User login
Tips for using lithium in bipolar disorder
Despite numerous drug treatment innovations, just about all patients with bipolar disorder that I have treated reported improvement after starting a lithium regimen.
In the 1970s, the clinical literature began highlighting numerous drug therapies for different bipolar symptoms. Before then, I had been taught to treat all “manic-depressive” patients with lithium—regardless of whether mood swings, bouts of anger, depression, or mania were the dominant symptoms.
So I experimented. I prescribed lithium to any potential bipolar patient who did not meet DSM criteria for another mental illness. I discovered the following:
- A family history of any mental illness, especially alcohol abuse and depression, is a strong indicator of bipolar disorder and of potential positive response to lithium.
- The existence of mood swings, especially without cause, confirms the diagnosis of bipolar disorder when paired with family history.
- Lithium, 900 mg/d, works fine as acute or maintenance therapy. I would decrease the dosage for smaller people (eg, 600 mg/d for a patient weighing approximately 125 lbs). I would only increase the dosage—to 1,200 mg/d—for patients with severe mania.
- Gauging lithium blood levels is a waste of time, assuming you have checked for kidney disease. Across 3 decades in practice, the only patient I have ever seen with an abnormally high lithium blood count also suffered renal failure.
- Side effects I have seen most commonly with lithium are:
- weight gain in women, in which case another medication should be prescribed
- tremor, which should warrant a check of the patient’s caffeine intake.
Other side effects (such as diarrhea and GI upset) are usually mild and easy to control by adding other medications.
Dr. Magnon practices general psychiatry in Bradenton, FL.
Despite numerous drug treatment innovations, just about all patients with bipolar disorder that I have treated reported improvement after starting a lithium regimen.
In the 1970s, the clinical literature began highlighting numerous drug therapies for different bipolar symptoms. Before then, I had been taught to treat all “manic-depressive” patients with lithium—regardless of whether mood swings, bouts of anger, depression, or mania were the dominant symptoms.
So I experimented. I prescribed lithium to any potential bipolar patient who did not meet DSM criteria for another mental illness. I discovered the following:
- A family history of any mental illness, especially alcohol abuse and depression, is a strong indicator of bipolar disorder and of potential positive response to lithium.
- The existence of mood swings, especially without cause, confirms the diagnosis of bipolar disorder when paired with family history.
- Lithium, 900 mg/d, works fine as acute or maintenance therapy. I would decrease the dosage for smaller people (eg, 600 mg/d for a patient weighing approximately 125 lbs). I would only increase the dosage—to 1,200 mg/d—for patients with severe mania.
- Gauging lithium blood levels is a waste of time, assuming you have checked for kidney disease. Across 3 decades in practice, the only patient I have ever seen with an abnormally high lithium blood count also suffered renal failure.
- Side effects I have seen most commonly with lithium are:
- weight gain in women, in which case another medication should be prescribed
- tremor, which should warrant a check of the patient’s caffeine intake.
Other side effects (such as diarrhea and GI upset) are usually mild and easy to control by adding other medications.
Despite numerous drug treatment innovations, just about all patients with bipolar disorder that I have treated reported improvement after starting a lithium regimen.
In the 1970s, the clinical literature began highlighting numerous drug therapies for different bipolar symptoms. Before then, I had been taught to treat all “manic-depressive” patients with lithium—regardless of whether mood swings, bouts of anger, depression, or mania were the dominant symptoms.
So I experimented. I prescribed lithium to any potential bipolar patient who did not meet DSM criteria for another mental illness. I discovered the following:
- A family history of any mental illness, especially alcohol abuse and depression, is a strong indicator of bipolar disorder and of potential positive response to lithium.
- The existence of mood swings, especially without cause, confirms the diagnosis of bipolar disorder when paired with family history.
- Lithium, 900 mg/d, works fine as acute or maintenance therapy. I would decrease the dosage for smaller people (eg, 600 mg/d for a patient weighing approximately 125 lbs). I would only increase the dosage—to 1,200 mg/d—for patients with severe mania.
- Gauging lithium blood levels is a waste of time, assuming you have checked for kidney disease. Across 3 decades in practice, the only patient I have ever seen with an abnormally high lithium blood count also suffered renal failure.
- Side effects I have seen most commonly with lithium are:
- weight gain in women, in which case another medication should be prescribed
- tremor, which should warrant a check of the patient’s caffeine intake.
Other side effects (such as diarrhea and GI upset) are usually mild and easy to control by adding other medications.
Dr. Magnon practices general psychiatry in Bradenton, FL.
Dr. Magnon practices general psychiatry in Bradenton, FL.
Treating bipolar disorder during pregnancy
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
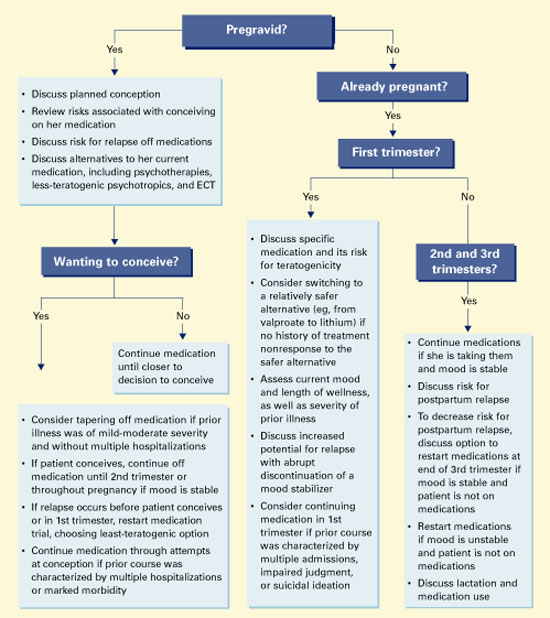
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
Prescribing drug therapy for pregnant bipolar women requires psychiatrists to balance the potential for neonatal malformations against the high risk of relapse when patients discontinue their medications.1 To help you achieve this balance, we offer an evidence-based approach that includes:
- analysis of the FDA’s teratogenicity categories for psychotropics
- review of the safety profiles of drugs used in mood stabilization
- an algorithm for managing patients who are considering conception or are pregnant.
PSYCHOTROPIC RISKS TO OFFSPRING
All psychotropic medications diffuse across the placenta, which exposes the fetus to some degree. Risks include teratogenicity, obstetrical complications, perinatal syndromes, and long-term postnatal behavioral sequelae.
Teratogenicity. A medication is considered teratogenic when prenatal exposure significantly increases the risk of congenital deformities over the baseline risk, which is 2% in the United States.2 The cause of most congenital malformations is unknown. Risk for teratogenicity occurs in the first 12 weeks of gestation, as organs are formed.
Table 1
FDA Use-in-Pregnancy ratings for medications The FDA system weighs the degree to which research findings have ruled out risk to the fetus
| Category | Interpretation |
|---|---|
| A | Controlled studies show no risk |
| B | No evidence of risk in humans |
| C | Risk cannot be ruled out |
| D | Positive evidence of risk |
| X | Contraindicated in pregnancy |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | |
Obstetrical complications include preterm delivery, low birth weight, and delivery complications such as low Apgar scores or behavioral effects requiring intensive care.
Perinatal syndromes include physical and behavioral symptoms noticed shortly after birth (such as jitteriness). These consequences are putatively related to drug use at or near birth and have limited duration.
Postnatal behavioral sequelae include long-term neurobehavioral abnormalities in children who were exposed to psychotropics in utero.
BALANCING RISKS
Risks with medication. The FDA’s “use in pregnancy” rating system (Table 1) uses available data to assess the degree of teratogenic risk. These guidelines can be confusing and are one of many tools to use when considering a possible drug treatment.
Most psychotropics are category “C” or “D,” which imply a chance of harm to the exposed fetus. Category “B” drugs would appear safer, but this rating could simply indicate a lack of adequate human data or that no data have shown harm in animals.
Moreover, a category “D” drug may be chosen more often during pregnancy than a category “C” drug. This may occur when more human data exist on using the category “D” drug in patients with a particular disorder (such as using lithium versus valproate or olanzapine in pregnant bipolar women).
No psychotropics are classified as “A,” meaning either some risks are associated with every psychotropic or the risk of some agents has not been adequately explored. Furthermore, no psychotropics are FDA-approved for use during pregnancy.
Risks without medication. Teratogenicity notwithstanding, psychotropic intervention is the most effective treatment for women with bipolar disorder. Patients who discontinue mood-stabilizing medication after conception increase their risk of relapse into depression or mania,3 either of which could lead to complications and untoward effects on the fetus.
Depression during pregnancy has been linked to low birth weight and preterm delivery.4,5 These effects may be mediated by the illness itself or by other factors that indirectly affect birth outcomes. For example, depression during pregnancy is associated with decreased appetite, substance use and abuse, and lower use of prenatal care.6
Untreated mania may also be associated with perinatal risks, as a pregnant patient in a manic state may engage in impulsive, high-risk behaviors that endanger her and the fetus.7
MOOD STABILIZERS
The FDA categorizes as “D” the three most commonly used mood stabilizers: lithium, valproate, and carbamazepine (Table 2). This rating implies that studies have demonstrated fetal risk but the drug’s potential benefit may still outweigh the risk.
Lithium. The International Registry of Lithium reported increased rates of cardiovascular malformations— such as Ebstein’s anomaly—in children whose mothers took lithium during pregnancy.
Relative risk for Ebstein’s anomaly in children with fetal exposure to lithium may be 20 times higher than the risk in unexposed children, although the absolute risk with lithium exposure remains low (1 in 1,000 births).1,8
No significant neurobehavioral teratogenicity has been reported in infants exposed in utero to lithium, although few cases have been studied. One study reported that 22 lithium-exposed infants attained developmental milestones at a pace comparable to that of unexposed controls.9
“Floppy baby” syndrome, in which infants experience hypotonicity and cyanosis, is the most recognized adverse effect in infants exposed to lithium in utero.10 Its frequency is unknown, but rare. Neonatal hypothyroidism and nephrogenic diabetes insipidus have also been documented.
Anticonvulsants. To date, no studies have examined the outcomes of children whose mothers took anticonvulsants for bipolar disorder during pregnancy, though the research concerning epileptic mothers is extensive.
Neural tube defects. Data associate anticonvulsant exposure with a significantly greater risk for malformations than in the general population. Specifically, anticonvulsants may cause neural tube defects such as spina bifida, ancephaly, and encephaly in 2 to 5% of those exposed, as well as craniofacial anomalies, microcephaly, growth retardation, and heart defects.11-14
Table 2
FDA’s teratogenicity ratings of mood stabilizers and other antimanic agents
| Category | Medication | Teratogenicity |
|---|---|---|
| Mood stabilizers | Lithium Carbamazepine Valproate | Category D Category D Category D |
| Anticonvulsants | Gabapentin Lamotrigine Topiramate | Category C Category C Category C |
| Antipsychotics | Olanzapine Risperidone Chlorpromazine Haloperidol Trifluoperazine | Category C Category C Safety in pregnancy not known Category C Safety in pregnancy not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
More minor malformations—such as rotated ears, depressed nasal bridge, short nose, elongated upper lip, and fingernail hypoplasia—have been reported in infants exposed to anticonvulsants in utero.14 These malformations disappear with age.13 Teratogenicity increases with the use of multiple anticonvulsants and possibly with higher maternal plasma levels and toxic metabolites.15
Conclusion. The three most commonly used mood stabilizers are all teratogenic. The least risk may occur with lithium (0.1%) versus valproate (2 to 5%) or carbamazepine (1 to 3%). These risks must be weighed against the up to 50% chance of relapse with medication discontinuation.3
ANTIPSYCHOTICS
Antipsychotics are often used to treat mania because of their rapid effects and sedative properties. Most antipsychotics—specifically, haloperidol, olanzapine, and risperidone—are labeled “C,” specifying that fetal risk cannot be ruled out.
Table 3
FDA’s teratogenicity ratings of common antidepressants
| Category | Medication | Teratogenicity |
|---|---|---|
| Tricyclics | Amitriptyline Clomipramine Desipramine Imipramine Nortriptyline | Category C Category C Safety in pregnancy not known Safety in pregnancy not known Safety in pregnancy not known |
| Selective serotonin reuptake inhibitors | Citalopram Fluoxetine Fluvoxamine Paroxetine Sertraline | Category C Category C Category C Category C Category C |
| Other antidepressants | Bupropion Phenelzine Tranylcypromine | Category B Safety in pregnancy and nursing not known Safety in pregnancy and nursing not known |
| Source: Physicians’ Desk Reference. Montvale, NJ: Medical Economics Co., 2003. | ||
Chlorpromazine and haloperidol have been most studied during pregnancy but in relation to treating hyperemesis gravidarum and psychosis, not bipolar disorder. Results regarding antipsychotics’ teratogenic and behavioral risks are mixed,16-21 probably because the various compounds have different effects on the fetus.
The underlying illness—rather than the medications—may increase the rate of anomalies seen with exposure to antipsychotics:
- Rieder et al22 reported an increased rate of perinatal death in infants of schizophrenic mothers but no significant association between the mothers’ use of antipsychotics and perinatal death.
- Sobel23 compared psychotic women with and without histories of chlorpromazine exposure during pregnancy. Rates of fetal damage were similar and approximately twice that of the general population.
A meta-analysis of 74,337 live births revealed that first-trimester exposure to low-potency antipsychotics increases the relative risk of fetal anomalies in nonpsychotic women. Phenothiazines may increase the 2% baseline incidence of malformations to 2.4%.1 No specific organ malformation following fetal exposure to phenothiazines has been consistently identified.
Olanzapine was recently approved for treating mania. Very little data exist regarding its impact on fetal development when used during pregnancy, although studies on small numbers of women have not revealed teratogenicity.24,25
Conclusion. Psychotic illness itself may increase the risk of poor fetal outcome to a greater extent than does antipsychotic use. Prenatal exposure to low-potency phenothiazines may further increase this risk, although only slightly. The effect of prenatal exposure to atypical antipsychotics requires further study.
BENZODIAZEPINES
Benzodiazepines are rarely a primary treatment for mania or depression. Thus, a comprehensive review of their effect on fetal outcome is beyond the scope of this review. A meta-analysis of exposure in the first trimester suggests a very small but significant increase in risk for cleft palate.1 The absolute risk is <1 in 1,000 cases.
ANTIDEPRESSANTS
Whereas treatment of acute mania is considered a medical emergency, women with bipolar disorder may also relapse into depression during pregnancy. An antidepressant should not be used without a mood stabilizer when treating bipolar I disorder, although a mood stabilizer alone may be inadequate to treat depression. Using tricyclics and selective serotonin reuptake inhibitors (SSRIs) during pregnancy has not been associated with teratogenicity (Table 3),26 although perinatal effects have been reported.1
Tricyclics. In case-control studies involving more than 300,000 live births, 414 incidences of first-trimester exposure to tricyclics were followed. Information from these patients found no significant association between fetal exposure to tricyclics and increased rates of congenital malformations.1 The few studies that have been performed suggest no long-term effects from in utero exposure.26 Although these results suggest that prenatal exposure to tricyclics is relatively safe, more research is needed.
SSRIs. To date, no significant teratogenic effects of SSRIs have been identified in offspring of treated women.
The manufacturer’s register for fluoxetine contains approximately 2,000 cases of treated patients, with no excess cases of congenital anomalies or malformations following prenatal exposure. Citalopram has the next largest database of in utero exposure (n=365), again with no increased risk for teratogenicity. Several smaller systematic reports are available on in utero exposure to sertraline, paroxetine, or escitalopram.26
Most studies of pregnant women taking fluoxetine in the first trimester have found no increased risk of obstetrical complications—including spontaneous pregnancy loss, preterm labor, or low birth weight—compared with women not taking fluoxetine. Taking fluoxetine during the third trimester may increase the risk for perinatal complications,27 although this has been inconsistently reported and requires further study. Effects of other SSRIs in the third trimester have not been systematically explored.
Case reports and one controlled study have addressed possible neonatal perinatal symptoms from in utero exposure to SSRIs.28,29 Preliminary data show no adverse neurobehavioral function in exposed neonates.26
Electroconvulsive therapy (ECT) has been proven effective for acute mania and depression, demonstrating few deleterious effects on neonates. ECT has few side effects and may be safer than drug therapy in this population. Two reviews support the efficacy and relative safety of ECT treatment during pregnancy, although more evidence is needed.30,31
RECOMMENDATIONS
Discuss pregnancy and medication risks with all bipolar women, regardless of proximal plans for pregnancy. If psychotropic medication is used, prescribe carefully during the first trimester, using the minimum number of drugs and the lowest dosages needed to restore or maintain well-being.32
Pros and cons of switching. Some clinicians may encourage a patient to taper a medication during the first trimester because of its unknown or high teratogenicity. Depending on the patient’s illness severity, this might not be the optimal decision. A more conservative option would be to switch to a lower-risk drug during pregnancy.
Lithium has both antidepressant and antimanic properties and is less teratogenic compared with first-trimester exposure to an anticonvulsant. However, if lithium has not been successful for the woman’s mania prophylaxis in the past and she has demonstrated antimanic response to an anticonvulsant, switching to lithium or another anticonvulsant is not recommended.
Algorithm Suggested approach to the bipolar patient who wishes to conceive or is pregnant
Folate and neural tube defects. As first-trimester exposure to carbamazepine or valproate increases the risk for neural tube defects, using the lowest available dosage may decrease the risk for spina bifida, at least with valproate.
Low maternal folate levels are often associated with neural tube defects from any cause.33 Valproate lowers folate levels by inhibiting one of the enzymes necessary for its formation, which may be a mechanism for the increased risk of spina bifida.34
Folate supplementation. To date, no study has demonstrated that giving folate supplements to women taking anticonvulsants during pregnancy reduces the risk of neural tube defects.35 Nonetheless, we recommend that women who continue to take valproate or carbamazepine during pregnancy receive folate, 3 to 4 mg/d, as a precaution.
Treating manic relapse. Data show high rates of relapse in patients who stop taking lithium, particularly if done abruptly.3 Counsel women taking lithium to plan their pregnancies to allow enough time to taper off the medication prior to conception, if they want to try this. Lithium should be decreased slowly—approximately 50% every 2 weeks—to avoid relapse.
Treat aggressively if relapse occurs during pregnancy. Consider:
- psychiatric hospitalization in case of suicidality or psychosis
- reinstituting drug therapy with a less-teratogenic agent
- ECT for a manic or depressive episode.
As the pregnancy advances and the mother’s volume of distribution increases, dosage increases may be needed to maintain therapeutic drug levels.
Treating depressive relapse. Should depression occur in pregnancy, SSRIs or tricyclics added to mood stabilizer therapy have been shown to be effective, with few teratogenic effects.
Cognitive-behavioral and interpersonal psychotherapies also have shown efficacy in pregnant women with major depressive disorder36 and may be effective for women with bipolar disorder in pregnancy. Cognitive psychotherapies, when used with medication, have been reported effective in preventing relapse in nongravid bipolar patients.36-37
Related resources
Psychiatric disorders during pregnancy. Massachusetts General Hospital Center for Women’s Health. Perinatal Resource Center. www.womensmentalhealth.org/topics/pregnancy_lib.html
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Tegretol
- Chlorpromazine • Thorazine
- Citalopram • Celexa
- Clomipramine • Anafranil
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Haloperidol • Haldol
- Imipramine • Tofranil
- Lamotrigine • Lamictal
- Lithium • Lithobid et al
- Methylphenidate • Ritalin et al
- Nortriptyline • Pamelor
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Phenelzine • Nardil
- Risperidone • Risperdal
- Sertraline • Zoloft
- Topiramate • Topamax
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproate • Depakote et al
Disclosure
Dr. Altshuler receives research support from Abbott Laboratories, is a consultant to Abbott Laboratories, Forest Laboratories, and Eli Lilly & Co., and is a speaker for GlaxoSmithKline and Janssen Pharmaceutica.
Ms. Richards reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Yonkers receives research support from GlaxoSmithKline and Berlex Laboratories, is a consultant to GlaxoSmithKline, and is a speaker for Eli Lilly and Co., Pfizer Inc., GlaxoSmithKline, and Wyeth Pharmaceuticals.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.
1. Altshuler L, Cohen L, Szuba, et al. Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. Am J Psychiatry 1996;153:592-606.
2. Nelson K, Holmes LB. Malformations due to presumed spontaneous mutations in newborn infants. N Engl J Med 1989;320:19-23.
3. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. Am J Psychiatry 2000;157:179-84.
4. Steer RA, Scholl TO, Hediger ML, Fischer RL. Self-reported depression and negative pregnancy outcomes. J Clin Epidemiol 1992;45(10):1093-9.
5. Orr ST, Miller CA. Maternal depressive symptoms and the risk of poor pregnancy outcome. Review of the literature and preliminary findings. Epidemiol Rev 1995;17(1):165-71.
6. Zuckerman B, Amaro H, Bauchner H, Cabral H. Depressive symptoms during pregnancy: relationship to poor health behaviors. Am J Obstet Gynecol 1989;160:1107-11.
7. Miller LJ. Psychotic denial of pregnancy: phenomenology and clinical management. Hosp Community Psychiatry 1990;41:1233-7.
8. Cohen LS, Friedman JM, Jefferson JW, et al. A reevaluation of risk of in utero exposure to lithium. JAMA 1994;271(2):146-50correction JAMA 1994;271(19):1485.
9. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand 1976;54(3):193-7.
10. Woody JN, London WL, Wilbanks GD. Lithium toxicity in a newborn. Pediatrics 1971;47:94-6.
11. Jones K, Lacro R, Johnson K, Adams J. Patterns of malformations in the children of women treated with carbamazepine during pregnancy. N Engl J Med 1989;320:1661-6.
12. Rosa F. Spina bifida in infants of women treated with carbamazepine during pregnancy. N Engl J Med 1991;324(10):674-7.
13. Koch S, Losche G, Jager-Roman E, et al. Major and minor birth malformations and antiepileptic drugs. Neurology 1992;42:83-8.
14. Jager-Roman E, Deichl A, Jakob S, et al. Fetal growth, major malformations, and minor anomalies in infants born to women receiving valproic acid. J Pediatr 1986;108:997-1004.
15. Nakane Y, Okuma T, Takahashi R, et al. Multi-institutional study on the teratogenicity and fetal toxicity of antiepileptic drugs: a report of a collaborative study group in Japan. Epilepsia 1980;21:663-80.
16. Edlund MJ, Craig TJ. Antipsychotic drug use and birth defects: an epidemiologic reassessment. Compr Psychiatry 1984;25:32-8.
17. Kris EB. Children of mothers maintained on pharmacotherapy during pregnancy and postpartum. Curr Ther Res 1965;7:785-9.
18. Clark CVH, Gorman D, Vernadakis A. Effects of prenatal administration of psychotropic drugs on behavior of developing rats. Dev Psychobiol 1970;3:225-35.
19. Golub M, Kornetsky C. Seizure susceptibility and avoidance conditioning in adult rats treated prenatally with chlorpromazine. Dev Psychobiol 1974;7:79-88.
20. Spear LP, Shalaby IA, Brick J. Chronic administration of haloperidol during development: behavioral and psychopharmacological effects. Psychopharmacology (Berl) 1980;70:47-58.
21. Cagiano R, Barfield RJ, White NR, et al. Subtle behavioral changes produced in rat pups exposed in utero to haloperidol. Eur J Pharmacol 1988;157:45-50.
22. Rieder RO, Rosenthal D, Wender P, Blumenthal H. The offspring of schizophrenics: fetal and neonatal deaths. Arch Gen Psychiatry 1975;32:200-11.
23. Sobel DE. Fetal damage due to ECT, insulin coma, chlorpromazine, or reserpine. Arch Gen Psychiatry 1960;2:606-11.
24. Dickson R. Olanzapine and pregnancy. Can J Psychiatry 1998;43:196-7.
25. Goldstein DJ, Corbin LA, Fung MC. Olanzapine-exposed pregnancies and lactation; early experience. J Clin Psychopharmacol 2000;24(4):399-403.
26. Altshuler LL, Cohen LS, Moline ML, et al. The expert consensus guideline series: treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-22.
27. Chambers CD, Johnson KA, Dick LM, et al. Birth outcomes in pregnant women taking fluoxetine. N Engl J Med 1996;335:1010-15.
28. Spencer MJ. Fluoxetine hydrochloride (Prozac) toxicity in the neonate. Pediatrics 1993;92:721-2.
29. Cabrera FM, Battaglia G. Delayed decreases in brain 5-HT 2a and 2c receptor density and function in male rat progeny following prenatal fluoxetine. J Pharmacol Exp Ther 1994;269:637-45.
30. Miller LJ. Use of electroconvulsive therapy during pregnancy. Hosp Community Psychiatry 1994;45:444-50.
31. Ferrill MJ, Kehoe WA, Jacisin JJ. ECT during pregnancy: physiologic and pharmacologic considerations. Convuls Ther 1992;8:186-200.
32. Yonkers K, Wisner K, Cohen L, et al. Management of bipolar disorder during pregnancy and the postpartum period. Bipolar Consensus Statement. Submitted for publication.
33. Dansky L, Rosenblatt D, Andermann E. Mechanisms of teratogenesis: folic acid and antiepileptic therapy. Neurology 1992;42(suppl 5):32-42.
34. Wegner C, Nau H. Alteration of embryonic folate metabolism by valproic acid during organogenesis: implications for mechanism of teratogenesis. Neurology 1992;42(suppl 5):17-24.
35. MRC Vitamin Study Research Group. Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet 1991;338:131-7.
36. Spinelli MG, Endicott J. Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women. Am J Psychiatry 2003;160:555-62.
37. Lam DH, Watkins ER, Hayward P, et al. A randomized controlled study of cognitive therapy for relapse prevention for bipolar affective disorder: outcome in the first year. Arch Gen Psychiatry 2003;60(2):145-52.
Treating bipolar disorder during pregnancy: No time for endless debate
To me, the main difference between MDs and PhDs* is that MDs—at some point—must stop gathering data and make decisions.
I once heard Dr. Albert (Mickey) Stunkard say that when he was a physician fellow at Stanford University’s Center for Advanced Studies in the Behavioral Sciences he was at first energized—and a little intimidated—by the scintillating conversations taking place around him. Eventually, though, all the discourse reminded him of those long, philosophical discussions he and his classmates had had in their college dorms (“Well, on one hand you have communism, and on the other hand you have fascism… ”).
Physicians do not have the luxury of endless debate. At some point, we need to do something or else let our patients die of old age while waiting. One issue about which I have had to make decisions over the years—and which has troubled me the most—is whether to treat pregnant patients with psychotropics. Generally, I try to avoid using drugs in these cases, but sometimes I decide that the mother’s need for drug therapy outweighs the potential risks to her offspring.
Dr. Lori Altshuler and colleagues’ article in this issue is the best summary I have seen of what is known about the risks of using psychotropics in pregnant bipolar women. Each time I treat a woman with bipolar disorder, I will remember this discussion and the algorithm these authors suggest for making therapeutic decisions.
This excellent article may not be the final word on the subject. It can, however, help us with an important clinical decision we often have to make—and that is what Current Psychiatry is all about.

James Randolph Hillard, MD
Editor-in-Chief
* PhD clinical psychologists are probably more like MDs in this regard.
James Randolph Hillard, MD
Editor-in-Chief
* PhD clinical psychologists are probably more like MDs in this regard.
James Randolph Hillard, MD
Editor-in-Chief
* PhD clinical psychologists are probably more like MDs in this regard.
To me, the main difference between MDs and PhDs* is that MDs—at some point—must stop gathering data and make decisions.
I once heard Dr. Albert (Mickey) Stunkard say that when he was a physician fellow at Stanford University’s Center for Advanced Studies in the Behavioral Sciences he was at first energized—and a little intimidated—by the scintillating conversations taking place around him. Eventually, though, all the discourse reminded him of those long, philosophical discussions he and his classmates had had in their college dorms (“Well, on one hand you have communism, and on the other hand you have fascism… ”).
Physicians do not have the luxury of endless debate. At some point, we need to do something or else let our patients die of old age while waiting. One issue about which I have had to make decisions over the years—and which has troubled me the most—is whether to treat pregnant patients with psychotropics. Generally, I try to avoid using drugs in these cases, but sometimes I decide that the mother’s need for drug therapy outweighs the potential risks to her offspring.
Dr. Lori Altshuler and colleagues’ article in this issue is the best summary I have seen of what is known about the risks of using psychotropics in pregnant bipolar women. Each time I treat a woman with bipolar disorder, I will remember this discussion and the algorithm these authors suggest for making therapeutic decisions.
This excellent article may not be the final word on the subject. It can, however, help us with an important clinical decision we often have to make—and that is what Current Psychiatry is all about.
To me, the main difference between MDs and PhDs* is that MDs—at some point—must stop gathering data and make decisions.
I once heard Dr. Albert (Mickey) Stunkard say that when he was a physician fellow at Stanford University’s Center for Advanced Studies in the Behavioral Sciences he was at first energized—and a little intimidated—by the scintillating conversations taking place around him. Eventually, though, all the discourse reminded him of those long, philosophical discussions he and his classmates had had in their college dorms (“Well, on one hand you have communism, and on the other hand you have fascism… ”).
Physicians do not have the luxury of endless debate. At some point, we need to do something or else let our patients die of old age while waiting. One issue about which I have had to make decisions over the years—and which has troubled me the most—is whether to treat pregnant patients with psychotropics. Generally, I try to avoid using drugs in these cases, but sometimes I decide that the mother’s need for drug therapy outweighs the potential risks to her offspring.
Dr. Lori Altshuler and colleagues’ article in this issue is the best summary I have seen of what is known about the risks of using psychotropics in pregnant bipolar women. Each time I treat a woman with bipolar disorder, I will remember this discussion and the algorithm these authors suggest for making therapeutic decisions.
This excellent article may not be the final word on the subject. It can, however, help us with an important clinical decision we often have to make—and that is what Current Psychiatry is all about.
Pediatric bipolar disorder: Mood swings, irritability are cues to this diagnosis
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
Pediatric bipolar disorder: Mood swings, irritability are cues to this diagnosis
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
Children and adolescents with bipolar disorder are often referred to psychiatrists because of disruptive behaviors at home and in school. They exhibit poor academic performance, disturbed interpersonal relationships, increased rates of substance abuse, legal difficulties, multiple hospitalizations, and high rates of suicide attempts and completions.1,2 Many have comorbid psychiatric problems—particularly attention-deficit/hyperactivity disorder (ADHD).
Although few studies have examined this complex diagnosis, we do know that bipolar disorder presents differently in children and adolescents than in adults. Prodromal symptoms can appear early—before kindergarten in some children. Early recognition therefore is key to effectively treating these sick and often complicated patients.
How often a clinician encounters a child or adolescent with bipolar disorder depends largely on the practice setting (Box).1,3,4 Wherever you practice, however, you can recognize and treat pediatric bipolar disorder if you keep in mind that its presentation and disease progression differ from the adult type.
Pediatric versus adult symptoms
Prodromal symptoms—such as episodes of depressed mood or hopelessness and excessive mood lability—have been detected in youths who later were diagnosed with bipolar disorder. More than one-half of 494 adult members of the Depression and Bipolar Support Alliance have reported that they first exhibited signs of bipolar illness before age 19, with distribution by age as follows:
- 5% before age 5
- 12% at ages 5 to 9
- 14% at ages 10 to 14
- 28% at ages 15 to 19.5
Pediatric bipolar disorder is seen much more commonly in specialized psychiatric settings than in general practice.
Overall prevalence. A large, well-designed population study of mood disorders in adolescents reported a lifetime prevalence of 1% for bipolar spectrum disorders, including bipolar I, bipolar II, and cyclothymia.1 Most adolescents in the bipolar group (84%) reported a distinct period of elevated, expansive, or irritable mood that best fit DSM-IV criteria for bipolar disorder not otherwise specified (NOS). These adolescents—who represented an overall prevalence of 5.7%—had extremely high rates of psychosocial impairment and use of mental health services, similar to those with bipolar I disorder.
In specialized settings. Bipolar disorder is seen much more frequently in specialized settings, such as a pediatric psychopharmacology clinic, than in general psychiatric practice. For example:
- Among 262 children referred consecutively to a specialty pediatric psychopharmacology clinic, 16% met DSM-III-R criteria for mania.3
- In a special education class, 8 of 12 students met DSM-III-R criteria for a bipolar disorder.4
- In child and adolescent psychiatry inpatient units, it is not uncommon to find 30 to 40% of patients with a bipolar disorder.
Table 1
COMMON PRESENTING SYMPTOMS OF PEDIATRIC BIPOLAR DISORDER
| Episodes of depressed mood/hopelessness |
| Excessive mood lability |
| Periods of increased or decreased energy |
| Episodes of decreased need for sleep |
| Anger dyscontrol |
| Markedly irritable moods |
| Frequent argumentativeness |
| Bold/intrusive/demanding behaviors |
In a similar study,6 58 adult patients with bipolar I disorder reported an average interval of 9 to 12 years between the emergence of bipolar symptoms and the onset of a major affective disorder.
Common initial symptoms of pediatric bipolar disorder are listed in Table 1. Most of these symptoms occur in discrete episodes and represent a change from the child’s normal functioning.
Many children and adolescents are labeled “bipolar” without careful consideration of this disorder’s diagnostic complexities and subtypes. Bipolarity in young patients can be difficult to establish because of:
- variability of symptom expression, depending on the illness’ context and phase
- effects of development on symptom expression
- mood and behavioral effects of psychotropic medications the patient is taking.
Pediatric bipolar patients often present with a mixed or “dysphoric” picture characterized by frequent short periods of intense mood lability and irritability rather than classic euphoric mania.3,7 Clinicians who evaluate children with pediatric bipolar disorders often try to fit them into the DSM-IV “rapid cycling” subtype. This subtype does not fit bipolar children very well, however, because they often lack clear episodes of mania. Rather, researchers are reporting that bipolar children cycle far more frequently than the four episodes/year in DSM-IV’s diagnostic criteria:
- Continuous, daily cycling from mania or hypomania to euthymia or depression was seen in 81% of a well-defined group of pediatric bipolar patients.7,8
- A high rate of rapid cycling and onset of a first manic episode at mean age 7 was reported in 90 children and adolescents (mean age 11) with bipolar I disorder.9
The picture that emerges from independent research groups is that multiple daily mood swings and irritability are much more common than euphoria in prepubertal children with bipolar disorder.8,10
Making the diagnosis
DSM-IV’s diagnostic classification system for bipolar disorders is complex, involving:
- five types of episodes (manic, hypomanic, mixed, depressed, unspecified)
- four severity levels (mild, moderate, severe without psychosis, severe with psychosis)
- and three course specifiers (with or without inter-episode recovery, seasonal pattern, rapid cycling).
Table 2
PEDIATRIC BIPOLAR DISORDER SUBTYPES: DIAGNOSTIC CHARACTERISTICS AND ASSOCIATED FEATURES
| DSM-IV subtype | Minimum duration of manic symptoms | Depression symptoms | Cardinal features |
|---|---|---|---|
| Bipolar I | Pure mixed or manic 1 week (or hospitalization needed) | Major depressive disorder presentation of bipolar may be the first disorder, particularly in adolescents | Multiple daily mood swings with severe irritability (mood lability) Short periods of euphoria Decreased need for sleep Hypersexuality Grandiosity Racing thoughts Pressured speech |
| Bipolar II | Hypomania 4 days | One or more prior episodes of major depressive disorder required, each with a duration of 2 weeks | Noticeable manic symptoms that do not cause significant dysfunction or lead to hospitalization |
| Cyclothymia | Hypomania cycling with depressive symptoms 1 year | Hypomania cycling with depressive symptoms, without manic, mixed, or major depressive episodes (1 year, with symptom-free intervals <2 months) | Chronic, low-level mood cycling |
| Bipolar NOS | < 4 days of bipolar symptoms | Rapid alternation (within days) between manic depressive symptoms without full manic, mixed, or major depressive episodes | May include hypomanic and episodes (but <4 days) without intercurrent depression May also be diagnosed when clinician determines bipolar disorder is present but cannot determine whether it is primary, due to a general medical condition, or substance-induced, such as severe mood lability secondary to fetal alcohol syndrome or alcohol-related neurodevelopmental disorder |
| NOS: not otherwise specified | |||
Table 3
COMPLICATING FACTORS IN PEDIATRIC BIPOLAR DISORDER
| Medical conditions that may mimic bipolar mania |
| Temporal lobe epilepsy |
| Hyperthyroidism |
| Closed or open head injury |
| Multiple sclerosis |
| Systemic lupus erythematosus |
| Alcohol-related neurodevelopmental disorder |
| Wilson’s disease (rare progressive disease caused by defective copper metabolism) |
| Medications that may increase mood cycling |
| Tricyclic antidepressants |
| Selective serotonin reuptake inhibitors |
| Serotonin and norepinephrine reuptake inhibitors |
| Aminophylline |
| Corticosteroids |
| Sympathomimetic amines, such as pseudoephedrine |
DSM-IV criteria for mania—which were developed from data on adults with bipolar disorders—do not take into account developmental differences between bipolar adults and bipolar children and adolescents.
Diagnostic characteristics of the pediatric bipolar disorder subtypes are compared in Table 2. Generally:
- Pediatric patients with bipolar I disorder have multiple daily mood swings, a “mixed” type of episode with short periods of euphoria and longer periods of irritability, and comorbidities such as ADHD, oppositional defiant disorder, or conduct disorder.3,11,12
- Bipolar II disorder presents more typically in adolescence and is usually noticed clinically as a major depressive episode. Past episodes of hypomania may have been missed unless a careful history was taken.
- Cyclothymia is difficult to diagnose because the hypomania and depressive symptoms are not as severe as in bipolar types I or II. Prospective mood charting can help the clinician diagnose cyclothymia (see “Related Resources”).
- Bipolar disorder NOS represents the largest group of patients with bipolar symptoms. This diagnosis is made when bipolar symptoms are present but not of sufficient severity or duration to warrant a diagnosis of bipolar I, II or cyclothymia. Bipolar NOS also can be diagnosed when a bipolar disorder is secondary to a general medical condition, such as fetal alcohol syndrome or alcohol-related neurodevelopmental disorder.
Differential diagnosis. Medications and medical disorders may exacerbate or mimic pediatric bipolar symptoms (Table 3), so it is important to assess these potential confounds before initiating treatment. Psychiatric comorbidities also frequently complicate the presentation of pediatric bipolar disorder and its response to treatment (Table 4). ADHD is the most common comorbidity, with rates as high as 98% in bipolar children.3,13
Outcomes
Long-term outcomes of children and adolescents with bipolar disorders have not been well studied. In the only prospective follow-up investigation of adolescent inpatients with mania, Strober et al found that most of 54 patients (96%) recovered from an index affective episode, but nearly one-half (44%) experienced one or more relapses within 5 years.14 The rate of recovery varied according to the index episode’s polarity. Recovery was faster in patients with pure mania or mixed states, and multiple relapses occurred more frequently in those with mixed or cycling episodes. Twenty percent of the patients attempted suicide.
Recently, Geller et al reported the results of the first large, prospective, follow-up study of children with bipolar disorder.15 In 89 outpatients (mean age 11) with bipolar I disorder, comprehensive assessments at baseline and at 6, 12, 18, and 24 months showed that 65% recovered from mania but 55% relapsed after recovery. Mean time to recovery was 36 weeks, and relapse occurred after a mean of 28.6 weeks. Children living with their intact biological families were twice as likely to recover as those in other living arrangements.
The poor outcomes of these bipolar children highlight the need for earlier recognition and more effective treatments.
Treating acute mania
Many psychotropic medications used to treat adults with bipolar disorders are also used for children and adolescents. To date, only two double-blind, placebo-controlled studies13,16 and one uncontrolled maintenance treatment study17 have examined treatment of acute mania in pediatric bipolar disorder.
Lithium is the most studied medication for pediatric bipolar disorder and the only FDA-approved medication for treating acute mania and bipolar disorder in patients ages 12 to 18. Approximately 40 to 50% of children and adolescents with bipolar disorder respond to lithium monotherapy.18,19
In general, lithium should be titrated to 30 mg/kg/d in two or three divided doses; this typically produces a serum level of 0.8 to 1.2 mEq/L. Common side effects in children and adolescents include nausea, polyuria, polydipsia, tremor, acne, and weight gain. Lithium levels and thyroid function should be monitored, as in adult patients.
Only one prospective, placebo-controlled study has examined lithium use in children and adolescents with bipolar disorders. Twenty-five adolescents with comorbid bipolar and substance use disorders were treated with lithium or placebo for 6 weeks. Positive urine toxicology screens decreased significantly, and global assessment of functioning improved in 46% of those receiving lithium vs. 8% of those receiving placebo.13 This study demonstrated lithium’s efficacy in treating bipolar adolescents with comorbid substance abuse but did not measure its effect on mood.
Risk factors for poor lithium response in children and adolescents with bipolar disorder include prepubertal onset and comorbid ADHD.20
Divalproex. No placebo-controlled studies of antiepileptics in pediatric bipolar disorder have been published. Open-label studies of divalproex have reported response rates of 53 to 82% in manic adolescents.18, 21-23 Several case reports and series have described successful use of carbamazepine as monotherapy and adjunctive treatment in children and adolescents with bipolar disorder.24,25
Table 4
RATES OF COMMON COMORBIDITIES IN PEDIATRIC BIPOLAR DISORDERS
| Disorder | Children (prepubertal) | Adolescents |
|---|---|---|
| ADHD | 70 to 90% | 30 to 60% |
| Anxiety disorders | 20 to 30% | 30 to 40% |
| Conduct disorders | 20 to 30% | 30 to 50% |
| Oppositional defiant disorder | 60 to 80% | 20 to 30% |
| Substance abuse | 10% | 40 to 80% |
| Learning disabilities | 30 to 40% | 30 to 40% |
One 6-week, random-assignment, prospective study compared lithium, divalproex, and carbamazepine in treating 42 acutely manic or hypomanic patients ages 8 to 18.18 In this open study, all three mood stabilizers demonstrated efficacy in treating a mixed or manic episode in youths with bipolar I or II disorder. Response rates—based on a 50% improvement in Young Mania Rating Scale baseline scores—were divalproex 53%, lithium 38%, and carbamazepine 38%.
In general, divalproex is started at 20 mg/kg/d, which typically produces a serum level of 80 to 120 μg/ml. Common side effects in children include weight gain, nausea, sedation, and tremor.
A possible association between divalproex and polycystic ovary syndrome (PCOS) has been reported in women with epilepsy.26 The mechanism for PCOS has been hypothesized to be obesity secondary to divalproex, resulting in elevated insulin and androgen levels. Recently, Rasgon et al27 reported that epilepsy—and not the anticonvulsants used to treat it—may increase the risk of PCOS. In contrast, O’Donovan et al reported higher rates of menstrual irregularities and PCOS in women with bipolar disorder who were taking divalproex than in those who were not taking divalproex and in healthy controls.28
Until we learn more about this association, clinicians should monitor bipolar female adolescents treated with divalproex for any signs of PCOS, which include menstrual abnormalities, hirsutism, and acne.
Carbamazepine is used widely for seizure management but less commonly than divalproex in pediatric bipolar disorder. This anticonvulsant must be titrated slowly and requires frequent monitoring of blood levels, which can be a problem in children with needle phobia.
Carbamazepine is usually titrated to 15 mg/kg/d to produce a serum level of 7 to 10 μg/ml. Its most common side effects are sedation, rash, nausea, and hyponatremia. Aplastic anemia and severe dermatologic reactions, such as Stevens-Johnson syndrome, occur uncommonly.28
Atypical antipsychotics. Recent case series and open-label reports suggest that atypical antipsychotics such as clozapine,29 risperidone,30 olanzapine,31-33 and quetiapine16 are effective in treating pediatric bipolar disorder. However, clinically significant weight gain may be associated with the use of olanzapine and risperidone.34 Ziprasidone may increase QTc prolongation, and safety data are limited in children and adolescents. Therefore, ziprasidone should be used with caution in pediatric bipolar disorder, and ECGs should be monitored.
In the only double-blind, placebo-controlled study of an atypical antipsychotic in pediatric bipolar disorder, manic symptoms were more greatly reduced in 15 adolescents given quetiapine plus divalproex than in 15 patients who received divalproex alone. Quetiapine was titrated to 450 mg/d across 7 days and was well-tolerated. The findings suggest that a mood stabilizer plus an atypical antipsychotic may be more effective than a mood stabilizer alone for treating adolescent mania.16
Long-term treatment
In addition to treating acute affective episodes, lithium may also help prevent recurrent affective episodes in younger patients. In the only maintenance treatment study for pediatric bipolar disorder, Strober et al prospectively evaluated 37 adolescents whose bipolar disorder had been stabilized with lithium during hospitalization.17 After 18 months of follow-up, 35% of patients had discontinued lithium, and their relapse rate was 92% (compared with 38% in patients who were lithium-compliant.
It is reasonable to maintain a child or adolescent who has had a single manic episode on mood-stabilizing treatment for several years and then—if the patient is euthymic and asymptomatic—to slowly taper the mood stabilizer(s) over several months. If mood symptoms recur, the agent(s) should be reintroduced.
If a child with bipolar disorder does not respond or only partially responds to a mood stabilizer, it may be necessary to add a second mood stabilizer or an atypical antipsychotic. A bipolar child or adolescent with psychotic symptoms should be maintained on an antipsychotic (typical or atypical) for at least 1 month, even if the psychosis has resolved.35
Treatment of comorbid ADHD. Most children with bipolar disorder have comorbid ADHD, and mood stabilization is necessary prior to starting stimulant medications.36 In bipolar patients, sustained-release psychostimulants may reduce rebound symptoms more effectively than immediate-release formulations. Typical dosages for a child with bipolar disorder and ADHD would be Concerta, 36 mg/d, or Adderall XR, 10 to 20 mg/d.
Psychosocial interventions
Most psychotherapeutic interventions have not been systematically studied in pediatric bipolar disorder but may be beneficial. In a recent study, Fristad et al reported the efficacy of multifamily psychoeducational group therapy for treating bipolar children and adolescents and their families.37
Other useful psychosocial tactics include:
- Minimize periods of overstimulation (for example, these patients do not do well at shopping malls).
- Maintain good sleep hygiene.
- Address medication nonadherence immediately.
- Discuss the risk of substance abuse with the patient.
- Encourage mood charting by the patient and or parent.
- Mood charts appropriate for pediatric patients.
- Child and Adolescent Bipolar Foundation. www.cabf.org
- Findling RF, Kowatch RA, Post RM. Pediatric bipolar disorders: a handbook for clinicians. London, Martin Dunitz Press, 2002.
- Geller B, DelBello MP (eds). Child and early adolescent bipolar disorder: theory, assessment, and treatment. New York: Guilford Publications, 2002.
Drug brand names
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Quetiapine • Seroquel
- Ziprasidone • Geodon
Disclosure
Dr. Kowatch receives grant support from, serves as a consultant to, or is on the speakers bureau of Novartis Pharmaceuticals Corp., Abbott Laboratories, Solvay Pharmaceuticals, Eli Lilly and Co., Janssen Pharmaceutica, GlaxoSmithKline, and AstraZeneca Pharmaceuticals.
Dr. DelBello receives grant support from, serves as a consultant to, or is on the speakers bureau of Abbott Laboratories, AstraZeneca Pharmaceuticals, Eli Lilly and Co., Ortho-McNeil Pharmaceutical, Shire Pharmaceutical Group, Janssen Pharmaceutica, Pfizer Inc., and GlaxoSmithKline.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
1. Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorders in a community sample of older adolescents: prevalence, phenomenology, comorbidity, and course. J Am Acad Child Adolesc Psychiatry 1995;34:454-63.
2. Nottelmann E. National Institute of Mental Health Research Roundtable on Prepubertal Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 2001;40:871-8.
3. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry 1995;34(7):867-76.
4. Isaac G. Misdiagnosed bipolar disorder in adolescents in a special educational school and treatment program. J Clin Psychiatry 1992;53(4):133-6.
5. Lish JD, Dime-Meenan S, et al. The National Depressive and Manic-depressive Association (DMDA) survey of bipolar members. J Affect Disord 1994;31(4):281-94.
6. Egeland JA, Hostetter AM, Pauls DL, Sussex JN. Prodromal symptoms before onset of manic-depressive disorder suggested by first hospital admission histories. J Am Acad Child Adolesc Psychiatry 2000;39(Oct):1245-52.
7. Geller B, Sun K, Zimerman B, Luby J, Frazier J, Williams M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord 1995;34:259-68.
8. Geller B, Zimerman B, Williams M, et al. Diagnostic characteristics of 93 cases of a prepubertal and early adolescent bipolar disorder phenotype by gender, puberty and comorbid attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 2000;10:157-64.
9. Findling RL, Gracious BL, McNamara NK, et al. Rapid, continuous cycling and psychiatric co-morbidity in pediatric bipolar I disorder. Bipolar Disord 2001;3:202-10.
10. Wozniak J, Biederman J. Childhood mania: insights into diagnostic and treatment issues. J Assoc Acad Minor Phys 1997;8(4):78-84.
11. West SA, McElroy SL, Strakowski SM, et al. Attention-deficit/hyperactivity disorder in adolescent mania. Am J Psychiatry 1995;152(2):271-3.
12. Kovacs M, Pollock M. Bipolar disorder and comorbid conduct disorder in childhood and adolescence. J Am Acad Child Adolesc Psychiatry 1995;34(6):715-23.
13. Geller B, Cooper TB, Sun K, et al. Double-blind and placebo-controlled study of lithium for adolescent bipolar disorders with secondary substance dependency. J Am Acad Child Adolesc Psychiatry 1998;37(2):171-8.
14. Strober M, Schmidt-Lackner S, Freeman R, Bower S, Lampert C, DeAntonio M. Recovery and relapse in adolescents with bipolar affective illness: a five-year naturalistic, prospective follow-up. J Am Acad Child Adolesc Psychiatry 1995;34(6):724-31.
15. Geller B, Craney JL, Bolhofner K, Nickelsburg MJ, Williams M, Zimerman B. Two-year prospective follow-up of children with a prepubertal and early adolescent bipolar disorder phenotype. Am J Psychiatry 2002;159(6):927-33.
16. DelBello M, Schwiers M, Rosenberg H, Strakowski S. Quetiapine as adjunctive treatment for adolescent mania associated with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2002;41(10):1216-23.
17. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry 1990;147(4):457-61.
18. Kowatch RA, Suppes T, Carmody TJ, et al. Effect size of lithium, divalproex sodium and carbamazepine in children and adolescents with bipolar disorder. J Amer Acad Child Adolesc Psychiatry 2000;39(6):713-20.
19. Youngerman J, Canino IA. Lithium carbonate use in children and adolescents. A survey of the literature. Arch Gen Psychiatry 1978;35(2):216-24.
20. Strober M. Mixed mania associated with tricyclic antidepressant therapy in prepubertal delusional depression: three cases. J Child Adolesc Psychopharmacol 1998;8:181-5.
21. Wagner KD, Weller E, Biederman J, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry 2002;41(10):1224-30.
22. West SA, Keck PE, Jr, McElroy SL, et al. Open trial of valproate in the treatment of adolescent mania. J Child Adolesc Psychopharmacol 1994;4:263-7.
23. Papatheodorou G, Kutcher SP, Katic M, Szalai JP. The efficacy and safety of divalproex sodium in the treatment of acute mania in adolescents and young adults: an open clinical trial. J Clin Psychopharmacol 1995;15(2):110-6.
24. Evans RW, Clay TH, Gualtieri CT. Carbamazepine in pediatric psychiatry. J Am Acad Child Adolesc Psychiatry 1987;26(1):2-8.
25. Puente RM. The use of carbamazepine in the treatment of behavioural disorders in children. In: Birkmayer W (ed). Epileptic seizures - behaviour - pain. Baltimore: University Park Press, 1975;243-52.
26. Isojarvi JI, Laatikainen TJ, Pakarinen AJ, Juntunen KT, Myllyla VV. Polycystic ovaries and hyperandrogenism in women taking valproate for epilepsy. N Engl J Med 1993;329(19):1383-8.
27. Rasgon NL, Altshuler LL, et al. Medication status and polycystic ovary syndrome in women with bipolar disorder: a preliminary report. J Clin Psychiatry 2000;61:173-8.
28. O'Donovan C, Kusumakar V, Graves GR, Bird DC. Menstrual abnormalities and polycystic ovary syndrome in women taking valproate for bipolar mood disorder. J Clin Psychiatry 2002;63:322-30.
29. Kowatch RA, Suppes T, Gilfillan SK, et al. Clozapine treatment of children and adolescents with bipolar disorder and schizophrenia: a clinical case series. J Child Adolesc Psychopharmacol 1995;5(4):241-53.
30. Frazier J, Meyer M, et al. Risperidone treatment for juvenile bipolar disorder: a retrospective chart review. J Am Acad Child Adolesc Psychiatry 1999;38:960-5.
31. Soutullo C, Sorter M, Foster K, et al. Olanzapine in the treatment of adolescent acute mania: a report of seven cases. J Affect Disord. 1999;53:279-83.
32. Khouzam H, El-Gabalawi F. Treatment of bipolar I disorder in an adolescent with olanzapine. J Child Adolesc Psychopharmacol 2000;10:147-51.
33. Chang K, Ketter T. Mood stabilizer augmentation with olanzapine in acutely manic children. J Child Adolesc Psychopharmacol 2000;10:45-9.
34. Ratzoni G, Gothelf D, Brand-Gothelf A, et al. Weight gain associated with olanzapine and risperidone in adolescent patients: a comparative prospective study. J Am Acad Child Adolesc Psychiatry 2002;41:337-43.
35. Kafantaris V, Dicker R, et al. Adjunctive antipsychotic treatment is necessary for adolescents with psychotic mania. J Child Adolesc Psychopharmacol 2001;11:409-13.
36. Biederman J, Mick E, Prince J, et al. Systematic chart review of the pharmacologic treatment of comorbid attention deficit hyperactivity disorder in youth with bipolar disorder. J Child Adolesc Psychopharmacol 1999;9(4):247-56.
37. Fristad MA, Goldberg-Arnold JS. Working with families of children with early-onset bipolar disorder. In: Geller B, DelBello M (eds). Child and early adolescent bipolar disorder: Theory, assessment, and treatment. New York: Guilford Publications, 2002.
Rediscovering the art of lithium therapy
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
Rediscovering the art of lithium therapy
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
Update on bipolar disorder: How to better predict response to maintenance therapy
What are we trying to accomplish in the maintenance treatment of patients with bipolar disorder? Given that the disorder recurs in more than 90% of patients who experience a manic episode,1 there are 5 important goals:
- Prevention of recurrent episodes;
- Amelioration of subsyndromal symptoms;
- Reduction of suicide risk;
- Compliance enhancement;
- Optimization of interpersonal, social, and vocational functioning.
There is a great premium on preventing mood episode recurrence in patients with bipolar disorder. Mood episodes themselves produce substantial morbidity, but morbidity is not confined to these episodes alone. Full recovery of functioning often lags many months behind remission of symptoms.2 Recurrent mood episodes also may lead to progressive loss of function between episodes. Mood episodes also carry risks of mortality from suicide, violence, and impulsive risk taking.
Clearly, mood-stabilizing medications form the cornerstone of maintenance treatment,3,4 along with a strong therapeutic alliance between patient and clinician and targeted psychosocial therapies. In the Expert Consensus Guidelines for medication treatment of bipolar I disorder, maintenance treatment was recommended for 1 year following an initial manic or mixed episode; longer (indefinite) treatment was recommended for patients with a family history of bipolar disorder or if 2 episodes occurred.3
Compared with clinical trials of agents for acute bipolar mania (and mixed episodes), there are relatively few randomized controlled trials of medications for the maintenance phase of bipolar disorder. Some naturalistic studies have provided data on relapse rates associated with treatment with a variety of different agents. Even fewer studies have examined psychosocial interventions designed specifically to reduce relapse rates.
But new data are beginning to emerge regarding the efficacy of divalproex, lamotrigine, and olanzapine as maintenance therapies. A number of clinical predictors of response to these agents have begun to be identified, as well as to lithium and carbamazepine. Eliciting these characteristics is important when making recommendations to patients about available drug therapies.
In addition, effective maintenance treatment often requires combinations of mood-stabilizing, antidepressant, and antipsychotic agents to control or eliminate subsyndromal and breakthrough symptoms.
In this review, we will cover the available new data on pharmacologic maintenance treatments of bipolar disorder and their clinical implications.
What the studies show
Lithium has been the mainstay of therapy for bipolar disorder for more than 35 years. Most randomized, controlled trials of lithium maintenance therapy were conducted in the 1960s and 1970s5 (Table 1). Unfortunately, these studies had several design limitations that inflated the expectations of lithium’s efficacy as a maintenance treatment.6 These included discontinuation designs in which patients stabilized on lithium were abruptly switched to placebo; exaggerated early placebo relapse rates; enrollment of both unipolar and bipolar patients; lack of specific diagnostic criteria; and reported results only for patients completing studies. Pooled data from these trials indicated that lithium reduced the risk of relapse fourfold compared with placebo at 6 months and 1 year.5
Two contemporary randomized, placebo-controlled maintenance studies utilizing more rigorous designs provided further evidence of lithium’s superiority over placebo in extending time to manic relapse.7,8 Both studies enrolled patients who were currently or had recently been manic and had been stabilized in open-label treatment that included study medications.
In the first study, comparing 1-year relapse rates among patients randomized to lithium, divalproex, or placebo, lithium extended time to recurrence of mania by 55% compared with placebo.7 In the second, an 18-month trial comparing lithium, lamotrigine, and placebo, lithium significantly increased the time to intervention for recurrence of mania compared with placebo.8 The overall manic relapse rates were 17% for lithium-treated patients and 41% for those on placebo. However, lithium did not significantly extend time to depressive relapse or intervention for depressive relapse, respectively, in either study. Moreover, in the first study, patients who received lithium tended to have greater subthreshold depressive symptoms.8
Table 1
What works in maintenance treatment of bipolar disorder (ranked by number of randomized, controlled trials)
| Medication RCTs (n) | Trial results | Strong evidence | Some evidence |
|---|---|---|---|
| Lithium (15) | Equal to divalproex and lamotrigine; equal to or better than carbamazepine; better than placebo | 4-fold reduction of relapse risk vs. placebo at 6, 12 months; more efficacious in mania than in depression; higher lithium level correlated with lower relapse rates, but more side effects | |
| Carbamazepine (7) | No significant benefit vs. lithium; better than placebo | May be more efficacious in mania than in depression; may be less tolerable than lithium; no data on serum levels | |
| Divalproex (4) | Equal to lithium and olanzapine; better than placebo | May be more efficacious in mania than in depression; may be more tolerable than lithium; data on serum levels pending | |
| Lamotrigine (2) | Better than placebo | More efficacious in depression than in mania | Dosage 200-400 mg/d |
| Olanzapine (1) | Equal to divalproex | Data on dosage and differential efficacy related to dosage pending | |
| Clozapine (1) | Better than treatment as usual | Efficacy in treatment-resistant mania (bipolar schizoaffective disorder, bipolar type) |
These findings were consistent with earlier placebo-controlled studies of lithium maintenance treatment and a recent crossover comparison trial with carbamazepine.9 Lithium was also recently compared with carbamazepine in a 2.5-year maintenance multisite study in Europe.10 There was no significant difference in efficacy between the two in time to hospitalization, the primary outcome measure. On other outcome measures, including time to relapse or need for additional medication, lithium was superior to carbamazepine.
Pooled results from a number of naturalistic studies, which mirror clinical practice, indicated that approximately one-third of patients maintained on lithium had good functional outcomes without relapses and only minimal symptoms.11 In general, these studies found higher rates of relapse with longer durations of follow-up.
Valproate maintenance treatment has been studied in two randomized, controlled trials (one vs. placebo,7 and one vs. olanzapine12) and two open-label comparison studies against lithium.13,14 In the placebo-controlled trial, which also included a lithium comparison group described earlier, there was no significant difference in the time to development of any mood episode among the three treatment groups.7 However, divalproex was superior to placebo on a number of other outcome measures, including rate of study termination for any mood episode, termination for depression, and termination for noncompliance.
Divalproex was superior to placebo in patients who received divalproex in the open-label treatment phase before randomization. This is clinically relevant, as this group reflects expected relapse rates in patients treated initially with divalproex for acute mania who then remain on the drug for maintenance therapy. Patients receiving divalproex had significantly lower rates of intolerance and noncompliance compared to those treated with lithium.
In the second comparison study, 167 patients initially randomized and responding to divalproex or olanzapine in a 3-week acute bipolar mania trial continued in a double-blind 44-week extension study.12 There were no significant differences in relapse into mania between the two groups (olanzapine 41%, divalproex 50%, p = 0.4) or time to manic relapse (olanzapine 270 days, divalproex 74 days, p = 0.4). There was no significant difference in tolerability between the two.
Two open-label studies compared valproate with lithium. In an 18-month study conducted in France, patients randomized to the valpromide formulation of valproate displayed a 20% lower relapse rate than those receiving lithium.13 The second open-label comparison trial found comparable efficacy between lithium and divalproex in a 1-year naturalistic pharmacoeconomic study that allowed additional medications as needed for recurrent symptoms.14
Carbamazepine has been evaluated in a limited number of studies for maintenance treatment of bipolar disorder. The results of many early randomized, controlled maintenance trials were criticized on methodologic grounds.15 But two recent comparison trials with lithium, as noted earlier, provided clinically important data regarding carbamazepine’s prophylactic efficacy.9,10 Several additional clinically relevant observations emerged from analyses of secondary outcome measures in these two trials.
In the first study, 52 patients with bipolar I or II disorder received lithium or carbamazepine for 1 year, crossed over to the alternate drug the second year, and received both drugs the third year.9 There was little difference in relapse rates during the first year between the lithium (31%) and carbamazepine (37%) groups. Similarly, in the overall trial, there was little difference in the percentage of patients who were rated as having a moderate or better response—33% on lithium, 31% on carbamazepine, and 55% on the combination. A higher proportion of patients receiving carbamazepine withdrew due to side effects. In the second trial, significantly more patients receiving carbamazepine required additional medications for breakthrough symptoms and experienced side effects requiring treatment discontinuation.10
Lamotrigine has been studied in two placebo-controlled, randomized maintenance studies in patients with bipolar disorder.8,16 The first evaluated bipolar I patients who had experienced a manic or hypomanic episode within 60 days of entry into an open-label treatment phase with lamotrigine.8 Patients who, in turn, improved or remained stable during the open-label treatment phase were then randomized to treatment with lamotrigine 200-400 mg/d, lithium, or placebo for up to 18 months. Both lamotrigine and lithium were superior to placebo on the primary outcome measure, which was time to need for additional medication for a mood episode. The median time until 25% of patients relapsed was 72 weeks for lamotrigine, 58 weeks for lithium, and 35 weeks for placebo.
Table 2
PUTATIVE PREDICTORS OF RESPONSE TO MAINTENANCE MEDICATIONS
| Medication | Predictor of response | Strength of evidence |
|---|---|---|
| Lithium | Nonrap id cycling Few episodes Few depressive symptoms Family history bipolar disorder Episode sequence M-D-I No substance/alcohol use disorder | ◊◊◊ ◊ ◊ ◊ ◊ ◊ |
| Divalproex | Equal efficacy in rapid & non-rapid cycling, manic & mixed, No personality disorder | ◊ ◊ |
| Carbamazepine | Equal efficacy in rapid & non-rapid cycling, manic & mixed Mood-incongruent symptoms | ◊◊ ◊ |
| Lamotrigine | Bipolar II > bipolar I Depression > mania | ◊ ◊◊ |
| Olanzapine | Equal efficacy in rapid & non-rapid cycling, manic & mixed, psychotic & nonpsychotic mania in acute studies; data pending in maintenance | ◊ |
| Clozapine | Efficacy in treatment-resistant mania rapid & nonrapid cycling, manic & mixed, psychotic & nonpsychotic in naturalistic studies | ◊◊◊ |
| Key ◊ = reported in 1 study; ◊◊ = reported in 2 studies; ◊◊◊ = reported in > 3 studies. | ||
On secondary outcome measures, lamotrigine, but not lithium, was superior to placebo in delaying time to depressive relapse. In contrast, lithium, but not lamotrigine, was superior to placebo in delaying time to manic relapse. Finally, lamotrigine, but not lithium, was superior to placebo in time to discontinuation for any reason.
From this study, it appears that lamotrigine is most effective in preventing depressive relapse, whereas lithium is most effective in preventing manic relapse. Thus, lithium and lamotrigine may complement each other in maintenance treatment by preventing manic and depressive episodes in combination.
The findings of the first trial were consistent with those of the second placebo-controlled lamotrigine (100-500 mg/d) maintenance study conducted specifically in patients with rapid cycling bipolar I and II disorders.16 In this 6-month trial, there was no significant difference in time to need for additional medications, the primary outcome measure, between the lamotrigine and placebo groups.
Median survival time was significantly greater for the lamotrigine group (18 weeks) than for the placebo group (12 weeks). The lamotrigine group had significantly longer time to need for additional medications in bipolar II, but not bipolar I, patients. Patients with bipolar II disorder also displayed significantly greater improvement with lamotrigine on global scales compared with bipolar I patients. Because bipolar II disorder is characterized predominantly by depressive episodes, these findings suggest that lamotrigine was again more beneficial in preventing recurrent depression, in this case, specifically, in rapid cycling bipolar II patients.
Taken together, the results of these studies are also consistent with the results of two placebo-controlled trials of lamotrigine in the treatment of acute bipolar depression.17,18 Its efficacy in acute bipolar I depression was first demonstrated in a 6-week, double-blind, randomized, parallel-group trial in which patients received lamotrigine 50 mg/d, 200 mg/d (after gradual titration over the first 4 weeks), and placebo.17
Both dosage groups of lamotrigine displayed significantly greater improvement in depressive symptoms as measured by the Montgomery-Asberg Depression Rating Scale (but not the Hamilton Depression Rating Scale) and by the Clinical Global Improvement Scale compared with the placebo group. There was a trend for the 200 mg/d group to have greater improvement than the 50 mg/d group, a trend that might have become significant had the study been longer, as the 200 mg/d group did not receive this dose for the full trial. There was no significant difference in the incidence of hypomanic or manic switches among the three study groups.
Frye and colleagues also found lamotrigine to be superior to placebo in global improvement in depressive (but not manic) symptoms in a crossover monotherapy trial in treatment-refractory bipolar I and II patients.18
Olanzapine, as described earlier, was comparable to divalproex in a head-to-head comparison 44-week extension trial in patients who responded to double-blind treatment in an acute mania study.12 These results were consistent with the preliminary findings of an open-label extension study of olanzapine.19 There are no placebo-controlled trials of olanzapine or any other atypical antipsychotic in the maintenance phase of bipolar disorder published to date.
Clozapine was more effective than “treatment as usual” (combinations of mood-stabilizers and typical antipsychotics) in patients with treatment-refractory bipolar and schizoaffective (bipolar subtype) disorders.20 Many patients with bipolar disorder now receive adjunctive maintenance treatment with typical antipsychotics, but the limited data from the few controlled trials of typical agents administered in combination with mood-stabilizers do not support the efficacy of this strategy.21 Moreover, some reports suggest that maintenance treatment incorporating typical antipsychotics may increase the frequency and severity of depressive episodes in patients with bipolar disorder.
Predicting response to pharmacologic treatment
Clinical experience and data from the randomized, controlled trials reviewed earlier have identified several tentative predictors of response—or nonresponse—to specific medications. Lithium, divalproex, and carbamazepine appear to have greater efficacy in the prevention of manic rather than depressive episodes.11 In contrast, lamotrigine appears to have greater efficacy in preventing depressive rather than manic episodes.
It is unclear whether olanzapine and perhaps other atypical antipsychotics may have a more favorable effect in preventing one pole of the illness over another (Table 2). The currently available atypicals (clozapine, risperidone, olanzapine, quetiapine, and ziprasidone) in general appear to differ from typical antipsychotics in having bidirectional (antimanic and antidepressant) effects on mood symptoms.

Atypicals may exert antidepressant effects via a number of different mechanisms, including 5HT2 receptor antagonism (a property shared by all atypicals and the antidepressants trazodone, nefazodone, and mirtazapine); alpha2-adrenergic antagonism (clozapine and risperidone); and 5HT1D antagonism, 5HT1A agonism, and 5HT and NE reuptake inhibition (ziprasidone).22
Patients with rapid-cycling bipolar disorder have a relatively poor response to lithium (response rates of approximately 20%).11 Patients with rapid-cycling bipolar I disorder may have a greater likelihood of response to combined treatment with lithium and carbamazepine,9 or divalproex.11 Alternately, patients with rapid-cycling bipolar II disorder have lower relapse rates on lamotrigine compared with placebo.16 Anecdotal reports and the results of acute treatment studies suggest that clozapine and olanzapine may be beneficial maintenance agents for rapid-cycling bipolar I patients.
Other predictors of favorable response to lithium prophylaxis include a family history of bipolar disorder, illness course characterized by maniadepression-euthymia episode sequence, and few prior mood episodes.21 Conversely, co-occurring alcohol or substance use disorder, multiple prior mood episodes, and familial negative affective style have been associated with poor response to lithium maintenance treatment.
Tentative predictors of response to divalproex maintenance treatment include mixed episodes, rapid cycling, and absence of co-occurring personality disorder. In one lithium comparison trial, patients with mixed episodes, bipolar II, and NOS disorders and mood-incongruent symptoms appeared to have a better response to carbamazepine.10
The dosage and relevant plasma concentrations of maintenance agents may also affect long-term efficacy. Gelenberg et al observed that the risk of relapse in bipolar patients maintained on low (0.4-0.6 mmol/L) serum concentrations was 2.6 times higher than for patients maintained on high (0.8-1.0 mmol/L) serum concentrations.23 However, there was a tradeoff in tolerability. Patients treated at the higher concentrations experienced significantly more and often treatment-limiting side effects.
No data are available regarding a possible plasma concentration-response relationship between maintenance treatment with divalproex or carbamazepine, but based on data from acute treatment trials, concentrations well within the therapeutic range of each drug appear essential.
The problem of subsyndromal symptoms
Evidence from a number of long-term outcome studies in bipolar disorder indicates that many patients spend protracted periods of time neither well nor in syndromal manic or depressive episodes, but rather experiencing chronic subsyndromal symptoms.24,25 In these studies, depressive symptoms were twice as prevalent as hypomanic symptoms between acute episodes of illness. Furthermore, persistent subsyndromal depressive symptoms were strongly associated with an increased risk for relapse and poor occupational functioning.
Keller et al26 found that patients maintained on low lithium serum concentrations (0.4-0.6 mmol/L) were more likely to experience subsyndromal symptoms and that their symptoms were more likely to worsen at any time than were symptoms of patients maintained at higher serum concentrations (0.8-10 mmol/L). The first occurrence of subsyndromal symptoms increased the risk of fullepisode relapse fourfold. These findings indicate that the optimal pharmacological maintenance treatment of bipolar disorder requires titration of mood-stabilizer medications to eradicate subsyndromal symptoms. Eliminating these residual or recurrent symptoms, in turn, substantially decreases the risk of relapse and of enduring functional impairment.
Conventional wisdom, in part supported by limited data from a small number of studies, suggests that antidepressants be used sparingly and for limited periods of time in conjunction with mood-stabilizers for bipolar depression. However, new data indicate that this strategy may significantly increase the risk of recurrence of depressive symptoms and episodes.27 Thus, combined treatment with mood-stabilizing agents and antidepressants for patients without rapid cycling and with recurrent depressive episodes may be indicated more often than previously thought.
In practice, perhaps the majority of patients with bipolar disorder require treatment with more than one mood-stabilizing medication to suppress subsyndromal symptoms as well as to prevent full episode recurrence. The use of combinations has been very poorly studied in randomized, controlled trials. In a pilot study of 12 patients with bipolar I disorder, Solomon et al compared the efficacy of lithium alone versus the combination of lithium and divalproex for 1 year.28 Not surprisingly, the combination significantly reduced the risk of recurrence of mania and depression but was also associated with more bothersome side effects.
Clinical practice has greatly outstripped the limited data available from formal studies. Recently reported as useful maintenance treatment strategies are combinations of:
- lithium and divalproex
- lithium and carbamazepine
- divalproex and carbamazepine
- lithium, divalproex, and carbamazepine
- lithium and/or divalproex with atypical antipsychotics, antidepressants, and lamotrigine.
Related resources
- Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. 2nd ed. New York: Oxford University Press, 2001.
- Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: the New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000.
- Goldberg JF, Harrow M. Bipolar Disorders. Clinical Course and Outcome. Washington, DC: American Psychiatric Press, 1999.
- Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
- Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of bipolar disorder (revision). Am J Psychiatry, in press.
Drug brand names
- Clozapine • Clozaril
- Divalproex • Depakote, Depakote Sprinkle
- Lamotrigine • Lamictal
- Mirtazapine • Remeron, Remeron Soltab
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate sodium • Depacon
- Ziprasidone • Geodon
Disclosure
Dr. Keck reports that he receives grant/research support from and serves as a consultant to Abbott Laboratories, AstraZeneca, Pfizer Inc., and Eli Lilly and Co. He also receives grant/research support from Merck and Co. and Otsuka America Pharmaceutical, and serves as a consultant to Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceutica.
Dr. McElroy reports that she receives grant/research support from and serves as a consultant to Abbott Laboratories, Elan Pharmaceuticals, Cephalon Inc. GlaxoSmithKline, and Eli Lilly and Co. She also receives grant/research support from Forest Pharmaceuticals and Solvay Pharmaceuticals, and serves as a consultant to Bristol-Myers Squibb Co., Ortho-McNeil Pharmaceutical, and Janssen Pharmaceutica.
Dr. Nelson reports no financial relationship with any company whose products are mentioned in this article.
1. Solomon DA, Keitner GI, Miller IW, et al. Course of illness and maintenance treatments for patients with bipolar disorder. J Clin Psychiatry 1995;56:5-13.
2. Keck PE, Jr, McElroy SL, et al. Twelve-month outcome of bipolar patients following hospitalization for a manic or mixed episode. Am J Psychiatry 1998;155:646-52.
3. Sachs GS, Printz DJ, et al. The Expert Consensus Guideline Series: medication treatment of bipolar disorders 2000. Postgrad Med Special Report 2000;4:1-104.
4. Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
5. Keck PE, Jr, Welge JA, et al. Placebo effect in randomized, controlled maintenance studies of patients with bipolar disorder. Biol Psychiatry 2000;47:756-65.
6. Calabrese JR, Rapport DJ, Shelton MD, et al. Evolving methodologies in bipolar disorder maintenance research. Br J Psychiatry 2001;178 [Suppl 41]:157-63.
7. Bowden CL, Calabrese JR, McElroy SL, et al. A randomized, placebo-controlled 12-month trial of divalproex and lithium in treatment of outpatients with bipolar I disorder. Arch Gen Psychiatry 2000;57:481-9.
8. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Lamictal 606 Study Group [Abstract]. Presented at the Annual Meeting of the American Psychiatric Association Meeting, New Orleans, LA, May 5-10, 2001.
9. Denicoff KD, et al. Comparative prophylactic efficacy of lithium, carbamazepine, and the combination in bipolar disorder. J Clin Psychiatry 1997;58:470-8.
10. Greil W, et al. Lithium versus carbamazepine in the maintenance treatment of bipolar disorders—a randomized study. J Affect Disord 1997;43:151-61.
11. Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry, in press.
12. Tohen M, Baker R. Olanzapine versus divalproex sodium for the treatment of acute mania and maintenance of remission: a 47-week study. Presented at the Annual Meeting of the American Psychiatric Association. New Orleans, La, May 5-10, 2001.
13. Lambert PA, Venaud G. Comparative study of valpromide versus lithium as prophylactic treatment in affective disorders. Nervure J Psychiatrie 1982;4:1-9.
14. Revicki DA, Hirschfeld RMA, Keck PE, Jr, et al. Cost-effectiveness of divalproex sodium vs. lithium in long-term therapy for bipolar disorder. Presented at the Annual Meeting of the American College of Neuropsychopharmacology. San Juan, Puerto Rico, Dec. 13-17, 1999.
15. Dardennnes R, Even C, et al. Comparison of carbamazepine and lithium in the prophylaxis of bipolar disorders. A meta-analysis. Br J Psychiatry 1995;166:375-81.
16. Calabrese JR, Suppes T, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
17. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. J Clin Psychiatry 1999;60:79-88.
18. Frye MA, Ketter TA, Kimbrell TA, et al. A double-blind, placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;24:133-40.
19. Tohen M. Olanazpine versus placebo in the treatment of acute bipolar mania. Presented at the XI World Congress of Psychiatry, World Psychiatric Association. Hamburg, Germany, Aug. 7, 1999.
20. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
21. Keck PE, Jr, McElroy SL. Pharmacological treatment of bipolar disorder. In: Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. New York: Oxford University Press, 2001, in press.
22. Keck PE, Jr, Licht R. Antipsychotic medications in the treatment of mood disorders. In: Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: The New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000;199-211.
23. Gelenberg AJ, Kane JM, et al. Comparison of standard and low serum levels of lithium for maintenance treatment of bipolar disorder. N Engl J Med 1989;321:1489-93.
24. Judd LL, Akiskal HS. Delineating the longitudinal structure of depressive illness: beyond clinical subtypes and duration thresholds. Pharmacopsychiatry 2000;33:3-7.
25. Goodnick PJ, Fieve RR, Schlegel A, et al. Inter-episode major and subclinical symptoms in affective disorder. Acta Psychiatr Scand 1987;75:592-600.
26. Keller MB, Lavori PW, et al. Subsyndromal symptoms in bipolar disorder: a comparison of standard and low serum lithium levels. Arch Gen Psychiatry 1992;49:371-6.
27. Post RM, Altshuler LL, Frye MA, et al. Rate of switch in bipolar patients prospectively treated with second-generation antidepressants as augmentation to mood stabilizers. Bipolar Disorders 2001;3:259-65.
28. Solomon DA, Ryan CE, Keitner GI, et al. A pilot study of lithium carbonate plus divalproex sodium for the continuation and maintenance treatment of patients with bipolar I disorder. J Clin Psychiatry 1997;58:95-9.
What are we trying to accomplish in the maintenance treatment of patients with bipolar disorder? Given that the disorder recurs in more than 90% of patients who experience a manic episode,1 there are 5 important goals:
- Prevention of recurrent episodes;
- Amelioration of subsyndromal symptoms;
- Reduction of suicide risk;
- Compliance enhancement;
- Optimization of interpersonal, social, and vocational functioning.
There is a great premium on preventing mood episode recurrence in patients with bipolar disorder. Mood episodes themselves produce substantial morbidity, but morbidity is not confined to these episodes alone. Full recovery of functioning often lags many months behind remission of symptoms.2 Recurrent mood episodes also may lead to progressive loss of function between episodes. Mood episodes also carry risks of mortality from suicide, violence, and impulsive risk taking.
Clearly, mood-stabilizing medications form the cornerstone of maintenance treatment,3,4 along with a strong therapeutic alliance between patient and clinician and targeted psychosocial therapies. In the Expert Consensus Guidelines for medication treatment of bipolar I disorder, maintenance treatment was recommended for 1 year following an initial manic or mixed episode; longer (indefinite) treatment was recommended for patients with a family history of bipolar disorder or if 2 episodes occurred.3
Compared with clinical trials of agents for acute bipolar mania (and mixed episodes), there are relatively few randomized controlled trials of medications for the maintenance phase of bipolar disorder. Some naturalistic studies have provided data on relapse rates associated with treatment with a variety of different agents. Even fewer studies have examined psychosocial interventions designed specifically to reduce relapse rates.
But new data are beginning to emerge regarding the efficacy of divalproex, lamotrigine, and olanzapine as maintenance therapies. A number of clinical predictors of response to these agents have begun to be identified, as well as to lithium and carbamazepine. Eliciting these characteristics is important when making recommendations to patients about available drug therapies.
In addition, effective maintenance treatment often requires combinations of mood-stabilizing, antidepressant, and antipsychotic agents to control or eliminate subsyndromal and breakthrough symptoms.
In this review, we will cover the available new data on pharmacologic maintenance treatments of bipolar disorder and their clinical implications.
What the studies show
Lithium has been the mainstay of therapy for bipolar disorder for more than 35 years. Most randomized, controlled trials of lithium maintenance therapy were conducted in the 1960s and 1970s5 (Table 1). Unfortunately, these studies had several design limitations that inflated the expectations of lithium’s efficacy as a maintenance treatment.6 These included discontinuation designs in which patients stabilized on lithium were abruptly switched to placebo; exaggerated early placebo relapse rates; enrollment of both unipolar and bipolar patients; lack of specific diagnostic criteria; and reported results only for patients completing studies. Pooled data from these trials indicated that lithium reduced the risk of relapse fourfold compared with placebo at 6 months and 1 year.5
Two contemporary randomized, placebo-controlled maintenance studies utilizing more rigorous designs provided further evidence of lithium’s superiority over placebo in extending time to manic relapse.7,8 Both studies enrolled patients who were currently or had recently been manic and had been stabilized in open-label treatment that included study medications.
In the first study, comparing 1-year relapse rates among patients randomized to lithium, divalproex, or placebo, lithium extended time to recurrence of mania by 55% compared with placebo.7 In the second, an 18-month trial comparing lithium, lamotrigine, and placebo, lithium significantly increased the time to intervention for recurrence of mania compared with placebo.8 The overall manic relapse rates were 17% for lithium-treated patients and 41% for those on placebo. However, lithium did not significantly extend time to depressive relapse or intervention for depressive relapse, respectively, in either study. Moreover, in the first study, patients who received lithium tended to have greater subthreshold depressive symptoms.8
Table 1
What works in maintenance treatment of bipolar disorder (ranked by number of randomized, controlled trials)
| Medication RCTs (n) | Trial results | Strong evidence | Some evidence |
|---|---|---|---|
| Lithium (15) | Equal to divalproex and lamotrigine; equal to or better than carbamazepine; better than placebo | 4-fold reduction of relapse risk vs. placebo at 6, 12 months; more efficacious in mania than in depression; higher lithium level correlated with lower relapse rates, but more side effects | |
| Carbamazepine (7) | No significant benefit vs. lithium; better than placebo | May be more efficacious in mania than in depression; may be less tolerable than lithium; no data on serum levels | |
| Divalproex (4) | Equal to lithium and olanzapine; better than placebo | May be more efficacious in mania than in depression; may be more tolerable than lithium; data on serum levels pending | |
| Lamotrigine (2) | Better than placebo | More efficacious in depression than in mania | Dosage 200-400 mg/d |
| Olanzapine (1) | Equal to divalproex | Data on dosage and differential efficacy related to dosage pending | |
| Clozapine (1) | Better than treatment as usual | Efficacy in treatment-resistant mania (bipolar schizoaffective disorder, bipolar type) |
These findings were consistent with earlier placebo-controlled studies of lithium maintenance treatment and a recent crossover comparison trial with carbamazepine.9 Lithium was also recently compared with carbamazepine in a 2.5-year maintenance multisite study in Europe.10 There was no significant difference in efficacy between the two in time to hospitalization, the primary outcome measure. On other outcome measures, including time to relapse or need for additional medication, lithium was superior to carbamazepine.
Pooled results from a number of naturalistic studies, which mirror clinical practice, indicated that approximately one-third of patients maintained on lithium had good functional outcomes without relapses and only minimal symptoms.11 In general, these studies found higher rates of relapse with longer durations of follow-up.
Valproate maintenance treatment has been studied in two randomized, controlled trials (one vs. placebo,7 and one vs. olanzapine12) and two open-label comparison studies against lithium.13,14 In the placebo-controlled trial, which also included a lithium comparison group described earlier, there was no significant difference in the time to development of any mood episode among the three treatment groups.7 However, divalproex was superior to placebo on a number of other outcome measures, including rate of study termination for any mood episode, termination for depression, and termination for noncompliance.
Divalproex was superior to placebo in patients who received divalproex in the open-label treatment phase before randomization. This is clinically relevant, as this group reflects expected relapse rates in patients treated initially with divalproex for acute mania who then remain on the drug for maintenance therapy. Patients receiving divalproex had significantly lower rates of intolerance and noncompliance compared to those treated with lithium.
In the second comparison study, 167 patients initially randomized and responding to divalproex or olanzapine in a 3-week acute bipolar mania trial continued in a double-blind 44-week extension study.12 There were no significant differences in relapse into mania between the two groups (olanzapine 41%, divalproex 50%, p = 0.4) or time to manic relapse (olanzapine 270 days, divalproex 74 days, p = 0.4). There was no significant difference in tolerability between the two.
Two open-label studies compared valproate with lithium. In an 18-month study conducted in France, patients randomized to the valpromide formulation of valproate displayed a 20% lower relapse rate than those receiving lithium.13 The second open-label comparison trial found comparable efficacy between lithium and divalproex in a 1-year naturalistic pharmacoeconomic study that allowed additional medications as needed for recurrent symptoms.14
Carbamazepine has been evaluated in a limited number of studies for maintenance treatment of bipolar disorder. The results of many early randomized, controlled maintenance trials were criticized on methodologic grounds.15 But two recent comparison trials with lithium, as noted earlier, provided clinically important data regarding carbamazepine’s prophylactic efficacy.9,10 Several additional clinically relevant observations emerged from analyses of secondary outcome measures in these two trials.
In the first study, 52 patients with bipolar I or II disorder received lithium or carbamazepine for 1 year, crossed over to the alternate drug the second year, and received both drugs the third year.9 There was little difference in relapse rates during the first year between the lithium (31%) and carbamazepine (37%) groups. Similarly, in the overall trial, there was little difference in the percentage of patients who were rated as having a moderate or better response—33% on lithium, 31% on carbamazepine, and 55% on the combination. A higher proportion of patients receiving carbamazepine withdrew due to side effects. In the second trial, significantly more patients receiving carbamazepine required additional medications for breakthrough symptoms and experienced side effects requiring treatment discontinuation.10
Lamotrigine has been studied in two placebo-controlled, randomized maintenance studies in patients with bipolar disorder.8,16 The first evaluated bipolar I patients who had experienced a manic or hypomanic episode within 60 days of entry into an open-label treatment phase with lamotrigine.8 Patients who, in turn, improved or remained stable during the open-label treatment phase were then randomized to treatment with lamotrigine 200-400 mg/d, lithium, or placebo for up to 18 months. Both lamotrigine and lithium were superior to placebo on the primary outcome measure, which was time to need for additional medication for a mood episode. The median time until 25% of patients relapsed was 72 weeks for lamotrigine, 58 weeks for lithium, and 35 weeks for placebo.
Table 2
PUTATIVE PREDICTORS OF RESPONSE TO MAINTENANCE MEDICATIONS
| Medication | Predictor of response | Strength of evidence |
|---|---|---|
| Lithium | Nonrap id cycling Few episodes Few depressive symptoms Family history bipolar disorder Episode sequence M-D-I No substance/alcohol use disorder | ◊◊◊ ◊ ◊ ◊ ◊ ◊ |
| Divalproex | Equal efficacy in rapid & non-rapid cycling, manic & mixed, No personality disorder | ◊ ◊ |
| Carbamazepine | Equal efficacy in rapid & non-rapid cycling, manic & mixed Mood-incongruent symptoms | ◊◊ ◊ |
| Lamotrigine | Bipolar II > bipolar I Depression > mania | ◊ ◊◊ |
| Olanzapine | Equal efficacy in rapid & non-rapid cycling, manic & mixed, psychotic & nonpsychotic mania in acute studies; data pending in maintenance | ◊ |
| Clozapine | Efficacy in treatment-resistant mania rapid & nonrapid cycling, manic & mixed, psychotic & nonpsychotic in naturalistic studies | ◊◊◊ |
| Key ◊ = reported in 1 study; ◊◊ = reported in 2 studies; ◊◊◊ = reported in > 3 studies. | ||
On secondary outcome measures, lamotrigine, but not lithium, was superior to placebo in delaying time to depressive relapse. In contrast, lithium, but not lamotrigine, was superior to placebo in delaying time to manic relapse. Finally, lamotrigine, but not lithium, was superior to placebo in time to discontinuation for any reason.
From this study, it appears that lamotrigine is most effective in preventing depressive relapse, whereas lithium is most effective in preventing manic relapse. Thus, lithium and lamotrigine may complement each other in maintenance treatment by preventing manic and depressive episodes in combination.
The findings of the first trial were consistent with those of the second placebo-controlled lamotrigine (100-500 mg/d) maintenance study conducted specifically in patients with rapid cycling bipolar I and II disorders.16 In this 6-month trial, there was no significant difference in time to need for additional medications, the primary outcome measure, between the lamotrigine and placebo groups.
Median survival time was significantly greater for the lamotrigine group (18 weeks) than for the placebo group (12 weeks). The lamotrigine group had significantly longer time to need for additional medications in bipolar II, but not bipolar I, patients. Patients with bipolar II disorder also displayed significantly greater improvement with lamotrigine on global scales compared with bipolar I patients. Because bipolar II disorder is characterized predominantly by depressive episodes, these findings suggest that lamotrigine was again more beneficial in preventing recurrent depression, in this case, specifically, in rapid cycling bipolar II patients.
Taken together, the results of these studies are also consistent with the results of two placebo-controlled trials of lamotrigine in the treatment of acute bipolar depression.17,18 Its efficacy in acute bipolar I depression was first demonstrated in a 6-week, double-blind, randomized, parallel-group trial in which patients received lamotrigine 50 mg/d, 200 mg/d (after gradual titration over the first 4 weeks), and placebo.17
Both dosage groups of lamotrigine displayed significantly greater improvement in depressive symptoms as measured by the Montgomery-Asberg Depression Rating Scale (but not the Hamilton Depression Rating Scale) and by the Clinical Global Improvement Scale compared with the placebo group. There was a trend for the 200 mg/d group to have greater improvement than the 50 mg/d group, a trend that might have become significant had the study been longer, as the 200 mg/d group did not receive this dose for the full trial. There was no significant difference in the incidence of hypomanic or manic switches among the three study groups.
Frye and colleagues also found lamotrigine to be superior to placebo in global improvement in depressive (but not manic) symptoms in a crossover monotherapy trial in treatment-refractory bipolar I and II patients.18
Olanzapine, as described earlier, was comparable to divalproex in a head-to-head comparison 44-week extension trial in patients who responded to double-blind treatment in an acute mania study.12 These results were consistent with the preliminary findings of an open-label extension study of olanzapine.19 There are no placebo-controlled trials of olanzapine or any other atypical antipsychotic in the maintenance phase of bipolar disorder published to date.
Clozapine was more effective than “treatment as usual” (combinations of mood-stabilizers and typical antipsychotics) in patients with treatment-refractory bipolar and schizoaffective (bipolar subtype) disorders.20 Many patients with bipolar disorder now receive adjunctive maintenance treatment with typical antipsychotics, but the limited data from the few controlled trials of typical agents administered in combination with mood-stabilizers do not support the efficacy of this strategy.21 Moreover, some reports suggest that maintenance treatment incorporating typical antipsychotics may increase the frequency and severity of depressive episodes in patients with bipolar disorder.
Predicting response to pharmacologic treatment
Clinical experience and data from the randomized, controlled trials reviewed earlier have identified several tentative predictors of response—or nonresponse—to specific medications. Lithium, divalproex, and carbamazepine appear to have greater efficacy in the prevention of manic rather than depressive episodes.11 In contrast, lamotrigine appears to have greater efficacy in preventing depressive rather than manic episodes.
It is unclear whether olanzapine and perhaps other atypical antipsychotics may have a more favorable effect in preventing one pole of the illness over another (Table 2). The currently available atypicals (clozapine, risperidone, olanzapine, quetiapine, and ziprasidone) in general appear to differ from typical antipsychotics in having bidirectional (antimanic and antidepressant) effects on mood symptoms.
Atypicals may exert antidepressant effects via a number of different mechanisms, including 5HT2 receptor antagonism (a property shared by all atypicals and the antidepressants trazodone, nefazodone, and mirtazapine); alpha2-adrenergic antagonism (clozapine and risperidone); and 5HT1D antagonism, 5HT1A agonism, and 5HT and NE reuptake inhibition (ziprasidone).22
Patients with rapid-cycling bipolar disorder have a relatively poor response to lithium (response rates of approximately 20%).11 Patients with rapid-cycling bipolar I disorder may have a greater likelihood of response to combined treatment with lithium and carbamazepine,9 or divalproex.11 Alternately, patients with rapid-cycling bipolar II disorder have lower relapse rates on lamotrigine compared with placebo.16 Anecdotal reports and the results of acute treatment studies suggest that clozapine and olanzapine may be beneficial maintenance agents for rapid-cycling bipolar I patients.
Other predictors of favorable response to lithium prophylaxis include a family history of bipolar disorder, illness course characterized by maniadepression-euthymia episode sequence, and few prior mood episodes.21 Conversely, co-occurring alcohol or substance use disorder, multiple prior mood episodes, and familial negative affective style have been associated with poor response to lithium maintenance treatment.
Tentative predictors of response to divalproex maintenance treatment include mixed episodes, rapid cycling, and absence of co-occurring personality disorder. In one lithium comparison trial, patients with mixed episodes, bipolar II, and NOS disorders and mood-incongruent symptoms appeared to have a better response to carbamazepine.10
The dosage and relevant plasma concentrations of maintenance agents may also affect long-term efficacy. Gelenberg et al observed that the risk of relapse in bipolar patients maintained on low (0.4-0.6 mmol/L) serum concentrations was 2.6 times higher than for patients maintained on high (0.8-1.0 mmol/L) serum concentrations.23 However, there was a tradeoff in tolerability. Patients treated at the higher concentrations experienced significantly more and often treatment-limiting side effects.
No data are available regarding a possible plasma concentration-response relationship between maintenance treatment with divalproex or carbamazepine, but based on data from acute treatment trials, concentrations well within the therapeutic range of each drug appear essential.
The problem of subsyndromal symptoms
Evidence from a number of long-term outcome studies in bipolar disorder indicates that many patients spend protracted periods of time neither well nor in syndromal manic or depressive episodes, but rather experiencing chronic subsyndromal symptoms.24,25 In these studies, depressive symptoms were twice as prevalent as hypomanic symptoms between acute episodes of illness. Furthermore, persistent subsyndromal depressive symptoms were strongly associated with an increased risk for relapse and poor occupational functioning.
Keller et al26 found that patients maintained on low lithium serum concentrations (0.4-0.6 mmol/L) were more likely to experience subsyndromal symptoms and that their symptoms were more likely to worsen at any time than were symptoms of patients maintained at higher serum concentrations (0.8-10 mmol/L). The first occurrence of subsyndromal symptoms increased the risk of fullepisode relapse fourfold. These findings indicate that the optimal pharmacological maintenance treatment of bipolar disorder requires titration of mood-stabilizer medications to eradicate subsyndromal symptoms. Eliminating these residual or recurrent symptoms, in turn, substantially decreases the risk of relapse and of enduring functional impairment.
Conventional wisdom, in part supported by limited data from a small number of studies, suggests that antidepressants be used sparingly and for limited periods of time in conjunction with mood-stabilizers for bipolar depression. However, new data indicate that this strategy may significantly increase the risk of recurrence of depressive symptoms and episodes.27 Thus, combined treatment with mood-stabilizing agents and antidepressants for patients without rapid cycling and with recurrent depressive episodes may be indicated more often than previously thought.
In practice, perhaps the majority of patients with bipolar disorder require treatment with more than one mood-stabilizing medication to suppress subsyndromal symptoms as well as to prevent full episode recurrence. The use of combinations has been very poorly studied in randomized, controlled trials. In a pilot study of 12 patients with bipolar I disorder, Solomon et al compared the efficacy of lithium alone versus the combination of lithium and divalproex for 1 year.28 Not surprisingly, the combination significantly reduced the risk of recurrence of mania and depression but was also associated with more bothersome side effects.
Clinical practice has greatly outstripped the limited data available from formal studies. Recently reported as useful maintenance treatment strategies are combinations of:
- lithium and divalproex
- lithium and carbamazepine
- divalproex and carbamazepine
- lithium, divalproex, and carbamazepine
- lithium and/or divalproex with atypical antipsychotics, antidepressants, and lamotrigine.
Related resources
- Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. 2nd ed. New York: Oxford University Press, 2001.
- Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: the New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000.
- Goldberg JF, Harrow M. Bipolar Disorders. Clinical Course and Outcome. Washington, DC: American Psychiatric Press, 1999.
- Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
- Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of bipolar disorder (revision). Am J Psychiatry, in press.
Drug brand names
- Clozapine • Clozaril
- Divalproex • Depakote, Depakote Sprinkle
- Lamotrigine • Lamictal
- Mirtazapine • Remeron, Remeron Soltab
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate sodium • Depacon
- Ziprasidone • Geodon
Disclosure
Dr. Keck reports that he receives grant/research support from and serves as a consultant to Abbott Laboratories, AstraZeneca, Pfizer Inc., and Eli Lilly and Co. He also receives grant/research support from Merck and Co. and Otsuka America Pharmaceutical, and serves as a consultant to Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceutica.
Dr. McElroy reports that she receives grant/research support from and serves as a consultant to Abbott Laboratories, Elan Pharmaceuticals, Cephalon Inc. GlaxoSmithKline, and Eli Lilly and Co. She also receives grant/research support from Forest Pharmaceuticals and Solvay Pharmaceuticals, and serves as a consultant to Bristol-Myers Squibb Co., Ortho-McNeil Pharmaceutical, and Janssen Pharmaceutica.
Dr. Nelson reports no financial relationship with any company whose products are mentioned in this article.
What are we trying to accomplish in the maintenance treatment of patients with bipolar disorder? Given that the disorder recurs in more than 90% of patients who experience a manic episode,1 there are 5 important goals:
- Prevention of recurrent episodes;
- Amelioration of subsyndromal symptoms;
- Reduction of suicide risk;
- Compliance enhancement;
- Optimization of interpersonal, social, and vocational functioning.
There is a great premium on preventing mood episode recurrence in patients with bipolar disorder. Mood episodes themselves produce substantial morbidity, but morbidity is not confined to these episodes alone. Full recovery of functioning often lags many months behind remission of symptoms.2 Recurrent mood episodes also may lead to progressive loss of function between episodes. Mood episodes also carry risks of mortality from suicide, violence, and impulsive risk taking.
Clearly, mood-stabilizing medications form the cornerstone of maintenance treatment,3,4 along with a strong therapeutic alliance between patient and clinician and targeted psychosocial therapies. In the Expert Consensus Guidelines for medication treatment of bipolar I disorder, maintenance treatment was recommended for 1 year following an initial manic or mixed episode; longer (indefinite) treatment was recommended for patients with a family history of bipolar disorder or if 2 episodes occurred.3
Compared with clinical trials of agents for acute bipolar mania (and mixed episodes), there are relatively few randomized controlled trials of medications for the maintenance phase of bipolar disorder. Some naturalistic studies have provided data on relapse rates associated with treatment with a variety of different agents. Even fewer studies have examined psychosocial interventions designed specifically to reduce relapse rates.
But new data are beginning to emerge regarding the efficacy of divalproex, lamotrigine, and olanzapine as maintenance therapies. A number of clinical predictors of response to these agents have begun to be identified, as well as to lithium and carbamazepine. Eliciting these characteristics is important when making recommendations to patients about available drug therapies.
In addition, effective maintenance treatment often requires combinations of mood-stabilizing, antidepressant, and antipsychotic agents to control or eliminate subsyndromal and breakthrough symptoms.
In this review, we will cover the available new data on pharmacologic maintenance treatments of bipolar disorder and their clinical implications.
What the studies show
Lithium has been the mainstay of therapy for bipolar disorder for more than 35 years. Most randomized, controlled trials of lithium maintenance therapy were conducted in the 1960s and 1970s5 (Table 1). Unfortunately, these studies had several design limitations that inflated the expectations of lithium’s efficacy as a maintenance treatment.6 These included discontinuation designs in which patients stabilized on lithium were abruptly switched to placebo; exaggerated early placebo relapse rates; enrollment of both unipolar and bipolar patients; lack of specific diagnostic criteria; and reported results only for patients completing studies. Pooled data from these trials indicated that lithium reduced the risk of relapse fourfold compared with placebo at 6 months and 1 year.5
Two contemporary randomized, placebo-controlled maintenance studies utilizing more rigorous designs provided further evidence of lithium’s superiority over placebo in extending time to manic relapse.7,8 Both studies enrolled patients who were currently or had recently been manic and had been stabilized in open-label treatment that included study medications.
In the first study, comparing 1-year relapse rates among patients randomized to lithium, divalproex, or placebo, lithium extended time to recurrence of mania by 55% compared with placebo.7 In the second, an 18-month trial comparing lithium, lamotrigine, and placebo, lithium significantly increased the time to intervention for recurrence of mania compared with placebo.8 The overall manic relapse rates were 17% for lithium-treated patients and 41% for those on placebo. However, lithium did not significantly extend time to depressive relapse or intervention for depressive relapse, respectively, in either study. Moreover, in the first study, patients who received lithium tended to have greater subthreshold depressive symptoms.8
Table 1
What works in maintenance treatment of bipolar disorder (ranked by number of randomized, controlled trials)
| Medication RCTs (n) | Trial results | Strong evidence | Some evidence |
|---|---|---|---|
| Lithium (15) | Equal to divalproex and lamotrigine; equal to or better than carbamazepine; better than placebo | 4-fold reduction of relapse risk vs. placebo at 6, 12 months; more efficacious in mania than in depression; higher lithium level correlated with lower relapse rates, but more side effects | |
| Carbamazepine (7) | No significant benefit vs. lithium; better than placebo | May be more efficacious in mania than in depression; may be less tolerable than lithium; no data on serum levels | |
| Divalproex (4) | Equal to lithium and olanzapine; better than placebo | May be more efficacious in mania than in depression; may be more tolerable than lithium; data on serum levels pending | |
| Lamotrigine (2) | Better than placebo | More efficacious in depression than in mania | Dosage 200-400 mg/d |
| Olanzapine (1) | Equal to divalproex | Data on dosage and differential efficacy related to dosage pending | |
| Clozapine (1) | Better than treatment as usual | Efficacy in treatment-resistant mania (bipolar schizoaffective disorder, bipolar type) |
These findings were consistent with earlier placebo-controlled studies of lithium maintenance treatment and a recent crossover comparison trial with carbamazepine.9 Lithium was also recently compared with carbamazepine in a 2.5-year maintenance multisite study in Europe.10 There was no significant difference in efficacy between the two in time to hospitalization, the primary outcome measure. On other outcome measures, including time to relapse or need for additional medication, lithium was superior to carbamazepine.
Pooled results from a number of naturalistic studies, which mirror clinical practice, indicated that approximately one-third of patients maintained on lithium had good functional outcomes without relapses and only minimal symptoms.11 In general, these studies found higher rates of relapse with longer durations of follow-up.
Valproate maintenance treatment has been studied in two randomized, controlled trials (one vs. placebo,7 and one vs. olanzapine12) and two open-label comparison studies against lithium.13,14 In the placebo-controlled trial, which also included a lithium comparison group described earlier, there was no significant difference in the time to development of any mood episode among the three treatment groups.7 However, divalproex was superior to placebo on a number of other outcome measures, including rate of study termination for any mood episode, termination for depression, and termination for noncompliance.
Divalproex was superior to placebo in patients who received divalproex in the open-label treatment phase before randomization. This is clinically relevant, as this group reflects expected relapse rates in patients treated initially with divalproex for acute mania who then remain on the drug for maintenance therapy. Patients receiving divalproex had significantly lower rates of intolerance and noncompliance compared to those treated with lithium.
In the second comparison study, 167 patients initially randomized and responding to divalproex or olanzapine in a 3-week acute bipolar mania trial continued in a double-blind 44-week extension study.12 There were no significant differences in relapse into mania between the two groups (olanzapine 41%, divalproex 50%, p = 0.4) or time to manic relapse (olanzapine 270 days, divalproex 74 days, p = 0.4). There was no significant difference in tolerability between the two.
Two open-label studies compared valproate with lithium. In an 18-month study conducted in France, patients randomized to the valpromide formulation of valproate displayed a 20% lower relapse rate than those receiving lithium.13 The second open-label comparison trial found comparable efficacy between lithium and divalproex in a 1-year naturalistic pharmacoeconomic study that allowed additional medications as needed for recurrent symptoms.14
Carbamazepine has been evaluated in a limited number of studies for maintenance treatment of bipolar disorder. The results of many early randomized, controlled maintenance trials were criticized on methodologic grounds.15 But two recent comparison trials with lithium, as noted earlier, provided clinically important data regarding carbamazepine’s prophylactic efficacy.9,10 Several additional clinically relevant observations emerged from analyses of secondary outcome measures in these two trials.
In the first study, 52 patients with bipolar I or II disorder received lithium or carbamazepine for 1 year, crossed over to the alternate drug the second year, and received both drugs the third year.9 There was little difference in relapse rates during the first year between the lithium (31%) and carbamazepine (37%) groups. Similarly, in the overall trial, there was little difference in the percentage of patients who were rated as having a moderate or better response—33% on lithium, 31% on carbamazepine, and 55% on the combination. A higher proportion of patients receiving carbamazepine withdrew due to side effects. In the second trial, significantly more patients receiving carbamazepine required additional medications for breakthrough symptoms and experienced side effects requiring treatment discontinuation.10
Lamotrigine has been studied in two placebo-controlled, randomized maintenance studies in patients with bipolar disorder.8,16 The first evaluated bipolar I patients who had experienced a manic or hypomanic episode within 60 days of entry into an open-label treatment phase with lamotrigine.8 Patients who, in turn, improved or remained stable during the open-label treatment phase were then randomized to treatment with lamotrigine 200-400 mg/d, lithium, or placebo for up to 18 months. Both lamotrigine and lithium were superior to placebo on the primary outcome measure, which was time to need for additional medication for a mood episode. The median time until 25% of patients relapsed was 72 weeks for lamotrigine, 58 weeks for lithium, and 35 weeks for placebo.
Table 2
PUTATIVE PREDICTORS OF RESPONSE TO MAINTENANCE MEDICATIONS
| Medication | Predictor of response | Strength of evidence |
|---|---|---|
| Lithium | Nonrap id cycling Few episodes Few depressive symptoms Family history bipolar disorder Episode sequence M-D-I No substance/alcohol use disorder | ◊◊◊ ◊ ◊ ◊ ◊ ◊ |
| Divalproex | Equal efficacy in rapid & non-rapid cycling, manic & mixed, No personality disorder | ◊ ◊ |
| Carbamazepine | Equal efficacy in rapid & non-rapid cycling, manic & mixed Mood-incongruent symptoms | ◊◊ ◊ |
| Lamotrigine | Bipolar II > bipolar I Depression > mania | ◊ ◊◊ |
| Olanzapine | Equal efficacy in rapid & non-rapid cycling, manic & mixed, psychotic & nonpsychotic mania in acute studies; data pending in maintenance | ◊ |
| Clozapine | Efficacy in treatment-resistant mania rapid & nonrapid cycling, manic & mixed, psychotic & nonpsychotic in naturalistic studies | ◊◊◊ |
| Key ◊ = reported in 1 study; ◊◊ = reported in 2 studies; ◊◊◊ = reported in > 3 studies. | ||
On secondary outcome measures, lamotrigine, but not lithium, was superior to placebo in delaying time to depressive relapse. In contrast, lithium, but not lamotrigine, was superior to placebo in delaying time to manic relapse. Finally, lamotrigine, but not lithium, was superior to placebo in time to discontinuation for any reason.
From this study, it appears that lamotrigine is most effective in preventing depressive relapse, whereas lithium is most effective in preventing manic relapse. Thus, lithium and lamotrigine may complement each other in maintenance treatment by preventing manic and depressive episodes in combination.
The findings of the first trial were consistent with those of the second placebo-controlled lamotrigine (100-500 mg/d) maintenance study conducted specifically in patients with rapid cycling bipolar I and II disorders.16 In this 6-month trial, there was no significant difference in time to need for additional medications, the primary outcome measure, between the lamotrigine and placebo groups.
Median survival time was significantly greater for the lamotrigine group (18 weeks) than for the placebo group (12 weeks). The lamotrigine group had significantly longer time to need for additional medications in bipolar II, but not bipolar I, patients. Patients with bipolar II disorder also displayed significantly greater improvement with lamotrigine on global scales compared with bipolar I patients. Because bipolar II disorder is characterized predominantly by depressive episodes, these findings suggest that lamotrigine was again more beneficial in preventing recurrent depression, in this case, specifically, in rapid cycling bipolar II patients.
Taken together, the results of these studies are also consistent with the results of two placebo-controlled trials of lamotrigine in the treatment of acute bipolar depression.17,18 Its efficacy in acute bipolar I depression was first demonstrated in a 6-week, double-blind, randomized, parallel-group trial in which patients received lamotrigine 50 mg/d, 200 mg/d (after gradual titration over the first 4 weeks), and placebo.17
Both dosage groups of lamotrigine displayed significantly greater improvement in depressive symptoms as measured by the Montgomery-Asberg Depression Rating Scale (but not the Hamilton Depression Rating Scale) and by the Clinical Global Improvement Scale compared with the placebo group. There was a trend for the 200 mg/d group to have greater improvement than the 50 mg/d group, a trend that might have become significant had the study been longer, as the 200 mg/d group did not receive this dose for the full trial. There was no significant difference in the incidence of hypomanic or manic switches among the three study groups.
Frye and colleagues also found lamotrigine to be superior to placebo in global improvement in depressive (but not manic) symptoms in a crossover monotherapy trial in treatment-refractory bipolar I and II patients.18
Olanzapine, as described earlier, was comparable to divalproex in a head-to-head comparison 44-week extension trial in patients who responded to double-blind treatment in an acute mania study.12 These results were consistent with the preliminary findings of an open-label extension study of olanzapine.19 There are no placebo-controlled trials of olanzapine or any other atypical antipsychotic in the maintenance phase of bipolar disorder published to date.
Clozapine was more effective than “treatment as usual” (combinations of mood-stabilizers and typical antipsychotics) in patients with treatment-refractory bipolar and schizoaffective (bipolar subtype) disorders.20 Many patients with bipolar disorder now receive adjunctive maintenance treatment with typical antipsychotics, but the limited data from the few controlled trials of typical agents administered in combination with mood-stabilizers do not support the efficacy of this strategy.21 Moreover, some reports suggest that maintenance treatment incorporating typical antipsychotics may increase the frequency and severity of depressive episodes in patients with bipolar disorder.
Predicting response to pharmacologic treatment
Clinical experience and data from the randomized, controlled trials reviewed earlier have identified several tentative predictors of response—or nonresponse—to specific medications. Lithium, divalproex, and carbamazepine appear to have greater efficacy in the prevention of manic rather than depressive episodes.11 In contrast, lamotrigine appears to have greater efficacy in preventing depressive rather than manic episodes.
It is unclear whether olanzapine and perhaps other atypical antipsychotics may have a more favorable effect in preventing one pole of the illness over another (Table 2). The currently available atypicals (clozapine, risperidone, olanzapine, quetiapine, and ziprasidone) in general appear to differ from typical antipsychotics in having bidirectional (antimanic and antidepressant) effects on mood symptoms.
Atypicals may exert antidepressant effects via a number of different mechanisms, including 5HT2 receptor antagonism (a property shared by all atypicals and the antidepressants trazodone, nefazodone, and mirtazapine); alpha2-adrenergic antagonism (clozapine and risperidone); and 5HT1D antagonism, 5HT1A agonism, and 5HT and NE reuptake inhibition (ziprasidone).22
Patients with rapid-cycling bipolar disorder have a relatively poor response to lithium (response rates of approximately 20%).11 Patients with rapid-cycling bipolar I disorder may have a greater likelihood of response to combined treatment with lithium and carbamazepine,9 or divalproex.11 Alternately, patients with rapid-cycling bipolar II disorder have lower relapse rates on lamotrigine compared with placebo.16 Anecdotal reports and the results of acute treatment studies suggest that clozapine and olanzapine may be beneficial maintenance agents for rapid-cycling bipolar I patients.
Other predictors of favorable response to lithium prophylaxis include a family history of bipolar disorder, illness course characterized by maniadepression-euthymia episode sequence, and few prior mood episodes.21 Conversely, co-occurring alcohol or substance use disorder, multiple prior mood episodes, and familial negative affective style have been associated with poor response to lithium maintenance treatment.
Tentative predictors of response to divalproex maintenance treatment include mixed episodes, rapid cycling, and absence of co-occurring personality disorder. In one lithium comparison trial, patients with mixed episodes, bipolar II, and NOS disorders and mood-incongruent symptoms appeared to have a better response to carbamazepine.10
The dosage and relevant plasma concentrations of maintenance agents may also affect long-term efficacy. Gelenberg et al observed that the risk of relapse in bipolar patients maintained on low (0.4-0.6 mmol/L) serum concentrations was 2.6 times higher than for patients maintained on high (0.8-1.0 mmol/L) serum concentrations.23 However, there was a tradeoff in tolerability. Patients treated at the higher concentrations experienced significantly more and often treatment-limiting side effects.
No data are available regarding a possible plasma concentration-response relationship between maintenance treatment with divalproex or carbamazepine, but based on data from acute treatment trials, concentrations well within the therapeutic range of each drug appear essential.
The problem of subsyndromal symptoms
Evidence from a number of long-term outcome studies in bipolar disorder indicates that many patients spend protracted periods of time neither well nor in syndromal manic or depressive episodes, but rather experiencing chronic subsyndromal symptoms.24,25 In these studies, depressive symptoms were twice as prevalent as hypomanic symptoms between acute episodes of illness. Furthermore, persistent subsyndromal depressive symptoms were strongly associated with an increased risk for relapse and poor occupational functioning.
Keller et al26 found that patients maintained on low lithium serum concentrations (0.4-0.6 mmol/L) were more likely to experience subsyndromal symptoms and that their symptoms were more likely to worsen at any time than were symptoms of patients maintained at higher serum concentrations (0.8-10 mmol/L). The first occurrence of subsyndromal symptoms increased the risk of fullepisode relapse fourfold. These findings indicate that the optimal pharmacological maintenance treatment of bipolar disorder requires titration of mood-stabilizer medications to eradicate subsyndromal symptoms. Eliminating these residual or recurrent symptoms, in turn, substantially decreases the risk of relapse and of enduring functional impairment.
Conventional wisdom, in part supported by limited data from a small number of studies, suggests that antidepressants be used sparingly and for limited periods of time in conjunction with mood-stabilizers for bipolar depression. However, new data indicate that this strategy may significantly increase the risk of recurrence of depressive symptoms and episodes.27 Thus, combined treatment with mood-stabilizing agents and antidepressants for patients without rapid cycling and with recurrent depressive episodes may be indicated more often than previously thought.
In practice, perhaps the majority of patients with bipolar disorder require treatment with more than one mood-stabilizing medication to suppress subsyndromal symptoms as well as to prevent full episode recurrence. The use of combinations has been very poorly studied in randomized, controlled trials. In a pilot study of 12 patients with bipolar I disorder, Solomon et al compared the efficacy of lithium alone versus the combination of lithium and divalproex for 1 year.28 Not surprisingly, the combination significantly reduced the risk of recurrence of mania and depression but was also associated with more bothersome side effects.
Clinical practice has greatly outstripped the limited data available from formal studies. Recently reported as useful maintenance treatment strategies are combinations of:
- lithium and divalproex
- lithium and carbamazepine
- divalproex and carbamazepine
- lithium, divalproex, and carbamazepine
- lithium and/or divalproex with atypical antipsychotics, antidepressants, and lamotrigine.
Related resources
- Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. 2nd ed. New York: Oxford University Press, 2001.
- Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: the New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000.
- Goldberg JF, Harrow M. Bipolar Disorders. Clinical Course and Outcome. Washington, DC: American Psychiatric Press, 1999.
- Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
- Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of bipolar disorder (revision). Am J Psychiatry, in press.
Drug brand names
- Clozapine • Clozaril
- Divalproex • Depakote, Depakote Sprinkle
- Lamotrigine • Lamictal
- Mirtazapine • Remeron, Remeron Soltab
- Nefazodone • Serzone
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate sodium • Depacon
- Ziprasidone • Geodon
Disclosure
Dr. Keck reports that he receives grant/research support from and serves as a consultant to Abbott Laboratories, AstraZeneca, Pfizer Inc., and Eli Lilly and Co. He also receives grant/research support from Merck and Co. and Otsuka America Pharmaceutical, and serves as a consultant to Bristol-Myers Squibb Co., GlaxoSmithKline, and Janssen Pharmaceutica.
Dr. McElroy reports that she receives grant/research support from and serves as a consultant to Abbott Laboratories, Elan Pharmaceuticals, Cephalon Inc. GlaxoSmithKline, and Eli Lilly and Co. She also receives grant/research support from Forest Pharmaceuticals and Solvay Pharmaceuticals, and serves as a consultant to Bristol-Myers Squibb Co., Ortho-McNeil Pharmaceutical, and Janssen Pharmaceutica.
Dr. Nelson reports no financial relationship with any company whose products are mentioned in this article.
1. Solomon DA, Keitner GI, Miller IW, et al. Course of illness and maintenance treatments for patients with bipolar disorder. J Clin Psychiatry 1995;56:5-13.
2. Keck PE, Jr, McElroy SL, et al. Twelve-month outcome of bipolar patients following hospitalization for a manic or mixed episode. Am J Psychiatry 1998;155:646-52.
3. Sachs GS, Printz DJ, et al. The Expert Consensus Guideline Series: medication treatment of bipolar disorders 2000. Postgrad Med Special Report 2000;4:1-104.
4. Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
5. Keck PE, Jr, Welge JA, et al. Placebo effect in randomized, controlled maintenance studies of patients with bipolar disorder. Biol Psychiatry 2000;47:756-65.
6. Calabrese JR, Rapport DJ, Shelton MD, et al. Evolving methodologies in bipolar disorder maintenance research. Br J Psychiatry 2001;178 [Suppl 41]:157-63.
7. Bowden CL, Calabrese JR, McElroy SL, et al. A randomized, placebo-controlled 12-month trial of divalproex and lithium in treatment of outpatients with bipolar I disorder. Arch Gen Psychiatry 2000;57:481-9.
8. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Lamictal 606 Study Group [Abstract]. Presented at the Annual Meeting of the American Psychiatric Association Meeting, New Orleans, LA, May 5-10, 2001.
9. Denicoff KD, et al. Comparative prophylactic efficacy of lithium, carbamazepine, and the combination in bipolar disorder. J Clin Psychiatry 1997;58:470-8.
10. Greil W, et al. Lithium versus carbamazepine in the maintenance treatment of bipolar disorders—a randomized study. J Affect Disord 1997;43:151-61.
11. Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry, in press.
12. Tohen M, Baker R. Olanzapine versus divalproex sodium for the treatment of acute mania and maintenance of remission: a 47-week study. Presented at the Annual Meeting of the American Psychiatric Association. New Orleans, La, May 5-10, 2001.
13. Lambert PA, Venaud G. Comparative study of valpromide versus lithium as prophylactic treatment in affective disorders. Nervure J Psychiatrie 1982;4:1-9.
14. Revicki DA, Hirschfeld RMA, Keck PE, Jr, et al. Cost-effectiveness of divalproex sodium vs. lithium in long-term therapy for bipolar disorder. Presented at the Annual Meeting of the American College of Neuropsychopharmacology. San Juan, Puerto Rico, Dec. 13-17, 1999.
15. Dardennnes R, Even C, et al. Comparison of carbamazepine and lithium in the prophylaxis of bipolar disorders. A meta-analysis. Br J Psychiatry 1995;166:375-81.
16. Calabrese JR, Suppes T, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
17. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. J Clin Psychiatry 1999;60:79-88.
18. Frye MA, Ketter TA, Kimbrell TA, et al. A double-blind, placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;24:133-40.
19. Tohen M. Olanazpine versus placebo in the treatment of acute bipolar mania. Presented at the XI World Congress of Psychiatry, World Psychiatric Association. Hamburg, Germany, Aug. 7, 1999.
20. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
21. Keck PE, Jr, McElroy SL. Pharmacological treatment of bipolar disorder. In: Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. New York: Oxford University Press, 2001, in press.
22. Keck PE, Jr, Licht R. Antipsychotic medications in the treatment of mood disorders. In: Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: The New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000;199-211.
23. Gelenberg AJ, Kane JM, et al. Comparison of standard and low serum levels of lithium for maintenance treatment of bipolar disorder. N Engl J Med 1989;321:1489-93.
24. Judd LL, Akiskal HS. Delineating the longitudinal structure of depressive illness: beyond clinical subtypes and duration thresholds. Pharmacopsychiatry 2000;33:3-7.
25. Goodnick PJ, Fieve RR, Schlegel A, et al. Inter-episode major and subclinical symptoms in affective disorder. Acta Psychiatr Scand 1987;75:592-600.
26. Keller MB, Lavori PW, et al. Subsyndromal symptoms in bipolar disorder: a comparison of standard and low serum lithium levels. Arch Gen Psychiatry 1992;49:371-6.
27. Post RM, Altshuler LL, Frye MA, et al. Rate of switch in bipolar patients prospectively treated with second-generation antidepressants as augmentation to mood stabilizers. Bipolar Disorders 2001;3:259-65.
28. Solomon DA, Ryan CE, Keitner GI, et al. A pilot study of lithium carbonate plus divalproex sodium for the continuation and maintenance treatment of patients with bipolar I disorder. J Clin Psychiatry 1997;58:95-9.
1. Solomon DA, Keitner GI, Miller IW, et al. Course of illness and maintenance treatments for patients with bipolar disorder. J Clin Psychiatry 1995;56:5-13.
2. Keck PE, Jr, McElroy SL, et al. Twelve-month outcome of bipolar patients following hospitalization for a manic or mixed episode. Am J Psychiatry 1998;155:646-52.
3. Sachs GS, Printz DJ, et al. The Expert Consensus Guideline Series: medication treatment of bipolar disorders 2000. Postgrad Med Special Report 2000;4:1-104.
4. Sachs GS, Thase ME. Bipolar disorder therapeutics: maintenance treatment. Biol Psychiatry 2000;48:573-81.
5. Keck PE, Jr, Welge JA, et al. Placebo effect in randomized, controlled maintenance studies of patients with bipolar disorder. Biol Psychiatry 2000;47:756-65.
6. Calabrese JR, Rapport DJ, Shelton MD, et al. Evolving methodologies in bipolar disorder maintenance research. Br J Psychiatry 2001;178 [Suppl 41]:157-63.
7. Bowden CL, Calabrese JR, McElroy SL, et al. A randomized, placebo-controlled 12-month trial of divalproex and lithium in treatment of outpatients with bipolar I disorder. Arch Gen Psychiatry 2000;57:481-9.
8. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Lamictal 606 Study Group [Abstract]. Presented at the Annual Meeting of the American Psychiatric Association Meeting, New Orleans, LA, May 5-10, 2001.
9. Denicoff KD, et al. Comparative prophylactic efficacy of lithium, carbamazepine, and the combination in bipolar disorder. J Clin Psychiatry 1997;58:470-8.
10. Greil W, et al. Lithium versus carbamazepine in the maintenance treatment of bipolar disorders—a randomized study. J Affect Disord 1997;43:151-61.
11. Hirschfeld RMA, Bowden CL, Gitlin MJ, et al. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry, in press.
12. Tohen M, Baker R. Olanzapine versus divalproex sodium for the treatment of acute mania and maintenance of remission: a 47-week study. Presented at the Annual Meeting of the American Psychiatric Association. New Orleans, La, May 5-10, 2001.
13. Lambert PA, Venaud G. Comparative study of valpromide versus lithium as prophylactic treatment in affective disorders. Nervure J Psychiatrie 1982;4:1-9.
14. Revicki DA, Hirschfeld RMA, Keck PE, Jr, et al. Cost-effectiveness of divalproex sodium vs. lithium in long-term therapy for bipolar disorder. Presented at the Annual Meeting of the American College of Neuropsychopharmacology. San Juan, Puerto Rico, Dec. 13-17, 1999.
15. Dardennnes R, Even C, et al. Comparison of carbamazepine and lithium in the prophylaxis of bipolar disorders. A meta-analysis. Br J Psychiatry 1995;166:375-81.
16. Calabrese JR, Suppes T, et al. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid-cycling bipolar disorder. J Clin Psychiatry 2000;61:841-50.
17. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. J Clin Psychiatry 1999;60:79-88.
18. Frye MA, Ketter TA, Kimbrell TA, et al. A double-blind, placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol 2000;24:133-40.
19. Tohen M. Olanazpine versus placebo in the treatment of acute bipolar mania. Presented at the XI World Congress of Psychiatry, World Psychiatric Association. Hamburg, Germany, Aug. 7, 1999.
20. Suppes T, Webb A, Paul B, et al. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry 1999;156:1164-9.
21. Keck PE, Jr, McElroy SL. Pharmacological treatment of bipolar disorder. In: Nathan PE, Gorman JM, eds. A Guide to Treatments that Work. New York: Oxford University Press, 2001, in press.
22. Keck PE, Jr, Licht R. Antipsychotic medications in the treatment of mood disorders. In: Buckley PF, Waddington JL, eds. Schizophrenia and Mood Disorders: The New Drug Therapies in Clinical Practice. Boston: Butterworth-Heiman, 2000;199-211.
23. Gelenberg AJ, Kane JM, et al. Comparison of standard and low serum levels of lithium for maintenance treatment of bipolar disorder. N Engl J Med 1989;321:1489-93.
24. Judd LL, Akiskal HS. Delineating the longitudinal structure of depressive illness: beyond clinical subtypes and duration thresholds. Pharmacopsychiatry 2000;33:3-7.
25. Goodnick PJ, Fieve RR, Schlegel A, et al. Inter-episode major and subclinical symptoms in affective disorder. Acta Psychiatr Scand 1987;75:592-600.
26. Keller MB, Lavori PW, et al. Subsyndromal symptoms in bipolar disorder: a comparison of standard and low serum lithium levels. Arch Gen Psychiatry 1992;49:371-6.
27. Post RM, Altshuler LL, Frye MA, et al. Rate of switch in bipolar patients prospectively treated with second-generation antidepressants as augmentation to mood stabilizers. Bipolar Disorders 2001;3:259-65.
28. Solomon DA, Ryan CE, Keitner GI, et al. A pilot study of lithium carbonate plus divalproex sodium for the continuation and maintenance treatment of patients with bipolar I disorder. J Clin Psychiatry 1997;58:95-9.
Rapid-cycling bipolar disorder: Which therapies are most effective?
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.

Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
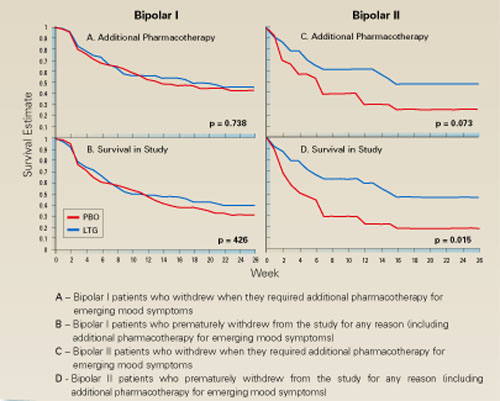
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
Disclosure
Dr. Muzina reports that he is a member of the Eli Lilly and Co. speaker’s bureau.
Dr. Calabrese reports that he receives research/grant support from Abbott Laboratories, GlaxoSmithKline, and Wyeth-Ayerst Pharmaceuticals, and serves as a consultant to Abbott Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Novartis Pharmaceuticals Corp., and Parke Davis/Warner Lambert.
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.
Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
Disclosure
Dr. Muzina reports that he is a member of the Eli Lilly and Co. speaker’s bureau.
Dr. Calabrese reports that he receives research/grant support from Abbott Laboratories, GlaxoSmithKline, and Wyeth-Ayerst Pharmaceuticals, and serves as a consultant to Abbott Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Novartis Pharmaceuticals Corp., and Parke Davis/Warner Lambert.
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.
Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
Disclosure
Dr. Muzina reports that he is a member of the Eli Lilly and Co. speaker’s bureau.
Dr. Calabrese reports that he receives research/grant support from Abbott Laboratories, GlaxoSmithKline, and Wyeth-Ayerst Pharmaceuticals, and serves as a consultant to Abbott Pharmaceuticals, Eli Lilly and Co., GlaxoSmithKline, Novartis Pharmaceuticals Corp., and Parke Davis/Warner Lambert.
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.
Rapid-cycling bipolar disorder: Which therapies are most effective?
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.
Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.
Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
Patients with rapid-cycling bipolar disorder (RCBD) can be frustrating to treat. Despite growing research and data, knowledge and effective therapies remain limited. How do you manage patients with rapid cycling who do not respond robustly to lithium, divalproex, or carbamazepine monotherapy? Are combination therapies likely to be more effective? Where does lamotrigine fit in? Is there a role for conventional antidepressants?
We’ll explore these and related questions—but the final answers are not yet in. Recognition of RCBD is important because it presents such difficult treatment challenges. Available evidence does suggest that rapid cycling as defined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (Box 1), describes a clinically specific course of illness that may require treatments different from currently used traditional drug therapies for nonrapid cycling bipolar disorder, particularly as no one agent appears to provide ideal bimodal treatment and prophylaxis of this bipolar disorder variant.
Rapid cycling is a specifier of the longitudinal course of illness presentation that is seen almost exclusively in bipolar disorder and is associated with a greater morbidity. Dunner and Fieve1 originally coined the term when evaluating clinical factors associated with lithium prophylaxis failure. Since that time the validity of rapid cycling as a distinct course modifier for bipolar disorder has been supported by multiple studies, leading to its inclusion in the fourth edition of the Diagnostic and Statistical Manual of the APA (1994).
According to DSM-IV, the course specifier of rapid cycling applies to “at least 4 episodes of a mood disturbance in the previous 12 months that meet criteria for a manic episode, a hypomanic episode, or a major depressive episode.” The episodes must be demarcated by a full or partial remission lasting at least 2 months or by a switch to a mood state of opposite polarity.
Early reports noted that patients suffering from RCBD did not respond adequately when treated with lithium.1 Other observations indicated that divalproex was more effective in this patient population, particularly for the illness’ hypomanic or manic phases.2 We hope that the following evaluation of these and other drug therapies will prove helpful.
Watch out for antidepressants
Most concerning has been the frequency and severity of treatment-refractory depressive phases of RCBD that may be exacerbated by antidepressant use (cycle induction or acceleration). Indeed, the frequent recurrence of refractory depression has been described as the hallmark of this bipolar disorder variant.3
Lithium: the scale weighs against it
Although an excellent mood stabilizer for most patients with bipolar disorder, lithium monotherapy is less than ideal for patients with the rapid-cycling variant, particularly in treatment or prevention of depressive or mixed episodes. The efficacy of lithium is likely decreased by the concurrent administration of antidepressant medication and increased when administered with other mood stabilizers.
The landmark article by Dunner and Fieve,1 which described a placebo-controlled, double-blind maintenance study in a general cohort of 55 patients, tried to clarify factors associated with the failure of lithium prophylaxis in bipolar disorder. Rapid cyclers comprised 20% of the subjects and 80% were nonrapid cyclers. Rapid cyclers were disproportionately represented in the lithium failure group. Lithium failures included 82% (9 of 11) of rapid cyclers compared to 41% (18 of 44) of nonrapid cyclers. Lithium failure was defined as (1) hospitalization for, or (2) treatment of, mania or (3) depression during lithium therapy, or as mood symptoms that, as documented by rating scales, were sufficient to warrant a diagnosis of mild depression, hypomania, or mania persisting for at least 2 weeks.
Kukopulos et al4 replicated the findings of Dunner and Fieve in a study of the longitudinal clinical course of 434 bipolar patients. Of these patients, 50 were rapid cyclers and had received continuous lithium therapy for more than a year, with good to partial prophylaxis in only 28%. Maj and colleagues5 published a 5-year prospective study of lithium therapy in 402 patients with bipolar disorder and noted the absence of rapid cycling in good responders to lithium but an incidence rate of 26% in nonresponders to lithium.
Other investigators have reported better response in RCBD. In a select cohort of lithium-responsive bipolar I and II patients, Tondo et al6 concluded that lithium maintenance yields striking long-term reductions in depressive and manic morbidity, more so in rapid cycling type II patients. This study, however, was in a cohort of lithium responders and excluded patients who had been exposed to antipsychotic or antidepressant medications for more than 3 months, those on chronic anticonvulsant therapy, and those with substance abuse disorders.
Although most studies do report poor response to lithium therapy in RCBD, Wehr and colleagues7 suggest that in some patients with rapid cycling, the discontinuation of antidepressant drugs may allow lithium to act as a more effective anticycling mood-stabilizing agent.
Divalproex: effective in manic phase
In contrast to lithium, an open trial of a homogenous cohort of patients with RCBD by Calabrese and colleagues3,8 found divalproex to possess moderate to marked acute and prophylactic antimanic properties with only modest antidepressant effects (Table 1). Data from 6 open studies involving 147 patients with rapid cycling suggest that divalproex possesses moderate to marked efficacy in the manic phase, but poor to moderate efficacy in the depressed phase. Positive outcome predictors were bipolar II and mixed states, no prior lithium therapy, and a positive family history of affective disorder. Predictors of negative response included increase in frequency and severity of mania, and borderline personality disorder.
Divalproex therapy in combination with lithium may improve response rates.9 Calabrese and colleagues, however, have examined large cohorts of patients, including those comorbid with alcohol, cocaine, and/or cannabis abuse, treated with a lithium-divalproex combination over 6-month study periods. The researchers found that only 25% to 50% of patients stabilized, and that of those not exhibiting a response, the majority (75%) did not respond because of treatment-refractory depression in the context of RCBD.3
Although experts believe divalproex to be more effective than lithium in preventing episodes associated with RCBD, such a conclusion awaits confirmation with the near completion of a double-blind, 20-month maintenance trial sponsored by the National Institute of Mental Health (NIMH).
Carbamazepine’s role in combination therapy
Early reports by Post and colleagues in 1987 suggested that rapid cycling predicted positive response to carbamazepine, but later findings by Okuma in 1993 refuted this. Other collective open and controlled studies suggest that this anticonvulsant possesses moderate to marked efficacy in the manic phase, and poor to moderate efficacy in the depressed phase of RCBD. Again, combination therapy with lithium may offer greater efficacy. Of significance, carbamazepine treatment outcomes have not been prospectively evaluated in a homogeneous cohort of rapid cyclers.
The limitations of carbamazepine therapy are well known and available evidence also does not seem to support monotherapy with this agent as being useful in RCBD, especially in the treatment and prophylaxis of depressive or mixed phases of the disorder. Thus, further controlled studies are needed to examine the agent’s potential role and safety in combination therapies for RCBD.
Table 1
SPECTRUM OF ACUTE AND PROPHYLACTIC EFFICACY OF DIVALPROEX IN RAPID-CYCLING BIPOLAR DISORDER
| Spectrum of marked responses to divalproex in bipolar rapid cycling | ||
|---|---|---|
| Acute | Prophylactic | |
| Dysphoric hypomania/mania | 87% | 89% |
| Elated hypomania/mania | 64% | 77% |
| Depression (n = 101, mean follow-up 15 months) | 21% | 38% |
| Adapted from Calabrese and Delucchi. Am J Psychiatry. 1990;147:431-434 and Calabrese et al. J Clin Psychopharmacol. 1993;13:280-283. | ||
Lamotrigine: best hope for monotherapy
Lamotrigine monotherapy has been reported to be effective in some RCBD cases. The data suggest that it possesses both antidepressant and mood-stabilizing properties.10
An open, naturalistic study of 5 women with treatment-refractory rapid cycling by Fatemi et al11 demonstrated both mood-stabilizing and antidepressant effects from lamotrigine monotherapy or augmentation at a mean dose of 185 ±33.5 mg/d. In 14 clinical reports involving 207 patients with bipolar disorder, 66 of whom had rapid cycling, lamotrigine was observed to possess moderate to marked efficacy in depression and hypomania, but only moderate efficacy in mania.
An open, prospective study compared the efficacy of lamotrigine add-on or monotherapy in 41 rapid cyclers to 34 nonrapid cyclers across 48 weeks. Improvement from baseline to last visit was significant between both subgroups for depressive and hypomanic symptoms. Patients presenting with more severe manic symptoms did less well.13
In the first double-blind, placebo-controlled study of lamotrigine in RCBD,12 182 of 324 patients with rapid cycling responded to treatment with open-label lamotrigine and were then randomized to the study’s double-blind phase. Forty-one percent of lamotrigine-treated vs. 26% of placebo-treated patients were stable without relapse during 6 months of monotherapy. Patients with rapid-cycling bipolar II disorder consistently experienced more improvement than their bipolar I counterparts (Figure 1). The results of this only prospective, placebo-controlled, acute-treatment study of rapid-cycling bipolar patients to date indicate that lamotrigine monotherapy is useful for some patients with RCBD, particularly those with bipolar II.
Frye et al14 conducted a double-blind, placebo-controlled study of 23 patients with rapid cycling utilizing a crossover series of three 6-week monotherapy evaluations of lamotrigine, gabapentin, and placebo. Marked antidepressant response on lamotrigine was seen in 45% of the participants compared with 19% of patients on placebo and a similar response rate among those on gabapentin.
A study evaluating the safety and efficacy of 2 dosages of lamotrigine (50 mg/d or 200 mg/d) compared with placebo in the treatment of a major depressive episode in patients with bipolar I disorder over 7 weeks demonstrated significant antidepressant efficacy.15 These bipolar outpatients displayed clinical improvement as early as the third week of treatment, and switch rates for both dosages did not exceed that of placebo. Patients with RCBD, however, were excluded from this initial trial. Subsequent studies have demonstrated similar magnitudes of efficacy in patients with RCBD, primarily in the prevention of depressive episodes, including the 6-month RCBD maintenance study10 and 2 recently completed 18-month maintenance studies of patients with bipolar I disorder, either recently manic or recently depressed.
Lamotrigine thus may have a special role in RCBD treatment. Its most significant side effect in bipolar disorder is benign rash, which has occurred in 9.0% (108 of 1,198) of patients randomized to lamotrigine vs. 7.6% (80 of 1,056) of those randomized to placebo in pivotal multicenter, double-blind, placebo-controlled bipolar trials.
In mood disorder trials conducted to date, the rate of serious rash, defined as requiring both drug discontinuation and hospitalization, has been 0.06% (2 of 3,153) on lamotrigine and 0.09% (1 out of 1,053) on placebo. No cases of Steven’s Johnson syndrome or toxic epidermal necrolysis were observed.16 A low starting dose and gradual titration of lamotrigine (Table 2) appear to minimize the risk of serious rash.
Levothyroxine: possible add-on therapy
Levothyroxine should be considered as add-on therapy in patients with known hypothyroidism, borderline hypothyroidism, or otherwise treatment-refractory cases.
The strategy of thyroid supplementation is derived from Gjessing’s 1936 report of success in administering hypermetabolic doses of thyroid hormone to patients with periodic catatonia. Stancer and Persad17 initially reported the potential efficacy of this therapeutic maneuver in rapid cyclers; remissions were induced by hypermetabolic thyroid doses in 5 of 7 patients with treatment-refractory bipolar disorder. No data currently support any prophylactic efficacy of thyroid supplementation monotherapy for RCBD treatment.
Bauer and Whybrow18 suggest that thyroid supplementation with T4 added to mood stabilizers augments efficacy independent of pre-existing thyroid function. The potential side effects of long-term levothryoxine administration, namely osteoporosis and cardiac arrhythmias, limit the usefulness of thyroid augmentation in RCBD.
Atypical antipsychotics: perhaps in combination
Coadministering atypical antipsychotics in other mood stabilizers may help rapid cyclers with current or past psychotic symptoms during their mood episodes, but further study is clearly needed.
Atypical antipsychotic medications may have specific mood-stabilizing properties, particularly in the management of mixed and manic states. In the first prospective trial of clozapine monotherapy in bipolar disorder, Calabrese and colleagues in 1994 reported that rapid cycling did not appear to predict nonresponse to treatment.
In the first randomized, controlled trial involving clozapine in bipolar disorder, Suppes et al19 noted significant improvement for symptoms of mania, psychosis, and global improvement. Subjects with nonpsychotic bipolar disorder showed a degree of improvement similar to that seen in the entire clozapine-treated group. These results support a mood-stabilizing role for clozapine.
Preliminary studies of risperidone and olanzapine further suggest therapeutic utility for atypical antipsychotics.
Figure 1 LAMOTRIGINE VS. PLACEBO IN RAPID-CYCLING BIPOLAR DISORDER
Table 2
DOSAGE PLAN FOR LAMOTRIGINE IN MONOTHERAPY AND COMBINATION
| Treatment period | Type of therapy | Daily dosage |
|---|---|---|
| Weeks 1-2 | Monotherapy With divalproex With carbamazepine | 25 mg 12.5 mg 50 mg |
| Weeks 3-4 | Monotherapy With divalproex With carbamazepine | 50 mg 25 mg 100 mg |
| Week 5 | Monotherapy With divalproex With carbamazepine | 100 mg 50 mg 200 mg |
| Thereafter | Monotherapy With divalproex With carbamazepine | 200 mg 100 mg 400 mg |
Topiramate: in patients with weight problems
Evidence from 12 open studies of 223 patients with bipolar disorder suggest that this anticonvulsant may possess mood-stabilizing properties while sparing patients the weight gain commonly seen with other pharmacotherapies.
Two studies of topiramate as an add-on therapy come to mind. Marcotte in 1998 retrospectively studied 44 patients with RCBD, 23 (52%) of whom demonstrated moderate or marked improvement on a mean topiramate dosage of 200 mg/d.
Sachs also reported that symptoms for some patients with a treatment-refractory bipolar disorder could be improved when topiramate was added to their medication regimen. Available data encourage further controlled studies of topiramate add-on therapy for RCBD, especially in obese patients.
Gabapentin: contradictory reports
Preliminary data from 14 open-label studies of gabapentin in 302 bipolar patients reported a response rate of around 67% when used as an add-on therapy, usually in mania or mixed states. A moderate antimanic effect was observed among a total of 23 rapid cyclers in 9 of the studies.
The reports are contradictory, however, and available data do not firmly support the agent’s efficacy in RCBD treatment.
Other potential uses for gabapentin are being investigated, such as antidepressant augmentation, anxiety, and chronic pain. Thus, patients with RCBD and a comorbid illness may benefit from add-on gabapentin.
ECT: Some limited success
Electroconvulsive therapy (ECT) has been implicated less frequently than antidepressants in the induction of rapid cycling, and when this does occur it is usually in the context of combined ECT/antidepressant therapies.
Berma and Wolpert in 1987 reported a case of successful ECT treatment of rapid cycling in an adolescent who had been treated with trimipramine for depression. Vanelle et al in 1994 suggested that maintenance ECT works well in 22 treatment-resistant bipolar patients, including 4 with rapid cycling, over an 18-month treatment period.
Behavioral intervention: changing sleep routines
NIMH research of 15 rapid cyclers who were studied for 3 months looked at behavioral interventions and their effect on switching (Feldman-Naim 1997). This study suggested that patients were more likely to switch from depression into hypomania/mania during daytime hours and from mania/hypomania into depression during nighttime.
The use of light therapy or activity and exercise during depression and the use of induced sleep or exposure to darkness during mania/hypomania may be therapeutic. Wehr and colleagues supported this in a 1998 report of one patient studied over several years, comparing this rapid-cycling patient’s regular sleep routine with prolonged (10 to 14 hours per night) and enforced bed rest in the dark.7 The promotion of sleep by scheduling regular nighttime periods of enforced bed rest in the dark may help prevent mania and stabilize mood in rapid cyclers.
Other add-on possibilities
Haykal in 1990 reported bupropion to be an effective add-on treatment in 5 of 6 patients with refractory, rapid-cycling bipolar II disorder. Benefit has also been reported from clorgyline, clonidine, magnesium, primidone, and acetazolamide.
Calcium-channel blockers may also offer clinical utility, although supportive evidence is limited. Nimodipine was evaluated for efficacy in 30 patients with treatment-refractory affective illness by the NIMH and Passaglia et al in 1998. Patients who improved on this agent had ultradian rapid cycling, defined in the study as those with affective episodes lasting as short as a week.
A recommended treatment strategy
Based on the available data in bipolar I rapid cycling, we recommend initial treatment with divalproex followed by augmentation with lithium if hypomanic or manic episodes persist, lamotrigine if breakthrough episodes are predominantly depressive, and atypical antipsychotics if psychotic symptoms or true mixed states remain.
For patients presenting with bipolar II rapid cycling, we recommend starting with lamotrigine, then augmenting with divalproex or lithium for breakthrough episodes. Lamotrigine shows more promise because of its reportedly greater antidepressant properties and lack of cycle induction or switching, but offers only modest antimanic therapy.
Pending further investigations, current application of the data suggests that when treating patients with RCBD, conventional antidepressants should be avoided and, if first-line therapies are not effective, the clinician should consider moving to combination drug therapy with 2 or more agents.
Related resources
- Bauer MS, Calabrese JR, Dunner DL, et al. Multi-site data reanalysis: validity of rapid cycling as a course modifier for bipolar disorder in DSM-IV. Am J Psychiatry. 1994;151:506-515.
- Calabrese JR, Kimmel SE, Woyshville MJ, et al. Clozapine in treatment refractory mania. Am J Psychiatry. 1996;153(6):759-764.
- Calabrese JR, Bowden CL, McElroy SL, et al. Spectrum of activity of lamotrigine in treatment refractory bipolar disorder. Am J Psychiatry. 1999;156(7):1019-1023.
- Sachs GS. Printz DJ. Kahn DA. Carpenter D. Docherty JP. The expert consensus guideline series: medication treatment of bipolar disorder 2000. Postgraduate Medicine. April 2000; Spec No:1-104.
Drug brand names
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clonidine • Catapres
- Clozapine • Clozaril
- Divalproex sodium • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid, Levothroid, Levoxyl
- Olanzapine • Zyprexa
- Nimodipine • Nimotop
- Primidonem • Mysoline
- Topiramate • Topamax
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.
1. Dunner DL, Fieve RR. Clinical factors in lithium carbonate prophylaxis failure. Arch Gen Psychiatry. 1974;20:229-233.
2. Calabrese JR, Delucchi GA. Spectrum of efficacy of valproate in 55 rapid-cycling manic depressives. Am J Psychiatry. 1990;147(4):431-434.
3. Calabrese JR, Shelton MD, Bowden CL, et al. Bipolar rapid cycling: Focus on depression as its hallmark. J Clin Psychiatry. 2001;62(Suppl 14):34-41.
4. Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic depressive cycle and changes caused by treatment. Pharmacopsychiatry. 1980;13:156-167.
5. Maj M, et al. Long-term outcome of lithium prophylaxis in bipolar disorder: a 5-year prospective study of 402 patients at a lithium clinic. Am J Psychiatry. 1998;155:30-35.
6. Tondo L, Baldessarini RJ, et al. Lithium maintenance treatment of depression and mania in bipolar I and bipolar II disorders. Am J Psychiatry. 1998;155:638-645.
7. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145:179-84.
8. Calabrese JR, Woyshville MJ, Kimmel SE. Rapport DJ: Predictors of valproate response in bipolar rapid cycling. J Clin Psychopharmacology. 1993;13(4):280-283.
9. Sharma V, Persad E, et al. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can J Psychiatry. 1993;38:137-139.
10. Calabrese JR, Suppes T, Bowden CL, et al. for the Lamictal 614 Study Group. A double-blind, placebo-controlled, prophylaxis study of lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry. 2000;61(11):841-850.
11. Fatemi SH, Rapport DJ, Calabrese JR, et al. Lamotrigine in rapid cycling bipolar disorder. J Clin Psychiatry 1997;58:522-527.
12. Calabrese JR, Bowden CL, et al. for the Lamictal 602 Study Group. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry 1999;60(2):79-88.
13. Bowden CL, Calabrese JR, McElroy SL, et al. Comparison of the efficacy of lamotrigine in rapid cycling and non-rapid cycling bipolar disorder. Biol Psychiatry. 1999;45(8):953-958.
14. Frye MA, et al. A placebo-controlled study of lamotrigine and gabapentin monotherapy in refractory mood disorders. J Clin Psychopharmacol. 2000;20:607-614.
15. Calabrese JR, Bowden CL, Sachs GS, et al. A double-blind placebo-controlled study of lamotrigine monotherapy in outpatients with bipolar I depression. Lamictal 602 Study Group. J Clin Psychiatry. 1999;60(2):79-88.
16. Calabrese JR, Bowden CL, DeVeaugh-Geiss J, et al. Lamotrigine demonstrates long term mood stabilization in recently manic patients. Annual meeting of the American Psychiatric Association, New Orleans, 2001.
17. Stancer HC, Persad E. Treatment of intractable rapid-cycling manic-depressive disorder with levothyroxine. Clinical observations. Arch Gen Psychiatry. 1982;39(3):311-312.
18. Bauer MS, Whybrow PC. Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study.. Arch Gen Psychiatry. 1990;47(5):435-40.
19. Suppes T, Webb A, Paul B, Carmody T, et al:. Clinical outcome in a randomized 1-year trial of clozapine versus treatment as usual for patients with treatment-resistant illness and a history of mania. Am J Psychiatry. 1999;156:1164-1169.