User login
Appeals court ruling protects marijuana doctors from prosecution
A new appellate ruling protects doctors from federal prosecution when they recommend medical marijuana in accordance with state law.
In an Aug. 16 opinion, the 9th U.S. Circuit Court of Appeals ruled that the U.S. Department of Justice cannot spend funding to prosecute physicians and patients who allegedly violate federal drug laws if their actions comply with state medical cannabis statutes.

The decision supports the longstanding policies of several medical specialty societies.
“The conflict between state and federal law regarding medical marijuana can be concerning for patients and physicians who may consider using or recommending marijuana as a treatment option,” Hilary Daniel, senior health policy analyst for the American College of Physicians, said in an interview. “We are encouraged that the decision by the 9th U.S. Circuit Court of Appeals may help to address some of these conflicts and remain cognizant of the potential challenges faced by physicians and patients outside the jurisdiction of the 9th Circuit.”
The ruling stems from a 2014 federal appropriations law that banned the Justice Department from interfering with state implementation of marijuana laws. Short-term measures since then have extended the prohibition, which now continues through Sept. 30, 2016. Defendants in 10 criminal cases sued the federal government, requesting their prosecutions be dismissed on the grounds that the Justice Department is prevented from spending funds to prosecute them. The parties were accused of various federal marijuana offenses, including conspiracy to manufacture and possession with intent to distribute. The Justice Department argued it is not preventing states from operating their medical marijuana laws by prosecuting private individuals. Three district courts declined to halt the prosecutions from proceeding.
But the appeals court ruled that the Justice Department is prohibited from spending funds from relevant federal appropriation to prosecute the defendants if their conduct was permitted by state medical marijuana laws. Judges remanded the cases to the district courts with instructions that if the Justice Department wishes to continue the cases, the appellants are entitled to hearings to determine whether their actions were authorized by state laws.
The decision is significant because it establishes an appellate level precedent regarding enforcement of the Congressional budget requirements, said Joshua Prober, general counsel and senior vice president for the American Osteopathic Association. However, the decision does not overturn federal criminal laws regarding marijuana use and is limited to the impact of Congress’ specific budgetary authorization measure, he said.
“As noted in the court’s opinion, it is quite possible that a future Congress will not put the same restrictions in place on federal prosecutorial activity,” Mr. Prober said in an interview. “And obviously there are the procedural limitations, i.e., the decision is only the view of one appellate circuit. It is possible that a different appellate court might find the Department of Justice’s arguments to be more persuasive.”
The appeals ruling comes less than a week after the U.S. Drug Enforcement Agency refused to reclassify marijuana under the Controlled Substances Act. Marijuana remains a schedule I controlled substance, noting in its decision that marijuana does not meet the criteria for currently accepted medical use in the United States, that there is a lack of accepted safety for its use under medical supervision, and that it has a high potential for abuse.
“The DEA and FDA continue to believe that scientifically valid and well-controlled clinical trials conducted under investigational new drug applications are the proper way to research all potential new medicines, including marijuana,” DEA Acting Administrator Chuck Rosenberg wrote in a letter to state governors. “Furthermore, we believe that the drug approval process is the proper way to assess whether a product derived from marijuana or its constituent parts is safe and effective for medical use.”
While tension between state and federal law regarding marijuana lingers, more states continue to approve marijuana for recreational and medical use, noted John A. DiNome, a health law attorney based in Philadelphia. So far, Oregon, Colorado, Washington, and Alaska allow recreational marijuana use, while 25 states have approved marijuana for medical use. At least 9 more states will consider recreational marijuana use in November.
“For the time being, the problem still exists,” Mr. DiNome said in an interview. “This temporarily keeps doctors off the hook from prosecution, but it doesn’t solve the underlying problem, which is: Is federal law going to change?”
On Twitter @legal_med
A new appellate ruling protects doctors from federal prosecution when they recommend medical marijuana in accordance with state law.
In an Aug. 16 opinion, the 9th U.S. Circuit Court of Appeals ruled that the U.S. Department of Justice cannot spend funding to prosecute physicians and patients who allegedly violate federal drug laws if their actions comply with state medical cannabis statutes.
The decision supports the longstanding policies of several medical specialty societies.
“The conflict between state and federal law regarding medical marijuana can be concerning for patients and physicians who may consider using or recommending marijuana as a treatment option,” Hilary Daniel, senior health policy analyst for the American College of Physicians, said in an interview. “We are encouraged that the decision by the 9th U.S. Circuit Court of Appeals may help to address some of these conflicts and remain cognizant of the potential challenges faced by physicians and patients outside the jurisdiction of the 9th Circuit.”
The ruling stems from a 2014 federal appropriations law that banned the Justice Department from interfering with state implementation of marijuana laws. Short-term measures since then have extended the prohibition, which now continues through Sept. 30, 2016. Defendants in 10 criminal cases sued the federal government, requesting their prosecutions be dismissed on the grounds that the Justice Department is prevented from spending funds to prosecute them. The parties were accused of various federal marijuana offenses, including conspiracy to manufacture and possession with intent to distribute. The Justice Department argued it is not preventing states from operating their medical marijuana laws by prosecuting private individuals. Three district courts declined to halt the prosecutions from proceeding.
But the appeals court ruled that the Justice Department is prohibited from spending funds from relevant federal appropriation to prosecute the defendants if their conduct was permitted by state medical marijuana laws. Judges remanded the cases to the district courts with instructions that if the Justice Department wishes to continue the cases, the appellants are entitled to hearings to determine whether their actions were authorized by state laws.
The decision is significant because it establishes an appellate level precedent regarding enforcement of the Congressional budget requirements, said Joshua Prober, general counsel and senior vice president for the American Osteopathic Association. However, the decision does not overturn federal criminal laws regarding marijuana use and is limited to the impact of Congress’ specific budgetary authorization measure, he said.
“As noted in the court’s opinion, it is quite possible that a future Congress will not put the same restrictions in place on federal prosecutorial activity,” Mr. Prober said in an interview. “And obviously there are the procedural limitations, i.e., the decision is only the view of one appellate circuit. It is possible that a different appellate court might find the Department of Justice’s arguments to be more persuasive.”
The appeals ruling comes less than a week after the U.S. Drug Enforcement Agency refused to reclassify marijuana under the Controlled Substances Act. Marijuana remains a schedule I controlled substance, noting in its decision that marijuana does not meet the criteria for currently accepted medical use in the United States, that there is a lack of accepted safety for its use under medical supervision, and that it has a high potential for abuse.
“The DEA and FDA continue to believe that scientifically valid and well-controlled clinical trials conducted under investigational new drug applications are the proper way to research all potential new medicines, including marijuana,” DEA Acting Administrator Chuck Rosenberg wrote in a letter to state governors. “Furthermore, we believe that the drug approval process is the proper way to assess whether a product derived from marijuana or its constituent parts is safe and effective for medical use.”
While tension between state and federal law regarding marijuana lingers, more states continue to approve marijuana for recreational and medical use, noted John A. DiNome, a health law attorney based in Philadelphia. So far, Oregon, Colorado, Washington, and Alaska allow recreational marijuana use, while 25 states have approved marijuana for medical use. At least 9 more states will consider recreational marijuana use in November.
“For the time being, the problem still exists,” Mr. DiNome said in an interview. “This temporarily keeps doctors off the hook from prosecution, but it doesn’t solve the underlying problem, which is: Is federal law going to change?”
On Twitter @legal_med
A new appellate ruling protects doctors from federal prosecution when they recommend medical marijuana in accordance with state law.
In an Aug. 16 opinion, the 9th U.S. Circuit Court of Appeals ruled that the U.S. Department of Justice cannot spend funding to prosecute physicians and patients who allegedly violate federal drug laws if their actions comply with state medical cannabis statutes.
The decision supports the longstanding policies of several medical specialty societies.
“The conflict between state and federal law regarding medical marijuana can be concerning for patients and physicians who may consider using or recommending marijuana as a treatment option,” Hilary Daniel, senior health policy analyst for the American College of Physicians, said in an interview. “We are encouraged that the decision by the 9th U.S. Circuit Court of Appeals may help to address some of these conflicts and remain cognizant of the potential challenges faced by physicians and patients outside the jurisdiction of the 9th Circuit.”
The ruling stems from a 2014 federal appropriations law that banned the Justice Department from interfering with state implementation of marijuana laws. Short-term measures since then have extended the prohibition, which now continues through Sept. 30, 2016. Defendants in 10 criminal cases sued the federal government, requesting their prosecutions be dismissed on the grounds that the Justice Department is prevented from spending funds to prosecute them. The parties were accused of various federal marijuana offenses, including conspiracy to manufacture and possession with intent to distribute. The Justice Department argued it is not preventing states from operating their medical marijuana laws by prosecuting private individuals. Three district courts declined to halt the prosecutions from proceeding.
But the appeals court ruled that the Justice Department is prohibited from spending funds from relevant federal appropriation to prosecute the defendants if their conduct was permitted by state medical marijuana laws. Judges remanded the cases to the district courts with instructions that if the Justice Department wishes to continue the cases, the appellants are entitled to hearings to determine whether their actions were authorized by state laws.
The decision is significant because it establishes an appellate level precedent regarding enforcement of the Congressional budget requirements, said Joshua Prober, general counsel and senior vice president for the American Osteopathic Association. However, the decision does not overturn federal criminal laws regarding marijuana use and is limited to the impact of Congress’ specific budgetary authorization measure, he said.
“As noted in the court’s opinion, it is quite possible that a future Congress will not put the same restrictions in place on federal prosecutorial activity,” Mr. Prober said in an interview. “And obviously there are the procedural limitations, i.e., the decision is only the view of one appellate circuit. It is possible that a different appellate court might find the Department of Justice’s arguments to be more persuasive.”
The appeals ruling comes less than a week after the U.S. Drug Enforcement Agency refused to reclassify marijuana under the Controlled Substances Act. Marijuana remains a schedule I controlled substance, noting in its decision that marijuana does not meet the criteria for currently accepted medical use in the United States, that there is a lack of accepted safety for its use under medical supervision, and that it has a high potential for abuse.
“The DEA and FDA continue to believe that scientifically valid and well-controlled clinical trials conducted under investigational new drug applications are the proper way to research all potential new medicines, including marijuana,” DEA Acting Administrator Chuck Rosenberg wrote in a letter to state governors. “Furthermore, we believe that the drug approval process is the proper way to assess whether a product derived from marijuana or its constituent parts is safe and effective for medical use.”
While tension between state and federal law regarding marijuana lingers, more states continue to approve marijuana for recreational and medical use, noted John A. DiNome, a health law attorney based in Philadelphia. So far, Oregon, Colorado, Washington, and Alaska allow recreational marijuana use, while 25 states have approved marijuana for medical use. At least 9 more states will consider recreational marijuana use in November.
“For the time being, the problem still exists,” Mr. DiNome said in an interview. “This temporarily keeps doctors off the hook from prosecution, but it doesn’t solve the underlying problem, which is: Is federal law going to change?”
On Twitter @legal_med

Obamacare marketplace shakeout rocks Arizona, Southeast
Some of the Affordable Care Act’s insurance marketplaces are in turmoil as the fourth open enrollment season approaches this fall, but what’s ahead for consumers very much depends on where they live.
Competition on these exchanges will be diminished next year when three of the nation’s largest health insurers – Aetna, UnitedHealthcare and Humana – will sell individual plans in many fewer markets. So too will several Blue Cross and Blue Shield plans in various states. That’s on top of the 16 nonprofit co-ops that have closed since January 2015.
The announcements, however, apply generally only to the individual market. The much larger market of employer-sponsored insurance is not part of the health law exchanges.
Aetna’s exit announcement Aug. 15 that blamed financial losses on its marketplace plans gave Obamacare opponents who have from the start predicted the ACA’s failure a fresh chance to proclaim “I told you so.”
That story line got more complicated Aug. 17 after the Huffington Post reported that Aetna CEO Mark Bertolini sent a letter to the Department of Justice (DOJ) on July 5 threatening to withdraw from the Obamacare marketplaces if the DOJ sued to block his company’s planned merger with Humana. The DOJ did just that a couple weeks later.
But most marketplace consumers won’t see any ill effects from insurers’ withdrawals, according to ACA advocates and independent experts.
“The effect on consumers is going to be mixed around the country,” said Katherine Hempstead, PhD, a senior adviser at the nonpartisan Robert Wood Johnson Foundation. “Most of these marketplaces are not dependent on” the large national carriers.
Many major metropolitan areas, such as those in California, New York, and Texas, will still have several insurers for individual health insurance consumers to choose from. In Texas, all major metro areas – including Austin, Dallas, Houston, and San Antonio – will have at least three insurers after Aetna and UnitedHealthcare exit.
That’s true also for most urban exchange customers living in the Northwest, the Midwest, and New England.
Most hurt will be marketplace consumers in Arizona, North and South Carolina, Georgia, and parts of Florida, where only one or two insurers will be left when open enrollment season begins Nov. 15.
Remaining insurers might raise their monthly premiums as a result, but more than eight in 10 consumers on the marketplaces who get government subsidies would be insulated. Subsidies increase as premiums rise.
Still, health experts worry that with less competition, insurers may tighten their provider networks and give these consumers fewer choices of hospitals and doctors. That trend started several years ago, and some states have responded with regulations requiring insurers to provide customers with reasonable access to doctors and hospitals in each county where they sell plans.
Nearly 13 million people signed up for Obamacare marketplace policies for 2016. Aetna, UnitedHealthcare, and Humana have 2 million members in total, but their exit from certain states is predicted to affect between 1 million and 1.5 million people who will have to choose new carriers.
While changing plans can force people to find new doctors, it’s also the best way for consumers get the best deals on coverage.
Aetna will exit 11 of 15 states where it sells plans on the exchanges. UnitedHealthcare has said it will quit 22 of 34 states, and Humana will leave 4 of the 15 states where it operates.
In late May, the Kaiser Family Foundation estimated the number of rural counties at risk of having one insurer on the exchanges would triple in 2017. That was before Humana and Aetna detailed their plans. (KHN is an editorially independent project of the foundation.)
Now, “we could be looking at about one in four counties in the U.S. with just one exchange insurer next year, though this could change between now and open enrollment in November,” said Cynthia Cox, associate director for the Kaiser Family Foundation Program for the Study of Health Reform and Private Insurance.
Overshadowed by the big insurers’ withdrawals is the prospect that other carriers will enter markets the three giants are leaving. Smaller insurers Molina and Centene have said they’re doing fine on the exchanges. And Cigna, a larger insurer, has said it will move into some North Carolina counties for 2017.
North Carolina will be left with just one or two plans in most of the state after it loses UnitedHealthcare and Aetna plans. Health insurance experts say three insurers are needed for a healthy competitive market.
“We’ve had a very robust enrollment under the ACA and hope consumers will still see benefits of having coverage even if they have fewer options,” said Ciara Zachary, health policy analyst for the North Carolina Justice Center’s Health Access Coalition.
Rural Americans had few health insurers to choose from even before Obamacare, but some suburban and urban parts of the Southeast will be in the same fix next year. In southeast Florida, consumers in counties near Naples and Fort Myers will have only one marketplace insurer – Florida Blue – next year, unless other insurers step in.
“There are some headwinds, but it’s not a question of whether the market will stabilize but how quickly and how well,” said Dr. Hempstead.
Strong winds are already blowing toward Arizona’s Pinal County, southeast of Phoenix, health care advocates say. Nearly 10,000 people enrolled in Obamacare marketplace policies this year and about 85% received a federal subsidy.
In 2017, Pinal stands to lose its only two insurers – UnitedHealthcare and Blue Cross and Blue Shield of Arizona.
“Clearly this is a big concern for consumers,” said Allen Gjersvig, director of navigator and enrollment services for the Arizona Alliance for Community Health Centers. He said he is hopeful, but not confident, that another insurer will step in.
Neighboring Maricopa County, which includes Phoenix, is expected to have just two relatively small insurers left on its marketplace next year. Mr. Gjersvig said that he questions whether those two – Cigna and Phoenix Health Plan – will have enough doctors and hospitals under contract to handle their new members after larger rival Blue Cross and Blue Shield of Arizona gives up its 40,000 customers.
At least a dozen other counties in Arizona will be left with just one health insurer, he said.
Arizona had eight insurers operating in various parts of the state this year, but four are leaving entirely – Aetna, UnitedHealthcare, Humana, and Health Choice. Two more, Blue Cross Blue Shield and Health Net, are scaling back their participation.
Despite the problems with the marketplaces, Mr. Gjersvig said thousands of people have gained coverage through them and he is confident they will survive.
“We do not see this as a death knell for the marketplace,” he said.
Tammie King, an insurance agent in Columbia, S.C., is less sure how insurer departures will affect consumers in the Palmetto State. Pullouts by UnitedHealthcare and Aetna mean only one carrier in the state in 2017 – Blue Cross and Blue Shield of South Carolina.
That’s a concern in Columbia, S.C., because the Blue Cross plan does not include one of the biggest hospitals, Lexington Medical Center, and its affiliated physicians, she said.
“People will be left unable to see the doctors they are now using,” she added.
Ms. King said she worried the Blue Cross plan will use its monopoly power to further reduce the number of doctors and hospitals in its network and limit its choice of prescription drugs. “You can’t blame them because … they have to do something to control costs,” she said.
This story appears courtesy of Kaiser Health News, a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Some of the Affordable Care Act’s insurance marketplaces are in turmoil as the fourth open enrollment season approaches this fall, but what’s ahead for consumers very much depends on where they live.
Competition on these exchanges will be diminished next year when three of the nation’s largest health insurers – Aetna, UnitedHealthcare and Humana – will sell individual plans in many fewer markets. So too will several Blue Cross and Blue Shield plans in various states. That’s on top of the 16 nonprofit co-ops that have closed since January 2015.
The announcements, however, apply generally only to the individual market. The much larger market of employer-sponsored insurance is not part of the health law exchanges.
Aetna’s exit announcement Aug. 15 that blamed financial losses on its marketplace plans gave Obamacare opponents who have from the start predicted the ACA’s failure a fresh chance to proclaim “I told you so.”
That story line got more complicated Aug. 17 after the Huffington Post reported that Aetna CEO Mark Bertolini sent a letter to the Department of Justice (DOJ) on July 5 threatening to withdraw from the Obamacare marketplaces if the DOJ sued to block his company’s planned merger with Humana. The DOJ did just that a couple weeks later.
But most marketplace consumers won’t see any ill effects from insurers’ withdrawals, according to ACA advocates and independent experts.
“The effect on consumers is going to be mixed around the country,” said Katherine Hempstead, PhD, a senior adviser at the nonpartisan Robert Wood Johnson Foundation. “Most of these marketplaces are not dependent on” the large national carriers.
Many major metropolitan areas, such as those in California, New York, and Texas, will still have several insurers for individual health insurance consumers to choose from. In Texas, all major metro areas – including Austin, Dallas, Houston, and San Antonio – will have at least three insurers after Aetna and UnitedHealthcare exit.
That’s true also for most urban exchange customers living in the Northwest, the Midwest, and New England.
Most hurt will be marketplace consumers in Arizona, North and South Carolina, Georgia, and parts of Florida, where only one or two insurers will be left when open enrollment season begins Nov. 15.
Remaining insurers might raise their monthly premiums as a result, but more than eight in 10 consumers on the marketplaces who get government subsidies would be insulated. Subsidies increase as premiums rise.
Still, health experts worry that with less competition, insurers may tighten their provider networks and give these consumers fewer choices of hospitals and doctors. That trend started several years ago, and some states have responded with regulations requiring insurers to provide customers with reasonable access to doctors and hospitals in each county where they sell plans.
Nearly 13 million people signed up for Obamacare marketplace policies for 2016. Aetna, UnitedHealthcare, and Humana have 2 million members in total, but their exit from certain states is predicted to affect between 1 million and 1.5 million people who will have to choose new carriers.
While changing plans can force people to find new doctors, it’s also the best way for consumers get the best deals on coverage.
Aetna will exit 11 of 15 states where it sells plans on the exchanges. UnitedHealthcare has said it will quit 22 of 34 states, and Humana will leave 4 of the 15 states where it operates.
In late May, the Kaiser Family Foundation estimated the number of rural counties at risk of having one insurer on the exchanges would triple in 2017. That was before Humana and Aetna detailed their plans. (KHN is an editorially independent project of the foundation.)
Now, “we could be looking at about one in four counties in the U.S. with just one exchange insurer next year, though this could change between now and open enrollment in November,” said Cynthia Cox, associate director for the Kaiser Family Foundation Program for the Study of Health Reform and Private Insurance.
Overshadowed by the big insurers’ withdrawals is the prospect that other carriers will enter markets the three giants are leaving. Smaller insurers Molina and Centene have said they’re doing fine on the exchanges. And Cigna, a larger insurer, has said it will move into some North Carolina counties for 2017.
North Carolina will be left with just one or two plans in most of the state after it loses UnitedHealthcare and Aetna plans. Health insurance experts say three insurers are needed for a healthy competitive market.
“We’ve had a very robust enrollment under the ACA and hope consumers will still see benefits of having coverage even if they have fewer options,” said Ciara Zachary, health policy analyst for the North Carolina Justice Center’s Health Access Coalition.
Rural Americans had few health insurers to choose from even before Obamacare, but some suburban and urban parts of the Southeast will be in the same fix next year. In southeast Florida, consumers in counties near Naples and Fort Myers will have only one marketplace insurer – Florida Blue – next year, unless other insurers step in.
“There are some headwinds, but it’s not a question of whether the market will stabilize but how quickly and how well,” said Dr. Hempstead.
Strong winds are already blowing toward Arizona’s Pinal County, southeast of Phoenix, health care advocates say. Nearly 10,000 people enrolled in Obamacare marketplace policies this year and about 85% received a federal subsidy.
In 2017, Pinal stands to lose its only two insurers – UnitedHealthcare and Blue Cross and Blue Shield of Arizona.
“Clearly this is a big concern for consumers,” said Allen Gjersvig, director of navigator and enrollment services for the Arizona Alliance for Community Health Centers. He said he is hopeful, but not confident, that another insurer will step in.
Neighboring Maricopa County, which includes Phoenix, is expected to have just two relatively small insurers left on its marketplace next year. Mr. Gjersvig said that he questions whether those two – Cigna and Phoenix Health Plan – will have enough doctors and hospitals under contract to handle their new members after larger rival Blue Cross and Blue Shield of Arizona gives up its 40,000 customers.
At least a dozen other counties in Arizona will be left with just one health insurer, he said.
Arizona had eight insurers operating in various parts of the state this year, but four are leaving entirely – Aetna, UnitedHealthcare, Humana, and Health Choice. Two more, Blue Cross Blue Shield and Health Net, are scaling back their participation.
Despite the problems with the marketplaces, Mr. Gjersvig said thousands of people have gained coverage through them and he is confident they will survive.
“We do not see this as a death knell for the marketplace,” he said.
Tammie King, an insurance agent in Columbia, S.C., is less sure how insurer departures will affect consumers in the Palmetto State. Pullouts by UnitedHealthcare and Aetna mean only one carrier in the state in 2017 – Blue Cross and Blue Shield of South Carolina.
That’s a concern in Columbia, S.C., because the Blue Cross plan does not include one of the biggest hospitals, Lexington Medical Center, and its affiliated physicians, she said.
“People will be left unable to see the doctors they are now using,” she added.
Ms. King said she worried the Blue Cross plan will use its monopoly power to further reduce the number of doctors and hospitals in its network and limit its choice of prescription drugs. “You can’t blame them because … they have to do something to control costs,” she said.
This story appears courtesy of Kaiser Health News, a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Some of the Affordable Care Act’s insurance marketplaces are in turmoil as the fourth open enrollment season approaches this fall, but what’s ahead for consumers very much depends on where they live.
Competition on these exchanges will be diminished next year when three of the nation’s largest health insurers – Aetna, UnitedHealthcare and Humana – will sell individual plans in many fewer markets. So too will several Blue Cross and Blue Shield plans in various states. That’s on top of the 16 nonprofit co-ops that have closed since January 2015.
The announcements, however, apply generally only to the individual market. The much larger market of employer-sponsored insurance is not part of the health law exchanges.
Aetna’s exit announcement Aug. 15 that blamed financial losses on its marketplace plans gave Obamacare opponents who have from the start predicted the ACA’s failure a fresh chance to proclaim “I told you so.”
That story line got more complicated Aug. 17 after the Huffington Post reported that Aetna CEO Mark Bertolini sent a letter to the Department of Justice (DOJ) on July 5 threatening to withdraw from the Obamacare marketplaces if the DOJ sued to block his company’s planned merger with Humana. The DOJ did just that a couple weeks later.
But most marketplace consumers won’t see any ill effects from insurers’ withdrawals, according to ACA advocates and independent experts.
“The effect on consumers is going to be mixed around the country,” said Katherine Hempstead, PhD, a senior adviser at the nonpartisan Robert Wood Johnson Foundation. “Most of these marketplaces are not dependent on” the large national carriers.
Many major metropolitan areas, such as those in California, New York, and Texas, will still have several insurers for individual health insurance consumers to choose from. In Texas, all major metro areas – including Austin, Dallas, Houston, and San Antonio – will have at least three insurers after Aetna and UnitedHealthcare exit.
That’s true also for most urban exchange customers living in the Northwest, the Midwest, and New England.
Most hurt will be marketplace consumers in Arizona, North and South Carolina, Georgia, and parts of Florida, where only one or two insurers will be left when open enrollment season begins Nov. 15.
Remaining insurers might raise their monthly premiums as a result, but more than eight in 10 consumers on the marketplaces who get government subsidies would be insulated. Subsidies increase as premiums rise.
Still, health experts worry that with less competition, insurers may tighten their provider networks and give these consumers fewer choices of hospitals and doctors. That trend started several years ago, and some states have responded with regulations requiring insurers to provide customers with reasonable access to doctors and hospitals in each county where they sell plans.
Nearly 13 million people signed up for Obamacare marketplace policies for 2016. Aetna, UnitedHealthcare, and Humana have 2 million members in total, but their exit from certain states is predicted to affect between 1 million and 1.5 million people who will have to choose new carriers.
While changing plans can force people to find new doctors, it’s also the best way for consumers get the best deals on coverage.
Aetna will exit 11 of 15 states where it sells plans on the exchanges. UnitedHealthcare has said it will quit 22 of 34 states, and Humana will leave 4 of the 15 states where it operates.
In late May, the Kaiser Family Foundation estimated the number of rural counties at risk of having one insurer on the exchanges would triple in 2017. That was before Humana and Aetna detailed their plans. (KHN is an editorially independent project of the foundation.)
Now, “we could be looking at about one in four counties in the U.S. with just one exchange insurer next year, though this could change between now and open enrollment in November,” said Cynthia Cox, associate director for the Kaiser Family Foundation Program for the Study of Health Reform and Private Insurance.
Overshadowed by the big insurers’ withdrawals is the prospect that other carriers will enter markets the three giants are leaving. Smaller insurers Molina and Centene have said they’re doing fine on the exchanges. And Cigna, a larger insurer, has said it will move into some North Carolina counties for 2017.
North Carolina will be left with just one or two plans in most of the state after it loses UnitedHealthcare and Aetna plans. Health insurance experts say three insurers are needed for a healthy competitive market.
“We’ve had a very robust enrollment under the ACA and hope consumers will still see benefits of having coverage even if they have fewer options,” said Ciara Zachary, health policy analyst for the North Carolina Justice Center’s Health Access Coalition.
Rural Americans had few health insurers to choose from even before Obamacare, but some suburban and urban parts of the Southeast will be in the same fix next year. In southeast Florida, consumers in counties near Naples and Fort Myers will have only one marketplace insurer – Florida Blue – next year, unless other insurers step in.
“There are some headwinds, but it’s not a question of whether the market will stabilize but how quickly and how well,” said Dr. Hempstead.
Strong winds are already blowing toward Arizona’s Pinal County, southeast of Phoenix, health care advocates say. Nearly 10,000 people enrolled in Obamacare marketplace policies this year and about 85% received a federal subsidy.
In 2017, Pinal stands to lose its only two insurers – UnitedHealthcare and Blue Cross and Blue Shield of Arizona.
“Clearly this is a big concern for consumers,” said Allen Gjersvig, director of navigator and enrollment services for the Arizona Alliance for Community Health Centers. He said he is hopeful, but not confident, that another insurer will step in.
Neighboring Maricopa County, which includes Phoenix, is expected to have just two relatively small insurers left on its marketplace next year. Mr. Gjersvig said that he questions whether those two – Cigna and Phoenix Health Plan – will have enough doctors and hospitals under contract to handle their new members after larger rival Blue Cross and Blue Shield of Arizona gives up its 40,000 customers.
At least a dozen other counties in Arizona will be left with just one health insurer, he said.
Arizona had eight insurers operating in various parts of the state this year, but four are leaving entirely – Aetna, UnitedHealthcare, Humana, and Health Choice. Two more, Blue Cross Blue Shield and Health Net, are scaling back their participation.
Despite the problems with the marketplaces, Mr. Gjersvig said thousands of people have gained coverage through them and he is confident they will survive.
“We do not see this as a death knell for the marketplace,” he said.
Tammie King, an insurance agent in Columbia, S.C., is less sure how insurer departures will affect consumers in the Palmetto State. Pullouts by UnitedHealthcare and Aetna mean only one carrier in the state in 2017 – Blue Cross and Blue Shield of South Carolina.
That’s a concern in Columbia, S.C., because the Blue Cross plan does not include one of the biggest hospitals, Lexington Medical Center, and its affiliated physicians, she said.
“People will be left unable to see the doctors they are now using,” she added.
Ms. King said she worried the Blue Cross plan will use its monopoly power to further reduce the number of doctors and hospitals in its network and limit its choice of prescription drugs. “You can’t blame them because … they have to do something to control costs,” she said.
This story appears courtesy of Kaiser Health News, a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Providing Effective Palliative Care in the Era of Value
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.
Although effective palliative care has always been a must-have for patients and caregivers facing serious illness, it hasn’t always been readily available. With the emergence of value-based healthcare models—and their potent incentives to reduce avoidable readmissions—there is renewed hope that such care will be accessible to those who need it.
Palliative and end-of-life care have long been promoted as core skills for hospitalists. The topic has regularly been included at SHM annual meetings and other prominent hospital medicine conferences, in the American Board of Internal Medicine blueprint for recognition of focused practice in hospital medicine, and in a number of influential references for hospitalists. Still, as I look at hospitalist programs around the country, there is a clear need to improve hospitalists’ delivery of palliative and end-of-life care.
Care of patients with chronic illness in their last two years of life accounts for a third of all Medicare spending.1 As hospitalists, we encounter many of these patients as they are hospitalized—and often re-hospitalized. Palliative care, which can improve quality of life and decrease costs for patients while leading to increased satisfaction and better outcomes for caregivers, can help alleviate unneeded and unwanted aggressive interventions like hospitalization.2,3
In its 2014 report, Dying in America, the Institute of Medicine (IOM) identified several areas for improvement, including better advance care planning and payment systems supporting high quality end-of-life care.4 As I write this column in mid 2016, there are two notable achievements since the IOM report: two E&M codes for advance care planning and a substantial and growing number of hospitalist patients in alternative payment models like bundled payments or ACOs.5 I believe we are entering a time when the availability of good palliative care will be accelerated due to broader forces in healthcare that for the first time align incentives between patients’ wishes and how care is paid for.
Palliative Care Skills for Hospitalists
The following are key actions for physicians in addressing palliative care for the hospitalized patient. At the risk of oversimplifying the discipline, I offer a few key actions for hospitalists to keep in mind.
Identify patients who would benefit from palliative care. The surprise question—“Would I be surprised if this patient died in the next year?”—has the ability to predict which patients would benefit from palliative care. In one observation from a group of patients with cancer, a “no” answer identified 60% of patients who died within a year.6 The surprise question has previously been shown to be predictive in other cancer and non-cancer populations.7,8
Weisman and Meier suggest using the following in a checklist at the time of hospital admission as “primary criteria to screen for unmet palliative care needs”:9
- The surprise question
- Frequent admissions
- Admission prompted by difficult-to-control physical or psychological symptoms
- Complex care requirements
- Decline in function, feeding intolerance, or unintended decline in weight
Hold a “goals of care” meeting. A notable step forward for supporting conversations between physicians and patients occurred on Jan. 1, when the Centers for Medicare & Medicaid Services (CMS) announced the Advance Care Planning E&M codes. These are CPT codes 99497 and 99498. They can be used on the same day as other E&M codes and cover discussions regarding advance care planning issues including discussing advance directives, appointing a healthcare proxy or durable power of attorney, discussing a living will, or addressing orders for life-sustaining treatment like the role of hydration or future hospitalizations. (For more information on how to use them, visit the CMS website and search for the FAQ.)
What should hospitalists concentrate on when having “goals of care” conversations with patients and caregivers? Ariadne Labs, a Harvard-affiliated health innovation group, offers the following as elements of a serious illness conversation:10
- Patients’ understanding of their illness
- Patients’ preferences for information and for family involvement
- Personal life goals, fears, and anxieties
- Trade-offs they are willing to accept
For hospitalists, an important area to pay particular attention to is the role of future hospitalizations in patients’ wishes for care, as some patients, if offered appropriate symptom control, would prefer to remain at home.
Two other crucial elements of inpatient palliative care—offer psychosocial support and symptom relief and hand off patient to effective post-hospital palliative care—are outside the scope of this article. However, they should be kept in mind and, of course, applied.
Understand the role of the palliative care consultation. Busy hospitalists might reasonably think, “I simply don’t have time to address palliative care in patients who aren’t likely to die during this hospitalization or soon after.” The palliative care consult service, if available, should be accessed when patients are identified as palliative care candidates but the primary hospitalist does not have the time or resources—including specialized knowledge in some cases—to deliver adequate palliative care. Palliative care specialists can also help bridge the gap between inpatient and outpatient palliative care resources.
In sum, the move to value-based payment models and the new advance care planning E&M codes provide a renewed focus—with more aligned incentives—and the opportunity to provide good palliative care to all who need it.
For hospitalists, identifying those who would benefit from palliative care and working with the healthcare team to ensure the care is delivered are at the heart of our professional mission. TH
References
- End-of-life care. The Darmouth Atlas of Health Care website. Accessed June 23, 2016.
- Gade G, Venohr I, Conner D, et al. Impact of an inpatient palliative care team: a randomized control trial. J Palliat Med. 2008;11(2):180-190.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Int Med. 2008;168(16):1783-1790.
- Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life. 2014.
- BPCI Model 2: Retrospective acute & post acute care episode. Centers for Medicare & Medicaid Services website. Accessed June 24, 2016.
- Vick JB, Pertsch N, Hutchings M, et al. The utility of the surprise question in identifying patients most at risk of death. J Clin Oncol. 2015;33(suppl):8.
- Moss AH, Ganjoo J, Sharma S, et al. Utility of the “surprise” question to identify dialysis patients with high mortality. Clin J Am Soc Nephrol. 2008;3:1379-1384.
- Moss AH, Lunney JR, Culp S, et al. Prognostic significance of the “surprise” question in cancer patients. J Palliat Med. 2010;13(7):837-840.
- Weissman D, Meier C. Identifying patients in need of a palliative care assessment in the hospital setting: a consensus report from the Center to Advance Palliative Care. J Palliat Med. 2011;14(1):17-23.
- Serious illness care resources. Ariadne Labs website. Accessed June 24, 2016.
5 tips to surviving Meaningful Use audits
The Meaningful Use (MU) program as doctors know it may soon be ending, but audits of past attestations are slated to continue for at least the next 6 years.
Experts offer the following guidance on how to successfully manage audits and subsequent appeals.
1. Expect an audit.

Assume that at some point, you will be audited, said Joshua J. Freemire, a health law attorney based in Baltimore who specializes in regulatory compliance matters.
“Have good procedures in place to ensure the audit is brought to the attention of management and responded to promptly,” Mr. Freemire said in an interview. “Similarly, it is important that practices understand, in advance, how information created by their EHR is stored and managed.”
Audits are not limited to the current or most recent year, he noted. Being able to promptly access the appropriate information is an important part of drafting appropriate responses.
2. Save records

Keep all relevant records electronically for at least 6 years after attestation, advised Carmiña Nitzki, a senior consultant with GE Healthcare Camden Group.
Some documentation, such as your security risk analysis, should be maintained in paper form, she added. It is also helpful to take screen shots of certain measures that address the functionality of your system.
Records should follow when a physician moves a practice or changes employment. Ms. Nitzki recently assisted a case in which an early adopter physician dissolved his practice, became employed, and moved offices. His 2011 attestation was later audited, and he did not have all of the requested information. The doctor came to Ms. Nitzki after failing an audit and being assessed an $18,000 recoupment payment. Together, they were able to recreate and locate much of the necessary records through old emails and past documentation.
“We won the appeal,” said Ms. Nitzki, who spoke about meaningful use audits at a recent American Bar Association meeting. “The takeaway is if you’re going to respond to an audit, make sure you understand everything that they’re asking for and that you’re confident that you’re responding with all of the appropriate documentation,” she said.
3. Meet deadlines
Promptly responding to audits and quickly addressing failed audits are critical, Mr. Freemire said.
“The [MU] program is very strict with regard to deadlines, and an appeal cannot be filed once the applicable deadline has passed,” he said.
Mr. Freemire said that he routinely encounters health providers who have missed deadlines or let too much time lapse after being contacted by the government. Failure to meet deadlines can result from various reasons, including that notices are not promptly brought to the physician’s attention, delays investigating the availability of requested materials, or a false assumption that the requested information is readily at hand, he said.
Ensure that all audit deadlines are recorded and work with staff and leadership to file responses on time. Factor in additional time if there could be difficulty in locating records, experts stressed.
“I see difficulty in effectively responding to audits where records are simply not maintained,” he said. “Again, this can happen for many reasons, including personnel turnover, but it can be difficult or impossible to effectively respond to audit requests” in this situation.
4. Appeal effectively
Swiftly and thoroughly appeal a failed audit.
When a doctor fails an audit, it’s usually because of incomplete responses or missing information, Ms. Nitzki said. Only those measures that were rejected or that failed to meet standards need to be addressed during an appeal. Sending a cover letter to CMS with the appeal, explaining why the doctor may have failed initially can strengthen the case, she said.
“The appeals process is done directly with CMS, so they’re a little more reasonable,” she said. “They tend to look at things on broader scale.”
Don’t wait to appeal, Mr. Freemire said. Practices have 30 days from the date of an adverse audit determination letter to submit an appeal. If time runs out, physicians must pay back any money requested by auditors, and CMS expects the recoupment in full.
“Following a negative decision, the most important step is prompt attention,” he said. “The sooner that process begins, the sooner it can be completed. The time line for audit appeals is not generous and providers need to ensure they react promptly to a negative finding.”
5. Get help
Ms. Nitzki recommends that physicians obtain professional assistance when responding to an audit.
Practices can hire a consulting company or find audit resources from their specialty society or state medical association. The American Academy of Family Physicians provides a tip sheet on responding to audits. Some state organizations, such as the Texas Medical Association, offer a helpline for doctors to call and ask questions related to meaningful use.
“Unless they have a very savvy person in their office who has taken care all of their meaningful use attestations and documentation, we recommend they get help because it’s in the details where they could fail,” she said.
Seeking help after a failed audit is also essential, notes Mr. Freemire. Experts who are familiar with the program and its requirements and procedures can be of great assistance when it comes organizing the facts into a persuasive argument, he said.
“A cost/benefit is necessary – as it is with all service providers,” he said. “But a provider’s chances for a successful appeal are increased when that appeal is prepared by someone who understands the history and intention behind program requirements, who can best identify and present the necessary evidence of compliance, and who can make a compelling argument as to the provider’s satisfaction of program requirements.”
On Twitter @legal_med
The Meaningful Use (MU) program as doctors know it may soon be ending, but audits of past attestations are slated to continue for at least the next 6 years.
Experts offer the following guidance on how to successfully manage audits and subsequent appeals.
1. Expect an audit.
Assume that at some point, you will be audited, said Joshua J. Freemire, a health law attorney based in Baltimore who specializes in regulatory compliance matters.
“Have good procedures in place to ensure the audit is brought to the attention of management and responded to promptly,” Mr. Freemire said in an interview. “Similarly, it is important that practices understand, in advance, how information created by their EHR is stored and managed.”
Audits are not limited to the current or most recent year, he noted. Being able to promptly access the appropriate information is an important part of drafting appropriate responses.
2. Save records
Keep all relevant records electronically for at least 6 years after attestation, advised Carmiña Nitzki, a senior consultant with GE Healthcare Camden Group.
Some documentation, such as your security risk analysis, should be maintained in paper form, she added. It is also helpful to take screen shots of certain measures that address the functionality of your system.
Records should follow when a physician moves a practice or changes employment. Ms. Nitzki recently assisted a case in which an early adopter physician dissolved his practice, became employed, and moved offices. His 2011 attestation was later audited, and he did not have all of the requested information. The doctor came to Ms. Nitzki after failing an audit and being assessed an $18,000 recoupment payment. Together, they were able to recreate and locate much of the necessary records through old emails and past documentation.
“We won the appeal,” said Ms. Nitzki, who spoke about meaningful use audits at a recent American Bar Association meeting. “The takeaway is if you’re going to respond to an audit, make sure you understand everything that they’re asking for and that you’re confident that you’re responding with all of the appropriate documentation,” she said.
3. Meet deadlines
Promptly responding to audits and quickly addressing failed audits are critical, Mr. Freemire said.
“The [MU] program is very strict with regard to deadlines, and an appeal cannot be filed once the applicable deadline has passed,” he said.
Mr. Freemire said that he routinely encounters health providers who have missed deadlines or let too much time lapse after being contacted by the government. Failure to meet deadlines can result from various reasons, including that notices are not promptly brought to the physician’s attention, delays investigating the availability of requested materials, or a false assumption that the requested information is readily at hand, he said.
Ensure that all audit deadlines are recorded and work with staff and leadership to file responses on time. Factor in additional time if there could be difficulty in locating records, experts stressed.
“I see difficulty in effectively responding to audits where records are simply not maintained,” he said. “Again, this can happen for many reasons, including personnel turnover, but it can be difficult or impossible to effectively respond to audit requests” in this situation.
4. Appeal effectively
Swiftly and thoroughly appeal a failed audit.
When a doctor fails an audit, it’s usually because of incomplete responses or missing information, Ms. Nitzki said. Only those measures that were rejected or that failed to meet standards need to be addressed during an appeal. Sending a cover letter to CMS with the appeal, explaining why the doctor may have failed initially can strengthen the case, she said.
“The appeals process is done directly with CMS, so they’re a little more reasonable,” she said. “They tend to look at things on broader scale.”
Don’t wait to appeal, Mr. Freemire said. Practices have 30 days from the date of an adverse audit determination letter to submit an appeal. If time runs out, physicians must pay back any money requested by auditors, and CMS expects the recoupment in full.
“Following a negative decision, the most important step is prompt attention,” he said. “The sooner that process begins, the sooner it can be completed. The time line for audit appeals is not generous and providers need to ensure they react promptly to a negative finding.”
5. Get help
Ms. Nitzki recommends that physicians obtain professional assistance when responding to an audit.
Practices can hire a consulting company or find audit resources from their specialty society or state medical association. The American Academy of Family Physicians provides a tip sheet on responding to audits. Some state organizations, such as the Texas Medical Association, offer a helpline for doctors to call and ask questions related to meaningful use.
“Unless they have a very savvy person in their office who has taken care all of their meaningful use attestations and documentation, we recommend they get help because it’s in the details where they could fail,” she said.
Seeking help after a failed audit is also essential, notes Mr. Freemire. Experts who are familiar with the program and its requirements and procedures can be of great assistance when it comes organizing the facts into a persuasive argument, he said.
“A cost/benefit is necessary – as it is with all service providers,” he said. “But a provider’s chances for a successful appeal are increased when that appeal is prepared by someone who understands the history and intention behind program requirements, who can best identify and present the necessary evidence of compliance, and who can make a compelling argument as to the provider’s satisfaction of program requirements.”
On Twitter @legal_med
The Meaningful Use (MU) program as doctors know it may soon be ending, but audits of past attestations are slated to continue for at least the next 6 years.
Experts offer the following guidance on how to successfully manage audits and subsequent appeals.
1. Expect an audit.
Assume that at some point, you will be audited, said Joshua J. Freemire, a health law attorney based in Baltimore who specializes in regulatory compliance matters.
“Have good procedures in place to ensure the audit is brought to the attention of management and responded to promptly,” Mr. Freemire said in an interview. “Similarly, it is important that practices understand, in advance, how information created by their EHR is stored and managed.”
Audits are not limited to the current or most recent year, he noted. Being able to promptly access the appropriate information is an important part of drafting appropriate responses.
2. Save records
Keep all relevant records electronically for at least 6 years after attestation, advised Carmiña Nitzki, a senior consultant with GE Healthcare Camden Group.
Some documentation, such as your security risk analysis, should be maintained in paper form, she added. It is also helpful to take screen shots of certain measures that address the functionality of your system.
Records should follow when a physician moves a practice or changes employment. Ms. Nitzki recently assisted a case in which an early adopter physician dissolved his practice, became employed, and moved offices. His 2011 attestation was later audited, and he did not have all of the requested information. The doctor came to Ms. Nitzki after failing an audit and being assessed an $18,000 recoupment payment. Together, they were able to recreate and locate much of the necessary records through old emails and past documentation.
“We won the appeal,” said Ms. Nitzki, who spoke about meaningful use audits at a recent American Bar Association meeting. “The takeaway is if you’re going to respond to an audit, make sure you understand everything that they’re asking for and that you’re confident that you’re responding with all of the appropriate documentation,” she said.
3. Meet deadlines
Promptly responding to audits and quickly addressing failed audits are critical, Mr. Freemire said.
“The [MU] program is very strict with regard to deadlines, and an appeal cannot be filed once the applicable deadline has passed,” he said.
Mr. Freemire said that he routinely encounters health providers who have missed deadlines or let too much time lapse after being contacted by the government. Failure to meet deadlines can result from various reasons, including that notices are not promptly brought to the physician’s attention, delays investigating the availability of requested materials, or a false assumption that the requested information is readily at hand, he said.
Ensure that all audit deadlines are recorded and work with staff and leadership to file responses on time. Factor in additional time if there could be difficulty in locating records, experts stressed.
“I see difficulty in effectively responding to audits where records are simply not maintained,” he said. “Again, this can happen for many reasons, including personnel turnover, but it can be difficult or impossible to effectively respond to audit requests” in this situation.
4. Appeal effectively
Swiftly and thoroughly appeal a failed audit.
When a doctor fails an audit, it’s usually because of incomplete responses or missing information, Ms. Nitzki said. Only those measures that were rejected or that failed to meet standards need to be addressed during an appeal. Sending a cover letter to CMS with the appeal, explaining why the doctor may have failed initially can strengthen the case, she said.
“The appeals process is done directly with CMS, so they’re a little more reasonable,” she said. “They tend to look at things on broader scale.”
Don’t wait to appeal, Mr. Freemire said. Practices have 30 days from the date of an adverse audit determination letter to submit an appeal. If time runs out, physicians must pay back any money requested by auditors, and CMS expects the recoupment in full.
“Following a negative decision, the most important step is prompt attention,” he said. “The sooner that process begins, the sooner it can be completed. The time line for audit appeals is not generous and providers need to ensure they react promptly to a negative finding.”
5. Get help
Ms. Nitzki recommends that physicians obtain professional assistance when responding to an audit.
Practices can hire a consulting company or find audit resources from their specialty society or state medical association. The American Academy of Family Physicians provides a tip sheet on responding to audits. Some state organizations, such as the Texas Medical Association, offer a helpline for doctors to call and ask questions related to meaningful use.
“Unless they have a very savvy person in their office who has taken care all of their meaningful use attestations and documentation, we recommend they get help because it’s in the details where they could fail,” she said.
Seeking help after a failed audit is also essential, notes Mr. Freemire. Experts who are familiar with the program and its requirements and procedures can be of great assistance when it comes organizing the facts into a persuasive argument, he said.
“A cost/benefit is necessary – as it is with all service providers,” he said. “But a provider’s chances for a successful appeal are increased when that appeal is prepared by someone who understands the history and intention behind program requirements, who can best identify and present the necessary evidence of compliance, and who can make a compelling argument as to the provider’s satisfaction of program requirements.”
On Twitter @legal_med

Nearly three-quarters of physician specialties saw compensation increases in 2015 – AMGA
Seventy-four percent of physician specialties saw increases in their compensation in 2015, led by emergency medicine, according to the American Medical Group Association.
Overall, the weighted average increase in median compensation across all physician specialties was 3.1%, according to the 2016 Medical Group Compensation and Productivity Survey. Results were based on responses from 260 medical groups representing more than 92,000 providers.

“Once again, we see that physician compensation in general has remained relatively flat, with an average increase around 3.0%,” AMGA President and CEO Donald Fisher, PhD, said in a statement.
“We’ve seen peaks in certain specialties, and dips in others, and much of this reflects the cyclical nature of health care economics,” he added. For example, data from the 2014 survey saw gastroenterology had the largest year-over-year increase and in the 2016 survey, it was one of four specialties to see a decrease in compensation.
Individual specialties seeing the largest median total compensation increase year over year include emergency medicine (9.65% to $355,280), cardiac/thoracic surgery (8.12% to $645,112), cardiology (6.88% to $483.653), and hypertension and nephrology (6.72% to $329,750). Total compensation captures base and variable compensation plus all voluntary salary reductions, but excludes fringe benefits and employer payments to any type of retirement, pension, SERP or tax-deferred profit-sharing plan.
Four specialties saw median decreases in their compensation, including dermatology (–4.27% to $434,520), ophthalmology (–4.17% to $385,149), cardiology-cath lab (–0.81% to $584,118), and gastroenterology (–0.16% to $505,194).
Seventy-four percent of physician specialties saw increases in their compensation in 2015, led by emergency medicine, according to the American Medical Group Association.
Overall, the weighted average increase in median compensation across all physician specialties was 3.1%, according to the 2016 Medical Group Compensation and Productivity Survey. Results were based on responses from 260 medical groups representing more than 92,000 providers.
“Once again, we see that physician compensation in general has remained relatively flat, with an average increase around 3.0%,” AMGA President and CEO Donald Fisher, PhD, said in a statement.
“We’ve seen peaks in certain specialties, and dips in others, and much of this reflects the cyclical nature of health care economics,” he added. For example, data from the 2014 survey saw gastroenterology had the largest year-over-year increase and in the 2016 survey, it was one of four specialties to see a decrease in compensation.
Individual specialties seeing the largest median total compensation increase year over year include emergency medicine (9.65% to $355,280), cardiac/thoracic surgery (8.12% to $645,112), cardiology (6.88% to $483.653), and hypertension and nephrology (6.72% to $329,750). Total compensation captures base and variable compensation plus all voluntary salary reductions, but excludes fringe benefits and employer payments to any type of retirement, pension, SERP or tax-deferred profit-sharing plan.
Four specialties saw median decreases in their compensation, including dermatology (–4.27% to $434,520), ophthalmology (–4.17% to $385,149), cardiology-cath lab (–0.81% to $584,118), and gastroenterology (–0.16% to $505,194).
Seventy-four percent of physician specialties saw increases in their compensation in 2015, led by emergency medicine, according to the American Medical Group Association.
Overall, the weighted average increase in median compensation across all physician specialties was 3.1%, according to the 2016 Medical Group Compensation and Productivity Survey. Results were based on responses from 260 medical groups representing more than 92,000 providers.
“Once again, we see that physician compensation in general has remained relatively flat, with an average increase around 3.0%,” AMGA President and CEO Donald Fisher, PhD, said in a statement.
“We’ve seen peaks in certain specialties, and dips in others, and much of this reflects the cyclical nature of health care economics,” he added. For example, data from the 2014 survey saw gastroenterology had the largest year-over-year increase and in the 2016 survey, it was one of four specialties to see a decrease in compensation.
Individual specialties seeing the largest median total compensation increase year over year include emergency medicine (9.65% to $355,280), cardiac/thoracic surgery (8.12% to $645,112), cardiology (6.88% to $483.653), and hypertension and nephrology (6.72% to $329,750). Total compensation captures base and variable compensation plus all voluntary salary reductions, but excludes fringe benefits and employer payments to any type of retirement, pension, SERP or tax-deferred profit-sharing plan.
Four specialties saw median decreases in their compensation, including dermatology (–4.27% to $434,520), ophthalmology (–4.17% to $385,149), cardiology-cath lab (–0.81% to $584,118), and gastroenterology (–0.16% to $505,194).

FBI questions legality of telemedicine compact laws
The FBI is raising concerns that language in the Interstate Medical Licensure Compact violates federal regulations over criminal background checks. The government pushback could mean implementation delays of telemedicine legislation that 17 states have enacted.
In a letter to the Minnesota Bureau of Criminal Apprehension, an FBI attorney wrote that the state’s compact law does not meet federal rules that allow the sharing of information with states for purposes of criminal background checks. In addition, no federal statutory authority exists for the FBI to share criminal files with a “private” entity such as the interstate commission, wrote Christopher B. Chaney, an attorney in the FBI Office of the General Counsel in Clarksburg, W.Va. The FBI sent a letter expressing the same concerns to the Montana Department of Justice regarding Montana’s compact law.
The Minnesota Board of Medical Practice has requested that the FBI reverse its findings, writing in an Aug. 3 letter that the agency does not appear to fully understand how the compact works. The board is scheduled to begin issuing licenses via the compact in January 2017, said Ruth Martinez, the board’s executive director.

“We believe it’s an erroneous conclusion that they’ve drawn,” Ms. Martinez said in an interview. “We are very actively engaged in rule-writing and in preparing technology and so forth to be ready to issue licenses, and we feel very confident that this determination will be overturned.”
The Montana Board of Medical Examiners meanwhile is aware of the FBI’s letter and is closely monitoring the situation in Minnesota before taking action, said Ian Marquand, executive officer for the Montana Board of Medical Examiners.
“We are still digesting this and are anxious to see what happens with the Minnesota situation,” Mr. Marquand said in an interview. “That may provide the road map.”
The Interstate Medical Licensure Compact is aimed at making it easier for telemedicine physicians to gain licenses in multiple states. Under the model legislation, developed by the Federation of State Medical Boards (FSMB), physicians designate a member state as the state of principal licensure and select the other states in which they wish to be licensed. The state of principal licensure then verifies the physician’s eligibility and provides credential information to the interstate commission, which collects applicable fees and transmits the doctor’s information to the other states. Upon receipt in the additional states, the physician would be granted a license.
In July 2015, the U.S. Health Resources and Services Administration awarded the FSMB a grant to support establishment of the commission and aid with the compact’s infrastructure.
There is nothing unique about Minnesota’s compact law, Ms. Martinez said. The statute is based on the same model legislation that passed in 16 other states. She believes that Minnesota’s law is merely one of the first to be reviewed by the FBI. Both Minnesota and Montana officials had requested that their respective state departments of justice determine if the compact laws met public law standards pertaining to criminal history records.
Ms. Martinez said that she hopes that the board’s letter to the FBI will help explain how the compact process works and prevent further federal rejections in other jurisdictions. She notes for example that the FBI incorrectly characterizes the interstate commission as a “private” entity in its letter, when the commission is a corporate body and a joint agency of the member states. The FBI also misunderstands how the commission interacts with the individual state licensing boards and the process of licensure, according to the board’s reply letter. It is not the commission that will be using FBI data, but the member states that will be utilizing the information in the course of verification, writes Rick Masters, special counsel to the National Center for Interstate Compacts.
The Federation of State Medical Boards is closely watching the matter and supports the Minnesota Board of Medical Practice, said Lisa A. Robin FSMB’s chief advocacy officer.
“The FSMB, along with the Council of State Governments (CSG), agrees with and supports the Minnesota board’s position in this matter,” Ms. Robin said in an emailed statement. “The compact’s statutory language does not alter state-based responsibility for the administration of criminal background checks, nor does it seek to extend this responsibility beyond individual state medical boards.”
At press time, the FBI’s Mr. Chaney had not responded to a message seeking comment.
On Twitter @legal_med
The FBI is raising concerns that language in the Interstate Medical Licensure Compact violates federal regulations over criminal background checks. The government pushback could mean implementation delays of telemedicine legislation that 17 states have enacted.
In a letter to the Minnesota Bureau of Criminal Apprehension, an FBI attorney wrote that the state’s compact law does not meet federal rules that allow the sharing of information with states for purposes of criminal background checks. In addition, no federal statutory authority exists for the FBI to share criminal files with a “private” entity such as the interstate commission, wrote Christopher B. Chaney, an attorney in the FBI Office of the General Counsel in Clarksburg, W.Va. The FBI sent a letter expressing the same concerns to the Montana Department of Justice regarding Montana’s compact law.
The Minnesota Board of Medical Practice has requested that the FBI reverse its findings, writing in an Aug. 3 letter that the agency does not appear to fully understand how the compact works. The board is scheduled to begin issuing licenses via the compact in January 2017, said Ruth Martinez, the board’s executive director.
“We believe it’s an erroneous conclusion that they’ve drawn,” Ms. Martinez said in an interview. “We are very actively engaged in rule-writing and in preparing technology and so forth to be ready to issue licenses, and we feel very confident that this determination will be overturned.”
The Montana Board of Medical Examiners meanwhile is aware of the FBI’s letter and is closely monitoring the situation in Minnesota before taking action, said Ian Marquand, executive officer for the Montana Board of Medical Examiners.
“We are still digesting this and are anxious to see what happens with the Minnesota situation,” Mr. Marquand said in an interview. “That may provide the road map.”
The Interstate Medical Licensure Compact is aimed at making it easier for telemedicine physicians to gain licenses in multiple states. Under the model legislation, developed by the Federation of State Medical Boards (FSMB), physicians designate a member state as the state of principal licensure and select the other states in which they wish to be licensed. The state of principal licensure then verifies the physician’s eligibility and provides credential information to the interstate commission, which collects applicable fees and transmits the doctor’s information to the other states. Upon receipt in the additional states, the physician would be granted a license.
In July 2015, the U.S. Health Resources and Services Administration awarded the FSMB a grant to support establishment of the commission and aid with the compact’s infrastructure.
There is nothing unique about Minnesota’s compact law, Ms. Martinez said. The statute is based on the same model legislation that passed in 16 other states. She believes that Minnesota’s law is merely one of the first to be reviewed by the FBI. Both Minnesota and Montana officials had requested that their respective state departments of justice determine if the compact laws met public law standards pertaining to criminal history records.
Ms. Martinez said that she hopes that the board’s letter to the FBI will help explain how the compact process works and prevent further federal rejections in other jurisdictions. She notes for example that the FBI incorrectly characterizes the interstate commission as a “private” entity in its letter, when the commission is a corporate body and a joint agency of the member states. The FBI also misunderstands how the commission interacts with the individual state licensing boards and the process of licensure, according to the board’s reply letter. It is not the commission that will be using FBI data, but the member states that will be utilizing the information in the course of verification, writes Rick Masters, special counsel to the National Center for Interstate Compacts.
The Federation of State Medical Boards is closely watching the matter and supports the Minnesota Board of Medical Practice, said Lisa A. Robin FSMB’s chief advocacy officer.
“The FSMB, along with the Council of State Governments (CSG), agrees with and supports the Minnesota board’s position in this matter,” Ms. Robin said in an emailed statement. “The compact’s statutory language does not alter state-based responsibility for the administration of criminal background checks, nor does it seek to extend this responsibility beyond individual state medical boards.”
At press time, the FBI’s Mr. Chaney had not responded to a message seeking comment.
On Twitter @legal_med
The FBI is raising concerns that language in the Interstate Medical Licensure Compact violates federal regulations over criminal background checks. The government pushback could mean implementation delays of telemedicine legislation that 17 states have enacted.
In a letter to the Minnesota Bureau of Criminal Apprehension, an FBI attorney wrote that the state’s compact law does not meet federal rules that allow the sharing of information with states for purposes of criminal background checks. In addition, no federal statutory authority exists for the FBI to share criminal files with a “private” entity such as the interstate commission, wrote Christopher B. Chaney, an attorney in the FBI Office of the General Counsel in Clarksburg, W.Va. The FBI sent a letter expressing the same concerns to the Montana Department of Justice regarding Montana’s compact law.
The Minnesota Board of Medical Practice has requested that the FBI reverse its findings, writing in an Aug. 3 letter that the agency does not appear to fully understand how the compact works. The board is scheduled to begin issuing licenses via the compact in January 2017, said Ruth Martinez, the board’s executive director.
“We believe it’s an erroneous conclusion that they’ve drawn,” Ms. Martinez said in an interview. “We are very actively engaged in rule-writing and in preparing technology and so forth to be ready to issue licenses, and we feel very confident that this determination will be overturned.”
The Montana Board of Medical Examiners meanwhile is aware of the FBI’s letter and is closely monitoring the situation in Minnesota before taking action, said Ian Marquand, executive officer for the Montana Board of Medical Examiners.
“We are still digesting this and are anxious to see what happens with the Minnesota situation,” Mr. Marquand said in an interview. “That may provide the road map.”
The Interstate Medical Licensure Compact is aimed at making it easier for telemedicine physicians to gain licenses in multiple states. Under the model legislation, developed by the Federation of State Medical Boards (FSMB), physicians designate a member state as the state of principal licensure and select the other states in which they wish to be licensed. The state of principal licensure then verifies the physician’s eligibility and provides credential information to the interstate commission, which collects applicable fees and transmits the doctor’s information to the other states. Upon receipt in the additional states, the physician would be granted a license.
In July 2015, the U.S. Health Resources and Services Administration awarded the FSMB a grant to support establishment of the commission and aid with the compact’s infrastructure.
There is nothing unique about Minnesota’s compact law, Ms. Martinez said. The statute is based on the same model legislation that passed in 16 other states. She believes that Minnesota’s law is merely one of the first to be reviewed by the FBI. Both Minnesota and Montana officials had requested that their respective state departments of justice determine if the compact laws met public law standards pertaining to criminal history records.
Ms. Martinez said that she hopes that the board’s letter to the FBI will help explain how the compact process works and prevent further federal rejections in other jurisdictions. She notes for example that the FBI incorrectly characterizes the interstate commission as a “private” entity in its letter, when the commission is a corporate body and a joint agency of the member states. The FBI also misunderstands how the commission interacts with the individual state licensing boards and the process of licensure, according to the board’s reply letter. It is not the commission that will be using FBI data, but the member states that will be utilizing the information in the course of verification, writes Rick Masters, special counsel to the National Center for Interstate Compacts.
The Federation of State Medical Boards is closely watching the matter and supports the Minnesota Board of Medical Practice, said Lisa A. Robin FSMB’s chief advocacy officer.
“The FSMB, along with the Council of State Governments (CSG), agrees with and supports the Minnesota board’s position in this matter,” Ms. Robin said in an emailed statement. “The compact’s statutory language does not alter state-based responsibility for the administration of criminal background checks, nor does it seek to extend this responsibility beyond individual state medical boards.”
At press time, the FBI’s Mr. Chaney had not responded to a message seeking comment.
On Twitter @legal_med

Most physician practices unsure about joining ACOs
The majority of physician practices are uncertain about joining or starting an accountable care organization (ACO), according to a survey.
Of nearly 400 hospital-owned and freestanding outpatient practices, 65% were unsure how to approach accountable care, a survey by Healthcare Information and Management Systems Society (HIMSS) Analytics found. About 13% of health providers said they expected to join an established ACO, while 14% planned to form an ACO, and 8% planned to create an ACO with a neighboring provider.

HIMSS Analytics director of research Brendan FitzGeraldand his team surveyed 436 health providers during June 23–July 12, 2016, regarding electronic health record (EHR) adoption, accountable care, and health information exchanges, among other subjects. The respondents included physicians, practice managers/administrators, physician assistants, nurse practitioners, and practice IT directors. Investigators also analyzed the HIMSS Analytics LOGIC database, which includes 47,084 hospital-owned practices and 57,909 freestanding practices.
Respondents also reported a high level of uncertainty around plans to join a health information exchange (HIE): 48% of health providers were unsure about whether to join an HIE, compared with 46% who were uncertain in 2015. Of respondents who plan to join an HIE, 10% plan to enter a hospital or health system HIE, 7% plan to enter a regional HIE, and 17% plan to join a state health information exchange.
As far as EHR adoption, nearly 78% of respondents representing a free standing outpatient facility (228 practices) reported having an EHR, a 30% increase since 2010. Data from the LOGIC database found 92% of hospital-owned outpatient facilities had a live and operational EHR. Of all survey respondents, 66% did not have plans to replace or upgrade their current outpatient solution, or purchase a new solution. Of health providers that planned to purchase a new EHR, 18% said they would be upgrading, 9% would be purchasing a new solution, and 7% would be replacing a their current EHR.
The survey shows that most doctors appear to be content with the EHR solutions they have adopted with no plans to change systems, said Mr. FitzGerald.
“The level of universal adoption is great, and it seems that physicians for the most part, are satisfied with the work they’ve done to implement and utilize these solutions the first time around,” he said in an interview. “While there may be some getting used to the process of using these particular solutions or even some functionality shortcomings, it seems likes physicians are moving forward with the solutions they have on hand.”
On Twitter @legal_med
The majority of physician practices are uncertain about joining or starting an accountable care organization (ACO), according to a survey.
Of nearly 400 hospital-owned and freestanding outpatient practices, 65% were unsure how to approach accountable care, a survey by Healthcare Information and Management Systems Society (HIMSS) Analytics found. About 13% of health providers said they expected to join an established ACO, while 14% planned to form an ACO, and 8% planned to create an ACO with a neighboring provider.
HIMSS Analytics director of research Brendan FitzGeraldand his team surveyed 436 health providers during June 23–July 12, 2016, regarding electronic health record (EHR) adoption, accountable care, and health information exchanges, among other subjects. The respondents included physicians, practice managers/administrators, physician assistants, nurse practitioners, and practice IT directors. Investigators also analyzed the HIMSS Analytics LOGIC database, which includes 47,084 hospital-owned practices and 57,909 freestanding practices.
Respondents also reported a high level of uncertainty around plans to join a health information exchange (HIE): 48% of health providers were unsure about whether to join an HIE, compared with 46% who were uncertain in 2015. Of respondents who plan to join an HIE, 10% plan to enter a hospital or health system HIE, 7% plan to enter a regional HIE, and 17% plan to join a state health information exchange.
As far as EHR adoption, nearly 78% of respondents representing a free standing outpatient facility (228 practices) reported having an EHR, a 30% increase since 2010. Data from the LOGIC database found 92% of hospital-owned outpatient facilities had a live and operational EHR. Of all survey respondents, 66% did not have plans to replace or upgrade their current outpatient solution, or purchase a new solution. Of health providers that planned to purchase a new EHR, 18% said they would be upgrading, 9% would be purchasing a new solution, and 7% would be replacing a their current EHR.
The survey shows that most doctors appear to be content with the EHR solutions they have adopted with no plans to change systems, said Mr. FitzGerald.
“The level of universal adoption is great, and it seems that physicians for the most part, are satisfied with the work they’ve done to implement and utilize these solutions the first time around,” he said in an interview. “While there may be some getting used to the process of using these particular solutions or even some functionality shortcomings, it seems likes physicians are moving forward with the solutions they have on hand.”
On Twitter @legal_med
The majority of physician practices are uncertain about joining or starting an accountable care organization (ACO), according to a survey.
Of nearly 400 hospital-owned and freestanding outpatient practices, 65% were unsure how to approach accountable care, a survey by Healthcare Information and Management Systems Society (HIMSS) Analytics found. About 13% of health providers said they expected to join an established ACO, while 14% planned to form an ACO, and 8% planned to create an ACO with a neighboring provider.
HIMSS Analytics director of research Brendan FitzGeraldand his team surveyed 436 health providers during June 23–July 12, 2016, regarding electronic health record (EHR) adoption, accountable care, and health information exchanges, among other subjects. The respondents included physicians, practice managers/administrators, physician assistants, nurse practitioners, and practice IT directors. Investigators also analyzed the HIMSS Analytics LOGIC database, which includes 47,084 hospital-owned practices and 57,909 freestanding practices.
Respondents also reported a high level of uncertainty around plans to join a health information exchange (HIE): 48% of health providers were unsure about whether to join an HIE, compared with 46% who were uncertain in 2015. Of respondents who plan to join an HIE, 10% plan to enter a hospital or health system HIE, 7% plan to enter a regional HIE, and 17% plan to join a state health information exchange.
As far as EHR adoption, nearly 78% of respondents representing a free standing outpatient facility (228 practices) reported having an EHR, a 30% increase since 2010. Data from the LOGIC database found 92% of hospital-owned outpatient facilities had a live and operational EHR. Of all survey respondents, 66% did not have plans to replace or upgrade their current outpatient solution, or purchase a new solution. Of health providers that planned to purchase a new EHR, 18% said they would be upgrading, 9% would be purchasing a new solution, and 7% would be replacing a their current EHR.
The survey shows that most doctors appear to be content with the EHR solutions they have adopted with no plans to change systems, said Mr. FitzGerald.
“The level of universal adoption is great, and it seems that physicians for the most part, are satisfied with the work they’ve done to implement and utilize these solutions the first time around,” he said in an interview. “While there may be some getting used to the process of using these particular solutions or even some functionality shortcomings, it seems likes physicians are moving forward with the solutions they have on hand.”
On Twitter @legal_med
Key clinical point: Most health providers don’t know how to go about joining or creating an accountable care organization.
Major finding: Sixty-five percent of health providers reported being unsure as how to approach accountable care.
Data source: A survey of 436 health providers.
Disclosures: The survey was conducted by HIMSS Analytics, of which Mr. FitzGerald is an employee.

Mayo Clinic tops hospital rankings for 2016-2017
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.

For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.
For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Mayo Clinic in Rochester, Minn., was named the top hospital in the United States, according to the U.S. News & World Report Best Hospitals ranking for 2016-2017.
After finishing second to Massachusetts General Hospital in Boston last year, the Mayo Clinic regained the top spot it earned in 2014-2015. This year, the Cleveland Clinic finished second in the U.S. News Honor Roll, with Massachusetts General third, Johns Hopkins Hospital in Baltimore fourth, and the University of California, Los Angeles, Medical Center in fifth.
For 2016-2017, there were 20 hospitals in the Honor Roll, which is reserved for those institutions that finish at or near the top among the 16 specialties included in the U.S. News rankings. This year, 153 hospitals did well enough to be nationally ranked in one or more specialties, which is up from the 144 that were ranked nationally in at least one specialty last year.
The 16 specialties used in the analysis are cancer, cardiology and heart surgery, diabetes and endocrinology, otolaryngology, gastroenterology and gastrointestinal surgery, geriatrics, gynecology, nephrology, neurology and neurosurgery, ophthalmology, orthopedics, psychiatry, pulmonology, rehabilitation, rheumatology, and urology.
This year’s ranking process initially included 4,667 nonfederal community hospitals. The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
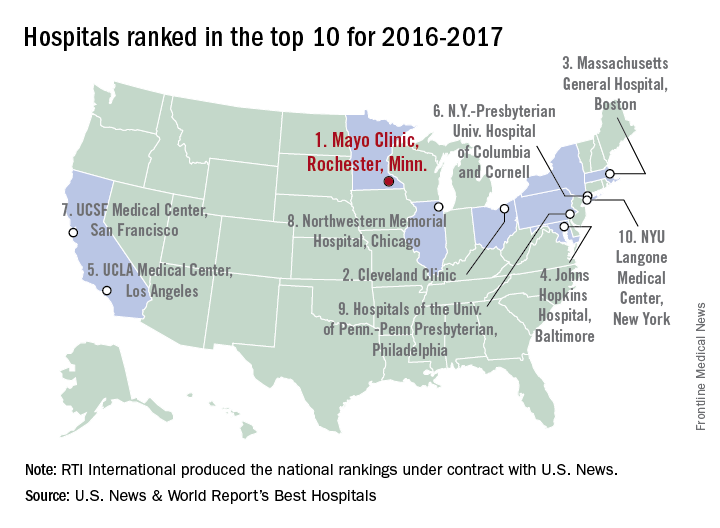
Medicaid expansion leads to better access to care
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.

Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Whether the premium assistance model proves to be durable and effective remains an open question. On the upside, the findings of Sommers et al suggest that the Arkansas initiative is living up to its promises. Moreover, the waiver seems to have increased the number of insurers participating in the marketplaces and contributed to lower premiums.
But other evidence concerning premium assistance waivers suggests the need for caution in assessing their effectiveness. The Government Accountability Office has questioned whether these waivers are budget neutral – a federal requirement. In this vein, the Congressional Budget Office has estimated that it will cost 50% more per enrollee to cover the expansion population on the exchanges than in the conventional Medicaid program. Nor are premium assistance waivers necessarily sustainable. In Pennsylvania, for instance, a newly elected Democratic governor worked to phase out that state’s existing alternative waiver, which had been negotiated by a prior Republican administration, in favor of a traditional expansion of the Medicaid entitlement.
Frank J. Thompson, PhD, and Joel C. Cantor, ScD, are both at Rutgers University in New Brunswick, N.J. They reported having no financial disclosures. Their comments were excerpted from a commentary in JAMA Internal Medicine (2016 Aug 8. doi: 10.1001/jamainternmed.2016.4422).
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
Low-income adults living in two states that expanded Medicaid enrollment are showing significant increases in outpatient utilization and preventive care, improved health care quality, and reductions in emergency department use, compared with those living in a state that did not expand Medicaid, according to a new study.
The study also found similar improvements in care whether a state expanded traditional Medicaid or increased coverage through a private insurance option.
Benjamin D. Sommers, MD, PhD, of Harvard University, Boston, and his colleagues examined outcomes for nearly 9,000 low-income Medicaid enrollees in Kentucky (where officials expanded traditional Medicaid), Arkansas (where the state used funds to purchase private insurance to expand coverage), and Texas (which did not expand Medicaid) in November and December of 2013, 2014, and 2015. They looked specifically at changes in use of healthcare services, preventive care, and self-reported health (JAMA Intern Med. 2016 Aug 8. doi: 10.1001/jamainternmed.2016.4419).
“By the end of 2015, we found marked increases in coverage and reduced cost-related barriers to care in the expansion states, with associated increases in preventive care, outpatient visits, annual checkups, and chronic disease care, as well as decreased reliance on the [emergency department],” the researchers wrote.
They found that by 2015 there was a 6 percentage point drop in the likelihood of ED visits (P = 0.04), an increase of 0.69 office visits per person in the outpatient setting (P = 0.04), and an increase likelihood of getting a checkup (16.1 percentage points, P less than .001) in Medicaid expansion states. In Medicaid expansion states the share of adults obtaining regular care for chronic conditions increased by 12 percentage points after expansion (P = .008), compared with Texas. Additionally, adults reporting fair or poor quality of care dropped by 7.1 percentage points (P = .03).
One significant difference between the expansion states was changes in glucose monitoring rates for patients with diabetes were lower in Arkansas than Kentucky (–11.6 percentage points, P = .04).
“Of note, we found improvements in receipt of checkups, care for chronic conditions, and quality of care even in areas with primary care shortages, suggesting that while clinician capacity is undoubtedly an important consideration, insurance expansion can have a demonstrable positive impact even in areas with relative shortages, perhaps partially due to increased use of safety net providers,” the researchers added.
The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Medicaid expansion improved self-reported health outcomes and access to care.
Major finding: By 2015 there was a 6 percentage point drop in the likelihood of emergency department visits (P = .04) and an increase of 0.69 outpatient office visits per person (P = .04).
Data source: A differences-in-differences analysis of survey data from Nov. 2013 through Dec. 2015 of 8,676 low-income adults in Kentucky, Arkansas, and Texas.
Disclosures: The study was supported by a research grant from the Commonwealth Fund and a grant from the Agency for Healthcare Research and Quality. The researchers reported having no financial disclosures.

Understanding, Counsel Can Help to Navigate Payor Audits
Receiving notice from a payor that you are being audited can be alarming. Questions will inevitably run through your mind, such as, Why? How? How much will this cost?

Understanding the types of payor audits and how to navigate the process can make answering those questions easier. In addition, advanced preparation and knowing when to engage legal counsel can be critical to a successful audit outcome.
Audit Types
There are three general types of audits that providers face: Medicare audits, Medicaid audits, and private payor audits.
Medicare audits: The agency responsible for Medicare audits is the Centers for Medicare & Medicaid Services (CMS). There are three types of Medicare audits. Comprehensive Error Rate Testing (CERT) audits focus on providers who deliver high-cost items or services, have high volume, and/or have atypical billing or coding practices. Private contractors perform Recovery Audit Contractor (RAC) program audits; these contractors are paid a percentage of the amount of any improper payment discovered. Finally, Zone Program Integrity Contractor (ZPIC) audits are the most serious of the three audit types. ZPIC audits are performed by CMS contractors who mine the provider’s data for compliance with Medicare coverage and coding policies, investigate fraud, and may prepare cases for civil or criminal referral to CMS or law enforcement agencies.
Medicaid audits: Medicaid audits evaluate compliance with both CMS and applicable state regulations and investigate fraud. Evidence of fraud will be reported to the state attorney general for further review and prosecution.
Private payor audits: Private payor audits consist of informal reviews and formal audits. These audits can be triggered by actual allegations or evidence of noncompliance, or they can be random, in which general compliance is assessed. Audit procedures are typically determined by contract or the payor’s provider handbook and in accordance with applicable state law. The process can consist of prepayment reviews, in which the sufficiency of a claim and its supporting documentation is determined before payment is made to the provider, or post-payment reviews, during which claims are analyzed after the provider has been paid to determine if an overpayment was made and the amount of such overpayment. In the event an overpayment is discovered, a recoupment will be sought from the provider.
Focus
Consistent billing by a provider of high volumes of certain high-level services, high volumes of evaluation and management services, or consistently referring patients for certain testing can create suspicion in mayors.
In recent years, the primary focus of audits has been medical necessity due to payor concerns about specific fraud and abuse issues. Documentation of medical necessity is required during an audit. However, proving medical necessity can be difficult as the definition of “medical necessity” can vary by payor and within a payor depending on the underlying plan. In addition, private payors often have arbitrary and vague guidelines for defining and determining medical necessity, particularly when dealing with physicians or ordering clinicians. For this reason, it is critical that providers read their payor contracts and manuals carefully. If those materials are unclear, it is best to confirm requirements with the payor.
Regardless of the definition, medical necessity is a precondition to coverage for all payors. Proof is required that the services were reasonable and necessary to diagnosis or treat a patient’s medical condition. To satisfy this standard, providers should document the diagnosis for all procedures performed and all diagnostic tests ordered. In the case of repeat procedures, providers should clearly note the outcome of the previous procedure and the basis for reordering.
Responding to an Audit Request
All audit requests must be taken very seriously. Payors tend to copy what other payors are doing, and a problematic audit with one payor can cause other payors to initiate their own audits. Therefore, it is critical to respond appropriately to each audit request. Also, auditors often only check a few billing records. If errors are found, they will then extrapolate those findings, and the provider may be penalized.
Upon receipt of an audit request, it is important to immediately engage legal counsel well-versed in handling payor audits. Having an attorney who understands the audit process and has experience responding to audit requests can help ensure the best possible audit outcome. A negative outcome could result in recovery of overpayments, civil and/or criminal penalties, and exclusion from government programs.
Providers should work with such legal counsel to review the audit request and supply everything reasonably requested. A concerted effort should be made to submit all information to the auditor at one time. If information is missing, the auditor may determine that a significant error rate exists, which could cause the auditor to review all CPT codes to calculate the overpayment made to the provider. If it is not possible to gather the requested material before the auditor’s deadline, an extension should be requested. Any extensions granted should be documented.
It is important that an audit response and supporting documentation be thorough, clear, and concise. It should be submitted in a manner that allows the auditor to quickly review the information and understand the provider’s arguments. It should clearly state what measures the provider has already taken to terminate existing problems and prevent future issues. Competent legal counsel will be able to address procedural, legal, or factual flaws in the auditor’s position.
Advanced Preparation
The best way to ensure compliance and audit readiness is to develop and implement a compliance plan well in advance of any audit. Experienced legal counsel should play a pivotal role in development of such plan. As always, periodic self-audits or independent audits are necessary to proactively identify compliance issues and mitigate their impact.
Finally, regular and periodic training and education should be conducted regarding audit response obligations and responsibilities. Performing these tasks will help ensure a smooth audit experience with minimal infractions and penalties. TH
Receiving notice from a payor that you are being audited can be alarming. Questions will inevitably run through your mind, such as, Why? How? How much will this cost?
Understanding the types of payor audits and how to navigate the process can make answering those questions easier. In addition, advanced preparation and knowing when to engage legal counsel can be critical to a successful audit outcome.
Audit Types
There are three general types of audits that providers face: Medicare audits, Medicaid audits, and private payor audits.
Medicare audits: The agency responsible for Medicare audits is the Centers for Medicare & Medicaid Services (CMS). There are three types of Medicare audits. Comprehensive Error Rate Testing (CERT) audits focus on providers who deliver high-cost items or services, have high volume, and/or have atypical billing or coding practices. Private contractors perform Recovery Audit Contractor (RAC) program audits; these contractors are paid a percentage of the amount of any improper payment discovered. Finally, Zone Program Integrity Contractor (ZPIC) audits are the most serious of the three audit types. ZPIC audits are performed by CMS contractors who mine the provider’s data for compliance with Medicare coverage and coding policies, investigate fraud, and may prepare cases for civil or criminal referral to CMS or law enforcement agencies.
Medicaid audits: Medicaid audits evaluate compliance with both CMS and applicable state regulations and investigate fraud. Evidence of fraud will be reported to the state attorney general for further review and prosecution.
Private payor audits: Private payor audits consist of informal reviews and formal audits. These audits can be triggered by actual allegations or evidence of noncompliance, or they can be random, in which general compliance is assessed. Audit procedures are typically determined by contract or the payor’s provider handbook and in accordance with applicable state law. The process can consist of prepayment reviews, in which the sufficiency of a claim and its supporting documentation is determined before payment is made to the provider, or post-payment reviews, during which claims are analyzed after the provider has been paid to determine if an overpayment was made and the amount of such overpayment. In the event an overpayment is discovered, a recoupment will be sought from the provider.
Focus
Consistent billing by a provider of high volumes of certain high-level services, high volumes of evaluation and management services, or consistently referring patients for certain testing can create suspicion in mayors.
In recent years, the primary focus of audits has been medical necessity due to payor concerns about specific fraud and abuse issues. Documentation of medical necessity is required during an audit. However, proving medical necessity can be difficult as the definition of “medical necessity” can vary by payor and within a payor depending on the underlying plan. In addition, private payors often have arbitrary and vague guidelines for defining and determining medical necessity, particularly when dealing with physicians or ordering clinicians. For this reason, it is critical that providers read their payor contracts and manuals carefully. If those materials are unclear, it is best to confirm requirements with the payor.
Regardless of the definition, medical necessity is a precondition to coverage for all payors. Proof is required that the services were reasonable and necessary to diagnosis or treat a patient’s medical condition. To satisfy this standard, providers should document the diagnosis for all procedures performed and all diagnostic tests ordered. In the case of repeat procedures, providers should clearly note the outcome of the previous procedure and the basis for reordering.
Responding to an Audit Request
All audit requests must be taken very seriously. Payors tend to copy what other payors are doing, and a problematic audit with one payor can cause other payors to initiate their own audits. Therefore, it is critical to respond appropriately to each audit request. Also, auditors often only check a few billing records. If errors are found, they will then extrapolate those findings, and the provider may be penalized.
Upon receipt of an audit request, it is important to immediately engage legal counsel well-versed in handling payor audits. Having an attorney who understands the audit process and has experience responding to audit requests can help ensure the best possible audit outcome. A negative outcome could result in recovery of overpayments, civil and/or criminal penalties, and exclusion from government programs.
Providers should work with such legal counsel to review the audit request and supply everything reasonably requested. A concerted effort should be made to submit all information to the auditor at one time. If information is missing, the auditor may determine that a significant error rate exists, which could cause the auditor to review all CPT codes to calculate the overpayment made to the provider. If it is not possible to gather the requested material before the auditor’s deadline, an extension should be requested. Any extensions granted should be documented.
It is important that an audit response and supporting documentation be thorough, clear, and concise. It should be submitted in a manner that allows the auditor to quickly review the information and understand the provider’s arguments. It should clearly state what measures the provider has already taken to terminate existing problems and prevent future issues. Competent legal counsel will be able to address procedural, legal, or factual flaws in the auditor’s position.
Advanced Preparation
The best way to ensure compliance and audit readiness is to develop and implement a compliance plan well in advance of any audit. Experienced legal counsel should play a pivotal role in development of such plan. As always, periodic self-audits or independent audits are necessary to proactively identify compliance issues and mitigate their impact.
Finally, regular and periodic training and education should be conducted regarding audit response obligations and responsibilities. Performing these tasks will help ensure a smooth audit experience with minimal infractions and penalties. TH
Receiving notice from a payor that you are being audited can be alarming. Questions will inevitably run through your mind, such as, Why? How? How much will this cost?
Understanding the types of payor audits and how to navigate the process can make answering those questions easier. In addition, advanced preparation and knowing when to engage legal counsel can be critical to a successful audit outcome.
Audit Types
There are three general types of audits that providers face: Medicare audits, Medicaid audits, and private payor audits.
Medicare audits: The agency responsible for Medicare audits is the Centers for Medicare & Medicaid Services (CMS). There are three types of Medicare audits. Comprehensive Error Rate Testing (CERT) audits focus on providers who deliver high-cost items or services, have high volume, and/or have atypical billing or coding practices. Private contractors perform Recovery Audit Contractor (RAC) program audits; these contractors are paid a percentage of the amount of any improper payment discovered. Finally, Zone Program Integrity Contractor (ZPIC) audits are the most serious of the three audit types. ZPIC audits are performed by CMS contractors who mine the provider’s data for compliance with Medicare coverage and coding policies, investigate fraud, and may prepare cases for civil or criminal referral to CMS or law enforcement agencies.
Medicaid audits: Medicaid audits evaluate compliance with both CMS and applicable state regulations and investigate fraud. Evidence of fraud will be reported to the state attorney general for further review and prosecution.
Private payor audits: Private payor audits consist of informal reviews and formal audits. These audits can be triggered by actual allegations or evidence of noncompliance, or they can be random, in which general compliance is assessed. Audit procedures are typically determined by contract or the payor’s provider handbook and in accordance with applicable state law. The process can consist of prepayment reviews, in which the sufficiency of a claim and its supporting documentation is determined before payment is made to the provider, or post-payment reviews, during which claims are analyzed after the provider has been paid to determine if an overpayment was made and the amount of such overpayment. In the event an overpayment is discovered, a recoupment will be sought from the provider.
Focus
Consistent billing by a provider of high volumes of certain high-level services, high volumes of evaluation and management services, or consistently referring patients for certain testing can create suspicion in mayors.
In recent years, the primary focus of audits has been medical necessity due to payor concerns about specific fraud and abuse issues. Documentation of medical necessity is required during an audit. However, proving medical necessity can be difficult as the definition of “medical necessity” can vary by payor and within a payor depending on the underlying plan. In addition, private payors often have arbitrary and vague guidelines for defining and determining medical necessity, particularly when dealing with physicians or ordering clinicians. For this reason, it is critical that providers read their payor contracts and manuals carefully. If those materials are unclear, it is best to confirm requirements with the payor.
Regardless of the definition, medical necessity is a precondition to coverage for all payors. Proof is required that the services were reasonable and necessary to diagnosis or treat a patient’s medical condition. To satisfy this standard, providers should document the diagnosis for all procedures performed and all diagnostic tests ordered. In the case of repeat procedures, providers should clearly note the outcome of the previous procedure and the basis for reordering.
Responding to an Audit Request
All audit requests must be taken very seriously. Payors tend to copy what other payors are doing, and a problematic audit with one payor can cause other payors to initiate their own audits. Therefore, it is critical to respond appropriately to each audit request. Also, auditors often only check a few billing records. If errors are found, they will then extrapolate those findings, and the provider may be penalized.
Upon receipt of an audit request, it is important to immediately engage legal counsel well-versed in handling payor audits. Having an attorney who understands the audit process and has experience responding to audit requests can help ensure the best possible audit outcome. A negative outcome could result in recovery of overpayments, civil and/or criminal penalties, and exclusion from government programs.
Providers should work with such legal counsel to review the audit request and supply everything reasonably requested. A concerted effort should be made to submit all information to the auditor at one time. If information is missing, the auditor may determine that a significant error rate exists, which could cause the auditor to review all CPT codes to calculate the overpayment made to the provider. If it is not possible to gather the requested material before the auditor’s deadline, an extension should be requested. Any extensions granted should be documented.
It is important that an audit response and supporting documentation be thorough, clear, and concise. It should be submitted in a manner that allows the auditor to quickly review the information and understand the provider’s arguments. It should clearly state what measures the provider has already taken to terminate existing problems and prevent future issues. Competent legal counsel will be able to address procedural, legal, or factual flaws in the auditor’s position.
Advanced Preparation
The best way to ensure compliance and audit readiness is to develop and implement a compliance plan well in advance of any audit. Experienced legal counsel should play a pivotal role in development of such plan. As always, periodic self-audits or independent audits are necessary to proactively identify compliance issues and mitigate their impact.
Finally, regular and periodic training and education should be conducted regarding audit response obligations and responsibilities. Performing these tasks will help ensure a smooth audit experience with minimal infractions and penalties. TH