User login
Hospitalist Rick Hilger, MD, SFHM, Discusses How the ACA Might Accelerate the Drive Toward ACO-style of Care
Click here to listen to more of our interview with Dr. Hilger
Click here to listen to more of our interview with Dr. Hilger
Click here to listen to more of our interview with Dr. Hilger
SHM Helps Hospitals Comply With Two-Midnight Rule for Patient Admissions

As many hospitalists are probably acutely aware, the Centers for Medicare & Medicaid Services (CMS) is putting a new rule into effect that will greatly impact how inpatient admission decisions are made. The rule, known as the “two-midnight rule,” states that if the admitting practitioner admits a Medicare beneficiary as an inpatient with the reasonable expectation that the beneficiary will require care that “crosses two midnights” and this decision is justified in the medical record, Medicare Part A payment is “generally appropriate.”
While there are multiple caveats, exceptions, and details, this rule can be simply articulated: If the admitting physician feels a patient will be in the hospital for a period longer than two midnights and the medical record supports this determination, the patient is an inpatient. Stays expected to be shorter than two midnights should be under observation status.
This new policy is an attempt to respond both to hospital calls for more guidance about when a beneficiary is appropriately treated as an inpatient—and paid by Medicare—and concerns about increasingly long hospital stays under observation status. Most hospitalists wrestle with status determination issues on a daily basis.
SHM is aware of the struggle and has been advocating on behalf of hospitalists to help shape observation status and the two-midnight rule. When the rule was first proposed, SHM voiced serious concerns about its utility and how it was unlikely to solve the overall confusion surrounding inpatient status determinations. Nevertheless, CMS finalized the rule as an attempt to begin addressing the problem.
Faced with an increasingly loud chorus of providers and hospitals concerned about the implementation of the new policy, CMS agreed to delay full enforcement from the original date of Oct. 1, 2013, until March 31, 2014.
During the delayed enforcement period, hospitals will be expected to begin implementing the two-midnight rule, and auditors will be giving hospitals non-punitive feedback on their application of the policy. To accomplish this, CMS is instructing Medicare Administrative Contractors (MACs) to review a sample of 10 to 25 inpatient hospital claims spanning less than two midnights after admission for each hospital. This probe sample will be used to assist hospitals with implementing the new requirements correctly. To give an additional level of comfort during this adjustment period, CMS has announced that it will not conduct post-payment patient status reviews for claims with dates of admission Oct. 1, 2013, through March 31, 2014.
Unfortunately, beyond the vague guidance CMS has offered thus far, there is no foolproof guide to establishing new hospital admissions policies that comply with the rule. As a result, there likely will be wide variation among hospitals.
To assist in sorting out the confusion, SHM will be hosting a webinar this month with case studies from several hospitals. The focus will be on the internal processes each hospital is using to implement the rule and how they were developed. Sharing and learning from national implementation experiences is a valuable way for hospitalists to gain new perspectives and to bring those experiences to their home institutions when considering their own roles in meeting the new admissions criteria head on.
For more information about the webinar and to register, visit www.hospitalmedicine.org today.
Josh Boswell is SHM’s senior manager of government relations.
As many hospitalists are probably acutely aware, the Centers for Medicare & Medicaid Services (CMS) is putting a new rule into effect that will greatly impact how inpatient admission decisions are made. The rule, known as the “two-midnight rule,” states that if the admitting practitioner admits a Medicare beneficiary as an inpatient with the reasonable expectation that the beneficiary will require care that “crosses two midnights” and this decision is justified in the medical record, Medicare Part A payment is “generally appropriate.”
While there are multiple caveats, exceptions, and details, this rule can be simply articulated: If the admitting physician feels a patient will be in the hospital for a period longer than two midnights and the medical record supports this determination, the patient is an inpatient. Stays expected to be shorter than two midnights should be under observation status.
This new policy is an attempt to respond both to hospital calls for more guidance about when a beneficiary is appropriately treated as an inpatient—and paid by Medicare—and concerns about increasingly long hospital stays under observation status. Most hospitalists wrestle with status determination issues on a daily basis.
SHM is aware of the struggle and has been advocating on behalf of hospitalists to help shape observation status and the two-midnight rule. When the rule was first proposed, SHM voiced serious concerns about its utility and how it was unlikely to solve the overall confusion surrounding inpatient status determinations. Nevertheless, CMS finalized the rule as an attempt to begin addressing the problem.
Faced with an increasingly loud chorus of providers and hospitals concerned about the implementation of the new policy, CMS agreed to delay full enforcement from the original date of Oct. 1, 2013, until March 31, 2014.
During the delayed enforcement period, hospitals will be expected to begin implementing the two-midnight rule, and auditors will be giving hospitals non-punitive feedback on their application of the policy. To accomplish this, CMS is instructing Medicare Administrative Contractors (MACs) to review a sample of 10 to 25 inpatient hospital claims spanning less than two midnights after admission for each hospital. This probe sample will be used to assist hospitals with implementing the new requirements correctly. To give an additional level of comfort during this adjustment period, CMS has announced that it will not conduct post-payment patient status reviews for claims with dates of admission Oct. 1, 2013, through March 31, 2014.
Unfortunately, beyond the vague guidance CMS has offered thus far, there is no foolproof guide to establishing new hospital admissions policies that comply with the rule. As a result, there likely will be wide variation among hospitals.
To assist in sorting out the confusion, SHM will be hosting a webinar this month with case studies from several hospitals. The focus will be on the internal processes each hospital is using to implement the rule and how they were developed. Sharing and learning from national implementation experiences is a valuable way for hospitalists to gain new perspectives and to bring those experiences to their home institutions when considering their own roles in meeting the new admissions criteria head on.
For more information about the webinar and to register, visit www.hospitalmedicine.org today.
Josh Boswell is SHM’s senior manager of government relations.
As many hospitalists are probably acutely aware, the Centers for Medicare & Medicaid Services (CMS) is putting a new rule into effect that will greatly impact how inpatient admission decisions are made. The rule, known as the “two-midnight rule,” states that if the admitting practitioner admits a Medicare beneficiary as an inpatient with the reasonable expectation that the beneficiary will require care that “crosses two midnights” and this decision is justified in the medical record, Medicare Part A payment is “generally appropriate.”
While there are multiple caveats, exceptions, and details, this rule can be simply articulated: If the admitting physician feels a patient will be in the hospital for a period longer than two midnights and the medical record supports this determination, the patient is an inpatient. Stays expected to be shorter than two midnights should be under observation status.
This new policy is an attempt to respond both to hospital calls for more guidance about when a beneficiary is appropriately treated as an inpatient—and paid by Medicare—and concerns about increasingly long hospital stays under observation status. Most hospitalists wrestle with status determination issues on a daily basis.
SHM is aware of the struggle and has been advocating on behalf of hospitalists to help shape observation status and the two-midnight rule. When the rule was first proposed, SHM voiced serious concerns about its utility and how it was unlikely to solve the overall confusion surrounding inpatient status determinations. Nevertheless, CMS finalized the rule as an attempt to begin addressing the problem.
Faced with an increasingly loud chorus of providers and hospitals concerned about the implementation of the new policy, CMS agreed to delay full enforcement from the original date of Oct. 1, 2013, until March 31, 2014.
During the delayed enforcement period, hospitals will be expected to begin implementing the two-midnight rule, and auditors will be giving hospitals non-punitive feedback on their application of the policy. To accomplish this, CMS is instructing Medicare Administrative Contractors (MACs) to review a sample of 10 to 25 inpatient hospital claims spanning less than two midnights after admission for each hospital. This probe sample will be used to assist hospitals with implementing the new requirements correctly. To give an additional level of comfort during this adjustment period, CMS has announced that it will not conduct post-payment patient status reviews for claims with dates of admission Oct. 1, 2013, through March 31, 2014.
Unfortunately, beyond the vague guidance CMS has offered thus far, there is no foolproof guide to establishing new hospital admissions policies that comply with the rule. As a result, there likely will be wide variation among hospitals.
To assist in sorting out the confusion, SHM will be hosting a webinar this month with case studies from several hospitals. The focus will be on the internal processes each hospital is using to implement the rule and how they were developed. Sharing and learning from national implementation experiences is a valuable way for hospitalists to gain new perspectives and to bring those experiences to their home institutions when considering their own roles in meeting the new admissions criteria head on.
For more information about the webinar and to register, visit www.hospitalmedicine.org today.
Josh Boswell is SHM’s senior manager of government relations.
Affordable Care Act Latest in Half-Century of Healthcare Reform
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Observation-Status Patients Are Clinically Heterogeneous, Costly to Hospitals
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.
Clinical question: What are the characteristics of a large cohort of patients under observation status?
Background: The use of observation hospital services has increased significantly. The Centers for Medicare and Medicaid Services (CMS) defines observation status as a “well-defined set of specific, clinically appropriate services,” usually lasting <24 hours and exceeding 48 hours in “only rare and exceptional cases.”
Study design: Retrospective descriptive study.
Setting: University of Wisconsin Hospital and Clinics, a 566-bed tertiary academic medical center.
Synopsis: A total of 43,853 hospitalizations were reviewed during the study period. Of those, 4578 (10.4%) were observation. The mean observation LOS was 33.3 hours, which included 16.5% of patients with LOS >48 hours. Although chest pain was the top observation diagnosis, 1141 distinct observation diagnosis codes were found.
These findings illustrate a significant disparity between the CMS definition for observation stay and the description of observation patients in this cohort, despite using CMS-endorsed InterQual criteria to determine status. While the cost per encounter for observation care was less than inpatient care, reimbursement was insufficient to cover those reduced costs. Ultimately, the net loss of revenue per observation encounter was $331, compared to a net gain in revenue per inpatient encounter of $2,163. This operating loss for hospitals is coupled with the fact that some of this cost is being transferred to patients.
Bottom line: Definitions and reimbursement models for observation status warrant continued research and discussion in the context of our evolving healthcare climate.
Citation: Sheehy AM, Graf B, Gangireddy S, et al. Hospitalized but not admitted: characteristics of patients with “observation status” at an academic medical center [published online ahead of print July 8, 2013]. JAMA Intern Med.
Hospital Strategies for Decreasing Readmissions for Heart Failure Patients
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Report on England’s Health System Mirrors Need for Improvement in U.S.

Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Don Berwick, MD, former president and CEO of the Institute for Healthcare Improvement (IHI) and former administrator for the Centers for Medicare and Medicaid Services (CMS), recently consulted with the National Health Service (NHS) on how to devise and implement a safer and better healthcare system for England. His services were solicited due to a number of high-profile scandals involving neglect in hospitals. His team’s work resulted in a report entitled “A Promise to Learn – A Commitment to Act: Improving the Safety of Patients in England.”1 The purpose of the consultative visit and resulting series of recommendations was to identify and recommend solutions to ailments and limitations in the current NHS.
Many of the “current state” ailments outlined in Dr. Berwick’s report would not sound terribly novel or unfamiliar to most U.S. healthcare systems. The report listed problems with:
- Systems-procedures-conditions-environments-constraints that lead people to make bad or incorrect decisions;
- Incorrect priorities;
- Not heeding warning signals about patient safety;
- Diffusion of responsibility;
- Lack of support for continuous improvement; and
- Fear, which is “toxic to both safety and improvement.”
Dr. Berwick and his team made a number of recommendations to reshape priorities and resources, enhance the safety of the system, and rebuild the confidence of its customers (e.g., patients and caregivers).
The consultant group’s core message was simple and inspiring:
“The NHS in England can become the safest healthcare system in the world. It will require unified will, optimism, investment, and change. Everyone can and should help. And, it will require a culture firmly rooted in continual improvement. Rules, standards, regulations, and enforcement have a place in the pursuit of quality, but they pale in potential compared to the power of pervasive and constant learning.”
To achieve improvement, Dr. Berwick’s team recommended 10 guiding principles. Similar to The 10 Commandments, they offer a way of thinking, acting, and living—to make the healthcare industry a better place. These healthcare 10 commandments include the following:
- “The NHS should continually and forever reduce patient harm by embracing wholeheartedly an ethic of learning.” While we should all aspire to zero harm, the reality is that getting there will be a long and difficult goal, more than likely a goal of continual reduction. Defining harm is also more difficult than looking just at what meets the eye; because the qualitative “you know it when you see it” will likely never be embraced widely, we are left with quantitative and imperfect measures, such as hospital-acquired conditions (HACs) and patient safety indicators (PSIs). Despite the imperfection of current measures, the goal for continual reduction is laudable and necessary.
- “All leaders concerned with NHS healthcare—political, regulatory, governance, executive, clinical, and advocacy—should place quality of care in general, and patient safety in particular, at the top of their priorities for investment, inquiry, improvement, regular reporting, encouragement, and support.” As with anything, leadership sets the vision, mission, and values of an organization or system. Leadership will have to commit to placing patient safety at the top of the priority list, without sacrificing other priorities.
- “Patients and their caregivers should be present, powerful, and involved at all levels of healthcare organizations, from the wards to the boards of trusts.” This directive is certainly ideal, but, realistically, it will take a while to develop a level of comfort from both the patients and the providers, because both are much more used to operating in parallel, with intermittent intersections. Involving patients in all organizational decision-making, and including the boards of trustees, will be prerequisite to true patient-caregiver-centered care.
- “Government, Health Education England, and NHS England should assure that sufficient staff are available to meet the NHS’ needs now and in the future. Healthcare organizations should ensure staff are present in appropriate numbers to provide safe care at all times and are well-supported." All healthcare organizations should be on a relentless pursuit to match workload and intensity to staffing, pursue work standardization and efficiency, and match work to human intellect. These are the founding tenets of Lean and Six Sigma and should be pursued for all disciplines, both clinical and non-clinical.
- “Mastery of quality and patient-safety sciences and practices should be part of initial preparation and lifelong education of all healthcare professionals, including managers and executives.” The U.S. has made great strides in incorporating at least a basic curriculum of quality and safety for most healthcare professionals, but we need to move the current level of understanding to the next level. We need to ensure that all healthcare professionals have at least a basic understanding of the fundamental principles.
- “The NHS should become a learning organization. Its leaders should create and support the capability for learning, and therefore change, at scale within the NHS.” Healthcare organizations should not just be willing to learn from individual and system opportunities; they should be eager to learn. Quality and safety missions should uniformly extend into educational and research missions in all organizations, to enhance learning opportunities and create best practice.
- “Transparency should be complete, timely, and unequivocal. All data on quality and safety, whether assembled by government, organizations, or professional societies, should be shared in a timely fashion with all parties who want it, including, in accessible form, with the public.” Many healthcare organizations equate transparency with marketing, where they tout their fanciest technology or latest innovation. And many also subscribe to the theory “if you’re gonna go bare, you better be buff” and only widely disseminate those metrics that make them appear superior. We all need to be more transparent across the board, because going “bare” can actually stimulate improvements more quickly and reliably than they would otherwise occur. Organizational metrics really should not belong to the organization; they should belong to the patients who created the metrics. As such, full transparency of organizational performance (on all the domains of quality) should be an organizational and patient expectation.
- “All organizations should seek out the patient and caregiver voice as an essential asset in monitoring the safety and quality of care.” Organizations should seek out patient-caregiver feedback and should be eager to learn from their words. Most other industries regularly and routinely seek out customer feedback to improve upon their products and services; some even pay customers for a chance to hear what they have to say. Too often, the theme from disgruntled patients is that no one is listening to them.
- “Supervisory and regulatory systems should be simple and clear. They should avoid diffusion of responsibility. They should be respectful of the goodwill and sound intention of the vast majority of staff. All incentives should point in the same direction.”
- U.S. regulatory agencies have an incredible amount of simplification to accomplish, along with a need to align incentives for the betterment of the patient. “We support responsive regulation of organizations, with a hierarchy of responses. Recourse to criminal sanctions should be extremely rare, and should function primarily as a deterrent to willful or reckless neglect or mistreatment.”
This commandment acknowledges the rarity of willful misconduct, by organizations and providers, and calls for a simplification of the governance needed for such rare events and situations.
In Sum As with The 10 Commandments, these guiding principles can help transform the way we in the healthcare industry think, act, and live—and put us on the road to making it a better place.
Reference
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
How to Handle Medicare Documentation Audits

The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
Why Hospitalists Should Focus on Patient-Care Basics


We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
We all are too familiar with the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized set of questions randomly deployed to recently discharged patients. More recently, hospitalists have noticed the introduction of the Clinician and Groups Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) survey, randomly deployed to recently evaluated ambulatory patients. HCAHPS has been publicly reported since 2008. CG-CAHPS will be in the near future. In addition to these, there are a variety of other types of CAHPS surveys, ranging from ambulatory surgery to patient-centered medical homes. For HCAHPS alone, there are more than 8,200 adult surveys completed every day from almost 4,000 different U.S. hospitals.1
In addition to these surveys being publicly reported and widely viewed online by patients, payors, and employers, the results now are tightly coupled to the reimbursement of hospitals and, in some cases, individual providers. As of October 2012, Medicare has relegated 30% of its hospital value-based purchasing (VBP) program to the results of hospitals’ HCAPHS survey results. For the foreseeable future, about one-third of the financial bonus—or penalty—of a hospital rests in the hands of how well our patients perceive their care. Many individual hospitals and practice groups have started coupling individual physicians’ compensation to their patients’ CAHPS scores. Within the (approximately) seven minutes it takes to complete the survey, our patients determine millions of dollars of physician and hospital reimbursement.1
With all of the financial and reputational emphasis on HCAHPS, it is vital that hospitalists understand what it is these surveys are actually measuring, and if they have any correlation with the quality of the care the patient receives. The questions currently address 11 different domains of hospital care:
- Communication with doctors;
- Communication with nurses;
- Responsiveness of hospital staff;
- Pain management;
- Communication about medicines;
- Discharge information;
- Cleanliness of hospital environment;
- Quietness of hospital environment;
- Transitions of care;
- Overall rating of the hospital; and
- Willingness to recommend the hospital.
As the domains of care are all very different, one can imagine a wide range of answers to the various questions; a patient can perceive that communication was excellent but the quietness and cleanliness was disgraceful. And, depending on what they consider the most important aspects of their stay, they therefore may rate their overall stay as excellent or disgraceful. Why? Because each of these rest in the eye of the beholder.
But to keep pace, hospitals and providers across the country have invested millions of hours dissecting the meaning of the results and trying to improve upon them. My hospital has struggled for years with the “cleanliness” question, trying to figure out what our patients are trying to tell us: that we need to sweep and mop more often, that hospital supplies are cluttering our patient rooms, that the trashcans are overflowing or within eyesight? When we ask focus groups, we often get all of the above—and then try to implement several solutions all at once.
The quietness question is much easier to interpret but certainly difficult to improve upon. We have implemented “yacker trackers,” “quiet time,” and soft-wheeled trash cans. And the results of the surveys take months to come back and get analyzed, so it is difficult to quickly know if your interventions are actually working. Given that so many hospitals and providers are back-flipping to “play to the test,” we really need some validation that care is truly improving based on this patient feedback.
A recent New York Times article calls to light a natural paradox in the medical field, in that patients who understand more about disease processes and medical information actually feel less, rather than more, informed. In other words, those who are actually the most well-informed may rate communication the lowest. The article also calls to light the natural paradox between providers being honest and providers being likable, especially considering they routinely have to deliver messages that patients do not want to hear:
- You need to quit smoking;
- Your weight is affecting your health; and
- Your disease is not curable.
Given these natural paradoxes, the article argues that it is difficult to reconcile why hospitals and providers should be held financially accountable for their patients’ perception of care, when that perception may not equate to “real” care quality.2
However, there is some evidence that patient satisfaction surveys may actually be good proxies for care quality. A large study found that hospitals with the highest quartile HCAHPS ratings also have about 2%-3% higher quality scores for acute MI, CHF, pneumonia, and surgery, compared to those in the lowest quartile. The highest scoring hospitals also have about 2%-3% lower readmission rates for acute MI, CHF, and pneumonia.3,4 And, similar to other quality metrics, there is evidence that the longer a hospital has been administering HCAHPS, the better are their scores. So maybe hospital systems and providers can improve not only the perception a patient has of the quality of the care they received, but improve the quality, as measured by the patient’s perception.
Although there are legitimate arguments on both sides as to whether a patient’s perception of care reflects “real” care quality, in the end these CAHPS surveys are, and have been publicly reported, and will be tightly coupled to reimbursement for hospitals and (likely) providers for the foreseeable future. So in the meantime, we should continue to focus on patient-centered care, take seriously any voiced concerns, and have a relentless pursuit of perfection for how patients perceive their care. Because in the end, you would do it for your family so we should do it for our patients.
References
- Centers for Medicare & Medicaid Services. Spring 2013 HCAHPS Executive Insight Letter. Available at: www.hcahpsonline.org/Executive_Insight. Accessed Aug. 15, 2013.
- Rosenbaum L. When doctors tell patients what they don’t want to hear. The New Yorker website. Available at: www.newyorker.com/online/blogs/elements/2013/07/when-doctors-tell-patients-what-they-dont-want-to-hear.html. Published July 23, 2013. Accessed Aug. 15, 2013.
- Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the US. New Eng J Med. 2008;359(18):1921-1931.
- Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R. Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care. 2011;17(1):41-48.
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
How To Avoid Medicare Denials for Critical-Care Billing

Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
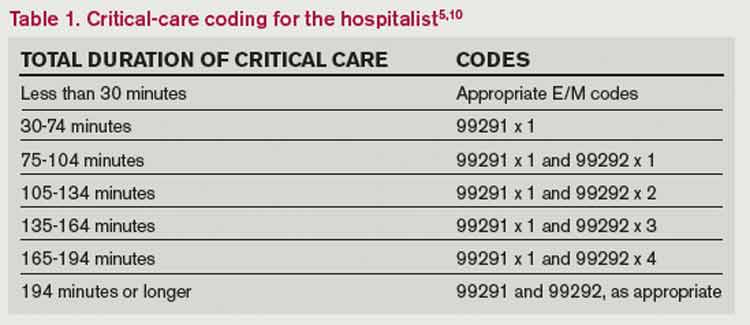
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
Are your critical-care claims at risk for denial or repayment upon review? Several payors have identified increased potential for critical-care reporting discrepancies, which has resulted in targeted prepayment reviews of this code.1 Some payors have implemented 100% review when critical care is reported in settings other than inpatient hospitals, outpatient hospitals, or emergency departments.2 To ensure a successful outcome, make sure the documentation meets the basic principles of the critical-care guidelines.
Defining Critical Illness/Injury
CPT and the Centers for Medicare & Medicaid Services (CMS) define “critical illness or injury” as a condition that acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient’s condition (e.g. central-nervous-system failure; circulatory failure; shock; renal, hepatic, metabolic, and/or respiratory failure).3 The provider’s time must be solely directed toward the critically ill patient. Highly complex decision-making and interventions of high intensity are required to prevent the patient’s inevitable decline if left untreated. Payment may be made for critical-care services provided in any reasonable location, as long as the care provided meets the definition of critical care. Critical-care services cannot be reported for a patient who is not critically ill but happens to be in a critical-care unit, or when a particular physician is only treating one of the patient’s conditions that is not considered the critical illness.4
Examples of patients who may not satisfy Medicare medical-necessity criteria, do not meet critical-care criteria, or who do not have a critical-care illness or injury and therefore are not eligible for critical-care payment:
- Patients admitted to a critical-care unit because no other hospital beds were available;
- Patients admitted to a critical-care unit for close nursing observation and/or frequent monitoring of vital signs (e.g. drug toxicity or overdose);
- Patients admitted to a critical-care unit because hospital rules require certain treatments (e.g. insulin infusions) to be administered in the critical-care unit; and
- Care of only a chronic illness in the absence of caring for a critical illness (e.g. daily management of a chronic ventilator patient; management of or care related to dialysis for an ESRD).
These circumstances would require using subsequent hospital care codes (99231-99233), initial hospital care codes (99221-99223), or hospital consultation codes (99251-99255) when applicable.3,5
Because critical-care time is a cumulative service, providers keep track of their total time throughout a single calendar day. For each date and encounter entry, the physician’s progress notes shall document the total time that critical-care services were provided (e.g. 45 minutes).4 Some payors impose the notation of “start-and-stop time” per encounter (e.g. 10 to 10:45 a.m.).
Code This Case
Consider the following scenario: A hospitalist admits a 75-year-old patient to the ICU with acute respiratory failure. He spends 45 minutes in critical-care time. The patient’s family arrives soon thereafter to discuss the patient’s condition with a second hospitalist. The discussion lasts an additional 20 minutes, and the decision regarding the patient’s DNR status is made.
Family meetings must take place at the bedside or on the patient’s unit/floor. The patient must participate, unless they are medically unable or clinically incompetent to participate. A notation in the chart should indicate the patient’s inability to participate and the reason. Meeting time can only involve obtaining a medical history and/or discussing treatment options or the limitations of treatment. The conversation must bear directly on patient management.5,6 Meetings that take place for family grief counseling (90846, 90847, 90849) are not included in critical-care time and cannot be billed separately.
Do not count time associated with periodic condition updates to the family or answering questions about the patient’s condition that are unrelated to decision-making.
Family discussions can take place via phone as long as the physician is calling from the patient’s unit/floor and the conversation involves the same criterion identified for face-to-face family meetings.6
Critically ill patients often require the care of multiple providers.3 Payors implement code logic in their systems that allow reimbursement for 99291 once per day when reported by physicians of the same group and specialty.8 Physicians of different specialties can separately report critical-care hours. Documentation must demonstrate that care is not duplicative of other specialists and does not overlap the same time period of any other physician reporting critical-care services.
Same-specialty physicians (two hospitalists from the same group practice) bill and are paid as one physician. The initial critical-care hour (99291) must be met by a single physician. Medically necessary critical-care time beyond the first hour (99292) may be met individually by the same physician or collectively with another physician from the same group. Cumulative physician time should be reported under one provider number on a single invoice in order to prevent denials from billing 99292 independently (see “Critical-Care Services: Time Reminders,”).
When a physician and a nurse practitioner (NP) see a patient on the same calendar day, critical-care reporting is handled differently. A single unit of critical-care time cannot be split or shared between a physician and a qualified NP. One individual must meet the entire time requirement of the reported service code.
More specifically, the hospitalist must individually meet the criteria for the first critical-care hour before reporting 99291, and the NP must individually meet the criteria for an additional 30 minutes of critical care before reporting 99292. The same is true if the NP provided the initial hour while the hospitalist provided the additional critical-care time.
Payors who recognize NPs as independent billing providers (e.g. Medicare and Aetna) require a “split” invoice: an invoice for 99291 with the hospitalist NPI and an invoice for 99292 with the NP’s NPI.9 This ensures reimbursement-rate accuracy, as the physician receives 100% of the allowable rate while the NP receives 85%. If the 99292 invoice is denied due to the payor’s system edits disallowing separate invoicing of add-on codes, appeal with documentation by both the hospitalist and NP to identify the circumstances and reclaim payment.
Critical-Care Services: Time Reminders
Two available codes:
99291: Critical care, evaluation and management of the critically ill or critically injured patient: first 30-74 minutes. It is reported only once per day, per physician or group member of the same specialty.
+99292: Critical care, evaluation and management of the critically ill or critically injured patient: each additional 30 minutes (list separately in addition to code for primary service). Categorized as an “add on” code, it must be reported on the same invoice as its “primary” code, 99291. Multiple units of code 99292 can be reported per day per physician/group (see Table 1).
Critical-care time constitutes bedside time and time spent on the patient’s unit/floor where the physician is immediately available to the patient. Also count physician time associated with the performance and/or interpretation of labs, diagnostic studies, and procedures inherent to the provision of critical care:
- Cardiac output measurements (93561, 93562);
- Chest X-rays (71010, 71015, 71020);
- Pulse oximetry (94760, 94761, 94762);
- Blood gases and interpretation of data stored in computers (e.g. ECGs, blood pressures, hematologic data [99090]);
- Gastric intubation (43752, 91105);
- Temporary transcutaneous pacing (92953);
- Ventilation management (94002-94004, 94660, 94662); and
- Vascular access procedures (36000, 36410, 36415, 36591, 36600).5
Other separately billable services or procedures cannot be added to critical-care time. A notation in the medical record is highly recommended (e.g. “central-line insertion is not included as critical-care time”) for validation to prevent payor inquiries.
Do not count time associated with indirect care provided outside of the patient’s unit/floor (e.g. reviewing data or calling the family from the office) toward critical-care time. Activities on the floor/unit that do not directly contribute to patient care or management (e.g. review of literature, teaching rounds) cannot be counted toward critical-care time.
—Carol Pohlig
References
- Cahaba Government Benefit Administrators LLC. Widespread prepayment targeted review notification—CPT 99291. Cahaba Government Benefit Administrators LLC website. Available at: http://www.cahabagba.com/news/widespread-prepayment-targeted-review-notification-part-b/. Accessed May 4, 2013.
- First Coast Service Options Inc. Prepayment edit of evaluation and management (E/M) code 99291. First Coast Service Options Inc. website. Available at: http://medicare.fcso.com/Medical_documentation/249650.asp. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12A. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12B. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 5, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12E. Centers for Medicare and Medicaid Services website. Available at http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 6, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012.
- Novitas Solutions Inc. Evaluation & management: service-specific coding instructions. Novitas Solutions Inc. website. Available at: http://www.novitas-solutions.com/em/coding.html. Accessed May 7, 2013.
- United Healthcare. Same day same service policy—adding edits. United Healthcare website. Available at: http://www.unitedhealthcareonline.com/ccmcontent/ ProviderII/ UHC/en-US/Assets/ProviderStaticFiles/ProviderStaticFilesPdf/News/Network_Bulletin_November _2012_Volume_52.pdf. Accessed May 7, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12I. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 10, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.12G. Centers for Medicare and Medicaid Services website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 4, 2013.
SHM Advocates for Medicare to Cover Skilled-Nursing Facilities
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.
The Centers for Medicare & Medicaid Services (CMS) recently issued a Final Rule for the Inpatient Prospective Payment System, which guides payment and programs associated with inpatient hospitalizations. In this year’s rule, CMS adjusted the criteria for inpatient admissions in an attempt to simplify and clarify the decision-making process.
The policy would allow physicians to admit a patient if they reasonably expect and document in the medical record that a beneficiary will need to stay in the hospital for more than two midnights. Admissions based on this time-limited expectation will be presumed to be appropriate for Medicare Part A payment. CMS cited concerns about the growing trend of longer observation stays to support this change.
With observation stays, there are two major financial concerns for patients: whether the hospital stay is paid under Medicare Part A or Part B, and whether Medicare will pay for post-acute care in a skilled-nursing facility (SNF). Medicare Part A reimburses for inpatient admissions, with a one-time deductible for the benefit period. Outpatient services, such as observation care and physician services, are covered under Medicare Part B, which has copays and co-insurance that greatly increase the costs for beneficiaries. In addition, SNF coverage through Medicare Part A is determined by the three-day rule; a patient must be an inpatient for three days to qualify for coverage.
While the long-term impacts of this regulatory change to the admission criteria remain to be seen, SHM is concerned that the rule does not adequately address the broader problems associated with inpatient and observation status. As we note in our comments to CMS on the new rule:1
Even with these changes, the central tension created by the bifurcation in admission status still remains.…Other policies and programs, such as the attempts to reduce admissions, may inadvertently add pressure to the admission decision.
Indeed, for beneficiaries, the barrier to SNF coverage remains. CMS takes care to note that, while time under emergency care and observation care count toward the two-midnight presumption for inpatient admission, it does not count toward the three-day rule for SNF coverage. This is particularly problematic; as advances in medicine allow for the treatment of higher-acuity and -severity conditions with observation stays or shorter inpatient stays, patients might not be getting the follow-up care they need. This puts them at risk for additional complications and, ultimately, readmissions to the hospital.
In an era of seeking value in the healthcare system, it seems like an opportunity lost to streamline and coordinate care across settings and to ensure that patients are getting the follow-up care they require. It is for this reason that hospitalists continue to push for passage of the Improving Access to Medicare Coverage Act, a bill sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio) that would count observation status as time toward the three-day requirement for SNF coverage.
A recent Office of Inspector General (OIG) report for the U.S. Department of Health and Human Services on observation status sums up the problem succinctly.2 The OIG states that “CMS should consider how to ensure that beneficiaries with similar post-hospital care needs have the same access and cost-sharing for SNF services.”2
SHM concurs.
Joshua Lapps is SHM’s government relations specialist.
References
- Society of Hospital Medicine. SHM submits comments in response to FY2014 inpatient prospective payment system proposed rule. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=34044. Accessed Sept. 9, 2013.
- Office of Inspector General. Memorandum report: Hospitals’ use of observations stays and short inpatient stays for Medicare beneficiaries, OEI-02-12-00040. U.S. Department of Health and Human Services website. Available at: http://oig.hhs.gov/oei/reports/oei-02-12-00040.pdf. Accessed Sept. 9, 2013.