User login
CDC Expert Discusses MRSA Infections and Monitoring for Anti-Microbial Resistance
Click here to listen to more of our interview with Dr. Patel
Click here to listen to more of our interview with Dr. Patel
Click here to listen to more of our interview with Dr. Patel
Pros and Cons of Clinical Observation Units

Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Clinical Vignettes 101

Check out winners of the HM13 Research, Innovation, and Clinical Vignette competition at www.hospitalmedicine2013.org/riv/vignettes.php. The site includes poster PDFs and presentations from the winners, as well as poster PDFs for all finalists.
Physicians are exposed to a wide variety of cases that pique our interest. Cases that make you go home and read just a little bit more. Cases that prompt you to seek out your classmates and colleagues for further discussion, or trigger a call to someone from your past. Residents and students often ask, “Should I write this case up?” Our answer is, “Yes!”
Why do we recommend that you write the case up? Much of medical education is a clinical- or case-based exercise. Clinical cases provide context for the principles being taught. We use real cases to point out the nuance in a presentation of a particular illness or the management of a disease.
In clinical conferences, such as morning report or clinical-pathologic conferences (CPCs), we highlight the choices we make as physicians to provide the best care. Respected physicians and master clinicians at our own institutions often lead these discussions, which form the building blocks for how many of us will practice in our careers.
At grand rounds, the best speakers start with a case. These vignettes grab our attention, making us realize the importance of what the speaker teaches us.
Writing up a vignette will give you a skill set you need. You learn how to select a case, create a “teachable moment,” or hone a series of teaching points. You develop your skills in searching and critically appraising the literature. You become a content expert among your peers. This activity helps you to develop and master the academic skills that will drive your career and will be pivotal in your success.
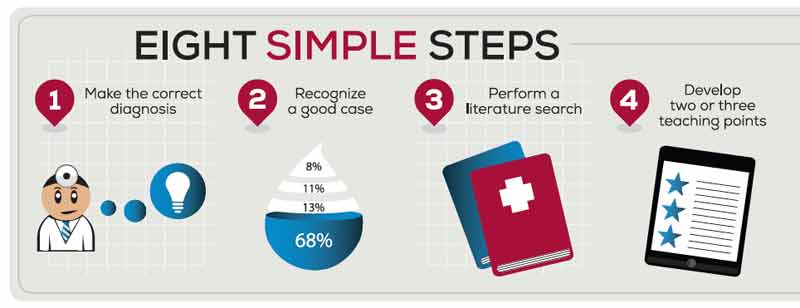
Follow these eight steps to produce successful clinical vignette submissions:
Step 1
Be a good doctor and make the correct diagnosis: Interesting cases will come to you. Don’t chase a zebra on every cough. Don’t send autoimmune panels for every rash. Read about each patient’s case that you see. Use the time to build your clinical acumen and develop your own illness scripts. Through the process of being a thoughtful student of medicine, you will come to distinguish the fascinoma from the merely fleeting infatuation with a diagnosis.
Step 2
Recognize the good case: The best way to recognize a good case is appreciate when it excites people locally. If you present it at morning report or CPC, are you inundated with requests to speak more after the conference has finished? Did it stump your colleagues (usually a pretty bright group)? Do you find that the consultants ask for others in their division to come and see the case? Clinically, did it take the team a while to come to the end diagnosis? If any of these are true, then you should move forward.
Step 3
Perform a literature search: How often does a similar situation arise? Is it 1 in 10,000, 1 in a million, or less? Even a case of 1 in 10,000 can be impactful to read about when you consider how long it may take a physician to see that many patients.
Step 4.
Develop two or three teaching points: Most abstracts for national and regional meetings have a restrictive word limit. When you consider all the information required of a thorough case presentation and adequate discussion, it can seem almost impossible to fit it all in. Start early, at least a month before the deadline if you can, and start big. Determine two or three key teaching points you wish to make. These will serve as your roadmap for the write-up.
Next, write down everything you want to say. Then cut the verbiage and descriptions that are not needed to tell your story. Focus on two or three take-home points. Each fact included or statement made should help to guide the reader to these lessons. As readers and authors, we also like to see prevalence and incidence of disease findings, or how good a test is with specificity and sensitivity values. Make sure the readers know what you want them to learn.
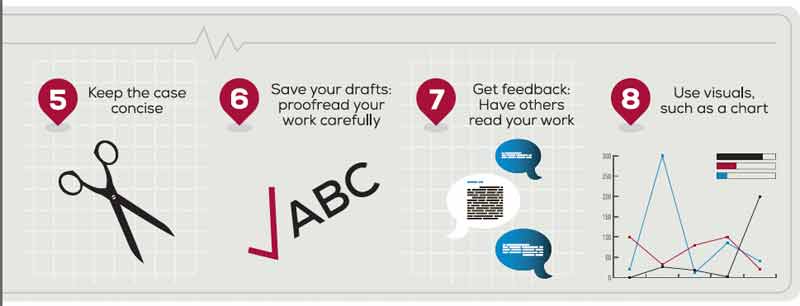
Step 5
Keep the case concise, and focus on the discussion: The best write-ups keep the case description short and focused. Avoid trying to tell your readers everything about your case. Highlight what makes your case different without including extraneous information that does not support your teaching points. This leaves more room to focus on your discussion and explain to the reader the importance of your case. The discussion is where you create the “teachable moment” by elaborating on your teaching points.
Step 6
Keep your drafts and proofread your work carefully: The process of writing a clear and concise vignette will take many drafts. To do a great job, plan for at least three or four versions. Through the process of revisiting every word you use, you will start to hone your mastery of the topic; you will see the case in a new way with each draft.
As you do this, keep each edit as a separate file. You will inevitably edit something out early on that you will want to put back in later. Keeping your drafts will make this much easier.
At the final version, proofread carefully! Most reviewers will deduct points for poor grammar and misspellings. If it looks sloppy, then a reader will assume it represents sloppy thoughts.
Step 7
Get feedback: Have others read your work. It is always hard to put your writing out there for critique, particularly when it is such a personal representation of your own clinical thought. Hopefully, you have collaborated with others involved in the case; however, to avoid any “group think” about the work, it is best to have uninvolved individuals (e.g., trusted faculty member, program director, division chief) review your work before submission. The point of these vignettes is to help you develop skills as an author and academician. Since most meetings do not provide any feedback on the review of your submission, outside of “accepted” or “rejected,” it is important to get this from your own institution. It will also heighten your chances of acceptance. Take their suggestions openly, and use them to refine your abstract.
Step 8
Consider the following keys to a poster or oral presentation: The presentation at the meeting should be an expansion on the abstract. Remember, you have described the situation, but now you have the opportunity to use a picture. The old adage that a picture is worth a thousand words really rings true here.
Avoid copying and pasting your text. Concise statements will grab people’s eyes and leave you more space for charts and images. Visuals grab the reader’s eye better than small-font text.
Conclusion
Your first clinical vignette can be a truly great experience. Although it is a lot of hard work, presenting clinical thought is a skill that you must learn. Once you do this, you might find that you have “caught the bug,” and will find yourself well on your way to a role in medical education. You might even start a larger project based on this experience.
Dr. Burger is associate program director of internal medicine residency in the Department of Medicine at Beth Israel Medical Center and assistant dean and assistant professor of medicine at Albert Einstein College of Medicine, both in New York City. Dr. Paesch is a comprehensive care physician in the section of hospital medicine at the University of Chicago, and assistant professor at the University of Chicago Pritzker School of Medicine. Dr. Miller is director of student programs, associate program director, residency, and associate professor of medicine in the Department of Medicine at Tulane Health Sciences Center in New Orleans.
Check out winners of the HM13 Research, Innovation, and Clinical Vignette competition at www.hospitalmedicine2013.org/riv/vignettes.php. The site includes poster PDFs and presentations from the winners, as well as poster PDFs for all finalists.
Physicians are exposed to a wide variety of cases that pique our interest. Cases that make you go home and read just a little bit more. Cases that prompt you to seek out your classmates and colleagues for further discussion, or trigger a call to someone from your past. Residents and students often ask, “Should I write this case up?” Our answer is, “Yes!”
Why do we recommend that you write the case up? Much of medical education is a clinical- or case-based exercise. Clinical cases provide context for the principles being taught. We use real cases to point out the nuance in a presentation of a particular illness or the management of a disease.
In clinical conferences, such as morning report or clinical-pathologic conferences (CPCs), we highlight the choices we make as physicians to provide the best care. Respected physicians and master clinicians at our own institutions often lead these discussions, which form the building blocks for how many of us will practice in our careers.
At grand rounds, the best speakers start with a case. These vignettes grab our attention, making us realize the importance of what the speaker teaches us.
Writing up a vignette will give you a skill set you need. You learn how to select a case, create a “teachable moment,” or hone a series of teaching points. You develop your skills in searching and critically appraising the literature. You become a content expert among your peers. This activity helps you to develop and master the academic skills that will drive your career and will be pivotal in your success.
Follow these eight steps to produce successful clinical vignette submissions:
Step 1
Be a good doctor and make the correct diagnosis: Interesting cases will come to you. Don’t chase a zebra on every cough. Don’t send autoimmune panels for every rash. Read about each patient’s case that you see. Use the time to build your clinical acumen and develop your own illness scripts. Through the process of being a thoughtful student of medicine, you will come to distinguish the fascinoma from the merely fleeting infatuation with a diagnosis.
Step 2
Recognize the good case: The best way to recognize a good case is appreciate when it excites people locally. If you present it at morning report or CPC, are you inundated with requests to speak more after the conference has finished? Did it stump your colleagues (usually a pretty bright group)? Do you find that the consultants ask for others in their division to come and see the case? Clinically, did it take the team a while to come to the end diagnosis? If any of these are true, then you should move forward.
Step 3
Perform a literature search: How often does a similar situation arise? Is it 1 in 10,000, 1 in a million, or less? Even a case of 1 in 10,000 can be impactful to read about when you consider how long it may take a physician to see that many patients.
Step 4.
Develop two or three teaching points: Most abstracts for national and regional meetings have a restrictive word limit. When you consider all the information required of a thorough case presentation and adequate discussion, it can seem almost impossible to fit it all in. Start early, at least a month before the deadline if you can, and start big. Determine two or three key teaching points you wish to make. These will serve as your roadmap for the write-up.
Next, write down everything you want to say. Then cut the verbiage and descriptions that are not needed to tell your story. Focus on two or three take-home points. Each fact included or statement made should help to guide the reader to these lessons. As readers and authors, we also like to see prevalence and incidence of disease findings, or how good a test is with specificity and sensitivity values. Make sure the readers know what you want them to learn.
Step 5
Keep the case concise, and focus on the discussion: The best write-ups keep the case description short and focused. Avoid trying to tell your readers everything about your case. Highlight what makes your case different without including extraneous information that does not support your teaching points. This leaves more room to focus on your discussion and explain to the reader the importance of your case. The discussion is where you create the “teachable moment” by elaborating on your teaching points.
Step 6
Keep your drafts and proofread your work carefully: The process of writing a clear and concise vignette will take many drafts. To do a great job, plan for at least three or four versions. Through the process of revisiting every word you use, you will start to hone your mastery of the topic; you will see the case in a new way with each draft.
As you do this, keep each edit as a separate file. You will inevitably edit something out early on that you will want to put back in later. Keeping your drafts will make this much easier.
At the final version, proofread carefully! Most reviewers will deduct points for poor grammar and misspellings. If it looks sloppy, then a reader will assume it represents sloppy thoughts.
Step 7
Get feedback: Have others read your work. It is always hard to put your writing out there for critique, particularly when it is such a personal representation of your own clinical thought. Hopefully, you have collaborated with others involved in the case; however, to avoid any “group think” about the work, it is best to have uninvolved individuals (e.g., trusted faculty member, program director, division chief) review your work before submission. The point of these vignettes is to help you develop skills as an author and academician. Since most meetings do not provide any feedback on the review of your submission, outside of “accepted” or “rejected,” it is important to get this from your own institution. It will also heighten your chances of acceptance. Take their suggestions openly, and use them to refine your abstract.
Step 8
Consider the following keys to a poster or oral presentation: The presentation at the meeting should be an expansion on the abstract. Remember, you have described the situation, but now you have the opportunity to use a picture. The old adage that a picture is worth a thousand words really rings true here.
Avoid copying and pasting your text. Concise statements will grab people’s eyes and leave you more space for charts and images. Visuals grab the reader’s eye better than small-font text.
Conclusion
Your first clinical vignette can be a truly great experience. Although it is a lot of hard work, presenting clinical thought is a skill that you must learn. Once you do this, you might find that you have “caught the bug,” and will find yourself well on your way to a role in medical education. You might even start a larger project based on this experience.
Dr. Burger is associate program director of internal medicine residency in the Department of Medicine at Beth Israel Medical Center and assistant dean and assistant professor of medicine at Albert Einstein College of Medicine, both in New York City. Dr. Paesch is a comprehensive care physician in the section of hospital medicine at the University of Chicago, and assistant professor at the University of Chicago Pritzker School of Medicine. Dr. Miller is director of student programs, associate program director, residency, and associate professor of medicine in the Department of Medicine at Tulane Health Sciences Center in New Orleans.
Check out winners of the HM13 Research, Innovation, and Clinical Vignette competition at www.hospitalmedicine2013.org/riv/vignettes.php. The site includes poster PDFs and presentations from the winners, as well as poster PDFs for all finalists.
Physicians are exposed to a wide variety of cases that pique our interest. Cases that make you go home and read just a little bit more. Cases that prompt you to seek out your classmates and colleagues for further discussion, or trigger a call to someone from your past. Residents and students often ask, “Should I write this case up?” Our answer is, “Yes!”
Why do we recommend that you write the case up? Much of medical education is a clinical- or case-based exercise. Clinical cases provide context for the principles being taught. We use real cases to point out the nuance in a presentation of a particular illness or the management of a disease.
In clinical conferences, such as morning report or clinical-pathologic conferences (CPCs), we highlight the choices we make as physicians to provide the best care. Respected physicians and master clinicians at our own institutions often lead these discussions, which form the building blocks for how many of us will practice in our careers.
At grand rounds, the best speakers start with a case. These vignettes grab our attention, making us realize the importance of what the speaker teaches us.
Writing up a vignette will give you a skill set you need. You learn how to select a case, create a “teachable moment,” or hone a series of teaching points. You develop your skills in searching and critically appraising the literature. You become a content expert among your peers. This activity helps you to develop and master the academic skills that will drive your career and will be pivotal in your success.
Follow these eight steps to produce successful clinical vignette submissions:
Step 1
Be a good doctor and make the correct diagnosis: Interesting cases will come to you. Don’t chase a zebra on every cough. Don’t send autoimmune panels for every rash. Read about each patient’s case that you see. Use the time to build your clinical acumen and develop your own illness scripts. Through the process of being a thoughtful student of medicine, you will come to distinguish the fascinoma from the merely fleeting infatuation with a diagnosis.
Step 2
Recognize the good case: The best way to recognize a good case is appreciate when it excites people locally. If you present it at morning report or CPC, are you inundated with requests to speak more after the conference has finished? Did it stump your colleagues (usually a pretty bright group)? Do you find that the consultants ask for others in their division to come and see the case? Clinically, did it take the team a while to come to the end diagnosis? If any of these are true, then you should move forward.
Step 3
Perform a literature search: How often does a similar situation arise? Is it 1 in 10,000, 1 in a million, or less? Even a case of 1 in 10,000 can be impactful to read about when you consider how long it may take a physician to see that many patients.
Step 4.
Develop two or three teaching points: Most abstracts for national and regional meetings have a restrictive word limit. When you consider all the information required of a thorough case presentation and adequate discussion, it can seem almost impossible to fit it all in. Start early, at least a month before the deadline if you can, and start big. Determine two or three key teaching points you wish to make. These will serve as your roadmap for the write-up.
Next, write down everything you want to say. Then cut the verbiage and descriptions that are not needed to tell your story. Focus on two or three take-home points. Each fact included or statement made should help to guide the reader to these lessons. As readers and authors, we also like to see prevalence and incidence of disease findings, or how good a test is with specificity and sensitivity values. Make sure the readers know what you want them to learn.
Step 5
Keep the case concise, and focus on the discussion: The best write-ups keep the case description short and focused. Avoid trying to tell your readers everything about your case. Highlight what makes your case different without including extraneous information that does not support your teaching points. This leaves more room to focus on your discussion and explain to the reader the importance of your case. The discussion is where you create the “teachable moment” by elaborating on your teaching points.
Step 6
Keep your drafts and proofread your work carefully: The process of writing a clear and concise vignette will take many drafts. To do a great job, plan for at least three or four versions. Through the process of revisiting every word you use, you will start to hone your mastery of the topic; you will see the case in a new way with each draft.
As you do this, keep each edit as a separate file. You will inevitably edit something out early on that you will want to put back in later. Keeping your drafts will make this much easier.
At the final version, proofread carefully! Most reviewers will deduct points for poor grammar and misspellings. If it looks sloppy, then a reader will assume it represents sloppy thoughts.
Step 7
Get feedback: Have others read your work. It is always hard to put your writing out there for critique, particularly when it is such a personal representation of your own clinical thought. Hopefully, you have collaborated with others involved in the case; however, to avoid any “group think” about the work, it is best to have uninvolved individuals (e.g., trusted faculty member, program director, division chief) review your work before submission. The point of these vignettes is to help you develop skills as an author and academician. Since most meetings do not provide any feedback on the review of your submission, outside of “accepted” or “rejected,” it is important to get this from your own institution. It will also heighten your chances of acceptance. Take their suggestions openly, and use them to refine your abstract.
Step 8
Consider the following keys to a poster or oral presentation: The presentation at the meeting should be an expansion on the abstract. Remember, you have described the situation, but now you have the opportunity to use a picture. The old adage that a picture is worth a thousand words really rings true here.
Avoid copying and pasting your text. Concise statements will grab people’s eyes and leave you more space for charts and images. Visuals grab the reader’s eye better than small-font text.
Conclusion
Your first clinical vignette can be a truly great experience. Although it is a lot of hard work, presenting clinical thought is a skill that you must learn. Once you do this, you might find that you have “caught the bug,” and will find yourself well on your way to a role in medical education. You might even start a larger project based on this experience.
Dr. Burger is associate program director of internal medicine residency in the Department of Medicine at Beth Israel Medical Center and assistant dean and assistant professor of medicine at Albert Einstein College of Medicine, both in New York City. Dr. Paesch is a comprehensive care physician in the section of hospital medicine at the University of Chicago, and assistant professor at the University of Chicago Pritzker School of Medicine. Dr. Miller is director of student programs, associate program director, residency, and associate professor of medicine in the Department of Medicine at Tulane Health Sciences Center in New Orleans.
Massachusetts Hospitalists Experiment with Unit-Based Rounding

Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at [email protected].
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at [email protected].
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Today marks the end of the second week of a three-month experiment we are embarking on to improve team-based care. The main elements of our experiment are two early career hospitalists dedicated to a single nursing unit who are present on the unit throughout the day, structured multidisciplinary rounds, pharmacists doing medication histories to help with medical reconciliation, and a veteran hospitalist serving as a coach, broadly overseeing care coordination and throughput on the unit. (I’m going to focus on multidisciplinary care and leave the coaching part for another day.)
Many have written about and many more have tried to establish unit-based hospitalist models, where a hospitalist is assigned to a single nursing unit. These models often incorporate multidisciplinary rounds, where the hospitalist, case management, social services, physical therapy, and perhaps pharmacy meet each day and review each patient’s progress through the hospitalization. The underlying premise for establishing a unit-based model is that all, or nearly all, of the hospitalist’s patients are located on the nursing unit.
It Can’t Be That Hard
Dedicated units and multidisciplinary rounds are designed to achieve better coordination between the hospitalists and the other members of the hospital team. Most healthcare professionals intuitively support this model; however, many hospitalists have concerns.
To provide the best care for their patients while maintaining career satisfaction, these hospitalists may feel the need for flexibility—the ability to be independent and roam unrestricted through the hallways and departments of the hospital. This goal can be at odds with being limited to a single nursing unit.
For these hospitalists to support the unit-based model, there had better be good reasons for doing so.
Measuring the Effects of Teamwork
Jody Hoffer Gittell, PhD, a professor of management at Brandeis University in Waltham, Mass., has studied relational coordination extensively in healthcare and other service industries. Relational coordination can be defined as “coordinating work through relationships of shared goals, shared knowledge and mutual respect, supported by frequent, timely, accurate, problem-solving communication.”1
Dr. Gittell has developed a validated questionnaire to be completed by each member of the healthcare team, quantifying their perspective on these dimensions for others on the team. I think of relational coordination as a rigorous way of quantifying teamwork.
In 2008, Dr. Gittell published an observational study with SHM senior vice president Joe Miller and hospitalist leader Adrienne L. Bennett, MD, PhD, conducted at a suburban Boston hospital.2 The study looked at relational coordination between members of the hospital team under hospitalist care compared to traditional, PCP-based hospital care. They measured relational coordination by asking the attending physician (hospitalist or PCP providing hospital care), medical resident, floor nurse, case manager, social worker, and therapist (occupational, physical, respiratory, speech) to complete questionnaires about the other team members for a cohort of patients.
The study concluded that relational coordination between other members of the team and the physician was significantly higher for patients treated by hospitalists than for patients treated by traditional PCPs. Further, they found that as relational coordination increased, for patients treated either by hospitalists or PCPs, length of stay, cost, and 30-day readmission rates decreased. I will add that the hospitalists were not unit-based in this study, but were assumed to be more available to the care team than traditional PCPs.
Subsequent studies of multidisciplinary rounds on a “hospitalist unit” conducted by Kevin O’Leary, MD, and colleagues at Northwestern University in Chicago have demonstrated a favorable effect on nurses’ ratings of teamwork and collaboration, as well as the rate of adverse events.3,4 The former study did not, however, find decreased costs or length of stay.
Keys to Success
Before our current experiment, I’ve had the privilege to witness, both at my home institution and at a number of outside ones, many permutations of multidisciplinary rounds and unit-based hospitalists. I’ve seen failures, some mixed results, and occasional success stories. In all cases, participants seem to agree that it takes extra effort to execute on this model, especially once the initial enthusiasm wanes. So, for these arrangements to succeed over time, including our current experiment, I see the following four factors as critical:
- Multidisciplinary rounds must be tightly organized, with case manager, nurse, and hospitalist providing input concisely. Average time per patient should not exceed about three minutes. The total time for rounds, no matter how many patients are under discussion, should not exceed one hour.
- Each team member must be prepared to provide critical information for rounds. For example, hospitalists and nurses should have seen/reviewed their patients, case managers should know expected length of stay and key disposition information, and pharmacists should know medical histories and other pertinent information.
- The fundamental concern of multidisciplinary rounds—that someone’s time is being wasted (when not talking about that team member’s patient at that moment)—must be mitigated one way or another. Solutions include rotating nurses or hospitalists in and out of rounds, and allowing hospitalists to enter orders and do other discreet multitasking during rounds. Careful attention to showing up for the rounds on time and on cue is crucial.
- Hospitalist autonomy and need to roam has to be programmed in by allowing them time to get off the unit, see the broader world, and interact with colleagues.
At the conclusion of three months, as a QI project (as opposed to rigorous research), we will measure a number of things, including cost, throughput, patient satisfaction, and team member satisfaction with the model. If you have predictions, please e-mail me. I’ll report our results in a subsequent column.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is co-founder and past president of SHM. E-mail him at [email protected].
References
- Relational Coordination Research Collaborative. Brandeis University website. Available at: http://rcrc.brandeis.edu/about-rc/What%20is%20Relational%20Coordination.html. Accessed September 23, 2013.
- Gittell JH, Weinberg DB, Bennett AL, Miller JA. Is the doctor in? A relational approach to job design and the coordination of work. Hum Resource Manag J. 2008;47(4):729-755.
- O’Leary KJ, Haviley C, Slade ME, Shah HM, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a hospitalist unit. J Hosp Med. 2011;6(2):88-93.
- O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Hospitalist-Led, Post-Discharge Clinic Improves Care Transitions
Two Research, Hospital Innovations, and Clinical Vignettes (RIV) scientific posters presented at HM13 shed new light on the opportunities and challenges of hospitalist-run post-discharge clinics, which a growing number of hospitals have adopted in an attempt to smooth care transitions and prevent rehospitalizations.
The Denver VA Medical Center (VAMC) started its post-discharge clinic, located on a floor above its medicine wards, in 2003. Open two afternoons, the clinic sees up to 16 patients a week. Discharging housestaff are paged to meet their patients in the clinic as part of required afternoon activities, explains the poster’s lead author, Robert Burke, MD, a hospitalist at the VAMC and assistant professor of medicine at affiliated University of Colorado. Every patient is seen by a rotating, supervising hospitalist attending.
The clinic is able to see patients for their first post-discharge clinical encounter within five days on average, much sooner than either urgent care clinics (9.4 days) or primary care physicians (13.7 days).
However, data presented at HM13 found no reduction in readmissions for the VA clinic’s patients.1 Dr. Burke suggests that this finding reflects the challenges of connecting patients to their PCPs after the clinic visit. “Also, it’s not a full, multidisciplinary clinic—just housestaff and attendings,” he says. “The patients we see in the clinic are very ill.”
A second poster from the same team presented data from a national survey of hospitalists’ attitudes regarding post-discharge clinics.2 Three-quarters of 228 respondents believed that these clinics would reduce ED visits, but only 38% said that hospitalists should be seeing patients after discharge, and about 75% said doing so should require additional compensation for the physician.
“In my experience, I find it very valuable to see patients post-discharge as part of the larger continuum of care,” Dr. Burke says.
Larry Beresford is a freelance writer in San Francisco.
References
Two Research, Hospital Innovations, and Clinical Vignettes (RIV) scientific posters presented at HM13 shed new light on the opportunities and challenges of hospitalist-run post-discharge clinics, which a growing number of hospitals have adopted in an attempt to smooth care transitions and prevent rehospitalizations.
The Denver VA Medical Center (VAMC) started its post-discharge clinic, located on a floor above its medicine wards, in 2003. Open two afternoons, the clinic sees up to 16 patients a week. Discharging housestaff are paged to meet their patients in the clinic as part of required afternoon activities, explains the poster’s lead author, Robert Burke, MD, a hospitalist at the VAMC and assistant professor of medicine at affiliated University of Colorado. Every patient is seen by a rotating, supervising hospitalist attending.
The clinic is able to see patients for their first post-discharge clinical encounter within five days on average, much sooner than either urgent care clinics (9.4 days) or primary care physicians (13.7 days).
However, data presented at HM13 found no reduction in readmissions for the VA clinic’s patients.1 Dr. Burke suggests that this finding reflects the challenges of connecting patients to their PCPs after the clinic visit. “Also, it’s not a full, multidisciplinary clinic—just housestaff and attendings,” he says. “The patients we see in the clinic are very ill.”
A second poster from the same team presented data from a national survey of hospitalists’ attitudes regarding post-discharge clinics.2 Three-quarters of 228 respondents believed that these clinics would reduce ED visits, but only 38% said that hospitalists should be seeing patients after discharge, and about 75% said doing so should require additional compensation for the physician.
“In my experience, I find it very valuable to see patients post-discharge as part of the larger continuum of care,” Dr. Burke says.
Larry Beresford is a freelance writer in San Francisco.
References
Two Research, Hospital Innovations, and Clinical Vignettes (RIV) scientific posters presented at HM13 shed new light on the opportunities and challenges of hospitalist-run post-discharge clinics, which a growing number of hospitals have adopted in an attempt to smooth care transitions and prevent rehospitalizations.
The Denver VA Medical Center (VAMC) started its post-discharge clinic, located on a floor above its medicine wards, in 2003. Open two afternoons, the clinic sees up to 16 patients a week. Discharging housestaff are paged to meet their patients in the clinic as part of required afternoon activities, explains the poster’s lead author, Robert Burke, MD, a hospitalist at the VAMC and assistant professor of medicine at affiliated University of Colorado. Every patient is seen by a rotating, supervising hospitalist attending.
The clinic is able to see patients for their first post-discharge clinical encounter within five days on average, much sooner than either urgent care clinics (9.4 days) or primary care physicians (13.7 days).
However, data presented at HM13 found no reduction in readmissions for the VA clinic’s patients.1 Dr. Burke suggests that this finding reflects the challenges of connecting patients to their PCPs after the clinic visit. “Also, it’s not a full, multidisciplinary clinic—just housestaff and attendings,” he says. “The patients we see in the clinic are very ill.”
A second poster from the same team presented data from a national survey of hospitalists’ attitudes regarding post-discharge clinics.2 Three-quarters of 228 respondents believed that these clinics would reduce ED visits, but only 38% said that hospitalists should be seeing patients after discharge, and about 75% said doing so should require additional compensation for the physician.
“In my experience, I find it very valuable to see patients post-discharge as part of the larger continuum of care,” Dr. Burke says.
Larry Beresford is a freelance writer in San Francisco.
References
Safety WalkRounds at Children's Hospital Improve Teamwork

A recent study in The Joint Commission Journal on Quality and Patient Safety describes unit-based Patient Safety Leadership WalkRounds conducted on six pilot units at the Children’s Hospital of Philadelphia (CHOP) and how they have helped clinical leaders identify and address safety concerns.1 The WalkRound team, made up of at least one senior executive, a patient safety officer, and the manager of each unit, engages frontline staff in safety assessments and concerns.
The concept was developed by Allan Frankel, MD, director of patient safety at Partners Healthcare System in Boston, to increase awareness of safety issues by all clinicians, make safety a high priority for senior leadership, and act on the safety information collected from frontline staff.
At CHOP, the WalkRounds led to improved nurse-physician relationships, workflow, and medical safety, and uncovered previously unidentified safety concerns.
Reference
A recent study in The Joint Commission Journal on Quality and Patient Safety describes unit-based Patient Safety Leadership WalkRounds conducted on six pilot units at the Children’s Hospital of Philadelphia (CHOP) and how they have helped clinical leaders identify and address safety concerns.1 The WalkRound team, made up of at least one senior executive, a patient safety officer, and the manager of each unit, engages frontline staff in safety assessments and concerns.
The concept was developed by Allan Frankel, MD, director of patient safety at Partners Healthcare System in Boston, to increase awareness of safety issues by all clinicians, make safety a high priority for senior leadership, and act on the safety information collected from frontline staff.
At CHOP, the WalkRounds led to improved nurse-physician relationships, workflow, and medical safety, and uncovered previously unidentified safety concerns.
Reference
A recent study in The Joint Commission Journal on Quality and Patient Safety describes unit-based Patient Safety Leadership WalkRounds conducted on six pilot units at the Children’s Hospital of Philadelphia (CHOP) and how they have helped clinical leaders identify and address safety concerns.1 The WalkRound team, made up of at least one senior executive, a patient safety officer, and the manager of each unit, engages frontline staff in safety assessments and concerns.
The concept was developed by Allan Frankel, MD, director of patient safety at Partners Healthcare System in Boston, to increase awareness of safety issues by all clinicians, make safety a high priority for senior leadership, and act on the safety information collected from frontline staff.
At CHOP, the WalkRounds led to improved nurse-physician relationships, workflow, and medical safety, and uncovered previously unidentified safety concerns.
Reference
San Francisco Medical Center Adapts Choosing Wisely List for Waste Reduction Campaign


A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
Hospitalists' Role in PQRS, Pay for Performance Gets Boost
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
Two Hospitalist Groups Join SHM's Hospital Medicine Exchange

HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
Submit Your HM14 Scientific Abstracts Soon

HM14: Submit Your Scientific Abstracts Soon
Abstracts are being accepted for SHM’s scientific poster and oral abstract competition, known as Research, Innovations, and Clinical Vignettes (RIV), until Sunday, Dec. 1. Visit the Academic Community page on the SHM website, or, for a full suite of resources for submitting your abstract, go directly to the abstract submission site (https://shm.confex.com/shm/HM14/cfp.cgi) to submit your abstract today.
For more on HM14, the biggest meeting in hospital medicine, visit www.hospitalmedicine2014.org.
Brendon Shank is SHM’s associate vice president of communications.
HM14: Submit Your Scientific Abstracts Soon
Abstracts are being accepted for SHM’s scientific poster and oral abstract competition, known as Research, Innovations, and Clinical Vignettes (RIV), until Sunday, Dec. 1. Visit the Academic Community page on the SHM website, or, for a full suite of resources for submitting your abstract, go directly to the abstract submission site (https://shm.confex.com/shm/HM14/cfp.cgi) to submit your abstract today.
For more on HM14, the biggest meeting in hospital medicine, visit www.hospitalmedicine2014.org.
Brendon Shank is SHM’s associate vice president of communications.
HM14: Submit Your Scientific Abstracts Soon
Abstracts are being accepted for SHM’s scientific poster and oral abstract competition, known as Research, Innovations, and Clinical Vignettes (RIV), until Sunday, Dec. 1. Visit the Academic Community page on the SHM website, or, for a full suite of resources for submitting your abstract, go directly to the abstract submission site (https://shm.confex.com/shm/HM14/cfp.cgi) to submit your abstract today.
For more on HM14, the biggest meeting in hospital medicine, visit www.hospitalmedicine2014.org.
Brendon Shank is SHM’s associate vice president of communications.