In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Although patients with blood clots are oftentimes not admitted to the hospital, there are some exceptions. Monal Shah, MD, physician advisor for Parkland Hospital in Dallas, Texas, and the former section head of hospital medicine at the University of Texas Southwestern Medical Center, discusses some exceptions.
Educational Opportunities for Hospitalists Beyond HM15
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
Whether you’re packing your bags for HM15 or following from afar, there are plenty of other opportunities to get the most up to date clinical, management, and quality improvement information in the specialty:
Leadership Academy 2015
October 19-22
Austin, Texas
Get the managerial confidence you need to take your hospital medicine career to the next level. All three Leadership Academy courses will be offered in what’s now called the “Live Music Capital of the World.” www.hospitalmedicine.org/leadership
Quality and Safety Educators Academy
May 7-9
Tempe, Ariz.
Medical students and residents are turning to hospitalists to learn about quality improvement and patient safety. The Quality and Safety Educators Academy (QSEA) is a great way to stay up to speed on the latest knowledge and tools to teach quality improvement. www.hospitalmedicine.org/qsea
Project BOOST
Ongoing Applications
Have you thought about enrolling your hospital in SHM’s award-winning Project BOOST only to find that you missed the enrollment deadline? SHM has now made Project BOOST’s application process more flexible by accepting rolling applications throughout the year. www.hospitalmedicine.org/boost
ABIM Maintenance of Certification
Deadline is August 1
Now is the time to start planning to enroll in the Focused Practice in Hospital Medicine Maintenance of Certification program. The enrollment deadline for the Fall 2015 exam is August 1, but don’t wait until the end of July to get started! http://www.hospitalmedicine.org/moc
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.
If you’re among the many physicians enrolled in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program, you have to earn a combined 100 points in medical knowledge and practice improvement throughout your 10-year certificate period. SHM wants to help you with this process.
SHM is pleased to announce that the ABIM has approved SHM’s Hospital Quality Improvement and Patient Safety Medical Knowledge Module for credit in the ABIM MOC program.
Take the QI and Patient Safety Medical Knowledge Module and many other online courses—free for members—at www.shmlearningportal.org.
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge.” —Dr. Maynard
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
Patients are not optimally mobilized;
Adherence to ordered mechanical prophylaxis is notoriously low; and
Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge.” —Dr. Maynard
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
Patients are not optimally mobilized;
Adherence to ordered mechanical prophylaxis is notoriously low; and
Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge.” —Dr. Maynard
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
Patients are not optimally mobilized;
Adherence to ordered mechanical prophylaxis is notoriously low; and
Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
Patient-safety guru Peter Pronovost, MD, PhD, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, talks about hospitalists’ role in improving the American healthcare system.
Patient-safety guru Peter Pronovost, MD, PhD, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, talks about hospitalists’ role in improving the American healthcare system.
Patient-safety guru Peter Pronovost, MD, PhD, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore, talks about hospitalists’ role in improving the American healthcare system.
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
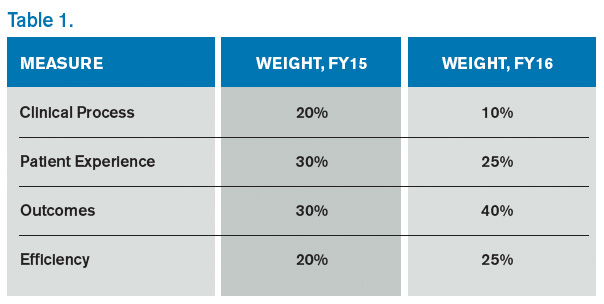
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
(click for larger image)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
Dr. Whitcomb is chief medical officer of Remedy Partners. He is co-founder and past president of SHM. E-mail him at [email protected].
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
(click for larger image)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
Dr. Whitcomb is chief medical officer of Remedy Partners. He is co-founder and past president of SHM. E-mail him at [email protected].
I have reported previously on major incentive programs under Medicare and the Affordable Care Act that affect hospitals and, by extension, their affiliated hospitalists. I’d like to provide you with an update on these programs. The bad news is that hospitals have more revenue than ever that is at risk based on performance. The good news is that such risk, and its mitigation, centers on performance measures in the sweet spot of hospitalists and the teams they work with to improve patient care.
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures.
Hospital-Acquired Conditions
On Dec. 17, 2014, the Centers for Medicare and Medicaid Services (CMS) announced that 724 U.S. hospitals—the lowest quartile—will have 1% of their reimbursement docked effective Oct. 1, 2014, as part of the Hospital-Acquired Condition Reduction Program (HACRP). The HACRP is divided into the following domains:
35%, Agency for Healthcare Research and Quality Patient Safety Indicators (PSI-90). This is a composite of eight claims-based harm measures.
65%, CDC National Health Safety Network measures. These are clinically derived metrics, currently central line-associated blood stream infection (CLABSI) and catheter-associated urinary tract infection (CAUTI).
The HACRP program, which debuted in October 2014, will continue at least through 2020. The 65% weight domain will change in FY16 with the addition of surgical site infections (colon, hysterectomy) and in FY17 with the addition of MRSA and Clostridium difficile infections.
Just two weeks prior to the CMS announcement, AHRQ announced some major accomplishments in efforts to address patient safety at U.S. hospitals. The agency reported that the number of hospital-acquired conditions in the Partnership for Patients (PfP) program in the U.S. declined 9% over a one-year period (2012 to 2013) and 17% over a three-year period (2010 to 2013). Hospital-acquired conditions are defined somewhat differently in the PfP than in the HACRP, with PfP targeting certain hospital-acquired infections, pressure ulcers, falls, and adverse drug effects.
The report noted that reductions in adverse drug events and pressure ulcers were the largest contributors to a reported 50,000 fewer in-hospital deaths over the 2010-2013 period.
Hospital Value-Based Purchasing
The Hospital VBP program continues to evolve. See Table 1 for a breakdown of the program for the next two years.
Unlike the HACRP and the Hospital Readmissions Reduction Program, which are pure penalty programs, VBP has hospitals at risk for 1.5% (for 2015) of Medicare payments, but they may earn back some, all, or an amount in excess of the 1.5% based on performance. For the years noted above, the VBP program metrics are as follows:
Clinical Process: selected heart failure (HF), pneumonia (PN), myocardial infarction (MI), and surgical care measures.
Patient Experience: a subset of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey questions.
Outcomes: HF, PN, MI, 30-day mortality, CLABSI, and PSI-90.
Efficiency: Medicare spending per beneficiary (spending from three days prior to an inpatient hospital admission through 30 days after discharge)
(click for larger image)
Readmission Penalties
CMS announced that in the latest round of the Hospital Readmissions Reduction Program, 2,610 hospitals were penalized in total, while 39 hospitals will receive the largest penalty allowed. For FY15, the program added chronic obstructive pulmonary disease and hip and knee arthroplasty to HF, PN, and MI as the conditions counting toward excess readmissions.
For FY15, the number of hospitals penalized and the amount of the penalty are expected to increase. In addition, 1% of hospitals are anticipated to receive the maximum penalty, while 77% are expected to have some penalty, and 22% will likely have no penalty. The maximum penalty has topped out at 3% of Medicare inpatient payments.
HCAHPS Star Ratings
The CMS Hospital Compare website will debut ‘star ratings’ in April 2015 to make it easier for consumers to decipher the site’s information. In a format similar to the one used by Nursing Home Compare, the website will use a five-star rating system based on the 11 publicly reported HCAHPS measures. The initial ratings will be based on discharges during the period ranging from July 2013 through June 2014.
What’s a Hospitalist to Do?
The latest version of CMS incentive programs should serve to reinforce your hospital medicine group’s strategy to be agents of collaboration and change. Link up with your quality department to align priorities, and make sure you have hospitalist representatives on key patient safety, patient experience, and quality improvement committees.
Because dollars are at stake for your hospital, have a clear understanding of the value your hospitalist group brings to the table, so you can secure the appropriate financial support for the time and work expended on these initiatives.
And don’t forget to keep the patient at the center of your efforts.
Dr. Whitcomb is chief medical officer of Remedy Partners. He is co-founder and past president of SHM. E-mail him at [email protected].
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
SHM convened a subcommittee of representatives from its Hospital Quality and Patient Safety Committee to consider 150 Choosing Wisely submissions from SHM committee members. These were narrowed down, ranked, and sent to all SHM members in a survey. Five evidence-based suggestions were adopted for adult patients. The recommendations are:
Don’t place, or leave in place, urinary catheters for incontinence or convenience or monitoring of output for non-critically ill patients (acceptable indications: critical illness, obstruction, hospice, peri-operatively for <2 days for urologic procedures; use weights instead to monitor diuresis).
Don’t prescribe medication for stress ulcer prophylaxis to medical inpatients unless at high risk for GI complications.
Avoid transfusions of red bloods cells for arbitrary hemoglobin or hematocrit thresholds and in the absence of symptoms of active coronary disease, heart failure, or stroke.
Don’t order continuous telemetry monitoring outside of the ICU without using a protocol that governs continuation.
Don’t perform repetitive CBC and chemistry testing in the face of clinical and lab stability.
Choosing Wisely is an initiative of the American Board of Internal Medicine Foundation to advocate for open dialogue between healthcare providers and patients to ensure appropriate care delivery at the right time.
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
SHM convened a subcommittee of representatives from its Hospital Quality and Patient Safety Committee to consider 150 Choosing Wisely submissions from SHM committee members. These were narrowed down, ranked, and sent to all SHM members in a survey. Five evidence-based suggestions were adopted for adult patients. The recommendations are:
Don’t place, or leave in place, urinary catheters for incontinence or convenience or monitoring of output for non-critically ill patients (acceptable indications: critical illness, obstruction, hospice, peri-operatively for <2 days for urologic procedures; use weights instead to monitor diuresis).
Don’t prescribe medication for stress ulcer prophylaxis to medical inpatients unless at high risk for GI complications.
Avoid transfusions of red bloods cells for arbitrary hemoglobin or hematocrit thresholds and in the absence of symptoms of active coronary disease, heart failure, or stroke.
Don’t order continuous telemetry monitoring outside of the ICU without using a protocol that governs continuation.
Don’t perform repetitive CBC and chemistry testing in the face of clinical and lab stability.
Choosing Wisely is an initiative of the American Board of Internal Medicine Foundation to advocate for open dialogue between healthcare providers and patients to ensure appropriate care delivery at the right time.
In 2015, reimbursement for physicians in large groups is subject to a value modifier that takes into account the cost and quality of services performed under the Medicare Physician Fee Schedule. By 2017, the modifier will apply to all physicians participating in fee-for-service Medicare.
It’s one more way the Centers for Medicare and Medicaid Services (CMS) and the federal government are attempting to tip the scales on skyrocketing healthcare costs. Their end goal is a focus on better efficiency and less waste in the healthcare system.
But in an environment of top-down measures, hospitalists on the front lines are leading the charge to reduce overuse and overtreatment, slow cost growth, and improve both the quality of care and outcomes for their patients.
“I think the hospitalist movement has prided itself on quality improvement and patient safety in the hospital,” says Chris Moriates, MD, assistant clinical professor in the division of hospital medicine at the University of California San Francisco (UCSF) and co-creator of the cost awareness curriculum for UCSF’s internal medicine residents. “Over the last few years…they are more focused and enthusiastic about looking at value.”
Dr. Moriates leads the UCSF hospitalist division’s High Value Care Committee and is director of implementation initiatives at Costs of Care. He’s also part of a UCSF program that invites all employees to submit ideas for cutting waste in the hospital while maintaining or improving patient care quality. Last year, the winning project tackled unnecessary blood transfusions and at the same time realized $1 million in savings due to lower transfusion rates. This year, the hospital will focus on decreasing money spent on surgical supplies, potentially saving millions of dollars, he says.
“Say a patient gets a prophylactic scan for abdominal pain,” says Vineet Arora, MD, MAPP, a hospitalist on faculty in the University of Chicago’s department of medicine and director of education initiatives for Costs of Care. “The patient gets better, but an incidental finding of the scan is a renal mass. Now, there is a work-up of that mass, the patient gets a biopsy, and they have a bleed. A lot of testing leads to more testing, and more testing can lead to harm.”
The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.
—LeRoi S. Hicks, MD, MPH
Doing less is often better, says John Bulger, DO, MBA, SFHM, chief quality officer for the Geisinger Health System in Danville, Pa. Dr. Bulger, who has led SHM’s participation in the Choosing Wisely campaign, cites a September 2014 study in JAMA Internal Medicine, in which Christiana Care Health System—an 1,100-bed tertiary care center in northern Delaware—built best practice telemetry guidelines into its electronic ordering system to help physicians determine when monitoring was appropriate.3 The health system also assembled multidisciplinary teams, which identified when medications warranted telemetry, and equipped nurses with tools to determine when telemetry should be stopped.
Appropriate use of telemetry is one of SHM’s five Choosing Wisely recommendations for adult patient care.
In addition to an overall 70% reduction in telemetry use without negative impact to patient safety, Christiana Care saved $4.8 million. Throughout its inpatient units, Christiana Care utilizes a multidisciplinary team approach to coordinate patient care. Daily rounds are attended by hospitalists, nurses, pharmacists, case managers, social workers, and others to ensure timely and appropriate patient care. The health system’s Value Institute evaluates hospital efforts and assesses process design to improve efficiency and, ultimately, outcomes.
“This is preparing for war in a time of peace, essentially,” says LeRoi S. Hicks, MD, MPH, a hospitalist, researcher, and educator at Christiana Care. “The goal will be, as we move to bundled payment and population health approaches, to minimize the time patients spend in the hospitals and limit the growth curve in spending on the hospital side. We are doing this and not taking on financial risk.”
Dr. Hicks adds that in its most simple form the project “reduces variation in the care we deliver” while improving efficiency and outcomes.
For many physicians, the best way to start is to begin a dialogue with patients who might also be at risk of financial harm due to unnecessary care, Dr. Arora says. “Patients are willing to change their minds and go with the more affordable and more evidence-based treatment and forgo expensive ones if they have that conversation,” she says.
Many resources exist for physicians interested in driving the frontline charge to improve healthcare quality and value. The Costs of Care curriculum provides training and tools for physicians at teachingvalue.org, as do SHM’s Center for Quality Innovation and the Institute for Healthcare Improvement. Dr. Moriates and Dr. Arora also have co-authored a book, along with Neel Shah, MD, founder and executive director of Costs of Care, called “Understanding Value Based Healthcare.” The book will be available this spring.
“We shouldn’t sit by the side of the road waiting for things to pass by,” Dr. Arora says. “I think the key is, we know the needle is shifting in Washington, we know system innovation models are being tested. It would be silly for us to say we’re going to continue the status quo and not look at ways to contribute as physicians.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
SHM convened a subcommittee of representatives from its Hospital Quality and Patient Safety Committee to consider 150 Choosing Wisely submissions from SHM committee members. These were narrowed down, ranked, and sent to all SHM members in a survey. Five evidence-based suggestions were adopted for adult patients. The recommendations are:
Don’t place, or leave in place, urinary catheters for incontinence or convenience or monitoring of output for non-critically ill patients (acceptable indications: critical illness, obstruction, hospice, peri-operatively for <2 days for urologic procedures; use weights instead to monitor diuresis).
Don’t prescribe medication for stress ulcer prophylaxis to medical inpatients unless at high risk for GI complications.
Avoid transfusions of red bloods cells for arbitrary hemoglobin or hematocrit thresholds and in the absence of symptoms of active coronary disease, heart failure, or stroke.
Don’t order continuous telemetry monitoring outside of the ICU without using a protocol that governs continuation.
Don’t perform repetitive CBC and chemistry testing in the face of clinical and lab stability.
Choosing Wisely is an initiative of the American Board of Internal Medicine Foundation to advocate for open dialogue between healthcare providers and patients to ensure appropriate care delivery at the right time.
The University of Vermont Medical Center (UVMC), a 562-bed academic facility in Burlington, has been honored with a Partnership in Prevention award for sustainable improvements to eliminate healthcare-associated infections (HAIs). The award, sponsored by the U.S. Department of Health and Human Services, the Association for Professionals in Infection Control and Epidemiology, and the Society for Healthcare Epidemiology of America, recognizes the concepts of the National Action Plan to Prevent Healthcare-Associated Infections: Roadmap to Elimination of the federal Office of Disease Prevention and Health Promotion.
UVMC was honored for creating a culture of safety and collaboration across ranks and disciplines, with a team of infection prevention advocates from the hospital, ambulatory clinics, and dialysis center, along with multi-disciplinary teams focused on infection prevention and control initiatives. The hospital posted a 77% reduction in reported central line-associated blood stream infections (CLABSI) in its medical ICU, and its neonatal ICU went 36 months without a CLABSI. Two surgeon-directed initiatives reduced surgical site infection rates for total knee and hip joint replacements by 81%—with 1,677 consecutive infection-free total knee arthroplasties.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
One key to its success, according to Anna Noonan, vice president of the Jeffords Institute for Quality and Operational Effectiveness at UVMC, is the fact that executive leadership, infection prevention specialists, clinicians, and quality experts are working together and using data to drive improvement. For example, the medical center implemented protocols for inserting central lines and offered mentored support in its simulation lab for clinicians—including hospitalists—to learn and practice correct insertion techniques.
For more information about UVMC’s award-winning commitment to zero infections, e-mail Noonan at [email protected].
The University of Vermont Medical Center (UVMC), a 562-bed academic facility in Burlington, has been honored with a Partnership in Prevention award for sustainable improvements to eliminate healthcare-associated infections (HAIs). The award, sponsored by the U.S. Department of Health and Human Services, the Association for Professionals in Infection Control and Epidemiology, and the Society for Healthcare Epidemiology of America, recognizes the concepts of the National Action Plan to Prevent Healthcare-Associated Infections: Roadmap to Elimination of the federal Office of Disease Prevention and Health Promotion.
UVMC was honored for creating a culture of safety and collaboration across ranks and disciplines, with a team of infection prevention advocates from the hospital, ambulatory clinics, and dialysis center, along with multi-disciplinary teams focused on infection prevention and control initiatives. The hospital posted a 77% reduction in reported central line-associated blood stream infections (CLABSI) in its medical ICU, and its neonatal ICU went 36 months without a CLABSI. Two surgeon-directed initiatives reduced surgical site infection rates for total knee and hip joint replacements by 81%—with 1,677 consecutive infection-free total knee arthroplasties.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
One key to its success, according to Anna Noonan, vice president of the Jeffords Institute for Quality and Operational Effectiveness at UVMC, is the fact that executive leadership, infection prevention specialists, clinicians, and quality experts are working together and using data to drive improvement. For example, the medical center implemented protocols for inserting central lines and offered mentored support in its simulation lab for clinicians—including hospitalists—to learn and practice correct insertion techniques.
For more information about UVMC’s award-winning commitment to zero infections, e-mail Noonan at [email protected].
The University of Vermont Medical Center (UVMC), a 562-bed academic facility in Burlington, has been honored with a Partnership in Prevention award for sustainable improvements to eliminate healthcare-associated infections (HAIs). The award, sponsored by the U.S. Department of Health and Human Services, the Association for Professionals in Infection Control and Epidemiology, and the Society for Healthcare Epidemiology of America, recognizes the concepts of the National Action Plan to Prevent Healthcare-Associated Infections: Roadmap to Elimination of the federal Office of Disease Prevention and Health Promotion.
UVMC was honored for creating a culture of safety and collaboration across ranks and disciplines, with a team of infection prevention advocates from the hospital, ambulatory clinics, and dialysis center, along with multi-disciplinary teams focused on infection prevention and control initiatives. The hospital posted a 77% reduction in reported central line-associated blood stream infections (CLABSI) in its medical ICU, and its neonatal ICU went 36 months without a CLABSI. Two surgeon-directed initiatives reduced surgical site infection rates for total knee and hip joint replacements by 81%—with 1,677 consecutive infection-free total knee arthroplasties.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
UVMC also joined the Centers for Disease Control and Prevention’s Dialysis Bloodstream Infection Prevention Collaborative in 2009 and has since reduced dialysis-related bloodstream infections by 83%.
One key to its success, according to Anna Noonan, vice president of the Jeffords Institute for Quality and Operational Effectiveness at UVMC, is the fact that executive leadership, infection prevention specialists, clinicians, and quality experts are working together and using data to drive improvement. For example, the medical center implemented protocols for inserting central lines and offered mentored support in its simulation lab for clinicians—including hospitalists—to learn and practice correct insertion techniques.
For more information about UVMC’s award-winning commitment to zero infections, e-mail Noonan at [email protected].