User login
The Hospitalist only
The Comanagement Conundrum

As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.

Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”

Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying

Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.

Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”

For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB
As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.
Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”
Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying
Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.
Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”
For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB
As patient care grows ever more complex, driven by demographic shifts and regulatory trends, hospitalists around the country continue to worry about the “dumping” practices of referring surgeons and other specialists. Negative nicknames like “admitologist,” “dischargologist,” or “glorified resident” reflect the concerns of some veteran physicians who find themselves doing what they perceive as “scut work”—merely processing the surgeons’ patients through the hospitalization.
Comanagement has been proposed as a solution to improve both patient care and professional satisfaction. But its promise can be eroded if the arrangement isn’t well planned and executed, experts say. Comanagement requires clearly defined roles, collaborative professional relationships, and some sense of equal standing with the surgeons or other specialists who call on hospitalists to care for their hospitalized patients’ medical needs.
“The growing formalization of comanagement agreements stems from prior tendency by some to view hospitalists as glorified house staff,” says Christopher Whinney, MD, FACP, FHM, director of comanagement at The Cleveland Clinic. “Hospitalists feel this is inappropriate, based on our skill set and scope of practice. There is also a concern that if a hospitalist group jumps in to do this without a clear service agreement in writing, that is where dumping can become a problem.”
Dr. Whinney is one of two expert mentors for hospitalists under a new SHM demonstration project called the Hospitalist Orthopedic Patient Service Comanagement Program, which is gathering data to evaluate its effectiveness on clinical and other outcomes. He has been working with five of the 10 participating HM groups, helping them define what it means to institutionalize formal comanagement relationships.
“Whatever your personal feelings about the comanagement relationship, pro or con, comanagement is going to be part of most hospital medicine groups’ repertoire of services,” says Hugo Quinny Cheng, MD, director of the comanagement with neurosurgery service at the University of California at San Francisco (UCSF) Medical Center. “You can try to avoid it, but if the medical center and the surgeons want it, there’s going to be pressure on your group to do it—or else they’ll look for another hospitalist group to do it.”
Dr. Cheng advises hospitalist group leaders make themselves aware of the trend and position themselves in a way to take advantage of it—or, at the very least, not be blindsided by it.
According to SHM data, 85% of hospitalist groups have done some kind of comanagement.1 It’s not explicitly listed by SHM as one of The Core Competencies in Hospital Medicine, but it might as well be, says Leslie Flores, MHA, SHM senior advisor, practice management, because aspects of comanagement are addressed throughout.2
Defined, Distinguished, Delineated
Comanagement is different from traditional medical consultations performed by hospitalists upon request, and also differs from cases in which the hospitalist is the admitting physician of record with sole management responsibilities while the patient is in the hospital. According to an SHM white paper, A Guide to Hospitalist/Orthopedic Surgery Comanagement, the concept involves shared responsibility, authority, and accountability for the care of hospitalized patients, typically with orthopedic surgeons or other specialties, and with the hospitalist managing the patient’s medical concerns, such as diabetes, congestive heart failure, or DVT.3 (SHM’s website is full of comanagement resources, including sample service agreements; visit www.hospitalmedicine.org/publications and click on the “comanagement” button.)
But just as HM programs can be diverse in their organization, structure, and leadership, there is no single definition of comanagement, says Sylvia McKean, MD, SFHM, senior hospitalist at Brigham and Women’s Hospital in Boston. “You can have a very formal relationship where there’s a contract and where people are paid by whatever group is initiating the comanagement. There may be clear definitions in terms of their roles,” says Dr. McKean, an SHM board member who chaired the advisory panel that developed the comanagement white paper. “At the other extreme may be an informal relationship where you have a group of people in a community hospital who are available to manage medical problems when requested by specialists on a subset of patients.
“What really seems to distinguish comanagement from traditional medical consultations is that it implies equality in the relationship, even though the surgeon is often the attending of record,” as is practiced at Brigham and Women’s, Dr. McKean says. The comanaging hospitalist might follow the patient until discharge, rather than just seeing the patient once regarding the consultation question. “It’s more of a robust involvement of the hospitalist or internist, who really takes responsibility to make sure that medical conditions are actively managed, ideally before complications emerge.”
Eric Siegal, MD, SFHM, an intensivist with Aurora Medical Group in Wisconsin and an SHM board member, recommended developing comanagement services “carefully and methodically, paying close attention to consequences, intended and unintended”1 in a 2008 Journal of Hospital Medicine article. He tries to avoid broad generalizations about comanagement because “it’s applied variably across the industry. You’re going to find hospitalist programs that comanage very well and others that do it poorly.”
Dr. Siegal says he doesn’t think anyone in the field is “categorically anti-comanagement.”
However, he says it should be done thoughtfully, with clear goals in mind, and clearly defined roles and responsibilities. “Just showing up to see the specialists’ patients and calling it comanagement doesn’t necessarily mean you’re doing anything to make those patients’ care better,” he says.
Expert-Recommended
Demographic trends driving the spread of comanagement include an aging population of hospitalized patients with multiple comorbidities receiving surgical or other procedures that might not have been offered to them in the past. It fits with broader healthcare reform trends toward enhanced coordination and greater efficiency, illustrated by accountable-care organizations (ACOs).
Comanagement can be a growth and expansion opportunity for hospitalist groups, one that offers a defined niche and cements a group’s value to a hospital that wants improved relationships with surgeons. It also addresses the need for standardization and improved patient care in response to quality and safety concerns, and is associated with higher reported rates of satisfaction for surgeons and other staff and for patients.
“There are compelling reasons to do this, related to the limitations placed on resident work hours, which have affected neurosurgery and other surgical specialties profoundly, and the need to provide on-the-floor physician coverage more often and more consistently,” says UCSF hospitalist Andrew Auerbach, MD, MPH.
Dr. Auerbach is the lead author of a recently published study of the neurosurgery comanagement service at UCSF, which found that the program did not result in changes in patient mortality, readmission rates, or lengths of stay (LOS), although it was associated with reduced costs and perceptions of higher quality by professionals.5 Previous research has identified similar results with regard to increased professional satisfaction but without improvements in hard clinical outcomes.6
“Our paper supports the idea that clinical benefits to patients are not there yet,” Dr. Auerbach says. “Maybe we haven’t comanaged the right kinds of patients. Is there something else we have to think about? Maybe the real action is to be found post-hospitalization.”
Comanagement Caveats
In his landmark 2008 JHM article, Dr. Siegal pointed to potential drawbacks associated with comanagement. For example, surgeons, other specialists, and residents can become disengaged from the medical care of their hospitalized patients. He also noted the exacerbation of hospitalist and generalist manpower shortages, as well as the theoretical risk of fragmentation of care that is provided by multiple physician managers. If hospitalists are asked to do things that are outside of their skill set, that can be a problem, too. But the biggest concerns seem to center on the potential negative impact on job satisfaction.
“A fair and robust comanagement structure is an optimal delivery model,” says Christopher Massari, MD, hospitalist at PHMG/PeaceHealth Hospital in Springfield, Ore. “But because most hospitalist services are staffed 24/7, there’s a tendency for specialists and nurses to take advantage of hospitalists because they are ‘available.’ ”
Dr. Massari says he has experienced the “dumping” phenomenon firsthand. “It happens frequently. In the past few years, I have gradually developed the confidence and experience not to let it happen to me,” he says, “but I may inherit patients admitted by my hospitalist colleagues who may not feel as empowered or as skilled at avoiding it.”
Hospitalist dissatisfaction with comanagement is a problem with imperfect solutions, Dr. Cheng explains. “From my view, the biggest risk of comanagement is the inequality in relationships. Not every hospitalist has the temperament to do comanagement. If there is a perception that the partnership is unequal—favoring the surgeon—and if you feel like the junior partner in the relationship, it can be disheartening,” he says. “If the patient is not that sick, or if you feel you don’t have much to add professionally, it might feel like doing grunt work.”
Dr. Cheng also points to a theoretical increase in medical legal risk that the individual hospitalist faces. “With comanagement, you are taking responsibility not just for recommending care but for ensuring that the care is appropriately carried out, monitoring responses to treatment and dealing with delays,” he says. “When I talk to hospitalists, this fear of medical legal exposure comes up regularly.”
Rules of Engagement
SHM’s white paper offers a checklist of important issues to address when developing a comanagement service agreement. Issues include identifying champions from both sides of the collaboration, as well as from the hospital’s administration—which is an essential third party.
“Rules of engagement,” which should be spelled out in a written service agreement, include clarifying a shared vision, mutual goals and expectations, and the identified value proposition for both sides from the arrangement. Appropriate patients should be defined, along with what happens at night and on weekends, lines of authority and communication channels, and how conflicts will be addressed.
For Dr. McKean, the process really starts with “reflecting on your own core values.” Have a clear sense of the group’s goals, current staffing levels and pressures, and ability to add staff for a growing caseload, she says. “That’s where the rubber meets the road,” she adds. “You may want to hire people with a special interest in comanagement, and don’t try to have everyone in the group do everything.”
Jeanne Huddleston, MD, FACP, FHM, clinical scholar at the Mayo Clinic in Rochester, Minn., and past president of SHM, recommends dipping into the hospital’s database to get a better sense of the patient population targeted by a planned comanagement agreement—numbers, demographics, severity of illness, level of symptoms, length of stay, costs, and the like. Hospitalists also need to clearly understand the goals and needs of their comanagement partners—surgeons and other specialists—and of hospital administrators, who are an essential third party to the arrangement (see “What Hospitalists’ Comanagement Partners Are Saying,” above).
For Dr. Auerbach, the fundamental question is: “What are we specifically being asked to fix, and are we the right resource to fix the problem? Are we qualified to do it? Are we staffed to do it? Are we being given appropriate resources and authority to do it? And fundamentally, how are we going to know if we’ve made an improvement?” Quality metrics for comanagement—which should be gathered from the outset to provide a baseline—include in-hospital morbidity and mortality rates, 30-day mortality, hospital readmissions, length of hospital stay, costs of care, and overall return on investment for the hospital, as well as improved patient and professional satisfaction.
Experts agree that comanagement arrangements are unlikely to be self-sustaining from billing revenues alone, and thus will need some kind of support. In some cases, specialist groups can contribute the needed support, but more likely it is up to the hospital’s administration, based on its commitment to keeping its surgeons happy and busy in the operating suite, and on outcomes documenting financial and other benefits.
Medicare currently pays surgeons a global fee to manage their patient’s care associated with the surgery. Hospitalist comanagers typically bill under different codes for managing the patient’s medical conditions. But in an era of heightened regulatory scrutiny, health reform, and increased bundling of payments, this approach could be in for some revision, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C.
ACOs will receive a global fee and apportion it among all the providers involved in a given episode of care, perhaps returning to capitation as a method to accomplish the apportionment, Dr. Ruhlen says. Hospitalists now developing comanagement agreements with surgeons should be aware that such changes are on the horizon, requiring all of the parties involved to rethink how their agreements are structured. In such cases, clearly demonstrating the value of both parties’ contributions to comanagement will be essential, he says.
Professional Impact
For The Cleveland Clinic’s Dr. Whinney, having a service agreement in place will help when physician reimbursement changes. “The thing you develop through these relationships is a sense of collegiality with your surgical colleagues, which is not something we’ve often seen before,” he says. “Particularly in large hospitals, where physicians don’t necessarily know each other, comanagement develops a true sense of collegiality.”
Felix Aguirre, MD, vice president of medical affairs for North Hollywood, Calif.-based IPC: The Hospitalist Company, says that a significant majority of hospitalized patients can benefit from an HM physician on the case.
“At IPC, we started with relationships [with the specialists], but as you go longer, you eventually move to more formal relationships, better defining what you are trying to do,” he says. “We’re still developing comanagement programs, and we’re trying to envision how they might relate to the readmission problem and to optimizing lengths of stay.”
Other industry leaders also ask how comanagement might contribute to the problem of hospital readmissions, perhaps with the hospitalist’s comanagement role continuing after the patient leaves the hospital. Others are exploring perioperative programs, broadly defined, with the hospitalist performing pre-operative assessments on an outpatient basis and helping to standardize processes and optimize the patient for surgery, thus reducing last-minute cancellations.
Ultimately, Dr. Huddleston says, these relationships should be built around putting the patient and the patient’s needs first, and patients don’t fit into neat boxes.
“Sometimes it’s comanagement, sometimes it’s just consultation. Each situation is discussed at the patient level,” she says. “As programs mature, all of these approaches can coexist. That’s where the service agreements become absolutely crucial, and they have to evolve as practice evolves. If you’re really basing it on patient need, you’ll probably end up with a hybrid of models.” TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Hospitalist co-management with surgeons and specialists. SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=25894. Accessed March 11, 2011.
- The core competencies in hospital medicine. ShM website. Available at: www.hospitalmedicine.org/Content/NavigationMenu/Education/CoreCurriculum/Core_Competencies.htm. Accessed March 11, 2011.
- SHM Co-Management Advisory Panel. A white paper on a guide to hospitalist/orthopedic surgery co-management, SHM website. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=25864.Accessed March 11, 2011.
- Siegal EM. Just because you can, doesn’t mean that you should: A call for the rational application of hospitalist comanagement. J Hosp Med. 2008;3(5):398-402.
- Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Burger MS. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22):2004-2010.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: A randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Pinzur MS, Gurza E, Kristopaitis T, et al. Hospitalist-orthopedic comanagement of high-risk patients undergoing lower extremity reconstruction surgery. Orthopedics. 2009; 32(7):495.
What Hospitalists’ Comanagement Partners Are Saying
Depending on local setting, culture, and HM group, hospital administrators often are very supportive of comanagement relationships, particularly if they improve satisfaction for surgeons practicing at the hospital, says Michael Ruhlen, MD, MHCM, FACHE, SFHM, chief medical officer of Carolinas Medical Centers in Charlotte, N.C. But that support is not a blank check.
“Administrators want to know that comanagement creates positive effects on quality, efficiency, and throughput. In this day and age, facilities are under the gun from many directions to demonstrate such improvements. We’re also responsible for ensuring patient satisfaction,” says Dr. Ruhlen, who was a member of SHM’s comanagement advisory group.
Michael Pinzur, MD, an orthopedic surgeon at Loyola University Medical Center in Chicago who was an advisory panel member, says the model for the comanagement agreement varies greatly from one facility to another. “There are some places where orthopedists want the hospitalists to do their scut work,” he says. “For us, we wanted to work together.
“When we developed our comanagement program for hip fracture patients, at the urging of the hospital’s administrators, we had an idea that this was a marriage both of us would benefit from,” he says.7 “As our hospitalists learned the unique needs of our patient population, we learned from their experience and then changed some of our treatment algorhythms. And they learned from us. We see this as real comanagement. Somebody from our group meets with one of the hospitalists every day, and periodically we sit down together and talk about our care processes. … They’re so in tune with issues of the orthopedic surgeon, they do very little unwanted testing.”
For Melbourne Boynton, MD, clinical director of Vermont Orthopedic Clinic in Rutland and a member of the Board of Councilors of the American Association of Orthopaedic Surgeons, what’s most important is what matters to the patient.
“Optimal comanagement is a team approach,” he says, and it has worked well at Rutland Regional Medical Center.
However, it is more informal, rather than under a specific service agreement, because variable situations arise with elderly patients.
“There isn’t much that can’t get fixed with communication, and with focusing on what you’d want for your own mother in this situation,” he says. Which service is primary depends on how active a role each has in the patient’s care. “The quality of care is what matters, not whose service the patient is on.”—LB
Letters to the Editor
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
Pennsylvania group director sounds the call for hospitalist emancipation
Terms such as partners, associates, and K-1 are much less common in HM than other specialties. Instead, we are more familiar with such terms as medical director, employee, corporation-owned, hospital-owned, W-2. In most HM practices, there tends to be more of a hierarchal structure with unequal distribution of say and authority; 100% of the decision-making authority lies with two or three people in the group or organization.
I look around at my friends’ practices in other fields, the majority being privately owned with partnership track and equitable standing in the group, and I contrast that with what I see in nearly every HM group in my area. In HM, our fellow hospitalist must answer to his or her medical director, who then answers to the hospital administration. In many of the large, multistate corporations, the medical director answers to hospital administration as well as to a regional director, who then answers to the CMO of the corporation, who then answers to the CEO.
Rarely do you see a field of medicine that has such little autonomy. I believe it is time for hospitalists to step up to the plate and create practices in which we answer to ourselves and determine our own destinies.
Another phenomenon in HM demonstrates how everyone wants a piece of the HM action. In a 20-mile radius of where I practice, there are HM groups that have been started by specialists in other fields, including infectious disease, pulmonary, emergency medicine, and anesthesia. A cardiology acquaintance of mine recently started three hospitalist practices—single-handedly. These new additions are in addition to the HM groups started by hospital administrations and large multistate corporations.
The majority, but certainly not all, of these people or entities have very little understanding of what running a hospitalist practice entails. They might understand an HM practice to the extent that I understand how a hip replacement is done, procedurally, from my reading of a textbook or an operative note. Unless one currently practices or has recently practiced as a hospitalist, then it is difficult to fully grasp all the nuances of running an HM practice. Never have I seen a GI physician start up a cardiology group, nor have I seen an ER group start up an endocrine practice. Yet the majority of HM practices nationwide are started and controlled by entities other than the hospitalists themselves.
This recent epiphany has prompted me to sound the call for hospitalist emancipation. With a new generation of HM leaders, who now have both clinical and administrative experience in HM, it is time for hospitalists, not other specialists nor hospital administrators, to pave the course of our future in light of emerging healthcare reforms. Of course, we still need to work intimately with our parent hospitals, align our goals and vision, and be mindful of the construct in which HM is practiced. But I believe it is time for us to take control of our practices, because only we know what’s best for our patients and our fellow hospitalists.
Edward Ma, MD, hospitalist,
managing partner, Medical Inpatient Care Associates,
West Chester, Pa.,
president, The Hospitalist Consulting Group, LLC
ACGME not the only game in town for graduate medical education
I enjoy reading your column, but feel I must correct you regarding graduate medical education. You stated in your January 2011 column (“Turn to ACGME for Transfer, Resident Supervision Rules,” p. 39) that all U.S. postgraduate physician-training programs are governed by rules of the ACGME. Please note that there are hundreds of osteopathic postgraduate training programs throughout the country that are governed by the rules of the American Osteopathic Association and the osteopathic specialty colleges that sponsor these residencies and fellowships. If you need more information regarding this segment of postgraduate training, I would be more than happy to share more information with you.
Joanne Kaiser-Smith, DO,
FACOI, FACP, assistant dean,
Graduate Medical Education,
University of Medicine and Dentistry New Jersey,
School of Osteopathic Medicine, Stratford, N.J.
Dr. Hospitalist responds:
Dr. Kaiser-Smith: Thank you for your letter to the editor. You are absolutely correct. My intention was not to overlook the postgraduate training of osteopathic physicians, which, as you pointed out, is governed differently from the postgraduate allopathic training programs.
Thank you for sharing this information with our readers.
New Zealanders have pharmaceutical choice, but most choose subsidized meds
Dr. Williams’ excellent article (see “Hospitalist Down Under,” Feb-ruary 2011, p. 1) about his experiences at a country hospital in New Zealand and comparisons with the U.S. system has had a warm reception in this country. However, one statement he makes needs correction.
Dr. Williams states that if a drug was not available on the New Zealand “formulary” (the Pharmaceutical Schedule), then it is not available. The New Zealand government has separate drug evaluation (Medsafe) and funding (PHARMAC) agencies, each of which has different remits. Medsafe decides which medicines are safe and effective to use in New Zealand. PHARMAC decides which medicines will be funded by the government, and publishes this list in the Pharmaceutical Schedule.
Any Medsafe-approved drug can be prescribed for New Zealand patients, even those not on the schedule. About 20% of medicines used in New Zealand are purchased privately.
Our experience is that when faced with a choice, New Zealanders usually opt for government-funded medicines (those subsidized by PHARMAC). For this reason, the majority of medicines prescribed for New Zealand patients are funded by the government.
Thanks again for the excellent article.
Simon England,
communications manager,
PHARMAC, Wellington,
New Zealand
ONLINE EXCLUSIVE: Listen to HM experts discuss comanagement opportunities
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
Click here to listen to Dr. McKean
Click here to listen to Dr. Wachter
Click here to listen to Dr. Siegal
Click here to listen to Dr. Cheng
Click here to listen to Dr. Auerbach
ONLINE EXCLUSIVE: Comanagement Business Models
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
One of the emerging trends in comanagement by hospitalists (see “The Comanagement Conundrum,” p. 1, April 2011) is an expanded role in the perioperative care of surgical patients—extending from before the operation into rehabilitation. To be successful, hospitalists should think more broadly than the usual focus on medical needs immediately post-surgery, says Burke Kealey, MD, director of perioperative comanagement at Regions Hospital in St. Paul, Minn.
The perioperative service at Regions includes staffing of a pre-operative clinic, a partnership with the hospital’s anesthesia department, and use of a pre-operative patient checklist. Many primary-care physicians (PCPs) want to retain a role in the pre-operative assessments of their patients, so the Regions service has tried to partner with physicians in the community to work on standardizing the process.
Dr. Kealey, an SHM board member, was hired by Regions’ orthopedic department right out of residency in 1995 to do medical comanagement of its patients. His service later was absorbed into an emerging HM department. It has experimented with models including the use of nurse practitioners and physician assistants.
—Burke Kealey, MD, director of perioperative comanagement, Regions Hospital, St. Paul, Minn., SHM board member
Today, Regions dedicates three of its 16 full-time hospitalist teams to comanagement services, largely on the orthopedics floor, but also for cardiovascular surgery and urology. “As hospitalists, we can help to facilitate using the best, up-to-date medical knowledge” both before and after surgery, he says.
At the University of Rochester School of Medicine in New York, a group of fellowship-trained geriatric hospitalists has taken on comanagement of hip fracture patients at the Geriatric Fracture Center, leading to improved processes and patient outcomes.1 According to hospitalist Susan M. Friedman, MD, MPH, the program began as a collaboration between a geriatrician and an orthopedic surgeon. They found that their patients’ outcomes seemed to be better when they worked together on a case, so they sat down to talk about what they were doing and how to standardize it.
“From the start, they set the tone for how this is supposed work, and when it doesn’t, they find out why and address it,” Dr. Friedman says. The program does not use a formal service agreement, but there is a strong emphasis on co-ownership, mutual respect, and communication. “One thing that has helped us a lot is data-gathering,” she adds. The hip fracture comanagement has cut lengths of stay and readmissions by half and complications by one-third for the mostly elderly patients.
Larry Beresford is a freelance writer based in Oakland, Calif.
Reference
- Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of co-managed geriatric fracture center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712-1717.
Q&A with Hospitalist Administrator Amit Prachand

Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Amit Prachand, MEng
Division Administrator, Hospital Medicine
Northwestern Memorial Hospital and Feinberg School of Medicine,
Northwestern University, Chicago
Question: What motivated you to join SHM’s Administrators Task Force (ATF)?
A: I wanted to be able to directly interface with the community of leaders in similar administrator roles in order to obtain a stronger perspective of the role, its rewards and challenges, and of the creative solutions different practices have implemented to address issues relevant to hospital medicine and the overall healthcare delivery model. I was also relatively new to hospital medicine practice management, and even healthcare, so I wanted to put myself in the best position to soak in as much as possible as well as help facilitate the sharing of ideas amongst my new group of peers.
Q: How is the Administrators Task Force moving HM forward?
A: One of our main thrusts in the task force is to help expand the administrative membership in SHM. As hospitalist programs mature and the environment in which hospital medicine is practiced evolves, it is imperative that we develop the community, the infrastructure, and the tools required to partner with our stakeholders—both internal and external—to help lead hospital medicine forward.
Q: Has your participation in the Administrators Task Force helped your group?
A: The ATF has helped develop direct lines of communication with peers. This helps when it come to issues for which we are finding the best solutions for; areas such as on-boarding of new physicians, negotiations with hospitals, coding and billing improvement, and meaningful performance reporting.
Q: How is the task force helping hospitals improve patient care?
A: By having a peer group on the administrative side, I believe we are now able to more readily share ideas that support the ideas around patient-care improvement that are being shared amongst the physician membership.
One of the key roles we play as an administrator is to help develop the systems and structures that help improve patient care. That may range from advocating for physician representation on certain hospital committees to facilitating a process/QI project that involves hospitalists and other members of the extended patient-care team, such as physicians from other medical specialties, nursing, pharmacists, case management, bed management, environmental services, and information technology.
Q: How is the task force helping hospitals improve healthcare overall?
A: We are continually improving the infrastructure for administrators to share ideas and solutions to address overall healthcare issues (payment reform, readmissions, compliance, cost). It is through this infrastructure that we can identify best implementation practices of ideas. The webinar series (www.hospitalmedicine.org/roundtables) that we’ve developed addresses many of the issues that healthcare in general is facing. This series has exceeded expectations for participation and interest.
Q: What do you like most about your job as an administrator?
A: It is never dull, always exciting. From the firefighting to the long-term planning, the role keeps me on my toes. I enjoy being in a position that is so tightly intertwined with so many critical functions and disciplines across the medical center in a profession—hospital medicine—that is continuing to lead advances in healthcare delivery.
—Brendon Shank
Q&A with Hospitalist Administrator Kristi Gylten

Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
Kristi Gylten, MBA
Director, Hospitalist Service,
Rapid City (S.D.) Regional Hospital
Question: What motivated you to join the Administrators Task Force (ATF)?
Answer: I wanted to have the opportunity to meet and network with my peers, and to be a part of developing resources and a place “on the map” for hospitalist administrators. The Administrators Task Force is bringing awareness to the administrative and business side of hospital medicine through the eyes of the hospitalist administrators.
Q: Has your participation on the task force helped out your group?
A: My group has benefited through the access and utilization of the available tools and resources to evaluate my own program, including tools like dashboards, job descriptions, patient communication, and marketing materials. The ATF has increased my awareness of the resources available, clinical and operational, to hospitalist groups, including my own.
Q: How is the ATF helping hospitals improve healthcare overall?
A: I believe the task force has its pulse on how healthcare could ideally be provided in the future. And, to me, it is extremely exciting to be part of the team that will help design the future of inpatient medicine and, in part, the continuum of care.
As hospitalist administrators, you have a close and collaborative relationship with the inpatient providers. And I think that because of that relationship and the fact that they live and breathe inpatient medicine, you are able to engage your team in improving many aspects of healthcare.
Q: What do you like most about your job as an administrator?
A: I like the wide variety of opportunities and challenges the role presents: human resources, contracting, recruitment, marketing and public relations, customer satisfaction, quality, and financials. The list goes on. No one day is like the previous, and it’s never dull. And most of all, I enjoy the challenge of strategizing and planning for the future of providing healthcare.
—Brendon Shank
The To-Don’t List

Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Last month, I wrote about the attributes of hospitalist practices that I associate with success. This month, I’ll do the opposite. That is, I’ll write about strategies your practice could, or even should, do without. Of course, all of these things are open to debate, and some thoughtful people might (and in my experience, probably will) arrive at different conclusions.
So I offer my list as food for thought, and if your practice relies on some of these strategies, you shouldn’t feel threatened by my opinion. But you might want to think about whether they’ve been made part of your practice by design, or if things just evolved this way without careful consideration of alternatives. I’ve listed them in no particular order.
Fixed-duration day shifts. My sense is that the majority of practices have a day shift with a predetermined start and end. That is, the hospitalist is expected to arrive and depart at the same time each day.
This seems to make a lot of sense, but it ignores the dramatic variations in workload a practice will have. For example, a practice that is appropriately staffed with four daytime hospitalists, and schedules each of them to work a 12-hour shift, provides 48 hours of daytime hospitalist manpower each day. But that will turn out to be precisely the right level of staffing only a few days a year. On all other days, daytime staffing will be optimal with a different number of hours. So it would make sense for the doctors to work more or less on those days.
Telling doctors that their shift always starts at the same time has significant lifestyle advantages. But it can inhibit the doctors who would be happy to start earlier to address more discharges early in the day and potentially go home earlier. So, just like most other doctors at your hospital have, why not let the doctors have significant latitude in when they start and stop working each day? In most cases, it might be necessary to have a time by which every doctor must be available to respond to pages (and one who must be on-site before the night doctor leaves), but they should feel free to actually arrive and start working when they choose. Most will make good choices and will likely feel a little more empowered and happy with their work.
And, at the end of the day, it might be reasonable to allow some of the day-shift doctors to leave when their work is done, and allow the others to stay to handle admissions until the night shift takes over. Those who leave early might still be required to respond to pages until a specified time.
Shifts that don’t involve rounding on “continuity” patients, such as night and evening (“swing”) shifts, usually should be arranged with predetermined start. I wrote in more detail on this topic in January 2007 and October 2010.
Contractual vacation provisions. Hospitalists should have significant amounts of time off. We work a lot of evenings, nights, and weekends, and we must have liberal amounts of time away from work. But for many practices, there is no advantage in classifying this time as vacation (or CME, etc.) time. In most cases, it makes the most sense to simply specify how much work (e.g. number of shifts) a doctor is to do each year and not specify a number of days or hours of vacation time. For more detail, read “The Vacation Conundrum” from March 2007.
If your practice has a vacation system that works well, then stick with it. But if you or your administrators are going nuts trying to categorize nonworking days between vacation and days the doctor simply wasn’t scheduled, then it might be best to stop trying. Just settle on the number of shifts (or some other metric) that a doctor is to work each year.
Tenure-based salary increases. It makes a lot of sense to pay doctors in most specialties an increasing salary based on his or her tenure with the practice. As they build a patient population and a referral stream, they generate more revenue and should benefit accordingly. But a new hospitalist who joins an existing group almost never has to build the referrals. In most cases, the group hired the doctor because the referrals are already coming and the practice needs more help, or the new doctor is replacing a departing one. So paying a new hospitalist a lower salary that increases automatically every few years isn’t really a raise earned by the doctor’s improved financial performance. Usually it’s just a system of withholding money that could be available for compensation for the doctor’s first few years in the practice. This lower starting salary might adversely impact recruiting. For more, see “Compensation Conundrum” from December 2009.
Poor roles for nonphysician providers (NPPs). I’ve worked with a lot of practices that have NPs and PAs (and, in some cases, RNs) who are doing what amounts to clerical work. They’re faxing discharge summaries, making calls to schedule patient appointments, dividing up the overnight admissions for the day rounders, etc.
Don’t make this mistake. Hire a secretary for that sort of work. And be sure that the roles occupied by trained clinicians (PAs, NPs, RNs, etc.) are professionally satisfying and will position them to make an effective contribution to the practice.
For more on this topic, see “The 411 on NPPs” from September 2008 and “Role Refinement” from September 2009; the latter features the perspective of Ryan Genzink, a thoughtful PA-C from Michigan.
Blinded performance reporting. First, make sure your practice provides regular, meaningful reports on each doctor’s performance and the group as a whole. This usually takes the form of a dashboard or report card. In my experience, too few practices do this. Make sure your group isn’t in that category.
Groups that do provide performance data often allow each doctor to see only his or her data. If data about other individuals in the group are provided, the names have often been removed. With exception of certain human resources issues (e.g. counseling a doctor to prevent termination), I think all performance data in the group should be shared by name with the whole group. In most practices, everyone should know by name which doctors are the high and low producers, each doctor’s compensation, and CPT coding practices (e.g. the portion of discharges coded at the high level).
When clinical performance can be attributed to individual providers, report those metrics openly, too. This usually creates greater cohesion within the group and helps foster a mentality of practice ownership. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Managerial Muscle
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.

Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.
Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
Ajay Kharbanda, MBA, CMPE, is regional director of Arlington-based Texas Health Resources, a nonprofit healthcare system that serves 16 counties in North and Central Texas with 4,100 beds at 24 acute-care and short-stay hospitals. Kharbanda, chair of SHM’s Administrators Task Force, chatted with The Hospitalist about his work, his involvement in SHM leadership, and how administrators can work with HM to improve the healthcare delivery.
Question: How would you characterize your role?
Answer: I work closely with the medical director of the hospitalist group to support physician practice operations for employed hospitalist physicians.
Q: What do you like most about your job as an administrator?
A: I serve professionals who make a difference in people’s lives, and I work with a specialty that is making a difference in how healthcare is being delivered in the country. Additionally, I work for a health system that has the mission to improve the health of the people in the communities we serve.
Q: What motivated you to join—and lead—SHM’s Administrators Task Force?
A: I have been a member of both MGMA (Medical Group Management Association) and SHM for many years, and I have seen SHM mature in the sense of meeting needs of nonclinicians who are looking for an avenue to network and seek answers to our common issues. I remember going to annual meetings, looking for familiar faces, and seeking out peers among the stream of physicians attending the event. Several of us saw the need for an avenue, especially at the annual meetings, for administrators to huddle and brainstorm.
As nonphysician administrators, we send a powerful message about our commitment to the specialty of hospital medicine by becoming a member of the society, and we do need to remember that this is a community unique to our needs as hospital medicine practice administrators.
Q: How is the task force moving HM forward?
A: The Administrators Task Force (ATF) is helping to develop initiatives and programs that promote and define the role of nonphysician practice administrators in hospital medicine. The ATF is charged with facilitating and enhancing the integration of administrators into the society. We strive to strengthen the society’s ability to fulfill its mission by developing and using the talents of current and future administrative leaders.
Q: How is the ATF helping hospitals improve patient care?
A: I believe it is by strengthening the role of the society. ATF has reached out to administrators nationwide to build awareness of the value of SHM resources, and we advised on the practice management [curriculum] for HM10. Plus, we have created the Web-based Practice Administrators’ Roundtable Series. These quarterly events provide an opportunity to discuss issues of common concern and share best practices around various topics. Following a brief formal presentation, participants are encouraged to take part in the discussion.
We all know that SHM offers a remarkable avenue for clinical knowledge, and we are helping to build an avenue for nonclinicians.
Q: Are there ways for other hospitalists and administrators to get involved with SHM?
A: First, visit the Practice Management Institute Web page at www.hospitalmedicine.org. It has information about the Practice Administrators’ Roundtable Series and resources on staffing and scheduling, career satisfaction, and coding and documentation.
Second, come to HM11, SHM’s annual meeting. We will be hosting a special-interest forum specifically designed for administrators. TH
Brendon Shank is vice president of communications for SHM.
NEW MEMBERS
Enter text here
Enter text here
Enter text here
CPT 2011 Update
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1

Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
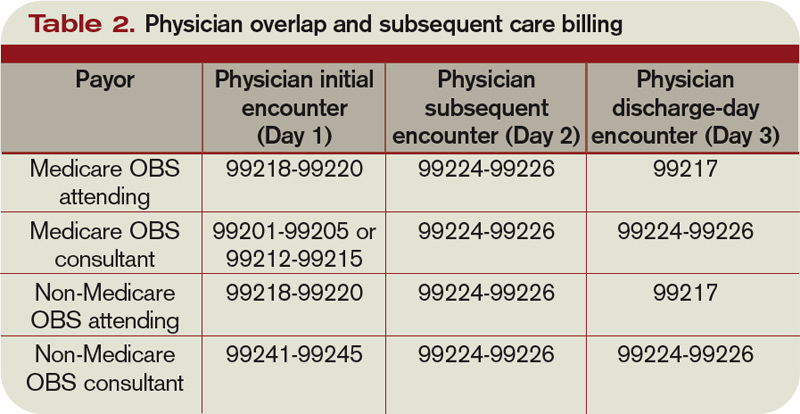
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1
Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.
In the past, observation services typically did not exceed 24 hours or two calendar days. However, changes in healthcare policy coupled with the impetus to reduce wasteful spending have spurred an atmosphere of scrutiny over hospital admissions. Sometimes there are discrepancies between a hospital’s utilization review committee and a payor’s utilization review committee in determining the appropriateness of healthcare services and supplies, in accordance with each party’s definition of medical necessity. This situation has caused an increase in both the number and cost of observation stays.
In response, subsequent observation-care codes (99224-99226) were developed and published in the 2011 edition of Current Procedural Terminology (CPT).1
Codes and Their Uses
CPT outlines three subsequent observation care codes:
- 99224: Subsequent observation care, per day, for the evaluation and management (E/M) of a patient, which requires at least two of these three key components: problem-focused interval history; problem-focused examination; and medical decision-making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
- 99225: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: expanded problem focused interval history; expanded problem focused examination; and medical decision-making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
- 99226: Subsequent observation care, per day, for the E/M of a patient, which requires at least two of these three key components: detailed interval history; detailed examination; and medical decision-making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Subsequent observation-care codes replicate the key components and time requirements established for subsequent hospital care services (99231-99233). However, the relative value units (RVUs) of physician work associated with subsequent observation care are not weighted equally (see Table 1, below). Subsequent observation care is a less-intense service, and therefore is valued at a lesser rate.
The attending of record writes the orders to admit the patient to observation (OBS); indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. Specialists typically are called onto an OBS case for their opinion/advice (i.e. consultants) but do not function as the attending of record.
According to CPT 2011, subsequent OBS care codes can be reported by both the attending physician of record and specialists who provide medically necessary, nonoverlapping care to patients on any day other than the admission or discharge day (see Table 2, above). At press time, CMS and private payors had not provided written clarification on the use of subsequent observation-care codes. Therefore, it is imperative to monitor payments, denials, and policy clarifications providing further billing instruction.
On the Horizon
Prior reporting guidelines required the reporting of subsequent observation-care days with established outpatient codes (99212-99215). Some member plans insisted on referrals for all outpatient visits regardless nature of the service. Without the mandated referral for established patient visits performed in the observation setting, physician services were denied for coverage.
The creation of subsequent observation codes might play a role in decreasing these denials. Be sure to review the private payors’ fee schedules for inclusion of 99224-99226 codes. If missing, contact the payor or include it as an agenda item during your contract negotiations.
For more information on observation care services, check out “Observation Care” in the July 2010 issue of The Hospitalist. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology: Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 16, 2011.