User login
Clear Identification Needed for Hospitalists in Medicare
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
In recent months, numerous articles have come out targeting high-billing physicians—looking for smoking guns in recently released 2012 Medicare fee-for-service physician claims data. These data include both the amount each individual physician billed and the amount Medicare paid on average for services performed by all physicians treating Medicare beneficiaries.
Many physician groups, including the AMA, criticized the data release as having significant limitations, including clinical and billing practice realities that confound the layperson’s understanding of the data’s implications. Still, there is much physicians can learn by exploring this information, particularly those in a still-growing field like hospital medicine (HM).
There is no clear method to identify hospitalists within these data. Hospitalists are dispersed throughout their respective board certifications—internal medicine, family practice, pediatrics. The designations come directly from the Medicare specialty billing code; the code associated with the largest number of services becomes that provider’s de facto specialty. For the majority of providers, this will correspond with their board certification and their professional identity. A hospitalist’s unique practice is lost within these general identifiers.
However, the contours of that unique practice may provide some tools to identify hospitalists, albeit roughly, within the data and in the absence of a specialty billing code. Things like practice location and commonly billed Healthcare Common Procedure Coding System (HCPCS) codes can help sketch the boundaries of the field. Certainly, any classification methodology will have its share of imperfections and may exclude individuals who would otherwise identify as hospitalists. Regardless, such an exercise could identify trends in hospital medicine while providing a better understanding of the field as a whole.
HM does not have the traditional hallmark signifiers—board certification and Medicare specialty billing code—used by many specialties and subspecialties to frame their fields and to classify and compare physicians. The Medicare specialty billing code is a unique code applied to Medicare billing claims that tells Medicare exactly how the provider would like to be identified.
Because of its relative specificity and ready accessibility, the Centers for Medicare and Medicaid Services (CMS) uses the specialty billing code to create specialty comparison groups in pay-for-performance programs. Under the value-based payment modifier, hospitalists are compared against outpatient internal medicine or family medicine physicians, which makes them seem all the more expensive and less efficient.
SHM has been attuned to this particular issue since the early days of the physician value-based payment modifier. For nearly two years, SHM has repeatedly admonished CMS to compare hospitalists against other hospitalists in order for a pay-for-performance scheme to fairly and reasonably evaluate quality and efficiency. CMS acknowledged that many specialties and subspecialties may be masked within the current listing of Medicare specialty billing codes but yielded only so far as to say that aggrieved specialties can apply for their own code. SHM, for its part, applied for a specialty billing code for hospitalists in May 2014.
SHM has been actively exploring the data and looking at ways to identify hospitalists within this Medicare data. There’s an inherent value to this sort of self-reflection—it explains who we are and where we have been.
More importantly, it helps inform where we are going.
Joshua Lapps is SHM’s government relations manager.
Medicare Billing Practices More Transparent as CMS Cracks Down on Overchargers

The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
The U.S. Department of Health and Human Services (HHS) is putting forth stricter interventions and penalties aimed at curbing acts of careless billing by physicians it refers to as “recalcitrant providers.” Webster’s defines recalcitrant as “obstinately defiant of authority or restraint…difficult to manage or operate.” According to Medicare, these “recalcitrants” are providers who routinely and repeatedly overcharge for services billed through Medicare, despite proper training on how to bill appropriately for these services.1
Medicare has long battled the issue of finding and curbing overcharging and overpayment. CMS estimates that such defiance accounts for up to $6 billion a year in unnecessary Medicare costs, which makes up about 10% of all physician fee payments, given the fact that total Medicare Part B payments are about $65 billion a year.2
Medicare has systems in place to prevent, detect, and/or mitigate improper payments, whether they result from mistakes or from intentional fraud. In 2011, CMS’ Center for Program Integrity implemented sophisticated technology, called the Fraud Prevention System (FPS), which uses predictive analytics to detect provider irregularities warranting further inspection. According to their 2012 report, the FPS generated 536 new investigations, assisted in providing additional information for 511 active investigations, and initiated thousands of verification interviews of beneficiaries and providers to validate the legitimate receipt of services and items. The center estimates that in the first year of this program, FPS prevented about $115 million in payments.3
So what is Medicare’s response to providers who are identified as outliers? For overpayments from mistakes, CMS generally aims to recover the overpayments and educate the providers. Tactics range from educational letters and phone calls to on-site reviews and “prepayment medical reviews.” For fraud, on the other hand, Medicare (obviously) pursues more disciplinary sanctions, including criminal or civil penalties.
A New Paradigm
Now CMS is stepping up its expectations of provider accountability, adding heftier penalties for infractions, including higher financial penalties and even expulsion from Medicare, Medicaid, and other federal programs. In addition to these disciplinary actions, the agency plans to utilize recently changed laws to maximize public transparency around provider billing practices.
As of March 2014, Medicare will be able to publicly report all federal payments that have been paid out to individual providers. Although it has not yet disclosed how or when these will be reported, CMS now has the authority, for the first time since 1979, to display this information publicly. The history on this topic is that a federal district judge in Florida in 1979 prohibited the disclosure of individual payments to physicians, based on the contention that such disclosure would be an invasion of physician privacy. This longstanding mandate, which was reversed in May 2012, now allows Medicare to weigh the risks and benefits of individual requests for information on charges/payments by individual physicians. According to a New York Times article, Medicare is now being pressured by advocacy groups (insurers, employers, consumers) to release as much of the data as possible, to aid in data dissection and analysis and prompt early identification of abusive providers.4
Understandably, many physician advocacy groups, such as the American Medical Association, are concerned that such unfiltered access to this raw data may lead to inaccurate and unnecessary conclusions about physician practice and billing patterns.
The good news is that the federal government currently estimates that the recalcitrant provider list comprises a relatively small group of providers, roughly 300 or so. Some of these providers have received up to $3 million in Medicare payments a year. They estimate that, overall, about 2% of total Medicare licensed providers charged 25% of total payments, and that the total volume of these high-charging outliers increased by 78% between the years 2008 to 2011. A 2009 audit found that more than half of these recalcitrants were internists; other “high offenders” were ophthalmology and radiation oncology.
The list of these particular high-outlier offenders will be turned over to the Office of the Inspector General (OIG) at HHS to impose the appropriate degree of penalty. Then the federal government will determine an appropriate process of “screening” for providers that may meet the criteria for penalties and will start with those at the highest levels of cumulative payments. The OIG acknowledges that high payments do not necessarily imply fraud or abuse but believes it is reasonable to start there when analyzing and investigating potential areas of fraud or abuse.
Transparency Is Coming
So, while it is not exactly clear when or how the data will be released, what is clear is that the federal government has been granted the authority to dissect and release the data as it sees fit, opening up a new era of transparency in pricing, cost, charges, billing, and payments.
This change should affect all types of providers that bill Medicare part B, including hospitalists and other physicians, as well as nurse practitioners and physical therapists.5 While this is likely to cause some degree of discomfort and generate many questions from the public, hospitalists should be willing to embrace such transparency and engage in the dialogue needed to help the lay public understand the data. Most hospitalists work in practices that routinely share their data about billing, at least among the group, if not with a larger audience.
This is just one of many examples of how transparency can and should identify those providers considered “recalcitrant” in a number of realms, including patient satisfaction, quality, utilization, or cost. And, similar to other publicly reported “metrics,” release of this data will likely generate more questions than answers in the short run. In the long run, we should all be prepared for the release of data that is coming, one that will usher us into a whole new era of transparency.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. CMS Manual System. Pub 100-08 Medicare program integrity. December 13, 2013. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R495PI.pdf. Accessed April 6, 2014.
- Levinson DR. Department of Health and Human Services. Office of Inspector General. Reviews of clinicians associated with high cumulative payments could improve Medicare program integrity efforts. December 2013. Available at: http://oig.hhs.gov/oas/reports/region1/11100511.pdf. Accessed April 6, 2014.
- Department of Health and Human Services. Centers for Medicare and Medicaid Services. Report to Congress: fraud prevention system—first implementation year, 2012. Available at: http://www.stopmedicarefraud.gov/fraud-rtc12142012.pdf. Accessed April 6, 2014.
- Pear R. Doctors abusing Medicare face fines and expulsion. January 25, 2014. The New York Times website. Available at: http://www.nytimes.com/2014/01/26/us/doctors-abusing-medicare-to-face-fines.html. Accessed April 6, 2014.
- Steinbrook R. Public disclosure of Medicare payments to individual physicians. The Journal of the American Medical Association website. April 2, 2014. Available at: http://jama.jamanetwork.com/article.aspx?articleID=1832217&utm_source=Silverchair%20Information%20Systems&utm_medium=email&utm_campaign=JAMA%3AOnlineFirst02%2F17%2F2014. Accessed April 6,
2014.
Medicare Rule Change Raises Stakes for Hospital Discharge Planning

When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.

Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.
Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
When she presents information to hospitalists about the little-known revision to Medicare’s condition of participation for discharge planning by hospitals, most hospitalists have no idea what Amy Boutwell, MD, MPP, is talking about. Even hospitalists who are active in their institutions’ efforts to improve transitions of care out of the hospital setting are unaware of the change, which was published in the Centers for Medicare & Medicaid Services’ Transmittal 87 and became effective July 19, 2013.
“I just don’t hear hospital professionals talking about it,” says Dr. Boutwell, a hospitalist at Newton-Wellesley Hospital and president of Collaborative Healthcare Strategies in Lexington, Mass. “When I say, ‘There are new rules of the road for discharge planning and evaluation,’ many are not aware of it.”
The revised condition states that the hospital must have a discharge planning process that applies to all patients—not just Medicare beneficiaries. Not every patient needs to have a written discharge plan—although this is recommended—but all patients should be screened and, if indicated, evaluated at an early stage of their hospitalization for risk of adverse post-discharge outcomes. Observation patients are not included in this requirement.
The discharge plan is different from a discharge summary document, which must be completed by the inpatient attending physician, not the hospital, and is not directly addressed in the regulation. The regulation does address the need for transfer of essential information to the next provider of care and says the hospital should have a written policy and procedure in place for discharge planning. The policy and procedure should be developed with input from medical staff and approved by the hospital’s governing body.
Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation.
—Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST
Transmittal 87 represents the first major update of the discharge planning regulation (Standard 482.43) and accompanying interpretive guidelines in more than a decade, Dr. Boutwell says. It consolidates and reorganizes 24 “tags” of regulatory language down to 13 and contains blue advisory boxes recommending best practices in discharge planning, drawn from the suggestions of a technical expert panel convened by CMS.
That panel included many of the country’s recognized thought leaders on improving care transitions, such as Mark Williams, MD, FACP, SFHM, principal investigator of SHM’s Project BOOST; Eric Coleman, MD, MPH, head of the University of Colorado’s division of health care policy and research and creator of the widely-adopted Care Transitions Program (caretransitions.org), and Dr. Boutwell, co-founder of the STAAR initiative (www.ihi.org/engage/Initiatives/completed/STAAR).
The new condition raises baseline expectations for discharge planning and elevates care transitions efforts from a quality improvement issue to the realm of regulatory compliance, Dr. Boutwell says.
“This goes way beyond case review,” she adds. “It represents an evolution from discharge planning case by case to a system for improving transitions of care [for the hospital]. I’m impressed.”
The recommendations are consistent with best practices promoted by Project BOOST, STAAR, Project RED [Re-Engineered Discharge], and other national quality initiatives for improving care transitions.
“Any hospitalist participating with a hospital QI team involved in Project BOOST is helping their hospital comply with this condition of participation,” Dr. Williams says.
In the Byzantine structure of federal regulations, Medicare’s conditions of participation are the regulations providers must meet in order to participate in the Medicare program and bill for their services. Condition-level citations, if not resolved, can cause hospitals to be decertified from Medicare. The accompanying interpretive guidelines, with survey protocols, are the playbook to help state auditors and providers know how to interpret and apply the language of the regulations. The suggestions and examples of best practices contained in the new condition are not required of hospitals but, if followed, could increase their likelihood of achieving better patient outcomes and staying in compliance with the regulations on surveys.
“If hospitals were to actually implement all of the CMS advisory practice recommendations contained in this 35-page document, they’d be in really good shape for effectively managing transitions of care,” says Teresa L. Hamblin, RN, MS, a CMS consultant with Joint Commission Resources. “The government has provided robust practice recommendations that are a model for what hospitals can do. I’d advise doing your best to implement these recommendations. Check your current processes using this detailed document for reference.”
Discharge planning starts at admission, Hamblin says. If the hospitalist assumes that responsibility, it becomes easier to leave a paper trail in the patient’s chart. Other important lessons for hospitalists include participation in a multidisciplinary approach to discharge planning (i.e., interdisciplinary rounding) and development of policies and procedures in this area.
“If the hospital has not elected to do a discharge plan on every patient, request this for your own patients and recommend it as a policy,” Hamblin says. “Go the extra mile, making follow-up appointments for your patients, filling prescriptions in house, and calling the patient 24 to 72 hours after discharge.”
Weekend coverage, when case managers typically are not present, is a particular challenge in care transitions.
“Encourage your hospital to provide reliable weekend coverage for discharge planning. Involve the nurses,” Hamblin says. “Anything the hospitalist can do to help the hospital close this gap is important.”
Larry Beresford is a freelance writer in Alameda, Calif.
SGR Reform, ICD-10 Implementation Delays Frustrate Hospitalists, Physicians
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”

The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Congress has once again delayed implementation of draconian Medicare cuts tied to the sustainable growth rate (SGR) formula. It was the 17th temporary patch applied to the ailing physician reimbursement program, so the decision caused little surprise.
But with the same legislation—the Protecting Access to Medicare Act of 2014—being used to delay the long-awaited debut of ICD-10, many hospitalists and physicians couldn’t help but wonder whether billing and coding would now be as much of a political football as the SGR fix.1
The upshot: It doesn’t seem that way.
“I think it’s two separate issues,” says Phyllis “PJ” Floyd, RN, BSN, MBA, NE-BC, CCA, director of health information services and clinical documentation improvement at Medical University of South Carolina (MUSC) in Charleston, S.C. “The fact that it was all in one bill, I don’t know that it was well thought out as much as it was, ‘Let’s put the ICD-10 in here at the same time.’
“It was just a few sentences, and then it wasn’t even brought up in the discussion on the floor.”
Four policy wonks interviewed by The Hospitalist concurred that while tying the ICD-10 delay to the SGR issue was an unexpected and frustrating development, the coding system likely will be implemented in the relative short term. Meanwhile, a long-term resolution of the SGR dilemma remains much more elusive.
“For about 12 hours, I felt relief about the ICD-10 [being delayed], and then I just realized, it’s still coming, presumably,” says John Nelson, MD, MHM, a co-founder and past president of SHM and medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash. “[It’s] like a patient who needs surgery and finds out it’s canceled for the day and he’ll have it tomorrow. Well, that’s good for right now, but [he] still has to face this eventually.”
“Doc-Pay” Fix Near?
Congress’ recent decision to delay both an SGR fix and the ICD-10 are troubling to some hospitalists and others for different reasons.
The SGR extension through this year’s end means that physicians do not face a 24% cut to physician payments under Medicare. SHM has long lobbied against temporary patches to the SGR, repeatedly backing legislation that would once and for all scrap the formula and replace it with something sustainable.
The SGR formula was first crafted in 1997, but the now often-delayed cuts were a byproduct of the federal sequester that was included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. The cuts were implemented as a doomsday scenario that was never likely to actually happen, but despite negotiations over the past three years, no long-term compromise can be found. Paying for the reform remains the main stumbling block.
“I think, this year, Congress was as close as it’s been in a long time to enacting a serious fix, aided by the agreement of major professional societies like the American College of Physicians and American College of Surgeons,” says David Howard, PhD, an associate professor in the department of health policy and management at the Rollins School of Public Health at Emory University in Atlanta. “They were all on board with this solution. ... Who knows, maybe if the economic situation continues to improve [and] tax revenues continue to go up...that will create a more favorable environment for compromise.”
Dr. Howard adds that while Congress might be close to a solution in theory, agreement on how to offset the roughly $100 billion in costs “is just very difficult.” That is why the healthcare professor is pessimistic that a long-term fix is truly at hand.
“The places where Congress might have looked for savings to offset the cost of the doc fix, such as hospital reimbursement rates or payment rates to Medicare Advantage plans—those are exactly the areas that the Affordable Care Act is targeting to pay for insurance expansion,” Dr. Howard adds. “So those areas of savings are not going to be available to offset the cost of the doc fix.”
ICD-10 Delays “Unfair”
The medical coding conundrum presents a different set of issues. The delay in transitioning healthcare providers from the ICD-9 medical coding classification system to the more complicated ICD-10 means the upgraded system is now against an Oct. 1, 2015, deadline. This comes after the Centers for Medicare & Medicaid Services (CMS) already pushed back the original implementation date for ICD-10 by one year.
SHM Public Policy Committee member Joshua Lenchus, DO, RPh, FACP, SFHM, says he thinks most doctors are content with the delay, particularly in light of some estimates that show that only about 20% of physicians “have actually initiated the ICD-10 transition.” But he also notes that it’s unfair to the health systems that have prepared for ICD-10.
“ICD-9 has a little more than 14,000 diagnostic codes and nearly 4,000 procedural codes. That is to be contrasted to ICD-10, which has more than 68,000 diagnostic codes ... and over 72,000 procedural codes,” Dr. Lenchus says. “So, it is not surprising that many take solace in the delay.”
–Dr. Lenchus
Dr. Nelson says the level of frustration for hospitalists is growing; however, the level of disruption for hospitals and health systems is reaching a boiling point.
“Of course, in some places, hospitalists may be the physician lead on ICD-10 efforts, so [they are] very much wrapped up in the problem of ‘What do we do now?’”
The answer, at least to the Coalition for ICD-10, a group of medical/technology trade groups, is to fight to ensure that the delays go no further. In an April letter to CMS Administrator Marilyn Tavenner, the coalition made that case, noting that in 2012, “CMS estimated the cost to the healthcare industry of a one-year delay to be as much as $6.6 billion, or approximately 30% of the $22 billion that CMS estimated had been invested or budgeted for ICD-10 implementation.”2
The letter went on to explain that the disruption and cost will grow each time the ICD-10 deadline is pushed.
“Furthermore, as CMS stated in 2012, implementation costs will continue to increase considerably with every year of a delay,” according to the letter. “The lost opportunity costs of failing to move to a more effective code set also continue to climb every year.”
Stay Engaged, Switch Gears
One of Floyd’s biggest concerns is that the ICD-10 implementation delays will affect physician engagement. The hospitalist groups at MUSC began training for ICD-10 in January 2013; however, the preparation and training were geared toward a 2014 implementation.
“You have to switch gears a little bit,” she says. “What we plan to do now is begin to do heavy auditing, and then from those audits we can give real-time feedback on what we’re doing well and what we’re not doing well. So I think that will be a method for engagement.”
She urges hospitalists, practice leaders, and informatics professionals to discuss ICD-10 not as a theoretical application, but as one tied to reimbursement that will have major impact in the years ahead. To that end, the American Health Information Management Association highlights the fact that the new coding system will result in higher-quality data that can improve performance measures, provide “increased sensitivity” to reimbursement methodologies, and help with stronger public health surveillance.3
“A lot of physicians see this as a hospital issue, and I think that’s why they shy away,” Floyd says. “Now there are some physicians who are interested in how well the hospital does, but the other piece is that it does affect things like [reduced] risk of mortality [and] comparison of data worldwide—those are things that we just have to continue to reiterate … and give them real examples.”
Richard Quinn is a freelance writer in New Jersey.
References
- Govtrack. H.R. 4302: Protecting Access to Medicare Act of 2014. https://www.govtrack.us/congress/bills/113/hr4302. Accessed June 5, 2014.
- Coalition for ICD. Letter to CMS Administrator Tavenner, April 11, 2014. http://coalitionforicd10.wordpress.com/2014/03/26/letter-from-the-coalition-for-icd-10. Accessed June 5, 2014.
- American Health Information Management Association. ICD-10-CM/PCS Transition: Planning and Preparation Checklist. http://journal.ahima.org/wp-content/uploads/ICD10-checklist.pdf. Accessed June 5, 2014.
Bill to Clarify Three-Midnight Rule for Medicare Patients Gains Support from Congress, Hospitalists
In 2010, my office received a call from a Norwich, Conn., family whose 89-year-old father had fallen and broken his hip. After he was treated in the local hospital for four days, his doctor prescribed follow-on skilled nursing facility (SNF) care. Upon his arrival at the nursing home, his family was informed that they would have to pay more than $10,000 up front to cover the cost of his care: Because he had never been admitted to the hospital as an inpatient, Medicare would not cover the prescribed rehabilitative care that he needed to return home safely.
I know that hospitalists are already far too familiar with stories like this. Together, we can work to make sure it doesn’t happen again.
Support Is Growing
For me, that family’s story was a call for action. Shortly after speaking with the family, I introduced the Improving Access to Medicare Coverage Act (H.R. 1179). The bill is simple: It would restore the three-day hospital stay standard for SNF coverage, whether the stay is coded as inpatient under Part A or outpatient observation under Part B. Two Congresses later, support for the proposal is growing. In the 113th Congress, the bill has 137 bipartisan cosponsors, an indication of how widespread this problem is for Medicare beneficiaries.
The outdated Medicare law on skilled nursing care coverage is creating financial and healthcare dilemmas for families across the country. Under current law, beneficiaries must have a hospital inpatient stay of at least three days in order to qualify for Medicare coverage SNF benefits; however, more and more patients are being coded under observation status, and access to post-acute SNF care is diminishing. Patients are suffering, and healthcare providers are caught in the middle.
In fact, the Office of the Inspector General at the Department of Health and Human Services released a report last fall that showed that Medicare beneficiaries in 2012 had more than 600,000 hospital stays that lasted three nights, yet none were admitted as inpatients. Even though these beneficiaries likely received the same care inpatients received, their observation status designation disqualified them from Medicare coverage of the SNF benefit. For their families, prescribed follow-on SNF care would have an out-of-pocket cost averaging more than $10,000. For seniors on fixed incomes, that is a devastating financial penalty for a service that should be covered by their health plans.

—Rep. Joe Courtney
Administrative Oversight
There are many reasons for the growth in observation status treatments, but a primary driver is increasing scrutiny of admitting practices by recovery audit contractors (RACs). The consequences of RAC review processes have created difficult situations for hospitals, because admitting decisions are reviewable for three years, and hospitals can be hit with claw-back penalties for payments on behalf of patients RACs determine were incorrectly admitted. To prevent costly penalties and protracted appeals of individual cases, many hospitals feel an understandable amount of pressure to err on the side of treating patients under outpatient observation status covered under Part B.
The original intent of the three-day inpatient stay requirement was to serve as a tangible measure of medical necessity of SNF care. And, when the three-day inpatient stay prerequisite was written into law, long-term hospital observation stays were nonexistent. This intent has been lost in a changing system of hospital oversight under RACs and admitting practices.
The impact on patients and families is tragic.
Ann Sheehy, MD, MS, FHM, a hospitalist speaking on behalf of the Society of Hospital Medicine on a recent conference call I hosted, detailed the scenes she sees every day with her own patients. She described how doctors, knowing that a patient lacks the means to pay for rehabilitative care out of pocket and the support system to recover safely at home, sometimes keep the patient in the hospital longer, at a higher cost to Medicare. In other cases, Dr. Sheehy noted that patients end up back in the hospital soon after being discharged, having foregone expensive SNF care and subsequently suffered preventable injuries and illnesses. Both of these outcomes are bad for patients—and bad for Medicare expenditures.
Three-Day Fix
While the problem of observation status treatment is complex, the solution is simple.
As observation status becomes more ingrained in the healthcare lexicon, a legislative fix to restore the three-day hospital stay standard is needed now more than ever. Three days in the hospital—whether as an inpatient or under outpatient observation—should count for three days in the hospital when Medicare determines eligibility for SNF coverage.
My bill, H.R. 1179, is the most direct solution to rectify the flaw that leaves hundreds of thousands of beneficiaries wondering how their stay in the hospital does not “count” and scrambling to figure out how to pay for care—or foregoing it entirely. The strong support in the advocacy community for this legislation—especially from SHM—and the sway of outside groups cannot be overstated. In Washington’s current climate, the only thing that moves bipartisan issues forward is outside pressure.
Together, I hope hospitalists and members of Congress will reach the critical mass needed to pass this legislation and ensure that Medicare beneficiaries are covered for medically necessary care.
Joseph “Joe” Courtney is the U.S. Representative for Connecticut’s second congressional district, serving since 2007. The district includes most of the eastern third of the state, including Norwich and New London.
In 2010, my office received a call from a Norwich, Conn., family whose 89-year-old father had fallen and broken his hip. After he was treated in the local hospital for four days, his doctor prescribed follow-on skilled nursing facility (SNF) care. Upon his arrival at the nursing home, his family was informed that they would have to pay more than $10,000 up front to cover the cost of his care: Because he had never been admitted to the hospital as an inpatient, Medicare would not cover the prescribed rehabilitative care that he needed to return home safely.
I know that hospitalists are already far too familiar with stories like this. Together, we can work to make sure it doesn’t happen again.
Support Is Growing
For me, that family’s story was a call for action. Shortly after speaking with the family, I introduced the Improving Access to Medicare Coverage Act (H.R. 1179). The bill is simple: It would restore the three-day hospital stay standard for SNF coverage, whether the stay is coded as inpatient under Part A or outpatient observation under Part B. Two Congresses later, support for the proposal is growing. In the 113th Congress, the bill has 137 bipartisan cosponsors, an indication of how widespread this problem is for Medicare beneficiaries.
The outdated Medicare law on skilled nursing care coverage is creating financial and healthcare dilemmas for families across the country. Under current law, beneficiaries must have a hospital inpatient stay of at least three days in order to qualify for Medicare coverage SNF benefits; however, more and more patients are being coded under observation status, and access to post-acute SNF care is diminishing. Patients are suffering, and healthcare providers are caught in the middle.
In fact, the Office of the Inspector General at the Department of Health and Human Services released a report last fall that showed that Medicare beneficiaries in 2012 had more than 600,000 hospital stays that lasted three nights, yet none were admitted as inpatients. Even though these beneficiaries likely received the same care inpatients received, their observation status designation disqualified them from Medicare coverage of the SNF benefit. For their families, prescribed follow-on SNF care would have an out-of-pocket cost averaging more than $10,000. For seniors on fixed incomes, that is a devastating financial penalty for a service that should be covered by their health plans.
—Rep. Joe Courtney
Administrative Oversight
There are many reasons for the growth in observation status treatments, but a primary driver is increasing scrutiny of admitting practices by recovery audit contractors (RACs). The consequences of RAC review processes have created difficult situations for hospitals, because admitting decisions are reviewable for three years, and hospitals can be hit with claw-back penalties for payments on behalf of patients RACs determine were incorrectly admitted. To prevent costly penalties and protracted appeals of individual cases, many hospitals feel an understandable amount of pressure to err on the side of treating patients under outpatient observation status covered under Part B.
The original intent of the three-day inpatient stay requirement was to serve as a tangible measure of medical necessity of SNF care. And, when the three-day inpatient stay prerequisite was written into law, long-term hospital observation stays were nonexistent. This intent has been lost in a changing system of hospital oversight under RACs and admitting practices.
The impact on patients and families is tragic.
Ann Sheehy, MD, MS, FHM, a hospitalist speaking on behalf of the Society of Hospital Medicine on a recent conference call I hosted, detailed the scenes she sees every day with her own patients. She described how doctors, knowing that a patient lacks the means to pay for rehabilitative care out of pocket and the support system to recover safely at home, sometimes keep the patient in the hospital longer, at a higher cost to Medicare. In other cases, Dr. Sheehy noted that patients end up back in the hospital soon after being discharged, having foregone expensive SNF care and subsequently suffered preventable injuries and illnesses. Both of these outcomes are bad for patients—and bad for Medicare expenditures.
Three-Day Fix
While the problem of observation status treatment is complex, the solution is simple.
As observation status becomes more ingrained in the healthcare lexicon, a legislative fix to restore the three-day hospital stay standard is needed now more than ever. Three days in the hospital—whether as an inpatient or under outpatient observation—should count for three days in the hospital when Medicare determines eligibility for SNF coverage.
My bill, H.R. 1179, is the most direct solution to rectify the flaw that leaves hundreds of thousands of beneficiaries wondering how their stay in the hospital does not “count” and scrambling to figure out how to pay for care—or foregoing it entirely. The strong support in the advocacy community for this legislation—especially from SHM—and the sway of outside groups cannot be overstated. In Washington’s current climate, the only thing that moves bipartisan issues forward is outside pressure.
Together, I hope hospitalists and members of Congress will reach the critical mass needed to pass this legislation and ensure that Medicare beneficiaries are covered for medically necessary care.
Joseph “Joe” Courtney is the U.S. Representative for Connecticut’s second congressional district, serving since 2007. The district includes most of the eastern third of the state, including Norwich and New London.
In 2010, my office received a call from a Norwich, Conn., family whose 89-year-old father had fallen and broken his hip. After he was treated in the local hospital for four days, his doctor prescribed follow-on skilled nursing facility (SNF) care. Upon his arrival at the nursing home, his family was informed that they would have to pay more than $10,000 up front to cover the cost of his care: Because he had never been admitted to the hospital as an inpatient, Medicare would not cover the prescribed rehabilitative care that he needed to return home safely.
I know that hospitalists are already far too familiar with stories like this. Together, we can work to make sure it doesn’t happen again.
Support Is Growing
For me, that family’s story was a call for action. Shortly after speaking with the family, I introduced the Improving Access to Medicare Coverage Act (H.R. 1179). The bill is simple: It would restore the three-day hospital stay standard for SNF coverage, whether the stay is coded as inpatient under Part A or outpatient observation under Part B. Two Congresses later, support for the proposal is growing. In the 113th Congress, the bill has 137 bipartisan cosponsors, an indication of how widespread this problem is for Medicare beneficiaries.
The outdated Medicare law on skilled nursing care coverage is creating financial and healthcare dilemmas for families across the country. Under current law, beneficiaries must have a hospital inpatient stay of at least three days in order to qualify for Medicare coverage SNF benefits; however, more and more patients are being coded under observation status, and access to post-acute SNF care is diminishing. Patients are suffering, and healthcare providers are caught in the middle.
In fact, the Office of the Inspector General at the Department of Health and Human Services released a report last fall that showed that Medicare beneficiaries in 2012 had more than 600,000 hospital stays that lasted three nights, yet none were admitted as inpatients. Even though these beneficiaries likely received the same care inpatients received, their observation status designation disqualified them from Medicare coverage of the SNF benefit. For their families, prescribed follow-on SNF care would have an out-of-pocket cost averaging more than $10,000. For seniors on fixed incomes, that is a devastating financial penalty for a service that should be covered by their health plans.
—Rep. Joe Courtney
Administrative Oversight
There are many reasons for the growth in observation status treatments, but a primary driver is increasing scrutiny of admitting practices by recovery audit contractors (RACs). The consequences of RAC review processes have created difficult situations for hospitals, because admitting decisions are reviewable for three years, and hospitals can be hit with claw-back penalties for payments on behalf of patients RACs determine were incorrectly admitted. To prevent costly penalties and protracted appeals of individual cases, many hospitals feel an understandable amount of pressure to err on the side of treating patients under outpatient observation status covered under Part B.
The original intent of the three-day inpatient stay requirement was to serve as a tangible measure of medical necessity of SNF care. And, when the three-day inpatient stay prerequisite was written into law, long-term hospital observation stays were nonexistent. This intent has been lost in a changing system of hospital oversight under RACs and admitting practices.
The impact on patients and families is tragic.
Ann Sheehy, MD, MS, FHM, a hospitalist speaking on behalf of the Society of Hospital Medicine on a recent conference call I hosted, detailed the scenes she sees every day with her own patients. She described how doctors, knowing that a patient lacks the means to pay for rehabilitative care out of pocket and the support system to recover safely at home, sometimes keep the patient in the hospital longer, at a higher cost to Medicare. In other cases, Dr. Sheehy noted that patients end up back in the hospital soon after being discharged, having foregone expensive SNF care and subsequently suffered preventable injuries and illnesses. Both of these outcomes are bad for patients—and bad for Medicare expenditures.
Three-Day Fix
While the problem of observation status treatment is complex, the solution is simple.
As observation status becomes more ingrained in the healthcare lexicon, a legislative fix to restore the three-day hospital stay standard is needed now more than ever. Three days in the hospital—whether as an inpatient or under outpatient observation—should count for three days in the hospital when Medicare determines eligibility for SNF coverage.
My bill, H.R. 1179, is the most direct solution to rectify the flaw that leaves hundreds of thousands of beneficiaries wondering how their stay in the hospital does not “count” and scrambling to figure out how to pay for care—or foregoing it entirely. The strong support in the advocacy community for this legislation—especially from SHM—and the sway of outside groups cannot be overstated. In Washington’s current climate, the only thing that moves bipartisan issues forward is outside pressure.
Together, I hope hospitalists and members of Congress will reach the critical mass needed to pass this legislation and ensure that Medicare beneficiaries are covered for medically necessary care.
Joseph “Joe” Courtney is the U.S. Representative for Connecticut’s second congressional district, serving since 2007. The district includes most of the eastern third of the state, including Norwich and New London.
Delays, Controversy Muddle CMS’ Two-Midnight Rule for Hospital Patient Admissions
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.

–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.
–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.
–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
How Will New Physician Value-Based Payment Modifier Affect Medicare Reimbursements?

We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
We talk a lot about value in healthcare—about how to enhance quality and reduce cost—because we all know both need an incredible amount of work. One tactic Medicare is using to improve the value equation on a large scale is aggregating and displaying physician-specific “value” metrics. These metrics, which will be used to deduct or enhance reimbursement for physicians, are known as the Physician Value-Based Payment Modifier (PVBM).
This program has been enacted fairly rapidly since the passage of the Affordable Care Act; it is being rolled out first to large physician practices, then to all groups by 2017. Those with superior performance in both quality and cost will experience as much as a 2% higher reimbursement, while groups with average performance will remain financially neutral and those who show lower performance or choose not to report will be penalized up to 1% of Medicare reimbursement. This first round, for larger groups of 100-plus physicians, will affect about 30% of all U.S. physicians. The second round, for groups of 10 or more physicians, will affect about another third of physicians. The last round, for groups with fewer than 10 physicians, will be applicable to the remaining physicians practicing in the U.S.
On the face of it, the program does seem to be a potentially effective tactic for improving value on a large scale, holding individual physicians accountable for their own individual patient-care performance. A few fatal flaws in the program as it currently stands make it extraordinarily unlikely to be universally adopted by all physicians, however. Here are a few of those flaws:1,2
1 Uncertain yield: Because it is essentially a “zero-sum game” for Medicare, the incentive or penalty for a physician (or the physician’s group) depends on the performance of all the other physicians’ or groups’ performance. As a result, there is incredible uncertainty as to how strong a physician’s performance actually needs to be, year to year, to result in a bonus payment. Given that many of the metrics will require some type of investment to perform well, such as information technology infrastructure or a quality coordinator, there is an equal amount of uncertainty about how much investment will be needed to get a certain budgetary yield. For smaller physician practices, taking a 1% to 2% reduction in Medicare reimbursements may be easier to weather financially than investing in the infrastructure needed to reliably hit the quality metrics for every relevant patient.
2 Uncertain benchmarks: Unlike many hospital quality metrics, which have been publicly displayed for years, physician-level value metrics are just now being reported publicly. This leaves uncertainty about how strong a physician’s performance needs to be in order to be better than average. In the hospital value-based purchasing program, “average” performance is extremely good, in the 98% to 99% compliance range for most metrics. It is less clear what compliance range will be “average” in the physician-based program.
3 Physician variability: More than a half million physicians in the U.S. bill Medicare, and their practice types range from primary care solo practice to multi-group specialty practice. Motivating all brands to understand, measure, report, and improve quality metrics is a yeoman’s task, unlikely to be successful in the short term. Most physicians have not received any formal education or training in quality improvement, so they may not even have the skill set required to improve their metrics into a highly reliable range, worthy of bonus designation.
4 Metric identity and attribution: Because the repertoire of physician types is broad, the ability of each physician type to have a set of metrics that they understand and can identify with is extremely unlikely. In addition, attribution of patients and their associated metrics to any single physician is complicated, especially for patients who are cared for by many different physicians across a number of settings. For hospitalists, the attribution issue is a fatal flaw, as many groups routinely “hand off” patients among other hospitalists in their group, at least once if not several times during a typical hospital stay. The same is true of many other hospital-based specialty physicians.
5 Playing to the test: As with other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to play to the test, so that their efforts to perform exceedingly well at a few metrics will crowd out and hinder their performance on unmeasured metrics. This tendency can result in lower-value care in the sum total, even if the metrics show stellar performance.
6 Reducing the risk: As seen in other pay-for-performance programs, there is a legitimate concern that physicians will be overwhelmingly motivated to avoid caring for patients who are likely to be unpredictable, including those with multiple co-morbid conditions or with complex social situations; these patients are likely to perform less well on any metric, despite risk adjusting (which is inherently imperfect). This is a well-known and documented risk of publicly reported programs, and there is no reason to believe the PVBM program will be immune to this risk.
In Sum
Because these flaws seem so daunting at first glance, many physicians and physician groups will be tempted to reject the program outright and take the financial hit induced by nonparticipation. An alternative approach is to embrace all of the value programs outright, investing time and energy in improving the metrics that are truly valuable to both patients and providers.
Regardless of which regulatory agency is demanding performance, we need to be active participants in foraging out what metrics and attribution logic are most appropriate. For hospitalists, these could include risk-adjusted device days, appropriate prescribing and unprescribing of antibiotics, judicious utilization of diagnostic testing, and measurements of patient functional status and/or mobility.
Value metrics are here to stay, including those attributable to individual physicians; our job now is to advocate for meaningful metrics and meaningful attribution, which can and should motivate hospitalists to enhance their patients’ quality of life at a lower cost.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
References
Shift from Productivity to Value-Based Compensation Gains Momentum
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
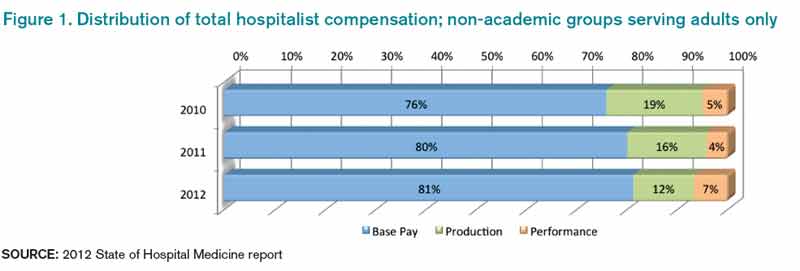
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.

At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
At the 2011 SHM annual meeting in Dallas, I served on an expert panel that reviewed the latest hospitalist survey data. Included in this review were the latest compensation and productivity figures. As the session concluded, I was satisfied that the panel had discussed important information in an accessible way; however, the keynote speaker who followed us to address an entirely different topic began his talk by pointing out that the data we had reviewed, including things like wRVUs, would very soon have little to do with compensation for any physician, regardless of specialty. He implied, quite persuasively, that we were pretty old school to be talking about wRVUs and compensation based on productivity; everyone should be prepared for and embrace compensation based on value, not production.
I hear a similar sentiment reasonably often. And I agree, but I think many make the mistake of oversimplifying the issue.
Physician Value-Based Payment
Measurement of physician performance using costs, quality, and outcomes has already begun and will influence Medicare payments to doctors beginning in 2015 for large groups (>100 providers with any mix of specialties billing under the same tax ID number) and in 2017 for smaller groups.
If Medicare is moving away from payment based on wRVUs, likely followed soon by other payors, then hospitalist compensation should do the same. But I don’t think that changes the potential role of compensation based on productivity.
Compensation Should Include Performance and Productivity Metrics
Survey data show a move from an essentially fixed annual compensation early in our field to an inclusion of components tied to performance several years before the introduction of the Physician Value-Based Payment Modifier program. Data from SHM’s 2010, 2011, and 2012 State of Hospital Medicine reports (www.hospitalmedicine.org/survey) show that a small, but probably increasing, part of compensation has been tied to performance on things like patient satisfaction and core measures (see “Distribution of Total Hospitalist Compensation,” below). Note that the percentages in the chart refer to the fraction of total compensation dollars allocated to each domain and not the portion of hospitalists who have compensation tied to each domain.
Over the same three years, the percentage of compensation tied to productivity has been decreasing overall, while “private groups are more likely to pay a higher proportion of compensation based on productivity, and hospital-employed groups are more likely to pay a higher proportion of compensation based on performance.”
Matching Performance Compensation to Medicare’s Value-Based Modifier
It makes sense for physician compensation to generally mirror Medicare and other payor professional fee reimbursement formulas. But, in that regard, hospitalists are ahead of the market already, because the portion of dollars allocated to performance (value) in hospitalist compensation plans already exceeds the 2% or less portion of Medicare reimbursement that is influenced by performance.
Medicare will steadily increase the portion of reimbursement allocated to performance (value) and decrease the part tied solely to wRVUs. So it makes sense that hospitalist compensation plans should do the same. Who knows, within the next 5-10 years, hospitalists, and potentially doctors in all specialties, might see 20% to 50% of their compensation tied to performance. I think that might be a good thing, as long as we can come up with effective measures of performance and value—not an easy thing to do in any business or industry.
Future Role of Productivity Compensation
I don’t think all the talk about value-based reimbursement means we should abandon the idea of connecting a portion of compensation to productivity. The first two practice management columns I wrote for The Hospitalist appeared in May 2006 (www.the-hospitalist.org/details/article/252413/The_Sweet_Spot.html) and June 2006 (www.the-hospitalist.org/details/article/246297.html) and recommended tying a meaningful portion of compensation to individual hospitalist productivity, and I think it still makes sense to do so.
Source: 2012 State of Hospital Medicine report
In any business or industry, financial performance is connected to the amount of product produced and its value. In the future, both metrics will determine reimbursement for even the highest performing healthcare providers. The new emphasis on value won’t ever make it unnecessary to produce at a reasonable level.
Unquestionably, there are many high-performing hospitalist practices with little or no productivity component in the compensation formula. So it isn’t an absolute sine qua non for success. But I think many practices dismiss it as a viable option when it might solve problems and liberate individuals in the group to exercise some autonomy in finding their own sweet spot between workload and compensation.
It will be interesting to see if future surveys show that the portion of dollars tied to hospitalist productivity continues to decrease, despite what I see as its potential benefits.
How Many Americans Will Remain Uninsured?
The question of whether health insurance equals healthcare access is complicated in the roughly two dozen states that have chosen not to expand Medicaid—an option granted by the U.S. Supreme Court in its June 2012 decision that upheld the law’s main tenets. Even with the federal government paying the full cost for the first three years (decreasing to 90% by 2020), some states have argued that the economic burden will be too great.
According to a recent analysis by the Kaiser Family Foundation, roughly five million uninsured adults may now fall into a “coverage gap” as a result. In essence, they will earn too much to be covered under the highly variable Medicaid caps established by individual states but too little to receive any federal tax credits to help pay for insurance in the exchanges. With limited options, the report suggests, they are likely to remain uninsured.
Safety net hospitals also may be squeezed between conflicting state and federal Medicaid priorities. During the initial Affordable Care Act (ACA) negotiations, hospitals agreed to $155 billion in cuts over 10 years, including sharp reductions in Disproportionate Share Hospital (DSH) payments, in anticipation of seeing a significant decrease in uninsured patients. Despite lower DSH payments, the hospitals expected to recoup the money through more Medicaid or private insurance reimbursements.
"The Medicaid expansion being optional throws a kink in all of that,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.
The ongoing open enrollment in insurance exchanges will make up part of the total. But in states that are not expanding Medicaid, the number of newly insured patients may not compensate for the DSH reductions. Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, says the resulting net loss could put some hospitals under additional financial strain.
"There will be pressure within the states from hospitals and from the business community to expand Medicaid because, otherwise, they’re bearing the burden of it,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
The question of whether health insurance equals healthcare access is complicated in the roughly two dozen states that have chosen not to expand Medicaid—an option granted by the U.S. Supreme Court in its June 2012 decision that upheld the law’s main tenets. Even with the federal government paying the full cost for the first three years (decreasing to 90% by 2020), some states have argued that the economic burden will be too great.
According to a recent analysis by the Kaiser Family Foundation, roughly five million uninsured adults may now fall into a “coverage gap” as a result. In essence, they will earn too much to be covered under the highly variable Medicaid caps established by individual states but too little to receive any federal tax credits to help pay for insurance in the exchanges. With limited options, the report suggests, they are likely to remain uninsured.
Safety net hospitals also may be squeezed between conflicting state and federal Medicaid priorities. During the initial Affordable Care Act (ACA) negotiations, hospitals agreed to $155 billion in cuts over 10 years, including sharp reductions in Disproportionate Share Hospital (DSH) payments, in anticipation of seeing a significant decrease in uninsured patients. Despite lower DSH payments, the hospitals expected to recoup the money through more Medicaid or private insurance reimbursements.
"The Medicaid expansion being optional throws a kink in all of that,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.
The ongoing open enrollment in insurance exchanges will make up part of the total. But in states that are not expanding Medicaid, the number of newly insured patients may not compensate for the DSH reductions. Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, says the resulting net loss could put some hospitals under additional financial strain.
"There will be pressure within the states from hospitals and from the business community to expand Medicaid because, otherwise, they’re bearing the burden of it,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
The question of whether health insurance equals healthcare access is complicated in the roughly two dozen states that have chosen not to expand Medicaid—an option granted by the U.S. Supreme Court in its June 2012 decision that upheld the law’s main tenets. Even with the federal government paying the full cost for the first three years (decreasing to 90% by 2020), some states have argued that the economic burden will be too great.
According to a recent analysis by the Kaiser Family Foundation, roughly five million uninsured adults may now fall into a “coverage gap” as a result. In essence, they will earn too much to be covered under the highly variable Medicaid caps established by individual states but too little to receive any federal tax credits to help pay for insurance in the exchanges. With limited options, the report suggests, they are likely to remain uninsured.
Safety net hospitals also may be squeezed between conflicting state and federal Medicaid priorities. During the initial Affordable Care Act (ACA) negotiations, hospitals agreed to $155 billion in cuts over 10 years, including sharp reductions in Disproportionate Share Hospital (DSH) payments, in anticipation of seeing a significant decrease in uninsured patients. Despite lower DSH payments, the hospitals expected to recoup the money through more Medicaid or private insurance reimbursements.
"The Medicaid expansion being optional throws a kink in all of that,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.
The ongoing open enrollment in insurance exchanges will make up part of the total. But in states that are not expanding Medicaid, the number of newly insured patients may not compensate for the DSH reductions. Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, says the resulting net loss could put some hospitals under additional financial strain.
"There will be pressure within the states from hospitals and from the business community to expand Medicaid because, otherwise, they’re bearing the burden of it,” he says.
Bryn Nelson is a freelance medical writer in Seattle.
Hospitalist Joshua Lenchus, DO, RPh, SFHM, Says Obamacare Might Impact Patient Access, Physician Workload
Click here to listen to more of our interview with Dr. Lenchus
Click here to listen to more of our interview with Dr. Lenchus
Click here to listen to more of our interview with Dr. Lenchus