User login
Correction: Acute pancreatitis
Dr. Todd Baron’s middle initial was omitted in his article, Managing severe acute pancreatitis. Cleve Clin J Med 2013; 80:354–359. His full name is Todd H. Baron, MD. This information has been added online.
Dr. Todd Baron’s middle initial was omitted in his article, Managing severe acute pancreatitis. Cleve Clin J Med 2013; 80:354–359. His full name is Todd H. Baron, MD. This information has been added online.
Dr. Todd Baron’s middle initial was omitted in his article, Managing severe acute pancreatitis. Cleve Clin J Med 2013; 80:354–359. His full name is Todd H. Baron, MD. This information has been added online.
Correction: Emergency contraception
Decimal points were misplaced in TABLE 1 in the article by Dr. Pelin Batur, Emergency contraception: Separating fact from fiction. Cleve Clin J Med 2012; 79:771–776. The correct dose of levonorgestrel (Plan B One-Step, Next Choice, generic) is 1.5 mg orally × 1 or 0.75 mg orally × 2. The table has been corrected online.
Decimal points were misplaced in TABLE 1 in the article by Dr. Pelin Batur, Emergency contraception: Separating fact from fiction. Cleve Clin J Med 2012; 79:771–776. The correct dose of levonorgestrel (Plan B One-Step, Next Choice, generic) is 1.5 mg orally × 1 or 0.75 mg orally × 2. The table has been corrected online.
Decimal points were misplaced in TABLE 1 in the article by Dr. Pelin Batur, Emergency contraception: Separating fact from fiction. Cleve Clin J Med 2012; 79:771–776. The correct dose of levonorgestrel (Plan B One-Step, Next Choice, generic) is 1.5 mg orally × 1 or 0.75 mg orally × 2. The table has been corrected online.
Correction: Aspirin
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
Peer-reviewers for 2012
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2012. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2012. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2012. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
Correction: Androgen deficiency in older men
In an article in the November 2012 issue (McGill JJ, Shoskes DA, Sabanegh ES Jr. Androgen deficiency in older men: Indications, advantages, and pitfalls of testosterone replacement therapy. Cleve Clin J Med 2012; 79:797–806), the final sentence of the abstract was omitted. The missing sentence should read as follows: “This article reviews androgen decline in men, focusing on those over age 40, and covers symptoms, indications, contraindications, diagnosis, treatments, and the risks and benefits of treatment.” The online version of the article has been corrected.
In an article in the November 2012 issue (McGill JJ, Shoskes DA, Sabanegh ES Jr. Androgen deficiency in older men: Indications, advantages, and pitfalls of testosterone replacement therapy. Cleve Clin J Med 2012; 79:797–806), the final sentence of the abstract was omitted. The missing sentence should read as follows: “This article reviews androgen decline in men, focusing on those over age 40, and covers symptoms, indications, contraindications, diagnosis, treatments, and the risks and benefits of treatment.” The online version of the article has been corrected.
In an article in the November 2012 issue (McGill JJ, Shoskes DA, Sabanegh ES Jr. Androgen deficiency in older men: Indications, advantages, and pitfalls of testosterone replacement therapy. Cleve Clin J Med 2012; 79:797–806), the final sentence of the abstract was omitted. The missing sentence should read as follows: “This article reviews androgen decline in men, focusing on those over age 40, and covers symptoms, indications, contraindications, diagnosis, treatments, and the risks and benefits of treatment.” The online version of the article has been corrected.
Correction: Anemia, leukocytosis, abdominal pain, flushing, and bone and skin lesion
In the June 2012 issue, on page 384 of the Clinical Picture article by Álvarez-Twose et al (Álvarez-Twose I, Vañó-Galván S, Sanchez-Muñoz L, Fernandez-Zapardiel S, Escribano L. The Clinical Picture: anemia, leukocytosis, abdominal pain, flushing, and bone and skin lesions. Cleve Clin J Med 2012; 79:384–386), Dr. Alvarez-Twose’s first name was spelled incorrectly. The correct spelling is Iván. This error has been corrected in the online version.
In the June 2012 issue, on page 384 of the Clinical Picture article by Álvarez-Twose et al (Álvarez-Twose I, Vañó-Galván S, Sanchez-Muñoz L, Fernandez-Zapardiel S, Escribano L. The Clinical Picture: anemia, leukocytosis, abdominal pain, flushing, and bone and skin lesions. Cleve Clin J Med 2012; 79:384–386), Dr. Alvarez-Twose’s first name was spelled incorrectly. The correct spelling is Iván. This error has been corrected in the online version.
In the June 2012 issue, on page 384 of the Clinical Picture article by Álvarez-Twose et al (Álvarez-Twose I, Vañó-Galván S, Sanchez-Muñoz L, Fernandez-Zapardiel S, Escribano L. The Clinical Picture: anemia, leukocytosis, abdominal pain, flushing, and bone and skin lesions. Cleve Clin J Med 2012; 79:384–386), Dr. Alvarez-Twose’s first name was spelled incorrectly. The correct spelling is Iván. This error has been corrected in the online version.
Correction: Advances in the management of PML
An error appeared in “Advances in the management of PML: focus on natalizumab” (Fox R. Cleve Clin J Med 2011; 78[Suppl 2]:S33–S37), in the November 2011 supplement to the Cleveland Clinic Journal of Medicine, Progressive Multifocal Leukoencephalopathy in the Biologic Era: Implications for Practice. On page S34, in the section “Experience with natalizumab,” the second sentence of the second paragraph included an incorrect percentage. The corrected paragraph appears below. The error has been corrected in the online version of the article.
“The mortality associated with natalizumab-related PML was 19% (29 deaths among the 150 confirmed cases) as of August 4, 2011.3 In cases with at least 6 months of follow-up, mortality has remained at about 20%. Many who survived were left with serious morbidity and permanent disability, although interpretation of disability is difficult because functional impairment is a hallmark of multiple sclerosis (MS) irrespective of PML. Survival in patients with natalizumab-associated PML appears to be better than with PML associated with other conditions, possibly because of early diagnosis achieved through clinical vigilance and swift immune reconstitution through natalizumab discontinuation and either plasmapheresis or immunoabsorption. Predictors of survival include younger age at diagnosis, less disability prior to onset of PML, more localized disease on magnetic resonance imaging (MRI) of the brain, and shorter time from symptom onset to PML diagnosis.”
An error appeared in “Advances in the management of PML: focus on natalizumab” (Fox R. Cleve Clin J Med 2011; 78[Suppl 2]:S33–S37), in the November 2011 supplement to the Cleveland Clinic Journal of Medicine, Progressive Multifocal Leukoencephalopathy in the Biologic Era: Implications for Practice. On page S34, in the section “Experience with natalizumab,” the second sentence of the second paragraph included an incorrect percentage. The corrected paragraph appears below. The error has been corrected in the online version of the article.
“The mortality associated with natalizumab-related PML was 19% (29 deaths among the 150 confirmed cases) as of August 4, 2011.3 In cases with at least 6 months of follow-up, mortality has remained at about 20%. Many who survived were left with serious morbidity and permanent disability, although interpretation of disability is difficult because functional impairment is a hallmark of multiple sclerosis (MS) irrespective of PML. Survival in patients with natalizumab-associated PML appears to be better than with PML associated with other conditions, possibly because of early diagnosis achieved through clinical vigilance and swift immune reconstitution through natalizumab discontinuation and either plasmapheresis or immunoabsorption. Predictors of survival include younger age at diagnosis, less disability prior to onset of PML, more localized disease on magnetic resonance imaging (MRI) of the brain, and shorter time from symptom onset to PML diagnosis.”
An error appeared in “Advances in the management of PML: focus on natalizumab” (Fox R. Cleve Clin J Med 2011; 78[Suppl 2]:S33–S37), in the November 2011 supplement to the Cleveland Clinic Journal of Medicine, Progressive Multifocal Leukoencephalopathy in the Biologic Era: Implications for Practice. On page S34, in the section “Experience with natalizumab,” the second sentence of the second paragraph included an incorrect percentage. The corrected paragraph appears below. The error has been corrected in the online version of the article.
“The mortality associated with natalizumab-related PML was 19% (29 deaths among the 150 confirmed cases) as of August 4, 2011.3 In cases with at least 6 months of follow-up, mortality has remained at about 20%. Many who survived were left with serious morbidity and permanent disability, although interpretation of disability is difficult because functional impairment is a hallmark of multiple sclerosis (MS) irrespective of PML. Survival in patients with natalizumab-associated PML appears to be better than with PML associated with other conditions, possibly because of early diagnosis achieved through clinical vigilance and swift immune reconstitution through natalizumab discontinuation and either plasmapheresis or immunoabsorption. Predictors of survival include younger age at diagnosis, less disability prior to onset of PML, more localized disease on magnetic resonance imaging (MRI) of the brain, and shorter time from symptom onset to PML diagnosis.”
Peer-reviewers for 2011
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2011. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2011. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
We thank those who reviewed manuscripts submitted to the Cleveland Clinic Journal of Medicine in the year ending December 31, 2011. Reviewing papers for scientific journals is an arduous task and involves considerable time and effort. We are grateful to these reviewers for contributing their expertise this past year.
—Brian F. Mandell, MD, PhD, Editor in Chief
Correction: Presumed premature ventricular contractions
In the article “Presumed premature ventricular contractions” by Drs. Moises Auron and Donald Underwood (Cleve Clin J Med 2011; 78:812–813), Figure 1 was incorrectly labelled. The corrected figure and legend appear below. The authors wish to thank Philippe Akhrass, MD, from the State University of New York, Brooklyn, and Shahrokh Rafii, MD, from Brookdale University Hospital and Medical Center, Brooklyn, NY, for pointing out this error.
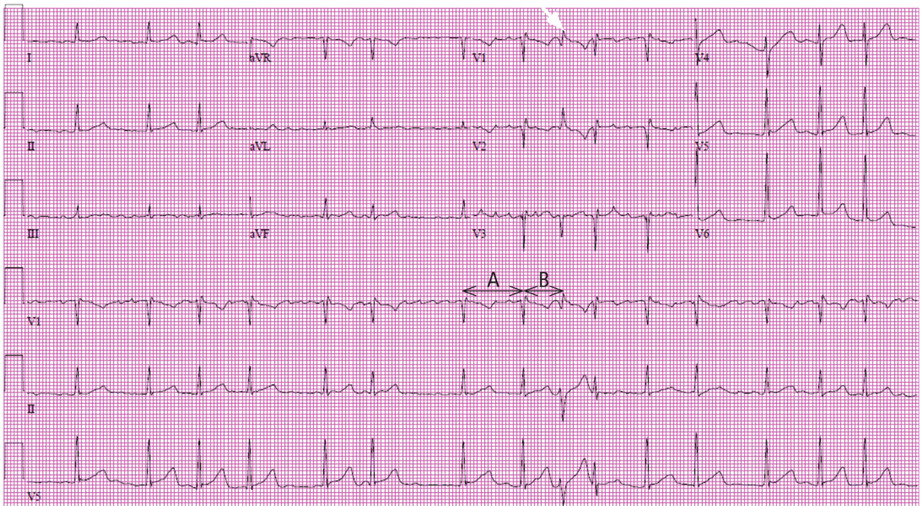
In the article “Presumed premature ventricular contractions” by Drs. Moises Auron and Donald Underwood (Cleve Clin J Med 2011; 78:812–813), Figure 1 was incorrectly labelled. The corrected figure and legend appear below. The authors wish to thank Philippe Akhrass, MD, from the State University of New York, Brooklyn, and Shahrokh Rafii, MD, from Brookdale University Hospital and Medical Center, Brooklyn, NY, for pointing out this error.
In the article “Presumed premature ventricular contractions” by Drs. Moises Auron and Donald Underwood (Cleve Clin J Med 2011; 78:812–813), Figure 1 was incorrectly labelled. The corrected figure and legend appear below. The authors wish to thank Philippe Akhrass, MD, from the State University of New York, Brooklyn, and Shahrokh Rafii, MD, from Brookdale University Hospital and Medical Center, Brooklyn, NY, for pointing out this error.
Correction: Measles