User login
Expedited Multistate Medical Licensure Promises Efficiency for Physicians
For hospitalists who want to relocate to another state, practice in multiple states, provide telemedicine services, or take on some per diem work, this should be of interest. As part of the feasibility study on an Interstate Medical Licensure Compact, the Federation of State Medical Boards (FSMB) “allied in common purpose to develop a comprehensive process that complements the existing licensing and regulatory authority of state medical boards” and, therefore, to provide physicians with an efficient process to become licensed in multiple states.
Put simply, FSMB intends to work with the states to simplify and expedite state licensure.
The compact boasts of positively impacting physician shortage areas, leveraging the portability of care and expertise, and, in the end, not just making licensure much easier, but also favorably influencing patient safety. In a press release, the CEO of FSMB, Humayun Chaudhry, DO, MS, MACP, FACOI, stated that the compact “offers an effective solution to the question of how best to balance patient safety and quality care with the needs of a growing and changing healthcare market.” The compact promises to systematize the ability of physicians to obtain licensure in multiple states.
From a hospitalist’s perspective, the compact has a lot to offer. Hospitalists do not have a “panel” of patients that we will follow indefinitely. This allows for an enormous amount of flexibility to consider additional work, to take on per diem opportunities, and also to practice telemedicine as a “telehospitalist” in multiple states. Such flexibility would invariably mean getting licensed in several states. Getting a license in a newer state (one that takes part in the compact) should become easier once all of your credentials have been duly verified and are readily accessible. Essentially, there will be a repository of verified credentials and any disciplinary actions that will be promptly available, simplifying the process quite a bit for the applicant, as well as for the state boards. At the end of the day, the jurisdiction, execution, and authority to issue the license will always belong to the state medical boards, maintaining the integrity of the Medical Practice Act. From a physician’s perceptive, participation is entirely voluntary.
At the time of writing this, upwards of 25 states have shown enthusiasm towards this compact, 15 states have introduced a bill for the compact, including Alabama, Idaho, Illinois, Iowa, Maryland, Minnesota, Montana, Nebraska, Nevada, Oklahoma, Rhode Island, South Dakota, Texas, Utah, Vermont, West Virginia, and Wyoming, and the support continues to grow. The compact already has cleared legislative houses in Wyoming and South Dakota, and are now awaiting the governor’s signature.
For example, some argue that the high licensing fees on initial issuance and reissuance by the state medical boards may be hard to justify once a simplified licensing mechanism is in place; despite this concern, momentum and enthusiasm for the compact continue to grow. SHM, having applauded the FSMB’s efforts in its letter of support, will also likely be calling upon local chapters to promote these initiatives. Generally speaking, the interstate compact would be beneficial, offering a multistate licensure process that would be exponentially quicker than the one we currently have. I applaud the FSMB’s efforts in spearheading this endeavor.
Want to further discuss the Interstate Medical Licensure Compact? Add to my discussion on HMX.
For more information, visit the FSMB website.
Dr. Deepak Asudani, MD, MPH, FHM, is an academic hospitalist at the University of California San Diego, and is a member of the SHM Public Policy Committee. At UCSD Hospital Medicine, he directs Global Health Initiatives and is involved in developing educational programs for international students including their clinical training and simulation experiences.
For hospitalists who want to relocate to another state, practice in multiple states, provide telemedicine services, or take on some per diem work, this should be of interest. As part of the feasibility study on an Interstate Medical Licensure Compact, the Federation of State Medical Boards (FSMB) “allied in common purpose to develop a comprehensive process that complements the existing licensing and regulatory authority of state medical boards” and, therefore, to provide physicians with an efficient process to become licensed in multiple states.
Put simply, FSMB intends to work with the states to simplify and expedite state licensure.
The compact boasts of positively impacting physician shortage areas, leveraging the portability of care and expertise, and, in the end, not just making licensure much easier, but also favorably influencing patient safety. In a press release, the CEO of FSMB, Humayun Chaudhry, DO, MS, MACP, FACOI, stated that the compact “offers an effective solution to the question of how best to balance patient safety and quality care with the needs of a growing and changing healthcare market.” The compact promises to systematize the ability of physicians to obtain licensure in multiple states.
From a hospitalist’s perspective, the compact has a lot to offer. Hospitalists do not have a “panel” of patients that we will follow indefinitely. This allows for an enormous amount of flexibility to consider additional work, to take on per diem opportunities, and also to practice telemedicine as a “telehospitalist” in multiple states. Such flexibility would invariably mean getting licensed in several states. Getting a license in a newer state (one that takes part in the compact) should become easier once all of your credentials have been duly verified and are readily accessible. Essentially, there will be a repository of verified credentials and any disciplinary actions that will be promptly available, simplifying the process quite a bit for the applicant, as well as for the state boards. At the end of the day, the jurisdiction, execution, and authority to issue the license will always belong to the state medical boards, maintaining the integrity of the Medical Practice Act. From a physician’s perceptive, participation is entirely voluntary.
At the time of writing this, upwards of 25 states have shown enthusiasm towards this compact, 15 states have introduced a bill for the compact, including Alabama, Idaho, Illinois, Iowa, Maryland, Minnesota, Montana, Nebraska, Nevada, Oklahoma, Rhode Island, South Dakota, Texas, Utah, Vermont, West Virginia, and Wyoming, and the support continues to grow. The compact already has cleared legislative houses in Wyoming and South Dakota, and are now awaiting the governor’s signature.
For example, some argue that the high licensing fees on initial issuance and reissuance by the state medical boards may be hard to justify once a simplified licensing mechanism is in place; despite this concern, momentum and enthusiasm for the compact continue to grow. SHM, having applauded the FSMB’s efforts in its letter of support, will also likely be calling upon local chapters to promote these initiatives. Generally speaking, the interstate compact would be beneficial, offering a multistate licensure process that would be exponentially quicker than the one we currently have. I applaud the FSMB’s efforts in spearheading this endeavor.
Want to further discuss the Interstate Medical Licensure Compact? Add to my discussion on HMX.
For more information, visit the FSMB website.
Dr. Deepak Asudani, MD, MPH, FHM, is an academic hospitalist at the University of California San Diego, and is a member of the SHM Public Policy Committee. At UCSD Hospital Medicine, he directs Global Health Initiatives and is involved in developing educational programs for international students including their clinical training and simulation experiences.
For hospitalists who want to relocate to another state, practice in multiple states, provide telemedicine services, or take on some per diem work, this should be of interest. As part of the feasibility study on an Interstate Medical Licensure Compact, the Federation of State Medical Boards (FSMB) “allied in common purpose to develop a comprehensive process that complements the existing licensing and regulatory authority of state medical boards” and, therefore, to provide physicians with an efficient process to become licensed in multiple states.
Put simply, FSMB intends to work with the states to simplify and expedite state licensure.
The compact boasts of positively impacting physician shortage areas, leveraging the portability of care and expertise, and, in the end, not just making licensure much easier, but also favorably influencing patient safety. In a press release, the CEO of FSMB, Humayun Chaudhry, DO, MS, MACP, FACOI, stated that the compact “offers an effective solution to the question of how best to balance patient safety and quality care with the needs of a growing and changing healthcare market.” The compact promises to systematize the ability of physicians to obtain licensure in multiple states.
From a hospitalist’s perspective, the compact has a lot to offer. Hospitalists do not have a “panel” of patients that we will follow indefinitely. This allows for an enormous amount of flexibility to consider additional work, to take on per diem opportunities, and also to practice telemedicine as a “telehospitalist” in multiple states. Such flexibility would invariably mean getting licensed in several states. Getting a license in a newer state (one that takes part in the compact) should become easier once all of your credentials have been duly verified and are readily accessible. Essentially, there will be a repository of verified credentials and any disciplinary actions that will be promptly available, simplifying the process quite a bit for the applicant, as well as for the state boards. At the end of the day, the jurisdiction, execution, and authority to issue the license will always belong to the state medical boards, maintaining the integrity of the Medical Practice Act. From a physician’s perceptive, participation is entirely voluntary.
At the time of writing this, upwards of 25 states have shown enthusiasm towards this compact, 15 states have introduced a bill for the compact, including Alabama, Idaho, Illinois, Iowa, Maryland, Minnesota, Montana, Nebraska, Nevada, Oklahoma, Rhode Island, South Dakota, Texas, Utah, Vermont, West Virginia, and Wyoming, and the support continues to grow. The compact already has cleared legislative houses in Wyoming and South Dakota, and are now awaiting the governor’s signature.
For example, some argue that the high licensing fees on initial issuance and reissuance by the state medical boards may be hard to justify once a simplified licensing mechanism is in place; despite this concern, momentum and enthusiasm for the compact continue to grow. SHM, having applauded the FSMB’s efforts in its letter of support, will also likely be calling upon local chapters to promote these initiatives. Generally speaking, the interstate compact would be beneficial, offering a multistate licensure process that would be exponentially quicker than the one we currently have. I applaud the FSMB’s efforts in spearheading this endeavor.
Want to further discuss the Interstate Medical Licensure Compact? Add to my discussion on HMX.
For more information, visit the FSMB website.
Dr. Deepak Asudani, MD, MPH, FHM, is an academic hospitalist at the University of California San Diego, and is a member of the SHM Public Policy Committee. At UCSD Hospital Medicine, he directs Global Health Initiatives and is involved in developing educational programs for international students including their clinical training and simulation experiences.
Ways Hospitalists Can Support Advocacy for Patients, Hospital Medicine
There are so many ways to advocate for your patients, for your profession, for the future of hospital medicine. The easiest way? Getting involved.
We know how important it is to you that your patients receive the best care possible. We know that you do your absolute best as their provider but that sometimes there are hurdles that can hinder your capabilities until some kind of legislative change is enacted. SHM does its best to foresee these obstacles and works rigorously to achieve positive legislative outcomes, but often there are details we cannot fathom without your input and expertise. That’s why we need you, our hospitalist members, to fill in the gaps.
On April 1, the final day of Hospital Medicine 2015, SHM is hosting another “Hospitalists on the Hill” in Washington, D.C. We are so excited to join members on Capitol Hill again. Discussing healthcare issues that impact your patients and the specialty by meeting personally with legislators and their staff is an opportunity to share your experiences as a frontline hospitalist and directly impact key policy issues.
Want to learn more about how you can impact the process prior to heading to the Hill? Unable to attend Hill Day, but still want a better understanding of the legislative process and how SHM gets involved? Come to our “Policy Basics 101” session March 31 at HM15, where you’ll hear from SHM’s Government Relations team and from members of the Public Policy Committee. You will not only learn about the legislative and regulatory processes, but you can also discover where hospitalists can take part and exert influence along the way.
If you find that you’re unable to attend the face-to-face meetings on April 1, or even if you are, make sure that you are a member of SHM’s Grassroots Network. SHM uses this venue to keep you informed of the healthcare policy decisions on the horizon and asks you to take only a few minutes to reach out to your representatives via e-mail to take action on the issues most important to hospital medicine.
The Grassroots Network has grown substantially over the past few years, but we are always looking for more hospitalists to take up the cause. Strength in numbers is the most effective way to tell Congress where change is needed. Sign up directly.
Whether you do it in person on Capitol Hill or through periodic e-mails to legislators, advocating for patients and the specialty of hospital medicine is important work, and we hope you’ll continue to help us in even greater numbers in the future. Hospitalists have a unique voice in the healthcare system—one that needs to be shared and engaged in critical policy discussions. We hope you’ll join us in the movement to advocate for hospitalists, for your patients, and for hospital medicine.
Ellen Boyer is SHM’s government relations project coordinator.
There are so many ways to advocate for your patients, for your profession, for the future of hospital medicine. The easiest way? Getting involved.
We know how important it is to you that your patients receive the best care possible. We know that you do your absolute best as their provider but that sometimes there are hurdles that can hinder your capabilities until some kind of legislative change is enacted. SHM does its best to foresee these obstacles and works rigorously to achieve positive legislative outcomes, but often there are details we cannot fathom without your input and expertise. That’s why we need you, our hospitalist members, to fill in the gaps.
On April 1, the final day of Hospital Medicine 2015, SHM is hosting another “Hospitalists on the Hill” in Washington, D.C. We are so excited to join members on Capitol Hill again. Discussing healthcare issues that impact your patients and the specialty by meeting personally with legislators and their staff is an opportunity to share your experiences as a frontline hospitalist and directly impact key policy issues.
Want to learn more about how you can impact the process prior to heading to the Hill? Unable to attend Hill Day, but still want a better understanding of the legislative process and how SHM gets involved? Come to our “Policy Basics 101” session March 31 at HM15, where you’ll hear from SHM’s Government Relations team and from members of the Public Policy Committee. You will not only learn about the legislative and regulatory processes, but you can also discover where hospitalists can take part and exert influence along the way.
If you find that you’re unable to attend the face-to-face meetings on April 1, or even if you are, make sure that you are a member of SHM’s Grassroots Network. SHM uses this venue to keep you informed of the healthcare policy decisions on the horizon and asks you to take only a few minutes to reach out to your representatives via e-mail to take action on the issues most important to hospital medicine.
The Grassroots Network has grown substantially over the past few years, but we are always looking for more hospitalists to take up the cause. Strength in numbers is the most effective way to tell Congress where change is needed. Sign up directly.
Whether you do it in person on Capitol Hill or through periodic e-mails to legislators, advocating for patients and the specialty of hospital medicine is important work, and we hope you’ll continue to help us in even greater numbers in the future. Hospitalists have a unique voice in the healthcare system—one that needs to be shared and engaged in critical policy discussions. We hope you’ll join us in the movement to advocate for hospitalists, for your patients, and for hospital medicine.
Ellen Boyer is SHM’s government relations project coordinator.
There are so many ways to advocate for your patients, for your profession, for the future of hospital medicine. The easiest way? Getting involved.
We know how important it is to you that your patients receive the best care possible. We know that you do your absolute best as their provider but that sometimes there are hurdles that can hinder your capabilities until some kind of legislative change is enacted. SHM does its best to foresee these obstacles and works rigorously to achieve positive legislative outcomes, but often there are details we cannot fathom without your input and expertise. That’s why we need you, our hospitalist members, to fill in the gaps.
On April 1, the final day of Hospital Medicine 2015, SHM is hosting another “Hospitalists on the Hill” in Washington, D.C. We are so excited to join members on Capitol Hill again. Discussing healthcare issues that impact your patients and the specialty by meeting personally with legislators and their staff is an opportunity to share your experiences as a frontline hospitalist and directly impact key policy issues.
Want to learn more about how you can impact the process prior to heading to the Hill? Unable to attend Hill Day, but still want a better understanding of the legislative process and how SHM gets involved? Come to our “Policy Basics 101” session March 31 at HM15, where you’ll hear from SHM’s Government Relations team and from members of the Public Policy Committee. You will not only learn about the legislative and regulatory processes, but you can also discover where hospitalists can take part and exert influence along the way.
If you find that you’re unable to attend the face-to-face meetings on April 1, or even if you are, make sure that you are a member of SHM’s Grassroots Network. SHM uses this venue to keep you informed of the healthcare policy decisions on the horizon and asks you to take only a few minutes to reach out to your representatives via e-mail to take action on the issues most important to hospital medicine.
The Grassroots Network has grown substantially over the past few years, but we are always looking for more hospitalists to take up the cause. Strength in numbers is the most effective way to tell Congress where change is needed. Sign up directly.
Whether you do it in person on Capitol Hill or through periodic e-mails to legislators, advocating for patients and the specialty of hospital medicine is important work, and we hope you’ll continue to help us in even greater numbers in the future. Hospitalists have a unique voice in the healthcare system—one that needs to be shared and engaged in critical policy discussions. We hope you’ll join us in the movement to advocate for hospitalists, for your patients, and for hospital medicine.
Ellen Boyer is SHM’s government relations project coordinator.
Hospitalists May Share Smaller Slice of Healthcare Spending Pie
Committee member Bradley Flansbaum, DO, MPH, SFHM, says he expects the amount of funding going to hospitalists to decrease in the coming years as healthcare reform focuses on keeping patients out of the hospital.
"The slice that's going to be dedicated to inpatient medicine in hospitals is going to shrink," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City. "From a hospitalist standpoint, I don't think it's kick back, flip open the beer lid, and turn the game on. Things are really going to change."
A report in this month's Health Affairs shows that spending growth in 2013 fell to 3.6%, down from 7.2% annually on average between 1990 and 2008. The decreased rate is attributed to a "sluggish economic recovery, the effects of sequestration, and continued increases in private health insurance cost-sharing requirements," according to the report.
However, the combination of money being pumped into healthcare reform and a growing economy is projected to push up spending by 5.6% this year and 6% annually each year from 2015 to 2023, according to the report. How much of that money will flow into HM depends, in part, on how well the specialty improves patient care and hospital bottom lines, Dr. Flansbaum says. "And teasing out that effect is tough," he says. "Mainly, is it that we're ordering less tests or are the prices going down or neither, and [are] other forces contributing to efficiency gains? Those are very different variables."
Committee member Bradley Flansbaum, DO, MPH, SFHM, says he expects the amount of funding going to hospitalists to decrease in the coming years as healthcare reform focuses on keeping patients out of the hospital.
"The slice that's going to be dedicated to inpatient medicine in hospitals is going to shrink," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City. "From a hospitalist standpoint, I don't think it's kick back, flip open the beer lid, and turn the game on. Things are really going to change."
A report in this month's Health Affairs shows that spending growth in 2013 fell to 3.6%, down from 7.2% annually on average between 1990 and 2008. The decreased rate is attributed to a "sluggish economic recovery, the effects of sequestration, and continued increases in private health insurance cost-sharing requirements," according to the report.
However, the combination of money being pumped into healthcare reform and a growing economy is projected to push up spending by 5.6% this year and 6% annually each year from 2015 to 2023, according to the report. How much of that money will flow into HM depends, in part, on how well the specialty improves patient care and hospital bottom lines, Dr. Flansbaum says. "And teasing out that effect is tough," he says. "Mainly, is it that we're ordering less tests or are the prices going down or neither, and [are] other forces contributing to efficiency gains? Those are very different variables."
Committee member Bradley Flansbaum, DO, MPH, SFHM, says he expects the amount of funding going to hospitalists to decrease in the coming years as healthcare reform focuses on keeping patients out of the hospital.
"The slice that's going to be dedicated to inpatient medicine in hospitals is going to shrink," says Dr. Flansbaum, a hospitalist at Lenox Hill Hospital in New York City. "From a hospitalist standpoint, I don't think it's kick back, flip open the beer lid, and turn the game on. Things are really going to change."
A report in this month's Health Affairs shows that spending growth in 2013 fell to 3.6%, down from 7.2% annually on average between 1990 and 2008. The decreased rate is attributed to a "sluggish economic recovery, the effects of sequestration, and continued increases in private health insurance cost-sharing requirements," according to the report.
However, the combination of money being pumped into healthcare reform and a growing economy is projected to push up spending by 5.6% this year and 6% annually each year from 2015 to 2023, according to the report. How much of that money will flow into HM depends, in part, on how well the specialty improves patient care and hospital bottom lines, Dr. Flansbaum says. "And teasing out that effect is tough," he says. "Mainly, is it that we're ordering less tests or are the prices going down or neither, and [are] other forces contributing to efficiency gains? Those are very different variables."
Clear Identification Needed for Hospitalists in Medicare
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
Society of Hospital Medicine Ranks Observation Status a Priority Advocacy Issue
The use of observation status within hospitals has risen over the last several years, creating the potential for negative financial impacts on patients and mounting headaches for hospitalists. Historically, the intent of observation status was to provide care in designated hospital units for short-stay patients with well-defined diagnoses, according to Medicare; however, as a result of complex federal policy and the realities of hospital care, patients under observation often receive care in general hospital beds, with stays that can extend past the 48-hour benchmark set by the Centers for Medicare & Medicaid Services (CMS).
Almost all hospitalists are familiar with the implications of observation status for their patients, and SHM has taken a leadership role in advocating for positive changes that benefit both the patient and hospitalist workflow.
Today, patients under observation often receive identical care to that received by inpatients but are billed as outpatients under Medicare Part B. This results in high deductibles, additional cost sharing, and out-of-pocket costs for medications. Complicating the issue more, hospitals in most states are not required to notify patients that they are coded as outpatients, leaving them with the impression that they have been admitted, until they receive their hospital bill.
In an attempt to curb the overuse of hospital observation status and clarify guidelines pertaining to inpatient admission decisions, CMS changed the rules for admitting patients in August 2013. Under what is now known as the “Two-Midnight Rule,” if a patient is expected to stay longer than two midnights and their stay is documented as medically necessary, they are an inpatient; fewer than two midnights constitutes outpatient services.
Even though the two-midnight rule is intended to simplify admission decisions, hospitalists have expressed a general apprehension regarding the impact of observation status. If a patient classified as an inpatient is discharged before two midnights, Medicare recovery auditors may deem the inpatient classification unnecessary, potentially resulting in loss of payment for medical services rendered.
For patients, the new rule does not remedy the fact that days spent under observation do not count toward the three-day inpatient stay requirement needed for skill nursing facility (SNF) post-acute care under Medicare. Consequently, thousands of patients classified under outpatient status have no choice but to pay for SNF care themselves, or forego the treatment altogether, creating possible complications in their care and delays in recovery.
Hospitalist concern over this issue has prompted SHM to rank observation status as a priority advocacy issue. Hospitalists are ideally situated to be part of a meaningful solution, and SHM’s Public Policy Committee has set out to do just that.
The first step will be to fully understand the experiences and perspectives regarding observation policy among hospitalists. SHM’s Public Policy Committee and government relations team have developed a survey for a group of randomized members. While individual anecdotal accounts are available, this is the first time the issue will be addressed on an aggregate level. Responses from survey participants will be used to frame the hospitalist perspective, help to bolster advocacy and educational efforts within SHM, and, ultimately, bring about possible policy revisions.
Hospitalists not receiving the survey can help by joining SHM’s Grassroots Network and lending their voice to the effort. To get involved, visit www.hospitalmedicine.org/advocacy.
NaDea Jeter is a member of SHM’s government relations team.
The use of observation status within hospitals has risen over the last several years, creating the potential for negative financial impacts on patients and mounting headaches for hospitalists. Historically, the intent of observation status was to provide care in designated hospital units for short-stay patients with well-defined diagnoses, according to Medicare; however, as a result of complex federal policy and the realities of hospital care, patients under observation often receive care in general hospital beds, with stays that can extend past the 48-hour benchmark set by the Centers for Medicare & Medicaid Services (CMS).
Almost all hospitalists are familiar with the implications of observation status for their patients, and SHM has taken a leadership role in advocating for positive changes that benefit both the patient and hospitalist workflow.
Today, patients under observation often receive identical care to that received by inpatients but are billed as outpatients under Medicare Part B. This results in high deductibles, additional cost sharing, and out-of-pocket costs for medications. Complicating the issue more, hospitals in most states are not required to notify patients that they are coded as outpatients, leaving them with the impression that they have been admitted, until they receive their hospital bill.
In an attempt to curb the overuse of hospital observation status and clarify guidelines pertaining to inpatient admission decisions, CMS changed the rules for admitting patients in August 2013. Under what is now known as the “Two-Midnight Rule,” if a patient is expected to stay longer than two midnights and their stay is documented as medically necessary, they are an inpatient; fewer than two midnights constitutes outpatient services.
Even though the two-midnight rule is intended to simplify admission decisions, hospitalists have expressed a general apprehension regarding the impact of observation status. If a patient classified as an inpatient is discharged before two midnights, Medicare recovery auditors may deem the inpatient classification unnecessary, potentially resulting in loss of payment for medical services rendered.
For patients, the new rule does not remedy the fact that days spent under observation do not count toward the three-day inpatient stay requirement needed for skill nursing facility (SNF) post-acute care under Medicare. Consequently, thousands of patients classified under outpatient status have no choice but to pay for SNF care themselves, or forego the treatment altogether, creating possible complications in their care and delays in recovery.
Hospitalist concern over this issue has prompted SHM to rank observation status as a priority advocacy issue. Hospitalists are ideally situated to be part of a meaningful solution, and SHM’s Public Policy Committee has set out to do just that.
The first step will be to fully understand the experiences and perspectives regarding observation policy among hospitalists. SHM’s Public Policy Committee and government relations team have developed a survey for a group of randomized members. While individual anecdotal accounts are available, this is the first time the issue will be addressed on an aggregate level. Responses from survey participants will be used to frame the hospitalist perspective, help to bolster advocacy and educational efforts within SHM, and, ultimately, bring about possible policy revisions.
Hospitalists not receiving the survey can help by joining SHM’s Grassroots Network and lending their voice to the effort. To get involved, visit www.hospitalmedicine.org/advocacy.
NaDea Jeter is a member of SHM’s government relations team.
The use of observation status within hospitals has risen over the last several years, creating the potential for negative financial impacts on patients and mounting headaches for hospitalists. Historically, the intent of observation status was to provide care in designated hospital units for short-stay patients with well-defined diagnoses, according to Medicare; however, as a result of complex federal policy and the realities of hospital care, patients under observation often receive care in general hospital beds, with stays that can extend past the 48-hour benchmark set by the Centers for Medicare & Medicaid Services (CMS).
Almost all hospitalists are familiar with the implications of observation status for their patients, and SHM has taken a leadership role in advocating for positive changes that benefit both the patient and hospitalist workflow.
Today, patients under observation often receive identical care to that received by inpatients but are billed as outpatients under Medicare Part B. This results in high deductibles, additional cost sharing, and out-of-pocket costs for medications. Complicating the issue more, hospitals in most states are not required to notify patients that they are coded as outpatients, leaving them with the impression that they have been admitted, until they receive their hospital bill.
In an attempt to curb the overuse of hospital observation status and clarify guidelines pertaining to inpatient admission decisions, CMS changed the rules for admitting patients in August 2013. Under what is now known as the “Two-Midnight Rule,” if a patient is expected to stay longer than two midnights and their stay is documented as medically necessary, they are an inpatient; fewer than two midnights constitutes outpatient services.
Even though the two-midnight rule is intended to simplify admission decisions, hospitalists have expressed a general apprehension regarding the impact of observation status. If a patient classified as an inpatient is discharged before two midnights, Medicare recovery auditors may deem the inpatient classification unnecessary, potentially resulting in loss of payment for medical services rendered.
For patients, the new rule does not remedy the fact that days spent under observation do not count toward the three-day inpatient stay requirement needed for skill nursing facility (SNF) post-acute care under Medicare. Consequently, thousands of patients classified under outpatient status have no choice but to pay for SNF care themselves, or forego the treatment altogether, creating possible complications in their care and delays in recovery.
Hospitalist concern over this issue has prompted SHM to rank observation status as a priority advocacy issue. Hospitalists are ideally situated to be part of a meaningful solution, and SHM’s Public Policy Committee has set out to do just that.
The first step will be to fully understand the experiences and perspectives regarding observation policy among hospitalists. SHM’s Public Policy Committee and government relations team have developed a survey for a group of randomized members. While individual anecdotal accounts are available, this is the first time the issue will be addressed on an aggregate level. Responses from survey participants will be used to frame the hospitalist perspective, help to bolster advocacy and educational efforts within SHM, and, ultimately, bring about possible policy revisions.
Hospitalists not receiving the survey can help by joining SHM’s Grassroots Network and lending their voice to the effort. To get involved, visit www.hospitalmedicine.org/advocacy.
NaDea Jeter is a member of SHM’s government relations team.
SHM Backs Medicare Reimbursement for End-of-Life Care Counseling

Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Although inevitable, death is often difficult to conceptualize and even more sensitive to discuss. For hospitalists and other care providers, conversations about the end of life with families and caregivers can be fraught with emotion. The fact that something is uncomfortable does not mean it is not useful or valuable, however. Patients must be able to vocalize their end-of-life wishes and should feel confident that the healthcare system is able to respond.
To help with this effort, the Society of Hospital Medicine is supporting legislation that would encourage voluntary end-of-life conversations between patients and their healthcare providers. Sponsored by U.S. Rep. Earl Blumenauer (D-Ore.), the Personalize Your Care Act of 2013 (H.R. 1173) would make Medicare reimbursement available for advance-care planning consultations, establish grants for state-level physician orders for life-sustaining treatment (POLST) programs, and require that advance directives be honored across state lines.
Hospitalists are integral team leaders for coordinating care and, as such, are often highly involved in end-of-life care for patients. They are at the front lines of these conversations, often tasked to plan end-of-life care and then carry out those plans. Many of their patients are acutely ill and need to face these critical decisions, often in real time.
End-of-life planning, like many other cognitive medical services, is not adequately reimbursed under current Medicare payment policy. This legislation would authorize Medicare to provide coverage for voluntary advance care consultations every five years or following changes in health, health-related condition, or care setting of the patient.
SHM is strongly supportive of adequate reimbursement for the counseling these patients require in planning their end-of-life care. The bill would make these conversations a practicable addition to the care and counseling workflow for healthcare providers and would ensure that they could occur at reasonable intervals and at significant changes in health or life events. These conversations would help ensure that patient wishes are respected at the end of life and prevent the use of unwanted treatments or interventions.
As the healthcare system works toward being more coordinated and more patient-centered, voluntary advance care planning is essential. Patients often see multiple providers at the end of their lives and—particularly as questions arise—it is imperative that providers have access to the most up-to-date advance care plans. H.R. 1173 works to address this gap by moving toward electronic health record display of advance directives and POLST.
Hospitalists may be eligible for reimbursement for these consultations, particularly in cases where these discussions did not occur in the outpatient setting. SHM is actively working with Rep. Blumenauer to ensure that all providers in a position to have these important conversations would be appropriately reimbursed. Patients need to have an active mechanism to ensure that their wishes are appropriately followed; this legislation would give them better access to these important and difficult conversations.
Joshua Lapps is SHM’s government relations specialist.
Hospitalists' Role in PQRS, Pay for Performance Gets Boost
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
With the voluntary and incentive period for participating in the Physician Quality Reporting System (PQRS) quickly coming to a close, hospitalists are finding a limited number of PQRS measures broadly applicable to their practice. SHM, through its Performance Measurement and Reporting Committee (PMRC), is actively working on behalf of hospitalists to change that. At the same time, it is critical that hospitalists be proactive and participate in PQRS, not just to avoid the 2015 penalty, but to position themselves for success as the Value-Based Payment Modifier (VBPM) expands to all physicians by 2017.
In the current PQRS, the PMRC has identified the following measures that have appropriate inpatient codes for reporting and have potential relevance to hospitalists:
- Congestive Heart Failure (CHF): #5, ACE/ARB for LV systolic dysfunction; #8, beta-blocker prescribed for LV systolic dysfunction; #228, assessment of LV function.
- Stroke: #31, DVT prophylaxis; #32, discharge on antiplatelet therapy; #33, anticoagulation for atrial fibrillation; #35, dysphagia screening; #36, consideration of rehab; #187, thrombolytic therapy.
- Others: #47, advance care plan documented; #76, use of a central venous catheter insertion protocol.
Some of these measures are only reportable by registry. For groups who do not take care of stroke patients, the field is clearly limited. More detail on PQRS reporting and available codes can be found at the Centers for Medicare and Medicaid Services (CMS) website (www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/MeasuresCodes.html).
The committee is deeply concerned about the limited number of PQRS measures broadly applicable to hospitalists, and we are working to change this disparity. Over the past several months, the PMRC has successfully advocated to add inpatient codes to existing measures that will expand the field for hospitalists. So far, we have achieved the following changes for future PQRS reporting years:
- Community-acquired pneumonia (CAP): Measures #56 (vital signs) and #59 (empiric antibiotics) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Osteoporosis/fractures: Measure #24 (communication with the outpatient provider) and #40 (DXA scan ordered or therapy initiated) will have discharge codes 99238 and 99239 added to their denominator, in recognition of the fact that many hospitalists partner with their orthopedic colleagues in the care of patients post-hip fracture.
- Medication reconciliation: Measure #130 (documentation of current medication list) will have admission codes 99221, 99222, and 99223 added to the denominator.
- Anticoagulation for acute pulmonary embolism: Measure #252, intended for use by ED physicians, is being retired by CMS due to a loss of National Quality Forum endorsement. SHM is working with the American College of Emergency Physicians (ACEP) to appeal the decision, possibly maintain the measure, and add inpatient admission codes to the denominator. This remains a work in progress.
Finally, in response to SHM advocacy efforts, the recent FY2014 Physician Fee Schedule proposed rule sought comments from stakeholders about retooling certain hospital-based measures to allow for physician-level reporting. SHM supports the concept of allowing physician-level performance reporting on hospital metrics and recommended the inclusion of multiple measures from the Inpatient Quality Reporting Program.
The PMRC is charged with monitoring the rapidly evolving provider performance and measurement landscape to ensure that hospitalists are adequately represented. We will continue to work diligently with key stakeholders on behalf of our field.
Dr. Seymann is chief of the division of hospital medicine at the University of California San Diego and chair of SHM’s Performance Measurement and Reporting Committee. Josh Boswell is SHM’s senior manager of government relations.
SHM Report Provides New Insights About Physician Practice Leaders
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
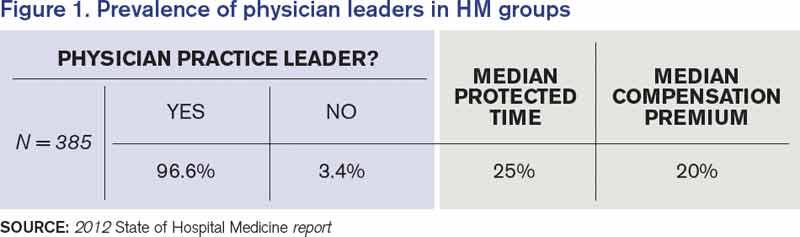
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.

Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
Two Hospitalist Groups Join SHM's Hospital Medicine Exchange

HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
HMX: Two New Communities, Lots of New Conversations
More than 2,500 hospitalists have logged in to HMX (www.hmxchange.org) to share their experiences and learn from the experiences of other hospitalists. And now, two other groups of hospitalists have a new reason to check out HMX.
The first community, for family medicine hospitalists, was launched in October. Approximately 10% of SHM’s active members are hospitalists trained in family medicine (HTFM), many of whom are very active within SHM. More than 60 hospitalists trained in family medicine are either Fellows in Hospital Medicine or Senior Fellows in Hospital Medicine.
And, in December, hospitalists who work in post-acute care can work together to tackle the challenges unique to post-acute care. This new community was an outgrowth of SHM’s Post-Acute Care Task Force.
Brendon Shank is SHM’s associate vice president of communications.
SHM Advocates for Medicare to Cover Skilled-Nursing Facilities
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.