she was transferred to another hospital, where she died.
ESTATE’S CLAIM The ObGyn failed to find the perforation during hysterectomy. He did not properly follow-up with the patient after surgery, and improperly discharged her despite abnormal blood work and vital signs; elevated temperature and pulse rate; and an increase in her white blood cell count. Both physicians failed to diagnose and treat the perforation in a timely manner. Delay in diagnosis and treatment led to the woman’s death.
PHYSICIANS’ DEFENSE The physicians denied negligence.
VERDICT A $7 million North Carolina verdict was returned against the ObGyn. A defense verdict was returned for the ICU physician.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: The NLRB and You
Questions have been streaming in about the recent National Labor Relations Board rule requiring private-sector employers to remind employees of their rights under the National Labor Relations Act with another lengthy, decorative government poster by Nov. 14. Will this new rule apply to the average medical private practice?
The answer proved more difficult to nail down than I anticipated. A National Labor Relations Board (NLRB) spokesperson said he thought that it would indeed apply to medical offices, but he would get back to me with an authoritative answer. (As of my early September deadline, he had not.) A prominent labor lawyer was fairly certain that it would not apply, in most cases; but another opined that the answer was irrelevant since it wouldn’t matter either way.
Before explaining this disparity and revealing who (if anyone) is right, let me start from the beginning. The National Labor Relations Act (NLRA) is the federal law that guarantees the rights of employees to organize and bargain collectively with their employers, or not, as they choose. The NLRB is the federal agency charged with enforcing the NLRA.
Last year the NLRB decided that labor rights should be spelled out – displayed in writing in virtually every private-sector business for all employees to see – and in late August of this year issued a ruling to that effect. The same notice must appear on the company’s Internet site, if one exists.
In essence, the notice informs employees that they have the right to act together to improve wages and working conditions, to form a union, to bargain collectively, and to refrain from any of these activities – and to not be penalized for whatever choices they make.
The NLRB noted that the new requirement applies to all private-sector work places, unionized or not, except for farms, railroads, airlines, and the U.S. Postal Service. That would seem to include private medical offices; however, according to the NLRB, they have "chosen not to assert [their] jurisdiction over very small employers whose annual volume of business is not large enough to have more than a slight effect on interstate commerce."
These days it’s hard not to engage in interstate commerce; most of the medical and office supplies you buy probably come from another state, for example; and you might send your billing or pathology services out of state – and so on. But the NLRB appears to be saying that such commerce is okay as long as it has no more than a "slight effect" on the grand scheme; but naturally, no one has defined "slight."
Common sense tells us that medical treatment and procedures performed in a small office within a single state are not "interstate commerce," and are unlikely to affect interstate commerce in any measurable way, no matter how many supplies you purchase or what services you outsource. (That’s why one lawyer told me the rule would not apply.) But if you have a large multispecialty clinic, or multiple offices in more than one state (or in one state that draws patients from more than one state), the NLRB would probably argue that you’re within its jurisdiction. Unions are irrelevant – the NLRA applies to all workplaces, unionized or not.
Complicating all of this are questions of whether the rule is necessary – or even legal – and whether it will withstand court challenge. The NLRA contains no provision authorizing the board to make such a rule. Indeed, after the rule was announced, one of the NLRB’s own members wrote a blistering dissent charging that the board had acted in excess of its authority, and predicting that a reviewing court would soon "save the Board from itself" by striking the rule. Even if the courts uphold the rule and it takes effect as scheduled in November, the NLRB has admitted that it has no authority to enforce it. (That’s why the other lawyer thought the answer wouldn’t matter.)
So what does all this mean for the average private medical practice?
In the absence of an official answer, small offices seem likely to be in the clear; and with a court challenge looming and no specific requirements until the middle of November, even if you run an operation big enough to have a measurable effect on interstate commerce, my suggestion is to wait and see.
Questions have been streaming in about the recent National Labor Relations Board rule requiring private-sector employers to remind employees of their rights under the National Labor Relations Act with another lengthy, decorative government poster by Nov. 14. Will this new rule apply to the average medical private practice?
The answer proved more difficult to nail down than I anticipated. A National Labor Relations Board (NLRB) spokesperson said he thought that it would indeed apply to medical offices, but he would get back to me with an authoritative answer. (As of my early September deadline, he had not.) A prominent labor lawyer was fairly certain that it would not apply, in most cases; but another opined that the answer was irrelevant since it wouldn’t matter either way.
Before explaining this disparity and revealing who (if anyone) is right, let me start from the beginning. The National Labor Relations Act (NLRA) is the federal law that guarantees the rights of employees to organize and bargain collectively with their employers, or not, as they choose. The NLRB is the federal agency charged with enforcing the NLRA.
Last year the NLRB decided that labor rights should be spelled out – displayed in writing in virtually every private-sector business for all employees to see – and in late August of this year issued a ruling to that effect. The same notice must appear on the company’s Internet site, if one exists.
In essence, the notice informs employees that they have the right to act together to improve wages and working conditions, to form a union, to bargain collectively, and to refrain from any of these activities – and to not be penalized for whatever choices they make.
The NLRB noted that the new requirement applies to all private-sector work places, unionized or not, except for farms, railroads, airlines, and the U.S. Postal Service. That would seem to include private medical offices; however, according to the NLRB, they have "chosen not to assert [their] jurisdiction over very small employers whose annual volume of business is not large enough to have more than a slight effect on interstate commerce."
These days it’s hard not to engage in interstate commerce; most of the medical and office supplies you buy probably come from another state, for example; and you might send your billing or pathology services out of state – and so on. But the NLRB appears to be saying that such commerce is okay as long as it has no more than a "slight effect" on the grand scheme; but naturally, no one has defined "slight."
Common sense tells us that medical treatment and procedures performed in a small office within a single state are not "interstate commerce," and are unlikely to affect interstate commerce in any measurable way, no matter how many supplies you purchase or what services you outsource. (That’s why one lawyer told me the rule would not apply.) But if you have a large multispecialty clinic, or multiple offices in more than one state (or in one state that draws patients from more than one state), the NLRB would probably argue that you’re within its jurisdiction. Unions are irrelevant – the NLRA applies to all workplaces, unionized or not.
Complicating all of this are questions of whether the rule is necessary – or even legal – and whether it will withstand court challenge. The NLRA contains no provision authorizing the board to make such a rule. Indeed, after the rule was announced, one of the NLRB’s own members wrote a blistering dissent charging that the board had acted in excess of its authority, and predicting that a reviewing court would soon "save the Board from itself" by striking the rule. Even if the courts uphold the rule and it takes effect as scheduled in November, the NLRB has admitted that it has no authority to enforce it. (That’s why the other lawyer thought the answer wouldn’t matter.)
So what does all this mean for the average private medical practice?
In the absence of an official answer, small offices seem likely to be in the clear; and with a court challenge looming and no specific requirements until the middle of November, even if you run an operation big enough to have a measurable effect on interstate commerce, my suggestion is to wait and see.
Questions have been streaming in about the recent National Labor Relations Board rule requiring private-sector employers to remind employees of their rights under the National Labor Relations Act with another lengthy, decorative government poster by Nov. 14. Will this new rule apply to the average medical private practice?
The answer proved more difficult to nail down than I anticipated. A National Labor Relations Board (NLRB) spokesperson said he thought that it would indeed apply to medical offices, but he would get back to me with an authoritative answer. (As of my early September deadline, he had not.) A prominent labor lawyer was fairly certain that it would not apply, in most cases; but another opined that the answer was irrelevant since it wouldn’t matter either way.
Before explaining this disparity and revealing who (if anyone) is right, let me start from the beginning. The National Labor Relations Act (NLRA) is the federal law that guarantees the rights of employees to organize and bargain collectively with their employers, or not, as they choose. The NLRB is the federal agency charged with enforcing the NLRA.
Last year the NLRB decided that labor rights should be spelled out – displayed in writing in virtually every private-sector business for all employees to see – and in late August of this year issued a ruling to that effect. The same notice must appear on the company’s Internet site, if one exists.
In essence, the notice informs employees that they have the right to act together to improve wages and working conditions, to form a union, to bargain collectively, and to refrain from any of these activities – and to not be penalized for whatever choices they make.
The NLRB noted that the new requirement applies to all private-sector work places, unionized or not, except for farms, railroads, airlines, and the U.S. Postal Service. That would seem to include private medical offices; however, according to the NLRB, they have "chosen not to assert [their] jurisdiction over very small employers whose annual volume of business is not large enough to have more than a slight effect on interstate commerce."
These days it’s hard not to engage in interstate commerce; most of the medical and office supplies you buy probably come from another state, for example; and you might send your billing or pathology services out of state – and so on. But the NLRB appears to be saying that such commerce is okay as long as it has no more than a "slight effect" on the grand scheme; but naturally, no one has defined "slight."
Common sense tells us that medical treatment and procedures performed in a small office within a single state are not "interstate commerce," and are unlikely to affect interstate commerce in any measurable way, no matter how many supplies you purchase or what services you outsource. (That’s why one lawyer told me the rule would not apply.) But if you have a large multispecialty clinic, or multiple offices in more than one state (or in one state that draws patients from more than one state), the NLRB would probably argue that you’re within its jurisdiction. Unions are irrelevant – the NLRA applies to all workplaces, unionized or not.
Complicating all of this are questions of whether the rule is necessary – or even legal – and whether it will withstand court challenge. The NLRA contains no provision authorizing the board to make such a rule. Indeed, after the rule was announced, one of the NLRB’s own members wrote a blistering dissent charging that the board had acted in excess of its authority, and predicting that a reviewing court would soon "save the Board from itself" by striking the rule. Even if the courts uphold the rule and it takes effect as scheduled in November, the NLRB has admitted that it has no authority to enforce it. (That’s why the other lawyer thought the answer wouldn’t matter.)
So what does all this mean for the average private medical practice?
In the absence of an official answer, small offices seem likely to be in the clear; and with a court challenge looming and no specific requirements until the middle of November, even if you run an operation big enough to have a measurable effect on interstate commerce, my suggestion is to wait and see.
Nocturnists’ Compensation Puzzles Practice Leaders
Welcome to “Survey Insights,” a new section devoted to exploring and interpreting information from the survey conducted jointly by SHM and the Medical Group Management Association (MGMA). Each month we will focus on a specific topic, providing not only the survey results, but also background information and commentary from members of SHM’s Practice Analysis Committee.
With this month’s release of the 2010-2011 State of Hospital Medicine report, we now have several useful data points regarding the work of nocturnists in HM. In the survey, nocturnist was defined as an individual hospitalist who predominantly works a schedule providing in-house night coverage for inpatients. The question “Does your practice include nocturnists?” was part of the survey’s HM Supplement, and was answered by 238 of the 307 supplement respondents. As was the case last year, 41% of HM practices responding to the survey reported having nocturnists working in their group.
Although less than half of respondent groups reported having nocturnists, more than 55% of the individual hospitalists in the data set worked in groups with nocturnists. This suggests that nocturnists tend to be found more often in larger HM groups.
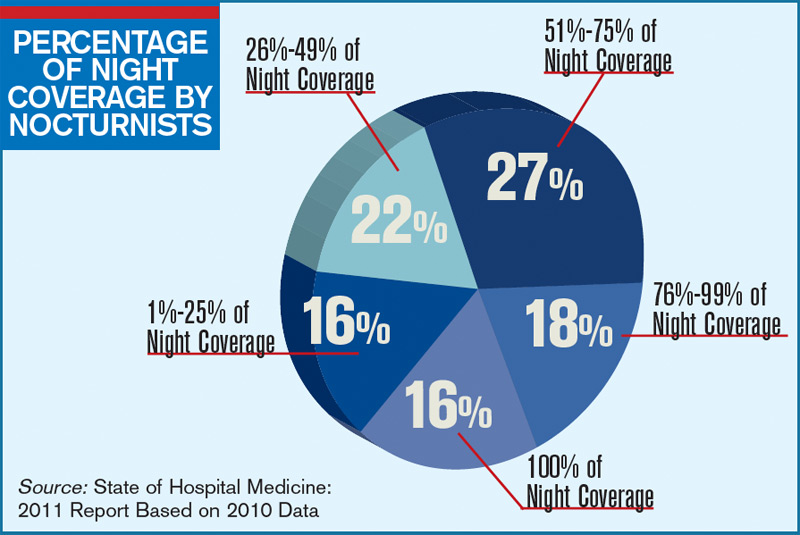
The proportion of night coverage provided by nocturnists varied widely among groups, as can be seen in the chart (see “Percentage of Night Coverage by Nocturnists,” p. 11). Only 16% of the groups with nocturnists used them for all of their night coverage. For about half the groups, the nocturnists provide from one-quarter to three-quarters of the night coverage. This year, data were also obtained on compensation and productivity for 131 nocturnists. Perhaps the most surprising finding is that the median compensation reported for nocturnists in practices that care for adults was $215,000, about 2.5% lower than the median compensation reported for all adult hospitalists. (There was not enough pediatric nocturnist data to report results.)
It’s no surprise, however, that median annual nocturnist productivity was 3,058 wRVUs, about 27% lower than the productivity reported for all adult hospitalists. This suggests that even though median compensation for nocturnists is a bit lower, the “juice to squeeze” ratio for working exclusively at night remains higher than for daytime work.
According to committee member Dan Fuller, president and cofounder of Alpharetta, Ga.-based InCompass Health Inc., “this data supports what we already know: that nocturnists are not as productive as the typical rounding hospitalist. However, they are necessary in most of the larger models, given the need for a physician to be in-house at night for both admissions and emergencies.”
Committee members weren’t sure how to interpret the lower nocturnist compensation, because for many the finding differs from the situation in their own practices. Chris Frost, MD, FHM, vice president of operations for Knoxville, Tenn.-based TeamHealth, postulates that “unless productivity thresholds are adjusted for nocturnists, they will rarely achieve productivity incentives” earned by daytime hospitalists. And PAC member John Nelson, MD, MHM, points out, “There’s more than one way of compensating nocturnists for the inconvenience of working at night. The three nocturnists in our practice, for example, make about the same as everyone else but only work 10 nights a month.”
Leslie Flores, SHM senior advisor, practice management
Welcome to “Survey Insights,” a new section devoted to exploring and interpreting information from the survey conducted jointly by SHM and the Medical Group Management Association (MGMA). Each month we will focus on a specific topic, providing not only the survey results, but also background information and commentary from members of SHM’s Practice Analysis Committee.
With this month’s release of the 2010-2011 State of Hospital Medicine report, we now have several useful data points regarding the work of nocturnists in HM. In the survey, nocturnist was defined as an individual hospitalist who predominantly works a schedule providing in-house night coverage for inpatients. The question “Does your practice include nocturnists?” was part of the survey’s HM Supplement, and was answered by 238 of the 307 supplement respondents. As was the case last year, 41% of HM practices responding to the survey reported having nocturnists working in their group.
Although less than half of respondent groups reported having nocturnists, more than 55% of the individual hospitalists in the data set worked in groups with nocturnists. This suggests that nocturnists tend to be found more often in larger HM groups.
The proportion of night coverage provided by nocturnists varied widely among groups, as can be seen in the chart (see “Percentage of Night Coverage by Nocturnists,” p. 11). Only 16% of the groups with nocturnists used them for all of their night coverage. For about half the groups, the nocturnists provide from one-quarter to three-quarters of the night coverage. This year, data were also obtained on compensation and productivity for 131 nocturnists. Perhaps the most surprising finding is that the median compensation reported for nocturnists in practices that care for adults was $215,000, about 2.5% lower than the median compensation reported for all adult hospitalists. (There was not enough pediatric nocturnist data to report results.)
It’s no surprise, however, that median annual nocturnist productivity was 3,058 wRVUs, about 27% lower than the productivity reported for all adult hospitalists. This suggests that even though median compensation for nocturnists is a bit lower, the “juice to squeeze” ratio for working exclusively at night remains higher than for daytime work.
According to committee member Dan Fuller, president and cofounder of Alpharetta, Ga.-based InCompass Health Inc., “this data supports what we already know: that nocturnists are not as productive as the typical rounding hospitalist. However, they are necessary in most of the larger models, given the need for a physician to be in-house at night for both admissions and emergencies.”
Committee members weren’t sure how to interpret the lower nocturnist compensation, because for many the finding differs from the situation in their own practices. Chris Frost, MD, FHM, vice president of operations for Knoxville, Tenn.-based TeamHealth, postulates that “unless productivity thresholds are adjusted for nocturnists, they will rarely achieve productivity incentives” earned by daytime hospitalists. And PAC member John Nelson, MD, MHM, points out, “There’s more than one way of compensating nocturnists for the inconvenience of working at night. The three nocturnists in our practice, for example, make about the same as everyone else but only work 10 nights a month.”
Leslie Flores, SHM senior advisor, practice management
Welcome to “Survey Insights,” a new section devoted to exploring and interpreting information from the survey conducted jointly by SHM and the Medical Group Management Association (MGMA). Each month we will focus on a specific topic, providing not only the survey results, but also background information and commentary from members of SHM’s Practice Analysis Committee.
With this month’s release of the 2010-2011 State of Hospital Medicine report, we now have several useful data points regarding the work of nocturnists in HM. In the survey, nocturnist was defined as an individual hospitalist who predominantly works a schedule providing in-house night coverage for inpatients. The question “Does your practice include nocturnists?” was part of the survey’s HM Supplement, and was answered by 238 of the 307 supplement respondents. As was the case last year, 41% of HM practices responding to the survey reported having nocturnists working in their group.
Although less than half of respondent groups reported having nocturnists, more than 55% of the individual hospitalists in the data set worked in groups with nocturnists. This suggests that nocturnists tend to be found more often in larger HM groups.
The proportion of night coverage provided by nocturnists varied widely among groups, as can be seen in the chart (see “Percentage of Night Coverage by Nocturnists,” p. 11). Only 16% of the groups with nocturnists used them for all of their night coverage. For about half the groups, the nocturnists provide from one-quarter to three-quarters of the night coverage. This year, data were also obtained on compensation and productivity for 131 nocturnists. Perhaps the most surprising finding is that the median compensation reported for nocturnists in practices that care for adults was $215,000, about 2.5% lower than the median compensation reported for all adult hospitalists. (There was not enough pediatric nocturnist data to report results.)
It’s no surprise, however, that median annual nocturnist productivity was 3,058 wRVUs, about 27% lower than the productivity reported for all adult hospitalists. This suggests that even though median compensation for nocturnists is a bit lower, the “juice to squeeze” ratio for working exclusively at night remains higher than for daytime work.
According to committee member Dan Fuller, president and cofounder of Alpharetta, Ga.-based InCompass Health Inc., “this data supports what we already know: that nocturnists are not as productive as the typical rounding hospitalist. However, they are necessary in most of the larger models, given the need for a physician to be in-house at night for both admissions and emergencies.”
Committee members weren’t sure how to interpret the lower nocturnist compensation, because for many the finding differs from the situation in their own practices. Chris Frost, MD, FHM, vice president of operations for Knoxville, Tenn.-based TeamHealth, postulates that “unless productivity thresholds are adjusted for nocturnists, they will rarely achieve productivity incentives” earned by daytime hospitalists. And PAC member John Nelson, MD, MHM, points out, “There’s more than one way of compensating nocturnists for the inconvenience of working at night. The three nocturnists in our practice, for example, make about the same as everyone else but only work 10 nights a month.”
Leslie Flores, SHM senior advisor, practice management
Conglomerate HM?
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.

—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”

For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
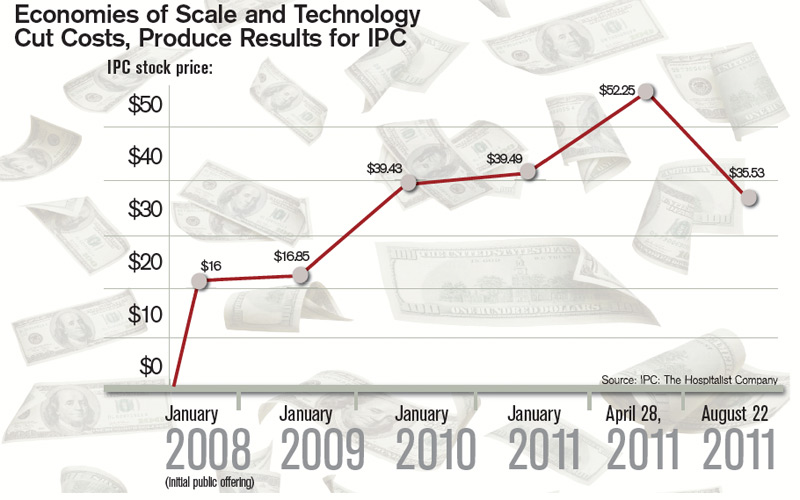
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM

Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine

When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
Modest Gains
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
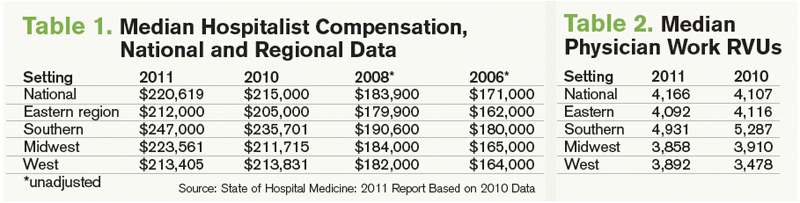
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).

The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time

Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.

—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
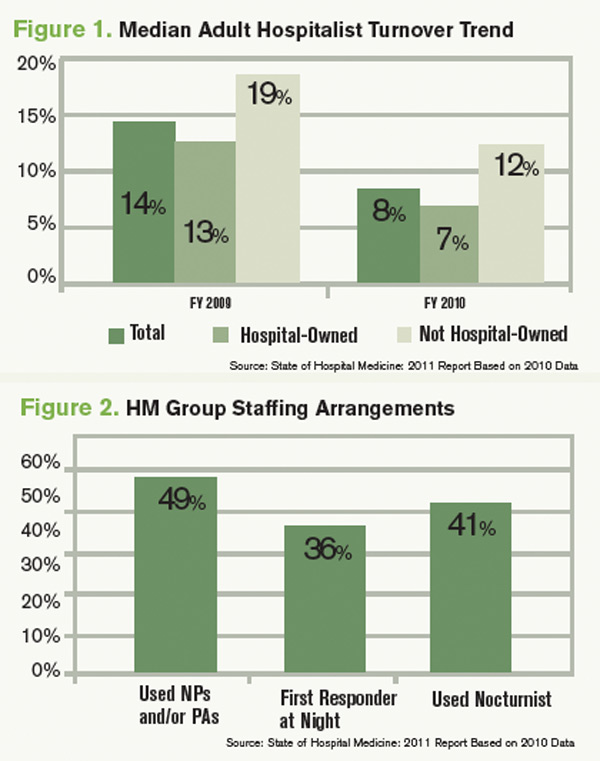
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy

A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Dr. Hospitalist

What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
What I am curious about are the current issues around using length of stay (LOS) or cost/case or the like as part of compensation packages. I have had discussions with several other folks, and I think I am getting the picture. However, it sounds like there has been some new interpretation of the laws around gainsharing, and that is what I am curious about.
K.S., Ohio
Dr. Hospitalist responds:
Tough question, and let me start by saying that I’m not a healthcare lawyer: This stuff is tricky. I’ll do my best to explain the current situation as I understand it, but I’m no expert on this.
So gainsharing, as generally defined in healthcare, is where a hospital and a group of physicians design a contract around services for which the two sides can share in any savings. Physicians are paid fee-for-service by Medicare, thus they are reimbursed per unit of work, with no incentive for cost control. Hospitals are paid on a per-case (or per-procedure) basis, so cost control means a lot to them: Because they get a set payment, any savings generated, they get to keep. Ideally, this means that better performance leads to more efficient care, less waste, and better outcomes. Unfortunately, that’s not always what happens, especially in the view of the federal government (you know, the guys who issue the bright orange jumpsuits for you to wear when you break the law).
Gainsharing has an interesting history as interpreted by the Office of the Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS). Back in 1999, the OIG explicitly stopped any gainsharing models between physicians and hospitals based on concerns that these contracts might reduce the care provided to patients. The opinion was that there might be a “race to the bottom” in terms of cutting expenses (read: services).
Since then, there has been only incremental movement forward in the form of demonstration projects. One project looked at two very specific procedures: cardiac catheterization and coronary artery bypass grafting (CABG). The results showed that gainsharing could be beneficial to the hospital-physician relationship, and, more important, not harmful to the patient. There has since been some movement toward gainsharing, but only in the context of specific procedures, with very clear safeguards around it, including an independent auditor. Nothing to this point has suggested that a cost per case or adjusted LOS gainsharing agreement would pass muster with the OIG.
So, at this point in time, I would caution against any contract that contained explicit references connecting compensation to a change in hospital costs, such as reducing LOS or cost per case. The new accountable-care organization (ACO) model might be a different prism through which to view this, but it’s a world apart from an individual physician or hospitalist group contract (see “A Chilly Reception,” August 2011, p. 23).
For contractual compensation, I think that quality metrics can fill a need, and there are lots of ways to be creative here. You could set a target around something measurable (appropriate DVT prophylaxis is just one example) and tie dollars to that specific performance. The key is avoiding any language that would imply additional physician compensation for a reduction in patient services.
Might things change in the future? Your guess is as good as mine.
ONLINE EXCLUSIVE: Emergency Medicine Companies Venture into Hospital Medicine
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when opportunity came knocking: Hospital administrators started asking, “Can you provide us with some hospitalists to go with our emergency-room doctors?”
Today, HPP is firmly in the HM business—and all signs point toward more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners,” says Ed Weinberg, HPP’s chief operating officer. “Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing. And that is something we are pursuing as vigorously as we are emergency medicine.”
HPP handling both emergency care and hospital medicine can help with the transition of patients from the ED to a hospital bed upstairs, he says.
“That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy,” he says.
Out of HPP’s 120 contracts, 15 are in hospital medicine. But the HM contract numbers are growing quickly, Weinberg notes.
EmCare has about 400 emergency-medicine programs and more than 50 HM programs, according to Mark Hamm, CEO of EmCare Inpatient Services. He says that it can be much more cost effective to contract with one company for both hospitalist and ED services, something hospitals find attractive.
EmCare service agreements range from completely separate emergency and HM staffs to small, rural hospitals where ED physicians also do rounds. Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare, he adds. If they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. But it’s a blip. Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, the executives agreed.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.”