User login
When your patient’s blood pressure won’t come down
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help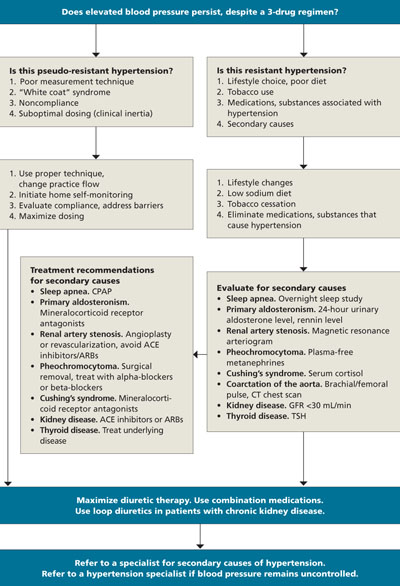
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; [email protected]
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; [email protected]
• Encourage home BP monitoring. Home readings are often lower than those taken in the office and closer to the average BP recorded by 24-hour ambulatory monitors. C
• Tell patients that reducing sodium intake not only reduces mortality, but it has positive cardiovascular effects separate from BP reduction, such as improved endothelium-dependent vasodilation. A
• Search for secondary causes of resistant hypertension, such as renal artery stenosis, pheochromocytoma, obstructive sleep apnea, and hyperaldosteronism. A
• Consider pseudohypertension in elderly patients who exhibit postural hypotension and fail to respond to increased doses of medication. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Mr. Brown is a 60-year-old African American man who works as a mid-level executive at a local bank. About a year and a half ago, he was diagnosed with hypertension, joining a number of other family members who also have the condition. Reviewing his chart, you note that at many of his visits—but not all of them—his systolic blood pressure runs close to 150 mm Hg, with diastolic pressure <90 mm Hg. Today his blood pressure is 148/88 mm Hg, numbers that exceed the parameters of the currently accepted definition of hypertension: blood pressure ≥140 mm Hg systolic or ≥90 mm Hg diastolic, taken on 2 separate occasions with the patient sitting down.1
Mr. Brown is one of the more than 65 million American adults suffering from high blood pressure—the No. 1 diagnosis reported in outpatient medical offices.2,3 Despite such prevalence, blood pressure control in the United States is suboptimal, with only one-third of hypertensive patients under adequate control.1 In 2007, the total estimated cost of treating high blood pressure in the United States exceeded $66 billion.4
When you tell Mr. Brown that his blood pressure doesn’t meet the therapeutic goal of <140/90 mm Hg, he gives you his reasons: He was late, he rushed, the traffic was bad, and the nurse rushed him into the exam room before he even had time to catch his breath. He insists his blood pressure is “normal” at home, and blames the elevated numbers on anxiety. He also tells you he was up working most of the night before, drinking coffee to stay awake to finish an urgent project.
Mr. Brown’s current medication regimen includes daily doses of lisinopril-hydrochlorothiazide (HCTZ) 20/25 mg daily and simvastatin 20 mg. He tells you he has no chest pain, shortness of breath, cough, edema, claudication, paroxysmal nocturnal dyspnea, or orthopnea. When you ask if he takes his lisinopril-HCTZ every day, he says Yes, but you have your suspicions.
Consider pseudo-resistance
Suboptimal blood pressure control can be classified as either pseudo-resistant or resistant hypertension. According to the definition used in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7), resistance is the “failure to achieve goal BP in patients who are adhering to full doses of an appropriate 3-drug regimen that includes a diuretic.”1
Hypertension is described as “pseudo-resistant” when persistent elevations in blood pressure are the result of a failure to comply with the medication regimen, “white-coat” syndrome, poor blood pressure technique, or a combination of these.5,6 Physician failure to prescribe adequate doses of medication, so-called clinical inertia, may also be a factor.5,7 Causes and remedies for pseudo-resistance are summarized in the algorithm.
In Mr. Brown’s case, he’s told you that he’s taking his lisinopril-HCTZ every day, but when you check your records, you see that the intervals between his refill requests range between 34 and 36 days. So you ask him, again, whether he is taking his lisinopril-HCTZ daily, and this time he says he takes the medication “at least 5 or 6 days a week.”
Encourage compliance. To motivate Mr. Brown, you tell him his blood pressure does not meet the goal of <140/90 mm Hg and that pressure higher than goal is a significant risk factor for cardiovascular disease. You emphasize the importance of taking his medication every day—a mantra you’ve repeated to countless patients over the years. In fact, it’s estimated that up to 40% of patients will discontinue their medication at some point during treatment.8 Patients’ reasons vary and may include medication side effects, the cost of treatment, or a patient’s personal philosophy. Cultural differences may also play a role in noncompliance.9
You talk with Mr. Brown a bit more and confirm that his poor compliance is due to simple forgetfulness and not another underlying reason that would need to be addressed. You hand him a pill calendar to help him keep track of his medication. You review the dosage and feel confident that you’ve prescribed a regimen simple enough for Mr. Brown to stick to and adequate to bring his pressure down.
When your white coat is the problem. Though not the case with Mr. Brown, a patient’s elevated readings could be a case of white coat hypertension—a conditioned response in some patients that is probably the result of anxiety in the medical setting.10 Patients with white coat hypertension have significantly less risk of death and reduced target organ damage than patients with truly resistant hypertension.11,12
If you suspect that a patient of yours has white coat hypertension, you can test your hypothesis by encouraging him or her to buy a blood pressure monitor to use at home, keep a log of the readings, and bring the log in to the next appointment. Improved technology has made home blood pressure monitoring an important tool in the treatment of high blood pressure.13-15
According to a 2008 statement issued jointly by the American Heart Association, the American Society of Hypertension, and the Preventive Cardiovascular Nurses Association, “There is a rapidly growing literature showing that measurements taken by patients at home are often lower than readings taken in the office and closer to the average blood pressure recorded by 24-hour ambulatory monitors, which is the blood pressure that best predicts cardiovascular risk.”14
Arm monitors are the most accurate because they measure brachial artery blood pressure.14 Most wrist monitors have not been validated in studies, but obese patients who cannot find a properly sized cuff may need to use them.14 Finger devices should never be used.14
Sometimes technique is at fault. To ensure that you get proper readings when your patient is in the office, advise the nursing staff not to take a patient’s blood pressure for at least 5 minutes after bringing him or her to an exam room. Specifically, the nurse can either make blood pressure measurement the last thing she (or he) does when “rooming” the patient, or she may prefer to go back to the exam room a few minutes after the patient is there to take the reading. The nurse should take care that the cuff is the right size and that the pressure is taken with the patient’s arm at heart level. In hypertensive patients, placing the arm below the horizontal in the dependent position can raise blood pressure 23/10 mm Hg.1,16,17
Newer blood pressure monitoring devices for the office are available that obviate artificially high readings caused by errors in technique and by white coat syndrome. Researchers have found that readings taken with the BpTRU automatic device, which obtains and records 5 blood pressure readings over a 5-minute period, are lower than those taken by office personnel, and that the white coat effect is eliminated.18,19
One pseudo-resistant case solved. At Mr. Brown’s next visit, you review his pill calendar with him and note that his blood pressure is now running 138/88 mm Hg and he is within his target goal of less than 140/90 mm Hg.
If Mr. Brown’s blood pressure control had continued to be suboptimal even after you’d taken steps to address cause(s) of pseudo-resistance, you would have had to shift gears and consider his case one of resistant hypertension.1
Consider resistant hypertension
Causes of resistant hypertension include lifestyle factors, side effects of medications, and secondary causes.5,6 Tobacco use, obesity, lack of exercise, a high sodium diet, and alcohol consumption can all contribute to hypertension.1,5,6,20,21 Dietary sodium in particular has significant adverse effects. Reducing dietary sodium not only reduces mortality, but has positive cardiovascular effects separate from blood pressure reduction, such as improved endothelium-dependent vasodilation.22-24
Medications including nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, sympathomimetics, glucocorticoids, and black licorice (found in some herbal supplements) may all raise blood pressure.5 Medications and other substances associated with increased blood pressure are listed in the TABLE. A search for such products, with changes or discontinuations that are clinically appropriate, should be part of any evaluation for resistant hypertension.
CASE 2 Ms. Stevens is a 30-year-old woman who was diagnosed with high blood pressure 7 months ago. She is currently taking triamterene-HCTZ 37.5/25 mg daily, amlodipine 10 mg daily, and metoprolol succinate 100 mg daily. She is compliant with medication, sticks to a low-sodium diet, and exercises 5 days a week. She does not drink alcohol. A review of her chart tells you her baseline serum chemistries, chest x-ray, and urinalysis are all normal. Today’s blood pressure taken in the sitting position after a 5-minute rest is 160/92 mm Hg. How should you proceed?
TABLE
Medications and other agents that may cause hypertension
| • Alcohol | • Cyclosporine | • Nicotine |
| • Antidepressants | • Erythropoietin | • NSAIDs |
| • Buspirone (Buspar) | • Estrogen preparations | • St. John’s wort |
| • Cocaine | • Licorice | • Tyramine-containing foods |
| • Corticosteroids | • Metoclopramide (Reglan) | |
| NSAIDs, nonsteroidal anti-infiammatory drugs. | ||
| Source: Chobanian A, et al. Hypertension. 2003.1 | ||
Is it resistant hypertension? Look for clues
You go over Ms. Stevens’ history carefully. Her hypertension medications should be adequate, and she is compliant with the prescribed regimen. Lifestyle factors are clearly not to blame: She’s not obese, she follows a low-sodium diet, doesn’t drink or smoke, and gets plenty of exercise. You ask her about other medications or over-the-counter supplements she takes, and nothing on her list raises a red flag. This doesn’t seem to be pseudo-resistance, and though you’re aware that only about 5% of cases of hypertension can be attributed to secondary causes, you think Ms. Stevens may be one of those patients.25
Numerous causes of secondary hypertension exist, and evaluations for such causes should be considered in all patients with resistant hypertension. Renal artery stenosis and pheochromocytoma are the most well-known causes, but less well known but significant contributors are obstructive sleep apnea and hyperaldosteronism.1,6,26,27
The relationship between obstructive sleep apnea and hypertension is not clear, and most of the studies linking the 2 conditions are population based.28 Nevertheless, because studies show that continuous positive airway pressure (CPAP) does improve blood pressure control in patients with obstructive sleep apnea, it is appropriate to investigate patients with resistant hypertension for this condition.29
Aldosterone’s role in resistant hypertension appears to be greatest in those with insulin resistance. The mechanism appears to be amplified sodium retention resulting in increased volume expansion, negative effects on oxidative stress, and elevated inflammation.27 Many patients with hypertension also have insulin resistance, so testing for hyperaldosteronism should be part of your investigation.
Test, and as necessary, test some more
Taking into consideration that 2 of the more common causes of secondary hypertension are obstructive sleep apnea and renal artery stenosis, you schedule an overnight sleep study for Ms. Stevens and a magnetic resonance arteriogram of the kidneys.26,30 (For more on the diagnostic tests and treatments for secondary causes of resistant hypertension, see the ALGORITHM.)
Reconsider medications. Ms. Stevens is already receiving the maximum dose of amlodipine, so you increase her metoprolol succinate to 200 mg daily and ask her to return in 1 month after the results of her tests come in.
Change medications and keep testing. At her next visit, Ms. Stevens’ blood pressure is 150/88 mm Hg, and her pulse rate is 64. Results of her overnight sleep study and magnetic resonance arteriogram are normal. At this juncture, with her work-up for common secondary causes of hypertension negative, you consider changes in her medication regimen. Because her pulse rate of 64 rules out any increase in the metoprolol, you decide to add lisinopril-HCTZ 10/12.5 mg to her regimen and discontinue her triamterene-HCTZ. Because her blood pressure is still elevated at this visit, you schedule additional testing to look for other secondary causes.
More tests, higher doses. One month later, Ms. Stevens returns with a blood pressure of 146/88 mm Hg. Appropriate testing for primary aldosteronism, pheochromocytoma, Cushing’s disease, and coarctation are all normal. Her lisinopril-HCTZ dose is increased to 20/12.5 mg, and when she returns 1 month later her blood pressure reading is 138/88 mm Hg.
You conclude that she is a patient with hard-to-control hypertension with no underlying cause who requires a significant amount of medication. That is not an uncommon situation. Although her blood pressure is now controlled to an appropriate level, you make a chart notation to consider referral to a hypertension specialist if her blood pressure become elevated again and treatment changes are not effective.6
ALGORITHM
Hard-to-control hypertension? This treatment algorithm can help
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CPAP, continuous positive airway pressure; CT, computed tomography; GFR, glomerular filtration rate; TSH, thyroid-stimulating hormone.
Adapted from: Calhoun DA, et al. Hypertension. 2008.6
Another consideration: Pseudohypertension
This uncommon condition sometimes occurs in elderly patients who suffer from a stiffened or thickened brachial artery.1 Because the blood pressure cuff cannot compress the artery, blood pressure readings overestimate true arterial pressure. The condition should be considered in patients when increased doses of medication fail to achieve the desired response, particularly in patients who exhibit postural hypotension.1
This was not a likely explanation for Ms. Stevens, however, given the clinical scenario and her young age.
CORRESPONDENCE Randy Wexler, MD, MPH, B0902B Cramblett Hall, 456 W 10th Avenue, Columbus, OH 43210; [email protected]
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
1. Chobanian A, Bakris GL, Black HR, et al. Seventh Report of The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7). Hypertension. 2003;42:1206-1252.
2. Fields L, Burt V, Cutler J, et al. The burden of adult hypertension in the United States 1999-2000: A rising tide. Hypertension. 2004;44:1-7.
3. Fang J, Alderman MH, Keenan NL, et al. Hypertension control at physicians’ offices in the United States. Am J Hypertens. 2008;21:136-142.
4. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics–2007 update. Circulation. 2007;115:e69-e171.
5. Sarafidis PA, Bakris GL. Resistant hypertension: an overview of evaluation and treatment. J Am Coll Cardiol. 2008;52:1749-1757.
6. Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403-1419.
7. Phillips LS, Branch WT, Book CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825-834.
8. Van Wijk BL, Klungel OH, Heerdink ER, et al. Rate and determinants of 10-year persistence with antihypertensive drugs. J Hypertens. 2005;23:2101-2107.
9. Wexler R, Pleister A, Feldman D. Sociology meets genetics: sociogenetic implications for future management of hypertension and heart failure. Curr Treat Options Cardiovasc Med. 2009;11:305-315.
10. Ogedegbe G, Pickering TG, Clemow L, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168:2459-2465.
11. Dawes MG, Bartlett G, Coats AJ, et al. Comparing the effects of white coat hypertension and sustained hypertension on mortality in a UK primary care setting. Ann Fam Med. 2008;6:390-396.
12. Pierdomenico SD, Lapenna D, Bucci A, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18:1422-1428.
13. Verberk WJ, Kroon AA, Kessels AGH, et al. Home blood pressure monitoring: a systematic review. J Am Coll Cardiol. 2005;46:743-751.
14. Pickering TG, Miller NH, Ogedegbe G, et al. AHA/ASH/PCNA scientific statement. Call to action on use and reimbursement for home blood pressure monitoring. Hypertension. 2008;52:10-29.
15. O’Brien E. Ambulatory blood pressure measurement: the case for implementation in primary care. Hypertension. 2008;51:1435-1441.
16. O’Brien E, Asmar R, Beilin L, et al. On behalf of the European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional ambulatory and home blood pressure measurements. J Hypertens. 2003;21:821-848.
17. Mourad A, Carney S, Gillies A, et al. Arm position and blood pressure: a risk factor for hypertension. J Hum Hypertens. 2003;17:389-395.
18. Myers MG. Automated blood pressure measurement in routine clinical practice. Blood Press Monit. 2006;11:59-62.
19. Myers MG, Valdivieso M, Kiss A. Use of automated office blood pressure measurement to reduce white coat hypertension. J Hypertens. 2009;27:280-286.
20. He J, Paul J, Whelton P, Appel L, et al. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544-549.
21. PREMIER Collaborative Research Writing Group. Effects of comprehensive lifestyle modification on blood pressure control. JAMA. 2003;289:2083-2093.
22. Cook NR, Cutler JA, Obarzanek E, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334:885-888.
23. Dickinson BD, Havas S. Reducing the population burden of cardiovascular disease by reducing sodium intake. Arch Intern Med. 2007;167:1460-1468.
24. Li J, White J, Guo L, et al. Salt inactivates endothelial nitric oxide synthase in endothelial cells. J Nutr. 2009;139:1-5.
25. Beevers G, Lip G, O’Brien E. ABCs of hypertension: the pathophysiology of hypertension. BMJ. 2001;322:912-916.
26. Peppard PE, Young T, Palta M, et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378-1384.
27. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med. 2009;150:776-783.
28. Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746-1752.
29. Haentjens P, Van Meerhaeghe A, Moscariello A. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167:757-764.
30. Kawashima A, Francis IR, Baumgarten DA, et al. For the Expert Panel on Urologic Imaging. Renovascular hypertension. Reston, Va: American College of Radiology; 2007. Available at: www.guideline.gov/summary/summary.aspx?ss=15&doc_id=11590&nbr=6003. Accessed April 4, 2009.
You can do more to slow the progression of heart failure
- Use B-type natriuretic peptide (BNP) levels as an aid not only in the diagnosis of heart failure (HF), but to track its progression as well (A).
- Prescribe exercise training for patients with stable heart failure; exercising at 40% to 70% of maximum capacity for 20 to 45 minutes several times a week offers benefits on par with pharmacotherapy (A).
- Consider using the Simplified Treatment Intervention to Control Hypertension (STITCH) algorithm for hypertensive patients or those who are at risk of developing HF; this step-care strategy is effective in treating hypertension, a leading cause of HF (C).
- Consult a specialist before prescribing both an angiotensin-converting enzyme (ACE) inhibitor and an angiotensin receptor blocker (ARB) for a patient with advanced HF; studies of combination therapy for this patient population have had mixed results (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians are all too familiar with heart failure (HF). This debilitating condition accounts for approximately 3.4 million outpatient visits to US physicians annually,1 and fully two-thirds of HF patients are cared for by primary care physicians.2
A host of comorbid conditions—coronary artery disease, valvular heart disease, diabetes, dyslipidemia, metabolic syndrome, obesity, chronic renal insufficiency, and hypertension chief among them—contribute to the development of HF.3 Of these, hypertension is the most important factor. In more than 75% of cases, high blood pressure precedes HF,1 and an individual’s lifetime risk of developing HF is strongly associated with poor blood pressure control.4 Hypertension is the most significant controllable factor in the management of HF as well. Because of the nexus between hypertension and HF, we encourage physicians to think of these 2 conditions as a single entity—and to recognize that a reduction of even a few millimeters of mercury can have huge clinical benefits.
This review, which highlights a recently tested hypertension algorithm along with other recent developments and long-established treatment strategies, will help you do everything possible to slow the progression of this debilitating and deadly disease.
BNP’s increasing role in evaluating heart failure
A diagnosis of HF in patients with known heart disease is based on functionality and symptoms, assessed with the help of 2 classification schemes5,6 ( TABLE 1 ) and a variety of tests. (Patients who present with the signs and symptoms of HF but no evidence of the comorbid conditions typically associated with it should be screened for other, noncardiac causes—human immunodeficiency virus, hepatitis C, hemochromatosis, hypothyroidism, and substance abuse among them.6 )
Diagnostic testing. Baseline serum chemistries include a complete blood count, urinalysis, electrolytes, magnesium, blood urea nitrogen, creatinine, and blood glucose levels, and liver and thyroid function tests.
B-type natriuretic peptide (BNP), a homeostatic marker secreted by the heart in an attempt to maintain stable blood pressure and plasma volume and avoid fluid retention, is increasingly recognized as an important aid, not only in diagnosing HF but in gauging its severity, managing symptoms, and determining the prognosis.7,8 BNP concentrations <80 pg/mL have been found to have a negative predictive value of 98%, and are also highly sensitive (98%) and specific (98%) for the diagnosis of HF.9,10

Testing may also include a 12-lead electrocardiogram as well as a posterior-anterior/lateral chest x-ray. Echocardiography is often used to evaluate left ventricular function and ejection fraction6 —a key to establishing whether the patient has systolic (reduced ejection fraction) or diastolic (preserved ejection fraction) HF.
An ejection fraction ≤40% is characteristic of systolic HF, which affects approximately 60% of patients with heart failure11 and is the focus of the following discussion of treatments.
TABLE 1
Classifying heart failure: 2 systems
| NEW YORK HEART ASSOCIATION |
| Class I: No limitation of physical activity; ordinary activity does not cause undue fatigue or dyspnea. Class II: Slight limitation of activity; comfortable at rest, but ordinary physical activity results in fatigue or dyspnea. Class III: Marked limitation in activity. Class IV: Unable to carry on any physical activity without symptoms; symptoms present even at rest. |
| AMERICAN COLLEGE OF CARDIOLOGY/AMERICAN HEART ASSOCIATION |
| Stage A: Conditions strongly associated with heart failure (HF); at high risk of HF. No identified structural or functional abnormalities of the pericardium, myocardium, or cardiac valves; no signs or symptoms of HF. Stage B: Structural heart disease strongly associated with HF, but no known signs or symptoms. Stage C: Current or prior symptoms of HF associated with underlying structural heart disease. Stage D: Advanced structural heart disease, with marked symptoms of HF at rest despite maximal medical therapy. Specialized interventions required. |
| Sources: Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. 1964;5 Hunt et al. Circulation. 2005.6 |
Early interventions: Get patients moving
For all patients with stable HF—and those at high risk of developingit—behavioral modification is a key component of treatment. Lifestyle intervention should be directed at weight loss and diet, including control of salt intake; increased physical activity; and smoking cessation.
Don’t shy away from exercise. Although many physicians hesitate to prescribe exercise to patients with HF, physical activity should be a routine recommendation for all but the most debilitated patients.6 Regular exercise has been shown to decrease symptoms, increase functional capacity, and improve the quality of life, with benefits comparable to those of pharmacotherapy.6,12,13
Studies of the beneficial effects of exercise were based on sustaining 40% to 70% of maximum capacity for 20 to 45 minutes, 3 to 5 days a week.6 A good walking program—of at least 30 minutes 4 to 5 days each week—should not be difficult for patients to maintain.
BP treatment guidelines: The old and the new
As noted earlier, controlling hypertension is crucial, not only to prevent HF but to attenuate its progress. But blood pressure management is suboptimal in the United States, with many patients failing to achieve recommended levels of pressure reduction. It’s been suggested that the complexity of standard treatment guidelines may be part of the problem.
STITCH step care is a newer option. Researchers designed the Simplified Treatment Intervention to Control Hypertension (STITCH) Trial, a cluster randomized study of patients at multiple family medicine clinics in Canada, to evaluate whether a simplified step-care algorithm would yield better results.
The STITCH algorithm has 4 treatment steps:
Step 1: Initiate therapy by pairing a diuretic with either an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB).
Step 2: Increase combination therapy to the highest dose tolerated.
Step 3: Add a calcium channel blocker and increase to the highest tolerated dose.
Step 4: Add a non-first-line antihypertensive agent (alpha-blocker, beta-blocker, or spironolactone).
Researchers found that after 6 months, 64.7% of patients on the STITCH protocol had achieved target blood pressure, compared with 52.7% of those whose treatment was based on the Canadian Hypertension Education Program (CHEP) guidelines (P=.03).14 The CHEP protocol is similar to that of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7);15 both offer numerous options for initial treatment.16
In presenting the STITCH results at the 2007 annual meeting of the American Heart Association, the lead author described the use of a simple step-care approach as “an important way forward in the treatment of hypertension [which] may be a paradigm for managing a range of chronic diseases.”16 Yet the STITCH algorithm has yet to be widely embraced; outside of the research community, most US physicians are relying on the JNC 7 guidelines.
ACC/AHA recommendations indicate that for patients at stage A—that is, those with conditions strongly associated with, and at high risk for, HF—management of hypertension should conform to national standards such as JNC 7. The JNC 7 guidelines recommend the use of a thiazide diuretic as the initial drug of choice for patients with essential hypertension. For those with diabetes, ACE inhibitors and ARBs are the first-line antihypertensive agents of choice.
Glucose control is also essential for stage A patients with diabetes. Treatment of lipid disorders and pharmacotherapy for metabolic syndrome are also recommended for stage A patients, as needed.
Treatment escalates as HF progresses
ACE inhibitors, ARBs, and beta-blockers are the preferred pharmacologic interventions for patients at stage B—those who have structural heart disease strongly associated with HF but are not yet symptomatic. Anyone who has had a myocardial infarction (MI) should be started on a beta-blocker and an ACE inhibitor, ACC/AHA recommends, unless a contraindication exists.6 Similarly, any patient with a reduced ejection fraction should be started on an ACE inhibitor regardless of symptoms.6
The Heart Outcomes Prevention Evaluation (HOPE) study demonstrated a 23% relative risk (RR) reduction with the use of an ACE inhibitor in patients with coronary artery disease, peripheral vascular disease, or diabetes, compared with patients receiving a placebo.17 The importance of a beta-blocker was established in a subanalysis of the Survival and Ventricular Enlargement Trial (SAVE), which found that patients taking beta-blockers in addition to an ACE inhibitor had a 32% RR reduction in progression of HF, compared with patients on an ACE inhibitor alone.18
We recommend an ACE inhibitor or an ARB and a beta-blocker, when appropriate, to slow the progression of HF pathophysiology. It is important to be aware of the potential adverse effects of certain beta-blockers in patients with HF. Only 3 beta-blockers are approved for use in this patient population in the United States—bisoprolol, carvedilol, and metoprolol succinate, which have been found to provide benefits that other beta-blockers do not.6,15
Stages C and D: Tx considerations and controversies
Treatment for patients at stage C should include all components of therapy for patients at stages A and B, but with a more aggressive use of pharmacotherapy ( TABLE 2 ). Patients with stage C HF, by definition, are symptomatic, and the ACC/AHA recommendations reflect concern about their increasingly compromised status. Thus, in addition to the use of ACE inhibitors or ARBs and beta-blockers, modest use of diuretics is recommended, as needed, for fluid volume control.6 Diuretics should be used judiciously, though, with ongoing evaluation to avoid the excessive loss of potassium and magnesium, which can lead to volume depletion and lethal arrhythmias. Limiting sodium consumption is an important dietary restriction for stage C patients.
Aldosterone antagonists may also be considered on a case-by-case basis for patients with stage C HF. Due to their potassium-sparing effects, aldosterone antagonists, used in conjunction with standard therapies, may have a positive effect on electrolyte balance. Potassium levels must be carefully monitored, however, and potassium supplementation reevaluated for patients who are put on an aldosterone antagonist.19
Digitalis may also be helpful in select patients who remain symptomatic despite maximal pharmacotherapy.20 While it does not affect mortality, digitalis has been shown to reduce hospitalizations.21
ACE inhibitor-ARB combination therapy, another possible treatment for advanced HF, remains controversial. The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET), detailed in “ACE inhibitors and ARBs: One or the other—not both” in the January 2009 issue of The Journal of Family Practice, evaluated use of this dual therapy; the trial was also designed to determine whether telmisartan (an ARB) is inferior to ramipril (an ACE inhibitor) in patients at high risk for vascular events.22 The researchers found that telmisartan is not, in fact, inferior to ramipril, and reported that for patients with HF, an ACE-ARB combination offers a potential benefit.
However, the clinical benefit of an ACE-ARB combination in this patient population was not clarified in this study, and may be potentially harmful. In the Valsartan Heart Failure Trial (ValHeFT), the combination of valsartan, an ARB, and an ACE inhibitor decreased hospitalizations but did not improve mortality.23 Indeed, an increase in mortality was found when an ACEARB combination was used in conjunction with beta-blockers. Because beta-blockers are indicated for routine use in patients with HF, this finding was of particular concern.
In a meta-analysis of randomized trials using both an ACE inhibitor and an ARB in patients with left ventricular dysfunction, researchers found a “marked” increase in adverse effects, including deteriorating renal function (RR=2.17), hyperkalemia (RR=4.87), and symptomatic hypotension (RR=1.05).24 Although an ACE-ARB combination may benefit a subset of patients with HF, it is best to initiate such treatment only with the guidance of an HF specialist.
TABLE 2
Treating heart failure: How the different drugs and devices rate
| STAGE | PHARMACOTHERAPY | LOE | DEVICE/INTERVENTION | LOE |
|---|---|---|---|---|
| A | Treat BP per JNC 7 ACE inhibitor or ARB for patients with vascular disease or diabetes | A | None | N/A |
| B | ACE inhibitor or ARB BB | A | None | N/A |
| C | Routine use: Diuretics ACE inhibitor BB Select use: Aldosterone antagonist ARB Digitalis | A | Consider: Biventricular pacer or ICD or both | B |
| D | Same as C | B | Consider: Heart transplant or LVAD; experimental protocols | C |
| ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BB, beta-blocker; BP, blood pressure; ICD, implantable cardioverter defibrillator; JNC 7, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; LOE, level of evidence; LVAD, left ventricular assist device. | ||||
| Adapted from: Hunt SA, et al. Circulation. 2005.6 | ||||
Beyond drug therapy: Assistive devices
Refractory end-stage HF requires a clear treatment plan, and should involve the recommendations of an HF specialist. Careful maintenance of fluid status is required, and an evaluation for cardiac transplantation may be considered.
A left ventricular assist device (LVAD) should also be considered for patients with an estimated 1-year mortality of >50%.6 LVADs are mechanical heart pumps that were initially utilized as a “bridge” to transplant, but are increasingly being used as a palliative alternative for severely ill patients.25
Other devices—an implantable cardioverter defibrillator (ICD) or a biventricular pacer—should also be considered for patients at stage D, as well as stage C patients who are at increased risk of sudden death despite maximal drug therapy.6 Patients who have had a previous MI or ventricular arrhythmia are at risk for a repeat episode.6
Use of an ICD can reduce mortality by 23% in selected patients.26 Potential candidates for the device are patients who have an ejection fraction of <30%, mild to moderate symptoms, and a life expectancy of at least 1 year.6
Biventricular pacing, also known as cardiac resynchronization therapy (CRT), has been found to improve the quality of life, functional status, and exercise capacity in some patients with advanced disease. CRT, which reduces symptoms of HF and improves cardiac function by reestablishing the mechanical sequence of ventricular activation and ventricular contraction, has also been associated with reductions in hospitalization and death from progressive HF.27,28
The Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) trial demonstrated a 20% reduction in the 12-month risk of death or hospitalization from any cause with CRT, and the Cardiac Resynchronization-Heart Failure (CARE-HF) trial established that patients receiving CRT had a significantly lower risk of death than those receiving medical therapy alone (40% reduction).29,30
However, not all patients with HF have problems with conduction delay that result in a dyssynchronous heart beat. CRT is indicated only for patients who are in sinus rhythm and have:
- NYHA class III or IV HF
- an ejection fraction of <35%
- a prolonged QRS complex (>120 m/sec), and
- continued symptoms despite maximal medical therapy.6
Under these criteria, approximately 10% of patients with HF would qualify for CRT.31 The restrictive criteria are due, in part, to the fact that this modality is relatively new and has been studied only in a small subset of patients.
Options for patients who are running out of them
For acutely decompensated hospitalized patients with volume overload, ultrafiltration (UF) is a useful alternative to diuretics. UF uses high pressure to “force” volume through the kidneys;32,33 the technique maximizes diuresis, and is best suited for patients who have significant renal dysfunction or are not responding to standard diuretic therapy. UF makes it easier to remove the desired amount of fluid, and has a positive impact on pulmonary wedge pressure and cardiac output.34 Its use in diuretic-resistant patients can decrease the length of stay and produce positive clinical benefits that may last up to 3 months.34
There are also a number of experimental strategies, surgical and otherwise. Among them are:
Cardiac wrap surgery, in which the heart is encased in a mesh bag attached with stitches, in an attempt to stop the progression of end-stage HF by preventing further dilation;25
Ventricular restoration surgery, a procedure in which scar tissue caused by MI is removed from the ventricular muscle and the left ventricle is reshaped and its size reduced in an attempt to restore some of the heart’s pumping ability;25 and
Enhanced external counterpulsation, or EECP, a noninvasive technique in which pressure cuffs are placed on the calves, thighs, and buttocks and inflated and deflated in an attempt to increase blood flow back to the heart.25
Correspondence
Randy Wexler, MD, MPH, FAAFP, The Ohio State University, B0902B Cramblett Hall, 456 W. 10th Avenue, Columbus, OH 43210; [email protected]
1. Rosamond W, Flegal K, Friday G, et al. American Heart Association: heart disease and stroke statistics–2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
2. Lloyd-Jones DM, Larson MG, Leip EP, et al. Framingham heart study. Lifetime risk for developing congestive heart failure. Circulation. 2002;106:3068-3072.
3. Burt CW, Schappert SM. Ambulatory care visits to physicians offices, hospital outpatient departments, and emergency departments: United states, 1999-2000. Vital Health Stat 13. 2004;157:1-70
4. Levit K, Stranges E, Ryan K, et al. HCUP facts and figures, 2006: Statistics on Hospital-based Care in the United States. Rockville, MD: Agency for Healthcare Research and Quality, 2008. Available at: http://www.hcup-us.ahrq.gov/reports.jsp. Accessed February 9, 2009.
5. Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. Boston: Little, Brown and Company; 1964.
6. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult. Circulation. 2005;112:e154-e235.
7. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74:1893-1898.
8. Maisel A, Krishnaswamy P, Nowak R, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161-167.
9. Maisel AS. B-type natriuretic peptide (BNP) levels: diagnostic and therapeutic potential. Rev Cardiovasc Med. 2001;2(suppl 2):S13-S18.
10. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide (BNP) in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001;37:379-385.
11. Philbin EF, Rocco TA, Jr, Lindenmuth NW, et al. Systolic versus diastolic heart failure in a community practice: clinical features, outcomes, and the use of angiotensin-converting enzyme inhibitors. Am J Med. 2000;109:605-613.
12. Piepoli MF, Flather M, Coats AJ. Overview of studies of exercise training in chronic heart failure: the need for a prospective randomized multicentre European trial. Eur Heart J. 1998;19:830-841.
13. Coats AJ, Adamopoulos S, Meyer TE, et al. Effects of physical training in chronic heart failure. Lancet. 1990;335:63-66.
14. Feldman RD, Zou G, Feagen BG, et al. The STITCH Investigators. The Simplified Treatment Intervention to Control Hypertension (STITCH) trial: A cluster randomized controlled trial of a step-care algorithm using initial fixed dose combination therapy for the management of hypertension. Presented at Scientific Sessions 2007 of the American Heart Association, November 4-7, 2007; Orlando, Fla.
15. Chobanian A, Bakris G, Black H, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Hypertension. 2003;42:1206-1252.
16. Brookes L. Hypertension highlights: new drug algorithms, new drug approvals, new drugs. Available at: http://canadiancpd.medscape.com/viewarticle/568786_print. Accessed January 27, 2009.
17. Yusuf S, Sleight P, Pogue J, et al. The Heart Outcomes Prevention Evaluation Study Investigators: effects of angiotensin converting enzyme inhibitor, ramipril, on cardiovascular events in high risk patients. N Engl J Med. 2000;342:145-153.
18. Vantrimpont P, Rouleau JL, Wun CC, et al. For the SAVE Investigators. Additive beneficial effects of beta-blockers to angiotensin converting enzyme inhibitors in the Survival and Ventricular Enlargement (SAVE) study. J Am Coll Cardiol. 1997;29:229-236.
19. Juurlink DN, Mamdani M, Kopp A, et al. Drug-drug interactions among elderly patients hospitalized for drug toxicity. JAMA. 2003;289:1652-1658.
20. Rahimtoola SH. Digitalis therapy for patients in clinical heart failure. Circulation. 2004;109:2942-2946.
21. Cayley W. Digitalis for the treatment of congestive heart failure in patients in sinus rhythm. Am Fam Physician. 2004;69:71-73.
22. The ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547-1559.
23. Cohn JN, Tognoni G. Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345:1667-1675.
24. Phillips CO, Kashani A, Ko DK, et al. Adverse effects of combination angiotensin II receptor blockers plus angiotensin-converting enzyme inhibitors for left ventricular dysfunction. Arch Intern Med. 2007;167:1930-1936.
25. Mayo Clinic. Heart failure: treatments and drugs. January 3, 2008. Available at: http://www.mayoclinic.com/health/heart-failure.DS00061/DSECTION=treatments-and-drugs. Accessed January 30, 2009.
26. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225-237.
27. Blanc J-J, Bertault-Valls V, Fatemi M, et al. Mid-term benefits of left univentricular pacing in patients with congestive heart failure. Circulation. 2004;109:1741-1744.
28. Bradley DJ, Bradley EA, Baughman KL, et al. Cardiac resynchronization and death from progressive heart failure: a meta-analysis of randomized controlled trials. JAMA. 2003;289:730-740.
29. Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140-2150.
30. Cleland JG, Daubert JC, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539-1549.
31. Farwell D, Patel NR, Hall A, et al. How many people with heart failure are appropriate for biventricular resynchronization? Eur Heart J. 2000;21:1246-1250.
32. Bart BA, Boyle A, Bank AJ, et al. Ultrafiltration versus usual care for hospitalized patients with heart failure: the relief for acutely fluid-overloaded patients with decompensated congestive heart failure (RAPD-HF). J Am Coll Cardiol. 2005;46:2043-2046.
33. Costanzo MR, Saltzberg M, O’Sullivan J, et al. Early ultrafiltration in patients with acutely decompensated heart failure and diuretic resistance. J Am Coll Cardiol. 2005;46:2047-2051.
34. Agostini PG, Marenzi GC, Lauri G, et al. Sustained improvement in functional capacity after removal of body fluid with isolated ultrafiltration in chronic cardiac insufficiency; failure of furosemide to provide same results. Am J Med. 1994;96:191-199.
- Use B-type natriuretic peptide (BNP) levels as an aid not only in the diagnosis of heart failure (HF), but to track its progression as well (A).
- Prescribe exercise training for patients with stable heart failure; exercising at 40% to 70% of maximum capacity for 20 to 45 minutes several times a week offers benefits on par with pharmacotherapy (A).
- Consider using the Simplified Treatment Intervention to Control Hypertension (STITCH) algorithm for hypertensive patients or those who are at risk of developing HF; this step-care strategy is effective in treating hypertension, a leading cause of HF (C).
- Consult a specialist before prescribing both an angiotensin-converting enzyme (ACE) inhibitor and an angiotensin receptor blocker (ARB) for a patient with advanced HF; studies of combination therapy for this patient population have had mixed results (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians are all too familiar with heart failure (HF). This debilitating condition accounts for approximately 3.4 million outpatient visits to US physicians annually,1 and fully two-thirds of HF patients are cared for by primary care physicians.2
A host of comorbid conditions—coronary artery disease, valvular heart disease, diabetes, dyslipidemia, metabolic syndrome, obesity, chronic renal insufficiency, and hypertension chief among them—contribute to the development of HF.3 Of these, hypertension is the most important factor. In more than 75% of cases, high blood pressure precedes HF,1 and an individual’s lifetime risk of developing HF is strongly associated with poor blood pressure control.4 Hypertension is the most significant controllable factor in the management of HF as well. Because of the nexus between hypertension and HF, we encourage physicians to think of these 2 conditions as a single entity—and to recognize that a reduction of even a few millimeters of mercury can have huge clinical benefits.
This review, which highlights a recently tested hypertension algorithm along with other recent developments and long-established treatment strategies, will help you do everything possible to slow the progression of this debilitating and deadly disease.
BNP’s increasing role in evaluating heart failure
A diagnosis of HF in patients with known heart disease is based on functionality and symptoms, assessed with the help of 2 classification schemes5,6 ( TABLE 1 ) and a variety of tests. (Patients who present with the signs and symptoms of HF but no evidence of the comorbid conditions typically associated with it should be screened for other, noncardiac causes—human immunodeficiency virus, hepatitis C, hemochromatosis, hypothyroidism, and substance abuse among them.6 )
Diagnostic testing. Baseline serum chemistries include a complete blood count, urinalysis, electrolytes, magnesium, blood urea nitrogen, creatinine, and blood glucose levels, and liver and thyroid function tests.
B-type natriuretic peptide (BNP), a homeostatic marker secreted by the heart in an attempt to maintain stable blood pressure and plasma volume and avoid fluid retention, is increasingly recognized as an important aid, not only in diagnosing HF but in gauging its severity, managing symptoms, and determining the prognosis.7,8 BNP concentrations <80 pg/mL have been found to have a negative predictive value of 98%, and are also highly sensitive (98%) and specific (98%) for the diagnosis of HF.9,10
Testing may also include a 12-lead electrocardiogram as well as a posterior-anterior/lateral chest x-ray. Echocardiography is often used to evaluate left ventricular function and ejection fraction6 —a key to establishing whether the patient has systolic (reduced ejection fraction) or diastolic (preserved ejection fraction) HF.
An ejection fraction ≤40% is characteristic of systolic HF, which affects approximately 60% of patients with heart failure11 and is the focus of the following discussion of treatments.
TABLE 1
Classifying heart failure: 2 systems
| NEW YORK HEART ASSOCIATION |
| Class I: No limitation of physical activity; ordinary activity does not cause undue fatigue or dyspnea. Class II: Slight limitation of activity; comfortable at rest, but ordinary physical activity results in fatigue or dyspnea. Class III: Marked limitation in activity. Class IV: Unable to carry on any physical activity without symptoms; symptoms present even at rest. |
| AMERICAN COLLEGE OF CARDIOLOGY/AMERICAN HEART ASSOCIATION |
| Stage A: Conditions strongly associated with heart failure (HF); at high risk of HF. No identified structural or functional abnormalities of the pericardium, myocardium, or cardiac valves; no signs or symptoms of HF. Stage B: Structural heart disease strongly associated with HF, but no known signs or symptoms. Stage C: Current or prior symptoms of HF associated with underlying structural heart disease. Stage D: Advanced structural heart disease, with marked symptoms of HF at rest despite maximal medical therapy. Specialized interventions required. |
| Sources: Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. 1964;5 Hunt et al. Circulation. 2005.6 |
Early interventions: Get patients moving
For all patients with stable HF—and those at high risk of developingit—behavioral modification is a key component of treatment. Lifestyle intervention should be directed at weight loss and diet, including control of salt intake; increased physical activity; and smoking cessation.
Don’t shy away from exercise. Although many physicians hesitate to prescribe exercise to patients with HF, physical activity should be a routine recommendation for all but the most debilitated patients.6 Regular exercise has been shown to decrease symptoms, increase functional capacity, and improve the quality of life, with benefits comparable to those of pharmacotherapy.6,12,13
Studies of the beneficial effects of exercise were based on sustaining 40% to 70% of maximum capacity for 20 to 45 minutes, 3 to 5 days a week.6 A good walking program—of at least 30 minutes 4 to 5 days each week—should not be difficult for patients to maintain.
BP treatment guidelines: The old and the new
As noted earlier, controlling hypertension is crucial, not only to prevent HF but to attenuate its progress. But blood pressure management is suboptimal in the United States, with many patients failing to achieve recommended levels of pressure reduction. It’s been suggested that the complexity of standard treatment guidelines may be part of the problem.
STITCH step care is a newer option. Researchers designed the Simplified Treatment Intervention to Control Hypertension (STITCH) Trial, a cluster randomized study of patients at multiple family medicine clinics in Canada, to evaluate whether a simplified step-care algorithm would yield better results.
The STITCH algorithm has 4 treatment steps:
Step 1: Initiate therapy by pairing a diuretic with either an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB).
Step 2: Increase combination therapy to the highest dose tolerated.
Step 3: Add a calcium channel blocker and increase to the highest tolerated dose.
Step 4: Add a non-first-line antihypertensive agent (alpha-blocker, beta-blocker, or spironolactone).
Researchers found that after 6 months, 64.7% of patients on the STITCH protocol had achieved target blood pressure, compared with 52.7% of those whose treatment was based on the Canadian Hypertension Education Program (CHEP) guidelines (P=.03).14 The CHEP protocol is similar to that of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7);15 both offer numerous options for initial treatment.16
In presenting the STITCH results at the 2007 annual meeting of the American Heart Association, the lead author described the use of a simple step-care approach as “an important way forward in the treatment of hypertension [which] may be a paradigm for managing a range of chronic diseases.”16 Yet the STITCH algorithm has yet to be widely embraced; outside of the research community, most US physicians are relying on the JNC 7 guidelines.
ACC/AHA recommendations indicate that for patients at stage A—that is, those with conditions strongly associated with, and at high risk for, HF—management of hypertension should conform to national standards such as JNC 7. The JNC 7 guidelines recommend the use of a thiazide diuretic as the initial drug of choice for patients with essential hypertension. For those with diabetes, ACE inhibitors and ARBs are the first-line antihypertensive agents of choice.
Glucose control is also essential for stage A patients with diabetes. Treatment of lipid disorders and pharmacotherapy for metabolic syndrome are also recommended for stage A patients, as needed.
Treatment escalates as HF progresses
ACE inhibitors, ARBs, and beta-blockers are the preferred pharmacologic interventions for patients at stage B—those who have structural heart disease strongly associated with HF but are not yet symptomatic. Anyone who has had a myocardial infarction (MI) should be started on a beta-blocker and an ACE inhibitor, ACC/AHA recommends, unless a contraindication exists.6 Similarly, any patient with a reduced ejection fraction should be started on an ACE inhibitor regardless of symptoms.6
The Heart Outcomes Prevention Evaluation (HOPE) study demonstrated a 23% relative risk (RR) reduction with the use of an ACE inhibitor in patients with coronary artery disease, peripheral vascular disease, or diabetes, compared with patients receiving a placebo.17 The importance of a beta-blocker was established in a subanalysis of the Survival and Ventricular Enlargement Trial (SAVE), which found that patients taking beta-blockers in addition to an ACE inhibitor had a 32% RR reduction in progression of HF, compared with patients on an ACE inhibitor alone.18
We recommend an ACE inhibitor or an ARB and a beta-blocker, when appropriate, to slow the progression of HF pathophysiology. It is important to be aware of the potential adverse effects of certain beta-blockers in patients with HF. Only 3 beta-blockers are approved for use in this patient population in the United States—bisoprolol, carvedilol, and metoprolol succinate, which have been found to provide benefits that other beta-blockers do not.6,15
Stages C and D: Tx considerations and controversies
Treatment for patients at stage C should include all components of therapy for patients at stages A and B, but with a more aggressive use of pharmacotherapy ( TABLE 2 ). Patients with stage C HF, by definition, are symptomatic, and the ACC/AHA recommendations reflect concern about their increasingly compromised status. Thus, in addition to the use of ACE inhibitors or ARBs and beta-blockers, modest use of diuretics is recommended, as needed, for fluid volume control.6 Diuretics should be used judiciously, though, with ongoing evaluation to avoid the excessive loss of potassium and magnesium, which can lead to volume depletion and lethal arrhythmias. Limiting sodium consumption is an important dietary restriction for stage C patients.
Aldosterone antagonists may also be considered on a case-by-case basis for patients with stage C HF. Due to their potassium-sparing effects, aldosterone antagonists, used in conjunction with standard therapies, may have a positive effect on electrolyte balance. Potassium levels must be carefully monitored, however, and potassium supplementation reevaluated for patients who are put on an aldosterone antagonist.19
Digitalis may also be helpful in select patients who remain symptomatic despite maximal pharmacotherapy.20 While it does not affect mortality, digitalis has been shown to reduce hospitalizations.21
ACE inhibitor-ARB combination therapy, another possible treatment for advanced HF, remains controversial. The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET), detailed in “ACE inhibitors and ARBs: One or the other—not both” in the January 2009 issue of The Journal of Family Practice, evaluated use of this dual therapy; the trial was also designed to determine whether telmisartan (an ARB) is inferior to ramipril (an ACE inhibitor) in patients at high risk for vascular events.22 The researchers found that telmisartan is not, in fact, inferior to ramipril, and reported that for patients with HF, an ACE-ARB combination offers a potential benefit.
However, the clinical benefit of an ACE-ARB combination in this patient population was not clarified in this study, and may be potentially harmful. In the Valsartan Heart Failure Trial (ValHeFT), the combination of valsartan, an ARB, and an ACE inhibitor decreased hospitalizations but did not improve mortality.23 Indeed, an increase in mortality was found when an ACEARB combination was used in conjunction with beta-blockers. Because beta-blockers are indicated for routine use in patients with HF, this finding was of particular concern.
In a meta-analysis of randomized trials using both an ACE inhibitor and an ARB in patients with left ventricular dysfunction, researchers found a “marked” increase in adverse effects, including deteriorating renal function (RR=2.17), hyperkalemia (RR=4.87), and symptomatic hypotension (RR=1.05).24 Although an ACE-ARB combination may benefit a subset of patients with HF, it is best to initiate such treatment only with the guidance of an HF specialist.
TABLE 2
Treating heart failure: How the different drugs and devices rate
| STAGE | PHARMACOTHERAPY | LOE | DEVICE/INTERVENTION | LOE |
|---|---|---|---|---|
| A | Treat BP per JNC 7 ACE inhibitor or ARB for patients with vascular disease or diabetes | A | None | N/A |
| B | ACE inhibitor or ARB BB | A | None | N/A |
| C | Routine use: Diuretics ACE inhibitor BB Select use: Aldosterone antagonist ARB Digitalis | A | Consider: Biventricular pacer or ICD or both | B |
| D | Same as C | B | Consider: Heart transplant or LVAD; experimental protocols | C |
| ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BB, beta-blocker; BP, blood pressure; ICD, implantable cardioverter defibrillator; JNC 7, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; LOE, level of evidence; LVAD, left ventricular assist device. | ||||
| Adapted from: Hunt SA, et al. Circulation. 2005.6 | ||||
Beyond drug therapy: Assistive devices
Refractory end-stage HF requires a clear treatment plan, and should involve the recommendations of an HF specialist. Careful maintenance of fluid status is required, and an evaluation for cardiac transplantation may be considered.
A left ventricular assist device (LVAD) should also be considered for patients with an estimated 1-year mortality of >50%.6 LVADs are mechanical heart pumps that were initially utilized as a “bridge” to transplant, but are increasingly being used as a palliative alternative for severely ill patients.25
Other devices—an implantable cardioverter defibrillator (ICD) or a biventricular pacer—should also be considered for patients at stage D, as well as stage C patients who are at increased risk of sudden death despite maximal drug therapy.6 Patients who have had a previous MI or ventricular arrhythmia are at risk for a repeat episode.6
Use of an ICD can reduce mortality by 23% in selected patients.26 Potential candidates for the device are patients who have an ejection fraction of <30%, mild to moderate symptoms, and a life expectancy of at least 1 year.6
Biventricular pacing, also known as cardiac resynchronization therapy (CRT), has been found to improve the quality of life, functional status, and exercise capacity in some patients with advanced disease. CRT, which reduces symptoms of HF and improves cardiac function by reestablishing the mechanical sequence of ventricular activation and ventricular contraction, has also been associated with reductions in hospitalization and death from progressive HF.27,28
The Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) trial demonstrated a 20% reduction in the 12-month risk of death or hospitalization from any cause with CRT, and the Cardiac Resynchronization-Heart Failure (CARE-HF) trial established that patients receiving CRT had a significantly lower risk of death than those receiving medical therapy alone (40% reduction).29,30
However, not all patients with HF have problems with conduction delay that result in a dyssynchronous heart beat. CRT is indicated only for patients who are in sinus rhythm and have:
- NYHA class III or IV HF
- an ejection fraction of <35%
- a prolonged QRS complex (>120 m/sec), and
- continued symptoms despite maximal medical therapy.6
Under these criteria, approximately 10% of patients with HF would qualify for CRT.31 The restrictive criteria are due, in part, to the fact that this modality is relatively new and has been studied only in a small subset of patients.
Options for patients who are running out of them
For acutely decompensated hospitalized patients with volume overload, ultrafiltration (UF) is a useful alternative to diuretics. UF uses high pressure to “force” volume through the kidneys;32,33 the technique maximizes diuresis, and is best suited for patients who have significant renal dysfunction or are not responding to standard diuretic therapy. UF makes it easier to remove the desired amount of fluid, and has a positive impact on pulmonary wedge pressure and cardiac output.34 Its use in diuretic-resistant patients can decrease the length of stay and produce positive clinical benefits that may last up to 3 months.34
There are also a number of experimental strategies, surgical and otherwise. Among them are:
Cardiac wrap surgery, in which the heart is encased in a mesh bag attached with stitches, in an attempt to stop the progression of end-stage HF by preventing further dilation;25
Ventricular restoration surgery, a procedure in which scar tissue caused by MI is removed from the ventricular muscle and the left ventricle is reshaped and its size reduced in an attempt to restore some of the heart’s pumping ability;25 and
Enhanced external counterpulsation, or EECP, a noninvasive technique in which pressure cuffs are placed on the calves, thighs, and buttocks and inflated and deflated in an attempt to increase blood flow back to the heart.25
Correspondence
Randy Wexler, MD, MPH, FAAFP, The Ohio State University, B0902B Cramblett Hall, 456 W. 10th Avenue, Columbus, OH 43210; [email protected]
- Use B-type natriuretic peptide (BNP) levels as an aid not only in the diagnosis of heart failure (HF), but to track its progression as well (A).
- Prescribe exercise training for patients with stable heart failure; exercising at 40% to 70% of maximum capacity for 20 to 45 minutes several times a week offers benefits on par with pharmacotherapy (A).
- Consider using the Simplified Treatment Intervention to Control Hypertension (STITCH) algorithm for hypertensive patients or those who are at risk of developing HF; this step-care strategy is effective in treating hypertension, a leading cause of HF (C).
- Consult a specialist before prescribing both an angiotensin-converting enzyme (ACE) inhibitor and an angiotensin receptor blocker (ARB) for a patient with advanced HF; studies of combination therapy for this patient population have had mixed results (C).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
Family physicians are all too familiar with heart failure (HF). This debilitating condition accounts for approximately 3.4 million outpatient visits to US physicians annually,1 and fully two-thirds of HF patients are cared for by primary care physicians.2
A host of comorbid conditions—coronary artery disease, valvular heart disease, diabetes, dyslipidemia, metabolic syndrome, obesity, chronic renal insufficiency, and hypertension chief among them—contribute to the development of HF.3 Of these, hypertension is the most important factor. In more than 75% of cases, high blood pressure precedes HF,1 and an individual’s lifetime risk of developing HF is strongly associated with poor blood pressure control.4 Hypertension is the most significant controllable factor in the management of HF as well. Because of the nexus between hypertension and HF, we encourage physicians to think of these 2 conditions as a single entity—and to recognize that a reduction of even a few millimeters of mercury can have huge clinical benefits.
This review, which highlights a recently tested hypertension algorithm along with other recent developments and long-established treatment strategies, will help you do everything possible to slow the progression of this debilitating and deadly disease.
BNP’s increasing role in evaluating heart failure
A diagnosis of HF in patients with known heart disease is based on functionality and symptoms, assessed with the help of 2 classification schemes5,6 ( TABLE 1 ) and a variety of tests. (Patients who present with the signs and symptoms of HF but no evidence of the comorbid conditions typically associated with it should be screened for other, noncardiac causes—human immunodeficiency virus, hepatitis C, hemochromatosis, hypothyroidism, and substance abuse among them.6 )
Diagnostic testing. Baseline serum chemistries include a complete blood count, urinalysis, electrolytes, magnesium, blood urea nitrogen, creatinine, and blood glucose levels, and liver and thyroid function tests.
B-type natriuretic peptide (BNP), a homeostatic marker secreted by the heart in an attempt to maintain stable blood pressure and plasma volume and avoid fluid retention, is increasingly recognized as an important aid, not only in diagnosing HF but in gauging its severity, managing symptoms, and determining the prognosis.7,8 BNP concentrations <80 pg/mL have been found to have a negative predictive value of 98%, and are also highly sensitive (98%) and specific (98%) for the diagnosis of HF.9,10
Testing may also include a 12-lead electrocardiogram as well as a posterior-anterior/lateral chest x-ray. Echocardiography is often used to evaluate left ventricular function and ejection fraction6 —a key to establishing whether the patient has systolic (reduced ejection fraction) or diastolic (preserved ejection fraction) HF.
An ejection fraction ≤40% is characteristic of systolic HF, which affects approximately 60% of patients with heart failure11 and is the focus of the following discussion of treatments.
TABLE 1
Classifying heart failure: 2 systems
| NEW YORK HEART ASSOCIATION |
| Class I: No limitation of physical activity; ordinary activity does not cause undue fatigue or dyspnea. Class II: Slight limitation of activity; comfortable at rest, but ordinary physical activity results in fatigue or dyspnea. Class III: Marked limitation in activity. Class IV: Unable to carry on any physical activity without symptoms; symptoms present even at rest. |
| AMERICAN COLLEGE OF CARDIOLOGY/AMERICAN HEART ASSOCIATION |
| Stage A: Conditions strongly associated with heart failure (HF); at high risk of HF. No identified structural or functional abnormalities of the pericardium, myocardium, or cardiac valves; no signs or symptoms of HF. Stage B: Structural heart disease strongly associated with HF, but no known signs or symptoms. Stage C: Current or prior symptoms of HF associated with underlying structural heart disease. Stage D: Advanced structural heart disease, with marked symptoms of HF at rest despite maximal medical therapy. Specialized interventions required. |
| Sources: Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. 1964;5 Hunt et al. Circulation. 2005.6 |
Early interventions: Get patients moving
For all patients with stable HF—and those at high risk of developingit—behavioral modification is a key component of treatment. Lifestyle intervention should be directed at weight loss and diet, including control of salt intake; increased physical activity; and smoking cessation.
Don’t shy away from exercise. Although many physicians hesitate to prescribe exercise to patients with HF, physical activity should be a routine recommendation for all but the most debilitated patients.6 Regular exercise has been shown to decrease symptoms, increase functional capacity, and improve the quality of life, with benefits comparable to those of pharmacotherapy.6,12,13
Studies of the beneficial effects of exercise were based on sustaining 40% to 70% of maximum capacity for 20 to 45 minutes, 3 to 5 days a week.6 A good walking program—of at least 30 minutes 4 to 5 days each week—should not be difficult for patients to maintain.
BP treatment guidelines: The old and the new
As noted earlier, controlling hypertension is crucial, not only to prevent HF but to attenuate its progress. But blood pressure management is suboptimal in the United States, with many patients failing to achieve recommended levels of pressure reduction. It’s been suggested that the complexity of standard treatment guidelines may be part of the problem.
STITCH step care is a newer option. Researchers designed the Simplified Treatment Intervention to Control Hypertension (STITCH) Trial, a cluster randomized study of patients at multiple family medicine clinics in Canada, to evaluate whether a simplified step-care algorithm would yield better results.
The STITCH algorithm has 4 treatment steps:
Step 1: Initiate therapy by pairing a diuretic with either an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB).
Step 2: Increase combination therapy to the highest dose tolerated.
Step 3: Add a calcium channel blocker and increase to the highest tolerated dose.
Step 4: Add a non-first-line antihypertensive agent (alpha-blocker, beta-blocker, or spironolactone).
Researchers found that after 6 months, 64.7% of patients on the STITCH protocol had achieved target blood pressure, compared with 52.7% of those whose treatment was based on the Canadian Hypertension Education Program (CHEP) guidelines (P=.03).14 The CHEP protocol is similar to that of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7);15 both offer numerous options for initial treatment.16
In presenting the STITCH results at the 2007 annual meeting of the American Heart Association, the lead author described the use of a simple step-care approach as “an important way forward in the treatment of hypertension [which] may be a paradigm for managing a range of chronic diseases.”16 Yet the STITCH algorithm has yet to be widely embraced; outside of the research community, most US physicians are relying on the JNC 7 guidelines.
ACC/AHA recommendations indicate that for patients at stage A—that is, those with conditions strongly associated with, and at high risk for, HF—management of hypertension should conform to national standards such as JNC 7. The JNC 7 guidelines recommend the use of a thiazide diuretic as the initial drug of choice for patients with essential hypertension. For those with diabetes, ACE inhibitors and ARBs are the first-line antihypertensive agents of choice.
Glucose control is also essential for stage A patients with diabetes. Treatment of lipid disorders and pharmacotherapy for metabolic syndrome are also recommended for stage A patients, as needed.
Treatment escalates as HF progresses
ACE inhibitors, ARBs, and beta-blockers are the preferred pharmacologic interventions for patients at stage B—those who have structural heart disease strongly associated with HF but are not yet symptomatic. Anyone who has had a myocardial infarction (MI) should be started on a beta-blocker and an ACE inhibitor, ACC/AHA recommends, unless a contraindication exists.6 Similarly, any patient with a reduced ejection fraction should be started on an ACE inhibitor regardless of symptoms.6
The Heart Outcomes Prevention Evaluation (HOPE) study demonstrated a 23% relative risk (RR) reduction with the use of an ACE inhibitor in patients with coronary artery disease, peripheral vascular disease, or diabetes, compared with patients receiving a placebo.17 The importance of a beta-blocker was established in a subanalysis of the Survival and Ventricular Enlargement Trial (SAVE), which found that patients taking beta-blockers in addition to an ACE inhibitor had a 32% RR reduction in progression of HF, compared with patients on an ACE inhibitor alone.18
We recommend an ACE inhibitor or an ARB and a beta-blocker, when appropriate, to slow the progression of HF pathophysiology. It is important to be aware of the potential adverse effects of certain beta-blockers in patients with HF. Only 3 beta-blockers are approved for use in this patient population in the United States—bisoprolol, carvedilol, and metoprolol succinate, which have been found to provide benefits that other beta-blockers do not.6,15
Stages C and D: Tx considerations and controversies
Treatment for patients at stage C should include all components of therapy for patients at stages A and B, but with a more aggressive use of pharmacotherapy ( TABLE 2 ). Patients with stage C HF, by definition, are symptomatic, and the ACC/AHA recommendations reflect concern about their increasingly compromised status. Thus, in addition to the use of ACE inhibitors or ARBs and beta-blockers, modest use of diuretics is recommended, as needed, for fluid volume control.6 Diuretics should be used judiciously, though, with ongoing evaluation to avoid the excessive loss of potassium and magnesium, which can lead to volume depletion and lethal arrhythmias. Limiting sodium consumption is an important dietary restriction for stage C patients.
Aldosterone antagonists may also be considered on a case-by-case basis for patients with stage C HF. Due to their potassium-sparing effects, aldosterone antagonists, used in conjunction with standard therapies, may have a positive effect on electrolyte balance. Potassium levels must be carefully monitored, however, and potassium supplementation reevaluated for patients who are put on an aldosterone antagonist.19
Digitalis may also be helpful in select patients who remain symptomatic despite maximal pharmacotherapy.20 While it does not affect mortality, digitalis has been shown to reduce hospitalizations.21
ACE inhibitor-ARB combination therapy, another possible treatment for advanced HF, remains controversial. The Ongoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial (ONTARGET), detailed in “ACE inhibitors and ARBs: One or the other—not both” in the January 2009 issue of The Journal of Family Practice, evaluated use of this dual therapy; the trial was also designed to determine whether telmisartan (an ARB) is inferior to ramipril (an ACE inhibitor) in patients at high risk for vascular events.22 The researchers found that telmisartan is not, in fact, inferior to ramipril, and reported that for patients with HF, an ACE-ARB combination offers a potential benefit.
However, the clinical benefit of an ACE-ARB combination in this patient population was not clarified in this study, and may be potentially harmful. In the Valsartan Heart Failure Trial (ValHeFT), the combination of valsartan, an ARB, and an ACE inhibitor decreased hospitalizations but did not improve mortality.23 Indeed, an increase in mortality was found when an ACEARB combination was used in conjunction with beta-blockers. Because beta-blockers are indicated for routine use in patients with HF, this finding was of particular concern.
In a meta-analysis of randomized trials using both an ACE inhibitor and an ARB in patients with left ventricular dysfunction, researchers found a “marked” increase in adverse effects, including deteriorating renal function (RR=2.17), hyperkalemia (RR=4.87), and symptomatic hypotension (RR=1.05).24 Although an ACE-ARB combination may benefit a subset of patients with HF, it is best to initiate such treatment only with the guidance of an HF specialist.
TABLE 2
Treating heart failure: How the different drugs and devices rate
| STAGE | PHARMACOTHERAPY | LOE | DEVICE/INTERVENTION | LOE |
|---|---|---|---|---|
| A | Treat BP per JNC 7 ACE inhibitor or ARB for patients with vascular disease or diabetes | A | None | N/A |
| B | ACE inhibitor or ARB BB | A | None | N/A |
| C | Routine use: Diuretics ACE inhibitor BB Select use: Aldosterone antagonist ARB Digitalis | A | Consider: Biventricular pacer or ICD or both | B |
| D | Same as C | B | Consider: Heart transplant or LVAD; experimental protocols | C |
| ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BB, beta-blocker; BP, blood pressure; ICD, implantable cardioverter defibrillator; JNC 7, the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; LOE, level of evidence; LVAD, left ventricular assist device. | ||||
| Adapted from: Hunt SA, et al. Circulation. 2005.6 | ||||
Beyond drug therapy: Assistive devices
Refractory end-stage HF requires a clear treatment plan, and should involve the recommendations of an HF specialist. Careful maintenance of fluid status is required, and an evaluation for cardiac transplantation may be considered.
A left ventricular assist device (LVAD) should also be considered for patients with an estimated 1-year mortality of >50%.6 LVADs are mechanical heart pumps that were initially utilized as a “bridge” to transplant, but are increasingly being used as a palliative alternative for severely ill patients.25
Other devices—an implantable cardioverter defibrillator (ICD) or a biventricular pacer—should also be considered for patients at stage D, as well as stage C patients who are at increased risk of sudden death despite maximal drug therapy.6 Patients who have had a previous MI or ventricular arrhythmia are at risk for a repeat episode.6
Use of an ICD can reduce mortality by 23% in selected patients.26 Potential candidates for the device are patients who have an ejection fraction of <30%, mild to moderate symptoms, and a life expectancy of at least 1 year.6
Biventricular pacing, also known as cardiac resynchronization therapy (CRT), has been found to improve the quality of life, functional status, and exercise capacity in some patients with advanced disease. CRT, which reduces symptoms of HF and improves cardiac function by reestablishing the mechanical sequence of ventricular activation and ventricular contraction, has also been associated with reductions in hospitalization and death from progressive HF.27,28
The Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) trial demonstrated a 20% reduction in the 12-month risk of death or hospitalization from any cause with CRT, and the Cardiac Resynchronization-Heart Failure (CARE-HF) trial established that patients receiving CRT had a significantly lower risk of death than those receiving medical therapy alone (40% reduction).29,30
However, not all patients with HF have problems with conduction delay that result in a dyssynchronous heart beat. CRT is indicated only for patients who are in sinus rhythm and have:
- NYHA class III or IV HF
- an ejection fraction of <35%
- a prolonged QRS complex (>120 m/sec), and
- continued symptoms despite maximal medical therapy.6
Under these criteria, approximately 10% of patients with HF would qualify for CRT.31 The restrictive criteria are due, in part, to the fact that this modality is relatively new and has been studied only in a small subset of patients.
Options for patients who are running out of them
For acutely decompensated hospitalized patients with volume overload, ultrafiltration (UF) is a useful alternative to diuretics. UF uses high pressure to “force” volume through the kidneys;32,33 the technique maximizes diuresis, and is best suited for patients who have significant renal dysfunction or are not responding to standard diuretic therapy. UF makes it easier to remove the desired amount of fluid, and has a positive impact on pulmonary wedge pressure and cardiac output.34 Its use in diuretic-resistant patients can decrease the length of stay and produce positive clinical benefits that may last up to 3 months.34
There are also a number of experimental strategies, surgical and otherwise. Among them are:
Cardiac wrap surgery, in which the heart is encased in a mesh bag attached with stitches, in an attempt to stop the progression of end-stage HF by preventing further dilation;25
Ventricular restoration surgery, a procedure in which scar tissue caused by MI is removed from the ventricular muscle and the left ventricle is reshaped and its size reduced in an attempt to restore some of the heart’s pumping ability;25 and
Enhanced external counterpulsation, or EECP, a noninvasive technique in which pressure cuffs are placed on the calves, thighs, and buttocks and inflated and deflated in an attempt to increase blood flow back to the heart.25
Correspondence
Randy Wexler, MD, MPH, FAAFP, The Ohio State University, B0902B Cramblett Hall, 456 W. 10th Avenue, Columbus, OH 43210; [email protected]
1. Rosamond W, Flegal K, Friday G, et al. American Heart Association: heart disease and stroke statistics–2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
2. Lloyd-Jones DM, Larson MG, Leip EP, et al. Framingham heart study. Lifetime risk for developing congestive heart failure. Circulation. 2002;106:3068-3072.
3. Burt CW, Schappert SM. Ambulatory care visits to physicians offices, hospital outpatient departments, and emergency departments: United states, 1999-2000. Vital Health Stat 13. 2004;157:1-70
4. Levit K, Stranges E, Ryan K, et al. HCUP facts and figures, 2006: Statistics on Hospital-based Care in the United States. Rockville, MD: Agency for Healthcare Research and Quality, 2008. Available at: http://www.hcup-us.ahrq.gov/reports.jsp. Accessed February 9, 2009.
5. Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. Boston: Little, Brown and Company; 1964.
6. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult. Circulation. 2005;112:e154-e235.
7. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74:1893-1898.
8. Maisel A, Krishnaswamy P, Nowak R, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161-167.
9. Maisel AS. B-type natriuretic peptide (BNP) levels: diagnostic and therapeutic potential. Rev Cardiovasc Med. 2001;2(suppl 2):S13-S18.
10. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide (BNP) in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001;37:379-385.
11. Philbin EF, Rocco TA, Jr, Lindenmuth NW, et al. Systolic versus diastolic heart failure in a community practice: clinical features, outcomes, and the use of angiotensin-converting enzyme inhibitors. Am J Med. 2000;109:605-613.
12. Piepoli MF, Flather M, Coats AJ. Overview of studies of exercise training in chronic heart failure: the need for a prospective randomized multicentre European trial. Eur Heart J. 1998;19:830-841.
13. Coats AJ, Adamopoulos S, Meyer TE, et al. Effects of physical training in chronic heart failure. Lancet. 1990;335:63-66.
14. Feldman RD, Zou G, Feagen BG, et al. The STITCH Investigators. The Simplified Treatment Intervention to Control Hypertension (STITCH) trial: A cluster randomized controlled trial of a step-care algorithm using initial fixed dose combination therapy for the management of hypertension. Presented at Scientific Sessions 2007 of the American Heart Association, November 4-7, 2007; Orlando, Fla.
15. Chobanian A, Bakris G, Black H, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Hypertension. 2003;42:1206-1252.
16. Brookes L. Hypertension highlights: new drug algorithms, new drug approvals, new drugs. Available at: http://canadiancpd.medscape.com/viewarticle/568786_print. Accessed January 27, 2009.
17. Yusuf S, Sleight P, Pogue J, et al. The Heart Outcomes Prevention Evaluation Study Investigators: effects of angiotensin converting enzyme inhibitor, ramipril, on cardiovascular events in high risk patients. N Engl J Med. 2000;342:145-153.
18. Vantrimpont P, Rouleau JL, Wun CC, et al. For the SAVE Investigators. Additive beneficial effects of beta-blockers to angiotensin converting enzyme inhibitors in the Survival and Ventricular Enlargement (SAVE) study. J Am Coll Cardiol. 1997;29:229-236.
19. Juurlink DN, Mamdani M, Kopp A, et al. Drug-drug interactions among elderly patients hospitalized for drug toxicity. JAMA. 2003;289:1652-1658.
20. Rahimtoola SH. Digitalis therapy for patients in clinical heart failure. Circulation. 2004;109:2942-2946.
21. Cayley W. Digitalis for the treatment of congestive heart failure in patients in sinus rhythm. Am Fam Physician. 2004;69:71-73.
22. The ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547-1559.
23. Cohn JN, Tognoni G. Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345:1667-1675.
24. Phillips CO, Kashani A, Ko DK, et al. Adverse effects of combination angiotensin II receptor blockers plus angiotensin-converting enzyme inhibitors for left ventricular dysfunction. Arch Intern Med. 2007;167:1930-1936.
25. Mayo Clinic. Heart failure: treatments and drugs. January 3, 2008. Available at: http://www.mayoclinic.com/health/heart-failure.DS00061/DSECTION=treatments-and-drugs. Accessed January 30, 2009.
26. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225-237.
27. Blanc J-J, Bertault-Valls V, Fatemi M, et al. Mid-term benefits of left univentricular pacing in patients with congestive heart failure. Circulation. 2004;109:1741-1744.
28. Bradley DJ, Bradley EA, Baughman KL, et al. Cardiac resynchronization and death from progressive heart failure: a meta-analysis of randomized controlled trials. JAMA. 2003;289:730-740.
29. Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140-2150.
30. Cleland JG, Daubert JC, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539-1549.
31. Farwell D, Patel NR, Hall A, et al. How many people with heart failure are appropriate for biventricular resynchronization? Eur Heart J. 2000;21:1246-1250.
32. Bart BA, Boyle A, Bank AJ, et al. Ultrafiltration versus usual care for hospitalized patients with heart failure: the relief for acutely fluid-overloaded patients with decompensated congestive heart failure (RAPD-HF). J Am Coll Cardiol. 2005;46:2043-2046.
33. Costanzo MR, Saltzberg M, O’Sullivan J, et al. Early ultrafiltration in patients with acutely decompensated heart failure and diuretic resistance. J Am Coll Cardiol. 2005;46:2047-2051.
34. Agostini PG, Marenzi GC, Lauri G, et al. Sustained improvement in functional capacity after removal of body fluid with isolated ultrafiltration in chronic cardiac insufficiency; failure of furosemide to provide same results. Am J Med. 1994;96:191-199.
1. Rosamond W, Flegal K, Friday G, et al. American Heart Association: heart disease and stroke statistics–2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
2. Lloyd-Jones DM, Larson MG, Leip EP, et al. Framingham heart study. Lifetime risk for developing congestive heart failure. Circulation. 2002;106:3068-3072.
3. Burt CW, Schappert SM. Ambulatory care visits to physicians offices, hospital outpatient departments, and emergency departments: United states, 1999-2000. Vital Health Stat 13. 2004;157:1-70
4. Levit K, Stranges E, Ryan K, et al. HCUP facts and figures, 2006: Statistics on Hospital-based Care in the United States. Rockville, MD: Agency for Healthcare Research and Quality, 2008. Available at: http://www.hcup-us.ahrq.gov/reports.jsp. Accessed February 9, 2009.
5. Criteria Committee of the New York Heart Association. Diseases of the Heart and Blood Vessels–Nomenclature and Criteria for Diagnosis. 6th ed. Boston: Little, Brown and Company; 1964.
6. Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult. Circulation. 2005;112:e154-e235.
7. Doust J, Lehman R, Glasziou P. The role of BNP testing in heart failure. Am Fam Physician. 2006;74:1893-1898.
8. Maisel A, Krishnaswamy P, Nowak R, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161-167.
9. Maisel AS. B-type natriuretic peptide (BNP) levels: diagnostic and therapeutic potential. Rev Cardiovasc Med. 2001;2(suppl 2):S13-S18.
10. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide (BNP) in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001;37:379-385.
11. Philbin EF, Rocco TA, Jr, Lindenmuth NW, et al. Systolic versus diastolic heart failure in a community practice: clinical features, outcomes, and the use of angiotensin-converting enzyme inhibitors. Am J Med. 2000;109:605-613.
12. Piepoli MF, Flather M, Coats AJ. Overview of studies of exercise training in chronic heart failure: the need for a prospective randomized multicentre European trial. Eur Heart J. 1998;19:830-841.
13. Coats AJ, Adamopoulos S, Meyer TE, et al. Effects of physical training in chronic heart failure. Lancet. 1990;335:63-66.
14. Feldman RD, Zou G, Feagen BG, et al. The STITCH Investigators. The Simplified Treatment Intervention to Control Hypertension (STITCH) trial: A cluster randomized controlled trial of a step-care algorithm using initial fixed dose combination therapy for the management of hypertension. Presented at Scientific Sessions 2007 of the American Heart Association, November 4-7, 2007; Orlando, Fla.
15. Chobanian A, Bakris G, Black H, et al. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Hypertension. 2003;42:1206-1252.
16. Brookes L. Hypertension highlights: new drug algorithms, new drug approvals, new drugs. Available at: http://canadiancpd.medscape.com/viewarticle/568786_print. Accessed January 27, 2009.
17. Yusuf S, Sleight P, Pogue J, et al. The Heart Outcomes Prevention Evaluation Study Investigators: effects of angiotensin converting enzyme inhibitor, ramipril, on cardiovascular events in high risk patients. N Engl J Med. 2000;342:145-153.
18. Vantrimpont P, Rouleau JL, Wun CC, et al. For the SAVE Investigators. Additive beneficial effects of beta-blockers to angiotensin converting enzyme inhibitors in the Survival and Ventricular Enlargement (SAVE) study. J Am Coll Cardiol. 1997;29:229-236.
19. Juurlink DN, Mamdani M, Kopp A, et al. Drug-drug interactions among elderly patients hospitalized for drug toxicity. JAMA. 2003;289:1652-1658.
20. Rahimtoola SH. Digitalis therapy for patients in clinical heart failure. Circulation. 2004;109:2942-2946.
21. Cayley W. Digitalis for the treatment of congestive heart failure in patients in sinus rhythm. Am Fam Physician. 2004;69:71-73.
22. The ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547-1559.
23. Cohn JN, Tognoni G. Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001;345:1667-1675.
24. Phillips CO, Kashani A, Ko DK, et al. Adverse effects of combination angiotensin II receptor blockers plus angiotensin-converting enzyme inhibitors for left ventricular dysfunction. Arch Intern Med. 2007;167:1930-1936.
25. Mayo Clinic. Heart failure: treatments and drugs. January 3, 2008. Available at: http://www.mayoclinic.com/health/heart-failure.DS00061/DSECTION=treatments-and-drugs. Accessed January 30, 2009.
26. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225-237.
27. Blanc J-J, Bertault-Valls V, Fatemi M, et al. Mid-term benefits of left univentricular pacing in patients with congestive heart failure. Circulation. 2004;109:1741-1744.
28. Bradley DJ, Bradley EA, Baughman KL, et al. Cardiac resynchronization and death from progressive heart failure: a meta-analysis of randomized controlled trials. JAMA. 2003;289:730-740.
29. Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140-2150.
30. Cleland JG, Daubert JC, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539-1549.
31. Farwell D, Patel NR, Hall A, et al. How many people with heart failure are appropriate for biventricular resynchronization? Eur Heart J. 2000;21:1246-1250.
32. Bart BA, Boyle A, Bank AJ, et al. Ultrafiltration versus usual care for hospitalized patients with heart failure: the relief for acutely fluid-overloaded patients with decompensated congestive heart failure (RAPD-HF). J Am Coll Cardiol. 2005;46:2043-2046.
33. Costanzo MR, Saltzberg M, O’Sullivan J, et al. Early ultrafiltration in patients with acutely decompensated heart failure and diuretic resistance. J Am Coll Cardiol. 2005;46:2047-2051.
34. Agostini PG, Marenzi GC, Lauri G, et al. Sustained improvement in functional capacity after removal of body fluid with isolated ultrafiltration in chronic cardiac insufficiency; failure of furosemide to provide same results. Am J Med. 1994;96:191-199.