The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Because of overlapping clinical manifestations, clinicians often order ultrasound to rule out deep vein thrombosis (DVT) in cases of cellulitis. Ultrasound testing is performed for 16% to 73% of patients diagnosed with cellulitis. Although testing is common, the pooled incidence of DVT is low (3.1%). Few data elucidate which patients with cellulitis are more likely to have concurrent DVT and require further testing. The Wells clinical prediction rule with D-dimer testing overestimates DVT risk in patients with cellulitis and is of little value in this setting. Given the overall low incidence, routine ultrasound testing is unnecessary for most patients with cellulitis. ultrasound should be reserved for patients with a history of venous thromboembolism (VTE), immobility, thrombophilia, congestive heart failure (CHF), cerebrovascular accident (CVA) with hemiparesis, trauma, or recent surgery, and for patients who do not respond to antibiotics.
CASE REPORT
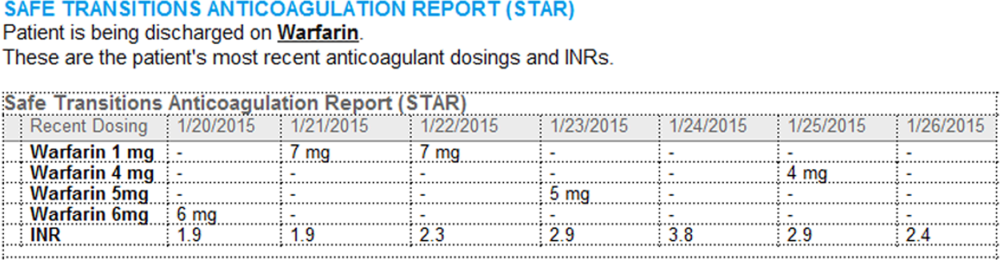
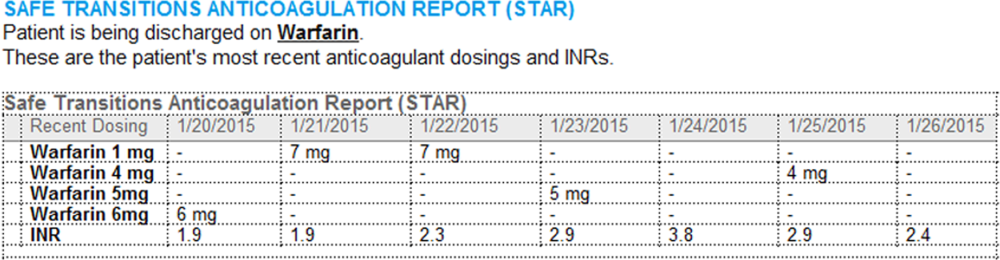
A 50-year-old man presented to the emergency department with a 3-day-old cut on his anterior right shin. Associated redness, warmth, pain, and swelling had progressed. The patient had no history of prior DVT or pulmonary embolism (PE). His temperature was 38.5°C, and his white blood cell count of 18,000. On review of systems, he denied shortness of breath and chest pain. He was diagnosed with cellulitis and administered intravenous fluids and cefazolin. The clinician wondered whether to perform lower extremity ultrasound to rule out concurrent DVT.
WHY YOU MIGHT THINK ULTRASOUND IS HELPFUL IN RULING OUT DVT IN CELLULITIS
Lower extremity cellulitis, a common infection of the skin and subcutaneous tissues, is characterized by unilateral erythema, pain, warmth, and swelling. The infection usually follows a skin breach that allows bacteria to enter. DVT may present similarly, and symptoms can include mild leukocytosis and elevated temperature. Because of the clinical similarities, clinicians often order compression ultrasound of the extremity to rule out concurrent DVT in cellulitis. Further impetus for testing stems from fear of the potential complications of untreated DVT, including post-thrombotic syndrome, chronic venous insufficiency, and venous ulceration. A subsequent PE can be fatal, or can cause significant morbidity, including chronic VTE with associated pulmonary hypertension. An estimated quarter of all PEs present as sudden death.1
WHY ULTRASOUND IS NOT HELPFUL IN THIS SETTING
Studies have shown that ultrasound is ordered for 16% to 73% of patients with a cellulitis diagnosis.2,3 Although testing is commonly performed, a meta-analysis of 9 studies of cellulitis patients who underwent ultrasound testing for concurrent DVT revealed a low pooled incidence of total DVT (3.1%) and proximal DVT (2.1%).4 Maze et al.2 retrospectively reviewed 1515 cellulitis cases (identified by International Classification of Diseases, Ninth Revision codes) at a single center in New Zealand over 3 years. Of the 1515 patients, 240 (16%) had ultrasound performed, and only 3 (1.3%) were found to have DVT. Two of the 3 had active malignancy, and the third had injected battery acid into the area. In a 5-year retrospective cohort study at a Veterans Administration hospital in Connecticut, Gunderson and Chang3 reviewed the cases of 183 patients with cellulitis and found ultrasound testing commonly performed (73% of cases) to assess for DVT. Only 1 patient (<1%) was diagnosed with new DVT in the ipsilateral leg, and acute DVT was diagnosed in the contralateral leg of 2 other patients. Overall, these studies indicate the incidence of concurrent DVT in cellulitis is low, regardless of the frequency of ultrasound testing.
Although the cost of a single ultrasound test is not prohibitive, annual total costs hospital-wide and nationally are large. In the United States, the charge for a unilateral duplex ultrasound of the extremity ranges from $260 to $1300, and there is an additional charge for interpretation by a radiologist.5 In a retrospective study spanning 3.5 years and involving 2 community hospitals in Michigan, an estimated $290,000 was spent on ultrasound tests defined as unnecessary for patients with cellulitis.6 A limitation of the study was defining a test as unnecessary based on its result being negative.
DOES WELLS SCORE WITH D-DIMER HELP DEFINE A LOW-RISK POPULATION?
The Wells clinical prediction rule is commonly used to assess the pretest probability of DVT in patients presenting with unilateral leg symptoms. The Wells score is often combined with D-dimer testing to help determine whether ultrasound is necessary. Studies of patients with suspected DVT have found that those considered low risk according to the Wells criteria had a 6.5% incidence of DVT.7 However, the predictive value is lower in the setting of presumed cellulitis. In a prospective cohort study of 200 patients with cellulitis, Maze et al.8 reported that use of the Wells score with D-dimer testing overestimated the DVT risk. D-dimer level was elevated for 74% of patients, and 20.5% were high-risk by Wells criteria. An algorithm determined that—among patients with a high-risk Wells score, a positive D-dimer result, or both—only 1 (0.5%) was diagnosed with ipsilateral DVT after ultrasound testing. Two patients were diagnosed with DVT in the contralateral leg. These results suggest that a strategy that incorporates the Wells score and D-dimer testing in the setting of acute cellulitis provides little value. The authors concluded that, in the absence of a known hypercoagulable state, ultrasound is not warranted. However, their study did not assess whether there are any specific hypercoagulable states for which further testing may be indicated.
WHEN MIGHT ULTRASOUND BE HELPFUL IN CELLULITIS?
Investigators have described possible DVT risk factors in patients with cellulitis, but definitive associations are lacking because of the insufficient number of patients studied.8,9 The most consistently identified DVT risk factor is history of previous thromboembolism. In a retrospective analysis of patients with cellulitis, Afzal et al.6 found that, of the 66.8% who underwent ultrasound testing, 5.5% were identified as having concurrent DVT. The authors performed univariate analyses of 15 potential risk factors, including active malignancy, oral contraceptive pill use, recent hospitalization, and surgery. A higher incidence of DVT was found for patients with history of VTE (odds ratio [OR], 5.7; 95% confidence interval [CI], 2.3-13.7), calf swelling (OR, 4.5; 95% CI, 1.3-15.8), CVA (OR, 3.5; 95% CI, 1.2-10.1), or hypertension (OR, 3.5; 95% CI, 0.98-12.2). Given the wide confidence intervals, paucity of studies, and lack of definitive data in the setting of cellulitis, clinicians may want to consider the risk factors established in larger trials in other settings, including known immobility (OR, <2); thrombophilia, CHF, and CVA with hemiparesis (OR, 2-9); and trauma and recent surgery (OR, >10).10
WHAT YOU SHOULD DO INSTEAD
As the incidence of concurrent VTE in patients with cellulitis is low, the essential step is to make a clear diagnosis of cellulitis based on its established signs and symptoms. A 2-center trial of 145 patients found that cellulitis was diagnosed accurately by general medicine and emergency medicine physicians 72% of the time, with evaluation by dermatologists and infectious disease specialists used as the gold standard. Only 5% of the misdiagnosed patients were diagnosed with DVT; stasis dermatitis was the most common alternative diagnosis. Taking a thorough history may elicit risk factors consistent with cellulitis, such as a recent injury with a break in the skin. On examination, cellulitis should be suspected for patients with fever and localized pain, redness, swelling, and warmth—the cardinal signs of dolor, rubor, tumor, and calor. An injury or entry site and leukocytosis also support the diagnosis of cellulitis. Distinct margins of erythema on the skin are highly suspicious for erysipelas.11 Other physical findings (eg, laceration, purulent drainage, lymphangitic spread, fluctuating mass) also are consistent with a diagnosis of cellulitis.
The patient’s history is also essential in determining whether any DVT risk factors are present. Past medical history of VTE or CVA, or recent history of surgery, immobility, or trauma, should alert the clinician to the possibility of DVT. Family history of VTE increases the likelihood of DVT. Acute shortness of breath or chest pain in the setting of concerning lower extremity findings for DVT should raise concern for DVT and concurrent PE.
If the classic features of cellulitis are present, empiric antibiotics should be initiated. Routine ultrasound testing for all patients with cellulitis is of low value. However, as the incidence of DVT in this population is not negligible, those with VTE risk factors should be targeted for testing. Studies in the setting of cellulitis provide little guidance regarding specific risk factors that can be used to determine who should undergo further testing. Given this limitation, we suggest that clinicians incorporate into their decision making the well-established VTE risk factors identified for large populations studied in other settings, such as the postoperative period. Specifically, clinicians should consider ultrasound testing for patients with cellulitis and prior history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery.10-12 Ultrasound should also be considered for patients with cellulitis that does not improve and for patients whose localized symptoms worsen despite use of antibiotics.
RECOMMENDATIONS
Do not routinely perform ultrasound to rule out concurrent DVT in cases of cellulitis.
Consider compression ultrasound if there is a history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery. Also consider it for patients who do not respond to antibiotics.
In cases of cellulitis, avoid use of the Wells score alone or with D-dimer testing, as it likely overestimates the DVT risk.
CONCLUSION
The current evidence shows that, for most patients with cellulitis, routine ultrasound testing for DVT is unnecessary. Ultrasound should be considered for patients with potent VTE risk factors. If symptoms do not improve, or if they worsen despite use of antibiotics, clinicians should be alert to potential anchoring bias and consider DVT. The Wells clinical prediction rule overestimates the incidence of DVT in cellulitis and has little value in this setting.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason”? Let us know what you do in your practice and propose ideas for other “Things We Do for No Reason” topics. Please join in the conversation online at Twitter (#TWDFNR)/Facebook and don’t forget to “Like It” on Facebook or retweet it on Twitter. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
References
1. Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21(1):23-29. PubMed 2. Maze MJ, Pithie A, Dawes T, Chambers ST. An audit of venous duplex ultrasonography in patients with lower limb cellulitis. N Z Med J. 2011;124(1329):53-56. PubMed 3. Gunderson CG, Chang JJ. Overuse of compression ultrasound for patients with lower extremity cellulitis. Thromb Res. 2014;134(4):846-850. PubMed 4. Gunderson CG, Chang JJ. Risk of deep vein thrombosis in patients with cellulitis and erysipelas: a systematic review and meta-analysis. Thromb Res. 2013;132(3):336-340. PubMed 5. Extremity ultrasound (nonvascular) cost and procedure information. http://www.newchoicehealth.com/procedures/extremity-ultrasound-nonvascular. Accessed February 15, 2016. 6. Afzal MZ, Saleh MM, Razvi S, Hashmi H, Lampen R. Utility of lower extremity Doppler in patients with lower extremity cellulitis: a need to change the practice? South Med J. 2015;108(7):439-444. PubMed 7. Goodacre S, Sutton AJ, Sampson FC. Meta-analysis: the value of clinical assessment in the diagnosis of deep venous thrombosis. Ann Intern Med. 2005;143(2):129-139. PubMed 8. Maze MJ, Skea S, Pithie A, Metcalf S, Pearson JF, Chambers ST. Prevalence of concurrent deep vein thrombosis in patients with lower limb cellulitis: a prospective cohort study. BMC Infect Dis. 2013;13:141. PubMed 9. Bersier D, Bounameaux H. Cellulitis and deep vein thrombosis: a controversial association. J Thromb Haemost. 2003;1(4):867-868. PubMed 10. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 suppl 1):I9-I16. PubMed 11. Rabuka CE, Azoulay LY, Kahn SR. Predictors of a positive duplex scan in patients with a clinical presentation compatible with deep vein thrombosis or cellulitis. Can J Infect Dis. 2003;14(4):210-214. PubMed 12. Samama MM. An epidemiologic study of risk factors for deep vein thrombosis in medical outpatients: the Sirius Study. Arch Intern Med. 2000;160(22):3415-3420. PubMed
The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Because of overlapping clinical manifestations, clinicians often order ultrasound to rule out deep vein thrombosis (DVT) in cases of cellulitis. Ultrasound testing is performed for 16% to 73% of patients diagnosed with cellulitis. Although testing is common, the pooled incidence of DVT is low (3.1%). Few data elucidate which patients with cellulitis are more likely to have concurrent DVT and require further testing. The Wells clinical prediction rule with D-dimer testing overestimates DVT risk in patients with cellulitis and is of little value in this setting. Given the overall low incidence, routine ultrasound testing is unnecessary for most patients with cellulitis. ultrasound should be reserved for patients with a history of venous thromboembolism (VTE), immobility, thrombophilia, congestive heart failure (CHF), cerebrovascular accident (CVA) with hemiparesis, trauma, or recent surgery, and for patients who do not respond to antibiotics.
CASE REPORT
A 50-year-old man presented to the emergency department with a 3-day-old cut on his anterior right shin. Associated redness, warmth, pain, and swelling had progressed. The patient had no history of prior DVT or pulmonary embolism (PE). His temperature was 38.5°C, and his white blood cell count of 18,000. On review of systems, he denied shortness of breath and chest pain. He was diagnosed with cellulitis and administered intravenous fluids and cefazolin. The clinician wondered whether to perform lower extremity ultrasound to rule out concurrent DVT.
WHY YOU MIGHT THINK ULTRASOUND IS HELPFUL IN RULING OUT DVT IN CELLULITIS
Lower extremity cellulitis, a common infection of the skin and subcutaneous tissues, is characterized by unilateral erythema, pain, warmth, and swelling. The infection usually follows a skin breach that allows bacteria to enter. DVT may present similarly, and symptoms can include mild leukocytosis and elevated temperature. Because of the clinical similarities, clinicians often order compression ultrasound of the extremity to rule out concurrent DVT in cellulitis. Further impetus for testing stems from fear of the potential complications of untreated DVT, including post-thrombotic syndrome, chronic venous insufficiency, and venous ulceration. A subsequent PE can be fatal, or can cause significant morbidity, including chronic VTE with associated pulmonary hypertension. An estimated quarter of all PEs present as sudden death.1
WHY ULTRASOUND IS NOT HELPFUL IN THIS SETTING
Studies have shown that ultrasound is ordered for 16% to 73% of patients with a cellulitis diagnosis.2,3 Although testing is commonly performed, a meta-analysis of 9 studies of cellulitis patients who underwent ultrasound testing for concurrent DVT revealed a low pooled incidence of total DVT (3.1%) and proximal DVT (2.1%).4 Maze et al.2 retrospectively reviewed 1515 cellulitis cases (identified by International Classification of Diseases, Ninth Revision codes) at a single center in New Zealand over 3 years. Of the 1515 patients, 240 (16%) had ultrasound performed, and only 3 (1.3%) were found to have DVT. Two of the 3 had active malignancy, and the third had injected battery acid into the area. In a 5-year retrospective cohort study at a Veterans Administration hospital in Connecticut, Gunderson and Chang3 reviewed the cases of 183 patients with cellulitis and found ultrasound testing commonly performed (73% of cases) to assess for DVT. Only 1 patient (<1%) was diagnosed with new DVT in the ipsilateral leg, and acute DVT was diagnosed in the contralateral leg of 2 other patients. Overall, these studies indicate the incidence of concurrent DVT in cellulitis is low, regardless of the frequency of ultrasound testing.
Although the cost of a single ultrasound test is not prohibitive, annual total costs hospital-wide and nationally are large. In the United States, the charge for a unilateral duplex ultrasound of the extremity ranges from $260 to $1300, and there is an additional charge for interpretation by a radiologist.5 In a retrospective study spanning 3.5 years and involving 2 community hospitals in Michigan, an estimated $290,000 was spent on ultrasound tests defined as unnecessary for patients with cellulitis.6 A limitation of the study was defining a test as unnecessary based on its result being negative.
DOES WELLS SCORE WITH D-DIMER HELP DEFINE A LOW-RISK POPULATION?
The Wells clinical prediction rule is commonly used to assess the pretest probability of DVT in patients presenting with unilateral leg symptoms. The Wells score is often combined with D-dimer testing to help determine whether ultrasound is necessary. Studies of patients with suspected DVT have found that those considered low risk according to the Wells criteria had a 6.5% incidence of DVT.7 However, the predictive value is lower in the setting of presumed cellulitis. In a prospective cohort study of 200 patients with cellulitis, Maze et al.8 reported that use of the Wells score with D-dimer testing overestimated the DVT risk. D-dimer level was elevated for 74% of patients, and 20.5% were high-risk by Wells criteria. An algorithm determined that—among patients with a high-risk Wells score, a positive D-dimer result, or both—only 1 (0.5%) was diagnosed with ipsilateral DVT after ultrasound testing. Two patients were diagnosed with DVT in the contralateral leg. These results suggest that a strategy that incorporates the Wells score and D-dimer testing in the setting of acute cellulitis provides little value. The authors concluded that, in the absence of a known hypercoagulable state, ultrasound is not warranted. However, their study did not assess whether there are any specific hypercoagulable states for which further testing may be indicated.
WHEN MIGHT ULTRASOUND BE HELPFUL IN CELLULITIS?
Investigators have described possible DVT risk factors in patients with cellulitis, but definitive associations are lacking because of the insufficient number of patients studied.8,9 The most consistently identified DVT risk factor is history of previous thromboembolism. In a retrospective analysis of patients with cellulitis, Afzal et al.6 found that, of the 66.8% who underwent ultrasound testing, 5.5% were identified as having concurrent DVT. The authors performed univariate analyses of 15 potential risk factors, including active malignancy, oral contraceptive pill use, recent hospitalization, and surgery. A higher incidence of DVT was found for patients with history of VTE (odds ratio [OR], 5.7; 95% confidence interval [CI], 2.3-13.7), calf swelling (OR, 4.5; 95% CI, 1.3-15.8), CVA (OR, 3.5; 95% CI, 1.2-10.1), or hypertension (OR, 3.5; 95% CI, 0.98-12.2). Given the wide confidence intervals, paucity of studies, and lack of definitive data in the setting of cellulitis, clinicians may want to consider the risk factors established in larger trials in other settings, including known immobility (OR, <2); thrombophilia, CHF, and CVA with hemiparesis (OR, 2-9); and trauma and recent surgery (OR, >10).10
WHAT YOU SHOULD DO INSTEAD
As the incidence of concurrent VTE in patients with cellulitis is low, the essential step is to make a clear diagnosis of cellulitis based on its established signs and symptoms. A 2-center trial of 145 patients found that cellulitis was diagnosed accurately by general medicine and emergency medicine physicians 72% of the time, with evaluation by dermatologists and infectious disease specialists used as the gold standard. Only 5% of the misdiagnosed patients were diagnosed with DVT; stasis dermatitis was the most common alternative diagnosis. Taking a thorough history may elicit risk factors consistent with cellulitis, such as a recent injury with a break in the skin. On examination, cellulitis should be suspected for patients with fever and localized pain, redness, swelling, and warmth—the cardinal signs of dolor, rubor, tumor, and calor. An injury or entry site and leukocytosis also support the diagnosis of cellulitis. Distinct margins of erythema on the skin are highly suspicious for erysipelas.11 Other physical findings (eg, laceration, purulent drainage, lymphangitic spread, fluctuating mass) also are consistent with a diagnosis of cellulitis.
The patient’s history is also essential in determining whether any DVT risk factors are present. Past medical history of VTE or CVA, or recent history of surgery, immobility, or trauma, should alert the clinician to the possibility of DVT. Family history of VTE increases the likelihood of DVT. Acute shortness of breath or chest pain in the setting of concerning lower extremity findings for DVT should raise concern for DVT and concurrent PE.
If the classic features of cellulitis are present, empiric antibiotics should be initiated. Routine ultrasound testing for all patients with cellulitis is of low value. However, as the incidence of DVT in this population is not negligible, those with VTE risk factors should be targeted for testing. Studies in the setting of cellulitis provide little guidance regarding specific risk factors that can be used to determine who should undergo further testing. Given this limitation, we suggest that clinicians incorporate into their decision making the well-established VTE risk factors identified for large populations studied in other settings, such as the postoperative period. Specifically, clinicians should consider ultrasound testing for patients with cellulitis and prior history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery.10-12 Ultrasound should also be considered for patients with cellulitis that does not improve and for patients whose localized symptoms worsen despite use of antibiotics.
RECOMMENDATIONS
Do not routinely perform ultrasound to rule out concurrent DVT in cases of cellulitis.
Consider compression ultrasound if there is a history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery. Also consider it for patients who do not respond to antibiotics.
In cases of cellulitis, avoid use of the Wells score alone or with D-dimer testing, as it likely overestimates the DVT risk.
CONCLUSION
The current evidence shows that, for most patients with cellulitis, routine ultrasound testing for DVT is unnecessary. Ultrasound should be considered for patients with potent VTE risk factors. If symptoms do not improve, or if they worsen despite use of antibiotics, clinicians should be alert to potential anchoring bias and consider DVT. The Wells clinical prediction rule overestimates the incidence of DVT in cellulitis and has little value in this setting.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason”? Let us know what you do in your practice and propose ideas for other “Things We Do for No Reason” topics. Please join in the conversation online at Twitter (#TWDFNR)/Facebook and don’t forget to “Like It” on Facebook or retweet it on Twitter. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
The “Things We Do for No Reason” series reviews practices which have become common parts of hospital care but which may provide little value to our patients. Practices reviewed in the TWDFNR series do not represent “black and white” conclusions or clinical practice standards, but are meant as a starting place for research and active discussions among hospitalists and patients. We invite you to be part of that discussion. https://www.choosingwisely.org/
Because of overlapping clinical manifestations, clinicians often order ultrasound to rule out deep vein thrombosis (DVT) in cases of cellulitis. Ultrasound testing is performed for 16% to 73% of patients diagnosed with cellulitis. Although testing is common, the pooled incidence of DVT is low (3.1%). Few data elucidate which patients with cellulitis are more likely to have concurrent DVT and require further testing. The Wells clinical prediction rule with D-dimer testing overestimates DVT risk in patients with cellulitis and is of little value in this setting. Given the overall low incidence, routine ultrasound testing is unnecessary for most patients with cellulitis. ultrasound should be reserved for patients with a history of venous thromboembolism (VTE), immobility, thrombophilia, congestive heart failure (CHF), cerebrovascular accident (CVA) with hemiparesis, trauma, or recent surgery, and for patients who do not respond to antibiotics.
CASE REPORT
A 50-year-old man presented to the emergency department with a 3-day-old cut on his anterior right shin. Associated redness, warmth, pain, and swelling had progressed. The patient had no history of prior DVT or pulmonary embolism (PE). His temperature was 38.5°C, and his white blood cell count of 18,000. On review of systems, he denied shortness of breath and chest pain. He was diagnosed with cellulitis and administered intravenous fluids and cefazolin. The clinician wondered whether to perform lower extremity ultrasound to rule out concurrent DVT.
WHY YOU MIGHT THINK ULTRASOUND IS HELPFUL IN RULING OUT DVT IN CELLULITIS
Lower extremity cellulitis, a common infection of the skin and subcutaneous tissues, is characterized by unilateral erythema, pain, warmth, and swelling. The infection usually follows a skin breach that allows bacteria to enter. DVT may present similarly, and symptoms can include mild leukocytosis and elevated temperature. Because of the clinical similarities, clinicians often order compression ultrasound of the extremity to rule out concurrent DVT in cellulitis. Further impetus for testing stems from fear of the potential complications of untreated DVT, including post-thrombotic syndrome, chronic venous insufficiency, and venous ulceration. A subsequent PE can be fatal, or can cause significant morbidity, including chronic VTE with associated pulmonary hypertension. An estimated quarter of all PEs present as sudden death.1
WHY ULTRASOUND IS NOT HELPFUL IN THIS SETTING
Studies have shown that ultrasound is ordered for 16% to 73% of patients with a cellulitis diagnosis.2,3 Although testing is commonly performed, a meta-analysis of 9 studies of cellulitis patients who underwent ultrasound testing for concurrent DVT revealed a low pooled incidence of total DVT (3.1%) and proximal DVT (2.1%).4 Maze et al.2 retrospectively reviewed 1515 cellulitis cases (identified by International Classification of Diseases, Ninth Revision codes) at a single center in New Zealand over 3 years. Of the 1515 patients, 240 (16%) had ultrasound performed, and only 3 (1.3%) were found to have DVT. Two of the 3 had active malignancy, and the third had injected battery acid into the area. In a 5-year retrospective cohort study at a Veterans Administration hospital in Connecticut, Gunderson and Chang3 reviewed the cases of 183 patients with cellulitis and found ultrasound testing commonly performed (73% of cases) to assess for DVT. Only 1 patient (<1%) was diagnosed with new DVT in the ipsilateral leg, and acute DVT was diagnosed in the contralateral leg of 2 other patients. Overall, these studies indicate the incidence of concurrent DVT in cellulitis is low, regardless of the frequency of ultrasound testing.
Although the cost of a single ultrasound test is not prohibitive, annual total costs hospital-wide and nationally are large. In the United States, the charge for a unilateral duplex ultrasound of the extremity ranges from $260 to $1300, and there is an additional charge for interpretation by a radiologist.5 In a retrospective study spanning 3.5 years and involving 2 community hospitals in Michigan, an estimated $290,000 was spent on ultrasound tests defined as unnecessary for patients with cellulitis.6 A limitation of the study was defining a test as unnecessary based on its result being negative.
DOES WELLS SCORE WITH D-DIMER HELP DEFINE A LOW-RISK POPULATION?
The Wells clinical prediction rule is commonly used to assess the pretest probability of DVT in patients presenting with unilateral leg symptoms. The Wells score is often combined with D-dimer testing to help determine whether ultrasound is necessary. Studies of patients with suspected DVT have found that those considered low risk according to the Wells criteria had a 6.5% incidence of DVT.7 However, the predictive value is lower in the setting of presumed cellulitis. In a prospective cohort study of 200 patients with cellulitis, Maze et al.8 reported that use of the Wells score with D-dimer testing overestimated the DVT risk. D-dimer level was elevated for 74% of patients, and 20.5% were high-risk by Wells criteria. An algorithm determined that—among patients with a high-risk Wells score, a positive D-dimer result, or both—only 1 (0.5%) was diagnosed with ipsilateral DVT after ultrasound testing. Two patients were diagnosed with DVT in the contralateral leg. These results suggest that a strategy that incorporates the Wells score and D-dimer testing in the setting of acute cellulitis provides little value. The authors concluded that, in the absence of a known hypercoagulable state, ultrasound is not warranted. However, their study did not assess whether there are any specific hypercoagulable states for which further testing may be indicated.
WHEN MIGHT ULTRASOUND BE HELPFUL IN CELLULITIS?
Investigators have described possible DVT risk factors in patients with cellulitis, but definitive associations are lacking because of the insufficient number of patients studied.8,9 The most consistently identified DVT risk factor is history of previous thromboembolism. In a retrospective analysis of patients with cellulitis, Afzal et al.6 found that, of the 66.8% who underwent ultrasound testing, 5.5% were identified as having concurrent DVT. The authors performed univariate analyses of 15 potential risk factors, including active malignancy, oral contraceptive pill use, recent hospitalization, and surgery. A higher incidence of DVT was found for patients with history of VTE (odds ratio [OR], 5.7; 95% confidence interval [CI], 2.3-13.7), calf swelling (OR, 4.5; 95% CI, 1.3-15.8), CVA (OR, 3.5; 95% CI, 1.2-10.1), or hypertension (OR, 3.5; 95% CI, 0.98-12.2). Given the wide confidence intervals, paucity of studies, and lack of definitive data in the setting of cellulitis, clinicians may want to consider the risk factors established in larger trials in other settings, including known immobility (OR, <2); thrombophilia, CHF, and CVA with hemiparesis (OR, 2-9); and trauma and recent surgery (OR, >10).10
WHAT YOU SHOULD DO INSTEAD
As the incidence of concurrent VTE in patients with cellulitis is low, the essential step is to make a clear diagnosis of cellulitis based on its established signs and symptoms. A 2-center trial of 145 patients found that cellulitis was diagnosed accurately by general medicine and emergency medicine physicians 72% of the time, with evaluation by dermatologists and infectious disease specialists used as the gold standard. Only 5% of the misdiagnosed patients were diagnosed with DVT; stasis dermatitis was the most common alternative diagnosis. Taking a thorough history may elicit risk factors consistent with cellulitis, such as a recent injury with a break in the skin. On examination, cellulitis should be suspected for patients with fever and localized pain, redness, swelling, and warmth—the cardinal signs of dolor, rubor, tumor, and calor. An injury or entry site and leukocytosis also support the diagnosis of cellulitis. Distinct margins of erythema on the skin are highly suspicious for erysipelas.11 Other physical findings (eg, laceration, purulent drainage, lymphangitic spread, fluctuating mass) also are consistent with a diagnosis of cellulitis.
The patient’s history is also essential in determining whether any DVT risk factors are present. Past medical history of VTE or CVA, or recent history of surgery, immobility, or trauma, should alert the clinician to the possibility of DVT. Family history of VTE increases the likelihood of DVT. Acute shortness of breath or chest pain in the setting of concerning lower extremity findings for DVT should raise concern for DVT and concurrent PE.
If the classic features of cellulitis are present, empiric antibiotics should be initiated. Routine ultrasound testing for all patients with cellulitis is of low value. However, as the incidence of DVT in this population is not negligible, those with VTE risk factors should be targeted for testing. Studies in the setting of cellulitis provide little guidance regarding specific risk factors that can be used to determine who should undergo further testing. Given this limitation, we suggest that clinicians incorporate into their decision making the well-established VTE risk factors identified for large populations studied in other settings, such as the postoperative period. Specifically, clinicians should consider ultrasound testing for patients with cellulitis and prior history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery.10-12 Ultrasound should also be considered for patients with cellulitis that does not improve and for patients whose localized symptoms worsen despite use of antibiotics.
RECOMMENDATIONS
Do not routinely perform ultrasound to rule out concurrent DVT in cases of cellulitis.
Consider compression ultrasound if there is a history of VTE; immobility; thrombophilia, CHF, and CVA with hemiparesis; or trauma and recent surgery. Also consider it for patients who do not respond to antibiotics.
In cases of cellulitis, avoid use of the Wells score alone or with D-dimer testing, as it likely overestimates the DVT risk.
CONCLUSION
The current evidence shows that, for most patients with cellulitis, routine ultrasound testing for DVT is unnecessary. Ultrasound should be considered for patients with potent VTE risk factors. If symptoms do not improve, or if they worsen despite use of antibiotics, clinicians should be alert to potential anchoring bias and consider DVT. The Wells clinical prediction rule overestimates the incidence of DVT in cellulitis and has little value in this setting.
Disclosure
Nothing to report.
Do you think this is a low-value practice? Is this truly a “Thing We Do for No Reason”? Let us know what you do in your practice and propose ideas for other “Things We Do for No Reason” topics. Please join in the conversation online at Twitter (#TWDFNR)/Facebook and don’t forget to “Like It” on Facebook or retweet it on Twitter. We invite you to propose ideas for other “Things We Do for No Reason” topics by emailing [email protected].
References
1. Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21(1):23-29. PubMed 2. Maze MJ, Pithie A, Dawes T, Chambers ST. An audit of venous duplex ultrasonography in patients with lower limb cellulitis. N Z Med J. 2011;124(1329):53-56. PubMed 3. Gunderson CG, Chang JJ. Overuse of compression ultrasound for patients with lower extremity cellulitis. Thromb Res. 2014;134(4):846-850. PubMed 4. Gunderson CG, Chang JJ. Risk of deep vein thrombosis in patients with cellulitis and erysipelas: a systematic review and meta-analysis. Thromb Res. 2013;132(3):336-340. PubMed 5. Extremity ultrasound (nonvascular) cost and procedure information. http://www.newchoicehealth.com/procedures/extremity-ultrasound-nonvascular. Accessed February 15, 2016. 6. Afzal MZ, Saleh MM, Razvi S, Hashmi H, Lampen R. Utility of lower extremity Doppler in patients with lower extremity cellulitis: a need to change the practice? South Med J. 2015;108(7):439-444. PubMed 7. Goodacre S, Sutton AJ, Sampson FC. Meta-analysis: the value of clinical assessment in the diagnosis of deep venous thrombosis. Ann Intern Med. 2005;143(2):129-139. PubMed 8. Maze MJ, Skea S, Pithie A, Metcalf S, Pearson JF, Chambers ST. Prevalence of concurrent deep vein thrombosis in patients with lower limb cellulitis: a prospective cohort study. BMC Infect Dis. 2013;13:141. PubMed 9. Bersier D, Bounameaux H. Cellulitis and deep vein thrombosis: a controversial association. J Thromb Haemost. 2003;1(4):867-868. PubMed 10. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 suppl 1):I9-I16. PubMed 11. Rabuka CE, Azoulay LY, Kahn SR. Predictors of a positive duplex scan in patients with a clinical presentation compatible with deep vein thrombosis or cellulitis. Can J Infect Dis. 2003;14(4):210-214. PubMed 12. Samama MM. An epidemiologic study of risk factors for deep vein thrombosis in medical outpatients: the Sirius Study. Arch Intern Med. 2000;160(22):3415-3420. PubMed
References
1. Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Thrombolysis. 2006;21(1):23-29. PubMed 2. Maze MJ, Pithie A, Dawes T, Chambers ST. An audit of venous duplex ultrasonography in patients with lower limb cellulitis. N Z Med J. 2011;124(1329):53-56. PubMed 3. Gunderson CG, Chang JJ. Overuse of compression ultrasound for patients with lower extremity cellulitis. Thromb Res. 2014;134(4):846-850. PubMed 4. Gunderson CG, Chang JJ. Risk of deep vein thrombosis in patients with cellulitis and erysipelas: a systematic review and meta-analysis. Thromb Res. 2013;132(3):336-340. PubMed 5. Extremity ultrasound (nonvascular) cost and procedure information. http://www.newchoicehealth.com/procedures/extremity-ultrasound-nonvascular. Accessed February 15, 2016. 6. Afzal MZ, Saleh MM, Razvi S, Hashmi H, Lampen R. Utility of lower extremity Doppler in patients with lower extremity cellulitis: a need to change the practice? South Med J. 2015;108(7):439-444. PubMed 7. Goodacre S, Sutton AJ, Sampson FC. Meta-analysis: the value of clinical assessment in the diagnosis of deep venous thrombosis. Ann Intern Med. 2005;143(2):129-139. PubMed 8. Maze MJ, Skea S, Pithie A, Metcalf S, Pearson JF, Chambers ST. Prevalence of concurrent deep vein thrombosis in patients with lower limb cellulitis: a prospective cohort study. BMC Infect Dis. 2013;13:141. PubMed 9. Bersier D, Bounameaux H. Cellulitis and deep vein thrombosis: a controversial association. J Thromb Haemost. 2003;1(4):867-868. PubMed 10. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 suppl 1):I9-I16. PubMed 11. Rabuka CE, Azoulay LY, Kahn SR. Predictors of a positive duplex scan in patients with a clinical presentation compatible with deep vein thrombosis or cellulitis. Can J Infect Dis. 2003;14(4):210-214. PubMed 12. Samama MM. An epidemiologic study of risk factors for deep vein thrombosis in medical outpatients: the Sirius Study. Arch Intern Med. 2000;160(22):3415-3420. PubMed
Address for correspondence and reprint requests: Hyung J. Cho, MD, Division of Hospital Medicine, Mount Sinai Health System, One Gustave L. Levy Place, Box 1086, New York, NY 10029; Telephone: 212-241-1653; Fax: 212-289-6393; E-mail: [email protected]
Content Gating
Open Access (article Unlocked/Open Access)
Alternative CME
Consolidated Pubs: Do Not Show Source Publication Logo
The care of hospitalized patients requires practitioners from multiple disciplines to assess and communicate the patient’s status in a dynamic manner during hospitalization. Although optimal teamwork is needed for patient care to be delivered reliably and efficiently, care within hospitals is typically delivered in a fragmented manner.1 A bedside model for daily interdisciplinary rounds (IDR) has been proposed as a method to provide a structured process and engage all team members in a patient-centered, system-of-care delivery.2 Specific advantages of convening rounds in the presence of the patient include the ability to directly assess care (eg, presence of a potentially unnecessary urinary catheter), patient engagement in key aspects of their care and disposition, and an increased opportunity for team members to develop a shared understanding of the patient’s views and needs.
Implementing dramatic changes to the workflow of multiple disciplines will require rigorous evidence to support a concerted effort from leadership and buy-in from stakeholders at the front line of patient care. Despite the urgency for evidence, there has been little investigation of this strategy. A systematic review3 identified 30 studies published between 1998 and 2013 addressing interdisciplinary interventions on medical wards, none of which examined a bedside IDR model. In a study performed after the period assessed by the systematic review, Stein et al4 described the restructuring of a medical ward as an accountable care unit (ACU), which included a bedside model for rounds by the interdisciplinary team. The change was associated with decreased mortality and length of stay (LOS), although the study did not isolate the impact of rounds or use a concurrent control group and presented aggregate rather than patient-level outcomes. The lack of convincing data may be a reason bedside rounds are not widely employed by hospitals. To provide high-quality evidence, we performed a large, prospective controlled trial comparing a structured bedside model (mobile interdisciplinary care rounds [MICRO]) with standard rounds.
METHODS
This study took place at the Mount Sinai Hospital, which is a 1171-bed tertiary care academic medical center in New York City, New York. A nonteaching unit offered the ability to use a prospective controlled design. Patients were assigned to the north and the south wings of the unit in a quasi-randomized manner, rather than based on diagnosis or acuity. We transformed IDR to a bedside model on the north side of the unit (MICRO group), while the south side of the unit continued using standard conference room-based IDR (control group). The north and south sides of the unit contain 17 and 14 beds, respectively. During the study period, nurses and hospitalists cared for patients on both sides of the study unit, although on any given day were assigned only patients on 1 side of the unit. The unit uses a clinical microsystem model, which has been defined as “a group of clinicians and staff working together with a shared clinical purpose to provide care for a population of patients,” and has a defined set of characteristics associated with high performance.5,6 Our microsystem model has incorporated features as described by Stein’s ACU model,4 including co-leadership by a hospitalist and a nurse manager, geographic assignment of patients to teams, and unit-level data reports. One hospitalist is assigned geographically to each area of the unit in a 2- to 4-week rotation. Coverage of the unit does not include house staff; patients are primarily assigned to hospitalists working with nurse practitioners. Patients were enrolled prospectively during their initial IDR by a research coordinator. Patient-level data and outcomes were collected prospectively by a research coordinator who attended IDR on the intervention and the control sides of the study unit daily.
Inclusion Criteria
All patients admitted to the medicine service on the study unit were eligible. Patients were greater than 18 years and admitted for an acute medical condition. Patients admitted to another unit and later transferred to the study unit were enrolled at the time of transfer. Patients could be included more than once if hospitalized on the study unit on more than 1 occasion. Most patients were covered by hospitalists, although patients covered by private physicians were included. Patients from other departments, including family medicine, are uncommonly admitted to the unit and were excluded. Patients were also excluded if they were admitted and discharged over the same weekend, because the MICRO rounds occur during weekdays and there was no opportunity to offer the intervention on Saturdays and Sundays.
MICRO Intervention
Interdisciplinary rounds occurred daily at 10:00 am for the control group and at 10:30 am for the MICRO group, and were attended by the hospitalist caring for the majority of patients on the unit, staff nurses, and the unit medical director, nurse manager, social worker, and case manager. Rounds on the control unit focused on the plan of care and disposition but did not follow any set structure and were typically 25 to 30 minutes in duration.
The MICRO rounds occurred at the bedside and followed a structured script (Appendix 1) that was designed to limit discussion of each patient to 3 minutes or less, and included speaking roles for the hospitalist, nurse, and social worker. For private physicians, the nurse practitioner assigned to the patient performed the role of the hospitalist. Rounds were expected to be approximately 50 minutes in duration. Patients were further engaged by asking for their main goal for the day. A patient safety checklist was reviewed. Initially, this task was performed by the nurse manager, who did not verbalize the items unless a deficiency was noted. After 6 months’ experience, this responsibility was given to the staff nurse, who reviewed the checklist verbally as part of the bedside script. Patients were seen daily, including those being discharged later that same day.
Staff and Clinician Education
We developed and implemented a curriculum based on a modified version of the Agency for Healthcare Research and Quality’s TeamStepps® program to ensure that all team members were provided with the basic principles of communication within the healthcare setting. The curriculum consisted of interactive didactics on essential elements of teamwork, including team structure, communication, situation monitoring, and mutual support, as well as the purpose and structure of the MICRO model. The curriculum was delivered to nurses at 3 monthly staff meetings on the study unit and to hospitalists during 3 hospital medicine grand rounds over a 3-month period. Nurses and physicians providing care on both geographic areas of the study unit received the education program because no group of practitioners was designated to only 1 geographic area.
Outcomes
Primary and Secondary Outcomes
The primary outcomes were clinical deterioration (CD) and length of stay. Clinical deterioration was a composite outcome defined a priori as death; escalation of care (ie, transfer to an intensive care unit, intermediate care unit, or teaching unit); or a hospital-acquired complication (ie, venous thromboembolism, fall, stage III-IV pressure ulcer, catheter-associated urinary tract infection, central-line associated bloodstream infection, or Clostridium difficile-associated diarrhea). The LOS was calculated as the mean LOS with outliers excluded (outliers defined as having a LOS 100 days or longer or 2.5 or more standard deviations from the expected LOS).
Process metrics on IDR, such as the duration of rounds, attendance by members of the interdisciplinary team, the percentage of patients discussed, or the effectiveness of communication, were not collected. We assessed patient satisfaction based on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Patient Safety Culture Survey
To assess the impact on the perceptions of patient safety, we administered the Agency for Healthcare Research and Quality (AHRQ) Hospital Survey on Patient Safety Culture toall staff and clinicians working on both sides of the study unit immediately before and 12 months after implementation of the MICRO model. Results are reported for the AHRQ dimensions that were most relevant to the MICRO intervention: “teamwork within units,” “overall perceptions of safety,” “communication,” “openness,” “overall patient safety grade,” and “handoffs and transitions.” The survey represents pre- and post-comparison. All nurses and hospitalists on both the MICRO and control sides of the study unit had received the TeamStepps curriculum and participated in MICRO rounds by the time of the postintervention survey. We added 3 questions specifically assessing the perception of the efficiency and effectiveness of IDR. Postintervention respondents reflected on their overall impression of IDR, which included their experiences on both sides of the unit, because no group of nurses or hospitalists was exposed only to the MICRO side or the control side of the unit. Responses to survey questions were recorded on a 5-point Likert scale (from “strongly disagree” to “strongly agree” for opinion questions; and “never,” rarely,” sometimes,” “most of the time,” and “always” for frequency questions) and given a score from 1 to 5. The question asking for an overall grade for patient safety was scored from 1 to 5 points corresponding to letter grade choices F, D, C, B, A.
Statistical Analysis
The sample size was based on the estimate of the baseline rate of the primary outcome of CD and the projected decrease by the MICRO intervention. A study using the Global Trigger Tool developed by the Institute for Healthcare Improvement provided a best estimate of 16% as the baseline rate for CD.7 A total of 2000 hospitalizations were planned to be included to have a power of at least 80% to detect a 25% reduction in the annual incidence of CD with a 2-tailed type I error rate of 0.05. Comparisons of dichotomous event rates were made using chi square tests at a 2-tailed level for significance of 0.05. The LOS was analyzed using the nonparametric median test and multivariable regression analysis. We used a generalized linear model with gamma distribution and log link for all analyses of LOS, where LOS was the outcome variable, and intervention vs. control unit type was the predictor variable. Age, sex, race, payer, case mix, and comorbidities defined with the Elixhauser algorithm were used as covariates.8 We used multivariable logistic regression for analysis of CD, where the dependent variable was CD. Predictor variables included intervention, patient age, sex, race, payer, case mix and comorbidities. Patient satisfaction data were compared using the chi square test. The Student t test for dependent means was used to analyze the patient safety culture survey data.
The study protocol was submitted to the Icahn Mount Sinai School of Medicine’s institutional review board and determined to be exempt from full review.
RESULTS
A total of 2005 hospitalizations were included over the 12-month study period, consisting of 1089 hospitalizations in the MICRO group and 916 in the control group. Bedside and standard IDR were completed daily, Monday through Friday without exception. The demographic characteristics and comorbidities were similar for the 2 groups (Table). Hospitalizations of patients who were initially admitted to another unit and subsequently transferred to the study unit accounted for 11.1% of hospitalizations.
Table
Risk-adjusted LOS was similar for the groups (6.6 vs 7.0 days, P = 0.17, for the MICRO and control groups, respectively). On subgroup analysis, a reduction in LOS was noted for patients transferred to the study unit (10.4 vs 14.0 days, P = 0.02, for the MICRO and control groups, respectively). The LOS was unchanged for patients admitted directly to the study unit (6.0 vs 5.8 days, P = 0.93). There was no difference in the incidence of clinical deterioration for the MICRO or control groups (7.7% vs 9.3%, odds ratio, 0.89; 95% confidence interval, 0.61-1.22, P = 0.46).
The finding of a LOS benefit for the MICRO group limited to patients transferred to the study unit prompted a comparison of patients transferred to the study unit and patients directly admitted to the study unit from the emergency department (Appendix 2). Compared to patients admitted directly to the study unit, patients transferred to the study unit were more likely to have Medicaid or no insurance, more likely to be discharged to a facility, had longer LOS, and were more likely to experience CD.
Patient Satisfaction
There were 175 and 140 responses to the HCAHPS survey for the MICRO and the control groups, respectively. Patients in the MICRO group were more likely to report that “doctors, nurses, or other hospital staff talk with you about whether you would have the help you needed when you left the hospital” (88% vs 78%, P = 0.01). Responses for all other HCAHPS items were similar for the 2 groups.
Figure 1
Clinician/Staff Survey
The response rate was 96% (30 nurses and 17 hospitalists) pre-intervention and 100% (30 nurses and 22 hospitalists) postintervention. Hospitalists and nurses gave significantly higher scores for the dimensions “teamwork within units,” “overall perception of patient safety,” and “patient safety grade” on the postintervention survey compared to the pre-intervention survey (Figure 1). Hospitalists and nurses rated the efficiency of IDR and the ability of IDR to identify safety issues higher on the postintervention survey compared to the pre-intervention survey (Figure 2).
Figure 2
DISCUSSION
We transformed daily IDR from a standard conference room model to a structured bedside model with scripted roles, and performed a rigorous comparison using patient-level data. Our finding that transforming daily IDR from a standard conference room model to a bedside model did not significantly reduce LOS suggests either that the model is ineffective or needs to be incorporated into more comprehensive efforts to improve clinical outcomes. Studies suggest that bedside rounding can improve outcomes when implemented in the context of comprehensive restructuring of patient care.4,9 Stein et al.4 have described the reorganization of a medical ward as an “accountable care unit.” The ACU model included daily IDRs at the bedside, as well as geographic-based teams, co-leadership by a hospitalist and nurse manager, and unit-level reporting. Although no definitive conclusions can be drawn based on their descriptive report, transformation of the unit was associated with reduced LOS and mortality. Similarly, Kara et al.9 found that the number of elements of an “accountable care team” model implemented by each unit was associated with greater reductions in LOS and cost. In contrast, our findings of a lack of an effect are consistent with a recent cluster-randomized trial by O’Leary et al,10 which found that implementation of patient-centered bedside rounds did not improve patient satisfaction or perceptions of shared decision-making compared to units using a model of structured IDRs in a conference room setting. It is notable that the control groups in both the O’Leary trial10 and this study did not represent usual care, because these groups featured localization of the clinical teams and high-quality IDR. In our trial, it is plausible that the control side of the unit was functioning at a high level, which would have decreased our ability to further improve outcomes. Whether restructuring unit processes, including implementation of bedside IDR, improves care compared to usual care without these processes is unknown.
We found that the MICRO intervention significantly decreased LOS compared to the control group for patients transferred to the study unit. This analysis was exploratory and the finding was unexpected. Patients were transferred to the study unit from units of higher acuity, and were more likely to have Medicaid or no insurance and be discharged to facilities rather than home, suggesting that these patients had substantial disposition challenges. It is plausible that this is the population for which bedside IDRs may have the greatest impact. This was a secondary analysis, however, and should be considered as hypothesis-generating for future investigations.
Although the impact on outcomes of bedside IDRs is uncertain, potential benefits and practical barriers have been examined. Gonzalo et al.11 surveyed inpatient physicians and nurses at a hospital employing bedside IDRs and found that the benefits ranked the highest were communication, coordination, and teamwork, and the lowest-ranked benefits were related to efficiency and outcomes. The 6 greatest barriers concerned the time required to complete bedside IDR. These results indicate that the time investiture by staff may be a barrier to widespread adoption. More modest changes, such as increasing the structure of standard conference room rounds, may improve care, although the data are mixed. O’Leary et al.12 assessed the value of a structured approach in a conference room setting, which primarily entailed implementing a checklist for newly admitted patients, and found no difference in LOS. Follow-up studies by these investigators found mixed results on the ability of structured IDR to decrease the incidence of adverse events.13,14
The results of our AHRQ survey of patient safety culture found that several important aspects of teamwork and safety were perceived as improved by the intervention, including the “overall grade on patient safety.” Other studies have similarly shown increases in teamwork and safety ratings through redesign of IDR. O’Leary et al.12 surveyed residents and nurses on a unit that implemented a structured, conference room-based IDR and found that providers on the intervention unit rated the teamwork climate higher than providers on the control unit. Our finding that hospitalists and nurses gave higher ratings for IDR being “efficient” and “a good use of my time” on the postintervention survey than the pre-intervention survey suggests that initial concerns about the additional time commitment may be offset by gains in overall efficiency and in development of an environment of enhanced communication, teamwork, and safety.
This study has several limitations. First, the trial may have been underpowered to find small differences between the groups. The trends for decreased LOS and clinical deterioration in the MICRO group may suggest that bedside IDR can provide a small but clinically significant benefit that would be statistically significant only in a larger trial. Second, patients were not randomized to the 2 groups. The impact is diminished, however, because the routine hospital process for assigning patients to the 2 areas in which the groups were located is random and based solely on bed availability. Third, nurses and hospitalists caring for patients in the control group likely experienced improved communication practices from the unit-wide TeamStepps education and from participating in the MICRO protocol when caring for patients on the intervention side of the unit. Fourth, we did not collect data on the effectiveness of communication and are unable to assess the fidelity with which the structured protocol was followed or whether interprofessional communication was fostered or hindered. Lastly, the study was implemented on a nonteaching unit at a single academic medical center. The protocol and the results may not be generalizable to other hospitals or units that include house staff.
In conclusion, transforming IDR from a conference room model to a bedside model did not reduce overall LOS or clinical deterioration on a unit using features of an ACU structure. Although several beneficial effects were noted, including a reduction in LOS for patients transferred to the study unit and higher ratings of the patient safety climate and efficiency of IDR, implementing bedside IDR in this setting has marginal benefit. Future studies should assess whether a comprehensive transformation of the inpatient model of care, including patient-centered bedside IDR, geographic cohorting of teams, and co-leadership, improves outcomes compared to models without these features.
Disclosures
This trial was funded by Medline’s Prevention Above All Discoveries Grant Program. The authors report no financial conflicts of interest.
1. O’Leary KJ, Sehgal NL, Terrell G, Williams MV; High Performance Teams and the Hospital of the Future Project Team. Interdisciplinary teamwork in hospitals: A review and practical recommendations for improvement. J Hosp Med. 2011;7(1):48-54. PubMed 2. Gonzalo JD, Wolpaw DR, Lehman E, Chuang CH. Patient-centered interprofessional collaborative care: factors associated with bedside interprofessional rounds. J Gen Intern Med. 2014;29(7):1040-1047. PubMed 3. Pannick S, Davis R, Ashrafian H, et al. Effects of interdisciplinary team care interventions on general medical wards. A systematic review. JAMA Intern Med. 2015;175(8):1288-1298. PubMed 4. Stein J, Payne C, Methvin A, et al. Reorganizing a hospital ward as an accountable care unit. J Hosp Med. 2015;10(1):36-40. PubMed 5. Mohr J, Batalden P, Barach P. Integrating patient safety into the clinical microsystem. Qual Saf Health Care. 2004;13(suppl 2):ii34-ii38. PubMed 6. Nelson EC, Batalden PB, Huber TP, et al. Microsystems in health care: Part 1. Learning from high-performing front-line clinical units. Jt Comm J Qual Improv. 2002;28:472-493. PubMed 7. Rutberg H, Borgstedt Risberg MB, Sjödahl R, Nordqvist P, Valter L, Nilsson L. Characterisations of adverse events detected in a university hospital: a 4-year study using the Global Trigger Tool method. BMJ Open. 2014;4(5):e004879. PubMed 8. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8-27. PubMed 9. Kara A, Johnson CS, Nicley A, Niemeier MR, Hui SL. Redesigning accountable care: testing the effectiveness of an accountable care team model. J Hosp Med. 2015;10(12):773-779. PubMed 10. O’Leary KJ, Killarney A, Hansen LO, Jones S, Malladi M, Marks K, et al. Effect of patient-centred bedside rounds on hospitalised patients’ decision control, activation and satisfaction with care. BMJ Qual Saf. 2016;25(12):921-928. PubMed 11. Gonzalo JD, Kuperman E, Lehman E, Haidet P. Bedside interprofessional rounds: perceptions of benefits and barriers by internal medicine nursing staff, attending physicians, and housestaff physicians. J Hosp Med. 2014;9(10):646-651. PubMed 12. O’Leary KJ, Wayne DB, Haviley C, Slade ME, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a medical teaching unit. J Gen Intern Med. 2010;25:826-832. PubMed 13. O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684. PubMed 14. O’Leary KJ, Creden AJ, Slade ME, et al. Implementation of unit-based interventions to improve teamwork and patient safety on a medical service. Am J Med Qual. 2015;30(5):409-416. PubMed
The care of hospitalized patients requires practitioners from multiple disciplines to assess and communicate the patient’s status in a dynamic manner during hospitalization. Although optimal teamwork is needed for patient care to be delivered reliably and efficiently, care within hospitals is typically delivered in a fragmented manner.1 A bedside model for daily interdisciplinary rounds (IDR) has been proposed as a method to provide a structured process and engage all team members in a patient-centered, system-of-care delivery.2 Specific advantages of convening rounds in the presence of the patient include the ability to directly assess care (eg, presence of a potentially unnecessary urinary catheter), patient engagement in key aspects of their care and disposition, and an increased opportunity for team members to develop a shared understanding of the patient’s views and needs.
Implementing dramatic changes to the workflow of multiple disciplines will require rigorous evidence to support a concerted effort from leadership and buy-in from stakeholders at the front line of patient care. Despite the urgency for evidence, there has been little investigation of this strategy. A systematic review3 identified 30 studies published between 1998 and 2013 addressing interdisciplinary interventions on medical wards, none of which examined a bedside IDR model. In a study performed after the period assessed by the systematic review, Stein et al4 described the restructuring of a medical ward as an accountable care unit (ACU), which included a bedside model for rounds by the interdisciplinary team. The change was associated with decreased mortality and length of stay (LOS), although the study did not isolate the impact of rounds or use a concurrent control group and presented aggregate rather than patient-level outcomes. The lack of convincing data may be a reason bedside rounds are not widely employed by hospitals. To provide high-quality evidence, we performed a large, prospective controlled trial comparing a structured bedside model (mobile interdisciplinary care rounds [MICRO]) with standard rounds.
METHODS
This study took place at the Mount Sinai Hospital, which is a 1171-bed tertiary care academic medical center in New York City, New York. A nonteaching unit offered the ability to use a prospective controlled design. Patients were assigned to the north and the south wings of the unit in a quasi-randomized manner, rather than based on diagnosis or acuity. We transformed IDR to a bedside model on the north side of the unit (MICRO group), while the south side of the unit continued using standard conference room-based IDR (control group). The north and south sides of the unit contain 17 and 14 beds, respectively. During the study period, nurses and hospitalists cared for patients on both sides of the study unit, although on any given day were assigned only patients on 1 side of the unit. The unit uses a clinical microsystem model, which has been defined as “a group of clinicians and staff working together with a shared clinical purpose to provide care for a population of patients,” and has a defined set of characteristics associated with high performance.5,6 Our microsystem model has incorporated features as described by Stein’s ACU model,4 including co-leadership by a hospitalist and a nurse manager, geographic assignment of patients to teams, and unit-level data reports. One hospitalist is assigned geographically to each area of the unit in a 2- to 4-week rotation. Coverage of the unit does not include house staff; patients are primarily assigned to hospitalists working with nurse practitioners. Patients were enrolled prospectively during their initial IDR by a research coordinator. Patient-level data and outcomes were collected prospectively by a research coordinator who attended IDR on the intervention and the control sides of the study unit daily.
Inclusion Criteria
All patients admitted to the medicine service on the study unit were eligible. Patients were greater than 18 years and admitted for an acute medical condition. Patients admitted to another unit and later transferred to the study unit were enrolled at the time of transfer. Patients could be included more than once if hospitalized on the study unit on more than 1 occasion. Most patients were covered by hospitalists, although patients covered by private physicians were included. Patients from other departments, including family medicine, are uncommonly admitted to the unit and were excluded. Patients were also excluded if they were admitted and discharged over the same weekend, because the MICRO rounds occur during weekdays and there was no opportunity to offer the intervention on Saturdays and Sundays.
MICRO Intervention
Interdisciplinary rounds occurred daily at 10:00 am for the control group and at 10:30 am for the MICRO group, and were attended by the hospitalist caring for the majority of patients on the unit, staff nurses, and the unit medical director, nurse manager, social worker, and case manager. Rounds on the control unit focused on the plan of care and disposition but did not follow any set structure and were typically 25 to 30 minutes in duration.
The MICRO rounds occurred at the bedside and followed a structured script (Appendix 1) that was designed to limit discussion of each patient to 3 minutes or less, and included speaking roles for the hospitalist, nurse, and social worker. For private physicians, the nurse practitioner assigned to the patient performed the role of the hospitalist. Rounds were expected to be approximately 50 minutes in duration. Patients were further engaged by asking for their main goal for the day. A patient safety checklist was reviewed. Initially, this task was performed by the nurse manager, who did not verbalize the items unless a deficiency was noted. After 6 months’ experience, this responsibility was given to the staff nurse, who reviewed the checklist verbally as part of the bedside script. Patients were seen daily, including those being discharged later that same day.
Staff and Clinician Education
We developed and implemented a curriculum based on a modified version of the Agency for Healthcare Research and Quality’s TeamStepps® program to ensure that all team members were provided with the basic principles of communication within the healthcare setting. The curriculum consisted of interactive didactics on essential elements of teamwork, including team structure, communication, situation monitoring, and mutual support, as well as the purpose and structure of the MICRO model. The curriculum was delivered to nurses at 3 monthly staff meetings on the study unit and to hospitalists during 3 hospital medicine grand rounds over a 3-month period. Nurses and physicians providing care on both geographic areas of the study unit received the education program because no group of practitioners was designated to only 1 geographic area.
Outcomes
Primary and Secondary Outcomes
The primary outcomes were clinical deterioration (CD) and length of stay. Clinical deterioration was a composite outcome defined a priori as death; escalation of care (ie, transfer to an intensive care unit, intermediate care unit, or teaching unit); or a hospital-acquired complication (ie, venous thromboembolism, fall, stage III-IV pressure ulcer, catheter-associated urinary tract infection, central-line associated bloodstream infection, or Clostridium difficile-associated diarrhea). The LOS was calculated as the mean LOS with outliers excluded (outliers defined as having a LOS 100 days or longer or 2.5 or more standard deviations from the expected LOS).
Process metrics on IDR, such as the duration of rounds, attendance by members of the interdisciplinary team, the percentage of patients discussed, or the effectiveness of communication, were not collected. We assessed patient satisfaction based on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Patient Safety Culture Survey
To assess the impact on the perceptions of patient safety, we administered the Agency for Healthcare Research and Quality (AHRQ) Hospital Survey on Patient Safety Culture toall staff and clinicians working on both sides of the study unit immediately before and 12 months after implementation of the MICRO model. Results are reported for the AHRQ dimensions that were most relevant to the MICRO intervention: “teamwork within units,” “overall perceptions of safety,” “communication,” “openness,” “overall patient safety grade,” and “handoffs and transitions.” The survey represents pre- and post-comparison. All nurses and hospitalists on both the MICRO and control sides of the study unit had received the TeamStepps curriculum and participated in MICRO rounds by the time of the postintervention survey. We added 3 questions specifically assessing the perception of the efficiency and effectiveness of IDR. Postintervention respondents reflected on their overall impression of IDR, which included their experiences on both sides of the unit, because no group of nurses or hospitalists was exposed only to the MICRO side or the control side of the unit. Responses to survey questions were recorded on a 5-point Likert scale (from “strongly disagree” to “strongly agree” for opinion questions; and “never,” rarely,” sometimes,” “most of the time,” and “always” for frequency questions) and given a score from 1 to 5. The question asking for an overall grade for patient safety was scored from 1 to 5 points corresponding to letter grade choices F, D, C, B, A.
Statistical Analysis
The sample size was based on the estimate of the baseline rate of the primary outcome of CD and the projected decrease by the MICRO intervention. A study using the Global Trigger Tool developed by the Institute for Healthcare Improvement provided a best estimate of 16% as the baseline rate for CD.7 A total of 2000 hospitalizations were planned to be included to have a power of at least 80% to detect a 25% reduction in the annual incidence of CD with a 2-tailed type I error rate of 0.05. Comparisons of dichotomous event rates were made using chi square tests at a 2-tailed level for significance of 0.05. The LOS was analyzed using the nonparametric median test and multivariable regression analysis. We used a generalized linear model with gamma distribution and log link for all analyses of LOS, where LOS was the outcome variable, and intervention vs. control unit type was the predictor variable. Age, sex, race, payer, case mix, and comorbidities defined with the Elixhauser algorithm were used as covariates.8 We used multivariable logistic regression for analysis of CD, where the dependent variable was CD. Predictor variables included intervention, patient age, sex, race, payer, case mix and comorbidities. Patient satisfaction data were compared using the chi square test. The Student t test for dependent means was used to analyze the patient safety culture survey data.
The study protocol was submitted to the Icahn Mount Sinai School of Medicine’s institutional review board and determined to be exempt from full review.
RESULTS
A total of 2005 hospitalizations were included over the 12-month study period, consisting of 1089 hospitalizations in the MICRO group and 916 in the control group. Bedside and standard IDR were completed daily, Monday through Friday without exception. The demographic characteristics and comorbidities were similar for the 2 groups (Table). Hospitalizations of patients who were initially admitted to another unit and subsequently transferred to the study unit accounted for 11.1% of hospitalizations.
Table
Risk-adjusted LOS was similar for the groups (6.6 vs 7.0 days, P = 0.17, for the MICRO and control groups, respectively). On subgroup analysis, a reduction in LOS was noted for patients transferred to the study unit (10.4 vs 14.0 days, P = 0.02, for the MICRO and control groups, respectively). The LOS was unchanged for patients admitted directly to the study unit (6.0 vs 5.8 days, P = 0.93). There was no difference in the incidence of clinical deterioration for the MICRO or control groups (7.7% vs 9.3%, odds ratio, 0.89; 95% confidence interval, 0.61-1.22, P = 0.46).
The finding of a LOS benefit for the MICRO group limited to patients transferred to the study unit prompted a comparison of patients transferred to the study unit and patients directly admitted to the study unit from the emergency department (Appendix 2). Compared to patients admitted directly to the study unit, patients transferred to the study unit were more likely to have Medicaid or no insurance, more likely to be discharged to a facility, had longer LOS, and were more likely to experience CD.
Patient Satisfaction
There were 175 and 140 responses to the HCAHPS survey for the MICRO and the control groups, respectively. Patients in the MICRO group were more likely to report that “doctors, nurses, or other hospital staff talk with you about whether you would have the help you needed when you left the hospital” (88% vs 78%, P = 0.01). Responses for all other HCAHPS items were similar for the 2 groups.
Figure 1
Clinician/Staff Survey
The response rate was 96% (30 nurses and 17 hospitalists) pre-intervention and 100% (30 nurses and 22 hospitalists) postintervention. Hospitalists and nurses gave significantly higher scores for the dimensions “teamwork within units,” “overall perception of patient safety,” and “patient safety grade” on the postintervention survey compared to the pre-intervention survey (Figure 1). Hospitalists and nurses rated the efficiency of IDR and the ability of IDR to identify safety issues higher on the postintervention survey compared to the pre-intervention survey (Figure 2).
Figure 2
DISCUSSION
We transformed daily IDR from a standard conference room model to a structured bedside model with scripted roles, and performed a rigorous comparison using patient-level data. Our finding that transforming daily IDR from a standard conference room model to a bedside model did not significantly reduce LOS suggests either that the model is ineffective or needs to be incorporated into more comprehensive efforts to improve clinical outcomes. Studies suggest that bedside rounding can improve outcomes when implemented in the context of comprehensive restructuring of patient care.4,9 Stein et al.4 have described the reorganization of a medical ward as an “accountable care unit.” The ACU model included daily IDRs at the bedside, as well as geographic-based teams, co-leadership by a hospitalist and nurse manager, and unit-level reporting. Although no definitive conclusions can be drawn based on their descriptive report, transformation of the unit was associated with reduced LOS and mortality. Similarly, Kara et al.9 found that the number of elements of an “accountable care team” model implemented by each unit was associated with greater reductions in LOS and cost. In contrast, our findings of a lack of an effect are consistent with a recent cluster-randomized trial by O’Leary et al,10 which found that implementation of patient-centered bedside rounds did not improve patient satisfaction or perceptions of shared decision-making compared to units using a model of structured IDRs in a conference room setting. It is notable that the control groups in both the O’Leary trial10 and this study did not represent usual care, because these groups featured localization of the clinical teams and high-quality IDR. In our trial, it is plausible that the control side of the unit was functioning at a high level, which would have decreased our ability to further improve outcomes. Whether restructuring unit processes, including implementation of bedside IDR, improves care compared to usual care without these processes is unknown.
We found that the MICRO intervention significantly decreased LOS compared to the control group for patients transferred to the study unit. This analysis was exploratory and the finding was unexpected. Patients were transferred to the study unit from units of higher acuity, and were more likely to have Medicaid or no insurance and be discharged to facilities rather than home, suggesting that these patients had substantial disposition challenges. It is plausible that this is the population for which bedside IDRs may have the greatest impact. This was a secondary analysis, however, and should be considered as hypothesis-generating for future investigations.
Although the impact on outcomes of bedside IDRs is uncertain, potential benefits and practical barriers have been examined. Gonzalo et al.11 surveyed inpatient physicians and nurses at a hospital employing bedside IDRs and found that the benefits ranked the highest were communication, coordination, and teamwork, and the lowest-ranked benefits were related to efficiency and outcomes. The 6 greatest barriers concerned the time required to complete bedside IDR. These results indicate that the time investiture by staff may be a barrier to widespread adoption. More modest changes, such as increasing the structure of standard conference room rounds, may improve care, although the data are mixed. O’Leary et al.12 assessed the value of a structured approach in a conference room setting, which primarily entailed implementing a checklist for newly admitted patients, and found no difference in LOS. Follow-up studies by these investigators found mixed results on the ability of structured IDR to decrease the incidence of adverse events.13,14
The results of our AHRQ survey of patient safety culture found that several important aspects of teamwork and safety were perceived as improved by the intervention, including the “overall grade on patient safety.” Other studies have similarly shown increases in teamwork and safety ratings through redesign of IDR. O’Leary et al.12 surveyed residents and nurses on a unit that implemented a structured, conference room-based IDR and found that providers on the intervention unit rated the teamwork climate higher than providers on the control unit. Our finding that hospitalists and nurses gave higher ratings for IDR being “efficient” and “a good use of my time” on the postintervention survey than the pre-intervention survey suggests that initial concerns about the additional time commitment may be offset by gains in overall efficiency and in development of an environment of enhanced communication, teamwork, and safety.
This study has several limitations. First, the trial may have been underpowered to find small differences between the groups. The trends for decreased LOS and clinical deterioration in the MICRO group may suggest that bedside IDR can provide a small but clinically significant benefit that would be statistically significant only in a larger trial. Second, patients were not randomized to the 2 groups. The impact is diminished, however, because the routine hospital process for assigning patients to the 2 areas in which the groups were located is random and based solely on bed availability. Third, nurses and hospitalists caring for patients in the control group likely experienced improved communication practices from the unit-wide TeamStepps education and from participating in the MICRO protocol when caring for patients on the intervention side of the unit. Fourth, we did not collect data on the effectiveness of communication and are unable to assess the fidelity with which the structured protocol was followed or whether interprofessional communication was fostered or hindered. Lastly, the study was implemented on a nonteaching unit at a single academic medical center. The protocol and the results may not be generalizable to other hospitals or units that include house staff.
In conclusion, transforming IDR from a conference room model to a bedside model did not reduce overall LOS or clinical deterioration on a unit using features of an ACU structure. Although several beneficial effects were noted, including a reduction in LOS for patients transferred to the study unit and higher ratings of the patient safety climate and efficiency of IDR, implementing bedside IDR in this setting has marginal benefit. Future studies should assess whether a comprehensive transformation of the inpatient model of care, including patient-centered bedside IDR, geographic cohorting of teams, and co-leadership, improves outcomes compared to models without these features.
Disclosures
This trial was funded by Medline’s Prevention Above All Discoveries Grant Program. The authors report no financial conflicts of interest.
The care of hospitalized patients requires practitioners from multiple disciplines to assess and communicate the patient’s status in a dynamic manner during hospitalization. Although optimal teamwork is needed for patient care to be delivered reliably and efficiently, care within hospitals is typically delivered in a fragmented manner.1 A bedside model for daily interdisciplinary rounds (IDR) has been proposed as a method to provide a structured process and engage all team members in a patient-centered, system-of-care delivery.2 Specific advantages of convening rounds in the presence of the patient include the ability to directly assess care (eg, presence of a potentially unnecessary urinary catheter), patient engagement in key aspects of their care and disposition, and an increased opportunity for team members to develop a shared understanding of the patient’s views and needs.
Implementing dramatic changes to the workflow of multiple disciplines will require rigorous evidence to support a concerted effort from leadership and buy-in from stakeholders at the front line of patient care. Despite the urgency for evidence, there has been little investigation of this strategy. A systematic review3 identified 30 studies published between 1998 and 2013 addressing interdisciplinary interventions on medical wards, none of which examined a bedside IDR model. In a study performed after the period assessed by the systematic review, Stein et al4 described the restructuring of a medical ward as an accountable care unit (ACU), which included a bedside model for rounds by the interdisciplinary team. The change was associated with decreased mortality and length of stay (LOS), although the study did not isolate the impact of rounds or use a concurrent control group and presented aggregate rather than patient-level outcomes. The lack of convincing data may be a reason bedside rounds are not widely employed by hospitals. To provide high-quality evidence, we performed a large, prospective controlled trial comparing a structured bedside model (mobile interdisciplinary care rounds [MICRO]) with standard rounds.
METHODS
This study took place at the Mount Sinai Hospital, which is a 1171-bed tertiary care academic medical center in New York City, New York. A nonteaching unit offered the ability to use a prospective controlled design. Patients were assigned to the north and the south wings of the unit in a quasi-randomized manner, rather than based on diagnosis or acuity. We transformed IDR to a bedside model on the north side of the unit (MICRO group), while the south side of the unit continued using standard conference room-based IDR (control group). The north and south sides of the unit contain 17 and 14 beds, respectively. During the study period, nurses and hospitalists cared for patients on both sides of the study unit, although on any given day were assigned only patients on 1 side of the unit. The unit uses a clinical microsystem model, which has been defined as “a group of clinicians and staff working together with a shared clinical purpose to provide care for a population of patients,” and has a defined set of characteristics associated with high performance.5,6 Our microsystem model has incorporated features as described by Stein’s ACU model,4 including co-leadership by a hospitalist and a nurse manager, geographic assignment of patients to teams, and unit-level data reports. One hospitalist is assigned geographically to each area of the unit in a 2- to 4-week rotation. Coverage of the unit does not include house staff; patients are primarily assigned to hospitalists working with nurse practitioners. Patients were enrolled prospectively during their initial IDR by a research coordinator. Patient-level data and outcomes were collected prospectively by a research coordinator who attended IDR on the intervention and the control sides of the study unit daily.
Inclusion Criteria
All patients admitted to the medicine service on the study unit were eligible. Patients were greater than 18 years and admitted for an acute medical condition. Patients admitted to another unit and later transferred to the study unit were enrolled at the time of transfer. Patients could be included more than once if hospitalized on the study unit on more than 1 occasion. Most patients were covered by hospitalists, although patients covered by private physicians were included. Patients from other departments, including family medicine, are uncommonly admitted to the unit and were excluded. Patients were also excluded if they were admitted and discharged over the same weekend, because the MICRO rounds occur during weekdays and there was no opportunity to offer the intervention on Saturdays and Sundays.
MICRO Intervention
Interdisciplinary rounds occurred daily at 10:00 am for the control group and at 10:30 am for the MICRO group, and were attended by the hospitalist caring for the majority of patients on the unit, staff nurses, and the unit medical director, nurse manager, social worker, and case manager. Rounds on the control unit focused on the plan of care and disposition but did not follow any set structure and were typically 25 to 30 minutes in duration.
The MICRO rounds occurred at the bedside and followed a structured script (Appendix 1) that was designed to limit discussion of each patient to 3 minutes or less, and included speaking roles for the hospitalist, nurse, and social worker. For private physicians, the nurse practitioner assigned to the patient performed the role of the hospitalist. Rounds were expected to be approximately 50 minutes in duration. Patients were further engaged by asking for their main goal for the day. A patient safety checklist was reviewed. Initially, this task was performed by the nurse manager, who did not verbalize the items unless a deficiency was noted. After 6 months’ experience, this responsibility was given to the staff nurse, who reviewed the checklist verbally as part of the bedside script. Patients were seen daily, including those being discharged later that same day.
Staff and Clinician Education
We developed and implemented a curriculum based on a modified version of the Agency for Healthcare Research and Quality’s TeamStepps® program to ensure that all team members were provided with the basic principles of communication within the healthcare setting. The curriculum consisted of interactive didactics on essential elements of teamwork, including team structure, communication, situation monitoring, and mutual support, as well as the purpose and structure of the MICRO model. The curriculum was delivered to nurses at 3 monthly staff meetings on the study unit and to hospitalists during 3 hospital medicine grand rounds over a 3-month period. Nurses and physicians providing care on both geographic areas of the study unit received the education program because no group of practitioners was designated to only 1 geographic area.
Outcomes
Primary and Secondary Outcomes
The primary outcomes were clinical deterioration (CD) and length of stay. Clinical deterioration was a composite outcome defined a priori as death; escalation of care (ie, transfer to an intensive care unit, intermediate care unit, or teaching unit); or a hospital-acquired complication (ie, venous thromboembolism, fall, stage III-IV pressure ulcer, catheter-associated urinary tract infection, central-line associated bloodstream infection, or Clostridium difficile-associated diarrhea). The LOS was calculated as the mean LOS with outliers excluded (outliers defined as having a LOS 100 days or longer or 2.5 or more standard deviations from the expected LOS).
Process metrics on IDR, such as the duration of rounds, attendance by members of the interdisciplinary team, the percentage of patients discussed, or the effectiveness of communication, were not collected. We assessed patient satisfaction based on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey.
Patient Safety Culture Survey
To assess the impact on the perceptions of patient safety, we administered the Agency for Healthcare Research and Quality (AHRQ) Hospital Survey on Patient Safety Culture toall staff and clinicians working on both sides of the study unit immediately before and 12 months after implementation of the MICRO model. Results are reported for the AHRQ dimensions that were most relevant to the MICRO intervention: “teamwork within units,” “overall perceptions of safety,” “communication,” “openness,” “overall patient safety grade,” and “handoffs and transitions.” The survey represents pre- and post-comparison. All nurses and hospitalists on both the MICRO and control sides of the study unit had received the TeamStepps curriculum and participated in MICRO rounds by the time of the postintervention survey. We added 3 questions specifically assessing the perception of the efficiency and effectiveness of IDR. Postintervention respondents reflected on their overall impression of IDR, which included their experiences on both sides of the unit, because no group of nurses or hospitalists was exposed only to the MICRO side or the control side of the unit. Responses to survey questions were recorded on a 5-point Likert scale (from “strongly disagree” to “strongly agree” for opinion questions; and “never,” rarely,” sometimes,” “most of the time,” and “always” for frequency questions) and given a score from 1 to 5. The question asking for an overall grade for patient safety was scored from 1 to 5 points corresponding to letter grade choices F, D, C, B, A.
Statistical Analysis
The sample size was based on the estimate of the baseline rate of the primary outcome of CD and the projected decrease by the MICRO intervention. A study using the Global Trigger Tool developed by the Institute for Healthcare Improvement provided a best estimate of 16% as the baseline rate for CD.7 A total of 2000 hospitalizations were planned to be included to have a power of at least 80% to detect a 25% reduction in the annual incidence of CD with a 2-tailed type I error rate of 0.05. Comparisons of dichotomous event rates were made using chi square tests at a 2-tailed level for significance of 0.05. The LOS was analyzed using the nonparametric median test and multivariable regression analysis. We used a generalized linear model with gamma distribution and log link for all analyses of LOS, where LOS was the outcome variable, and intervention vs. control unit type was the predictor variable. Age, sex, race, payer, case mix, and comorbidities defined with the Elixhauser algorithm were used as covariates.8 We used multivariable logistic regression for analysis of CD, where the dependent variable was CD. Predictor variables included intervention, patient age, sex, race, payer, case mix and comorbidities. Patient satisfaction data were compared using the chi square test. The Student t test for dependent means was used to analyze the patient safety culture survey data.
The study protocol was submitted to the Icahn Mount Sinai School of Medicine’s institutional review board and determined to be exempt from full review.
RESULTS
A total of 2005 hospitalizations were included over the 12-month study period, consisting of 1089 hospitalizations in the MICRO group and 916 in the control group. Bedside and standard IDR were completed daily, Monday through Friday without exception. The demographic characteristics and comorbidities were similar for the 2 groups (Table). Hospitalizations of patients who were initially admitted to another unit and subsequently transferred to the study unit accounted for 11.1% of hospitalizations.
Table
Risk-adjusted LOS was similar for the groups (6.6 vs 7.0 days, P = 0.17, for the MICRO and control groups, respectively). On subgroup analysis, a reduction in LOS was noted for patients transferred to the study unit (10.4 vs 14.0 days, P = 0.02, for the MICRO and control groups, respectively). The LOS was unchanged for patients admitted directly to the study unit (6.0 vs 5.8 days, P = 0.93). There was no difference in the incidence of clinical deterioration for the MICRO or control groups (7.7% vs 9.3%, odds ratio, 0.89; 95% confidence interval, 0.61-1.22, P = 0.46).
The finding of a LOS benefit for the MICRO group limited to patients transferred to the study unit prompted a comparison of patients transferred to the study unit and patients directly admitted to the study unit from the emergency department (Appendix 2). Compared to patients admitted directly to the study unit, patients transferred to the study unit were more likely to have Medicaid or no insurance, more likely to be discharged to a facility, had longer LOS, and were more likely to experience CD.
Patient Satisfaction
There were 175 and 140 responses to the HCAHPS survey for the MICRO and the control groups, respectively. Patients in the MICRO group were more likely to report that “doctors, nurses, or other hospital staff talk with you about whether you would have the help you needed when you left the hospital” (88% vs 78%, P = 0.01). Responses for all other HCAHPS items were similar for the 2 groups.
Figure 1
Clinician/Staff Survey
The response rate was 96% (30 nurses and 17 hospitalists) pre-intervention and 100% (30 nurses and 22 hospitalists) postintervention. Hospitalists and nurses gave significantly higher scores for the dimensions “teamwork within units,” “overall perception of patient safety,” and “patient safety grade” on the postintervention survey compared to the pre-intervention survey (Figure 1). Hospitalists and nurses rated the efficiency of IDR and the ability of IDR to identify safety issues higher on the postintervention survey compared to the pre-intervention survey (Figure 2).
Figure 2
DISCUSSION
We transformed daily IDR from a standard conference room model to a structured bedside model with scripted roles, and performed a rigorous comparison using patient-level data. Our finding that transforming daily IDR from a standard conference room model to a bedside model did not significantly reduce LOS suggests either that the model is ineffective or needs to be incorporated into more comprehensive efforts to improve clinical outcomes. Studies suggest that bedside rounding can improve outcomes when implemented in the context of comprehensive restructuring of patient care.4,9 Stein et al.4 have described the reorganization of a medical ward as an “accountable care unit.” The ACU model included daily IDRs at the bedside, as well as geographic-based teams, co-leadership by a hospitalist and nurse manager, and unit-level reporting. Although no definitive conclusions can be drawn based on their descriptive report, transformation of the unit was associated with reduced LOS and mortality. Similarly, Kara et al.9 found that the number of elements of an “accountable care team” model implemented by each unit was associated with greater reductions in LOS and cost. In contrast, our findings of a lack of an effect are consistent with a recent cluster-randomized trial by O’Leary et al,10 which found that implementation of patient-centered bedside rounds did not improve patient satisfaction or perceptions of shared decision-making compared to units using a model of structured IDRs in a conference room setting. It is notable that the control groups in both the O’Leary trial10 and this study did not represent usual care, because these groups featured localization of the clinical teams and high-quality IDR. In our trial, it is plausible that the control side of the unit was functioning at a high level, which would have decreased our ability to further improve outcomes. Whether restructuring unit processes, including implementation of bedside IDR, improves care compared to usual care without these processes is unknown.
We found that the MICRO intervention significantly decreased LOS compared to the control group for patients transferred to the study unit. This analysis was exploratory and the finding was unexpected. Patients were transferred to the study unit from units of higher acuity, and were more likely to have Medicaid or no insurance and be discharged to facilities rather than home, suggesting that these patients had substantial disposition challenges. It is plausible that this is the population for which bedside IDRs may have the greatest impact. This was a secondary analysis, however, and should be considered as hypothesis-generating for future investigations.
Although the impact on outcomes of bedside IDRs is uncertain, potential benefits and practical barriers have been examined. Gonzalo et al.11 surveyed inpatient physicians and nurses at a hospital employing bedside IDRs and found that the benefits ranked the highest were communication, coordination, and teamwork, and the lowest-ranked benefits were related to efficiency and outcomes. The 6 greatest barriers concerned the time required to complete bedside IDR. These results indicate that the time investiture by staff may be a barrier to widespread adoption. More modest changes, such as increasing the structure of standard conference room rounds, may improve care, although the data are mixed. O’Leary et al.12 assessed the value of a structured approach in a conference room setting, which primarily entailed implementing a checklist for newly admitted patients, and found no difference in LOS. Follow-up studies by these investigators found mixed results on the ability of structured IDR to decrease the incidence of adverse events.13,14
The results of our AHRQ survey of patient safety culture found that several important aspects of teamwork and safety were perceived as improved by the intervention, including the “overall grade on patient safety.” Other studies have similarly shown increases in teamwork and safety ratings through redesign of IDR. O’Leary et al.12 surveyed residents and nurses on a unit that implemented a structured, conference room-based IDR and found that providers on the intervention unit rated the teamwork climate higher than providers on the control unit. Our finding that hospitalists and nurses gave higher ratings for IDR being “efficient” and “a good use of my time” on the postintervention survey than the pre-intervention survey suggests that initial concerns about the additional time commitment may be offset by gains in overall efficiency and in development of an environment of enhanced communication, teamwork, and safety.
This study has several limitations. First, the trial may have been underpowered to find small differences between the groups. The trends for decreased LOS and clinical deterioration in the MICRO group may suggest that bedside IDR can provide a small but clinically significant benefit that would be statistically significant only in a larger trial. Second, patients were not randomized to the 2 groups. The impact is diminished, however, because the routine hospital process for assigning patients to the 2 areas in which the groups were located is random and based solely on bed availability. Third, nurses and hospitalists caring for patients in the control group likely experienced improved communication practices from the unit-wide TeamStepps education and from participating in the MICRO protocol when caring for patients on the intervention side of the unit. Fourth, we did not collect data on the effectiveness of communication and are unable to assess the fidelity with which the structured protocol was followed or whether interprofessional communication was fostered or hindered. Lastly, the study was implemented on a nonteaching unit at a single academic medical center. The protocol and the results may not be generalizable to other hospitals or units that include house staff.
In conclusion, transforming IDR from a conference room model to a bedside model did not reduce overall LOS or clinical deterioration on a unit using features of an ACU structure. Although several beneficial effects were noted, including a reduction in LOS for patients transferred to the study unit and higher ratings of the patient safety climate and efficiency of IDR, implementing bedside IDR in this setting has marginal benefit. Future studies should assess whether a comprehensive transformation of the inpatient model of care, including patient-centered bedside IDR, geographic cohorting of teams, and co-leadership, improves outcomes compared to models without these features.
Disclosures
This trial was funded by Medline’s Prevention Above All Discoveries Grant Program. The authors report no financial conflicts of interest.
References
1. O’Leary KJ, Sehgal NL, Terrell G, Williams MV; High Performance Teams and the Hospital of the Future Project Team. Interdisciplinary teamwork in hospitals: A review and practical recommendations for improvement. J Hosp Med. 2011;7(1):48-54. PubMed 2. Gonzalo JD, Wolpaw DR, Lehman E, Chuang CH. Patient-centered interprofessional collaborative care: factors associated with bedside interprofessional rounds. J Gen Intern Med. 2014;29(7):1040-1047. PubMed 3. Pannick S, Davis R, Ashrafian H, et al. Effects of interdisciplinary team care interventions on general medical wards. A systematic review. JAMA Intern Med. 2015;175(8):1288-1298. PubMed 4. Stein J, Payne C, Methvin A, et al. Reorganizing a hospital ward as an accountable care unit. J Hosp Med. 2015;10(1):36-40. PubMed 5. Mohr J, Batalden P, Barach P. Integrating patient safety into the clinical microsystem. Qual Saf Health Care. 2004;13(suppl 2):ii34-ii38. PubMed 6. Nelson EC, Batalden PB, Huber TP, et al. Microsystems in health care: Part 1. Learning from high-performing front-line clinical units. Jt Comm J Qual Improv. 2002;28:472-493. PubMed 7. Rutberg H, Borgstedt Risberg MB, Sjödahl R, Nordqvist P, Valter L, Nilsson L. Characterisations of adverse events detected in a university hospital: a 4-year study using the Global Trigger Tool method. BMJ Open. 2014;4(5):e004879. PubMed 8. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8-27. PubMed 9. Kara A, Johnson CS, Nicley A, Niemeier MR, Hui SL. Redesigning accountable care: testing the effectiveness of an accountable care team model. J Hosp Med. 2015;10(12):773-779. PubMed 10. O’Leary KJ, Killarney A, Hansen LO, Jones S, Malladi M, Marks K, et al. Effect of patient-centred bedside rounds on hospitalised patients’ decision control, activation and satisfaction with care. BMJ Qual Saf. 2016;25(12):921-928. PubMed 11. Gonzalo JD, Kuperman E, Lehman E, Haidet P. Bedside interprofessional rounds: perceptions of benefits and barriers by internal medicine nursing staff, attending physicians, and housestaff physicians. J Hosp Med. 2014;9(10):646-651. PubMed 12. O’Leary KJ, Wayne DB, Haviley C, Slade ME, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a medical teaching unit. J Gen Intern Med. 2010;25:826-832. PubMed 13. O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684. PubMed 14. O’Leary KJ, Creden AJ, Slade ME, et al. Implementation of unit-based interventions to improve teamwork and patient safety on a medical service. Am J Med Qual. 2015;30(5):409-416. PubMed
References
1. O’Leary KJ, Sehgal NL, Terrell G, Williams MV; High Performance Teams and the Hospital of the Future Project Team. Interdisciplinary teamwork in hospitals: A review and practical recommendations for improvement. J Hosp Med. 2011;7(1):48-54. PubMed 2. Gonzalo JD, Wolpaw DR, Lehman E, Chuang CH. Patient-centered interprofessional collaborative care: factors associated with bedside interprofessional rounds. J Gen Intern Med. 2014;29(7):1040-1047. PubMed 3. Pannick S, Davis R, Ashrafian H, et al. Effects of interdisciplinary team care interventions on general medical wards. A systematic review. JAMA Intern Med. 2015;175(8):1288-1298. PubMed 4. Stein J, Payne C, Methvin A, et al. Reorganizing a hospital ward as an accountable care unit. J Hosp Med. 2015;10(1):36-40. PubMed 5. Mohr J, Batalden P, Barach P. Integrating patient safety into the clinical microsystem. Qual Saf Health Care. 2004;13(suppl 2):ii34-ii38. PubMed 6. Nelson EC, Batalden PB, Huber TP, et al. Microsystems in health care: Part 1. Learning from high-performing front-line clinical units. Jt Comm J Qual Improv. 2002;28:472-493. PubMed 7. Rutberg H, Borgstedt Risberg MB, Sjödahl R, Nordqvist P, Valter L, Nilsson L. Characterisations of adverse events detected in a university hospital: a 4-year study using the Global Trigger Tool method. BMJ Open. 2014;4(5):e004879. PubMed 8. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8-27. PubMed 9. Kara A, Johnson CS, Nicley A, Niemeier MR, Hui SL. Redesigning accountable care: testing the effectiveness of an accountable care team model. J Hosp Med. 2015;10(12):773-779. PubMed 10. O’Leary KJ, Killarney A, Hansen LO, Jones S, Malladi M, Marks K, et al. Effect of patient-centred bedside rounds on hospitalised patients’ decision control, activation and satisfaction with care. BMJ Qual Saf. 2016;25(12):921-928. PubMed 11. Gonzalo JD, Kuperman E, Lehman E, Haidet P. Bedside interprofessional rounds: perceptions of benefits and barriers by internal medicine nursing staff, attending physicians, and housestaff physicians. J Hosp Med. 2014;9(10):646-651. PubMed 12. O’Leary KJ, Wayne DB, Haviley C, Slade ME, Lee J, Williams MV. Improving teamwork: impact of structured interdisciplinary rounds on a medical teaching unit. J Gen Intern Med. 2010;25:826-832. PubMed 13. O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684. PubMed 14. O’Leary KJ, Creden AJ, Slade ME, et al. Implementation of unit-based interventions to improve teamwork and patient safety on a medical service. Am J Med Qual. 2015;30(5):409-416. PubMed
Address for correspondence and reprint requests: Andrew S. Dunn, MD, MPH, Chief, Division of Hospital Medicine, Mount Sinai Health System, 1468 Madison Ave, Box 1087, New York, NY 10029; Telephone: 212-241-2920; Fax: 212-289-6393; E-mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)
Anticoagulants are among the prescriptions with the highest risk of an adverse drug event (ADE) after discharge, and many of these events are preventable.[1, 2, 3] In recognition of the high risk for adverse events, the Institute for Healthcare Improvement Map details several key features of a safe anticoagulation management program, including the recommendation during the transition period that clinicians ensure proper lab monitoring and establish capacity for follow‐up testing.[4]
Despite the potential for harm, most hospitals do not have a structured process for the transmission of vital information related to warfarin management from the inpatient to the ambulatory setting. Our aim was to develop a concise report containing the essential information regarding the patient's anticoagulation regimen, the Safe Transitions Anticoagulation Report (STAR), and a process to ensure the report can be readily accessed and utilized by ambulatory clinicians.
METHODS
We assembled an interdisciplinary team to develop a new report and workflow to ensure that information on inpatient warfarin management was transmitted to outpatient providers in a reliable and structured manner. Explicit goals were to maximize use of the electronic medical record (EMR) to autopopulate aspects of the new report and create a process that worked seamlessly into the workflow. The final items were selected based on the risk of harm if not conveyed and feasibility of incorporation through the EMR:
Warfarin doses: the 7 warfarin doses immediately prior to discharge
International normalized ratio (INR) values: the 7 INR values immediately prior to discharge
Bridging anticoagulation: the low‐molecular‐weight heparin (LMWH) prescribed as a bridging anticoagulant, if any
The STAR resides in both the discharge summary and the after visit summary (AVS) for patients discharged on warfarin. At our institution, the AVS contains a medication list, discharge instructions, and appointments, and is automatically produced through our EMR. Our institution utilizes the Epic EMR (Epic Systems Corp., Verona, WI) in the hospital, ambulatory clinics, and faculty practices.
A process was developed where a structured table is automatically created (Figure 1). A field was added to our EMR's discharge summary template asking whether the patient is being discharged on warfarin. Answering yes produces a second question asking whether the patient is also being discharged on bridging anticoagulation with LMWH. The STAR is not inserted into the discharge summary if the clinician completing the discharge summary deletes the anticoagulation question. The STAR is automatically created for patients discharged on warfarin and inserted into the AVS by the EMR regardless of whether the discharge summary has been completed. Patients are instructed by their nurse to bring their AVS to their follow‐up appointments.
Figure 1
The Safe Transitions Anticoagulation Report (STAR) as it appears in the discharge summary. Abbreviations: INR, international normalized ratio.
The STAR project team utilized plan‐do‐study‐act cycles to test small changes and make revisions. The workflow was piloted on 2 medical/surgical units from January 2014 through March 2014, and revised based on feedback from clinicians and nursing staff. The STAR initiative was fully implemented across our institution in April 2014.
The study was evaluated by the institutional review board of the Icahn School of Medicine at Mount Sinai, and full review was waived.
Outcomes
Our primary outcomes were the timeliness of laboratory monitoring and quality of anticoagulation management for patients with an established relationship at 1 of the main outpatient practices in our system. Our institution has an anticoagulation clinic for patients followed at the general medicine clinic. We defined an established relationship as having been seen in the same practice on at least 2 occasions in the 12 months prior to admission. The primary outcomes were the percentage of patients who had an INR measurement done and the percentage who had a therapeutic INR value within 10 days after discharge. As the 10‐day period is arbitrary, we also assessed these outcomes for the 3‐, 7‐, and 30‐day periods after discharge. The therapeutic range was defined for all patients as an INR of 2.0 to 3.0, as this is the target range for the large majority of patients on warfarin in our system. Outcomes during the intervention period were compared to baseline values during the preintervention period. For patients with multiple admissions, the first admission during each period was included.
Ambulatory Physician Survey
We surveyed ambulatory care physicians at the main practices for our health system. The survey assessed how often the STAR was viewed and incorporated into decision making, whether the report improved workflow, and whether ambulatory providers perceived that the report increased patient safety. The survey was distributed at the 6‐month interval during the intervention phase. The survey was disseminated electronically on 3 occasions, and a paper version was distributed on 1 occasion to housestaff and general medicine faculty.
Statistical Analysis
Comparisons for categorical data were performed using the 2 test. P values were based on 2‐tailed tests of significance, and a value 0.05 was considered significant.
RESULTS
The STAR was embedded in the discharge summary for 1370 (78.6%) discharges during the intervention period. A total of 505 patients in the preintervention period and 292 patients in the intervention period were established patients at an affiliated practice and comprised the study population. Demographics and indications for warfarin for the preintervention and intervention groups are listed in the Table 1.
Patient Demographics and Warfarin Indications
Preintervention Group, N=505
Intervention Group, N=292
P Value
NOTE: Abbreviations: INR, international normalized ratio. *Total sums to greater than 100% as categories are not mutually exclusive. Including but not limited to prevention of venous thromboembolism after orthopedic or other surgical procedure and prevention of arterial thromboembolism after left ventricular assist device implantation. No indication listed in the order field for warfarin within the electronic medical record.
Age, y
66.7
68.0
0.29
Male gender, n (%)
236 (46.7)
153 (52.4)
0.12
Discharged on bridging agent, n (%)
90 (17.8)
36 (12.3)
0.04
Average length of stay, d
7.1
7.6
0.46
Newly prescribed warfarin, n (%)
147 (29.1)
62 (21.2)
0.01
INR 2.03.0 range at discharge, n (%)
187 (37.0)
137 (46.9)
0.02
Warfarin indication, n (%)*
Venous thromboembolism
93 (18.4)
39 (13.4)
Atrial fibrillation
204 (40.3)
127 (43.5)
Mechanical heart valve
19 (3.8)
17 (6.5)
Prevention of thromboembolism
142 (28.1)
94 (32.2)
Intracardiac thrombosis
3 (0.5)
6 (2.1)
Thrombophilia
4 (0.8)
5 (1.7)
Other
19 (3.8)
12 (4.1)
No indication
32 (6.3)
1 (3.8)
The frequency of INR testing within 10 days of discharge was similar for the preintervention and intervention periods (41.4% and 47.6%, respectively, P=0.09). Similarly, the likelihood of having at least 1 therapeutic INR value within 10 days of discharge was not statistically different for the groups (17.0% and 21.2%, P=0.14). The pattern was similar for the 3‐, 7‐, and 30‐day periods; a higher percentage of the intervention group had INR testing and attained a therapeutic INR value, though for no time period did this reach statistical significance. This pattern was also found when limiting the analysis to patients discharged home rather than to a facility, patients on warfarin, prior to admission, and patients started on warfarin during the hospitalization.
A total of 87of 207 (42.0%) clinicians responded to the survey. Of respondents, 75% reported that they had seen 1 patient who had been discharged on warfarin since the STAR initiative had begun, 58% of whom reported having viewed the STAR. Most respondents who viewed the STAR found it to be helpful or very helpful in guiding warfarin management (67%), improving their workflow and efficiency (58%), and improving patient safety (77%). Approximately one‐third of respondents who had viewed the STAR (34%) reported that they selected a different dose than they would have chosen had the STAR not been available.
DISCUSSION
We developed a concise report that is seamlessly created and inserted into the discharge summary. Though the STAR was perceived as improving patient safety by ambulatory care providers, there was no impact on attaining a therapeutic INR after discharge. There are several possible explanations for a lack of benefit. Most notably, our intervention was comprised of a stand‐alone EMR‐based tool and focused on 1 component of the transitions process. Given the complexity of healthcare delivery and anticoagulant management, it is likely that broader interventions are required to improve clinical outcomes over the transition period. Potential targets of multifaceted approaches may include improving access to care, providing greater access to anticoagulation clinics, enhancing patient education, and promoting direct physician‐physician communication. Bundled interventions will likely need to include involvement of an interdisciplinary team, such as pharmacist involvement in the medication reconciliation process.
The transition period from the hospital to the outpatient setting has the potential to jeopardize patient safety if vital information is not reliably transmitted across venues.[5, 6, 7, 8] Forster and colleagues noted an 11% incidence of ADEs in the posthospitalization period, of which 60% were either preventable or ameliorable.[3] To decrease the risk to patient safety during the transitions period, the Transitions of Care Consensus policy statement by the Society of Hospital Medicine and other medical organizations called for incorporation of standard data transfer forms (templates and transmission protocols).[9] Despite the high risk and preventable nature of many of the events, few specific tools have been developed. As part of broader initiatives to improve the transitions process, the STAR may have the potential to be a means for health systems to improve the quality of the transition of care for patients on anticoagulants.
Our study has several limitations. First, it was performed at a single health system. It is unknown whether the EMR‐based report could be similarly employed at other systems. Second, our study was unable to assess clinical endpoints. Given the lack of effect on attaining a therapeutic INR, it is unlikely that downstream outcomes, such as thromboembolism, were impacted. Lastly, we were unable to examine whether our intervention improved the care of patients whose outpatient provider was external to our system.
The STAR is a concise tool developed to provide essential anticoagulant‐related information to ambulatory providers. Though the report was perceived as improving patient safety, our finding of a lack of impact on attaining a therapeutic INR after discharge suggests that the tool would need to be a component of a broader multifaceted intervention to impact clinical outcomes.
Disclosures
This project was funded by a grant from the Cardinal Health E3 Foundation. The authors report no conflicts of interest.
Santell JP, Hicks R, McMeekin J, Cousins DD.Medication errors: experience of the United States Pharmacopeia (USP) MEDMARX reporting system. J Clin Pharm.2003;43:760–767.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161–167.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.Adverse drug events occurring following hospital discharge. J Gen Int Med. 2005;204:317–323.
IHI Improvement Map. Available at: http://app.ihi.org/imap/tool/#Process=54aa289b‐16fd‐4a64‐8329‐3941dfc565d1. Accessed February 20 2015.
Kripalani S, Jackson AT, Schnipper JL, Coleman EA.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2:314–323.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831–841.
Johnson MP.Transitions of care in patients receiving oral anticoagulants: general principles, procedures, and impact of new oral anticoagulants. J Cardiovasc Nurs. 2013;28:54–65.
Deitelzweig SB.Care transitions in anticoagulation management for patients with atrial fibrillation: an emphasis on safety. Oschner J. 2013;13:419–427.
Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College Of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med.2009;4:364–370.
Anticoagulants are among the prescriptions with the highest risk of an adverse drug event (ADE) after discharge, and many of these events are preventable.[1, 2, 3] In recognition of the high risk for adverse events, the Institute for Healthcare Improvement Map details several key features of a safe anticoagulation management program, including the recommendation during the transition period that clinicians ensure proper lab monitoring and establish capacity for follow‐up testing.[4]
Despite the potential for harm, most hospitals do not have a structured process for the transmission of vital information related to warfarin management from the inpatient to the ambulatory setting. Our aim was to develop a concise report containing the essential information regarding the patient's anticoagulation regimen, the Safe Transitions Anticoagulation Report (STAR), and a process to ensure the report can be readily accessed and utilized by ambulatory clinicians.
METHODS
We assembled an interdisciplinary team to develop a new report and workflow to ensure that information on inpatient warfarin management was transmitted to outpatient providers in a reliable and structured manner. Explicit goals were to maximize use of the electronic medical record (EMR) to autopopulate aspects of the new report and create a process that worked seamlessly into the workflow. The final items were selected based on the risk of harm if not conveyed and feasibility of incorporation through the EMR:
Warfarin doses: the 7 warfarin doses immediately prior to discharge
International normalized ratio (INR) values: the 7 INR values immediately prior to discharge
Bridging anticoagulation: the low‐molecular‐weight heparin (LMWH) prescribed as a bridging anticoagulant, if any
The STAR resides in both the discharge summary and the after visit summary (AVS) for patients discharged on warfarin. At our institution, the AVS contains a medication list, discharge instructions, and appointments, and is automatically produced through our EMR. Our institution utilizes the Epic EMR (Epic Systems Corp., Verona, WI) in the hospital, ambulatory clinics, and faculty practices.
A process was developed where a structured table is automatically created (Figure 1). A field was added to our EMR's discharge summary template asking whether the patient is being discharged on warfarin. Answering yes produces a second question asking whether the patient is also being discharged on bridging anticoagulation with LMWH. The STAR is not inserted into the discharge summary if the clinician completing the discharge summary deletes the anticoagulation question. The STAR is automatically created for patients discharged on warfarin and inserted into the AVS by the EMR regardless of whether the discharge summary has been completed. Patients are instructed by their nurse to bring their AVS to their follow‐up appointments.
Figure 1
The Safe Transitions Anticoagulation Report (STAR) as it appears in the discharge summary. Abbreviations: INR, international normalized ratio.
The STAR project team utilized plan‐do‐study‐act cycles to test small changes and make revisions. The workflow was piloted on 2 medical/surgical units from January 2014 through March 2014, and revised based on feedback from clinicians and nursing staff. The STAR initiative was fully implemented across our institution in April 2014.
The study was evaluated by the institutional review board of the Icahn School of Medicine at Mount Sinai, and full review was waived.
Outcomes
Our primary outcomes were the timeliness of laboratory monitoring and quality of anticoagulation management for patients with an established relationship at 1 of the main outpatient practices in our system. Our institution has an anticoagulation clinic for patients followed at the general medicine clinic. We defined an established relationship as having been seen in the same practice on at least 2 occasions in the 12 months prior to admission. The primary outcomes were the percentage of patients who had an INR measurement done and the percentage who had a therapeutic INR value within 10 days after discharge. As the 10‐day period is arbitrary, we also assessed these outcomes for the 3‐, 7‐, and 30‐day periods after discharge. The therapeutic range was defined for all patients as an INR of 2.0 to 3.0, as this is the target range for the large majority of patients on warfarin in our system. Outcomes during the intervention period were compared to baseline values during the preintervention period. For patients with multiple admissions, the first admission during each period was included.
Ambulatory Physician Survey
We surveyed ambulatory care physicians at the main practices for our health system. The survey assessed how often the STAR was viewed and incorporated into decision making, whether the report improved workflow, and whether ambulatory providers perceived that the report increased patient safety. The survey was distributed at the 6‐month interval during the intervention phase. The survey was disseminated electronically on 3 occasions, and a paper version was distributed on 1 occasion to housestaff and general medicine faculty.
Statistical Analysis
Comparisons for categorical data were performed using the 2 test. P values were based on 2‐tailed tests of significance, and a value 0.05 was considered significant.
RESULTS
The STAR was embedded in the discharge summary for 1370 (78.6%) discharges during the intervention period. A total of 505 patients in the preintervention period and 292 patients in the intervention period were established patients at an affiliated practice and comprised the study population. Demographics and indications for warfarin for the preintervention and intervention groups are listed in the Table 1.
Patient Demographics and Warfarin Indications
Preintervention Group, N=505
Intervention Group, N=292
P Value
NOTE: Abbreviations: INR, international normalized ratio. *Total sums to greater than 100% as categories are not mutually exclusive. Including but not limited to prevention of venous thromboembolism after orthopedic or other surgical procedure and prevention of arterial thromboembolism after left ventricular assist device implantation. No indication listed in the order field for warfarin within the electronic medical record.
Age, y
66.7
68.0
0.29
Male gender, n (%)
236 (46.7)
153 (52.4)
0.12
Discharged on bridging agent, n (%)
90 (17.8)
36 (12.3)
0.04
Average length of stay, d
7.1
7.6
0.46
Newly prescribed warfarin, n (%)
147 (29.1)
62 (21.2)
0.01
INR 2.03.0 range at discharge, n (%)
187 (37.0)
137 (46.9)
0.02
Warfarin indication, n (%)*
Venous thromboembolism
93 (18.4)
39 (13.4)
Atrial fibrillation
204 (40.3)
127 (43.5)
Mechanical heart valve
19 (3.8)
17 (6.5)
Prevention of thromboembolism
142 (28.1)
94 (32.2)
Intracardiac thrombosis
3 (0.5)
6 (2.1)
Thrombophilia
4 (0.8)
5 (1.7)
Other
19 (3.8)
12 (4.1)
No indication
32 (6.3)
1 (3.8)
The frequency of INR testing within 10 days of discharge was similar for the preintervention and intervention periods (41.4% and 47.6%, respectively, P=0.09). Similarly, the likelihood of having at least 1 therapeutic INR value within 10 days of discharge was not statistically different for the groups (17.0% and 21.2%, P=0.14). The pattern was similar for the 3‐, 7‐, and 30‐day periods; a higher percentage of the intervention group had INR testing and attained a therapeutic INR value, though for no time period did this reach statistical significance. This pattern was also found when limiting the analysis to patients discharged home rather than to a facility, patients on warfarin, prior to admission, and patients started on warfarin during the hospitalization.
A total of 87of 207 (42.0%) clinicians responded to the survey. Of respondents, 75% reported that they had seen 1 patient who had been discharged on warfarin since the STAR initiative had begun, 58% of whom reported having viewed the STAR. Most respondents who viewed the STAR found it to be helpful or very helpful in guiding warfarin management (67%), improving their workflow and efficiency (58%), and improving patient safety (77%). Approximately one‐third of respondents who had viewed the STAR (34%) reported that they selected a different dose than they would have chosen had the STAR not been available.
DISCUSSION
We developed a concise report that is seamlessly created and inserted into the discharge summary. Though the STAR was perceived as improving patient safety by ambulatory care providers, there was no impact on attaining a therapeutic INR after discharge. There are several possible explanations for a lack of benefit. Most notably, our intervention was comprised of a stand‐alone EMR‐based tool and focused on 1 component of the transitions process. Given the complexity of healthcare delivery and anticoagulant management, it is likely that broader interventions are required to improve clinical outcomes over the transition period. Potential targets of multifaceted approaches may include improving access to care, providing greater access to anticoagulation clinics, enhancing patient education, and promoting direct physician‐physician communication. Bundled interventions will likely need to include involvement of an interdisciplinary team, such as pharmacist involvement in the medication reconciliation process.
The transition period from the hospital to the outpatient setting has the potential to jeopardize patient safety if vital information is not reliably transmitted across venues.[5, 6, 7, 8] Forster and colleagues noted an 11% incidence of ADEs in the posthospitalization period, of which 60% were either preventable or ameliorable.[3] To decrease the risk to patient safety during the transitions period, the Transitions of Care Consensus policy statement by the Society of Hospital Medicine and other medical organizations called for incorporation of standard data transfer forms (templates and transmission protocols).[9] Despite the high risk and preventable nature of many of the events, few specific tools have been developed. As part of broader initiatives to improve the transitions process, the STAR may have the potential to be a means for health systems to improve the quality of the transition of care for patients on anticoagulants.
Our study has several limitations. First, it was performed at a single health system. It is unknown whether the EMR‐based report could be similarly employed at other systems. Second, our study was unable to assess clinical endpoints. Given the lack of effect on attaining a therapeutic INR, it is unlikely that downstream outcomes, such as thromboembolism, were impacted. Lastly, we were unable to examine whether our intervention improved the care of patients whose outpatient provider was external to our system.
The STAR is a concise tool developed to provide essential anticoagulant‐related information to ambulatory providers. Though the report was perceived as improving patient safety, our finding of a lack of impact on attaining a therapeutic INR after discharge suggests that the tool would need to be a component of a broader multifaceted intervention to impact clinical outcomes.
Disclosures
This project was funded by a grant from the Cardinal Health E3 Foundation. The authors report no conflicts of interest.
Anticoagulants are among the prescriptions with the highest risk of an adverse drug event (ADE) after discharge, and many of these events are preventable.[1, 2, 3] In recognition of the high risk for adverse events, the Institute for Healthcare Improvement Map details several key features of a safe anticoagulation management program, including the recommendation during the transition period that clinicians ensure proper lab monitoring and establish capacity for follow‐up testing.[4]
Despite the potential for harm, most hospitals do not have a structured process for the transmission of vital information related to warfarin management from the inpatient to the ambulatory setting. Our aim was to develop a concise report containing the essential information regarding the patient's anticoagulation regimen, the Safe Transitions Anticoagulation Report (STAR), and a process to ensure the report can be readily accessed and utilized by ambulatory clinicians.
METHODS
We assembled an interdisciplinary team to develop a new report and workflow to ensure that information on inpatient warfarin management was transmitted to outpatient providers in a reliable and structured manner. Explicit goals were to maximize use of the electronic medical record (EMR) to autopopulate aspects of the new report and create a process that worked seamlessly into the workflow. The final items were selected based on the risk of harm if not conveyed and feasibility of incorporation through the EMR:
Warfarin doses: the 7 warfarin doses immediately prior to discharge
International normalized ratio (INR) values: the 7 INR values immediately prior to discharge
Bridging anticoagulation: the low‐molecular‐weight heparin (LMWH) prescribed as a bridging anticoagulant, if any
The STAR resides in both the discharge summary and the after visit summary (AVS) for patients discharged on warfarin. At our institution, the AVS contains a medication list, discharge instructions, and appointments, and is automatically produced through our EMR. Our institution utilizes the Epic EMR (Epic Systems Corp., Verona, WI) in the hospital, ambulatory clinics, and faculty practices.
A process was developed where a structured table is automatically created (Figure 1). A field was added to our EMR's discharge summary template asking whether the patient is being discharged on warfarin. Answering yes produces a second question asking whether the patient is also being discharged on bridging anticoagulation with LMWH. The STAR is not inserted into the discharge summary if the clinician completing the discharge summary deletes the anticoagulation question. The STAR is automatically created for patients discharged on warfarin and inserted into the AVS by the EMR regardless of whether the discharge summary has been completed. Patients are instructed by their nurse to bring their AVS to their follow‐up appointments.
Figure 1
The Safe Transitions Anticoagulation Report (STAR) as it appears in the discharge summary. Abbreviations: INR, international normalized ratio.
The STAR project team utilized plan‐do‐study‐act cycles to test small changes and make revisions. The workflow was piloted on 2 medical/surgical units from January 2014 through March 2014, and revised based on feedback from clinicians and nursing staff. The STAR initiative was fully implemented across our institution in April 2014.
The study was evaluated by the institutional review board of the Icahn School of Medicine at Mount Sinai, and full review was waived.
Outcomes
Our primary outcomes were the timeliness of laboratory monitoring and quality of anticoagulation management for patients with an established relationship at 1 of the main outpatient practices in our system. Our institution has an anticoagulation clinic for patients followed at the general medicine clinic. We defined an established relationship as having been seen in the same practice on at least 2 occasions in the 12 months prior to admission. The primary outcomes were the percentage of patients who had an INR measurement done and the percentage who had a therapeutic INR value within 10 days after discharge. As the 10‐day period is arbitrary, we also assessed these outcomes for the 3‐, 7‐, and 30‐day periods after discharge. The therapeutic range was defined for all patients as an INR of 2.0 to 3.0, as this is the target range for the large majority of patients on warfarin in our system. Outcomes during the intervention period were compared to baseline values during the preintervention period. For patients with multiple admissions, the first admission during each period was included.
Ambulatory Physician Survey
We surveyed ambulatory care physicians at the main practices for our health system. The survey assessed how often the STAR was viewed and incorporated into decision making, whether the report improved workflow, and whether ambulatory providers perceived that the report increased patient safety. The survey was distributed at the 6‐month interval during the intervention phase. The survey was disseminated electronically on 3 occasions, and a paper version was distributed on 1 occasion to housestaff and general medicine faculty.
Statistical Analysis
Comparisons for categorical data were performed using the 2 test. P values were based on 2‐tailed tests of significance, and a value 0.05 was considered significant.
RESULTS
The STAR was embedded in the discharge summary for 1370 (78.6%) discharges during the intervention period. A total of 505 patients in the preintervention period and 292 patients in the intervention period were established patients at an affiliated practice and comprised the study population. Demographics and indications for warfarin for the preintervention and intervention groups are listed in the Table 1.
Patient Demographics and Warfarin Indications
Preintervention Group, N=505
Intervention Group, N=292
P Value
NOTE: Abbreviations: INR, international normalized ratio. *Total sums to greater than 100% as categories are not mutually exclusive. Including but not limited to prevention of venous thromboembolism after orthopedic or other surgical procedure and prevention of arterial thromboembolism after left ventricular assist device implantation. No indication listed in the order field for warfarin within the electronic medical record.
Age, y
66.7
68.0
0.29
Male gender, n (%)
236 (46.7)
153 (52.4)
0.12
Discharged on bridging agent, n (%)
90 (17.8)
36 (12.3)
0.04
Average length of stay, d
7.1
7.6
0.46
Newly prescribed warfarin, n (%)
147 (29.1)
62 (21.2)
0.01
INR 2.03.0 range at discharge, n (%)
187 (37.0)
137 (46.9)
0.02
Warfarin indication, n (%)*
Venous thromboembolism
93 (18.4)
39 (13.4)
Atrial fibrillation
204 (40.3)
127 (43.5)
Mechanical heart valve
19 (3.8)
17 (6.5)
Prevention of thromboembolism
142 (28.1)
94 (32.2)
Intracardiac thrombosis
3 (0.5)
6 (2.1)
Thrombophilia
4 (0.8)
5 (1.7)
Other
19 (3.8)
12 (4.1)
No indication
32 (6.3)
1 (3.8)
The frequency of INR testing within 10 days of discharge was similar for the preintervention and intervention periods (41.4% and 47.6%, respectively, P=0.09). Similarly, the likelihood of having at least 1 therapeutic INR value within 10 days of discharge was not statistically different for the groups (17.0% and 21.2%, P=0.14). The pattern was similar for the 3‐, 7‐, and 30‐day periods; a higher percentage of the intervention group had INR testing and attained a therapeutic INR value, though for no time period did this reach statistical significance. This pattern was also found when limiting the analysis to patients discharged home rather than to a facility, patients on warfarin, prior to admission, and patients started on warfarin during the hospitalization.
A total of 87of 207 (42.0%) clinicians responded to the survey. Of respondents, 75% reported that they had seen 1 patient who had been discharged on warfarin since the STAR initiative had begun, 58% of whom reported having viewed the STAR. Most respondents who viewed the STAR found it to be helpful or very helpful in guiding warfarin management (67%), improving their workflow and efficiency (58%), and improving patient safety (77%). Approximately one‐third of respondents who had viewed the STAR (34%) reported that they selected a different dose than they would have chosen had the STAR not been available.
DISCUSSION
We developed a concise report that is seamlessly created and inserted into the discharge summary. Though the STAR was perceived as improving patient safety by ambulatory care providers, there was no impact on attaining a therapeutic INR after discharge. There are several possible explanations for a lack of benefit. Most notably, our intervention was comprised of a stand‐alone EMR‐based tool and focused on 1 component of the transitions process. Given the complexity of healthcare delivery and anticoagulant management, it is likely that broader interventions are required to improve clinical outcomes over the transition period. Potential targets of multifaceted approaches may include improving access to care, providing greater access to anticoagulation clinics, enhancing patient education, and promoting direct physician‐physician communication. Bundled interventions will likely need to include involvement of an interdisciplinary team, such as pharmacist involvement in the medication reconciliation process.
The transition period from the hospital to the outpatient setting has the potential to jeopardize patient safety if vital information is not reliably transmitted across venues.[5, 6, 7, 8] Forster and colleagues noted an 11% incidence of ADEs in the posthospitalization period, of which 60% were either preventable or ameliorable.[3] To decrease the risk to patient safety during the transitions period, the Transitions of Care Consensus policy statement by the Society of Hospital Medicine and other medical organizations called for incorporation of standard data transfer forms (templates and transmission protocols).[9] Despite the high risk and preventable nature of many of the events, few specific tools have been developed. As part of broader initiatives to improve the transitions process, the STAR may have the potential to be a means for health systems to improve the quality of the transition of care for patients on anticoagulants.
Our study has several limitations. First, it was performed at a single health system. It is unknown whether the EMR‐based report could be similarly employed at other systems. Second, our study was unable to assess clinical endpoints. Given the lack of effect on attaining a therapeutic INR, it is unlikely that downstream outcomes, such as thromboembolism, were impacted. Lastly, we were unable to examine whether our intervention improved the care of patients whose outpatient provider was external to our system.
The STAR is a concise tool developed to provide essential anticoagulant‐related information to ambulatory providers. Though the report was perceived as improving patient safety, our finding of a lack of impact on attaining a therapeutic INR after discharge suggests that the tool would need to be a component of a broader multifaceted intervention to impact clinical outcomes.
Disclosures
This project was funded by a grant from the Cardinal Health E3 Foundation. The authors report no conflicts of interest.
References
Santell JP, Hicks R, McMeekin J, Cousins DD.Medication errors: experience of the United States Pharmacopeia (USP) MEDMARX reporting system. J Clin Pharm.2003;43:760–767.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161–167.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.Adverse drug events occurring following hospital discharge. J Gen Int Med. 2005;204:317–323.
IHI Improvement Map. Available at: http://app.ihi.org/imap/tool/#Process=54aa289b‐16fd‐4a64‐8329‐3941dfc565d1. Accessed February 20 2015.
Kripalani S, Jackson AT, Schnipper JL, Coleman EA.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2:314–323.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831–841.
Johnson MP.Transitions of care in patients receiving oral anticoagulants: general principles, procedures, and impact of new oral anticoagulants. J Cardiovasc Nurs. 2013;28:54–65.
Deitelzweig SB.Care transitions in anticoagulation management for patients with atrial fibrillation: an emphasis on safety. Oschner J. 2013;13:419–427.
Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College Of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med.2009;4:364–370.
References
Santell JP, Hicks R, McMeekin J, Cousins DD.Medication errors: experience of the United States Pharmacopeia (USP) MEDMARX reporting system. J Clin Pharm.2003;43:760–767.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161–167.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW.Adverse drug events occurring following hospital discharge. J Gen Int Med. 2005;204:317–323.
IHI Improvement Map. Available at: http://app.ihi.org/imap/tool/#Process=54aa289b‐16fd‐4a64‐8329‐3941dfc565d1. Accessed February 20 2015.
Kripalani S, Jackson AT, Schnipper JL, Coleman EA.Promoting effective transitions of care at hospital discharge: a review of key issues for hospitalists. J Hosp Med. 2007;2:314–323.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW.Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831–841.
Johnson MP.Transitions of care in patients receiving oral anticoagulants: general principles, procedures, and impact of new oral anticoagulants. J Cardiovasc Nurs. 2013;28:54–65.
Deitelzweig SB.Care transitions in anticoagulation management for patients with atrial fibrillation: an emphasis on safety. Oschner J. 2013;13:419–427.
Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus policy statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College Of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med.2009;4:364–370.
Address for correspondence and reprint requests: Andrew S. Dunn, MD, Chief, Division of Hospital Medicine, Mount Sinai Health System, 1468 Madison Ave., Box 1087, New York, NY 10029; Telephone: 212‐241‐2920; Fax: 212‐289‐6393; E‐mail: [email protected]
Content Gating
Gated (full article locked unless allowed per User)