These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
“My census is too high.”
“I don’t have enough time to talk to patients.”
“These are outside our scope of practice.”
Dr. Sowmya Kanikkannan
These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
Kathleen Finn, MD, FHM and Jeffrey Greenwald, MD, SFHM engaged the audience with their playful banter while reviewing medical literature of clinical significance for the hospitalist in Update in Hospital Medicine. The studies presented were high-quality, practical and addressed questions that arise in our day-to-day practice. A wide variety of topics were addressed and key points are summarized below.
Key takeaways
In the PARADIGM-HF study, Angiotensin Receptor Blocker (ARB) + Neprilysin Inhibitor decreased cardiovascular mortality and reduced CHF hospitalization by 20% when compared to Enalapril alone in heart failure patients. The combination drug is an alternative choice to ACE inhibitors. FDA approval is forthcoming.
Is the risk of contrast-induced nephrotoxicity really as great as we have come to believe? Review of propensity matched studies suggests that AKI, 30 day need for emergent hemodi
alysis and death are unrelated to contrast. If CT with contrast makes a difference to the patient, consider using it if GFR>30 ml/min.
SAGES trial and Project Recovery developed a delirium screening method in hospitalized patients. The CAM (Confusion Assessment Method) scoring system assesses delirium severity in elderly patients (70+). Hospital and post-hospital outcomes in delirious vs. non-delirious patients showed that the more severe the delirium, the longer the patient stayed in the hospital. Further, the rate of new SNF placement and 90 day mortality was higher in the delirious group. The CAM score correlates with prognosis in medical patients. Addressing long-term goals of care in this patient population may be warranted.
A randomized placebo-controlled trail looked at the preventive effects of Ramelteon (melatonin receptor agonist) on delirium. Ramelteon 8mg was given to patients at 9pm for 7 days (or d/c). Although this was a small and short study, Ramelteon appears to reduce incident delirium in medical and non-intubated ICU patients.
The HELP randomized clinical trial compared Lactulose vs. Polyethylene Glycol (PEG) electrolyte solution for treatment of overt hepatic encephalopathy. Patients received either PEG (4L in 4 hours) or Lactulose (20-30g 3+doses/24hrs). Primary outcome was an improvement in HESA (Hepatic Encephalopathy Scoring Algorithm ) score by 1 at 24 hours. HESA score improved and patients had a shorter length of stay in the PEG group. In addition, patients requested PEG at discharge because it tasted better.
A retrospective study looked at Nonselective beta blockers (NSBB) in patients with Spontaneous Bacterial Peritonitis (SBP). It suggests that the use of NSBB after SBP onset increases the risk of AKI, Hepatorenal Syndrome and mortality by 58%. NSBB appear beneficial before SBP onset suggesting that as cirrhosis becomes more severe, NSBB may not be effective.
A retrospective cohort trial (Michigan Hospital Medicine Safety Consortium) assessed hospital performance of VTE prophylaxis. The rate of clinically evident, confirmed VTE was measured. There was no difference in VTE occurrence during hospitalization, 90 day VTE rates and PE vs. DVT rates. No clear benefit was evident from VTE prophylaxis for medical patients. This could indicate the need to risk stratify patients’ VTE risk.
Direct oral anticoagulants (DOACs) were compared with Vitamin K antagonists (VKA) for treatment of acute VTE in a meta-analysis reviewed by the speakers. Death, safety and bleeding were assessed. DOACs seem to work as well as VKAs for VTE. They also had a better safety profile. In cancer patients, DOACs vs. LMWH study is still needed. In patients with atrial fibrillation (AF), DOACs prevent AF-associated strokes better than VKAs. They also reduce hemorrhagic stroke and intracranial hemorrhage.
In the elderly (75 or older) patient, DOACs are as safe as VKAs and LMWH for AF and VTE treatment.
Randomized control trails compared once weekly Dalbavancin or single-dose Oritavancin vs. daily conventional therapy for acute bacterial skin infections (cellulitis, major abscess, wound infection, 75cm² erythema). Outcomes measured were cessation of spread of erythema and no fever X3 readings in 48-72 hours. Dalbavancin once weekly was non-inferior to Vancomycin in safety profile and outcome measures. Direct cost of Dalbavancin was higher although patients on this drug had shorter length of stays which is cost effective. FDA approved for skin infections.
The presence of family during CPR decreased PTSD, anxiety and depression symptoms in family members. Outcomes were similar when participants were assesses at 90 days and 1 year. While this study was conducted in an out of hospital setting, it may be worthwhile to assess if it is applicable to patients who code in the hospital.
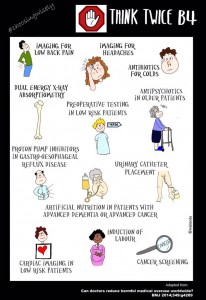
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
John Bulger, DO, MBA reviewed the components of the Choosing Wisely campaign and SHM’s recommendations in an era where providing high value cost-conscious care is key to optimizing the health of our patients. Choosing Wisely is an initiative of the ABIM foundation to foster communication between physicians and patients about common tests and procedures that may fail to provide value or enhance patient outcomes. It’s a partnership with 70-plus medical societies including an innovative partnership with Consumer Reports. SHM’s evidence-based recommendations are:
Don’t leave urinary catheters in place for convenience or monitoring of output for non-critically ill patients.
Don’t prescribe stress ulcer prophylaxis to hospitalized patients unless they are at high risk for GI complications.
Avoid transfusion of PRBC for arbitrary hemoglobin in the absence of CAD, CHF or CVA.
Don’t order continuous telemetry monitoring outside of the ICU without a protocol.
Don’t perform repetitive CBC and chemistry testing in a clinically stable patient.
Dr. Bulger highlighted that the Choosing Wisely campaign is designed to encourage conversations to
improve patient care. While cost-conscious care is a natural by-product of this effort, the primary focus when these guidelines were developed was to provide better healthcare for our patients. This year, SHM’s Choosing Wisely Case Competition has triggered the application of the above recommendations in institutions across the country. A summary of these efforts will be published in the near future to assist fellow hospitalists with their efforts to minimize waste and improve care in their own institutions. Look for the Hospitalist Guide to Choosing Wisely which is expected to be published in spring 2015. Choosing Wisely has now become a world-wide effort with Canada, Europe and Brazil implementing similar recommendations to improve healthcare.
Dr.Bulger concluded that while tradition is hard to change, it is of paramount importance to think differently to find innovative solutions to common problems in healthcare. Join the conversation using #ChoosingWisely or #LessIsMore on twitter.
Key Takeaways
Choosing Wisely is an ABIM campaign developed to address and promote conversations about common tests and procedures that are of low-value.
SHM’s recommendations were implemented in institutions with positive results as evidenced by the Choosing Wisely case competition at #HospMed15.
Look for a summary of these efforts to be published in the spring of 2015.
Use these guidelines to educate, provoke dialogue and achieve optimal patient outcomes in your institution.
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH
In this session, Drs. Michelle Mourad and Christopher Moriates took a systematic approach to answer quality questions that we commonly encounter in our hospitalist practice. They reviewed current evidence including meta-analyses and systematic reviews to arrive at an answer for various quality-related questions. These are summarized below:
What are the common features of interventions that have successfully reduced re-admissions? Effective interventions that enhance patient capacity to reliably access and engage in post-discharge care has been associated with success in decreasing re-admissions.
Does patient engagement correlate with decreased resource use or readmissions? Patient activation is defined as knowledge, skills, confidence and inclination to assume responsibility for managing one’s own health. A higher patient activation score reduced the risk of 30-day hospital re-utilization.
Does patients’ report of their healthcare experience reflect quality of care? Patient satisfaction scores may be a reflection of their desires (for example, to get pain medications) regardless of clinical benefit. In these situations, quality should be based on achieving a mutual understanding of patient situation and treatment plan between the provider and patient.
Is there any relationship between quality of care and health outcomes? Positive associations were found between patient experience and safety/effectiveness. Including patient experience in quality improvement, therefore, may lead to improvements in safety and effectiveness. Reducing the trauma of hospitalization could improve patient satisfaction and outcomes. Efforts such as personalization, providing rest and nourishment, reducing stress disruption and surprises as well as providing a post discharge safety net are strategies to reduce the trauma of hospitalization, improve satisfaction and patient outcomes.
Is there anything we can do to make hand-offs safer? The I-PASS hand-off bundle for a systematic hand-off process was reviewed (Illness severity, Patient summary, Action list, Situation awareness, Synthesis by receiver) as a means of reducing medical errors. When used in conjunction with training, faculty development and a culture-change campaign, this was associated with improving patient safety without negatively affecting workflow.
How can hospitalists deflate medical bills? Patient expectations of the benefits and harms of clinical interventions influences physician decision making and contributes to overuse and increased healthcare costs. Harm of excessive testing was underestimated in such situations. Conversations with patients, colleagues and the public are crucial to decreasing low value care. Physicians should discuss potential benefits and risks to address patient expectations. In addition, they should seek opportunities to better understand healthcare costs.
How big of a problem is antibiotic overuse in hospitals and can we do better? In a national database review, more than half of all patients (55.7%) discharged from a hospital received antibiotics during their stay. There is a wide variation in antibiotic use across hospital wards. Reducing this exposure to broad spectrum antibiotics would lead to a 26% reduction in C. diff infections and reduce antibiotic resistance. To improve this over-utilization, stewardship programs should actively engage and educate clinicians, encourage clear antibiotic documentation in daily progress notes and use 72-hour antibiotic time-out during multidisciplinary rounds. TH